For personal use only. Reproduce with permission from The Lancet Publishing Group. ARTICLES 592 THE LANCET • Vol 357 • February 24, 2001 Summary Background Risk factors for lipodystrophy in patients infected with HIV-1 treated with highly active antiretroviral therapy (HAART) containing HIV-1 protease inhibitors are poorly understood. We aimed to identify the risk factors for lipodystrophy in antiretroviral-naïve HIV-1-infected adults on HAART. Methods Moderate or severe body-fat changes were clinically assessed and categorised as subcutaneous lipoatrophy, central obesity, or both, in all consecutive antiretroviral-naïve HIV-1-infected adults who began HAART with two nucleoside reverse transcriptase inhibitors plus at least one protease inhibitor from October, 1996, to September, 1999. A person- years analysis was used to calculate the incidence of types of lipodystrophy, and Cox proportional hazards models were used to describe the univariate and multivariate factors associated with progression to any lipodystrophy. Findings After a median follow-up of 18 months, 85 (17%) of the 494 patients developed some type of lipodystrophy. The incidences of any lipodystrophy, lipodystrophy with subcutaneous lipoatrophy, and lipodystrophy with central obesity were 11·7 (95% CI 9·2–14·2), 9·2 (7·0–11·4), and 7·7 (5·7–9·7) per 100 patient-years. An increased risk for any lipodystrophy was found among women as compared with men (relative hazard 1·87 [1·07–3·28]), heterosexuals (2·86 [1·50–5·48]), and homosexuals (2·17 [1·07–4·42]) as compared with intravenous drug users, with increasing age (1·33 per 10 years older [1·08–1·62]), and with the duration of exposure to antiretroviral therapy (1·57 per 6 months extra [1·30–1·88]) but not with any individual antiretroviral agent. The factors associated with an increased risk for lipodystrophy with subcutaneous lipoatrophy or lipodystrophy with central obesity were very similar to those associated with any lipodystrophy. The duration of indinavir use may represent an additional contribution for the development of lipodystrophy with central obesity (1·26 per 6 months extra [0·99–1·60]); p0·064). Interpretation Risk factors associated with development of any lipodystrophy, lipodystrophy with subcutaneous lipoatrophy, and lipodystrophy with central obesity in patients infected with HIV-1 who were receiving HAART containing protease inhibitors are multifactorial and overlapping, and cannot be exclusively ascribed to the duration of exposure to an particular antiretroviral agent. Lancet 2001; 357: 592–98 Introduction After the publication of several case reports, abnormal fat distribution in HIV-1-infected patients receiving antiretroviral therapy was formally described as a clinical entity in 1998, under the name of lipodystrophy syndrome. 1 Soon after lipodystrophy was recognised as one of the major limiting factors for long-term antiretroviral therapy. Initially described as a single entity, at least two different syndromes were found to exist: lipoatrophy or loss of subcutaneous fat; 2 and central or visceral fat accumulation. 3 Despite the difficulties in defining lipodystrophy, a high level of concordance has been seen between the doctor and patient diagnosis of moderate or severe lipodystrophy and the results of dual-energy X-ray absorptiometry (DEXA) 4 or sonography. 5 Lipodystrophy was initially considered to be only due to HIV-1 protease inhibitors. 6 However, lipodystrophy does not invariably develop in all patients treated with protease inhibitors and it has been also described in patients who had never received protease inhibitors. Moreover, reversion of lipodystrophy does not occur after withdrawal of protease inhibitors. 7,8 More recently, several studies have linked the development of lipodystrophy with specific nucleoside reverse transcriptase inhibitors (NRTI). 9–13 Interference with the lipid metabolism and mitochondrial toxicity associated with protease inhibitors 6 and NRTI, 14 respectively, are postulated to be involved in the pathogenesis of lipodystrophy. Current studies on risk factors for lipodystrophy have important design limitations. 4,9–13 Small and sometimes biased population samples have been included, or cross- sectional analysis of mixed retrospective and prospectively followed cohort have been done. In addition, antiretroviral agents have usually been included in the analysis either as the initial prescribed drugs or as the current drugs when the analysis was undertaken. We report on a prospective cohort study specifically designed to identify risk factors for moderate or severe lipoatrophy and fat accumulation including total exposition to individual antiretroviral agents in a large, unselected sample of antiretroviral-naive patients who were started on highly active antiretroviral therapy (HAART) including two NRTI plus at least one protease inhibitor. Methods Patients All consecutive antiretroviral-naive HIV-1-infected adults who started triple therapy with two NRTIs plus at least one protease inhibitor from October, 1996, to September, 1999, were eligible if they granted oral informed consent to be assessed for clinical lipodystrophy at baseline and in subsequent routine medical visits. Data on body changes Risk of lipodystrophy in HIV-1-infected patients treated with protease inhibitors: a prospective cohort study Esteban Martinez, Amanda Mocroft, Miguel A García-Viejo, José B Pérez-Cuevas, José L Blanco, José Mallolas, Luis Bianchi, Ignacio Conget, Jordi Blanch, Andrew Phillips, José M Gatell Department of Infectious Diseases (E Martínez MD, M A García-Viejo MD, J B Pérez-Cuevas MD, J L Blanco MD, J Mallolas MD, J Blanch MD, J M Gatell MD), Radiology (L Bianchi MD), and Endocrinology (I Conget MD), Institut d’Investigacions Biomèdiques August Pi i Sunyer Hospital Clínic Universitari, Barcelona 08036, Spain; and Royal Free Centre for HIV Medicine and Department of Primary Care and Population Sciences, Royal Free and University College Medical School, University College London, London NW3 2PF, UK (A Mocroft PhD, A Phillips MD) Correspondence to: Dr Esteban Martínez, Infectious Diseases Unit, Hospital Clínic, C/Villarroel 170, 08036 Barcelona, Spain (e-mail: [email protected])

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

For personal use only. Reproduce with permission from The Lancet Publishing Group.
ARTICLES
592 THE LANCET • Vol 357 • February 24, 2001
Summary
Background Risk factors for lipodystrophy in patients infectedwith HIV-1 treated with highly active antiretroviral therapy(HAART) containing HIV-1 protease inhibitors are poorlyunderstood. We aimed to identify the risk factors forlipodystrophy in antiretroviral-naïve HIV-1-infected adults onHAART.
Methods Moderate or severe body-fat changes were clinicallyassessed and categorised as subcutaneous lipoatrophy,central obesity, or both, in all consecutive antiretroviral-naïveHIV-1-infected adults who began HAART with two nucleosidereverse transcriptase inhibitors plus at least one proteaseinhibitor from October, 1996, to September, 1999. A person-years analysis was used to calculate the incidence of types oflipodystrophy, and Cox proportional hazards models wereused to describe the univariate and multivariate factorsassociated with progression to any lipodystrophy.
Findings After a median follow-up of 18 months, 85 (17%) ofthe 494 patients developed some type of lipodystrophy. Theincidences of any lipodystrophy, lipodystrophy withsubcutaneous lipoatrophy, and lipodystrophy with centralobesity were 11·7 (95% CI 9·2–14·2), 9·2 (7·0–11·4), and7·7 (5·7–9·7) per 100 patient-years. An increased risk for anylipodystrophy was found among women as compared withmen (relative hazard 1·87 [1·07–3·28]), heterosexuals (2·86[1·50–5·48]), and homosexuals (2·17 [1·07–4·42]) ascompared with intravenous drug users, with increasing age(1·33 per 10 years older [1·08–1·62]), and with the durationof exposure to antiretroviral therapy (1·57 per 6 months extra[1·30–1·88]) but not with any individual antiretroviral agent.The factors associated with an increased risk forlipodystrophy with subcutaneous lipoatrophy or lipodystrophywith central obesity were very similar to those associated withany lipodystrophy. The duration of indinavir use may representan additional contribution for the development oflipodystrophy with central obesity (1·26 per 6 months extra[0·99–1·60]); p�0·064).
