KSNACC KSAP KSOA KSPA KNRS KSCVA KSTA KSPS KSRA KSAM Vol. 16/No. 1 Jan. 2021 http://anesth-pain-med.org REVIEW ARTICLES 1 Who are at high risk of mortality and morbidity among children with congenital heart disease undergoing noncardiac surgery? 8 Perioperative glucocorticoid management based on current evidence 16 Safety of epidural steroids: a review pISSN: 1975-5171 eISSN: 2383-7977 Vol. 16/No. 1 Jan. 2021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

http://anesth-pain-med.orghttp://anesth-pain-med.orghttp://anesth-pain-med.orghttp://anesth-pain-med.orghttp://anesth-pain-med.orghttp://anesth-pain-med.org
KSNACC KSAP KSOA KSPA KNRS KSCVA KSTA KSPS KSRA KSAM
Vol. 16/N
o. 1 Jan. 2021
http://anesth-pain-med.org
REVIEW ARTICLES
1 Who are at high risk of mortality and morbidity among children with congenital heart disease undergoing noncardiac surgery?8 Perioperative glucocorticoid management based on current evidence16 Safety of epidural steroids: a review
pISSN: 1975-5171eISSN: 2383-7977
Vol. 16/No. 1Jan. 2021

THE K
OREA
N SOCIETY OF OBSTETRIC A
NES
THES
IOLO
GI S
T S
Aims and ScopeAnesthesia and Pain Medicine (APM) is the official scientific journal of Korean Society of Neuroscience in Anesthesiology and Critical Care (KSNACC), The Korean Society for Anesthetic Pharmacology (KSAP), The Korean Society of Obstetric Anesthesiologists (KSOA), The
Korean Society of Pediatric Anesthesiologists (KSPA), Korean Neuromuscular Research Society (KNRS), Korean Society of Cardiothoracic
and Vascular Anesthesiologists (KSCVA), Korean Society of Transplantation Anesthesiologists (KSTA), The Korean Spinal Pain Society
(KSPS), Korean Society of Regional Anesthesia (KSRA), and Korean Society for Airway Management (KSAM). The abbreviated title is
"Anesth Pain Med". It is published four times a year on the last day of January, April, July, and October in English.
The mission of APM is to improve safety and quality of care of related patients and clinical practice of anesthesiologists by publishing
definitive articles in the field of anesthesiology including practice of perioperative management, critical care, and pain medicine. The
scopes of APM are as follows : anesthesia-related issues from affiliated neuroanesthesiology (KSNACC), experimental, laboratory
works or clinical relevance of anesthetic pharmacology (KSAP), anesthesia for operative delivery, pain relief in labor, care of the
critically ill parturient, perinatal physiology and pharmacology (KSOA), anesthetic care, perioperative management, and alleviation
of pain in children (KSPA), physiology of neuromuscular transmission and block, pharmacology of neuromuscular blocking agents
and their reversal agents, principles and applications of neuromuscular monitoring, and drug interaction between neuromuscular
blocking agents and other substances (KNRS), anesthesia for cardiothoracic and vascular surgery and management of patients
undergoing various surgeries for patients with cardiac, pulmonary, and vascular diseases (KSCVA), perioperative anesthesia care
of transplantation surgery, physiology or pharmacology related with transplantation anesthesiology (KSTA), pathophysiology,
pharmacology, and all respects of spine related pain (KSPS), clinical techniques of regional blocks, anatomy, patient safety issues,
basic sciences such as pharmacology of local anesthetics or sedative drugs (KSRA), all fields of airway management including difficult
airway and complications (KSAM).
All or part of the Journal is indexed/tracked/covered by PubMed, PubMed Central (PMC), KoreaMed, KoMCI, Google Scholar, Science
Central.
Full text is freely available from http://anesth-pain-med.org
The circulation number per issue is 400.
Anesthesia and Pain Medicine January 2021; Volume 16, Number 1, Serial No. 59ⓒ 2021 the Korean Society of Anesthesiologists.
Korean Society of Neuroscience in Anesthesiologyand Critical Care
The Korean Society for Anesthetic Pharmacology
Korean Neuromuscular Research Society Korean Society of Cardiothoracic and VascularAnesthesiologists
The Korean Society of Obstetric Anesthesiologists The Korean Society of Pediatric Anesthesiologists
Korean Society of Transplantation Anesthesiologists The Korean Spinal Pain Society
Korean Society for Airway ManagementKorean Society of Regional Anesthesia
pISSN: 1975-5171eISSN: 2383-7977

iAnesth Pain Med
Vol.16 No.1 January 2021
PublisherJae-Hwan Kim (Korea University, Korea)
Editor-in-ChiefYoung-Cheol Woo (Chung-Ang University, Korea)
Associate EditorChong Wha Baek (Chung-Ang University, Korea)
Jung-Won Hwang (Seoul National University, Korea)Hyun Kyo Lim (Yonsei University, Korea)
Editorial BoardHyunjoo Ahn (Sungkyunkwan University, Korea)
Randal S. Blank (University of Virginia, USA)Yong Seon Choi (Yonsei University, Korea)
Woo-jong Choi (University of Ulsan, Korea)Yang Hoon Chung (Soonchunhyang University, Korea)Seongtae Jeong (Chonnam National University, Korea)
Jae Hun Kim (Konkuk University, Korea)Ju Hwan Lee (Wonkwang University, Korea)
Jeong-Rim Lee (Yonsei University, Korea)
Wonjin Lee (Inje University, Korea)Chaeseong Lim (Chungnam National University, Korea)Jung Hyun Park (The Catholic University of Korea, Korea)Hyungseok Seo (Kyung Hee University, Korea)Young Duck Shin (Chungbuk National University, Korea)Peter D. Slinger (University of Toronto, Canada)Weipeng Wang (Shanghai Deltahealth Hospital, China)Laurence Weinberg (University of Melbourne, Australia)Young Ju Won (Korea University, Korea)
Ethics EditorYoung Yoo (Korea University, Korea)
Statistics EditorEun-Jin Ahn (Chung-Ang University, Korea), Junyong In (Dongguk University, Korea),
Jong Hae Kim (Daegu Catholic University, Korea), Dong-Kyu Lee (Korea University, Korea)
Illustrated EditorYong Beom Kim (Gachon University of Medicine and Science, Korea)
Manuscript EditorJi Youn Ha (The Korean Society of Anesthesiologists, Korea), Se Jueng Kim (MEDrang Inc., Korea)
Contacting the Anesthesia and Pain Medicine
All manuscripts must be submitted online through the APM e-Submission system (http://submit.anesth-pain-med.org).Electronic files of the manuscript contents must be uploaded at the web site.Items pertaining to manuscripts submitted for publication, as well as letters or other forms of communication regarding the editorial
management of APM should be sent to:
