doi: 10.1152/ajpheart.00555.2009 297:H1752-H1759, 2009. First published 4 September 2009; Am J Physiol Heart Circ Physiol Anton Vonk-Noordegraaf Boer, Warner S. Simonides, Walter J. Paulus, Nico Westerhof, Cornelis P. Allaart and M. Louis Handoko, Regis R. Lamberts, Everaldo M. Redout, Frances S. de Man, Christa the isolated heart in experimental pulmonary arterial hypertension: a study Right ventricular pacing improves right heart function in You might find this additional info useful... 35 articles, 17 of which you can access for free at: This article cites http://ajpheart.physiology.org/content/297/5/H1752.full#ref-list-1 7 other HighWire-hosted articles: This article has been cited by http://ajpheart.physiology.org/content/297/5/H1752#cited-by including high resolution figures, can be found at: Updated information and services http://ajpheart.physiology.org/content/297/5/H1752.full can be found at: Physiology American Journal of Physiology - Heart and Circulatory about Additional material and information http://www.the-aps.org/publications/ajpheart This information is current as of October 19, 2012. 1522-1539. Visit our website at http://www.the-aps.org/. Pike, Bethesda MD 20814-3991. Copyright © 2009 the American Physiological Society. ISSN: 0363-6135, ESSN: molecular levels. It is published 12 times a year (monthly) by the American Physiological Society, 9650 Rockville cardiovascular function at all levels of organization ranging from the intact animal to the cellular, subcellular, and physiology of the heart, blood vessels, and lymphatics, including experimental and theoretical studies of publishes original investigations on the American Journal of Physiology - Heart and Circulatory Physiology at Vrije Universiteit, Library on October 19, 2012 http://ajpheart.physiology.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
doi: 10.1152/ajpheart.00555.2009297:H1752-H1759, 2009. First published 4 September 2009;Am J Physiol Heart Circ Physiol
Anton Vonk-NoordegraafBoer, Warner S. Simonides, Walter J. Paulus, Nico Westerhof, Cornelis P. Allaart and M. Louis Handoko, Regis R. Lamberts, Everaldo M. Redout, Frances S. de Man, Christathe isolated heart
inexperimental pulmonary arterial hypertension: a study Right ventricular pacing improves right heart function in
You might find this additional info useful...
35 articles, 17 of which you can access for free at: This article citeshttp://ajpheart.physiology.org/content/297/5/H1752.full#ref-list-1
7 other HighWire-hosted articles: This article has been cited by http://ajpheart.physiology.org/content/297/5/H1752#cited-by
including high resolution figures, can be found at: Updated information and serviceshttp://ajpheart.physiology.org/content/297/5/H1752.full
can be found at: PhysiologyAmerican Journal of Physiology - Heart and Circulatory about Additional material and information
http://www.the-aps.org/publications/ajpheart
This information is current as of October 19, 2012.
1522-1539. Visit our website at http://www.the-aps.org/. Pike, Bethesda MD 20814-3991. Copyright © 2009 the American Physiological Society. ISSN: 0363-6135, ESSN:molecular levels. It is published 12 times a year (monthly) by the American Physiological Society, 9650 Rockville cardiovascular function at all levels of organization ranging from the intact animal to the cellular, subcellular, andphysiology of the heart, blood vessels, and lymphatics, including experimental and theoretical studies of
publishes original investigations on theAmerican Journal of Physiology - Heart and Circulatory Physiology
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from

Right ventricular pacing improves right heart function in experimentalpulmonary arterial hypertension: a study in the isolated heart
M. Louis Handoko,1,2 Regis R. Lamberts,1,3 Everaldo M. Redout,1 Frances S. de Man,2 Christa Boer,3
Warner S. Simonides,1 Walter J. Paulus,1 Nico Westerhof,1,2 Cornelis P. Allaart,4
and Anton Vonk-Noordegraaf2
Departments of 1Physiology, 2Pulmonology, 3Anesthesiology, and 4Cardiology, VU University Medical Center, Institute forCardiovascular Research, Amsterdam, The Netherlands
Submitted 22 June 2009; accepted in final form 31 August 2009
Handoko ML, Lamberts RR, Redout EM, de Man FS, Boer C,Simonides WS, Paulus WJ, Westerhof N, Allaart CP, Vonk-Noordegraaf A. Right ventricular pacing improves right heart function inexperimental pulmonary arterial hypertension: a study in the isolatedheart. Am J Physiol Heart Circ Physiol 297: H1752–H1759, 2009. Firstpublished September 4, 2009; doi:10.1152/ajpheart.00555.2009.—Rightheart failure in pulmonary arterial hypertension (PH) is associatedwith mechanical ventricular dyssynchrony, which leads to impairedright ventricular (RV) function and, by adverse diastolic interaction,to impaired left ventricular (LV) function as well. However, therapiesaiming to restore synchrony by pacing are currently not available. Inthis proof-of-principle study, we determined the acute effects of RVpacing on ventricular dyssynchrony in PH. Chronic PH with rightheart failure was induced in rats by injection of monocrotaline (80mg/kg). To validate for PH-related ventricular dyssynchrony, rats (6PH, 6 controls) were examined by cardiac magnetic resonance imag-ing (9.4 T), 23 days after monocrotaline or sham injection. In a secondgroup (10 PH, 4 controls), the effects of RV pacing were studied indetail, using Langendorff-perfused heart preparations. In PH, septumbulging was observed, coinciding with a reversal of the transseptalpressure gradient, as observed in clinical PH. RV pacing improvedRV systolic function, compared with unpaced condition (maximal firstderivative of RV pressure: �8.5 � 1.3%, P � 0.001). In addition, RVpacing markedly decreased the pressure-time integral of the transsep-tal pressure gradient when RV pressure exceeds LV pressure, an indexof adverse diastolic interaction (�24 � 9%, P � 0.01), and RVpacing was able to resynchronize time of RV and LV peak pressure(unpaced: 9.8 � 1.2 ms vs. paced: 1.7 � 2.0 ms, P � 0.001). Finally,RV pacing had no detrimental effects on LV function or coronaryperfusion, and no LV preexcitation occurred. Taken together, wedemonstrate that, in experimental PH, RV pacing improves RVfunction and diminishes adverse diastolic interaction. These findingsprovide a strong rationale for further in vivo explorations.
right ventricular dysfunction; artificial cardiac pacing; magnetic res-onance imaging; Langendorff preparation
PULMONARY ARTERIAL HYPERTENSION (PH) is characterized byprogressive pulmonary vascular remodeling. During the pro-gression of the disease, right ventricular (RV) afterload con-tinues to rise and eventually right heart failure develops in themajority of patients.
In PH patients, signs of mechanical RV dyssynchrony, alongwith signs of adverse interventricular diastolic interaction, areoften observed (19, 25, 32). This results in inefficient pumpingof the heart (3, 9, 22). In essence, the duration of RV contrac-tion is lengthened due to increased RV afterload (14). As a
consequence, time-to-peak shortening of the RV free wall isdelayed, even beyond closure of the pulmonary valves (9, 21,22). Loss of a coordinated ventricular contraction results inimpaired RV systolic function (18, 21). In addition, the pro-longed RV contraction in early left ventricular (LV) diastolecauses the already relaxing interventricular septum to bulgeinto the LV. This negatively influences early LV filling, even-tually contributing to the impairment of LV diastolic functionas well (12, 28).
