ORIGINAL ARTICLE Robotic whole body stereotactic radiosurgery: clinical advantages of the CyberKnifeH integrated system E ` Coste-Manie ` re, D Olender, W Kilby, R A Schulz E ` Coste-Manie `re Accuray Europe, Paris, France D Olender, W Kilby and R A Schulz Accuray Inc., Sunnyvale, California, USA Correspondence to: R Schulz, E-mail: [email protected] Abstract Radiosurgery is defined as the delivery of high doses of ionising radiation, in mono- or hypo- fractionated treatments, to destroy tumours or focal areas of pathology. The clinical requirements of designing a radiosurgical treatment system include providing: a) a highly precise beam delivery to targets located throughout the body, b) a highly conformal dose distribution, c) the ability to irradiate both small and/or large complex-shaped lesions while minimising the dose to adjacent radiosensitive tissues and d) the ability to interactively track lesion motion due to normal patient motion. To accomplish this, the CyberKnifeH radiosurgery system has pioneered in this area by taking advantage of the inherent geometrical targeting precision of a commercial arm-based robotic system carrying a compact X-band linear accelerator and integrated with X-ray imaging and visualisation feedback systems. The arm-mounted linear accelerator, equipped with patient specific anatomical models, registered to the patient in real-time with image guidance, dynamically and safely delivers conformal and homogeneous radiation for therapeutic benefit. This paper details the components of the CyberKnife system and their integration in the clinical workflow of radiosurgery. Keywords: Radiosurgery, medical robotics, image-guided treatment, CyberKnife Paper accepted: 1 December 2004 Published online: 15 January 2005. Available from: www.roboticpublications.com DOI: 10.1581/mrcas.2005.010211 INTRODUCTION: THE REVOLUTION OF ROBOTICS IN MEDICINE A robot is defined as a sensor-based tool capable of performing precise, accurate and versatile actions on its environment. Robots were initially developed to spare humans from performing burdensome, repe- titive or risky tasks. They have yielded substantial productivity benefits within a variety of manufac- turing fields. Robots have progressed from the research lab to the factory to medical devices. In medicine, in their most sophisticated form, robots have recently evolved into complex systems integrating perception (medical images and infor- mation) and action (precise spatial positioning and sensory feedback) by mechanically controlled systems and image-guided devices (1) . Robots are becoming revolutionary tools for surgeons in a variety of clinical applications. In addition, they can extend capabilities that transcend human limitations such as tremor reduction, repeatability, precision and accuracy. In doing so, they provide a new level of minimally invasive access to a variety of anatomical targets. These new capabilities have the potential to give better consistency to surgical treatments resulting in improved patient outcome and added economic benefit. A number of robots have been successfully applied to several areas of medicine. Historically, rigid or rigidly constrained organs were the first to benefit from the geometrical precision of robotic 28 Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39 E 2005 Robotic Publications Ltd. www.roboticpublications.com

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ORIGINAL ARTICLE
Robotic whole body stereotactic radiosurgery: clinicaladvantages of the CyberKnifeH integrated system
E Coste-Maniere, D Olender, W Kilby, R A Schulz
E Coste-ManiereAccuray Europe, Paris, FranceD Olender, W Kilby and R A SchulzAccuray Inc., Sunnyvale, California, USACorrespondence to: R Schulz, E-mail: [email protected]
AbstractRadiosurgery is defined as the delivery of high doses of ionising radiation, in mono- or hypo- fractionatedtreatments, to destroy tumours or focal areas of pathology. The clinical requirements of designing aradiosurgical treatment system include providing: a) a highly precise beam delivery to targets locatedthroughout the body, b) a highly conformal dose distribution, c) the ability to irradiate both small and/orlarge complex-shaped lesions while minimising the dose to adjacent radiosensitive tissues and d) the ability tointeractively track lesion motion due to normal patient motion. To accomplish this, the CyberKnifeHradiosurgery system has pioneered in this area by taking advantage of the inherent geometrical targetingprecision of a commercial arm-based robotic system carrying a compact X-band linear accelerator andintegrated with X-ray imaging and visualisation feedback systems. The arm-mounted linear accelerator,equipped with patient specific anatomical models, registered to the patient in real-time with image guidance,dynamically and safely delivers conformal and homogeneous radiation for therapeutic benefit. This paperdetails the components of the CyberKnife system and their integration in the clinical workflow ofradiosurgery.
Keywords: Radiosurgery, medical robotics, image-guided treatment, CyberKnife
Paper accepted: 1 December 2004
Published online: 15 January 2005. Available from: www.roboticpublications.com
DOI: 10.1581/mrcas.2005.010211
INTRODUCTION: THE REVOLUTION OFROBOTICS IN MEDICINEA robot is defined as a sensor-based tool capable ofperforming precise, accurate and versatile actions onits environment. Robots were initially developed tospare humans from performing burdensome, repe-titive or risky tasks. They have yielded substantialproductivity benefits within a variety of manufac-turing fields. Robots have progressed from theresearch lab to the factory to medical devices.
In medicine, in their most sophisticated form,robots have recently evolved into complex systemsintegrating perception (medical images and infor-mation) and action (precise spatial positioningand sensory feedback) by mechanically controlled
systems and image-guided devices (1). Robots arebecoming revolutionary tools for surgeons in avariety of clinical applications. In addition, they canextend capabilities that transcend human limitationssuch as tremor reduction, repeatability, precisionand accuracy. In doing so, they provide a new levelof minimally invasive access to a variety ofanatomical targets. These new capabilities have thepotential to give better consistency to surgicaltreatments resulting in improved patient outcomeand added economic benefit.