Editor-in-Chief
Young-Cheol Woo
Publishing/Editorial Office
The Korean Society of Anesthesiologists101-3503, Lotte Castle President, 109 Mapo-daero, Mapo-gu, Seoul 04146, KoreaTel +82-2-795-5129, Fax +82-2-792-4089, E-mail [email protected]
Printed by M2PI
8th FL, DreamTower, 66 Seongsui-ro, Seongdong-gu, Seoul 04784, KoreaTel +82-2-2190-7300, Fax +82-2-2190-7333, E-mail [email protected]

Anesth Pain Medii
Vol.16 No.1 January 2021
Table of Contents
Reviews
1 Who are at high risk of mortality and morbidity among children with congenital heart disease undergoing noncardiac surgery?In-Kyung Song, Won-Jung Shin
8 Perioperative glucocorticoid management based on current evidence Kwon Hui Seo
16 Safety of epidural steroids: a review Min Soo Lee, Ho Sik Moon
Neuroanesthesia
Clinical Research
28 Pharmacological strategies to prevent postoperative delirium: a systematic review and network meta-analysisJun Mo Lee, Ye Jin Cho, Eun Jin Ahn, Geun Joo Choi, Hyun Kang
Obstetric Anesthesia
Clinical Research
49 Comparison of the effect of general and spinal anesthesia for elective cesarean section on maternal and fetal outcomes: a retrospective cohort studyTae-Yun Sung, Young Seok Jee, Hwang-Ju You, Choon-Kyu Cho
pISSN: 1975-5171eISSN: 2383-7977
Neuromuscular Research
Case Report
56 Treatment of rocuronium-induced anaphylaxis using sugammadexSun-Min Kim, Sei-hoon Oh, Seung-Ah Ryu
Cardiothoracic and Vascular Anesthesia
Clinical Research
60 Comparison of postoperative pulmonary complications between sugammadex and neostigmine in lung cancer patients undergoing video-assisted thoracoscopic lobectomy: a prospective double-blinded randomized trialTae Young Lee, Seong Yeop Jeong, Joon Ho Jeong, Jeong Ho Kim, So Ron Choi
http://anesth-pain-med.orghttp://anesth-pain-med.orghttp://anesth-pain-med.orghttp://anesth-pain-med.orghttp://anesth-pain-med.orghttp://anesth-pain-med.org
KSNACC KSAP KSOA KSPA KNRS KSCVA KSTA KSPS KSRA KSAM

iiiAnesth Pain Med
General Article
Clinical Research
108 An exploratory study of risk factors for pressure injury in patients undergoing spine surgeryDaeHee Suh, Su Yeon Kim, Byunghoon Yoo, Sangseok Lee
Spinal Pain
Clinical Research
81 Prolotherapy for the patients with chronic musculoskeletal pain: systematic review and meta-analysisGeonhyeong Bae, Suyeon Kim, Sangseok Lee, Woo Yong Lee, Yunhee Lim
Case Report
96 Paraplegia after transforaminal epidural steroid injection in a patient with severe lumbar disc herniation Seok Ho Jeon, Won Jang, Sun-Hee Kim, Yong-Hyun Cho, Hyun Seok Lee, Hyun Cheol Ko
103 Unexpected extrusion of the implantable pulse generator of the spinal cord stimulator Eun-Ji Choi, Hyun-Su Ri, Hyeonsoo Park, Hye-Jin Kim, Ji-Uk Yoon, Gyeong-Jo Byeon
Transplantation Anesthesia
Clinical Research
68 Changes in the allocation policy for deceased donor livers in Korea: perspectives from anesthesiologists Seung Yeon Yoo, Gaab Soo Kim
Case Report
75 Capillary leak syndrome and disseminated intravascular coagulation after kidney transplantation in a patient with hereditary angioedema Jeong Wook Park, Jinyoung Seo, Sang Hun Kim, Ki Tae Jung
Letters to the Editor
116 Change of inspired oxygen concentration and temperature in low flow anesthesia To The editorHong Seuk Yang, Dong Ho Park, Chang Young Jeong
117 In replyJiwook Kim, Hochul Lee, Sungwon Ryu, Donghee Kang, Siejeong Ryu, Doosik Kim


C
M
Y
CM
MY
CY
CMY
K
나제아_리플렛(2p)_A4(출력용).pdf 1 2019. 12. 9. 오후 5:42

KS
PA
INTRODUCTION
The incidence of congenital heart disease (CHD) is re-
ported to be about 6 per 1,000 full-term live births in the
United States [1]. With advances in the perinatal diagnosis
of CHD and improvement in surgical and medical man-
agement, the survival rate and life expectancy in children
with CHD have been increasing [2]. These children fre-
quently require noncardiac surgeries, including laparo-
scopic, urogenital, and otolaryngological surgeries. During
the first year of life, 41% of infants who underwent congen-
ital heart surgery had undergone noncardiac surgery by
the age of 5 years [3]. With an increasing demand for surgi-
cal procedures under general anesthesia in these patients,
it is not uncommon for anesthesiologists to encounter chil-
dren with an unrepaired CHD or residual pathologic con-
ditions, as well as children with a repaired CHD. Therefore,
it is important to identify children at risk of perioperative
Corresponding author Won-Jung Shin, M.D., Ph.D.Department of Anesthesiology and Pain Medicine, Laboratory for Cardiovascular Dynamics, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea Tel: 82-2-3010-5644 Fax: 82-2-3010-6790E-mail: [email protected]
With advances in the development of surgical and medical treatments for congenital heart disease (CHD), the population of children and adults with CHD is growing. This population requires multiple surgical and diagnostic imaging procedures. Therefore, general anesthesia is inevitable. In many studies, it has been reported that children with CHD have increased anesthesia risks when undergoing noncardiac surgeries compared to children without CHD. The highest risk group included patients with functional single ventricle, suprasystemic pul-monary hypertension, left ventricular outflow obstruction, and cardiomyopathy. In this re-view, we provide an overview of perioperative risks in children with CHD undergoing noncar-diac surgeries and anesthetic considerations in patients classified as having the highest risk.
Keywords: Anesthesia; Child; Congenital heart defect; Risk.
Who are at high risk of mortality and morbidity among children with congenital heart disease undergoing noncardiac surgery?
In-Kyung Song and Won-Jung Shin
Department of Anesthesiology and Pain Medicine, Laboratory for Cardiovascular
Dynamics, Asan Medical Center, University of Ulsan College of Medicine, Seoul,
Korea Received November 25, 2020Accepted December 7, 2020
ReviewAnesth Pain Med 2021;16:1-7https://doi.org/10.17085/apm.20090pISSN 1975-5171 • eISSN 2383-7977
morbidity and mortality and to understand their patho-
physiologic and hemodynamic status when preparing their
general anesthetic plan. In the following review, we discuss
the current knowledge regarding children with CHD who
have high anesthesia and surgical risks and also focus on
the perioperative considerations for these high-risk pa-
tients.
