Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

May 2005
Document of the World Bank
Report No. 32354-ECA
Review of Experience of Family Medicinein Europe and Central Asia(In Five Volumes) Volume III: Bosnia and Herzegovina Case Study
Human Development Sector UnitEurope and Central Asia Region
Rep
ort N
o. 3
23
54
-ECA
Review
of Exp
erience o
f Family M
edicin
e in Eu
rop
e and
Cen
tral Asia V
olu
me III
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
FMP
FMSP FMT GDP
GP HE HIF HI1
HSEP IDA JICA MDG
Family Medicine Physician
Family Medicine Specialization Program Family Medicine Team Gross domestic product
General Practitioner Health Expenditure Health Insurance Fund Health Insurance Institute
Health Sector Enhancement Project International Development Association Japanese International Cooperation Agency Millennium Development Goals
SITAP
STI TA THE
TOR UK us USAID
VTS WB WBBHP WHO
WB Social Insurance Technical Assistance Project Sexually Transmitted I l lness Technical Assistance Total Health Expenditure
Terms o f Reference The United Kingdom The United States o f America United States Agency for International Development Vocational Training Scheme The World Bank The World Bank Basic Health Project in B IH World Health Organization

REVIEW OF EXPERIENCE OF FAMILY MEDICINE IN EUROPE AND CENTRAL ASIA: BOSNIA AND HERZEGOVINA CASE STUDY
CONTENTS
...................
............................................................................................................... 2 Physician Task Profile
.................................................................................................................... 3
........................................................................................................... 5
2.1.
2.3. Economic Changes and Incre ........................................................................................ 5 2.4. Changes in Health Indicators ........................................................................................ 7 2.5. Prior to the War ............................................................. 8
2.7. Reform Challenges in the H e ........................................................................................ 8
The Impact ofthe War Between 1992-1995 .......................................................................................................... 5 2.2. Post-War Governance Arrangements. .............................. ....... ...... 5
Background to Bosnia and Herzego 2.6. Health Expenditure in Bosnia and Herzegovina. ............................... ...... 8
Key Legislative Changes and Health Reform Initiatives in the BIH Health System .................................................. 11 3.1. Key Legislative Changes in the Federation o f BIH .......................... .................... 11
Financing o f the Health System and PHC in the FBIH ........................................................................................ 12
3.
3.2. 3.2.1. Collection. 3.2.2. Pooling ..... 3.2.3. Health Expenditure Trends .................
.............................................................................................................................. 13
Out-of-pocket Payments in PHC ............................................................................................................. 15 3.2.4. 3.3. 3.4. Financing o f the
3.4.1. Collection ............... 3.4.2. Pooling. 3.4.3. Health E 3.4.4. Out-of-P Key Developments in PHC in FBIH ...........
4.2.1. Undergraduate Training in FBIH .............. ............................... Training o f Health Managers in FBIH ...............................
Key Changes in the Delivery o f PHC Services in FBIH ........................................... PHC Gatekeeping, First Contact Function and Comprehensiveness ..... Prescribing and Dispensing o f Drugs in PHC ......................................
Key Legislative Changes in RS .
4. 4.1, Organization o f PHC in FBIH ............................................................................................................................. 19 4.2. Development o f PHC Human Resources in FBIH ................................................................................... 20
4.2.2.
4.3.1. 4.3.2. 4.3.3. Role o f PHC Nurses ....... ..................................................................................................... 23 4.3.4. Emergency Out-of-Hour Services ................................... ........... .............................. 24
Resource Allocation for PHC in FBIH ................................................................................................................ 24
4.3.
4.4.
4.6. Infrastructure and Equipment at PHC Facilities in FBIH . ........................................ 4.7. PHC Information Systems in FBIH ................................................ .................
5. Key Developments in 5.1. 5.2. Development o f
Organisation o f PHC in RS ......................................
5.2.1. Undergraduate Training in RS ......................................................
............................................................................ 29 ...................... 29
5.3.3, Comprehensiveness o f Care 5.3.4. Coordination o f Care ...........................
5.3.6. Role o f FM Nurses .............................. ................
...................................................................... 31
............................................................................ 32 5.6. 5.7.
Infrastructure and Equipment at PHC Facilities in RS Licensing and Revalidation in RS ...................................................
...................................................................... 33
6.1. Characteristics o f the Ordinations ........................ 34 6. Task Profile and Facility Survey Results ............................
6.2.1. Education and Training .... 6.2. Respondent
6.3. Patient List 6.4. Contacts wi th Patients .......
6.7. Collaboration with Other Medical Professionals ... ..................... 6.8. Face-to-Face Interaction with Other Health Profes ................................................ ....................... 41 6.9. Responsibility for Emergency Health Care ...... ......................................... 41
.............................................................................. 54 7.
7.1.4. Improved Commu ...................
........................................................................ ..........................
7.3. Critical Success Factors .... ...........................
8.
9.
10
........................ 58 7.3.2. “Improved Work Environment” 7.3.3. Effective Communication ......... ....................................................... 59
7.3.6. “Developing Trust” ............................................................ 7.3.7. “Bottom Up Versus T
......................................................................... 60
Understanding Stakeholder Needs ...................................................................................................................... . 6 1 7.5.1. 7.5.2. “Incentives Matter” .................................................................................................................... 62
7.6.1. 7.6.2. .................................... 7.6.3. “Demonstrating Success - Quic ................................ 63
“Importance o f Networks and Exposure” ............................................................................................................ 63 “Health System As a Means to Maintaining Social Peace”
7.5.
7.6. Managing Strategic Change ..................................... ........................
7.7. “The role o f International Agents” .................... ........................... 7.8. 7.9.
Key Achievements o f PHC Reforms ................................................................................................................ 8.1, Organization .................................................................................... 65 8.2. Resource Alloc ........................................ 8.3. Financing ........ ................................................................................ 66 8.4. Service Provi
.................................................................................................................... 68
8.5. Resource Generation .............................................................................................. 68
9.1, Challenges Which Remai .......................
Asymmetry in the Pace o
............................................................................. 70 ............................................................................................................................................ 71
Incentives and Retention ...................................................................................................................................... 71 9.6. Quality .....................................................................................................................................
9.8. Communicating the Reforms ............... ...................... .................... 71 9.7.
................
....................... ......................
10.2. Being Strategic
............................................................................................... 73 10.5. Beyond Pilots
10.7. Institutions Versus Institutionalization ............................... 10.8. 10.9. Coordination 10.10. Communicati
Reading the Context ............................................................................................................................................. 74
10.1 1. Responsiveness ........................................................................................ 74
10.12. Monitoring an ............................................................................ 74 10.13. Dissemination 75 10.14. Exit Strategy .. ..................................................................................... 75
Annex 1 : Family Medicine Contract from FBIH Annex 2: An Example o f a Contract in the Republika Srpska ...............
......................................................... 94 Annex 4: F M Clinical Guidelines Introduced in Annex 5: Curriculum for F M Specialist Training Program ....................................................................................................... 97
Annex 7: Family Medicine Curriculum at Undergraduate M Annex 8: Data Regularly Collected at PHC Level ........
Annex3 : Standard Medical and Non-Medical Equipment for GeneralIF
Annex 6: In-Service Program for Advance Training (PAT). ......................
Endnotes .................................................................................................................................................................................. 106
Boxes
Box 1: Box 2: Box 3: Box 4: Box 5 : Box 6:
Figure 1: Figure 2: Figure 3 : Figure 4: Figure 5 : Figure 6: Figure 7: Figure 8: Figure 9: Figure 10: Figure 11: Figure 12:
Key Problems Identified With the Health System in the Federation of Bosnia and Herzegovina Goals o f the Health Reform Reasons for Reforming PHC Level in FBIH ...... PHC Reform Objectives in FBIH ...... Goals o f the Health Reform and Heal argets ............................... .......................... 16
.................................................................................................. 1 1
................................................................................................... 12
....................................................................................... 16 PHC Reform Objectives in
Figures
A Framework for Analyzing Health Systems.
L i fe Expectancy, 1992-2002 Infant and Under-five Morta
GDP Growth ( percent), 1998-2003 ............................................................ ................................................ 6
.................
Health Insurance Fund Expenditure by Category .................................................
Management o f Common Conditions ................ ................... 45 Y
Figure 13: Involvement o f FPs and GPS in Managing Chronic I l lness with No Difference .............................................. 5 1
Tables
Table 1 : Interviewees Distribution ................................................................................................................................. 2
Table 3: ............................................................... 3
Table 5: Table 6: of the Total
Table 2: Informants Categorization ............................................... .....................
Table 4: Poverty Levels in Bosnia and Herzegovina .... ................. Bosnia and Herzegovina: Number o f Facilities and Phys
Number o f F M Doctors in the FBiH by June 30, 2004 .......................................................................................... 21
....................................................................................................... ................... 23 Analysis o f General Practice and FM Specialist Service Delivery Patterns: Service Types
Table 7: Table 8: Table 9: Table 10: Table 11: Table 12: Table 13: Table 14: Table 15: Table 16: Table 17: Table 18: Table 19: Table 20: Table 2 1 : Table 22: Table 23: Table 24: Table 25: Table 26: Table 27: Table 28: Table 29: Table 30: Table 3 1 : Table 32: Table 33: Table 34: Table 35: Table 36: Table 37: Table 38: Table 39: Table 40: Table 4 1 : Table 42: Table 43: Table 44: Table 45: Table 46: Table 47: Table 48: Table 49:
Analysis o f General Practice and F M Specialist Service Delivery Patterns: Service Types .................................. 23 Number o f F M Doctors in RS by June 30, 2004 ............................................................ Number and Type Services Provided at Emergency Department o f DZ Banja Luka in 2001 ............................... 3 1
.............. .. 28
Accreditation Standards ..................................................................... Bosnia and Herzegovina: Number o f Facilities and Family Physicia Distribution o f Ordinations with Family Physicians or GPs .................................... Estimated Number o f Citizens in Places Where Ordinations Location of An Ordination ................................................... Distance to the Nearest General Hospital ............................. Age Distribution ...................................................
Salaried or Self- employment and Additional Position ...................
Hours Worked Weekly on Main Position ..........
Length o f Training in Family Medicine ................. Year When Training in Family Medicine Was ................................... 37 Years Worked As A Medical Doctor ............... Years Worked As A Family PhysicianiGP Specialist ....................................................................................... 38 Number o f Patients on a Doctor’s L i s t .............................................................................................................. 38
................. 38 Average Number o f Consultations Per Do
....................................... 39 ............................................................................ 39
Specialization of Family Medicine Program ..................................................................................................... 36
Number o f Medical Doctors in Shared Accom
Number o f Hours Spent on Professional Development Per D Hours Spent on Professional Development Per Month by Professional Category
.........................
Number o f Patients Not on the List That Request Medical Care ........................................
Frequency o f Meetings with Other H e ................ Responsibility for Out-of-Hours Eme
.........................
................ Orthopaedic Procedures ....................................................................................................................... 44
Management o f Common Gynecological Conditions .....
General Conditions ............................................................................................................................................ 48
.................. 49 ........................................................................ 49
Neurodegenerative Conditions and Mental I l lness ............ ......... ................................. 48 Psychosocial and Family Problems ..................................................................... Measuring Blood Pressure ......
Table 50: Table 5 1 : Table 52: Table 53: Table 54: Table 55: Table 56: Table 57: Table 58: Table 59: Table 60: Table 6 1 : Table 62: Table 63:
Measuring Blood Cholesterol Level ............................... ...................... ..,...... .... ................................................ 50 Involvement in Health Education Activities
Neurological and Psychiatric Conditions . .
Curriculum Structure and the Units o f Teaching for the Program for Advanced Training .. Family Medicine Curriculum Structure at Undergraduate Level ......... .................................... ...........
This volume is a product o f the staff o f the International Bank for Reconstruction and Development I The World Bank. The findings, interpretations, and conclusions expressed in this paper do not necessarily reflect the views o f the Executive Directors o f The World Bank or the governments they represent.
The World Bank does not guarantee the accuracy o f the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status o f any territory or the endorsement or acceptance o f such boundaries.

ACKNOWLEDGMENTS
This report reviews the experience o f family medicine in Bosnia and Herzegovina. It i s part o f a study comprising five volumes that reviews the experience o f family medicine in four countries in the Europe and Central Asia (ECA) Region - Armenia, Bosnia and Herzegovina, Kyrgyz Republic and Moldova. The report reviews the experience, draws lessons, and establishes an evidence base for detailed analysis. The study presents best practices for policy dialogue and future investments by the Bank and other financial institutions. The detailed case studies compare these countries and draw common themes and issues. Comparisons are made with best-developed or existing models in the Organization for Economic Cooperation and Development (OECD) and other E C A countries that have already undertaken family medicine reform.
The report was prepared with financing from a Dutch trust fund. It was prepared by Rifat Atun (Imperial College). Drazenka Rados-Malicbegovic, Gordan Jelic, and Ioannis Kyratsis assisted with data collection. The Task Profile Instrument was designed by Wienke Boerma. The study was prepared under the leadership o f Betty Hanan, Kees Kostermaans and Juan Pablo Ur ibe were the peer reviewers. Valuable comments were provided by Betty Hanan and Nedim Jaganjac. Carmen Laurente helped to prepare the document for publication.
EXECUTIVE SUMMARY
INTRODUCTION
1. The objective o f the study was to review the experience o f family medicine in Europe and Central Asia (ECA), present best practices, and make recommendations for policy dialogue and future investments. Five countries were reviewed as part o f the study. Estonia was selected as pi lot country to test the analytical framework and the instruments developed for research, which were subsequently refined. Four IDA countries -- Armenia, Bosnia and Herzegovina, Kyrgyz Republic, and Moldova were studied in detail. The findings o f the study are presented as four case studies -- one for each o f the four countries studied -- and a synthesis report (Executive Summary) that aggregates the findings and identifies policy implications for the Wor ld Bank and the transition countries undertaking primary health care (PHC) reforms in the E C A Region.
2. methods o f inquiry.
The study comprises primary and secondary research and employed both qualitative and quantitative
3. The study explored changes in four key health system levers as a result o f health care reforms: the regulatory environment and organizational structures, health system financing, resource allocation and provider payment systems, and service provision.
KEY FINDINGS
4. A key finding o f the study i s the paucity o f meaningful, systematically collected, and reliable data to ascertain impact o f policy interventions. Even when data are available, they are not analyzed (often due to resource constraints and limited analytical capacity) to inform decisions or to ascertain whether reform objectives have been achieved. In a l l f ive countries studied, there were no baseline studies to allow pre-and post-intervention studies. Further, there were no quasi-experimental designs that might have allowed comparison o f intervention sites with non-intervention sites.
5. Available monitoring and evaluation (M&E) systems in Bosnia and Herzegovina (BIH) are inadequate for monitoring and evaluating reform impact as they tend to focus on input activities rather than system outputs and outcomes and do not map onto reform objectives. Hence, data generation was challenging, but proprietary instruments were used to generate both qualitative and quantitative data to inform the study.
6. very good progress with PHC reforms and rapidly expanded to cover 23 percent o f the country.
The study findings show that despite a post-conflict setting and resource constraints, BIH has made
7. An enabling environment has been established through appropriate regulatory changes and laws for the reforms to be further extended and scaled up. There i s evidence o f institutionalization o f family medicine (FM) team-centered PHC in both entities, in contrast to other countries in the region, which have established family doctor-centered PHC systems. The laws have established FM as a specialty, defined core and unified curricula for their training in specialist residency and retraining programs, specified the infrastructure and the equipment needed to enable them to practice, and established chambers with responsibility for licensing and revalidation. Further, FM Associations have been developed in both entities and have been admitted to the membership o f Wor ld Family Medicine Association (WONCA). Following appropriate legislation, Agencies for Accreditation and Quality Improvement (AAQIs) have been established and operationalized in both entities.
8. At the end o f June 2004, around 413 FM doctors/specialists and 286 FM nurses have been trained in the Federation o f Bosnia and Herzegovina (FBIH). In addition, 168 FM doctors/specialists and 154 FM
ii
nurses have been trained in Republika Sprska. Further, over 250 health professionals have been trained in health management through programs supported by the Bank-financed Basic Health Project (BHP).
9 . Organizationally, there i s separation o f purchasing and provision, with purchasing devolved to the Health Insurance Fund (HIF) in Republika Srpska (RS) and Cantonal Health Insurance Institutes (CHIIs) in FBIH. Family medicine teams have been established as the basic building block for PHC provider units in both entities. In the pilot regions, the HIF/CHII have established service contracts directly with dom zdravljas (health centers - (DZ) or through DZ with the FM teams. The ambulantas (doctors’ offices) in pilot sites have been refurbished and appropriately equipped and are functioning. The users have been granted the right to choose their family physicians.
10. I n terms o f financing, there i s a shift to a health insurance-based system. Both entities have specified in law that 40 percent o f the revenues o f the CHI1 and HIF (which come predominantly f rom health insurance contributions) should be allocated to PHC.
11. Changes have been made to resource allocation and provider payment systems. A simple per capita payment system has been successfully introduced in the demonstration sites to remunerate FM teams. The per capita model i s weighted by age and in RS includes a performance-related element for health promotion and prevention activities.
12. In the pi lot regions, the contracts between the CHII /HIF and the DZ/FM teams specify in detail the services to be provided by the FM teams as wel l as the equipment they need to use when delivering services. The scope o f services and the equipment used are broader than those specified for non-specialist general practitioners (GPs). Evidence-based guidelines have been introduced for 20 conditions to enhance the quality of services in PHC. The A A Q I s have commenced accreditation o f PHC providers in RS. The accreditation, which i s voluntary, attracts a bonus payment for the PHC provider.
13. The study shows that the family physicians, as compared with the non-specialist GPs, have expanded the scope and content o f their services, and the observed differences are statistically significant. Family physicians are more l ikely to: use an appointment system for consultations; provide health education, promotion, and prevention services; manage a wider range o f acute conditions; provide services for common chronic illnesses; use a broader range o f equipment; and apply a wider range o f medical techniques when managing patients. They are more l ikely to visit their patients in hospital but have been shown to reduce referrals for investigations and prescriptions.
14. The perceived benefits o f the FM for the users identified by key informants include, among others, a user focus; enhanced choice; holistic care; improved continuity; higher quality services; better doctor-patient communication and relationship; a broader set o f services with more health prevention and promotion activities; a shift from a biomedical model to a psychosocial model o f care; and having a named physician to whom the user can relate for a l l problems.
15. Key benefits o f the team-centric FM model for health professionals have been identified as, among others, empowerment o f the health professionals and in particular the FM nurses; enhanced professionalism through improved knowledge and skills; more transparent payment systems; abil ity to provide a broader set o f services, which helps increase status o f the professional; and improved teamwork.
KEY CHALLENGES
16. Despite impressive achievements, a substantial number o f challenges remain if the PHC reforms are to be fully scaled up or sustained. There i s clearly an asymmetry in the pace o f development and the rate at which new laws and regulations have been developed. Rapid pace o f development o f the FM model has
... 111
meant that the existing laws and regulations need to be modified to take into account the current level o f development and the expansion needs. N e w laws and regulations have to be developed to define the legal status o f FM teams in relation to the DZ and contracting institutions. The roles and responsibilities o f the FM team members need to be expanded and defined in law. The scope o f services for FM teams and the PHC level need to be clearly articulated.
17. Organizationally, the FBIH health system i s adversely affected by the premature decentralization to a cantonal structure. Cantons have responsibility for managing health services for their populations and have their own ministers o f health and health insurance institutes. This has led to fragmentation o f the health system, created small risk pools, thinly spread available expert human resources, caused duplication o f services, fractured horizontal linkages, and a created a cumbersome administrative system that i s too inefficient and costly to be sustained. On the other hand, RS has a more centralized organizational structure, with a Ministry o f Health and Social Welfare (MOHSW) responsible for delivery o f health services. Although the M O H S W regulates and manages secondary and tertiary care providers, PHC i s devolved to local governments. Financing and purchasing i s the responsibility o f the Health Insurance Fund. This structure has led to a fragmentation o f services by separating primary and secondary care levels into silos with separate financing flows.
18. Financially, key problems relate to: small risk pools, inter-cantonal and interregional inequities in financing levels and access; high expenditure levels for the health sector, estimated to be 12.5 percent o f the gross domestic product (GDP); despite high expenditure levels, inability o f a substantial proportion o f the population to access freely an essential set o f services, hence creating a high risk factor for poverty; lack o f transportability o f the health insurance entitlements; high out-of-pocket expenditure; and poor tadinsurance collection capacity.
19. The resource allocation systems do not take into account need or poverty levels. Thus, large interregional and inter-cantonal differences in the per capita expenditure for health care exist. Although the Federal Solidarity and Reinsurance Institute covers certain catastrophic expenses and vertical programs, it does not function as an equalization fund to correct interregional inequities in resource allocation.
20. Although per capita pay systems have been introduced in both entities, laws in FBIH do not allow for creation o f incentive systems linked to improved performance. In both entities, there are no M&E systems or adequate capacity at CHI I /HIF to progress to more advanced payment systems with greater performance- related elements based on fee-for-service and target payments.
2 1. The biggest barrier t o development o f FM-centered PHC i s the organization o f service delivery at the PHC level, where a large number o f narrow specialists provide services for common PHC conditions and can be accessed directly by the population. These narrow specialists act as substitutes for family physicians -- often crowding out the FM specialists, fragmenting first contact care, and fracturing gate keeping, continuity, and the comprehensiveness function o f the PHC system. Further, in PHC centers that have not yet adopted the model, services are delivered according to age, gender, and condition o f the users, hindering development o f holistic care and continuous care.
22. A further barrier to the development o f PHC i s poor vertical linkages between PHC and secondary level and lack o f referral and counter-referral mechanisms. These impede the development o f integrated services and frustrate any attempts to establish a continuum o f care.
LESSONS LEARNED
23. The study has identified a number o f critical success factors for expanding PHC: (a) branding FM and image building; (b) improved work environment; (c) improved communication between and within levels o f
iv
the health system and with the public; (d) improved coordination o f key institutions; (e) developing a holistic approach to reform; (0 developing trust through better engagement o f the operational level to create ownership; and (g) better coordination between donors.
24. The study clearly demonstrates the importance o f a multifaceted, multi level approach to reform: developing an enabling legal environment for change to occur while simultaneously intervening to refine organizational structures, financing, resource allocation, provider payment systems, and service provision.
25. Balancing short-term success and sustainability i s important. Achieving system change takes time, and sustained support over a five- to eight-year period i s a realistic time scale to adopt for new PHC projects in the region.
26. health system reform.
Moving out o f “pilot” and “experiment” mode i s key to institutionalizing changes needed to sustain
27. Vertical and horizontal links should be formed to work simultaneously at both policy and operational levels -- the former to institutionalize changes and the latter to create shared ownership to implement policies.
28. balanced with efforts to widely engage stakeholders to achieve consensus o n reform objectives.
While it i s necessary to invest in key individuals to develop champions o f reform, this must be
29. The fluidity o f the sociopolitical and economic environment in BIH means that the political economy o f health reforms and factors influencing strategic change must be analyzed and addressed in the design phase and throughout implementation o f programs.
30. duplicated, but to achieve this objective, the ministries o f health must be actively supported.
Coordination o f international agencies i s necessary to ensure that activities are not fragmented and
31. communication strategy must be aimed at users, health professionals, managers, and decision makers.
Poor communication creates a fear o f the unknown and breeds resistance. A well-developed
32. adapt to changes and respond to windows o f opportunity, but without sacrificing a strategic approach.
Given the fluidity o f the context, programs should adopt a flexible approach to implementation to
33. o f PHC reforms and systematically gather information to verify progress against objectives.
There i s an urgent need to develop appropriate metrics and information systems to monitor progress
34. The Basic Health Project was a highly successful project. I t demonstrates that the World Bank can add much value to the reform process, but success brings with it responsibility. A clear exit strategy needs to be developed to ensure that there are no gaps in support and to sustain the transformation process.
V

1. INTRODUCTION
1. The objectives o f the study are to review the experience o f family medicine (The term “family medicine” i s used here, but other terms such as “primary health care (PHC)” or “general practice” are used frequently and interchangeably) in Europe and Central Asia (ECA), present best practices, and make recommendations for policy dialogue and future investments.
1.1. THE EVALUATION FRAMEWORK
2. Kutzin suggests a three-step approach to evaluating health reforms, describing clearly: (a) key contextual factors driving reform, (b) the reform itself and i t s objectives, and (c) the process by which the reform was (is being) implemented.’ To this approach, three further elements can be added: (a) describing clearly the changes introduced by the reforms, (b) analyzing the impact o f these changes on health system objectives and goals, and (c) establishing whether the reforms have achieved the policy objectives set by the government - or the agency leading the reforms.
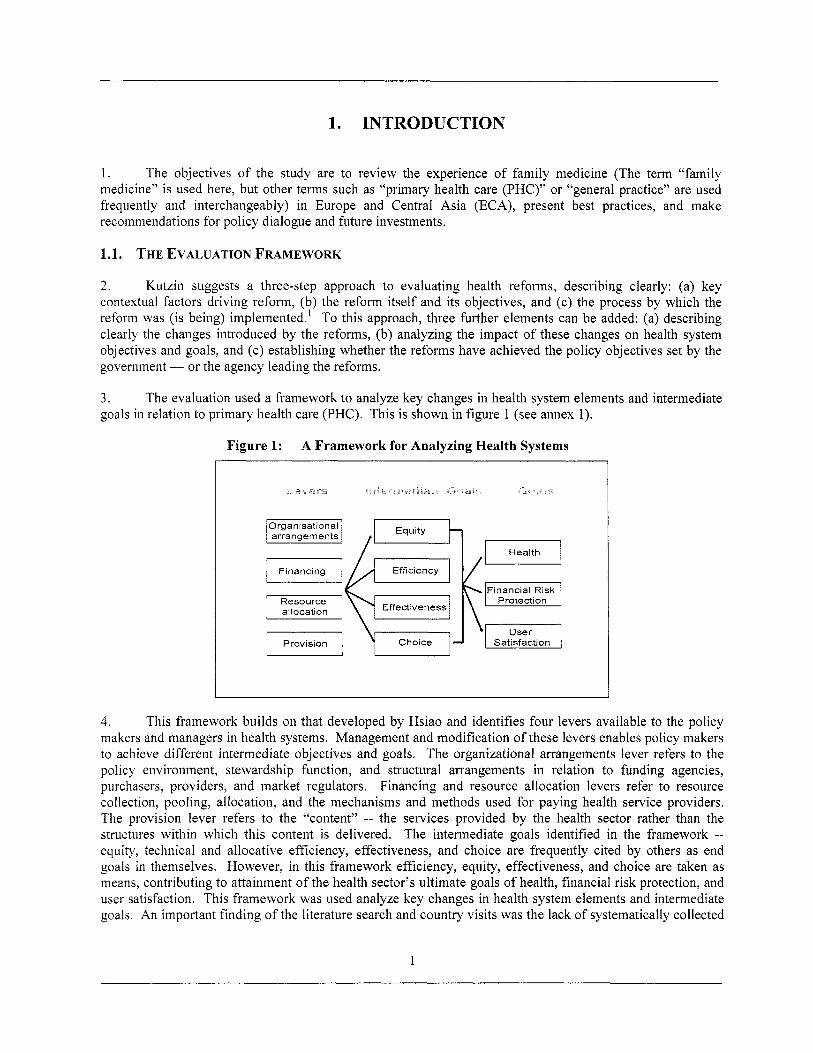
3 , goals in relation to primary health care (PHC). This i s shown in figure 1 (see annex 1).
The evaluation used a framework to analyze key changes in health system elements and intermediate
Figure 1: A Framework for Analyzing Health Systems
I I Organisational ~~h arrangements
Effectiveness allocation
I I I
4. This framework builds on that developed by Hsiao and identifies four levers available to the policy makers and managers in health systems. Management and modification o f these levers enables policy makers to achieve different intermediate objectives and goals. The organizational arrangements lever refers to the policy environment, stewardship function, and structural arrangements in relation to funding agencies, purchasers, providers, and market regulators. Financing and resource allocation levers refer to resource collection, pooling, allocation, and the mechanisms and methods used for paying health service providers. The provision lever refers to the “content” -- the services provided by the health sector rather than the structures within which this content i s delivered. The intermediate goals identified in the framework -- equity, technical and allocative efficiency, effectiveness, and choice are frequently cited by others as end goals in themselves, However, in this framework efficiency, equity, effectiveness, and choice are taken as means, contributing to attainment o f the health sector’s ultimate goals o f health, financial risk protection, and user satisfaction. This framework was used analyze key changes in health system elements and intermediate goals. An important finding o f the literature search and country visits was the lack o f systematically collected
1
data at the PHC level. Therefore, primary research was undertaken to generate original data to complement secondary research findings.
Number o f Informants Republika Srpska Federation o f Bosnia & Herzegovina
Visit 1 9 10 Visit 2 18 21 Total 21 3 1
1.2. PRIMARY RESEARCH
Bosnia & Herzegovina
19 39 58
5. Survey; and (c) Physician Task Profile Survey.
Primary research comprised three elements: (a) qualitative research; (b) Primary Health Care Facility
1.2.1. Qualitative Research
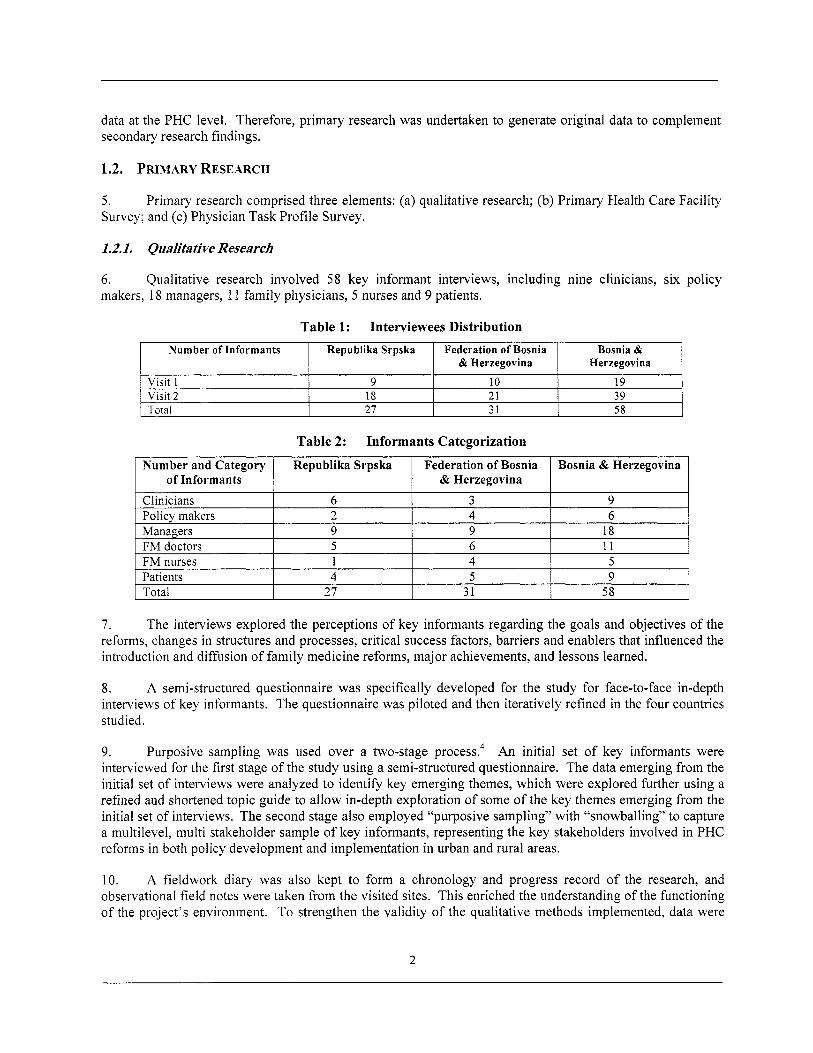
6, makers, 18 managers, 1 1 family physicians, 5 nurses and 9 patients.
Qualitative research involved 5 8 key informant interviews, including nine clinicians, six policy
Table 2: Informants Categorization
7. The interviews explored the perceptions o f key informants regarding the goals and objectives o f the reforms, changes in structures and processes, critical success factors, barriers and enablers that influenced the introduction and diffusion o f family medicine reforms, major achievements, and lessons learned.
8. A semi-structured questionnaire was specifically developed for the study for face-to-face in-depth interviews o f key informants. The questionnaire was piloted and then iteratively refined in the four countries studied.
9. Purposive sampling was used over a two-stage p r o ~ e s s . ~ An init ial set o f key informants were interviewed for the first stage o f the study using a semi-structured questionnaire. The data emerging from the initial set o f interviews were analyzed to identify key emerging themes, which were explored further using a refined and shortened topic guide to al low in-depth exploration o f some o f the key themes emerging from the initial set o f interviews. The second stage also employed “purposive sampling” with “snowballing” to capture a multilevel, multi stakeholder sample o f key informants, representing the key stakeholders involved in PHC reforms in both policy development and implementation in urban and rural areas.
10. A fieldwork diary was also kept to form a chronology and progress record o f the research, and observational f ield notes were taken from the visited sites. This enriched the understanding o f the functioning o f the project’s environment. T o strengthen the validity o f the qualitative methods implemented, data were
2
triangulated by comparing the results o f interviews from different groups o f stakeholders wi th the outcome of the analysis o f official documents,
Federation o f Bosnia and Herzegovina
Bosnia and Herzegovina Total Republika Srpska
1 1, The analysis informed the detailed case study by capturing information o n key structural and process changes, issues related to design and implementation o f PHC reforms, the drivers and barriers to reform, the factors influencing the establishment o f an enabling environment for change, and the lessons learned.
Ordinations (Facilities) Physicians Surveyed 42 100
45 99 87 199
1.2.2. Primary Health Care Facility and Physician Task Profile
12. These two elements o f primary research were done concurrently to explore changes in service delivery and practice o f family physicians as a result o f the PHC reforms and training o f physicians as family medicine specialists. I t was not possible to do a pre- and post-intervention study as there were no data or baseline studies that analyzed service delivery patterns and physician practices before the reforms and after the introduction o f changes.
13. and (b) Physician Task Profi le survey.
Two cross-sectional studies were carried out simultaneously: (a) Primary Health Care Facility survey
14. Each o f the instruments was translated into Bosnian and Serbo-Croat (local language). Local research teams were trained in the use and application o f the instruments. Data analysis was undertaken in Bosnia and London.
15. geography and the relative stage o f development o f PHC reforms.
Purposive sampling was used to provide a diverse sample. The dom zdravjlas were selected based on
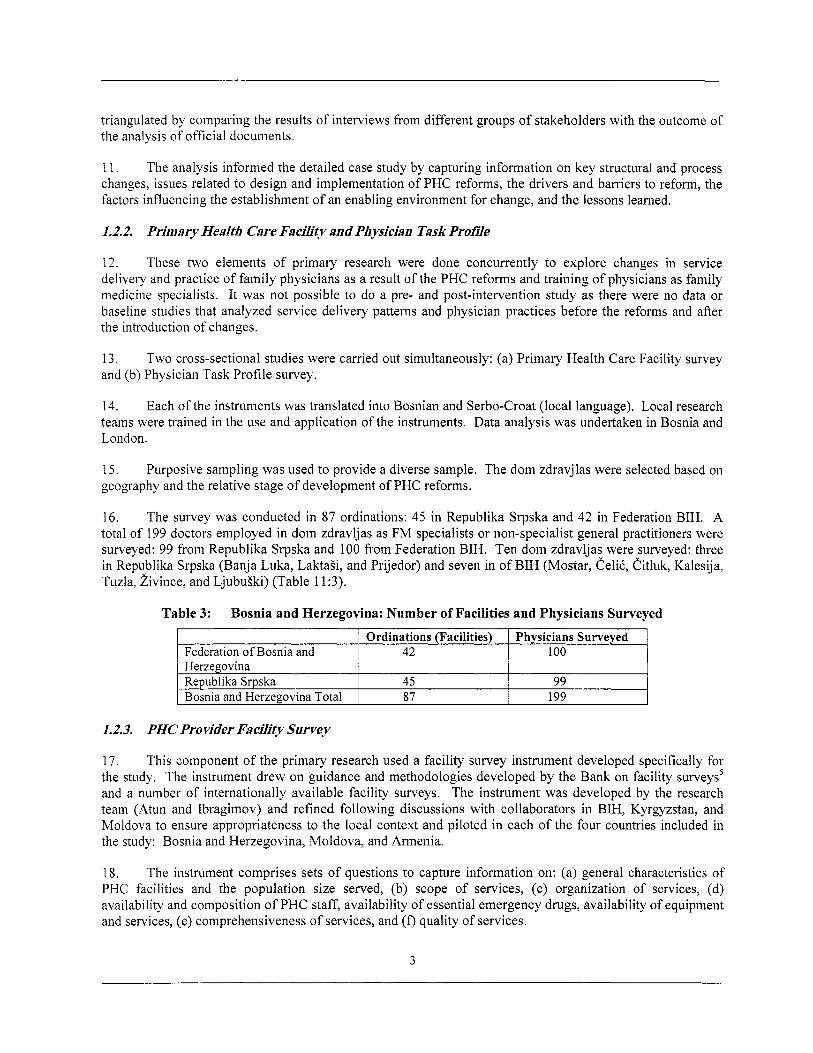
16. The survey was conducted in 87 ordinations: 45 in Republika Srpska and 42 in Federation BIH. A total o f 199 doctors employed in dom zdravljas as FM specialists or non-specialist general practitioners were surveyed: 99 from Republika Srpska and 100 from Federation BIH. Ten dom zdravljas were surveyed: three in Republika Srpska (Banja Luka, LaktaSi, and Prijedor) and seven in o f BIH (Mostar, CeliC, Citluk, Kalesija, Tuzla, i iv ince, and LjubuSki) (Table 11:3).
Table 3: Bosnia and Herzegovina: Number o f Facilities and Physicians Surveyed
1.2.3. PHC Provider Facility Survey
17. This component o f the primary research used a facility survey instrument developed specifically for the study. The instrument drew on guidance and methodologies developed by the Bank on facility surveys’ and a number o f internationally available facility surveys. The instrument was developed by the research team (Atun and Ibragimov) and refined following discussions with collaborators in BIH, Kyrgyzstan, and Moldova to ensure appropriateness to the local context and piloted in each o f the four countries included in the study: Bosnia and Herzegovina, Moldova, and Armenia.
18. The instrument comprises sets o f questions to capture information on: (a) general characteristics of PHC facilities and the population size served, (b) scope o f services, (c) organization o f services, (d) availability and composition o f PHC staff, availability o f essential emergency drugs, availability o f equipment and services, (e) comprehensiveness o f services, and ( f ) quality o f services.
3
19. The instrument also initially had a section on financing o f the facilities, but this was later omitted as field testing revealed that most facilities did not have financing data at the facility level. A summary o f the elements o f the instrument i s attached in Annex 2.
20. analysis. We performed statistical analysis (descriptive statistics and T-test) to test for observed differences.
The instrument was coded and a computer program was written in Access@ for data entry and
1.2.4, Survey o f Task Profiles ofFamily Physicians
2 1. The second component o f the primary research was a cross-sectional survey o f family physicians to explore their “Task Profiles” using a validated instrument developed by the NIVEL Group in the Netherlands.6 The instrument, previously tested and validated in 32 European countries, i s available in several languages, including Russian and other Slavic languages. I t enables collection o f detailed data on the preventative, promotive, and curative services provided by family physicians, their skills, knowledge base, attitudes, and workload. The latter i s captured by use o f a seven-day workload diary. The instrument was obtained from the author, Dr. W. G. W. Boerma, and with his kind permission used in the study. A summary o f the instrument i s shown in Annex 3.
22. The survey o f the Task Profiles o f Family Physicians aimed to identify the scope and availability o f services and sk i l ls o f doctors working at PHC level and to identify similarities and differences between FM specialists and non-specialist GPs.
23. The instrument was tested in the four study countries and minor modifications made to ensure contextual sensitivity. The instrument was coded and a data collection and entry program developed in Microsoft Access. Data were transferred to SPSSO for statistical analysis.
1.3. SECONDARY RESEARCH
24. Secondary research consisted o f a review o f international and in-country published literature to ascertain key legislative changes related to the reforms and to identify changes in financing, resource allocation, provider payment systems, organizational changes and regulation, and service provision. There were no a cross-sectional or longitudinal data on referrals and admissions for conditions commonly managed in PHC setting for analysis.
1.3.1. Literature Review
25. The literature review comprised analysis o f published articles in peer-reviewed journals, supplemented by documentary analysis o f published reports, key legal instruments and policy documents from the four countries, Bank publications, country Health Care Systems in Transition (HIT) published by the European Observatory on Health Systems Research, and other relevant studies (e.g. evaluation o f Bank- financed health projects in the E C A Region by Dr. D. Miller).’
4
2. THE CHALLENGES FACED BY THE HEALTH SYSTEM IN BOSNIA AND HERZEGOVINA
2.1. THE IMPACT OF THE W A R BETWEEN 1992 AND 1995
26. The four-year war caused widespread physical damage and had a devastating effect on Bosnia and Herzegovina. Over 10 percent o f the population was ki l led or wounded and over two mi l l ion people -- nearly hal f the pre-war population were forced from or chose to leave their homes and became refugees, either abroad or displaced internally within BIH. With these population movements, community- and family-based social networks were seriously disrupted. Two-thirds o f homes were damaged, with one-fifth totally destroyed. An estimated 30 to 40 percent o f hospitals and 70 percent o f schools were destroyed or severely damaged, and 30 percent o f health care professionals and a similar share o f teachers were lost to death or emigration.
27. Economic situation deteriorated rapidly during the war. The economy collapsed and the per capita GDP fell five-fold, f rom US$2,429 in 1990 to US$456 in 1995.’
2.2. POST-WAR GOVERNANCE ARRANGEMENTS
28. Following three years o f c i v i l war, a peace agreement, the Dayton Accord, was negotiated in November 1995. The Accord acknowledged the bitter ethnic divides that had led to war by establishing a government structure with a weak central state in which the ethnically based “entities” retained political, military, and economic authority. The Accord also provided for a strong international policy and military presence and an international overseer - the Office o f the High Representative (OHR).
29. Under the 1995 Dayton Accord, four levels o f government were established in the Federation o f Bosnia and Herzegovina and three in Republika Srpska: (a) At the highest level, the state o f Bosnia and Herzegovina (the state); (ii) at the next level two constituent political entities, the Federation o f Bosnia and Herzegovina (FBIH) and the Republika Srpska (RS), covering 5 1 percent and 49 percent o f the land area o f Bosnia and Herzegovina, respectively; and (iii) FBIH was divided into ten cantons, which in turn were divided into municipalities. In the RS, no cantons were established and local government was assumed directly by municipalities. In addition, Brcko, with three municipalities, was designated as a District.
