PROCEEDINGS ABSTRACT BOOK

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTSPROCEEDINGSBELGRADE, OCTOBER 23-26, 2014
ABSTRACTSBELGRADE, OCTOBER 23-26, 2014
SERBIAN ASSOCIATION OF ANESTHESIOLOGISTS AND INTESIVISTS,BELGRADEMILITARY MEDICAL ACADEMY,BELGRADE
PROCEEDINGS ABSTRACT BOOK
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
1
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS
PROCEEDINGS
ABSTRACT BOOK
BELGRADE
OCTOBER 23-26, 2014
SERBIAN ASSOCIATION OF ANESTHESIOLOGISTS AND INTESIVISTS, BELGRADE MILITARY MEDICAL ACADEMY,BELGRADE

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
2
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS CONGRESS PROCEEDINGS BELGRADE, OCTOBER 23-26, 2014 Editorial board Prof. Zoran Slavkovic, MD, PhD Dusica Stamenkovic, MD, PhD Vojislava Neskovic, MD, PhD Associate Professor Milic Veljovic Associate Professor Nebojsa Ladjevic, MD,PhD Ana Popadic, MD Publisher Military Medical Academy,Belgrade, Serbia For the publisher Prof.Zoran Slavkovic, MD, PhD Editor Dusica Stamenkovic, MD,PhD Technical Editor Nebojša Colić Printed by Domino,Belgrade, Serbia C štampa, Belgrade, Serbia Circulation 500
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
3
TABLE OF CONTENTS DEPARTMENT OF ANESTHESIOLOGY, WASHINGTON UNIVERSITY SCHOOL OF MEDICINE, ST.LOUIS – FREE TOPICS
Liver Transplantation in the US in 2014-Update for Anesthesiologists
Ivan M.Kangrga
Ongoing Issues in Difficult Airways Management Andrea Vannucci ANESTHESIA IN CARDIOVASCULAR AND THORACIC SUREGRY
Volatile vs. intravenous anesthesia in noncardiac surgical patients with coronary artery disease M.Seeberger
Role of biomarkers in cardiac risk assessment for non-cardiac surgery R.Janković
Myocardial Ischemia: Challenges in Preoperative Assessment V.Nešković
Perioperative beta-blocking therapy: state of the art S. de Hert
PATIENT SAFETY – STANDARDS -EDUCATION IN ANESTHESIA
Why are we not using checklists properly? D. Wilkinson Excellence in Anesthesiology: The Patient Safety Goal M.Milenovic Fluid guidelines for Hospitals-our NICE guidelines N.Soni ULTRASOUND IN ANESTHESIA & INTENSIVE CARE
Echocardiography as a tool for hemodynamic monitoring: gold standard, surrogate or complementary to standard monitoring tools? G.Voga
Critical Ultrasound in prehospital settings: where the benefit of ultrasound use is even greater G. Prosen
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
4
DIFFICULT AIRWAY EAMS
Clinical Use of High Frequency Jet Ventilation D. Janjevic (Novi Sad, Serbia)
The art of sedation for difficult airway D. Stamenkovic (Belgrade, Serbia)
TRANSFUSION & HAEMOSTASIS
Fluid therapy and volume therapy S. Koszek
Bleeding in patients with congenital disorders of haemostasis. D. Filipescu
SEPSIS UPDATE
Innate immunity, infection and sepsis D.Djordjevic
Fluid resuscitation in sepsis: What do the data show M.Veljovic
Supportive Therapy of Severe Sepsis: Myths and Evidence J.Velickovic
Diagnosis and preventive strategies of ICU infection B.Jovanovic
ANESTHESIA IN OBSTETRICS
Anesthetic management for preterm delivery and interactions between drugs T. Mostic
Ultrasound of the lumbar spine - a new challenge for obstretic anaesthetists M. Kendrisic
Peripartum cardiomyopathy I. Velickovic
Morphine renesanse for postcaesarean pain releif – spinal and epidural application B. Pujić
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
5
MECHANICAL VENTILATION Mechanical ventilation in patients with COPD and asthma patients: an update D. Markovic
Minimal flow techniques in anesthesia C.Hoenemann Airway management and prevention of Ventilatory Associated Pneumonia N.Popovic
ANESTHESIA IN ENDOCRINE SURGERY A difficult airway in Endocrine Surgery N.Kalezic
Specifics of anaesthesia in surgeries on the pituitary gland B.Milakovic
Assessment of perioperative risk in patients with diabetes mellitus V. Malenkovic
Hemodynamic disturbances during thyroidectomy M. Stojanovic
Risk factors for perioperative hypertension in patients undergoing parathyroidectomy V. Sabljak
Anesthesia aspects of surgical treatment of pheochromocytoma M. Kažić
TRANSPLANTATION
Liver transplantation: The anaesthesiologist's agony! E.Katsika
Management of Bleeding and Coagulopathy during Orthotopic Liver Transplantation M. Bogdanović Dvorščak
Fungal infections after orthotopic liver transplantation G.Jovanovic
Heart transplantation – anesthesia and perioperative treatment M.Jovic
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
6
SELECTED TOPICS IN ANESTHESIA General versus regional anesthesia in carotid endarterectomy D.Unic
Sub-Tenon’s Anaesthesia-anaesthetic of choice for anterior segment of the eye surgery S.Gligorijevic
ANESTHESIA IN PEDIATRICS
Anesthetic related neurotoxicity in children
R.Flick
Safety in Paediatric Anaesthesia
E. Schindler
ARDS in children - a modern approach B.Drasković
Anesthesia for diagnostic procedures in children I.Budić
Perioperative Hypothermia in the Paediatric Population V.Stevanović Transfusion in children - a modern approach D. Simic
TRAUMA – CPR
Cardiopulmonary Resuscitation Research. Were are the gaps? T Xanthos
Post-resuscitation Care: current therapeutic concepts J.Jevđić
Airway Management in Trauma: An Update I. Krstić Lečic
PAIN THERAPY
Analgesia after liver transplantation Z.Milan
Interventional treatment for musculoskeletal pain Z.Petrovic
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
7
Neuropathic pain in patients with malignancy
N. Ladjevic
Imagine living without pain…Understanding pain genetics D. Stamenkovic
ABSTRACTS

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
8
ADULT LIVER TRANSPLANTATION IN THE UNITED STATES IN 2014 –AN UPDATE FOR ANESTHESIOLOGISTS (US LIVER TRANSPLANT) IVAN KANGRGA Department of Anesthesiology, Washington University in St. Louis - School of Medicine, St. Louis, USA E-mail: [email protected] Introduction
Orthotopic liver transplantation (OLT) is the only definitive treatment for end-stage liver disease (ESLD). Since the first successful OLT in 1967 [1], the number of liver transplants has been steadily increasing, both in the United Sates and globally. Almost 24,00 liver transplants were performed worldwide in 2012 according to the World Health Organization [2], and more than one fourth of those were performed in the US. [3] Organization of US Liver Transplant
Liver transplantation in the United Statesisoverseen bythe United Network for Organ Sharing (UNOS, established in 1984) [4], a private organization working under the auspices of the US Department of Health and Human Services. UNOS maintains transplant databases, including the National Transplant Waiting List,and publishesoutcomes via the Scientific Registry of Transplant Recipients (SRTR). [3] UNOS also facilitates organ distribution and transplantation, establishes equitable policiesand monitors for compliance with Federal regulatory standards. A2012UNOS bylaw mandates that transplant centers appoint a Director of Liver Transplant Anesthesia and establishes the directorship criteria, based largely on the recommendations by the American Society of Anesthesiologists. This decision by UNOS was motivated by the emerging evidence that standardized care by a dedicated liver transplant anesthesia team may influence outcomes and resource utilization, including blood transfusion, length of mechanical ventilation, and ICU and hospital stay. [5,6] Organization of institutional liver transplant anesthesia service was assessed in recent surveys. [7,8] All responding US academic programs reported having a director of liver transplant anesthesia and distinct liver transplant anesthesia team. Most had perioperative protocols. Variability in team membership criteria, structure and responsibilities were associated with center volume, likely reflecting resource availability. US Liver Transplant Volumes and Outcomes
In 2012, 6,256adult liver transplants and 473 pediatric liver transplants were performed in the US.[3]Almost96% (6,010)of adult transplants utilized a cadaveric organ and 4% (246) living donation. Over 95% (5747) of the cadaveric organswere from donation after brain death (DBD) and5% (263)were from donation after circulatory death (DCD). The limited utilization of living donation in the US may reflect access to deceased donors, living donor safety concerns and increased cost. Similarly, the percentage of DCD donations has plateaued, largely due to outcome and resource utilization concerns.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
9
The number of OLTs in the US has been increasing annually, but the demand for organs continues to exceed the number of available donors by a wide margin and the waiting list continues to grow. Over 16 000 patients were on the US waiting for OLT in 2012. It is estimated that about 5-10% of the waiting list patients expire without receiving an organ. The outcomes of OLT have improved dramatically over the years, reflecting advances in perioperative care and immune suppression. Current US unadjusted 1-, 3- and 5-year survival rates are 88%, 80% and 74%, respectively. [4]As of June 2012, more than 65,000 liver transplant recipients were alive, testifying to the success of the liver transplant program in the US.[3]This success is remarkable in the context of the severity of illness-based allocation system and broader use of marginal donors. Despite the overall success of the national organ transplant program, transplant centers and perioperative teams face multiple challenges maintaining OLT outcomes in the changing regulatory and economic environment.Recipient data analysis demonstrates rapidly changing demographics of liver transplant candidates, with continued trend towards older and sicker recipients. In 2012 more than 70% of OLT recipients were older than 50 years (HR 1.27), and more than 13% were 65 years or older (HR 1.64), doubling from the 2002 census. [3] Introduction of the Model for End-stage Liver Disease (MELD) [9], which prioritizes organ allocation based on the severity of illness (i.e., the “sickest first” principle),has also substantially impactedthe complexity of liver transplant recipients. Whereas implementation of MELD has been highly successful in its primary goal, reduction of waiting list mortality and the number of patients on the active waiting list, it has resulted in much sicker patients presenting for OLT. This increased severity of recipient illnessis associated with worse outcomes, longer lengths of hospital stay and greater utilization of intensive care unit, ventilator support and dialysis [10], thus putting more pressure on transplant centers. The sustained shortage of liver donors has necessitated the expansion of the donor pool. As general indices of donor quality,such as the donor risk index (DRI) [10], correlate with outcomes and resource utilization, use of extended-criteria donors has significant implications. Medical and economic implications of recipient severity of illness and donor quality vary markedly within the US. The median national MELD score in 2012 was 27, ranging from 21 to 35, reflecting the wide geographic disparity. [3] In higher recipient density donation service areas, recipient are transplanted with higher MELD score and are more likely to receive a higher DRI organ. Both MELD and the DRI score synergistically impact the outcomes and the cost of liver transplantation. [10] Select Clinical Updates
ESLD patients often present with hyperdynamic circulation, a high cardiac output vasodilatory state. [11] A disproportionate distribution of intravascular volume into the splanchnic circulation and contraction of central blood volume mimic hypovolemia and result in activation of a neuroendocrine axis, including renovascular vasoconstriction. Stroke volume response to volume loading is blunted as administered fluids are quickly redistributed to splanchnic circulation, worsening bleeding during the dissection phase of OLT. Understanding of these circulatory

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
10
derangements has had direct implications on perioperative recipient management and outcomes in OLT. Restrictive fluid management and use of vasopressors, such as vasopressin- or adrenergic-receptor agonists, restore central filling volume, stroke volume and organ perfusion, but decrease portal flow and splanchnic hyperemia, and contribute to reduced bleeding during the dissection phase. [12] Cirrhotic cardiomyopathy, an increasingly recognized sequel of ESLD,may involve impaired systolic and diastolic function, and electromechanical abnormalities in cirrhotic patients without known cardiac diseases. [11]It is now appreciated that diastolic dysfunctionmay be present in up to 50% of OLT recipients with advanced ESLD. Diastolic dysfunction is associated with severity of the post-reperfusion syndrome [13], and with development of post-transplant heart failure. [14] Current view of coagulation in ESLD favors the concept of a rebalanced hemostatic system. [15] Both pro-coagulant and anticoagulant factors are reduced, and the resulting rebalanced state is more fragile, with higher propensity towards either bleeding or thrombosis. Similarly, platelet numbers are often reduced but upregulation of Factor VIII and von Willebrand Factor may offset the effects of thrombocytopenia. Clinically, both coagulopathy and pro-thrombotic states are common in ESLD. Low-grade fibrinolysis occurs frequently in OLT recipients providing a rationale for the use of antifibrinolytics. Conventional tests, prothrombin time and activated thromboplastin time do not reflect the clotting function or predict bleeding in OLT [15]. Whole blood clotting assays, such as rotational thromboelastometry or thromboelastography, may better inform of the status of the clotting function and are commonly used as point-of-care tests to help guide a protocolized hemostatic management strategy [16]. Prothormbin complex and fibrinogen concentrates are being investigated as attractive alternatives to fresh frozen plasma and cryoprecipitate, as the association of transfusion with morbidity and mortality in ELSD is well established. [16] Quality Improvement Program in Liver Transplantation
Liver transplantation is a niche subspecialty. The number of transplants performed in individual centers is relatively small compared to other major surgeries. Consequently,most of the current evidence is based on data from small, non-randomized series.Consensus on the best approach to common perioperative practices in OLT, such as transfusion practices, fluid management, etc., is lacking. Few health care disciplines are scrutinized as rigorously as the US transplant. Mandatory data reporting and state of the art analysis, result in the largest national outcomes report, the SRTR. [3] SRTRreports national, regional and center-specific gross transplant quality metrics: overall wait list mortality, transplant rates and risk-adjusted post-transplant patient and graft survival. Thereport comparestrue outcomes with a rigorously developed, risk-adjusted model based on multiple donor and recipient risk factors.Whereas the SRTR report provides critical information to inform governmental regulatory agencies, insurers and policymakers, it falls short of a comprehensive outcomes and quality database that would allow systematic examination of current practice and lead to quality improvement processes in liver transplantation [17]. A notable deficiency of the model is omission ofmanyrecipient comorbidities and relevant
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
11
peritransplant datawith known association to outcomes. One good example is perioperative blood transfusion,a factor strongly associated with mortality after liver transplantation. [18] To address these deficiencies the transplant community has initiatedcollaboration with the National Surgical Quality Improvement Program (NSQIP), instituted by the American College of Surgeons. The program has developed a standardized approach to quality improvement with demonstrated potential for reduction in postoperative morbidity and mortality.The joint initiative, referred to asTRANSQIP, has not yet been formally introduced.Another attractive direction would be active participation in the National Anesthesia Clinical Outcomes Registry (NACOR) maintained by the Anesthesia Quality Institute (AQI). Conclusions Orthotopic liver transplantation is a well-established, effective treatment for patients with ESLD. Although outcomes of liver transplantation are robust, transplant centers face significant challenges, including trends toward sicker and older recipients, increased use of marginal donors due to persistent donor shortage, and stricter regulatory and financial environment. Current efforts are directed towards refining quality metrics and risk-adjusted outcomes, and developing a standardized approach to quality improvement in perioperative care of liver transplant patients. REFERENCES 1. Starzl TE, Marchioro TL, Porter KA, Brettschneider L. Homotransplantation of the liver.
Transplantation 1967; 5 (Suppl): 790–803. 2. WHO statistics: http://issuu.com/o-n-t/docs/2012ad, accessed August 3, 2014. 3. http://srtr.transplant.hrsa.gov/annual_reports/2012/flash/03_liver_13/v2index.html#/4/
accessed August 3, 2014. 4. www.UNOS.org, accessed August 3, 2014 5. Hevesi ZG, Lopukhin SY, Mezrich JD, Andrei AC, Lee M. Designated liver transplant
anesthesia team reduces blood transfusion, need for mechanical ventilation, and duration of intensive care. Liver Transpl 2009;15:460-465.
6. Mandell MS, Lezotte D, Kam I, Zamudio S. Reduced use of intensive care after liver transplantation: influence of early extubation. Liver Transpl 2002;8:676-681.
7. Mandell SM, Pomfret EA, Stedman R, Hirose R, et al. Director of Anesthesiology for Liver Transplantation: existing practices and recommendations by the United Network for Organ Sharing. Liver Transpl 2013; 19:425-30.
8. Walia A, Mandell MS, Mercaldo N, et al. Anesthesia for liver transplantation in US academic centers: institutional structure and perioperative care. Liver Transpl 2012; 18(6): 737-43.
9. Kamath PS, Weisner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, et al. A model to predict survival in patients with end-stage liver disease. Hepatol 2001; 33:464-70.
10. Axelrod D. Economic and financial outcomes in transplantation: whose dime is it anyway? Curr Opin Organ Transplant. 2103; 18: 1-7.
11. Möller S, Henricksen JH. Cardiovascular complications of cirrhosis. Postgrad Med J. 2009; 85: 44-55.
12. Hong SH, Park CS, Jung HS, et al. A comparison of intra-operative blood loss and acid-base balance between vaso- pressor and inotrope strategy during living donor liver transplantation. Anaesthesia 2012; 67: 1091–100.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
12
13. Xu Z-D, Xu H-T, Li W-W, Zou Z, et al. Influence of preoperative diastolic dysfunction on hemodynamics and outcomes of patients undergoing liver transplantation. Int J Clin Exp Med 2013; 6: 351-7.
14. Dowsley TF, Bayne DB, Langnas AN, et al. Diastolic dysfunction in patients with end-stage liver disease is associated with development of heart failure early after liver transplantation. Transplantation 2012; 94: 646-51.
15. Lisman T, Porte RJ. Rebalanced hemostasis in patients with liver disease: evidence and clinical consequences. Blood 2010; 116(6): 878-85.
16. Kirchner C, Dirkmann D, Treckmann JW, Paul A, et al. Coagulation management with factor concentrates in liver transplantation: a single center experience. Transfusion 2014; e-published: doi:10.1111/trf.12707
17. Englesbe MJ, Pelletier SJ, Kheterpal S, O’Riley M, et al. A call for National Transplant Surgical Quality Improvement Program. Am J Transpl 2006; 6: 666-70.
18. Rana A, Petrowsky H, Hong JC, Agopian AG, et al. Blood transfusion requirement during liver transplantation is an important risk factor for mortality. J Am Coll Surg 2013; 1-6.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
13
ONGOING PATIENT SAFETY ISSUES IN THE MANAGEMENT OF DIFFICULT AIRWAYS ANDREA VANNUCCI, LAURA F. CAVALLONE Department of Anesthesiology, Washington University in St. Louis - School of Medicine, St. Louis, USA E-mail [email protected] DEFINITIONS: Terminology has an important role in supporting clear understanding and effective communication;here we report a list of pertinent definitions and concepts that we are going to refer to in this paper to describe issues related to difficult airway management. -Difficult Airway: the American Society of Anesthesiology (ASA)(1) states that“a difficult airway…[is a] clinical situation in which a conventionally trained anesthesiologist experiences difficulty with facemask ventilation of the upper airway, difficulty with tracheal intubation, or both”. - Difficult laryngoscopy: the ASA defines this condition as when:“It is not possible to visualize anyportion of the vocal cords after multiple attempts atconventional laryngoscopy”. Conventional, or direct, laryngoscopy is based on the visualization of the glottisby aligning one’s line of sightwith the laryngeal axis and by displacing the epiglottis and the tongue via the laryngoscope blade.While apparently a simple principle, the mechanisms of success and failure with direct laryngoscopy are still actively debated (2) Video-laryngoscopy is performed with instruments that allow visualization of the glottis independently from the alignment of the line of sight with the laryngealstructures (glottis and supporting cartilages). - Difficult tracheal intubation: the ASA elaborates:“Tracheal intubationrequires multiple attempts, in the presence or absenceof tracheal pathology”. Of note, “tracheal intubation involves 3 distinct challenges: laryngeal sighting, delivering the tube to the glottis opening, and advancing the tube beyond the target and into the trachea”(3). These three separate components of a successful intubation have become more recognized by clinicians since the widespread adoption of video-laryngoscopes in the clinical practice. In fact, it is a quite common problemwith the use of these devices tobe able to easily visualize the glottis,while facing difficulties in advancing the tube beyond the vocal cords. -Intubation failure: the ASA defines intubation failure as: “Placement of the endotracheal tubethat fails after multiple[three for the Canadian Airway Focus Group(3)] attempts”. In this context, the issue is that multipleattempts at intubation may cause direct trauma to the airway, edema and bleeding resulting in impossibile mask ventilation, hypoxemia(“cannot ventilate, cannot oxygenate” situation), aspiration and long-term sequelae.Prevention of intubation failure strictly depends on the preparation and timely implementation of an “exit strategy” to prevent further patient harm (4). -Extubation failure and Weaning failure:Extubation failure has been defined as “the inability to tolerate removal of the translaryngeal tube,”(5) and it is generallytreated with tracheal reintubation. It needs to be recognized as a separate problem from “Weaning failure”, which is the inability to tolerate spontaneous breathing without ventilatorysupport,”and its treatment includes tracheal reintubation and invasive ventilation or, in selected patients, noninvasive ventilation(6, 7)
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
14
STATUS OF THE PROBLEM: Recent data from the Anesthesia Closed Claims Project in the US and the results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society in the UK (NAP4) show that adverse events related to difficult airway management can be associated with severe patient outcomes (8), can arise throughout the perioperative period (9) and are relatively common, occurring approximately in one case per 22,000 anesthetics (10). While adverse events at the induction of anesthesia have become progressively less frequent and severe, problems at the extubation appear to be an unresolved patient safety issue(9-11).Analysis of Closed Claims data(8) show that 12% of severe airway complications occur at extubation, and the comparison of the time intervals 1985-1992 and 1993-1999 (and even in later years, as reported as “personal communication” by a member of the same research group in another article (11)) does not show any meaningful change in the number of extubation events leading to either brain damage or patient death. The results of the NAP4 study show that 16% of severe airway adverse events (leading to brain damage, death, or patient ICU admission) occur at or shortly after extubation. Importantly, in a significant percentage of these circumstances “…the reviewers noted evidence of poor anticipation and planning for management after extubation in the face of known problems”. In the two following paragraphs, we will discuss these two “situations” separately to try to understand what factors account for the improvements in tracheal intubation outcomes and the absence of such progress with issues atextubation of the trachea. AIRWAY-RELATED EVENTS AT INTUBATION: There are several possible reasons why intubation-related adverse outcomes are becoming less common:
• Development and adoption into clinical practice of the ASA “difficult airway” algorithm and similar guidelines by other groups and societies(4, 12, 13). Practice guidelines have had an important role in reinforcing the principle of planning in advance, suggesting modalities for airway assessment, establishing priorities in difficult airway management, proposing a sequence ofinterventions to adopt in case of difficulties, and endorsing the use of advanced tools to gain control of the airway, or, at least, to maintain oxygenation.
• Widespread utilization of bedside screening tools that allow the identification of a significant percentage of patientswith difficult airways(14), reducing the cases of unanticipated difficult airway: the most difficult clinical situation associated with intubation failure and severe adverse outcomes.
• Increasingfamiliarity of providers with advanced airway devices like fiberscope, supraglotticairway devices and video laryngoscopes(15, 16).
• Possible expanding role of sugammadex as a rescue treatment after failed intubation and impossible mask ventilation (17).
Still, it is recognized that available practice guidelines and tools present several limitations: • Current voiced critiques to the last ASA difficult airways algorithm(1) underscore the
importance of updating the following definitions: 1) the concept of “difficult mask ventilation”should be replaced by a broader definition of “difficult non-invasive ventilation” to include difficulties encountered during ventilation with supraglottic devices; 2) difficult laryngoscopy should indicate the lack of visualization of vocal cords even with the use of new video-laryngoscopes. Additionally, several experts have pointed out that the algorithm should explicitly address: the risk of aspiration in
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
15
individual patient and circumstances; the pre-existing patient conditions and co-morbidities that may influence patient tolerance to apnea; the anticipated difficulties in the use of trans-laryngeal techniques (goiter, status post-radiation, etc.), and, finally,the re-introduction of the rigid laryngoscope in the difficult airway armamentarium.
• Limited sensitivity, specificity, and positive and negative predictive value of current available tests even in apparently normal patient populations, without a known pathology of the airway (2, 14).
• Inadequate understanding of the indications(18),limitations(19)and complications(20-22) resulting from the use of the different video-laryngoscope bladesavailable on the market as well as the absence of standardization in the use of video-laryngoscopes (primary versus rescue devices).
Possible further improvements may result from: • Fine tuning of difficult airway algorithms, especially in selected patient populations:
obese, pregnant women, children, subjects affected by specific comorbidities (e.g. rheumatoid arthritis, syndromes characterized by craniofacial abnormalities), subjects undergoing specific surgical procedures (e.g. cervical spine and head and neck procedures). .
• Developing and implementingmore advanced methods for the assessment ofdifficult airway that can be utilized in unconscious or uncooperative patients, both in emergent situations and/or elective situations: endoscopic airway evaluation (23), cervical ultrasound(24) and analysis of overall facial appearance (25), also supplemented by computer imaging reconstruction(26).
• Developing and adopting predictive tests for difficult airway when approached with different video-laryngoscopes
• Combining the use of different advanced airway devices like video-laryngoscope and fibroscope(27).
• Recognizing evidence-based criteria for the use of Sugammadex. • Consistently adopting monitors of neuromuscular function and recovery(28, 29)
AIRWAY-RELATED EVENTS AT EXTUBATION Extubation related events are still prevalent because:
• Until recently no extubation guidelines were available. Recently, the Difficult Airway Society of the United Kingdom has made available an extubation algorithm divided into a “basic”, a “low risk” and an “at risk” section, to be applied in different clinical scenarios. However, there is still a limited experience with the use of this algorithm and, at this point, it is not known if it is having an impact on clinician practices and patient outcomes.
• Tests to identifyairwaysat riskof post-extubation obstruction in intubated patientshave limited predictive value(11).
• Many clinicians have limited familiaritywith the proper use of tube exchangers andare at risk of having to deal withsevere complications from their use(30).
Possible future improvements may resultfrom: • Development and use of patient and circumstance-specific strategies for safe extubation:
i.e., as mentioned for airwayalgrithms in general, extubation strategies directed to selected populations (e.g. obese subjects, patients with obstructive sleep apnea (OSA), pregnant females, subjects with cervical instability, ICU patients after prolonged

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
16
intubation) and specific surgical procedures (e.g. major head and neck, cervical spine, prone procedures).
• Widespread implementation of postoperativemonitoring of gas exchange not limited to pulse-oximetry but includingcontinuous respiratory rate,End-Tidal CO2, and/or transcutaneous CO2 to the goal of timely recognizing inadequateventilation(31, 32).
CONCLUSIONS Difficulties with airway management continue to represent a patient safety concern. Developing technology and increasing efforts by National and International Societies in designing and diffusing effective guidelines have significantly contributed to reduce adverse outcomes. However, it is the task and continuous challenge of the single providers to adapt general guidelines to the specific clinical scenarios and make the final choices regarding appropriate devices and “best strategy” to adoptto the benefit of their individual patients. References: 1. Apfelbaum JL, Hagberg CA, Caplan RA, Blitt CD, Connis RT, Nickinovich DG, et al. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2013;118(2):251-70. Epub 2013/02/01. 2. Greenland KB. A proposed model for direct laryngoscopy and tracheal intubation. Anaesthesia. 2008;63(2):156-61. Epub 2008/01/24. 3. Levitan RM. The mystique of direct laryngoscopy. Respiratory care. 2007;52(1):21-3. Epub 2006/12/30. 4. Law JA, Broemling N, Cooper RM, Drolet P, Duggan LV, Griesdale DE, et al. The difficult airway with recommendations for management--part 1--difficult tracheal intubation encountered in an unconscious/induced patient. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2013;60(11):1089-118. Epub 2013/10/18. 5. Epstein SK. Decision to extubate. Intensive Care Med. 2002;28(5):535-46. Epub 2002/05/25. 6. Burns KE, Adhikari NK, Keenan SP, Meade M. Use of non-invasive ventilation to wean critically ill adults off invasive ventilation: meta-analysis and systematic review. BMJ. 2009;338:b1574. Epub 2009/05/23. 7. Blackwood B, Alderdice F, Burns K, Cardwell C, Lavery G, O'Halloran P. Use of weaning protocols for reducing duration of mechanical ventilation in critically ill adult patients: Cochrane systematic review and meta-analysis. BMJ. 2011;342:c7237. Epub 2011/01/15. 8. Peterson GN, Domino KB, Caplan RA, Posner KL, Lee LA, Cheney FW. Management of the difficult airway: a closed claims analysis. Anesthesiology. 2005;103(1):33-9. 9. Metzner J, Posner KL, Lam MS, Domino KB. Closed claims' analysis. Best practice & research Clinical anaesthesiology. 2011;25(2):263-76. Epub 2011/05/10. 10. Cook TM, Woodall N, Frerk C. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia. British journal of anaesthesia. 2011;106(5):617-31. Epub 2011/03/31. 11. Cavallone LF, Vannucci A. Extubation of the Difficult Airway and Extubation Failure. Anesth Analg. 2013. Epub 2013/01/11.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
17
12. Law JA, Broemling N, Cooper RM, Drolet P, Duggan LV, Griesdale DE, et al. The difficult airway with recommendations for management - Part 2 - Difficult airway. Canadian Journal of Anesthesia. 2013;60(11):1119-38. 13. Frova G, Sorbello M. Algorithms for difficult airway management: a review. Minerva Anestesiol. 2009;75(4):201-9. Epub 2008/10/24. 14. Shiga T, Wajima Z, Inoue T, Sakamoto A. Predicting difficult intubation in apparently normal patients: a meta-analysis of bedside screening test performance. Anesthesiology. 2005;103(2):429-37. Epub 2005/07/30. 15. Paolini JB, Donati F, Drolet P. Review article: video-laryngoscopy: another tool for difficult intubation or a new paradigm in airway management? Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2013;60(2):184-91. Epub 2012/12/13. 16. Wahlen BM, Roewer N, Kranke P. A survey assessing the procurement, storage and preferences of airway management devices by anaesthesia departments in German hospitals. Eur J Anaesthesiol. 2010;27(6):526-33. Epub 2010/04/21. 17. Mendonca C. Sugammadex to rescue a 'can't ventilate' scenario in an anticipated difficult intubation: is it the answer? Anaesthesia. 2013;68(8):795-9. Epub 2013/09/21. 18. Crosby ET. An evidence-based approach to airway management: is there a role for clinical practice guidelines? Anaesthesia. 2011;66 Suppl 2:112-8. Epub 2011/12/07. 19. Levitan RM, Heitz JW, Sweeney M, Cooper RM. The complexities of tracheal intubation with direct laryngoscopy and alternative intubation devices. Annals of emergency medicine. 2011;57(3):240-7. Epub 2010/08/03. 20. Cooper RM. Complications associated with the use of the GlideScope videolaryngoscope. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2007;54(1):54-7. Epub 2007/01/02. 21. Chin KJ, Arango MF, Paez AF, Turkstra TP. Palatal injury associated with the GlideScope. Anaesthesia and intensive care. 2007;35(3):449-50. Epub 2007/06/27. 22. van Zundert A, Pieters B, van Zundert T, Gatt S. Avoiding palatopharyngeal trauma during videolaryngoscopy: do not forget the 'blind spots'. Acta anaesthesiologica Scandinavica. 2012;56(4):532-4. Epub 2012/02/01. 23. Rosenblatt W, Ianus AI, Sukhupragarn W, Fickenscher A, Sasaki C. Preoperative endoscopic airway examination (PEAE) provides superior airway information and may reduce the use of unnecessary awake intubation. Anesth Analg. 2011;112(3):602-7. 24. Kristensen MS. Ultrasonography in the management of the airway. Acta anaesthesiologica Scandinavica. 2011;55(10):1155-73. Epub 2011/11/19. 25. Connor CW, Segal S. The importance of subjective facial appearance on the ability of anesthesiologists to predict difficult intubation. Anesth Analg. 2014;118(2):419-27. Epub 2013/12/24. 26. Connor CW, Segal S. Accurate classification of difficult intubation by computerized facial analysis. Anesth Analg. 2011;112(1):84-93. Epub 2010/11/18. 27. Lenhardt R, Burkhart MT, Brock GN, Kanchi-Kandadai S, Sharma R, Akca O. Is video laryngoscope-assisted flexible tracheoscope intubation feasible for patients with predicted difficult airway? A prospective, randomized clinical trial. Anesth Analg. 2014;118(6):1259-65. Epub 2014/05/21. 28. Brull SJ, Murphy GS. Residual neuromuscular block: lessons unlearned. Part II: methods to reduce the risk of residual weakness. Anesth Analg. 2010;111(1):129-40. Epub 2010/05/06.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
18
29. Murphy GS, Brull SJ. Residual neuromuscular block: lessons unlearned. Part I: definitions, incidence, and adverse physiologic effects of residual neuromuscular block. Anesth Analg. 2010;111(1):120-8. Epub 2010/05/06. 30. Duggan LV, Law JA, Murphy MF. Brief review: Supplementing oxygen through an airway exchange catheter: efficacy, complications, and recommendations. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2011;58(6):560-8. Epub 2011/04/06. 31. Lagow EE, Leeper BB, Jennings LW, Ramsay MA. Incidence and severity of respiratory insufficiency detected by transcutaneous carbon dioxide monitoring after cardiac surgery and intensive care unit discharge. Proc. 2013;26(4):373-5. 32. Ramsay MA, Usman M, Lagow E, Mendoza M, Untalan E, De Vol E. The accuracy, precision and reliability of measuring ventilatory rate and detecting ventilatory pause by rainbow acoustic monitoring and capnometry. Anesth Analg. 2013;117(1):69-75.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
19
VOLATILE VS. INTRAVENOUS ANESTHESIA IN NONCARDIAC SURGICAL PATIENTS WITH CORONARY ARTERY DISEASE MANFRED D. SEEBERGER University Hospital Basel & Hirslanden Klinik Zürich, Zürich, Switzerland. e-mail: [email protected] Cardiac complications due to coronary artery disease (CAD) are the leading cause of morbidity and mortality after major surgery.1-3 Multiple efforts have been made to improve outcome by modifying perioperative management. Studies performed in these efforts have investigated the effects of perioperative administration of β-receptor blockers4, 5 and statins,6 and of choice of anesthetic technique7 or anesthetic agent8, 9 on the incidence of cardiac complications. In vitro- and animal models suggested that administration of volatile anesthetic prior to myocardial ischemia reduced myocardial infarct size.10-12 This effect called “anesthetic preconditioning” is characterized by a short-term memory phase with immediate protection 10 and by a late protection phase 12 – 72 hours after exposure.13 There is a lack of sufficiently large randomized, controlled trials investigating whether this anesthetic preconditioning effect results in better outcome in surgical patients at cardiac risk. Nevertheless, a recent meta-analysis of randomized trials strongly suggest that volatile anesthetics provide clinically relevant anesthetic preconditioning in patients undergoing coronary artery bypass graft surgery.14 Effects found in patients undergoing coronary artery bypass surgery include better preserved left ventricular function, reduced length of stay in the intensive care unit and in the hospital,15-18 and even a lower incidence of late cardiac events.19 Based on this evidence obtained in patients undergoing coronary artery bypass surgery, current AHA/ACC guidelines20 recommend the use of volatile anesthetics as beneficial in hemodynamically stable patients undergoing noncardiac surgery. However, studies on the clinical value of preconditioning by volatile anesthetics in noncardiac surgery are scarce. To obtain scientific data on the value of preconditioning in patients at coronary risk who undergo major noncardiac surgery, we performed a study in three centers in Switzerland (University Hospital Basel, Kantonsspital Solothurn, Kantonsspital Liestal). Between 2006 and 2010, we enrolled 380 patients at increased cardiovascular risk. Patients were randomized to maintenance of anesthesia either with sevoflurane or propofol. To assess occurrence of perioperative ischemia, we recorded continuous ECG for 48 hours perioperatively and measured troponin T on postoperative day 1 and 2. In addition, we measured NT-proBNP on postoperative day 1 and 2 as an indicator of cardiac function. We used the Confusion Assessment Method (CAM) to assess occurrence of delirium on day 1, 2, and 7 after surgery. To assess the occurrence of major adverse cardiac events (MACE), the patients were contacted by phone 6 and 12 months after surgery. MACE were defined as a composite of cardiac death, acute coronary events syndrome, and congestive heart failure or arrhythmia requiring hospitalization. The primary endpoint was a composite of myocardial ischemia, as indicated by ECG changes in the 48-hour continuous ECG and/or troponin elevation. Additional endpoints were postoperative
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
20
NT-proBNP, MACE and delirium. Patients and outcome assessors were blinded. Myocardial ischemia occurred in 75 (41.4%) patients in the sevoflurane and 81 (40.7%) in the propofol group (RR 0.98, 95%, confidence interval [CI] 0.76-1.27). NT-proBNP release did not differ between the sevoflurane and propofol groups on postoperative day 1 or 2 (p=0.85). Within 12 months, 14 (7.7%) patients suffered a MACE after sevoflurane and 17 (8.5%) after propofol (RR 0.91, 95% CI 0.43-1.89). The incidence of delirium did not differ (11.6% vs 14.6%, p=0.392) We concluded that sevoflurane compared to propofol did not reduce myocardial ischemia in high- risk patients undergoing major noncardiac surgery. In addition, we failed to detect any effect of sevoflurane on postoperative NTproBNP release, MACE at 1 year, or delirium. The results of this study were published in the journal Circulation in 2012.21 References 1. Mangano DT, Browner WS, Hollenberg M, London MJ, Tubau JF, Tateo IM. Association of perioperative myocardial ischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. The Study of Perioperative Ischemia Research Group. N Engl J Med 1990;323:1781-8. 2. Bartels C, Bechtel JF, Hossmann V, Horsch S. Cardiac risk stratification for high-risk vascular surgery. Circulation 1997;95:2473-5. 3. Sprung J, Abdelmalak B, Gottlieb A, et al. Analysis of risk factors for myocardial infarction and cardiac mortality after major vascular surgery. Anesthesiology 2000;93:129-40. 4. Mangano DT, Layug EL, Wallace A, Tateo I. Effect of atenolol on mortality and cardiovascular morbidity after noncardiac surgery. Multicenter Study of Perioperative Ischemia Research Group. N Engl J Med 1996;335:1713-20. 5. Devereaux PJ, Yang H, Yusuf S, et al. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet 2008;371:1839-47. 6. O'Neil-Callahan K, Katsimaglis G, Tepper MR, et al. Statins decrease perioperative cardiac complications in patients undergoing noncardiac vascular surgery: the Statins for Risk Reduction in Surgery (StaRRS) study. J Am Coll Cardiol 2005;45:336-42. 7. Christopherson R, Beattie C, Frank SM, et al. Perioperative morbidity in patients randomized to epidural or general anesthesia for lower extremity vascular surgery. Perioperative Ischemia Randomized Anesthesia Trial Study Group. Anesthesiology 1993;79:422-34. 8. Slogoff S, Keats AS. Randomized trial of primary anesthetic agents on outcome of coronary artery bypass operations. Anesthesiology 1989;70:179-88. 9. Tuman KJ, McCarthy RJ, Spiess BD, DaValle M, Dabir R, Ivankovich AD. Does choice of anesthetic agent significantly affect outcome after coronary artery surgery? Anesthesiology 1989;70:189-98. 10. Cason BA, Gamperl AK, Slocum RE, Hickey RF. Anesthetic-induced preconditioning: previous administration of isoflurane decreases myocardial infarct size in rabbits. Anesthesiology 1997;87:1182-90. 11. Kersten JR, Schmeling TJ, Pagel PS, Gross GJ, Warltier DC. Isoflurane mimics ischemic preconditioning via activation of K(ATP) channels: reduction of myocardial infarct size with an acute memory phase. Anesthesiology 1997;87:361-70. 12. Cope DK, Impastato WK, Cohen MV, Downey JM. Volatile anesthetics protect the ischemic rabbit myocardium from infarction. Anesthesiology 1997;86:699-709.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
21
13. de Klaver MJ, Buckingham MG, Rich GF. Isoflurane pretreatment has immediate and delayed protective effects against cytokine-induced injury in endothelial and vascular smooth muscle cells. Anesthesiology 2003;99:896-903. 14. Landoni G, Greco T, Biondi-Zoccai G, et al. Anaesthetic drugs and survival: a Bayesian network meta-analysis of randomized trials in cardiac surgery. Br J Anaesth 2013;111:886-96. 15. De Hert SG, Cromheecke S, ten Broecke PW, et al. Effects of propofol, desflurane, and sevoflurane on recovery of myocardial function after coronary surgery in elderly high-risk patients. Anesthesiology 2003;99:314-23. 16. De Hert SG, Van der Linden PJ, Cromheecke S, et al. Cardioprotective properties of sevoflurane in patients undergoing coronary surgery with cardiopulmonary bypass are related to the modalities of its administration. Anesthesiology 2004;101:299-310. 17. Zaugg M, Lucchinetti E, Garcia C, Pasch T, Spahn DR, Schaub MC. Anaesthetics and cardiac preconditioning. Part II. Clinical implications. Br J Anaesth 2003;91:566-76. 18. Bein B, Renner J, Caliebe D, et al. Sevoflurane but not propofol preserves myocardial function during minimally invasive direct coronary artery bypass surgery. Anesth Analg 2005;100:610-6, table of contents. 19. Garcia C, Julier K, Bestmann L, et al. Preconditioning with sevoflurane decreases PECAM-1 expression and improves one-year cardiovascular outcome in coronary artery bypass graft surgery. Br J Anaesth 2005;94:159-65. 20. Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery): Developed in Collaboration With the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation 2007;116:1971-96. 21. Lurati Buse GA, Schumacher P, Seeberger E, et al. Randomized comparison of sevoflurane versus propofol to reduce perioperative myocardial ischemia in patients undergoing noncardiac surgery. Circulation 2012;126:2696-704.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
22
ROLE OF BIOMARKERS IN CARDIAC RISK ASSESSMENT FOR NON-CARDIAC SURGERY
RADMILO J JANKOVIĆ 1,2, IVANA ZDRAVKOVIĆ 3, DANICA MARKOVIĆ 2 1School of Medicine, University of Niš,2Center for Anesthesiology and Reanimatology, Clinical Center of Niš,3Department of Anesthesia and Reanimation, Clinical Hospital Center “Zvezdara”, Beograd Email: [email protected]
Introduction The number of patients with cardiovascular comorbiditiesscheduled for non-cardiac surgery and withperi-operative complications is high, and real dimensions of the problem are problematic to measure in detail. For Europe, with an overall population of over 500 million, there are approximately 19 million major surgical procedures per year, approximately 30% of which are performed in presence of cardiovascular co-morbidity (around 5.7 million procedures/year). Complication rate is between 7 and 11%, and mortality rate ranges from 0.8 to 1.5%, whereas up to 42% of these are caused by cardiac complications. It is estimated that the number of patients undergoing surgery will increase by 25% by the year 2020, and in the same time period, the elderly population will increase by 50% [1-4]. Recently published guidelines on non-cardiac surgery by European Society of Cardiology (ESC)/European Society of Anaesthesiology (ESA)highlight important keypoints: Anaesthesiologist have a leading role in perioperative cardiovascular assessment and management, through identifying patients who require pre-operative evaluation by a team of integrated multi-disciplinary specialists including anaesthesiologists, cardiologists and surgeons, and, when appropriate, by an extended team (e.g. internists, pulmonologists or geriatricians) [5-6]. Risk scores and indices In the past 30 years, several risk indices, based on multivariable analyses of observational datato represent the relationship between clinical characteristics and perioperative cardiac mortality and morbidity, have been developed. Between them, the indices developed by Goldman et al. (1977) [7], Detsky et al. (1986) [8], and Lee et al. (1999) [9] have become well known and mostly used. The Lee index, or revised cardiac risk index, is a modified version of the original Goldman index and it was designed to predict complications such as postoperative myocardial infarction, pulmonary oedema, ventricular fibrillation or cardiac arrest, and complete heart block. The Lee index has been developed from prospectively collected data from a total of 4315 patients divided into a derivation and a validation cohort,and it was considered by many clinicians and researchers to be the best currently available cardiac-risk prediction index in noncardiac surgery. It takes account of six variables: high-risk type of surgery, history of heart failure, history of IHD (ischaemic heart disease) , history of cerebrovascular disease, preoperative treatment with insulin and preoperative creatinine>170mmol/L (>2 mg/dL. It) [9]. Recently, using the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, a new predictive model has been developed to assess the risk of intraoperative/postoperative myocardial infarction or cardiac arrest.This risk assessment model is
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
23
based on five predictors of perioperative myocardial infarction/cardiac arrest: type of surgery, functional status, elevated creatinine (>130mmol/L or >1.5 mg/dL), age and American Society of Anesthesiologists (ASA) class (class I, patient is completely healthy; class II, patient has mild systemic disease; class III, patient has severe systemic disease that is not incapacitating; class IV, patient has incapacitating disease that is a constant threat to life; and class V, a moribund patient who is not expected to live for 24 hours with or without the surgery). This model is presented as an interactive risk calculator, so that the risk could be calculated at patients’ bedside or in clinic activity in a simple and accurate way [10]; furtherly, both models (Lee risk index and NSQIP), providing complementary prognostic perspectives,might help the clinician in the decision-making process [11-12]. In light of recently published ESC/ESA guidelines, use of clinical risk indices for perioperative risk stratification isstrongly recommended, and between them, the NSQIP model or the Lee risk index are recommended for cardiac perioperative risk stratification. (Class of recommendation Ia/Level of evidence B) [6]. Biomarkers A biomarker (biological marker) is defined as a substance used as an indicator of a biological state, which can be objectively measured and evaluated as an indicator of normal biological processes, pathologic processes, or pharmacologic responses to a therapeutic intervention. According to World Health Organization (1993) definition, a biomarker is any parameter (chemical, physical or biological) which can be used to measure the interaction of environmental agents and biological systems. National Institutes of Health (2002) defines biomarkers as molecular indicators of specific biological and biochemical characteristics which can be used to assess disease progression or treatment effects. For these reasons, biomarkers are considered as basis of “Evidence Based Medicine”; furthermore, helping decision-making process, they improve patient treatment effectiveness and increase possibility to achieve the best clinical outcome for each patient. The ideal biomarker should have specific characteristics: a) ability to differentiatewith high accuracy healthy and a illpatient; b) opportunity to be present in early stage of disease (so to achieve effective and early therapeutic interventions); c) to be present in high enough level and in an easily accessible tissue fluid; d) tolead to the development of tests that will ultimately impact in reduced mortality. Due to these precise characteristics, an ideal biomarker is difficult to find. In the perioperative setting, especially in cardiac risk assessment for non-cardiac surgery, biomarkers can be divided into markers focusing on myocardial ischaemia and damage, inflammation and LV function. Inflammatory markers, such is C reactive protein (CRP), might pre-operatively identify those patients with increased risk of unstable coronary plaque. CRP has been implicated in many aspects of atherogenesis and plaque vulnerability, and it is also expressed in smooth muscle cells within diseased atherosclerotic arteries. However, in the surgical setting, no data are currently available to recommend use of CRP as a marker for the initiation of risk reduction strategies [13]. Brain natriuretic peptide (BNP) and N-terminal pro-BNP (NT-proBNP) are produced in cardiac myocytes in response to increases in myocardial wall stress. Plasma BNP and NT-proBNP have emerged as important prognostic indicators in patients with heart failure, ACS (Acute Coronary Syndrome) and stable IHD in non-surgical settings. Pre-operative determination of BNP and NT-

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
24
proBNP levels has additional prognostic value for cardiac events and long-term mortality after major non-cardiac vascular surgery. Accordingly to previously published ESC/ESA guidelines, NT-proBNP and BNP measurements should be considered for obtaining independent prognostic information for perioperative and late cardiac events in high-risk patients (Class of recommendation IIb/Level of evidence B) [14]. Cardiac troponins T and I (cTnT and cTnI, respectively) remain the preferred markers for the diagnosis of myocardial infarction because of demonstrated higher sensitivity and tissue specificity if compared with other available biomarkers. Existing evidence suggests that even small increases in cTnT in the perioperative period reflect clinically relevant myocardial injury with worsened cardiac prognosis and outcome[12,15-16]. Development of new biomarkers, including high-sensitivity troponins, will likely further enhance the assessment of myocardial damage. Comparing different biomarkers, Weber’s study found no difference between NT-proBNP and the Lee index, whereas a significant higher Area Under curve (AUC) of hsTnT (high sensitivity troponins T) compared with the Lee index for the prediction of mortality was detected. However, for the combined endpoint, the AUC for hsTnT was larger but this difference did not reach statistical significance [12]. Therefore, assessment of cardiac troponins in high-risk patients, both before and 48–72 hours after major surgery, may be considered (Class of recommendation II b/Level of evidence B) [5-6]. It must be underlined that routine pre-operative biomarker sampling in all patients for risk stratification and to prevent cardiac events is not recommended (Class of recommendation III/ Level of evidence C). Conclusion Today, biomarkers play pivotal role in cardiac risk assessment for non-cardiac surgery. Very recent guidelines stipulate that the assessment of both cardiac troponins and natriuretic peptides measurements may be considered for obtaining independent prognostic information for peri-operative and late cardiac events in high-risk patients. The impact of these guidelines on perioperative management of patients who must undergo non-cardiac surgery is still to be determined, but these recommendations clearly set up the beginning of use of biomarkers as part of peri-operative management. References:
1. Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 2008; 372:139–144.
2. Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med 2009; 360:491–499.
3. Devereaux PJ, Chan MT, Alonso-Coello P, et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA 2012; 307:2295– 2304.
4. Naughton C, Feneck RO. The impact of age on 6-month survival in patients with cardiovascular risk factors undergoing elective noncardiac surgery. Int J ClinPract 2007; 61:768–776.
5. Langrois D, Hoeft A, De Hert S. 2014 European Society of Cardiology/European Society of Anaesthesiology guidelines on non-cardiac surgery: cardiovascular assessment and management. A short explanatory statement from the European Society of
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
25
Anaesthesiology members who participated in the European Task Force. Eur J Anaesthesiol 2014; 31: 513 -516.
6. Kristensen SD, Knuuti J, Saraste A, et al. 2014 European Society of Cardiology/European Society of Anaesthesiology guidelines on non-cardiac surgery: cardiovascular assessment and management. The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur J Anaesthesiol 2014; 31:517–573.
7. Goldman L, Caldera DL, Nussbaum SR, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med 1977; 297:845–850.
8. Detsky AS, Abrams HB, Forbath N, et al. Cardiac assessment for patients undergoing noncardiac surgery. A multifactorial clinical risk index. Arch Intern Med 1986; 146:2131–2134.
9. Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 100:1043– 1049.
10. Gupta PK, Gupta H, Sundaram A, et al. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Circulation 2011; 124:381–387.
11. Ford MK, Beattie WS, Wijeysundera DN. Systematic review: prediction of perioperative cardiac complications and mortality by the revised cardiac risk index. Ann Intern Med 2010; 152:26–35.
12. Weber M, Luchner A, Seeberger M, et al. Incremental value of highsensitive troponin T in addition to the revised cardiac index for perioperative risk stratification in noncardiac surgery. Eur Heart J 2013; 34:853–862.
13. Tsimikas S, Willerson JT, Ridker PM. C-reactive protein and other emerging blood biomarkers to optimize risk stratification of vulnerable patients. J Am CollCardiol 2006;47(8 Suppl):C19–C31.
14. Poldermans D, Bax JJ, Boersma E, et al. Guidelines for preoperative cardiac risk assessment and perioperative cardiac management in noncardiac surgery. Eur Heart J 2009; 30:2769–2812.
15. Maisel AS, Bhalla V, Braunwald E. Cardiac biomarkers: a contemporary status report. Nat ClinPractCardiovasc Med 2006; 3:24–34.
16. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Eur Heart J 2012; 33:2551–2567.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
26
MYOCARDIAL ISCHEMIA: CHALLENGES IN PREOPERATIVE ASSESSMENT
VOJISLAVA NEŠKOVIĆ Klinika za anesteziju i intenzivnu terapiju, Vojnomedicinska akademija, Beograd, Srbija email: [email protected]
Introduction
The major cause of morbidity and mortality in patients undergoing non-cardiac surgery are cardiac events, such as: sudden cardiac death, myocardial infarction, acute heart failure and cardiac arrhythmias. Myocardial infarction (MI) holds much of the interest during the perioperative period due to its high hospital mortality rate (15-25%).1Additionally, nonfatal perioperative MI is an independent risk factor for MI and cardiovascular death during six months following surgery.1The magnitude of the problem is very high, considering that about 200 million of adults worldwide undergo non-cardiacsurgery every year.1,2At the same time,the number of patients with high risk burden of coronary artery disease,carrying the risk for experiencing cardiac event during the perioperative period, is increasing. The incidence of perioperative MI ranges from 1 to 17%, but the true incidence may be underestimated because many of them can be silent or unrecognized.3 As a matter of fact, the most of the perioperative MIs occur during the first three days after the surgery, when typical signs and symptoms of the disease may be masked (mechanical ventilation, sedation, narcotics, etc.).3,4Diagnosis of perioperative MI requires high index of vigilance and any hemodynamic instability and hypotension that does not respond to treatment should imply more thorough search for diagnosis.3,4 Preoperative assessment
The pathophysiology of perioperative MI is not clear; in fact, the cause is often multifactorial. Around half of the cases of perioperative MI are the consequence ofincrease in catecholamine levels, tachycardia, hypotension, anaemiaand hypothermiathat lead to myocardial oxygen supply/demand mismatch. In addition, increased procoagulant activity, inflammation, as well as the plaque rupture and subsequent thrombosis may be the pathophysiological mechanism as well. 1,2 Recognizing patient population that carries increased risk for perioperative cardiac morbidity is a good starting point in creating the strategy for decreasing the incidence of new events. However, ideal strategy remains unattainable. The European guidelines for perioperative risk assessment and perioperative cardiac management in non-cardiac surgery have been published recently.2 Generally speaking, identification of patients at increased risk for perioperative MI requires stepwise evaluation of exercises capacity, surgical risk, clinical risk factors and additional noninvasive testing.2,4 Type of surgery, particularly some factors related to surgery, such as urgency, duration of the procedure, blood loss, fluid shifts and body temperature are considered as risk factors for cardiac complications. Also, stress response to surgery may lead to neuroendocrine disturbances, catecholamine release and consequent cardiovascular response (tachycardia and hypertension), as well as altered balance between prothrombotic and fibrinolytic factors. All these elements, individually or combined, may cause heart failure and coronary thrombosis.2,5With regard to cardiac risk related, surgical interventions can be divided into low-risk, intermediate-risk, and

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
27
high-risk groups. Vascular surgery is considered as one with the highest risk for the new cardiac events.2 Although risk related to surgery is important and may influence decisions during the perioperative treatment, risk factors related to the patient’s characteristics remain pivotal. Determination of functional capacity is indispensable step in assessing cardiac risk. It is measured in metabolic equivalents (METs), where one MET equals the basal metabolic rate. Without testing, estimation of functional reserve is usually based on the patient`s daily activities. Climbing two stairs equals 4 METs and this is used as a cutoff point for poor functional capacity. Patients with less than 4METs are considered as patients with poor functional capacity, which can be related to increased mortality. On the other hand, prognosis is excellent when the functional capacity is high, even in the presence of stable coronary artery disease.6 However, if the functional capacity cannot be determined (due to poor physical activity) and the patient carries a number of risk factors, additional testing is indicated. Several risk indices have been developed in order to define the relationship between clinical characteristics of the patients and new perioperative cardiac events. Nowadays, the Lee index,which is a modificationof the original Goldman index,is considered the best currently available.2,6 This index contains five independent clinical determinants: a history of ischemic heart disease, cerebrovascular disease and heart failure, presence of insulin-dependent diabetes mellitus and impaired renal function. All factors are marked with one point and total sum of points gives the estimation of incidence of major perioperative cardiac complications (0.4, 0.9, 7,and 11% in patients with an index of 0, 1, 2, and 3 points, respectively). Identifying the risk has major implications for perioperative care of the patients. Patients considered carrying low cardiac risk after the assessment could be operated on safely without any additional strategies for reducing the risk any further. Patients at higher risk could benefit from pharmacological treatment. Also, they could be candidates for additional testing such as non-invasive cardiac imaging techniques. However, any noninvasive testing which leads to surgery delay should be reserved only for those patients in whom results would influence management. All efforts to assess perioperative cardiac risk in the past were focused in detection of myocardium at risk of ischemia that could lead to some cardiac treatment before surgery. Now, the focus has been put on cardioprotective measures during the surgery, which led to different pharmacological measures on order to decrease perioperative cardiac risk. The most controversial topic in recent years was perioperative management with β-blockers. European guidelines continue to emphasize perioperative use of β-blockers in high-risk patients, while American guidelines have more restrictive approach and are focused on haemodynamic titration.2,8 Other perioperative strategies to reduce or prevent perioperative ischemic events are still not well defined. The use of statins and α2-agonists have also been linked to improved perioperative outcome, while the role of volatile anesthetics in preventing myocardial ischemia in non-cardiac surgerystill waits to be better understood.2,9,10 Obviously, there are lots of questions to be answered and successful management of perioperative myocardial ischemia and infarction is still developing.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
28
Conclusion
Recognizing patient population that carries increased risk for perioperative cardiac morbidity is a good starting point in creating the strategy for decreasing the incidence of new events. Stepwise evaluation of exercises capacity, surgical risk, clinical risk factors and additional noninvasive testing has been used for assessing the perioperative cardiac risk. Cardio-protective measures in order to reduce the incidence of major cardiac complications are of particular interest. However, ideal strategy remains unattainable. Literature
1) Devereaux P.J., Goldman L, Cook DJ, Gilbert K, Leslie K, Guyatt GH. Perioperative cardiac events in patients undergoingnoncardiac surgery: a review of the magnitudeof the problem, the pathophysiology of the eventsand methods to estimate and communicate risk. CMAJ 2005;173(6):627-34
2) Poldermans D, Bax JJ, Boersma E, et al. Guidelines for preoperative cardiac risk assessment and perioperative cardiac management in noncardiac surgery. Eur Heart J 2009; 30:2769–2812.
3) Devereaux P.J, Goldman L, Yusuf S, Gilbert K, Leslie K, Guyatt GH. Surveillance and prevention of major perioperativeischemic cardiac events in patients undergoingnoncardiac surgery: a review. CMAJ 2005;173(7):779-88.
4) Bakker EJ, Ravensbergen NJC, Poldermans D. Perioperative cardiac evaluation, monitoring, and risk reduction strategies in noncardiac surgery patients. Current Opinion in Critical Care 2011, 17:409–415
5) Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof E, Fleischmann KE,Freeman WK, Froehlich JB, Kasper EK, Kersten JR, Riegel B, Robb JF,Smith SC Jr., Jacobs AK, Adams CD, Anderson JL, Antman EM, Buller CE,Creager MA, Ettinger SM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF,Hunt SA, Lytle BW, Md RN, Ornato JP, Page RL, Riegel B, Tarkington LG,Yancy CW. ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary: A Report ofthe American College of Cardiology/American Heart Association Task Forceon Practice Guidelines (Writing Committee to Revise the 2002 Guidelines onPerioperative Cardiovascular Evaluation for Noncardiac Surgery): Developedin Collaboration With the American Society of Echocardiography, AmericanSociety of Nuclear Cardiology, Heart Rhythm Society, Society of CardiovascularAnesthesiologists, Society for Cardiovascular Angiography and Interventions,Society for Vascular Medicine and Biology, and Society for Vascular Surgery. Circulation2007;116:1971–1996.
6) Biccard BM. Relationship between the inability to climb two flights of stairs andoutcome after major non-cardiac surgery: implications for the pre-operativeassessment of functional capacity. Anaesthesia 2005;60:588–593.
7) Lee TH, Marcantonio ER, Mangione CM, Thomas EJ, Polanczyk CA, Cook EF, Sugarbaker DJ, Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L.Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation. 1999;100(10):1043-9.
8) Flynn BC, Vernick WJ, Ellis JE. β-Blockade in the perioperative management of the patient with cardiac disease undergoing non-cardiac surgery. Br J Anaesth 2011;107(S1):i3-i15.
9) Bein B. Clinical application of the cardioprotective effects of volatileanaesthetics: PRO – get an extra benefit from a provenanaesthetic free of charge. Eur J Anaesthesiol 2011;28:620–622.
10) Van Rompaey N, Barvais L. Clinical application of the cardioprotective effects of volatileanaesthetics: CON – total intravenous anaesthesia or not totalintravenous anaesthesia to anaesthetise a cardiac patient?Eur J Anaesthesiol 2011;28:623–627.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
29
PERIOPERTIVE BETA-BLOCKING THERAPY: STATE OF THE ART STEFAN DE HERT Department of Anesthesiology Ghent University Hospital,Ghent,Belgium email: [email protected] The publication in 1996 by Mangano et al.1 of the finding that the perioperative administration of a beta-blocker was associated with a decreased early and late perioperative mortality challenged the common believe that negative inotropic interventions were to be avoided in the perioperative period. Although this study has from the beginning been critisized because of major methodological issues2 the publication a few years later of another study demonstrating a similar beneficial effect of perioperative beta-blocking therapy3 seemed to confirm the protective effects of such therapy. In the following years several randomized controlled trials were published, some of them showing a beneficial effect of perioperative beta-blocking therapy4-10, whereas others failed to demonstrate such an effect11-15 and even reported adverse effects such as perioperative bradycardia and hypotension and an increased rate of perioperative stroke. Despite these contradictory findings, it became generally accepted that beta-blockers provided protection against perioperative cardiac events and improved perioperative morbidity and mortality16-18 finally resulting in guidelines that recommended very liberal use of beta-blocking therapy in the perioperative period19,20. In the meantime critical signals with respect to the liberal use of perioperative beta-blockade came from systematic reviews and meta-analyses.21,22Then in 2008 the famous POISE study23 was published. In this study over 10,000 patients with increased cardiac risk undergoing non-cardiac surgery were randomized to receive either placebo or metoprolol. The results were straightforward: beta-blocked patients suffered less perioperative myocardial infarction but this was at the expense of an increased mortality duet o perioperative stroke which seemed to be initiated by the occurrence of intra-operative hypotension and bradycardia. These observations underscored the call for caution expressed in recent meta-analyses and shifted the attitude towards peri-operative beta-blocking therapy together with a call to revise the current guidelines on this topic,24 which in the meantime has been done.25
How should all these data be interpreted and what should our attitude be with respect to perioperative beta-blocking therapy? There are several issues to take into account when analyzing data form randomized controlled trials with regard to perioperative beta-blocking therapy. These issues will be discussed in the presentation and include: 1. risk of bias in the individual trials It appears that beneficial effects of perioperative beta-blockade therapy were mainly observed in trials at high risk of bias. In those trials with low risk of bias the magnitude of the beneficial effects on perioperative beta-blocking therapy on occurrence and extent of myocardial ischemic events and myocardial infarction rate are far less prominent and risk of stroke important.22,26

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
30
2. timing of administration In the POISE trial, the first dose of beta-blocking therapy was given 2 to 4 hrs before the start of surgery. There are several data indicating that there is an inverse relationship between the occurrence of adverse events and the length of the titration period.26-29 Giving a first dose of a beta-blocker immediately before surgery is likely tob e associated with hemodynamic instability and an increased risk for perioperative stroke. 3. metabolism of beta-blockers Beta-blockers are metabolized in a different way. Especially metoprolol is dependent on metabolization by the cytochrome P450 CYP2D6 isoenzyme. The gene coding fort his enzyme is highly polymorphic resulting in an important variation in acticvity. As a consequence patients can be divided in thos who are good metabolizers and those who are poor metabolizers of for instance metoprolol. The consequence is that for the same dose plama concntrations may vary substantially and hence hemodynamic side-effects may occur in some patients and not in others.30-33 4. ratio of beta-1 to beta-2 blocking activity The risk of developing perioperative stroke seems to be related to the ratio of beta-1 to beta-2 selectivity of the beta-blocker with a higher risk with those beta-blockers that have a lower 1 to 2 ratio.34-40 5. perioperative anemia The risk of adverse events under perioperative beta-blocking therapy seems to be triggered by the occurrence of perioperative anemia.38,41,42 5. others Finally other variables such as type of surgery39,43 or genotype of beta-adrenergic receptors44 may influence the effects of perioperative beta-blocking therapy on occurrence of adeverse events. Conclusions • Chronic beta-blocker therapy for class I indicationsaccording to the ESC, AHA and ACC should be continued. • If a medical indication for beta-blockade arises preoperatively, it should be started well before surgery and the dose be titrated to effect. • Initiation of fixed dose beta-blockade shortly before surgery must be avoided. • Beta-blockers other than metoprolol should be considered. • During beta-blockade, there is probably less tolerance to systemic hypotension and anaemia. Suggested literature 1. Mangano DT et al. N Engl J Med 1996; 335: 1713 – 1720 2. Devereaux PJ. CMAJ 2004; 171: 245 – 7 3. Poldermans D et al. N Engl J Med 1999; 341: 1789 – 94 4. Raby KE et al. Anesth Analg 1999; 88: 477 – 82 5. Urban MK et al. Anesth Analg 2000; 90: 1257 – 61 6. Poldermans D et al. Eur Heart J 2001; 22: 1353 – 8 7. Kertai MD et al. Arch Int Med 2003; 163: 2230 – 5 8. Schouten O et al. Am Heart J 2004; 148: 1047 – 52 9. Poldermans D et al. J Am Coll Cardiol 2007; 49: 1763 – 9 10. Dunkelgrun M. Ann Surg 2009; 249: 621 – 6
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
31
11. Juul AB et al. Am Heart J 2004; 147: 677 – 83 12. Brady AR et al. J Vasc Surg 2005; 41: 602 – 9 13. Lindenauer PK et al. N Engl J Med 2005; 353: 349 – 61 14. Juul AB et al. Br Med J 2006; 332: 1482 – 9 15. Yang H et al. Am Heart J 2006; 152: 983 – 90 16. Warltier D. Anesthesiology 1998; 88: 2 – 5 17. Jones KG et al. Br J Surg 2000; 87: 689 – 90 18. Kertai MD et al. Anesthesiology 2004; 100: 4 – 7 19. Fleisher LA et al. Circulation 2007; 116: e418 – e500 20. Poldermans D et al. Eur Heart J 2009; 30: 2769 – 812 21. Devereaux PJ et al. Br Med J 2005; 331: 313 – 21 22. Bangalore S et al. Lancet 2008; 372: 1962 – 76 23. POISE study group. Lancet 2008; 371: 1839 – 47 24. Bouri S et al. Heart 2014; 100: 456 – 64 25. Kristensen SD et al. Eur Heart J 2014; in press 26. Badgett RG et al. Anesthesiology 2010; 113: 585 – 92 27. Poldermans D et al. Anesthesiology 2009; 111: 940 – 5 28. Flu WJ et al. J Am Coll Cardiol 2010; 56: 1922 – 9 29. Ellenberger C et al. Anesthesiology 2011; 114: 817 – 23 30. Nozawe T et al. J Cardiovasc Pharmacol 2005; 46: 713 – 20 31. Shin J et al. Pharmacotherapy 2007; 27: 874 – 87 32. Bijl MJ et al. Clin Pharmacol Ther 2009; 85: 45 – 50 33. Rau T et al. Clin Pharmacol Ther 2009; 85: 269 – 72 34. Baker JG. Br J Pharmacol 2005; 144: 317 – 22 35. Poldermans D et al. Anesthesiology 2009; 111; 940 – 5 36. Poldermans D et al. Clev Clin J Med 2009; 76 (Suppl 4): 584 – 92 37. Wallace AW et al. Anesthesiology 2011; 114: 824 – 36 38. Ashes C et al. Anesthesiology 2013; 119: 777 – 87 39. London MJ et al. JAMA 2013; 309: 1704 – 13 40. Mashour A et al. Anesthesiology 2013; 119: 1340 – 6 41. Beattie WS et al. Anesthesiology 2010; 112: 25- 33 42. Le Manach Y et al. Anesthesiology 2012; 117: 1203 – 11 43. Andersson C et al. JAMA Int Med 2014; 174: 336 – 44 44. Zaugg M et al. Anesthesiology 2007; 107: 33 – 44

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
32
WHY ARE WE NOT USING CHECKLISTS PROPERLY? DAVID J WILKINSON President, WFSA Barts Health NHS Trust. St.Bartholomew’s Hospital, London , Member of the Faculty of History and Philosophy of Medicine and Pharmacy, Worshipful Society of Apothecaries of London Set up in September 2007 by the World Health Organisation (WHO), Safe Surgery Saves Lives is the second Global Patient Safety Challenge and followed on from the first such challenge which was to increase hand washing as a major effort to decrease infection transmission. The basic tool in this second challenge is the WHO Checklist. Designed to be used for every patient coming for any surgical procedure it has three separate sections which have to be completed before the patient undergoes any form of anaesthesia, before skin incision and once the surgical procedure is completed but before the patient leaves the operating area. It was designed by a group of health care professionals, surgeons, anaesthetists and nurses, from all around the world. The first form of the checklist was trialled in 8 locations, both affluent and less affluent areas were chosen, and the results were carefully evaluated before the final checklist was ‘released’ for general use. The group evaluated the 30 day morbidity and mortality in over 7700 patients divided into two groups; the first under normal procedures and the second after introduction of the checklist. Hospitals in London UK, Toronto Canada, New Delhi India, Amman Jordan, Auckland New Zealand, Ifakara Tanzania, Seattle USA and Manila Philippines were studied. The results were spectacular; morbidity and mortality in both affluent and less affluent regions dropped markedly after introduction of the checklist.1. This highly influential study was widely highlighted by those involved and the WHO encouraged launches of the checklist around the world. The use of checklists is not new in anaesthesia or theatre practice and has followed on from their use in areas like the aviation and the nuclear power industries. However simple checklist procedures like the counting of instruments and theatre swabs have tended to be focussed on single parts of the theatre team, in this case the nursing staff who then ‘report’ their findings to the surgeon. In anaesthesia there are multiple nationally approved checklists for everyday use like the preparation of the anaesthesia workstation and others which can be used in acute but unusual/life threatening situations like anaphylaxis or malignant hyperthermia.2Routine use of checklists by individual anaesthetists remain a source of concern. Many, while realising the importance of the process, tend to skip over all of the written checks or assume that other personnel who are assisting them have performed the checks. This is so different from the use of checklists in the aviation industry where pilot and co-pilot patiently work through and complete long checklists before every flight. It is interesting to speculate on the rationale for this difference when all recognise the importance of the basic safety procedures and yet many doctors seem willing to assume the responsibility for the equipment they use without performing the checks as mandated. There are no excuses that can be made for errors that then ensue and the medical, moral, ethical and legal sequelae can be devastating for all, including the patient. One of the most influential aspects included in the pre-anaesthesia aspect of this WHO checklist was the check that a pulse oximeter had been attached to the patient. This apparatus was

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
33
unavailable in large sectors of the world and this lack of what is rightly regarded in the affluent world as a mandatory monitoring device gave rise to the WHO Global Oximetry Project which developed into the LifeBox Foundation ©. Supported by the WFSA, the Association of Anaesthetists of Great Britain and Ireland, Brigham and Women’s Hospital and the Harvard School of Public Health this charity seeks to close the current 77000 gap in theatre sites around the world still lacking pulse oximeters for patient care.3 Within a short period of time 17 countries were utilising the WHO checklist as a matter of national agreement. These again included affluent and less affluent countries. In the UK the National Patient Safety Agency made it mandatory that the checklist be used in every theatre situation in 2009 and this was implemented rapidly. But such a statement hides a huge variation in activity and practice. Operating theatres in the UK are very complex hierarchical structures and not all those who worked within them welcomed the changes that the introduction of the checklist required. This then was the first difficulty that this checklist required with its use that of a culture change of everyone working in a single team instead of a series of hierarchical subsets. Secondly it required everyone in the operating theatre environment being equally supportive and thirdly it needed to be done correctly by everyone. There was a report of a pilot study of its implementation in one hospital early in 2010. 4The authors found that surgeons were initially reluctant to participate but after persuasion by senior colleagues it became more straightforward. Despite a series of training sessions, initial use of the checklist was fraught with problems amongst which incomplete areas particularly the sign out part, hurried utilisation because of perceived time pressure on the operating list, dismissive replies and absence of key team members during completion were all highlighted. It was difficult to inculcate the concept that this was not just a ‘tick-box exercise’ but was a method of sharing vital information, creating a better team spirit and thus improving patient safety. Also the presence of a research team in theatre collecting data artificially increased the rate of completion which fell immediately the research team left. This pilot study did not see the improvements in morbidity seen in the original NEJM published study but there were noticeable improvements in some aspects of care like the timely administration of perioperative antibiotics. Poor implementation of a checklist, for whatever reason, can cause severe problems particularly by creating a false sense of security. This has been reported in the airline industry.5 Successful implementation requires diligent training, organisational leadership, the development of local champions in all professions, regular audit with feedback, clarification of roles and the ability for local modifications of the checklist provided these do not oversimplify. As the use of this checklist had been mandated as compulsory throughout the UK it was obviously going to take time to provide the required levels of training and an understanding of the required change from a hierarchical structure to one of a unified team all of whom were focussed on the patient. Other papers soon demonstrated similar effects with poor compliance in completing the forms being directly related to an ability to demonstrate a change in mortality. Good compliance with the checklist could demonstrate a positive outcome but not as high as with some earlier studies in one such paper from The Netherlands. 6 NHS England then decided to ‘label’ a series of patient safety lapses that they believed should not take place in the NHS as “Never events”. Such events are defined as ‘serious, largely

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
34
preventable patient safety incidents that should not occur if existing national guidance or safety recommendations had been implemented by healthcare providers.’ Many of these are not applicable to the operating theatre environment but several are. Examples of these theatre ‘never events’ are wrong site surgery, surgery on the wrong patient, leaving surgical instruments or swabs within a patient after surgery and failure to respond to a low oxygen saturation. The use of the WHO Checklist should have presumably removed these from any future listing but this is not the case. The provisional NHS listing of ‘never events’ for 1 April to 30 June shows 56 incidents in the UK including 23 cases of wrong site surgery, 20 cases of retained foreign object post procedure and 9 cases of use of wrong implant or prosthesis used.7 Now these are only provisional listings but do represent a source of considerable concern. There must be multiple reasons why the use of the WHO checklist is not effective in preventing what can only be considered by anyone as preventable mistakes. Patients could not believe that if a ‘tool’ has been introduced to try to prevent such errors it is not being used with appropriate diligence. The hierarchical historical basis for theatre activity is one of the major challenges to the success of this type of work. Despite superficial agreement from senior people within the operating theatre environment that there is a need to promote team working, if any anaesthetist or surgeon does not fully accept the process then the use of the checklist is doomed. Indeed what is worse is the false sense of security it creates. I do not believe this is an age related phenomenon. There are plenty of young people who do not rigorously apply the checklist and plenty of older people who do. Checklists work but only if they are adhered to in a rigorous manner. Their use needs to be audited and the results of those audits need to be fed back to those involved and behaviours modified as required. Patients, their relatives and all of the general public would not believe that corners were being cut and it is to them that all in the operating theatre are responsible. This should be a prime focus for improved education around the globe so that ‘tick-box mentality’ can be replaced with a patient safety centred team working attitude. References:
1. Haynes AB., Weiser TG., Berry WR., Lipsitz SR., Breizat A-HS., Dellinger EP., Herbosa T., Joseph S., Kibatala PL., Lapitan MCM., Merry AF., Moorthy K., Reznick RK., Taylor B., Gwande AA. A surgical safety checklist to reduce morbidity and mortality in a global population. The New England Journal of Medicine. 2009; 360: 491-499.
2. http://www.aagbi.org/publications/publications-guidelines 3. http://www.lifebox.org/ 4. Vats A., Vincent CA., Nagpal K., Davies RW., Darzi A., Moorthy K. Practical challenges
of introducing WHO surgical checklist: UK pilot experience. British Medical Journal 2010; 340: b5433.
5. Degani A., Wiener EL. Cockpit checklists: concepts, design and use. Human Factors 1993; 35: 345-359.
6. 6. van Klei WA., Hoff RG., van Aarnhem EE., Simmermacher RK., Regli LP., Kappen TH., van Wolfswinkel L., Kalkman CJ., Buhre VVF., Peelen LM. Effects of the introduction of the WHO “Surgical Safety Checklist” on in-hospital mortality: a cohort study. Annals of Surgery 2012; 255: 44-49.
7. http://www.england.nhs.uk/ourwork/patientsafety/never-events/ne-data/
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
35
FLUID GUIDELINES FOR HOSPITALS - OUR NICE GUIDELINES NEIL SONI Chelsea and Westminster Hospital, Imperial College Medical School, London, UK
The National Institute of Health and Care Excellence (NICE) commissions the National Clinical Guideline Centre (NCGC) to develop evidence based clinical guidelines. They rigorously assess the quality of the evidence for interventions using GRADE. GRADE classifies evidence as
High: We are very confident that the true effect lies close to that of the estimate of the effect
Moderate: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different
Low: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect
Very low: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect
Fluid management in hospitals is fundamental to patient care but paradoxically has been largely ignored. Medical students get taught a little, very little, about the physiology of fluid compartments but on qualifying the practical use and prescription of fluids is often handed down rather than taught. Many senior clinicians are relatively ignorant of fluid physiology, tend to leave fluid management to the juniors and hence perpetuate a cycle of ignorance.
This major dilemma is then made worse by the fact that the individuals most interested in fluids and fluid research focus on the erudite. They discuss which fluid and why, how much fluid in certain special circumstancesand argue over relative minutia. Examples include the use of albumin, the problems of starch whether restrictive or liberal is best and whether saline causes problems. Meanwhile complications with basic fluid management are very common in the wards.This well known to all, but yet there is little data to support this statement as it has rarely been audited.
Such information as exists highlights the following. Poor documentation, too much fluid, too little fluid and major electrolyte disturbances such as hyponatraemia. Renal failure and pulmonary oedema are often the consequence. The intrinsic mortality is unknown and nor is the morbidity beyond thinking it is major. The 199 NCEPOD report suggested 1 in 5 patients in the UK had complications from fluid yet nothing changed.
The NICE guidelines is the first step in correcting this anomaly in health care. They are aimed at junior doctors and nurses as the individuals who are most likely to be involved and provide basic guidance on the principle and practice of fluid management that should help standardise
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
36
this in the UK. They are not intended to dictate to specialist units or specialities where fluid management is their specialist area but rather are for general use. The main problem is in the wards and that is what needs correcting.
The aims are to educate people administering fluid as follows; physiological principles that underpin fluid prescribing
pathophysiological changes that affect fluid balance in disease states indications for IV fluid therapy reasons for the choice of the various fluids available principles of assessing fluid balance. Of these assessment is key. Assessment and regular reassessment. The practical application can be summarised as the 5 R’s.
Resuscitation, Routine maintenance, Replacement, Redistribution Reassessment.
There are appropriate algorithms for each and these provide a basis for understanding and
a framework for management. The individual algorithms are all linked so it provides a very useful and pragmatic teaching aide. Interestingly the comment “ SEEK HELP EARLY’ appears regularly.
The principles are simple. Assessment and reassessment determines which algorithm to use and also indicates how things progress.
History and examination are very important. Assessing fluid status involves: pulse, blood pressure, capillary refilland jugular venous pressure presence of pulmonary or peripheral oedema presence of postural hypotension I In particular is the patient hypovolaemic ? Do they need IV fluid resuscitation. Urgent resuscitation: SBP < 100 mmHg HR > 90 beats per minute capillary refill time > 2 seconds or peripheries are cold to touch RR > 20 breaths per minute National Early Warning Score (NEWS) is 5 or more passive leg raising test is positive.
Then monitoring which recognises that fluid management is dynamic, requirements change and so monitoring is also dynamic.
Clinical monitoring - status and trends : NEWS fluid balance charts weight.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
37
Lab tests : FBC U +E + electrolytes. IV fluids = regular monitoring.
Of course if resuscitation is involved then additional tests such as Lactate and base excess may be helpful. Routine maintenance is most common and least studied. Only give IV fluid if needed and reassess need regularly. Limit fluid to 25-30 ml/kg/day and monitor so adjust if needed. Use Dextrose saline as it meets sodium and water requirements if at low volume and hyponatraemia is rare and will be identified if it is being monitored. The old days of 3 litres a day for everyone should be long gone. If a patient has unusual and or excessive losses then assessment and replacement should be appropriate to their losses. Different bodily fluids have different compositions and this should be taken into account along with clinical and biochemical monitoring as identifying volume and content of some fluids can be difficult. Again key in this advice is seeking help early. A significant part of the guidelines addresses the need for formalising training in this area. It recognises that it will take time to make fluid administration as important as , for example, infection control and it will require establishing this new ethos in the new generation of hospital doctors. It will require an individual in each hospital to take responsibility for teaching training auditing and correcting fluid management in each Hospital. It will be difficult but it will reduce morbidity rapidly.
Identification and recognition of complications is emphasised as is the need to record and audit fluid management. This is long overdue as standard practice. Complications include;
Dehydration Pulmonary oedema Hyponatraemia Hypernatraemia Peripheral oedema Hyperkalaemia Hypokalaemia
The Guidelines do not pretend to be a complete fix of the problem. They provide a sound basis for changing the cultural approach to fluids in the wards, to recognising the importance of doing it well and the problems with doing it badly. It takes time to alter behaviour but it is a start. To be successful requires compliance with the guidelines but they are simple and easy to understand and along with education and audit should be a good start to sorting out a major previously ignored yet fundamentally vital part of hospital management. NICE Guideline .. http://www.nice.org.uk/guidance/cg174 Quality Standard http://www.nice.org.uk/Guidance/QS66 NCEPOD 1999. http://www.ncepod.org.uk/pdf/1999/99full.pdf
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
38
EXCELLENCE IN ANAESTHESIOLOGY: THE PATIENT SAFETY GOAL
MIODRAG MILENOVIĆ1, ZLATIBOR LONČAR2,6, NATAŠA PETROVIĆ1, DUŠICA SIMIĆ3,6, IVANA BUDIĆ4,7, BOJANA MATEJIĆ5,6 1Center for Anaesthesiology and Resuscitation, Emergency Center, Clinical Center of Serbia, 2Clinic for Emergency Surgery, Emergency Center, Clinical Center of Serbia, 3University Children's Hospital, Belgrade, Serbia, 4Center for Anaesthesiology and Resuscitation, Clinical Center of Nis, 5Institute of Social Medicine, 6Faculty of Medicine, University of Belgrade, Serbia, 7Faculty of Medicine, University of Nis, Serbia
Introduction
Beside knowledge and clinical skills, the anaesthesiologist should have some capabilities for teamwork, qualities related to their own behaviour, empathy for patients and their families. Anaesthesiologists often work closely with the team members. Because of the manpower problem in anaesthesia, residents and nurses in some countries are allowed to administer anaesthetics with supervision. [1] After years of observing and assisting anaesthesiologists in the operating theatre, the other team members, particularly anaesthesia nurses have become experienced in anaesthesia clinical practice and capable to describe the characteristics of the excellent anaesthesiologist, as skills and behaviours in the operating theatre environment. Up to some extent, all the team members could be helpful in observational evaluation of clinical and theoretical characteristics and anaesthesiologists behaviour in the operating theatre.
Methodology
This paper is based on review of existing relevant observational studies on this topic. With intention to explore the connection between Excellence in Anaesthesiology and Patient Safety, we searched the US National Library of Medicine, National Institutes of Health database (PubMed), looking for the articles related to this topic in last 10 years. Initially we detected 53 articles. Later on, we reduced the number down to 5 with a selection of observational studies in anaesthesiology education. Long term observation has high face validity and can give valuable information’s into someone’s behaviour. The special effort to conduct interviews of all the team members, or the special designed questioner and methodology considerations have to be implemented to get refine expert opinion, sublimated from the surveyed number of experts involved in education, together with the authors’ efforts to differentiate between visible behaviour and anaesthesiologists personality. [2, 3]
Desired characteristics of excellent anaesthesiologist
Analyzing available studies, we identified several items as preferred characteristics of anaesthesiologists from the interviews performed among team members: organization, communication, situation awareness, leadership, and described by the interviewed: ‘patient-centered’, and ‘humble to the complexity of anaesthesia’, ‘admitting own fallibility’. All of them

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
39
relate more to values and attitudes than to skills. [4] Patient-centered approach, suggests respect of patients’ autonomy, shared information, decision-making inclusion, compassion, and has been identified as a desirable characteristic in several researches. Anaesthesiologist with an empathic manner during the perioperative time, significantly improved the patient’s perception of anaesthesiologist attitude and the quality of information delivered. Empathic approach tended to decrease patient concern. In the operating room, patients who had the same anaesthesiologist (continuing care) expressed greater satisfaction levels regarding anaesthesiologist behaviour and quality of care. [5]
According to refine expert opinion [3], sublimated from the surveyed number of experts involved in education, anaesthesia tutors, instructors, heads of university anaesthesia departments as well as from the anaesthesia trainees, important characteristics of excellent anaesthesiologist are: clinical skills, ‘strives for excellence’, innovation and originality, ‘good communicator’ and teacher, followed by: leadership, ‘relationship with patients’, ‘liked and respected’, organizational efficiency. To describe each of the characteristics, surveyed individuals explained what exactly they expect in particular situations. Related to ‘clinical skills’, they expected excellent one to be able to demonstrate practical knowledge, to complete required tasks. ‘Striving for excellence’ was described as personal effort in constant review of its own practice and improvement, which may be redefined as ‘striving for perfection’.
Innovation and originality were described as constant effort to resist ‘the status quo’ and individual enthusiasm to innovate, in correlation with patient safety standards. Good communicator referred to interaction with patients and other staff members and included the capability to resolve any problem situation in a diplomatic manner with intercession. He also needs to know to apologize. Few major elements where categorized under the anaesthesia excellence teaching: ability to inspire through enthusiasm for the subject; a willingness to teach not only trainee anaesthesiologists, but also other team members and students and finally, specific role in supporting trainees. Academic excellence was not felt to be the indicator of universal excellence. Still, lots of the statements presumed applied knowledge. [6]
Patient safety considerations
Formed in 1985 the Anesthesia Patient Safety Foundation (APSF) has prepared simple mission statement: "That no patient shall be harmed by anaesthesia". Errors in medical practice could be avoided by systematic collection of data, conduction of methodologically well organized research, interventions for improvement, as well as targeted education to health care personnel, patients and their families. Achieving the higher standards in education and knowledge has encouraged changes in practice and behaviour and consequently provoked declining in adverse outcomes. All these efforts need endorsement of local governments, health care institutions and professional associations, as well as support of private foundations. [7]

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
40
Enlargement and deepness of the gap between ongoing demands to perform the number of surgery or other invasive procedures on one side, and the need to do it on the already achieved or higher level of safety, made the highly developed medical system in the well provided affluent world, to work hard to promote excellence in patient care, with the intention to enhance the patient safety, which is strongly related to excellence in anaesthesiology. The American Medical Association made great effort to promote educational ‘Initiative to Transform Medical Education (ITME): Recommendations for change in the system of medical education’. The result was proposed reform of the medical education and training, from premedical preparation and medical school admission through continuing physician professional development. They systematically analyzed the educational system and identified areas with possible need for intervention: a) enhancement of health system safety and quality, b) the need for improvement of education in training institutions, and c) the inadequacy of physician theoretical and practical preparedness in required specialists’ area. [8, 9]
Joined European and Global effort
A number of less affluent nations made huge effort to achieve an adequate level of trained anaesthesia professionals, equipment and safety regulations, but political instability and economic crisis opposed that process. [10, 11] Pioneer efforts have been made to unite a political and professional influence, knowledge and experience and to launch the first international declaration on patient safety - The Helsinki Declaration on Patient Safety in Anaesthesiology. The main initiative came from the two major European Anaesthesia bodies: European Board of Anaesthesiology (EBA) and the European Society of Anaesthesiology (ESA). The endorsement of this important initiative came from the World Health Organization (WHO), the World Federation of Societies of Anaesthesiologists (WFSA), and the European Patients' Federation (EPF).The Declaration gave strategic foundation and short term plan for improvement to all parties in the safety process: anaesthesiology professionals, industry and patients. [12, 13]
Conclusion
Desired high level of Excellence in Anaesthesiology can be achieved by the strategically and systematically improved human resource policy, with proactive, positive selection of high professional and ethical standards of anaesthesiologists, development of stimulating and collaborative team environment and constant improvement of education in training institutions. The concept of Excellence in Anaesthesiology can become one of the major patient safety goals, because it has been proven in everyday clinical and teaching practice.
Reference
1. Smith AF, Mishra K. Interaction between anaesthetists, their patients, and the anaesthesia team. Br J Anaesth. 2010 Jul;105(1):60-8.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
41
2. Larsson J, Holmström IK. How excellent anaesthetists perform in the operating theatre: a qualitative study on non-technical skills. Br J Anaesth. 2013 Jan;110(1):115-21.
3. Murphy MK, Black NA, Lampling DL, et al. Consensus development methods and their use in clinical guideline development. Health Technol Assess 1998; 2: 1–88
4. Smith AF, Pope C, Goodwin D, Mort M. Communication between anesthesiologists, patients and the anesthesia team: a descriptive study of induction and emergence. Can J Anaesth. 2005 Nov;52(9):915-20.
5. Soltner C, Giquello JA, Monrigal-Martin C, Beydon L. Continuous care and empathic anaesthesiologist attitude in the preoperative period: impact on patient anxiety and satisfaction. Br J Anaesth. 2011 May;106(5):680-6.
6. Smith AF, Glavin R, Greaves JD. Defining excellence in anaesthesia: the role of personal qualities and practice environment. Br J Anaesth. 2011 Jan;106(1):38-43.
7. Eichhorn JH. The Anesthesia Patient Safety Foundation at 25: a pioneering success in safety, 25th anniversary provokes reflection, anticipation. Anesth Analg. 2012 Apr;114(4):791-800.
8. Papadimos TJ, Murray SJ. Foucault's "fearless speech" and the transformation and mentoring of medical students. Philos Ethics Humanit Med. 2008 Apr 17;3:12.
9. American Medical Association Initiative to Transform Medical Education [http://www.ama-assn.org/ama1/pub/upload/mm/377/finalitme.pdf]
10. Milenović M, Nešković V, Simić D, Jovanović G. Anaesthesia teachers training – advanced approach. Fourth annual spring Scientific Symposium in Anaesthesiology and Intensive Care. Proceeding. Scientific symposium, 2012, 30-31.
11. Milenović M. Training of teachers in anaesthesiology: the less affluent society – the more
challenging results. 5th All Africa Anaesthesia Congress „Knowledge for Tomorrow“, 2013, 123-125.
12. Mellin-Olsen J, Staender S, Whitaker DK, Smith AF. The Helsinki Declaration on Patient Safety in Anaesthesiology. Eur J Anaesthesiol. 2010 Jul;27(7):592-7.
13. Staender S, Smith A, Brattebø G, Whitaker D. Three years after the launch of the Helsinki Declaration on patient safety in anaesthesiology: the history, the progress and quite a few challenges for the future. Eur J Anaesthesiol. 2013 Nov;30(11):651-4.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
42
ECHOCARDIOGRAPHY AS A TOOL FOR HEMODYNAMIC MONITORING: GOLD STANDARD, SURROGATE OR COMPLEMENTARY TO STANDARD MONITORING TOOLS? ECHOCARDIOGRAPHY IN THE ICU GORAZD VOGA Medical ICU, General Hospital Celje, Slovenia E: [email protected] Introduction Hemodynamic instability is the common reason for ICU admission. In order achieve rapid hemodynamic stability without overtreatment, which can have serious side effects, balanced used of proper hemodynamic variables should be used for hemodynamic assessment and monitoring. Hemodynamic assessment is a “snapshot” of actual hemodynamic status by measuring various hemodynamic variables on admission and should be frequently repeated even in hemodynamic stable patients.Hemodynamic monitoring, on the other hand, represents continuous measurement of relevant hemodynamic variables in order to detect unexpected deterioration and titratethe treatment. The basic purpose of hemodynamic assessment/monitoring is to assess, if oxygen transport meets the actual demands and if not, which component is failing and why,in order to correct it properly and ensure normal organ function.Correct treatment with fluids, vasopressors and inotropic agents should rely on proper assessment of arterial pressure, preload, flow and flow adequacy. Basic hemodynamic assessment
On admission basic hemodynamic assessment should be made by clinical examination and classical vital signs: non-invasive blood pressure, heart rate, frequency of breathing, body temperature and saturation measured by pulse oximeter. Basic vital signs do not allow conclusions about preload, flow and flow adequacy, and non-invasive measurement of arterial blood pressure is frequently inaccurate and inadequate in critically ill patients. Tachycardia and tachypnea can be associated with all kind of shock, sepsis, pain, anxiety, febrile state, hyperthyrosis, hypo and hypervolemia, heart failure, anaemia, hypoxia and many other conditions. Hypotension, on the other hand, can be normal, result of incorrect measurement and caused by vasodilation, inadequate vasoconstriction and by various drugs. The low value of arterial oxygen saturation is diagnostic for hypoxia, but gives no information concerning its etiology. So, it is clear that such assessment is inadequate for hemodynamic stabilisation. Hemodynamic assessment before volume loading
Since the first step in hemodynamic stabilisation is optimisation of preload by volume loading, the basic question is which variables are required for safe use of fluids. It seems logical that assessment of preload and fluid responsiveness is mandatory. Assessment of preload can rely on pressures or volumes. Unfortunately pressures (central venous pressure and pulmonary artery occlusion pressure) are not accurate measures of preload and they cannot predict fluid responsiveness. Nevertheless,they should be measured as safety parameters: i.e. steep rise of filling pressures after volume loading indicates immediate stop of volume treatment. Therefore, for correct volume assessment, static pressure and volume variables (intrathoracic blood volume, global end-diastolic volume, end-diastolic areas and volumes) must be measured, together with dynamic variables which can predict fluid responsiveness. However, the usual dynamic
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
43
parameters of fluid responsiveness are predictive only in in approximately 50% of critically ill patients. The increase of stroke volume after volume challenge depends on thefunction of right and left ventricle and both should be assessed before giving fluids to the patient. Finally, there is no need to increase oxygen delivery if it is adequate, and determination of at least one marker of flow adequacy (lactate level, mixed venous oxygen saturation, central venous oxygen saturation) is mandatory. The decision for volume loading should therefore rely on determination of preload, fluid responsiveness, cardiac function and flow adequacy. Role of echocardiography in initial hemodynamic assessment and hemodynamic monitoring
At the point of initial hemodynamic assessment echocardiography is mandatory for estimation of preload (diameter of inferior vena cava, areas and volumes of cardiac chambers), fluid responsiveness (respiratory variation of inferior/superior vena cava or aortic flow) and assessment of right and left ventricular function. Most information can be provided by transthoracic echocardiography but transesophageal echocardiography can be performed in patients with bad visibility. In hemodynamic unstable patients in whom after preload optimisation cardiac output (estimated by transthoracic echocardiography)remains low and the inotropic support is considered, monitoring of cardiac output is mandatory. Since there are many methods for measurement, relatively reliable value of cardiac output can be obtained very easily in most critically ill patients, but the problem is proper interpretation. Basically, echocardiography is mandatory for selection of most appropriate method for cardiac output monitoring. We believe that in patients with similar preload and function of both ventricles methods based on arterial pulse contour analysis are preferred. On the other hand, in patients with different right and left ventricle preload and function we prefer monitoring with pulmonary artery catheter. There are no normal or optimal values for cardiac output and many factors should be considered for its interpretation such as preload, afterload, flow adequacy, heart rate and rhythm and microcirculation. They should be therefore interpreted together with other hemodynamic variables, but assessment of preload and adequacy of tissue perfusion is most important and mandatory. The measurement and monitoring of cardiac output without assessment of preload and flow adequacy is needless and can lead to erroneous therapeutic decisions. Hemodynamic assessment requires therefore integrative approach with measurement of variables by various methods. Hemodynamic assessment/monitoring should provide reliable estimation of preload, flow and flow adequacy. Unfortunately, the monitoring of microcirculation is not ready for routine use, nevertheless, its improvement and normalisation remains the main goal of hemodynamic support stabilisation. Finally, hemodynamic assessment and monitoring, despite being mandatory, are only the first step of hemodynamic stabilisation. They have to be followed by proper treatment in order to improve the outcome of critically ill patients. It should be pointed out the after hemodynamic assessment by echocardiography treatment is changed in 40 – 60% of patients. Assessment of cardiac performance
Inadequate cardiac performance is one of the most frequent causes of hemodynamic instability and circulatory failure in critically ill patients. Prompt and exact diagnosis of heart diseases and assessment of cardiac function is therefore an integral part of intensive care medicine. M-mode,

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
44
2-D-mode, pulse and continuous wave Doppler spectral analysis and color Doppler flow imaging constitute the essential elements of transthoracic echocardiography (TTE). The method provides high-quality real time images of heart, great vessels and mediastinal structures and enables qualitative and quantitative blood flow assessment. TTE is noninvasive, can be performed immediately at the bedside and frequently repeated. In patients with inadequate visibility and in specific indications transesophageal echocardiography (TEE) is successfully employed. Assessment of cardiac function represents the most frequent indication for TTE in the hemodynamically unstable critically ill patients. Increasingly important indication for TEE is becoming intraoperative diagnostic evaluation and cardiac function monitoring in patients with cardiac or non-cardiac surgery during hemodynamic instability. Cardiac output can be calculated simply by measuring flow over valves and the diameter of the valve opening. However, it can be replaced by velocity time integral, which is closely related to stroke volume. Global and regional left and right ventricular systolic function can be assessed by TTE. Beside traditional measurements of left ventricular function (ejection fraction/fractional shortening) ventricular long axis function and tissue Doppler imaging can be additionally performed. In patients with inadequate visibility the simple measurement of TAPSE (tricuspid annulus plane systolic excursion) and MAPSE (mitral annulus plane systolic excursion) reflects right and left ventricular function respectively. Nevertheless, in majority of critically ill patients the visual estimation of systolic function (eye balling) is performing. Segmental wall motion abnormalities can significantly impair global cardiac function. Regional hypokinesis or akinesis detected by TTE is the earliest sign of myocardial ischemia. Assessment of preload
Left ventricular diastolic area can be easily measured by TTE in the short axis at the mid-papillary level and correlates closely with the left ventricular end diastolic volume. It estimates preloadmore reliably than other methods and is suitable also for bedside assessment the fluid responsiveness. End-diastolic left ventricular area less than 5, 5 cm2/m2 signifies hypovolemia in patients without diastolic dysfunction or hypercontractility. In patients with chronic heart failure, inadequate preload can be associated with normal or even large left ventricular end-diastolic area. The usual initial assessment of preload is performed by measuring diameter and respiratory change of inferior vena cavain the subcostal view. Evaluation of left ventricular filling pattern (transmitral flow and pulmonary venous flow pattern) must be included in the assessment of left ventricular function since it provides valuable information about left ventricular diastolic function and left ventricular filling pressure. Abnormal compliance is a frequent problem in critically ill and cannot be detected or assessed with the pulmonary artery catheter. TTE should be routinely used for assessment of cardiac function, but cannot simply replace several other already established technologies in the ICU. Echocardiography gives us different information comparing to invasive methods (pulmonary artery catheter or methods that use arterial pressure contour analysis) and the methods are therefore not competitive but rather
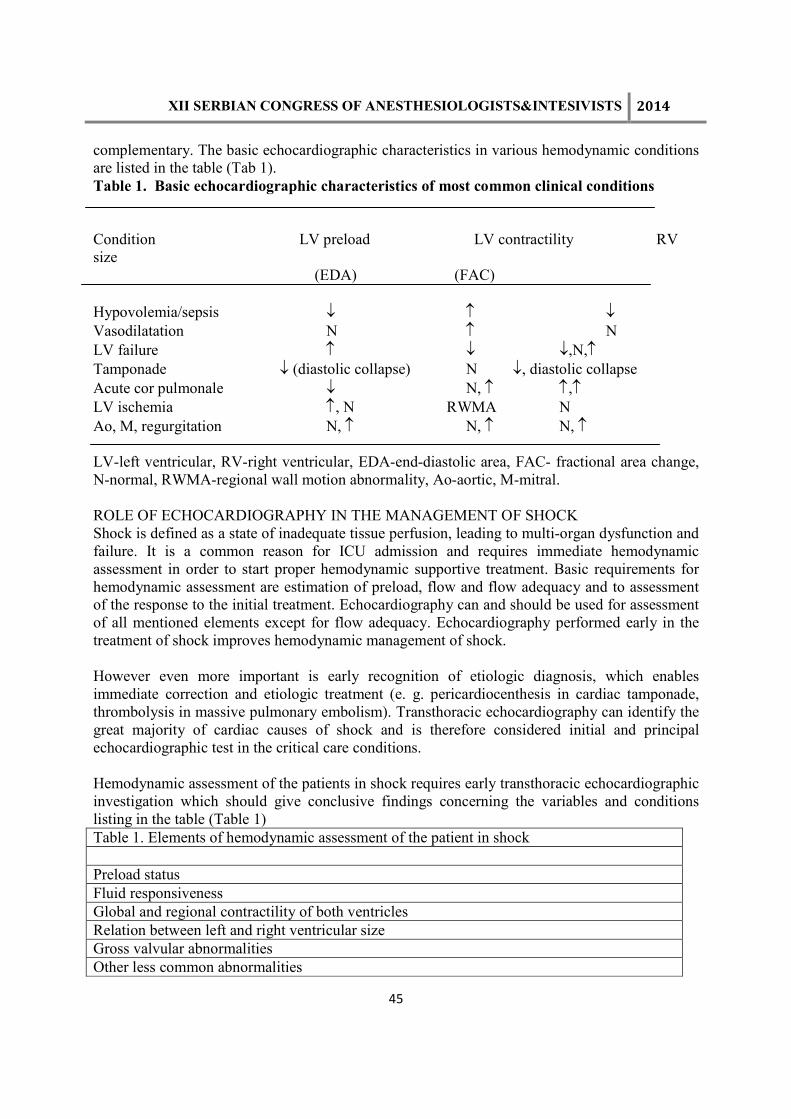
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
45
complementary. The basic echocardiographic characteristics in various hemodynamic conditions are listed in the table (Tab 1). Table 1. Basic echocardiographic characteristics of most common clinical conditions Condition LV preload LV contractility RV size (EDA) (FAC) Hypovolemia/sepsis ↓ ↑ ↓ Vasodilatation N ↑ N LV failure ↑ ↓ ↓,N,↑ Tamponade ↓ (diastolic collapse) N ↓, diastolic collapse Acute cor pulmonale ↓ N, ↑ ↑,↑ LV ischemia ↑, N RWMA N Ao, M, regurgitation N, ↑ N, ↑ N, ↑ LV-left ventricular, RV-right ventricular, EDA-end-diastolic area, FAC- fractional area change, N-normal, RWMA-regional wall motion abnormality, Ao-aortic, M-mitral. ROLE OF ECHOCARDIOGRAPHY IN THE MANAGEMENT OF SHOCK Shock is defined as a state of inadequate tissue perfusion, leading to multi-organ dysfunction and failure. It is a common reason for ICU admission and requires immediate hemodynamic assessment in order to start proper hemodynamic supportive treatment. Basic requirements for hemodynamic assessment are estimation of preload, flow and flow adequacy and to assessment of the response to the initial treatment. Echocardiography can and should be used for assessment of all mentioned elements except for flow adequacy. Echocardiography performed early in the treatment of shock improves hemodynamic management of shock. However even more important is early recognition of etiologic diagnosis, which enables immediate correction and etiologic treatment (e. g. pericardiocenthesis in cardiac tamponade, thrombolysis in massive pulmonary embolism). Transthoracic echocardiography can identify the great majority of cardiac causes of shock and is therefore considered initial and principal echocardiographic test in the critical care conditions. Hemodynamic assessment of the patients in shock requires early transthoracic echocardiographic investigation which should give conclusive findings concerning the variables and conditions listing in the table (Table 1) Table 1. Elements of hemodynamic assessment of the patient in shock Preload status Fluid responsiveness Global and regional contractility of both ventricles Relation between left and right ventricular size Gross valvular abnormalities Other less common abnormalities

