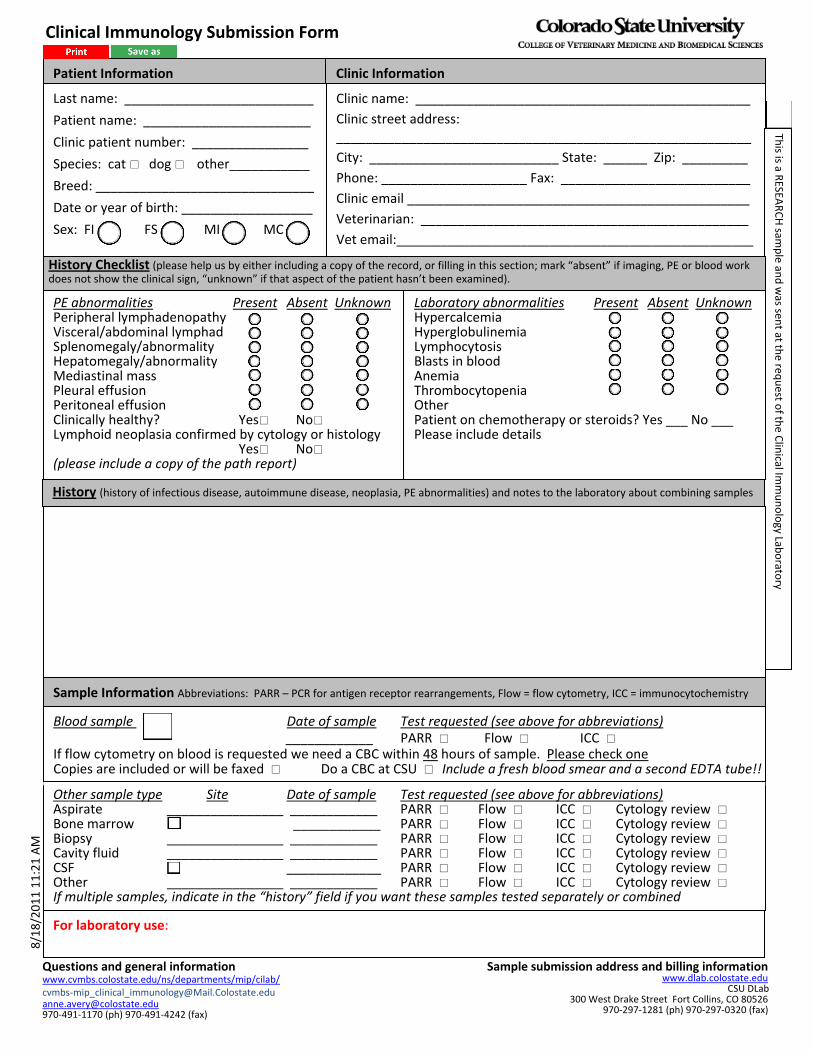
Other sample type Site Date of sample Test requested (see above for abbreviations) Aspirate ________________ ____________ PARR Flow ICC Cytology review Bone marrow ____________ PARR Flow ICC Cytology review Biopsy ________________ ____________ PARR Flow ICC Cytology review Cavity fluid ________________ ____________ PARR Flow ICC Cytology review CSF _____________ PARR Flow ICC Cytology review Other ________________ ____________ PARR Flow ICC Cytology review If multiple samples, indicate in the “history” field if you want these samples tested separately or combined Last name: __________________________ Patient name: _______________________ Clinic patient number: ________________ Species: cat dog other___________ Breed: ______________________________ Date or year of birth: __________________ Sex: FI FS MI MC Clinic name: ______________________________________________ Clinic street address: _________________________________________________________ City: __________________________ State: ______ Zip: _________ Phone: ____________________ Fax: __________________________ Clinic email _______________________________________________ Veterinarian: _____________________________________________ Vet email:_________________________________________________ Clinic Information For laboratory use: Patient Information Questions and general information www.cvmbs.colostate.edu/ns/departments/mip/cilab/ cvmbs‐[email protected] [email protected] 970‐491‐1170 (ph) 970‐491‐4242 (fax) Sample submission address and billing information www.dlab.colostate.edu CSU DLab 300 West Drake Street Fort Collins, CO 80526 970‐297‐1281 (ph) 970‐297‐0320 (fax) 8/18/2011 11:21 AM This is a RESEARCH sample and was sent at the request of the Clinical Immunology Laboratory History Checklist (please help us by either including a copy of the record, or filling in this section; mark “absent” if imaging, PE or blood work does not show the clinical sign, “unknown” if that aspect of the patient hasn’t been examined). PE abnormalities Present Absent Unknown Peripheral lymphadenopathy Visceral/abdominal lymphad Splenomegaly/abnormality Hepatomegaly/abnormality Mediastinal mass Pleural effusion Peritoneal effusion Clinically healthy? Yes No Lymphoid neoplasia confirmed by cytology or histology Yes No (please include a copy of the path report) Laboratory abnormalities Present Absent Unknown Hypercalcemia Hyperglobulinemia Lymphocytosis Blasts in blood Anemia Thrombocytopenia Other Patient on chemotherapy or steroids? Yes ___ No ___ Please include details History (history of infectious disease, autoimmune disease, neoplasia, PE abnormalities) and notes to the laboratory about combining samples Sample Information Abbreviations: PARR – PCR for antigen receptor rearrangements, Flow = flow cytometry, ICC = immunocytochemistry Blood sample Date of sample Test requested (see above for abbreviations) ____________ PARR Flow ICC If flow cytometry on blood is requested we need a CBC within 48 hours of sample. Please check one Copies are included or will be faxed Do a CBC at CSU Include a fresh blood smear and a second EDTA tube!! Clinical Immunology Submission Form