Interpretation Risk factors associated with development ofany lipodystrophy, lipodystrophy with subcutaneouslipoatrophy, and lipodystrophy with central obesity in patientsinfected with HIV-1 who were receiving HAART containing
protease inhibitors are multifactorial and overlapping, andcannot be exclusively ascribed to the duration of exposure toan particular antiretroviral agent.
Lancet 2001; 357: 592–98
IntroductionAfter the publication of several case reports, abnormalfat distribution in HIV-1-infected patients receivingantiretroviral therapy was formally described as a clinicalentity in 1998, under the name of lipodystrophysyndrome.1 Soon after lipodystrophy was recognised as oneof the major limiting factors for long-term antiretroviraltherapy. Initially described as a single entity, at least twodifferent syndromes were found to exist: lipoatrophy orloss of subcutaneous fat;2 and central or visceral fataccumulation.3 Despite the difficulties in defininglipodystrophy, a high level of concordance has been seenbetween the doctor and patient diagnosis of moderate orsevere lipodystrophy and the results of dual-energy X-rayabsorptiometry (DEXA)4 or sonography.5
Lipodystrophy was initially considered to be only due toHIV-1 protease inhibitors.6 However, lipodystrophy doesnot invariably develop in all patients treated with proteaseinhibitors and it has been also described in patients whohad never received protease inhibitors. Moreover,reversion of lipodystrophy does not occur after withdrawalof protease inhibitors.7,8 More recently, several studies havelinked the development of lipodystrophy with specificnucleoside reverse transcriptase inhibitors (NRTI).9–13
Interference with the lipid metabolism and mitochondrialtoxicity associated with protease inhibitors6 and NRTI,14
respectively, are postulated to be involved in thepathogenesis of lipodystrophy.
Current studies on risk factors for lipodystrophy haveimportant design limitations.4,9–13 Small and sometimesbiased population samples have been included, or cross-sectional analysis of mixed retrospective and prospectivelyfollowed cohort have been done. In addition, antiretroviralagents have usually been included in the analysis either asthe initial prescribed drugs or as the current drugs whenthe analysis was undertaken.
We report on a prospective cohort study specificallydesigned to identify risk factors for moderate or severelipoatrophy and fat accumulation including totalexposition to individual antiretroviral agents in a large,unselected sample of antiretroviral-naive patients whowere started on highly active antiretroviral therapy(HAART) including two NRTI plus at least one proteaseinhibitor.
MethodsPatientsAll consecutive antiretroviral-naive HIV-1-infected adultswho started triple therapy with two NRTIs plus at leastone protease inhibitor from October, 1996, to September,1999, were eligible if they granted oral informed consentto be assessed for clinical lipodystrophy at baseline and insubsequent routine medical visits. Data on body changes
Risk of lipodystrophy in HIV-1-infected patients treated withprotease inhibitors: a prospective cohort study
Esteban Martinez, Amanda Mocroft, Miguel A García-Viejo, José B Pérez-Cuevas, José L Blanco, José Mallolas, Luis Bianchi,Ignacio Conget, Jordi Blanch, Andrew Phillips, José M Gatell
Department of Infectious Diseases (E Martínez MD,M A García-Viejo MD, J B Pérez-Cuevas MD, J L Blanco MD,J Mallolas MD, J Blanch MD, J M Gatell MD), Radiology (L Bianchi MD),and Endocrinology (I Conget MD), Institut d’InvestigacionsBiomèdiques August Pi i Sunyer Hospital Clínic Universitari,Barcelona 08036, Spain; and Royal Free Centre for HIV Medicineand Department of Primary Care and Population Sciences, RoyalFree and University College Medical School, University CollegeLondon, London NW3 2PF, UK (A Mocroft PhD, A Phillips MD)
Correspondence to: Dr Esteban Martínez, Infectious Diseases Unit,Hospital Clínic, C/Villarroel 170, 08036 Barcelona, Spain(e-mail: [email protected])

For personal use only. Reproduce with permission from The Lancet Publishing Group.
ARTICLES
THE LANCET • Vol 357 • February 24, 2001 593
were prospectively collected as part of a protocoladdressed to analyse the incidence of increased abdominalgirth or fat accumulation since the initiation of the study.In June, 1997, when initial data on fat loss and fataccumulation became available15 we introduced a new setof more detailed and specific variables, designed into theprotocol to assess the incidence of both fat accumulationand fat loss. During the period of study, availableantiretroviral agents for routine prescription werezidovudine, zalcitabine, didanosine, stavudine,lamivudine, hard-gel saquinavir, indinavir, and ritonavir.Nelfinavir became available from April, 1998, and patientsstarting on two NRTIs plus nelfinavir were also included.Patients taking nevirapine and two NTIs were notincluded in the present study.
Patients were assessed at baseline and every 3 months bythe same team of doctors. The assessment includedcollecting demographic data, and carrying out a clinicalassessment and physical examination to specifically identifybody-fat changes. Blood analysis at each visit included atleast plasma viral load, CD4-cell count, and fastingglucose, cholesterol, and triglyceride concentrations. Thestudy was done in the AIDS department of a single referralhospital in Barcelona, Spain.
CriteriaLipodystrophy was considered a diagnosis only if body-fatchanges were moderate or severe enough to be clearlyrecognised. For the purpose of this study, we definedmoderate or severe lipodystrophy as changes in body-fatdistribution reported by the patient and confirmed by thedoctor, or identified by the doctor and accepted by thepatient. The opinion of a third person was required in acase of discrepancy.
Body-fat changes were categorised as subcutaneouslipoatrophy (fat loss alone), central obesity(fat accumulation alone), or mixed lipodystrophy (both fatloss and fat accumulation). For the purpose of severalanalyses including the analysis of risk factor forlipodystrophy we classified the patients as: (1)lipodystrophy with subcutaneous lipoatrophy—patientswith fat loss alone or with fat loss plus fat accumulation;and (2) lipodystrophy with central obesity—patients withcentral obesity alone or patients with central obesity plusfat loss. Consequently, those patients with both fat lossand fat accumulation are included in both categories. Thediagnosis of fat loss reported by the patient required theconfirmation of hollow cheeks, prominent superficial veinsin the limbs, or flattening of the buttocks by the doctor.Any complaint by the patient consisting of increasedabdominal girth, breast enlargement, or development ofcervical fat pads was confirmed on examination by thedoctor. When available, previous photographs wererequested to further confirm body changes. Sonography orcomputed tomography was tried out in some patients torule out malignancy, visceromegaly, or ascites. Objectivemeasurements of regional fat were not routinely done.However, regional fat thickness was assessed bysonography as previously described5 in a subgroup ofpatients with lipodystrophy to validate the clinicaldiagnosis of body-fat changes.
Antiretroviral therapy could be modified at thediscretion of the treating physician, and patients remainedin the study as long as the newer regimen containedprotease inhibitors. The censoring date was the medicalvisit performed during the last quarter of 1999. Othercensoring reasons were death, loss to follow-up,withdrawal of protease inhibitors, or development oflipodystrophy—whichever came first.
