Role of RAAS inhibition Role of RAAS inhibition in the Management of in the Management of Hypertension Hypertension Dr KyawSoe Win MBBS, M Med Sc (Int Med), MRCPUK, FRCPE, FAsCC, FAPSIC Asso: Prof / Senoir Consultant Cardiologist Department of Cardiovascular Medicine Mandalay General Hospital Hot Topic In Hypertension 2013 12 th January 2013

Role of raas inhibition in management of hypertension
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Role of RAAS inhibition Role of RAAS inhibition in the Management of in the Management of
HypertensionHypertension
Dr KyawSoe WinMBBS, M Med Sc (Int Med), MRCPUK, FRCPE, FAsCC, FAPSIC
Asso: Prof / Senoir Consultant CardiologistDepartment of Cardiovascular Medicine
Mandalay General Hospital
Hot Topic In Hypertension 2013
12th January 2013

RAAS: Central Role in the Pathogenesis
of Cardiovascular Disease

Ang II effect in target organ damage
McFarlane SI et al. Am J Cardiol. 2003;91(suppl):30H-7.
Angiotensinogen
Angiotensin I
Angiotensin II
Renin
ACE
Aldosterone(Adrenal/CV tissues)
Stroke HFKidneyfailure
↑BP
VSMC
Fat cells
Reduced baroreceptor sensitivity

RAAS: Sites of intervention with RAAS modulators
Angiotensinogen
Angiotensin I
Renin
ACEinhibitors
Angiotensin-convertingenzyme (ACE)
Angiotensin II
AT1 receptor
Angiotensin receptorblockers
AT2 receptor
Atherosclerosis, hypertension Vascular protection?
Adapted from Nickenig G. Circulation. 2004;110:1013-20.
Direct renin inhibitor
Aldosterone
Aldo antagonist

Atherosclerosis-promoting actions of Ang II and protective effects of bradykinin
↑↑ VasodilationVasodilation↑↑ ProstacyclinProstacyclin↑↑ Nitric oxideNitric oxide
↑↑ tPAtPA
↑↑ Vasoconstriction Vasoconstriction ↑↑ ICAM-1, VCAM-1 ICAM-1, VCAM-1
↑↑ Growth factorsGrowth factors↑ Oxyradical formationOxyradical formation
↑ PAI-1PAI-1↑ Smooth muscle cellSmooth muscle cell
proliferation proliferation↑ Matrix degradationMatrix degradation
Protection against Protection against the effects the effects
of Ang IIof Ang II
↑ Endothelial dysfunctionEndothelial dysfunction↑ Inflammation Inflammation ↑ CoagulationCoagulation
↑ AtherogenesisAtherogenesis
BradykininBradykinin
Ang IIAng II
Inactive peptidesInactive peptides
Ang IAng I
--
--
ACEinhibitor
Ferrari R. Expert Rev Cardiovasc Ther. 2005;3:15-29.

AT1R blockade upregulates both Ang II levels and AT2R expression
Ang I
Strauss MH, Hall AS. Circulation. 2006;114:838-54.
Ang II
AT2
ACE
ARB
AT1 AT4
Ang I
Ang II
AT2
ACE
ARB
AT1 AT4
+
Both physiologic and pathologic effects have been proposed for AT2R stimulation
Vasodilation Hypertrophy Inflammation

ImpairedNO synthase
Ang II and mechanisms of atherosclerosis
Jacoby DS, Rader DJ. Arch Intern Med. 2003;163:1155-64.
IL-6MCP-1PDGF
LOX-1
PAI-1TF
TGF-β
VCAMICAM
Angiotensin II
Lipid oxidation
Thrombosis
Inflammation
Proliferation fibrosis
Adhesion
EndothelialdysfunctionEndothelialdysfunction

PERTINENT: ACE inhibition ↑ NO via ↑ eNOS activity
Ferrari R et al. www.europa-trial.org
0
1
2
3
4
2.5
3.5
2.4
2.93.3
Controlsn = 45
Placebon = 44
Placebon = 44
Perindopriln = 43
Perindopriln = 43
P < 0.01*P < 0.05†
Baseline 1 Year
eNOSactivity in HUVECs
(pmol/min/mg protein)
Controls CAD patients
* vs baseline† ∆ perindopril vs ∆ placebo
PERindopril – Thrombosis, InflammatioN, Endothelial dysfunction and Neurohormonal activation Trial (substudy of EUROPA)
HUVEC = human umbilical vein endothelial cell

Schwartzkopff B et al. Hypertension. 2000;36:220-5.
0
200
400
600
800
Periarteriolar collagen
P = 0.04
53%
558 ± 270
260 ± 173
µm2
0
2
4
6
8
Total interstitial collagen
P = 0.04
22%5.5 ± 3.8
4.3 ± 3.2Vv%
Pretreatment(n = 14)
Post-treatment*(n = 14)
Coronary reserve
+67%
P = 0.001
Baseline 2.1
3.5Perindopril
*Perindopril 4–8 mg for 12 months
ACEI normalizes structure of resistance arteries in CAD patients
At treatment end (12 mo)

AT1 receptor blockade improves flow-mediated vasodilation122 Hypertensive patients treated for 2 months
*P < 0.05 vs baseline and vs placebo Koh KK et al. Am J Cardiol. 2004;93:1432-5.
0.15
1.14
1.66
1.32
0.0
0.5
1.0
1.5
2.0
Placebo(n = 30)
Irbesartan300 mg(n = 30)
Losartan100 mg(n = 31)
Candesartan16 mg
(n = 31)
∆FMD
inbrachialartery(%)
2.5
*
*
*

Inflammation
IL-6MCP-1PDGF
Inflammation
Ang II and mechanisms of atherosclerosis
Jacoby DS, Rader DJ. Arch Intern Med. 2003;163:1155-64.
ImpairedNO synthase LOX-1
PAI-1TF
TGF-β
VCAMICAM
Lipid oxidation
Thrombosis
Proliferation fibrosis
Endothelialdysfunction
Adhesion
Angiotensin II

ACE inhibition reduces oxidative stress and inflammation
20 Patients with type 2 diabetes
Marketou ME et al. J Am Coll Cardiol. 2005;45 (suppl A):396A.
Baseline Perindopril 4 mg x 6 mos
* P < 0.05 vs baseline
TNF-α IL-6Lipid peroxides
3.3
2.0
0
1
2
3
4
2.9
1.8
370
264
0
100
200
300
400
µmol/L pg/mL
** *

LOX-1
VCAMICAM
Jacoby DS, Rader DJ. Arch Intern Med. 2003;163:1155-64.
Ang II and mechanisms of atherosclerosis
IL-6MCP-1PDGF
ImpairedNO synthase
PAI-1TF
TGF-β
Thrombosis
Inflammation
Proliferation fibrosis
Endothelialdysfunction
Angiotensin II
Lipid oxidationLipid oxidation
AdhesionAdhesion

Ang II upregulates LOX-1 expression via lipoxygenase pathway
* P < 0.0001 vs control† P < 0.0001 vs Ang II‡ P < 0.05 vs Ang II
Bai = baicalein (12-lipoxygenase inhibitor)
Human vascular smooth muscle cells
Limor R et al. Am J Hypertens. 2005;18:299-307.
Ang II10-7 mol/L+
losartan 10-5 mol/L
0
100
200
300
Control Ang II10-7 mol/L
Ang II10-7 mol/L+
Bai 10-5 mol/L
LOX-1mRNA
*† ‡
400

TGF-β
Jacoby DS, Rader DJ. Arch Intern Med. 2003;163:1155-64.
Ang II and mechanisms of atherosclerosis
IL-6MCP-1PDGF
ImpairedNO synthase LOX-1
PAI-1TF
VCAMICAM
Angiotensin II
Lipid oxidation
Thrombosis
Inflammation
Endothelialdysfunction
Adhesion
ProliferationProliferation fibrosis

HOPE: Dose-dependent effects of ramipril on LV mass and function
5.31
2.9
–1.9–3
0
2
4
68.21 7.86
–3.53–4
0
5
10
LV end-systolic volumeLV mass
Lonn E et al. J Am Coll Cardiol. 2004;43:2200-6.Mean baseline LVEF 58%, all groups
∆(mL)
∆(g)
PTrend = 0.001PTrend = 0.03
N = 446 follow-up, 4 years
Placebo Ramipril 2.5 mg
Ramipril 10 mg

LIFE: Greater reduction in LV mass with angiotensin receptor blockade vs beta-blockade
Devereux RB et al. Circulation. 2004;110:1456-62.
Patients with hypertension and LVH
Change inLV mass
(g)
–50
–20
Year
–10
0
Losartan 50–100 mg (n = 457)
Atenolol 50–100 mg (n = 459)
–30
–40
1 2 3 4 5Lastvisit
P = 0.009 for all time points

