REVISIÓ BIBLIOGRÀFICA: REVISIÓ BIBLIOGRÀFICA: TRAUMATISMES AL TRAUMATISMES AL TRAUMATISMES AL TRAUMATISMES AL COLL COLL CLARA CANELA CLARA CANELA GRUP DE SESSIONS CLÍNIQUES GRUP DE SESSIONS CLÍNIQUES D’EMERGÈNCIES D’EMERGÈNCIES SEM BARCELONA CIUTAT SEM BARCELONA CIUTAT

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
REVISIÓ BIBLIOGRÀFICA:REVISIÓ BIBLIOGRÀFICA:TRAUMATISMES AL TRAUMATISMES AL TRAUMATISMES AL TRAUMATISMES AL
COLLCOLL
CLARA CANELACLARA CANELAGRUP DE SESSIONS CLÍNIQUES GRUP DE SESSIONS CLÍNIQUES
D’EMERGÈNCIESD’EMERGÈNCIESSEM BARCELONA CIUTAT SEM BARCELONA CIUTAT
INTRODUCCIÓINTRODUCCIÓ
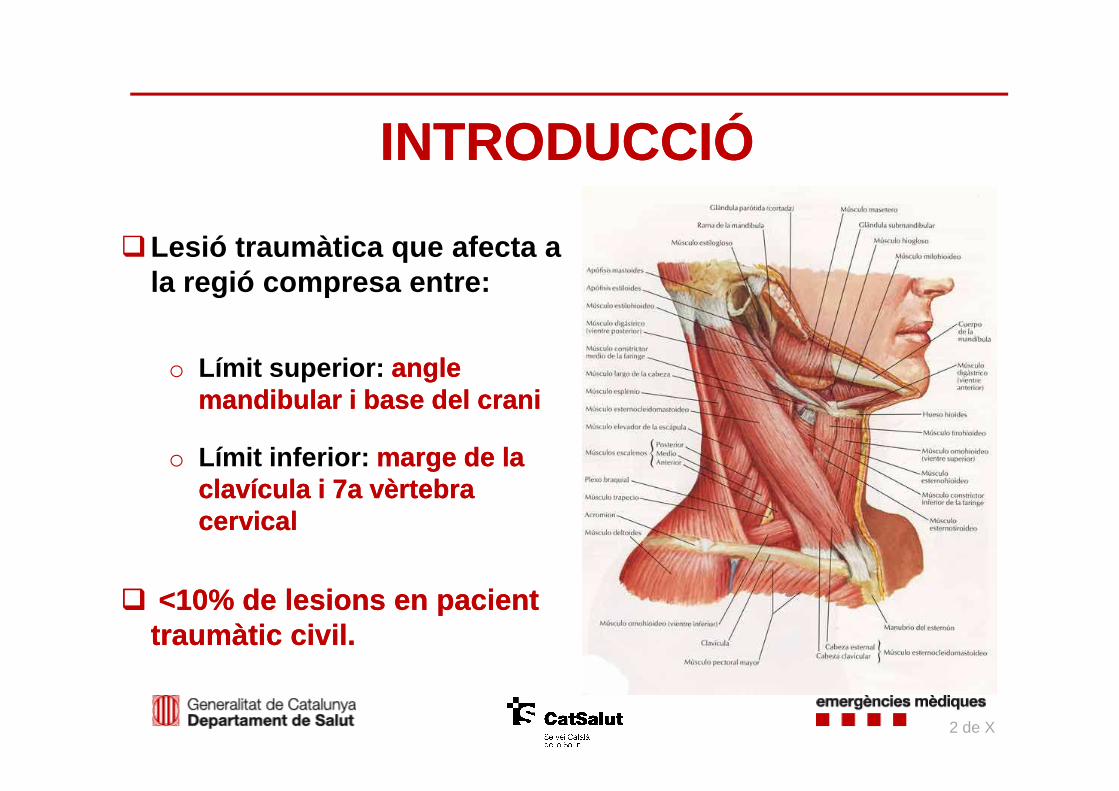
�Lesió traumàtica que afecta a la regió compresa entre:
o Límit superior: angle angle mandibular imandibular i base del cranibase del crani
2 de X
mandibular imandibular i base del cranibase del crani
o Límit inferior: marge de la marge de la clavícula i 7a vèrtebra clavícula i 7a vèrtebra cervicalcervical
�� <10% de lesions en pacient <10% de lesions en pacient traumàtic civil.traumàtic civil.