A number of robots have been successfullyapplied to several areas of medicine. Historically,rigid or rigidly constrained organs were the first tobenefit from the geometrical precision of robotic
28
Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39 E2005 Robotic Publications Ltd.
www.roboticpublications.com

systems. Orthopaedic and neurosurgical applicationshave utilised robots and image guidance for totaljoint replacement (hip, knee), brain surgery andspine surgery. Some robots such as RobodocH(Integrated Surgical Systems, Inc., USA, www.robodoc.com) have had varying degrees of com-mercial success in this area. Tele-operated robotssuch as the da VinciH (Intuitive SurgicalH, Inc.,USA, www.intuitivesurgical.com) have allowed softtissue procedures to start benefiting from roboticenhancement. These systems have successfully madetheir way into cardiac and abdominal applications asan enhancement to traditional minimally invasivesurgery.
The delivery of ionising radiation for radio-surgical purposes has been an enhancement to theuse of radiation for general therapeutic uses. TheCyberKnifeH radiosurgery system (AccurayTM, Inc,USA, www.accuray.com), has pioneered the field ofrobotic radiosurgery by introducing the advantagesof medical robots to perform more precise andaccurate delivery of ionising radiation. Intracranialrobotic radiosurgery was first achieved on neuro-pathology within the skull. This was followed byradiosurgery of generally static extra-cranial targetssuch as spine lesions. More recently, the designof innovative, target-tracking technologies hasextended clinical applications to tumours and lesionswithin soft tissues which are affected by respiratorymotion.
RADIOSURGICAL REQUIREMENTS: ANOVERALL GEOMETRICAL PROBLEMChallenges to the adoption of robotics into currentclinical practice include clinical benefit, ease of usein the clinical environment and total economicefficacy for society. Without these benefits, newmedical devices, including those that involverobotics, will have scant chance of being adoptedby the medical community. Both clinical andeconomic benefits of any revolutionary medicaldevice must be realizable for a technology to besuccessfully integrated into standard medicalpractice.
Introduced in the 1950’s by Lars Leksell, MD,radiosurgery has been defined as precisely targeteddoses of radiation for tumour ablation as a substitutefor procedures using traditional surgical instruments.These early ‘‘virtual scalpel’’ procedures were ableto perform ablations for a variety of intracranial
abnormalities. Recently, radiosurgery has beenextended to the whole body applications. Thesequence of product development events for radio-surgery is analogous to the progression of CT in theearly 70s and MR in the early 80s. In the formercase CT imaging systems were confined to only thehead for almost a decade from inception. In thelatter case MR systems were not generally used inthe body for at least 5 years from inception. Theknifeless, minimally invasive, procedure of radio-surgery eliminates the trauma of traditional surgerywith little swelling, no blood or tissue loss and noinfection. Furthermore, the morbidity and mortalityassociated with general anaesthesia is eliminated andpatients can be treated in ambulatory environmentswith their associated economic and clinical benefits.
These advantages become fully realised whenradiosurgery, the equivalent of abnormal tissuedissection, is performed. This technique maximisestarget resection and minimises normal tissuedestruction. For example, the radiosensitive spinalcord must be protected when targeting lesions inthe vertebrae due to the cord’s proximity to thetumour. The radiation dose has to optimally fit thetumour shape, while reducing the damage tocollateral organs. This requires focusing the radia-tion on the target in a precise, conformal, andaccurate manner (2). From a robotics and medicalimaging viewpoint, this process may be seen as anoverall ray-tracing geometrical problem. Manyparameters have to be adjusted to optimize radio-surgical workflow.
Pre-operative lesion identification phaseThe targeted lesion and its surrounding criticaltissues must be identified in 3-D space relative to thepatient’s reference frame. Sophisticated medicalimaging techniques are key to optimum targetlesion identification. Enhanced medical imagingtechnologies such as functional imaging (CT/PET,fMRI and spectroscopy) can help provide preciseand thorough modelling of the patient’s radio-surgical target site.
Pre-operative planning phaseThe goal of this step is to sculpt a conformal dosevolume around the target while minimising the dosedelivered to adjacent healthy tissues. To do this, thesystem uses a combination of beam positions whoserelative weights, or dose contributions, have been
Robotic whole body stereotactic radiosurgery: clinical advantages of the CyberKnifeH integrated system 29
E2005 Robotic Publications Ltd. Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39
www.roboticpublications.com

scaled to volumetrically shape the dose accordingly.In the model known as forward planning, this isdone manually by the user specifying the desiredweight of the various beams. More commonly,inverse planning is employed. This planing methodutilises an algorithm to automatically calculate theoptimum combination of beams and weights basedupon user-defined dose constraints to the target andhealthy tissues.
System registration phaseThe lesion and the radiation source must beregistered to one another in 3D space, so as toaccurately preoperatively plan for optimal radio-surgical results. Six degrees of freedom are necessaryto describe the spatial position (x, y, z) and thedirectional orientation (yaw, pitch, roll) of the targetrelative to the source. Various hardware and soft-ware strategies for positioning the radiation sourcewith respect to the patient have been implemented.
In Leksell’s precursor radiosurgical system, theGammaKnife (Elekta, Sweden, www.elekta.com),the (Cobalt-60) radiation sources are fixed in spaceand the patient’s head is moved and registered so asto expose the anatomical target to the focal point ofthe 201 pencil like gamma radiation beams. Thisscenario requires the rigid fixation of the patient’sskull within a pin based stereotactic frame, withsubstantial discomfort to the patient. By relocatingthe frame within the machine, the patient’s skullis repeatedly repositioned relative to the fixedradiation reference frame based on a pre-calculatedradiation plan.