PAI-1TF
Jacoby DS, Rader DJ. Arch Intern Med. 2003;163:1155-64.
Ang II and mechanisms of atherosclerosis
IL-6MCP-1PDGF
ImpairedNO synthase LOX-1
TGF-β
VCAMICAM
Angiotensin II
Lipid oxidation
Inflammation
Proliferation fibrosis
Endothelialdysfunction
AdhesionThrombosisThrombosis

Brown NJ et al. Hypertension. 2002;40:859-65.P = 0.043, drug × time interaction
ACE inhibition (ramipril) AT1 receptor blockade (losartan)
10
0
–10
20
Week 1
–20
∆PAI-1
antigen(ng/mL)
30
Week 3 Week 4
Sustained decrease in PAI-1 antigen over time with ACEI vs ARB
Week 6

Greater decrease in PAI-1 over time with ACEI vs ARB
85 Hypertensive diabetic patients treated for 12 weeks
Fogari R et al. Am J Hypertens. 2002;15:316-20.
10
–10
5
0
–5
Losartan 50 mg
4Perindopril 4 mg
–10
P < 0.01
*P = 0.028 perindopril vs placebo
∆PAI-1ng/dL
*

Change in PAI-1 antigen levels: Differing effects of ARBs
Koh KK et al. Atherosclerosis. 2004;177:155-60.
%Change
–40
20
40
60
Placebo
80
–20
0
Irbesartan 300 mg
Losartan 100 mg
Candesartan 16 mg
P < 0.01
P = 0.012P = 0.163
126 Patients with hypertension

Pretorius M et al. Circulation. 2003;107:579-85.
*P < 0.05 vs baseline†P < 0.05 vs vehicle or baseline
‡P < 0.05 vs enalaprilat + vehicleHOE 140 = bradykinin B2 receptor antagonist
Greater effect in women vs men
Women (n = 7) Men (n = 5)
Baseline
‡
HOE 140 + Enalaprilat
HOE 140
2
1
0
3
Net tPArelease(ng/min/100 mL)
2
1
0Baseline
*†
Vehicle + Enalaprilat
Vehicle
3
ACEI increases tPA release through endogenous bradykinin

tPA release: Differing effects of ACEinhibition vs AT1 receptor blockade
Matsumoto T et al. J Am Coll Cardiol. 2003;41:1373-9.*P < 0.05 vs baseline
20
10
15
5
0.2
0
0 0.6 2.0
tPA antigenin coronary
sinus (ng/mL)
Bradykinin (µg/min)
Perindopril 4 mg(n = 16)
Losartan 50 mg(n = 15)
Control(n = 14)
P < 0.05
*
**
**
* *
25

Antiatherosclerotic effect of RAAS modulation: Clinical and experimental evidence
• Studies in several animal models of atherosclerosis demonstrated reduced lesion progression with ACE inhibitor or AT1 receptor blocker1
• Regression of human carotid plaque demonstrated with ramipril (SECURE2), losartan (LAARS3), and fosinopril (PHYLLIS4)
1Jacoby DS, Rader DJ. Arch Intern Med. 2003;163:1155-64.2Lonn E et al. Circulation. 2001:103;919-25.
3Ludwig M et al. Clin Ther. 2002;24:1175-93.4Zanchetti A et al. Stroke. 2004;35:2807-12.

Lonn EM et al. Circulation. 2001;103:919-25.
0
0.005
0.010
0.015
0.020
0.025
Ramipril 10 mg
Ramipril 2.5 mg
Placebo
0.022
0.018
0.014
NS
37% Reduction
P = 0.028
Mean maximum IMT slope
(mm/y)
SECURE
ACEI reduces atherosclerosis progression

ARB blunts MMP expression in human carotid plaques: Potential role in plaque stabilization
25.828.2
25.1
22.4
5.8 6.2 7.25.6
0
10
20
30
MMP-2 MMP-9 COX-2 mPGES-1
P < 0.0001 all comparisonsARB = AT1 receptor blockade
MMP = matrix metalloproteinase
% Positive staining
Chlorthalidone Irbesartan
Cipollone F et al. Circulation. 2004;109:1482-8.
Carotid endarterectomy specimens

Role of RAAS Modulation:Evidence from Clinical Trials
• CAD• Heart Failure

ACEIs: Evolution of benefits
BP reduction
Cardioprotection
Improved glycemic control (?)
Vascular protection
Lonn E et al. Eur Heart J Suppl. 2003;5(suppl A):A43-8.DREAM Trial Investigators. N Engl J Med. 2006;355:1551-62.
Renal protection

Benefit of ACE inhibition in CADBenefit of ACE inhibition in CAD
EUROPA
HOPE
All CAD patientsAll CAD patients
Post-MI, HF, LVEF <40%
SOLVDSAVEAIRETRACE
SOLVD(prev)
High risk
Bertrand ME. Curr Med Res Opin. 2004;20:1559-69.

ACEI trials in CAD without HF: Primary outcomes
HOPE Study Investigators. N Engl J Med. 2000;342:145-53.Pitt B et al. Am J Cardiol. 2001;87:1058-63.
PEACECV death/MI/CABG/PCI
HOPECV death/MI/stroke
15
5
10
0
20
0
Placebo
Ramipril 10 mg
Time (years)
%
2 41
22% Risk reductionHR 0.78 (0.70–0.86)
P < 0.001
3Time (years)
12
4
10
0
1 3 4
14
0
Placebo
Perindopril 8 mg
86
2
52
EUROPACV death/MI/cardiac arrest
20% Risk reductionHR 0.80 (0.71–0.91)
P = 0.0003
40
20
30
0
50
0
Placebo
Quinapril 20 mg
Time (years)1
4% Risk increaseHR 1.04 (0.89–1.22)
P = 0.6
10
2 3
QUIETAll CV events
Time (years)
Trandolapril4 mg
Placebo30
20
10
15
5
1 2 3 4 5
25
06
4% Risk reductionHR 0.96 (0.88–1.06)
P = 0.43
EUROPA Investigators. Lancet. 2003;362:782-8.PEACE Trial Investigators. N Engl J Med. 2004;351:2058-68.
%
%
%

HOPE EUROPA PEACE QUIET
Antiplatelet agents (%) 76 92 91 73
β-Blockers (%) 40 62 60 26
Lipid-lowering agents (%) 29/49* 58/68† 70 0/14*
Calcium antagonists (%) 47 32 36 0/7*
Diuretics (%) 15 10 13 NA
EUROPA Investigators. Lancet. 2003;362:782-8.HOPE Study Investigators. N Engl J Med. 2000;342:145-53.
PEACE Trial Investigators. N Engl J Med. 2004;351:2058-68.Pitt B et al. Am J Cardiol. 2001;87:1058-63.
*at study end†at 3 yrs
ACEI outcome trials in CAD patients without HF: CV therapies at entry/during study

ACE inhibitor Key inclusion criteria Primary outcome
EUROPA N = 12,218 (4.2 years)
Perindopril 8 mg CAD No heart failure Age ≥18 years
CV death, MI, cardiac arrest
PEACE N = 8290 (4.8 years)
Trandolapril 4 mg CAD LVEF ≥40% Age ≥50 years
CV death, MI, coronary revascularization
QUIET N = 1750 (2.25 years)
Quinapril 20 mg PTCA, atherectomy Normal LVEF
CV death, MI, coronary revasc, cardiac arrest, hosp for angina
EUROPA Investigators. Lancet. 2003;362:782-8.HOPE Study Investigators. N Engl J Med. 2000;342:145-53.
PEACE Trial Investigators. N Engl J Med. 2004;351:2058-68.Pitt B et al. Am J Cardiol. 2001;87:1058-63.
ACEI outcome trials in CAD patients without HF
HOPE N = 9297 (4.5 years)
Ramipril 10 mg Vascular disease (80% had CAD) LVEF ≥40%, or No heart failure Age ≥55 years
CV death, MI, stroke

ACEI outcome trials in CAD patients without HF: Totality of trial evidence
MI
Stroke
All-cause death
Event rate (%)
Favors ACEIACEI
Revascularization
Favors placeboPlacebo
7.5
6.4
2.1
15.5
8.9
7.7
2.7
16.3
0.86
0.86
0.77
0.93
0.0004
0.0004
0.0004
0.025
0.5 0.75 1.251Odds ratio
P
Pepine CJ, Probstfield JL. Vasc Bio Clin Pract. CME Monograph; UF College of Medicine. 2004;6(3).
HOPE, EUROPA, PEACE, QUIET

