Richard M. Hoffman, MD, MPH DOIM Thursday School October 30, 2014

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Richard M. Hoffman, MD, MPHDOIM Thursday SchoolOctober 30, 2014
“But I’m admitting that American medicine has overpromised when it comes to screening. The advantages to screening have been exaggerated.”
Otis Brawley, MD Chief Medical Officer American Cancer Society
New York Times (10/21/09)
Screening definitionCriteria for implementing screeningEvaluating the efficacy of screeningCritical review of prostate cancer
screening Evidence Guidelines
USPSTF cancer screening recommendations
Applying a diagnostic test to asymptomatic people to classify their likelihood of having a particular disease

“Likelihood of disease”
“Likelihood of disease” Persons with abnormal tests
require further diagnostic studies Gold standard tests usually
invasive, riskier, and more expensive

“Asymptomatic”
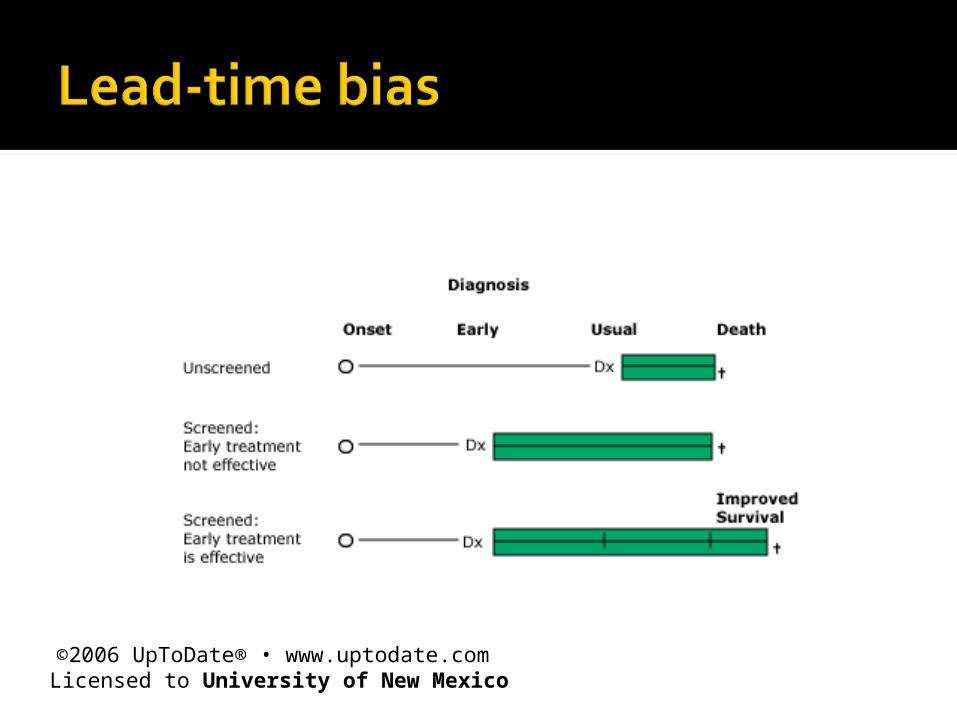
“Asymptomatic” Patient expectations Screening helpful only if early
detection and treatment is effective▪ First do no harm (primum non nocere)▪ Merely advancing the time of diagnosis
is harmful (lead time)
“Asymptomatic” Target high-risk population▪ Behaviors▪Smoking▪ Risk factors▪Family history
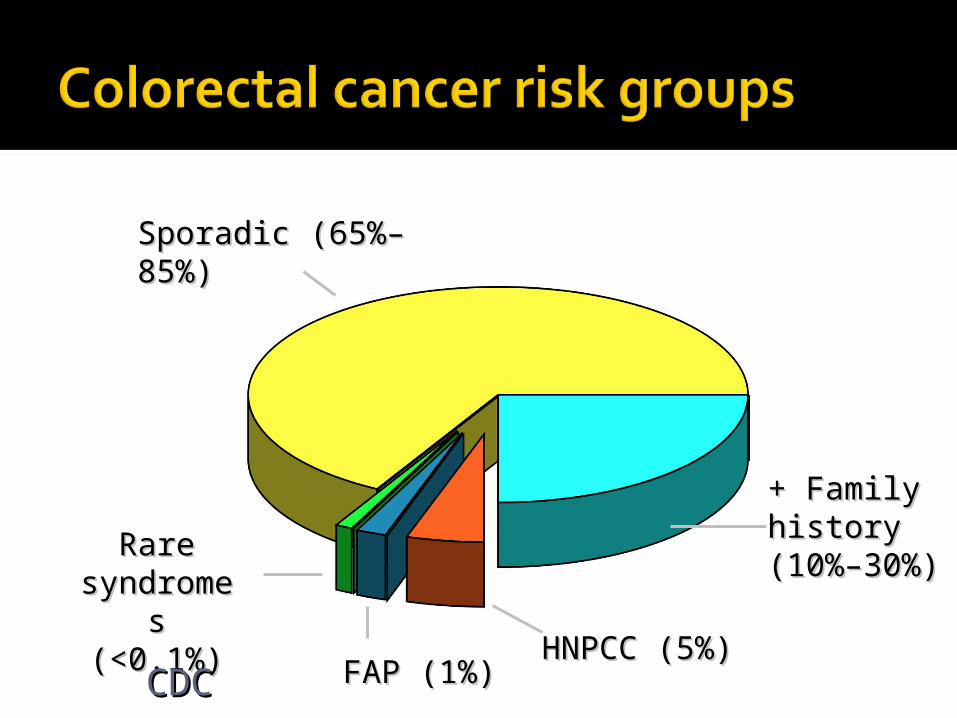
Sporadic (65%–Sporadic (65%–85%)85%)
+ Family+ Familyhistoryhistory(10%–30%)(10%–30%)
HNPCC (5%)HNPCC (5%)FAP (1%)FAP (1%)
Rare Rare syndromesyndromes (<0.1%)s (<0.1%)
CDCCDC
“Asymptomatic” Older age (> 50 years)▪ 70+ million

