Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved. C URRENT O PINION Are all fluids bad for the kidney? Johan Ma ˚rtensson a,b and Rinaldo Bellomo a,c Purpose of review To describe the harmful effects of intravenous fluids on kidney structure and function and summarize recent comparisons between different fluids and their effect on kidney outcome. Recent findings Administration of intravenous fluids may contribute to the development and sustention of acute kidney injury. In excess, fluids cause kidney interstitial edema and venous congestion, which prevents renal blood flow and glomerular filtration rate. In contrast to balanced crystalloids, chloride-rich solutions impair renal blood flow via autoregulatory mechanisms. Synthetic colloids, such as hydroxyethyl starches, gelatins, and dextrans are potentially nephrotoxic because they can cause osmotic nephrosis, which, in susceptible patients, might precede permanent kidney damage. Albumin solutions appear well tolerated to use in septic patients, although their renal efficacy over balanced crystalloids is not established. In contrast, administration of albumin solutions to patients with decompensated liver failure effectively prevents and ameliorates hepatorenal syndrome. Summary Being nephrotoxic, synthetic colloids should be avoided in patients with reduced renal reserve, such as in critically ill patients and in patients with preexisting renal dysfunction. Suggested adverse effects with chloride-rich solutions need confirmation from ongoing trials. Albumin solutions are well tolerated in patients with sepsis and/or liver failure and improve outcomes in the latter. Keywords acute kidney injury, colloids, crystalloids, dextrans, gelatins, hydroxyethyl starches INTRODUCTION Intravenous fluids are frequently administered to critically ill patients with deteriorating kidney function. The rationale for such fluid therapy is to improve cardiac output, renal blood flow (RBF), and glomerular filtration rate (GFR). This is a log- ical approach in fluid deplete patients who present after diarrhea or vomiting or both or other clear decompensated fluid losses. However, when fluids are given in excess or given to patients who are not actually fluid deplete, renal interstitial edema, and worsening kidney dysfunction may develop [1 && ]. Even in clinically applied doses some fluids are potentially nephrotoxic. In fact, fluid-induced acute kidney injury (AKI) is associated with delays in recovery from acute illness and with significant and independent links with increased mortality [2]. Unfortunately, unlike many other supportive therapies commonly used in the ICU, the duration of the unwanted side-effects from fluid adminis- tration may occur over a longer timeframe (days to weeks) than the time frame associated with the physiological effects of fluid therapy (minutes to hours). Importantly, fluid removal is much harder to achieve and less predictably successful in terms of fluid balance than fluid administration. There- fore, all fluids must be considered drugs and be prescribed, and carefully dose-adjusted within their therapeutic safety and physiological efficacy window. In this review, we summarize key pathophysio- logical mechanisms behind fluid-induced AKI. We describe the impact of colloid and crystalloid solutions on kidney function in humans and a Department of Intensive Care, Austin Hospital, Melbourne, Victoria, Australia, b Section of Anaesthesia and Intensive Care Medicine, Depart- ment of Physiology and Pharmacology, Karolinska Institutet, Stockholm, Sweden and c Australian and New Zealand Intensive Care Research Centre, School of Preventive Medicine and Public Health, Monash University, Melbourne, Victoria, Australia Correspondence to Professor Rinaldo Bellomo, MD, FRACP, FCICM, Department of Epidemiology and Preventive Medicine, Australian and New Zealand Intensive Care Research Centre, Monash University, Melbourne, VIC, Australia. Tel: +61 3 94965992; fax: +61 3 94963932; e-mail: [email protected]; [email protected] Curr Opin Crit Care 2015, 21:292–301 DOI:10.1097/MCC.0000000000000214 www.co-criticalcare.com Volume 21 Number 4 August 2015 REVIEW

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

REVIEW
CURRENTOPINION Are all fluids bad for the kidney?
Copyright
www.co-criticalcare.com
a,b a,c
Johan Martensson and Rinaldo BellomoPurpose of review
To describe the harmful effects of intravenous fluids on kidney structure and function and summarize recentcomparisons between different fluids and their effect on kidney outcome.
Recent findings
Administration of intravenous fluids may contribute to the development and sustention of acute kidneyinjury. In excess, fluids cause kidney interstitial edema and venous congestion, which prevents renal bloodflow and glomerular filtration rate. In contrast to balanced crystalloids, chloride-rich solutions impair renalblood flow via autoregulatory mechanisms. Synthetic colloids, such as hydroxyethyl starches, gelatins, anddextrans are potentially nephrotoxic because they can cause osmotic nephrosis, which, in susceptiblepatients, might precede permanent kidney damage. Albumin solutions appear well tolerated to use inseptic patients, although their renal efficacy over balanced crystalloids is not established. In contrast,administration of albumin solutions to patients with decompensated liver failure effectively prevents andameliorates hepatorenal syndrome.
Summary
Being nephrotoxic, synthetic colloids should be avoided in patients with reduced renal reserve, such as incritically ill patients and in patients with preexisting renal dysfunction. Suggested adverse effects withchloride-rich solutions need confirmation from ongoing trials. Albumin solutions are well tolerated inpatients with sepsis and/or liver failure and improve outcomes in the latter.