HOPE, EUROPA, PEACE: Benefit of ACEIs across broad spectrum of risk
Dagenais GR et al. Lancet. 2006;368:581-8.
TrialPatients
(n)Annual rates in placebo groups
OR(95% CI) P
-5 20 405 3015 35Odds reduction (%)
25100
PEACE 8290 2.13 7 (-8 to 19) 0.328
HOPE total 9297 3.95 25 (16 to 32) 0.0001HOPE lower risk 3083 2.17 18 (-4 to 35)HOPE med risk 3100 3.58 20 (3 to 33)HOPE high risk 3114 5.98 24 (12 to 34)
EUROPA total 12,218 2.60 19 (8 to 28) 0.0007
EUROPA lower risk 3976 1.40 19 (-5 to 38)EUROPA med risk 3975 2.41 28 (11 to 41)EUROPA high risk 3975 4.00 10 (-4 to 22)
AIRE 1986 22.6 24 (7 to 38) 0.0068
TRACE 1749 17.0 25 (9 to 33) 0.0028
SOLVD-P 4228 7.4 15 (2 to 27) 0.0252SOLVD-T 2569 13.1 23 (10 to 33) 0.0009SAVE 2231 9.8 20 (4 to 33) 0.0168
CV death,* nonfatal MI or strokeACEI worse
ACEI better
*Or total mortality in AIRE, TRACE, SOLVD, SAVE trials
HOPE Study Investigators. N Engl J Med. 2000;342:145-53. EUROPA Investigators. Lancet. 2003;362:782-8.
PEACE Trial Investigators. N Engl J Med. 2004;351:2058-68.Pitt B et al. Am J Cardiol. 2001;87:1058-63.
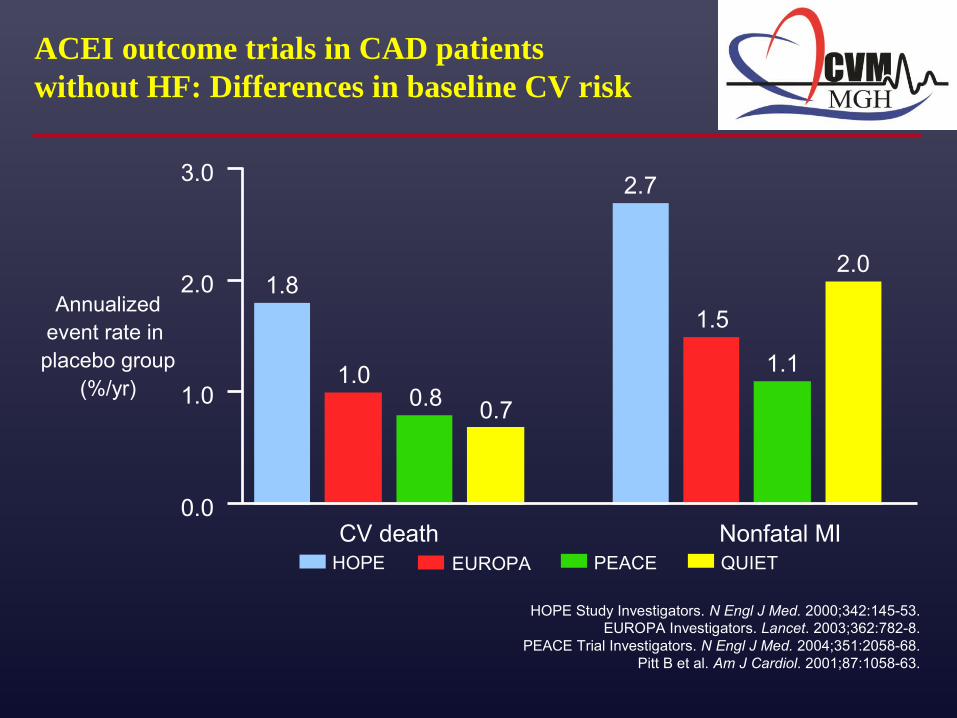
ACEI outcome trials in CAD patients without HF: Differences in baseline CV risk
HOPE EUROPA PEACE
Annualizedevent rate in placebo group
(%/yr)
CV death Nonfatal MIQUIET
1.8
1.00.8 0.7
2.7
1.5
1.1
2.0
0.0
1.0
2.0
3.0

EUROPA: EUropean trial on Reduction Of cardiac events with Perindopril in stable coronary Artery disease
EUROPA Investigators. Lancet. 2003;362:782-8.
Objective: Assess effects of the ACEI perindopril on CV risk in a broad-spectrum population with stable CAD and without HF
Design: N = 12,218, age ≥18 years, with CAD/without HF at randomization
Treatment: Perindopril 8 mg or placebo
Follow-up: 4.2 years
Primary outcome: CV death, nonfatal MI, cardiac arrest

EUROPA: Baseline characteristics
EUROPA Investigators. Lancet. 2003;362:782-8.
Female History of CAD – MI – PCI – CABGDocumented CAD – Angiographic evidence (stenosis >70% )
14.5 100 64.9 29.0 29.3
60.4
14.710064.729.529.4
60.5
– Positive stress test (in men w/chest pain) History of stroke/TIAPVDHypertension DiabetesHypercholesterolemia
22.6
3.4 7.1 27.0 11.8 63.3
23.3
3.3 7.427.212.863.3
Placebo (%)(n = 6108)
Perindopril (%)
(n = 6110)

EUROPA: Concomitant medications
Platelet inhibitors
Beta-blockers
Lipid-lowering agents
Nitrates
Calcium channel blockers
Diuretics
92
62
58
43
32
9
91
63
69
NA
NA
NA
EUROPA Investigators. Lancet. 2003;362:782-8.
Baseline (%) 3 Years (%)*
*Concomitant medications recorded in 11,547 patients

EUROPA Investigators. Lancet. 2003;362:782-8.Fox KM. Br J Cardiol. 2004;11:195-204.
EUROPA: Primary outcome
12
4
10
0
1 3 4
14
0
Placebo
Perindopril 8 mg8
6
2
52
Primary outcome
(%)
Time (years)
10%
11%
14%
20%
CV death, MI, cardiac arrest
RRR 20% (95% CI: 9%–29%)AR 8.0% vs 9.9%
P = 0.0003
P < 0.05
P = 0.35
AR = absolute risk (perindopril vs placebo)

RRR 24%AR 5.2% vs 6.8%
P < 0.001
EUROPA Investigators. Lancet. 2003;362:782–8.
Fatal and nonfatal MI
RRR 39%AR 1.0% vs 1.7%
P = 0.002
2
4
Events(%)
0
10
6
8
0 1 2 3 4 5
Years
Placebo
Perindopril8 mg
0.5
1.0
0.0
2.0
1.5
0 1 2 3 4 5
Years
Placebo
Perindopril8 mg
HF hospitalization
EUROPA: Effect of ACEI on fatal/nonfatal MI and HF hospitalizations
AR = absolute risk (perindopril vs placebo)

EUROPA Investigators. Lancet. 2003;362:782-8.
8.0
14.8
7.9
6.1
3.5
5.2
CV mortality, MI, cardiac arrest
Total mortality, MI, UA, cardiac arrest
CV mortality, MI
Total mortality
CV mortality
Fatal/nonfatal MI
Favorsperindopril
Favorsplacebo
Perindopril (%)(n = 6110)
Placebo (%)(n = 6108)
9.9
17.1
9.8
6.9
4.1
6.8
0.5 1.0 2.0
EUROPA: Benefit of ACEI on primary and secondary outcomesN = 12,218

EUROPA Investigators. Lancet. 2003;362:782-8.
5.6
0.1
1.6
9.4
1.0
Unstable angina
Cardiac arrest
Stroke
Revascularization
HF w/hospital admission
Favorsperindopril
Favorsplacebo
Perindopril (%)(n = 6110)
Placebo (%)(n = 6108)
6.0
0.2
1.7
9.8
1.7
0.5 1.0 2.0
EUROPA: Benefit of ACEI on selected secondary outcomesN = 12,218

EUROPA: Benefit of perindopril was on top of recommended medications
EUROPA Investigators. Lancet. 2003;362:782-8.
7.0
9.3
7.6
8.7
9.9
7.1
0.5 1.0 2.0
8.3
11.9
10.2
9.4
11.7
9.0
Lipid-lowering drug
No lipid-lowering drug
β-blockers
No β-blockers
Calcium channel blockers
No calcium channel blockers
Favorsperindopril
Favorsplacebo Perindopril
(n = 6110) Placebo
(n = 6108)
Primary events (%)

EUROPA HOPE
Age, mean (yrs) 60 66
BP (mm Hg) 137/82 139/79
Known CAD (%) MI (%) PVD (%) Stroke/TIA (%) Revascularization (%)Diabetes (%)Hypertension (%)Hypercholesterolemia (%)
1006573
58122763
8053431144394766
EUROPA Investigators. Lancet. 2003;362:782-8.HOPE Study Investigators. N Engl J Med. 2000;342:145-53.
EUROPA vs HOPE: Study populations

EUROPA vs HOPE: Inclusion criteria
HOPE • Age ≥55 years • Females: 27%• No HF or LV dysfunction • High-risk of CV events
with history of – CAD, stroke, or peripheral
vascular disease– Diabetes + ≥1 CV risk factor
(hypertension, dyslipidemia, smoking, microalbuminuria)
EUROPA • Age ≥18 years• Females: 15% • No clinical HF• Documented CAD including
– Previous MI, PCI/CABG– Angiographic evidence of
CAD with/without previous coronary event
– Positive stress test (men)
EUROPA Investigators. Lancet. 2003;362:782-8.HOPE Study Investigators. N Engl J Med. 2000;342:145-53.
HOPE patients were at higher risk than EUROPAHOPE patients were at higher risk than EUROPA