To this date, no specific treatment is available for thefailing RV (33). Cardiac resynchronization therapy is awell-established treatment for LV dyssynchrony related toleft heart failure (23) and might be an interesting therapeuticoption for right heart failure as well. However, our labora-tory recently demonstrated that the origin of PH-relatedventricular dyssynchrony lies in regional differences in theduration of the contraction, rather than regional differencesin the onset of the contraction (e.g., due to a conductancedelay) (22). For this reason, PH-related ventricular dyssyn-chrony is essentially different from dyssynchrony associatedwith left heart failure (23).
In the present proof-of-principle study, we tested whetherRV pacing could synchronize pressure generation across theseptum, resulting in an improvement of RV systolic functionand a reduction of adverse diastolic interaction. First, wevalidated the monocrotaline (MCT) rat model, a well-estab-lished model for chronic PH, for the presence of ventriculardyssynchrony. Subsequently, we evaluated the acute effects ofRV pacing on cardiac performance and PH-related ventriculardyssynchrony in isolated Langendorff-perfused heart prepara-tions. This approach allows relatively easy manipulation andoffers a high degree of preparation stability in which LV andRV load can be varied independently, with derivation ofcardiac-specific functional data (20).
MATERIALS AND METHODS
All experiments were approved by the Institutional Animal Careand Use Committee of the VU University Amsterdam.
Experimental model of PH. In total, 26 male Wistar rats wereincluded in the study (150–175 g; Harlan, Horst, the Netherlands). PHwas induced (n � 16) by a single subcutaneous injection of MCT (80mg/kg dissolved in sterile saline; Sigma-Aldrich, Zwijndrecht, TheNetherlands). This resulted in a PH phenotype, followed by right heartfailure �23 days after injection (8, 15). The control group wasinjected with saline only (n � 10).
Cardiac magnetic resonance imaging. Twenty-three days afterMCT injection, the presence of ventricular dyssynchrony in vivo wasassessed in PH rats and compared with controls (6 for each group), bymeasuring cardiac function and the behavior of the interventricular
Address for reprint requests and other correspondence: A. Vonk Noordegraaf,Dept. of Pulmonology, VU Univ. Medical Center, De Boelelaan 1117, 1081 HVAmsterdam, The Netherlands (e-mail: [email protected]).
Am J Physiol Heart Circ Physiol 297: H1752–H1759, 2009.First published September 4, 2009; doi:10.1152/ajpheart.00555.2009.
0363-6135/09 $8.00 Copyright © 2009 the American Physiological Society http://www.ajpheart.orgH1752
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from
septum with cardiac magnetic resonance imaging (CMR; 9.4 T;Varian Medical Systems, Palo Alto, CA), as previously described(26). After CMR scanning, all rats were euthanized, and their organsweighed.
Images were analyzed offline using Segment (version 1.698; http://segment.heiberg.se) (16). Endocardial borders of both ventricles wereautomatically detected for all slices of the heart and for each frame inthe heart cycle. LV and RV volume curves were constructed using themodified Simpson’s rule, from which end-diastolic and end-systolicvolume, peak filling rate, stroke volume, heart rate, cardiac output,and ejection fraction were derived (11, 12). Septum curvature wascalculated as previously described (25). In short, the anterior, middle,and posterior positions of the interventricular septum at midventricu-lar level were determined, through which a circle was fitted. Thereciprocal of the radius of this circle was used to quantify septumcurvature (1/R) and was defined positive, if the septum bowed towardthe RV.
Isolated Langendorff-perfused heart preparation. To characterizethe hearts of PH rats and controls (10 PH rats, 4 controls; no CMRperformed) and to study ventricular dyssynchrony in detail, a Lange-ndorff setup was used, as previously described, with balloons in LVand RV (Fig. 1) (20). The heart was perfused (at 35–37°C) using amodified Krebs-Henseleit solution (composition in mM: 118.5 NaCl,4.7 KCl, 1.4 CaCl2, 25 NaHCO3, 1.2 MgCl2, 1.2 KH2PO4, and 11glucose) that was continuously gassed with 95% O2-5% CO2 (pH7.4). Coronary perfusion pressure was set at a constant value of 80mmHg to minimize edema formation (27, 29). Electrodes were placedat the right atrium and at a vessel-free area of the LV and RV free wall(LV: posterolateral-midventricular; RV: RV “anterolateral”, oppositethe LV electrode), after which normal atrial and subsequent ventric-ular activation were checked to verify that the intrinsic conductancesystem was intact. In addition, signals of LV and RV electrodes werecompared to detect potential differences in electrical activation of LVand RV. Atrial and ventricular threshold stimuli were determined, andthe heart was atrial paced at 4.0 Hz (pulse duration 1.0 ms, at twice thethreshold). During the whole experiment, electrical activity and stim-uli, LV and RV pressures, and coronary flow were continuouslyrecorded with a sample rate of 2.0 kHz.
After stabilization (10 min), the volumes at maximal developedpressure (Vmax) of both ventricles were determined by small stepwiseincreases and decreases in balloon volume [in analogy to length atmaximal developed force, used in isolated muscle studies (31)].Subsequently, the pressure-volume (PV) relationship of the LV wasdetermined (in the physiological range of 70–100% Vmax), with theRV volume set at 75% Vmax, and this was repeated for the RV, nowwith the LV volume set at 75% Vmax (20).
RV pacing protocol. RV pacing was only performed in PH hearts;RV pacing experiments in normal hearts were not performed, since itis known that this results in loss of synchrony and worsening ofcardiac function (30). LV volume was set at 75% Vmax, and RVvolume was set at 95% Vmax. These volumes correspond with LV andRV end-diastolic pressures of 5 and 10 mmHg, respectively (Fig. 2),as observed in PH patients (11) and in MCT-treated rats in vivo (15).
The intrinsic atrioventricular delay (AV time) was defined as the timeinterval between atrial and (right) ventricular activation (Fig. 1).
RV pacing was performed by direct stimulation of the RV free wall(using the RV electrode), triggered from atrial activation, starting withan AV time equal to the intrinsic AV time. Subsequently, AV timewas shortened in steps of 10 ms (AV shortening). Effects of RVpacing stabilized within 5 s. After the experiment, all hearts weredissected in LV (including interventricular septum) and RV andweighed.
Functional assessment of RV pacing. The isovolumic pressurerecordings were evaluated offline using MATLAB (version R2007b,The MathWorks, Natick, MA). Signals were averaged over �100beats (25 s). The effects of RV pacing on both intra- as well asinterventricular aspects of PH-related dyssynchrony were evaluated(13). Intraventricular dyssynchrony was measured by the maximalfirst derivative of RV pressure (RV dP/dtmax) and RV systolic pres-sure (RV SP). The time difference between RV and LV peak pressurewas used as an index for interventricular dyssynchrony (�tpeak).
The pressure-time integral of the transseptal pressure gradientwhen RV pressure exceeds LV pressure (PTIRVP�LVP) was used toquantify the interventricular diastolic interaction in isolated hearts. Itmeasures the degree as well as the duration of reversed pressuredifferences across the interventricular septum (i.e., RV pressure � LVpressure) during a heartbeat, which is considered the driving force thatcauses the septum to bulge into the LV (25), impairing LV filling (12,28). This parameter is especially sensitive (it decreases) for improve-ments in synchronic pressure generation across the septum (due to RVpacing). PTIRVP�LVP was calculated by:
PTIRVP�LVP � 1 beat
RV pressure � LV pressure�dt,
when RV pressure � LV pressure � 0
The onset of LV and RV contraction was defined as the time pointat which pressure rose to 5% of developed pressure above diastolicpressure (DP). The difference between the onset in RV and LVcontraction was used to identify the presence of LV preexcitation. LVpreexcitation refers to depolarization of the LV myocardium that isearlier than would occur by conduction of an impulse through the AVnode (in this case, LV depolarization triggered by artificial pacing ofthe RV free wall) and is known to be detrimental for LV function inthe long term (30). This phenomenon can be recognized from pressurerecordings, when the difference in onset no longer changes at largerAV shortening intervals (see Figs. 1 and 5D); in that case, RV pacingno longer solely advances RV contraction, but prematurely activatesthe LV as well.
