1 Roche Committed to Innovation Jean-Jacques Garaud, M.D.| Global Head of pharma. Research & Exploratory Development Roche Pharmaceuticals 2010 Citi Investment Research Global Health Care Conference May 26, 2010, New York

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
RocheCommitted to Innovation
Jean-Jacques Garaud, M.D.|Global Head of pharma. Research & Exploratory DevelopmentRoche Pharmaceuticals
2010 Citi Investment Research Global Health Care Conference
May 26, 2010, New York

2
Roche: Focused on medically differentiated therapies
Generics
Differentiation
Focus
MedTech
OTC
Value
DiaPharma
3
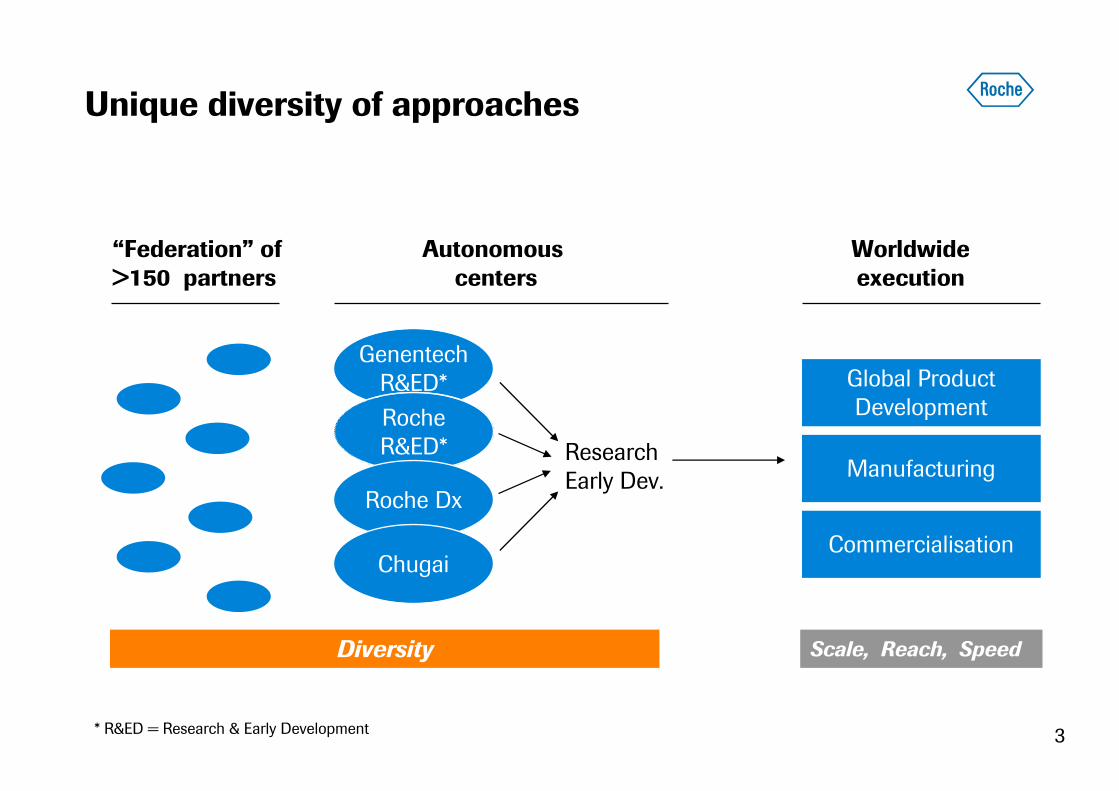
Unique diversity of approaches
Autonomous centers
GenentechR&ED*
Diversity Scale, Reach, Speed
“Federation” of >150 partners
* R&ED = Research & Early Development
RocheR&ED* Research
Early Dev.
Worldwideexecution
Roche Dx
Chugai
Global Product Development
Manufacturing
Commercialisation