EUROPA vs HOPE: Event rates in placebo groups reflect differences in baseline risk
80% higher annual rate of CV and total mortality in HOPE80% higher annual rate of CV and total mortality in HOPE
EUROPA Investigators. Lancet. 2003;362:782-8.HOPE Study Investigators. N Engl J Med. 2000;342:145-53.
CV mortality Total mortality
Annualizedevent ratein placebo
groups(%)
HOPEEUROPA
1.8
2.7
1.0
1.5
0.0
0.5
1.0
1.5
2.0
2.5
3.0

Are all ACEIs the same: Survival post-MI by ACEI at discharge
P < 0.001 log-rank
100
90
80
70121086420
Months
Captopril
Ramipril
Quinapril
Fosinopril
Lisinopril
Enalapril
Perindopril
Unadjusted cumulative
survival(%)
N = 7512
Pilote L et al. Ann Intern Med. 2004;141:102-12.
n = 421
n = 905
n = 276
n = 889
n = 2201
n = 2577
n = 243

Factors that may lead to divergent results in ACEI trials
• Underdosing – Dose-related effects on vascular and myocardial tissue
– Dose for CAD patients can’t be predicted from studies in HF or hypertension
• Differences may exist among ACEIs
• Differences in baseline risk (age, diabetes, HTN, PAD)
• Inclusion of revascularization in primary outcome
• Lack of power
• Poor adherence to assigned treatmentPitt B et al. Am J Cardiol. 2004;87:1058-63.
Yusuf S, Pogue J. N Engl J Med. 2005;352:937-8.Pitt B. N Engl J Med. 2004;351:2115-7.
Pepine CJ, Probstfield JL. Vasc Bio Clin Pract. CME Monograph; UF College of Medicine. 2004;6(3).

• Cumulative evidence supports ACE inhibitors for stable CAD patients with/without clinical signs of HF
• Not all ACE inhibitors can be assumed to have comparable effects for all indications – Dose and individual properties of ACEIs are important
• Benefit may depend on risk level – Benefit may be less in patients with well controlled risk factors
• Randomized clinical trial evidence and guidelines should guide selection of effective ACE inhibitor and dose for CAD patients without HF
Pitt B. N Engl J Med. 2004;351:2115-7.
ACEI outcome trials in CAD patients without HF: Clinical implications

• Totality of clinical trial evidence supports ACEI for treatment of stable CAD patients with/without HF
• Benefits have been shown in patients at all levels of risk
• All ACEIs may not have comparable effects for all indications
• Consider evidence and guidelines in selection of an ACEI and dose.
• Both ramipril and perindopril reduce risk of CV events in stable CAD patients without HF
– Ramipril 10 mg has proven efficacy in CAD patients ≥55 yrs
– Perindopril 8 mg has proven efficacy in CAD patients ≥18 yrs
Pitt B. N Engl J Med. 2004;351:2115-7.EUROPA Investigators. Lancet. 2003;362:782-8.
HOPE Study Investigators. N Engl J Med. 2000;342:145-53.PEACE Trial Investigators. N Engl J Med. 2004;351:2058-68.
Should all patients with stable CAD without HF receive an ACEI? Interpreting evidence

Evidence-based medicine: Updated guide-lines for ACEI in CAD patients without HF
“ACE inhibitors should be used as routine secondary prevention for patients with known CAD, particularly in diabetics without severe renal disease.” . . . R.J. Gibbons et al.
“The HOPE trial…confirms that the ACE inhibitor ramipril reduced CV death, MI, and stroke in patients who were at high risk for, or had, vascular disease in the absence ofheart failure.” . . . R.J. Gibbons et al.
EUROPA “showed that an ACE inhibitor can have a vasculoprotective effect in patients at lower risk than those enrolled in the HOPE study.” . . . V. Snow et al.
Gibbons RJ et al. 2002 ACC/AHA Practice Guidelines. www.acc.org; July 2005.Snow V et al. Ann Intern Med. 2004;141:562-7.

Role of RAAS Modulation in
CAD Patients with heart failure
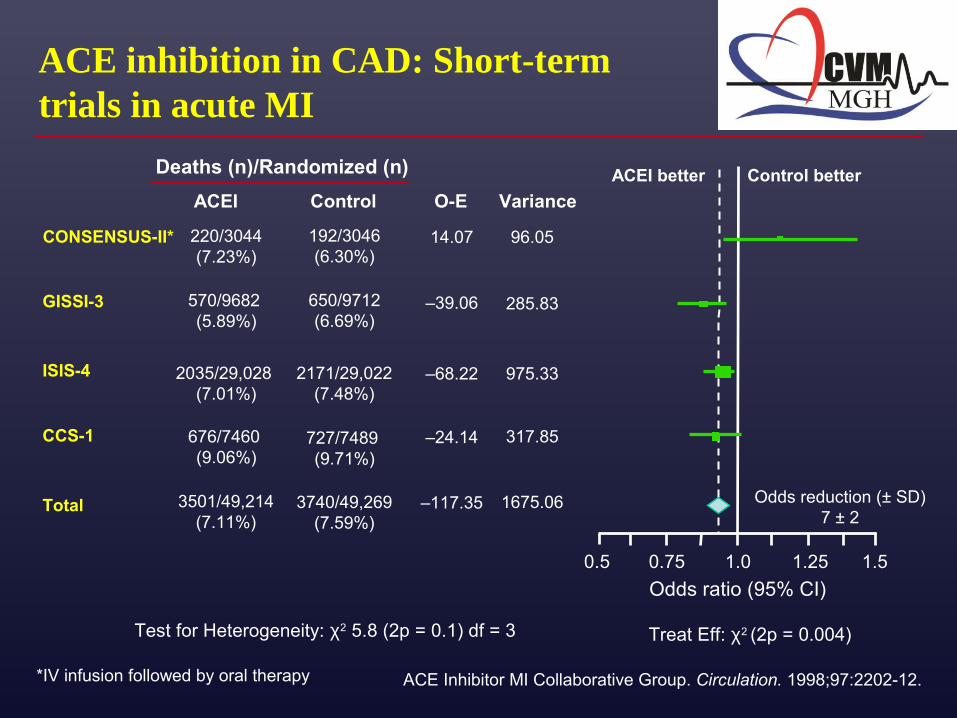
ACE inhibition in CAD: Short-term trials in acute MI
Odds ratio (95% CI)
220/3044 (7.23%)
570/9682 (5.89%)
2035/29,028 (7.01%)
676/7460 (9.06%)
CONSENSUS-II*
Test for Heterogeneity: χ2 5.8 (2p = 0.1) df = 3
Deaths (n)/Randomized (n)
GISSI-3
ISIS-4
CCS-1
Total
Control O-E Variance
1.0 1.25 1.50.750.5
727/7489 (9.71%)
650/9712(6.69%)
192/3046(6.30%)
2171/29,022(7.48%)
3501/49,214(7.11%)
3740/49,269(7.59%)
14.07
–39.06
–68.22
–24.14
–117.35
96.05
285.83
975.33
317.85
1675.06
ACEI
ACEI better Control better
Odds reduction (± SD)7 ± 2
Treat Eff: χ2 (2p = 0.004)
ACE Inhibitor MI Collaborative Group. Circulation. 1998;97:2202-12.*IV infusion followed by oral therapy

ACE inhibition in CAD: Long-term trials in post-MI LV dysfunction and HF
AIRE Study Investigators. Lancet. 1993;342:821-8.Køber L et al. N Engl J Med. 1995;333:1670-6.
SOLVD Investigators. N Engl J Med. 1991;325:293-302.SOLVD Investigators. N Engl J Med. 1992;327:685-91.
Pfeffer MA et al. N Engl J Med. 1992;327:669-77.
AIRE
TRACE
SOLVD(Treatment)
SAVE
0.002
0.001
0.0036
0.019
0 5 10 15 20 25
Risk reduction in total mortality (%)
P
30
SOLVD(Prevention)
0.30
27%
22%
8%
16%
19%

Aldosterone blockade and AT1 receptor blockade: Trials in post-MI/LV dysfunction or HF
Pitt B et al. N Eng J Med. 1999;341:709-17.Pitt B et al. N Eng J Med. 2003;348:1309-21.
Pitt B et al. N Eng J Med. 2003;349:1893-906.
VALIANT
Months
CaptoprilValsartan
0.4
0.1
0.2
6 12 24 30 36
0.3
0.0
Probability of event
0% RR V vs CHR 1.00 (0.90–1.11)
P = 0.98
RALES
0.75
0.60
1.00
0
Placebo
Spironolactone
Months
Probability of survival
24 366
30% Risk reductionRR 0.70 (0.60–0.82)
P < 0.001
300.00
12 18
0.90
0.45
180
Valsartan/captopril
22
10
2
6 24 300
Eplerenone
Months
18
14
6
3612
EPHESUS15% Risk reductionRR 0.85 (0.75–0.96)
P = 0.008
Cumulativeincidence
(%)
Placebo
018
2% RR V/C vs CHR 0.98 (0.89–1.09)
P = 0.73)