“Asymptomatic” Expensive▪ Screening▪ Gold-standard diagnosis
“Asymptomatic” Policy decision▪ Limited health care resources▪ Competing demands

Epidemiology
Natural history
Screening tests
Treatments

Important clinical problem Common Substantial burden of suffering▪ Impairs quality of life ▪ Hospitalizations▪ Death
Time course of disease Long asymptomatic period to make
early diagnosis
Acceptable
Available
Accurate: valid and reproducible
Detects clinically important disease
Acceptable
Available
Efficacious Reduces disease-specific mortality
and morbidity in randomized controlled trial

Outcomes Decreased disease mortality and
morbidity▪ Decreased incidence of advanced-
stage disease▪ Prevents disease (sometimes)
Screening study designs Randomized controlled trial: least
biased Observational▪ Cohort▪ Case-control
Selection
Lead-time Overdiagnosis bias
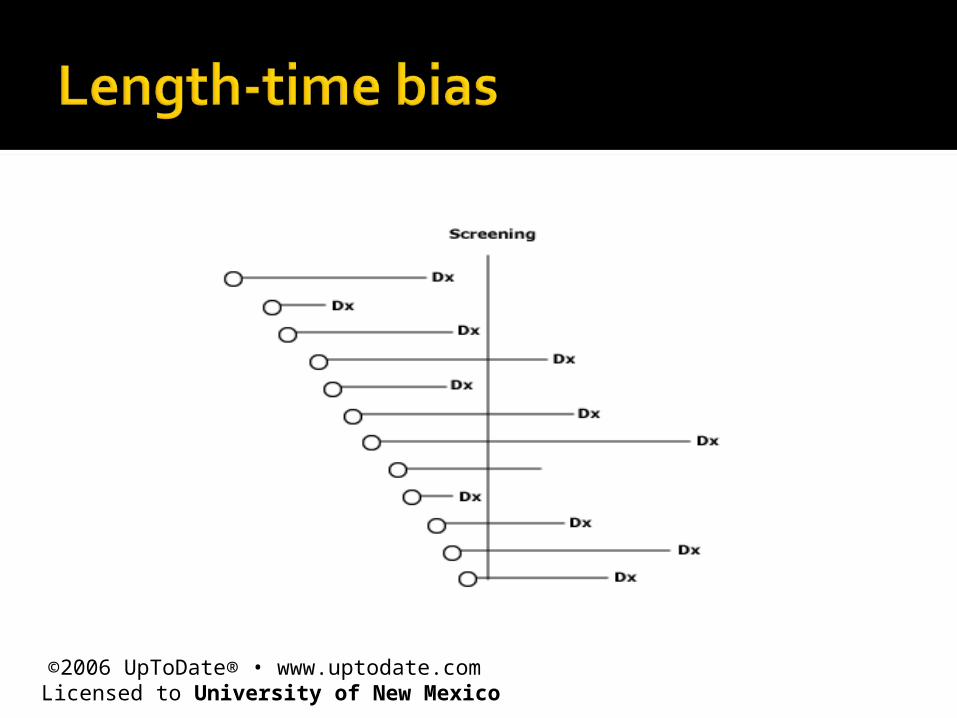
Length-time
Healthy volunteer
Adherent
Worried well
©2006 UpToDate® • www.uptodate.com Licensed to University of New Mexico