In later systems, a linear accelerator producinghigh energy X-rays is attached to a gantry-basedsystem. The resultant device generates arbitrarilyshaped beams of radiation, which intersect oneanother to define a relatively uniform dose distribu-tion at the target. In these systems, fixed stereotacticframes remain necessary to register pre-operativepatient information to the intra-operative conflu-ence of the treatment beams. Both of thesetechnologies have the additional constraint oflimiting the treatment to single fractions due tothe invasive nature of the frame, eliminating theoption of hypo-fractionated radiosurgical strategies.
Relocatable stereotactic frames have been devel-oped to avoid this limitation, but these also achievelower alignment accuracy than is possible with thefixed frames.
Robotic stereotactic radiosurgeryThe CyberKnife robotic stereotactic radiosurgeryintegrated system provides a clever solution to theproblems encountered in other systems. Employingreal-time frameless registration (3) with six degrees ofrobotic positioning, this system provides precisespatial positioning. This results in a variety ofadvantages over other systems.
Using advanced robotic systems, the treatmentbeam distribution may be eloquently controlled.Such technologies allow radiation beams to bedelivered to one or more irregularly shaped lesionswhile avoiding irregularly shaped radiosensitiveareas. Treatment may involve beam paths with asingle isocenter, with multiple isocenters, or withcompletely non-isocentric approaches. The latterapproach will always provide the most conformaltreatment for irregularly shaped target lesions.Treatment can be delivered in either a single session(mono-fractionation) or in a small number ofsessions (hypo-fractionation) as determined duringtreatment planning. Treatment plans may beoptimized for any combination of treatment time,dose conformality or dose homogeneity, by varyingthe planning constraints. Integration of the overalltreatment workflow is key (4). The inherentcomplexity of the information may be managed inan elegantly structured way prior to its adoption anduse by multi-disciplinary teams of surgeons, oncol-ogists, physicists and technologists.
THE CYBERKNIFE SYSTEMThe CyberKnifeH system is a non-invasive radio-surgical device for tumour ablation. It is a uniquedevice that integrates robotics with image-guidancetechnology. It is used to destroy lesions or tumourswith large doses of accurately targeted megavoltageX-radiation. During treatment, multiple radiationbeams are delivered according to a pre-definedtreatment plan. A 6MV linear accelerator mountedon a robotic positioning arm (KUKA, Germany,www.kuka.de) accurately targets the beams attumours and other lesions in the head and body.The radiation beams, and their resultant dosedistribution, are designed to destroy the tumourwhile minimising exposure to nearby healthy tissue.Prior to and during treatment, a system composed oftwo orthogonal imaging chains made of diagnostic(kV) X-ray sources and digital amorphous silicondetectors provides a continuous update of thepatient’s position. This system allows the robotic
30 Coste-Maniere, Olender, Kilby, Schulz
Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39 E2005 Robotic Publications Ltd.
www.roboticpublications.com

manipulator to correct for changes in patientposition during treatment beam delivery. A five-degree of freedom treatment table (AxumTM) is alsoavailable for automatic patient (re)positioning priorto or during treatment. A real time optical trackingsubsystem is used for dynamic compensation oftumour movement due to respiration duringtreatment delivery. Figure 1 illustrates the overallsystem hardware within the radiosurgical suite.Planning, monitoring and system control equipmentare located outside the shielded treatment room.
The CyberKnife system was developed to over-come both the geometrical limitations of gantry-based systems and the invasive aspect of frame-basedstereotactic systems. A detailed history of the Cyber-Knife system can be found in ‘‘Accuray: TightlyTargeting Tumours’’ (5). Using the CyberKnifesystem, the radiosurgical procedure requires noanaesthesia and the technology is available for
ambulatory patients. Patients typically resumenormal activities immediately after treatment.
CYBERKNIFE TREATMENT WORKFLOWThe adoption of medical robots in regular clinicalpractice has been limited by a dearth of formalizedclinical workflow. Too often workflow is inefficientand disseminated into many steps lacking integrationand synchronization (6). The CyberKnife system’sworkflow incorporates automated subsystems, tech-nologies and techniques which efficiently integratethe different steps found in traditional radiosurgicalprocedures. This workflow employs a multi-dis-ciplinary clinical team composed of surgeons,radiation oncologists, medical physicists and radia-tion therapists working together prior to and duringtreatments.
In the preoperative phase, the workflow beginswith patient preparation. In intracranial surgery, a
Figure 1 Overview of the CyberKnife System and localization setup. Two X-ray images of the patient positioned via theAxum automated treatment couch.
Robotic whole body stereotactic radiosurgery: clinical advantages of the CyberKnifeH integrated system 31
E2005 Robotic Publications Ltd. Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39
www.roboticpublications.com

soft retention mask is moulded on the patient’s faceprior to their medical imaging examination. Inextracranial procedures, radiopaque fiducials maybe implanted in close proximity to, or inside,the tumour or lesion in a minimally invasiveinterventional procedure. Patients may also be fittedwith a custom moulded body cradle to stabilize thepatient on the treatment table.
The second step of the workflow consistsof medical imaging studies. These examinationsrequire at least a CT scan. Additional imagingprocedures such as MRI, 3D angiography orfunctional imaging techniques (fMRI, PET orPET/CT, etc.) may be required to better definespecific pathologies. These imaging examinationsare used as inputs for segmentation (contouring)of both the target and radiosensitive normalanatomy.
