Rosuvastatin: A Highly Effective New HMG-CoA Reductase Inhibitor Anders G. Olsson, *Fergus McTaggart, and *Ali Raza University Hospital, Linköping, Sweden, and *AstraZeneca, Alderley Park, Cheshire, United Kingdom Key words: Atherosclerosis—Cholesterol—HMG-CoA reductase inhibitors— Hypercholesterolemia—Rosuvastatin. ABSTRACT Rosuvastatin, a new statin, has been shown to possess a number of advantageous phar- macological properties, including enhanced HMG-CoA reductase binding characteristics, relative hydrophilicity, and selective uptake into/activity in hepatic cells. Cytochrome P450 (CYP) metabolism of rosuvastatin appears to be minimal and is principally mediated by the 2C9 enzyme, with little involvement of 3A4; this finding is consistent with the absence of clinically significant pharmacokinetic drug-drug interactions between rosuva- statin and other drugs known to inhibit CYP enzymes. Dose-ranging studies in hypercho- lesterolemic patients demonstrated dose-dependent effects in reducing low-density lipo- protein cholesterol (LDL-C) (up to 63%), total cholesterol, and apolipoprotein (apo) B across a 1- to 40-mg dose range and a significant 8.4% additional reduction in LDL-C, compared with atorvastatin, across the dose ranges of the two agents. Rosuvastatin has also been shown to be highly effective in reducing LDL-C, increasing high-density lipo- protein cholesterol (HDL-C), and producing favorable modifications of other elements of the atherogenic lipid profile in a wide range of dyslipidemic patients. In patients with mild to moderate hypercholesterolemia, rosuvastatin has been shown to produce large de- creases in LDL-C at starting doses, thus reducing the need for subsequent dose titration, and to allow greater percentages of patients to attain lipid goals, compared with available statins. The substantial LDL-C reductions and improvements in other lipid measures with rosuvastatin treatment should facilitate achievement of lipid goals and reduce the re- quirement for combination therapy in patients with severe hypercholesterolemia. In addi- tion, rosuvastatin’s effects in reducing triglycerides, triglyceride-containing lipoproteins, non–HDL-C, and LDL-C and increasing HDL-C in patients with mixed dyslipidemia or elevated triglycerides should be of considerable value in enabling achievement of LDL-C 303 Cardiovascular Drug Reviews Vol. 20, No. 4, pp. 303–328 © 2002 Neva Press, Branford, Connecticut Address correspondence and reprint requests to: Fergus McTaggart, B.Sc., Ph.D., Principal Scientist, CV & GI Discovery, AstraZeneca, Mereside Alderley Park, Macclesfield, Cheshire SK10 4TG, UK. Tel: +44 (1625) 515-124. Fax: +44 (1625) 516-667. E-mail: [email protected].

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Rosuvastatin: A Highly EffectiveNew HMG-CoA Reductase Inhibitor
Anders G. Olsson, *Fergus McTaggart, and *Ali Raza
University Hospital, Linköping, Sweden, and
*AstraZeneca, Alderley Park, Cheshire, United Kingdom
Key words: Atherosclerosis—Cholesterol—HMG-CoA reductase inhibitors—
Hypercholesterolemia—Rosuvastatin.
ABSTRACT
Rosuvastatin, a new statin, has been shown to possess a number of advantageous phar-
macological properties, including enhanced HMG-CoA reductase binding characteristics,
relative hydrophilicity, and selective uptake into/activity in hepatic cells. Cytochrome
P450 (CYP) metabolism of rosuvastatin appears to be minimal and is principally mediated
by the 2C9 enzyme, with little involvement of 3A4; this finding is consistent with the
absence of clinically significant pharmacokinetic drug-drug interactions between rosuva-
statin and other drugs known to inhibit CYP enzymes. Dose-ranging studies in hypercho-
lesterolemic patients demonstrated dose-dependent effects in reducing low-density lipo-
protein cholesterol (LDL-C) (up to 63%), total cholesterol, and apolipoprotein (apo) B
across a 1- to 40-mg dose range and a significant 8.4% additional reduction in LDL-C,
compared with atorvastatin, across the dose ranges of the two agents. Rosuvastatin has
also been shown to be highly effective in reducing LDL-C, increasing high-density lipo-
protein cholesterol (HDL-C), and producing favorable modifications of other elements of
the atherogenic lipid profile in a wide range of dyslipidemic patients. In patients with mild
to moderate hypercholesterolemia, rosuvastatin has been shown to produce large de-
creases in LDL-C at starting doses, thus reducing the need for subsequent dose titration,
and to allow greater percentages of patients to attain lipid goals, compared with available
statins. The substantial LDL-C reductions and improvements in other lipid measures with
rosuvastatin treatment should facilitate achievement of lipid goals and reduce the re-
quirement for combination therapy in patients with severe hypercholesterolemia. In addi-
tion, rosuvastatin’s effects in reducing triglycerides, triglyceride-containing lipoproteins,
non–HDL-C, and LDL-C and increasing HDL-C in patients with mixed dyslipidemia or
elevated triglycerides should be of considerable value in enabling achievement of LDL-C
303
Cardiovascular Drug ReviewsVol. 20, No. 4, pp. 303–328© 2002 Neva Press, Branford, Connecticut
Address correspondence and reprint requests to: Fergus McTaggart, B.Sc., Ph.D., Principal Scientist, CV & GI
Discovery, AstraZeneca, Mereside Alderley Park, Macclesfield, Cheshire SK10 4TG, UK.
Tel: +44 (1625) 515-124. Fax: +44 (1625) 516-667. E-mail: [email protected].

and non–HDL-C goals in the numerous patients with combined dyslipidemias or meta-
bolic syndrome who require lipid-lowering therapy. Rosuvastatin is well tolerated alone,
and in combination with fenofibrate, extended-release niacin, and cholestyramine, and has
a safety profile similar to that of currently marketed statins. A large, long-term clinical
trials program is under way to investigate the effects of rosuvastatin on atherosclerosis and
cardiovascular morbidity and mortality.
INTRODUCTION
Low-density lipoprotein (LDL) is the primary atherogenic lipoprotein. A wealth of ex-
perimental, epidemiological, and clinical data indicate that elevated LDL cholesterol
(LDL-C) or total cholesterol, as a surrogate for LDL-C, is associated with increased risk
of atherosclerosis and coronary heart disease (CHD) and that reduction of LDL-C is asso-
ciated with reduced CHD morbidity and mortality (21). Statin drugs reduce cholesterol
biosynthesis by inhibiting the activity of the HMG-CoA reductase enzyme in converting
HMG-CoA to mevalonate, an early and rate-limiting step in cholesterol synthesis. Statins
are the major pharmacological treatment for a number of dyslipidemias, primarily on the
basis of their ability to effectively reduce LDL-C. A number of large clinical trials have
unequivocally demonstrated the ability of statin therapy to reduce CHD events in indi-
viduals with or without established CHD across a wide range of initial LDL-C levels
(17,33,43,52,53,56).
The observation that the relationship between LDL-C level and CHD risk is continuous
from low to high LDL-C values and the relative failure to achieve guideline-recom-
mended LDL-C levels in clinical practice (20,51,63) have prompted attempts to develop
statins with improved pharmacology profiles, with the objective of greater efficacy in re-
ducing LDL-C. Rosuvastatin (AstraZeneca, Alderley Park, Macclesfield, Cheshire, UK;
licensed from Shionogi & Co., Ltd., Osaka, Japan) is a new statin with pharmacological
and clinical features that distinguish it from other currently available statins. This agent
has been shown to be highly effective in lowering LDL-C and improving other elements
of the atherogenic lipid profile in patients with a variety of dyslipidemias.
CHEMISTRY
Rosuvastatin (rosuvastatin calcium) is a synthetic compound that consists of a single
enantiomer formulated and administered as the calcium salt of the active hydroxy acid; its
chemical name is bis{(E)-7-[4-(4-fluorophenyl)-6-isopropyl-2-[methyl(methylsulfonyl)ami-
no]pyrimidin-5-yl](3R,5S )-3,5-dihydroxyhept-6-enoic acid} calcium salt. The empirical
formula for rosuvastatin calcium is (C22H27FN3O6S)2Ca. Its molecular weight is 1001.14.
The structural formula is shown in Fig. 1. Rosuvastatin calcium is a white amorphous
powder that is sparingly soluble in water and methanol and slightly soluble in ethanol.
HMG-CoA REDUCTASE BINDING AND INHIBITION
In chemical structure rosuvastatin shows similarity to other compounds of the statin
class but also important differences. Rosuvastatin and other statins contain a dihydroxy
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
304 A. G. OLSSON ET AL.
heptenoic (heptanoic in some cases) acid chain that mimics the HMG portion of the
HMG-CoA substrate. However, the additional ring structures and substituents of rosuva-
statin differ from those of other statins. Of particular note is the polar methane sulfon-
amide group that confers to the molecule a relatively low lipophilicity.
The additional components of the molecule are also important in enzyme binding, and
subtle differences in the way different statins interact with the enzyme have been revealed
by x-ray crystallography of the statin-enzyme complexes (28). In addition to a number of
interactions with the active site that are common among the statins, rosuvastatin exhibits
a hydrogen bond between a sulfone oxygen atom and the enzyme Ser565, a binding trait
otherwise observed only with atorvastatin (involving its carbonyl oxygen atom), and a
unique polar interaction between the rosuvastatin electronegative sulfone group and the
enzyme Arg568 side chain.
Consistent with these findings, rosuvastatin was found to be a relatively potent in-
hibitor of HMG-CoA reductase, as measured in experiments using a cloned catalytic
fragment of human HMG-CoA reductase. As with other statins, inhibition was compet-
itive for HMG-CoA reductase and noncompetitive with NADPH. The inhibition constant
(Ki) was approximately 0.1 nM. In the presence of a fixed concentration of HMG-CoA
reductase, 50% inhibitory concentration (IC50) values were 5.4 nM for rosuvastatin, com-
pared with 8.2 nM for atorvastatin, 10.0 nM for cerivastatin, 11.2 nM for simvastatin,
27.6 nM for fluvastatin, and 44.1 nM for pravastatin (24,41). Thus, rosuvastatin is a rela-
tively potent inhibitor of HMG-CoA reductase, consistent with some differences in the
way the molecule binds the active site of the enzyme in comparison with other statins.
CELL AND TISSUE SELECTIVITY
Assessment of relative lipophilicity of statins showed that the statin octanol-water coef-
ficients were –0.84 log D at pH 7.4 for pravastatin and –0.33 log D for rosuvastatin, com-
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 305
2
N
N
N
OO
S
OH OH O
O
F
Ca2+
FIG. 1. Chemical structure of rosuvastatin.

pared with values of >1.0 to <2.0 for atorvastatin, fluvastatin, simvastatin (sodium salt),
and cerivastatin, indicating greater lipophilicity on the part of these latter drugs (11,41).
Consistent with its hydrophilic properties, rosuvastatin was found to be highly selective
for effect in hepatocytes, compared with a range of non-hepatic cells. Thus, when incu-
bated with freshly prepared rat hepatocytes, rosuvastatin inhibited cholesterol synthesis in
these cells with an IC50 of 0.2 nM (95% confidence limits, 0.1–0.3 nM), and was found to
be significantly (P < 0.001) more potent than the other statins (IC50 range, 1.2–6.9 nM)
(8). Studies assessing inhibitory effects in hepatic and non-hepatic cells showed that rosu-
vastatin had an approximately 1,000-fold reduced potency in rat fibroblasts, compared
with primary hepatocytes. The log10 ratio for IC50 values in hepatocytes:fibroblasts was
3.3 for rosuvastatin and pravastatin, the other relatively hydrophilic compound, compared
with 2.2 for atorvastatin, 0.54 for simvastatin, –0.04 for fluvastatin, and –0.14 for ceriva-
statin (8,11). Thus, the marked hepatic cell selectivity of both rosuvastatin and pravastatin
is in contrast with that of the more lipophilic compounds.
Studies with 14C-labeled rosuvastatin in rat hepatocytes showed uptake by both non-
specific diffusion and active transport, with a specific uptake Km of 9.2 ìM; comparison
with pravastatin showed that the rate of active uptake clearance (Vmax�Km) for rosuvastatin
was greater and that rosuvastatin competitively inhibited pravastatin uptake with a Ki
value close to the Km for uptake (11,44).
Additional studies indicate high affinity of rosuvastatin for liver-specific organic anion
transport proteins (OATPs), which may mediate efficient uptake into hepatocytes (4).
Measurement of uptake of 3H-labeled rosuvastatin in oocytes expressing OATP-A, which
is expressed in the basolateral membrane of hepatocytes and widely expressed in other
tissues, and in those expressing the predominantly liver-specific OATP-C showed that
uptake was 20-fold greater in oocytes expressing OATP-C than in those expressing
OATP-A or in H2O-injected control oocytes. The apparent Km for interaction between ro-
suvastatin and OATP-C was 7.3 ìM; cis-inhibition studies of 3H-labeled rosuvastatin
uptake indicated that the affinity of rosuvastatin for OATP-C was greater than that for pra-
vastatin (30.3 ìM) and simvastatin (43.1 ìM), but not significantly different from that for
the lipophilic statin atorvastatin (2.5 ìM).