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
46
Echocardiographic approach to the patient in shock should be systematic
1. Pre-existing cardiac diseases such as dilative cardiomyopathy can be suspected in patients with dilated left ventricle and atrium and hypertensive heart disease, hypertrophic cardiomyopathy or aortic stenosis in patients with concentric left ventricular hypertrophy. RV dilation and hypertrophy indicates chronic cor pulmonale.
2. With examination of inferior vena cava clear hypovolemia can be confirmed if there is a complete inspiratory collapse of the vein, but dilated and fixed vena cava gives no reliable information concerning hypovolemia. Small left ventricle with left ventricular end diastolic area smaller than 5, 5 cm2/m2 is strongly suggestive for hypovolemia. Nevertheless, in patients with pre-existing dilation of the left ventricle, hypovolemia can occur also with much larger end-diastolic area.
3. Estimation of fluid responsiveness is even more important than preload assessment. It is usually based on the respiratory collapsibility of inferior vena cava in spontaneously breathing patients or its distensibility in mechanically ventilated patients. Despite wide use of these variables for assessment of fluid responsiveness, one should realized that they are nor very reliable because of following reasons:
a. Inferior vena cava is placed in the abdominal cavity and therefore the change of the diameter does not reflect always the change of the intrathoracic pressure. In that sense the changes of superior vena cava are more reliable.
b. Estimation of fluid responsiveness by distensibility is more reliable than by collapsibility.
c. For reliable estimation of fluid responsiveness the assessment of right and left ventricular function is mandatory.
4. Dilated right ventricle with severely impaired contractility is suggestive for the right ventricular dysfunction due to biventricular failure, right ventricular infarction or acute cor pulmonale. The assessment of tricuspid regurgitation and estimation of pulmonary artery pressure is mandatory for differentiation of right ventricular failure. D shape of the right ventricle is typical for tight ventricular pressure overload. The right ventricular function should be expressed according to eye balling or/and according to measurements of TAPSE (tricuspid annulus systolic excursion) or systolic velocity of tricuspid annulus movement measured by tissue Doppler.
5. Patients with severely depressed left ventricular contractility can have coronary artery disease, septic myocardial dysfunction, fulminant myocarditis and cardiomyopathy. Severe functional and morphological valvular disorders should be detected and categorised as acute (e.g. mitral and aortic regurgitation) or chronic (e.g. aortic stenosis). Severe and clear regional wall motion abnormalities are suggestive for acute myocardial ischemia. Global left ventricular systolic function is usually estimated by eye balling, extensive and sophisticated measurements and calculations are not necessary. However, quantitative measurements of left ventricular systolic function include calculation of fractional shortening, fractional area change and ejection fraction. In selected patients (i.e. patients with preserved systolic function and congestive symptoms) left ventricular diastolic function should be determined, usually by analysis of transmitral flow and velocity of movement of mitral annulus by tissue Doppler. Assessment of contractility, volume status and basic morphological characteristics allows differentiation of four major categories of circulatory shock.
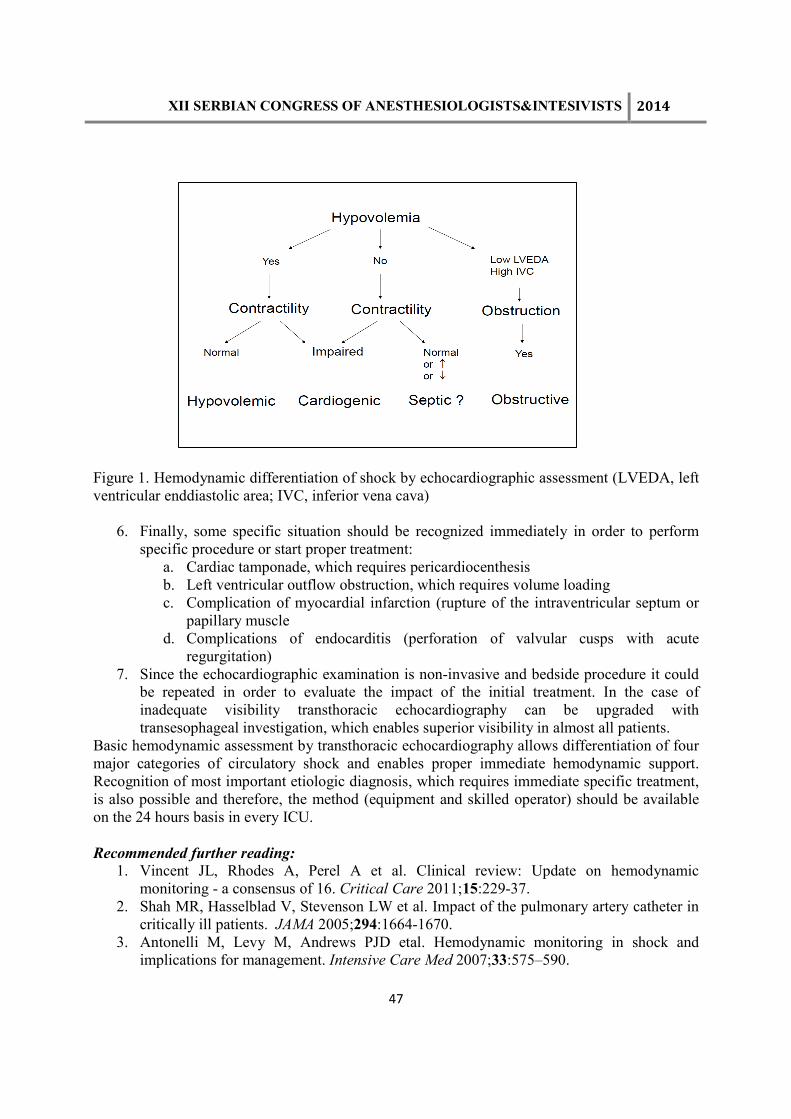
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
47
Figure 1. Hemodynamic differentiation of shock by echocardiographic assessment (LVEDA, left ventricular enddiastolic area; IVC, inferior vena cava)
6. Finally, some specific situation should be recognized immediately in order to perform specific procedure or start proper treatment:
a. Cardiac tamponade, which requires pericardiocenthesis b. Left ventricular outflow obstruction, which requires volume loading c. Complication of myocardial infarction (rupture of the intraventricular septum or
papillary muscle d. Complications of endocarditis (perforation of valvular cusps with acute
regurgitation) 7. Since the echocardiographic examination is non-invasive and bedside procedure it could
be repeated in order to evaluate the impact of the initial treatment. In the case of inadequate visibility transthoracic echocardiography can be upgraded with transesophageal investigation, which enables superior visibility in almost all patients.
Basic hemodynamic assessment by transthoracic echocardiography allows differentiation of four major categories of circulatory shock and enables proper immediate hemodynamic support. Recognition of most important etiologic diagnosis, which requires immediate specific treatment, is also possible and therefore, the method (equipment and skilled operator) should be available on the 24 hours basis in every ICU. Recommended further reading:
1. Vincent JL, Rhodes A, Perel A et al. Clinical review: Update on hemodynamic monitoring - a consensus of 16. Critical Care 2011;15:229-37.
2. Shah MR, Hasselblad V, Stevenson LW et al. Impact of the pulmonary artery catheter in critically ill patients. JAMA 2005;294:1664-1670.
3. Antonelli M, Levy M, Andrews PJD etal. Hemodynamic monitoring in shock and implications for management. Intensive Care Med 2007;33:575–590.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
48
4. Pearse R, Dawson D, Fawcett J et al. Early goal-directed therapy after major surgery reduces complications and duration of hospital stay. A randomised, controlled trial. Critical Care 2005;9:R687-R693.
5. Sakka SG, Reinhart K, Meier-Hellmann A: Comparison of pulmonary artery and arterial thermodilution cardiac output in critically ill patients. Intensive Care Med 1999;25:843-846.
6. Reinhart K, Kuhn HJ, Hartog C, Bredle DL: Continuous central venous and pulmonary artery oxygen saturation monitoring in the critically ill. Intensive Care Med 2004;30:1572-1578.
7. Pinsky MR, Payen D: Functional hemodynamic monitoring. Crit Care 2005;9:566-572. 8. Senn A, Button D, Zollinger A, Hofer C. Assessment of cardiac output using a modified
FloTrac/Vigileo algorithm in cardiac surgery patients. Critical Care 2009;13:R32. 9. Takala J, Ruokonen E, Tenhunen JJ, Parviainen I, Jakob SM: Early non-invasive cardiac
output monitoring in hemodynamically unstable intensive care patients: a multi-center randomized controlled trial.Crit Care 2011;15:R148.
10. Cecconi M, Bennett D: Should we use early less invasive hemodynamic monitoring in unstable ICU patients? Critical Care 2011;15:173.
11. Rhodes A, Cusack RJ, Newman PJ, Grounds RM, Bennett ED: A randomised, controlled trial of the pulmonary artery catheter in critically ill patients. Intensive Care Med 2002;28:256-264.
12. Harvey SE, Welch CA, Harrison DA, Rowan KM, Singer M: Post hoc insights from PACMan--the U.K. pulmonary artery catheter trial. Crit Care Med 2008;36:1714-1721.
13. Joseph MX, Disney PJ, Da Costa R, Hutchison SJ. Transthoracic echocardiography to identify or exclude cardiac cause of shock. Chest 2004;126:1592-7.
14. Manasia A, Cucu D, Oropello J, DelGiudice R, Hufanda J Benjamin E. Clinical impact of early goal-directed echocardiography in shock patients performed by non-cardiologist intensivists free to view. Chest 2005;128:222S.
15. Muller L, Bobbia X, Toumi M, Louart G, Molinari N,Ragonnet B, QuintardH,Leone M, Zoric L, Lefrant JY, and the AzuRea group. Respiratory variations of inferior vena cava diameter to predict fluid responsiveness in spontaneously breathing patients with acute circulatory failure: need for a cautious use. Crit Care 2012; 16:R188.
16. Bergenzaun L, Gudmundsson P, Öhlin H, Düring J, Ersson A, Ihrman L, Willenheimer R, Chew MS. Assessing left ventricular systolic function in shock: evaluation of echocardiographic parameters in intensive care. Critical Care 2011, 15:R200.
17. De Backer D. Ultrasonic evaluation of the heart. Curr Opin Crit Care 2014, 20:309-3014.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
49
CRITICAL ULTRASOUND IN PREHOSPITAL SETTINGS: WHERE THE BENEFIT OF ULTRASOUND USE IS EVEN GREATER GREGOR PROSEN1,2,3, MATEJ STRNAD 1,2 Center for emergency medicine, Community health centre Maribor, C. Proletarskih brigad 22, 2000 Maribor, Slovenia email: [email protected] “Critical illness does not respect geography” (Peter Safar)
Nothing has generated as much change in emergency medicine in past 15 years as the
introduction of bedside ultrasound
Christian J Fox (1)
Introduction Emergency medicine is distinct speciality where time and correct decision-making are critical (1). Since decisions for (or against) specific treatment or procedures can make a difference between Life and Death or cause major morbidity, physicians in whole spectrum of critical care need as many useful informations as possible, to make correct, beneficial decisions. Ultrasound (US) can provide such important informations in many situations, especially, since sensitivity and specificity of focused US exam is generally much higher then that of “classical” propedeutic physical exam (2). Ultrasound use in Emergency medicine (EM) context, specifically in trauma, was probably first application of focused bedside ultrasound. First such specific use was FAST algorithm (Focused Assessment with Sonography in Trauma) (3), searching for free fluid, presumably blood in trauma patient. This focused US applications in specific clinical problems heralded distinct, new use of this potent diagnostic tool - bedside, problem-based, focused US examinations, performed by clinicians, that by their training are non-imaging specialists. Such US exams are thus focused on specific pathology in question, mainly dichotomous in answering simple question “is this pathology present; yes/no?”, problem based (“is this cause of
shock/respiratory failure/swollen leg etc…”) and transversal, unbound by “classical”, region-based division of sonographic assessment (abdomen being assessed by radiologists, heart by cardiologists, etc). They can be done at the point-of-care, wherever that might be (prehospital, emergency department (ED), intensive care unit (ICU), hospital wards, operating room, helicopter, etc…) Thus, new concept of point-of-care ultrasound (POCUS) (4) was born, encompassing whole spectrum of such focused sonographic applications in different medical specialities, from anaesthesiology to different surgical specialities to internal, family and emergency medicine and beyond. From this perspective of bedside, point-of-care ultrasound use, emergency US use in prehospital arena is in essence no different than it’s use in emergency departments or in-hospital critical care wards.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
50
In contrast, since prehospital medical systems by design lack most of sophisticated diagnostic/imaging modalities that can be found in hospitals, POCUS is actually first true equaliser in spectrum of critical care from pre-hospital to in-hospital environments. Thus, our present article deliberately makes no clear distinction between POCUS applications in prehospital or in-hospital arenas. All of POCUS applications performed in emergency departments/ICUs can also be performed out-of-hospital, albeit under less ideal physical, spacial and hygienic conditions. Performing focused, bedside US in pre- or in-hospital arenas is bound to same conceptual laws that have to be obeyed; First, safe and meaningful use of POCUS is unavoidably based on assessment of pre-test probability for distinct clinical entity we are assessing for. Thus, history trumps everything! Secondly, based on history, clinician performing POCUS has to clearly know what pathology they are looking for and how will they recognise it sonographically! Third comes solid sonographic body of knowledge and skills. From everything written so far, it is clear, that actual sonographic skills are but a part of whole POCUS use in emergency/critical care. Of equal importance is knowing indications, limitations, pitfalls and pearls of POCUS applications and most importantly, rock-solid, core clinical base is needed! POCUS examinations is “just” an extension of physical examination and clinical acumen and should be viewed as such! What can be viewed by POCUS in emergencies?
Although specific (sub)indications (and variations) of US use in EM/critical care are expanding almost weekly, it is appropriate to review core US applications that ACEP (American College of Emergency physicians)proposes (5) in Table 1: Table 1: Applications of bedside ultrasound in emergency medicine; ACEP 2009 - FAST examination of the traumatized patient - AAA - emergency cardiac US - pregnancy - hepatobiliary US - kidney US - DVT - lung US - musculo-skeletal US - eye US - procedural US Legend: ACEP: American College of Emergency physicians Based on that, we can expand on specifics of these regional POCUS examinations: Given below are specific pathologies, we can look for in pertinent regions at the basic-mid level of POCUS knowledge:

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
51
- lung EUS: Pneumothorax, pleural effusion, consolidations, “interstitial syndrome” (eg. pulmonary edema, contusion, fibrosis), diaphragmatic (dys)function - cardiac EUS: pericardial effusion/tamponade, IVC (V. cava inferior)colapsibility/preload (marker of fluid responsiveness), gross assessment of left ventricular (dys)function, relative size and function of the right ventricle (ac. cor pulmonale) (6), marked morphological changes (valves, chamber sizes, hypertrophy) - FAST: presence of free fluid in intraperitoneal space? - AAA: diameter of abdominal aorta? - DVT: proximal deep vein thrombosis? - gallbladder EUS: features of cholecystitis? - kidney EUS: hydronephrosis? - gynecological EUS (transabdominal): free fluid in the Douglas pouch? Intrauterine pregnancy? Fetal position? - skeletal and soft tissue EUS: fractures? Abscess/cellulitis? Foreign body? Achilles tendon rupture? - eye EUS: intracranial pressure assessment (optic nerve sheath diameter)? Retinal/vitreousdetachment? Foreign body? Lens dislocation? Pupillary reflex? - procedural EUS: intravenous access (central/peripheral), foreign body evacuation, thoracic
tube placement, endotracheal intubation and checking for correct position. Based on these specific, focused regional POCUS applications, we can clearly see potential uses in variety of clinical presentations/context, dealing with undifferentiated patients - the sine qua
non of patients we help in prehospital arena. For sake of systematic approach, we list different clinical uses in ABCDE sequence, followed by different symptoms. Airway management: - real-time confirmation of endotracheal tube position (7) - confirmation of correct tube position (exclusion of right mainstem intubation by confirmation
of bilateral “lung sliding”/“lung pulse” and diaphragmatic excursions - assessment of prandial status/gastric fullness (RSI context) - identification of crycothyroid membrane position and avoidance of overlying structures (8) Breathing/respiratory failure/dyspnea: - diagnosis of pneumothorax (PTx); spontaneus, traumatic, post procedures (9) - diagnosis of fluidothorax(FTx); “medical”, haematothorax - diagnosis of pneumonia(PNA); lobar pneumonia (sonographic appearance of consolidation
usually with some minimal FTx)(10) or interstitial pneumonia (sonographic appearance of “interstitial syndrome”)
- diagnosis of pulmonary edema(cardiogenic or ARDS, each with distinct sonographic features) (11,12,13)
- diagnosis of pulmonary contusion (sonographic appearance of localised “interstitial
syndrome”) (14) - diagnosis of pulmonary fibrosis/other chronic interstitial diseases (sonographic appearance of
global “interstitial syndrome”) - diagnosis of bronchiolitis

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
52
- in lieau with transversal, problem-based approach, we can also diagnose pulmonary embolism, both by findings of DVT with/with-out signs of ac. cor pulmonale and/or sonographic identification of pulmonary infarcts (sonographic appearance of small un-airated consolidations) (15)
- although being bronchial processes, asthma/COPD exacerbations can be indirectly presumed by sonographic appearance of well-aerated, “dry” lungs without sonographic findings of other aforementioned pathologies.
Circulation/shock/syncope:
• focused cardiac ultrasound (FOCUS) (6) - diagnosis of pericardial effusion/tamponade present? - assessment of size & respiratory collapsibility (in spontaneously breathing) of V. cava
inferior (IVC) as marker of fluid responsiveness/(preload) - rough assesment of left-ventricular function (inotropy) - rough assessment of right-ventricular function and relative size (diagnosing acute for
pulmonale) - identification of obvious gross anatomic abnormalities (valve abnormalities, chamber sizes,
ventricular hypertrophy) • diameter of abdominal aorta (risk of rupture in AAA) (16) • diagnosis of DVT (deep venous trombosis)(17) • diagnosis of tension PTx • diagnosis of hematothorax (HTx), (haemorhagic shock in trauma) • diagnosis of free intraperitoneal fluid, presumably blood in trauma (FAST; haemorhagic
shock in trauma) • identifying foci of sepsis (look below) specifically cardiac arrest: - diagnosis of tension PTx - diagnosis of cardiac tamponade - diagnosis of massive pulmonary embolism (mPE) Disability/eye ultrasound: - diameter of optic nerve sheath diameter (ONSD) as marker of increased intracranial pressure
(ICP) (18) - diagnosis of retinal/vitreous detachment - identifying foreign body in the eye - diagnosis of globe rupture - assessing pupillary reflex (under overt lid edema) chest pain: - diagnosis of cardiac tamponade (non-traumatic, due to aortic dissection?) - diagnosis of massive pulmonary embolism (mPE) - diagnosis of pneumothorax - diagnosis of wall motion abnormalities (acute coronary syndrome) - advanced application! - diagnosis of pneumonia
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
53
abdominal pain: - diameter of abdominal aorta (risk of rupture in AAA) - diagnosis of free intraperitoneal fluid - diagnosis of cholecystitis - diagnosis of hydronephrosis (surrogate confirmation in renal colic syndrome) - diagnosis of pregnancy (intra-uterine, possibly extrauterine, identification of free fluid, fetal
position) sepsis: - diagnosis most frequent foci: pneumonia, hydronephrosis/pyelonephritis, absces, celulitis,
necrotising fasciitis, cholecystitis - haemodynamic monitoring during early sepsis resuscitation (i.e. early goal-directed therapy
(EGDT) swollen leg: - diagnosis of deep venous thrombosis (DVT) - diagnosis of celulitis MSK/musculo-skeletal: - diagnosis of bone fractures (and bedside confirmation of correct repositioning) - diagnosis of tendon rupture (mainly Achile’s) - diagnosis joint effusion (and needle aspiration guidance) procedures: - aid in IV line placement (peripheral or central) - abscess confirmation and drainage - aid in pericardiocentesis - aid in thoracocentesis - peripheral nerve block/regional anaesthesia But truly revolutionary and synergistic benefits of POCUS use can only be gained by ubiquitous use in whole spectrum of critical care, from prehospital arena, to emergency departments and intensive care units. Following are few cases of different clinical scenarios, presented to convey magnitude of POCUS impact in prehospital emergency medicine. For more in-depth discussion of specific POCUS application in critical care, reader is kindly invited to read other original resources. Case vignettes with discussion Case No. 1: 62 year-old male was found unresponsive in his cellar. Bystanders did not perform BLS, yet arrival time of EMS, accompanied by physician, was relatively short (8 minutes from time of collapse). ALS was commenced immediately, initial rhythm being asystole. After roughly 10 minutes of standard ALS procedures, planned rhythm check showed PEA rythm, without palpable pulse, yet capnography during that pulse check pause remained stable (28 mmHg).
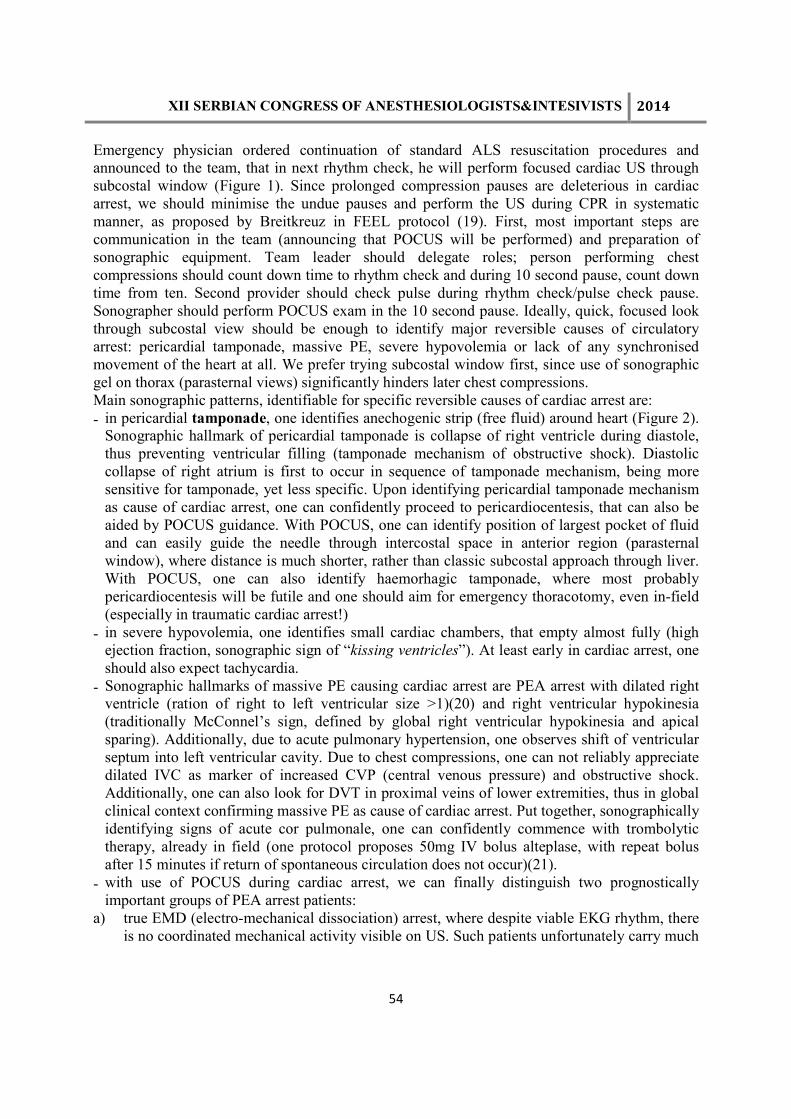
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
54
Emergency physician ordered continuation of standard ALS resuscitation procedures and announced to the team, that in next rhythm check, he will perform focused cardiac US through subcostal window (Figure 1). Since prolonged compression pauses are deleterious in cardiac arrest, we should minimise the undue pauses and perform the US during CPR in systematic manner, as proposed by Breitkreuz in FEEL protocol (19). First, most important steps are communication in the team (announcing that POCUS will be performed) and preparation of sonographic equipment. Team leader should delegate roles; person performing chest compressions should count down time to rhythm check and during 10 second pause, count down time from ten. Second provider should check pulse during rhythm check/pulse check pause. Sonographer should perform POCUS exam in the 10 second pause. Ideally, quick, focused look through subcostal view should be enough to identify major reversible causes of circulatory arrest: pericardial tamponade, massive PE, severe hypovolemia or lack of any synchronised movement of the heart at all. We prefer trying subcostal window first, since use of sonographic gel on thorax (parasternal views) significantly hinders later chest compressions. Main sonographic patterns, identifiable for specific reversible causes of cardiac arrest are: - in pericardial tamponade, one identifies anechogenic strip (free fluid) around heart (Figure 2).
Sonographic hallmark of pericardial tamponade is collapse of right ventricle during diastole, thus preventing ventricular filling (tamponade mechanism of obstructive shock). Diastolic collapse of right atrium is first to occur in sequence of tamponade mechanism, being more sensitive for tamponade, yet less specific. Upon identifying pericardial tamponade mechanism as cause of cardiac arrest, one can confidently proceed to pericardiocentesis, that can also be aided by POCUS guidance. With POCUS, one can identify position of largest pocket of fluid and can easily guide the needle through intercostal space in anterior region (parasternal window), where distance is much shorter, rather than classic subcostal approach through liver. With POCUS, one can also identify haemorhagic tamponade, where most probably pericardiocentesis will be futile and one should aim for emergency thoracotomy, even in-field (especially in traumatic cardiac arrest!)
- in severe hypovolemia, one identifies small cardiac chambers, that empty almost fully (high ejection fraction, sonographic sign of “kissing ventricles”). At least early in cardiac arrest, one should also expect tachycardia.
- Sonographic hallmarks of massive PE causing cardiac arrest are PEA arrest with dilated right ventricle (ration of right to left ventricular size >1)(20) and right ventricular hypokinesia (traditionally McConnel’s sign, defined by global right ventricular hypokinesia and apical sparing). Additionally, due to acute pulmonary hypertension, one observes shift of ventricular septum into left ventricular cavity. Due to chest compressions, one can not reliably appreciate dilated IVC as marker of increased CVP (central venous pressure) and obstructive shock. Additionally, one can also look for DVT in proximal veins of lower extremities, thus in global clinical context confirming massive PE as cause of cardiac arrest. Put together, sonographically identifying signs of acute cor pulmonale, one can confidently commence with trombolytic therapy, already in field (one protocol proposes 50mg IV bolus alteplase, with repeat bolus after 15 minutes if return of spontaneous circulation does not occur)(21).
- with use of POCUS during cardiac arrest, we can finally distinguish two prognostically important groups of PEA arrest patients:
a) true EMD (electro-mechanical dissociation) arrest, where despite viable EKG rhythm, there is no coordinated mechanical activity visible on US. Such patients unfortunately carry much

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
55
worse prognosis (22), although this prognostication tool is not validated enough yet, to be of single decision tool.
b) on the other side of PEA (pulseless electrical activity) spectrum is “pseudo-PEA”; where viable EKG rhythm is accompanied by coordinated mechanical activity of the heart (despite no palpable pulse). Despite small studies (23, 24), these patients carry much prognosis, and should probably be seen as end-spectrum of severe shock, with search for specific causes and probably strong vasopressor support (vasopressin?) Treatment options in such patients are off course not yet matter of general CPR guidelines, thus demanding additional knowledge and expertise in management of these patients! (19)
Case No. 2 72-year old male was found in his bed unresponsive. He was found with normal oxygenation and ventilation,elevated blood pressure, normal sinus rhythm, normal blood glucose, yet decreased pain responsiveness on right side of the body. History given by family was unrevealing as to cause of coma. Presumptive diagnosis of intracranial haemorrhage was made and decision taken to secure patient’s airway by RSI (rapid sequence intubation). Emergency physician chose ketamine and rocuronium for induction and paralysis. After tube placement, correct position in the trachea was confirmed by capnography. In addition to tube position confirmation by capnography, POCUS was used for additional confirmation of appropriate position in trachea. Since Lichtenstein has shown that “lung sliding” sign confirms adherence of visceral pleura to parietal (and excludes pneumothorax)(9), presence of lung sliding on anterior portion of thorax on both sides, implies successful ventilation of both lungs, thus confirms correct tube placement above carina. Similarly, visualising clear diaphragmatic excursion on both sides while mechanically ventilating the patient, confirms correct position above carina. In addition to these two POCUS applications, after tube placement, one can also make use prior or during intubation. Most important step in whole RSI cascade in first step of preparation, that must also include preparations for case of unanticipated difficult airway, including possibility and feasibility of cryco-thyrotomy. Although identification of crycothyroid membrane (CTM) is usually straight-forward with classical anatomic landmarks, difficulty can arise in case of neck trauma, obesity, malignancies, post radiation therapy etc. Since CTM is always very superficial structure with quit distinct sonographic features and it can be easily identified in longitudinal section, identifying thyroid and crycoid cartilages and membrane in-between, which length can also be measured and confirm its exact anatomical position. Additionally, with POCUS one can observe passage of endotracheal tube in real-time, either passing into trachea or into oesophagus. This technique off-course demand additional sonographer, apart from actual “intubator”, since placement of tube into trachea produces only faint movement in are of trachea, in contrast with distinct appearance of “second lumen” (“double lumen sign”) in case of oesophageal intubation. (7) Case 3: syncope/mPE Prehospital team was called on scene, where 74-year old female was found after syncope. She was alert, appeared mildly distressed, although she complained of no specific symptom, apart from “passing out on her sofa”. She was mildly tachy-dyspneic (30 breaths/minute), SpO2 of
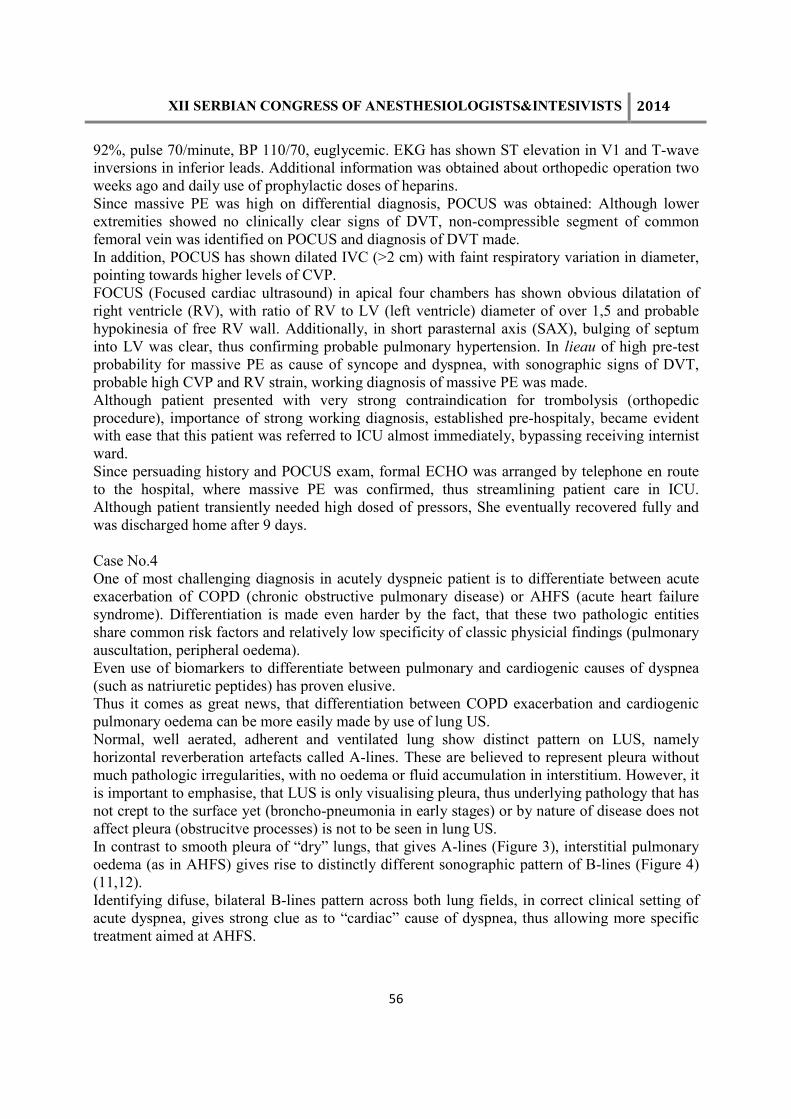
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
56
92%, pulse 70/minute, BP 110/70, euglycemic. EKG has shown ST elevation in V1 and T-wave inversions in inferior leads. Additional information was obtained about orthopedic operation two weeks ago and daily use of prophylactic doses of heparins. Since massive PE was high on differential diagnosis, POCUS was obtained: Although lower extremities showed no clinically clear signs of DVT, non-compressible segment of common femoral vein was identified on POCUS and diagnosis of DVT made. In addition, POCUS has shown dilated IVC (>2 cm) with faint respiratory variation in diameter, pointing towards higher levels of CVP. FOCUS (Focused cardiac ultrasound) in apical four chambers has shown obvious dilatation of right ventricle (RV), with ratio of RV to LV (left ventricle) diameter of over 1,5 and probable hypokinesia of free RV wall. Additionally, in short parasternal axis (SAX), bulging of septum into LV was clear, thus confirming probable pulmonary hypertension. In lieau of high pre-test probability for massive PE as cause of syncope and dyspnea, with sonographic signs of DVT, probable high CVP and RV strain, working diagnosis of massive PE was made. Although patient presented with very strong contraindication for trombolysis (orthopedic procedure), importance of strong working diagnosis, established pre-hospitaly, became evident with ease that this patient was referred to ICU almost immediately, bypassing receiving internist ward. Since persuading history and POCUS exam, formal ECHO was arranged by telephone en route to the hospital, where massive PE was confirmed, thus streamlining patient care in ICU. Although patient transiently needed high dosed of pressors, She eventually recovered fully and was discharged home after 9 days. Case No.4 One of most challenging diagnosis in acutely dyspneic patient is to differentiate between acute exacerbation of COPD (chronic obstructive pulmonary disease) or AHFS (acute heart failure syndrome). Differentiation is made even harder by the fact, that these two pathologic entities share common risk factors and relatively low specificity of classic physicial findings (pulmonary auscultation, peripheral oedema). Even use of biomarkers to differentiate between pulmonary and cardiogenic causes of dyspnea (such as natriuretic peptides) has proven elusive. Thus it comes as great news, that differentiation between COPD exacerbation and cardiogenic pulmonary oedema can be more easily made by use of lung US. Normal, well aerated, adherent and ventilated lung show distinct pattern on LUS, namely horizontal reverberation artefacts called A-lines. These are believed to represent pleura without much pathologic irregularities, with no oedema or fluid accumulation in interstitium. However, it is important to emphasise, that LUS is only visualising pleura, thus underlying pathology that has not crept to the surface yet (broncho-pneumonia in early stages) or by nature of disease does not affect pleura (obstrucitve processes) is not to be seen in lung US. In contrast to smooth pleura of “dry” lungs, that gives A-lines (Figure 3), interstitial pulmonary oedema (as in AHFS) gives rise to distinctly different sonographic pattern of B-lines (Figure 4) (11,12). Identifying difuse, bilateral B-lines pattern across both lung fields, in correct clinical setting of acute dyspnea, gives strong clue as to “cardiac” cause of dyspnea, thus allowing more specific treatment aimed at AHFS.
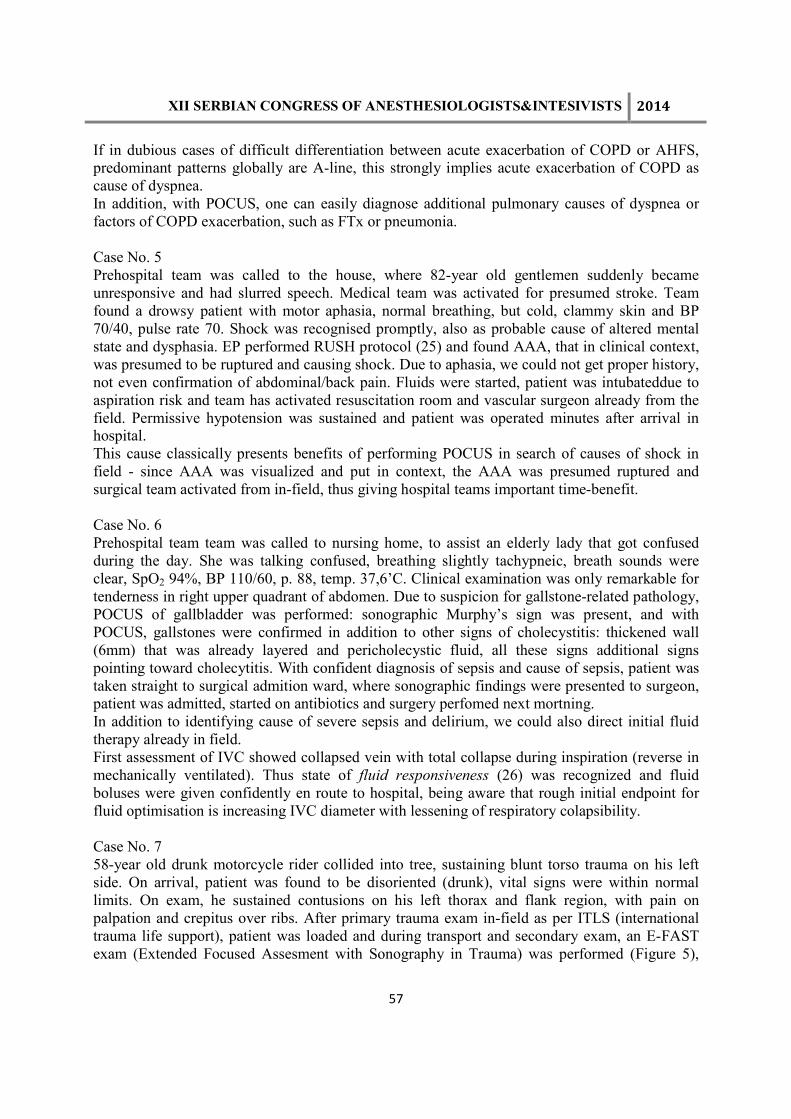
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
57
If in dubious cases of difficult differentiation between acute exacerbation of COPD or AHFS, predominant patterns globally are A-line, this strongly implies acute exacerbation of COPD as cause of dyspnea. In addition, with POCUS, one can easily diagnose additional pulmonary causes of dyspnea or factors of COPD exacerbation, such as FTx or pneumonia. Case No. 5 Prehospital team was called to the house, where 82-year old gentlemen suddenly became unresponsive and had slurred speech. Medical team was activated for presumed stroke. Team found a drowsy patient with motor aphasia, normal breathing, but cold, clammy skin and BP 70/40, pulse rate 70. Shock was recognised promptly, also as probable cause of altered mental state and dysphasia. EP performed RUSH protocol (25) and found AAA, that in clinical context, was presumed to be ruptured and causing shock. Due to aphasia, we could not get proper history, not even confirmation of abdominal/back pain. Fluids were started, patient was intubateddue to aspiration risk and team has activated resuscitation room and vascular surgeon already from the field. Permissive hypotension was sustained and patient was operated minutes after arrival in hospital. This cause classically presents benefits of performing POCUS in search of causes of shock in field - since AAA was visualized and put in context, the AAA was presumed ruptured and surgical team activated from in-field, thus giving hospital teams important time-benefit. Case No. 6 Prehospital team team was called to nursing home, to assist an elderly lady that got confused during the day. She was talking confused, breathing slightly tachypneic, breath sounds were clear, SpO2 94%, BP 110/60, p. 88, temp. 37,6’C. Clinical examination was only remarkable for tenderness in right upper quadrant of abdomen. Due to suspicion for gallstone-related pathology, POCUS of gallbladder was performed: sonographic Murphy’s sign was present, and with POCUS, gallstones were confirmed in addition to other signs of cholecystitis: thickened wall (6mm) that was already layered and pericholecystic fluid, all these signs additional signs pointing toward cholecytitis. With confident diagnosis of sepsis and cause of sepsis, patient was taken straight to surgical admition ward, where sonographic findings were presented to surgeon, patient was admitted, started on antibiotics and surgery perfomed next mortning. In addition to identifying cause of severe sepsis and delirium, we could also direct initial fluid therapy already in field. First assessment of IVC showed collapsed vein with total collapse during inspiration (reverse in mechanically ventilated). Thus state of fluid responsiveness (26) was recognized and fluid boluses were given confidently en route to hospital, being aware that rough initial endpoint for fluid optimisation is increasing IVC diameter with lessening of respiratory colapsibility. Case No. 7 58-year old drunk motorcycle rider collided into tree, sustaining blunt torso trauma on his left side. On arrival, patient was found to be disoriented (drunk), vital signs were within normal limits. On exam, he sustained contusions on his left thorax and flank region, with pain on palpation and crepitus over ribs. After primary trauma exam in-field as per ITLS (international trauma life support), patient was loaded and during transport and secondary exam, an E-FAST exam (Extended Focused Assesment with Sonography in Trauma) was performed (Figure 5),

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
58
where PTx was confidently ruled out on both sides, as was haemothorax. On the side of thoracic contusion, sonographic sign called “B-lines” was found, indication “interstitial syndrome”. In clinical context of blunt thoracic trauma, pointing to lung contusion. On further FAST sonographic exam, free intraperitoneal fluid was identified around spleen, and cardiac tamponade excluded. Both sonographic findings were later confirmed by CT. In this case, performing E-FAST exam in field has enabled to diagnose pulmonary contusion and peritoneal haemorrhage in minutes! Although diagnosis of pulmonary contusion carried no immediate management repercussions, finding of free intraperitoneal fluid added important information; patient was recognised as immediately higher risk and information about positive FAST exam was communicated to receiving trauma center, among other things. As per modern trauma management, patients with positive FAST exam deserve to receive CT scan if “stable” and need prompt laparotomy if haemodinamically unstable (Figure 6)(7). Receiving aforementioned information en route to hospital, trauma team could better prepare, anticipating possible consequences of internal bleeding and lung contusion, alerting radiology dept. and blood bank. In addition, emergency physician in field, by very sensitive exclusion of PTx, was more confident of indication for mechanical ventilation if need arose. References: 1. http://www.eusem.org/whatisem/ 2. Lichtenstein D, Goldstein I, Mourgeon E, Cluzel P, Grenier P, Rouby JJ. Comparative
diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004;100(1): 9-15
3. Beck-Razi N, Gaitini D. Focused assessment with sonography for trauma. Ultrasound Clinics 2008; 3(1): 23–31
4. Moore CL, Copel JA. Point-of-care ultrasonography. NEJM 2011;364(8):749-57 5. Various. Emergency ultrasound guidelines-ACEP clinical policy. Ann Emerg Med 2009;
53:550-70 6. Via G, Hussain A, Wells M, Reardon R, ElBarbary M, Noble VE et al. International
Evidence-based recommendations for Focused Cardiac Ultrasound. J A Soc Echo 2014; 27(7): 683e1-e32
7. Chou HC, ChongKM, SimSS, MaMH, LiuSH, ChenNC et al. Real-time tracheal ultrasonography for confirmation of endotracheal tube placement during cardiopulmonary resuscitation. Resuscitation2013; doi:10.1016/j.resuscitation.2013.06.018
8. OsmanAB, ChuanTW, ManikamR. A feasibility study on bedside upper airway ultrasonography compared to waveform capnography for verifying endotracheal tube location after intubation. Crit Ultrasound J 2013; 5(1):7
9. Lichtenstein D, MenuY. A Bedside Ultrasound Sign Ruling Out Pneumothorax in the Critically III: Lung Sliding. Chest 1995; 108:1345–1353
10. Parlamento S, Copetti R, Di Bartolomeo S. Evaluation of lung ultrasound for the diagnosis of pneumonia in the ED. The American Journal of Emergency Medicine 2009;27(4): 379–384
11. Lichtenstein et al. The comet-tail artifact. An ultrasound sign of alveolar-interstitial syndrome. American journal of respiratory and critical care medicine 1997,156 (5):1640-9
12. Lichtenstein DA, Mezière GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 2008, 134 (1):117-25
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
59
13. Xirouchaki N, GeorgopoulosD. The use of lung ultrasound: A brief review for critical care physicians and pneumonologists. Pneumonology 2012; 35: 212-25
14. RoccoM, CarboneI, Morelli A, Bertoletti L, RossiSS, Vitale M et al.Diagnostic accuracy of bedside ultrasonography in the ICU: feasibility of detecting pulmonary effusion and lung contusion in patients on respiratory support after severe blunt thoracic trauma. Ac Anaesth Scand2008; 52(6): 776–84
15. Mathis G,Blank W, Reißig A. Thoracic ultrasound for diagnosing pulmonary embolism: a prospective multicenter study of 352 patients; Chest 2005 Sep;128(3):1531-8
16. TayalVS, GrafCD, GibbsMA.Prospective study of accuracy and outcome of emergency ultrasound for abdominal aortic aneurysm over two years. AcEmerg Med2003; 10(8): 867–71
17. Burnside PR, Brown MD, Kline JA. Systematic review of emergency physician-performed ultrasonography for lower-extremity deep vein thrombosis. Acad Emerg Med 2008;15(6): 493–498
18. DubourgJ, Javouhey E, Geeraerts T, MessererM, Kassai B. Ultrasonography of optic nerve sheath diameter for detection of raised intracranial pressure: a systematic review and meta-analysis. Intensive Care Med2011; 37(7): 1059–68
19. Breitkreutz R; Walcher F, Seeger FH. Focused echocardiographic evaluation in resuscitation management: Concept of an advanced life support–conformed algorithm. CritCare Med 2007; 35: S150–S161
20. Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a Scientific Statement from the American Heart Association. Circulation 2011;123:1788-1830
21. Fengler BT, Brady WJ. Fibrinolytic therapy in pulmonary embolism: an evidence- based treatment algorithm. Am J Emerg Med 2009;27:84-95
22. Salen P, Melniker L, Chooljian C, et al. Does the presence or absence of sonographically identified cardiac activity predict resuscitation outcomes of cardiac
arrest patients? Am J Emerg Med 2005;23:459–62 23. ProsenG, Križmarić M, Završnik J, Grmec S. Impact of modified treatment in
echocardiographically confirmed pseudo-pulseless electrical activity in out-of-hospital cardiac arrest patients with constant end-tidal carbon dioxide pressure during compression pauses. J Int Med Research2010; 38(4): 1458–67.
24. BreitkreutzR, Price S, SteigerHV, SeegerFH, lIperH, AckermannH et al. Focused echocardiographic evaluation in life support and peri-resuscitation of emergency patients: a prospective trial. Resuscitation2010; 81(11): 1527–33
25. Perera P, Mailhot T, Riley D, Mandavia D. The RUSH Exam: Rapid Ultrasound in SHock in the evaluation of the critically ill. Emerg Med Clin N Am 2010; 28: 29–56
26. Lanspa MJ, GrissomK, HirshbergEL, JonesJP, BrownSM. Applying Dynamic Parameters to Predict Hemodynamic Response to Volume Expansion in Spontaneously Breathing Patients With Septic Shock. Shock. 2013;39(2):155-60
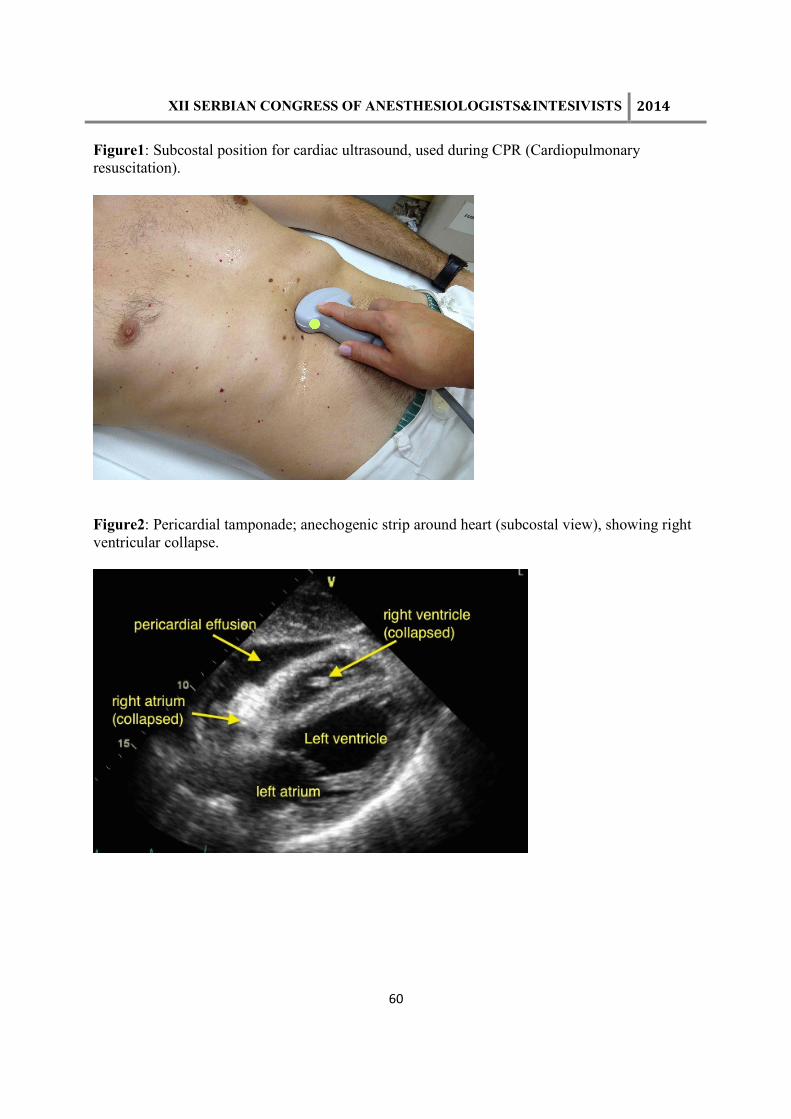
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
60
Figure1: Subcostal position for cardiac ultrasound, used during CPR (Cardiopulmonary resuscitation).
Figure2: Pericardial tamponade; anechogenic strip around heart (subcostal view), showing right ventricular collapse.
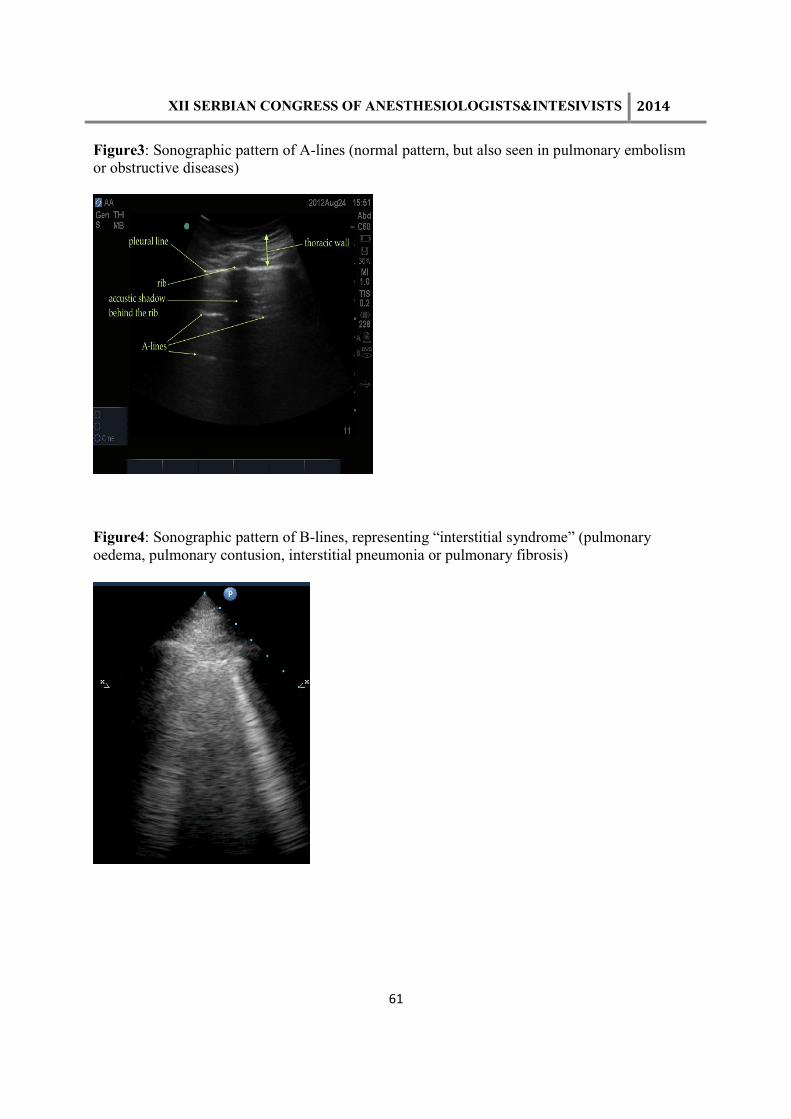
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
61
Figure3: Sonographic pattern of A-lines (normal pattern, but also seen in pulmonary embolism or obstructive diseases)
Figure4: Sonographic pattern of B-lines, representing “interstitial syndrome” (pulmonary oedema, pulmonary contusion, interstitial pneumonia or pulmonary fibrosis)
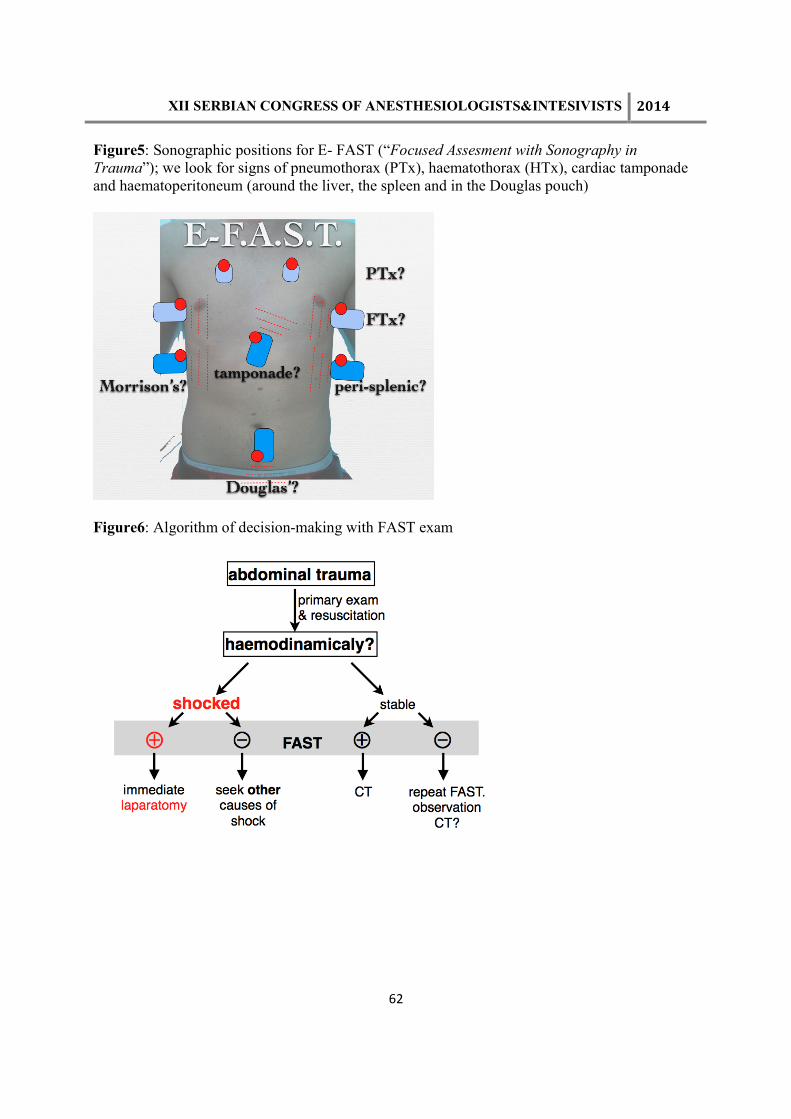
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
62
Figure5: Sonographic positions for E- FAST (“Focused Assesment with Sonography in
Trauma”); we look for signs of pneumothorax (PTx), haematothorax (HTx), cardiac tamponade and haematoperitoneum (around the liver, the spleen and in the Douglas pouch)
Figure6: Algorithm of decision-making with FAST exam

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
63
CLINICAL USE OF HIGH FREQUENCY JET VENTILATION DUSANKA JANJEVIC ENT Clinic, Dept of Anaesthesiology,Clinical Centre of Vojvodina,Novi Sad,Serbia E-mail:[email protected] Jet ventilation (JV) is an alternative ventilatory technique with specific advantages when used for diagnostic or surgical procedures in patients with airway pathology. Direct examination and surgical procedures involving the larynx require close cooperation between the laryngologist and the anaesthetist as a balance must be achieved between adequate surgical access and safe, effective ventilation JV was introduced for that purpose in three different modes:
• transtracheal jet ventilation – skin and trachea are punctured by the jet needle below the larynx
• supraglottic jet ventilation – the jet blows into the laryngoscope, which is tightly positioned to the larynx
• translaryngeal (subglottic) jet ventilation – a small catheter is introduced through the larynx into the trachea.
Endolaryngeal surgery with rigid laryngoscopes has an important place in solving various pathologic conditions of the larynx and trachea. Advantages offered by HFJV for intraoperative ventilation of anaesthetized patients were reported as follows: positioning of small bore catheter or cannula in the presence of airway lesions with less effort than large tubes, performance of laser surgery with less risk, by avoiding the use of flammable plastic materials, improvement of surgical access and viewing of the larynx due to the small-bore tubes, simplifying access to a near motionless surgical field and smoother process of surgery, reduced risk of aspiration of blood and debris due to continuous outflow of gases. Jet ventilation vs. Conventional ventilation. During JV gas from a high pressure source is delivered through a small-bore cannula positioned in the airway. Because of the narrow outflow orifice, a jet effect is produced, entraining gas around the cannula. HFJV achieves gas exchange by using subphysiologic tidal volumes applied at extreme rates. The traditional concepts of applied physiology to the mechanisms of normal or conventional mechanical ventilation (CV) are not completely applicable to JV. During the JV good gas exchange and the efficiency of CO2 elimination can be maintained with a tidal volume not larger than the dead space. The principles of oxygenation during HFV are similar to those during (CV) and oxygenation is dependent on an optimal lung volume recruitment strategy and consequent reduction of intrapulmonary shunting of blood. In contrast to CV, where a bulk gas volume is rather slowly pushed forward into the airway via a large bore tube (an endotracheal tube) that is fitted airtight to the trachea, JV consists of the rapid gas insufflations with high velocity via a narrow nozzle into the open airway.
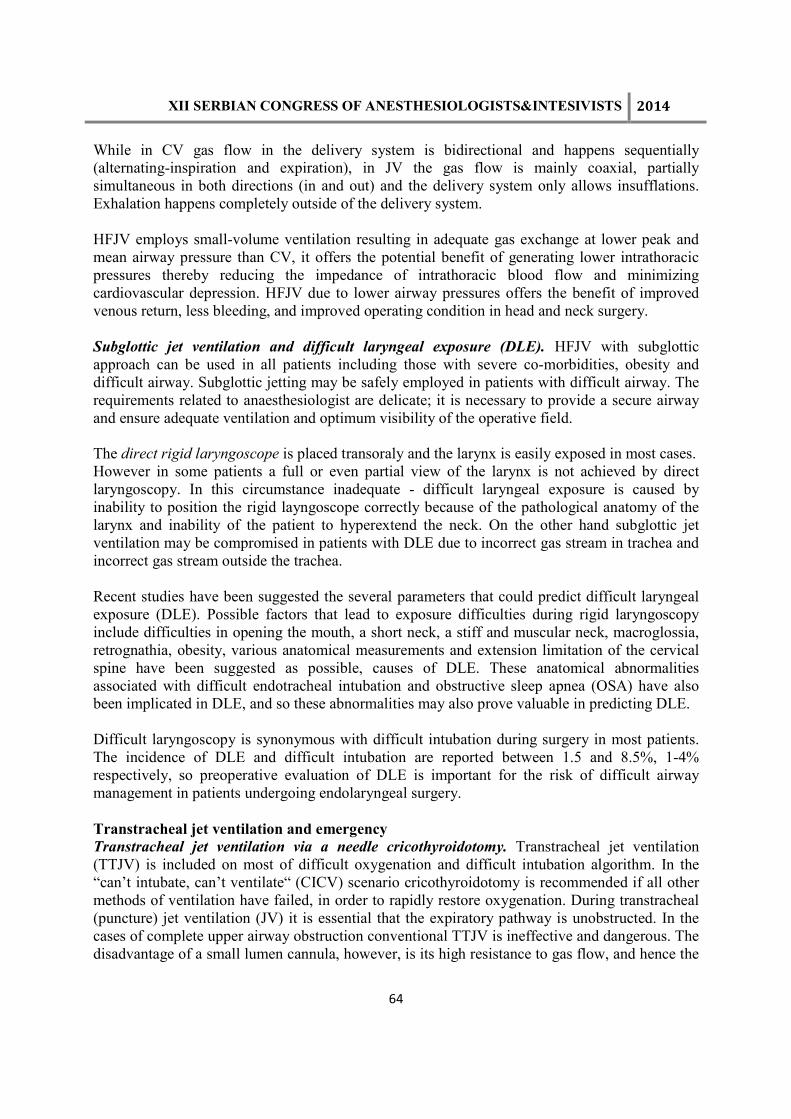
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
64
While in CV gas flow in the delivery system is bidirectional and happens sequentially (alternating-inspiration and expiration), in JV the gas flow is mainly coaxial, partially simultaneous in both directions (in and out) and the delivery system only allows insufflations. Exhalation happens completely outside of the delivery system. HFJV employs small-volume ventilation resulting in adequate gas exchange at lower peak and mean airway pressure than CV, it offers the potential benefit of generating lower intrathoracic pressures thereby reducing the impedance of intrathoracic blood flow and minimizing cardiovascular depression. HFJV due to lower airway pressures offers the benefit of improved venous return, less bleeding, and improved operating condition in head and neck surgery.
Subglottic jet ventilation and difficult laryngeal exposure (DLE). HFJV with subglottic approach can be used in all patients including those with severe co-morbidities, obesity and difficult airway. Subglottic jetting may be safely employed in patients with difficult airway. The requirements related to anaesthesiologist are delicate; it is necessary to provide a secure airway and ensure adequate ventilation and optimum visibility of the operative field. The direct rigid laryngoscope is placed transoraly and the larynx is easily exposed in most cases. However in some patients a full or even partial view of the larynx is not achieved by direct laryngoscopy. In this circumstance inadequate - difficult laryngeal exposure is caused by inability to position the rigid layngoscope correctly because of the pathological anatomy of the larynx and inability of the patient to hyperextend the neck. On the other hand subglottic jet ventilation may be compromised in patients with DLE due to incorrect gas stream in trachea and incorrect gas stream outside the trachea. Recent studies have been suggested the several parameters that could predict difficult laryngeal exposure (DLE). Possible factors that lead to exposure difficulties during rigid laryngoscopy include difficulties in opening the mouth, a short neck, a stiff and muscular neck, macroglossia, retrognathia, obesity, various anatomical measurements and extension limitation of the cervical spine have been suggested as possible, causes of DLE. These anatomical abnormalities associated with difficult endotracheal intubation and obstructive sleep apnea (OSA) have also been implicated in DLE, and so these abnormalities may also prove valuable in predicting DLE. Difficult laryngoscopy is synonymous with difficult intubation during surgery in most patients. The incidence of DLE and difficult intubation are reported between 1.5 and 8.5%, 1-4% respectively, so preoperative evaluation of DLE is important for the risk of difficult airway management in patients undergoing endolaryngeal surgery. Transtracheal jet ventilation and emergency Transtracheal jet ventilation via a needle cricothyroidotomy. Transtracheal jet ventilation (TTJV) is included on most of difficult oxygenation and difficult intubation algorithm. In the “can’t intubate, can’t ventilate“ (CICV) scenario cricothyroidotomy is recommended if all other methods of ventilation have failed, in order to rapidly restore oxygenation. During transtracheal (puncture) jet ventilation (JV) it is essential that the expiratory pathway is unobstructed. In the cases of complete upper airway obstruction conventional TTJV is ineffective and dangerous. The disadvantage of a small lumen cannula, however, is its high resistance to gas flow, and hence the
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
65
need for a high driving pressure to achieve adequate flow. The occlusion of the expiratory pathway rapidly leads to hypoventilation, manifested by hypercarbia and hypoxemia, and interferes with cardiac output by increasing the intrathoracic pressure, with the risk of producing
serious barotrauma to the lung. Recently reviews (Hamaekers at al.) suggested the ejectors capable of creating suction by the Bernoulli principle, which facilitate expiration through small-bore catheters. Further research may confirm the clinical the clinical applicability Prophylactic placement of cricothyroidotomy cannula. Transtracheal jet ventilation (TTJV) must be viewed as procedure providing adequate gas-exchange and ensuring the patency of the airway until a definitive procedure such as oral intubation or surgical tracheotomy can be performed especially in laryngeal (upper airway) surgery. With transtracheal JV it is vital to keep the upper airway as open as possible with jaw thrust and to verify deflation of the lungs and exhalation through the upper airway. If the system is closed barotrauma becomes a real and serious risk.
Conclusion. JV can be a valuable and highly effective tool to optimize conditions during airway surgery. The usage of this technique requires: clinical training of skill, profound knowledge of basic physical properties of JV and clinical experience. References
1. Ihra G, Gockner G, Kashanipour A, Aloy A. High-frequency jet ventilation in European and North American institutions: developments and clinical practice. Eur J Anaesthesiol. 2000;17(7):418-30.
2. Bacher A, Lang T, Weber J, Aloy A. Respiratory efficacy of subglottic low-frequency, subglottic combined-frequency, and supraglottic combined-frequency jet ventilation during microlaryngeal surgery. Anesth Analg. 2000;91(6):1506-12.
3. Hunsaker DH. Anesthesia for microlaryngeal surgery: the case for subglottic jet ventilation. Laryngoscope 1994;104( Suppl 65):1-30.
4. Rezai-Majd A, Bigenzahn W, Denk D-M, et al. Superimposed high-frequency jet ventilation (SHFJV) for endoscopic laryngotracheal surgery in more than 1500 patients. Br J Anaesth 2006;96:650-9.
5. Brooker CR, Hunsaker DH, Zimmerman AA. A new anesthetic system for microlaryngeal surgery. Otolaryngol Head Neck Surg 1998;118(1):55-60.
6. Santos P, Ayuso A, Luis M, Martinez G, Sala X. Airway ignition during CO2 laser laryngeal surgery and high frequency jet ventilation. Eur J Anaesthesiol. 2000;17(3):204-7.
7. Lanzenberger-Schragl E, Donner A, Grasl MC, Zimpfer M, Aloy A. Superimposed high-frequency jet ventilation for laryngeal and tracheal surgery. Arch Otolaryngol Head Neck Surg. 2000;126(1):40-4.
8. Leiter R, Aliverti A, Priori R, Staun P, Lo Mauro A, Larsson A, Frykholm P. Comparison of superimposed high-frequency jet ventilation with conventional ventilation for laryngeal surgery. Br J Anaesth 2012;108(4):690-7.
9. Ihra G, Aloy A. On the use of Venturi's principle to describe entrainment during jet ventilation. J Clin Anesth. 2000;12(5):417-9.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
66
10. Janjevic D: Jet ventilation for difficult intubationsand Emergencies, joined Papers on Jet Ventilation. Edited by Baer GA.Tampere, Tampere University Press, 2011.
11. Henderson JJ., Popat MT., LattoIP., Pearce AC. Difficult Airway Society quidelines for management of the unanticipated difficult intubation. Anaesthesia 2004;59:675-94.
12. Popet M., Dudnikov S. Management of the obstructed upper airway. In Current Anaesthersia and Critical Care. Focus on Difficult Airway, ed Pollard BJ.Harcourt Publicher Ltd, London 2001;12:225-3.
13. Patel R. Percutaneous transtracheal jet ventilation:a safe, quick and temporary way to provide oxygenation and ventilation when convencional methods are unsuccessful. Chest 1999;116:1689-94.
14. Mace SE., Khan N. Needle cricothyroidotomy. Emerg.Med Clin.Nort Am 2008;26(4):1085-101.
15. Ross-Anderson DJ., Ferguson C, Patel A. Transtracheal jet ventilation in 50 patients with severe airway compromise and stridor. Br J Anaesth 2011;106 (1):140-144.
16. Schuh JR., Bettendorf R., Shapiro D. et al. Comfirmation of needle cricothyroidotomy using an esophageal detector devices in a porcian model. Mil Med 2010;275(9):686-687.
17. Roh JL, Lee YW. Prediction difficult laryngeal exposure in patients undergoing microlaryngosurgery. Ann Otol Rhinol Laryngol 2005;114:614-20.
18. Pinar E, Calli C, Oncel S, Selek B, Tatar B. Preoperative clinical prediction of difficult laryngeal exposure in suspension laryngoscopy. Eur Arch Otorhinolaryngol 2009;266:699-703.
19. Hsiung MW, Pai L, Kang BH, Wang BL, Wong CS, Wang HW. Clinical predictors of difficult laryngeal exposure. Laryngoscope 2004;114:358-63.
20. Bourgain JL, Chollet M, Fischler M, Gueret M, Mayne A. Guide for the use of jet ventilation during ENT and oral surgery. Ann Fr Anaesth Reanim. 2010;29(10):720-727.
21. Bouldi M, Bearfield P. Techniques for emergency ventilation through a needle cricithyroidotomy. Anaesthesia 2008;63:535-9.
22. Gulleth Y. TTJV as an option in airway management in head and neck surgery. Arch Otolaryngol Head Neck Surg. 2005;131(10):886-90
23. Friedrich G, Kiesler K, Gugatschka M. Curved rigid laryngoscope: missing link between direct suspension laryngoscopy and indirect techniques? Eur Arch Otorhinolaryngol 2009;266(10):1583-8.
24. Chandradeva K, Palin C, Ghosh SM. Perccutaneous transtracheal jet ventilation as a guide in severe upper airway obstruction from supraglottic oedema. Br J Anaesth 2005;94:683-6.
25. Cook TM, Alexander R. Major complications during anaesthesia for elective laryngeal surgery in the UK: a national survey of the use of high-pressure source ventilation. Br J Anaesth 2008;101:266-72.
26. Mausser G, Friedrich G, Schwarz G. Airway management and anesthesia in neonatus, infants and children during endolaryngotracheal surgery. Paediatr Anaesth 2007;17:942-7.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
67
THE ART OF SEDATION FOR DIFFICULT AIRWAY DUSICA STAMENKOVIC1, NEBOJSA LADJEVIC2,3, ALEKSANDAR TOMIC4, IVAN MARJANOVIC4, GORAN RONDOVIC1 1Department of Anesthesiology and Intensive Care, Belgrade, Serbia, 2Centre for anesthesia and resuscitation, Clinical Center Serbia, Belgrade, Serbia, 3Medical School, University of Belgrade, Serbia, 4Department of Vascular and Endovascular Surgery, Belgrade, Serbia E mail:[email protected]. Introduction
The safety of patient with difficult airway is the most important issue during tracheal intubation. In the situation where both, patient’s safety and commodity are desirable, possibility for alternative method must be assured 1. Spontaneous breathing with adequate oxygenation and sedated but easy arousable patient are “must” in sedation for difficult airway. General anesthesia and muscle relaxation is suggested for educational purposes only in patient with regular airway. The major risk of sedation is the danger that light sedation can become profound sedation with compromised airway. This is possible scenario in uncooperative and exaggerated patient where additional dose of medication can lead to excessive sedation and compromised oxygenation. Moreover, the expert’s advice is implementation of method preferred and well known by provider for difficult airway situation. Even general anesthesia with adequate oxygenation and planned options for difficult airway are better solution than situation of excessive sedation with risk of emergency general anesthesia in hypoxic patients after numerous unsuccessful attempts for intubation. High risk patients including severe comorbid states, obesity and pregnancy are prone to desaturation and vigorous preoxygenation and oxygenation throughout the procedure is mandatory 2. In the literature medications used for sedation are classified as medications used for pretreatment and treatment. Pretreatment medications
Pretreatment medications are used three minutes before the actual act of intubation and the main aim for their use is to blunt stress response to laryngoscopy and tracheal intubation. Usually, tracheal intubation causes stimulation of sympathetic and parasympathetic nerves responsible for airway innervation and physiological response as hypertension, tachycardia, intracranial pressure increase, bronchoconstriction and cough. These changes can lead to exacerbation of comorbidities and even worsening the state that was reason for intubation. Numerous medications used for blunting the reflexes during intubation were analyzed in the clinical practice. Lidocaine, an amide local anesthetic (1.5 mg/kg IV) needs up to 45-90 s for effect. It is shown that lidocaine decreases level of intracranial pressure elevation and decreases the airway resistance in patients with reactive airway. Fentanyl, an opioid (1-3 µg kg-1) needs 2-3 mins for effect which lasts for up to 60 mins and reduces sympathetic response during tracheal intubation. This is of special concern in patients with ischemic heart or brain disease, abdominal aneurysm and existing hypertension.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
68
“Awake” intubation
Awake intubation is preferred way for difficult airway, this term covers regional anesthesia, in combination with sedative and opioid medications. Additional medications suggested to be ready for use are opioid and benzodiazepine antagonists in case of oversedation and vasopressores in case of hypotension. Usual medications used for sedation during difficult airway intubation are benzodiazepines, opioids, propofol, ketamine and dexmedetomidine. Use of sedation enables better intubation conditions during rapid sequence intubation. Hypotension increases morbidity and mortality during intubation, and phenylephrine or ephedrine use is suggested in this situation. The major rules for fiberoptic intubation are adequate oxygenation with spontaneous breathing, sedated patient and deprived laryngeal reflexes. It is vital to explain the complete procedure to patient including the possibility of emergency tracheostomy if necessary. Airway cleared of blood and saliva is important, so antisialogogue is the first medication used, usually 20 mins before intubation if use of video equipment is planned. Atropine, glyccopyrolate and scopolamine are used as antisialogogues 3. Midazolam (0.025-0.05 mg kg-1), is effective after 1 to 2 mins intravenous application and at least minimum two minutes period is suggested between successive doses. Beside sedation, midazolam provides amnesia. If excessive sedation occurs, flumazenil 0.5 mg in one minute period time with maximum of 3 mg is used. Haloperidol, butirophenon (2-3 mg IV or 5-10 mg IM), needs 5-20 mins for its action to start. Potential complications are extrapyramidal symptoms, hypotension and arrhythmia4. Dexmedetomidine (DEX), an α-2 agonist, is an ideal medication for sedation in patients with compromised airway 4. No respiratory depression occurs, but bradycardia and hypotension can jeopardize its use, and only infusion is suggested (1-7 µg kg-1 h-1). Combination of midazolam and DEX are superior combination for “awake” intubation 4. Remifentanyl used as target controlled infusion (TCI, 0.8 ng mL-1) or manually controlled infusion (0.02-0.075 µg kg-1 min-1) is the first line opioid in sedation for difficult airway 5,6. Propofol used as TCI or manually controlled infusion and sevoflurane are also used successfully for sedation in the case of difficult airway 7. Regional anesthesia
Regional anesthesia includes airway topicalization and regional blocks. Lidocaine 4% can be used as aerosole and gel. Three regional blocks are performed for upper airway anesthesia: n. glossopharyngeus, n. laryngeus superior and transtracheal block. Muscular relaxation drugs
The avoidance of muscle relaxation medications is generally advised. If rocuronim was used, sugammadex selective relaxant binding agent reversing rocuronium-induced neuromuscular blockade provides rapid reversal of deep muscular block 8. Sugammadex 16 mg kg⁻¹ can be used

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
69
for the immediate reversal of neuromuscular block, 3 mins after administration of rocuronium and could be used in place of succinylcholine for emergency intubation 9. Special problem is difficult airway in out of hospital situation. Usually difficult airway problem arises in facial injury, obesity, tumors, previous surgery and additional problems are medical staff expertise and patient’s position. Supralaryngeal devices and combitube are suggested for use in these patients, with etomidate and low dose midazolam if needed 10. Conclusion
Combination of antisialogogue, midazolam with DEX or remifentanyl and regional anesthesia can provide good condition for tracheal intubation with preserved spontaneous breathing and oxygenation. The ideal choice depends from patient’s characteristics and situation. Literature
1. Johnston KD, Rai MR. Conscious sedation for awake fibreoptic intubation: a review of the literature. Can J Anaesth. 2013;60:584-99. 2.Kristensen MS. Airway management and morbid obesity. Eur J Anaesthesiol. 2010;27:923-7. 3.Rosenstock CV, Thøgersen B, Afshari A, Christensen AL, Eriksen C, Gätke MR. Awake fiberoptic or awake video laryngoscopic tracheal intubation in patients with anticipated difficult airway management: a randomized clinical trial. Anesthesiology. 2012;116:1210-6. 4.Celis-Rodríguez E, Birchenall C, de la Cal MÁ, Castorena Arellano G, Hernández A, Ceraso D, et al. Clinical practice guidelines for evidence-based management of sedoanalgesia in critically ill adult patients. Med Intensiva. 2013; 37:519-74. 4. Bergese SD1, Candiotti KA, Bokesch PM, Zura A, Wisemandle W, Bekker AY; AWAKE Study Group. A Phase IIIb, randomized, double-blind, placebo-controlled, multicenter study evaluating the safety and efficacy of dexmedetomidine for sedation during awake fiberoptic intubation. Am J Ther. 2010;17:586-95. 5.Zhang X, He W, Wu X, Zhou X, Huang W, Feng X. TCI remifentanil vs. TCI propofol for awake fiber-optic intubation with limited topical anesthesia. Int J Clin Pharmacol Ther. 2012;50:10-6. 6.Fotopoulou G, Theocharis S, Vasileiou I, Kouskouni E, Xanthos T. Management of the airway without the use of neuromuscular blocking agents: the use of remifentanil. Fundam Clin Pharmacol. 2012;26:72-85. 7.Péan D, Floch H, Beliard C, Piot B, Testa S, Bazin V, Lejus C, Asehnoune K. Propofol versus sevoflurane for fiberoptic intubation under spontaneous breathing anesthesia in patients difficult to intubate. Minerva Anestesiol. 2010;76:780-6. 8.Sørensen MK, Bretlau C, Gätke MR, Sørensen AM, Rasmussen LS. Rapid sequence induction and intubation with rocuronium-sugammadex compared with succinylcholine: a randomized trial. Br J Anaesth. 2012;108:682-9. 9. Chambers D, Paulden M, Paton F, Heirs M, Duffy S, Hunter JM, Sculpher M, Woolacott N. Sugammadex for reversal of neuromuscular block after rapid sequence intubation: a systematic review and economic assessment. Br J Anaesth. 2010;105:568-75. 10.Gaither JB, Spaite DW, Stolz U, Ennis J, Mosier J, Sakles JJ. Prevalence of Difficult Airway Predictors in Cases of Failed Prehospital Endotracheal Intubation. J Emerg Med. 2014. pii: S0736-4679(14)00378-3. doi: 10.1016/j.jemermed.2014.04.021.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
70
PERI-OPERATIVE STRATEGY IN PATIENTS WITH INHERITED BLEEDING DISORDERS DANIELA FILIPESCU University of Medicine Carol Davila. Emergency Institute for Cardiovascular Diseases Bucharest, Romania Once considered prohibitive, surgery in patients with inherited bleeding disorders (IBDs) is considered a challenge nowadays, due to the risk of haemorrhagic complications. However, good outcome is possible if patients are carefully cared by an experienced team (1-4). Although the anesthesiologist should work together with the hematologist the perioperative management plan, a thorough understanding of these diseases is necessary. Bleeding disorders can be classified as disorders of primary hemostasis which include von Willebrand disease (vWD) and platelet defects, and disorders of secondary hemostasis which include coagulation factor deficiencies. Von Willebrand disease (VWD) is the most common IBD with an estimated prevalence of 0.6-1.3% (5). It affects both sexes and is caused by deficiency or abnormality of von Willebrand factor (vWF), which facilitates adhesion of platelets to the endothelium, and also carries and stabilizes factor VIII (FVIII) in the circulation. The current classification of inherited VWD (types 1, 2A, 2B, 2N, 2M and 3) is important to determine the risk of bleeding and to select the best therapeutic approach (6). The bleeding phenotype is variable, but generally, mild to moderate, except for type 3, which is usually severe (7). The most frequent bleeding symptoms are epistaxis and menorrhagia, but surgery may increase dramatically the risk of bleeding. If vWD is suspected, laboratory screening tests include measurements of von Willebrand antigen and ristocetin cofactor activity along with FVIII coagulant activity (5). A low level of vWF is not sufficient for defining the disease, as low level can be encountered in normal people, especially in those with blood group type 0 (8). The mainstays of therapy in vWD related bleedings include desmopressin and exogenous factor replacement. Desmopressin is a vasopressin synthetic analogue which stimulates endogenous release of vWF and FVIII from the endothelium (9). Desmopressin is effective in most cases of vWD type 1, variable effective in type 2A, 2N and 2M vWD, because any increase in vWF is dysfunctional, and ineffective in type 3 vWD, because there are no releasable stores of vWF (6). A test-infusion should be given to all patients with clinically relevant vWD to predict clinical efficacy during procedure (10). The usual dose is 0.3 µg kg−1 in 30–50 mL of normal saline given iv. over 30 min. and repeated every 12 to 24 hours, generally 2-4 doses. Peak increases in VWF and FVIII are observed between 30 and 90 min after infusion and should be monitored by factor levels and possibly by a platelet function point of care devices (5,9). The main adverse effects of desmopressin are tachyphylaxis, fluid retention and hyponatremia (9). Standard replacement therapy for vWD is represented by plasma-derived, viral-inactivated concentrates which contain vWF (11). Patients undergoing elective surgery should receive a concentrate infusion 6 to 8 hours before the procedure in order to allow enough time for new synthesis of endogenous FVIII (5,6). In emergency situations, concentrates containing large quantities of FVIII are preferred to obtain a more rapid effect. The recommended perioperative target levels and duration of therapy depend on the type of surgery (Table 1). Perioperative

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
71
monitoring of VWF/FVIII levels is recommended to avoid supernormal levels of vWF/FVIII which may increase the risk of VTE (12). Cryoprecipitate represents an alternative to concentrates for treating vWD-related bleeding when desmopressin is inefficient and factor concentrates are not available. Platelet concentrates are effective, particularly in patients with type 3 vWD, probably because of their role in transporting vWF to sites of vascular injury (13). Antifibrinolytics are useful adjuvants to clot stabilization. In dental surgery they can be used alone or along with desmopressin (5). Inherited platelet defects (IPD) are uncommon and heterogeneous conditions that can alter circulating platelet numbers, function or both. Due to the multiple roles of platelets in hemostasis there are many classifications of IPD (14). However, they are less relevant in practice, as most of defects have mild to moderate bleeding phenotype and they are usually referred as mild bleeding disorders (MBDs) (15). The exceptions are represented by Glanzmann’s thrombasthenia and Bernard-Soulier syndrome, which may result in severe bleeding. Glanzmann’s thrombasthenia is characterized by a deficiency or functional defect of glycoprotein (GP) IIb/IIIa platelet membrane receptor, resulting in impaired platelet adhesion and aggregation. Bernard-Soulier syndrome is due to dysfunction or absence of the GP Ib/IX/V, resulting in abnormal adhesion of platelets to subentothelial-bound VWF (14). The diagnosis of IPD is based on classical aggregometry. The new point-of-care devices for platelet function are not validated in clinical practice for the diagnosis of these disorders (16). Most MBDs are responsive to desmopressin and/or antifibrinolytics given prior to dental extractions and minor surgery regardless of their specific defect (17). If these agents are not effective, patients with IPD should receive HLA-selected platelets or possibly recombinant activated FVII (rFVIIa) (18). Recombinant FVIIa is licensed for use in Glanzmann’s thrombasthenia, where refractoriness to platelet transfusions has been demonstrated. A suggested regime would be a dose of 90 µg kg-1 given immediately prior to the procedure and repeated every 2 hours for 12 hours, then at increasing intervals of 3-4 hours, until the patient is considered to be no longer at risk of bleeding (19). Haemophilias are the most frequent IBDs. Haemophilia A is characterized by a reduced plasma FVIII coagulant activity and haemophilia B by the deficiency of FIX. Both are X-linked recessive disorders with a prevalence of 1:10 000 and 1:60 000 male births, respectively (20). The severity of haemophilias relate directly to the degree of deficiencies, classified according to the factor level, as: severe (< 0.01 IU mL-1), moderate (0.01-0.05 IU mL-1) or mild (> 0.05-0.40 IU mL-1) (21). However, there is a discrepancy between the level of factor and bleeding phenotype, and some female-carriers may also have reduced coagulation factor levels. The haemostatic response in patients who develop antibodies (also known as “inhibitors”) against FVIII or FIX, after receiving treatment with exogenous factors, is also difficult to predict. The clinical manifestations of haemophilias include spontaneous bleeding into joints, skin, muscles, soft tissues, mucous membranes, and prolonged bleeding post-surgery or trauma. There is a lack of excessive hemorrhage from minor cuts or abrasions, due to normalcy of platelet function. However, bleeding in haemophilias can be life-threatening, if occurring intra-cerebrally or at the airway level. The diagnosis in haemophilias is classically based on the level of factors, but recently global tests of hemostasis, such as generation of thrombin and vascoelastic tests were used for characterization of the disease (22).
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
72
The mainstay of haemophilia treatment is represented by substitution of factor VIII or IX by exogenous specific factor concentrates. Whether plasma-derived or recombinant products are preferable remains controversial (23,24). Cryoprecipitate can be used for substitution when the factor concentrates are not available (21). Desmopressin may release enough FVIII for mild cases (25) and antifibrinolytics are usually used as adjuvants (21). The target preoperative levels of FVIII are around 100 Units dL-1 and they are tapered down after the first 3 days. However, 30-50% of normal levels are recommended until healing, about 2 weeks post-procedure (21,26)(Table 2). The target levels are lower for FIX. FVIII is administered every 8-12 hours and FIX every 18 hours, based on their pharmacokinetics. Perioperative continuous infusion of replacement factors of coagulation could be advantageous by decreasing the amount of the concentrate and by avoiding the sub-therapeutic concentrations induced by bolus injections (27). For invasive diagnostic procedures, such as lumbar puncture, arterial blood gas determination, bronchoscopy with brushings or biopsy, and gastrointestinal endoscopy with biopsy the factor concentrates should be infused just before the procedures (21). The adverse effects related to replacement therapy include thrombotic complications, allergic reactions and development of inhibitors (28,29). The later is the most serious complication of haemophilia (21). Bleeding in patients with inhibitors can be treated with by-passing agents, such as activated prothrombin complex concentrates (aPCCs) and rFVIIa (20). Mainly, these agents induce thrombin formation without any requirement for FVIII. It seems that by-passing agents have a similar perioperative haemostatic effect (30). However there are concerns about potential risk of thrombo-embolic events secondary to their administration. Antifibrinolytic drugs (AFs) inhibit the fixation of plasminogen to fibrin and slow the plasmin formation. Recently it was shown that tranexamic acid dramatically increases the stability of clots that have been formed (31) justifying the adjunctive administration of AFs in IBDs, as long as the bleeding risk exists. AFs alone may be sufficient in the management of less severe forms of mucosal bleeding and in dental surgery (32). Other coagulation factor deficiencies are referred as rare bleeding disorders (RBDs). These disorders have a low prevalence in the general population, ranging from 1:500,000 to 1:2 million inhabitants (20). The bleeding phenotype is variable, generally mild to moderate, except for afibrinogenemia and severe FVII, FX, and FXIII deficits which can induce severe bleeding (33). Recent analysis of registries showed that there is a heterogeneous association between coagulation factor activity level and clinical bleeding severity in different RBDs (34). The management of bleeding in patients with RBD is based on substitution of the deficient factor (Table 3). Fibrinogen and other factors are found in plasma and/or in cryoprecipitate. However these blood products are not virally safe and are indicated only when the plasma-derived, virally inactivated concentrates or recombinant factors are not available. There is insufficient data to recommend routine perioperative or peripartum substitutive therapy of deficient factors in patients with RBDs (35). As a general rule, substitutive treatment seems advisable for values less of 1 g L-1 for fibrinogen and for levels less than 20-30% for other factors, depending on the severity of trauma or surgery (33). FXIII needs even lower levels for hemostasis. The frequency of administration depends on the pharmacokinetic of the agent. Recombinant FVIIa seems to be effective in surgical bleeding resistant to substitutive treatment in patients with various RBDs (36). The association with tranexamic acid proved effective for hemostasis but it might increase the risk of thrombosis (37).
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
73
Perioperative strategy Surgery in patients with IBDs should be carried out by an experienced surgeon under the supervision or in consultation with a haematologist specialized in coagulation disorders, preferably in dedicated haemophilia centres with appropriate facilities for investigation and treatment (1-4,26,38). It is recommended that the care team, including the anaesthesiologist, write down a detailed plan for preoperative, intra-operative, and postoperative patient management. Some important points of the perioperative plan are summarized in Table 4. One important issue for the anaesthesiologist is the venous access which is essential for the correct replacement therapy. This could be problematic in patients receiving frequent factor infusions, especially in very young children. Recent data demonstrated that good surgical results are achievable in a full range of procedures when there is appropriate factor replacement. Haemorrhagic complications rate was 4 to 10% (1-3) and postoperative outcome was similar to matched pairs without IBDs (38). Further evidence of the safety and efficacy of necessary surgical procedures comes from a review of children with IBDs (4). All these studies stress the importance of careful preoperative planning and multidisciplinary team management. Neuraxial techniques are usually contraindicated in patients with IBDs (39). However, regional anaesthesia may be considered if there are serious concerns against general anaesthesia, provided the coagulation defect has normalized by prophylactic treatment or during pregnancy, no other defects are present, and the coagulation screen is normal and can be monitored frequently (35). A major concern of substitution of deficient factors in IBDs is thrombosis and there are some reports on thrombotic events related to fibrinogen, VWF, FVIII, and FXI concentrate administration (40-42). Therefore, the perioperative risk of venous thromboembolism (VTE) should be taken into account, especially for major orthopaedic procedures in older patients. Low molecular weight heparin should be considered at the same regimen that is recommended for patients without IBDs who are undergoing a similar procedure (43). In conclusion, surgery can be performed safely in patients with IBDs. These patients should be managed perioperatively in collaboration with a haematologist as appropriate perioperative replacement of pro-coagulant factors is the mainstay of therapy. Antifibrinolytic drugs are recommended perioperatively as adjunctive therapy. References 1. Solimeno LP, Mancuso ME, Pasta G, Santagostino E, Perfetto S, Mannucci PM. Factors influencing the long-term outcome of primary total knee replacement in haemophiliacs: a review of 116 procedures at a single institution. British Journal of Haematology 2009; 145:227-34 2. Goldmann G, Holoborodska Y, Oldenburg J et al. Perioperative management and outcome of general and abdominal surgery in haemophiliacs. The American Journal of Surgery 2010; 199:702-7 3. Aryal KR, Wiseman D, Siriwardena AK, Bolton-Maggs PH, Hay CR, Hill J. General surgery in patients with a bleeding diathesis: how we do it. World Journal of Surgery 2011; 35:2603-10 4. Watts RG, Cook RP. Operative management and outcomes in children with congenital bleeding disorders: a retrospective review at a single haemophilia treatment centre. Haemophilia 2011; 18(3):421-5
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
74
5. Nichols WL, Hultin MB, James AH et al. von Willebrand disease (VWD): evidence-based diagnosis and management guidelines, the National Heart, Lung, and Blood Institute (NHLBI) Expert Panel report (USA). Haemophilia 2008; 14(2):171-232 6. Mannucci PM. Treatment of von Willebrand's Disease. The New England of Journal Medicine 2004; 351:683-94 7. Mannucci PM, Franchini M, Castaman G, Federici AB, Italian Association of Hemophilia Centers. Evidence-based recommendations on the treatment of von Willebrand disease in Italy. Blood Transfusion 2009; 7:117-267.
8. Sadler JE. Low von Willebrand factor: sometimes a risk factor and sometimes a disease. Hematology Am Soc Hematol Educ Program 2009: 106-12
9. Federici AB. The use of desmopressin in von Willebrand disease: the experience of the first 30 years (1977-2007). Haemophilia 2008; 14:5-14 10. Castaman G, Lethagen S, Federici AB et al. Response to desmopressin is influenced by the genotype and phenotype in type 1 von Willebrand disease (VWD): results from the European Study MCMDM-1VWD. Blood 2008; 111(7):3531-9 11. Castaman G Treatment of von Willebrand disease with FVIII/VWF concentrates. Blood Transfus 2011; Suppl 2:s9-13. 12. Michiels JJ, van Vliet HH, Berneman Z, Schroyens W, Gadisseur A. Managing patients with von Willebrand disease type 1, 2 and 3 with desmopressin and von Willebrand factor-factor VIII concentrate in surgical settings. Acta Haematologica 2009; 121:167-76 13. Castillo R, Escolar G, Monteagudo J, Aznar-Salatti J, Reverter JC, Ordinas A. Hemostasis in patients with severe von Willebrand disease improves after normal platelet transfusion and normalizes with further correction of the plasma defect. Transfusion 1997; 37:785-90 14. Bolton-Maggs PH, Chalmers EA, Collins PW et al. A review of inherited platelet disorders with guidelines for their management on behalf of the UKHCDO. British Journal of Haematology 2006; 135(5):603-33 15. Quiroga T, Mezzano D. Is my patient a bleeder? A diagnostic framework for mild bleeding disorders. Hematology Am Soc Hematol Educ Program. 2012;2012:466-74 16. Alamelu J, Liesner R. Modern management of severe platelet function disorders. British Journal of Haematology 2010; 149(6):813-23 17. Coppola A, Di Minno G. Desmopressin in inherited disorders of platelet function. Haemophilia 2008; 14:31-9 18. Seligsohn U. Treatment of inherited platelet disorders. Haemophilia 2012;18 Suppl 4:161-5 19. Poon MC, D'Oiron R, Von Depka M et al. Prophylactic and therapeutic recombinant factor VIIa administration to patients with Glanzmann's thrombasthenia: results of an international survey. Journal of Thrombosis and Haemostasis 2004; 2:1096-103 20. Keeling D, Tait C, Makris M. Guideline on the selection and use of therapeutic products to treat haemophilia and other hereditary bleeding disorders A United Kingdom Haemophilia Center Doctors' Organisation (UKHCDO) guideline approved by the British Committee for Standards in Haematology. Haemophilia 2008; 14(4):671-84 21. World Federation of Hemophilia. Guidelines for the Management of Hemophilia. Available at: http://www.wfh.org. Accessed August 2014. 22. Young G, Sørensen B, Dargaud Y, Negrier C, Brummel-Ziedins K, Key NS. Thrombin generation and whole blood viscoelastic assays in the management of hemophilia: current state of art and future perspectives. Blood 2013;121(11):1944-50.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
75
23 Mannucci PM. Plasma-derived versus recombinant factor VIII concentrates for the treatment of haemophilia A: plasma-derived is better. Blood Transfusion 2010; 8:288-91 24. Franchini M. Plasma-derived versus recombinant Factor VIII concentrates for the treatment of haemophilia A: recombinant is better. Blood Transfusion 2010; 8:292-96 25. Franchini M, Favaloro EJ, Lippi G. Mild haemophilia A. Journal of Thrombosis and Haemostasis 2010; 8:421-3222 26. Hermans C, Altisent C, Batorova A et al. European Haemophilia Therapy Standardisation Board. Replacement therapy for invasive procedures in patients with haemophilia: literature review, European survey and recommendations. Haemophilia 2009; 15(3):639-58 27. Batorova A, Holme P, Gringeri A, et al. Continuous infusion in haemophilia: current practice in Europe. Haemophilia 2012;5:753-9 28. Coppola A, Franchini M, Makris M, Santagostino E, Di Minno G, Mannucci PM. Thrombotic adverse events to coagulation factor concentrates for treatment of patients with haemophilia and von Willebrand disease: a systematic review of prospective studies. Haemophilia 2012; 18(3):e173-87 29. Franchini M, Makris M, Santagostino E, Coppola A, Mannucci PM. Non-thrombotic-non-inhibitor-associated adverse reactions to coagulation factor concentrates for treatment of patients with hemophilia and von Willebrand's disease: a systematic review of prospective studies. Haemophilia 2012; 18(3):e164-72 30. Iorio A, Matino D, D'Amico R, Makris M. Recombinant Factor VIIa concentrate versus plasma derived concentrates for the treatment of acute bleeding episodes in people with haemophilia and inhibitors. Cochrane Database Systematic Review 2010; 4;(8):CD004449 31. Hvas AM, Sørensen HT, Norengaard L, Christiansen K, Ingerslev J, Sørensen B. Tranexamic acid combined with recombinant factor VIII increases clot resistance to accelerated fibrinolysis in severe hemophilia A. Journal of Thrombosis and Haemostasis 2007; 5:2408-14 32. Hewson I, Makhmalbaf P, Street A, McCarthy P, Walsh M. Dental surgery with minimal factor support in the inherited bleeding disorder population at the Alfred Hospital. Haemophilia 2011; 17:e185-830. 33. Peyvandi F, Bolton-Maggs PH, Batorova A, De Moerloose P. Rare bleeding disorders. Haemophilia. 2012;18 Suppl 4:148-53 34. Peyvandi F, Palla R, Menegatti M, et al. Coagulation factor activity and clinical bleeding severity in rare bleeding disorders: results from the European Network of Rare Bleeding Disorders. Journal of Thrombosis and Haemostasis 2012; 10(4):615-21 35. Kadir R, Chi C, Bolton-Maggs P. Pregnancy and rare bleeding disorders. Haemophilia 2009; 15(5):990-1005 36. Johansson PI, Ostrowski SR. Evidence supporting the use of recombinant activated factor VII in congenital bleeding disorders. Drug Design, Development and Therapy 2010; 4:107-16 37. Livnat T, Tamarin I, Mor Y et al. Recombinant activated factor VII and tranexamic acid are haemostatically effective during major surgery in factor XI-deficient patients with inhibitor antibodies. Journal of Thrombosis and Haemostasis 2009; 102:487-92 38. Sikkema T, Boerboom AL, Meijer K. A comparison between the complications and long-term outcome of hip and knee replacement therapy in patients with and without haemophilia; a controlled retrospective cohort study. Haemophilia 2011; 17(2):300-3. 39. Choi S, Brull R. Neuraxial techniques in obstetric and non-obstetric patients with common bleeding diatheses. Anaesthesia and Analgesia 2009; 109:648-60

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
76
40. Makris M, Colvin B, Gupta V, Shields ML, Smith MP. Venous thrombosis following the use of intermediate purity FVIII concentrate to treat patients with von Willebrand's disease. Journal of Thrombosis and Haemostasis 2002; 88:387-8 41, Ruiz-Saez A. Occurrence of thrombosis in rare bleeding disorders. Semin Thromb Hemost 2013; 39(6):684-92 42. Hermans C, Hammer F, Lobet S, Lambert C. Subclinical deep venous thrombosis observed in 10% of hemophilic patients undergoing major orthopedic surgery. Journal of Thrombosis and Haemostasis 2010; 8:1138-40 43. Mannucci PM, Schutgens RE, Santagostino E, Mauser-Bunschoten EP. How I treat age-related morbidities in elderly persons with hemophilia. Blood 2009; 114(26):5256-63. Table 1. Recommendations of peri-procedural prophylaxis of bleeding in patients with von Willebrand disease (5,6,11) Type of haemorrhage Target levels of VWF/
FVIII (IU dL-1) Frequency of administration
initial subsequent
Major surgery 100 > 50 Every 8-24 hours, until healing is complete
Minor surgery > 30-50 > 30-50 Every 12-48 hours, until healing is complete Diagnostic procedures > 50 Single dose Delivery > 50 > 50 Daily before delivery and 3-4 days postpartum Table 2. Perioperative replacement therapy recommended for haemophilia A patients (21,26) Type of procedure Target FVIII levels Duration (days) Major surgery 80–100 % 10-14 Liver biopsy 70-100 % 1-7
Tonsillectomy 90-100 % 5-11 Central venous device insertion 100 % 3-10 Circumcision 50-60 % 2-4 Dental >50 % Single dose Table 3. Therapeutic options rare bleeding disorders Factor deficiency Therapeutic options Fibrinogen Concentrate, Plasma, Cryoprecipitate Prothrombin PCC, Plasma V Plasma VII rFVIIa, pd-concentrate, Plasma, PCC X PCC plasma XI pd-concentrate, tranexamic acid , Plasma
rFVIIa, Desmopressin XIII pd or r-concentrate, Plasma, Cryoprecipitate V + VIII Plasma, FVIII concentrates, Desmopressin, ,rFVIIa Vitamin K dependent multiple deficiency
Vitamin K, Plasma, PCC, rFVIIa
PCC - prothrombin complex concentrate; rFVIIa - recombinant activated FVII pd - plasma derived; r – recombinant; a activated
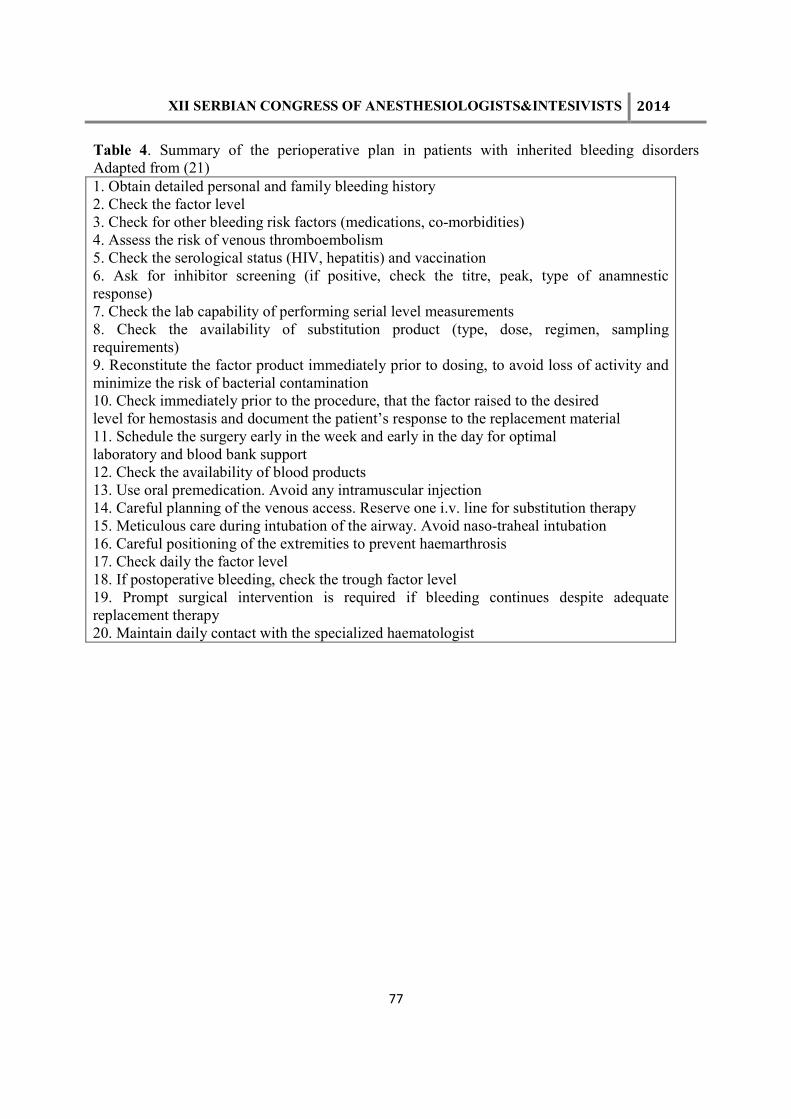
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
77
Table 4. Summary of the perioperative plan in patients with inherited bleeding disorders Adapted from (21) 1. Obtain detailed personal and family bleeding history 2. Check the factor level 3. Check for other bleeding risk factors (medications, co-morbidities) 4. Assess the risk of venous thromboembolism 5. Check the serological status (HIV, hepatitis) and vaccination 6. Ask for inhibitor screening (if positive, check the titre, peak, type of anamnestic response) 7. Check the lab capability of performing serial level measurements 8. Check the availability of substitution product (type, dose, regimen, sampling requirements) 9. Reconstitute the factor product immediately prior to dosing, to avoid loss of activity and minimize the risk of bacterial contamination 10. Check immediately prior to the procedure, that the factor raised to the desired level for hemostasis and document the patient’s response to the replacement material 11. Schedule the surgery early in the week and early in the day for optimal laboratory and blood bank support 12. Check the availability of blood products 13. Use oral premedication. Avoid any intramuscular injection 14. Careful planning of the venous access. Reserve one i.v. line for substitution therapy 15. Meticulous care during intubation of the airway. Avoid naso-traheal intubation 16. Careful positioning of the extremities to prevent haemarthrosis 17. Check daily the factor level 18. If postoperative bleeding, check the trough factor level 19. Prompt surgical intervention is required if bleeding continues despite adequate replacement therapy 20. Maintain daily contact with the specialized haematologist

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
78
UROĐENA IMUNOST, INFEKCIJA I SEPSA INNATE IMUNITY, INFECTION AND SEPSIS DRAGAN ĐORĐEVIĆ Univerzitet Odbrane u Beogradu, Medicinski fakultet VMA, Klinika za anesteziologiju i intenzivnu terapiju VMA Beograd, Beograd, E-mail: [email protected] SUMMARY Innate immunity is the first line of defense against infections. It has very important function to control and eliminate infection of the host by many microbes. Also, it stimulates adaptive immune response and can influence the nature of the adaptive response. The invasion of microbial pathogens and/or cytokines into the bloodstream, is characterized by a systemic proinflammatory response, which can lead to severe sepsis and septic shock. Sepsis, severe sepsis and septic shock are major health care problems worldwide; they affect millions of people each year, and their incidence increases annually. Despite significant advances in intensive care treatment over the last years, septic shock remains associated with high mortality rates. The epidemiologic studies reported that septic shock is the most common cause of death in noncoronary intensive care units, and the tenth leading cause of death overall in high income countries. The outcome of sepsis is particularly unfavorable in elderly, immune compromised, and critically ill patients. UVOD
Sistem urođene imunosti prepoznaje invazivne mikroorganizme (bakterije, virusi, gljive) preko receptora za prepoznavanje mikroorganizma (eng. pathogen recognition receptors -PRRs), koji se nalaze na epitelnim barijerama, odnosno na imunskim ćelijama kao što su dendritske ćelije i makrofage (1). Do sada su opisane 4 vrste ovih receptora, koji se nalaze na površini ili unutar ćelija. Specifična familija ovih receptora – receptori slični Tolu (eng. Toll-like receptors -TLRs) prepoznaju konzervirane makromolekulske motive sa mikroorganizma – molekulski obrazci (eng.pathogen-associated molecular patterns- PAMPs). Primeri ovih bakterijskih molekulskih obrazaca su: lipopolisaharid (LPS; glavni faktor virulencije Gram-negativnih bakterija), peptidoglikan, lipoteiholična kiselina (komponenta ćelijskog zida Gram-pozitivnih bakterija), flagelin i bakterijska DNK (2).
Takođe, ćelije urođene imunosti mogu prepoznati i molekulske obrazce oštećenja ćelija ili alarmine (eng. damage associated molecular pattern- DAMPs) kao što su High mobility group box 1 (HMGB-1), heat shok protein, mokraćna kiselina, aneksini i interleukin-1 alfa. HMGB1 je jedarni protein koji ima fiziološku ulogu u stabilizaciji nukleozoma i uvijanju molekula DNK. Kod oštećenja ćelija to je snažni proinflamatorni citokin koji napušta jedro i vezuje se za specifični receptore- receptori slični Toll-u i to za TLR -2, -4 i -9 kao i za RAGE receptore (eng. receptor for advanced glycation end- products) (3, 4). Takođe, ćelije urođene imunosti, pre svih makrofage, prelaze u tkiva i luče različite proinflamatorne citokine kao što su faktor nekroze tumora (TNF), IL-1, IL-6 i IL-12, hemokine kao što su IL-8, makrofagni inflamatorni proteini MIP1 i MIP2, kao i monocitni hemotaktički protein MPC-1.U odgovoru na infekciju ili traumu, urođena imunost odgovara neposrednim biološkim odgovorom- inflamacijom, sa nakupljanjem ćelija urođene imunosti (neutrofili, monociti, makrofage) u cilju eliminacije patogena. Posle
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
79
njihove eliminacije, inflamatorni odgovor može da slabi u cilju uspostavljanja imunske homeostaze. U suprotnom procesu, egzogeni patogeni ili oslobođeni endogeni proinflamatorni medijatori mogu ući u cirkulaciju i izazvati sistemski inflamatorni odgovor koji može dovest do teške inflamatorne vaskularne bolesti tj. do sepse (5). Sepsa je dakle, sindrom sistemskog inlamatorornog odgovora izazvana infekcijom mikroorganizmima, i može se razviti u tešku sepsu ili septički šok (6).
Teška sepsa se javlja kao rezultat bolničkih ali i vanbolničkih infekcija. Najčešći uzrok sepse je pneumonija (kod skoro 50% bolesnika), zatim slede intraabdominalne infekcije kao I infekcije urinarnog sistema. Kod trećine bolesnika hemokulture su pozitivne, a kod trećine bolesnika sve uzete kulture su negativne. Najčešći Gram-pozitivni izolati bakterija su Staphylococcus aureus I Streptococcus pneumonia dok su od Gram-negativnih bakterija najčešće Echerichia coli, Klebsiella species i Pseudomonas aeruginosa. Gram-negativne bakterije su češći uzročnice sepse u odnosu na Gram- pozitivne bakterije i glive (7).
CITOKINI U PATOFIZIOLOGIJI SEPSE
Termin citokini opisuje funkcionalnu klasu malih proteina- medijatora ( molekulske mase <40 kDa), koji imaju regulatornu ulogu u aktivaciji i diferencijaciji imunskog odgovora i predstavalju tzv. međućelijske glasnike (8). Jednom oslobođeni, proinflamatorni citokini dovode do aktivacije urođenog i stečenog imunskog sistema, što dovodi do dalje produkcije regulatornih ili efektorskih citokina. Postepeno oslobađanje ovih specifičnih citokina naziva se citokinska kaskadea. Tokom 1990s, za sepsu se verovalo da je udružena sa povećanim oslobađanjem uglavnom proinflamatornih citokina kao što su faktor nekroze tumora (TNF)-�, interleukin(IL)-1 ,IL-6, IL-12, interferon (IFN)-�, and faktor inhibicije migracije makrofaga (MIF). Desetak godina kasnije, patofiziološka teorija sepse se menja u pravcu da proinlfamatorni odgovor prati kompenzatorni anti-inflamatorni odgovor I da se oslobađaju citokini sa anti-inflamatornim dejstvom, kao što su IL-10, transformišući faktor rasta (TGF)-�, i IL-4, sa ciljem da se uspostavi imunska ravnoteža (9). NOVA IMUNSKA TEORIJA SEPSE Imunska teorija sepse je i dalje predmet velikih rasprava (10). Tradicionalno, imunski odgovor domaćina na infekciju se karakteriše početnom hiperinflamatornom fazom, koja traje nekoliko dana i nastavlja se produženom imunosupresivnom fazom (TEORIJA 1). Međutim, nedavne studije su pokazale da se i proinflamatorni i antiiflamatorni odgovor dešavaju rano i simultano u sepsi, mada se početni efekat ovog procesa tipično manifestuje kao rani, dominantni, hiperinflamatorni odgovor, koji se karakteriše groznicom, hipermetabolizom i šokom. Jačina ovog odgovora zavisi od brojnih faktora kao što su postojeći komorbiditeti, nutricioni status, broj mikroorganizma i njihova virulencija. Rana smrt bolesnika sa sepsom nastaje zbog prejakog hiperiflamatornog odgovora i razvoja disfunkcije organa. U daljoj fazi bolesti dolazi do slabljenja i urođenog i stečenog imunskog odgovora, te do razvoja značajnog imunosupesivog stanja. Kasna smrt bolesnika sa sepsom nastaje zbog nemogućnosti eliminacije primarne infekcije i razvoja sekundarnih infekcija (11, 12).
Istraživači iz Kine (13) su nedavno saopštili novu imunsku teoriju sepse, koja opisuje imunski odgovor domaćina kod trauma i sepse (TEORIJA 2). Podaci iz studije genske ekspresije cirkulišućih leukocita su pokazali, da bolesnici sa traumom i opekotinama pokazaju brzi i stalni porast ekskpresije gena koji regulišu urođeni imunski odgovor i simultano smanjenje ekspresije

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
80
gena koji regulišu stečeni (adaptivni) imunski odgovor. Njihov zaključak ukazuje da je za razvoj organske disfunkcije značajna produžena i neoslabljena inflamacija izazvana reakcijom urođenog imunskog sistema. Iako je stečeni imunski odgovor oštećen, bolesnici koji umiru od sepse imaju dug tok i veliki stepen oštećenja organa, izazvanog neadekvatnim odgovorom urođenog imunskog sistema.
Iako su ovi nalazi vrlo provokativni, većina autora i dalje veruje da bolesnici koji umiru od sepse imaju vrlo izraženu imunosupresiju (14). Gore navedena studija je rađena na populaciji mlađih pacijenata sa traumom i opekotinama, što se značajno razlikuje od starije populacije sa sepsom čiji je uzročnik difuzni peritonitis. Post mortem studije su pokazale da ovi bolesnici u plućima i slezini imaju snižene nivoe i proinflamatornih i antiinflamatornih citokina, povećanu ekspresiju inhibitornih receptora kao i ekspanziju regulatornih T limfocita i mijeloidnih supresorskih ćelija. Gotovo sve ćelije urođenog i stečenog imunskog sistema imaju skraćeni životni vek (rana apoptoza) i pokazuju značajna funkcionalna oštećenja, što se posebno odnosi na populaciju T i B limfocita. ZAKLJUČAK
Aktuelni koncept uloge sistema urođene imunosti u infekciji se zasniva na vezivanju specifičnih molekulskih obrazaca mikroorganizama i oštećenih ćelija za receptore na makrofagama i dendridskim ćelijama uz aktivaciju intracelularnih signalnhih mehanizama koji dovode do oslobađanja proinflamatornih citokina. Ova saznanja u proteklih dve decenije su izmenila klasičnu sliku patofiziologije sepse.
Odgovor svakog pacijenta na infekciju zavisi od vrste i karakteristika mikroorganizma (broj i virulencija) kao i od odgovora domaćina (genetske karakteristike i prateće bolesti) sa različitim odgovorima na lokalnom, regionalnom i sistemskom nivou (15). Intenzitet i oblik ovog odgovora se mogu menjati tokom vremena, sinhrono sa kliničkim tokom infekcije i sepse. Uopšte, proinflamatorni odgovor je odgovoran za kolateralno oštećenje tkiva u teškoj sepsi, dok je antiinflamatorni odgovor odgovoran za povećanu sklonost ka sekundarnim infekcijama.
LITERATURA
1) Cinel I, Opal SM. Molecular biology of inflammation and sepsis: A primer. Crit Care Med 2009; 37(1): 291- 304
2) Uematatsu S, Akira S. Tool- like receptors and innate immunity. J Mol Med 2007; 84: 712-25 3) Klune JR, Dhupar R, Cardinal J. Billiar T, Tsung A. HMBG1: endogenous danger signaling. Mol
Med 2008; 14(7-8): 476-84 4) Wang H, Ward M, Sama AE. Targeting HMGB1 in the treatment of sepsis. Expert Opin Ther Targets
2014; 18(3): 257-68 5) Djordjević D, Surbatović M, Ugrinović D, Radaković S, Jevdjić J, Filipović N, Romić P, Jovanović
D. New aspects of sepsis pathophysiology in critically ill. Vojnosanit Pregl. 2012 Jan; 69(1): 58-68 6) Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM et al. Surviving Sepsis
Campaign: International Guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med 2013; 41(2): 580-63
7) Angus DC, Van der Poll T. Severe Sepsis and Septic Shock. N Engl J Med 2013; 369: 840-51 8) Bernhagen J, Bucala R. Cytokines in Sepsis: Potent Immunoregulators and Potential Therapeutic
Targets—An Updated View. Mediators Inflamm 2013; 2013: 165974 9) Bone RC, Grodyin CJ, Balk RA. Sepsis: A new hypotesis for pathogenesis of the disease process.
Chest 1997; 112: 235-43