In the normal workflow, the surgeon is in chargeof anatomical contouring. Models of the lesionand surrounding tissues, displayed on the medicalimages, are used as inputs to the pre-operativeplanning phase. The treatment beam arrangement isthen optimised to deliver the required dosedistribution at the target lesion(s) while minimisingnormal tissue irradiation. Medical physicists andradiation oncologists are both involved in planningthe radiosurgical treatment including determiningthe optimal number of treatment fractions. Thesystem optimises the robot’s positional sequencingand those orientations required to render thattreatment. Once this treatment plan is complete,the radiosurgical treatment can begin.
For treatment, the patient is positioned on thetreatment table. Their face mask or other immobi-lisation device is used to limit movement whilemaintaining the patient in a comfortable position.Next, real time X-ray images of the patient in thesurgical position are acquired. Target localisationinformation based on skull or fiducial identification,is extracted automatically and compared withinformation available from the preoperative medicaldata. Geometrical transformations are computed toguide the operator to manually or automaticallymanoeuvre the patient and the treatment table so asto approximately align the patient’s real positionwith the position of the preoperative imaging data.This procedure continues iteratively until an initialalignment threshold is met. The final, precisealignment is then achieved by compensating withthe robotic manipulator.
The robot is positioned around the patient andtherapeutic beam delivery can start in a sequentialmanner. The manipulator follows a given patharound the patient as computed by the planningsystem. Prior to the delivery of each beam inthe path, the imaging system rechecks patientalignment. Following the same image registrationprocess as employed for patient positioning, thesystem calculates the patient’s position to 0.1 mmand 0.1 degrees. Patient displacement information isreturned to the manipulator, allowing the robot toautomatically modify its delivery path to compen-sate for patient movement during the treatment. Incases where patient movement is minimized, theoperator can reduce the imaging frequency (typi-cally to every third beam) in order to expeditethe treatment. Should patient motion exceed anacceptable displacement threshold, the treatmentis stopped and the patient can be repositionedmanually or using the automatic couch. Beamdelivery, localization and co-registration processesare performed continuously until the treatment iscompleted. For radiosurgical treatments that requiremore than one fraction, the same workflow isrepeated by the clinical team during subsequentlyscheduled treatment sessions.
THE CYBERKNIFE SUBSYSTEMS AS USEDIN THE TREATMENT WORKFLOWThe individual elements of the CyberKniferadiosurgical system are detailed in their order ofappearance in the clinical workflow.
Patient modeling: The CyRISTM InView image fusionand contouring stationThe CyRISTM InView platform is an interactivesoftware package enabling clinicians to completethe critical step of visualization and segmenting(contouring) anatomical structures in an efficientmanner. This procedure (Figure 2) may beperformed remotely from the physician’s practice,clinic, or hospital via computer network connec-tions, thus maximising clinical efficiency.
A set of slices from medical images (CT, MRIscans, 3D Angiography (7), PET, SPECT,…) areused as inputs to the CyRIS InView subsystem.State-of-the-art multi-modality image fusion algo-rithms (8) are integrated in the treatment planningsystem to make optimal use of the capability of eachimaging modality. Sophisticated drawing tools allowthe clinician to quickly and accurately define the
32 Coste-Maniere, Olender, Kilby, Schulz
Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39 E2005 Robotic Publications Ltd.
www.roboticpublications.com
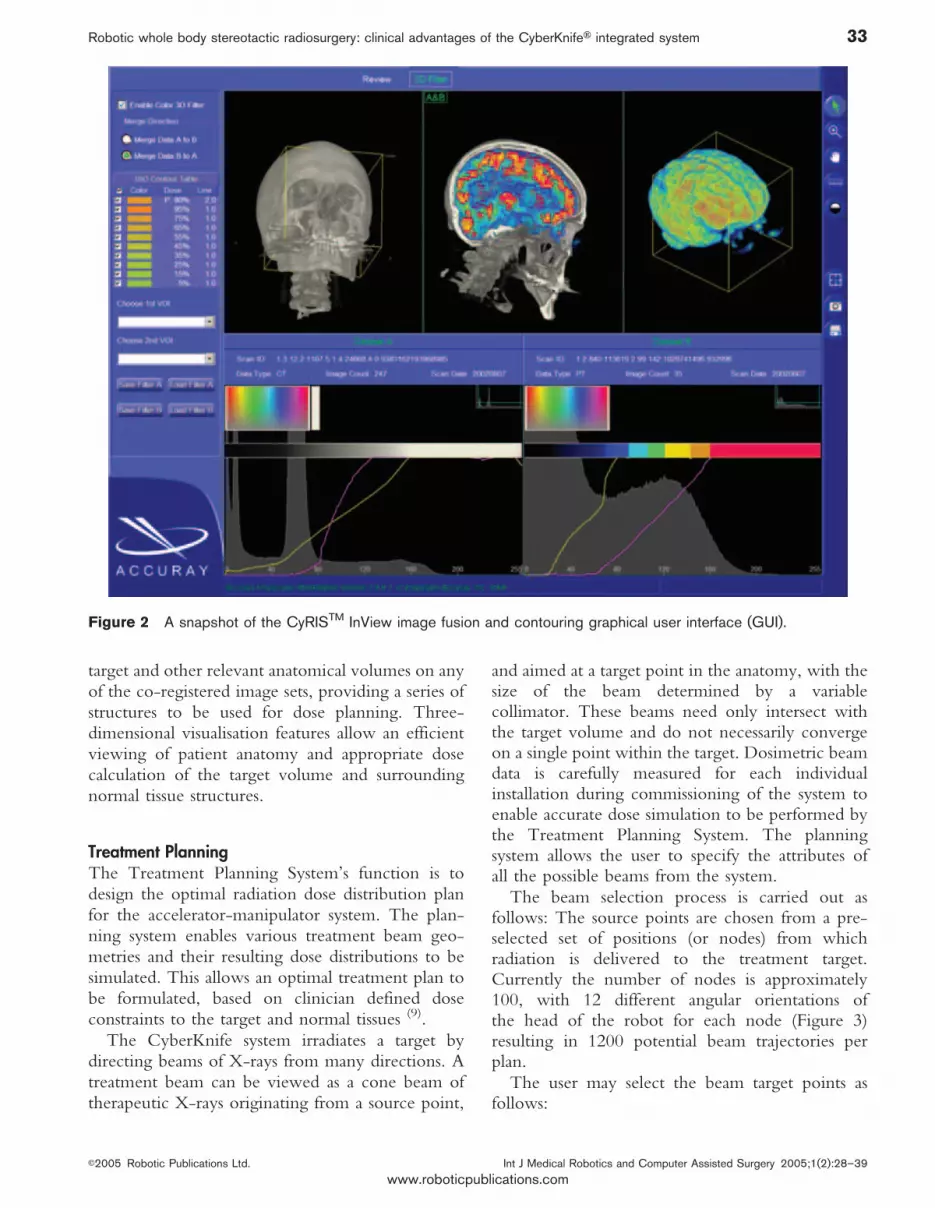
target and other relevant anatomical volumes on anyof the co-registered image sets, providing a series ofstructures to be used for dose planning. Three-dimensional visualisation features allow an efficientviewing of patient anatomy and appropriate dosecalculation of the target volume and surroundingnormal tissue structures.