Failure to adjust for detecting “pseudo-disease” Subclinical disease that would not
have been detected during the person’s lifetime▪ No chance of dying from the disease▪ Survival time is misleading
Welch HG. JGIM 1997;12:118
©2006 UpToDate® • www.uptodate.com Licensed to University of New Mexico


2014 ACS estimates (men) 233,000 cases (1st) 29,480 deaths (2nd)
Lifetime risks Diagnosis: 1 in 6 Death: 1 in 30
American Cancer Society. Cancer Facts & Figures 2014.
Microscopic cancer (found with PSA testing) to clinical detection 5 to 15 year interval
Prostate-specific antigen (PSA) PPV: 30%
Digital rectal exam PPV: 28%
Randomized controlled trials Surgery vs. watchful waiting: 2 studies▪ RP effective for clinically detected cancers▪ Only for men < 65
▪ RP not effective for screen-detected cancers▪ Possible benefit for high-risk cancers
Radiation vs. watchful waiting: 1 study▪ No benefit
Dahabrah IJ. Ann Intern Med 2012;156:582
High burden of disease
Long asymptomatic stage
Available screening tests
Available treatments
European Randomized Study of Screening for Prostate Cancer (ERSPC)
Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (PLCO)
Randomized controlled trial of 182,160 men ages 50-74 7 European countries
Screening group PSA every 4 years
Control group Usual care
Schröder FH. N Engl J Med 2009; 360:1320
Biopsy referral PSA > 3 ng/mL
Treatment Local standards
Endpoints (9-year follow up) Cancer incidence and mortality
Schröder FH. N Engl J Med 2009; 360:1320
Initial report 162,243 in core age group 55-69
Prostate cancer incidence Screening: 8.2% Control: 4.8% ▪ Rate ratio = 1.70 (95% CI, 1.64 – 1.77)
Schröder FH. N Engl J Med 2009; 360:1320
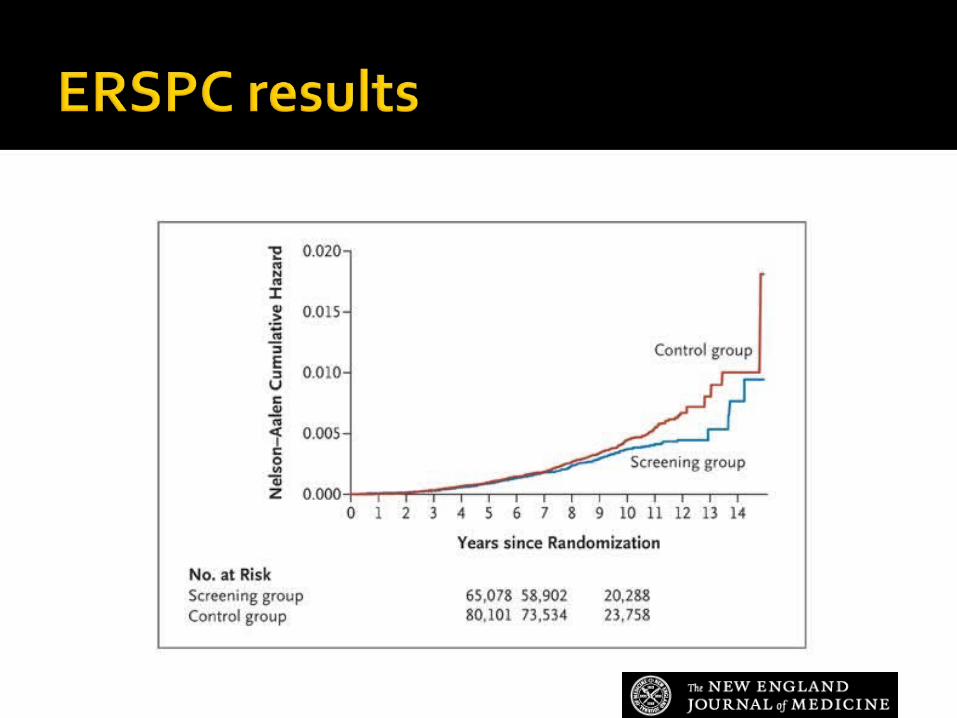
Relative risk = 0.80 (95% CI 0.65 – 0.98)
Relative risk reduction: 20%Absolute risk reduction: 0.71
deaths/1000 menNeed to invite 1410 men to be
screened twice over 9 years to prevent 1 PCa death Need to diagnose 48 cancers to
prevent 1 PCa death
Schröder FH. N Engl J Med 2009; 360:1320