4
Roche pharma Research & Early Development Legacy
Six transitions to late-stage over 2007-2009
GA101
Aleglitazar
Taspoglutide
B-RAF antagonist
Gly T-1 inhibitor
Dalcetrapib

5
The pRED mission
Science and patients: our focus, our passion
Deepen understanding of disease biology and the molecular basis of heterogeneity of diseases
Leverage technologies and capabilities to develop new compounds to Lifecycle Investment Point (LIP)
Deliver on individual patient needs through the implementation of PHC strategies

6
Three critical steps for innovation in drug discovery and early development
We know what to target
(Understanding disease, new pathways, Biomarkers, PHC)
We have a powerful multiplier
(Therapeutic Modalities)
World-Class skills inTranslational Medicine
(PoM and PoC)
Small Molecules
Therapeutic Proteins
RNA Interference
Therapeutic stem cells
Peptides
7
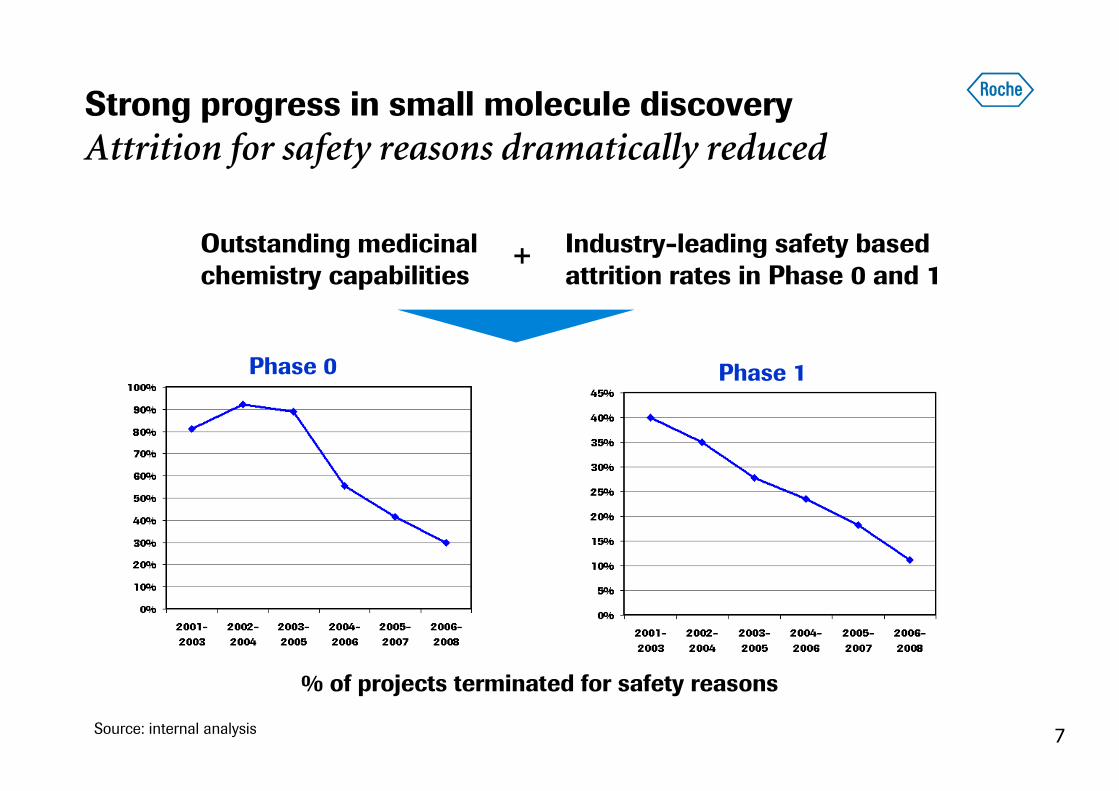
Strong progress in small molecule discovery
Attrition for safety reasons dramatically reduced
% of projects terminated for safety reasons
Phase 0 Phase 1
Industry-leading safety based attrition rates in Phase 0 and 1
Outstanding medicinal chemistry capabilities
+
Source: internal analysis