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
81
10) Hotchkiss RS, Monneret G, Payen D. Immunosuppression in sepsis: a novel understanding of the disorder and a new therapeutic approach. Lancet Infect Dis 2013; 13: 260-268
11) Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N. Engl. J. Med. 2003; 348: 138-150
12) Asehnoune K, Roquilly A, Abraham E. Innate immune dysfunction in trauma patients. Anesthesiology 2012; 117(2): 411-16
13) Xiao W, Mindrinos MN, Seok J, Cuschieri J, Cuenca AG, Gao H et al. A genomic storm in critically injured humans. J Exp Med 2011; 208: 2581-90
14) Surbatovic M, Jevdjic J, Veljovic M, Popovic N, Djordjevic D, Radakovic S. Immunoinflammatory response in critically ill patients: Severe sepsis and/or trauma. Mediators Inflamm 2013; 2013: 362793
15) Van der Poll T, Opal SM. Host- pathogen interaction in sepsis. Lancet Infect Dis 2008; 8: 32-43
SLIKA 1 – IMUNSKE TEORIJE SESPE. TEORIJA 1 – Aktivacija proinflamatornog i antiinflamatornog
odgovora u sepsi se dešava brzo i istovremeno. Rana smrt u sepsi nastaje zbog prejakog hiperinlamatornog odgovora (disfunkcija organa). Kasna smrt u sepsi nastaje zbog slabosti i urođenog i stečenog imunskog odgovora i razvoja značajnog imunosupresivnog stanja (nemogućnost eliminacije primarne infekcije i razvoj sekundarnih infekcija). TEORIJA 2 – Rana aktivacija urođenog imunskog odgovora i supresija stečenog imunskog odgovora kod bolesnika sa traumom i opekotinama. Produžena inflamacija dovodi do razvoja disfunkcije organa i smrti.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
82
NADOKNADA TEČNOSTI U SEPSI: ŠTA PODACI POKAZUJU FLUID RESUSCITATION IN SEPSIS: WHAT DO DATA SHOW 1M. VELJOVIĆ, 1U. PETROVIĆ, 1A. RISTANOVIĆ, 2T. DJORDJEVIĆ, I 1I. UDOVIČIĆ 1Vojnomedicinska akademija, Beograd, 2KBC Zvezdara, Beograd Email: [email protected] Abstract Fluid resuscitation is one of the most important treatment for patients with severe sepsis, but the optimal choice, the amount and manner of giving fluids is still cause for debate. In the early hours of sepsis, venodilatation and transudation of fluid from the intravascular space into the tissues, reduced oral intake of fluids and fluid loss leading to hypovolemia perspiration. Cardiac dysfunction, dilatation of arterioles, vascular obstruction, decreased volume leads to a deterioration of perfusion and thus the functioning of the body. Treatment of hypovolemia is a major goal of severe sepsis. Infusions to increase intravascular volume, improve tissue perfusion, prevent organ failure and improve survival. Most studies of sepsis emphasize the central role of early and aggressive fluid resuscitation. However, there is little credible policies that lead clinicians to the best method of treatment fluids in septic patients. You need to determine the right time, quantity, type of fluid for optimal therapy and monitor the effectiveness of treatment fluids. During the first six hours of the initial goals of treatment fluids, tissue hypoperfusion in patients with sepsis, were: central venous pressure of 8 -12 mmHg, mean arterial pressure ≥ 65 mmHg, urine output ≥ 0.5 ml / kg / h and oxygen saturation of blood in the vena cava superior and mixed venous blood oxygen saturation of 70% or 65%. Such infusions should be normalized lactate levels as parameters of tissue perfusion. Uvod Sepsa je sistemski, štetan odgovor domaćina na infekciju koja može dovesti do teške sepse (akutna disfunkcija organa sekundarna u odnosu na dokumentovanu ili suspektnu infekciju) i septičkog šoka (teška sepsa, plus hipotenzija nekompenzovana uprkos nadoknadi tečnosti). Teška sepsa i septički šok su ozbiljni problem zdravstvene zaštite i pogađa milione ljudi širom sveta svake godine, dovodeći do smrtnog ishoda jednog od četiri (a često i više) pacijenata [1-5]. Slično politraumi, akutnoj infekciji miokarda ili infarktu, brzina i prikladnost terapije u inicijalnim satima po razvoju teške sepse utiče na ishod. Inicijalni tretman tečnostima U prvim satima teške sepse, kombinacija venodilatacije, transudacije tečnosti iz vaskularnog prostora u tkiva, smanjen oralni unos i pojačan gubitak dovode do hipovolemije. Disfunkcija srca, arteriolarna dilatacija, vaskularna opstrukcija i hipovolemija dovode do globalnog oštećenja perfuzije i insuficijencije vitalnih organa. Tretiranje hipovolemije je glavni princip lečenja sepse u početnom periodu [6]. Nadoknadom tečnosti treba da se podigne intravaskularni volumen, povećava perfuzija tkiva, spreči organska insuficijencija i poveća preživljavanje. Radovi u vezi sa nadoknadom volumena kod septičkih pacijenata naglašavaju ključnu ulogu rane i agresivne terapije tečnostima.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
83
Preporučuje [7] se protokolizovano zbrinjavanje pacijenata sa hipoperfuzijom tkiva izazvanom sepsom (definisanu kao hipotenzija koja perzistira posle inicijalnog opterećenja tečnostima ili koncentracija laktata u krvi ≥ 4 mmol/L). Ovaj protokol se mora započeti čim se otkrije hipoperfuzija i ne sme se odlagati prijem u jedinicu za intenzivno lečenje. Tokom prvih šest sati reanimacije, ciljevi inicijalnog zbrinjavanja hipoperfuzije indukovane sepsom moraju da uključuju sve od sledećeg, kao deo protokola terapije:
a) CVP 8-12 mm Hg b) MAP ≥ 65 mm Hg c) Diureza ≥ 0.5 mL-kg-h d) Zasićenost hemoglobina kiseonikom gornje šuplje vene (ScvO2) >70% ili zasićenost
hemoglobina kiseonikom mešane venske krvi (SVO2) > 65%. Rano zbrinjavanje popravlja stopu preživljavanja za pacijente sa septičkim šokom [8]. Zbrinjavanje usmereno na fiziološke ciljeve koji su gore navedeni za inicijalni period od šest sati je povezano sa apsolutnim smanjenjem smrtnosti od 15.9% tokom perioda od 28 dana8. Ova strategija, nazvana rana ciljana terapija (early goal-directed therapy), bila je ispitivana i u studiji sa teškom sepsom u osam kineskih centara [9]. Ova studija je utvrdila apsolutno smanjenje smrtnosti od 17.7% u roku od 28 dana. Veliki broj drugih studija koje su koristile slične oblike ranog zbrinjavanja na uporedivim populacijama pacijenata pokazale su značajno smanjenje smrtnosti [10]. Izbor tečnosti Preporuka je da kristaloidi budu inicijalni izbor u teškoj sepsi i septičnom šoku. Ne preporučuje se upotreba hidroksietil skroba (HES) za nadoknadu tečnosti u teškoj sepsi i septičnom šoku. Ova preporuka se zasniva na rezultatima VISEP [11], CRYSTMAS [12], 6S [13] i CHEST [14] studija. Odsustvo bilo kakvog jasnog benefita od upotrebe koloida u odnosu na kristaloide, zajedno sa troškovima koji su povezani sa upotrebom koloida, podržava preporuke o inicijalnoj upotrebi kristaloida kod pacijenata sa teškom sepsom i septičnim šokom. Objavljene su tri skorašnje multicentrične studije o evaluaciji 6% HES-a 130/04 rastvora (tetra skrob). CRYSTMAS studija [12] je pokazala da ne postoji razlika u mortalitetu pri upotrebi HES-a naspram 0.9% slanog rastvora (31% naspram 25,3%, p=0.37) kod pacijenata sa septičnim šokom. Skandidavska multicentrična studija septičnih pacijenata (6S Trial Group) [13] pokazuje porast stope mortaliteta pri upotrebi 6% HES-a 130/0.42 u poređenju sa upotrebom Ringer acetata (51% prema 43%, p=0.03). CHEST studija [14], vodjena u heterogenoj populaciji pacijenata koji su primljeni u jedinicu intenzivnog lečenja (HES prema izotonom slanom rastvoru, n=7000 kritično obolelih pacijenata), ne pokazuje razliku u 90-odnevnom mortalitetu između nadoknade 6% HES-om 130/0.4 i izotoničnim slanim rastvorom (18% prema 17%, p=0.26), potreba za primenu hemodijalizene trapije je bila veća u grupi sa HES-om. Meta analiza 56 randomiziranih studija generalno nije otkrila razliku u mortalitetu između kristaloida i veštačkih koloida (modifikovani želatin, HES, dekstran) kada se koriste u inicijalnoj nadoknadi tečnosti [15]. Informacije iz tri randomizirane studije (n=704 pacijenata sa ozbiljnom sepsom/septičnim šokom) nisu pokazale benefit u preživljavanju pri upotrebi heta-, hexa- ili pentaskroba u poređenju sa drugim tečnostima [16-18]. Dokazi iz studija 6S [13] i CHEST [14]

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
84
podržavaju preporuku da se HES rastvori ne koriste kod pacijenata sa ozbiljnom sepsom i septični šokom, naročito kada postoje druge opcije za nadoknadu tečnosti. Preporučuje se upotreba albumina za nadoknadu tečnosti u teškoj sepsi i septičnom šoku kada pacijenti zahtevaju znatnu količinu kristaloida. SAFE studija pokazuje da je administracija albumina bezbedna i podjednako efikasna kao i upotreba 0.9% slanog rastvora [19]. Meta analiza je skupila podatke iz 17 randomiziranih studija (n=1977) o upotrebi albumina naspram drugih tečnosti za nadoknadu volumena kod pacijenata sa teškom sepsom i septičnim šokom [20]; 279 smrtnih slučajeva je zabeleženo kod 961 pacijenta koji su tretirani albuminima naspram 343 smrtna slučaja kod 1016 pacijenata koji su tretirani drugim tečnostima što favorizuje upotrebu albumina. Kada se grupa pacijenata koji su tretirani albuminimа uporedi sa grupom onih koji su primali kristaloide (sedam studija), odnos umirućih bio je značajno snižen za pacijente koji su primali albumine. Način davanja tečnosti Preporučuje se početni unos tečnosti u pacijenata sa tkivnom hipoperfuzijom indukovanom sepsom kod sumnje na hipovolemiju. Potrebno je postići unos od minimalno 30 ml/kg kristaloidnih rastvora (ekvivalentna doza albumina može zameniti deo ovog volumena) [7]. Brža primena i veće količine tečnosti mogu biti potrebne kod pojedinih pacijenata. Hemodinamska nestabilnost ima važnu ulogu u progresiji sistemske inflamacije, tkivne hipoksije i otkazivanja više organa u sepsi. Hitna nadoknada tečnosti je ključna intervencija za ostvarivanje hemodinamske stabilnosti u teškoj sepsi. Obnavljanje ravnoteže izmedju dopremanja i potrošnje kiseonika, i obnavljanje mikrocirkulacije sa sprečavanjem endotelijalne disfunkcije u ranoj fazi sepse dovodi do smanjenja smrtnosti [7,21]. Tehniku unosa tečnosti bolusima (fluid challenge) treba produžiti sve dok se njome postiže poboljšanje bilo dinamičkih (npr. promene u pulsnom pritisku, varijacije udarnog volumena) bilo statičkih (npr. arterijski pritisak, srčana frekvenca) hemodinamskih parametara. Kod pacijenata sa hipovolemijom, treba dati 500 – 1000 ml kristaloidnih rastvora u bolusima. Odluka o daljoj nadoknadi volumena se donosi na osnovu efekata (porast krvnog pritiska, diureza, ScvO2) i tolerancije (znaci intravaskularne hipervolemije)[7] (Slika 1.) Monitoring nadoknade tečnosti Postoje priznata ograničenja procene statičnog ventrikularnog pritiska punjenja kao surogata za nadoknadu tečnosti [22], ali merenje CVP je trenutno najlakše ostvariv cilj za monitoring nadoknade tečnosti i procenu stanja intravaskularnog volumena. Na nizak CVP se u osnovi može osloniti ako postoji pozitivni trend kao odgovor na nadoknadu tečnostima. Kod mehanički ventiliranih pacijenata, ili onih kod kojih je poznato da od ranije postoji smanjena ventrikularna elastičnost miokarda, mora se postići viša ciljna vrednost CVP od 12 do 15 mm Hg, da bi se nadoknadila ograničenost punjenja [23]. Slično se mora uzeti u obzir okolnost povećanog abdominalnog pritiska [24]. Povećana vrednost CVP se takođe može videti u slučaju od ranije postojeće klinički značajne hipertenzije plućne arterije, što čini upotrebu ove varijable neodrživom za procenjivanje statusa intravaskularnog volumena. Bilo intermitentna, ili kontinuirana merenja zasićenosti hemoglobina kiseonikom procenjena su kao prihvatljiva. Tokom prvih 6 h reanimacije, ukoliko perzistira ScvO2 manja od 70% ili SvO2
ekvivalentna ili manja od 65%, sa onim što je procenjeno kao adekvatna nadoknada intravaskularnog volumena u prisustvu perzistirajuće hipoperfuzije tkiva, onda su opravdane opcije infuzija dobutamina (do maksimuma od 20 µg/kg/min), ili transfuzija koncentrovanih

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
85
eritrocita (da se postigne hematokrit veći ili jednak 30%) u pokušajima da se postigne ciljna ScvO2 ili SvO2 [7]. Ako SCVO2 nije raspoloživa, monitoring nivoa laktata može da bude izvodljiva opcija u slučaju pacijenata sa teškom sepsom indukovanom hipoperfuzijom tkiva. Iako uzrok tahikardije kod septičkih pacijenata može da bude multifaktorski, smanjenje povećanog broja srčanih otkucaja po nadoknadi tečnosti je često koristan marker popravljanja intravaskularnog punjenja [7]. Dinamički paramatri kojima se ispituje odgovor pacijenta na nadoknadu tečnosti poslednjih godina dobili su na popularnosti kod lekara koji rade u jedinicama intenzivnog lečenja. Ovi se testovi baziraju na praćenju promena udarnog volumena. Sistematskim pregledom (29 studija, n=685 kritično obolelih pacijenata) uočena je povezanost između varijacija udarnog volumena, pulsnog pritiska i/ili varijacija udarnog volumena i promena odnosa udarni volumen/srčani indeks posle bolusa tečnosti ili uspostavljanja pozitivnog pritiska na kraju ekspirijuma (PEEP) [25]. Korisnost praćenja varijacija pulsnog pritiska i udarnog volumena je ograničena u prisustvu pretkomorske fibrilacije, spontanog disanja i malog pritiska asistiranog disanja. Raspoložive tehnologije omogućavaju merenje protoka pored bolničkog kreveta [26]. Međutim, uticaj ovih tehnika monitoringa na kliničke ishode još od nadoknade tečnostima u ranoj sepsi ostaje nekompletna i zahteva dalje studije pre usvajanja. Transfuzija krvi i derivata krvi Preporučuje se transfuzija eritrocita kada su vrednosti hemoglobina < 70g/l, ili do postizanja ciljnih vrednosti od 70 do 90 g/l kod odraslih osoba po hemodinamskoj stabilizaciji i oporavku tkivne hipoperfuzije ( u odsustvu miokardne ishemije, teške hipoksemije, akutnog krvavljenja, ili ishemijske koronarne arterijske bolesti) [27]. Optimalna koncentracija hemoglobina kod bolesnika sa teškom sepsom nije specifično istraživana, ali rezultati studije Transfusion Requirements in Critical Care pokazali su da nivo hemoglobina od 70 do 90 g/l, u poređenju sa 100 do 120 g/dl, nije udružen sa povećanjem mortaliteta kod kritično obolelih odraslih pacijenata [28]. Nisu uočene statistički značajne razlike u mortalitetu između dve terapijske grupe (posle 30 dana) kao ni u podgrupi bolesnika sa teškom infekcijom i septičnim šokom. Transfuzija eritrocita kod bolesnika sa sepsom povećava isporuku kiseonika tkivima, ali ne povećava i njegovo iskorišćavanje [29-31]. Prag za primenu transfuzije od 70g/l je u suprotnosti sa protokolom rane terapije, u kome je ciljna vrednost hematokrita 30% kod bolesnika sa septičnim šokom i niskom ScvO2, tokom prvih 6 sati reanimacije [8]. Iako kliničkim studijama nije utvrđen uticaj transfuzije sveže zamrznute plazme na ishod kritično obolelih, stručna udruženja su dala preporuke za primenu plazme kada postoji dokumentovan deficit faktora koagulacije (produženo protrombinsko vreme, INR ili parcijalno tromboplastinsko vreme), aktivno krvavljenje kao i pre hirurške intervencije ili invazivne procedure[32-34]. Štetni efekti nadoknade tečnosti Tečnost ubrizgana u vaskularni prostor postiže ravnotežu sa drugim telesnim prostorima prema Starlingovom zakonu. Stoga, višak tečnosti ( tj., tečnost koja ne poboljša perfuziju ) će izazvati ili pogoršati edem u plućima, srcu, crevima, koži, mozgu i drugih tkiva. S vremena na vreme, to dovodi do otkazivanja organa, kao što su respiratorna insuficijencija, abdominalni kompartment sindrom ili cerebralni edem i hernijaciju [36, 37]. Mnogobrojna istraživanja su u
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
86
korelaciji da pozitivnu ravnotežu tečnosti prati smanjenje preživljavanja u ARDS-u [38, 39] i, takođe, može da ometa oslobođenje od mehaničke ventilacija. Pozitivan bilans tečnosti, zajedno u ranoj nadoknadi i tokom četiri dana lečenja, je u vezi sa povećanim rizikom od smrtnosti u septičkom šoku. Centralni venski pritisak može biti koristan monitoring i vodič adekvatne nadoknade tečnosti u prvih 12 sati reanimacije septičkog šoka, ali postaje nepouzdan marker balansa tečnosti nakon toga. Optimalano preživljavanje u VASST studiji je postignuto sa pozitivnim balansom tečnosti od oko 3 L na 12 sati [40]. Literatura
1. Angus DC, Linde-Zwirble WT, Lidicker J, et al: Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care
Med 2001; 29:1303–1310. 2. Dellinger RP: Cardiovascular management of septic shock. Crit Care Med 2003; 31:946–
955 3. Martin GS, Mannino DM, Eaton S, et al: The epidemiology of sepsis in the United States
from 1979 through 2000. N Engl J Med 2003; 348:1546–1554. 4. Linde-Zwirble WT, Angus DC: Severe sepsis epidemiology: Sampling, selection, and
society. Crit Care 2004; 8:222–226. 5. Dombrovskiy VY, Martin AA, Sunderram J, et al: Rapid increase in hospitalization and
mortality rates for severe sepsis in the United States: A trend analysis from 1993 to 2003. Crit Care Med 2007; 35:1414–1415.
6. Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med 2004; 32:858–8731.
7. Dellinger RP, Levy MM, Rhodes A,et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med 2013; 41:580–637.
8. Rivers E, Nguyen B, Havstad S, et al; Early Goal-Directed Therapy Collaborative Group: Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J
Med 2001; 345:1368–1377. 9. Early Goal-Directed Therapy Collaborative Group of Zhejiang Province:The effect of
early goal-directed therapy on treatment of critical patients with severe sepsis/septic shock: A multi-center, prospective,randomized, controlled study [in Chinese]. Zhongguo
Wei Zhong Bing Ji Jiu Yi Xue 2010; 6:331–334. 10. Supplemental Digital Content 2, http://links.lww.com/CCM/A615. 11. Brunkhorst FM, Engel C, Bloos F, et al; German Competence Network Sepsis (SepNet):
Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med
2008; 358:125–139. 12. Guidet B, Martinet O, Boulain T, et al: Assessment of hemodynamic efficacy and safety
of 6% hydroxyethylstarch 130/0.4 vs. 0.9% NaCl fluid replacement in patients with severe sepsis: The CRYSTMAS study. Crit Care 2012; 16:R94.
13. Perner A, Haase N, Guttormsen AB, et al; 6S Trial Group; Scandinavian Critical Care Trials Group: Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N
Engl J Med 2012; 367:124–134. 14. Myburgh JA, Finfer S, Bellomo R, et al; CHEST Investigators; Australian and New
Zealand Intensive Care Society Clinical Trials Group: Hydroxyethyl starch or saline for fluid resuscitation in intensive care. N Engl J Med 2012; 367:1901–1911.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
87
15. Perel P, Roberts I: Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database Syst Rev 2011; 3:CD000567.
16. Schortgen F, Lacherade JC, Bruneel F, et al: Effects of hydroxyethylstarch and gelatin on renal function in severe sepsis: A multicentre randomised study. Lancet 2001; 357:911–916.
17. McIntyre LA, Fergusson D, Cook DJ, et al; Canadian Critical Care Trials Group: Fluid resuscitation in the management of early septic shock (FINESS): A randomized controlled feasibility trial. Can J Anaesth 2008; 55:819–826.
18. Brunkhorst FM, Engel C, Bloos F, et al; German Competence Network Sepsis (SepNet): Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med
2008; 358:125–139. 19. Finfer S, Bellomo R, Boyce N, et al; SAFE Study Investigators: A comparison of
albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 2004; 350:2247–2256.
20. Delaney AP, Dan A, McCaffrey J, et al: The role of albumin as a resuscitation fluid for patients with sepsis: A systematic review and metaanalysis. Crit Care Med 2011; 39:386–391.
21. Bozza FA, Carnevale R, Japiassu AM, et al. Early fluid resustitation in sepsis: Evidence and perspectives. Shock 2010; 34:40-43.
22. Magder S: Central venous pressure: A useful but not so simple measurement.Crit Care
Med 2006; 34:2224–2227. 23. Bendjelid K, Romand JA: Fluid responsiveness in mechanically ventilated patients: A
review of indices used in intensive care. Intensive Care Med 2003; 29:352–360. 24. Malbrain ML, Deeren D, De Potter TJ: Intra-abdominal hypertension in the critically ill:
It is time to pay attention. Curr Opin Crit Care 2005; 11:156–171. 25. Marik PE,Cavallazzi R, Vasu T at al: Dynamic changes in arterial waveformderived
variables and fluid responsiveness in mechanically ventilated patients: A systemic review of the literature. Crit Care Med 2009; 37:2642-2647.
26. Pinsky MR, Payen D: Functional hemodynamic monitoring. Crit Care 2005; 9:566–572. 27. Levy MM, Dellinger RP, Townsend SR, et al; Surviving Sepsis Campaign: The
Surviving Sepsis Campaign: Results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med 2010; 38:367–374.
28. Hébert PC, Wells G, Blajchman MA, et al: A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999; 340:409–417.
29. Marik PE, Sibbald WJ: Effect of stored-blood transfusion on oxygen delivery in patients with sepsis. JAMA 1993; 269:3024–3029.
30. Lorente JA, Landín L, De Pablo R, et al: Effects of blood transfusion on oxygen transport variables in severe sepsis. Crit Care Med 1993; 21:1312–1318.
31. Fernandes CJ Jr, Akamine N, De Marco FV, et al: Red blood cell transfusion does not increase oxygen consumption in critically ill septic patients. Crit Care 2001; 5:362–367.
32. College of American Pathologists: Practice parameter for the use of fresh-frozen plasma, cryoprecipitate, and platelets. JAMA 1994; 271:777–781.
33. Canadian Medical Association Expert Working Group: Guidelines for red blood cell and plasma transfusion for adults and children.Can Med Assoc J 1997; 156:S1–S2.
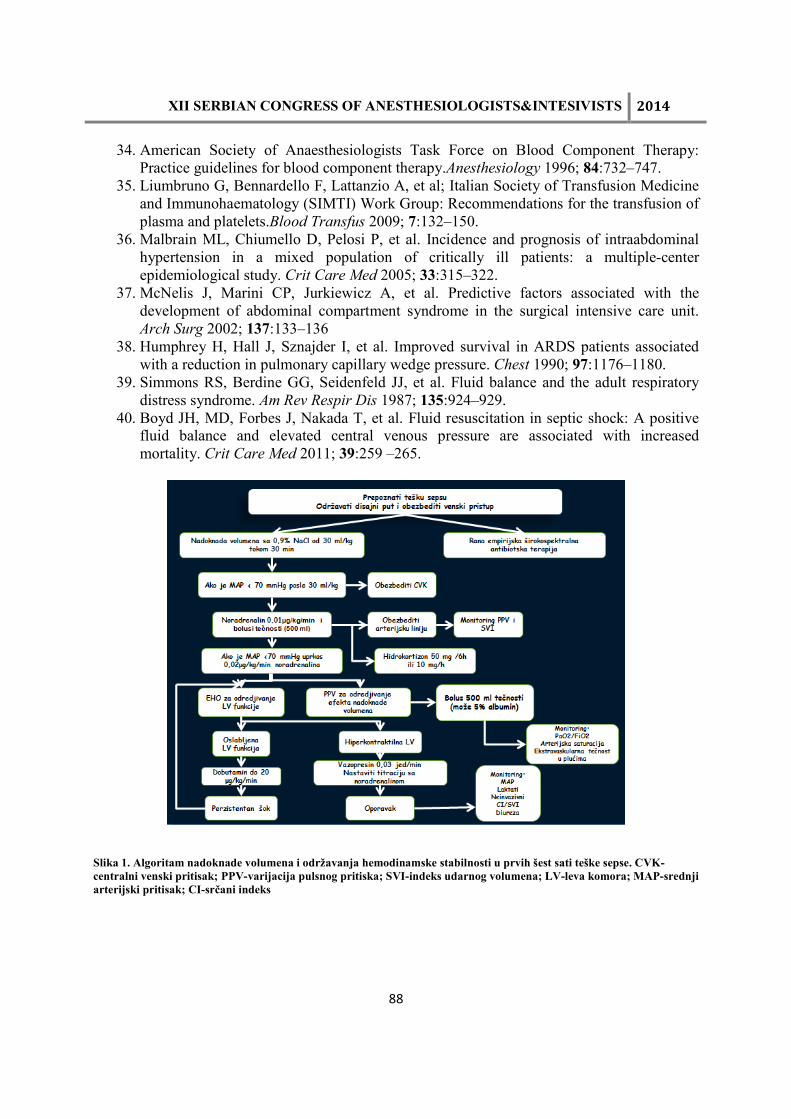
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
88
34. American Society of Anaesthesiologists Task Force on Blood Component Therapy: Practice guidelines for blood component therapy.Anesthesiology 1996; 84:732–747.
35. Liumbruno G, Bennardello F, Lattanzio A, et al; Italian Society of Transfusion Medicine and Immunohaematology (SIMTI) Work Group: Recommendations for the transfusion of plasma and platelets.Blood Transfus 2009; 7:132–150.
36. Malbrain ML, Chiumello D, Pelosi P, et al. Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: a multiple-center epidemiological study. Crit Care Med 2005; 33:315–322.
37. McNelis J, Marini CP, Jurkiewicz A, et al. Predictive factors associated with the development of abdominal compartment syndrome in the surgical intensive care unit. Arch Surg 2002; 137:133–136
38. Humphrey H, Hall J, Sznajder I, et al. Improved survival in ARDS patients associated with a reduction in pulmonary capillary wedge pressure. Chest 1990; 97:1176–1180.
39. Simmons RS, Berdine GG, Seidenfeld JJ, et al. Fluid balance and the adult respiratory distress syndrome. Am Rev Respir Dis 1987; 135:924–929.
40. Boyd JH, MD, Forbes J, Nakada T, et al. Fluid resuscitation in septic shock: A positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med 2011; 39:259 –265.
Slika 1. Algoritam nadoknade volumena i održavanja hemodinamske stabilnosti u prvih šest sati teške sepse. CVK-centralni venski pritisak; PPV-varijacija pulsnog pritiska; SVI-indeks udarnog volumena; LV-leva komora; MAP-srednji arterijski pritisak; CI-srčani indeks
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
89
POTPORNA TERAPIJA U SEPSI: VEROVANJA I ČINJENICE
JELENA VELIČKOVIĆ1, VESNA BUMBAŠIREVIĆ1,2, BOJAN JOVANOVIĆ1,2, DEJAN VELIČKOVIĆ2,3, BILJANA DRAŠKOVIĆ 4,5, GORAN RAKIĆ 4,5
1Centar za anesteziju Kliničkog centra Srbije, Beograd,2Medicinski fakultet Univerziteta u Beogradu, 3Klinika za digestivnu hirurgiju Kliničkog centra Srbije, Beograd, 4Služba za anesteziju, intenzivnu terapiju i terapiju bola, Klinika za dečju hirurgiju, Institut za zdravstvenu zaštitu dece i omladine Vojvodine, Novi Sad,5Medicinski fakultet Univerziteta u Novom Sadu
Email: [email protected]
SUMMARY
Sepsis represents huge health problem and an economic burden worldwide because of the growing incidence, costly treatment and high mortality. Multiorgan failure due to tissue hypoperfusion is still a major cause of death. Antibiotic treatment and hemodynamic support are the cornerstone of severe sepsis therapy, but patients who survive hemodynamic instability and organ dysfunction may still suffer from complications and be in need for various supportive treatments. Although there is no clear evidence to quantify the importance of such complications on outcome, the anticipated impact is huge having in mind the exhausted physiologic reserves of critically ill patients.
Supportive therapies of sepsis represent heterogenous therapeutic modalities such as: administration of blood products, immunoglobulins, mechanical ventilation, sedation and muscle relaxants, nutrition, stress ulcer and deep venous thrombosis prophylaxis, renal replacement therapy, and other. There is much controversy and lack of prospective studies regarding their impact on outcome of sepsis. This review summarises current evidence contained in the international and domestic guidelines for diagnostics, prevention and treatment of sepsis and septic shock.
Uvod
Sepsa je veliki zdravstveni i ekonomski problem u celom svetu zbog toga što je incidenca u porastu, lečenje skupo a smrtnost velika.1Najznačajniji uzrok mortaliteta u sepsi je razvoj multiorganske disfunkcije zbog tkivne hipoperfuzije koja karakteriše tešku sepsu i septični šok. Antibiotska terapija i medikamentozna hemodinamska potpora predstavljaju osnovu lečenja ali se kod bolesnika koji prežive cirkulatornu insuficijenciju i organsku disfunkciju mogu javiti komplikacije poput plućne embolije ili stres ulkusa.2 Iako uticaj tih komplikacija na mortalitet nije jasno kvantifikovan u literaturi, on je nesumnjivo značajan imajući u vidu smanjene fiziološke rezerve ovih bolesnika.
Postoje brojne kontroverze i nedostatak prospektivnih istraživanja koja se odnose na efekte potporne terapije na ishod kod bolesnika sa teškom sepsom. Savremena saznanja su objedinjena i

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
90
na osnovu njih su sačinjene preporuke sadržane u međunarodnom i domaćem vodiču za dijagnostiku, prevenciju i lečenje sepse, teške sepse i septičnog šoka.1,3
Primena produkata krvi
Transfuzije eritrocita se koriste kod kritično obolelih sa ciljem povećanja kapaciteta krvi za transport kiseonika i izbegavanja ozbiljnih posledica kiseoničnog duga.4 Nekoliko studija je pokazalo da transfuzije eritrocita kod septičnih bolesnika povećavaju transport ali ne i iskorišćavanje kiseonika u tkivima.5,6 Pored toga, septični bolesnici su izloženi rizicima od imunosupresivnih i mikrocirkulatornih efekata transfuzije.7,8 Optimalna koncentracija hemoglobina kod bolesnika sa teškom sepsom nije specifično istraživana, ali su rezultati velike randomizovane studije koja je poredila efekte liberalne i restriktivne strategije za transfuziju eritrocita pokazali da nivo hemoglobina od 70 do 90g/l u poređenju sa 100 do 120 g/l nije udružen sa povećanjem mortaliteta niti komplikacija kod kritično obolelih i septičnih bolesnika.9 I rezultati drugih studija govore u prilog restriktivnoj transfuzionoj terapiji, uz ograde koje se odnose na bolesnike sa miokardnom ishemijom i infarktom miokarda.10
Velika prospektivna, opservaciona, multicentrična studija je pokazala da 12.4% kritično obolelih primi zamrznutu svežu plazmu (ZSP) tokom lečenja, kao i da se 31% ZSP primeni kod bolesnika bez produženog INRa a 41% kod bolesnika bez krvarenja i sa INRom ispod 2.5.11 Takođe, prikazano je i veliko variranje u doziranju ZSP. Dokazano je da transfuzija ZSP kod bolesnika sa blagim koagulacionim poremećajem i bez aktivnog krvavljenja ne dovodi do korekcije protrombinskog vremena.12 Nema dokaza ni da primena ZSP ima koristi u korekciji težih poremećaja koagulacije kod bolesnika koji nemaju aktivno krvavljenje.
Septični bolesnici sa trombocitopenijom imaju povećan rizik od krvavljenja. Pored apsolutnog broja trombocita na potrebu za transfuzijom utiču i funkcija trombocita, planiranje invazivne procedure, priroda i mesto krvavljenja i prateći koagulacioni poremećaji.13,14 Savremeni vodiči preporučuju primenu trombocita u profilaktičke svrhe kod bolesnika sa teškom sepsom kada je njihov broj manji od 10000/mm3, dok se veći broj trombocita (≥50000/mm3) savetuje kada postoji aktivno krvavljenje ili se planira invazivna procedura.1,3,15
Tešku sepsu odlikuje aktivacija koagulacione kaskade, formiranje mikrotromba i potrošnja endogenih antikoagulantnih supstanci. Antitrombin III je potentan prirodni antikoagulans sa izraženim antiinflamatornim delovanjem. Zbog toga se verovalo da bi primena antitrombina III mogla biti od koristi kod bolesnika sa sepsom. Rezultati faze III kliničkog istraživanja su pokazali da primena antitrombina III nema nikakav efekat na 28-dnevni mortalitet kod bolesnika sa teškom sepsom.16 Iako je post-hoc analiza bolesnika sa najvišim rizikom za smrtni ishod pokazala bolje preživljavanje posebno kada se primenjuje bez heparina, potrebna su dodatna ispitivanja kako bi se AT III mogao preporučiti kao potporna terapija u stanju sepse.17

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
91
Imunoglobulini
Primena imunoglobulina u lečenju sepse je otvoreno pitanje godinama. Patofiziološko opravdanje za dodavanje poliklonalnih imunoglobulinaG (IvIg) odnosi se na neutralizaciju endotoksina, pojačanje fagocitoze i modifikaciju oslobađanja citokina iz stimulisanih mononuklearnih ćelija krvi.18 Uprkos ranijim ohrabrujućim rezultatima, meta-analiza izrađena u okviru Cochrane-ove kolaboracije koja je uključila i dve nove, velike randomizovane studije koje se odnose na primenu IvIg u terapiji adultne i neonatalne sepse pokazala je da IvIg ne doprinose smanjenju mortaliteta od sepse kod odraslih i novorođenčadi.19 Preparati imunoglobulina obogaćeni IgM mogli bi imati prednost nad poliklonalnim IvIg, te se ohrabruju istraživanja u tom smeru.20,21
Mehanička ventilacija
Akutni respiratorni distres sindrom (ARDS) je jedan od najčešćih oblika organske disfunkcije u sepsi a sprovođenje mehaničke ventilacije je od suštinskog značaja za preživljavanje septičnih bolesnika sa ARDSom. Neadekvatna mehanička ventilacija može izazvati dodatno oštećenje pluća putem prekomerne distenzije ventiliranih regiona pluća posebno u toku ventilacije visokim disajnim volumenom.22 Takođe, ponavljano otvaranje i kolabiranje alveola zbog neprilagođenih vrednosti end-ekspiratornog pritiska podstiče inflamaciju i oštećuje parenhim.
Iako postoje brojni ventilatorni i neventilatorni terapijski modaliteti za ARDS, jedina mera za koju je pokazano da smanjuje mortalitet je protektivna mehanička ventilacija. Ona podrazumeva ventiliranje pluća malim disajnim volumenom (do 6 ml/kg predviđene telesne mase) sa ciljem postizanja plato pritiska manjeg od 30 cmH2O.(23,24) Kod veoma teških formi ARDSa, može postojati potreba za redukcijom disajnog volumena do 4 ml/kg u cilju održavanja pomenutog plato pritiska, što obično ide na račun hiperkapnije koju treba dopustiti ukoliko ne postoje kontraindikacije.
Nije pokazana prednost bilo kog režima ventilacije (volumenom ili pritiskom kontrolisana) ukoliko su na jednak način ispoštovani principi protektivne ventilacije.
Primena PEEPa u cilju poboljšanja oksigenacije i prevencije atelektotraume je imperativ kod bolesnika sa ARDSom.25,26 Titrovanje PEEPa vrši se ili sa ciljem postizanja najbolje komplijanse ili najbolje oksigenacije pri datom FiO2 .
27
Pokazano je da konzervativna strategija u nadoknadi tečnosti u ARDSu ima prednosti u odnosu na liberalnu, jer iako ne utiče na 60-dnevni mortalitet, uzrokuje poboljšanje plućne funkcije, skraćuje trajanje mehaničke ventilacije i boravak u jedinici intenzivnog lečenja.28
Sedacija, analgezija i neuromišićna blokada
Dugogodišnja je praksa da se kod bolesnika na mehaničkoj ventilaciji koristi duboka sedacija. Međutim, pokazano je da ograničeno korišćenje sedacije putem intermitentne primene, dnevnog

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
92
prekida kontinuirane sedacije ili titrovanja do željenih efekata doprinosi kraćem trajanju mehaničke ventilacije, bržem otpustu iz JIL i kraćoj hospitalizaciji.29
Rezultati ACURASYS studije ukazuju na korist od kratkotrajne miorelaksacije (do 48h) u ranoj fazi teškog ARDSa.30 Moguće je da se uočeno poboljšanje preživljavanja i bolja gasna razmena mogu objasniti manjom učestalošću VALIja što u ovoj studiji potvrđuje manja učestalost barotraume i pneumotoraksa u cisatrakurijumskoj grupi. Takođe, relaksacija omogućava neometano izvođenje protektivne ventilacije pluća koja putem manje biotraume rezultuje u nižoj koncentraciji proinflamatornih citokina.
Glikoregulacija
Prethodnu deceniju obeležile su brojne studije iz oblasti glikoregulacije kod kritično obolelih kojima je nesumnjivo potvrđen štetan uticaj hiperglikemije na ishod kod ovih bolesnika.31,32
Početno oduševljenje protokolima sa ciljem održavanja glikemije u normalnom opsegu zamenili su pragmatičniji algoritmi sa ciljem održavanja glikemije ispod 10 mmol/l uz obavezan intenzivan monitoring šećera u krvi.1,3
Nutricija
Iako postoje brojne smernice za parenteralnu i enteralnu ishranu kod kritično obolelih, opservacione studije pokazuju da čak 40% kritično obolelih nema nikakvu nutritivnu potporu tokom boravka u jedinicama intenzivnog lečenja a da preko 60% obolelih ne dobije bilo kakvu ishranu tokom prvih 48h.33 Novi internacionalni i nacionalni vodič za lečenje sepse sugeriše ranu primenu oralne ili enteralne ishrane, u prvih 48h od postavljanja dijagnoze teške sepse.1,3 Iako nema mnogo studija koje ispituju uticaj ranog uvođenja enteralne ishrane na mortalitet, dokazan je povoljan efekat na incidencu infekcije, dužinu mehaničke ventilacije, boravka u JIL i hospitalizacije.34,35 Ipak rano započinjanje ne znači i uvođenje punog kalorijskog unosa. Rezultati EDEN studije pokazuju da je pun kalorijski unos rano u toku sepse, povezan sa češćom gastrointestinalnom intolerancijom i većim rizikom za infekcije.36 Rezultati novijih istraživanja ne preporučuju primenu omega-3 masnih kiselina kod septičnih bolesnika na mehaničkoj ventilaciji, jer je pokazan nepovoljan uticaj na mortalitet, kao ni primenu imunonutricije.37
Ostalo
Stavovi vezani za primenu nekih oblika potporne terapije u teškoj sepsi, poput potpore bubrežnoj funkciji, profilaksi duboke venske tromboze i profilaksi stres ulkusa nisu se značajnije menjali u godinama između dve revizije internacionalnog vodiča za lečenje sepse, teške sepse i septičnog šoka.3 Nasuprot tome, rezultati kliničkih studija doprineli su drastičnoj promeni stava o primeni rekombinantnog aktiviranog proteina C i uzrokovali povlačenje preporuke za njegovu primenu u sepsi.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
93
Kritično oboleli koji se leče od teške sepse u jedinicama intenzivnog lečenja često dobijaju pored osnovne i veoma raznovrsne oblike potporne terapije. Nekada je to svrsishodno a nekada, kao u stanju uznapredovaale multiorganske disfunkcije ne doprinosi preživljavanju a značajno narušava kvalitet života pacijenata i njihovih porodica uz enormno povećanje troškova.38
Zato bi bilo poželjno da se rano u toku lečenja postave realni terapijski ciljevi u skladu sa prognozom i eventualno sprovede palijativno lečenje.
Kako bi se jasno mogao proceniti zbirni efekat različitih oblika potporne terapije na ishod lečenja teške sepse, neophodna su dodatna istraživanja u okviru kojih bi se na dokazima zasnovani protokoli testirali u kliničkoj praksi.
Literatura:
1. Nacionalni vodič dobre kliničke prakse za dijagnostikovanje i lečenje sepse, teške sepse i septičnog šoka, Republička stručna komisija za izradu i implementaciju vodiča dobre kliničke prakse, Ministarstvo zdravlja republike Srbije; Beograd, 2013
2. Perez J, Dellinger RP, International Sepsis Forum. Other supportive therapies in sepsis. Intensive Care Med. 2001; 27 Suppl 1:S116-27.
3. Dellinger RP, Levy MM, Rhodes A, et al: Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013; 41:580-637
4. Russell JA, Phang PT. The oxygen delivery/consumption controversy: an approach to management of the critically ill. Am J Respir Crit Care Med 1994;149:533-7.
5. Lorente JA, Landin L, De Pablo R, et al. Effects of blood transfusion on oxygen transport variables in severe sepsis. Crit Care Med 1993;21:1312-1318.
6. Fernandes CJ Jr, Akamine N, De Marco FV, et al. Red blood cell transfusion does not increase oxygen consumption in critically ill septic patients. Crit Care 2001;5:362-7
7. Bordin JO, Heddle NM, Blajchman MA. Biologic effects of leukocytes present in transfused cellular blood products. Blood 1994;84:1703-21
8. Langenfeld JE, Livingston DH, Machiedo GW. Red cell deformability is an early indicator of infection. Surgery 1991;110:398-404
9. Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999;340:409-17
10. Hajjar LA, Vincent JL, Galas FR, et al. Transfusion requirements after cardiac surgery: The TRACS randomized controlled trial. JAMA 2010;304:1559-67
11. Stanworth JS, Walsh TS, Prescott RJ et al. A national study of plasma use in critical care: clinical indications, dose and effect on prothrombin time. Critical Care 2011; 15:R108
12. Abdel-Wahab OI, Healy B, Dzik WH: Effect of fresh-frozen plasma transfusion on prothrombin time and bleeding in patients with mild coagulation abnormalities. Transfusion 2006;46:1279-85
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
94
13. Schiffer CA, Anderson KC, Bennett CL, et al. American Society of Clinical Oncology: Platelet transfusion in patients with cancer: Clinical practice guidelines of the american society of clinical oncology. J Clin Oncol 2001; 19:1519-38
14. Katz JN, Kolappa KP, Becker RC. Beyond thrombosis. The versatile platelet in critical Illness. Chest 2011; 139(3):658–668
15. Liumbruno G, Bennardello F, Lattanzio A, et al; Italian Society of Transfusion Medicine and Immunohaematology (SIMTI) Work Group: Recommendations for the transfusion of plasma and platelets.BloodTransfus2009; 7:132–150
16. Warren BL, Eid A, Singer P, et al; KyberSept Trial Study Group: Caring for the critically ill patient. High-dose antithrombin III in severesepsis: A randomized controlled trial. JAMA 2001; 286:1869–1878
17. Wiedermann CJ, Hoffmann JN, Juers M, et al; KyberSept Investigators: High-dose antithrombin III in the treatment of severe sepsis in patients with a high risk of death: Efficacy and safety. Crit Care Med 2006; 34:285–292
18. Andersson J, Skansen-Saphir U, Sparrelid E, et al. Intravenous immune globulin affects cytokine production in T lymphocytes and monocytes/macrophages. ClinExpImmunol 1996;104(Suppl):1:10-20
19. Alejandria MM, Lansang MAD, Dans LF, Mantaring III JB. Intravenous immunoglobulin for treating sepsis, severe sepsis and septic shock. Cochrane Database of Systematic Reviews 2013; 9:CD001090
20. Molnar Z, Nierhaus A, Esen F. Immunoglobulins in Sepsis: Which patients will benefiit the most? Annual Update in intensive Care and emergency Medicine. Edited by J.-L.Vincent,Springer 2013;145-152.
21. Berlot G, Vassallo MC, Busetto N et al. Relationship between the timing of administratin of IgM and IgA enriched immunoglobulins in patients with severe sepsis and sepstic shock and the outcome: A retrospective analysis. J Crit Care 2012;27:167-171
22. Tsuno K, Miura K, Takeya M, Kolobow T, Morioka T. Histopathologic pulmonary changes from mechanical ventilation at high peak airway pressures. Am Rev Respir Dis 1991;143:1115-20
23. Acute Respiratory Distress Syndrome Network: Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308
24. Amato MB, Barbas CS, Medeiros DM, et al: Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome.N Engl J Med 1998; 338:347–354
25. Meade MO, Cook DJ, Guyatt GH, et al; Lung Open Ventilation Study Investigators: Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. JAMA 2008; 299:637–645
26. Pesenti A, Marcolin R, Prato P, et al: Mean airway pressure vs. Positive end-expiratory pressure during mechanical ventilation. Crit Care Med 1985; 13:34–37d 2000;162(4Pt1) :1361–1365
27. Mercat A, Richard JC, Vielle B, et al; Expiratory Pressure (Express)Study Group: Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: A randomized controlled trial. JAMA 2008; 299:646–655
28. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDSARDS) Clinical Trials Network; Wiedemann HP, Wheeler AP, Bernard GR, et al:

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
95
Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006; 354:2564–2575
29. Girard TD, Kress JP, Fuchs BD, et al: Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): A randomised controlled trial. Lancet 2008; 371:126–134
30. Papazian L, Forel JM, Gacouin A, et al; ACURASYS Study Investigators: Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med
2010; 363:1107–1116 31. Annane D, Cariou A, Maxime V, et al; COIITSS Study Investigators: Corticosteroid
treatment and intensive insulin therapy for septic shock in adults: A randomized controlled trial. JAMA 2010; 303:341–348
32. The NICE-SUGAR Study Investigators: Intensive versus conventional glucose control in critically ill patients. N Engl J Med 2009; 360:1283–1297
33. Heyland DK, Schroter –Noppe D, Drover JW,et al. Nutrition support in the critical care setting: current practice in Canadian ICUs-opportunities for improvement? J Parenter Enteral Nutr 2003;27:74-83
34. Kompan L, Vidmar G, Spindler-Vesel A, et al: Is early enteral nutrition a risk factor for gastric intolerance and pneumonia? ClinNutr2004;23:527–532
35. Doig GS, Heighes PT, Simpson F, et al: Early enteral nutrition, provided within 24 h of injury or intensive care unit admission, significantly reduces mortality in critically ill patients: A meta-analysis of randomised controlled trials. Intensive Care Med
2009;35:2018–2027 36. The National Heart, Lung and Blood Institute ARDS Clinical Trial Network. Initial
trophic vs full enteral feeding in patients with acute lung injury. The EDEN randomized trial. JAMA 2012;307(8):795-803
37. Pontes-Arruda A, Martins LF, de Lima SM, et al; Investigating Nutritional Therapy with EPA, GLA and Antioxidants Role in Sepsis Treatment (INTERSEPT) Study Group: Enteral nutrition with eicosapentaenoic acid, -linolenic acid and antioxidants in the early treatmentof sepsis: Results from a multicenter, prospective, randomized, double-blinded, controlled study: The INTERSEPT study. Crit Care 2011; 15:R144
38. Thompson BT, Cox PN, Antonelli W, et al. American Thoracic Society. European Respiratory Society. European Society of Intensive Care Medicine. Society of Critical care Medicine. Societe de Reanimation de langue Francaise: Challenges in end-of-life care in the ICU: statement of the 5th International Consensus Conference in Critical Care: Brussels, Belgium, April 2003: executive summary. Crit Care Med 2004;32:1781-4.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
96
DIAGNOSIS AND PREVENTIVE STRATEGIES OF ICU INFECTION BOJAN JOVANOVIĆ (1), VESNA BUMBAŠIREVIĆ (1), JELENA VELIČKOVIĆ (2), LJILJANA MARKOVIĆ – DENIĆ (3), MILIĆ VELJOVIĆ (4), GORAN RAKIĆ (5) 1Urgentni centar, Centar za anesteziologiju i reanimatologiju, Klinički centar Srbije, Beograd,2Klinika za digestivne bolesti, Centar za anesteziologiju i reanimatologiju, Klinički centar Srbije, Beograd,3 Institut za epidemiologiju, Medicinski fakultet, Univerziteta u Beogradu,4Klinika za anesteziologiju i intenzivno lečenje, VMA,5 Služba za anesteziju, intenzivnu terapiju i terapiju bola, Klinika za dečiju hirurgiju, Institut za zdravstvenu zaštitu dece i omladine vojvodine, Novi Sad Abstract: Infections are frequent in intensive care units (ICUs) because the patients are likely to have chronic illnesses and acute physiologic derangements, indwelling catheterization is common, and multidrug resistant pathogens that are difficult to eradicate are isolated with increasing frequency due to enhanced selective antimicrobial and colonization pressure. Restricted and judicious antibiotic utilization, often implemented as part of a global institutional antimicrobial stewardship program, can decrease selective pressure that promotes emergence of resistant bacterial strains. The most common infections in the ICU are those associated with indwelling devices, namely catheter associated urinary tract infection, ventilator-associated pneumonia, and intravascular catheter-related bloodstream infection.Infection control measures to prevent the spread of multidrug-resistant organisms include hand hygiene, barrier precautions, chlorhexidine bathing and active surveillance for certain pathogens and reduction of catheterization utilization. UVOD Iako se u proseku manje od 10%bolničkih posteljanalazi u jedinicama intenzivnog lečenja (JIL), više od 20% bolničkih infekcija nastaje upravo tamo (1). Bolničke infekcija povećavaju mortalitet ali i dužinu lečenja. Infekcije i sepsa su vodeći uzrok smrti van kardioloških JIL i više od 40% novca u JIL se potroši na njihov tretman (2).Najčešće infekcije u JIL su pneumonije udružene sa mehaničkom ventilacijom(ventilator associated pneumonia - VAP), sepsa nastala usled prisustva centralnih venskih katetera i urinarnih katetera. Incidencija varira u svetu u zavisnosti od razvijenosti zdravstvenog sistema, i veća je u zemljama u razvoju, gde na primer incidencija VAP-a može da iznosi i do 52%. U razvijenim zemljama je međutim obrnuta situacija, i u JIL su infekcije urinarnog trakta najčešće nozokomnijalne infekcije, sa stopom od40% (3). Faktori koji utiču na povećanu incidenciju infekcija ali i loš ishod lečenja su pre svega veća prevalencija multirezistentnih uzročnika (među kojima su od značaja meticilin rezistentni Staphylococcus aureus, vancomycin-rezistentne enterococce kao i carbapenem-rezistentni Acinetobacter baumannii) (4). Međutim,od značaja su i stanje pacijenata na prijemu u JIL sa pratećim bolestima, kao i dugotrajno korišćenje katetera i ostalih invazivnih procedura (2). Prevalenca multirezistentnih bakterija je u stalnom rastu svuda u svetu, te je primena preventivnih mera kao i poboljšanje dijagnostičkih postupaka i protokola neophodna radi adekvatnog zaustavljanja ovog procesa koji značajno povećava morbiditet i mortalitet u JIL. U cilju poboljšanja dijagnostikovanja i tretmana teške sepse i septičnog šoka publikovan je vodič
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
97
2013. po uzoru na svetske standarde. U njemu su, između ostalog, navedene i preporuke za dijagnostiku uzročnika i mesta infekcije kao i najefikasnije preventivne mere (5). U cilju identifikacije uzročnika i mesta infekcije uzimaju se hemokulture kao i drugi biološki materijali, i primenjuju se radiološke kao i druge “imaging” tehnike (5). Kod svake sumnje na postojanje bakterijemije bilo u bolničkim uslovima, bilo kod pacijenata na prijemu predlaže se uzimanje hemokulture. Preporučeno je uzimanje krvi za hemokulturu pre započinjanja primene antibiotika ako je to moguće i to sa najmanje 2 mesta (dve venepunkcije) (6).Međutim, i u slučajevima kada postoji normalan broj leukocita i ne tako klinički jasna slika bakterijemije, uzimanje hemokulture je od značaja (osteomijelitis, meningitis, artritis, endokarditis, febrilnost nepoznate etiologije i slično) (7). Tehnika uzorkovanja, broj uzoraka i volumen krvi koji se uzorkuje su od najvećeg značaja. Kod odraslih se uzima uzorak od minimalno 10 ml (poželjno 20 ml) krvi, dok kod dece to zavisi od telesne težine i varira od 1 ml do 20 ml. Treba uzimati u obzir da je bakterijemija najčešće intermitentnog tipa, međutim uzimanje uzorka tokom skoka telesne temperature nije ni senzitivna niti specifična za dijagnostikovanje bakterijemije. Takođe postoje bakterije za koje je teško diferencirati da li se radi o patogenu koji je uzročnik infekcije ili o kontaminaciji uzorka kao što su Corynebacterium species, Bacillus species, i koagulaza-negativan stafilokok(8). Dijagnostikovanje infekcije i sepse nastale usled prisustva centralnih venskih katetera se sastoji od kliničke evaluacije i mikrobioloških nalaza. Nastaje najčešće na četiri načina: kolonizacija kože, kontaminacija katetera, sekundarna infekcija usled bakterijemije iz drugog fokusa i kontaminacija infuzomatom (veoma retko, ali treba posumnjati ako pacijent ne spada u rizičnu grupu za nastanak ove komplikacije). Svaka pojava bakterijemije bez očiglednog uzročnika infekcije treba da uputi kliničara da posumnja na ovu vrstu infekcije. Povišena temperatura nije senzitivan parametar kod ove vrste infekcija (9). Obično se javlja hemodinamska nestabilnost, izmenjen mentalni status, klinički znaci sepse ali i disfunkcija katetera naglo nakon započinjanja infuzije. Uzorci krvi se uzimaju i iz katetera kao i sa periferije i to najbolje pre započinjanja ili promene antibiotske terapije. U slučaju hemokultura pozitivnih na Staph. aureus, koagulaza-negativan stafilokok ili Candidu u odsustvu drugog mogućeg izvora infekcije uvek treba sumnjati na kateter infekciju. U slučaju da laboratorija nije u mogućnosti da obavi kvantitativnu analizu kultura, savetuje se određivanje diferencijalno vreme pozitivnosti (differential time to positivity – DTP) (10). Time se detektuje rast bakterija iz uzorka iz katetera najmanje 2 sata pre detekcije iz uzorka iz periferne vene. U slučaju sumnje treba ukloniti kateter i eventualno poslati vrh katetera na mikrobiološku analizu. Pneumonije udružene sa mehaničkom ventilacijom (Ventilator associated pneumonia – VAP) mogu nastati nakon 48 sati od započinjanja mehaničke ventilacije. Uglavnom se klinički uočava postepen ili nagao početak novog ili progresivnog plućnog infiltrata i jednog ili više od sledećih znakova i simptoma: povišena temperatura, purulentna traheobronhijalna sekrecija, leukocitoza, tahipnea, izmenjena ventilacija pluća kao i poremećena oksigenacija. Radiografski snimak pluća je neophodno uraditi kod svake sumnje na VAP (11). Radi precizne identifikacije uzročnika potrebno je uzorkovati sputum i poslati ga na mikrobiološku analizu. Postoje razne metode za uzorkovanje sekreta iz donjih partija disajnog puta, i one se uglavnom dele na nebronhoskopske (slepe) i bronhoskopske. Nebronhoskopske tehnike su traheobronhijalni aspirat i mini-BAL (mini - bronhoalveolarna lavaža). U bronhoskopske metode spada bronhoalveolarna lavaža.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
98
Uzorak se šalje na analizu. Preporučuje se kvantitativna ili semi-kvantitativna tehnika za postavljanje dijagnoze. Kvantitativna metoda podrazumeva detekovanje kolonija bakterija iznad praga od 1000 do milion na ml uzorka u zavisnosti kojom metodom je uzet aspirat (12). Strategije za prevenciju intrahospitalnih infekcijapodrazumevaju primenu standardnih mera (higijena ruku, upotreba maski i rukavica, higijena sredine JIL, monitoring primenjenih mera) kao i mera izolacije (kontakt sa pacijentom, telesnim tečnostima kao i potpuna izolacija). Ne treba zaboraviti značaj edukacije osoblja koji su uključeni u tretman kritično obolelih pacijenata, kroz treninge o primeni protokola i ranom prepoznavanju infekcije. Preporučuje se da sve mere prevencije kao i monitoring vrši za to adekvatnoedukovani tim (13). Antibiotici se pažljivo primenjuju na osnovu epidemioloških i mikrobioloških karakteristika određene jedinice intenzivnog lečenja stalnom evaluacijom i primenom odgovarajućih protokola. Lokalni protokol određuje pre svega tim na čijem je čelu intenzivista uz konsultacije infektologa, farmakologa i mikrobiologa (14). Higijena ruku je najznačajnija mera prevencije transmisije mikroorganizama sa jednog mesta na drugo u sredini JIL. SZO je u okviru “Save Lives” kampanje definisala pet korakakada zdravstveni radnici treba da operu ruke: pre dodira pacijenta, pre započinjanja aseptične procedure, nakon kontakta sa telesnim tečnostima, nakon dodira pacijenta i nakon dodira sredine oko pacijenta. Sredstvo za pranje ruku treba da bude na bazi alkohola. Voda i sapun se ne preporučuju samostalno zbog smanjene efikasnosti ali i dokaza da neke rezistente bakterije (VRE) zahtevaju minimalno 30 sekundi pranja da bi došlo do eradikacije, jedino u slučaju prevencije širenja Clostridium difficile infekcije kada je dokazano da alkohol ne uništava spore (16). Sredstva na bazi alkohola su podjednako efikasna i protih gram pozitivnih i gram negativnih mikoorganizama, za razliku od hlorheksidina, kao i protiv virusa (npr. influenca), i zahtevaju manje vremena do potpunog dejstva (17). Problem sa sredstvima za dezinfekciju, a naročito hloheksidinom, je mogućnost transmisije u slučaju da se preparat ne koristi jednokratno i na samo jednom pacijentu, usled kontaminacije samog sredstva neadekvatnim rukovanjem (to se odnosi na sva sredstva za dezinfekciju) . Upravo zbog toga je FDA donela određene preporuke kojima se ističe značaj prevencije kontaminacije preparata i proizvodnje u pakovanjima za jednokratnu upotrebu (18). U poslednje vreme se dosta raspravlja o značaju monitoringa adekvatne prevencije transmisije kao iedukacijiosoblja koji bi učestvovali u tome. Kupanje (nega) pacijenata hlorheksidinom se preporučuje svakog dana, jer je hlorheksidin glukonat antiseptično sredstvo sa širokim spektrom dejstva i kao efektivna metoda smanjenja incidencije infekcija kao i kolonizacije rezistentnim mikroorganizmima. Efikasnost je dokazana u mnogim studijama, ali zabrinjava činjenica pojave rezistencije na hlorheksidin (19). Od ostalih preventivnih mera, navedenih u vodiču, izdvajaju se aseptična tehnika plasiranja centralnih venskih i drugih katetera, upotreba endotrahealnih tubusa sa subglotičnom aspiracijom, položaj sa podignutim uzglavljem kod intubiranih pacijenata, selektivna oralna i digestivna dekontaminacija, kao i upotreba oralnog hlorheksidin glukonata (0,2%) (5). Treba na kraju naglasiti još jednom, da je epidemiološko praćenje nozokomnijalnih infekcija kamen temeljac uspešnog programa kontrole bolničkih infekcija. To podrazumeva precizan uvid u stopu i prevalenciju određenih infekcija kao i prouzrokovača, praćenje doslednosti primene

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
99
svih preventivnih mera od strane medicinskog osoblja u JIL. Ovo najčešće obavljaju epidemiolozi i podrazumeva sledeće: rutinska kontrola mikrobioloških nalaza, redovne vizite u JIL, pregled otpusnih lista, patoloških i obdukcionih nalaza, kao i evaluacija pacijenata pri ponovnom prijemu u JIL. Reference:
1. Fridkin SK, Welbel SF, Weinstein RA. Magnitude and prevention of nosocomial infections in the intensive care unit. Infect Dis Clin North Am. 1997;11(2):479
2. Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, Reinhart K, EPIC II Group of Investigators. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302(21):2323.
3. Lo E, Nicolle L, Classen D, Arias KM, Podgorny K, et all. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals. Infect Control Hosp Epidemiol. 2008 Oct;29 Suppl 1:S41-50.
4. Schwaber MJ, Carmeli Y. The effect of antimicrobial resistance on patient outcomes: importance of proper evaluation of appropriate therapy. Crit Care. 2009;13(1):106. Epub 2009 Jan 12.
5. Bumbaširević V et all. Sepsa, teška sepsa i septični šok. Nacionalni vodič dobre kliničke prakse. Ministarstvo zdravlja Republike Srbije 2013.
6. Dellinger RP, Levy MM, Rhodes A et all. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Intensive Care Med. 2013 Feb;39(2):165-228
7. Seigel TA, Cocchi MN, Salciccioli J et all. Inadequacy of temperature and white blood cell count in predicting bacteremia in patients with suspected infection. J Emerg Med. 2012 Mar;42(3):254-9. Epub 2010 Jul 31.
8. Baron EJ, Miller JM, Weinstein MP et all. A guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2013 recommendations by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). Clin Infect Dis. 2013;57(4):e22.
9. Marschall J, Mermel LA, Fakih M, Hadaway L, Kallen A et all. Strategies to prevent central line-associated bloodstream infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014 Jul;35(7):753-71.
10. Safdar N, Fine JP, Maki DG. Meta-analysis: methods for diagnosing intravascular device-related bloodstream infection. Ann Intern Med. 2005;142(6):451.
11. American Thoracic Society, Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171(4):388.
12. Canadian Critical Care Trials Group. A randomized trial of diagnostic techniques for ventilator-associated pneumonia. N Engl J Med. 2006;355(25):2619.
13. Dellit TH, Owens RC, McGowan JE Jr, Infectious Diseases Society of America, Society for Healthcare Epidemiology of America. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44(2):159
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
100
14. Kollef MH, Fraser VJ. Antibiotic resistance in the intensive care unit. Ann Intern Med. 2001;134(4):298.
15. World Health Organization. WHO guidelines on hand hygiene in health care : first global patient safety challenge : clean care is safer care. Geneva, Switzerland: World Health Organization, Patient Safety; 2009.
16. Stelfox HT, Bates DW, Redelmeier DA. Safety of patients isolated for infection control. JAMA. 2003;290(14):1899.
17. Climo MW, Yokoe DS, Warren DK, Perl TM, Bolon M, Herwaldt LA. Effect of daily chlorhexidine bathing on hospital-acquired infection. N Engl J Med. 2013 Feb;368(6):533-42.
18. Over-the-Counter Topical Antiseptic Products: Drug Safety Communication - FDA Requests Label Changes and Single-Use Packaging to Decrease Risk of Infection
19. Climo MW, Yokoe DS, Warren DK, Perl TM, Bolon M, Herwaldt LA. Effect of daily chlorhexidine bathing on hospital-acquired infection. N Engl J Med. 2013 Feb;368(6):533-42.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
101
ANESTEZIOLOŠKI PRISTUP ZA PREVREMENI POROĐAJ I INTERAKCIJE LEKOVA ANESTHETIC MANAGEMENT FOR PRETERM DELIVERY AND INTERACTIONS BETWEEN DRUGS TATJANA ILIĆ MOSTIĆ¹,², MIROSLAVA GOJNIĆ DUGALIĆ²,3, BORISLAVA PUJIĆ4, DANKA MOSTIĆ 3, MARIJA KUTLEŠIĆ5, RADAN STOJANOVIĆ 2,6
¹ Centar za anesteziologiju i reanimatologiju, Klinički Centar Srbije, Beograd,² Medicinski Fakultet, Univerzitet u Beogradu,3 Klinika za ginekologiju i akušerstvo, Klinički Centar Srbije, Beograd, 4 Klinika za ginekologiju i akušerstvo, Klinički Centar Vojvodine, Novi Sad, 5 Centar za anesteziologiju i reanimatologiju, Klinički Centar Niš, Niš, 6 Institut za farmakologiju, kliničku farmakologiju i toksikologiju, Univerzitet u Beogradu email:[email protected] Summary. The ideal method of delivery for the preterm infant remains controversial. Some studies suggest that the pretem fetus is at higher risk for acidosis during labor and delivery, and
the preterm infant is at higher risk for intraventricular hemorrhage. Preterm fetus is more
vulnerable than the term fetus to the depressant effects of analgesic and anesthetic drugs for the
following reasons: decreased protein available for drug binding and decreased protein drug
affinity by the protein that is present; higher levels of bilirubin, which may compete with the
drug for protein binding; greater drug access to the central nervous system because of the
presence of an incomplete blood-brain barrier; decreased ability to metabolize and excrete
drugs and higher incidence of acidosis during labor and delivery.
Uvod
Filozofija i pristup pacijentu u obstetriciji menjao se kroz prve dekade 20-og veka, što je imalo uticaja i na primenu anestezije u akušerstvu. Do 1900. akušeri su rođenje deteta smatrali fiziološkim procesom u koji je najbolje bilo ne mešati se, ni kao lekar, ni kao babica. Kritikovali su ’’nametljive metode’’ u normalnom porođaju. Nakon toga, nova generacija akušera zabrinuta za visok procenat komplikacija povezanih sa rutinskim porođajima počela je da zagovara aktivniji pristup porođaju. Prvaci ovog pokreta, kao što je Joseph Delee iz Čikaga, snažno su zagovarali rutinsku upotrebu epiziotomije, korišćenje forcepsa u porođaju i manuelno uklanjanje placente. Naravno, ove mere su takođe zahtevale veću potrebu za anestezijom.1
Definicije
Prevremeno rođeno dete je dete rođeno izmedju 20 i 37 nedelje od poslednje menstruacije (npr. najmanje tri nedelje pre očekivanog termina).2 Gestaciona starost je često nepoznata ili ju je tesko ustanoviti kod neonatusa koji su male telesne težine. Neki od ovih novorođenčadi su male telesne tezine (Small for Gestational Age -SGA) pre nego prevremeno rođeni. Novorođenče koje tezi manje od 2500 grama se smatra onim sa malom telesnom težinom (Low Birth Weight- LBW), bez obzira na gestacionu starost. Takodje, novorođenče koje teži manje od 1500 g na rođenju se smatra novorođenčetom sa veoma malom telesnom tezinom (Very Low Birth Weight-VLBW).
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
102
Dijagnoza i terapija
Inicijalna procena i terapija podrazumevaju pregled, intravensku rehidrataciju, odmor u postelji, monitoring srca bebe (Fetal Heart Rate-FHR) i ultrazvučnu procenu stanja. Ultrazvučna procena nije invazivna i može odrediti gestacionu starost i fetalnu težinu. Ako je potrebno, može se uraditi amniocenteza da bi se odredio stepen plućne maturacije i tražila eventualna infekcija. Jednom kad se uspostavi dijagnoza pretećeg PP, akušer određuje da li će započeti sa terapijom. Fiziologija kontrakcija uterusa
Kontraktilni elementi miometrijuma, glatki misići se sastoje od debelih (miozinskih) i tankih (aktinkskih) vlakana koji su u dodiru i prelaze jedan preko drugog, stvarajući silu za kontrakciju uterusa. Miometrijum ima pejsmejkerske ćelije sa spontanom kontraktilnom aktivnosću, koja utiče na aktivnost širom uterusa, pomoću gep junction veza između njih. Kontrakcija se može predvideti porastom intracelularnog kalcijuma preko influksa kalcijuma duž sarkoleme i/ili otpuštanjem iz sakroplazmatskog retikuluma. Hormoni i neurotransmiteri igraju ulogu regulacije uterusne aktivnosti izazivajući ponovno oslobađanje kalcijuma ili drugih jona preko receptorskih kanala i oslobađanjem skladištenog kalcijuma. Metode porođaja i anestezija
Asfiksija fetusa3 dodatno izaziva sledeće promene: 1) smanjen kapacitet vezujućih proteina (povećava se nivo slobodnog leka), 2) povećava se fetomaternalna razlika jona, koja izaziva “vezivanje jona” (npr. lokalne anestetike, opioide) u fetalnoj cirkulaciji, 3) povećanu propustljivst krvno-moždane barijere, 4) povećana je osetjivost miokarda na depresivne efekte anestetika.4
Vaginalni porođaj Anestetik upotrebljen tokom vaginalnog porođaja prevremnog deteta treba da uključi sledeće:1) zaustavljanje ekspulzionih napona pre kompletne cervikalne dilatacije, posebno kod karlične prezentacije, 2) izbegavanje prebrzog porođaja, koji rezultira u brzoj dekompenzaciji fetalnog srca i povećava rizik od intrakranijalne hemoragije, i 3) pomoć karličnom dnu i perineumu u olakšanju mekanog i kontrolisanog porođaja fetalne glave, što je posebno važno kod karlične prezentacije. Carski rez Većina anestetika koja se koristi za indukciju i održavanje opšte anestezije prolazi kroz placentu, i može dovesti do depresije već kompromitovanog prevremenog fetusa. Ako je carki rez neophodan, konvencionalno pravilo je da se primeni spinal ili epidural kako bi se izbegli depresivni efekti ovih supstanci.5 Međutim, ugroženost majke i fetalni distres, zahtevaju primenu opšte anestezije. Mnoge studije su pokazale da su prematurusi nakon spinalnih i epiduralnih anestezija u boljem stanju na porođaju nego oni izloženi opštoj anesteziji. Slično tome, Rolbin i saradnici 6 ukazuju da prevremeno rođena deca sa primenom epidruralne anestezije na carskom rezu, imaju viši Apgar skor u prvom i petom minutu, nego slična novorođenčad nakon opšte anestezije. Naposletku, primena kiseonika je od esencijalne važnosti, bez obzira na tip anestezije.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
103
Intereakcije između tokolitičke terapije i anestezije
Postoje najmanje tri situacije u kojima je akušerskim pacijentima potrebna anestezija nakon tokolitičke terapije. Prvo, kada nema efekta nakon primene tokolitika. U ovom slučaju pacijentima je potrebno ukinuti bol tokom porođaja i vaginalnog rađanja. Zatim, nekim pacijentima je potrebna anestezija za carski rez. Drugo, povremeno akušeri daju tokolitike pre i posle stavljanja serklaža. Treće, neki akušeri daju bolus dozu tokolitičkog agensa da poboljšaju stanje fetusa u slučaju distresa. Uteroplacentarna perfuzija je najoptimalnija tokom uterine dijastole. Zbog toga, relaksacija uterusa treba da dovede do poboljšanja uteroplacentne perfuzije. Beta- adrenergički agonisti
Ritodrin, terbutalin i fenoterol su najčesće korisćeni tokolitički lekovi. Oni efektivno odlažu porođaj za 48-72 sata, što omogućava primenu glikokortikoida za ubrzano sazrevanje pluća fetusa (maturacija). Preporučen lek od strane Američke agencije za lekove (U.S. Food and Drug Administration – FDA) je Ritodrin i njegova upotreba je ograničena na 48h. Takođe, treba naglasiti da se ovi lekovi isključivo daju u stanjima kada nema kontraindikacija.7
Primena anestetika Poželjno je odložiti primenu anestetika do hemodinamske stabilizacije majke. Međutim, ubrzan porođaj, abnormalna prezentacija i fetalni distres često zahtevaju hitnu primenu anestezije. Registruje se pojava intraoperativnog plućnog edema, sinusne tahikardije i ventrikularne aritmije tokom opšte anestezije kod pacijenata koji su primili terapiju beta-adrenergkim agonostima neposredno pre uvođenja u anesteziju. Preporuka je da se odloži uvođenje u anesteziju najmanje 10 minuta po prekidu primanja beta-adrenergičkih agonista. Kod primene regionalne anestezije neophodno je izbegavati agresivnu hidrataciju. Dati mali bolus tecnosti (npr. 250-500 ml. Ringer laktata), zatim postepenu epiduralnu anesteziju. Dodatni intravenski kristaloid i vazopresor je potrebno davati za održavanje maternalnog krvnog pritiska. Efedrin je najčeće vazopresor izbora. Efedrin, mešavina alfa i beta adrenergičkih agonista, je lek izbora za hipotenziju kod većine pacijenata zbog protektivnog efekta na uterini krvni protok (UBF). Međutim, treba biti oprezan kod davanja efedrina jer može pogoršati tahikardiju kod pacijentkinja koje su skoro primale beta-adrenergičkuu tokolitičku terapiju. Kod registrujemo poremećaje srčanog ritma, primenjujemo fenilefrin. Tokom primene opšte anestezije kod pacijenata koji su neposredno primili beta-adrenergičku tokolizu, treba izbegavati agense koji mogu pogoršati tahikardiju majke. Rezidualna maternalna tahikardija moze otežati procenu volumena, kao i dubinu anestezije. Može se primeniti i intravenski bolus lidokaina (1 mg/kg) tokom brzog uvođenja u opštu anesteziju, radi eventualnog smanjenja mogućnosti pojave aritmija tokom laringoskopije i intubacije. Hiperventilaciju treba izbegnuti, jer može ubrzati nastanak hipokalemije i potencijalnu hiperpolarizaciju membrane ćelija. Prati se neuromuskulatorna aktivnost stimulatorom perifernih nerava tokom opšte anestezije. Magnezijum sulfat
Dugogodišnje je iskustvo u upotrebi Mg-sulfata u akušerstvu. Godine 1959., Hall i saradnici8 su prvi obajavili da hipermagnezemija produžava dužinu porođaja kod pacijentkinja koje imaju

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
104
hipertenziju u trudnoći. Dalje studije su pokazale da Mg-sulfat deluje i smanjuje uterusnu aktivnost. On je tokolitik prve linije u mnogim centrima zbog svoje aktivnosti, a delom i zato što daje manje kardiovaskularnih neželjenih efekata kod pacijentkinja, nego kad su u pitanju beta-adrenergički tokolitici.9
Neželjeni efekat magnezijum sulfata može biti i promenjena neuromuskularna funkcija. Magnezijum usporava oslobađanje acetilholina u neuromuskularnoj sinapsi, smanjuje senzitivnost platoa za acetilholin i povećava ekscitabilnost membrane mišića. Takođe, potencira dejstvo i polarišućih i nedepolarišućih mišićnih relaksanata.
Doza nedepolarišućih mišićnih relaksanata za defascikulaciju ne bi trebalo da se daje pre doze sukcinilholina kod žena sa hipermagnezemijom. Uobičajena doza mišićnog relaksanta za intubaciju ( na primer sukcinilholin 1mg/kg) trebalo bi da se koristiti, jer je obim dejstva magnezijum sulfata varijabilan. Međutim, potrebno je smanjiti dozu nedepolarišućeg mišićnog relaksanta, pošto su pacijentkinje sa terapijom magnezijuma posebno osetljive na ove mišićne relaksante. Neuromuskularna blokada trebalo bi da se prati uz stimulator perifernog nerva. Procenjivani odnosi magnezijum sulfata i ritodrina sa minimalnom alveolarnom koncentracijom (MAC) ukazali su na 20% smanjenja MAK-a kod nivoa magnezijuma u serumu od 7-11 mg/dL. Upotreba magnezijum sulfata u terapiji smanjuje kako intraoperativne, tako i postoperativne potrebe za analgeticima .10
Inhibitori ciklooksigenaze Inhibitori ciklooksigenaze –COX (prostaglandin sintaze) su uspešni lekovi za tokolizu, bilo da se daju sami ili u kombinaciji sa drugim lekovima. Lekovi se lako aplikuju oralnim ili rektalnim putem, a majka ih dobro podnosi. Indometacin je prototip za ove inhibitore koji se koriste kao tokolitici.11 Efekat indometacina na trombocite je kratkotrajan. Poželjno je meriti vreme krvarenja kod pacijentkinja koje su skorije dobijali inhibitore sinteze prostaglandina kao tokolizu, a koje se porađaju ili se trudnoća operativno završava.
Postoji nekoliko objavljenih slučajeva epiduralnog hematoma posle regionalne anestezije kod pacijenata koji su dobijali inhibitore sinteze prostaglandina. Ali ne postoji objavljeni prikaz slučaja epiduralnog hematoma nakon primanja epiduralne anestezije kod obstetričkog pacijenta koji je nedavno primao inhibitore sinteze prostaglandina. Blokatori kalcijumskih kanala Blokatori kalcijumskih kanala - nifedipin, nikardipin, verapamil dobri su lekovi za inhibiranje kontrakcija uterusa. Od ove grupe lekova, nifedipin je najviše ispitan kao tokolitik. Među blokatorima kalcijumskih kanala nifedipin ima manje efekata na sprovodljivost srca, specifičnije delovanje na kontraktilnost miometrijuma i manje efekte na elektrolite u serumu. Godine 1980., Ulmsten i saradnici12 publikovali su prvo kliničko istraživanje vezano za upotrebu nifedipina kao tokolitika. Usporili su preveremeno rađanje za najmanje 72h, što je omogućavalo primenu glukokortikoida za ubrzavanja sazrevanja fetalnih pluća. Neželjeni efekti kod majke bili su blagi, i obuhvatali su crvenilo lica i ubrzanu frekvencu rada srca. Nisu zapažene značajne promene fetalne frekvence srca (FHR). Smatra se da kratkotrajna aplikacija nifedipina nema nepovoljan uticaj na uteroplacentalnu ili fetalnu cirkulaciju.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
105
Iako nifedipin ima manje neželjenih efekata na sprovodni sistem srca od drugih inhibitora kalcijumskih kanala, ovaj lek ima potencijal da izazove vazodilataciju, hipotenziju, depresiju miokarda i defekte u sprovođenju, ako se koristi u kombinaciji sa nekim od halogenih anestetičkih lekova.19
Poseban osvrt je poželjan kod pacijentkinja koje su primale nifedipin i magnezijum sulfat, a kada se ordiniraju mišićni relaksanti jer može doći do prolongiranja neuromišićne blokade. Postpartalno krvarenje može biti rezultat postpartalne atonije uterusa koja ne reaguje na oksitocin i prostaglandin F2-alfa. Kod takvih pacijentkinja neophodno je sprovesti intenzivan hemodinamski i monitoring hemostaze. Antagonisti oksitocina Proteklih decenija istraživači su napravili značajan napredak u razumevanju molekularnih mehanizama započinjanja porođaja. Kao rezultat razvili su nove lekove koji se još uvek procenjuju u tretmanu prevremenog porođaja. Atosiban (1-deamino-2-D-tyr-[OEt]-4-thr-8-orn-vaso-tocin/oxytocin) je oksitocinski antagonist koji se ispituje kao tokolitik.20 Atosiban je kompetitivni inhibitor oksitocina koji se vezuje za receptore i miometrijuma i decidue. Naknadno ne menja senzitivnost miometrijuma prema oksitocinu. Klinički, ovo je velika prednost i trebalo bi da smanji rizik od postpartalne atonije uterusa i hemoragije. Preliminarne studije pokazuju da je atosiban efektivan tokolitik. Za sad se pokazao kao lek koji ima velikih prednosti u odnosu na druge tokolitike zbog: malih maternalnih neželjenih efekata, minimalnog prolaska kroz placentu, ne izaziva neželjene efekte na fetus i ne povećava gubitak krvi majke pri porođaju. Za sad ne postoje podaci koji se tiču interakcije atosibana i anestetika.
Zaključak
Kako je sve veća učestalost preterminskih porođaja, kao i prevremeno rođene dece koja su male telesne težine, neophodno je sagledati sve aspekte primenjene anestezije koja može dodatno uticati na stanje fetusa. Takođe, primena sve većeg broja lekova u okviru tokolitičke terapije, zahteva sagledavanje intereakcija između primenjenih aktivnih supstanci i anestetika, kako bi se izbegla neželjena dejstva tokom primene regionalne ili opšte anestezije za završavanje trudnoće. Literatura
1. Ventura SJ, Martin JA, Mathews TJ, Clarke SC. Advance report of final natality statistics, 1994. Mon Vital Stat Rep 1996; 44:S75.
2. Creasy RK. Preterm birth prevention:Where are we? Am J Obstet Gynecol 1993; 168:1223-30.
3. Chesnut DH. Anesthesiafor preterm laborand delivery. In Hood D, quest editor. Anesthesia in Obstetrics and Gynecology: Problems in Anesthesia. Philadelphia, JB Lippincott, 1989:32-34.
4. Santos AC, Yun EM, Bobby PD, et al. The effects of bupivacainie, 1-nitro-1-arginine-methil ester, and phenylephrine on cardiovascular adptacions to asphyxia in the preterm fetal lamb. Anesth Analg 1997; 85:1299-306.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
106
5. Albright GA,Forster RM. Does combinedspinal-epidural analgesia with subarachnoid sufentanil increase theincidence og emergency cesarean delivery? Reg Anesth 1997; 22:400-5.
6. Rolbin SH, Cohen MM, Levinton Cm, et al. The premature infant: Anesthesia for cesarean delivery. Anesth Analg 1994; 78:912-7.
7. Lamant RF. The contemporary use of ß-agonists. Br J Obstet Anesth 1995; 4:238-43 8. Hall DG, McGaughey HS Jr, Corey EL, Thornton WN Jr. The effects of magnesium therapy
on the duration of labor. Am J Obstet Gynecol 1959; 78:27-32. 9. Chau AC, Gabert HA, Miller JM Jr. A prospective comparasion of terbutaline and
magnesium for tocolysis. Obstet Gynecol 1992; 80:847-51. 10. Koinig H, Walner T, Marhofer P, et al. Magnesium sulfate reduces intra- and postoperative
analgesic requirements. Anesth Analg 1998; 87:206-10. 11. Niebyl JR, Witter FR. Neonatal outcome after indomethacintreatment for preterm labor. AM
J Obstet Gynecol 1986; 155:747-9. 12. Ulmsten U, Andersson K-E, Wingerup L. Treatment of premature labor with the calcium
antagonist nifedipine. Arch Gynecol 1980; 229:1-5.
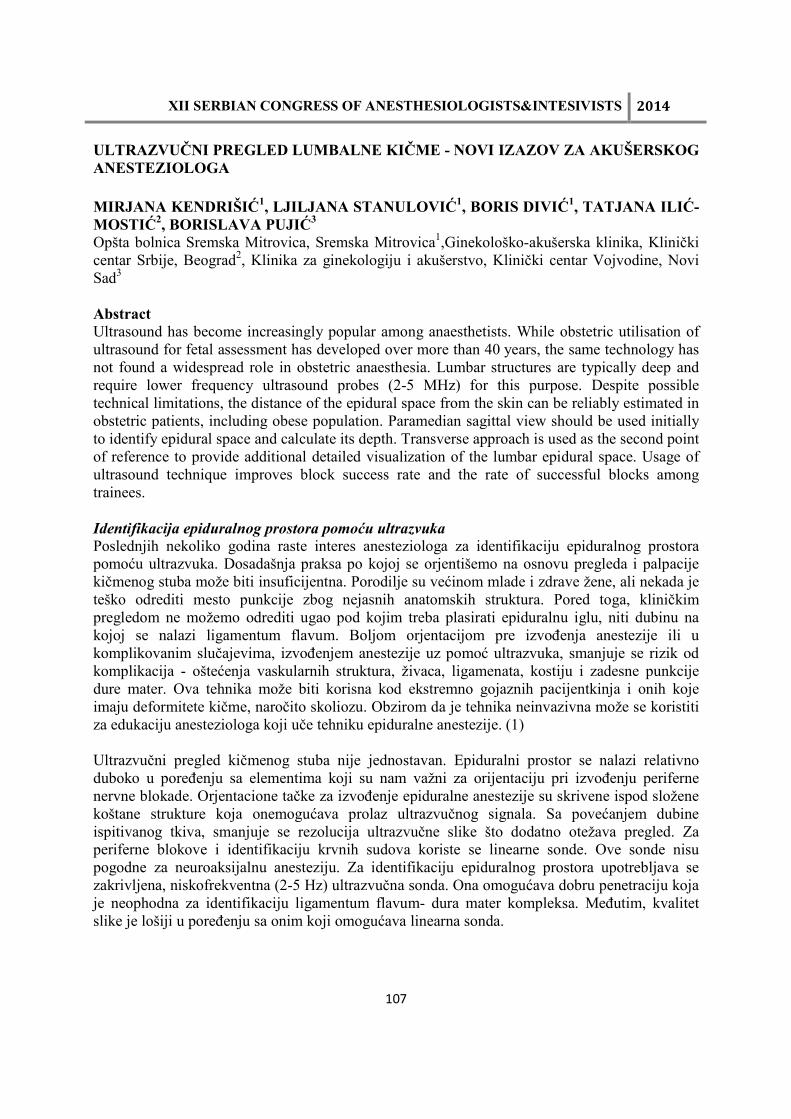
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
107
ULTRAZVUČNI PREGLED LUMBALNE KIČME - NOVI IZAZOV ZA AKUŠERSKOG ANESTEZIOLOGA
MIRJANA KENDRIŠIĆ1, LJILJANA STANULOVIĆ1, BORIS DIVIĆ1, TATJANA ILIĆ- MOSTIĆ2, BORISLAVA PUJIĆ3 Opšta bolnica Sremska Mitrovica, Sremska Mitrovica1,Ginekološko-akušerska klinika, Klinički centar Srbije, Beograd2, Klinika za ginekologiju i akušerstvo, Klinički centar Vojvodine, Novi Sad3 Abstract Ultrasound has become increasingly popular among anaesthetists. While obstetric utilisation of ultrasound for fetal assessment has developed over more than 40 years, the same technology has not found a widespread role in obstetric anaesthesia. Lumbar structures are typically deep and require lower frequency ultrasound probes (2-5 MHz) for this purpose. Despite possible technical limitations, the distance of the epidural space from the skin can be reliably estimated in obstetric patients, including obese population. Paramedian sagittal view should be used initially to identify epidural space and calculate its depth. Transverse approach is used as the second point of reference to provide additional detailed visualization of the lumbar epidural space. Usage of ultrasound technique improves block success rate and the rate of successful blocks among trainees. Identifikacija epiduralnog prostora pomoću ultrazvuka
Poslednjih nekoliko godina raste interes anesteziologa za identifikaciju epiduralnog prostora pomoću ultrazvuka. Dosadašnja praksa po kojoj se orjentišemo na osnovu pregleda i palpacije kičmenog stuba može biti insuficijentna. Porodilje su većinom mlade i zdrave žene, ali nekada je teško odrediti mesto punkcije zbog nejasnih anatomskih struktura. Pored toga, kliničkim pregledom ne možemo odrediti ugao pod kojim treba plasirati epiduralnu iglu, niti dubinu na kojoj se nalazi ligamentum flavum. Boljom orjentacijom pre izvođenja anestezije ili u komplikovanim slučajevima, izvođenjem anestezije uz pomoć ultrazvuka, smanjuje se rizik od komplikacija - oštećenja vaskularnih struktura, živaca, ligamenata, kostiju i zadesne punkcije dure mater. Ova tehnika može biti korisna kod ekstremno gojaznih pacijentkinja i onih koje imaju deformitete kičme, naročito skoliozu. Obzirom da je tehnika neinvazivna može se koristiti za edukaciju anesteziologa koji uče tehniku epiduralne anestezije. (1) Ultrazvučni pregled kičmenog stuba nije jednostavan. Epiduralni prostor se nalazi relativno duboko u poređenju sa elementima koji su nam važni za orijentaciju pri izvođenju periferne nervne blokade. Orjentacione tačke za izvođenje epiduralne anestezije su skrivene ispod složene koštane strukture koja onemogućava prolaz ultrazvučnog signala. Sa povećanjem dubine ispitivanog tkiva, smanjuje se rezolucija ultrazvučne slike što dodatno otežava pregled. Za periferne blokove i identifikaciju krvnih sudova koriste se linearne sonde. Ove sonde nisu pogodne za neuroaksijalnu anesteziju. Za identifikaciju epiduralnog prostora upotrebljava se zakrivljena, niskofrekventna (2-5 Hz) ultrazvučna sonda. Ona omogućava dobru penetraciju koja je neophodna za identifikaciju ligamentum flavum- dura mater kompleksa. Međutim, kvalitet slike je lošiji u poređenju sa onim koji omogućava linearna sonda.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
108
Postoje dva akustična “prozora” koji se koriste za UZ pregled lumbalne kičme. Kroz jedan “prozor” se unutrašnjost kičmenog stuba ispituje sondom postavljenom paramedijalno u sagitalnoj ravni. Kroz drugi “prozor” se epiduralnom prostoru pristupa sondom postavljenom u transverzalnoj ravni. Informacije koje dobijamo iz obe ravni se dopunjuju. Tipična ultrazvučna slika u sagitalnoj ravni podseća na testeru. (Slika 2.) Tipična ultrazvučna slika u transverzalnoj ravni podseća na slepog miša raširenih krila. (Slika 6.)
Paramedijalni sagitalni pristup: Najpre treba postaviti sondu paramedijalno u sagitalnoj ravni. (Slika 1.) Koštane strukture koje se na ovaj način identifikuju su sakrum i višestruke lamine. Kroz interspinozne prostore mogu se vizualizovati zadnja dura mater i/ili ligamentum flavum, spinalni kanal i kompleks pršljensko telo/zadnji longitudinalni ligament /prednja dura mater. (Slika 2.) Vizualizacija u sagitalnoj ravni je često bolja nego u transverzalnoj ravni jer se ligamentum flavum i zadnja dura mater mogu razlikovati kao dve odvojene strukture. (Slika 3.)
Paramedijalni sagitalni ultrazvučni pristup
Slika 1.
Tipičan sonogram dobijen paramedijalnim sagitalnim ultrazvučnim pristupom - izgled
Lamine
Ligamentum flavum / prednja
dura Telo pršljena / zadnja dura
Slika 2.
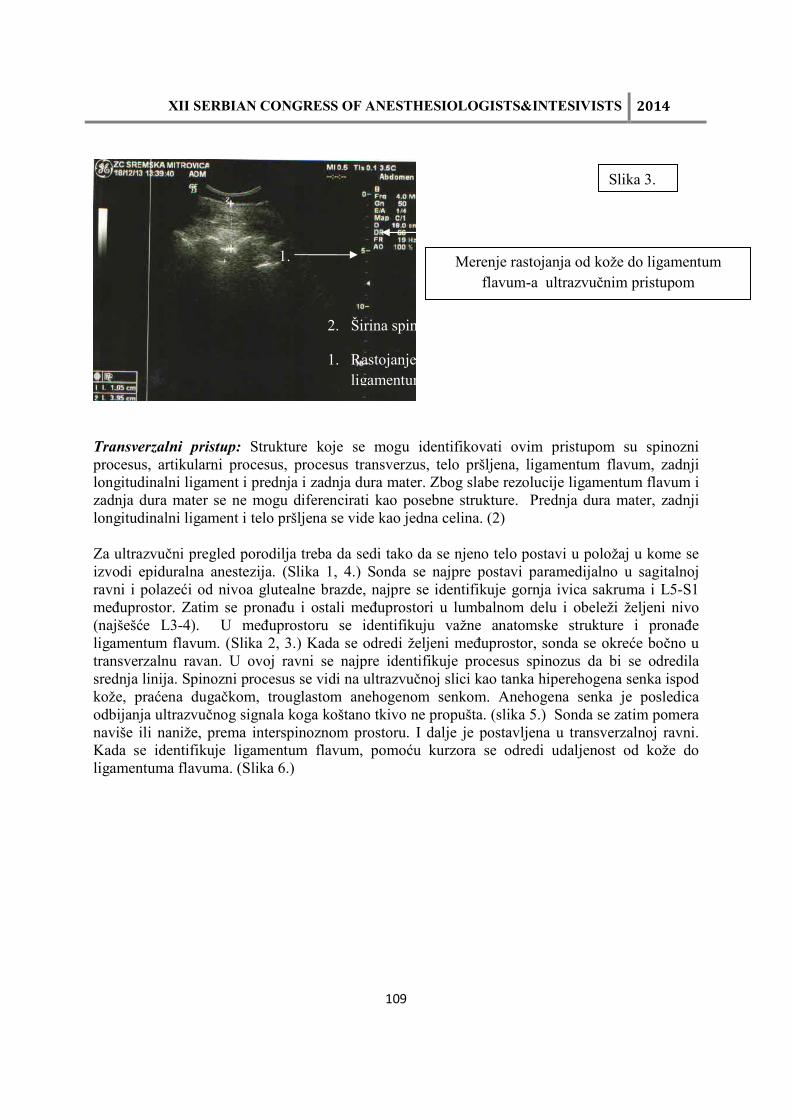
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
109
Transverzalni pristup: Strukture koje se mogu identifikovati ovim pristupom su spinozni procesus, artikularni procesus, procesus transverzus, telo pršljena, ligamentum flavum, zadnji longitudinalni ligament i prednja i zadnja dura mater. Zbog slabe rezolucije ligamentum flavum i zadnja dura mater se ne mogu diferencirati kao posebne strukture. Prednja dura mater, zadnji longitudinalni ligament i telo pršljena se vide kao jedna celina. (2) Za ultrazvučni pregled porodilja treba da sedi tako da se njeno telo postavi u položaj u kome se izvodi epiduralna anestezija. (Slika 1, 4.) Sonda se najpre postavi paramedijalno u sagitalnoj ravni i polazeći od nivoa glutealne brazde, najpre se identifikuje gornja ivica sakruma i L5-S1 međuprostor. Zatim se pronađu i ostali međuprostori u lumbalnom delu i obeleži željeni nivo (najšešće L3-4). U međuprostoru se identifikuju važne anatomske strukture i pronađe ligamentum flavum. (Slika 2, 3.) Kada se odredi željeni međuprostor, sonda se okreće bočno u transverzalnu ravan. U ovoj ravni se najpre identifikuje procesus spinozus da bi se odredila srednja linija. Spinozni procesus se vidi na ultrazvučnoj slici kao tanka hiperehogena senka ispod kože, praćena dugačkom, trouglastom anehogenom senkom. Anehogena senka je posledica odbijanja ultrazvučnog signala koga koštano tkivo ne propušta. (slika 5.) Sonda se zatim pomera naviše ili naniže, prema interspinoznom prostoru. I dalje je postavljena u transverzalnoj ravni. Kada se identifikuje ligamentum flavum, pomoću kurzora se odredi udaljenost od kože do ligamentuma flavuma. (Slika 6.)
1.
2.
2. Širina spinalnog kanala
1. Rastojanje od kože do ligamentuma flavuma
Slika 3.
Merenje rastojanja od kože do ligamentum flavum-a ultrazvučnim pristupom

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
110
Transverzalni ultrazvučni pristup
Slika 4.
Identifikacija procesusa spinozusa transverzalnim pristupom
Slika 5.
1.
2. 1. Procesus spinosus 2. Trouglasta anehogena senka
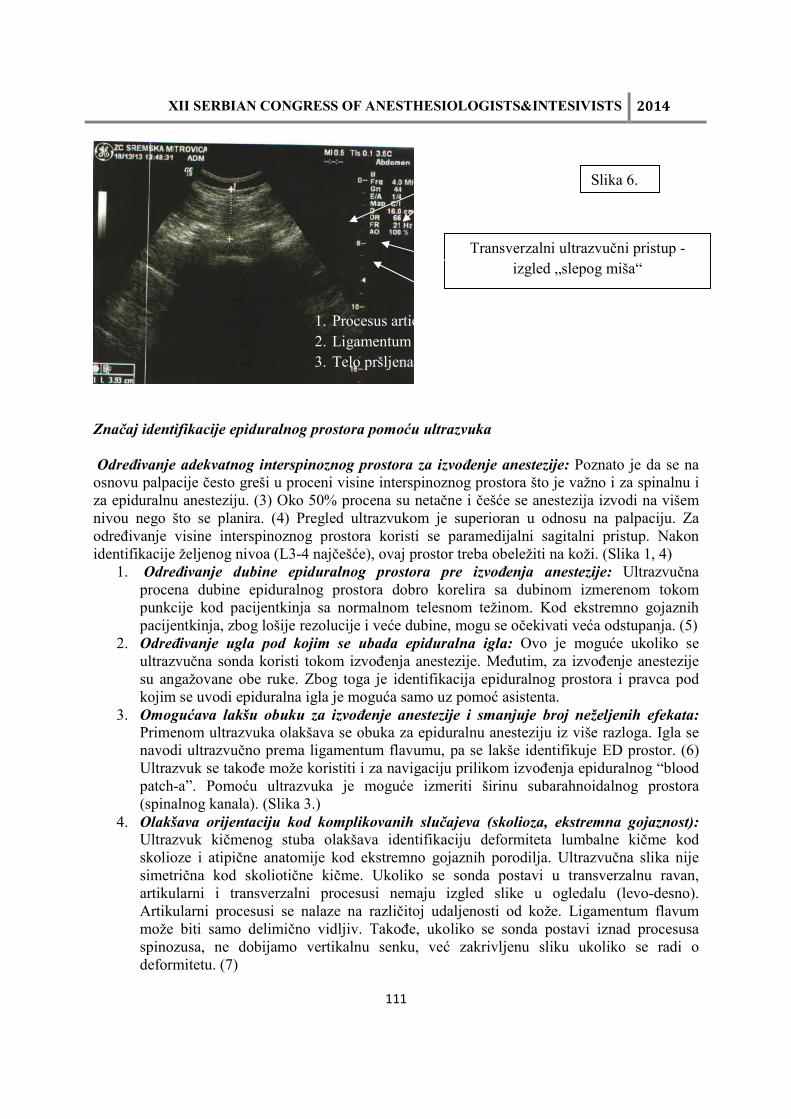
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
111
Značaj identifikacije epiduralnog prostora pomoću ultrazvuka
Određivanje adekvatnog interspinoznog prostora za izvođenje anestezije: Poznato je da se na osnovu palpacije često greši u proceni visine interspinoznog prostora što je važno i za spinalnu i za epiduralnu anesteziju. (3) Oko 50% procena su netačne i češće se anestezija izvodi na višem nivou nego što se planira. (4) Pregled ultrazvukom je superioran u odnosu na palpaciju. Za određivanje visine interspinoznog prostora koristi se paramedijalni sagitalni pristup. Nakon identifikacije željenog nivoa (L3-4 najčešće), ovaj prostor treba obeležiti na koži. (Slika 1, 4)
1. Određivanje dubine epiduralnog prostora pre izvođenja anestezije: Ultrazvučna procena dubine epiduralnog prostora dobro korelira sa dubinom izmerenom tokom punkcije kod pacijentkinja sa normalnom telesnom težinom. Kod ekstremno gojaznih pacijentkinja, zbog lošije rezolucije i veće dubine, mogu se očekivati veća odstupanja. (5)
2. Određivanje ugla pod kojim se ubada epiduralna igla: Ovo je moguće ukoliko se ultrazvučna sonda koristi tokom izvođenja anestezije. Međutim, za izvođenje anestezije su angažovane obe ruke. Zbog toga je identifikacija epiduralnog prostora i pravca pod kojim se uvodi epiduralna igla je moguća samo uz pomoć asistenta.
3. Omogućava lakšu obuku za izvođenje anestezije i smanjuje broj neželjenih efekata:
Primenom ultrazvuka olakšava se obuka za epiduralnu anesteziju iz više razloga. Igla se navodi ultrazvučno prema ligamentum flavumu, pa se lakše identifikuje ED prostor. (6) Ultrazvuk se takođe može koristiti i za navigaciju prilikom izvođenja epiduralnog “blood patch-a”. Pomoću ultrazvuka je moguće izmeriti širinu subarahnoidalnog prostora (spinalnog kanala). (Slika 3.)
4. Olakšava orijentaciju kod komplikovanih slučajeva (skolioza, ekstremna gojaznost):
Ultrazvuk kičmenog stuba olakšava identifikaciju deformiteta lumbalne kičme kod skolioze i atipične anatomije kod ekstremno gojaznih porodilja. Ultrazvučna slika nije simetrična kod skoliotične kičme. Ukoliko se sonda postavi u transverzalnu ravan, artikularni i transverzalni procesusi nemaju izgled slike u ogledalu (levo-desno). Artikularni procesusi se nalaze na različitoj udaljenosti od kože. Ligamentum flavum može biti samo delimično vidljiv. Takođe, ukoliko se sonda postavi iznad procesusa spinozusa, ne dobijamo vertikalnu senku, već zakrivljenu sliku ukoliko se radi o deformitetu. (7)
Transverzalni ultrazvučni pristup - izgled „slepog miša“
Slika 6. 1.
2.
3. 1. Procesus articularis 2. Ligamentum flavum 3. Telo pršljena

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
112
Zaključak
Prednosti ultrazvuka za izvođenje centralnih neuroaksijalnih blokova su višestruke: lakše pronalaženje željenog interspinoznog prostora, određivanje mesta punkcije u interspinoznom prostoru, određivanje ugla pod kojim se punktira, određivanje udaljenosti od kože do ligamentuma flavuma i pomoć kod deformiteta kičme Literatura
1. Royal College of Obstetricians and Gynaecologists, Royal College of Midwives, Royal College of Anaesthetists, Royal College of Paediatrics and Child Health. Safer Childbirth: Minimum Standards for the Organisation and Delivery of Care in Labour. London: RCOG Press at the Royal College of Obstetricians and Gynaecologists; 2007.
2. Carvalho JC. Ultrasound-facilitated epidurals and spinals in obstetrics. Anesthesiol Clin 2008; 26(1): 145-58
3. Balki M, Lee Y, Halpern S, Carvalho JC. Ultrasound imaging of the lumbar spine in the transverse plane: the correlation between estimated and actual depth to the epidural space in obese parturients. Anesth Analg 2009 Jun; 108(6): 1876-81.
4. Balki M. Locating the epidural space in obstetric patients-ultrasound a useful tool: continuing professional development. Can J Anaesth 2010; 57(12): 1111-26.
5. The lumbar epidural space in pregnancy: visualization by ultrasonography. Grau T, Leipold RW, Horter J, Conradi R, Martin E, Motsch J. The lumbar epidural space in pregnancy: visualization by ultrasonography. Br J Anaesth 2001; 86(6):798-804.
6. Gambling DR. Lumbar ultrasound: useful gadget or time-consuming gimmick? Int J Obstet Anesth 2011; 20(4): 318-20.
7. Whitty R, Moore M, Macarthur A. Identification of the lumbar interspinous spaces: palpation versus ultrasound. Anesth Analg 2008; 106(2): 538-40

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
113
PERIPARTUM CARDIOMIOPATHY IVAN VELIČKOVIĆ¹, BORISLAVA PUJIĆ² ¹SUNY Downstate Medical Center, NY, USA, ² Klinika za ginekologiju i akušerstvo, Kliničkog centra Vojvodine, Novi Sad E-mail: [email protected] Summary
PPCM is a serious idiopathic myocardial disease, which typically presents as heart failure secondary to left ventricular dysfunction towards the end of pregnancy or the following months postpartum, when no other cause of heart failure can be found. The incidence of PPCM is noted to vary between studies due to sample size differences but trends towards 1:2500-4000 in the US, 1:1000 in South Africa, and 1:300 in Haiti. The etiology of PPCM is unknown. Associated risk factors include multiparity, advanced maternal age, multiple gestation, preeclampsia, dysfunctional adaptation to the hemodynamic stresses of the pregnancy, prolonged tocolysis, malnutrition, chronic hypertension, diabetes, smoking, and black race. PPCM may present as fatigue, dyspnea on exertion, orthopnea, palpitations, dizziness, orthostatic hypotension, edema, embolic phenomena, chest pain, , cough, cardiomegaly, tachycardia, or murmur of mitral regurgitation. The diagnosis of PPCM should be performed, including ECG, BNP, and echocardiography. Pregnancy has been discouraged in patients with a previous diagnosis of PPCM, due to the high risk of recurrence and the mortality rate of up to 20%. Principles of anesthetic management for these parturients should be similar to that for other types of severe cardiomyopathies: oxygen administration, diuretics, vasodilatators, beta blockers, anticoagulant therapy and new therapies may include bromocriptine. Cesarean Section should be done only for obstetric indications. There are no indications that one type of anesthesia is preferable over the other. We believe that regional anesthesia, especially CSA and CSE can be successfully employed for patients with PPCM.
Introduction
PPCM is a serious idiopathic myocardial disease, which typically presents as heart failure secondary to left ventricular dysfunction towards the end of pregnancy or the following months postpartum, when no other cause of heart failure can be found. 1 Heart failure may occur with or without left ventricular dilation. The incidence of PPCM is noted to vary between studies due to sample size differences but trends towards 1:2500-4000 in the US, 1:1000 in South Africa, and 1:300 in Haiti.1 The incidence of PPCM in Asia, Australia, and Europe is uncertain and requires epidemiological study.2
Ethiology
The etiology of PPCM is unknown, but viral myocarditis, autoimmune, and idiopathic causes may contribute. Recent studies have been published regarding the possible link between oxidative stress which triggers cathepsin D in cardiomyocytes. Cathepsin D cleaves prolactin into a pro-apoptotic 16 kDa subfragment. In one animal model the administration of bromocriptine, a dopamine D2 receptor agonist which suppresses the production of prolactin, prevented the onset of PPCM1. Another recent study of 90 families with familial dilated cardiomyopathy suggest a small set of PPCM may be the initial manifestation of familial DCM
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
114
which may bode well for future screening in these specific families.3 Current recommendations, however, do not include routine genetic testing. Associated risk factors include multiparity, advanced maternal age, multiple gestation, preeclampsia, dysfunctional adaptation to the hemodynamic stresses of the pregnancy, prolonged tocolysis, malnutrition, chronic hypertension, diabetes, smoking, and black race.1,4 Symptoms
PPCM may present as fatigue, dyspnea on exertion, orthopnea, abdominal pain in association with hepatic congestion, palpitations, dizziness, orthostatic hypotension, edema, embolic phenomena, chest pain, hemoptysis, cough, increased JVD, pulmonary rales, cardiomegaly, tachycardia, S3 gallop, or murmur of mitral regurgitation.
Diagnosis
Echocardiographic criteria for diagnosis include ejection fraction of less than 45%, M-mode fractional shortening less than 30%, or both, and end-diastolic dimension more than 2.7 cm/m.4.5 Severe mitral regurgitation, as a consequence of left ventricular dilatation is often present. This may render the cardiac output data obtained by the thermodilution method less reliable, but the PA catheter and thermodilution method, and to a lesser degree CVP, may be used as an effective measurement of trends or responses to specific therapeutic interventions. MRI has a higher sensitivity in detection of ventricular thrombus and allows more accurate evaluation of ventricular functions and volumes, however, gadolinium should not be used until after delivery.1 Diagnosis of an early disease might be a challenge because many normal women experience dyspnea, orthopnea, persistent cough, fatigue, and pedal edema in the last month of pregnancy. PPCM is a diagnosis of exclusion, distinguished by rapid onset, occurrence in the peripartum period, and the significant improvement in up to 50% of affected women. The diagnosis of PPCM should be considered whenever women present with heart failure during the peripartum period6 and a thorough cardiac workup looking for alternate causes should be performed, including ECG, BNP, and echocardiography.
Pregnancy has been discouraged in patients with a previous diagnosis of PPCM, due to the high risk of recurrence and the mortality rate of up to 20%. Symptoms of heart failure occurred in 21% of those who entered the subsequent pregnancy with normal left ventricular systolic function and 44% of those who entered the subsequent pregnancy with abnormal left ventricular systolic function.7 Patients with persistent left ventricular dysfunction are at particular risk of premature delivery, therapeutic abortion, heart failure and death.7 The etiology of recurrent disease is not known: symptoms may represent an intolerance of the normal physiologic changes of pregnancy or a true recurrence of a distinct syndrome. However, many women who survive a severe episode of PPCM will continue to have decreased cardiac function, as evidenced by dobutamine stress tests and echocardiographic studies, while others may continue to improve over time.8 An LV end-diastolic diameter of >60 mm and LVEF <30% predicts poor recovery of LV function.1 Anesthetic management
Principles of anesthetic management for these parturients should be similar to that for other types of severe cardiomyopathies; that is, rapid treatment, oxygen administration with a goal of
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
115
maintaining arterial oxygen saturation 95% or greater, avoidance of myocardial depressants and cautious fluid management with judicious use of diuretics, vasodilatators and beta blockers.
Treatment of PPCM
Hydralazine, furosemide and metoprolol are the drugs of choice prepartum, and angiotensin-converting enzyme inhibitors are the mainstay of treatment post-partum. Initial boluses of furosemide should be 20-40 mg I.V. 1 In the treatment of acutely ill or highly symptomatic patients, intravenous preload and afterload reducing agents (nitroprusside, nitroglycerin) or inotropic agents in low output states (dobutamine, dopamine, milrinone) should be considered.9,10 Nitroglycerin can be started at 10-20 µg/min and titrated up to 200 µg/min to achieve a SBP between 90-110 mmHg.1 Persistently severe disease may necessitate a cardiac transplant or mechanical assist device as a bridge to transplantation. Anticoagulant therapy is often indicated due to increased risk of thromboembolic events.8 Anticoagulation with subcutaneous heparin (i.e., 5000 U heparin subcutaneously twice daily) should be strongly considered in this population. Warfarin should be avoided until the antepartum period.
As discussed earlier, new therapies may include bromocriptine. Although there have been reports of bromocriptine associated myocardial infarctions, dosages of 2.5 mg twice daily for two weeks followed by 2.5 mg daily for four weeks have shown promise. A high recovery rate (96 %) was observed in patients obtaining combination therapy with beta-blocker, angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor-blockers (ARBs) and bromocriptine. Larger RCTs are needed to accept this regimen as a recommendation.11
Anesthesia for Cesarean delivery
Cesarean Section should be done only for obstetric indications. There are no indications that one type of anesthesia is preferable over the other. Initial hemodynamic goals during Cesarean Section sometimes can be achieved with careful induction of regional anesthesia. Titration of a vasodilatator, e.g., nitroglycerin, can be also used with general anesthesia or in addition to regional anesthesia for hemodynamic control. The autotransfusion subsequent to the delivery of fetus and placenta potentially resulting in an increase in filling pressures could have adverse consequences. Therefore, an intentional decrease in filling pressures with a single IV dose of furosemide immediately before delivery should be considered.
Regional anesthesia in the form of epidural, combined spinal-epidural or continuous spinal anesthesia should be considered for these patients. Epidural analgesia is the preferred anesthetic for labour as it stabilizes cardiac output. 1 The ability to titrate the anesthetic is critical. Continuous spinal anesthesia appears to offer more hemodynamic stability compared with single dose spinal for Cesarean Section,12 as has also been shown to be the case with knee and hip surgery. Hemodynamic stability, similar to that of epidural anesthesia, has also been reported. Furthermore, CSA may be more rapidly and effectively titratable than epidural or combined-spinal epidural anesthesia. The goal of providing reliable, rapidly titratable, profound analgesia with minimal hemodynamic changes may be most easily achieved with continuous spinal anesthesia. As with combined spinal-epidural anesthesia, we believe that CSA has a lower failure rate than epidural anesthesia
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
116
and also provides for lower maternal and umbilical cord blood concentrations of local anesthetics. Potential disadvantages of this technique include the risks of postdural puncture headache and cauda equina syndrome. Small gauge catheters are currently not commercially available. However a 19/20-gauge epidural catheter can be use for the CSA for these patients. The patients are usually monitored in the intensive care unit post-operatively, and are not expected to ambulate immediately. The use of larger gauge catheters and the choice of local anesthetic (bupivacaine/ropivacaine over lidocaine) may be associated with less risk of cauda equina syndrome. This is probably because the larger catheters allow for more rapid injection, and much better mixing of anesthetic drug with the CSF. Furthermore, the larger size facilitates more effective aspiration of CSF to confirm proper catheter placement. Finally, the intrathecal catheter may be left in place post-operatively for analgesia and postdural puncture headache protection, as has been previously postulated. Conclusion We believe that regional anesthesia, especially CSA and CSE can be successfully employed for patients with PPCM. This technique should be considered an anesthetic option for patients with PPCM and other significant cardiac diseases, provided that the anesthesia personnel have sufficient experience with this technique. References
1. Sliwa K, Hilfiker-Kleiner D, Petrie M, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of peripartum cardiomyopathy: a position statement from the Heart Failure Association of the European Society of Cardiology Working Group on peripartum cardiomyopathy. Eur J of Heart Failure. 2010;12:767-778
2. Hilfiker-Kleiner D, Sliwa K. Pathophysiology and epidemiology of peripartum cardiomyopathy. Nat Rev Cardiol. 2014 Jun;11(6):364-70.
3. Van Spaendonck-Zwarts K, van Tintelen J, van Veldhuisen DJ, et al. Peripartum cardiomyopathy as part of familial dilated cardiomyopathy. Circulation. 2010;121:2169-2175
4. Sliwa K, Fett J, Elkayam U. Peripartum cardiomyopathy.Lancet. 2006; 368: 687-93. 5. Hibbard JU, Lindheimer M, Lang RM. A modified definition for peripartum
cardiomyopathy and prognosis based on echocardiography. Obstet Gynecol. 1999; 94: 311-6
6. Abboud J, Murad Y, Chen-Scarabelli C, et al. Peripartum cardiomyopathy: a comprehensive review. Int J Cardiol. 2007;118:295-303.
7. Elkayam U, Tummala P, Rao K, et al. Maternal and fetal outcomes of subsequent pregnancies in women with peripartum cardiomyopathy. N Engl J Med 2001; 344: 1567-1571.
8. Reimold SC, Rutherford JD. Peripartum cardiomyopathy. N Engl J Med 2001; 344:1629-1630
9. Lata I, Gupta R, Sahu S, Singh H. Emergency management of decompensated peripartum cardiomyopathy. J Emerg Trauma Shock. 2009; 2: 124-8
10. Pryn A, Bryden F, Reeve W, et al. Cardiomyopathy in pregnancy and caesarean section: four case reports. Int J Obstet Anesth. 2007;16:68-73