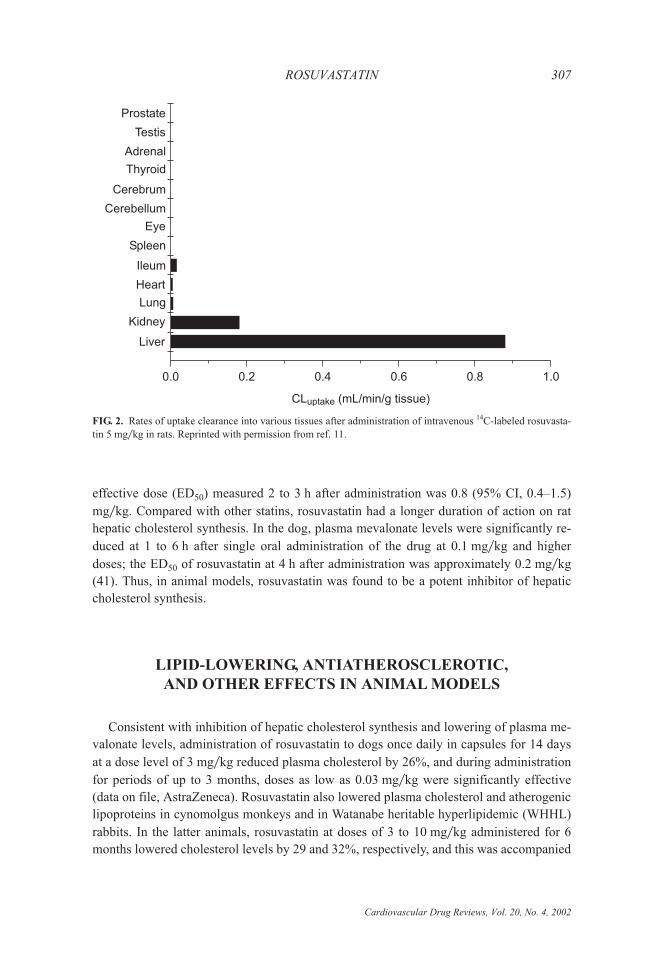
After intravenous administration of 14C-labeled rosuvastatin, 5 mg�kg, to rats, uptake
clearance rates as determined from plasma and tissue radioactivity levels were approxi-
mately 0.9 mL�min�g into the liver, approximately 0.2 mL�min�g into the kidney, and
<0.02 mL�min�g into other tissues (Fig. 2). Pravastatin also exhibited liver uptake selec-
tivity, whereas simvastatin exhibited high uptake into liver and such other tissues as the
adrenals and spleen (11). In summary, effective and selective delivery of rosuvastatin to
the liver is suggested by the combination of the compound’s relative hydrophilicity and its
selectivity for hepatic cells.
INHIBITION OF HEPATIC CHOLESTEROL SYNTHESIS
IN ANIMAL MODELS
Rosuvastatin was found to be a potent inhibitor of hepatic cholesterol synthesis after
oral administration to the rat with a maximal effect at 1 h after administration. The 50%
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
306 A. G. OLSSON ET AL.
effective dose (ED50) measured 2 to 3 h after administration was 0.8 (95% CI, 0.4–1.5)
mg�kg. Compared with other statins, rosuvastatin had a longer duration of action on rat
hepatic cholesterol synthesis. In the dog, plasma mevalonate levels were significantly re-
duced at 1 to 6 h after single oral administration of the drug at 0.1 mg�kg and higher
doses; the ED50 of rosuvastatin at 4 h after administration was approximately 0.2 mg�kg
(41). Thus, in animal models, rosuvastatin was found to be a potent inhibitor of hepatic
cholesterol synthesis.
LIPID-LOWERING, ANTIATHEROSCLEROTIC,
AND OTHER EFFECTS IN ANIMAL MODELS
Consistent with inhibition of hepatic cholesterol synthesis and lowering of plasma me-
valonate levels, administration of rosuvastatin to dogs once daily in capsules for 14 days
at a dose level of 3 mg�kg reduced plasma cholesterol by 26%, and during administration
for periods of up to 3 months, doses as low as 0.03 mg�kg were significantly effective
(data on file, AstraZeneca). Rosuvastatin also lowered plasma cholesterol and atherogenic
lipoproteins in cynomolgus monkeys and in Watanabe heritable hyperlipidemic (WHHL)
rabbits. In the latter animals, rosuvastatin at doses of 3 to 10 mg�kg administered for 6
months lowered cholesterol levels by 29 and 32%, respectively, and this was accompanied
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 307
Cerebellum
Prostate
Testis
Adrenal
Thyroid
Cerebrum
Eye
Spleen
Ileum
Liver
Kidney
Lung
Heart
0.80.0 0.2 0.4 0.6 1.0
CL (mL/min/g tissue)uptake
FIG. 2. Rates of uptake clearance into various tissues after administration of intravenous 14C-labeled rosuvasta-
tin 5 mg�kg in rats. Reprinted with permission from ref. 11.

by reductions in the surface coverage of the aortic arch by atherosclerotic lesions of 29
and 24%, respectively (data on file, AstraZeneca).
In addition to its lipid-lowering and antiatherosclerotic properties, rosuvastatin has
been found to exert a number of potentially beneficial effects in animal models that are not
obviously the result of lipid lowering. Administration of rosuvastatin has been shown to
result in anti-inflammatory action in the microvascular endothelium (59), upregulate en-
dothelial nitric oxide synthase, and protect against tissue damage in models of cerebral
and cardiac ischemia (30,32), and increase the numbers of circulating endothelial progeni-
tor cells and accelerate vascular reendothelialization (65). The clinical relevance of these
interesting observations in animal models has yet to be evaluated.
PHARMACOKINETICS�PHARMACODYNAMICS
Rosuvastatin is administered orally, once daily. No clinically relevant differences in
pharmacokinetics are observed between older and younger patients, between male and
female patients, or between morning and evening dosing. The drug undergoes minimal
metabolism in vivo. No clinically significant interactions with known inhibitors of cyto-
chrome P450 (CYP) 3A4 or other isoenzymes have been observed in drug interaction
studies.
Rosuvastatin is administered orally in the active form. Peak plasma concentrations of
the parent compound are reached at 3 to 5 h after oral dosing. Both peak plasma concen-
tration (Cmax) and area under the plasma concentration-time curve (AUC) increase in pro-
portion to dose (61). In this study, after 7 days of administration of 40 mg rosuvastatin
once daily for 7 days, the geometric mean Cmax and AUC values were 37.0 (38.1) ng�mL
and 255.9 (24.6) (ng � h)�mL, respectively (% coefficient of variation in parentheses). The
absolute bioavailability of rosuvastatin is approximately 20%. The mean volume of distri-
bution at steady state is approximately 134 L. Rosuvastatin is 88% bound to plasma pro-
teins, primarily albumin; binding is reversible and independent of plasma concentrations.
The elimination half-life (t1�2) is approximately 19 h. The relatively long t1�2 compared
with some other statins may possibly reflect a degree of enterohepatic recirculation, a phe-
nomenon that has been documented for rosuvastatin in the rat (data on file, AstraZeneca).
Pharmacokinetic studies in subjects receiving rosuvastatin, 40 mg, showed no clini-
cally relevant differences between its effects in younger (18 to 35 years) and older (>65
years) subjects. Cmax was increased by 12% in younger subjects and AUC was increased
by 6% in younger subjects. There were also no significant differences in the effect of the
drug in males and females on these parameters (Cmax reduced by 18% and AUC by 9% in
males) (36). Study of the pharmacokinetics and pharmacodynamics of rosuvastatin,
10 mg, administered at 7:00 a.m. or at 6:00 p.m. showed no differences in Cmax (4.6 and
4.5 ng�mL) or AUC [40.1 and 42.7 (ng � h)�mL]. There was also no difference in urinary
excretion of mevalonic acid or AUC for plasma mevalonic acid and no difference in
LDL-C reduction (41 and 44%) after morning, as compared with evening dosing (39).
These findings suggest that, unlike the case with several members of the statin class, the
pharmacokinetics and pharmacodynamics of rosuvastatin do not appear to be affected by
time of administration.
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
308 A. G. OLSSON ET AL.

Rosuvastatin is not extensively metabolized, with approximately 10% of an oral dose
being recovered as metabolite. In studies with 14C-labeled rosuvastatin, 90% of an oral
dose was recovered in feces and 10% in urine (37). In feces, 92% of radioactivity was the
parent compound, with N-desmethyl and 5S-lactone metabolites accounting for 6 and 2%,
respectively. In urine, the parent compound accounted for approximately 50% of radioac-
tivity, with N-desmethyl and 5S-lactone metabolites accounting for 20 and 10%, respec-
tively. Overall, 85–95% of active plasma HMG-CoA reductase inhibitory activity is ac-
counted for by the parent compound.
Unlike most marketed statins, rosuvastatin exhibits minimal interaction with CYP iso-
enzymes and undergoes minimal hepatic metabolism. Study of the effect of rosuvastatin
50 ìM on CYP isoenzyme 1A2, 2C9, 2C19, 2D6, 2E1, and 3A4 activity in human hepatic
microsomes showed no significant inhibitory effect on any enzymes; the most potent inhi-
bition was for CYP 2C9, for which a 10% decrease in activity was observed (40). Investi-
gation of the metabolism of 14C-labeled rosuvastatin 1 to 4 ìM showed no metabolism in
human hepatic microsomes (3-h incubation) or heterologously expressed human CYP en-
zymes (1-h incubation), with very slow metabolism (5–50% over 3 d) being observed in
cultured human hepatocytes. In the latter case, a single N-desmethyl metabolite was
formed; inhibition of this metabolism by sulfaphenazole indicated that CYP 2C9 was the
primary enzyme involved, with less inhibition by omeprazole indicating a lesser role of
the 2C19 enzyme. The N-desmethyl metabolite exhibits one sixth to one half the HMG-
CoA reductase inhibition of the parent compound. Overall, these findings suggest that
rosuvastatin is unlikely to cause clinically significant metabolically mediated drug
interactions.
The absence of clinically significant interactions of rosuvastatin with inhibitors of CYP
enzymes has been confirmed by drug interaction studies. Coadministration of rosuva-
statin, 80 mg, and ketoconazole (CYP 3A4 inhibitor), 200 mg, resulted in virtually no
effect on rosuvastatin Cmax (4.6% decrease) or AUC (1.6% increase) (13). Itraconazole
(CYP 3A4 inhibitor), 200 mg, increased Cmax of rosuvastatin by 36 and 15%, and AUC by
39 and 28%, at 10- and 80-mg doses, respectively (35). These changes are thought to be
due not to interaction with CYP enzymes but rather to the effect of an as-yet undefined
transporter. Coadministration of rosuvastatin 80 mg with 500 mg of erythromycin (CYP
3A4 inhibitor) reduced rosuvastatin Cmax by 31% and AUC by 20% (14); this effect is
likely due to increased gastrointestinal motility induced by erythromycin. Coadministra-
tion of rosuvastatin 80 mg with 200 mg of fluconazole (a potent CYP 2C9 inhibitor) in-
creased rosuvastatin Cmax by 9% and AUC by 14% (12); this small effect supports limited
metabolism of rosuvastatin via the 2C9 enzyme.
In other drug-interaction studies, coadministration of rosuvastatin 10 mg and feno-
fibrate 67 mg three times daily increased rosuvastatin Cmax by 7% and AUC by 21% and
decreased fenofibric acid Cmax by 9% and AUC by 4%. No clinically significant change in
digoxin Cmax (4% increase) or AUC (4% increase) was observed with digoxin 0.5 mg and
rosuvastatin 40 mg (38).
In studies in patients with hepatic insufficiency, rosuvastatin Cmax and AUC were mod-
estly increased in patients with mild to moderate hepatic impairment, compared with con-
trols (63.7 vs. 60.7 for AUC, 9.3 vs. 6.0 for Cmax). Patients with the highest scores (8 and
9) in the Child-Pugh B category, however, had the highest Cmax and AUC values (73.3 for
AUC, 12.8 for Cmax), indicating that rosuvastatin exposure increased with greater hepatic
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 309
impairment. A trend toward reduced LDL-C–lowering effectiveness was observed with
greater hepatic impairment (58).
CLINICAL TRIALS IN DYSLIPIDEMIC PATIENTS
Rosuvastatin has been extensively evaluated in clinical trials in adult patients with mild
to moderate hypercholesterolemia and mixed hyperlipidemia (Fredrickson’s type IIa �IIb),
severe hypercholesterolemia (heterozygous familial hypercholesterolemia or homozygous
familial hypercholesterolemia), or hypertriglyceridemia (Fredrickson’s type IIb or IV),
and in combination with other lipid-modifying agents in dyslipidemic patients. A con-
sistent feature of the randomized, controlled trials is that patients underwent a 6-w dietary
lead-in phase with discontinuation of all cholesterol-lowering drugs or supplements; pa-
tients were instructed in the National Cholesterol Education Program (NCEP) step I diet,
and compliance with diet (Eating Pattern Assessment Tool score <28) was a requirement
for entry into the study treatment phase.
Mild to Moderate Hypercholesterolemia
Rosuvastatin has been assessed in dose-ranging studies and comparative trials with
other statins in patients with mild to moderate hypercholesterolemia (type IIa�IIb).
Dose-ranging studies
Dose-ranging studies with rosuvastatin have demonstrated marked dose-related reduc-
tions in LDL-C of up to 63% at 40 mg (46). A comparative dose-ranging study with ator-
vastatin, which has been considered the most effective LDL-C–lowering statin (1,29),
showed that rosuvastatin produces a significantly greater reduction in LDL-C across the
dose range.
In a randomized, placebo-controlled, dose-ranging program, 206 patients with LDL-C
>160 and <220 mg�dL (>4.14 and <5.69 mmol�L) and triglycerides <300 mg�dL (<3.39
mmol�L) received double-blind placebo or rosuvastatin 1, 2.5, 5, 10, 20, or 40 mg or
open-label atorvastatin (used as a benchmark, with no statistical comparisons performed)
for 6 w (46). An intent-to-treat analysis of those patients receiving placebo or rosuvastatin,
10, 20, or 40 mg, showed that rosuvastatin produced marked, dose-related reductions in
LDL-C, total cholesterol, and apolipoprotein (apo) B from baseline, compared with place-
bo (Table 1) (data on file, AstraZeneca). Increases in high-density lipoprotein cholesterol
(HDL-C), reductions in triglycerides, and reductions in lipid ratios were also observed for
all three doses.
In a randomized, double-blind trial (31), 374 patients with LDL-C �160 and <250
mg�dL (�4.14 and <6.46 mmol�L) and triglycerides <400 mg�dL (<4.52 mmol�L) re-
ceived rosuvastatin 5, 10, 20, 40, or 80 mg or atorvastatin 10, 20, 40, or 80 mg for 6 w.