RISKS OF NONCARDIAC SURGERIES IN CHILDREN WITH CHD
Recently, mortality and perioperative adverse events re-
lated to noncardiac surgeries have been reported in chil-
dren studies with large sample populations, including
those with and without CHD. Baum et al. [4] showed that
the overall 30-day mortality after noncardiac procedures
was higher in patients with CHD (6.0%) than in those with-
out CHD (3.8%). They also found that age, complexity of
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
1

the operation, and CHD, were associated with periopera-
tive mortality. In the Pediatric Perioperative Cardiac Arrest
(POCA) Registry, causes of anesthesia-related cardiac ar-
rest were reported from nearly 80 voluntarily enrolled
North American institutions that provide anesthesia for
children over a period of 10 years [5]. In this study, children
with CHD had a higher mortality rate (33%) than those
without CHD (26%). Cardiac arrest was strongly associated
with surgical complexity and the patient’s underlying func-
tional status. Among the types of CHD, single ventricular
physiology, aortic stenosis, and cardiomyopathy were as-
sociated with the highest mortality following a cardiac ar-
rest. In another study, the incidence of perioperative cardi-
ac arrest was 2.9 per 10,000 anesthetic episodes among pa-
tients undergoing noncardiac surgeries, and of these, 27%
had CHD [6]. In addition, they found that the most com-
mon causes of cardiac arrest during noncardiac surgeries
were hypovolemia, bleeding, and massive transfusion.
These findings suggest that intrinsic surgical factors and
the associated hemodynamic deterioration are important
for estimating the risk of cardiac arrest. In a study investi-
gating 101,885 anesthetic cases, the overall 24-h mortality
after anesthesia was 13.4 per 10,000 [7]. The highest inci-
dence of death was in children younger than 30 days. Col-
lectively, children with CHD are faced with a high risk of
mortality and adverse events related to anesthesia when
undergoing noncardiac surgeries. In particular, the com-
plexity of CHD is regarded as an important factor influenc-
ing high risk of mortality. Therefore, children with CHD
may be at higher risk of mortality and morbidity during
and after noncardiac surgeries. In addition, age, anatomi-
cal and functional status according to CHD complexity,
and intrinsic surgical risks are points that must be consid-
ered with care when estimating the risks of mortality and
morbidity.
The other issue to consider is how to define and stratify
the risk factors. According to the American College of Sur-
geons who collected data on noncardiac surgeries as a part
of its National Surgical Quality Improvement Program for
the classification of CHD, CHD can be stratified as minor,
major, and severe, based on the residual lesion burden and
the functional status of the heart [8]. According to this clas-
sification, children who have maintained good cardiac
conditions with or without medication and children with a
repaired CHD are classified as having minor CHD; patients
with a repaired CHD but who have residual abnormalities
in hemodynamic status are considered to have major CHD;
patients with an unrepaired cyanotic CHD, pulmonary hy-
pertension, or ventricular dysfunction or children awaiting
transplantation are classified to have severe CHD. After
propensity matching for age, sex, physical status, surgical
emergency, and surgical complexity, severe CHD was sig-
nificantly associated with 30-day mortality and overall
mortality [8]. However, there was no difference between
children with minor CHD and their matched controls. In
addition to perioperative mortality, morbidities including
postoperative reintubation, infections, renal failure, neuro-
logic complications, thrombotic events, reoperation, and
readmission were more frequent in patients with major
and severe CHD. In a recent study regarding surgical com-
plexity, children with CHD younger than 1 year showed a
greater risk of postoperative complications, with an incre-
mental increase in odds ratios in the order of minor, major,
and severe CHD [9]. In another study of 3,010 children with
CHD undergoing noncardiac surgeries, major and severe
CHD remained significant risk factors for perioperative
cardiovascular events after adjusting for the American So-
ciety of Anesthesiologists physical status, emergency cases,
and surgical types [10].
In a previous study using a risk stratification tool to clas-
sify risk levels for perioperative cardiac complications, re-
paired atrial defects and ventricular septal defects were
considered low risk, maintenance cardiac medications;
and repaired cyanotic or complex CHD were classified as
moderate risk; and unrepaired cardiac anomalies, Williams
syndrome, pulmonary hypertension, valvular heart disease
with significant valvular gradients, hypertrophic cardiomy-
opathy with obstruction, congestive heart failure, or chil-
dren with ventricular-assisted devices were considered
high risk [11]. To further determine the anesthesia risk, age
less than 1 year, comorbidities, and surgical complexity
were included as the next step. Similarly, results from
non-validated data of anesthesia for noncardiac surgeries
indicated that children with CHD were classified as low,
intermediate, and high risk, and further discriminated
based on physiological decompensation, complexity of the
CHD, major surgery, age under 2 years, emergency, preop-
erative hospital stay more than 10 days, and American So-
ciety of Anesthesiologists physical status [12,13].
To date, only one study has reported a risk assessment
model using a validation cohort. This study identified eight
preoperative factors that were significant in determining
in-hospital mortality: 1) emergency procedure, 2) severe
CHD, 3) previous surgery within the last 30 days, 4) single
2 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PA
ventricular physiology, 5) inotropic use, 6) cardiopulmo-
nary resuscitation, 7) kidney injury, and 8) mechanical
ventilation [14]. Based on the variables obtained from mul-
tivariable logistic regression analyses, scores from 0 to 10
were determined. This scoring system showed good dis-
crimination and calibration with an area under the receiver
operating characteristic curve of 0.831 (95% confidence in-
terval: 0.787–0.875) in the validation cohort. Briefly, scores
≤ 3 were associated with low risk, scores of 4–6 were asso-
ciated with medium risk, and scores ≥ 7 were associated
with a high risk for mortality (odds ratios 1.54, 4.19, and
22.15, respectively) [14]. Notably, major and severe CHD,
including single ventricular physiology, were found to be
major determinants of perioperative outcomes [14]. In
contrast, surgical complexity was not significant [14]. They
also highlighted that scoring-based risk stratification for
mortality may be necessary to help guide the perioperative
management of patients with high-risk CHD.
Herein, we reviewed the perioperative considerations of
children undergoing noncardiac surgeries who were classi-
fied as having high-risk CHD, in common with most of the
previously reported studies.
SINGLE VENTRICULAR PHYSIOLOGY
It is critical that anesthesiologists understand the physi-
ology of each palliative stage of a single ventricle, which in-
cludes truncus arteriosus, large and multiple ventricular
septal defects, and hypoplastic left heart syndrome
(HLHS). Patients who have not undergone completion of
superior cavopulmonary anastomosis (SCPA) are known to
have the highest risks during noncardiac surgeries and
congenital heart surgery. Especially in HLHS, the mortality
rate of patients younger than 2 years has been reported to
be up to 19% after noncardiac surgeries [15]. Hemodynam-
ic derangement is caused by excessive pulmonary blood
perfusion and poor systemic perfusion from imbalanced
circulation, decreased coronary perfusion, impairment of
the systemic right ventricle, and atrioventricular valve dys-
function. As the single ventricle concurrently operates both
the pulmonary and systemic circulations, hemodynamic
balance is frequently disrupted by alterations in pulmo-
nary and systemic vascular resistance (PVR and SVR, re-
spectively), ventilatory strategy including hypoxia and hy-
percapnia, acid-base balance, and intravascular volume
status. Therefore, postponing elective noncardiac proce-
dures under after SCPA is recommended. If the patient
could not postpone due to an emergent condition, Pulmo-
nary-to-systemic blood flow ratio should be at or just below
1 to maintain systemic perfusion and optimize oxygen de-
livery, consequently resulting in arterial oxygen saturation
of 80–90% [16].