EPHESUS: New subgroup analysis
Pitt B et al. Am J Cardiol. 2006;97(suppl):26F-33F.
N = 6632 with post-MI LVSD, mean follow-up 16 months
Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study
History of hypertensionAll-cause mortalityCV mortality/hospitalizationSudden cardiac death
History of diabetesAll-cause mortalityCV mortality/hospitalizationSudden cardiac death
LVEF ≤30%All-cause mortalityCV mortality/hospitalizationSudden cardiac death
P
0.0010.0020.022
0.1270.03
0.641
0.0120.001
0.010.2 1.0 1.2 1.8
Eplerenone better Placebo better
1.4 1.60.4 0.6 0.8Odds ratio (95% Cl)

Greenberg B et al. Am J Cardiol. 2006;97(suppl):34F-40F.
EMPHASIS-HF: Study design
Eplerenone+ standard therapy
N = 2584 with NYHA class II chronic systolic HF
Results in 2010
Placebo+ standard therapy
Primary end point:CV death, hosp for HF
Follow-up: 4 years
Effect of Eplerenone in Chronic Systolic Heart Failure

EMPHASIS-HF: Major results
EMPHASIS-HF
Outcome Eplerenone (%) Placebo (%) Adjusted hazard ratio (95% CI)
p
Cardiovascular death/heart-failure hospitalization
18.3 25.9 0.63 (0.54–0.74) <0.001
Cardiovascular death 10.8 13.5 0.76 (0.61–0.94) 0.01
Heart-failure hospitalization 12.0 18.4 0.58 (0.47–0.70) <0.001
Hospitalization for hyperkalemia 0.3 0.2 1.15 (0.25–5.31) 0.85
NYHA Class II HF (N=2737)LV EF < 30%
Eplerenone 25-50mg QD vs. Placebo

Greenberg B et al. Am J Cardiol. 2006;97(suppl):34F-40F.
TOPCAT: Study design
Spironolactone
N ≅ 4500 with HF and LVEF >45%
Results anticipated 2011
Placebo
Primary end point:CV death, hosp for HF
Follow-up: ≥2 years
Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist
Enrollment: 3445Study Start Date: August 2006Estimated Study Completion Date: June 2013Estimated Primary Completion Date: June 2013

RAAS Modulation in Patients With Diabetes

Potential role of RAAS activation in metabolic syndrome and diabetes
Adapted from Henriksen EJ, Jacob S. J Cell Physiol. 2003;196:171-9.Paul M et al. Physiol Rev. 2006;86:747-803.
RAAS activation
Skeletal muscle Pancreatic β cells
↑MetS ↑T2DM
MetS = metabolic syndromeT2DM = type 2 diabetes
Obesity

RAAS activation in obesity
Engeli S et al. Hypertension. 2005;45:356-62.
Circulating RAAS, N = 38 menopausal women
*P < 0.05
Renin(ng/l)
ACE(U/l)
Aldosterone (ng/l)
Ang II(nmol/l)
Lean Obese0
3
6
12
9
0
15
30
60
45
0
90
0.00
0.05
0.10
30
60
Lean Obese
Lean Obese Lean Obese
* *
*

Obesity
Volume expansion
Arterial hypertension
Sharma AM. Hypertension. 2004;44:12-19.
↑Leptin Renal medullary compression
↑RAAS activation
Sodium reabsorption
Renal vasodilation ↑SNS activation
SNS = sympathetic nervous system
RAAS activation contributes to obesity-related hypertension

Adipocyte and vasculature interactionsAdipocyte and vasculature interactions
Courtesy of W. Hseuh; 2005.
IL-6
PAI-1TNF-α
AdiponectinLeptin
Insulin sensitivity Insulin resistance
Vascular inflammation Endothelial dysfunction
Angiotensinogen
FFA
Visfatin

Furuhashi M et al. Hypertension. 2003;42:76-81.
• Insulin sensitivity, BMI, and HDL-C independent determinants of adiponectin concentrations
• ACEI and ARB increased insulin sensitivity and adiponectin (P < 0.05)
• Changes in insulin sensitivity correlated with changes in adiponectin (r = 0.59, P < 0.05)
*P < 0.05
N = 16 with essential hypertension and insulin resistance
RAAS blockade increases adiponectin
6
4
10
Adiponectin(µg/mL)
0
8
2
Before After Before After
6
4
10
0
8
2
Temocapril 4 mg(n = 9)
Candesartan 8 mg(n = 7)
*
*

ACEIs: Potential mechanisms of improved glucose metabolism
Henriksen EJ, Jacob S. J Cell Physiol. 2003;196:171-9.
Angiotensin I
ACE/Kininase II
Degradation products
↑Nitric oxide
Angiotensin II
↓Angiotensin II
ACE inhibitors
Bradykinin
↑Bradykinin
↑Skeletal muscleblood flow
↑Glucose metabolism
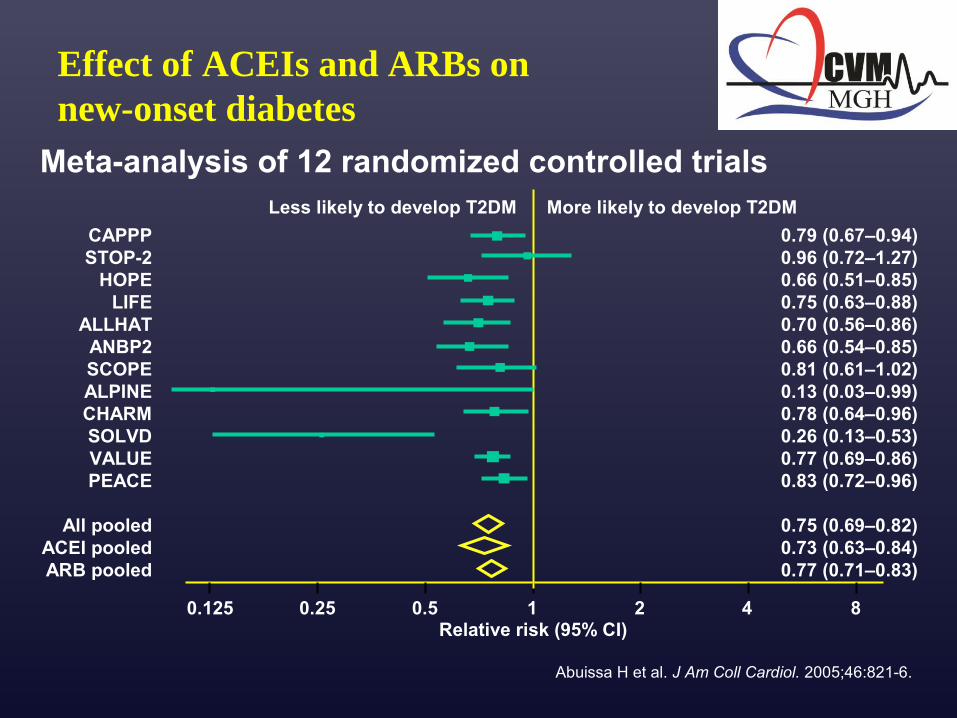
Effect of ACEIs and ARBs on new-onset diabetes
Abuissa H et al. J Am Coll Cardiol. 2005;46:821-6.
Meta-analysis of 12 randomized controlled trials
CAPPPSTOP-2
HOPELIFE
ALLHATANBP2SCOPEALPINECHARMSOLVDVALUEPEACE
All pooledACEI pooledARB pooled
0.79 (0.67–0.94)0.96 (0.72–1.27)0.66 (0.51–0.85)0.75 (0.63–0.88)0.70 (0.56–0.86)0.66 (0.54–0.85)0.81 (0.61–1.02)0.13 (0.03–0.99)0.78 (0.64–0.96)0.26 (0.13–0.53)0.77 (0.69–0.86)0.83 (0.72–0.96)
0.75 (0.69–0.82)0.73 (0.63–0.84)0.77 (0.71–0.83)
0.125 0.25 0.5 1 2 4 8
Less likely to develop T2DM
Relative risk (95% CI)
More likely to develop T2DM

HOPE, EUROPA, PEACE: Reduction in new-onset diabetes (placebo-controlled trials)
0
2
4
6
8
10
12
14
HOPE EUROPA PEACE Pooled data
New-onset diabetes
(%)
Placebo ACEI
Dagenais GR et al. Lancet. 2006;368:581-8.
n = 23,340 free from diabetes* at baseline
Ramipril 10 mg
Perindopril 8 mg
Trandolapril 4 mg
Overall14% RRRRR 0.86 (0.78–0.95)P = 0.0023
(all trials)
*Not a prespecified end point

PERSUADE: PERindorpil SUbstudy of coronary Artery disease and DiabEtes: The diabetic substudy of EUROPA
Objective: Investigate the effect of long-term treatment with perindopril added to standard therapy on CV
events in diabetic patients with CAD and without heart failure
Population: N = 1502 with known diabetes at randomization
Treatment: Perindopril 8 mg (n = 721) or placebo (n = 781)
Follow-up: 4.2 years
Daly CA et al. Eur Heart J. 2005;26:1369-78.