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
117
11. Haghikia A, Podewski E, Libhaber E, et al. Phenotyping and outcome on contemporary management in a German cohort of patients with peripartum cardiomyopathy. Basic Res Cardiol. 2013;108:366
12. Pittard A, Vucevic M. Regional anaesthesia with a subarachnoid microcatheter for caesarean section in a parturient with aortic stenosis. Anaesthesia 1998; 53: 169-173.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
118
SPINALNI MORFIN I NJEGOVA RENESANSA U AKUŠERSKOJ ANESTEZIJI BORISLAVA PUJIĆ¹, IVAN VELIČKOVIĆ², TATJANA ILIĆ-MOSTIĆ3,4 , MIRJANA KENDRIŠIĆ5
¹ Klinika za ginekologiju i akušerstvo, Kliničkog centra Vojvodine, Novi Sad, ² SUNY Downstate Medical Center, NY, USA, ³Medicinski fakultet Univerziteta u Beogradu, 4Centar za anesteziologiju i reanimatologiju, Kliničkog centra Srbije, Beograd, 5Služba za anesteziologiju i intenzivno lečenje Opšte bolnice Sremska Mitrovica E-mail: [email protected]
INTRATHECAL MORPHINI RENESANSE IN OBSTETRIC ANESTHESIA Summary. The analgesic effect of morphine has been known from the period B.C. when people found that poppy seeds have been used as medication. In the beginning of the XIX century, the young and courious pharmaceutical assistant Friedrich Serturner synthesized a substance from the opium poppy, called morphine. Morphine is an opioid analgesic, with very powerfull and long lasting effects, which causes almost immideate pain relief and creates a good mental feeling resulting in psychological dependence. It is on the World Health Organization's List of Essential Medicines. In the early XX century, Oscar Kreis used the first spinal analgesia for delivery. Spinal or epidural morphine (0.1-0-2mg vs. 3-4mg) with bupivacaine can cause a longer-lasting analgesic effect than other pain killers. Usually it is enough for 12-24h. Morphine side-effects are common, but mild (constipation, nausea, vomiting, and pruritus). Serious side-effects are very rare (respiratory depression and addiction) because the intrathecal dose is very small, but then it is necessary to administer naloxone. Patient satisfaction is essential and it is not recommended to avoid morphine in post-cesarean analgesia.
Uvod
Analgetski efekti morfina poznati su od davnina. Čim su ljudi spoznali da se biljke mogu upotrebljavati kao lekovi, započela je eksploatacija maka u medicinske svrhe. Još davne 3400g. pre nove ere u Mesopotamiji postojali su nasadi kulture maka. Sumeri su mak nazivali biljka za uživanje. Iz Mesopotamije je kultura preneta u ostale delove sveta, prvenstveno u Asiriju, Vavilon i Egipat. Od 1300.g. pre nove ere u Egiptu je započeta proizvodnja opijuma. Naziv Tebaikum dobio je po glavnom gradu Tebi. Iz Egipta je započela distribucija po Evropi i Srednjem Istoku. U vreme Hipokrata, u staroj Grčkoj se znalo da je opijum magični lek za otklanjanje bola, ali otkrivena su i njegova dejstva u zaustavljanju krvavljenja. Zahvaljujući Aleksandru Velikom, opijum je oko 330. godine nove ere dopremljen u Kinu. Posledica osvajanja novih prostora bila je trgovina između Arapa i stanovnika novoosvojenih zemalja. Kina je vekovima posle bila najbolji i najveći potrošač opijuma. U Evropu su ga tokom srednjeg veka doneli portugalski moreplovci, koji su ga pušili. Zbog tadašnjih stavova, da sve što je stiglo sa istoka je đavolsko, opijum je dugo godina u Evropi bio poznat samo malom broju ljudi. Tada se već znalo da pušenje opijuma dovodi do trenutnog efekta, za razliku od efekta ako se koristi kao piće ili jelo. Nekoliko vekova se nije znalo da opijum izaziva zavisnost kod onih, koji ga redovno upotrebljavaju.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
119
Istorijat morfina
Početkom dvadesetih godina XIX veka mladi znatiželjni farmaceutski asistent Fridrih Serturner izolovao je supstancu iz opijuma, koja je izazivala san, te je zato nazvana Morfin. Ime je dato po grčkom bogu sna, Morfeusu. Emanuel Merk (Merck) je prvi prepoznao snagu ovog alkaloida i započeo njegovu proizvodnju u svojoj maloj laboratoriji. Tek kasnije su mu se pridružili i drugi proizvođači. Ovo je bio revolucionarni pronalazak, jer je od tada (pa sve do danas) morfin jedan od najčešće zastupljenih lekova za ublažavanje jakog bola, kako akutnog (postoperativni bol, bol nakon infarkta miokarda, plućni edem, porođajni bol), tako i hroničnog (kancerski i nekancerski bol).1 Svetska Zdravstvena Organizacija (SZO) uvrstila ga je u grupu neophodnih lekova u medicini. Morfin je opioidni analgetik, snažnog i dugotrajnog dejstva, koji direktno i trenutno deluje vezujući se za receptore u mozgu. Skoro trenutno otklanja bol i stvara osećaj blaženstva, te se zbog toga brzo razvija jaka psihička zavisnost od leka. Ipak, potrebni su meseci da bi se razvila fizička zavisnost. U mozgu deluje tako što se vezuje za µ-receptore, imitira dejstvo endorfina, te stvara prekid bolnih impulsa, pospanost i osećaj blaženstva. Jedan deo se vezuje za κ-receptore, koji su odgovorni za spinalnu analgeziju, kao i za miozu zenica, a jedan deo se vezuje za δ-receptore, odgovorne za bol. Efekat nastupa nakon 20-30min, zavisno da li je dat oralno ili parenteralno. Morfin se metabolizuje u jetri, a 87% se izlučuje preko urina u roku od 72h nakon uzimanja. Poluživot mu je oko 120min. Ako se upotrebljava peroralno efekat mu traje od 4-6h, dok nakon parenteralne upotrebe traje 3-4h. Upotreba morfina u akušerstvu
Prvobitna upotreba morfina u akušerstvu bila je u vidu supkutane ili intramuskularne inekcije. Tek krajem XIX veka, kada je Kvinke (Quinke) izumeo prvu iglu za lumbalnu punkciju, stekli su se uslovi za drugačije davanje lekova za ublažavanje bola. Tada je data prva spinalna anestezija, pod vođstvom nemačkog hirurga Avgusta Bira (August Bear), a nedugo nakon toga data je i prva spinalna analgezija za porođaj. Izveo ju je Oskar Krajs (Oskar Kreis). Neposredno pre prvog svetskog rata, u SAD je osnovano udruženje žena iz viših društvenih slojeva, koje su se zalagale za upotrebu specijalnog koktela lekova za ublažavanje porođajnog bola pod nazivom New England Twilight Sleep Association. Kombinacija morfina i skopolamina bila je vrlo delotvorna i bila je rezervisana samo za privilegovane slojeve društva. Morfin je otklanjao porođajni bol, a skopolamin je izazivao amneziju za događaje vezane za porođaj. Ovakva kombinacija je bila pozdravljena kao napredak u akušerskoj analgeziji, iako su se kasnije pokazali njeni negativni efekti, koji su i publikovani.2,3
Upotreba morfina u spinalnoj i epiduralnoj anesteziji
Razvoj različitih anestezioloških tehnika i njihiva primena u raznim vrstama hirurgije neminovno je primenjena i u akušerskoj anesteziji. Vekovna težnja da se ženama pomogne u obezboljavanju pri aktu samog porođaja konačno je našla svoje mesto. Sve veći procenat završavanja porođaja operativnim putem doprineo je da se primenjuju različite strategije u otklanjanju postoperativnog bola kod porodilja. Primena lokalnih anestetika u akušerstvu omogućilo je da se putem epiduralne i spinalne anestezije porodilji omogući da doživi porođaj na sasvim drugi način nego vekovima ranije.4,5 To je, neminovno dovelo do uvođenja novih analgetika za postoperativno obezboljavanje. Sam lopkalni anestetik omogućava da se izvrši operacija, ali nakon prestanka

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
120
njegovog dejstva nastaje jak i često vrlo neprijatan i nepodnošljiv bol. Zbog toga je započeto sa dodavanjem različitih supstanci lokalnim anesteticima, da bi se njihovo analgetsko dejstvo produžilo u postoperativnom periodu.6,7
Upotreba morfina spinalno i epiduralno doprinela je obezboljavanju porodilja, koje je trajalo duži vremenski period nego nakon upotrebe drugih analgetika (primenjenih intramuskularno ili intravenski), a efekat je trajao od 12-24h. Kombinacija sa lokalnim anesteticima, najčešće bupivakainom, doprinosi boljoj analgeziji za vreme carskog reza i u postoperativnom periodu. Pomoću fentanila dobijemo bolju analgeziju za vreme same operacije, a morfin obezbeđuje analgeziju tokom naredna 24h. U SAD i nekim drugim zemljama Zapada više od dvadeset godina u upotrebi je morfin bez prezervativa (preservative-free morphini). Kod nas ovaj oblik morfina nije registrovan, kao ni u drugim delovima istočne Evrope. Pre pojave morfina bez prezervativa na Zapadu je godinama korišćen „obični“ morfin u spinalnom prostoru bez ikakvih posledica (ne postoje publikacije koje dokazuju da je bilo neželjenih posledica upotrebe ovog oblika morfina). U zadnjih nekoliko godina objavljeno je nekoliko naučnih radova gde je sa uspehom primenjen „obični“ morfin u spinalnom prostoru. Doza spinalnog morfina je izmedju 0.1-0.2 mg, a epiduralnog 3-4 mg. Vrlo često kod tih pacijentkinja ova jednokratna doza bude dovoljna da pokrije bol za narednih 24 sata i nije potrebno dodavati druge analgetike.8.9
Kontraindikacije za upotrebu morfina
Naravno da se morfin ne sme davati svakoj porodilji, jer postoje stanja gde je njegova upotreba kontraindikovana. To su:
1. akutna respiratorna depresija 2. oštećenje bubrega 3. žučne kolike 4. povišen intrakranijalni pritisak 5. hemijska toksičnost (može dovesti do smrtnog ishoda)
Neželjeni efekti
Jedino na čega moramo misliti, pri davanju morfina je da kod ovih pacijentkinja može doći do ispoljavanja blažih neželjenih efekata samog morfina ( konstipacija, mučnina, povraćanje, svrab), koje se dalje tretiraju simptomatski.10 Ozbiljniji neželjeni efekti (depresija disanja i zavisnost) obično ne budu ispoljeni, zbog malih doza koje se daju intratekalno. U slučaju predoziranja ili jako ispoljenih neželjenih efekata, koji ne prolaze na simptomatsku terapiju treba dati nalokson, koji je specifični antidot za opioide (1/10 doze za intravnsko davanje je često dovoljno da otkloni neželjene efekte morfina).
Zaključak
Bez obzira na sve kontraindikacije i neželjene efekte ne treba izbegavati davanje morfina za postoperativnu analgeziju nakon carskog reza. Zadovoljstvo samih pacijentkinja je satisfakcija da se što jednostavnije, sa manje sredstava postigne odgovarajući nivo analgezije.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
121
Literatura
1. Morphine Sulfate. The American Society of Health-System Pharmacists. Retrieved 3 April 2011.
2. Wong JY, Carvalho B, Riley ET. Intrathecal morphine 100 and 200µg for post-cesarean delivery analgesia- a trade-off between analgesic efficacy and side- effects. Int I Obstet Anaesth 2013; 22(1): 36-41.
3. Gehling M, Tryba M. Risks and side-effects of intrathecal morphine combined with spinal anaesthesia: a meta-analysis. Anaesthesia 2009;64(6): 643–651.
4. Girgin NK1, Gurbet A, Turker G, Aksu H, Gulhan N. Intrathecal morphine in anesthesia for cesarean delivery: dose-response relationship for combinations of low-dose intrathecal morphine and spinal bupivacaine. J Clin Anesth. 2008; 20(3):180-5.
5. Gehling M, Tryba M. Risks and side-effects of intrathecal morphine combined with spinal anaesthesia: a meta-analysis. Anaesthesia 2009;64(6): 643–651.
6. Bujedo BM. A Clinical Approach to Neuraxial Morphine for the Treatment of Postoperative Pain. Pain Research and Treatment Volume 2012 (2012), Article ID 612145, 11 pages http://dx.doi.org/10.1155/2012/612145
7. Carvalho B, Drover DR, Ginosar Y, Cohen SE, Riley ET. Intrathecal fentanyl added to bupivacaine and morphine for cesarean delivery may induce a subtle acute opioid tolerance. Int I Obstet Anaesth 2012; 21: 29-34.
8. Vercauteren M, Vereecken K, La Malfa M, Coppejans H, Adriaensen H. Cost-effectiveness of analgesia after Caesarean section. A comparison of intrathecal morphine and epidural PCA. Acta Anaesthesiol Scand. 2002; 46: 85-89.
9. Kato R, Shimamoto H, Terui K, Yokota K, Miyao H. Delayed respiratory depression associated with 0.15 mg intrathecal morphine for cesarean section: a review of 1915 cases. J Anesth 2008; 22: 112-116.
10. Verstraete S, Van de Velde M. Post-cesarean section analgesia. Acta Anaesth. Belg., 2012, 63, 147-167.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
122
MEHANIČKA VENTILACIJA KOD BOLESNIKA SA HRONIČNOM OPSTRUKTIVNOM BOLEŠĆU PLUĆA I ASTMOM DEJAN MARKOVIĆ
Centar za anesteziologiju i reanimatologiju Kliničkog Centra Srbije, Medicinski fakultet Univerziteta u Beogradu E-mail: [email protected] Abstract Acute exacerbation of asthma and chronic obstructive pulmonary disease (COPD) can require tracheal intubation and mechanical ventilation of patient. A good understanding of the pathophysiology these disorders provides adequate medical treatment and mechanical ventilator settings in order to treat respiratory failure. In this paper will be presented basic pathophysiological mechanisms of asthma and COPD as well as parameters of mechanical ventilation adjustment. Uvod
Hronična opstruktivna bolest pluća (HOBP) je po definiciji oboljenje koga karakteriše stalno ograničenje protoka vazduha u disajnim putevima koje je obično progresivno i udruženo sa povećanim inflamatornim odgovorom na štetne čestice i gasove u disajnim putevima i plućima.1 HOBP nastaje kao posledica hronične inflamacije u malim disajnim putevima i inflamacije u plućnom parenhimu usled čega dolazi do suženja lumena disajnih puteva, destrukcije zida alveola, smanjenja elastičnosti alveola, a zbog svega toga dolazi do zarobljavanja vazduha u njima što remeti razmenu gasova. Ovo oboljenje predstavlja veliki zdravstveni problem širom sveta, a smatra se da će 2020. godine HOBP biti treći uzročnik svih smrtnih ishoda. Astma po definiciji predstavlja hroničnu inflamatornu bolest koja difuzno zahvata disajne puteve dovodeći do smanjenja protoka vazduha usled njihove hiperreaktivnosti na različite stimuluse iz spoljašnje sredine.2 Ovo smanjenje protoka kod bolesnika sa astmom je najčešće reverzibilno i prestaje spontano ili usled primene lekova. Medikamentna terapija kod bolesnika sa HOBP i astmom je ključna kako u hroničnom lečenju tako i za vreme egzacerbacije bolesti, dok je mehanička ventilacija neophodna u onim slučajevima kada i pored primenjene medikamentne terapije dolazi do pogoršanja u kliničkoj slici. U tim situacijama ventilatorna podrška često predstavlja životno spašavajući tretman. Ona može da bude neinvazivna i invazivna. Neinvazivna ventilacija je rezervisana za bolesnike sa lakšom kliničkom slikom i prisutnom dispnejom i hipoksemijom, dok je invazivna ventilacija rezervisana za bolesnike sa težom kliničkom slikom. Iako patogeneza i klinički tok kod bolesnika sa hroničnom opstruktivnom bolešću pluća i kod bolesnika sa astmom nisu isti, ventilatorna podrška i podešavanje parametara invazivne ventilacije se bitno ne razlikuju. Neinvazivna ventilacija Neinvazivna ventilacija pozitivnim pritiskom podrazumeva mehaničku ventilaciju koja se primenjuje najčešće putem facijalne maske ili nazalne maske. Kliničke studije su pokazale da rana primena neinvazivne mehaničke ventilacije može da odloži potrebu za primenom invazivne ventilacije i kod bolesnika sa astmatičnim statusom i kod bolesnika sa egzacerbacijom HOBP.3
Postoji nekoliko različitih modova neinvazivne ventilacije (BiLevel positive airway pressure, pressure support, volume preset ventilation), a ventilacija preko facijalne maske se pokazala kao
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
123
bolja (naročito kod bolesnika koji dišu sa otvorenim ustima) u odnosu na neinvazivnu ventilaciju preko nazalne kanile iako je mrtvi prostor veći kod facijalne maske. Invazivna mehanička ventilacija Podešavanje parametara invazivne ventilacije se vrši uzimajući u obzir dve osnovne patofiziološke promene koje se viđaju kod ovih bolesnika - povećan otpor u disajnim putevima i dinamičku hiperinflaciju pluća. Povećanje otpora u disajnim putevima nastaje kao posledica suženja disajnih puteva usled njihove inflamacije, povećane količine sekreta i usled pritiska okolnog tkiva na male disajne puteve zbog povišenog intrapleuralnog pritiska za vreme ekspirijuma. Dinamička hiperinflacija pluća nastaje kao posledica suženja disajnih puteva i limitiranog protoka gasa za vreme ekspirijuma. Ukoliko ekspiratorno vreme nije dovoljno dugo, u plućima ostaje određena količina vazduha koja ne može da bude izdahnuta, a započinjanjem novog inspirijuma količina vazduha u plućima postaje sve veća. Zbog toga se povećava funkcionalni rezidualni kapacitet pluća i njegova vrednost premašuje vrednosti uobičajenog volumena relaksacije pluća na kraju ekspirijuma. Ovako zarobljeni gas u alveolama dovodi do nastanka pozitivnog pritiska na kraju ekspirijuma koji se naziva auto-PEEP, unutrašnji ili intrinzički PEEP.4 Iako inicijalno autoPEEP može da bude od koristi u sprečavanju nastanka kolapsa alveola i održavanju disajnih puteva prohodnim, on zapravo ima brojne negativne posledice. Auto-PEEP značajno povećava disajni rad bolesnika.5 Da bi alveole sa zarobljenim vazduhom bile ventilirane potrebno je da intrapleuralni pritisak (njegova negativna vrednost kod bolesnika na spontanom disanju) nadmaši vrednost auto-PEEP-a čime se stvaraju uslovi da započne protok gasa. Povećanje disajnog rada potrebno da se generiše toliki intrapleuralni pritisak dovodi do povećane potrošnje kiseonika i povećane produkcije ugljen dioksida, a poremećaj ventilacije alveola dovodi do nastanka hipoksemije što se u gasnim analizama arterijske krvi ovih bolesnika vidi kao smanjenje Ph, povećanje PaCO2 i smanjenje PaO2. Pored povećanja disajnog rada, auto-PEEP dovodi do manje efikasnog rada respiratorne muskulature zato što je radna dužina mišića skraćena zbog hiperinflacije pluća. Ovo se naročito vidi u radu dijafragme koja obzirom da se nalazi najniže u grudnom košu nije u stanju da pravi velike dodatne descedentne ekskurzije za vreme inspirijuma. Takođe auto-PEEP može da kompromituje povratak venske krvi u desnu komoru, a zbog distenzije alveola povećava kompresiju na alveolarne kapilare što može da poveća otpor u plućnoj cirkulaciji i dovede do opterećenja desne komore. Smanjen priliv krvi u srce kao i opterećenje desne komore mogu da dovedu do hemodinamske nestabilnosti.6 Hiperinflacija i auto-PEEP mogu još da uzrokuju i nastanak barotraume, pneumotoraksa, pneumomedijastinuma i pneumoperitoneuma. Podešavanje parametara ventilacije Inicijalno podešavanje parametara ventilacije i odabir moda mehaničke ventilacije zavise od protokola bolnice. Najčešće podešavanje ventilatora nakon intubacije podrazumeva mali disajni volumen (od 5 do 8 ml/kg) i disajnu frekvencu od 10-14 respiracija u minutu uz održavanje adekvatnog odnosa između inspirijuma i ekspirijuma.7 Procenat kiseonika u udahnutoj smeši gasova najpre se podešava na 100%, a zatim ako je moguće smanjuje se ispod 50% uz uslov da se saturacija arterijske krvi održi na vrednostima većim od 88%. Inspiratorni protok treba podesiti na vrednosti od 80-100 l/min kako bi se obezbedila adekvatna dužina ekspirijuma. Senzitivnost trigera se podešava na minimalne vrednosti (- 1 do 2 cm H2O za pritisak ili 2 l/min ukoliko je triger protok) jer u slučaju postojanja auto-PEEP-a bolesnik možda neće biti u stanju da generiše dovoljan negativni pritisak ili protok koji bi služio kao triger. Vršni pritisak u
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
124
disajnim putevima (peak airway pressure) kod bolesnika sa opstrukcijom ne korelira dobro sa pritiskom u alveolama, mnogo bolji pokazatelj pritiska u alveolama je plato pritisak u disajnim putevima i njegova vrednost ne bi trebalo da prelazi 30 cm H2O čime se smanjuje rizik od nastanka barotraume. I kod ovih bolesnika na mehaničkoj ventilaciji podešavaju se vrednosti pozitivnog pritiska na kraju ekspirijuma - PEEP (ovo je spoljašnji PEEP za razliku od auto-PEEP-a). Dodavanjem PEEP-a bolesniku koji već ima auto-PEEP na prvi pogled može da deluje nelogično, međutim dodavanjem spoljašnjeg PEEP-a mogu se otkloniti ili bar ublažiti neki negativni efekti auto-PEEP-a. Naime, dodavanje PEEP-a sprečava nastanak kolapsa disajnih puteva u ekspirijumu što olakšava ekspirijum, a za vreme sledećeg spontanog inspirijuma omogućava da se uz manji napor bolesnika i manji disajni rad generiše protok vazduha prema alveolama. Ovo važi samo ako je vrednost spoljašnjeg PEEP-a manja od vrednosti auto-PEEP-a. Mogućnost protoka gasa kod postojanja auto-PEEP-a uz dodavanje spoljašnjeg PEEP-a objašnjava se efektom vodopada.8 Naime, voda teče niz vodopad samo ako postoji visinska razlika, auto-PEEP predstavlja gornji nivo vodopada, a spoljašnji PEEP donji nivo. Protok gasa iz alveola u spoljašnju sredinu postoji sve dok je spoljašnji PEEP manji od unutrašnjeg, pa se zato preporučuje podešavanje spoljašnjeg PEEP-a na vrednosti od oko 80% auto-PEEP-a. Vrednosti auto-PEEP-a je moguće meriti uz pomoć ventilatora. Pritiskom na komandu “ekspiratorno zadržavanje” (expiratory hold) moguće je kod relaksiranih bolesnika bez spontanog disanja odrediti vrednost takozvanog statičkog auto-PEEP-a. Aparat u tom slučaju meri prosečnu vrednost pritisaka iz svih alveola na kraju ekspirijuma. Pored statičkog postoji i dinamički auto-PEEP. Vrednosti dinamičkog auto-PEEP-a se registruju kod bolesnika sa spontanim disanjem i njegove vrednosti su uvek manje od vrednosti statičkog auto-PEEP-a zato što on predstavlja pritisak u onim alveolama koje imaju najmanji auto-PEEP (protok gasa u tim alveolama započinje kada pritisak u disajnim putevima nadvlada najmanju vrednost auto-PEEP-a). Treba imati u vidu da i za vreme mehaničke ventilacije ovih bolesnika može da nastane dinamička hiperinflacija. Značajne determinante nastanka dinamičke hiperinflacije za vreme mehaničke ventilacije pluća predstavljaju minutna ventilacija pluća, disajni volumen, ekspiratorno vreme i stepen opstrukcije disajnih puteva. Iako minutna ventilacija može da bude zadovoljavajuća, skraćenje ekspiratornog vremena bilo smanjenjem inspiratornog protoka ili povećanjem frekvence disanja dovodi do zarobljavanja vazduha i nastanka dinamičke hiperinflacije. Potrebno je obezbediti adekvatnu dužinu trajanja ekspiratornog protoka ali i smanjiti stepen opstrukcije disajnih puteva korišćenjem kortikosteroida i bronhodilatatora. Od velike pomoći u svakodnevnom radu može da bude poznavanje i praćenje ventilacionih kriva na displeju ventilatora zato što se promene na njima mogu videti ranije nego što to pokažu klinička slika i laboratorijski nalazi (tahikardija, hipertenzija, korišćenje pomoćne musculature, znojenje, hipotenzija, hipoksemija, hiperkapnija), a moguća je i brza procena postojanja i veličine auto-PEEP-a. Završetak mehaničke ventilacije i odvajanje bolesnika od mehaničkog ventilator
Bolesnike sa HOBP i astmom potrebno je što pre odvojiti od ventilatora. Kada su ispunjeni nerespiratorni preduslovi za završetak ventilacije kao što su hemodinamska stabilnost i adekvatan neurološki status procenjuju se respiratorni parametri bolesnika kao i kod drugih bolesnika na mehaničkoj ventilaciji. Progresivno smanjenje inspiratorne koncentracije kiseonika, smanjenje nivoa podrške spontanom disanju i PEEP-a uz zadovoljavajuće gasne analize su preduslovi uspešnog odvajanja bolesnika. Svakodnevno je potrebna procena sposobnosti bolesnika za spontano disanje i procena mogućnosti ekstubacije (korišćenjem T nastavka ili

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
125
nekog od modova spontane ventilacije PAV, NAVA, PPS) a ukoliko odvajanje nije moguće bolesnik se odmara a sledeće odvajanje se planira za 24h.9 Za vreme mehaničke ventilacije potrebna je redovna procena bola i administracija analgetika (fentanil, morfin), kao i sedativa kod agitiranih bolesnika (lorazepam, midazolam, propofol). Zaključak
Mehanička ventilacija bolesnika sa astmom i HOBP zahteva dobro poznavanje patofizioloških procesa ovih oboljenja kako bi se odabrao adekvatan mod ventilacije, a parametri ventilatora podesili tako da omoguće adekvatnu razmenu gasova uz dobru sinhronizaciju između bolesnika i ventilatora. Literatura:
1. Bošnjak-Petrović V, Rebić P. Globalna inicijativa za hroničnu opstruktivnu bolest pluća - džepni vodič za dijagnostikovanje, lečenje i prevenciju. Beograd 2007.
2. Nestorović B. et al. Vodič kliničke prakse za dijagnostikovanje, lečenje i praćenje astme u dečijem uzrastu.Beograd 2002.
3. Ram FSF, Picot J, Lightowler J, et al. Non-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews,2004; CD004104.
4. Ranieri VM, Giuliani R, Cinnella G, et al. Physiologic effects of positive end-expiratory pressure in patients with chronic obstructive pulmonary disease during acute ventilatory failure and controlled mechanical ventilation. Am Rev Respir Dis,1993;147:5–13.
5. Tobin MJ. Respiratory monitoring in the intensive care unit. Am Rev Respir Dis, 1988;138:1625–42.
6. Scharf SM, Iqbal M, Keller C, et al. Hemodynamic characterization of patients with severe emphysema. Am J Respir Crit Care Med,2002;166:314–22.
7. Garcia Vicente E. Sandoval Almengor JC, Diaz Caballero JA, Salgado Campo JC. Invasive mechanical ventilation in COPD and asthma. Med Intensiva. 2011;35(5):288-298.
8. Tobin MJ, Lodato RF. 1989. PEEP, auto-PEEP, and waterfalls. Chest, 96:449–51. 9. Reddy R, Guntupalli K. Review of ventilatory techniques to optimize mechanical
ventilation in acute exacerbation of chronic obstructive pulmonary disease International Journal of COPD 2007:2(4) 441–452.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
126
LOW FLOW ANAESTHESIA THEORY, PRACTICE, TECHNICAL PRECONDITIONS, ADVANTAGES, FOREIGN GAS ACCUMULATION JAN A.BAUM,CHRISTIAN HÖNEMANN Department of Anaesthesia and Intensive Care Hospital St. Elisabeth-Stift and Marioenhospital Vechta, Germany
Short history of the rebreathing technique in anaesthesiology
As early as in 1850 John Snow recognized that a considerable amount of inhalation anaesthetics were exhaled unchanged in the expired air of anaesthetized patients. He concluded and could proof that the narcotic effect really could be markedly prolonged by reinhaling these unused vapours (1). About 75 years later, in 1924, rebreathing systems equipped with carbon dioxide absorbers were introduced into anaesthetic practice. While Ralph Waters used a to-and-fro system (2), the German gynecologist Carl J. Gauss and the chemist Hermann D. Wieland did advocate the use of a circle system for application of purified acetylene as an inhalation anaesthetic (3). The introduction of the highly combustible anaesthetic gas cyclopropane in 1933 urged anaesthetists to use fresh gas flows as low as possible to reduce pollution of the operating room and, thus, to minimize the risk of inadvertent explosions (4).
In 1954 halothane was introduced, a new volatile anaesthetic characterized by high anaesthetic potency yet narrow therapeutical width. To ensure patients safety, the use of this anaesthetic was bound to the knowledge of the applied vapour concentration. Its estimation, however, only was simple and easy if a high fresh gas flow was used and the proportion of rebreathing was kept rather low. The more, as the vaporizers, available at that time, didn´t work sufficiently reliably and precisely in the low flow range. Thus, although nearly all anaesthetic machines were already equipped with sophisticated rebreathing circle systems, paradoxically, it became clinical routine to use fresh gas flows as high as 4 to 6 l/min, completely excluding any significant rebreathing (4). In many countries this is still the routine way to execute inhalational anaesthesia (5). However, due to the development of modern anaesthetic apparatus, the availability of comprehensive gas monitoring, an increasing environmental awareness, the introduction of new advantageous but expensive inhalational anaesthetics, and the world wide restriction of economical ressources in medical care, since about fifteen years an increasingly strong recollection towards low flow techniques can be observed - and should be encouraged (6).
2. Low flow anaesthesia - the theory
Rebreathing systems can be used in different ways: If used with a fresh gas flow equal to the minute volume of the patient, the share of rebreathing will be neglectible. Nearly completely the expired air will vented out off the system as excess gas via the APL-valve. The patient gets nearly pure fresh gas. If a flow of 4.0 l/min is used, the share of rebreathing will increase to about 20%. The patient inhales a gas the composition of which still resembling that of the fresh
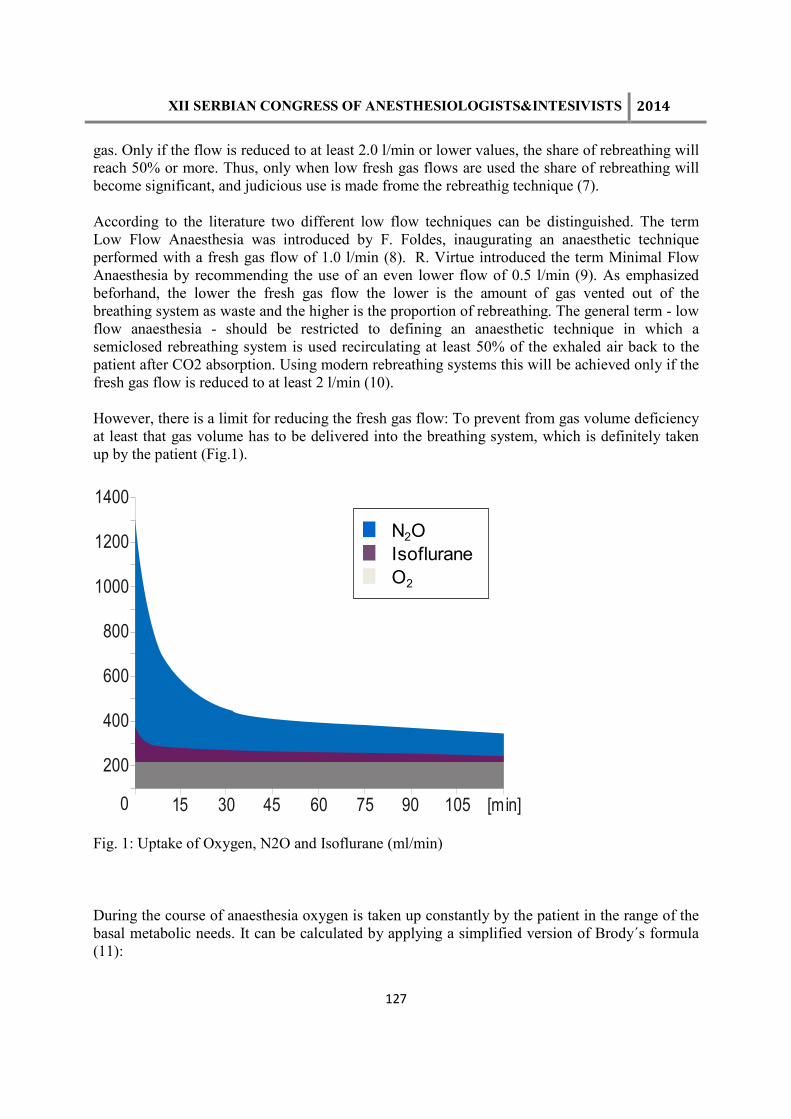
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
127
gas. Only if the flow is reduced to at least 2.0 l/min or lower values, the share of rebreathing will reach 50% or more. Thus, only when low fresh gas flows are used the share of rebreathing will become significant, and judicious use is made frome the rebreathig technique (7).
According to the literature two different low flow techniques can be distinguished. The term Low Flow Anaesthesia was introduced by F. Foldes, inaugurating an anaesthetic technique performed with a fresh gas flow of 1.0 l/min (8). R. Virtue introduced the term Minimal Flow Anaesthesia by recommending the use of an even lower flow of 0.5 l/min (9). As emphasized beforhand, the lower the fresh gas flow the lower is the amount of gas vented out of the breathing system as waste and the higher is the proportion of rebreathing. The general term - low flow anaesthesia - should be restricted to defining an anaesthetic technique in which a semiclosed rebreathing system is used recirculating at least 50% of the exhaled air back to the patient after CO2 absorption. Using modern rebreathing systems this will be achieved only if the fresh gas flow is reduced to at least 2 l/min (10).
However, there is a limit for reducing the fresh gas flow: To prevent from gas volume deficiency at least that gas volume has to be delivered into the breathing system, which is definitely taken up by the patient (Fig.1).
1400
1200
1000
800
600
400
200
15 30 45 60 75 90 105 [min]0
Fig. 1: Uptake of Oxygen, N2O and Isoflurane (ml/min)
During the course of anaesthesia oxygen is taken up constantly by the patient in the range of the basal metabolic needs. It can be calculated by applying a simplified version of Brody´s formula (11):
N2O
Isoflurane
O2

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
128
VO2 = 10 x BW [kg] 3/4 .
The uptake of nitrous oxide and the volatile anaesthetic, however, follows a power function. Nitrous oxide uptake of a normal body weight adult patient can be roughly estimated by applying Severinghaus´ formula (12)
VN2O = 1000 x t-1/2 ,
and the uptake of inhalational anaesthetics may be calculated by H. Lowe´s formula (13):
VAN = f x MAC x λλλλB/G x Q x t-1/2 .
Thus, assuming a constant gas composition circulating within the breathing system, the total gas uptake, the sum of oxygen, nitrous oxide and inhalational anaesthetic uptake, is following a power function. Initially it is high and declines sharply during the first 30 minutes, but is comparatively low and decreases only delayed during the following time course of anaesthesia. This exponential characteristic of the gas uptake results from the fact that the partial pressure difference of anaesthetic gases between the alveolar space and the blood, being initially high, decreases continuously with increasing saturation of the blood and the tissues. If the anaesthetist, by frequent alterations of the settings at the gas controls, could succeed to approximate the total gas uptake, anaesthesia with closed rebreathing system would be realized. In clinical practice, however, continuous adaptations of the fresh gas flow according to the continuously changing individual gas uptake will be impossible. Whereas, applying very simple and safe standardized dosing schemes, low flow techniques like Minimal Flow and Low Flow Anaesthesia can be performed safely with already available anaesthetic equipment in routine clinical work (7,14).
3. Low flow anaesthesia - the practice 3.1 Induction
Premedication and induction of low flow anaesthesia is performed according to the usual induction scheme. Preoxigenation by applying pure oxygen via a face mask is followed by intravenous injection of a hypnotic. After neuromuscular relaxation and endotracheal intubation or insertion of a laryngeal mask the patient is connected to the breathing system. In about 85% of all cases the gas tightness of the laryngeal mask will allow the fresh gas flow to be reduced to 0.5 l/min, even if controlled ventilation is performed (7,15). There are no procedure specific requirements for premedication and induction.
3.2 Initial high flow phase
According to the guidelines given by Foldes or Virtue, during the first initial phase lasting 10 to 15 minutes a high fresh gas flow has to be used. The author himself (7,16) recommends to set the oxygen flow to 1.4 l/min and the nitrous oxide flow to 3.0 l/min. This fresh gas composition guarantees in most of all patients an inspired oxygen concentration of at least 30%, meeting the recommendations of Barton and Nunn (17,18). The following settings of the vaporizers are used

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
129
routinely during the initial phase: enflurane 2.5 Vol%, isoflurane 1.5 Vol%, sevoflurane 2.5 Vol%, and desflurane 4.0 to 6.0%. If these settings are used over the first 10 to 15 minutes an expired concentration of about 0.7 to 0.8 times the MAC of the respective volatile agent will be gained. In addition to a nitrous oxide MAC of about 0.6, corresponding to a nitrous oxide concentration of 60%, this will result in a common MAC of 1.3 representing the AD95, the anaesthetic gas concentration guaranteeing a sufficient anaesthetic depth for 95% of all patients to tolerate the skin incision without any movement. To initially use a high fresh gas flow is furthermore indispensable for sufficient denitrogenation and wash in of the aspired gas composition into the whole gas containing space. Last but not least, if the flow to early would be reduced to too low values, inevitably gas volume deficiency would result compromizing adequate ventilation (7,16).
3.3 Flow reduction
If Low Flow Anaesthesia is to be performed, the fresh gas flow can be reduced to 1.0 l/min already after 10 minutes. Flow reduction will lead to a significant increase of rebreathing. The inspired gas, thus, contains a markedly increased proportion of the exhaled gas which already had passed the patient´s lung and contains less oxygen. The resulting decrease of oxygen content in the gas mixture has to be compensated by increasing the fresh gas oxygen content, which must be the higher the lower is the flow. Thus, to maintain a safe inspired oxygen concentration of about 30 % in Low Flow Anaesthesia, the fresh gas oxigen concentration has to be increased to 50%, but at least to 40%. With the fresh gas flow reduction, furthermore, the amount of anaesthetic vapour delivered into the system is markedly reduced. This has to be compensated by a corresponding significant increase of the agent´s concentration in the fresh gas. Only in this way the aspired anaesthetic concentration within the breathing system can be kept constant. In Low Flow Anaesthesia the fresh gas enflurane concentration is increased to 3.0 Vol%, isoflurane to 2.0 Vol% and sevoflurane to 3.0 Vol% (7,16,19). Due to its specific pharmacokinetic properties, only the fresh gas desflurane concentration can be maintained unchanged (20). Executing these standardized schemes, the expired anaesthetic concentrations will be maintained in the aspired range of 0.7 to 0.8 times the MAC.
If Minimal Flow Anaesthesia is to be performed, the initial high flow phase should last about 15 minutes. A sufficiently long initial high flow phase will prevent from accidental gas volume deficiency, which always will result whenever the gas loss via individual uptake and leakages is higher than the gas volume delivered into the system. To maintain a safe inspired oxygen concentration of at least 30%, oxygen fresh gas concentration has to be increased to 60%, but at least to 50%, when the flow is reduced to 0.5 l/min. Simultaneously the anaesthetic concentration of the fresh gas has to be increased: When enflurane is used to 3.5 Vol%, isoflurane to 2.5 Vol%, sevoflurane to 3.5 Vol%, and the Desflurane concentration standardizedly is raised by 1 Vol%. By applying this dosing scheme again an expired agent's concentration in the range of 0.7 to 0.8 times of the respective MAC will be maintained too (7,16,19,20).

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
130
3.3.1 Inspired oxygen and nitrous oxide concentration
After flow reduction from 4.4 to 0.5 l/min an initial increase of the FIO2 over the following period of 30 to 45 minutes can be observed. It will be more pronounced in small or elderly patients with low oxygen uptake than in strong young and athletic patients. This initial increase is followed by a slow but continuous decline of the inspired oxygen concentration to lower values, on its part being the more pronounced the higher is the oxygen uptake of the patient. Whenever the lower alarm limit of the oxygen monitoring is reached, which carefully must be adjusted to 30%, the oxigen flow has to be increased by 10% of the total fresh gas flow, whereas the nitrous oxide flow must be decreased by the same amount. Thus, in Minimal Flow Anaesthesia, the oxygen flow has to be increased by 50 ml/min and the nitrous oxide flow to be reduced by 50 ml/min likewise. After these adjustments, again, first a slow increase of the FIO2 will be followed by its slow but continuous decrease. Whenever the lower alarm threshold is reached anew, the oxygen flow again has to be increased by 10% of the total fresh gas flow and the nitrous oxide flow to be reduced by the same amount. In Low and Minimal Flow Anaesthesia the oxygen concentration within the breathing system is changing slowly but continuously during the course of the anaesthetic procedure (7,16).
3.3.2 Concentration of inhalational anaesthetics
If, with reduction of the flow, the fresh gas concentration of the volatile anaesthetic is increased according to the given standardized schemes, a slight decrease of the inspired and expired anaesthetic concentration can be observed. The vaporizers of all modern anesthetic apparatus are switched into the fresh gas line (VOC). Thus, the reduction of the flow results in a corresponding significant decrease of the amount of anaesthetic vapour delivered into the system. In all the different anaesthesia machines, likewise, the breathing system, the ventilator, the connecting hoses and the patient hose assembly contain a gas volume of about 5 to 6 liter. This, in addition to the gas volume of about 2.5 liter contained in the lung of an adult patient, is the distribution space for the anaesthetic vapour delivered into the system (7). A fresh gas flow as low as 500 ml/min assumed, a change of the vaporizer's setting from zero to 5 Vol% only will raise the amount of vapour from 0 to 25 ml/min, a considerably small volume if compared with the distribution space. Thus, in low flow anaesthesia there is a marked difference between the anaesthetic´s fresh gas concentration and its concentration within the breathing system, and this difference is the higher the lower is the fresh gas flow, but the lower the less soluble is the anaesthetic agent (19-21). If the concentration of the volatile anaesthetic shall be changed, the vaporizer has to be adjusted to a concentration considerably exceeding the aspired nominal value.
3.3.3 Time constant
The time constant is a measure for the time it takes, that alterations of the fresh gas composition will lead to corresponding alterations of the gas composition within the breathing system. According to a formula given by Conway (22) the time constant (T) can be calculated by the division of the system's volume (VS) by the difference between the amount of anaesthetic agent delivered into the system with the fresh gas (VD) and the individual gas uptake (VU):
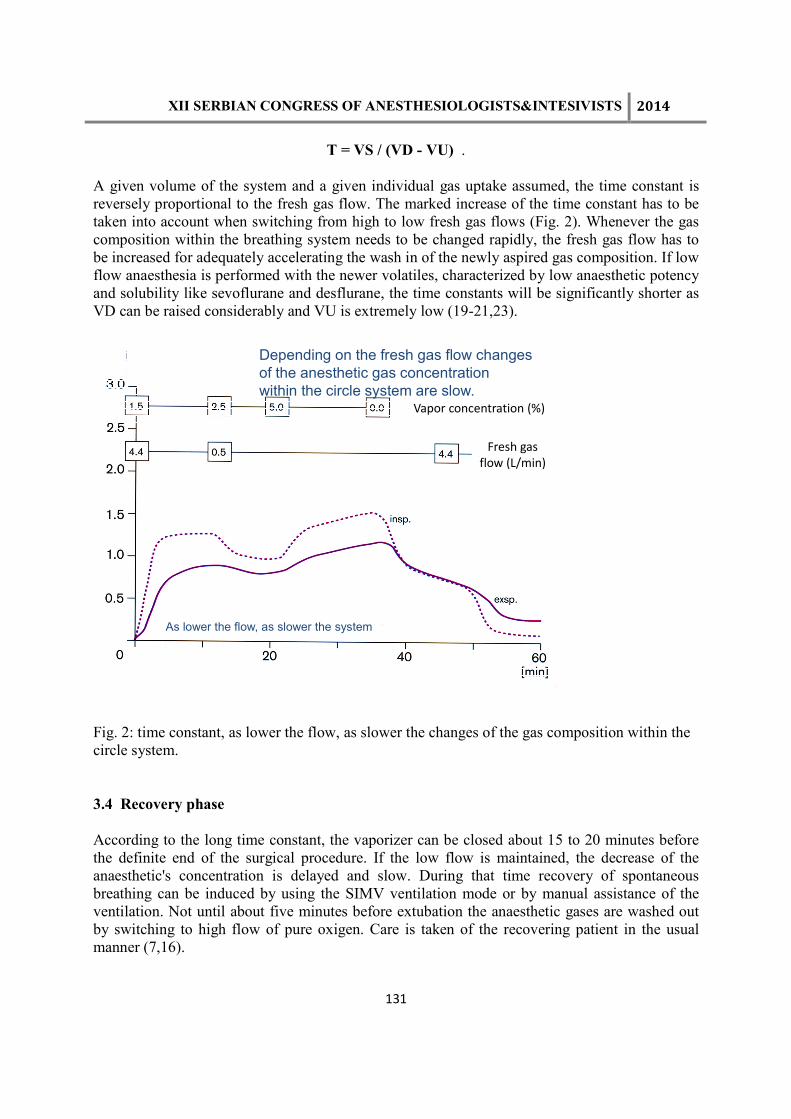
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
131
T = VS / (VD - VU) .
A given volume of the system and a given individual gas uptake assumed, the time constant is reversely proportional to the fresh gas flow. The marked increase of the time constant has to be taken into account when switching from high to low fresh gas flows (Fig. 2). Whenever the gas composition within the breathing system needs to be changed rapidly, the fresh gas flow has to be increased for adequately accelerating the wash in of the newly aspired gas composition. If low flow anaesthesia is performed with the newer volatiles, characterized by low anaesthetic potency and solubility like sevoflurane and desflurane, the time constants will be significantly shorter as VD can be raised considerably and VU is extremely low (19-21,23).
Depending on the fresh gas flow changes
of the anesthetic gas concentration
within the circle system are slow.
As lower the flow, as slower the system
Fresh gas flow (L/min)
Vapor concentration (%)
Fig. 2: time constant, as lower the flow, as slower the changes of the gas composition within the circle system.
3.4 Recovery phase
According to the long time constant, the vaporizer can be closed about 15 to 20 minutes before the definite end of the surgical procedure. If the low flow is maintained, the decrease of the anaesthetic's concentration is delayed and slow. During that time recovery of spontaneous breathing can be induced by using the SIMV ventilation mode or by manual assistance of the ventilation. Not until about five minutes before extubation the anaesthetic gases are washed out by switching to high flow of pure oxigen. Care is taken of the recovering patient in the usual manner (7,16).
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
132
3.4.5 Characteristics of low flow anaesthesia
If commercially available anaesthetic machines are used, with Low and Minimal Flow Anaesthesia the maximum of flow reduction is reached which can be gained in routine clincal practice. Both techniques are extreme variants of semiclosed use of rebreathing systems, as still a small amount of excess gas is used.
The performance of Low and Minimal Flow Anaesthesia becomes very simple if standardized schemes are used to controll the fresh gas flow and its composition. This schemes require only rare adjustments at the gas flow controls and vaporizers. The anaesthetist, however, must accept that the gas concentrations within the breathing system not will remain constant at the aspired values, but rather will change slowly but continuously during the course of anaesthesia.
Last but not least, standardized schemes for the performance of low flow anaesthesia only can be guidelines. The fresh gas flow and its composition always must be adapted to the individual patient's reaction and the current requirements of the surgical procedure.
4. Technical preconditions for safe performance of low flow anaesthesia
4.1. Monitoring and alarm thresholds
Due to its specific characteristics following monitoring is essential for safe performance of low flow anaesthesia (6,7,16): As the difference between the gas concentrations in the breathing system and the fresh gas increases with the extend of flow reduction, the anaesthetic gas composition can't be reliably assessed from the composition of the fresh gas. Thus, continuous monitoring of the inspired oxigen concentration is absolutely indispensable. The same applies for the concentration of volatile anaesthetics, if a fresh gas flow lower than 1 l/min is used. The lower threshold for the inspired oxigen concentration should be set to 30%, and the upper alarm limit of inspired anaesthetic concentration to 2.0-3.0 Vol% for Halothane, Enflurane and Isoflurane likewise, to 5.0 Vol% for Sevoflurane and 8.0 Vol% for Desflurane. Always the fresh gas volume must be as large as to sufficiently compensate the gas loss via individual uptake and leakages. Otherwise gas volume deficiency will occure, inevitably leading to an alteration of the ventilation. Continuous monitoring of the air way pressure or, alternatively, the minute volume therefore also is indispensable. The disconnect alarm should be set to a value 5 mbar lower than the peak pressure, the lower alarm limit of the minute volume monitoring to 0.5 l/min lower than the aspired minute volume. If low flow techniques are performed consistently the soda lime consumption will increase fourfold. By continuous monitoring of the inspired carbon dioxide concentration soda lime exhaustion reliably can be detected. If this monitoring is not available jumbo or double absorber canisters should be used and the soda lime changed after each day of work (7,24).
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
133
4.2. Anaesthetic apparatus
The technical features of the anaesthetic apparatus have to comply with following requirements (7,10):
The flow control system must feature needle valves and flow meter tubes calibrated and reliably working even in the low flow range, the vaporizers must be fresh gas flow compensated. The rebreathing system has to be sufficiently gas tight: The leackage must not exceed 100 ml/min at a pressure of 20 mbar to meet the requirements for Minimal Flow Anaesthesia. The performance of low flow techniques is significantly facilitated by the availability of an anaesthetic gas reservoir, by which small accidental gas volume deficiencies can be balanced. Such gas reservoir can be, alternatively, the endinspiratory volume contained in the bag of a bag-in-bottle ventilator, or the bellows of a ventilator with standing or hanging „floating“ bellows, or the manual ventilation bag in machines equipped with a fresh gas decoupling valve. If an anaesthetic apparatus is used, featuring continuous flow of the fresh gas into the breathing system, furthermore, it has to be considered that each alteration of the fresh gas flow will lead to a corresponding alteration of the tidal volume. Only if an anaesthetic ventilator is used, featuring fresh gas flow compensation, the preset tidal volume will be delivered independently from the fresh gas flow range. Fresh gas flow compensation can be realized, alternatively, by discontinuous delivery of the fresh gas into the breathing system, or by automatic electronical control of the ventilator´s performance corresponding to the fresh gas flow rate.
Using modern anaesthetic equipment even in pediatric anaesthesia low flow techniques are advantageous and can be executed safely (7,25,26).
5. Advantages of low flow anaesthesia
The advantages of low flow anaesthesia are obvious and indisputable and were already comprehensively listed in Waters´ paper (2): the reduction of anaesthetic gas and vapour consumption, the decrease of atmospheric pollution with inhalation anaesthetics, the improvement of anaesthetic gas climate, and the significant reduction of costs.
Comparing two hours of continuous high flow (4.5 l/min) with minimal flow (0.5 l/min) isoflurane anaesthesia, the consumption of oxygen is reduced by 115 l, that of nitrous oxide by 300 l, and that of isoflurane vapour by 5.6 l (7). If high flow techniques, using fresh gas flows of about 4.5 l/min, would be replaced consistently by low flow anaesthesia, in Germany and the UK the resulting reduction in gas and anaesthetic vapour consumption were projected to be about 350 million liters of oxygen, 1000 million liters of nitrous oxide, 33500 liters of fluid isoflurane and 46250 liters of fluid enflurane (10). The conclusion is very simple and obvious: The lower the flow the less the gas consumption (27,28).
Anaesthetists also have to deal with increasingly stringent official regulations on the maximum acceptable workplace concentrations of anaesthetic gases (29). Careful maintenance of the anaesthetic apparatus and scrupulous attention on leaks from breathing systems provided, even the extremely low anaesthetic gas concentrations stipulated by the US National Institute of Occupational Safety and Health can be achieved easily only by the use of low flow techniques
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
134
(30,31). Most operating theatres, however, are equipped with central gas-scavenging systems, and it is possible to stay within the defined limits even if high fresh gas flows are used. Nevertheless, high flow anaesthesia will inevitably result in pollution of the atmosphere beyond the operating theatre. Both, nitrous oxide and the volatile anaesthetics contribute to the destruction of the ozone layer and to the greenhouse effect. The ozone destructive potential of the volatile anaesthetics halothane, enflurane and isoflurane, which are partially halogenated chlorofluorocarbons (CFCs), is assumed to be only 0.1-1 % of all fully substituted CFCs. Furthermore, the proportion of nitrous oxide, emitted from hospitals, is only about 1 % of the total amount of nitrous oxide polluting the atmosphere. Most is derived from bacterial metabolism in fertilised soil. Nevertheless, even if the emission of anaesthetic gases is a comparatively small fraction of the total polluting gases, anaesthetists are morally obliged to minimize pollution in an age of increasing environmental awareness, and it is their duty to use all technical facilities available to achieve this (32-36). Desflurane and sevoflurane, which are halogenated only with fluorine, are assumed to have nearly no ozone depleting potential but may contribute considerably to the greenhouse effect.
Appropriate humidification and warming of anaesthetic gases have significant impact on the function and the integrity of the ciliated epithelium of the respiratory tract. During anaesthesia, the absolute humidity of the inspired gas should range preferably between 17-30 mgH2O/l, and its temperature between 28-32 °C. After an initial period of 30-45 minutes in an actively heated compact breathing system, the values referred to above can be achieved solely by the use of a low flow technique (37-41).
Cost savings directly result from the decrease of gas and anaesthetic consumption. They are related to the duration of the anaesthetic procedure, the price of the respective anaesthetic agent and the extend of flow reduction (42-44). Comparing high flow (4.5 l/min) with a minimal flow (0.5 l/min) technique lasting 2 hours, assuming the inspired anaesthetic concentration at MAC, savings of about US$ 15 can be gained if enflurane, about US$ 21 if isoflurane and about US$ 47 if desflurane is used (16). By comparison, the additional cost of about US$ 0.60 resulting from increased consumption of soda lime during 2 hours is negligible (7). Relating to the beforehand mentioned projection, the annual financial savings resulting from reduced gas and anaesthetic consumption in Germany and UK are assumed to total more than US$ 65,36 million if low flow anaesthetic techniques would be performed consistently (10). It seems to be realistic to assume a cost saving in the range of 50 - 75% if low flow techniques would be used consistently in clinical routine practice (7,45,46). Even the more costly anaesthetics like desflurane could be used without significant increase in costs (47).
5.1 Efficiency of inhalation anaesthetic techniques
One of the most striking aguments in favour for low flow anaesthesia is the marked increase in efficiency of inhalational anaesthesia (48). The efficiency (Eff) can be calculated by dividing the amount of agent taken up by the patient (VU) by the amount of agent delivered into the breathing system (VD):
Eff = VU / VD .
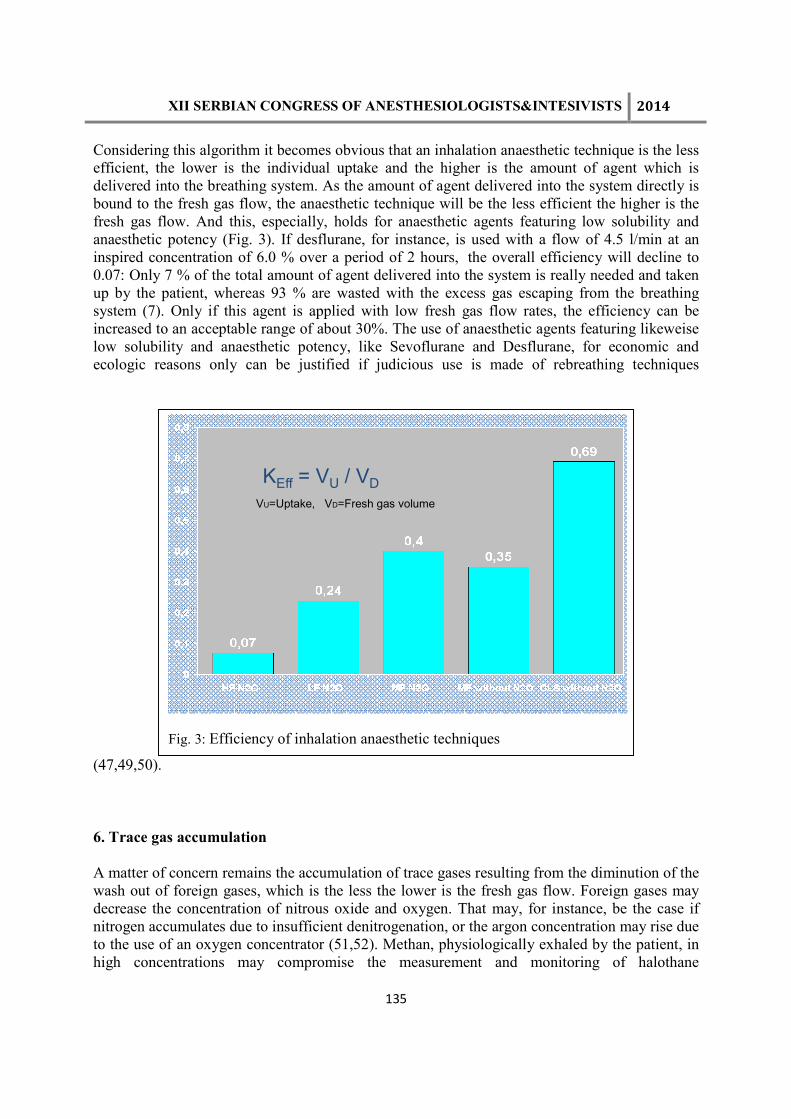
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
135
Considering this algorithm it becomes obvious that an inhalation anaesthetic technique is the less efficient, the lower is the individual uptake and the higher is the amount of agent which is delivered into the breathing system. As the amount of agent delivered into the system directly is bound to the fresh gas flow, the anaesthetic technique will be the less efficient the higher is the fresh gas flow. And this, especially, holds for anaesthetic agents featuring low solubility and anaesthetic potency (Fig. 3). If desflurane, for instance, is used with a flow of 4.5 l/min at an inspired concentration of 6.0 % over a period of 2 hours, the overall efficiency will decline to 0.07: Only 7 % of the total amount of agent delivered into the system is really needed and taken up by the patient, whereas 93 % are wasted with the excess gas escaping from the breathing system (7). Only if this agent is applied with low fresh gas flow rates, the efficiency can be increased to an acceptable range of about 30%. The use of anaesthetic agents featuring likeweise low solubility and anaesthetic potency, like Sevoflurane and Desflurane, for economic and ecologic reasons only can be justified if judicious use is made of rebreathing techniques
(47,49,50).
6. Trace gas accumulation
A matter of concern remains the accumulation of trace gases resulting from the diminution of the wash out of foreign gases, which is the less the lower is the fresh gas flow. Foreign gases may decrease the concentration of nitrous oxide and oxygen. That may, for instance, be the case if nitrogen accumulates due to insufficient denitrogenation, or the argon concentration may rise due to the use of an oxygen concentrator (51,52). Methan, physiologically exhaled by the patient, in high concentrations may compromise the measurement and monitoring of halothane
KEff = VU / VD
VU=Uptake, VD=Fresh gas volume
Fig. 3: Efficiency of inhalation anaesthetic techniques

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
136
concentration (53). Accumulation of acetone may prolong the emergence from anaesthesia and provoke nausea or vomiting. However, only in the very rare cases of severely ketoacidotic patients this really may become clinically relevant (54). Accumulation of these trace gases even in prolonged low flow anaesthesia, up to now, have not been shown to be of real clinical importance (55).
All inhalational anaesthetics react with carbon dioxide absorbents by absorption and degradation, most eagerly if the absorbent is desiccated (56). The new volatiles desflurane and sevoflurane are more liable to react with the alkaline absorbents than the older anaesthetics halothane, enflurane or isoflurane. Desflurane more than enflurane and isoflurane react with absolutely dry carbon dioxide absorbents by generating carbon monoxide. Only partial wetting markedly reduces this chemical reaction, and if soda lime contains only 4.8% and Baralyme only 9.5% water, carbon monoxide generation is suppressed completely (57). It had been concluded, consistently not to use fresh gas flows lower than 5 l/min to safely avoid accidental carbon monoxide intoxication resulting from trace gas accumulation (58). This conclusion, however, strongly must be rejected, as just high fresh gas flows are liable to dry out the absorbents. Contrarily, low flow anaesthesia, preserving the moisture content of the absorbents, just can be taken as a measure preventing from carbon monoxide generation (59). Sevoflurane more eagerly than halothane reacts with dry absorbents too (60,61). Both agents, however, also react with normally wet carbon dioxide absorbents by generating haloalkenes: Halothane by forming BCDFE = 1,bromo-1,chloro-2,2,difluoro-ethylene (62) and sevoflurane by forming compound A = fluoromethyl-2,2,difluoro-1,trifluoromethyl-vinylether. Compound A concentration was found to increase with the extend of flow reduction, with the absorbent´s temperature and the agent´s concentration (63,64). Some authors regard a compound A load of 150 to 240 ppmh as potentially nephrotoxic in humans (65-67) and emphasize not to use this anaesthetic with flows lower than 2.0 l/min. Contrarily, some authors estimate Low Flow Anaesthesia with sevoflurane to be safe, arguing that mean peak concentrations in different studies did not exceed 25 ppm and no signs of renal impairment were observed in any patient (49, 68,69). Mazze recently published the results of an investigation on nephrotoxicity of compound A in primates demonstrating that only at a load of at least 800 ppmh nephrotoxic effects occured (70). Accepting this threshold for nephrotoxic load with compound A absolutely no flow restriction would be justified. Even long lasting Minimal Flow Anaesthesia with sevoflurane could be performed safely, although compound A peak concentrations were found to reach 50 to 60 ppm with this technique (71). Unlike in the United States, sevoflurane was approved for clinical use without any fresh gas flow restriction in all countries of the European Common Market. Nevertheless, whenever in clinical practice there might be assumed the possibility of accumulation of potentially harmful trace gases, for safety reasons, a low flow technique using a flow of at least 1 l/min should be performed, guaranteeing a sufficient continuous wash out effect (7).
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
137
7. Literature
1. Snow J. On Narcotism by the Inhalation of Vapours. Part XV. The effects of Chloroform and Ether Prolonged by Causing the Exhaled Vapour to be reinspired. London Medical Gazette 1850; 11: 749-754
2. Waters RM. Clinical Scope and Utility of Carbon Dioxid Filtration in Inhalation Anaesthesia. Anesth Analg 1924; 3: 20-2
3. Baum JA. Who introduced the Rebreathing System into Clinical Practice? In Schulte am Esch J., M. Goerig, eds. Proceedings of the Fourth International Symposium on the History of Anaesthesia. Lübeck: Dräger 1998: 441-450
4. Onishchuk, JL. The early History of Low-Flow Anaesthesia. In Fink, B.R., L.E. Morris, C.R. Stephen, eds. The History of Anesthesia. Third International Symposium, Proceedings. Park Ridge, Illinois: Wood Library-Museum of Anesthesiology, 1992: 308-313
5. Cravero J, Suida E, Manzi DJ, Rice LJ. Survey of low flow anesthesia in the United States. Anesthesiology 1996; 85: A995
6. Baxter A. Low and minimal flow inhalation anaesthesia. Can J Anaesth 1997; 44: 643-653
7. Baum JA. Low Flow Anaesthesia. The Theory and Practice of Low Flow, Minimal Flow and Closed System Anaesthesia. Oxford: Butterworth Heinemann, 1996
8. Foldes FF, Ceravolo AJ, Carpenter SL. The administration of nitrous oxide - oxigen anesthesia in closed systems. Ann Surg 1952; 136: 978-981
9. Virtue RW. Minimal flow nitrous oxide anesthesia. Anesthesiology 1974; 40: 196-198
10. Baum JA, Aitkenhead AR. Low-flow anaesthesia. Anaesthesia 1995; 50 (Suppl.): 37-44
11. Kleiber M. Body size and metabolic rate. Physiol Rev 1945; 27: 511-539
12. Severinghaus J W. The rate of uptake of nitrous oxide in man. J Clin Invest 1954; 33: 1183-1189
13. Lowe H J, Ernst E A. The Quantitative Practice of Anesthesia. Williams& Wilkins, Baltimore 1981
14. Baker AB. Back to the basics - a simplified non-mathematical approach to low flow techniques in anaesthesia. Anaesth Intensive Care 1994; 22: 394-395

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
138
15. Fröhlich D, Schwall B, Funk W, Hobbhahn J. Laryngeal mask airway and uncuffed tracheal tubes are equally effective for low flow or closed system anaesthesia in children. Br J Anaesth 1997; 79: 289-292
16. Baum JA. Low Flow Anaesthesia with Dräger Machines. Questions and Answers. 3rd ed. Lübeck, Dräger Medizintechnik, 1998
17. Barton F, Nunn JF. Totally closed circuit nitrous oxide/oxygen anaesthesia. Br J Anaesth 1975; 47: 350-357
18. Don H. Hypoxemia and hypercapnia during and after anesthesia. In: Orkin F K, Cooperman L H, eds. Complications in Anesthesiology. Lippincott, Philadelphia 1983, pp. 183- 207
19. Baum J, Stanke HG. Low flow and minimal flow anaesthesia with sevoflurane (German). Anaesthesist 1998; 47 (Supplement 1): S70-S76
20. Baum J, Berghoff M, Stanke HG, Petermeyer M, Kalff G. Low-flow anaesthesia with desflurane (German). Anaesthesist 1997; 46: 287-293
21. Hargasser S, Hipp R, Breinbauer B, Mielke L, Entholzner E, Rust M. A lower solubility recommends the use of desflurane more than isoflurane, halothane, and enflurane under low-flow conditions. J Clin Anesth 1995; 7: 1-5
22. Conway CM. Closed and low flow systems. Theoretical considerations. Acta Anaesth Belg 1984; 34: 257-263
23. Avramov MN, Griffin JD, White PF. The effect of fresh gas flow and anaesthetic technique on the ability to control hemodynamic responses during surgery. Anesth Analg 1998; 87: 666-670
24. Morris LE. Closed carbon dioxide filtration revisited. Anaesth Intensive Care 1994; 22: 345-358
25. Peters JWB, Bezstarosti J, van Eden, Erdman W, Meursing AEE. Safety and efficacy of semi-closed circle ventilation in small infants. Pediatric Anaesthesia 1998; 8: 299-304
26. Igarashi M, Watanabe H, Iwasaki H, Namiki A. Clinical evaluation of low-flow sevoflurane anaesthesia for pediatric patients. Acta Anaesth Scand 1999; 43: 19-23
27. Feiss P, Demontoux MH, Colin D. Anesthetic gas and vapour saving with minimal flow anesthesia. Acta Anesth Belg 1990; 41: 249-251
28. Pedersen FM, Nielsen J, Ibsen M, Guldager H. Low-flow isoflurane-nitrous oxide anaesthesia offers substantial economic advantages over high-flow and medium flow isoflurane-nitrous oxide anaesthesia. Act Anaesth Scand 1993; 37: 509-512
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
139
29. Spence AA. Environmental pollution by inhalation anaesthetics. Br J Anaesth 1987; 59: 96-103
30. Virtue RW. Low flow anesthesia: advantages in its clinical application, cost and ecology. In: Aldrete JA, Lowe HJ, Virtue RW, eds. Low Flow and Closed System Anesthesia. Grune & Stratton, New York 1979, pp. 103-108
31. Imberti R, Preseglio I, Imbriani M, Ghittori S, Cimino F, Mapelli A. Low flow anaesthesia reduces occupational exposure to inhalation anaesthetics. Acta Anaesth Scand 1995; 39: 586-591
32. Logan M, Farmer JG. Anaesthesia and the ozone layer: Br J Anaesth 1989; 53: 645-646
33. Noerreslet J, Frieberg S, Nielsen TM, Römer U. Halothane anaesthetic and the ozone layer. Lancet 1989; 719
34. Pierce JMT, Linter SPK. Anaesthetic agents and the ozone layer. Lancet 1989; 1011-1012
35. Sherman SJ, Cullen BF. Nitrous oxide and the greenhouse effect. Anesthesiology 1988; 68: 816-817 36. Solomon S, Albritton D. Time-dependent ozone depletion potentials for short and long-term forecasts. Nature 1992; 357: 33-37
37. Bengtson JP, Sonander H, Stenqvist O. Preservation of humidity and heat of respiratory gases during anaesthesia - a laboratory investigation. Acta Anaesthesiol Scand 1987; 31: 127-131
38. Bengtson JP, Bengtson A, Stenqvist O. The Circle System as a Humidifier. Br J Anaesth 1989; 63: 453-457
39. Branson RD, Campbell RS, Davis K, Porembka DT. Anesthesia circuits, humidity output, and mucociliary structure and function. Anesth Intens Care 1998; 26: 178-183
40. Chalon J, Ali M, Turndorf H, Fischgrund GK. Humidification of anesthetic gases. Charles C. Thomas, Sprigfield 1981
41. Kleemann PP. Humidity of Anesthetic Gases with Respect to Low Flow Anaesthesia. Anaesth Intens Care 1994; 22: 396-408
42. Bengtson JP, Sonander H, Stenqvist O. Comparison of costs of different anaesthetic techniques. Acta Anaesth Scand 1988; 32: 33-35
43. Christensen KN, Thomsen A, Jorgensen S, Fabricius J. Analysis of Costs of Anaesthetic Breathing Systems. Br J Anaesth 1987; 59: 389-390
44. Loke J, Shearer WAJ. Cost of anaesthesia. Can J Anaesth. 1993; 40: 472-474
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
140
45. Cotter SM, Petros AJ, Doré CJ, Berber ND, White DC. Low-flow anaesthesia. Anaesthesia 1991; 46: 1009-1012
46. McKenzie AJ. Reinforcing a „low flow“ anaesthesia policy with feedback can produce a sustained reduction in isoflurane consumption. Anaesth Intensive Care 1998; 26: 371-376
47. Eger EI. Economic analysis and pharmaceutical policy: a consideration of the economics of the use of desflurane. Anaesthesia 1995; 50 (Supplement): 45-48
48. Ernst EA, Spain JA. Closed-circuit and high-flow systems: Examining alternatives. In: Brown BR, ed. Future Anesthesia Delivery Systems. Contemporary Anesthesia Practice, Vol. 8. F. A. Davies, Philadelphia 1984, pp. 11-38 49. Mazze RI, Jamison RL. Low-flow (1 l/min) sevoflurane - Is it safe?. Anesthesiology 1997; 86: 1225-1227
50. Smith I, Nathanson M, White PF. Sevoflurane - a long-awaited volatile anaesthetic. Brit J Anaesth 1996; 76: 435-445
51. Morita S, Latta W, Hambro K, Snider M. Accumulation of methane, acetone and nitrogen in the inspired gas during closed-circuit anesthesia. Anesth Analg 1985; 64: 343-347
52. Parker CJR, Snowdon SL. Predicted and measured oxygen concentrations in the circle system using low fresh gas flows with oxygen supplied by an oxygen concentrator. Br. J Anaesth 1988; 61: 397-402
53. Rolly G, Versichelen LF, Mortier E. Methane Accumulation During Closed-Circuit Anesthesia. Anesth Analg 1994; 79: 545-547
54. Strauß JM, Hausdörfer J. Accumulation of Acetone in Blood During Long-Term Anaesthesia with Closed System. Br J Anaesth 1993; 70: 363-364
55. Baumgarten RK, Reynolds WJ. Much Ado About Nothing: Trace Gaseous Metabolites in the Closed Circuit. Anesth Analg 1985; 64: 1029-1030
56. Strum DP, Eger II EI. The degradation, absorption and solubility of volatile anesthetics in soda lime depends on the water content. Anesth Analg 1994; 78: 340-348 57. Fang ZX, Eger II EI, Laster MJ, Chortkoff BS, Kandel L, Ionescu P. Carbon monoxide production from degradation of desflurane, enflurane isoflurane, halothane and sevoflurane by soda lime and baralyme. Anesth Anlag 1995; 80: 1187-1193
58. Moon RE. Carbon monoxide gas may be linked to CO2 absorbent. Anesth Patient Safety Found Newslett 1991; 6: 8
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
141
59. Baum J, Sachs G, v. d. Driesch C, Stanke HG. Carbon monoxide generation in carbon dioxide absorbents. Anesth Analg 1995; 81: 144-146
60. Baum J, Sitte Th, Strauß JM, Forst H, Zimmermann H, Kugler B. Absorption and degradation of sevoflurane in dry soda lime (German). Anästh Intensivmed 1998; 39: 11-16
61. Funk W, Gruber M, Wild K, Hobbhahn J. Dry soda lime markedly degrades sevoflurane during simulated inhalation induction. Br J Anaesth 1999; 82: 193-198
62. Sharp HJ, Trudell JR, Cohen EN. Volatile metabolites and decomposition products of halothane in man. Anesthesiology 1979; 50: 2-8
63. Fang ZX, Eger II EI. Factors affecting the concentration of compound A resulting from degradation of sevoflurane by soda lime and Baralyme Ò in a standard anesthetic circuit. Anesth Analg 1995; 81: 564-568
64. Fang ZX, Kandel L, Laster MJ, Ionescu P, Eger II EI. Factors affecting production of compound A from the interaction of sevoflurane with Baralyme Ò and soda lime. Anesth Analg 1996; 82: 775-781
65. Eger EI, Gong D, Koblin DD, Bowland T, Ionescu P, Laster MJ, Weiskopf RB. Dose-related biochemical markers of renal injury after sevoflurane versus desflurane anesthesia in volunteers. Anesth Analg 1997; 85: 1154-1163
66. Eger EI, Gong D, Koblin DD, Bowland T, Ionescu P, Laster MJ, Weiskopf RB. The effect of anesthetic duration on kinetic and recovery characteristics of desflurane versus sevoflurane, and on the kinetic characteristics of compound A in volunteers. Anesth Analg 1998; 86: 414-421
67. Goldberg ME, Cantillo J, Gratz I, Deal E, Vekeman D, McDougall R, Afshar M, Zafeiridis A, Larijani G. Dose of compound A, not sevoflurane, determines changes in the biochemical markers of renal injury in healthy volunteers. Anesth Analg 1999; 88: 437-445
68. Bito H, Ikeuchi Y, Ikeda K: Effects of low-flow sevoflurane anesthesia on renal function. comparison with high-flow sevoflurane and low-flow isoflurane anesthesia. Anesthesiology 86 (1997) 1231-1237
69. Kharash ED, Frink EJ, Zager R, Bowdle TA, Artru A, Nogami WM: Assessment of low-flow sevoflurane and isoflurane effects on renal function using sensitive markers of tubular toxicity. Anesthesiology 86 (1997) 1238-1253
70. Mazze RI, Friedman M, Delgado-Herrera L, Galvez ST, Mayer DB. Renal toxicity of compound A plus sevoflurane compared with isoflurane in non-human primates. Anesthesiology 1998; 89: A490
71. Reinhardt C, Gronau E, Wüsten R, Goeters C, Vrana S, Baum J, van Aken H. Compound A in Minimal Flow Sevoflurane. Anesthesiology 1998, 89 (No 3A): A142
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
142

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
143

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
144
ODRŽAVANJE DISAJNOG PUTA I PREVENCIJA PNEUMONIJE POVEZANE SA MEHANIČKOM VENTILACIJOM AIRWAY MANAGEMENT AND PREVENTION OF VENTILATOR ASSOCIATED PNEUMONIA NADA POPOVIĆ1,3, BRANKA TERZIĆ1, ALEKSANDAR KARAMARKOVIĆ2,3, NEBOJŠA LAĐEVIĆ1,3, MARINA STOJANOVIĆ1, DANIJELA STOJMIROVIĆ1, MILAN STOJIČIĆ3,4
1Centar za anesteziologiju i reanimatologiju Kliničkog centra Srbije, Beograd,2Klinika za urgentnu hirurgiju, KCS,3Medicinski fakultet Univerziteta u Beogradu,4Klinika za opekotine, plastičnu i rekonstruktivnu hirurgiju Abstract
Ventilator-associated pneumonia-VAPis the most commonhospitalinfection whichhas a significant impacton thefinal outcome oftreatment ofcritically ill patients. The prevalenceofVAPis6-50of 100patients. Diagnosis ofVAPis made based onthe clinical, radiological, andlaboratory test results, and microbiological findingsareusedas aconfirmation of a diagnosisbased on thelessspecific clinicalcriteria. Recently,significantemphasis is placed onthe use of differentstrategiesaimed at reducing thefrequency and /orprevents the development ofVAP.The most importantrisk factor forVAP isthe presence ofthe endotracheal tubein theairwayduring the prolonged time period, as well asre-intubation. The use ofdifferent strategies, such as the so-called"VAP package" (headelevation, oral administrationof hlorhexidin, interruptionof sedationand application of protocolsforweaningfrom the ventilator), selectivedecontaminationof the digestivetract, hand hygieneandother,significantlyreducesthe incidence ofVAP. Also it is veryimportantthe tube shape, the shape of the coffee, the pressurein thecoffee, as well as theapplication ofintermittentsubglottic drainage.It was shownthat the application ofpreventive measuresforVAPreducesmortalityandimproves theoutcome of patientsin theICU. Preventivemeasures includethe simultaneous use ofmultiplemethodsso-called VAPpackage. Uvod
Pneumonija povezana sa mehaničkom ventilacijom (ventilator-associated pneumonia-VAP) je najčešća bolnička infekcija koja ima značajan uticaj kako na morbiditet, tako i na mortalitet kritično obolelih bolesnika u jedinici intenzivnog lečenja (JIL). Ona produžava dužinu trajanja mehaničke ventilacije, ostanak bolesnika u JILi dužinu hospitalizacije, cenu lečenja tih bolesnika, kao i mortalitet1-4. VAP ima varijabilnu prevalencu, odnosno VAP se razvije kod 6-50 bolesnika na 100 primljenih u JIL4,5,6. Tako veliki varijabilitet je posledica nepostojanja tačnih dijagnostičkih kriterijuma, jer nekoliko kliničkih stanja veoma liče na VAP. Takođe, tačnost za dijagnozu VAP izostaje najviše kao posledica subjektivnosti u evaluaciji važnih komponenti kliničke dijagnoze7. Dijagnoza pneumonije povezane sa mehaničkom ventilacijom se postavlja na osnovu kliničkih, radioloških i laboratorijskih testova koji su nespecifični i zajednički i za postavljanje drugih dijagnoza kao i za potvrdu komplikacija koje se razvijaju kod kritično obolelih bolesnika koji zahtevaju ventilatornu potporu. Klinički kriterijumi podrazumevaju prisustvo nove ili progresivne infiltracije/konsolidacije/kavitacije kao i prisustvo bar dva od sledećih kriterijuma: febrilnost (aksilarna telesna temperatura iznad 380C, leukopenija (< 4x109) ili leukocitoza (> 12x109), ili prisustvo purulentne sekrecije, ili promena karakteristika i obima
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
145
sekrecije. Prisustvo funkcionalnog pogoršanja npr. hipoksije ili pogoršanje odnosa P02/Fi02, povišeni biomarkeri infekcije, izmenjen mentalni status bolesnika ili pojava sepse/septičnog šoka su dodatni faktori koje treba uzeti u obzir4. Dijagnoza VAP se postavlja na osnovu kliničkih, radioloških i laboratorijskih nalaza, a mikrobiološki nalazi se koriste kao potvrda dijagnoze postavljene na osnovu manje specifičnih kliničkih kriterijuma. Mikrobiološka potvrda VAP podrazumeva prisustvo bar jednog od sledećih kriterijuma:
- pozitivna hemokultura bez nekog drugog vidljivog izvora infekcije - pozitivna kultura punktata pleuralne tečnosti - pozitivna kultura bronhoalveolarne lavaže - pozitivna kultura trahealnog aspirata - histopatološki nalaz infekcije plućnog parenhima - pozitivan dijagnostički test za Legionelu
Monitoring
U aprilu 2013. godine Centar za kontrolu i prevenciju bolesti (Center for Disease Control and Prevention (CDC) objavioje nove vodiče za monitoring bolesnika koji se mehanički ventiliraju. U tim vodičima značajno se menjaju kriterijumi za praćenje tih bolesnika. Do sada su praćeni samo znaci koji ukazuju na razvoj pneumonije, a u novim vodičima praćenje bolesnika je sveobuhvatnije i uzimaju se u razmatranje sve komplikacije koje su povezane sa mehaničkom ventilacijom. Taj pristup ima za cilj da minimalizuje subjektivnost u postavljanju dijagnoze. Radiografski kriterijumi za pneumoniju i specifični znaci i simptomi (npr. promena obima sekrecije) pokazuju veliku varijabilnost u interpretaciji, opisu i registrovanju podataka. Najnoviji algoritam je baziran na objektivnim i jednostavnim kriterijumima čiji je cilj da identifikuje širok dijapazon komplikacija kod bolesnika koji se mehanički ventiliraju8. U algoritmu su dati novi termini, a to su:
1. Novo funkcionalno respiratorno pogoršanje-ventilator-associated condition (VAC)-
podrazumeva da posle perioda funkcionalne respiratorne stabilnosti ili poboljšanja u trajanju ≤ dva dana, dolazi do razvoja pogoršanja oksigenacije zbog čega je potrebno povećati pozitivni end-ekspiratorni pritisak (PEEP) za ≥ 3 cm H20 ili povećati Fi02 za 20% u trajanju ≥ dva dana
2. Novo funkcionalno respiratorno pogoršanje sa znacima infekcije - infection-related
ventilator-associated complication (IVAC)-podrazumeva VAC udružen sa telesnom temperaturom < 360C ili > 380C ili brojem leukocita ≤ 4x109 ili ≥ 12x109 sa primenom jednog ili više novih antibiotika u trajanju najmanje četiri dana, u periodu dva dana pre ili posle početka VAC, ne računajući prva dva dana od početka primene mehaničke ventilacije
3. Novo funkcionalno respiratorno pogoršanje sa mogućom infekcijom pluća – possible
VAP-podrazumeva IVAC udružen sa purulentnim respiratornim sekretom (≥ 25 neutrofila i ≤ 10 epitelnih ćelija) ili pozitivna kultura sputuma, endotrahealnog aspirata, bronhoalveolarne lavaže i histopatološki nalaz infekcije plućnog parenhima
4. Novo funkcionalno respiratorno pogoršanje sa verovatnom infekcijom pluća – probable
VAP-podrazumevaIVAC udružen sa purulentnim respiratornim sekretom što podrazumeva pozitivnu kulturu endotrahealnog aspirata sa ≥ 105 CFU/ml ili pozitivnu kulturu bronhoalveolarne lavaže sa ≥ 104 CFU/ml ili pozitivna kultura plućnog
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
146
parenhima ≥ 104 CFU/g. U ovoj grupi su i bolesnici koji nemaju purulentan sekret, ali imaju pozitivnu kulturu punktata pleuralne tečnosti, pozitivan histopatološki nalaz plućnog parenhima, pozitivan dijagnostički test za Legionelu i pozitivan dijagnostički test za virus influence, respiratorni sincicijelni virus, adenovirus, rinovirus, korona virus itd.
Nove strategije u prevenciji VAP
U poslednje vreme značajan akcenat se stavlja na primenu različitih strategija čiji je cilj smanjenje učestalosti i/ili sprečavanje razvoja VAP kod bolesnika u jedinici intenzivnog lečenja9.Poznata je činjenica da prisustvo endotrahealnog tubusa u disajnom putu u dužem vremenskom periodu, kao i reintbacija povećavaju učestalost razvoja VAP. Prisustvo tubusa ometa normalne fiziološke mehanizme koji sprečavaju kontaminaciju i kolonizaciju disajnih puteva bakterijama, odnosno izostaje refleks kašlja i mukocilijarna aktivnost. Takođe, tubus održava komunikaciju između traheje i orofarinksa, pa je širenje bakterija lako. Zbog toga se mislilo da jedna od preventivnih mera za VAP može biti rana traheostomija. Tačno je da traheostoma smanjuje trajanje ventilatorne potpore i skraćuje boraval u JIL10, ali nedavna randomizirana studija nije pokazala smanjenje incidence razvoja VAP kod bolesnika kod kojih je rađena rana traheostomija (6-8 dana posle intubacije)11.Simultana primena više tretmana koji spadaju u tzv. „VAP paket“ značajno smanjuju učestalost nastanka VAP. Taj paket podrazumeva: elevaciju glave, oralnu primena hlorhexidin gela, prekid sedacije i primenu protokola za odvikavanje od ventilatora12.Iako nema podataka, trenutno dostupnih,koji dokazuju da je incidenca razvoja VAP smanjena sa smanjenom primenom sedativa, ipak je predložena primena redukovanih dnevnih doza sedativa kao preventivna mera13. Selektivna dekontaminacija digestivnog trakta antibioticima smanjuje incidencu razvoja VAP, ali se ne preporučuje zbog razvoja rezistentnosti bakterija. Međutim, danas je standard kod intubiranih bolesnika orofaringealno ispiranje hlorheksidinom, jer je pokazano da smanjuje trahealnu kolonizaciju i VAP incidencu14.Preventivna mera koji treba uvek primeniti kod intubiranih bolesnika pri aspiraciji sekreta iz tubusa jeste adekvatna higijena ruku zdravstvenih radnika15. Posleintubacijeunutrašnjosttubusa, naročito u zonikafa,veomabrzobudepokrivenaslojemmukusa i ćelijatrahealnogstablačinećitkz. biofilm. Dokazan je velikiznačajbiofilmazanastanak i razvoj VAP, jersučakkod 70% bolesnikasa VAP izolovaniistipatogeniizbiofilma i trahealnog sekreta16. Zato se u prevenciji VAP svevećiznačajdajeizgledutubusa, oblikukafa, pritisku u kafu i intermitentnojsubglotičnojsukciji.Kodbolesnika,zakoje se zna da ćebitipotrebnaventilatornapotporaduža od 48 sati,poželjno je koristititubusečija je unutrašnjostobloženasrebrom, jer je srebrobiološkikompatibilno, lakozananošenje,efikasno u smanjenjutrahealnekolonizacije i bakterijskog rasta17,18. Smatra se da je oblikkafatakođeznačajan u prevenciji VAP, pa se preporučujekorišćenjetubusačiji se kaf u distalnomdelusužava-“tapered cuff”, jertajoblikonemogućavaprolazaksekreta pored kafa i nakupljanjesekretana kafu19. Pritisak u kafutrebastalnoodržavatiizmeđu 20-30 mmHg jerako je pritisakispod 20 mmHg olakšano je slivanjesekreta i prolaz u distalnepartijedisajnogstabla, dokpritisakpreko 30mmHgmožedovesti do oštećenja sluzokože20.Istražuje se i značajmaterijalaodkoga se pravikaf (ispituju se poliuretanski, silikonski, lateks i likrakafovi), alijošuveknijepotvrđennjihov benefit za VAP, osim u kardiohirurgiji21. Intermitentnasubglotičnadrenažaimaznačajnomesto u smanjenju incidence razvoja VAP, kraćemboravku u JIL ismanjenombrojudanaprimenemehaničke ventilacije22,23.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
147
Stalnasubglotičnaaspiracija se ne preporučuje, jermožedovesti dooštećenjasluzokože. Osobljekojeučestvuje u lečenjuintubiranogbolesnikakome je neophodnaventilatornapotpora, treba da vodiračuna i o pozicioniranjubolesnika u krevetu.Preporuka je da bolesnikatrebastaviti u polusedećipoložaj (450), alinajnovijipodacisugerišu da je zaprevenciju VAP superiornijibočni položaj25,26.
Zaključak
Da bi incidenca pneumonije povezane sa mehaničkom ventilacijom bila što niža, neophodna je rana dijagnostika komplikacija koje su povezane sa mehaničkom ventilacijom, primena odgovarajuće antibiotske terapije, stalna edukacija osoblja i primena protokola za menaničku ventilaciju. Dokazano je da primena preventivnih mera za VAP smanjuje mortalitet i poboljšava ishod lečenja bolesnika u JIL. Preventivne mere podrazumevaju istovremenu primenu više postupaka tzv.VAP paket.
Literatura
1. Juneja D, Singh O, Javeri Y, Arora V, Dang R, Kaushal A. Prevention and management of ventilator-associated pneumonia: A survey on current practices by intensivists practicing in the Indian subcontinent. Indian J Anaesth 2011; 55(2):122-8.
2. Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in combined medical-surgical intensive care units in the United States. Infect Control Hosp Epidemiol 2000; 21:510-5.
3. American ThoracicSociety; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia.Am J RespirCrit Care Med 2005; 171(4):388-416.
4. Dalmora CH, Deutschendorf C, Nagel F, Santos RP, Lisboa T. Defining ventilator-associated pneumonia: a construction concept.Rev Bras TerIntensiva 2013; 25(2):81-86.
5. American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Comment in Am J RespirCrit Care Med. 2006;173(1):131-3.
6. Rello J, Diaz E. Pneumonia in the intensive care unit. Crit Care Med. 2003;31(10):2544-51. Review.
7. Klompas M. Does this patient have ventilator-associated pneumonia? JAMA 2007; 297(14):1583-93. Review.
8. Center of Disease Control and Prevention. Protocol Correction, Clarification, and Additions. http://www.cdc.gov/nhsn/pdf/pscmanual/errata 2013.pdf
9. Coppadoro A, Bittner E, Berra L. Novel preventive strategies for ventilator-associated pneumonia. Critical Care 2012; 16:210.
10. Griffiths J, Barber VS, Morgan L, Young JD. Systematic review and metaanalysis of studies of the timing of tracheostomy in adult patients undergoing artificial ventilation. BMJ 2005; 330:1243.
11. Terragni PP, Antonelli M, Fumagalli R, et al. Early vs late tracheotomy for prevention of pneumonia in mechanically ventilated adult ICU patients: a randomized controlled trial. JAMA 2010; 303:1483–89.
12. Morris AC,Hay AW, Swann DG, et al. Reducing ventilator-associated pneumonia in intensive care: Impact of implementing a care bundle. CritCare Med 2011; 39:2218–24.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
148
13. Blackwood B, Alderdice F, Burns KE, Cardwell CR, Lavery G, O’Halloran P. Protocolized versus non-protocolized weaning for reducing the duration of mechanical ventilation in critically ill adult patients. Cochrane Database Syst Rev 2010; 12:CD006904.
14. Koeman M, van der Ven AJ, Hak E, et al. Oral decontamination with chlorhexidine reduces the incidence of ventilator-associated pneumonia. Am J RespirCrit Care Med2006; 173:1348–55.
15. Flanagan ME, Welsh CA, Kiess C, Hoke S, Doebbeling BN. Agency for Healthcare Research and Quality Hospital-Acquired Infections Collaborative: A national collaborative for reducing health care-associated infections: current initiatives, challenges, and opportunities. Am J Infect Control 2011; 39:685–89.
16. Adair CG, Gorman SP, Feron BM, et al.: Implications of endotracheal tube biofi lm for ventilator-associated pneumonia. Intensive Care Med 1999; 25:1072–76.
17. Kollef MH, Afessa B, Anzueto A, et al. Silver-coated endotracheal tubes and incidence of ventilator-associated pneumonia: the NASCENT randomized trial. JAMA 2008; 300:805–813.
18. Shorr AF, Zilberberg MD, Kollef M. Cost-effectiveness analysis of a silvercoated endotracheal tube to reduce the incidence of ventilator-associated pneumonia. Infect Control HospEpidemiol2009; 30:759–63.
19. Dave MH, Frotzler A, Spielmann N, Madjdpour C, Weiss M. Effect of tracheal tube cuff shape on fluid leakage across the cuff : an in vitro study. Br J Anaesth2010; 105:538–43.
20. Nseir S, Brisson H, Marquette CH, et al. Variations in endotracheal cuff pressure in intubated critically ill patients: prevalence and risk factors. Eur J Anaesthesiol2009; 26:229–34.
21. Poelaert J, Poelaert J, Depuydt P, De Wolf A, Van de Velde S, Herck I, Blot S. Polyurethane cuff ed endotracheal tubes to prevent early postoperative pneumonia after cardiac surgery: a pilot study. J ThoracCardiovascSurg2008; 135:771–76.
22. Lacherade JC, De Jonghe B, et al. Intermittent subglottic secretion drainage and ventilator-associated pneumonia: a multicenter trial. Am J RespirCrit Care Med 2010; 182:910–17.
23. Muscedere J, Rewa O, McKechnie K, Jiang X, Laporta D, Heyland DK. Subglottic secretion drainage for the prevention of ventilator-associated pneumonia: a systematic review and meta-analysis. Crit Care Med2011; 39:1985–91.
24. Miller MA, Arndt JL, Konkle MA, et al. A polyurethane cuff ed endotracheal tube is associated with decreased rates of ventilator-associated pneumonia. J Crit Care2011; 26:280–86.
25. Mauri T, Berra L, Kumwilaisak K, et al. Lateral-horizontal patient position and horizontal orientation of the endotracheal tube to prevent aspiration in adult surgical intensive care unit patients: a feasibility study. Respir Care 2010; 55:294–02.
26. Li Bassi G, Torres A. Ventilator-associated pneumonia: role of positioning. CurrOpinCrit Care 2011; 17:57–63.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
149
PROBLEMATIČAN DISAJNI PUT U ENDOKRINOJ HIRURGIJI DIFFICULT AIRWAY IN ENDOCRINE SURGERY NEVENA KALEZIĆ1,2,3, VERA SABLJAK,1,2,3 ANKA TOŠKOVIĆ,2,3 MARINA STOJANOVIĆ,2 KSENIJA STEVANOVIĆ,2 MAJA MILINIĆ,2,3 VESNA ANTONIJEVIĆ,2 DEJAN MARKOVIĆ1,2 1.Medicinski fakultet Univerziteta u Beogradu, 2Centar za anesteziologiju i reanimatologiju Kliničkog centra Srbije, Beograd,3Centar za endokrinu hirurgiju KCS, Beograd E-mail: [email protected] Abstract
Endocrine disturbances are well known acquired causes of difficult airway. In patients with endocrine disturbances the incidence of difficult and impossible intubation is higher, not only in endocrine surgery, but in other surgical areas, when patients have these disturbances as a comorbidity. The biggest problems in this area are the patients with thyroid gland diseases which leadto thyromegaly and the consequent dislocation of the trachea and/orlarynx. Pituitary gland diseases or tumors, which lead tothe abnormal secretion of pituitary hormones, may also be a cause of difficult intubation, if there has been a development of acromegaly, gigantism, or Cushing's syndrome. Cushing’s syndromemay occur in the absence of pituitary gland dysfunction, as result of hyperplasiaorhormonally active tumors of adrenal cortex. Hyperparathyroidism, as a hormonal disorder and indication for total or subtotal parathyroidectomy, can contribute to the difficult tracheal intubation due to marked osteoporosis in these patients, and sometimes significant disorders of the musculoskeletal system, which limit proper positioning of these patients on the operating table and restrict the extension of the head and neck during laryngoscopy. In patients with diabetes mellitus, especially if not under controland in the presence of chronic complications of these disease, tracheal intubation can be difficult and risky- on the one hand because of the stiff jointssyndrome , and on the other hand due to gastroparesis, which is associated with an increased risk of aspiration of gastric content. In patients with endocrine disorders, a careful evaluation of the airway is necessary, as well as assessment of the risk of difficult intubation and its complications, in order to prevent adverse events, and in the case of their occurrence-to promptly treat them.
Uvod
Problematičan disajni put podrazumeva otežanu intubaciju traheje ili otežanu ventilaciju na masku ili i jedno i drugo. Ukoliko je u pitanju ova poslednja opcija, to može voditi nemogućnosti intubacije i nemogućnosti oksigenacije (CICO, cannnot intubate, cannot oxygenate), koja je jedna od najdramatičnijih situacija u radu anesteziologa jer predstavlja potencijalno životno ugrožavajuće stanje.1 Prema različitim izveštajima, učestalost CICO situacije kreće se od veoma velike(1:1.000) do veoma male (1:100.000), ali je ta incidenca najčešće 1-2: 10.000 opštih anestezija.2,3 To, praktično, znači da se svaki anesteziolog, u toku svoje radne karijere, može susresti sa ovom situacijom bar jednom ili više puta. Pored urođenih anomalija, koje mogu biti uzrok problematičnog disajnog puta, brojna stečena oboljenja i stanja mogu dovesti do toga. Flečer, u 5. izdanju Milerove “Anestezije” navodi endokrine poremećaje kao vodeće razloge otežane intubacije (OI) traheje među stečenim

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
150
oboljenjima.4 Brojnim radovima je pokazano da gotovo svi endokrini i metabolićki poremećaji, mogu dovesti do OI.1Učestalost otežane ventilacije na masku i OI je različita i zavisi od težine endokrinog poremećaja, drugih pridruženih poremećaja i oboljenja, vrste i hitnosti operacije, iskustva anesteziologa, tehničke opremljenosti ustanove i niza drugih faktora.1,2,3 Među endokrinim poremećajima, kao razlozima otežane intubacije traheje, svakako vodeće mesto zauzimaju oboljenja štitaste žlezde.5 Međutim do OI mogu dovesti i poremećaji funkcije hipofize, paraštitastih i nadbubrežnih žlezda.Takođe i bolesnici sa dijabetesom melitusom mogu imati ovaj problem. Iako su kreirani mnogi skorovi za procenu disajnog puta, kao i algoritmi za rešavanje (očekivane i neočekiane) OI,6,7,8,9,10,11 posedovanje informacije šta je kod konkretnog bolesnika bio (konkretan) problem prilikom prethodne (teške) intubacije, može spasiti život tom bolesniku.U tom smislu, mnoge razvijene zemlje imaju nacionalne baze podataka, koje omogućavaju prepoznavanje tih bolesnika (kao i razloga prethodne OI) prilikom njihove svake naredne hospitalizacije.To svakako poboljšava bezbednost i ishod lečenja tih bolesnika.
Oboljenja tireoideje kao razlog problematičnog disajnog puta
Oboljenja tireoideje imaju vodeće mesto među svim endokrinim i metaboličkim poremećajima kao razlog problematičnog disajnog puta.5 Naša iskustva12, kao i iskustva drugih autora13,14,15,16,17,18 pokazuju da je učestalost otežane intubacije traheje daleko češća kod bolesnika sa tireomegalijom nego kod drugih subpopulacija bolesnika.
Imajući u vidu ovu činjenicu, potrebna je pažljiva preoperativna evaluacija ovih bolesnika od strane svih članova tima koji učestvuju u hirurškom lečenju ovih bolesnika i anesteziološka procena disajnog puta, kako bi se izbegli neželjini ishodi, kao što su nemoguća intubacija, CICO ili pojava različitih komplikacija.19,20,21,22
U tom smislu, u Centru za endokrinu hirurgiju Kliničkog centra Srbije (CEH KCS) izvodi se skrining, sastavljen od 14 testova/pregleda (7 kvantitativnih i 7 kvalitativnih), koji se boduju sa 0 (nema rizika, 1 (umeren rizik) I 2 (visok rizik). Skor veći od 5 ukazuje na mogućnost OI. U obavezan skrining spada i radiografija grudnog koša (i vrata), mada ima autora koji osporavaju rutinsku RTG dijagnostiku u sklopu procene rizika za OI kod tireomegalije.23
Oboljenja paratireoideje kao razlog problematičnog disajnog puta
Među oboljenjima paratireoideje koja mogu biti razlog problematičnog disajnog puta, vodeće mesto zauzima hiperparatireoidizam (HPT) i to prvenstveno sekundarni, ali i primarni, mada u nešto manjoj meri.24,25,26 Ovo je razumljivo kada se ima u vidu da HPT dovodi do osteoporoze, povećane sklonosti ka patološkim frakturama, a može dovesti i do drugih, težih komplikacija na koštano-zglobnom i mišićnom sistemu (i na svim drugim organskim sistemima, ali je to od manjeg značaja sa aspekta problematičnog disajnog puta), pa je i kod ovih bolesnika neophodna pažljiva preoperativna evaluacija i procena disajnog puta.27,28 Iz ovoga, dalje, prozilazi činjenica da pozicioniranje bolesnika na operacionom stolu mora biti veoma pažljivo i oprezno, kako ne bi došlo do patoloških fraktura. Ovo se naročito odnosi na postavljanje glave i vrata bolesnikau položaj koji omogućuje olakšanu laringoskopiju i intubaciju (maksimalna ekstenzija). To je, često, nemoguće postići zbog opasnosti od frakture cervikalnih pršljenova, pa se intubacija izvodi u veoma blagoj ekstenziji ili u neutralnom položaju. Ovi, nekonformni intubacioni uslovi, pored koštano-zglobnih deformiteta, dodatno doprinose povećanju incidence OI kod HPT24,25,26,29,30 Poseban problem predstavljaju bolesnici sa sekundarni HPT, koji najčešče imaju terminalnu hroničnu bubrežnu insuficijenciju, sa svim karakteristikama i posledicama tog
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
151
oboljenja, uključujući i multiple, teške deformitete koštano-zglobnog sistema, koji dodatno otežavaju uspostavljanje disajnog puta i obezbeđivanje ventilacije pluća.31,32,33
Oboljenja hipofize i /ili nadbubrega kao razlog problematičnog disajnog puta
Akromegalija, kao jedan od znakova poremećaja funkcije hipofize, među svim oboljenjima hipofize koja doprinose problematičnom disajnom putu, svakako zauzima vodeće mesto.34,35,36 Preoperativna procena disajnog puta akromegaličnih bolesnika doprinosi bezbednosti ovih bolesnika u anesteziji i smanjenju broja komplikacija povezanih sa OI.37,38Imajući u vidu da osim akromegaličnih bolesnika i svi drugi bolesnici koji se podvrgavaju operativnom lečenju hipofize, mogu imati problem sa OI, uključujuči i one sa hipogonadizmom,39 neophodno je da svi bolesnici sa bolestima hipofize budu podvrgnuti pažljivom skriningu, a naročito oni koji se podvrgavaju hitnim hirurškim intervencijama.40,41
Kušingov sindrom, bilo da je nastao zbog primarnog poremećaja na nivou hipofize ili na nivou nadbubrežne žlezde, ili da je do njega došlo sekundarno (najčešće zbog glukokortikoidne terapije nekog drugog oboljenja), predstavlja dobro poznati razlog problematičnog disajnog puta.42 Tipični simptomi i znaci ove bolesti, kao što su gojaznost, kratak i širok vrat, osteoporoza, sami po sebi ukazuju na mogućnost OI, pa se pažljiva preoperativna evaluacija disajnog puta ovih bolesnika podrazumeva, iako se OI ne javlja tako često.43,44,45
Kada su u pitanju druga oboljenja nadbubrežne žlezde, koja nisu povezana sa hiperkorticizmom, učestalost OI je daleko manja i ne razlikuje se od drugih subpopulacija bolesnika (koji nemaju anatomske anomalije i metabolički komorbiditet).43,46,47,48,49
Dijabetes mellitus kao razlog problematičnog disajnog puta
Dijabetes melitus (DM) je najčešći endokrini/metabolički poremećaj, sa tendencijom daljeg porasta. Iako učestalost DM iznosi “svega” 6,4%, kod hirurških bolesnika ona je daleko veća i kreće se od 15-20%, a u nekim granama hirurgije, kao što je vaskularna, čak i do 50%.50 Problematičan disajni put karakterističan je za dijabetičare kod kojih su razvijene hronične komplikacije DM, ali se može javiti kod svih dijabetičara, uključujuči i dečji uzrast.51Od hroničnih komplikacijaDM, najveći značaj za mogućnost problematičnog disajnog puta ima okoštavanje zglobova (“stiff joint” sydroma), koje se uglavnom odnosi na male zglobove, ali i na atlanto-okcipitalni zglob. Imajući u vidu da se kod dijabetičara može javiti gastropareza, tj.usporeno i odloženo gastrično pražnjenje (“pun stomak”), ova činjenica, udružena sa mogućnošću OI, može rezultirati aspiracijom gastričnog sadržaja prilikom intubacije traheje, sa svim posledicama koje kasnije mogu proizaći iz toga.52 Naravno, rizik se uvećava, ako su u pitanju hitna stanja.53 Standardna primena Selikovog manevra (pritiska na krikoidnu hrskavicu) već dugi niz godina je prilično osporavana metoda zaštite disajnog puta od aspiracije.54 Osim iskustva i spretnosti anesteziologa, fiberoptička intubacija ostaje suverena metoda povećanja bezbednosti bolesnika u anesteziji, ne samo sa DM i ankilozom temporo-mandibularnog zgloba, već i u svim drugim slučajevima očekivane i neočekivane otežane intubacije traheje.55
Zaključak
U cilju prevencije i lečenja komplikacija koje mogu biti povezane sa otežanom i nemogućom intubacijom, potrebna je pažljiva preoperativna evaluacija disajnog puta bolesnika bolesnika sa endokrinim i metaboličkim poremečajima i procena rizika od neželjenih događaja. Takođe, neophodno je etablirati nacionalnu bazu podataka o bolesnicima visokog rizika, kako bi ovi podaci bili dostupni svim anesteziolozima. Istovremeno, i sam bolesnik koji je imao