Keywords
acute kidney injury, colloids, crystalloids, dextrans, gelatins, hydroxyethyl starches
aDepartment of Intensive Care, Austin Hospital, Melbourne, Victoria,Australia, bSection of Anaesthesia and Intensive Care Medicine, Depart-ment of Physiology and Pharmacology, Karolinska Institutet, Stockholm,Sweden and cAustralian and New Zealand Intensive Care ResearchCentre, School of Preventive Medicine and Public Health, MonashUniversity, Melbourne, Victoria, Australia
Correspondence to Professor Rinaldo Bellomo, MD, FRACP, FCICM,Department of Epidemiology and PreventiveMedicine, Australian andNewZealand Intensive Care Research Centre, Monash University, Melbourne,VIC, Australia. Tel: +61 3 94965992; fax: +61 3 94963932;e-mail: [email protected]; [email protected]
Curr Opin Crit Care 2015, 21:292–301
DOI:10.1097/MCC.0000000000000214
INTRODUCTION
Intravenous fluids are frequently administered tocritically ill patients with deteriorating kidneyfunction. The rationale for such fluid therapy isto improve cardiac output, renal blood flow (RBF),and glomerular filtration rate (GFR). This is a log-ical approach in fluid deplete patients who presentafter diarrhea or vomiting or both or other cleardecompensated fluid losses. However, when fluidsare given in excess or given to patients who are notactually fluid deplete, renal interstitial edema, andworsening kidney dysfunction may develop [1
&&
].Even in clinically applied doses some fluids arepotentially nephrotoxic. In fact, fluid-inducedacute kidney injury (AKI) is associated with delaysin recovery from acute illness and with significantand independent links with increased mortality[2]. Unfortunately, unlike many other supportivetherapies commonly used in the ICU, the durationof the unwanted side-effects from fluid adminis-tration may occur over a longer timeframe (days toweeks) than the time frame associated with thephysiological effects of fluid therapy (minutes tohours). Importantly, fluid removal is much harder
© 2015 Wolters Kluwer
to achieve and less predictably successful in termsof fluid balance than fluid administration. There-fore, all fluids must be considered drugs and beprescribed, and carefully dose-adjusted withintheir therapeutic safety and physiological efficacywindow.
In this review, we summarize key pathophysio-logical mechanisms behind fluid-induced AKI. Wedescribe the impact of colloid and crystalloidsolutions on kidney function in humans and
Health, Inc. All rights reserved.
Volume 21 � Number 4 � August 2015

KEY POINTS
� Fluid-induced acute kidney injury can be caused bykidney interstitial edema, renal venous congestion,osmotic nephrosis, and activation oftubuloglomerular feedback.
� Synthetic colloids, such as hydroxyethyl starches,gelatins, and dextrans may induce irreversible osmoticnephrosis and should therefore be avoided.
� As chloride-rich solutions can reduce kidney functionvia activation of tubuloglomerular feedback, potentialrenal benefits of balanced crystalloids are currentlyunder investigation.
� Among colloids, albumin solutions appear welltolerated and potentially beneficial to use in patientswith or at risk of acute kidney injury because of sepsisor liver failure.
Are all fluids bad for the kidney? Martensson and Bellomo
explain why some fluids do more harm to the kid-neys than others.
PATHOPHYSIOLOGY OF FLUID-INDUCEDACUTE KIDNEY INJURY
The pathogenesis of fluid-induced AKI involvesmultiple potential mechanisms. Below, we suggestfour such mechanisms: activation of the tubuloglo-merular feedback (TGF), increased intravascularoncotic pressure, osmotic nephrosis, and kidneyparenchymal edema and/or venous congestion.All of the above mechanisms are not mutually exclu-sive and may occur in any combination of some or
Copyright © 2015 Wolters Kluwe
TGF
Afferent arteriole
NaCI
Macula densa
PC
Distal tubule
Net filtration pressure = PC–PB–πC
πC
PB
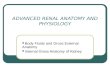
FIGURE 1. Pathophysiology of fluid-induced acute kidney injurpressure; PB, pressure within Bowman’s space; pC, capillary onco
1070-5295 Copyright � 2015 Wolters Kluwer Health, Inc. All rights rese
all of these. The first three mechanisms are mostlyrelated to type of fluid, whereas the last mechanismis caused by fluid overdose (Fig. 1).
Administration of solutions with supraphysio-logic chloride concentrations such as 0.9% salineincreases the filtered load of sodium chloride, lead-ing to increased chloride delivery to the ‘chloride-detecting’ macula densa cells in the distal part of thenephron. This is followed by the release of signalingsubstances (e.g., adenosine) from the macula densa.These mediators increase the tone of the afferentarteriole (vasoconstriction) and thereby lower theRBF and GFR. This is the so-called TGF (Fig. 1). Thistheoretical, yet logical, link between excessivesodium chloride administration, afferent arteriolarcontraction, reduced GFR and AKI is supported byanimal and human studies [3–5,6
&
]. The untowardeffect on kidney function is likely amplified inacutely and chronically injured kidneys as impairedproximal tubular sodium chloride reabsorption willincrease chloride delivery to macula densa [7].
The net filtration pressure (NFP) over the glo-merular filtration barrier is the driving force for GFR.NFP is determined by the hydraulic pressure inthe glomerular capillaries (PC), which is a resultof the systemic blood pressure and the relative tonein the afferent and efferent arterioles, and is opposedby plasma oncotic pressure (pC). Plasma oncoticpressure is determined mainly by the serum albuminconcentration. NFP is then controlled by the threeforces of Pc, pC, and the hydraulic back-pressure inBowman’s space (PB). In other words,
NFP ¼ PC � PB � pC:
r Health, Inc. All rights reserved.
Vacuole
Proximal tubular cell
Interstitial edema
y. TGF, tubuloglomerular feedback; PC, glomerular capillarytic pressure.
rved. www.co-criticalcare.com 293

Intravenous fluids
Intravenous administration of fluids contain-ing osmotically active substances, such as albuminsolutions or artificial colloid solutions, inevitablytransiently increases pC (Fig. 1). During this timeframe, a GFR reduction should logically beexpected [8].
The above-mentioned notion has, however,been elegantly refuted by Tomita et al. [9]. In theirtrial, no difference in renal function was seen whenpatients with brain edema were randomly allocatedto receive supranormal oncotic pressure treatmentwith 25% albumin or maintain a normal oncoticpressure over a 2-week period. In addition, largetrials have failed to show harmful effects on kidneyfunction after normalization of serum albumin, andhence pC, in septic patients [10,11
&&
]. The lack ofrelation between intravascular oncotic pressureelevations and kidney dysfunction in these studiescan be theoretically explained. Increasing plasmaoncotic pressure to approximately 28 mmHg, as inTomita’s study, from normal values of approxi-mately 25 mmHg may not sufficiently counteractPc to create filtration equilibrium (i.e., zero NFP).Moreover, colloid infusion leads to elevated plasmaoncotic pressure, but logically also to a parallelincrease in circulating volume, amplified by the factthat hyperoncotic solutions draw water from theinterstitium into the plasma compartment. Aug-mented RBF and Pc, resulting from such volumeexpansion, may offset the increase in oncotic pres-sure, thereby maintaining NFP and GFR. In contrast,increased incidence of cardiac surgery-associatedAKI was associated with albumin administrationin a propensity-matched analysis suggesting thatthe renal response to albumin depends on the popu-lation under study [12
&
] or that albumin therapy incardiac surgery patients is a marker of illnessseverity, which in turn is associated with AKI.
