)RUP 'HSDUWPHQW RI WKH 7UHDVXU\ ,QWHUQDO 5HYHQXH 6HUYLFH 'HSDUWPHQW RI /DERU (PSOR\HH %HQHILWV 6HFXULW\ $GPLQLVWUDWLRQ 3HQVLRQ %HQHILW *XDUDQW\ &RUSRUDWLRQ $QQXDO 5HWXUQ5HSRUW RI (PSOR\HH %HQHILW 3ODQ 7KLV IRUP LV UHTXLUHG WR EH ILOHG IRU HPSOR\HH EHQHILW SODQV XQGHU VHFWLRQV DQG RI WKH (PSOR\HH 5HWLUHPHQW ,QFRPH 6HFXULW\ $FW RI (5,6$ DQG VHFWLRQV H E DQG D RI WKH ,QWHUQDO 5HYHQXH &RGH WKH &RGH &RPSOHWH DOO HQWULHV LQ DFFRUGDQFH ZLWK WKH LQVWUXFWLRQV WR WKH )RUP 20% 1RV 7KLV )RUP LV 2SHQ WR 3XEOLF ,QVSHFWLRQ 3DUW , $QQXDO 5HSRUW ,GHQWLILFDWLRQ ,QIRUPDWLRQ )RU FDOHQGDU SODQ \HDU RU ILVFDO SODQ \HDU EHJLQQLQJ DQG HQGLQJ $ 7KLV UHWXUQUHSRUW LV IRU D PXOWLHPSOR\HU SODQ D PXOWLSOHHPSOR\HU SODQ RU D VLQJOHHPSOR\HU SODQ D ')( VSHFLI\ % 7KLV UHWXUQUHSRUW LV WKH ILUVW UHWXUQUHSRUW WKH ILQDO UHWXUQUHSRUW DQ DPHQGHG UHWXUQUHSRUW D VKRUW SODQ \HDU UHWXUQUHSRUW OHVV WKDQ PRQWKV & ,I WKH SODQ LV D FROOHFWLYHO\EDUJDLQHG SODQ FKHFN KHUH ' &KHFN ER[ LI ILOLQJ XQGHU )RUP DXWRPDWLF H[WHQVLRQ WKH ')9& SURJUDP VSHFLDO H[WHQVLRQ HQWHU GHVFULSWLRQ 3DUW ,, %DVLF 3ODQ ,QIRUPDWLRQ²HQWHU DOO UHTXHVWHG LQIRUPDWLRQ D 1DPH RI SODQ E 7KUHHGLJLW SODQ QXPEHU 31 F (IIHFWLYH GDWH RI SODQ D 3ODQ VSRQVRU¶V QDPH DQG DGGUHVV LQFOXGH URRP RU VXLWH QXPEHU HPSOR\HU LI IRU D VLQJOHHPSOR\HU SODQ E (PSOR\HU ,GHQWLILFDWLRQ 1XPEHU (,1 F 6SRQVRU¶V WHOHSKRQH QXPEHU G %XVLQHVV FRGH VHH LQVWUXFWLRQV &DXWLRQ $ SHQDOW\ IRU WKH ODWH RU LQFRPSOHWH ILOLQJ RI WKLV UHWXUQUHSRUW ZLOO EH DVVHVVHG XQOHVV UHDVRQDEOH FDXVH LV HVWDEOLVKHG 8QGHU SHQDOWLHV RI SHUMXU\ DQG RWKHU SHQDOWLHV VHW IRUWK LQ WKH LQVWUXFWLRQV , GHFODUH WKDW , KDYH H[DPLQHG WKLV UHWXUQUHSRUW LQFOXGLQJ DFFRPSDQ\LQJ VFKHGXOHV VWDWHPHQWV DQG DWWDFKPHQWV DV ZHOO DV WKH HOHFWURQLF YHUVLRQ RI WKLV UHWXUQUHSRUW DQG WR WKH EHVW RI P\ NQRZOHGJH DQG EHOLHI LW LV WUXH FRUUHFW DQG FRPSOHWH 6,*1 +(5( 6LJQDWXUH RI SODQ DGPLQLVWUDWRU 'DWH (QWHU QDPH RI LQGLYLGXDO VLJQLQJ DV SODQ DGPLQLVWUDWRU 6,*1 +(5( 6LJQDWXUH RI HPSOR\HUSODQ VSRQVRU 'DWH (QWHU QDPH RI LQGLYLGXDO VLJQLQJ DV HPSOR\HU RU SODQ VSRQVRU 6,*1 +(5( 6LJQDWXUH RI ')( 'DWH (QWHU QDPH RI LQGLYLGXDO VLJQLQJ DV ')( 3UHSDUHU¶V QDPH LQFOXGLQJ ILUP QDPH LI DSSOLFDEOH DQG DGGUHVV LQFOXGH URRP RU VXLWH QXPEHU RSWLRQDO 3UHSDUHU¶V WHOHSKRQH QXPEHU RSWLRQDO )RU 3DSHUZRUN 5HGXFWLRQ $FW 1RWLFH DQG 20% &RQWURO 1XPEHUV VHH WKH LQVWUXFWLRQV IRU )RUP )RUP 07/01/2013 06/30/2014 X X Columbia College Retirement Plan 001 07/01/1989 Columbia College 1001 Rogers Street Columbia MO 65216 43-0655867 573-875-7251 611000 Bruce Boyer

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
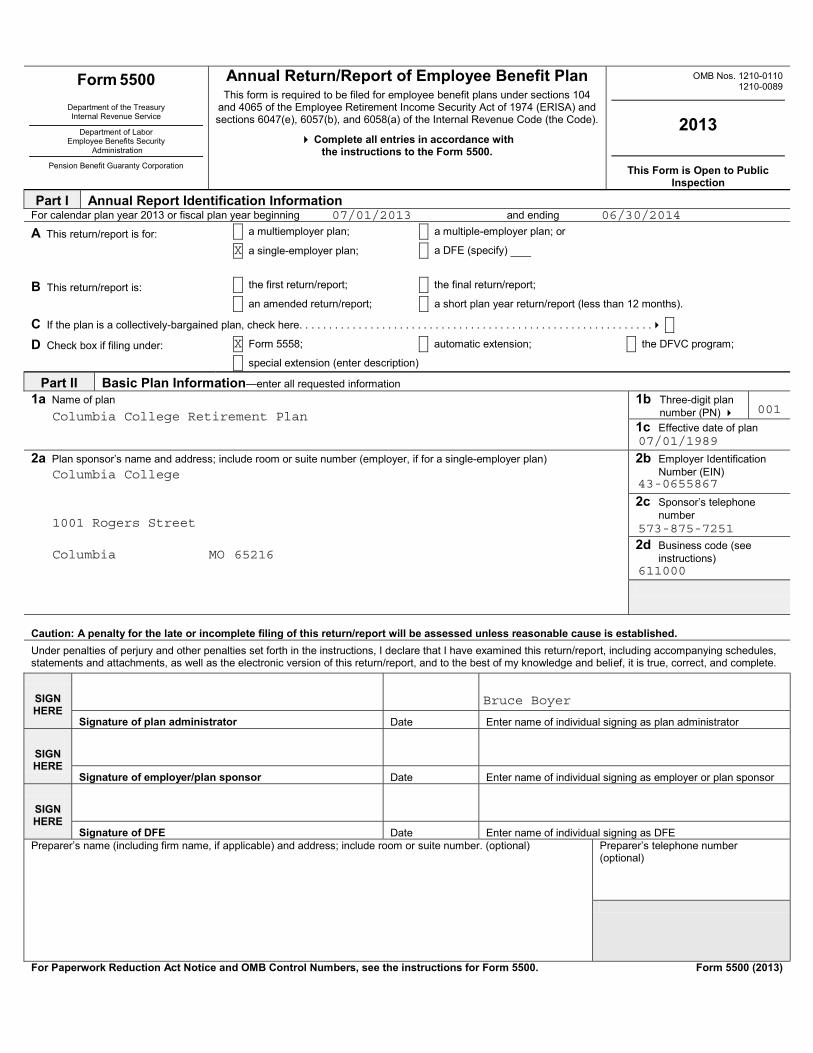
07/01/2013 06/30/2014
X
X
Columbia College Retirement Plan 001
07/01/1989
Columbia College
1001 Rogers Street
Columbia MO 65216
43-0655867
573-875-7251
611000
Bruce Boyer

X X
887
652
27
256
935
0
935
935
45
2G 2L 2M
X
X
X
X
X X
X 3
XX
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE FGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
001
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE FGHI ABCDEFGHI
012345678
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
012345678 ABCDE ABCDE0123456789 1234567 YYYY-MM-DD YYYY-MM-DD
123456789012345 123456789012345
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
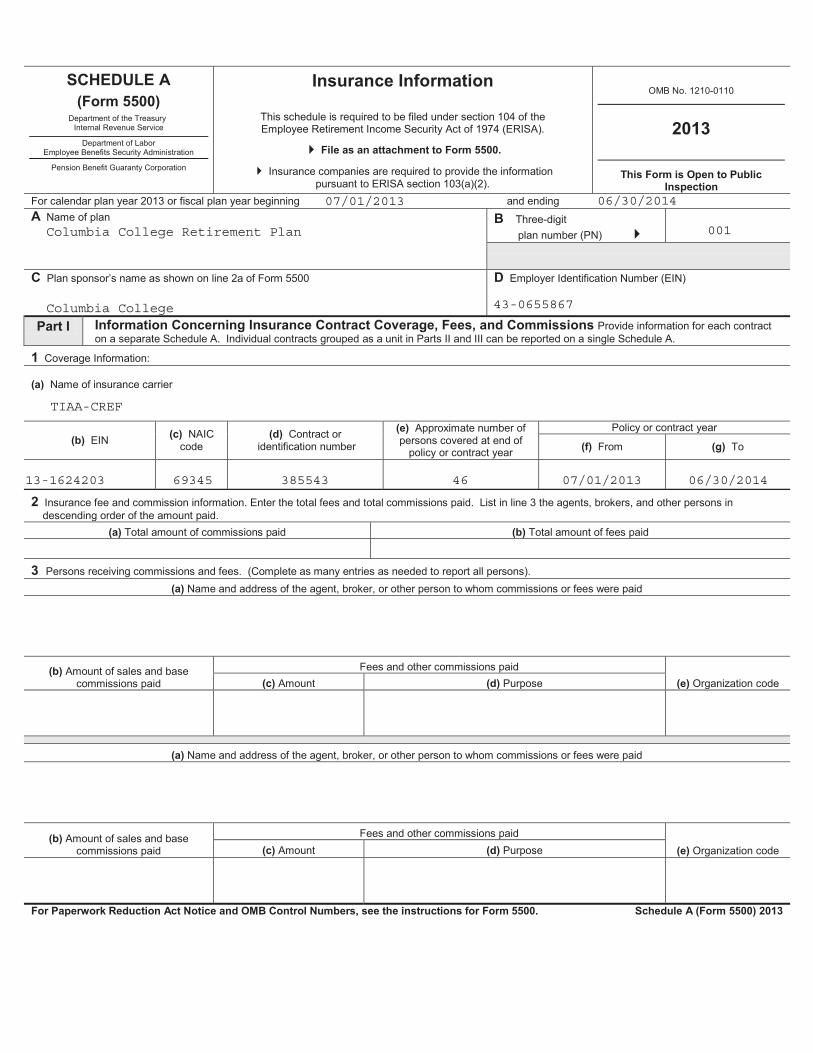
07/01/2013 06/30/2014
Columbia College Retirement Plan 001
Columbia College 43-0655867
TIAA-CREF
13-1624203 69345 385543 46 07/01/2013 06/30/2014
1 x
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1

-123456789012345 -123456789012345
-123456789012345 -123456789012345
-123456789012345
X X
X
X
X X X X
-123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
53567674386
X
36043614514
016571452628
483713844149
8382
300091
308473535676

X X X XX X X XX X X XX ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCKEFGHI ABCDEFGHI ABCDEFGHI ABCDE
-123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345 -123456789012345
123456789012345 123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 X X -123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
X X
