Role of Satvavajaya Chikitsa and Guduchyadi Yoga in the management of Madatyayaja Yakrit Vikara. By Dr. NIRANJANA. H. P. Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore In partial fulfilment of the requirements for the degree of AYURVEDA VACHASPATI (DOCTOR OF MEDICINE - AYURVEDA) In MANASA ROGA Under the guidance of Dr. NARAYANA PRAKASH. B. M.D. (Ayu) Professor & H.O.D. DEPARTMENT OF MANASA ROGA SHRI DHARMASTHALA MANJUNATHESHWARA COLLEGE OF AYURVEDA & HOSPITAL HASSAN 2011

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Role of Satvavajaya Chikitsa and Guduchyadi Yoga
in the management of Madatyayaja Yakrit Vikara.
By
Dr. NIRANJANA. H. P.
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfilment of the requirements for the degree of
AYURVEDA VACHASPATI
(DOCTOR OF MEDICINE - AYURVEDA)
In
MANASA ROGA
Under the guidance of
Dr. NARAYANA PRAKASH. B. M.D. (Ayu)
Professor & H.O.D.
DEPARTMENT OF MANASA ROGA SHRI DHARMASTHALA MANJUNATHESHWARA
COLLEGE OF AYURVEDA & HOSPITAL HASSAN
2011
DDEEPPAARRTTMMEENNTT OOFF MMAANNAASSAA RROOGGAA SHRI DHARMASTHALA MANJUNATHESHWARA
COLLEGE OF AYURVEDA & HOSPITAL, HASSAN – 573 201
(Affiliated to RGUHS, Karnataka, Bangalore)
CCeerrttiiffiiccaattee
This is to certify that the dissertation entitled “Role of Satvavajaya
chikitsa and Guduchyadi yoga in the management of Madatyayaja Yakrit
Vikara ” is the record of research work conducted by Dr. Niranjana H P
under our direct supervision and guidance as a partial fulfilment for the
award of the degree of Doctor of Medicine (Ayurveda) in Manasa Roga.
The candidate has fulfilled all the requirement of ordinances laid down
in the prospectus of Rajiv Gandhi University of Health Sciences, Karnataka,
Bangalore, for the award of Degree of Doctor of Medicine (Ayurveda) in
Manasa Roga.
We are fully satisfied with his work and recommend this thesis to
be submitted for adjudication.
Co Guide: Guide:
Dr. Suhas Kumar Shetty Dr. Narayana Prakash B. Reader Professor & H.O.D.
Dept.of Manasa Roga Dept.of Manasa Roga
S D M College of Ayurveda, S D M College of Ayurveda,
Hassan. 573 201 Hassan. 573 201
Date: Date:
Place: Hassan Place: Hassan
DDEEPPAARRTTMMEENNTT OOFF MMAANNAASSAA RROOGGAA SHRI DHARMASTHALA MANJUNATHESHWARA
COLLEGE OF AYURVEDA & HOSPITAL,HASSAN – 573 201
(Affiliated to RGUHS, Karnataka, Bangalore)
EENNDDOORRSSEEMMEENNTT BBYY TTHHEE HH OO DD &&
PPRRIINNCCIIPPAALL // HHEEAADD OOFF TTHHEE IINNSSTTIITTUUTTIIOONN
This is to certify that the dissertation entitled “Role of
Satvavajaya chikitsa and Guduchyadi yoga in the management of
Madatyayaja Yakrit Vikara ” is a bonafide research work done by
Dr. Niranjana H P under the guidance of Dr. Narayana Prakash B.,
Professor, Department of Manasa Roga, S.D.M. College of Ayurveda
and Hospital, Hassan - 573201.
Dr. Narayana Prakash B. Dr. Prasanna N. Rao
Professor & Head Principal
Dept.of Manasa Roga S D M College of Ayurveda
S D M College of Ayurveda & Hospital.
Hassan. Hassan.
Date: Date:
Place: Hassan Place: Hassan
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
KARNATAKA, BANGALORE
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “Role of
Satvavajaya chikitsa and Guduchyadi yoga in the management of
Madatyayaja Yakrit Vikara”is a bonafide and genuine research work
carried out by me under the guidance of Dr. Narayana Prakash B.,
Professor & H.O.D., Department of Manasa Roga, S. D. M. College of
Ayurveda and Hospital, Hassan – 573 201.
Date :
Place : Hassan Dr. NIRANJANA H P
COPYRIGHT
I hereby declare that the Rajiv Gandhi University of Health
Sciences, Karnataka shall have the rights to preserve, use and disseminate
this dissertation / thesis in print or electronic format for academic /
research purpose.
Date : Dr. NIRANJANA H P
Place : Hassan .
© Rajiv Gandhi University of Health Sciences, Karnataka.
ACKNOWLEDGEMENT
At the outset, I bow my head at the feet of Lord Dhanvantari and Lord
Manjunatha for giving me strength to complete this academic venture in time and
style.
With the blessings and words of inspiration from Poojya Dr.D. Veerendra
Heggade, I would like to express my deepest gratitude and heartfelt thanks to all the
people and the heavenly powers that have helped me in making my dream a reality.
I am indebted to Prof. Gurudip Singh, for his functional freedom, encouragement,
guidance and support that he showed on me throughout my association with him.
I am greatly indebted to Dr. Prasanna Narasimha.Rao. Principal, for supporting
me in every walk of my life at Hassan. He is the person who was instrumental in
building my basis and sharpening my professional skills.
From the innermost recess of my heart, come sincere gratitude, thankfulness and
immense indebtedness to my esteemed teacher and elite guide Dr.Narayana
Prakash B. HOD & Professor. Dept of Manasa roga under whose guidance, I had
the privilege of carrying out this work, his parental affection and vigilant care have
always encouraged me to right path throughout my work. His constructive valuable
suggestions will always inspire me in my future endeavors.
I express my deep sense of gratitude to my co-guide Dr.Suhas Kumar Shetty, for his
valuable guidelines, concern and genuine interaction towards my study.
It’s my pleasure to convey my gratitude to Dr.Savitha.H.P and Dr. Hrishikesh
Rangnekar, for their precious suggestions and co-operation throughout dissertation
work.
I take this opportunity to thank Dr.Muralidhar P Pujar, Dr.P Hemantha Kumar,
Dr.T.B. Tripathy, Dr.Mallika K.J, Dr.Ashwini Kumar M, Dr.Shailaja.U,
Dr.Prakash L.Hegde, Dr.Harini.A, Dr Prathibha K, who extended their valuable
suggestions and support.
I am extremely greatful to Dr.Girish.K.J, HOD Dept of Kayachikitsa and Dr.Ravi
Bhat for their help and support to carry out all the technical work of thesis.
I am thankfull to all the teaching and non teaching staffs of S.D.M College of
Ayurveda and Hospital. Hassan, for their support and co-operation.
I express my sincere gratitude to Dr.B.G.Gopinath, Dr.Raghvendra R. Bhat,
Dr.Naveen B.S who helped me to gain seat in this esteemed institution.
I am greatfull to Dr.Pankaj Patil, Dr.Geetha.L.Jaiswal and all my classmates for
their never ending encouragement.
I take this opportunity to thank my seniors, Dr.Abhinandan Patil, Dr.Narayan
Namboothiri, Dr.Drisya Ravindran, Dr.Sunil Kumar and my jouniors Dr.Issac
Paul, Dr.Toolika, Dr.Rinjin G Krishna, Dr.Aditya Subrahmanyam,
Dr.JayaKrishnan, Dr.Chitrangana, Dr.Unni, Dr.Vikram C and Dr.VinayShankar
for their love and help.
I thank my patients who subjected themselves for this study and co-operating with
me in every stage of my clinical work.
I am extremely great full to my friends Mr.Akshay Pandith, Mr.Anil, Dr Deepthi
H, Dr.Ashwini Ravishankar, Dr.Hemachandra Shetty, Dr.Niveditha P.N, Miss
Shruthi R Sharma, Miss Abhignya Deshikachar and Mr.Vivek Solapurkar for
their encouragement, love, moral support and co-operation.
I remain thankful to Student Council-2010&2011 and Student Community of
S.D.M College Of Ayurveda Hassan, for their support and co-operation in every step
of my life at this institution.
I feel immensely privileged to credit this work to my parents Mr.H.A.Prabhakar
Rao, Mrs Shantha Prabhakara Rao, sisters Rajashree, Usha Raman, Vani Arun
& Veena Ananth and brother in- laws Mr.R.K.Hegde, Mr.T S Raman,
Mr.T.S.Arun and Mr.B.Ananthmurthy who constantly kept supporting me against
all odds.
Finally I thank all who helped me directly and indirectly in this research work.
NIRANJANA H.P
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara
ABBREVIATIONS
Bhai. Ra : Bhiashajya Ratnavali
BP : Bhava Prakash
Sa. Sam : Sharngadhara Samhita
YR : Yoga Ratnakara
Bhe.Sa : Bhela Samhita
Ch : Charaka
Su : Sushruta
A.H : Ashtanga Hridaya
A.S : Ashtanga Sangraha
B.T : Before treatment
AV : After Vamana
A.T : After treatment
S.D. : Standard Deviation
S.E : Standard Error
G. S : Grading score
Sl. No : Serial Number
Symbols
+ : Present
- : Absent
df : Degree of freedom
< : Lesser than
> : Greater than
% : Percentage
p : Probability
t : Test of significance
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara
Contents Page no.
1. INTRODUCTION 01- 04
2. CONCEPTUAL CONTRIVE
Review of Ayurveda:
Madya 05-11
Madatyaya 12 -28
Madatyayaja Yakrit Vikara 29-31
Satvavajaya Chikitsa 32-41
Review of the Modern science
Alcohol 42 – 56
Alcohol – Related Disorder 57 – 94
Alcoholic Liver Disorder 95 - 100
3. DRUG CONTRIVE 101 - 108
4. CLINICAL CONTRIVE
Objectives 109
Methodology 110 - 119
5. OBSERVATIONS 120 - 132
6. RESULTS 133 - 147
7. DISCUSSION 148 - 158
8. SUMMARY AND CONCLUSION 159 - 161
9. BIBLIOGRAPHIC REFERENCES 162 - 178
10. ANNEXURE- 1(Model case Performa) 177 -182
11. ANNEXURE -2(Synopsis) 183- 192
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara
LIST OF TABLES
Table no.
Table Contents Page no.
1. General Properties of Madya 8
2. Comparison of Guna of Ojas, Madya and Visha 9
3. Showing Lakshana of Vatapraya Madatyaya 14
4. Showing Lakshana of Pittapraya Madatyaya 16
5. Showing Lakshana of Kaphapraya Madatyaya 17
6. Showing application of Satvavajaya 38
7. Epidemiology of alcohol 60
8. Data Supporting Genetic Influences in Alcoholism 65
9. DSM-IV-TR Alcohol-Related Disorders and Corresponding
ICD-10 Disorders
68
10. DSM-IV-TR Diagnostic Criteria for Alcohol Intoxication 71
11. Impairment Likely to be Seen at Different Blood Alcohol
Concentrations
72
12. DSM-IV-TR Diagnostic Criteria for Alcohol Withdrawal 73
13. State Markers of Heavy Drinking Useful in Screening for
Alcoholism
75
14. Clinical Course of Alcohol Dependence 81
15. Parameters 115
16. Showing Gradation Index 116
17. Severity of MYV 118
18. Showing incidence of Age 121
19. Showing incidence of Sex 121
20. Showing incidence of Occupation 121
21. Showing incidence of Socio – economic status 123
22. Showing incidence of Marital status 123
23. Incidence of Educational status 123
24. Showing incidence of Age of starting of Alcohol. 124
25. Showing incidence of Duration of daily drinking of Alcohol
in years.
124
26. Showing incidence of Type of Alcohol 125
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara
27. Showing incidence of Time of first drink in a day 127
28. Showing incidence of Prakriti 127
29. Showing incidence of Sara 127
30. Showing incidence of Samhanana 128
31. Showing incidence of Satva and Satmya(30.1) 128
32. Showing incidence of Vyayama Shakti 129
33. Showing incidence of Abhyavarana Shakti 129
34. Showing incidence of Jarana Shakti 129
35. Showing incidence of Pramana 130
36. Showing incidence of other habits. 130
37. Showing incidence of Psychiatric complications 130
38. Showing incidence of Relationship with Spouse 131
39. Showing incidence of signs and symptoms 131
40. Effect of Satvavajaya Chikitsa with Placebo on symptoms
of Madatyayaja Yakrit Vikara.
134
41. effect of Satvavajaya Chikitsa with Placebo on Liver function Test
135
42. Overall effect of Satvavajaya Chikitsa 136
43. effect of Guduchyadi Yoga on symptoms of Madatyayaja Yakrit Vikara
137
44. Effect of Guduchyadi Yoga on Liver function test 138
45. Overall effect of Guduchyadi Yoga 139
46. effect of Satvajaya Chikitsa and Guduchyadi Yoga 140
47. Satvavajaya chikitsa and Guduchyadi Yoga on Liver
function Test.
141
48. Overall combined effect 142
49. Severity of Madatyayaja Yakrit Vikara 142
50. Overall effect 142
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara
LIST OF GRAPHS
Graph
no. Graph Contents
Page
no.
1. Effect of Therapy on Symptoms of Madatyayaja Yakrit
Vikara 143
2. Effect of Therapy on Symptoms of Madatyayaja Yakrit
Vikara 144
3. Effect of Therapy on Liver Function Test 145
4. Effect of Therapy on Liver Function Test 145
5. Showing the severity of Madatyayaja Yakrit Vikara 146
6. Overall Effect Of Therapy 147
Introduction
Introduction
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 1
INTRODUCTION
Since the antiquity the man is using Madya and it is the part of social and cultural life.
The Madya has nectar like properties when used judicially following all norms,
otherwise it acts as poison1. Man is experiencing the ill effects of Madya since
beginning and invented the modes of overcoming its ill effects.
Now a days alcohol use disorders are common, lethal conditions that often cover-up
as other psychiatric syndromes. The average alcohol-dependent person decreases his
or her life span by 10 to 15 years, and alcohol contributes to 22,000 deaths and two
million nonfatal injuries each year. At least 20 percent of the patients in mental health
settings have alcohol abuse or dependence, including individuals from all
socioeconomic strata and both genders.2
According to US Census Bureau International Data Base 2004, 106,50,70,607
persons in the world were using alcohol and out of which 78,31,407 persons were
affected by Alcoholic liver disease. It manifests as a clinical spectrum ranging from
non specific symptoms to hepatic failure. Classically, alcoholic liver injury comprises
three major forms, 1.fatty liver, 2.alcoholic hepatitis and 3.cirrhosis.
However, any amount of alcohol is considered harmful to the developing fetus,
recovering alcoholics, people taking medications that may adversely interact with
alcohol. Individuals with certain medical disorders or psychiatric syndromes (such as
major depressive disorder or schizophrenia) might be intensified by alcohol. Also, the
intake of more than two drinks a day is likely to increase low-density lipoprotein
(LDL) cholesterol and triglycerides and to increase blood pressure, with the overall
result of increasing the risk of cardiac disorders, and even low levels of alcohol may
increase the risk for breast cancer.3
Introduction
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 2
Alcoholic liver disease is the major cause of liver disease in Western countries, (in
Asian countries, viral hepatitis is the major cause). It arises from the excessive
ingestion of alcohol. Even though millions of individuals drink alcohol on a regular
basis, only chronic heavy drinkers develop liver damage. How alcohol damages the
liver is not completely understood. It is known that alcohol produces toxic chemicals
like acetaldehyde which can damage liver cells, but why this occurs in only a few
individuals is still in debate. When alcohol damages the liver, the function of the
organ is not immediately compromised as the liver has a tremendous capacity to
regenerate and even when 75% of the liver is damaged, it continues to function as
normal. When alcohol is consumed chronically, it eventually results in liver scarring
or what is known as cirrhosis or end-stage alcoholic liver disease.
That which produces Mada is called Madya, the disease produced due to improper use
of Madya is called Madatyaya. One should take the Madya with food materials and
judiciously. Madatyaya is produced when person takes the Madya without
considering Prakriti, Satmya, Agni, etc. Continuing same amount of alcohol intake
leads to Madatyayaja Yakrit Vikara. It is a Pitta pradhana Tridoshaja Vyadhi mainly
Pitta Sthana is vitiated along with Agni.
Acharya Bhavaprakasha mentions Yakrit-Vruddhi (hepatomegaly) as one of the
symptoms of Yakrit Vikara due to excessive intake of Vidahi and Abhishyandi
Aharas and Madya (alcohol).
Ayurveda has many options to treat Madatyaya . All the texts mention
Pittahara and Deepana Pachana Dravyas to treat Yakrit-Vikaras. Guduchyadi Yoga
mentioned by Charaka comprising of Guduchi (Tinospora cordifolia), Musta (Cyperus
Introduction
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 3
rotundus), Patola(Tricosanthes dioica) and Nagara(Gingeber officinalis) may relieve
the adverse effects of Madatyaya as well as liver disorders caused by it.
Satvavajaya Chikitsa may help people to address psychological issues
involved in their drinking problem. Astanga Hrudaya explains Vismapana,
Samsmarana, Priyadarshana, Priyashravana, Geeta, Vadya and Charaka advises
Harshanee Kriya and restrain from the things which are harmful to body and mind as
the treatment modalities in the management of Madatyaya.
Alcohol related disorders are earlier called as alcoholism. Diagnostic and Statistical
Manual of Mental Disorders (DSM-IV-TR) in 1994 listed alcohol related disorders as
below- Alcohol use disorders and alcohol induced disorders.
Alcohol use disorders are Alcohol dependence and abuse. Alcohol induced disorders
are Alcohol intoxication, Alcohol intoxication delirium, Alcohol withdrawal, Alcohol
withdrawal delirium, Alcohol-induced persisting dementia, Alcohol-induced
persisting amnestic disorder, Alcohol-induced psychotic disorder, with delusions,
Alcohol-induced psychotic disorder, with hallucinations, Alcohol-induced mood
disorder, Alcohol-induced anxiety disorder, Alcohol-induced sexual dysfunction,
Alcohol-induced sleep disorder and Alcoholic liver disorder.9 The treatment for
alcohol withdrawal is only pacifying the symptoms by tranquilizers; there is no
specific treatment modality available in conventional science for detoxifying the
effects of alcohol. In Ayurveda many drugs are explained for detoxifying,
Guduchyadi Yoga is one among them.
By taking into consideration of the above facts, In this study 54 patients of
Madatyayaja Yakrit Vikara were registered, 16 patients in Satvavajaya(S)group,19
Introduction
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 4
patients in Guduchyadi Yoga(GY)group and 19 patients in Combined (S&GY) group,
out of which 3 patients of GY group and 3 patients of S&GY group were drop out. In
this way 16 patients in each group completed full courses of the treatment.
This study revealed Satvavajaya chikitsa and Guduchyadi Yoga combined group is
better than Guduchyadi Yoga group and Guduchyadi Yoga group is better than
Satvavajaya chikitsa with placebo group.
The overall effect shows no patients got cured, where as marked improvement of 6.25
% &37.5% in GuduchyadiYoga and Satvavajaya & GuduchyadiYoga group
respectively. 75.0% and 62.5% had moderate improvement in GuduchyadiYoga and
(Combined) Satvavajaya & Guduchyadi Yoga group respectively, where as 18.75 %
and 56.25% got mild improvement in GuduchyadiYoga and Satvavajaya with placebo
group respectively and but 43.75 % patient remained uncured in Satvavajaya with
placebo group.
This study has been presented in the following headings, literary review, Clinical
study, Discussion, Summary and conclusion. Literary review is again divided mainly
into Ayurveda review and Modern review. Ayurveda review has Madya review,
Madatyaya review, Madatyayaja Yakrit Vikara review and Satvavajaya chikitsa
review. Modern review has Alcohol review, Alcohol related disorders review and
Alcoholic liver disorder review. Clinical study has divided into Materials and
methodology, observations, results, discussion and conclusion.
Conceptual
Contrive
Review of
Ayurveda
Madya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 5
MADYA
The one which causes Mada by ingestion is called Madya. Mada means any
exhilarating or intoxicating condition
Nirukti and Nirvacana:
‘Mada’ is derived from the word ‘Madee’ which gives the meaning ‘Harsha’ –
‘Made Harshe’.
Madya is defined as ‘Madyatyanena Karaņe Yat Madya ’i.e., which does the action
of Mada is called Madya.10
Sharngadhara says,
Buddhim Lumpati Yaddravyam Madakari Taducyate |
Tamoguņa Pradhanasca Yatha Madyam Suradikam || 11
Madakari Dravya is that intake of which produces disturbance of the intellect faculty
by its virtue of Tamo-guņa like Madya, Sura etc.
Types of Madya:
All most all Acharyas has explained Madya Varga, and explained many types of
Madya. Those can be classified as based on their use viz.
a) Used as medicine
b) Used as drinking beverage
Madya used as Medicine:
Arishta: When drugs mixed with water are heated to make the decoction which is
then fermented and filtered, the liquid thus obtained is called as Arishta. It is Laghu
and best among the Madya. Depending upon the medicinal drugs added, its properties
vary.12, 13
Madya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 6
Asava: Preparation prepared without heating the water and drugs and fermented is
called Asava. Its qualities depend upon the drugs those are added. 14, 15
Caraka explains 84 types of Asava based on the following 9 Yonis (souece
materials): : The following nine are the Yonis (sources) from which Madya is
prepared viz., Dhanya (grain), Phala (fruit), Moola (root), Sara (pith), Pushpa
(flower), Kaņda (stalks), Patra (leaves), Tvaca (bark) and Sharkara (sugar).
84 Types of Madya: There are innumerable varieties of Madya resulting from
different Samyoga (combinations) and Samskara. Among them, some important 84
types of Madya are described by Charaka. They are -
Six from Dhanya - Sura, Sauvera, Tushodaka, Maireya, Medaka, Dhanyaamla
Twenty six types from Phala - Mrdveeka, Kharjura, Kashmarya, Dhanva, Rajadana,
Triņashunya, Parooshaka, Abhaya, Amalaka, Mrigaliņdika, Jambava, Kapittha,
Kuvala, Badara, Karkandu, Peelu, Priyala, Panasa, Nyagrodha, Ashvattha, Plaksha,
Kapitana, Udumbara, Ajamoda And Shankhini.
Eleven type from Moola - Vidari Gandha, Ashvagandha, Krishņa Gandha, Shatavari,
Shyaama, Trivrt, Danti, Dravanti, Bilva, Urubuka, Citrakamoola
Twenty from Sara - Shaala, Priyala, Ashvakarņa, Candana, Syandana, Kshadira,
Kadara, Saptaparņa, Arunasana, Arimeda, Tinduka, Kiņihi, Shami, Shukti,
Shimshapa, Shireesha, Vanjala, Dhanvana, Madhooka
Ten from Pushpa - Padma, Utpala, Nalina, Kumuda, Saugandhika, Puņdreeka,
Shatapatra, Madhooka, Priyangu, Dhataki
Four from Kaņda - Ikshu, Kaņdekshu, Ikshuvalika, Puņdraka,
Two from Patra - Patola, Tada
Four from Tvak - Tilvaka, Lodhra, Elavaluka, Kramuka and
Madya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 7
One from Sharkara. 16
Tushambu, Souviraka, Dhanyamla.17
Madya used as Drinking Beverage:
Sura: The Madya prepared from the Shali, Shashtika etc is called Sura. It is having
the properties of Guru, Balakara, Stanyajanana, Pushtikara, Medokara and Kaphakara,
and is indicated in Grahaņi, Shotha, Gulma, Arshas, and Motrakrichra.18, 19
Varuņi: Madya prepared from the water added with Shilapishta of Punarnava is
called Varuņi or Madya prepared from the Rasa of Tala, Kharjura etc, is also called
Varuņi. It is having the same properties that of Sura.20,
Seedhu: Madya prepared from sugarcane juice is called Seedhu. It is of two types, if
prepared from Apakvarasa, it is Sheetarasa Seedhu; and if prepared from Pakvarasa, it
is called Pakvarasa Seedhu. Pakvarasa Seedhu is the best with the actions of Svarya,
Agnikara, Balakara, Varņakara, Vata and Pittakara, Sadya-Snehakara, Rocaka,
Malabandhahara, Medohara, Shophahara, Arsohara, Udarahara and other Kapha-
rogahara actions. Sheetarasa seethu is having Lekhana property 21, 22
Acharya
Sushruha mentioned some more types of seedhu they are Gudaseedhu,
Sharkaraseedhu, Pakvarasaseedhu, Apakvarasaseedhu, Akshikaseedhu,
Jambavaseedhu, Puspayoni Seedhu. 23
PROPERTIES AND ACTIONS OF MADYA:
Guna of Madya in General:
Madya is having the following ten Guna:
Laghu, Ushņa, Tikshņa, Sukshma, Vishada, Amla, Vyavayi, Ashu, Vikashi and
Ruksha. All the Madya are generally Pittakara and Vatahara in nature24

Madya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 8
Table - 1
General Properties of Madya According to Brihad-Trayi
Guna Charaka24
Sushruta25
Vagbhata26
Laghu + - +
Ushņa + + +
Tikshņa + + +
Sukshma + + +
Vishada + + +
Amla + - +
Vyavayi + + +
Aashu + + +
Vikashi + + +
Ruksha + + +
Madya are prepared of different types of ingredients, accordingly they have different
Guna and Karma, but all are intoxicating in nature. Charaka and Vagbhata say that
Madya has ten Gunas but Sushruta says only eight Gunas except Laghu and Amla.
Commenting on the Guna of Visha, Charaka, Sushruta and Vagbhata say that the
Gunas of Madya are just opposite to the Gunas of Ojas.
Gunas of Madya verses Ojas:
Madya is having Guna which are just opposite to that of Ojas. Therefore when Madya
reaches the Hridaya, it afflicts the ten Gunas of Ojas, which is located in Hridaya.
Madya by virtue of its ten Guna give rises to mental distortion.
Madya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 9
The ten Guna of Madya are Laghu, Ushņa, Tikshņa, Sukshma, Amla, Vyavayi,
Ashuga, Ruksha, Vikashi and Vishada.
The ten qualities of Ojas are Guru, Sheeta, Mridu, Shlakshna, Bahala, Madhura,
Sthira, Prasanna, Picchila, and Snigdha.
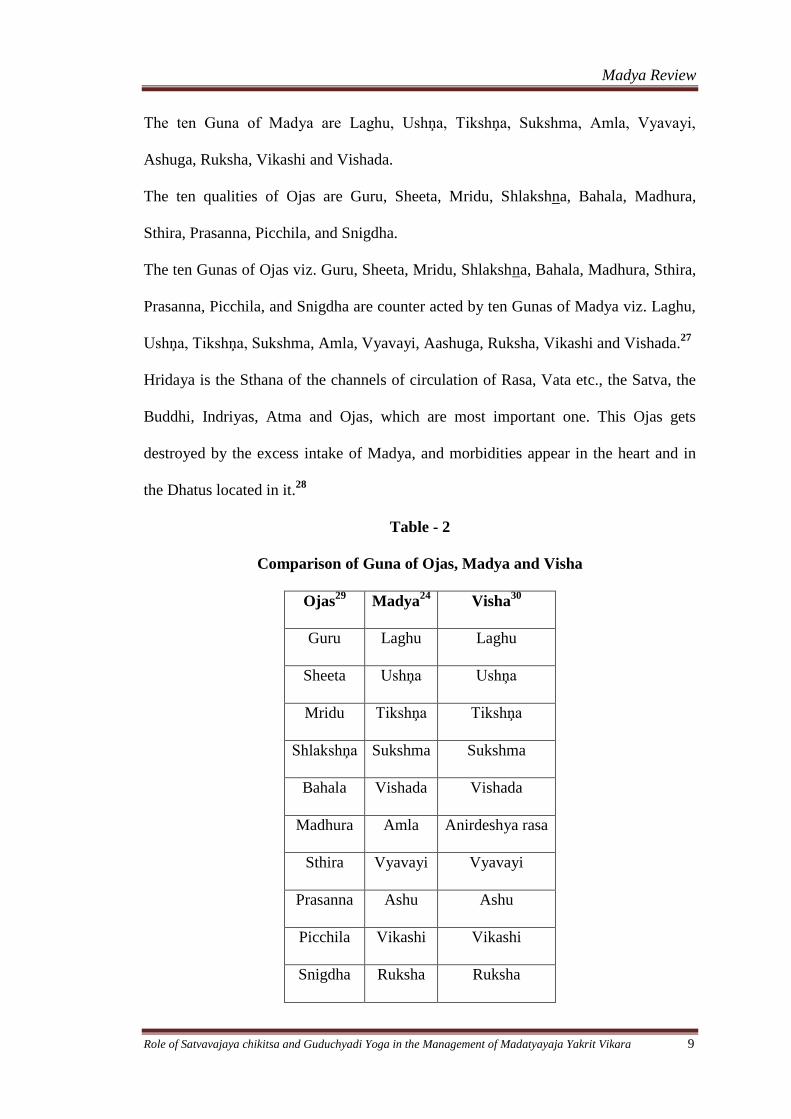
The ten Gunas of Ojas viz. Guru, Sheeta, Mridu, Shlakshna, Bahala, Madhura, Sthira,
Prasanna, Picchila, and Snigdha are counter acted by ten Gunas of Madya viz. Laghu,
Ushņa, Tikshņa, Sukshma, Amla, Vyavayi, Aashuga, Ruksha, Vikashi and Vishada.27
Hridaya is the Sthana of the channels of circulation of Rasa, Vata etc., the Satva, the
Buddhi, Indriyas, Atma and Ojas, which are most important one. This Ojas gets
destroyed by the excess intake of Madya, and morbidities appear in the heart and in
the Dhatus located in it.28
Table - 2
Comparison of Guna of Ojas, Madya and Visha
Ojas29
Madya24
Visha30
Guru Laghu Laghu
Sheeta Ushņa Ushņa
Mridu Tikshņa Tikshņa
Shlakshņa Sukshma Sukshma
Bahala Vishada Vishada
Madhura Amla Anirdeshya rasa
Sthira Vyavayi Vyavayi
Prasanna Ashu Ashu
Picchila Vikashi Vikashi
Snigdha Ruksha Ruksha
Madya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 10
Pharmacology of Madya:
For living beings, food is the sustainer of life, but when taken inappropriately, it
causes death. Similarly, poison, which causes death, works like Rasayana when used
appropriately.
Madya taken following the rules and regulations produces exhilaration, energy,
happiness, nourishment, good health, excellent virility and pleasant intoxication
(Sukha Mada Prada) instantaneously. It promotes appetite, stimulates the power of the
digestion, tones up the heart, promotes the voice and complexion, produces the
feeling of refreshment and corpulence, increases strength, and removes fear and
fatigue. Patients suffering from insomnia enjoy sound sleep by taking Madya and it
stimulates speech in Mooka (who talks less). It helps persons having excessive sleep
to remain awake and causes bowel movements in constipated patients. It renders the
mind insensitive to the miseries of injury and fatigue.31
In moderate dose and taken with food or after food Madya tends to promote digestion
by direct stimulation of the fundus of stomach causing an abundant secretion of
gastric juice.
Since it causes dilatation of vessels especially of the skin and increases the functional
activity of different organs.
Actions of Madya According to three types of Sattva: 32
A person having Sāttvika type of mental faculty drinks Madya in pleasant conditions
and good quality Madya with wholesome and delicious food and drinks. While taking
Madya, he always engages himself in delightful conversations. He takes Madya in
happy mood leading to a pleasing type of intoxication, which promotes cheerfulness

Madya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 11
and passion. It terminates as a pleasing event, and it does not lead to the third stage of
intoxication.
Sattvika type of person does not exhibit perverted activities immediately after taking
Madya because Madya is incapable of adversely afflicting the powerful minds of
Sattvika persons instantaneously.
A person having Rajasika type of mental faculty talks some time gently and at times
rudely, some time distinctly and at times indistinctly and so demonstrates his irregular
varieties of behaviour after taking Madya. It terminates as a tragic event.
A person of Tamasika mental faculty, after taking Madya, becomes excited and
passionate in his talks, he never gets satisfaction in eating and drinking, and his
alcoholic intoxication terminates in unconsciousness, anger and sleep.
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 12
MADATYAYA
Word Madatyaya is composed of two terms i.e. Mada - any exhilarating or
intoxicating condition. Atyaya – suffering.
Hence suffering from intoxicating drink is
known as Madatyaya. Madatyaya or the alcoholic disorders are completely based on
stability of one’s own Satva. So mind plays an important role in the de-addiction of
alcohol.
Nirukti of Madatyaya:
“Madena Atyayo Madatyayah |
Madahetuko Vyadhirityarthah |
The Atyayata (disorder) produced by Madya is called as Madatyaya.33
Nidana of Madatyaya:
The general Nidana for Madatyaya are not given separately, but while explaining
various types of Madatyaya the Nidanas of each type are mentioned, which will be
dealt with that particular type of Madatyaya.
General Samprapti of Madatyaya:
Intake of excessive alcohol which is Tikshņa, Ushņa, Amla and Vidahi makes the
Annarasa Utkleda and will be digested improperly which ultimately turns Kshara and
causes Antardaha (burning sensation in the interior of the body), Jvara (fever),
Trishņa (morbid thirst), Pramoha (loss of orientation), Vibhrama (completely
deranged mental faculty) and Mada (intoxication).
The Dosha incited by alcohol causes obstruction to the movement of Vayu in the
Srotas (channels of circulation) because of which the patient suffers from excruciating
pain in the head, bones and joints
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 13
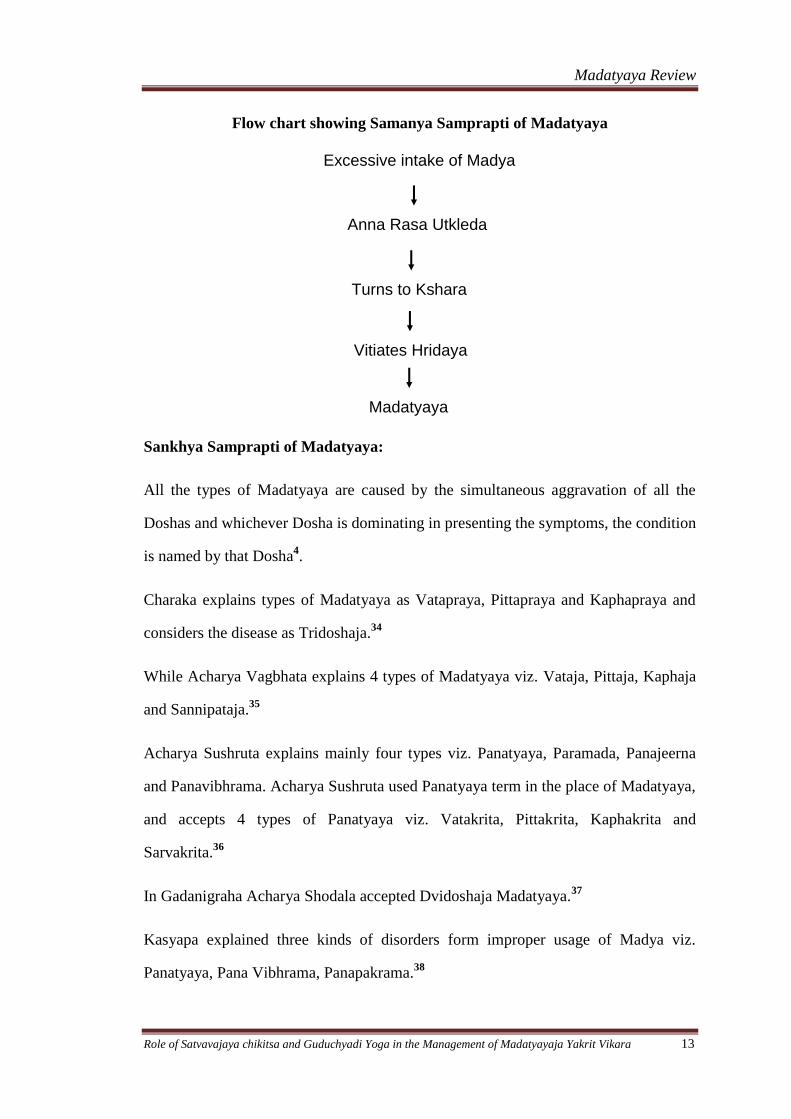
Excessive intake of Madya
Anna Rasa Utkleda
Turns to Kshara
Vitiates Hridaya
Madatyaya
Flow chart showing Samanya Samprapti of Madatyaya
Sankhya Samprapti of Madatyaya:
All the types of Madatyaya are caused by the simultaneous aggravation of all the
Doshas and whichever Dosha is dominating in presenting the symptoms, the condition
is named by that Dosha4.
Charaka explains types of Madatyaya as Vatapraya, Pittapraya and Kaphapraya and
considers the disease as Tridoshaja.34
While Acharya Vagbhata explains 4 types of Madatyaya viz. Vataja, Pittaja, Kaphaja
and Sannipataja.35
Acharya Sushruta explains mainly four types viz. Panatyaya, Paramada, Panajeerna
and Panavibhrama. Acharya Sushruta used Panatyaya term in the place of Madatyaya,
and accepts 4 types of Panatyaya viz. Vatakrita, Pittakrita, Kaphakrita and
Sarvakrita.36
In Gadanigraha Acharya Shodala accepted Dvidoshaja Madatyaya.37
Kasyapa explained three kinds of disorders form improper usage of Madya viz.
Panatyaya, Pana Vibhrama, Panapakrama.38
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 14
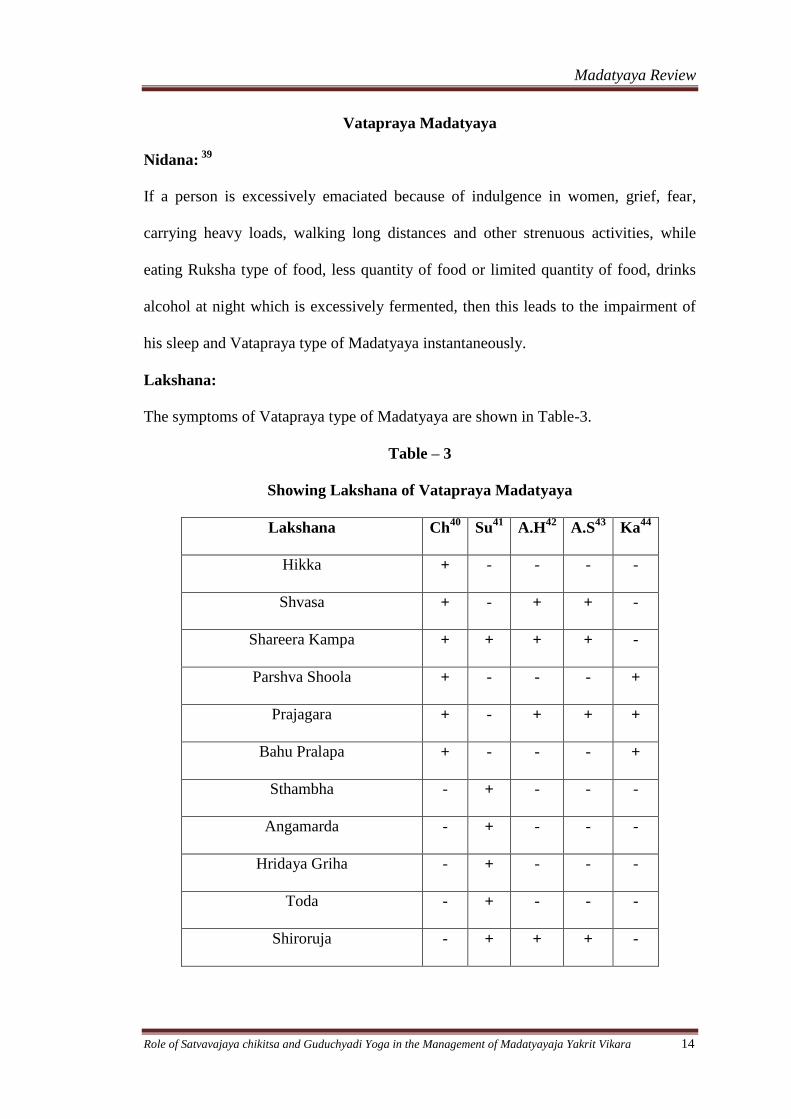
Vatapraya Madatyaya
Nidana: 39
If a person is excessively emaciated because of indulgence in women, grief, fear,
carrying heavy loads, walking long distances and other strenuous activities, while
eating Ruksha type of food, less quantity of food or limited quantity of food, drinks
alcohol at night which is excessively fermented, then this leads to the impairment of
his sleep and Vatapraya type of Madatyaya instantaneously.
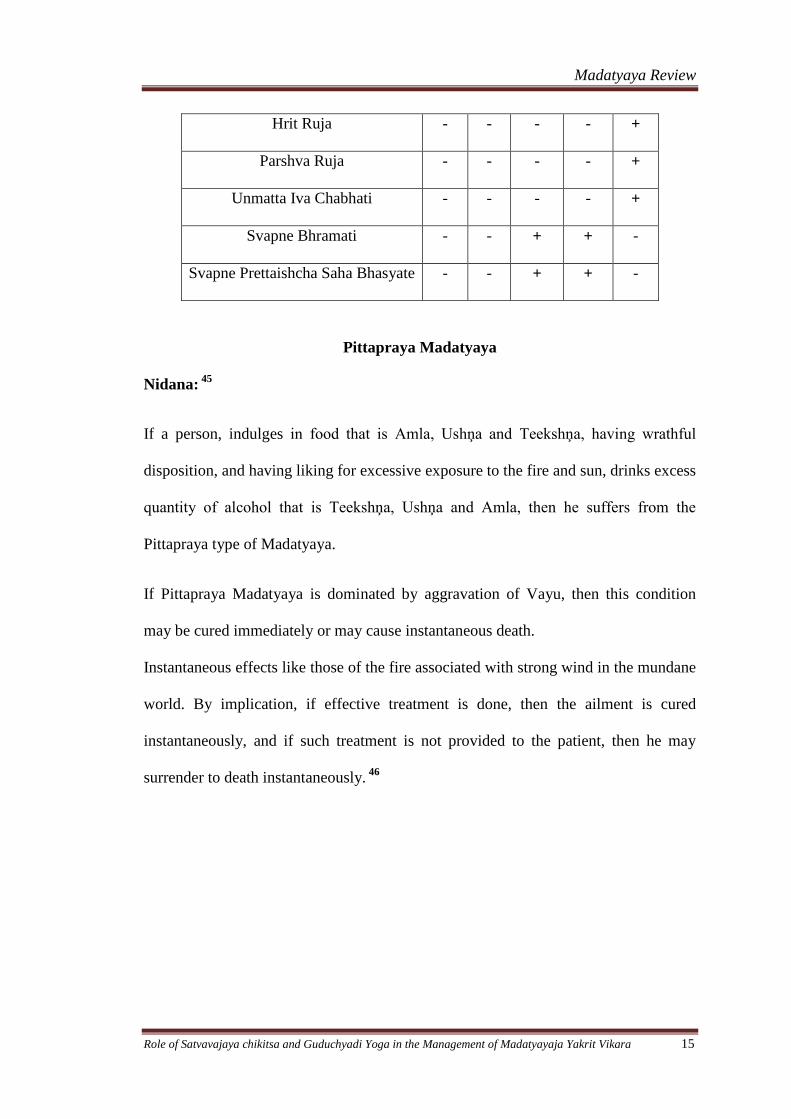
Lakshana:
The symptoms of Vatapraya type of Madatyaya are shown in Table-3.
Table – 3
Showing Lakshana of Vatapraya Madatyaya
Lakshana Ch40
Su41
A.H42
A.S43
Ka44
Hikka + - - - -
Shvasa + - + + -
Shareera Kampa + + + + -
Parshva Shoola + - - - +
Prajagara + - + + +
Bahu Pralapa + - - - +
Sthambha - + - - -
Angamarda - + - - -
Hridaya Griha - + - - -
Toda - + - - -
Shiroruja - + + + -
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 15
Hrit Ruja - - - - +
Parshva Ruja - - - - +
Unmatta Iva Chabhati - - - - +
Svapne Bhramati - - + + -
Svapne Prettaishcha Saha Bhasyate - - + + -
Pittapraya Madatyaya
Nidana: 45
If a person, indulges in food that is Amla, Ushņa and Teekshņa, having wrathful
disposition, and having liking for excessive exposure to the fire and sun, drinks excess
quantity of alcohol that is Teekshņa, Ushņa and Amla, then he suffers from the
Pittapraya type of Madatyaya.
If Pittapraya Madatyaya is dominated by aggravation of Vayu, then this condition
may be cured immediately or may cause instantaneous death.
Instantaneous effects like those of the fire associated with strong wind in the mundane
world. By implication, if effective treatment is done, then the ailment is cured
instantaneously, and if such treatment is not provided to the patient, then he may
surrender to death instantaneously. 46
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 16
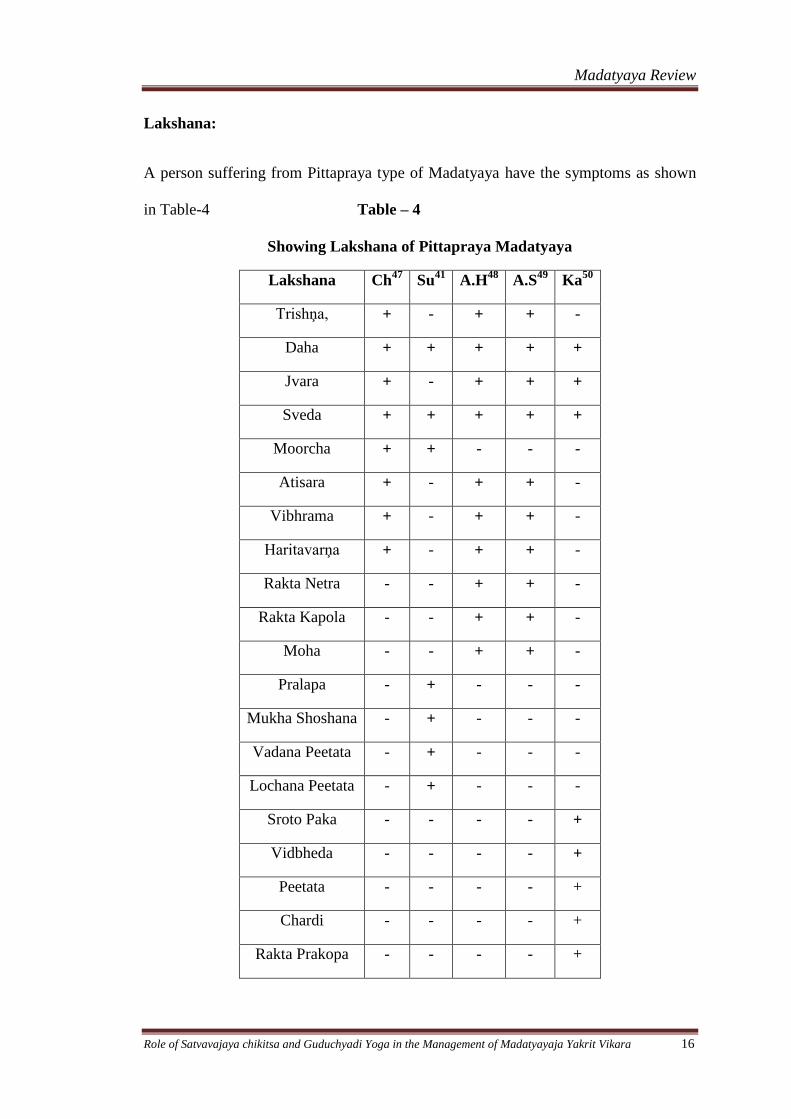
Lakshana:
A person suffering from Pittapraya type of Madatyaya have the symptoms as shown
in Table-4 Table – 4
Showing Lakshana of Pittapraya Madatyaya
Lakshana Ch47
Su41
A.H48
A.S49
Ka50
Trishņa, + - + + -
Daha + + + + +
Jvara + - + + +
Sveda + + + + +
Moorcha + + - - -
Atisara + - + + -
Vibhrama + - + + -
Haritavarņa + - + + -
Rakta Netra - - + + -
Rakta Kapola - - + + -
Moha - - + + -
Pralapa - + - - -
Mukha Shoshana - + - - -
Vadana Peetata - + - - -
Lochana Peetata - + - - -
Sroto Paka - - - - +
Vidbheda - - - - +
Peetata - - - - +
Chardi - - - - +
Rakta Prakopa - - - - +
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 17
Kaphapraya Madatyaya
Nidana: 51
If a person who is habituated to Madhura, Snigdha and Guru Ahara, who does not
perform exercise, who sleeps during the daytime and who indulges in comforts of
beds and seats, if excessively drinks alcohol which is not an old one or which is
prepared of Guda, and Paishtika, then he immediately develops Kaphapraya
Madatyaya.
