
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript



Incidence and prevalence
Risk factors for breast CA
New Treatments
New medications
Oral Care
New Products

2009:
USA: 1,479,350 new cancer diagnoses (all types)
SC: 22,100 new cancer diagnoses (all types)
USA: 562,340 deaths from cancer
SC: 9,100 deaths from cancer
2012:
USA: 1,638,910 new diagnoses anticipated (all types)
SC: 26,570 new cancer diagnoses (all types)
USA: 577,190 deaths from cancer
SC: 9670 deaths from cancer
*these numbers are slightly higher than last year’s

Breast Cancer (2012)
USA new – 229,060 -2,190 men (1%)
SC new – 3,570
USA incidence/100,000 -120
SC incidence/100,000 -121
USA deaths – 39,920
SC deaths - 660
Oral Cancer (2012)
USA new – 40,250
USA (2009) – 35,700
SC new - ?
USA deaths – 7,850
USA (2009) – 7,600
SC deaths - ?

Decrease in all BC incidence since 2000
7% decrease from
2002-3
› May be related to
reduced use of
hormone therapy
for menopause
Stable 2004-2008
For early stage breast CA
› CA in situ
Stable for white women
Increasing for
African American
Is this a good thing?
› Perhaps more early
diagnoses????

Arizona: 104*
Utah: 108
New Mexico: 109
Mississippi: 110
South Carolina: 120
Oregon, Washington, Vermont: 130
Connecticut: 134
› *per 100,000

1975 -77
All races
› 75%
White
› 76%
African American
› 68%
Today:
All races
› 90% overall,
› 99% for localized
White
› 91%
African American
› 78%
Note: 5-year survival was only 63% in the 1960’s !!!!!
-African American survival rates have not increased at the same rate
as survival of white American women.

10 year = 82%
15 year = 77%
*Remember : a 15 year survivor who dies
this year had her initial diagnosis and
treatment 15 years ago….Sooooo,
advances in diagnosis and treatment
should lead to even longer survival for
women diagnosed this year!

2.5 million
U.S. breast cancer
survivors were
alive in 2010 !

Non-modifiable
› Gender
› Age Long menstrual history
No pregnancies or 1st child
after 30
› Family history:
Genetic
predisposition
Race/ethnicity ?

Lifetime probability of developing breast
cancer = 1 in 8
Probability before age 39 = 1 in 207
Between ages 40-59 = 1 in 27
> age 70 = 1 in 15

Breast Cancer susceptibility gene mutations – BRCA1 and BRCA2
Accounts for 5-10% of all new BCA › Family clusters
› Eastern European Jewish descent
› Males who develop BC

HER2 - a gene gone wild!
All women have the HER2 gene
“Human Epithelial growth factor Receptor 2” = HER2
Normal HER2 receptors help control growth and maintenance of healthy breast tissue.
25% of all breast cancers have an overproduction of HER2 which causes accelerated growth of the tumor.

Newer studies of Latina women:
Links between known BC risk factors are not as clear for Latinas as for non-Hispanic white women
Only common risk is age

Compared to African American women, white women are slightly more likely to develop breast cancer, but less likely to die of it.
African American women tend to have more aggressive tumors. Why this is the case is not known

Women of other ethnic backgrounds
— Asian, Latino, and
Native American — have a lower risk of
developing and
dying from breast cancer than white
women and African
American women

Educational level is the
greatest predictor of unnecessary cancer
death.
Even with racial and demographic data
factored in, lower
education level = higher death rate from
cancer.
Dr. Baker’s perio students?????
Potentially Modifiable:
› Overweight Especially older women
› Hormone exposure HRT – estrogen/progesterone
combos
High dosage BCP
› Couch potato
› Nighttime work* Exposure to light
› Alcohol > 1 drink per day
› Smoking – tobacco exposure* NEW research in this area
Limited evidence, but suggestive

To Decrease Risk:
› Breastfeeding
› Healthy weight
› 4-7 hours / week of physical
activity
› 7-9 servings / day of fruits
and veggies
› Limit alcohol consumption to
less than one drink per day,
2-4 per week.

Body weight and
activity level
› impacts both
risk of disease
and survival
rates.