�� +/+/--1% àrea superfície 1% àrea superfície corporalcorporal
� Estructures i Estructures i òrgansòrgans vitalsvitals: : faringe, esòfag, laringe, tràquea, canal toràcic, a. caròtides i v.
INTRODUCCIÓINTRODUCCIÓ
canal toràcic, a. caròtides i v. jugulars, a/v. subclàvies i vertebrals, columna cervical i medul·la espinal, nervis cranials, plexes nerviosos, tiroides, paratiroides i glàndulessalivals.
� Lesions potencialment Lesions potencialment letalsletals
3 de X

CLASSIFICACIÓ ANATÒMICACLASSIFICACIÓ ANATÒMICA
4 de X
Roon AJ, Christensen N. 1979
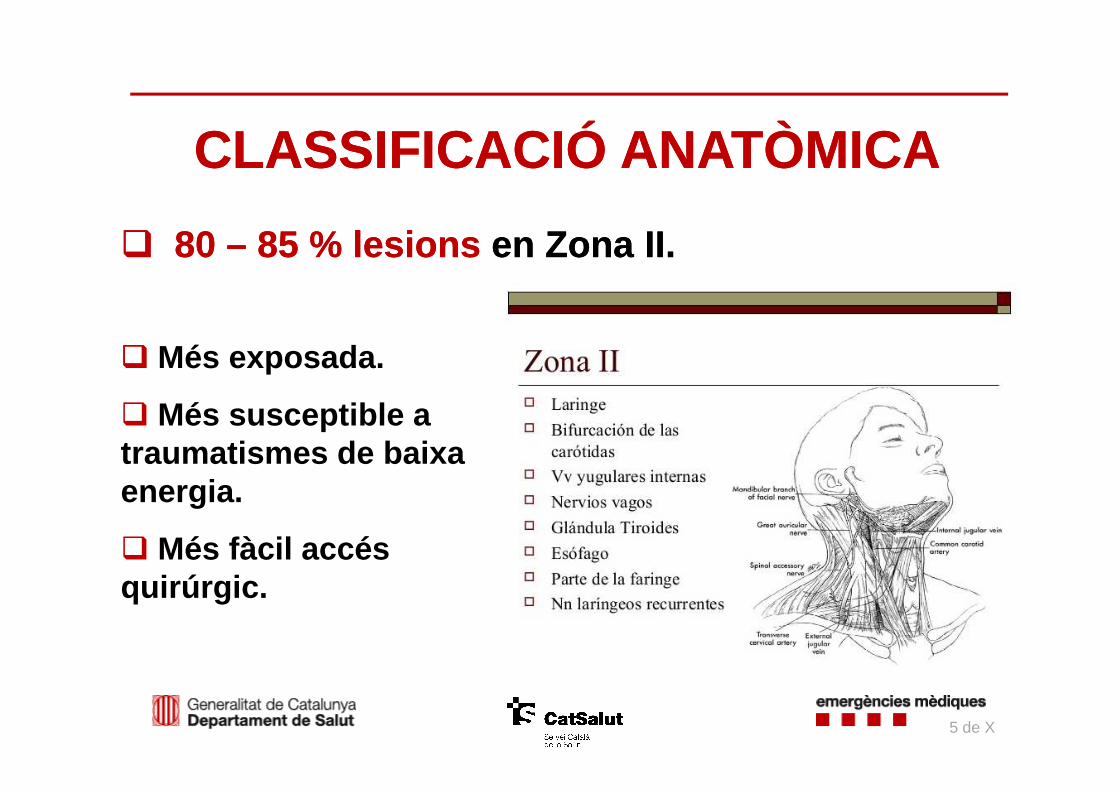
�� 80 80 –– 85 % 85 % lesionslesions en Zona II. en Zona II.
CLASSIFICACIÓ ANATÒMICACLASSIFICACIÓ ANATÒMICA
�� Més exposada.
5 de X
� Més susceptible a traumatismes de baixa energia.
� Més fàcil accés quirúrgic.

�� TANCAT: TANCAT: Accident trànsit (acceleració/desacceleració, contusió directa, compressió cinturó seguretat), estrangulament (escanyament, penjament, “choke hold”...), agressió amb contusió directa .
TIPUS DE TRAUMATISMETIPUS DE TRAUMATISME
6 de X
�� PENETRANT:PENETRANT:Lesions per arma blanca (tall o punxant) o de foc , accident de trànsit (projectil).