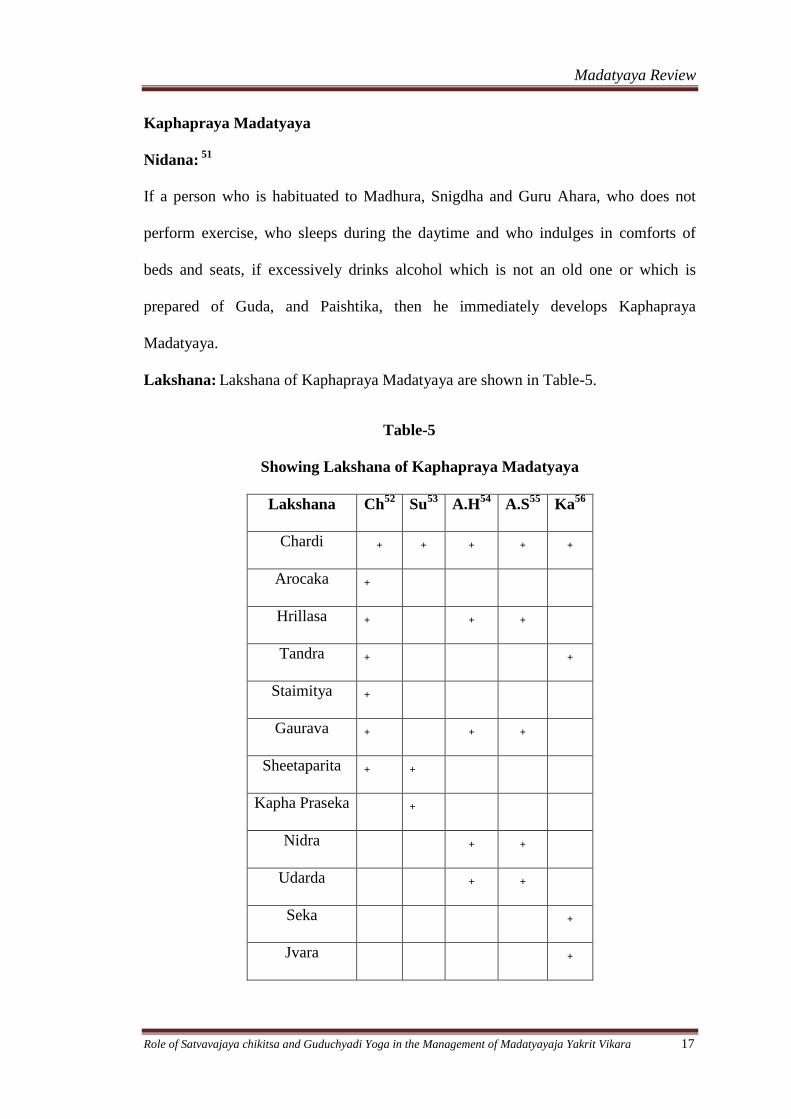
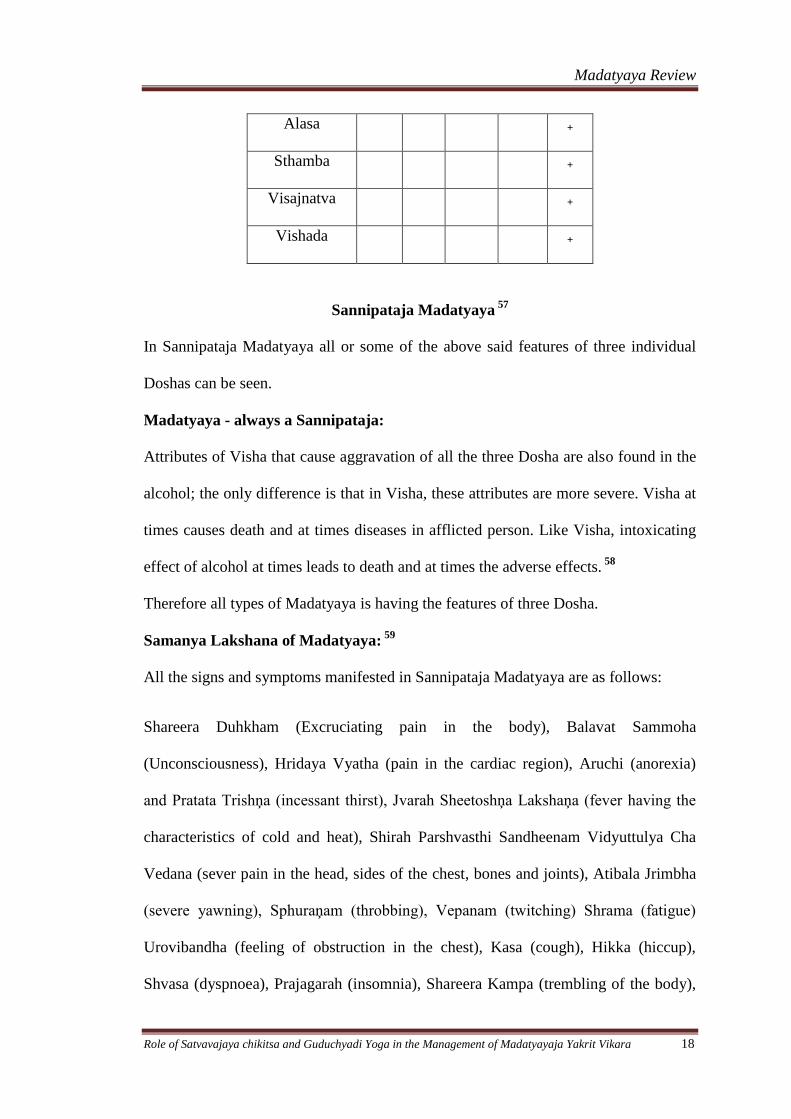
Lakshana: Lakshana of Kaphapraya Madatyaya are shown in Table-5.
Table-5
Showing Lakshana of Kaphapraya Madatyaya
Lakshana Ch52
Su53
A.H54
A.S55
Ka56
Chardi + + + + +
Arocaka +
Hrillasa + + +
Tandra + +
Staimitya +
Gaurava + + +
Sheetaparita + +
Kapha Praseka +
Nidra + +
Udarda + +
Seka +
Jvara +
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 18
Alasa +
Sthamba +
Visajnatva +
Vishada +
Sannipataja Madatyaya 57
In Sannipataja Madatyaya all or some of the above said features of three individual
Doshas can be seen.
Madatyaya - always a Sannipataja:
Attributes of Visha that cause aggravation of all the three Dosha are also found in the
alcohol; the only difference is that in Visha, these attributes are more severe. Visha at
times causes death and at times diseases in afflicted person. Like Visha, intoxicating
effect of alcohol at times leads to death and at times the adverse effects. 58
Therefore all types of Madatyaya is having the features of three Dosha.
Samanya Lakshana of Madatyaya: 59
All the signs and symptoms manifested in Sannipataja Madatyaya are as follows:
Shareera Duhkham (Excruciating pain in the body), Balavat Sammoha
(Unconsciousness), Hridaya Vyatha (pain in the cardiac region), Aruchi (anorexia)
and Pratata Trishņa (incessant thirst), Jvarah Sheetoshņa Lakshaņa (fever having the
characteristics of cold and heat), Shirah Parshvasthi Sandheenam Vidyuttulya Cha
Vedana (sever pain in the head, sides of the chest, bones and joints), Atibala Jrimbha
(severe yawning), Sphuraņam (throbbing), Vepanam (twitching) Shrama (fatigue)
Urovibandha (feeling of obstruction in the chest), Kasa (cough), Hikka (hiccup),
Shvasa (dyspnoea), Prajagarah (insomnia), Shareera Kampa (trembling of the body),

Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 19
Karņakshimukharoga (diseases of ears, eyes and mouth), Trikagraha (stiffness of
sacro-iliac joint), Chardi, Atisara and Hrilasa of Tridoshatmaka, Bhrama (giddiness),
Pralapa (delirium), Roopaaņaamasastaanaam Darshanam (visual hallucinations like if
the body is covered with grass, creepers, leaves or dust; and afraid of birds as if they
are colliding with his body), Vyakulanamashastaanaam Svapnaanam Darshanani
(dreaming of terrifying and inauspicious objects).
Madatyaya according Sushruta:
According to Sushruta, the adverse effects of chronic usage of alcohol against the
rules and regulations prescribed for alcohol intake are classified into four types. They
are Panatyaya, Paramada, Panajeerņa and Panavibhrama60
.
Panatyaya: 61
Panatyaya is divided in to four types depending upon the characteristic features of
Dosha predominance.
a) Vatika Panatyaya: It is characterized by Stambha, Angamarda, Hridaya Graha,
Toda, Kampa and Shiroruja
b) Paittika Panatyaya: It is characterized by Sveda, Pralapa, Mukha Shoshaņa,
Daha, Moorcha, Vadana and Locana Peetata.
c) Kaphaja Panatyaya: It is characterized by Vamathu, Sheetata and Kaphapraseka
d) Sannipataja Panatyaya: It characterized by the symptomatology of three
Doshas.
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 20
Paramada: 62
Paramada is characterized by Oshmanam, Angagurutam, Virasananatvam,
Shleshmadhikatvam, Aruchim, Malamootrasanga, Trishņa, Shiro and Sandhi ruja.
Panajeerņa: 63
Aadhmanam, Udgiranamamlarasa, Vidahi and other features of aggravated Pitta
characterize Panajeerņa.
Panavibhrama: 64
Panavibhrama is characterized by Hrit, Gatra Toda, Vamathu, Jvara, Kantha Dhooma,
Moorcha, Kaphasravanam, Shiroruja, Vidahi, and Sura, Anna Vikruteshu dvesha.
Dhvamsaka & Vikshaya:
Nidana:
If a person, who has stopped drinking alcohol, suddenly takes recourse to drinking
alcohol in excess, he suffers from Dhvamsaka and Vikshaya. 65
Lakshana:
Dhvamsaka: Shleshma Praseka (excessive salivation), Kaņthasya Shosha (dryness of
the throat and mouth), Shabdasahishņuta (intolerance to noise), Atitandra (excessive
drowsiness) and Nidra (sleep) characterize the Dhvamsaka. 66
Vikshaya: Hritkaņtha Roga (thoracolaryngial disorders), Sammoha (loss of
orientation), Chardi (vomiting), Anga Ruja (body pains), Jvara (fever), Trishņa
(thirst), Kasa (cough) and Shirashoola (headache) characterize the Vikshaya. 67
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 21
Prognosis:
Since a person suffering from Dhvamsaka or Vikshaya who is already emaciated
because of his earlier drinking habit, these two diseases appearing in him are difficult
to be cured. 68
Duration of severity of Madatyaya / Panatyaya:
According to Yogaratnakara the severity of disease Madatyaya will persist for seven
or eight days. 69
Upadrava of Madatyaya:
The following are the complications of Madatyaya- Hikkaa associated with Jvara,
Vamathu, Vepathu, Paarshvashoola, Kaasa and Bhrama.70
Asadhya Lakshanani (Characters of bad prognosis):
The following are the characteristics of bad prognosis:
Hinottaraushtham (thinner upper lip), Atisheetam (excessive cold), Amandadaham
(mild burning sensation), Tailaprabhasyam (oily glistering of face), Jihvaushtha
Dantamasitam Vaa Neelam (black or blue tongue, lips and teeth), and Peete Nayana
Rudhirata (reddish eyes immediately after taking alcohol). 71
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 22
CHIKITSA OF MADATYAYA
General treatment principles
1. All the varieties of Madatyaya are of Tridoshaja. Therefore, in the beginning,
treatment should be done for the most predominant Dosha. If all the Doshas are
equally aggravated, then the treatment should be done first for the location of
Kapha, followed by that of Pitta and lastly that of Vata.6
2. The ailments caused by the drinking of alcohol in Mithyaa Yoga or in Atiyoga
or in Heena Yoga can be cured by taking the alcohol in appropriate manner and
quantity (Samayoga). Here the same type of Madya or other varieties of Madya
can also be given. 72
3. According to Kaashyapa, Madatyaya is Aamaja. That is why while treating
Madatyaya, Langhana should be done first. 73
4. Why Madya in Madatyaya
Intake of excessive alcohol which is Teekshņa, Ushņa, Amla and Vidaahi
makes the Annarasa Utkleda and will be digested improperly which ultimately
turns Kshaara and causes Antardaaha (burning sensation in the interior of the
body), Jvara (fever), Trishņaa (morbid thirst), Pramoha (loss of orientation),
Vibhrama (completely deranged mental faculty) and Mada (intoxication). To
correct these ailments, alcohol should be administered because when a Kshaara
(alkaline) substance gets mixed with a sour substance, the outcome becomes
sweet in taste, and alcohol is the best among the substances having the Amla
taste. Alcohol by nature is sour in taste and it has four subsidiary tastes like
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 23
Madhura (sweet), Kashaaya (astringent), Tikta (bitter) and Katu (pungent). Thus
along with other ten qualities, alcohol has fourteen attributes in total. It is because
of these fourteen attributes, alcohol stands supreme among all the article of sour
taste.
The Dosha incited by alcohol causes obstruction of the movement of Vayu in
the Srotas (channels of circulation) because of which the patient suffers from
excruciating pain in the head, bones and joints. In spite of the availability of other
sour ingredients, alcohol should specifically be administered to such a patient for
the liquefaction of the Dosha because of its Vyavaayi, Teekshņa and Ushņa
properties. Alcohol removes the obstruction in the channels of circulation, helps
in the downward movement of Vaayu, acts as an appetizer, stimulates the power
of digestion and becomes wholesome (Satmya) when consumed habitually
(Abhyaasa). When the obstruction in the channel is removed, and Vaayu moves
downwards, the pain subsides and the ailments caused by intake of alcohol get
cured.74
5. For Vatika type of Madatyaya, Piashtika type of alcohol (prepared of the paste
of cereals) mixed with Beeja Pooraka, Vrikshamla, Kola and Dadima, some
quantity of Yavani, Hapusha, Ajaji and Shringavera should be taken along with
salt. In addition, snacks prepared of Saktu should be taken.
For Vatika type of Madatyaya the following also should be administered: meat
soup, Veshavaara with ghee. After taking food if patient feels thirsty, he should
be given Varuņi Maņda, Dadima juice, Pancamoola Siddha Jala etc. Other
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 24
measures which can be followed are Abhyanga, Utsaadana, Agarulepa, residing
with women etc.
6. For Paittika type of Madatyaya Sharkara or Mardveeka type of alcohol which
is diluted with large quantity of water along with the juice of Kharjoora,
Mridveeka, Parooshaka, Daadima should be given. This type of patients should
take sweet and sour type of food, Shaali and Shashthika type of rice, Maamsa and
soups prepared of meat of goat adding the soup of Patola, Mudga, Daadima, and
Aamalaka. Different types of Tarpanas, Yooshas also should be given.
If, in the patient of Paittika type of Madatyaya, Kapha, Pitta located in
Aamaasaya are incited, if there is excessive morbidity and if he is suffering from
burning sensation and morbid thirst, then alcohol, grape juice and other Tarpaka
Dravyas should be given and there after Vamana Karma should be administered
to eliminate the morbid Doshas completely. This gives instant results in this type
of patient. For other complications Kashayas prepared of Guduchi, Bhadra
Mustaa, Patola, Naagara, Daadima, Laaja, or Parņacatushka should be given.
Baahyopacaaras compatible for Pitta also should be done.
7. For Kaphaja type of Madatyaya, Vamana Karma and Upavaasa should be
administered. If the patient suffers from morbid thirst, then the Kashaayas
prepared of Hreebera, Bala, Prishņiparņi, Kaņtakaari together with Naagara
should be given. For Dosha Paacana, Kashaaya prepared of Dussparsha, Musta, or
Parpaataka should be given. When the patient is free from Aama, he should be
given the alcohol prepared of Sharkara, Madhu and old Arishtas, and Seedhu
along with honey. He should be given the food prepared of Yava, Godhooma and
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 25
Rooksha type of Yooshas like Kulattha Yoosha etc. meat prepared with profuse
quantity of Marica and other Amla, Katu and Lavaņa Dravyas. Digestive
stimulants and Srotoshodhakas like Ashtaanga Lavaņa should also be given.
8. For Sannipaataja Madatyaya, which can be of thirteen types, according to the
Dosha dominance, the appropriate treatment should be done. When there is
involvement of three Doshas with equal dominance, then first treatment should be
dome for Kapha Dosha followed by Pitta Dosha and Vaata Dosha.
9. The following psychological measures also can be applied for the patients
suffering from Madatyaya because, alcohol cannot cause the disorders related to
improper alcohol intake without causing agitation of the mind and without causing
morbidity in the body. 75
The psychological measures are -
a) Beautiful forests
b) Ponds and lakes with lotus flowers
c) Clean food and drinks
d) Pleasing and delightful companions
e) Use of garlands and perfumes
f) Clean garments
g) Musical performances
h) Exposition of refreshing stories, jokes and songs and
i) Company of lovely and devoted women. 76
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 26
10. Dugdha for Madatyaya:
After giving up alcohol, because of Langhana, Paacana, Dosha Shodhana,
Shamana Kapha gets diminished, and body of the patient becomes Durbala and
Laaghava. For this type of patient, whose body is burnt by alcohol, and in whose
body Vaayu and Pitta are aggravated, milk is exceedingly wholesome like the rain
for a tree afflicted with hot summer. 77
11. Re-administration of alcohol:
After the disease is cured by the administration of milk, and after the patient
has strength, the milk should be gradually withdrawn, and alcohol should be
substituted in its place little by little.
12. According to Kaashyapa, for the Madatyaya patients suffering from Pipasa,
Jvara and Daha, the treatment principles of Visarpa, Daha and Jvara should be
applied.78
13. For Panatyaya, Paramada, Panajeerņa and Panavibhrama, the above said
principles can be applied accordingly.
14. Treatment for Dhvamsaka & Vikshaya:
As emaciated and weak persons are suffered from these two types of
disorders, their treatment should be done on the line suggested for the
treatment of Vaatika type of Madatyaya. Such a patient should be given Vasti,
Sarpi, Dugdha, Ghrita, Abhyanga, Snehana, Snaana, food and drinks which
cause alleviation of Vayu. 79
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 27
APATHYA
According to Kashyapa, the following are prohibited in patients suffering from
Madatyaya: Ushņa, Rooksha and Guru Anna and Paana; Agni, Aatapa, Divaasvapna,
other activities which does emaciate the bodily tissues, Shoka, Adhva, Maithuna,
other laborious works, excessive exercise, food preparations like Yavagu, Maņda,
Yusha. 80
In Bhelasamhita the following are contraindicated in patients suffering from
Madatyaya:
Ushņodakam, Svedanam, Dhoopanam, Sarpirpaanam, all types of Jvaala and Analam,
Yavaagu, Dadhi, Dugdham, Graamya, Anoopa and Udaka Maamsa, preparations
made up of Tilapishta. 81
In Bhashajyaratnavali, apart from above said descriptions, Dantadhavana, Navana and
Anjana are also contraindicated in patients suffering from Madatyaya. 82
DISCOURAGING ALCOHOL INTAKE:
A wise person who has control over the sense organs and who abstains from drinking
all types of alcoholic preparations never gets afflicted with physical and mental
disorders.
He who is addicted to alcohol is unaware of right and wrong, happiness and
unhappiness, beneficial and non-beneficial, suitable and unsuitable and who do the
wise indulge in it? 83
Madatyaya Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 28
Some important Yogas for Madatyaya:
Kharjooradi Mantha in all types of Madatyaya, Punarnavadi Ghritam for
Ojovardhana, Ashtanga Lavaņa in Kaphaja Madatyaya. (Cakradatta)
Karkandhoobadara Panakam, Kashmaryadi Panakam, Amritadya Panakam,
Drakshadya Panakam, Triphaladya Kashaya with Madya for Pittaja Madatyaya
(Bhe.Sa.).
Cavyadicoorņa with Madya, Katphaladi Ghritam, Sharkara and Ghrita for acute
intoxication. (YR.)
Phalatrikadi Choorņa, Eladi Modaka, Mahakalyanaka Vati, Sreekhandasava (Bhai.
Ra.)
Madatyayaja Yakrit Vikara Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 29
MADATYAYAJA YAKRIT VIKARA
In Brihatrayi there is no direct reference of Yakrit Vikara but while explaining
the diseases like Pandu, Kamala, Udara, Yakridalyodara etc , Acharyas explained
some of the signs and symptoms which are manifested because of Yakrit impairment.
In so many contexts they explained the symptoms of Yakrit Vikara indirectly.
Both Charaka and Sushrutha Acharyas have explained that Yakrit is the moola of
Rakta Vaha srotas. As Rakta dhatu and Pitta doshas are Ashrayaashrayi , it can be
consider that the Nidanas for Pitta or Pittakaraka Ahara Vihara leads to Rakta
pradoshaja vikaras and simultaneously it affects the moola of Raktavaha srotas and
thereby leads to the vitiation of Yakrit or Yakrit vikara.
Ranjaka pitta is a type of pitta which is responsible for the rasa ranjana and gives
colour to the rakta, mutra and pureesha. In madatyayaja yakrit vikara, colour of the
puresha and mutra are deranged and rakta dhatu is one among the main dushya. As
Yakrit and pleeha are the moola of rakta vaha srotas, it is very clear that ranjaka pitta
is the main dosha which is responsible for the samprapti of Madatyayaja Yakrit
Vikara.
As Kamala is the Rakta pradoshaja vikara and that leads to the impairment of the
functions of Yakrit. We can consider the symptoms of Kamala for understanding
Yakrit Vikara. Mainly Pitta dosha is involved in the samprapti of Kamala that leads to
the vitiation of Rakta Dhatu and thereby affects the Hridaya and Yakrit.
As Madya is Abhishyandi , Vyavayi, Vikashi, Teekshna, ushna, vidahi and
amlarasayukta , which leads to the vitiation of Pitta and thereby form the Raktadusti
Madatyayaja Yakrit Vikara Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 30
and can affects the Yakrit. So Madya can be considered as the Nidana for the
Madatyayaja Yakrit Vikara and it may generate Yakrit Vikara.
As Madya is having the gunas like Vyavayi, Vikashi, Ashukari etc. it immediately
affects the Ojas and Hridaya and thereby causing Uttarottara Dhatu Hrāsa and leads to
many types of symptoms.
Exessive intake of madya leads to agni dusti and mandagni by its vidahi, teekshna,
usna, and drava guna. Severe agni dusti leads to the samprapti of Udara (accumulation
of fluid in twank-mamsantara pradesha), Kukshimadmapana and mainly
Yakridalyodara and resulting in Madatyayaja Yakrit Vikara, which is similar to that
of alcoholic liver cirrhosis.
There is a direct reference of Yakrit Vikara in BhavaPrakasha, he mentions Yakrit
vriddhi (can be compared with hepatomegaly) is the main feature of Yakrit vikara and
nidana for Yakrit vikara is vidahi, abhishyandi Āharas. Madya being the abhishyandi
and vidahi, it can cause Yakrit vikara and Yakrit vriddi and thereby leads to different
pathological symptoms of Yakrit.
By all these explanations we can consider that Madya leads to Madatyaya and
Madatyaya leads to Yakrit vikara, therefore the study or clinical trials taken on
Madatyayaja Yakrit Vikara.
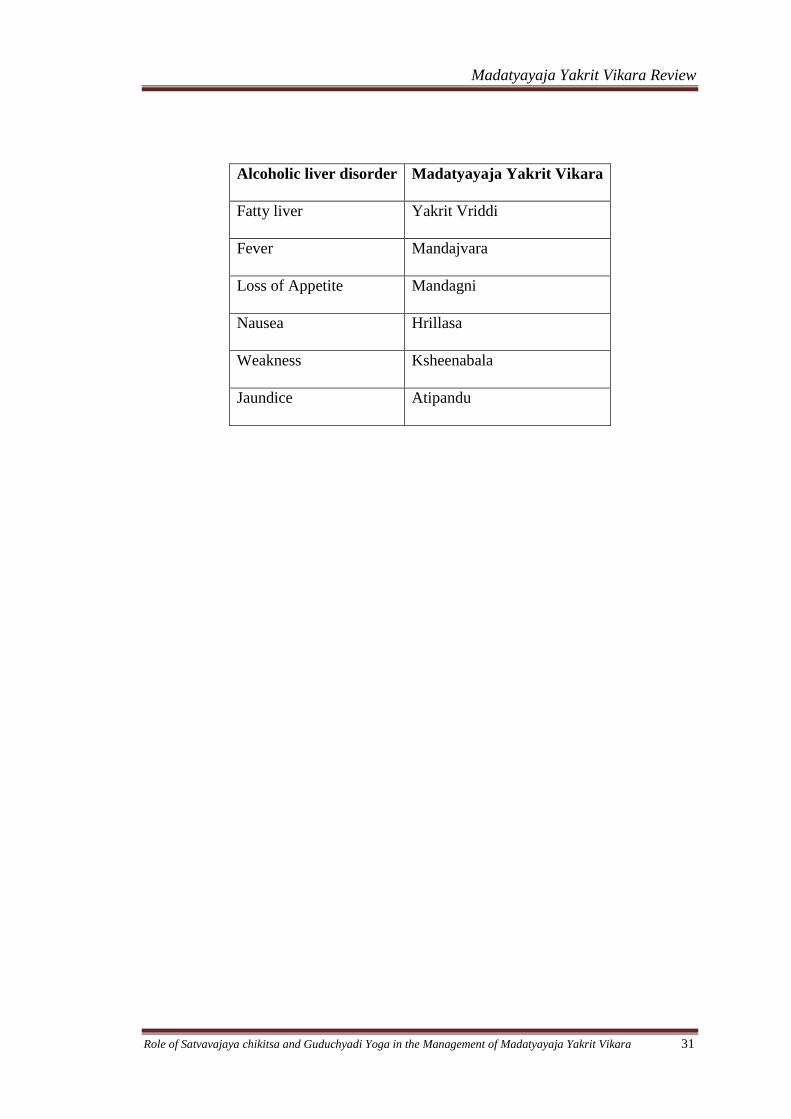
Symptoms of alcoholic liver disorder and symptoms of Madatyayaja Yakrit Vikara
appears to be same. Hence Madatyayaja Yakrit Vikara can be considerd as Alcoholic
liver disorder.
Madatyayaja Yakrit Vikara Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 31
Alcoholic liver disorder Madatyayaja Yakrit Vikara
Fatty liver Yakrit Vriddi
Fever Mandajvara
Loss of Appetite Mandagni
Nausea Hrillasa
Weakness Ksheenabala
Jaundice Atipandu
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 31
Concept of Satvavajaya Chikitsa
Trividha Aushadha
“Trividham Aushadham Iti Daivavyapashrayam Yuktivyapashrayam
Satvavajayascha167”
Three types of treatment modalities have been explained in
Ayurvedic science for the management of the various ailments related to the body as
well as the mind. They are – Daivavyapashraya, Yuktivyapashraya and Satvavajaya
Chikitsa.
a) Daivavyapashraya - It is termed the divine therapy or the therapy by faith. It
includes mainly the use of Mantra, Aushadha, Mani, Mangala, Bali, Homa, etc.
Detailed description of the Daivavyapashraya Chikitsa can be found in Atharvana-
Veda.
b) Yuktivyapashraya - It is the intellectual adoption of the treatment which includes
planned usage of medicines and the food.
c) Satvavajaya Chikitsa -The Satvavajaya Chikitsa includes various psychotherapies
which help in controlling of the Manas from moving towards the Ahita Arthas.
Satvavajaya Chikitsa
Satvavajaya Chikitsa is mainly aimed at controlling of the Manas from moving
towards the Ahita Arthas.
“Satvavajayam Punar Ahitebhyo Arthebhyo Mano Nigrahah”
The Satvavajaya chikitsa includes all the measures which help in restraining of
the Manas from craving towards the Ahita Arthas (unwholesome objects), and avoid
the involvement of the Manas in abnormal mental faculties i.e. Ati, Heena and Mithya
yoga.
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 32
Aims of Satvavajaya Chikitsa:
1. To help individual to discriminate between thoughts and actions.
2. To divert mind and make the person to involve with commitment in other
or next activity.
3. To help individual to discriminate between objective and imagined
dangers and to respond selectively to each.
4. To initiate Bhakti or regard or strengthen his believes in Ishta-Daivam.
5. To take out phobic nucleus by making awareness of subject knowledge
and true facts.
Need for the Satvavajaya Chikitsa
Among the three basic types of treatment explained for the treatment of
diseases–
a) Daivavyapashreya chikitsa – which is mainly aimed in the management of Bhuta
Abhishyanga Vyadhis and the neurotic type of disorders.
b) Yuktivyapshraya chikitsa - is mainly aimed at the somatic and the psycho somatic
disorders.
c) Satvavajaya chikitsa - is mainly aimed for the treatment of the Manasika Vikaras
by restraining the Manas from craving towards the unwholesome objects.
Techniques of the Satvavajaya Chikitsa
a)“Manasam Prati Bhaishajyam, Tadvidyaseva Vijnanamatmadinam Ca Sarvashah”168
b) “Dhi Dhairyatmaadi Vijnanam Manodoshoushadham Param”. 169
The Satvavajaya chikitsa includes
i) Jnana - The word Jnana denotes the application of various techniques in the
management of the mental ailments.
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 33
ii) Vijnana – The word Vijnana indicates various types of special techniques which
are applied in the treatment of the various conditions, such as-
a) Relaxation- Deep-muscle relaxation, Jacobsons relaxation, progressive muscle
relaxation, Yogic relaxation, etc
b) Hypnotherapy – Age regression, past life regression therapies etc.
iii) Dhi – The word Dhi indicates various techniques applied in improving the
intellect of the patient. Such as
a) Pancha tantra stories.
b) Play therapy.
c) Group therapy.
iv) Dhairya- “Dhairyam Unnatischetasah”
Charaka mentioned Dhairya as one of the methods of treatment of mental
diseases. Dhairya includes all the measures applied for the upliftment of ones Satva,
such as by direct, simple advice and reassurance, encouragement etc. The supportive
and cognitive psychotherapy of the modern psychology can be compared to the
Dhairya Chikitsa.
Atma Jnana – Providing the knowledge about the self is termed the Atma Jnana.
Such as,” Who am I, what are my aims, what is good and what is bad for me” etc.
Desha Jnana – Providing the knowledge about the Desha i.e.,
i) Dwelling place.
ii) Seasons.
iii) Rituals.
iv) Rules and regulations of the place etc.
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 34
Kulajnana – Providing the knowledge about the Kula i.e. the family to which he is
related to and the, Rituals of the family etc
Kala jnana- Providing knowledge about the Kala i.e knowledge about facts and
circumstances at that particular time.
Balajnana – The word Bala here indicates the Sharirika Bala as well as the Mano
Bala and the Vachika Bala. The Manasika Bala is said to be of three types, i.e. the
a) Pravara
b) Madhyama
c) Avara
i) The Bala Jnana includes the various techniques applied to improve the Manasika
Bala of the person and also to provide the knowledge of the self capacity to make him
aware of the dos and the don'ts.
Shakti jnana- Providing knowledge about strength and capacity according to the
situations and show the way towards the opportunities.
II) Psycho-phylaxis, which refers to the development of healthy mental and
emotional habits, attitude and behavior and is concerned with the prevention of
emotional problems and mental illness.
Samadhi-
The Samadhi includes implementation of Yoga, Pranayama, and Meditation etc
“Samadhih Samatavastha Jeevatma Paramatmanoh Yogah Samyoga
Ityuchyate Jeevatma Paramatmanoh”170
.
The union of Jeevatma and Paramatma is called the Samadhi and the state of oneness
of the Jeevatma and Paramatma is called the Yoga.
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 35
Yoga- “Yogah Chittavrutti Nirodhah”171
. The controlling of the Chittavrittis (i.e. the
activities of the Manas) is termed the Yoga.
The Yoga has got 8 Steps, they are
“Yama Niyama Asana Pranayama Pratyahara Dharana Dhyana Samadhiretani
Astavangani Yogasya”172
a) Yama, b) Niyama, c) Asana d) Pranayama
e) Pratyahara, f) Dharana, g) Dhyana, and h) Samadhi.
a)Yama (Self control) “Dehendrieshu Vairagyam Yama Ityucchate”.
Detachment from the Indriya Vishayas which yields to the self- control is called the
Yama.
For attaining the state of Yama, five steps have been explained. They are-
a) Ahimsa (Non-Violence),
b) Satya (Speaking truth),
c) Asteya (Abstinence from stealing),
d) Bramhacharya (Abstinence from sex)
e) Aparigraha (Disowning of possessions).
Niyama (Regulation)-
“Anuraktih Paretatve Satatam Niyamah Smrutah”.173
Means the state of continued attachment with the Paramatma is called as Niyama. The
Niyama has got 5 steps. They are
“Shoucha Santosha Tapa Svadhyaya Ishvara Pranidhanani Niyamani.”.174
a) Shoucha (Purity).
b) Santosha (Contentment).
c) Tapa (Right aspiration).
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 36
d) Svadhyaya (Study).
e) Ishvarapranidhana (Devotion to God).
Asana (Control of the Limbs)-
“Sthira Sukham Aasanam”
The control of the limbs ting in a stable and a comfort position is termed the Asana.
Pranayama (Cotrolled Breathing)-
“Yasmin Sati Svasa Prasvasa Yorgativicchedah Pranayama”175
The controlled breathing with the ultimate object of suspending it is termed the
Pranayama.
Pratyahara (Withdrawal of the Mind)-
“Chittasyantarmukhi Bhavah Pratyaharastu Satamah”.
In Mandala Bramhopanishad the Pratyahara is explained as the withdrawal of the
Manas from the Indriya Vishayas.
Dhyana (Meditation) –
“Tatra Pratyaikatanata Dhyanam”. 176
Dhyana is keeping the Manas fixed on one subject till a habit and a disposition
grows up.
Dharana –
“Deshabandha Chittasya Dharanah”177
Binding of the Manas with any subject, such as towards God is termed, in a
sense to bring a state of autohypnosis without external suggestion is Dharana.
Samadhi (Super Conscious State) –
“Tadevarthamaatra NirbhasamSvaroopa Shoonyameva Samadih”.178
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 37
Concentrating the Manas by getting detached from all sorts of worldly
thoughts is termed the Samadhi.
Importance of the Astanga Yoga –
By the practice of the Astanga Yoga one becomes free from all the sorts of the
disorders of the mind as well as the body, as there by one attains the control over all
his Jnanendriyas as well as Karmendriyas which helps to restrain from the disease of
the mind as well as the body.
Preventive Aspects of Satvavajaya Chikitsa -
The Preventive aspects of the Satvavajaya Chikitsa can be considered as the
Sadvrtta which have been explained in order to maintain the normal mental health.
They are as follows-
a) Respecting the God, teacher, elders, Yogis etc
b) Maintaining the physical and mental hygiene.
c) Avoid the Kayika, Vachika, and the Manasika Papa Karmas, such as
i) Kayika- Physically hurting other, theft, etc.
ii) Vaachika- Telling lies, insulting others by using bad words, etc.
iii) Manasika-Bad thoughts about others, thinking bad about others mentally.
d) Withhold the Dharaniya Vegas.
Summary of the Satvavajaya Chikitsa
The Satvavajaya chikitsa in brief can be explained in the following way.
1) Assurance (Dhairya).
2) By replacing the thought process (Chintya).
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 38
3) By regulating the ideas (Vicharya).
4) By channeling the presumptions (Oohya).
5) By polishing the objectives (Dhyeya).
6) By proper guidance and advice for taking the decision (Sankalpa).
7) Reframing the ideas.
8) Proper control of patience.
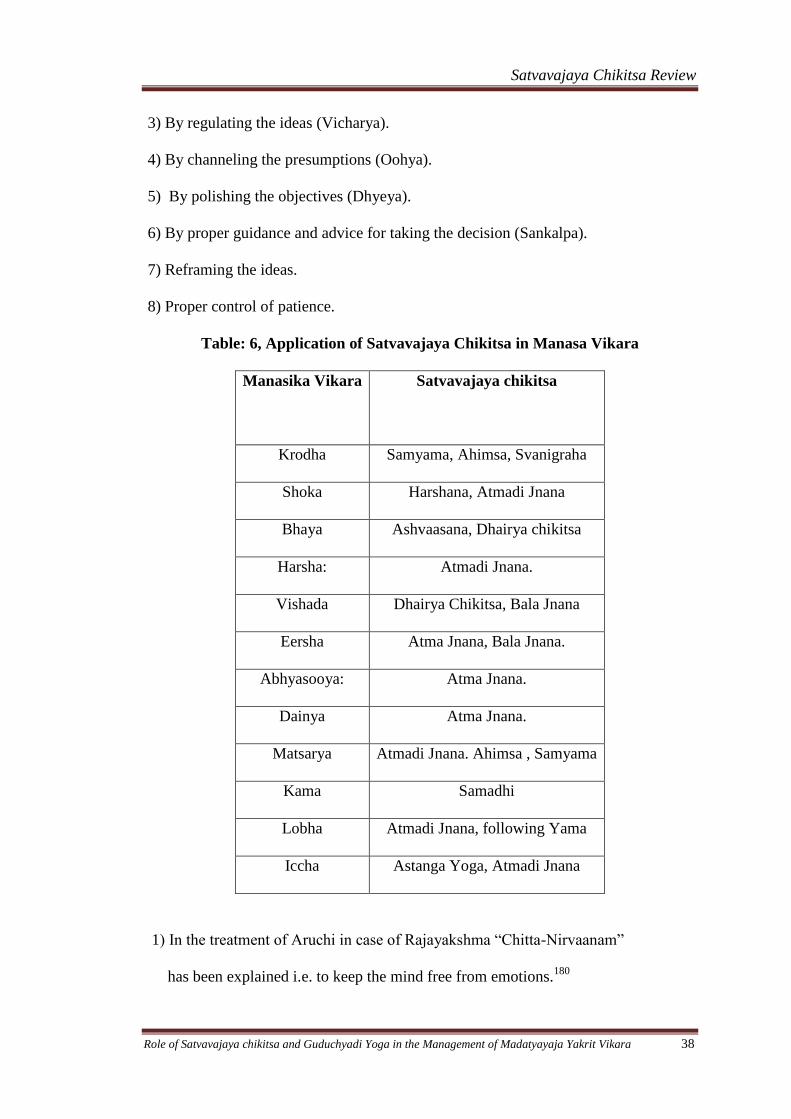
Table: 6, Application of Satvavajaya Chikitsa in Manasa Vikara
Manasika Vikara Satvavajaya chikitsa
Krodha Samyama, Ahimsa, Svanigraha
Shoka Harshana, Atmadi Jnana
Bhaya Ashvaasana, Dhairya chikitsa
Harsha: Atmadi Jnana.
Vishada Dhairya Chikitsa, Bala Jnana
Eersha Atma Jnana, Bala Jnana.
Abhyasooya: Atma Jnana.
Dainya Atma Jnana.
Matsarya Atmadi Jnana. Ahimsa , Samyama
Kama Samadhi
Lobha Atmadi Jnana, following Yama
Iccha Astanga Yoga, Atmadi Jnana
1) In the treatment of Aruchi in case of Rajayakshma “Chitta-Nirvaanam”
has been explained i.e. to keep the mind free from emotions.180
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 39
2) In case of the treatment of the “Dvistarthajanya Chardi” “Anukuulopachara” has
been adviced.181
3) In case of the treatment of the Bhayaja and Shokaja Atisara
“Ashvaasana and Harshana” i.e. creating confidence and happiness are
mentioned.182
4) In case of treatment of the Kustha some of the rituals like “Vruta Dama Seva
Tyaga Sheelabhiyoga” i.e. observance of vows, avoiding of anger and other
emotions, control of the senses, disciplined life, serving others, cultivating habit of
charity have been explained.183
5) In case of the treatment of the Bhutabhishyanga, the Bhuta which is not involved
in causing hurt, harm, should be won by-
“Bhutam Jayed Tapah Sheela Samadana Jnana Danadayadibih”. i.e. by observing
Tapa i.e. Penance, virtuous behavior, right conduct, good knowledge, charity, and by
showing mercy.
Psychotherapies
1) Behaviour therapy –The behavior therapy is mainly based on the theories of
learning (operant and classical), aims at changing maladaptive behavior and
substituting it with adaptive behavior. It involves the methods like
a) Systemic desensitization.
i) Relaxation. ii) Hierarchy construction. iii) Systemic desensitization.
b) Aversion therapy.
c) Operant conditioning procedures for increasing the behavior-
i) Positive reinforcement .ii) Negative reinforcement. iii) Modeling.
d) Flooding.
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 40
2) Cognitive Therapy:
Cognitive or cognitive behavior therapy is mainly aimed at correcting the
maladaptive methods of thinking.
The cognitive therapy is used for the treatment of depression, anxiety disorder,
panic disorder, phobias, eating disorders, etc. Techniques followed are teaching of the
problem solving skills, identifying and testing, maladaptive assumptions, activity
scheduling, homework assignments, behavioral rehearsal etc.
3) Supportive Therapy:
The supportive therapy mainly focuses on the existing symptoms or current
life situations. The aims of the therapy are-
i) Correction of situational problems.
ii) Symptom rectification.
iii) Strengthening defenses.
iv) Prevention of emotional breakdown.
v) Teaching new coping skills.
4) Family Therapy or Marital Therapy.-
Can be applied in cases of-
i) Family conflicts.
ii) Drug abuse.
iii) Spouse conflicts.
5) Group therapy-
The group therapy is a-
i) Less time consuming.
ii) Involves at least 8- 10 people at a time in treatment.
Satvavajaya Chikitsa Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 41
iv) The participants mainly suffer from the similar type of disorders such as diabetes,
hypertension, depression, anxiety etc. Which gives them a chance to know that there
are many other people who suffer from a similar disorder, and they will get a chance
to interact with all those people which give them a moral support and help them to
come out of their sufferings.
5) Rehabilitation- In case of chronic disorders.
6) Hypnotherapy– Hypnosis is a state of artificially induced increase state of
suggestibility. In this condition there will be constriction in the peripheral awareness
with increased focal concentration. The hypnotherapy involves providing of positive
thoughts and detachment from the negative thoughts.
Indications-
i) Conversion disorders.
ii) Dissociative disorder (Hysteria).
iii) Eating disorder.
iv) Habit disorder
v) Pain.
vi) Anxiety disorder.
Review of
Modern
Science
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 42
ALCOHOL REVIEW
Definition of Alcohol:
Alcohols are hydroxyl derivatives of aliphatic hydrocarbons. Alcohols exists naturally
either free or combined as esters; like phenols they generally have names ending „-ol‟
e. g. ethanol, glycerol and mannitol.151
Alcohol is one of the most widely used psychoactive drugs, and alcoholism is
characterized by chronic, repetitive, excessive use of alcohol such that it interferes
with the health, personal relationships, and livelihood of the drinker.
The active ingredient in most common alcoholic beverages is ethanol or ethyl alcohol,
yet other impurities including enanthic eathers, amyl alcohol, and acetaldehyde may
be contained in some liquor152
Types of Alcohol
The alcohols are classified mainly based on their number of hydroxyl group as
follows
Monohydric aromatic alcohols: benzyl alcohol, C6H5CH2OH and Cinnamyl alcohol,
C6H5CH = CHCH2OH, occur both free and as esters of benzoic and cinnamic acids.
Polyhydric aliphatic alcohols: the following are the alcohols with either four or six
hydroxyl groups. Erythritol, CH2OHCHOHCHOH CH2OH, is found in certain lichens
both free and combined with lecanoric acid.
Monohydric terpene alcohols: 1) noncyclic terpene alcohols occur in many volatile
oils for example, geraniol in otto of rose 2) monocyclic terpene alcohols aree
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 43
represented by terpineol and its acetate in neroli nad menthol 3) dicyclic terpene
alcohols are particularly abundant in the Coniferae (e.g sabinol and its acetate in
Juniperus Sabina)
Amino alcohols: Ecgonine and hydroxyl derivates of tropine are basic heterocyclic
compounds which occur either free or as esters in some of the Erythroxylacea,
Convolvulaceae and Solanaceae.153
Different Alcoholic Beverages:154
There are many alcoholic beverages available in the market those are differ from one
another based on the starch used for their preparation.
A. Malted liquors: produced by fermentation of germinating cereals: are undistilled
– alcohol content is low (3 – 6 %) e. g. Beers, Stout.
B. Wines: produced by fermentation of natural sugars as present in grapes and other
fruits. These are also undistilled.
Light wines: Claret, Cider alcohol content is 9 – 12 % cannot exceed 15%
Fortified wines: Port, Sherry (alcohol 16 – 22 %): distilled beverages are added
from outside
Effervescent wines: Champagne (12 – 16 % alcohol): bottled before fermentation is
complete
Wines are called „Dry‟ when all sugar present has been fermented and „Sweet‟ when
some is left.
C. Spirits: These are distilled after fermentation, alcohol content 40 – 55 %, eg. –
Rum, Gin, Whiskey, Brandy, vodka etc.
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 44
The taste, flavour and value of alcoholic beverages depend not only on alcohol
content but on presence of higher ethers, higher alcohols, aldehydes, esters, and
volatile oils: many of these are formed during the „maturation‟ of the beverage.
Other forms of alcohol:
i. Absolute alcohol: 99 % w/w/ ethanol (dehydrated alcohol).
ii. Rectified spirit: 90 % w/w ethyl alcohol – produced from mollases, by
distillation.
PHARMACOLOGY:
One cannot understand alcohol-related disorders without knowing something about
alcohol itself, what is alcohol, how it digests, absorbed, metabolise and excreted out
of the body.
Wine, beer, and such distilled spirits as whiskey, gin, and vodka differ in their content
of components other than alcohol. These congeners are responsible for much of the
characteristic taste of the beverage and consist of combinations of methanol, butanol,
aldehydes, phenols, tannins, lead, cobalt, iron, and other substances. Under certain
circumstances, congeners can have physiological effects, but their potency pales in
comparison with the effects of alcohol.
Properties and Metabolism of Alcohol155
Absorption:
Ethanol (beverage alcohol) is a simple molecule that is well absorbed through the
mucosal lining of the digestive tract in the mouth, esophagus, and stomach. The most
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 45
prominent area of uptake, however, is in the proximal small intestine, which is also
the site of absorption of many of the B vitamins. Ethanol rapidly enters the
bloodstream and, as a result of its high solubility in water, is distributed to almost
every body system. As a consequence of its modest fat solubility, alcohol is likely to
have effects on body membranes rich in fat, including neurons.
A Drink: 156
A standard drink of an alcoholic beverage is usually defined as containing 10 to 12
gm of ethanol. In round figures, this is the amount of alcohol contained in
approximately 12 oz of beer (which, in the United States, has approximately 3.6
percent ethanol), 4 oz of table wine (containing approximately 12 percent ethanol),
and between 1.0 and 1.5 oz of 80-proof spirits (containing 40 percent ethanol).
Blood alcohol level: 155
For an average 70-kg (155 lb) person who has an average amount of body fat, one
drink is likely to raise the blood alcohol level by approximately 15 to 20 mg/dL (the
same as 0.015 to 0.020 g/dL). The body subsequently metabolizes and excretes
approximately one drink per hour.
Factors influencing the absorption of alcohol:
The rate of absorption of alcohol from the digestive tract is likely to be faster on an
empty stomach than after a full meal, especially one rich in fats and carbohydrates.
Metabolism:
The major site of alcohol metabolism is the liver; small amounts are also metabolized
in the stomach, and kidneys. The most important enzyme is alcohol dehydrogenase
(ADH), which converts alcohol into acetaldehyde.
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 46
Metabolism in that organ occurs mostly through four pathways, with each resulting in
the production of acetaldehyde. Most of the process occurs through the actions of
alcohol dehydrogenase (ADH) in the cytosol of hepatic cells. Especially at high blood
alcohol levels, some of the alcohol is also broken down in the microsomes of the
smooth endoplasmic reticulum (the microsomal ethanol oxidizing system [MEOS]).
The ADH process is the usual rate-limiting metabolic step, occurring relatively slowly
because of the liver's need to handle the produced hydrogen ions through use of a
cofactor that is in relatively short supply, nicotinamide adenine dinucleotide (NAD).
The acetaldehyde produced primarily by ADH and MEOS is then destroyed by the
enzyme aldehyde dehydrogenase (ALDH) in both the liver cell cytosol and
mitochondria. This step occurs rapidly, with the result that the average person does
not have substantial levels of this substance. This is fortunate because, at high levels,
acetaldehyde can produce histamine release and other effects that, through a variety of
mechanisms, contribute to an increase and subsequent decrease in blood pressure
along with nausea and vomiting.
The ALDH and ADH isoenzyme patterns of an individual are related to the risk for
developing alcoholism. This is especially relevant to Asian (e.g., Japanese, Chinese,
Korean) men and women, although the impact of genes that control ADH also extends
to some other groups.
Gastric metabolism:
Alcohol metabolism begins in the stomach by the activity of gastric (ADH). The
degree of metabolism depends upon several factors. It is greater with beverages such
as whisky with high ethanol content compared to low concentration drinks like beer.
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 47
Alcohol metabolism is less on empty stomach, because of rapid gastric emptying,
which explains the quick „high‟ people experience when drinking without food.
Gastric ADH is inhibited by drugs such as aspirin and H2 receptor blockers, resulting
in higher blood alcohol levels.
Hepatic metabolism:
In the liver, alcohol metabolism is carried out by two different enzyme systems.
Hepatic ADH located in the cytoplasm of the cells, plays the dominant role. Ethanol is
also metabolized in the endoplasmic reticulum by the microsomal ethanol
metabolizing system (MEOS), a part of the P450 enzymes. Acetaldehyde is again
produced but in addition, free oxygen radicals are released which are damaging to the
tissues. MEOS has a lower affinity for ethanol compared to ADH, therefore, at low
blood alcohol levels; ADH is responsible for most of the ethanol metabolism, while at
higher levels, and MEOS also plays an important role.
Excreation: After absorption into the bloodstream from the small intestine, between 2
and 10 percent of the alcohol is then excreted unchanged from the lungs or the
kidneys or through sweat, but the majority is broken down in the liver.