The primary analysis was change in LDL-C across the dose range of the two study drugs
assessed by linear regression analysis. The LDL-C–lowering response with rosuvastatin
was significantly greater (P < 0.001) than that with atorvastatin by 8.4% across the dose
range (Table 2). At doses of 10–80 mg, reductions in LDL-C were 47 to 62% with
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
310 A. G. OLSSON ET AL.
rosuvastatin and 38 to 53.5% with atorvastatin. Rosuvastatin also produced significantly
greater reductions than atorvastatin across the dose range (P < 0.001) in total cholesterol
(4.9%), non–HDL-C (7.0%), apo B (6.3%), and LDL-C:HDL-C (9.5%), total choleste-
rol:HDL-C (6.9%), non–HDL-C:HDL-C (8.4%), and apo B:apo A-I (7.8%).
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 311
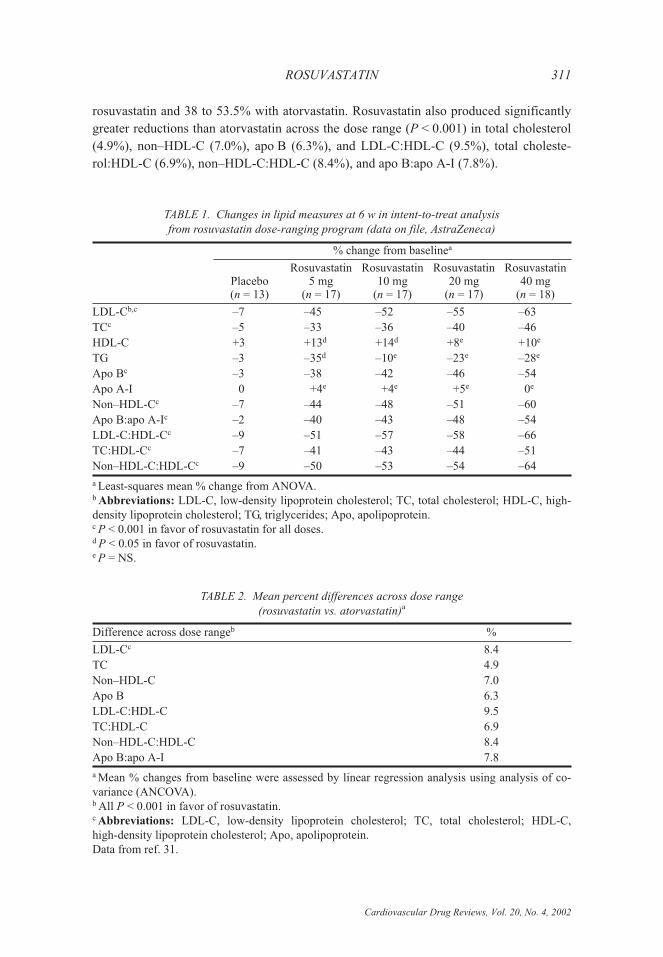
TABLE 1. Changes in lipid measures at 6 w in intent-to-treat analysis
from rosuvastatin dose-ranging program (data on file, AstraZeneca)
% change from baselinea
Placebo(n = 13)
Rosuvastatin5 mg
(n = 17)
Rosuvastatin10 mg
(n = 17)
Rosuvastatin20 mg
(n = 17)
Rosuvastatin40 mg
(n = 18)
LDL-Cb,c –7 –45 –52 –55 –63
TCc –5 –33 –36 –40 –46
HDL-C +3 +13d +14d +8e +10e
TG –3 –35d –10e –23e –28e
Apo Bc –3 –38 –42 –46 –54
Apo A-I 0 +4e +4e +5e 0e
Non–HDL-Cc –7 –44 –48 –51 –60
Apo B:apo A-Ic –2 –40 –43 –48 –54
LDL-C:HDL-Cc –9 –51 –57 –58 –66
TC:HDL-Cc –7 –41 –43 –44 –51
Non–HDL-C:HDL-Cc –9 –50 –53 –54 –64
a Least-squares mean % change from ANOVA.b Abbreviations: LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; HDL-C, high-
density lipoprotein cholesterol; TG, triglycerides; Apo, apolipoprotein.c P < 0.001 in favor of rosuvastatin for all doses.d P < 0.05 in favor of rosuvastatin.e P = NS.
TABLE 2. Mean percent differences across dose range
(rosuvastatin vs. atorvastatin)a
Difference across dose rangeb %
LDL-Cc 8.4
TC 4.9
Non–HDL-C 7.0
Apo B 6.3
LDL-C:HDL-C 9.5
TC:HDL-C 6.9
Non–HDL-C:HDL-C 8.4
Apo B:apo A-I 7.8
a Mean % changes from baseline were assessed by linear regression analysis using analysis of co-
variance (ANCOVA).b All P < 0.001 in favor of rosuvastatin.c Abbreviations: LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; HDL-C,
high-density lipoprotein cholesterol; Apo, apolipoprotein.
Data from ref. 31.
Randomized, double-blind comparative trials
Rosuvastatin was compared with atorvastatin or with simvastatin and pravastatin in tri-
als assessing initial doses and dose titration in patients with LDL-C �160 and <250 mg�dL
(�4.14 and <6.46 mmol�L) and triglycerides �400 mg�dL (�4.52 mmol�L) (data on file,
AstraZeneca). These trials were prospectively designed to allow pooling of data from
12-w fixed-dose treatment phases (see pooled data analyses below). Together with results
from the comparative dose-ranging study, the comparative trials vs. atorvastatin demon-
strate that rosuvastatin significantly reduces LDL-C and significantly increases HDL-C,
compared with atorvastatin at the usual starting dose, and enables more patients to achieve
guideline LDL-C goals with reduced need for dose titration. Similarly, comparative trials
with simvastatin and pravastatin show that rosuvastatin markedly improves lipid mea-
sures, compared with starting doses of these agents, and enables more patients to reach
LDL-C goals.
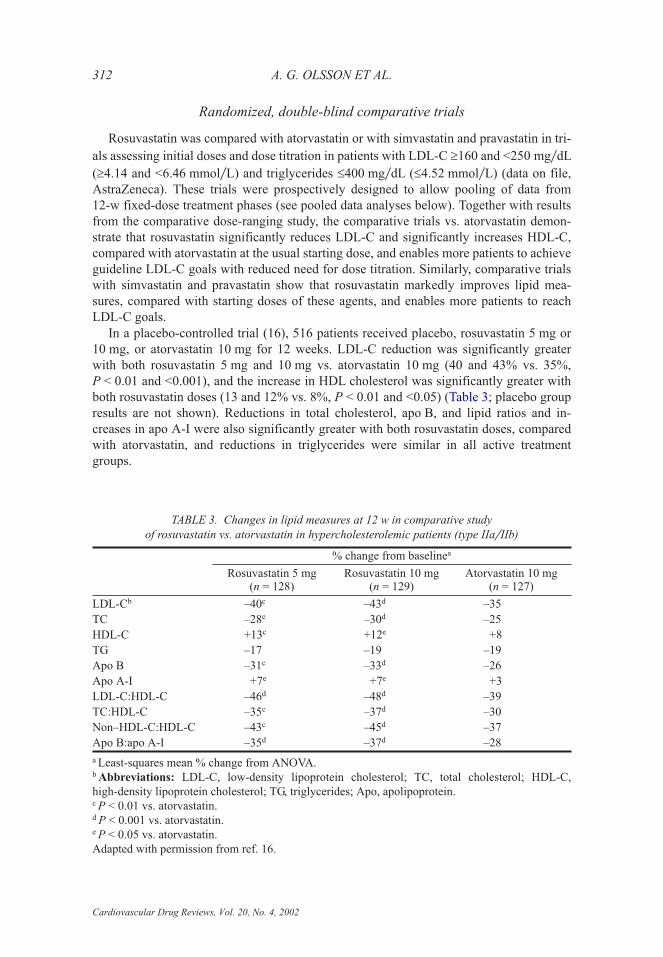
In a placebo-controlled trial (16), 516 patients received placebo, rosuvastatin 5 mg or
10 mg, or atorvastatin 10 mg for 12 weeks. LDL-C reduction was significantly greater
with both rosuvastatin 5 mg and 10 mg vs. atorvastatin 10 mg (40 and 43% vs. 35%,
P < 0.01 and <0.001), and the increase in HDL cholesterol was significantly greater with
both rosuvastatin doses (13 and 12% vs. 8%, P < 0.01 and <0.05) (Table 3; placebo group
results are not shown). Reductions in total cholesterol, apo B, and lipid ratios and in-
creases in apo A-I were also significantly greater with both rosuvastatin doses, compared
with atorvastatin, and reductions in triglycerides were similar in all active treatment
groups.
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
312 A. G. OLSSON ET AL.
TABLE 3. Changes in lipid measures at 12 w in comparative study
of rosuvastatin vs. atorvastatin in hypercholesterolemic patients (type IIa�IIb)
% change from baselinea
Rosuvastatin 5 mg(n = 128)
Rosuvastatin 10 mg(n = 129)
Atorvastatin 10 mg(n = 127)
LDL-Cb –40c –43d –35
TC –28e –30d –25
HDL-C +13c +12e +8
TG –17 –19 –19
Apo B –31c –33d –26
Apo A-I +7e +7e +3
LDL-C:HDL-C –46d –48d –39
TC:HDL-C –35c –37d –30
Non–HDL-C:HDL-C –43c –45d –37
Apo B:apo A-I –35d –37d –28
a Least-squares mean % change from ANOVA.b Abbreviations: LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; HDL-C,
high-density lipoprotein cholesterol; TG, triglycerides; Apo, apolipoprotein.c P < 0.01 vs. atorvastatin.d P < 0.001 vs. atorvastatin.e P < 0.05 vs. atorvastatin.
Adapted with permission from ref. 16.
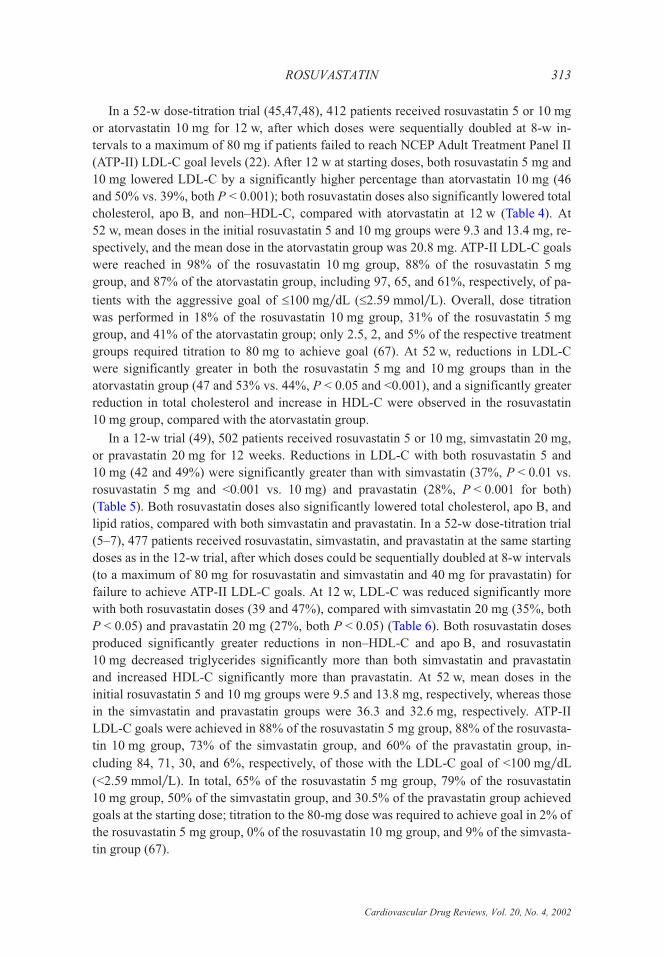
In a 52-w dose-titration trial (45,47,48), 412 patients received rosuvastatin 5 or 10 mg
or atorvastatin 10 mg for 12 w, after which doses were sequentially doubled at 8-w in-
tervals to a maximum of 80 mg if patients failed to reach NCEP Adult Treatment Panel II
(ATP-II) LDL-C goal levels (22). After 12 w at starting doses, both rosuvastatin 5 mg and
10 mg lowered LDL-C by a significantly higher percentage than atorvastatin 10 mg (46
and 50% vs. 39%, both P < 0.001); both rosuvastatin doses also significantly lowered total
cholesterol, apo B, and non–HDL-C, compared with atorvastatin at 12 w (Table 4). At
52 w, mean doses in the initial rosuvastatin 5 and 10 mg groups were 9.3 and 13.4 mg, re-
spectively, and the mean dose in the atorvastatin group was 20.8 mg. ATP-II LDL-C goals
were reached in 98% of the rosuvastatin 10 mg group, 88% of the rosuvastatin 5 mg
group, and 87% of the atorvastatin group, including 97, 65, and 61%, respectively, of pa-
tients with the aggressive goal of �100 mg�dL (�2.59 mmol�L). Overall, dose titration
was performed in 18% of the rosuvastatin 10 mg group, 31% of the rosuvastatin 5 mg
group, and 41% of the atorvastatin group; only 2.5, 2, and 5% of the respective treatment
groups required titration to 80 mg to achieve goal (67). At 52 w, reductions in LDL-C
were significantly greater in both the rosuvastatin 5 mg and 10 mg groups than in the
atorvastatin group (47 and 53% vs. 44%, P < 0.05 and <0.001), and a significantly greater
reduction in total cholesterol and increase in HDL-C were observed in the rosuvastatin
10 mg group, compared with the atorvastatin group.