8
MDM2 antagonist (RG7112) induces apoptosis
Nutlins: a novel approach to cancer therapy
• p53 is a major tumor suppressor protein that induces apoptosis in tumors
– MDM2 naturally inhibits the activity of p53
– Nutlins prevent MDM2 from inactivating p53
• Nutlins represent a breakthrough in cancer drug research
– small molecule that specifically blocks the interaction between the two proteins
• Roche is the leader in the field
Xenografts model results
• RG7112 currently in late Phase 1
• Companion diagnostics in co-development with Diagnostics (p53 chip & MDM2 expression)
L Vassilev et al. (2004) Science, 303, 844-848; L Vassilev (2006) Trends in Molecular Medicine 13, 1 23-31; Rosisnki, J., etal., Proc. Natl. Acad. Sci. 103 1888-93 (2006); Xia M., etal., Cell Cycle 7 1604-12 (2008); Huang B, etal., Mol Cancer Res. 2009 Sep;7(9):1497-509.

9
Enhancing antibody performance
NK
or MØØØØ
Bi-specific antibodybinds to two different targetsand enhances specificity
Antibody inhibits or activates signaling
Naked Antibodies
bi-specific Antibodies
Bi-specific antibodybinds to two different targets in different cells
bi-specific Antibodiesdrugdrug
drugdrug
Antibody recruits immune effectorcell and induces cytotoxicity
ADCC enhanced Antibody
Antibody specifiesdelivery of drug
Armed Antibodies

10
T-DM1
HER2 suppression meets cytotoxic potency
• A novel anti-cancer agent
– Herceptin’s biologic activity
– Targeted intracellular delivery of a potent cell-killing agent, DM1
• Unprecedented efficacy inheavily pre-treated HER2+ mBC
– 33% ORR
• Single agent data indicates better tolerability than standard chemotherapy-containing regimens
In collaboration with ImmunoGen