Mechanism of action of Alcohol: 156
The mechanism of action of alcohol on the nervous system has been debated for
decades, and since the turn of the century, some investigators have speculated that
alcohol acts as a non specific drug, producing its action via perturbation of neuronal
membrane lipids. More recently, it has been suggested that ethanol acts at the
interface between membrane lipids and integral membrane proteins
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 48
Neurotransmitter gated ion channels have also been focus of attention regarding the
potential site of alcohol action, including nicotinic acetylcholine, GABAA, and N –
methyl – D – aspartate (NMDA) receptor – ion channels. Alcohol affects the function
of these receptors - ion channels mostly via direct interactions, yet the molecular
structure of the alcohol binding site has yet to be determined.
Tolerance to alcohol is defined as an acquired resistance to the effects of the drug,
which can be related to pharmacokinetics, pharmacodynamic, environmental and
behavioral factors. It has been hypothesized that tolerance represents an adaptive
changes in the CNS with mechanistic similarities to learning or memory function.
EFFECTS ON THE BODY: 157
Alcohol as a Depressant Drug; Neurochemical Effects of Ethanol:
Alcohol has major effects on most neurochemical systems, depending on the dose,
with opposite actions during intoxication and withdrawal. One series of theories on
the mechanisms underlying intoxication and subsequent craving focuses on changes
in dopamine, tying in the effects of alcohol to the pleasure centers in the limbic
system. Alcohol acutely increases dopamine and its metabolites, brain imaging
reveals enhanced activity in relevant areas of the brain, and chronic drinking changes
dopamine receptor numbers and sensitivity. Another key neurochemical is serotonin,
with alcohol causing changes in key aspects of this transmitter and associated
receptors, and levels of serotonin impact on the amount of alcohol consumed.
Additional studies point out the indirect actions that alcohol has on the
benzodiazepine receptor–sensitive γ-aminobutyric acid (GABA) complexes in the
brain. These effects, especially actions on the GABA type A receptor (GABAA),
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 49
enhance the acute sedating, sleep-inducing, anticonvulsant, and muscle-relaxing
effects of alcohol. Alcohol has potent effects on glutamate-gated ionophoric receptors,
especially those that bind N- methyl-D-aspartate (NMDA), which are muted during
intoxication and overactive during alcohol withdrawal. Finally, alcohol also acutely
enhances the functioning of the opioid-related brain systems and impacts on
adenosine, neurosteroids, and acetylcholine.
Tolerance:
With repeated administration of alcohol, larger and larger doses of the drug are
required to produce the desired effect. This phenomenon, called tolerance, is also the
ability to tolerate higher and higher doses of the substance and is the result of at least
three processes. Behavioral tolerance reflects the ability of a person to learn how to
perform tasks effectively despite the effects of alcohol. Pharmacokinetic tolerance is
an adaptation of the metabolizing systems, including ADH and MEOS, to rid the body
of alcohol rapidly. Finally, and most important, pharmacodynamic or cellular
tolerance is an adaptation of the nervous system so that it can function, despite very
high blood alcohol concentrations (e.g., as much as 600 mg/dL), by resisting the
actions of alcohol on the cell.
Once tolerance has developed for one of the brain depressants, an individual is likely
to demonstrate a similar reaction to a second drug of that class (cross-tolerance).
Therefore, a person who has been drinking heavily has tolerance for alcohol, and then
stops drinking can be expected to require a higher dose of benzodiazepines for sleep
induction. If the individual took two depressant drugs at the same time, tolerance is
not likely to be observed, and the mixing of the two substances can have lethal
effects.
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 50
Aspects of tolerance decrease and even disappear with consecutive weeks of
abstinence. In addition, some clinicians and researchers have described a phenomenon
of reverse tolerance, increased sensitivity, or sensitization. This is a complex situation
that might relate to neurochemical adaptations or other mechanisms. For example,
whether alcoholic or not, as people grow older, they have increasing levels of reaction
to most brain depressants, including alcohol. Even more dramatic examples of
increased reaction to alcohol are seen after severe brain damage (e.g., the consequence
of an auto accident or alcohol-related brain deterioration) and after impairment in any
of the major alcohol-metabolizing systems, as occurs in cirrhosis.
Craving:
The state of motivation to seek out alcohol is an important component of drinking
behavior. This phenomenon of craving, however, fluctuates with time and can be
difficult to measure. Aspects of the drive to drink are believed to relate to classical
conditioning and to also reflect neurochemical changes
Blackout:
Blackout indicates memory impairment (anterograde amnesia) for the period when
the person was drinking heavily but remained awake. This common phenomenon is
related to the ability of any brain depressant at high enough doses to interfere with the
acquisition of memory. Perhaps 40 percent of teenaged and young adult males have
had a blackout, and memory loss does not by itself indicate a high likelihood of
alcohol abuse or dependence. The blackout, which is temporary and limited to
memory problems involving a short period is not part of the DSM-IV-TR diagnosis
and is distinct from alcohol-induced persisting amnestic disorder, formerly known as
Wernicke-Korsakoff syndrome.
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 51
Effect on Sleep:
Alcohol intoxication can help a person fall asleep more quickly, but if the intake in an
evening is more than one or two drinks, the sleep pattern can be significantly
impaired. Most heavy drinkers awaken after several hours and can have problems
falling back asleep. Alcohol also tends to depress rapid eye movements (REMs) and
inhibit stage 4 sleep and, thus, is likely to be associated with frequent alternations
between sleep stages (sleep fragmentation) and with more dreams late in the night as
the blood alcohol level falls. Exaggerated forms of similar problems are seen in
alcoholics in whom sleep stages might not return to normal for 3 or more months of
abstinence.
Effect on nervous system: on Cerebellum:
Characterized by unsteadiness of gait, problems with standing, and mild nystagmus,
cerebellar degeneration is probably caused by a combination of the effects of ethanol
and acetaldehyde along with vitamin deficiencies. Treatment usually consists of total
abstinence and vitamin supplementation, although complete recovery is not usual.
Other Effects on the Central Nervous System:
Several rare but serious neurological and cognitive syndromes can also be observed in
alcohol-dependent men and women. A thiamine deficiency, especially in the context
of a preexisting vulnerability, such as a transketolase deficiency, can present as any of
several neurological syndromes, including a sixth cranial nerve palsy (Wernicke's)
and a severe anterograde amnesia that is out of proportion to the alcohol level of
confusion (Korsakoff's). Two additional central nervous system (CNS) syndromes are
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 52
often fatal, including a loss of myelin in the central pons that can present as
quadriplegia, lethargy, and cognitive impairment (central pontine myelinolysis) and a
thinning of the corpus callosum along with a change in consciousness, ataxia, and
possible dementia (Marchiafava-Bignami syndrome).
Beneficial Effects on the Body:
Under certain circumstances, one to two drinks per day can have some beneficial
effects. Low doses of ethanol appear to decrease the risk for myocardial infarction and
thrombotic stroke, probably through decreasing platelet aggregation and enhancing
the beneficial impact of high-density lipoprotein cholesterol. Additional
cardioprotective action may occur through antioxidant flavinoids or the inhibition of
the vasoconstrictor, endothelin-1, in the components of red wine. Low doses of
alcohol have also been reported to decrease the risks for some old-age dementias,
peripheral arterial disease, and gallstones.
Peripheral Neuropathy:
Approximately 10 percent of alcoholic people develop a deterioration of nerve
functioning to the hands and feet called peripheral neuropathy. The symptoms
include numbness of the hands and feet, often bilateral, frequently accompanied by
tingling and paresthesias. Although the condition is usually relatively mild and often
improves with abstinence, the pain and the numbness can result in a permanent
impairment.
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 53
Gastrointestinal Problems
The gastrointestinal (GI) system can be severely affected by heavy drinking, with a
relatively common problem of an acute and at times severe inflammation of the
esophagus or the stomach, often accompanied by vomiting and bleeding. If gastritis
occurs in the presence of dilated esophageal veins, as seen with cirrhosis, it can
induce potentially lethal bleeding.
Effect on Liver:
The liver and the pancreas are especially vulnerable to alcohol. In the liver, increasing
alcohol doses result in the accumulation of fats and proteins in the cells, producing a
reversible swelling often described as a fatty liver. Inflammation of the liver cells
accompanied by a subsequent intense increase in some liver function tests and other
signs of alcohol-induced inflammation, or hepatitis, can lead to the deposition of
excessive amounts of hyalin and collagen near blood vessels, an early stage of
cirrhosis, a condition only seen in approximately 15 percent of alcoholics. As damage
progresses, the normal flow of blood through the liver is impaired, dilated veins or
varices develop from the increased abdominal venous pressure, and fluid seeps from
the liver capsule, accumulating in the abdomen as ascites. As liver failure progresses,
secondary cognitive impairment can develop as various levels of hepatic
encephalopathy.
Effect on pancreas:
Perhaps 10 percent of alcoholic people develop an inflammation of the pancreas that
can present as the abdominal emergency of acute pancreatitis, which can lead to a
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 54
chronic irreversible condition with associated signs of insufficiency of both sugar
metabolism (a form of diabetes) and digestive enzymes. One corollary of even early-
stage effects of alcohol on the liver and pancreas is an abnormality in blood sugar
levels that often reverts to normal glucose tolerance with maintained abstinence.
Cardiovascular Problems:
Heavy intake of alcohol increases the blood pressure and elevates both LDL
cholesterol and triglycerides, thus enhancing the risk for myocardial infarction and
thrombosis. At high doses, alcohol is also a striated-muscle toxin with a resulting
deterioration in the heart muscle that manifests itself as beating irregularities and
signs of heart failure (alcoholic cardiomyopathy). Thus, it is not surprising that the
leading cause of early deaths in alcoholics is cardiovascular disease. Similar levels of
swelling of muscle cells and subsequent muscle pain can be observed in the skeletal
muscles.
Blood-Producing Systems
Alcohol intake of four to eight drinks or more per day decreases the production of
white blood cells and impairs the ability of those cells to migrate to sites of infection.
Such drinking can also affect the stem cells that produce the red blood components,
significantly increasing the average size of the red cell (the mean corpuscular volume
[MCV]), and can impair the production and the efficiency of blood platelets.
Cancer:
High rates of most cancers are seen in alcoholic people, especially those of the head,
neck, esophagus, stomach, liver, colon, lungs, and breast tissue. An enhanced risk for
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 55
breast malignancies might be seen with as few as two drinks per day, especially in
women with family histories of this disease. The association with cancer probably
reflects alcohol-related immune system suppression and the direct effects of ethanol
on mucosal membranes. The heightened rates of malignant tumors in alcoholic people
remain significant even when the possible effects of smoking and poor nutrition are
considered, and this is the second leading cause of premature death in alcohol-
dependent men and women.
Withdrawal syndromes:
The manifestation of alcohol withdrawal occur when a person decreases or stops a
high level alcohol intake, either after a binge lasting a matter of days or after the
regular ingestion of alcohol sustained over many months. Although the exact
mechanism are not known, most symptoms appear related to over activity of various
portions of the nervous system resembling a “rebound” phenomenon after profound
suppression, and its basis may relate to alterations in the functions of GABA or
NMDA receptor system. The earliest findings of alcohol withdrawal typically occur
within 6 to 8 hours of alcohol cessation. Tremulousness is the earliest and most
common complaint, and many alcoholics view their so called shakes as an indication
that it is time to resume drinking in order to avoid more severe complications of
withdrawal. Tremors appear within hours of cessation of alcohol ingestion and
gradually increase to peak within 1 or 2 days. The tremor is postural and appears to be
irregular due to its variable but large amplitude. The amplitude may increase at the
end points of an action, and the typical frequency varies from 6 to 11 Hz. This
movement abnormality mainly involves by hands it can cause titubation. The tremor
remits during relaxation and sleep but often persists for weeks after discontinuation of
Alcohol Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 56
alcohol consumption. The pathophysiological mechanisms of tremors are not known,
but it probably represents an exaggerated physiological tremor. The tremulousness is
associated with hyperacuity of all sensory modalities, hyper - reflexia, hypervigilince,
anxiety, tachycardia, hypertension and insomnia. The severity of these signs and
symptoms vary with the intensity and duration of the previous alcohol exposure. In
mild forms of withdrawal, the signs and symptoms usually resolve after 48 hours.
In severe reactions, patient may experience additional symptoms including
auditory hallucinations, which usually take the form of identifiable voices saying
critical or threatening things to the patients. When they occur, hallucinations generally
appear within 24 hours of withdrawal. At first, patients tend to accept the voice as real
and react accordingly, but as the intensity of hallucinations wanes, they recognize
their true origin. The hallucinations may be accompanied by global confusions, and
the autonomic hyperactivity continues and may become more pronounced.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 57
ALCOHOL-RELATED DISORDERS 158
The alcohol-related disorders impact on all aspects of health care delivery systems,
especially psychiatric practice. At least 20 percent of the patients in mental health
settings have alcohol abuse or dependence, including individuals from all
socioeconomic strata and both genders. A recent national evaluation of students on
college campuses reported a 12-month prevalence for alcohol dependence of 6
percent and for abuse more than 20 percent—and alcohol has been estimated to have
contributed to at least 15,000 deaths in students per year. Of particular importance to
the psychiatrist are the estimated 40 to 50 percent of alcoholics who develop alcohol-
induced, but temporary, clinical syndromes that resemble major depressive disorder,
panic disorder, generalized anxiety disorder, and additional mood or anxiety
conditions. In addition, men and women with several independent psychiatric
disorders have elevated risks for the future development of alcohol-related disorders,
including those with manic-depressive disease, schizophrenia, antisocial personality
disorder, panic disorder, and possibly generalized anxiety disorder.
These data emphasize the need for all health care providers, especially psychiatrists,
to develop and maintain skills for diagnosing and treating alcohol-related disorders.
Definition:
Alcohol Use Disorder: 159
In all diagnostic systems, the definition of alcoholism (i.e., alcohol abuse and
dependence) relates to evidence of repeated impairments from alcohol in multiple
areas of life functioning, despite which the person returns to drinking. According to
DSM-IV-TR, alcohol dependence is diagnosed as the repeated presence of at least
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 58
three of seven major areas of life impairment related to alcohol that cluster together in
the same 12-month period. These difficulties include tolerance, evidence of a
withdrawal syndrome when the drug is discontinued or intake is decreased, potential
interference with life functioning associated with spending a great deal of time using
the substance, and returning to use despite evidence of physical or psychological
problems. It is the syndrome of dependence for which the best data are available
regarding the usual clinical course of problems, appropriateness of treatment, and
potential importance of genetic factors. All patients with a possible alcohol use
disorder should first be evaluated for the presence of alcohol dependence. For those
who do not meet the criteria for this disorder, however, there is a second potential
syndrome to consider, abuse. Here, an individual who is not dependent on alcohol
demonstrates repeated problems within any 12-month period in any one or more of
four potential areas of difficulties. These include repeated legal, interpersonal, social,
or occupational impairments related to alcohol as well as use of alcohol in physically
unsafe situations. DSM-IV-TR reformulated the concept of abuse to identify criteria
that were not just a subset of those noted for dependence.
A similar definition of dependence is offered in the tenth revision of the International
Statistical Classification of Diseases and Related Health Problems (ICD-10). Here,
however, the threshold for diagnosis is any three of six (rather than seven) items.
ICD-10 also lists a second and less intense alcohol use disorder known as harmful
use. The definition of this second syndrome is quite different from DSM-IV-TR abuse
because the ICD-10 approach is based on evidence of repeated interference with
psychological and physical health functioning and does not include social impairment,
legal problems, or use in physically hazardous situations.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 59
Attempts have been made to further divide alcohol dependence into additional
clinically meaningful subgroups. Some authors have called for the recognition of a
more severe early-onset alcohol dependence syndrome, often accompanied by
criminality and dependence on other drugs, which has been labeled as type II or type
B alcoholism.
Epidemiology: 160
Psychiatrists need to be concerned about alcoholism because this condition is
common, intoxication and withdrawal mimic many major psychiatric disorders, and
the usual alcoholic person does not fit the common stereotype.
Prevalence of Drinking:
At some time during life, 90 percent of the population in the United States drinks,
with most people beginning their alcohol intake in the early to middle teens. By the
end of high school, 80 percent of students have consumed alcohol, and more than 60
percent have been intoxicated. At any time, two out of three men are drinkers, with a
ratio of persisting alcohol intake of approximately 1.3 men to 1.0 woman, and the
highest prevalence of drinking is from the middle or late teens to the mid-20s.
Very high rates of alcohol problems are found among most, but not all, American
Indian and Inuit tribes.
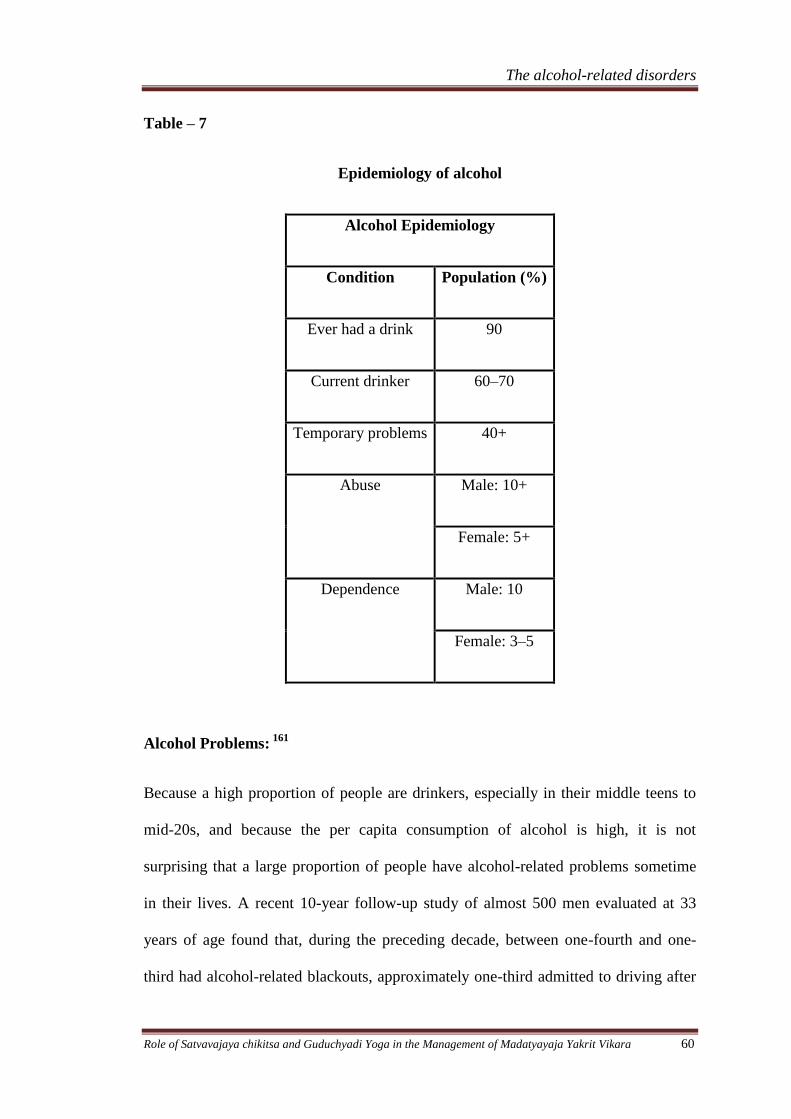
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 60
Table – 7
Epidemiology of alcohol
Alcohol Epidemiology
Condition Population (%)
Ever had a drink 90
Current drinker 60–70
Temporary problems 40+
Abuse Male: 10+
Female: 5+
Dependence Male: 10
Female: 3–5
Alcohol Problems: 161
Because a high proportion of people are drinkers, especially in their middle teens to
mid-20s, and because the per capita consumption of alcohol is high, it is not
surprising that a large proportion of people have alcohol-related problems sometime
in their lives. A recent 10-year follow-up study of almost 500 men evaluated at 33
years of age found that, during the preceding decade, between one-fourth and one-
third had alcohol-related blackouts, approximately one-third admitted to driving after
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 61
consuming enough alcohol to be impaired, and 20 percent reported missing school or
work because of either a hangover or a desire to party with alcohol rather than work.
As common and costly as these problems are, most people mature out of less severe
alcohol problems with the passage of time. Thus, the average person is likely to
experience fewer alcohol-related difficulties during their 30s than during their 20s,
and even fewer difficulties in their 40s and 50s.
Alcohol Abuse or Dependence: 161
The lifetime risk for alcohol dependence is approximately 10 to 15 percent for men
and 3 to 5 percent for women. The rate of alcohol abuse and dependence combined
may be as high as 20 percent for men and more than 10 percent for women. These
high rates have been reported for all socioeconomic and educational levels.
The age of peak onset of alcohol problems severe enough to lead to a diagnosis of
alcohol dependence is probably in the middle 20s to approximately 40 years of age.
Despite multiple difficulties, most alcohol-dependent people have jobs, families, and
relatively high levels of functioning. Thus, the stereotypical alcoholic person who is a
homeless street person is very much the exception rather than the rule, representing
only 5 percent of all people with severe, recurring alcohol-related difficulties.
Age-related differences are found in the pattern of alcohol-related problems. Earlier
the onset of alcoholism, greater the severity and higher the probability of a preexisting
independent psychiatric condition. Therefore, when alcohol dependence is noted in a
teenager, the person usually also has conduct disorder (e.g., early antisocial
personality disorder). In that instance, the alcohol-related problems are likely to be
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 62
associated with severe drug difficulties and antisocial problems in school and with
family or peers that occurred before the onset of alcohol dependence. At the other
extreme, although most alcoholic people have their problems early in life, possibly 10
percent or so have an onset of recurring difficulties after the age of 55 years. The late
onset of the disorder tends to be associated with less severe social difficulties and
more subtle signs and symptoms, but a greater likelihood of associated medical
problems than among younger alcoholic people.
Etiology162
Many factors affect the decision to drink, the development of temporary alcohol-
related difficulties in the teenage years and the 20s, and the development of alcohol
dependence. The initiation of alcohol intake probably depends largely on social,
religious, and psychological factors, although genetic characteristics might also
contribute. However, the factors that influence the decision to drink or those that
contribute to temporary problems might be different from those that add to the risk for
the severe, recurring problems of alcohol dependence.
It is likely that a series of genetic influences combine to explain approximately 60
percent of the proportion of risk for alcoholism, with environment responsible for the
remaining proportion of the variance. Therefore, the divisions are more heuristic than
real, as it is the combination of a series of psychological, sociocultural, biological, and
other factors that are responsible for the development of severe, repetitive alcohol-
related life problems.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 63
Psychological Theories:
A variety of theories relate to the use of alcohol to reduce tension, increase feelings of
power, and decrease the effects of psychological pain. Perhaps the greatest interest
has been paid to the observation that people with alcohol-related problems often
report that alcohol decreases their feelings of nervousness and helps them cope with
the day-to-day stresses of life. The psychological theories are built in part on the
observation among nonalcoholic people that the intake of low doses of alcohol in a
tense social setting or after a difficult day can be associated with an enhanced feeling
of well-being and an improved ease of interactions. However, in high doses,
especially at falling blood alcohol levels, most measures of muscle tension and
psychological feelings of nervousness and tension are increased. Thus, tension-
reducing effects of this drug might impact most on light to moderate drinkers or add
to the relief of withdrawal symptoms but play a minor role in causing alcoholism. The
theories that focus on alcohol's potential to enhance feelings of being powerful and
sexually attractive and to decrease the effects of psychological pain are difficult to
definitively evaluate.
Psychodynamic Theories:
Perhaps related to the inhibiting or anxiety-lowering effects of lower doses of alcohol
is the hypothesis that some people may use this drug to help them deal with self-
punitive harsh superegos and to decrease unconscious stress levels. Also, classic
psychoanalytical theory hypothesizes that at least some alcoholic people may have
become fixated at the oral stage of development and use alcohol to relieve their
frustrations by taking the substance by mouth. However, hypotheses regarding
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 64
arrested phases of psychosexual development, although heuristically useful, have had
little effect on the usual treatment approaches and are not the focus of extensive
ongoing research. Similarly, most studies have not been able to document an
―addictive personality‖ present in the majority of alcoholics and associated with a
propensity to lack of control of intake over a wide range of substances and foods.
Although pathological scores on personality tests are often seen during intoxication,
withdrawal, and early recovery, many of these characteristics are not found to predate
alcoholism, and most disappear with abstinence. Similarly, prospective studies of
children of alcoholics who themselves have no co-occurring disorders usually
document high risks mostly for alcoholism. As described below, one partial exception
to these comments occurs with the extreme levels of impulsivity seen in the 15 to 20
percent of alcoholic men with antisocial personality disorder, as these people have
high risks for criminality, violence, and multiple substance dependencies.
Behavioral Theories:
Expectations about the rewarding effects of drinking, cognitive attitudes toward
responsibility for one's behavior, and subsequent reinforcement after alcohol intake all
contribute to the decision to drink again after the first experience with alcohol and to
continue to imbibe despite problems. These issues are important in efforts to modify
drinking behaviors in the general population, and they contribute to some important
aspects of alcoholic rehabilitation.
Sociocultural Theories:
Sociocultural theories are often based on extrapolations from social groups that have
high and low rates of alcoholism. Theorists hypothesize that ethnic groups, such as
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 65
Jews, who introduce children to modest levels of drinking in a family atmosphere and
eschew drunkenness have low rates of alcoholism. Some other groups, such as Irish
men or some American Indian tribes with high rates of abstention but a tradition of
drinking to the point of drunkenness among drinkers, are believed to have high rates
of alcoholism. However, these theories often depend on stereotypes that tend to be
erroneous, and there are prominent exceptions to these rules. For example, some
theories based on observations of the Irish and the French have incorrectly predicted
high rates of alcoholism among the Italians.
Yet, environmental events, presumably including cultural factors, account for as much
as 40 percent of the alcoholism risk. The cultural attitudes toward drinking,
drunkenness, and personal responsibility for consequences are important contributors
to the rates of alcohol-related problems in a society. In the final analysis, social and
psychological theories are probably highly relevant, as they outline factors that
contribute to the onset of drinking, the development of temporary alcohol-related life
difficulties, and even alcoholism. The problem is how to gather relatively definitive
data to support or refute the theories.
Table – 8
Data Supporting Genetic Influences in Alcoholism
Close family members have a fourfold increased risk.
The identical twin of an alcoholic person is at higher risk than is a fraternal twin.
Adopted-away children of alcoholic people have a fourfold increased risk.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 66
Possible Biological Mediators of the Alcoholism Risk:
There appears to be a series of independent characteristics that impact the alcoholism
risk. First, as discussed earlier, genes on chromosome 12 that control ALDH and
those on chromosome 4 that relate to ADH can decrease the alcoholism risk. The
most relevant isoenzyme is the low Km ALDH2 located in the mitochondria of cells,
and the gene responsible for the ALDH2*2 polymorphism is seen in approximately 50
percent of Japanese, Chinese, and Korean individuals. If a person carrying this gene is
an ALDH2*2, 2*2 homozygote, they have inherited a disulfiram (or Antabuse)–like
aversive reaction to alcohol because they cannot metabolize low to moderate levels of
acetaldehyde and have almost no alcoholism risk. Heterozygotes (e.g., with
ALDH2*2, 2*1 alleles) have a mild to modest facial flush, enhanced heart rate, and a
moderately more intense (although not more aversive) response to alcohol. It has been
hypothesized that the higher response may contribute to a significant decreased risk
for alcohol use disorders, although the level of protection is much less for that seen
for homozygotes. However, if a person with this heterozygous genotype does develop
alcohol dependence, he or she may carry higher risks for damage to the brain, liver,
pancreas, and testes, perhaps as a consequence of higher acetaldehyde levels when
they drink. In addition, genes that impact on ADH2 and ADH3, which are more
prevalent among Asian, black, and Jewish individuals, might be responsible for a
slight increase in the rapidity of breakdown of alcohol, with a possible modest
increase in acetaldehyde. This has been hypothesized to have a relatively small
protective effect against alcohol use disorders, perhaps through enhancing the level of
response to alcohol.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 67
A second potentially important genetically influenced mechanism appears to relate to
genes that impact on impulsivity, sensation seeking, and disinhibition. Studies using
personality profiles and investigations incorporating electrophysiological measures of
disinhibition both report that these characteristics are seen at a higher-than-expected
prevalence among alcoholics, are observed in a substantial minority of children of
alcohol-dependent individuals, and are strongly related to yet-to-be-identified genes.
These findings might reflect the fact that more impulsive or disinhibited individuals,
who, at the extreme, have the antisocial personality disorder, are both more likely to
drink and less likely to demonstrate self-control when under the influence of alcohol.
Consistent with this hypothesis is the fact that this type of predisposition toward
substance-related disorders extends to all substances of abuse. An alternative
hypothesis is that alcohol or other drugs have specific brain effects that ameliorate
some of the consequences of the biological aspects of the disinhibition.
DIAGNOSIS AND CLINICAL FEATURES163
Alcohol use disorders are among the most common of the serious life-threatening
behavioral or psychiatric syndromes. It is difficult to know whether the person is
having alcohol related disorders or not because the average man or woman presenting
with severe and repetitive alcohol problems is likely to be neatly dressed, to show no
signs of severe alcohol withdrawal. The alcohol-related disorders in DSM-IV-TR and
also presents a comparable listing from ICD-10.
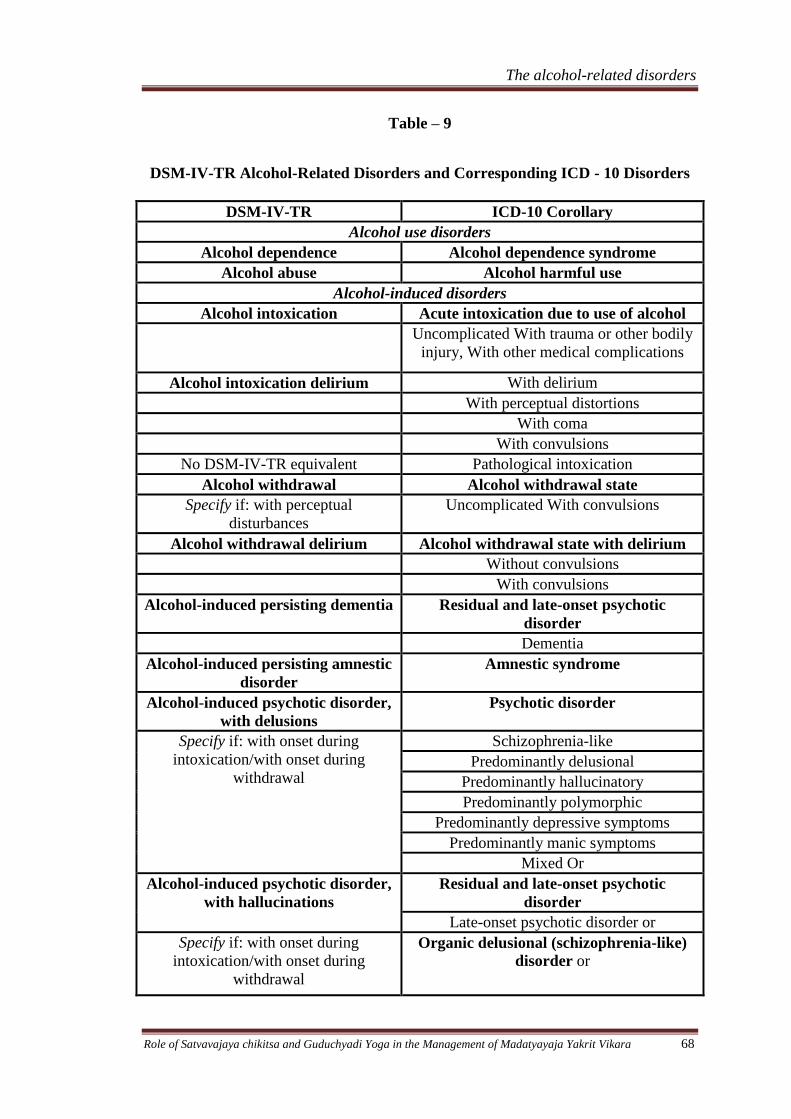
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 68
Table – 9
DSM-IV-TR Alcohol-Related Disorders and Corresponding ICD - 10 Disorders
DSM-IV-TR ICD-10 Corollary
Alcohol use disorders
Alcohol dependence Alcohol dependence syndrome
Alcohol abuse Alcohol harmful use
Alcohol-induced disorders
Alcohol intoxication Acute intoxication due to use of alcohol
Uncomplicated With trauma or other bodily
injury, With other medical complications
Alcohol intoxication delirium With delirium
With perceptual distortions
With coma
With convulsions
No DSM-IV-TR equivalent Pathological intoxication
Alcohol withdrawal Alcohol withdrawal state
Specify if: with perceptual
disturbances
Uncomplicated With convulsions
Alcohol withdrawal delirium Alcohol withdrawal state with delirium
Without convulsions
With convulsions
Alcohol-induced persisting dementia Residual and late-onset psychotic
disorder
Dementia
Alcohol-induced persisting amnestic
disorder
Amnestic syndrome
Alcohol-induced psychotic disorder,
with delusions
Psychotic disorder
Specify if: with onset during
intoxication/with onset during
withdrawal
Schizophrenia-like
Predominantly delusional
Predominantly hallucinatory
Predominantly polymorphic
Predominantly depressive symptoms
Predominantly manic symptoms
Mixed Or
Alcohol-induced psychotic disorder,
with hallucinations
Residual and late-onset psychotic
disorder
Late-onset psychotic disorder or
Specify if: with onset during
intoxication/with onset during
withdrawal
Organic delusional (schizophrenia-like)
disorder or
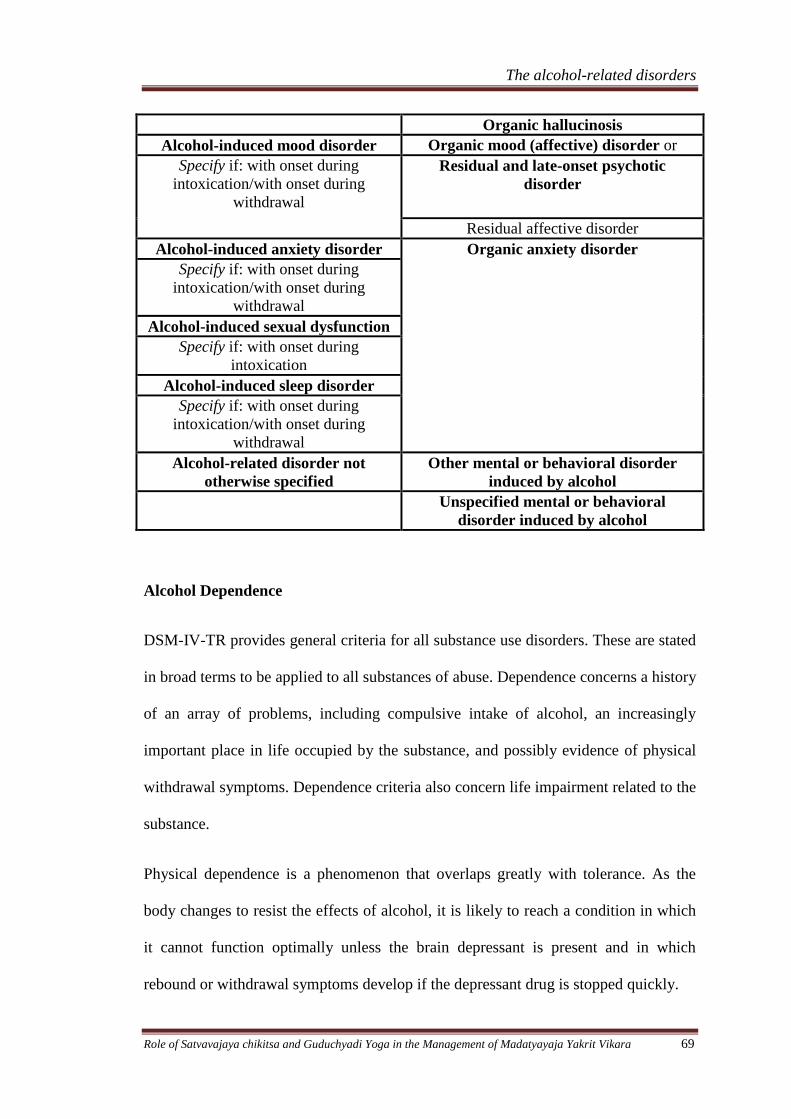
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 69
Organic hallucinosis
Alcohol-induced mood disorder Organic mood (affective) disorder or
Specify if: with onset during
intoxication/with onset during
withdrawal
Residual and late-onset psychotic
disorder
Residual affective disorder
Alcohol-induced anxiety disorder Organic anxiety disorder
Specify if: with onset during
intoxication/with onset during
withdrawal
Alcohol-induced sexual dysfunction
Specify if: with onset during
intoxication
Alcohol-induced sleep disorder
Specify if: with onset during
intoxication/with onset during
withdrawal
Alcohol-related disorder not
otherwise specified
Other mental or behavioral disorder
induced by alcohol
Unspecified mental or behavioral
disorder induced by alcohol
Alcohol Dependence
DSM-IV-TR provides general criteria for all substance use disorders. These are stated
in broad terms to be applied to all substances of abuse. Dependence concerns a history
of an array of problems, including compulsive intake of alcohol, an increasingly
important place in life occupied by the substance, and possibly evidence of physical
withdrawal symptoms. Dependence criteria also concern life impairment related to the
substance.
Physical dependence is a phenomenon that overlaps greatly with tolerance. As the
body changes to resist the effects of alcohol, it is likely to reach a condition in which
it cannot function optimally unless the brain depressant is present and in which
rebound or withdrawal symptoms develop if the depressant drug is stopped quickly.
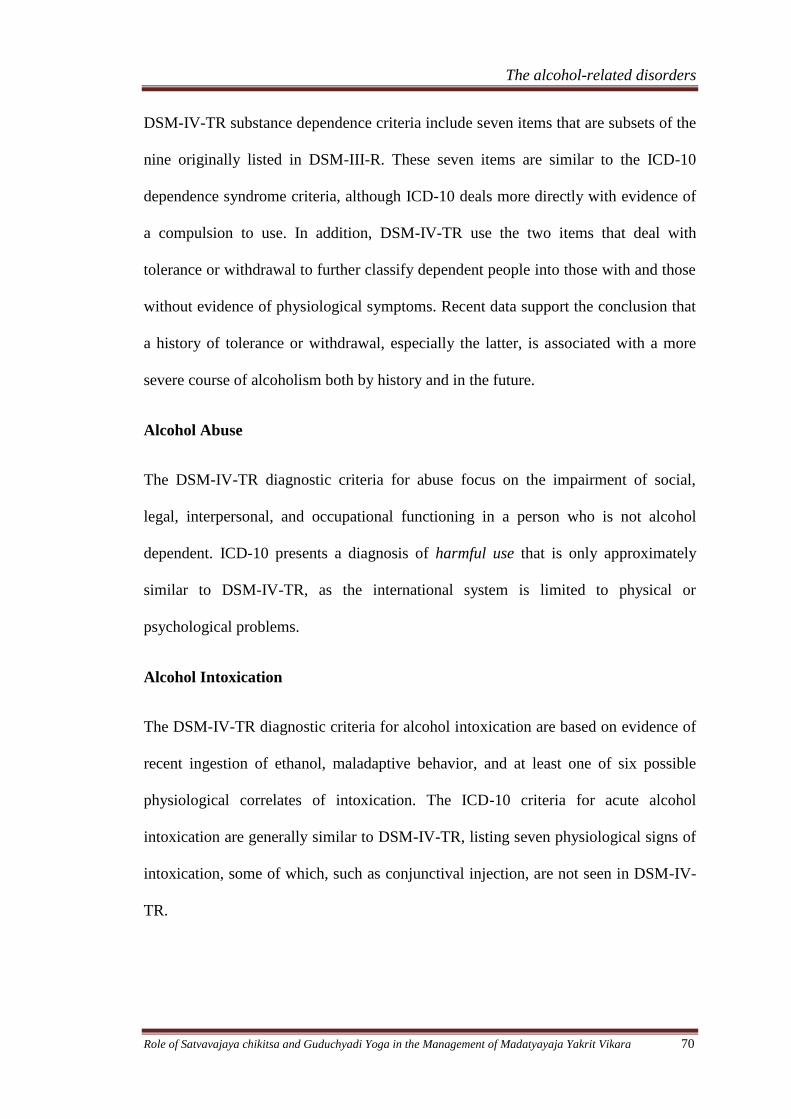
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 70
DSM-IV-TR substance dependence criteria include seven items that are subsets of the
nine originally listed in DSM-III-R. These seven items are similar to the ICD-10
dependence syndrome criteria, although ICD-10 deals more directly with evidence of
a compulsion to use. In addition, DSM-IV-TR use the two items that deal with
tolerance or withdrawal to further classify dependent people into those with and those
without evidence of physiological symptoms. Recent data support the conclusion that
a history of tolerance or withdrawal, especially the latter, is associated with a more
severe course of alcoholism both by history and in the future.
Alcohol Abuse
The DSM-IV-TR diagnostic criteria for abuse focus on the impairment of social,
legal, interpersonal, and occupational functioning in a person who is not alcohol
dependent. ICD-10 presents a diagnosis of harmful use that is only approximately
similar to DSM-IV-TR, as the international system is limited to physical or
psychological problems.
Alcohol Intoxication
The DSM-IV-TR diagnostic criteria for alcohol intoxication are based on evidence of
recent ingestion of ethanol, maladaptive behavior, and at least one of six possible
physiological correlates of intoxication. The ICD-10 criteria for acute alcohol
intoxication are generally similar to DSM-IV-TR, listing seven physiological signs of
intoxication, some of which, such as conjunctival injection, are not seen in DSM-IV-
TR.
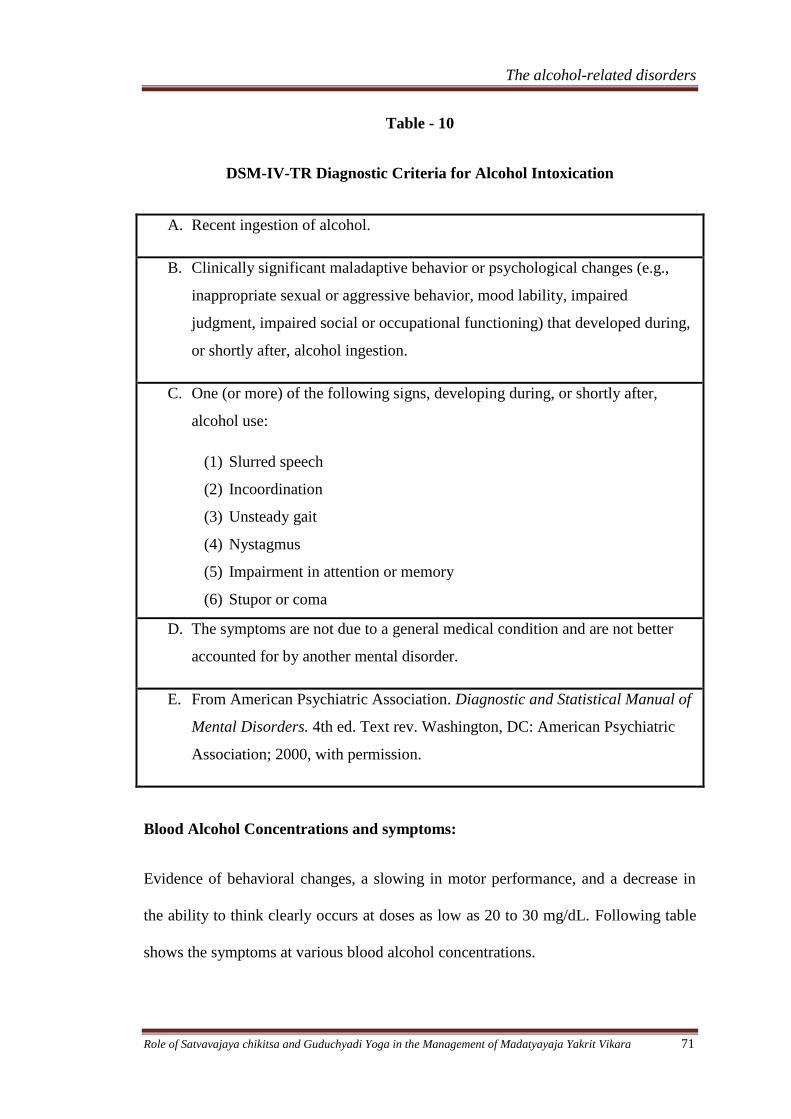
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 71
Table - 10
DSM-IV-TR Diagnostic Criteria for Alcohol Intoxication
A. Recent ingestion of alcohol.
B. Clinically significant maladaptive behavior or psychological changes (e.g.,
inappropriate sexual or aggressive behavior, mood lability, impaired
judgment, impaired social or occupational functioning) that developed during,
or shortly after, alcohol ingestion.
C. One (or more) of the following signs, developing during, or shortly after,
alcohol use:
(1) Slurred speech
(2) Incoordination
(3) Unsteady gait
(4) Nystagmus
(5) Impairment in attention or memory
(6) Stupor or coma
D. The symptoms are not due to a general medical condition and are not better
accounted for by another mental disorder.
E. From American Psychiatric Association. Diagnostic and Statistical Manual of
Mental Disorders. 4th ed. Text rev. Washington, DC: American Psychiatric
Association; 2000, with permission.
Blood Alcohol Concentrations and symptoms:
Evidence of behavioral changes, a slowing in motor performance, and a decrease in
the ability to think clearly occurs at doses as low as 20 to 30 mg/dL. Following table
shows the symptoms at various blood alcohol concentrations.
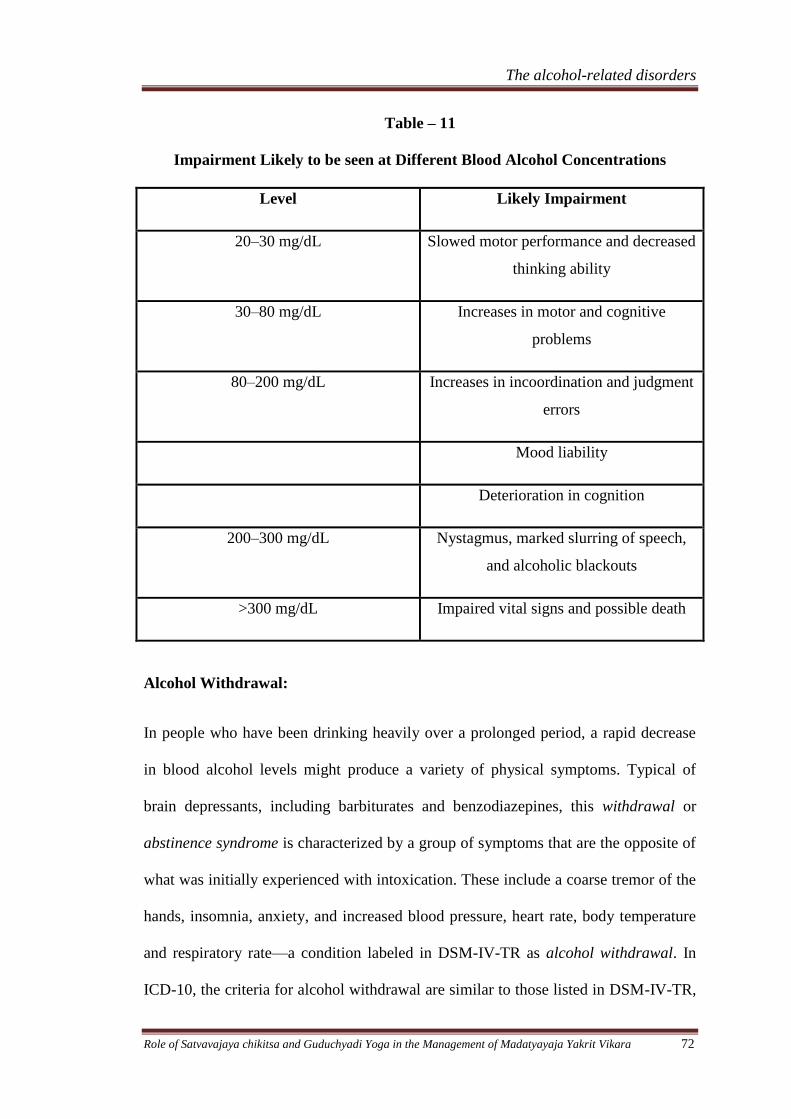
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 72
Table – 11
Impairment Likely to be seen at Different Blood Alcohol Concentrations
Level Likely Impairment
20–30 mg/dL Slowed motor performance and decreased
thinking ability
30–80 mg/dL Increases in motor and cognitive
problems
80–200 mg/dL Increases in incoordination and judgment
errors
Mood liability
Deterioration in cognition
200–300 mg/dL Nystagmus, marked slurring of speech,
and alcoholic blackouts
>300 mg/dL Impaired vital signs and possible death
Alcohol Withdrawal:
In people who have been drinking heavily over a prolonged period, a rapid decrease
in blood alcohol levels might produce a variety of physical symptoms. Typical of
brain depressants, including barbiturates and benzodiazepines, this withdrawal or
abstinence syndrome is characterized by a group of symptoms that are the opposite of
what was initially experienced with intoxication. These include a coarse tremor of the
hands, insomnia, anxiety, and increased blood pressure, heart rate, body temperature
and respiratory rate—a condition labeled in DSM-IV-TR as alcohol withdrawal. In
ICD-10, the criteria for alcohol withdrawal are similar to those listed in DSM-IV-TR,
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 73
with some differences in the specific items listed and the number of signs required
(i.e., three) to make a diagnosis. The DSM-IV-TR criteria for alcohol withdrawal also
require that the symptoms must cause clinically significant distress or impairment.
Although 95 percent or more of withdrawals are limited to these mild or moderate
symptoms, for 3 to 5 percent, the symptoms include convulsions or delirium.