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
0
0
0
X

ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE FGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
001
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE FGHI ABCDEFGHI
012345678
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
012345678 ABCDE ABCDE0123456789 1234567 YYYY-MM-DD YYYY-MM-DD
123456789012345 123456789012345
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
07/01/2013 06/30/2014
Columbia College Retirement Plan 001
Columbia College 43-0655867
Lincoln National life Insurance Company
35-0472300 65676 CR18693 896 07/01/2013 06/30/2014
210153 0
Lincoln Financial Advisors1300 S Clinton St, Ste 150
Fort Wayne IN 46802-9999
210153 4
1 x
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1

-123456789012345 -123456789012345
-123456789012345 -123456789012345
-123456789012345
X X
X
X
X X X X
-123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
6827896
X
58849651004052
0201445404113132034
Loan Repayments, Forfeitures, Takeovers,and/or Adjustments
17416447626609
4811251102
147441169045
Loans Issued, Forfeitures, Fees,Correctives and/or Adjustments
7987136827896
X X X XX X X XX X X XX ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCKEFGHI ABCDEFGHI ABCDEFGHI ABCDE
-123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345 -123456789012345
123456789012345 123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 X X -123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
X X
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
0
0
0
X
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE FGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
001
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE FGHI ABCDEFGHI
012345678
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
012345678 ABCDE ABCDE0123456789 1234567 YYYY-MM-DD YYYY-MM-DD
123456789012345 123456789012345
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
07/01/2013 06/30/2014
Columbia College Retirement Plan 001
Columbia College 43-0655867
USAA Life Insurance Company
74-1472662 69663 008602561 4 07/01/2013 06/30/2014
1 x
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE 123456789 ABCDEFGHI ABCDEFGHI ABCDE CITY56789 ABCDEFGHI AB, ST 021345678901
-123456789012345 -123456789012345 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
1
-123456789012345 -123456789012345
-123456789012345 -123456789012345
-123456789012345
X X
X
X
X X X X
-123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
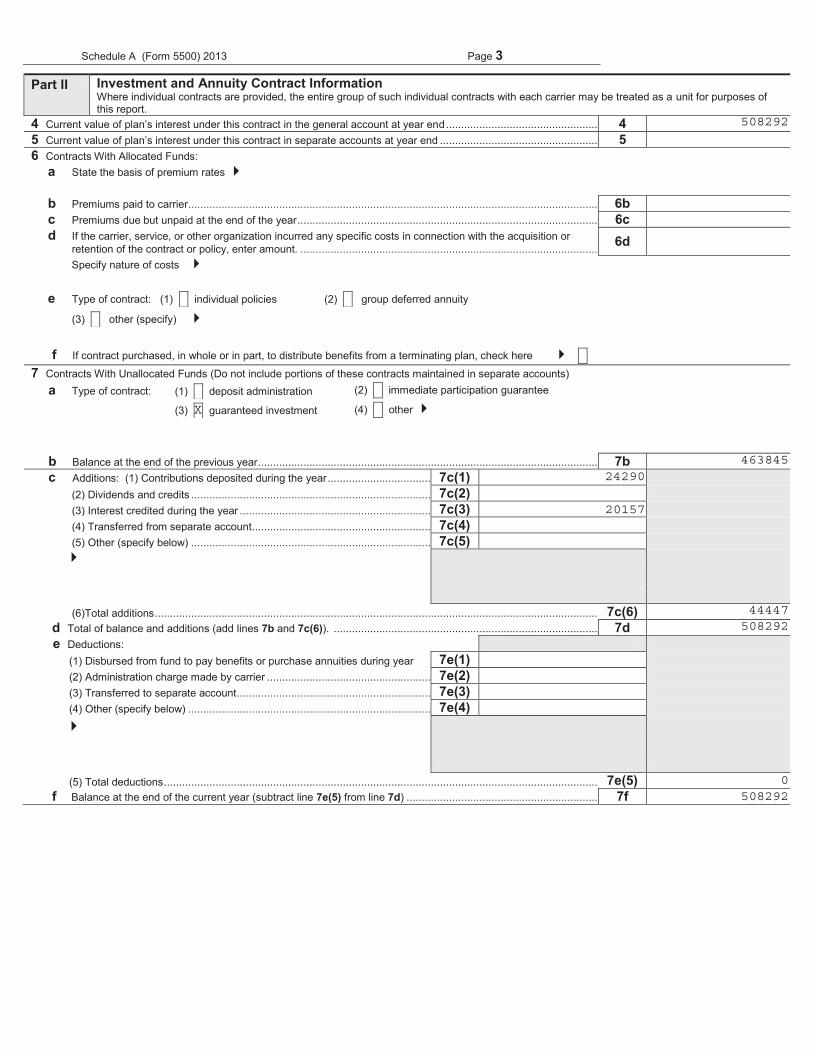
508292
X
46384524290
20157
44447508292
0508292
X X X XX X X XX X X XX ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCKEFGHI ABCDEFGHI ABCDEFGHI ABCDE
-123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345 -123456789012345
123456789012345 123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 X X -123456789012345
-123456789012345 -123456789012345 -123456789012345 -123456789012345
-123456789012345 -123456789012345
X X
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
0
0
0
X

ABCDEFGHI 001
Plan sponsor’s name as shown on line 2a of Form 5500ABCDEFGHI 012345678
X XIf you answered line 1a “Yes,” enter the name and EIN or address of each person providing the required disclosures for the s
07/01/2013 06/30/2014
Columbia College Retirement Plan 001
Columbia College43-0655867
X
TIAA 13-1624203
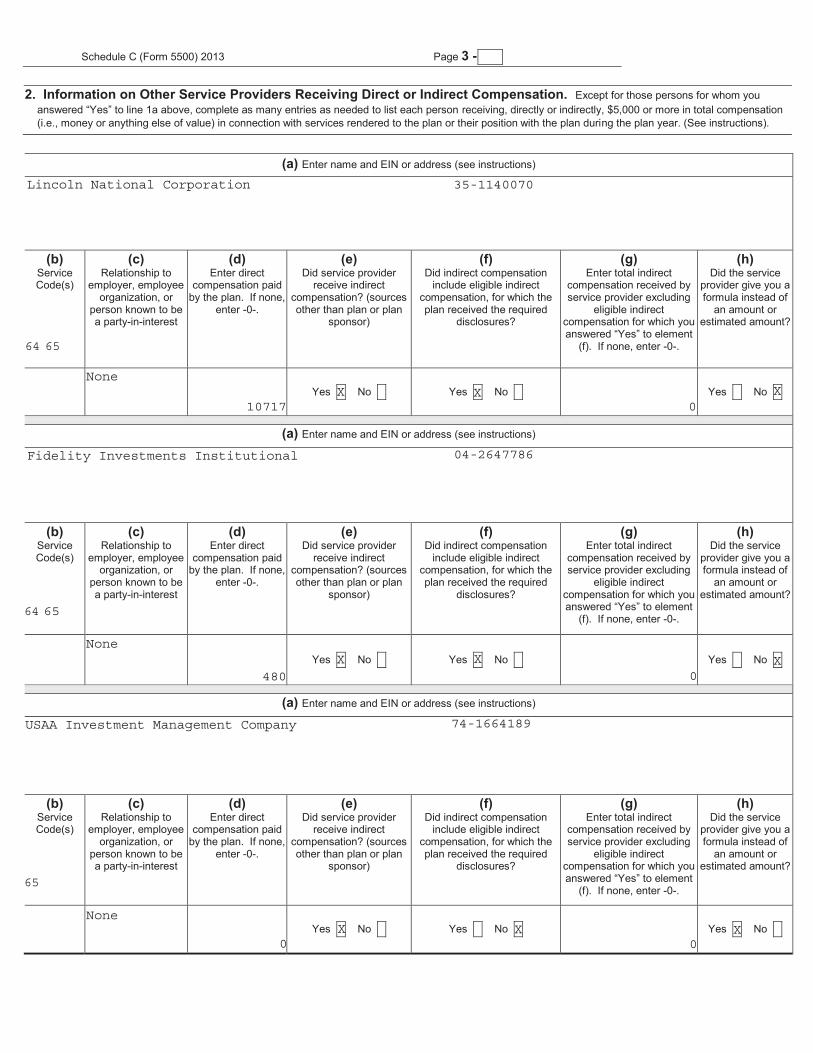
Lincoln National Corporation 35-1140070
Fidelity Institutional Operations 04-2647786
1 x
1 x
answered “Yes” to line 1a above, complete as many entries as needed to list each person
answered “Yes” to element
ABCDEFGHI ABCDEFGHI ABCD
123456789012345 X X X X
123456789012345 X X
answered “Yes” to element
ABCDEFGHI ABCDEFGHI ABCD
123456789012345
X X X X123456789012345
X X
answered “Yes” to element
ABCDEFGHI ABCDEFGHI ABCD
123456789012345 X X X X
X X
Lincoln National Corporation 35-1140070
64 65
None
10717X X
0X
Fidelity Investments Institutional 04-2647786
64 65
None
480X X
0X
USAA Investment Management Company 74-1664189
65
None
0X X
0X