PERSUADE: Primary outcome
Cumulative frequency
(%)
Perindopril8 mg
Placebo
2 3 4 510
Years from randomization
0
4
8
12
16
20
RRR: 19%95% CI: –7% to 38%
P = 0.13
CV death, MI, cardiac arrest
Daly CA et al. Eur Heart J. 2005;26:1369-78.

PERSUADE: Clinical implications
• Perindopril 8 mg once daily reduced CV events in
patients with CAD and diabetes
• Relative risk reduction in primary and secondary
outcomes with perindopril was similar to EUROPA
• Results extend the benefit of ACEI shown in MICRO-
HOPE to a lower-risk population with diabetes and
CAD
Daly CA et al. Eur Heart J. 2005;26:1369-78.

HOPE Study Investigators. Lancet. 2000;355:253-9.
3.0
2.5
2.0
1.5
1.0
0.5
0 1 2 3 4.5
Placebo
Ramipril 10 mg
Mean albumin-creatinine ratio
Years
P = 0.001
P = 0.02
0
10
20
30
40
Overtnephro-pathy
CV deathStrokeMI
Riskreduction
(%)P = 0.027
P = 0.0001
P = 0.007
P = 0.01
22
3337
24
N = 3577 (32% with microalbuminuria)
MICRO-HOPE: ACEI improves renal and CV outcomes in type 2 diabetes

HOPE Study Investigators. Lancet. 2000;355:253-9.Daly CA et al. Eur Heart J. 2005. In press.
PERSUADE(N = 1502)
CV death/MI/cardiac arrest
MICRO-HOPE(N = 3577)
CV death/MI/stroke
MICRO-HOPE, PERSUADE: Primary outcome
Placebo
Ramipril10 mg
25
20
15
10
5
0
%
Follow-up (years)
0 1 2 3 4 5
25% Risk reductionRR 0.75 (0.64–0.88)
P = 0.000420
15
10
5
00 1 2 3 4 5
Follow-up (years)
Placebo
Perindopril8 mg
19% Risk reductionP = 0.131
25

MICRO-HOPE, PERSUADE: Consistency of benefit
HOPE Study Investigators. Lancet. 2000;355:253-9.Daly CA et al. Eur Heart J. 2005. In press.
Primary outcome
Total mortality
CV mortality
All MI
Stroke
0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8
Favors ACEI Favors placebo
Relative risk (95% CI)
MICRO-HOPE(N = 3577)
PERSUADE(N = 1502)
Effects of ACEI on endothelial function: EUROPA substudies
• PERTINENT: PERindopril Thrombosis, InflammatioN, Endothelial dysfunction and Neurohormonal activation Trial
– Determined the mechanisms by which the ACEI perindopril improved outcomes in patients with stable coronary artery disease
• PERFECT: PERindopril-Function of the Endothelium in Coronary artery disease Trial
– Evaluated whether long-term administration of perindopril improves endothelial dysfunction
Ferrari R. ESC 2004; Munich.Bots ML et al. Cardiovasc Drugs Ther. 2002;16:227-36.

PERTINENT: Study design
Endothelial cell (EC) studiesEndothelial cell (EC) studiesECs incubated with serum from CAD ECs incubated with serum from CAD patients at baseline and at 1 year* patients at baseline and at 1 year*
Plasma studiesPlasma studiesMeasure substances in plasma that Measure substances in plasma that
modulate ecNOS and apoptosismodulate ecNOS and apoptosis
Ang IIAng IIBradykininBradykinin
TNF-TNF-ααvon Willebrand factorvon Willebrand factor
ecNOSecNOSEC apoptosis rateEC apoptosis rate
*Human umbilical vein ECsecNOS = EC nitric oxide synthase Ferrari R. ESC 2004; Munich.
Levels measured at baseline vs 1 year
Objective: Objective: Evaluate effects of perindopril on endothelial function and markers of Evaluate effects of perindopril on endothelial function and markers of inflammation and thrombosis in EUROPA subgroup of CAD patientsinflammation and thrombosis in EUROPA subgroup of CAD patients
EUROPA substudy

↑ ecNOS activity
↓ Endothelial cell apoptosis
↓ Ang II
↑ Bradykinin
↓ TNF-α↓ von Willebrand factor
Ferrari R. ESC 2004; Munich.*Incubated with patients’ serum
Endothelial cells* Patients’ plasma
EUROPA substudy
• The only significant correlation was between bradykinin and ecNOS
• Results suggest perindopril modifies inflammation and thrombosis and endothelial function through bradykinin-dependent mechanisms
PERTINENT: Effects of treatment with perindopril for 1 year

PERFECT: Study design
Objective: Determine effect of perindopril on brachial artery endothelial function in patients with stable CAD and without clinical HF
Design: Double-blind randomized controlled trial
Population: N = 333 at 20 centers
Treatment: Perindopril 8 mg or placebo
Follow-up: 3 years
Primary outcome: Change in flow-mediated vasodilation of
brachial artery assessed over 36 months
EUROPA substudy
Bots ML et al. J Am Coll Cardiol. 2005;45A(suppl):409A.Bots ML et al. Cardiovasc Drugs Ther. 2002;16:227-36.

• Mean FMD* increased (baseline vs 36 months) Perindopril 2.7% to 3.3% (+37%)Placebo 2.8% to 3.0% (+7%)
• Endothelial function (rate of change per 6 months) Perindopril 0.14% (P < 0.05 vs baseline) Placebo 0.02% (P = 0.74 vs baseline) (P = 0.07 for perindopril vs placebo)
• Conclusion: Part of the beneficial effect of perindopril on CV morbidity and mortality in the EUROPA study may be explained by improvement in endothelial function
*Brachial artery vasodilation in response to reactive hyperemia Bots ML et al. J Am Coll Cardiol. 2005;45A(suppl A):409A.
PERFECT: ACEI and endothelial functionEUROPA substudy

Effects of ARBs in type 2 diabetes: Renal and CV outcomes
Lewis EJ et al. N Engl J Med. 2001;345:851-60.Brenner BM et al. N Engl J Med. 2001;345:861-9.Parving HH et al. N Engl J Med. 2001;345:870-8.
*Doubling of baseline serum creatinine, end-stage renal disease (IDNT, RENAAL): progression to
diabetic nephropathy (IRMA-2)
Study(N) ARB
Primary outcome: Renal disease progression*
Secondaryoutcomes
(CV)
Average duration(years)
IDNT (N = 1715)
Irbesartan 300 mg/d vs amlodipine 10 mg
↓20% vs placebo, (P = 0.02) and ↓23% vs amlodipine (P = 0.006)
Combined CV outcomes: NS
2.6
RENAAL(N = 1514)
Losartan 100 mg/d vs placebo†
↓16% (P = 0.02) CV morbidity and mortality: NS HF hospitalization ↓32%
3.4
IRMA-2(N = 590)
Irbesartan 150–300 mg vs placebo
↓39% with 150 mg (P = 0.08)↓70% with 300 mg (P < 0.001)
Nonfatal CV events: NS
2

Clinical trials of ARBs: CV outcomes
Similar ↓
Greater ↓ with amlodipine (2.0/1.6 mm Hg)
Losartan vs atenolol
Valsartan vs amlodipine
Essential HTN
N = 9193
(4.8 years)
Essential HTN, high CV risk
N = 15,245
(4.3 years)
LIFE (2002)
VALUE (2004)
BPTreatment
Patients
(Follow-up)Trial (year)
HTN = hypertension
13% ↓ in primary outcome (CV death, MI, stroke) with ARB (P = 0.021) driven by 25% ↓ in stroke (P = 0.001)
No difference in CV death/MI
CV outcomes
Primary outcome similar at study end
Trend favors amlodipine at 3 and 6 months
Difficult to interpret due to BP difference
Dahlöf B et al. Lancet. 2002;359:995-1003. Julius S et al. Lancet. 2004;363:2022-31.