2.3. ECONOMIC CHANGES AND INCREASING POVERTY
30. Immediately after the war a postwar Priority Reconstruction and Recovery Program (1996-1999) was put in place by the donors and development agencies. By the end o f 1999, around US$3.5 bi l l ion o f the US$5 bil l ion pledged for reconstruction had been d i s b ~ r s e d . ~
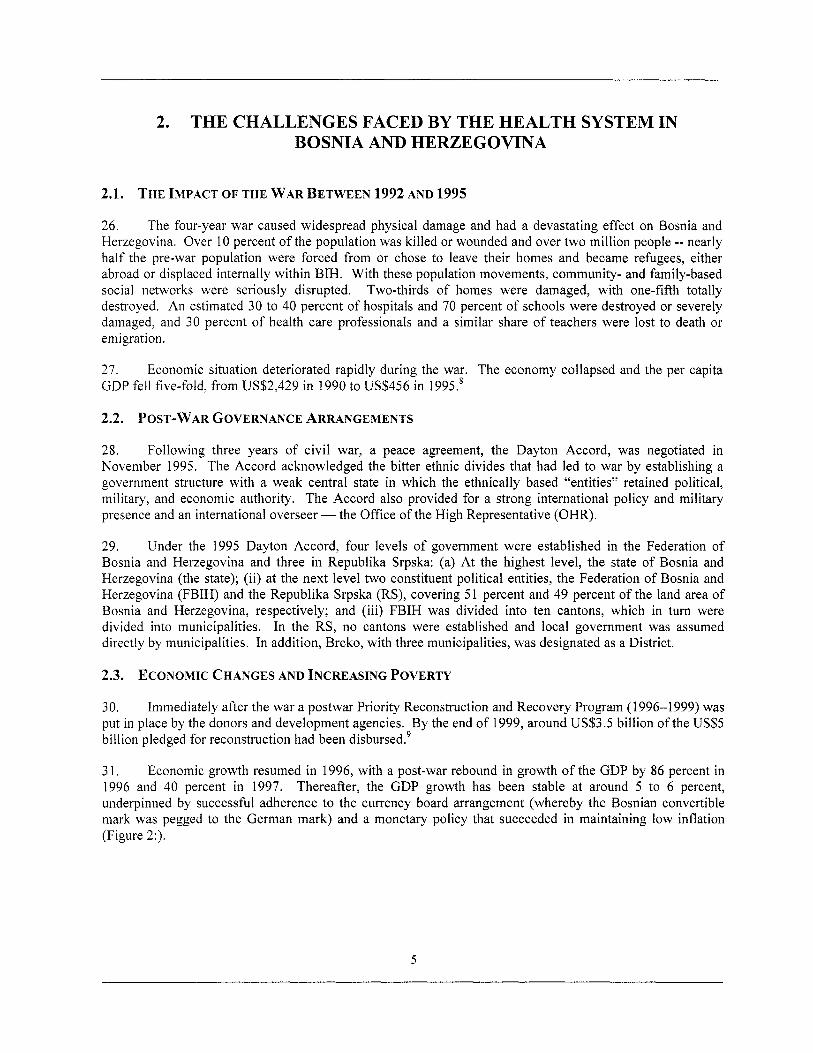
3 1. Economic growth resumed in 1996, with a post-war rebound in growth o f the GDP by 86 percent in 1996 and 40 percent in 1997. Thereafter, the GDP growth has been stable at around 5 to 6 percent, underpinned by successful adherence to the currency board arrangement (whereby the Bosnian convertible mark was pegged to the German mark) and a monetary policy that succeeded in maintaining l ow inflation (Figure 2:).
5
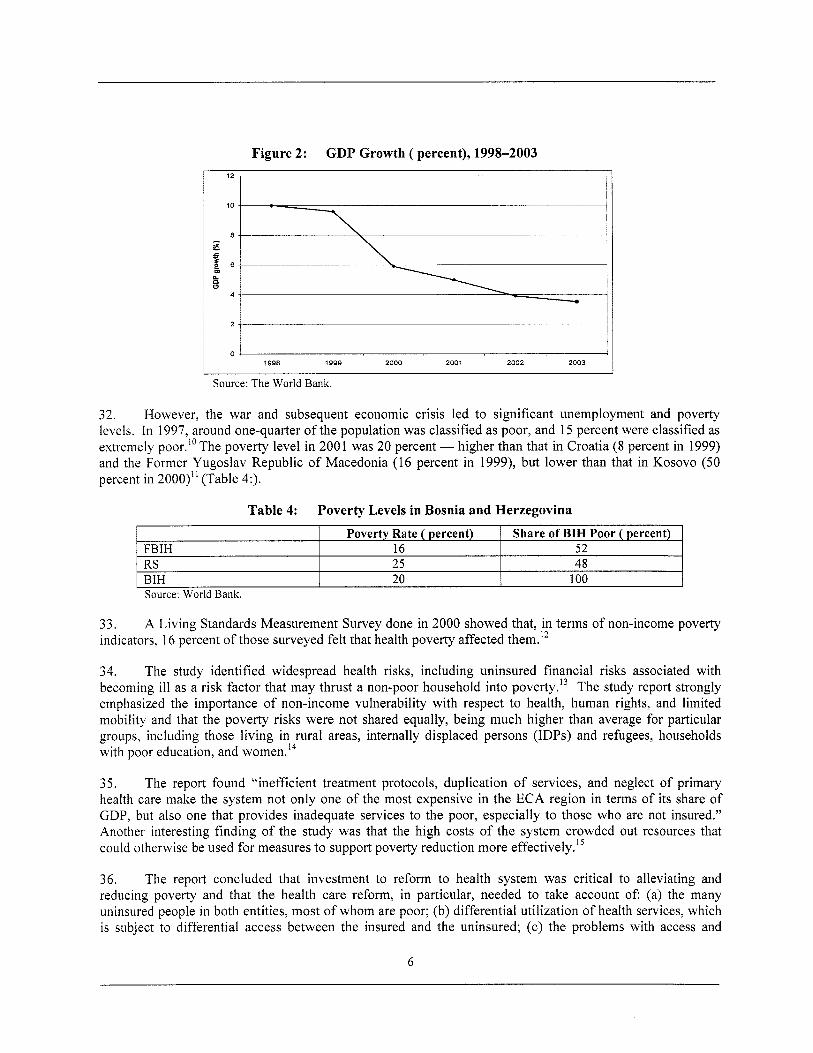
Figure 2: GDP Growth ( percent), 1998-2003 12 -
10
a - E I e, 6 - B W
4 -
---
-- I I
I I
1998 1999 zoo0 2001 2002 2003
Source: The World Bank.
FBIH RS BIH
32. However, the war and subsequent economic crisis led to significant unemployment and poverty levels. In 1997, around one-quarter o f the population was classified as poor, and 15 percent were classified as extremely poor.I0The poverty level in 2001 was 20 percent - higher than that in Croatia (8 percent in 1999) and the Former Yugoslav Republic o f Macedonia (16 percent in 1999), but lower than that in Kosovo (50 percent in 2000)” (Table 4:).
Poverty Rate ( percent) Share of BIH Poor ( percent) 16 52 25 48 20 100
33. indicators, 16 percent o f those surveyed felt that health poverty affected them.’*
A Living Standards Measurement Survey done in 2000 showed that, in terms o f non-income poverty
34. The study identified widespread health risks, including uninsured financial risks associated with becoming ill as a risk factor that may thrust a non-poor household into poverty.13 The study report strongly emphasized the importance o f non-income vulnerability with respect to health, human rights, and limited mobility and that the poverty risks were not shared equally, being much higher than average for particular groups, including those living in rural areas, internally displaced persons (IDPs) and refugees, households with poor education, and women.I4
35. The report found “inefficient treatment protocols, duplication o f services, and neglect o f primary health care make the system not only one o f the most expensive in the ECA region in terms o f i t s share o f GDP, but also one that provides inadequate services to the poor, especially to those who are not insured.” Another interesting finding o f the study was that the high costs o f the system crowded out resources that could otherwise be used for measures to support poverty reduction more ef fe~t ive1y. l~
36. The report concluded that investment to reform to health system was critical to alleviating and reducing poverty and that the health care reform, in particular, needed to take account o f (a) the many uninsured people in both entities, most o f whom are poor; (b) differential utilization o f health services, which i s subject to differential access between the insured and the uninsured; (c) the problems with access and
6
equity in a system that i s supposed to ensure universal coverage; (d) financial consequences o f health risks for the poor, who allocate a greater proportion o f their consumption to health care than the rich, and thus are more exposed to these risks; (e) the prevalence o f large out-of-pocket expenditures, which negatively affected access to health services; and (f) substantial public expenditures on health services.I6
37. 1998, among the highest in the ECA region. ”
In 1998, registered unemployment reached 37 percent in FBIH and 36 percent in Republika Srpska in
2.4. CHANGES IN HEALTH INDICATORS
38. In the post-war period, the population suffered significant post-traumatic stress due to ravages o f the war, the subsequent socio-economic crisis, unemployment, migration, and displacement. However, general population indicators such as infant mortality, under-five mortality, and l i fe expectancy have remained stable (Figure 3: ) .
Figure 3: Life Expectancy, 1992-2002
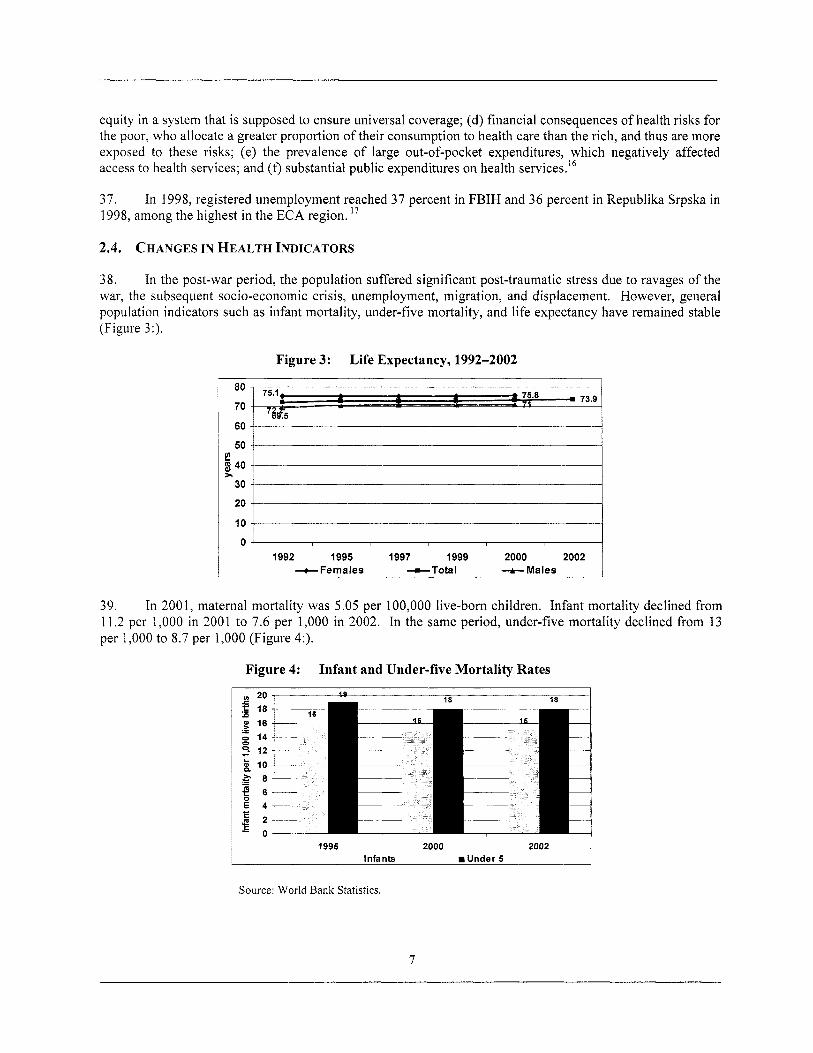
39. In 2001, maternal mortality was 5.05 per 100,000 live-born children. Infant mortality declined from 11.2 per 1,000 in 2001 to 7.6 per 1,000 in 2002. In the same period, under-five mortality declined from 13 per 1,000 to 8.7 per 1,000 (Figure 4:).
Figure 4: Infant and Under-five Mortality Rates
l I 1995 2000 2002 Infants m Under 5
Source: World Bank Statistics.
7
40. percent), and injuries and poisoning (around 5 percent) - similar to those in the pre-war period.
The leading causes o f death in 2000 were cardiovascular diseases (52 percent), malignancies (18
41. 8 1.3 percent; and MMR 86.0 percent,
In 2002, immunization coverage in children for B C G was 91.2 percent; for DTP3 73.9 percent, OPV3
42. No systematic data are available on the quality o f antenatal services and heath outcomes. The Federal Public Health Institute estimates that in 2001 only 2.1 percent o f mothers were breastfeeding at six months - a very low figure by international standards.
2.5. BACKGROUND ON BOSNIA AND HERZEGOVINA HEALTH SYSTEM PRIOR TO THE WAR
43. The former Federal Socialist Republic o f Yugoslavia had a well-developed health care system with a large network o f clinics, hospitals, and public health facilities. The population health indicators were comparable to those o f OECD countries. In Bosnia and Herzegovina, there were 5.8 beds and 2.6 doctors per 1,000 people.
44. Prior to the war, BIH had a well-established network o f PHC centers comprising dom zdravljas (DZs), doctors’ offices for ambulatory PHC services (podrucna ambulantas), and f i rst aid and emergency service units (hitne pomoci).
45. Each municipality had i t s health center (a DZ), which coordinated a network o f smaller PHC community facilities (as outposts o f the DZ). The DZ was located in the main city or town and the smaller clinics (ambulantas) in smaller communes and villages. There were 109 DZs, each covering a commune o f 30,000 to 50,000 inhabitants. The DZs coordinated 900 doctors’ offices (ambulantas), usually staffed by one doctor and a few nurses, which provided basic and first-line services to local populations.
46. Within the DZ, PHC was divided into seven distinct functions: (a) general practice; (b) occupational medicine; (c) pre-school pediatrics; (d) school pediatrics; (e) gynecology/obstetrics; (0 laboratory/)(-ray, and (g) hygiene and epidemiological unit. The PHC system was coordinated by the Ministry o f Health and Social Affairs and supplemented by additional health clinics that served special groups such as the police and military personnel. In addition, almost every large company had organized i t s own health services.
47. Public health services were also responsible for monitoring health status and epidemiological indicators, control o f communicable diseases and immunization, radiation control, water quality and sanitation control, nutrition monitoring, and health promotion. Public health services were provided through epidemiological surveillance departments within DZs and a network o f regional public health institutes throughout Bosnia and Herzegovina - with a main Public Health Institute in Sarajevo.
2.6. HEALTH EXPENDITURE IN BOSNIA AND HERZEGOVINA
48. Bosnia and Herzegovina allocates around 12 percent o f i t s total GDP to health: o f this, about 8 percent comes from the Compulsory Health Insurance System, State Budget Transfers, and donations; and around 4 percent comes from out-of-pocket expenditures in form o f co-payments for health services and drugs and under-the-table payments and fees for service in private sector. The total allocation to health, as a proportion o f GDP, i s high compared with developed countries in Western Europe.I8
2.7. REFORM CHALLENGES IN THE HEALTH SYSTEM
49. Following the post-war Priority Reconstruction and Recovery Program (1996-1999), the donors began to identify sector specific programs to support sustainable development. The Wor ld Bank Bosnia and
8
Herzegovina Country Assistance Strategy (CAS) in 2000 for the financial years 2000 to 2002 identified key medium-term development challenges that needed addressing to increase economic opportunity and improve the quality o f l i f e for a l l B o ~ n i a n s . ' ~ These challenges were identified as (a) strengthening governance and public sector management; (b) Fostering private sector led-growth; (c) building social sustainability; and (d) completing reconstruction.
50. The CAS in 2000 identified weak and fragmented governance as the most serious impediment to implementing reforms needed for sustainable economic growth. Specifically for the health sector, the CAS identified key challenges as implementation o f laws that provide universal access to a basic package o f health care, equal access to services, and efficient financing and delivery. The CAS also noted that the post-war decentralization had resulted in an unreasonably l ow level o f risk pooling for health insurance funds despite a very large share o f GDP (over 12 percent) spent on health care, with over one-third o f these expenditures covered out o f pocket by private citizens (disproportionately by the poor, who identify the cost o f health care as a key concern). The CAS identified as priorities institutional reforms to enhance risk pooling, build capacity, and increase use o f modern health management methods.20
51. The "Strategic Health Systems Plan for the Federation o f BIH," published in 1998, identified a number o f key structural problems with the FBIH health system and articulated the need for health reforms2' (Box 1:).
Box 1: Key Problems Identified With the Health System in the Federation o f Bosnia and Herzegovina
Inadequate access with inequalities in the use o f health services Large numbers o f inappropriate procedures performed in the system Poor coordination between care providers and sub sectors o f the system Inability o f the system to meet the demands o f an increasingly assertive population wishing to exercise choice anc participation in decision making Low income and poor working conditions for health professionals with consequent low morale and emigration Huge demographic shifts with refugees and intemally displaced persons Health facilities and equipment destroyed in the war Large number o f wounded and disabled people as a consequence o f the war Worsening environmental conditions for health - waste disposal, water supply Excessive health expenditures Fragmentation o f the PHC level with multiple providers
52. The Appraisal in 1999 for the World Bank-financed Basic Health Project identified the principal issues in the health sector as (a) the absence o f a sustainable health finance system; (b) a mismatch between health needs and health services; and (c) a weak coordination o f international donor activity in primary health care and public health care. These problems were attributed to multiple factors related to the weak economy, political and social context, infrastructure, incentives, and management systems, as wel l as training and deployment o f staff.22
53. Financing problems were identified as high levels o f expenditure (as a proportion o f GDP), highly fragmented risk pools in FBIH (especially in small cantons), and wide variation in resource mobilization and expenditures among cantons and between the two entities. In terms o f the health care delivery system, the appraisal identified, among others, fragmented delivery systems, inequitable access, and wide variations in the scope, content, and quality o f services among different cantons as key problems that needed a d d r e ~ s i n g . ~ ~
54. A further important problem identified by the appraisal was the proliferation o f large number o f training programs for doctors and nurses in PHC without any common or agreed standards in scope, content, quality, and length o f training.24
9
55. The difficulties with co-coordinating the activities o f the donors working at the PHC level were attributed to large number o f donors active in BIH (around 140) and limited capacity at the Ministries o f Health in both entities.25
56. A rapid appraisal o f the primary care equipment, undertaken with support f rom the World Bank in 1998, revealed wide variations among health facilities in availability, status, and use. In most cases, the installed equipment was found to be obsolete, not working, or unused due to lack o f consumables and personnel.26
57. The analysis undertaken for the Social Insurance Technical Assistance Project (SITAP) identified a number o f systemic and health sector specific problems that needed to be addressed to enhance development o f the health sector. The systemic issues identified were: (a) high wage tax and contribution burden, leading to tax evasion; (b) low compliance with wage tax obligations by those in the large informal economy; (c) inadequate contributions from farmers and the self-employed; (d) inadequate mechanisms for dealing with the uninsured non-working populations; (e) inadequate data access and exchange among agencies involved in contribution collection; and ( f ) lack o f portability o f health insurance benefits.27 K e y health system issues identified were: (a) premature decentralization, which led to l imited institutional capacity and institutional fragmentation; (b) financial instability f rom the proportion o f GDP allocated to the health sector - as a result o f the high cost o f operating a fragmented and muttered structure with allocative and technical inefficiency - but with a low tax base, inadequate inclusion o f the self-employed and farmers as health insurance contributors, and a large proportion o f beneficiaries who are exempt from contribution; (c) inequities due to the substantial proportion o f the population not covered by health insurance; (d) small risk pools due to the devolution o f health insurance function to entities and cantons; (e) high variability in economic status and revenue generation capacity o f the cantons in FBIH; (0 inefficient service delivery; and (g) unequal access to care.28
58. Inequitable access to health services and excessive fragmentation o f the health system has been identified as key problems in subsequent analyses2’, 30 -- although empirical evidence demonstrating the direction and magnitude o f these problems i s lacking.
59. The fragmentation i s not confined to financing o f the health system. Service delivery i s fragmented by level o f care but also highly verticalized within these levels. For instance, at the PHC level, separate services exist for different age groups (e.g., dispensary for children), gender (e.g., dispensary for women), occupational groups (e.g., occupational medicine departments in different companies), as wel l as for specific illnesses (e.g., tuberculosis dispensary).
60. Although the Bosnian government i s aware o f many o f these problems and, with donor support, has made efforts to address them, the complexity o f governance arrangements and premature decentralization, wi th consequent managerial inadequacy, have led to delays in implementing interventions to address priorities in the health sector.31
10
3. KEY LEGISLATIVE CHANGES AND HEALTH REFORM INITIATIVES IN THE BIH HEALTH SYSTEM
61. The Government o f BIH has tried to respond systematically t o the socio-economic challenges by developing a number o f overarching frameworks and approaches that wil l guide i t s response, These included the Global Framework for Economic Development and Social Protection32 (as a prelude to the Economic Development Strategy) and the Poverty Reduction Strategy Paper (PRSP), which was preceded by an interim paper.
62. The PRSP identifies a number o f priorities for health reform: (a) new health legislation to regulate health services, especially to improve solidarity and patient mobility; (b) reform o f the Health Insurance Funds system; (c) regulation o f the private health services; (d) more rational capacity utilization to improve referral between levels and reduce duplication; (e) improvement o f operational transparency and expansion o f public services; ( f ) increasing the accountability o f health workers to the general public; and (g) improving the quality o f health services throughout the country.33
63. The post-war reconstruction and development programs in both entities, supported by the World Bank, aimed to develop a Basic Health Program comprising (a) primary health care based on the family medicine concept; (b) a shift from the pre-war emphasis on large hospitals and polyclinics toward more efficient use o f outpatient facilities and home-based care; and (c) a greater emphasis on cost-effective public health and disease prevention and control. A number o f policy and strategy documents were developed to articulate objectives and plans.
3.1. KEY LEGISLATIVE CHANGES IN THE FEDERATION OF BIH
64. In the Federation, elements o f the reform strategy were outlined in several laws and strategy documents including: Federation Health Program: Health Reform and R e c o n s t r ~ c t i o n ~ ~ and Public Health and Health Care: Federation o f Bosnia and Herzegovina. 35
65. The 1997 Health Care Law36 and Health Insurance Law37 were enacted. These, along with the related bylaws and regulations, divided the responsibilities o f the Federation and canton levels. The Federation level was given the authority to formulate policy and pass laws and the canton level the authority to formulate local policies, implement laws, and be responsible for financing and provision o f health services.
66, the objectives for health system reform38 (Box 2:).
In 1998, the “Strategic Health System Plan for the Federation o f Bosnia and Herzegovina” articulated
Box 2: Goals o f the Health Reform
System sustainability - affordable Equity and solidarity - universal coverage for a “basic package” o f services Efficiency - fair allocation o f resources to priorities and maximizing available resources through effective management Satisfaction o f users and health professionals - higher quality health care with transparency and accountability Pluralism and ownership - recognizing the need for public/private balance
67, The Strategic Health Systems Plan also identified the major reasons for reforming the PHC sector and set a number o f reform objectives to address these reasons (Box 3: and 4).
11

Box 3: Reasons for Reforming the PHC Level in F B M
Fragmented PHC system - care delivery segmented by gender and age Poor gatekeeping - due to direct first contact with a large number o f sub specialists working at the PHC level and a high hospital referral rate Limited continuity o f care - due to frequent changes o f general practitioners and multiple providers at the PHC level Low problem resolution capacity - with only 40 to 60 percent o f problems solved at the PHC level, compared with over 90 percent in well-developed PHC systems Physician-centered system - undervaluing other health professionals Biomedical service model with curative focus -with insufficient disease prevention and health promotion activities Inequity in coverage and access - urban-rural and intercantonal differences
1 Poor infrastructure with low-quality, outdated, and poorly maintained equipment --compared with secondary and tertiarv care facilities
Box 4: PHC Reform Objectives in F B M
Developing a universal “basic package” o f good-quality services that i s equitable, affordable, and cost-effective Providing freedom o f choice with family physiciadgeneral practitioner Strengthening continuity o f care Strengthening doctor-patient relationship Enhancing gatekeeping to reduce unnecessary referrals to the secondary care level by establishing the family doctor as the point o f first contact in the health system, and improving the capacity for problem resolution at the PHC level Improving the capacity o f the family physicians to coordinate health care services Improving the quality o f PHC facilities and equipping them appropriately
68. Under the 1997 L a w on Health Care3’, PHC was defined in FBIH to include activities o f the family doctor and general practitioner, school medicine, hygiene and epidemiology, dental care, occupational medicine, care o f women and children, and diagnostic and pharmaceutical activities. The Health Care and Health Insurance elements o f the law stipulated that each insured person was entitled to the “basic package of services” regardless o f available resources within a canton4’ and that resources should be allocated to family medicine teams on the basis o f the number o f people served by each team. However, the law did not stipulate any entitlements for the uninsured and hence created huge inequities in access to an essential set o f services,
69. The 1997 L a w on Health Care broadly defined the activities for family physicians and the PHC teams, as wel l as the knowledge base and the skill sets they were expected to acquire. The law stated that one family medicine team should care for 1,800 to 2,000 residents. (As the population o f FBIH i s around 2.4 million, the entity wi l l require over 1,200 FM teams to achieve full coverage-a target set by the Federal Ministry o f Health to be achieved by 2007.)
70. The Program for Specialization in FM developed by the Faculties o f Medicine in FBIH and RS was adopted by the respective Ministries o f Education and Health. (See section on resource generation and Annex 5). In FBIH the regulations (“The Rulebook”) stipulating the curriculum and duration o f training for the Family Medicine Specialization was published in the Off ic ia l Gazette in February 1999.41 (See section on FM training in FBIH,)
3.2. FINANCING OF THE HEALTH SYSTEM AND PHC IN THE FBIH
3.2.1. Collection
7 1. In accordance with the FBIH L a w on Health Insurance,42 health care i s financed almost exclusively from the Compulsory Health Insurance (CHI) scheme. There are 10 Cantonal Health Insurance Institutes (CHIIS) and one Federation Health Insurance and Reinsurance Institute (FHIRI).
12
72. income accounts for 94 percent o f the total income o f the CHII .
Income for the C H I scheme comes from the contributions paid by employers and employees. This
73. The FHIRI has the responsibility for producing a financial plan for the FBIH health sector, drawing on the projections o f the CHII . The FHIRI, in collaboration with the Federation Solidarity Fund (FSF), estimates the total health expenditures and funds flow within the health sector.
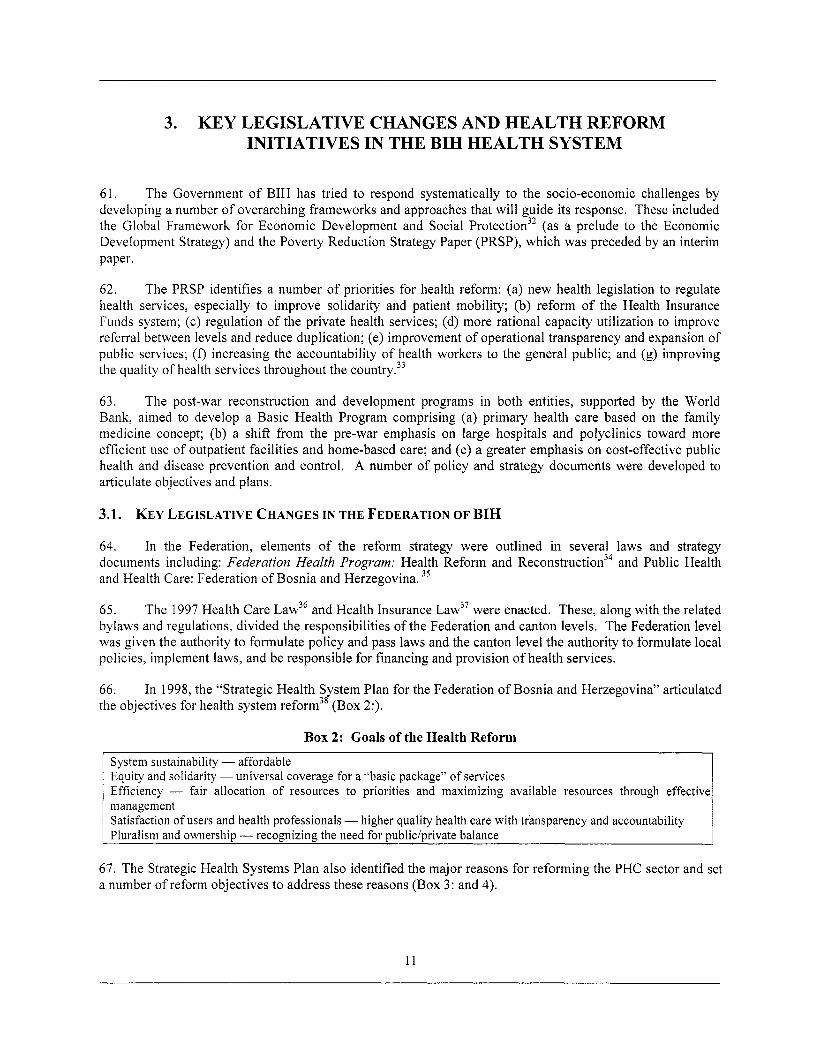
74. percent) came from the C H I and KM 171 mi l l ion (26.5 percent) f rom other sources (Figure 5:).
In 2002, the total health insurance income was KM 694.5 mill ion. Of this, KM 523 mi l l ion (73.5
Figure 5: Sources of Income for Health Insurance Institutions in FBIH
Sources of income for FBIH Health Insurance Institutions
80
70
60
50
40
30
20
10
0 Income from Income from Budget Income Other
Contributions CMI co-payment
Source
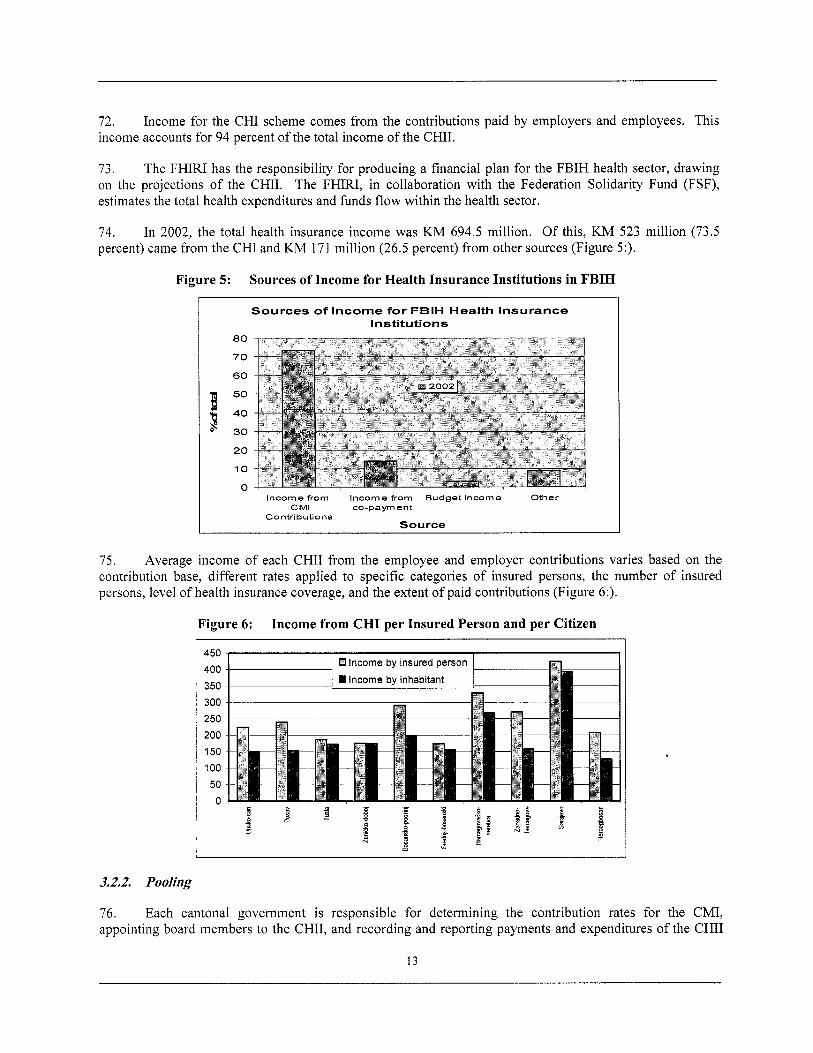
75. Average income o f each C H I I f rom the employee and employer contributions varies based on the contribution base, different rates applied to specific categories o f insured persons, the number o f insured persons, level o f health insurance coverage, and the extent o f paid contributions (Figure 6:).
Figure 6: Income from C H I per Insured Person and per Citizen
400 350 300 250 200 150 100 50 n
1 1 0 Income by insured person 1 I
3.2.2. Pooling
76. Each cantonal government i s responsible for determining the contribution rates for the CMI, appointing board members to the CHII, and recording and reporting payments and expenditures o f the C H I I
13
to the Federation government. The FHIRI i s responsible for implementing conventions and international agreements and providing reinsurance.
77. The FSF was established in 2002 to reduce duplication o f services financed by insurance agencies and enable intercanton movement o f patients to receive health services when needed. This scheme i s designed to reduce the fragmentation o f services between cantons and along ethnic lines, but also has an equity-enhancing effect, as patients from lower income cantons can access costly interventions previously available only to patients from better-off cantons. The FSF has eliminated the justification for ethnically based risk pooling. Consequently, in 2002, the Croat Inter-cantonal Health Insurance Fund ceased to exist.
78. The CHIIs contribute 8 percent o f their revenue to the FSF. This amount i s supposed to be matched by contributions from the Federation budget, but in reality this does not happen. The FSF was established to finance priority vertical health care programs and help equalize health expenditures across the Federation. The FSF also finances complex and expensive health services, which are reviewed on an annual basis. Since the beginning o f 2004, the FSF has also started to finance some preventive programs, including immunization and the operating costs o f the Agency for Accreditation and Quality Assurance.
3.2.3. HeaIth Expenditure Trends
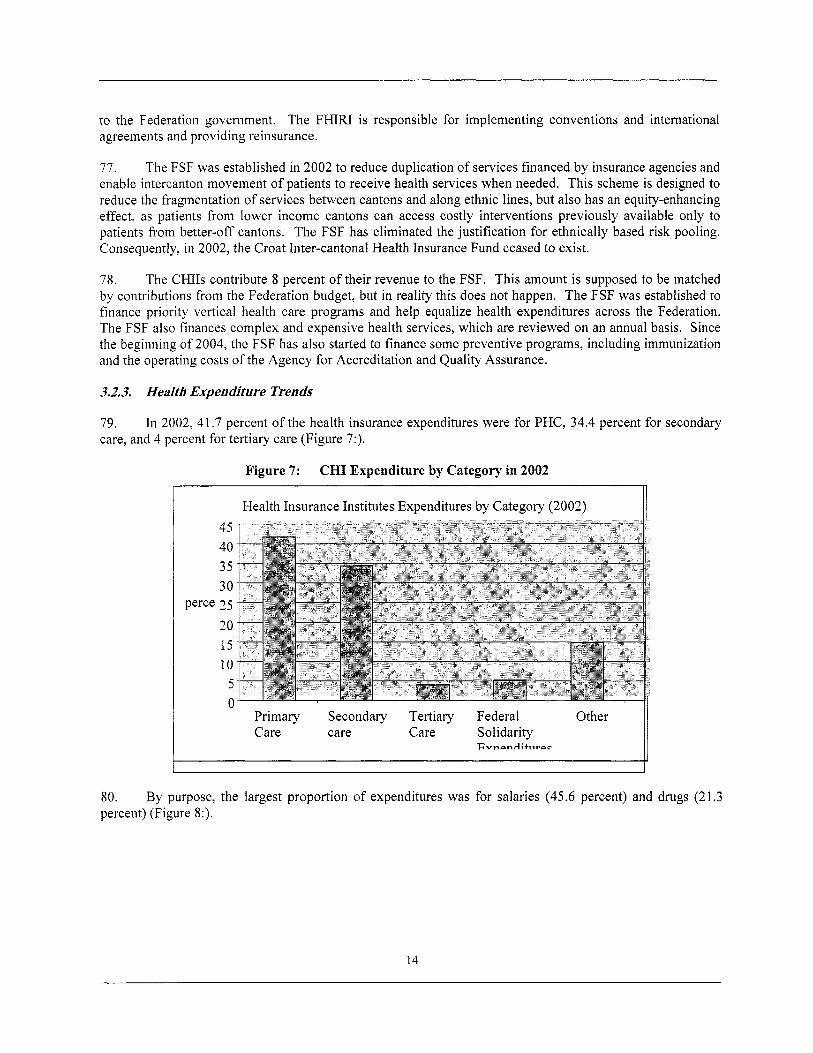
79. care, and 4 percent for tertiary care (Figure 7:).
In 2002, 41.7 percent o f the health insurance expenditures were for PHC, 34.4 percent for secondary
Figure 7: CHI Expenditure by Category in 2002 ~~
Health Insurance Institutes Expenditures by Category (2002) 45 40 35 30
Perce 2 5 20 15 10
5 0
Other li Primary Secondary Tertiary Federal Care care Care Solidarity
E"nPnf4;tllt.PC
80. percent) (Figure 8:).
By purpose, the largest proportion o f expenditures was for salaries (45.6 percent) and drugs (21.3
14
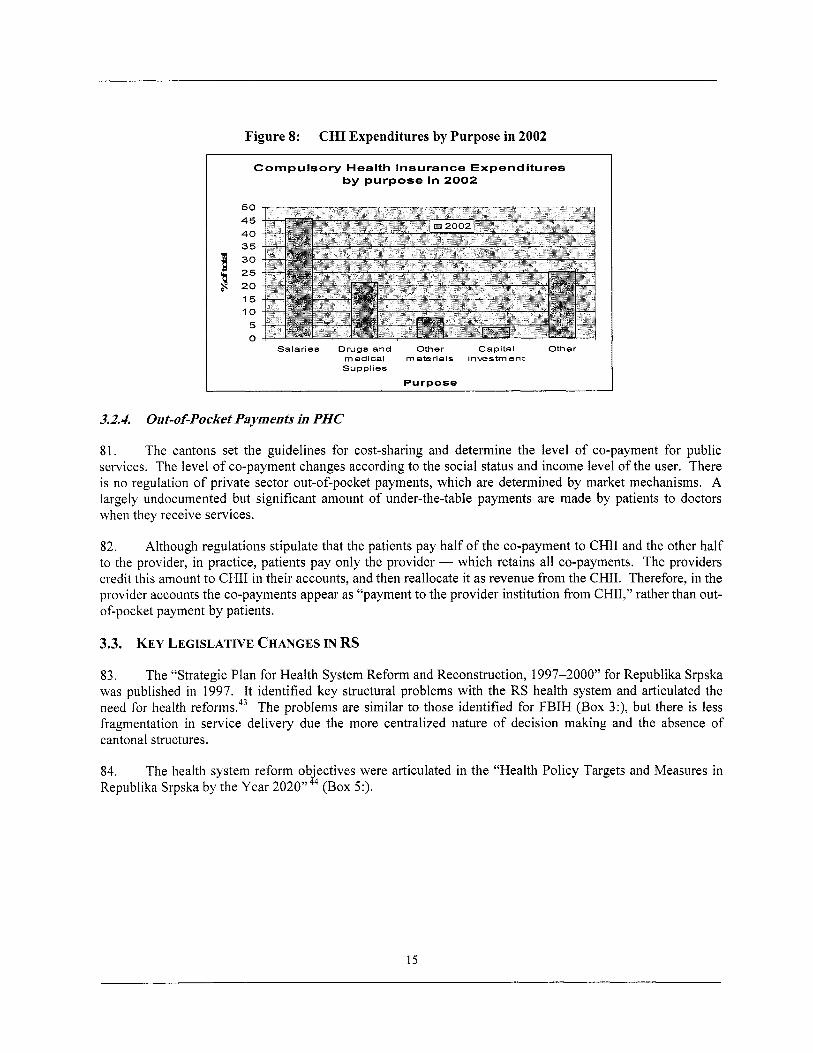
Figure 8: CHI Expenditures by Purpose in 2002 I
Compulsory Health Insurance Expenditures by purpose in 2002
50 45 40 35 30 25 20 15 10
5 0
Salaries Drugs and Other Capital Other medical materials investment Supplies
Purpose
3.2.4. Out-of-Pocket Payments in PHC
81. The cantons set the guidelines for cost-sharing and determine the level o f co-payment for public services. The level o f co-payment changes according to the social status and income level o f the user. There i s no regulation o f private sector out-of-pocket payments, which are determined by market mechanisms. A largely undocumented but significant amount o f under-the-table payments are made by patients to doctors when they receive services.
82. Although regulations stipulate that the patients pay hal f o f the co-payment to C H I I and the other ha l f to the provider, in practice, patients pay only the provider - which retains al l co-payments. The providers credit this amount to C H I I in their accounts, and then reallocate it as revenue from the CHII. Therefore, in the provider accounts the co-payments appear as “payment to the provider institution f rom CHII,” rather than out- of-pocket payment by patients.
3.3. KEY LEGISLATIVE CHANGES IN RS
83. The “Strategic Plan for Health System Reform and Reconstruction, 1997-2000” for Republika Srpska was published in 1997. It identified key structural problems with the RS health system and articulated the need for health reforms.43 The problems are similar to those identified for FBIH (Box 3:), but there i s less fragmentation in service delivery due the more centralized nature o f decision making and the absence o f cantonal structures.
84. Republika Srpska by the Year 2020”44 (Box 5:).
The health system reform objectives were articulated in the “Health Policy Targets and Measures in
15
Box 5: Goals of the Health Reform and Health Policy Targets
Health equity and solidarity Healthy l i f e start - reduce infant and child mortality Reduce risk factors for health Reorientation to PHC Develop sustainable financing Establish need-based and fair resource allocation system Manage for quality o f care Develop human resources for health
Source: Ministry o f Health and Social Welfare, Republika Srpska. Health Policy Targets and Measures in Republika Srpska by the Year 2020. Banja Luka, 1999.
85 . The “Strategic Plan for Health System Reform and Reconstruction, 1997-2000” and the “Health Policy Targets and Measures in Republika Srpska by the Year 2020” identified reasons for reforming PHC and the interventions to reform PHC. The reasons and objectives for reform are similar to those in FBIH (Boxes 3 and 4), but the policy documents identify clear targets in addition to general reform objectives (Box 6:).
Box 6: PHC Reform Objectives in RS
Organizational reforms - restructuring PHC, refbrbishing centers, improving management capacity, introducing appointments for consultation, and new data collection system Education reform - Establish Chair o f F M at Banja Luka, develop new post-graduate curricula to train FM specialists, introduce F M training in undergraduate studies, training program for nurses Gradual introduction o f the family doctor (FD) and the FM team - create 700 teams throughout RS, each serving approximately 1,800 to 2,000 patients Freedom o f choice with family physicianigeneral practitioner Enhance doctor-patient relationship to strengthen continuity o f care Enhancing gatekeeping to reduce unnecessary referrals to the secondary care level - by establishing family doctors as the point o f first contact in the health system and improving the capacity for problem resolution at the PHC level Improve capacity o f family physicians to coordinate health care services PHC financing reforms - introduce weighted per capita and performance-related pay
86. In July 1999, the RS Parliament adopted The L a w on Health Care, which introduced family medicine as a specialty.45 Article 23 o f the L a w on Health Care stipulated, “The fami ly medicine ambulanta (ordination) i s the basic component o f primary health care in terms o f i t s organization. The family medicine team i s the first point o f contact for citizens accessing the health care system.”
3.4. FINANCING OF THE HEALTH SYSTEM AND PHC IN RS
3.4.1. Collection
87. Following the introduction o f the 1999 L a w on Health Insurance, the CHI system was established in RS, The family and household members o f the contributor to the Health Insurance Fund (HIF) are entitled to health insurance benefits.
88. The sources o f revenue for the HIF are (a) contributions to compulsory and extended health insurance (the extended health insurance has not yet been introduced); (b) budget contributions for the entity; (c) donations; (d) contributions f rom sales taxes on alcohol and tobacco (not yet introduced); (e) funds derived by way o f applicable conventions; (0 funds from state transfers; and (f) other funds, in accordance with the law.