answered “Yes” to line 1a above, complete as many entries as needed to list each person
answered “Yes” to element
ABCDEFGHI ABCDEFGHI ABCD
123456789012345 X X X X
123456789012345 X X
answered “Yes” to element
ABCDEFGHI ABCDEFGHI ABCD
123456789012345
X X X X123456789012345
X X
answered “Yes” to element
ABCDEFGHI ABCDEFGHI ABCD
123456789012345 X X X X
X X
1 x
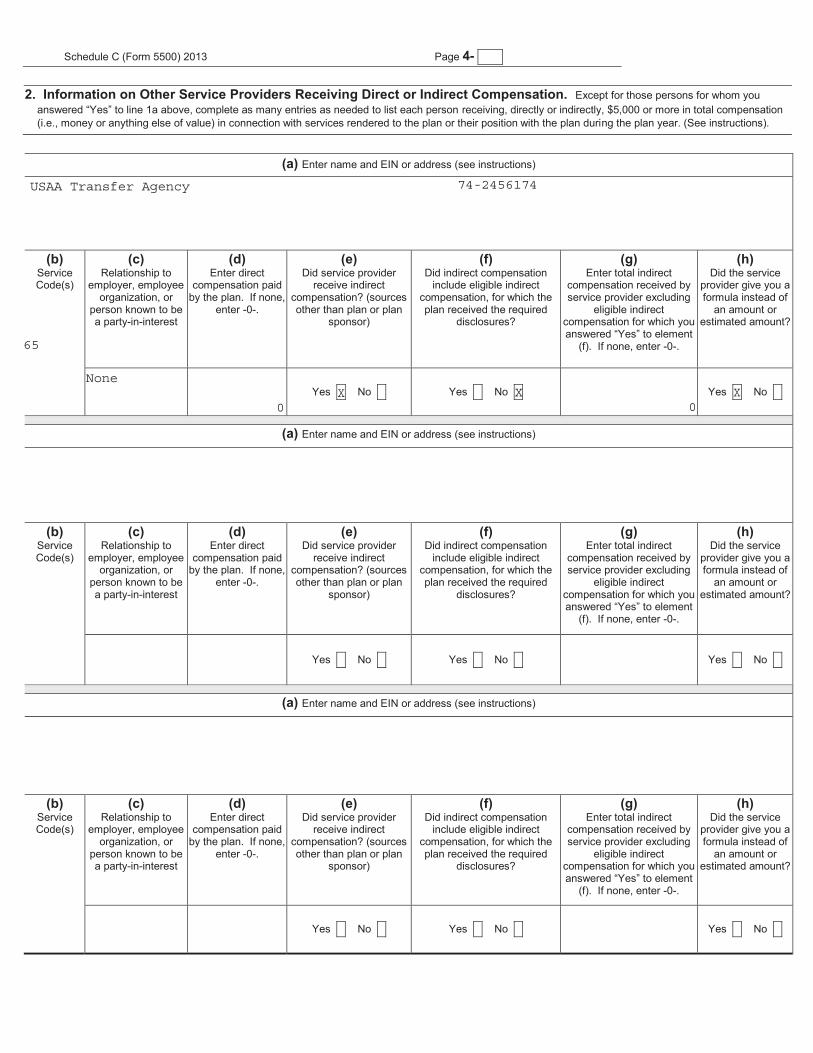
USAA Transfer Agency 74-2456174
65
None
0X X
0X

formula used to determine the service provider’s eligibility
formula used to determine the service provider’s eligibility
formula used to determine the service provider’s eligibility
1 x
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 10 11 12 13
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 10 11 12 13
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 10 11 12 13
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 10 11 12 13
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 10 11 12 13
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDE
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 1234567890
1 x

ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 123456789 ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 123456789
ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 123456789
ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 123456789
ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD 123456789
ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD
1234567890
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
7-

SCHEDULE D(Form 5500)
DFE/Participating Plan Information
File as an attachment to Form 5500.
2013
This Form is Open to Public Inspection.
AABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
B001
CABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
D012345678
Part I Information on interests in MTIAs, CCTs, PSAs, and 103-12 IEs (to be completed by plans and DFEs)
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
07/01/2013 06/30/2014
Columbia College Retirement Plan 001
Columbia College 43-0655867
TIAA Real Estate
TIAA-CREF
13-1624203 004 P 74386
2 - 1 xa ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDb ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHIc 123456789-123
d 1
e-123456789012345
3 - 1 x6
Part II Information on Participating Plans (to be completed by DFEs)
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123
a ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
b
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
c 123456789-123

SCHEDULE H(Form 5500)
Department of the TreasuryInternal Revenue Service
Department of LaborEmployee Benefits Security Administration
Pension Benefit Guaranty Corporation
Financial Information
This schedule is required to be filed under section 104 of the Employee Retirement Income Security Act of 1974 (ERISA), and section 6058(a) of the
Internal Revenue Code (the Code).
File as an attachment to Form 5500.
OMB No. 1210-0110
2013
This Form is Open to Public Inspection
For calendar plan year 2013 or fiscal plan year beginning and ending A Name of planABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
B Three-digitplan number (PN) 001
C Plan sponsor’s name as shown on line 2a of Form 5500 ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
D Employer Identification Number (EIN)012345678
Part I Asset and Liability Statement1 Current value of plan assets and liabilities at the beginning and end of the plan year. Combine the value of plan assets held in more than one trust. Report
the value of the plan’s interest in a commingled fund containing the assets of more than one plan on a line-by-line basis unless the value is reportable on lines 1c(9) through 1c(14). Do not enter the value of that portion of an insurance contract which guarantees, during this plan year, to pay a specific dollar benefit at a future date. Round off amounts to the nearest dollar. MTIAs, CCTs, PSAs, and 103-12 IEs do not complete lines 1b(1), 1b(2), 1c(8), 1g, 1h, and 1i. CCTs, PSAs, and 103-12 IEs also do not complete lines 1d and 1e. See instructions.