Table - 12
DSM-IV-TR Diagnostic Criteria for Alcohol Withdrawal
A. Cessation of (or reduction in) alcohol use that has been heavy and prolonged.
B. Two (or more) of the following, developing within several hours to a few days
after Criterion A:
(1) Autonomic hyperactivity (e.g., sweating or pulse rate greater than 100)
(2) Increased hand tremor
(3) Insomnia
(4) Nausea or vomiting
(5) Transient visual, tactile, or auditory hallucinations or illusions
(6) Psychomotor agitation
(7) Anxiety
(8) Grand mal seizures
C. The symptoms in Criterion B cause clinically significant distress or impairment in
social, occupational, or other important areas of functioning.
D. The symptoms are not due to a general medical condition and are not better
accounted for by another mental disorder.
Specify if: With perceptual disturbances
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 74
Withdrawal phenomena are likely to begin within approximately 8 hours of
abstinence, reach peak intensity on the second or third day, and markedly diminish by
the fourth or fifth day. The symptoms persist in a more mild form for as many as 3 to
6 months or more as part of a protracted withdrawal syndrome, which might
contribute to relapse.
Alcohol Withdrawal Delirium
For the small proportion of intoxications and withdrawals that are accompanied by
severe cognitive symptoms, both DSM-IV-TR and ICD-10 list criteria for alcohol
intoxication delirium and alcohol withdrawal delirium When this agitated confusion
is associated with tactile or visual hallucinations, the diagnosis of alcohol withdrawal
delirium (also called delirium tremens) can be made. During withdrawal, some
alcoholic people show one or several grand mal convulsions, sometimes called rum
fits.
Identification in Clinical Settings:
Patients should be asked about patterns of problems related to accidents, interpersonal
difficulties, problems at work, encounters with the law and so on. When a problem is
apparent, one can then determine the time of day, the situation and the complaints
voiced by others. If an alcohol use disorder appears probable, the diagnostic criteria
can be reviewed along with a history of the quantity and frequency of alcohol intake.
Several relatively simple questionnaires can be used to preliminarily survey relevant
problem areas. Two useful examples are the Alcohol Use Disorders Identification
Test (AUDIT) and the Michigan Alcohol Screening Test (MAST), each of which
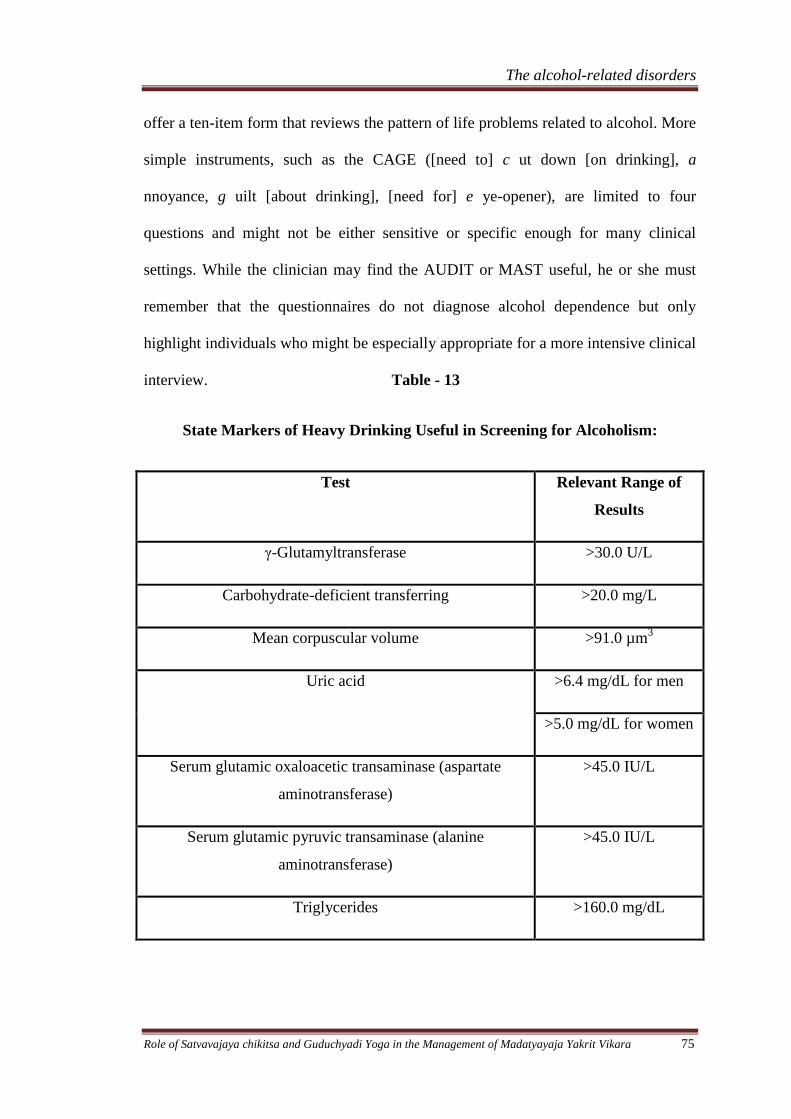
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 75
offer a ten-item form that reviews the pattern of life problems related to alcohol. More
simple instruments, such as the CAGE ([need to] c ut down [on drinking], a
nnoyance, g uilt [about drinking], [need for] e ye-opener), are limited to four
questions and might not be either sensitive or specific enough for many clinical
settings. While the clinician may find the AUDIT or MAST useful, he or she must
remember that the questionnaires do not diagnose alcohol dependence but only
highlight individuals who might be especially appropriate for a more intensive clinical
interview. Table - 13
State Markers of Heavy Drinking Useful in Screening for Alcoholism:
Test Relevant Range of
Results
γ-Glutamyltransferase >30.0 U/L
Carbohydrate-deficient transferring >20.0 mg/L
Mean corpuscular volume >91.0 µm3
Uric acid >6.4 mg/dL for men
>5.0 mg/dL for women
Serum glutamic oxaloacetic transaminase (aspartate
aminotransferase)
>45.0 IU/L
Serum glutamic pyruvic transaminase (alanine
aminotransferase)
>45.0 IU/L
Triglycerides >160.0 mg/dL
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 76
The MCV blood test, with perhaps 70 percent sensitivity and specificity, is useful
when the size of the red blood cell is 91 µm3 or more. The 120-day life span of the red
cell does not allow the test to be useful as an indicator of a return to drinking. Other
tests that can be helpful in identifying patients who are regularly consuming heavy
doses of alcohol include high normal values of uric acid (e.g., greater than 6.4
mg/dL), even mild elevations in the usual liver function tests, including aspartate
aminotransferase and alanine aminotransferase, and elevated levels of triglycerides or
LDL cholesterol.
A number of physical findings can also be useful. These include modest elevations in
blood pressure; frequent bruising; cancer of the head, neck, and upper digestive tract;
an enlarged liver; evidence of cirrhosis; and symptoms consistent with pancreatitis.
Differential Diagnosis:
Once the pattern of alcohol-related life problems has been established, the diagnosis
of alcohol abuse or dependence may be fairly obvious. To determine whether an
independent major psychiatric disorder exists or not; briefly, individuals who present
with clinically significant levels of depression, anxiety, or psychotic symptoms in
addition to their alcoholism should be evaluated using the timeline approach to
determine whether the psychiatric symptoms are likely to have been substance
induced (and are thus temporary) or represent independent and longer-term
psychiatric disorders.
Antisocial Personality Disorder:
When the emphasis on the chronological development of symptoms is used, at least
three diagnoses—antisocial personality disorder, schizophrenia, and bipolar I
disorder— are likely to run a course independent of alcohol abuse or dependence and
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 77
be true co morbid conditions. Antisocial personality disorder, listed on Axis II, begins
early in life and has major effects on many aspects of life functioning. The diagnosis
is based on evidence of severe antisocial behaviors in many areas beginning before
the age of 15 years and continuing into adulthood. People with antisocial personality
disorder are described as impulsive, frequently violent, highly likely to take risks, and
unable to learn from their mistakes or to benefit from punishment. A person who
carries these characteristics into adolescence, typically the time for experimentation
with alcohol and drugs, can be expected to have difficulty controlling substance use.
Thus, perhaps 80 percent or more of people with antisocial personality disorder are
likely to develop severe alcohol problems in the course of their lives. A diagnosis of
preexisting antisocial personality disorder with subsequent alcohol abuse or
dependence indicates someone who is more likely than the average alcohol-dependent
person to have severe coexisting drug problems, to be violent, to discontinue
treatment prematurely, and to have a less-than-optimistic prognosis.
Schizophrenia
A second disorder in which alcohol problems are more common than in the general
population is schizophrenia. Characterized by what is usually a slow onset of paranoid
delusions and auditory hallucinations in a clear sensorium and typically beginning in
the mid-teens to the 20s, schizophrenia is likely to be severe, long lasting, and
debilitating. Possibly because of a lack of long-term treatment facilities, people with
schizophrenia are likely to live in inner-city areas and to spend a great deal of time on
the streets. Because most alcohol treatment programs exclude actively psychotic
patients, people with schizophrenia rarely appear in inpatient alcohol settings, but
alcohol-related disorders are observed in 30 percent or so of schizophrenic people
being treated in public mental health facilities.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 78
Bipolar I Disorder
The third disorder in which severe alcohol problems are overrepresented is bipolar I
disorder. In a manic episode, the patient is hyperexcited and impulsive, carries out
most activities to excess, has poor judgment, and is likely to develop temporary
alcohol problems. Although the severity of the manic symptoms usually precludes
inpatient alcohol rehabilitation, alcohol-related difficulties must be evaluated in
histories taken from people with manic features entering mental health facilities.
However, bipolar II is difficult to evaluate in substance-dependent patients, as
intoxication, withdrawal, and adjustment to frequent changes in living situations can
easily mimic hypomania. This label should be reserved only for those with clear
hypomanic episodes antedating the alcoholism.
Major Anxiety Disorders
Finally, there are data from recent studies that support a small but statistically
significant association between independent (i.e., not alcohol induced) panic disorder
and perhaps independent social phobia and alcohol dependence. Although
approximately 90 percent of alcohol-dependent men and women did not have an
independent major anxiety disorder, and there was no evidence for a significant
increased risk for most major anxiety disorders, the rates of independent panic
disorder and independent social phobia were significantly higher than in controls.
Other Disorders
Debate in the literature continues about whether major depressive disorder,
agoraphobia, obsessive-compulsive disorder (OCD), posttraumatic stress disorder
(PTSD), and other major psychiatric diagnoses are overrepresented in the histories of
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 79
alcoholic people. Several studies indicate that, when the timeline method is used and a
history is obtained from multiple informants, little evidence is found for very high
rates of most independent psychiatric disorders among alcoholic people other than the
disorders noted above. Therefore, although the majority of alcoholic people have
temporary psychiatric symptoms, they are not more likely than are people in the
general population to carry an independent psychiatric syndrome other than the three
exceptions discussed above.
Finally, there are interesting and complex relations between alcoholism and
dependence on other drugs. Men and women with antisocial personality disorder
demonstrate a marked increased risk for dependence on multiple substances,
including alcohol. It is also probable that individuals with dependence on opioids and
stimulants (such as cocaine and amphetamines) exhibit an increased risk for alcohol
dependence, even in the absence of antisocial personality disorder. However,
although, as is true for the general population, many have used other substances, most
alcohol-dependent people do not meet the criteria for dependence on illicit drugs.
Several recent investigations of children of alcohol-dependent men and women, as
well as the large Collaborative Study on the Genetics of Alcoholism (COGA),
indicated that, once the effects of antisocial personality disorder were controlled,
alcohol dependence appeared to run relatively true within families, without evidence
of a marked crossover between alcoholism and most other dependencies. An
exception to this general rule is nicotine dependence, which has long been noted to be
elevated among alcohol-dependent individuals, a finding that has been hypothesized
to relate to either attempts to use nicotine to try to moderate some of the effects of
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 80
high doses of alcohol or withdrawal or a possible genetic relationship between
nicotine and alcohol dependence syndromes.
Course and Prognosis:
Several recent large-scale evaluations suggest that most subgroups of alcoholics are
more similar than different on the time course and prevalence of alcohol-related life
difficulties. The clinical courses of alcohol-dependent men and women are relatively
similar. Older alcohol-dependent individuals are more likely to have medical
problems, to take multiple medications, to experience more severe withdrawal
syndromes, and have a less extensive social support system. Again, these
characteristics reflect differences between older and younger individuals in general
more than they indicate unique aspects of alcoholism in the geriatric population.
Early Course
Patients with antisocial personality disorder who go on to develop alcoholism have an
early onset of drinking, intoxication, and alcohol-related problems, but that scenario is
not applicable to the other 80 to 90 percent of alcoholic men and 95 percent of
alcoholic women. Usually, alcoholic people have their first drink (other than taking a
sip from a parent's glass) between the ages of 13 and 15 years, the first intoxication is
likely to occur at 15 or 16 years of age, and the first evidence of a minor alcohol-
related problem is usually observed in the late teenage years. These milestones do not
differ significantly from what is expected for people in the general population who do
not later go on to develop alcohol abuse or dependence.
For the average person, the pattern of severe difficulties becomes apparent in the
middle 20s to the middle 30s when a constellation of symptoms of relatively great
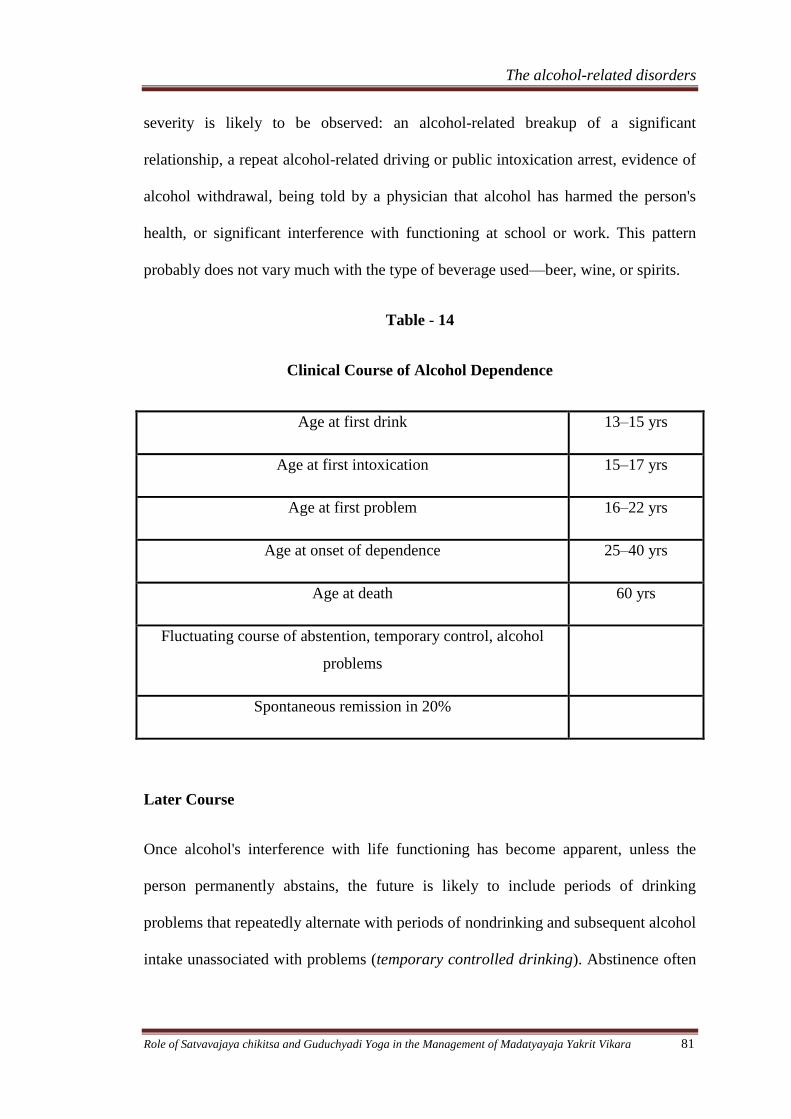
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 81
severity is likely to be observed: an alcohol-related breakup of a significant
relationship, a repeat alcohol-related driving or public intoxication arrest, evidence of
alcohol withdrawal, being told by a physician that alcohol has harmed the person's
health, or significant interference with functioning at school or work. This pattern
probably does not vary much with the type of beverage used—beer, wine, or spirits.
Table - 14
Clinical Course of Alcohol Dependence
Age at first drink 13–15 yrs
Age at first intoxication 15–17 yrs
Age at first problem 16–22 yrs
Age at onset of dependence 25–40 yrs
Age at death 60 yrs
Fluctuating course of abstention, temporary control, alcohol
problems
Spontaneous remission in 20%
Later Course
Once alcohol's interference with life functioning has become apparent, unless the
person permanently abstains, the future is likely to include periods of drinking
problems that repeatedly alternate with periods of nondrinking and subsequent alcohol
intake unassociated with problems (temporary controlled drinking). Abstinence often
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 82
develops in response to some interpersonal, social, or legal crisis and is likely to
produce only mild withdrawal symptoms. The usual alcoholic person is then likely to
use the temporary cessation of drinking problems to convince themselves that alcohol
is not really a cause for concern after all. Those periods of abstinence, lasting days to
months, are usually followed by times during which drinking rules are established and
are temporarily followed. The person is likely to consume only beer or wine (ignoring
that a glass of beer, a glass of wine, and a shot of whiskey have similar amounts of
alcohol) and tries to drink only at certain times of the day and under certain
conditions. This period of temporary control soon leads to an escalation of alcohol
intake, the accumulation of a new set of problems, and a subsequent crisis. These
events, in turn, are likely to precipitate a new period of temporary abstinence, and the
cycle begins again.
Thus, controlled drinking is a common but temporary condition for most alcoholic
people. Those who have less severe alcohol problems, such as abuse, are probably
more likely to have long-term and even permanent periods of control. However,
several research projects have indicated that long-term continued control is not likely
to be seen once a person meets the diagnostic criteria for alcohol dependence.
However, if drinking continues, the alcoholic is likely to decrease his or her life span
by 10 to 15 years as a result of many causes, including the marked increased risks for
heart disease, cancer, accidents, and suicide among alcoholic individuals. The reasons
for these enhanced mortality rates are likely to reflect the effects of alcohol described
in this chapter.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 83
Prognosis
Between 10 and 40 percent of alcoholic people enter some form of treatment during
the course of their alcohol problems. Although anyone might do well, there are a
number of favorable prognostic signs. First is the absence of preexisting antisocial
personality disorder or a diagnosis of other substance abuse or dependence. Second,
evidence of general life stability with a job, continuing close family contacts, and the
absence of severe legal problems also bodes well. Third, if the person stays for the
full course of the initial rehabilitation (perhaps 2 to 4 weeks), the chances of
maintaining abstinence are good. The combination of these three attributes predicts at
least a 60 percent chance for 1 or more years of abstinence. Few studies have
documented the long-term course, but researchers agree that 1-year rates are
associated with a good chance for continued abstinence over an extended period.
TREATMENT164
The elements of treatment appropriate for patients with severe alcohol problems are
fairly straightforward. The core of these efforts involves steps to maximize motivation
for abstinence, helping alcoholics to restructure their lives without alcohol, and taking
steps to minimize a return, or relapse, to substance-using behaviors. This cognitive
and behavioral approach is similar to efforts appropriate for any long-term disorder
that requires changes in lifestyles such as diabetes or hypertension. Much of the
clinical challenge comes in recognizing how prevalent the alcohol-related disorders
are, how often those conditions present with temporary symptoms of other psychiatric
syndromes, and how to use clinical clues, physical findings, and laboratory tests to
identify alcoholism.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 84
Three general steps are involved in treating the alcoholic person once the disorder has
been diagnosed: intervention, detoxification, and rehabilitation. Those approaches
assume that all possible efforts have been made to optimize medical functioning and
to address psychiatric emergencies. Thus, for example, the alcoholic person with
symptoms of depression severe enough to be suicidal requires inpatient
hospitalization for at least several days until the suicidal ideation disappears, even if it
is a temporary alcohol-induced mood disorder. Similarly, the person presenting with
cardiomyopathy, liver difficulties, or GI bleeding first needs adequate attention paid
to the medical emergency.
The patient with alcohol abuse or dependence must then be brought face to face with
the reality of the disorder (intervention), be detoxified if needed, and begin
rehabilitation. The essentials of these three steps for alcoholic people with and
without independent psychiatric syndromes are quite similar. However, in the former
case, the treatments are often applied after the psychiatric disorder has been stabilized
to the maximum degree possible.
Intervention:
The goal in this step is to break through feelings of denial and to help the patient
recognize the adverse consequences likely to occur if the disorder is not treated.
Intervention is a process aimed at increasing to as high a level as possible the levels of
motivation for treatment and for continued abstinence.
This procedure often involves convincing patients that they are responsible for their
own actions while reminding them how alcohol has created significant life
impairments. The psychiatrist often finds it useful to take advantage of the person's
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 85
chief presenting complaint, whether it is insomnia, difficulties with sexual
performance, an inability to cope with life stresses, depression, anxiety, or psychotic
symptoms. The emphasis is then placed in teaching the patient how alcohol has either
created or contributed to these problems and reassuring the patient that abstinence can
be achieved with a minimum of discomfort.
A more systematic approach to this process has been described as various forms of
intervention that might fall under the heading of a brief intervention using
motivational interviewing. Here, the clinician gains an alliance with the patient by
demonstrating an understanding of his or her viewpoint while encouraging the
individual to think through consequences associated with alcohol and the way that
changing behaviors might produce benefits. During this process, it is important to
recognize the patient's ambivalence toward abstinence and to show sensitivity in
monitoring the person's readiness to change. Resistance on the part of the patient is
best handled through discussion and problem solving rather than direct confrontation.
Reaching out to the Family:
The family can be of great help in the intervention. Members must learn not to protect
the patient from the problems caused by alcohol, or else the patient may not be able to
generate the energy and the motivation necessary to stop drinking.
During the intervention stage, the family can suggest that the patient meet with people
who are themselves recovering from alcoholism, perhaps through AA, and they
themselves can attend groups, such as Al-Anon, that reach out to family members.
Those support groups help family members and friends see that they are not alone in
their fears, worry, and feelings of guilt. Members share coping strategies and help
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 86
each other find community resources. The groups can be most useful in helping
family members rebuild their lives, even if the alcoholic person refuses to seek help.
Detoxification:
Most people with alcohol dependence have relatively mild symptoms when they stop
drinking. If the patient is in relatively good health, adequately nourished, and has a
good social support system, the depressant withdrawal syndrome usually resembles a
mild case of the flu. Even intense withdrawal syndromes rarely approach the severity
of symptoms described by some early textbooks.
The essential first step in detoxification is a thorough physical examination. In the
absence of a serious medical disorder or combined drug dependence, severe alcohol
withdrawal is unlikely. The second step is to offer rest, adequate nutrition, and
multiple vitamins, especially those containing thiamine.
Mild or Moderate Withdrawal:
Withdrawal develops because the brain has physically adapted to the presence of a
brain depressant and cannot function adequately in the absence of the drug. Giving
enough of a brain depressant on the first day to diminish symptoms and then weaning
the patient off the drug over the next 5 days offers most patients optimal relief and
minimizes the possibility that a severe withdrawal will develop. Any depressant,
including alcohol, barbiturates, or a benzodiazepine, can work, but most clinicians
choose a benzodiazepine for its relative safety. Adequate treatment can be given with
either short-acting drugs, such as lorazepam (Ativan), or long-acting substances such
as chlordiazepoxide (Librium) and diazepam (Valium).
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 87
A social model program of detoxification saves money by avoiding medications while
using social supports. This less expensive regimen can be helpful for mild or
moderate withdrawal syndromes. Some clinicians have also recommended β-
adrenergic receptor antagonists, such as propranolol (Inderal), or α-adrenergic
receptor agonists, such as clonidine (Catapres), although these medications do not
appear to be superior to the benzodiazepines. Unlike the brain depressants, these other
agents do little to decrease the risk of seizures or delirium.
Severe Withdrawal:
For less than 1 percent of alcoholic patients with extreme autonomic dysfunction,
agitation, and confusion—that is, those with alcoholic withdrawal delirium, also
called delirium tremens—no perfect treatment has been found. The first key step is to
ask why such a severe and relatively uncommon withdrawal syndrome has occurred;
the answer often relates to a concomitant medical problem that needs immediate
treatment. The withdrawal symptoms can then be minimized either through the use of
benzodiazepines (in which case high doses are sometimes required), or through
antipsychotic agents such as haloperidol (Haldol). Once again, doses are used on the
first or second day to control behavior, and the patient can be weaned off the
medication by approximately the fifth day.
Another 1 percent or so of patients may have a single grand mal convulsion; the rare
person has multiple fits, and the peak incidence is on the second day of withdrawal.
Such patients require a neurological evaluation, but in the absence of evidence of a
seizure disorder, they do not benefit from anticonvulsant drugs.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 88
Protracted Withdrawal:
Finally regarding withdrawal, symptoms of anxiety, insomnia, and mild autonomic
over activity are likely to continue for 2 to 6 months after the acute withdrawal has
disappeared. Although no pharmacological treatment for this syndrome appears
appropriate, it is possible that some of the medications discussed below, especially
acamprosate (Campral), may work, at least in part, by diminishing some of these
symptoms. In any event, it is important that the clinician warn the patient that some
levels of sleep problems or feelings of nervousness might remain after acute
withdrawal and discuss cognitive and behavioral approaches that might be appropriate
to helping the patient feel more comfortable. At least theoretically, these protracted
withdrawal symptoms may enhance the probability of relapse.
Rehabilitation:
For most patients, rehabilitation includes three major components: (1) continued
efforts to increase and maintain high levels of motivation for abstinence, (2) work to
help the patient readjust to a lifestyle free of alcohol, and (3) relapse prevention.
Because these steps are carried out in the context of distractions inherent in acute and
protracted withdrawal syndromes and life crises, treatment requires repeated
presentations of similar materials that remind the patient how important abstinence is
and that help the patient develop new day-to-day support systems and coping styles.
No single major life event, traumatic life period, or identifiable psychiatric disorder is
known to be a unique cause of alcoholism. In addition, the effects of any causes of
alcoholism are likely to have been diluted by the effects of alcohol on the brain and
the years of an altered lifestyle so that the alcoholism has developed a life of its own.
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 89
This is true even though many alcoholic people believe that the cause was depression,
anxiety, life stress, or pain syndromes. Research, data from records, and resource
people usually reveal that the alcohol contributed to the mood disorder, accident, or
life stress, not vice versa.
The same general treatment approach is used in inpatient, as well as outpatient,
settings. The selection of the more expensive and intensive and perhaps a bit more
effective inpatient mode often depends on evidence of additional severe medical or
psychiatric syndromes, the absence of appropriate nearby outpatient groups and
facilities, and the patient's history of having tried but failed in outpatient care. The
treatment process in either setting involves intervention, optimizing physical and
psychological functioning, enhancing motivation, reaching out to family, and using
the first 2 to 4 weeks of care as an intensive period of help. Those efforts must be
followed by at least 3 to 6 months of less frequent outpatient care. The latter uses a
combination of individual and group counseling, the judicious avoidance of
psychotropic medications unless needed for independent disorders, and involvement
in such self-help groups as AA.
There are few data that indicate that it is necessary to carefully match specific aspects
of the patient's history with a particular type of treatment program. In general, most
investigations demonstrate relatively high rates of abstinence and improvement in life
functioning regardless of the type of therapeutic approach involved.
Counseling:
Counseling efforts in the first several weeks to months should focus on day-to-day life
issues to help patients maintain a high level of motivation for abstinence and to
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 90
enhance their levels of functioning. Psychotherapy techniques that provoke anxiety or
that require deep insights have not been shown to be of benefit during the early phases
of recovery and, at least theoretically, may impair efforts at maintaining abstinence.
Much time in counseling deals with how to build a lifestyle free of alcohol.
Discussions cover the need for a sober peer group, a plan for social and recreational
events without drinking, and approach for reestablishing communication with family
members and friends.
Many clinicians believe that cognitive and behavioral approaches can form a solid
base to these counseling sessions. The goal of these efforts is to help the patient learn
ways of coping while focusing on approaches for identifying life stresses. The
clinician can use role rehearsal, modeling, and role playing while encouraging
patients to practice these skills between sessions. At the same time, individuals are
encouraged to identify areas of problems in day-to-day functioning, paying special
attention to how they react to these challenges and the impact that substance use
might have on the outcomes.
Relapse Prevention:
The third major component of rehabilitation efforts, relapse prevention, begins with
identifying situations in which the risk for relapse is high. The counselor must help
the patient to develop modes of coping to be used when the craving for alcohol
increases or when any event or emotional state makes a return to drinking more likely.
An important part of relapse prevention is reminding the patient about the appropriate
attitude toward slips in which short-term experiences with alcohol can never be used
as an excuse for returning to regular drinking. Rather, recovery is a process of trial
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 91
and error; patients use slips when they occur to identify high-risk situations and to
develop more appropriate coping techniques.
Importance of the Family:
Most treatment efforts recognize the effects that alcoholism has on the significant
people in the patient's life, and an important aspect of recovery involves helping
family members and close friends to understand alcoholism and how rehabilitation is
an ongoing process that lasts for 6 to 12 months or more. Couples and family
counseling and support groups for relatives and friends help the people involved to
rebuild relationships, to learn how to avoid protecting the patient from the
consequences of any drinking in the future, and to be as supportive as possible of the
alcoholic patient's recovery program.
Medications:
If detoxification has been completed, and the patient is not one of the 10 to 15 percent
of alcoholic people who have an independent mood disorder, schizophrenia, or
anxiety disorder, there is little evidence in favor of prescribing psychotropic
medications for the treatment of alcoholism. Levels of anxiety and insomnia that can
linger for 6 months or more as part of a reaction to life stresses and protracted
abstinence should be treated with behavior modification approaches and reassurance.
Medications, including benzodiazepines, for these symptoms are likely to lose their
effectiveness much faster than the insomnia disappears; as a result, the patient may
increase the dose and have subsequent problems related to the prescribed drug.
Similarly, although low levels of sadness and mood swings can linger several months,
controlled clinical trials indicate no benefit in prescribing antidepressant medications
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 92
or lithium to treat the average alcoholic person who has no independent or long-
lasting psychiatric disorder. The mood disorder clears before the medications can take
effect, and patients who resume drinking while on the medications face significant
potential dangers. With little or no evidence that the medications are effective, the
dangers significantly outweigh any potential benefits from their routine use.
Data from recent years support the probable modest effect of two medications in
addition to the usual cognitive-behavioral approaches for treating alcohol dependence.
These have been hypothesized to possibly decrease the rewarding effects of alcohol if
an individual returns to drinking, diminish the symptoms of the protracted withdrawal
syndrome, or, perhaps, diminish feelings of craving.
The first drug is acamprosate, which is an analog of the amino acid neurotransmitter
taurine and structurally resembles GABA. Although the mechanism of action in
alcoholics is unknown, acamprosate does antagonize neuronal overactivity related to
the actions of the excitatory neurotransmitter glutamate, at least in part by acting as an
antagonist to NMDA receptors. Thus, one possibly important mechanism for this drug
may be in diminishing anxiety, mood swings, and other sleep difficulties associated
with the subacute and protracted withdrawal syndrome observed after the first 4 to 5
days of alcohol abstinence.
The second promising medication is the long-acting, oral, opioid antagonist
naltrexone. This agent has been marketed for many years for the treatment of acute
opioid overdose as well as to help more highly motivated opioid-dependent
individuals maintain abstinence through knowledge that because of the use of this
blocking drug they could not achieve intoxication. Naltrexone works by blocking
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 93
opioid receptors in the brain and, thus, at least indirectly changing the levels of brain
activity regarding dopamine and serotonin. In alcohol-dependent individuals,
naltrexone and its cousin nalmefene have been hypothesized to decrease the
rewarding effects of a drink or to diminish craving.
A third drug of possible interest in the treatment of alcoholism is the alcohol-
sensitizing agent disulfiram which is usually given in doses of 250 mg per day. The
goal is to place the patient in a condition in which drinking alcohol precipitates an
uncomfortable physical reaction, including nausea, vomiting, and changes in blood
pressure. However, few data convincingly prove that disulfiram is more effective than
a placebo, probably because most people stop taking the disulfiram when they resume
drinking. Many clinicians have stopped routinely prescribing the agent, partly in
recognition of the dangers associated with the drug itself, including mood swings, rare
instances of psychosis, the possibility of an increase in peripheral neuropathies, the
relatively rare occurrence of other significant neuropathies, and a rare but potentially
fatal hepatitis. Moreover, patients with preexisting heart disease, cerebral thrombosis,
diabetes, and a number of other conditions cannot be given disulfiram because an
alcohol reaction to the disulfiram could be fatal.
Several additional medications are worth brief mention. First, a recent study evaluated
the possibility that an antagonist of the serotonin 3 receptor, ondansetron, might be
better than placebo in treating alcoholics who have an early-onset severe form of their
disorder associated with multiple drug dependencies and criminality. However, this
drug showed no superiority to placebo for the treatment of the usual alcoholic. A
second medication with some potential promise in the treatment of alcoholism is the
nonbenzodiazepine antianxiety drug buspirone, although the effect of this drug on
The alcohol-related disorders
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 94
alcohol rehabilitation is inconsistent between studies. However, at the same time,
there is no evidence that antidepressant medications, such as the selective serotonin
reuptake inhibitors (SSRIs), lithium, or antipsychotic medications, are significantly
effective in the treatment of alcoholism. Another physical treatment, acupuncture, has
been evaluated, although the results are not promising.
Self-Help Groups:
Clinicians must recognize the potential importance of self-help groups such as
Alcoholic Anonymous (AA). Members of AA have help available 24 hours a day,
associate with a sober peer group, learn that it is possible to participate in social
functions without drinking, and are given a model of recovery by observing the
accomplishments of sober members of the group. Learning about AA usually begins
during inpatient or outpatient rehabilitation. The clinician can play a major role in
helping patients understand the differences between specific groups. Some are
comprised only of men or women, and others are mixed; some meetings are
comprised mostly of blue collar men and women, whereas others are mostly for
professionals; some groups place great emphasis on religion, and others are eclectic.
Patients with coexisting psychiatric disorders may need some additional education
about AA. The clinician should remind them that some members of AA may not
understand their special need for medications and should arm the patients with ways
of coping when group members inappropriately suggest that the required medications
be stopped. Although difficult to evaluate using double-blind controls, most studies
indicate that participation in AA is associated with improved outcomes, and
incorporation into treatment programs saves money.
Alcoholic Liver Disease Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 95
ALCOHOLIC LIVER DISORDER
Alcoholic liver disease is the major cause of liver disease in Western countries, (in
Asian countries, viral hepatitis is the major cause). It arises from the excessive
ingestion of alcohol. Even though millions of individuals drink alcohol on a regular
basis, only chronic heavy drinkers develop liver damage. How alcohol damages the
liver is not completely understood. It is known that alcohol produces toxic chemicals
like acetaldehyde which can damage liver cells, but why this occurs in only a few
individuals is still in debate. When alcohol damages the liver, the function of the
organ is not immediately compromised as the liver has a tremendous capacity to
regenerate and even when 75% of the liver is damaged, it continues to function as
normal. When alcohol is consumed chronically, it eventually results in liver scarring
or what is known as cirrhosis or end-stage alcoholic liver disease.
The risk factors presently known are: quantity of alcohol taken, type of alcohol (beer
and spirits have increased risk), gender (females are twice as susceptible to alcohol
related liver disease, presently explained by the difference in the ability to metabolize
it), hepatitis C infection, genetic factors (changes in the profiles of various enzymes
involved in the metabolism of alcohol, such as ADH, ALDH, CYP4502E1 ,
mitochondrial dysfunction, and cytokine polymorphism) and malnutrition and diet
(particularly vitamin A and E deficiencies). Generally it is believed that certain genes
increase metabolism of alcohol, which may increase risk of cirrhosis and even alcohol
related cancers. Alcohol-induced liver injury can be worsened by hepatitis. If one has
hepatitis B or hepatitis C and consumes alcohol, cirrhosis occurs sooner. Alcohol-
induced liver disease is also worsened in people who have iron overload. Malnutrition
can worsen alcohol-induced liver damage. Most alcoholics tend to eat poorly and
Alcoholic Liver Disease Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 96
often substitute alcohol as a meal. The liver has a great capacity to regenerate, but
without proper nutrition, it quickly fails.
Fatty liver
Fatty change or steatosis is the accumulation of fatty acids in liver cells which can be
seen as fatty globules under the microscope. Alcoholism causes development of large
fatty globules (macrovesicular steatosis) throughout the liver and can begin to occur
after a few days of heavy drinking. Development of Macrovesicular steatosis, small
fatty acid globules may have different causes, such as diabetes, obesity and starvation.
The mechanism of action in alcohol induced fatty liver involves an above average
NADH:NAD ratio caused by the heavy demands of alcohol metabolism, including
other damaging metabolites such as free radicals and acetaldehyde that are very toxic,
(Higuchi, Kato, Miura, & Ishi, 1996) Alcohol is metabolized by alcohol
dehydrogenase (ADH)into highly toxic acetaldehyde, then further metabolized by
aldehyde dehydrogenase (ALDH) into acetic acid which is oxidized into Carbon
Dioxide (CO2) and water (H2O). A higher NADH concentration induces fatty acid
synthesis (creation) while a decreased NAD level results in decreased fatty acid
oxidation (processing). Consequently, the higher levels of fatty acids signal the
hepatocytes (liver cells) to compound it to glycerol to form triglycerides.
Alcoholic hepatitis
Between 10% and 35% of heavy drinkers develop alcoholic hepatitis (NIAAA, 1993).
Acute hepatitis or inflammatory reaction of cells affected by fatty change. While
development of hepatitis is not directly related to the dose of alcohol, some people
seem more prone to this reaction than others. This is called alcoholic steatonecrosis
and the inflammation appears to predispose to liver fibrosis.
Alcoholic Liver Disease Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 97
Cirrhosis
Between 10% to 20% of heavy drinkers will develop Cirrhosis of the liver.(NIAAA,
1993) Cirrhosis is a late stage of serious liver disease marked by inflammation
(swelling), fibrosis (cellular hardening) and damaged membranes preventing
detoxification of chemicals in the body, ending in scarring and necrosis (cell death.)
Symptoms include jaundice (yellowing), liver enlargement, and pain and tenderness
from the structural changes in damaged liver architecture. It is progressive and
without total abstinence from alcohol use, (80% of alcohol passes through the liver to
be detoxified) will eventually lead to liver failure. Late complications of cirrhosis or
liver failure include portal hypertension (high blood pressure related to kidney
problems), coagulation disorders blood clotting is impaired, ascites (heavy abdominal
swelling due to build up of fluids in the tissues) and other complications, including
hepatic encephalopathy and the hepatorenal syndrome.
Cirrhosis can also result from other causes than alcohol abuse, such as viral hepatitis
and heavy exposure to toxins other than alcohol. The late stages of cirrhosis may look
similar medically, regardless of cause. This phenomenon is termed the "final common
pathway" for the disease.
Fatty change and alcoholic hepatitis with abstinence can be reversible. The later
stages of fibrosis and cirrhosis tend to be irreversible, but can usually be contained
with abstinence for long periods of time.
Diagnosis:
There are many tests to assess alcoholic liver damage. Besides blood examination,
doctors use ultrasound and a CT scan to assess liver damage. In some cases a liver
Alcoholic Liver Disease Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 98
biopsy is performed. This minor procedure is done under local anesthesia, and
involves placing a small needle in the liver and obtaining a piece of tissue. The tissue
is then sent to the laboratory to be examined under a microscope.
Treatment:
The first treatment of alcohol-induced liver disease is cessation of alcohol
consumption. This is the only way to reverse liver damage or prevent liver injury
from worsening. Without treatment, most patients with alcohol-induced liver damage
will develop liver cirrhosis.
Other treatment for alcoholic hepatitis include:
Nutrition:
Doctors recommend a calorie-rich diet to help the liver in its regeneration process.
Dietary fat must be reduced because fat interferes with alcohol metabolism. The diet
is usually supplemented with vitamins and dietary minerals (including calcium and
iron).
Many nutritionists recommend a diet high in protein, with frequent small meals eaten
during the day, about 5-6 instead of the usual 3. Nutritionally, supporting the liver and
supplementing with nutrients that enhance liver function is recommended. These
include carnitine, which will help reverse fatty livers, and vitamin C, which is an
antioxidant, aids in collagen synthesis, and increases the production of
neurotransmitters such as norepinephrine and serotonin, as well as supplementing
with the nutrients that have been depleted due to the alcohol consumption.
Eliminating any food that may be manifesting as an intolerance and alkalizing the
Alcoholic Liver Disease Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 99
body is also important. There are some supplements that are recommended to help
reduce cravings for alcohol, including choline, glutamine, and vitamin C. As research
shows glucose increases the toxicity of centrilobular hepatotoxicants by inhibiting cell
division and repair, it is suggested fatty acids are used by the liver instead of glucose
as a fuel source to aid in repair; thus, it is recommended the patient consumes a diet
high in protein and essential fatty acids, e.g. omega 3. Cessation of alcohol
consumption and cigarette smoking, and increasing exercise are lifestyle
recommendations to decrease the risk of liver disease caused by alcoholic stress.
Drugs
Abstinence from alcohol intake and nutritional modification form the backbone in the
management of ALD. Symptom treatment can include: corticosteroids for severe
cases, anticytokines (infliximab and pentoxifylline), propylthiouracil to modify
metabolism and colchicine to inhibit hepatic fibrosis.
Antioxidants
It is widely believed that alcohol-induced liver damage occurs via generation of
oxidants. Thus alternative health care practitioners routinely recommend natural
antioxidant supplements like milk thistle Unfortunately, there is no valid clinical data
to show that milk thistle truly works. Rambaldi A, Jacobs BP, Iaquinto G, Gluud C
(2005). "Milk thistle for alcoholic and/or hepatitis B or C liver diseases--a systematic
cochrane hepato-biliary group review with meta-analyses of randomized clinical
trials". Am. J. Gastroenterol. 100 (11): 2583–91. doi:10.1111/j.1572-
0241.2005.00262.x. PMID 16279916
Alcoholic Liver Disease Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 100
Transplant
When all else fails and the liver is severely damaged, the only alternative is a liver
transplant. While this is a viable option, liver transplant donors are scarce and usually
there is a long waiting list in any given hospital. One of the criteria to become eligible
for a liver transplant is to discontinue alcohol consumption for a minimum of six
months.[2]
Complications and prognosis
As the liver scars, the blood vessels become noncompliant and narrow. This leads to
increased pressure in blood vessels entering the liver. Over time, this causes a backlog
of blood (portal hypertension), and is associated with massive bleeding. Enlarged
veins also develop to bypass the blockages in the liver. These veins are very fragile
and have a tendency to rupture and bleed (varices). Variceal bleeding can be life-
threatening and needs emergency treatment. Once the liver is damaged, fluid builds
up in the abdomen and legs. The fluid buildup presses on the diaphragm and can make
breathing very difficult.[3]
As liver damage progresses, the liver is unable to get rid of
pigments like bilirubin and both the skin and eyes turn yellow (jaundice). The dark
pigment also causes the urine to appear dark; however, the stools appear pale. Also
with the progression of the disease, the liver can release toxic substances (including
ammonia) which then lead to brain damage. This results in altered mental state, and
may cause behavior and personality changes.
Drug Contrive
Drug Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 101
DRUG REVIEW
Many drugs have been explained in the management of complications of Madatyaya.
As Madatyayaja Yakrit Vikara is one of the complications and in this particular
condition mainly Pitta dosha is affected, agni dusti and ama are the main causes,
hence Guduchyadi Yoga is selected as the drug because of its deepana, pachaka and
pitta rechaka qualities. Guduchyadi Yoga is explained by Acharya Charaka, while
stating the yogas for the complication of Madatyaya in the Madatyaya chikitsa. The
ingredients and their compositions are explained below.
Guduchyadi Yoga:
This medicine contains four drugs viz. Guduchi, Bhadramusta, Nagara and Patola in
equal parts. This choorna can be given before food with luke warm water.
Guduchi:
Latin Name : Tinospora Cordifolia
Family : Menispermaceae
Synonyms : Madhuparni, Amrita, Chinnaruha,
Vatsadani, Tantrika, Kundalini,
Chakralakshanika
Habitat : All over India upto the height of 1000
Feet
Habit: Climber
Chemical composition: Alkaloid - Berberine
Glycoside - Giloin
Volatile oil and fatty acids present
Guna - Guru Snigdha
Drug Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 102
Rasa – Tikta, Kashaya
Vipaka - Madhura
Virya - Ushna
Doshkarma - Tridosha Shamak
Properties – Rasayana,Balya,Daurbalya hara,Daha Trishnahara.
Part used - Kaanda
Pharmacological Action :
The drug has been observed to relax smooth muscles of intestine, uterus and inhibit
constrictor response of histamine and acetyle choline on smooth muscles (Gupta et al.
1967).
Alcoholic extract of the stem shows activity against Eschorchia Coli. Oral
administration of the aqueous and alcoholic extract of the plant caused reduction in
fasting blood sugar in rabbit and rats. The bitter fraction of the aqueous extract caused
insignificant reduction in blood sugar level, it inhibited the adrenalin induced-hyper
glycaemic significantly (Gupta et al.1967).
Favourable influence on glucose tolerance was observed in rats administered aqueous
extract of Tinospora cordifolia for a month (Gupta et al. 1964).
The drug has further proved to be effective as anti-rheumatic and diuretic (Sisodia and
Laxmi narayan 1961) as well as having anti-inflammatory properties (Rai and Gupta
1966). They (1967) have further carried out experimental evaluation of the drug for
dissolution of urinary calculi.
Recently Patel et al. (1978) reported that the aqueous extract of the stem was found to
antagonise the effects of various agonists such as histamine,5 H-T bradykinin and
prostaglandins E1 and F2X on the smooth muscles of guinea pig and rat.
Drug Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 103
(Pharmacognosy of Indigenous drugs CCRAI).
Musta:
Botanical name:Cyperus rotundus
Family: Cyperaceae
Kula: Mustaka Kula
Synonyms: Jalada, Nagaramusta Ghana, Shirhira, Bhadra, Gudagranthi, Sugandhi,
Hima.
Classical categorization :
Charaka : Truptighna, Trushnanigrahana, Lekhaneeya, Kandughna, Stanya, Shodhana
Sushruta: Mustadi, Vachadi
Major chemical constituents :
Cyperotundone, Cyperolone, Stearic Acids, Myristic Acid, Starch, Gum,
Sugar.
Properties :
Rasa: Tikta , Katu , Kashaya
Guna : Ruksha , laghu
Virya : Sheeta
Vipaka : Katu
Karma : Kaphahara, lekhana, vishaghna, varnya, Twakdoshahara, Shothahara,
Stanyajanana, Medhya, Deepana, Pachana, Grahi.
Indications : Twakvikara, Apasmara, Aruchi, Agnimandhya, Ajeerna, Kasa,
Swasa, kandu, Jwara, Daurbalya.
Strotogamitva:
Dosha: Kaphahara, Pittahara
Drug Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 104
Dhatu: Rasa, Meda, Raktha
Mala: Purisha.
Organs : GIT.
Pharmacological Activities:
Tranquilizing, Anti-inflammatory, Antipyretic, Diuretic, Smooth muscle
relaxant.
Used part : Moola
Dose:
Churna : 1-3 grms
Shunti/Nagara:
Botanical name: Zinziber Officinale Roscoe
Family: Scitaminaceae
Synonyms: Shunti, Vishva, Nagara, Vishvabheshaja, Vishvoushadha, Katuranthi,
Katubhadra, Katushana, Sauparna.
Classical categorization:
Charaka : Truptighna, Arshoghna, Deepaniya, Shoolaprashamana, Trushnanigrahana,
Sushruta:Pippalyadi, Trikatu
Bhavaprakasha: Panchakola, Shadushana
Major chemical constituents:
Votatile Oil, Gingerol, Gingerin, Haeptane, Zingiberene.
Properties :
Rasa: Katu
Guna : Laghu, Singdha
Drug Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 105
Virya : Ushna
Vipaka : Madhura
Karma : Sheeta prashamana, Shothahara, Vedanasthapana, Deepana, Rochana,
Pachana, Bhedana, Grahi, Hridya, Jwaraghna.
Indication : Amavata, Gulma, Chardi, Vishamajwara, Ajeerna, Pratisyaya.
Strotogamitva:
Dosha: Kapha-Vatahara
Dhatu: Rasa, Shukra, Raktha
Mala: Purisha.
Organs : GIT, Heart.
Pharmacological Activities:
Anti-inflammatory, Antipyretic, Antiatherosclerotic, Hepatoprotective,
Hypouricemic, Hypolipidaemic.
Used part : Kanda, Rhizomes
Dose:
Churna : 0.75-1.5 grms
Swarasa : 2-4 ml
Yoga:
Ardrakhanda
Saubhagyashunthipaka
Drug Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 106
Patola:
Botanical name: Trichosanthes dioica
Family: Curcurbitaceae
Synonyms: Karkasacchad, Kulaka, Bijagarbha, Pancha Rajiphala, Rajiphala,
Amritaphala, Panduphala, Tiktottama, Nagaphala.
Classical categorization :
Charaka : Truptighna, Trushnanigrahana,
Sushruta: Patoladi, Aragvadhadi.
Vagbhata: Patoladi, Aragvadhadi
Major chemical constituents:
Nicotinic acid, riboflavin, vit.C, thiamine, linoleic acid, colocynthin, oleic
acid, trichosanthin, cucurbita-5.
Properties :
Rasa: Tikta , Katu
Guna : Ruksha , laghu
Virya : Ushna
Vipaka : Katu
Karma : Kapha-Pittahara, Vrishya, Varnya, Dipana.