�� 11--5%5% dels pacients traumàtics.
� Mortalitat 33--6%6%: : 50% per exanguinació.
� Arma blanca Arma blanca vs. arma de focarma de foc :o 70%70% vsvs. . 22% 22% (mitjana darreres revisions)
o Diferències entre països: EUA 40% EUA 40% vsvs 49%.49%.
TRAUMATISME PENETRANTTRAUMATISME PENETRANT
o Diferències entre països: EUA 40% EUA 40% vsvs 49%.49%.
�� Lesions via aèria/digestivavia aèria/digestiva :o Rares. Digestives (5%):
�������� Diagnòstic demorat per baixa sospita.
o Alta energia (arma de foc).
� Lesions vascularsvasculars :o Més freqüents. Majors causants de mortalitat.o Formació de pseudoaneurisma, dissecció, fístula AV,
transecció completa, trombos oclusius per ruptura de placa ateroescleròtica (tromboembolisme cerebral).
7 de X
Profunditat: Profunditat: fins a múscul fins a múscul PlatismaPlatisma..

TRAUMATISME PENETRANT: SignesTRAUMATISME PENETRANT: Signes
VIA AÈRIA ESÒFAG VASCULAR
Dispnea
Estridor
Disfonia
Disfàgia
Odinofàgia
Baveig
FrèmitFrèmit o bufo buf
HematomaHematoma expansiu o expansiu o pulsàtilpulsàtil
8 de X
Disfonia
Ronquera
Patró respiratori anormal
Hemoptisi
Emfisema subcutanimassiu
Bombolles aire per ferida
Baveig
Hematemesi
Emfisema subcutani massiu
Hemorràgia severa o Hemorràgia severa o pulsàtilpulsàtil
Dèficit polsDèficit pols
Hipotensió i xoc
Hematoma no pulsàtil
Isquèmia SNC o SNP
Proximitat a gran vas
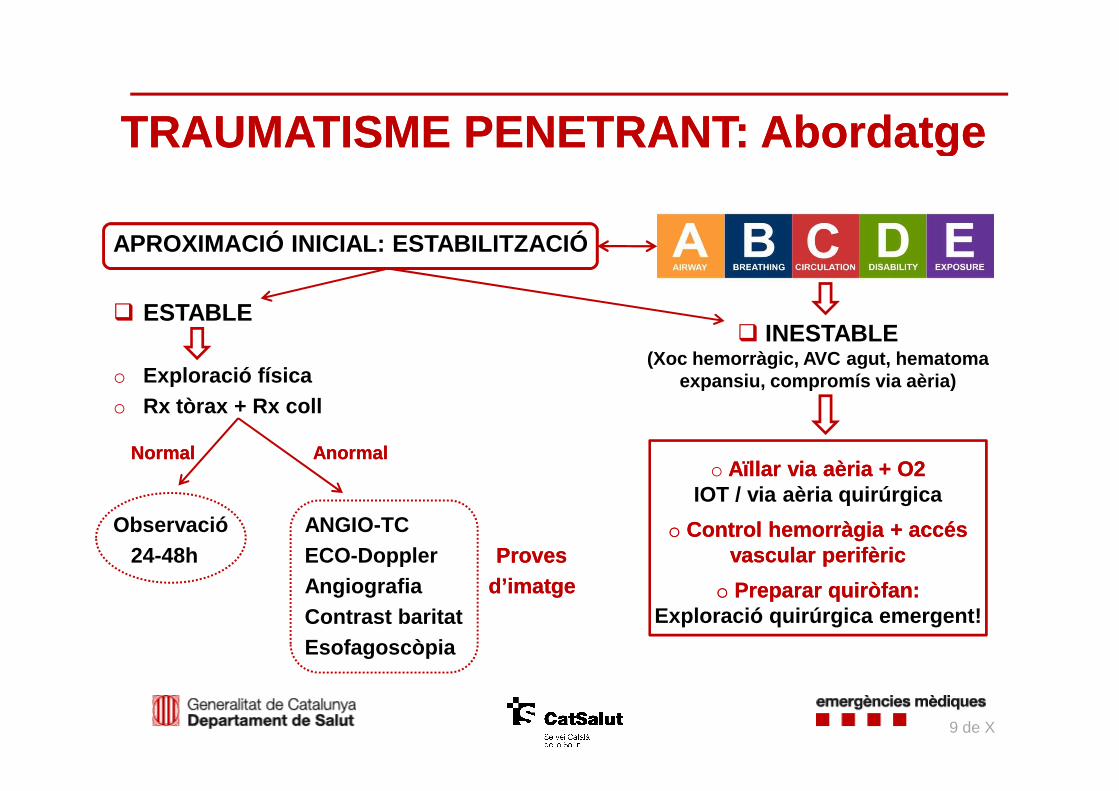
APROXIMACIÓ INICIAL: ESTABILITZACIÓ
� ESTABLE
o Exploració físicaRx tòrax + Rx coll
TRAUMATISME PENETRANT: Abordatge TRAUMATISME PENETRANT: Abordatge
� INESTABLE(Xoc hemorràgic, AVC agut, hematoma
expansiu, compromís via aèria)o Rx tòrax + Rx coll
Normal AnormalNormal Anormal
Observació ANGIO-TC24-48h ECO-Doppler ProvesProves
Angiografia d’imatged’imatgeContrast baritatEsofagoscòpia
9 de X
o Aïllar via aèria + O2Aïllar via aèria + O2IOT / via aèria quirúrgica
oo Control hemorràgia + accés Control hemorràgia + accés vascular perifèricvascular perifèric
oo Preparar quiròfan:Preparar quiròfan:Exploració quirúrgica emergent!