Assets (a) Beginning of Year (b) End of Year
a Total noninterest-bearing cash ...................................................................... 1a -123456789012345 -123456789012345 b Receivables (less allowance for doubtful accounts):
(1) Employer contributions.......................................................................... 1b(1) -123456789012345 -123456789012345 (2) Participant contributions........................................................................ 1b(2) -123456789012345 -123456789012345 (3) Other..................................................................................................... 1b(3) -123456789012345 -123456789012345
c General investments: (1) Interest-bearing cash (include money market accounts & certificates
of deposit)............................................................................................ 1c(1) -123456789012345 -123456789012345 (2) U.S. Government securities .................................................................. 1c(2) -123456789012345 -123456789012345 (3) Corporate debt instruments (other than employer securities):
(A) Preferred ........................................................................................ 1c(3)(A) -123456789012345 -123456789012345(B) All other .......................................................................................... 1c(3)(B) -123456789012345 -123456789012345
(4) Corporate stocks (other than employer securities): (A) Preferred ........................................................................................ 1c(4)(A) -123456789012345 -123456789012345(B) Common......................................................................................... 1c(4)(B) -123456789012345 -123456789012345
(5) Partnership/joint venture interests ......................................................... 1c(5) -123456789012345 -123456789012345 (6) Real estate (other than employer real property)..................................... 1c(6) -123456789012345 -123456789012345 (7) Loans (other than to participants) .......................................................... 1c(7) -123456789012345 -123456789012345 (8) Participant loans.................................................................................... 1c(8) -123456789012345 -123456789012345 (9) Value of interest in common/collective trusts ......................................... 1c(9) -123456789012345 -123456789012345
(10) Value of interest in pooled separate accounts ....................................... 1c(10) -123456789012345 -123456789012345 (11) Value of interest in master trust investment accounts ............................ 1c(11) -123456789012345 -123456789012345 (12) Value of interest in 103-12 investment entities....................................... 1c(12) -123456789012345 -123456789012345 (13) Value of interest in registered investment companies (e.g., mutual funds).................................................................................... 1c(13) -123456789012345 -123456789012345 (14) Value of funds held in insurance company general account (unallocated
contracts).............................................................................................. 1c(14) -123456789012345 -123456789012345 (15) Other..................................................................................................... 1c(15) -123456789012345 -123456789012345
For Paperwork Reduction Act Notice and OMB Control Numbers, see the instructions for Form 5500 Schedule H (Form 5500) 2013
07/01/2013 06/30/2014
Columbia College Retirement Plan 001
Columbia College 43-0655867
0 00 0
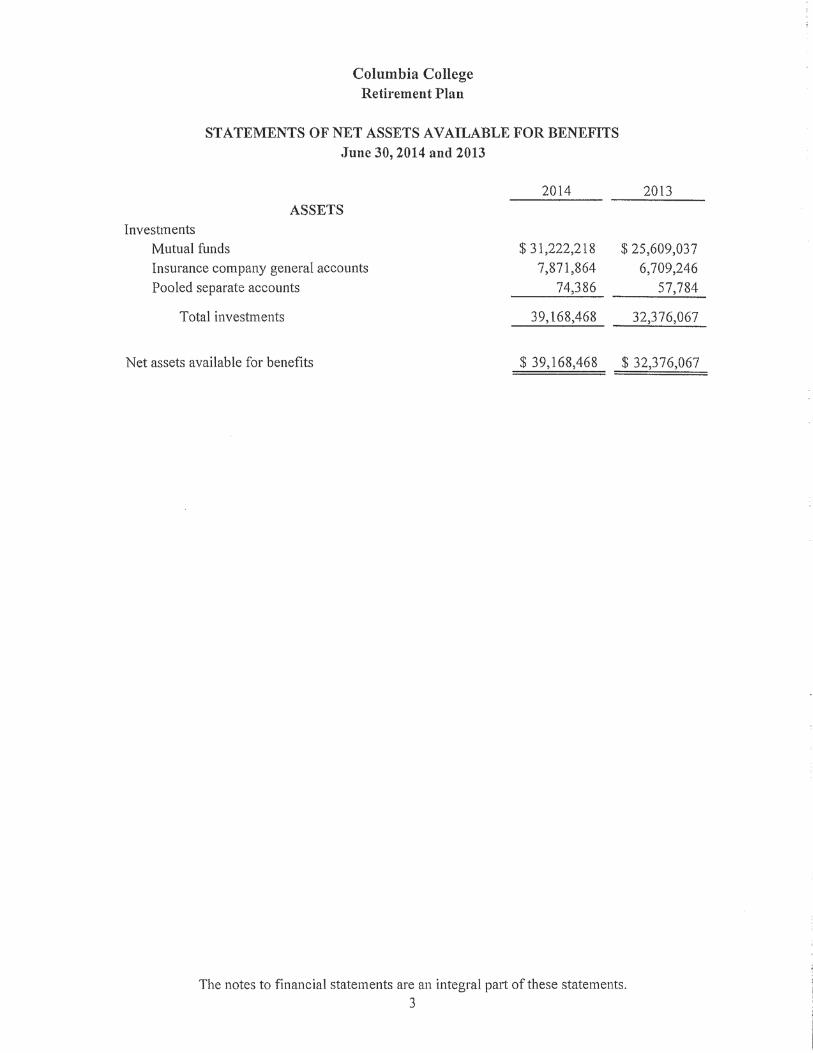
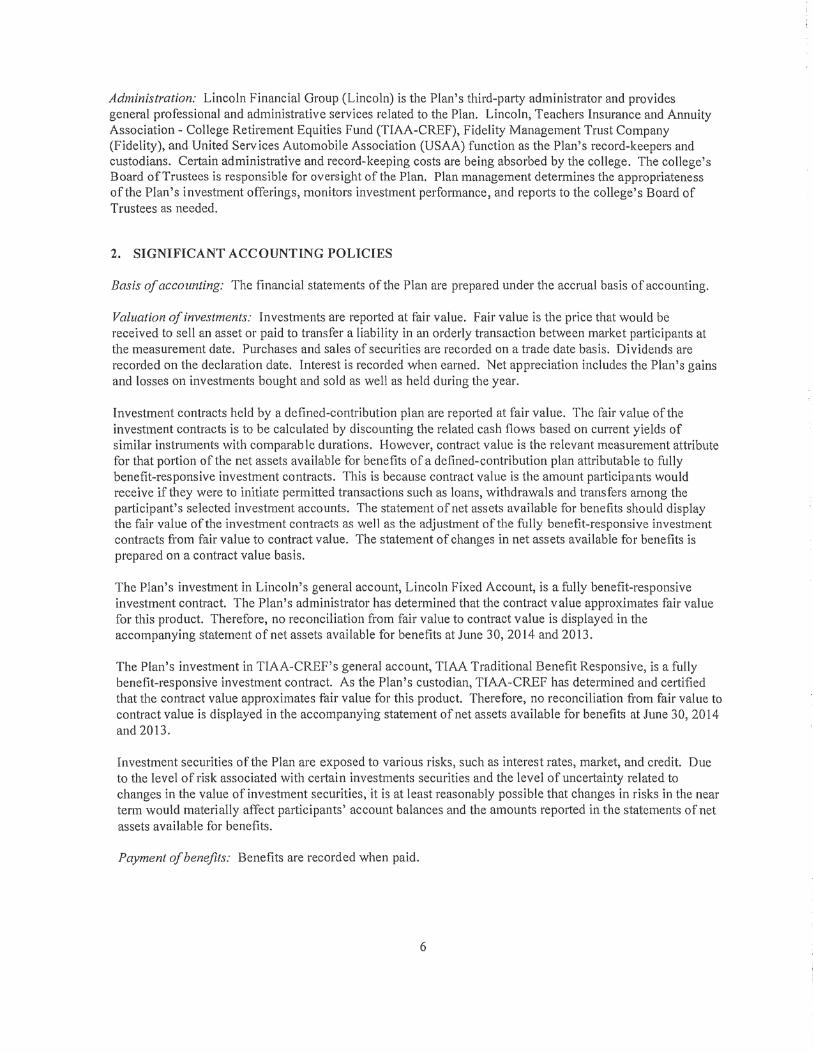
57784 74386
25609037 31222218
6709246 7871864
Schedule H (Form 5500) 2013 130118 Page 2
(5) Unrealized appreciation (depreciation) of assets: (A) Real estate........................ 2b(5)(A) -123456789012345 (B) Other ................................................................................................ 2b(5)(B) -123456789012345
(C) Total unrealized appreciation of assets. Add lines 2b(5)(A) and (B)................................................................ 2b(5)(C) -123456789012345
1d Employer-related investments: (a) Beginning of Year (b) End of Year
(1) Employer securities.................................................................................. 1d(1) -123456789012345 -123456789012345 (2) Employer real property ............................................................................. 1d(2) -123456789012345 -123456789012345
1e Buildings and other property used in plan operation ....................................... 1e -123456789012345 -123456789012345 1f Total assets (add all amounts in lines 1a through 1e) ..................................... 1f -123456789012345 -123456789012345
Liabilities1g Benefit claims payable.................................................................................... 1g -123456789012345 -123456789012345 1h Operating payables ........................................................................................ 1h -123456789012345 -123456789012345 1i Acquisition indebtedness................................................................................ 1i -123456789012345 -123456789012345 1j Other liabilities................................................................................................ 1j -123456789012345 -123456789012345 1k Total liabilities (add all amounts in lines 1g through1j) .................................... 1k -123456789012345 -123456789012345
Net Assets1l Net assets (subtract line 1k from line 1f) ......................................................... 1l -123456789012345 -123456789012345
Part II Income and Expense Statement2 Plan income, expenses, and changes in net assets for the year. Include all income and expenses of the plan, including any trust(s) or separately maintained
fund(s) and any payments/receipts to/from insurance carriers. Round off amounts to the nearest dollar. MTIAs, CCTs, PSAs, and 103-12 IEs do not complete lines 2a, 2b(1)(E), 2e, 2f, and 2g.