Osmotic nephrosis is a histological diagnosis.This condition is characterized by vacuolizationand swelling of the proximal tubular cells (Fig. 1)[13]. Tubular uptake of filtered substances by pino-cytosis with subsequent storage in vacuoles is theproposed mechanism. In severe cases when vacuolesfill the cytoplasm, the nucleus may become dis-placed and even distorted. Several substances,including dextrans, iodinated contrast media, man-nitol, and, perhaps more important and relevant tointensive care practice, hydroxyethyl starches (HES),have been shown to cause osmotic nephrosis [13].
Osmotic nephrosis is potentially reversible andfunctional recovery may occur. However, osmoticnephrosis may contribute to permanent kidneydysfunction in patients with multiple AKI risk fac-tors such as chronic kidney disease, advanced age,sepsis, and major surgery [13]. Osmotic nephrosis
Copyright © 2015 Wolters Kluwer
294 www.co-criticalcare.com
may be a major mechanism by which HES inducesrenal injury.
Increased renal volume because of renal inter-stitial edema can already be detected after infusionof moderate fluid volumes (2 l over 1 h) in healthyindividuals [5]. As the kidneys are enclosed within alow-compliance capsule, intrarenal pressures willlogically increase rapidly with increasing renal inter-stitial volume [14
&
]. In this regard, the kidney, likethe brain, should have a volume pressure relation-ship that, once the capsular distension has reachedmaximum stretch, leads to a rapid exponentialincrease in intraparenchymal pressure. In addition,overzealous fluid administration can cause centraland renal venous congestion, especially in combi-nation with myocardial diastolic dysfunction [15
&
].RBF depends on the transrenal pressure gra-
dient, that is the difference between mean arterialpressure (MAP) and renal venous pressure (RVP).Elevated central venous pressure (CVP), translatedinto elevated RVP, hence reduces the transrenalpressure gradient, RBF and GFR [16,17]. A lineardecrease in kidney function with increasing CVPabove 10–12 mmHg was observed in patients withcardiovascular disease [18]. In addition, a strongrelation between elevated CVP and worsening kid-ney function was shown in patients with decom-pensated heart failure [19].
Taken together, interstitial edema and venouscongestion counteract RBF, increase PB, and, con-sequently, decrease NFP and GFR. Unfortunately,fluid accumulation is common in ICU patients,especially after major surgery because of generousadministration of fluid boluses and maintenancefluids [20
&
]. Given the logical mechanistic linksbetween fluid overload and AKI, and a frequentlyreported independent association of fluid overloadwith development and progression of AKI [21,22], itappears logical to advocate the cautious adminis-tration of fluids and close monitoring of fluid bal-ance in patients at risk.
BALANCED VERSUS UNBALANCEDCRYSTALLOIDS
Electroneutrality, that is the balance betweenpositive and negative ions, is a fundamental prop-erty for intravenous fluids. Isotonicity with plasmais another desirable feature of such fluids. Isotonic(0.9%) saline contains 154 mmol/l of sodium andchloride with an effective osmolality similar toplasma. It is, however, well established that infusionof fluids with such a nonphysiological chlorideconcentration induces hyperchloremic metabolicacidosis [23]. Hence, balanced solutions withphysiological concentrations of strong ions have
Health, Inc. All rights reserved.
Volume 21 � Number 4 � August 2015

Table 1. Electrolyte composition and osmolality of human plasma and widely available crystalloid solutions
Humanplasma
0.9%saline
Ringer’slactatea
Ringer’sacetateb Plasmalytec Jonosterilb Sterofundina
Sodium (mmol/l) 142 154 130 131 140 137 145
Potassium (mmol/l) 4.5 4 4 5 4 4
Calcium (mmol/l) 2.5 3 2 1.7 2.5
Magnesium (mmol/l) 1.25 1 1.5 1.3 1
Chloride (mmol/l) 103 154 110 110 98 110 127
Bicarbonate (mmol/l) 24
Lactate (mmol/l) 1.5 28
Acetate (mmol/l) 30 27 37 24
Gluconate (mmol/l) 23
Malate (mmol/l) 5
Osmolalityd (mosm/kg) H2O 290 308 275 270 295 291 309
aB Braun (Melsungen, Germany).bFresenius Kabi (Bad Homburg, Germany).cBaxter International (Deerfield, Illinois, USA).dCalculated osmolality for the different solutions. Actual osmolality is lower.
Are all fluids bad for the kidney? Martensson and Bellomo
emerged on the market as a possible response to thisbiochemical problem. In these solutions, chloridehas been partly replaced by bicarbonate precursorssuch as lactate, acetate, or gluconate (Table 1).
Infusion of chloride-rich solutions has beenassociated, although not consistently, with poor
Copyright © 2015 Wolters Kluwe
Table 2. Saline compared to balanced solutions and kidney outc
Reference Design Population N Balanced fl
[24] Before-and-after General ICU 1533 Chloride-po
[5] RCT Healthy volunteers 12 Plasmalyte
[25] Retrospective DKA 23 Plasmalyte
[26] Retrospective Major abdominalsurgery
3704 Plasmalyte
[27] RCT DKA 54 Ringer’s lac
[28] RCT Kidneytransplantation
74 Ringer’s lac
[29] Observational Dehydration dueto diarrhea
40 Ringer’s lac
[30] RCT Kidneytransplantation
60 Plasmalyte
[31&] RCT Trauma 65 Plasmalyte
[32&&] Retrospective Sepsis 6730 Balanced crþ0.9% s
AKI, acute kidney injury; DKA, diabetic ketotic acidosis; RCT, randomized controlle
1070-5295 Copyright � 2015 Wolters Kluwer Health, Inc. All rights rese
kidney outcomes [e.g., creatinine increase andincreased need for renal replacement therapy(RRT); Table 2] [5,24–30,31
&
,32&&
].In a sequential before-and-after study, the use
of balanced (Hartmann solution or Plasmalyte) orchloride-poor (20% albumin) solutions during a
r Health, Inc. All rights reserved.