� Maneig pacient inestablepacient inestable :
o Control hemorràgia amb compressió externacompressió externa (valorar hemostàtic).
oo Via aèriaVia aèria: Precoç. IOTIOT: Laringoscòpia directa, videolaringoscopi, fibrolaringoscòpia flexible (hospitalari). SRI indicada SRI indicada ((Alerta amb relaxació!).
���� Si IOT fallida, lesions significatives maxil·lofaci als o disrupció laríngia: Indicació via aèria quirúrgica via aèria quirúrgica (cricotiroidectomia o traqueostomia ).
TRAUMATISME PENETRANT: Abordatge TRAUMATISME PENETRANT: Abordatge
Indicació via aèria quirúrgica via aèria quirúrgica (cricotiroidectomia o traqueostomia ).
10 de X

TRAUMATISME PENETRANT: TRAUMATISME PENETRANT: Exploració quirúrgica emergentExploració quirúrgica emergent
� Història:Història:o A partir de II GM: Exploració quirúrgica obligatòri a a tots els
traumatismes penetrants. o Més del 50%: exploracions negatives.
o Avenços en tècniques d’imatge Maneig selectiu!!Maneig selectiu!!
� Indicacions actuals: Indicacions actuals: o Compromís via aèriao Emfisema subcutani massiuo Bombolles aire per ferida
o Hemorràgia profusa activao Hematoma ràpidament expansiuo Xoc hemorràgic refractari
11 de X
o Avenços en tècniques d’imatge Maneig selectiu!!Maneig selectiu!!

� Sospita lesió Sospita lesió via aèriavia aèria : : oo TOMOGRAFIA TOMOGRAFIA COMPUTARITZADACOMPUTARITZADA: : aire extrapulmonar, disrupció paret
traqueal, herniació baló IOT.oo FIBROBRONCOSCÒPIAFIBROBRONCOSCÒPIA: : completar exploració. Extensió lesions.
Comparativament amb TC poques diferències.
TRAUMATISME PENETRANT: TRAUMATISME PENETRANT: Exploracions complementàries en pacient estableExploracions complementàries en pacient estable
Comparativament amb TC poques diferències.
� Sospita lesió Sospita lesió faringoesofàgicafaringoesofàgica ::o FIBROESOFAGOSCÒPIAFIBROESOFAGOSCÒPIA: : S100%.o CONTRAST CONTRAST BARITATBARITAT: : Menys sensible.
Dificultós si pacient intubat. Permet mesurar fugue s.
12 de X