After the SCPA, the single ventricle is no longer operating
with the volume overloading required to sustain parallel
circulations. Accordingly, cardiac output and systemic per-
fusion are not entirely dependent on pulmonary blood
flow, which makes the hemodynamic performance rela-
tively stable. However, hypercarbia, acidosis, and elevated
airway pressure should be avoided because pulmonary
blood flow remains dependent on PVR. However, hypocar-
bia may exacerbate a decrease in cerebral blood flow and
reduce venous return from the brain and upper body [17].
If there is high pressure in the superior vena cava, the head
and the tongue may become congestive due to disturbance
in venous return. In these patients, the goal of anesthetic
management is to maintain systemic oxygenation with ad-
equate pulmonary blood flow, which is secured by opti-
mizing intravascular volume, minimizing airway pressure,
and ensuring a low PVR.
Finally, the destination of single ventricular physiology is
the completion of successful Fontan circulation, in which all
systemic venous return is composed of pulmonary blood
flow. Even though systemic arterial saturation is maintained
above 90%, cardiac output relies on pulmonary blood flow
that runs down passively because there is no pump func-
tion producing a pulsatile driving pressure. Pulmonary
blood flow and cardiac output are strictly influenced by
mechanical ventilation with positive end-expiratory pres-
sure [18,19]. In addition, the pressure of the systemic ve-
nous system is elevated, and its capacitance is decreased,
and accompanied by diminished recruitment reserve of
the vascular volume [20]. Consequently, patients with a
Fontan circulation are intolerant of vasodilation from anes-
thetic agents, surgical bleeding, and dehydration. It may be
beneficial to prepare inotropic agents and vasopressors for
the treatment of hypotension and avoid excessive volume
challenges [20]. Unfortunately, bleeding tendency may be
increased due to persistent high venous pressure and anti-
coagulant therapy. However, they also have thrombosis
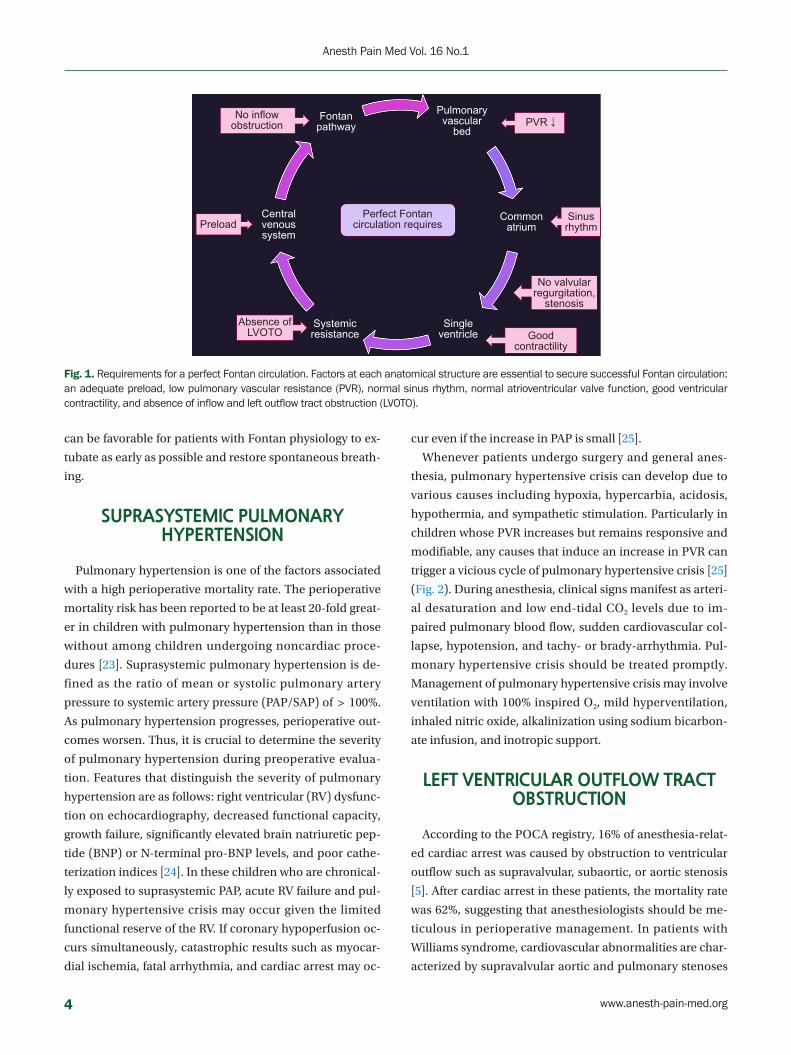
risks [21]. Along with preloading, other factors are required
to achieve the perfect Fontan circulation as follows: low
PVR, sinus rhythm, normal atrioventricular valve function,
good ventricular performance, and the absence of inflow
and outflow tract obstruction [22] (Fig. 1). After surgery, it
www.anesth-pain-med.org 3
Risks associated with congenital heart disease
can be favorable for patients with Fontan physiology to ex-
tubate as early as possible and restore spontaneous breath-
ing.
SUPRASYSTEMIC PULMONARY HYPERTENSION
Pulmonary hypertension is one of the factors associated
with a high perioperative mortality rate. The perioperative
mortality risk has been reported to be at least 20-fold great-
er in children with pulmonary hypertension than in those
without among children undergoing noncardiac proce-
dures [23]. Suprasystemic pulmonary hypertension is de-
fined as the ratio of mean or systolic pulmonary artery
pressure to systemic artery pressure (PAP/SAP) of > 100%.
As pulmonary hypertension progresses, perioperative out-
comes worsen. Thus, it is crucial to determine the severity
of pulmonary hypertension during preoperative evalua-
tion. Features that distinguish the severity of pulmonary
hypertension are as follows: right ventricular (RV) dysfunc-
tion on echocardiography, decreased functional capacity,
growth failure, significantly elevated brain natriuretic pep-
tide (BNP) or N-terminal pro-BNP levels, and poor cathe-
terization indices [24]. In these children who are chronical-
ly exposed to suprasystemic PAP, acute RV failure and pul-
monary hypertensive crisis may occur given the limited
functional reserve of the RV. If coronary hypoperfusion oc-
curs simultaneously, catastrophic results such as myocar-
dial ischemia, fatal arrhythmia, and cardiac arrest may oc-
cur even if the increase in PAP is small [25].