11
T-DM1
Changing paradigm in a broad clinical program
HER2-positive Metastatic Breast Cancer
Third-line
Treatment
Second-line
Treatment
First-line
Treatment
First-line
Treatment
Phase IIPhase III
EMILIA
Randomised
Phase II
Preparing for
Phase III
• Single ARM: T-DM1
• Potential US submission
2010
• ARM A: T-DM1
• ARM B: Xeloda plus lapatinib
• Potential submission 2012
• ARM A: T-DM1
• ARM B: Herceptin plus docetaxel
• ARM A: Herceptin plus taxane
• ARM B: T-DM1
• ARM C: T-DM1 plus pertuzumab
• Potential submission
beyond 2014
Phase II 1L HER2+ mBC data submitted for presentation at
ESMO 2010In collaboration with ImmunoGen
12
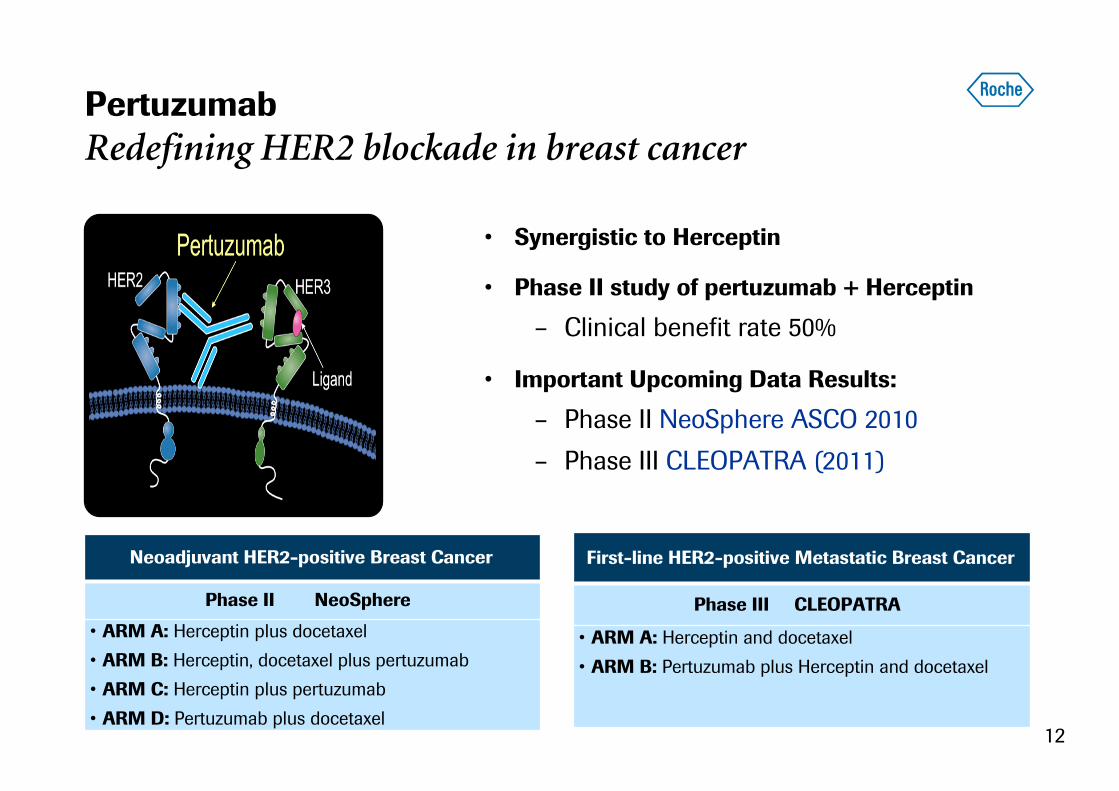
Pertuzumab
Redefining HER2 blockade in breast cancer
• Synergistic to Herceptin
• Phase II study of pertuzumab + Herceptin
– Clinical benefit rate 50%
• Important Upcoming Data Results:
– Phase II NeoSphere ASCO 2010
– Phase III CLEOPATRA (2011)
First-line HER2-positive Metastatic Breast Cancer
Phase III CLEOPATRA
• ARM A: Herceptin and docetaxel
• ARM B: Pertuzumab plus Herceptin and docetaxel
Neoadjuvant HER2-positive Breast Cancer
Phase II NeoSphere
• ARM A: Herceptin plus docetaxel
• ARM B: Herceptin, docetaxel plus pertuzumab
• ARM C: Herceptin plus pertuzumab
• ARM D: Pertuzumab plus docetaxel

13
GA101: a glycoengineered, type II anti-CD20 antibody
Enhanced ADCC and direct cell induction
GA101 in patients with relapsed/refractory CD20+B-CLL
Glycoengineered
Type II epitope
Mossner E., etal., Blood, Mar 2010 GA101 B-CLL data presented at ASH, December, 2009

14
GA201
Anti-EGFR glycoengineered antibody for enhanced ADCC
• A potential breakthrough in cancer therapy
– opportunity to treat k-ras mutant tumors
• Will allow to demonstrate the utility of glycoengineering antibodies
• Roche could become the leader in ADCC–enhanced antibody therapy
GA201
Fully humanEGFR mAb
Cetuximab
-20
0
20
40
60
80
100
1500 300 60 12 2.40 0.48 0.096
Antibody Concentration (ng/ml)
AD
CC
(%
)
GA201 vs. other EGFR Abs(NK92/FcgRIIIA-158F effector cells)
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68
Study day
0
20
40
60
80
100
120
Sur
viva
l %
CetuximabVehicleGA201
Superior efficacy in CRC (kRAS mut liver met model in Scid-bg mice)
Patient 1696 (kRAS WT, EGFR mut CRC): complete response
after 12 cyclesGerdes C., etal., Presentation at AACR Meeting, April 2009; Abstract 5476.Data on file, Roche