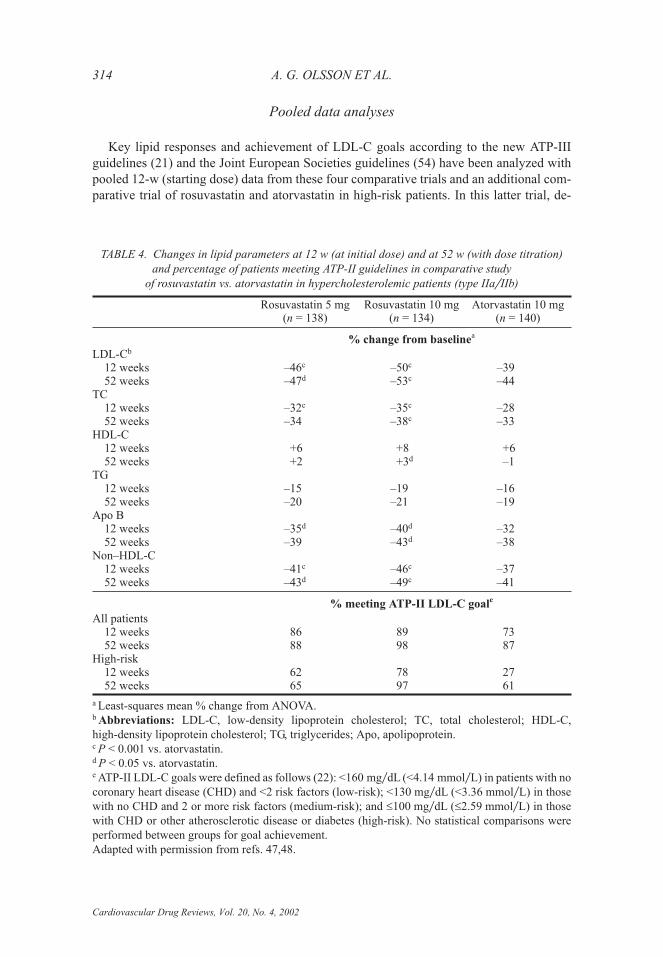
In a 12-w trial (49), 502 patients received rosuvastatin 5 or 10 mg, simvastatin 20 mg,
or pravastatin 20 mg for 12 weeks. Reductions in LDL-C with both rosuvastatin 5 and
10 mg (42 and 49%) were significantly greater than with simvastatin (37%, P < 0.01 vs.
rosuvastatin 5 mg and <0.001 vs. 10 mg) and pravastatin (28%, P < 0.001 for both)
(Table 5). Both rosuvastatin doses also significantly lowered total cholesterol, apo B, and
lipid ratios, compared with both simvastatin and pravastatin. In a 52-w dose-titration trial
(5–7), 477 patients received rosuvastatin, simvastatin, and pravastatin at the same starting
doses as in the 12-w trial, after which doses could be sequentially doubled at 8-w intervals
(to a maximum of 80 mg for rosuvastatin and simvastatin and 40 mg for pravastatin) for
failure to achieve ATP-II LDL-C goals. At 12 w, LDL-C was reduced significantly more
with both rosuvastatin doses (39 and 47%), compared with simvastatin 20 mg (35%, both
P < 0.05) and pravastatin 20 mg (27%, both P < 0.05) (Table 6). Both rosuvastatin doses
produced significantly greater reductions in non–HDL-C and apo B, and rosuvastatin
10 mg decreased triglycerides significantly more than both simvastatin and pravastatin
and increased HDL-C significantly more than pravastatin. At 52 w, mean doses in the
initial rosuvastatin 5 and 10 mg groups were 9.5 and 13.8 mg, respectively, whereas those
in the simvastatin and pravastatin groups were 36.3 and 32.6 mg, respectively. ATP-II
LDL-C goals were achieved in 88% of the rosuvastatin 5 mg group, 88% of the rosuvasta-
tin 10 mg group, 73% of the simvastatin group, and 60% of the pravastatin group, in-
cluding 84, 71, 30, and 6%, respectively, of those with the LDL-C goal of <100 mg�dL
(<2.59 mmol�L). In total, 65% of the rosuvastatin 5 mg group, 79% of the rosuvastatin
10 mg group, 50% of the simvastatin group, and 30.5% of the pravastatin group achieved
goals at the starting dose; titration to the 80-mg dose was required to achieve goal in 2% of
the rosuvastatin 5 mg group, 0% of the rosuvastatin 10 mg group, and 9% of the simvasta-
tin group (67).
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 313
Pooled data analyses
Key lipid responses and achievement of LDL-C goals according to the new ATP-III
guidelines (21) and the Joint European Societies guidelines (54) have been analyzed with
pooled 12-w (starting dose) data from these four comparative trials and an additional com-
parative trial of rosuvastatin and atorvastatin in high-risk patients. In this latter trial, de-
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
314 A. G. OLSSON ET AL.
TABLE 4. Changes in lipid parameters at 12 w (at initial dose) and at 52 w (with dose titration)
and percentage of patients meeting ATP-II guidelines in comparative study
of rosuvastatin vs. atorvastatin in hypercholesterolemic patients (type IIa�IIb)
Rosuvastatin 5 mg(n = 138)
Rosuvastatin 10 mg(n = 134)
Atorvastatin 10 mg(n = 140)
% change from baselinea
LDL-Cb
12 weeks –46c –50c –3952 weeks –47d –53c –44
TC12 weeks –32c –35c –2852 weeks –34 –38c –33
HDL-C12 weeks +6 +8 +652 weeks +2 +3d –1
TG12 weeks –15 –19 –1652 weeks –20 –21 –19
Apo B12 weeks –35d –40d –3252 weeks –39 –43d –38
Non–HDL-C12 weeks –41c –46c –3752 weeks –43d –49c –41
% meeting ATP-II LDL-C goale
All patients12 weeks 86 89 7352 weeks 88 98 87
High-risk12 weeks 62 78 2752 weeks 65 97 61
a Least-squares mean % change from ANOVA.b Abbreviations: LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; HDL-C,
high-density lipoprotein cholesterol; TG, triglycerides; Apo, apolipoprotein.c P < 0.001 vs. atorvastatin.d P < 0.05 vs. atorvastatin.e ATP-II LDL-C goals were defined as follows (22): <160 mg�dL (<4.14 mmol�L) in patients with no
coronary heart disease (CHD) and <2 risk factors (low-risk); <130 mg�dL (<3.36 mmol�L) in those
with no CHD and 2 or more risk factors (medium-risk); and �100 mg�dL (�2.59 mmol�L) in those
with CHD or other atherosclerotic disease or diabetes (high-risk). No statistical comparisons were
performed between groups for goal achievement.
Adapted with permission from refs. 47,48.
tails of which have yet to be reported, 383 high-risk patients (with documented atheroscle-
rotic disease or diabetes) meeting lipid entry criteria identical to those of the other four
studies received rosuvastatin 5 mg or 10 mg or atorvastatin for 12 w, followed by a 12-w
dose-titration period (data on file, AstraZeneca). Pooled analysis of the three comparative
trials with atorvastatin (66) showed that both rosuvastatin 5 mg (n = 390) and rosuvastatin
10 mg (n = 389) doses produced significantly greater reductions in LDL-C, compared
with atorvastatin (n = 393) (42 and 47% vs. 36%, both P < 0.001), and that both produced
significantly greater increases in HDL-C (8 and 9% vs. 5.5%, both P < 0.01). Overall,
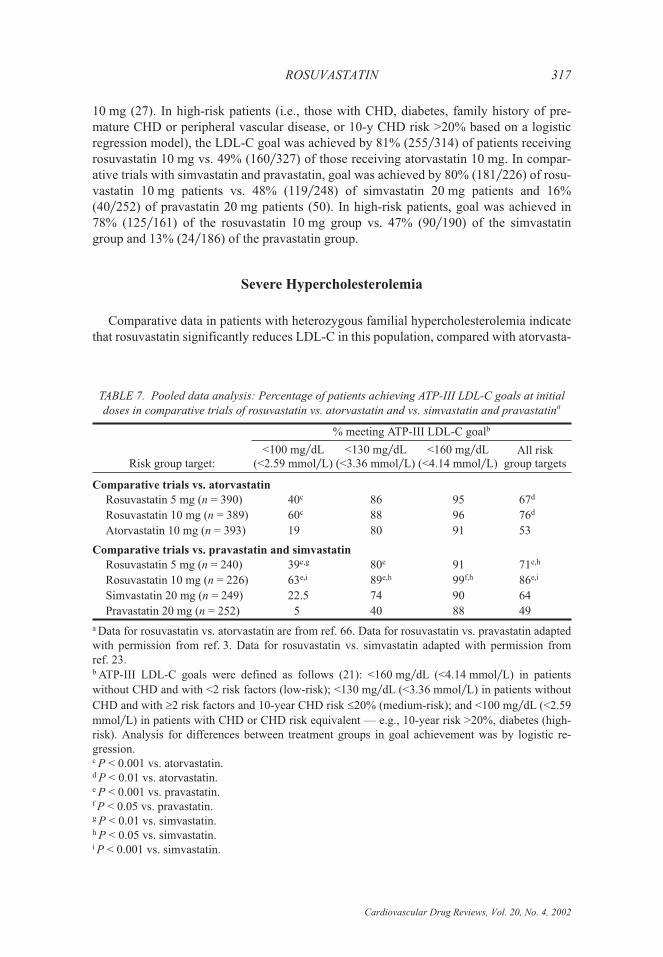
ATP-III LDL-C goals were achieved by 67% of rosuvastatin 5 mg patients, 76% of rosu-
vastatin 10 mg patients, and 53% of atorvastatin 10 mg patients (both P < 0.01 vs. atorva-
statin) (Table 7). Both rosuvastatin doses were also associated with a significantly greater
achievement of the aggressive LDL-C goal of <100 mg�dL (<2.59 mmol�L) in patients
with CHD or CHD risk equivalents.
In analysis of pooled data from the two trials comparing rosuvastatin with simvastatin
and pravastatin, both rosuvastatin 5 mg (n = 240) and rosuvastatin 10 mg (n = 226) pro-
duced significantly greater reductions in LDL-C, compared with simvastatin 20 mg
(n = 249) (41 and 48% vs. 36%, both P < 0.001) and pravastatin 20 mg (n = 252) (41 and
48% vs. 27%, both P < 0.001) (3,23). Rosuvastatin 10 mg increased HDL-C significantly
more than simvastatin 20 mg (9 vs. 6%, P < 0.05) or pravastatin 20 mg (9 vs. 6%,
P < 0.05). Overall, ATP-III LDL-C goals were achieved in 71% of rosuvastatin 5 mg pa-
tients, 86% of rosuvastatin 10 mg patients, 64% of simvastatin 20 mg patients (P < 0.05
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 315
TABLE 5. Changes in lipid measures at 12 w in comparative study of rosuvastatin vs. simvastatin
and pravastatin in hypercholesterolemic patients (type IIa�IIb)
% change from baselinea
Rosuvastatin5 mg (n = 119)
Rosuvastatin10 mg (n = 111)
Simvastatin20 mg (n = 129)
Pravastatin20 mg (n = 136)
LDL-Cb –42c –49d –37 –28
TC –30c –34d –26 –20
HDL-C +6 +7 +4 +4
TG –12 –18 –14 –13
Apo B –33e –40d –30 –21
Apo A-I +7 +5 +4 +4
LDL-C:HDL-C –45c –51d –39 –29
TC:HDL-C –33c –38d –28 –22
Non–HDL-C:HDL-C –41f –47d –35 –27
Apo B:apo A-I –37f –42d –32 –23
a Least-squares mean % change from ANOVA.b Abbreviations: LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; HDL-C, high-
density lipoprotein cholesterol; TG, triglycerides; Apo, apolipoprotein.c P < 0.001 vs. pravastatin, P < 0.005 vs. simvastatin.d P < 0.001 vs. pravastatin, P < 0.001 vs. simvastatin.eP < 0.001 vs. pravastatin, P < 0.05 vs. simvastatin.fP < 0.001 vs. pravastatin, P < 0.01 vs. simvastatin.
Adapted with permission from ref. 49.
and <0.001), and 49% of pravastatin 20 mg patients (both P < 0.001) (Table 7). Both
rosuvastatin doses also brought significantly more patients to their LDL-C goal of
<100 mg�dL (<2.59 mmol�L).
