ROBIN LUNGE DIRECTOR OF HEALTH CARE REFORM NOVEMBER 18, 2011 Integration of Medicaid and the Exchange

ROBIN LUNGE DIRECTOR OF HEALTH CARE REFORM NOVEMBER 18, 2011 Integration of Medicaid and the Exchange.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
ROBIN LUNGEDIRECTOR OF HEALTH CARE REFORM
NOVEMBER 18 , 2011
Integration of Medicaid and the Exchange
Purpose & Agenda
Overview of issues & options for how to integrate Medicaid and the Exchange
Summary of analysis underwayYour thoughts and input!

Goals
Universal coverage (for low and moderate income Vermonters)
Comprehensive High Quality Benefits / Innovative services to meet individuals’ needs
Focus on Better Consumer ExperienceProvider Access and QualityPayment ReformSimplified AdministrationControlling Health Care Costs

STAGE 3:
Vermont Single Payer (2017 and
beyond – 2014 if ACA waiver date
changed in
federal law)
Two financing plans
developed for
universal
coverage under: 1.
Green Mountain Care (single payer) and 2.
Exchange –
report back to legislatu
re in 2013
STAGE 2:
Vermont Health Benefit Exchan
ge become
s operatio
nal (2014)
Integration Plan Developed for
“Single Payer
Exchange” – report back to legislature in 2012
STAGE 1:
Vermont Health Benefit Exchange and Vermont Health Reform Board
(established
2011)
Stages of Vermont Health Reforms

Medicaid Changes in 2014
Medicaid income eligibility increases to 133% FPL $1226/month
Income calculation changes for some people “MAGI” – modified adjusted gross income from tax
returnMore verification done electronically
Reduction in paperwork, we hope!!Web-based enrollment
Can still do phone & in person

Health Benefits Exchange in 2014
Individuals without employer-sponsored insurance
Small businesses & their employeesFederal tax subsidies for people with incomes
under 400% FPL $3684/month

Medicaid & the Exchange in 20147
What happens to VHAP, Catamount Health, and employer-sponsored insurance assistance? Individuals with incomes under 133% move to Medicaid Individuals with incomes over this amount – either
Basic Health Plan (option – next slide more details) Health Benefit Exchange with subsidies
Very much like Catamount Health & ESIA
What happens to coverage for individuals with disabilities and seniors? This coverage need not change Anticipate filing Medicaid waiver request to continue
coverage for certain populations currently covered

Children <19
SSI (Aged, Blind and Disabled)
Parents and Caretaker Relatives
Pregnant Women
Und
rinsurdM
edicaid
UninsuredC
HIP
Adults ≥19 but < 65 Medically Needy
QHP without Subsidy
Medicare
PIL
SSI Income Level
AFDC
QHP with Tax Credits Only
300%
400%
225%
Vermont Health Benefit Programs
Options Under Consideration
QHP with Tax Credits and Cost-Sharing
250%
200%
133%
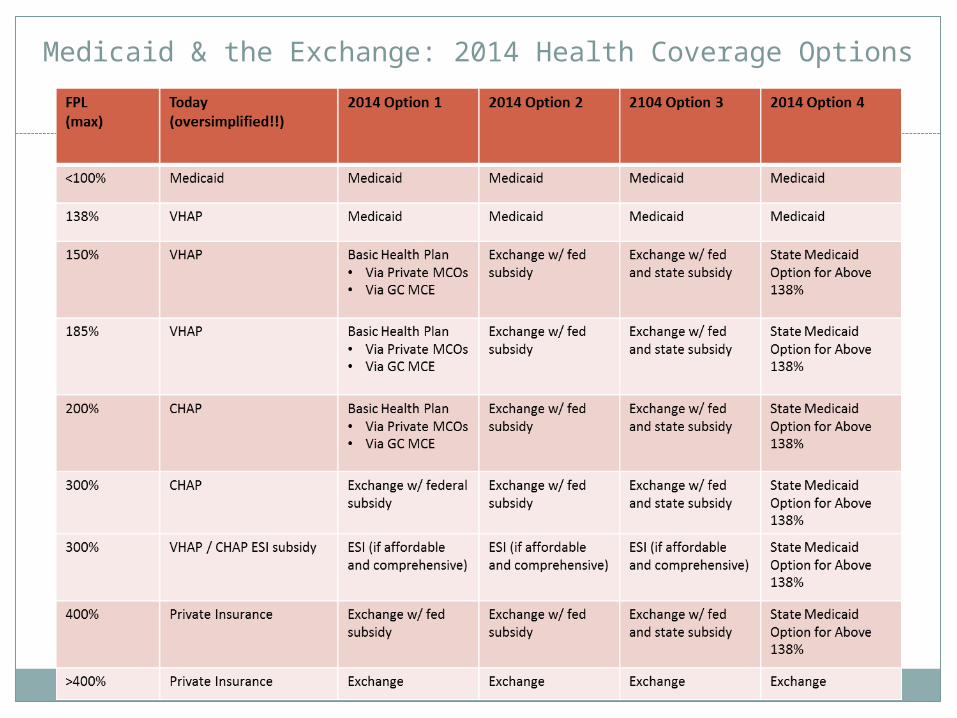
Medicaid & the Exchange: 2014 Health Coverage Options
Exchange with federal subsidies
100% federal funds In process of creating complete financial model
Premiums are lower than VHAP/CHAP for very low income & for 2 person families
Premiums are a bit higher at upper income levels of CHAP

Comparison of Subsidies: Exchange Subsidy & Current Vermont
Exchange with federal subsidies12
Cost-sharing (deductibles, co-payments, co-insurance) Higher in Exchange than for VHAP
Approx. 70-80% of people in VHAP move to Medicaid VHAP has no deductible or co-insurance, limited co-pays
Hard to compare CHAP & Catamount Need detailed benefit designs to compare deductibles,
etc Out of pocket maximums (total you MIGHT have to pay)
higher in the Exchange w/ subsidy than Catamount Health
Provider rates – by insurer
Possible solutions to cost-sharing issues
State subsidy “wrap” in addition to federal subsidy Similar to wrap for employer-sponsored insurance
program now Could provide additional assistance so people don’t
have dramatic increases In process of costing this out
Flexibility in income phase-out 60-40 if included in new Medicaid waiver request
Basic Health Plan (see next slides)

Basic Health Plan
95% federal funds that would have been received in Exchange
More protective of consumers financially More chance of people losing coverage due to
transitionsImpacts on Exchange financial sustainability
& viabilityProvider rates uncertain at this point
Could be Medicaid; could be Catamount Health level; could be private insurance level

Medicaid Option above 133%
May cover populations above 133% in Medicaid
60/40 fed/state split More expensive – lose 100% fed funds
Issues with Exchange viability and sustainability
Provider rates at Medicaid level
Related Documents