Treatment PlanningThe Treatment Planning System’s function is todesign the optimal radiation dose distribution planfor the accelerator-manipulator system. The plan-ning system enables various treatment beam geo-metries and their resulting dose distributions to besimulated. This allows an optimal treatment plan tobe formulated, based on clinician defined doseconstraints to the target and normal tissues (9).
The CyberKnife system irradiates a target bydirecting beams of X-rays from many directions. Atreatment beam can be viewed as a cone beam oftherapeutic X-rays originating from a source point,
and aimed at a target point in the anatomy, with thesize of the beam determined by a variablecollimator. These beams need only intersect withthe target volume and do not necessarily convergeon a single point within the target. Dosimetric beamdata is carefully measured for each individualinstallation during commissioning of the system toenable accurate dose simulation to be performed bythe Treatment Planning System. The planningsystem allows the user to specify the attributes ofall the possible beams from the system.
The beam selection process is carried out asfollows: The source points are chosen from a pre-selected set of positions (or nodes) from whichradiation is delivered to the treatment target.Currently the number of nodes is approximately100, with 12 different angular orientations ofthe head of the robot for each node (Figure 3)resulting in 1200 potential beam trajectories perplan.
The user may select the beam target points asfollows:
Figure 2 A snapshot of the CyRISTM InView image fusion and contouring graphical user interface (GUI).
Robotic whole body stereotactic radiosurgery: clinical advantages of the CyberKnifeH integrated system 33
E2005 Robotic Publications Ltd. Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39
www.roboticpublications.com

1. Single Centre Planning: A single target pointis to be used by all the beams. This processresults in an approximately spherical dosedistribution.
2. Multiple Centre Planning: Multiple (up to ten)target points are to be used by the multiplebeams. This process is used for the treatment ofmultiple lesions with spherical distributions ormultiple spherical treatments for a single irre-gular lesion.
3. Conformal Planning: Multiple independent tar-get points are distributed according to thegeometry of the lesion (i.e. each beam is targetedat a different point within the target volume).This process results in highly conformal dosedistributions.
One or more secondary collimators can be usedto give the beams the diameter required to achievethe desired clinical result. Beam trajectories andrelative weights must then be assigned. In forwardplanning, the beam-weights for each beam areselected by the user and an algorithm computesthe dose distribution. In inverse planning, thealgorithm incorporates a two step process to arriveat the desired dose distribution. First, the system
adjusts the robot’s angular orientation for each nodalposition such that the beam’s central axis intersectsthe target volume. Next, the algorithm computesthe weights for each beam so that the compositedose from all beams complies with the doseconstraints for each volume of interest (target andcritical structures). The resulting dose distribution isdisplayed on the monitor and can be fine tuned andthen stored in the patient’s files as shown (Figure 4)
The treatment plan computed as a result of theabove beam selection and weighting processes isthen converted into a set of paths that the roboticmanipulator can safely follow. The treatmentinformation is in turn communicated to the deliverysystem for treatment.
Registration: Patient alignment and targetlocalisationThe graphical user interface (GUI) of the maintreatment delivery software is the primary controlpoint of the CyberKnife operational system. It is atthe heart of the integrated architecture approach.The treatment delivery software initiates andmonitors operations in the different subsystems.During treatment delivery, the software monitorsthe system status and safety controls, reports errors,manages the patient database and records treatmentdata log files for post-treatment assessment andanalysis.
Registration makes use of the localization systemcomposed of two diagnostic X-ray beams and twoamorphous silicon plates, orthogonally positioned.They provide near real-time digital X-ray images ofthe patient in the treatment position. After verifica-tion of the target position, this subsystem providesthe requested information to the control algorithmsallowing them to dynamically reposition the patienttable and/or the manipulator arm. Afterwards, thetreatment will then be activated and the 6MV beamscan be triggered iteratively as calculated during theplanning phase.
The system uses a movable table to support thepatient. The table, with imbedded safety switches,can be moved automatically in five orientations(three translations and two rotations). The finalrotational movement can be applied manually.Figure 1 illustrates the overall system configurationfor patient alignment and target localization.