The duration of RV and LV contraction was defined as the timeinterval between 5% rise and 95% fall in developed pressure. Coro-nary perfusion was measured by average total coronary flow.
Statistical analyses. All data were verified for normal distribution,and values were expressed as means � SE, unless stated otherwise. AP value �0.05 was considered significant. Group differences were
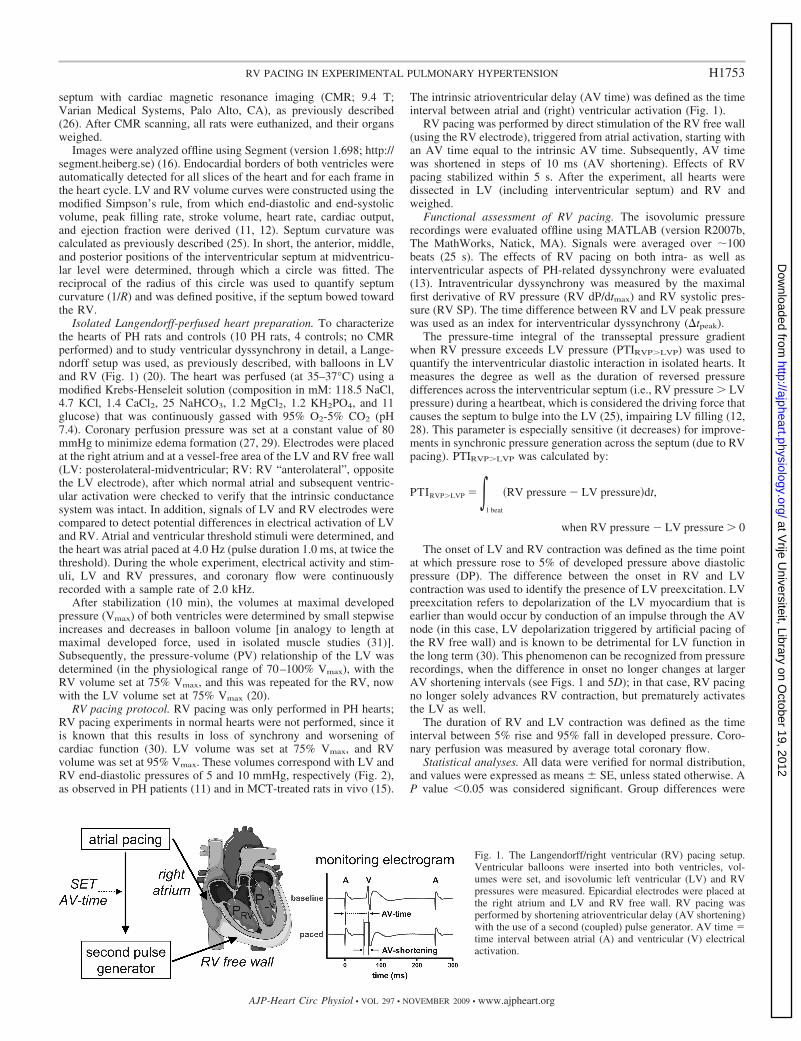
Fig. 1. The Langendorff/right ventricular (RV) pacing setup.Ventricular balloons were inserted into both ventricles, vol-umes were set, and isovolumic left ventricular (LV) and RVpressures were measured. Epicardial electrodes were placed atthe right atrium and LV and RV free wall. RV pacing wasperformed by shortening atrioventricular delay (AV shortening)with the use of a second (coupled) pulse generator. AV time �time interval between atrial (A) and ventricular (V) electricalactivation.
H1753RV PACING IN EXPERIMENTAL PULMONARY HYPERTENSION
AJP-Heart Circ Physiol • VOL 297 • NOVEMBER 2009 • www.ajpheart.org
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from
analyzed by unpaired Student T-test. Septum curvature, ventricularvolume curves, and PV relationships were analyzed by two-wayANOVA for repeated measurements. Paired Student T-test was per-formed to evaluate the effect of RV pacing.
RESULTS
General characteristics of PH rats vs. controls. In PH rats,CMR revealed significantly smaller cardiac output, strokevolume, lower heart rate, and RV ejection fraction, and signif-icantly larger RV end-diastolic volumes, compared with con-trol (Table 1). Autopsy showed a significant increase in (wet)
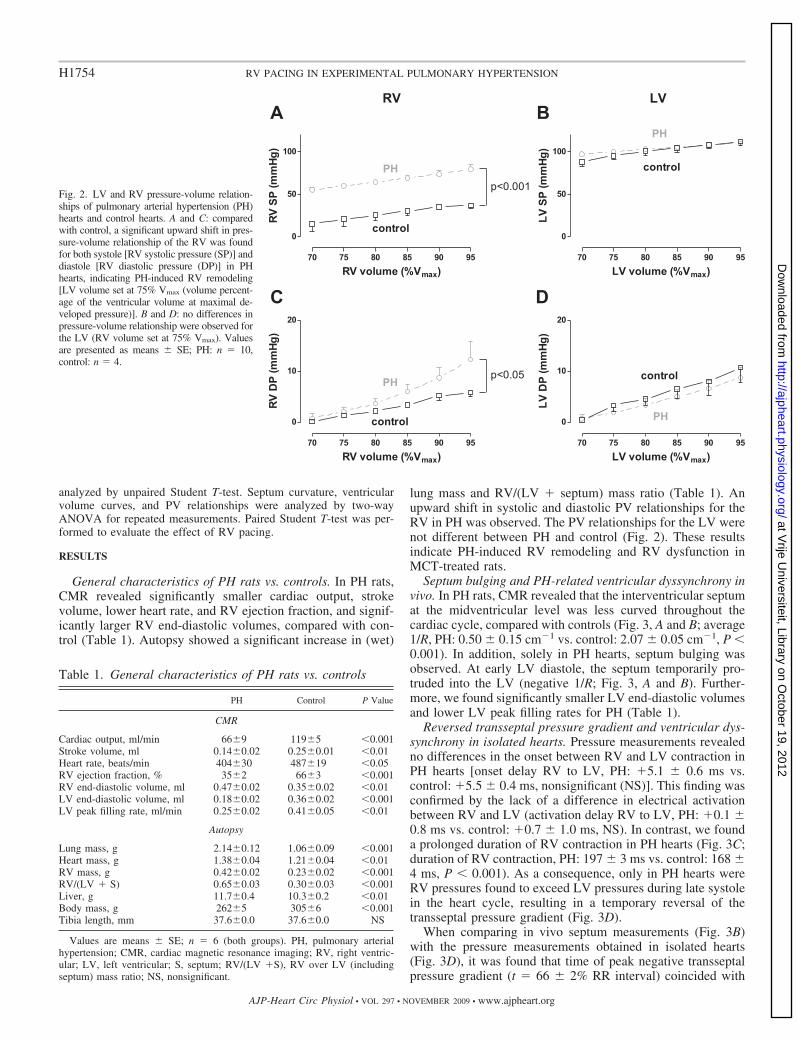
lung mass and RV/(LV � septum) mass ratio (Table 1). Anupward shift in systolic and diastolic PV relationships for theRV in PH was observed. The PV relationships for the LV werenot different between PH and control (Fig. 2). These resultsindicate PH-induced RV remodeling and RV dysfunction inMCT-treated rats.