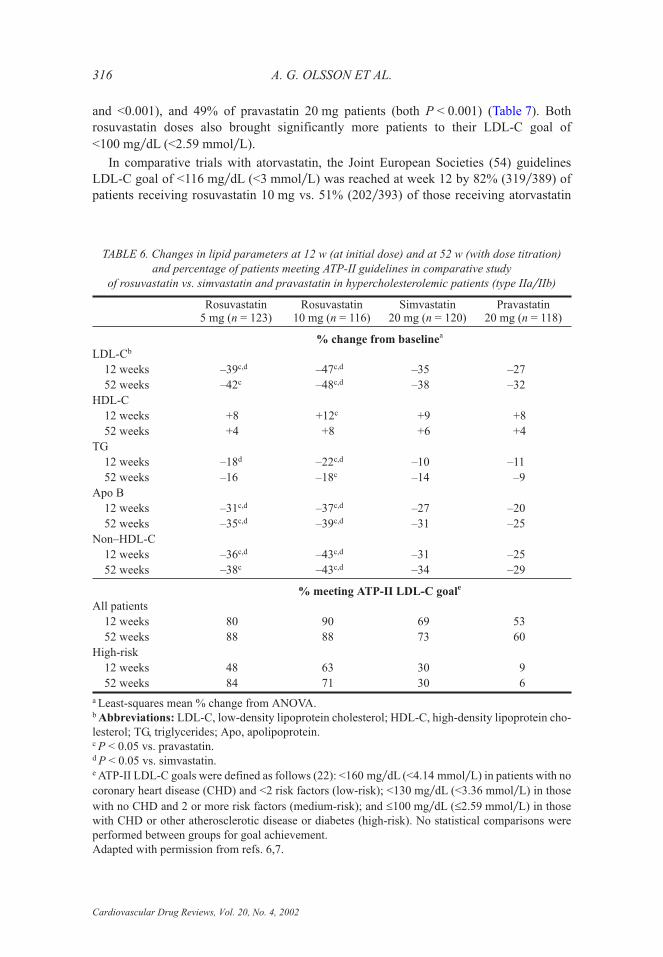
In comparative trials with atorvastatin, the Joint European Societies (54) guidelines
LDL-C goal of <116 mg�dL (<3 mmol�L) was reached at week 12 by 82% (319�389) of
patients receiving rosuvastatin 10 mg vs. 51% (202�393) of those receiving atorvastatin
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
316 A. G. OLSSON ET AL.
TABLE 6. Changes in lipid parameters at 12 w (at initial dose) and at 52 w (with dose titration)
and percentage of patients meeting ATP-II guidelines in comparative study
of rosuvastatin vs. simvastatin and pravastatin in hypercholesterolemic patients (type IIa�IIb)
Rosuvastatin5 mg (n = 123)
Rosuvastatin10 mg (n = 116)
Simvastatin20 mg (n = 120)
Pravastatin20 mg (n = 118)
% change from baselinea
LDL-Cb
12 weeks –39c,d –47c,d –35 –27
52 weeks –42c –48c,d –38 –32
HDL-C
12 weeks +8 +12c +9 +8
52 weeks +4 +8 +6 +4
TG
12 weeks –18d –22c,d –10 –11
52 weeks –16 –18c –14 –9
Apo B
12 weeks –31c,d –37c,d –27 –20
52 weeks –35c,d –39c,d –31 –25
Non–HDL-C
12 weeks –36c,d –43c,d –31 –25
52 weeks –38c –43c,d –34 –29
% meeting ATP-II LDL-C goale
All patients
12 weeks 80 90 69 53
52 weeks 88 88 73 60
High-risk
12 weeks 48 63 30 9
52 weeks 84 71 30 6
a Least-squares mean % change from ANOVA.b Abbreviations: LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cho-
lesterol; TG, triglycerides; Apo, apolipoprotein.c P < 0.05 vs. pravastatin.d P < 0.05 vs. simvastatin.e ATP-II LDL-C goals were defined as follows (22): <160 mg�dL (<4.14 mmol�L) in patients with no
coronary heart disease (CHD) and <2 risk factors (low-risk); <130 mg�dL (<3.36 mmol�L) in those
with no CHD and 2 or more risk factors (medium-risk); and �100 mg�dL (�2.59 mmol�L) in those
with CHD or other atherosclerotic disease or diabetes (high-risk). No statistical comparisons were
performed between groups for goal achievement.
Adapted with permission from refs. 6,7.
10 mg (27). In high-risk patients (i.e., those with CHD, diabetes, family history of pre-
mature CHD or peripheral vascular disease, or 10-y CHD risk >20% based on a logistic
regression model), the LDL-C goal was achieved by 81% (255�314) of patients receiving
rosuvastatin 10 mg vs. 49% (160�327) of those receiving atorvastatin 10 mg. In compar-
ative trials with simvastatin and pravastatin, goal was achieved by 80% (181�226) of rosu-
vastatin 10 mg patients vs. 48% (119�248) of simvastatin 20 mg patients and 16%
(40�252) of pravastatin 20 mg patients (50). In high-risk patients, goal was achieved in
78% (125�161) of the rosuvastatin 10 mg group vs. 47% (90�190) of the simvastatin
group and 13% (24�186) of the pravastatin group.
Severe Hypercholesterolemia
Comparative data in patients with heterozygous familial hypercholesterolemia indicate
that rosuvastatin significantly reduces LDL-C in this population, compared with atorvasta-
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 317
TABLE 7. Pooled data analysis: Percentage of patients achieving ATP-III LDL-C goals at initial
doses in comparative trials of rosuvastatin vs. atorvastatin and vs. simvastatin and pravastatina
Risk group target:
% meeting ATP-III LDL-C goalb
<100 mg�dL(<2.59 mmol�L)
<130 mg�dL(<3.36 mmol�L)
<160 mg�dL(<4.14 mmol�L)
All riskgroup targets
Comparative trials vs. atorvastatin
Rosuvastatin 5 mg (n = 390) 40c 86 95 67d
Rosuvastatin 10 mg (n = 389) 60c 88 96 76d
Atorvastatin 10 mg (n = 393) 19 80 91 53
Comparative trials vs. pravastatin and simvastatin
Rosuvastatin 5 mg (n = 240) 39e,g 80e 91 71e,h
Rosuvastatin 10 mg (n = 226) 63e,i 89e,h 99f,h 86e,i
Simvastatin 20 mg (n = 249) 22.5 74 90 64
Pravastatin 20 mg (n = 252) 5 40 88 49
a Data for rosuvastatin vs. atorvastatin are from ref. 66. Data for rosuvastatin vs. pravastatin adapted
with permission from ref. 3. Data for rosuvastatin vs. simvastatin adapted with permission from
ref. 23.b ATP-III LDL-C goals were defined as follows (21): <160 mg�dL (<4.14 mmol�L) in patients
without CHD and with <2 risk factors (low-risk); <130 mg�dL (<3.36 mmol�L) in patients without
CHD and with �2 risk factors and 10-year CHD risk �20% (medium-risk); and <100 mg�dL (<2.59
mmol�L) in patients with CHD or CHD risk equivalent — e.g., 10-year risk >20%, diabetes (high-
risk). Analysis for differences between treatment groups in goal achievement was by logistic re-
gression.c P < 0.001 vs. atorvastatin.d P < 0.01 vs. atorvastatin.e P < 0.001 vs. pravastatin.f P < 0.05 vs. pravastatin.g P < 0.01 vs. simvastatin.h P < 0.05 vs. simvastatin.i P < 0.001 vs. simvastatin.
tin, and enables more patients to achieve LDL-C goals. Rosuvastatin treatment in patients
with homozygous familial hypercholesterolemia produces clinically significant LDL-C
reductions in the majority of patients.
Heterozygous familial hypercholesterolemia
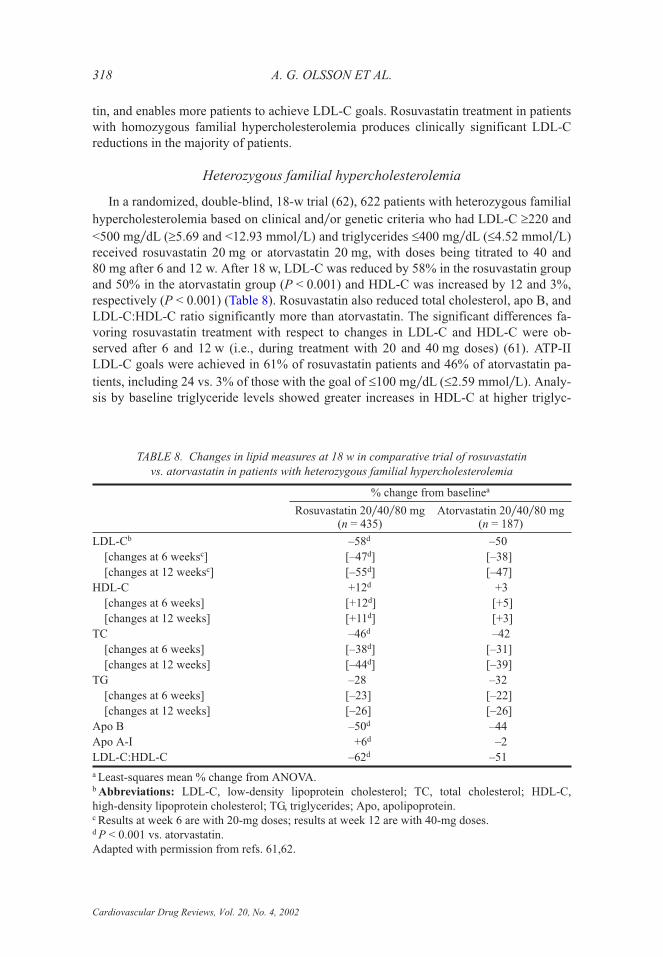
In a randomized, double-blind, 18-w trial (62), 622 patients with heterozygous familial
hypercholesterolemia based on clinical and�or genetic criteria who had LDL-C �220 and
<500 mg�dL (�5.69 and <12.93 mmol�L) and triglycerides �400 mg�dL (�4.52 mmol�L)
received rosuvastatin 20 mg or atorvastatin 20 mg, with doses being titrated to 40 and
80 mg after 6 and 12 w. After 18 w, LDL-C was reduced by 58% in the rosuvastatin group
and 50% in the atorvastatin group (P < 0.001) and HDL-C was increased by 12 and 3%,
respectively (P < 0.001) (Table 8). Rosuvastatin also reduced total cholesterol, apo B, and
LDL-C:HDL-C ratio significantly more than atorvastatin. The significant differences fa-
voring rosuvastatin treatment with respect to changes in LDL-C and HDL-C were ob-
served after 6 and 12 w (i.e., during treatment with 20 and 40 mg doses) (61). ATP-II
LDL-C goals were achieved in 61% of rosuvastatin patients and 46% of atorvastatin pa-
tients, including 24 vs. 3% of those with the goal of �100 mg�dL (�2.59 mmol�L). Analy-
sis by baseline triglyceride levels showed greater increases in HDL-C at higher triglyc-
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
318 A. G. OLSSON ET AL.
TABLE 8. Changes in lipid measures at 18 w in comparative trial of rosuvastatin
vs. atorvastatin in patients with heterozygous familial hypercholesterolemia
% change from baselinea
Rosuvastatin 20�40�80 mg(n = 435)
Atorvastatin 20�40�80 mg(n = 187)
LDL-Cb –58d –50
[changes at 6 weeksc] [–47d] [–38]
[changes at 12 weeksc] [–55d] [–47]
HDL-C +12d +3
[changes at 6 weeks] [+12d] [+5]
[changes at 12 weeks] [+11d] [+3]
TC –46d –42
[changes at 6 weeks] [–38d] [–31]
[changes at 12 weeks] [–44d] [–39]
TG –28 –32
[changes at 6 weeks] [–23] [–22]
[changes at 12 weeks] [–26] [–26]
Apo B –50d –44
Apo A-I +6d –2
LDL-C:HDL-C –62d –51
a Least-squares mean % change from ANOVA.b Abbreviations: LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; HDL-C,
high-density lipoprotein cholesterol; TG, triglycerides; Apo, apolipoprotein.c Results at week 6 are with 20-mg doses; results at week 12 are with 40-mg doses.d P < 0.001 vs. atorvastatin.
Adapted with permission from refs. 61,62.

eride levels, with increases of 9, 15, and 22% being observed according to triglyceride
levels of <150, 150–250, and >250 mg�dL (<1.69, 1.69–2.82, and >2.82 mmol�L), re-
spectively (60).
Homozygous familial hypercholesterolemia
In an open-label, 18-w trial, 44 patients with homozygous familial hypercholester-
olemia, aged 8 to 63 y, received rosuvastatin 20 mg increased to 40 and 80 mg after 6 and
12 w after completing a 4-w dietary lead-in phase (34). Mean LDL-C level at baseline was
515 mg�dL (13.32 mmol�L). After 18 weeks, LDL-C and total cholesterol were reduced
by means of 21% and 20%, respectively, with most of the decreases occurring within the
first 6 w of treatment with rosuvastatin 20 mg. Clinically relevant decreases in LDL-C
(15% or greater) occurred in 29 (72.5%) of 40 patients, and reductions of greater than 30%
occurred in 13 (32.5%).
Hypertriglyceridemia
In studies involving hypertriglyceridemic patients, rosuvastatin significantly reduced
triglycerides, very-low-density lipoprotein cholesterol (VLDL-C), non–HDL-C, and
LDL-C, with analysis of changes in apo B–containing lipoprotein fractions indicating
marked reductions in all measures and normalization of particle composition.
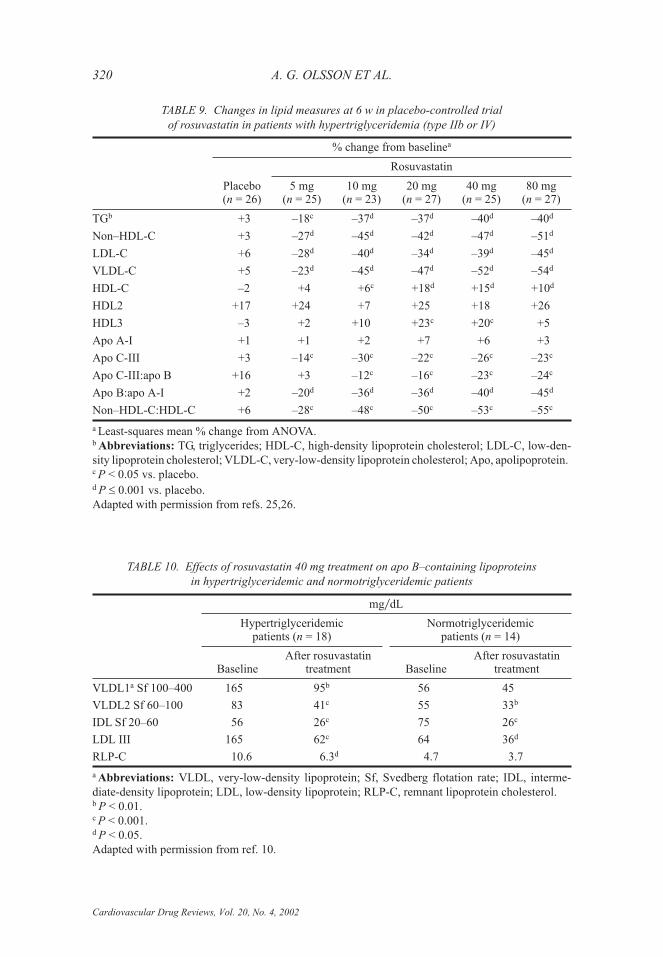
In a randomized, double-blind, placebo-controlled trial (25,26), 156 patients with
triglyceride levels �300 and <800 mg�dL (�3.39 and <9.03 mmol�L; type IIb or IV dys-
lipidemia) received placebo or rosuvastatin 5–80 mg for 6 w. Triglyceride levels were sig-
nificantly reduced, compared with placebo, at all rosuvastatin dose levels, with reductions
ranging from 18 to 40% (Table 9). Significant reductions in LDL-C, non–HDL-C,
VLDL-C, apo C-III, and non–HDL-C:HDL-C and apo B:apo A-I ratios occurred at each
dose level, and significant increases in HDL-C occurred at all dose levels except 5 mg
(range, 4–18%). All doses reduced the triglyceride content of LDL, VLDL, and HDL and
the apo B content of LDL and VLDL.
