Route-to-route extrapolation of VOCs

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Route-to-route extrapolation of VOCs
Components of this package
• Guidance document (2006)
• White paper
• Spreadsheet for simple r-to-r extrapolation

Purpose
The purpose of this guidance document and the white paper is to provide a consistent approach in risk extrapolation of chemicals through different routes of exposure.

What is R-to-R extrapolation?
Route-to-route extrapolation techniques are used to quantify the chemical concentration to produce similar magnitude of the effect through different routes of exposure
Exposure route 1
Exposure route 3
Exposure route 2
Similar Internal dose Similar magnitude of effect
R-to-r R-to-r
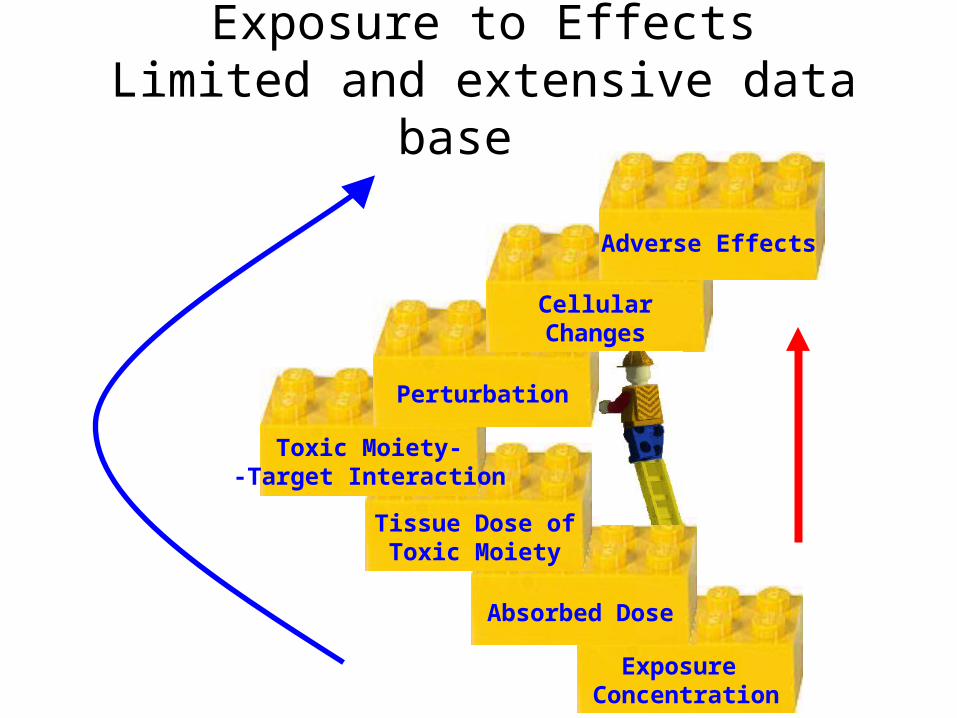
Exposure Concentration
Absorbed Dose
Tissue Dose ofToxic Moiety
Toxic Moiety--Target Interaction
Perturbation
CellularChanges
Adverse Effects
Exposure to EffectsLimited and extensive data base

Internal dosimetry
Conc. mg*L-1
Time (Hr)
Blood concentration profiles of a hypothetical chemical following oral, inhalation and dermal exposure
oral
inhalation
dermal
Route-to-route extrapolation – a quantitative toxicity data base
• Route-to-route extrapolation quantifies the toxicological equivalent dose of a chemical through different routes of exposure.
• This requires quantitative chemical specific data base - e.g. ADME data.
• Route-to-route extrapolation is generally carried out at concentrations equivalent to the LOAEL or NOAEL doses.

Why should we do R-to-R extrapolation?
• In the absence of chemical specific dose-response information through any route of exposure and if there is a need to assess the toxicity through this route of exposure, r-to-r extrapolation becomes necessary.
• To reduce the uncertainties by using advanced r-to-r extrapolation.
• Potentially be used as a tool for mechanistic understanding.

Methods of R-to-R extrapolation and the order of preference
Internal dosimetry (critical organ - e.g. blood, CNS), which Internal dosimetry (critical organ - e.g. blood, CNS), which can also include the metabolitescan also include the metabolites
Absorbed doseAbsorbed dose
Administered doseAdministered dose

Application of TK data for route-to- route extrapolation
Extrapolation using TK data and PBTK model – data rich situation
Extrapolation using route/chemical specific absorption data
Extrapolation using basic physiological data

Dose calculations
Exposed Dose• Doseinhaled = Cair x Qp
BW
• NOAELinhalation = NOAELoral x Body weight / Qp
Absorbed Dose• Doseinhaled (mg/kg/d) = Cair x Qp x t x Fi
BW
• NOAELinhalation = NOAELoral x BW x Fo Qp x Fi
Fi = fraction inhaledFo = fraction absorbed orallyQp = Alveolar ventilation rate

Equations for converting the dose from one route of exposure to another on the basis of the fraction absorbed
Dermal
To
Oral Inh.
Dermal
NOAELdermal*Fd
Fo
NOAELdermal*BW*Fd
Qp*t*Fi
F Oralrom
NOAELoral*Fo
Fd
NOAELoral*BW*Fo
Qp*t*Fi
Inh.NOAELinh* Qp*t*Fi BW*Fd
NOAELinh* Qp*t*Fi BW*Fo

The decision tree showing the level of sophistication in carrying out r-to-r extrapolation.