15
2007 2008 2009 2010E
Late-stage pipeline continues to build up
Expanding into new therapeutic areas
Number of NMEs
2
4
10Metabolic
Oncology
Inflammation
ocrelizumab
dalcetrapib
pertuzumab
dalcetrapib
taspoglutide
Actemra
ocrelizumab
aleglitazar
dalcetrapib
taspoglutide
aleglitazar
SGLT2 inh*
CNS
taspoglutide
ocrelizumab
GlyT-1 inh
ocrelizumab MS*
pertuzumab
T-DM1
Hedgehog inh
BRAF inhibitor
RG7159 (CLL)
GlyT-1 inh
pertuzumab
BRAF inhibitor
T-DM1
Hedgehog inh
RG7159 (CLL, NHL)
up to 13
lebrikizumab *
HCV pol inh *
Virology
* LIP or phase III decision pending

16
Metabolism/CV: High Unmet Need Remains
> 65% of CV events not prevented despite wide use of statins
Major clinical trials aimed at reducing cardiovascular risk
0%
20%
40%
60%
80%
100%
4S Lipid Care HPS WOSCOP AFCAPS/TexCAPS
TNT
% event not prevented % event prevented
4S, The Lancet, 1994 - Lipid, NEJM, 1998 - Care, NEJM, 1996 - HPS, The Lancet, 2002WOSCOP, NEJM, 1999 - AFCAPS/TexCAPS, JAMA, 1998 - TNT, NEJM, 2005
17
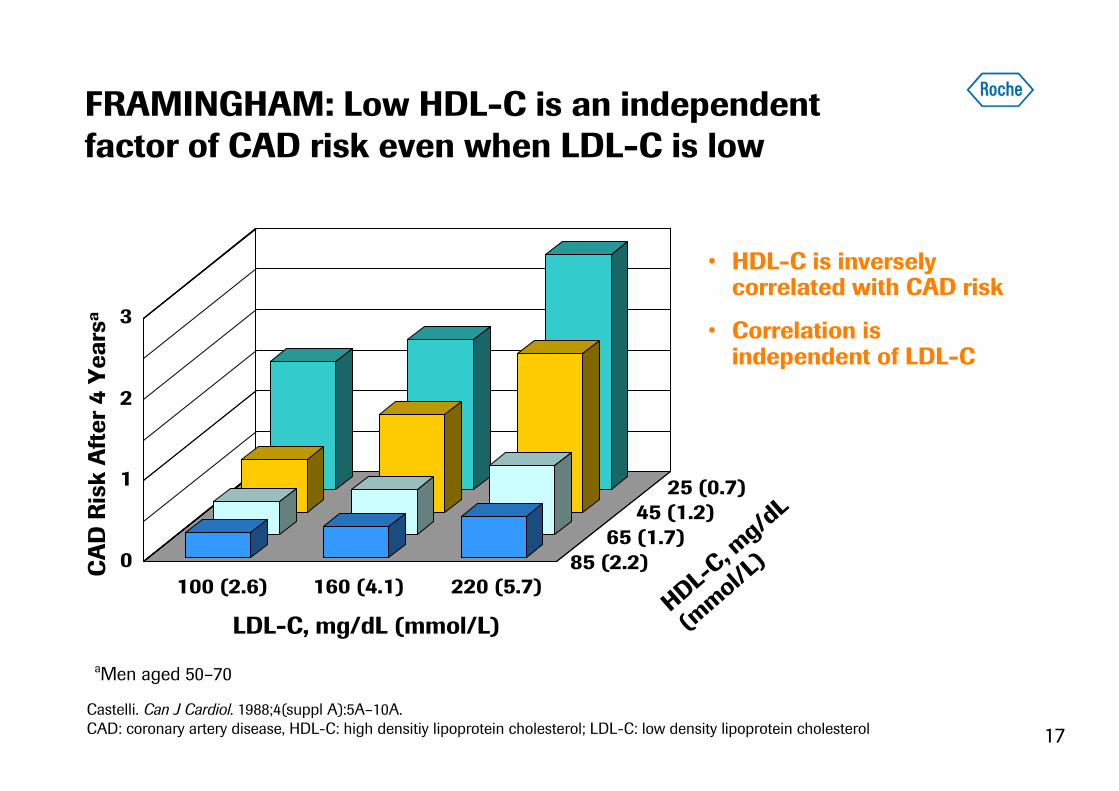
HDL-C, mg/dL
(mmol/L)
FRAMINGHAM: Low HDL-C is an independent factor of CAD risk even when LDL-C is low
CAD Risk After 4 Years
a
85 (2.2)65 (1.7)
45 (1.2)25 (0.7)
100 (2.6) 160 (4.1) 220 (5.7)
LDL-C, mg/dL (mmol/L)
0
1
2
3
• HDL-C is inversely correlated with CAD risk
• Correlation is independent of LDL-C
aMen aged 50–70
Castelli. Can J Cardiol. 1988;4(suppl A):5A–10A.CAD: coronary artery disease, HDL-C: high densitiy lipoprotein cholesterol; LDL-C: low density lipoprotein cholesterol