Statistical analysesThe median baseline values of laboratory markers werecompared between demographic groups by means of thenon-parametric Kruskal-Wallis or Wilcoxon test. Aperson-years analysis was used to calculate the incidenceof lipodystrophy. Follow-up of patients started at the dateof starting HAART and ended at date of censoring or atthe date of developing lipodystrophy. CIs were calculatedusing a normal approximation or the exact Poissondistribution when there was less than 20 events.
A cross-sectional analysis considered whether those thatdeveloped lipodystrophy had a significantly differentchange in any of their markers compared with those whodid not develop lipodystrophy. For each patient, the finalvalue measured immediately before censoring or at thedevelopment of lipodystrophy was compared to the valueat the start of HAART. A further analysis consideredwhether there were any significant differences in change ofthese values according to type of lipodystrophy amongthose patients who developed lipodystrophy. Fourmeasures of change were considered: the absolute changein laboratory marker from baseline, the percentage changein laboratory marker from baseline, the absolute change inlaboratory marker from baseline per month of follow-up,and the percentage change in laboratory marker frombaseline per month of follow-up. All four measures ofchange gave similar results, in terms of significance levels.
Kaplan-Meier analysis was used to identify theproportion of patients estimated to have anylipodystrophy, and specific types of lipodystrophy. Follow-up of patients started at the date of starting HAART andended at date of censoring or the date of developinglipodystrophy. Cox proportional hazards models wereused to describe the univariate and multivariate factorsassociated with progression to any lipodystrophy,progression to lipodystrophy with subcutaneouslipoatrophy, and progression to lipodystrophy with centralobesity. Patient follow-up was up to the first manifestationof lipodystrophy. Time on HAART was the intervalbetween initiation of therapy and censoring. Cumulativeexposure for each individual agent was also calculated foreach patient. In order to include the time on HAART andspecific antiretrovirals in the Cox proportional hazardsmodels, all patients were assigned a dummy date ofstarting HAART of Oct 1, 1996, and were left censoreduntil the date of actually starting HAART. All therecorded variables were considered in univariate analyses,including demographic variables, laboratory values, andchanges to HAART regimens after starting HAART (suchas stopping any antiretroviral or starting any newantiretroviral), included as time-dependent covariates.Any variables which were significant in univariate analyseswith p<0·25 were then included in multivariate analyses.Sensitivity analyses were also done. In particular, bothforward and backward selection models which included allthe recorded variables and with an entry/removal criteriaof p>0·25 identified the same factors related tolipodystrophy. The time on HAART was not adjusted forthe time on each individual drug in the multivariateanalysis, because this was not felt to be appropriate. Allanalyses were done with SAS (version 6.12).
ResultsStudy groupDuring the period of study, 494 antiretroviral-naive adultsstarted HAART containing protease inhibitors. Themedian CD4-lymphocyte count at baseline was204 cells per mm3 (IQR 96–342) and median viral load was4·9 log copies/mL (4·4–5·4). Median known duration of
For personal use only. Reproduce with permission from The Lancet Publishing Group.
ARTICLES
594 THE LANCET • Vol 357 • February 24, 2001
HIV-1 infection was 33 months (3–87), and the mediandate of starting HAART was December, 1997 (May, 1997,to July, 1998). During a median follow-up of 18 months(10–24), 85 (17%) of the patients developedlipodystrophy. There were seven (1%) deaths duringfollow-up. 58 (12%) patients were lost to follow-up, and 18(4%) discontinued protease inhibitors before the end of thestudy for reasons other than developing lipodystrophy.Most patients were men (n=375 [76%]), with roughlyequal proportions of patients infected via intravenous druguse (n=193 [39%]), homosexual (n=140 [28%]), andheterosexual sex (n=136 [28%]). Baseline median glucoseconcentration was higher in men (0·92 g/L) than in women(0·86 g/L), p<0·0001. Baseline median cholesterol waslower in patients infected through intravenous drug use(1·51 g/L) than in those through heterosexual sex(1·65 g/L), homosexual sex (1·66 mg/dL), or other routes(1·62 g/L), p<0·0001. There were no significantdifferences between demographic groups in other baselinelaboratory markers.