Indication : Jwara, Kusta, Kandu, Amlapitta, Daha
Strotogamitva:
Dosha: Kaphahara, Pittahara
Dhatu: Rasa, Raktha
Mala: Purisha.
Organs : GIT.
Drug Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 107
Therapeutic Uses:
Indralupta, Medoroga, Netraroga.
Pharmocological action:
Antipyretic, Antiatherosclerotic, Hepatoprotective, Hypouricemic, Hypolipidaemic.
Used part : Moola, Phala, Patra
Dose:
Churna : 1-3 grms
Svarasa: 10-20ml
Kvatha : 30-50 ml.

Drug Review
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 108
Guduchyadi Yoga (Choorna)
Guduchi Musta
Nagara Patola
Clinical
Contrive
Objectives
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 109
OBJECTIVES OF THE STUDY
1. To evaluate the efficacy of Satvavajaya chikitsa in Madatyayaja Yakrit Vikara
(Alcoholic liver disorder).
2. To evaluate the efficacy of Guduchyadi yoga in Madatyayaja Yakrit Vikara
(Alcoholic liver disorder).
3. To evaluate the efficacy of combined effect of Satvavajaya Chikitsa and
Guduchyadi yoga in Madatyayaja Yakrit Vikara (Alcoholic liver disorder).
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 110
METHODOLOGY
Madatyaya or the alcoholic dependency is completely based on stability of
one’s own Satva. So mind plays an important role in the de-addiction of alcohol.
Word Madatyaya is composed of two terms i.e. Mada -any exhilarating or
intoxicating condition. Atyaya – suffering.
Hence suffering from intoxicating drink
is known as Madatyaya.
Chronic and excessive alcohol ingestion is one of the major causes of liver
disorders across the world. Despite the untoward effect of alcohol, alcoholism is a
major problem in India. The different drug abuse surveys have shown the prevalence
of alcoholism as 5 to 20 percent worldwide. In India, general population surveys
shows the prevalence rate as high as 16 to 50 percent . Atleast 20% of the patients in
mental settings have alcohol abuse or dependence or withdrawal , including
individuals from all socioeconomic conditions and both the genders.
According to US Census Bureau International Data Base 2004, 106,50,70,607
persons in the world were using alcohol and out of which 78,31,407 persons were
affected by Alcoholic liver disease. It manifests as a clinical spectrum ranging from
non specific symptoms to hepatic failure. Classically, alcoholic liver injury comprises
three major forms, 1.fatty liver, 2.alcoholic hepatitis and 3.cirrhosis.
Bhavaprakasha mentions Yakrit-Vruddhi (hepatomegaly) as one of the
symptoms of Yakrit Vikara due to excessive intake of Vidahi and Abhishyandi
Aharas and Madya (alcohol).
Ayurveda has many options to treat Madatyaya . All the texts mention
Pittahara and Deepana Pachana Dravyas to treat Yakrit-Vikaras. Guduchyadi Yoga
mentioned by Charaka comprising of Guduchi (Tinospora cordifolia), Musta(Cyperus
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 111
rotundus), Patola(Tricosanthes dioica) and Nagara(Gingeber officinalis) may relieve
the adverse effects of Madatyaya as well as liver disorders caused by it.
Satvavajaya Chikitsa may help people to address psychological issues
involved in their drinking problem. Astanga Hrudaya explains Vismapana,
Samsmarana, Priyadarshana, Priyashravana, Geeta, Vadya and Charaka advises
Harshanee Kriya and restrain from the things which are harmful to body and mind as
the treatment modalities in the management of Madatyaya.
The three therapies i.e. cognitive behavioral coping skills, motivational enhancement
therapy and 12 step facilitation approaches of alcoholics anonymous has been found
to be helpful for the people to boost their motivation to stop drinking.
As the number of alcohol related disorders are increasing in the society and till
date no study has been conducted , hence it is decided to carry out the present study to
evaluate the effect of Guduchyadi Yoga and Satvavajaya Chikitsa in the management
of Madatyayaja Yakrit Vikara.
Material and Methods
Source of data :
54 patients of Madatyaya were selected from the Out Patient Department and In
Patient Department of ManasaRoga of the S D M College of Ayurveda and Hospital,
Hassan.
Method of Collection of Data :
54 patients of Madatyaya with liver disorder who fulfills the inclusion criteria
were selected and randomly assigned into the following 3 groups; each group
comprising of 16 patients and 6 were dropouts.
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 112
Group A: The patients of this group were subjected to Satvavajaya Chikitsa
daily along with placebo capsule 500 mg starch thrice daily for 1 month. Satvavajaya
Chikitsa was carried out as follows:
Jnana- 12 Step facilitation (Atmadi Jnana) approach.
1. We admit we are powerless over alcohol- that our lives have become
unmanageable.
2. We believe that a Power greater than ourselves can restore us to sanity.
3. We make a decision to turn our will and our lives over to the care of God as we
understand Him.
4. We make a search and fearless moral inventory of ourselves.
5. We admit to God, to ourselves and to another human being the exact nature of
our wrong doings.
6. We’re entirely ready to have God remove all these defects of character.
7. We shall humbly ask Him to remove our shortcomings.
8. We shall make a list of all persons we have harmed and become willing to
make amends to them all.
9. We shall make direct amends to such people wherever possible, except when to
do so would injure them or others.
10. We shall continue to take personal inventory and when we are wrong,
promptly admit it.
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 113
11. We will search through prayer and meditation to improve the conscious
contact with God as we understood Him, praying only for knowledge of Him for
us and the power to carry it out.
12. After experiencing this, we shall carry this message to alcoholics, and to
practice these principles in all their affairs.
Vijnana- Specific information about effect of alcohol on various organs.
Dhairya- Supportive Psychotherapy – motivational enhancement therapy.
Smriti - Methods to cope with high-risk drinking situations and develop social
support systems.
Samadhi – Yoga for 30 minutes and Pranayama for 15 minutes daily for 1 month.
Yogasana – Standing Asana- Vrikshasana , Pada Hastasana, Ardha Chakrasana,
Trikonasana.
Supine Asana – Pavana Muktasana, Matsyasana.
Prone Asana - Bhujangasana, Dhanurasana.
Sitting Asana – Vajrasana, Ushtrasana, Vakrasana.
Pranayama - Kapalabhati, Bhastrika, Anuloma-Viloma, Shitali, Shithkari and
Bhramari.
Dhairya Chikitsa will be also done on 15th
and 30th
day of treatment.
Group B: The patients of this group were given Guduchyadi yoga in the dose of
5 gm, before food with warm water thrice daily for 1 month.
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 114
Group C: The patients of this group were subjected to Satvavajaya Chikitsa as
mentioned above and simultaneously Guduchyadi Yoga was given in the dose of 5gm
before food with warm water thrice daily for 1 month
Diagnostic Criteria:
Diagnosis was made on the basis of Lakshanas of Alcoholic liver disorder and
Madatyayaja Yakrit Vikara.
Fatty liver Yakrit vruddhi
Right upper quadrant discomfort. Manda jvara
Tender hepatomegaly. Mandagni.
Nausea Ksheenabala.
Jaundice Atipandu.
Fever and Abdominal pain
Elevated AST (Aspartate amino transferace)
Elevated ALT (Alanine amino transferace)
Inclusion Criteria:
1.Patients presenting with symptoms of Madatyaya along with Alcoholic liver
disorder.
2. Age group of 16-70 years of either sex.
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 115
Exclusion Criteria:
1.Patients suffering from any Organic brain disorder.
2.Patients suffering from complications of Alcoholic liver disorders.
3.Patients suffering from other types of addictions.
4.Patients suffering from other Systemic or Psychiatric illnesses.
Assessment Criteria:
Assessment of clinical study was done based on subjective and objective
parameters. Self scoring of symptoms of Madatyayaja Yakrit Vikara were done and
self prepared scale was used for assessment.
Table: 15: Parameters
Subjective parameters : Objective parameters:
Aruchi. Chardi
Prajagara Manda jvara
Hrillasa Atipanduta
Pralapa Atisara
Bhrama Shareera kampa
Mandagni. USG Abdomen
Liver Function Test
Hepatomegaly.
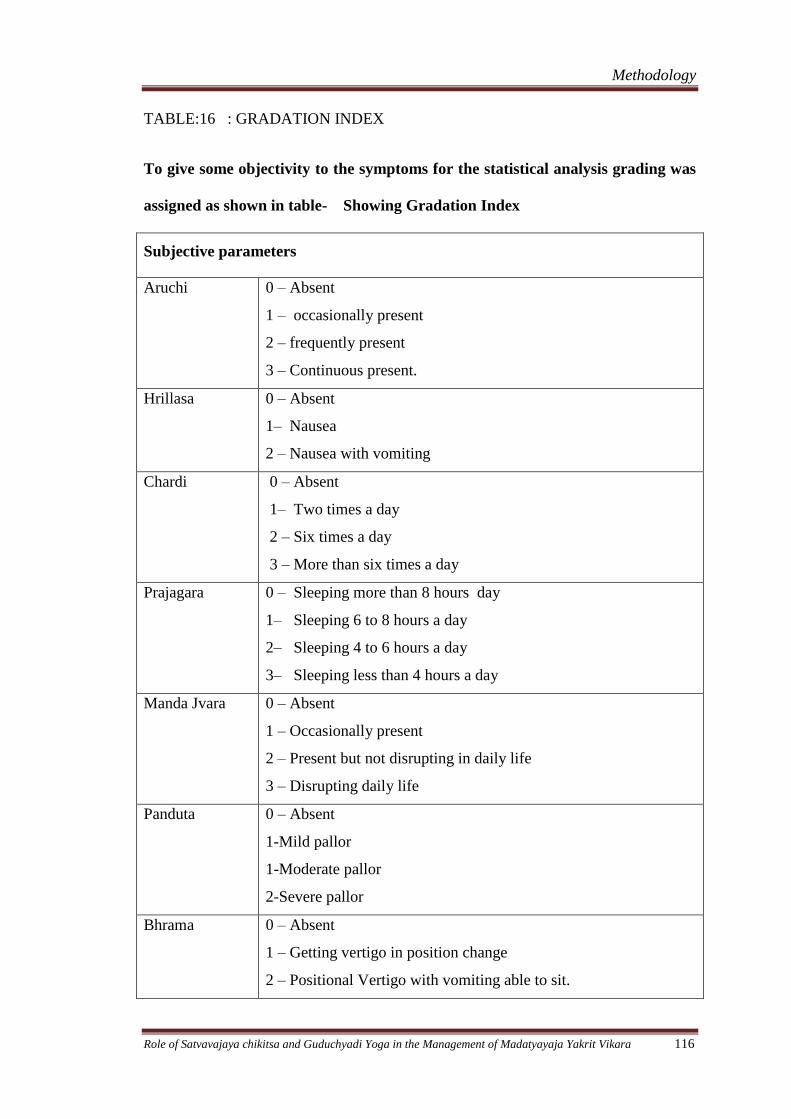
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 116
TABLE:16 : GRADATION INDEX
To give some objectivity to the symptoms for the statistical analysis grading was
assigned as shown in table- Showing Gradation Index
Subjective parameters
Aruchi 0 – Absent
1 – occasionally present
2 – frequently present
3 – Continuous present.
Hrillasa 0 – Absent
1– Nausea
2 – Nausea with vomiting
Chardi 0 – Absent
1– Two times a day
2 – Six times a day
3 – More than six times a day
Prajagara 0 – Sleeping more than 8 hours day
1– Sleeping 6 to 8 hours a day
2– Sleeping 4 to 6 hours a day
3– Sleeping less than 4 hours a day
Manda Jvara 0 – Absent
1 – Occasionally present
2 – Present but not disrupting in daily life
3 – Disrupting daily life
Panduta 0 – Absent
1-Mild pallor
1-Moderate pallor
2-Severe pallor
Bhrama 0 – Absent
1 – Getting vertigo in position change
2 – Positional Vertigo with vomiting able to sit.
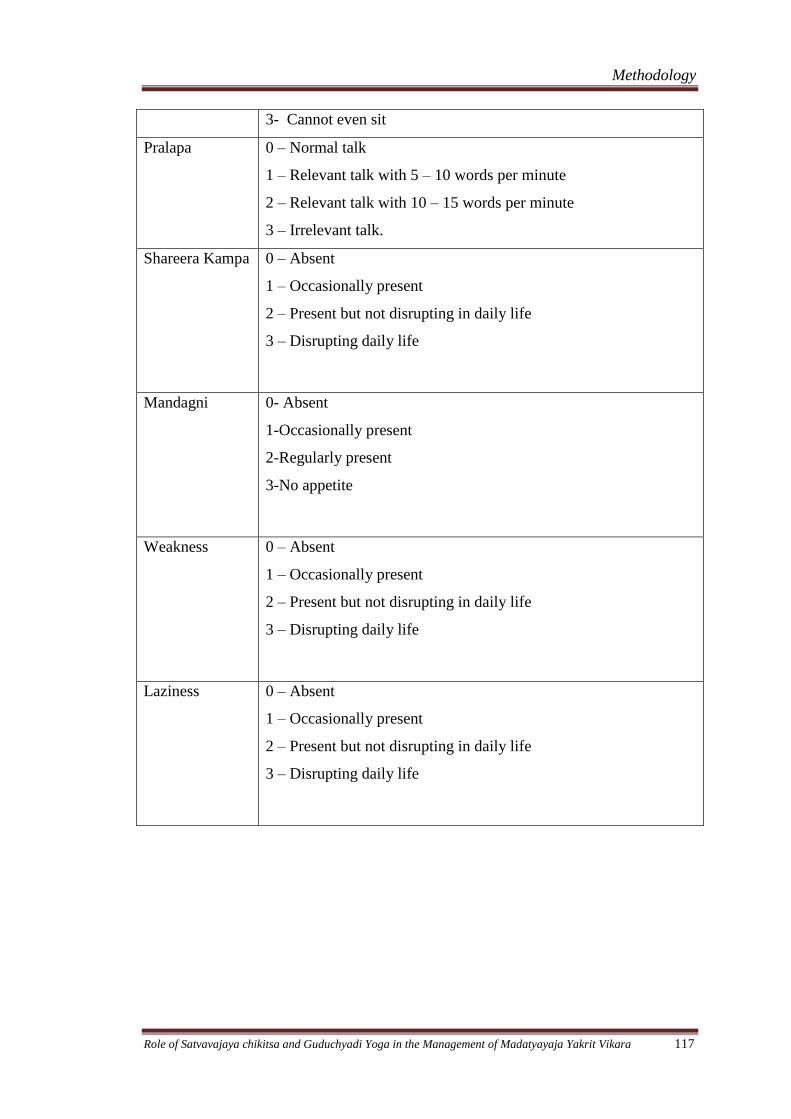
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 117
3- Cannot even sit
Pralapa 0 – Normal talk
1 – Relevant talk with 5 – 10 words per minute
2 – Relevant talk with 10 – 15 words per minute
3 – Irrelevant talk.
Shareera Kampa 0 – Absent
1 – Occasionally present
2 – Present but not disrupting in daily life
3 – Disrupting daily life
Mandagni 0- Absent
1-Occasionally present
2-Regularly present
3-No appetite
Weakness 0 – Absent
1 – Occasionally present
2 – Present but not disrupting in daily life
3 – Disrupting daily life
Laziness 0 – Absent
1 – Occasionally present
2 – Present but not disrupting in daily life
3 – Disrupting daily life
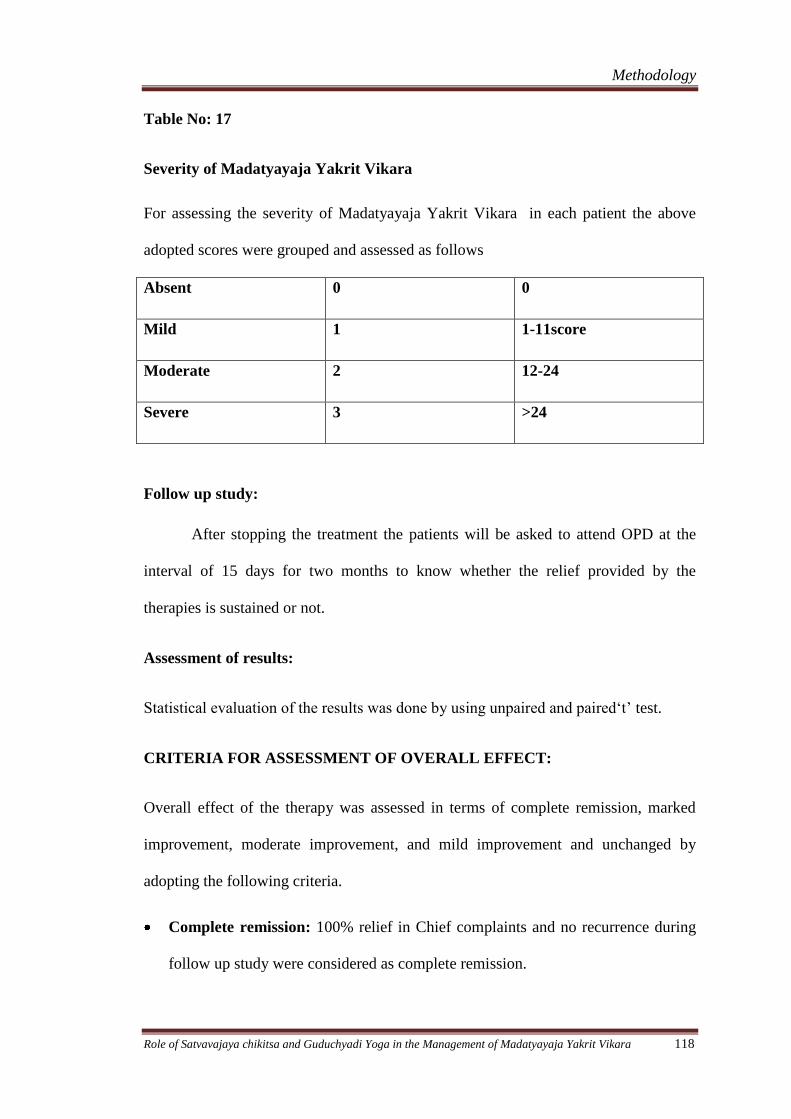
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 118
Table No: 17
Severity of Madatyayaja Yakrit Vikara
For assessing the severity of Madatyayaja Yakrit Vikara in each patient the above
adopted scores were grouped and assessed as follows
Absent 0 0
Mild 1 1-11score
Moderate 2 12-24
Severe 3 >24
Follow up study:
After stopping the treatment the patients will be asked to attend OPD at the
interval of 15 days for two months to know whether the relief provided by the
therapies is sustained or not.
Assessment of results:
Statistical evaluation of the results was done by using unpaired and paired‘t’ test.
CRITERIA FOR ASSESSMENT OF OVERALL EFFECT:
Overall effect of the therapy was assessed in terms of complete remission, marked
improvement, moderate improvement, and mild improvement and unchanged by
adopting the following criteria.
Complete remission: 100% relief in Chief complaints and no recurrence during
follow up study were considered as complete remission.
Methodology
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 119
Marked improvement: 75 – 99 % improvement in chief complaints is
considered as marked improvement.
Moderate improvement: 50 - 74% improvement in chief complaints is
considered as moderate improvement.
Mild improvement: 25 - 49% improvement in chief complaints is considered as
mild improvement.
Unchanged: Less than 24% reduction in chief complaints or recurrence of the
symptoms to the similar extent of severity is noted as unchanged.
Observations
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 120
OBSERVATIONS
54 patients of Madatyaya were registered for this clinical study, out of which 6
patients were dropouts and totally 48 patients completed the study plan. They were
treated in three groups as Satvavajaya Group (S), Guduchyadi Yoga Group (GY) and
Combined (S&GY). The age, sex, religion, Socio – Economic Status, occupation, etc.
noted in the patients of this study were as follows.
Incidence of Age: In this study maximum number (34.70 %) of patients were
belonging to 30 – 40 years age group, 27.30 % to 20 – 30 years age group, 27.30% to
40 – 50 years age group, 8.60 % to 50 – 60 years age group and only 2.10 % were
belonging to 60 – 70 years age group (Table - 18).
Incidence of Sex: In this study the prevalence of Madatyayaja Yakrit Vikara was
found only in males, out of 48 patients all were males only (Table - 19).
Incidence of occupation: This study reveals that prevalence of Madatyayaja Yakrit
Vikara is more in Business people with 48.2 %, then Agriculturist were 27.6 %, 25.2
% were of Students. (Table - 20).
Socio – economic status: 91.6 % of patients were belonging to Middle class income
group, 6.3% to higher income group and 2.1 % to lower income group (Table - 21).
Incidence of Marital Status: Out of 48 patients 76.8% were married and only 23.2
% were unmarried (Table - 22
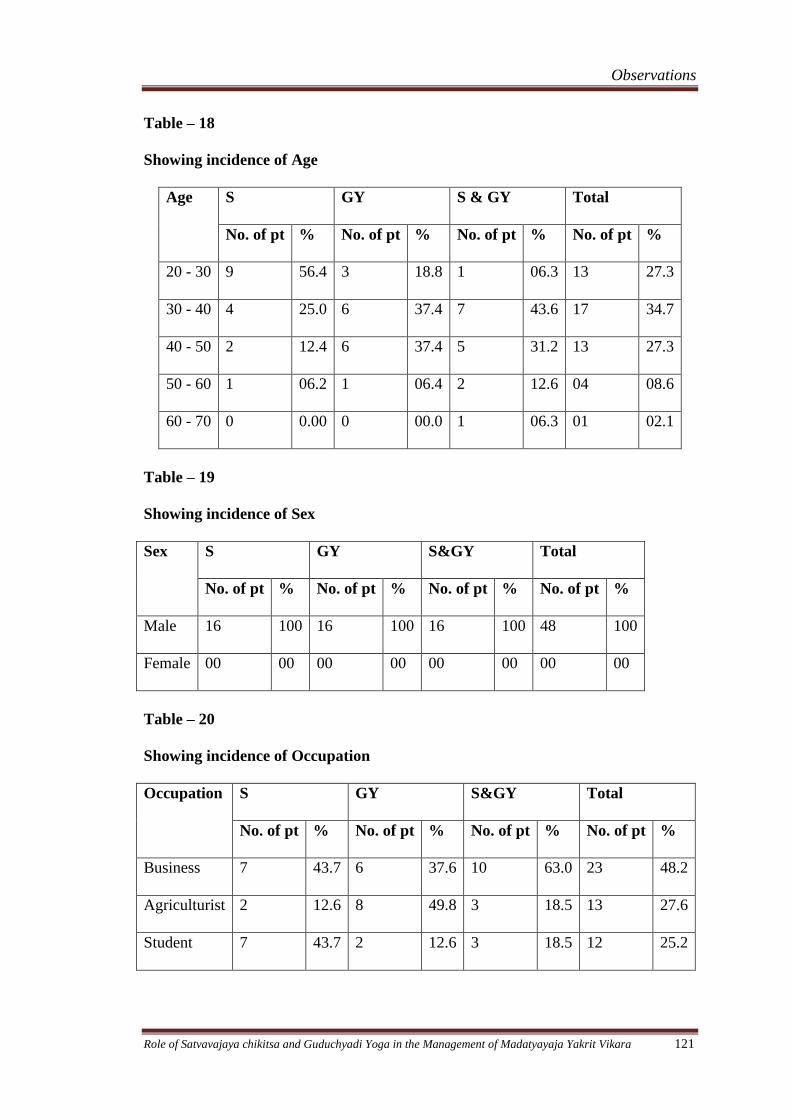
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 121
Table – 18
Showing incidence of Age
Age S GY S & GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
20 - 30 9 56.4 3 18.8 1 06.3 13 27.3
30 - 40 4 25.0 6 37.4 7 43.6 17 34.7
40 - 50 2 12.4 6 37.4 5 31.2 13 27.3
50 - 60 1 06.2 1 06.4 2 12.6 04 08.6
60 - 70 0 0.00 0 00.0 1 06.3 01 02.1
Table – 19
Showing incidence of Sex
Sex S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Male 16 100 16 100 16 100 48 100
Female 00 00 00 00 00 00 00 00
Table – 20
Showing incidence of Occupation
Occupation S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Business 7 43.7 6 37.6 10 63.0 23 48.2
Agriculturist 2 12.6 8 49.8 3 18.5 13 27.6
Student 7 43.7 2 12.6 3 18.5 12 25.2
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 122
Incidence of education status: Educational status of this study revealed maximum
(65.1%) patients were educated till higher secondary while 2.1 % of patients educated
till primary level. 14.4 % of patients were graduates and 12.3% were educated till post
graduate level. Only one person (2.1%) was up to primary level.(Table - 23).
Age of starting of first drink: Among total no of subjects (48 patients), 46.2 % of
people had their first drink in between 10 – 20 years of age of life, 45.2 % people had
their first drink in between 20 – 30 years of age of life, where as 8.6 % had their first
drink in between 30 – 40 years of age of life (Table - 24).
Incidence of period of daily drinking: In this study 79.0 % of people were having
alcohol daily since 1 – 5 years, 8.4% were having since 5 – 10 years, where as 10.5%
since 10 – 15 years and 2.1% since 15 – 20 years. (Table - 25).
Incidence of type of alcohol: This study shown maximum people (64.3 %) took
Whisky, 12.6 % of people took Brandy, 8.4 % people had Beer, 8.4 % people had
Rum and 6.3% had Vodka. (Table - 26).
Incidence of time of first drink in a day: Out of 48 patients 48.0 % of patients start
days drink at morning and 42.0 % of patients drink at evening. (Table – 27).
Incidence of Prakruti: Vatapitta Prakruti patients were more with 35.7 %,
Vatakapha Prakruti patients were 27.3 %, only 6.3 % of patients were of Vataja
Prakruti and 30.7 % of patients belong to Pittakaphaja Prakruti (Table – 28).
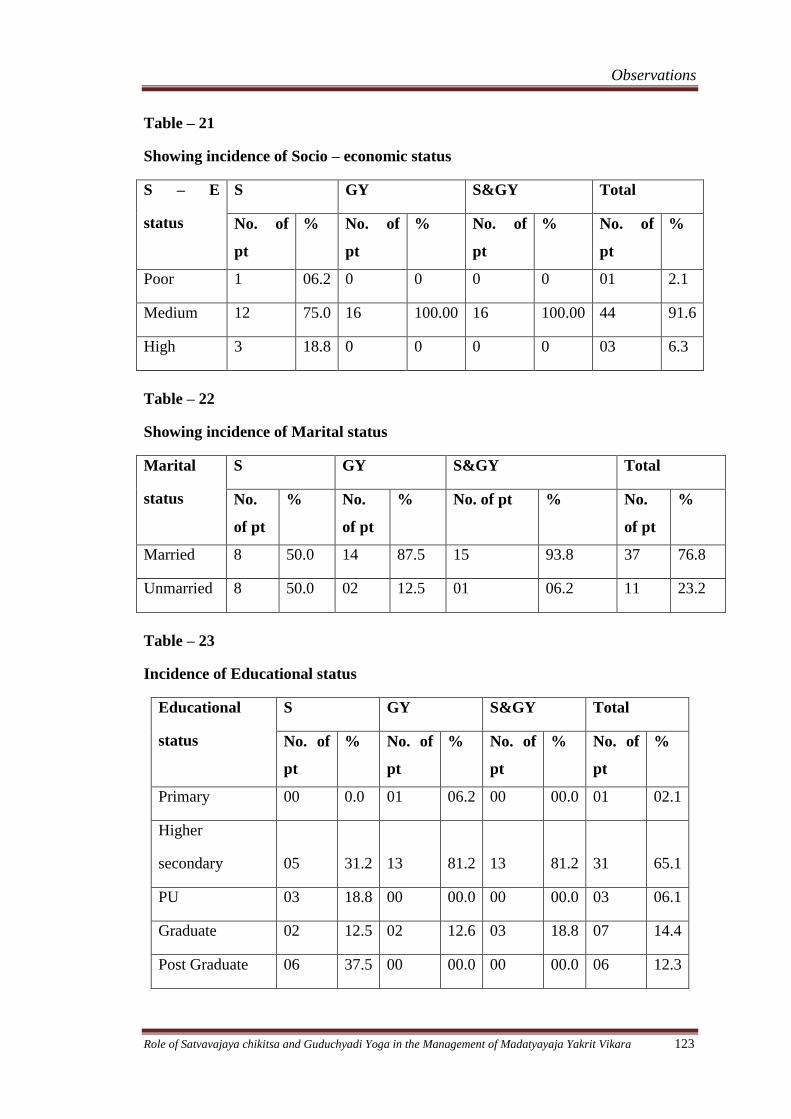
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 123
Table – 21
Showing incidence of Socio – economic status
S – E
status
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
Poor 1 06.2 0 0 0 0 01 2.1
Medium 12 75.0 16 100.00 16 100.00 44 91.6
High 3 18.8 0 0 0 0 03 6.3
Table – 22
Showing incidence of Marital status
Marital
status
S GY S&GY Total
No.
of pt
% No.
of pt
% No. of pt % No.
of pt
%
Married 8 50.0 14 87.5 15 93.8 37 76.8
Unmarried 8 50.0 02 12.5 01 06.2 11 23.2
Table – 23
Incidence of Educational status
Educational
status
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
Primary 00 0.0 01 06.2 00 00.0 01 02.1
Higher
secondary 05 31.2 13 81.2
13
81.2 31 65.1
PU 03 18.8 00 00.0 00 00.0 03 06.1
Graduate 02 12.5 02 12.6 03 18.8 07 14.4
Post Graduate 06 37.5 00 00.0 00 00.0 06 12.3
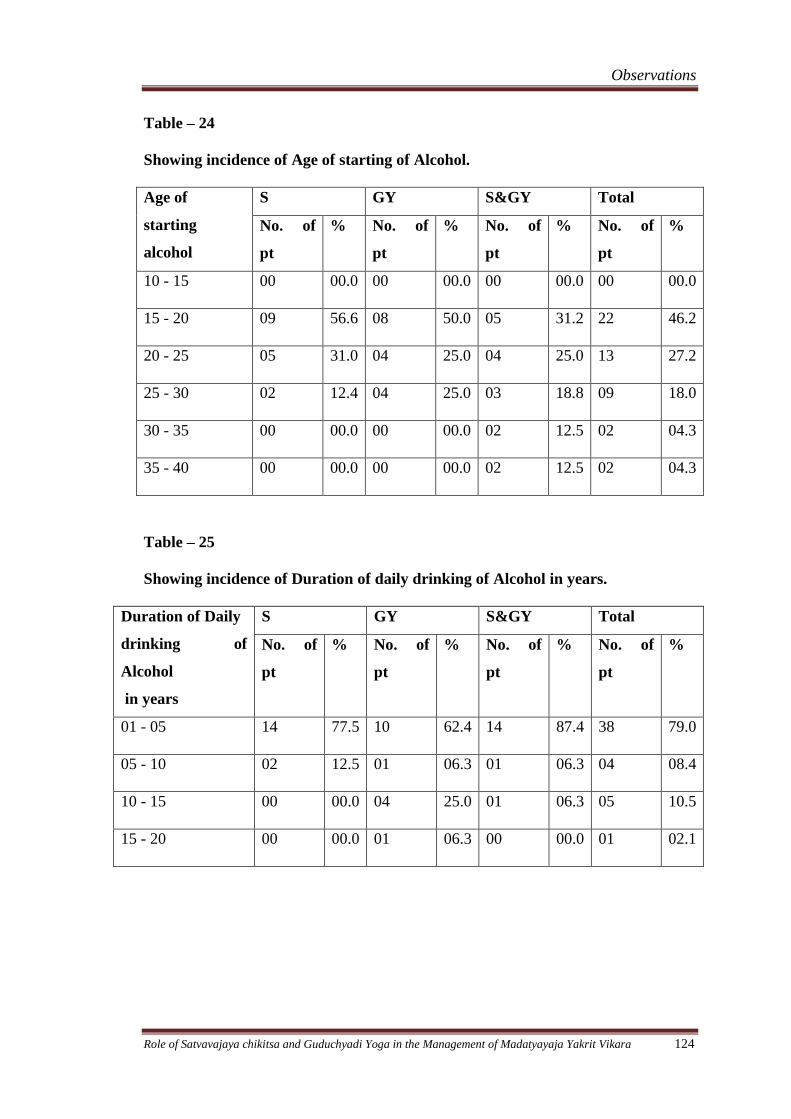
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 124
Table – 24
Showing incidence of Age of starting of Alcohol.
Age of
starting
alcohol
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
10 - 15 00 00.0 00 00.0 00 00.0 00 00.0
15 - 20 09 56.6 08 50.0 05 31.2 22 46.2
20 - 25 05 31.0 04 25.0 04 25.0 13 27.2
25 - 30 02 12.4 04 25.0 03 18.8 09 18.0
30 - 35 00 00.0 00 00.0 02 12.5 02 04.3
35 - 40 00 00.0 00 00.0 02 12.5 02 04.3
Table – 25
Showing incidence of Duration of daily drinking of Alcohol in years.
Duration of Daily
drinking of
Alcohol
in years
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
01 - 05 14 77.5 10 62.4 14 87.4 38 79.0
05 - 10 02 12.5 01 06.3 01 06.3 04 08.4
10 - 15 00 00.0 04 25.0 01 06.3 05 10.5
15 - 20 00 00.0 01 06.3 00 00.0 01 02.1
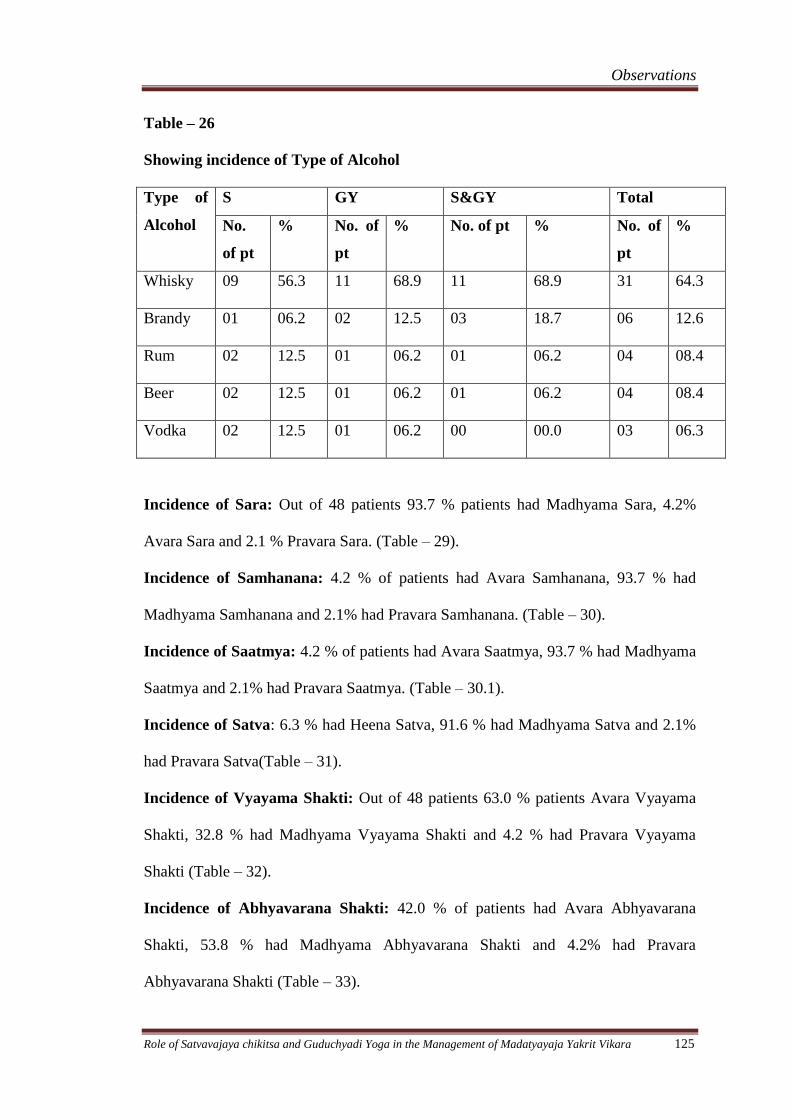
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 125
Table – 26
Showing incidence of Type of Alcohol
Type of
Alcohol
S GY S&GY Total
No.
of pt
% No. of
pt
% No. of pt % No. of
pt
%
Whisky 09 56.3 11 68.9 11 68.9 31 64.3
Brandy 01 06.2 02 12.5 03 18.7 06 12.6
Rum 02 12.5 01 06.2 01 06.2 04 08.4
Beer 02 12.5 01 06.2 01 06.2 04 08.4
Vodka 02 12.5 01 06.2 00 00.0 03 06.3
Incidence of Sara: Out of 48 patients 93.7 % patients had Madhyama Sara, 4.2%
Avara Sara and 2.1 % Pravara Sara. (Table – 29).
Incidence of Samhanana: 4.2 % of patients had Avara Samhanana, 93.7 % had
Madhyama Samhanana and 2.1% had Pravara Samhanana. (Table – 30).
Incidence of Saatmya: 4.2 % of patients had Avara Saatmya, 93.7 % had Madhyama
Saatmya and 2.1% had Pravara Saatmya. (Table – 30.1).
Incidence of Satva: 6.3 % had Heena Satva, 91.6 % had Madhyama Satva and 2.1%
had Pravara Satva(Table – 31).
Incidence of Vyayama Shakti: Out of 48 patients 63.0 % patients Avara Vyayama
Shakti, 32.8 % had Madhyama Vyayama Shakti and 4.2 % had Pravara Vyayama
Shakti (Table – 32).
Incidence of Abhyavarana Shakti: 42.0 % of patients had Avara Abhyavarana
Shakti, 53.8 % had Madhyama Abhyavarana Shakti and 4.2% had Pravara
Abhyavarana Shakti (Table – 33).
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 126
Incidence of Jarana Shakti: 68.5 % of patients had Avara Jarana Shakti, 27.3 % had
Madhyama Jarana Shakti and 4.2% had Pravara Jarana Shakti (Table – 34).
Incidence of Pramana: 6.3 % patients had Avara Pramana, 91.6 % had Madhyama
Pramana and 2.1 % had Pravara Pramana (Table – 35).
Incidence of other habits: Out of 48 patients 62.2 % people were smokers, 25.2 %
were not having any other habits, 6.3 % were having habit of Tobacco chewing, and
6.3 % of patients were having habit of taking Gutka. (Table – 36).
Incidence of Psychiatric complications: Out of 48 patients 79.0% of patients were
not having Psychiatric complications while 12.6 % of patients were having
Depression, 6.3% of patients were having Suicidal ideation and 2.1% had
Aggression.(Table – 37).
Incidence of Relationship with spouse: Out of 48 patients 68.0 % patients were
having cordial, 14.7 % patients were having moderate and 27.3% patients were
having unaffectionate relationship with their spouse. (Table – 38).
Incidence of Signs and symptoms: Out of 48 patients 100 % had Aruchi, 87.5% had
Hrillasa, 75% had Chardi, and 95.8 % had Prajagara, while 20.8 % patients had
Mandajvara, 20.8% had Panduta, 22.9% Bhrama, 12.5 % had Pralapa, 66.7% had
Shareera Kampa, 85.4% had Mandagni, 87.5% had weakness and 58.3% had
Laziness. (Table – 39).
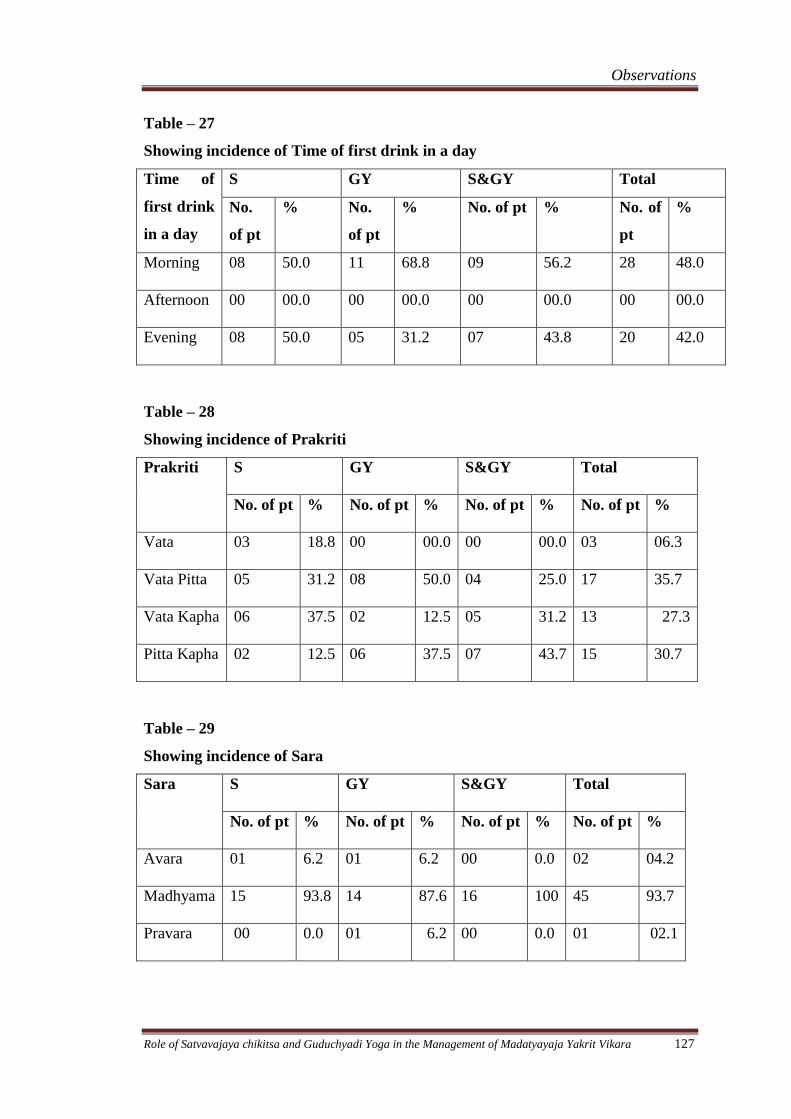
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 127
Table – 27
Showing incidence of Time of first drink in a day
Time of
first drink
in a day
S GY S&GY Total
No.
of pt
% No.
of pt
% No. of pt % No. of
pt
%
Morning 08 50.0 11 68.8 09 56.2 28 48.0
Afternoon 00 00.0 00 00.0 00 00.0 00 00.0
Evening 08 50.0 05 31.2 07 43.8 20 42.0
Table – 28
Showing incidence of Prakriti
Prakriti S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Vata 03 18.8 00 00.0 00 00.0 03 06.3
Vata Pitta 05 31.2 08 50.0 04 25.0 17 35.7
Vata Kapha 06 37.5 02 12.5 05 31.2 13 27.3
Pitta Kapha 02 12.5 06 37.5 07 43.7 15 30.7
Table – 29
Showing incidence of Sara
Sara S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Avara 01 6.2 01 6.2 00 0.0 02 04.2
Madhyama 15 93.8 14 87.6 16 100 45 93.7
Pravara 00 0.0 01 6.2 00 0.0 01 02.1
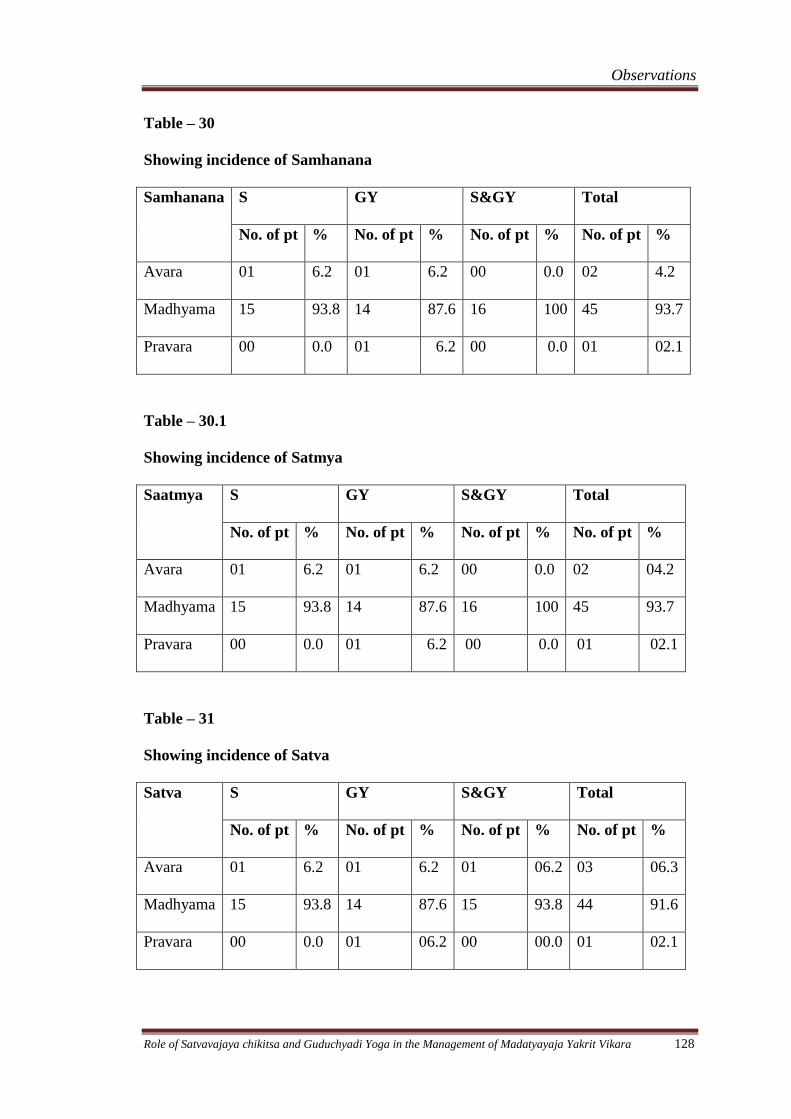
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 128
Table – 30
Showing incidence of Samhanana
Samhanana S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Avara 01 6.2 01 6.2 00 0.0 02 4.2
Madhyama 15 93.8 14 87.6 16 100 45 93.7
Pravara 00 0.0 01 6.2 00 0.0 01 02.1
Table – 30.1
Showing incidence of Satmya
Saatmya S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Avara 01 6.2 01 6.2 00 0.0 02 04.2
Madhyama 15 93.8 14 87.6 16 100 45 93.7
Pravara 00 0.0 01 6.2 00 0.0 01 02.1
Table – 31
Showing incidence of Satva
Satva S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Avara 01 6.2 01 6.2 01 06.2 03 06.3
Madhyama 15 93.8 14 87.6 15 93.8 44 91.6
Pravara 00 0.0 01 06.2 00 00.0 01 02.1
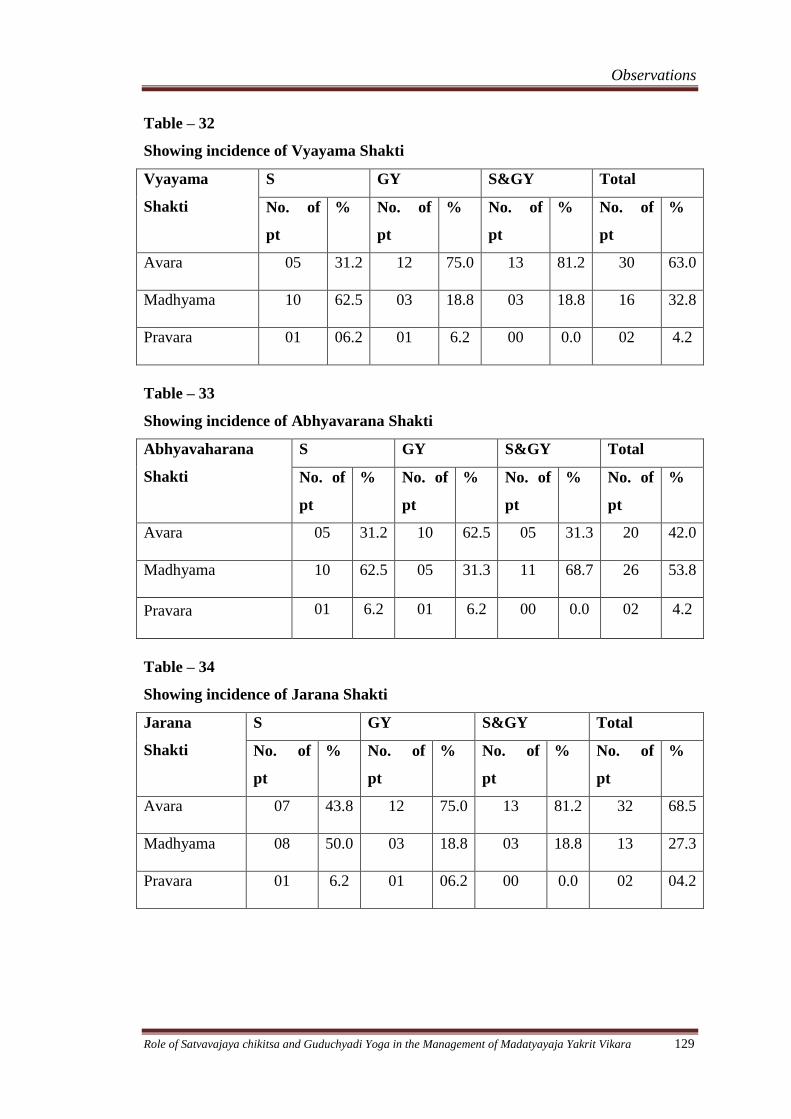
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 129
Table – 32
Showing incidence of Vyayama Shakti
Vyayama
Shakti
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
Avara 05 31.2 12 75.0 13 81.2 30 63.0
Madhyama 10 62.5 03 18.8 03 18.8 16 32.8
Pravara 01 06.2 01 6.2 00 0.0 02 4.2
Table – 33
Showing incidence of Abhyavarana Shakti
Abhyavaharana
Shakti
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
Avara 05 31.2 10 62.5 05 31.3 20 42.0
Madhyama 10 62.5 05 31.3 11 68.7 26 53.8
Pravara 01 6.2 01 6.2 00 0.0 02 4.2
Table – 34
Showing incidence of Jarana Shakti
Jarana
Shakti
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
Avara 07 43.8 12 75.0 13 81.2 32 68.5
Madhyama 08 50.0 03 18.8 03 18.8 13 27.3
Pravara 01 6.2 01 06.2 00 0.0 02 04.2
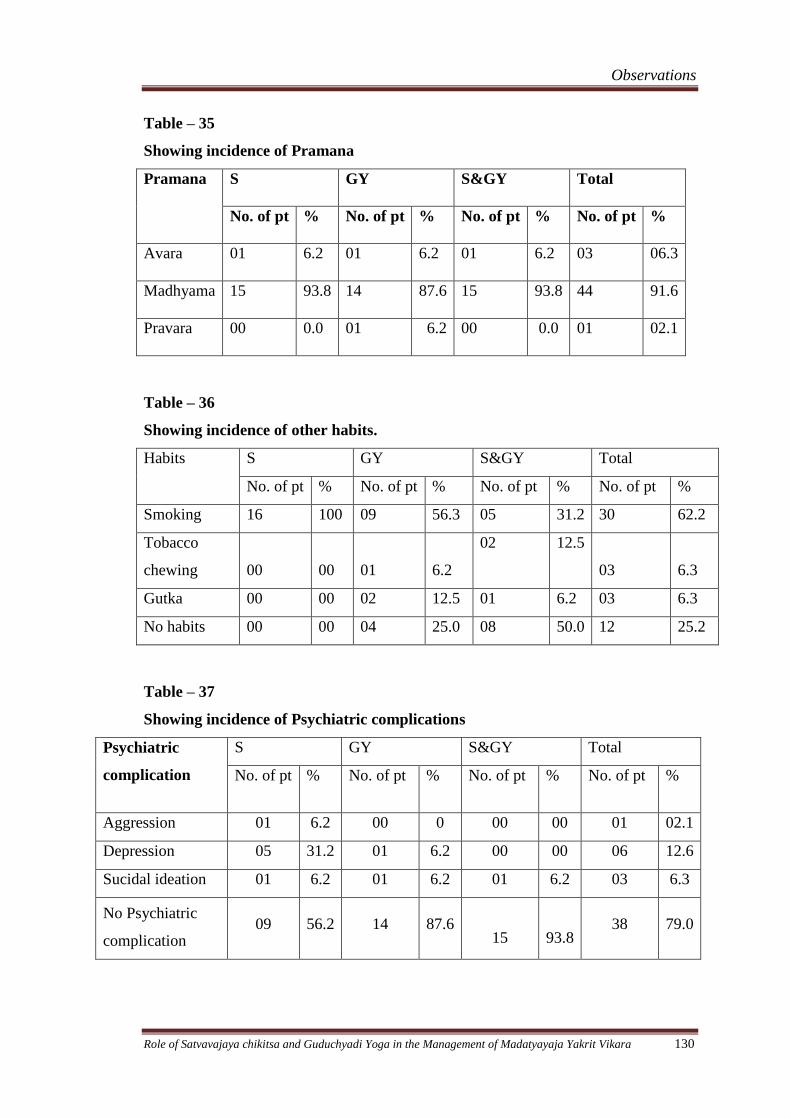
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 130
Table – 35
Showing incidence of Pramana
Pramana S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Avara 01 6.2 01 6.2 01 6.2 03 06.3
Madhyama 15 93.8 14 87.6 15 93.8 44 91.6
Pravara 00 0.0 01 6.2 00 0.0 01 02.1
Table – 36
Showing incidence of other habits.