18
LIVER
PERIPHERAL TISSUEBile Excretion
Reverse
Cholesterol Transport
LDL
PLASMA
Cholesterol Efflux
CETP Athero-sclerosis
HDL removes cholesterol from atherosclerotic plaque
CETP inhibition: next breakthrough in CV risk reduction?
Hypothesis tested with CETP inhibition
• Increases HDL
• Promotes cholesterol efflux from macrophages in atherosclerotic plaque
• Promotes reverse cholesterol transport
Cardiovascular Morbidity and Mortality benefits
HDL
?

19
dalHDL
torcetrapib
CETP
HDL
• Dalcetrapib binds to CETP, inducing aconformational change of CETP1
• HDL generated is of normal composition
• Torcetrapib binding to CETP results in a highaffinity complex of torcetrapib, HDL and CETP2,3,4
• HDL generated is different from physiological
1 Okamoto et al. Nature. 2000;406:203–207; 2Niesor et al. Atheroslerosis. 2008;199:231;3 Clark et al. J. Lipid Res. 2006;47:537–552; 4Barter et al. N Engl J Med. 2007;357:2109–2122.
Dalcetrapib and torcetrapib
Different mechanisms of CETP inhibition

20
• Patients with acute coronary syndrome and diabetes: at highest risk of recurring CV events
• Patients with ACS and diabetes are characterized by atherogenic dyslipidemia:
– Triglycerides ↑
– HDL ↓
– small, dense LDL ↑
– Apo-B ↑
RR=1.99 (1.52 -2.60)
RR=1.71 (1.44 - 2.04)
RR=1.00
RR=2.88 (2.37– 3.49)
Event rate
6 9 153 18 2112 24
Diabetes/CVD (n = 1148)
No Diabetes/CVD (n = 3503)
