ROLE OF SURGERY IN METASTATIC COLORECTAL CANCER Dr.A.Joseph Stalin M.Ch PG PROF.DR.R.RAJARAMAN’S UNIT CENTRE FOR ONCOLOGY GOVT.ROYAPETTAH HOSPITAL CHENNAI

Role of surgery in metastatic colorectal cancer
Aug 07, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ROLE OF SURGERY IN METASTATIC COLORECTAL CANCER
Dr.A.Joseph Stalin M.Ch PG
PROF.DR.R.RAJARAMAN’S UNITCENTRE FOR ONCOLOGY
GOVT.ROYAPETTAH HOSPITALCHENNAI

CONTENTS
• HISTORY OF COLORECTAL METASTASIS• RATIONALE FOR SURGERY• ROLE OF SURGERY IN -ISOLATED LIVER METASTASIS -ISOLATED METASTASIS –OTHER SITES
• CONCLUSION

NATURAL HISTORY OF COLORECTAL METASTASIS

INCIDENCE
• 25 - 35% of patients presents with synchronous metastasis.
• 50 – 60 % of patients will eventually develop metastasis, mostly within 2 years of detecting the primary.

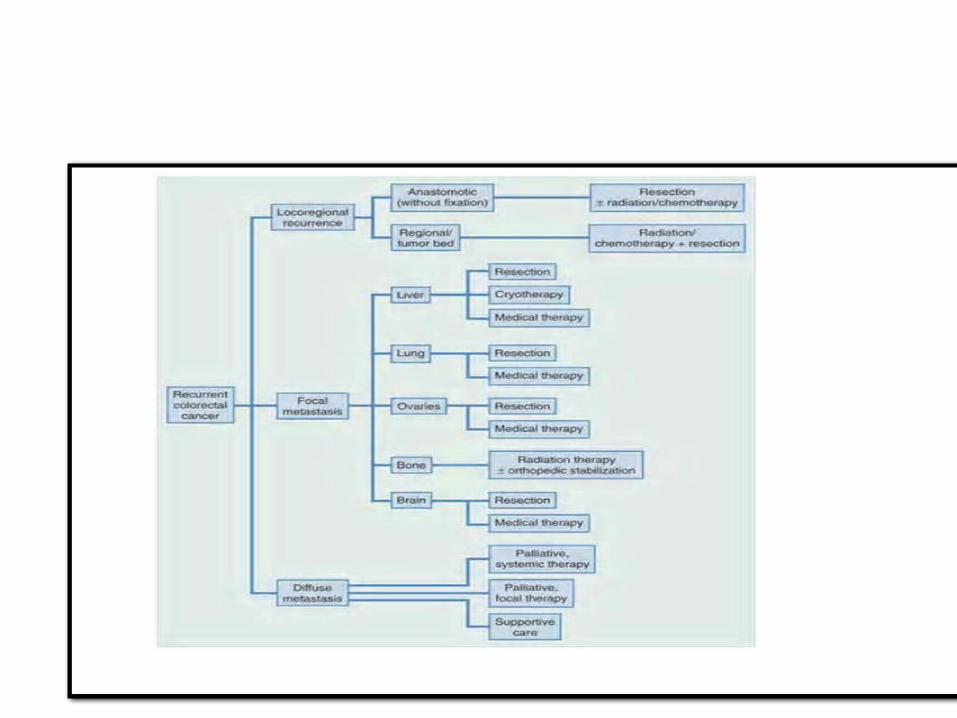
SITES OF RECURRANCE
• Liver (most common site)• Locoregional • Lung• Peritoneal deposits• Non-regional nodes• Bones• Brain• Thyroid• Subcutaneous tissues
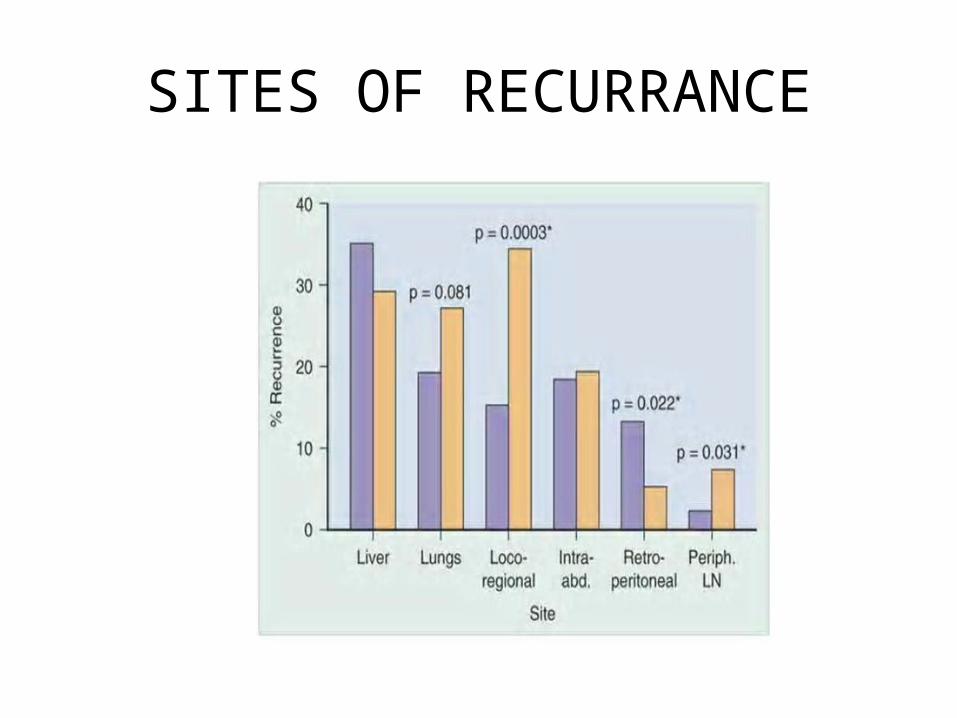
SITES OF RECURRANCE