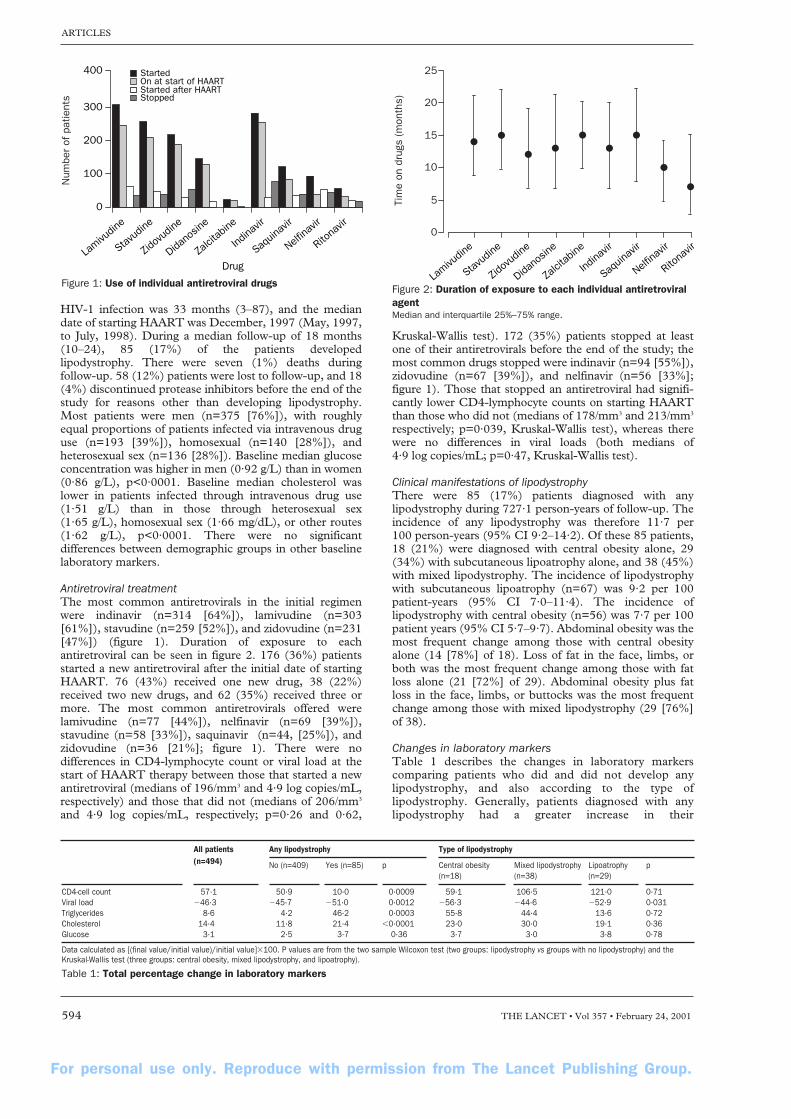
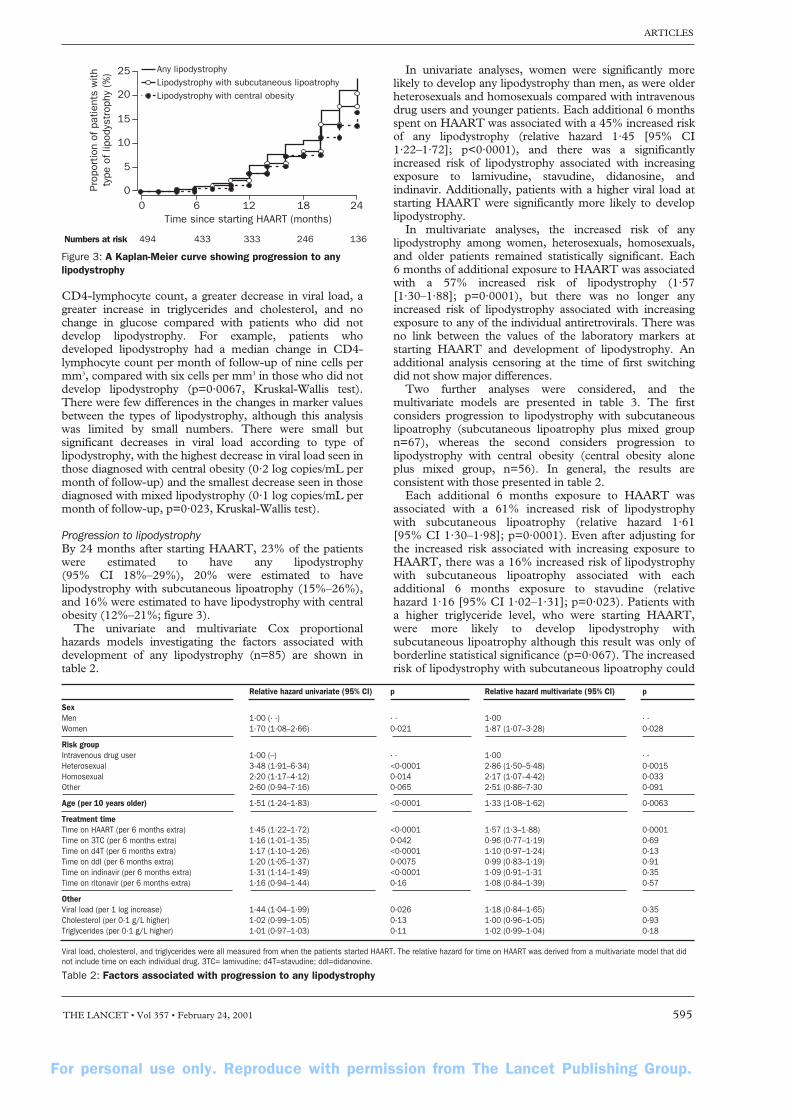
Antiretroviral treatmentThe most common antiretrovirals in the initial regimenwere indinavir (n=314 [64%]), lamivudine (n=303[61%]), stavudine (n=259 [52%]), and zidovudine (n=231[47%]) (figure 1). Duration of exposure to eachantiretroviral can be seen in figure 2. 176 (36%) patientsstarted a new antiretroviral after the initial date of startingHAART. 76 (43%) received one new drug, 38 (22%)received two new drugs, and 62 (35%) received three ormore. The most common antiretrovirals offered werelamivudine (n=77 [44%]), nelfinavir (n=69 [39%]),stavudine (n=58 [33%]), saquinavir (n=44, [25%]), andzidovudine (n=36 [21%]; figure 1). There were nodifferences in CD4-lymphocyte count or viral load at thestart of HAART therapy between those that started a newantiretroviral (medians of 196/mm3 and 4·9 log copies/mL,respectively) and those that did not (medians of 206/mm3
and 4·9 log copies/mL, respectively; p=0·26 and 0·62,
Kruskal-Wallis test). 172 (35%) patients stopped at leastone of their antiretrovirals before the end of the study; themost common drugs stopped were indinavir (n=94 [55%]),zidovudine (n=67 [39%]), and nelfinavir (n=56 [33%];figure 1). Those that stopped an antiretroviral had signifi-cantly lower CD4-lymphocyte counts on starting HAARTthan those who did not (medians of 178/mm3 and 213/mm3
respectively; p=0·039, Kruskal-Wallis test), whereas therewere no differences in viral loads (both medians of4·9 log copies/mL; p=0·47, Kruskal-Wallis test).
Clinical manifestations of lipodystrophyThere were 85 (17%) patients diagnosed with anylipodystrophy during 727·1 person-years of follow-up. Theincidence of any lipodystrophy was therefore 11·7 per100 person-years (95% CI 9·2–14·2). Of these 85 patients,18 (21%) were diagnosed with central obesity alone, 29(34%) with subcutaneous lipoatrophy alone, and 38 (45%)with mixed lipodystrophy. The incidence of lipodystrophywith subcutaneous lipoatrophy (n=67) was 9·2 per 100patient-years (95% CI 7·0–11·4). The incidence oflipodystrophy with central obesity (n=56) was 7·7 per 100patient years (95% CI 5·7–9·7). Abdominal obesity was themost frequent change among those with central obesityalone (14 [78%] of 18). Loss of fat in the face, limbs, orboth was the most frequent change among those with fatloss alone (21 [72%] of 29). Abdominal obesity plus fatloss in the face, limbs, or buttocks was the most frequentchange among those with mixed lipodystrophy (29 [76%]of 38).
Changes in laboratory markersTable 1 describes the changes in laboratory markerscomparing patients who did and did not develop anylipodystrophy, and also according to the type oflipodystrophy. Generally, patients diagnosed with anylipodystrophy had a greater increase in their
400
300
200
100
0
Lamivu
dine
Stavud
ine
Zidov
udine
Didano
sine
Zalci
tabine
Indina
vir
Saquin
avir
Nelfina
vir
Ritona
vir
Drug
StartedOn at start of HAARTStarted after HAARTStopped
Num
ber
of p
atie
nts
Figure 1: Use of individual antiretroviral drugs
25
20
15
10
5
0
Tim
e on
dru
gs (
mon
ths)
Lamivu
dine
Stavud
ine
Zidov
udine
Didano
sine
Zalci
tabine
Indina
vir
Saquin
avir
Nelfina
vir
Ritona
vir
Figure 2: Duration of exposure to each individual antiretroviralagentMedian and interquartile 25%–75% range.
All patients Any lipodystrophy Type of lipodystrophy(n=494) No (n=409) Yes (n=85) p Central obesity Mixed lipodystrophy Lipoatrophy p
(n=18) (n=38) (n=29)
CD4-cell count 57·1 50·9 10·0 0·0009 59·1 106·5 121·0 0·71Viral load �46·3 �45·7 �51·0 0·0012 �56·3 �44·6 �52·9 0·031Triglycerides 8·6 4·2 46·2 0·0003 55·8 44·4 13·6 0·72Cholesterol 14·4 11·8 21·4 �0·0001 23·0 30·0 19·1 0·36Glucose 3·1 2·5 3·7 0·36 3·7 3·0 3·8 0·78
Data calculated as [(final value/initial value)/initial value]�100. P values are from the two sample Wilcoxon test (two groups: lipodystrophy vs groups with no lipodystrophy) and theKruskal-Wallis test (three groups: central obesity, mixed lipodystrophy, and lipoatrophy).
Table 1: Total percentage change in laboratory markers
For personal use only. Reproduce with permission from The Lancet Publishing Group.