Habits S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Smoking 16 100 09 56.3 05 31.2 30 62.2
Tobacco
chewing 00 00 01 6.2
02 12.5
03 6.3
Gutka 00 00 02 12.5 01 6.2 03 6.3
No habits 00 00 04 25.0 08 50.0 12 25.2
Table – 37
Showing incidence of Psychiatric complications
Psychiatric
complication
S GY S&GY Total
No. of pt % No. of pt % No. of pt % No. of pt %
Aggression 01 6.2 00 0 00 00 01 02.1
Depression 05 31.2 01 6.2 00 00 06 12.6
Sucidal ideation 01 6.2 01 6.2 01 6.2 03 6.3
No Psychiatric
complication 09 56.2 14 87.6
15
93.8 38 79.0
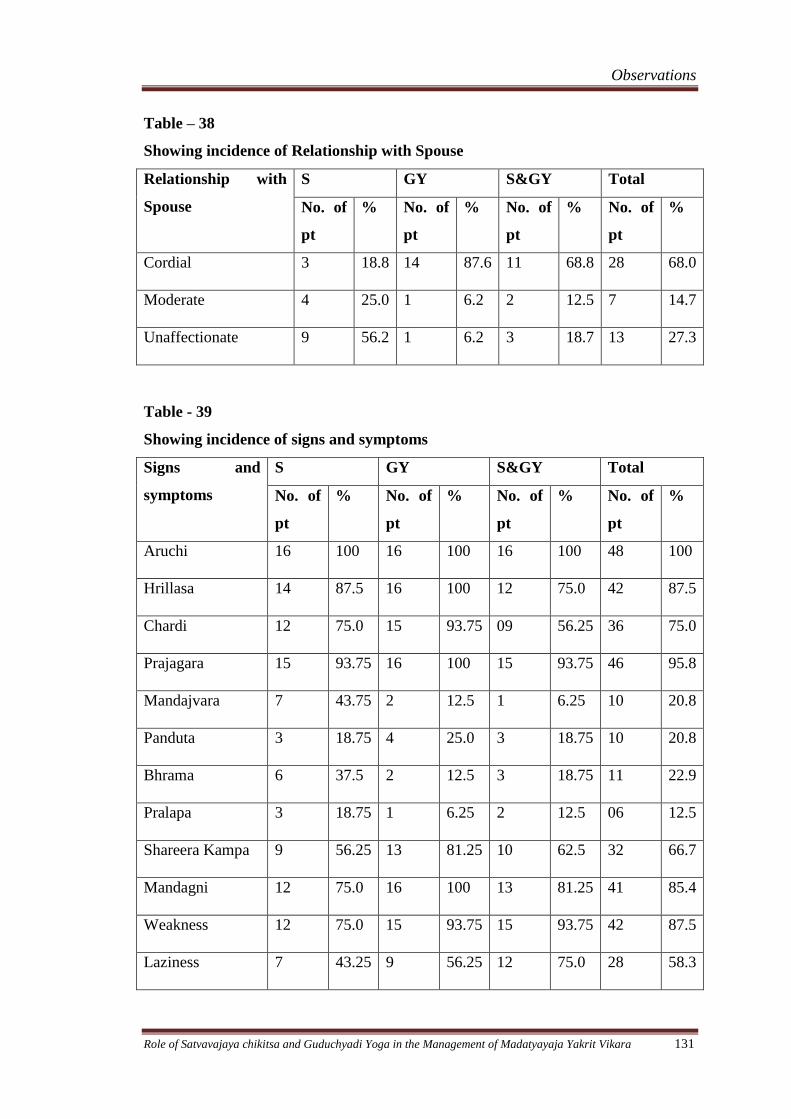
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 131
Table – 38
Showing incidence of Relationship with Spouse
Relationship with
Spouse
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
Cordial 3 18.8 14 87.6 11 68.8 28 68.0
Moderate 4 25.0 1 6.2 2 12.5 7 14.7
Unaffectionate 9 56.2 1 6.2 3 18.7 13 27.3
Table - 39
Showing incidence of signs and symptoms
Signs and
symptoms
S GY S&GY Total
No. of
pt
% No. of
pt
% No. of
pt
% No. of
pt
%
Aruchi 16 100 16 100 16 100 48 100
Hrillasa 14 87.5 16 100 12 75.0 42 87.5
Chardi 12 75.0 15 93.75 09 56.25 36 75.0
Prajagara 15 93.75 16 100 15 93.75 46 95.8
Mandajvara 7 43.75 2 12.5 1 6.25 10 20.8
Panduta 3 18.75 4 25.0 3 18.75 10 20.8
Bhrama 6 37.5 2 12.5 3 18.75 11 22.9
Pralapa 3 18.75 1 6.25 2 12.5 06 12.5
Shareera Kampa 9 56.25 13 81.25 10 62.5 32 66.7
Mandagni 12 75.0 16 100 13 81.25 41 85.4
Weakness 12 75.0 15 93.75 15 93.75 42 87.5
Laziness 7 43.25 9 56.25 12 75.0 28 58.3
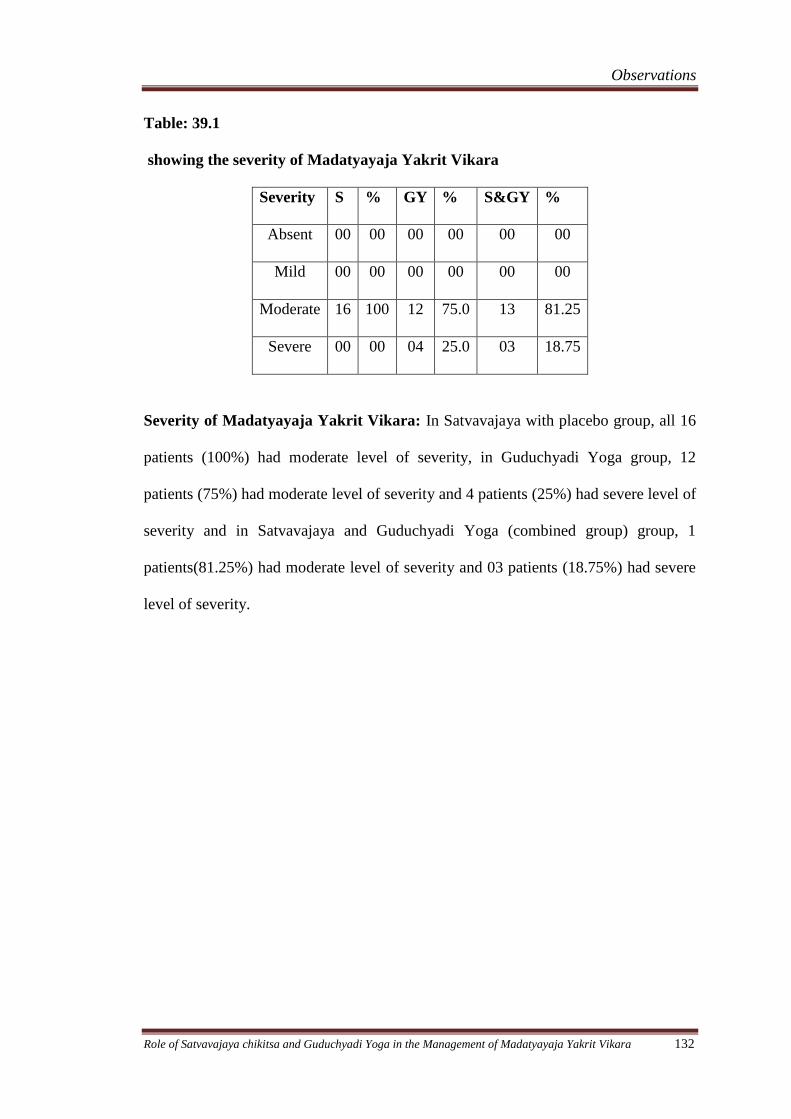
Observations
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 132
Table: 39.1
showing the severity of Madatyayaja Yakrit Vikara
Severity S % GY % S&GY %
Absent 00 00 00 00 00 00
Mild 00 00 00 00 00 00
Moderate 16 100 12 75.0 13 81.25
Severe 00 00 04 25.0 03 18.75
Severity of Madatyayaja Yakrit Vikara: In Satvavajaya with placebo group, all 16
patients (100%) had moderate level of severity, in Guduchyadi Yoga group, 12
patients (75%) had moderate level of severity and 4 patients (25%) had severe level of
severity and in Satvavajaya and Guduchyadi Yoga (combined group) group, 1
patients(81.25%) had moderate level of severity and 03 patients (18.75%) had severe
level of severity.
Results
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 133
Effect of Therapies
In this study 54 patients of Madatyayaja Yakrit Vikara were registered, 16 patients in
Satvavajaya(S)group,19 patients in Guduchyadi Yoga(GY)group and 19 patients in
Combined (S&GY) group, out of which 3 patients of GY group and 3 patients of
S&GY group were drop out. In this way 16 patients in each group completed full
courses of the treatment. The effects of the therapies are described according to the
group on respective symptoms
1.Effect of Satvavajaya Chikitsa with Placebo on symptoms of Madatyayaja
Yakrit Vikara.
In S group, it was observed that statistically highly significant improvements were
seen in Aruchi i.e 51.44% improvement, 38.16% in Hrillasa, 44.58% in Prajagara and
44.81% in Mandagni with p value < 0.001. Statistically significant results were
observed in the following; 46.0% relief in Chardi(P<0.01),50% in Manda jwara,
54.64% in Bhrama and 42.18% in Shareera kampa (P<0.02), 30.18% relief in laziness
(P<0.05). Statistically insignificant results with p>0.10 were observed in Panduta and
Pralapa.(Table.40)
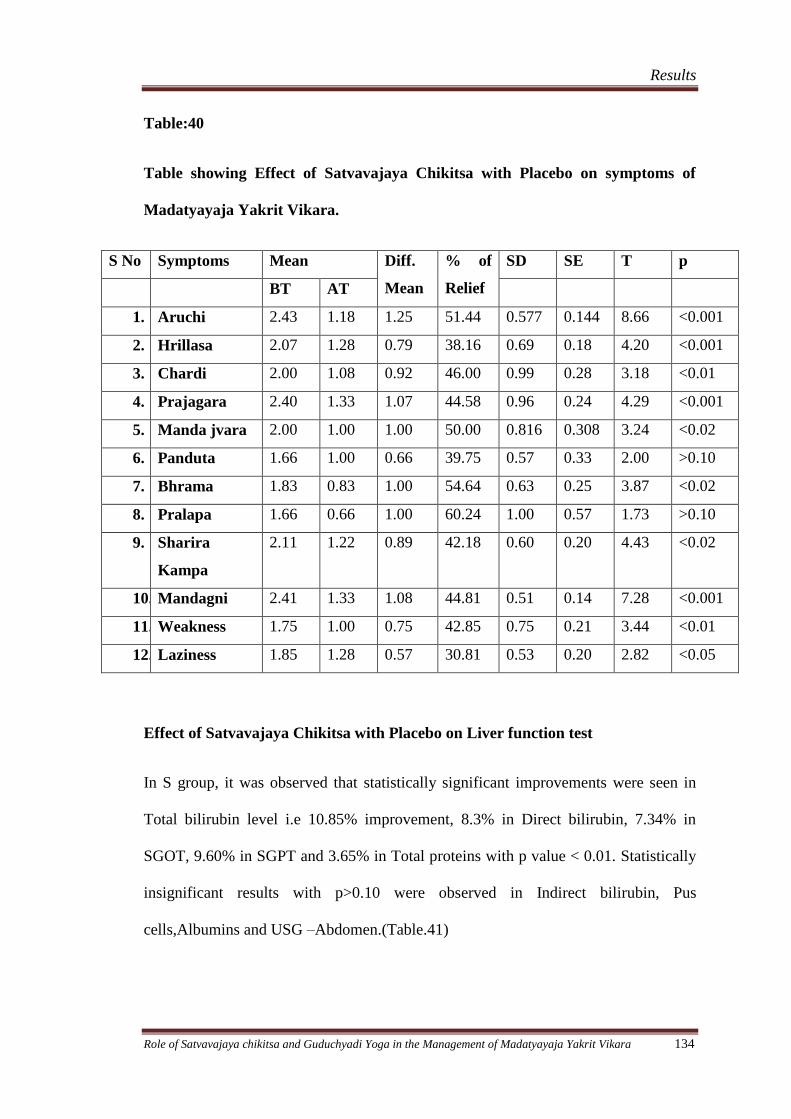
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 134
Table:40
Table showing Effect of Satvavajaya Chikitsa with Placebo on symptoms of
Madatyayaja Yakrit Vikara.
S No Symptoms Mean Diff.
Mean
% of
Relief
SD SE T p
BT AT
1. Aruchi 2.43 1.18 1.25 51.44 0.577 0.144 8.66 <0.001
2. Hrillasa 2.07 1.28 0.79 38.16 0.69 0.18 4.20 <0.001
3. Chardi 2.00 1.08 0.92 46.00 0.99 0.28 3.18 <0.01
4. Prajagara 2.40 1.33 1.07 44.58 0.96 0.24 4.29 <0.001
5. Manda jvara 2.00 1.00 1.00 50.00 0.816 0.308 3.24 <0.02
6. Panduta 1.66 1.00 0.66 39.75 0.57 0.33 2.00 >0.10
7. Bhrama 1.83 0.83 1.00 54.64 0.63 0.25 3.87 <0.02
8. Pralapa 1.66 0.66 1.00 60.24 1.00 0.57 1.73 >0.10
9. Sharira
Kampa
2.11 1.22 0.89 42.18 0.60 0.20 4.43 <0.02
10. Mandagni 2.41 1.33 1.08 44.81 0.51 0.14 7.28 <0.001
11. Weakness 1.75 1.00 0.75 42.85 0.75 0.21 3.44 <0.01
12. Laziness 1.85 1.28 0.57 30.81 0.53 0.20 2.82 <0.05
Effect of Satvavajaya Chikitsa with Placebo on Liver function test
In S group, it was observed that statistically significant improvements were seen in
Total bilirubin level i.e 10.85% improvement, 8.3% in Direct bilirubin, 7.34% in
SGOT, 9.60% in SGPT and 3.65% in Total proteins with p value < 0.01. Statistically
insignificant results with p>0.10 were observed in Indirect bilirubin, Pus
cells,Albumins and USG –Abdomen.(Table.41)
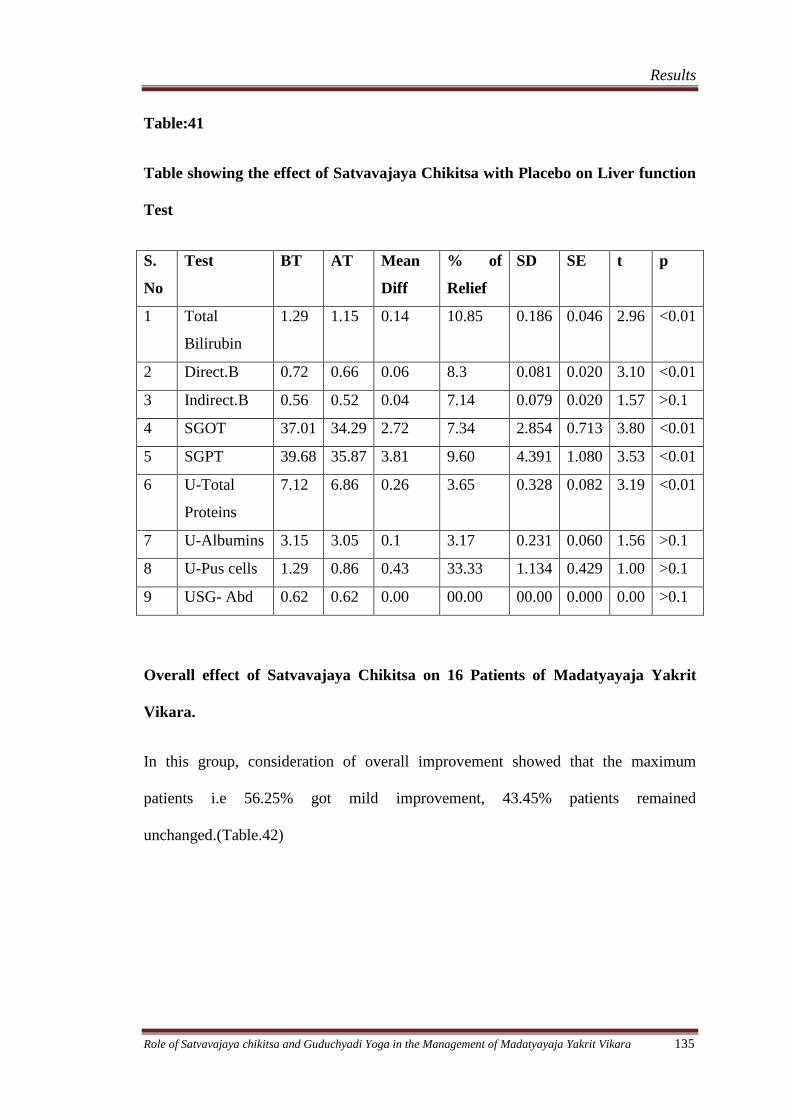
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 135
Table:41
Table showing the effect of Satvavajaya Chikitsa with Placebo on Liver function
Test
S.
No
Test BT AT Mean
Diff
% of
Relief
SD SE t p
1 Total
Bilirubin
1.29 1.15 0.14 10.85 0.186 0.046 2.96 <0.01
2 Direct.B 0.72 0.66 0.06 8.3 0.081 0.020 3.10 <0.01
3 Indirect.B 0.56 0.52 0.04 7.14 0.079 0.020 1.57 >0.1
4 SGOT 37.01 34.29 2.72 7.34 2.854 0.713 3.80 <0.01
5 SGPT 39.68 35.87 3.81 9.60 4.391 1.080 3.53 <0.01
6 U-Total
Proteins
7.12 6.86 0.26 3.65 0.328 0.082 3.19 <0.01
7 U-Albumins 3.15 3.05 0.1 3.17 0.231 0.060 1.56 >0.1
8 U-Pus cells 1.29 0.86 0.43 33.33 1.134 0.429 1.00 >0.1
9 USG- Abd 0.62 0.62 0.00 00.00 00.00 0.000 0.00 >0.1
Overall effect of Satvavajaya Chikitsa on 16 Patients of Madatyayaja Yakrit
Vikara.
In this group, consideration of overall improvement showed that the maximum
patients i.e 56.25% got mild improvement, 43.45% patients remained
unchanged.(Table.42)
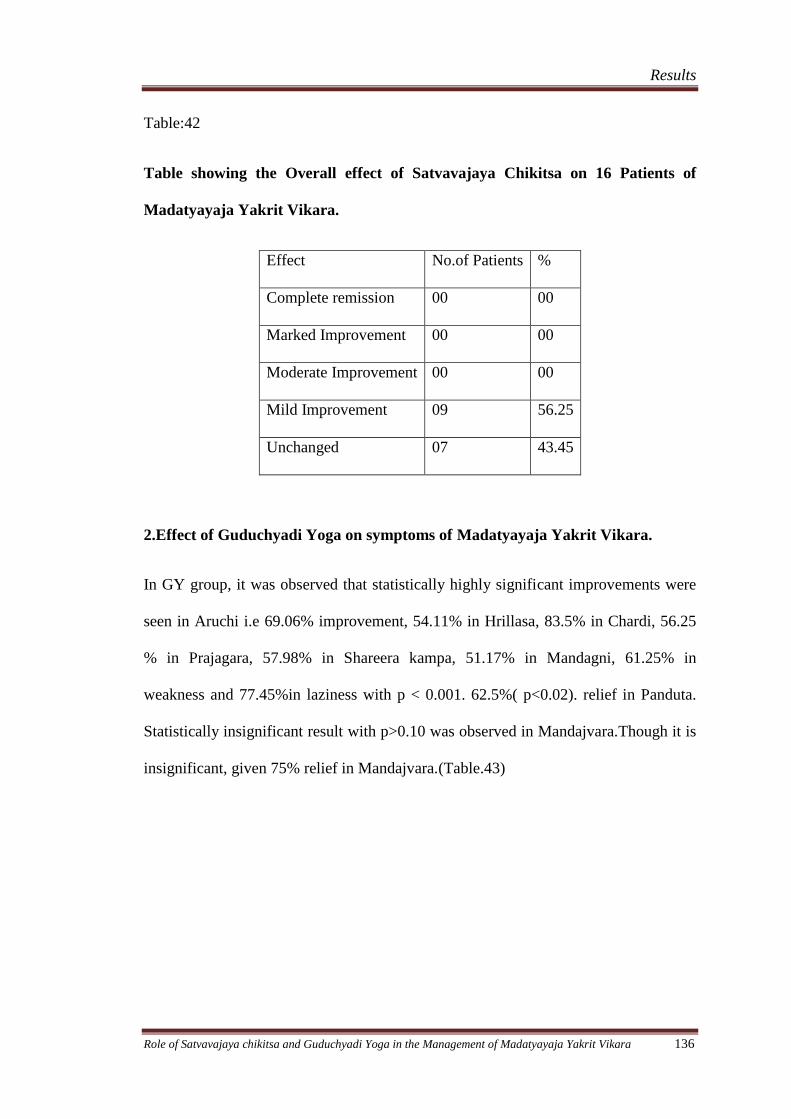
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 136
Table:42
Table showing the Overall effect of Satvavajaya Chikitsa on 16 Patients of
Madatyayaja Yakrit Vikara.
Effect No.of Patients %
Complete remission 00 00
Marked Improvement 00 00
Moderate Improvement 00 00
Mild Improvement 09 56.25
Unchanged 07 43.45
2.Effect of Guduchyadi Yoga on symptoms of Madatyayaja Yakrit Vikara.
In GY group, it was observed that statistically highly significant improvements were
seen in Aruchi i.e 69.06% improvement, 54.11% in Hrillasa, 83.5% in Chardi, 56.25
% in Prajagara, 57.98% in Shareera kampa, 51.17% in Mandagni, 61.25% in
weakness and 77.45%in laziness with p < 0.001. 62.5%( p<0.02). relief in Panduta.
Statistically insignificant result with p>0.10 was observed in Mandajvara.Though it is
insignificant, given 75% relief in Mandajvara.(Table.43)
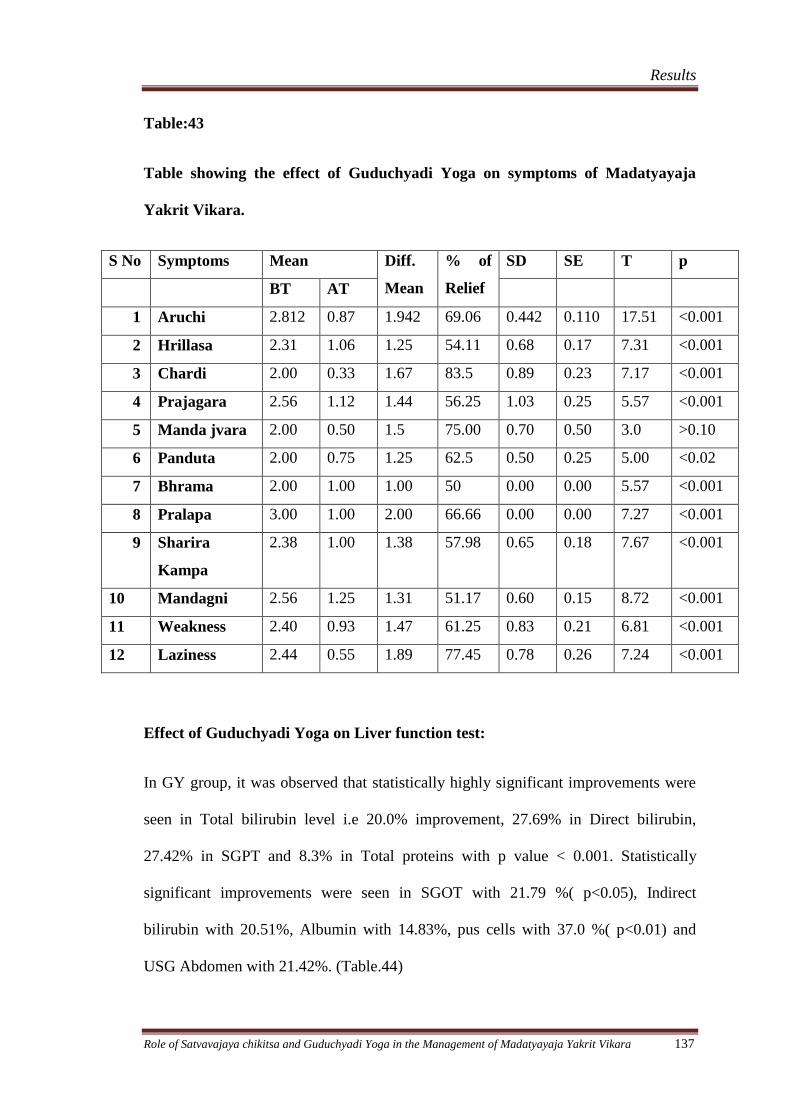
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 137
Table:43
Table showing the effect of Guduchyadi Yoga on symptoms of Madatyayaja
Yakrit Vikara.
S No Symptoms Mean Diff.
Mean
% of
Relief
SD SE T p
BT AT
1 Aruchi 2.812 0.87 1.942 69.06 0.442 0.110 17.51 <0.001
2 Hrillasa 2.31 1.06 1.25 54.11 0.68 0.17 7.31 <0.001
3 Chardi 2.00 0.33 1.67 83.5 0.89 0.23 7.17 <0.001
4 Prajagara 2.56 1.12 1.44 56.25 1.03 0.25 5.57 <0.001
5 Manda jvara 2.00 0.50 1.5 75.00 0.70 0.50 3.0 >0.10
6 Panduta 2.00 0.75 1.25 62.5 0.50 0.25 5.00 <0.02
7 Bhrama 2.00 1.00 1.00 50 0.00 0.00 5.57 <0.001
8 Pralapa 3.00 1.00 2.00 66.66 0.00 0.00 7.27 <0.001
9 Sharira
Kampa
2.38 1.00 1.38 57.98 0.65 0.18 7.67 <0.001
10 Mandagni 2.56 1.25 1.31 51.17 0.60 0.15 8.72 <0.001
11 Weakness 2.40 0.93 1.47 61.25 0.83 0.21 6.81 <0.001
12 Laziness 2.44 0.55 1.89 77.45 0.78 0.26 7.24 <0.001
Effect of Guduchyadi Yoga on Liver function test:
In GY group, it was observed that statistically highly significant improvements were
seen in Total bilirubin level i.e 20.0% improvement, 27.69% in Direct bilirubin,
27.42% in SGPT and 8.3% in Total proteins with p value < 0.001. Statistically
significant improvements were seen in SGOT with 21.79 %( p<0.05), Indirect
bilirubin with 20.51%, Albumin with 14.83%, pus cells with 37.0 %( p<0.01) and
USG Abdomen with 21.42%. (Table.44)
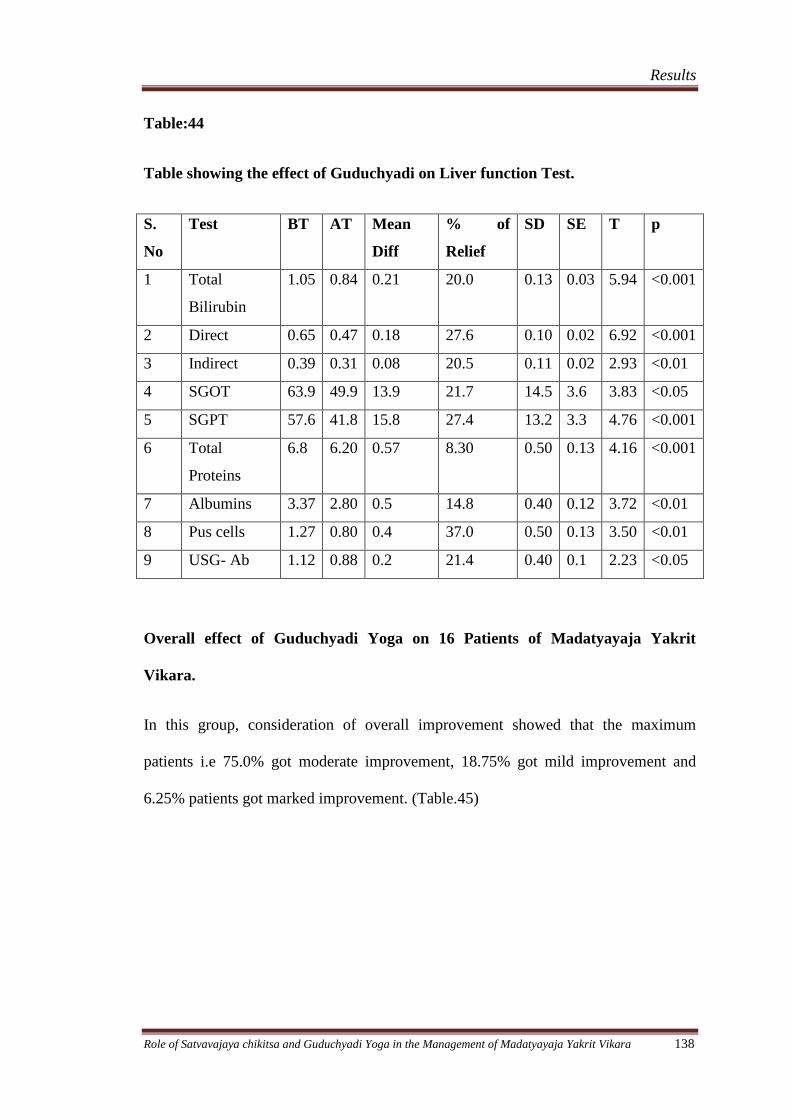
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 138
Table:44
Table showing the effect of Guduchyadi on Liver function Test.
S.
No
Test BT AT Mean
Diff
% of
Relief
SD SE T p
1 Total
Bilirubin
1.05 0.84 0.21 20.0 0.13 0.03 5.94 <0.001
2 Direct 0.65 0.47 0.18 27.6 0.10 0.02 6.92 <0.001
3 Indirect 0.39 0.31 0.08 20.5 0.11 0.02 2.93 <0.01
4 SGOT 63.9 49.9 13.9 21.7 14.5 3.6 3.83 <0.05
5 SGPT 57.6 41.8 15.8 27.4 13.2 3.3 4.76 <0.001
6 Total
Proteins
6.8 6.20 0.57 8.30 0.50 0.13 4.16 <0.001
7 Albumins 3.37 2.80 0.5 14.8 0.40 0.12 3.72 <0.01
8 Pus cells 1.27 0.80 0.4 37.0 0.50 0.13 3.50 <0.01
9 USG- Ab 1.12 0.88 0.2 21.4 0.40 0.1 2.23 <0.05
Overall effect of Guduchyadi Yoga on 16 Patients of Madatyayaja Yakrit
Vikara.
In this group, consideration of overall improvement showed that the maximum
patients i.e 75.0% got moderate improvement, 18.75% got mild improvement and
6.25% patients got marked improvement. (Table.45)
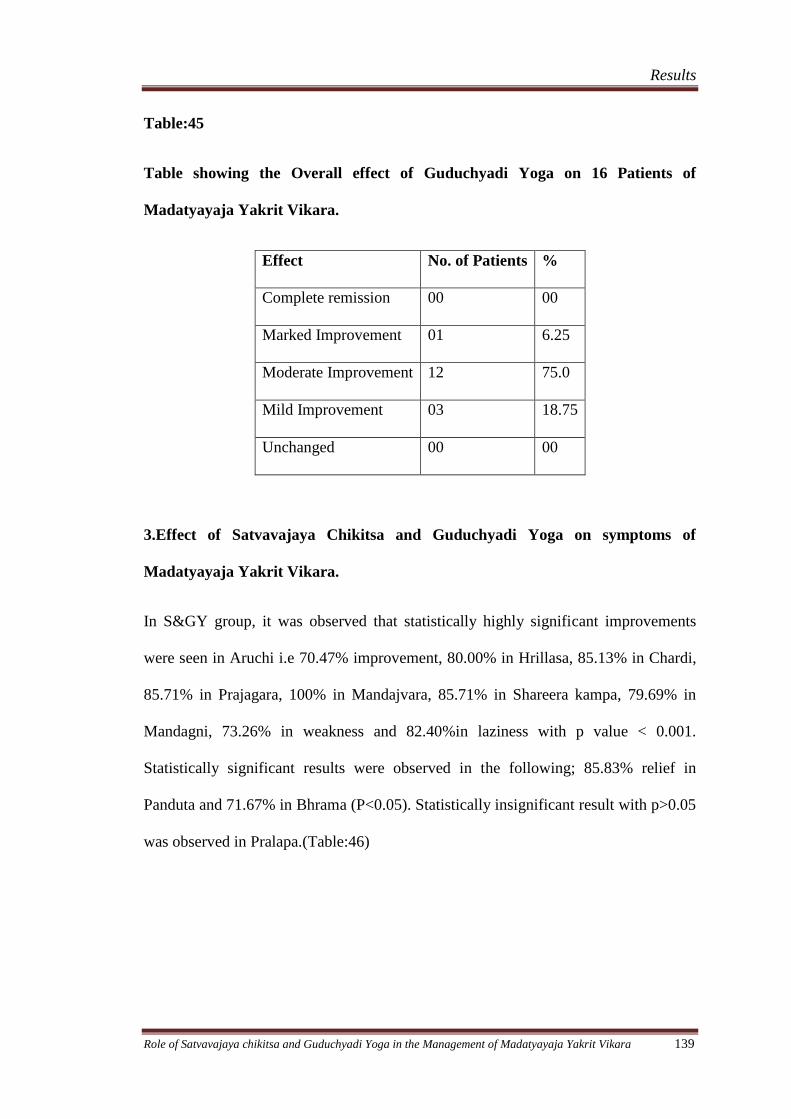
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 139
Table:45
Table showing the Overall effect of Guduchyadi Yoga on 16 Patients of
Madatyayaja Yakrit Vikara.
Effect No. of Patients %
Complete remission 00 00
Marked Improvement 01 6.25
Moderate Improvement 12 75.0
Mild Improvement 03 18.75
Unchanged 00 00
3.Effect of Satvavajaya Chikitsa and Guduchyadi Yoga on symptoms of
Madatyayaja Yakrit Vikara.
In S&GY group, it was observed that statistically highly significant improvements
were seen in Aruchi i.e 70.47% improvement, 80.00% in Hrillasa, 85.13% in Chardi,
85.71% in Prajagara, 100% in Mandajvara, 85.71% in Shareera kampa, 79.69% in
Mandagni, 73.26% in weakness and 82.40%in laziness with p value < 0.001.
Statistically significant results were observed in the following; 85.83% relief in
Panduta and 71.67% in Bhrama (P<0.05). Statistically insignificant result with p>0.05
was observed in Pralapa.(Table:46)
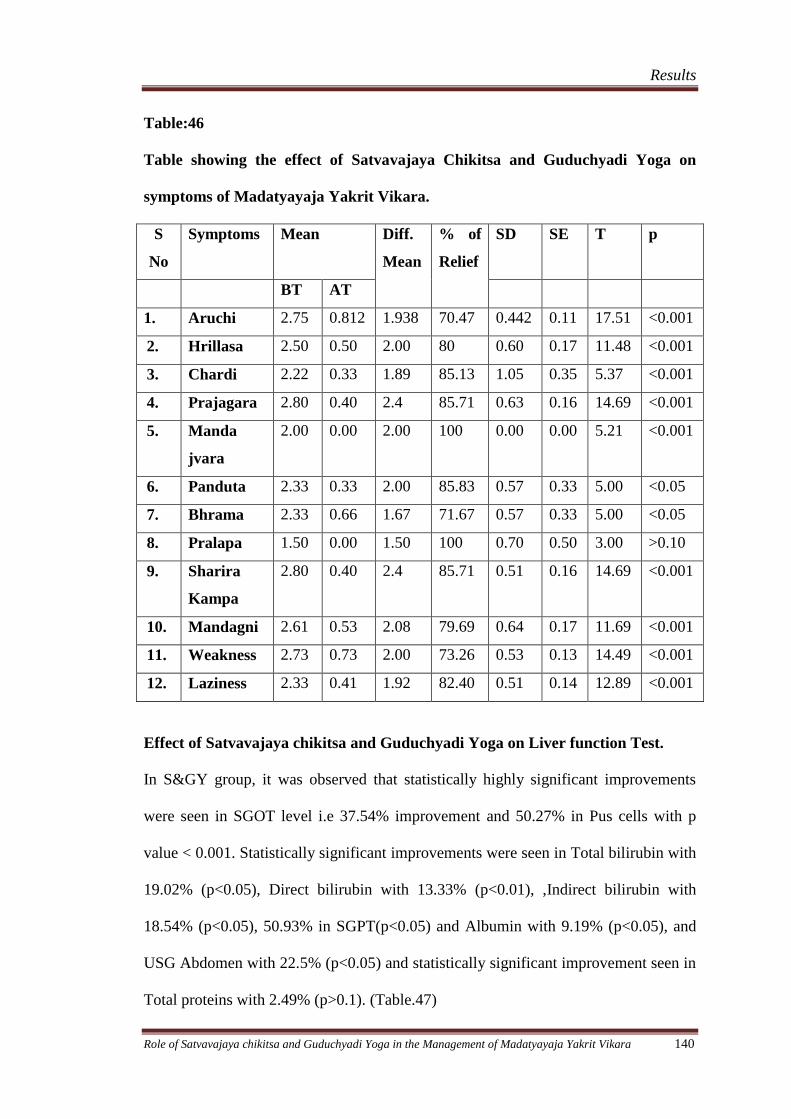
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 140
Table:46
Table showing the effect of Satvavajaya Chikitsa and Guduchyadi Yoga on
symptoms of Madatyayaja Yakrit Vikara.
S
No
Symptoms Mean Diff.
Mean
% of
Relief
SD SE T p
BT AT
1. Aruchi 2.75 0.812 1.938 70.47 0.442 0.11 17.51 <0.001
2. Hrillasa 2.50 0.50 2.00 80 0.60 0.17 11.48 <0.001
3. Chardi 2.22 0.33 1.89 85.13 1.05 0.35 5.37 <0.001
4. Prajagara 2.80 0.40 2.4 85.71 0.63 0.16 14.69 <0.001
5. Manda
jvara
2.00 0.00 2.00 100 0.00 0.00 5.21 <0.001
6. Panduta 2.33 0.33 2.00 85.83 0.57 0.33 5.00 <0.05
7. Bhrama 2.33 0.66 1.67 71.67 0.57 0.33 5.00 <0.05
8. Pralapa 1.50 0.00 1.50 100 0.70 0.50 3.00 >0.10
9. Sharira
Kampa
2.80 0.40 2.4 85.71 0.51 0.16 14.69 <0.001
10. Mandagni 2.61 0.53 2.08 79.69 0.64 0.17 11.69 <0.001
11. Weakness 2.73 0.73 2.00 73.26 0.53 0.13 14.49 <0.001
12. Laziness 2.33 0.41 1.92 82.40 0.51 0.14 12.89 <0.001
Effect of Satvavajaya chikitsa and Guduchyadi Yoga on Liver function Test.
In S&GY group, it was observed that statistically highly significant improvements
were seen in SGOT level i.e 37.54% improvement and 50.27% in Pus cells with p
value < 0.001. Statistically significant improvements were seen in Total bilirubin with
19.02% (p<0.05), Direct bilirubin with 13.33% (p<0.01), ,Indirect bilirubin with
18.54% (p<0.05), 50.93% in SGPT(p<0.05) and Albumin with 9.19% (p<0.05), and
USG Abdomen with 22.5% (p<0.05) and statistically significant improvement seen in
Total proteins with 2.49% (p>0.1). (Table.47)
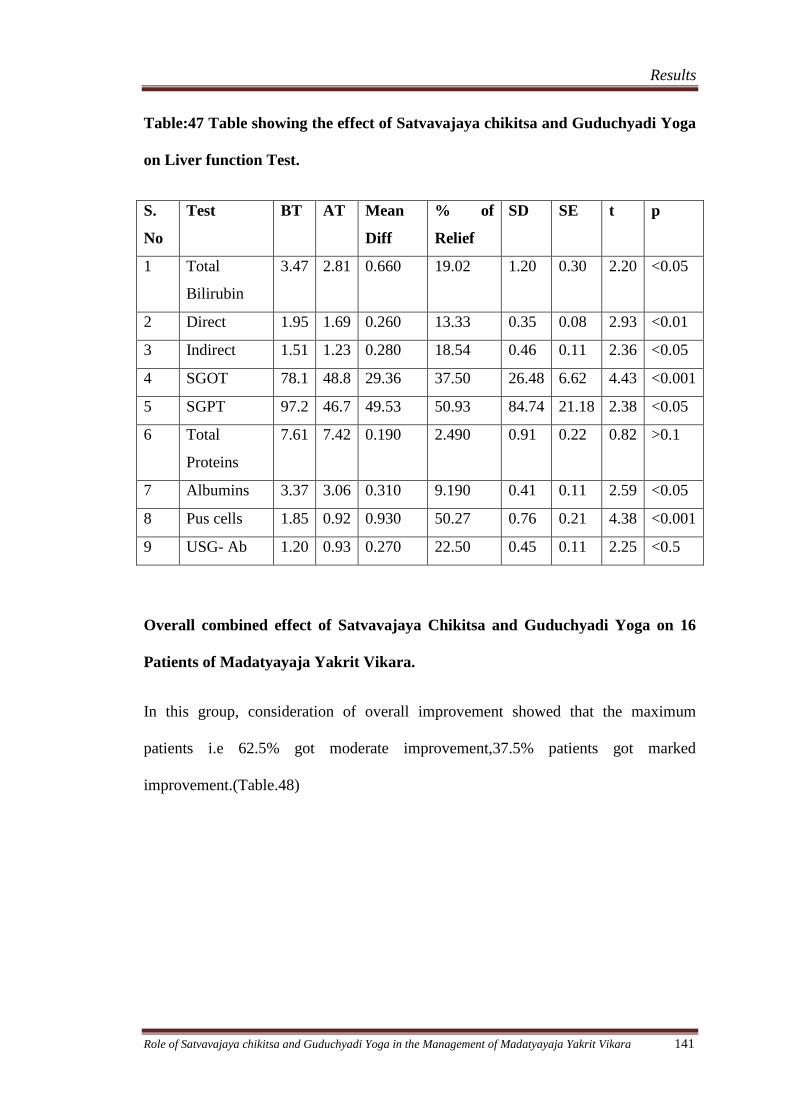
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 141
Table:47 Table showing the effect of Satvavajaya chikitsa and Guduchyadi Yoga
on Liver function Test.
S.
No
Test BT AT Mean
Diff
% of
Relief
SD SE t p
1 Total
Bilirubin
3.47 2.81 0.660 19.02 1.20 0.30 2.20 <0.05
2 Direct 1.95 1.69 0.260 13.33 0.35 0.08 2.93 <0.01
3 Indirect 1.51 1.23 0.280 18.54 0.46 0.11 2.36 <0.05
4 SGOT 78.1 48.8 29.36 37.50 26.48 6.62 4.43 <0.001
5 SGPT 97.2 46.7 49.53 50.93 84.74 21.18 2.38 <0.05
6 Total
Proteins
7.61 7.42 0.190 2.490 0.91 0.22 0.82 >0.1
7 Albumins 3.37 3.06 0.310 9.190 0.41 0.11 2.59 <0.05
8 Pus cells 1.85 0.92 0.930 50.27 0.76 0.21 4.38 <0.001
9 USG- Ab 1.20 0.93 0.270 22.50 0.45 0.11 2.25 <0.5
Overall combined effect of Satvavajaya Chikitsa and Guduchyadi Yoga on 16
Patients of Madatyayaja Yakrit Vikara.
In this group, consideration of overall improvement showed that the maximum
patients i.e 62.5% got moderate improvement,37.5% patients got marked
improvement.(Table.48)
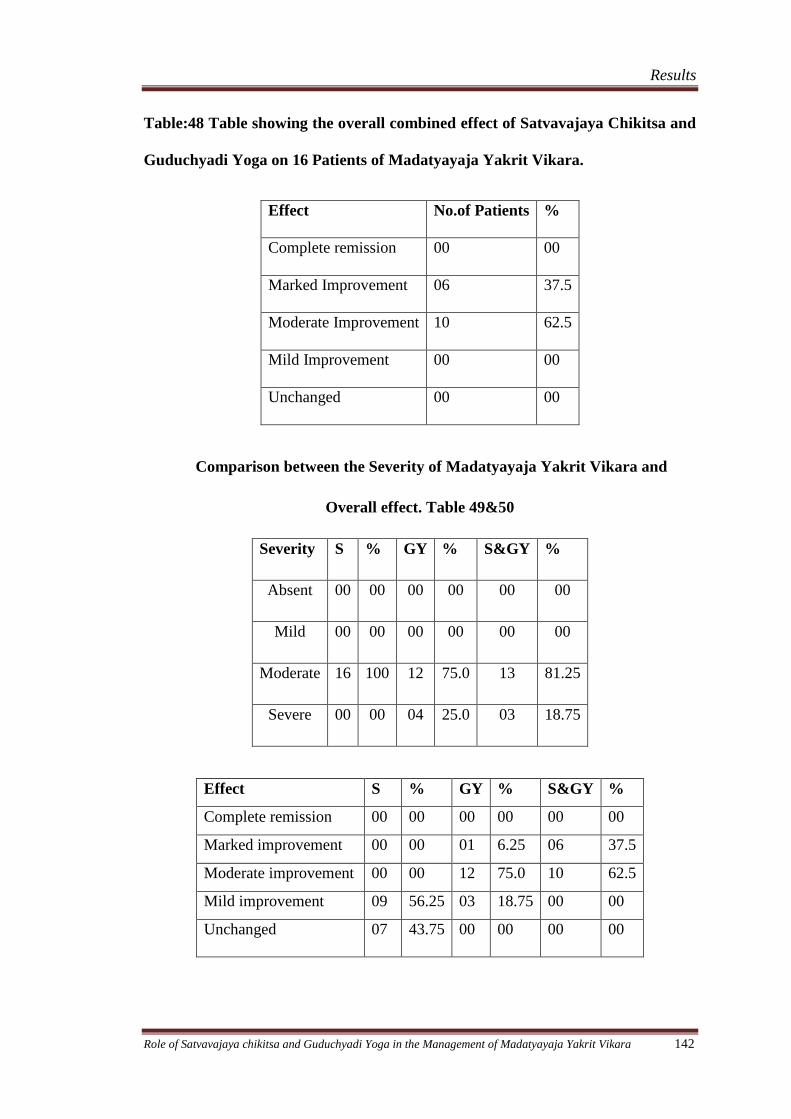
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 142
Table:48 Table showing the overall combined effect of Satvavajaya Chikitsa and
Guduchyadi Yoga on 16 Patients of Madatyayaja Yakrit Vikara.