PATTERN OF SPREAD
• Hematogenous/Lymphatic
• Directly to liver via portal venous circulation.
• Lymph node – Central lymphatic chain –hematogenous spread.
• Metastasis occur in a stepwise pattern.

Published in: Jelena Urosevic; Angel R Nebreda; Roger R Gomis; Cell Cycle 2014, 13, 2641-2642.DOI: 10.4161/15384101.2014.946374Copyright © The Author(s)

RISK FACTORS Tumor Factors Disease stage
High-grade tumor (poorly differentiated) Tumor location Obstruction/perforation Venous invasion Perineural invasion Mucin production Diminished stromal immune reaction Aneuploidy Mutant p53 gene expression Low microsatellite instability
Technical Factors Inadequate resection margins (radial, distal, mesorectal)
Implantation of exfoliated cells Tumor location (pelvis and splenic flexure is anatomically and technically more difficult)
ISOLATED LIVER METASTASIS

What are the options for patients with colorectal liver metastasis?
• Do nothing– median survival of 6 to 9 months.
• Chemotherapy – 14.5-month median survival,
• RFA – 40% 3-year survival rate,
• Resection– 5-year survival rate of 45% to 60%

RATIONALE FOR SURGERY
• Spread of colorectal cancer occurs in a step wise pattern-primarily to liver and then from liver to other sites.
• Treatment of liver metastasis with the ability of liver to regenerate results in prevention of metastasis to other sites and results in increased survival.
• In 1986, Ekberg et al defined resectability as less than four metastases (even if bilobar), absence of extrahepatic disease, and a resection margin of at least 1 cm.
• Today, resections are based on the remnant liver. A sufficient future remnant liver volume (>20% of the total estimated liver volume) is a prerequisite.
• If R0 with negative surgical margins (≥1mm) is possible and sufficient liver parenchyma remains to maintain liver function, resection should be considered
The Role of Liver Resection in Colorectal Cancer Metastases
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Report Date: June 15, 2012
What is a Resectable Tumor?

INDICATIONS
• The patient has no extrahepatic disease
• The intrahepatic disease is safely resectable and the patient must also be in good medical condition.