89. Contributions are based on a payroll tax and amount to 15 percent o f net pay (7.5 percent contributed by the employee and 7.5 percent by the employer). The self-employed contribute 15 percent o f net income,
16
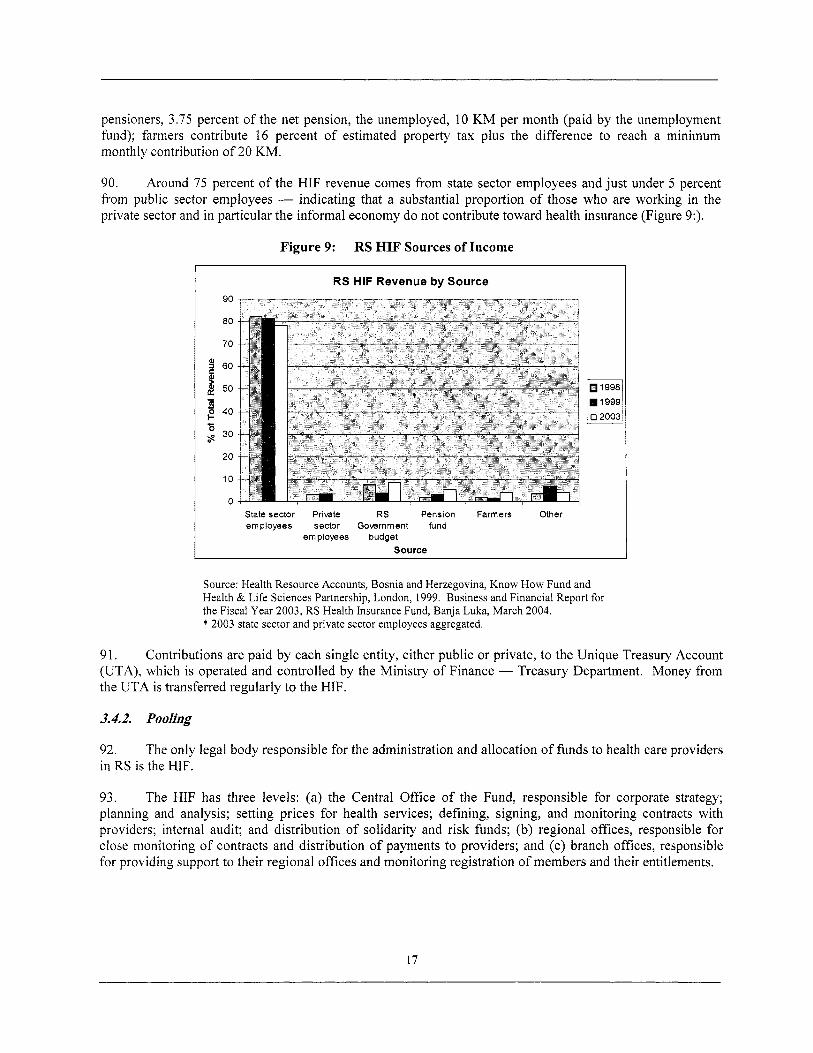
pensioners, 3.75 percent o f the net pension, the unemployed, 10 Kh4 per month (paid by the unemployment fund); farmers contribute 16 percent o f estimated property tax plus the difference to reach a minimum monthly contribution o f 20 KM.
90. Around 75 percent o f the HIF revenue comes from state sector employees and just under 5 percent from public sector employees - indicating that a substantial proportion of those who are working in the private sector and in particular the informal economy do not contribute toward health insurance (Figure 9:) .
Figure 9: RS HIF Sources of Income
I RS HIF Revenue by Source 90
80
70
3 60
50 E
30
20
10
0 State sector Private RS Pension Farmers Other employees sector Government fund
employees budget Source
1998 1999
0 2003 -
Source: Health Resource Accounts, Bosnia and Herzegovina, Know How Fund and Health & L i f e Sciences Partnership, London, 1999. Business and Financial Report for the Fiscal Year 2003, RS Health Insurance Fund, Banja Luka, March 2004. * 2003 state sector and private sector employees aggregated.
91 Cnntrihiitinnc are naid hv each cinole entitv either niihlir nr nrivate tn the TTniniie T r e a c i i n i A r r n i i n t
(U IA), which i s operated and controlled by the Ministry 01 Finance - lreasury uepartment. Money rrom the UTA i s transferred regularly to the HIF.
3.4.2. Pooling
92. in RS i s the HIF.
The only legal body responsible for the administration and allocation of funds to health care providers
93. The HIF has three levels: (a) the Central Office o f the Fund, responsible for corporate strategy; planning and analysis; setting prices for health services; defining, signing, and monitoring contracts with providers; internal audit; and distribution o f solidarity and risk funds; (b) regional offices, responsible for close monitoring o f contracts and distribution o f payments to providers; and (c) branch offices, responsible for providing support to their regional offices and monitoring registration o f members and their entitlements.
17
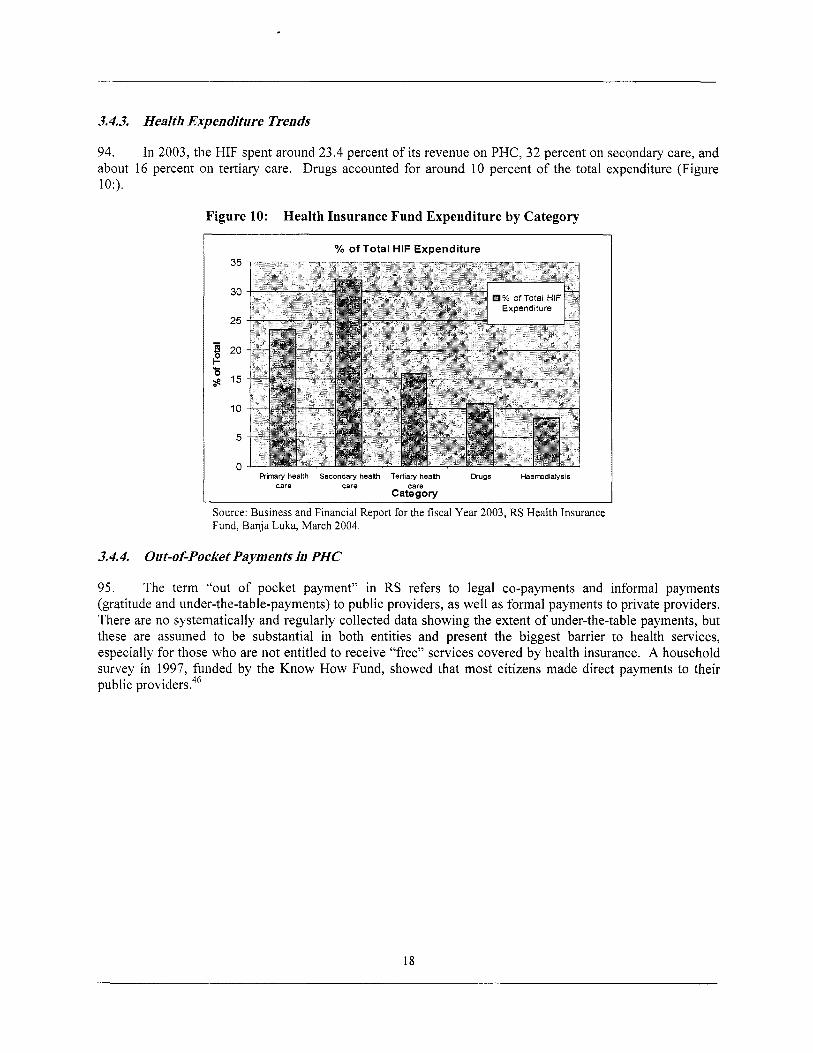
3.4.3. HeaIth Expenditure Trends
94. In 2003, the HIF spent around 23.4 percent of i t s revenue on PHC, 32 percent on secondary care, and about 16 percent on tertiary care. Drugs accounted for around 10 percent o f the total expenditure (Figure 10:).
Figure 10: Health Insurance Fund Expenditure by Category
I YO of Total HIF Expenditure 35
30
25
1 20 e ’s $ ’5
10
5
n
% of Total HIF
- R i m r y health Secondary health Tertiary heaith Drugs Haemdialysis
care care cere Category
Source: Business and Financial Report for the fiscal Year 2003, RS Health Insurance Fund, Banja Luka, March 2004.
3.4.4. Out-of-Pocket Payments in PHC
95. The term “out o f pocket payment” in RS refers to legal co-payments and informal payments (gratitude and under-the-table-payments) to public providers, as wel l as formal payments to private providers. There are no systematically and regularly collected data showing the extent o f under-the-table payments, but these are assumed to be substantial in both entities and present the biggest barrier to health services, especially for those who are not entitled to receive “free” services covered by health insurance. A household survey in 1997, funded by the K n o w H o w Fund, showed that most citizens made direct payments to their public providers.46
18
4. KEY DEVELOPMENTS IN PHC IN FBIH
4.1. ORGANIZATION OF PHC IN FBIH
96. Each o f the 87 municipalities in FBIH has a DZ, staffed by general practitioners, occupational medicine specialists, epidemiologists, obstetricians and gynecologists, pediatricians, and internal medicine specialists.
97. endoscopes, electrocardiographs, and specialist advanced X-ray equipment.
The DZs usually have a small laboratory and X-ray facilities, and in some cases ultrasound,
98. Narrow specialists visit DZs on a regular basis to provide specialist services to patients. The frequency o f these visits depends on the size o f the DZ but also on influence o f local politicians and the DZ director.
99. There i s a high referral o f patients f rom PHC to secondary-level hospitals or tertiary-level clinical centers because of: the l ow capacity o f the PHC level t o resolve problems; the basic level o f training o f general practitioners; and disincentives created by the salary-based provider payment systems. Patients can go to hospitals directly without referral f rom GPs, further fracturing the gate keeping function o f the PHC level.
100. Ambulantas are satellite units o f a DZ, located in rural areas and many villages. Usually staffed by a nurse and a GP, they provide basic ambulatory PHC services to a local population o f 2,000 to 6,000 people. Except for those refurbished by the Wor ld Bank and other donors, most ambulantas are structurally in poor condition and have only basic medical equipment.
101. First aid and emergency services are provided by dedicated emergency medicine units usually co- located with a DZ; some have their own premises. Very few o f these units have well-equipped emergency vehicles or ambulances.
102. medicine, well short o f the 1,400 needed.
Currently in FBIH, a total o f 2,220 doctors work in PHC - but o f these, only 316 work in family
103. Primary health care professionals work in collaboration with specialists (such as the general internist, respiratory physicians, ophthalmologist, general and ear nose and throat (ENT) surgeons), who provide consultations in the PHC centers and take referrals f rom GPs and FM specialists. Even the PHC centers that have introduced the new FM model s t i l l have a large number o f narrow specialists. There are, as yet, no regulations stipulating the relationship between FM practitioners and narrow specialists. However, a bylaw stipulating j o b description and minimum standards for FM specialists i s being developed.
104. physicians, but the role o f these nurses and the scope o f services they can provide are not defined.
There are plans to develop a system o f “patronage nurses’’ who work independently o f the family
105. cantons with 133 FM teams covering a population o f approximately 267,000.
Currently, the FM concept i s being implemented in 60 rehabilitated FM ambulantas in three pilot
106. A bylaw enabling establishment o f private practice was passed in 2004. Regulating private practice i s the responsibility o f Cantonal Ministries o f Health. Private providers can j o i n together to form private group practices, but are not entitled to sign contracts with the health insurance funds. Private practice i s often organized in specialist polyclinics, but private FM does not yet exist.
19
4.2. DEVELOPMENT OF PHC HUMAN RESOURCES IN FBIH
107. development o f medical specialists. specialization and have invested in in-service training programs.
The Cantonal Ministries o f Health have the responsibility to develop an annual plan for training and Since 1999, the cantons have prioritized the development o f FM
108. A substantial proportion o f the large number of sub specialists in PHC centers do not want to be retrained as FM specialists. This has hindered the transformation o f these PHC centers into FM centers. Reducing the numbers o f sub specialists through natural attrition or redundancy is, at present, politically not feasible, and the FBIH government appears to have adopted a gradualist policy to address this issue.
109. The 1997 L a w on Health Care, which established FM as a specialty, created FM departments as independent chairs (cathedra) within the faculties o f medicine. FM chairs have been appointed in Mostar and Tuzla but not Sarajevo. Teaching centers have been established at Sarajevo, Tuzla, and Mostar, wi th three satellite centers in Bihac, Ljubuski, and Zenica, operating effectively and providing training programs for FM teams. The teaching centers in Tuzla and Mostar are affiliated with the respective medical faculties.
110. The curriculum for specialist training in FM was developed in 1999 by the faculties o f medicine in BIH and adopted by both the Federation and RS Ministries o f Health. The details o f the curriculum are published in both entities in the Rulebooks for FM, which specify the content and methods o f training for specialist and in-service FM training programs delivered by the FM chairs.47 The curriculum o f the FM specialist training program i s based on internationally recognized principles (Annex 5).
1 1 1. Three training programs exist for family medicine: (a) a three-year FM specialist training program for new graduates with no work experience; (b) a two-year training program for PHC doctors who have less than 10 years’ work experience and doctors who have over 10 years o f work experience and who have been granted the Certificate o f Doctor o f Family Medicine; and (c) a one-year in-service Program for Additional Training (PAT) for those who already have had training in related specialties and have a certificate from the Federal Ministry o f Health recognizing their specialty (Annexes 5 and 6).
112. Postgraduate studies for masters and doctorates in FM have not yet been introduced, although some FM specialists have postgraduate training in social medicine and public health. In FBIH, there are one family physician with a doctorate and six family physicians with master’s degrees.
113. In F B I H in any one year, the number o f residents training in FM ranges from 40 to 50: clearly not adequate to meet current and future needs. This number i s determined by the Rulebook on FM specialization and the capacity o f the FM chair responsible for the residency training. T o overcome this supply-demand gap, the World Bank Basic Health Project has supported the development o f PAT, in close collaboration with the Queen’s University o f Canada, for in-service training o f physicians and nurses currently working in PHC centers.48
114. The curriculum for PAT, adopted in 2002, i s used throughout Bosnia and Herzegovina (Annex 6). On successful completion o f PAT, doctors receive a Certificate o f FM Doctor or one-year credit toward the three-year F M specialist training Program.
115. In FBIH between 1995 and 2004, a total o f 413 FM doctors/specialists were trained (Table 5:) representing around 30 percent o f the 1,200 FM teams needed. In the same period, a total o f 286 nurses graduated from PAT.
20
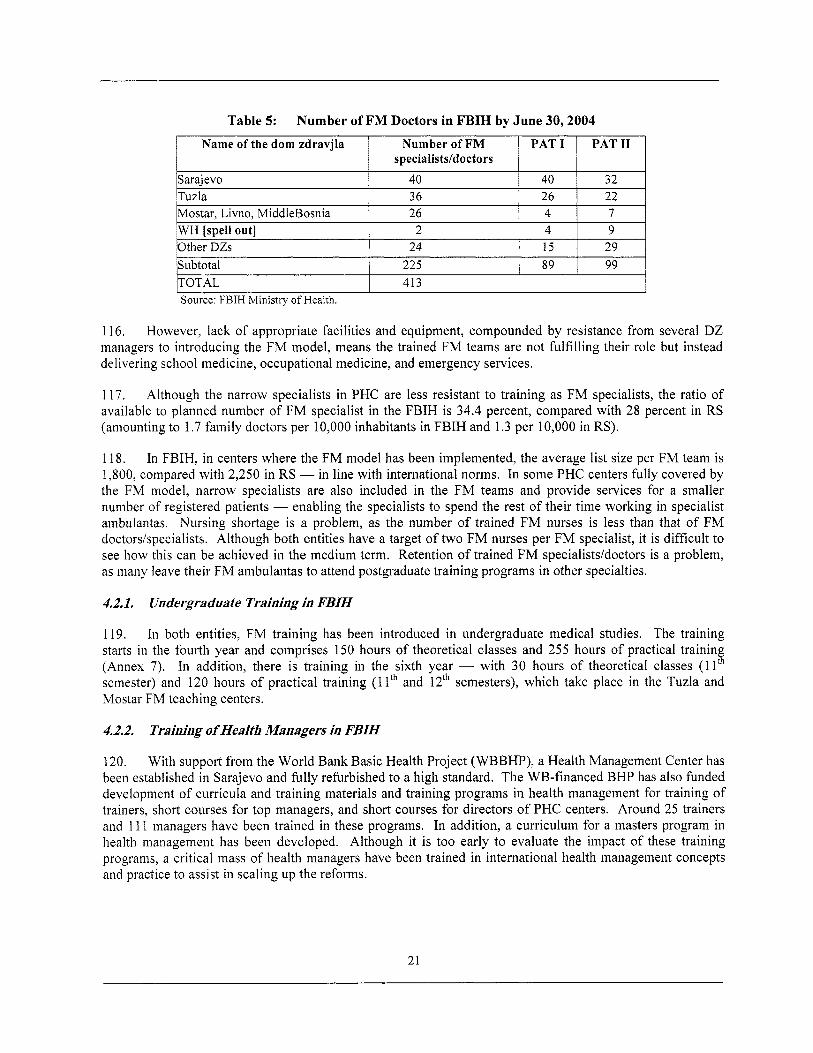
Name of the dom zdravjla Number o f FM PAT1 PAT11 specialists/doctors
Sarajevo 40 40 32 Tuzla 36 26 22 Mostar. Livno. MiddleBosnia 26 4 7 WH [spell out] Other DZs Subtotal TOTAL
116. However, lack o f appropriate facilities and equipment, compounded by resistance from several DZ managers to introducing the FM model, means the trained FM teams are not fulfilling their role but instead delivering school medicine, occupational medicine, and emergency services.
2 4 9 24 15 29
225 89 99 413
117. Although the narrow specialists in PHC are less resistant to training as FM specialists, the ratio o f available to planned number o f FM specialist in the FBIH i s 34.4 percent, compared with 28 percent in RS (amounting to 1.7 family doctors per 10,000 inhabitants in FBIH and 1.3 per 10,000 in RS).
118. In FBIH, in centers where the FM model has been implemented, the average l i s t size per FM team i s 1,800, compared with 2,250 in RS - in line with international norms. In some PHC centers fully covered by the FM model, narrow specialists are also included in the FM teams and provide services for a smaller number o f registered patients - enabling the specialists to spend the rest o f their time working in specialist ambulantas. Nursing shortage i s a problem, as the number o f trained FM nurses i s less than that o f FM doctors/specialists. Although both entities have a target o f two FM nurses per FM specialist, it i s diff icult to see how this can be achieved in the medium term. Retention o f trained FM specialists/doctors i s a problem, as many leave their FM ambulantas to attend postgraduate training programs in other specialties.
4.2.1. Undergraduate Training in FBIH
119. starts in the fourth year and comprises 150 hours o f theoretical classes and 255 hours o f practical trainin (Annex 7). In addition, there i s training in the sixth year - with 30 hours o f theoretical classes (1 1 semester) and 120 hours o f practical training (1 lth and 12'" semesters), which take place in the Tuzla and Mostar FM teaching centers.
In both entities, FM training has been introduced in undergraduate medical studies. The training
i
4.2.2. Training ofwealth Managers in FBIH
120. With support f rom the Wor ld Bank Basic Health Project (WBBHP), a Health Management Center has been established in Sarajevo and fully refurbished to a high standard. The WB-financed BHP has also funded development o f curricula and training materials and training programs in health management for training o f trainers, short courses for top managers, and short courses for directors o f PHC centers. Around 25 trainers and 1 11 managers have been trained in these programs. In addition, a curriculum for a masters program in health management has been developed, Although it i s too early to evaluate the impact o f these training programs, a critical mass o f health managers have been trained in international health management concepts and practice to assist in scaling up the reforms.
21
4.3. KEY CHANGES IN THE DELIVERY OF PHC SERVICES IN FBIH
121. The FM model introduced in FBIH extends the scope o f services delivered in the PHC setting to include health, education, promotion, prevention, diagnostic, curative, and rehabilitative services - enabling the FM team to perform a gate keeping function and to provide comprehensive and continuous health care to i t s registered population,
122. their equipment (Annexes 1 and 3).
Contracts between the FM teams and CHI1 specify the roles and responsibilities o f FM teams and
123. An important feature o f the FM model in FBIH i s that it i s team- and not doctor-centric. The model emphasizes a psychosocial (as opposed to biomedical) approach, with a focus on holistic health, prevention, and promotion activities and the doctor-patient relationship. The FM specialists act as advocates for their clients - at both individual and family levels - to guide them through the health system and function as the link between different service providers.
124. The regulations do not clarify the boundaries between primary and secondary care. There are no guidelines on referral and counter-referral mechanisms or how hospital-based services can be shifted to the PHC. I n most PHC centers, FM i s provided as an “add-on,” along with general practice and narrow specialists’ services. The result i s fragmentation o f services, weakened gate keeping, and compromised first- contact functions o f the PHC.
4.3.1. PHC Gate keeping, First Contact Function, and Comprehensiveness
125. i s the FM specialist with whom they are registered. specialists fo l lowing referral by the FM specialist - except in case o f emergencies.
In the DZ where the FM model i s established, the f i rst point o f contact for PHC services for patients They usually access other PHC professionals or
126. In PHC centers where the FM model i s not yet established, the gate keeping function i s compromised and first-contact access highly fragmented, as the services are organized according to age, gender, and health problems (as in the past) and in addition to non-specialist GPs, patients have direct access to a range o f narrow specialists (such as pediatricians, gynecologists, pre-school and school medicine specialists, occupational medicine specialists, and respiratory physicians). This i s a source o f considerable inefficiency, as the narrow specialists generally have a narrow and curative approach to patient care, with a tendency to excessive investigations and prescribing. In these centers, cervical smear tests for screening o f cancer o f the cervix are done by gynecologists, and immunization o f children i s done by pediatricians. In rural ambulantas without an FM specialist, immunization o f school children i s organized in an intermittent fashion.
127. In PHC centers that have implemented that FM model, there i s emerging evidence o f improved patterns o f service provision by FM specialists compared with non-specialist GPs. For example, analysis o f services delivered by 24 FM specialists and 22 non-specialist GPs in PHC centers in Zenica-Doboj canton - covering 168,000 citizens, or 43 percent o f the cantonal population - showed that FM specialists were more l ikely to provide preventive services, refer less to hospitals, use fewer laboratory investigations, and undertake more home visits (Table 6: and 7).
22
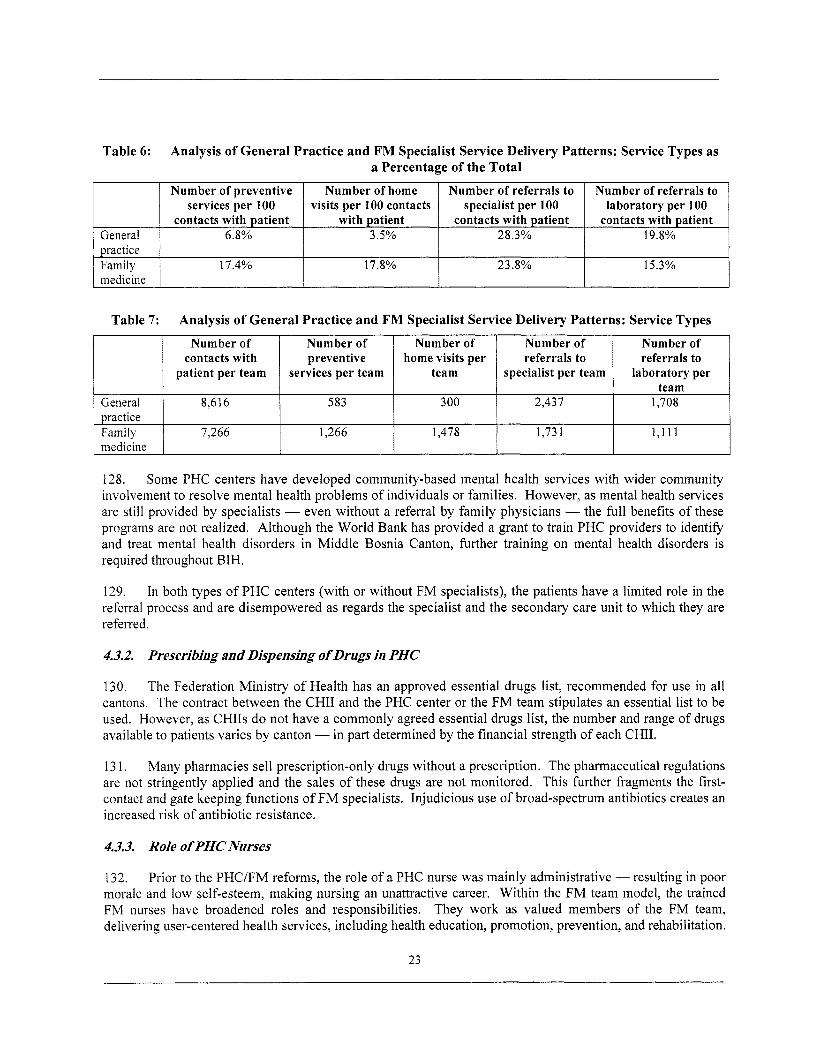
Number of preventive Number of home Number of referrals to services per 100 visits per 100 contacts specialist per 100
contacts with patient with patient contacts with patient General 6.8% 3.5% 28.3% practice Family 17.4% 17.8% 23.8% medicine
Number of referrals to laboratory per 100
contacts with patient 19.8%
15.3%
Number of Number of Number o f contacts with preventive home visits per
patient per team services per team team
Number of Number of referrals to referrals to
specialist per team laboratory per
128. Some PHC centers have developed community-based mental health services with wider community involvement to resolve mental health problems o f individuals or families. However, as mental health services are s t i l l provided by specialists - even without a referral by family physicians - the full benefits o f these programs are not realized. Although the Wor ld Bank has provided a grant t o train PHC providers to identify and treat mental health disorders in Middle Bosnia Canton, further training o n mental health disorders i s required throughout BIH.
General 1 8,6 16 583
129. In both types o f PHC centers (with or without FM specialists), the patients have a limited role in the referral process and are disempowered as regards the specialist and the secondary care unit to which they are referred.
300 2,437 1,708
4.3.2. Prescribing and Dispensing o f Drugs in PHC
practice
medicine Family
130. The Federation Ministry o f Health has an approved essential drugs list, recommended for use in all cantons. The contract between the CHI1 and the PHC center or the FM team stipulates an essential l is t to be used. However, as CHIIs do not have a commonly agreed essential drugs l ist , the number and range o f drugs available to patients varies by canton - in part determined by the financial strength o f each C H I .
7,266 1,266 1,478 1,73 1 1,111
13 1. Many pharmacies sell prescription-only drugs without a prescription. The pharmaceutical regulations are not stringently applied and the sales o f these drugs are not monitored. This further fragments the first- contact and gate keeping functions o f FM specialists. Injudicious use o f broad-spectrum antibiotics creates an increased risk o f antibiotic resistance.
4.3.3. Role o f PHC Nurses
132. Prior to the PHC/FM reforms, the role o f a PHC nurse was mainly administrative - resulting in poor morale and low self-esteem, making nursing an unattractive career. Within the FM team model, the trained FM nurses have broadened roles and responsibilities. They work as valued members o f the FM team, delivering user-centered health services, including health education, promotion, prevention, and rehabilitation.
23
They work closely with families to provide necessary psycho-social and medical support. The FM nurses now play an important role in maintaining up-to-date records o f patient care, enhancing the continuity and coordination o f health care.
4.3.4. Emergency Out-of-Hour Services
133. PHC centers are responsible for providing emergency care to patients in their catchment area between 4 pm and 8 am. In small health centers, emergency care i s provided by FM physicians who organize a duty rota. In large health centers, ambulance services provide f i rst aid services, emergency care, and support to the emergency departments attached to the DZ. When necessary, the ambulances transport patients to general hospitals, or in severe cases, directly to clinical centers (university hospitals).
4.4. RESOURCE ALLOCATION FOR PHC IN FBIH
134. In 2003, total expenditure on PHC in the FBIH, without prescribed drugs, was KM161 million, accounting for 33.1 percent o f the total C H I I health expenditures. The expenditure on prescribed drug was KM53.4 million, accounting for 11 percent o f the total C H I I expenditures.
135. In the same year, the expenditures on secondary and tertiary care (in-patients and out-patients) were KM177 mi l l ion and KM20.4 mill ion, respectively, accounting for 36.4 percent and 4.18 percent, respectively, o f the total C H I I expenditures.
136. tertiary care and vertical and priority health care program^.^'
In addition to the C H I I expenditures, the FSF spent a similar amount (around KM20.4 million) on
4.5. PROVIDER PAYMENT SYSTEMS AND CONTRACTS FOR PHC IN FBIH
137. The CHIIs contract health institutions to provide services to the beneficiaries - although most contracts specify the scope o f services to be provided, in some cases the CHIIs merely pay a fixed amount o f money to the providers.
138. health providers for priority vertical health care programs and complex health services.
The Federal Solidarity and Reinsurance Institute are responsible for contracting with specialized
139. The scope o f the FM team health care program i s determined according to the FM standards and norms defined in law, which specify (a) the structure o f health care services, (b) scope o f health care services by number o f users (insured persons), (c) the quality o f health care services, and (d) staffing norms, space, and equipment as a precondition for appropriate quality o f services.
140. According to regulations, the cost o f an annual health care program provided to a defined population by an FM team should be determined according to (a) the average time spent by the FM team on service delivery, their salary level, employment benefits, transport costs, and subsistence expenses; (b) recurrent operating costs; (c) depreciation o f f ixed assets (space and equipment); (d) investment; (e) continuous maintenance; (0 the content o f services, and (g) the number o f users served by the FM team. However, in reality, the program costs do not take al l o f these factors into account due to a lack o f data.
141. The WBBHP aimed to test two payment mechanisms: (a) direct contracting between the C H I I and an FM team led by an FM specialist (Herzegovina-Neretva and West Herzegovina cantons) and (b) indirect contracting with contracts at two levels - between the C H I I and a DZ and then between the DZ and an FM team led by an FM specialist. Although it was not possible to implement direct contracting due to inadequacy o f laws, new payment mechanisms based on weighted capitation have been developed and successfully
24
introduced in Tuzla, Herzegovina-Neretva, and West Herzegovina cantons. Up to 66 FM teams have signed contracts with the CHI1 based o n weighted capitation, providing them somewhat higher income compared with GPs. The weighted capitation formula uses varied weights for different age groups: for 0 to 7 years o f age, a coefficient o f 2 (KM35.18); for 7 -to 18 years o f age, a coefficient o f 1 (KM17.59); for 18 to 65 years o f age, a coefficient o f 1.5 (KM26.39); for over 65 years o f age, a coefficient o f 2.5 (KM43.98).
142. The contract defines the rights and responsibilities o f the contracting parties as regards provision o f PHC services, and stipulates (a) type and scope o f services; (b) structure o f family medicine team; (c) framework for physician accountability; (d) place for service delivery; (e) method o f delivering services; ( f ) funds allocated by the health insurance institute; (g) payment methods; (h) method by which the payment i s calculated; (i) contract payment terms; 0) infrastructure specifications; (k) required documentation for reporting; (1) monitoring o f performance and quality; (m) obligations regarding fulfil lment o f relevant decrees; and (n) contract rights and responsibilities. An example o f an FM contract i s appended in Annex 1.
143. The contracts in FBIH do not cover preventive services or allow for bonus payments - unlike the contracts in RS, which do. Further, absence o f appropriate legislation means that introducing performance- related element to these contracts has not been possible.
144. Operationalizing these contracts has been challenging due to a deficient legislative base regarding the status o f the FM teams; a lack o f management and financial ski l ls at DZ and FM team levels; absence o f appropriate monitoring and evaluation systems; and no indicators for measuring quality, effectiveness, or efficiency o f services. The authorities are testing the new provider payment systems for FM teams within the bounds o f the regulations so as not to create asymmetry with the prevailing pay levels in the PHC system. Preliminary evaluations show that the FM teams contracted by the new scheme have attracted new patients for registration.
145. The expansion o f the new payment mechanisms and contracts will require consensus o f key stakeholders and changes in existing legislation to (a) clearly define the roles and responsibilities o f the FM teams and other health providers; (b) address and correct anomalies in laws and standards relating to the contradictory definitions o f a “user” (according to the L a w o n Health Insurance, a health care user i s a person covered by health insurance, but according to the 2003 Health Care Standards and Norms, a user i s defined as a citizen o f FBIH); (iii) clearly stipulate health care entitlements for C H I beneficiaries and non-insured citizens - for instance, specifying an “essential benefits package” for a l l citizens and an “additional benefits package” for C H I beneficiaries; (d) clearly define who i s responsible for covering the costs o f health services provided to the uninsured; (e) define the scale and scope o f services to be provided by FM teams; and ( f ) specify provider payment methods that can be used, along with incentives for performance related pay.
4.6. INFRASTRUCTURE AND EQUIPMENT AT PHC FACILITIES IN FBIH
146. There i s a standard l i s t o f equipment adopted by both entities for FM specialists and PHC centers. Prior to the war, PHC centers had access to essential equipment, but after the war much o f the equipment was destroyed or became obsolete.
147. The FM ambulantas refurbished under the WBBHP have been provided equipment appropriate for FM practice. The equipment varies according to the number o f FM teams working in the ambulanta. The number o f FM teams working in a PHC center depends on the catchment’s population. FM ambulantas situated at a distance o f 10 kilometers or further from a DZ have a mini-laboratory as wel l as test-strips for urinalysis. Plans to establish mini-reference-pharmacies in these ambulantas were prevented by lack o f legislation. FM ambulantas refurbished by other donor projects have medical equipment commonly used by family physicians.
25
4.7. PHC INFORMATION SYSTEMS IN FBIH
148. Data collection in PHC centers i s uneven due to lack o f coordination among cantons and absence o f commonly agreed metrics and a shared core data set for PHC, among other things. Changes introduced by one canton are not adopted by others. Data collection forms currently in use generate an excessive amount o f data o f variable quality, which are collected and sent to the Ministry o f Health and Public Health Institute. However, many o f these data are not analyzed, and when they are analyzed, very l imited information i s fed back to the PHC level. There is, hence, no incentive for PHC providers to collect accurate and timely data.
149. New reporting forms are being designed by the Federation Health Insurance Institute (HII) for the newly restructured health centers to meet the needs o f the PHC level, the Ministry o f Health, and the HII. With the introduction o f performance-based contracts between the HIF and the PHC providers, there will be incentives to collect accurate and timely data.
150. A proprietary software program designed for collection o f patient information and other relevant data was piloted in some o f the FM ambulantas established with support f rom the WBBHP. The program i s being used by the FM ambulantas for daily operations However, due to coordination problems between the Federation HI1 and the Public Health Institute, the software program i s not yet used to aggregate data at a higher level, Further, the existing laws require paper-based data submission, limiting the utility o f the electronically collected data.
4.8. LICENSING AND REVALIDATION IN FBIH
15 1. The 1997 L a w on Health Care stipulated that the Chambers o f Medical Professionals are responsible for issuing licenses for health professionals. The Cantonal Ministries o f Health have the responsibility for monitoring the work o f these Chambers. However, as Chambers have not been established in all cantons, the licensing o f health professionals i s uneven and there are no mechanisms for revalidation.
4.9. ACCREDITATION IN FBIH
152. An Agency for Health Care Quality and Accreditation was established n 2004 under the WBBHP but not yet formally approved, as the Federation Parliament i s currently considering the L a w on Health Care Quality and Safety and Accreditation. With international technical assistance, the Agency has designed a framework for assessing quality standards in health provider institutions in three main areas: (a) organization governance; (b) risk management, and (c) patient-focused care, and specific services for both patient and team.
153. An information package on accreditation has been developed for PHC institutions, explaining the accreditation process and terms and conditions for contracts for accreditation. Quality standards have been developed for hospitals. A set o f basic tools for assessing quality standards o f health care providers has been developed and a cadre o f assessors trained. However, to date, accreditation has focused on hospitals.
4.10. PROFESSIONAL ASSOCIATIONS IN FBIH
154. counterpart in RS, and in 2002 accepted to the membership o f W O N C A - Europe.
The F B I H Association o f Family Medicine Physicians was established in 2000, along with i ts
26
5. KEY DEVELOPMENTS IN PHC IN REPUBLIKA SRPSKA
5.1. ORGANIZATION OF PHC IN RS
15.5. modifications to the law, this i s changing.
The organizational structure o f PHC in RS i s similar to that in FBIH, although following recent
1.56. According to the L a w on Health Care, the FM ambulanta was the basic organizational unit at the PHC level: covering villages and rural areas usually wi th one or more FM teams and organizationally part o f a DZ. Cities and towns had a DZ with multidisciplinary teams. DZ Banja Luka, the biggest in RS, covers approximately 250,000 citizens. DZs and FM ambulantas are owned by local municipal authorities and employ salaried staff, except for pilot sites where contracts for FM teams have been introduced.
157. According to the planned new law on PHC, ambulantas will become autonomous FM units and have an option to create a group practice independent o f the DZ. Group practices were recently introduced in DZ Laktasi - a pi lot municipality for PHC reforms.
158. An FM team in RS i s composed o f two nurses and a family medicine doctor, who leads the team. The FM ambulantas are responsible for (a) organizing health education; (b) monitoring the health o f the population and taking steps to detect, prevent, and combat infectious and non-communicable disease; (c) diagnosing and treating common illnesses; (d) providing home-based treatment for those not requiring hospital care; and (e) providing extended care and rehabilitation fo l lowing discharge from hospital.
5.2. DEVELOPMENT OF PHC HUMAN RESOURCES IN RS
159. In August 1999, the RS Ministry o f Health and Social Welfare (MOHSW) adopted “The Rulebook on Family Medicine Specialization Program” (FMSP).” The Rulebook specifies in detail the curriculum for the FMSP.
160. a d ~ p t e d . ~ ’ The Rulebook on P A T also covers the training o f PHC nurses.52
In M a y 2003, “The Rulebook on Program o f Additional Training in Family Medicine” (PAT) was
161. T w o training centers established by the WBBHP, Banja Luka Teaching Center and Doboj Satellite Teaching Center, work effectively. A pi lot FM center has been established at Laktasi. Training in RS i s supported by the WBBHP, the Canadian International Development Agency (CIDA), the Swiss Cooperation, Project Hope, and MCdecins Sans Frontihes (MSF), with Queens University o f Canada providing technical assistance.
162. recently joined the P A T to become FM doctors.
There i s a healthy demand for FM training - for instance, 11 narrow specialists in DZ Laktasi
163. In RS, to date, a total 168 FM doctors and 154 nurses have been trained through the P A T (Table 8:). The required number o f FM teams in RS i s estimated to be around 600, although no PHC human resources plans exist.
27
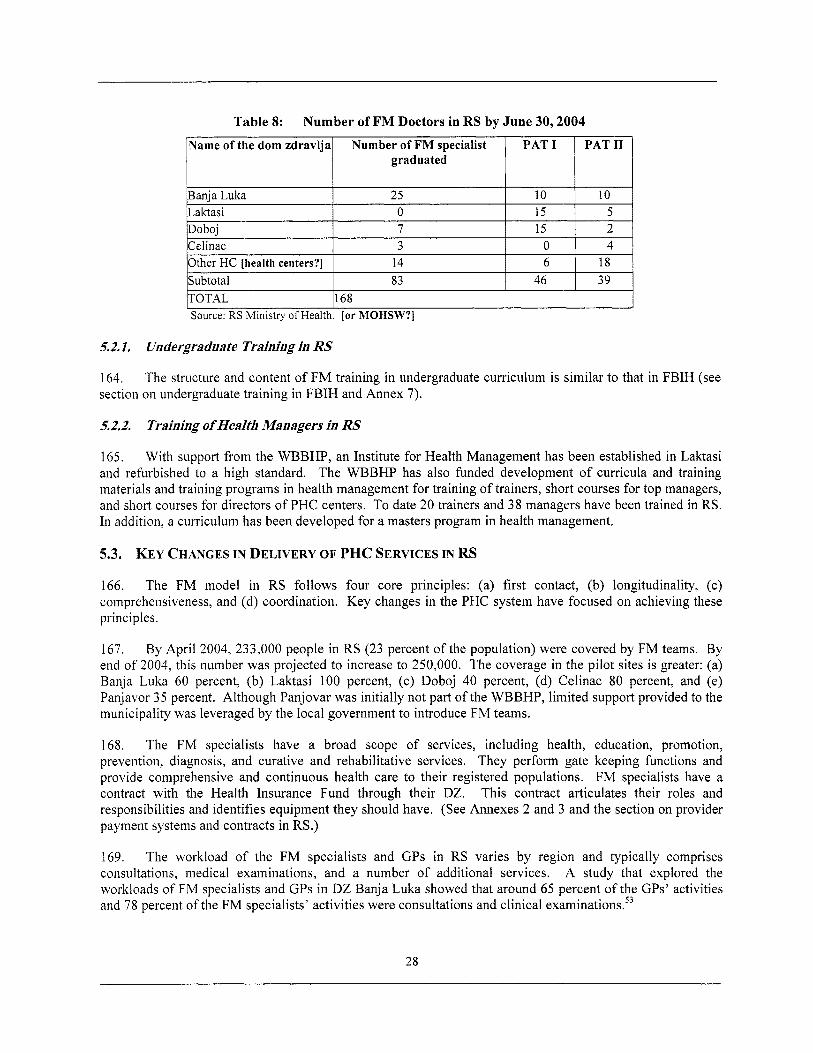
Table 8: Number of FM Doctors in RS by June 30,2004
Source: RS Ministry o f Health. [or MOHSW?]
5.2.1. Undergraduate Training in RS
164. section on undergraduate training in FBIH and Annex 7).
The structure and content o f FM training in undergraduate curriculum i s similar to that in FBIH (see
5.2.2. Training o f Health Managers in RS
165. With support f rom the WBBHP, an Institute for Health Management has been established in Laktasi and refurbished to a high standard. The WBBHP has also funded development o f curricula and training materials and training programs in health management for training o f trainers, short courses for top managers, and short courses for directors o f PHC centers. To date 20 trainers and 38 managers have been trained in RS. In addition, a curriculum has been developed for a masters program in health management.
5.3. KEY CHANGES IN DELIVERY OF PHC SERVICES IN RS
166. The FM model in RS follows four core principles: (a) f i r s t contact, (b) longitudinality, (c) comprehensiveness, and (d) coordination. K e y changes in the PHC system have focused on achieving these principles.
167. By April 2004, 233,000 people in RS (23 percent o f the population) were covered by FM teams. By end o f 2004, this number was projected to increase to 250,000. The coverage in the pi lot sites i s greater: (a) Banja Luka 60 percent, (b) Laktasi 100 percent, (c) Doboj 40 percent, (d) Celinac 80 percent, and (e) Panjavor 3 5 percent. Although Panjovar was init ially not part o f the WBBHP, limited support provided to the municipality was leveraged by the local government to introduce FM teams.
168. The FM specialists have a broad scope o f services, including health, education, promotion, prevention, diagnosis, and curative and rehabilitative services. They perform gate keeping functions and provide comprehensive and continuous health care to their registered populations. FM specialists have a contract with the Health Insurance Fund through their DZ. This contract articulates their roles and responsibilities and identifies equipment they should have. (See Annexes 2 and 3 and the section on provider payment systems and contracts in RS.)
169. The workload o f the FM specialists and GPs in RS varies by region and typically comprises consultations, medical examinations, and a number o f additional services. A study that explored the workloads o f FM specialists and GPs in DZ Banja Luka showed that around 65 percent o f the GPs’ activities and 78 percent o f the FM specialists’ activities were consultations and clinical examination^.^^
28
5.3.1. First Contact and Gatekeeper Role o f FM
170. In i t s “Strategic Plan for the Reform and Reconstruction o f the Health Care System,” published in 1997,54 the M O H S W specified that each family should be registered with a named FM specialistldoctor and that the citizens should have the right and the freedom to register with an FM specialist o f their choice. This objective has been achieved to a large extent,
171. In the DZ where the FM model has been implemented, the users access their FM doctor as the first point o f contact and the narrow-specialists in PHC centers and hospitals fo l lowing a referral by their FM specialist (except for emergencies). In the PHC centers where the FM model i s not established, the gate keeping function i s compromised and first-contact access fragmented, as the services are organized according to age, gender, and health problems (as in the past). In addition to non-specialist GPs, the citizens have direct access to pediatricians, gynecologists, pre-school and school medicine specialists, occupational medicine specialists, and respiratory physicians.
5.3.2. Longitudinal Care and Continuity o f Care
172. In PHC centers where the FM model i s established, a patient appointment system has been introduced. Having named FM specialists has strengthened the doctor-patient relationship and enhanced continuity o f care.
5.3.3. Comprehensiveness o f Care
173. In the refurbished PHC centers piloting the FM model, new equipment and infrastructure improvements have created a favorable environment for expanded service delivery for chronic illness, infectious diseases, pediatrics, gynecology, sexually transmitted diseases, mental health, tuberculosis, and minor surgery.