Septum bulging and PH-related ventricular dyssynchrony invivo. In PH rats, CMR revealed that the interventricular septumat the midventricular level was less curved throughout thecardiac cycle, compared with controls (Fig. 3, A and B; average1/R, PH: 0.50 � 0.15 cm�1 vs. control: 2.07 � 0.05 cm�1, P �0.001). In addition, solely in PH hearts, septum bulging wasobserved. At early LV diastole, the septum temporarily pro-truded into the LV (negative 1/R; Fig. 3, A and B). Further-more, we found significantly smaller LV end-diastolic volumesand lower LV peak filling rates for PH (Table 1).
Reversed transseptal pressure gradient and ventricular dys-synchrony in isolated hearts. Pressure measurements revealedno differences in the onset between RV and LV contraction inPH hearts [onset delay RV to LV, PH: �5.1 � 0.6 ms vs.control: �5.5 � 0.4 ms, nonsignificant (NS)]. This finding wasconfirmed by the lack of a difference in electrical activationbetween RV and LV (activation delay RV to LV, PH: �0.1 �0.8 ms vs. control: �0.7 � 1.0 ms, NS). In contrast, we founda prolonged duration of RV contraction in PH hearts (Fig. 3C;duration of RV contraction, PH: 197 � 3 ms vs. control: 168 �4 ms, P � 0.001). As a consequence, only in PH hearts wereRV pressures found to exceed LV pressures during late systolein the heart cycle, resulting in a temporary reversal of thetransseptal pressure gradient (Fig. 3D).
When comparing in vivo septum measurements (Fig. 3B)with the pressure measurements obtained in isolated hearts(Fig. 3D), it was found that time of peak negative transseptalpressure gradient (t � 66 � 2% RR interval) coincided with
Fig. 2. LV and RV pressure-volume relation-ships of pulmonary arterial hypertension (PH)hearts and control hearts. A and C: comparedwith control, a significant upward shift in pres-sure-volume relationship of the RV was foundfor both systole [RV systolic pressure (SP)] anddiastole [RV diastolic pressure (DP)] in PHhearts, indicating PH-induced RV remodeling[LV volume set at 75% Vmax (volume percent-age of the ventricular volume at maximal de-veloped pressure)]. B and D: no differences inpressure-volume relationship were observed forthe LV (RV volume set at 75% Vmax). Valuesare presented as means � SE; PH: n � 10,control: n � 4.
Table 1. General characteristics of PH rats vs. controls
PH Control P Value
CMR
Cardiac output, ml/min 66�9 119�5 �0.001Stroke volume, ml 0.14�0.02 0.25�0.01 �0.01Heart rate, beats/min 404�30 487�19 �0.05RV ejection fraction, % 35�2 66�3 �0.001RV end-diastolic volume, ml 0.47�0.02 0.35�0.02 �0.01LV end-diastolic volume, ml 0.18�0.02 0.36�0.02 �0.001LV peak filling rate, ml/min 0.25�0.02 0.41�0.05 �0.01
Autopsy
Lung mass, g 2.14�0.12 1.06�0.09 �0.001Heart mass, g 1.38�0.04 1.21�0.04 �0.01RV mass, g 0.42�0.02 0.23�0.02 �0.001RV/(LV � S) 0.65�0.03 0.30�0.03 �0.001Liver, g 11.7�0.4 10.3�0.2 �0.01Body mass, g 262�5 305�6 �0.001Tibia length, mm 37.6�0.0 37.6�0.0 NS
Values are means � SE; n � 6 (both groups). PH, pulmonary arterialhypertension; CMR, cardiac magnetic resonance imaging; RV, right ventric-ular; LV, left ventricular; S, septum; RV/(LV �S), RV over LV (includingseptum) mass ratio; NS, nonsignificant.
H1754 RV PACING IN EXPERIMENTAL PULMONARY HYPERTENSION
AJP-Heart Circ Physiol • VOL 297 • NOVEMBER 2009 • www.ajpheart.org
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from
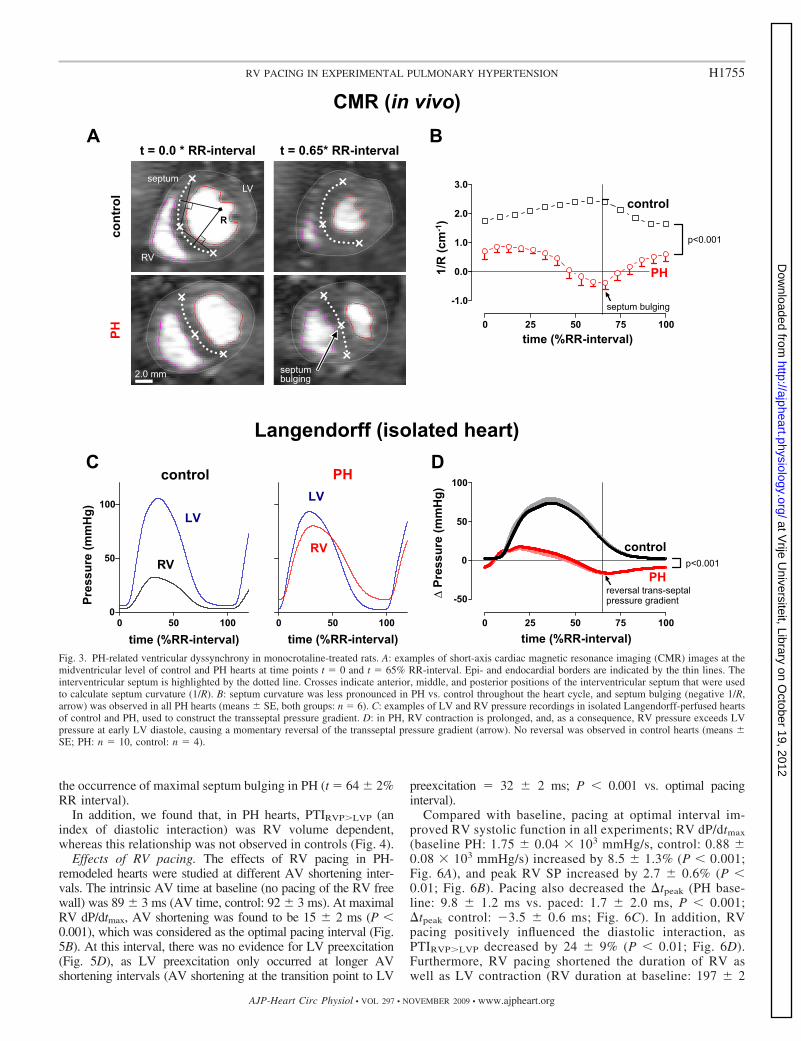
the occurrence of maximal septum bulging in PH (t � 64 � 2%RR interval).
In addition, we found that, in PH hearts, PTIRVP�LVP (anindex of diastolic interaction) was RV volume dependent,whereas this relationship was not observed in controls (Fig. 4).