Randomization methods, screening protocols, and biopsy criteria varied across countries and over time Considered a meta-analysis▪ Positive results only in Netherlands,
Sweden
Unable to exclude treatment effect Control subjects with localized PCa,
particularly with high-risk features, were less likely than screening subjects to receive radical prostatectomy—which is effective.
Control subjects more likely to receive androgen deprivation therapy—which is harmful.
Wolters T. Int J Cancer 2010; 126:2387; Barry MJ. NEJM 2009;360:1351Haines IE. J Natl Cancer Inst 2013;105:1534
Randomized controlled trial of 76,685 men ages 55-74
Screening group Annual PSA and DRE
Control group Usual care
Andriole GL. N Engl J Med 2009; 360:1310
Biopsy referral PSA > 4 ng/mL, abnormal DRE
Treatment Local standards
Endpoints (7-year follow up) Cancer incidence and mortality
Andriole GL. N Engl J Med 2009; 360:1310
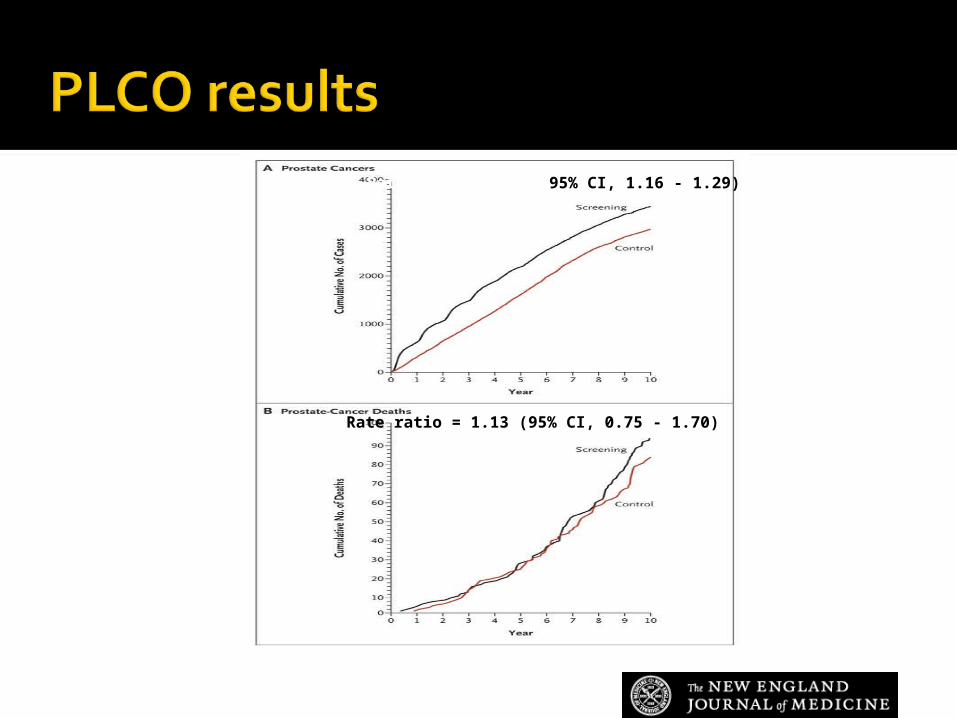
Rate ratio = 1.22 (95% CI, 1.16 - 1.29)
Rate ratio = 1.13 (95% CI, 0.75 - 1.70)