174. Further, fo l lowing the implementation o f the Program for Prevention and Control o f Non- communicable Diseases (adopted by the M O H S W in 2002)55 and “Guidelines for Detection and Reduction o f Risks Factors and Early Detection o f Non-Communicable disease^,"^' the FM specialists now provide a broad spectrum o f health education, promotion, and prevention services to the populations they serve.
5.3.4. Coordination of Care
175. problem-oriented medical records and a referral counter-referral system.
Coordination o f health services has been enhanced through introduction and improvement o f
176. During the implementation o f the WBBHP, the RS Project Coordination Unit team, together with the management o f pilot DZs, enforced the regular and systematic use o f patient medical records and introduced a proprietary software program for FMs to capture accurate and reliable patient information on patients, activities, and trends, This information will enable the FM teams to improve decision making by providing them timely information on health care needs o f their individual patients and the population they cover.
177. The “Rulebook on Referral System in Health Care o f Republika Srpska,” produced with input from the FM specialists in RS and subsequently adopted by RS MOHSW,56 has introduced evidence-based clinical guidelines for 20 o f the most common conditions encountered at the PHC level. The guidelines define management o f these conditions by FM specialists and thresholds for referral to the specialist and secondary level (Annex 4).
29
178. Analysis o f the work o f FM teams in DZ Laktasi (the f i rs t DZ in the RS with a functioning FM model) following the introduction o f guidelines shows, when compared with levels for other DZs, a decline in referrals to hospitals and specialist services, reduced laboratory and imaging diagnostics tests, and fewer prescriptions.
5.3.5. Prescribing and Dispensing o f Drugs
179. A “List o f Essential Drugs” was introduced in 1997 and revised in 1999 in collaboration with the World Health Organization (WHO). The manual, “‘The Essential Drugs o f Republika Srpska (247),” published in collaboration with UNICEF in 1999, has been distributed to al l health professionals in RS, including general/FM doctors, to promote rational pre~cr ib ing.~’ However, the FM training curriculum i s not aligned with the essential drugs list, an issue that needs to be addressed.
180. Every year, the HIF in RS decides on a positive drug l i s t o f over 300 drugs that can be used by general/FM doctors working at the PHC level. The state pharmacies are reimbursed for dispensing the drugs on this l i s t according to a reimbursement system based on a reference price l i s t that averages the prices o f drugs from the 10 largest wholesalers. The private pharmacies are excluded from the HIF reimbursement system.
5.3.6. Role o f FM Nurses
18 1. As in the FBIH, prior to the PHC/FM reforms the role o f the FM nurse was mainly administrative, with consequent adverse effects on morale, self-esteem, and the attractiveness o f nursing as a career. Within the FM team model, the trained FM nurses have broadened roles and responsibilities and work as members o f the F M team, delivering user-centered health services, including health education, promotion prevention, and rehabilitation. The trained FM nurses work closely with families to provide psycho-social and medical support and play an important role in maintaining up-to-date records o f patient care, enhancing continuity and coordination o f health care.
5.3.7. Out-of-Hours Emergency Services
182. PHC centers are responsible for providing emergency care to patients in their catchment area between 4 pm and 8 am. In small health centers, emergency care i s provided by FM physicians who organize a duty rota, and in large health centers by full-time physicians.
183. Ambulance services provide f i rst aid services, emergency care, and support to the emergency departments attached to the DZ. When necessary, the ambulances transport patients to general hospitals, or in severe cases, directly to clinical centers.
184. In areas where the FM model has not been introduced, the emergency care system functions as an expensive substitute for the FM system. Analysis o f the type and range o f services provided by the emergency services at DZs where the FM model has not been fully implemented shows that over 65 percent of the services could be provided by an FM specialist. An analysis o f the number and structure o f health services provided at the emergency department in the DZ Banja Luka demonstrates the extent o f this problem, with emergency services substituting for FM (Table 9:).
30
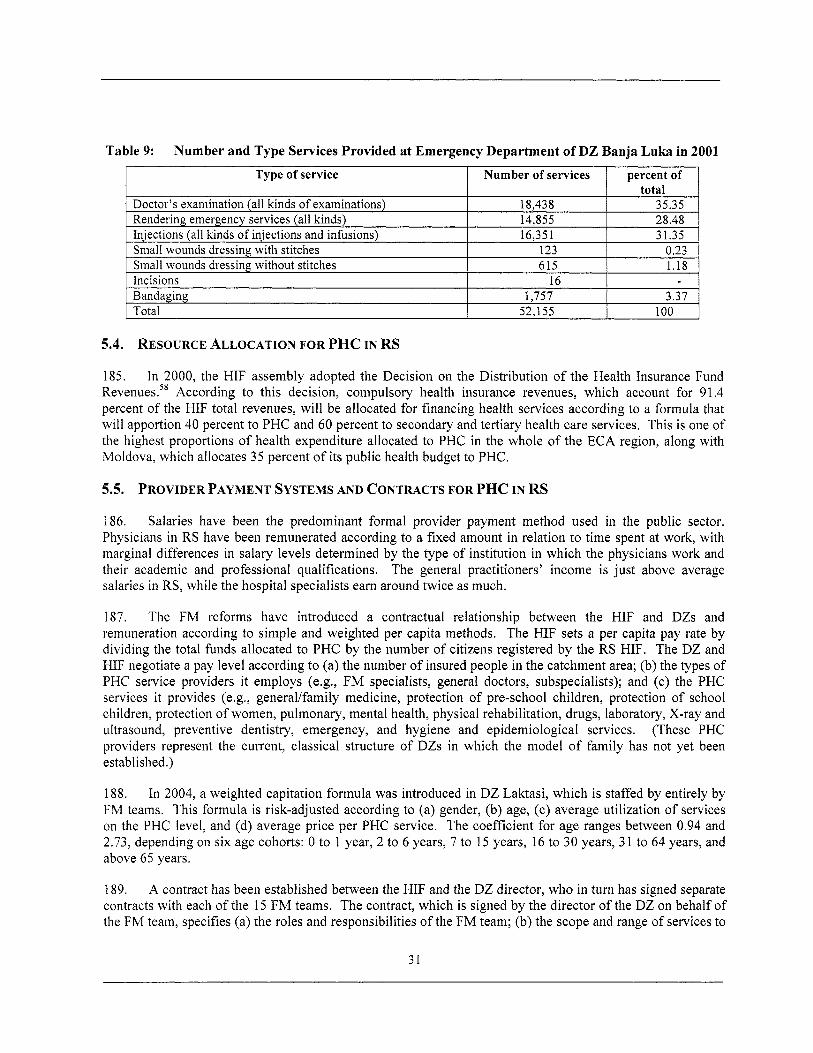
Table 9: Number and Type Services Provided at Emergency Department of DZ Banja Luka in 2001
I Type of service 1 Number of services 1 percent of 1 Doctor’s examination (all kinds o f examinations) Rendering emergency services (all kinds) Injections (all kinds o f injections and infusions) Small wounds dressing with stitches
Incisions Small wounds dressing without stitches
18,438 35.35 14,855 28.48 16,351 31.35
123 0.23 615 1.18
16 Bandaging Total
5.4. RESOURCE ALLOCATION FOR PHC IN RS
..
1,757 3.37 52,155 100
185. In 2000, the HIF assembly adopted the Decision on the Distribution o f the Health Insurance Fund Revenues.s8 According to this decision, compulsory health insurance revenues, which account for 9 1.4 percent o f the HIF total revenues, will be allocated for financing health services according to a formula that w i l l apportion 40 percent to PHC and 60 percent to secondary and tertiary health care services. This i s one o f the highest proportions o f health expenditure allocated to PHC in the whole o f the ECA region, along with Moldova, which allocates 35 percent o f i ts public health budget to PHC.
5.5. PROVIDER PAYMENT SYSTEMS AND CONTRACTS FOR PHC IN RS
186. Salaries have been the predominant formal provider payment method used in the public sector. Physicians in RS have been remunerated according to a fixed amount in relation to time spent at work, with marginal differences in salary levels determined by the type o f institution in which the physicians work and their academic and professional qualifications. The general practitioners’ income i s just above average salaries in RS, while the hospital specialists earn around twice as much.
187. The FM reforms have introduced a contractual relationship between the HIF and DZs and remuneration according to simple and weighted per capita methods. The HIF sets a per capita pay rate by dividing the total funds allocated to PHC by the number o f citizens registered by the RS HIF. The DZ and HIF negotiate a pay level according to (a) the number o f insured people in the catchment area; (b) the types o f PHC service providers it employs (e.g., FM specialists, general doctors, subspecialists); and (c) the PHC services it provides (e.g., general/family medicine, protection o f pre-school children, protection o f school children, protection o f women, pulmonary, mental health, physical rehabilitation, drugs, laboratory, X-ray and ultrasound, preventive dentistry, emergency, and hygiene and epidemiological services. (These PHC providers represent the current, classical structure o f DZs in which the model o f family has not yet been established.)
188. In 2004, a weighted capitation formula was introduced in DZ Laktasi, which i s staffed by entirely by FM teams. This formula i s risk-adjusted according to (a) gender, (b) age, (c) average utilization o f services on the PHC level, and (d) average price per PHC service. The coefficient for age ranges between 0.94 and 2.73, depending on six age cohorts: 0 to 1 year, 2 to 6 years, 7 to 15 years, 16 to 30 years, 3 1 to 64 years, and above 65 years.
189. A contract has been established between the HIF and the DZ director, who in turn has signed separate contracts with each o f the 15 FM teams. The contract, which i s signed by the director o f the DZ on behalf o f the FM team, specifies (a) the roles and responsibilities o f the FM team; (b) the scope and range o f services to
31
be provided; (c) population covered; (d) quality standards to be observed; (e) prescribing l i s ts (positive l i s t and the essential l i s t o f drugs); (f) opening hours; (g) reporting mechanisms; (h) payment method and amount; (i) payment duration; and (‘j) mechanisms for arbitration in case o f disputes (Annex 2). Provision o f preventive services i s part o f this contract and attracts additional remuneration. Further, a 10 percent bonus payment i s payable to each FM team if it i s satisfactorily accredited by the RS AAQI.
5.6. INFRASTRUCTURE AND EQUIPMENT AT PHC FACILITIES IN RS
190. The L a w on Health Care allows M O H S W to implement quality control programs for health services and to set standards for functioning health care institutions - specifying the number and structure o f human resources, infrastructure, and equipment - and ensure use of modern evidence-based interventions for health care.
19 1. The “Rulebook on Family Medicine Specialization Program” defines normative standards - in terms o f space, equipment, and personnel - for every type o f health facility.59 The L a w on Health Care and the contract between the HIF and the DZ specify different equipment lists for ordinary ambulantas staffed by non-specialist general doctors and FM ambulantas staffed by FM specialists - reflecting the extended role and responsibilities o f the FM specialist as regards clinical care (Annex 3).
192. environment according to the needs o f the FM teams, and this has improved the privacy o f consultations.
In the DZs that have introduced the new FM model, physical changes have been made to the work
5.7. LICENSING AND REVALIDATION IN RS
193. In July 2001, RS Parliament adopted The L a w on Health Chambers,60 which established a unified Chamber for licensing o f health professionals working in RS. This law was amended in 2002, enabling the division o f the unified health Chamber into three Chambers - one each for doctors, dentists, and pharmacists. Article 1 o f the amended law obliges doctors who are working in public and private health facilities to be members o f the Doctors’ Chamber. Article 5 stipulates that the “Doctors’ Chamber has the responsibility to issue certificates (licenses) to i t s members.”
194. The Chamber has an important role in quality assurance o f health services and i s responsible for (a) determining professional rights and obligations, ethical and deontological rules o f conduct for health professionals; (b) verifying medical knowledge of health professionals and providing appropriate certification; (c) renewal or cancellation o f medical licenses o f health professionals; and (d) issuing opinions on medical training curricula.
195. Licenses are renewed every five years. Members o f the Chamber are required to engage in continuing professional development activities organized or approved by the Chamber and accumulate 60 points each year to renew their license to practice..
All practicing medical doctors are obliged to become members o f the Chamber.
5.8. ACCREDITATION IN RS
196. Following the L a w o n Changes and Additions on the L a w on Health Care6’ adopted by RS Parliament in 2001, the A A Q I was established in 2002 and operationalized in 2003.62 The AAQI i s a state agency that has a trained a cadre o f assessors, Accreditation i s voluntary. The AAQI provides support to FM teams, practices, or departments o f FM in the PHC centers registered with the RS M O H S W that wish to be accredited. There are 11 accreditation standards, grouped into five main areas, which must be met by the FM team or PHC center to secure full accreditation (Table 10:).
32
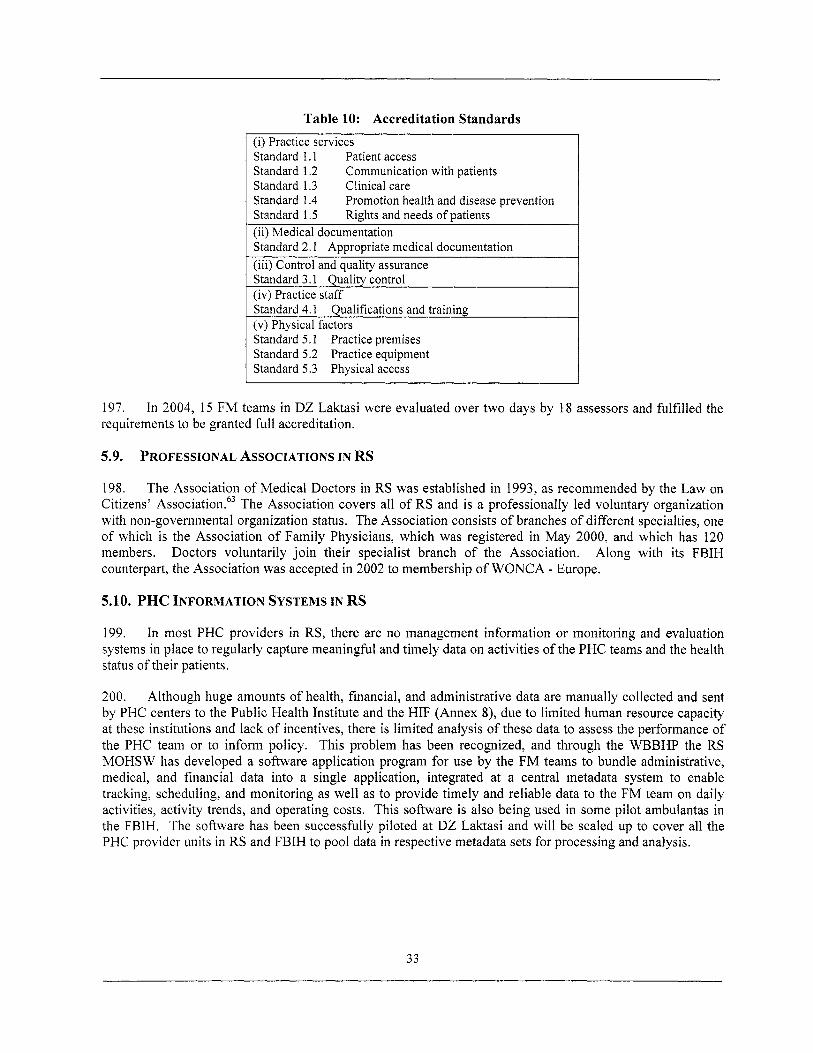
Table 10: Accreditation Standards (i) Practice services Standard 1.1 Patient access Standard 1.2 Communication with patients Standard 1.3 Clinical care Standard 1.4 Standard 1.5 (ii) Medical documentation Standard 2.1 Appropriate medical documentation (iii) Control and quality assurance Standard 3.1 Quality control (iv) Practice staff Standard 4.1 Qualifications and training (v) Physical factors Standard 5.1 Practice premises Standard 5.2 Practice equipment Standard 5.3 Physical access
Promotion health and disease prevention Rights and needs o f patients
197. requirements to be granted full accreditation.
In 2004, 15 FM teams in DZ Laktasi were evaluated over two days by 18 assessors and fulf i l led the
5.9. PROFESSIONAL ASSOCIATIONS IN RS
198. The Association o f Medical Doctors in RS was established in 1993, as recommended by the L a w on Citizens’ A ~ s o c i a t i o n . ~ ~ The Association covers al l o f RS and i s a professionally led voluntary organization wi th non-governmental organization status. The Association consists o f branches o f different specialties, one o f which i s the Association o f Family Physicians, which was registered in M a y 2000, and which has 120 members. Along with i t s FBIH counterpart, the Association was accepted in 2002 to membership o f W O N C A - Europe.
Doctors voluntarily j o i n their specialist branch o f the Association.
5.10. PHC INFORMATION SYSTEMS IN RS
199. In most PHC providers in RS, there are no management information or monitoring and evaluation systems in place to regularly capture meaningful and timely data on activities o f the PHC teams and the health status o f their patients.
200. Although huge amounts o f health, financial, and administrative data are manually collected and sent by PHC centers to the Public Health Institute and the HIF (Annex 8), due to l imited human resource capacity at these institutions and lack o f incentives, there i s l imited analysis o f these data to assess the performance o f the PHC team or to inform policy. This problem has been recognized, and through the WBBHP the RS M O H S W has developed a software application program for use by the FM teams to bundle administrative, medical, and financial data into a single application, integrated at a central metadata system to enable tracking, scheduling, and monitoring as wel l as to provide timely and reliable data to the FM team on daily activities, activity trends, and operating costs. This software i s also being used in some pilot ambulantas in the FBIH. The software has been successfully piloted at DZ Laktasi and will be scaled up to cover all the PHC provider units in RS and FBIH to pool data in respective metadata sets for processing and analysis.
33
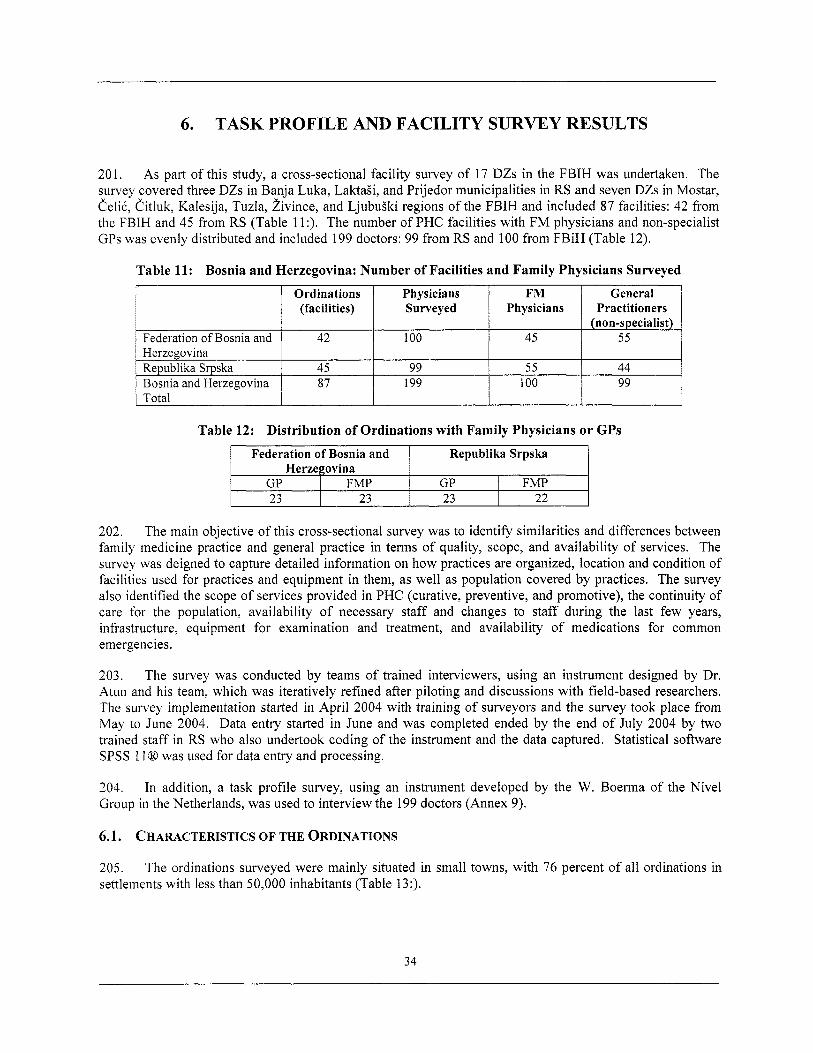
6. TASK PROFILE AND FACILITY SURVEY RESULTS
Ordinations Physicians FM (facilities) Surveyed Physicians
201. As part o f this study, a cross-sectional facility survey o f 17 DZs in the FBIH was undertaken. The survey covered three DZs in Banja Luka, Laktagi, and Prijedor municipalities in RS and seven DZs in Mostar, CeliC, Citluk, Kalesija, Tuzla, i iv ince, and Ljubugki regions o f the FBIH and included 87 facilities: 42 from the FBIH and 45 from RS (Table 1 1 :). The number o f PHC facilities with FM physicians and non-specialist GPs was evenly distributed and included 199 doctors: 99 f rom RS and 100 from FBiH (Table 12).
General Practitioners
Federation o f Bosnia and 1 42 100 45 55 Herzegovina Republika Srpska Bosnia and Herzegovina
Table 12: Distribution of Ordinations with Family Physicians or GPs 1 Federation of Bosnia and I Republika Srpska
45 99 5 5 44 87 199 100 99
Herzegovina GP FMP 23 23
202. The main objective o f this cross-sectional survey was to identify similarities and differences between family medicine practice and general practice in terms o f quality, scope, and availability o f services. The survey was deigned to capture detailed information on how practices are organized, location and condition o f facilities used for practices and equipment in them, as wel l as population covered by practices. The survey also identified the scope o f services provided in PHC (curative, preventive, and promotive), the continuity o f care for the population, availability o f necessary staff and changes to staff during the last few years, infrastructure, equipment for examination and treatment, and availability o f medications for common emergencies.
GP I FMP 23 22
203. The survey was conducted by teams o f trained interviewers, using an instrument designed by Dr. Atun and his team, which was iteratively refined after piloting and discussions with field-based researchers. The survey implementation started in April 2004 with training o f surveyors and the survey took place from M a y to June 2004. Data entry started in June and was completed ended by the end o f July 2004 by two trained staff in RS who also undertook coding o f the instrument and the data captured. Statistical software SPSS 11Q was used for data entry and processing.
204. Group in the Netherlands, was used to interview the 199 doctors (Annex 9).
In addition, a task profi le survey, using an instrument developed by the W. Boerma o f the Nive l
6.1. CHARACTERISTICS O F THE ORDINATIONS
205. settlements wi th less than 50,000 inhabitants (Table 13:).
The ordinations surveyed were mainly situated in small towns, with 76 percent o f a l l ordinations in
34
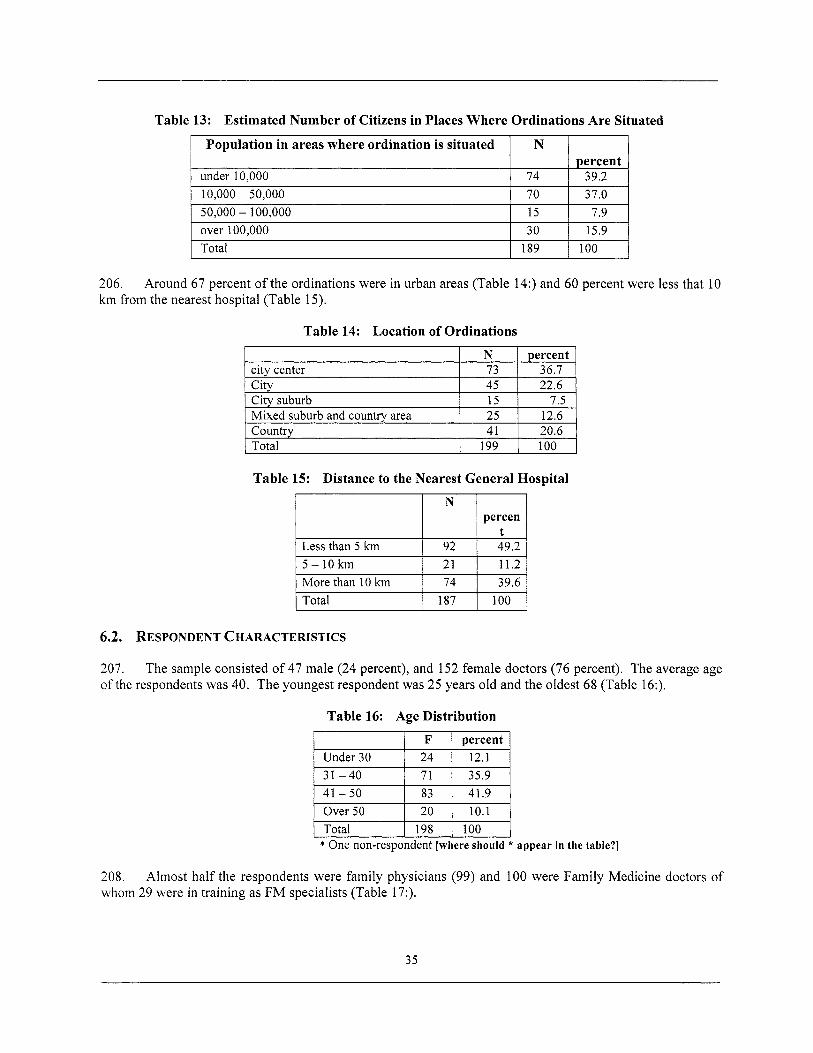
Table 13: Estimated Number of Citizens in Places Where Ordinations Are Situated
10,000 - 50,OO.O 50,000 - 100,000 over 100,000 Total
I Population in areas where ordination i s situated I N 1 I
70 37.0 15 7.9 30 15.9
189 100
1 percent under 10,000 1 74 I 39.2
city center City
Mixed suburb and country area Country Total
City suburb
N percent 73 36.7 45 22.6 15 7.5 25 12.6 41 20.6
199 100
206. km from the nearest hospital (Table 15).
Around 67 percent o f the ordinations were in urban areas (Table 14:) and 60 percent were less that 10
Table 14: Location of Ordinations
Table 15: Distance to the Nearest General Hospital
N percen
Less than 5 km 5-10km More than 10 km 74 39.6 Total 187 100
6.2. RESPONDENT CHARACTERISTICS
207. o f the respondents was 40. The youngest respondent was 25 years old and the oldest 68 (Table 16:).
The sample consisted o f 47 male (24 percent), and 152 female doctors (76 percent). The average age
Table 16: Age Distribution
I F I Dercent I Under 30 31 -40 41 -50 Over 50 Total 100 * One non-respondent [where should * appear in the table?]
208. whom 29 were in training as FM specialists (Table 17:).
Almost hal f the respondents were family physicians (99) and 100 were Family Medicine doctors o f
35
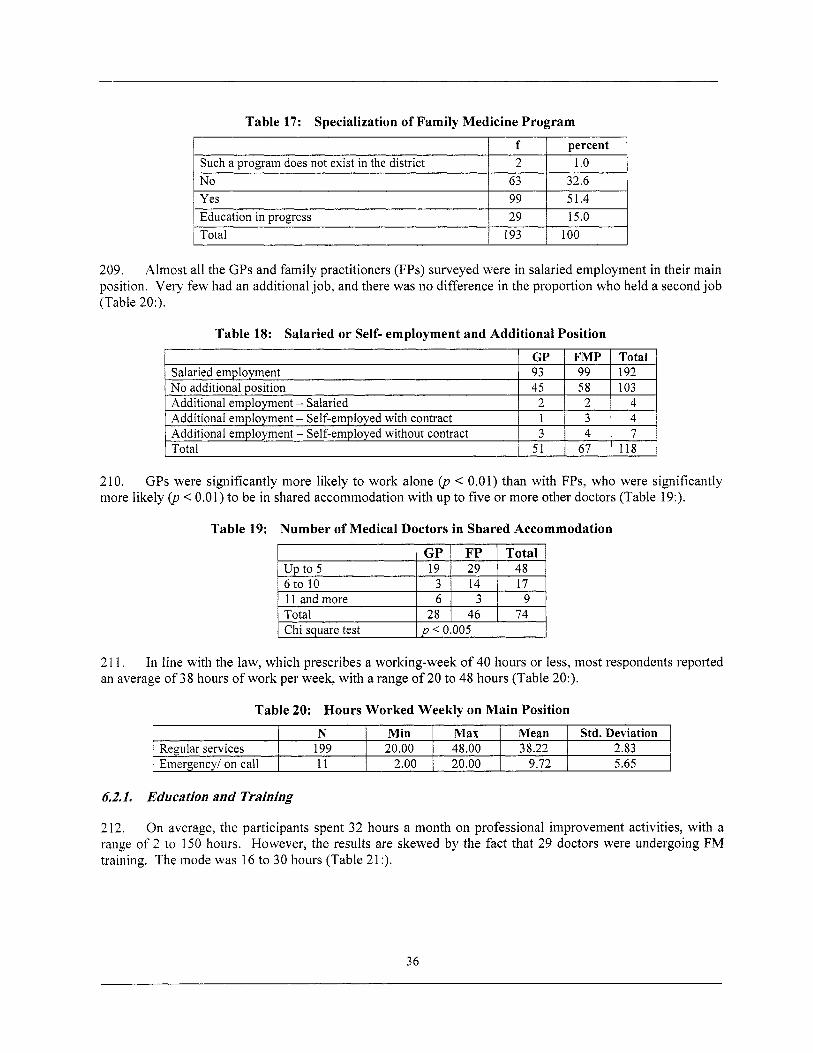
Table 17: Specialization of Family Medicine Program
Such a program does not exist in the district N o
f percent 2 1 .o
63 32.6 Yes
Total Education in progress
99 51.4 29 15.0
193 100
210. more likely (p < 0.01) to be in shared accommodation with up to five or more other doctors (Table 19:).
GPs were significantly more likely to work alone (p < 0.01) than with FPs, who were sign ficanf
Salaried employment No additional position Additional employment - Salaried 5 Additional employment - Self-employed without contract
Y
GP FMP Total 93 99 192 45 58 103
2 2 4 1 3 4 3 4 7
______-
GP u p to 5 19 6 to 10 3 11 and more I 6 1 3 1 9 Total I 28 I 46 1 74
FP Total 29 48 14 17
I Chi square test 1 p < 0.005 I
N Min M a x Regular services 199 20.00 48.00 Emergency1 on call 11 2.00 20.00
2 1 1. an average o f 38 hours o f work per week, with a range o f 20 to 48 hours (Table 20:).
In line with the law, which prescribes a working-week o f 40 hours or less, most respondents reported
M e a n Std. Deviation 38.22 2.83
9.72 5.65
62.1. Education and Training
212. On average, the participants spent 3 2 hours a month on professional improvement activities, with a range o f 2 to 150 hours. However, the results are skewed by the fact that 2 9 doctors were undergoing FM training. The mode was 16 to 30 hours (Table 21:).
36
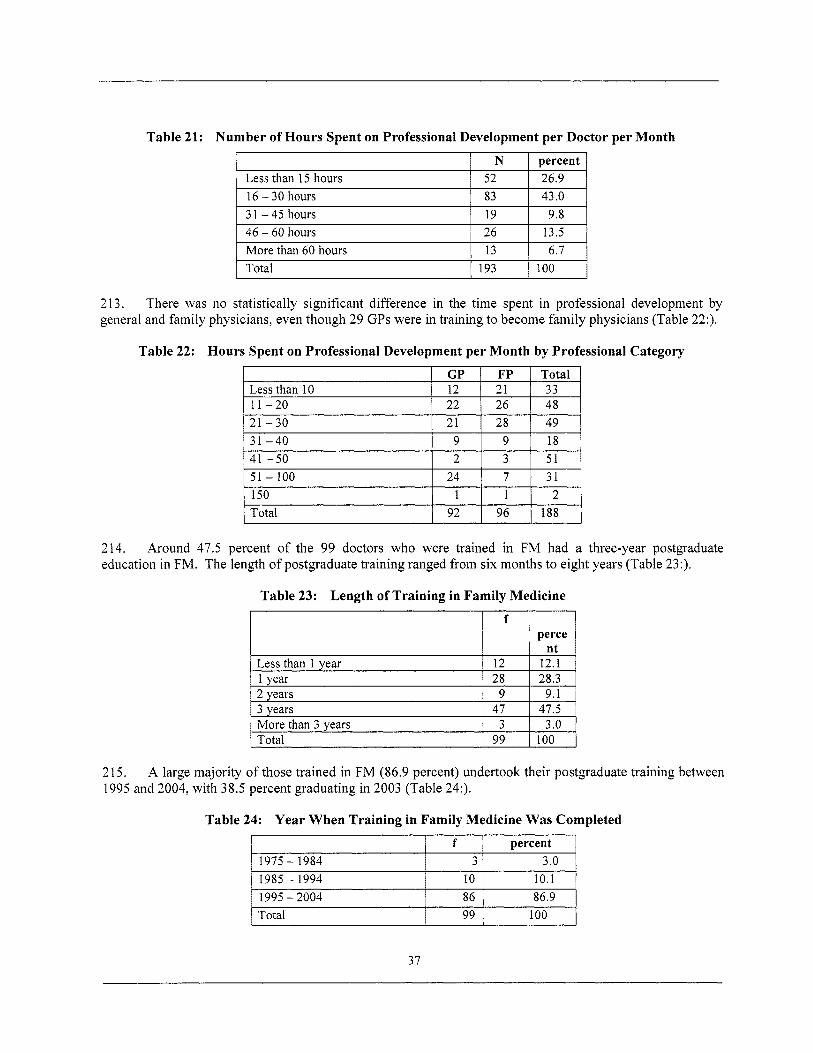
Table 21: Number of Hours Spent on Professional Development per Doctor per Month
Less than 10 11 -20
I 1 N I percent 1
GP FP Total 12 21 33 22 26 48
1 Less than 15 hours 1 52 I 26.9 1
21 -30 3 1 -40
16 - 30 hours 3 1 - 45 hours 46 - 60 hours More than 60 hours Total 193 100
21 28 49 9 9 18
213. general and family physicians, even though 29 GPs were in training to become fami ly physicians (Table 22:).
There was no statistically significant difference in the time spent in professional development by
Table 22: Hours Spent on Professional Development per Month by Professional Category
I 4 1 -50 I 2 I 3 1 5 1 I
1 Total 1 92 I 96 1 188 1 214. education in FM. The length o f postgraduate training ranged from six months to eight years (Table 23:).
Around 47.5 percent o f the 99 doctors who were trained in FM had a three-year postgraduate
Table 23: Length of Training in Family Medicine
perce f
47.5 3 .O More than 3 years
Total
215. 1995 and 2004, with 38.5 percent graduating in 2003 (Table 24:).
A large majority o f those trained in FM (86.9 percent) undertook their postgraduate training between
Table 24: Year When Training in Family Medicine Was Completed
percent 1975 - 1984 1985 - 1994 1995 - 2004 86 86.9 Total 99 100
37
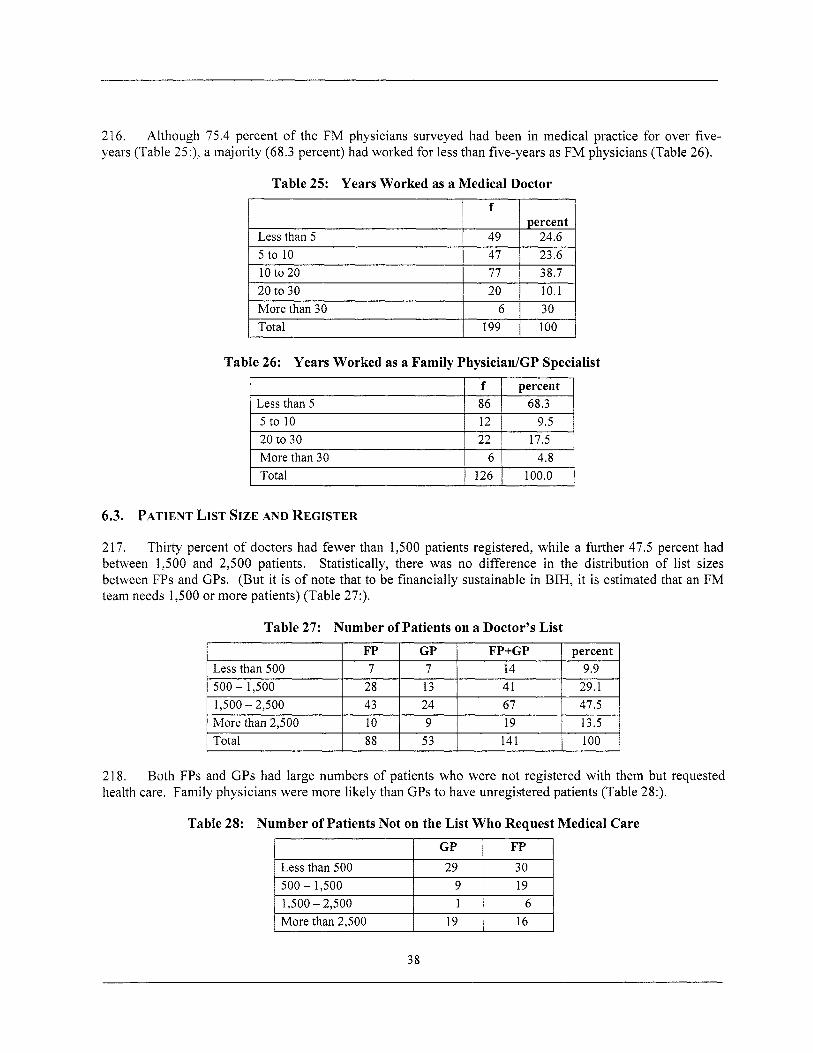
216. years (Table 25:), a majority (68.3 percent) had worked for less than five-years as FM physicians (Table 26).
Although 75.4 percent o f the FM physicians surveyed had been in medical practice for over five-
Less than 5
Table 25: Years Worked as a Medical Doctor
f
49 I 24.6
10 to 20 20 to 30 More than 30 Total
I 5 t o 1 0 1 47 I 23.6 1 77 38.7 20 10.1
6 30 199 100
Less than 500 500 - 1,500 1,500 - 2,500 More than 2,500 Total
I I I I
FP GP FP+GP percent 7 7 14 9.9
28 13 41 29.1 43 24 67 47.5 10 9 19 13.5 88 53 141 100
Tabie 26: Years Worked as a Family Physician/GP Specialist
I f I percent I
Less than 500
Less than 5 5 to 10 20 to 30 More than 30 4.8 Total
GP FP
29 30
6.3. PATIENT LIST SIZE AND REGISTER
217. Thirty percent o f doctors had fewer than 1,500 patients registered, while a further 47.5 percent had between 1,500 and 2,500 patients. Statistically, there was no difference in the distribution o f l i s t sizes between FPs and GPs. (But it i s o f note that to be financially sustainable in BIH, it i s estimated that an FM team needs 1,500 or more patients) (Table 27:).
Table 27: Number of Patients on a Doctor’s L ist
218. health care. Family physicians were more likely than GPs to have unregistered patients (Table 28:).
Both FPs and GPs had large numbers o f patients who were not registered with them but requested
1 500 - 1,500 I 9 1 1 9 1 1 1,500 - 2,500 I 1 1 6 1 1 M o r e than 2,500 1 19 1 16
38
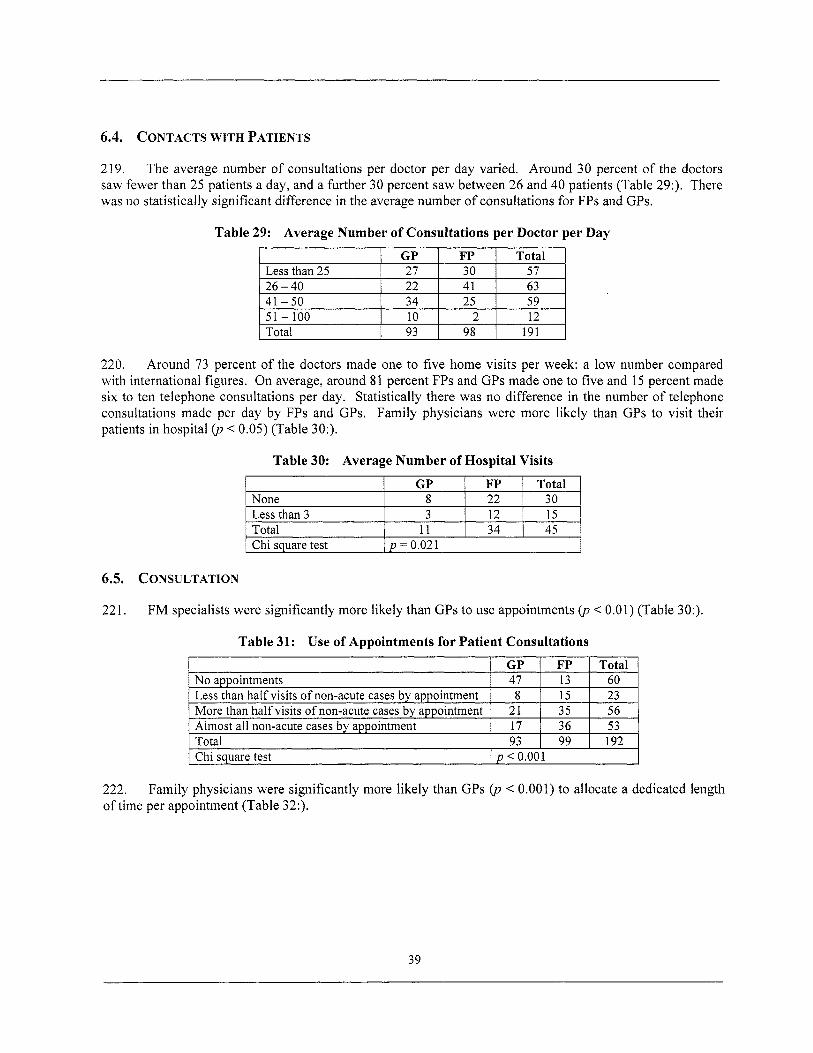
6.4. CONTACTS WITH PATIENTS
None Less than 3 Total
219. The average number o f consultations per doctor per day varied. Around 30 percent o f the doctors saw fewer than 25 patients a day, and a further 30 percent saw between 26 and 40 patients (Table 29:). There was no statistically significant difference in the average number o f consultations for FPs and GPs.
GP FP Total 8 22 30 3 12 15
11 34 45
Table 29: Average Number o f Consultations per Doctor per Day
GP FP No appointments 47 13 Less than half visits o f non-acute cases by appointment 15 More than half visits o f non-acute cases by appointment 35
Total 93 99
8 2 1
Almost all non-acute cases by appointment 17 36
Total Less than 25 26 - 40 41 -50 51 - 100 Total 93 98 191
Total 60 23 56 53 192
220, Around 73 percent o f the doctors made one to f ive home visits per week: a l ow number compared with international figures. On average, around 8 1 percent FPs and GPs made one to five and 15 percent made six to ten telephone consultations per day. Statistically there was no difference in the number o f telephone consultations made per day by FPs and GPs. Family physicians were more l ikely than GPs to visit their patients in hospital (p < 0.05) (Table 30:).
Table 30: Average Number o f Hospital Visits
1 Chi sauare test I D = 0.021 I
6.5. CONSULTATION
221. FM specialists were significantly more l ikely than GPs to use appointments 0, < 0.01) (Table 30:).
1 Chi sauare test I D < 0.001
222. of time per appointment (Table 32:).