ome
uid Chloride rich Kidney outcome
or Chloride-rich Lower AKI incidence and lower need forRRT during chloride-poor period
0.9% saline Reduced kidney perfusion and urineoutput with saline
0.9% saline Lower urine output with saline. Similarchanges in serum creatinine
0.9% saline Increased need for RRT with saline
tate 0.9% saline Similar changes in serum creatinine
tate 0.9% saline Higher postoperative serum creatininewith saline. Similar urine output
tate 0.9% saline Similar changes in serum creatinine
0.9% saline Postoperative serum creatinine, urineoutput and incidence of graft failurewere similar
0.9% saline Nonsignificant trend towards higherurine output in the first 6 h and lowerdelta creatinine within the first 5 dayswith Plasmalyte
ystalloidaline
0.9% saline Similar incidence of acute renal failurewith or without need for dialysis.Balanced fluids associated with lowerin-hospital mortality
d trial; RRT, renal replacement therapy.
rved. www.co-criticalcare.com 295

Intravenous fluids
6-month period reduced AKI incidence and RRTrequirements compared to the previous periodwhen chloride-rich crystalloid and colloidsolutions were used [24,33
&&
]. Moreover, saline infu-sion around the time of major abdominal surgerywas associated with increased need for RRT in a largepropensity-matched case–control study [26].Finally, in a recent randomized controlled trial(RCT) in which trauma patients were resuscitatedwith either Plasmalyte or saline, a trend towardsimproved kidney outcomes was found in thePlasmalyte Group [31
&
]. In their aggregate, thesestudies support the notion that there may beadverse effects of chloride overload on kidney func-tion as reported in previous experiments. Althoughresults from large RCTs comparing saline andbalanced solutions are underway [34
&
], chloride-rich solutions should be prescribed with caution.
In addition to chloride overload, ICU-acquiredhypernatremia is common [35,36
&
] and clinicallyimportant as it is associated with AKI [37
&
] andmortality [38
&
]. Hypernatremia is traditionallyregarded a phenomenon secondary to dehydration.In ICU patients, in whom persistent dehydration israre, other mechanisms are likely more responsiblefor such sodium overload. In fact, cumulative sodiumbalance seems to poorly reflect fluid balance in crit-ically ill patients [39]. In this setting, removal of water
Copyright © 2015 Wolters Kluwer
Table 3. Large randomized controlled trials comparing colloids w
Study Population N Colloid volume (l)
CRISTAL [40] General ICU 2857 Any colloid 2.0 [1.0–3.5]a
VISEP [41] Severe sepsis 537 HES 200/0.5
0.07 [0.03–0.14]b
6S [2] Severe sepsis 804 HES 130/0.42
3.0 [1.5–5.1]c
CHEST [42] General ICU 7000 HES 130/0.4
0.52�0.43d
SAFE [43] General ICU 6997 4% albumin
2.2e
EARSS [10] Septic shock 798 20% albumin
100 ml 8 hourly for 3 days
ALBIOS [11&&] Severe sepsis 1818 20% albuminþ crystalloids
3.7 [3.2–4.4]f
AKI, acute kidney injury; HES, hydroxyethyl starches; RRT, renal replacement therapaMedian cumulative volume of study fluid during the first 7 days.bMedian cumulative volume of study fluid during study period in l/kg.cMedian cumulative volume in ICU.dMean daily average during the first 4 days.eMean cumulative volume of study fluid during first 4 days.fMedian total daily amount of administered fluid in the first 7 days.
296 www.co-criticalcare.com
inexcess of sodiumthroughdiuretic-induceddiuresisor RRT together with a lavish use of sodium-richsolutions likely contributes to ICU-acquired hyper-natremia. We further acknowledge that such cumu-lative sodium balance, dissociated from waterbalance, may negatively impact kidney functionpossibly by activation of TGF.
COLLOIDS VERSUS CRYSTALLOIDS
Results from large RCTs comparing the effect ofcolloid versus crystalloid solutions on kidney out-comes are shown in Table 3 [2,10,11
&&
,40–43] anddescribed below.
Hydroxyethyl starch
HES is a modified polysaccharide derived frommaize or potato. Intravenous HES solutions areclassified based on their molecular weight (range130–450 kDa) and degree of molar substitution,that is mean number of hydroxyethyl residues perglucose unit (range 0.4–0.7; Table 4). After degra-dation in plasma, smaller HES molecules are filteredby the kidneys. In addition, HES is cleared from thecirculation by uptake into hematopoietic cells andother tissues, where HES molecules may be storedfor years.
Health, Inc. All rights reserved.
ith crystalloids and kidney outcome
Crystalloid volume (l) Kidney outcome
Any crystalloid Similar need for RRT
3.0 [0.5–5.2]a
Ringer’s lactate Higher AKI risk and needfor RRT with HES
1.32 � HES volume
Ringer’s acetate Increased need for RRT with HES
3.0 [2.0–5.8]c
0.9% saline Increased need for RRT with HES
0.62�0.49d
0.9% saline Similar need for RRT
3.1e
0.9% saline Similar AKI incidence
100 mL 8 hourly for 3 days
Crystalloids Similar AKI incidence andneed for RRT
3825 [3205–4533]f
y.