Prevalent screening 44% 1+ PSA tests within past 3
yearsContamination in control group
52% underwent PSA testing36% of those with elevated
baseline PSA not biopsied within 3 years (Pinsky PF. J Urol 2005;173:746)
American Cancer Society (ACS)
American College of Physicians (ACP)
American Urological Association (AUA)
United States Preventive Services Task Force (USPTF)
Shared/informed decision making Address screening average-risk men at
50/55▪ 10- to 15-year life expectancy
DRE optional Consider 2-year screening interval
Wolf AMD. Ca Cancer J Clin 2010;60:70; Qaseem A. Ann Intern Med 2013;158:761; Carter HB. J Urol 2013;190:419
Grade D recommendation The USPSTF recommends against
providing [PSA screening] to men without suspicious symptoms regardless of age, race, or family history
An individual man may choose to be screened. The decision should be an informed decision, preferably made in consultation with a regular care provider.
Moyer VM. Ann Intern Med 2012;157:120

Don’t ask, don’t tell (unless they ask)
Complex decisions Multiple acceptable options
involving significant tradeoffs among different possible outcomes
Extensive effect on the patient Controversial
Braddock CH. JAMA 1999; 282:2313

Elements required for complex decisions Discuss▪ Patient’s role in decision making ▪ Clinical issue or nature of decision▪ Alternatives ▪ Potential benefits and harms of the
alternatives▪ Uncertainties associated with the
decisionBraddock CH. JAMA 1999; 282:2313
Collaborative process that allows patients and their providers to make health care decisions together, taking into account the best scientific evidence available, as well as the patient’s values and preferences
http://informedmedicaldecisions.org/

PSA screening is controversial
For most men, chances of harms of screening outweigh chances benefits
Most prostate cancers are indolent
Most men, even if not screened, will not be diagnosed with or die from prostate cancer
Qaseem A. Ann Intern Med 2013;158:761
PSA testing increases risk of cancer diagnosis
PSA does not identify high-risk cancers
Small potential benefit
Many potential harms
Not “just a blood test”Qaseem A. Ann Intern Med 2013;158:761
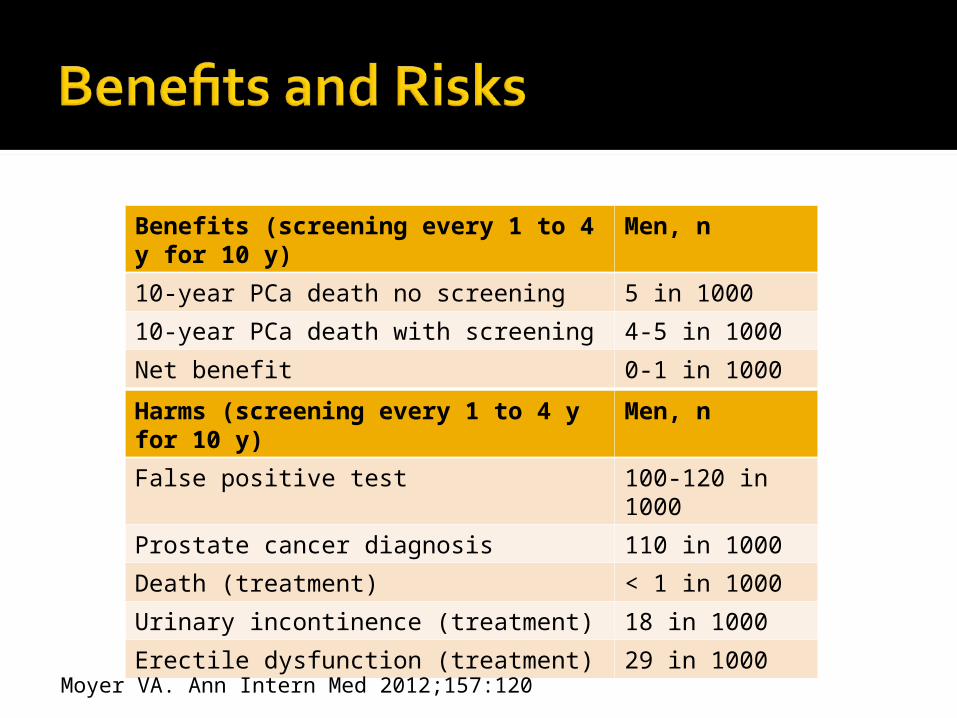
Benefits (screening every 1 to 4 y for 10 y)
Men, n
10-year PCa death no screening 5 in 1000
10-year PCa death with screening 4-5 in 1000
Net benefit 0-1 in 1000
Harms (screening every 1 to 4 y for 10 y)
Men, n
False positive test 100-120 in 1000
Prostate cancer diagnosis 110 in 1000
Death (treatment) < 1 in 1000
Urinary incontinence (treatment) 18 in 1000
Erectile dysfunction (treatment) 29 in 1000Moyer VA. Ann Intern Med 2012;157:120
Shared decision making Given the complexity of the issues
involved and the time constraints faced by health care providers, we encourage providers and patients to use prostate cancer screening decision aids to facilitate the process
Wolf AMD. Ca Cancer J Clin 2010;60:70
Tools to support decision making when evidence is uncertain and/or very sensitive to patient preferences
Formats: written, video, interactive computer programs, Web-based
Rimer BK. Cancer 2004; 101:1214. Barry MJ. Ann Intern Med 2002; 136:127
Provide evidence-based information about a health condition, the options, associated benefits, harms, probabilities, and uncertainties
O ’Connor AM. Cochrane Database Syst Rev 2009;Jul 8;(3):CD001431