Diabetes/No CVD (n = 569)
No Diabetes/No CVD (n = 2796)
6 9 153 18 2112 24
Months
0.00
0.05
0.10
0.15
0.20
0.25
The true unmet medical need in type 2 diabetes is cardiovascular risk reduction
Malmberg K et al. Circulation 2000;102:1014-1019; Results of the OASIS(Organisation to Assess Strategies for Ischemic Syndromes) Registry
21
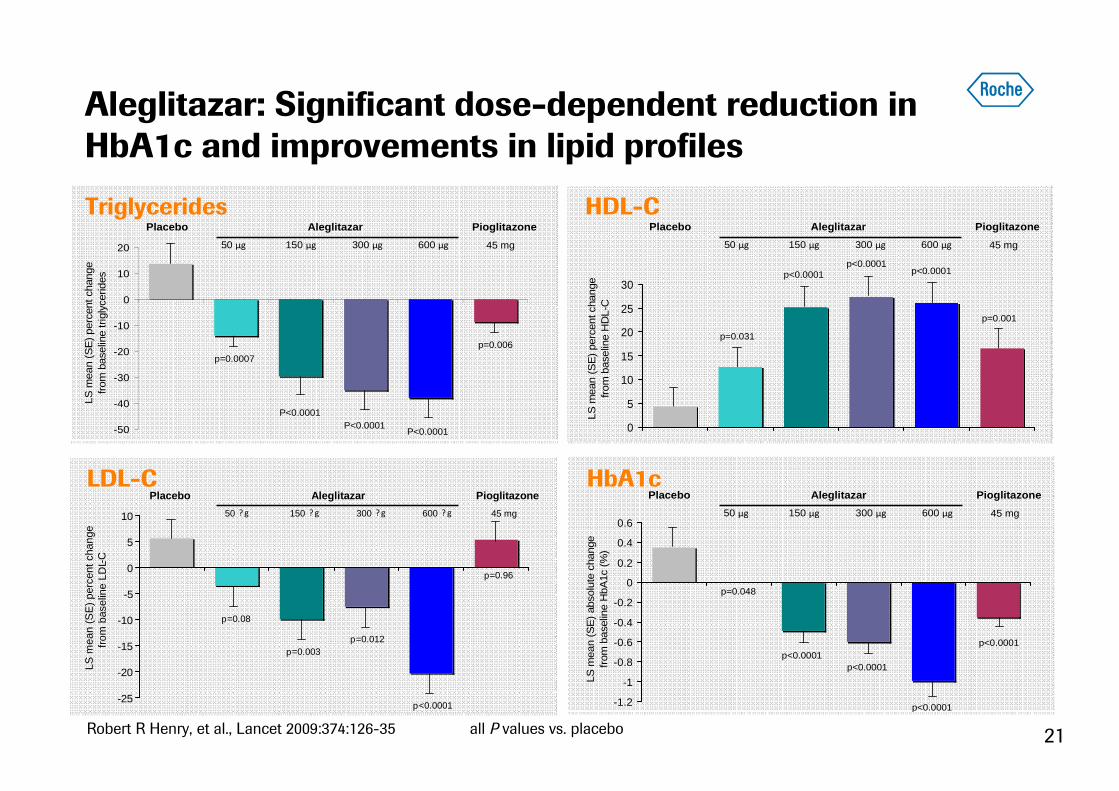
Aleglitazar: Significant dose-dependent reduction in HbA1c and improvements in lipid profiles
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
LS m
ean
(SE
) ab
solu
te c
hang
e fr
om b
asel
ine
HbA
1c (
%)
Placebo
50 μg 150 μg 300 μg 600 μg
Aleglitazar Pioglitazone
45 mg
p<0.0001
p=0.048
P values vs. placebo.
p<0.0001p<0.0001
p<0.0001
Placebo
50 μg 150 μg 300 μg 600 μg
Aleglitazar Pioglitazone
45 mg
LS m
ean
(SE
) pe
rcen
t cha
nge
from
bas
elin
e tr
igly
cerid
es
p=0.0007
P<0.0001
p=0.006
P<0.0001P<0.0001-50
-40
-30
-20
-10
0
10
20
LS m
ean
(SE
) pe
rcen
t cha
nge
from
bas
elin
e H
DL-
C
p=0.001
p=0.031
p<0.0001
Placebo
50 μg 150 μg 300 μg 600 μg
Aleglitazar Pioglitazone
45 mg
p<0.0001 p<0.0001
0
5
10
15
20
25
30
Triglycerides HDL-C
LDL-C HbA1c
Robert R Henry, et al., Lancet 2009:374:126-35 all P values vs. placebo
-25
-20
-15
-10
-5
0
5
10
LS m
ean
(SE
) pe
rcen
t cha
nge
from
bas
elin
e LD
L-C
p=0.08
p=0.003p=0.012
p<0.0001
p=0.96
Placebo
50 ?g 150 ? g 300 ?g 600 ? g
Aleglitazar Pioglitazone
45 mg