Whenever patients undergo surgery and general anes-
thesia, pulmonary hypertensive crisis can develop due to
various causes including hypoxia, hypercarbia, acidosis,
hypothermia, and sympathetic stimulation. Particularly in
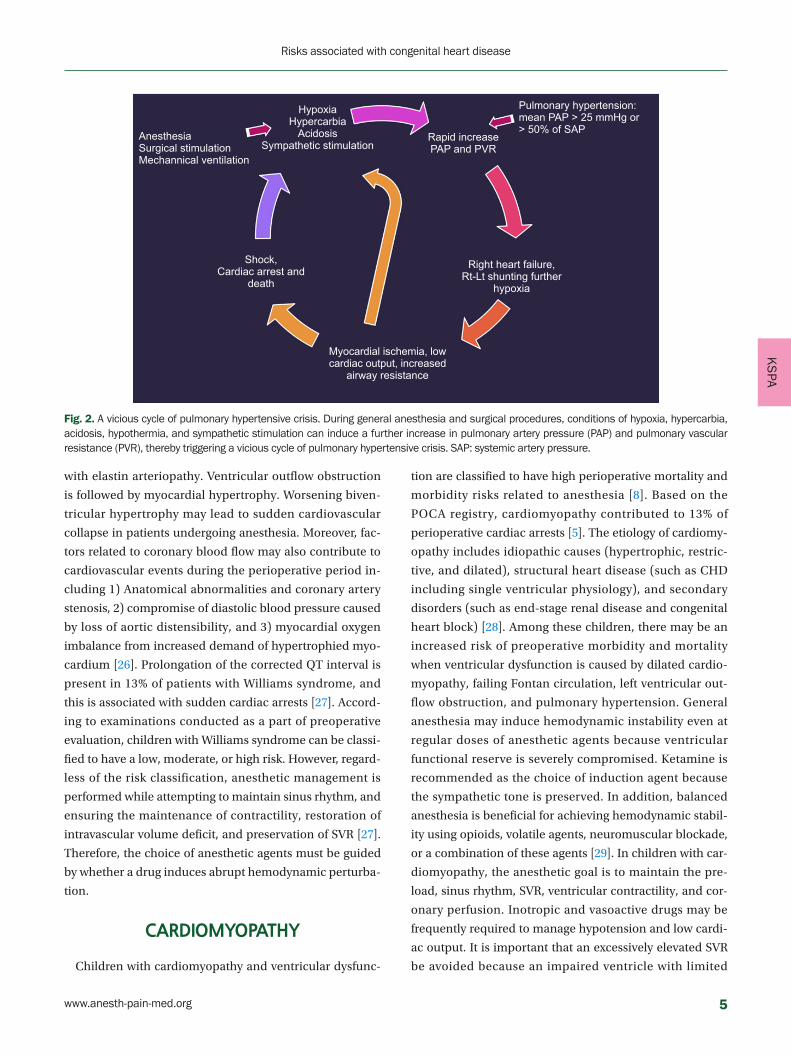
children whose PVR increases but remains responsive and
modifiable, any causes that induce an increase in PVR can
trigger a vicious cycle of pulmonary hypertensive crisis [25]
(Fig. 2). During anesthesia, clinical signs manifest as arteri-
al desaturation and low end-tidal CO2 levels due to im-
paired pulmonary blood flow, sudden cardiovascular col-
lapse, hypotension, and tachy- or brady-arrhythmia. Pul-
monary hypertensive crisis should be treated promptly.
Management of pulmonary hypertensive crisis may involve
ventilation with 100% inspired O2, mild hyperventilation,
inhaled nitric oxide, alkalinization using sodium bicarbon-
ate infusion, and inotropic support.
LEFT VENTRICULAR OUTFLOW TRACT OBSTRUCTION
According to the POCA registry, 16% of anesthesia-relat-
ed cardiac arrest was caused by obstruction to ventricular
outflow such as supravalvular, subaortic, or aortic stenosis
[5]. After cardiac arrest in these patients, the mortality rate
was 62%, suggesting that anesthesiologists should be me-
ticulous in perioperative management. In patients with
Williams syndrome, cardiovascular abnormalities are char-
acterized by supravalvular aortic and pulmonary stenoses
No inflow obstruction
Fontan pathway
Pulmonary vascular
bed
Perfect Fontan circulation requires
Common atrium
Single ventricle
Systemic resistance
Central venous system
Sinus rhythmPreload
Absence of LVOTO
No valvular regurgitation,
stenosis
Good contractility
PVR ↓
Fig. 1. Requirements for a perfect Fontan circulation. Factors at each anatomical structure are essential to secure successful Fontan circulation: an adequate preload, low pulmonary vascular resistance (PVR), normal sinus rhythm, normal atrioventricular valve function, good ventricular contractility, and absence of inflow and left outflow tract obstruction (LVOTO).
4 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
KS
PA
with elastin arteriopathy. Ventricular outflow obstruction
is followed by myocardial hypertrophy. Worsening biven-
tricular hypertrophy may lead to sudden cardiovascular
collapse in patients undergoing anesthesia. Moreover, fac-
tors related to coronary blood flow may also contribute to
cardiovascular events during the perioperative period in-
cluding 1) Anatomical abnormalities and coronary artery
stenosis, 2) compromise of diastolic blood pressure caused
by loss of aortic distensibility, and 3) myocardial oxygen
imbalance from increased demand of hypertrophied myo-
cardium [26]. Prolongation of the corrected QT interval is
present in 13% of patients with Williams syndrome, and
this is associated with sudden cardiac arrests [27]. Accord-
ing to examinations conducted as a part of preoperative
evaluation, children with Williams syndrome can be classi-
fied to have a low, moderate, or high risk. However, regard-
less of the risk classification, anesthetic management is
performed while attempting to maintain sinus rhythm, and
ensuring the maintenance of contractility, restoration of
intravascular volume deficit, and preservation of SVR [27].
Therefore, the choice of anesthetic agents must be guided
by whether a drug induces abrupt hemodynamic perturba-
tion.
CARDIOMYOPATHY
Children with cardiomyopathy and ventricular dysfunc-
tion are classified to have high perioperative mortality and
morbidity risks related to anesthesia [8]. Based on the
POCA registry, cardiomyopathy contributed to 13% of
perioperative cardiac arrests [5]. The etiology of cardiomy-
opathy includes idiopathic causes (hypertrophic, restric-
tive, and dilated), structural heart disease (such as CHD
including single ventricular physiology), and secondary
disorders (such as end-stage renal disease and congenital
heart block) [28]. Among these children, there may be an
increased risk of preoperative morbidity and mortality
when ventricular dysfunction is caused by dilated cardio-
myopathy, failing Fontan circulation, left ventricular out-
flow obstruction, and pulmonary hypertension. General
anesthesia may induce hemodynamic instability even at
regular doses of anesthetic agents because ventricular
functional reserve is severely compromised. Ketamine is
recommended as the choice of induction agent because
the sympathetic tone is preserved. In addition, balanced
anesthesia is beneficial for achieving hemodynamic stabil-
ity using opioids, volatile agents, neuromuscular blockade,
or a combination of these agents [29]. In children with car-
diomyopathy, the anesthetic goal is to maintain the pre-
load, sinus rhythm, SVR, ventricular contractility, and cor-
onary perfusion. Inotropic and vasoactive drugs may be
frequently required to manage hypotension and low cardi-
ac output. It is important that an excessively elevated SVR
be avoided because an impaired ventricle with limited
Anesthesia Surgical stimulationMechannical ventilation
HypoxiaHypercarbia
AcidosisSympathetic stimulation
Rapid increase PAP and PVR
Right heart failure, Rt-Lt shunting further
hypoxia
Myocardial ischemia, low cardiac output, increased
airway resistance
Shock,Cardiac arrest and
death
Pulmonary hypertension:mean PAP > 25 mmHg or > 50% of SAP
Fig. 2. A vicious cycle of pulmonary hypertensive crisis. During general anesthesia and surgical procedures, conditions of hypoxia, hypercarbia, acidosis, hypothermia, and sympathetic stimulation can induce a further increase in pulmonary artery pressure (PAP) and pulmonary vascular resistance (PVR), thereby triggering a vicious cycle of pulmonary hypertensive crisis. SAP: systemic artery pressure.
www.anesth-pain-med.org 5
Risks associated with congenital heart disease
contractile reserve is not tolerant of a high afterload [30].