The comparison of the real time orthogonal [leftanterior oblique (LAO) and right anterior oblique
Figure 3 Sample available nodal locations within apartial spherical surface around the patient, for anintracranial radiosurgical procedure.
34 Coste-Maniere, Olender, Kilby, Schulz
Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39 E2005 Robotic Publications Ltd.
www.roboticpublications.com

(RAO)] X-ray images and the digitally recon-structed radiographs (DRRs) in the same LAO andRAO positions from the preoperatively obtainedCT scans is highly accurate and eliminates therequirement for frame based stereotactic treatment.Replacing the function of frame based systemsprovides greater comfort to the patient andallows for treatments of multiple fractions whereindicated. Either bones or fiducials can be localizedand registered to the perioperative images inreal-time.
A table of DRRs samples the full range of motionof the target centre with six degrees of freedom. Theregistration process verifies that the real-time imagesrepresent an acceptable position within the rangesampled by the reference images. It interpolates theactual position and orientation of the real imagewith respect to the reference. The correct treatmentis obtained in two stages: i) prior to treatment,approximate alignment is obtained by automatic ormanual repositioning of the table, and ii) finalalignment during treatment is achieved by auto-matic adjustment of the robot’s position.
After the initial registration is performed, thesoftware tracks the target centre, via the fiducials orbony landmarks of the skull and sends any positionalcorrection data to the manipulator.
Surgical guidance: 6D skull tracking and 6D fiducialtrackingTracking the full range of motion of the targetcentre is feasible with six degrees of freedom definedin the CT image reference frame. Skull or fiducialtracking is performed using an image processingalgorithm which compares pairs of live orthogonal(LAO/RAO) images to sets of equivalent referenceimages generated from the preoperative CT scan.Both rotational and translational movements of thepatient can be tracked for enhanced treatmentaccuracy.
During initial patient alignment, translational androtational information is displayed on the patientalignment screen of the control monitor. Thetracking information is then used to assist theoperator in aligning the patient manually or maybe used as inputs to the automatic alignment featureprovided by the Axum, five-degree of freedom,patient table. During treatment, changes in align-ment within certain limits (¡10 mm in x, y and z;¡1˚ pitch and roll, ¡3˚ yaw) are compensated forautomatically by the robot. If a movement exceedsthese limits an error warning is triggered allowingthe system to pause for patient realignment.
Fiducial tracking enables treatment in bodyregions other than skull. Radiopaque fiducial
Figure 4 Top left image: the patient model with the tumour to be targeted and the spinal cord radiosensitive area.Bottom left: CyberKnife radiation beams for treatment. Right: Isodose lines for treatment.
Robotic whole body stereotactic radiosurgery: clinical advantages of the CyberKnifeH integrated system 35
E2005 Robotic Publications Ltd. Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39
www.roboticpublications.com

markers (small gold seeds or stainless steel screws) areimplanted in close proximity to, or within, thelesion one to seven days prior to preoperativeimaging. Based on these reference points, thefiducial tracking algorithm searches the pair ofX-ray images, detects the fiducial markers, andcalculates translations and rotations of the target. Aswith skull tracking, when the specified limits areexceeded the system pauses for manual realignment.
While only one fiducial is required to trackanatomical translations, three or more are necessaryto compute both translational and rotationalmotions. Fiducial locations are detected in the X-ray images and motion is computed by comparingtheir positions to the preoperative position of thefiducials as computed in the DRR (Figure 6)
Surgical guidance: with or without compensation forrespirationThe CyberKnife system uses a six-axis manipulatorfor positioning and manoeuvring the compact
X-band 6MV linear accelerator to up to 1200treatment positions defined in the treatment plan-ning phase. Interchangeable collimators, rangingfrom 5 mm to 60 mm in diameter, deliver radiationin corresponding circular fields at the treatmentdistance. High end multi-processor computersprovide the computational power to control thedevice for treatment delivery according to thetreatment plan.
The robotic manipulator (Figure 7) is capable ofpositioning the linear accelerator and pointing thebeam at the treatment target within a treatmenthemisphere at a source to axis distance (SAD)ranging from 100 cm to 65 cm. The robotictargeting precision is better than 0.2 mm. Theoverall precision of treatment delivery (CT, treat-ment planning, image guidance, robot and linearaccelerator), is better than 0.95 mm (10) for cranial/spinal lesions and 1.5 mm for moving targets trackedwith the SynchronyTM respiratory tracking module.More recent multi-center phantom studies for spinal
Figure 5 Synchrony Tumor Tracking: The combination of the LED camera system, the LEDs on the patient vest, theDRR derived images and real time LAO/RAO images allow for real time dose delivery to the tumor (Insert).
36 Coste-Maniere, Olender, Kilby, Schulz
Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39 E2005 Robotic Publications Ltd.
www.roboticpublications.com

radiosurgery report a mean error of 0.7¡0.3 mm,a treatment delivery precision of 0.3¡0.1 mm, anda spine fiducial tracking error of ,0.3 mm for radialtranslations of up to 14 mm and ,0.7 mm forrotations of up to 4.5˚ (11).
Early robot designs assumed fixed targets andenvironments. Likewise early surgical robotsassumed that the anatomy was a rigid target. Theability to sense and react to soft tissue motion (12)
which eluded surgical robot design in the past hasbeen solved with Synchrony. Synchrony is anautomated lesion tracking system which tracks bothexternal and internal fiducials during the course oftreatment and modifies the beam position, in realtime, during that tracking process (Figure 5).Traditionally, compensating for respiratory motionof tumours involved including safety marginsaround the tumour of up to 2 cm or more in thetreatment (13, 14). With Synchrony, these marginsare significantly reduced, allowing treatment ofsmaller volumes and the associated sparing ofadjacent normal tissues. This motion trackingsubsystem provides the capability to maintain thesystem’s high dose conformality index (CI) while
simultaneously treating targets that move withrespiration. The manipulator arm is dynamicallycontrolled, compensating for target motion due torespiration, while radiation is being delivered.