Volume 21 � Number 4 � August 2015

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Tab
le4
.C
ompo
sitio
nan
dos
mol
ality
ofw
idel
yav
aila
ble
collo
idso
lutio
ns
Hu
ma
na
lbu
min
Hy
dro
xy
ethy
lst
arc
hG
ela
tin
Tra
de
na
me
Alb
um
ex4
aA
lbu
mex
20
aH
emo
hes
bH
exte
ndc
Vo
luve
nd
Vo
luly
ted
Ven
ofu
ndin
bTe
tra
spa
nbG
elo
fusi
neb
Ha
ema
ccel
e
Col
loid
cont
ent
4%
albu
min
20%
albu
min
10%
pota
tost
arch
6%
Mai
zest
arch
6%
Mai
zest
arch
6%
Mai
zest
arch
6%
Pota
tost
arch
6%
Pota
tost
arch
4%
Bovi
nege
latin
3.5
%Bo
vine
gel
atin
MW
/sub
stitu
tion
200/0
.5450/0
.7130/0
.4130/0
.4130/0
.42
130/0
.42
30
30
Sodi
um(m
mol
/l)
140
40
–100
154
143
154
137
154
140
154
145
Pota
ssiu
m(m
mol
/l)
34
45.1
Cal
cium
(mm
ol/l
)5
2.5
6.2
5
Mag
nesi
um(m
mol
/l)
0.9
1.5
1
Chl
orid
e(m
mol
/l)
128
19
154
124
154
110
154
118
120
145
Bica
rbon
ate
(mm
ol/l
)
Lact
ate
(mm
ol/l
)28
Ace
tate
(mm
ol/l
)34
24
Glu
cona
te(m
mol
/l)
Mal
eate
(mm
ol/l
)5
Oct
anoa
te(m
mol
/l)
6.4
32
Theo
retic
alos
mol
ality
(mos
m/k
g)H
2O
250
308
304
308
286.5
309
297
274
301
aC
SLBe
hrin
g(M
elbo
urne
,A
ustra
lia).
bB.
Brau
n(M
elsu
ngen
,G
erm
any)
.c H
ospi
ra(L
ake
Fore
st,
Illin
ois,
USA
).dFr
esen
ius
Kab
i(B
adH
ombu
rg,
Ger
man
y).
ePi
ram
al(B
ethl
ehem
,Pe
nnsy
lvan
ia,
USA
).
Are all fluids bad for the kidney? Martensson and Bellomo
1070-5295 Copyright � 2015 Wolters Kluwer Health, Inc. All rights reserved. www.co-criticalcare.com 297

Intravenous fluids
Large RCTs have confirmed a dose-dependentAKI risk and excess need for RRT with HES comparedto balanced [2,41] or unbalanced [42] crystalloids.Fluid resuscitation with colloids (70% received HES)or crystalloids (86% received 0.9% saline) was com-pared in a recent RCT [40]. This unblinded trialfailed to show any group differences in 28-daymortality or acute dialysis requirements. The factthat patients in the crystalloid group were given50% more resuscitation fluids and that most of thesepatients received chloride-rich saline may have con-tributed to more AKI in this group and hence offsetthe difference in RRT requirements between the twogroups. Moreover, as stated in the subsequent studycorrespondence [44
&
–46&
], there were imbalances inbaseline characteristics between the two studygroups, possibly due to a lack of allocation conceal-ment. In particular, marked differences in the num-ber of patients receiving crystalloids and colloidsprerandomization likely biased the results. Inaddition, absent information about hemodynamicresponses beyond the first 24 h raised concernsabout whether patients were treated differently inthe two study groups. In summary, based on evi-dence from two large blinded trials [2,42], HES ispotentially nephrotoxic and should therefore beavoided in patients susceptible to develop AKI, suchas elderly patients, patients with CKD, and criticallyill patients.
Albumin
Albumin is the major determinant of plasma colloidosmotic force. Additional features include the abil-ity to bind and transport biologically active mol-ecules such as drugs, scavenge free radicals, andprotect the endothelial surface layer [47]. Albuminis available in two different preparations. The nearisoooncotic 4–5% albumin solutions containsodium at concentrations of 140–160 mmol/l andchloride at concentrations of 100–130 mmol/l. Incontrast, the concentrated 20–25% solutions con-tain only 100–125 mmol sodium and 20–100 mmolchloride per liter, depending on manufacturer.
The Saline versus Albumin Fluid Evaluation(SAFE) study reported similar mortality andduration of RRT in critically ill patients resuscitatedwith 4% albumin or 0.9% saline [43]. The fact thattwo chloride-rich solutions were compared couldhave attenuated any differences in clinical out-comes between the two solutions. In addition,although significantly less study fluids were admin-istered to patients in the albumin group, the differ-ence by day 4 (<900 ml) was not pronounced.
Volume resuscitation with concentrated 20%albumin offers a number of theoretical advantages
Copyright © 2015 Wolters Kluwer
298 www.co-criticalcare.com
over resuscitation with diluted albumin solutions.First, their volume expanding effect may be up tofive times the volume of administered fluid as inter-stitial fluid is drawn towards the hyperoncotic pres-sure in plasma provided by infused albumin [48].This will potentially reduce fluid accumulation,interstitial edema, and organ failure in patientsrequiring multiple fluid boluses. Second, their lowerchloride concentration makes them attractive froma kidney perspective. In contrast, hyperoncoticsolutions, such as 20% albumin, could, as discussedabove, impair GFR by raising pC and thereby coun-teracting NFP (Fig. 1). The safety of low-volumeresuscitation with 20% albumin compared to0.9% saline in patients with septic shock was pre-viously confirmed [10]. In fact, infusion of identicalvolumes of albumin and saline (300 ml/day) for 3days resulted in similar mortality and AKI incidence.More recently, in the Albumin Italian OutcomeSepsis (ALBIOS) study, 20% albumin was used totarget a serum albumin level of at least 30 g/l inpatients with severe sepsis [11
&&
]. On average, thetarget was reached and levels were significantlyhigher than in the untreated group. However, suchtargeted albumin infusion did not reduce the totaldaily amount of administered fluid or affectedclinical outcomes including AKI.
Based on results from RCTs and meta-analyses,guidelines recommend resuscitation with albuminin combination with terlipressin, a selective vaso-pressin-1 receptor agonist, for treatment of hepa-torenal syndrome (HRS) type-1 (doubling of serumcreatinine within 2 weeks in patients with advancedcirrhosis) [49]. In patients with liver failure under-going large-volume paracentesis (4–6 l/day), a com-mon precipitator of HRS, concomitant albumininfusion attenuated its development [50]. Moreover,treatment with albumin and antibiotics in patientswith spontaneous bacterial peritonitis (SBP) reducedAKI incidence compared to treatment with anti-biotics alone [51]. Finally, in two RCTs, terlipressinin combination with albumin reversed HRS in morethan two thirds of patients, whereas monotherapywith albumin achieved HRS reversal in less than15% [52,53]. Given that septic AKI shares manypathophysiological features with HRS, it is surpris-ing that albumin infusion has not proved to be AKI-protective in sepsis. Notably, patients with liverfailure were excluded from SAFE [43] and were infre-quent in ALBIOS [11
&&
]. One possible explanationcould be that cirrhotic patients have more severehypoalbuminemia and would therefore benefitmore from albumin replacement. However, baselineserum albumin levels were identical in SAFE andALBIOS and in the study investigating liver failurepatients with SBP [51], suggesting that albumin may
Health, Inc. All rights reserved.