In a study examining the effects of rosuvastatin 40 mg on concentration and compo-
sition of apo B–containing lipoprotein subfractions (10), patients were divided into a
hypertriglyceridemic group (triglycerides >177 mg�dL [>2.00 mmol�L] and LDL-C
106–215 mg�dL [2.75–5.55 mmol�L], n = 18) and a normotriglyceridemic group (triglyc-
erides <177 mg�dL [<2.00 mmol�L] and LDL-C 131–220 mg�dL [3.40–5.70 mmol�L],
n = 14). In all patients, rosuvastatin reduced LDL-C by a mean of 59% and triglycerides
by a mean of 28%; the reduction in LDL-C was inversely related to baseline triglycerides,
and the reduction in triglycerides was positively related to baseline triglycerides. Rosuva-
statin reduced both cholesteryl ester and free cholesterol contents of all apo B–containing
lipoproteins, including remnants and small dense LDL, in both hypertriglyceridemic and
normotriglyceridemic groups (Table 10) and normalized particle composition. Some of
the effects (e.g., those on VLDL2 and LDL-C) were phenotype independent, whereas
some (e.g., those on VLDL1, remnant lipoprotein cholesterol, and LDL III) were de-
pendent on the baseline lipid profile. In the hypertriglyceridemic group, rosuvastatin
largely corrected the atherogenic LDL profile, with LDL III concentrations falling to
�100 mg�dL (�2.59 mmol�L) in 16 of 18 patients.
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 319
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
320 A. G. OLSSON ET AL.
TABLE 9. Changes in lipid measures at 6 w in placebo-controlled trial
of rosuvastatin in patients with hypertriglyceridemia (type IIb or IV)
% change from baselinea
Placebo(n = 26)
Rosuvastatin
5 mg(n = 25)
10 mg(n = 23)
20 mg(n = 27)
40 mg(n = 25)
80 mg(n = 27)
TGb +3 –18c –37d –37d –40d –40d
Non–HDL-C +3 –27d –45d –42d –47d –51d
LDL-C +6 –28d –40d –34d –39d –45d
VLDL-C +5 –23d –45d –47d –52d –54d
HDL-C –2 +4 +6c +18d +15d +10d
HDL2 +17 +24 +7 +25 +18 +26
HDL3 –3 +2 +10 +23c +20c +5
Apo A-I +1 +1 +2 +7 +6 +3
Apo C-III +3 –14c –30c –22c –26c –23c
Apo C-III:apo B +16 +3 –12c –16c –23c –24c
Apo B:apo A-I +2 –20d –36d –36d –40d –45d
Non–HDL-C:HDL-C +6 –28c –48c –50c –53c –55c
a Least-squares mean % change from ANOVA.b Abbreviations: TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-den-
sity lipoprotein cholesterol; VLDL-C, very-low-density lipoprotein cholesterol; Apo, apolipoprotein.c P < 0.05 vs. placebo.d P � 0.001 vs. placebo.
Adapted with permission from refs. 25,26.
TABLE 10. Effects of rosuvastatin 40 mg treatment on apo B–containing lipoproteins
in hypertriglyceridemic and normotriglyceridemic patients
mg�dL
Hypertriglyceridemicpatients (n = 18)
Normotriglyceridemicpatients (n = 14)
BaselineAfter rosuvastatin
treatment BaselineAfter rosuvastatin
treatment
VLDL1a Sf 100–400 165 95b 56 45
VLDL2 Sf 60–100 83 41c 55 33b
IDL Sf 20–60 56 26c 75 26c
LDL III 165 62c 64 36d
RLP-C 10.6 6.3d 4.7 3.7
a Abbreviations: VLDL, very-low-density lipoprotein; Sf, Svedberg flotation rate; IDL, interme-
diate-density lipoprotein; LDL, low-density lipoprotein; RLP-C, remnant lipoprotein cholesterol.b P < 0.01.c P < 0.001.d P < 0.05.
Adapted with permission from ref. 10.

Combination Studies
Rosuvastatin has been evaluated alone and in combination with fenofibrate in mixed
dyslipidemia patients (type IIb�IV) with type 2 diabetes (18,19), with extended-release
niacin (ERN) in patients with mixed dyslipidemia (type IIb �IV) (9,40), and with chole-
styramine in hypercholesterolemic patients (2). In diabetic patients and patients with
mixed dyslipidemia, rosuvastatin monotherapy improved most lipid measures as much as,
or more than, combinations of lower-dose rosuvastatin with fenofibrate or ERN, sug-
gesting a potential role for monotherapy in some patients in these settings. Advantages of
combination therapy included a significantly greater reduction in triglycerides with the ro-
suvastatin�fenofibrate combination and a significantly greater increase in HDL-C with the
rosuvastatin�ERN combination. No differences in changes in lipid measures were ob-
served between high-dose rosuvastatin alone and in combination with cholestyramine in
hypercholesterolemic patients. Rosuvastatin monotherapy was generally better tolerated
than combined treatment, but the combination did not produce any unexpected or serious
adverse events.
In a 24-w trial (18,19), 216 hyperlipidemic (type IIb or IV dyslipidemia) type 2 diabetic
patients with triglycerides �200 and <800 mg�dL (�2.26 and <9.03 mmol�L), total cho-
lesterol �200 mg�dL (�5.17 mmol�L), and HbA1c <10% were randomized to double-blind
rosuvastatin 5 or 10 mg or one of two placebo groups for 6 w. During the subsequent
18-w, open-label, dose-titration phase, fenofibrate titrated from 67 mg once daily to three
times daily was added to both rosuvastatin groups, one placebo group received rosuvasta-
tin 10–40 mg, and one placebo group received fenofibrate 67 mg one to three times daily
if LDL-C remained above 50 mg�dL (1.29 mmol�L). After 6 w, both rosuvastatin groups
had significantly reduced triglycerides, LDL-C, total cholesterol, and apo B and signifi-
cantly increased HDL-C, compared with the combined placebo groups (all P < 0.001).
After 24 w, combined treatment with rosuvastatin 10 mg�fenofibrate 67 mg three times
daily produced a significantly greater reduction in triglycerides, compared with rosuvasta-
tin 10–40 mg alone (47 vs. 30%, P = 0.001) (Table 11). Rosuvastatin 10–40 mg alone re-
duced LDL-C significantly more than both combination treatment with rosuvastatin
5 mg�fenofibrate and fenofibrate monotherapy. Increases in HDL-C were comparable in
all groups. All groups exhibited favorable changes in lipid subfractions. Combination
treatment was well tolerated.
In a 24-w, open-label trial (9,40), 270 patients with total cholesterol �200 mg�dL
(�5.17 mmol�L), triglycerides �200 and �800 mg�dL (�2.26 and �9.03 mmol�L; type IIb
or IV dyslipidemia), and HDL-C <45 mg�dL (<1.16 mmol�L) were randomized to one of
four dose-titrated monotherapy or combination therapy arms: rosuvastatin 10–40 mg;
ERN 0.5–2 g; rosuvastatin 10–40 mg + ERN 0.5–1 g; and rosuvastatin 10 mg + ERN
0.5–2 g. Rosuvastatin alone reduced LDL-C by 48%, significantly more than ERN alone
(0%, P < 0.017) and significantly more than combined treatment with rosuvastatin
10 mg�ERN 2 g (36%, P < 0.017) (Table 12); similar differences in reductions were ob-
served in apo B (42 vs. 9 and 34%, both P < 0.017) and non–HDL-C (49 vs. 11% and
38%, both P < 0.017). Combination treatment with rosuvastatin 10 mg�ERN 2 g produced
significantly greater increases than rosuvastatin alone in HDL-C (24 vs. 11%), HDL2 (41
vs. 9%), and apo A-I (11 vs. 5%; all P < 0.017). Rosuvastatin alone was better tolerated
than ERN alone or rosuvastatin�ERN combinations, with most withdrawals due to ad-
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 321
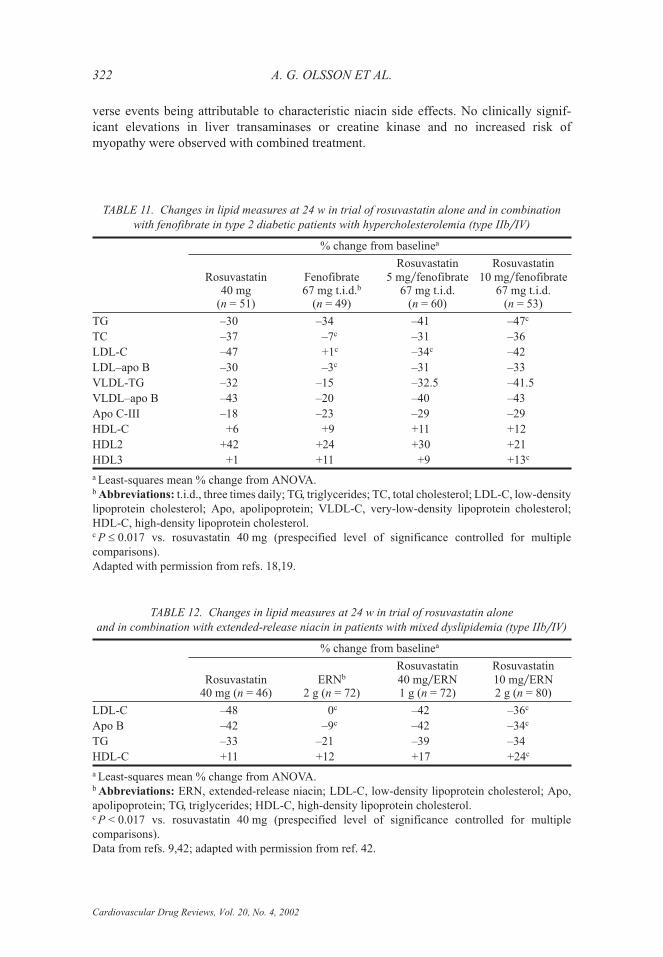
verse events being attributable to characteristic niacin side effects. No clinically signif-
icant elevations in liver transaminases or creatine kinase and no increased risk of
myopathy were observed with combined treatment.
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
322 A. G. OLSSON ET AL.
TABLE 11. Changes in lipid measures at 24 w in trial of rosuvastatin alone and in combination
with fenofibrate in type 2 diabetic patients with hypercholesterolemia (type IIb�IV)
% change from baselinea
Rosuvastatin40 mg
(n = 51)
Fenofibrate67 mg t.i.d.b
(n = 49)
Rosuvastatin5 mg�fenofibrate
67 mg t.i.d.(n = 60)
Rosuvastatin10 mg�fenofibrate
67 mg t.i.d.(n = 53)
TG –30 –34 –41 –47c
TC –37 –7c –31 –36
LDL-C –47 +1c –34c –42
LDL–apo B –30 –3c –31 –33
VLDL-TG –32 –15 –32.5 –41.5
VLDL–apo B –43 –20 –40 –43
Apo C-III –18 –23 –29 –29
HDL-C +6 +9 +11 +12
HDL2 +42 +24 +30 +21
HDL3 +1 +11 +9 +13c
a Least-squares mean % change from ANOVA.b Abbreviations: t.i.d., three times daily; TG, triglycerides; TC, total cholesterol; LDL-C, low-density
lipoprotein cholesterol; Apo, apolipoprotein; VLDL-C, very-low-density lipoprotein cholesterol;
HDL-C, high-density lipoprotein cholesterol.c P � 0.017 vs. rosuvastatin 40 mg (prespecified level of significance controlled for multiple
comparisons).
Adapted with permission from refs. 18,19.
TABLE 12. Changes in lipid measures at 24 w in trial of rosuvastatin alone
and in combination with extended-release niacin in patients with mixed dyslipidemia (type IIb�IV)
% change from baselinea
Rosuvastatin40 mg (n = 46)
ERNb
2 g (n = 72)
Rosuvastatin40 mg�ERN1 g (n = 72)
Rosuvastatin10 mg�ERN2 g (n = 80)
LDL-C –48 0c –42 –36c
Apo B –42 –9c –42 –34c
TG –33 –21 –39 –34
HDL-C +11 +12 +17 +24c
a Least-squares mean % change from ANOVA.b Abbreviations: ERN, extended-release niacin; LDL-C, low-density lipoprotein cholesterol; Apo,
apolipoprotein; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol.c P < 0.017 vs. rosuvastatin 40 mg (prespecified level of significance controlled for multiple
comparisons).
Data from refs. 9,42; adapted with permission from ref. 42.
In a 12-w trial (2), 147 patients with LDL-C �190 and �400 mg�dL (�4.91 and �10.34
mmol�L) and triglycerides <400 mg�dL (<4.52 mmol�L; heterozygous familial or nonfa-
milial hypercholesterolemia) received rosuvastatin 40 mg for 6 w and were subsequently
randomized to rosuvastatin 80 mg alone or rosuvastatin 80 mg + cholestyramine 8 g twice
daily for 6 w. After 12 w, there were no significant differences between the rosuvastatin
group and the rosuvastatin�cholestyramine group in reductions in LDL-C (56 vs. 61%),
total cholesterol (43 vs. 46%), triglycerides (23 vs. 26%), or apo B (47 vs. 48%) or in in-
creases in HDL-C (11 vs. 10%) or apo A-I (8 vs. 10%). No unexpected safety issues arose
with combined treatment.