ARTICLES
THE LANCET • Vol 357 • February 24, 2001 595
25
20
15
10
5
0Prop
ortio
n of
pat
ient
s w
ithty
pe o
f lip
odys
trop
hy (
%)
0
Numbers at risk
6 12Time since starting HAART (months)
18 24
494 433 333 246 136
Any lipodystrophyLipodystrophy with subcutaneous lipoatrophyLipodystrophy with central obesity
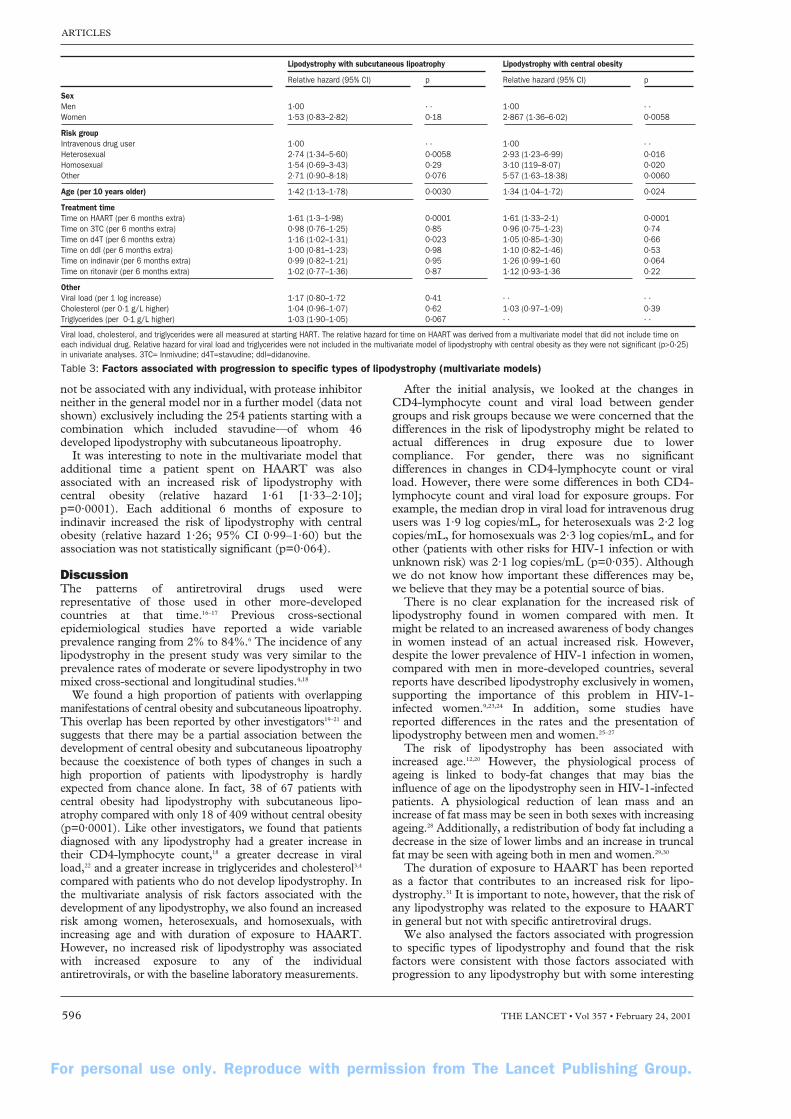
Figure 3: A Kaplan-Meier curve showing progression to anylipodystrophy
Relative hazard univariate (95% CI) p Relative hazard multivariate (95% CI) p
SexMen 1·00 (· ·) · · 1·00 · ·Women 1·70 (1·08–2·66) 0·021 1·87 (1·07–3·28) 0·028
Risk groupIntravenous drug user 1·00 (–) · · 1·00 · ·Heterosexual 3·48 (1·91–6·34) <0·0001 2·86 (1·50–5·48) 0·0015Homosexual 2·20 (1·17–4·12) 0·014 2·17 (1·07–4·42) 0·033Other 2·60 (0·94–7·16) 0·065 2·51 (0·86–7·30 0·091
Age (per 10 years older) 1·51 (1·24–1·83) <0·0001 1·33 (1·08–1·62) 0·0063
Treatment timeTime on HAART (per 6 months extra) 1·45 (1·22–1·72) <0·0001 1·57 (1·3–1·88) 0·0001Time on 3TC (per 6 months extra) 1·16 (1·01–1·35) 0·042 0·96 (0·77–1·19) 0·69Time on d4T (per 6 months extra) 1·17 (1·10–1·26) <0·0001 1·10 (0·97–1·24) 0·13Time on ddI (per 6 months extra) 1·20 (1·05–1·37) 0·0075 0·99 (0·83–1·19) 0·91Time on indinavir (per 6 months extra) 1·31 (1·14–1·49) <0·0001 1·09 (0·91–1·31 0·35Time on ritonavir (per 6 months extra) 1·16 (0·94–1·44) 0·16 1·08 (0·84–1·39) 0·57
OtherViral load (per 1 log increase) 1·44 (1·04–1·99) 0·026 1·18 (0·84–1·65) 0·35Cholesterol (per 0·1 g/L higher) 1·02 (0·99–1·05) 0·13 1·00 (0·96–1·05) 0·93Triglycerides (per 0·1 g/L higher) 1·01 (0·97–1·03) 0·11 1·02 (0·99–1·04) 0·18
Viral load, cholesterol, and triglycerides were all measured from when the patients started HAART. The relative hazard for time on HAART was derived from a multivariate model that didnot include time on each individual drug. 3TC= lamivudine; d4T=stavudine; ddI=didanovine.
Table 2: Factors associated with progression to any lipodystrophy
CD4-lymphocyte count, a greater decrease in viral load, agreater increase in triglycerides and cholesterol, and nochange in glucose compared with patients who did notdevelop lipodystrophy. For example, patients whodeveloped lipodystrophy had a median change in CD4-lymphocyte count per month of follow-up of nine cells permm3, compared with six cells per mm3 in those who did notdevelop lipodystrophy (p=0·0067, Kruskal-Wallis test).There were few differences in the changes in marker valuesbetween the types of lipodystrophy, although this analysiswas limited by small numbers. There were small butsignificant decreases in viral load according to type oflipodystrophy, with the highest decrease in viral load seen inthose diagnosed with central obesity (0·2 log copies/mL permonth of follow-up) and the smallest decrease seen in thosediagnosed with mixed lipodystrophy (0·1 log copies/mL permonth of follow-up, p=0·023, Kruskal-Wallis test).
Progression to lipodystrophyBy 24 months after starting HAART, 23% of the patientswere estimated to have any lipodystrophy(95% CI 18%–29%), 20% were estimated to havelipodystrophy with subcutaneous lipoatrophy (15%–26%),and 16% were estimated to have lipodystrophy with centralobesity (12%–21%; figure 3).
The univariate and multivariate Cox proportionalhazards models investigating the factors associated withdevelopment of any lipodystrophy (n=85) are shown intable 2.
In univariate analyses, women were significantly morelikely to develop any lipodystrophy than men, as were olderheterosexuals and homosexuals compared with intravenousdrug users and younger patients. Each additional 6 monthsspent on HAART was associated with a 45% increased riskof any lipodystrophy (relative hazard 1·45 [95% CI1·22–1·72]; p<0·0001), and there was a significantlyincreased risk of lipodystrophy associated with increasingexposure to lamivudine, stavudine, didanosine, andindinavir. Additionally, patients with a higher viral load atstarting HAART were significantly more likely to developlipodystrophy.
In multivariate analyses, the increased risk of anylipodystrophy among women, heterosexuals, homosexuals,and older patients remained statistically significant. Each6 months of additional exposure to HAART was associatedwith a 57% increased risk of lipodystrophy (1·57[1·30–1·88]; p=0·0001), but there was no longer anyincreased risk of lipodystrophy associated with increasingexposure to any of the individual antiretrovirals. There wasno link between the values of the laboratory markers atstarting HAART and development of lipodystrophy. Anadditional analysis censoring at the time of first switchingdid not show major differences.
Two further analyses were considered, and themultivariate models are presented in table 3. The firstconsiders progression to lipodystrophy with subcutaneouslipoatrophy (subcutaneous lipoatrophy plus mixed groupn=67), whereas the second considers progression tolipodystrophy with central obesity (central obesity aloneplus mixed group, n=56). In general, the results areconsistent with those presented in table 2.