Contraindications to liver resection
• Non-treatable primary tumor.• Widespread pulmonary disease.• Peritoneal disease. • Extensive nodal disease, such as retroperitoneal
or mediastinal nodes. • Bone or CNS metastases.
Guidelines for resection of colorectal cancer liver metastases. Gut 2006; 55 (Suppl 3):iii1–iii8

Clinical Risk Score
• Nodal status of the primary disease• Free interval from the discovery of the primary to the discovery
of the liver metastases of <12 months• Number of tumors >1• Preoperative CEA level of >200 ng/mL• Size of the largest tumors >5 cm
• Each positive criterion is assigned one point. 5-year survival is 60% with score of 0 points, and falls to 14% in patients with 5 points.
• Fong , et al.,Ann Surg 1999;230:309–318; discussion 318–321

CLINICAL RECURRANCE SCORE

Bittoni, Giampieri et al, CROH 2012

Principles of Resection in Colorectal Liver Metastases
• An R0 resection of both the intra- and extrahepatic disease sites must be feasible.
• At least two adjacent liver segments need to be spared.
• Vascular inflow and outflow, as well as biliary drainage to the remaining segments, must be preserved.
• The volume of the liver remaining after resection (i.e., the future liver remnant) must be adequate
TECHNIQUE
• Anatomical resection
• Non Anatomical resection
• Anatomical resection preferred due to low recurrance rate.
Preoperative Patient Evaluation
• Colonoscopy • Chest / abdominal/ pelvic CT• CBC, Platelets, Chemistry• CEA• Determination of tumor K- RAS status• Needle biopsy – if clinically indicated• PET – CT only if potentially surgically curable M1
disease

TIMING OF HEPATECTOMY IN PATIENTS PRESENTING WITH SYNCHRONOUS METASTASES
• Staged – Allows biological behavior of the metastatic disease become evident, improving the selection of patients
• Simultaneous resection of the primary and metastatic disease - preferable from the patient's perspective
No proof of inferior survival or greater morbidity for a
one-stage procedure as compared to delayed (staged) hepatic resection

How to increase RESECTABILITY
• Portal Vein Occlusion• Two-Stage Hepatectomy• Downstaging chemotherapy• Local Ablation Techniques

Synchronous tumors
What are the possible options?• Colon first: Staged approach
• Colon and liver: Simultaneous approach
• “Reverse Strategy”

Criteria for synchronous approach
• Age<70 years • good surgical fitness.• an adequate tumor-free margin, • lesions that are not advanced(T4), • less than 4 colorectal lymph node metastases• histology that is not poorly differentiated or mucinous
adenocarcinoma.• 3 or fewer liver metastases.• a minor liver resection (less than 3 segments) is planned Ann Acad Med Singapore 2010;39:719-33

Surgical incisions according to primary tumor and liver metastases

Advantages of simultaneous resection
• The performance of only a single surgical procedure.
• Reduced length of hospital stay• The removal of all neoplastic foci and
interruption of the “metastatic cascade”.• The avoidance of immunodepression after
isolated primary tumor resection• No delay in initiating systemic treatment

Disadvantages of simultaneous resections
• The combination of a “clean” and a “contaminated” surgical procedure and thus the higher risk of septic complications, which could cause or worsen a liver dysfunction
• The increased risk of anastomotic leak due to splanchnic congestion if prolonged pedicle clamping is needed.
• The inadequate surgical exposure through a single incision.

• The need for a double surgical team for liver and colorectal surgery/inadequate treatment if a single team performs the entire procedure.
• Small occult metastases may not be evident during the evaluation and therefore not addressed during the operation.
“Test of time”
• Scheele et al suggested a “test of time” approach of waiting up to 6 months to observe the tumor biology and evolution of metastases as a means of natural selection for operable disease.
• World J Surg 1995;19:59-71.

“Reverse Strategy”
• Brouquet et al. and the group from M.D. Anderson Cancer Center
• preoperative chemotherapy is followed by resection of the hepatic metastases and then by resection of the colorectal primary at a second operation.
• J Am Coll Surg 2010;210:934-41.