LIFE: Effects of ARB vs β-blockade on primary outcome and components
Dahlöf B et al. Lancet. 2002;359:995-1003.
N = 9193 with hypertension and ECG-LVH
LIFE = Losartan Intervention for Endpoint Reduction in Hypertension
16
Proportionof patientswith first
event (%)
12
8
4
0
60 18 30 5442 66
AtenololLosartan
Primary composite endpoint(CV death/MI/stroke)
Adjusted RR 13.0%P = 0.021
(losartan vs atenolol)
Time (months)
5
10Risk
increase(%)
0
5
10
15
20
25
Primary outcome components
(Losartan vs atenolol)
Riskreduction
(%)
P = 0.206
CV death
P = 0.491
Stroke
MI
P = 0.001

LIFE: Comparison of treatment effects in overall population vs with diabetes
Patients with hypertension and LVH
Dahlöf B et al. Lancet. 2002;359:995-1003. Lindholm LH et al. Lancet. 2002;359:1004-10.
0.5 1.0 1.5
Overall (n = 9193)
Diabetes (n = 1195)0.206
0.028
0.001
0.204
0.491
0.373
Favors losartan50–100 mg
Favors atenolol50–100 mg
P
CV death
Stroke
MI
Hazard ratio

VALUE: Similar treatment effectson primary outcome at study end
14
4
2
0
Proportionof patientswith first
event (%)
0 12 3018 24 54 60 66
Time (months)
6
8
10
12
6 36 42 48
HR = 1.03; 95% CI 0.94–1.14; P = 0.49
Valsartan-based regimen
Amlodipine-based regimen
Julius S et al. Lancet. 2004;363:2049-51

Timeinterval(mos)
∆ SBP(mm Hg)
Odds ratio Odds ratio
Favorsvalsartan
Favorsamlodipine
Favorsvalsartan
Favorsamlodipine
Primary outcome Myocardial infarction
0.5 1.0 2.0 4.0 0.5 1.0 2.0 4.0
All study 2.20–3 3.83–6 2.36–12 2.012–24 1.824–36 1.6
Study end 1.736–48 1.4
Julius S et al. Lancet. 2004;363:2022-31.
VALUE: SBP and outcome differences during consecutive time periods
VALUE = Valsartan Antihypertensive Long-Term Use Evaluation

Direct Renin InhibitorAliskerin
pre-clinical data




Aliskerin preclinical dataSummary
• Aliskerin demonstrates organ protective effects in animal models
• Renoprotection comparable with ACEIs and ARBs
• LVH reductions comparable with ARBs• Suppresses markers of renal damage in
diabetic nephropathy• Atherogenesis prevention

Direct Renin InhibitorAliskerin
Clinical data






Direct Renin InhibitorAliskerin
Outcome data
EFFECT OF THE DIRECT RENIN INHIBITOR ALISKIREN ON LEFT VENTRICULAR
REMODELING FOLLOWING MYOCARDIAL INFARCTION WITH LEFT VENTRICULAR
DYSFUNCTION
ASPIRE TrialScott D. Solomon, MD, FACC, Sung Hee Shin, MD, Amil Shah, MD, Lars Kober, MD, Aldo P.
Maggioni, MD, Jean Rouleau, MD, FACC, John J. V. McMurray, MD, FACC, Roxzana Kelly, Allen Hester, Marc A. Pfeffer, MD, PhD, FACC for the Aliskiren Study in Post-MI Patients to Reduce
Remodeling (ASPIRE) investigators
Brigham and Women’s Hospital, Boston, MA; Rigshospitalet Copenhagen University Hospital, Copenhagen, Denmark; ANMCO Research Center, Firenze, Italy; University of Montreal, Montreal,
Canada; Western Infirmary, Glasgow, Scotland; Novartis Pharmaceuticals, East Hanover, NJ

Cardiovascular Outcomes ASPIRE Trial
EndpointPlacebo
n=397n (%)
Aliskiren n=423n (%)
CV Death 6 (1.5) 13 (3.1)
Resuscitated Sudden Death 4 (1.0) 1 (0.2)
HF Hospitalization 17 (4.3) 12 (2.8)
Myocardial Infarction 16 (4.0) 11 (2.6)
Stroke 2 (0.5) 7 (1.7)
Any of the above 34 (8.6) 39 (9.2)
No Significant between group differences

Conclusions ASPIRE Trial
• In high risk post-MI patients with LV systolic dysfunction, the addition of aliskiren to a standard optimal medical regimen, including an ACE-I or an ARB, did not result in benefit with respect to ventricular remodeling compared to placebo and was associated with more adverse events
• Although ASPIRE utilized a surrogate endpoint, and was not powered to assess hard clinical outcomes, these results do not provide support for testing the use of aliskiren in a morbidity and mortality trial in the high-risk post-MI population
• Ongoing outcomes trials with aliskiren in patients with heart failure and diabetic kidney disease are well underway and will further assess the role for direct renin inhibition in these populations

Evidence of Dual RAA inhibition

RAAS: Pathways of ACE inhibition and angiotensin receptor blockade
Dzau V. J Hypertens. 2005;23(suppl 1):S9-S17.
ACE inhibitor
Bradykinin/NO
Inactivefragments
Chymase,tPA,
cathepsin
‘Angiotensin IIescape’
ARB
AT1 receptor AT2 receptor
Angiotensin I
Angiotensin II

ONTARGET/TRANSCEND Investigators. Am Heart J. 2004;148:52-61.
ONTARGET: Study design
Ramipril 10 mg Telmisartan 80 mg
N = 25,620≥55 years with coronary, cerebrovascular, or peripheral vascular disease,
or diabetes + end-organ damage
Results in 2007
Ramipril 10 mg + telmisartan 80 mg
Primary end point:CV death, MI, stroke, hosp for HF
Secondary end point:Newly diagnosed diabetes
ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial

ONTARGET/TRANSCEND Investigators. Am Heart J. 2004;148:52-61.
TRANSCEND: Study design
Telmisartan 80 mg
N = 5776 ACEI-intolerant≥55 years with coronary, cerebrovascular, or peripheral vascular disease,
or diabetes + end-organ damage
Results in 2007
Placebo
Primary end point:CV death, MI, stroke, hosp for HF
Secondary end point:Newly diagnosed diabetes
Telmisartan Randomized AssessmeNt Study in aCE iNtolerant subjects with cardiovascular Disease

Yusuf S et al. N Engl J Med 2008: 358:1547-1559.
ONTARGET: Key results Outcome Ramipril,
n=8576 (%)Telmisartan, n=8542 (%)
Combination, n=8502 (%)
CV death/MI/stroke/ CHF hospitalizationa
16.5 16.7 16.3
CV death/MI/strokeb 14.1 13.9 14.1
MI 4.8 5.2 5.2
Stroke 4.7 4.3 4.4
CHF hospitalization 4.1 4.6 3.9
CV death 7.0 7.0 7.3
Any death 11.8 11.6 12.5
Renal impairment 10.2 10.6 13.5
a. Primary end pointb. Primary end point in the HOPE trial

Yusuf S et al. N Engl J Med 2008: 358:1547-1559.
ONTARGET: Key results Outcome Risk ratio (95% CI),
telmisartan vs ramipril Risk ratio (95% CI), combination therapy vs ramipril
CV death/MI/stroke/ CHF hospitalizationa
1.01 (0.94–1.09) 0.99 (0.92–1.07)
CV death/MI/strokeb 0.99 (0.91–1.07) 1.00 (0.93–1.09)
MI 1.07 (0.94–1.22) 1.08 (0.94–1.23)
Stroke 0.91 (0.79–1.05) 0.93 (0.81–1.07)
CHF hospitalization 1.12 (0.97–1.29) 0.95 (0.82–1.10)
CV death 1.00 (0.89–1.12) 1.04 (0.93–1.17)
Any death 0.98 (0.90–1.07) 1.07 (0.98–1.16)
Renal impairment 1.04 (0.96–1.14) 1.33 (1.22–1.44)
a. Primary end pointb. Primary end point in the HOPE trial

ONTARGET: Reasons for permanent discontinuations
Yusuf S et al. N Engl J Med 2008: 358:1547-1559.
Outcome Ramipril (%)
Telmisartan (%)
Combination (%)
p, telmisartan vs ramipril
p, combination therapy vs ramipril
Hypotensive symptoms
1.7 2.7 4.8 <0.001 <0.001
Syncope 0.2 0.2 0.3 0.49 0.03
Cough 4.2 1.1 4.6 <0.001 0.19
Diarrhea 0.1 0.2 0.5 0.20 <0.001
Angioedema 0.3 0.1 0.2 0.01 0.30
Renal impairment
0.7 0.8 1.1 0.46 <0.001

Conclusions: Telmisartan vs. Ramipril
1. Telmisartan is clearly “non-inferior” to ramipril,with most ( 95-100%) of the benefits preserved
2. Consistent results on a range of:• Secondary outcomes• Subgroups
3. Telmisartan exhibits slightly superior overall tolerability:
• Less cough and angioneurotic edema• More mild hypotensive symptoms, but no
difference in severe hypotensive symptoms, such as syncope

Conclusions: Telmisartan plus Ramipril vs. Ramipril
1. Combination therapy does not reduce the primary outcome to a greater extent compared to ramipril alone and has higher adverse events.
Implications• Telmisartan is as effective as ramipril, with a slightly
better tolerability.
• Combination therapy is not superior to ramipril, and has increased side effects.