Effect No.of Patients %
Complete remission 00 00
Marked Improvement 06 37.5
Moderate Improvement 10 62.5
Mild Improvement 00 00
Unchanged 00 00
Comparison between the Severity of Madatyayaja Yakrit Vikara and
Overall effect. Table 49&50
Severity S % GY % S&GY %
Absent 00 00 00 00 00 00
Mild 00 00 00 00 00 00
Moderate 16 100 12 75.0 13 81.25
Severe 00 00 04 25.0 03 18.75
Effect S % GY % S&GY %
Complete remission 00 00 00 00 00 00
Marked improvement 00 00 01 6.25 06 37.5
Moderate improvement 00 00 12 75.0 10 62.5
Mild improvement 09 56.25 03 18.75 00 00
Unchanged 07 43.75 00 00 00 00
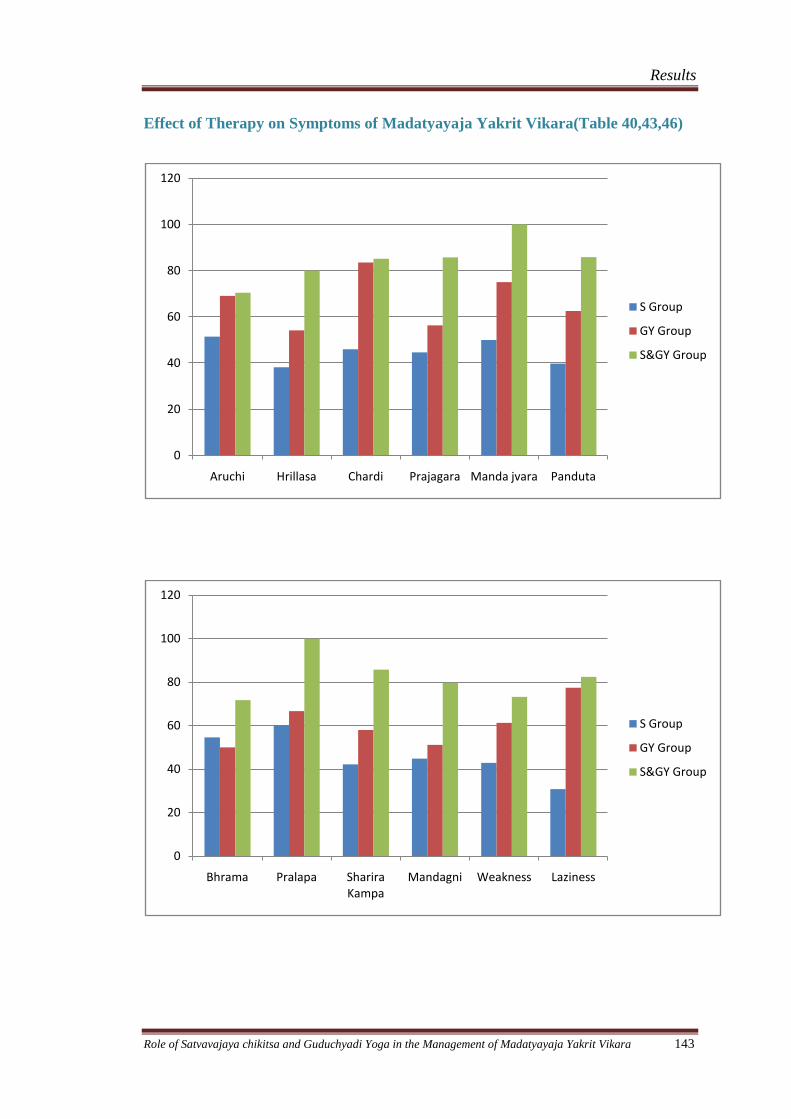
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 143
Effect of Therapy on Symptoms of Madatyayaja Yakrit Vikara(Table 40,43,46)
0
20
40
60
80
100
120
Aruchi Hrillasa Chardi Prajagara Manda jvara Panduta
S Group
GY Group
S&GY Group
0
20
40
60
80
100
120
Bhrama Pralapa Sharira Kampa
Mandagni Weakness Laziness
S Group
GY Group
S&GY Group
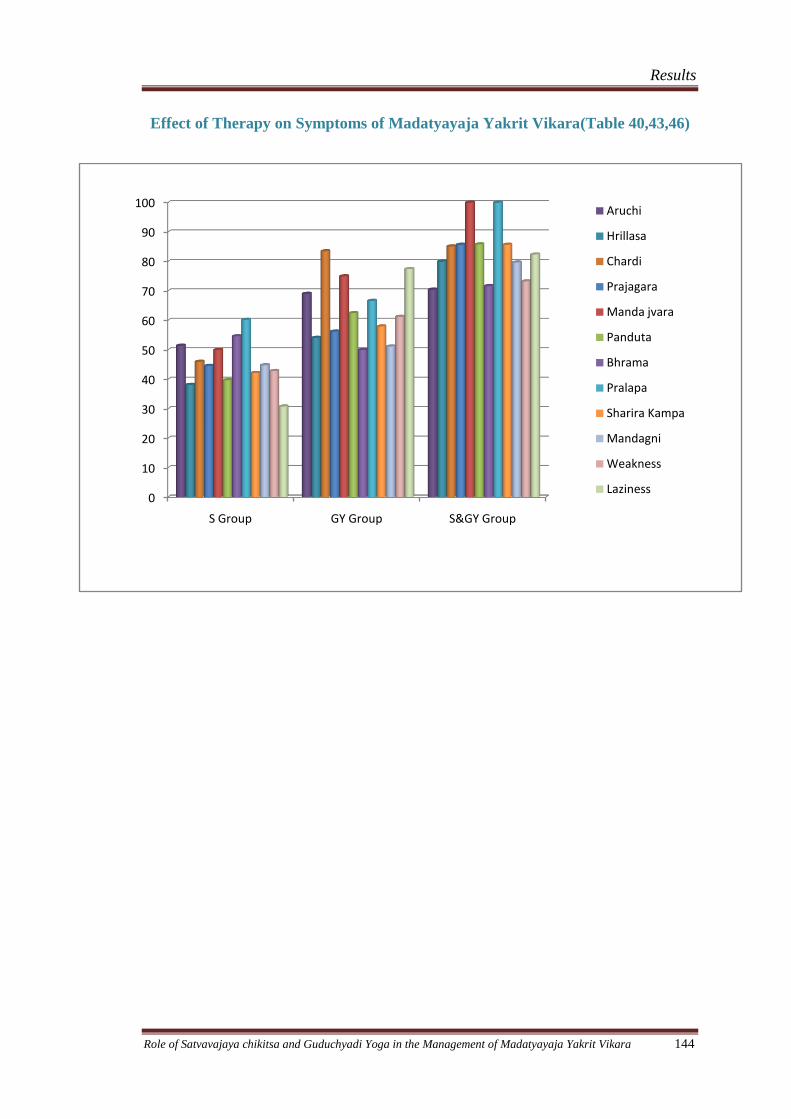
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 144
Effect of Therapy on Symptoms of Madatyayaja Yakrit Vikara(Table 40,43,46)
0
10
20
30
40
50
60
70
80
90
100
S Group GY Group S&GY Group
Aruchi
Hrillasa
Chardi
Prajagara
Manda jvara
Panduta
Bhrama
Pralapa
Sharira Kampa
Mandagni
Weakness
Laziness
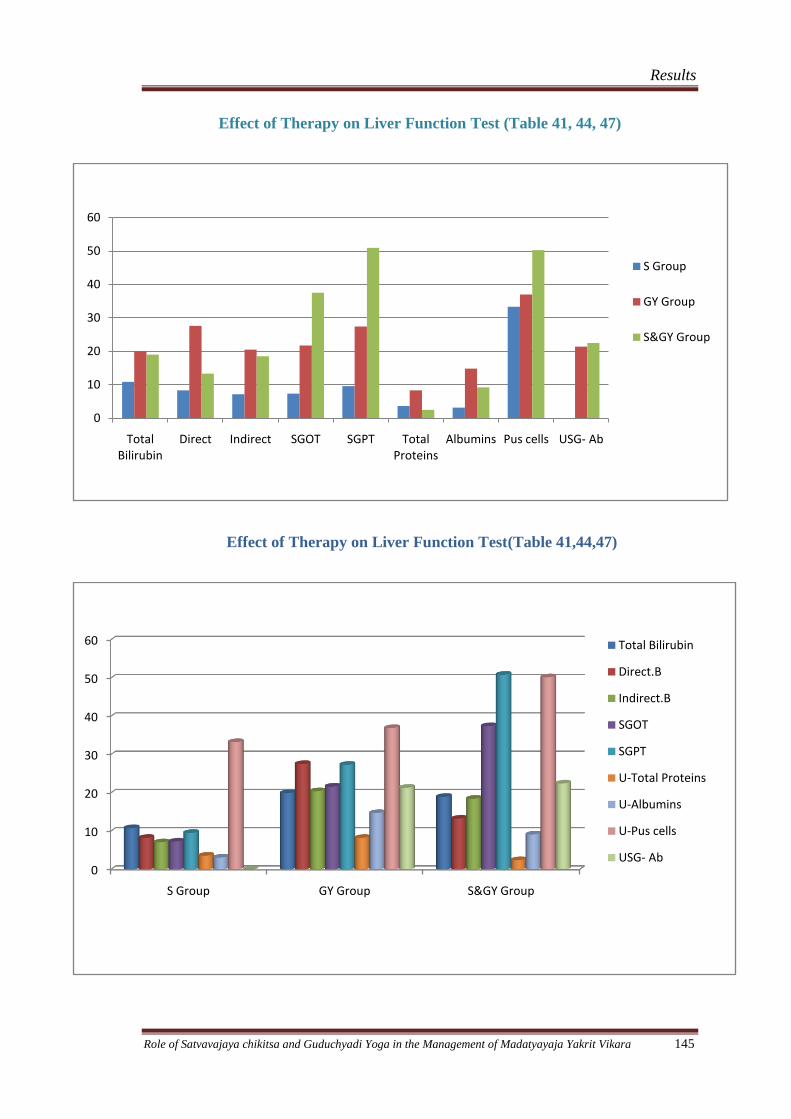
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 145
Effect of Therapy on Liver Function Test (Table 41, 44, 47)
Effect of Therapy on Liver Function Test(Table 41,44,47)
0
10
20
30
40
50
60
Total Bilirubin
Direct Indirect SGOT SGPT Total Proteins
Albumins Pus cells USG- Ab
S Group
GY Group
S&GY Group
0
10
20
30
40
50
60
S Group GY Group S&GY Group
Total Bilirubin
Direct.B
Indirect.B
SGOT
SGPT
U-Total Proteins
U-Albumins
U-Pus cells
USG- Ab
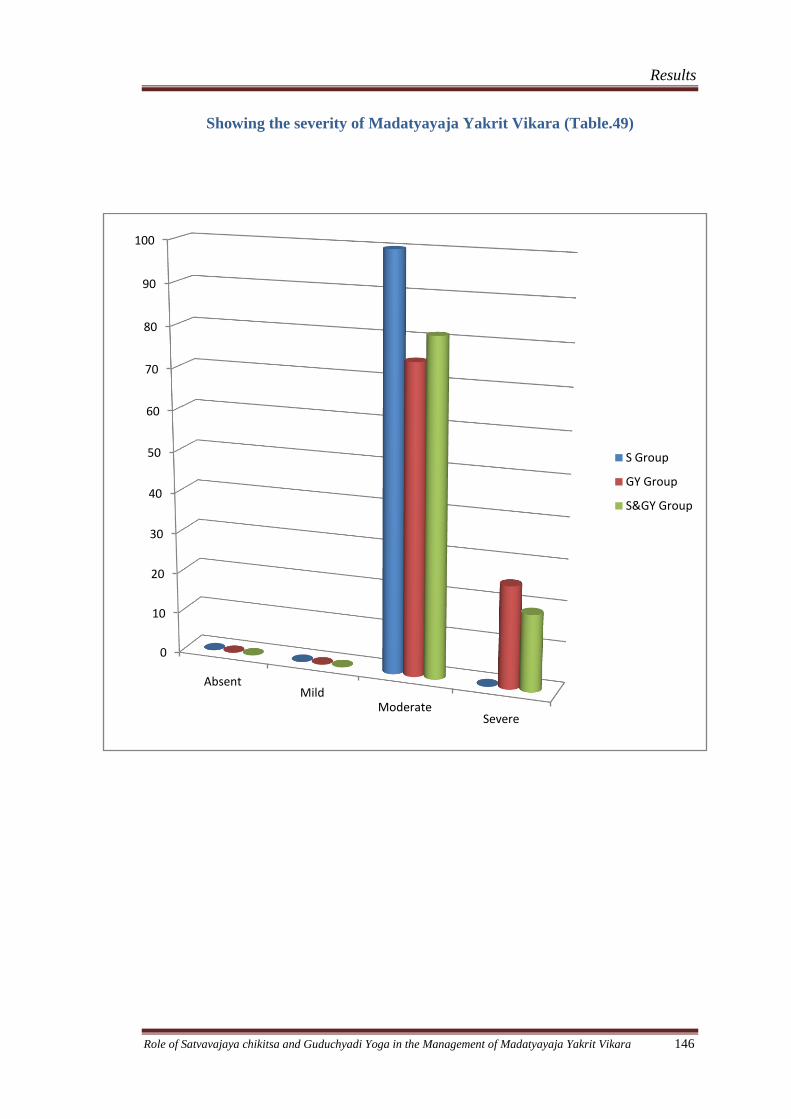
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 146
Showing the severity of Madatyayaja Yakrit Vikara (Table.49)
0
10
20
30
40
50
60
70
80
90
100
AbsentMild
ModerateSevere
S Group
GY Group
S&GY Group
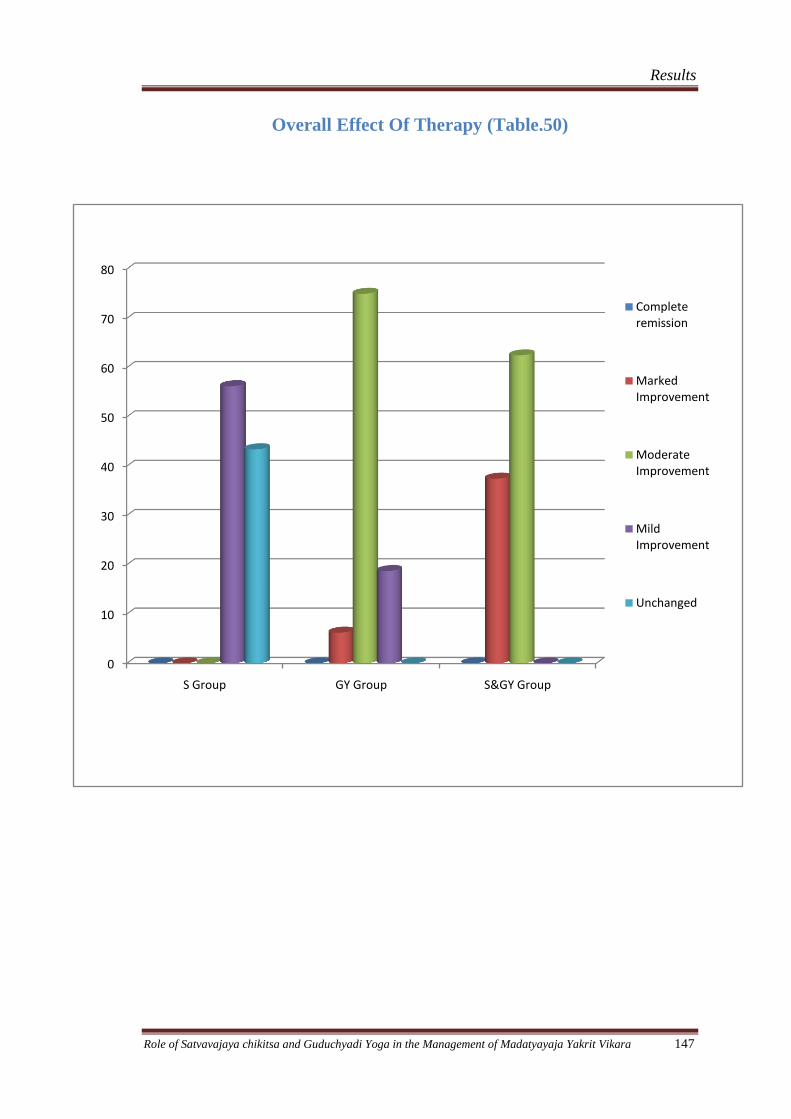
Results
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 147
Overall Effect Of Therapy (Table.50)
0
10
20
30
40
50
60
70
80
S Group GY Group S&GY Group
Complete remission
Marked Improvement
Moderate Improvement
Mild Improvement
Unchanged
Discussion
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 148
DISCUSSION
Day by day the prevalence of alcohol liver disorders is increasing in India may be
because of effect of media or attraction towards the western culture. An increasing
rate of consumption of alcohol is a major problem with extensive legal, social, moral,
ethical consequences all over the world irrespective of cultural, geographical,
educational, and economic differences. Indiscriminate and repeated use of alcohol
produces a gradual, physical and moral deterioration of the individual and leads to
crimes or perversions. This alcohol abuse interferes with the health, social
relationships, economic stability which have effects further in other areas in terms of
illness, disability, decreased productivity, accidents, crimes, family disorientation,
economic and psychological hardships, and lastly death in all classes of the society.
According to Ayurveda, the good qualities of alcohol when used judiciously well for
health but when used against the rules and regulations it may lead to adverse effects.
The other factors like nutritional deficiency, poor physical health, other systemic
pathologies, lack of emotional and family support etc increase the severity of the
withdrawal state.
For the person suffering from Madatyayaja yakrit vikara due to heavy and prolonged
consumption of alcohol, the first aim of the treatment should be safer resolution of
withdrawal state. That is why this study entitled “Role of Satvavaja chikitsa and
Guduchyadi Yoga in the management of Madatyayaja Yakrit Vikara” was carried out.
Satvavajaya Chikitsa may help people to address psychological issues involved in
their drinking problem. Astanga Hrudaya explains Vismapana, Vismarana,
Priyadarshana, Priyashravana, Geeta, Vadya and Charaka advises Harshanee Kriya
and restrain from the things which are harmful to body and mind as the treatment
modalities in the management of Madatyaya.
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 149
The patients of this group were subjected to Satvavajaya Chikitsa daily along with
placebo capsule 500 mg starch thrice daily for 1 month.
Ayurveda has many options to treat Madatyayaja yakrit vikara . All the texts mention
Pittahara and Deepana Pachana Dravyas to treat Yakrit-Vikaras. Guduchyadi Yoga
mentioned by Charaka comprising of Guduchi (Tinospora cordifolia), Musta(Cyperus
rotundus), Patola(Tricosanthes dioica) and Nagara(Gingeber officinalis) may relieve
the adverse effects of Madatyaya as well as liver disorders caused by it.
Guduchyadi Yoga which is mentioned as Madatyaya upadrava nashaka, is also has
Agni Deepana property. In Madatyaya due to Madya along with Agni Dusthi, Pitta
dosha is also increased. To treat that Guduchyadi Yoga was selected. The patients of
this group were given Guduchyadi yoga in the dose of 5 gm, before food with warm
water thrice daily for 1 month.
Satvavaja chikitsa and Guduchyadi Yoga combined group is taken to study to see the
effect of combined group and to see the difference among other groups.
48 patients of Madatyayaja Yakrit vikara were studied in this series; the significance
of their demographic is being discussed here under in each heading:
Age: This study shows the prevalence of Madatyayaja Yakrit Vikara is more
(34.7%,27.3% and 27.3 %) in 3rd
, 4th
and 5th decade, its prevalence goes down in
elderly people may be either by this time most of the people has left the habit of
alcohol because of their health problem or the problems produced due to alcohol itself
(Table - 18).
A large scale study (Karan Gaur, 2002) showed 21% incidence in
second decade, 42% in third decade and 26.5% in the fourth decade.
Sex: In this study all patients were male, this may be because of the Male dominancy
and addiction are more seen in males around the Hassan or the females may not
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 150
approach the hospital for taking treatment for such problems (Table - 19). Edwin
Sharon (2006) in his study on “Is Alcohol provokes liver disorder in men than in
women?” reported that male patients were more likely to experience liver disorders
than female.
Occupation: This study reveals the prevalence of Madatyaya is more in Business
people with 48.2 %, then Agriculturist were 27.65 % out of 48 patients. This may
because of stress of business and strain of agriculture, Friends Company and Students
were 25.2% out of 48, because of curiosity and peer group pressure. (Table - 20).
Bidadar (2003) in large sample of more than 2000 patients reported that Business men
(51%) were more prone to alcoholic addictions.
Socio – economic status: 91.6% of patients were belonging to Middle class income
group, this may be because of the more people surrounding Hassan are belonging to
Medium income group, worries and stresses are more in middle class people (Table -
21).
Marital status: Out of 48 patients 76.8 % were married, this may be because the
more incidences were found in the age group of 30 – 40 years in this study, by this
time the most of the people in India were got married, only 23.2% were unmarried
that is because they were belonging to below 30 years of age. The family tensions,
quarrels and conflicts make the married to start or continue the habit of alcohol to get
rid of these problems (Table - 22).
Education status: Educational status of this study revealed maximum ( 65.1%)
patients were educated till higher secondary, this may be because the education status
in the mid 1970s, the only one person has not been educated that was because of his
socio – economic status (Table - 23).
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 151
Age of starting of alcohol: 46.2 % of people had their first drink in between 10 – 20
years of age of life, this may be because of the first time most people expose to
society individually at this age or the first drink is usually starts at the college days
because a high proportion of people are drinkers, especially in their middle teens to
mid-20s (Table - 24). 161
Duration of daily drinking: In this study 79.0 % of people were having alcohol daily
since 1 – 5 years, this may be because the people come / brought to hospital in the
initial stage of disease, and this study reveals even taking alcohol daily only for few
years will produce noticeable disturbance in health, social, and occupational life
(Table - 25).
Type of alcohol: This study shown maximum people (64.3%) take Whisky, 12.6 % of
people take brandy, this may be because of cost, the Whisky being cheaper and
produces maximum kick hence maximum people use it and local beverages are still in
use in spite of ban over it. (Table - 26).
First drink of the day: Out of 48 patients 48.0 % of patients start drink at morning,
42.0 % of patients drink at evening. Even less number of subjects starts their first
drink at night but they have more serious problems than other may be because of
other factors like their stressful life style, co morbid disorders like Hypertension,
Diabetes. As there are many patients start their first drink at morning so they have
noticeable problems so have approached hospital for assistance. That also shows the
dependency on alcohol or the severity of addiction to the alcohol (Table - 27).
Prakriti: Vatapitta Prakriti patients were more with 35.7%, may be because the
patients with this Prakriti may suffer with Madatyayaja Yakrit Vikara more often
than other Prakriti (Table - 28).
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 152
Sara, Samhanana, Pramana, Saathmya: Out of 48 patients 93.7% patients had
Madhyama Sara, 93.7 % of patients had Madhyama Samhanana, 91.6 % patients had
Madhyama Pramana and 93.7% patients had Madhyama Saathmya. (Table 29, 30,
30.1, 35) The judicious usage of alcohol improves the health on the contrary the
dependence, excessive usage and improper usages reduces the compactness,
nutritional state and quality of tissues. This may be because of vitiation of Agni and
the Srotosanga which are produced due to Madya.
Jarana Shakti, Abhyavarana Shakti and Vyayama Shakti: Out of 48 patients 68.5
% of patients had Avara Jarana Shakti, 42 % of patients had Avara Abhyavarana
Shakti, 63.0 % patients Avara Vyayama Shakti (Table 34, 33, 32). It’s quite evident
that the Madya directly vitiates the Agni and the persons capacity of quantity of
consumption of food reduces and also the digestion power. Because of the reduced
nutritional status a physical power also hampers. The observations of the present
study also prove the same.
Satva: In the present study 91.6% had Madhyama Satva, followed by 6.3 % had
Avara Satva (Table - 31). The addictions and abuses are commonly seen in the weak
and moderate level minded persons. Though the Pravara Satva people may be
addicted but they may easily overcome the consequences of addiction. The Avara
Satva and Madhyama Satva people needs the help or motivation to overcome the
addiction.
Other habits: Out of 48 patients 62.2% people were smokers, because of alcohol
drinkers’ smoke more often during the time of alcohol intake (Table - 36).
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 153
Psychiatric complications: Out of 48 patients 12.6% of patients were having
depression, that shows that alcohol dependency causes Vishada because of increased
Tamo guna by Madya.(Table - 37).
Relationship with spouse: Out of 48 patients 27.3% patients were having
unaffectionate relationship with spouse. This clearly shows alcohol addiction directly
affect the healthy family relationships. (Table-38)
Discussion on results:
Satvavajaya chikitsa group, Guduchyadi Yoga group and Combined group showed
different amount of relief on the symptoms of Madatyayaja Yakrit Vikara and
improvement amount of each symptoms and their differences discussed below.
Effect on Aruchi:
S group provided 51.44% improvement, GY group provided 69.06% improvement
and S&GY group provided 70.47% improvement on Aruchi which is statistically
highly significant (p<0.001) .It shows that combined group is given more relief
because the action of therapy acts both on the mind and vitiated condition of the
body. Guduchyadi Yoga showed very good Deepaka- pachaka action and Agni
deepaka property.
Effect on Hrillasa:
S group provided 38.16% improvement , GY group provided 54.11% improvement
and S&GY group provided 80.0% improvement on Hrillasa which is statistically
highly significant (p<0.001). It shows that combined group is given more relief
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 154
because the Guduchyadi Yoga acts as very good deepaka- pachaka and pitta rechaka
action and satvavajaya chikitsa helped in controlling the nidana.
Effect on Chardi: S group provided 46.0% improvement, GY group provided 83.5%
improvement and S&GY group provided 85.13% relief on chardi which is statistically
highly significant (p<0.001) .It shows that combined group is given more relief
because the action of therapy acts physically and psychologically. Guduchyadi Yoga
acts Deepaka- pachaka, Agni deepaka and Vatanulomaka property. Tikta rasa of
Guduchyadi yoga acts as Pitta shamaka.
Effect on Prajagara: S group provided 44.58% improvement , GY group provided
56.25% improvement and S&GY group provided 85.71% improvement on Prajagara
which is statistically highly significant (p<0.001). It shows that combined group is
given more relief because the action of therapy acts Manah prasadakara and Pitta
shamaka. After therapy food intake become normal which in turn regulate the sleep.
Effect on Mandajvara: S group provided 50.0% relief (p<0.02), GY group provided
75.0% relief and S&GY group provided 100% relief on Mandajvara which is
statistically highly significant (p<0.001) .It shows that Aashwasana therapy and Tikta
rasa of Guduchyadi yoga acted as Jvaragna thereby decreased the body temperature.
Effect on Panduta: S group provided 39.75% improvement which is statistically
insignificant, GY group provided 62.5% (p<0.02) improvement and S&GY group
provided 85.83% improvement on Panduta which is statistically significant (p<0.05).
It shows that Guduchyadi yoga acts as Pittarechaka and removed Amshamsha
Samprapti of Panduta.
Effect on Bhrama: S group provided 54.64% improvement (p<0.02), GY group
provided 50.0% (p<0.05) improvement and S&GY group provided 71.67%
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 155
improvement on Bhrama which is statistically significant (p<0.05). It shows that
Guduchyadi yoga acts as Pitta shamaka and thereby Bhrama nashaka.
Effect on Pralapa: S group provided 60.24% improvement, , S&GY group provided
100% improvement on Bhrama which is statistically insignificant (p>0.10) which is
statistically insignificant and GY group provided 66.0% (p<0.05) improvement and .It
shows that Guduchyadi yoga alone acted on Pralapa.
Effect on Shareera kampa: S group provided 42.18% improvement (p<0.02) which
is statistically significant, GY group provided 57.98% improvement and S&GY
group provided 85.71% improvement on Shareera kampa which is statistically highly
significant (p<0.001). This data clarifies Satvavajaya given mental streangth to
withhold the Indriya and Guduchyadi yoga acted as Vatanulomaka and Rasayana.
Effect on Mandagni: S group provided 44.81% improvement , GY group provided
51.17% improvement and S&GY group provided 79.69% improvement on Mandagni
which is statistically highly significant (p<0.001). It shows that combined group is
given more relief because the action of therapy acts both on the mind and vitiated
condition of the body. Guduchyadi Yoga showed very good Deepana- pachana action.
Effect on Weakness: : S group provided 42.85% improvement (p<0.01) which is
statistically significant, GY group provided 61.25% improvement and S&GY group
provided 73.26% improvement on weakness which is statistically highly significant
(p<0.001). Satvavajaya given mental strength and that confirms mental stability is
directly influences on physical strength and Guduchyadi yoga acted as Agnivardhaka
and Rasayana.
Effect on Laziness: : S group provided 30.81% improvement (p<0.05) which is
statistically significant, GY group provided 77.45% improvement and S&GY group
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 156
provided 82.40% improvement on laziness which is statistically highly significant
(p<0.001). Satvavajaya given enthusiasm and helped to start new style of life.
Guduchyadi yoga acted as Agnivardhaka and Rasayana.
Effect on Liver Function Test:
Effect on Total Billirubin:
S group provided 10.85% improvement, GY group provided 20.00% improvement
and S&GY group provided 19.02% improvement on Total bilirubin which is
statistically significant (p<0.05) .
Effect on Direct Billirubin:
S group provided 8.3% improvement , GY group provided 27.69% improvement and
S&GY group provided 13.33% improvement on Direct billirubin which is
statistically significant (p<0.01)
Effect on Indirect Billirubin:
S group provided 7.14% improvement (p>0.1) which is statistically insignificant, GY
group provided 20.51% improvement and S&GY group provided 18.54%
improvement on Indirect billirubin which is statistically significant (p<0.05) .
Effect on SGOT:
S group provided 7.34% improvement, GY group provided 21.79% improvement and
S&GY group provided 37.54% improvement on SGOT which is statistically
significant (p<0.05) .
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 157
Effect on SGPT:
S group provided 9.60% improvement , GY group provided 27.42% improvement and
S&GY group provided 50.93% improvement on SGPT which is statistically
significant (p<0.05) .
Effect on Total Protein:
S group provided 3.65% improvement, GY group provided 8.3% improvement which
is statistically significant (p<0.05) and S&GY group provided 2.49% improvement in
Total proteins which is statistically insignificant (p>0.1).
Effect on Albumin:
S group provided 3.17% improvement which is statistically insignificant (p>0.1) ,
GY group provided 14.83% improvement and S&GY group provided 9.19%
improvement on Albumins which is statistically significant (p<0.05)
Effect on Pus cells:
S group provided 33.33% improvement which is statistically insignificant (p>0.1) ,
GY group provided 37.00% and S&GY group provided 50.27% improvement on Pus
cells which is statistically significant (p<0.05)
Effect on USG Abdomen:
S group provided 0% improvement which is statistically insignificant (p>0.1) , GY
group provided 21.42% and S&GY group provided 22.5% improvement on Pus cells
which is statistically significant (p<0.05)
As the Liver is one of the major organ related to digestion and metabolism and also
detoxification. Guduchyadi Yoga contains Deepana, Pachana and Srotoshodhan drugs
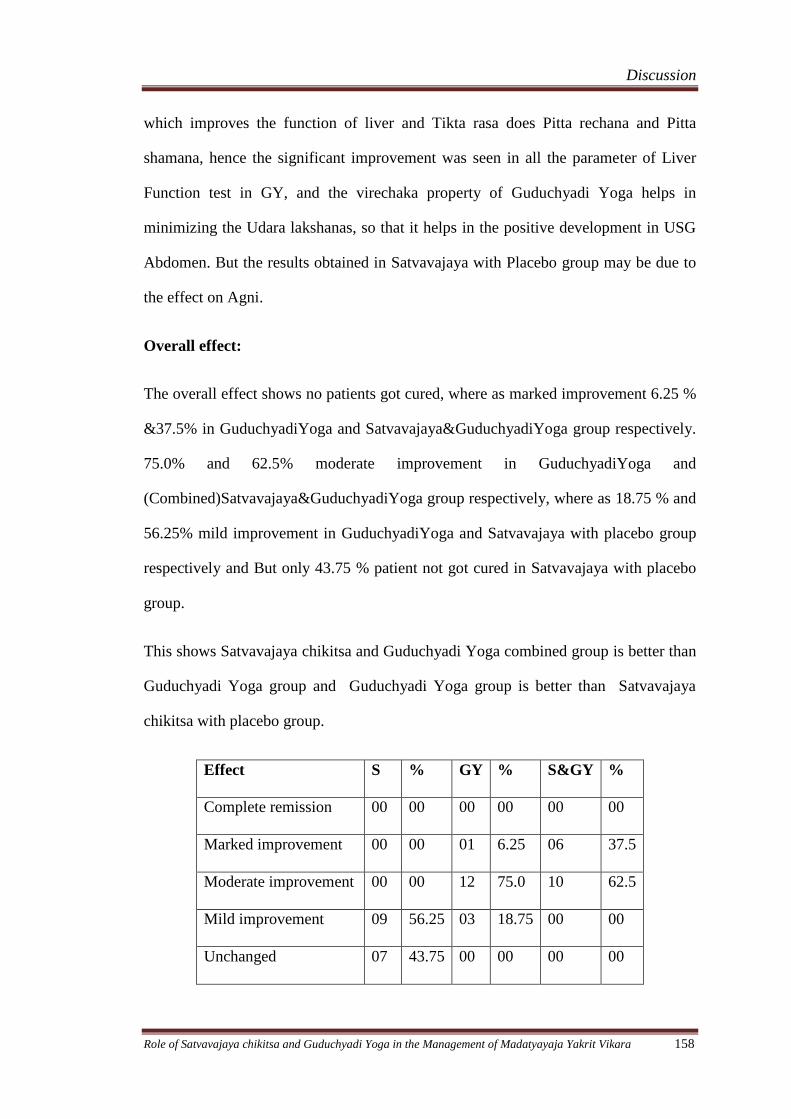
Discussion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 158
which improves the function of liver and Tikta rasa does Pitta rechana and Pitta
shamana, hence the significant improvement was seen in all the parameter of Liver
Function test in GY, and the virechaka property of Guduchyadi Yoga helps in
minimizing the Udara lakshanas, so that it helps in the positive development in USG
Abdomen. But the results obtained in Satvavajaya with Placebo group may be due to
the effect on Agni.
Overall effect:
The overall effect shows no patients got cured, where as marked improvement 6.25 %
&37.5% in GuduchyadiYoga and Satvavajaya&GuduchyadiYoga group respectively.
75.0% and 62.5% moderate improvement in GuduchyadiYoga and
(Combined)Satvavajaya&GuduchyadiYoga group respectively, where as 18.75 % and
56.25% mild improvement in GuduchyadiYoga and Satvavajaya with placebo group
respectively and But only 43.75 % patient not got cured in Satvavajaya with placebo
group.
This shows Satvavajaya chikitsa and Guduchyadi Yoga combined group is better than
Guduchyadi Yoga group and Guduchyadi Yoga group is better than Satvavajaya
chikitsa with placebo group.
Effect S % GY % S&GY %
Complete remission 00 00 00 00 00 00
Marked improvement 00 00 01 6.25 06 37.5
Moderate improvement 00 00 12 75.0 10 62.5
Mild improvement 09 56.25 03 18.75 00 00
Unchanged 07 43.75 00 00 00 00
Summary
&
Conclusion
Summary and Conclusion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 159
SUMMARY & CONCLUSION
For good health among various factors, Ahara is one important factor. Madya is
considered as one of the Aharadravya and it acts like ambrosia if taken properly
following the rules and regulations, otherwise it acts like a poison. In all the classics,
the adverse effects are described beautifully with suitable similes.
The present study entitled “Role of Satvavajaya chikitsa and Guduchyadi Yoga in the
management of Madatyayaja Yakrit Vikara” has been carried out with two objectives
viz., to study Madatyaya conceptually in detail and to clinically study the efficacy of
Satvavajaya Chikitsa and Guduchyadi Yoga in the management of Madatyayaja
Yakrit Vikara.
The work is presented in four sections viz., Conceptual study, Clinical study,
Observation, Results and Discussion with a brief Introduction as the preface of the
dissertation and Summary & Conclusion at the end.
Introduction gives the details of the study about its need and significance, statement of
the problem, objectives of the study.
In first major section conceptual study, classical descriptions of Madya, Madatyaya,
Madatyayaja Yakrit Vikaras and Satvavajaya chikitsa are explained including
modern explanations.
The second major section Clinical study comprises of two subsections Methodology
of the study and Observations & results.
Under the methodology of the study, the details about statement of the problem,
research design, selection of subjects - inclusion criteria and exclusion criteria,
research techniques and tools, treatment schedule, follow up, assessment & statistical
analysis and total effect of therapy are discussed.
Summary and Conclusion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 160
General Observations:
In this study maximum number (34.7%) of patients were belonging to 30 – 40 years
of age, all the patients were male (100 %), occupation wise maximum (48.2%,)
patients were Businessmen, socio – economic status wise 91.6 % of people were
belonging to Middle class income group, 76.8 % were married, 65.1 % patients were
educated till higher secondary, The average age of the starting of alcohol was 46.2 %
of people had their first drink in between 10 – 20 years of age of life, 79.0 % of
people were having alcohol daily since 1 – 5 years, maximum patients (64.3 %) take
Whisky as their drink, 48.0 % of patients start days drink at morning, Vatapitta
Prakruti subjects were more with 35.7 %.
Effect of Satvajaya chikitsa with placebo group:
Improvement were seen on Aruchi i.e 51.44% , 38.16% in Hrillasa, 44.58% in
Prajagara and 44.81% in Mandagni ,46.0% relief in chardi,50% in Manda jwara,
54.64% in Bhrama, 42.18% in Shareera kampa, 30.18% relief in Laziness and In total
bilirubin level i.e 10.85% improvement, 8.3% in Direct bilirubin, 7.34% in SGOT,
9.60% in SGPT ,3.65% in Total proteins, 7.14% in Indirect bilirubin, 33.33% in Pus
cells,3.17% in Albumins and 0% in USG –Abdomen
Effect of Guduchyadi Yoga group:
Improvements were seen in Aruchi i.e 69.06% , 54.11% in Hrillasa,83.5% in Chardi,
56.25 % in Prajagara, 57.98% in Shareera kampa, 51.17% in Mandagni, 61.25% in
Weakness, 77.45%in Laziness, 62.5% relief in Panduta,75.0% Mandajvara and in
Total bilirubin level i.e 20.0% improvement, 27.69% in Direct bilirubin, 27.42% in
SGPT , 8.3% in Total proteins, SGOT with 21.79% ,Indirect bikirubin with 20.51%,
Albumin with 14.83%, pus cells with 37.0% and USG Abdomen with 21.42%.
Summary and Conclusion
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 161
Effect of Combined group (Satvavajaya and Guduchyadi Yoga group):
Improvements were seen in Aruchi i.e 70.47% improvement, 80.00% in
Hrillasa,85.13% in Chardi, 85.71% in Prajagara, 100% in Mandajvara, 85.71% in
Shareera kampa, 79.69% in Mandagni, 73.26% in Weakness and 82.40%in Laziness,
85.83% relief in Panduta, 71.67% in Bhrama, 100% in Pralapa and SGOT level i.e
37.54% improvement, 50.27% in Pus cells, Total bilirubin with 19.02%,Direct
bilirubin with 13.33%,Indirect bilirubin with 18.54% , 50.93% in SGPT, Albumin
with 9.19%, Total proteins with 2.49% and USG Abdomen with 22.5%.
Overall effect:
The overall effect shows no patients got cured, where as marked improvement 6.25 %
&37.5% in GuduchyadiYoga and Satvavajaya&GuduchyadiYoga group respectively.
75.0% and 62.5% moderate improvement in GuduchyadiYoga and
(Combined)Satvavajaya&GuduchyadiYoga group respectively, where as 18.75 % and
56.25% mild improvement in GuduchyadiYoga and Satvavajaya with placebo group
respectively and But only 43.75 % patient not got cured in Satvavajaya with placebo
group.
This shows Satvavajaya chikitsa and Guduchyadi Yoga combined group is better than
Guduchyadi Yoga group and Guduchyadi Yoga group is better than Satvavajaya
chikitsa with placebo group.
Advises for further study:
Number of the patients should be increased.
Duration of the study should be minimum of six months.
Bibliographic
References
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 162
Bibliographic References
1. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana24/59
2. Kaplan & Sadock: Comprehensive textbook of psychiatry, Lippincott Williams
& Wilkins publication, eighth edition, 2005, 11.2 Alcohol – Related
Disorders,Page No - 1168.
3. Ibid; Page No - 1172
4. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/107
5. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Uttaratantra 47/17.
6. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/108
7. Ibid; Chikitsa Sthana 24/177
8. Ibid; Chikitsa Sthana 24/178
9. Kaplan & Sadock: Comprehensive textbook of psychiatry, Lippincott Williams
& Wilkins publication, eighth edition, 2005, 11.2 Alcohol – Related
Disorders,Page No - 1176.
10. Amarasimha: Amarakosha with Ramasrami commentary of Bhanuji Diksita
edited by Pt. Haragovinda Sastri, . Chaukhambha Sanskrit Sansthan Varanasi,
Fourth edition 2001, 3/2/12 page no. – 530.
11. Sharngadhara: Sarngadhara Samhita Edited by Dr Brahmanand Tripathi,
published by Chaukhamba Surabharati Prakashan varanashi. Pu 4/21 PN – 50
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 163
12. Sri Bhava Misra: Bhavaprakasha edited with Vidyotini Hindi commentary by Sri
Brahmasankara Misra Chaukhambha Sanskrit Sansthan Varanasi, seventh edition
1990, Page No - 785
13. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Sutrasthana 45/194, 195.
14. Ibid: 45 / 187 - 191 page no 211.
15. Sri Bhava Misra: Bhavaprakasha edited with Vidyotini Hindi commentary by Sri
Brahmasankara Misra Chaukhambha Sanskrit Sansthan Varanasi, seventh edition
1990, Page No – 786
16. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 25/49
17. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Sutrasthana 45/210 – 213
18. Ibid; Sutrasthana 45/175 – 176
19. Sri Bhava Misra: Bhavaprakasha edited with Vidyotini Hindi commentary by Sri
Brahmasankara Misra Chaukhambha Sanskrit Sansthan Varanasi, seventh edition
1990, Page No – 785 – 786
20. Ibid; Page no – 785
21. Ibid; Page no – 786
22. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Sutrasthana 45/182 – 187.
23. Ibid; Sutrasthana 45/171 – 181
24. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/30
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 164
25. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Uttaratantra 47/3
26. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Nidana Sthana 6 / 1
27. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/31 – 33
28. Ibid; Chikitsa Sthana 24/35
29. Ibid; Chikitsa Sthana 24/31
30. Ibid; Chikitsa Sthana 23/24
31. Ibid; Chikitsa Sthana 24/61 – 64
32. Ibid; Chikitsa Sthana 24/74 - 78
33. Vagbhata: Astanga Sangraha Induvykhyasahita, by Acharya V.J. Thakkar,
published by Central council for Research in Ayurveda and Siddha, New Delhi,
publication 1991, Indu on Nidana Sthana 6/1
34. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/89 – 97
35. Vagbhata: Astanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Nidana Sthana 6/14.
36. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Uttara Tantra 47/17 -18.
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 165
37. Vaidya Sodhala: Gada nigraha with the Vidyotini Hindi Commentary Vol. two,
by Sri Indradeva Tripathi. Chaukhambha Sanskrit sansthan, Varanasi. 3rd
edition
1999 (Kayachikitsa khand 17/21) page no. 451.
38. Kasyapa: Kasyapa Samhita edited by prof (Km) P.V.Tewari, Chaukhambha
Visvabharati Varanasi, Reprint 2002, Chikitsa Sthana Madatyaya Chikitsa
Adhyaya / 3, page no – 234
39. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/89 – 90
40. Ibid; Chikitsa Sthana 24/91
41. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Uttara Tantra 47/18.
42. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Nidana Sthana 6 / 18
43. Vagbhata: Astanga Sangraha Induvykhyasahita, by Acharya V.J. Thakkar,
published by Central council for Research in Ayurveda and Siddha, New Delhi,
publication 199,1 Indu on Nidana Sthana 6/16
44. Kasyapa: Kasyapa Samhita edited by prof (Km) P.V.Tewari, Chaukhambha
Visvabharati Varanasi, Reprint 2002, Chikitsa Sthana Madatyaya Chikitsa
Adhyaya / 19, page no – 235
45. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/92 – 93
46. Ibid; Chakrapani commentary on Chikitsa Sthana 24/93
47. Ibid; Chikitsa Sthana 24/ 94
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 166
48. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Nidana Sthana 6 / 19
49. Vagbhata: Astanga Sangraha Induvykhyasahita, by Acharya V.J. Thakkar,
published by Central council for Research in Ayurveda and Siddha, New Delhi,
publication 1991, Indu on Nidana Sthana 6/17
50. Kasyapa: Kasyapa Samhita edited by prof (Km) P.V.Tewari, Chaukhambha
Visvabharati Varanasi, Reprint 2002, Chikitsa Sthana Madatyaya Chikitsa
Adhyaya / 20, page no – 235
51. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/95 – 96
52. Ibid; Chikitsa Sthana 24/ 97
53. Sushruta: Sushruta Samhita with Nibandha Sangraha Commentary of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Uttara Tantra 47/19.
54. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Nidana Sthana 6 / 20
55. Vagbhata: Astanga Sangraha Induvykhyasahita, by Acharya V.J. Thakkar,
published by Central council for Research in Ayurveda and Siddha, New Delhi,
publication 199, Indu on Nidana Sthana 6/18
56. Kasyapa: Kasyapa Samhita edited by prof (Km) P.V.Tewari, Chaukhambha
Visvabharati Varanasi, Reprint 2002, Chikitsa Sthana Madatyaya Chikitsa
Adhyaya / 21, page no – 235
57. Ibid; Chikitsa Sthana 24/100
58. Ibid; Chikitsa Sthana 24/98 – 100
59. Ibid; Chikitsa Sthana 24/98 – 101 - 106
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 167
60. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Uttara Tantra 47/17.
61. Ibid; Uttara Tantra 47/18 - 19
62. Ibid; Uttara Tantra 47/19,20
63. Ibid; Uttara Tantra 47/20,21
64. Ibid; Uttara Tantra 47/21,22
65. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/ 199
66. Ibid; Chikitsa Sthana 24/ 201
67. Ibid; Chikitsa Sthana 24/ 202
68. Ibid; Chikitsa Sthana 24/ 203
69. Yogaratnakara: Yogaratnakara with Vidyotini Hindi commentary by Vaidya
Laksmipati Sasrti edited by Bhisagratna Brahmasankar Sastri, Chaukhambha
Sanskrit Samsthan Varanasi, Seventh edition 1999, page no 478
70. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Uttara Tantra 47/23
71. Ibid; , Uttara Tantra 47/22
72. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/ 109
73. Kasyapa: Kasyapa Samhita edited by prof (Km) P.V.Tewari, Chaukhambha
Visvabharati Varanasi, Reprint 2002, Chikitsa Sthana Madatyaya Chikitsa
Adhyaya 23, page no – 236
74. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/ 112-120
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 168
75. Ibid; Chikitsa Sthana 24/ 194.
76. Ibid; Chikitsa Sthana 24/191-193.
77. Ibid; Chikitsa Sthana 24/ 195-198.
78. Kasyapa: Kasyapa Samhita edited by prof (Km) P.V.Tewari, Chaukhambha
Visvabharati Varanasi, Reprint 2002, Chikitsa Sthana Madatyaya Chikitsa
Adhyaya 51, page no – 239
79. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chikitsa Sthana 24/ 204,205
80. Kasyapa: Kasyapa Samhita edited by prof (Km) P.V.Tewari, Reprint 2002,
Chikitsa Sthana Madatyaya Chikitsa Adhyaya 39 - 41, page no – 239
81. Bhela: Bhela Samhita edited by Dr K.H. Krishnamurthy Chaukhambha
Visvabharati Varanasi, First edition 2000, Chikitsa Sthana 28/ 57 – 58
82. Govinda Dasa Sen: Bhaishajyaratnavali with Hindi Tika, Khemaraj Shrikrishna
Das Prakashan Bombay,edition 2004,Madatyaya Roga Chikitsa 25, page no – 585.
83. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Nidana Sthana 6/ 8.
84. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Kalpa sthana 1/4.