Income (a) Amount (b) Total
a Contributions:
(1) Received or receivable in cash from: (A) Employers................................. 2a(1)(A) -123456789012345
(B) Participants ...................................................................................... 2a(1)(B) -123456789012345 (C) Others (including rollovers)............................................................... 2a(1)(C) -123456789012345
(2) Noncash contributions .............................................................................. 2a(2) -123456789012345 (3) Total contributions. Add lines 2a(1)(A), (B), (C), and line 2a(2)................. 2a(3) -123456789012345
b Earnings on investments: (1) Interest:
(A) Interest-bearing cash (including money market accounts and certificates of deposit)....................................................................... 2b(1)(A) -123456789012345
(B) U.S. Government securities .............................................................. 2b(1)(B) -123456789012345 (C) Corporate debt instruments .............................................................. 2b(1)(C) -123456789012345 (D) Loans (other than to participants) ..................................................... 2b(1)(D) -123456789012345 (E) Participant loans ............................................................................... 2b(1)(E) -123456789012345 (F) Other ................................................................................................ 2b(1)(F) -123456789012345 (G) Total interest. Add lines 2b(1)(A) through (F).................................... 2b(1)(G) -123456789012345
(2) Dividends: (A) Preferred stock.................................................................. 2b(2)(A) -123456789012345
(B) Common stock.................................................................................. 2b(2)(B) -123456789012345 (C) Registered investment company shares (e.g. mutual funds) ............. 2b(2)(C) (D) Total dividends. Add lines 2b(2)(A), (B), and (C) 2b(2)(D)
-123456789012345
(3) Rents........................................................................................................ 2b(3) -123456789012345 (4) Net gain (loss) on sale of assets: (A) Aggregate proceeds ...................... 2b(4)(A) -123456789012345
(B) Aggregate carrying amount (see instructions) ................................... 2b(4)(B) -123456789012345 (C) Subtract line 2b(4)(B) from line 2b(4)(A) and enter result ................. 2b(4)(C) -123456789012345
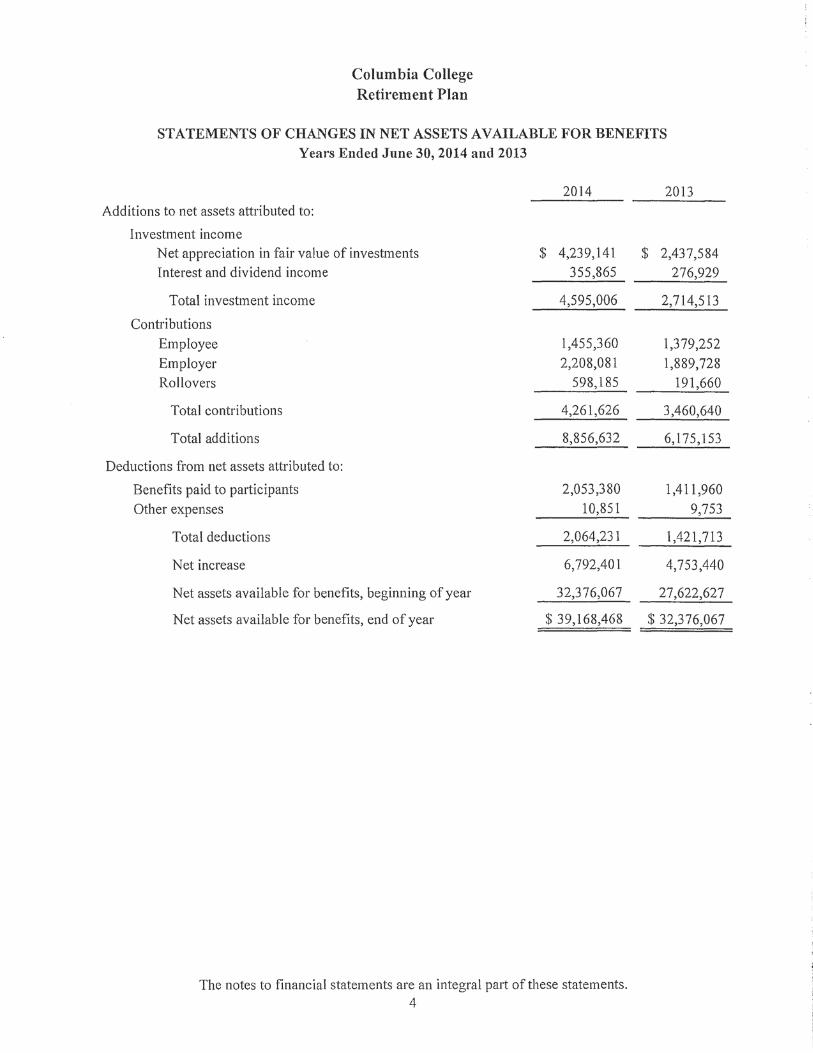
32376067 39168468
0 0
32376067 39168468
2208081
1455360
598185
4261626
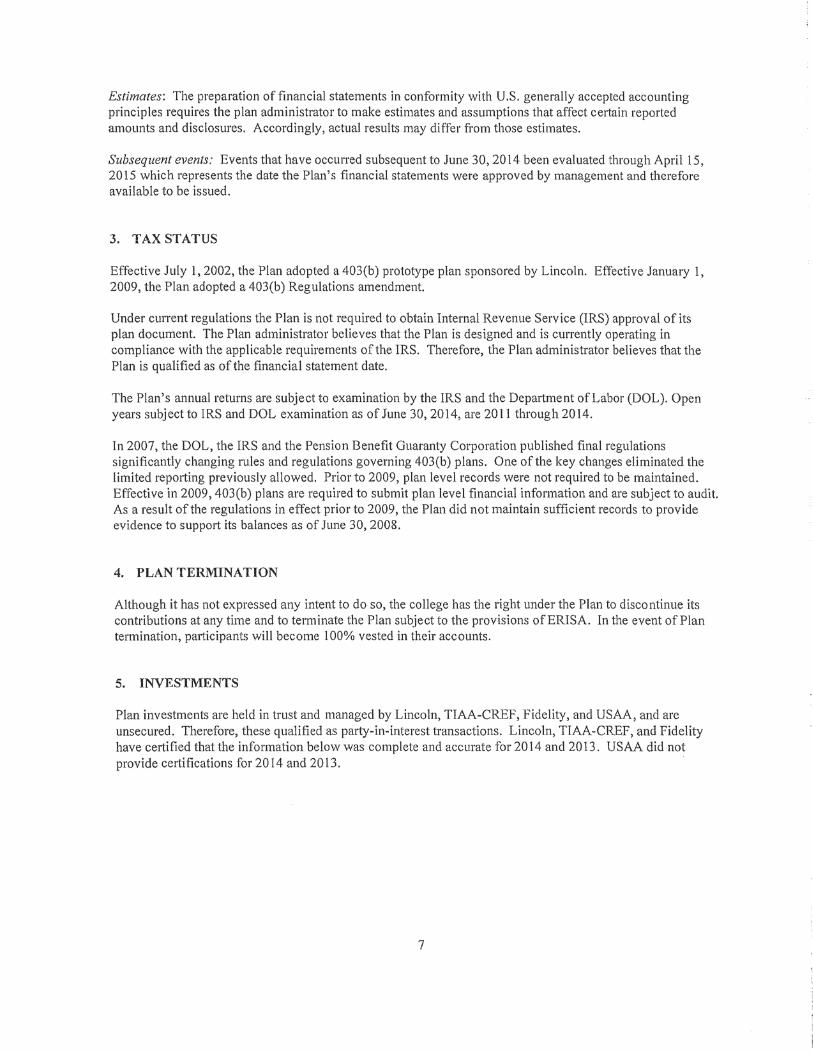
238173
238173
117692
117692
0
0
Schedule H (Form 5500) 2013 Page 3
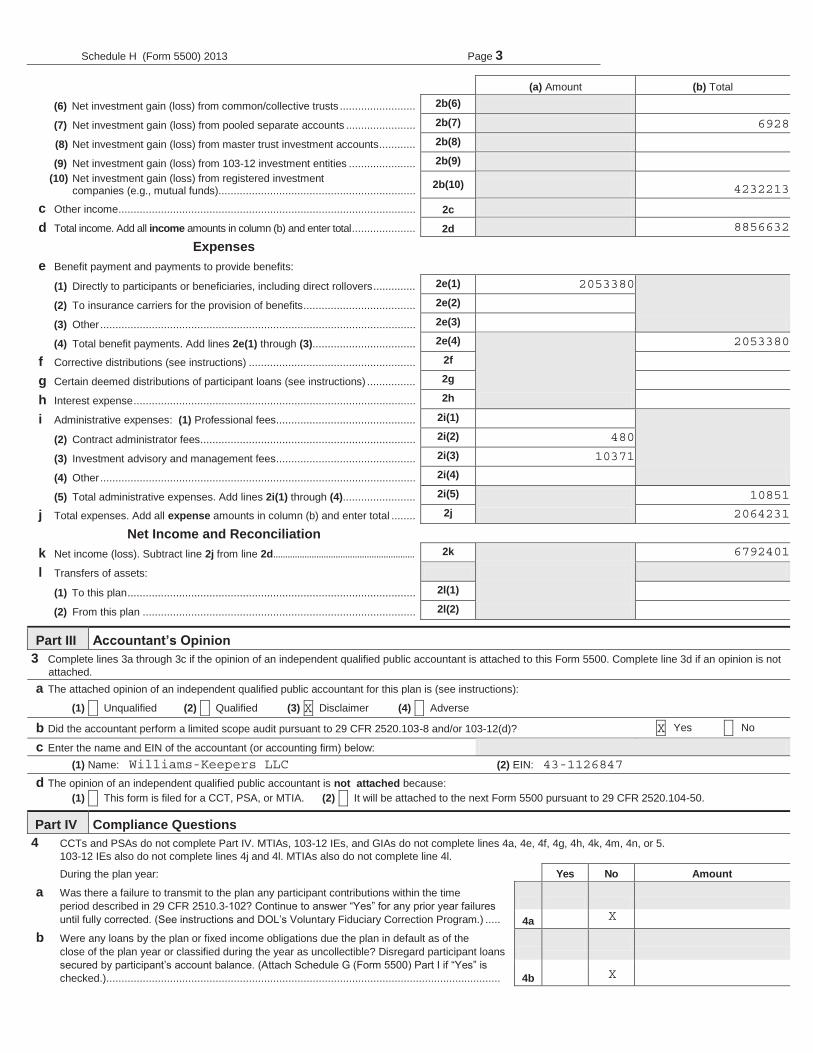
(a) Amount (b) Total (6) Net investment gain (loss) from common/collective trusts ......................... 2b(6) -123456789012345(7) Net investment gain (loss) from pooled separate accounts ....................... 2b(7) -123456789012345(8) Net investment gain (loss) from master trust investment accounts............ 2b(8) -123456789012345 (9) Net investment gain (loss) from 103-12 investment entities ...................... 2b(9) -123456789012345
(10) Net investment gain (loss) from registered investment companies (e.g., mutual funds)................................................................. 2b(10) -123456789012345
c Other income.................................................................................................. 2c -123456789012345d Total income. Add all income amounts in column (b) and enter total..................... 2d -123456789012345
Expensese Benefit payment and payments to provide benefits:
(1) Directly to participants or beneficiaries, including direct rollovers.............. 2e(1) -123456789012345
(2) To insurance carriers for the provision of benefits..................................... 2e(2) -123456789012345 (3) Other........................................................................................................ 2e(3) -123456789012345 (4) Total benefit payments. Add lines 2e(1) through (3).................................. 2e(4)
-123456789012345f Corrective distributions (see instructions) ....................................................... 2f -123456789012345g Certain deemed distributions of participant loans (see instructions) ................ 2g -123456789012345h Interest expense............................................................................................. 2h -123456789012345i Administrative expenses: (1) Professional fees.............................................. 2i(1) -123456789012345
(2) Contract administrator fees....................................................................... 2i(2) -123456789012345 (3) Investment advisory and management fees.............................................. 2i(3) -123456789012345 (4) Other........................................................................................................ 2i(4) -123456789012345 (5) Total administrative expenses. Add lines 2i(1) through (4)........................ 2i(5) -123456789012345
j Total expenses. Add all expense amounts in column (b) and enter total ........ 2j -123456789012345 Net Income and Reconciliation
k Net income (loss). Subtract line 2j from line 2d........................................................... 2k -123456789012345 l Transfers of assets:
(1) To this plan............................................................................................... 2l(1) -123456789012345 (2) From this plan .......................................................................................... 2l(2) -123456789012345
Part III Accountant’s Opinion3 Complete lines 3a through 3c if the opinion of an independent qualified public accountant is attached to this Form 5500. Complete line 3d if an opinion is not
attached.a The attached opinion of an independent qualified public accountant for this plan is (see instructions):
(1) X Unqualified (2) X Qualified (3) X Disclaimer (4) X Adverse
b Did the accountant perform a limited scope audit pursuant to 29 CFR 2520.103-8 and/or 103-12(d)? X Yes X No
c Enter the name and EIN of the accountant (or accounting firm) below: (1) Name: ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCD (2) EIN: 123456789
d The opinion of an independent qualified public accountant is not attached because:(1) X This form is filed for a CCT, PSA, or MTIA. (2) X It will be attached to the next Form 5500 pursuant to 29 CFR 2520.104-50.