Family physicians were significantly more l ikely than GPs (p < 0.001) to allocate a dedicated length
39
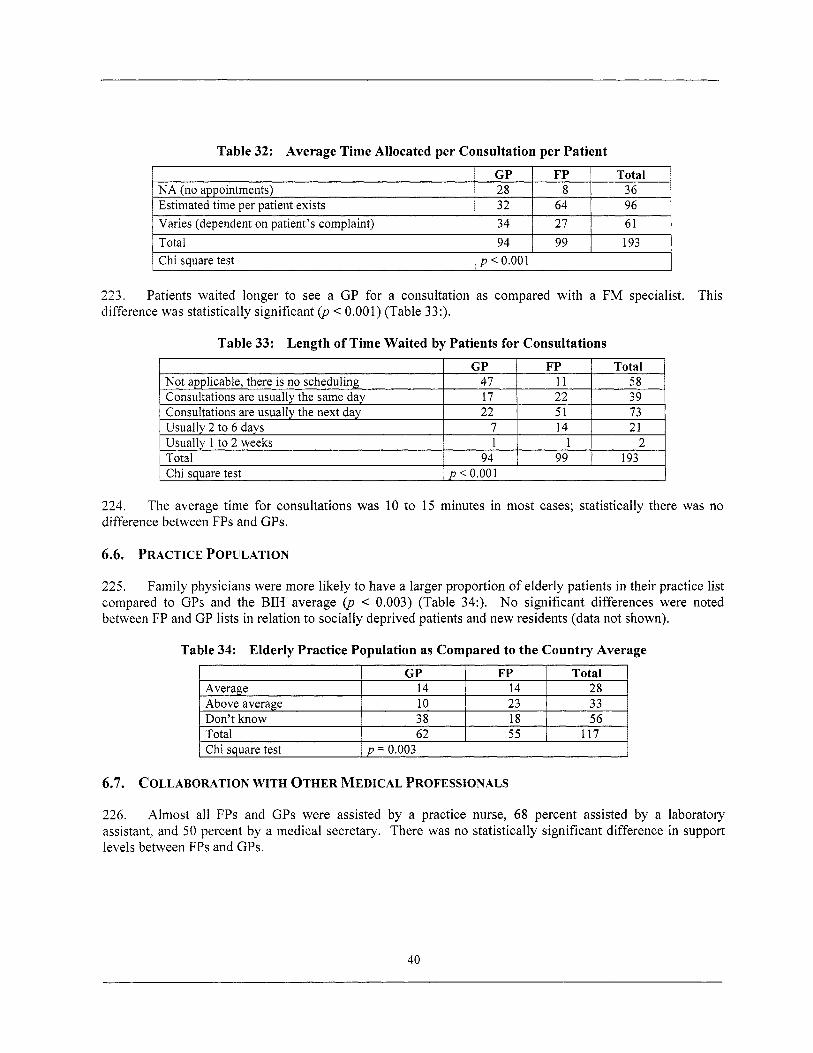
GP FP N A (no appointments) 28 8 Estimated time per patient exists 32 64 Varies (dependent on patient’s complaint) 34 27
Total 36 96 61
223. difference was statistically significant (p < 0.00 1) (Table 33:).
Patients waited longer to see a GP for a consultation as compared with a FM specialist. This
Total Chi square test
Table 33: Length of Time Waited by Patients for Consultations
I I
94 I 99 I 193 p < 0.00 1
224. difference between FPs and GPs.
The average time for consultations was 10 to 15 minutes in most cases; statistically there was no
GP Average 14
Don’t know 38 Total 62
Above average 10
6.6. PRACTICE POPULATION
FP Total 14 28 23 33 18 56 55 117
225. Family physicians were more l ikely to have a larger proportion o f elderly patients in their practice l i s t compared to GPs and the BIH average (p < 0.003) (Table 34:). No significant differences were noted between FP and GP l ists in relation to socially deprived patients and new residents (data not shown).
Chi square test
Table 34: Elderly Practice Population as Compared to the Country Average
p = 0.003
6.7. COLLABORATION WITH OTHER MEDICAL PROFESSIONALS
226. Almost a l l FPs and GPs were assisted by a practice nurse, 68 percent assisted by a laboratory assistant, and 50 percent by a medical secretary. There was no statistically significant difference in support levels between FPs and GPs.
40
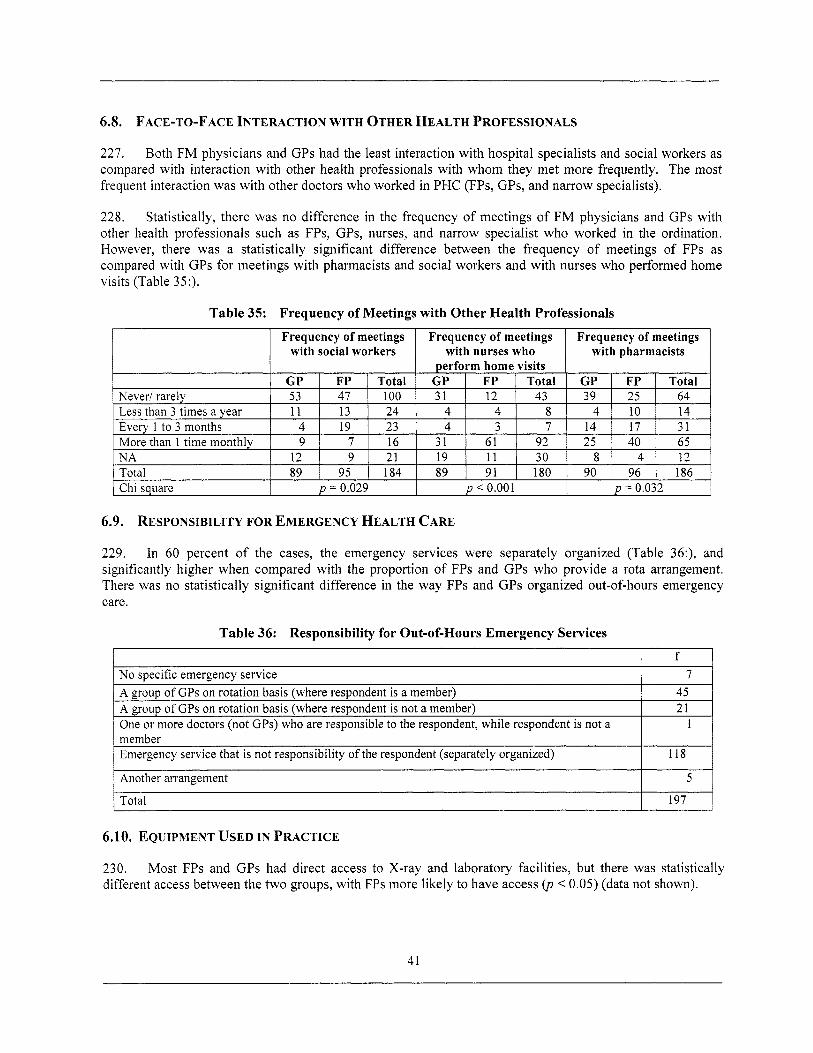
6.8. FACE-TO-FACE INTERACTION WITH OTHER HEALTH PROFESSIONALS
N A Total Chi square
227. Both FM physicians and GPs had the least interaction with hospital specialists and social workers as compared with interaction with other health professionals with whom they met more frequently. The most frequent interaction was with other doctors who worked in PHC (FPs, GPs, and narrow specialists).
12 I 9 I 21 19 1 11 1 30 8 1 4 1 12 89 1 95 I 184 89 I 91 I 180 90 I 96 1 186
p = 0.029 p < 0.001 p = 0.032
228. Statistically, there was no difference in the frequency o f meetings o f FM physicians and GPs with other health professionals such as FPs, GPs, nurses, and narrow specialist who worked in the ordination. However, there was a statistically significant difference between the frequency o f meetings o f FPs as compared with GPs for meetings with pharmacists and social workers and with nurses who performed home visits (Table 35:).
No specific emergency service A group o f GPs on rotation basis (where respondent i s a member) A group o f GPs on rotation basis (where respondent i s not a member) One or more doctors (not GPs) who are responsible to the respondent, while respondent i s not a
Emergency service that i s not responsibility o f the respondent (separately organized) member
Table 35: Frequency of Meetings with Other Health Professionals
f 7
45 21
1
118
Another arrangement
Total
6.9. RESPONSIBILITY FOR EMERGENCY HEALTH CARE
5
197
229. In 60 percent o f the cases, the emergency services were separately organized (Table 36:), and significantly higher when compared with the proportion o f FPs and GPs who provide a rota arrangement. There was no statistically significant difference in the way FPs and GPs organized out-of-hours emergency care.
6.10. EQUIPMENT USED IN PRACTICE
230. different access between the two groups, with FPs more l ikely to have access (p < 0.05) (data not shown).
Most FPs and GPs had direct access to X-ray and laboratory facilities, but there was statistically
41
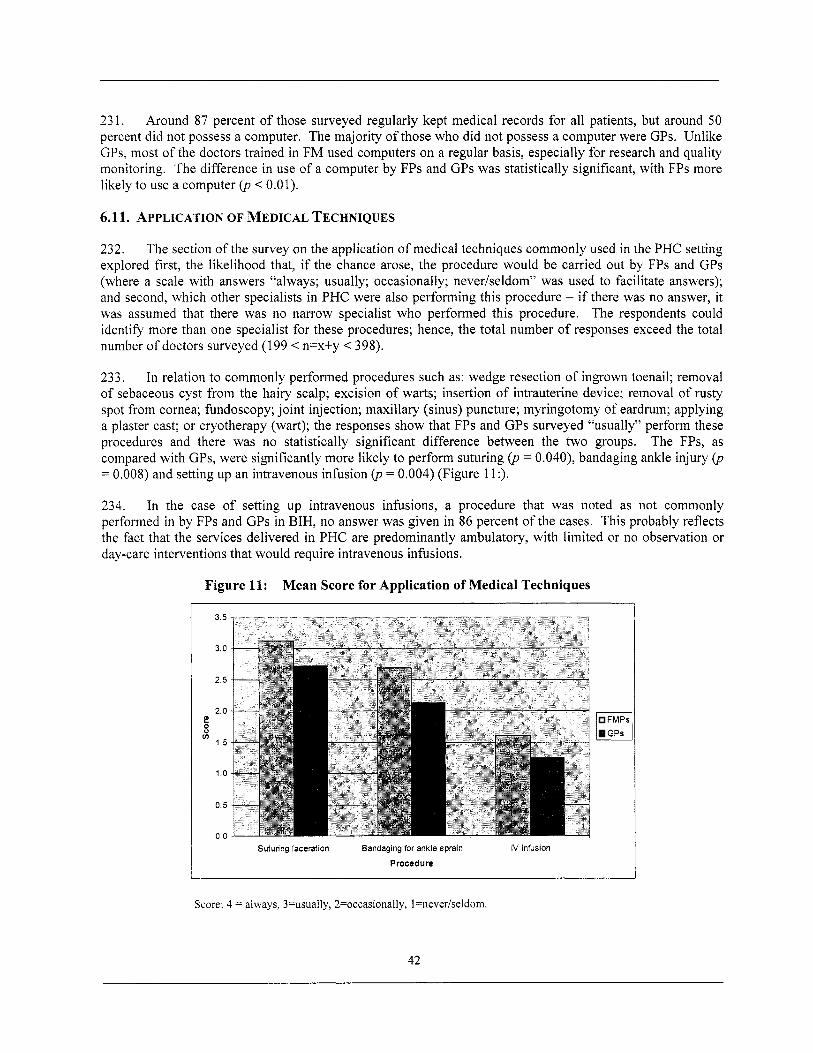
23 1. Around 87 percent o f those surveyed regularly kept medical records for a l l patients, but around 50 percent did not possess a computer. The majority o f those who did not possess a computer were GPs. Unlike GPs, most o f the doctors trained in FM used computers on a regular basis, especially for research and quality monitoring. The difference in use o f a computer by FPs and GPs was statistically significant, with FPs more likely to use a computer (p < 0.01).
6.11. APPLICATION OF MEDICAL TECHNIQUES
232. The section o f the survey on the application o f medical techniques commonly used in the PHC setting explored first, the likelihood that, if the chance arose, the procedure would be carried out by FPs and GPs (where a scale with answers “always; usually; occasionally; never/seldom” was used to facilitate answers); and second, which other specialists in PHC were also performing this procedure - if there was no answer, it was assumed that there was no narrow specialist who performed this procedure. The respondents could identify more than one specialist for these procedures; hence, the total number o f responses exceed the total number o f doctors surveyed (199 < n=x+y < 398).
233. In relation to commonly performed procedures such as: wedge resection o f ingrown toenail; removal o f sebaceous cyst f rom the hairy scalp; excision o f warts; insertion o f intrauterine device; removal o f rusty spot f rom cornea; fundoscopy; jo int injection; maxillary (sinus) puncture; myringotomy o f eardrum; applying a plaster cast; or cryotherapy (wart); the responses show that FPs and GPs surveyed “usually” perform these procedures and there was no statistically significant difference between the two groups. The FPs, as compared with GPs, were significantly more l ikely to perform suturing (p = 0.040), bandaging ankle injury (p = 0.008) and setting up an intravenous infusion (p = 0.004) (Figure 11:).
234. In the case o f setting up intravenous infusions, a procedure that was noted as not commonly performed in by FPs and GPs in BIH, no answer was given in 86 percent o f the cases. This probably reflects the fact that the services delivered in PHC are predominantly ambulatory, with limited or no observation or day-care interventions that would require intravenous infusions.
Figure 11: Mean Score for Application of Medical Techniques I
FMPs GPs
Suturing laceration Bandaging for ankle sprain iV infusion
Procedure
Score: 4 = always, 3=usually, 2=occasionally, l=never/seldom.
42
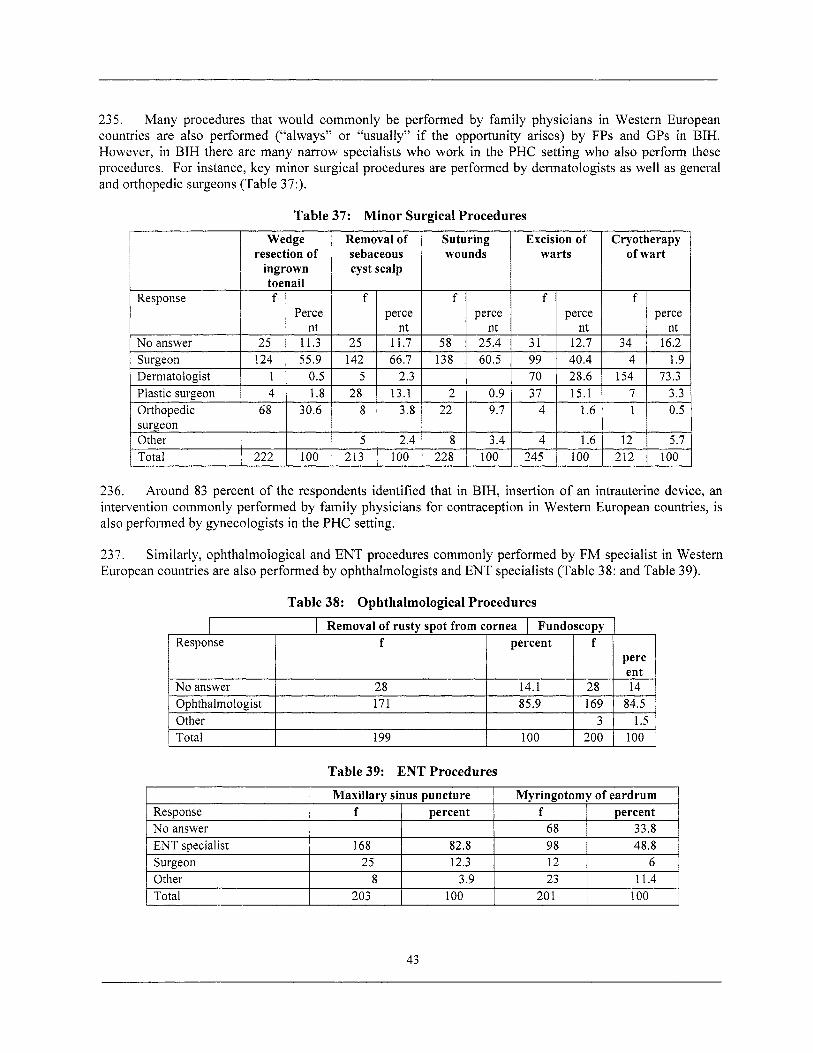
235. Many procedures that would commonly be performed by family physicians in Western European countries are also performed (“always” or “usually” if the opportunity arises) by FPs and GPs in BIH. However, in BIH there are many narrow specialists who work in the PHC setting who also perform these procedures. For instance, key minor surgical procedures are performed by dermatologists as wel l as general and orthopedic surgeons (Table 37:).
7 1
12 212
Table 37: Minor Surgical Procedures
3.3 0.5
5.1 100
Cryotherapy of wart
Response
perce
1.9
f percent 1 f percent No answer
236. Around 83 percent o f the respondents identified that in BIH, insertion o f an intrauterine device, an intervention commonly performed by fami ly physicians for contraception in Western European countries, i s also performed by gynecologists in the PHC setting.
68 33.8
237. European countries are also performed by ophthalmologists and ENT specialists (Table 38: and Table 39).
Similarly, ophthalmological and ENT procedures commonly performed by FM specialist in Western
ENT specialist Surgeon Other Total
Table 38: Ophthalmological Procedures
168 82.8 98 48.8 25 12.3 12 6
8 3.9 23 11.4 203 100 20 1 100
Table 39: ENT Procedures
I I Maxillarv sinus puncture I Mvringotomv of eardrum I
43
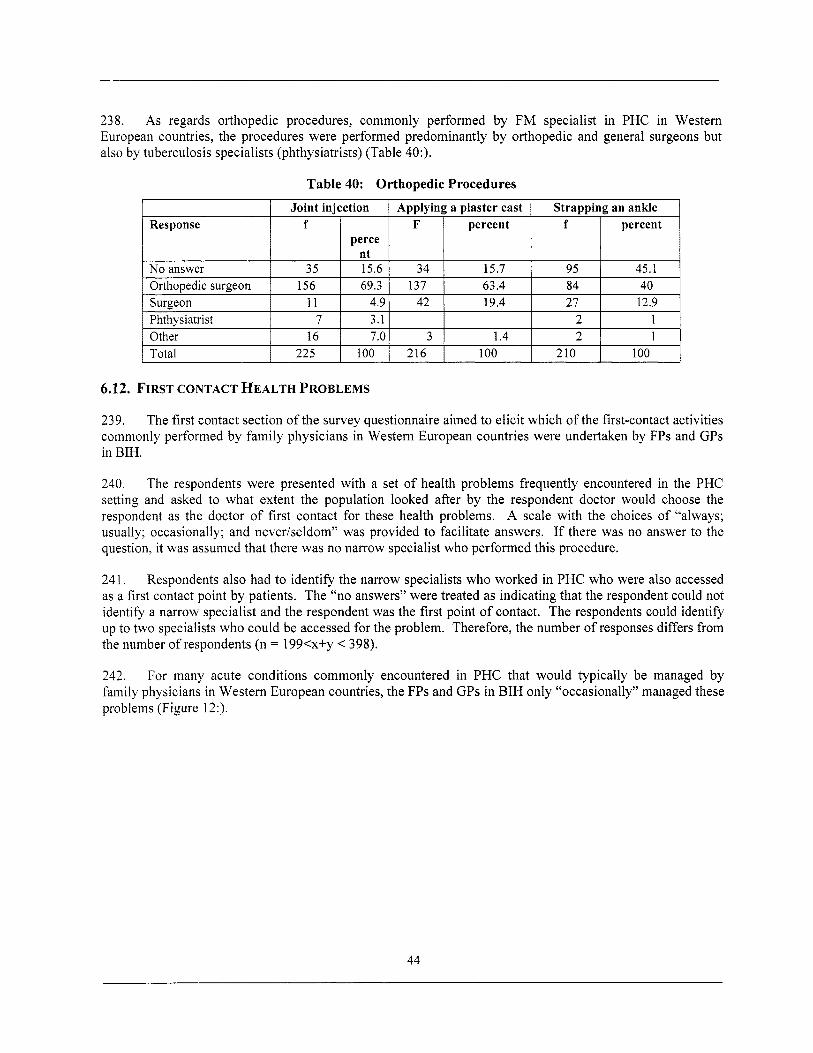
238. As regards orthopedic procedures, commonly performed by FM specialist in PHC in Western European countries, the procedures were performed predominantly by orthopedic and general surgeons but also by tuberculosis specialists (phthysiatrists) (Table 40:).
Response
Table 40: Orthopedic Procedures
Joint injection Applying a plaster cast Strapping an ankle f F percent f percent
perce
6.12. FIRST CONTACT HEALTH PROBLEMS
239. The first contact section o f the survey questionnaire aimed to elicit which o f the first-contact activities commonly performed by family physicians in Western European countries were undertaken by FPs and GPs in BIH.
240, The respondents were presented with a set o f health problems frequently encountered in the PHC setting and asked to what extent the population looked after by the respondent doctor would choose the respondent as the doctor o f f i rst contact for these health problems. A scale with the choices o f “always; usually; occasionally; and neveriseldom” was provided to facilitate answers. If there was no answer to the question, it was assumed that there was no narrow specialist who performed this procedure.
241. Respondents also had to identify the narrow specialists who worked in PHC who were also accessed as a first contact point by patients. The “no answers” were treated as indicating that the respondent could not identify a narrow specialist and the respondent was the f irst point o f contact. The respondents could identify up to two specialists who could be accessed for the problem. Therefore, the number o f responses differs from the number o f respondents (n = 199<x+y < 398).
242. For many acute conditions commonly encountered in PHC that would typically be managed by family physicians in Western European countries, the FPs and GPs in BIH only “occasionally” managed these problems (Figure 12:).
44
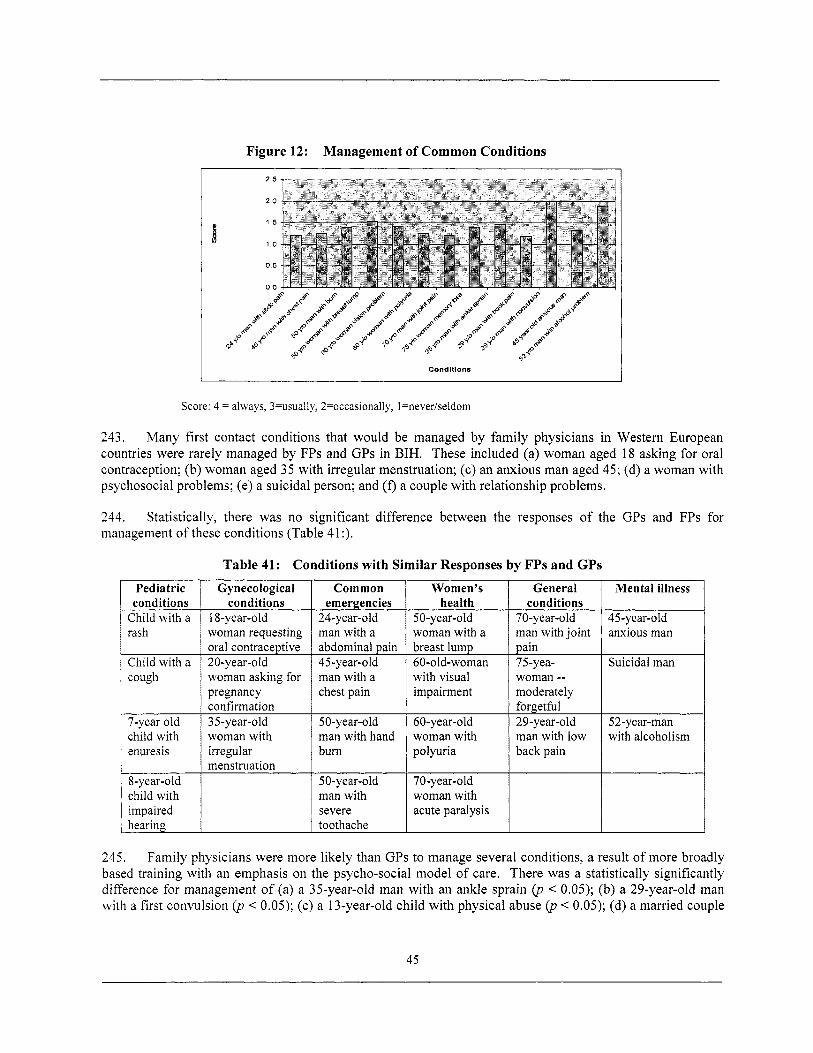
Figure 12: Management of Common Conditions
Gynecological conditions
18-year-old woman requesting oral contraceptive 20-year-old woman asking for pregnancy confirmation 35-year-old woman with irregular menstruation
Conditions
Common Women's emergencies health
24-year-old 50-year-old man with a woman with a abdominal pain breast lump 45-year-old 60-old-woman man with a with visual chest pain impairment
50-year-old 60-year-old man with hand woman with bum polyuria
50-year-old 70-year-old man with woman with severe acute paralysis toothache
Score: 4 = always, 3=usually, 2=occasionally, l=never/seldom
243. Many first contact conditions that would be managed by family physicians in Western European countries were rarely managed by FPs and GPs in BIH. These included (a) woman aged 18 asking for oral contraception; (b) woman aged 35 with irregular menstruation; (c) an anxious man aged 45; (d) a woman with psychosocial problems; (e) a suicidal person; and (f) a couple with relationship problems.
244. management o f these conditions (Table 41 :).
Statistically, there was no significant difference between the responses o f the GPs and FPs
Pediatric conditions
Child with a rash
Child with a cough
7-year old child with enuresis
8-year-old child with impaired hearing
Table 41: Conditions with Similar Responses by FPs and GPs General
conditions 70-year-old man with joint pain 75-yea- woman -- moderately forgethi 29-year-old man with low back pain
Mental illness
45 -year-o Id anxious man
Suicidal man
52-year-man with alcoholism
for
245. Family physicians were more l ikely than GPs to manage several conditions, a result o f more broadly based training with an emphasis on the psycho-social model o f care. There was a statistically significantly difference for management o f (a) a 35-year-old man with an ankle sprain (p < 0.05); (b) a 29-year-old man with a first convulsion (p < 0.05); (c) a 13-year-old chi ld with physical abuse (p < 0.05); (d) a married couple
45
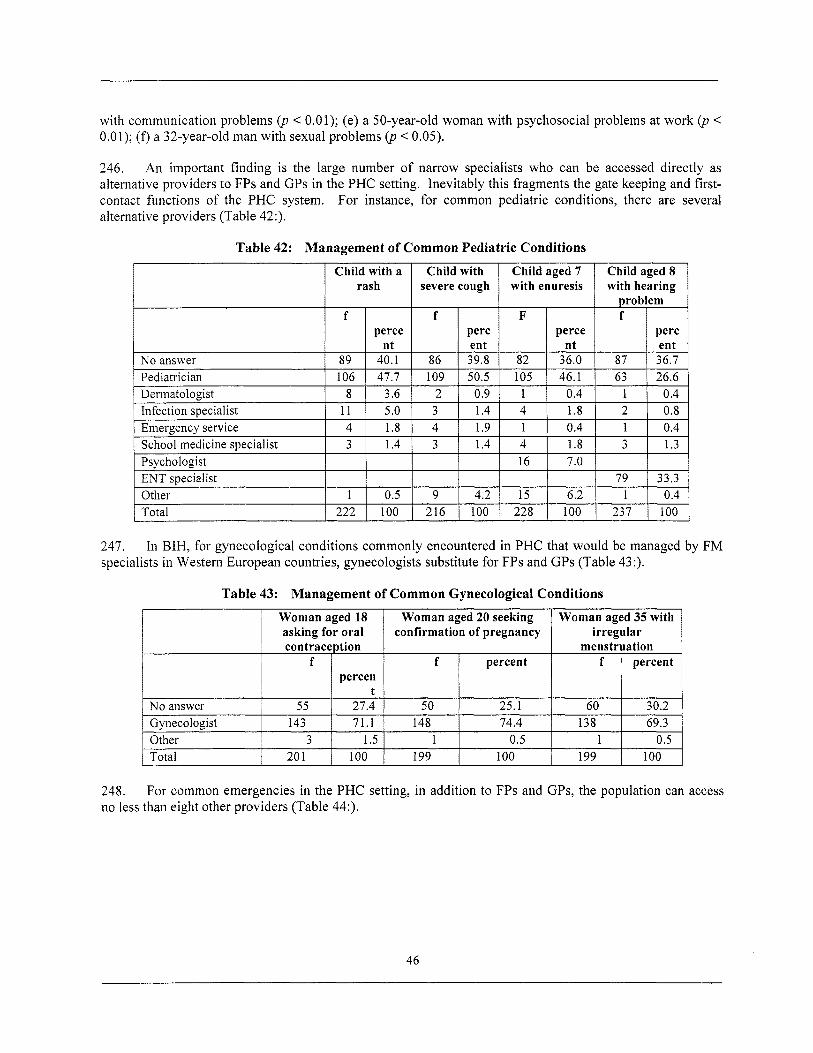
with communication problems (p < 0.01); (e) a 50-year-old woman with psychosocial problems at work (p < 0.01); (f) a 32-year-old man with sexual problems (p < 0.05).
246. An important finding i s the large number o f narrow specialists who can be accessed directly as alternative providers to FPs and GPs in the PHC setting. Inevitably this fragments the gate keeping and first- contact functions o f the PHC system. For instance, for common pediatric conditions, there are several alternative providers (Table 42:).
Table 42: Management o f Common Pediatric Conditions
247. specialists in Western European countries, gynecologists substitute for FPs and GPs (Table 43 :).
In BIH, for gynecological conditions commonly encountered in PHC that would be managed by FM
Table 43: Management o f Common Gynecological Conditions
248. no less than eight other providers (Table 44:).
For common emergencies in the PHC setting, in addition to FPs and GPs, the population can access
46
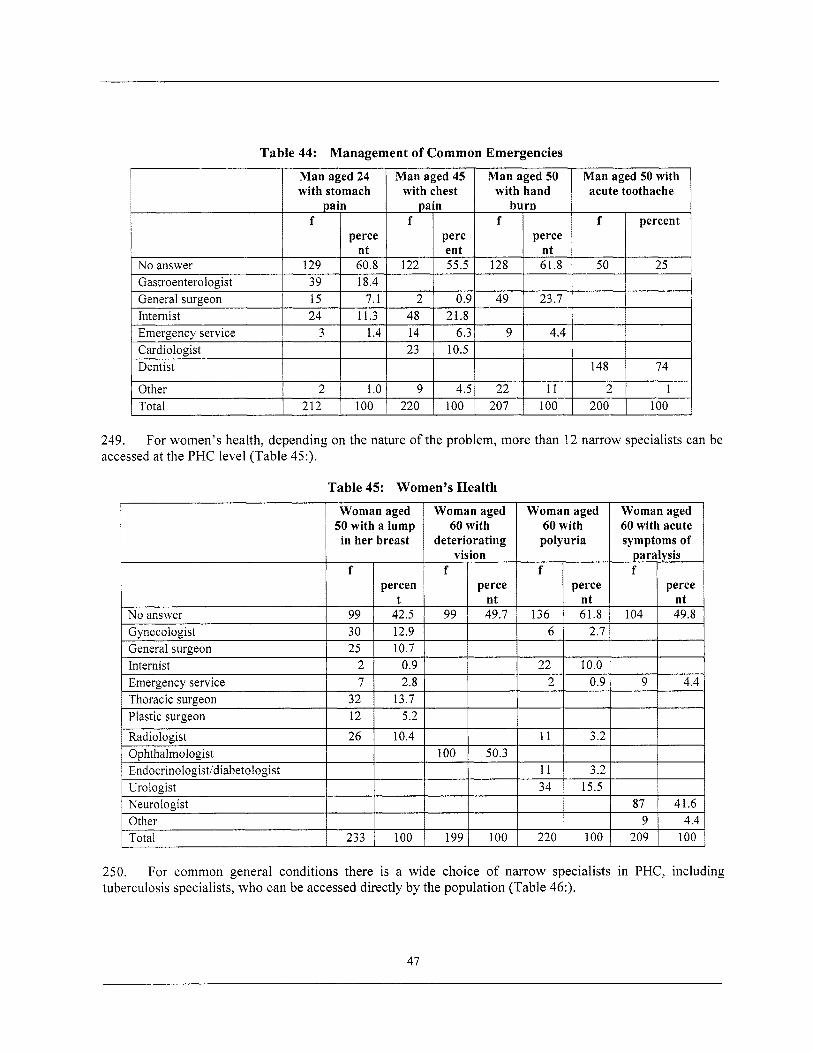
Table 44: Management o f Common Emergencies
acute toothache
Woman aged 60 with polyuria
f perce
nt 136 61.8
249. For women’s health, depending on the nature o f the problem, more than 12 narrow specialists can be
Woman aged 60 with acute symptoms of
paralysis f
perce nt
104 49.8
accessed at the PHC level (Table 45:).
Table 45: Women’s Heal th
No answer Gvnecologist
Woman aged Woman aged 50 with a lump in her breast deteriorating
60 with
vision f f
percen perce t nt
99 42.5 99 49.7 30 12.9
Internist 2 1 0.9 1 - -
Thoracic surgeon Plastic surgeon
I I I I 1 Radiologist I 26 I 10.4 I
32 13.7 12 5.2
Ophthalmologist 1 100 I 50.3
Neurologist Other Total
6 1 2.7 1
233 100 199 100
22 I 10.0 I I I I
2 1 0.9 1 9 1 4.4
I I I
11 I 3.2 I
11 I 3.2 1 34 1 15.5 I ~1 220 100 209 100
250. tuberculosis specialists, who can be accessed directly by the population (Table 46:).
For common general conditions there i s a wide choice o f narrow specialists in PHC, including
47
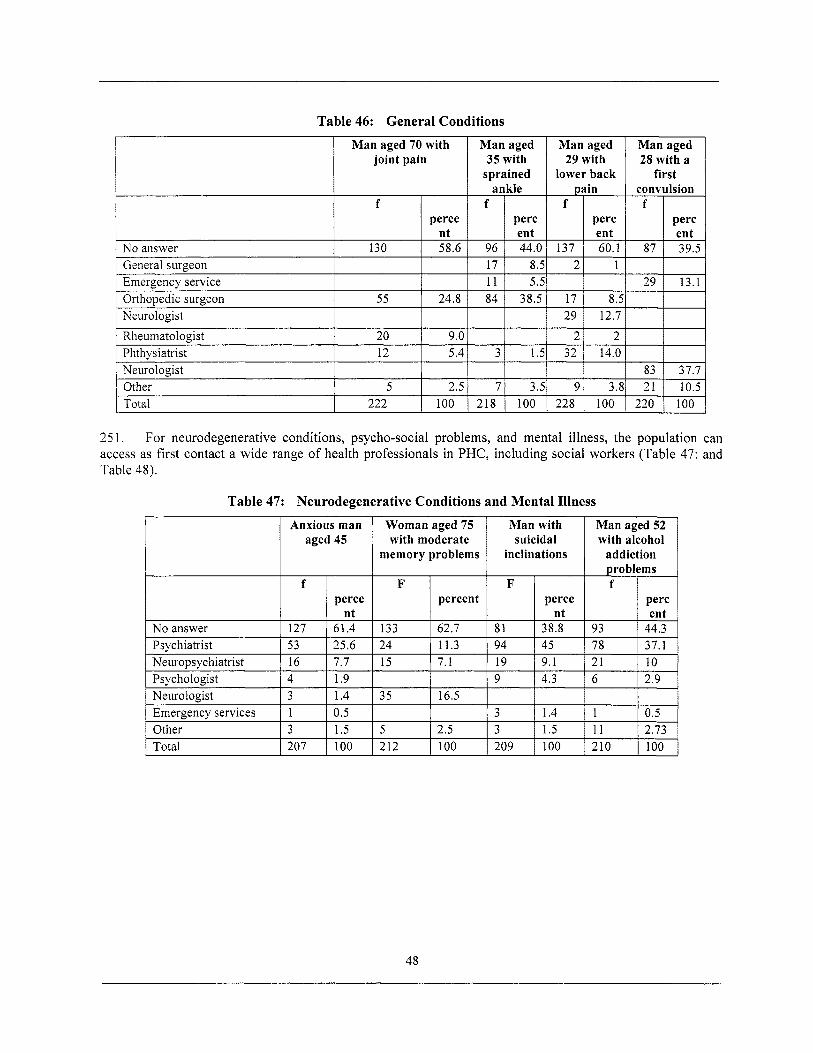
Table 46: General Conditions
No answer
M a n aged 70 with joint pain
f perce
nt 130 58.6
Orthopedic surgeon Neurologist
Rheumatologist
I General surgeon I I
55 24.8
20 9.0
1 -Emergency service I I
v
Other Total
5 2.5 222 100
1 Phthysiatrist I 12 I 5.4 1 Neuroloeist I I
M a n aged 35 with
sprained ankle
I perc
M a n aged 29 with
lower back Dain
1 perc
~
12.7
Man aged 28 with a
first convulsion
25 1. For neurodegenerative conditions, psycho-social problems, and mental illness, the population can access as f i r s t contact a wide range o f health professionals in PHC, including social workers (Table 47: and Table 48).
Table 47: Neurodegenerative Conditions and Mental Illness
48
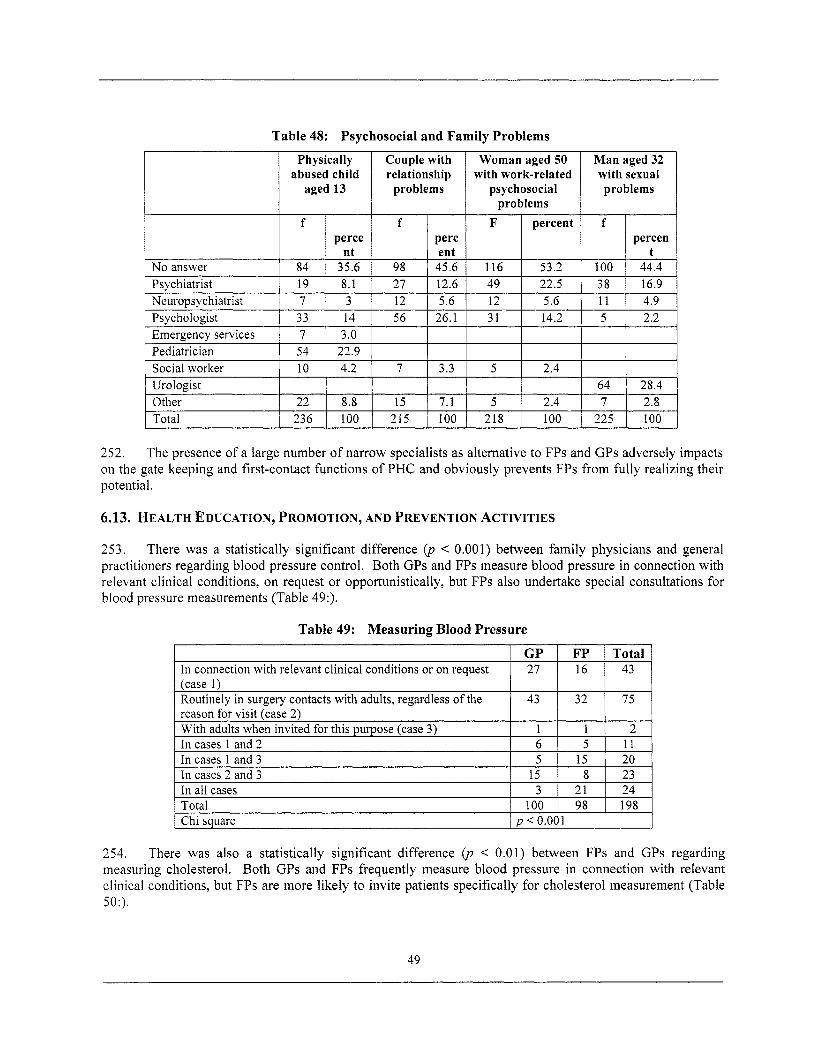
Table 48: Psychosocial and Family Problems
Routinely in surgery contacts with adults, regardless o f the
With adults when invited for this purpose (case 3) reason for visit (case 2)
In cases 1 and 2 In cases 1 and 3 In cases 2 and 3 In all cases Total
1 Chi sauare
abused child aged 13
43 32 75
1 1 2 6 5 11 5 15 20
15 8 23 3 21 24
100 98 198 D < 0.001
I 1 perce nt
No answer 84 35.6 Psvchiatrist 19 8.1 Neuropsychiatrist 1 7 I 3 Psychologist 1 33 j 14 Emergency services I 7 1 3 .O - - I
Pediatrician 1 54 22.9 Social worker 1 10 4.2 Urologist I I - Other 22 8.8 Total 236 100
Couple with relationship
problems
27 I 12.6
I
lit;i 215 100
Woman aged 50 with work-related
psychosocial problems
percent
22.5
218 100
M a n aged 32 with sexual problems
percen
16.9
64 I 28.4
252. The presence o f a large number o f narrow specialists as alternative to FPs and GPs adversely impacts on the gate keeping and first-contact functions o f PHC and obviously prevents FPs from fully realizing their potential.
6.13. HEALTH EDUCATION, PROMOTION, AND PREVENTION ACTIVITIES
253. There was a statistically significant difference (p < 0.001) between family physicians and general practitioners regarding blood pressure control. Both GPs and FPs measure blood pressure in connection with relevant clinical conditions, on request or opportunistically, but FPs also undertake special consultations for blood pressure measurements (Table 49:).
Table 49: Measuring Blood Pressure
I GP 1 FP I Total In connection with relevant clinical conditions or on request I 43
254. There was also a statistically significant difference (p < 0.01) between FPs and GPs regarding measuring cholesterol. Both GPs and FPs frequently measure blood pressure in connection with relevant clinical conditions, but FPs are more l ikely to invite patients specifically for cholesterol measurement (Table 50:).
49
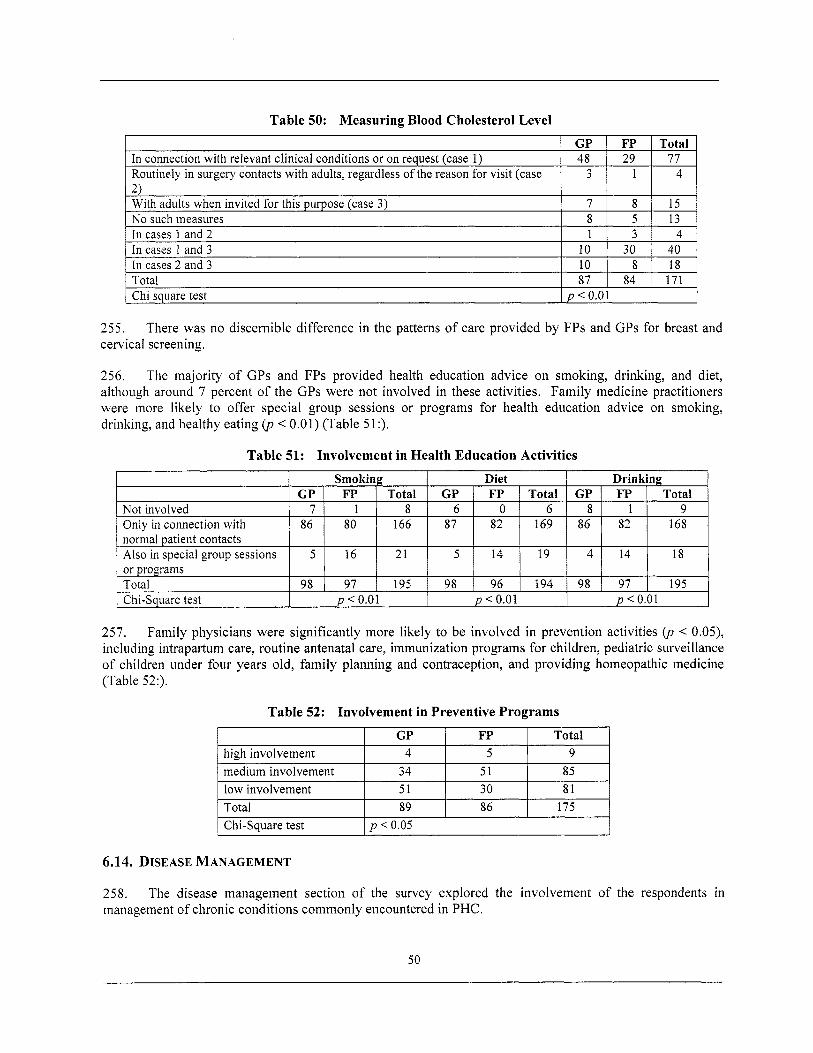
Table 50: Measuring Blood Cholesterol Level
In connection with relevant clinical conditions or on request (case 1) Routinely in surgery contacts with adults, regardless o f the reason for visit (case 2) With adults when invited for this purpose (case 3) No such measures In cases 1 and 2 In cases 1 and 3 In cases 2 and 3
GP FP Total 48 29 77
3 1 4
7 8 15 8 5 13 1 3 4
10 30 40 10 8 18
Total I 87 I 84 I 171 I p < 0.01 Chi square test
255. cervical screening.