85. Sarngadhara: Sarngadhara Samhita with the commentary of Adamalla’s Dipika
and Kasirama’s Gudharth parasurama Sastri, Vidyasagar Dipika edited by Pandit
Chaukhambha Orientalia Varanasi, fifth edition 2002, Uttara Khanda 3 / 2
86. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana – 4 /13.
87. Ibid; Kalpasthana 1 / 5
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 169
88. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Sutra Sthana 42/10.
89. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 9/ 11
90. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/33.
91. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana – 16/20
92. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana– 15/3.
93. Ibid; Siddhi Sthana 2 / 8 – 10
94. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/14 – 15, 18
95. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 18/ 1 - 6
96. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/46.
97. Ibid; Chikitsa Sthana. 33/47
98. Bhela: Bhela Samhita edited by Dr K.H. Krishnamurthy Chaukhambha
Visvabharati Varanasi, First edition 2000, Sutra Sthana 14/ 11.
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 170
99. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 6/11
100. Ibid; Sutra Sthana 13 / 37
101. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 31/26.
102. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 16/ 17 – 18
103. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 30/30.
104. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 13/61
105. Ibid; Siddhi Sthana 1/7
106. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 18/ 58
107. Ibid; Sutra Sthana 16/25
108. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 13/60
109. Ibid; Sutra Sthana 13/81
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 171
110. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/35.
111. Ibid; Dalhana Commentary Chikitsa Sthana. 33/6
112. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 15/9
113. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/7.
114. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Kalpa Sthana 1/14
115. Ibid; Sutra Sthana 15/10
116. Sarngadhara: Sarngadhara Samhita with the commentary of Adamalla’s Dipika
and Kasirama’s Gudharth parasurama Sastri, Vidyasagar Dipika edited by Pandit
Chaukhambha Orientalia Varanasi, fifth edition 2002, Uttara Khanda 3 / 16 - 17
117. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Kalpa Sthana 15/11
118. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 27/ 14
119. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 16/12
120. Ibid; Chakrapani commentary on Siddhi Sthana 1 / 14
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 172
121. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/9.
122. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 15/14
123. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 18 / 24
124. Vagbhata: Astanga Sangraha Induvykhyasahita, by Acharya V.J. Thakkar,
published by Central council for Research in Ayurveda and Siddha, New Delhi,
publication 1991, Sutra Sthana 27/19
125. Sarngadhara: Sarngadhara Samhita with the commentary of Adamalla’s Dipika
and Kasirama’s Gudharth parasurama Sastri, Vidyasagar Dipika edited by Pandit
Chaukhambha Orientalia Varanasi, fifth edition 2002, Uttara Khanda 3 / 32
126. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 15/13
127. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/8.
128. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 18 / 23 - 24
129. Vagbhata: Astanga Sangraha Induvykhyasahita, by Acharya V.J. Thakkar,
published by Central council for Research in Ayurveda and Siddha, New Delhi,
publication 1991, Sutra Sthana 27/18
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 173
130. Sarngadhara: Sarngadhara Samhita with the commentary of Adamalla’s Dipika
and Kasirama’s Gudharth parasurama Sastri, Vidyasagar Dipika edited by Pandit
Chaukhambha Orientalia Varanasi, fifth edition 2002, Uttara Khanda 3 / 25
131. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 15/13
132. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/8.
133. Vagbhata: Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 18 / 25 - 26
134. Vagbhata: Astanga Sangraha Induvykhyasahita, by Acharya V.J. Thakkar,
published by Central council for Research in Ayurveda and Siddha, New Delhi,
publication 1991, Sutra Sthana 27/20
135. Sarngadhara: Sarngadhara Samhita with the commentary of Adamalla’s Dipika
and Kasirama’s Gudharth parasurama Sastri, Vidyasagar Dipika edited by Pandit
Chaukhambha Orientalia Varanasi, fifth edition 2002, Uttara Khanda 3 / 25 – 26
136. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 15/15
137. Ibid; Sutra Sthana 15/16
138. Ibid; Chakrapani commentary on Siddhi Sthana 1 / 11
139. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 33/11
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 174
140. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Chakrapani commentary on Siddhi Sthana 6/11
141. Vagbhata : : Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, collated by late Dr Anna
Moreswara Kunte and Krsna Ramachandra Shastri Navare, Chaukhambha
Orientalia Varanasi, reprint ninth edition 2005, Sutra Sthana 18/ 46
142. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 23/36 – 38
143. Sarngadhara: Sarngadhara Samhita with the commentary of Adamalla’s Dipika
and Kasirama’s Gudharth parasurama Sastri, Vidyasagar Dipika edited by Pandit
Chaukhambha Orientalia Varanasi, fifth edition 2002, Uttara Khanda 3 / 33
144. Charaka : Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992,Siddhi Sthana 1/12
145. Ibid; Siddhi Sthana 6/10
146. Ibid; Siddhi Sthana 6/30
147. Ibid; Chakrapani Commentary on Siddhi Sthana 6/29 – 30
148. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Chikitsa Sthana. 34/3
149. Ibid; Dalhana commentary onChikitsa Sthana. 34/16 – 18
150. Trease and Evans: Pharmacognosy, Thirteenth edition William Charles Evans
ELBS with bailliere tindall, PN 320 -321
151. Christopher G. Goetz: Text book of Clinical Neurology, Saunders publications,
Second edition, Chapter 40 PN 885
152. Trease and Evans: Pharmacognosy, Thirteenth edition William Charles Evans
ELBS with bailliere tindall, PN 320 -321
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 175
153. Tripathy: Textbook of pharmacology
154. Kaplan & Sadock: Comprehensive textbook of psychiatry, Lippincott Williams
& Wilkins publication, eighth edition, 2005, 11.2 Alcohol – Related
Disorders,Page No – 1169 - 70.
155. Peoples RW, Li C, Weight FF: Lipid vs protein theories of alcohol action in the
nervous system. Annu Rev Pharmacol Toxicol 1996;36:185 – 201
156. Kaplan & Sadock: Comprehensive textbook of psychiatry, Lippincott Williams
& Wilkins publication, eighth edition, 2005, 11.2 Alcohol – Related
Disorders,Page No – 1171
157. Ibid: 1168 – 1188
158. Ibid: Page no – 1169
159. Ibid: Page no – 1173
160. Ibid: Page no – 1170
161. Ibid: Page no – 1171
162. Ibid: Page no – 1175
163. Ibid: Page no – 1184
164. Ibid: Page no – 1185
165. Charaka: Charaka Samhita of Agnivesha, revised by Charaka and Dridhabala
with the Ayurveda – Dipika commentary of Chakrapanidatta, edited by Vaidya
Jadavji Trikamji Acharya, Munshiram Manoharlal Publishers pvt. Ltd. Fifth
edition 1992, Sutra Sthana 27/34
166. Sushruta: Sushruta Samhita with Nibanda Sangraha Commentry of Sri
Dalhanacharya, edited by Vaidya Jadavji Trikamji Acharya. Chaukhambha
Orientalia Varanasi, Seventh edition 2002, Sutra Sthana. 46/13
167. Charaka- Charaka Samhita with Ayurveda Dipika commentary of
Chakrapanidatta, Chaukhambha Sanskrit Sansthan, 5th
edition, Varanasi, 2001
Su. 11/54.
168. Charaka- Charaka Samhita with Ayurveda Dipika commentary of
Chakrapanidatta, Chaukhambha Sanskrit Sansthan, 5th
edition, Varanasi, 2001
Su. 11/47.
Bibliographic References
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 176
169. Vagbhata- Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, Chaukhambha Orientalia,
Varanasi. Su. 1/26.
170. Patanjali Yoga Sutra. Su.2/26.
171. Patanjali Yoga Sutra. 2/46.
172. Patanjali Yoga Sutra. 2/29
173. Patanjali Yoga Sutra. 2/30
174. Patanjali Yoga Sutra. 2/32
175. Patanjali Yoga Sutra. 2/45.
176. Patanjali Yoga Sutra. 3/2.
177. Patanjali Yoga Sutra. 3/1.
178. Patanjali Yoga Sutra. 3/3.
179. Vagbhata- Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, Chaukhambha Orientalia,
Varanasi. Chi.1/191. Chi.5/47.
180. Vagbhata- Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, Chaukhambha Orientalia,
Varanasi. Chi.5/47.
181. Vagbhata- Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, Chaukhambha Orientalia,
Varanasi. Chi.6/21.
182. Vagbhata- Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, Chaukhambha Orientalia,
Varanasi. Chi.7/9.
183. Vagbhata- Ashtanga Hridaya with the commentaries Sarvangasundara of
Arunadatta and Ayurvedarasayana of Hemadri, Chaukhambha Orientalia,
Varanasi. Chi.19/98.
Annexures
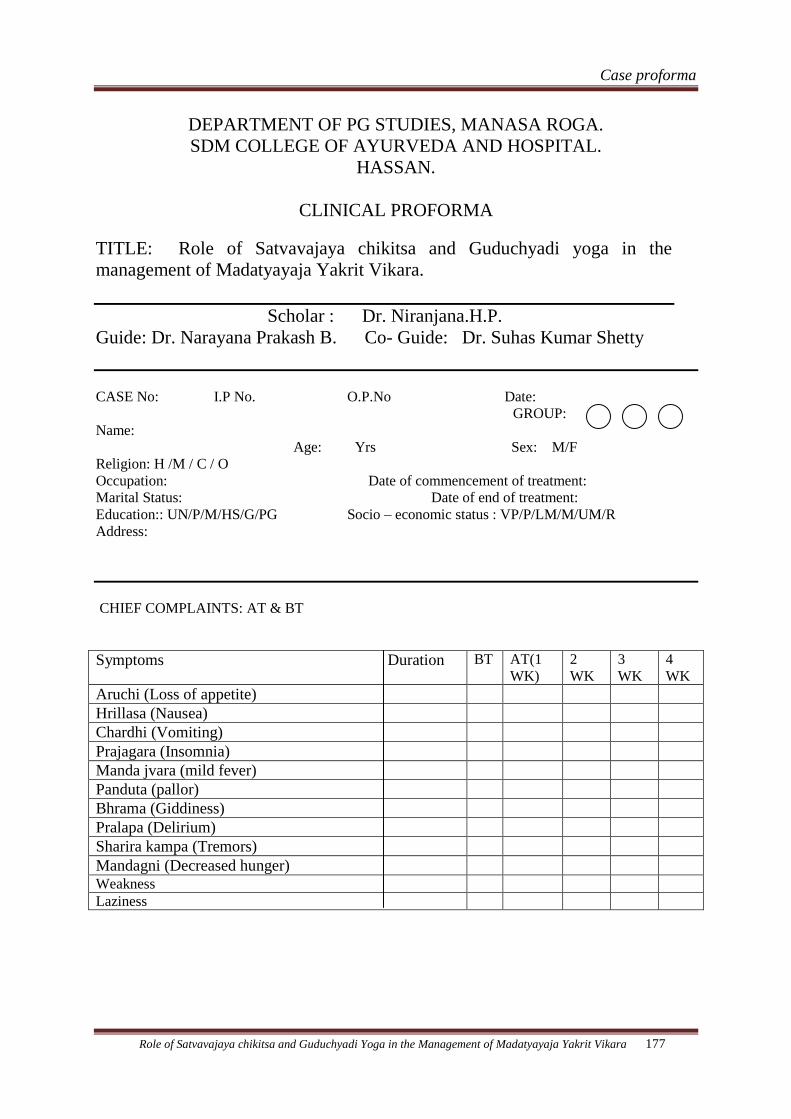
Case proforma
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 177
DEPARTMENT OF PG STUDIES, MANASA ROGA.
SDM COLLEGE OF AYURVEDA AND HOSPITAL.
HASSAN.
CLINICAL PROFORMA
TITLE: Role of Satvavajaya chikitsa and Guduchyadi yoga in the
management of Madatyayaja Yakrit Vikara.
Scholar : Dr. Niranjana.H.P.
Guide: Dr. Narayana Prakash B. Co- Guide: Dr. Suhas Kumar Shetty
CASE No: I.P No. O.P.No Date:
GROUP:
Name:
Age: Yrs Sex: M/F
Religion: H /M / C / O
Occupation: Date of commencement of treatment:
Marital Status: Date of end of treatment:
Education:: UN/P/M/HS/G/PG Socio – economic status : VP/P/LM/M/UM/R
Address:
CHIEF COMPLAINTS: AT & BT
Symptoms Duration BT AT(1
WK)
2
WK
3
WK
4
WK
Aruchi (Loss of appetite)
Hrillasa (Nausea)
Chardhi (Vomiting)
Prajagara (Insomnia)
Manda jvara (mild fever)
Panduta (pallor)
Bhrama (Giddiness)
Pralapa (Delirium)
Sharira kampa (Tremors)
Mandagni (Decreased hunger)
Weakness
Laziness
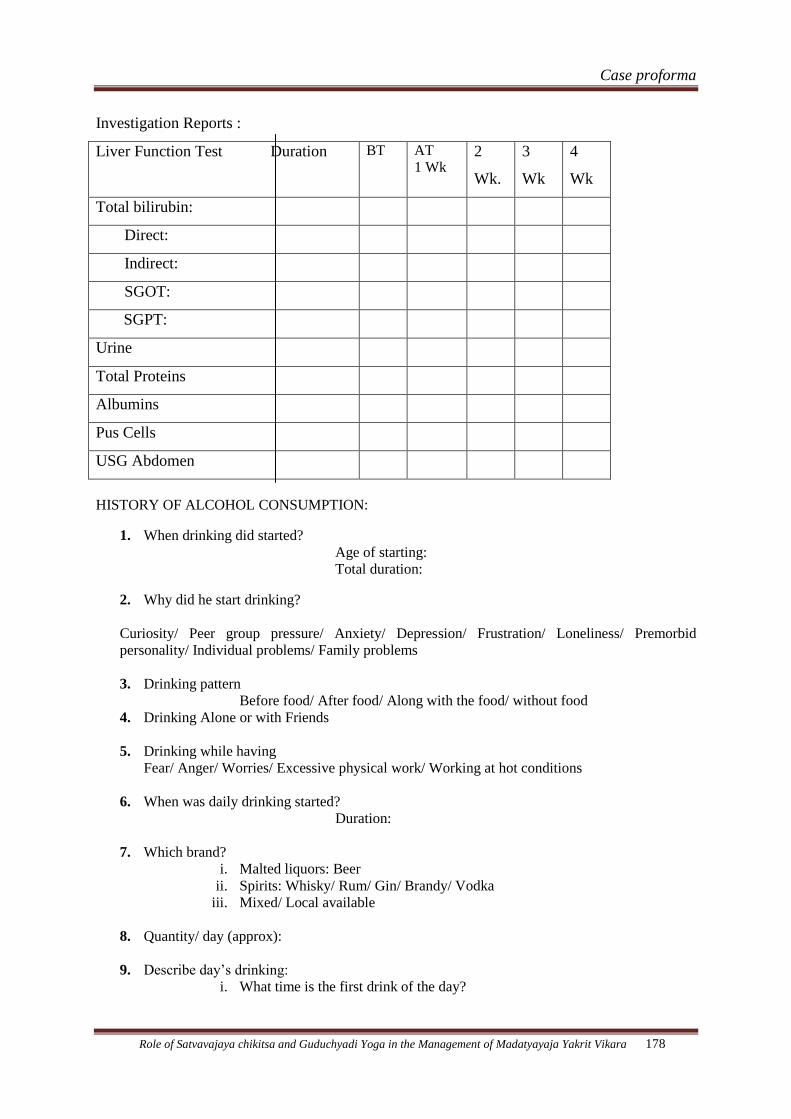
Case proforma
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 178
Investigation Reports :
Liver Function Test Duration BT
AT
1 Wk 2
Wk.
3
Wk
4
Wk
Total bilirubin:
Direct:
Indirect:
SGOT:
SGPT:
Urine
Total Proteins
Albumins
Pus Cells
USG Abdomen
HISTORY OF ALCOHOL CONSUMPTION:
1. When drinking did started?
Age of starting:
Total duration:
2. Why did he start drinking?
Curiosity/ Peer group pressure/ Anxiety/ Depression/ Frustration/ Loneliness/ Premorbid
personality/ Individual problems/ Family problems
3. Drinking pattern
Before food/ After food/ Along with the food/ without food
4. Drinking Alone or with Friends
5. Drinking while having
Fear/ Anger/ Worries/ Excessive physical work/ Working at hot conditions
6. When was daily drinking started?
Duration:
7. Which brand?
i. Malted liquors: Beer
ii. Spirits: Whisky/ Rum/ Gin/ Brandy/ Vodka
iii. Mixed/ Local available
8. Quantity/ day (approx):
9. Describe day’s drinking:
i. What time is the first drink of the day?
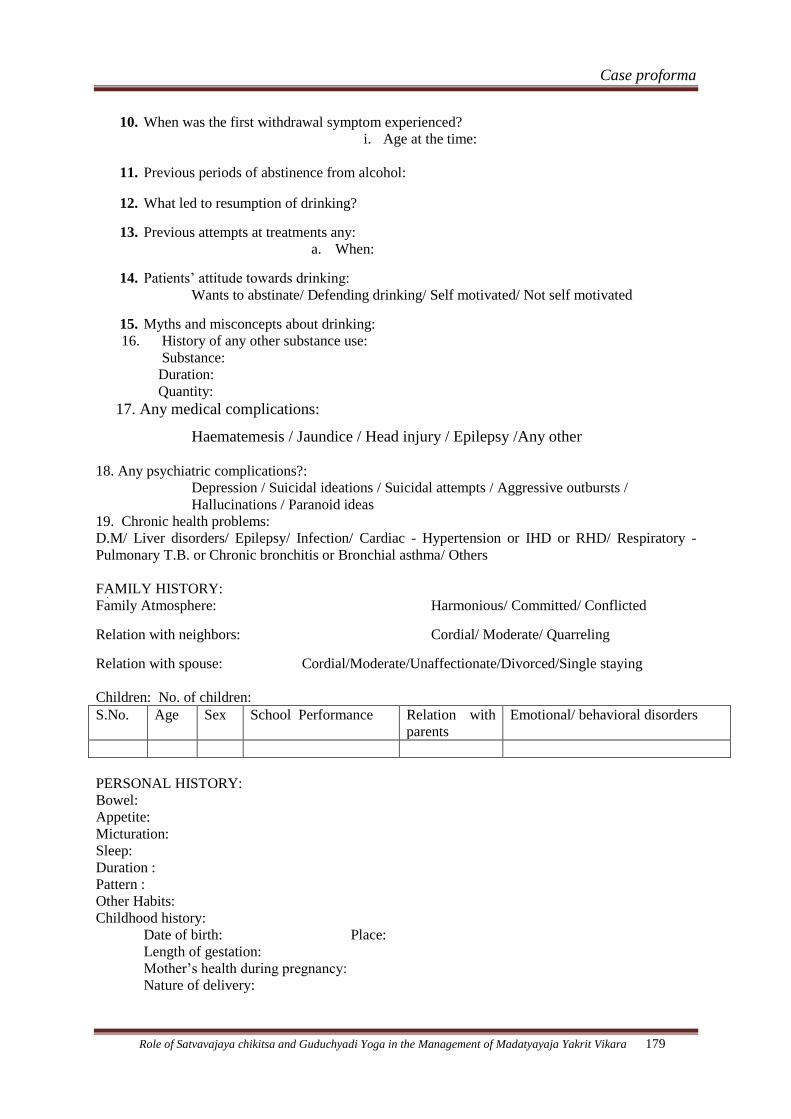
Case proforma
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 179
10. When was the first withdrawal symptom experienced?
i. Age at the time:
11. Previous periods of abstinence from alcohol:
12. What led to resumption of drinking?
13. Previous attempts at treatments any:
a. When:
14. Patients’ attitude towards drinking:
Wants to abstinate/ Defending drinking/ Self motivated/ Not self motivated
15. Myths and misconcepts about drinking:
16. History of any other substance use:
Substance:
Duration:
Quantity:
17. Any medical complications:
Haematemesis / Jaundice / Head injury / Epilepsy /Any other
18. Any psychiatric complications?:
Depression / Suicidal ideations / Suicidal attempts / Aggressive outbursts /
Hallucinations / Paranoid ideas
19. Chronic health problems:
D.M/ Liver disorders/ Epilepsy/ Infection/ Cardiac - Hypertension or IHD or RHD/ Respiratory -
Pulmonary T.B. or Chronic bronchitis or Bronchial asthma/ Others
FAMILY HISTORY:
Family Atmosphere: Harmonious/ Committed/ Conflicted
Relation with neighbors: Cordial/ Moderate/ Quarreling
Relation with spouse: Cordial/Moderate/Unaffectionate/Divorced/Single staying
Children: No. of children:
S.No. Age Sex School Performance Relation with
parents
Emotional/ behavioral disorders
PERSONAL HISTORY:
Bowel:
Appetite:
Micturation:
Sleep:
Duration :
Pattern :
Other Habits:
Childhood history:
Date of birth: Place:
Length of gestation:
Mother’s health during pregnancy:
Nature of delivery:
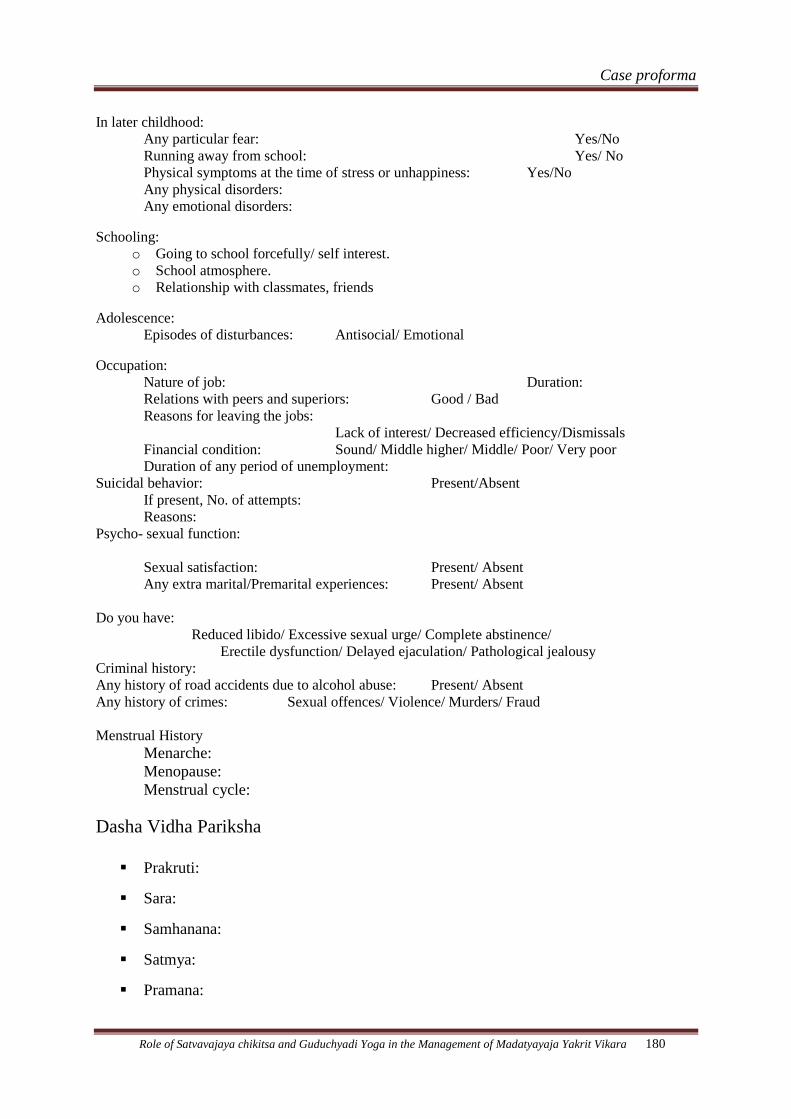
Case proforma
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 180
In later childhood:
Any particular fear: Yes/No
Running away from school: Yes/ No
Physical symptoms at the time of stress or unhappiness: Yes/No
Any physical disorders:
Any emotional disorders:
Schooling:
o Going to school forcefully/ self interest.
o School atmosphere.
o Relationship with classmates, friends
Adolescence:
Episodes of disturbances: Antisocial/ Emotional
Occupation:
Nature of job: Duration:
Relations with peers and superiors: Good / Bad
Reasons for leaving the jobs:
Lack of interest/ Decreased efficiency/Dismissals
Financial condition: Sound/ Middle higher/ Middle/ Poor/ Very poor
Duration of any period of unemployment:
Suicidal behavior: Present/Absent
If present, No. of attempts:
Reasons:
Psycho- sexual function:
Sexual satisfaction: Present/ Absent
Any extra marital/Premarital experiences: Present/ Absent
Do you have:
Reduced libido/ Excessive sexual urge/ Complete abstinence/
Erectile dysfunction/ Delayed ejaculation/ Pathological jealousy
Criminal history:
Any history of road accidents due to alcohol abuse: Present/ Absent
Any history of crimes: Sexual offences/ Violence/ Murders/ Fraud
Menstrual History
Menarche:
Menopause:
Menstrual cycle:
Dasha Vidha Pariksha
Prakruti:
Sara:
Samhanana:
Satmya:
Pramana:
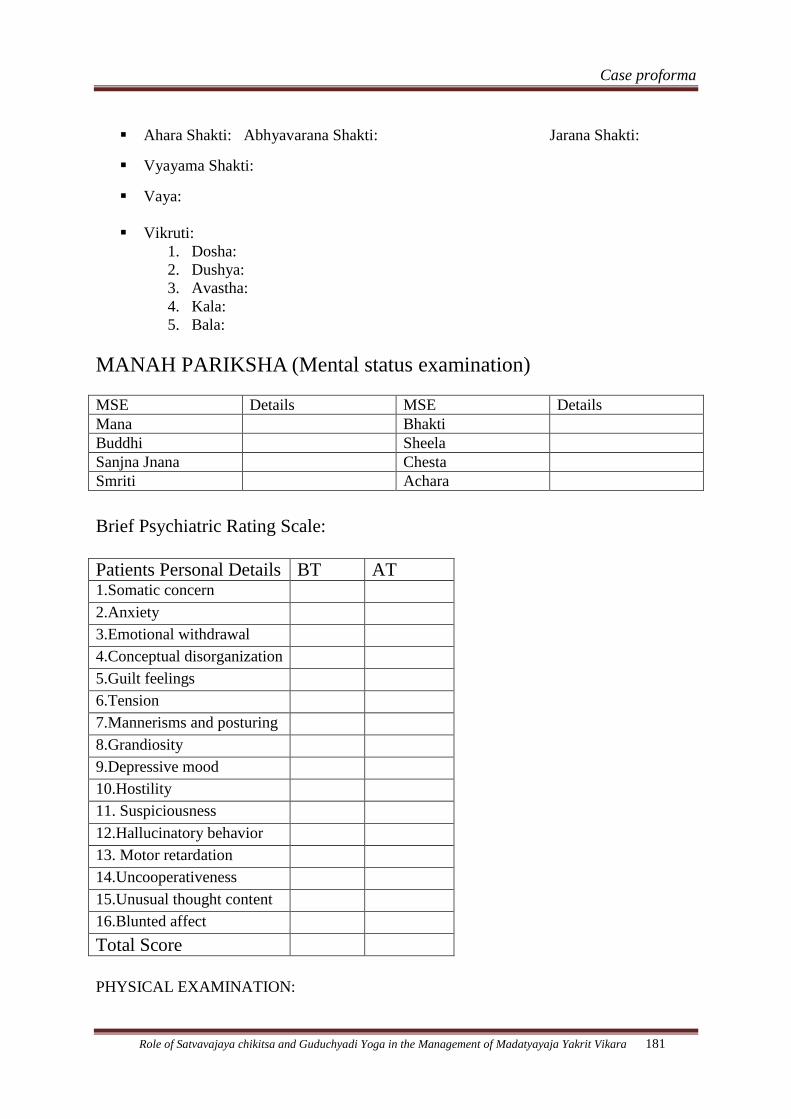
Case proforma
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 181
Ahara Shakti: Abhyavarana Shakti: Jarana Shakti:
Vyayama Shakti:
Vaya:
Vikruti:
1. Dosha:
2. Dushya:
3. Avastha:
4. Kala:
5. Bala:
MANAH PARIKSHA (Mental status examination)
MSE Details MSE Details
Mana Bhakti
Buddhi Sheela
Sanjna Jnana Chesta
Smriti Achara
Brief Psychiatric Rating Scale:
Patients Personal Details BT AT 1.Somatic concern 2.Anxiety 3.Emotional withdrawal 4.Conceptual disorganization 5.Guilt feelings 6.Tension 7.Mannerisms and posturing 8.Grandiosity 9.Depressive mood 10.Hostility 11. Suspiciousness 12.Hallucinatory behavior 13. Motor retardation 14.Uncooperativeness 15.Unusual thought content 16.Blunted affect
Total Score
PHYSICAL EXAMINATION:
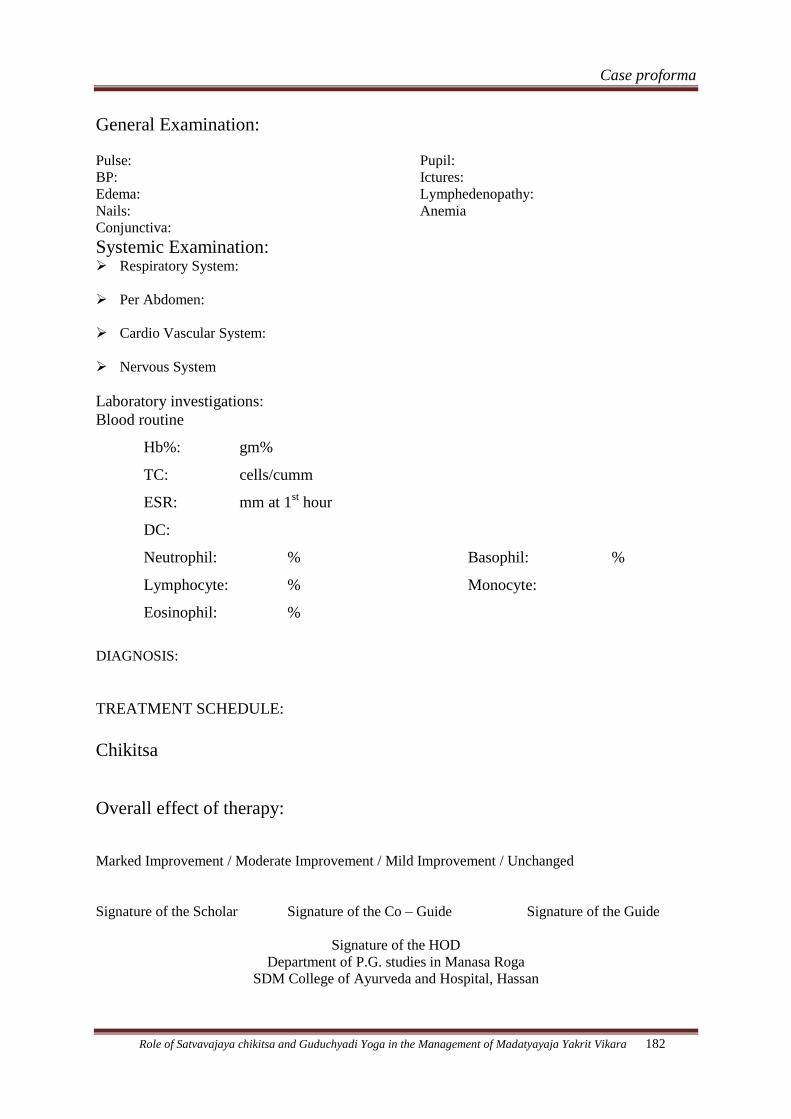
Case proforma
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 182
General Examination:
Pulse:
BP:
Edema:
Nails:
Conjunctiva:
Pupil:
Ictures:
Lymphedenopathy:
Anemia
Systemic Examination: Respiratory System:
Per Abdomen:
Cardio Vascular System:
Nervous System
Laboratory investigations:
Blood routine
Hb%: gm%
TC: cells/cumm
ESR: mm at 1st hour
DC:
Neutrophil: %
Lymphocyte: %
Eosinophil: %
Basophil: %
Monocyte:
DIAGNOSIS:
TREATMENT SCHEDULE:
Chikitsa
Overall effect of therapy:
Marked Improvement / Moderate Improvement / Mild Improvement / Unchanged
Signature of the Scholar Signature of the Co – Guide Signature of the Guide
Signature of the HOD
Department of P.G. studies in Manasa Roga
SDM College of Ayurveda and Hospital, Hassan
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 183
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,KARNATAKA.
BANGALORE
ANNEXURE – II
COMPLETED PROFORMA FOR REGISTRATION OF SUBJECT FOR
DISSERTATION.
1.NAME OF THE CANDIDATE: NIRANJANA.H.P.
ADDRESS PRELIMINARY M.D (AYU) SCHOLAR.
DEPARTMENT OF P.G STUDIES IN
MANASA ROGA.
SDM COLLEGE OF AYURVEDA AND
HOSPITAL.
HASSAN – 573201
PERMANENT ADDRESS: S/O MR.H.A.PRABHAKARA.RAO.
NO.03, HOSABALE
POST: HOSABALE.
TALUK: SORABA.
DISTRICT:SHIMOGA
KARNATAKA.
PIN: 577-434.
2.NAME OF THE INSTITUTION: SDM COLLEGE OF AYURVEDA AND
HOSPITAL HASSAN – 573-201
KARNATAKA
3.COURSE OF STUDY IN SUBJECT: M.D.(AYU) IN MANASA ROGA.
4.DATE OF ADMISSION TO THE
COURSE : 15TH
JUNE 2009.
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 184
5.TITLE OF THE DISSERTATION : “ROLE OF SATVAVAJAYA
CHIKITSA AND GUDUCHYADI
YOGA IN THE MANAGEMENT OF
MADATYAYAJA YAKRIT VIKARA
(ALCOHOLIC LIVER DISORDER)”
6. BRIEF RESUME OF THE STUDY:
6.1 Need For The Study:
Excessive intake of alcohol leads to affliction of heart resulting in
exhilaration, passionate desire, erotic stimulation, sense of pleasure and varieties of
psychic morbidities of Rajasika and Tamasika nature depending upon the mental
attitude of the person and finally resulting in Moha nidra(coma). This type of mental
perversion caused by alcohol is called Mada. And whatever supreme for attaining
salvation are based on the tranquility of the mind of an individual.Alcohol
considerably agitates this mind like a strong wind shakes the tree located on the bank
of the river.1.
Madatyaya or the alcoholic dependency is completely based on stability of
one’s own Satva. So mind plays an important role in the de-addiction of alcohol.2
Word Madatyaya is composed of two terms i.e. Mada -any exhilarating or
intoxicating condition.3 Atyaya – suffering.
4 Hence suffering from intoxicating drink
is known as Madatyaya.
Chronic and excessive alcohol ingestion is one of the major causes of liver
disorders across the world. Despite the untoward effect of alcohol, alcoholism is a
major problem in India. The different drug abuse surveys have shown the prevalence
of alcoholism as 5 to 20 percent worldwide. In India, general population surveys
shows the prevalence rate as high as 16 to 50 percent .5
Atleast 20% of the patients in
mental settings have alcohol abuse or dependence or withdrawal , including
individuals from all socioeconomic conditions and both the genders.6
According to US Census Bureau International Data Base 2004, 106,50,70,607
persons in the world were using alcohol and out of which 78,31,407 persons were
affected by Alcoholic liver disease.7
It manifests as a clinical spectrum ranging from
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 185
non specific symptoms to hepatic failure. Classically, alcoholic liver injury comprises
three major forms, 1.fatty liver, 2.alcoholic hepatitis and 3.cirrhosis.8
Bhavaprakasha mentions Yakrit-Vruddhi (hepatomegaly) as one of the
symptoms of Yakrit Vikara due to excessive intake of Vidahi and Abhishyandi
Aharas and Madya (alcohol).9
Ayurveda has many options to treat Madatyaya . All the texts mention
Pittahara and Deepana Pachana Dravyas to treat Yakrit-Vikaras. Guduchyadi Yoga
mentioned by Charaka comprising of Guduchi (Tinospora cordifolia), Musta(Cyperus
rotundus), Patola(Tricosanthes dioica) and Nagara(Gingeber officinalis) may relieve
the adverse effects of Madatyaya as well as liver disorders caused by it.10
Satvavajaya Chikitsa may help people to address psychological issues
involved in their drinking problem. Astanga Hrudaya explains Vismapana,
Samsmarana, Priyadarshana, Priyashravana, Geeta, Vadya 11
and Charaka advises
Harshanee Kriya and restrain from the things which are harmful to body and mind as
the treatment modalities in the management of Madatyaya.12
The three therapies i.e. cognitive behavioral coping skills, motivational
enhancement therapy and 12 step facilitation approaches of alcoholics anonymous has
been found to be helpful for the people to boost their motivation to stop drinking.
As the number of alcohol related disorders are increasing in the society and till
date no study has been conducted , hence it is decided to carry out the present study to
evaluate the effect of Guduchyadi Yoga and Satvavajaya Chikitsa in the management
of Madatyayaja Yakrit Vikara.
6.2 Review of literature
o The Dukha produced due to Madya is called as Madatyaya.13
o Charakacharya explained types of Madatyaya as Vatapraya, Pittapraya ,
Kaphapraya and considered the disease as Tridoshaja.14
o Vagbhata explains 4 types of Madatyaya viz. Vataja, Pittaja, Kaphaja and
Sannipataja.15
o Sushruta explains mainly 4 types viz. Panatyaya, Paramada, Panajeerna and
Panavibhrama. Sushruta used Panatyaya term in place of Madatyaya and
accepts 4 types of Panatyaya viz. Vatakrita, Pittakrita,Kaphakrita and
Sarvakrita.16
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 186
o Acharya Charaka explained the qualities of Satvika , Rajasika and Tamasika
Madatyaya rogi as Uttama, Asaumya and Sammohakrodhitha respectively.
o In Gadanigraha Acharya Shodala accepted Dvidoshaja Madatyaya also.17
o Charaka has mentioned Hrudaya Vyatha, Aruchi, Trishna, Jrimbha, Sphurana,
Vepana, Shrama, Prajagara, Sharirakampa, Chardi, Atisara, Hrillasa, Bhrama,
Pralapa 18
etc as symptoms of Madatyaya.
o Madyapana will affect all aspects of life i.e., physically, psychologically,
socially, economically, occupationally etc.
o Sushruta has mentioned Hikka, Jvara, Vamathu, Vepathu, Parshvashoola,
Kasa and Bhrama as its Upadrava.19
o In allied science they have explained clinical features of alcoholic liver
disorders as fatty liver, right upper quadrant discomfort, tender hepatomegaly,
nausea, jaundice, abdominal pain, malnutrition, severe illness and ascitis.20
o The ingredients of Guduchyadi yoga are Guduchi, Mustha, Patola and Nagara
– equal quantity of all these drugs. It acts as Pittahara, Pitta Rechaka and
Rakta Prasadaka, Pachaka, Deepaka and plays an important role in Yakrit
Vikara and Madatyaya.
o Satvavajaya includes Vismapana, Samsmarana, Priyashravanadarshana,
Vadya, Geeta and Harshanee kriya.
o Charaka has defined Satvavajaya and considerd Jnana, Vijnana, Dhairya,
Smriti and Samadhi as techniques of psychological therapies .
6.3 Objective of the study
1. To evaluate the efficacy of Satvavajaya chikitsa in Madatyayaja Yakrit Vikara
(Alcoholic liver disorder).
2. To evaluate the efficacy of Guduchyadi yoga in Madatyayaja Yakrit Vikara
(Alcoholic liver disorder).
3. To evaluate the efficacy of combined effect of Satvavajaya Chikitsa and
Guduchyadi yoga in Madatyayaja Yakrit Vikara (Alcoholic liver disorder).
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 187
7. Material and Methods
7.1. Source of data :
45 patients of Madatyaya will be selected from the Out Patient Department and
In Patient Department of ManasaRoga of the S D M College of Ayurveda and
Hospital, Hassan.
7.2 Method of Collection of Data :
45 patients of Madatyaya with liver disorder who fulfills the inclusion criteria
will be selected and randomly assigned into the following 3 groups; each group
comprising of 15 patients.
Group A: The patients of this group will be subjected to Satvavajaya Chikitsa daily
along with placebo capsule 500 mg starch thrice daily for 1 month. Satvavajaya
Chikitsa will be carried out as follows:
Jnana- 12 Step facilitation (Atmadi Jnana) approach.
1. We admit we are powerless over alcohol- that our lives have become
unmanagable.
2. We believe that a Power greater than ourselves can restore us to sanity.
3. We make a decision to turn our will and our lives over to the care of God as we
understand Him.
4. We make a search and fearless moral inventory of ourselves.
5. We admit to God, to ourselves and to another human being the exact nature of
our wrong doings.
6. We’re entirely ready to have God remove all these defects of character.
7. We shall humbly ask Him to remove our shortcomings.
8. We shall make a list of all persons we have harmed and become willing to
make amends to them all.
9. We shall make direct amends to such people wherever possible, except when to
do so would injure them or others.
10. We shall continue to take personal inventory and when we are wrong,
promptly admit it.
11. We will search through prayer and meditation to improve the conscious
contact with God as we understood Him, praying only for knowledge of Him for
us and the power to carry it out.
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 188
12. After experiencing this, we shall carry this message to alcoholics, and to
practice these principles in all their affairs.
Vijnana- Specific information about effect of alcohol on various organs.
Dhairya- Supportive Psychotherapy – motivational enhancement therapy.
Smriti - Methods to cope with high-risk drinking situations and develop social
support systems.
Samadhi – Yoga for 30 minutes and Pranayama for 15 minutes daily for 1 month.
Yogasana – Standing Asana- Vrikshasana , Pada Hastasana, Ardha Chakrasana,
Trikonasana.
Supine Asana – Pavana Muktasana, Matsyasana.
Prone Asana - Bhujangasana, Dhanurasana.
Sitting Asana – Vajrasana, Ushtrasana, Vakrasana.
Pranayama - Kapalabhati, Bhastrika, Anuloma-Viloma, Shitali, Shithkari and
Bhramari.
Dhairya Chikitsa will be also done on 15th
and 30th
day of treatment.
Group B: The patients of this group will be given Guduchyadi yoga in the dose of
5 gm, before food with warm water thrice daily for 1 month.
Group C: The patients of this group will be subjected to Satvavajaya Chikitsa as
mentioned above and simultaneously Guduchyadi Yoga will be given in the dose of
5gm before food with warm water thrice daily for 1 month
Follow up study:
After stopping the treatment the patients will be asked to attend OPD at the
interval of 15 days for two months to know whether the relief provided by the
therapies is sustained or not.
Diagnostic Criteria:
Diagnosis will be made on the basis of Lakshanas of Alcoholic liver disorder
and Madatyayaja Yakrit Vikara.
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 189
Fatty liver Yakrit vruddhi
Right upper quadrant discomfort. Manda jvara
Tender hepatomegaly. Mandagni.
Nausea Ksheenabala.
Jaundice Atipandu.09.
Fever and Abdominal pain
Elevated AST (Aspartate amino transferace)
Elevated ALT (Alanine amino transferace)08.
Inclusion Criteria:
1.Patients presenting with symptoms of Madatyaya along with Alcoholic liver
disorder.
2. Age group of 16-70 years of either sex.
Exclusion Criteria:
1.Patients suffering from any Organic brain disorder.
2.Patients suffering from complications of Alcoholic liver disorders.
3.Patients suffering from other types of addictions.
4.Patients suffering from other Systemic or Psychiatric illnesses.
Assessment Criteria:
Assessment of clinical study will be done based on subjective and objective
parameters. Self scoring of symptoms of Madatyayaja Yakrit Vikara will be done and
self prepared scale will be used for assessment.
Subjective parameters : Objective parameters:
Aruchi. Chardi
Prajagara Manda jvara
Hrillasa Atipanduta
Pralapa Atisara
Bhrama Shareera kampa
Mandagni. USG Abdomen
Liver Function Test
Hepatomegaly.
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 190
Statistical evaluation of the results will be done by using Unpaired and Paired ‘t’ test.
7.3.Laboratory Investigations
Blood routine
Urine routine
Liver Function Test
USG Abdomen.
7.4 Has ethical clearance been obtained from your institution?. YES.
8.List of References:
1.Charaka: Charaka Samhitha with the ‘Ayurveda deepika’ commentary by
Chakrapanidatta edited by Trivikrimatmajena Yadav Sharma, Choukambha Sanskrit
Sansthana,Publications,Varanasi, 1994 year edition. Chikitsaasthana 24/39,40,53.
page no584-585.
2. Ibid. Chikitsa sthana 24/52-55. page no.585.
3.Sir Monier Williams : A Sanskrit –English dictionary, Motilal Banarasidas
publishers, Pvt. Ltd.Delhi. Reprint -1993.Page no. 777.
4. Ibid. Page no 17.
5.Dr. M.S.Bhatia : Essential of Psychiatry, CBS publishers and distributors, New
Delhi. 4th
edition 2004.Page no. 8.6.
6. Kaplan and Saddock: Comprehensive text book of Psychiatry , 8th
edition ,
volume 1, by Lippincott Williams and Wilkings , Page no.1168.
7. US Census Bureau International Data Base.2004.
8.Harrison’s Principles of Internal Medicine . Volume.2, 15th
edition Published by
Times Roman by monotype composition Company. Page no. 1752&1753.
9.BhavaPrakasha : Vidyothini Teeka , Choukambha Sanskrit Sansthana,
Publications, Varanasi. Uttarardha.Chapter.33 ./10.Page no. 346.
10.Charaka: Charaka Samhitha with the ‘Ayurveda deepika’ commentary by
Chakrapanidatta edited by Trivikrimatmajena Yadav Sharma, Choukambha Sanskrit
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 191
Sansthana, Publications,Varanasi, 1994 year edition. Chikitsasthana 24/145.Page
no.589.
11.Vagbhata: Astanga Hrudaya , with the Commentaries Sarvanga Sundari of
Arunadatta and Ayurveda Rasayana of Hemadri edited by Harishastri Padakar vaidya,
Krishnadas Academy, Varanasi. Reprint 2000.Chikitsa stana,7/113-114.Page no.642.
12.Charaka: Charaka Samhitha with ‘Ayurveda deepika’ commentary by
Chakrapanidatta edited by Trivikrimatmajena Yadav Sharma, Choukambha Sanskrit
Sansthana.Publications. Varanasi, 1994 year edition. Chikitsa sthana 24/194.Page
no.590.
13. Ibid. Chikitsa sthana 24/101-106.Page no.587.
14. Ibid. Chikitsa sthana 24/89-97.Page no.587.
15. Vagbhata: Astanga Hrudaya , with the Commentaries Sarvanga Sundari of
Arunadatta and Ayurveda Rasayana of Hemadri edited by Harishastri Padakar vaidya,
Krishnadas Academy, Varanasi. Reprint 2000.Nidana Stana 6/14..Page.no.487.
16.Sushrutha : Sushrutha Samhitha with the Nibandhasangraha, commentary of Shri
Dalhanacharya and the Nyayachandrika Panjika of Shri Gayadasacharya on
Nidanasthana , edited by Vaidya Jadavji Trikamji Acharya . Chaukambha Orientalia ,
Varanasi.7th
edition 2002. UttaraTantra 47/17-18.Page.no.743.
17.Vaidya Shodala : Gada nigraha with the Vidyothini Hindi commentary Vol.2 by
Sri Indradeva Tripathi, Chaukambha Sanskrit Sanstan,Publications. Varanasi. 3rd
edition 1999.Page no.451.
18.Charaka: Charaka Samhitha with the ‘Ayurveda deepika’ commentary by
Chakrapanidatta edited by Trivikrimatmajena Yadav Sharma, Choukambha Sanskrit
Sansthana. Varanasi, Publications. 1994 year edition. Chikitsa stana 24/101-106.Page
no.587.
19. Sushrutha : Sushrutha Samhitha with the Nibandhasangraha, commentary of
Shri Dalhanacharya and the Nyayachandrika Panjika of Shri Gayadasacharya on
Nidanastana , edited by Vaidya Jadavji Trikamji Acharya . Chaukambha Orientalia ,
Varanasi.7th
edition 2002. UttaraTantra 47/23 .Page.no.743.
20.Davidson’s Principles and Practice of Medicine 19th
edition Page
no.867.Published by Churchill Livingstone,An imprint of Elsevier Science Limited.
Synopsis
Role of Satvavajaya chikitsa and Guduchyadi Yoga in the Management of Madatyayaja Yakrit Vikara 192
9.SIGNATURE OF CANDIDATE :
10. REMARKS OF GUIDE :
11. NAME AND DESIGNATION OF
11.1 GUIDE : Dr.NARAYANA PRAKASH. B. M.D.(AYU)
Professor & H.O.D.
Dept.of PG Studies in Manasa Roga.
S.D.M.College of Ayurveda.
Hassan. (Karnataka)
11.2 SIGNATURE :
11.3 CO-GUIDE : Dr.SUHAS KUMAR SHETTY. M.D.(AYU)
Reader,
Dept.of PG Studies in Manasa Roga.
S.D.M.College of Ayurveda.
Hassan. (Karnataka)
11.4 SIGNATURE :
11.5 H.O.D. : Dr.NARAYANA PRAKASH. B.
Professor & H.O.D.
Dept.of PG Studies in Manasa Roga.
S.D.M.College of Ayurveda.
Hassan. (Karnataka)
11.6 SIGNATURE :
12.
12.1 REMARKS OF CHAIRMAN
& PRINCIPAL : Dr. PRASANNA. N. RAO
Related Documents