� Sospita lesió Sospita lesió vascularvascular ::
oo ANGIOANGIO--TCTC: : Darrerament de 1a elecció1a elecció . � Menys invasiva, escassa preparació, major dispo. �� Útil detecció lesions Útil detecció lesions aeroaero--digestivesdigestives . � Alta sensibilitat (100%) i especificitat (94 -99%).
TRAUMATISME PENETRANT: TRAUMATISME PENETRANT: Exploracions complementàries en pacient estableExploracions complementàries en pacient estable
� Alta sensibilitat (100%) i especificitat (94 -99%).
oo ANGIOGRAFIA per catèter: ANGIOGRAFIA per catèter: Considerada ““GoldGold--standardstandard””. � Possibilitat de tractament tractament intravascularintravascular .� Inconvenients : disponibilitat, preparació, complicacions (AVC).
oo ECOECO--DOPPLERDOPPLER: : � Menys invasiva. � Inconvenient: operador depenent. (S91%, E99%)
13 de X

� Lesió Lesió VIA AÈRIAVIA AÈRIA : : oo AÏLLAMENT VIA AÈRIA COMPROMESA: AÏLLAMENT VIA AÈRIA COMPROMESA:
�� IOTIOT per laringoscòpia directa (SRI) �������� 12% fallides
�� CRICOTIROIDECTOMIA D’EMERGÈNCIACRICOTIROIDECTOMIA D’EMERGÈNCIA�� TRAQUEOSTOMIA TRAQUEOSTOMIA : si disrupció d’anatomia laringotraqueal
TRAUMATISME PENETRANT: TRAUMATISME PENETRANT: TractamentTractament
�� TRAQUEOSTOMIA TRAQUEOSTOMIA : si disrupció d’anatomia laringotraquealIncisió 1 anella per sota la lesió.
oo REPARACIÓ QUIRÚRGICAREPARACIÓ QUIRÚRGICA
� Lesió Lesió FARINGOESOFÀGICAFARINGOESOFÀGICA ::o Antibiòtics, nutrició parenteral o enteral per SNG.
o Reparació quirúrgica vs. maneig conservador segons mida lesions.
14 de X
� Lesió Lesió VASCULARVASCULAR ::
oo ““DAMAGEDAMAGE--CONTROLCONTROL” ” (control provisional):
1. Compressió externa.2. Sonda Foley 18/20 per trajecte de ferida, inflar baló 5ml aigua , fixar amb sutura.
TRAUMATISME PENETRANT: TRAUMATISME PENETRANT: TractamentTractament
2. Sonda Foley 18/20 per trajecte de ferida, inflar baló 5ml aigua , fixar amb sutura. Fins a 48-72h.
3. Si fallida ���� exploració quirúrgica immediata.
o Pacient estable amb angio-TC +: plantejar intervenció intervenció intravascularintravascular (angioplàstia) o externa.(angioplàstia) o externa.
�� Lesió caròtidaLesió caròtida : REVASCULARITZACIÓ REVASCULARITZACIÓ (85% evolució favorable)�� LLligadura indicada en pacients en coma previ i mal pronòstic.
�� Lesió jugular: Lesió jugular: Majoria resolució espontàniaresolució espontània . � Si hemorràgia severa: LLIGADURALLIGADURA .
15 de X
� Molt poc freqüent. o 0.15% de ferides pen. en coll per arma blanca. o Sempre acompanyades de dèficit NRL dèficit NRL evident.
� Requereix alta energia alta energia (p.ex. arma de foc).
TRAUMATISME PENETRANT: TRAUMATISME PENETRANT: COLUMNA CERVICALCOLUMNA CERVICAL
�� PrioritatPrioritat: TRACTAMENT DE FERIDA PENETRANTTRACTAMENT DE FERIDA PENETRANT. o Immobilització cervical NO indicada NO indicada en estabilització inicial.o Associada a major risc de mort!!!major risc de mort!!!
�������� signes clínics ocults, intubació dificultosa, retar d evacuació, reticència a retirar collaret per tractar lesions de risc vital.
�� Via aèria:Via aèria: IOT (laringoscòpia directa)IOT (laringoscòpia directa) . Alineació i tracció manual cervical.
�� Tècnica d’imatge: Tècnica d’imatge: TC cervicalTC cervical .
16 de X

�� 55--20%20% dels traumatismes al coll. Mortalitat 2020--30%30%..
� 95% associats a lesions toràciques majors o comalesions toràciques majors o coma .
� 37-58% pacients desenvolupen dèficit NRL per isquèmia isquèmia SNC SNC (lesions vascularslesions vasculars !!).
TRAUMATISME TANCATTRAUMATISME TANCAT
� Lesions aeroaero--digestivesdigestives molt poc freqüents (alta energia).
� Lesió vascularvascular : o Pseudoaneurisma, dissecció, fístula AV,
transecció completa, trombos oclusius per ruptura de placa ateroescleròtica(tromboembolisme cerebral).
17 de X