Part IV Compliance Questions4 CCTs and PSAs do not complete Part IV. MTIAs, 103-12 IEs, and GIAs do not complete lines 4a, 4e, 4f, 4g, 4h, 4k, 4m, 4n, or 5.
103-12 IEs also do not complete lines 4j and 4l. MTIAs also do not complete line 4l.During the plan year: Yes No Amount
a Was there a failure to transmit to the plan any participant contributions within the time period described in 29 CFR 2510.3-102? Continue to answer “Yes” for any prior year failures until fully corrected. (See instructions and DOL’s Voluntary Fiduciary Correction Program.) ..... 4a -123456789012345
b Were any loans by the plan or fixed income obligations due the plan in default as of the close of the plan year or classified during the year as uncollectible? Disregard participant loanssecured by participant’s account balance. (Attach Schedule G (Form 5500) Part I if “Yes” is checked.).................................................................................................................................. 4b -123456789012345
6928
4232213
8856632
2053380
2053380
480
10371
10851
2064231
6792401
X
X
Williams-Keepers LLC 43-1126847
X
X
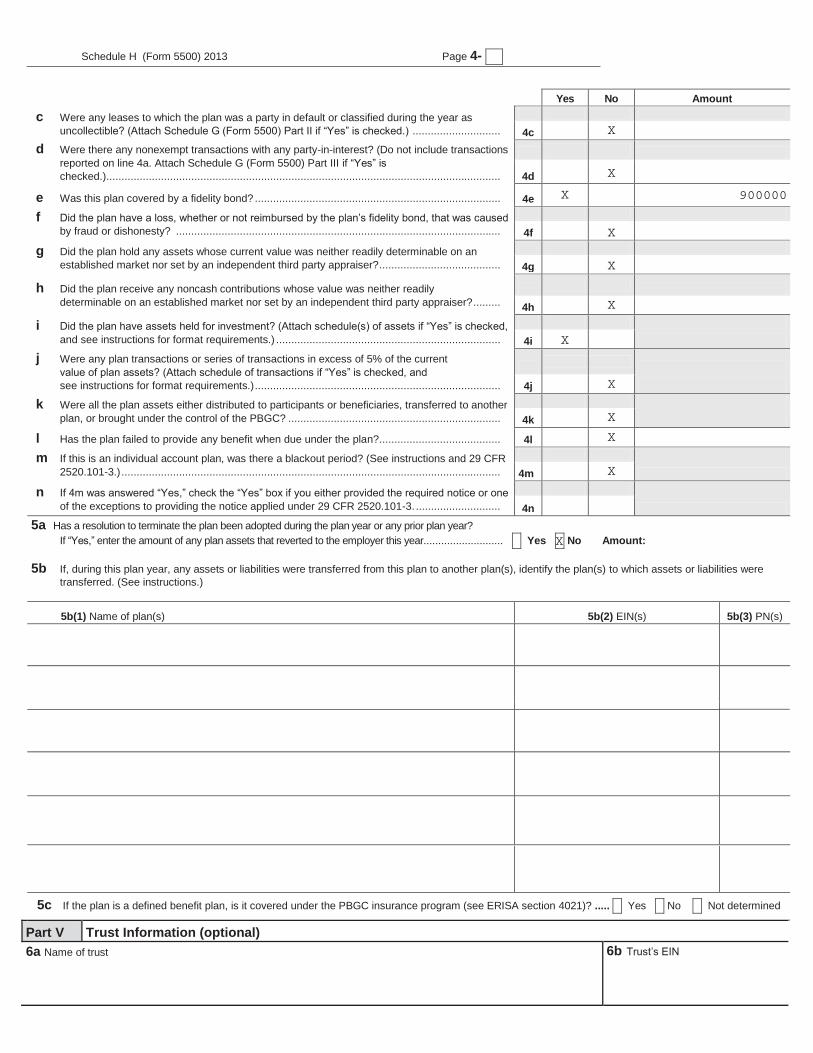
Schedule H (Form 5500) 2013 Page 4- X
Yes No Amount
c Were any leases to which the plan was a party in default or classified during the year as uncollectible? (Attach Schedule G (Form 5500) Part II if “Yes” is checked.) ............................. 4c -123456789012345
d Were there any nonexempt transactions with any party-in-interest? (Do not include transactions reported on line 4a. Attach Schedule G (Form 5500) Part III if “Yes” is checked.).................................................................................................................................. 4d -123456789012345
e Was this plan covered by a fidelity bond? ................................................................................. 4e -123456789012345f Did the plan have a loss, whether or not reimbursed by the plan’s fidelity bond, that was caused
by fraud or dishonesty? ........................................................................................................... 4f -123456789012345 g Did the plan hold any assets whose current value was neither readily determinable on an