There was no discernible difference in the patterns o f care provided by FPs and GPs for breast and
256. The majority o f GPs and FPs provided health education advice on smoking, drinking, and diet, although around 7 percent o f the GPs were not involved in these activities. Family medicine practitioners were more l ikely to offer special group sessions or programs for health education advice on smoking, drinking, and healthy eating (p < 0.01) (Table 5 1 :).
Table 51: Involvement in Health Education Activities
257. Family physicians were significantly more likely to be involved in prevention activities (p < 0.05), including intrapartum care, routine antenatal care, immunization programs for children, pediatric surveillance o f children under four years old, family planning and contraception, and providing homeopathic medicine (Table 52:).
Table 52: Involvement in Preventive Programs
Total high involvement medium involvement low involvement 51 30 Total 89 86 175
I Chi-square test I p < 0.05 I
6.14. DISEASE MANAGEMENT
258. management o f chronic conditions commonly encountered in PHC.
The disease management section o f the survey explored the involvement o f the respondents in
50
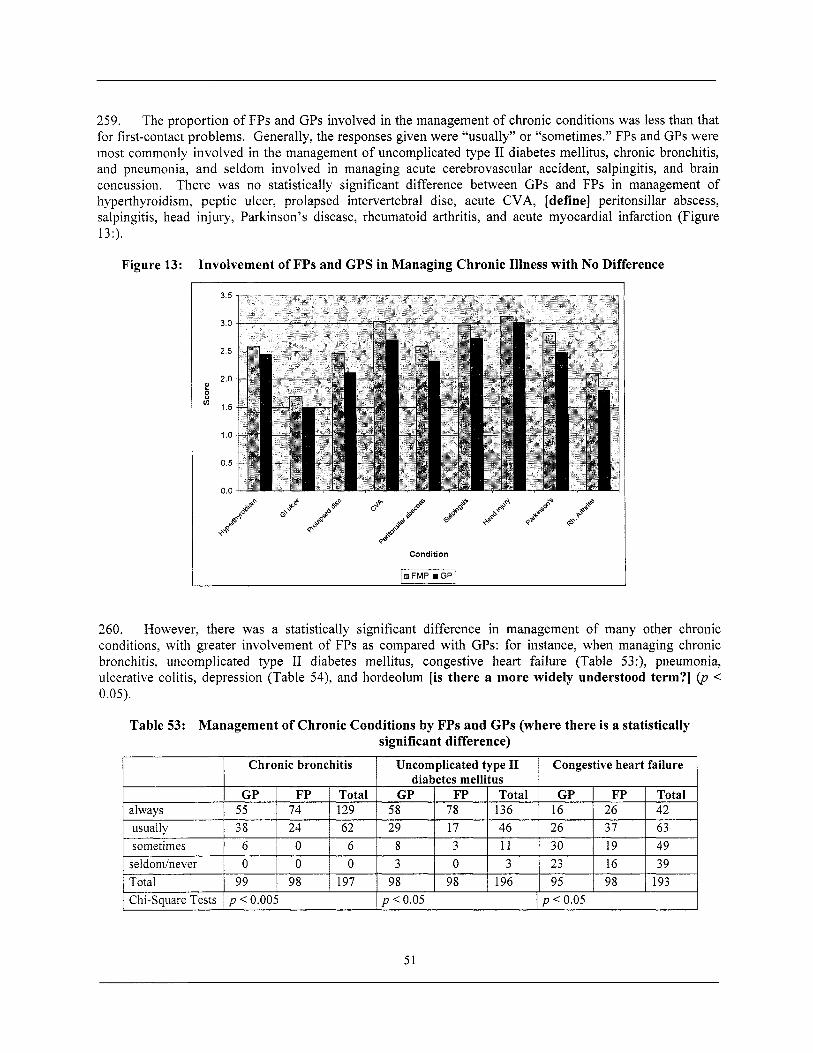
259. The proportion o f FPs and GPs involved in the management o f chronic conditions was less than that for first-contact problems. Generally, the responses given were “usually” or “sometimes.” FPs and GPs were most commonly involved in the management o f uncomplicated type I1 diabetes mellitus, chronic bronchitis, and pneumonia, and seldom involved in managing acute cerebrovascular accident, salpingitis, and brain concussion. There was no statistically significant difference between GPs and FPs in management o f hyperthyroidism, peptic ulcer, prolapsed intervertebral disc, acute CVA, [define] peritonsillar abscess, salpingitis, head injury, Parkinson’s disease, rheumatoid arthritis, and acute myocardial infarction (Figure 13:).
Figure 13: Involvement o f FPs and GPS in Managing Chronic Illness with N o Difference
Condition
-1
260. However, there was a statistically significant difference in management o f many other chronic conditions, with greater involvement o f FPs as compared with GPs: for instance, when managing chronic bronchitis, uncomplicated type I1 diabetes mellitus, congestive heart failure (Table 53:), pneumonia, ulcerative colitis, depression (Table 54), and hordeolum [is there a more widely understood term?] (p < 0.05).
Table 53: Management o f Chronic Conditions by FPs and GPs (where there i s a statistically significant difference)
51
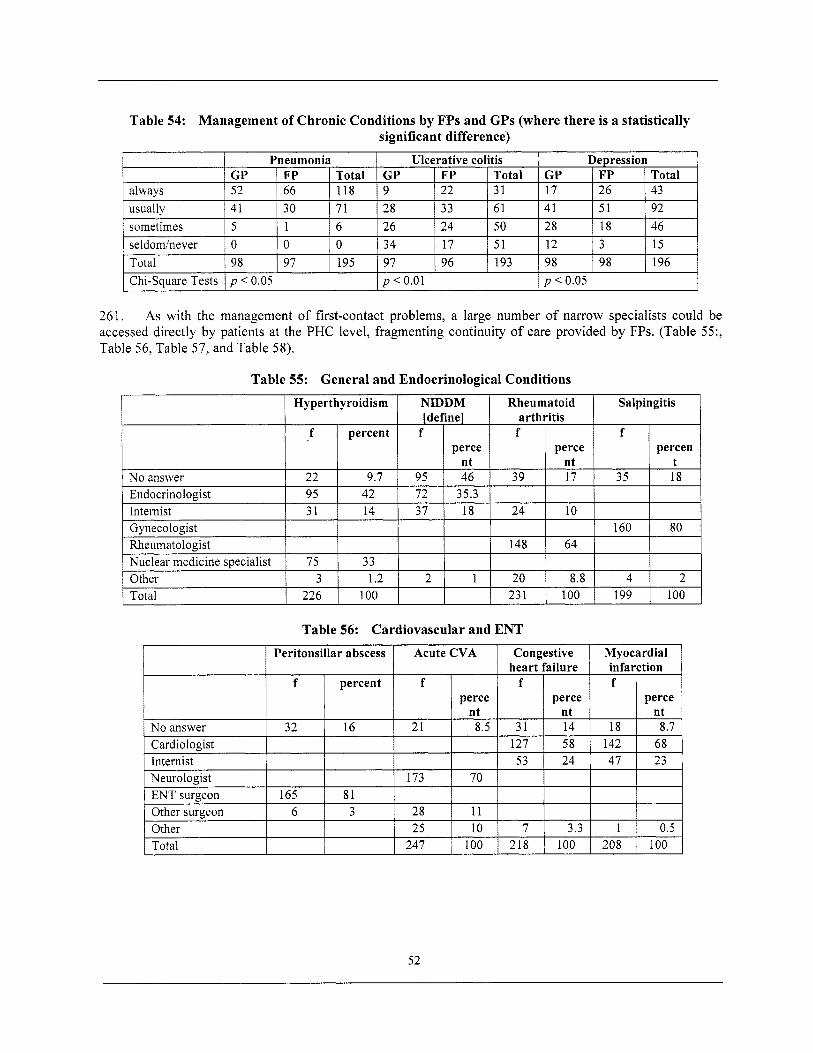
Table 54: Management of Chronic Conditions by FPs and GPs (where there i s a statistically significant difference)
I Chi-square Tests I p < 0.05 I p < 0.01 1 p < 0.05 I
Rheumatologist 148 Nuclear medicine specialist 75 33 Other 3 1.2 2 1 20 Total 226 100 23 1
261. As with the management o f first-contact problems, a large number o f narrow specialists could be accessed directly by patients at the PHC level, fragmenting continuity o f care provided by FPs. (Table 55:, Table 56, Table 57, and Table 58).
64
8.8 4 2 100 199 100
ENT surgeon 165 81 Other surgeon 6 3 28 11 Other 25 10 7 Total 247 100 218
3.3 1 0.5 100 208 100
52
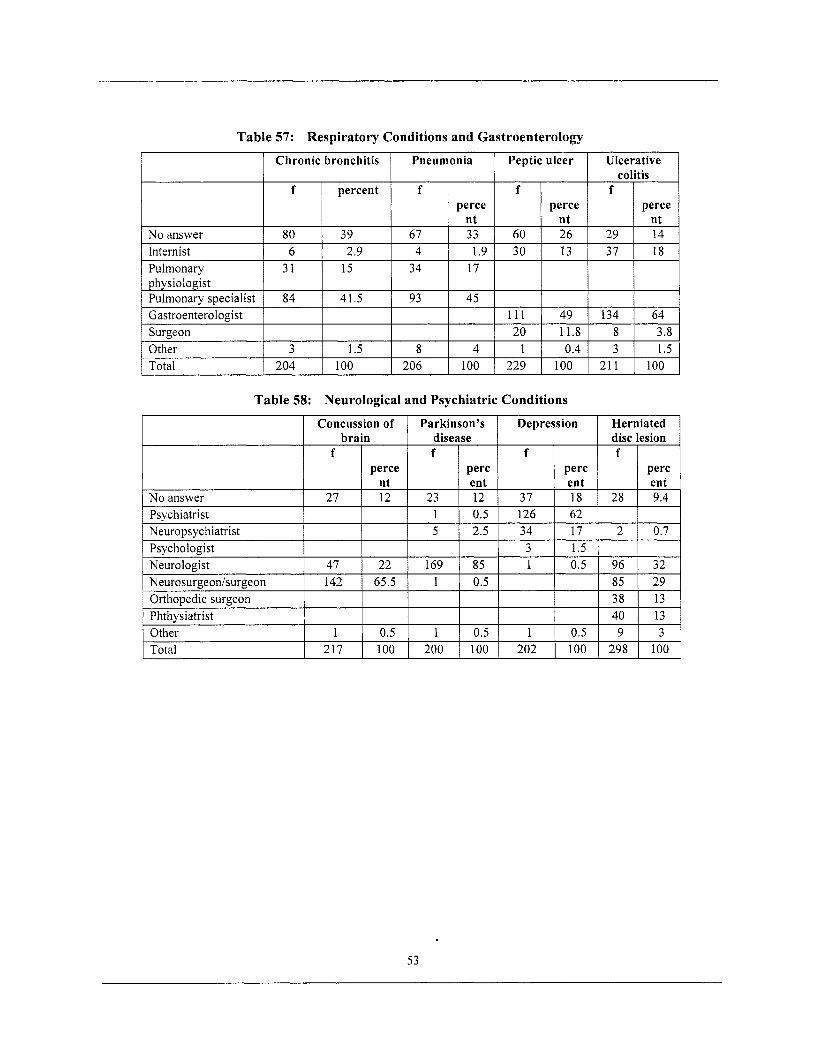
Table 57: Respiratory Conditions and Gastroenterology
I Chronic bronchitis I Pneumonia I Peptic ulcer I Ulcerative 1
Other
I ~ percent
3 1.5
No answer 80 1 39 Internist 6 2.9 Pulmonary physiologist ~ :: 1 :l.5 Pulmonary specialist Gastroenterologist
Total I 204 I 100
perce
1.9 34 17
93 45 I I 111
206
perce nt 26 13
49 11.8 0.4
100
f
29 37
134 8 3
21 1
perce nt 14 18
64 3.8 1.5
100
Table 58: Neurological and Psychiatric Conditions
53
7. FINDINGS OF THE QUALITATIVE RESEARCH
7.1. PERCEIVED BENEFITS OF FM
262. Most o f the respondents interviewed felt that family medicine was beneficial to the users, health professionals, and the health system. Perceived benefits for the users most frequently cited by the respondents included, “improved access to the system,” “improved doctor-patient relationship,” “an increased individual responsibility for the health professionals towards the user,” and “a respect for one’s time.” Greater emphasis on holistic health care, health promotion, and prevention activities were cited as distinct advantages o f FM.
263. Family medicine was seen to be a “more human friendly health care model” with a “holistic approach to population’s health needs,” which gave the users simultaneously more “choice” and “responsibility with health decisions.” The family orientation o f the model allowed “personal problems to be seen in a broader context.”
264. Perceived benefits for the health professionals included a “more meritocratic payment system” with introduction o f “performance related pay,” which created “an opportunity for promotion o f those who perform well.’’
265. cost-effective” and introduced “gate keeping” to reduce unnecessary hospitalizations.
Health system benefits included improved productivity, as FM was seen to be “more rational and
ZI.1. Empowering the Health Professionals
266. and an opportunity to exercise more control over their professional duties, which motivated them.
A key perception o f the respondents was that FM gave more responsibility to the heath professionals
“Now doctors know that their destiny i s in their hands.” (FI-9, MoH)
“In the old system nurses did most o f the administrative tasks and there were just a few clinical services provided directly to the patients. N o w , . . they talk to patients, seek to identify problems, and perform clinical procedures.” (RSI-2, Project Coordination Unit/Ministry o f Health (PCU/MOH))
Empowering health professionals helped improve performance by increasing self-esteem, morale, and 267. confidence:
‘‘After two years o f training we updated our knowledge ... developed new treatment skil ls, but the most importantly we now feel much more confident to apply these.” (RSI-14, Clinician)
7.1.2. “Broadening the Skill Base”
268. increased efficiency o f daily work and a boost in confidence - as one nurse remarked:
The FM model was seen to have expanded the knowledge and skill base o f health professionals, with
“With the new model we had to upgrade our knowledge and improve our clinical and communication skills. With now have a completely new type o f nurse: more advanced, more confident and efficient.” (FI- 1 1, FM Nurse)
269. These sentiments were echoed by doctors:
54
“Not to mention the ski l ls that we have gained; we had the knowledge, but we lacked some practical and communication ski l ls. N o w we have made great improvement and get great satisfaction from managing our patients.” (FI-4, FM Doctor)
However, concerns were expressed by a DZ director that broadening the responsibilities o f family medicine specialists may adversely affect quality o f services:
“FM model deals with a very wide area o f medical knowledge and I am afraid that not many o f my peers will be able to cope with this demand and manage to perform accordingly.” (FI-6, DZ Director)
7.1.3. “Team work”
270, among health professionals, which enhanced quality and efficiency o f services:
Most respondents felt that the FM model promoted development o f teams with increased cooperation
“Teamwork i s also one o f the greatest things; Now.. .the doctor can just concentrate on the medical work, which helps effectiveness and efficiency o f the team’s work.” (RSI-2, PCU/MOH)
“There i s a big change in the functioning o f the teams; we now work as real teams, al l o f us: doctors, nurses and patients. There i s good co-operation and that helps to deliver better quality services”, (FI- 1 1, FM Nurse)
7.1.4. Improved Communication
27 1. a key benefit o f the FM reforms.
Improved communication between FM team members and between doctors and patients was noted as
“We have learned new communication techniques to use when we are with the patients, to show a friendlier and accessible face and the patients are really thri l led about that.” (FI-3, FM Doctor)
7.1.5. “Transforming Roles”
272. transformation in the role o f doctors at the PHC level:
Probably the most important change noted with the introduction o f the new model was the
“In the old system there was general practice without really any practice. The GP in the previous system only used to refer patients to the other specialists. But now doctors in FM, with the new education, can solve over 80 percent o f the clinical problems.” (FI-13, Clinician - Professor in Medical Depart.)
273, develop their competencies to provide quality service to their patients. They felt more valued:
This evolution o f roles motivated doctors to actively become involved in the new model and further
“GPs in the o ld system had a similar role to that o f a railway traffic controller. They used to simply divert patients to specialists; who, in reality, provided treatment services to patients. In that way we were just bypassing GPs.” (FI-9, CMOH)
“In the new model, the doctor i s not someone who just f i l l s in prescriptions, or just refers patients to the hospital.” (FI-8, FMOH [define])
55
7.1.6. Sensitivity to User Needs
274. Many interviewees acknowledged that the new model was user-friendly and more beneficial to users than to health professionals. The new system provided an incentive for health professionals to be more sensitive to the quality o f services they provide to users: a shift in line with the changing expectations o f the population and valued, as it encouraged greater involvement o f the users in the health promotion process:
“Now they are face to face, eye to eye with patients and each patient now expects a proper explanation and a proper treatment: and I say proper, not simply a good one.” (RSI-14, Clinician)
“The new approach (model) i s better for the patients, because they can choose the doctor, or team depending if they are satisfied with the quality o f the doctor, the quality o f the nurses, the organization o f the whole service, for example if they do not have to wait for long time to receive the service they require.” (FI-8, FMOH)
7.1. Z “Choice”
275, position o f patients in the system and helped drive forward the reform process:
The ability o f patients to choose their doctor was seen as a revolution, which strengthened the
“If patients are not satisfied with the service, or the doctor’s knowledge they can change their doctor after one year. Many doctors, who are not competent, will lose patients and subsequently money.” (FI-8, FMOH)
“The most innovative thing with FM model i s the fact that patients can choose where to go, they have the opportunity to choose their own practitioner.” (FI-5, DZ Director)
Many respondents identified that with the FM model patients feel a vital component o f the system and are willing to actively participate in further development o f the model and reforms.
“This i s the f i rst time that patients can actually choose their own doctors and it i s one o f the key elements that will enable the reform to move forward.” (FI-9, CMOH)
Z1.8. Economic Benefits
276. and socio-economic situation in the country were acknowledged by most o f the informants:
The benefits t o the wider macro-environment and appropriateness o f the model to the current political
“Our political structures have backed the model, as we are now a poor country and poor countries do not have money to waste. So, the system must become rational and optimal and FM model i s more efficient without duplications.” (RSI-11, GP)
Z1.9. Improving the Image and Quality of PHCServices
277. quality:
Introduction o f guidelines for FM teams was identified as a positive development for improving
“There are guidelines for every illness and I don’t need to have everything in my head, I can check everything on my computer. My service has now definitely more quality than before, I have more confidence, I feel more certain with what I do and patients can feel that too.” (FI-I, FM Doctor)
56

7.2. BARRIERS TO CHANGE
7.21. Resistance from Users and Heal th Professionals
278. Two sources o f resistance were identified: f rom users (patients) and from professionals.
279. Resistance from the users was attributed to “reluctance,” “inadequate information,” “fear o f the unknown,” “habit,” and even the “shock o f change.” The views expressed by a GP from RS and a FM specialist from FBIH are shared many o f the respondents:
“People are not well-informed, they fear the unknown and don’t want changes.” (RSI- 1 1, GP)
“Patients are s t i l l not ready and are reluctant about the new reforms and the new doctors. They s t i l l don’t fully accept the nurse as an equal member o f the FM team, and s t i l l have not got rid o f the old habit o f visiting many clinicians - they don’t like to be limited to just one doctor.” (FI-IO, FM Doctor)
280. Considerable resistance was noted to be coming from pediatricians, gynecologists, and to a lesser extent hospital specialists, and attributed to their perception that the change had been “imposed” and to their “fear o f the unknown”:
“People didn’t accept it, because they thought it was being imposed. People are afraid o f changes and new things.” (RSI-10, Nurse)
“Habit,” “culture,” adherence to “routine,” and insecurity due to “uncertainty” were quoted frequently as roots o f resistance. The majority o f informants identified “close-minded‘’ and “self-interested” professional groups as the main source o f resistance, worsened by a “lack o f adequate information” and even provision o f “wrong information”:
“It i s inherent in human nature to oppose anything new: as people are used to the previous system that has become a habit and a routine and don’t l ike something new as it requires additional effort to adapt to it and i s associated with uncertainty.. .some people obstruct as they have a personal interest and with the new situation will lose privileges.” (FI-12, HIF)
28 1. were cited as reasons for resistance from clinicians but also the mangers:
“Threat” o f loss o f “existing status,” “power base,” “authority,” and the need for “additional effort”
“We had resistance, people were skeptical, especially the management o f DZ, as in the new system they w i l l lose the authority and the money which they manage today.” (FI-8, CMOH)
The reform challenges the status quo. N e w opportunities emerge, especially for the young, while the older participants are threatened as they feel less able to adapt to the new circumstances:
“One o f the obstacles to the process may be old doctors, because they are too old to learn.” (FI-8, FMOH)
“There was a lot o f resistance at the beginning, mainly due to ignorance, but then, when people became familiar they got involved. Among doctors the youngest accepted it wel l as they saw a better chance with a new system.” (RSI- 10, Nurse)
57
The threat to “job security” was the most commonly quoted reason for resistance to implementing the FM model:
“, . .people f rom the secondary and tertiary levels fear that as PHC level strengthens they wil l probably lose their j o b ... they were the rulers in the system and don’t want to lose that position and power.” (RSI- 1 1, GP)
282. Resistance was unpredictable and often concealed:
“Resistance i s often invisible, but somewhere it exists, hidden behind corners.” (RSI-13, GP)
“Suddenly we were exposed to the fire coming from the management board o f that institution; tremendous resistance was coming from the specialists working at PHC and secondary levels. They just don’t understand what i s going on in the system and they are protecting their vested interests” (RSI-2, PCU/MOH)
283. content:
A few respondents expressed a negative attitude toward the reforms as they didn’t believe in the
“It i s reasonable to believe that one man cannot know everything; there should be teams with skills.” (RSI-9, Clinician)
7.3. CRITICAL SUCCESS FACTORS
Z3.1. “Branding and Image Building”
284. by many respondents:
The need to improve the status o f FM doctors as compared with narrow specialists was emphasized
“The view o f population regarding GPs i s that they are not real doctors; the real doctors are in the secondary and tertiary levels. This belief undermines the real value o f FM doctors and their reputation and it i s an impediment to the expansion o f the model.” (RSI-11, GP)
285. remuneration:
Therefore, it was felt necessary to signal that FM i s valued, for instance, through financial
“If you want to change the status o f the FM doctor, you could pay FM doctors 5,000 KM salary and hospital specialists 2,000 KM. This would automatically change the status o f the two categories o f doctors, and people would respect FM doctors more.” (FI-6, DZ Director)
Z3.Z. Tmproved Work Environment”
286. reforms and acceptance o f the new model:
Improvements in working conditions o f the FM teams were seen as critical to the success o f the
“Just the knowledge i s not enough, without the necessary equipment one cannot work.. .refurbishing ambulantas and new equipment have greatly helped.. .even patients realized the change and they really l ike it.” (FI-14 FM Doctor)
“We have, for the first time, fully equipped FM teams, an evolution that makes people much more happy and willing to work under such conditions.” (RSI-22, FM Doctor)
58
7.3.3. Effective Comm unica tion
287. Communication was identified as a key factor for successful introduction and diffusion o f the F M :
“We recognized at the beginning that it i s absolutely necessary to include in the [FM] project a sub- component o f communication.” (RSI-2)
The “media,” especially the “local media” for active dissemination o f the model to the wider public, “interpersonal contacts,” “peers,” and “high-profile senior people” were identified as the main ways for effective communication:
“The actual problem was that they didn’t spread the word to their colleagues. So, just we, the early adopters o f FM were the promoters o f the new model.” (FI-4, FM Doctor)
“After providing some information to people, you can see how questions become more precise and to the point.” (RSI-2, PCU/MOH)
288. cited as a critical problem:
A lack o f communication between and within levels o f the health system and with the public was
“There are no official communication procedures in place between FM doctors and the secondary level and no official referral system; the communication among teams in the same DZ i s insufficient.”(FI- 10, FM Doctor)
“The communication between the [medical] faculty, the ministry [o f health] and the health insurance fund i s not very good; it appears that they are detached.” (RSI-19, PHI)
289. model was successfully implemented in Laktasi, RS:
The presence o f an effective communication strategy was cited as one o f the reasons why the FM
“In Laktasi, the promotion campaign o f the new model was really very good. They visited almost every family in the municipality and individually informed them about the new model. In Banja Luka people s t i l l do not know many things about the FM concept, and this i s a problem. I t i s obvious now that the promotion o f the model in Laktasi was successful. But we don’t have any promotion activity here in Banja Luka at all.” (RSI-14, Clinician)
Z3.4. “Speaking the Same Language”
290. objectives and shared values on FM reforms as an issue that needed to be addressed:
Many respondents cited “misunderstanding” or “lack o f understanding” o f the terminology,
“Our previous director didn’t have an understanding about our efforts and the scope o f the [FM] reform, as with many o f our colleagues and especially those working in hospitals, who do not understand our role.” (FI-4, FM Doctor)
Z3.5. “Holistic Approach to Reform”
291. Many informants stressed the need for a holistic approach to the reform that was comprehensive in scope, communicated a clear strategic vision, had a balanced management o f various stakeholders, and adopted a pragmatic approach to implementation. As one GP from the RS commented:
59
“I clearly said it f rom the very beginning that it i s not a good idea to do this [reform] in segments ....... If medicine i s separated to eyes, nose and legs then we lose the entity: we lose the person.” (RSI-11, GP)
292. The importance o f inter-sectoral collaboration and aligning institutions involved in policy development to share the same strategic direction was passionately highlighted by a clinician:
“The problem i s wider [than health sector], The Ministries o f Education and Health have no co- operation at all. So, we are currently producing some vague kind o f doctors who as students are trained mainly at the clinical centre [tertiary level]. . . I t i s l ike we are s t i l l producing the old fashioned car Yugo45; without ABS system, without air conditioning, without the innovations that took place in the car industry. But the new concepts and the new needs in our lives demand a completely new car, which is faster, safer, and more comfortable. And we are s t i l l producing the o ld car.” (RSI-14, Clinician)
7.3.6. “Developing Trust’’
293. family physician:
The importance o f developing trust was seen as a critical f i rs t step in reform, as commented by a
“The development o f a good and trustful relationship with patients i s crucial ... for success o f reforms.” (FI-14, FM Doctor)
Z3. 7. c‘Bottom Up Versus Top Down: Engaging the Operational Level and Creating Ownership”
294. There was a commonly shared view that the engagement o f frontline staff (those most affected by the reforms) was the most critical factor impacting the diffusion o f the FM model, but it was felt by many that in BIH there was insufficient involvement o f the operational level in the reform process:
“So far, we have mainly been just objects o f the reform: not agencies that implement it. Therefore, the results o f the reform initiatives are not in accordance with the real needs in the field.” (RSI-3, DZ Director)
“Usually all the proposals come l ike orders from the top, instead o f having proposals from FM teams.. . . . . . They s t i l l don’t think that we are serious partners.” (RSI-21, DZ Director)
7.4. UNDERSTANDING THE CONTEXT
7.4. I. “Con text Matters”
295. Most informants expressed the view that the war and i t s consequences resulted in an inherently complex reform context and the FM model in the pilot sites was profoundly influenced by the immaturity o f the political system and broader contextual factors:
“FM reform i s very complex because it i s very diff icult to have a complete agreement o f all the actors involved in the system.” (FI-19, FMOH)
“We are an immature society: a vulnerable society. Democracy here has a different meaning to that in the UK or other European countries.”(RSI- 14, Clinician)
60
296. cooperation were identified as reasons for inconsistent policy implementation, especially in the FBIH:
Deficiencies in administrative and governance systems, and inadequate inter-cantonal and inter-entity
“Dayton agreement created a country with two entities and ten cantons in one o f the entities. Health policy was delegated to cantonal level in the Federation. It i s diff icult t o develop policies which can embrace al l these peculiarities.” (FI- 19, FMOH)
“We haven’t got exact data to inform policy, as the administrative system in the Federation i s very complicated. There are 10 Cantons and 11 different [health insurance] Institutions. Each follows different reporting practices.” (FI-7, HIF)
“There i s no national BIH healthcare system, a fact that adversely affects the development o f FM.” (RSI-2 1, DZ Director)
7.4.1.1. “Adjusting Reforms to the Local Context”
297. circumstances to increase ownership rather than replicating a model imported from other settings:
Many informants pointed out that the adoption the new model was enhanced by adjusting it to local
“We adjusted the model to local needs: that o f the patients. You cannot apply exactly the same model everywhere; you have to adjust it to people you are working with, the area and the needs o f the local population.” (FI-5, DZ Director)
298. The introduction o f the model in Laktasi municipality was cited as a creative example o f how adjustment o f the model to the local context made it more attractive to the specialists, thereby reducing resistance, improving ownership, and accelerating adoption:
“The creativity and abilities o f the director in the particular DZ managed to find a solution to this problem. So, now in Laktasi the system has been adapted to the local needs.” (RSI-14, Clinician)
299. Many informants pointed out to the dangers o f directly replicating models from other countries:
“People who worked o n the [FM] project went to Canada, saw the system there and wanted to literally copy it and transfer it to our system. But they forgot an important dimension: the GDP in that country i s 15-20 times higher than here.” (RSI-18, HIF)
7.5. UNDERSTANDING STAKEHOLDER NEEDS
300. Understanding stakeholders and their expectations i s critical to successfully managing them.
7.5.1. ‘‘Cultural Issues”
301. the introduction o f FM was highlighted by al l key informants.
The importance o f national, local, and professional cultural factors and peer recognition influencing
“If we were Germans or Japanese, it [the FM reforms] would probably have been done sooner, as people from these countries always stick to regulations, it i s part o f their culture. But here we allow people to think, to use their heads and their hearts and therefore, the process takes more time and requires patience.” (RSI-11, GP)
61
“The failure we encountered when introducing the new model in [one] region was due to the mentality o f the people there - where it i s hard to promote new ideas and implement something new in an environment where people s t i l l l ive in the 17th or 18th centuries. They don’t recognize the new age - new things promoted in Western countries 50 or 100 years ago.” (RSI-2, P C U Director)
302. example:
There are traditions that prevail among patients in BIH which need to be taken into account, for
‘‘. . .as regards provision o f gynecological services, we need to bear in mind the tradition [of women going to gynecologists]. . .” (RSI-22, FM Doctor)
7.52. ‘Clncentives Matter”
303. highlighted by many respondents as critical to encourage trial and adoption o f the new model:
Understanding needs o f the stakeholders enables promotion o f reforms with appropriate incentives -
“YOU have to stimulate people.. .not only talk about reform but provide support in the field.” (FI-11, FM Nurse)
“Doctors now have an FM department.. .[and] know that there i s a possibility o f becoming a professor - this means FM has become a profession.” (RSI-13, GP)
“As a director, I provided money for the development o f satellite ambulantas, because I believe that you have to stimulate people to make them accept something.” (FI-5, DZ Director)
304. The pi lot financing scheme and quality accreditation were considered by many as incentives:
“There i s [now] an incentive to attract more patients and for FM teams to upgrade their skills.” (FI-8, FMOH)
7.6. MANAGING STRATEGIC CHANGE
7.6.1. 46Transformation Versus Incremental Change”
305. There were contrasting views on the change approach associated with reforms. Some respondents expressed the view that an incremental approach, building on past strengths, was appropriate; in contrast, others supported a rapid and transformational change:
“We are trying not to destroy everything from the old model, but rather to keep what was good in the old system and bring that into the new model.” (FI-20, DZ Director)
“. , . [reform] requires patience and takes time. W e should not try to jump too far, too quickly.” (RSI- 11, GP)
“I personally expected more radical changes from the very beginning, we lost time (pauses) three years have passed and we are sti l l , more or less, at the same level.”(FI-10, FM Doctor)
Z6.2. “Using Windows o f Opportunity”
306. system as an opportunity to trigger change:
Many o f the respondents saw the post-war economic crisis and consequent problems in the health
62
“It i s not easy to implement a reform if it has not started in a crisis situation”, (RSI-13, GP)
“The diff icult economic situation we live in compelled us to introduce innovations in health system.. . to make it more rational and use the funds in the most cost-effective way to have quality services.” (RSI-20, M O H )
7.6.3. “Demonstrating Success - Quick Wins”
307. o f and securing interest in the reform:
Demonstration o f successful examples was considered to be critically important in raising awareness
“We should implement the program and bring those, who are suspicious about, it to see what it looks like [in practice]. It makes me really happy to be able to bring here any group and show them that the new [FM] model really makes a difference.” (RSI-1, DZ Director)
“The positive example o f Laktasi, to some extent Banja Luka and Doboj as wel l as some DZs in the Federation, l ike in Kladanji, have helped to change the attitude o f people.” (RSI-13, GP)
7.7. “THE ROLE OF INTERNATIONAL AGENTS”
308. Effective collaboration between international agencies involved in the health reform led to a cohesive approach to reform, catalyzed rapid institutionalization o f policies, and increased the chances o f sustainability o f the project. The role o f the international agencies, according to the majority o f the participants, was mainly the provision o f both technical and financial assistance:
“This assistance has been the most important and crucial factor for the introduction and diffusion o f the model.” (RSI-10, Nurse)
“[People] accepted the new model as it has strong support o f organizations l ike the World Bank and the World Health Organization. [Given this support] the politicians felt pressure to make some changes.” (FI- 13, Clinician -- Professor in Medical Department)
7.8. “IMPORTANCE OF NETWORKS AND EXPOSURE’’
3 09. enhanced the diffusion o f innovations:
Networking and international exposure enriched the experience o f the participating actors and
“Among the factors which enabled the diffusion o f the model was the communication with the rest o f the world; people visited other countries and saw how systems were organized and how the model worked.” (RSI- 13, GP)
“. . . importantly, the Wor ld Bank helped us to create connections with other European countries and the world-wide FM network.. . participate in conferences, exchange experiences and invite people here for lectures. This i s really very important.” (FI-13, Clinician -- Professor in Medical Department)
7.9. “HEALTH SYSTEM AS A MEANS TO MAINTAINING SOCIAL PEACE”
310. A particularly interesting finding emerging from the qualitative research was the perception o f the overwhelming majority o f informants on the “vital” role played by the health care system within the wider societal context in solving wider social problems:
63
“Politicians have always cared about social peace, but it costs a lot o f money to keep this peace. So, expensive medical examinations are performed even when not necessary.” (RSI-11, GP)
“If we are rigid with what we need to do then we wil l have riots in the streets. Social peace i s always bought at the expense o f the efficiency o f the health care system.” (FI-20, DZ Director)
64
8. KEY ACHIEVEMENTS OF PHC REFORMS
3 1 1. Within a very short time, despite a very complex post-conflict and resource-constrained environment, there have been remarkable achievements in FM/PHC reforms in both entities. There i s very strong high- level and local support for FM reforms, with significant financial contributions by cantons and municipalities - as counterpart financing - toward refurbishment o f FM ambulantas at the FM pi lot sites. This indicates strong support for the reforms and i s an encouraging signal for sustainability o f the changes introduced.
3 12. It i s important t o note that there i s an attempt to institutionalize many o f the changes introduced by the Pilot Project by developing an appropriate legal framework - creating an enabling environment for the FM centered PHC model and new financing mechanisms to be rolled out to BIH and sustained.
8.1. ORGANIZATION AND REGULATION
3 13. reforms to be sustained. For instance:
Several laws have been enacted and regulations passed to create an enabling environment for FM
(a) Family medicine i s recognized in law as a specialty.
(b) faculties o f medicine in BIH.
Chairs o f family medicine have been established and are functioning within the three o f the four
(c) The team-centered FM model has been developed and team compositions adopted in law.
(d) The scope and content o f FM services have been defined in law - this greatly extends the role and responsibilities o f the family medicine team, although this law needs to be changed in light o f the rapid development o f FM.
(e) Institutions or “indirectly” with the dom zdravjlas.
FM teams have been established and are legally able to contract “directly” with Health Insurance
314. A number o f organizational changes have been made to enhance the gate keeping function o f PHC with the FM team acting as the first point o f contact for patients - although the presence o f multiple narrow specialists at the PHC level who can be accessed directly means that the gate keeping and first-contact functions o f PHC are seriously hampered - encourage continuity, improve user-centeredness o f services, and provide a greater choice for users. For instance:
(a) Users have been given the freedom to choose their family physicians and change if they so wish.
(b) “patient-friendly” and functional PHC units.
A large number o f FM centers have been refurbished in the pi lot sites o f both entities to create
(c) model.
Appointment systems have been introduced in the PHC centers that have adopted the family medicine
(d) address serious shortcomings in the monitoring and evaluation systems.
There are initiatives to develop new electronic data collection systems in the pi lot PHC centers to
3 15. Laws have been enacted in both entities enabling the establishment o f Agencies for Accreditation and Quality Improvement for accreditation o f health care providers. With international technical assistance, these
65
agencies have developed frameworks, mechanisms, and tools for accreditation, trained assessors for accreditation, and have already undertaken accreditation o f some FM centers.
316. The L a w on Medical Chambers has enabled the establishment o f medical chambers that have the responsibility for licensing and revalidation o f a l l practicing doctors. Doctors are obliged to receive a license before they can practice but also have an obligation to undertake continuing medical education programs approved by the medical chambers before they can be revalidated.
8.2. RESOURCE ALLOCATION AND PROVIDER PAYMENT SYSTEMS
3 17. The Cantonal Health Insurance Institutions and RS Health Insurance Fund allocate a significant proportion o f their revenues to PHC. This amounts to 43 percent o f the CHI1 expenditure in FBIH and 23 percent o f the HIF expenditure in RS.
3 18. Both entities have a target o f allocating 40 percent o f the health insurance expenditures to PHC. This figure i s higher than the proportion o f health system funds allocated, o n average, to PHC by the countries in the ECA region and OECD. Allocation o f such a high proportion o f health funding to PHC indicates a strong commitment to the development o f a PHC system.
3 19. There has been significant local counterpart investment to refurbish infrastructure for FM ambulantas: for instance, the local authorities in the three pilot cantons o f the FBIH have committed higher levels o f counterpart funding than anticipated in the Credit Agreement - 77 percent in West Herzegovina, 58 percent in Tuzla, and 37 percent in Herzegovina-Neretva Canton.
320, successfully introduced in the pi lot sites.
New provider payment methods, based on simple and weighted per capita models, have been
321. Direct and indirect contracts between the CHII/HIF and DZ/FM teams have been successfully piloted - one pilot includes a performance-related pay element in addition to per capita pay. The contracts specify the scope o f services to be provided by FM teams and in include RS incentives to provide health prevention and promotion services and demonstrate increased quality through accreditation by the AAQI.
322. It i s too early to judge the effect o f new provider payment methods, but qualitative research findings suggest that new models used in the pi lot areas are perceived by key informants to be more meritocratic and transparent.
8.3. FINANCING
323. Health expenditure as a proportion o f GDP i s high by OECD and ECA region standards and certainly unusual for a country at the stage o f economic development o f BIH. There are four main problems with health systems financing: (a) highly fragmented risk-pooling in FBIH; (b) l ow tax base and an inability to capture adequately al l the citizens who should be making health insurance contributions; (c) A large population segment who are not covered by CHI; and (4) a high level o f out-of-pocket expenditures.
324. to be made to selectively reduce expenditure in the hospital sector.
It i s unlikely that such a high level o f expenditure can be macro-economically sustained. Efforts need
8.4. SERVICE PROVISION
325. significantly.
In the pi lot sites that have introduced the FM model, the scope and content o f services have expanded The task profi le survey demonstrates statistically significant difference in the breadth o f
66
preventive, first-contact, and chronic disease management services provided by FM specialists as compared with non-specialist GPs.
326. There i s strong evidence from the qualitative research that the new model i s welcomed by the users. Many o f the key informants identify benefits o f the new system for the users, such as user-centeredness o f the model; holistic approach to health and the person; emphasis on health education, promotion, and prevention; having a named doctor; user choice; more comprehensive nature o f FM model; empowerment o f FM team to increase quality; and an increased emphasis on teamwork with enhanced continuity.
327. The presence o f multiple providers as entry points at the PHC level and a large number o f narrow specialists who can be directly accessed by users are probably the greatest barriers to developing FM team- centered PHC. This issue needs to be urgently addressed.
8.4.1. Increased Emphasis on Health Education, Promotion, and Prevention
328. In the services provided by FPs, as compared with GPs, there i s a clear shift from a curative biomedical care model to one that emphasizes prevention, promotion, and holistic care. There i s empirical evidence from the study demonstrating this shift: the task profi le survey findings show a statistically significant difference in the level o f health education, promotion, and prevention activities delivered by FPs as compared with GPs. Family physicians are more l ikely to provide promotive and preventive activities and organize special sessions for health education programs on a healthy lifestyle, in particular smoking, drinking, and diet.
329. Qualitative research findings identify the provision o f health promotion, education, and prevention activities as key strengths o f the FM model and that these services are valued by users and FM providers. The emphasis on health education, promotion, and prevention i s being reinforced and institutionalized through the contracts between the HIF/HII and the FM teams. For instance, in RS, contracts between the HIF and PHC centers stipulate a penalty for failure to perform specified preventive tasks and include a bonus payment for promotion and prevention activities.
8.4.2. Management o f First-Contact Conditions
330. Both FM physicians and GPs “usually” manage many o f the common conditions encountered at PHC settings. FM physicians are more l ikely to manage some conditions as compared with GPs, with a statistically significant difference for managing (a) 35-year-old-man with an ankle sprain (p < 0.05); (b) 29- year-old man with a f i rst convulsion 0) < 0.05); (c)l3-year-old chi ld with physical abuse 0) < 0.05); (d) married couple with communication problems (p < 0.0 1); (e) 50-year-old woman with psychosocial problems at work (p < 0.01); and (f) 32-year-old man with sexual problems (p < 0.05). The findings are in line with the evidence from the study demonstrating the psychosocial approach adopted by FPs and also show that FPs provide more comprehensive care than GPs.
8.4.3. Management o f Chronic Conditions
33 1. The task profile survey shows a greater involvement o f FM specialists, as compared with GPs, in the management o f many chronic conditions. This difference in breadth o f service provision i s statistically significant for chronic bronchitis, uncomplicated type I1 diabetes mellitus, congestive heart failure, pneumonia, ulcerative colitis, depression, and hordeolum. This difference signals that the FM specialists are applying the knowledge and sk i l ls gained during their training.
67
8.4.4. Secondary to Primary Shift
332. number o f hospital admissions, or a reduction in the length o f hospital stay.
There is, as yet, no evidence to demonstrate a shift from secondary to primary level, a decline in the
333. The health information systems do not capture timely and meaningful information on referral patterns. Unfortunately, there has been no baselining or subsequent monitoring and evaluation to undertake pre- and post-intervention comparisons in pilot and non-pilot sites to ascertain the impact o f FM. Although a study from one o f the pilot sites demonstrates reduced hospital referral rates by family physicians as compared with GPs, the study size was small and design not robust enough to show any statistically significant changes.
8.4.5. Team work
334. In BIH, an F M model based on teamwork has been introduced. This i s in contrast to many countries in the region that have developed family doctor-centric PHC models. The teamwork approach i s highly valued by the members o f the FM team, who identify benefits such as improved productivity and communication.
8.4.6. Evidence-based Care Guidelines
3 3 5. This wi l l enhance quality o f care delivered and also reduce unnecessary interventions.
Evidence-based guidelines have been introduced for 20 common conditions encountered in PHC.
8.5. RESOURCE GENERATION
336. With financial assistance from CIDA and technical assistance from Queens University, the faculties o f medicine o f Sarajevo, Mostar, Tuzla, and Banja Luka universities have jointly developed two postgraduate training programs for training FM specialist in BIH: a one-year in-service training program and a three-year specialization program. Both o f these programs are o f high standards and in line with internationally accepted training programs for FM. These two programs have been approved by the Federation and RS Ministr ies o f Health and appropriate Rulebooks issued specifying the curricula in detail. Hence, for BIH as a whole, a uniform curriculum and training program for FM exists. Both o f the FM training programs (specialist and PAT) have been successfully implemented in both entities. Further, regardless o f the donor providing financing, the same curricula are used for FM training, in contrast to the period prior to the WBBHP, when varied approaches and several curricula were used in programs funded by different donors.