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
152
problematičan disajni put, trebalo bi da bude obavešten o tome na prikladan način i da poseduje dokument koji bi pomogao lakšem rešavanju ovog vitalnog problema, prilikom sledeće, naročito hitne, operacije/anestezije.
Literatura
1. Kalezić N, Palibrk I, Videnović N, Sabljak V, Janjević D, Simić D. Disajni put i arteficijalna ventilacija pluća. U: Kalezić N: Inicijalni tretman urgentnih stanja u medicini, Medicinski fakultet, Beograd, 2013; 1:21-84.
2. Kheterpal S, Han R, Tremper KK, Shanks A, Tait AR, O'Reilly M, Ludwig TA. Incidence and predictors of difficult and impossible mask ventilation. Anesthesiology, 2006;105(5), 885-91.
3. Shah PN, Sundaram V. Incidence and predictors of difficult mask ventilation and intubation. J Anaesthesiol Clin Pharmacol, 2012;28(4):451-5.
4. Fleisher LA. Risk of Anesthesia. In: Miller RD, editor. Anesthesia. 5th Edition. Churchill Livingstone 2000.p.821-22
5. Kalezić N, Palibrk I, Nešković V, Grković S, Subotić D, Ugrinović Đ. Otežana intubacija kod bolesnika sa tireomegalijom, u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 7:125-50
6. Combes X, Jabre P, Margenet A, Merle JC, Leroux B, Dru M, et al. Unanticipated difficult airway management in the prehospital emergency setting: prospective validation of an algorithm. Anesthesiology, 2011;114(1):105-10.
7. De Jong A, Molinari N, Terzi N, Mongardon N, Arnal JM, Guitton C, et al. Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. Am J Respir Crit Care Med, 2013;187(8):832-9.
8. Seo SH, Lee JG, Yu SB, Kim DS, Ryu SJ, Kim KH. Predictors of difficult intubation defined by the intubation difficulty scale (IDS): predictive value of 7 airway assessment factors. Korean J Anesthesiol, 2012;63(6),491-7.
9. Mahmoodpoor A, Soleimanpour H, Nia KS, Panahi JR, Afhami M, Golzari SE, Majani K. Sensitivity of +Palm Print, Modified Mallampati Score and 3-3-2 Rule in Prediction of Difficult Intubation. Int J Prev Med, 2013;4(9):1063-9.
10. Martin LD, Mhyre JM, Shanks AM, Tremper KK, Kheterpal S. 3,423 emergency tracheal intubations at a university hospital: airway outcomes and complications. Anesthesiology, 2011;114(1):42-8.
11. McKeen MD, George RB, O’Connell CM, Allen VM, Yazer M, Wilson M, Phu TC. Difficult and failed intubation: Incident rates and maternal, obstetrical, and anesthetic predictors. Can J Anesth, 2011; 58:514–24.
12. Kalezić N, Milosavljević R, Paunović I, Živaljević V, Diklić A, Matić D, Ivanović B, Nešković V. The incidence of difficult intubation in 2000 patients undergoing thyroid surgery: single center experience. Vojnosanit Pregl 2009; 66(5):377-82.
13. Amathieu R, Smail N, Catineau J, Poloujadoff MP, Samii K, Adnet F. Difficult intubation in thyroid surgery: myth or reality?. Anesth Analg, 2006;103(4):965-8.
14. Agarwal A, Agarwal S, Tewari P, Gupta S, Chand G, Mishra A, et al. Clinicopathological profile, airway management, and outcome in huge multinodular

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
153
goiters: an institutional experience from an endemic goiter region. World J Surg, 2012; 36(4):755-60.
15. Shaha A, Ferlito A, Owen RP, Silver CE, Rodrigo JP, Haigentz Jr M, Mendenhall WM, Rinaldo A, Smallridge RC. Airway management in anaplastic thyroid carcinoma. Eur Arch Otorhinolaryngol, 2013;118(7):1195-8.
16. Shen WT, Kebebew E, Duh QY, Clark OH. Predictors of airway complications after thyroidectomy for substernal goiter. Arch Surg, 2004;139(6):656-60.
17. Wakeling HG, Ody A, Ball A. Large goitre causing difficult intubation and failure to intubate using the intubating laryngeal mask airway: lessons for next time. Br J Anaesth, 1998;81(6):979-81.
18. Niels JF, Benumof JL. The difficult airway in head and neck tumor surgery. Anesthesiology clinics of North America, 1993; 11:475-75.
19. Carty SE, Doherty GM, Inabnet III WB, Pasieka JL, Randolph GW, Shaha AR, et al. For the Surgical Affairs Committee of the American Thyroid Association. American Thyroid Association statement on the essential elements of interdisciplinary communication of perioperative information for patients undergoing thyroid cancer surgery. Thyroid, 2012;22(4):395-9.
20. Sabljak V, Kalezić N, Ivanović B, Živaljević V, Diklić A, Paunović I. Modern concepts of preoperative preparation of patients with thyroid gland disease, Acta Chir Iugoslav, 2011; 58:103-8.
21. Russell S. Managing the Airway in Thyroid Surgery. In: Tips and Tricks in Endocrine Surgery. Springer London, 2014. 195-8.
22. Rosato L, Avenia N, Bernante P, De Palma M, Gulino G, Nasi PG, et al. Complications of thyroid surgery: analysis of a multicentric study on 14,934 patients operated on in Italy over 5 years. World J Surg, 2004;28(3):271-6.
23. Hong BW, Mazeh H, Chen H, Sippel RS. Routine chest X-ray prior to thyroid surgery: is it always necessary? World J Surg, 2012;36(11): 2584-9.
24. Bajwa SJS, Sehgal V. Anesthetic management of primary hyperparathyroidism: A role rarely noticed and appreciated so far. Indian J Endocrinol Metab, 2013;17(2):235-9.
25. Kiverniti E, Kazi R, Rhys-Evans P, Nippah R. Airway obstruction due to giant non-parathyroid hormone-producing parathyroid adenoma. J Can Res Ther, 2008;4:197-9.
26. Schroeder KM, Joffe AJ, Andrei AC, Thomas KD, Arndt GA. Hyperparathyroidism, hypercalcemia and difficult laryngoscopy: a retrospective review. Middle East journal of anesthesiology,2012;21(5):665-71.
27. Živaljević V, Kalezić N, Sabljak V, Diklić A, Jovanović D, Paunović I. Preoperative preparation of patients with hyperparathyroidism as comorbidity, Acta Chir Iugoslav, 2011; 58:109-15.
28. Sabljak V, Veličković J, Gvozdenović Lj, Joksimović S, Pajtić V, Marković D, Kalezić N. Anestezija za operacije paratireoidnih žlezda zbog primarnog hiperparatireoidizma, Medicina danas, 2010; 9(4-6): 188-193.
29. Gvozdenović Lj, Kalezić N, Malenković V, Palibrk I. Specifičnosti anestezije kod bolesnika sa primarnim hiperparatireoidizmom, u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 15:243-8.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
154
30. Melenković V, Kalezić N, Živaljević V, Sabljak V, Marković D, Paunović I. Hiperparatireoidizam i anestezija, Anestezija i intenzivna terapija, 2011; 33(1-2):37-42.
31. Kalezić N, Gvozdenović Lj, Milošević Z, Živaljević V, Diklić A, Paunović I.
Preoperativna evaluacija bolesnika sa sekundarnim hiperparatireoidizmom. Medicina danas, Novi Sad, 2008; 4-6:161-8.
32. Kalezić N, Jovanović D, Živaljević V, Gvozdenović Lj, Malenković V, Vučović D. Preoperativna evaluacija bolesnika sa sekundarnim hiperparatireoidizmom i bubrežnom insuficijencijom, u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 16:249-66.
33. Kalezić N. Anestezija kod bolesnika sa sekundarnim hiperparatireoidizmom u endokrinoj hirurgiji (za paratireoidektomije) i u neendokrinoj hirurgiji (za elektivne i hitne operacije), u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 17:267-76.
34. Schmitt H, Buchfelder M, Radespiel-Tröger M, Fahlbusch R. Difficult intubation in acromegalic patients: incidence and predictability. Anesthesiology, 2000;93(1):110-4.
35. Lim M, Williams D, Maartens N. Anaesthesia for pituitary surgery.Journal of clinical neuroscience, 2006, 13.4: 413-18.
36. Malhotra SK, Sharma K, Saini V. Pituitary Surgery and Anesthetic Management: An Update. WJOES, 2013;5(1):1-5.
37. Bindra A, Prabhakar H, Bithal PK, Singh GP, Chowdhury T. Predicting difficult laryngoscopy in acromegalic patients undergoing surgery for excision of pituitary tumors: A comparison of extended Mallampati score with modified Mallampati classification. J Anaesthesiol Clin Pharmacol, 2013;29(2):187-90.
38. Seidman PA, Kofke WA, Policare R, Young M. Anaesthetic complications of acromegaly. Br J Anaesth, 2000;84(2):179-82.
39. Yaman F, Arslan B, Yuvanç E, Büyükkoçak Ü. Unexpected difficult airway with hypogonadotropic hypogonadism. Int Med Case Rep J, 2014;7:75-7.
40. Malenković V, Gvozdenović Lj, Milaković B, Sabljak V, Palibrk I, Živaljević V. Preparation of patients with pituitary gland disorders, Acta Chir Iugoslav, 2011; 58:93-6.
41. Kalezić N, Malenković V, Živaljević V, Sabljak V, Milaković B, Šumarac-Dumanović M. Akutni poremećaji funkcije hormona hipofize. U: Kalezić N: Inicijalni tretman urgentnih stanja u medicini, Medicinski fakultet, Beograd, 2013; 20:443-52.
42. Kalezić N, Palibrk I, Dimitrijević I, Paunović I, Malenković V, Živaljević V. Preoperativna evaluacija bolesnika sa Kušingovim sindromom u endokrinoj hirurgiji (za adrenalektomije) i neendokrinoj hirurgiji (za elektivne i hitne operacije), u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 25:367-78.
43. Kalezić N, Malenković V, Živaljević V, Sabljak V, Diklić A, Paunović I. Contemporary approach to preoperative preparation of patients with adrenal cortex hormones dysfunction, Acta Chir Iugoslav, 2011; 58:117-22.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
155
44. Khan ZH, Gharabaghian M, Nilli F, Ghiamat M, Mohammadi M. Easy endotracheal intubation of a patient suffering from both Cushing's and Nelson's syndromes predicted by the upper lip bite test despite a Mallampati Class 4 airway. Anesthesia & Analgesia, 2007;105(3):786-7.
45. Domi R, Sula H. Cushing syndrome and the anesthesiologist, two case reports. Indian J Endocrinol Metab, 2011;15(3):209-13.
46. Malenković V, Kalezić N. Anestezija kod bolesnika sa Konovim sindromom u endokrinoj hirurgiji (za adrenalektomije) i u neendokrinoj hirurgiji (za elektivne i hitne operacije), u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 28:399-407.
47. Kalezić N. Anestezija za operacije feohromocitoma, u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 35:491-510.
48. Griesdale DEG, Henderson WR, Green RS. Airway Management in Critically Ill Patients. Lung 189.3, 2011; 181-92.
49. Hua M, Brady SJ, Li G. The epidemiology of upper airway injury in patients undergoing major surgical procedures. Anesth Analg, 2012;114(1):148-51.
50. Bajwa SJS, Kalra S. Diabeto-anaesthesia: A subspecialty needing endocrine introspection. Indian J Anaesth, 2012;56(6):513-7.
51. Stevanović V, Milosavljević N, Stevanović D, Vasiljević S, Mandraš A, Kalezić N. Preoperativna priprema dece sa dijabetesom melitusom, SJAIT, 2012; 34(3-4):219-26
52. Kalezić N, Veličković J, Janković R, Sabljak V, Živaljević V, Vučetić Č. Preoperative preparation of patients with diabetes mellitus, Acta Chir Iugoslav, 2011; 58:97-102
53. Kalezić N. Emergences related to diabetes mellitus: differential diagnosis and treatment. Fifth spring scientific symposium in anesthesiology and intensive care, Proceeding Scientific Symposium, Niš, 2013; p-153-7.
54. Bhatia N, Bhagat H, Sen I. Cricoid pressure: Where do we stand? J Anaesthesiol Clin Pharmacol, 2014 Jan-Mar; 30(1): 3–6.
55. Mishra, M, Bhavsar M M, Patel C, Parikh H, Upadhyaya R, Parmar MH. A comparative study of intubating condition and hemodynamic changes during blind nasal intubation versus fibre optic intubation in cases of temporo-mandibular joint ankylosis. International Journal of Biomedical and Advance Research, 2014;5(1):01-04.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
156
SPECIFIČNOSTI ANESTEZIJE U HIRURGIJI HIPOFIZE ANESTHESIA IN SURGERY OF PITUITARY GLAND BRANKO MILAKOVIĆ Centar za anesteziologiju i reanimatologiju Kliničkog centra Srbije Klinika za neurohirurgiju KCS – Odeljenje anesteziologije i reanimatologije E-mail: [email protected] Summary
Airway management is likely to be difficult in patients with excess production of growth hormone. A conservative, awake approach to airway management in these patients is recommended. Significant hypertension is anticipated during placement of surgical instruments thru the nasal cavity and during topicalization of the nasal mucosa with epinephrine and lydocaine, which should be treated expectantly. Intraoperative treatment with hydrocortisone will prevent the postoperative physiologic consequences of low ACTH levels in the immediate postoperative period. Before extubation, confirm no material or blood clots on the base of the patient’s pharynx, in addition to confirm no airway obstruction due to additional edema. Treatment of diabetes insipidus in the postoperative period must take into consideration the three phases of this disease in patients immediately following pituitary surgery. Postoperative diagnosis of either visual field abnormality or cerebrospinal fluid leak requires immediate evaluation and treatment. Key words: Surgery, pituitary gland, diabetes insipidus; Anaesthesia, airway management. Uvod
Hipofiza (pituitarna žlezda) smeštena je u turskom sedlu (sella turcica), na bazi mozga, u neposrednoj blizini: sfenoidnog sinusa, hipotalamusa, optičke hijazme i velikih krvnih sudova (unutrašnja karotidna arterija, kavernozni sinus). Čine je dva dela: prednji – adenohipofiza, i zadnji – neurohipofiza. Hipotalamus kontroliše funkciju adenohipofize – vaskularnim putem, odnosno funkciju neurohipofize – putem nervnih vlakana. Sekrecijom svojih hormona hipofiza utiče na mnoge, udaljene, ciljne organe. Poremećaji u njenoj funkciji ispoljavaju se kroz sindrome nenormalno pojačane sekrecije pojedinih hormona, tj. smanjene ili potpuno nestale sekrecije istih. Tumori hipofize, svojim fizičkim rastom, izazivaju i simptome povećanog intrakranijalnog pritiska: glavobolju, slepilo i obstruktivni hidrocefalus. Hirurško lečenje hipofize vezano je, najčešće, za tumore ove žlezde. Tumori hipofize čine skoro 1/5 svih primarnih tumora mozga. Za skoro dve trećine njih konačna dijagnoza je benigni adenom hipofize. Najčešći primeri hiperfunkcije adenohipofize su: prekomerno lučenje prolaktina (amenoreja, galaktoreja, nemogućnost rađanja), adrenokortikotropnog (ACTH) hormona (Kušingova bolest), i hormona rasta, somatotropina (akromegalija) 1. Hirurgija hipofize može da izazove jatrogene komplikacije, kao i promene u endokrinoj funkciji, tokom i posle same intervencije. Perioperativni rizik Transkranijalni pristup, sa supraselarnim prilazom žlezdi, može da izazove: curenje cerebrospinalne tečnosti – likvoreju, ishemiju čeonih režnjeva mozga i gubitak vida.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
157
Transsfenoidalni pristup može da izazove vazdušnu emboliju i likvoreju kroz nosne hodnike. Transnazalni, endoskopski pristup – koji se smatra minimalno invazivnim, takođe može izazvati vazdušnu emboliju, kao i leziju kože i sluzokože nosa endoskopom. Zajednička, moguća posledica sva tri pristupa je neurogeni insipidni dijabet (diabetes insipidus – DI) 2. Neurogeni DI javlja se kod približno svakog petog bolesnika, posle transsfenoidalne resekcije adenoma hipofize – u neposrednom postoperativnom periodu. Česte komplikacije hirurgije hipofize su i hipofunkcija hipotalamo – hipofizne osovine, poremećaji vida, krvarenje i lokalni edem 3.
Preanestetička priprema
Pacijentu kome je dijagnostikovan tumor selarne regije, pogotovo ako taj tumor potiče iz same hipofize ili hipotalamusa, potrebno je uraditi detaljnu procenu endokrinog statusa. Iako i funkcionalni i nefunkcijski tumori hipofize retko kad dovode do skoka intrakranijalnog pritiska (IKP), rast tumora u ograničenom prostoru turskog sedla može dovesti do kliničkih znakova poremećaja vida, usled pritiska na optičku hijazmu. Endokrini status i odgovarajuća hormonska supstitucija određuju se od strane specijaliste endokrinologa. Ako je neophodna, supstitucija nedostajućim hormonima treba da se započne bar dve nedelje pre termina operacije. Hirurška intervencija dovodi do manipulacije tkivom prednjeg režnja hipofize (adenohipofiza), ponekad i do potpunog uklanjanja žlezde. Da bi se sprečile posledice deficita lučenja glikokortikoida u perioperativnom periodu, pacijentu se, u preoperativnoj pripremi, uvodi supstitucija kortizola (hidrokortizona) i to po šemi: 50 mg i.m., uveče pred operaciju, i 100 mg i.m. ujutro, pred operaciju, u sklopu rutinske premedikacije 4. Važan deo preoperativne pripreme pacijenta je upoznavanje sa intraoperativnim postupkom i onim što ga očekuje u trenutku posle buđenja iz anestezije. Sve veći procenat operacija selarne regije obavlja se transfenoidalnim ili transnazalnim, endoskopskim pristupom, što suočava pacijenta sa neprijatnošću disanja na usta u postoperativnom periodu od nekoliko dana. Pacijenta upozoravamo na mogućnost da će tokom buđenja morati možda, još par trenutaka, da trpi endotrahealni tubus dok se anesteziolog ne uveri da je gornji disajni put oslobođen sekreta i spreman za ekstubaciju. Preoperativno upozoren pacijent, informisan o manje prijatnim neminovnostima tokom postupka buđenja iz anestezije, spremnije izvršava naloge anesteziologa i time skraćuje neprijatni interval tolerisanja endotrahealnog tubusa in situ 5.
Tehnike anestezije
Po dolasku u operativni blok pacijent se rutinski priprema za intrakranijalni operativni zahvat. Postavljaju se najmanje dve periferne venske linije. Na vensku liniju odmah priključujemo 500 mL slanog, kristaloidnog rastvora (sol. Hartmann ili sol. 0.9% NaCl) koji ima funkciju da polaganom, "kap po kap," infuzijom održava vensku liniju stalno prolaznom i obezbedi nadoknadu tečnosti i elektrolita u perioperativnom periodu. Ukoliko pacijent ne boluje od Kušingovog sindroma (hiperkorticizma), infuzionom rastvoru se dodaje i 100 mg hidrokortizona kojim želimo da preveniramo nedovoljnu intraoperativnu reakciju hipofizo-adrenokortikalne osovine na operativni stres 4, 5. Dok je pacijent još budan postavljamo manžetnu za neinvazivno merenje arterijskog krvnog pritiska i elektrode za jednokanalni monitoring EKG-a. Posle kratkotrajne preoksigenacije na masku (6 – 8 L min-1), pristupa se rutinskom uvodu u anesteziju. Po nastupanju paralize poprečno-prugaste muskulature, duboko uspavanom pacijentu se, transoralnim putem, uvodi endotrahealni tubus (obični ili ojačan žicom – "armirani").

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
158
Proverava se da li je tubus korektno postavljen i fiksiran. Ovim postupcima bolesnik je pripremljen za kontrolisanu (mehaničku) ventilaciju intermitentnim pozitivnim pritiskom (IPPV) u perioperativnom toku. Dalja mišićna relaksacija bolesnika odvija se bilo davanjem IV bolusa, bilo kontinuiranim davanjem nedepolarizujućeg relaksanta, putem špric-pumpe 6. Varijante ovog rutinskog uvoda u anesteziju su česte i uslovljene: uzrastom pacijenta, preope-rativnim fizikalnim statusom, preosetljivošću na određene medikamente i afinitetima samog anesteziologa. Decu mlađu od godinu dana, telesne težine: < 10 kg, obično uvodimo u anesteziju inhalacionim anestetikom (Sevofluran). Po utvrđivanju znakova da je dete u dovoljno dubokoj anesteziji (optimalno je postići srednje duboku hiruršku anesteziju – po Guedelu) uvodimo endotrahealni tubus. Dete se tokom operacije ostavlja da spontano diše smesu O2 i N2O kojoj se
dodaje potrebna koncentracija inhalacionog anestetika. Kao sistem za disanje tokom anestezije koristimo Kuhnov sistem, jednu modifikaciju Ayreovog poluotvorenog sistema sa T-nastavkom. Kod starijih pacijenata (>65 g.) i pacijenata sa značajno smanjenom miokardijalnom rezervom izbegavamo thiopental ili propofol i umesto njih uvod izazivamo etomidatom, u dozi od 0.3 mg kg1, IV, u bolusu. Umesto fentanila, kao analgetik možemo da koristimo remifentanil u kontinuiranoj infuziji, 0.05 – 0.5 µg kg-1 min-1 4–6. Uspavanom pacijentu, sa obezbeđenim disajnim putem, tamponiramo oro- i hipofarinks. Ovo je obavezna mera predostrožnosti tokom transsfenoidalnih i transnazalnih, endoskopskih operacija ("kroz nos") gde postoji intraoperativno slivanje krvi iz nosnih hodnika u nazo-, oro-, hipofarinks i želudac, a time i rizik aspiracije krvi u traheobronhijalno stablo ukoliko dođe do popuštanja tubusnog balončića. Tamponadu izvodimo navlaženim i dobro isceđenim pamučnim zavojem (1 – 2 komada). Pacijentu koji će biti operisan "kroz nos" urinarni kateter obično nije potreban. Intervencija je kratka, ukoliko se ne iskomplikuje, 1 – 1.5 h u proseku, pacijent je potpuno budan i ekstubiran odmah po završetku intervencije, tako da može spontano da mokri čim stigne u odelenje intenzivne nege. Po prenošenju pacijenta u operacionu salu, on se priključuje za mehanički ventilator, odnosno na kružni, poluzatvoreni sistem za disanje tokom perioda anestezije. Kao gasna smesa služi nam kombinacija O2 /vazduh (sa 50% inspiratorne frakcije
O2).
Anesteziju održavamo na dva načina: -potentnim inhalacionim anestetikom iz grupe halogeniranih ugljovodonika (izofluran, sevofluran); -"balansiranom" anestezijom: malim intravenskim dozama snažnog analgetika (fentanil, remifentanil) i mišićnog relaksanta (rokuronijum hlorid, cis-atrakurijum), kojima, po potrebi, dodajemo i male koncentracije inhalacionog anestetika 7. Za transfenoidalni pristup selarnoj regiji pacijent se namešta u varijantu polusedećeg položaja (semi-Fowler position – glava je 20 – 30 cm iznad nivoa ostatka tela). Zbog potrebe za intraoperativnim rentgenskim snimanjem selarnog regiona aparat za anesteziju se mora odmaknuti od pacijenta, odn. opremiti kombinacijom inspiratornog i ekspiratornog creva dužom nego za klasične operacije. Za endoskopski, transnazalni, minimalno invazivni pristup, bolesnik je u sličnom, poluležećem položaju – spavača sa unazad zabačenom glavom. Još uvek se dosta koristi transkranijalni pristup za operacije selarne regije. Za ovakav pristup, istovetan pristupu velikim krvnim sudovima prednjeg sliva na bazi lobanje (pterionalni pristup), pacijent se postavlja u ležeći, dorzalni položaj (supinatio) 4, 5, 8.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
159
Posle postavljanja na kružni sistem kontrolisane ventilacije, priključujemo sisteme za rutinsko praćenje vitalnih funkcija pacijenta tokom perioperativnog perioda. Merenje centralnog venskog pritiska (CVP) rutinski se ne koristi kod neurohirurškog bolesnika jer hiperventilacija (kao najčešći režim ventiliranja ovih bolesnika) izaziva refleksnu vazokonstrikciju koja čini vrednosti CVP, dobijene tokom operativnog zahvata, nepouzdanim. Ipak, u specifičnim situacijama, kada postoji rizik od vazdušne embolije, postavljanje centralnog venskog katetera (CVK ) u desnu srčanu pretkomoru ima svoje opravdanje. Perioperativne specifičnosti vezane za različite endokrine tipove tumora selarne regije
Bolesnici mlađi od 40 godina, sa dokazanom Kušingovom bolešću, najčešće imaju pojačanu sekreciju hormona kore nadbubrega, kao posledicu nenormalnog stvaranja ACTH od strane hromofobnog (bazofilnog) adenoma hipofize. Posle 60. godine života Kušingova bolest daleko češće je posledica karcinoma nadbubrežne žlezde. Bolesniku sa Kušingovom bolešću, preoperativno, treba kontrolisati vrednosti arterijskog krvnog pritiska i korigovati eventualnu hipertenziju. Kontrola serumskih vrednosti elektrolita i glukoze takođe je potrebna radi proce rizika od eventualnog dizbalansa tokom operativnog i ranog postoperativnog perioda. Izbor tehnike anestezije izgleda da nema veći uticaj na oslobađanje kortizola, izazvano operativnim stresom 8. Bolesnici sa Kušingovom bolešću ili prolaktinomom ništa nisu teži za intubaciju od bolesnika sa nefunkcijskim tumorima hipofize. Akromegalija suočava anesteziologa sa više potencijalnih problema koji su posledica povećanog lučenja somatotropina, obično iz mikroskopski malog tumora adenohipofize. Od ove retke bolesti obolevaju ljudi srednje životne dobi. Prvenstveni značaj imaju promene u anatomiji gornjeg disajnog puta. Prenaglašenost svih izbočina facijalnog masiva i makroglosija otežavaju priljubljivanje maske za oksigenaciju uz lice bolesnika 9. Uvećani jezik i epiglotis otežavaju direktnu laringoskopiju i dobru vizualizaciju glasnih žica. Uvećanje glasnih žica dovodi do suženja glotisnog otvora, a nije retkost ni pojava subglotičnog suženja. Učestalost otežanog vazdušnog puta, kod akromegaličnih bolesnika, više od tri puta je veća nego kod bolesnika sa ostalim oblicima tumora hipofize (9.1% vs. 2.6%) 10. Nekada se ovi bolesnici intubiraju budni i sa spontanim disanjem, odnosno pod lokalnom anestezijom farinksa, glotisa i traheje. Od koristi je imati mogućnost primene fiberoptičkog laringoskopa 11. Nazalnu intubaciju treba izbegavati zbog čestog prisustva uvećanih nazalnih konhi 12. Bolesnici sa akromegalijom često imaju izraženu netoleranciju skoka glukoze u krvi. Ako bolesnik ima dijagnostikovan diabetes mellitus, indikovana je intraoperativna kontrola nivoa glukoze u serumu. Budući da se ovi bolesnici obično operišu transnazalnim putem, hirurg može da primeni adrenalin (odn. lokalni anestetik sa adrenalinom) u sluzokožu nosnog hodnika što će dovesti do hipertenzivne reakcije bolesnika, tahikardije, pa čak i aritmije miokarda. Na ove "jatrogene" skokove krvnog pritiska reagujemo pravovremenim produbljivanjem anestezije, primenom bolusa lidokaina ili nekog beta-blokatora (propranolol, metoprolol) 13. Operisani bolesnik često razvije znake insipidnog dijabeta u ranom postoperativnom periodu. Arteficijelna osmotska diureza (manitol, furosemid) može da maskira znake ranog diabetesa insipidusa, zato je uglavnom i ne primenjujemo tokom operacija mikroadenoma hipofize. Jedinice intenzivnog lečenja moraju imati na raspolaganju sintetski vazopresin, za slučaj neophodne supstitucione terapije. Ukoliko krvni pritisak intraoperativno pratimo invazivnom
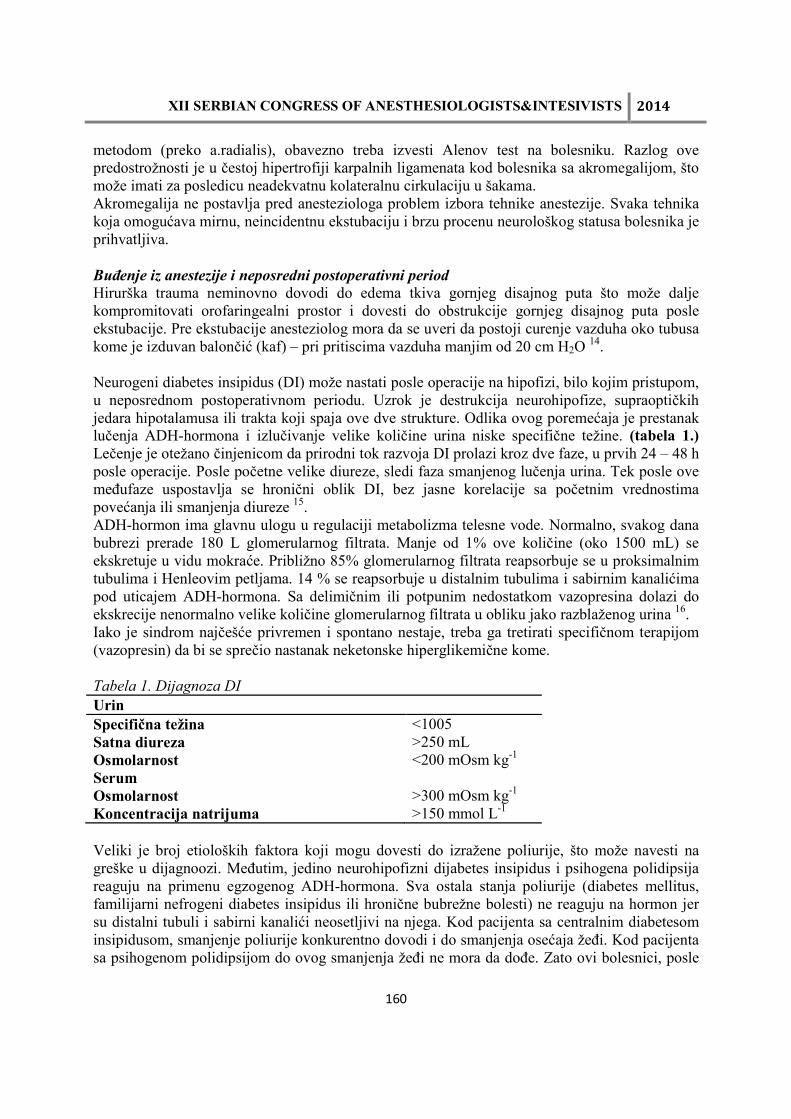
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
160
metodom (preko a.radialis), obavezno treba izvesti Alenov test na bolesniku. Razlog ove predostrožnosti je u čestoj hipertrofiji karpalnih ligamenata kod bolesnika sa akromegalijom, što može imati za posledicu neadekvatnu kolateralnu cirkulaciju u šakama. Akromegalija ne postavlja pred anesteziologa problem izbora tehnike anestezije. Svaka tehnika koja omogućava mirnu, neincidentnu ekstubaciju i brzu procenu neurološkog statusa bolesnika je prihvatljiva. Buđenje iz anestezije i neposredni postoperativni period
Hirurška trauma neminovno dovodi do edema tkiva gornjeg disajnog puta što može dalje kompromitovati orofaringealni prostor i dovesti do obstrukcije gornjeg disajnog puta posle ekstubacije. Pre ekstubacije anesteziolog mora da se uveri da postoji curenje vazduha oko tubusa kome je izduvan balončić (kaf) – pri pritiscima vazduha manjim od 20 cm H2O 14. Neurogeni diabetes insipidus (DI) može nastati posle operacije na hipofizi, bilo kojim pristupom, u neposrednom postoperativnom periodu. Uzrok je destrukcija neurohipofize, supraoptičkih jedara hipotalamusa ili trakta koji spaja ove dve strukture. Odlika ovog poremećaja je prestanak lučenja ADH-hormona i izlučivanje velike količine urina niske specifične težine. (tabela 1.) Lečenje je otežano činjenicom da prirodni tok razvoja DI prolazi kroz dve faze, u prvih 24 – 48 h posle operacije. Posle početne velike diureze, sledi faza smanjenog lučenja urina. Tek posle ove međufaze uspostavlja se hronični oblik DI, bez jasne korelacije sa početnim vrednostima povećanja ili smanjenja diureze 15. ADH-hormon ima glavnu ulogu u regulaciji metabolizma telesne vode. Normalno, svakog dana bubrezi prerade 180 L glomerularnog filtrata. Manje od 1% ove količine (oko 1500 mL) se ekskretuje u vidu mokraće. Približno 85% glomerularnog filtrata reapsorbuje se u proksimalnim tubulima i Henleovim petljama. 14 % se reapsorbuje u distalnim tubulima i sabirnim kanalićima pod uticajem ADH-hormona. Sa delimičnim ili potpunim nedostatkom vazopresina dolazi do ekskrecije nenormalno velike količine glomerularnog filtrata u obliku jako razblaženog urina 16. Iako je sindrom najčešće privremen i spontano nestaje, treba ga tretirati specifičnom terapijom (vazopresin) da bi se sprečio nastanak neketonske hiperglikemične kome. Tabela 1. Dijagnoza DI
Urin Specifična težina <1005 Satna diureza >250 mL Osmolarnost <200 mOsm kg-1 Serum Osmolarnost >300 mOsm kg-1 Koncentracija natrijuma >150 mmol L-1 Veliki je broj etioloških faktora koji mogu dovesti do izražene poliurije, što može navesti na greške u dijagnoozi. Međutim, jedino neurohipofizni dijabetes insipidus i psihogena polidipsija reaguju na primenu egzogenog ADH-hormona. Sva ostala stanja poliurije (diabetes mellitus, familijarni nefrogeni diabetes insipidus ili hronične bubrežne bolesti) ne reaguju na hormon jer su distalni tubuli i sabirni kanalići neosetljivi na njega. Kod pacijenta sa centralnim diabetesom insipidusom, smanjenje poliurije konkurentno dovodi i do smanjenja osećaja žeđi. Kod pacijenta sa psihogenom polidipsijom do ovog smanjenja žeđi ne mora da dođe. Zato ovi bolesnici, posle
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
161
tretmana egzogenim hormonom (dezmopresin, pitresin tanat), mogu da razviju sliku trovanja vodom, jer i pored normalizovanja diureze, njihova neumerena žeđ se ne smanjuje! Zaključak
Anestezija za operacije na hipofizi ima niz specifičnosti, sa kojima anesteziolog mora biti familijaran, kako bi izvršio valjanu preoperativnu evaluaciju i pripremu bolesnika, izabrao adekvatne medikamente i tehniku anestezije i bio spreman za prevenciju i lečenje mogućih komplikacija, povezanih sa ovom oblašću neurohirurgije. Održavanje gornjeg vazdušnog puta može biti otežano kod bolesnika sa akromegalijom. Kod ovih bolesnika izvršićemo budnu intubaciju, pod lokalnom anestezijom farinksa, glotisa i traheje, uz primenu fiberoptičkog laringoskopa. Kod operacija transsfenoidalnim i transnazalnim, endoskopskim pristupom može se očekivati snažna sistemska hipertenzivna reakcija bolesnika, bilo na infiltraciju sluzokože nosa rastvorom lokalnog anestetika i adrenalina, bilo samim prolaskom instrumenata do prednjeg zida turskog sedla. U tom periodu hirurške intervencije anesteziju treba produbiti i primeniti lekove koji smanjuju hemodinamski odgovor organizma. Intraoperativna infuzija hidrokortizona sprečava postoperativne komplikacije niskog nivoa ACTH u neposrednom postoperativnom periodu. Lečenje postoperativnog DI mora se bazirati na prepoznavanju tri faze u razvoju sindroma, neposredno posle izvršene hirurške intervencije na hipofizi.
Literatura
1. The Committee of Brain Tumor Registry of Japan: Report of brain tumor registry of Japan (1969 – 1993) 10th edition. Neurol Med Chir 2000; 40: 1 – 102.
2. Atkinson JL, Young Jr WF, Meyer FB, Davis DH, Nippoldt TB, Erickson D, et al. Sublabial transseptal vs. transnasal combined endoscopic microsurgery in patients with Cushing disease and MRI-depicted microadenomas. Mayo Clin Proc 2008; 83: 550 – 3.
3. Abhoud CF, Laws ER. Clinical endocrinological approach to hypothalamic-pituitary disease. J eurosurg 1979; 51: 271 – 91.
4. Milaković B. Specifičnosti u anesteziji selarnih tumora. U: Ivanović SP, urednik. Tumori
hipofize i kraniofaringeomi. Beograd: Nova Evropa, 1995: 223 – 232. 5. Antunović V, Milaković B. Anestezija u neurohirurgiji. Beograd: Zavod za udžbenike i
nastavna sredstva, 1995. 6. Dinsmore J. Anaesthesia for elective neurosurgery. Br J Anaesth 2007; 99: 68 – 74. 7. Ali Z, Prabhakar H, Bithal PK, Dash HH. Bispectral index-guided administration of
anesthesia for transsphenoidal resection of pituitary tumors: a comparison of 3 anesthetic techniques. J Neurosurg Anesthesiol 2009; 21: 10 – 15.
8. Dohi Sh. Perioperative Challenges During Pituitary Surgery. In: Brambrink AM, Kirsch JR, Eds. Essentials of Neurosurgical Anesthesia & Critical Care. New York; Springer, 2012.
9. Cucchiara RF, Messick JM. Airway management in patients with acromegaly (letter). Anesthesiology 1982; 56: 157.
10. Schmitt H, Buchfelder M, Radespiel-Tröger M, Fahlbusch R. Difficult intubation in acromegalic patients: incidence and predictability. Anesthesiology 2000; 93: 110 – 14.
11. Ovassapian A, Doka JC, Romsa DE. Acromegaly-uses of fiberoptic laryngoscopy to avoid tracheostomy. Anesthesiology 1981; 54: 429 – 30.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
162
12. Nemergut EC, Zuo Z. Airway management in patients with pituitary disease: a review of 746 patients. J Neurosurg Anesthesiol 2006; 18: 73 – 7.
13. Laws ER, Abhoud CF. Perioperative management of patients with pituitary microadenomas. Neurosurgery 1980; 7: 566 – 73.
14. Frost EAM. Postanesthetic care. In: Frost EAM, ed. Clinical Anesthesia in Neurosurgery,
2nd ed. Boston: Butterworth-Heinemann, 1991: 507 – 8. 15. Osborn I. The patient with pituitary disease. In: Frost EAM, ed. Preanesthetic Assessment,
Vol.2. Boston: Birkhauser, 1989. 16. Streeten DHP, Moses AM, Miller M. Disorders of the neurohypophysis. In: Harrison's
Principles of Internal Medicine, 11th ed. New York: McGraw-Hill, 1987: 1724 – 29.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
163
PROCENA PERIOPERATIVNOG RIZIKA KOD BOLESNIKA SA DIAJBETES MELITUSOM ASSESSMENT OF PERIOPERATIVE RISK IN PATIENTS WITH DIABETES MELLITUS
VESNA MALENKOVIĆ1, NEVENA KALEZIĆ2,3 1Služba anestezije i intenzivnog lečenja, KBC “Bežanijska kosa”, Beograd, 2Centar za anesteziologiju i reanimatologiju Kliničkog centra Srbije, Beograd,3Medicinski fakultet Univerziteta u Beogradu E-mail: [email protected] Abstract
Incidence of diabetes mellitus (DM) is constantly increasing both in our country and abroad. Approximately 10% of all surgical patients have DM, but in some surgical areas more than 10%. On the other hand, surgical procedure is often required in diabetic complications. Patients with DM are at increased risk of surgical procedures due to a number of co-morbidities; those pts. have delay wound helding and higher risk of complications such as infections. The aim of this paper is to point out the most important parameter for the assessment of perioperative risk in patients with diabetes in order to take prophylactic diagnostic and therapeutic procedures in the prevention of complications, further organ failure and increasing costs of hospitalization. Uvod
Američka asocijacija za dijabetes (ADA) procenjuje da 12-25% hospitalizovanih odraslih pacijenata ima dijabetes melitus (DM). Sa sve većim brojem pacijenata obolelih od dijabetesa raste i broj hirurških intervencija zbog njihovih komplikacija, a povećava se rizik od nastanka komplikacija povezanih sa DM tokom drugih operacija. Zbog ovih razloga procena perioperativnog rizika bolesnika sa DM, perioperativno praćenje i kontrola metaboličkih i kliničkih parametara su neophodni. Procenjuje se da se oko 25% pacijenata obolelih od DM mora podvrgnuti operaciji. Stopa mortaliteta kod ovih pacijenata je do 5 puta veća, nego kod pacijenata koji ne boluju od DM, a često to ima veze sa oštećenjem organa usled DM. Hronične komplikacije koje dovode do mikroangiopatije (retinopatije, nefropatije i neuropatije) i makroangiopatije (ateroskleroza) direktno uvećavaju potrebu za hiruškom intervencijom i dovode do hiruških komplikacija usled infekcija i vaskulopatije. Infekcije uzrokuju 66% postoperativnih komplikacija i skoro četvrtinu perioperativnih smrti pacijenata sa DM. Podaci ukazuju na oštećenu funkciju leukocita, uključujući i izmenjenu hemotaksu i fagocitne aktivnosti. Kontrola glikemije je veoma značajna za smanjenje učestalosti infekcije.1,2,3 Postoperativna ishemija miokarda je u porastu kod pacijenata sa DM koji se podvrgavaju kardiološkim i nekardiološkim operacijama. Ozbiljnija kontrola glikemije ima veliki uticaj na smanjenje incidence mnogih od ovih komplikacija prilikom različitih hiruških intervencija. Van der Berg i njegove kolege 2001.godine ukazali su na značajno smanjenje mortaliteta usled kontinuiranog korišćenja infuzije insulina zarad kontrole glikemije na 80-110/mg/dL. Učestalost perioperativnih komplikacija kod bolesnika sa dijabetesom zavisi od regulacije glikemije i postojanja komplikacija dijabetesa na različitim organima u preoperativnom periodu. Hirurški stres dovodi do poremećaja glikoregulacije usled povećanog tonusa simpatikusa i povećane sekrecije stres hormona: epinefrina, kortizola, glukagona, hormona rasta. Mehanizam
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
164
delovanja ovih hormona je suprotan dejstvu insulina. Hirurški pacijenti bez dijabetesa mogu povećati sekreciju insulina i održati homeostazu glukoze tokom perioperativnog perioda. Pacijenti sa DM nemaju kompenzatorne mehanizme zbog neadekvatne sekrecije insulina, tako da stres kod njih proizvodi hiperglikemiju različitog stepena koju treba regulisati perioperativno. Najčešće uzroci perioperativnog morbiditeta su hipo i hiperglikemija, kardiovaskularni poremećaji, renalna insuficijencija, infekcija, kompleksna primena lekova, neodgovarajuća intravenska insulinska terapija, greške u prevođenju bolesnika sa intravenskog insulin na uobičajenu medikamentnu terapiju. Lekari i pacijenti treba da preduzmu sve mere koje mogu pomoći da se broj postoperativnih komplikacija smanji. Pre operativnog lečenja, detaljan pregled pacijenta treba da utvrdi tekuću metaboličku kontrolu dijabetesa i postojanje komplikacija. Poremećaj renalne funkcije, bolesti srca, prisustvo autonomne neuropatije, učestalost hiperglikemijskih komplikacija dijabetesa melitusa ukazuju na uznapredovalu i loše kontrolisanu bolest.
Preoperativna procena rizika pacijenata sa dijabetes melitusom
Preoperativna procena rizika za nastanak perioperativnih komplikacija ima cilj da poboljša ishod hirurškog lečenja. Procena perioperativnog rizika zavisi od dugoročne metabolićke kontrole dijabetesa u preoperativnom period i postojanja komplikacija dijabetesa. Koronarna bolest je češća kod žena u odnosu na muškarce sa dijabetesom. Dijabetes je najčešći uzrok infarkta miokarda kod pacijenata mlađih od 30g. Bolest perifernih arterija je uglavnom asimptomatska, ali je dijabetes važan marker sistemske vaskularne bolesti i nalazi se kod 70% pacijenata umrlih od koronarne bolesti i 5-10% pacijenata koji su imali šlog.5,6,7,8 Dijabetična nefropatija prisutna je kod 40% pacijenata sa DM tip 1 i 5% do 40% sa DM tip 2. Dijabetična retinopatija je prisutna kod 30% pacijenata, a isti je procenat učestalosti periferne neuropotaije bolesnika sa DM. Autonomna neuropatija, mada ne tako česta, jako je važna jer može biti uzrok refrakterne hipotenzije u anesteziji i maskirati autonomni odgovor na hipoglikemiju. Bolesnici sa DM imaju povećanu sklonost ka perioperativnim infekcijama. Evaluacija metaboličke kontrole podrazumeva praćenje nivoa glikoziranog hemoglobina (HbA1c). Važna je evidencija koju vodi sam pacijent o kretanju glikemija i epizodama hipo i hiperglikemije tokom dana i noći. Obavezno je poznavanje lekova koje pacijent uzima, doza i vremena aplikacije. Često je neophodna promena terapije pre operacije, dok je tokom i posle hirurške intervencije, neophodna insulinska terapija, bazirana na različitim režimima, u zavisnosti od nivoa hiperglikemije, težine stanja bolesnika i druge terapije koju prima, u periodu dok pacijent ne jede.9,10,11,12,13 Metabolička kontrola dijabetesa preoperativno kao prediktor perioperativnog morbiditeta
Loša regulacija glikemije je udružena sa povećanim rizikom za nastanak kardiovaskularnih komplikacija i prestavlja važan marker lošeg ishoda u postoperativnom periodu. Studije su pokazale veću učestalost infarkta miokarda, drugih kardiooloških komplikacija, kao i viši mortalitet kod pacijenata podvrgnutim velikim vaskularnim operacijama koji su imali lošu dugoročnu metaboličku kontrolu DM. Studije su pokazale da pacijenti sa povišenim bazalnim nivoom glukoze, koji su operisani zbog nevaskularnih oboljenja, imaju povećan rizik od perioperativnih komplikacija.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
165
Postoperativna hiperglikemija pokazala se kao prediktor nepovoljnog ishoda lečenja. Hiperglikemija ima brojne neželjene efekte. Usporava zarastanje rana usled smanjenja perfuzije u tkivima i inhibicije ćeliske funkcije. Hiperglikemija povećava sklonost ka infekciji putem redukcije ćelijskog imuniteta. Pored toga, hiperglikemija može dovesti do egzacerbacije ishemičnih moždanih lezija kod starijih osoba. Porast glikemije preko 250mg/dl blokira hemotaksu leukocita i fagocitozu, dovodi do promena funkcije trombocita, što dalje ima za posledicu poremećaje u koagulaciji. Zbog toga bi trebalo da rutinske analize bolesnika sa DM, planiranih za operativno lečenje, obuhvate, pored glikemije, i celokupnu krvnu sliku, protrombinsko i trombinsko vreme, hepatogram.
Preoperativna evaluacija kardiovaskularnog sistema pacijenata sa DM
Za procenu rizika za pojavu perioperativnih komplikacija kod pacijenata sa DM su neophodni podaci o insulinskoj terapiji, koji predstavljaju vezu između kliničkih karakteristika i perioperativnog kardijalnog mortaliteta i morbiditeta. “Tiha” (“silent”) miokardna ishemija je posledica dijabetične neuropatije, čak i kod pacijenata sa dobro kontrolisanom glikemijom. Studije su pokazale da bolesnici sa DM, podvrgnuti nekardijalnoj hirurgiji, imaju povećani rizik od mortaliteta zbog kardiovaskularnih poremećaja. Procena rizika vrši se na osnovu istorije bolesti, fizikalnog pregleda, neinvazivnih testova, elektrokardiografije ehokardiografije, nivoa serumskog kreatinina. U svrhu procene kardijalnoj rizika, kreirani su različiti indeksi procene, među kojima su najpoznatiji Goldmanov indeks rizika, a u novije vreme Lijev indeks. Budući da dijabetičari često u osnovi imaju hiperholesterolemiju, makrovaskularne bolesti, i neuropatije, verovatnoća od postojanja pritajene ishemije se povećava. Preoperativna procena rizika bi trebalo da počne se sa elektrokardiogram (EKG) u položaju mirovanja kod svih pacijenata. Ukoliko je potrebno, kardiološka evaluacija mođe uključiti i osetljivije dijagnostičke testova i procedure pre operacije, kao što su ehokardiografija, koronarna angiografija i laboratorijske testove, kao što su BNP (moždani natriuretski peptid) i NT-proBNP, ACS, i IHD. Pre-operativni BNP i NT-proBNP nivoi, kao pokazatelji srčane insuficijencije, imaju značajnu prognostičku vrednost za dugoročni mortalitet i kardijalne smetnje nakon velikih nekardijalnih vaskularnih operacija.14,15,16,17 Analiza interakcije između kliničkih varijabila i pojave perioperativnog kardijalnog morbiditeta dala je više modela za procenu perioperativnih komplikacija kod pacijenata sa dijabetesom. Goldman kardijalni indeks je jedan od prvih modela procene kardijalnih faktora rizika. Ovaj indeks je u uzeo u obzir kardijalne faktore rizika kod pacijenata, kao i njihovo opšte zdravstveno stanje. Visok skor ukazuje na visok stepen rizika. Izmenjeni Goldman model uključuje i vrstu operacije, istoriju ishemijskog srčanog oboljenja, istoriju cerebrovaskularnog oboljenja, preoperativno lečenje insulinom i preoperativni serumski kreatinin >2.0 mg/dl. 18,19,20 Indeks rizika Eagle izdvaja pet kliničkih pokazatelja: Q-talase, istoriju ventrikularne ektopične aktivnosti, dijabetes, starost i anginu. Odsustvo ovih faktora rizika pomaže u utvrđivanju pacijenata sa manjim rizikom od kardioloških smetnji. U opštoj populaciji, istorija nedavnih infarkta miokarda (MI) je klinički pokazatelj povećanog rizika od kardioloških perioperativnih smetnji. Stopa ponovnog infarkta ili smrtnog ishoda kod pacijenata je 6%, ako se operacija izvrši u roku od 3 meseca od MI. Stopa verovatnoće ponovnog infarkta ili smrtnog ishoda opada na 2%, ukoliko se operacija izvrši u roku od 6 meseci, a stopa dalјe opada na 1,5%, ako se operacija
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
166
izvrši više od 6 meseci nakon MI. Elektivne operacije bi, ukoliko je to moguće, trebalo odložiti nakon kardioloških poremećaja.21,22,23,24,25 Preoperativna evaluacija hroničnih komplikacija DM
Prisustvo dijabetične nefropatije usmerava preoperativnu pripremu bolesnika u pravcu dodatne evaluacije bubrežne funkcije. Najčešći test, određivanje kreatinina u serumu, ne može biti pouzdan pokazatelj. Prvi korak u renalnoj proceni je skrining mikroalbuminurije. Ukoliko je pozitivan, trebalo bi, iz 24-h urina, odrediti klirens kreatinina. Pacijenti sa sniženim klirensom kreatinina imaju povećan rizik od bubrežne insuficijencije. Renalna disfunkcija je sigurna ako je kreatinin u serumu 170 mmol/L ili 2 mg/dL ili klirens kreatinina od, 60 mL/min. Smanjenje klirensa kreatinina na 10 mL/min povećava rizik od perioperativnog mortaliteta za 40%. Zbog toga je neophodno intenzivno praćenje ovih bolesnika u perioperativnom periodu. 26,27,28,29,30
Dijabetična autonomna neuropatija je predisponirajući faktor za pojavu perioperativne hipotenzije kod pacijenata sa dijabetesom. Simptomi su: vrtoglavica, rasejanost, zamućenje vida u stojećem položaju i sinkope. Simptomi uklјučuju i pad sistolnog krvnog pritiska > 30 mmHg nakon stajanja. Dijagnostički testovi obuhvataju merenja krvnog pritiska u ležećem i stojećem položaju. Kod pacijenata sa ortostatskom hipotenzijom neophodno je pažlјivo praćenje krvnog pritiska i volumena, nekada i vazoaktivna potpora u slučaju refrakterne hipotenzije, naročito u anesteziji. Podaci o sporom pražnjenju želuca ukazuju na dijabetičnu gastroparezu. Ovi pacijenti imaju rizik od aspiracije, a postoperativna peroralna nutricija može biti otežana. Zaključak
Pacijenti sa dijabetesom melitusom imaju veći stepen rizika od operacije u odnosu na nedijabetičare zbog usporenog zarastanja rana, povećane sklonosti ka infekcijama, pojave hipoglikemije tokom primene insulinske terapije itd. Loše regulisani dijabet, sa razvijenim hroničnim komplikacijama, uvećava rizik za perioperativni morbiditet i mortalitet. Adekvatna preoperativna evaluacija i procena rizika od pojave preoperativnih komplikacija kod bolesnika sa DM, omogućuju bolju pripremu ovih bolesnika i bolji ishod lečenja.
Literatura
1. Poldermans D, Bax JJ, Boersma E. et al. Guidelines for pre-operative cardiac risk assessment and perioperative cardiac management in non-cardiac surgery. Eur Heart J, 2009; 30:2769–812 doi:10.1093/eurheartj/ehp337
2. Diehm C, Lawall H. Diabetes, heart surgery and the peripheral arteries. Clin Res Cardiol. 2006; 95:63-9.
3. Lanzer P, Weser R, Prettin C. Carotid-artery stenting in a high-risk patient population--single centre, single operator results, Clin Res Cardiol, 2006; 95(1):4-12.
4. Axelrod DA, Upchurch GR Jr, DeMonner S, et al. Perioperative cardiovascular risk stratification of patients with diabetes who undergo elective major vascular surgery. J Vasc Surg. 2002; 35(5): 894-901.
5. Antunes PE, de Oliveira JF, Antunes MJ. Coronary surgery in patients with diabetes mellitus: a risk-adjusted study on early outcome. Eur J Cardiothorac Surg. 2008; 6.
6. Filsoufi F, Rahmanian PB, Castillo JG, et al. Diabetes is not a risk factor for hospital mortality following contemporary coronary artery bypass grafting, Interact Cardiovasc Thorac Surg. 2007; 6(6):753-8.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
167
7. Mohammadi S, Dagenais F, Mathieu P, et al. Long-term impact of diabetes and its comorbidities in patients undergoing isolated primary coronary artery bypass graft surgery. Circulation. 2007; 116(11 Suppl):1220-5.
8. Humar A, Kerr SR, Ramcharan T, et al. Peri-operative cardiac morbidity in kidney transplant recipients: incidence and risk factors. Clin Transplant, 2001;15(3):154-8.
9. Aziz I, Lewis RJ, Baker JD, et al. Cardiac morbidity and mortality following carotid endarterectomy: the importance of diabetes and multiple Eagle risk factors. Ann Vasc Surg. 2001;15(2):243-6.
10. Schluter M, Reimers B, Castriota F, et al. Impact of diabetes, patient age, and gender on the 30-day incidence of stroke and death in patients undergoing carotid artery stenting with embolus protection: a post-hoc subanalysis of a prospective multicenter registry. J Endovasc Ther. 2007; 14(3): 271-8.
11. Roghi A, Palmieri B, Crivellaro W, et al. Relationship of unrecognised myocardial infarction, diabetes mellitus and type of surgery to postoperative cardiac outcomes in vascular surgery. Eur J Vasc Endovasc Surg, 200; 21(1): 9-16.
12. Weber FD, Schneider H, Wiemer M, et al. Sirolimus eluting stent (Cyphertrade mark) in patients with diabetes mellitus: results from the German Cypher Stent Registry. Clin Res Cardiol. 2008; 97(2):105-9.
13. De Servi S, Guastoni C, Mariani M, et al. Chronic renal failure in acute coronary syndromes. G Ital Cardiol (Rome), 2006; 7(4 Suppl 1):30S-35S.
14. Arabshahi KS, Koohpayezade J. Investigation of risk factors for surgical wound infection among teaching hospitals in Tehran. Int Wound J, 2006; 3(1):59-62.
15. Malmstedt J, Wahlberg E, Jorneskog G, et al. Influence of perioperative blood glucose levels on outcome after infrainguinal bypass surgery in patients with diabetes. Br J Surg. 2006; 16.
16. Ouattara A, Lecomte P, Le Manach Y, et al. Poor intraoperative blood glucose control is associated with a worsened hospital outcome after cardiac surgery in diabetic patients. Anesthesiology. 2005;103(4):687-94.
17. Gandhi GY, Nuttall GA, Abel MD.; Intraoperative hyperglycemia and perioperative outcomes in cardiac surgery patients. Mayo Clin Proc, 2005; 80(7):862-6.
18. Ghotkar SV, Grayson AD, Fabri BM, et al. Preoperative calculation of risk for prolonged intensive care unit stay following coronary artery bypass grafting. J Cardiothorac Surg. 2006; 31:1(1):14.
19. Tamai D, Awad AA, Chaudhry HJ, et al. Optimizing the medical management of diabetic patients undergoing surgery. Conn Med. 2006; 70(10):621-30
20. Sugarbaker DJ, Donaldson MC, Poss R, Ho KK, Ludwig LE, Pedan A, Goldman L. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery. Circulation 1999; 100:1043–9.
21. Boersma E, Kertai MD, Schouten O, Bax JJ, Noordzij P, Steyerberg EW, Schinkel AF, van Santen M, Simoons ML, Thomson IR, Klein J, van Urk H, Poldermans D. Perioperative cardiovascular mortality in noncardiac surgery: validation of the Lee cardiac risk index. Am J Med 2005;118:1134–41.
22. Poldermans D, Bax JJ, Schouten O, Neskovic AN, Paelinck B, Rocci G, van Dortmont L, Durazzo AES, van de Ven LLM, van Sambeek MRHM. Should major vascular surgery be delayed because of preoperative cardiac testing in intermediate-risk patients receiving beta-blocker therapy with tight heart rate control? J Am Coll Cardiol 2006; 48:964–9.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
168
23. Naughton C, Feneck RO. The impact of age on 6-month survival in patients with cardiovascular risk factors undergoing elective non-cardiac surgery. Int J Clin Pract 2007; 61:768–76.
24. Hoeks SE, Scholte op Reimer WJ, Lenzen MJ, van Urk H, Jorning PJ, Boersma E, Simoons ML, Bax JJ, Poldermans D. Guidelines for cardiac management in noncardiac surgery are poorly implemented in clinical practice: results from a peripheral vascular survey in the Netherlands. Anesthesiology 2007;107:537–44.
25. Goldman L, Caldera DL, Nussbaum SR, Southwick FS, Krogstad D, Murray B, Burke DS, O’Malley TA, Goroll AH, Caplan CH, Nolan J, Carabello B, Slater EE. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med 1977; 297:845–50.
26. Maisel AS, Bhalla V, Braunwald E. Cardiac biomarkAuerbach A, Goldman L. Assessing and reducing the cardiac risk of noncardiac surgery. Circulation 2006; 113:1361-76.
27. Detsky AS, Abrams HB, Forbath N, et al: Cardiac assessment for patients undergoing noncardiac surgery. A multifactorial clinical risk index. Arch Intern Med 1986; 146:2131-4.
28. Donati A, Ruzzi M, Adrario E, et al: A new and feasible model for predicting operative risk. Br J Anaesth, 2004; 93:393-9.
29. Eagle KA, Berger PB, Calkins H. et al. American College of Cardiology; American Heart Association: ACC/AHA guideline update for perioperative cardiovascular evaluation for noncardiac surgery-executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1996 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). J Am Coll Cardiol 2002; 39:542-53.
30. Polanczyk CA, Marcantonio E, Goldman L. et al. Impact of age on perioperative complications and length of stay in patients undergoing noncardiac surgery. Ann Intern Med 2001;134:637-64.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
169
HEMODINAMSKI POREMEĆAJI U TOKU TIREOIDEKTOMIJA HEMODYNAMIC DISTURBANCES DURING THYROIDECTOMY MARINA STOJANOVIĆ¹, VERA SABLJAK1,2, KSENIJA STEVANOVIĆ¹, ANKA TOŠKOVIĆ1,2, VLADAN ŽIVALJEVIĆ2,3, NEVENA KALEZIĆ1,2,3 ¹ Centar za anesteziologiju i reanimatologiju, Klinički centar Srbije, Beograd, ² Centar za endokrinu hirurgiju, Klinički centar Srbije, Beograd, ³ Medicinski fakultet Univerziteta u Beogradu E-mail: [email protected] Summary
Intraoperative hemodynamicdisturbances(IOHP) representsignificant fluctuationsof blood pressureand heart rateandthe occurrence ofdysrhythmias. Their appearancehas a significant impacton the finaloutcome of the treatmentof surgicalpatients. Thyroid surgery anesthesia and the operation itselfhavecertain characteristicsthatinfluence the occurrence ofthese disorders. Thisis primarily relatedto thehigh incidenceof difficult intubation, hemostasiscontrolatthe end of the operation by methodcalled"hiperpresija" directsurgicalstimulation ofn.vagus, whichmay result inbradycardia, and in the immediate postoperativeperiodmay develop cervical hematoma orother postoperative complications that require urgent anesthetic treatment.
Uvod
Intraoperativni hemodinamski poremećaji (IOHP) u značajnoj meri utiču na konačan ishod lečenja hirurških bolesnika.Učestalost ovih poremećaja je veoma različita i podaci iz literature govore da se kreće između 4.9% i 17.5%1,2. Razike u učestalosti postoje, pre svega, zbog razlika u definiciji određenog intraoperativnog hemodinamskog poremećaja, a takođe se učestalost razlikuje i u određenim granama hirurgije. Anestezija u tireoidnoj hirurgiji i sama hirurška tehnikaimaju određene specifičnosti koje utiču na pojavu intraoperativnih hemodinamskih poremećaja. To se pre svega odnosi naotežanu intubaciju, položaj bolesnika na operacionom stolu, izbor anestetika, direktna mehanička stimulacija n.vagusa tokom hirurškog rada koja može rezultirati pojavom intraoperativne bradikardije, moguće pojave kardiovaskularne i respiratorne nestabilnosti u toku i posle operacije, kontrola hemostaze pri kraju operacije metodom tzv. “hiperpresije”, koju manuelno izvodi anesteziolog insuflacijom ispiratornih gasova pod povišenim pritiskom,a u neposrednom postoperativnom toku mogu se javiti komplikacije, kao što su edem larinksa, lezija laringealnih nerava, traheomalacija, cervikalni hematom idr., koje zahtevaju hitan anesteziološki tretman.3,4
Jedan od najčešćih razloga pojave hemodinamske nestabilnosti, u smislu velikih oscilacija vrednosti krvnog pritiska i frekvence pulsa i pojave disritmija, tokom uvoda u anesteziju u ovoj grani hirurgije, je pre svega velika učestalost otežane intubacije (OI). Za raziliku od opšte populacije gde je učestalot oko 1%, u tireoidnoj hirurgiji je učestalost OI znatno veća i kreće se od 5,5% do 17,5% 5-9. Takođe, poput ostalih grana hirurgije, hemodinamska nestabilnost može biti posledica i pridruženog kardiovaskularnog komorbiditeta, lošeg izbora anestetika i neadekvanto vođene anestezije.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
170
Intraoperativna hipertenzija
Intraopeartivna hipertenzija je česta i uzrokovana je brojnim činiocima.Ukoliko je značajna, i ukoliko dugo traje može izazvati značajne posledice.Populacione studije, velike multicentrične kliničke studije, kao i meta analize su pokazale da je izolovana sistemska hipertenzija faktor rizika za šlog, koronarnu bolest i povećani mortalitet10. Rič (Reich) i sar. su u svojoj studiji pokazali da SKP>160 mmHg utiče na pojavu negativnih ishoda (mortaliteta i morbiditeta) samo kod operacija koje traju duže od 220min11. Kada je reč o tireoidnoj hirurgiji, pojava intraoperativne hipertenzije i hipertenzivne krize su naročito značajne zbog moguće pojave postoperativnog cerviklanog hematoma.Naime, cervikalni postoperativni hematom je životno-ugrožavajuća komplikacija, koju karakteriše kompresija traheje i moguća asfiksija. Tretman se sastoji u hitnoj intubaciji i hirurškoj reviziji hemostaze. Iako je ova kompikacija retka, sa učestalošću od 0,32-1,3%12, zbog visokog procenta otežane i/ili nemoguće reintubacije traheje, ne treba žuriti sa ekstubacijom bolesnika.Takođe je primećeno da neadekvatno lečena intraoperativna hipertenzija, koja se održava i u postoperativnom period, može doprineti pojavi cervikalnog hematoma. Kalo (Calò) je u svojoj studiji pokazao da je čak 50% bolesnika kod kojih je došlo do pojave hematoma nakon tireoidektomije, imalo postoperativnu hipertenziju i da je ona bila faktor rizika za pojavu cervikalnog hematoma13,14.
Intraoperativna hipotenzija
Intraoperativna hipotenzija (IOH) predstavlja čest neželjeni efekat anetstetika. Ukoliko dugo traje, može poremetiti perfuziju organa i dovesti do ireverzibilnih ishemičnih oštećenja. Ranije studije su pokazale povezanost IOH i perioperativnog infarkta miokarda i šloga15-17, kao i uticaj na mortalitet, kako u kardijalnoj tako i u nekardijalnoj hirurgiji2. Potvrđen je uticaj IOH i u transplatacionoj hirurgiji, IOH je nezavistan prediktor odbacivanja bubrega18, kao i pojave novo-nastale atrrijalne fibrilacije (new onset atrial fibrillation, NOAF) nakon endarterektomije karotida19. Intraoperativna hipotenzija je česta u tireoidnoj hirurgiji.Ono što je specifično za intraoperativnu hipotenziju u tireoidnoj hirurgiji je da se različito leči kod bolesnika sa hiper i hipotireozom. Kod hipertireoze je lek izbora alfa adrenergički agonist fenilefrin, dok je kod hipotireoze efedrin, epinefrin, norepinefrin, dopamin. Ukoliko je intraoperativna hipotenzija kod bolesnika sa hipotireozom rezistentna na primenu vazopresora i nadoknadu volumena,potrebno je primeniti steroide zbog moguće udružene adrenalne insuficijencije. Tokom tireoidne hirurgije, intraoperativna hipotenzija može nastati i kao posledica produžene "hiperpresije". Kontrola hemostaze metodom hiperpresije predstavlja jednu od specifičnosti tireoidne hirurgije. Sastoji se u tome, da se pri kraju operacije, bolesnik manuleno ventilira pod povećanim pozitivnim pritiskom, pri čemu se pritisak zadržava 10-20s. Ovaj postupak se ponavlja nekoliko puta, vodeći računa da intratorakalni pritisak ne bude veći od 40 mBar-a. Suština je da se povišen intratorakalni pritisak prenosi na krvne sudove grudnog koša i vrata, pa do tada neprimećeno vensko krvarenje postaje uočljivo. Takođe treba voditi računa da suviše energična i produžena hiperpresija ne dovede do velikog pada krvnog pritiska, zbog smanjenog dotoka venske krvi u desno srce, a time i do efekta suprotnog od željenog: da krvarenje bude nedovoljno uočljivo.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
171
Intraoperativni poremećaji srčanog ritma
Najčešći intraoperativni poremećaj srčanog ritma u tireoidnoj hirurgiji je intraoperativna
bradikardija. Bradikardija se tokom tireoidektomije i drugih operacija na vratu može javiti, između ostalog, i zbog direktne hirurške stimulacije n. vagusa. Zbog toga je važno pratiti tok operacije i u slučaju pojave bradikardije ukazati hirurgu, kako bi se prestankom hirurške stimulacije, ili eventualnom primenom atropina, normalizovala srčana frekvenca. Obično se registruje kao neželjeno dejstvo lekova (inhalacionih agenasa, opijata, mišićnih relaksanata-sukcinil holina), zatim se može javiti usled hipoksije i hipoventilacije itd. Najčešći razlog pojave intraoperativne tahikardije je hipovolemija usled dehidratacije, gubitka krvi, zatim problemi sa ventilacijom, hipoksija, hipoventilacija, neželjena dejstva lekova i inhalcionih anestetika, a može biti refleksna, tokom laringoskopije ili usled hirurške stimulacije itd.Studija Reich-a i sar. je pokazala takođe da je intraoperativna tahikardija, definisana kao fr>100/min, prediktor perioperativnog infarkta miokarda.Pokazano je, takođe, da je perioperativna tahikardija uzrokproduženog bolničkog lečenja i većeg morbiditeta bolesnika podvrgnutih nekardijalnoj hirurgiji, ali samo u slučajevima dugog trajanja operacije(duže od 220 minuta)11. Tireoidna disfukcija je važan faktor rizika za nastanak atrijalne fibrilacije (AF)20. Učestalost AF je znatno veća kod bolesnika sa hipertireoidizmom u odnosu na eutireoidne bolesnike, krece se i do 13.8%20,21. Takođe je pokazano da je učestalost AF veoma visoka i kod bolesnika sa subkliničkim hipertireoidizmom (abnormalne vrednosti TSH uz normalne vrednosti tireoidnih hormona T3 i T4) iznosi i do 12%22.Najvažniji faktori rizika za nastanak AF su starije životno doba i prisustvo komorbiditeta poput hipertenzije, kardiomiopatije, srčane insuficijencije, bolesti srčanih zalistaka, dijabetes melitus, koronarna bolest i dr.
Zaključak
Kako pojava intraoperativnih hemodinamskih poremećaja značajno utiče na veći morbiditet i mortalitet bolesnika, čak i kada je reč o manjim operacijama i procedurama koje nose manji rizik, poput tireoidne hirurgije, neophodno je adekvatna priprema i perioperativni monitroing ovih bolesnika.
Literatura
1. Forrest JB, Rehder K, Cahalan Mket al. Multicenter study of general anesthesia III. Predictors of severe perioperative adverse outcomes.Anesthesiology1992:76; 3-15.
2. Röhrig R, Junger A, Hartmann B et al. The Incidence and Prediction of Automatically Detected Intraoperative Cardiovascular Events in Noncardiac Surgery. Anesth
Analg2004;98:569-77. 3. Sabljak V, Kalezić N, Ivanović B. et al. Modern concepts of preoperative preparation of
patients with thyroid gland disease. Acta Chir Iugoslav 2011; 18(2):103-8 4. Kalezić N,Živaljević V, Diklić A et al. Preoperativna evaluacija bolesnika sa oboljenjima
štitaste žlezde u endokrinoj i neendokrinoj hirurgiji, u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 5:89-108
5. Kalezić N, Palibrk I, Nešković V. et al. Otežana intubacija kod bolesnika sa tireomegalijom, u knjizi: Anesteziološki aspekti endokrinih i metaboličkih poremećaja

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
172
(štitasta žlezda, paraštitaste i nadbubrežne žlezde), urednika N. Kalezić, Medicinski fakultet, Beograd, 2009; 7:125-50
6. Kalezić N, Milosavljević R, Paunović I. et al. The incidence of difficult intubation in 2000 patients undergoing thyroid surgery: single center experience. Vojnosanit Pregl 2009; 66(5):377-82.
7. Bouaggad A, Nejmi SE, Bouderka MA, Abbassi O. Prediction of Difficult Intubation in Thyroid Surgery. Anesth Analg 2004;99:603-6.
8. Amathieu R, Smail N, Catineau J et al. Difficult intubation in Thyroid surgery: Myth or reality? Anesth Analg 2006;103:965-8.
9. Adnet F.et al. The intubacion difficulty Scale (IDS): proposal and evaluation of a new score characterizingthe complexity of endotracheal intubation. Anestesiology 1997;87;1290-7
10. Wongprasartsuk P, Sear JW. Anaesthesia and Isolated Systolic Hypertension-Pathophysiology and Anaesthesia Risk. Anaesthesia and Intensive Care 2003:619-28.
11. Reich D, Bennett-Guerrero E, Bodin C. Intraoperative Tachycardia and Hypertension Are Independently Associated with Adverse Outcome in Noncardiac Surgery of Long Duration. Anesth Analg 2002;95:273-277.
12. Lacoste L, Gineste D, Karayan J. et al. Airway complication in thyroid surgery. Ann Otol
Rhinol Laryngol 1993; 102: 441-6. 13. Calò PG, Pisano G, Piga G. et al. Postoperative hematomas after thyroid surgery.
Incidence and risk factors in our experience. Ann Ital Chir. 2010;81:343-7. 14. Kalezić N, Veličković J, Sabljak V. et al. Prevencija i lečenje komplikacija
tireoidektomije, Medicina danas, Novi Sad, 2010; 9(7-12): 253-9. 15. Lienhart A, Auroy Y, Pequignot F et al. Survey of anaesthesia-related mortality in
France. Anesthesiology 2006; 105: 1087-97. 16. Barone EJ, Bull BM, Cussatti HE et al. Perioperative Myocardial Infarction in Low-Risk
Patients Undergoing Noncardiac Surgery Is Associated With Intraoperative Hypotension. J Intensive Care Med 2002; 17: 250-5.
17. Bijker BJ, Persoon S, Peelen L et al. Intraoperative Hypotension and Perioperative Ischemic Stroke after General Surgery: A Nested Case-control Study. Anesthesiology
2012; 116: 658-64. 18. Sandid MS, Assi MA, Hall S. Intraoperativehypotension and prolonged operative time as
risk factors for slow graft function in kidney transplant recipients. Clin Transplant. 2006; 20: 762-8.
19. Sposato LA, Suárez A, Jáuregui A et al. Intraoperativehypotension, new onset atrial fibrillation, and adverse outcome after carotid endarterectomyJ NeurolSci 2011; 309: 5-8.
20. Gammage MD, Parle JV, Holder RL et al. Association between serum free thyroxine concentration and atrial fibrillation. ArchIntern Med 2007;167:928-34
21. Frost L, Vestergaard P, Mosekilde L. Hyperthyroidism and risk of atrial fibrillation or flutter: A population-based study. Arch InternMed 2004; 164:1675 – 1678.
22. Canaris GJ, Manowitz NR, Mayor G,et al. The Colorado thyroid disease prevalence study. Arch Intern Med. 2000;160:526-534.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
173
FAKTORI RIZIKA ZA POJAVU PERIOPERATIVNE HIPERTENZIJE KOD BOLESNIKA PODVRGNUTIH PARATIREOIDEKTOMIJI RISK FACTORS FOR PERIOPERATIVE HYPERTENSION IN PATIENTS UNDERGOING PARATHYROIDECTOMY VERA SABLJAK1,2, VLADAN ŽIVALJEVIĆ,2,3, MARINA STOJANOVIĆ1, ANKA TOŠKOVIĆ1,2, KSENIJA STEVANOVIĆ1,2, NEVENA KALEZIĆ1,2,3 1Centar za anesteziologiju i reanimatologiju KCS, Beograd, 2Centar za endokrinu hirurgiju KCS, Beograd, 3Medicinski fakultet Univerziteta u Beogradu E-mail: [email protected] Summary: Primary hyperparathyroidism (PHPT) is the most common indication for parathyroidectomy. PHPT is characterized by hypercalcemia, resulting from excessive secretion of parathyroid hormone (PTH). It is estimated that PHPT affects approximately 1% of adult population. In patients with PHPT there is an increased probability of occurrence of cardiovascular disease, especially arterial hypertension. Different authors reported the presence of hypertension in patients with PHPT in the range between 10-70%, although the mechanism of its occurrence in these patients has not been fully understood. The only form of therapy that involves healing of these patients is surgical treatment, which carries the risk of many life-threatening complications, of which certainly the most important ones are functional disorders of the cardiovascular system - primarily hypertension and hypertensive crisis, then disturbances of heart rhythm, up to cardiac arrest. For now, there is no sufficient number of studies which investigated precipitating factors that lead to such complications. However, there is no doubt that the most significant risk factors for the occurrence of numerous complications, primarily for the occurrence of intraoperative hypertension in patients with PHPT, respectively are age, gender and associated comorbidities. Insufficient literature data indicate that the incidence of intraoperative hypertension during parathyroidectomy is higher in elderly patients, female patients, patients with pre-existing hypertension and those with associated comorbidities. Additional studies are certainly needed in order to clarify the mechanisms of hypertension occurrence in PHPT, to examine and detect risk factors for complications during parathyroidectomy, and to confirm (or refute) the beneficial effect of parathyroidectomy on hypertension in patients with PHPT. Uvod
Primarni hiperparatireoidizam (PHPT) je oboljenje koje se karakteriše hiperkalcemijom, nastalom usled prekomerne sekrecije paratireoidnog hormona (PTH). PHPT je najčešći uzrok hiperkalcemije, pa je potrebno izvršiti evaluaciju u tom pravcu kod svih bolesnika koji imaju povišen nivo kalcijuma u serumu.1 Patoanatomski supstrat za nastanak PHPT najčešće je adenom paratireoidne žlezde, u 80-85% slučajeva (dvostruki adenom se nalazi kod oko 5%), hiperplazija paratireoidnih žlezda se opisuje u oko 10-15% slučajeva, a karcinom paratiroidne žlezde u oko 1% slučajeva. PHPT se sve češće otkriva zahvaljujući rutinskom određivanju nivoa kalcijuma prilikom uzimanja laboratorijskih analiza, pa je i njegova incidenca sve veća. Od ranih 1970-ih, od kada je u kliničku praksu uvedeno rutinsko laboratorijsko merenje nivoa serumskog kalcijuma, PHPT se u SAD dijagnostikuje kod 100 000 novo-obolelih godišnje.2
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
174
Procenjuje se da PHPT ima oko 1% adultne populacije. Incidenca javljanja PHPT je slična u oba pola pre 45. godine života, a povećava se višestruko posle 55. godine, kada oboljenje postaje nekoliko puta češće kod žena.3
Dijagnoza primarnog hiperparatireoidizma
U najvećem broju slučajeva, pažljivo uzeta anamneza, fizikalni pregled i laboratorijsko ispitivanje omoguju razlikovanje PHPT od drugih uzroka hiperkalcemije.2 Zahvaljujući rutinskom određivanju kalcemije, PHPT se danas ipak najčešće otkriva u asimptomatskoj fazi bolesti. U ovoj fazi bolesti se najveći broj bolesnika danas i operiše. Kod bolesnika sa simptomatskim PHPT postoje različite kliničke forme bolesti u zavisnosti od toga na kom su organu ili sistemu organa ispoljeni efekti povećane produkcije PTH, mada je najčešće u pitanju mešovita forma bolesti. Simptomi vezani za ovo oboljenje su: bubrežni kalkulusi, renalna disfunkcija, osteopenija ili osteoporoza, bol u kostima, patološke frakture, koštani cistični tumori, proksimalna mišićna slabost (posebno donjih estremiteta), hipertenzija ili nespecifični simptomi kao što su depresija, letargija i neodređeni bolovi. Ovakvi, klasični simptomi i znaci su danas veoma retki, ali nefrolitijaza i dalje postoji u 4-15% slučajeva.4
Primarni hiperparatireoidizam i hipertenzija
Poznato je da su bolesnici koji pate od simptomatske forme PHPT pod povećanim rizikom za nastanak smrtnog ishoda, uglavnom usled povećane incidence kardiovaskularnih bolesti.5,6 Pored dobro poznatih ciljnih organa, PTH ima uticaja i na povećanje rizika za nastanak kardiovaskularnih bolesti.7 Opservacione studije su pokazale da su hronično visoki nivoi PTH povezani sa hipertenzijom, hipertrofijom miokarda i miokardnom disfunkcijom.8,9,10,11,12 Receptori za PTH prisutni su i u miokardu, i ispoljavaju hipertrofične efekte na kardiomiocite.13 PHPT je povezan sa povećanim rizikom za nastanak arterijske hipertenzije. Različiti autori prijavljuju prisustvo hipertenzije kod bolesnika sa PHPT u opsegu između 10-70%.14
Velike varijacije mogu biti povezane sa različitim metodama merenja krvnog pritiska, dijagnostičkim kriterijumima, vrstom hiperparatireoidizma i izborom bolesnika. Bez obzira na to, prevalenca hipertenzije u ovih bolesnika veća je nego u opštoj populaciji, nevezano za godine starosti.15,16 Mehanizmi koji su u osnovi nastanka hipertenzije u bolesnika sa PHPT, još uvek nisu dovoljno proučeni. Sistemska hipertenzija u hiperkalcemičnih bolesnika sa PHPT karakteriše se povećanjem ukupnog perifernog otpora. Mehanizmi koji dovode do hipertenzije u PHPT podrazumevaju poremećaje na nivou simpatičkog nervnog sistema i na osovini renin-angiotenzin-aldosteron, i disfunkciju ili strukturne promene zida krvnih sudova.17 Pokazano je da infuzija PTH rezultira trajnom hiperkalcemijom i hipertenzijom u zdravih ispitanika.18 Genari (Gennari) i saradnici u svojoj studiji nisu uspeli da pokažu značajne promene u aktivnosti plazmatskog renina, mada dalja istraživanja sugerišu da postoji direktan efekat PTH na sekreciju renina.19 Rezultati ove studije su u skladu sa hipotezom direktnog dejstva PTH na sekreciju renina, koji bi mogao da doprinese patogenezi hipertenzije. Pokazano je da u PHPT dolazi do strukturnih i funkcionalnih promena u zidu krvnih sudova, koje nastaju kao krajnji rezlutat i direktna posledica dejstva PTH na vaskularne glatke mišiće, usled poremećenog metabolizma kalcijuma.20 Pored toga, do hipertenzije može dovesti povećan nivo kalcijuma u krvi, povišen intracelularni kalcijum, kao i hipomagneziemija. U nedavnoj studiji, akutna hiperkalcemija izazvana infuzijom kalcijuma kod zdravih ispitanika, rezultirala je dozno-zavisnim poremećajima u vazodilatatornoj funkciji endotela i povećanjem sistolnog krvnog pritiska.21
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
175
Paratireoidektomija i hipertenzija
Operativno lečenje bolesnika sa PHPT je jedini vid terapije koji podrazumeva izlečenje ovih bolesnika, pa predstavlja lečenje izbora za sve simptomatske bolesnike, kao i za bolesnike sa već postojećim komplikacijama PHPT.22 Kada su asimptomatski bolesnici u pitanju, postoje razne kontroverze, ali prema poslednjim preporukama, ovakvi bolesnici se podvrgavaju hirurškom lečenju ukoliko su mlađi od 50 godina, ukoliko imaju nivo serumskog kalcijuma preko 0,25 mmol/L iznad referentnih vrednosti, imaju vrednosti kalcijuma u urinu preko 400 mg/24h, imaju smanjenje bubrežne funkcije za preko 30% ili imaju komplikacije PHPT.23 Hipertenzija je poznati faktor rizika za perioperativni morbiditet i mortalitet. Hipertenzija u perioperativnom periodu se najčešće definiše kao odstupanje od inicijalnih, preoperativnih vrednosti arterijskog pritiska, za više od 20%, iako i dalje postoje kontroverzna mišljenja u pogledu definisanja ovog entiteta. Perioperativna hipertenzija je čest problem, sa kojim se susreću anesteziolozi, hirurzi, internisti i intenzivisti.24 Prisustvo hipertenzije u perioperativnom periodu dovodi do teže kontrolu hemodinamskog statusa bolesnika pre, tokom i posle hirurškog lečenja. Iz tog razloga je prisustvo hipertenzije u hirurškog bolesnika samo po sebi faktor rizika za nastanak kardiovaskularnih, cerebrovaskularnih, metaboličkih i poremećaja funkcije bubrega u perioperativnom periodu.25 Prilikom hirurškog lečenja bolesnika sa PHPT, može doći do potencijalno životno-ugrožavajućih komplikacija, od kojih su, svakako najznačajniji poremećaji funkcije kardiovaskularnog sistema. Tu se na prvom mestu nalaze hipertenzija i hipertenzivna kriza, potom različiti poremećaji srčanog ritma, sve do srčanog zastoja. Za sada ne postoji dovoljan broj studija koje se bave ispitivanjem precipitirajućih faktora koji dovode do ovakvih komplikacija. Međutim, nesumnjivo je da su među najznačajnijim faktorima rizika za pojavu brojnih komplikacija, prvenstveno intraoperativne hipertenzije u bolesnika sa PHPT, na prvom mestu godine starosti, a odmah potom pol bolesnika i pridruženi komorbitideti. Podaci iz Framingamske studije pokazuju da postoji linearna povezanost između vrednosti KP i godina starosti. Mogu se uočiti tri hemodinamske faze. Tokom sve tri faze sistolni KP raste linearno sa godinama starosti. Do 50. godine, postoji dominacija stabilnog rasta sistemskog vaskularnog otpora, koja se ogleda u povećanju dijastolnog i pulsnog pritiska. Između 50. i 60. godine, zbog istovremenog povećanja sistemskog otpora, ali i arterijske krutosti, dijastolni pritisak je konstantan, srednji arterijski pritisak dostiže plato i dolazi do porasta pulsnog pritiska. Nakon 60. godine, dominira arterijska krutost, dolazi do pada dijastolnog, porasta sistolnog i pulsnog pritiska.26,27 Studija Bahara (Bachar) i saradnika, koja je poredila perioperativne komplikacije i ishod paratireoidektomije među grupama mlađih i starijih bolesnika, pokazala je da je nivo PTH bio viši u starijih bolesnika, kao i da je trajanje hospitalizacije bilo duže u ovih bolesnika.28 Obzirom na činjenicu da se PHPT najčešće javlja posle 55. godine života, i na povezanost ovog oboljenja i hipertenzije, jasno je zašto je učestalost pojave intraoperativne hipertenzije veća kod starijih bolesnika. Brojnim studijama je pokazano da osobe ženskog pola u premenopauzi imaju niže vrednosti krvnog pritiska u odnosu na muškarce. Međutim, sa početkom perioda menopauze, vrednosti arterijskog pritska u žena se povećavaju, i postaju slične vrednostima u muškaraca, što ukazuje na važnu ulogu polnih hormona u regulaciji arterijskog pritiska.29 Obzirom na činjenicu da se PHPT najčešće javlja u postmenopauzalnih žena, odnosno u žena kod kojih izostaje zaštitna

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
176
uloga estrogenih hormona, može se zaključiti da su osobe ženskog pola pod povećanim rizikom za nastanak komplikacija od strane kardiovaskularnog sistema, tj. da su u povećanom riziku za nastanak intra- i postoperativne hipertenzije. U svakoj grani hirurgije, pa i u hirurgiji paratireoidnih žlezda, bolesnici sa pratećim komorbiditetima zahtevaju posebnu pažnju. Obzirom da su kardiovaskularne bolesti jedan od vodećih uzroka smrti današnjice, i da na globalnom nivou dostižu razmere epidemije, najveći perioperativni mortalitet sreće se upravo kod onih bolesnika koji pored osnovnog oboljenja imaju i komorbiditete od strane ovog sistema. Procenjeno je da je od hipertenzije obolelo više od 30% procenata svetske populacije, životnog doba iznad 20 godina. Iz tog razloga, smatra se da je to najčešće hronično oboljenje. Kao što je pokazano mnogim studijama, prethodno postojeća hipertenzija, posebno ukoliko nije regulisana terapijom, povećava verovatnoću pojave intraoperativne hipertenzije i perioperativnih komplikacija.30 U meta-analizi koja je uključila 24 studije, Hovel (Howell) i saradnici pokazali su da prethodno hipertenzivni bolesnici imaju 1.31 puta veći rizik za nastanak kardiovaskularnih komplikacija, u poređenju sa normotenzivnim bolesnicima.31 Klof (Clough) i saradnici su pokazali da preko 60% bolesnika ima hipertenziju, kao komorbiditet.32 Prema istraživanjima Centra za endokrinu hirurgiju Kliničkog centra Srbije, sprovedenom na 200 bolesnika, intraoperativna hipertenzija i poremećaji ritma nastali su isključivo kod bolesnika ASA (American Society of Anesthesiologists) 2 i 3 statusa, tj. kod onih koji pored osnovnog oboljenja imaju još neki značajni komorbiditet.33 U skorijoj studiji, sprovedenoj takođe u Centru za endokrinu hirurgiju KCS, na 2559 bolesnika podvrgnutih tireoidektomiji, koji su bili ASA 2 i ASA 3 statusa, pokazano je da je 66,5% bolesnika imalo prethodno dijagnostikovanu hipertenziju, i da je kod tih bolesnika češće dolazilo do pojave intraoperativne hipertenzije.34 Iako je već pokazan uticaj PTH na pojavu novo-otkrivene hipertenzije (de novo), kao i na povišenje vrednosti arterijskog pritiska u bolesnika sa PHPT, postavlja se pitanje da li kod bolesnika sa PHPT postoperativno (posle učinjene paratireoidektomije, odnosno ekstirpacije hiperaktivne žlezde) dolazi do smanjenja vrednosti arterijskog pritiska? Na žalost, na to pitanje, za sada, ne postoji definitivan odgovor. Nekoliko studija se bavilo ispitivanjem uticaja paratireoidektomije na hipertenziju u postoperativnom periodu. Fildstajn (Feldstein) i saradnici nisu pokazali povoljan uticaj paratireoidektomije na postoperativnu hipertenziju u bolesnika koji su i preoperativno bili hipertenzivni. Oni su, takođe, pokazali da je postoperativno došlo do nastanka hipertenzije u preoperativno normotenzivnih bolesnika, što objašnjavaju postojanjem drugih mehanizama u bolesnika sa PHPT, koji doprinose nastanku hipertenzije.15 Takođe, ni prospektivne studije Piovesana (Piovesan)35 i Nilsena (Nillsen)36 nisu pokazale smanjenje arterijskog pritiska posle paratireoidektomije. Za razliku od njih, Hejliger (Heyliger) i saradnici su pokazali sniženje krvnog pritiska u bolesnika sa PHPT, šest meseci posle paratireoidektomije.37 Kovač (Kovacs) i saradnici su pokazali da u toku prve nedelje posle paratireoidektomije dolazi do dramatičnog sniženja arterijskog pritiska.38 Brulik (Broulik) i saradnici su pokazali značajno sniženje i sistolnog i dijastolnog arterijskog pritiska kod 86 hipertenzivnih bolesnika sa PHPT posle paratireoidektomije.39 Dajmond (Diamond) i saradnici su, takođe, pokazali značajno smanjenje vrednosti sistolnog arterijskog pritiska u 75 normotenzivnih bolesnika sa asimptomatskim PHPT, u periodu od 30 meseci posle paratireoidektomije.14 Iz navedenog je jasno da i dalje postoje

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
177
kontroverzna mišljenja u pogledu uticaja same operacije paratireoidnih žlezda na hipertenziju u postoperativnom periodu, i da su potrebne dodatne studije koje će se baviti ovom problematikom. Zaključak
U bolesnika sa PHPT povećan je kardiovaskularni mortalitet i morbiditet, što je nesumnjivo pokazano brojnim istraživanjima. Iako je hipertenzija ključni faktor rizika za nastanak smrtnog ishoda od strane kardiovaskularnog sistema u bolesnika sa PHPT, ne bi trebalo zanemariti strukturne promene, kao što je hipertrofija leve komore, kao ni funkcionalne poremećaje, kao što su usporeno provođenje u sinusnom i AV čvoru i povećanje ekcitabilnosti i smanjen period refraktornosti, koji dovode do razvoja kompleksnih ventrikularnih aritmija. Malobrojni literaturni podaci ukazuju na činjenicu da je pojava intraoperativne hipertenzije tokom paratireoidektomije veća u bolesnika starijeg životnog doba, osoba ženskog pola, kod bolesnika sa postojećom hipertenzijom i kod bolesnika sa pridruženim komorbiditetima. Svakako su potrebne dodatne studije koje će razjasniti mehanizme nastanka hipertenzije u PHPT, ispitati i otkriti faktore rizika za nastanak brojnih komplikacija tokom paratireoidektomije, i razjasniti uticaj paratireoidektomije na hipertenziju bolesnika sa PHPT.
Literatura
1. Bilezikian JP. Primary hyperparathyroidism. 2011; (http://www.endotext.org/parathyroid/parathyroid5/parathyroidframe5.htm).
2. Lal G, Clark OH. Primary hyperparathyroidism: controversies in surgical management. Trends Endocrinol Metab, 2003; 14(9):417-22.
3. Marcocci C, Cetani F. Primary hyperparathyroidism. NEJM, 2011; 365(25): 2389-97. 4. Rejnmark L, Vestergaard P, Mosekilde L. Nephrolithiasis and renal calcifications in
primary hyperparathyroidism. J Clin Endocrinol Metab 2011; 96:2377-85. 5. Hedbach G, Tisell LE, Bengtsson BÅ, Hedman I, Oden A. Premature death in patients
operated on for primary hyperparathyroidism. World J Surg 1990; 14:829-36. 6. Hedback G, Ode’n A. Increased risk of death from primary hyperparathyroidism - an
update. Eur J Clin Invest 1998; 28: 277-8. 7. van Ballegooijen AJ, Reinders I, Visser M, Brouwer IA. Parathyroid hormone and
cardiovascular disease events: A systematic review and meta-analysis of prospective studies. Am Heart J, 2013; 165(5):655-64.
8. Fraser WD. Hyperparathyroidism. Lancet, 2009; 374:145-58. 9. Snijder MB, Lips P, Seidell JC, Visser M, Deeg DJ, Dekker JM, et al. Vitamin D status
and parathyroid hormone levels in relation to blood pressure: a population-based study in older men and women. J Intern Med, 2007; 261:558-65.
10. Saleh FN, Schirmer H, Sundsfjord J, Jorde R. Parathyroid hormone and left ventricular hypertrophy. Eur Heart J, 2003; 24:2054-60.
11. Kamycheva E, Sundsfjord J, Jorde R. Serum parathyroid hormone levels predict coronary heart disease: the Tromso Study. Eur J Cardiovasc Prev Rehabil, 2004; 11:69-74.
12. Walker MD, Fleischer JB, Di Tullio MR, Homma S, Rundek T, Stein EM, et al. Cardiac structure and diastolic function in mild primary hyperparathyroidism. J Clin Endocrinol Metab, 2010; 95:2172-9.
13. Potthoff SA, Janus A, Hoch H, Frahnert M, Tossios P, Reber D, et al. PTH-receptors regulate norepinephrine release in human heart and kidney. Regul Pept, 2011;171:35-42.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
178
14. Diamond TW, Botha JR, Wing J. Parathyroid hypertension: a reversible disorder. Arch Intern Med, 1986;146(9):1709–12.
15. Feldstein CA, Akopian M, Pietrobelli D, Olivieri A, Garrido D. Long-term effects of parathyroidectomy on hypertension prevalence and circadian blood pressure profile in primary hyperparathyroidism. Clin Exp Hypertens, 2010; 32(3):154–8.
16. Tordjman KM, Yaron M, Izkhakov E, Osher E, Shenkerman G, Marcus-Perlman Y, Stern N. Cardiovascular risk factors and arterial rigidity are similar in asymptomatic normocalcemic and hypercalcemic primary hyperparathyroidism. Eur J Endocrinol, 2010; 162(5):925–33.
17. Schiffl H, Lang SM. Hypertension secondary to PHPT: cause or coincidence? Int J Endocrinol, 2011; 2011:974647.
18. Kovacs L, Goth MI, Szabolc I, Dohan O, Ferencz A, Szilgyi G. The effect of surgical treatment on secondary hyperaldosteronism and relative hyperinsulinemia in primary hyperparathyroidism. Eur J Endocrinol 1998; 138: 543-7.
19. Gennari C, Nami R, Gonnelli S. Hypertension and primary hyperparathyroidism: the role of adrenergic and rennin-angiotensin-aldosteron systems. Miner Electrol Metab, 1995; 21:77-81.
20. Nuzzo V, Tauchmanova L, Fonderico F, Trotta R, Fittpaldi MR, Fontana MR, et al. Increased intima media thicknes of the carotid artery wall, normal blood pressure profile and normal left ventricular mass in subjects with primary hyperparathyroidism. Eur J Endocrinol 2002; 147:453-9.
21. Nilsson IL, Rastad J, Johansson K, Lind L. Endothelial vasodilatatory function and blood pressure response to local and systemic hypercalcemia. Surgery 2001; 130: 986-90.
22. Živaljević V. Hirurško lečenje oboljenja paraštitastih žlezda. U: Anesteziološki aspekti endokrinih i metaboličkih poremećaja (štitasta žlezda, parštitaste i nadbubrežne žlezde), Medicinski fakultet, Beograd, 2009; 13:225-32.
23. Bilezikian JP, Khan AA, Potts Jr JT. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the third international workshop. J Clin Endocrinol Metab, 2009; 94(2):335-9.
24. Marik PE, Varon J. Perioperative hypertension: a review of current and emerging therapeutic agents. J Clin Anesth 2009; 21:220-9.
25. Varon J, Marik PE. Perioperative hypertension management. Vasc Health Risk Manag 2008; 4:615-27.
26. Kannel WB. Elevated systolic blood pressure as a cardiovascular risk factor. Am J Cardiol 2000; 85:251-5.
27. Franklin SS, Gustin W, Wong ND et al. Hemodynamic patterns of age-related changes in blood pressure. Circulation 1997; 96:308-15.
28. Bachar G, Gilat H, Mizrachi A, Shimon I, Feinmesser R, Kaizerman I, Shpitzer T. Comparison of perioperative management and outcome of parathyroidectomy between older and younger patients. Head Neck, 2008; 30:1415–21.
29. Vincent A, Riggs BL, Atkinson EJ, Oberg AL, Khosla S. Effect of estrogen replacement therapy on parathyroid hormone secretion in elderly postmenopausal women. Menopause, 2003; 10(2):165-71.
30. Prys-Roberts C. Hypertension and anaesthesia – fifty years on. Anaesthesiology 1979; 50:281–4.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
179
31. Howell SJ, Sear JW, Hypertension FP. Hypertensive heart disease and perioperative cardiac risk. Br J Anaesth 2004; 92:570–83.
32. Clough RA, Leavitt BJ, Morton JR, Plume SK, Hernandez F, Nugent W et al. The Eeffect of Comorbid Iillness on Mortality Outcomes in Cardiac Surgery. Arch Surg 2002; 137:428–33.
33. Dimitrijević N, Nešković V, Obrenović-Kirćanski B, Gvozdenović LJ, Diklić A. Cardiovascular complications during anaesthesia in thyroid surgery, in “Proceedings Surgery 2000”, 127-30, Monduzzi Editore, International Proceeding Division, Istanbul, Turkey, 2000.
34. Kalezic N, Stojanovic M, Milicic B, Antonijevic V, Sabljak V, Markovic D, Zivaljevic V. The Incidence of Intraoperative Hypertension and Risk Factors for its Development during Thyroid Surgery. Clin and Exp Hyperten, 2013; 35(7):523-7.
35. Piovesan A, Molineri N, Casasso F, Emmolo I, Ugliengo G, Cesario F, et al. Left ventricular hypertrophy in primary hyperparathyroidism. Effects of successful parathyroidectomy. Clin Endocrinol (Oxf) 1999; 50:321–28.
36. Nilsson IL, Aberg J, Rastad J, Lind L. Maintained normalization of cardiovascular dysfunction 5 years after parathyroidectomy in primary hyperparathyroidism. Surgery, 2005; 137:632–38.
37. Heyliger A, Tangpricha V, Weber C, Sharma J. Parathyroidectomy decreases systolic and diastolic blood pressure in hypertensive patients with primary hyperparathyroidism. Surgery, 2009; 146(6):1042-7.
38. Kovács L, Góth MI, Szabolcs I, Dohán O, Ferencz A, Szilágyi G. The effect of surgical treatment on secondary hyperaldosteronism and relative hyperinsulinemia in primary hyperparathyroidism. Eur J Endocrinol, 1998; 138:543–7.
39. Broulik PD, Horký K, Pacovský V. Blood pressure in patients with primary hyperparathyroidism before and after parathyroidectomy. Exp Clin Endocrinol, 1985; 86:346–52.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
180
ANESTEZIOLOSKI ASPEKTI HIRURŠKOG LEČENJA FEOHROMOCITOMA ANAESTHETHIC ASPECTS IN SURGICAL TREATMENT OF PHEOCHROMOCYTOMA MILENA KAŽIĆ1, NEVENA KALEZIĆ1,2
1Centar za anesteziologiju i reanimatologiju Kliničkog centra Srbije, Beograd,2 Medicinski fakultet Univerziteta u Beogradu
E-mail: [email protected] Summary
Phaeochromocytoma is rare catecholamine-producing tumour.Currative surgery is recommended for these tumours, but it carries a high risk due to life treaatening cardiovascular disturbances during surgery which are provoked by catecholamine release from the tumour.The aim of this review is to describe the problems anaesthesist is confronting with during this type of surgery,and to show our experiences. Uvod Feohromocitomi su tumori koji luče kateholamine. Potiču iz hromafinog tkiva i najčešće(85%) se nalaze u srži nadbubrežne žlezde. Mogu se naći i u ganglijama simpatičnog sistema (15%), kada se nazivaju paragangliomi.Učestalost je 2-8 slučajeva na 100 000 stanovnika godišnje. Medjutim, na obdukcionim serijama je učestalost mnogo veća,od 250 na milion do 1300 na milion na obdukcionoj seriji Mejo klinike.1 Zbog lučenja kateholamina ti tumori ugrožavaju život bolesnika,i uzrok su velikog broja neočekivanih i neobjašnjivih smrti. Jedino efikasno lečenje je hirurško odstranjivanje tumora. Operacija nosi veliki rizik jer se tokom hirurškog pristupa tumoru velika količina kateholamina izbacuje u cirkulaciju. Smrtnost tokom ovih operacija bila je 50-tih godina prošlog veka oko20%2 , da bi se u današnje vreme kretala oko 3%3 do 0%.4,5
Značajno smanjenje perioperativne smrtnosti pripisuje se uvodjenju alfa blokatora u preoperativnu pripremu, otkriću potentnih vazodilatatora za promptno kupiranje intraoperativnih hipertenzivnih kriza, primeni unapredjenog hemodinamskog monitoringa i uznapredovalih tehnika za lokalizaciju tumora.
Preoperativna priprema
Pre operacije ovi se bolesnici pripremaju alfa blokatorima, od kojih je najčešće korišćen fenoksibenzamin (Phenoxybenzamine).6 On ima nekompetitivni i neselektivni karakter vezivanja za alfa 1 i alfa 2 receptore i dugotrajno dejstvo (oko 24h).6 Vazodilatacija koju alfa blokeri izazivaju dovodi do pada arteijskog pritiska, a takođe i do popunjavanja prethodno redukovanog intravaskularnog volumena, zbog vazokonstrikcije uzrokovane visokim nivoima kateholamina. Ovo preoperativno popunjavanje volumena čini dobru rezervu i prevenciju nekontrolisane hipotenzije posle ekstirpacije tumora (jer, kada se tumor izvadi nastupa snažna vazodilatacija i posledična hipotenzija). Uobičajeno trajanje preoperativne pripreme je 2-3 nedelje, ali se u poslednjih nekoliko godina javljaju autori koji zastupaju kraće trajanje preoperativne pripreme-samo do korekcije arterijskog pririska. Preoperativna priprema se može vršiti i selektivnim alfa 1 blokatorima (prazosin, doxazosin, terazosin), a kao dopuna koriste se i drugi medikamenti (beta blokatori, blokatorimi kalcijumovih kanala, sedativi idr). Američki autori daju prednost fenoksibenzaminu,4 a engleski doksazosinu.7
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
181
Neki francuski autori zastupaju davanje nikardipina (nicardipin) 2-3 dana pre operacije, čime se snižava arterijski pritisak, a zatim se pristupa operaciji i arterijski pritisak se intraoperativno kontroliše (takođe nikardipinom) intravenski.3,8Međutim, u ogromnoj većini slucajaeva, svuda u svetu, koristi se fenoksibenzamin, a tako je i u Kliničkom centru Srbije. U literaturi ne postoje kontrolisane randomizovane studije koje bi dokazale koji je metod preoperativne pripreme bolji.
Intraoperativni problemi
Tokom operacije feohromocitoma veoma je važan monitoring. Osim standardnog monitoringa, neophodno je da svaki bolesnik ima arterijsku liniju i monitor koji omogućava kontinuirano invazivno merenje arterijskog pritiska. Veoma je korisno postaviti i centralni venski kateter.
Problemi sa kojima se anesteziolog susreće tokom operacije su: hipertenzija, hipotenzija i poremećaji srčanog ritma (od kojih je najčešći tahikardija).
Hipertenzija može nastati tokom uvoda u anesteziju (najčešće intubacije), ali je češća tokom
preparisanja tumora. Za kupiranje hipertenzije najčešće se koristenatrijum nitroprusid i/ili nitroglicerin,9 a mogu se koristiti i fenoksibenzamin i labetalol. Kao dopuna, mogu se koristitit i manje potentni antihipertenzivi, kao što su nikardipin, magnezijum sulfat, urapidil i dr.
Hipotenzija se javlja posle podvezivanja adrenalne vene, a pogotovu posle ekstirpacije
tumora. Ona može biti veoma duboka (do nemerljivosti), a ako je protrahirana (24-48 sati u postoperativnom periodu), onda je najčešći uzrok morbiditeta i mortaliteta. Kod naših bolesnika nismo zabeležili niži arteijski sistolni pritisak od 60 mmHg. Karakteristika ove hipotenzije da ona vrlo slabo reaguje na vazoaktivne lekove (dopamin, noradrenalin, fenilefrin). To jeverovatno zato što je jedan deo alfa receptora blokiran, a i ukupan broj alfa receptora je smanjen, jer je došlo do nishodne (tzv. down) regulacije receptora usled dugotrajne izloženosti velikoj količini kateholamina u cirkulaciji. Prva linija terapije hipotenzije su velike količine kristaloidnih rastvora, zatim plazma ekspanderi, a ako je neophodno, infuzija inotropnih lekova. Kod naših bolesnika, post-ekstirpacioni sistolni pritisak se kretao od 60-80 mmHg, i uglavnom se regulisao do vrednosti od 90-100 mmHg tokom 10-ak min posle budjenja iz anestezije, a sistolnii pritisak oko100mmHg nije trajao duže od 12-24h posle operacije.
Tahikardija, kao najčešći poremećaj srčanog ritma tokom operacije feohromocitoma, se
kupira beta blokatorima. Lek prvog izbora je esmomolol, zbog mogućnosti najprikladnijeg titriranja doze (kratak poluživot, bez kumulativnog efekta), ali se mogu koristiti i drugi beta blokatori. Kod naših bolesnika najčešće je korišćen metoprolol.5
Iskustva Centra za endokrinu hirurgiju KCS
Svi anesteziolozi koji češće rade ove vrste operacija primetili su da nema svaki bolesnik sa feohromocitomom izražene hemodinamske promene tokom operacije.U našoj seriji od 145 bolesnika, 15-oro njih nije tokom operacije,primilo ni antihipertenzive niti beta blokere, jer nije bilo potrebe. Mi smo, kao i mnogi drugi autori3,4,9,10 pokušali da identifikujemo faktore rizika koji utiču na pojavu značajnih hemodinamskih fluktuacija tokom operacije. Ispitali smo uticaj preoperativne doze fenoksibenzamina, nivoa i vrste preoperativnih urinarnih kateholamina, veličine tumora, karaktera tumora (maligni vs. benigni), dužine operacije, pola, životnog doba i drugih faktora rizika. U našoj seriji, veća dužina trajanja operacije se izdvojila kao jedini

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
182
statistički značajan faktor za pojavuznačajne i produžene hipertenzije (arterijski pritisak>220 mmHg).5
Zaključak
Složenost i kompleksnost preoperativne pripreme, anestezije i neposrednog postoperativnog toka bolesnika podvrgnutih operaciji zbog feohromocitom, nameću imPerativ da ove operacije treba raditi u tercijarnoj zdravstvenoj ustanovi, sa iskusnim timom lekara među kojima postoji tesna saradnja.
Literatura
1. Sutton MG,Sheps SG,Lie JT. Prevalence of clinically unsuspected pheochromocytoma.review of a 50 year autopsy series Mayo Clin Proc 1981;56:354 2. Apgar V, Papper EM. Pheochromocytoma: anesthetic management during surgical treatment.
Arch Surg 1951;62:634-648. 3. Lebuffe G, Dosseh ED, Tek G. The effect of calcium channel blockers on outcome following the surgical treatment of pheochromocytomas and paragangliomas. Anaesthesia 2005 ; 60 : 439-444. 4. Kinney MAO, Warner ME, vanHeerden JA, et al. Perianesthetic risks and outcomes of pheochromocytoma and paraganglioma resection. Anesth Analg 2000 ; 91 : 1118–1120 5. Kazic M, Zivaljevic V, Milan Z, Paunovic I. Perioperative risk factors, morbidity, and outcome of 145 patients during phaeochromocytoma resection. Acta Chir Belg 2011; 111:223-71. 6. Roizen MF, Hunt TK, Beaupre PN, et al. The effect of alpha-adrenergic blockade on cardiac performance and tissue oxygen delivery during excision of pheochromocytoma. Surgery 1983; 94:941-5. 7.Prys-Roberts C: Pheochromocytoma – recent progress in its managemant.Br J Anaesth 2000; 85: 44-57 8. Lentschener C et all. Increased arterial pressure is not predictive of haemodynamic instability in patients undergoing adrenalectomy for phaeochromocytoma. Acta Anaesthesiol Scandin 2009; 53:522-7 9. Tauzin-Fin P, Sesay M, Gosse P, Ballanger P. Effects of perioperative α1 block on haemodynamic control during laparoscopic surgery for phaeochromocytoma. Br J Anaesth 2004; 92:512-7. 10. Atallah F,Bastide-Heulin T,Soulie M, et al. Haemodynamic changes during retroperitoneoscopic adrenalectomy for phaeochromocytoma.Br J Anesth 2001; 86:

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
183
LIVER TRANSPLANTATION: THE ANAESTHESIOLOGIST'S AGONY ELENI KATSIKA Hippokratio Hospital Thessaloniki, Greece
Liver transplantation is a long lasting very demanding operation and many unexpected events can take place during the whole procedure. The anesthetic working environment is often complex and dynamic place and range of tasks both mental and practical are required to be undertaken simultaneously1. When life and death decisions are made under these conditions, human error, lack of appropriate equipments or equipments failure and organizational disturbances can lead to disastrous consequences2. The agony of the anesthesiologist is to minimize human error by limiting factors that decrease vigilance as well as by early recognition of preventable events. So, safe “working conditions”, appropriate preoperative evaluation of the patients with end stage liver disease, point of care intraoperative monitoring and careful intraoperative anesthetic management are mandatory for improving patients care and outcome in liver transplantation. Besides the complexity of the operation, most patients have an already disturbed physiology because liver disease has affected all major organ systems.Τhe knowledge of management of some special critical situations during liver transplantation contribute significantly for decreasing morbidity and mortality of the patients.
Working conditions Anesthesiologists work round the clock to provide efficient and timely services and universally are the “sleep providers in a sleep debt themselves. A fatigued anesthesiologist results in impaired judgment, late and inadequate responses to clinical changes, poor communication and inadequate record keeping. The implications of sleep debt on patient safety are profound and preventive strategies are very essential3. The anesthesiologists role of monitoring the patient in a vigilant manner may be particularly vulnerable to the effects of fatigues. The word “vigilance” is the motto of anesthetic specialty. If anesthesiologist becomes disengaged from his/her environment (such as “microsleep” that happen when he/she is sleep-deprived) all vigilance is lost4. Humans are programmed for two periods of least vigilance between 3-7 am and 1-4pm every day and the maximal alertness is approximately 9-11am and 9-11pm5. Although, liver transplantation is an emergency operation, it can be planned to be performed during the day for patients safety and better overall outcome. Liver transplantation is the definition of “team work”. Anaesthesiologists, surgeons and nurses, healthcare professionals from different disciplines, share common patients and goals. They have to collaborate in an effort to improve the overall care-giving experience through coordination, communication and responsibility.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
184
Preoperative assessment Cardiovascular system. Cirrhotic patients are characterized by hyperdynamic circulation
Coronary artery disease (CAD). The last decade the criteria for orthotopic liver transplantation (OLT) have expanded, so the prevalence of CAD in patients with cirrhosis is much greater, than previously believed. CAD is found in 27% of patients over 50 years old, referred for liver transplant evaluation6. Dobutamine stress ECHO has been shown to be sensitive and specific for diagnosing CAD in patients with multiple cardiac risk factors, undergoing OLT. The most common risk factors for CAD, in liver transplant candidates are: age >50 years, male gender diabetes and obesity. In addition, altered lipid metabolism and other unknown factors make cirrhosis an independent risk factor. The presence of two or more factors (other than age) places patients of moderate to severe risk of CAD. A diagnosis of non-alcoholic steatohepatitis independently increases the risk of CAD7,8. In patient with symptomatic CAD, 3 year mortality is reported to be as high as 50%, and those with left ventricular systolic dysfunction are poor candidate for OLT8,9.
Cirrhotic cardiomyopathy is defined as “form of chronic cardiac dysfunction in patients with cirrhosis, characterized by blunted contractile responsiveness to stress, and/ or altered diastolic relaxation with electrophysiological abnormalities in the absence of other known cardiac disease”. Most of cirrhotic cardiomyopathy are not clinically obvious and patients are asymptomatic because of the cirrhotic pathophysiology. The diagnosis is performed by two-dimensional ECHO, ECG (prolonged QT interval) and serum markers (brain natriuretic peptide, levels of cardiac troponin 1)10. The use of non-selective b-blockers has been assessed in cirrhotic patients with prolonged QT interval. During the OLT, the rapid increase in arterial pressure and systemic vascular resistance in the postreperfusion period may uncover undiagnosed cardiomyopathy. Patients who survive the initial post transplant period have a complete reversal of both diastolic and systolic dysfunction at a mean time of 9 months post-transplant11. Respiratory system The pulmonary complications associated with liver disease, include restrictive lung disease, intrapulmonary shunts, ventilation – perfusion (V/Q) abnormalities and pulmonary hypertension.
Hepatopulmonory syndrome: Hypoxemia occurring in the absence of ascites or intrinsic lung disease is referred as hepatopulmonary syndrome (HPS). A contrast (bubble) ECHO may define the cause of room hypoxemia. Although HPS resolves after transplantation, the persistence of hypoxemia with 100% oxygen administration is a contraindication for OLT.
Porto Pulmonary hypertension (PPHTN):Porto-pulmonary hypertension is an elevation in pulmonary artery pressures, evolving in the presence of portal hypertension and in the absence of any other known causes of pulmonary hypertension. This occurs in 1% of patients with portal hypertension and probably more often in adult liver recipients TEE or transthoracic ECHO in expert hands should detect PPHTN, but it may appear after listing. Repeated echo every 6-12 months is recommended. The mPAP >50mmHg may not be a contraindication for OLT, if right
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
185
ventricular function is preserved. Patients with PPHTN must be treated before OLT and should be reevaluated after the treatment for its efficacy12. Severe PPHTN (mPAP >50mmHg) is associated with prohibitive preoperative mortality, because of right heart failure during surgery. Epoprostenol has been shown to improve pulmonary hemodynamics in PPHTN and inhaled nitric oxide or nitrates seem to be less effective alternatives. Oral alternatives are endothelin receptor antagonists and phosphodiertarase inhibitors12. Severe PPHTN (mPAP>40mmHg), beside the administration of epoprostenol, is a contraindication for OLT12. Coagulation Coagulation defects result from multiple causes, including quantitative and qualitative platelets defects, decreased synthesis of procoagulant and anticoagulant factors, vitamin K deficiency, synthesis of abnormal clotting factors, decreased clearance of activated factor fibrinolysis and disseminated intravascular coagulation (DIC). The decreased synthesis of anticoagulants is responsible for the hypercoagulable state that is occasionally found in cirrhotic patients and demonstrated by thromboelastograph (TEG) and not by PT or a PTT13,14. Intraoperotive management
Monitoring Full invasive monitoring including direct arterial blood pressure, central venous pressure and pulmonary artery pressure are obligatory. TEE is used for cardiac monitoring and has proved sensitive in detecting altered myocardial function and empolization of air or thrombus in OLT. Coagulation monitoring is essential. Thromboelastography (TEG) is a sensitive bedside technique, quantifying the rate and quality of fibrin formation, platelet function and fibrinolysis14. Post reperfusion syndrome During OLT, a marked decrease in blood pressure following unclamping of the portal vein and liver reperfusion is frequently observed and is termed postreperfusion syndrome (PRS). Predictors of PRS are cold ischemia time, marginal donors, large grafts and hyperkalemia in pre and postreperfusion period15,16,17. PRS must be differentiated (even though is not so easy) from vasoplegic syndrome which characterized by hypotension, tachycardia, low PCWP and PVR and high cardiac output. In vasoplegic syndrome, for patient who do not respond to noradrenaline, methylene blue is a logical therapeutic choice18,19. Transfusion requirements Historically significant blood loss at the time of OLT has been treated with large autologous transfusion of packed red blood cells (RBC), fresh frozen plasma (FFP), platelets and cryoprecipitate. Transfusions, however – especially large volume transfusions – are associated with a range of complications so, alternative therapies and approaches to transfusion are being investigated in transplantation20.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
186
Antifibrinolytic drugs
Hyperfibrinolysis plays a significant role in non-surgical blood loss requiring massive transfusion. Antifibrinolytics will decrease bleeding only in cases where it is caused by enhanced fibrinolysis. They are potentially harmful and they must be used only under TEG monitoring in patients with prothrombotic states like Budd-Chiari Syndrome, retransplantation, primary biliary cirrhosis, primary sclerosing cholangitis, transplant for malignancy, portal rein thrombosis.Of the two groups of antifibrinolytics available, lysine analogues (epsilon aminocoproic acid (EACA) and tranexamic acid) are more commonly used. Epsilon aminocaproic acid (EACA) has been used intraoperatively to inhibit fibrinolysis. It has been found effective for decreasing blood requirements in some studies but not in others. Tranexamic acid prevents plasmin-mediated conversion of fibrinogen to fibrinogen split products by competitively binding to the lysine binding sites on the plasminogen molecule. Comparing with EACA, tranexamic acid is 6-10 times more potent. Fibrinogen concentrate Fibrinogen levels in cirrhotic patients are reduced due to both decreased synthesis and increased turnover. The best and safest treatment in clinically relevant fibrinogen deficiency is the replacement with fibrinogen concentrate. A targeted fibrinogen increase by 1g/L requires the fibrinogen concentrate to be dosed at 50mg/kgr. It is crucial to maintain the fibrinogen concentration in the normal range in the presence of thrombocytopenia for avoiding bleeding. Before the application of fibrinogen concentrate, hyperfibrinolysis should be stopped with antifibrinolytics, because otherwise the generation of fibrin and fibrinogen degradation products will be amplified by fibrinogen administration and coagulation disorder may be exacerbated20. Prothrombine Complex Concentrate (PCC) Whereas fibrinogen concentration and the platelets are the most important determinants of clot firmness, the other clotting factors are responsible for the rate of thrombin generation. Transfusion of FFPs overcomes this problem. A major disadvantage of transfusion of FFPs is volume overload. PCC are hemostatically active highly purified concentrates, prepared from pooled plasma. They contain four vitamin-K dependent clotting factors (II, VII, IX, X). A major advantage of PCC is their low volume blood and quick normalization of prothrombine time (PT)21. Recombinant factor VIIa (Novo Seven) FVIIa is used in off-label status in clinical situations with manifested diffuse bleeding, which cannot be stopped by standard therapy. The recommended dosage is 90µg/kg. If the treatment is not sufficient, repetition of administration is required after 15 minutes. It is necessary to repeat the treatment after 1 to 3 hours because of the short half-life time of rFVIIa13.
Preconditions for the off-label use of rFVIIa are: - massive diffuse bleeding - pH > 7,2 - no heparin effect - no hyperfibrinolysis

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
187
- fibrinogen > 150mg/dl - platelets > 80.000µl
Besides all these managements and interventions, hypothermia, acidosis, hypocalcaemia and anemia deteriorate the preconditions of haemostasis, significantly. Thus, hypothermia at a body core temperature below 35oC has to be avoided and treated.Many coagulation factors have their optimum pH in alcaline conditions, so acidosis may leads to a significant reduction in thrombin generation. Anemia with a Hb < 8gr/dl can influence primary haemostasis significantly. Therefore, patients with manifested diffuse bleeding should have at least Hb 8-10gr/dl. Finally, monitoring of Ca++ and administration of CaCl2 is mandatory, as large amounts of FFPs may lead to hypocalcaemia with a concentration of lionized calcium of less than 1mol/lt. Beside the anticoagulational effect, hypocalcaemia can impact essentially the cardiovascular system, too. Special Situations Fulminant Hepatic Failure
Fulminant hepatic failure is frequently associated with brain edema and concominant intracranial hypertension. The placement of an epidural intracranial catheter is sometimes very useful for monitoring intracranial pressure (ICP). Non invasive methods of assessing cerebral hemodynamics include transcranial Doppler Ultrasonography and jugular venous oximetry. The intraoperative anaesthetic targets are: ICP to be maintained below 20mmHg and cerebral perfusion pressure (CPP = MAP-ICP) above 60mmHg. The targets can be achieved by hyperventilating the patients, fluid restriction, and by administering mannitol and muscle relaxants as needed. These patients are characterized by hypoglycemia, severe coagulopathy and cardiovascular instability. Inotropes are usually necessary and administration of FFP or rFVIIa (80γ/kgr) are mandatory for correction the coagulopathy, especially prior to the placement of the ICP monitor. Hypothermia (33o – 35oC) is induced, if ICP remains high. Cerebral edema with sustained elevation of ICP and decrease in CPP(<40mmHg) unresponsive to conventional therapy, irreversible brain damages, uncontrolled extrahepatic sepsis and multiorgan failure are contraindication to O.L.T. References
1. Leedal JM, Smith AF. Methodological approaches to anaesthetists’ workload in the operating theatre. British Journal of Anaesthesia, 2005;94:702-709.
2. Aggarwal R, Undre S, Moorthy K, Vincent C, Darzi A. The simulated operating theatre: comprehensive training for surgical teams. Quality and safety in health care , 2004;13:i27-i32
3. Sinha A, Singh A, Tewari A. The fatigued anesthesiologist: A threat to patient safety? J Anaesthesiol Clin Pharacol, 2013;29:151-159.
4. Howard S. Fatigue and the practice of anesthesiology. www. Apsf.org/newsletters, 2005. 5. Cao C, Weinger M, Slagle J, et al. Differences in day and night shift clinical performance
in anesthesiology. Human factors, 2008;50:276-290. 6. Keeffe B, Valantine H, Keeffe E. Detection of coronary artery disease in liver transplant
candidates. Liver transplantation 2001;7:755-761.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
188
7. Ehtisham J, Altieri M, Salame E, et al. Coronary artery disease in orthotopic liver transplantation: pretransplant assessment and management, Licer transplantation, 2010;16:550-557.
8. Mandell M.S, Lindenfeld J, Tsou M, et al. Cardiac evaluation of liver transplant candidates. World J Gastroenterology, 2008;14:3445-3451.
9. Appleton C, Hurst T. Reducing coronary artery disease events in liver transplant patients: moving toward identifying the vulnerable patient. Livet transplantation, 2008;14:1691-1693.
10. Biancofiore G, Mandell M , Rocca G. Perioperative considerations in patients with cirrhotic cardiomyopathy. Current opinion in anaesthesiology, 2010;23:128-32
11. Wong F. Cirrhotic cardiomyopathy. Hepatol int, 2009;3:294-304. 12. Ozier Y, Klinck J. Anesthetic management of liver transplantation. Current opinion in
anaesthesiology, 2008;21:391-400. 13. Goerlinger K.. Coagulation management during liver transplantation. Hamostaseologie
,2006; 3a:S64-S75. 14. Hakan F, Gieseler R, Akiz H, et al. Delicate balance of bleeding and thrombosis in end-
stage liver disease and liver transplantation. Digestion, 2013;88:135-144. 15. Paugam-Burtz C, Kavafyan J, Merckx P et al. Postreperfusion syndrome during liver
transplantation for cirrhosis: Outcome and predictors. Liver transplantation, 2009;15:522-529
16. Xia V, Ghobrial R, Du B et al.Predictors of hyperkalemia in the prereperfusion, early postreperfusion annd late postreperfusion period during adult liver transplantation. International anesthesia research society, 2007;105:780-785.
17. Xia V, Obaidi R, Park C, et al. Insulin therapy in doses with blood transfusion versus large bolus doses in patients at high risk for hyperkalemia during liver transplantation. Journal of cardiothracic and vascular anesthesia, 2010;24:80-3.
18. Cao Z, Cao Y, Tao G. Vasoplegic syndrome during liver transplantation.International anesthesia researsh society, 2009;108:1941-1943
19. Shanmugam G. Vasoplegic syndrome-the role of methylene blue. Eur. J. CCardiothorac. Surg., 2005;28:705-710
20. Goodnough L, Shander A. Current status of pharmacologc therapies in patient blood management. Anesthesia and analgesia, 2013;116:15-34.
21. Arshad F, Ickx B, R. T van Beem et al. Prothrombin complex concentrate in the reduction of blood loss during orthotopic liver transplantation: PROTON-trial. BMC surgery, 2013;13:22.
Proposed References 1. R. Steadman. Anesthesia for liver transplant surgery. Anesthesiology Clin. N. Am. 2004;687-711. 2. K. Kohn. Pitfalls in anethesia for liver transplantation. Transplantation proceedings , 2000;32:1515-6. 3. J. Manley, J. Plotkin, J. Yosaitis et al. Controversies in anesthetic management of liver transplantation. HPB(oxford), 2005;7:183-5. 4. K. Murray, R. Carithers. AASLD Practice guidelines : Evaluation of the patient for liver disease. Hepatology, 2005;41:1-26. 5. G. Biancofiore, M. Mandell, G. Rocca. Perioperative considerations in patients with
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
189
cirrhotic cardiomyopathy. Current opinion in anaesthesiology, 2010;23:128-32 6. Z. Raval, M.Harinstein, A.Skaro et al.Cardiovascular Risk Assessment of the Liver Transplant Candidate .J Am Coll Cardiol, 2011; 58:223-31 7. M.Mandell, J. Lindenfeld, Mei-Yung Tsou, et al.Cardiac evaluation of liver transplant candidatesWorld J Gastroenterol 2008 June 14; 14(22): 3445-3451 8. R. Planinsic, R. Raducu, B. Eghtesad et al. Diagnosis and treatment of intracardial thrombosis during orthotopic liver transplantation. Anesth analg, 2004;99:353-6 9. C. Paugam-Burtz, J. Kavafyan, P. Merckx et al. Postreperfusion syndrome during liver transplantation for cirrhosis: Outcome and predictors. Liver transplantation, 2009;15:522-9 10. V.Xia,R.Ghobrial,B.Du et al.Predictors of hyperkalemia in the prereperfusion, early postreperfusion annd late postreperfusion period during adult liver transplantation. International anesthesia research society, 2007;105:780-5 11. Z. Cao, Y. Gao, G. Tao. Vasoplegic syndrome during liver transplantation.International anesthesia researsh society, 2009;108:1941-3 12. G. Shanmugam. Vasoplegic syndrome-the role of methylene blue. Eur. J. CCardiothorac. Surg., 2005;28:705-10 13. V. Xia, R. Obaidi, C. Park et al.Insulin therapy in doses with blood transfusion versus large bolus doses in patients at high risk for hyperkalemia during liver transplantation. Journal of cardiothracic and vascular anesthesia, 2010;24:80-3 14. V. Olcese. Transfusion requirements in liver transplantation. Emedicine.medscape,2011 15. M. Senzolo, P. Burra, E. Cholongitas. New insights into the coagulopathy of liver disease and liver transplantation. World j. Gastroenterol, 2006;12:7725-36.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
190
MANAGEMENT OF BLEEDING AND COAGULOPATHY DURING ORTHOTOPIC LIVER TRANSPLANTATION MATEA BOGDANOVIĆ DVORŠČAK,TAMARA LUPIS,VANJA CRNICA Department of anesthesia and intensive care, KB Merkur, Zagreb, Croatia E-mail:[email protected]
Introduction
Orthotopic liver transplantation (OLT) is the biggest challenge in sustaining hemodynamic and hemostatic balance in the organism of a patient with end stage liver disease. A new dynamic bond between low levels of pro coagulant and anticoagulant factors results in a small hemostatic reserve.1Longer lasting procedures combined with extensive trauma and severe blood loss can easily distort the hemostatic balance. Blood loss and transfusion requirements depend on etiology and severity of liver disease, preoperative coagulation function, clinical status of the recipient, quality of the donor liver and experience of the transplantation team.2,3 The amount of blood loss often surpasses the definition of massive bleeding.4Whilethe average amount of blood loss has gradually been reduced over the past years, neither conventional nor point-of-care tests enable foreseeing the amount of blood loss for an individual patient. Conventional tests include prothrombin time (PT), international normalized ratio (INR), activated partial thromboplastintime (APTT), thrombocyte number (Tr) and fibrinogen, while point-of-care tests (POC) refer tothromboelastography (TEG) and rotation thromboelastometry(ROTEM).5,6 Understanding the specificitiesof stages of OLT is what enables adequate care. It is thus necessary to frequently repeat tests following a coagulation intervention and reinterpret results with respect to current surgical situation. There is a substantial variability between transplant centers in perioperative transfusion therapy during OLT.7The differences in coagulation surveillance between transplantation centers contribute to differing transfusion treatment during OLT.8 Transfusion of erythrocytes and thrombocytes is an independent predictor of a poor OLT outcome.9Any method that may contribute to reduce empirical, often excessive transfusion treatment would be more than helpful. Administration of blood and derivatives during OLT may be reduced by using ROTEM/TEG tests. Goerlinger and all. demonstrated in a retrospective study an 89% reduction in administering FFP, as well as a 60% and 58% decrease in the expenditure of erythrocytes and thrombocytes, respectively.10
Liver and hemostasis
Most of the proteins involved in the hemostatic system are synthesized in the liver, namely, pro-coagulant proteins (fibrinogen, FXI, factors that depend on vitamin K (II, VII, IX, X)) and anticoagulant proteins (antithrombin, proteins that depend on vitamin K (protein C, protein S)). All profibrinolytic (plasminogen) and antifibrinolytic (α2- antiplasmin) proteins, except for tissue plasminogen activator (tPA), are also synthesized in the liver.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
191
Liver disease and hemostasis
When liver function is lowered due to acute or chronic failure, the hemostatic system can be severely disrupted. Coagulation disorders that can result in bleeding include thrombocytopenia, disorder of thrombocyte function, reduced levels of coagulation factors,hypofibrinogenemia and low levels of antifibrinolitics (α2- antiplasmin). There is a simultaneous reduction in the levels of anticoagulant proteins (antithrombin, protein C, protein S) and the profibrinolytic protein (plasminogen), while the level of coagulation factor VIII (FVIII) is increased. All of this moves the balance towards hemostasis.As the liver failure progresses further the delicate balance between bleeding and coagulation is repeatedly reestablished. But, unlike in a healthy liver, the reserve of a patient with advanced liver failure is relatively small and likely to decompensate in either direction-bleeding or thrombosis, especially with added influence of contributing factors (e.g. sepsis, surgical procedure, renal failure…).11 In fact, contrary to the traditional notion of increased bleeding tendency in liver disease, there is increasing evidence of pro-thrombotic imbalance resulting in peripheral or portal venous thrombosis and liver fibrosis.12 Conventional tests (PT, INR, APTT, Tr and fibrinogen) are not sensitive to detect deficits in anticoagulant proteins. They can only detect deficits of pro coagulant factors and therefore suggest a hypocoagulabile state.13,14 Budd-Chiari syndrome (protein C deficit), autoimmune hepatitis (AIH) and chronic inflammation of biliary tract are at larger risk of thrombotic incidents. Patients with acute liver failure (ALF) have a decrease in coagulation factors coupled with an extremely severe fibrinolysis disorder, which explains a higher risk of thrombotic complications.12On the other hand, patients with Wilson’s disease, viral hepatitis (HCV, HBV), hemochromatosis and toxic liver diseases (e.g. alcohol) have a higher risk of bleeding.
Management of bleeding and coagulopathy during orthotopic liver transplantation
Factors like hypothermia, ionized hypocalcaemia and pH changes may impair coagulation.15 Hypothermia induces coagulopathy. A core temperature of ≤34°C inhibits thrombin generation, fibrinogen synthesis and platelet function, and increases fibrinolysis. Even mild hypothermia (>35.5°C) increases blood loss for around 16%, and the relative risk for transfusion for around 22%.16 Acidosis (pH<7.1) inhibits thrombin generation and platelet function, while accelerating degradation of fibrinogen. A pH decrease from 7.4 to 7.0 can reduce factor VII (FVII) activity in vitro by >90% and TF/FVIIa complex activity by >60% (tissue factor/activated factor VII complex).17Reversal of acidosis does not correct acidosis-induced coagulopathy.In other words, pH correction and treatment of acidotic coagulopathy should be performed simultaneously. Calcium ions (Ca2+) enhance fibrin polymerisation, coagulation factor activity and platelet activity. Activated factor VII (FVIIa) activity is calcium dependent. Ca2+ concentrations had an inverse concentration-dependent relationship with mortality of patients with critical bleeding requiring massive transfusion. Both acidosis and the amount of fresh frozen plasma transfused

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
192
were the main risk factors for severe hypocalcaemia.18,19During massive transfusion, calcium should be administered if Ca2+ concentration falls below the value 0.9 mmol/Lrequired for adequate coagulation. Red blood cells (RBC) are considered to be positioned centrally in a blood vessel, while blood platelets are mainly concentrated near the wall.20At high hemoglobin concentrations, erythrocytes congregate in the inner lumen of blood vessels, resulting in localization of thrombocytes at the vessel wall. This may improve clot formation. Furthermore, erythrocytes stimulate thrombin generation, thereby providing material for clot formation.21Although there is no consensus about transfusion trigger; most transplant centers use hemoglobin level of 70-90 g/L as threshold for RBC transfusion during active bleeding.22,23,24,25,26 Traditionally, liver transplantation is divided in four stages:
♣ preanhepatic phase ♣ anhepatic phase ♣ neohepatic or postreperfusional phase ♣ postoperative phase
♣ Preanhepaticphase– hepatectomy
Removing abdominal adhesions and cutting through numerous collateral blood vessels (portocaval shunts) for liver mobilization results in extensive surgical trauma during this stage. “Surgical” bleeding is the main characteristic of this stage. The blood loss correlates with a degree of “surgical” severity. Coagulopathy progresses mainly due to dilution and depletion of coagulation factors. Both pro-coagulant and anticoagulant levels are diminished. “Prophylactic” administration of blood and derivatives before and during OLT is still practiced in many transplantation centers. Excessive volume replacement, including administering fresh frozen plasma (FFP), can paradoxically contribute to further blood loss as central venous pressure (CVP) and pressure in portal circulation increase. Volume reduction combined with vasopressor treatment and transfusion protocol implementation can result with reduced transfusion requirements.23On the other hand, extreme volume reduction can aggravate renal failure.27 Optimization of cardiac preload throughout the surgical procedure appears beneficial to the patient. Recent Guidelines from the European Society of Anesthesiology for management of severe perioperative bleeding recommend against the use of central venous pressure and pulmonary artery occlusion pressure as the only variables to guide fluid therapy and preload during severe bleeding.Dynamic assessment of fluid responsiveness and non-invasive measurement of cardiac output should be considered instead. Replacement of extracellular fluid losses with isotonic crystalloids and iso-oncotic colloids, such as human albumin and hydroxyethyl starch, in a timely and protocol-based manner is recommended.28 When using colloids, third-generation starch solutions are recommended because of their smaller effect on coagulation and blood loss compared with second-generation starches.29,30
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
193
Usually the cell salvage use is recommended when the anticipated blood loss is 20% or more of the patient’s estimated blood volume. Because of the difficulty associated with the accurate prediction of substantial blood loss and the possible need for allogenic transfusion, in the majority of cases it would be appropriate to set up the cell salvage device in a “stand-by” mode.31
Utilization of intraoperative blood salvage and autologous blood transfusion is an important method required to reduce the need for allogenic blood and the associated complications during OLT.32Blood should be collected for autotransfusion only after ascitic fluid has been removed and should cease once the suturing of biliary anastomosis begins. Cell salvage autotransfusion during OLT in patients with liver tumor is controversial. The presence of hepatocellular carcinoma is considered a contraindication for the use of blood salvaging techniques due to theoretical risk of reintroducing neoplastic cells into the circulation and disseminating the tumor. In 1986 the American Medical Councils stated that cell salvage was contraindicated in cases of malignancy.33Others recommend cell salvage autotransfusion during hepatocellular tumor surgery when the risk of major bleeding is significant.34,35,36 ♣ Anhepatic stage – from hepatal vasculature occlusion to new liver reperfusion Although all of the major blood vessels are surgically clumped with consequently limited blood loss, major hemorrhage is still possible. This is mainly a consequence of termination in the synthesis of coagulation factors synthesis as well as certain extent off coagulation factors consumption. At the same time, tPAlevels are increased, as it is released from highly damaged endothelial cells and as there is a lack of tPA clearance because of absence of liver perfusion. All of this may shift the balance of coagulation towards hiperfibrinolisys and lead to massive bleeding.37,38 Currently, antifibrinolytic drugs are used for treatment of fibrinolysis (evident from microvascular oozing or TEG/ROTEM clot lysis measurement) and not for routine prophylaxis.28Another subject that deserves further attention is optimal dosing of antifibrinolytic drugs in liver transplant recipients. Various dosing schemes have been used in different studies and the total amount of drug administered per patient may differ accordingly. Future studies should aim at identifying the lowest effective doses.39
In severe bleeding, fibrinogen reaches critical concentrations early on, and hemorrhagic tendency is increased when fibrinogen concentration is <1.5–2 g/L.40,41,42,43The Rahe-Meyer study shows that administering concentrates of fibrinogen optimizes coagulation, reduces perioperative bleeding and significantly reduces transfusion.44,45A recent recommendation is that either plasma fibrinogen concentration of <1.5–2.0 g/L or ROTEM/TEG signs of functional fibrinogen deficit should be triggers for fibrinogen substitution.28
Another characteristic of the anhepaticphase is a progression in metabolic acidosis, hypocalcaemia and hypothermia. If not continuously and consistently corrected, this derangement can lead to a complete breakdown of hemostasis. ♣ Neohepatic or post reperfusion stage– begins with the release of vascular clump from
portal vein and inferior v. cava. This stage is marked with hemodynamic instability and hyperkalemia following releasing of the clump, and persisting during several continuous measurements. Coagulopathy may occur during
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
194
this stage as well. This is possibly a consequence of endogenous heparinoids and fibrinolytic substances from ischemic donor liver.46 The possibility of hyperfibrinolysis after reperfusion is approximately 60%. In one third of the cases, there can be a spontaneous recovery of hyperfibrinolysis due totPA uptake and synthesis of tPA inhibitors in the new liver. In remaining two thirds of patients a diffuse bleeding caused by fibrinolysis occurs and does not recover spontaneously, hence requiringantifibrinolytic treatment.47 Residual heparin, used to heparinize the donor liver prior to explanation may also be found in the receivers’ circulation and adds to probability of bleeding. Thrombocytopenia usually occurs as thrombocytes are sequestrated in sinusoids of donor liver. The discrepancy in the number of thrombocytes between arterial and venous circulation can be up to 50%. Consequently, microvascular diffusion bleeding may occur. The degree and duration may vary, depending also on the quality of the donor graft, which sometimes can cause uncontrollable diffuse bleeding in the first few minutes following reperfusion. Two randomized controlled trials (RCTs) investigated prophylactic rFVIIa inOLT.Both of them demonstrate a correction of INR but not a reduction in transfusion.48,49Off-label ‘rescue’ therapy with rFVIIa may help control hemorrhage. However, systematic reviews show no mortality reduction but increased risk of arterial thromboembolism. Recombinant activated factor VII (rFVIIa) should be used only as rescue therapy for uncontrolled bleeding. Prerequisites that must be met for successful use of rVIIa are pH > 7,2, fibrinogen> 1,5 – 2g/L and Tr> 50x 109/L.50,51
Usually in the first 30-90 minutes after reperfusion hemodynamic and coagulation stabilization occurs, together with a spontaneous recovery of hyperfibrinolysis. ♣ Postoperative stage Thrombocytopenia caused by hypersplenism and utilization and activation of thrombocytes inside the new liver gradually recovers in about 14 days.52 Early recovery of coagulation factors and postponed recovery of anticoagulant proteins can lead to hypercoagulability in some patients.53Postoperative prophylaxis of thromboembolic complications with low-molecular-weight heparin (LMWH) is not common in all transplantation centers. Recent studies support prophylactic doses of LMWH.54Patients with Budd-Chiari syndrome (deficit of protein C) are still at risk of hypercoagulability after OLT. Thus anticoagulant therapy is usually introduced (e.g. therapeutic doses of LMWH followed by peroral anticoagulants).
Occasionally extensive bleeding may also occur in this stage. Treatment depends on etiology (revision in case of “surgical bleeding” or specific treatment in case „coagulation bleeding” appears). In case of extensive coagulation bleeding the “off label” administration of rFVIIa remains a last resort.50

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
195
Conclusion
Blood loss and transfusion requirements depend on the etiology and severity of liver disease, preoperative coagulation function, clinical status of the recipient, quality of the donor liver and experience of the transplantation team. Blood loss during OLT cannot be predicted. The understanding that perioperative blood loss and blood transfusions may have a negative impact on postoperative outcome has contributed to develop various strategies to reduce blood loss. During past years considerable progress has been made on properly balancing intraoperative fluid, preventing and treating clotting abnormalities as well as on tailoring the transfusion triggers.A precise correction of coagulation disorders can be achieved in a suitable time frame by using point-of-care coagulation monitoring devices, thus decreasing the consumption of blood derivatives during liver transplantation. Intraoperative blood salvage and auto-transfusion can further contribute to reducing the requirement for heterologous transfusion. Presently, more and more OLT are performed without any blood or blood derivatives transfused and with satisfactory outcomes. Reference List 1. Lisman T, Porte RJ: Rebalanced hemostasis in patients with liver disease: evidence and clinical consequences. Blood 2010 Aug 12;116(6):878–85. 2. Feltracco P,Brezzi M, Barbieri S, et al. Bleeding and autotransfusion in liver transplantation, World J Hepatol 2013 January 27; 5(1): 1-15. 3. Agarwal A, Sharma N, Vij V. Point-of-care coagulation monitoring duringlivertransplantation. TrendsAnaesthCrit Care. 2013;3(1):42-48. 4. Martinowitz U, Michaelson M. IsraeliMultidisciplinaryrFVIIaTaskForce. Guidelines for the use ofrecombinantactivatedfactor VII (rFVIIa) inuncontrolledbleeding: a reportbytheIsraeliMultidisciplinaryrFVIIaTaskForce. J ThrombHaemost. 2005 Apr;3(4):640-8. 5. Feltracco P, Brezzi M, Barbieri S, et al.Bloodloss, predictorsofbleeding, transfusionpracticeandstrategiesofbloodcellsalvagingduringlivertransplantation. World J Hepatol.2013 Jan 27;5(1):1-15. 6. Steib A, Freys G, Lehmann C, Meyer C, Mahoudeau G. Intraoperativebloodlossesandtransfusionrequirementsduringadultlivertransplantationremain difficult to predict. Can J Anaesth. 2001 Dec;48(11):1075-9. 7. Ozier Y, Pessione F, Samain E, Courtois F. FrenchStudy Group on Blood Transfusionin Liver Transplantation. Institutional variability intransfusionpractice for livertransplantation. AnesthAnalg. 2003 Sep;97(3):671-9. 8. Coakley M, Reddy K, Mackie I, Mallett S.Transfusiontriggersinorthotopiclivertransplantation: a comparisonofthethromboelastometryanalyzer, thethromboelastogram, andconventionalcoagulationtests. J CardiothoracVascAnesth. 2006 Aug;20(4):548-53. 9. de Boer MT, Christensen MC, Asmussen M, et al. Theimpactofintraoperativetransfusionofplateletsand red bloodcells on survivalafterlivertransplantation. AnesthAnalg. 2008 Jan;106(1):32-44. 10. Gorlinger K, Dirkmann D, Müller-Beissenhirtz H, Paul A, Hartmann M, Saner F: Thromboelastometry-based perioperative coagulation management in visceral surgery and liver transplantation: experience of 10 years and 1105 LTX. Liver Transpl 2010 June;16:S86.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
196
11. Lisman T, Porte RJ. Rebalancedhemostasisinpatientswithliverdisease: evidenceandclinicalconsequences. Blood. 2010 Aug 12;116(6):878-85. 12. Roberts LN, Patel RK, Arya R. Haemostasisandthrombosisinliverdisease.Br J Haematol. 2010 Feb;148(4):507-21. 13. Tripodi A, Salerno F, Chantarangkul V, et al. Evidenceofnormalthrombingenerationincirrhosisdespiteabnormalconventional coagulation tests.Hepatology. 2005 Mar;41(3):553-8. 14. Thachil J.Relevanceofclottingtestsinliverdisease. Postgrad Med J. 2008 Apr;84(990):177-81. 15. Ramaker AJ, Meyer P, van der Meer J, et al. Effectsofacidosis, alkalosis, hyperthermiaandhypothermia on haemostasis: resultsofpoint-of-care testingwiththethromboelastographyanalyser. BloodCoagulFibrinolysis. 2009 Sep;20(6):436-9. 16. Rajagopalan S, Mascha E, Na J, Sessler DI. The effects of mild perioperative hypothermia on blood loss and transfusion requirement. Anesthesiology 2008 Jan; 108:71–7. 17. Meng ZH, Wolberg AS, Monroe DM 3rd, Hoffman M. The effect of temperature and pH on the activity of factor VIIa: implications for the efficacy of high-dose factor VIIa in hypothermic and acidotic patients. J Trauma 2003 Nov; 55(5):886–91. 18. Ho KM, Leonard AD.Concentration-dependenteffectofhypocalcaemia on mortalityofpatientswithcriticalbleedingrequiringmassivetransfusion: a cohortstudy.AnaesthIntensive Care. 2011 Jan;39(1):46-54. 19. Fukuda T, Nakashima Y, Harada M, et al. Effectofwholebloodclotting time inratswithionizedhypocalcemiainducedbyrapidintravenouscitrateinfusion. J Toxicol Sci. 2006 Aug;31(3):229-34. 20. Aarts PA, van denBroek SA, Prins GW, Kuiken GD, Sixma JJ, Heethaar RM. Bloodplatelets are concentratednearthewalland red bloodcells, inthecenterinflowingblood. Arteriosclerosis. 1988 Nov-Dec;8(6):819-24. 21. Sagesaka T. Influenceofred bloodcellconcentration on theinitiation time ofblood coagulation: riskofthrombusformationbyhemoconcentration.ClinHemorheolMicrocirc. 2004;31(4):243-9. 22. Murphy MF, Stanworth SJ, Yazer M. Transfusionpracticeandsafety: current status andpossibilities for improvement.VoxSang. 2011 Jan;100(1):46-59. 23. Massicotte L, Lenis S, Thibeault L, Sassine MP, Seal RF, Roy A. Reductionofbloodproducttransfusionsduringlivertransplantation. Can J Anaesth. 2005 May;52(5):545-6. 24. Klinck JR. Liver transplantation: anesthesia. In: Klinck JR, Lindop MJ, editors. Anesthesia and intensive care for organ transplantation. London: Chapman & Hall; 1998. p.169–99. 25. Dupont J, Messiant F, Declerck N, et al. Livertransplantationwithoutthe use offreshfrozenplasma.AnesthAnalg. 1996 Oct;83(4):681-6. 26. Kang YG, Gasior TA. Blood coagulation during liver, kidney, pancreas, and lung transplantation. In: Spiess BD, Counts RB, Gould SA, editors. Perioperative transfusion medicine.eds. Baltimore: Williams &Wilkins; 1998. p.471–92. 27. Schroeder RA, Collins BH, Tuttle-Newhall E, et al. Intraoperative fluid management during orthotopic liver transplantation. J CardiothoracVascAnesth 2004 Aug; 18(4):438–41. 28. Kozek-Langenecker SA, Afshari A, Albaladejo P, et al. Management of severe perioperative bleeding: guidelines from the European Society of Anaesthesiology. Eur J Anaesthesiol 2013 Jun; 30(6): 270-382.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
197
29. Bang SR, Kim YH, Kim GS. The effects of in vitro hemodilution with 6% hydroxyethyl starch (HES) (130/0.4) solution on thrombelastograph analysis in patients undergoing liver transplantation. Clin Transplant 2011 May-Jun;25(3):450–6. 30. Kozek-Langenecker SA, Jungheinrich C, Sauermann W, Van der Linden P. The effects of hydroxyethyl starch 130/0.4 (6%) on blood loss anduse of blood products in major surgery: a pooled analysis of randomized clinical trials. AnesthAnalg 2008 Aug;107(2):382–90. 31. Esper SA, Waters JH. Intra-operativecellsalvage: a fresh look at theindicationsandcontraindications. BloodTransfus. 2011 Apr;9(2):139-47. 32. Massicotte L, Thibeault L, Beaulieu D, Roy JD, Roy A. Evaluationofcellsalvage autotransfusion utilityduringlivertransplantation.HPB (Oxford). 2007;9(1):52-7. 33. Council on ScientificAffairs. Autologousbloodtransfusions. JAMA. 1986 Nov 7;256(17):2378-80. 34. AssociationofAnaesthetistsof Great Britainand Ireland. Bloodtransfusionandtheanaesthetist: intra operative cellsalvage [Internet]. London: AssociationofAnaesthetistsof Great Britainand Ireland; 2009 [cited 2014 July 28]. Availablefrom: http://www.aagb.org/sites/default/files/cell%20.salvage_2009_amended.pdf 35. Liang TB, Li DL, Liang L, et al. Intraoperativebloodsalvageduringlivertransplantationinpatientswithhepatocellularcarcinoma: efficiencyofleukocytedepletionfiltersintheremovalof tumor cells.Transplantation. 2008 Mar 27;85(6):863-9. 36. Muscari F, Suc B, Vigouroux D, et al. Bloodsalvage autotransfusion duringtransplantation for hepatocarcinoma: doesitincreasetheriskofneoplasticrecurrence? TransplInt. 2005 Nov;18(11):1236-9. 37. Porte RJ, Bontempo FA, Knot EA, Lewis JH, Kang YG, Starzl TE. Systemiceffectsoftissueplasminogenactivator-associatedfibrinolysisanditsrelation to thrombingenerationinorthotopiclivertransplantation. Transplantation. 1989 Jun;47(6):978-84. 38. Dzik WH, Arkin CF, Jenkins RL, Stump DC. Fibrinolysisduringlivertransplantationinhumans: role oftissue-typeplasminogenactivator. Blood. 1988 Apr;71(4):1090-5. 39. Molenaar IQ, Warnaar N, Groen H, Tenvergert EM, Slooff MJ, Porte RJ. Efficacyandsafetyofantifibrinolyticdrugsinlivertransplantation: a systematicreviewand meta-analysis. Am J Transplant. 2007 Jan;7(1):185-94. 40. Charbit B, Mandelbrot L, Samain E, et al; PPH Study Group. Thedecreaseoffibrinogen is anearlypredictoroftheseverityofpostpartumhemorrhage. J ThrombHaemost. 2007 Feb;5(2):266-73. 41. Fries D, Innerhofer P, Reif C, et al. Theeffectoffibrinogensubstitution on reversalofdilutionalcoagulopathy: aninvitro model.AnesthAnalg. 2006 Feb;102(2):347-51. 42. De Lorenzo C, Calatzis A, Welsch U, Heindl B. Fibrinogenconcentratereversesdilutionalcoagulopathyinducedinvitrobysaline but notbyhydroxyethylstarch 6%. AnesthAnalg. 2006 Apr;102(4):1194-200. 43. Kalina U, Stöhr HA, Bickhard H, et al. Rotationalthromboelastography for monitoring offibrinogenconcentratetherapyinfibrinogendeficiency. BloodCoagulFibrinolysis. 2008 Dec;19(8):777-83. 44. Rahe-Meyer N, Pichlmaier M, Haverich A, et al. Bleedingmanagementwithfibrinogenconcentratetargeting a high-normalplasmafibrinogenlevel: a pilot study.Br J Anaesth. 2009 Jun;102(6):785-92.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
198
45. Rahe-Meyer N, Solomon C, Winterhalter M, et al. Thromboelastometry-guidedadministrationoffibrinogenconcentrate for thetreatmentofexcessiveintraoperativebleedinginthoracoabdominalaorticaneurysmsurgery.J ThoracCardiovascSurg. 2009 Sep;138(3):694-702. 46. Porte RJ. Coagulationandfibrinolysisinorthotopiclivertransplantation: currentviewsandinsights.SeminThrombHemost. 1993;19(3):191-6. 47. Görlinger K. Coagulationmanagementduringlivertransplantation. Hamostaseologie. 2006 Aug;26(3 Suppl 1):S64-76. 48. Planinsic RM, van der Meer J, Testa G, et al. Safetyandefficacyof a singlebolusadministrationofrecombinantfactorVIIainlivertransplantationdue to chronicliverdisease. LiverTranspl. 2005 Aug;11(8):895-900. 49. Lodge JP, Jonas S, Jones RM, et al; rFVIIa OLT Study Group. EfficacyandsafetyofrepeatedperioperativedosesofrecombinantfactorVIIainlivertransplantation. LiverTranspl. 2005 Aug;11(8):973-9. 50. Yank V, Tuohy CV, Logan AC, et al. Systematicreview: benefitsandharmsofin-hospital use ofrecombinantfactorVIIa for off-labelindications. AnnIntern Med. 2011 Apr 19;154(8):529-40. 51. Levi M, Levy JH, Andersen HF, Truloff D. Safetyofrecombinantactivatedfactor VII inrandomizedclinicaltrials. N Engl J Med. 2010 Nov 4;363(19):1791-800. 52. Richards EM, Alexander GJ, Calne RY, Baglin TP. Thrombocytopeniafollowinglivertransplantation is associatedwithplateletconsumptionandthrombingeneration. Br J Haematol. 1997 Aug;98(2):315-21. 53. Stahl RL, Duncan A, Hooks MA, Henderson JM, Millikan WJ, Warren WD. A hypercoagulablestatefollowsorthotopiclivertransplantation. Hepatology. 1990 Sep;12(3 Pt 1):553-8. 54. Lisman T, Porte RJ. Towards a rational use oflow-molecular-weightheparininpatientswithcirrhosis. LiverInt. 2011 Aug;31(7):1063.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
199
INVAZIVNE GLJIVIČNE INFEKCIJE NAKON ORTOTOPSKE TRANSPLANTACIJE JETRE GORDANA JOVANOVIĆ Klinika za anesteziju i intenzivnu terapiju, Klinički centar Vojvodine, Medicinski fakultet , Univerzitet Novi Sad E-mail:[email protected] INVASIVE FUNGAL INFECTION AFTER ORTOTOPIC LIVER TRANSPLANTATION Abstract In spite of diagnostic and improvement in therapy of invasive fungal infections(IFI) they are devastating complication after orthotopic liver transplantation. Overall incidence is 5%to 42%. Most common fungal infection is candidiasis, followed by aspergillosis and cryptococcosis. Lungs and urinary tract are most frequent involved organ systems. Most fungal infections are developed during first 2 months post transplantation, apart from aspergillosis which is developed after 90 days post transplant. Early diagnosis of IFI is challenging because symptoms are nonspecific and microbiology cultures of fungi grows slowly. Prophylactic measures decrease overall incidence of IFI, but there are no evidence of decreasing overall mortality. Routine prophylaxis with antifungal drugs is still controversial issue. The most commonly used antifungal in therapy of IFI the triazole antifungals (fluconasole, itraconasole, and voriconasole), polyene antifungals (conventional amphotericyn B and amphotericin B lipid complex) and most recent antifungals the echinocandins (caspofungin and micafungin). The therapeutic option and duration of antifungal agent are choose by severity of clinical presentation and causative fungi. Uvod Invazivne gljivične infekcije nakon ortotopske transplantacije jetre (OTJ), predstavljaju jedan od značajnih problema sa kojima se ovi bolesnici susreću u postoperativnom periodu. U poslednjih nekoliko decenija dijagnostičke i terapijske mere u lečenju invazivnih gljivičnih infekcija su značajno napredovale, ali uprkos tome još uvek su praćene značajnim morbiditetom i mortalitetom (1). Epidemiologija Na razvoj gljivičnih infekcija nakon transplantacije jetre utiče više faktora, prvo to je izloženost gljivicama i prethodna kolonizacija recipijenta,drugo, upotreba antifugalne profilakse koja može promeniti vrstu gljivica koji su najčešći izazivači kao i stepen imunosupresije, kaja je integralni vid lečenja ovih bolesnika. Incidenca gljivičnih infekcija koje se javljaju nakon transplantacije jetre se kreće po podacima koji se sreću u literaturi između 5% i 42%. U poslednjim decenijama incidenca se smanjuje i to smanjenje je multifaktorijalno , pre svega vezano za unapređeno lečenje u postoperativnom periodu, bolju hiruršku tehniku, prevenciju i bržu dijagnozu. Najčesći su sojevi iz roda Candida
a zatim slede Aspergillus pa Cryptoccus i na kraju Phaeohyphomycetes.(2).Organi koji su najčesće zahvaćeni su pluća i urinarni trakt (1,2).
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
200
Rod Candida
Rod kandida (albicans) je daleko najčeći uzročnik gljivičnih infekcija nakon transplantacije jetre. Zbog toga što se često koristi rutinska profilaksa flukonalzolom, u poslednje vreme predominaciju su preuzeli non- albikans sojevi(C.glabrata i C.krusei).Najćešće se javlja kandidijaza oralne sluzokože ali se može klinički pojaviti i u formi invazivne kandidijaze.
Rod Aspergillus
Ovo je druga po redu gljivična infekcija koja se javlja nakon transplantacije jetre. Značaj aspergiloze je u njenom visokom mortalitetu. U 90% slučajeva ima plućnu prezentaciju. Vreme javljanja invazivnih gljivičnih infekcija je najčešće u prvih dva meseca nakon transplantaacije, najčešće oko petnaestog postoperativnog dana. Međutim, kada je u pitanju aspergiloza, infekcija se obično javlja nakon 90-tog dana posle transplantacije jetre (3). Faktori rizika Najvažniji riziko–faktori su povišen serumski kreatinin ( više od 265 µmol/l), vreme hirurgije duže od 11 časova, retransplantacija, rana kolonizacija, masivna upotreba krvnih produkata, infekcija hepatitisom C. Dijagnoza Ranu dijagnozu gljivične infekcije nakon transplantacije jetre nije jednostavno postaviti. Klinički simptomi mogu biti nespecifični i slabog intenziteta sve dok infekcija ne uđe u poodmaklu fazu. Mikrobiološke nalaze je nekada teško tumačiti jer zbog sveprisutnosti gljivica nekada nije lako razlučiti kontaminaciju od infekcije. Takođe u mikrobiološkim kulturama kolonije gljivica mogu rasti veoma sporo. Tokom 2002g, konsenzus grupa Evropske organizacije za istraživanje i tretman kancera i nacionalni institut za alergiju i infektivne bolesti (the European Organization for Research and
Treatment ofCancer/Invasive Fungal Infections Cooperative Group (EORTC) and the National
Institute of Allergy and Infectious Diseases Mycoses Study Group (MSG) ) publikoval i su definiciju invazivnih gljivičnih infekcija. Ova definicija je tokom 2008. godine revidirana. Definišu se tri kategorije invazivne gljivične infekcije:dokazana, verovatna i moguća. Dokazana gljivična infekcija je ona kod koje je prisustvo gljivice dokazano u mikrobiološkom ili histopatološkom uzorku tkiva sa obolelog mesta. Definicija verovatne i moguće invazivne gljivične infekcije se temelje na tri grupe elemenata: predisponirajući faktori vezani za domaćina, klinički znaci i simptomi bolesti i mikološki dokazi(kultura, mikroskopija, galaktomanan i beta D glikan ) (3-5). Mere prevencije Dobro poznavanje faktora rizika je neophodno da bi se primenjivala odgovarajuća ciljana antifugalna profiaksa kod ovih bolesnika. Pošto su u pitanju imunokompromitovani bolesnici ovo nekada može biti komplikovan proces. Preoperativno se mogu sprovoditi mere za smanjenje kolonizacije gljivicama, što podrazumeva selektivnu dekontaminaciju digestivnog trakta gde se primenjuje nistatin, klotrimazol ili oralni amfotericin B, međutim sprovođenje ovih mera za sada nije dovelo do značajnijeg smanjenja invazivnih gljivičnih infekcija kod ovih bolesnika (4,5). U nekim transplantacionim centrima se sprovodi rutinska prevencija flukonazolom i drugim triazolima, rutinska terapija svih bolesnika može dovesti do bujanja i predominacije ne-kandida

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
201
sojeva i aspergilusa. U nekim transplantacionim centrima se sprovodi profilaksa samo visokorizičnih bolesnika za pojavu invazivnih gljivičnih infekcija. Iako su mere profilakse dovele do smanjenja ukupnog broja invazivnih gljivičnih infekcija, nema još dokaza da smanjuje i mortalitet. Pitanja vezana za mere prevencije još uvek ostaju predmet kontroverze (4-6). Terapija U terapiji invazivnih gljivičnih infekcija najčeše se koriste antifungicidni lekovi iz tri grupe a to su: azoli (flukonazol, vorikonazol, itrakonazol..), polienski antimikotici (amfotericin B, amfotericin B lipid kompleks) i najnoviji ehinokanadini (kaspofungin i micafungin) (7-8). Antimikotici uglavnom deluju na elemente ćelijskog zida i dovode do osmotskog stresa koji izaziva lizu i smrt gljivice. Polienski antimikotici se vezuju za ergosterol - glavnu sterolsku komponentu ćelijske membrane gljivice, rezutirajući gubitkom integriteta ćelijske membrane. Azoli inhibišu enzime involvirane u sintezu ergosterola. Ehinokanadini inhibišu sintezu gukana. Vrsta antimikotika i dužina terapije se odabiraju u odnosu na potencijalnog uzročnika (8). Literatura
1. Liu X, Ling Z, Li L, Ruan B. Invasive fungal infections in liver transplantation. International Journal of Infectious Diseases 2011;15:e298-e304.
2. Green M. Introduction: Infections in solid organ transplantation. American Journal of tranplantation 2013;13:3-8.
3. Raghuram A, Restepo A, Safadjou S, Cooley J, Orlof M et al. Invasive fungal infections following liver transplantation: Incidence,risk factors, survival, and impact of fluconasole –resistant Candida parapsilosis (2003-2007). Liver Transpl 2012;18:1100-1109.
4. Shoham S, A Marr K. Invasive fungal infection in solid organ transplant recipients. Future Microbiol 2012;7(5):639-55.
5. Hellinger W, Bonatti H, Yao J, Alvarez S, Brumble L, et al. Risk stratification and targeted antifugal prophylaxis for prevention of aspergillosis and other invasive mold infections after liver transplantation. Liver transpl 2005;11(6):656-62.
6. Eschenauer G, Lam S, Carver P. Antifugal propxylaxis in liver transplant patients. Liver Transpl 2009;15:842-58.
7. Silveira F.P, Kusne S. Candida infections in Solid organ transplantation. American Journal of Transplantaion 2013;13:220-7.
8. Singh N, Wagener M, Cacciarelli T, Levitsky J. Antifugal management practices in liver transplant recipients. American Journal of Transplantation 2008;8:426-31.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
202
HEART TRANSPLANTATION – ANESTHESIA AND PERIOPERATIVE TREATMENT MIOMIR JOVIC Clinic for cardiovascular anesthesia and intensive therapy, Dedinje Cardiovascular Institute-Belgrade.Faculty of Medicine, University of Belgrade, Serbia Introduction In last decade nearly 5 million Americans had heart failure (HF), with an incidence of 10 per 1000 population among persons older than 65 years of age. HF is the reason of at least 20% of all hospital admission among older persons. On the other side, HF is largely preventable, due to control of blood pressure and other vascular risk factors. Recent years, interdisciplinary approach to heart failure treatment has made significant improvement. The staging of HF and combined therapy with ACE inhibitors, angiotensin receptor blockers, beta blockers, aldosterone antagonists, diuretics and neseritide have a direct beneficial effect on the myocardium improving its functional capacity and enhancing reverse remodeling. Cardiac resynchronization therapy with biventricular pacing improves left ventricular function and favors reverse remodeling associated with the great improvement made in VAD– ventricular assisst device technology. Based on recent clinical data, criteria for heart transplantation has to be redefined. Additional effort was made with different surgical techniques for left ventricular remodeling, with idea to reduce volume overloading and work stress of the left ventricle and to improve work efficacy. Mechanically assisted circulation is worldwide accepted option for patients with extended heart failure, as a prolonged therapy or as a bridge to heart transplantation. Heart transplantation is, still, option for end stage heart failure. In Europe, about 2000 heart transplant procedures are performed per year, 2004 in 2012 and some additional in heart - lung transplanted patients, with the increasing shortage of suitable donors. According to the reports the 1 and 3 years survivals after heart transplantation (HT) in USA, for period 1999-2001, were approximately 81% and 69%, respectively. Despite the innovations in left ventricular assist devices as well as in artificial heart technology, simultaneously with improvement in medical treatment of the heart failure, heart transplantation is still “the golden standard” in the end stage heart failure, resistant to the medical treatment. Pathophysiology before HT Candidates for HT are usually patients with idiopathic or ischemic cardiomyopathy, with both systolic and diastolic dysfunction. Left ventricular ejection fraction (LVEF) below 20% with increased pulmonary and systemic vascular resistance. Therapy of heart failure consists of: diuretics, vasodilators (nitrates, hydralazine or ACE inhibitors) and incremental β– blockade. Some pts often require inotropic therapy, intravenous infusion of direct β-adrenergic agonists (dopamine or dobutamine) or phosphodiesterase inhibitors (milrinone) sometimes combined with mechanically assisted circulation (intra-aortic balloon pump or other short or long term mechanical devices).
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
203
Preoperative donor evaluation has to assess the stage of heart failure as well as other organs functional reserve. Anesthetic Management Immediately after the admission to hospital, donor has to be evaluated, his medical records at last examination (renal, hepatic or pulmonary dysfunction), while some laboratory findings, TEE and chest x-ray should be repeated. Premedication and induction to anesthesia should be managed according to actual hemodynamics (some hospital patients will be supported with inotropic infusions and/or IABP and should be considered to have a “full stomach”. Induction has to provide minimal myocardial depression, (moderate dose of narcotic with short acting hypnotic or high-dose narcotic technique with or without benzodiazepines). Direct β-agonists (epinephrine) should be readily available as well as α-agonists (phenylephrine, norepinephrine) to compensate vasodilatory effects of anesthesia. Usual invasive hemodynamic monitoring should be used (arterial, central venous and/or pulmonary artery catheter) sometimes with transesophageal echocardiography. Pre cardiopulmonary bypass period is usually stabile, with proper volume loading and inotropic support. Most patients will have an excess of intravascular volume, and administration of diuretics with/or hemofiltration may be beneficial. After the graft implantation has been done, aortic cross clamping released, the period of graft reperfusion starts. In this period of CPB patient has to be prepared for the weaning of CPB. Inotropic support has to be considered. Patients with pulmonary hypertension are at risk of right heart failure, and may benefit from a pulmonary vasodilator (isoprenaline, milrinone, prostaglandin E1). Due to heart denervation, pace maker for rhythm control is mandatory. Despite to heparin neutralization by infusion of protamine, meticulous attention has to be paid to surgical hemostasis, with empiric administration of platelets, fresh frozen plasma and cryoprecipitate due to coagulopathy, guided by coagulation studies ( thrombelastography, platelet function assessment).
Patophysiology after Transplantation
Cardiac denervation is unavoidable during HT. The consequence is substantially altered response to demands for increased CO. So, the maintenance of adequate preload, during perioperative period, is crucial. Denervation has the direct implication on the choice of inotropic support after the transplantation. Agents with direct cardiac effects (epinephrine or isoproterenol) are the first choice, supported by pace maker controlled rhythm if it is necessary. Early complications after HT include hyperacute and acute rejection, cardiac failure, pulmonary and systemic hypertension, cardiac arrhythmias and renal failure. All of these complications may be part of rejection while hypertension and renal failure may be the consequence of immunosuppressive regimen (cyclosporine). Acute rejection is a constant threat in the early postoperative period (6 months) and may be presented in different forms (low CO, arrhythmias). Clinical evaluation and regular endomyocardial biopsies are the first step of control. Detection of rejection indicates aggressive
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
204
treatment, usually with pulse of glucocorticoid with eventual switch from cyclosporine to tacrolimus. Postoperative Therapy During the first few postoperative days, principles of treatment are very similar to periopartive strategy. Invasive monitoring of right and/or left ventricle failure, low CO, rhythm disturbances, renal failure and clinical signs of eventual rejection are mandatory. Aggressive immunosuppression and monitoring of its effects is the most important (the signs of rejection on one side and deleterious effects on white blood cells and T-cells on the other side). Prevention and treatment of any infection are of the equal importance. Bacterial pneumonia is frequent in firs days, but patients are susceptible to opportunistic viral and fungal infections in firs several weeks too. Hypertension and renal failure, impaired by immunosuppression (cyclosporine, tacrolimus) are permanent threat during postoperative period. Allograft coronary vasculopathy remains the most important and frequent complication after heart transplantation in firs 3 to 5 years, with incidence up to 80% after 5 years. Lymphoma of malignant etiology is less frequent, but still often during first years after heart transplantation. Conclusion Increasing number of recepients and long weiting lists are burning problem for organ transplantation. Better understandung of heart failure and left ventricular remodeling, development of different modalities for LV mechanical assistence, based on current scientific results improved the management of the heart insuficiency. However, national transplant organ service need well predefined organization and financial supplies as predispositin for success. Improvement in cardiopulmanary bypass technology, prevention of SIRS and fibrinilysis, and strategy of intraoperative blood conservation strategy as well as oregan protection has to be reconsidered. New era in heart failure tretmment is directed toward new strateges: HF support therapy, new immunosupresive drugs with fine tuning of immunosupresion, initiating reconstruction of criteria and protocols for recepient selection. Literature: 1. Kriet JM, Kaye MP. The Registry of the International Society for Heart Transplantation:
seventh officila report-1990. J Heart Transplant 1991; 10:491-98. 2. Deuse T, Sista R, Weill D et all. Review of heart-lung transplantation at Stanford. Ann
Thorac Surg 2010; 90(1):329-37. 3. Mc Allister FA, Lawson FM, Teo KK, Armstrong PW. A systemic review of randomized
trials of disease management programs in heart failure. Am J Med 2001; 110:378-84. 4. Meyns B, Sergeant P, Herijgers P, et al. Bridging procedures to heart transplantation. World
J Surg 2002; 26(2): 212-7. 5. http://www.eurotransplant.org/files/annual_report/ar_2012.pdf

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
205
6. Schmid C, Welp H, Klotz S, Baba HA, Wilhelm MJ, Scheld HH. Outcome of patients surviving to heart transplantation after being mechanically bridged for more than 100 days. J Heart Lung Transplant. 2003; 22(9): 1054-8.
7. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines J Am Coll Cardiol 2001; 38:2101-13.
8. Ellman PI, Ronson RS, Kron IL. Modern concepts in heart transplantation. J Long Term Eff Med Implants 2003; 13(6):46-83.
9. Bunzel B, Laederach-Hofmann K, Grimm M. Survival, clinical data and quality of life 10 years after heart transplantation: a prospective study. Z Kardiol 2002; 91(4):319-27.
10. JuffeA, Rodriguez MA, Caputo E, Cuenca J, Crespo M. Long-term results of cardiac transplantation. J Card Surg 2003; 18(3):183-9.
11. Ranjit J, Mandigo C, Weinberg A. Et all. Survival after heart transplantation: are pretransplant risk factors important ? Transplantation 1999;97(9):pS641.
12. Jessup M, Brozena S. Heart failure. N Engl J Med 2003; 348: 2007-18. 13. Vitali E, Lanfranconi M, Bruschi G, Russo C, Colombo T , Ribera E. Left ventricular assist
devices as bridge to heart transplantation: The Niquarda Experience. J Card Surg 2003; 18(2): 107-13.
14. Chang V. Calcineurun inhibitors in heart transplantation. J Herat Lung Transplantation 2004; 23 (5Suppl): S202-6.
15. Berman M, Erman A, Ben-GalT, Dvir T, et al. Coenzyme Q10 in patients with end-stage heart failure awaiting cardiac transplantation: a randomized, placebo-controlled study. Clin Cardiol 2004; 27(5): 295-9.
16. Pohwani AL, Murali S, Matheir MM et al. Impact of beta-blocker therapy on functional capacity for heart transplant listing. J Heart Lung Transplant 2003; 22(1):78-86.
17. Peterson RL, Schechtman KB, Ewald GA, et al. Timing of cardiac transplantation in patients with heart failure receivingbeta-adrenergic blockers. J Heart Lung Transplant 2003; 22(10): 1141-8.
18. Massad MG. Current trends in heart transplantation. Cardiology 2004; 101(1-3): 79-92. 19. Harringer W, Haverich A. Heart and heart-lung transplantation: standards and
improvements. World J Surg 2002; 26(2):218-25. 20. Butler J, Khadim G, Paul KM, et al. Selection of patients for heart transplantation in the
current era of heart failure therapy. J Am Coll Cardiol 2004; 43(5): 787-93. 21. Komoda T, Drews T, Hetzer R, Lehmkuhl HB. New prioritization of heart transplant
candidates on mechanical circulatory support in an era of severe donor shortage. J Heart Lung Transplant 2010;Jun 4
22. Kirklin KJ, Young BJ, McGiffin CD.(eds) Heart Transplantation.Philadelphia: Churchill Livingstone, 2002;
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
206
GENERAL VERSUS REGIONAL ANESTHESIA FOR CAROTID ENDARTERECTOMY DRAGANAUNIC-STOJANOVIC Cardiovascular Institute Dedinje Belgrade, Serbia E-mail: [email protected] Carotid endarterectomy (CEA) is a surgical procedure performed to reduce theincidences of embolic and thrombotic stroke1. To reduce the incidences of morbidity and mortality, there is a constant search for optimalanesthetic and surgical techniques1.There is a widespread view amongst anesthetists, surgeons, patients and other healthcare professionals that major surgery is inherently safer, if it can be performed under local or regional anaesthesia (RA) rather than general anaesthesia (GA), particularly if the patient has multiple comorbidities. Carotid endarterectomy is one such procedure, where such views are often polarised, such that in some centres a GA is not be offered as an option at all.However is there any real evidence to support such a stance, either for this or other procedures in the medically fit or unfit patient. There are both pros and cons to each anesthetic technique. Regional anesthesia (RA) is the only technique that will correctlyidentify all patients requiring a shunt insertion forcarotid artery crossclamping. Consequently, fewer shunts are used1,2. Although shunts should protect the brain from stroke that results from low cerebral-blood flow during carotid clamping, they can damage the arteria wall causing embolism to the brain1,2. Other possible benefits may include theavoidance of tracheal intubation in patients with chronicobstructive lung disease, and avoidance of negative inotropic anesthetic agents in patients with limited cardiac reserves, immediate postoperative neurological assessment, preserved cerebral autoregulationof perfusion, and avoidance of some adverse consequences ofGA on health-related quality of life and cancer recurrencepossibly associated with GA1. But, each regional technique has its complications3. The main advantages of GA are a safe airway throughout theprocedure with controlled ventilation and arterial carbon dioxideconcentrations1. Both inhalation and intravenous agents areused for maintaining anesthesia. There is no outcome-based evidence favoring any particular generalanesthetic agent during carotid clamping.The disadvantages of GA include the usual complications of GA, requirement for indirect methods of neurological monitoring and more importantly, the residual effects of GA in the early postoperative period that canmask the symptoms or signs of neurologic complications fromsurgery1. A large number of studies compares RA and GA techniques in CEA surgery patients. The primary outcome in these studies was the proportion of patients with stroke (including retinal infarction), myocardial infarction, or death. General Anaesthesia versus Local Anaesthesia for carotid surgery (GALA) is a largest, multicenter, randomized, controlled trial that included 3,526 patients with symptomatic or asymptomatic carotid stenosis from 95 centers in 24 countries4. This study showed no definite differences in primary outcome: stroke, myocardial infarction, or death between randomization and 30 days after surgerybeetwenthe two types of anesthesia. Although the GALA trial is a very

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
207
good, large randomized controlled trial, the GALA trial results have not silencedthe debate as to which anesthetic technique gives the best results. A meta-analysis of 14 randomisedtrials that included 4596 operations, of which 3526 were from the single largesttrial (GALA) showed that there was no statistically significant differencein the incidence ofoperative stroke and stroke or death between the 2 typesof anesthetic technique during CEA.There was a non-significant trend towards lower operative mortality with RA. In the RA group 0.9% of patients died within 30 days of surgery compared to 1.5% of patients in the GAgroup (Peto OR 0.62, 95% CI 0.36 to 1.07). However, neither the GALA trial or the pooled analysis were adequately powered toreliably detect an effect on mortality. Analysis of nonrandomized studies showed consistently lower risks of operative stroke and death when CEA was performed on patients under RA. Randomized trials showed that there was no evidence of advantages of one anesthesia technique over the other. This does not mean that the anesthetic technique is unimportant because GA and RA performed well (or badly) contribute to a good (or bad) outcome.Because of that, several additional outcomes need to be taken into account when comparing the 2 procedures including cost effectiveness, the incidence of postoperative cognitive dysfunction, the long-term effects of the difference in shunt usage between the 2 procedures, and postoperative blood pressure differences. In conclusion, individual choice is ideal choice. The mode of anesthesia should be determined at the discretion of the surgeon, anesthesiologist and patient. References:
1. Unic-Stojanovic D, Babic S, Neskovic V: General versus regional anesthesia forcarotid endarterectomy. J CardiothoracVascAnesth 2013; 27: 1379-1383.
2. McCarthy RJ, Walker R, McAteer P, et al: Patient and hospitalbenefits of local anesthesia for carotid endarterectomy. Eur J VascEndovascSurg 2011; 22:13-18.
3. Pandit JJ, Satya-Krishna R, Gration P: Superficial or deep cervicalplexus block for carotid endarterectomy: A systematic review ofcomplications. Br J Anaesth 2007; 99:159-169.
4. Lewis SC, Warlow CP, Bodenham AR, et al: General anaesthesia versus local anaesthesia for carotid surgery (GALA): A multicentre,randomised controlled trial. Lancet 2008; 372:2132-2142.
5. Vaniyapong T, Chongruksut W, Rerkasem K.Local versus general anaesthesia for carotid endarterectomy. Cochrane Database of Systematic Reviews 2013 (12). Art. No: CD000126.DOI: 10.1002/14651858.CD000126.pub4
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
208
SUB-TENON’S ANAESTHESIA - ANAESTHETIC OF CHOICE FOR ANTERIOR SEGMENT OF THE EYE SURGERY N. TOMANOVIC East Kent Hospitals University NHS Foundation Trust, Canterbury UK There has been a dramatic change of anaesthetic practice for ophthalmic surgery over the last twelve years. The use of local anaesthesia (LA) has risen from around 20% in 1991 to over 75% in 1996 and 86% in 1997. LA is the anaesthetic of choice nowadays unless contraindicated. Sub-Tenon’s anaesthesia, anaesthetic of choice, is a new method of direct infiltration of local anaesthetic into sub-Tenon’s space using a blunt cannula. The new technique was introduced because of serious concerns over the complication of sharp needle bulb perforation. Sub Tenon’s blocks avoid blind sharp needle penetration into space of the orbit. Although still a relatively new technique, sub-Tenon’s anaesthesia is becoming increasingly popular. Sub-Tenon’s anaesthesia is a simple, easy to teach method. A small volume of local anaesthetic provides excellent anaesthesia and akinesia and reliable eyelid block. There is no risk of bulb perforation, subarachnoid injection or intravascular injection. Real complications have not been described. Cataract operations are carried out as day cases. Uvod Operacije prednjeg segmenta oka najčešće su operacije u oftalmologiji. Operacije katarakte su najčešće elektivne operacije uopšte u hirurgiji i samo u Velikoj Britaniji 2007 godine uradjeno je vise od 368 000 operacija (1). U poslednjih 20-ak god. svedoci smo dramatičnih promena u anesteziološkoj praksi u očnoj hirurgiji u svetu. Udeo lokalne anestezije (LA) je porastao sa 20% 1991. na 75% 1996 i 86% 1997 (2, 3). Danas se praktično sve operacije prednjeg segmenta oka ,osim onih gde postoje kontraindikacije, izvode u lokalnoj anesteziji. U isto vreme korišćenje sedacije je drastično smanjeno tako da se izuzetno retko koristi. Do ovih promena je došlo usavrsavanjem hirurških i anestezioloških tehnika sto je omogućilo da se anesteziolozi prvo uključe a zatim i potpuno preuzmu izvodjenje lokalne anestezije u očnoj hirurgiji. Indikacije i kotraindikacije Lokalna anestezija je anestezija izbora u očnoj hirurgiji, ukoliko nema kontraindikacija a to su: 1. Pacijent koji odbija LA, 2. Dementan i konfuzan pacijent koji ne može da saradjuje i prati instrukcije, 3. Pacijent sa nekontrolisanim tremorom, 4. Pacijent koji ne može da leži na ravnom ( uglavnom teški srčani i plućni bolesnici- na kiseoniku), 5. Mladji pacijenti (traumatska katarakta n.pr.), 6. Pacijenti sa prethodnim alergijskim reakcijama ili komplikacijama LA – veoma retko. Preoperativna priprema
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
209
Pacijenti se pripremaju kao i za opštu anesteziju, što znači da svako prateće obolenje treba da bude pod kontrolom. Na dan operacije izmeri se puls, arterijski pritisak, prekontroliše šećer kod dijabetičara kao i koagulacioni status pacijenata na antikoagulantnoj terapiji. Premedikacija i sedacija se izuzetno retko koriste. Tehnike lokalne anestezije Tehnike lokalne anestezije koje su danas u upotrebi su:
a) Topikalna b) Subkonjunktivalna c) Retrobulbarna d) Peribulbarna e) Sub-Tenon – anestezija izbora
Topikalna i subkonjunktivalna anestezija Neakinetičke metode lokalne anestezije uvedene su 1988 u USA i Velikoj Britaniji. Retrobulbarna anestezija Akinetička metoda plasiranjem igle duzine 38 mm inferotemporalno čime se dobija solidna analgezija i akinezija. Metoda je uglavnom napuštena zbog čestih ozbiljnih komplikacija ( retrobulbarni hematom, oštećenje optičkog živca,perforacija očnog bulbusa) Peribulbarna anestezija Peribulbarna tehnika uvedena je 1986 kao sigurnija alternativa retrobulbarnom bloku (8). Blok se zove peribulbarni zato što vrh igle ostaje van mišićnog konusa (u peribulbarnom a ne retrobulbarnom prostoru), ali lokalni anestetik difunduje u retrobulbarni prostor.Komplikacije su mnogo redje i praktično jedina ozbiljnija, ali potencijalno katastrofalna komplikacija je perforacija bulbusa. Sub -Tenon anestezija Sub-Tenon anestezija je nova metoda direktnog ubrizgavanja lokalnog anestetika u sub-Tenon prostor korišćenjem tupe kanile. Tehnika otvaranja subtenonovog prostora poznata je već stotinak godina,dugo je bila zapostavljena, da bi ponovo ušla u kliničku praksu 1992 (9). Uvedena je kao izraz želje da se nadje alternativa retrobulbarnom pa i peribulbarnom bloku kao metodama anestezije vezanim sa retkom , ali teškom komplikacijom, perforacijom bulbusa. Ovo je metoda kojom se izbegava plasiranje oštre igle ‘na slepo’ u prostor orbite tako da je mogućnost perforacije bulbusa praktično isključena. Sub-Tenon anestezija, iako relativno nova metoda, veoma brzo dobija na popularnosti. 1997 god. svega 7% svih očnih klinika praktikovala je izvodjenje ove tehnike, dok se danas sub-Tenon anestezija primenjuje u 51% bolnica (podaci iz 2001 – UKISCRS).
Anatomska razmatranja
Tenonova kapsula (fascija očne jabučice) je relativno čvrsta fibroelastična membrana koja obavija očnu jabučicu i ekstraokularne mišiće, a pruža se od limbusa kornee do optičkog nerva (10). Svi ekstraokularni mišići pre pripajanja na skleru perforiraju Tenonovu kapsulu. Četiri rektusa se pripajaju neposredno iza ekvatora očne jabučice. Deo Tenonove kapsule ispred ovih
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
210
pripoja, anteriorni deo, odvojen je od sklere intermuskularnim septumom koji se pruža izmedju ekstraokularnih mišića. Posteriorni deo Tenonove kapsule je tanji i čvrsto priljubljen uz skleru. Difuzijom lokalnog anestetika, prekidaju se senzitivni impulsi blokadom kratkih cilijarnih nerava na njihovom putu kroz Tenonovu kapsulu do očne jabučice. Akinezija se postiže direktnom blokadom nervnih vlakana koji inervišu očne mišiće.Refleks treptanja, blokiran je direktnim širenjem lokalnog anestetika prema orbikularnom mišiću, tako da dodatna blokada nervusa facijalisa nije potrebna. Materijal
1. Očni spekulum (Barraquers) 2. Bezubi forceps (Moorfields) 3. Makazice zatupljenog vrha (Westcott – spring) 4. Sub-Tenon kanila (19 G) 5. Špric 5ml 6. Topikalni anestetik (0.4% Benoksinat ili 1% Ametokain) 7. Lokalni anestetik (2% Lignokain i 0.5% Bupivakain 50:50) 8. Hyaluronidaza (15-150 IU/ml) 9. 5% Jodni rastvor
Metoda
• Procedura se izvodi pod sterilnim uslovima. • Topikalna anestezija se aplikuje na inferonazalni deo konjunktive. • Oko se očisti sa nekoliko kapi 5% vodenog rastvora joda. • Očni spekulum se nežno plasira da drži očne kapke razmaknute. • Konjunktiva i Tenonova kapsula se čvrsto povuku nagore forcepsom na oko 5 mm od
limbusa kornee inferonazalno. • Makazicama se napravi mali prorez na konjunktivi i Tenonovoj kapsuli. • Zatvorenim makazicama se tupo preparira i proširi postojeći otvor tako da se napravi
mali tunel u subtenon prostoru. • Gledajući kroz otvor, belilo sklere bi trebalo da je vidljivo. • Zakrivljena, tupa, subtenon kanila spojena sa špricem od 5 ml napunjenim mešavinom
lokalnog anestetika ubaci se u otvoreni subtenon prostor. Iglom se napreduje dok se ne naidje na otpor, pri nailasku na posteriorni deo Tenonove kapsule koji je čvrsto priljubljen uz skleru.
• Lokalni anestetik se polako ubrizgava i hidrodisekcijom se lokalni anestetik širi u ostala tri kvadranta vidljivog dela očne jabučice kao i posteriorno i u očne kapke.
• Inferonazalni kvadrant je izabran da se ne bi interferiralo sa hirurškim operativnim poljem.
• Koristi se volumen od 3-5 ml lokalnog anestetika. • Anestezija nastupa u roku od 1-2 min.
Tehnika izvodjenja sub-Tenon bloka je relativno jednostavna i brza,lako se savladava i pruža, uglavnom,odličnu anesteziju i akineziju. Izbegavanjem korišćenja oštre igle rizik od perforacije očnog bulbusa, akcidentalne injekcije u subarahnoidalni prostor ili intravaskularnog ubrizgavanja lokalnog anestetika je praktično eliminisan.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
211
Oftalmološka i anesteziološka asocijacija Velike Britanije ( Royal College of Ophthalmologists,Royal College of Anaesthetists) publikovale su 2001 godine zajedničku brošuru preporuka u kojoj se zaključuje da dobro obučeni medicinski tehničari mogu samostalno da izvode sub-Tenon blok ukoliko u bolnici postoji dezurni anesteziolog. Postoji generalna tendencija u Velikoj Britaniji da neke hirurške i anesteziološke procedure postanu delokrug rada obučenog višeg medicinskog osoblja. Neželjeni efekti Prave komplikacije subtenon anestezije nisu opisane. Neželjeni efekti su:
• Subkonjunktivalno krvarenje koje se opisuje i kao 'neizbežno' a može se umanjiti pažljivim sečenjem ,odnosno izbegavanjem vidljivih krvnih sudova.
• Subkonjunktivalna injekcija - hemoza koja se takodje veoma često javlja, posledica je anteriornog ubrizgavanja lokalnog anestetika i brzo se resorbuje pogotovu ako se koristi hyaluronidaza i aplikuje pritisak na očnu jabučicu.
Zaključak Katarakte su najčešće elektivne operacije u hirurgiji. Anestezija i hirurgija se izvodi u ambulantnim uslovima - pacijenti se primaju, operišu i otpuštaju iz bolnice u roku od nekoliko sati. Obzirom da su u pitanju stariji pacijenti, ovom jednostavnom i efikasnom organizacijom minimalno se remeti njihov ustaljeni ritam.Značajno se smanjuje mogućnost komplikacija vezanih za dugotrajno ležanje u bolničkim uslovima. Dobro obučeni medicinski tehničari mogu da izvode samostalno sub-Tenon blok. Sve ovo doprinosi ogromnoj uštedi za zdravstvenu sluzbu. Reference
1. Desai P., Reidy A., Minassian D.C.: Profile of patients presenting for cataract surgery: National Data Collection., Br. J. Ophthalmol. 1999; 83: 893-896.
2. Hodgkins P.R. et. al.: Current practice of cataract extraction and anaesthesia. Br. J. Ophthalmol. 1992; 76: 323-326.
3. Eke T., Thompson J.R.: The National Survey of Local Anaesthesia for Ocular Surgery. I. Survey Methodology and Current Practice., Eye 1999a; 13: 189-195.
4. Dutton J.J.: Clinical and Surgical Orbital Anatomy, Philadelphia, W.B. Saunders, 1994. 5. Donaxas M.T., Anderson R.L.: Clinical Orbital Anatomy, Baltimore,.M.D., Williams and
Wilkins,. 1984, p 232. 6. Koorneef L., Grizzard W.S.: Ophthalmic Anesthesia, in Reinecke
RD(ed):.Ophthalmology Annual, New York, N.Y., Raven Press, 1989, 265-294. 7. Hamilton R.C.: Regional Anaesthesia of the Eye, Curr. Opin. Anaesthesiol. 3: 740-
744,1990. 8. Davis D.B., Mandel D.M.: Posterior Peribulbar Anaesthesia: An alternative to retrobulbar
anaesthesia. Journal of Cataract & Refractive Surgery, 1986 ; 12: 182-4. 9. Stevens J.D.: A new anaesthesia technique for cataract extraction by one quadrant sub-
Tenon's infiltration. Br. J. Ophthalmol.1992;76:670-674. 10. Kumar C.M.: How to do a sub-Tenon's block. CPD Anaesthesia.2001;.3(2):56-61.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
212
ANESTHETIC RELATED NEURAL INJURY IN CHILDREN R.FLICK Department of Anesthesiology, Mayo Clinic, Rochester, Minnesota, USA Introduction
Exposure of the developing animal brain to anesthetic and sedative medications may cause neurodegenerative changes with adverse effects on learning and behavior.(1-8) Implicated drugs include N-methyl-D-aspartate (NMDA) glutamate receptor agonists and gamma-aminobutyric acid (GABA) antagonists encompassing virtually every medication used for anesthesia including volatile anesthetics, benzodiazepines, nitrous oxide, and propofol. When these drugs are administered to young animals (including primates) using clinically-relevant regimens, apoptotic neurodegeneration results. (2, 4, 5, 7, 9-11) Few studies are available that can provide insight into the clinical significance of these observations.(12-14) Recently, we reported an association between multiple, but not single anesthetic exposure prior to age 4 years and subsequent learning disabilities in a population-based birth cohort.(15) However, there were two major limitations of this work. First, the need for anesthesia may be a marker for other potentially causal factors, such as the condition necessitating surgery or co-existing disease and our prior work did not account for differences in the burden of illness between those exposed and those not exposed to anesthesia. Second, we examined only a single outcome (learning disability) and it is unclear if other outcomes may better correspond to the pattern of neural injury observed in animals.(12-14) Assessment of multiple outcomes within a single study has not been previously performed and may provide clues to the underlying mechanism of neural injury. In a more recent study, we utilized a population-based birth cohort and employed a matched cohort design that includes methods to adjust for health status. We examined learning disabilities (LD), the need for an individualized education program (IEP) and group achievement tests as outcomes to determine if an association exists between exposure to anesthesia during the first 2 years of life and the development of outcomes potentially associated with neurodegeneration.
The major finding of the study is that after adjustment for health status and matching for other factors associated with LD, exposure to anesthesia prior to age 2 years was a risk factor for the development of LD in children receiving multiple, but not single, anesthetics. A similar pattern of results was observed for most scales of group-administered tests of cognitive ability and achievement and the need for an IEP for speech/language impairments, but not the need for an IEP for emotional and behavioral disorders.
Although GABA agonists and NMDA antagonists can produce widespread apoptotic neurodegeneration in young animals, the significance in humans is not known. The few extant human studies have relied upon observational methodologies in existing datasets and have examined several outcomes. DiMaggio et. al. examined a birth cohort of Medicaid patients undergoing hernia repair and found, compared with an unexposed cohort, an increased risk (HR=2.3) of diagnoses consistent with behavioral abnormalities.(12) In contrast, Bartels analyzed the Netherlands Twins Registry and reported that group achievement test scores for unexposed twins from pairs discordant for anesthetic exposure did not differ between anesthesia-exposed and unexposed co-twins.(13) In a pilot study, Kalkman found a small increase in hazard ratio for “deviant behavior” in children exposed prior to 24 months of age.(14) Subsequent studies from our group, Dimaggio, Davidson, Block and others have each demonstrated an effect.(16-18)
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
213
Hansen however was not able to demonstrate and effect in a large European cohort.(19) However, all previous studies including ours are limited by the fact that confounding factors associated with the need for anesthesia and surgery may influence outcomes; children requiring multiple anesthetic exposures may have a higher burden of illness potentially affecting learning.(15, 20)
This and our previous studies utilized a birth cohort that is unique in that all members reside in the same community, attended the same schools, and received virtually all of their health care either at Mayo Clinic (>90%) or at Olmsted County Medical Center (<10%) ensuring that all medical and educational records could be directly reviewed.(20-24) The construction of this cohort, including potential effects of migration have been previously described.(25) Compared with our prior study, the current work incorporated four key distinctions. (15) First, a matched cohort design was employed using children matched for those factors known to be associated with LD and who were not exposed to anesthesia. Second, health status as determined in all children using two methods was used as an adjuster (not feasible in the prior study). Third, in the current study we examined anesthesia prior to age 2 years rather than prior to age 4 years, as animal data suggests that risk increases as the age at exposure decreases.(26) Finally, this study examined group-administered measures of performance not examined in our previous work, and represents the only available study that includes multiple outcomes that may be related to anesthetic related neurodegeneration.
We also analyzed outcomes beyond the occurrence of any LD, including LD sub-types (reading, written language, and mathematics), group-administered tests of cognitive ability and achievement and the need for IEP’s for speech/language and behavioral disorders. The rationale for this extended analysis included 1) determining whether a similar pattern of results observed for LDs (diagnosed using individually administered tests of cognitive ability and achievement) would be present in group-administered tests, and 2) whether there was any differential effect of anesthetic exposure on different outcomes. The pattern of injury identified in animals is variable, and it is not yet possible to predict what specific defects in learning or behavior would arise in humans with similar injury. In general, a similar pattern of results was observed in most group achievement test scores; although the comparison of multiple anesthetic exposures verses no exposure was often not statistically significant. This may reflect that not all members of the cohort received every group test, such that power to detect effects is lessened, or that group-administered tests are less sensitive than individually-administered tests in detecting the association. Nonetheless, we find little evidence of a differential pattern of effect on the various domains measured by these instruments. The only possible exception is the phonics subscale of the California Achievement Test, in which the parameter estimate for the effect of multiple exposure compared to no exposure was close to zero (see Table 3). We also find no evidence of differential effects on the three forms of LD, although there is considerable overlap between these three (i.e., children are frequently diagnosed with multiple LD sub-types). The profound effect of multiple anesthetic exposures on the need for a speech/language IEP is consistent with the increase in LD diagnosed by research criteria. This finding suggests that if multiple exposures to anesthesia and surgery are causing effects, these effects may be limited to learning and memory impairment, rather than a general category of behavioral disorders.
We concluded that, in this population-based birth cohort analyzed using a matched cohort
design and controlling for differences in health status, repeated exposure to anesthesia and
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
214
surgery prior to age 2 years was a significant independent risk factor for the later development of LD.
This lecture will discuss this study and review the other clinical evidence for and against an association between early exposure to anesthesia and later development of cognitive deficiency. Also discussed will be a general approach to understanding the strengths and limitations of the epidemiologic research upon which ours and others work is dependent.(27) References 1. Wang C, Sadovova N, Fu X, Schmued L, Scallet A, Hanig J, et al. The role of the N-methyl-D-aspartate receptor in ketamine-induced apoptosis in rat forebrain culture. Neuroscience. 2005;132(4):967-77. 2. Slikker W, Jr., Zou X, Hotchkiss CE, Divine RL, Sadovova N, Twaddle NC, et al. Ketamine-induced neuronal cell death in the perinatal rhesus monkey. Toxicol Sci. 2007;98(1):145-58. 3. Wang C, Slikker W, Jr. Strategies and experimental models for evaluating anesthetics: effects on the developing nervous system. Anesth Analg. 2008;106(6):1643-58. 4. Olney JW, Wozniak DF, Jevtovic-Todorovic V, Farber NB, Bittigau P, Ikonomidou C. Drug-induced apoptotic neurodegeneration in the developing brain. Brain Pathol. 2002;12(4):488-98. 5. Jevtovic-Todorovic V, Benshoff N, Olney JW. Ketamine potentiates cerebrocortical damage induced by the common anaesthetic agent nitrous oxide in adult rats. Br J Pharmacol. 2000;130(7):1692-8. 6. Young C, Jevtovic-Todorovic V, Qin YQ, Tenkova T, Wang H, Labruyere J, et al. Potential of ketamine and midazolam, individually or in combination, to induce apoptotic neurodegeneration in the infant mouse brain. Br J Pharmacol. 2005;146(2):189-97. 7. Ikonomidou C, Bosch F, Miksa M, Bittigau P, Vockler J, Dikranian K, et al. Blockade of NMDA receptors and apoptotic neurodegeneration in the developing brain. Science. 1999;283(5398):70-4. 8. Jevtovic-Todorovic V, Hartman RE, Izumi Y, Benshoff ND, Dikranian K, Zorumski CF, et al. Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci. 2003;23(3):876-82. 9. Rizzi S, Carter LB, Ori C, Jevtovic-Todorovic V. Clinical anesthesia causes permanent damage to the fetal guinea pig brain. Brain Pathol. 2008;18(2):198-210. 10. Zou X, Patterson TA, Divine RL, Sadovova N, Zhang X, Hanig JP, et al. Prolonged exposure to ketamine increases neurodegeneration in the developing monkey brain. Int J Dev Neurosci. 2009;27(7):727-31. 11. Slikker W, Jr., Zou X, Hotchkiss CE, Divine RL, Sadovova N, Twaddle NC, et al. Ketamine-induced neuronal cell death in the perinatal rhesus monkey. Toxicological Sciences. 2007;98(1):145-58. 12. DiMaggio C, Sun LS, Kakavouli A, Byrne MW, Li G. A Retrospective Cohort Study of the Association of Anesthesia and Hernia Repair Surgery With Behavioral and Developmental Disorders in Young Children. J Neurosurg Anesth. 2009;21(4):286-91 10.1097/ANA.0b013e3181a71f11. 13. Bartels M, Althoff RR, Boomsma DI. Anesthesia and cognitive performance in children: no evidence for a causal relationship. Twin Res Hum Genet. 2009;12(3):246-53.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
215
14. Kalkman CJ, Peelen L, Moons KG, Veenhuizen M, Bruens M, Sinnema G, et al. Behavior and development in children and age at the time of first anesthetic exposure. Anesthesiology. 2009;110(4):805-12. 15. Wilder RT, Flick RP, Sprung J, Katusic SK, Barbaresi WJ, Mickelson M, et al. Early Exposure to Anesthesia and Learning Disabilities in a Population-Based Birth Cohort. Anesthesiology. 2009;110. 16. DiMaggio C, Sun LS, Li G. Early childhood exposure to anesthesia and risk of developmental and behavioral disorders in a sibling birth cohort. Anesth Analg. 2011;113(5):1143-51. 17. Ing C DC, Whitehouse A, Hegarty M, Davidson A, Sun LY. . Long-term differences in cognitive and language ability after exposure to surgery and anesthesia in infancy. . International Anesthesia Research Society; 20112011. 18. Block RI, Thomas JJ, Bayman EO, Choi JY, Kimble KK, Todd MM. Are Anesthesia and Surgery during Infancy Associated with Altered Academic Performance during Childhood? Anesthesiology. 2012. 19. Hansen TG, Pedersen JK, Henneberg SW, Pedersen DA, Murray JC, Morton NS, et al. Academic performance in adolescence after inguinal hernia repair in infancy: a nationwide cohort study. Anesthesiology. 2011;114(5):1076-85. 20. Sprung J, Flick RP, Wilder RT, Katusic SK, Pike TL, Dingli M, et al. Anesthesia for cesarean delivery and learning disabilities in a population-based birth cohort. Anesthesiology. 2009;111(2):302-10. 21. St Sauver JL, Katusic SK, Barbaresi WJ, Colligan RC, Jacobsen SJ. Boy/girl differences in risk for reading disability: potential clues? Amer J Epidemiol. 2001;154(9):787-94. 22. Katusic SK, Colligan RC, Barbaresi WJ, Schaid DJ, Jacobsen SJ. Incidence of reading disability in a population-based birth cohort, 1976-1982, Rochester, Minn. Mayo Clin Proc. 2001;76(11):1081-92. 23. Katusic SK, Colligan RC, Weaver AL, Barbaresi WJ. The forgotten learning disability: epidemiology of written-language disorder in a population-based birth cohort (1976-1982), Rochester, Minnesota. Pediatrics. 2009;123(5):1306-13. 24. Barbaresi WJ, Katusic SK, Colligan RC, Weaver AL, Jacobsen SJ. Math learning disorder: incidence in a population-based birth cohort, 1976-82, Rochester, Minn. Ambul Pediatr. 2005;5(5):281-9. 25. Katusic SK, Colligan RC, Barbaresi WJ, Schaid DJ, Jacobsen SJ. Potential influence of migration bias in birth cohort studies. Mayo Clin Proc. 1998;73(11):1053-61. 26. Loepke AW, Soriano SG. An assessment of the effects of general anesthetics on developing brain structure and neurocognitive function. Anesth Analg. 2008;106(6):1681-707. 27. Flick RP, Warner DO. A Users' Guide to Interpreting Observational Studies of Pediatric Anesthetic Neurotoxicity: The Lessons of Sir Bradford Hill. Anesthesiology. 2012.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
216
SAFETY ASPECTS IN PAEDIATRIC ANAESTHESIA EHRENFRIED SCHINDLER Dept. of Paediatric Anaesthesiology, Children´s Hospital Asklepios Klinik Sankt Augustin, visiting Professor University of Belgrade, Serbia
E-mail: [email protected] Introduction
Patient safety in the Operating Room and beyond has long been a driving force in anaesthesia care. Technical innovations such as pulse oximetry and end-tidal capnography combined with better trainee and practitioner education to dramatically increase the safety of our patients and the quality of our anaesthesia over the years and newer medications, technologies and monitoring modalities continue to advance the field. As a result of these systematic changes, anaesthesia-related patient morbidity and mortality has steadily declined across all patient populations. Non-technical attempts to reduce perioperative complications have become another major focus of various organizations such as the World Health Organization (WHO) and the Joint Commission for the Accreditation of Hospital Organizations (JCAHO). Efforts to delineate the frequency of complications related to anaesthesia in patients undergoing congenital cardiac surgery and procedures in the cardiac catheterization laboratory and elsewhere have been difficult because of the low occurrence of this surgery compared to other surgeries on children and the relatively rare incidence of anaesthesia-related complications1-3. Anaesthesia related mortality in children
The Mayo Clinic in Rochester, USA reviewed their experience with cardiac arrests in children4. A consistent factor in all of these studies is that children with underlying congenital cardiac defects are at a much higher risk of cardiac arrest than children without these defects. The incidence of cardiac arrest at the Mayo Clinic for children during non-cardiac procedures was 2.9 per 10,000 versus 127 per 10,000 for children undergoing cardiac procedures, a 30-fold increase in risk. Sub-analysis related to causality, age, and type of surgery further stratified their data. Of their 92,881 patients, 4,242 were for cardiac procedures. Within the 54 children who suffered a cardiac arrest or death undergoing a cardiac procedure, age played a significant role, with neonates having the highest risk. Anesthesia was not identified as a causative factor in any of the cardiac surgical arrests or death. At the Royal Children’s Hospital, Melbourne, Australia, van der Griend and colleagues examined anesthesia-related mortality in 101,885 anesthetics administered to 56,263 children from January 1, 2003 through August, 20085. They too utilized an expert review panel of 3 senior anesthesiologists examining the record of every patient who died during this time period who had received an anesthestic in the preceding 30 days. Overall anesthesia-related mortality was found to be 1 in 10,188 cases (0.98 per 10,000). All 10 deaths where anesthesia was found to be contributing factor had significant pre-existing conditions, with pulmonary hypertension present in 50%. There were no anesthetic-related morbidities in children without underlying medical problems. Overall mortality was significantly higher in children < 30 days and those with cardiac disease (particularly after 30 days of life).As is evident from the most recent data, even the busiest of programs only infrequently have anesthesia-related cardiac arrests or death because of the low incidence of these events. As a consequence, it is necessary to harvest data over many years to collect any meaningful numbers, during which time

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
217
major changes in patient management may occur. The APRICOT (Anaesthesia PRacticeIn Children Observational Trial) study is currently collecting observational data in paediatric anaesthesia practice all over Europe. APRICOT isincluding all children from birth to 15 years old scheduled for an elective or urgent diagnostic or surgical procedure under sedation (PSA included) or general anaesthesia with or without regional analgesia. Beside the child’s medical history, the occurrence of selected severe critical events during and up to 60 minutes after anaesthesia or sedation and requiring immediate intervention will be recorded. So far more than 5000 cases are in this database waiting for analysis. First results can be expected in late 2015.
Errors and Outcome in Paediatric Anaesthesia
The perioperative management of paediatric patients is fraught with times where even small decision making errors may have catastrophic outcomes. James Reason has described the “Swiss Cheese Model” for evaluating patient complications due to human errors. For a complication to occur, all the “holes” in the cheese have to line up – i.e. a sequential failure of various defense mechanisms in place to prevent, recognize and/or treat unwanted physiologic changes. Many “anaesthesia” complications are multi-factorial in origin and it can be difficult to assign the relative contributions of different clinical services. These system factors are further exacerbated if there are communication difficulties between the various parties, including surgeons, anaesthesiologists, paediatrician, and the pre- and post-operative medical and nursing teams6;7. “Near Misses” are important as they are 10 - 100 times more common than documented adverse events and yet share the same organizational and cognitive sources of error as major adverse events. Determining the frequency and nature of “Near Miss” events is potentially far more important than just looking at system failures resulting in patient injury. However, “Near Miss” analysis is difficult as it requires a trained, independent observer to accompany the patient through the entire care continuum.
The six ´C`s: Communication and Teamwork
In complex environments like paediatric operating rooms, errors cannot and will not be avoided nor eliminated. In his book “Normal Accidents: Living With High-Risk Technologies” Perrow has postulated that even the best teams cannot eliminate every error (ISBN 978-0691004129). What they can achieve at best is to prolong the time interval in between errors. Therefore it is of high importance for successful hospitals to create a culture of safety similar to the culture that the aviation industry promulgated to minimize the risk of human errors. More than a decade was required before hospitals were able to embed the concepts of checklists, team-time-outs and sign in/sign out procedures as components of daily safety procedures. The six “Cs” - Communication, Cooperation, Coordination, Cognition (simulation and cross-training), Conflict (managing disruptive behaviour) and Coaching (team-training) are the key goals for successful working interdisciplinary teams8.
Team Training and Simulation
Clinical training usually focuses on the individual execution of tasks. Safe and efficient patient care requires the co-ordination of activity amongst physicians, nurses, respiratory therapists, pharmacists, and other healthcare professionals6;7;9. However, all of these team members are rarely trained together. Effective teamwork is not reliably learned without formal training and cultivation. Team training teaches a set of tools and strategies that requires a mental shift from an individual perspective to a team perspective. Several different medical team training programs

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
218
have been developed. Medical team training programs can be categorized into high-fidelity simulator-based programs and classroom-based programs10. The high-fidelity simulator-based programs rely upon patient simulators and include courses such as anaesthesia crisis resource management (ACRM). The classroom-based team training programs rely upon lectures, videos, demonstrations, and role play11-13. There is considerable overlap between all of these training programs, and there is no evidence that one training program or method is superior to another. Advocates of high-fidelity simulator-based programs list several advantages. Simulators provide hands-on training in a realistic environment. The environment mandates the integration of decision skills, procedural skills, and teamwork skills in a scenario that actually challenges and stresses the clinician. Advocates of classroom-based programs highlight the lower cost, mobility, and ability to train large numbers of students simultaneously. From our experience during repeated courses during the Anaesthesia Summer School held in Belgrade University Hospital we know that these classroom trainings were highly effective and audience participation was remarkably high. Post congress ratings revealed the high quality of these courses. Simulation like the one in Belgrade can easily be transferred also to other units.
Checklists
The World Health Organization (WHO) recognizes that surgical complications are common and often preventable. It has been estimated that over 230 million major surgeries take place per year. Of these, 7 million major complications occur, including 1 million deaths. A team of experts created the WHO Surgical Safety Checklist, designed to improve teamwork and prevent common causes of perioperative morbidity and mortality14-16. The WHO Surgical Safety Checklist promotes and facilitates good teamwork by helping the team develop a shared mental model with the use of a brief before anesthesia induction and a time out before skin incision. Before the procedure begins, the entire team introduces themselves by name in order to flatten hierarchy. The checklist also empowers team members to speak up if they notice any safety concerns. Several components of the WHO Surgical Safety Checklist are related to the practice of anaesthesiologists. The Checklist specifically encourages vigilance related to the presence of a difficult airway, risk of aspiration, risk of significant blood loss, the presence of allergies, and timely administration of prophylactic antibiotics14. A redesigned Children oriented checklist can be downloaded from the website of the European Society for Paediatric Anaesthesia (ESPA) Summary
In the last years patient safety is becoming a major goal in medical all day practice. To avoid near misses and severe adverse events an open “error” culture of discussion and trust is mandatory. Simulation, patient safety workshops and specialist training is becoming more and more popular. It is on our own to initiate “safety systems” in our hospitals to increase and establish a more safe environment for our patients. Reference List 1. Morray JP: Cardiac arrest in anesthetized children: recent advances and challenges for the
future. Paediatr.Anaesth. 2011; 21: 722-9 2. Bognar A, Barach P, Johnson JK, Duncan RC, Birnbach D, Woods D, Holl JL, Bacha EA:
Errors and the burden of errors: attitudes, perceptions, and the culture of safety in pediatric cardiac surgical teams. Ann.Thorac.Surg. 2008; 85: 1374-81
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
219
3. Barach P, Small SD: Reporting and preventing medical mishaps: lessons from non-medical near miss reporting systems. BMJ 2000; 320: 759-63
4. Flick RP, Sprung J, Harrison TE, Gleich SJ, Schroeder DR, Hanson AC, Buenvenida SL, Warner DO: Perioperative cardiac arrests in children between 1988 and 2005 at a tertiary referral center: a study of 92,881 patients. Anesthesiology 2007; 106: 226-37
5. van der Griend BF, Lister NA, McKenzie IM, Martin N, Ragg PG, Sheppard SJ, Davidson AJ: Postoperative mortality in children after 101,885 anesthetics at a tertiary pediatric hospital. Anesth.Analg. 2011; 112: 1440-7
6. Christian CK, Gustafson ML, Roth EM, Sheridan TB, Gandhi TK, Dwyer K, Zinner MJ, Dierks MM: A prospective study of patient safety in the operating room. Surgery 2006; 139: 159-73
7. Gurses AP, Kim G, Martinez EA, Marsteller J, Bauer L, Lubomski LH, Pronovost PJ, Thompson D: Identifying and categorising patient safety hazards in cardiovascular operating rooms using an interdisciplinary approach: a multisite study. BMJ Qual.Saf 2012; 21: 810-8
8. Dickerman KN, Barach P: Designing the Built Environment for A Culture and System of Patient Safety - A Conceptual, New Design Process. 2008;
9. Papaspyros SC, Javangula KC, Adluri RK, O'Regan DJ: Briefing and debriefing in the cardiac operating room. Analysis of impact on theatre team attitude and patient safety. Interact.Cardiovasc.Thorac.Surg. 2010; 10: 43-7
10. Fehr JJ, Boulet JR, Waldrop WB, Snider R, Brockel M, Murray DJ: Simulation-based assessment of pediatric anesthesia skills. Anesthesiology 2011; 115: 1308-15
11. Gillon S, Radford S, Chalwin R, Devita M, Endacott R, Jones D: Crisis resource management, simulation training and the medical emergency team. Crit Care Resusc. 2012; 14: 227-35
12. Carlson J, Min E, Bridges D: The impact of leadership and team behavior on standard of care delivered during human patient simulation: a pilot study for undergraduate medical students. Teach.Learn.Med. 2009; 21: 24-32
13. Robertson B, Kaplan B, Atallah H, Higgins M, Lewitt MJ, Ander DS: The use of simulation and a modified TeamSTEPPS curriculum for medical and nursing student team training. Simul.Healthc. 2010; 5: 332-7
14. Saturno PJ, Soria-Aledo V, Da Silva Gama ZA, Lorca-Parra F, Grau-Polan M: Understanding WHO surgical checklist implementation: tricks and pitfalls. An observational study. World J.Surg. 2014; 38: 287-95
15. Fudickar A, Horle K, Wiltfang J, Bein B: The effect of the WHO Surgical Safety Checklist on complication rate and communication. Dtsch.Arztebl.Int. 2012; 109: 695-701
16. Alnaib M, Al SA, Bhattacharya V: The WHO surgical safety checklist. J.Perioper.Pract. 2012; 22: 289-92

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
220
AKUTNI RESPIRATORNI SINDROM KOD DECE – SAVREMENI PRISTUP ACUTE RESPIRATORY DISTRESS SYNDROME IN CHILDREN - A MODERN APPROACH BILJANA DRAŠKOVIĆ Institut za zdravstvenu zaštitu dece i omladine Vojvodine,Klinika za dečju hirurgiju Služba za anesteziju intenzivnu terapiju i terapiju bola,Medicinski fakultet Novi Sad E-mail:[email protected] Abstract Acute respiratory distress syndrome (ARDS) is a heterogeneous syndrome that lacks definitive treatment. The cornerstone of management is sound intensive care treatment and early anticipatory ventilation support. A mechanical ventilation strategy aiming at optimal alveolar recruitment, judicious use of positive end-respiratory pressure (PEEP) and low tidal volumes (VT) remains the mainstay for managing this lung disease. Several treatments have been proposed in rescue settings, but confirmation is needed from large controlled clinical trials before they be recommended for routine care. Non-invasive ventilation (NIV) is suggested with a cautious approach and a strict selection of candidates for treatment. The extra-corporeal carbon dioxide removal (ECCO2 R), used as an integrated tool with conventional ventilation, is playing a new role in adjusting respiratory acidosis and CO2. The proposed benefits of ECCO2 R over extra-corporeal membrane oxygenation (ECMO) consist in a reduction of artificial surface contact, avoidance of pump- related side effects and technical complications, as well as lower costs. The advantages and disadvantages of inhaled nitric oxide (iNO) are better recognized today and iNO is not recommended for ARDS in children and adults because iNO results in a transient improvement in oxygenation but does not reduce mortality, and may be harmful. Several trials have found no clinical benefit from various surfactant supplementation methods in adult patients with ARDS. However, studies which are still controversial have shown that surfactant supplementation can improve oxygenation and decrease mortality in pediatric and adolescent patients in specific conditions and, when applied in different modes and doses, also in neonatal respiratory distress syndrome (RDS) of preemies. Management of ARDS remains supportive, aimed at improving gas exchange and preventing complications.
Uvod
Akutni respiratorni distress sindrom (ARDS) je heterogeni sindrom sa složenom patologijom i mehanizmima nastanka koji za lekare kliničare predstavlja veliki izazov, posebno kada su u pitanju terapijske mogućnosti kod dece. ARDS ima manju učestalost kod odojčadi i dece nego kod odraslih i ređe se javlja težak oblik respiratorne insuficijencije.Kritična primena pozitivnog pritiska na kraju ekspirijuma (PEEP), inspiratorne koncentracije kiseonika (FiO2) i disajnog volumena (VT) poslednjih decenijaučinile su da se ARDS retko viđa u modernoj pedijatrijskoj jedinici intenzivnog lečena (ICU). Ranadijagnostika,adekvatne mere intenzivnog lečenja mogu poboljšati ishod, izbeći neželjene efekte i komplikacije i povećati preživljavanje.Neophodno je lečiti primarni uzrok (npr. sepsa, pneumonija), smanjiti rizikod multiple organske disfunkcije (MODS), kao i ventilatorom indukovane plućne povrede (VILI) (1).
Definicija ARDS-a kod odojčadi, male dece, adolescenatai I odraslih u osnovi je ista. Međutim, postoje razlike između pedijatrijskih bolesnika I odraslih koje u osnovi mogu uticati
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
221
na strategiju lečenja.Mlađa deca imaju veći otpor u disajnim putevima, veću komplijansu zida grudnog koša, niži funkcionalni rezidualni kapacitet. Imaju pluća koja su još uvek u fazi rasta I razvoja sa većim rizikom od razvoja VILI uz niže pritiske u disajnim putevima od odraslih. Niže vrednosti hematokrita – što može uticati na globalno dopremanje kiseonika, veće potrebe za sedacijom idrugo (2).
Kod dece kao i kod odraslih najčešći uzrok ARDS-a su infekcije (virusne ili bakterijske), sistemske infekcije, opsežne trauma, aspiracije. Ređe je uzrok pankreatitis, transfuzije, reakcija na lekove, gljivične infekcije. Rizik je svakakao veći ako postoji više faktora I komorbiditeta.(3)
Učestalost ARDS-a u celokupnoj pedijatrijskoj populaciji je relativno mala I kreće se od 2,9 do 9,5 na 100 000 dece godišnje. Međutim, učestalost je daleko veća ako se gleda samo u PICU.Velika prospektivna studija rađena u Španiji beleži ARDS kod 1,4% primljene dece u ICU, I 8,4% dece koja su bila na MV. U Nemačkoj 3,2% dece primljene u PICU razvije ARDS, dok u Kini 1,4%. Smrtnost se kreće od 22 do 35% I svakako zavisi od uzroka I predhodnog zdravstvenog stanja.(2, 4,5,6)
ARDS je nedavno dobio novu, Berlinsku, definiciju, po kojoj je klasifikovan u tri kategorije, zasnovane na stepenu hipoksemije, eliminišuću na taj način termin akutna plućna povreda (ALI). Blagi (200 mm Hg < PaO2/FiO2 ≤ 300 mm Hg), umereno teški (100 mm Hg < PaO2/FiO2 ≤ 200 mm Hg) i teški oblik (PaO2/FiO2 ≤ 100 mm Hg). Četiri pomoćne varijable [težina plućne radiografije, PEEP ≥ 10 cm H2O, komplijansa respiratornog sistema (Crs) ≤ 40 mL/cm H2O, korigovana vrednost izdahnutog volume u minuti (VEcorr) ≤ 10L/min)] uz indeks oksigenacije (OI) predložene su za procenu teškog ARDS-a, I ako ove varijable ne dobripose prognozi preživljavanja.(7) Berlinska definicija olakšava definisanje terapijskih strategija u odnosu na težinu bolesti. Deca čine oko 12% ukupne populacije I sprovođenje velikih studija, vezane za relativno retke bolesti, je teško. Tako da kod odojčadi i male dece ne postoji adekvatni literaturni podaci o terapijskoj strategiji te se uglavnom koriste podaci dobijeni iz iskustva na odraslima. Protektivna mehanička ventilacija pluća Osnovna strategija lečenja kod odraslih je primena protektivne ventilacije sa primenom nižih vrednosti disajnog volumena (VT) I pritiska, adekvatnog nivoa PEEP-a kakobi se sprečila VILI i poboljšalo preživljavanje. Ova strategija ventilacije prihvaćena je I kod akutne respiratorne insuficijencije u pedijatrijskom uzrastu. VT≤ 6-7 mL/kg, I sa nivoom PEEP-a najmanje 2-3 cm H2O iznad gornje najniže tačke na krivi volumen/pritisak kako bi se terminalne bronhiole održale otvorenim. (8)Optimalna vrednost o PEEP-a nije definisana, ali sigurno je najpoželjniji onaj nivo kojim možemo izbeći ponavljajuće kolapse pluća i održavati alveole otvorenim (9). Kod ventilacije niskim VT postoji rizik od hipoventilacije i ventilacije samo mrtavog prostora.Permisivna hiperkapnija je prihvatljiva I kod dece, ali vrednost PaCO2 treba da ispod 50-55 mm Hg. Minutna ventilacija može se smanjiti snižavanjem disajnog volumena, dokle god je PaCO2 u ravnoteži sa nivoom serumskih bikarbonata kako bi pH ostao iznad 7.20. Ovo je naročito važno u neonatalnom i odojčadskom uzrastu kada postoji povećani rizik odintrakranijalnog krvarenja.(10)
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
222
Potrbušni položaj Potrbušni položaj se predlaže za poboljšanje oksigenacije, respiratorne mehanike,
alveolarne inflacije i ventilatorne distribucije, za homogenizaciju gradijenta pleuralnog pritiska i sprečavanje prekomerne inflacije pluća.
Potrbušni položaj doprinosi povećanju plućnog volumena, smanjenju atelektaza i poboljšanju drenaže sekreta (11).
U ovom položaju plućna gustina se redistribuira od zavisnih delova pluća, dok se u leđnom (proksimalno od kičme) redistribuira ka zavisnim delovima pluća (bliže sternumu). Potrbušnipoložaj menja alveolarnu inflaciju i ventilatornu distribuciju reverzijom hidrostatskog pritiska koji se nalazi preko plućnog parenhima, reverzijom pritiska koji je posledica težine srca i promenama u obliku zida grudnog koša i njegovoj mehanici. Vraćajući se u supinaciju, alveole u dorzalnoj regiji mogu ostati otvorene zato što PEEP rezultuje konstantinim odgovorom.(12,13)
Neefikasnost ovog položaja može biti posledica kašnjenja u primeni (kad su pluća već konsolidovana te ne mogu biti ponovo otvorena), kao i nedovoljnog trajanja potrbušnog položaja.Neke studije navode da držanje pacijenta 12h sati u potrbušnom položaju može indukovati promene koje su slične onima koji se povezuju saleđnim. U zavisnosti od razvoja rane atelektaze pacijenata na mehaničkoj ventilaciji pluća, potrbušni položaj se mora započeti što je pre moguće da bi se povećala efikasnost. (1)
Postoje deca koja ne reaguju naovu metodu što se dešava i kod odraslih. Neinvazivna ventilacija Uprkos kontroverznim i ponekad neohrabrujućim rezultatima velikih studija koje je trebalo da kliničarima stvore oprezne stavove i usku selekciju pacijenata koje treba lečiti neinvazivnom ventilacijom (NIV), ovaj metod se sve češće primenjuje kod pacijenata u ICU obolelih od ALI ili ARDS-a. (14,15) Ventilacija kontinuiranim pozitivnim pritiskom
Početkom '70ih godina, počeli su se pojavljivati radovi o primeni ventilacije kontinuranim pozitivnim pritiskom (CPAP) za otvaranje neventiliranih alveola i povećanje funkcionalnog rezidalnog kapaciteta, posledično smanjivanje desno-levog intrapulmunarnog šanta i poboljšavanje plućne mehanike [3-32]. CPAP je široko korišćen i postigao je uspeh u lečenju pediatrijskih pacijenata, najviše među prevremeno rođenom decom, sa ili bez idiopatskog respiratornog distres sindroma (16,17).
Kod pacijenata sa blagim ARDS-om, CPAP može poboljšati oksigenaciju, redukovati dispneu (18).
Visokofrekventna oscilatorna ventilacija
Visokofrekventna oscilatorna ventilacija (HFOV) predstavlja metodu izbora kod odojčadi i dece sa ARDS-om kada konvencionalni modovi ventilacije nemaju uspeha. Podrazumeva primenu visokog PEEP-a, malog disajogi volumena, velike respiratorne frekvence. Primenjeni vid ventilacije redukuje nastanak VILI.Do sada nema pouzdanih podataka koji potvrđuju veću efikasnost od konvencionalnih metoda i protektivne stretegije ventilacije pluća.(1).
Bolja oksigenacija primenom HFOV kod dece, zabeležena je u okvirunekontrolisanih studija i prikaza slučajeva.(19).
Dve skorašnje multicentrične studije rađene na adultnoj populaciji ne ukazuju na prednost HFOV u odnosu na konvencionalnu populaciju. (20)