established market nor set by an independent third party appraiser?........................................ 4g -123456789012345 h Did the plan receive any noncash contributions whose value was neither readily
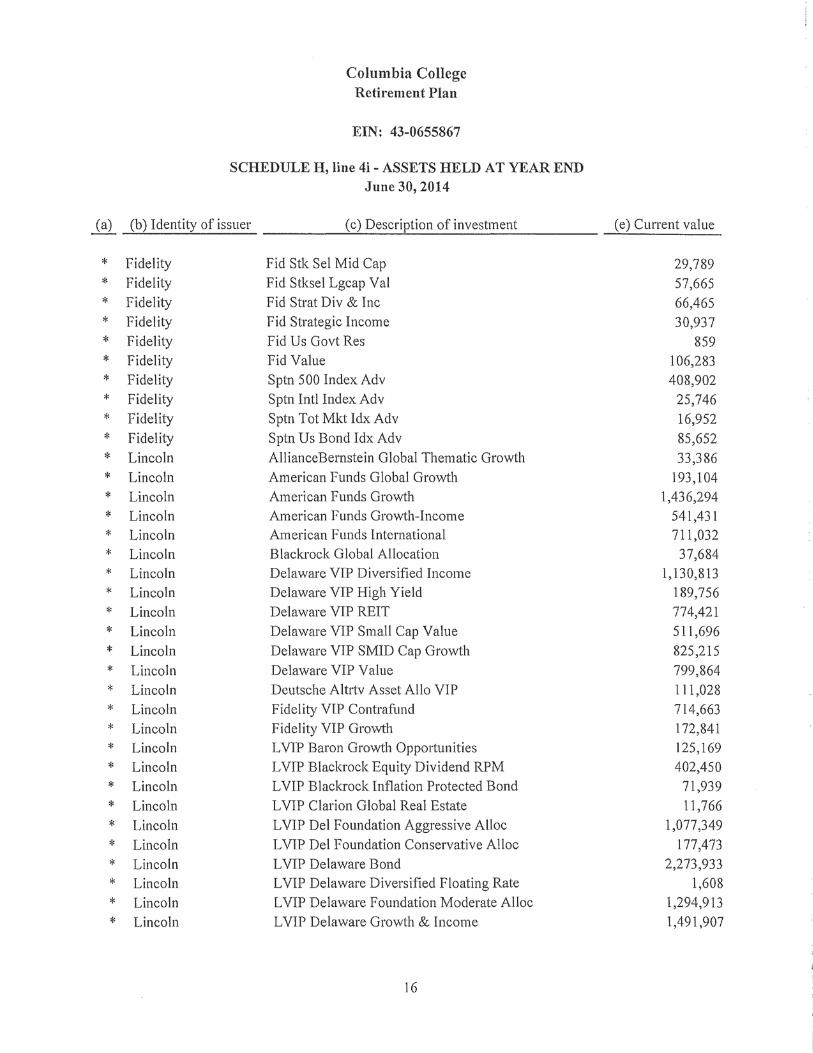
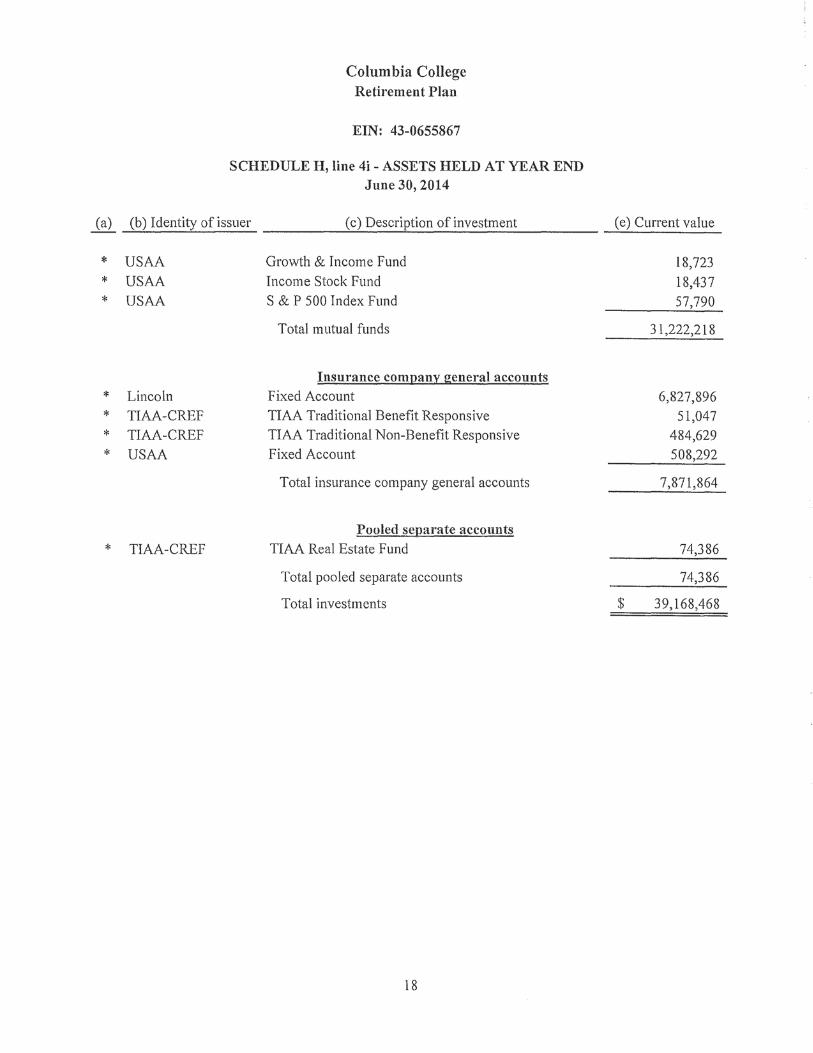
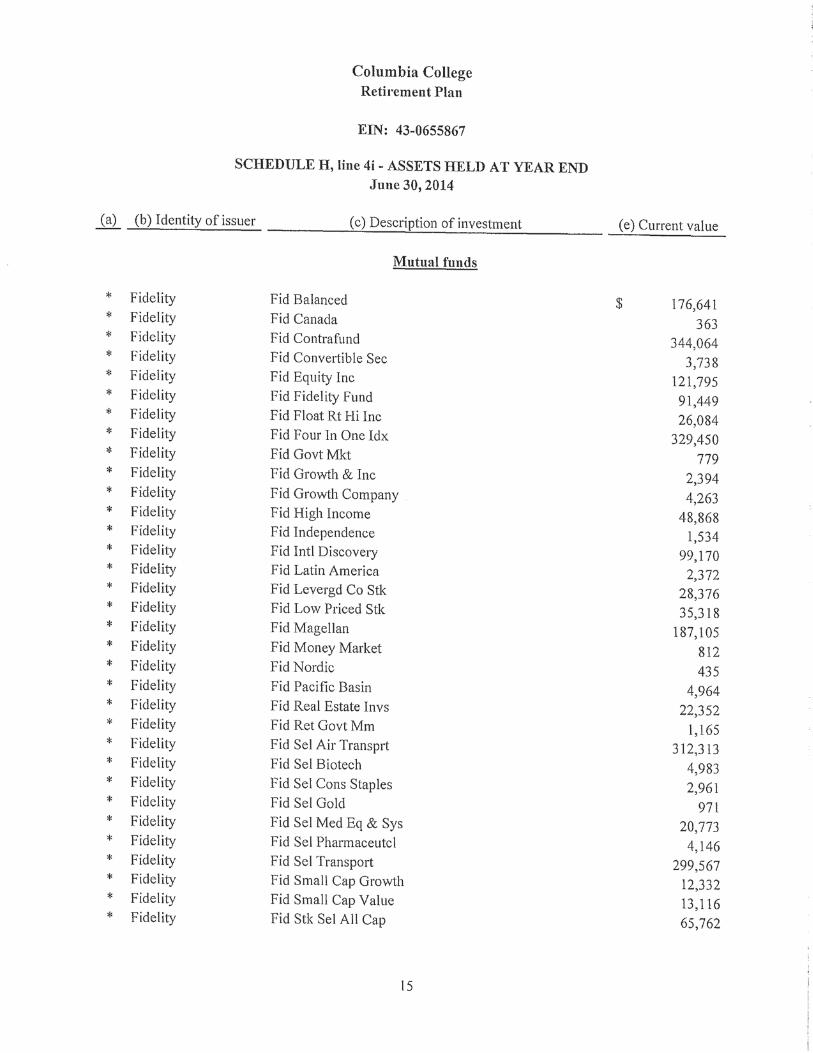
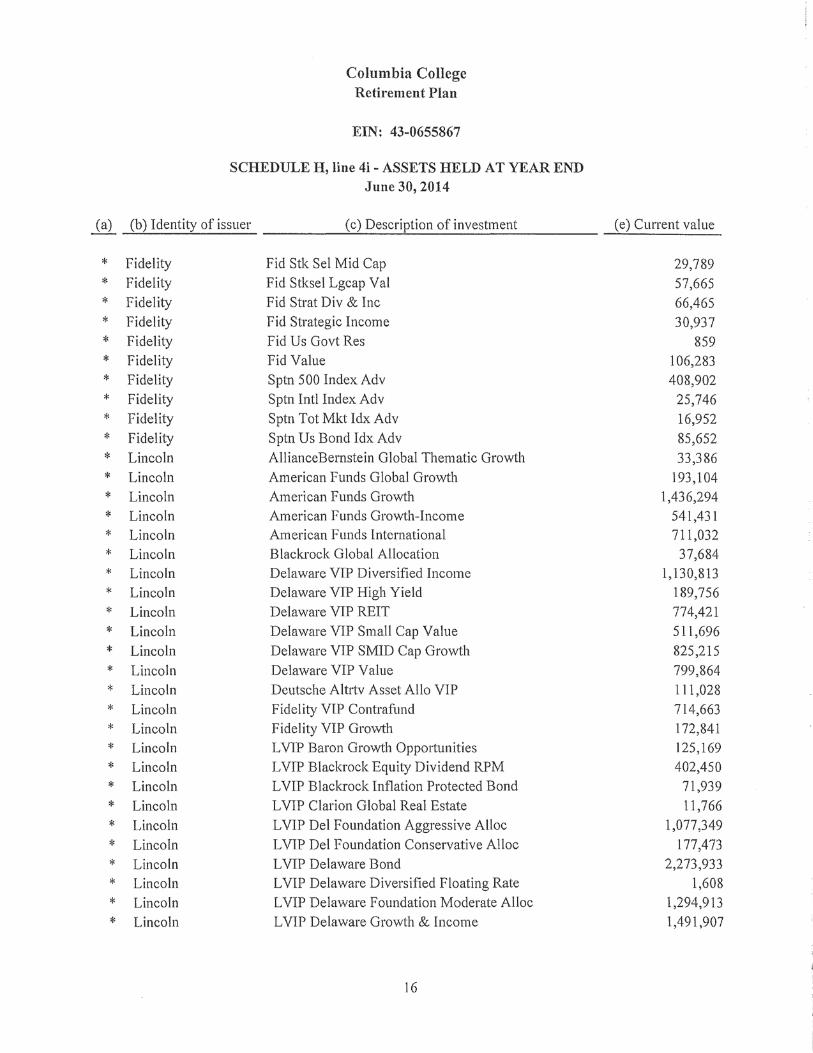
determinable on an established market nor set by an independent third party appraiser?......... 4h -123456789012345 i Did the plan have assets held for investment? (Attach schedule(s) of assets if “Yes” is checked,
and see instructions for format requirements.) .......................................................................... 4i j Were any plan transactions or series of transactions in excess of 5% of the current
value of plan assets? (Attach schedule of transactions if “Yes” is checked, and see instructions for format requirements.)................................................................................. 4j
k Were all the plan assets either distributed to participants or beneficiaries, transferred to another plan, or brought under the control of the PBGC? ...................................................................... 4k
l Has the plan failed to provide any benefit when due under the plan?........................................ 4l -123456789012345 m If this is an individual account plan, was there a blackout period? (See instructions and 29 CFR
2520.101-3.) ............................................................................................................................. 4m
n If 4m was answered “Yes,” check the “Yes” box if you either provided the required notice or one of the exceptions to providing the notice applied under 29 CFR 2520.101-3. ............................ 4n
5a Has a resolution to terminate the plan been adopted during the plan year or any prior plan year? If “Yes,” enter the amount of any plan assets that reverted to the employer this year........................... X Yes X No Amount:-123
5b If, during this plan year, any assets or liabilities were transferred from this plan to another plan(s), identify the plan(s) to which assets or liabilities were transferred. (See instructions.)