�� Mecanisme Mecanisme lesionallesional::oo Accident trànsitAccident trànsit :
� Acceleració/ desacceleració + hiperflexió/ hiperext ensió/ rotació, contusió directa, compressió cinturó segur etat.
EstrangulamentEstrangulament :
TRAUMATISME TANCATTRAUMATISME TANCAT
oo EstrangulamentEstrangulament : � Penjament: Pèrdua de consciència per pressió sobre jugulars i augment
de PIC ���� asfíxia per compressió sobre tràquea. Isquèmia per compressió de caròtides. “Fractura del penjat”.
� Escanyament, “choke hold”.
oo Agressió/esportsAgressió/esports :� Cop de peu o de puny, objecte contundent...
18 de X

TRAUMATISME TANCATTRAUMATISME TANCAT
VIA AÈRIA ESÒFAG VASCULAR
SupraglotisSupraglotis::
Emfisema subcutani
OVA progressiva
Disrupció cartílag tiroides
DisfàgiaDisfàgia
HematemesiHematemesi o sang o sang en aspirat SNGen aspirat SNG
Emfisema subcutaniEmfisema subcutani
Isquèmia SNC o SNPIsquèmia SNC o SNP
Criteris alt risc d’isquèmia:Criteris alt risc d’isquèmia:
Hiperextensió /flexió/rotació
19 de X
Disrupció cartílag tiroides palpable
Ronquera
Emfisema subcutaniEmfisema subcutani
�Detecció retardada
�ALERTA població envellida, tractament anticoagulantanticoagulant de base
Hiperextensió /flexió/rotació cervical
Gran hematoma
Fractura espinal cervical
Signe del cinturó de seguretat
Epistaxi massiva
Buf o frèmit
AIT o AVC
Fractura de base de crani
InfraglotisInfraglotis::
Hemoptisi
Fuga aire TOT

APROXIMACIÓ INICIAL: ESTABILITZACIÓ
� ESTABLE
o Immobilització cervicalo Exploració física (atenció NRL)
TRAUMATISME TANCAT: Abordatge TRAUMATISME TANCAT: Abordatge
� INESTABLE
o Exploració física (atenció NRL)o Rx tòrax + Rx coll
Normal AnormalNormal Anormal
Observació ANGIO-TC coll + cerebral
Normal (Alta sospita) Anormal
Angiografia cerebral anormal Anticoagulaciónormal Esofagoscòpia Stent
Cirurgia
20 de X
o Immobilització cervical Immobilització cervical
oo Assegurar via aèriaAssegurar via aèria
oo Accés venós perifèricAccés venós perifèric
Tractar xoc hemorràgic!!Tractar xoc hemorràgic!!
Valorar signes lesió Valorar signes lesió
vascular + risc isquèmiavascular + risc isquèmia

� Lesió Lesió VIA AÈRIAVIA AÈRIA : : oo AÏLLAMENT VIA AÈRIA COMPROMESA: AÏLLAMENT VIA AÈRIA COMPROMESA:
�� IOTIOT per laringoscòpia directa (SRI) �������� 12% fallides
�� CRICOTIROIDECTOMIA D’EMERGÈNCIACRICOTIROIDECTOMIA D’EMERGÈNCIA�� TRAQUEOSTOMIA TRAQUEOSTOMIA : si disrupció d’anatomia laringotraqueal
TRAUMATISME TANCAT: TRAUMATISME TANCAT: TractamentTractament
�� TRAQUEOSTOMIA TRAQUEOSTOMIA : si disrupció d’anatomia laringotraquealIncisió 1 anella per sota la lesió.
oo REPARACIÓ QUIRÚRGICAREPARACIÓ QUIRÚRGICA
� Lesió Lesió FARINGOESOFÀGICAFARINGOESOFÀGICA ::o Antibiòtics, nutrició parenteral o per SNG.
o Reparació quirúrgica vs. maneig conservador segons mida lesions.
21 de X