Volume 21 � Number 4 � August 2015

Are all fluids bad for the kidney? Martensson and Bellomo
have important properties beyond simply restoringthe colloid osmotic force.
Gelatin
Gelatin is a polypeptide derived from bovine col-lagen. Three types of commercially prepared gela-tin solutions are available: succinylated gelatin,urea-linked gelatin, and oxypolygelatin. With anaverage molecular weight of 30 kDa, gelatin iseliminated from the circulation by glomerularfiltration. Renal effects of fluid resuscitation withgelatin solutions have not been investigated inadequately powered RCTs. However, animal exper-iments suggest harmful effects on kidney structureand function similar to the effects seen with HES[54]. Furthermore, in prospective before-and-afterstudies, AKI incidence and RRT requirement washigher when 4% gelatin was used for fluid resus-citation in septic and cardiac surgery patientscompared to subsequent periods when crystalloidswere used [55,56]. Given these finding and therelatively high risk of allergic reactions, the useof gelatin solutions in critically ill patients remainsquestionable.
Dextrans
Dextrans are polysaccharides with a mean molecu-lar weight ranging from 40 to 70 kDa. Infuseddextrans are mainly eliminated by glomerular filtra-tion and partly through the gastrointestinal tract.Cellular uptake and storage is also suggested [57].Whether dextran-induced AKI is a reality is uncer-tain. Yet, osmotic nephrosis following resuscitationwith dextran solutions has been reported in theliterature [13] and case reports have suggested anassociation with acute renal failure [8]. In addition,given its significant side-effect profile includingtrue allergic reactions and compromised hemosta-sis, it is difficult to justify the use of dextrans in theICU setting.
CONCLUSION
Intravenous fluids are drugs and like drugs they havespecific compositions, potential benefits and poten-tial risks. Like drugs they can be under-dosed andover-dosed. They should be prescribed with carebased on available evidence. Chloride-rich solutionsinduce metabolic acidosis, may have a negativeimpact on the renal circulation and function andmay negatively affect kidney outcomes. HES isnephrotoxic and, given the lack of any benefit incomparison to other fluids, should not be pre-scribed. Other synthetic colloids are potentially
Copyright © 2015 Wolters Kluwe
1070-5295 Copyright � 2015 Wolters Kluwer Health, Inc. All rights rese
nephrotoxic and may trigger the developmentand progression of AKI. Thus, from a renal pointof view, all synthetic crystalloids are injurious andshould be avoided. Although the renal safety ofusing albumin solutions in septic patients has beenestablished, their renal efficacy over balanced crys-talloids has never been shown. It is possible, how-ever, that there may be a role for albumin basedvolume expansion in patients with liver disease andsepsis or patients with liver disease developing hep-atorenal syndrome or receiving a large volume para-centesis. Finally, whether balanced crystalloidsdeliver any clinically important renal benefit willcontinue to be the subject of debate and hopefullywell designed RCTs.
Acknowledgements
None.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
REFERENCES AND RECOMMENDEDREADINGPapers of particular interest, published within the annual period of review, havebeen highlighted as:
& of special interest&& of outstanding interest1.&&
Prowle JR, Kirwan CJ, Bellomo R. Fluid management for the prevention andattenuation of acute kidney injury. Nat Rev Nephrol 2014; 10:37–47.
This comprehensive review describes the pathophysiological and clinical con-sequences of fluid accumulation on kidney function. A tailored goal-directed fluidmanagement strategy is suggested.2. Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42
versus Ringer’s acetate in severe sepsis. N Engl J Med 2012; 367:124–134.3. Wilcox CS. Regulation of renal blood flow by plasma chloride. J Clin Invest
1983; 71:726–735.4. Hansen PB, Jensen BL, Skott O. Chloride regulates afferent arteriolar
contraction in response to depolarization. Hypertension 1998; 32:1066–1070.5. Chowdhury AH, Cox EF, Francis ST, Lobo DN. A randomized, controlled,
double-blind crossover study on the effects of 2-L infusions of 0.9% salineand plasma-lyte(R) 148 on renal blood flow velocity and renal cortical tissueperfusion in healthy volunteers. Ann Surg 2012; 256:18–24.
6.&
Zhou F, Peng ZY, Bishop JV, et al. Effects of fluid resuscitation with 0.9%saline versus a balanced electrolyte solution on acute kidney injury in a ratmodel of sepsis. Crit Care Med 2014; 42:e270–e278.
This study shows that resuscitation of 0.9% saline results in a more pronouncedincrease in serum creatinine and injury biomarkers, and more severe histologicalchanges as compared to Plasmalyte in septic rats.7. Zuk A, Bonventre JV, Brown D, Matlin KS. Polarity, integrin, and extracellular
matrix dynamics in the postischemic rat kidney. Am J Physiol 1998;275:C711–C731.
8. Moran M, Kapsner C. Acute renal failure associated with elevated plasmaoncotic pressure. N Engl J Med 1987; 317:150–153.
9. Tomita H, Ito U, Tone O, et al. High colloid oncotic therapy for contusionalbrain edema. Acta Neurochir Suppl (Wien) 1994; 60:547–549.
10. Charpentier J, Mira JP, Group ES. Efficacy and tolerance of hyperoncoticalbumin administration in septic shock patients: the EARSS study. IntensiveCare Med 2011; 37 (Suppl 1):S115.
11.&&
Caironi P, Tognoni G, Masson S, et al. Albumin replacement in patients withsevere sepsis or septic shock. N Engl J Med 2014; 370:1412–1421.
This is the largest RCT exploring the efficacy of 20% albumin infusion to maintain aserum albumin level of at least 30 g/l in patients with severe sepsis. This inter-vention did not improve survival or renal outcomes.
r Health, Inc. All rights reserved.
rved. www.co-criticalcare.com 299

Intravenous fluids
12.&
Frenette A, Bouchard J, Bernier P, et al. Albumin administration is associatedwith acute kidney injury in cardiac surgery: a propensity score analysis. CritCare 2014; 18:602.