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Other sample type Site Date of sample Test requested (see above for abbreviations)Aspirate ________________ ____________ PARR Flow ICC Cytology review Bone marrow ____________ PARR Flow ICC Cytology review Biopsy ________________ ____________ PARR Flow ICC Cytology review Cavity fluid ________________ ____________ PARR Flow ICC Cytology review CSF _____________ PARR Flow ICC Cytology review Other ________________ ____________ PARR Flow ICC Cytology review If multiple samples, indicate in the “history” field if you want these samples tested separately or combined
Last name: __________________________
Patient name: _______________________
Clinic patient number: ________________
Species: cat dog other___________
Breed: ______________________________
Date or year of birth: __________________
Sex: FI FS MI MC
Clinic name: ______________________________________________
Clinic street address: _________________________________________________________
City: __________________________ State: ______ Zip: _________
Phone: ____________________ Fax: __________________________
Clinic email _______________________________________________
Veterinarian: _____________________________________________
Vet email:_________________________________________________
Clinic Information
For laboratory use:
Patient Information
Questions and general information www.cvmbs.colostate.edu/ns/departments/mip/cilab/ cvmbs‐[email protected] [email protected] 970‐491‐1170 (ph) 970‐491‐4242 (fax)
Sample submission address and billing informationwww.dlab.colostate.edu
CSU DLab300 West Drake Street Fort Collins, CO 80526
970‐297‐1281 (ph) 970‐297‐0320 (fax)
8/18/2011 11:21 AM
This is a R
ESEARCH sam
ple an
d was sen
t at the req
uest o
f the Clinical Im
munology Lab
orato
ry
History Checklist (please help us by either including a copy of the record, or filling in this section; mark “absent” if imaging, PE or blood work does not show the clinical sign, “unknown” if that aspect of the patient hasn’t been examined).
PE abnormalities Present Absent UnknownPeripheral lymphadenopathy Visceral/abdominal lymphad Splenomegaly/abnormality Hepatomegaly/abnormality Mediastinal mass Pleural effusion Peritoneal effusion Clinically healthy? Yes No Lymphoid neoplasia confirmed by cytology or histology Yes No (please include a copy of the path report)
Laboratory abnormalities Present Absent UnknownHypercalcemia Hyperglobulinemia Lymphocytosis Blasts in blood Anemia Thrombocytopenia Other Patient on chemotherapy or steroids? Yes ___ No ___ Please include details
History (history of infectious disease, autoimmune disease, neoplasia, PE abnormalities) and notes to the laboratory about combining samples
Sample Information Abbreviations: PARR – PCR for antigen receptor rearrangements, Flow = flow cytometry, ICC = immunocytochemistry
Blood sample Date of sample Test requested (see above for abbreviations) ____________ PARR Flow ICC If flow cytometry on blood is requested we need a CBC within 48 hours of sample. Please check one Copies are included or will be faxed Do a CBC at CSU Include a fresh blood smear and a second EDTA tube!!
Clinical Immunology Submission Form
initiator:[email protected];wfState:distributed;wfType:email;workflowId:cb53a62d41f5fe47bebaed8f867dcbf9
aavery
Typewritten Text
aavery
Typewritten Text
For all other sample types use boxes below
aavery
Typewritten Text
aavery
Typewritten Text
aavery
Typewritten Text
Related Documents