CONCLUSION
Children with CHD, particularly single ventricular physi-
ology, suprasystemic pulmonary hypertension, left ventric-
ular outflow obstruction, and cardiomyopathy with ven-
tricular dysfunction, have the highest morbidity and mor-
tality risks following noncardiac surgeries. During the pre-
operative evaluation of these patients, it is necessary to
identify whether residual functional or anatomical impair-
ment is present at the time of surgery. To prevent poor out-
comes and avoid worse-case scenarios, anesthesiologists
should be fully acquainted with the pathophysiology of
CHD and be able to respond to intraoperative events and
complications during surgery in a timely manner.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Won-Jung Shin, In-Kyung Song. Writ-
ing - original draft: In-Kyung Song. Writing - review & edit-
ing: Won-Jung Shin.
ORCID
In-Kyung Song, https://orcid.org/0000-0002-7699-2005
Won-Jung Shin, https://orcid.org/0000-0002-6790-3859
REFERENCES
1. Hoffman JI, Kaplan S. The incidence of congenital heart dis-
ease. J Am Coll Cardiol 2002; 39: 1890-900.
2. Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N,
Kaouache M. Lifetime prevalence of congenital heart disease
in the general population from 2000 to 2010. Circulation 2014;
130: 749-56.
3. Sulkowski JP, Cooper JN, McConnell PI, Pasquali SK, Shah SS,
Minneci PC, et al. Variability in noncardiac surgical procedures
in children with congenital heart disease. J Pediatr Surg 2014;
49: 1564-9.
4. Baum VC, Barton DM, Gutgesell HP. Influence of congenital
heart disease on mortality after noncardiac surgery in hospi-
talized children. Pediatrics 2000; 105: 332-5.
5. Ramamoorthy C, Haberkern CM, Bhananker SM, Domino KB,
Posner KL, Campos JS, et al. Anesthesia-related cardiac arrest
in children with heart disease: data from the Pediatric Periop-
erative Cardiac Arrest (POCA) registry. Anesth Analg 2010; 110:
1376-82.
6. Flick RP, Sprung J, Harrison TE, Gleich SJ, Schroeder DR, Han-
son AC, et al. Perioperative cardiac arrests in children between
1988 and 2005 at a tertiary referral center: a study of 92,881 pa-
tients. Anesthesiology 2007; 106: 226-37.
7. van der Griend BF, Lister NA, McKenzie IM, Martin N, Ragg
PG, Sheppard SJ, et al. Postoperative mortality in children after
101,885 anesthetics at a tertiary pediatric hospital. Anesth An-
alg 2011; 112: 1440-7.
8. Faraoni D, Zurakowski D, Vo D, Goobie SM, Yuki K, Brown ML,
et al. Post-operative outcomes in children with and without
congenital heart disease undergoing noncardiac surgery. J Am
Coll Cardiol 2016; 67: 793-801.
9. Miller R, Tumin D, Tobias JD, McKee C. Estimating surgical risk
in younger and older children with congenital heart disease. J
Surg Res 2018; 232: 298-307.
10. Lee S, Reddington E, Koutsogiannaki S, Hernandez MR, Ode-
gard KC, DiNardo JA, et al. Incidence and risk factors for
perioperative cardiovascular and respiratory adverse events in
pediatric patients with congenital heart disease undergoing
noncardiac procedures. Anesth Analg 2018; 127: 724-9.
11. Saettele AK, Christensen JL, Chilson KL, Murray DJ. Children
with heart disease: risk stratification for non-cardiac surgery. J
Clin Anesth 2016; 35: 479-84.
12. Ng SM, Jin X, Yates R, Kelsall AW. Outcome of noncardiac sur-
gery in children with congenital heart disease performed out-
side a cardiac center. J Pediatr Surg 2016; 51: 252-6.
13. White MC, Peyton JM. Anaesthetic management of children
with congenital heart disease for non-cardiac surgery. Contin
Educ Anaesth Crit Care Pain 2012; 12: 17-22.
14. Faraoni D, Vo D, Nasr VG, DiNardo JA. Development and vali-
dation of a risk stratification score for children with congenital
heart disease undergoing noncardiac surgery. Anesth Analg
2016; 123: 824-30.
15. Torres A Jr, DiLiberti J, Pearl RH, Wohrley J, Raff GW, Bysani GK,
et al. Noncardiac surgery in children with hypoplastic left heart
syndrome. J Pediatr Surg 2002; 37: 1399-403.
16. Gottlieb EA, Andropoulos DB. Anesthesia for the patient with
congenital heart disease presenting for noncardiac surgery.
Curr Opin Anaesthesiol 2013; 26: 318-26.
17. Mott AR, Alomrani A, Tortoriello TA, Perles Z, East DL, Stayer
SA. Changes in cerebral saturation profile in response to me-
6 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PA
chanical ventilation alterations in infants with bidirectional
superior cavopulmonary connection. Pediatr Crit Care Med
2006; 7: 346-50.
18. Penny DJ, Hayek Z, Redington AN. The effects of positive and
negative extrathoracic pressure ventilation on pulmonary
blood flow after the total cavopulmonary shunt procedure. Int
J Cardiol 1991; 30: 128-30.
19. Redington AN, Penny D, Shinebourne EA. Pulmonary blood
flow after total cavopulmonary shunt. Br Heart J 1991; 65: 213-
7.
20. Yuki K, Casta A, Uezono S. Anesthetic management of noncar-
diac surgery for patients with single ventricle physiology. J
Anesth 2011; 25: 247-56.
21. Odegard KC, McGowan FX Jr, Zurakowski D, Dinardo JA, Cas-
tro RA, del Nido PJ, et al. Procoagulant and anticoagulant fac-
tor abnormalities following the Fontan procedure: increased
factor VIII may predispose to thrombosis. J Thorac Cardiovasc
Surg 2003; 125: 1260-7.
22. Windsor J, Townsley MM, Briston D, Villablanca PA, Alegria JR,
Ramakrishna H. Fontan palliation for single-ventricle physiol-
ogy: perioperative management for noncardiac surgery and
analysis of outcomes. J Cardiothorac Vasc Anesth 2017; 31:
2296-303.