Each additional 6 months exposure to HAART wasassociated with a 61% increased risk of lipodystrophy with subcutaneous lipoatrophy (relative hazard 1·61 [95% CI 1·30–1·98]; p=0·0001). Even after adjusting forthe increased risk associated with increasing exposure toHAART, there was a 16% increased risk of lipodystrophywith subcutaneous lipoatrophy associated with eachadditional 6 months exposure to stavudine (relative hazard 1·16 [95% CI 1·02–1·31]; p=0·023). Patients witha higher triglyceride level, who were starting HAART,were more likely to develop lipodystrophy withsubcutaneous lipoatrophy although this result was only ofborderline statistical significance (p=0·067). The increasedrisk of lipodystrophy with subcutaneous lipoatrophy could
For personal use only. Reproduce with permission from The Lancet Publishing Group.
ARTICLES
596 THE LANCET • Vol 357 • February 24, 2001
not be associated with any individual, with protease inhibitorneither in the general model nor in a further model (data notshown) exclusively including the 254 patients starting with acombination which included stavudine—of whom 46developed lipodystrophy with subcutaneous lipoatrophy.
It was interesting to note in the multivariate model thatadditional time a patient spent on HAART was alsoassociated with an increased risk of lipodystrophy withcentral obesity (relative hazard 1·61 [1·33–2·10];p=0·0001). Each additional 6 months of exposure toindinavir increased the risk of lipodystrophy with centralobesity (relative hazard 1·26; 95% CI 0·99–1·60) but theassociation was not statistically significant (p=0·064).
DiscussionThe patterns of antiretroviral drugs used wererepresentative of those used in other more-developedcountries at that time.16–17 Previous cross-sectionalepidemiological studies have reported a wide variableprevalence ranging from 2% to 84%.6 The incidence of anylipodystrophy in the present study was very similar to theprevalence rates of moderate or severe lipodystrophy in twomixed cross-sectional and longitudinal studies.4,18
We found a high proportion of patients with overlappingmanifestations of central obesity and subcutaneous lipoatrophy.This overlap has been reported by other investigators19–21 andsuggests that there may be a partial association between thedevelopment of central obesity and subcutaneous lipoatrophybecause the coexistence of both types of changes in such ahigh proportion of patients with lipodystrophy is hardlyexpected from chance alone. In fact, 38 of 67 patients withcentral obesity had lipodystrophy with subcutaneous lipo-atrophy compared with only 18 of 409 without central obesity(p=0·0001). Like other investigators, we found that patientsdiagnosed with any lipodystrophy had a greater increase intheir CD4-lymphocyte count,18 a greater decrease in viralload,22 and a greater increase in triglycerides and cholesterol3,4
compared with patients who do not develop lipodystrophy. Inthe multivariate analysis of risk factors associated with thedevelopment of any lipodystrophy, we also found an increasedrisk among women, heterosexuals, and homosexuals, withincreasing age and with duration of exposure to HAART.However, no increased risk of lipodystrophy was associatedwith increased exposure to any of the individualantiretrovirals, or with the baseline laboratory measurements.
After the initial analysis, we looked at the changes inCD4-lymphocyte count and viral load between gendergroups and risk groups because we were concerned that thedifferences in the risk of lipodystrophy might be related toactual differences in drug exposure due to lowercompliance. For gender, there was no significantdifferences in changes in CD4-lymphocyte count or viralload. However, there were some differences in both CD4-lymphocyte count and viral load for exposure groups. Forexample, the median drop in viral load for intravenous drugusers was 1·9 log copies/mL, for heterosexuals was 2·2 logcopies/mL, for homosexuals was 2·3 log copies/mL, and forother (patients with other risks for HIV-1 infection or withunknown risk) was 2·1 log copies/mL (p=0·035). Althoughwe do not know how important these differences may be,we believe that they may be a potential source of bias.
There is no clear explanation for the increased risk oflipodystrophy found in women compared with men. Itmight be related to an increased awareness of body changesin women instead of an actual increased risk. However,despite the lower prevalence of HIV-1 infection in women,compared with men in more-developed countries, severalreports have described lipodystrophy exclusively in women,supporting the importance of this problem in HIV-1-infected women.9,23,24 In addition, some studies havereported differences in the rates and the presentation oflipodystrophy between men and women.25–27
The risk of lipodystrophy has been associated withincreased age.12,20 However, the physiological process ofageing is linked to body-fat changes that may bias theinfluence of age on the lipodystrophy seen in HIV-1-infectedpatients. A physiological reduction of lean mass and anincrease of fat mass may be seen in both sexes with increasingageing.28 Additionally, a redistribution of body fat including adecrease in the size of lower limbs and an increase in truncalfat may be seen with ageing both in men and women.29,30
The duration of exposure to HAART has been reportedas a factor that contributes to an increased risk for lipo-dystrophy.31 It is important to note, however, that the risk ofany lipodystrophy was related to the exposure to HAARTin general but not with specific antiretroviral drugs.
We also analysed the factors associated with progressionto specific types of lipodystrophy and found that the riskfactors were consistent with those factors associated withprogression to any lipodystrophy but with some interesting
Lipodystrophy with subcutaneous lipoatrophy Lipodystrophy with central obesity
Relative hazard (95% CI) p Relative hazard (95% CI) p
SexMen 1·00 · · 1·00 · ·Women 1·53 (0·83–2·82) 0·18 2·867 (1·36–6·02) 0·0058
Risk groupIntravenous drug user 1·00 · · 1·00 · ·Heterosexual 2·74 (1·34–5·60) 0·0058 2·93 (1·23–6·99) 0·016Homosexual 1·54 (0·69–3·43) 0·29 3·10 (119–8·07) 0·020Other 2·71 (0·90–8·18) 0·076 5·57 (1·63–18·38) 0·0060
Age (per 10 years older) 1·42 (1·13–1·78) 0·0030 1·34 (1·04–1·72) 0·024
Treatment timeTime on HAART (per 6 months extra) 1·61 (1·3–1·98) 0·0001 1·61 (1·33–2·1) 0·0001Time on 3TC (per 6 months extra) 0·98 (0·76–1·25) 0·85 0·96 (0·75–1·23) 0·74Time on d4T (per 6 months extra) 1·16 (1·02–1·31) 0·023 1·05 (0·85–1·30) 0·66Time on ddI (per 6 months extra) 1·00 (0·81–1·23) 0·98 1·10 (0·82–1·46) 0·53Time on indinavir (per 6 months extra) 0·99 (0·82–1·21) 0·95 1·26 (0·99–1·60 0·064Time on ritonavir (per 6 months extra) 1·02 (0·77–1·36) 0·87 1·12 (0·93–1·36 0·22
OtherViral load (per 1 log increase) 1·17 (0·80–1·72 0·41 · · · ·Cholesterol (per 0·1 g/L higher) 1·04 (0·96–1·07) 0·62 1·03 (0·97–1·09) 0·39Triglycerides (per 0·1 g/L higher) 1·03 (1·90–1·05) 0·067 · · · ·
Viral load, cholesterol, and triglycerides were all measured at starting HART. The relative hazard for time on HAART was derived from a multivariate model that did not include time oneach individual drug. Relative hazard for viral load and triglycerides were not included in the multivariate model of lipodystrophy with central obesity as they were not significant (p>0·25)in univariate analyses. 3TC= Inmivudine; d4T=stavudine; ddI=didanovine.
Table 3: Factors associated with progression to specific types of lipodystrophy (multivariate models)

For personal use only. Reproduce with permission from The Lancet Publishing Group.