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
223
Ekstrakorporalnaeliminacija ugljen-dioksida Ekstrakorporalna gasna razmena, naročito ekstrakorporalna membranska oksigenacija (ECMO), ekstenzivno je proučavana sedamdesetih godina dvadesetog veka. Primena ECMO menjala se kroz vreme u zavisnosti od rezultata većih studija i manjih grupa bolesnika(21). Koncept ekstrakorporalne elimanacije ugljen-dioksida (ECCO2 R- Extracorporeal CO2- removal) primenjuje se kao sastavni deo konvencionalne ventilacije u terapiji respiratorne acidoze uz smanjenjedisajnog volumena.(22,23) Bezpumpna ekstrakorporalna asistirana plućna terapija (ili intervencijska plućna podrška (iLA)), koristi nisko rezistentnu gasno razmensku membranu (plućni asistirajući uređaj-lung assist device-LAD) interponiranu između dve kanile koje su povezane kratkim cevčicama da omogući artero-venski šant u femoralnim krvnim sudovima. Faza gasa je locirana unutar, dok krv teče izvan šupljeg sistema. Gasna razmena se dešava duž cele semipermeabilne membrane i omogućena je gradijentima parcijalnih pritisaka ugljen dioksida i kiseonika između krvi i gasne faze, koja je povezana sa izvorom kiseonika (12-13 L/min). Protok krvi kroz sistem cevi i membranu za gasnu razmenu posledica je isključivo razlike između arterijskog i venskog krvnog pritiska.(24) Predviđene prednosti ECCO2 R u poređenju sa ECMO su redukcija kontakta sa veštačkom površinom, izbegavanje neželjenih efekata povezanih sa pumpom, kao i tehničkih komplikacija i redukovanje troškova.(25) Ova metodologija se čini korisnomali zahteva još studija i istraživanja u pedijatrijskom uzrastu. Inhalatorni azot oksid Korišćenje inhalatornog azot oksida (iNO) predlagano je u lečenju teških plućnih bolesti, uključujući i ARDS, poslednjih petnaest godina i to u cilju smanjenja plućne hipertenzije i plućne hipoksijske vazokonstrikcije, što bi moglo da dovede do poboljšanja ventilacije pluća i potencijalno smanji potrebu za ventilacijskom podrškom i favorizuje oksigenaciju redukcijom FiO2, pri čemu se limitira toksičnost visokih koncentracija kiseonika (1). Posle inicijalnog entuzijazma nakon uptrebe iNO u ALI-a i ARDS-u, koristi i nedostaci ovog tretmana su sada bolje procenjeni. Poboljšanje u ventilaciji i redukciji FiO2, dva glavna benefita, sugerisana od brojnih autora, dovedena su u pitanje u Cochrane pregledu koji nije pokazao statistički značajne efekte na stopu mortaliteta i na tranzitorno poboljšanje oksigenacije u hipoksemijskoj respiratornojinsuficijenciji kod dece i odraslih tretiranih iNO. Postoji jasno dokazan rizik od toksičnosti, kako za pacijente tako i za blisko okruženje (uključujući i medicinsko osoblje). Posebna pažnja je posvećena mogućnosti indukovanja iNO zavisnosti koja je praćena produženim odvikavanjemod respiratora kao i toksičnim efektima iNO na egzogeni plućni surfaktant koji oboje mogu negativno da utiču na ishod lečenja.(26,27). iNO ne može biti preporučen za ARDS i ALI kod dece i odraslih. iNO rezultuje u prolaznom poboljšanju oksigenacije ali ne redukuje mortalitet i potencijalno može biti štetan.(28) Suplementacija surfaktanta Različite abnormalnosti surfaktanta su opisane kod pacijenata sa ARDS-om. Misli se da su alteracije u strukturi i funkciji surfaktanta rezultat različitih medijatora uključujući i kiseonične radikale, proteaze, lipaze, bioaktvne lipide i serumske proteine. Neuobičajena funkcija surfaktanta čini da neki delovi pluća kolabiraju, što dovodi do toga da deo udahnutog disajnog volumena biva usmeren u komplijantnije, neatelektatične delove pluća. Do tada nepovređeni delovi pluća mogu biti predistendirani i povređeni ako parametri ventilacije nisu adekvatno

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
224
podešeni. Suplementacija egzogenog surfaktanta može teoretski poboljšati rešavanje mnogih od navedenih problema.(1,29) Nekoliko randomizovanih studija kod odraslih došloje do zaključka da nema kliničkog benefita od različitih vrsta surfaktanata ako se primene u dozama i modalitetima koje se primenjuju kod prematurusa sa RDS-om i odraslih sa ARDS-om. Druge studije, naprotiv, nalaze da suplementacija surfaktanta poboljšava oksigenaciju i značajno smanjuje mortalitet kod pedijatrijskih pacijenata.(30,31,32) Malo je verovatno da je korišćenje surfaktanta na isti način kao kod prematurusa (u bolusima i visokim dozama) najbolji modalitet suplementacije u kasnijem životnom dobu (kod dece i odraslih) obzirom na različitu etiologiju nedostataka surfaktanta u ovim različitim starosnim grupama. Po sadašnjim saznanjima, nedostatak surfaktanta kod prematurusa sa RDS nastaje zbog nezrelosti pneumocita tipa II, dok je kod ARDS-a u odojčadi i dece glavni razlog poremećena produkcija i/ili povećana inaktivacija surfaktanta. Iz tih razloga, moguće je da se drugi načini suplementacije, kao što je bronhoalveolarna lavaža (BAL), mogu primeniti sa mnogo više uspeha jer se surfaktant primenjuje kada je većina inhibitora surfaktanta u plućima uklonjena. (33,34) Finalna razmatranja Napravljen je znatan napredak u razumevanju osnovnih mehanizama ARDS-a, njegovom definisanju I dijagnostifikovanju. Glavne preporuke lečenja su strategije mehaničke ventilacije: optimalno angažovanje alveola, uz razumnuupotrebu PEEP-a i niskedisajne volumenesa ciljem poboljšanja gasne razmene i prevencije komplikacija dok se uporedo leči bolest koja predstavlja uzrok nastajanja ARDS-a. Potencijalne ARDS-specifične terapije se i dalje istražuju i do sada nisu pokazale značajnija unapređenja u tretmanu ove bolesti, pa se ne mogu ni preporučiti u rutinskoj praksi. Napredak u preživljavanju čiji smo svedoci je verovatno rezltat savremenih metoda intenzivnog lečenja bolesnika i veće pažnje posvećene vidovima ventilacije. Ne postoji jedinstven metod u lečenju pacijenata sa ARDS-om, tretman mora biti prilagođen godinama pacijenta i težini plućne patologije. Literatura: 1. Marraro GA, Chengshui Chen, Maria Antonella PigaYan Qian, Claudio Spada, Umberto enovese1 Acute respiratory distress syndrome in the pediatric age: an update on advanced treatment. Chin J Contemp Pediatr 2014, 6 (5): 437- 447 2. Cheifetz MI, FAARC MD Pediatric Acute Respiratory Distress Syndrome. Respiratory Care 2011: 56(10) 1589-1599. 3. Cornfield DN Acute respiratory distress syndrome in children:physiology and management. Crr Opin Pediatr 2013, 25(3): 338-343. 4. Randolf AG Wypij D, VenkataramanST, Hanson JH Gedeit RG, Meert KL, et al;on behalv of thePediatric Acute Lung Injuty and Sepsis Investigators (PALISI) Network. Effect of mechanical ventilator weaning protocols on respiratory outcomes in infants and children: a randomized controlled trial. JAMA 2002;288(20):2561-2568. 5. Flori HR, Glidden EV, RutherfordGW, Matthay MA. Pediatric acute lung injury: Prospective evaluation of risk factors associated with mortality. Am J Respir Crit Care Med 2005;17(9):995-1001.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
225
6. Curley MA, Hibberd PL, Fineman LD, Wypij D, Shih MC, Thompson JE et al. Effect of prone position on clinical outcomes in children with acute lung injury: randomized controlled trial. JAMA 2005;294(2):229-237.
7. ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin Definition[J]. JAMA, 2012, 307(23): 2526--2533.
8. Kneyber MCJ, Rimensberger PC: The need for and feasibility of a pediatric ventilation trial: Reflection on a survey among pediatric intensivists[J]. Pediatric Crit Care Med, 2012, 13(6): 632--638.
9. Briel M, Meade M, Mercat A, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta--analysis[J]. JAMA, 2010, 303(9): 865--873.
10. Hagen EW, Sadek--Badawi M, Carlton DP, et al. Permissive hypercapnia and risk for brain injury and developmental impairment[J]. Pediatrics, 2008, 122(3): e583--e589.
11. Abroug F, Ouanes-Besbes L, Dachraoui F, et al. An updated study-level meta-analysis of randomised controlled trials on proning in ARDS and acute lung injury[J]. Crit Care, 2011, 15(1): R6.
12. Dickinson S, Park PK, Napolitano LM. Prone-positioning therapy in ARDS[J]. Crit Care Clin, 2011, 27(3): 511--523.
13. Gillies D, Wells D, Bhandari AP. Positioning for acute respiratory distress in hospitalised infants and children(J) Cchrane Database Syst Rev, 2012, 7: CD003645
14. Schonhofer B, Kuhlen R, Neumann P, et al. Non-invasive ventilation as treatment for acute respiratory insufficiency. Essentials from the new S3 guidelines[J]. Anaesthesist, 2008, 57(11): 1091--1102.
15. Wang S, Singh B, Tian L, et al. Epidemiology of noninvasive mechanical ventilation in acute respiratory failure a retrospective population-based study [J) BMC Emerg Med, 2013,13:6.
16. Tapia JL, Urzua S, Bancalari A, et al. Randomized trial of early bubble continuous positive airway pressure for very low birth weight infants[J]. J Pediatr, 2012,161(1):75-80.
17. Saxena A, Thapar RK, Sondhi V, et al. Continuous airway pressure for spontaneously breathing premature infants with respiratory distress syndrome[J]. Indian J Pediatr, 2012, 79(9): 1185--1191.
18. L Her E, Deye N, Lellouche F et al. Physilogic effect of noninvasive ventilation during acute lung injury(J). Am J Respir Crit Care Med, 2005, 172(9):1112-1118.
19. Ben Jaballah N, Khaldi A, Mnif K, et al. High-frequency oscillatory ventilation in pediatric patients with acute respiratory failure(J) Pedijatr Crit Care Med, 2006, 7(4):362-367.
20. Ferguson ND, Cook DJ, Guyatt GH, et al- High- frecvency oscillation in early acute respiratory distress syndrome[J]. N Engl J Med, 2013, 386(9): 795--805.
21. Kaushik M, Wojewodzka.Zelezniakowicz M, Cruz DN. Et al. Extracorporeal carbon dioxide removal: the future of lung support lies in the history(J). Blood Purif, 2012, 34(2):94-106.
22. Moerer O, Quintel M. Protective and ultra-protective ventilation: using pumpless interventional lung assist (iLA) (J). Minerva Anestesiol,. 2011, 77(5): 537-544.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
226
23. Gómez-Caro A, Badia JR, Ausin P. Extracorporeal lung assist in severe respiratory failure and ARDS. Current situation and clinical applications[J]. Arch Bronconeumol,. 2010, 46(10): 531-537.
24. Walles T. Clinical experience with the iLA Membrane Ventilator pumpless extracorporeal lung-assist device[J]. Expert Rev Med Devices, 2007, 4(3): 297-305.
25. Bein T, Weber F, Philipp A, et al. A new pumpless extracorporeal interventional lung assist in critical hypoxemia/hypercapnia[J]. Crit Care Med, 2006, 34(5): 1372-1377.
26. Sokol J, Jacobs SE, Bohn D. Inhaled nitric oxide for acute hypoxemic respiratory failure in children and adults[J]. Cochrane Database Syst Rev, 2003, (1): CD002787.
27. Marraro GA. Do we really need more confirmation on the usefulness of inhaled nitric oxide in children's acute respiratory distress syndrome? [J]. Pediatric Crit Care Med, 2004, 5(5): 496-497.
28. Afshari A, Brok J, Moller AM, et al. Inhaled nitric oxide for acute respiratory distress syndrome (ARDS) and acute lung injury in children and adults[J]. Cochrane Database Syst Rev, 2010, (7): CD002787.
29. Seeger W, Pison U, Buchhorn R, et al: Surfactant abnormalities and adult respiratory failure[J]. Lung, 1990, 168(Suppl): 891- 902. Spragg RG, Lewis JF, Walmrath HD, et al.
30. Effect of recombinant surfactant protein C-based surfactant on the acute respiratory distress syndrome[J]. N Engl J Med, 2004, 351(9): 884-892.
31. Wirbelauer J, Speer CP. The role of surfactant treatment in preterm infants and term newborns with acute respiratory distress syndrome[J]. J Perinatol, 2009, 29(Suppl 2): S18-22.
32. Raghavendran K, Willson D, Notter RH. Surfactant therapy for acute lung injury and acute respiratory distress syndrome[J]. Crit Care Clin, 2011, 27(3): 525-559.
33. Strohmaier W, Marraro G. Surfactant treatment in the ICU: alternative interpretations of existing evidence[J]. Pediatr Anesth, 2006, 16(8): 813-815.
34. Marraro GA. Surfactant in child and adult pathology: is it time to review our acquisitions? [J]. Pediatr Crit Care Med, 2008, 9(5): 537-538.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
227
ANESTHESIA FOR DIAGNOSTIC PROCEDURES IN CHILDREN IVANA BUDIC1,2, VESNA MARJANOVIC1, MIODRAG MILENOVIC3, IVANA PETROV BOJICIC4, DUSICA SIMIC4,5
1 Centre for Anesthesia and Resuscitation, Clinical Centre Nis, Serbia,2 Medical School, University of Nis, Serbia,3 Emergency Centre, Clinical Centre of Serbia, Belgrade,4 University Children’s Hospital, Belgrade, Serbia,5 Medical School, University of Belgrade, Serbia e-mail: [email protected] Introduction
Provision of general anesthesia and deep sedation for children outside of the traditional operating room setting has become increasingly common in the past few years. Imaging and diagnostic techniques like MRI and endoscopy as well as performance of special procedures are often done under anesthesia in infants and children who cannot remain immobile or cannot tolerate the pain and discomfort as well as adult patients.1 Multicenter data suggest that more than 60% of pediatric procedural sedation outside the operating room is related to radiological procedures.2 Radiological procedures
Magnetic resonance imaging (MRI)
MRI is a noninvasive, radiation-free diagnostic procedure. Depending on the diagnostic needs an MRI scan takes about 10–30 min, is quite noisy and the patient is moved into a narrow tube with limited access. For optimum image quality enabling precise diagnosis patients have to remain motionless. Metallic materials have to be removed as they impair image quality and may induce undesirable side effects, e.g. warming. The high-frequency radio impulses can cause damage to or dysfunction of medical devices. If young patients are unable to cooperate or to be at rest, either sedation or anesthesia is required. Most children who need MRI diagnostic procedures have neurological diseases, vascular malformation or oncological tumour growth. Epilepsy and spastic or mental retardation are common symptoms in these patients. These facts must be taken into account when sedation or anaesthesia for MRI in children is required. The main goals to be achieved are maximum patient safety, successful scanning and paramount image quality.3 In 2008 the American Society of Anesthesiologists (ASA) assembled a task force composed of anesthesiologists, a radiologist with MRI expertise, and two methodologists; a Practice Advisory on Anesthetic Care for Magnetic Resonance Imaging followed.4 This document establishes important recommendations for safe practice as well as consistency of anesthesia care in the MRI environment. Computerized tomography (CT) scan
CT differentiates between high density (calcium, iron, bone, contrast-enhanced vascular and cerebrospinal fluid (CSF) spaces) and low density (oxygen, nitrogen, carbon in air, fat, CSF, muscle, white matter, gray matter, and water-containing lesions) structures. Once the decision has been made to obtain a CT examination, sufficiently interpretable images are necessary to
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
228
make that diagnostic test (imaging) effective.2 The actual scanning sequences are short and can range from 10-40 seconds. These short scan times enable many children to complete a CT scan without any sedation, especially with parental presence and distraction techniques.5 When an anesthesiologist is involved, it is often for sedation issues, general anesthesia or for a medically complicated patient. Because the scan time is quick, CT may be preferable for patients who are medically unstable and in need of rapid diagnosis, for example, the child being evaluated for abuse, an intracranial hemorrhage or abdominal or thoracic mass.6
Other indications for emergency CT scans may include encephalopathy and a change in neurological status. In these situations, full stomach and increased intracranial pressure (ICP) issues usually necessitate a rapid sequence induction with tracheal intubation. Head CT scan is often the preferred study in emergency situations where head trauma is involved.
Anesthesia and sedation in children undergoing radiological procedures
Prerequisites for sedation and general anesthesia are the same: fasting, intravenous access, vital signs monitoring, emergency equipment and physicians who are experienced in using the technical equipment and trained in paediatric airway management. It must be pointed out that disabled children do not need higher doses of sedatives but are three times more at risk of hypoxia under sedation.7 A very safe and simple technique for newborns is “feed and wrap” technique in which children are fed and one has to wait until the young patient falls asleep. Disadvantages of this technique are the unpredictable ‘induction times’ and the high failure rates of the scanning procedure. Concerning infants and children (especially for MRI, because of noise and tube narrowness) deep sedation or anesthesia are required for examination in most cases. Infants are more likely to require deep sedation or anesthesia to keep them still during MRI studies, and they are also considered at higher risk for cardiorespiratory side effects of given drugs.8 Current advances in physiological monitors and anesthesia machines for the MRI environment have optimized the ability of the anesthesia care provider to provide safe care in the MRI suite. But, despite the advancing technology in physiological monitors and anesthesia equipment, the MRI environment continues to pose some limitations for anesthesia care. The ventilator in the MRI setting has to be equipped with compliance compensation, resuscitation equipement has to be within reach, difficult airway management must occur outside the MRI, core temperature monitoring cannot be monitored. The chest excursions cannot be observed easily and saturation might fall late after cessation of breathing, particularly if oxygen is insufflated (if end tidal CO2 monitoring is not available another alternative is to measure respiratory excursions with a special respiratory belt that monitors chest excursions during MRI scanning). If hypoventilation occurs, stopping the scan, pulling the scan desk outside the tube and attending to the patient in this special surrounding is time consuming and needs to be practised.3 The need for a cool room to ensure functioning of the MRI scanner and the lack of MRI-compatible forced-air warming systems, combined with the frequent need for small infants to undergo MRI scanning, frequently results in hypothermia.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
229
The advent of special MRI-compatible infusion pumps for agents such as propofol allows the pump to be deployed in the scan room itself, with short tubing lengths to allow accurate delivery of the intended drug or fluid dose. An alternative is to utilize standard infusion pumps just outside the door of the scanner room with multiple lengths of infusion tubing threaded under the door. Gadolinium (contrast agent for MRI) should not be administered to patients with acute or severe renal insufficiency because of the elevated risk of nephrogenic systemic fibrosis. Nonionic iodinated radiographic contrast medium (RCM) used for CT imaging could cause severe allergic reactions. When choosing an adequate sedative for CT or MRI in children the review of Krauss et al.9,10 about procedural sedation and analgesia is helpful. The advantage of general anesthesia for MRI scanning is that the whole process, including preparation and scan time, is more predictable, and the scan quality may benefit because the child is immobilized and scan interruptions are minimized. In addition, it is possible to perform breath-holding maneuvers for images that need complete immobilization.3 On the other hand general anesthesia results in a longer duration of recovery in the hospital.11
Anesthesia and sedation in children undergoing gastrointestinal endoscopic procedures
Gastrointestinal endoscopy constitutes the bulk of procedures performed by a pediatric gastroenterologist. Depending upon the patient and the type of procedure contemplated (therapeutic versus diagnostic), children may require no sedation, minimal to moderately deep sedation or general anesthesia.5,6 It has been recommended that deep sedation and general anesthesia should be performed by an anesthesiologist. Propofol sedation by non-anesthesiologists was an sedation regimen in several countries throughout Europe but this issue remained highly controversial.12 In 2011 European Society of Anesthesiology (ESA) General Assembly retracted the endorsement for the “European Society of Gastrointestinal Endoscopy, European Society of Gastroenterology and Endoscopy Nurses and Associates, and the European Society of Anaesthesiology Guideline: Non-anesthesiologist administration of propofol for GI endoscopy” published in December 2010 issue of European Journal of Anesthesiology (EJA) as well as in Endoscopy.13 The anesthetic technique depends on the procedure, the patient and the skill of the endoscopist as well as the limitations and capabilities of the endoscopy suite. However, regardless of the sedation regimen used, the overall immediate non-fatal hypoxia-related reversible complication rate of pediatric GI endoscopic procedures is 2.3% .14 Dar and Shah15 reported a complication rate of 1.2% associated with procedures performed under general anesthesia, as compared to 3.7% of complications associated with IV sedation. Children with more complex medical problems, anticipated airway difficulties, morbid obesity or behavioral problems should undergo their procedure in the operating room. Most endoscopy - related respiratory complications occur during esophagogastroduodenoscopy (EGD), especially in infants and younger children, when compared to colonoscopy. A combination of factors may contribute, including the large size of the endoscope, partial airway
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
230
obstruction, and abdominal distension due to air introduced into the stomach as well as sedation, leading to hypoventilation. Due to higher respiratory complication rate, 6 month of age is the time prior to which general anesthesia with endotracheal intubation is required. Targeted controlled intravenous infusions (TCI) of propofol have been used effectively in children (3 – 10 years) who underwent EGD with spontaneous ventilation without endotracheal intubation. Access to the airway is unimpeded during a colonoscopy. Deep sedation can be achieved more readily and if respiratory problems occur, airway interventions are straightforward to manage. Patients undergoing colonoscopy will experience increased stimulation during certain parts of the procedure such as traversing the colon to the splenic flexure and the ileocecal valve. The depth of the anesthetic should be adjusted accordingly.5,6 Conclusion
MRI and CT procedures themselves pose little risk for children, but sedation or general anesthesia, when used to facilitate these procedures, may add substantial risk. Of greatest concern is the risk of respiratory depression and hypoxemia that may have potentially long term consequences. Increased awareness of the complications associated with sedation during gastrointestinal endoscopy in children, and involving the anesthesiologists in caring for these children, may be optimal for safety.
References
1. Fiset P. Pediatric anesthesia and analgesia outside of the OR: what you need to know. IARS 2011; 47-49.
2. Macias CG, Chumpitazi CE. Sedation and anesthesia for CT: emerging issues for providing high-quality care. Pediatr Radiol. 2011; 41 Suppl 2:517-22.
3. Schulte-Uentrop L, Goepfert MS. Anaesthesia or sedation for MRI in children. Current Opinion in Anaesthesiology 2010; 23:513–517.
4. American Society of Anesthesiologists Task Force on Anesthetic Care for Magnetic Resonance Imaging. Practice advisory on anesthetic care for magnetic resonance imaging. Anesthesiology 2009; 110:459–79.
5. Mason KP, Zgleszewski SE. Anesthesia and sedation for procedures outside the operating room. In: Motoyama EK and Davis PJ editors. Smith’s Anesthesia for Infants and Children 7th edition. Philadelphia: Mosby Elsevier; 2006.p.685-722.
6. Holzman RS, Mason KP. Anesthesia and sedation outside the operating room. In: Gregory GA and Andropoulos DB editors. Gregory's Pediatric Anesthesia 5th edition. Oxford-Chichester-New York: Blackwell Publishing; 2012.p.919-945.
7. Kannikeswaran N,Mahajan P, Sethurman U, et al. Sedation medication received and adverse events related to sedation for brain MRI in children with and without developmentally disabilities. Paediatr Anaesth 2009; 19:250–256.
8. Dalal PG, Murray D, Cox T, McAllister J, Snider R. Sedation and anesthesia protocols used for magnetic resonance imaging studies in infants: provider and pharmacologic considerations. Anesth Analg. 2006; 103(4):863-8.
9. Krauss B, Green SM. Procedural sedation and analgesia in children. Lancet 2006; 367:766–780.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
231
10. Krauss BS, Krauss BA, Green SM. Procedural sedation and analgesia in children. N Engl J Med 2014; e23:1-6.
11. Malviya S, Voepel-Lewis T, Eldevik OP, Rockwell DT, Wong JH, Tait AR. Sedation and general anaesthesia in children undergoing MRI and CT: adverse events and outcomes. Br J Anaesth. 2000; 84(6):743-8.
12. Dumonceau JM, Riphaus A, Aparicio JR, Beilenhoff U, Knape JT et al. European Society of Gastrointestinal Endoscopy, European Society of Gastroenterology and Endoscopy Nurses and Associates, and the European Society of Anaesthesiology Guideline: Non-anesthesiologist administration of propofol for GI endoscopy. Endoscopy. 2010; 42(11):960-74.
13. Pelosi P. Retraction of endorsement: European Society of Gastrointestinal Endoscopy, European Society of Gastroenterology and Endoscopy Nurses and Associates, and the European Society of Anaesthesiology Guideline: Non-anesthesiologist administration of propofol for GI endoscopy. Endoscopy. 2012; 44(3):302.
14. Thakkar K, El-Serag HB, Mattek N, Gilger MA. Complications of pediatric EGD: a 4-year experience in PEDS-CORI. Gastrointest Endosc 2007; 65:213-221.
15. Dar AQ, Shah ZA. Anesthesia and sedation in pediatric gastrointestinal endoscopic procedures: A review. World J Gastrointest Endosc. 2010; 2(7):257-62.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
232
PERIOPERATIVNA HIPOTERMIJA U PEDIJATRIJSKOJ POPULACIJI PERIOPERATIVE HYPOTHERMIA IN THE PEDIATRIC POPULATION VESNA STEVANOVIĆ , IGOR KRUNIĆ , MAJA MIRČETIĆ , SLAĐANA PETROVIĆ, NIKOLA STANKOVIĆ Institut za zdravstvenu zaštitu majke i deteta Srbije „dr Vukan Čupić“ Beograd e-mail:[email protected] Abstract Hypothermia is the most common perioperative disturbance in pediatric patients. Inadverent hypothermia can be up to 20% among patients undergoing major surgical procedures. Neonates and infants have been shown to be at an increased risk for perioperative hypothermia for many reasons. These factors include: a high surface area to weight ratio, increased heat loss from head, limited stores of subcutaneous fat and poor thermoragulatory capacity. Perioperative hypothermia has been associated with a number of serious complication in children, e.g. metabolic acidosis, hypoxemia cardiac and respiratory disturbances, coagulopathy,wound infection, hypoglycemia. Strategies to minimize the incidence of hypothermia in pediatric patients are body temperature monitoring and methods of controlling body temperature. Uvod
Neželjena perioperativna hipotermija je veliki problem u pedijatrijskoj anesteziji jer uzrokuje ozbiljne komplikacije koje mogu uticati na ishod lečenja. Posebno ugrožena uzrasna grupa su novorođenčad i odojčad.1 Osim uzrasta, rizik od hipotermije povećajaju vrsta i dužina hirurškog zahvata, komorbiditet, preoperativna telesna temperatura niža od 36°C i svakako nesprovođenje preventivnih mera grejanja bolesnika. Smatra se da je incidenca značajne hipotemije oko 20% u slučaju velikih operacija u pedijatrijskih bolesnika, a na ukupan broj operisane dece svih uzrasta kreće se i do 50%.2
Hipotermijom smatramo telesnu temperaturu nižu od 36°C. U odnosu na normotermiju hipotermija može biti blaga (<1-2 °C), umerena (=35°C), ozbiljna (< 35°C) i duboka (< 28°C).
Regulacija telesne temperature
Regulacija telesne temperature čoveka je pod kontrolom autonomnog nervnog sistema kada se putem negativne povratne sprege reguliše optimum ( između 36,5-37,5°C) bez obzira na „neuslove“ koje diktira temperatura okoline. Kompleksni put obuhvata: termalne receptore (za tople i hladne senzacije), aferentne puteve (Aδ nervna vlakna za hladne draži i nemijelizovana C vlakna za tople draži), prednji spinotalamični put kičmene moždine i prednji hipotalamus u kome se nalazi termoregulacioni centar. 80% informacija o temperaturnom statusu stiže iz unutrašnjosti tela, a 20% sa kože i od kičmene moždine. Kičmena moždina pokazuje u izvesnim funkcijama termoregulacije autonomiju u odnosu na hipotalamus. Na finu funkciju termoregulacionog centra utiču cirkardijalni ritam, vežbe, unos hrane, infekcija, hormoni štitaste žlezde, polni hormoni, anestetici, alkohol, nikotin, oblačenje, položaj tela itd. Kada je telesna temperatura ispod praga termoregulacionog centra nastaje: vazokonstrikcija, hemijska termogeneza i drhtanje tela. U odraslih su glavni izvori noradrenalinom uzrokovane

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
233
termogeneze skeletni mišići i braon masno tkivo. Drhtanje u odraslih povećava metaboličku proizvodnju toplote za 50-100%, što se ne viđa u dece sve do uzrasta malog deteta. Razlog je manje mišićnoskeletne mase u odnosu telo u poređenju sa odraslima, zbog čega hemijska termogeneza iz braon masnog tkiva predstavlja glavni izvor stvaranja toplote. Suprotno, u slučaju pregrejavanja tela nastaje aktivna vazodilatacija i znojenje što je pod kontrolom parasimpatikusa. Osim hipertermijom znojenje može biti aktivirano anksioznošću, bolnim dražima i vagalnom reakcijom.3
Regulacija telesne temperature u anesteziji
U anesteziji telo uvek gubi toplotu radijacijom, evaporacijom, kondukcijom i kovnekcijom, kao i usled nemogućnosti da bihejvioralnim aktivnostima utiče na temperaturu tela. U normalnim okolnostima radijacijom se gubi 60% toplote tela (zavisi od protoka krvi u koži i veličine izložene površine), dok je u anesteziji to najveći gubitak (do 40%). U dečijem uzrastu ovi gubitci su još značajniji zbog veće površine tela u odnosu na telesnu masu, veličine dečije glave u odnosu na telo, tanje kože i potkožnog masnog tkiva. Evaporacija u normalnim okolnostima daje 20% gubitaka toplote tela usled isparavanja tečnosti iz mukoza, seroznih površina i iz pluća, što zavisi od veličine izložene površine i okolne temperature. U anesteziji je to značajan gubitak, posebno u slučaju otvorenih telesnih duplji,a manje značajno iz pluća. Kondukcijom se gubi 5% toplote što zavisi od veličine kontaktne površine tela (gubitak u anesteziji je najmanje značajan). Konvekcija u normalnim okolnostima daje 15% gubitaka telesne temperature tela, dok je u anesteziji zbog laminarnog kretanja vazduha preko pacijenta na zavidnom drugom mestu načina gubljenja toplote. Lekovi koji se koriste u anesteziji blokiraju fiziološke autonomne procese termoregulacije na više načina: deluju direktno depresivno na termoregulacioni centar, izazivaju vazodilataciju – opioidi simpatikolitičkim osobinama blokiraju vazokonstrikciju, mišićni relaksanti blokiraju drhtanje, lokalni anestetici u regionalnoj anesteziji daju simpatičku blokadu, mišićnu relaksaciju i senzornu blokadu ( najmanji uticaj ima midazolam).4
U toku opšte anestezije dramatični i karakteristični pad temperature dešava se u prvoj polovini anestezije kada nastaje redistribucija centralne temeperature ka periferiji zbog vazodilatacije koju uzrokuju anestetici. U dečijem uzrastu stepen redistribucije je niži jer su ekstremiteti manji u odnosu na telo poredeći sa odraslim. Volatilni anestetici to čine nelineranom,a propofol i opioidi linearnom inhibicijom. Termoregulacioni prag se dejstvom anestetika „baždari“ na 33-35°C. Posle te inicijalno brze faze nastaje sporija linearna redukcija telesne temperature koja nastaje zbog toga što je gubitak toplote veći od termogeneze. U 3-4. satu anestezije sledi stabilizacija nižih vrednosti centralne telesne temperature kada je gubitak jednak stvaranju toplote. Što se tiče regionalne anestezije centralni neuroblokovi centralnim delovanjem smanjuju prag termoregulacionog centra za vazokonstrikciju i drhtanje za 0,6°C. Osim centralnim mehanizmom lokalni anestetik blokira prenos osećaja hladnoće od periferije ka centralnom nervnom sistemu, zbog čega bolesnik doživljava vazodilataciju kao paradoksni osećaj toplote, iako gubi centralnu temperaturu.U dečijem uzrastu do 5. godine ovi efekti su manje izraženi zbog nezrelosti autonomnog nervnog sistema.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
234
Perioperativna hipotermija: posledice,mere prevencije,monitoring
Posledice hipotermije su mnogobrojne.4,5 Kardiovaskularni sistem reaguje povećanjem: pulsa i krvnog pritiska, sistemske i plućne vaskularne rezistence, kontaktilnosti i iritabilnosti srca, miokardne depresije i lučenjem noradrenalina. U novorođene dece često nastaje postoperativna bradikardija i apneja. Usled usporene cirkulacije kroz jetru usporen je metabolizam lekova zbog čega viđamo produženo buđenje iz anestezije. Na nivou bubrega povećana je vaskularna rezistenca i smanajena reapsorpcija Na, K i ADH. Smanjen protok krvi kroz mozak smanjuje vrednosti MAC za 5% za svaki stepen niže centralne temperature što uz povećanje koeficijenta solubilnosti krv/gas takođe odlaže buđenje iz anestezije. Usporava se metabolizam, nastaje metabolička acidoza, povećava se potrošnja kiseonika zbog drhtanja, razvija se hipoksemija. Povećana je viskoznost krvi, krivulja disocijacije hemoglobina skreće u levo, koagulacija je poremećena, smanjena je funkcija trombocita, podstaknuta fibrinoliza. Odlože se zarastanje rana, povećana je sklonost ka infekciji, smanjeno je odlaganje kolagena u ranu. Sveukupno povećan je mortalitet usled miokardnih incidenata, infekcije rane i produžene hospitalizacije, povećanog intraoperativnog krvarenja i masivnih transfuzija već u slučaju blage hipotermije (33.0°C-36.4°C).6
Zbog pogubnih efekata hipotermije posebne anesteziološku pripreme u smislu prevencije hipotermije zahtevaju srpasta anemija, hipokalijemična periodična paraliza, plućna alveolarna proteinoza i bolesti vezivnog tkiva. U današnje vreme hipotermiji su više izložena starija dece obzirom da je prevencija hipotermije u mlađim uzrastima postala rutinska procedura. Smatra se da je 60% dece uzrasta 12-18 godina izloženo neželjenoj intraoperativnoj hipotermiji posebno u ortopedskoj hirurgiji. I pored pažljive prevencije hipotermije ona će se izvesnom stepenu desiti u anesteziranih pacijenata. Sprečavanje gubitaka toplote preko kože treba da je imperativ,a cilj je centralna temperatura preko 36°C. Prevencija podrazumeva adekvatno oblačenje pacijenata ,preoperativno merenje temperature, održavanje adekvatne temperature operacione sale (24°C tokom indukcije kod pedijatrijskih slučajeva), pažljivo pozicionirane pacijenta, upotreba zatvorenih, low flow sistema u anestezijskom krugu, ovlaženih i zagrejanih gasova, zagrejanih iv tečnosti i najvažnije grejača tela (vazduhom ili vodom ili zračnim mehanizmima). U postoperativnom periodu gubi se vazodilatacija uzrokovana anesteticima,a zbog hipotermije nastaje vazokonstrikcija sa redistribucijom telesne temperature. Zato je zagrejavanje pacijenata u ovom periodu sporije nego tokom anestezije kada domonira vazodilatacija. Postoperativno drhtanje sprečava se grejanjem pacijenta i medikamentozno meperidinom, klonidinom, neostgminom i ketanserinom u odraslih pacijenata. Monitoring se rutinski i kontinuirano treba sprovoditi kod svih vidova anestezije. Merenje centralne temperature sprovodi se postavljanjem senzora na timpaničnu membranu, u plućnu arteriju, distalnu porciju jednjaka, nazofarings, oralno, rektalno, aksilarno, u mokraćnu bešiku i putem kože.7
Naučno je dokazan i benefit od indukovane hipotermije kod: ishemijskih lezija i operacija na mozgu i kičmenoj moždini, kod kardiohirurških operacija sa upotrebom by pass-a, kod hipoksično- ishemične encefalopatije novorođenčeta i nakon kardiak aresta.4
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
235
Zaključak
Dečiji uzrast pripada rizičnoj grupi bolesnika za razvoj perioperativne hipotermije. Mnogobrojni faktori predisponiraju brzom nastanaku ovog neželjenog poremećaja koji posledično daje mnogobrojne komplikacije. Rutinski monitoring telesne temperature i sprovođenje preventivnih mera zagrejavanja bolesnika imperativ su u pedijatrijskoj anesteziji za sve uzrasne grupe. Literatura:
1. Bajwa SJS,Swati.Peri-operative Hypothermis in pediatric patients:diagnosis, prevention and management.Anesth Pain&Intensive Care 2014;18(1):97-100
2. Pearce B,Christensen R,Voepel.Lewis T. (2010) Perioperative Hypothermia in the Pediatric Population: Prevalence, Risk Factors and Outcomes.J Anesthe Clinic Res1:102 doi:10.4172/2155-6148.1000102
3. Buggy DJ,Crossley AWA. Thermoregulation, mild perioperative hypothermia and post-anaesthestic shivering.Br J Anaesth 2000;84:615-28
4. Frank SM. Consequences of Hypothermia.Current Anaesthesia&Critical Care 2001;12:79-86
5. Kim P, Taghon T,Fetzer M et al. Perioperative Hypothermia in the Pediatric population: A Quality Improvement Project.American Journal of Medical Quality XX(X)1-7 DOI:10.1177/1062860612473350 http://ajmq.sagepub.com
6. Tander B,Baris S,Karakaya D et al. Risk factores influencing inadverent hypothermia in infants and neonates during anesthesia.Paediatr Anaesth 2005;15:574-79
7. Craig JV,Lancaster GA, Taylor S et al. Infrared ear thesrmometry compared with rectal thermometry in children:systematic rewiew. Lancet 2002;360:603-609
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
236
TRETMAN KRVARENJA U PEDIJATRIJSKOJ ANESTEZIJI DUŠICA SIMIĆ1, 2, MIRJANA KNEŽEVIĆ1, IRINA MILOJEVIĆ1, MARIJA STEVIĆ1, IVANA PETROV1, IVANA BUDIĆ3, 4 1 Univerzitetska dečja klinika,2 Medicinski fakultet Univerziteta u Beogradu,3 Klinika za dečju hirurgiju i ortopediju KC Niš,4 Medicinski fakultet Univerziteta u Nišu E-mail: [email protected] BLEEDING MANAGEMENT IN PEDIATRIC SURGERY
Abstract
Hypovolemia caused by massive per operative bleeding is a main cause of mortality in children. Preoperative evaluation and identification of children with high risk of bleeding is essential for prevention of bleeding. It is necessary to get PT, PTT and platelet count before any extensive operation and to do coagulation tests and consultation of hematologist, if there is diagnosed blood coagulation disorder. Crystalloids are first choice in per operative fluid therapy in children. After 30-50 ml/kg crystalloids given, colloids are administrated. Decision to start transfusion of erythrocytes depends of amount of bleeding, oxygenation and estimated potential consequences. Indications for platelet transfusion are qualitative and quantitative platelet deficiency, acute bleeding and invasive procedures when platelet count is under 50000 mm3, neurosurgical interventions when platelet count is less than 100000mm3. New guides do not recommend use of fresh frozen plasma. Fibrinogen needs to be kept on his haemostatic level of 1,5-2.0 g/l by using fibrinogen concentrate or cryoprecipitate (5 ml/kg) and thromboelastography should be done, if possible. The use of Tranexamic acid is recommended in pediatric surgery (cardio surgery, scoliosis surgery) in order to reduce per operative bleeding and the need for transfusion. Planed surgery is also a very important factor in preoperative evaluation.
Uvod
Hipovolemija uzrokovana masivnim perioperativnim krvarenjem je vodeći uzrok mortaliteta kod dece. Nehirurško krvarenje može biti posledica urođenih koagulacionih poremećaja koji nisu otkriveni preoperativno (hemofilija A i B , vW bolest i poremecaji funkcije trombocita); stečenih koagulacionih poremećaja (deficit vitamina K kod novorođenčeta, malapsorpcija, atrezija ekstrahepatićnih žučnih puteva i teške hronične bolesti); poremećaja u koagulaciji uzrokovanim specificnim hirurškim intervencijama kao sto su transplantacija jetre ili operacija kongenitalnih srčanih mana sa kardiopulmonalnim bypass-om ili masivnog gubitka krvi kod multiplih teških trauma. Perioperativno krvarenje hirurškog porekla je posledica izvođenja operacija u dobro vaskularizovanim tkivima i otežane kontrole krvarenja u hiruškom polju.1

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
237
Specifičnosti hemostaze kod dece
Postoji značajna kvantitativna i kvalitativna razlika između novorođenčeta i odraslih iako su sve ključne komponente hemostatskog sistema prisutne na rođenju. Nivoi faktora koagulacije (FXII, FXI) i HMWK (High molecular weight kininogen, kininogen velike molekulske mase) su niži na rođenju i te vrednosti se zadržavaju do 6 meseci starosti. To se manifestuje produženjem aPTT-a. Vitamin K zavisni faktori koagulacije (FII, FVII, FIX i FX) su takođe niži na rođenju i takođe dostižu adultni nivo do 6 meseca starosti, stoga su u tom periodu PT, PTT i INR blago produženi. Nivoi FV I FXIII su inicijalno niski, ali se rapidno povećavaju 5. dana života. FVIII i vWF su jedina dva prokoagulantna proteina sa izrazito povišenim nivoom na rođenju u odnosu na adultne vrednosti.2 Nivoi glavnih antikoagulantnih faktora su niski na rođenju i sa približno 3 meseca starosti dostižu adultne vrednosti. Nasuprot tome, alfa-2 makroglobulin, upadljivo je povišen kod novorođenčadi i često dostiže dvostruke vrednosti od onih izmerenih u odraslih. Broj i zapremina trombocita se ne razlikuju od adultnih, ali neonatalni trombociti pokazuju značajno smanjenje funkcije prvih 2 do 4 nedelje posle rođenja. U poređenju sa odraslima, novorođenčad nemaju samo veću koncentraciju cirkulišućeg vWF, već i veći procenat velikih vWF multimera. Srednja vrednost fibrinogena novorođenčadi i odraslih su uporedive, međutim neonatalni fibrinogen je kvalitativno disfunkcionalan do kraja prve godine. Plazminogen je jedini koagulacioni protein kod novorođenčadi koji se kvalitativno i kvantitativno razlikuje od adultnog. Plazminogena ima 50% do kraja 6. meseca kada dostiže adultnu vrednost. Međutim, primarni inhibitor fibrinolize, faktor inhibicije plazminogena (PIF) je normalan ili povišen u neonatalnom periodu. Stoga kod neonatusa postoji smanjeno stvaranje plazmina i smanjena fibrinoliticka aktivnost.1,2 Uprkos ovim kvantitativnim i kvalitativnim razlikama u koagulacioim komponentama novorođenčad i deca imaju dobru hemostazu. Dokazano je da se, osim tokom kardiohiruških zahvata, ne očekuje prekomerno krvarenje.
Preoperativna evaluacija i identifikacija dece sa visokim rizikom od krvarenja
U cilju prevencije krvarenja neophodna je preoperativna evaluacija i identifikacija dece sa visokim rizikom od krvarenja. Potrebno je uzeti dobru ličnu i porodičnu anamnezu. Posebno treba obratiti pažnju na podatke o krvarenjima. Planirana operacija je takođe bitan faktor u preoperativnoj evaluaciji. Ukoliko nema zabrinjavajućih podataka, a tokom operacije se ne očekuje krvarenje, nije potrebno raditi koagulacione testove. Međutim, ukoliko je operacija opsežnija, preoperativno treba uraditi PT, PTT i broj trombocita. Oni predstavljaju kvantitativne in vitro testove koji ne uzimaju u obzir koagulacionu kaskadu i ne daju podatke o tome šta se dešava sa pacijentom. Ukoliko iz anamneze saznamo za poremećaje krvarenja, neophodno je uraditi koagulacione testove i konsultovati hematologa. Predlaže se korišćenje perioperativnih testova koagulacije visko-elastrometrijskim monitoringom za pravovremeno otkrivanje poremećaja koagulacije, uključujući dilucionu koagulopatiju i hiperfibrinolizu. Dijagnostikovanje perioperativne koagulopatije u pedijatriji zahteva brz i adekvatan monitoring koagulacije, uz određene starosno-specifične referentne vrednosti.3,4

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
238
Priprema pedijatrijskog pacijenta za elektivnu hirurgiju
Pre operacije sa povišenim rizikom od krvarenja neophodno je proveriti kompletnu krvnu sliku (Ht, Hb, Tr) i uraditi koagulacione testove. Uvek treba proceniti volemiju i ukupan volumen krvi pedijatrijskog pacijenta, kao i dozvoljeni gubitak, te trebovati odgovarajući volumen eritrocita. Predlaže se, ukoliko se očekuje 30-50% gubitka cirkulatornog volumena, plasiranje urinarnog katetera i 2 periferne venske linije. Ako se očekuje još veći gubitak, potrebno je plasirati i arterijsku i centralnu vensku liniju. Ukoliko se očekuje masivni gubitak krvi, neophodno je pripremiti opremu za brzu nadoknadu krvi, kontrolisati acido-bazni i elektrolitni status, koagulacione parametre i prevenirati hipotermiju.3
Nadoknada volumena
Nadoknada volumena je od suštinskog značaja za održavanje kardiovaskularne stabilnosti, perfuzije i oksigenacije. Ona se vrši infuzionim rastvorima, komponentama i derivatima krvi.
Tečnosti
Intraoperativna nadoknada tečnosti ima za cilj održavanje fizioloških potreba, nadoknadu preoperativnog deficita i gubitaka u treći prostor. Gubici u treći prostor predstavljaju sekvestraciju tečnosti u nefunkcionalnim odeljcima i mogu da variraju od 1ml/kg/h do 15-20 ml/kg/h (velike intraabdominalne operacije) ili čak do 50 ml/kg/h (napr. kod nekrotizirajućeg enterokolitisa u prevremeno rođene dece).5 Mlađa deca imaju veće gubitke zbog većeg obima ekstracelularne tečnosti u odnosu na stariju decu i odrasle. I dalje se savetuje da kristaloidi budu prvi izbor za perioperativnu nadoknadu tečnosti kod dece. Naravno, treba voditi računa da ne dođe do preopterećenja tečnošću i dilucione koagulopatije. Intraoperativne tečnosti kod dece treba da imaju osmolarnost blizu fiziološke kako bi se izbegla hiponatremija, da sadrže anjone (acetat, laktat) kao prekursore bikarbonata za sprečavanje hiperhloremijske acidoze, posebno kod novorođenčadi. Ukoliko je indikovano, treba dodati i glukozu (1-2,5%) u cilju sprečavanja hipoglikemije. U velikoj većini pacijenata nema potrebe za glukozom u perioperativnom periodu, sem kod novorođenčeta (terminskog i prematurusa), dece koja su pothranjena, dece sa renalnom insuficijencijom i kod dece koja su na parenteralnoj ishrani.6 Hiperglikemija može izazvati osmotsku diurezu, posledičnu dehidraciju i elektrolitni disbalans, tako da je moramo sprečiti. Nakon davanja 30-50 ml/kg kristaloida, indikovana je administracija koloidnog rastvora u cilju održavanja intravaskularnog osmotskog pritiska. Koloidne tečnosti se mogu podeliti na prirodne koloide (albumine) i sintetske koloide (HES, želatina i dekstrani). Negativni efekat koloida na hemostazu je poznat i treba ga pažljivo pratiti. Hidroksietil starč (HES) izaziva prelazak krvnih proteina u intersticijum, smanjuje koncentraciju FVIII i vWF, smanjuje funkciju trombocita i inhibira interreakciju FXIII – polimeri fibrina, mada nove generacije ovih rastvora izazivaju manje poremećaje. Dekstrani uzrokuju vW sindrom i povećavaju fibrinolizu, te ih ne treba davati u dozi većoj od 20ml/kg/dan kod dece. Želatini ometaju koagulaciju i treba ih zabraniti kod dece. I albumin ometa koagulaciju inhibicijom agregacije trombocita ili efektom na antitrombin III koji je sličan heparinu, ali u manjoj meri nego sintetski koloidi.6
Eritrociti
Koncentracije hemoglobina variraju u zavisnosti od starosti i pola i transfuziju eritrocita treba tome prilagoditi. Bebe uzrasta preko 4 meseca tolerišu pad hemoglobina do 7g/dl ukoliko su hemodinamski stabilne. Kod dece uzrasta ispod 4 meseca, dece sa cijanogenim srčanim manama,
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
239
hroničnom pneumonijom i hemoglobinopatijama prag za transfuziju je 12 g/dl. Maksimalni dozvoljeni gubitak krvi se proračunava na osnovu formule:
[ (početni Ht-ciljni Ht)/početni Ht] x procenjen volumen krvi Može se nadoknaditi kristaloidima (1,3-1,4:1) ili koloidima (1:1). Odluku da započnemo transfuziju eritrocita donosimo na osnovu brzine krvarenja, smanjene oksigenacije i procenjene opasnosti od posledica.Volumen za transfuzudovanje se izračunava na sledeće načine3: VTT (volumen to transfuze) : VTT=10-15 ml/kg TT ili procenjena zapremina krvi x (željeni hematokrit – trenutna vrednost hematokrita)/ hematokrit u jedinici koncentrovanih eritrocita (60-70) ili TT(kg) x željeni porast Hb(g/dl) x 5 Suboptimalni transfudovani volumen izlaže dete riziku ponovljenje transfuzije od drugog donora. Ukoliko je potrebna masivna transfuzija, savetuje se da odnos eritrocita:SSP:Tr bude1:1:1 i da, po mogućstvu, budu od istog donora. Ukoliko se očekuje masivna nadoknada, eritrociti ne bi trebalo da budu stariji od nedelju dana, kako ne bi došlo do elektrolitnog disbalansa, a pre svega hiperkalijemije. Kalijum progresivno napušta eritrocite. Doza eritrocita odmah po uzimanju sadrži 12mEq/L K+, 21.dana 32mEq/L, a 35. dana 50mEq/L. Da bi se prevenirala hipokalcemija (usled prisustva citratnih konzervanasa) savetuje se primena 5-10mg/kg Ca++ hlorida ili 15-30mg/kg Ca++ glukonata IV.
Trombociti
Indikacije za nadoknadu trombocita su kvalitativna ili kvantitativna deficijencija trombocita, akutna krvarenja kod trombocita ispod 50.000 mm3, invazivne procedure kod trombocita ispod 50.000 mm3, neurohiruške intervencije kod trombocita ispod 100.000 mm3. U pogledu doziranja, nadoknada trombocita vrši se po šemi: 1-2 jedinice/10 kg ili 10-15 ml/kg. Očekivani efekat transfuzije trombocita je sledeći4,7: jedna jedinice koncentrata trombocita na 10 kg telesne težine ili 5ml / kg afereznog koncentrata trombocita bi trebalo da podigne broj trombocita za 20.000-50. 000µl -1.
Plazma
Novi vodiči ne opravdavaju upotrebu plazme. Prethodni vodiči su preporučivali 1 jedinicu/10 kg ili 10–15 ml/kg SSP kod stečenih krvarenja gde je PTT i PT >1,5 puta produžen.3 Međutim, sada se smatra da je to nedovoljno da bi se postigla hemostaza, a da bi veća količina dovela do preopterećenja tečnošću. Opisani su i teški neželjeni efekti kao što su TRALI, povećan mortalitet kod dece sa ALI, preopterećenje srca povezano sa transfuzijom, sepsa kod teških opekotina, transfuzijom uzrokovana imunomodulacija i multipla organska insuficijencija. Primena SSP se savetuje samo ukoliko nije dostupan fibrinogen ni krioprecipitat.8 Faktori koagulacije
Fibrinogen je prvi faktor koagulacije koji dostiže kritično niske koncentracije tokom životno ugrožavajućih krvarenja. Kod dece treba održavati hemostatski nivo fibrinogena (1,5-2,0 g/L) primenom koncentrata fibrinogena (30-50 mg/kgTT) ili krioprecipitata (5 ml/kgTT), a ukoliko je moguće, pratiti hemostazu tromboelastografijom.4 Ona obezbeđuje sveobuhvatne informacije o svim fazama koagulacije, formiranju i retrakciji ugruška i fibrinolizi. Nema preporuka za bezbednu primenu koncentrovanog protrombinskog kompleksa ni FXIII. rFVIIa se ne

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
240
preporučuje za primenu kod dece, osim kod leukemija sa AT protiv FVIII. Takođe se ne savetuje ni rutinska primena dezmopresina ukoliko ne postoji hemofilija A ili blag oblik vW bolesti. Međutim, savetuje se perioperativna primena antfibrinolitika (traneksamična kiselina) u dečjoj hirurgiji (operacija srca i skolioze) radi smanjivanja perioperativnog gubitaka krvi i potrebe za transfuzijom. Optimalna doza je i dalje neizvesna, uz velike varijacije udarnih doza (10-100mg/kg praćenih infuzijom od 1-10mg/kg/h). Smatra se da su u dečjoj kardio-hirurgiji ponovljenje doze efikasnije od pojedinačnih bolusa.
Zaključak
Uprkos razvojnim promenama u sistemu koagulacije hemostatski kapacitet kod novorođenčadi i dece je odličan. Prepoznavanje razvojnih promena može da poboljša kontrolu stečenih koagulopatija u pedijatriju. Planirana operacija je takođe bitan faktor u preoperativnoj evaluaciji. Plan intraoperativne nadoknade tečnosti kod pedijatrijskih pacijenata treba da obuhvata procenu intraoperativnog gubitka i precizan proračun količine datih tečnosti. Adekvatnost nadoknade tečnosti se najbolje procenjuje stalnim praćenjem kardiovaskularnih parametara, acido-baznog statusa i diureze. Perioperativnu nadoknadu tečnosti treba prilagoditi statusu pacijenta, vrsti hirurške intervencije i očekivanim događajima u postoperativnom periodu. Literatura
1. Giraldo MZ. Pediatric perioperative bleeding-Basic consideration. Rev Colomb Anestesiol 2013;41 (1):44-49.
2. Guzzetta N, Miller B. Principls of hemostasis in children: models and maturation. Pediat Anesth 2011;21:39
3. Giraldo MZ. Management of perioperative bleeding in children. Step by step review. Rev Colomb Anestesiol 2013;41 (1):50-56.
4. ESA guidelines: managements of severe bleeding. Eur J Anaesth 2013; 30:270-382. 5. Arya VK. Basic of fluid and blood transfusion therapy in paediatric surgical patients.
Indian J Anaesth 2012; 56 (5):454-62. 6. Isabelle Murat, Marie Claude Dubois. Perioperative fluid therapy in pediatrics. Pediat
Anesth 2008; 18 (5): 363-370. 7. Hemlata VA. Transfusion principles in children. Anesth Intens Care. 2009; 10:71-5. 8. Casino R, Luban N. Blood component therapy. Pediatr Clin North Am. 2008:421-45.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
241
CARDIOPULMONARY RESUSCITATION: WHERE ARE THE GAPS? THEODOROS XANTHOS1,2 1. School of Medicine, University of Athens, Greece, 2. Hellenic Society of Cardiopulmonary Resuscitation Summary Cardiac arrest is a daunting medical emergency with more than 1 million of victims in Europe and the United States of America. Survival to hospital discharge is however very poor and has not improved significantly the last two decades. International Organizations such as the European Resuscitation Council and the American Heart Association collaborate and publish guidelines every 5 years. The current manuscript aims at briefly highlighting the current knowledge gaps in cardiopulmonary resuscitation and hopes to initiate creative thinking from researchers around the globe. Introduction Cardiac arrest remains the ultimate medical emergency with more than one million victims every year in the United States of America and Europe1. Its incidence has been reported in various countries in Europe and each of the countries has variable survival to hospital discharge depending on many different factors, such as implementation of cardiopulmonary resuscitation (CPR) guidelines, training of healthcare professionals, availability of automated external defibrillators and sufficient legislation to permit usage of these defibrillators by trained lay people, just to name a few2. The annual incidence of out-of-hospital cardiac arrest is 38 per 100,000 population and the incidence of in-hospital cardiac arrest ranges from 1 to 5 per 1,000 admissions3. The International Liaison Committee on Resuscitation (ILCOR) is a joined initiative from various continents, including the European Resuscitation Council (ERC) and the American Heart Association (AHA), aiming at harmonization of the guidelines on CPR. These guidelines are reviewed every 5 years and they are updated to mirror both advancement in science and the current consensus of experts. Despite the fact that every possible measure is taken in the formulation of the consensus statements, the guidelines only include data derived from human studies; and while this is easily understood for any other discipline in medicine, human randomized trials are scarce in resuscitation, because of the difficulty from the part of the researchers to obtain consent from people who are “recruited” in these studies. As cardiac arrest victims are unconscious, this means that informed consent needs to be weaved and several ethical committees are reluctant to allow inclusion of patients in studies. This lack of human data often results in guidelines that show little or minimal change from the previous versions. In CPR, the most daring change was noted in 2010 when the compression ventilation ratio changed from 15 compressions to 2 ventilations to 30 compressions to 2 ventilations in a non-secured airway. On the other hand, researchers who do mainly animal research have found several promising receptors, pharmacological agents among others that await evaluation in humans. In addition, the way scientists understand science is culturally and socially bound; and this is especially the case for CPR4. The daring experiments of Safar have created the landscape of modern resuscitation and the 20th century marked the era of a new discipline that goes beyond ventilation and chest compressions. As we start to understand the phases of cardiac arrest and the

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
242
pathophysiology of resuscitation, we need strong studies that will advance the guidelines from consensus to analysis of new data. Redefinition of the terminology When considering terminology in cardiac arrest, one realizes that the scientific community needed almost 45 years to change the term “closed-chest cardiac massage” to the term we are currently using “external chest compressions”. Other than this major change, no other term has been reconsidered despite the fact that our understanding of the physiology has changed. We know that cardiac arrest represents cessation of the respiration and the cardiac function. This is the reason why the terms cardiac arrest and cardiorespiratory arrest are used interchangeably. Kouwenhoven, Safar and Jude proposed the term cardiopulmonary resuscitation more than 50 years ago. The term is composed by 2 words cardio (heart) and pulmonary (lung) resuscitation. At the time the term was proposed, the 3 scientists had not yet realized that it was the respiratory function that needed resuscitation and not just the pulmonary function. We now know that during cardiac arrest it is the gas exchange that ceases leading to anaerobic cellular metabolism and combined respiratory and metabolic acidosis. Moreover, recommendations for ventilation were made based on the studies from 1950 and 1960 in living humans with normal cardiac output5. At the time, these studies theorized that the goal of CPR was to achieve near normal tidal volume and minute ventilation. The 2010 guidelines on the other hand, pointed that excessive ventilation may inhibit venous return and as result inhibit return of spontaneous circulation (ROSC). As a result, another terminology has been proposed for CPR which is cardiorespiratory resuscitation. Despite the fact that this opinion was published in 20116, no real discussion has been initiated yet for the terminology we are using in CPR. As our understanding of the phenomenon is changing and we understand basic science better than in 1950s, it is time to reconsider all the terminology we are taking for granted in resuscitation science. Policy makers in resuscitation should follow the initiatives of every major scientific organization which developed committees to redefine their respective terminology. The controversial role of drugs in resuscitation Although it is not the aim of this short article to discuss every single scientific gap, as the author believes it is more suitable for an International Organization to publish a consensus statement of what the current gaps are, this article will provide a short discussion on the role of adrenaline in the setting of ventricular fibrillation (VF) cardiac arrest and CPR. Despite the fact that VF is the electrocardiographic rhythm recorded in 40% of the victims of cardiac arrest when help arrives, it is estimated that it may be the initial underlying rhythm in as many as 70% of cardiac arrest victims7. During CPR, the coronary perfusion pressure (CPP), which is the major determinant for ROSC, is defined as the pressure gradient between the aorta and the right atrium at decompression8. Even in optimal CPR, cardiac output rarely exceeds 30% of the normal cardiac output and as a result, there was an apparent need for a vasopressor. Adrenaline is the medication still recommended by the ERC and AHA (even if the latter has also accepted the role of vasopressin as an alternative in VF cardiac arrest). Adrenaline is a mixed alpha and beta agonist, and while its beneficial actions have been largely attributed to the alpha agonism, the beta agonism can cause a number of deleterious effects that have been proven in many animal models and human trials. Of note, adrenaline has not been positively correlated with survival to hospital discharge, but recently has been shown to improve ROSC in the recommended doses. Nevertheless, AHA and ERC seem to disagree on where adrenaline should be in the algorithm of
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
243
VF arrest. ERC posits that adrenaline should be administered after the third defibrillation attempt whereas AHA states that adrenaline should be given after the second defibrillation attempt with vasopressin being the reasonable alternative. This conflict simply mirrors the different interpretations either organization is giving to the same studies. Adrenaline has been used historically in CPR; however, if it were a new drug, it would be doubtful if it could obtain approval from FDA in resuscitation. The recommended dose for adrenaline is 1 mg for a 70 kg adult, but the optimum dose is not yet known8. It has been shown that higher doses have not been associated with better survival to hospital discharge9. More animal data are coming to light showing that adrenaline can be useful when co-administered with an intravenous beta-blocker10. Novel pharmacological strategies include co-administration of various regimens, such as glucagon, erythropoietin, levosimendan12, nitroglycerin and adrenaline and vasopressin13. One has to bear in mind though that animal studies should extrapolated with caution in human VF arrest and moreover, the conditions in the laboratory are always ideal, with chest compressions being optimal all the time, whereas this is rarely the case in human cardiac arrest. One of the reasons why pharmacology in human CPR shows controversial results can be attributed to the fact that poor quality chest compressions do not allow the drugs to exhibit their full pharmacologic properties. Are we ventilating properly? Recent guidelines propose positive pressure ventilation for every patient who is in cardiac arrest. In addition, automated ventilators are considered important for the cardiac arrest setting as they provide an inspiratory-time dependent volume and have been associated with lower peak airway pressures than manual ventillation14. In the setting of cardiac arrest, ventilation should be considered as a complement to resuscitation rather than its primary goal, because several studies have shown that excessive ventilation inhibit venous return and as a result, they minimize CPP and consequently ROSC. However, the current recommendation on providing ventilation rate of 10 per minute and limiting the tidal volume makes physiological sense, but it is based on very few and rather weak animal data15.Considering, however, the potentially negative haemodynamic effects ofartificial ventilation, the question that arises is: could positive pressure ventilation be a way to control intrathoracicpressure and enhance cardiac output during CPR14? Intrathoracic pressure should be increased during chest compressions and when positive pressure ventilation is applied. On the other hand this increase in intrathoracic pressure, as with all physiological parameters reaches a plateau when the outcome is beneficial and when this plateau is exceeded, then the outcome can be devastating. It becomes more and more obvious to physiologists that intrathoracic pressure should be optimized if we want to optimize coronary and cerebral perfusion pressure. Thoracic pump theory advocates that at the start of chest compression intrathoracic pressure rises and establishes an arteriovenous pressure gradientacross the heart forcing blood to move down the gradient through the heart and to flow from the thoracic to the systemic circulation16. If blood moves due to changes in intrathoracic pressure, then lateral pleural pressure and intrathoracic arterial and venous pressures are similar and nearly equal to extrathoracic arterial pressure, which is in turn significantly higher thanextrathoracic venous pressure17. Despite this data, it remains unknown whether the current theory is the only explanation for forward blood flow, as the cardiac pump theory advocates that blood is simply forwarded by external compressions and the direct compression of the heart between the sternum and the inferior thoracic cavity. Interestingly in several animal models mitral valve closure was

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
244
demonstrated when intrathoracic pressure was elevated. This is a paradox, as thoracic pulp theory advocates that atrioventricular valves should remain open for blood flow to occur. On the other hand guidelines advocate that chest compressions and ventilations need to be asynchronous when the airway has been “secured”. This raises significant concerns as simultaneous ventilation caused an abrupt drop in the coronary perfusion gradients which was related to a significant rise in right atrial pressure18. So a very logical assumption is that the mechanism of blood flow during CPR may be dependent on the stage and momentum of compression or decompression, without forgetting that the effect of ventilation, as well as that of compression force and rate, may vary during CPR14. So rather than the axiomatic guideline stating that even when any supraglottic airway has been placed the ventilations need to by asynchronous with chest compressions has never been proven and certainly it makes no sense from a physiological point of view. Research should focusespecially in relation totime, because both compressions and insufflationsincrease the intrathoracic pressure, which reaches a peak value and then gradually decreases. It appears that during positive-pressure ventilation, blood flow is promoted by the ‘thoracic pump’, but by the beginning of the expiratory phase (ventilator pause) the ‘thoracic pump’ effect decreases as the ‘cardiac pump’ begins to take over, reaching a peak effect by the end of ventilator pause and just before the inspiratory phase. Research is needed to identify whether proper timing of compression and ventilation may actually improve the circulation and as a final outcome ROSC. Conclusion These 3 examples from terminology to pharmacology and ventilation simply demonstrate the fact that we may know less than we had originally thought. Guidelines in 2015 will not show great changes, but serious research identifying key issues in resuscitation should be performed, if we are to create guidelines athat are robust and cannot be scientifically challenged. References 1. Koster RW, Baubin MA, Bossaert LL, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 2. Adult basic life support and use of automated external defibrillators. Resuscitation2010; 81:1277-92. 2. Eisenberg MS, Mengert TJ. Cardiac resuscitation. N Engl J Med 2001; 344:1304-13. 3. Neumar RW, Nolan JP, Adrie C, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology,treatment, and prognostication. A consensus statementfrom the International Liaison Committee on Resuscitation(American Heart Association, Australian and New ZealandCouncil on Resuscitation, European Resuscitation Council,Heart and Stroke Foundation of Canada, InterAmericanHeart Foundation, Resuscitation Council of Asia, and theResuscitation Council of Southern Africa); the AmericanHeart Association Emergency Cardiovascular Care Committee;the Council on Cardiovascular Surgery and Anesthesia;the Council on Cardiopulmonary, Perioperative, and CriticalCare; the Council on Clinical Cardiology; and the StrokeCouncil. Circulation 2008; 118:2452-83. 4. Ekmektzoglou KA, Johnson EO, Syros P et al. Cardiopulmonary Resuscitation: A historical perspercive leading up to the end of the 19th century. Acta med-histAdriat 2011; 10:83-100. 5. Safar P, Brown TC, Hotley WJ, et al. Ventilation and circulation with closed chest cardiac massage in man. JAMA 1961; 176:574-6. 6. Xanthos T, Iacovidou N, Ekmektzoglou KA. From cardiopulmonary to cardiorespiratory resuscitation. Resuscitation 2011;82:1360.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
245
7. CobbLA, FahrenbruchCE, OlsufkaM, et al. Changing incidence of out-of-hospital ventricular fibrillation 1980-2000. JAMA 2002;288: 3008–13. 8. Xanthos T, Pantazopoulos I, Demestiha T, et al.Epinephrine in ventricular fibrillation: friend or foe? A review for the Emergency Nurse.J EmergNurs.2011;37:408-12. 9. NiemannJT, Cairns CB, Sharma J, et al. Treatment of prolonged ventricular fibrillation, immediate countershock versus high-dose epinephrine and CPR preceding countershock. Circulation 1992;85:281–7. 10. Bassiakou E, Xanthos T, Papadimitriou L.The potential beneficial effects of beta adrenergic blockade in the treatment of ventricular fibrillation.Eur J Pharmacol. 2009;616:1-6. 11. Raffay V, Chalkias A, Lelovas P, et al. Addition of glucagon to adrenaline improves hemodynamics in a porcine model of prolonged ventricular fibrillation.Am J EmergMed. 2014;32:139-43. 12. Varvarousi G, Stefaniotou A, Varvaroussis D, et al. The role of Levosimendan in cardiopulmonary resuscitation.Eur J Pharmacol. 2014 Jun 24.pii: S0014-2999(14)00466-X.[Epub ahead of print]. 13. Xanthos T, Bassiakou E, Koudouna E, et al. Combination pharmacotherapy in the treatment of experimental cardiac arrest.Am J EmergMed. 2009;27:651-9. 14. Chalkias A, Xanthos T.Timing positive-pressure ventilation during chest compression: the key to improving the thoracic pump?Eur Heart J Acute Cardiovasc Care. 2013 Dec 12.[Epub ahead of print]. 15. Deakin CD, Nolan JP, Soar J, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 4. Adult advanced life support. Resuscitation 2010; 81:1305–52. 16. Weisfeldt M and Chandra N. Physiology of cardiopulmonary resuscitation. Annu Rev Med 1981; 32:435–42. 17. Werner JA, Greene HL, Janko CL, et al. Visualization of cardiac valve motion in man during external chest compression using two-dimensional echocardiography. Implications regarding the mechanism of blood flow. Circulation 1981; 63:1417–21. 18. Swenson RD, Weaver WD, Niskanen RA, etal. Hemodynamics in humans during conventional and experimental methods of cardiopulmonary resuscitation. Circulation 1988; 78:630–9.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
246
AKTUELNI TERAPIJSKI KONCEPTI I KONTROVERZE U POSTRESUSCITACIONOM LEČENJU CURRENT THERAPEUTIC CONCEPTS AND CONTROVERSIES IN POST-RESUSCITATION CARE JASNA JEVĐIĆ Centar za anesteziju i reanimaciju KC Kragujevac, Fakultet medicinskih nauka, Kragujevac Abstract Post-cardiac arrestsyndromeis the result ofischemicandreperfusioninjury causedbycessation ofcirculationorafterROSC (Return of Spontaneous Circulation). It manifests itself byseverecardiocirculatoryandneurological dysfunction, which leads todeath.The aimof postresuscitation treatment isto reduce theconsequences ofboth cessation of circulation/reperfusionandan inflammatory responseon the function of vital organs. Therapeutichypothermiaand earlycoronary angiographywithPCIform the basis forpostresuscitationtreatment. However,thevalidity oftheseaggressivemethodsin allcomatose patientsaftercardiac arrestof apparentcardiacetiology is being questioned lately.Several other interventions are strongly recommended in thepostresuscitation period, such as mantaininghemodynamicstability, control of blood glucoseandelectrolytestatus, ventilatory support to maintainoxygenand carbondioxidelevels within thereference range. Uvod Vodeći uzrok smrti u Evropi je vanbolnički srčani zastoj1. I pored značajnog napretka, tokom poslednje decenije u prehospitalnoj resuscitaciji, i značajnom povećanju procenta bolesnika koji u bolnicu dolazi sa uspotavljenom srčanom radnjom, krajnji ishod srčanog zastoja je loš. Kod oko 25-35% pacijenata sa vanbolničkim srčanim zastojem, nakon primenjenih mera kardiopulmonalne resuscitacije (KPR) dolazi do povratka spontane cirkulacije (ROSC), dok je procenat preživelih na otpustu iz bolnice oko 10%. Pri tome je procenat preživelih sa dobrim neurološkim ishodom i niži2. Danas je jasno, da se u cilju poboljšanja prognoze srčanog zastoja, pored mera koje se odnose na širu društvenu zajednicu i unapređenje prehospitalne resuscitacije, mora obezbediti adekvatan, integrisan, timski nastavak lečenja ovih pacijenat u bolnici. Po uspostavljanju spontane cirkulacije, nakon perioda globalne hipoksije i ishemije koja se javlja usled srčanog zastoja, uz procese kompenzacije, dolazi i do daljih reperfuzionih oštećenja. Ishemična/reperfuziona oštećenja su posledica kompleksnih procesa koji nastaju usled sintetizovanja i oslobađanja brojnih inflamatornih citokina, aktivacije kaskade komplementa, hemotaksisa i aktivacije polimorfonuklearnih leukocita. Posledica ovih procesa su aktivacija trombocita i intravaskularna koagulacija, endotelijalna oštećenja i povećanje vaskularnog permeabiliteta. Intracelularna anoksija dovodi do prekida oksidativne fosforilacije u mitohondrijama i započinjanja procesa anaerobne glikolize, usled čega dolazi do porasta nivoa laktata i intracelularne acidoze, uz dalje elektrolitne poremećaje3. Ova kompleksana oštećenja, su zapravo oblik sistemskog inflamatornog odgovora organizma (SIRS) koji dovodi do progresivne destrukcije ćelija i multiple disfunkcije organa, stanja poznatog kaoPost-cardiac arrest sindrom. Postresuscitaciono lečenje treba usmeriti ka minimiziranju Post-cardiac arrest sindroma.Prema preporukama za lečenje International Liaison Committee on Resuscitation ( ILCOR) iz 2010 godine, uz terapijsku hipotermiju, najvažniji ciljevi postresuscitacionog lečenja

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
247
su: rano lečenje uzroka srčanog zastoja, hemodinamska stabilizacija, adekvatna oksigenacija i ventilacija, regulisanje glikemije i elektrolitnog statusa. Terapijska hipotermija
Smatra se da primena terapijske hipotermije dovodi do smanjenja cerebralnog metabolizmauz čuvanje zaliha visko-energetskih fosfata i smanjenog oslobađanja inflamatornih citokina i ekscitatornih aminokiselina, stabilizuje endotelijalnu membranu i redukuje edem mozga. Nakon publikovanja dve randomizovane, prospektivne, kontrolisane studije koje su pokazale veće preživljavanje i bolji neurološki ishod nakon primene terapijske hipotermije kod VF vanbolničkog srčanog zastoja4,5, ona postaje preporuručena metoda u postresuscitacionom lečenju. Preporučuje se rashlađivanje pacijenta na 32-34°C, tokom 12-24h, koje treba započeti što pre, po mogućstvu još prehospitalno.Međutim dve nedavno objavljene, randomizovane, kontrolisane studije dovode u pitanje ovaj stav. U prvoj od ovih studija koja je objavljena u JAMA6, i koja je obuhvatila 1359 pacijenata, autori su pokazali da prehospitalno rashlađivanje primenom 2l fiziološkog rastvora, temperature 4°C, na terenu, odmah nakon ROSC, nije dovelo do većeg preživljavanja na otpustu iz bolnice, kao ni do boljeg neurološkog ishoda, uodnosu na grupu pacijenata koje su hladili tek pri dolasku u bolnicu. Osim toga u ovoj grupi pacijenata je bilo značajno više ponovnih zastoja srca na terenu, kao i plućnih edema na prvoj radiografiji grudnog koša.Diao je u svojoj meta-analizi 5 randomizovanih, kontrolisanih studija, na ukupno 633 pacijenta došao do istog zaključka7. Druga značajna multicentrična, randomizovana studija8 obuhvatila je 939 pacijenata bez svesti nakon srčanog zastoja van bolnice, koji su randomizovani u grupu pacijenata čija je telesna temperatura održavana na 33°C ili u grupu pacijenata čija je telesna temperatura održavana na 36°C. Među grupama nije bilo statistički značajne razlike u preživljavanju, kao ni u neurološkom ishodu. Nakon perioda praćenja od 180 dana, u grupi 33°C, 54% pacijenata je umrlo ili imalo loš neurološki ishod, prema CPC (Cerebral Performance Category) skali, u odnosu na 52% pacijenata sa smrtnim ishodom u grupi 36°C. Ovo istraživanje ukazuje da je značajnije, za dobar ishod, održavati ciljnu telesnu temperaturu u određenim granicama i sprečiti groznicu, tokom prva 3 dana nakon srčanog zastoja, nego rashlađivati pacijenta do 32-34°C. Ne treba zaboraviti da hipotermija utiče na sve sisteme organa, i da kod pojedinih pacijenata može dovesti do neželjenih posledica, te je zbog toga moža bolje primeniti manje agresivan pristup. Da je upravo hipertermija ta koja doprinosi lošem ishodu srčanog zastoja, bilo da se javlja nakon primene terapijske hipotermije (rebound pyrexia) ili kod pacijenata koji nisu hlađeni, dokazuju brojne studije9,10,11,12. Koronarna angiografija i PCI
Otklanjanje uzroka koji je doveo do srčanog zastoja je važan segment postresuscitacionog lečenja, jer se tako znatno smanjuje verovatnoća ponovnog srčanog zastoja i pogoršanja bolesti.Preporuke za KPR iz 2010 snažno preporučuju, u slučaju da je uzrok srčanog zastoja bio infarkt miokarda sa ST-elevacijom (STEMI), hitnu (u okviru 90 min) koronarografiju i po potrebiperkutanu koronarnu intervenciju (PCI), koja bi omogućila reperfuziju miokarda i očuvanje kontraktilnosti miokarda i na taj način bolju perfuziju mozga. Ne postoje randomizovane kliničke studije koje bi potvrdile benefit primene ove metode, ali na osnovu
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
248
brojnih opservacionih studija se došlo do zaključka da primena hitne PCI kod STEMI udvostručava šanse za preživljavanje i doprinosi dobrom neurološkom ishodu13. Međutim postoji dilema šta raditi ukoliko u post-resuscitacionom EKG-u nema ST-elevacije. Ne postojanje ST-elevacije kao ni kliničke slike akutnog koronarnog sindroma, nakon resuscitacije, nije siguran dokaz da značajne okluzijekoronarnih arterija nema. Kod pacijenata koji su imali srčani zastoj kardijalne etiologije van bolnice incidenca okluzije koronarnih arterija je veoma velika, i kada se to ne manifestuje elevacijom ST-segmenta u postresustitacionom EKG-u. Ukoliko bi svim pacijentima nakon srčaniog zastoja kardijalne etiologije, radili hitnu koronarografiju, i onima koji nemaju evidentne kliničke i EKG znake koronarne bolesti bi omogućili ranu revaskularizaciju miokarda i sve kliničke benefite koje to nosi. Sa druge strane ovakvim neselektivnim pristupom bi pojedine pacijente izložili veoma invazivnoj i potencijalno opasnoj proceduri a da to nije neophodno. Randomizovane kontrolisane studije koje ocenjuju efekat primene rane koronarografije i PCI kod pacijenata sa srčanim zastojem bez ST-elevacije ne postoje, a rezultati retrospektivnih opservacionih studija su oprečni. Pojedine od ovih studija pokazuju da rana koronarografija i PCI povećavaju preživljavanje14,15,16, dok druge negiraju bilo kakav benefit primene ovih metoda kod pacijenata kod kojih ne postoje jasni znaci koronarne okluzije17. Kardiovaskularna stabilizacija
Pojava kardiovaskularne nestabilnosti je uobičajena nakon srčanog zastoja. Obično spontano prolazi nakon 48-72h 18 i udružena je sa lošim neurološkim ishodom kod preživelih. Ciljni arterijski pritisak tokom postresuscitacionog perioda nije precizno definisan, ali on mora biti dovoljan da obezbedi dobru perfuziju mozga, čiji je mehanizam autoregulacije narušen. Krvni pritisak ne treba da bude previsok jer se time povećava miokardi rad i potrebe miokarda za kiseonikom. Stabilizacju kardivaskularnog sistema postižemo nadoknadom cirkulatornog volumena tečnostima, primenom inotropnih i vazoaktivnih lekova.U eksperimentalnim, animalnim modelima najbolji efekat na poboljšanje srčane sistolne i dijastolne funkcije nakon zastoja, pokazao je dobutamin. Ispitivanja drugih inotropnih i vazoaktivnih lekova nisu dokazala njihovu komparativnu prednost u odnosu na dobutamin19.Kao veoma dobra pokazala se kombinacija dobutamina i noradrenalina. Ukoliko medikamentozna terapija nije efikasna, može se primeniti mehanička potpora, odnosno intra-aortna balon pumpa. Kod teške ventrikularne insuficijencije, često ni mehanička potpora nije dovoljna. U tim slučajevima se može primeniti perkutani kardiopulmonalni bajpas sa ekstrakorporalnom oksigenacijom. Danas su dostupni ovakvi portabilni ekstrakorporalni oksigenatori krvi, čija je primena moguća ina terenu, u slučaju dugotrajnog rezistentnog srčanog zastoja20, 21, 22. Hemodinamski monitoring (srčana frekvenca, krvni pritisak,kardijak autput,SvO2 ili ScvO2, laktati i arteriske gasne analize) je neophodan da bi se postigla optimizacija cirkulacije i adekvatna dostava kiseonika tkivima. Ventilacija i oksigenacija
Eksperimentalne studije na životinjama su dokazale da se u uslovima hiperoksije nakon ROSC, stvara više reaktivnih kiseoničnih jedinjenja koja dovode do oksigenacije lipida i proteina i narušavanja integriteta ćelijskih membrana i normalne aktivnosti enzima. U krajnjem ishodu ovo znači veće neuronalno oštećenje i lošiji neurološki ishod nakon ROSC. Velike multicentrične, retrospektivne, kohortne studije su pokazale da su pacijenti koji su postresuscitaciono bili
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
249
hiperoksični imali značajno veći mortalitet u odnosu na normoksemične, pa čak i hipoksemične pacijente23, 24. Hipokapnija i hiperkapnija su česte nakon ROSC i obe su udružene sa lošim neurološkim ishodom25. Zato se tokom postresustitacionog lečenja preporučuje održavanje normokapnije. Metabolička kontrola
Zbog endokrinog i neurogenog odgovora organizma na stres nakon srčanog zastoja, u periodu nakon ROSC, hiperglikemija je uobičajen nalaz. Iako brojne studije ukazuju na poveznost hiperglikemije i smrtnog ishoda kod kritično obolelih, kod pacijenta nakon srčanog zastoja se ne može preporučiti striktna kontrola glikemije. Na neurološki ishod, kod ove grupe kritično obolelih, mnogo nepovoljniji uticaj od hiperglikemije ima hipoglikemija, pa je po svaku cenu treba izbeći. Zbog toga je napušten koncept intenzivne insulinske terapije26. Na ove pacijente nepovoljno dejstvo imaju i varijacije u vrednostima glikemije i njih takođe treba sprečiti27. Nivo glikemije treba često meriti, posebno u slučaju primene terapijske hipotermije. Dovoljno je glikemiju održavati ispod 10 mmol/l. Elektrolitni disbalans je takođe moguć i treba ga izbeći, posebno one koji mogu dovesti do ponovnog srčanog zastoja. Treba voditi računa i o nivou magnezijuma u krvi jer on utiče na funkcionisanje centralnog nervnog i kardiovaskularnog sistema, kao i na vrednosti drugih elektrolita u krvi. Zaključak
Ishod srčang zastoja u najvećoj meri zavisti od brzine uspostavljanja i održavanja cirkulacije. Edukacija određenih ciljnih grupa stanovništva i telefonom vođena CPR doprinele su da se u većem procentuprimenjuju visokokvalitetne kompresije grudnog koša,odmah nakon srčanog zastoja. Uz pravovremene mere KPR, veća dostupnost automatskih spoljašnjih defibrilatora na javnim mestima,omogućila je povećanje stope inicijalnog preživljavanja nakon srčanog zastoja. Da bi i dugoročno preživljavanje sa dobrim neurološkim ishodom bilo veće neophodno je lečiti komplikacije post-kardijak arest sindroma i omogućiti neuroprotekciju. Primena mera terapijske hipotermije, urgrntne koronarografije i PCI, održavanje hemodinamske i metaboličke homeostaze, kao i adekvatna oksigencija i ventilacija su najvažniji modaliteti postresuscitacionog lečenja. Reference
1. Atwood C, Eisenberg MS, Herlitz J, Rea TD. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 2005;67:75-80.
2. Nurnberger A, Sterz F, Malzer R, et al. Out of hospital cardiac arrest in Vienna: Incidence and outcome. Resustitation 2013; 84:42-47.
3. Adrie C, Adib-Conquy M, Laurent I et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation 2002;106:562-8.
4. The Hypothermia Afther Cardiac Arrest (HACA) study group: Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. New England Journal of Medicine 2002;346:549-56.
5. Bernard SA, Gray TW, Buist MD, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. New England Journal of Medicine 2002;346:557-63.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
250
6. Kim F, Nichol G, Maynard C, et al. Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: A randomized clinical trial. JAMA 2014; 311(1):45-52.
7. DiaoM, Huang F, Guan J, et al. Prehospital therapeutic hypothermia after cardiac arrest: a systematic review and meta-analysis of randomized controlled trials. Resuscitation 2013;84:1021–8.
8. Nielsen N, Wetterslev J, Cornberg T, et al. Targeted temperature management at 33˚C versus 36˚C after cardiac arrest. N Engl J Med 2013; 369:2197-206.
9. Leary M, Grossestreuer AV, Iannacone S, et al. Pyrexia and neurologic outcomes after therapeutic hypothermia for cardiac arrest. Resuscitation 2013;84:1056–61.
10. Gebhardt K, Guyette FX, Doshi AA, Callaway CW, Rittenberger JC, Post Cardiac Arrest Service. Prevalence and effect of fever on outcome following resuscitation from cardiac arrest. Resuscitation 2013;84:1062–7.
11. Bro-Jeppesen J, Hassager C, Wanscher M, et al. Post-hypothermia fever isassoci-ated with increased mortality after out -of-hospital cardiac arrest. Resuscitation 2013;84:1734–40.
12. Winters SA, Wolf KH, Kettinger SA, Seif EK, Jones JS, Bacon-Baguley T. Assessment of risk factors for post-rewarming “rebound hyperthermia” in cardiac arrest patients undergoing therapeutic hypothermia. Resuscitation 2013;84:1245–9.
13. Garot P, Lefevre T, Eltchaninoff H, et al. Six-month outcome of after emergency percutaneous coronary intervention in resuscitated patients cardiac arrest complicating ST-elevation myocardial infarction. Circulation 2007; 115:1354-1362.
14. Dumas F, Cariou A, Manzo-Silberman S, Grimaldi D, Vivien B, Rosencher J, Empana J-P, Carli P, Mira J-P, Jouven X, Spaulding C. Immediate percutaneous coronary intervention is associated with better survival after out-of-hospital cardiac arrest: insights from the PROCAT (Parisian Region Out of hospital Cardiac ArresT) registry. CircCardiovascInterv 2010; 3:200–207.
15. Larsen JM, Ravkilde J. Acute coronary angiography in patients resuscitated from out-of-hospital cardiac arrest–a systematic review and meta-analysis. Resuscitation 2012; 83:1427–1433.
16. Hollenbeck RD, McPherson JA,Mooney MR, et al. Early cardiac catheterization is associated with improved survival in comatose survivors of cardiac arrest without STEMI. Resuscitation 2014; 85:88–95.
17. Bro-Jeppesen J, Kjaergaard J, Wanscher M, Pedersen F, Holmvang L, Lippert F, Møller J, Køber L, Hassager C. Emergency coronary angiography in comatose cardiac arrest patients: do real-life experiences support the guidelines? Eur Heart J Acute Cardiovasc Care 2012; 1:291–301.
18. LaurentI, MonchiM, ChicheJD, et al. Reversible myocardial dysfunction in survivors of out-of-hospital cardiac arrest. J Am CollCardiol2002; 40: 2110–6.
19. Huang L, Weil MH, Tang, W, etal.Comparison between dobutamine and levosimendan for management of postresuscitation myocardial dysfunction. Crit Care Med 2005; 33:487-491.
20. Fagnoul D, Taccone FS, Belhaj A, et al. Extracorporeal life support associated with hypothermia and normoxemia in refractory cardiac arrest. Resuscitation 2013;84:1519–24.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
251
21. Wallmuller C, Sterz F, Testori C, et al. Emergency cardio-pulmonary bypass in cardiac arrest: seventeen years of experience. Resuscitation 2013;84:326–30.
22. Muller T, LubnowM. The future of E-CPR: a joint venture. Resuscitation 2013;84:1463–4.
23. KilgannonJH, JonesAE, ShapiroNI, et al. Emergency Medicine Shock Research Network (EMShockNet) Investigators. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA2010; 303:
2165–71 24. Kilgannon JH, Jones AE, ParrilloJE,et al.Emergency Medicine Shock Research
Network (EMShockNet) Investigators. Relationship between supranormal oxygen tension and outcome after resuscitation from cardiac arrest. Circulation 2011;123:2717–2722.
25. Roberts B, Kilgannon H, Chansky M, et al. Association between postresuscitation partial pressure of arterial carbon dioxide and neurological outcome in patients with post cardiac arrest syndrome.Circulation 2013; 127:2107-2113.
26. Beiser D, David G, Gordon E, et al. Derangements in blood glucose following initial resuscitation from in-hospital cardiac arrest: A report from the national registry of cardiopulmonary resuscitation. Resuscitation 2009;80(6):624-630.
27. Cueni-Villoz N, Devigili A, Dellodder F, et al. Increased blood glucose variability during therapeutic hypothermia and outcome after cardiac arrest. Crit Care Med 2011; 39:2225-2231.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
252
AIRWAY MANAGEMENT IN TRAUMA:AN UPDATE OBEZBEĐENJE DISAJNOG PUTA KOD TRAUMATIZOVANIH PACIJENATA
IVANA KRSTIĆ-LEČIĆ, DUSICA STAMENKOVIC, MILIC VELJOVIC, KATARINA MLADENOVIC Klinika za anesteziologiju i intenzivnu terapiju, Vojnomedicinska Akademija, Beograd, Srbija E-mail:[email protected] Airway management of the trauma victim is intervention of first level priority and must be carrying out in basic life suport. The potential for cervical spine injury makes airway management more complex in the trauma patient. Cervical spine injury is often occult, and secondary injury to the spinal cord must be avoided. When we have patien with head injury, orofacial cervical spin and chest trauma, special conifideration of secondary injury must be avoided. Which technique of airway management will be use, depends of patient level injury, experience and equipment available.Tracheal intubation (orotracheal or nasotracheal) is gold standard for airway mangment in trauma.Numerous appliances and device for easier establishment and maintenance of problematic airway are available today such as for example various types of LMAs, combitubes and sets for cricothyroidotomy. Each of these appliance and device are of a greate help in cases of expectedly or unexpectedly problematic airway, but only in hands of skilled, educated and experienced stuff. It is very important not to waste time with repeated attempts at intubation while the patient is desaturating. Alternative methods of securing the airway should be instituted as soon as a problem is recognized. Uvod Kod traumatizovanog pacijenta, učestalost povrede vratne kičme čini obezbeđenje disajnog puta komplikovanijim. Na povredu vratne kičme moramo posumnjati u svim mehanizmima povređivanja uključujući i tupe povrede. Naročito treba da pobude sumnju povrede udružene sa ozledom klavikule i ramenog pojasa, kao i sve traume glave sa Glazgov koma skalom manjom od 9 (GCS < 9). Povrede vratne kičme su najčešće prikrivene, a sekundano oštećenje mora biti na vreme prevenirano. Imobilizacija vratne muskulature mora biti obavezna i pre nego što se pristupi kliničkoj i dijagnostičkoj evaluaciji povrede. Procena
1. Svestan, orjentisan pacijent, bez poremećaja u govoru i gutanju ne zahteva primarno zbrinjavanje već kliničko praćenje i procenu.
2. Sledeći klinički znaci zahtevaju adekvatno obezbeđenje disajnog puta: a. Apnea/dispnea b. Glazgov koma skala <9 c. Nestabilne traume ličnog masiva (Le Fort I, II i III) d. Direktne/indirektne povrede disajnog puta e. Različiti nivoi repiratorne slabosti f. Visok rizik za aspiraciju g. Nemogućnost obezbeđenja adekvatne oksigenacije traumatizovanog
3. Stepen hitnosti obezbeđenja disajnog puta je najvažniji faktor planiranja najbezbednije i najprikladnije tehnike.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
253
Obezbeđenje vazdušnog puta Inicijalno disajni put se mora osloboditi od krvi, sekreta i tkivnog detritusa. Po potrebi primeniti dvostruki manevar sa minimalnom ekstenzijom vratne kičme. Ventilacija i intubacija u „snifing“ položaju se apsolutno preporučije ukoliko postoji čak i minimalna sumnja na lezije atlantookcipitalnog zgloba kao i C5/6 nestabilni segment kičmenog stuba. Primenom spoljašnjih cervikalnih stabilizatora dodatno smanjujemo mogućnost naknadnih lezija vratne kičme. Zlatni standard obezbeđenja disajnog puta u traumi je oralna odnosno nazotrahealna intubacija. Ventilacija na masku može prouzrokovati značajan stepen pomeranja u zoni nestabilnosti i dodatno ugroziti pacijenta. Trahealna intubacija Koju tehniku trahealne intubacije primeniti zavisi od obučenosti i iskustva onoga ko obezbeđuje disajni put. ATLS preporučuje nasotrahealnu intubaciju kod povređenog sa očuvanim spontanim disanjem i orotrahealnu intubaciju kod pacijenta u apnei. Naravno, moraju se poštovati preporuke vezane za povrede orofacijalne regije sa nestabilnim segmentima i krvarenjem koje nasotrahealnu intubaciju svode na kontraindikovanu. Orotrahealna intubacija sa „rapid sequence induction“ tehnikom, uz preoksigenaciju i pritisak na krikoid je generalno najprimenjivanija tehnika obezbeđenja disajnog puta kod traumatizovanih. Idealno sredstvo za indukciju treba da deluje brzo, obezbedi hemodinamsku stabilnost, ne utiče na skok intrakranijalnog pritiska i deluje protektivno na nervni sistem. U tom smislu thiopenton ima prednost u odnosu na propofol i etomidat, dok se upotreba ketamina preporučuje za izrazito hemodinamski nestabilne pacijente. Intubacija budnog pacijenta je takođe potencijalni način obezbeđenja disajnog puta, naročito ukoliko se primenjuje nasotrahealni put i fiberoptička tehnika. Ipak, uspešnost fiberoptičke trahealne intubacije može biti kompromitovana prisustvom krvi, sekreta kao i postojanjem supra i infraglotičkog edema. Naravno, primena lokalnog anestetika dodatno moze povećati rizik od aspiracije. Neuspešna trahealna intubacija Neuspešna ili otežana trahealna intubacija uvek predstavlja problem i veoma je značajno ne gubiti vreme uz napomenu da ne smemo zaboraviti da ono sto ugrožava pacijenta nije neuspešna intubacija već desaturacija tako da uvek moramo imati rezervni plan i na vreme primeniti alternativne tehnike obezbeđenja disajnog puta. Laringealna maska Upotreba laringealne maske (LMA) ima sve širu primenu u zbrinjavanju disajnog puta kod traumatizovanih, naročito verzija intubacione laringealne maske za trahealne tube promera 6 i manje. Ipak, jednostavnost njene primene ograničena je činjenicom da ne štiti disajni put od aspiracije i može dodatno uzrokovati relaksaciju donjeg ezofagealnog sfinktera („BOLUS efekat ) čime dodatno provocira refluks. Ipak, i pored ovog značajnog ograničavajućeg faktora, laringealna maska nalazi svoje mesto u uslovima otežane/nemoguće intubacije.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
254
Kombituba Kombituba je dvolumenska tuba koja se naslepo plasira u ezofagus ili traheju. Primena dvolumenske kombitube takođe ima svoje mesto u primarnom zbrinjavanju disajnog puta kod trautomatizovanih uz iste ograničavajuće faktore koji se odnose na primenu laringealne maske čime se svrstava u red alternativnih sredstava naročito u uslovima otežane/onemogućene intubacije i/ili neadekvatne ventilacije. Krikotiroidotomija Potreba za hirurškim obezbeđenjem vazdušnog puta mora biti brzo prepoznata i bez odlaganja izvršena od strane iskusnih osoba. Primenjuje se kao primarni metod obezbeđenja disajnog puta u povredama koje zahvataju traheju i orofaringealne strukture, odnosno kao sekundarni metod u uslovima neuspešne oro/nazotrahealne intubacije. Izvodi se kao klasična hirurška traheotomija ili se primenjuje perkutana tehnika uz visok protok kiseonika. Za sada nema studija koje daju prednost jednoj od pomenutih tehnika kao i učestalost neuroloških sekvela nakon zbrinjavanja disajnog puta na ovaj način. Potvrda ispravne pozicije tube Od vitalnog značaja je potvrda da se tuba nalazi u traheji. Primenom određene metode obezbeđenja disajnog puta (oro/nazotrahealna intubacija, LMA, kombi tuba...) neophodno je adekvatnim monitoringom, kapnografijom dokazati ispravno pozicioniranje tube i adekvatnu ventilaciju, naročito ukoliko imamo udruženu povredu glave, vrata i grudnog koša gde se ne možemo osloniti samo na spoljašnje kliničke znake.
Literatura
1. Abrams K.J., Grande C.M. "Airway Management of the trauma patient with cervical spine injury", Current Opinion in Anesthesiology 1994;7:184-190. 2. Aphramian C. et al "Experimental Cervical Spine Injury Model : Examination of Airway Management and Splinting Techniques", Ann Emerg Med 1984;13:584-587. 3. Bivins H. et al "The Effect of Axial Traction during Orotracheal Intubation of the Trauma Victim with an Unstable Cervical Spine". Ann Emerg Med 1988;17:25-9. 4. Crosby E, Lui A "The Adult Cervical Spine : Implications for Airway Management" Can J Anaesth 1990;37:77-93. 5. Grande C.M., Barton C.R., Stene J.K. "Appropriate Techniques for Airway Management of Emergency Patients with Suspected Spinal Cord Injury." Anesth Analg 1988;67:714-715. 6. Hastings R.H., Marks J.D. "Airway Management for Trauma Patients with Potential Cervical Injuries", Anesth Analg 1991;73:471-82. 7. Majernick T. et al "Cervical Spine Movement during Orotracheal Intubation" Ann Emerg Med 1986;15:417-20. 8. Meschino A. et al "The Safety of Awake Tracheal Intubation in Cervical Spine Injury" Can J Anaesth 1992;39:114-117. 9.Ross S.E. et al "Clinical Predictors of Unstable Cervical Spine Injury in Multiply Injured Patients", Injury 1992;23:317-319. 10. Abrams KJ. General management issues in severe head injuries: Airway management and mechanical ventilation. New Horizons 1995;3:479-487

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
255
ANALGESIA AFTER LIVER TRANSPLANTATION ZOKA MILAN King’s College Hospital, London, UK, King’s College School of Medicine, London, UK E-mail:[email protected]
Introduction
Liver transplantation (LT) surgery is a major surgery performed in very ill patients with end-stage liver disease. In terms of haemodynamic variations, fluid shift and replacement, metabolic derangements, bleeding tendency, duration and potential complications, it is probably the most challenging abdominal operation. Although there is an abundance of material in the literature on LT surgery and on certain aspects of anaesthesia, there is very little in the literature regarding postoperative analgesia following LT surgery. The first part of this paper will address the intensity and treatment of postoperative pain in LT recipients. The second part will address postoperative pain treatment in a completely different but related patient population: healthy people undergoing large right or small left liver lobe resection for donation to patients with end-stage liver disease. Specificity of pain intensity following LT surgery
There are several factors identified as contributing to a high analgesia requirement following LT surgery. Firstly, the large Mercedes-Benz incision that is routinely used for LT surgery is one of the longest and consequently most painful incisions. The subcostal component of that incision is particularly painful during deep breaths, coughing and movement. Secondly, the long surgical time, the use of surgical retractors and the pressure applied to the lower ribs with the retractors contribute to an intense pain sensation following surgery. Thirdly, the hyperdynamic circulation characteristic of end-stage liver disease is associated with a higher distribution clearance of analgesic medications administered intraoperatively.1 Consequently,theintraoperative analgesia requirement is increased in patients with end-stage liver disease undergoing LT. Fourthly, when massive blood loss and transfusion during surgery occurs, there is a need for more analgesia, as some analgesic drugs are lost with blood loss.Fifthly, when the newly transplanted liver is working, the drug metabolism that was decreased by the non-functioning liver returns to normal. Finally, there are less-frequent but still-present causes for a high analgesia requirement, such as the fact that a small proportion of LT recipients are methadone-maintained and require significantly more intra- and postoperative analgesia. 2 However, there are also factors that contribute to lower analgesia requirements following LT surgery. Firstly, patients with more severe end-stage liver disease generally require less analgesia.3Secondly, during the anhepatic phase, there is no analgesic drug metabolism and therefore there is a decreased requirement for analgesic medication.4 There is only one retrospective study comparing morphine requirements post-liver resection versus morphine requirements post-LT. That study found a slightly lower morphine consumption only on the first postoperative day in the LT group.5Thirdly, when patients are kept sedated post-LT, they receive

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
256
generous intravenous analgesia without fear of opioid overdose. The first few postoperative days are the most painful, and if patients are sedated for thosefirst few days, the pain is less intense when they wake up. Postoperative analgesia in LT surgery is largely dependent on intraoperative analgesia. The type of intraoperative analgesia used depends on the transplantation centre or the individual anaesthetist’s preference. It is mainly a continuous infusion of fentanyl, remifentanil or morphine or intermittent boluses of fentanyl or morphine.6A small proportion of LT recipients are eligible for intraoperative epidural analgesia.7 Postoperative analgesia is multimodal, with opioids as the main component. This is mainly continuous intravenous opioids (fentanyl, remifentanil, morphine or oxycodone) or patient-controlled analgesia (PCA). For example, at the King’s College Hospital Liver Intensive Care Unit, a continuous infusion of fentanyl is administered when patients are intubated, and oxycodone 2.5-5mgPRN is used when patients are extubated. When this is not sufficient, oxycodone PCA is used. Other components of multimodal analgesia are regular paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs) and a variety of other analgesics in the transitional period from PCA or epidural analgesia to regular or as-required analgesia. Other options, which are rarely used, are epidural analgesia or transversus abdominis plane (TAP) block in addition to PCA. Epidural analgesia and LT
Thoracic epidural analgesia (TEA) has been used as a mode of postoperative pain relief for LT in a selected group of patients. It is not widely practiced in view of the impaired haemostasis associated with end-stage liver disease and severe unpredictable intraoperative coagulopathy. TEA in LT may not be the technique of choice for routine administration of postoperative analgesia, but can be considered in patients who have normal coagulation profile preoperatively. Safe conduct of TEA in LT involves anaesthetic expertise and stringent monitoring in the postoperative period.8
Transversus Abdominis Plane (TAP) block and LT
Ultrasound guided subcostal TAP block can be used as a part of multimodal postoperative analgesia in LT patients. Retrospective study of Milan et al. has shown significant reduction in 24h morphine consumption when TAP block was performed (46 ± 24mg) compared with morphine consumption when TAP block was not performed (72 ± 40mg) , as well as lower pain scores and median time to extubation. 9 Analgesia for live related liver donors
Due to a lack of cadaveric donors and the religious beliefsof some countries, liver transplantation from live related or non-related donors is becoming increasingly popular. Acquired experience

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
257
has led to improvement in all aspects of this operation apart from postoperative pain treatment. Although the same postoperative analgesia is used for live related donors as for all other liver resection patients, there is a belief amongst clinicians that postoperative pain is more intense after liver resection for liver donation than for liver resection for tumour removal . A recent study from Lee et al. has shown that trait anxiety in liver donors is significantly associated with postoperative pain.10It is understandable that liver donors are more anxious before surgery and that they do not feel a sense of relief following surgery in the same way as patients do who underwent liver resection for liver tumour. Donors receive more attention from recipient transplant coordinators, other medical staff and relatives, mainly because they were fit and well before surgery and because they underwent the surgery only for the benefit of another person. Despite this attention and all other efforts, donors experience pain. A recent French study has shown that severe acute postoperative pain, apart from being unpleasant, can lead to chronic pain. A retrospective analysis of 65 patients who underwent liver resection for liver donation has shown the incidence of severe acute pain is 11% at rest and 37% with movement.11Chronic pain affected six patients without any link to gender or type of analgesia used. 11Acute pain was a risk factor for developing chronic pain.11 The modes of analgesia for liver donations are the same as for liver resections for tumours: epidural, PCA, wound infiltration + PCA or intrathecal opioids + PCA. Epidural analgesia
Epidural analgesia is the most efficient and most commonly used type of analgesia in liver donors. Clarke et al. performed a retrospective study on 226 consecutive patients who underwent living donor right hepatectomy. Epidural analgesia provided better postoperative pain relief over three days, and less sedation but more pruritus than with PCA. 12 Other downsides of epidural analgesia in donors include technical difficulties, non-working epidurals, patchy blocks, inability to cover all areas of pain (e.g., neck pain, shoulder pain) and pain following catheter removal.13Some anaesthetist are reluctant to insert epidural catheters in donors due to fear of the risk of epidural haematoma . Intrathecal opioids combined with intravenous patient-controlled analgesia
Clinicians are continually challenged to come up with an analgesic technique that is effective yet that ensures donor safety. Intrathecal opioid analgesia in combination with postoperative PCA has been used for liver resection surgery and even has advantages over epidural analgesia.14 Ko et al. performed a prospective randomised controlled study comparing the analgesic effect of 400 mcg of intrathecal morphine followed by fentanyl PCA,compared to fentanyl PCA only, for pain treatment following donor hepatectomy.15There was significantly less pain at rest and coughingfor up to 30 and 24 hours, respectively, in the intrathecal +PCA group and less cumulative consumption of meperidine as additional analgesia.15 All side effects were similar in both groups, apart from pruritus being more pronounced in the intrathecal + PCA group. 16

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
258
Patient-controlled analgesia
Generally, the classic morphine PCA still has a role in the donor’s postoperative analgesia. Although it is the least efficient method according to many studies, it is simple and cost-effective. There have been attempts to improve this type of analgesia by adding, for example, ketorolac. A recent study from Kao et al. has shown acceptable pain control with a daily Visual Analogue Scale pain (VAS)of less than 3 when morphine PCA was used for postoperative analgesia in live related donor hepatectomy patients. The addition of ketorolac significantly reduced the requirement for rescue doses of fentanyl (25µg), which subsequently reduced the work load of personnel in the pain-control service . Local anaesthetic infiltration via wound catheter infusion
Last year’s prospective randomised study on 40 patients compared the quality of postoperative analgesia and its side effects when using local anaesthetic-based analgesia (PainBuster) with the efficacy of opioid-based analgesia (intrathecal morphine with intravenous fentanyl) in liver donors. The researchers found more satisfactory analgesia with intrathecal opioid and fentanyl versus PainBuster during the first 12 hours after surgery and comparable analgesia after that time. The side effects were similar. Bowel recovery was faster with PainBuster. 17 Moreover, a recent meta-analysis has shown that local anaesthetic infiltration via wound catheters combined with PCA provides pain relief comparable to continuous epidural analgesia except for the first postoperative day. Both techniques are associated with a similar-length hospital stay, and opioid use with wound catheter isassociated with a lower complication rate. 18
Reference list
1. Jin SJ, Jung JY, Noh MH et al. The population pharmacokinetics of fentanyl in patients undergoing living-donor liver transplantation. Clin Pharmacol Ther 2011; 90(3): 423-31 2. Veinrieb RM, Bernett R, Lynch KG. et al. A matched comparison study of medical and psychiatric complications and anesthesia and analgesia requirements in methadone-maintaned liver transplant recipients. Liver Transpl 2004; 10(1): 97-106 3. Ko JS, Shin YH, Gwak MS et al. The relationship between postoperative intravenous patient-controlled fentanyl analgesic requiremnets and severity of liver disease. Transplant Proc 2012; 44(2): 445-7 4.Kang JG, Ko JS, Kim GS, Gwak MS, Kim YR, Lee SK. The relationship between inhalational anesthetic requirements and severity of liver disease in liver transplant recipients according to three phases of liver transplantation. Transplant Proc 2010; 42(3): 854-7 5. Chen JP, Jawan B, Chen CL, Wang CH, Cheng KW, Wang CC, Concejero AM, Villagomeza E, Huang CJ. Comparison of postoperative morphine requirements in healthy living liver donors, patients with hepatocellular carcinoma undergoing partial hepatectomy, and liver transplant recipients. Transplant proc 2010; 42(3): 701-2