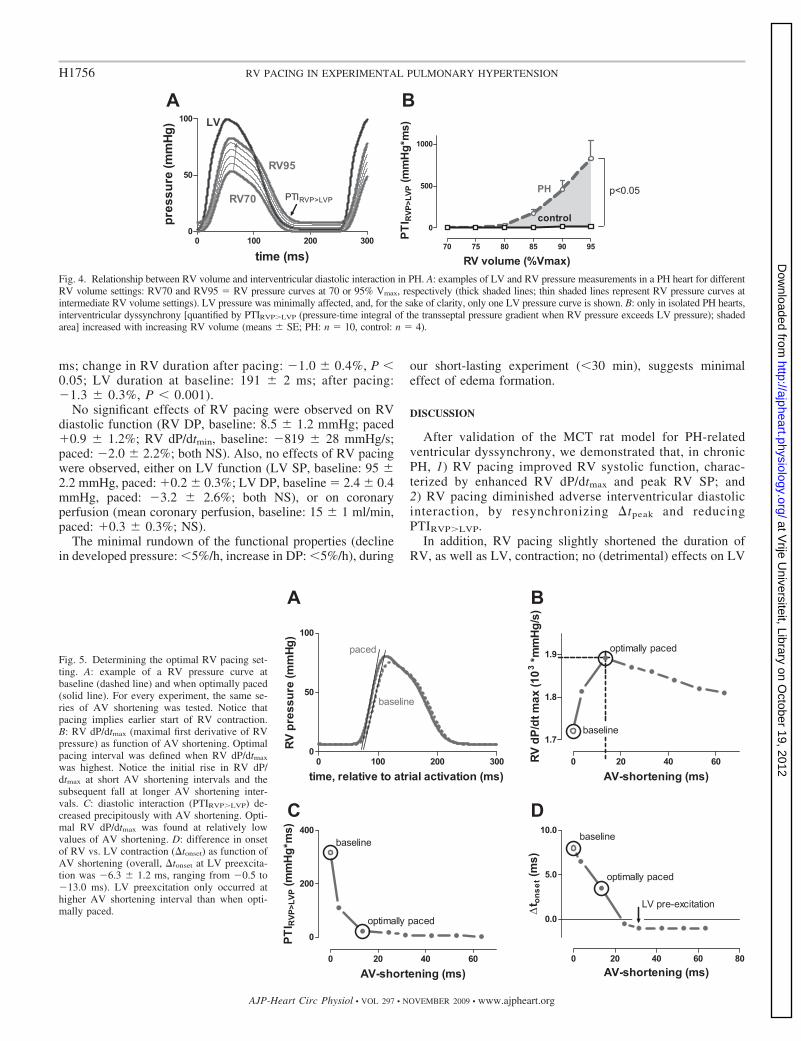
Effects of RV pacing. The effects of RV pacing in PH-remodeled hearts were studied at different AV shortening inter-vals. The intrinsic AV time at baseline (no pacing of the RV freewall) was 89 � 3 ms (AV time, control: 92 � 3 ms). At maximalRV dP/dtmax, AV shortening was found to be 15 � 2 ms (P �0.001), which was considered as the optimal pacing interval (Fig.5B). At this interval, there was no evidence for LV preexcitation(Fig. 5D), as LV preexcitation only occurred at longer AVshortening intervals (AV shortening at the transition point to LV
preexcitation � 32 � 2 ms; P � 0.001 vs. optimal pacinginterval).
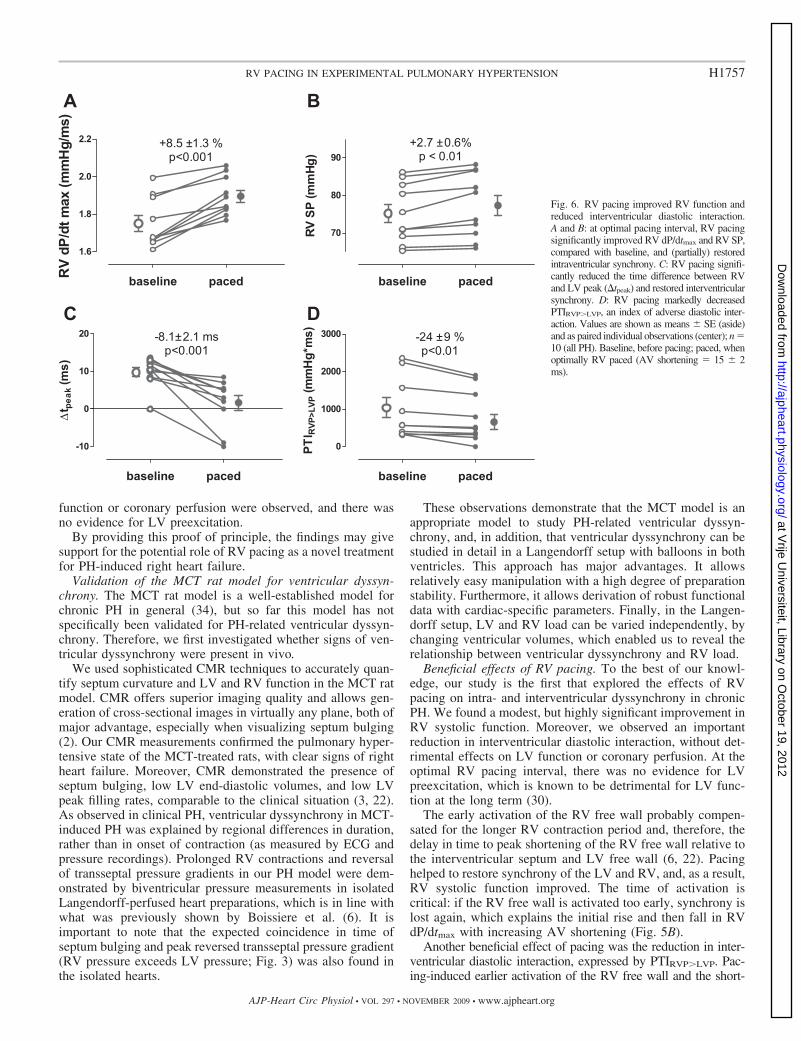
Compared with baseline, pacing at optimal interval im-proved RV systolic function in all experiments; RV dP/dtmax
(baseline PH: 1.75 � 0.04 � 103 mmHg/s, control: 0.88 �0.08 � 103 mmHg/s) increased by 8.5 � 1.3% (P � 0.001;Fig. 6A), and peak RV SP increased by 2.7 � 0.6% (P �0.01; Fig. 6B). Pacing also decreased the �tpeak (PH base-line: 9.8 � 1.2 ms vs. paced: 1.7 � 2.0 ms, P � 0.001;�tpeak control: �3.5 � 0.6 ms; Fig. 6C). In addition, RVpacing positively influenced the diastolic interaction, asPTIRVP�LVP decreased by 24 � 9% (P � 0.01; Fig. 6D).Furthermore, RV pacing shortened the duration of RV aswell as LV contraction (RV duration at baseline: 197 � 2
Fig. 3. PH-related ventricular dyssynchrony in monocrotaline-treated rats. A: examples of short-axis cardiac magnetic resonance imaging (CMR) images at themidventricular level of control and PH hearts at time points t � 0 and t � 65% RR-interval. Epi- and endocardial borders are indicated by the thin lines. Theinterventricular septum is highlighted by the dotted line. Crosses indicate anterior, middle, and posterior positions of the interventricular septum that were usedto calculate septum curvature (1/R). B: septum curvature was less pronounced in PH vs. control throughout the heart cycle, and septum bulging (negative 1/R,arrow) was observed in all PH hearts (means � SE, both groups: n � 6). C: examples of LV and RV pressure recordings in isolated Langendorff-perfused heartsof control and PH, used to construct the transseptal pressure gradient. D: in PH, RV contraction is prolonged, and, as a consequence, RV pressure exceeds LVpressure at early LV diastole, causing a momentary reversal of the transseptal pressure gradient (arrow). No reversal was observed in control hearts (means �SE; PH: n � 10, control: n � 4).