ARTICLES
THE LANCET • Vol 357 • February 24, 2001 597
differences. The duration of exposure to stavudine wasindependently associated with a subsequent risk forlipodystrophy with subcutaneous lipoatrophy. Severalrecent studies have described this association.9–13,19 Althoughwe must be cautious in our interpretation, because moststudies have not allocated treatments at random, thesestudies would appear to implicate stavudine as a cause oflipoatrophy. However, such results do not exonerate anyother cause. In fact, the association with stavudine wasgreater in the study by Mallal and colleagues12 butprogression was faster when associated with proteaseinhibitors compared with nucleoside analogues alone. If weexclude from the analysis those patients who ever tookstavudine we still find a significantly increased risk oflipodystrophy with subcutaneous lipoatrophy withincreasing time on HAART (data not shown). Neither theduration of antiretroviral therapy nor any specificantiretroviral drug was associated with lipodystrophy withcentral obesity, although exposure to indinavir was ofborderline significance. Abdominal-fat accumulation mayalso be a marker for other effects induced by HAARTcontaining protease inhibitors in patients with advancedHIV-1 infection.32–34 Another potential explanation is thatthe diagnosis of increased abdominal girth our presentstudy might have been unable to properly identify the intra-abdominal fat accumulation. Recently, Saint-Marc andcolleagues19 distinguished two types of central obesity inHIV-1-infected patients who had body-fat changes afterHAART. One was classic visceral obesity where fat ispredominantly deposited intra-abdominally, the otherconsisted of an increased abdominal subcutaneousadiposity without an increase in visceral adipose tissue. Theintra-abdominal obesity associated with insulin resistanceand the subcutaneous adiposity was attributed to anincreased caloric intake. As we did not routinely carry outobjective measurements of regional fat, all patients withincreased abdominal girth were classified homogeneously,although they might actually have had different processes.
Only moderate or severe cases of clinical lipodystrophywere included in our analysis and we did not routinely carryout measurements of regional fat. However, suchmeasurements are not standardised and they are notincluded in the definition of lipodystrophy most commonlyaccepted at present—a diagnosis that relies on reports fromboth patients and doctor confirmation. Moreover, thisdefinition has been found to be highly concordant withobjective measurements of regional fat in two differentstudies that used DEXA4 and sonography.5 Antiretroviraldrugs were not homogeneously distributed among patients,although their prescription was not biased by any potentialconcern for lipodystrophy. It is possible that the lownumbers of patients treated with some specificantiretrovirals does not allow the investigation of the drugspotential association with an increased risk forlipodystrophy. Finally, the results of this study may not beapplicable to other HIV-1-infected patients receivingHAART regimens without protease inhibitors.
ContributorsE Martínez, A Mocroft, and J M Gatell were the main contributors to studydesign and wrote the paper. A Mocroft and A Phillips did the statisticalanalysis. M A García-Viejo, J B Pérez-Cuevas, J L Blanco, J Mallolas,L Bianchi, I Conget and J Blanch gave ideas for analyses, helped to write tothe paper, and contributed to protocol design and data collection.J M Gatell supervised the project.
AcknowledgmentsSupported in part by grants FIS 98/1227, SAF 98/0021, and CIRITSCR99/398. Presented in part at the Second International Workshop onLipodystrophy and Adverse Events in HIV Infection, Toronto, September,2000, and in the Fifth International Congress on Drug Therapy in HIVInfection, Glasgow, October, 2000.
References1 Martínez E, Gatell JM. Metabolic abnormalities and body fat
redistribution in HIV-1 infected patients: the lipodystrophy syndrome.Curr Opin Infect Dis 1999; 12: 13–19.
2 Carr A, Samaras K, Burton S, et al. A syndrome of peripherallipodystrophy, hyperlipidaemia and insulin resistance in patientsreceiving HIV protease inhibitors. AIDS 1998; 12: F51–59.
3 Miller KK, Jones E, Yanovski JA, et al. Visceral abdominal-fataccumulation associated with use of indinavir. Lancet 1998; 351:871–75.
4 Carr A, Samaras K, Thorisdottir A, Kaufmann GR, Chisholm DJ,Cooper DA. Diagnosis, prediction, and natural course of HIV-1protease-inhibitor-associated lipodystrophy, hyperlipidaemia, anddiabetes mellitus: a cohort study. Lancet 1999; 353: 2093–99.
5 Martínez E, Bianchi L, García-Viejo MA, Bru C, Gatell JM.Sonographic assessment of regional fat in HIV-1-infected people. Lancet2000; 356: 1412–13.
6 Carr A, Samaras K, Chisholm DJ, Cooper DA. Pathogenesis of HIV-1-protease inhibitor-associated peripheral lipodystrophy, hyperlipidaemia,and insulin resistance. Lancet 1998; 352: 1881–83.
7 Martínez E, Conget I, Lozano L, Casamitjana R, Gatell J. Reversion ofmetabolic abnormalities after switching from HIV-1 protease inhibitorsto nevirapine. AIDS 1999; 13: 805–10.
8 Martínez E, García-Viejo MA, Blanco JL, et al. Impact of switchingfrom Human Immunodeficiency Virus type 1 protease inhibitors toefavirenz in successfully treated adult with lipodystrophy. Clin Infect Dis2000; 31: 1266–73.
9 Gervasoni C, Ridolfo AL, Trifirò G, et al. Redistribution of body fat inHIV-infected women unergoing combined antiretroviral therapy. AIDS1999; 13: 465–71.
10 Saint-Marc T, Poizot-Martin I, Partisani M, Fabre J, Touraine JL.A syndrome of peripheral fat wasting (lipodystrophy) in patientsreceiving long-term nucleoside analogue therapy. AIDS 1999; 13:1659–67.
11 Carr A, Miller J, Law M, Cooper DA. A syndrome of lipoatrophy, lacticacidaemia and liver dysfunction associated with HIV nucleosideanalogue therapy: contribution to protease inhibitor-relatedlipodystrophy syndrome. AIDS 2000; 14: F25–32.
12 Mallal SA, John M, Moore CB, et al. Contribution of nucleosideanalogue reverse transcriptase inhibitors to subcutaneous fat wasting inpatients with HIV infection. AIDS 2000; 14: 1309–16.
13 Galli M, Ridolfo AL, Gervasoni C, et al. Incidence of fat tissueabnormalities in protease inhibitor-naive patients treated with NRTIcombinations. San Diego: First International Workshop on AdverseDrug Reactions and Lipodystrophy in HIV, 1999 (abstr 20).
14 Brinkman K, Smeitink JA, Romjin JA, Reiss P. Mitochondrial toxicityinduced by nucleoside-analogue reverse-transcriptase inhibitors is a keyfactor in the pathogenesis of antiretroviral-therapy-related lipodystrophy.Lancet 1999; 354: 1112–15.
15 Carr A, Samaras K, Burton S, et al. Syndrome of peripherallipodystrophy, hyperlipidemia and insulin resistance due to HIVprotease inhibitors, Adelaide: 9th Annual Conference of theAustralasian Society for HIV Medicine, October, 1997.
16 Carpenter CC, Fischl MA, Hammer SM, et al. Antiretroviral therapyfor HIV infection in 1997: updated recommendations of theInternational AIDS Society-USA panel. JAMA 1997; 277: 1962–69.
17 Kirk O, Mocroft A, Katzenstein TL, et al. Changes in use ofantiretroviral therapy in regions of Europe over time. AIDS 1998; 12:2031–39.
18 Ward DJ, Delancy KM, Moorman AC, et al. Description oflipodystrophy in the HIV Outpatient Study (HOPS). San Diego: FirstInternational Workshop on Adverse Drug Reactions and Lipodystrophyin HIV, 1999 (abstr 14).