SAFETY
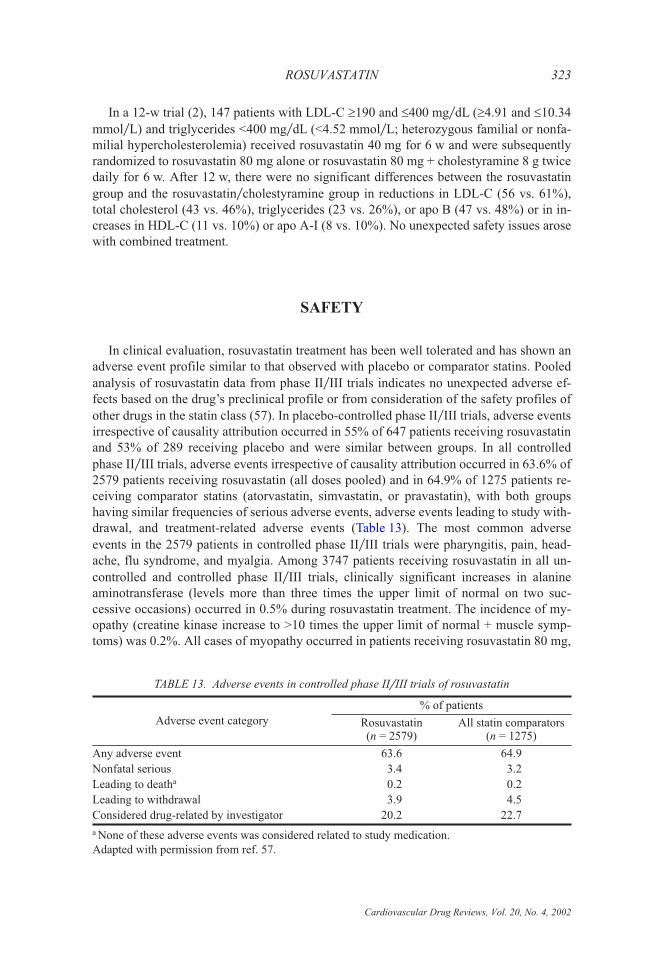
In clinical evaluation, rosuvastatin treatment has been well tolerated and has shown an
adverse event profile similar to that observed with placebo or comparator statins. Pooled
analysis of rosuvastatin data from phase II�III trials indicates no unexpected adverse ef-
fects based on the drug’s preclinical profile or from consideration of the safety profiles of
other drugs in the statin class (57). In placebo-controlled phase II �III trials, adverse events
irrespective of causality attribution occurred in 55% of 647 patients receiving rosuvastatin
and 53% of 289 receiving placebo and were similar between groups. In all controlled
phase II�III trials, adverse events irrespective of causality attribution occurred in 63.6% of
2579 patients receiving rosuvastatin (all doses pooled) and in 64.9% of 1275 patients re-
ceiving comparator statins (atorvastatin, simvastatin, or pravastatin), with both groups
having similar frequencies of serious adverse events, adverse events leading to study with-
drawal, and treatment-related adverse events (Table 13). The most common adverse
events in the 2579 patients in controlled phase II�III trials were pharyngitis, pain, head-
ache, flu syndrome, and myalgia. Among 3747 patients receiving rosuvastatin in all un-
controlled and controlled phase II�III trials, clinically significant increases in alanine
aminotransferase (levels more than three times the upper limit of normal on two suc-
cessive occasions) occurred in 0.5% during rosuvastatin treatment. The incidence of my-
opathy (creatine kinase increase to >10 times the upper limit of normal + muscle symp-
toms) was 0.2%. All cases of myopathy occurred in patients receiving rosuvastatin 80 mg,
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 323
TABLE 13. Adverse events in controlled phase II�III trials of rosuvastatin
Adverse event category
% of patients
Rosuvastatin(n = 2579)
All statin comparators(n = 1275)
Any adverse event 63.6 64.9
Nonfatal serious 3.4 3.2
Leading to deatha 0.2 0.2
Leading to withdrawal 3.9 4.5
Considered drug-related by investigator 20.2 22.7
a None of these adverse events was considered related to study medication.
Adapted with permission from ref. 57.
and all occurred in patients who were randomized directly to or force-titrated to this dose
(i.e., dose increase was not based on LDL-C response to treatment).
Following a regularly scheduled review of the benefit:risk ratio for rosuvastatin, Astra-
Zeneca is not seeking approval of the 80-mg dose at the current time. Most patients had
reached the 80-mg dose through forced titration or direct randomization, with very few re-
quiring titration to the maximum dose to achieve LDL-C goals, and the optimal use of this
dose has not yet been shown. The 80-mg dose will be reviewed for possible introduction
at a future date.
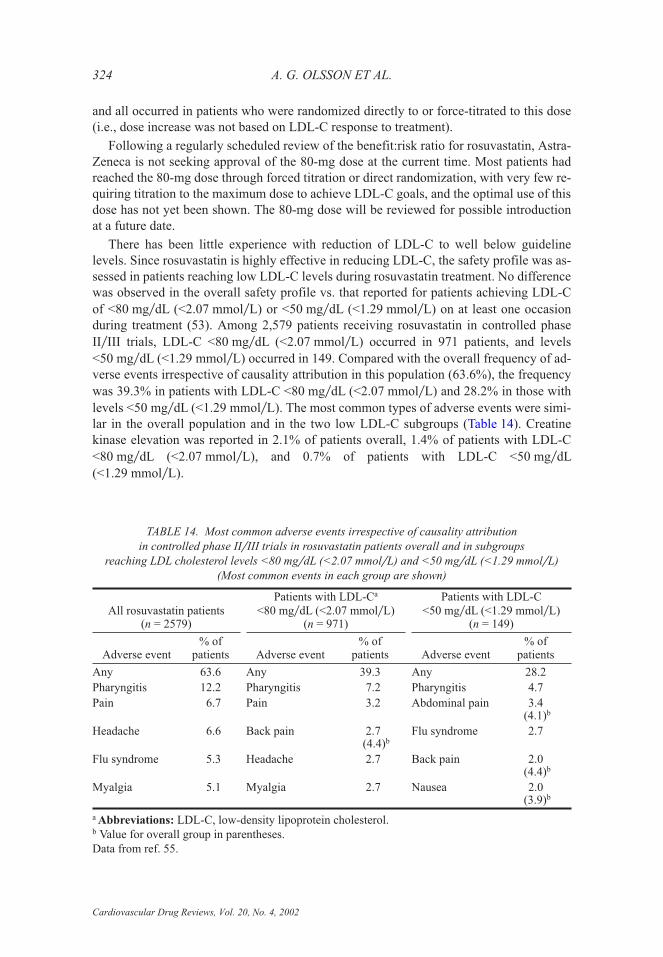
There has been little experience with reduction of LDL-C to well below guideline
levels. Since rosuvastatin is highly effective in reducing LDL-C, the safety profile was as-
sessed in patients reaching low LDL-C levels during rosuvastatin treatment. No difference
was observed in the overall safety profile vs. that reported for patients achieving LDL-C
of <80 mg�dL (<2.07 mmol�L) or <50 mg�dL (<1.29 mmol�L) on at least one occasion
during treatment (53). Among 2,579 patients receiving rosuvastatin in controlled phase
II�III trials, LDL-C <80 mg�dL (<2.07 mmol�L) occurred in 971 patients, and levels
<50 mg�dL (<1.29 mmol�L) occurred in 149. Compared with the overall frequency of ad-
verse events irrespective of causality attribution in this population (63.6%), the frequency
was 39.3% in patients with LDL-C <80 mg�dL (<2.07 mmol�L) and 28.2% in those with
levels <50 mg�dL (<1.29 mmol�L). The most common types of adverse events were simi-
lar in the overall population and in the two low LDL-C subgroups (Table 14). Creatine
kinase elevation was reported in 2.1% of patients overall, 1.4% of patients with LDL-C
<80 mg�dL (<2.07 mmol�L), and 0.7% of patients with LDL-C <50 mg�dL
(<1.29 mmol�L).
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
324 A. G. OLSSON ET AL.
TABLE 14. Most common adverse events irrespective of causality attribution
in controlled phase II�III trials in rosuvastatin patients overall and in subgroups
reaching LDL cholesterol levels <80 mg�dL (<2.07 mmol�L) and <50 mg�dL (<1.29 mmol�L)
(Most common events in each group are shown)
All rosuvastatin patients(n = 2579)
Patients with LDL-Ca
<80 mg�dL (<2.07 mmol�L)(n = 971)
Patients with LDL-C<50 mg�dL (<1.29 mmol�L)
(n = 149)
Adverse event% of
patients Adverse event% of
patients Adverse event% of
patients
Any 63.6 Any 39.3 Any 28.2
Pharyngitis 12.2 Pharyngitis 7.2 Pharyngitis 4.7
Pain 6.7 Pain 3.2 Abdominal pain 3.4(4.1)b
Headache 6.6 Back pain 2.7(4.4)b
Flu syndrome 2.7
Flu syndrome 5.3 Headache 2.7 Back pain 2.0(4.4)b
Myalgia 5.1 Myalgia 2.7 Nausea 2.0(3.9)b
a Abbreviations: LDL-C, low-density lipoprotein cholesterol.b Value for overall group in parentheses.
Data from ref. 55.

CONCLUSIONS
Rosuvastatin is a new statin with a number of advantageous pharmacological prop-
erties, including enhanced HMG-CoA reductase binding characteristics, relative hydro-
philicity, and selective uptake into, and activity in, hepatic cells. CYP metabolism of rosu-
vastatin, which appears to be minimal, is principally mediated by the 2C9 enzyme, with
little involvement of 3A4; consistent with these observations is the absence of clinically
significant pharmacokinetic drug-drug interactions with other drugs known to inhibit CYP
enzymes.
Dose-ranging studies in hypercholesterolemic patients showed dose-dependent effects
in reducing LDL-C (up to 63%), total cholesterol, and apo B across a 1- to 40-mg dose
range and a significant 8.4% additional reduction in LDL-C, compared with atorvastatin,
across the dose ranges of the two agents.
Rosuvastatin has been shown to be highly effective in reducing LDL-C, increasing
HDL-C, and favorably modifying other elements of the atherogenic lipid profile in a wide
range of dyslipidemic patients. In patients with mild to moderate hypercholesterolemia,
rosuvastatin treatment has produced large decreases in LDL-C at starting doses and re-
duced the need for subsequent dose titration. The large reductions in LDL-C and improve-
ments in other lipid measures with rosuvastatin treatment promise to facilitate goal
achievement and reduce the need for combination therapy in patients with severe hyper-
cholesterolemia. Moreover, the effects of rosuvastatin in reducing triglycerides, triglyc-
eride-containing lipoproteins, non–HDL-C, and LDL-C and increasing HDL-C in patients
with mixed dyslipidemia or elevated triglycerides should be of considerable utility in
achieving LDL-C and non–HDL-C goals in the many patients with combined dyslipide-
mias or metabolic syndrome who require lipid-lowering therapy. Rosuvastatin is well tol-
erated alone, and in combination with fenofibrate, ERN, and cholestyramine, and has a
safety profile similar to that of currently marketed statins.
A large, long-term clinical trials program has been initiated to investigate the effects of
rosuvastatin on atherosclerosis and cardiovascular morbidity and mortality. This initiative,
known as the GALAXY Program, will assess the efficacy and safety of rosuvastatin in a
wide range of patients and pathological processes (15). Areas of investigation will include
the slowing of atherosclerosis progression in low-risk asymptomatic patients, assessment
of lipids and pleiotropic effects in patients with acute coronary syndrome, reduction in ep-
isodes of myocardial ischemia in patients with proven coronary artery disease, and the use
of rosuvastatin in patients with�at risk of cardiovascular disease for whom there is cur-
rently no evidence of benefit from statin therapy. The GALAXY Program will also ex-
amine the relationship between lipid control and cardiovascular risk reduction, the attain-
ment of guideline treatment goals, and initiatives designed to improve patient compliance
with statin therapy.
REFERENCES
1. Andrews TC, Ballantyne CM, Hsia JA, Kramer JH. Achieving and maintaining National Cholesterol Edu-
cation Program low-density lipoprotein cholesterol goals with five statins. Am J Med 2001;111:185–191.
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 325
2. Ballantyne C, Miller E, Chitra R. Rosuvastatin alone produces similar lipid benefits compared with rosuva-
statin plus cholestyramine in patients with primary hypercholesterolemia. Int J Clin Pract 2002;124(Suppl):13.
3. Barter P, Shepherd J, Brown WV, Bays H, Southworth H, Strutt K. Rosuvastatin significantly improves lipid
parameters and ability to achieve low-density lipoprotein cholesterol goals compared with pravastatin. J Am
Coll Cardiol 2002;39(Suppl B):142B.
4. Brown CDA, Windass A, Bleasby K, Lauffart B. Rosuvastatin is a high affinity substrate of hepatic organic
anion transporter OATP-C. Atherosclerosis 2001;Suppl 2:88.
5. Brown WV, Bays HE, Hassman, DR. Efficacy and safety of rosuvastatin compared with pravastatin and sim-
vastatin in patients with hypercholesterolemia: A randomized, double-blind, 52-week trial. Am Heart J
2002; in press.
6. Brown WV, Chitra RR, Zedler BK, Bays HE, Hassman HA. Long-term efficacy and safety of rosuvastatin:
Results of a 52-week comparator-controlled trial versus pravastatin and simvastatin. Eur Heart J 2001;
22(Suppl):270.
7. Brown WV, McKenney JM, Zedler BK, et al. A 52-week trial of rosuvastatin versus pravastatin and simva-
statin in patients with primary hypercholesterolemia. Int J Clin Pract 2002;124(Suppl):12.
8. Buckett L, Ballard P, Davidson R, et al. Selectivity of ZD4522 for inhibition of cholesterol synthesis in he-
patic versus non-hepatic cells. Atherosclerosis 2000;151:41.