Use default extrapolation factors based on administered dose
Is a valid BBDR model available for the routes and species of interest?
Are route-specific TK data or models available?
Route-to-route extrapolation not recommended
Toxicity -based assessment
Internal dose based assessment
Is the POD based on a ‘’systemic’’ toxic effect?
Is the fraction absorbed by both routes known for the chemical of concern or a closely related chemical?
Absorbed dose-based assessment
YES NO, DNK
YES NO
YES NO
YES NO

Availability of chemical specific data• Physicochemical and Biochemical Parameters used in PBTK Modeling of
Toluene (Haddad et al., 2001)-
Human Parameters Values
– Blood: air 15.6
– Fat: air 1021
– SPT: air 27.7
– RPT: air 83.6
– Liver: air 83.6
– Vmax (mg/h/kg) 3.44
– Km (mg/L) 0.13

Internal Dose (inhalation)
b
pc
vcinhpa
PQ
Q
CQCQC ss
Ca = Arterial blood concentrationQp = Alveolar ventilation rateCinh = Concentration in inhaled air, Cv = Concentration in mixed venous blood,Pb = Blood:air partition coefficient, and Qc = Cardiac output

PBTK Model schematic
(Mumtaz et al., 2011)

Internal Dosimetry
Ca = Arterial blood concentrationQLC = the ratio between blood flow rate to the liver and the rate of cardiac output Ci = Concentration in inhaled airPb = Blood:air partition coefficientE = Metabolic extraction ratio
EQLCP
CCa
b
iss
*1

Effect of Metabolic Clearance
0, Ewhen
b
i
P
CCass
11
1, Ewhen
biss PCCa *
Factors affecting r-to-r extrapolation on top of chemical specific info.
• Chemical Mixture
Interference due to metabolism and elimination
• Alveolar ventilation rate –
Increased respiration

Limitations of R-to-R extrapolation
• Lack of toxicokinetic data especially for metals (eg. Nickel oral absorption factor)
• Lack of mechanistic understanding for chemical toxicity, especially through different routes of exposure
• Lack of data to validate route to route extrapolation
• Limited to chemicals that exhibits systemic toxicity
When do we require r-to-r extrapolation
• Site specific human health risk assessment.
• Development of media-specific chemical standards
• Providing toxicological opinion
HHRA
• Human-health-risk-assessment (HHRA): Risk quantification during HHRA requires both chemical specific exposure data and chemical specific toxicological benchmark dose (e.g. RfD).
• SSRA are usually carried out considering all the possible media of exposure.
• However, the benchmark dose may not be available for all the
routes of exposure for many chemicals.
• Hence, a route-to-route extrapolation should be carried out during the process of risk assessment. HHRA can range from EA, Brownfields, CBRA, GLC.
Media specific chemical standards
When setting media specific standards, toxicological information may predominantly be available with any one specific route of exposure (e.g. benzene – inhalation route). In such cases, route-to-route extrapolation becomes a mandate to extrapolate toxicological information from one route of exposure to the other.

Others
When expressing a toxicological opinion in a briefing note or as an expert witness or in a emergency situation, if detailed toxicological dose response information is not available for a particular route of exposure for a chemical, route-to-route extrapolation is essential.

What did we get from here?
• A decision tree
• A table of conversion factors
Explained in,
• A guidance document
• A white paper
• A spreadsheet to carryout quantitative r-to-r extrapolation
Additional reading
• Chiu W.A., White P. (2006): Steady-state solutions to PBPK models and their applications to risk assessment I: Route-to-route extrapolation of volatile chemicals. Risk Analysis. 26(3): 769-780.
• Falk-Filipsson A., Hanberg A., Victorin K., Warholm M., Wallen M. (2007): Assessment factors – applications in health risk assessment of chemicals. Environ. Res. 104(1): 108-127.
• Chiu W.A., Barton H.A., DeWoskin R.S., Schlosser P., Thompson C.M., Sonawane B., Lipscomb J.C., Krishnan K. (2007): Evaluation of physiologically based pharmacokinetic models for use in risk assessment. J. Appl. Toxicol. 27(3): 218-237.

• Lu Y., Rieth S., Lohitnavy M., Dennison J., El-Masri H., Barton H.A., Bruckner J., Yang R.R. (2008): Application of PBPK modeling in support of the derivation of toxicity reference values for 1,1,1-trichloroethane. Regul. Toxicol. Pharmacol. 50(2): 249-260.
• Borghoff S.J., Parkinson H., Leavens T.L. (2010): Physiologically based pharmacokinetic rat model for methyl tertiary-butyl ether; comparison of selected dose metrics following various MTBE exposure scenarios used for toxicity and carcinogenicity evaluation. Toxicol. 275(1-3): 79-91.
• Mielke H., Abraham K., Gotz M., Vieth B., Lampen A., Luch A., Gundert-Remy U. (2011): Physiologically based toxicokinetic modeling as a tool to assess target organ toxicity in route-to-route extrapolation – the case of coumarin. Toxicol. Lett. 202(2): 100-110.
Related Documents