19 Saint-Marc T, Partisani M, Poizot-Martin I, et al. Fat distributionevaluated by computed tomography and metabolic abnormalities inpatients undergoing antiretroviral therapy: preliminary results of theLIPOCO study. AIDS 2000; 14: 37–49.
20 Daucourt V, Thiébaut R, Mercié P, et al. Prevalence of lipodystrophyand relation with clinical, anthropometric data and treatment, AquitaineCohort, 1999. San Diego: First International Workshop on AdverseDrug Reactions and Lipodystrophy in HIV, 1999 (abstr 16).
21 Viard JP, Rakotoambinina B. Lipodystrophic syndromes in a cohort ofHIV-1-infected patients receiving HAART with a protease inhibitor.San Diego: First International Workshop on Adverse Drug Reactionsand Lipodostrophy in HIV, 1999: (abstr 26).
22 Kotler DP, Rosenbaum K, Wang J, Pierson RN. Studies of bodycomposition and fat distribution in HIV-infected and control subjects. J AIDS 1999; 20: 228–37.
23 Dong KL, Bausserman LL, Flynn MM, et al. Changes in body habitusand serum lipid abnormalities in HIV-positive women on highly activeantiretroviral therapy. J AIDS 1999; 21: 107–13.
24 Hadigan C, Miller K, Corcoran C, et al. Fasting hyperinsulinemia andchanges in regional body composition in human immunodeficiencyvirus-infected women. J Clin Endocrinol Metab 1999; 84: 1932–37.
For personal use only. Reproduce with permission from The Lancet Publishing Group.
ARTICLES
598 THE LANCET • Vol 357 • February 24, 2001
25 Falutz J, Turcot D. Considerations in the development of a casedefinition for HIV/HAART-associated lipodystrophy syndrome. SanDiego: First International Workshop on Adverse Drug Reactions andLipodystrophy in HIV, 1999: (abstr 21).
26 Muurahainen N, Falutz J, Santos G, et al. The SALSA (self-ascertained lipodystrophy syndrome assessment) cohort abnormalitiesin cases compared to controls. San Diego: First InternationalWorkshop on Adverse Drug Reactions and Lipodystrophy in HIV, 1999(abstr 22).
27 Muurahainen N, Pettit R, Kotler D, et al. Abnormalities in HIV-associated lipodystrophy syndrome that vary by weight status. SanDiego: First International Workshop on Adverse drug Reactions andLipodystrophy in HIV, 1999: (abstr 63).
28 Flynn MA, Nolph GB, Baker AS, et al. Total body potassium in aginghumans: a longitudinal study. Am J Clin Nutr 1989; 50: 713–17.
29 Shimokata H, Tobin JD, Muller DC, et al. Studies in the distribution ofbody fat: effects of the age, sex and obesity. J Gerontol 1989; 44: 66–73.
30 Schwartz RS, Shuman WP, Bradbury VL, et al. Body fat distribution inhealthy young and older men. J Gerontol 1990; 45: 181–85.
31 Safrin S, Grunfeld C. Fat distribution and metabolic changes in patientswith HIV infection. AIDS 1999; 13: 2493–505.
32 Silva M, Skolnik P, Gorbach S, et al. The effect of protease inhibitorson weight and body composition in HIV-infected patients. AIDS 1998;12: 1645–51.
33 Carbonnel F, Maslo C, Beaugerie L, et al. Effect of indinavir on HIV-related wasting. AIDS 1998; 12: 1777–84.
34 Pernerstorfer-Schoen H, Schindler K, Parschalk B, et al. Beneficialeffects of protease inhibitors on body composition and energyexpenditure: a comparison between HIV-infected and AIDS patients.AIDS 1999; 13: 2389–96.
Clinical picture: Hair repigmentation inlentigo maligna
Reinhard Dummer
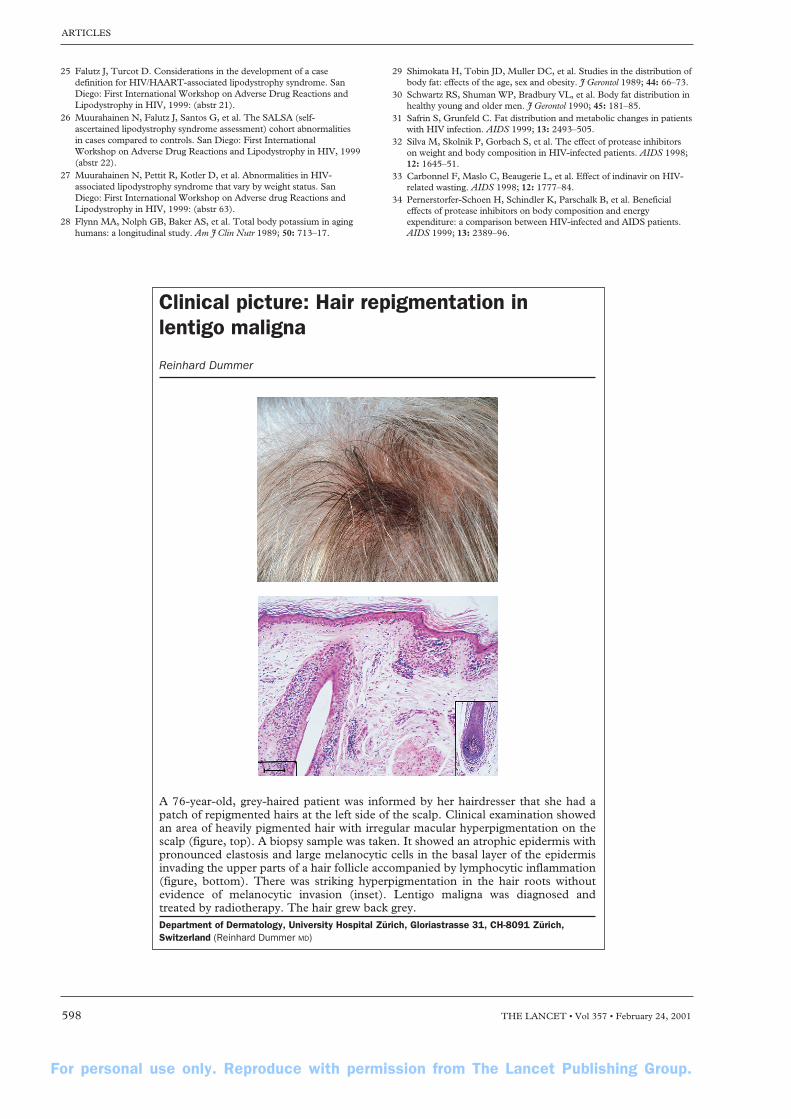
A 76-year-old, grey-haired patient was informed by her hairdresser that she had apatch of repigmented hairs at the left side of the scalp. Clinical examination showedan area of heavily pigmented hair with irregular macular hyperpigmentation on thescalp (figure, top). A biopsy sample was taken. It showed an atrophic epidermis withpronounced elastosis and large melanocytic cells in the basal layer of the epidermisinvading the upper parts of a hair follicle accompanied by lymphocytic inflammation(figure, bottom). There was striking hyperpigmentation in the hair roots withoutevidence of melanocytic invasion (inset). Lentigo maligna was diagnosed andtreated by radiotherapy. The hair grew back grey.Department of Dermatology, University Hospital Zürich, Gloriastrasse 31, CH-8091 Zürich,Switzerland (Reinhard Dummer MD)
Related Documents