Surgeries
Chemotherapy
Radiation
Most women undergo a
combination of these

Mastectomy with Lymph Node Dissection › With chemotherapy and/or radiation
Mastectomy with Terminal Node Biopsy › Newer technique
› Fewer complications!!! – more later
Lumpectomy + Radiation › With or without chemotherapy

Range of motion
› If muscles or nerves were lost or damaged in
surgery
Poor circulation in arm on affected side
Lymphedema
› Risk increases with increase in number of
lymph nodes removed.

swelling of the soft
tissues of the arm and
or hand
accumulation of
lymphatic fluid and
damaged drainage
system
5-40% of BC survivors
will have some degree
of lymphedema
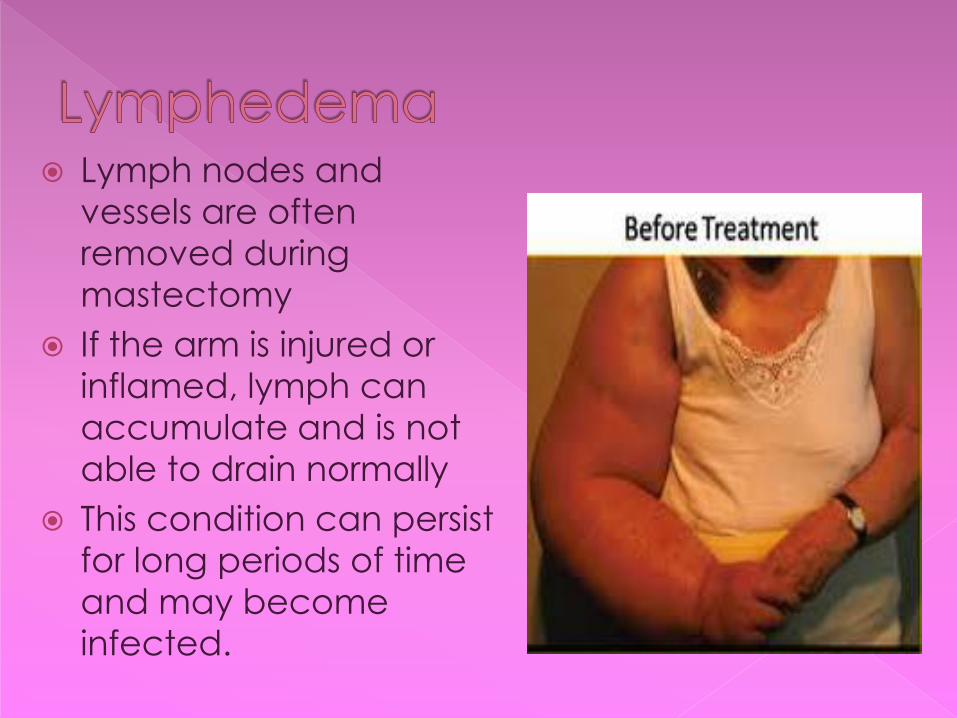
Lymph nodes and
vessels are often removed during
mastectomy
If the arm is injured or inflamed, lymph can
accumulate and is not
able to drain normally
This condition can persist
for long periods of time
and may become infected.

Injury to affected side after:
› mastectomy with
lymph node dissection
› Radiation treatment
that results in scarring
of lymphoid area
Lymphedema compression bandage

Do’s:
› Use protective gloves for gardening or
cleaning
› Use oven mitts
› Use mild soaps and moisturizers
› Avoid insect bites (use non-drying repellants)
› Use an electric razor
› Rest the arm in an elevated position
› Control blood sugar levels if you are diabetic

Don’ts:
› Carry a heavy shoulder bag
› Use hot tubs or saunas
› Apply heat or vigorous massage to affected arm
› Have BP taken on affected arm
› Have blood draws or injections on affected arm
› Have tattoos or piercing of affected area.

Sentinel node biopsy and dissection › Requires high level of surgical skill
› Radioactive dye injected into tumor prior to surgery
› Dye drains into lymph nodes – sentinel is first node in line
› Surgeon uses a special instrument to track the flow of the dye
› Sentinel node removed and checked under microscope – if clear – no further nodes removed
› If sentinel is positive for CA, further nodes removed and checked a few at a time.


Evista (raloxifine)
› estrogen receptor blocker
Novaldex (tamoxifen)
› estrogen receptor blocker
Both are given to women in high risk
families
› Tamoxifen is also used to prevent recurrence
of BC, but Evista is only used to prevent a first occurrence

IV chemo drugs:
Adriamycin*
Cytoxen
Taxol* / Taxotere
› made from bark of the Pacific yew tree
› may cause allergic reactions
Herceptin
› For HER2 positive cancers
Oral drugs:
Tamoxifen
Xeloda
Avastin
Arimidex
*Known oral side effects

Zofran
› Wonderful for nausea
› Expensive – must justify for some insurance
companies
Procrit
› stimulates bone marrow to make red blood cells.
› used to treat anemia caused by
chemotherapy. Helps with energy levels.
Neupogen, Neulasta
› Stimulates bone marrow to produce neutrophils

Tamoxifen (older, but still common)
› Blocks estrogen receptors
› Provides some protection against osteoporosis
Arimedex (newer)
› Aromatase (estrogen pre-curser)
› More effective than tamoxifen at preventing
recurrence
› No protective action for bones

Patients should receive a complete oral evaluation, debridement and oral hygiene instructions BEFORE chemotherapy begins.
-Eliminate potential sources of infection / inflammation
-Rough or sharp surfaces should be smoothed.