H1755RV PACING IN EXPERIMENTAL PULMONARY HYPERTENSION
AJP-Heart Circ Physiol • VOL 297 • NOVEMBER 2009 • www.ajpheart.org
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from
ms; change in RV duration after pacing: �1.0 � 0.4%, P �0.05; LV duration at baseline: 191 � 2 ms; after pacing:�1.3 � 0.3%, P � 0.001).
No significant effects of RV pacing were observed on RVdiastolic function (RV DP, baseline: 8.5 � 1.2 mmHg; paced�0.9 � 1.2%; RV dP/dtmin, baseline: �819 � 28 mmHg/s;paced: �2.0 � 2.2%; both NS). Also, no effects of RV pacingwere observed, either on LV function (LV SP, baseline: 95 �2.2 mmHg, paced: �0.2 � 0.3%; LV DP, baseline � 2.4 � 0.4mmHg, paced: �3.2 � 2.6%; both NS), or on coronaryperfusion (mean coronary perfusion, baseline: 15 � 1 ml/min,paced: �0.3 � 0.3%; NS).
The minimal rundown of the functional properties (declinein developed pressure: �5%/h, increase in DP: �5%/h), during
our short-lasting experiment (�30 min), suggests minimaleffect of edema formation.
DISCUSSION
After validation of the MCT rat model for PH-relatedventricular dyssynchrony, we demonstrated that, in chronicPH, 1) RV pacing improved RV systolic function, charac-terized by enhanced RV dP/dtmax and peak RV SP; and2) RV pacing diminished adverse interventricular diastolicinteraction, by resynchronizing �tpeak and reducingPTIRVP�LVP.
In addition, RV pacing slightly shortened the duration ofRV, as well as LV, contraction; no (detrimental) effects on LV
Fig. 4. Relationship between RV volume and interventricular diastolic interaction in PH. A: examples of LV and RV pressure measurements in a PH heart for differentRV volume settings: RV70 and RV95 � RV pressure curves at 70 or 95% Vmax, respectively (thick shaded lines; thin shaded lines represent RV pressure curves atintermediate RV volume settings). LV pressure was minimally affected, and, for the sake of clarity, only one LV pressure curve is shown. B: only in isolated PH hearts,interventricular dyssynchrony [quantified by PTIRVP�LVP (pressure-time integral of the transseptal pressure gradient when RV pressure exceeds LV pressure); shadedarea] increased with increasing RV volume (means � SE; PH: n � 10, control: n � 4).
Fig. 5. Determining the optimal RV pacing set-ting. A: example of a RV pressure curve atbaseline (dashed line) and when optimally paced(solid line). For every experiment, the same se-ries of AV shortening was tested. Notice thatpacing implies earlier start of RV contraction.B: RV dP/dtmax (maximal first derivative of RVpressure) as function of AV shortening. Optimalpacing interval was defined when RV dP/dtmax
was highest. Notice the initial rise in RV dP/dtmax at short AV shortening intervals and thesubsequent fall at longer AV shortening inter-vals. C: diastolic interaction (PTIRVP�LVP) de-creased precipitously with AV shortening. Opti-mal RV dP/dtmax was found at relatively lowvalues of AV shortening. D: difference in onsetof RV vs. LV contraction (�tonset) as function ofAV shortening (overall, �tonset at LV preexcita-tion was �6.3 � 1.2 ms, ranging from �0.5 to�13.0 ms). LV preexcitation only occurred athigher AV shortening interval than when opti-mally paced.
H1756 RV PACING IN EXPERIMENTAL PULMONARY HYPERTENSION
AJP-Heart Circ Physiol • VOL 297 • NOVEMBER 2009 • www.ajpheart.org
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from
function or coronary perfusion were observed, and there wasno evidence for LV preexcitation.
By providing this proof of principle, the findings may givesupport for the potential role of RV pacing as a novel treatmentfor PH-induced right heart failure.
Validation of the MCT rat model for ventricular dyssyn-chrony. The MCT rat model is a well-established model forchronic PH in general (34), but so far this model has notspecifically been validated for PH-related ventricular dyssyn-chrony. Therefore, we first investigated whether signs of ven-tricular dyssynchrony were present in vivo.
We used sophisticated CMR techniques to accurately quan-tify septum curvature and LV and RV function in the MCT ratmodel. CMR offers superior imaging quality and allows gen-eration of cross-sectional images in virtually any plane, both ofmajor advantage, especially when visualizing septum bulging(2). Our CMR measurements confirmed the pulmonary hyper-tensive state of the MCT-treated rats, with clear signs of rightheart failure. Moreover, CMR demonstrated the presence ofseptum bulging, low LV end-diastolic volumes, and low LVpeak filling rates, comparable to the clinical situation (3, 22).As observed in clinical PH, ventricular dyssynchrony in MCT-induced PH was explained by regional differences in duration,rather than in onset of contraction (as measured by ECG andpressure recordings). Prolonged RV contractions and reversalof transseptal pressure gradients in our PH model were dem-onstrated by biventricular pressure measurements in isolatedLangendorff-perfused heart preparations, which is in line withwhat was previously shown by Boissiere et al. (6). It isimportant to note that the expected coincidence in time ofseptum bulging and peak reversed transseptal pressure gradient(RV pressure exceeds LV pressure; Fig. 3) was also found inthe isolated hearts.
These observations demonstrate that the MCT model is anappropriate model to study PH-related ventricular dyssyn-chrony, and, in addition, that ventricular dyssynchrony can bestudied in detail in a Langendorff setup with balloons in bothventricles. This approach has major advantages. It allowsrelatively easy manipulation with a high degree of preparationstability. Furthermore, it allows derivation of robust functionaldata with cardiac-specific parameters. Finally, in the Langen-dorff setup, LV and RV load can be varied independently, bychanging ventricular volumes, which enabled us to reveal therelationship between ventricular dyssynchrony and RV load.
Beneficial effects of RV pacing. To the best of our knowl-edge, our study is the first that explored the effects of RVpacing on intra- and interventricular dyssynchrony in chronicPH. We found a modest, but highly significant improvement inRV systolic function. Moreover, we observed an importantreduction in interventricular diastolic interaction, without det-rimental effects on LV function or coronary perfusion. At theoptimal RV pacing interval, there was no evidence for LVpreexcitation, which is known to be detrimental for LV func-tion at the long term (30).
The early activation of the RV free wall probably compen-sated for the longer RV contraction period and, therefore, thedelay in time to peak shortening of the RV free wall relative tothe interventricular septum and LV free wall (6, 22). Pacinghelped to restore synchrony of the LV and RV, and, as a result,RV systolic function improved. The time of activation iscritical: if the RV free wall is activated too early, synchrony islost again, which explains the initial rise and then fall in RVdP/dtmax with increasing AV shortening (Fig. 5B).
Another beneficial effect of pacing was the reduction in inter-ventricular diastolic interaction, expressed by PTIRVP�LVP. Pac-ing-induced earlier activation of the RV free wall and the short-
Fig. 6. RV pacing improved RV function andreduced interventricular diastolic interaction.A and B: at optimal pacing interval, RV pacingsignificantly improved RV dP/dtmax and RV SP,compared with baseline, and (partially) restoredintraventricular synchrony. C: RV pacing signifi-cantly reduced the time difference between RVand LV peak (�tpeak) and restored interventricularsynchrony. D: RV pacing markedly decreasedPTIRVP�LVP, an index of adverse diastolic inter-action. Values are shown as means � SE (aside)and as paired individual observations (center); n �10 (all PH). Baseline, before pacing; paced, whenoptimally RV paced (AV shortening � 15 � 2ms).