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
259
6. Paugam-Burtz C, Chatelon J, Follin A et al. Perioperative anaesthetic practices in liver transplantation in France: Evolution between 2004 and 2008. Ann Fr Anesth Reanim 2010 Jun 5 [Epub ahead of print]] 7. Tzebicki J, Nicinska B, Blaszczyk B. et al. Thoracic epidural analgesia in anaesthesia for liver transplantation: the 10-year experience of a single centre. Ann Transplant 2010; 15(2): 35-9 8. Milan Z, Rewari V. Epidurals for liver transplantation-Where are we? Periodicum Biologorum 2011; 113(2): 163-6 9. Milan ZB, Duncan B, Rewari V, Kocarev M, Collin R. Subcostal transversus abdominis plane block for postoperative analgesia in liver transplant recipients. Transplant Proc 2011; 43: 2687-90 10. Lee SH, Lim KC, Jeon MK. Et al. Postoperative pain and influencing factors among living liver donors. Transplant Proc 2012; 44(2): 563-5 11. Bonnet A, Lavand’homme P, France MN, reding R, DeKock M. Postoperative pain trajectories to identify risk of chronic postsurgical pain in living donors for liver transplantation. Ann Fr Anesth Reanim 2012; 31(12): 945-9 12. Clarke H, Chandy T, Srinivas C. et al. Epidural analgesia provides better pain management after live liver donation: a retrospective study. Liver Transpl 2011; 17 (3): 315-23 13. Milan Z, Kalami T, Harbis A. et all. An audit on postoperative pain in liver resection surgery following epidural catheter removal. J Pain manage 2011; 4(4): 381-6 14. Koea JB, Young Y, Gunn K. Fast track liver resection: the effect of a comprehensive care package and analgesia with single dose intrathecal morphine with gabapentin or continuous epidural analgesia. HPB Surg 2009; Article ID 271986 15. Ko JS, Choi SJ, Gwak MS. Et al. Intrathecal morphine combined with intravenous patient-controlled analgesia is an effective and safe method for immediate postoperative pain control in live liver donors. Liver Transpl 2009; 15(4): 381-9 16. Kao CW, Wu SC, Lin KC. Et al. Pain management of living liver donors with morphine with or without ketorolac. Transplant Proc 2012; 44(2): 360-2 17. Lee SH, Gwak MS, Choi SJ. Et al. Prospective, Randomized study of ropivacaine wound infusion versus intrathecal morphine with intravenous fentanyl for analgesia in living donors for liver transplantation. Liver Transpl 2013; 19(9): 1036-45 18. Bell R, Pandanaboyana S, Prasad KR. Epidural versus local anaesthetic infiltration via wound catheters in open liver resection: a meta-analysis. ANZ J Surg. 2014 May 29. doi:10.1111/ans.12683. [Epub ahead of print]

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
260
INTERVENTIONAL TREATMENT FOR MUSCULO-SKELETAL PAIN – MYTH OR REALITY? Z PETROVIC Medway NHS Foundation Trust, UK Introduction Musculo-skeletal pain originates from the following anatomical structures: vertebrae, facet joints, sacroiliac joint, intervertebral disc, nerve roots, ligaments and tendons and muscles. Epidemiological studies commonly report that up to 20% of people complain of widespread pain and around 10% suffer from regional pain. If American College of Rheumatology diagnostic criteria are used, approximately 3-5% of females and 1% of males suffer from fibromyalgia.2 The prevalence of chronic musculo-skeletal pain is consistent across North America, the UK and Europe. Accurate localisation of the origin of pain is essential in targeting the correct anatomical structures. The pain may also be referred from surrounding or distant areas. Management of musculo-skeletal pain may be challenging as it often leads to chronicity. Acute low back pain gets better in 1 week in 40-50% of patients, resolves in 1 month in 80-90%, remains ‘chronic’ in 20-30% and becomes ‘disabling’ in 5-10%.3,4
Interventional treatment is attempted when other aspects of management have failed or have resulted in unsatisfactory pain relief. Discussion The latest evidence gathered from the systematic reviews, Cochrane database and national guidelines for the management of common musculo-skeletal conditions have been collected. Cervical Radicular Pain Epidural corticosteroid administration
There are two possible administration routes: the interlaminar and transforaminal. The recent systematic review of interlaminar route included 3 randomised controlled trials (RCT) and 5 observational studies.5 The RCTs compared interlaminar vs. intramuscular corticosteroid injection, addition of morphine to the standard mixture of local anaesthetic and corticosteroid, and single injection vs. continuous infusion. The general conclusion was that interlaminar corticosteroid administration for (sub)acute cervical radicular pain is effective and recommended. There was one major RCT on transforaminal approach which did not prove advantage.6 Also, there are numerous reports of complications, mainly neurologic, but also fatal. The particle size of the depot corticosteroid may have a role so non-particulate dexamethasone may be used instead. The recommendation for this approach is overall negative.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
261
(Pulsed) radiofrequency treatment
In 3 RCTs looking at the RF adjacent to the dorsal root ganglion (DRG) or PRF treatment to the DRG the technique proved to be efficient with the RF in one trial producing such a good pain relief 8 weeks post-intervention that a Number Needed to Treat (NNT) was 1.4.7
The recommendation is positive for the chronic cervical radicular pain. Surgical treatment
In a randomised study comparing surgical vs. conservative treatment there was a significant pain relief 3 months after surgery but not a year after.8
Cervical Facet Pain Intra-articular steroid injection
No quality studies available for this technique Local infiltration of the medial branch of the ramus dorsalis
Can be either diagnostic or therapeutic proving efficacy with duration of pain relief for 14-16 weeks.9 It appears that addition of corticosteroid to local anaesthetic does not provide better outcome. The treatment is recommended but may be impractical for the patients in view of frequent visits for repeat injections. RF treatment of the medial branch of the ramus dorsalis
Seven systematic reviews supported the effectiveness of RF treatment. After each intervention chronic neck pain was satisfactorily reduced in more than 90% of patients and the effect lasted between 8 and 12 months.10
The treatment is recommended if the conservative treatment failed. Low Back Pain The biomechanics of the spine may be best considered by studying the single Functional Spinal Unit (FSU) consisting of two adjacent vertebrae, their three connecting joints (disc and two facet joints) and ligaments. When the intradiscal pressure exceeds the absorbing capacity of the disc, damage occurs to the FSU. In only 5-10% of the low back patients a specific cause such as herniated disc, spondylolisthesis, discitis, Bechterew disease etc. can be identified. The non-specific low back pain is sub-classified as mechanical low back pain that may emanate from the facet or zygapophyseal joints 15% (15-40), internal disc disruption 39% (29-49%) and sacroiliac joint 15% (7-23%).11
Sciatica is subdivided into radicular pain, neuropathic pain with objective signs of nerve damage and sympathetic maintained pain. Lumbosacral Radicular Pain Epidural corticosteroid administration
There are three approaches: interlaminar, transforaminal or caudal.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
262
The interlaminar has been a mainstream choice for many years, though with mixed indicators of efficacy. One study calculated the NNT to achieve 50% pain reduction. The NNT=3 was obtained for short-term pain reduction (1-3 months) and NNT=13 for long-term pain reduction (3-12 months).12
Transforaminal approach is believed to allow more precise application of steroids to the inflamed nerve root. A study comparing effectiveness of caudal, interlaminar and tranforaminal epidural steroid administration in patients with radicular pain showed the best clinical results with the latter approach.13 Therefore, the transforaminal approach is recommended in ‘contained herniation’ (herniation with a broad base, which is still contained within the ligamentum longitudinale posterior), but not in the ‘extruded herniation’. Pulsed radiofrequency treatment
Two retrospective studies indicated beneficial effect of RF treatment for a radicular pain as a result of disc herniation (NNT=1.38), spinal canal stenosis (NNT=1.19) but not in those with Failed Back Surgery Syndrome –FBSS (NNT=6.5).14
Adhesiolysis
In cases of peridural fibrosis, fluoroscopic-guided adhesiolysis with navigable, radio-opaque, kink-resistant and soft-tipped catheters is possible. Three RCTs and one observational study found positive short- and long-term outcome with either mixture of hypertonic or isotonic saline with hyaluronidase os saline alone. Therefore, the technique is recommended in specialised centres. Spinal cord stimulation in FBSS
Spinal cord stimulation (SCS) consists of percutaneous application of electrodes at the level of the spinal cord segment involved. These electrodes are then connected to a generator that delivers electrical pulses to stimulate the painful dermatomes and to induce altered pain conductivity, transmissibility and perception. A systematic review of the effectiveness of SCS for the FBSS included an RCT, a cohort study and 72 case reports. The RCT showed clear advantage of SCS, but the case reports were heterogeneous.15
Overall, the SCS is recommended for the FBSS in specialised centres. Pain originating from the Lumbar Facet Joints Intra-articular corticosteroid injections
This application is controversial. There is no clear long-term benefit in majority of patients. Also, there is not much difference whether the local anaesthetic alone, mixture with steroid, or a saline alone are injected. The recommendation is to perform intra-articular facet injection as a diagnostic block or as one-off therapeutic injection. RF treatment of the lumbar medial branches of the dorsal ramus
In 7 controlled studies published to 2009, the RF treatment showed benefit in selected patients after the positive diagnostic block with duration of pain relief up to 12 months.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
263
A recent meta-analysis confirmed the superiority of RF treatment after the conventional treatment failed or was with unsatisfactory pain relief and after the diagnostic block relieved the pain for at least 50%.16
Discogenic Low Back Pain Intradiscal corticosteroid injection
They are not recommended as the available evidence from only cohort studies and case reports do not support its efficacy. Intradiscal electrothermal therapy (IDET)
The procedure consists of percutaneous insertion of a thermocoil into the disc under radiographic control. The distal portion of the catheter (5cm) is heated for 16 min to 90°C and possible local denervation. The systematic review from 2006 supported effectiveness of IDET procedure.17 Subsequent studies and RCTs are with mixed recommendations mainly due to different patient selection criteria used which remains the critical factor for achieving useful results. It seems that better results are obtained if no more than 2 discs are degenerative. Biacuplasty
The technique consists of placement of 2 electrodes under the radiographic control to the posterior annulus fibrosus of the intervertebral disc. The RF current between the electrodes heats the area for 7 minutes at 50-65°C. There are no yet sham controlled, prospective randomized studies, but available pilot studies and case series indicate effectiveness. There may be an advantage over IDET as this technique is less invasive and there is minimal disruption to the native tissue architecture. Intradiscal radiofrequency (RF) thermocoagulation
The studies are inconclusive as there are both with a positive or negative outcome. Selection criteria and position of the RF electrode are the subject of controversy. RF of the ramus communicans
Recent study demonstrated that low lumbar disci intervertebrales may be chiefly innervated by L1-L2 dorsal root ganglions via the truncus sympathicus and the ramus communicans. Nakamura successfully blocked L2 nerve root in 33 patients with discogenic pain. RF destruction of ramus communicans in the treatment of discogenic pain has been successfully demonstrated and is recommended.18
Sacroiliac Joint Pain Intra-articular corticosteroid injection
All available studies showed good pain relief lasting for up to 12 months with local anaesthetic and steroid injected either intra- or extra-articular hence strong recommendation.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
264
RF treatment of the SI joint
The sacroiliac joint receives variable and extensive innervation from different sources. Therefore, the several prospective observational and retrospective studies and a few RCTs varied wildly in selection criteria, definition of success and RF parameters (ie. temperature, duration and location of RF treatment). Cohen demonstrated a good pain relief in his RCT with cooled RF treatment of the S1 to S3 rami laterals and ‘classic’ RF treatment on L4 and L5 rami dorsales which remain as generally accepted positive recommendation once the intra-articular injection effect has been explored.19
Muscle Pain Injured muscles often meet the diagnostic criteria for myofascial pain syndrome, characterized by muscles that are in a shortened or contracted state, with increased tone and stiffness and that contain tender, firm, 3-6mm nodules (trigger points). Following a correct identification of affected muscles in the neck or low back they can injected with local anaesthetic and steroid. A recent retrospective study showed major improvement in pain control with extensive muscle treatment protocol in patients scheduled for spinal surgery leading to cancellation of surgery.20
Conclusion The interventional pain management techniques described above are to a ceratin degree supported by evidence justifying their use in specific conditions. Recommendations should weight the potential benefits versus the potential risks. Radiofrequency treatment is recognised as beneficial for the management of chronic facet pathology at cervical and lumbar level. (Sub)acute radicular pain at cervical level is preferentially treated with fluoroscopy guided interlaminar steroid injection. At lumbar level the transforaminal route seems to have superiority. For the management of chronic radicular pain, pulsed radiofrequency to the dorsal root ganglion at the affected level is a possibility before considering the spinal cord stimulation or surgery.21
References
1. Pain in Europe Survey. 2003 2 Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990
Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum 33:160-172, 1990
3 Palmer KT, Walsh K, et al. Back pain in Britain: comparison of two prevalence surveys at an interval of 10 years BMJ 2000;320:1577-1578.
4 NICE Low back pain: Early management of persistent non-specific low back pain. NICE clinical guidelines 88. Issue date: May 2009
5 Peloso P, Gross A, Haines T, Trinh K, Goldsmith CH, Burnie S. Medicinal and injection therapies for mechanical neck disorders. Cochrane Database Syst Rev. 2007;3:CD000319.
6 Anderberg L, Annertz M, Persson L, Brandt L, Saveland H. Transforaminal steroid injections for the treatment of cervical radiculopathy: a prospective and randomised study. Eur Spine J.2007;16:321-328
7 Van Kleef M, Liem L, Lousberg R, Barendse G, Kessels F, Slujiter M. Radiofrequency lesion adjacent to the dorsal root ganglion for cervicobrachial pain:a prospective double

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
265
blind randomized study. Neurosurgery. 1996;38:1127-1131; discussion 1131-1132. 8 Persson LC, Carlsson CA, Carlsson JY. Long-lasting cervical radicular pain managed
with surgery, physiotherapy, or a cervical collar. A prospective, randomized study. Spine. 1997;22:751-758
9 Manchikanti L, Singh V, Falco FJ, et al. Cervical medial branch blocks for chronic cervical facet joint pain: a randomized, double blind, controlled trial with one-year follow-up. Spine. 2008;33:1813-1820
10 Husted DS, Orton D, Schofferman J, et al. Effectiveness of repeated radiofrequency neurotomy for cervical facet joint pain. J Spinal Disord Tech. 2008;21:406-408
11 Jan Van Zundert, Koen Van Boxem, Pieter De Vooght, Martine Puylaert, Pascal Vanelderen, Maarten van Kleef. Interventional pain management techniques – are they Evidence Based. ESRA –European Society of Regional Anaesthesia and Pain Therapy – 2008
12 McQuay HJ, Moore RA. Epidural corticosteroids for Sciatica. Oxford, New York, Tokyo: Oxford University Press; 1998.
13 Ackerman WE, 3rd, Ahmad M. The efficacy of lumbar epidural steroid injections in patients with lumbar disc herniations. Anesth Analg. 2007;104:1217-1222, table of contents.
14 Abejon D, Garcia-del-Valle, Fuentes ML, et al. Pulsed radiofrequency in lumbar radicular pain: clinical effects in various etiological groups. Pain Pract. 2007;7:21-26
15 Taylor RS, Van Buyten JP, Buchser E. Spinal cord stimulation for chronic back and leg pain and failed back surgery syndrome: a systematic review and analysis of prognostic factors. Spine. 2005;30:152-160.
16 Van Zundert J, Vanelderen P, Kessels A, Re: Chou R, Atlas SJ, Stanos SP, et al. Nonsurgical interventional therapies for low back pain: a review of the evidence for an American Pain Society clinical practice guideline. Spine (Phila Pa 1976) 2009;34:1078-1093. Spine (phila Pa 1976) 2010;35:841; author reply 841-842
17 Appleby D, Anderson G, Totta M. Meta-analysis of the efficacy and safety of intradiscal electrothermal therapy (IDET). Pain Med. 2006;7:308-316
18 Slujiter ME. Radiofrequency lesions of the communicating ramus in the treatment of low back pain. In: Raj PP, ed. Current Management of Pain. Philadelphia: Kluwer Academic publishers; 1989:145-159.
19 Cohen SP, Hurley RW, Buckenmaier CC 3rd, et al. Randomized placebo-controlled study evaluating lateral branch radiofrequency denervation for sacroiliac joint pain. Anesthesiology. 2008;109:279-288.
20 Marcus JN, Shrikhande AA, McCarberg B, Gracely E. A preliminary study to determine if a muscle pain protocol can produce long-term relief in chronic back pain patients. Pain Medicine 2013;14:1212-1221.
21 Van Zundert J, Patijn J, Hartrick TC, Lataster A, Huygen JPMF, Mekhail N, van Kleef M. Evidence-based interventional pain medicine according to clinical diagnoses, Wiley-Blackwell, 2012

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
266
NEUROPATSKI BOL KOD BOLESNIKA SA MALIGNOM BOLESTI NEUROPATHIC PAIN IN PATIENTS WITH MALIGNANCY NEBOJŠA LAĐEVIĆ1,2, DUŠICA STAMENKOVIĆ3, DEJAN NEŠIĆ2, ANA MIMIĆ1, DEJAN MARKOVIĆ1,2, IVANA LIKIĆ LAĐEVIĆ2,4
1Centar za anesteziologiju i reanimatologiju KC Srbije,2Medicinski fakultet u Beogradu, 3Vojnomedicinska akademija Beograd, 4Klinika za ginekologiju i akušerstvo KC Srbije Abstract Neuropathic pain is a direct result of the disease or lesion, which covers part of the somatosensory nervous system. When we say LESIONS, we describe the damage which can be identified by macroscopic or microscopic methods, and the DISEASE is related to a pathological process that can be identified as an inflammation, or an autoimmune condition or channelopathies. The definition applies only to the "somatosensory system" because the lesions of other parts of the nervous system may cause other types of pain, like a spastic hypertonia or rigor, where the pain occurs by activation of nociceptors in muscle and should not be confused with term neuropathic pain. Neuropathic pain exceeds the duration of painful stimuli, occurs and persists after the stimulus that caused the pathological tissue damage and after complete recovery of pathological changes. Etiologicaly, the greatest number of patients had nociceptive pain (59%), and neuropathic (19%), mixed (20%), and unknown etiology (2%). The above data shows that as much as 39% of patients have a component of neuropathic pain that occurs either isolated or combined with nociceptive pain. Uvod Bol je neprijatan senzorni ili emocionalni doživljaj udružen sa postojećim ili potencijalnim ostećenjem tkiva, ili iskazan rečima koje opisuju takvo oštećenje. Bol je svakako najčešći simptom zbog koga se pacijent obraća lekaru i skoro uvek je manifestacija nekog patološkog procesa. I sama definicija nam govori o tesnoj povezanosti izmedju objektivne, senzorne, komponente i veoma prisutne subjektvne, psihološke komponente. Zbog toga i odgovor na bol izrazito varira kod različitih osoba, ali i kod iste osobe u različito vreme. Bol možemo posmatrati i podeliti na više načina. Ukoliko gledamo prema dužini trajanja onda ga delimo na akutni i hronični. Ukoliko posmatramo etiologiju možemo ga grubo podeliti na postoperativni i kancerski. Možemo ga podeliti i prema mestu nastanka, odnosno zahvaćenosti dela tela pa tada govorimo o bolu u leđima, glavoboljama i slično. Međutim, veoma je bitna podela prema patofiziološkom nastanku bola i tada govorimo o nociceptivnom, neropatskom i mešovitom (udružen nociceptivni i neuropatski bol) bolu. Upravo ova podela je veoma značajna za pacijente sa malignom bolesti (1). Nociceptivni bol nastaje nadražajem nociceptora usled povrede, bolešću ili abnormalnom funkcijom organa ili mišića. Znači, javlja se kada su specifični receptori - nocioceptori izloženi
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
267
štetnom nadražaju (hemijski, toplotni ili mehanički) koji pri dužem delovanju može da ošteti tkivo. Oštećenje tkiva na periferiji dovodi do stimulacije nervnih završataka i aktivacije lokalnih inflamatornih ćelija (makrofaga, mast ćelija, limfocita i trombocita), dolazi do oslobađanja mnogih alogenih supstanci koje direktno izazivaju bol kao što su:
• bradikinin, citokini interleukini i NGF (nerve growth factor) iz makrofaga • serotonin i histamin iz trombocita i mast ćelija • adenozin i H+ joni iz tkiva • prostaglandini iz tkiva i puta ciklooksigenaze • leukotrijeni iz tkiva i puta leukotrijena • neurotransmiteri (glutamat, supstanca P) iz aferentnih vlakana antidromnim
oslobađanjem Nociceptivni put je aferentan, ascedentan, 3-neuronski sistem, sa descedentnom modulacijom od strane korteksa i talamusa. Možemo ga grubo podeliti na sledeće komponente:
• nociceptore, primarna aferentna vlakna, sinapse i biohemijske medijatore u dorzalnom rogu kičmene moždine
• ascedentni nociceptivni trakt – spinotalamički i spinohipotalamički trakt • viši centri u CNS-u – uključeni u obradu bolnog stimulusa, afektivne komponente bola,
memoriju bola, momentalne agresivne odgovore na bolnu draž • nishodni sistem koji omogućava CNS-u da modifikuje nociceptivnu informaciju
na više nivoa. Neuropatski bol je direktna posledica lezije ili bolesti koja zahvata somatosenzorni deo nervnog sistema. Kada kažemo LEZIJA mislimo na oštećenja koje se mogu identifikovati makroskopski ili mikroskopskim metodama a BOLEST se odnosi na patološke procese koji se mogu identifikovati kao inflamacije, autoimunska stanja ili kanalopatije. Definicija se odnosi isključivo na “somatosenzorni sistem” jer lezije drugih delova nervnog sistema mogu uzrokovati druge tipove bola, kao kod spastične hipertonije ili rigora, gde bol nastaje aktivacijom nociceptora iz mišića i ne sme se zameniti sa neuropatskim bolom. Neuropatski bol prevazilazi vremensko trajanje bolne draži, nastaje i traje i nakon prestanka draži koja je izazvala patološko oštećenje tkiva kao i nakon potpune restitucije patoloških promena (2). Neuropatski bol se može podeliti na:
a. Periferni neuropatski bol - uzrokovan bolešću ili lezijom perifernih nerava i korenova kičmene moždine uključujući i senzorne neurone dorzalnih ganglija kičmene moždine
b. Centralni neuropatski bol - uzrokovan bolešću ili lezijom mozga i kičmene moždine c. Kombinovani neuropatski bol - uzrokovan sistemskim bolestima koje istovremeno
oštećuju periferni i centralni nervi sistem Promene koje nastaju usled oštećenja perifernog nerva mogu biti (2):

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
268
• Anatomske
Uglavnom je to aksonska degeneracija, regeneracija aksona i stvaranje neuroma
• Farmakološke
Oštećenje nerava povećava ekspresiju raznih proteinskih receptora kao što je i tranzitorni receptorski potencijal V1 (TRPV1). TRPV1 je lokalizovan na pojedinim subtipovima perifernih nociceptivnih završetaka i fiziološki se aktivira delovanjem termičkih draži od 41oC. Na oštećenim nervima se smanjuje a na neoštećenim C-vlaknima povećava ekspresija TRPV1 i bolesnici ispoljavaju hiperalgeziju na normalno tople draži po tipu žarećeg bola. Kod neuropatije sa hiperalgezijom na normalno hladne draži postoji povećana ekspresija receptorskog proteina TRP8. Nakon povrede nerva nastaje promene u osobinama jonskih kanala za natrijum kao i ekspresija različitih tipova jonskih kanala za natrijum. Nastaje redistribucija i akumulacija jonskih kanala za natrijum duž aksona povredjenog nerva. Različite izoforme natrijumovog kanala imaju različite kinetske i farmakološke osobine. Nav1.8 i 1.9 a subjedinice su eksprimirane isključivo na tankim nemijeliniziranim vlaknima i otporni su na blokirajuće dejstvo tetrodotoksina (TTX). Nav1.7 a subjedinica nije otporna na blokirajuće dejstvo TTX i eksprimirana je na senzornim neuronima ganglija dorzalnih korenova (DRG) i na simpatičkim neuronima. Duž povredjenih aksona i na neuromima dolazi do translokacije, insercije i grupisane akumulacije Nav1.8 i 1.9 a subjedinica kao i do ekspresije ambrionalne subjedinice Nav1.3 a koja je osetljiva na blokirajuće dejstvo TTX. Ektopično izbijanje akcionih potencijala senzitivnih vlakana se ostvaruje preko sujedinice Nav1.3 a.
• Elektrofiziološke
Pojačana ektopična aktivnost u neoromu, zadnjim rogovima kičmene moždine ali i u neoštećenim aksonima, prenos akcionog potencijala na susedne aksone i smanjen prag nadražljivosti.
• Neurohemijske
Povećanje neurotrofičkih faktora: faktor rasta (NGF), moždani faktor (BDNF), Neutrofin (NT-4) i Citokina (TNF).
Kao posledica oštećenja perifernog nerva može doći i do oštećenja centralnog neurona i to se manifestuje kao (2):
1. Strukturna reorganizacija kičmene moždine Dolazi do razvoja alodinije zato što vlakna koja ne prenose bolni nadražaj i koja se završavaju u lamini IV sada prorastaju u laminu II gde se završavaju vlakna koja prenose bol. Na taj način se stimulusi koji nisu bolni prelivaju u laminu II i postaju bolni.
2. Reorganizacija somatosenzornog korteksa. Bazira se na funkcionalnim sinaptičkim promenama i promenama telesnih mapa u korteksu (prepokrivanje telesnih mapa, kao posledica aktiviranja postojećih neaktivnih sinapsi, ili usled stvaranje novih sinapsi). Dolazi do ekspanzije reprezentacije bolnih područja.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
269
3. Promene u ekspresiji jonskih kanala za kalcijum na nivou kičmene moždine
a. Kompenzatorno povećanje Ca++ kanala kao posledica smanjenja aferentnih signala iz povređenog nerva
b. Povećana ekspresija α2δ subjedinice N-tip Ca++ kanala c. Povećana aktivnost visoko voltažnih N-tip Ca++ kanala d. Povećanje intracelularnog Ca++ dovodi do povećanog oslobadjanje transmitera iz
sinaptičkih vezikula i povećava membransku ekscitabilnost
4. Smanjenje inhibitorne GABA 5. Povećanje koncentracije glutamata 6. Promene koncentracije opioidnih receptora (povećanje ili smanjenje)
Detaljnim pregledom literature prevalenca bola kod pacijenata sa malignitetom se kreće (3):
o od 33% kod pacijenata posle terapije o do 59% kod pacijenata na atikancerskoj terapiji i o do 64% kod pacijenata sa metastazama, u uznapredovaloj ili terminalnoj fazi bolesti
Hronični bol se može javiti i kod bolesnika koji su uspešno završili terapiju karcinoma a faktori koji na to utiču su (4):
a. Periferna neuropatija zbog hemoterapije, b. Radijacijom izazvana brahijalna pleksopatija, c. postradijacioni hronični pelvični bol i d. Postoperativni bol
Bol ima veliku prevalencu u određenim specifičnim tipovima karcinoma kao što je karcinom pankreasa (44%) i karcinom glave i vrata (40%) (5). Skorašnje studije pokazuju da se različite vrste bola i bolnih sindroma javljaju u svim fazama karcinomske bolesti (i ranoj i metastatskoj) i da bol nije adekvatno lečen kod velikog broja pacijenata, u rasponu od 56% do 82.3% (6). Veliki broj pacijenata sa limfomima i leukemijom može imati bol i ne samo u poslednjim mesecima života (83%), već on može biti prisutan već u vreme postavljanja dijagnoze ili tokom terapije (7). Etiološki posmatrano najveći broj pacijenata ima nociceptivni bol (59%), zatim neuropatski (19%), mešoviti (20%) i nepoznate etiologije (2%). Iz iznetih podataka se vidi da čak 39% pacijenata ima neuropatsku komponentu bola koja se javlja ili izolovana ili udružena sa nocicceptivnim bolom (8). Ne smemo zaboraviti da se kod kancerskog bola može javiti i inflamatorni bol, kao reaktivna upala oko nerva koji je komprimovan, zahvaćen procesom. Pacijenti koji imaju neuropatski bol se mogu žaliti na (9, 10):

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
270
1. Negativne simptome i znake a. Hypoaesthesia - Smanjen osećaj bezbolnih draži b. Pal-hypoaesthesia - Smanjen osećaj vibracijskih draži c. Hypoalgesia - Smanjen osećaj bolnih draži d. Therm-hypoaesthesia - Smanjen osećaj termičkih (i toplih i hladnih) draži.
2. Spontane Pozitivne simptome
a. Paraesthesia - Bezbolni abnormalni osećaj trnjenja ili mravinjanja b. Paroksizmalni bol - Udarni kratkotrajni osećaj strujanja poput električnog udara c. Površni bol - Bolni površni osećaj pečenja ili žarenja
3. Evocirane pozitivne simptome
a. Mehanička dinamička alodinija - Osećaj bola na kretanje lake bezbolne draži po koži b. Mehanička statička hiperalgezija - Osećaj bola na normalni bezbolni blagi pritisak na
kožu c. Mehanička tačkasta hiperalgezija na dodir i ubod - Osećaj bola na bockanje
bezbolnim dražima d. Vremenska sumacija - Povećanje osećaja bola pri repetitivnoj primeni identičnih
pojedinačnih stimulusa e. Hiperalgezija na hladne i tople draži - Osećaj bola pri draženju normalno hladnim ili
toplim bezbolnim dražima f. Mehanička duboka somatska hiperalgezija - Osećaj bola pri normalnom bezbolnom
pritisku dubokih tkiva Glavni simptomi koji prate bol kod ovih pacijenata su nesanica i anksioznost pa su i glavni farmakološki ciljevi lečenja neuropatskog bola: smanjenje jačine bola, otklanjanje nesanice – poboljšanje sna, otklanjanje udružene depresije i anksioznosti, poboljšanje kvaliteta života. Reference:
1. Melzak R, Wall P. Pain management. Elsevier Churchill Livingstone (5th Ed), Philadelphia, USA, 2006.
2. Treede RD, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffin JW, Hansson P, Hughes R, Nurmikko T, Serra J. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology 2008;70(18):1630-5.
3. Van den Beuken-van Everdingen MHJ, De Rijke JM, Kessels AG et al. Prevalence of pain in patients with cancer: a systematic review of the past 40 years. Ann Oncol 2007;18:1437–49.
4. Sun V, Borneman T, Piper B et al. Barriers to pain assessment and management in cancer survivorship. J Cancer Surviv 2008;2:65–71.
5. Burton AW, Fanciullo GJ, Beasley RD et al. Chronic pain in cancer survivor: a new frontier. Pain Med 2007;8:189–98.
6. Higginson IJ, Murtagh F. Cancer pain epidemiology. In Bruera E, Portenoy RK (eds), Cancer Pain. Assessment and Management. Cambridge University Press 2010;3:37–52.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
271
7. Costantini M, Ripamonti C, Beccaro M et al. Prevalence, distress, management and relief of pain during the last three months of cancer patients’ life. Results of an Italian mortality follow-back survey. Ann Oncol 2009;20:729–735.
8. Benett MI, Rayment C, Hjermstad M, Aass N, Caraceni A, Kaasa S. Prevalence and aetiology of neuropathic pain in cancer patients: a systematic review. Pain 2012:153(2);359-65.
9. Haanpaa M et al. NeuPSIG guidelines on neuropathic pain assessment. Pain 2011;152:14-27.
10. Ripamonti CI et al. Management of cancer pain: ESMO clinical practiceguidelines. Annals of oncology 2012;23(7):139-54.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
272
IMAGINE LIVING WITHOUT PAIN...UNDERSTANDING PAIN GENETICS DUSICA STAMENKOVIC1, NEBOJSA LADJEVIC2,3, MILIC VELJOVIC1, VLADIMIR BANCEVIC 4 , PREDRAG ALEKSIC 4 1Department of Anesthesiology and Intensive Care, Military Medical Academy,Belgrade, Serbia 2Centre for anesthesia and resuscitation, Clinical Center Serbia, Belgrade, Serbia 3Medical School, University of Belgrade, Serbia 4Department of Urology, Military Medical Academy,Belgrade, Serbia E-mail:[email protected].
Introduction
Pain perception, opioid analgesic effects as well as incidence of opioid side effects are widely variable in the human population. So far more than 358 genes are found to be connected with pain1. Pain gene database and pain network connecting pain genes and phenotypes were constructed to assist in understanding pain genetics knowledge2. In this paper we present basic knowledge of genetic basis for pain variability and it’s implication on clinical practice. Pain is a complex phenomenon and result of multiple factors including gene interactions (gene x gene), environmental influence (gene x environment), micro RNAs and epigenetics3. Based on literature data, 30-60% of different chronic pain states such as neck pain, carpal tunnel syndrome, chronic pelvic pain are genetically determined4. Single-gene pain disorders are well investigated and classified as syndromes featuring absence of pain and syndromes featuring pain. Syndromes featuring absence of pain are channelopathy-associated indifference to pain (CAIP) and hereditary sensory and autonomic neuropathy (HSAN) types I to IV. Syndromes featuring pain are familial periodic fever, familial Mediterranean fever (FMF), familial hemiplegic migraine (FHM) types I-III, hereditary pancreatitis, hereditary neuralgic amyotrophy (HNA), and paroxysmal extreme pain disorder (PEPD) and primary erythermalgia3. Genes are responsible for production of different protein classes including ion channels, enzyme transcript factors and trophic factors. Numerous genes are connected with experimental and clinical painful states and pain phenotypes (cortical activation “pain matrix”, wind up phenomenon and pain modulation)3. SCN9A gene is responsible for voltage sensitive Nav 1.7 channel and today represents the most popular target for analgesic development. This gene is connected with individual susceptibility for development of different chronic pain states and variety in reaction to painful stimuli 5,6. Pharmacogenomics is dedicated to the study of gene influence on pharmacodynamic and pharmacokinetic characteristics of medication and body’s individual response to certain medication 7. Pharmacodynamic is dedicated to study of different mechanisms of medication’s action from the moment of receptors activation to receptors’ role and secondary messenger’s role. Pharmacokinetics includes observation of medication route from intake, absorption,
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
273
distribution, metabolism and elimination. Phenotype expressed as response to opioid, is complex and includes medication’s analgesic effect, gastrointestinal and central side effects. In pharmacokinetics the central role belongs to genes responsible for cytochrome P450 2D6 (CYP2D6) and P450 3A (CYP3A), and UDP-glucuronosyltransferase 2B7 (UGT 2B7). Polymorphism of genes coding CYP, is responsible for four phenotypes based on CYP function: slow metabolizers, medium, extensive and ultra fast metabolizers. CYP 450 is responsible for metabolism of numerous analgesics and therefore their action. CYP2D6 are family of enzymes involved in codeine, tramadol and oxicodone metabolism. CYP 3A is super family of enzymes involved in metabolism of almost 50% of known medications. CYP3A4 and CYP3A5 enzymes are involved in fentanyl metabolism on equal bases, and interaction between these two is additive and influences postoperative analgesia 8. UGT 2B7 is hepatic isoenzyme primarly responsible for morphine metabolism. UGT 2B7 gene expresion is variable in population with different mRNA expression and different metabolic products ratio 9. OPRM1 gene is responsible for Mu opioid receptor sinthesis. OPRM1 polymorhisam is responsible for different response after opioid analgesic application in postoperative pain, chronic non-cancer and cancer pain 10,11,12. G alel OPRM1 cariers need higher morphine dose for cancer and postoperative pain, while in A alel cariers morphine is more efficient for cancer pain treatment 12,13. Catechol-O-methyltransferase, HTR3B and cytokins genes are responsible for neurotransmiters function. COMT is responsible for catecholamine metabolism, and gen Val158Met, rs4680 increases sensitivity to pain and increases activity of mu opioid system 14, while Val158Met, rs4680 gene increases morphine requirement 15. HTR3B gene is responsible for 5-HT (serotnin) receptor synthesis. rs1176744G, rs3782025T, rs1672717T variants are responsible for lower incedence of nusea and vomiting after opioid use 16.
Mismatch of pro-inflamatory i anti-inflamatory cytokins ratio is responsible for peripheral neuropathies, fibromilagia and chronic regional pain syndrome. Epigenetics is term which assumes DNA or hromatine modification and therefore influnce on gene expression 17. Hope for more dynamic view on pain states lies in epigenetics. For expample DNA, methilation and post-translacional histone modification influences gene expression and cell characteristics 18.
Conclusion
Individual genotype can help us to predict response to certain medications. Personalized pain therapy is based on individual genomic information. Knowledge of chronic pain risk, postperative pain severity and analgesia effects will help medical providers in better pain treatment planning.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
274
Literature
1.LaCroix-Fralish, M.L., Ledoux, J.B. and Mogil, J.S. The Pain Genes Database: an interactive web browser of pain-related transgenic knockout studies. Pain 2007; 131:3.e1-3.e4. 2.Perkins JR, Lees J, Antunes-Martins A, Diboun I, McMahon SB, Bennett DL, Orengo C. PainNetworks: a web-based resource for the visualisation of pain-related genes in the context of their network associations.Pain. 2013;154:2586.e1-12. 3.Mogil JS. Pain genetics: past, present and future.Trends Genet. 2012;28:258-66. 4.Young EE, Lariviere WR, Belfer I. Genetic basis of pain variability: recent advances. J Med Genet. 2012 Jan;49(1):1-9. 5.Wood JN. Results in analgesia--Darwin 1, pharma 0. N Engl J Med. 2013;369:2558-60. 6.Cox JJ, Sheynin J, Shorer Z, Reimann F, Nicholas AK, Zubovic L, Baralle M, Wraige E, Manor E, Levy J, Woods CG, Parvari R. Congenital insensitivity to pain: novel SCN9A missense and in-frame deletion mutations.Hum Mutat. 2010;31:E1670-86. 7.Branford R, Droney J, Ross JR. Opioid genetics: the key to personalized pain control? Clin Genet. 2012 ;82:301-10. 8.Zhang W1, Chang YZ, Kan QC, Zhang LR, Li ZS, Lu H, Wang ZY, Chu QJ, Zhang J. CYP3A4*1G genetic polymorphism influences CYP3A activity and response to fentanyl in Chinese gynecologic patients.Eur J Clin Pharmacol. 2010;66:61-6. 9.Innocenti F1, Liu W, Fackenthal D, Ramírez J, Chen P, Ye X, Wu X, Zhang W, Mirkov S, Das S, Cook E Jr, Ratain MJ. Single nucleotide polymorphism discovery and functional assessment of variation in the UDP-glucuronosyltransferase 2B7 gene. Pharmacogenet Genomics. 2008;18:683-97. 10.Sia AT, Lim Y, Lim EC, Goh RW, Law HY, Landau R, Teo YY, Tan EC.A118G single nucleotide polymorphism of human mu-opioid receptor gene influences pain perception and patient-controlled intravenous morphine consumption after intrathecal morphine for postcesarean analgesia. Anesthesiology. 2008;109:520-6. 11.Janicki PK, Schuler G, Francis D, Bohr A, Gordin V, Jarzembowski T, Ruiz-Velasco V, Mets B.A genetic association study of the functional A118G polymorphism of the human mu-opioid receptor gene in patients with acute and chronic pain. Anesth Analg. 2006;103:1011-7. 12.Klepstad P, Rakvåg TT, Kaasa S, Holthe M, Dale O, Borchgrevink PC, Baar C, Vikan T, Krokan HE, Skorpen F.The 118 A > G polymorphism in the human mu-opioid receptor gene may increase morphine requirements in patients with pain caused by malignant disease. Acta Anaesthesiol Scand. 2004;48:1232-9. 13.Campa D, Gioia A, Tomei A, Poli P, Barale R. Association of ABCB1/MDR1 and OPRM1 gene polymorphisms with morphine pain relief.Clin Pharmacol Ther. 2008;83:559-66. 14.Zubieta JK, Heitzeg MM, Smith YR, Bueller JA, Xu K, Xu Y, Koeppe RA, Stohler CS, Goldman D.COMT val158met genotype affects mu-opioid neurotransmitter responses to a pain stressor. Science. 2003 Feb 21;299(5610):1240-3. 15.Rakvåg TT, Klepstad P, Baar C, Kvam TM, Dale O, Kaasa S, Krokan HE, Skorpen F.The Val158Met polymorphism of the human catechol-O-methyltransferase (COMT) gene may influence morphine requirements in cancer pain patients. Pain. 2005;116:73-8. 16.Laugsand EA, Fladvad T, Skorpen F, Maltoni M, Kaasa S, Fayers P, Klepstad P.Clinical and genetic factors associated with nausea and vomiting in cancer patients receiving opioids. Eur J Cancer. 2011;47:1682-91.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
275
17.Sun Y, Sahbaie P, Liang DY, Li WW, Li XQ, Shi XY, Clark JD. Epigenetic regulation of spinal CXCR2 signaling in incisional hypersensitivity in mice. Anesthesiology. 2013;119:1198-208. 18.Crow M, Denk F, McMahon SB. Genes and epigenetic processes as prospective pain targets.Genome Med. 2013;5:12.
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
276
ABSTRACTS
UAIS Final Four! Residents Corner-The Best Abstract Case Report Competition
FF1 Esophageal Doppler monitoring in esophageal surgery: is it necessarily a contraindication? Đukanović Marija1, Veličković Jelena1,3, Stojakov Dejan2,3, Palibrk Ivan1,3, Miljković Bojana1, Janjić Nataša1, Kosanović Momčilo1
1Center for Anesthesia, Clinic for Digestive Surgery, Clinical Center of Serbia, Belgrade, Serbia
2Clinic for Digestive Surgery, Clinical Center of Serbia, Belgrade, Serbia 3University of Belgrade, School of Medicine Introduction:We aimed to highlight the possibility of esophageal Doppler monitoring use for the operation on the esophagus, albeit formal contraindication for use in esophageal surgery. Case report:A 83-year old woman with history of hypertension and cardiomyopathy presented with dull chest pain and vomiting was diagnosed Boerhaave syndrome. The diagnosis was confirmed by CT findings and evacuation of gastric contents on chest drain placed in the left hemithorax. On admission,she was conscious,hemodynamicaly unstabile (BP-70/50mmHg,HR-110/min) with shortness of breath and chest pain. ECG revealed ST-elevation in D1,D2,avL,V5-V6. Myocardial infarction(MI) was suspected and it created dilemma for surgical team. If MI had been confirmed, surgeon would have decided for (less efficient) conservative treatment. Otherwise,she required an emergency operation. Troponin essay was obtained,but we couldn’t wait for the result,as the patient’s condition rapidly deteriorated. We performed transthoracic echocardiography which revealed no segmental wall motion abnormalities. In agreement with surgeon,we placed esophageal Doppler probe (CardioQ) above the site of esophageal rupture and obtained a waveform typical for hypovolemia (narrow complexes,CO-4.1L/min,SV-37ml,FTc-268ms,PV-34cm/s) and not cardiogenic shock. After fluid challenge (bolus of 200ml of saline) we noticed 10% rise of stroke volume (CO-4.9L/min,SV-49ml,FTc-290ms,PV-53cm/s). Patient was fluid responsive and was administered only fluids until resolution of shock state. The esophageal probe was under direct visual and manual control of surgeon during operation (transthoracic esophageal suture). Conclusion:We demonstrated that esophageal Doppler monitoring can be safe and helpful in decision making in some types of esophageal operations. To our knowledge it is the first case of CardioQ use in esophageal surgery.
FF2 A young anesthesiologist experience: extra-adrenal pheochromocytoma of urinary bladder. Oops…surprise! Radovic Nevena, Vaskovic Igor, Petrovic Uros, Veljovic Milic, Stamenkovic Dusica Department of anesthesia and intensive care, Military Medical Academy, Belgrade, Serbia. Introduction. Pheochromocytoma of the urinary bladder constitutes 1% of all pheochrocytomas. Surgical excision of extraadrenally localized or accidentally discovered pheocromocytomas is accompanied with high risk of bleeding and consequences of hypertension crises including acute heart failure and surgical mortality rate of 2-3%. Case report. We present two cases. 49 year old patient was scheduled for transurethral tumor resection (TUR). She complained of hypertension attacks after morning micturition. Blood levels of epinephrine, norepinephrine, metanephrine and vanil-mandelic acid were normal. Perioperatively, the first hypertension episode was noticed during urinary bladder tumor (UBT) biopsy and was treated with nitroprusside. Patient underwent pheochromocytoma preparation protocol after positive MIBG-J 131scanning. Partial cystectomy was performed uneventfully. The second case was 54 year old female patient with UBT treated for last two years with TUR. She was complaining of headaches, hypertension crises, tachycardia, postmicturition weakness and disuria. Her medical history included rheumatoid arthritis and insulin non dependent diabetes. Increased blood levels of metanephrin, normetanephrin, chromogranin A, ACTH and cortizol were measured and positive MIBG-J 131 scanning was recorded. After alpha- and beta- blockers preparation, and several hypertension crisis during preopertive period, she was scheduled for the surgery. Perioperatively, during urinary bladder manipulation, hypertension was controlled with nitropruside until tumor removal. Subsequent hypotension was treated with dopamine. Both patients were discharged from a hospital in a good state.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
277
Conclusion. During extraadrenal pheochromocythomas removal, hypertension and bleeding risks persist until tumour removal. Unsuspected or extraadrenal pheochromocytoma deserve exeprienced anesthesia provider and fast adequate treatment.
FF3 Fat embolism syndrome/diagnostic and management challenge even today! Igor Vasković, Uroš Petrović, Nevena Radović, Ivan Zlatkovic, Milić Veljović, Departement of Anesthesia and Intensive Care, Military Medical Academy, Belgrade, Serbia. Introduction. Fat embolism syndrome (FES) is presenting as a triad of respiratory insufficiency, neurological disorders and petechial rash. FES is associated with long bone and pelvic fractures. Case report. We present a case of 24 years old male with closed right femur fracture and bilateral open fractures of tibia and fibula. Surgical procedure was performed immediately. On the second postoperative day, patient was agitated (GCS 12), hemodynamically stable with spontaneous breathing. Several hours later, clinical status deteriorated, with loss of consciousness (GCS 5), pyrexia, tachycardia, dyspnea and hypoxemia requiring mechanical ventilation. Conjuctival petechial rash appeared 24 hours after ICU admission. Based on clinical signs developed postoperativly, FES was suspected. The chest computed tomography with pneumoangiography revealed focal area of ground glass (fat embolus) in the right pulmonary vessels with similar changes in bilateral basal segmental branches. Treatment includeded oxygenation and ventilation, reimbursement of blood and blood products, prevention of deep venous thrombosis and stress ulcers, and the patient state subsequently improved. Percutaneous tracheostomy was performed on day 8. Mechanical ventilation was terminated on day 14 and tracheostomy tube was removed on day 16. The patient remained in the ICU for 26 days and was discharged from the hospital three months later. Conclusion. FES is diagnosed on the basis of clinical features and the exclusion of other disease. Treatment for FES is supportive and includes adequate oxygenation and ventilation, and prophylaxis of possible complications. The key step in FES prevention is within 24 hours fixation of long bone fractures. Abstract FF4 Well known, but “tricky” to recognize: Transurethral resection of the prostate syndrome Petrovic Uros, Vaskovic Igor, Radovic Nevena, Veljovic Milic, Stamenkovic Dusica Department of Anesthesia and Intensive Care, Military Medical Academy, Belgrade, Serbia. Introduction. Transurethral resection of the prostate (TURP) syndrome is the term that unifies the symptoms that occur due to excessive absorption of irrigating fluid used during variety of endoscopic procedures, although classically on the prostate and bladder. Case report. 74 years old critically ill patient was transferred from the private hospital. On the admission, following parametars were recorded GCS 3, nonreactive pupils, tachypnoe, hypotension, tachycardia. Blood analysis showed leucocytosis, blood glucose level 23.9 mmol/L, creatinine 266 umol/L, urea 12,5 mmol/L, LDH 273 U/L, Na 102 mmol/L, Ca 1,85mol/L, Cl 72mmol/L, osmolarity 238 mOsm/K. Following scenario was reported: sudden hypotension and patient’s complain of chest pain were the reasons for conversion to general anesthesia during two hours TURP procedure performed under spinal anesthesia. Postoperative period was complicated with loss of consciousness, hypotension and tachycardia. After tracheal intubation, brain computed tomography was performed and revealed no changes. During this period, the first epileptic attack happened. Treatment was started with 3% NaCl (1 ml/kg/h) and sodium correction of 1 mmol/L/h. After 48 hours sodium level of 145 mmol/L and osmolarity 297 mOsm/K were achieved. Vancomycin and meropenem were introduced as signs of infective syndrome appeared (39°C, CRP (109 mg/L), leukocytosis (28.80 109 1/L)). On the second day, patient was conscious (GCS 12) and afebrile, trachea was extubated. Patient was discharged from hospital after 21 days with no signs of disease. Conclusion. Despite the progression made in physiologic understanding, TURP syndrome still remains in certain cases unrecognized. Variability in presentation still makes diagnosis and treatment difficult.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
278
FF5 Epidermolysis bullosa in children-challenging task for anesthesiologist Bojana D. Slavković, Igor M. Krunić Institut za zdravstvenu zaštitu majke i deteta “Dr Vukan Čupić“, Beograd Introduction: (EB) is a heterogeneous group of hereditary disorders caracterized by the hypersensitivity of the skin and mucous membranes to mechanical trauma. It is reflected by creating a bull in places that are exposed to the slightest pressure. Case report: In March 2014, girl aged 9 years was hospitalized at the Institute for Mother and Child, for the treatment of multiple stenoses of the esophagus. Dilation of the esophagus was required to be done under general anesthesia (GA). As part of the routine assessment and plan of performing GA, it was necessary to especially consider the position of the patient, airway and monitoring. Conclusion: Patients with EB challenge anesthesiologists in both introducing general anesthesia and perioperative monitoring. With the right preparation, successful managing a general anesthesia is possible with these patients.
FF6 Massive blood transfusion in children-a case report Jovana Simin, Marina Pandurov, Biljana Drašković Institute for the healthcare of children and youth of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Republic of Serbia Introduction: Acute hemorrhage leading to acute hypovolemic shock is a medical emergency carrying high mortality. A single replacement of the blood volume (80 ml/kg) in the first 24 hours of resuscitation is considered massive transfusion. Metabolic disturbances may occur to a greater degree in children than in adults. Case report: Adrenalectomy was performed on a fifteen year old boy weighing 53 kg with diagnosis of pheochromocytoma. The procedure was complicated by a lesion of inferior vena cava which eventually led to massive blood loss, extreme hypotension and hemoragic shock. The moment hypotension was detected, vigorous resuscitation was started, along with continuous vasoactive therapy. All intravenous fluids were warmed, as well as the operating room and the patient himself. Intraoperatively, 16 packed red blood cell units, 12 units of fresh frozen plasma (FFP) and 13 units of platelets were administered in total. Eventually the patient received 21 litres of fluids intraoperatively, almost 6 times his circulatory blood volume. The observed metabolic acidosis, hypocalcemia and hyperkalemia were corrected with appropriate resuscitation, 10% calcium gluconate and 8,4% sodium hydrogen-carbonat. After five-hour surgery laboratory findings showed complex posthemoragic disorder of hemostatic mechanism. After consulting our hematologist, the patient was given FFP, cryoprecipitate, tranexamic acid and kybernin. Postoperatively, patient was administered to the intensive care unit where he spent 8 days. Conclusions: Acute massive blood loss is accompanied by a number of metabolic disorders and high mortality rate, especially in pediatric age group. Timely treatment and anticipation of possible disorders is vital, making this a huge challenge for the anesthetist. In this case good team work and appropriate treatment resulted in a great outcome for our patient. FF7 Hageman factor deficiency in a patient who underwent umbilical hernia repair surgery: a case report Nenad ČJovanović1, Ines ŠVeselinović1, Milan V Lazarević2, RadmiloJ Janković1,3
1 Centre for Anesthesiology and Resuscitation, Clinical Centre Niš, Serbia 2Vascular Surgery Clinic, Clinical Centre Niš, Serbia 3 Faculty of Medicine, University of Niš, Serbia Introduction. Hageman factor (HF) deficiency (Hageman trait) is a rare genetic blood disorder that causes prolonged clotting of blood in a test tube, without the presence of prolonged clinical bleeding tendencies. Since no symptoms usually occur, many individuals remain undiagnosed. HF deficiency affects people of

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
279
Asian descent more often than other ethnicities. The incidence in general population is approximately 1 in 1 million individuals. Case presentation. A 64-years-old Romany man was scheduled for umbilical hernia repair at General Surgery in Clinical Center Nišin may 2012. During the preoperative anesthetist's visit, the patient gave a history of blood clotting disorder, without any medical records. After consulting a transfusiology specialist and performing additional laboratory tests, the following results occurred: immeasurable(“out of range”) activated partial thromboplastin time (aPTT)in three separate blood samplesand reduced HF levelsin the assay (20%), measured in the laboratory of Blood Transfusion Institute Nišand Vascular Surgery Laboratory in Clinical Center Niš. In order to detectan abnormality of coagulation, ROTEM test was also performed. INTEM test,that representsintrinsinc coagulation path, was alsoimmeasurable(Figure 1). The patient underwent surgery the next day. During the operation and postoperative period, there were no bleeding or thrombotic complications. Conclusion.Definite role of HF is still unclear, since many cases of severe HF deficiency experience thrombotic and thromboembolic phenomena instead of a bleeding problem. Moreover most of them are asymptomatic. Treatment for this disorder is usually not necessary since bleeding abnormalities are only mild or nonexistent.
FF8 Prothrombin complex concentrate versus fresh-frozen plasma in dilutional coagulopathy: a case report Marković Z. Danica1, Lazarević V. Milan2, Janković J. Radmilo2
1Center for Anaesthesiology and reanimatology, Clinical center in Niš, Serbia 2Clinic for cardiovascular and thoracic surgery, Clinical center in Niš, Serbia INTRODUCTION.Ruptured abdominal aortic aneurysm (AAA) is a life-threatening condition with an overall mortality rate of 65%. Massive haemorrhage requires infusion of fluids that do not contain clotting factors which develops dilutional coagulopathy. Rotational thrombelastometry (ROTEM) permits differential diagnosis of the underlying pathomechanism of coagulopathy. PCC showed much efficiency in the treatment of intraoperative massive bleeding . CASE REPORT. A 79-year-old man was addmited to Vascular Surgery Department, Clinical center in Nis as an emergency with the symptoms of AAA rupture. After resuscitation he was trasported to the operation room (Hgb: 45 g/L, HCT: 15%, BP: 80/40 mmHg). Massive infusion of crystalloids, colloids and plasma expanders kept the patient hemodinamically stable but led to dilutional coagulopathy. Transfusion of platelets, cryoprecipitate and fresh-frozen plasma (FFP) were provided together with tranexamic acid. Total blood loss during the surgery was 5L and 1.85L was returned to the patient by autotransfusion. Coagulation status was checked by ROTEM. The greatest deviation was found in the INTEM, CFT=3374s and α=12o (Picture 1) and in the EXTEM, CFT=169s and α=66o (Picture 2). After the infusion of 500IJ PCC, the results of INTEM went back to normal ranges (CFT=71s, α=76o) (Picture 3), as well as the results of EXTEM (CFT=71s, α=77o) (Picture 4). After the extensive operation, the patient spend 5 days in the Intensive care unit and was discharget from hospital after 26 days. CONCLUSION. PCC improves coagulation stability faster and more efficient than FFP without the risk of transfusion, volume load and infectious complications.
Figure 1 above shows INTEM test in a patient with FXII deficiency; Thecoagulation cascade is blocked at the start of the intrinsic coagulation pathway.
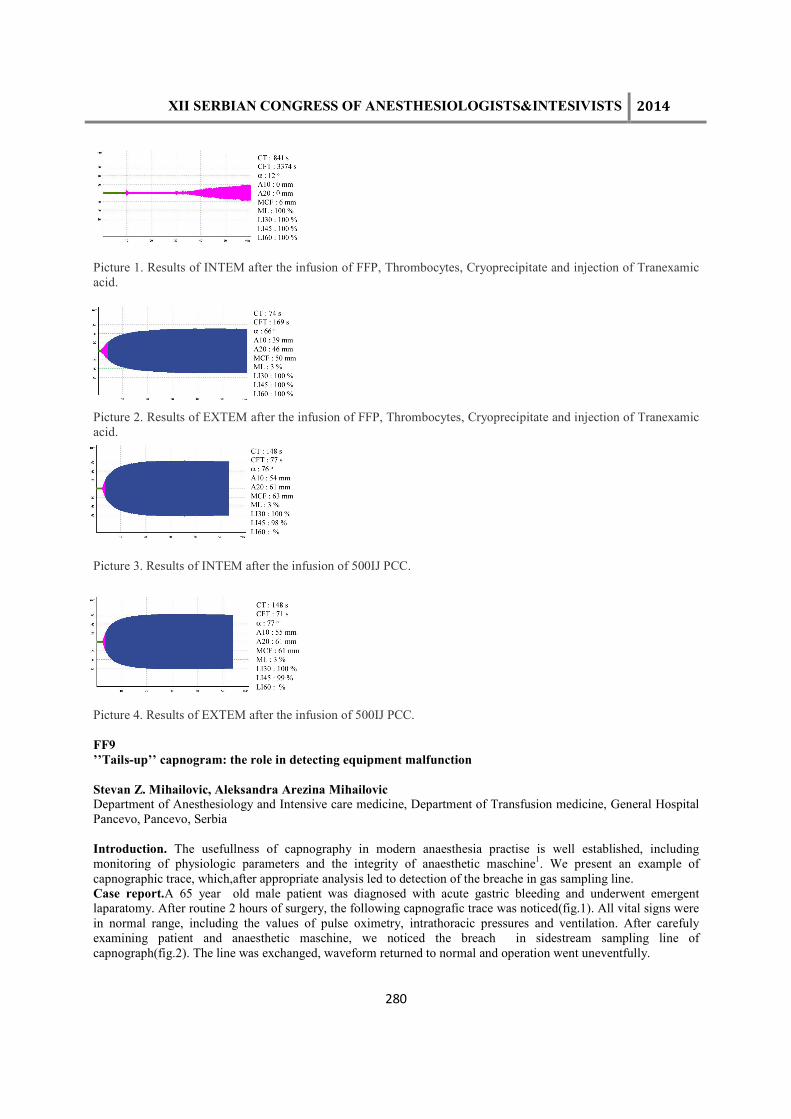
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
280
Picture 1. Results of INTEM after the infusion of FFP, Thrombocytes, Cryoprecipitate and injection of Tranexamic acid.
Picture 2. Results of EXTEM after the infusion of FFP, Thrombocytes, Cryoprecipitate and injection of Tranexamic acid.
Picture 3. Results of INTEM after the infusion of 500IJ PCC.
Picture 4. Results of EXTEM after the infusion of 500IJ PCC. FF9 ’’Tails-up’’ capnogram: the role in detecting equipment malfunction Stevan Z. Mihailovic, Aleksandra Arezina Mihailovic Department of Anesthesiology and Intensive care medicine, Department of Transfusion medicine, General Hospital Pancevo, Pancevo, Serbia Introduction. The usefullness of capnography in modern anaesthesia practise is well established, including monitoring of physiologic parameters and the integrity of anaesthetic maschine1. We present an example of capnographic trace, which,after appropriate analysis led to detection of the breache in gas sampling line. Case report.A 65 year old male patient was diagnosed with acute gastric bleeding and underwent emergent laparatomy. After routine 2 hours of surgery, the following capnografic trace was noticed(fig.1). All vital signs were in normal range, including the values of pulse oximetry, intrathoracic pressures and ventilation. After carefuly examining patient and anaesthetic maschine, we noticed the breach in sidestream sampling line of capnograph(fig.2). The line was exchanged, waveform returned to normal and operation went uneventfully.
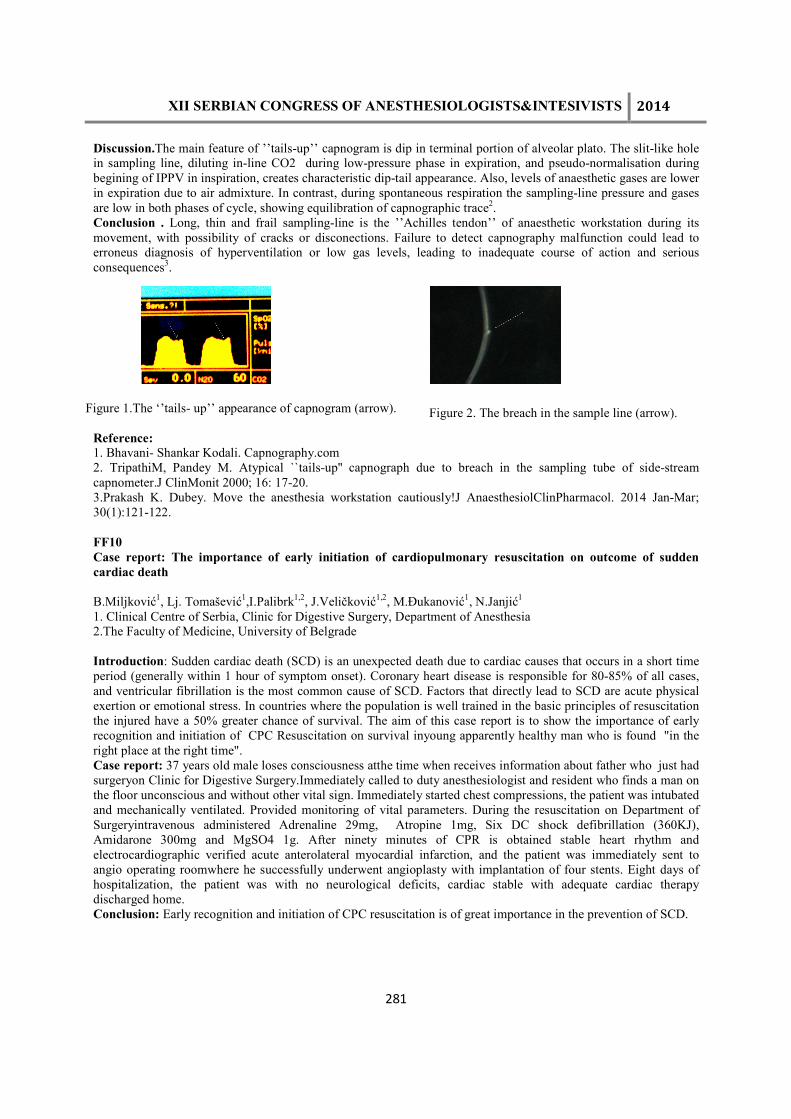
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
281
Discussion.The main feature of ’’tails-up’’ capnogram is dip in terminal portion of alveolar plato. The slit-like hole in sampling line, diluting in-line CO2 during low-pressure phase in expiration, and pseudo-normalisation during begining of IPPV in inspiration, creates characteristic dip-tail appearance. Also, levels of anaesthetic gases are lower in expiration due to air admixture. In contrast, during spontaneous respiration the sampling-line pressure and gases are low in both phases of cycle, showing equilibration of capnographic trace2. Conclusion . Long, thin and frail sampling-line is the ’’Achilles tendon’’ of anaesthetic workstation during its movement, with possibility of cracks or disconections. Failure to detect capnography malfunction could lead to erroneus diagnosis of hyperventilation or low gas levels, leading to inadequate course of action and serious consequences3.
Reference: 1. Bhavani- Shankar Kodali. Capnography.com 2. TripathiM, Pandey M. Atypical ``tails-up'' capnograph due to breach in the sampling tube of side-stream capnometer.J ClinMonit 2000; 16: 17-20. 3.Prakash K. Dubey. Move the anesthesia workstation cautiously!J AnaesthesiolClinPharmacol. 2014 Jan-Mar; 30(1):121-122. FF10 Case report: The importance of early initiation of cardiopulmonary resuscitation on outcome of sudden cardiac death B.Miljković1, Lj. Tomašević1,I.Palibrk1,2, J.Veličković1,2, M.Đukanović1, N.Janjić1 1. Clinical Centre of Serbia, Clinic for Digestive Surgery, Department of Anesthesia 2.The Faculty of Medicine, University of Belgrade Introduction: Sudden cardiac death (SCD) is an unexpected death due to cardiac causes that occurs in a short time period (generally within 1 hour of symptom onset). Coronary heart disease is responsible for 80-85% of all cases, and ventricular fibrillation is the most common cause of SCD. Factors that directly lead to SCD are acute physical exertion or emotional stress. In countries where the population is well trained in the basic principles of resuscitation the injured have a 50% greater chance of survival. The aim of this case report is to show the importance of early recognition and initiation of CPC Resuscitation on survival inyoung apparently healthy man who is found "in the right place at the right time". Case report: 37 years old male loses consciousness atthe time when receives information about father who just had surgeryon Clinic for Digestive Surgery.Immediately called to duty anesthesiologist and resident who finds a man on the floor unconscious and without other vital sign. Immediately started chest compressions, the patient was intubated and mechanically ventilated. Provided monitoring of vital parameters. During the resuscitation on Department of Surgeryintravenous administered Adrenaline 29mg, Atropine 1mg, Six DC shock defibrillation (360KJ), Amidarone 300mg and MgSO4 1g. After ninety minutes of CPR is obtained stable heart rhythm and electrocardiographic verified acute anterolateral myocardial infarction, and the patient was immediately sent to angio operating roomwhere he successfully underwent angioplasty with implantation of four stents. Eight days of hospitalization, the patient was with no neurological deficits, cardiac stable with adequate cardiac therapy discharged home. Conclusion: Early recognition and initiation of CPC resuscitation is of great importance in the prevention of SCD.
Figure 1.The ‘’tails- up’’ appearance of capnogram (arrow). Figure 2. The breach in the sample line (arrow).

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
282
FF11 Reflex cough induced by intravenous bolus doses of fentanyl-case report Tijana Smiljković, Danijela Stojmirović, Marina Stojanović, Nada Popović Clinic for burns, plastic and reconstructive surgery, Department of Anesthesia,Clinical Centre of Serbia, Belgrade, Serbia Introduction. The use of fentanyl during induction may lead to coughing, depending on dose, age, general condition and ethnic origin of patients. Cough can be induced by central inhibition of sympathetic predominance on vagal stimulation, reflex bronchoconstriction due to stimulation of tracheobronchial tree receptors or histamine surge. Case report. Patient aged 27 years was admitted to the Clinic for Burns, Plastic and Reconstructive Surgery with 28% total body surface burns (IIa and IIb degree; front side of the chest, abdomen, upper arms and neck). On admission SaO2 was 99%. Personal history negative. The first three days during dressing changes in intravenous anesthesia, there was no occurrence of adverse effects of fentanyl. On the fourth day, after the administration of fentanyl patient started to cough, hiccup, had shortness of breath which resulted in drop of Sa02 to 64% and after adminisstration of 6 l / min O2 through face mask he had recovered. Next two dressings done with fentanyl, despite previously prescribed therapy (corticosteroid), resulted with the same symptoms and decrease in SaO2 to 84%. Next dressings were carried out without the use of fentanyl using other analgesics and was without adverse symptoms, and SaO2 was satisfactory (99-100%). Conclusion. Reflex cough induced by fentanyl occurs in 31% of patients and it is not serious anesthetic complication, however it can present a problem due to spasms followed by a decline in saturation, petechiae on the skin, increased intra-abdominal, intraocular and intracranial pressure. References: 1. El Baissari MC, Taha SK, Siddik-Sayyid SM. Fentanyl-induced cough-pathophysiology and prevention. Middle East J Anesthesiol 2014; 22(5):449-56. 2. Kim JE, Min SK, Chae YJ, Lee YJ, Moon BK, Kim JY. Pharmacological and nonpharmacological prevention of fentanyl-induced cough: a meta-analysis. J Anesth 2014; 28(2):257-66. 3. Tweed WA, Dakin D. Explosive couging after bolus fentanyl injection. Anesth Analg 2001; 92:1442-3. 4. Lim KJ, Lee SK, Lee HM et all. Aspiration pneumonia caused by fentanyl-induced cough-a case report. Korean J Anesthesiol 2013; 65(3):251-253. Abstract FF12 Anesthetic management of patient wih anterior mediastinal mass: a case report Slađana M. Vasiljević Mother and Child Health Care Institute of Serbia “Dr Vukan Čupić”, Belgrade, Serbia Background: General anesthesia in patients with anterior mediastinal mass may be accompanied by serious life-treating complications, as a result of compression of the airway and large blood vessels. Case report: An 11 years old boy was admitted to the Mother and Child Health Care Institute with acute dyspnea, tachycardia and malaise. Radiographic, ehosonographic and CT examination of the thorax visualized a large tumor mass in the mediastinum, superior vena cava syndrome, compression of the pulmonary trunk, distal trachea and left bronchus and compressive atelectasis of the left lung parenchyma. Echocardiography detected significant pericardial effusion around the left ventricle with EF of 56% and no signs of tamponade. Consilium indicated biopsy of the tumor mass under general anesthesia. Corticosteroids were not administered before biopsy, since can interfere with histological diagnosis. Patient was premedicated with midazolam. Induction of anesthesia was with midazolam, ketamine and sevoflurane. Patient was intubated without the use of neuromuscular blocking agents. Maintenance of anesthesia was with sevoflurane, bolus doses of ketamine (1mg/kg) and fentanyl in dose of 50µg. Spontaneous ventilation was maintaining. Monitoring included ECG, pulse oximetry, NIBP, IBP, capnography. Anterior mini thoracothomy, tumor and bone marrow biopsy were done. A transient fall in blood pressure was registered, corrected by a fluid bolus (20ml/kg). There were no other complications. Patient was extubated and transported to Intensive Care Unit. Conclusion: Patients with anterior mediastinal mass have a high risk for serious compications in general anesthesia. Induction and maintenance of anesthesia with sevoflurane, ketamine and midazolam, maintaining spontaneous ventilation, may be an appropriate choice for these patients.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
283
ANESTHESIA FOR CARDIOVASCULAR AND THORACIC SURGERY
1ACT-1 Discrepancy Between Superior Vena Cava Oxygen Saturation and Mixed Venous Oxygen Saturation in Cardiac Surgery Patient Tanasić R. Milja, JovićDj. Miomir, Sagić D.Jelena,Vuković M. Petar, Unić-StojanovićR.Dragana Cardiovascular Institute Dedinje Belgrade, Serbia Background. The mixed venous oxygen saturation (SvO2) is a valuable measurement of tissue oxygenation. Central venous oxygen saturation (ScvO2), obtained in a less risky manner from a central venous catheter, may be a useful alternative to SvO2 measurement.We report a case of the significant discrepancy between values of ScvO2 and SvO2in a patient with cardiogenic shockafter the emergency heart surgery. Case report. A 69-year-old woman with a history of acute myocardial infarctionand 90% left main stenosis, presented for emergency coronary artery bypass grafting.The patient was weaned from cardiopulmonary bypasswith inotropic therapy (dobutamine, epinephrine).During three hours after the surgery, the patient was on mechanical ventilation andhemodinamically stable. This was based on standard invasive monitoring parameters: heart rate 90/min,arterial pressure 118/75 mmHg, urine output 1.0 ml/kg, lactate level immediately after surgery 8.5mmol/l which started decreasing (after 2h –6.6 mmol/l), ScvO2 65.6%, ABG pO2 112mmHg, pCO238.5 mmHg, FiO2 0.4. Afterward, use of pulmonary artery catheter revealed presence of cardiogenic shock(CI 1.5 l/m2, SvO2 46.2%). The administered therapy included additional inotropic drug milrinone. The patient’s clinical and hemodynamic status improved,she was extubated after 24h of mechanical ventilation and dischargedon the 6thpostoperative day to a ward. Conclusion. The difference between SvO2 and ScvO2 is related to variations in regional perfusion and oxygen consumption In patients with low cardiac index and filling pressures after coronary artery surgery, ScvO2 could not be used as a direct alternative for SvO2. 1ACT-2 Acute Aortic Dissection in patient with suspected pheochromocytoma Sagić D. Jelena , Jović Dj. Miomir, Tanasić R. Milja, Unić-Stojanović R. Dragana Cardiovascular Institute Dedinje Belgrade, Serbia Background. Aortic dissection is one of the most fatal vascular emergencies. We report a case of a young man presented with acute aortic dissection and suspected pheochromocytoma whom was preformed an urgent aortic ascending surgery. Case report. A 37-year old man was admitted to hospital with severe anterior chest pain which lasted for over two hours. Past medical history included hypertension, and heavy cocaine and alcohol abuse for over a decade, followed by a two year drug-free period. Suspected aortic dissection was confirmed using imaging modalities, that also discovered adrenal incidentaloma defined as malignant, pheochromocytoma like mass. There was not enough time for further endocrinological testing and an urgent surgical procedure was performed. Perioperative fluctuation of BP was managed by IV fluid overload and intravenous phentolamine. Anesthesia, surgery and postoperative recovery was uneventful and patient was discharged after 8 days without complications. Conclusion. Aortic dissection is the most common life-threatening disorder affecting the aorta; If left untreated, about 33% of patients die within the first 24 hours, and 50% die within 48 hours. When treating patients with pheochromocytoma, it is crucial to provide a stable hemodynamic state. Several anesthetic drugs or techniques are proposed to blunt sympathetic response such as opioids, nitroprusside, nitroglycerin, magnesium sulfate, urapidil, esmolol, nicardipine, remifentanil, and propofol. Cocaine is one of the possible causes for aortic dissection, due to the vasoconstriction similar to atherosclerotic vascular damage. Both dissection of aorta and pheochromocytoma present challenges for anesthesiologists and early recognition of symptoms is essential in establishing the diagnosis and reducing the mortality rate.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
284
1ACT-3 Suspected Amiodarone Hepatotoxicity After Cardiac Surgery DraganaUnic-Stojanovic, Vukovic Petar, Miroslav Milicic, Tanasic Milja, Djokovic Ljubomir, Miomir Jovic Cardiovascular Institute Dedinje Belgrade, Serbia Background and aim.Acute hepatotoxicity is a rare but potentially fatal complication of amiodarone use. We report a case of liver injury after intravenous amiodaroneadministration in a patient with atrial fibrillation after heart surgery. Case report. A 62-year-old man with a history of dissection of the ascending aortic aneurysm presentedfor emergency ascendingaortic surgery. Patientwas underwentto uncomplicated surgery, and was extubated after 17h of mechanical ventilation. On the 3rdpostoperative day, the patient developed rapid atrial fibrillation, which was treated with a 150-mg loading dose of intravenous amiodarone followed by infusion (1 mg/min for 6 hours followed by 0.5 mg/min). On the evening of postoperative day 3, the patient became hypotensive for approximately 4 hours and required phenylephrine and norepinephrine to maintain an MAP >60 mmHg. The patient’s lactate had increased to 3.8 mmol/L, the international normalized ratio increased to 3.12, alanine aminotransferase rose to 4401 IU/L, aspartate aminotransferase - 7355 IU/L, lactate dehydrogenase- 30043 IJ/L and creatinine increased from 96 to 190 µg/l. Metoprolol and amiodarone were discontinued. Possible etiologies included ischemia, infection, and drug-induced injury. N-acetylcystine was administered and started continuous furosemide infusion. Vancomycin and Imipenem/cilastatin were started empirically. Liver parameters significantly improved and returned to normal. On the13thpostoperative day, patient was discharged to a rehabilitation facility. Conclusion.Amiodarone loading should be adapted to the necessity of an immediate effect of the drug, and liver function should be monitored closely in critically ill patients. References. 1.Thiele RH.JCVA 2012; 26(4):729-732.
1ACT-4 Emergent coronary intervention for perioperative STEMI: hazardous or life saving? Janjić Nataša1, Veličković Jelena1,2, Čutura Đuro3, Đukanović Marija1, Sumrak Sanela1, Miljković Bojana1 1Center for anesthesia, Clinical Center of Serbia, Belgrade, Serbia 2 University of Belgrade, School of Medicine 3 Emergency Center, Clinical Center of Serbia, Belgrade, Serbia Introduction: Perioperative myocardial infarction(PMI) represents a major adverse cardiac event with high mortality rate(30-70%) due to atypical presentation,late diagnosis and limited treatment options.Wepresent a rare type of ST-elevation PMI successfuly treated with PCI immediately after non-cardiac,non-vascular surgery. Case report: A 59 years old man was admitted to ER with signs of ileus and scheduled for urgent surgery.He was smoker with history of HTA treated with beta-blocker.He underwent Ao-F bypass grafting two years ago,and ventral hernioplasty complicated with peritonitis and intestinal resection two months ago.Due to prolonged vomiting,he discontinued aspirin for three days. Intraoperative course was uneventful until the last 15 min when multifocal VES and nonsustained VT were registered on monitor.They were initially treated with lidocain.After completion of surgery(adhesiolysis and intestinal resection),patient was awake and spontaneously breathing,monitored in PACU.He was given MgSO4 and amiodarone bolus followed by a continuous infusion.When VT resolved,ST-elevation was noticed in leads D2,D3,avF,and cardiologist was consulted.He suggested conservative treatment because of concern for bleeding.The surgeon and the anesthetist estimated that PMI posed a higher risk,and allowed PCI.Troponin level was 47.9ng/ml.Antiplatelet therapy was given(clopidogrel and aspirin) via NG tube.Coronary angiography revealed ostial thrombotic occlusion of RCA with 90-99% occlusion of RCA mid and 50% occlusion of LAD.Successful PCI was performed with implantation of 3 bare metal stents in RCA 3 hours after surgery.Patient had no bleeding complications,he fully recovered and was discharged home after 16 days. Conclusion: Although coronary intervention is rarely indicated for PMI it can be done safely with careful estimation of bleeding risk.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
285
REGIONAL ANESTHESIA
2RA-1 Ultrasound guided regional anaesthesia for knee arthroscopy in children Dragan Marinković, Jovana Simin, Biljana Drašković, Goran Rakić, Marina Pandurov Institute for the healthcare of children and youth of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Republic of Serbia Introduction:Ultrasound guided regional anesthesia is a safe technique of perioperative pain treatment in children. The aim was to see if peripheral nerve blocks (PNB) reduce the amount of propofol and opiod analgesics used intraoperatively, as well as the level of pain and consumption of systemic analgesics postoperatively. Materials and methods:Randomised, prospective clinical trial was carried out. It included 60 children aged 11 to 18 years old scheduled for elective knee arthroscopy. Patients were devided in two groups. Group A received general anaesthesia, group B received a PNB with sedation or general anaesthesia. Postoperative level of pain was assessed using visual analogue scale (VAS). Results:Less propofoland fentanyl was used for induction and maintanance of anaesthesia in group B(p<0.001). Consequently, no adverse reactions such as nausea or vomitting were recorded and oral intake was started earlier in group B. Level of postoperative pain was significantly lower in group B (p<0.001). The average level of pain in group B ranged from 0,4 to 1,9, while in group A it was 2,8 to 5,93. Consumption of analgesics was lower in group B(p<0.001) and even 47% of the patients were discharged without receiving any analgesics postoperatively. The average duration of PNB was 468 minutes. Conclusions:Ultrasound guided PNB is a safe techinque of regional anaesthesia in children (no complications were recoreded in our trial). It reduces the amount of general anesthetics and opiod analgesics needed intraoperatively, as well as the level of postoperative pain and consumption of analgesics postoperatively.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
286
OBSTETRIC ANESTHESIA
3OB-1 Spinal versus general anesthesia for Cesarean section at patients with preeclampsia Sasho Spasovski, Dr.V.Bozinovska, D. Karadzova, A. Kuch University Clinic of Gynecology and Obsterics Introduction: Preeclampsia is a medical condition which manifests through higher blood pressure in pregnant women. In recent time the number of pregnant women with preeclampsia has gone up significantly and this prompted us to another more serious contemplation regarding the choice of anesthesia. Aim of the study: This study included 40 patients at the age between 20 -35, from which 10 were treated with general anesthesia and 30 with spinal. The aim was to see how the spinal anesthesia has advantages in comparison to the cardio-respiratory and chemo-dynamic stability, as well as the apgar score of newborn children. Material and method: For the spinal anesthesia they used 0,5% marcaine. After previous pre-hydration with 1000 ml 0, 9% NaCl and premedication with Reglan ampoules and ampoules Ranital i.v. at L3 and L4 level with 26-27 G needle, 0, 5% marcaine was applied from 1, 4 to 2, 4 ml depending on the height of the pregnant woman with adjuvant Fentanyl 20 mkqr. For the general anesthesia with previous premedication with ampoules Reglan and Ranital i.v., in the beginning they used Propofol 1,5-2 mg/kg, relaxant Leptosuccin 1, 5 mg/kg and they continued with Esmeron, rac Izoflurane 0, 6% I opioid Fentanyl. Results: Patients lead with spinal anesthesia, before the beginning of the Cesarean section had TA from 165-185 mm/hg systole and 100-120 mm/hg diyasole and pulse 90-100/min. After applying low doses of 0,5% marcaine with adjuvant Fentanyl there was minimal deviation from 10-15 % in relation of the TA and pulse as well as continuously good SaO2 from 98-100% and a better apgar score of the newborn child. When using general anesthesia there were bigger deviations from 25-30% in relation of the TA and pulse as well as bigger variations of SaO2 from 95-97% which had its effect on the apgar score of the newborn baby, which was lower. Conclusion: We can conclude that patients lead with spinal anesthesia have a lower fall of tension and pulse with a better SaO2 which is especially important, because a part of the tested people had asthma bronchial as well as a better apgar at birth which shows a better cardio-respiratory and chemo-dynamic stability in a general sense.
3OB-2 Deep vein thrombosis (DVT) in pregnancy and HELLP syndrome- case report Tatjana Ilić-Mostić1, Ana Slavković1, Žana Ivanković1, Aleksandra Suvajdžić1, Dušan Milenković1, Mirjana Pavlović1
1Center for Anaesthesia and resuscitation Clinical Center of Serbia, Belgrade
Background: Deep vein thrombosis (DVT) and pulmonary thromboembolism remains a major cause of direct maternal mortality, with many deaths associated with a failure to obtain objective diagnoses and lack of adequate treatment. Case report: A 37 years old and 36 weeks pregnant woman was admitted to our clinic. She had pain in her left leg. Her lef leg was completely swollen. Initial ultrasound investigations showed presence of unorganized DVT of the left leg. We performed complete clinical and laboratory examination. Low molecular weight heparinadministration was initiated and regulated to maintain anti Xa levels in therapeutic range. On 10th hospital day we verified organization of DVT. However, acute thrombocytopenia (69 x 109/L), with high levels of liver enzymes (AST: 90 J/L; ALT: 88 J/L) and laboratory proven hemolysis (haptoglobin: 1,3 g/L), indicated the development of HELLP syndrome. Consultative, we made a decision for emergent cesarean section, resulting in an excellent fetal outcome. In postoperative period, patient had no complication and laboratory essays returned into the normal range. On 13th postoperative day patient was released, with recommendation for oral anticoagulant therapy.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
287
Conclusion: Physicians should be of high vigilance to DVT in pregnant women, and should consider other life threating conditions associated with pregnancy. Right time decision for emergent cesarean section could be crucial for optimal fetal and mother outcome. 3OB-3 Herpes simplex virus 1 encephalitis in pregnancy- case report Tatjana Ilić-Mostić1, Ana Slavković1, Žana Ivanković1, Aleksandra Suvajdžić1, Dušan Milenković1, Danka Mostić2
1Center for Anaesthesia and resuscitation Clinical Center of Serbia, Belgrade 2 Clinic for Gynecology and Obstetrics of the Clinical Center of Serbia Introduction: Complications and maternal morbidity from pre-existing disease or from a disease that developed during the pregnancy and peripartal are very frequent. During the pregnancy, women are more sensitive to viral infection, which can affect both, mother and fetus. However, herpes simplex virus 1 (HSV1) encephalitis during the pregnancy is rare, so initial diagnose can be difficult. Case report: A 23 year old pregnant women emergency transferred from regional hospital. She was pregnant 39 weeks. She had a fever, tachycardia, left hemiparesis, hemianopsia. Her mental status was changed. She was somnolent, disoriented, agitated. Based on patient clinical condition and examinations with NMR endocranii and analysis of cerebro-spinal fluid, made the diagnosis of herpes simplex encephalitis. Patient was healthy and without comorbidity before and during the pregnancy. The patient was clinicaly and laboratory completely examinated. PCR was performed, such as serology of blood and cerebro-spinal fluid. The antiviral, edematous, antibiotic, corticosteroid and symptomatic therapy is started. The condition of mother and fetus intensively monitored. Consultative, we made decission for emergent Cesarean section. PCR for Herpes simplex virus 1 was positive. Postoperative period mother was at intensive care unit. Initial therapy is continued, and patient general condition was better, such as analyses of cerebro-spinal fluid, NMR of endocranium, EEG and PCR. Antiviral therapy is continued for two weeks, and the eighteenth postoperative day she had no neurological disorders, and she was dismissed from the clinic. Conclusion: With an early diagnosis and prompt initiation of antiviral treatment, as well as enhanced neurocritical care, a favorable outcome can now be expected in both mother and child.
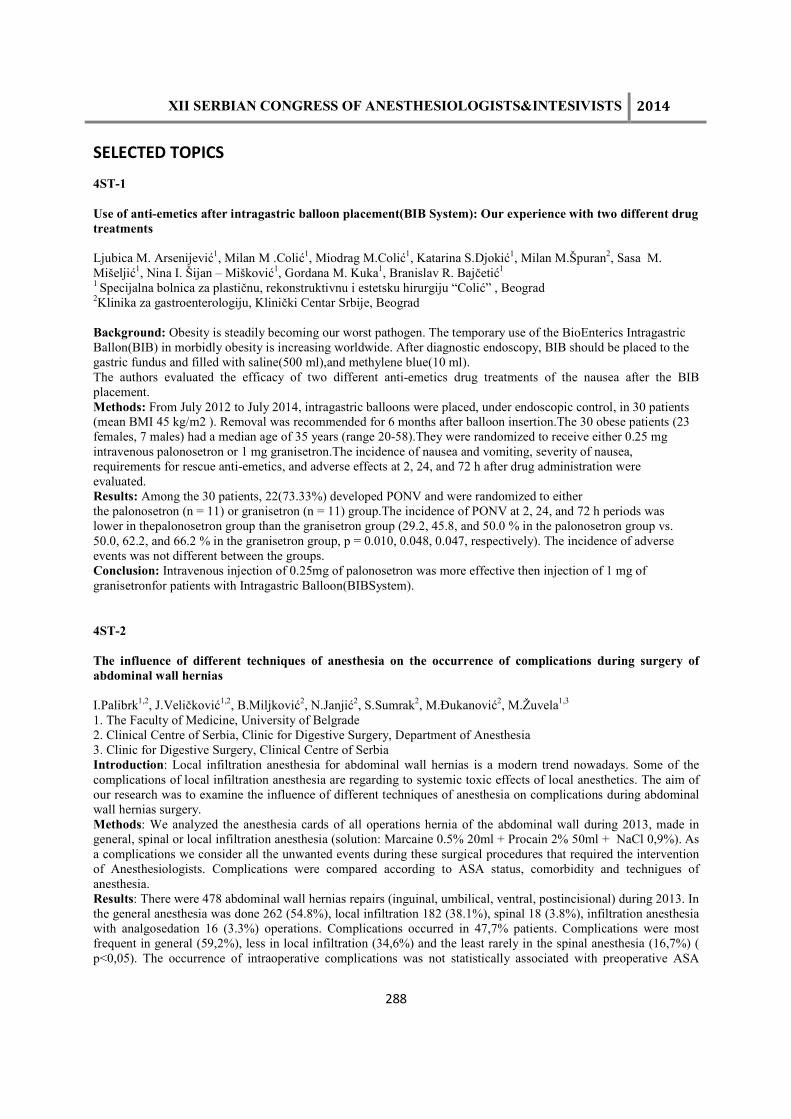
XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
288
SELECTED TOPICS
4ST-1
Use of anti-emetics after intragastric balloon placement(BIB System): Our experience with two different drug treatments Ljubica M. Arsenijević1, Milan M .Colić1, Miodrag M.Colić1, Katarina S.Djokić1, Milan M.Špuran2, Sasa M. Mišeljić1, Nina I. Šijan – Mišković1, Gordana M. Kuka1, Branislav R. Bajčetić1
1 Specijalna bolnica za plastičnu, rekonstruktivnu i estetsku hirurgiju “Colić” , Beograd 2Klinika za gastroenterologiju, Klinički Centar Srbije, Beograd Background: Obesity is steadily becoming our worst pathogen. The temporary use of the BioEnterics Intragastric Ballon(BIB) in morbidly obesity is increasing worldwide. After diagnostic endoscopy, BIB should be placed to the gastric fundus and filled with saline(500 ml),and methylene blue(10 ml). The authors evaluated the efficacy of two different anti-emetics drug treatments of the nausea after the BIB placement. Methods: From July 2012 to July 2014, intragastric balloons were placed, under endoscopic control, in 30 patients (mean BMI 45 kg/m2 ). Removal was recommended for 6 months after balloon insertion.The 30 obese patients (23 females, 7 males) had a median age of 35 years (range 20-58).They were randomized to receive either 0.25 mg intravenous palonosetron or 1 mg granisetron.The incidence of nausea and vomiting, severity of nausea, requirements for rescue anti-emetics, and adverse effects at 2, 24, and 72 h after drug administration were evaluated. Results: Among the 30 patients, 22(73.33%) developed PONV and were randomized to either the palonosetron (n = 11) or granisetron (n = 11) group.The incidence of PONV at 2, 24, and 72 h periods was lower in thepalonosetron group than the granisetron group (29.2, 45.8, and 50.0 % in the palonosetron group vs. 50.0, 62.2, and 66.2 % in the granisetron group, p = 0.010, 0.048, 0.047, respectively). The incidence of adverse events was not different between the groups. Conclusion: Intravenous injection of 0.25mg of palonosetron was more effective then injection of 1 mg of granisetronfor patients with Intragastric Balloon(BIBSystem).
4ST-2
The influence of different techniques of anesthesia on the occurrence of complications during surgery of abdominal wall hernias I.Palibrk1,2, J.Veličković1,2, B.Miljković2, N.Janjić2, S.Sumrak2, M.Đukanović2, M.Žuvela1,3
1. The Faculty of Medicine, University of Belgrade 2. Clinical Centre of Serbia, Clinic for Digestive Surgery, Department of Anesthesia 3. Clinic for Digestive Surgery, Clinical Centre of Serbia Introduction: Local infiltration anesthesia for abdominal wall hernias is a modern trend nowadays. Some of the complications of local infiltration anesthesia are regarding to systemic toxic effects of local anesthetics. The aim of our research was to examine the influence of different techniques of anesthesia on complications during abdominal wall hernias surgery. Methods: We analyzed the anesthesia cards of all operations hernia of the abdominal wall during 2013, made in general, spinal or local infiltration anesthesia (solution: Marcaine 0.5% 20ml + Procain 2% 50ml + NaCl 0,9%). As a complications we consider all the unwanted events during these surgical procedures that required the intervention of Anesthesiologists. Complications were compared according to ASA status, comorbidity and technigues of anesthesia. Results: There were 478 abdominal wall hernias repairs (inguinal, umbilical, ventral, postincisional) during 2013. In the general anesthesia was done 262 (54.8%), local infiltration 182 (38.1%), spinal 18 (3.8%), infiltration anesthesia with analgosedation 16 (3.3%) operations. Complications occurred in 47,7% patients. Complications were most frequent in general (59,2%), less in local infiltration (34,6%) and the least rarely in the spinal anesthesia (16,7%) ( p<0,05). The occurrence of intraoperative complications was not statistically associated with preoperative ASA

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
289
status (p = 0.167). Bradycardia as the most common complication (26.2%) was statistically more frequent in general anesthesia ( p=0,001), and preoperative use of beta blockers and other antiarrhythmic drugs is not associated with the intraoperative bradycardia ( p>0,05). Conclusion: Despite the use of large dose of local anesthetics during local infiltration anesthesia, intraoperative complications were statistically more frequent during general anesthesia compering to other techniques. Complications were the least frequent in spinal anesthesia. Local infiltration anesthesia is safe for this kind of surgery but the presence of Anesthesiologist is necessary.
4ST-3
BARIATRIC SURGERY IN ADOLESCENT PATIENTS, FIRST EXPERIENCES Dejan Dimitrijević, Biljana Drašković, Jovana Simin, Marina Pandurov Institute for the healthcare of children and youth of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Republic of Serbia Introduction: Obesity is a major health problem with clearly established health implications, including an increased risk of coronary artery disease, hypertension, dyslipidemia, diabetes mellitus, gallbladder disease, obstructive sleep apnea and socioeconomic and psychological impairment. Bariatric surgery is a surgical weight loss procedure used to treat extreme obesity (BMI more than 40 kg/m2 ) and individuals who have failed conventional weight control programs. Method: Gastric sleeve procedure is a laparoscopic operation which carries potential for numerous complications such as leakage along the suture line of the sleeve, bleeding, infection, atelectasis, pneumonia, embolism, heart failure and arrhythmias. Due to numerous comorbidities, preoperative evaluation is multidisciplinary and requires evaluation of an anesthesiologist, pulmologist, cardiologist and endocrinologist. In the obese patients difficult airway management and mechanical ventilation are expected, so optimal positioning (ramped position, reversed Trendeleburg), availability of different airway management devices, the usage of PEEP during ventilation and short acting anesthetic drugs are of great importance. In order to prevent postoperative atelectasis and pneumonia a good postoperative pain therapy is essential. Gastric sleeve procedure has been performed in our hospital on three patients aged 15 to 17 years, one male and two female, all with BMI more than 39 kg/m2. After the thorough preoperative preparation, careful positioning of the patient, induction of anesthesia has been performed with propofol, remifentanyl and with or without succinylcholine. Maintenance of anesthesia was provided with sevoflurane, remifentanyl and rocuronium. All three patients have been woken up and extubated in the operating room, postoperatively placed in ICU for the next two days. There were no major complications in these three cases. Results: In all three patients there has been a significant weight loss, particularly in the first patient who was operated on two years ago. This patient lost almost half of his original weight and records a great improvement of physical and mental condition. Conclusion: Gastric sleeve procedure is highly efficient, and less invasive bariatric operation with excellent long term effects. However, it is greatly challenging for the anesthesiologist and requires vigilance, great skill and a thorough anesthetic plan. 4ST-4 Incidence and risk factors for postoperative arrhythmia after esophagectomy for esophageal or cardiac carcinoma Veličković Jelena1,2, Palibrk Ivan1,2, Đukanović Marija1, Miljković Bojana1, Đorović Dubravka1, Stojakov Dejan2,3, Veličković Dejan2,3, Šljukić Vladimir3 1 Center for anesthesia, Clinical Center of Serbia,Belgrade,Serbia 2 Medical Faculty,University of Belgrade,Belgrade,Serbia 3Clinic for Digestive Surgery, Clinical Center of Serbia, Belgrade, Serbia Introduction:Cardiac events are common complications after radical esophagectomy. The aim of our study was to determine the incidence, type and risk factors for cardiac arrhythmias after esophagectomy and to investigate their impact on postoperative outcome.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
290
Methods:We performed a retrospective review of 74 patients who underwent esophagectomy for carcinoma during 2011. Demographic, clinical and therapeutic data were analysed. The occurrence of arrhythmia was assessed during the ICU stay. SPSS 19.0 was used for data analysis. Results:Postoperative arrhythmia (PA) occurred in 23 patients (31.08%). Supraventricular tachycardia was the most frequent (72.7%), followed by atrial fibrillation (18.2%) and ventricular ectopics (4.5%). The most common timing for PA occurrence was the second postoperative day (36.4%). They were usually transient lasting less than 24h (41.2% of patients)but in 23.5% of patients their duration was more than 4 days. The first choice antiarrhythmic drug was beta-blocker in 79.2% , followed by amiodarone and digoxine in 8.3%.Treatment success was achieved in 85.7% of patients. Univariate analysis revealed that female gender, non-smoking status, history of hypertension, abnormal pulmonary function tests, higher postoperative CRP level,intraoperative hypoxia and postoperative acid-base disequilibriumwere associated with PA. Logistic regression identified smoking status (OR 0.21), history of HTA (6.65),acid-base imbalance (12.8), intraoperative hypoxia (1.35) and abnormal pulmonary function tests (1.88) to be the independent predictors of PA.The occurrence of other complications was significantly influenced by PA (p=0.012). PA have shown a strong association with mortality (p=0.009), but they didn’t influence the length of ICU and hospital stay. Conclusion:PA affect nearly a third of patients after esophagectomy. Identification of patients at risk might help in choosing candidates suitable for preventive antiarrhythmic therapy.
4ST-5 Anaesthetic management of a patient with severe copd and giant pulmonary bulla undergoing non-thoracic surgery Sumrak Sanela1, Veličković Jelena1,2, Palibrk Ivan1,2, Miljković Bojana1, Đukanović Marija1,Pavlov Maja2,3, Ćeranić Miljan2,3 1 Center for anesthesia, Clinical center of Serbia, Clinic for digestive surgery 2 University of Belgrade, School of Medicine, Belgrade, Serbia 3 Clinic for Digestive Surgery, Clinical Center of Serbia, Belgrade, Serbia Introduction:COPD is a risk factor for postoperative pulmonary complications. It can be associated with bullous lung changes and these patients deserve special attention because of acute enlargement of bulla and its rupture. We present anaesthetic management of patient with very severe COPD and giant lung bulla undergoing elective and urgent major abdominal surgery. Case report: A 68 years old male (87 kg, BMI 30.8) was admitted for surgical treatment of rectal carcinoma.He was a former smoker with history of emphysema and low functional capacity. He was also diagnosed as having a giant bulla on his left lung that occupied more than half of his hemithorax. Pulmonary function tests done prior to surgery revealed a very severe airflow limitation (FEV1 30%,FVC 43%,PEF 27% of predicted) with significantly decreased DLCO(53%). Room air oxygen saturation was 93%. Patient was referred for preoperative physiotherapy. Anesthetic management consisted of: -placement of thoracic epidural catheter (Th8) and bolus of 0.5% bupivacaine -induction : iv lidocain(80mg), fentanyl(0.1mg),midazolam(3mg) and propofol(80mg). -NM blockade: succinylcholine(100mg)+rocuronium -BIS guided maintenance of anaesthesia with sevoflurane/air/oxygen. -US guided CVC placement in the left jugular vein. -IPPV:Vt of 480ml at the rate of 9/min and I:E ratio of 1:2.5. -Chest tube kept ready for the case of inadvertent pneumothorax. -NM block reversal with Sugammadex -Spontaneous ventilation quickly resumed and trachea extubated. Postoperative SpO2 was 98%. Epidural analgesia provided a good pain control. Nine days later patient had to be urgently reoperated due to intestinal fistula. He was placed thoracic epidural again and abdominal cavity was explored under regional anesthesia with maintenance of spontaneous ventilation and continuous infusion of 0.125% bupivacaine. Patient's perioperative course was uneventful and he was discharged home after 10 days.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
291
Conclusion: Abdominal surgery can be safely performed in patients with severe COPD with use of regional anesthesia and meticulous control of ventilation. Precautionary measures for patients with large thoracic bullae include: keeping low airway pressures, avoidance of nitrous oxide and readiness to perform chest drainage promptly in the case of pneumothorax.
4ST-6 Determination of meropenem in serum by liquid chromatography with mass spectrometric detection
Djordjevic Snezana, Peric Aneta, Denic Kristina, Rusic Branislava, Antunovic Marko, Kilibarda Vesna Poisoning Control Centre, Military Medical Academy, Belgrade, Serbia Background.Meropenem is semisynthetic carbapenem antibiotic. It has a broad spectrum of activity against Gram-positive and negative bacteria and it is resistant to hydrolysis by β-lactamases. Activity of meropenem is related to its serum concentration which has to be above the minimal inhibition concentration (MIC) for the offending organism. Time during the concentration of meropenem is above MIC is important parameter which determine its efficacy. Determination of meropenem serum concentration and comparison with MIC of microorganism cousing infection is effective tool in individualizing antimicrobial therapy. The mean peak serum concentration of meropenem in serum is 26mg/L with 500 mg iv dose. The aim of this work was to develop reliable analytical method for determination of meropenem in serum of patients after applying of meropenem. Methods. Determination of meropenem was performed after solid-phase extraction of patiens serum samples. Results.The mean analytical recovery was 64.5%. Extracts were analized by liquid chromatography with mass spectrometric detector in single ion recording mode with m/z 384 for meropenem. Quantitation of meropenem was done by calibration curve of serum spiked with meropenem solution in the range of 5-50 mg/L. Limit of quantitation of LC-MS method was 2.5 mg/L which is significantly lower then expected meropenem concentration in serum samples. Conclusion.Described LC-MS method is fast, precise, simple and reliable. It can be applied in everyday routine analysis of serum samples for improving and optimizing meropenem therapy.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
292
INTENSIVE CARE MEDICINE
5IC-1 The impact of postoperative lactate values on various complications and length of stay following major abdominal surgery Veličković Jelena1,2, Marjanović Slavko3, Miljković Bojana1, Đukanović Marija1, Sumrak Sanela1, Janjić Nataša1, Kosanović Momčilo1, Palibrk Ivan1,2, Filipović Sanja1
1 Center for anesthesia, Clinical Center of Serbia,Belgrade, Serbia 2 University of Belgrade, School of Medicine 3General Hospital Pljevlja, Pljevlja, Montenegro Introducion: The value of lactate measurements for outcome prediction is well recognized in critically ill patients. We aimed to investigate prognostic value of postoperative lactate levels for prediction of different postoperative complications (POC) and length of ICU and hospital stay after major abdominal surgery. Methods: We prospectively evaluated patients undergoing major abdominal surgery with expected ICU stay of 24h. Lactate values were obtained from blood samples taken on admission in the ICU(L0), 4h(L4), 12h(L12) and 24h(L24) after operation. Lactate area (LA; mmol×h/l) representing cumulative lactate values was calculated afterwards. Patients were screened for different POC(Clavien-Dindo ≥ 2) and length of stay until discharge. SPSS 19.0 was used for statystical analysis. ROC curves were constructed to demonstrate predictive ability of different lactate measurements on POCs. Results: The survey enrolled 195 patients of whom 76 (39%) developed a total of 184 complications including death in 18 patients. Mean ICU and hospital length of stay were 2.02(±2.69) and 13.21(±6.47) days. Blood lactate values were higher in patients with POC(p<0.001) in all time points. L12 and LA demonstrated the highest predictive ability for overall POCs (AUROC12=0.722; 95%CI 0.706-0.937;p<0.001) and mortality (AUROC12=0.821). Discriminative power of L12 was best for cardiac (AUROC=0.801), respiratory (0.722), neurologic (0.783), infectious (0.729) and renal (0.764) complications while L0 and LA discriminated the best in the case of surgical complications. Higher L12 values were associated with longer ICU and hospital stay and longer mechanical ventilation. (p<0.001) Conclusion: Postoperative lactate levels during the first 24 postoperative hours have shown predictive value for POCs after major abdominal surgery. L12 had the best power to discriminate between patients with and without POCs for majority of complication types. An elevated postoperative L12 is associated with higher duration of mechanical ventilation, ICU and hospital stay.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
293
PAEDIATRIC ANAESTHESIA AND INTENSIVE CARE
6PA-1 The incidence and risk factors of arrhythmias in the early postoperative period after cardiac surgery in neonates Zecevic V. Tatjana, Vulicevic M. Irena, Mimic D. Branko, Vukomanovic V. Goran, Milovanovic B. Vladimir, Parezanovic M. Vojislav, Ilic G. Slobodan, University Children’s Hospital, Belgrade Background:Rhythm disturbances following congenital heart surgery are frequent and may significantly increase early mortality and morbidity. The aim of this study was to determine incidence and identify risk factors of different arrhythmias in the early postoperative period in neonates. Methods: The study involved 50 neonates who underwent open heart surgery at University Children’s Hospital in Belgrade. Twelve-lead electrocardiography and holter monitoring were used to evaluate hemodinamically significant arrhythmias. Risk factors such as gender, type of congenital heart defect and surgical procedure, serum electrolite level, CPB and aortic clamp duration, inotropic and vasoactive score were analysed. Results:Eighteen patients (36%) developed postoperative arrhythmias. Out of that, 83.33% had supraventricular and 16,67% had junctional ectopic tachycardia. The incidence of arrhythmias after certain procedures were as follows: 77,78% after arterial switch operation, 16.67% after first-stage palliation of hypoplastic left heart syndrome, and 5,55% after total anomalous pulmonary venous return repair. Four out of five neonates with TGA who underwent VSD closure developed arrhythmias. The mean CPB time was slightly higher in patients with dysrhythmias (240.5 minutes versus 215.15 minutes). Vasoactive-inotropic score was higher in patients with arrhytmias (11.97 versus 7.22). The average length of hospital stay was shorter in patients without postoperative dysrhythmias (21.06 versus 34.25 days). Conclusion:Neither one of the risk factors was statistically significant in occurence of arrhythmias. Life-threatening arrhythmias are frequent after cardiac surgery but no precipitating factor has been identified.

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
294
ACUTE AND CHRONIC PAIN MANAGEMENT
7ACP-1 Postoperative pain management on the ward, surgeons’ perspective-An audit Stamenkovic D1,2, Jordanov A1, Ilic M1, Vaskovic I1, Veljovic M1,2, Popovic Z1,2, Kosutic M 1, Aleksic P 1,2, Rondovic G1,2, Bancevic V1,2, Ladjevic N3,4. 1Military Medical Academy, Belgrade, Serbia, 2Faculty of Medicine, University of Defence, Belgrade, Serbia, 3Clinical Center Serbia, Belgrade, Serbia, 4Faculty of Medicine, University of Belgrade, Belgrade, Serbia Background. The postoperative pain management (POPM) in developing countries is still widely neglected field. An audit carried out in two wards, as part of POPM improvement process for second part of PAINOUT study conducted at orthopedics and urology. Methods. Specialist surgeons on orthopedics and urology wards, were given questionnaire and submission of the questionnaire was anonymous. Questionnaire included surgeons’ view on POPM at present, opinion about patients’ pain intensity, practice in analgesics prescription and suggestion for POPM improvement. Results. All the questionnaires were fulfilled and returned, the results are presented in the Table 1. The NSAIL are still the most used analgesics. Diclofenac intramuscular and metamizol intravenous are the most frequently used medications on orthopedic (100%, 94.1%) and urology (90%, 80%) wards. Wider intravenous paracetamol use was noted in urology (40%). Opioids, pethidin and morphine are rarely used. Suggestions for POPM improvement were development of pain management protocol (orthopedic, 11.8%) and implamentation in the practice (10%), and on urology ward, education (10%) and epidural analagesia use (10%). Conclusion. The high return rate of the fulfilled questionnaires and suggestions for analgesia improvement indicate that POPM is recognized and analyzed from surgical point of view. Pain protocol development and education are suggested as valuable help. Moreover, recognition of epidural analgesia need is noted and it’s wider use is suggested. Table 1. Surgeons’ opinion of POPM. Data Ortopedic ward
(n=17) Urology word (n=10)
Satisfaction with postoperative recovery
15 (88%) 8(80%)
Analgesia medications prescribed by anesthesiologist
15 (88%) 8(80%)
Number of patients in pain 17 (100%) 6(60%) Assumed patients’ VAS score 5 (3-8) 3.5 (2-5) Percentage of patients complaining of pain at the arrival on the ward
50% (10%-100%) 30% (10%-70%)
The need for anesthesiologist involvement in postoperative pain management
7 (41%) 100%
Suggestions for pain management improvement on the ward
14 (82%) 4(40%)

XII SERBIAN CONGRESS OF ANESTHESIOLOGISTS&INTESIVISTS 2014
295
NEUROSCIENCES
8NS-1 Modified Pathology Scoring System in the assessment of the patients with aer or solid blast injury Olivera Jovanikic¹, Goran Pavlicevic¹, Jovana Obradovic², Nebojsa Damjanovic² ¹ Neurosurgery Clinic , Military Medical Academy, Belgrade, Serbia ² Clinic for Anesthesiology and Intensive Therapy, Military Mediac Academy, Belgrade, Serbia Background: Growing number of blast injuried patients, in both military and civilian ICU, need to be understood. A Pathology Scoring System(PSS) , initially developed by the J.T. Yelverton in the Walter Reed Army Institute of Research for assessment blast injuried patients by using the alfa numeric code, modified to arrive at a severity of injury index in blast injuried patients.The aim of the study was to assess all leasions by the PSS in 30 patients with primary, pure, aer or solid blast injury( 24 and 16 respectively) and correlation PSS with the GCS, TRISS, RTS,ISS. Methods: External lesions, burns, fractures,injury of pharinx/larinx, trachea, lungs, heart, hollow and solid abdominal organs were assigned numerical scores; lesions were graded as trace, slight, moderate, extensive. The score was divided by maximum possible score to arrive severity of injury ratio( for organ/ system). In the presence of the pneumo- or hemothorax, hemoperitoneum, coronary or cerebral air summed and added summ of the ratios. The results multiplied by 1 or 2 ( surviving or fatality respectively) and arrive severity injury index. The value of the PSS compare to other scores. Results: The mean value of PSS was 10,6±5,6; and for aer 11,2±6,0 and 8,4±3,5 for solid blast, respectively: in the limit 0-36. The analysis was make it clear that correlation is sigificant (p<0.05)betweeen PSS and GCS( r=-0,76), TRISS ( r=-0,66),RTS(r=0,51) and ISS(r=0,59). The correlation is significant ( p<0.05) between PSS and outcome ( p<0.05, r=0.74). Conclusion: The PSS is usefull and precise scale in blast injury assessment in daily clinical practice.


Related Documents