The Synchrony respiratory tracking subsystem isone of the most advanced subsystems within theCyberKnife system’s product configuration (15).With Synchrony, implanted fiducials measureinternal tumour movement. This is accomplishedas follows. Fiducials are imaged preoperativelyduring the CT scan. During perioperative proce-dures, fiducials are imaged, detected and locatedusing the pair of orthogonal diagnostic X-rayimages. The indirectly computed preoperativeCT-based LAO and RAO DRR images are thenco-registered to the continuously acquired perio-perative LAO and RAO images.
Multiple light emitting diodes (LEDs) are fibreoptically connected to optical lenses strategicallypositioned on the patient’s chest and/or abdomen.These light sources are monitored in real time (32frames per second) by 3 Charged Coupled Device(CCD) cameras, housed in a single structureand mounted on the ceiling. Classic localization
Figure 6 An example of fiducial tracking is shown on the left part of this snapshot of the user interface during spinesurgery. The left images are DRR images generated from a preoperative CT scan. The middle images correspond to thetwo orthogonal real time X-ray images acquired while the patient was on the treatment table. The right set of images is theoverlay of the two previous images.
Robotic whole body stereotactic radiosurgery: clinical advantages of the CyberKnifeH integrated system 37
E2005 Robotic Publications Ltd. Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39
www.roboticpublications.com

algorithms are used to accurately measure thelocation of each marker in space. Next a corre-spondence model based on the locations of bothimplanted fiducials and LED markers is created. Thiscorrespondence model between internal and exter-nal movements is updated and verified throughoutthe treatment by comparing estimated motions andcurrent locations of the fiducials while delays arecompensated for with a prediction model. Anydisplacement errors higher than a user prescribedvalue, based on an analysis of tumour motion (16),will trigger the system to stop so that adjustmentscan be made before continuing on with radiosurgery.
CLINICAL APPLICATIONS OF CYBERKNIFEHThe CyberKnife radiosurgical system is being usedas a minimally invasive alternative to traditionalsurgery in a variety of clinical areas. It offers aneffective treatment option for patients who cannotundergo traditional open surgery or whose lesionsare inaccessible with traditional surgical approaches.Residual tumours left after partial resection may also
be treated. It has also been used as a boost tostandard radiation therapy and to treat failed surgicalor radiotherapy techniques.
For intracranial conditions, the CyberKnifesystem has been used to radiosurgically treat avariety of tumours such as menigiomas, acousticneuromas, pituitary tumours, and metastases as wellas other abnormalities such as arteriovenous mal-formations (AVMs) and intractable pain such as inTrigeminal Neuralgia. With the SynchronyTM
motion tracking system, tumours in organs movingwith respiration such as lung, pancreas, liver andkidney can be successfully targeted. Other tumoursbased in more rigid body anatomy, where minimalmotion is expected, may be tracked via rigidlyimplanted fiducials including those in the spine,osteosarcomas and prostate. The CyberKnife sys-tem’s range of applications is limited only by theimagination of clinicians who currently have, or willeventually have access to this technology. To date,more than 10,000 patients have benefited from therevolutionary concept of marrying robotics toimage-guided radiosurgery. Scientific presentationsand publications on the clinical advantages of theCyberKnife are numerous – including intracranial(17), spine (18), paediatric (19) prostate (20), pancreas (21),kidney (22) and lung (23)
SUMMARYThe CyberKnife system’s integrated roboticapproach offers compelling treatment optionspreviously unavailable to many cancer patients. Anumber of new clinical applications are currentlybeing explored. For many of clinical conditions, itprovides an alternative to conventional procedures.Its unique features add capabilities to treatmentsotherwise non-existent. By using the combinationof i) a compact X-band linear accelerator, ii)connected to a six-degree of freedom robotic armcapable of freely moving in 3D space, and iii) guidedby real-time images of internal and externalanatomy patients can be treated in a highlyconformal hypo-fractionated radiosurgical manner.These patients do not need cumbersome head-mounted frames required by traditional radiosurgicalsystems for precise and accurate targeting ofintracranial tumours and lesions. Alignment proce-dures are also possible for extracranial treatment siteswhich are not accessible with frame based systems.The motion-tracking algorithm integrated withinthe Synchrony subsystem allows one to safely
Figure 7 Six axes of robotic arm motion provideunparalleled radiation beam directionality for maximumdose weighting and optimal dose conformality, especiallyfor complex lesion shapes.
38 Coste-Maniere, Olender, Kilby, Schulz
Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39 E2005 Robotic Publications Ltd.
www.roboticpublications.com

compensate for respiratory induced motion duringradiation delivery procedures.
The CyberKnife system’s unique features and itswide array of treatment capabilities are currentlybeing assessed by visionary clinicians for a widerange of clinical conditions. Dramatic patientbenefits have already been demonstrated in a broadrange of clinical areas, and there is considerableanticipation regarding its further adoption intomany new clinical areas.
REFERENCES1 Brady M, Paul R. Robotics Research: The First International
Symposium, The intelligent connection of perception toaction. Artificial Intelligence, MIT press, 1984.
2 Adler Jr. JR. Surgical guidance now and in the future: Thenext generation of instrumentation. Clin Neurosurg.2002;49:105–14.