H1757RV PACING IN EXPERIMENTAL PULMONARY HYPERTENSION
AJP-Heart Circ Physiol • VOL 297 • NOVEMBER 2009 • www.ajpheart.org
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from

ened RV contraction resulted in an earlier start of RV relaxation.The partially restored synchrony in the relaxation of both ventri-cles explains the observed reduction of the PTIRVP�LVP. Althoughisovolumic pressure measurements in our Langendorff setup can-not directly provide this information, a marked decrease inPTIRVP�LVP, together with a shortened duration of LV contrac-tion, would predict less septum bulging and improvement in earlyLV filling (12, 28).
Recently, Quinn et al. also reported positive effects ofpacing in a different model of RV pressure overload (24).However, their findings are only partially applicable to the PHpatient group, because they applied an acute pressure overloadin a pig model with the conductance system artificially dam-aged by ethanol injection. A few clinical studies have exploredthe effect of RV pacing on RV dysfunction secondary tocongenital heart disease (studies on systemic RVs are notdiscussed here) (7, 10). These studies aimed to restore RVelectromechanical dyssynchrony related to a complete rightbundle branch block, a late complication of surgical repair.However, as mentioned earlier, ventricular dyssynchrony inPH is based on prolonged contraction, rather than disturbancesin the electrical conductance system (22).
Limitations: the isolated heart vs. in vivo. This study sup-ports the potential role of RV pacing for the treatment ofPH-related ventricular dyssynchrony and right heart failure.However, the results cannot be translated directly to the in vivosituation yet. Future studies in a large-animal model or (acute)RV pacing experiments in PH patients are necessary.
In the Langendorff preparation, the mediating role of RVafterload remains unknown, which limits the prediction of theeffects of RV pacing and improved RV contractility on strokevolume and cardiac output. Nonetheless, related studies re-ported an improvement of cardiac output after RV pacing to thesame extent as the improvement in RV contractility (10, 24).RV pacing could also potentially worsen tricuspid regurgita-tion through elevation of RV SPs. On the other hand, it wasrecently shown that resynchronization therapy in left heartfailure actually reduced preexisting mitral regurgitation (35).
Another important issue is the role of the pericardium. In ourisolated Langendorff-perfused hearts, the pericardium was re-moved, which is known to reduce the interventricular diastolicinteraction in the case of RV pressure overload (4). This mightexplain why we did not observe a significant reduction in LVDP/LV filling pressures by RV pacing (that were already lowat baseline) in our isolated heart preparations (5). The effects ofRV pacing will probably be more pronounced in vivo with thepericardium intact.
Crystalloid-based Langendorff-perfused hearts are prone toedema formation, which could affect diastolic properties. How-ever, with a coronary perfusion pressure of 80 mmHg, this wasreduced to a minimum (27, 29). In addition, edema formationwas found to have only limited functional effects during ourexperiments, as we observed a minimal rundown of the func-tional properties during our short-lasting experiments, and wewere also able to detect clear differences in diastolic propertiesbetween control and PH heart.
We found longer PR intervals than are reported for (PH) ratsin vivo (�90 vs. �60 ms) (17). However, no differences wereobserved between PR intervals of isolated PH and controlhearts. We, therefore, conclude that the prolonged PR interval,compared with the in vivo situation, is most likely to be
attributed to the Langendorff setup in general and unlikely tobe related to differences in cardiac condition between PHhearts and controls. Furthermore, the apparently prolonged PRinterval is of little relevance for the interpretation of ourfinding, as the intervention studied involves ventricular activa-tion, which follows after the PR interval.
As a last point, clinical effective medical therapies, such asepoprostenol, are known to have a relatively small impact onhemodynamic measures, which, nonetheless, translate to im-proved survival (1). Therefore, the small acute improvementsin RV function found here may, in the long term, translate intosubstantial benefit.
Conclusions. In our experimental PH model, RV pacingimproved cardiac performance through alleviation of PH-re-lated ventricular dyssynchrony. The promising results of thisstudy identify RV pacing as a potential novel treatment forright heart failure in PH and provide a strong rationale forfuture investigations evaluating the effects of RV pacing invivo.
ACKNOWLEDGMENTS
We thank Taco Kind and Ingrid Schalij (Pulmonology, VU UniversityMedical Center) for assistance.
GRANTS
This work was supported by the Netherlands Organization for ScientificResearch, The Hague, The Netherlands (M. L. Handoko, A. Vonk-Noorde-graaf).
REFERENCES
1. Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, Badesch DB,Groves BM, Tapson VF, Bourge RC, Brundage BH, Koerner SK,Langleben D, Keller CA, Murali S, Uretsky BF, Clayton LM, JobsisMM, Blackburn SD Jr, Shortino D, Crow JW. A comparison ofcontinuous intravenous epoprostenol (prostacyclin) with conventionaltherapy for primary pulmonary hypertension. The Primary PulmonaryHypertension Study Group. N Engl J Med 334: 296–302, 1996.
2. Benza R, Biederman R, Murali S, Gupta H. Role of cardiac magneticresonance imaging in the management of patients with pulmonary arterialhypertension. J Am Coll Cardiol 52: 1683–1692, 2008.
3. Beyar R. Heart inefficiency in pulmonary hypertension: a double jeopardy.J Am Coll Cardiol 51: 758–759, 2008.
4. Beyar R, Dong SJ, Smith ER, Belenkie I, Tyberg JV. Ventricularinteraction and septal deformation: a model compared with experimentaldata. Am J Physiol Heart Circ Physiol 265: H2044–H2056, 1993.
5. Bleasdale RA, Turner MS, Mumford CE, Steendijk P, Paul V, TybergJV, Morris-Thurgood JA, Frenneaux MP. Left ventricular pacingminimizes diastolic ventricular interaction, allowing improved preload-dependent systolic performance. Circulation 110: 2395–2400, 2004.
6. Boissiere J, Gautier M, Machet MC, Hanton G, Bonnet P, Eder V.Doppler tissue imaging in assessment of pulmonary hypertension-inducedright ventricle dysfunction. Am J Physiol Heart Circ Physiol 289: H2450–H2455, 2005.
7. Bordachar P, Iriart X, Chabaneix J, Sacher F, Lafitte S, Jais P,Haissaguerre M, Clementy J, Dos SP, Thambo JB. Presence of ven-tricular dyssynchrony and haemodynamic impact of right ventricularpacing in adults with repaired Tetralogy of Fallot and right bundle branchblock. Europace 10: 967–971, 2008.
8. Buermans HP, Redout EM, Schiel AE, Musters RJ, Zuidwijk M, EijkPP, van Hardeveld C, Kasanmoentalib S, Visser FC, Ylstra B, Simo-nides WS. Microarray analysis reveals pivotal divergent mRNA expres-sion profiles early in the development of either compensated ventricularhypertrophy or heart failure. Physiol Genomics 21: 314–323, 2005.
9. Dohi K, Onishi K, Gorcsan J III, Lopez-Candales A, Takamura T,Ota S, Yamada N, Ito M. Role of radial strain and displacement imagingto quantify wall motion dyssynchrony in patients with left ventricularmechanical dyssynchrony and chronic right ventricular pressure overload.Am J Cardiol 101: 1206–1212, 2008.
H1758 RV PACING IN EXPERIMENTAL PULMONARY HYPERTENSION
AJP-Heart Circ Physiol • VOL 297 • NOVEMBER 2009 • www.ajpheart.org
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from
10. Dubin AM, Feinstein JA, Reddy VM, Hanley FL, Van Hare GF,Rosenthal DN. Electrical resynchronization: a novel therapy for thefailing right ventricle. Circulation 107: 2287–2289, 2003.