23. Chau DF, Gangadharan M, Hartke LP, Twite MD. The post-an-
esthetic care of pediatric patients with pulmonary hyperten-
sion. Semin Cardiothorac Vasc Anesth 2016; 20: 63-73.
24. Abman SH, Hansmann G, Archer SL, Ivy DD, Adatia I, Chung
WK, et al. American Heart Association Council on Cardiopul-
monary, Critical Care, Perioperative and Resuscitation; Coun-
cil on Clinical Cardiology; Council on Cardiovascular Disease
in the Young; Council on Cardiovascular Radiology and Inter-
vention; Council on Cardiovascular Surgery and Anesthesia;
and the American Thoracic Society. Pediatric pulmonary hy-
pertension: guidelines from the American Heart Association
and American Thoracic Society. Circulation 2015; 132: 2037-
99.
25. Latham GJ, Yung D. Current understanding and perioperative
management of pediatric pulmonary hypertension. Paediatr
Anaesth 2019; 29: 441-56.
26. Brown ML, DiNardo JA, Nasr VG. Anesthesia in pediatric pa-
tients with congenital heart disease undergoing noncardiac
surgery: defining the risk. J Cardiothorac Vasc Anesth 2020; 34:
470-8.
27. Matisoff AJ, Olivieri L, Schwartz JM, Deutsch N. Risk assess-
ment and anesthetic management of patients with Williams
syndrome: a comprehensive review. Paediatr Anaesth 2015; 25:
1207-15.
28. Kipps AK, Ramamoorthy C, Rosenthal DN, Williams GD. Chil-
dren with cardiomyopathy: complications after noncardiac
procedures with general anesthesia. Paediatr Anaesth 2007; 17:
775-81.
29. Murphy TW, Smith JH, Ranger MR, Haynes SR. General anes-
thesia for children with severe heart failure. Pediatr Cardiol
2011; 32: 139-44.
30. Ing RJ, Ames WA, Chambers NA. Paediatric cardiomyopathy
and anaesthesia. Br J Anaesth 2012; 108: 4-12.
www.anesth-pain-med.org 7
Risks associated with congenital heart disease

INTRODUCTION
Synthetic glucocorticoids were first introduced in 1949
after the development of a purified preparation, known as
cortisone, and became a revolutionary treatment for pa-
tients with primary adrenal failure and other acute-chronic
inflammatory and autoimmune diseases. In anesthesiolo-
gy, it is widely used to treat reactive airway diseases, acute
nerve injury, nausea or vomiting, inflammatory diseases,
and excessive immunosuppression during organ trans-
Corresponding author Kwon Hui Seo, M.D., Ph.D. Department of Anesthesiology and Pain Medicine, Hallym University Sacred Heart Hospital, Hallym University School of Medicine, 22 Gwanpyeong-ro 170beon-gil, Dongan-gu, Anyang 14068, Korea Tel: 82-31-380-5959 Fax: 82-31-385-3244 E-mail: [email protected]
Glucocorticoid preparations, adreno-cortical steroids, with strong anti-inflammatory and im-munosuppressive effects, are widely used for treating various diseases. The number of pa-tients exposed to steroid therapy prior to surgery is increasing. When these patients present for surgery, the anesthesiologist must decide whether to administer perioperative steroid supplementation. Stress-dose glucocorticoid administration is required during the perioper-ative period because of the possibility of failure of cortisol secretion to cope with the in-creased cortisol requirement due to surgical stress, adrenal insufficiency, hemodynamic in-stability, and the possibility of adrenal crisis. Therefore, glucocorticoids should be supple-mented at the same level as that of normal physiological response to surgical stress by eval-uating the invasiveness of surgery and inhibition of the hypothalamus-pituitary-adrenal axis. Various textbooks and research articles recommend the stress-dose of glucocorticoids during perioperative periods. It has been commonly suggested that glucocorticoids should be administered in an amount equivalent to about 100 mg of cortisol for major surgery be-cause it induces approximately 5 times the normal secretion. However, more studies, with appropriate power, regarding the administration of stress-dose glucocorticoids are still re-quired, and evaluation of patients with possible adrenal insufficiency and appropriate gluco-corticoid administration based on surgical stress will help improve the prognosis.
Keywords: Adrenal glands; Adrenal insufficiency; Glucocorticoids; Hypothalmus; Periopera-tive period; Pituitary gland; Steroids.
Perioperative glucocorticoid management based on current evidence
Kwon Hui Seo
Department of Anesthesiology and Pain Medicine, Hallym University Sacred Heart
Hospital, Hallym University School of Medicine, Anyang, KoreaReceived November 16, 2020Accepted November 30, 2020
ReviewAnesth Pain Med 2021;16:8-15https://doi.org/10.17085/apm.20089pISSN 1975-5171 • eISSN 2383-7977
plantation or cardiopulmonary bypass [1]. Shortly after the
development of synthetic cortisone, there were two case
reports of perioperative secondary adrenal crisis. The two
young patients on chronic cortisone therapy stopped ste-
roids before the surgery; they suddenly died after the sur-
gery, and the result of the autopsy showed bilateral adrenal
atrophy [2,3]. Since then, it has become common practice
to perioperatively administer glucocorticoids at a su-
pra-physiological dose, the so-called stress-dose, to pa-
tients on steroid therapy for long duration and in suspected
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
8

KS
AP
adrenal failure cases.
The number of patients exposed to steroid therapy prior
to surgery is increasing as corticosteroids are widely used
for systemic administration and as inhalation and topical
drugs [4]. Accordingly, clinical trials and retrospective
analyses have been conducted regarding stress-dose glu-
cocorticoids administration in the perioperative period for
patients on steroid therapy [5,6]. However, many clinical
trials had a low level of evidence, including unclear criteria
for adrenal failure with a limited number of patients, re-
sulting in various proposed recommendations for the ad-
ministration of glucocorticoids in the perioperative periods
[7]. Therefore, this article reviews the physiology of adre-
no-cortical hormones and indications and applications of
stress-dose glucocorticoids in the perioperative periods
based on recently published recommendations [7,8].
PHYSIOLOGY OF ADRENOCORTICAL HORMONE SECRETION:
HYPOTHALAMUS-PITUITARY-ADRENAL AXIS
Adrenocorticosteroids are steroid derivatives produced in
the adrenal cortex and include three endogenous hormones:
glucocorticoid, mineralocorticoid, and androgen. All of
them are synthesized when cholesterol is converted to preg-
nenolone by the cytochrome P450 enzyme [1]. Of these, glu-
cocorticoids are secreted from the zona fasciculata of the
adrenal cortex and the most important glucocorticoid is cor-
tisol. Cortisol is an essential hormone for maintaining life. It
mediates carbohydrate and protein metabolism, fatty acid
transfer, electrolyte and fluid balance, and anti-inflammato-
ry reactions. Cortisol enables the synthesis and release of
catecholamines and contributes to normal vascular perme-
ability, vascular tone, and myocardial contraction by regu-
lating β-receptor synthesis and regulation [1].