3 Adler JR. Frameless radiosurgery. In: Goetsch SJ, De SallesAAF, editors. Stereotactic Surgery and Radiosurgery.Wisconsin: Medical Physics Publishing; 1993;17:237–248.
4 Coste-Maniere E, Simmons R. Architecture: the backbone ofrobotic systems. Proceedings of IEEE InternationalConference of Robotics and Automation, ICRA2000. SpecialSession in Control Architecture; 2000 Apr; San Francisco,USA. IEEE; 2000. p 67–72.
5 Levin S. Accuray: Tightly Targeting Tumours. In Vivo: thebusiness and medicine report. Windhover Information Inc.2001;19(04).
6 Adhami L., Coste-Maniere E. A versatile system for computerintegrated mini-invasive robotic surgery. In: Dohi T, Kikinis Reditors. Lecture Notes in Computer Sciences, Medical ImageComputing and Computer Assisted Intervention(MICCAI’02). Springer-Verlag. 2002;2488:272–281.
7 Stancanello J, Cavedon C, Francescon P, Cerveri P, FerrignoG, Colombo F et al. Development and Validation of a CT-3Drotational angiography registration method for AVMradiosurgery. Medical Physics. June 2004;31(6):1363–71.doi:10.1118/1.1751252
8 Sonka M, Fitzpatrick JM. Handbook of Medical Imaging, Vol2. Medical Image Processing and Analysis, SPIE-International Society for Optical Engine; June 2000.
9 Schweikard A, Adler JR, Latombe JC. Motion planning instereotaxic radiosurgery. IEEE Transactions on Robotics andAutomation. 1993;9(6):764–774.doi:10.1109/70.265920
10 Chang SD, Main W, Martin DP, Gibbs IC, Heilbrun MP. Ananalysis of the accuracy of the CyberKnife: a roboticframeless stereotactic radiosurgical system. Neurosurgery.
2003;52(1):140–7.doi:10.1097/00006123-200301000-00018
11 Yu C, Main W, Taylor D, Kuduvalli G, Wang MY, Apuzzo MLJ,et al. An Anthropomorphic Phantom Study of the Accuracy ofCyberKnife Spinal Radiosurgery. Neurosurgery. Nov2004;55:1138–49.doi:10.1227/01.NEU.0000141080.54647.11
12 Taylor RH, Stoianovici D. ‘‘Medical Robotics in Computer-Integrated Surgery’’, IEEE Transactions on Robotics andAutomation. 2003;19(5):765–81.doi:10.1109/TRA.2003.817058
13 Wong JW, et al. Int J Radiat Oncol Biol Phys.1999;44(4):911–19.doi:10.1016/S0360-3016(99)00056-5
14 Dawson L, et al. Int J Radiat Oncol Biol Phys.2001;51(5):1410–21.doi:10.1016/S0360-3016(01)02653-0
15 Schweikard A, Glosser G, Bodduluri M, Murphy MJ, Adler JR.Robotic motion compensation for respiratory movementduring radiosurgery. Computer Aided Surgery.2000;5(4):263–77.
16 Murphy MJ. Tracking moving organs in real time. SeminRadiat Oncol. Jan 2004;14(1):91–100.doi:10.1053/j.semradonc.2003.10.005
17 Chang SD, Lee E, Sakamoto GT, Brown NP, Adler JR.Stereotactic radiosurgery in patients with multiple brainmetastases. Neurosurgical Focus. 2000;9(2):Article 3.
18 Gerszten PC, Ozhasoglu C, Burton SA, Vogel W, Atkins BKalnicki S, et al. CyberKnife frameless stereotacticradiosurgery for spinal lesions: Clinical experience in 125patients. Neurosurgery. 2004;55(1):1–11.
19 Giller CA, Berger BD, Gilio JP, Delp JL, Gall KP, Weprin B, etal. Feasibility of Radiosurgery for Malignant Brain Tumors inInfants by Use of Image-Guided Robotic Radiosurgery:Preliminary Report. Neurosurgery. Oct 2004;55(4):916–25.doi:10.1227/01.NEU.0000137332.03970.57
20 King CR, Lehmann J, Adler JR, Hai J. CyberKnife radiotherapyfor localized prostate cancer: rationale and technicalfeasibility. Technology in Cancer Research & Treatment.2003;2(1):25–9.
21 Koong AC, Le QT, Ho A, Fong B, Fisher G, Cho C, et al.Phase I Study of Stereotactic Radiosurgery in Patients withLocally Advanced Pancreatic Cancer. Int J RadiationOncology Bio Phys. 2004;58(4):1017–21.doi:10.1016/j.ijrobp.2003.11.004
22 Ponsky LE, Crownover RL, Rosen MJ, Rodebaugh RF,Castilla EA, Brainard J, et al. Initial evaluation of CyberKnifetechnology for extracorporeal renal tissue ablation. Urology.2003;61(3):498–501.doi:10.1016/S0090-4295(02)02442-1
23 Whyte RI, Crownover R, Murphy MJ, Martin DP, Rice TW,DeCamp MM Jr, et al. Stereotactic radiosurgery for lungtumours: Preliminary report of phase I trial. Ann ThoracicSurg. 2003;75(4):1097–1101.doi:10.1016/S0003-4975(02)04681-7
Robotic whole body stereotactic radiosurgery: clinical advantages of the CyberKnifeH integrated system 39
E2005 Robotic Publications Ltd. Int J Medical Robotics and Computer Assisted Surgery 2005;1(2):28–39
www.roboticpublications.com
Related Documents