11. Gan CT, Holverda S, Marcus JT, Paulus WJ, Marques KM,Bronzwaer JG, Twisk JW, Boonstra A, Postmus PE, Vonk-Noorde-graaf A. Right ventricular diastolic dysfunction and the acute effects ofsildenafil in pulmonary hypertension patients. Chest 132: 11–17, 2007.
12. Gan CT, Lankhaar JW, Marcus JT, Westerhof N, Marques KM,Bronzwaer JG, Boonstra A, Postmus PE, Vonk-Noordegraaf A. Im-paired left ventricular filling due to right-to-left ventricular interaction inpatients with pulmonary arterial hypertension. Am J Physiol Heart CircPhysiol 290: H1528–H1533, 2006.
13. Ghio S, Constantin C, Klersy C, Serio A, Fontana A, Campana C,Tavazzi L. Interventricular and intraventricular dyssynchrony are com-mon in heart failure patients, regardless of QRS duration. Eur Heart J 25:571–578, 2004.
14. Gillebert TC, Sys SU, Brutsaert DL. Influence of loading patterns onpeak length-tension relation and on relaxation in cardiac muscle. J AmColl Cardiol 13: 483–490, 1989.
15. Handoko ML, Schalij I, Kramer K, Sebkhi A, Postmus PE, van derLaarse WJ, Paulus WJ, Vonk-Noordegraaf A. A refined radio-teleme-try technique to monitor right ventricle or pulmonary artery pressures inrats: a useful tool in pulmonary hypertension research. Pflugers Arch 455:951–959, 2008.
16. Heiberg E, Wigstrom L, Carlsson M, Bolger AF, Karlsson M. Timeresolved three-dimensional automated segmentation of the left ventricle.Proc IEEE Comput Cardiol 32: 599–602, 2005.
17. Henkens IR, Mouchaers KT, Vliegen HW, van der Laarse WJ,Swenne CA, Maan AC, Draisma HH, Schalij I, van der Wall EE,Schalij MJ, Vonk-Noordegraaf A. Early changes in rat hearts withdeveloping pulmonary arterial hypertension can be detected with three-dimensional electrocardiography. Am J Physiol Heart Circ Physiol 293:H1300–H1307, 2007.
18. Kalogeropoulos AP, Georgiopoulou VV, Howell S, Pernetz MA,Fisher MR, Lerakis S, Martin RP. Evaluation of right intraventriculardyssynchrony by two-dimensional strain echocardiography in patientswith pulmonary arterial hypertension. J Am Soc Echocardiogr 21: 1028–1034, 2008.
19. Kingma I, Tyberg JV, Smith ER. Effects of diastolic transseptal pressuregradient on ventricular septal position and motion. Circulation 68: 1304–1314, 1983.
20. Lamberts RR, Vaessen RJ, Westerhof N, Stienen GJ. Right ventricularhypertrophy causes impairment of left ventricular diastolic function in therat. Basic Res Cardiol 102: 19–27, 2007.
21. Lopez-Candales A, Dohi K, Rajagopalan N, Suffoletto M, Murali S,Gorcsan J, Edelman K. Right ventricular dyssynchrony in patients withpulmonary hypertension is associated with disease severity and functionalclass. Cardiovasc Ultrasound 3: 23, 2005.
22. Marcus JT, Gan CT, Zwanenburg JJ, Boonstra A, Allaart CP, GotteMJ, Vonk-Noordegraaf A. Interventricular mechanical asynchrony inpulmonary arterial hypertension: left-to-right delay in peak shortening is
related to right ventricular overload and left ventricular underfilling. J AmColl Cardiol 51: 750–757, 2008.
23. McAlister FA, Ezekowitz J, Hooton N, Vandermeer B, Spooner C,Dryden DM, Page RL, Hlatky MA, Rowe BH. Cardiac resynchroniza-tion therapy for patients with left ventricular systolic dysfunction: asystematic review. JAMA 297: 2502–2514, 2007.
24. Quinn TA, Berberian G, Cabreriza SE, Maskin LJ, Weinberg AD,Holmes JW, Spotnitz HM. Effects of sequential biventricular pacingduring acute right ventricular pressure overload. Am J Physiol Heart CircPhysiol 291: H2380–H2387, 2006.
25. Roeleveld RJ, Marcus JT, Faes TJ, Gan TJ, Boonstra A, Postmus PE,Vonk-Noordegraaf A. Interventricular septal configuration at MR imag-ing and pulmonary arterial pressure in pulmonary hypertension. Radiology234: 710–717, 2005.
26. Schneider JE, Lanz T, Barnes H, Medway D, Stork LA, Lygate CA,Smart S, Griswold MA, Neubauer S. Ultra-fast and accurate assessmentof cardiac function in rats using accelerated MRI at 9.4 Tesla. Magn ResonMed 59: 636–641, 2008.
27. Skrzypiec-Spring M, Grotthus B, Szelag A, Schulz R. Isolated heartperfusion according to Langendorff–still viable in the new millennium.J Pharmacol Toxicol Methods 55: 113–126, 2007.
28. Stojnic BB, Brecker SJ, Xiao HB, Helmy SM, Mbaissouroum M,Gibson DG. Left ventricular filling characteristics in pulmonary hyper-tension: a new mode of ventricular interaction. Br Heart J 68: 16–20,1992.
29. Sutherland FJ, Hearse DJ. The isolated blood and perfusion fluidperfused heart. Pharmacol Res 41: 613–627, 2000.
30. Sweeney MO, Prinzen FW. A new paradigm for physiologic ventricularpacing. J Am Coll Cardiol 47: 282–288, 2006.
31. Sys SU, De Keulenaer GW, Brutsaert DL. Physiopharmacologicalevaluation of myocardial performance: how to study modulation bycardiac endothelium and related humoral factors? Cardiovasc Res 39:136–147, 1998.
32. Tanaka H, Tei C, Nakao S, Tahara M, Sakurai S, Kashima T,Kanehisa T. Diastolic bulging of the interventricular septum toward theleft ventricle. An echocardiographic manifestation of negative interven-tricular pressure gradient between left and right ventricles during diastole.Circulation 62: 558–563, 1980.
33. Voelkel NF, Quaife RA, Leinwand LA, Barst RJ, McGoon MD,Meldrum DR, Dupuis J, Long CS, Rubin LJ, Smart FW, Suzuki YJ,Gladwin M, Denholm EM, Gail DB. Right ventricular function andfailure: report of a National Heart, Lung, and Blood Institute workinggroup on cellular and molecular mechanisms of right heart failure. Cir-culation 114: 1883–1891, 2006.
34. Wilson DW, Segall HJ, Pan LC, Lame MW, Estep JE, Morin D.Mechanisms and pathology of monocrotaline pulmonary toxicity. Crit RevToxicol 22: 307–325, 1992.
35. Ypenburg C, Lancellotti P, Tops LF, Boersma E, Bleeker GB, HolmanER, Thomas JD, Schalij MJ, Pierard LA, Bax JJ. Mechanism ofimprovement in mitral regurgitation after cardiac resynchronization ther-apy. Eur Heart J 29: 757–765, 2008.
H1759RV PACING IN EXPERIMENTAL PULMONARY HYPERTENSION
AJP-Heart Circ Physiol • VOL 297 • NOVEMBER 2009 • www.ajpheart.org
at Vrije U
niversiteit, Library on October 19, 2012
http://ajpheart.physiology.org/D
ownloaded from
Related Documents