22
Patients
• Type 2 diabetes (known and recently diagnosed)
• Hospitalized for acute coronary syndrome
Primary endpoint• Composite endpoint of reduction in cardiovascular mortality, non-fatal myocardial infarction and non-fatal stroke (MACE)
Design
• Double-blind, placebo-controlled study on top of standard of care
• Treatment duration: At least 2.5 years
• N = 6,000
Treatment periodScreening/ placebo run-in period
Follow-up period
At least 2.5 years 4 weeks
Aleglitazar 150 µg or placebo
Standard of care (diabetes and other cardiovascular risk factors)
Aleglitazar development in patients with high CV risk
Phase III CV outcomes study: recruitment started Q1 2010

23
Schizophrenia, a devastating disease
The clock stops when schizophrenia starts
• Average life expectancy ~20 years shorter
– Attributed to suicide andcardiovascular co-morbidities
• Patient faced with invalidility
– Loss of job, hobbies, friends
– Heavily dependent on support
– Poor insurance coverage in the US
• High burden for caregivers
– Isolation
– Loss of previous life, often job
– Depression and stress

24
Features of schizophrenia syndrome
Heterogeneity requires specific treatment of symptoms
Social Dysfunction• Work
• Interpersonal relationships
• Self-care
Positive Symptoms
• Delusions
• Hallucinations
• Disorganized speech
• Catatonia
Primary Negative Symptoms
• Affective flattening
• Alogia
• Avolition
• Anhedonia
• Social withdrawal
Cognitive Deficits
• Attention
• Memory
• Executive functions(eg, abstraction)
Comorbid Substance Abuse
Mood Symptoms
• Depression
• Hopelessness
• Suicidality
• Anxiety
• Agitation
• Hostility
• InsomniaMaguire GA. Am J Health-Syst Pharm. 2002;59:S4-S11.

25
GlyT-1 inh. phase II data in schizophreniaPrimary endpoint: PANSS negative symptom factor score
-7
-6
-5
-4
-3
-2
-1
0
Placebo GlyT-1
-5.11
-6.45
�� ��Im
provement
ITT Population
-7
-6
-5
-4
-3
-2
-1
0
Placebo GlyT-1
-4.86
-6.50 *
�� ��Im
provement
p < 0.05
Per-Protocol Population
Three doses were tested in Phase II – data shown is for the most effective dose
p = 0.07
Change from Baseline at Week 8

26
Strong late-stage portfolio of NMEs
Limited risk due to rigorous proof of concept studies
Probability of technical success
Peak sales
CHF 2 bn
0% 50% 100%
aleglitazarocrelizumab MS*
GlyT-1 inhGA101
pertuzumabtaspoglutide
T-DM1
BRAF inh (Melanoma)Hedgehog inh (BCC)
CHF 5 bn
dalcetrapib
T-DM1 (early launch)
* Phase III “go/no go” decision pending

27
Changing the practice of medicine!
Improve outcomes in cardiovascular disease (taspoglutide, aleglitazar, dalcetrapib)
New therapies for Schizophrenia and MS (GlyT-1 inh. and ocrelizumab)
Better therapies for cancer (antibody drug conjugates, glycoengineered Abs-GA101, pertuzumab, BRAF and hedgehog inhibitors)
Prevent blindness with Lucentis(AMD, RVO and DME)
Launch at least 6 new products (NMEs) by end 201435 Line extensions of existing products could be filed by end 2014

28
Related Documents