This retrospective study analyzed almost 1000 patients who underwent cardiacsurgery of which 5.2% developed AKI according to RIFLE. Use of albumin wasassociated with an almost fourfold higher odds of having RIFLE-AKI.13. Dickenmann M, Oettl T, Mihatsch MJ. Osmotic nephrosis: acute kidney injury
with accumulation of proximal tubular lysosomes due to administration ofexogenous solutes. Am J Kidney Dis 2008; 51:491–503.
14.&
Cruces P, Salas C, Lillo P, et al. The renal compartment: a hydraulic view.Intens Care Med Exp 2014; 2:26.
This study nicely describes the intrarenal pressure-volume relationship afterinjection of fluid into the renal pelvis in pigs.15.&
Rajendram R, Prowle JR. Venous congestion: are we adding insult to kidneyinjury in sepsis? Crit Care 2014; 18:104.
This commentary discuss the consequences of elevated central and renal venouspressure on kidney function.16. Doty JM, Saggi BH, Sugerman HJ, et al. Effect of increased renal venous
pressure on renal function. J Trauma 1999; 47:1000–1003.17. Li X, Liu M, Bedja D, et al. Acute renal venous obstruction is more
detrimental to the kidney than arterial occlusion: implication for murinemodels of acute kidney injury. Am J Physiol Renal Physiol 2012; 302:F519–525.
18. Damman K, van Deursen VM, Navis G, et al. Increased central venouspressure is associated with impaired renal function and mortality in a broadspectrum of patients with cardiovascular disease. J Am Coll Cardiol 2009;53:582–588.
19. Mullens W, Abrahams Z, Francis GS, et al. Importance of venous congestionfor worsening of renal function in advanced decompensated heart failure.J Am Coll Cardiol 2009; 53:589–596.
20.&
Parke RL, McGuinness SP, Gilder E, McCarthy LW. Intravenous fluid use aftercardiac surgery: a multicentre, prospective, observational study. Crit CareResusc 2014; 16:164–169.
This study in patients admitted to five ICUs in Australia and New Zealand showedthat fluid boluses were commonly administered after cardiac surgery and oftencontributed to a positive fluid balance.21. Payen D, de Pont AC, Sakr Y, et al. A positive fluid balance is associated
with a worse outcome in patients with acute renal failure. Crit Care 2008;12:R74.
22. Grams ME, Estrella MM, Coresh J, et al. Fluid balance, diuretic use,and mortality in acute kidney injury. Clin J Am Soc Nephrol 2011; 6:966–973.
23. Volta CA, Trentini A, Farabegoli L, et al. Effects of two different strategies offluid administration on inflammatory mediators, plasma electrolytes and acid/base disorders in patients undergoing major abdominal surgery: a randomizeddouble blind study. J Inflamm 2013; 10:29.
24. Yunos NM, Bellomo R, Hegarty C, et al. Association between a chloride-liberalvs chloride-restrictive intravenous fluid administration strategy and kidneyinjury in critically ill adults. JAMA 2012; 308:1566–1572.
25. Chua HR, Venkatesh B, Stachowski E, et al. Plasma-Lyte 148 vs 0.9% salinefor fluid resuscitation in diabetic ketoacidosis. J Crit Care 2012; 27:138–145.
26. Shaw AD, Bagshaw SM, Goldstein SL, et al. Major complications, mortality,and resource utilization after open abdominal surgery: 0.9% saline comparedto Plasma-Lyte. Ann Surg 2012; 255:821–829.
27. Van Zyl DG, Rheeder P, Delport E. Fluid management in diabetic-acidosis—Ringer’s lactate versus normal saline: a randomized controlled trial. QJM2012; 105:337–343.
28. Modi MP, Vora KS, Parikh GP, Shah VR. A comparative study of impact ofinfusion of Ringer’s lactate solution versus normal saline on acid-base balanceand serum electrolytes during live related renal transplantation. Saudi J KidneyDis Transpl 2012; 23:135–137.
29. Cieza JA, Hinostroza J, Huapaya JA, Leon CP. Sodium chloride 0.9% versusLactated Ringer in the management of severely dehydrated patients withcholeriform diarrhoea. J Infect Dev Ctries 2013; 7:528–532.
30. Kim SY, Huh KH, Lee JR, et al. Comparison of the effects of normal salineversus Plasmalyte on acid-base balance during living donor kidney transplan-tation using the Stewart and base excess methods. Transplant Proc 2013;45:2191–2196.
31.&
Young JB, Utter GH, Schermer CR, et al. Saline versus Plasma-Lyte A in initialresuscitation of trauma patients: a randomized trial. Ann Surg 2014;259:255–262.
This RCT demonstrates that resuscitation of trauma patients with Plasma-Lyte A,compared with 0.9% saline, results in a more rapid normalization of acid–basestatus. Nonsignificant trend towards better kidney function was observed withPlasma-Lyte.32.&&
Raghunathan K, Shaw A, Nathanson B, et al. Association between the choiceof IV crystalloid and in-hospital mortality among critically ill adults with sepsis�.Crit Care Med 2014; 42:1585–1591.
This is the largest observational study on mortality, length of stay, AKI, and RRT inseptic patients resuscitated with balanced or unbalanced crystalloids. Lowestmortality risk was seen in patients receiving the highest proportion of balanced/unbalanced crystalloids. No differences in AKI, RRT or length of stay were observed.
Copyright © 2015 Wolters Kluwer
300 www.co-criticalcare.com
33.&&
Yunos NM, Bellomo R, Glassford N, et al. Chloride-liberal vs. chloride-restrictive intravenous fluid administration and acute kidney injury: an ex-tended analysis. Intensive Care Med 2015; 41:257–264.
This before-and-after study found that a 1-year period of restricting chlorideadministration to ICU patients decreased the incidence of moderate to severeAKI (KDIGO stage 2 and 3) compared to the preceeding chloride-liberal 1-yearperiod.34.&
Reddy SK, Bailey MJ, Beasley RW, et al. A protocol for the 0.9% saline versusPlasma-Lyte 148 for intensive care fluid therapy (SPLIT) study. Crit CareResusc 2014; 16:274–279.