The rationale for this approach
• complications related to the primary colorectal tumor are rare and treatment of metastatic disease is not delayed by local therapy for the primary tumor or complications associated with treatment of the primary tumor
• It can be considered as an alternative option in patients with advanced hepatic metastases and an asymptomatic primary.
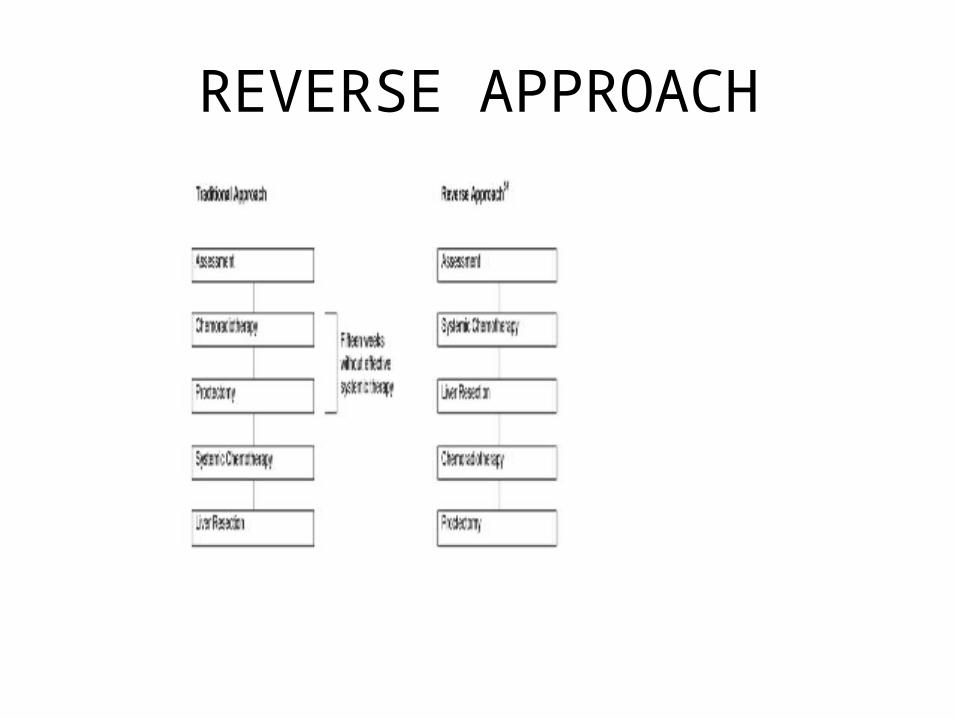
REVERSE APPROACH

STUDIES ON LIVER RESECTION
Gayowski et al. (1994) - Pitt sburg Medical Center
0 33 32%
Jamison et al. (1997) - Mayo Clinic
4 33 27%
Fong et al. (1999) - Memorial Sloan Katering
3 42 36%
Choti et al. (2002) - Johns Hopkins
1 46 40%
Fernandez et al. (2004) - Washington University
1 – 59%
Pawlik et al. (2005) - M.D. Anderson
1 74 58%
Hospital A.C. Camargo (2005)
0 – 51%
Hospital A.C. Camargo (2010)
1.8 – 66.2%
Author (year) Mortality % Mean
survival (months)
Five-year survival

– Neoadjuvant chemotherapy• Resectable liver metastases:
– Facilitate surgery– Obtain predictive and prognostic information– Early systemic therapy for poor-prognosis pts
– Conversion chemotherapy• Unresectable liver metastases:
– Allow R0 resection via downsizing
– Postoperative (adjuvant) chemotherapy
ROLE OF CHEMOTHERAPY

– 5-FU: hepatic steatosis, associated with increased postoperative morbidity - yellow liver
– Irinotecan: non-alcoholic steatohepatitis (especially in obese patients), can affect hepatic reserve and increase morbidity and mortality after hepatectomy - orange liver
– Oxaliplatin: hepatic sinusoidal obstruction syndrome, does not appear to be associated with increased risk of perioperative death - blue liver
– Both response rate and toxicity should be considered when selecting preoperative CT in patients with colorectal liver metastases
Adapted from Zorzi D, et al. Br J Surg 2007;94:274-86.
Liver Toxicities
CHEMO
• There is not a chemotherapy schedule indicated as standard treatment in neoadjuvant setting of colorectal liver metastases: all schedules could be used
• Triplet seems to be more effective
• Adding molecular drugs, there is an activity increase in term of response rate and resectability
• Prospective studies on predictive factors of response and resectability could be useful to select the better treatment for each patient

Selecting patients for neoadjuvant therapy
• Resection was always preferred, if possible, over local ablation strategies (cryosurgery, radiofrequency ablation [RFA], laser techniques).
• Immediate resection appropriate if adequate margins could be radiographically defined, there was no portal lymph node involvement, and four or fewer lesions. Resection could be considered for more than four lesions if they were localized to a single lobe.
• For patients with more than four metastases or bilobar involvement, resection considered appropriate only after tumor shrinkage using neoadjuvant chemotherapy.