Help patients to recognize the values-sensitive nature of the decision and clarify their preferences
O ’Connor AM. Cochrane Database Syst Rev 2009;Jul 8;(3):CD001431
Provide structured guidance in the steps of decision making and communicating informed values
O ’Connor AM. Cochrane Database Syst Rev 2009;Jul 8;(3):CD001431
Systematic review (18 randomized trials) Increase knowledge Reduce decisional conflict Decrease testing interest ▪ Relative risk = 0.88 (95% CI, 0.81 - 0.97)
Volk RJ. Am J Prev Med 2007;33:428



USPSTFhttp://www.uspreventiveservicestaskforce.org
American College of Physicians Guidance Statementshttp://www.acponline.org/clinical_information/guidelines/guidance/


Independent panel of nonfederal experts in prevention and evidence-based medicine Volunteer members represent
primary care disciplines▪ No substantial financial, intellectual, or
other conflicts that would impair the scientific integrity of the work of the Task Force
Rigorous review of existing peer-reviewed evidence Ratings reflect the strength of the
evidence on the harms and benefits of a preventive service▪ Task Force does not consider the costs
of providing the service or make recommendations for coverage

Grade
Evidence Recommendation
A High certainty of substantial net benefit Provide
B High certainty of moderate net benefitModerate certainty of moderate/substantial net benefit
Provide
C Moderate certainty that net benefit is small
Selectively offer/provide
D No benefit or harms outweigh benefits Do not provide
I Insufficient evidence regarding balance of benefits and harms
Patient Protection and Affordable Care Act Requires private insurers and Medicaid
to cover preventive services that have a grade of “A” or “B” from the USPSTF
Secretary of HHS can modify Medicare coverage of prevention services to be consistent with USPSTF
Grade A Cervical cancer Colorectal cancer
Grade B Breast cancer Lung cancer (LDCT)
Grade I Bladder cancer Skin cancer Oral cancer
Grade D Ovarian cancer Pancreatic cancer Prostate cancer Testicular cancer

Screening programs have important clinical and public health implications
Screening programs should be based on Burden of suffering Natural history Diagnostic tests Treatments
Screening efficacy is best demonstrated by randomized controlled trials showing Decreased mortality Decreased morbidity Preventing disease (sometimes)
Absolute benefits of screening are small
Most people face only potential harms from screening
Physicians should support patients in making informed decisions about cancer screening

Screening guidelines change Use USPSTF, ACP to prepare for
Boards
Related Documents