9. Capuzzi DM, Morgan JM, Weiss R, Chitra RR, Cressman MD, Hutchinson HG. Effects of rosuvastatin alone
and combined with extended-release niacin on apo B- and apo A-containing lipoproteins and triglycerides in
atherogenic dyslipidemia. Atherosclerosis Suppl 2002;3:82.
10. Caslake MJ, Stewart G, Day S, et al. Rosuvastatin normalises atherogenic levels of apo B-containing lipo-
protein subfractions. Int J Clin Pract 2002;124(Suppl):8.
11. Chapman MJ, McTaggart F. Optimizing the pharmacology of statins: Characteristics of rosuvastatin. Athero-
sclerosis Suppl 2002;2:33–37.
12. Cooper KJ, Martin PD, Dane AL, Warwick MJ, Schneck DW, Cantarini M. Fluconazole has no clinically
relevant effect on the pharmacokinetics of rosuvastatin. Pharmacol Toxicol 2001;89(Suppl 1):75.
13. Cooper KJ, Martin PD, Dane AL, Warwick MJ, Schneck DW. Lack of effect of ketoconazole on the pharma-
cokinetics of rosuvastatin. Br J Clin Pharmacol 2002; in press.
14. Cooper KJ, Martin PD, Dane AL, Warwick MJ, Schneck DW, Nwose OM. Erythromycin has no clinically
relevant effect on the pharmacokinetics of rosuvastatin. Eur J Clin Pharmacol 2002; in press.
15. Crouse JR, Grobbee DE, O’Leary DH, et al. Measuring effects on intima media thickness: An evaluation of
rosuvastatin — the METEOR study. Atherosclerosis Suppl 2002;3:94.
16. Davidson M, Ma P, Stein EA, Gotto AM Jr, Raza A, Chitra R, Hutchinson HG. Comparison of effects on
low-density lipoprotein cholesterol and high-density lipoprotein cholesterol with rosuvastatin versus atorva-
statin in patients with type IIa or IIb hypercholesterolemia. Am J Cardiol 2002;89:268–275.
17. Downs JR, Clearfield M, Weis S, et al. Primary prevention of acute coronary events with lovastatin in men
and women with average cholesterol levels. Results of AFCAPS�TexCAPS. JAMA 1998;279:1616–1622.
18. Durrington P, Hamann A, Tuomilehto J, Smith K, Kallend D. Rosuvastatin alone and in combination with
fenofibrate in hyperlipidaemic patients with type 2 diabetes. Diabetologia 2001;44(Suppl 1):A165.
19. Durrington PN, Tuomilehto J, Hamann A, Southworth H, Pears J, Kallend D. Effects of rosuvastatin alone
and in combination with fenofibrate on lipid subfractions in patients with type 2 diabetes: Results at 24
weeks. Circulation 2001;104(Suppl II):II-177.
20. EUROASPIRE I and II Group. Clinical reality of coronary prevention guidelines: A comparison of
EUROASPIRE I and II in nine countries. Lancet 2001;357:995–1001.
21. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive
summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on De-
tection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA
2001;285:2486–2497. Full report available at www.nhlbi.nhi.gov.
22. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Summary of
the second report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Eva-
luation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). JAMA 1993;269:
3015–3023.
23. Hamilton-Craig I, Schaefer E, Farnier M, Koren M, Southworth H, Pears J. Rosuvastatin produces signifi-
cantly greater reductions in low-density lipoprotein cholesterol and more patients achieve treatment goals
compared with simvastatin. J Am Coll Cardiol 2002;39(Suppl B):146B.
24. Holdgate GA, Ward WHJ, Davidson M, Thornton M, March R, McTaggart F. Kinetics of inhibition of
HMG-CoA reductase by a new statin, rosuvastatin. Atherosclerosis 2001;2(Suppl):90.
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
326 A. G. OLSSON ET AL.
25. Hunninghake DB, Chitra RR, Simonson SG, Schneck DW. Effects of rosuvastatin on serum lipids and lipid
subfractions in patients with hypertriglyceridemia. Int J Clin Pract 2002;124(Suppl):10.
26. Hunninghake DB, Chitra RR, Simonson SG, Schneck DW. Rosuvastatin markedly improved the atherogenic
profile in hypertriglyceridaemic patients. Eur Heart J 2001;22(Suppl):270.
27. Istad H, Ose L, Stender S, Southworth H, Pears J. Achievement of the Joint European Societies LDL-choles-
terol goal by hypercholesterolaemic patients receiving rosuvastatin or atorvastatin. Atherosclerosis Suppl
2002;3:130.
28. Istvan ES, Deisenhofer J. Structural mechanism for statin inhibition of HMG-CoA reductase. Science 2001;
292:1160–1164.
29. Jones P, Kafonek S, Laurora I, et al. Comparative dose efficacy study of atorvastatin versus simvastatin,
pravastatin, lovastatin, and fluvastatin in patients with hypercholesterolemia (the CURVES Study). Am J
Cardiol 1998;81:582–587.
30. Jones SP, Gibson MF, Rimmer DM 3rd, Gibson TM, Sharp BR, Lefer DJ. Direct vascular and
cardioprotective effects of rosuvastatin, a new HMG-CoA reductase inhibitor. J Am Coll Cardiol 2002;40:
1172–1178.
31. Knopp RH, Ballantyne CM, McPherson R, Chitra RR, Schneck DW, Simonson SG. Comparing rosu-
vastatin and atorvastatin across their dose ranges in patients with hypercholesterolemia. Eur Heart J 2002;
23(Suppl):19.
32. Laufs U, Gertz K, Dirnagl U, Bohm M, Nickenig G, Endres M. Rosuvastatin, a new HMG-CoA reductase in-
hibitor, upregulates endothelial nitric oxide synthase and protects from ischemic stroke in mice. Brain Res
2002;942:23–30.
33. Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardio-
vascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial
cholesterol levels. N Engl J Med 1998;339:1349–1357.
34. Marais D, Raal F, Stein E, et al. Effect of rosuvastatin on LDL-cholesterol, mevalonic acid and other lipid
measurements in patients with homozygous familial hypercholesterolaemia. Atherosclerosis Suppl
2002;3:159.
35. Martin PD, Cooper KW, Dane AL, Warwick MJ, Nwose OM, Cantarini M. Itraconazole produces modest in-
creases in rosuvastatin plasma concentrations. Pharmacol Toxicol 2001;89(Suppl 1):77–78.
36. Martin PD, Dane AL, Nwose D, Schneck DW, Warwick MJ. No effects of age or gender on the pharmacoki-
netics of rosuvastatin — a new HMG-CoA reductase inhibitor. J Clin Pharmacol 2002; in press.
37. Martin PD, Dane AL, Schneck DW, Warwick MJ. Disposition of new HMG-CoA reductase inhibitor
ZD4522 following dosing in healthy subjects. J Clin Pharmacol 2000;40:1056.
38. Martin PD, Kemp J, Dane AL, Warwick MJ, Schneck DW. No effect of rosuvastatin on the pharmacoki-
netics of digoxin in healthy volunteers. J Clin Pharmacol 2002; in press.
39. Martin PD, Mitchell PD, Schneck DW. Pharmacodynamic effects and pharmacokinetics of a new HMG-
CoA reductase inhibitor, rosuvastatin, after morning or evening administration in healthy subjects. Br J Clin
Pharmacol 2002; in press.
40. McCormick AD, McKillop D, Butters CJ, et al. ZD4522 — an HMG-CoA reductase inhibitor free of meta-
bolically mediated drug interactions: Metabolic studies in human in vitro systems. J Clin Pharmacol
2000;40:1055.
41. McTaggart F, Buckett L, Davidson R, et al. Preclinical and clinical pharmacology of rosuvastatin, a new
3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor. Am J Cardiol 2001;87(Suppl):28B–32B.
42. Morgan JM, Cressman MD, Hutchinson HG, Capuzzi DM. Beneficial effects of combination therapy with
rosuvastatin and extended-release niacin in patients with a mixed dyslipidemia. Int J Clin Pract 2002;
124(Suppl):14.
43. MRC�BHF Heart Protection Study: Preliminary results. Conference report. Int J Clin Pract 2002;56:53–56.
44. Nezasa K, Higaki K, Hasegawa H, et al. Uptake of HMG-CoA reductase inhibitor ZD4522 into hepatocytes
and distribution into liver and other tissues of the rat. Atherosclerosis 2000;151:39.
45. Olsson AG, Istad H, Luurila O. Effects of rosuvastatin and atorvastatin compared over 52 weeks of treatment
in hypercholesterolemic patients. Am Heart J 2002; in press.
46. Olsson AG, Pears J, McKellar J, Mizan J, Raza A. Effect of rosuvastatin on low-density lipoprotein choles-
terol in patients with hypercholesterolemia. Am J Cardiol 2001;88:504–508.
47. Olsson AG, Southworth H, Wilpshaar JW. A 52-week trial of rosuvastatin versus atorvastatin in patients with
primary hypercholesterolemia. Int J Clin Pract 2002;124(Suppl):11.
48. Olsson AG, Southworth H, Wilpshaar JW. Long-term efficacy and safety of rosuvastatin: Results of a 52-
week comparator-controlled trial versus atorvastatin. Eur Heart J 2001;22(Suppl):253.
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
ROSUVASTATIN 327
49. Paoletti R, Fahmy M, Mahla G, Mizan J, Southworth H. Rosuvastatin demonstrates greater reduction of
low-density lipoprotein cholesterol compared with pravastatin and simvastatin in hypercholesterolaemic pa-
tients: A randomized, double-blind study. J Cardiovasc Risk 2001;8:383–390.
50. Paoletti R, Pisciotta L, Southworth H, Carbarns I. Achievement of the Joint European Societies LDL-choles-
terol goal by hypercholesterolaemic patients receiving rosuvastatin, pravastatin or simvastatin. Atheroscle-
rosis Suppl 2002;3:180.
51. Pearson TA, Laurora I, Chu H, et al. The Lipid Treatment Assessment Project (L-TAP): A multicenter
survey to evaluate the percentages of dyslipidemic patients receiving lipid-lowering therapy and achieving
low-density lipoprotein cholesterol goals. Arch Intern Med 2000;160:459–467.
52. Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin on coronary events after myocardial in-
farction in patients with average cholesterol levels. N Engl J Med 1996;335:1001–1009.
53. Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 pa-
tients with coronary heart disease: The Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:
1383–1389.
54. Second Joint Task Force. Prevention of coronary heart disease in clinical practice. Recommendations of the
Second Joint Task Force of European and other Societies on Coronary Prevention. Eur Heart J 1998;19:
1434–1503.
55. Shepherd J, Carbarns I, Harris S, Caplan R, Pears J. Safety of rosuvastatin in patients developing LDL-C
<80 mg�dL and <50 mg�dL in clinical trials. Atherosclerosis Suppl 2002;3:205.
56. Shepherd J, Cobbe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hy-
percholesterolemia. N Engl J Med 1995; 333:1301–1307.
57. Shepherd J, Hunninghake D, Harris S, Hutchinson H, Pears J. A review of the safety profile of rosuvastatin
in an international phase II�III clinical trial programme. Int J Clin Pract 2002;124(Suppl):15.
58. Simonson SG, Martin PD, Mitchell PD, Schneck DW. Pharmacokinetics and pharmacodynamics of
rosuvastatin in hepatically impaired subjects. Clin Pharmacol Ther 2001;69:86.
59. Stalker TJ, Lefer AM, Scalia R. A new HMG-CoA reductase inhibitor, rosuvastatin, exerts anti-inflam-
matory effects on the microvascular endothelium: The role of mevalonic acid. Br J Pharmacol 2001;133:
406–412.
60. Stein EA, Strutt KL, Miller E, Southworth H. Effect of rosuvastatin on high density lipoprotein cholesterol
and apolipoprotein A-I in patients with heterozygous familial hypercholesterolemia. Int J Clin Pract 2002;
124(Suppl):9.
61. Stein E, Strutt KL, Miller E, Southworth H. Rosuvastatin (20, 40 and 80 mg) reduces LDL-C, raises HDL-C
and achieves treatment goals more effectively than atorvastatin (20, 40 and 80 mg) in patients with hetero-
zygous familial hypercholesterolaemia. Atherosclerosis 2001;Suppl 2:90.
62. Stein E, Strutt KL, Miller E, Southworth H. ZD4522 is superior to atorvastatin in the treatment of patients
with heterozygous familial hypercholesterolemia. J Am Coll Cardiol 2001;37(Suppl A):292A.
63. Vale MJ, Jelinek MV, Best JD. How many patients with coronary heart disease are not achieving their
risk-factor targets? Experience in Victoria 1996–1998 versus 1999–2000. Med J Aust 2002;176:211–215.
64. Warwick MJ, Dane AL, Raza A, Schneck DW. Single- and multiple-dose pharmacokinetics and safety of the
new HMG-CoA reductase inhibitor ZD4522. Atherosclerosis 2000;151:39.
65. Werner N, Priller J, Laufs U, et al. Bone marrow-derived progenitor cells modulate vascular reendotheliali-
zation and neointimal formation. Effect of 3-hydroxy-3-methylglutaryl coenzyme inhibition. Arterioscler
Thromb Vasc Biol 2002;22:1567–1572.
66. Wiklund O, Davidson M, Chitra R, Hutchinson H, Raza A. Rosuvastatin is more effective than atorvastatin
in modifying lipid profiles and achieving National Cholesterol Education Program Adult Treatment Panel III
LDL-cholesterol goals. Atherosclerosis Suppl 2002;3:237.
67. Zedler B, Davidson M, Ose L, Chitra R, Carbarns I. Rosuvastatin improves ability to achieve low-density li-
poprotein cholesterol goals compared with atorvastatin, pravastatin, and simvastatin. J Am Coll Cardiol
2002;39(Suppl B):143B.
Cardiovascular Drug Reviews, Vol. 20, No. 4, 2002
328 A. G. OLSSON ET AL.
Related Documents