� Lesió Lesió VASCULARVASCULAR ::
oo CIRURGIA: CIRURGIA: Lesions caròtida interna més freq., menys accessibl es.
oo ANGIOPLÀSTIA PERCUTÀNIA: ANGIOPLÀSTIA PERCUTÀNIA: alt risc de AVC isquèmic iatrogènic.
oo ANTICOAGULACIÓ ANTICOAGULACIÓ �������� Reducció morbiditat per isquèmia.
TRAUMATISME TANCAT: TRAUMATISME TANCAT: TractamentTractament
22 de X

�� NONO indicació IMMOBILITZADOR CERVICAL IMMOBILITZADOR CERVICAL en ferides penetrants ferides penetrants �������� si no existeix focalitat neurològica o alta sospita de lesió espinal.
� SÍ SÍ indicació IMMOBILITZADOR CERVICAL IMMOBILITZADOR CERVICAL en trauma tancattrauma tancat .
� IOT PRECOÇ IOT PRECOÇ si via aèria amenaçada o pacient inestable .
�� Laringoscòpia directa Laringoscòpia directa segura i efectiva. Alternativa:
CONCLUSIONSCONCLUSIONS
�� Laringoscòpia directa Laringoscòpia directa segura i efectiva. Alternativa:cricotiroidectomiacricotiroidectomia d’urgència d’urgència o traqueostomiatraqueostomia .
� Pacients estables sense signes de lesió de risc vit al: ANGIOANGIO--TCTC.
�� Atenció:Atenció: Signes i símptomes en trauma tancat vasculartrauma tancat vascular .
� Sovint 1r símptoma: ISQUÈMIA CEREBRALISQUÈMIA CEREBRAL .
� Traumatismes tancats Traumatismes tancats associats a lesions toràciques majors o coma.
ABCDE complet!ABCDE complet!
23 de X

� Rathlev NK, Medzon R, Bracken ME. Evaluation and Manag ement of Neck Trauma. Emerg Med Clin N Am 2007; 25: 679–694
� Burgess CA, Dale OT, Almeyda R, Corbridge RJ. An evide nce based review of the assessment and management of penetrating neck trauma. Clin. Otolaryn gol. 2012; 37: 44–52
� Brywczynski JJ, Barrett TW, Lyon JA, Cotton BA. Manage ment of penetrating neck injury in the emergency department: a structured literature review. Emerg Me d J 2008; 25: 711–715
� Desjardins G, Varon AJ. Airway management for penet rating neck injuries: the Miami experience. Resuscitation 2001; 48: 71–75
� Feliciano DV. Penetrating Cervical Trauma. World J Su rg 2014.� Castillo F, Moraga J, Pérez P, Borel C. Trauma cervical penetrante. Rev Chil Cir. 2015; 67(6): 584-589
BIBLIOGRAFIABIBLIOGRAFIA
� Castillo F, Moraga J, Pérez P, Borel C. Trauma cervical penetrante. Rev Chil Cir. 2015; 67(6): 584-589� Irish J, Hekkenberg R, Gullane P, Brown D, Rotstein L, Neligan P, Ali J. Penetrating and blunt neck trauma: 10 -
year review of a Canadian experience. CJS 1997; 40(1 ): 33-39� Nason R, Assuras G, Gray P, Lipschitz J, Burns C. Penet rating neck injuries: analysis of experience fron a
Canadian trauma centre. CJS 2001; 44(2): 122-128� Youssef N, Raymer KE. Airway management of an open pen etrating neck injury. CJEM 2015;17(1): 89-93� Fisher L, Callaway D, Sztajnkrycer M. Incidence of fa tal airway obstruction in police officers felonious ly killed
in the line of duty: a 10-year retrospective analys is. Prehosp Disaster Med. 2013;28(5): 466-470.� Jin Pyeong Kim, Sang Jae Cho, Hee Young Son, Jung Je Par k, Seung Hoon Woo. Analysis of Clinical Feature
and Management of Laryngeal Fracture: Recent 22 Cas e Review. Yonsei Med J 2012; 53(5): 992-998� Asennsio-Sánchez VM, Sánchez-Rodríguez JC, Macías-Pasc ual J. Síndrome de Horner traumático. Arch Soc
Esp Oftalmol 2007; 82: 171-174� Dubois-Marshall S, De Kock S. Two days with a broken knife blade in the neck – an interesting case of
Horner’s syndrome. BMJ Case Reports 2010.
24 de X

GRÀCIESGRÀCIES
Related Documents