When patients call… Attempt to schedule within 24 hours. › Patients often do not have much time
between a diagnosis of cancer and the beginning of treatment.
› “Put on your happy face; chances are that this person is having a worse day than you are.” Susan Calderbank, DMD
› YOU can make a difference!!

Consult with the oncologist.
Ask for current blood counts. Patient may be immunosuppressed › Premedication may be necessary.
Attempt to schedule 1 day before chemo day - this is when the patient should be strongest.
Do not schedule when the office will be crowded. › First patient in the morning

Nadir:
Approximately 10 days after
each treatment, the
patient’s blood counts are at
their lowest levels.
This period is called the
nadir.
If the white cells are
affected, the patient will be
most susceptible to infection
at this time
Neupogen/Neulasta help!!!!

Xerostomia
pH changes: more acidic
Fragile, friable tissues
› Generalized “mucositis”
Susceptible to candidiasis
› And other opportunistic infections
Dysgeusia = bad taste

xerostomia

pH changes
Oral environment
becomes more
acidic
Combined with
xerostomia
= Increased caries

oral mucositis: ALL mucosa of the oral
cavity is inflamed.
Changes may be subtle in appearance, but still significant to the patient.
Ulcers may or may not be visible.
Patients will report that the mouth feels “raw” or “scalded”

Candidiasis:
Xerostomia and pH changes alter the oral flora.
The patient’s immune system is suppressed by chemotherapy.
May not present classic appearance

Complications: Oral changes caused by chemotherapy
increase risk of mucositis, candidiasis, gingivitis, periodontitis and caries.
Destruction of blood cells during
chemotherapy places the patient at greater risk for infection.
Infection in the mouth can easily
become systemic in an immunosuppressed patient.

RINCINOL™ P.R.N., THE FIRST
BIO-ADHERENT NON-PRESCRIPTION MOUTH
RINSE FOR ORAL PAIN RELIEF

Non-prescription Aloe Vera based site
specific gel
no alcohol and no Benzocaine

Finally!

G U M Expanding floss:
soft and does not cut
G U M Sensitive Care TB


Xerostomia Xeropthalmia
Lubricant Eye drops
› Refresh
› Refresh PM
Avoid irritants:
› Smoke
› Chlorine

And nose care too…..
…especially at night.
Nose dryness leads to
mouth breathing

Negative effects of chemotherapy will
resolve partially or totally…..eventually
› Xerostomia and delicate tissues may take some time
For survivors of Head/Neck cancer,
effects of radiation therapy are
permanent.
Breast Cancer survivors have some long-
term effects

Chemotherapy for breast cancer will
bring on early and
sudden menopause.
Maintenance drugs
for breast cancer
keep the patient in a
hormone deprived
state. Survivors have
hormone levels of a
much older woman
To menopause and beyond!!!

Loss of estrogen contributes to other health problems such as osteoporosis
Long-term use of bisphosphonate medications for osteoporosis is associated with osteonecrosis of the bone (ONJ).
Rx names:
Fosamax, Actonel,
Boniva
*Reclast (IV)

Patients who have had
› IV bisphosphonates
or
› long term oral
bisphosphonates
are not good
candidates for tooth
extraction or
implants
Prevention and
maintenance is
key!!!

American Cancer Society, Cancer Facts and Figures 2009, www.cancer.org
American Cancer Society, Cancer Facts and Figures 2011, www.cancer.org
American Cancer Society, Cancer Facts and Figures 2012, www.cancer.org
Breastcancer.org
U.S Dept. of Health and Human Services, National Institutes of Health, National Institute of Dental and Craniofacial Research, Three Good Reasons to See a Dentist Before Cancer Treatment, March 2011.
U.S Dept. of Health and Human Services, National Institutes of Health, National Institute of Dental and Craniofacial Research, Head and Neck Radiation Treatment and Your Mouth, March 2011.
U.S Dept. of Health and Human Services, National Institutes of Health, National Institute of Dental and Craniofacial Research, Chemotherapy and Your Mouth, Dec.2010.
Related Documents