• 364 patients randomized• Potentially resectable (≤ 4 liver
metastases)• Goal: Improve PFS• Interim objective: Evaluate tumor
response to perioperative CT• Perioperative CT (n = 182)
– 159 (87.3%) underwent surgery – 151 (83.0%) resected
• Surgery (n=182)– 170 (93.4%) underwent surgery – 152 (83.0%) resected
R
Nordlinger B, et al. Lancet 2008
FOLFOX4 for 6 cycles (12 wks)(n = 182)
Surgery FOLFOX4 for 6 cycles (12 wks)
Surgery(n = 182)
Colon Cancer: EORTC 40983 (the EPOC trial)

Efficacy Results
No. ptsCT
No. pts Surgery
% absolute differencein 3-year PFS
Hazard ratio (confidence interval) p Value
All patients 182 182 +7.2% (28.1% to 35.4%)
0.79(0.62-1.02) 0.058
All eligiblepatients 171 171 +8.1%
(28.1% to 36.2%)0.77
(0.60-1.00) 0.041
All resectedpatients 151 152 +9.2%
(33.2% to 42.4%)0.73
(0.55-0.97) 0.025
Adapted from Nordlinger B, et al. Lancet 2008;371(9617):1007-16.

•High (anatomical) response rate
•Good toxicity profile– No hepatotoxicity– No interference with surgery– No interference with liver regeneration
What Do We Expect from Ideal Conversion Chemo?

• The use of chemotherapy as an adjunct to liver resection has resulted in a 5-year survival in the range of 37 to 58%. ¹
• Ten-year survival is reported to be between 16 to 30%.²
1. Clin Colon Rectal Surg 2009;22:225–232.2. Ann Surg Oncol 2008;15(9): 2458–2464

RECURRANT LEISION
• Common site of recurrance after hepatic resection is liver.
• Liver is the sole site of recurrance in 15-40 % of cases.
• Repeat hepatectomy considered in patient with good clinical reserve and absence of extra hepatic disease

VANISHING HEPATIC LEISION
• Complete radiological response occurs in 6-9% of patients after noeadjuvant chemo.
• Due to pathologically complete response or inability of imaging to pick leision due to hepatic stenosis.
• OBSERVATION OR RESECTION ?

ISOLATED METASTASIS IN LUNG
• Incidence less than 10 %
• Only 2% will be eligible for resection.
• In resectable patients, 5 yr survival is around 27-40 %.
• Guidelines are similar to that of liver.

ISOLATED METS IN PERITONEUM
• Cytoreductive surgery with HIPEC in pateints with localised leisions.
• 5 yr survival of about 20-45 %

ISOLATED METS IN BRAIN
• Rare incidence(<1%).
• If resectable patient should undergo resection.
• Unresectable patients treated with steroids and RT

ISOLATED METS IN BONE
• If unstable,internal fixation done.• Palliative RT given.
SURVEILLANCE AFTER METASTECTOMY
Surveillance strategy for patients with stage IV disease who are rendered surgically NED (no evidence of disease)
• CEA every three months for two years, then every six months for three to five years
• CT of the chest/abdomen and pelvis every three to six months for two years, then every 6 to 12 months up to a total of five years
• Colonoscopy in one year; if no adenoma repeat in three years, then every five years; if adenoma is found, repeat in one year

CONCLUSION
• Metastasis in colorectal cancer follows a stepwise pattern.
• Liver is the most common site and most often the first site to get involved.
• Median survival is around 15 months and 5 yr survival less than 2 % in patients without any treatment.
• Surgical resection improves the 5 yr survival rate to around 50 % .

• Intent of surgical resection is cure.
• Resectable metastatic leisions are best managed with surgical resection.

Thank U ……….
Related Documents