5b(1) Name of plan(s) 5b(2) EIN(s) 5b(3) PN(s) ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHIABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
123456789 123
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHIABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
123456789 123
ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHIABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
123456789
123ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHIABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
ABCDEFGHI ABCDEFGHI ABCDEFGHI
123456789 123
5c If the plan is a defined benefit plan, is it covered under the PBGC insurance program (see ERISA section 4021)? ..... X Yes X No X Not determined Part V Trust Information (optional)6a Name of trust ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
6b Trust’s EIN
X
X
X 900000
X
X
X
X
X
X
X
X
X
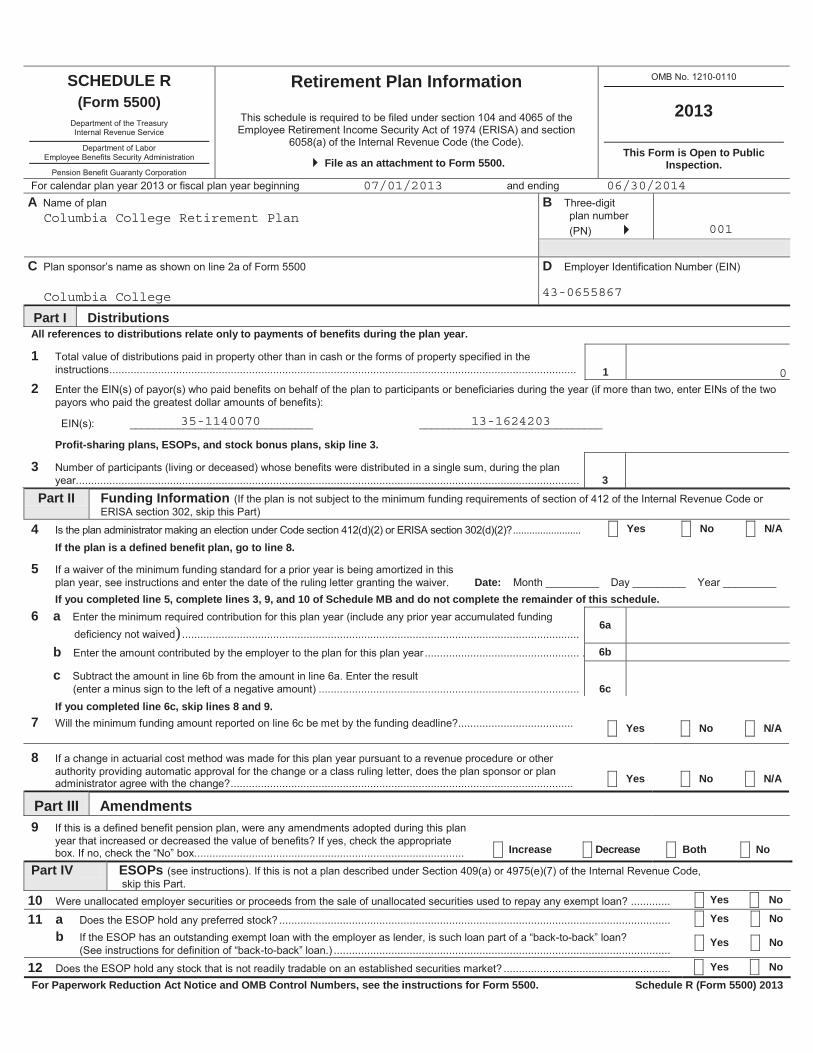
SCHEDULE R(Form 5500)
Retirement Plan Information
File as an attachment to Form 5500.
2013
This Form is Open to Public Inspection.
AABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
B
001
CABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI ABCDEFGHI
D012345678
Part I Distributions
11 -123456789012345
Part II Funding Information
If you completed line 5, complete lines 3, 9, and 10 of Schedule MB and do not complete the remainder of this schedule.
If you completed line 6c, skip lines 8 and 9.7 X Yes X No X N/A
8 X Yes X No X N/A
Part III Amendments9
X Increase X Decrease X Both X No Part IV ESOPs
10 X Yes X No 11 a X Yes X No
b X Yes X No 12 X Yes X No For Paperwork Reduction Act Notice and OMB Control Numbers, see the instructions for Form 5500. Schedule R (Form 5500) 2013
All references to distributions relate only to payments of benefits during the plan year.
2
Profit-sharing plans, ESOPs, and stock bonus plans, skip line 3. 3
3 12345678
4 X Yes X No X N/A If the plan is a defined benefit plan, go to line 8.
5Date:
6 a) 6a -123456789012345
b 6b -123456789012345 c
6c -123456789012345
07/01/2013 06/30/2014
Columbia College Retirement Plan001
Columbia College 43-0655867
0
35-1140070 13-1624203
2 - 1 x
Part V Additional Information for Multiemployer Defined Benefit Pension Plans13
Complete as many entries as needed to report all applicable employers.a b cd (If employer contributes under more than one collective bargaining agreement, check box X
and see instructions regarding required attachment. Otherwise, enter the applicable date.)
e (If more than one rate applies, check this box X and see instructions regarding required attachment. Otherwise, complete lines 13e(1) and 13e(2).) X X X X
a b cd (If employer contributes under more than one collective bargaining agreement, check box X
and see instructions regarding required attachment. Otherwise, enter the applicable date.)
e (If more than one rate applies, check this box X and see instructions regarding required attachment. Otherwise, complete lines 13e(1) and 13e(2).) X X X X
a b cd (If employer contributes under more than one collective bargaining agreement, check box X
and see instructions regarding required attachment. Otherwise, enter the applicable date.)
e (If more than one rate applies, check this box X and see instructions regarding required attachment. Otherwise, complete lines 13e(1) and 13e(2).) X X X X
ab cd (If employer contributes under more than one collective bargaining agreement, check box X
and see instructions regarding required attachment. Otherwise, enter the applicable date.)
e (If more than one rate applies, check this box X and see instructions regarding required attachment. Otherwise, complete lines 13e(1) and 13e(2).) X X X X
ab cd (If employer contributes under more than one collective bargaining agreement, check box X
and see instructions regarding required attachment. Otherwise, enter the applicable date.)
e (If more than one rate applies, check this box X and see instructions regarding required attachment. Otherwise, complete lines 13e(1) and 13e(2).) X X X X
ab cd (If employer contributes under more than one collective bargaining agreement, check box X
and see instructions regarding required attachment. Otherwise, enter the applicable date.)
e (If more than one rate applies, check this box X and see instructions regarding required attachment. Otherwise, complete lines 13e(1) and 13e(2).) X X X X
3
14
a 14a 123456789012345 b 14b 123456789012345 c 14c 123456789012345
15
a 15a 123456789012345 b 15b 123456789012345
16 a 16a 123456789012345 b 16b 123456789012345
17X
Part VI Additional Information for Single-Employer and Multiemployer Defined Benefit Pension Plans18
X19
a_____ _____ _____ _____ _____
bX X X X X X X X
cX X X X
0.00

Form 5558(Rev. August 2012)
Application for Extension of Time To File Certain Employee Plan Returns
Department of the Treasury Internal Revenue Service
For Privacy Act and Paperwork Reduction Act Notice, see instructions.
Information about Form 5558 and its instructions is at www.irs.gov/form5558
OMB No. 1545-0212
File With IRS Only
Part I Identification
A Name of filer, plan administrator, or plan sponsor (see instructions)
Number, street, and room or suite no. (If a P.O. box, see instructions)
City or town, state, and ZIP code
B Filer’s identifying number (see instructions)
Employer identification number (EIN) (9 digits XX-XXXXXXX)
Social security number (SSN) (9 digits XXX-XX-XXXX)
Plan year ending—
MM DD YYYY
CPlan name Plan
number
1Check this box if you are requesting an extension of time on line 2 to file the first Form 5500 series return/report for the plan listed in Part 1, C above.
Part II Extension of Time To File Form 5500 Series, and/or Form 8955-SSA
2 I request an extension of time until / / to file Form 5500 series (see instructions).Note. A signature IS NOT required if you are requesting an extension to file Form 5500 series.
3 I request an extension of time until / / to file Form 8955-SSA (see instructions).Note. A signature IS NOT required if you are requesting an extension to file Form 8955-SSA.
The application is automatically approved to the date shown on line 2 and/or line 3 (above) if: (a) the Form 5558 is filed on or before the normal due date of Form 5500 series, and/or Form 8955-SSA for which this extension is requested, and (b) the date on line 2 and/or line 3 (above) is not later than the 15th day of the third month after the normal due date.
Part III Extension of Time To File Form 5330 (see instructions)
4 I request an extension of time until / / to file Form 5330.You may be approved for up to a 6 month extension to file Form 5330, after the normal due date of Form 5330.
a Enter the Code section(s) imposing the tax . . . . . . . . . . . a
b Enter the payment amount attached . . . . . . . . . . . . . . . . . . . . . . b
c For excise taxes under section 4980 or 4980F of the Code, enter the reversion/amendment date . . . c
5 State in detail why you need the extension:
Under penalties of perjury, I declare that to the best of my knowledge and belief, the statements made on this form are true, correct, and complete, and that I am authorized to prepare this application.
Signature Date
Cat. No. 12005T Form 5558 (Rev. 8-2012)
Columbia College
1001 Rogers Street
Columbia, MO 65216
43-0655867
Columbia College Retirement Plan0 0 1 06 30 2014
04 15 2015
04 15 2015







Related Documents









![D } o ^ À ] } v P } Ç d ] o W W ] o P u › government › ... · 2019-06-10 · 6wdqgdug 7 &v dv rssrvhg wr wkh 0rgho 6huylfhv &rqwudfw wkhvh frqwudfwv kdyh vwdqgdug 7 &v wr zklfk](https://static.cupdf.com/doc/110x72/5f04068c7e708231d40bf2d1/d-o-v-p-d-o-w-w-o-p-u-a-government-a-2019-06-10.jpg)