3 3 7 . By June 2004, 80 FM trainers had been trained and a total o f 368 health professionals (173 doctors and 195 nurses from both entities) had completed the PAT in family medicine in programs supported by Swiss Development Corporation (SDC).
338. By 2005, Queens University-supported FM specialist and PAT programs w i l l graduate 1,215 health professionals, including 410 FM specialists, 212 doctors trained in PAT, 465 nurses trained in PAT, and an additional 141 nurses trained in F M training courses.
339. students) had received education in family medicine.
As o f June 2004, 18 generations o f sixth-year medical students (representing over 750 medical
340. trained in family medicine in programs supported by MSF-Belgium, WHO, and PHARE.
In addition to the World Bank, SDC, and CIDA-supported programs, a further 85 doctors have been
68
341. population.
A critical mass o f FM teams has been established in both entities, covering 23 percent o f the entire
342. Health Management Centers have been established and fully refurbished in both entities. A cadre o f 30 trainers has been trained in a train-the-trainers program. In addition, around 150 middle- to senior-level managers have been trained in modern health management subjects (1 11 mangers in FBIH and 38 in RS).
69
9. CHALLENGES THAT REMAIN TO BE ADDRESSED
9.1. ASYMMETRY IN THE PACE OF DEVELOPMENT
343. The pace o f development in FM has far exceeded the rate at which the legislative changes have been achieved. This i s a source o f tension and anxiety for many stakeholders who wish to see acceleration o f the rate at which new laws are enacted - in particular t o (a) define the role o f the FM team in the health system and articulate more clearly the scope o f services provided by the FM team; (b) establish a legal base for the new payment mechanisms to create incentives for FM teams; (c) clarify the role o f narrow specialists at the PHC level, the boundaries with secondary care, and referral and counter-referral mechanisms; (d) resolve the confusion surrounding the rights o f citizens and the insured and (e) redefine the status o f FM teams in relation to dom zdravljas as regards contracts.
9.2. STRATEGIC PLANNING FOR SCALING U P
344. FM reforms have been rapidly introduced and now cover 23 percent o f the population. There are, as yet, no clear strategic plans that identify human and financial resources needed for scaling up the FM model, which will require significant managerial resources at the PHC, Ministry o f Health, and CHII /HIF levels. Although around 200 health professionals have been trained in health management, there needs to be rapid scale-up o f health management training to prepare a cadre o f professionals to manage change, the scale-up process, and the transition f rom pi lot status to a fully institutionalized FM model. The World Bank Health Sector Enhancement Project, expected to be approved in 2005, will support the expansion o f managerial capacity.
9.3. SERVICE PROVISION
345. The first-contact function o f PHC in BIH i s significantly compromised due to presence o f a large number o f narrow specialists who work in PHC and participate in management o f acute and chronic conditions commonly encountered in PHC. In effect, these narrow specialists act as substitutes for FM specialists, fragment gate keeping, and compromise key FM functions o f f i rst contact, comprehensiveness, continuity, and coordination.
346. Further, other provider units, such as the emergency services and occupational health system, act as parallel PHC service delivery mechanisms, further weakening the first contact and gate keeping functions o f PHC . 347. The narrow specialists in PHC are probably the most important obstacle to fully scaling up the FM- centered PHC system in BIH. I t i s important to ensure that when scaling up FM reforms ,the narrow specialists who work in DZs are either retrained as FM physicians or shifted to the secondary care level.
9.4. INTEGRATION, CONTINUUM OF CARE, AND REFERRAL SYSTEMS
348. Although an effective FM-centered PHC system i s being introduced in BIH, the boundaries between primary and secondary levels and the regulatory environment for referral and counter-referral systems have not yet been established.
349. There are, as yet, no incentives to achieve a secondary-to-primary shift. This deficiency o f incentives limits the ability o f the PHC level to develop extended primary care and move beyond gate keeping. The World Bank Health Sector Enhancement Project will support the development o f an interface between PHC and higher levels o f care.
70
3 50. Horizontal integration remains a problem - adversely impacting o n risk pooling, freedom o f movement o f citizens, and development o f entity-wide strategic plans for optimizing resource utilization and allocation.
Decentralization in FBIH has fragmented the health system.
3 5 1. Vertical integration i s limited, with PHC and the hospital levels operating as two subsystems with precarious links between them. As the financing o f the two systems i s unlinked, there i s a risk o f cost-shifting between levels - especially as a per capita payment system without performance indicators wi l l eventually lead to increased referrals to reduce workload at the PHC level. This wil l undermine the gate keeping, continuity, and comprehensiveness functions o f the PHC level.
352. to develop an integrated system with a continuum o f care.
Without development o f effective interface between primary and secondary levels, it will be diff icult
9.5. CONTRACTING
353. Detailed contracts have been successfully introduced in the pi lot sites. This i s to be commended, as the platforms have been put in place to use contracting as a tool to improve service quality, efficiency, and effectiveness. However, to achieve these objectives, there needs to be a move from simple cost-volume contracts based on inputs to more sophisticated contracts based on performance, outputs, and outcomes. This shift will require (a) significant analytical and execution capacity at the PHC and CHIUHIF levels to manage and monitor more sophisticated contracts; (b) robust information systems in these domains to capture relevant and timely data on activities and outcomes; and (c) appropriate incentive systems to improve performance, develop extended PHC, and achieve the secondary to primary shift.
9.6. QUALITY
354. Currently in BIH, the quality o f services delivered in PHC i s not monitored. I t i s very encouraging to witness the development o f the AAQIs that have started accrediting PHC facilities. However, contracts and the provider payment systems should be used as instruments to drive quality improvement. I t i s necessary to develop more sophisticated contracts between CHII /HIF and the family medicine teams with explicit criteria for improving quality but with commensurate performance-related incentives to reward teams that improve quality.
9.7. INCENTIVES AND RETENTION
355. Unsystematic anecdotal evidence suggests that some o f the health professionals trained in FM specialist training programs and in PAT may be leaving or planning to leave FM to j o i n training for other specialties. I t i s important that in the early stage o f the reforms, incentives be introduced to retain the “early adopters” and leaders. Failure to do so will result in rapid demoralization o f the FM team and adversely affect sustainability o f the reforms.
356. Although the new payment mechanisms in pilot sites provide some incentives, there needs to be a much stronger indication that FM i s valued on par with hospital specialties. A visible salary differential between GPs and FPs, as wel l as between the narrow specialist who work in PHC and FPs, would send a strong signal to show FM i s valued and help attract doctors to FM.
9.8. COMMUNICATING THE REFORMS
357. A lack o f communication between and within levels o f the health system and with the public was cited by most o f the respondents interviewed as a critical problem. In particular, the population has not been adequately informed about the nature o f the reforms, the reasons for reform, and the expected benefits,
71
358. Due to inadequate communication and poor engagement o f the operational level in decision making, many perceive the reforms to be “top-down” and “imposed.” This i s a major barrier t o successful scale-up and sustainability o f an FM team-centered PHC system.
359. and inform users and other key stakeholders o f the expected benefits t o increase ownership o f the process.
A clear and all-embracing communication strategy i s necessary to increase visibility o f PHC reforms
9.9. BRANDING FAMILY MEDICINE
360. An effective communication strategy should be combined with a strategy o f re-branding dom zdravljas and ambulantas that have been converted to family medicine centers. This will signal to the users that the move to the FM model i s a comprehensive change program. Indeed, the Wor ld Bank Health Sector Enhancement Project will support communication activities, among other things, to communicate the rationale and the substance o f the FM reforms to the public at large; develop ways o f assessing and benchmarking customer satisfaction; and, through surveys o f users, elicit their expectations o f and experiences with PHC services.
9.10. MANAGING STRATEGIC CHANGE
361. placed on change management to balance a predominantly technical approach or one driven by training.
362. I t i s necessary to rapidly develop a critical mass o f middle- and senior-level managers and health professionals who can act as a cadre o f change agents. Exposure to international experience and experts was highly valued by key respondents, and this exposure will help increase acceptability o f the reforms among the new cadre o f professionals trained to implement the reforms.
Introduction o f the PHC reforms i s a complex strategic change process. More emphasis needs to be
363. Demonstration o f “quick wins” and effective communication o f success stories will catalyze the development process. Lack o f role models in the BIH context i s a problem, but the emergence o f dom zdravljas managed solely by FM teams (such as the one in Laktasi) i s an encouraging development and provides an opportunity to demonstrate what can be achieved.
9.11. MONITORING AND EVALUATION
364. As with the other countries in this study, a fundamental problem with the PHC reforms in the E C A region i s the lack o f meaningful and systematically collected data that can be analyzed to demonstrate if there have been changes in health system objectives (such as equity, efficiency, effectiveness, and choice) and health outcomes that can be attributed to developments in PHC.
365. In the PHC reforms in BIH, as in other countries studied, there was no baselining in the pilot sites to enable before-and after-intervention analysis or studies to compare and contrast p i lot sites with matched non- pilot sites.
366. A rather surprising finding in the study was the weakness o f monitoring and evaluation systems in place, and with the exception o f Kyrgyzstan, l imited investment in developing M&E systems that can capture relevant, reliable, and timely data to inform policy decisions. Further, in the BIH context, although large amounts o f data o f variable quality are collected regularly, due to l imited analytical capacity, they are not analyzed to generate meaningful information to inform decisions. I t i s encouraging to see that the new World Bank Health Sector Enhancement Project plans to invest in developing M&E systems for PHC in BIH.
1 2
10. LESSONS LEARNED
10.1. CRITICAL SUCCESS FACTORS
367. The study has identified a number o f critical success factors. These include, among others identified below, (a) branding FM and image building to improve the status o f FM doctors as compared with narrow specialists; (b) improved work environment o f the FM teams to improve acceptance o f the new model; (c) improved communication between and within levels o f the health system and with the public to share objectives and values o f FM reforms; (d) improved coordination o f key institutions - cited by many to be rather inefficient in BIH, but with significant improvements in the last two years at inter-entity and cantonal levels; (e) developing a holistic approach to reform; (f) developing t rust through better engagement o f the operational level to create ownership; and (g) better coordination between donors.
10.2. BEING STRATEGIC
368. There i s good opportunity for the World Bank to be more strategic in the E C A region, where it has a valued presence. Countries with World Bank-supported PHC reforms in the region can significantly benefit from one another’s experience through well-supported experience-sharing and dissemination strategies. This study i s a good vehicle to achieve this objective, but much more needs to be done.
10.3. HOLISTIC APPROACH
369. The study clearly demonstrates the importance o f a multifaceted and multi level approach to reform. While new laws and regulations are developed and existing ones modified to create an enabling environment for change to occur, simultaneous interventions are needed to refine organizational structures, health system financing, resource allocation, provider payment systems, and service provision.
10.4. TIME HORIZON
370. Balancing short-term success and sustainability i s important. Achieving system change takes time. Short-term projects have value, but sustained support over a five- to eight-year period i s a realistic time scale to achieve and institutionalize change in the BIH context.
10.5. BEYOND PILOTS TO SYSTEM CHANGE
371. Moving out o f “pilot” and “experiment” mode i s necessary to institutionalize and systematize changes to sustain health system reform. Continuing in a pi lot mode with multiple projects wi l l result in sprinklings o f pockets o f innovation without coherent systemic change.
10.6. LINKAGES
372. Strong vertical and horizontal links are needed to simultaneously work both at policy and operational levels - the former to institutionalize changes and the latter to create shared ownership to implement policies. Governance structures can limit what can be achieved at regional or organizational levels if there i s not a clear link to the national policy level. Without vertical and horizontal linkages, local-level initiatives and innovations have no impact on central policies and cannot diffuse to other regions. In the PHC reform program in BIH, there has been a visible effort by the Ministries o f Health and the World Bank to work at both policy and operational levels and share lessons from success stories.
73
10.7. INSTITUTIONS VERSUS INSTITUTIONALIZATION
373. While it i s necessary to invest in key individuals to develop champions o f reform, this must be balanced with efforts to widely engage stakeholders to achieve consensus o n reform objectives. The experience o f BIH confirms the importance o f combining bottom-up and top-down approaches with simultaneous investment in key individuals, institutional development at different levels, and institutionalization through appropriate laws and regulations.
10.8. READING THE CONTEXT
374. The fluidity o f the socio-political and the economic environment in BIH means that the political economy o f health reforms and factors influencing strategic change must be adequately analyzed and addressed in the design phase and throughout implementation o f programs. This analysis and monitoring should be continuous to ensure that generic technical solutions are not applied to complex socio-political contexts.
10.9. COORDINATION
375. Close coordination o f international agencies by the Ministries o f Health i s necessary to ensure activities a shared and coherent sector investment program and prevent fragmentation or duplication o f activities. The Ministries o f Health in both entities have made considerable efforts in this direction to ensure a comprehensive and coordinated approach to international assistance.
376. In BIH, a Reform Coordination Group, comprising the key development partners and multilaterals such as the World Bank, WHO, European Union, CIDA, Japanese International Cooperation Agency, and SDC i s moving toward a loose “‘operational Swap.” However, the complexity o f co-coordinating donor agencies should not be overlooked and appropriate support should be provided to the Ministries o f Health in both entities to achieve effective coordination.
10.10. COMMUNICATION
377, Inadequate and ineffective communication results in fear o f the unknown and breeds resistance. A well-developed communication strategy aimed at users, health professionals, managers, and decision makers i s needed. The planned Wor ld Bank Health Sector Enhancement Project has a large communication and advocacy component to address the communication gaps.
10.1 1. RESPONSIVENESS
378. to adapt to changes and respond to windows o f opportunity, but without sacrificing a strategic approach.
Given the fluidity o f the context, future programs should adopt a flexible approach to implementation
10.12. MONITORING AND EVALUATION
379. Perhaps the most important finding o f this study was the paucity o f appropriate systems for monitoring and evaluation o f interventions and program. As with the other countries studied, in BIH there was no baseline information against which PHC reforms or program success could be measured. There i s an urgent need to develop appropriate metrics and information systems to monitor progress o f PHC reforms and systematically gather information to verify progress against objectives.
74
10.13. DISSEMINATION AND CROSS-LEARNING
3 80. country and from countries implementing similar reforms in the region.
Many o f the respondents highlighted the value o f cross-learning and experience-sharing within the
381. There i s currently inadequate dissemination o f experience and sharing within and between countries. Regional collaborations, regular exchanges, and dissemination o f achievements and lessons should be encouraged and supported. K e y documents (such as technical reports) should be available in local languages and disseminated widely to local counterparts.
10.14. EXIT STRATEGY
382. This is a highly successful project and demonstrates that the Wor ld Bank can add much value to the reform process, but success brings with it responsibility. A clear exit strategy, agreed with local counterparts, i s needed, to ensure that there are no gaps in support to sustain the transformation process.
75
ANNEX 1: FAMILY MEDICINE CONTRACT FROM FBIH
In accordance with the Article 42, Paragraph 1 o f the L a w on Health Care (“Official Gazette o f the Federation o f BIH’, no 29/97) and the Provisions o f the Decision on Establishing Interim Standards and Norms o f Health Care under Compulsory Health Insurance (“Official Gazette o f the Federation o f BIH’, no 21/00), the
CONTRACT ON THE PROVISION OF FAMILY M E D I C I N E SERVICES IN P R I M A R Y HEALTH CARE has been concluded in .............. on .................. between:
1. Dr ....................... ., name and family name, (hereinafter: Family Doctor, Party in the Contract)
2. Health Insurance Fund o f Western Herzegovina Canton, represented by i t s director, ................ (hereinafter: the Fund).
The Parties in the Contract have concluded the following:
1. General Provisions
Article 1
The Contract regulates mutual rights and duties o f the Parties in the Contract with regard to the provision o f family medicine services in Primary Health Care in the course o f the year 2002 as follows:
Types and scope o f family medicine services, which are the subject o f this Contract;
Structure o f the family medicine team;
The scope o f work o f the family medicine team, the responsibility o f the fami ly medicine doctor, the Party in the Contract, and the family medicine team in provision o f services which are the subject o f the Contract;
Time o f commencement and place o f provision o f family medicine services;
The manner o f providing health care in the family medicine;
The amount allocated by the Fund for the provision o f family medicine services, and methods o f calculation and compensation payment;
Payment terms for contracted monthly compensation, i.e. average value o f the family medicine team; Infrastructure provision;
Documentation needed for monitoring and performance o f activities and teams for submitting the documentation;
Supervision over execution o f the provisions in this Contract;
Rights and duties o f the Parties in the Contract with regard to the abrogation o f the Contract; Other rights and duties.
76
Article 2
The Parties in the Contract agree to promote the concept o f family medicine based on the role o f a doctor as a “gatekeeper” towards higher levels o f health care system. The family medicine team wil l respond to all requirements concerning the contracted health services at the level o f the Primary Health Care for which it i s competent.
Article 3
In accordance with the Article 64 o f the L a w on Health Insurance (“Official Gazette o f the Federation o f BIH’, no 30/97 and 7/02), the insured persons select their family doctor for a period o f one year.
The Parties in the Contract are bound to insure the registration o f up to 2500 insured persons per family medicine team.
In extraordinary cases, a bigger number o f the insured persons than the above stated may be registered.
The terms and the manner o f registration o f a bigger number o f patients and the increased compensation for each registered person over the stated maximum number o f the insured persons will be regulated by the Fund in a special decision. However, the capitation amount shall not be lower than the amount corresponding to the capitation for the age group from 7-18 years o f age.
Until 30th September o f the ongoing year, the insured persons state the doctor they are choosing for the following year in writing. The insured person delivers hidher written statement to the Fund, which creates records according to the l is t o f the family doctor. The insured person i s provided health care with the chosen family doctor beginning with 1st January o f the following year. If the insured person does not state the wish to choose another family medicine doctor in writing until 30th September o f the ongoing year, it will be considered that he/she wishes to choose the same doctor again.
(Note: Registration o f a l l the insured persons related to the contribution payers (family members) i s recommendable.)
Article 4
For the provision o f health services that are the subject o f this Contract, the family doctor f rom the Contract i s bound to provide adequate business premises in the D o m Zdravlja that meet the standards and norms in the health work.
Provision o f the premises in the paragraph 1 o f this Article i s accomplished by concluding a separate Lease agreement for business premises between the family doctor in the Contract and the D o m Zdravlja.
All financial obligations based o n the separate Lease agreement from the paragraph 2 o f this Article are the responsibility o f the family doctor and he fulfils them using the resources allocated to him/her by the Fund, in accordance with this Contract.
Article 5
It i s the obligation o f the family doctor to provide optimal access to h isher practice by defining the working hours that most suit the majority o f hidher patients.
The following information should be on the door o f the practice:
77

Working hours
Names and family names o f the health workers, the team members.
If there i s a need for provision o f specific services that are the subject o f the Contract outside the working hours set in the Item 2 o f this Article, the family doctor in the Contract i s bound ensure their provision by concluding a separate contract with the D o m Zdravlja or other health institutions, which will establish the manners and modalities o f provision o f the health services in those health units.
Article 6
In case o f hidher absence that i s longer than a week or in case o f a temporary cessation o f work, the family doctor in the Contract i s bound to provide to hislher patients a substitute through a contract with a health worker who i s a specialist in the same field and performs private practice, or with a PHC institution that will provide services to hidher patients during hidher absence.
2. Types, Scope and Quality o f Health Services
Article 7
Health services that are the subject o f this contract are the following:
Outpatient and home treatment
Diagnostics, i.e. therapy at the level o f the doctor’s activity
Patronage supervision
Keeping o f the prescribed records and documentation
Health education and promotion measures
Prevention-promotion health services.
The family doctor i s bound to spend 40 percent o f hidher time on preventive health services related to disease prevention, diagnostics, early detection o f illness or condition, therapy control at home, education o f population on self-aid and self-care, prescribed in the line 6 o f the Paragraph 1 o f this Article.
The family doctor in the Contract i s bound to provide health services within the scope prescribed by the Basic Health Rights Package.
The family doctor in the Contract i s bound to provide health services o f standard quality and equal content to the patients, which implies co-ordination o f the health services provided with the up-to-date medical knowledge, technology and standards, in accordance with the special regulations in the field.
The family doctor in the Contract i s bound to participate in provision o f the emergency aid within the working schedule o f the associated D o m Zdravlja, for which he/she may receive compensation in accordance with a separate contract with the D o m Zdravlja.
78
Article 8
The family doctor in the Contract undertakes the obligation to provide health services from the Article 7 o f this Contract, with the assistance o f the family medicine team, in the D o m Zdravlja practice, and in compliance with the Provisions o f the L a w on Health Care, L a w on Health Insurance, general decrees o f the Fund, rules o f profession stipulated by the competent chamber on the principle o f free selection o f the family doctor on the basis o f the place o f residence o f the insured persons, in accordance with the standards and norms for this level o f health care.
Article 9
The family doctor in the Contract undertakes the obligation to make a l i s t o f the family medicine team, which i s the enclosure to the contract and represents i t s integral part. The Parties in the Contract agree on the structure o f the family medicine team depending on the number o f persons registered.
The norm for the structure o f the family medicine team from the paragraph 1 o f this Article that covers 2000 insured persons i s the following:
Family medicine doctor - 1
Nurse who has completed a training in the family medicine (hereinafter referred to: family medicine nurse)- 1
Family medicine nurse or nurse working on the tasks related to medical information - 0.5
Family medicine intervention nurse - 0.5
3. The Scope o f Work o f The Family Medicine Team, Responsibilities, Rights and Duties o f The Family Doctor, Party in the Contract, and the Family Medicine Team
Article 10
The scope o f the work o f family medicine team, pursuant to the health services set out in the Article 7 o f this Contract implies the following:
a. Treatment services
Orientation diagnostics, therapy and rehabilitation o f the lead mass diseases;
Referring to and supervision o f patients during their specialisuhospital treatment;
Prescription o f essential drugs;
Parenteral injection o f drugs (subcutanum, intramuscular, intravenous injection);
Surface wound treatment without stitches:
Removal o f stitches;
Second-degree-burn treatment;
Removal o f foreign body from skin or under-skin tissue;
79
Catheter replacement;
Ear flush (cerumen);
Immunization;
Prevention o f bleeding;
Reanimation measures;
Primary care, distortion, fracture immobilization;
Other services.
b. Prevention-promotion services
Control and supervision o f the lead risk factors defined through socio-medical diagnosis;
Systematic check-up o f the grown-ups, infants, pre-school children, school children;
Patronage visit to a pregnant woman, woman who has just given birth, infant, child, infectious patient, the old and weak;
Specialist check up o f school children for enrollment in school;
Medical check up o f children for kindergarten;
Medical check up for immunization;
Individual instruction to mothers on feeding;
Target check up;
Scheduled target conversation;
Health education work in small groups;
Health lecture by a health technician;
Health lecture by a doctor;
Forming o f socio-medical diagnosis for the field o f responsibility;
Monitoring o f the family medicine nurse diagnosis;
Collection o f data necessary for the further planning o f work, monitoring and evaluation by the family medicine doctor in the Contract;
Direct participation in a l l the prevention-promotion programs with the a im o f removing the risk factors that could directly affect the health o f the population at their territory o f operation;
80
Cooperation with schools, social institutions, municipal communities and other institutions in the implementation o f the prevention-promotion activities;
Other prevention-promotion services.
On the basis o f the scope o f work o f a family medicine team set in the I tem 1 o f this Article, the Parties in the Contract shall compose annual operation plan. It will contain individual types o f services, as wel l as the anticipated number o f services in the course o f 2002, and the point value o f the services.
Article 11
The family doctor and other family medicine team members are especially responsible for the following:
All activities which may cause deterioration o f the health condition o f the insured person, wrong and incomplete provision o f diagnostic and therapeutic services, control o f effect on the therapy prescribed or untimely referring to other health institution. All the above-mentioned represent reasons to unnecessarily long treatments, deterioration o f the patient’s condition, disability or death o f an insured person,
Provision o f health services by persons who are not qualified, except in emergency situations,
Beginning o f the working time later or finishing earlier than regulated, or any other form o f non-observance o f the work schedule or failure in internal organization, which can be the reason why an insured person did not satisfy hidher health needs, and was forced to wait and come several times for the same health service, or it was more diff icult for him/her to get the health care needed,
Untimely provision o f emergency health care according to the case,
Protection o f personal status o f an insured person during treatment, h idher dignity, honor and reputation, with stress on provision o f adequate health care without discrimination, on the right to adequate information about personal health condition, diagnosis and treatment, possible after-effects, o n the right to accepting medical treatment, as wel l as the right to personal physical integrity, the right to access to hidher personal medical information, and other rights regulated by the Patients’ Rights Charter.
Equal treatment o f a l l the insured persons with the same level o f health needs and prevention o f corruption or provision o f better treatment based on personal relations and other non-medical criteria.
In the case o f the established responsibility o f the family doctor in the Contract, that i s one o f the members o f the family medicine team, the Fund may, unilaterally, abrogate the contract without any obligation to compensate for the damage, and in the case o f more serious violations, the Fund may initiate the procedure wi th the competent health chamber to deprive the doctor o f h idher work permit.
Article 12
The family doctor in the Contract i s bound to provide a required medicine team and medical equipment for diagnostic and therapeutic procedures that are a part o f primary health care.
When the family doctor in the Contract assesses that the health condition o f an insurant requires more complex diagnostic and therapeutic procedures at the level o f specialist-consultative and hospital health care, he/she w i l l refer the patient to the specialist examination or stationary treatment in the closest polyclinic, that i s stationary health institution with which the Fund has concluded a contract.
81
When referring the patient to the polyclinic or stationary health institution for target check-ups, the family doctor in the Contract i s bound to complete the referral and enclose the history o f disease with all the data.
Article 13
The family doctor in the Contract i s bound to implement a rational policy o f drug prescription.
Only those drugs registered in the Federation o f BIH, as wel l as the drugs whose prescription and payment i s at the expense o f the compulsory health insurance (positive l i s t o f drugs in the Canton), in accordance with the Article 83 o f the L a w on Drugs (“Official Gazette o f the Federation o f BIH”, no 51/01) may be prescribed.
If the drug prescription costs are lower than the average o f the same costs o f other family medicine doctors in the Municipality / Canton, the family doctor in the Contract wi l l be paid a bonus, whose amount will depend on the amount that has been saved.
If the drug prescription costs considerably exceed the average consumption per doctor in the Municipality / Canton, the Fund will ask for the written explanation from the doctor, and if necessary, undertake adequate steps in accordance with the Law, with the aim o f sanctioning irrational prescription practice.
Article 14
The family medicine doctor in the Contract, as wel l as the family medicine team members are bound to check continually the quality o f the services provided by defining the program o f internal quality and health care service control in the family medicine, in accordance with the current and explicit standards, and by preparing reports on quality improvement o f health services, as wel l as on the results o f their work.
The family doctor in the Contract, as we l l as other members o f the team are bound to engage themselves in the quality improvement system and accreditation in health, conducted by the authorized body in the Federation o f BIH - Agency for Quality Improvement and Accreditation in Health.
4. Prescribed Records and Contract Implementation Monitoring
Article 15
The family doctor undertakes the obligation that the family medicine team will keep al l the necessary documentation and daily reports according to the codes from the L i s t o f Diagnostic and Therapeutic Procedures - timely and personnel norm for the performance monitoring needs o f the Fund. They are to be submitted by the 10th o f each month for the previous month.
In addition to the forms from regular statistic researches in health, the family doctor i s bound to submit the following data to the Fund: the number o f referrals for specialist-consultative examinations, number o f referrals for hospital treatment, drug consumption, referrals for diagnostic investigations, number o f patients in some vulnerable population groups (new-born babies, diabetes patients, hypertonic patients, chronic patients), data on the health promotion work.
The above data are delivered in the prescribed forms, which are enclosed in the Contract.
82
Article 16
Upon the receipt o f the monthly reports from the Article 15 o f this Contract, the Fund wi l l review the documentation and inform the family doctor on possible shortcomings and needs for adjustments within the period o f 15 days.
Article 17
Upon expiration o f the three months, the Fund makes a comparison o f the Contract and the results stated in the monthly reports.
Article 18
The Fund i s bound to inform the family doctor in the Contract on all alterations o f the general acts o f the Fund referring to the execution o f the contracted obligations on time.
Article 19
The Fund controls the fulfilled obligations o f the family doctor regulated by this Contract through:
An inspection o f the documents submitted
Direct insight o f the control service (monitoring service) into the work and documents o f the family doctor from this Contract.
A report i s made on the control, which includes the findings on the actual situation and a proposal for removing any shortcomings and irregularities in the execution o f the obligations from the Contract.
The director o f the Fund decides on the steps to be taken in the anticipated period for the purpose o f removing the shortcomings.
5. The Amount o f Resources for Health Services and The Payment Method
Article 20
The family doctor in the Contract i s entitled to compensation for the provided health services that are the subject o f this Contract. The compensation i s calculated as follows:
Age group Capitation No. o f insured persons Total compensation 1. 0 - 7 years o f age 2. 7 - 18 years o f age 3. 18 - 65 years o f age 4. > 65 years o f age T o t a l
3.6 KM 6.8 KM 5.2 KM 42.0 KM
The compensation for the capitation i s paid monthly: 1/12 o f the total compensation amount from the Paragraph 1 o f this Article. The total compensation i s adjusted to the change in the number and structure o f the insured persons registered by the family doctor in the Contract each January 1 s t o f the ongoing year.
83
Article 2 1
In the period until the family medicine doctor in the Contract has registered the minimum number o f the insured persons, he/she shall hold the status o f an employee in the D o m Zdravlja and receive the usual salary for hidher work.
When the doctor has registered the minimum number o f the insured persons and completed the registration o f a private practice, the payment o f hidher salary as regulated in the Article 20 shall commence.
Article 22
The family doctor in the Contract submits a monthly invoice prepared in compliance with the compensation from the Article 20 o f this Contract.
In accordance with the monthly invoice in the Item 1 o f this Article, the Fund remits the compensation amount for the ongoing month directly to the account number o f the family doctor in the Contract: . . . . . . . , . . . . , . . . . . . . . . . , , . . . . , . . , , . . , . . .., registered at the transaction bank . , . . . . . . . . . . . . . . . . , . , . . , . , . . . . . , . , . . . , . . . . . . ,
Article 23
The family medicine doctor in the Contract i s bound to settle al l the costs o f work at the ambulanta f rom the collected compensation amount. These are as follows:
Salaries for the family medicine nurses with the contribution and taxes
Costs o f the ampuled drugs and sanitary supplies
Management expenses
Costs o f rent o f the ambulanta
Costs o f the forms (fi les, referrals).
Article 24
The insured persons participate in covering a part o f the health care costs in accordance with the Decision on Direct Co-payment o f the Insured Persons in the Use o f Health Care (co-payment).
The family doctor withholds keeps the resources from the co-payments collected, f rom the paragraph 1 o f this Article (co-payment).
6. Rights and Duties o f the Parties in The Contract with Regard to Abrogation o f The Contract
Article 25
The parties in the Contract may abrogate this Contract before the expiration o f the Contract period in the following cases:
The family doctor may abrogate the Contract if the Fund fails to fulfill i t s contracted duties
84
The Fund may abrogate the Contract if the family doctor does not recognize and does not execute the Provisions o f this Contract.
The Contract wi l l be abrogated within 30 days from the day o f determining the abrogation circumstances.
Notification on the Contract abrogation i s published in the media for the purpose o f enabling the insured persons to select a new family doctor within 30 days.
Article 26
The Parties in the Contract wi l l attempt to solve amicably any disputes related to the Contract. In case o f an unresolved dispute, a jo in t commission consisting o f the representatives o f the Parties in the Contract will intervene.
Each Party in the Contract nominates two representatives to the jo int commission.
The Party in the Contract that i s dissatisfied with the decision o f the Commission from the Paragraph 1 o f this Article may, within 30 days from the date the decision i s passed, initiate court proceedings at the competent court.
7. Final Provisions
Article 27
The rights and duties f rom this Contract take effect f rom 1st October 2002.
Article 28
This Contract has six (6) identical copies. Each Party keeps two copies.
Article 29
This Contract takes effect o n the date o n which it i s signed. It i s applicable f rom the day o f conclusion o f a separate Lease Agreement for premises from the Article 4 o f the Contract.
Family medicine doctor, Party in the Contract:
Health Insurance Fund:
85
ANNEX 2: AN EXAMPLE OF A CONTRACT IN THE REPUBLIKA SRPSKA
Contract signed between the Director o f the DZ Laktasi on behalf o f FM team and the Director o f the HIF in the RS.
On the basis o f Article 60 paragraph 3 o f the L a w on Health Insurance (Official Gazette o f the Republic o f Srpska, N o 18/99, 5 1/01, 70/01 and 51/03) the Health Insurance Fund o f the Republic o f Srpska, represented by Dr, Svetozar Radulovic, and the Laktasi Health Center, represented by Dr. Ljubomir Sormaz, on behalf o f family medicine team 1 led by Dr. Drasko Josic, signed a contract in Banja Luka on 10 M a y 2004.
CONTRACT
on rights and obligations in provision o f health care and financing o f family medicine team’s work
1. GENERAL PROVISIONS
Article 1
This contract defines the rights and obligations between the Health Insurance Fund o f the Republic o f Srpska (hereinafter: the Fund) and the Laktasi Health Center represented by Dr. Ljubomir Sormaz, on behalf o f Family medicine team 1 (hereinafter: the Team) led by Dr. Drasko Josic, in provision o f health services to people insured with the Fund, and financing o f the Family medicine team in primary health care in 2004.
Article 2
The contract i s based on:
The L a w on Health Insurance, the L a w on amendments and additions to the L a w on Health Insurance (Official Gazette o f the Republic o f Srpska N o : 18/99; 5 1/0 1 and 62/02), the L a w o n Health Care and the Law on amendments and additions to the L a w on Health Care (Official Gazette o f the Republic o f Srpska N o : 18/99; 58/01; 70/01 and 51/03)
Objectives o f Health for All in the 2 1st Century - a WHO document
Decision on Heath Institutions Network (Official Gazette o f the Republic o f Srpska No: 2/01) and the Decision on amendments and additions to the Decision on Health Institutions (Official Gazette o f the Republic o f Srpska No : 65/01; 1/03)
The Rulebook o f regulations and registries in the health sector (Official Gazette o f the Republic o f Srpska No : 4/95)
The Fund’s financial plan for 2004
The Rulebook on the scope, content and ways o f realization o f health care (Official Gazette o f the Republic o f SrpskaNo: 21/01)
The Decision on the minimum package o f health care service (Official Gazette o f the Republic o f Srpska N o : 21/01)
86
Decision on payment participation o f insured people in the costs o f heath care services (Official Gazette o f the Republic o f Srpska N o : 21/01) and the Decision o n amendments and additions to the Decision on payment participation o f insured people in the costs o f heath care services (Official Gazette o f the Republic o f Srpska No: 42/0 1 and 1 1/02)
The Decision on determination o f criteria for financing the rights deriving f rom compulsory health insurance and other costs related to i t s implementation (Official Gazette o f the Republic o f SrpskaNo: 21/01),
The Decision on determination o f the Positive l i s t o f drugs (Official Gazette o f the Republic o f Srpska No: 34/00 and 38/02) and the Decision on amendments and additions to the Decision on determination o f the Positive l i s t o f drugs (Official Gazette o f the Republic o f Srpska No : 38/02)
The Decision on the List o f essential drugs for health centers and family medicine ambulantas (Official Gazette o f the Republic o f Srpska No : 1 1/02 and 6/03)
The Health Services Quotations
The RS Health Policy Program and the Health Strategy in the Republic o f Srpska until 2010 (Official Gazette o f the Republic o f Srpska No : 56/02)
Individuals and Groups Health Improvement Program (Official Gazette o f the Republic o f Srpska No: 4/01)
The Strategy for Prevention and Control o f Mass Non-contagious Diseases
The Strategy for Prevention and Control o f Non-contagious Diseases
The Program for prevention and Control o f Non-contagious Diseases
Professional instructions for detection and reduction o f risk-factors and early detection o f diseases from the Program for Prevention and Control o f Non-contagious Diseases in the Republic o f Srpska
Program for containment and detection o f cardiovascular and malignant diseases and other mass and non- contagious diseases risk factors (Official Gazette o f the Republic o f SrpskaNo: 4/01 and 10/02),
The Rulebook on Conditions for Performance o f Health Activities in Health Institutions (Official Gazette o f the Republic o f Srpska No : 6/94),
The Rulebook on Referral System in Health Care System o f the Republic o f Srpska (Official Gazette o f the Republic o f Srpska No: 15/02),
Strategy for reduction o f diversity in condition o f health and accessibility o f health care to the population, for reorientation o f health care and reorganization o f health services and for increase in efficiency and quality o f work o f health institutions (Official Gazette o f the Republic o f Srpska N o : 77/03).
Article 3
The contractual parties define: type and scope o f health services o f family medicine team, which are the subject o f this agreement, in accordance with Article 23 o f the L a w on Health Care in the RS,
87
personnel structure o f the family medicine team in accordance with Article 24 o f the Law on Health Care in the RS,
fulfillment o f conditionality stipulated in the Rulebook on Conditions for Performance o f Health Care Activities in Health Institutions and Other Forms o f Performance o f Health Care Activities,
responsibility of the doctor and the family medicine team in the provision o f health services that are the subject o f this agreement,
contractor period and the location where the services are provided,
amount o f funds that the Fund will secure for provision o f services in family medicine and the accounting and payment technique,
payment deadlines for agreed monthly disbursements,
documentation for monitoring o f execution of tasks, and the reporting form and deadlines,
contract implementation supervision,
ways o f contract termination,
other rights and obligations.
Article 4
Insured people referred to in Article 1 of this Contract are deemed al l the people who permanently reside in the territory o f Laktasi municipality and who have registered with the Team, concluded on the day of signing o f this Contract.
2. OBLIGATIONS OF THE FAMILY MEDICINE TEAM
Article 5
The Team i s obliged to have a resolution by the Ministry o f Health on organization o f i t s activity in compliance with the Rulebook on Conditions for Performance o f Health Care Activities in Health Institutions and Other Forms o f Performance o f Health Care Activities,
Apart form the general conditionality, the Team needs to fulfill the following conditions: education (the Rulebook on Specialization or the Rulebook on additional Education in Family Medicine), the population that chose it and registered with it in a special form with signatures o f the people who registered their families.
The total number o f citizens - insured people referred to in paragraph 2 o f this Article, registered with a family medicine team cannot exceed 2000.
The Team i s obliged to submit to the Fund data on registered people in accordance with age and sex. Article 6 The Team i s obliged to display:
working hours
88
names and surnames o f employees - members o f the Team.
Article 7
Health services that are the subject o f this Contract are contained in the following measures, activities and tasks:
health promotion measures in accordance with programs for improvement o f health o f individuals and groups o f population,
measures for removal and containment o f risk factors o f certain diseases in accordance with the Ministry o f Health and Social Welfare Program,
specific health care for women during pregnancy, birth and afterbirth period,
specific health care for infants, small and school children,
immunization in accordance with the Immunization Provision I
examinations and treatments o f sick and injured people in all cases which do not require more complex examination and hospitalization,
complete primary level treatment for the sick who are referred to examinations and treatments in organizational units or health institutions o f the f i rs t referral level,
continuation o f treatment and rehabilitation o f patients discharged f rom hospitals,
determination o f causes o f death,
maintenance o f the prescribed registries, documentation and submission o f the prescribed or agreed reports.
Article 8
The Team i s obliged to design an operation work plan in accordance with the programs o f the Ministry o f Health and Social Welfare o f the Republic o f Srpska and the structure o f choice o f the population as follows:
Prevention and Control o f Non-contagious Diseases Program,
Program for improvement o f health o f individuals and groups o f population,
Compulsory immunization program
The Team i s obliged to execute the activities foreseen in the operation plan.
In the event o f forfeit o f the operation plan, the funds will be decreased commensurately.
Article 9
Family medicine doctors in accordance with the Rulebook on the Referral System and Health Care shall only do referrals to the f i rst referral level in the Republic o f Srpska (Articles 13 and 14).
89

The criteria for referrals to specialist consultations are 20 percent o f the total number o f patients examined in the Team.
Out o f the total number o f referrals f rom the previous paragraph, exemptions shall be made for referrals for control by specialist consultants, which wi l l be separately noted on the referral slip.
Article 10
Prescribed drugs, which can be prescribed and reimbursed by the Fund, can only be prescribed by family medicine doctors for the citizens registered with the Team.
The planned amount for prescribed drugs for insured people with the Team i s KM 17.600 for the year.
The risk o f spending more or less funds allocated to prescribed drugs wil l be shared between the Team - 70 percent; the hospital 20 percent and the clinic 10 percent.
The positive l i s t o f prescribed drugs i s an integral part o f this Contract.
Article 11
The Team i s obliged to secure for family medicine ambulantas, through the Health Center, the necessary drugs in veils and sanitary materials f rom the L i s t o f basic drugs for health centers.
The family medicine doctor i s obliged to issue a confirmation to insured people if there i s a shortage o f a certain drug in vei l f rom the L i s t o f basic drugs for health centers.
The L is t o f basic drugs for health centers i s an integral part o f this Contract.
Article 12
The Team i s obliged to submit to the Health Center separate reports for provision o f health services to insured people injured in traffic accidents, injuries at work, poisoning, professional diseases etc., due to pursue compensation in a court proceedings.
Article 13
The Team wil l organize provision o f health services within the scope o f i t s activities during the working hours, and wil l take part in provision o f health services 24 hours a day, in a way and schedule determined by the Health Center.
3. OBLIGATIONS OF THE FUND
Article 14
The Fund i s obliged to pay compensations to the Team regularly in determined monthly amounts and deadlines, through the Health Center’s account.
: :The agreed annual amount per one insured person based on the weighted capitation i s (Table 59):
90
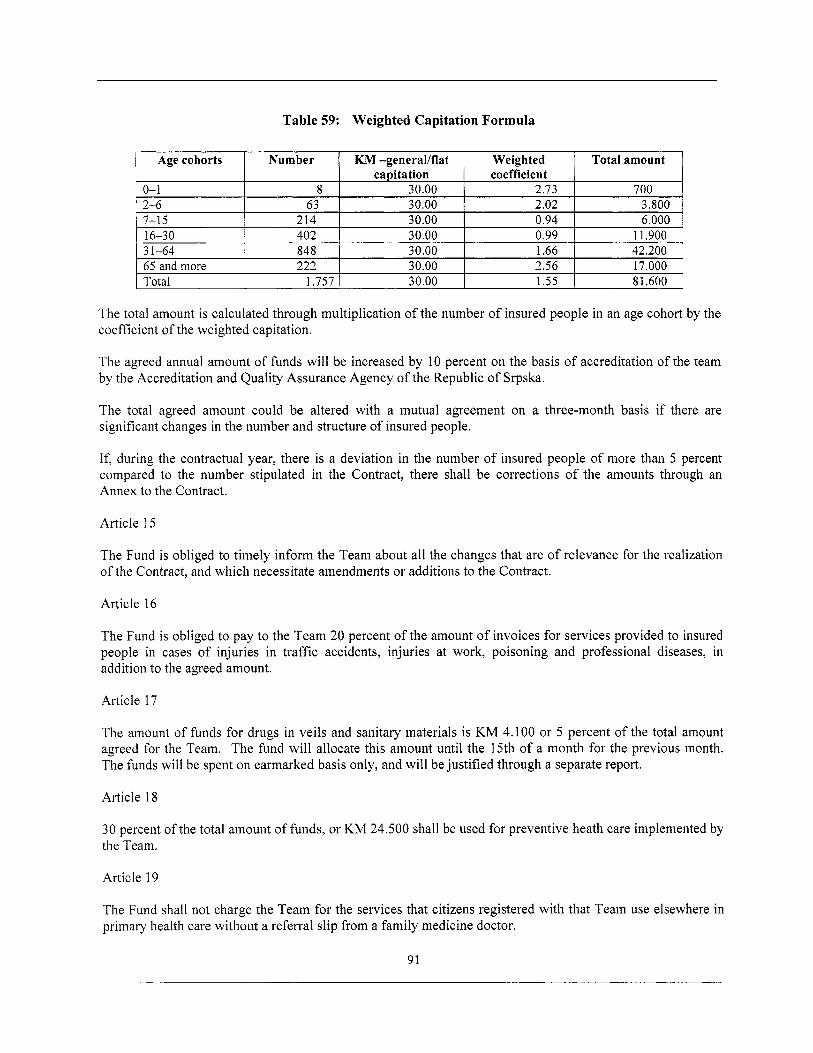
Table 59: Weighted Capitation Formula
0- 1 2-6 7-1 5 16-30 3 1-64 65 and more Total
' Agecohorts ' Number 1 KM-general/flat I Weighted I Total amount ' capitation coefficient
8 30.00 2.73 700 63 30.00 2.02 3.800
214 30.00 0.94 6.000 402 30.00 0.99 1 1.900 848 30.00 1.66 42.200 222 30.00 2.56 17.000
1.757 30.00 1.55 8 1.600
The total amount i s calculated through multiplication o f the number o f insured people in an age cohort by the coefficient o f the weighted capitation.