This ongoing (since 1 April 2014) RCT will be the largest to explore the impact of0.9% saline versus Plasma-Lyte on AKI development in ICU patients. The aim is toenroll approximately 2300 patients.35. Bihari S, Peake SL, Seppelt I, et al. Sodium administration in critically ill
patients in Australia and New Zealand: a multicentre point prevalence study.Crit Care Resusc 2013; 15:294–300.
36.&
Bihari S, Festa M, Peake SL, et al. Sodium administration in critically illpaediatric patients in Australia and New Zealand: a multicentre point pre-valence study. Crit Care Resusc 2014; 16:112–118.
This is a single-day point prevalence study in 10 Australian and New Zealandpaediatric ICUs. The study describes the sources and amount of sodium admin-istration to critically ill children.37.&
Kumar AB, Shi Y, Shotwell MS, et al. Hypernatremia is a significant risk factorfor acute kidney injury after subarachnoid hemorrhage: a retrospective ana-lysis. Neurocrit Care 2014.
This observational study on 736 patients with subarachnoid hemorrhage showedthat for every 1 mmol/l increase in peak daily serum sodium concentration, thehazard of developing AKI increased by 5.4%.38.&
Darmon M, Pichon M, Schwebel C, et al. Influence of early dysnatremiacorrection on survival of critically ill patients. Shock 2014; 41:394–399.
This observational study investigated 1830 patients with hyponatremia and 634with hypernatremia on ICU admission. Sodium correction by day 3 was indepen-dently associated with improved survival at 28 days. In addition, faster correctionrate was independently associated with survival.39. Bihari S, Baldwin CE, Bersten AD. Fluid balance does not predict estimated
sodium balance in critically ill mechanically ventilated patients. Crit CareResusc 2013; 15:89–96.
40. Annane D, Siami S, Jaber S, et al. Effects of fluid resuscitation with colloidsvs crystalloids on mortality in critically ill patients presenting withhypovolemic shock: the CRISTAL randomized trial. JAMA 2013; 310:1809–1817.
41. Brunkhorst FM, Engel C, Bloos F, et al. Intensive insulin therapy and pentas-tarch resuscitation in severe sepsis. N Engl J Med 2008; 358:125–139.
42. Myburgh JA, Finfer S, Bellomo R, et al. Hydroxyethyl starch or saline for fluidresuscitation in intensive care. N Engl J Med 2012; 367:1901–1911.
43. Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and saline forfluid resuscitation in the intensive care unit. N Engl J Med 2004; 350:2247–2256.
44.&
Perner A, Haase N, Wetterslev J. Mortality in patients with hypovolemic shocktreated with colloids or crystalloids. JAMA 2014; 311:1067.
Insightful comment highlighting some problems with the CRISTAL trial with specialreference to the randomization process.45.&
Bellomo R, Finfer S, Myburgh J. Mortality in patients with hypovolemic shocktreated with colloids or crystalloids. JAMA 2014; 311:1067–1068.
Insightful comment highlighting some problems with the CRISTAL trial with specialreference to the lack of physiology and biochemistry data beyond 24 h afterrandomization.46.&
Brun-Buisson C, Sun J, Natanson C. Mortality in patients withhypovolemic shock treated with colloids or crystalloids. JAMA 2014; 311:1068–1069.
Insightful comment highlighting some problems with the CRISTAL trial with specialreference to the statistical analysis of secondary endpoints.47. Taverna M, Marie AL, Mira JP, Guidet B. Specific antioxidant properties of
human serum albumin. Ann Intensive Care 2013; 3:4.48. Jacob M, Chappell D, Hofmann-Kiefer K, et al. The intravascular volume effect
of Ringer’s lactate is below 20%: a prospective study in humans. Crit Care2012; 16:R86.
49. Nadim MK, Kellum JA, Davenport A, et al. Hepatorenal syndrome: the 8thInternational Consensus Conference of the Acute Dialysis Quality Initiative(ADQI) Group. Crit Care 2012; 16:R23.
50. Gines P, Tito L, Arroyo V, et al. Randomized comparative study of therapeuticparacentesis with and without intravenous albumin in cirrhosis. Gastroenter-ology 1988; 94:1493–1502.
51. Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renalimpairment and mortality in patients with cirrhosis and spontaneous bacterialperitonitis. N Engl J Med 1999; 341:403–409.
52. Sanyal AJ, Boyer T, Garcia-Tsao G, et al. A randomized, prospective, double-blind, placebo-controlled trial of terlipressin for type 1 hepatorenal syndrome.Gastroenterology 2008; 134:1360–1368.
53. Martin-Llahi M, Pepin MN, Guevara M, et al. Terlipressin and albumin vsalbumin in patients with cirrhosis and hepatorenal syndrome: a randomizedstudy. Gastroenterology 2008; 134:1352–1359.
Health, Inc. All rights reserved.
Volume 21 � Number 4 � August 2015

Are all fluids bad for the kidney? Martensson and Bellomo
54. Schick MA, Isbary TJ, Schlegel N, et al. The impact of crystalloid and colloidinfusion on the kidney in rodent sepsis. Intensive Care Med 2010; 36:541–548.
55. Bayer O, Reinhart K, Kohl M, et al. Effects of fluid resuscitation with syntheticcolloids or crystalloids alone on shock reversal, fluid balance, and patientoutcomes in patients with severe sepsis: a prospective sequential analysis.Crit Care Med 2012; 40:2543–2551.
Copyright © 2015 Wolters Kluwe
1070-5295 Copyright � 2015 Wolters Kluwer Health, Inc. All rights rese
56. Bayer O, Schwarzkopf D, Doenst T, et al. Perioperative fluid therapy withtetrastarch and gelatin in cardiac surgery—a prospective sequential analysis�.Crit Care Med 2013; 41:2532–2542.
57. Bergonzi G, Paties C, Vassallo G, et al. Dextran deposits in tissuesof patients undergoing haemodialysis. Nephrol Dial Transplant 1990; 5:54–58.
r Health, Inc. All rights reserved.
rved. www.co-criticalcare.com 301
Related Documents