•The combination of aliskiren (Rasilez) with angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) has been associated with serious adverse cardiovascular and renal outcomes in a recent large clinical trial (ALTITUDE). •This combination is now contraindicated in: diabetic patients (type I or type II); and non-diabetic patients with an estimated glomerular filtration rate (eGFR) <60 mL/min per 1•73 m2
•In all other patient groups, aliskiren in combination with an ACE inhibitor or an ARB is not recommended•Any use of aliskiren (either as monotherapy or in combination with other medicines) is no longer recommended in any patient with severe renal impairment: eGFR <30 mL/min per 1•73 m2

RAA inhibition
? ACEI? ARB? DRI
Evidences from Recent Analysis

Aliskiren in HypertensionClinical summary
•Aliskerin provides long- term suppression of PRA
•Aliskerin effectively reduces PRA from baseline as monotherapy, and blocks the rise in PRA seen during treatment with other antihypertensives such as ARB
•Aliskerin monotherapy provides dose-dependent reductions in DBP and SBP
•Additional BP lowering when combined with other antihypertensives but more side effects

Meta-analyses show consistency of ACEI benefit in preventing CV events
No. of trials N
Relative risk reduction (%)
CV death MI
Danchin, 2006 7 33,960 19 18
Al-Mallah, 2006 6 33,500 17 16
Dagenais, 2006 3 29,805 18 18
Danchin N et al. Arch Intern Med. 2006.Al-Mallah MH et al. J Am Coll Cardiol. 2006.
Dagenais GR et al. Lancet. 2006.
Randomized, placebo-controlled trials in patients with CAD without HF or LV dysfunction

Meta-analysis of trials comparing ARB vs placebo, non-ACEI comparators, or ACEI
Strauss MH, Hall AS. Circulation. 2006;114:838-54.
9 of 11 trials show excess MI for ARB
TrialARB
n/N (MI)Controln/N (MI)
ELITE 3/352 4/370
DETAIL 9/120 6/130
ELITE II 31/1578 28/1574
IDNT 39/579 66/1136
CHARM-Alt 75/1013 48/1015
SCOPE 70/2477 63/2460
RENAAL 50/751 68/762
LIFE 198/4605 188/4588
VALUE 369/7649 313/7596
OPTIMAAL 384/2744 379/2733
VALIANT 587/4909 559/4909
Total 26,777 27,273
0.5 1.0 1.5 2.0Odds ratio (95% Cl)
Favors ARB
Favors control
1.08 (1.01–1.16)

Meta-analyses of ACEI and ARB trials
StraussStrauss TsuyukiTsuyuki VolpeVolpe VerdecchiaVerdecchia
NACEIACEI
150,943150,943ARBARB
55,05055,050ARBARB
68,71168,711ARBARB
56,25456,254ARBARB
64,38164,381
MIMI ↓↓14%14%(P < 0.00001)(P < 0.00001)
Event Rate 5.8%Event Rate 5.8%
↑8%(P = 0.03)(P = 0.03)
Event Rate 6.3%Event Rate 6.3%
↑3%(P = ns)
↑4%(P = ns)
↑2% (P = ns)
CV deathCV death ↓↓12%12%(P < 0.0005)(P < 0.0005)
Event Rate 8.4%Event Rate 8.4%
↑↑1%(P = ns)
Event Rate 9.2%Event Rate 9.2%
NA NA ↓1%
Strauss MH, Hall AS. Circulation. 2006.Tsuyuki RT, McDonald MA. Circulation. 2006.
Volpe M et al. J Hypertension. 2005.Verdecchia P et al. Eur Heart J. 2005.
Relative risk

ACEIs vs ARBs: Comparative effect on stroke, HF, and CHD
Turnbull F. 15th European Meeting on Hypertension. 2005.Adapted by Strauss MH, Hall AS. Circulation. 2006;114:838-54.CHD = MI and CV death
Blood Pressure Lowering Treatment Trialists’ Collaboration meta-analysisN = 137,356; 21 randomized clinical trials
ACEI
ARB
Stroke -1% (9% to -10%)
HF 10% (10% to 0%)
CHD 9% (14% to 3%)
Stroke 2% (33% to -3%)
HF 16% (36% to -5%)
CHD -7% (7% to -24%)
30% 0 30%Decrease Increase
StrokeP = 0.6
HFP = 0.4
CHDP = 0.001
Risk
RRR (95%)

Eur Heart J 2012
Van Vark LC, Bertrand M, Fox K, Mourad JJ, Boersma E, et al. Eur Heart J 2012; published online April 17.

All-cause mortality: effect of ACE inhibitors
ASCOT-BPLA
ADVANCE
HYVET
Overall
1.03 (0.90-1.15)
0.90 (0.75-1.09)
0.99 (0.62-1.58)
1.32 (0.61-2.86)
0.89 (0.81-0.99)
0.86 (0.75-0.98)
0.79 (0.65-0.95)
0.90 (0.84-0.97)
ACE inhibitor better Control better
Random effects model HR (95% CI) P
N= 76 6150.50 0.75 1.33 2.01HR (log scale)
0.03
0.03
0.02
0.87(0.81-0.93)
0.004
<0.001
ALLHAT (lisinopril)
ANBP-2 (enalapril)
pilot HYVET (lisinopril)
JMIC-B (lisinopril, enalapril)
(perindopril)
Van Vark LC, Bertrand M, Fox K, Mourad JJ, Boersma E, et al. Eur Heart J 2012; published online April 17.

All-cause mortality: effect of ARBs
RENAAL (losartan)
IDNT (irbesartan)
LIFE (losartan)
SCOPE (candesartan)
VALUE (valsartan)
MOSES (eprosartan)
JIKEI HEART (valsartan)
PRoFESS (telmisartan)
TRANSCEND (telmisartan)CASE-J (candesartan)
HIJ-CREATE (candesartan)
KYOTO HEART (valsartan)
NAVIGATOR (valsartan)
Overall
HR (log scale) Control betterARB better0.50 0.75 1.33 2.01
1.03 (0.83-1.29)
0.92 (0.69-1.23)
0.88 (0.77-1.01)
0.96 (0.81-1.14)
1.04 (0.94-1.14)
1.07 (0.73-1.57)
1.09 (0.64-1.85)
1.03 (0.93-1.14)
1.05 (0.91-1.22)
0.85 (0.62-1.16)
1.18 (0.83-1.67)
0.76 (0.40-1.30)
0.90 (0.77-1.05)
0.99 (0.94-1.04)
Random effects model HR (95% CI) P
N=82 383
0.683
Van Vark LC, Bertrand M, Fox K, Mourad JJ, Boersma E, et al. Eur Heart J 2012; published online April 17.

Among RAAS inhibitors, only ACE inhibitors have demonstrateda significant 10% mortality reduction in hypertensive patients (P=0.004).
No significant reduction in all-cause mortality could be demonstrated with ARBs (HR, 0.99 (0.95-1.04); P=0.683).
The difference in treatment effect between ACE inhibitors and ARBs was statistically significant (P-value for interaction 0.036).
The largest mortality reductions were observed in ASCOT-BPLA, ADVANCE, and HYVET, which studied the ACE inhibitor perindopril (pooled HR, 0.87 [0.81-0.93]; P<0.001).
Because of the high prevalence of hypertension, the widespread use of ACE inhibitors may result in an important gain in lives saved.
Van Vark LC, Bertrand M, Fox K, Mourad JJ, Boersma E, et al. Eur Heart J 2012; published online April 17.

Savarese G,et al.J Am Coll Cardiol.In press.doi:10.1016/i.iacc.2012.10.011

Savarese G,et al.J Am Coll Cardiol.In press.doi:10.1016/i.iacc.2012.10.011

Savarese G,et al.J Am Coll Cardiol.In press.doi:10.1016/i.iacc.2012.10.011
Conclusion From Saverese G,et al Conclusion From Saverese G,et al Meta-analysisMeta-analysis
End Points ACEI ARB
Composite outcome
-14.9%p=0.001
-7%p=0.005
CV death -10%p=0.112
No benefit
MI -17.7%p<0.001
-9.5%NS
Stroke -19.6%p=0.004
-9.1%p=0.011
All cause death -8.3%p=0.008
No benefit
New-onset HF -20.5%p=0.001
No benefit
New-onset DM -13.7%p=0.012
-10.6%P<0.001

RAAS modulation in high-risk patients: Summary
• Opportunity for greater use of RAAS modulation in patients at high risk for CV events
• ACEIs reduce CV death, MI, HF, and stroke across a broad range of patients with vascular disease– With/without LVSD or HF– With/without other proven CV therapies– Annual event rates of 1.4%–22.6% in untreated
groups• ARBs reduce HF and stroke• ACEIs may be considered in all patients with
vascular disease• ARBs are an alternative in ACEI-intolerant patients• Dual RAAS inhibition is not better than single
therapy and causes more side effects
AHA/ACC secondary-prevention guidelines: ACEIs and ARBs
ACEIs• All patients with LVEF ≤40%, hypertension, diabetes,
or chronic kidney disease (IA)• Consider for all other patients (IB)• Optional: Lower-risk, post-revascularization patients
with normal LVEF and well-controlled risk factors (IIaB)
ARBs• ACEI-intolerant patients with HF or post-MI LVEF
≤40% (IA)• Consider in DM and other ACEI-intolerant patients
(IB)• Consider use in combination with ACEIs in systolic
dysfunction HF (IIbB)

Thank You
Related Documents