The agreed annual amount o f funds wil l be increased by 10 percent on the basis o f accreditation o f the team by the Accreditation and Quality Assurance Agency o f the Republic o f Srpska.
The total agreed amount could be altered with a mutual agreement on a three-month basis if there are significant changes in the number and structure o f insured people.
If, during the contractual year, there i s a deviation in the number o f insured people o f more than 5 percent compared to the number stipulated in the Contract, there shall be corrections o f the amounts through an Annex to the Contract.
Article 15
The Fund i s obliged to timely inform the Team about a l l the changes that are o f relevance for the realization o f the Contract, and which necessitate amendments or additions to the Contract.
Article 16
The Fund i s obliged to pay to the Team 20 percent o f the amount o f invoices for services provided to insured people in cases o f injuries in traffic accidents, injuries at work, poisoning and professional diseases, in addition to the agreed amount.
Article 17
The amount o f funds for drugs in veils and sanitary materials i s KM 4.100 or 5 percent o f the total amount agreed for the Team. The fund wil l allocate this amount until the 15th o f a month for the previous month. The funds w i l l be spent on earmarked basis only, and will be justified through a separate report.
Article 18
30 percent o f the total amount o f funds, or KM 24.500 shall be used for preventive heath care implemented by the Team.
Article 19
The Fund shall not charge the Team for the services that citizens registered with that Team use elsewhere in primary health care without a referral slip from a family medicine doctor.
91
The Fund Shall not burden the Team for prescribed drugs nor for referrals to diagnostic units and specialist ambulantas if there i s n o stamp or signature o f the family medicine doctor on the prescriptions and referrals.
4. ACCOUNTING AND P A Y M E N T METHODOLOGY
Article 20
The Team wil l submit invoices to the Fund, on monthly basis, in amount o f 1/12 o f the contractual amount, through the Health Centre.
Along with the invoice f rom paragraph 1 o f this Article, the Team wil l submit reports on services executed in the previous month per team, that is, with names and surnames and unique ID numbers o f insured people, and in accordance with the nomenclature f rom the Health service quotations, until the 15th day o f the month for the previous month.
If the Team fails to submit the invoice and report on time, it will not be allocated the funds for the previous month.
Article 2 I
The Fund i s obliged to pay monthly invoice for the previous month within 30 days from the day o f reception o f the invoice.
The Fund will carry out accounting o f health care expenses o f the Team quarterly and upon the final account, in accordance with provisions o f this Contract and with obligations in relation to implementation o f the program referred to in Article 8.
The Fund i s obliged to pay separate invoices (traffic accidents, injuries at work, poisoning, etc.) within 30 days from the day o f reception o f an invoice.
5. MONITORING, CONTROL AND REPORTING
Article 22
In order to protect the rights o f the insured people, and due to rational and purposeful expenditure o f the contractual funds, the Fund and the Health Center, that i s the Team agree that the authorized representatives o f the Fund, the Health Center, that i s the Team, can at any time have insight into relevant documentation o f the Fund, that i s the Team, which i s related to the provisions o f this Contract.
Article 23
The team will, through the Health Center, submit three-month reports to the Fund about al l the changes in the numbers and structure o f the registered citizens.
The Team will, through the Health Center, additionally monitor and report to the Fund about the following: the number and structure o f the total number o f services rendered in accordance with age, sex and Programs from Article 8, the number o f patients referred to consultations, diagnostic services and hospitals, in accordance with age and gender cohorts.
92
The Team will submit, through the Health Center, and for the needs o f the Fund, monthly reports on the implementation o f Programs from Article 8 to the Public Health Institute o f Republic o f Srpska.
The Public Health Institute o f the Republic o f Srpska shall do Monitoring and evaluation o f the implementation o f the Programs from paragraph 3 o f this Article for the needs o f the Fund.
Article 24
The Fund wil l submit to the Team quarterly reports on the number o f prescriptions issued in accordance with codes o f the family medicine doctor and funds spent.
6. W A Y S OF SETTLING DISPUTES
Article 25
The Contractual parties assume the responsibility to amicably resolve al l the disputes ensuing from this Contract.
In those disputes that cannot be resolved in a manner referred to in paragraph 1 o f this Article, jurisdiction shall be yielded to the competent court,
7. IMPLEMENTATION OF THE CONTRACT
Article 26
This Contract shall be deemed concluded once authorized representatives o f the Contractual parties have signed it, and it shall be in force for 2004.
Upon the expiry o f the contractual year, the Fund’s liabilities toward the Health Center, that i s the Team, wi l l be regulated through the Decision o f temporary financing o f health institutions, until the conclusion o f a new contract.
Article 27
If there are any changes in the elements o f the Contract during i t s implementation, the Contractual parties shall regulate the new terms through an Annex to the Contract, which will conform to the new changes.
Article 28
This Contract i s produced in six identical copies, three o f which belong to each o f the Contractual parties.
93
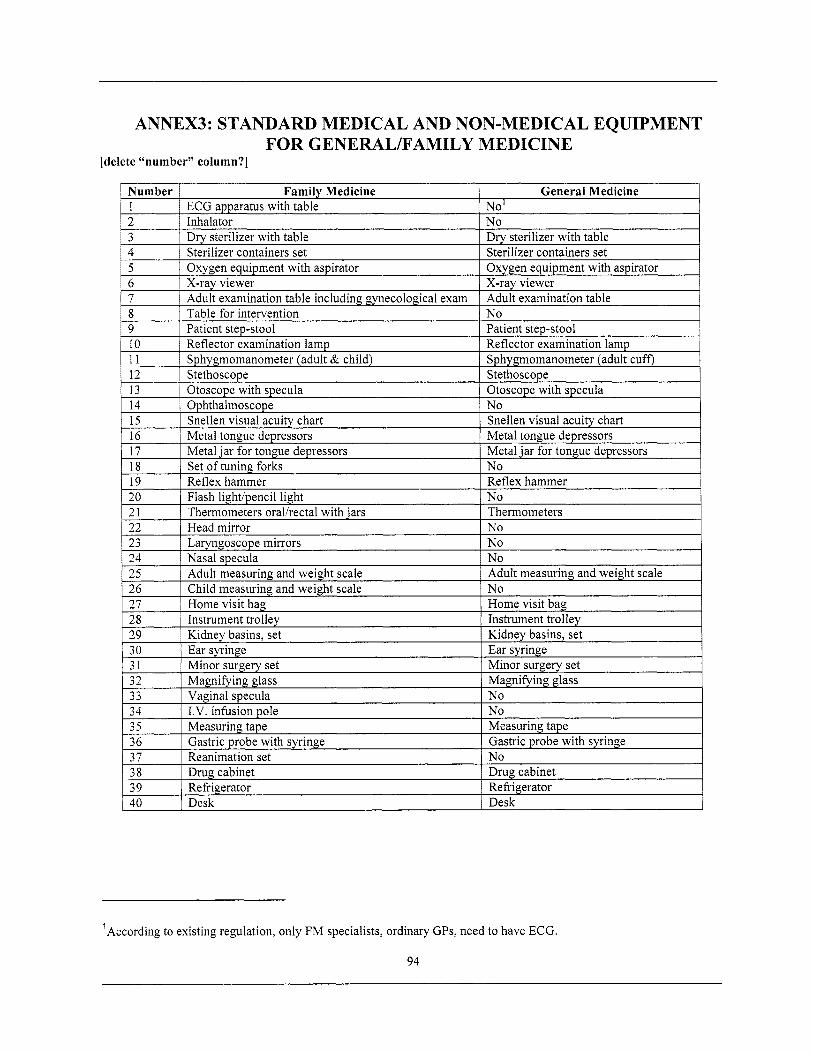
Number 1 2 3
1 4 I Sterilizer containers set I Sterilizer containers set
Family Medicine General Medicine ECG apparatus with table No’ Inhalator N o Drv sterilizer w i th table Drv sterilizer with table
’According to existing regulation, only FM specialists, ordinary GPs, need to have ECG.
94
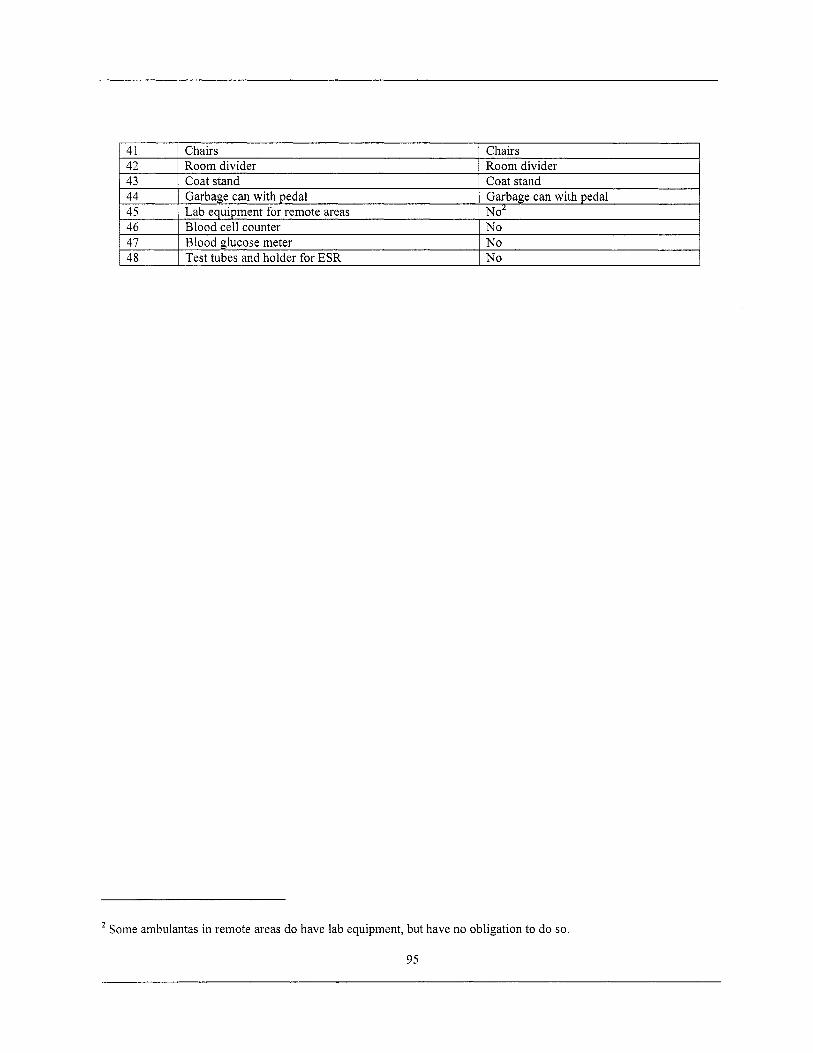
'Some ambulantas in remote areas do have lab equipment, but have no obligation to do so.
95
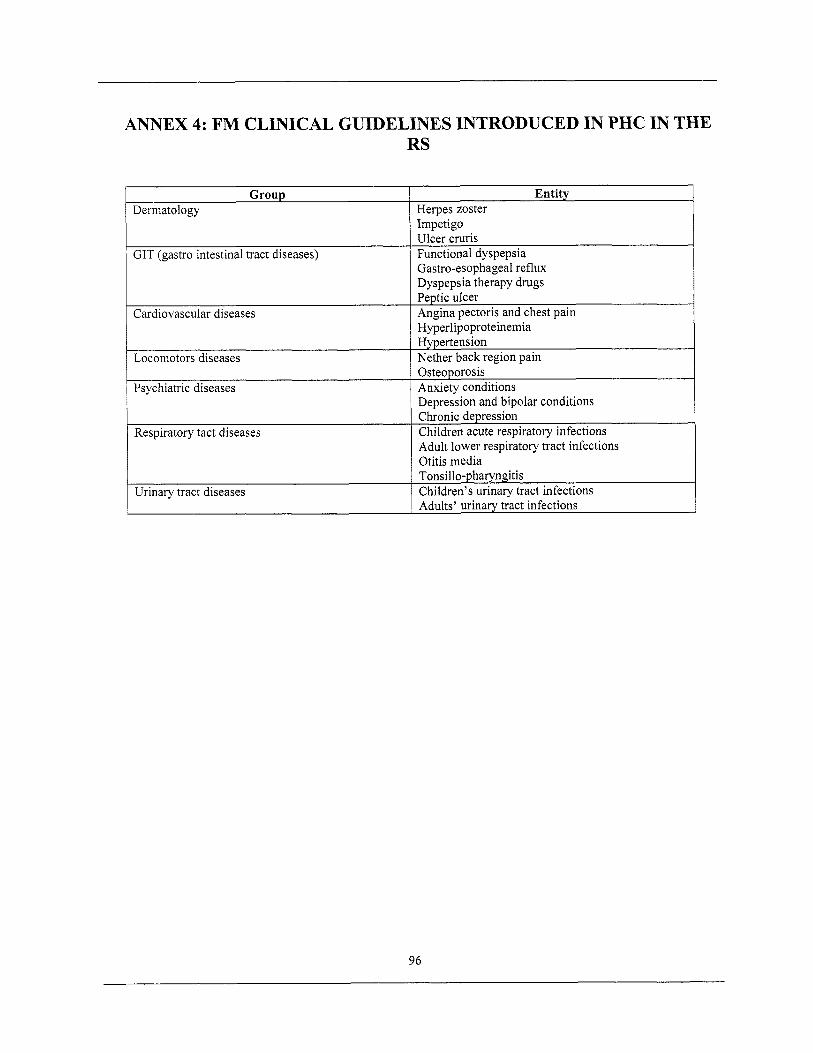
ANNEX 4: FM CLINICAL GUIDELINES INTRODUCED IN PHC IN THE
Group Dermatology
GIT (gastro intestinal tract diseases)
Cardiovascular diseases
Locomotors diseases
RS
Entity Herpes zoster Impetigo Ulcer cruris Functional dyspepsia Gastro-esophageal reflux Dyspepsia therapy drugs Peptic ulcer Angina pectoris and chest pain Hyperlipoproteinemia Hypertension Nether back region pain
Respiratory tact diseases
Urinary tract diseases
1 Osteoporosis Psychiatric diseases I Anxiety conditions
Depression and bipolar conditions Chronic depression Children acute respiratory infections Adult lower respiratory tract infections Otitis media Tonsillo-pharyngitis Children’s urinary tract infections Adults’ urinary tract infections
96
ANNEX 5: CURRICULUM FOR FM SPECIALIST TRAINING PROGRAM
Family medicine education i s aimed at providing a holistic approach to patient care rather than to a specific disease, symptom, or part o f the body.
The education includes:
1. Theoretical classes 648 classes
2. Practical classes 3276 classes
The specialization training methods include lectures, seminars, tutorials, self-directed work, clinical ski l ls training, and training on medical and surgical procedures.
The seminar program i s undertaken in the f i rst two years o f the training. The f i rs t year involves training in: principles and practice o f family medicine, doctor-patient relationship, utilization o f medical literature, and work on computers. The second year involves training in palliative care, geriatric care, psychosocial aspects o f medicine, occupational medicine, and organization and supervision o f fami ly medicine.
Clinical competencies, procedures, and ski l ls elements o f the program include consultation with patients, advising patients, organization and management o f family medicine teams, managing and utilizing fileddatabases and patients’ health charts, minor surgical and ambulance procedures, geriatric assessment procedures, and assessment o f mental condition.
Internship i s done in FM health centers in cycles which last six months in each year o f the specialist study.
Internal medicine
At internal medicine departments and in specialist internal clinics. rheumatology, endocrinology, and oncology.
Covers hematology, nephrology,
General internal medicine
1. Theoretical classes 36 classes
2. Practical classes 146 classes
Key areas: (a) primary treatment o f patients (history-taking); (b) diagnostic plan (diagnosis, differential diagnosis); (c) screening and interpreting ECG - especially in emergencies; (d) therapeutic procedures; (e) laboratory procedures; (f) emergency situations in internist practice and their treatment; (g) work in admission clinics and specialized clinics.
Cardiology
1. Theoretical classes 36 classes
2. Practical classes 146 classes
97
Key areas: (a) acute and chronic heart failure; (b) arrhythmias; (c) coronary heart disease; (d) rheumatic fever; (e) cardiomyopathy; ( f ) arterial hypertension; (g) cardiology drugs.
Pulmonary medicine
1. Theoretical classes 36 classes
2, Practical classes 146 classes
Key areas: (a) obstructive pulmonary diseases - asthma, COPD; (b) principles o f treating nonspecific respiratory diseases; (c) Cor pulmonale; (d) principles o f treating specific diseases.
Gastroenterology
1. Theoretical classes 36 classes
2. Practical classes 146 classes
Key areas: (a) diseases o f mouth, esophagus, stomach, duodenum, ileum; (b) colonic diseases; (c) pancreatic diseases; (d) liver diseases.
Infectious diseases
1. Theoretical classes 18 classes
2. Practical classes 73 classes
Key areas: (a) acute and chronic contagious diseases; (b) streptococcal infections; (c) other respiratory diseases; (d) influenza and other viral infections; (e) sepsis; ( f ) tetanus; (g) AIDS; (h) viral hepatitis.
Dermatology
1. Theoretical classes 18 classes
2. Practical classes 73 classes
Key areas: (a) performance of the acute allergy test; (b) taking samples o f epidermis when suspecting scabies; (c) taking smears f rom vulva, urethra, and vagina; (d)preparation o f genital discharge, paint it medicinal blue and recognize it under microscope; (e) taking samples for mycological analysis.
Gynecology
1. Theoretical classes 36 classes
2. Practical classes 146 classes
Key areas: (a) diagnostic and therapeutic methods; (b) microbiological analysis, basis o f cytological diagnostics, and general laboratory diagnostics; (c) acute gynecologic diseases; (d) menstrual cycle irregularities; (e) sterility; ( f ) fami ly planning and contraception methods; (g) sexually transmitted diseases, prevention and treatment; (h) basic methods for early detection o f malignant gynecologic and breast diseases.
Obstetrics
98
1. Theoretical classes 36 classes
2. Practical classes 146 classes
Key areas: (a) basic methods of pregnancy diagnostics; (b) pregnancy risks and premature birth; (c) managing normal pregnancy; (d) basic ski l ls for managing vaginal deliveries and care for newborns in the f i rs t few days after birth,
Pediatrics
1. Theoretical classes 72 classes
2. Practical classes 292 classes
Key areas: (a) prevention-promotion activities; (b) irregularities in growth and development; (c) psychomotor development o f children; (d) digestion system diseases; (e) infective diarrhea syndrome; (f) advantages and necessity o f breast feeding; artificial, diet, and parenteral food only when necessary; (g) diagnosing gastrointestinal tract diseases with children; (h) children urinary infections and kidney diseases; (i) children rheumatic diseases; G ) inborn heart anomalies; (k) respiratory distress syndrome with differential diagnosis; (I) neonatal hepatitis, physiological hepatitis, and hemolytic diseases; (m) noninfectious CNS diseases; (n) children convulsions and differential diagnosis; (0) febrile child; (p) hematological diseases at child age: anemia, thrombocytopenia, bleeding diseases, lymph glands, diseases, leucosis.
Emergency medicine
1. Theoretical classes 72 classes
2. Practical classes 292 classes
Key areas: (a) treatment o f unconscious and comatose patients, knowledge o f basic ECG, diagnostic principles, and laboratory diagnostics; (b) sk i l ls o f performing basic reanimation procedures with application o f breathing techniques and heart massage, as we l l as the usage o f the basic reanimation test; (c) procedures and processes in very anxious and convulsive conditions and illnesses, as wel l as procedures in acute and chronic psychosis; (d) ski l ls o f treating minor injuries, wounds dressing, and basic immobilization procedures; (e) procedures and skills in cardiopulmonary emergency situations.
Surgical disciplines
General surgery with orthopedics and reanimation
1. Theoretical classes 40 classes
2. Practical classes 162 classes
Ophthalmology
1. Theoretical classes 9 classes
2. Practical classes 36 classes
Surgical emergencies
99
1. Theoretical classes 9 classes
2. Practical classes 36 classes
Key areas: (a) basic bleeding stopping and the frontal nose tamponade skills; (b) preparation and sterilization o f primary wound dressing sets, primary wound treatment, and dressing technique; (c) insertion o f urinary catheter and gastric tube; (d) immobilization ski l ls with utilization o f standard and at-hand devices, abdominal and chest puncture; (e) procedures in diagnostics and differential diagnostics o f acute abdominal conditions; ( f ) procedures with comatose and pre-comatose patients; (g) reanimation procedures and skills (artificial breathing), heart massage, and utilization o f the basic massage set; (h) measures and procedures in shock conditions o f any etiology, procedures in acute heart conditions and injuries; (i) treatment and supervision o f chronic conditions in surgery disciplines; (i) immobile patient care and decubitus treatment; (k) procedures in acute conditions and diseases o f ear, throat, and nose, with acquisition o f minor surgery skil ls; (1) the skill o f removing alien bodies from ear and nose; (m) preoperational preparation with participation in operation risk assessment; (n) basic procedures in observation and diagnostics o f postoperative conditions; (0) support for the patient and the family before and after the operation; (p) close cooperation with specialists in specialized clinics and hospital departments.
Neurology
1. Theoretical classes 36 classes
2. Practical classes 146 classes
Key areas: (a) central and peripheral nervous system lesions; (b) cervical-bronchial syndrome; (c)consciousness disruptions in neurological diseases; (d) stroke; (e) polyneuropathy; ( f ) neurological complications in systemic diseases.
Psychiatry
1. Theoretical classes 36 classes
2. Practical classes 146 classes
Key areas: (a) delirium; (b) mental rehabilitation; (c) amnesia (confused-disoriented conditions); (d) psychotic conditions; (e) organic depressive conditions; ( f ) somatically induced anxious-depressive conditions.
Public health
1. Theoretical classes 36 classes
2. Practical classes 146 classes
Elective
1. Theoretical classes 72 classes
2. Practical classes 292 classes
100
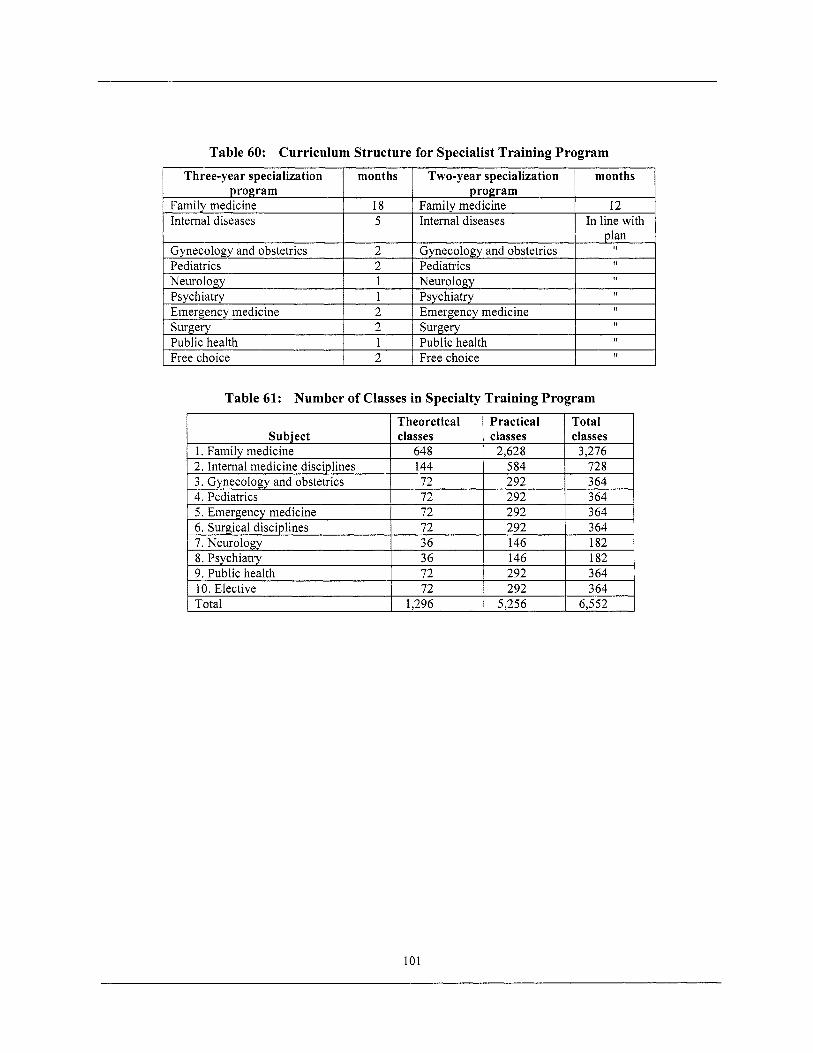
Table 60: Curriculum Structure for Specialist Training Program
1 Family medicine 18 I Family medicine 12
I Three-year specialization I months I Two-year specialization I months 1
1 Intemal diseases I 5 I Internal diseases I In line with 1
program program program program
Table 61: Number of Classes in Specialty Training Program
Family medicine Intemal diseases
101
18 Family medicine 12 5 Internal diseases In line with
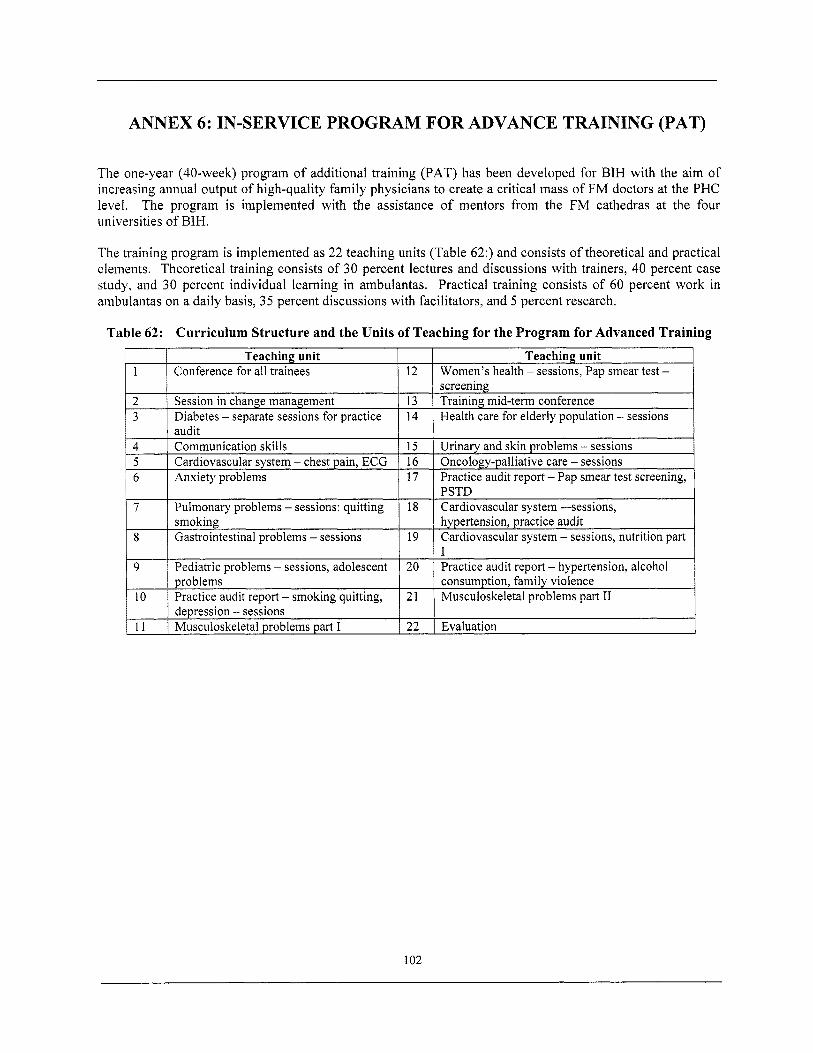
ANNEX 6: IN-SERVICE PROGRAM FOR ADVANCE TRAINING (PAT)
The one-year (40-week) program o f additional training (PAT) has been developed for BIH with the aim o f increasing annual output o f high-quality family physicians to create a critical mass o f FM doctors at the PHC level. The program i s implemented with the assistance o f mentors f rom the FM cathedras at the four universities o f BIH,
The training program i s implemented as 22 teaching units (Table 62:) and consists o f theoretical and practical elements. Theoretical training consists o f 3 0 percent lectures and discussions with trainers, 40 percent case study, and 30 percent individual learning in ambulantas. Practical training consists o f 60 percent work in ambulantas on a daily basis, 35 percent discussions with facilitators, and 5 percent research.
Table 62: Curriculum Structure and the Units of Teaching for the Program for Advanced Training
102
General Learning Objectives for Doctors
On completion o f the PAT, the Family Medicine Doctor will:
Understand and apply the principles o f Family Medicine in daily work with patients in the ambulanta.
Understand and apply the relevant practice changes to be able to provide continuing and comprehensive care to all registered patients in the ambulanta.
Perform as a skillful and supportive member o f the family medicine team, uti l izing the knowledge and ski l ls o f the Family Medicine Nurse.
Understand the important role o f Patient education and health promotion in the care o f patients in all age groups.
Demonstrate the ability to organize the ambulanta practice to maximize opportunities for prevention and screening.
Be able to identify local public health/ prevention priorities.
Understand and apply risk factor determination in individuals and vulnerable populations.
Understand and apply Case finding strategies for common health problems in the ambulanta population.
Have improved knowledge o f the diagnosis and treatment o f the common acute problems (infancy through old age, males and females) that are prevalent locally, including an evidence-based approach to use o f investigations and treatment resources.
Have improved knowledge o f the diagnosis and treatment o f the common chronic problems (infancy through old age, males and females) that are prevalent locally, including evidence-based use o f resources, effective referral mechanisms, use o f problem-oriented medical records and appointment systems to ensure continuity and coordination o f care.
Have improved knowledge and skill in the identification and init ial management o f common psychosocial problems including the needs o f special populations including refbgees, displaced people, the unemployed, and victims o f violence.
Have improved relevant physical examination skills, clinical skills, and communication sk i l ls to practice a more comprehensive model o f patient-centered medical care.
Understand the importance o f developing skill in critical appraisal o f the literature, and habits o f lifelong self- directed learning.
Understand and effectively apply concepts o f quality assurance and clinical audit o f aspects o f daily clinical work.
103
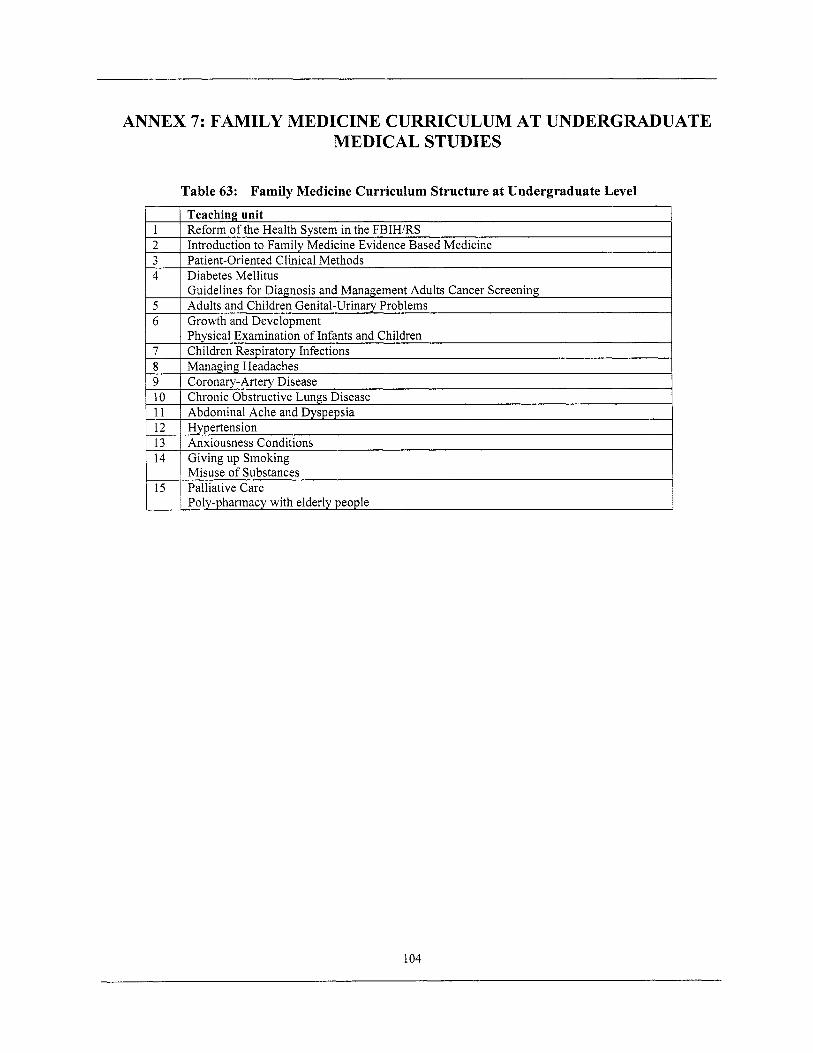
ANNEX 7: FAMILY MEDICINE CURRICULUM AT UNDERGRADUATE MEDICAL STUDIES
Table 63: Family Medicine Curriculum Structure at Undergraduate Level
104
ANNEX 8: DATA REGULARLY COLLECTED AT PHC LEVEL
Daily Record, form 2-01 RS Daily Record on Chest Diseases, form 3-04 RS Daily Record on Home Visits, form 3-06 RS Daily Record on Visits to Adult’s Consulting Room, form 3-02 RS Daily Record on Health Education Services, form 3-05 RS Daily Record on Visits to Children and Youth Consulting Room, form 3-01 RS Daily Record on Visits to Gynecology Consulting Room, form 3-03 RS Malign Neoplasm Report; Report on diseases, cases and injuries, form 3-05/1 RS Report on conducted ambulatory-polyclinics health services Communicable Diseases Report Death Certificate
105
ENDNOTES
1. Kutzin J, McPake B. “Methods for Evaluating Effects o f Health Reforms”, Current Concerns, Ara Paper number 13, World Health Organization, WHO/ARA/CC/97.3
2. Atun, R, Lennox-Chhuggani, N. Health System Development: A Review o f the Tools Used in Analysis and to Support Decision Making. Discussion Paper. 2003 Centre for Health Management. Imperial College London.
3. Hsiao, W. What Should Macroeconomists Know about Health Care Policy? IMF Working Paper. 2003. Washington, D.C., IMF.
4, Strauss, A, Corbin, J. Basics o f Qualitative Research Techniques and Procedures for Developing Grounded Theory (2nd edition). London: Sage Publications, 1998.
5. Lindelow, M, Wagstaff, A. Health Facility Surveys: An Introduction. Public Services, Development Research Group. Policy Research Working Paper 2953. The World Bank. January 2003.
6, Boerma, WGW. Profiles o f General Practice in Europe. An International Study o f Variation in the Tasks o f General Practitioners. Utrecht, Netherlands: NIVEL, 2003.
7. Miller, D. ECA Business Plan. PHC Chapter. World Bank 2004.
8. Memorandum o f the President o f the International Development Association to the Executive Directors on a Country Assistance Strategy o f the World Bank Group for Bosnia and Herzegovina. June 14, 2000. Southeast Europe Country Unit. Europe and Central Asia Region. Report No. 20592 BIH. The World Bank. 2000.
9. Ibid.
10. Bosnia and Herzegovina - Country assistance strategy progress report Vol. 1. Memorandum o f the President o f the International Development Association to the Executive Directors on A Country Assistance Strategy Progress Report o f The World Bank Group for Bosnia and Herzegovina. Report No. 22863. September 2001. South East Europe Country Unit. Europe and Central Asia Region. The World Bank.
1 1. Bosnia and Herzegovina Poverty Assessment (Volumes I and 11). Main Report. Poverty Reduction and Economic Management Unit. Europe and Central Asia Region. The World Bank. Report No. 25343- BIH. 2003.
12. Ibid.
13. Bisogno, M, Chong, S. “Bosnia and Herzegovina: Labor Market Study”. Mimeo. The World Bank, 2000.
14. Bosnia and Herzegovina Poverty Assessment (Volumes I and 11). Ma in Report. Poverty Reduction and Economic Management Unit. Europe and Central Asia Region. The World Bank. Report No. 25343- BIH. 2003.
15. Ibid.
16. Ibid.
17. Ibid.
106
18. Memorandum o f the President o f the International Development Association to the Executive Directors on a Country Assistance Strategy o f the World Bank Group for Bosnia and Herzegovina. June 14, 2000. Southeast Europe Country Unit. Europe and Central Asia Region. Report No. 20592 BIH. The World Bank. 2000.
19. Bosnia and Herzegovina: Interim Poverty Reduction Strategy Paper (I-PRSP). Bosnia and Herzegovina Ministry for Foreign Trade and Economic Relation. 2001
20. Memorandum o f the President o f the International Development Association to the Executive Directors on a Country Assistance Strategy o f the World Bank Group for Bosnia and Herzegovina. June 14, 2000. Southeast Europe Country Unit. Europe and Central Asia Region. Report No. 20592 BIH. The World Bank, 2000.
2 1. Strategic Health System Plan for the Federation o f BIH. Bosnia and Herzegovina, Federation o f BIH. Federal Ministry o f Health 1998. Sarajevo.
22. Project Appraisal Document on a Proposed Credit in the Amount o f Sdr 7.4 Mil l ion to Bosnia and Herzegovina for a Basic Health Project. APRIL 15, 1999. Human Development Sector Unit. Bosnia and Herzegovina Country Unit. Europe and Central Asia Region. The World Bank. Report No: 18637-BIH.
23. Ibid.
24. Ibid.
25. Ibid.
26. Giribona, P. Bosnia and Herzegovina, Basic Health Program. Primary Health Care Component, Medical
27. The World Bank, Bosnia and Herzegovina Social Insurance Technical Assistance Project. 2003. Human
28. Ibid.
29. The World Bank, International Development Association Country Assistance Strategy for Bosnia and
30. The European Union CARDS Programme for Bosnia and Herzegovina. Functional Review o f the Health
3 1, World Bank Health Sector Enhancement Project. Project Appraisal Document. Europe and Central Asia
32. Global Framework for Economic Development and Social Protection in Bosnia and Herzegovina, 2000-
33. Ibid.
34. Federation Health Program: Health Reform and Reconstruction. January 1998.
35. Public Health and Health Care: Federation o f Bosnia and Herzegovina. January 1997.
36. Law on Health Care. “Official Gazette o f the Federation o f Bosnia and Herzegovina,” No. 30/97.
37. Law on Health Insurance. “Official Gazette o f the Federation o f Bosnia and Herzegovina,” No. 32a/97.
38. Ibid.
39. Law on Health Care. “Official Gazette o f the Federation o f Bosnia and Herzegovina,” No. 30/97.
40. Ibid.
Equipment. Appraisal Report. The World Bank, 1998.
Development Unit. Europe and Central Asia Region. (Technical Annex May 27,2003)
Herzegovina. Europe and Central Asia Region. The World Bank Report No: 29196-BA. 2004
Sector in Bosnia and Herzegovina. EuropeAid/ll6649/C/SV/BA. Inception Report. May 2004.
Region, The World Bank, December 2004.
2004, March 2000, BH Ministry o f Foreign Trade and Economic Relations.
107
41. The Rulebook on Family Medicine Specialization Program” (FMSP). - Minister o f Health o f the
42. Law on Health Insurance. “Official Gazette o f the Federation o f Bosnia and Herzegovina,” No. 32aJ97.
43. Republika Srpska. Strategic Plan for Health System Reform and Reconstruction. 1997-2000. Ministry o f Health & Social Affairs o f the Republika Srpska, with the assistance o f the World Health Organization. May 1997.
44. Health Policy Targets and Measures in Republic o f Srpska by the Year 2020. Ministry o f Health and Social Welfare, Republic o f Srpska. Banja Luka 1999. h~://www.pcuhealth.orgien/docs/cm2020En.pdf last accessed September 18,2004.
45. Law on health care. Banja Luka, Republika Srpska Ministry o f Health and Social Welfare Expert Group (led by Prof. Dr D, Jakovljevic), 1999.
46. The Rulebook on Family Medicine Specialization Program” (FMSP). - Minister o f Health o f the Federation o f Bosnia and Herzegovina. Sarajevo 1999.
47. The Rulebook on Programme o f Additional Training in Family Medicine. - Minister o f Health o f the Federation o f Bosnia and Herzegovina, 2003.
48. The Health Resources Account Report for the Federation Solidarity Fund, 01.07 - 31.12.2003. Federation o f the Bosnia and Herzegovina.
49. The Rulebook on Family Medicine Specialization Program” (FMSP). - Minister o f Health and Social Welfare, AUGUST 27, 1999, with amendments and additions at JULY 25,2002 and JUNE 3,2003.
50, “The Rulebook on Programme o f Additional Training in Family Medicine” - Minister o f Health and
Federation o f Bosnia and Herzegovina. Sarajevo 1999.
51
52
53
Social Welfare, April 30,2003.
Ibid.
Inception report related to the implementation o f family medicine model in D Z Banja Luka, PCU Banja Luka, July 2002. Note: D Z Banja Luka i s the biggest DZ in Republika Srpska, covering app. 250,000 citizens . Strategic plan for health care reform and reconstruction in Republic o f Srpska 1997-2000. Banja Luka, Republika Srpska Ministry o f Health and Social Welfare Expert Group (led by Dr C. Aleksic), 1997.
-
54. Program for Prevention and Control o f Non-Communicable Diseases. Ministry o f Health and Social
55. Guidelines for Detection and Reduction o f Risks Factors and Early Detection o f Non-Communicable
56. Rulebook on Referral System in Health Care o f Republika Srpska. Ministry o f Health and Social
57. The Essential Drugs o f the Republika Srpska (247). Faculty o f Medicine. Republika Srpska. Banja
58, Decision on the Distribution o f the Health Insurance Fund Revenues. Health Insurance Fund, 2001.
59, The Rulebook on Family Medicine Specialization Program (FMSP). - Minister o f Health and Social Welfare, AUGUST 27, 1999, with amendments and additions at JULY 25, 2002 and JUNE 3,2003
60, Law on medical chambers (draft document). Banja Luka, Republika Srpska Ministry o f Health and Social Welfare Expert Group (led by Dr M. Balaban), 2000.
6 1. Law on “Changes and Additions on the Law on Health Care”. Republika Srpska. Banja Luka, 200 1.
Welfare, Republika Srpska. Banja Luka, 2002.
Diseases. Institute o f Public Health. Republika Srpska. Banja Luka, 2003.
Welfare. Republika Srpska. Banja Luka, 2002.
Luka, 1999.
108
62. Agency for Accreditation and Quality Improvement o f Health Care in Republika Srpska. Ministry o f
63, The Law on Citizens’ Association. Republika Srpska. Banja Luka, 1993.
Health and Social Welfare. Republika Srpska. Banja Luka, April 24, 2002.
109
Related Documents