The secretion of adrenal cortical hormones is regulated
by the hypothalamic-pituitary-adrenal (HPA) axis. The cor-
ticotropin-releasing hormone (CRH) secreted from the hy-
pothalamus stimulates the secretion of adrenocortico-
tropic hormone (ACTH) in the anterior pituitary gland, and
ACTH stimulates the adrenal gland. This positive feedback
for cortisol secretion and negative feedback for inhibiting
the secretion of CRH and ACTH due to increased cortisol
concentration regulates the secretion of cortisol [1].
The secretion of cortisol changes depending on the pul-
satile secretion of CRH and ACTH according to the circadi-
an rhythm. Serum cortisol concentration reaches the high-
est concentration of about 15 μg/dl around 6–9 am, then
drops to the lowest concentration of below 2 μg/dl around
11 pm to 1 am. The median value of the 24-h period is ap-
proximately 5.2 μg/dl [9]. In normal adults, the adrenal
glands produce approximately 5 to 10 mg/m2/day (body
surface area per day) of cortisol, which is equivalent to 5 to
7 mg of oral prednisone or 20 to 30 mg of hydrocortisone
[10,11]. In plasma, approximately 90% of circulating corti-
sol binds to corticosteroid-binding globulin (CBG), an
α2-globulin binding protein synthesized in the liver [12].
The remaining 5–10% binds to albumin or circulates freely
and exerts an effect on target cells. When plasma cortisol
concentration exceeds 20–30 μg/dl, CBG is saturated, and
the concentration of free cortisol increases rapidly [12].
Sudden physiological and mental stress such as trauma,
burns, major surgery, hypoglycemia, high fever, low blood
pressure, severe exercise, and cold exposure activates the
HPA axis and increases blood ACTH and cortisol levels. In
a normal response to stress, the blood cortisol concentra-
tion increases to 18–20 μg/dl and adrenal cortisol secretion
increases up to 30–45 μg/dl during moderately stressful sit-
uations and about 260 μg/dl in a highly stressful life-threat-
ening situation. Increased cortisol levels normalize within
approximately 24 to 48 h after the stress is resolved [11].
ADRENAL INSUFFICIENCY
Adrenal insufficiency (AI) is the inability of the adrenal
glands to produce adequate amounts of corticosteroids in
response to various pathophysiologic states; this condition
can be classified into primary, secondary, and tertiary AI
depending on the cause [11]. Primary AI is an abnormality
in the adrenal gland itself and is caused by the destruction
of the adrenal cortex due to autoimmune diseases, viral
and tuberculosis infection, hemorrhage, metastatic cancer,
and sepsis. Secondary AI is rare but is caused by impaired
production of ACTH or CRH due to damage or dysfunction
caused by diseases of the pituitary gland or hypothalamus.
Tertiary AI is the most common form, widely included in
secondary AI, and is typically caused by inhibition of the
hypothalamus or pituitary due to iatrogenic corticosteroid
therapy; the degree of adrenal dysfunction is variable and
sometimes reversible. In these patients, mineralocorticoid
secretion is not affected and only cortisol production is re-
versibly inhibited [13]. Tertiary AI rarely occurs when oral
prednisone dosage is less than 5 mg or when steroid is tak-
www.anesth-pain-med.org 9
Perioperative glucocorticoid management

en for a short period of less than 2 weeks, regardless of the
dosage. However, AI has been reported to occur in more
than 60% of patients taking high-dose oral prednisone ( >
40 mg) even after only about 6 days [11,14].
Clinical signs of adrenal crisis
Patients with long-term steroid administration or severe
illness have a reduced cortisol response to stress, which
causes risk of an acute adrenal crisis. Symptoms of acute
adrenal crisis in awake patients are presented in Table 1
[15]. In patients under anesthesia, hypotension, which
does not respond to fluid administration, has been consid-
ered the most important sign of perioperative adrenal crisis
[7]. Symptoms and signs that occur earlier than hypoten-
sion include non-specific changes in consciousness and
cognitive decline and persistent fever [8]. Laboratory ex-
aminations may show hypoglycemia, hyponatremia, and
hyperkalemia. Since most of these symptoms are non-spe-
cific, it is necessary to exclude causes other than AI. How-
ever, since adrenal crisis is a life-threatening condition, it
should be immediately recognized and corrected by the
administration of stress-doses of steroids, fluids, and vaso-
pressors [8].
SURGERY INDUCED CORTISOL STRESS RESPONSE
Surgery causes a stress response with a wide range of en-
docrine, immune, and cardiovascular effects. During major
surgery, proinflammatory cytokines, CRH, ACTH, and cor-
tisol levels increase proportionally, resulting in an increase
in cortisol secretion up to approximately 5–10 times the
normal secretion, that is, 75–150 mg/day [16,17]. After sur-
gery, the diurnal secretion of cortisol malfunctions tempo-
rarily, and the serum concentration of cortisol rises due to
surgical stress [11].
In a recent meta-analysis, the change in serum cortisol
concentration before and after surgery in patients without
steroid therapy was analyzed in 71 studies since the 1990s
[18]. In this study, the invasiveness of surgery was divided
into three stages from grade 1 to 3 according to the modi-
fied Johns Hopkins surgical criteria [19]. Minor to moder-
ately invasive procedures with less bleeding (potential
blood loss < 500 ml) were included in grade 1; for example,
breast biopsy, removal of minor skin or subcutaneous le-
sions, myringotomy tubes, hysteroscopy, cystoscopy, va-
sectomy, circumcision, fiberoptic bronchoscopy, diagnos-
tic laparoscopy, dilatation, and curettage. Moderately to
significantly invasive procedures (potential blood loss 500–
1,500 ml) were included in grade 2; for example, thyroidec-
tomy, hysterectomy, myomectomy, cystectomy, cholecys-
tectomy, laminectomy, hip/knee replacement, nephrecto-
my, and major laparoscopic procedures. Highly invasive
procedures (potential blood loss > 1,500 ml) were included
in Grade 3, for example, major reconstruction of the gas-
trointestinal tract, major genitourinary surgery, cardiotho-
racic procedures, and intracranial procedures. In this re-
view, it was found that the grade of surgery significantly af-
fected cortisol secretion [18]. Patients undergoing grade 1
surgery did not show an intraoperative cortisol peak, and
postsurgical cortisol concentrations were similar to those
at baseline. Nevertheless, when compared to published
data on healthy, unstressed adults, the mean cortisol out-
put over the first 24 h after grade I surgical procedure was
approximately doubled. Patients undergoing grade 2 and 3
surgery had 3.5–4 times higher cortisol output than that of
healthy, unstressed individuals within the first 24-h post-
operative period. Moreover, in both grade 2 and 3 surger-
ies, mean cortisol values remained elevated in comparison
with the baseline measurements up to postoperative day 7.
Due to ethical issues, only a few studies have investigated
the change in cortisol concentration and the incidence of
AI after discontinuation of steroids in patients taking ste-
roids. In 1973, Kehlet and Binder [16] investigated the oc-
currence of acute AI after steroid discontinuation in 73 pa-
tients undergoing major surgery, including splenectomy
and colon resection. Patients took 5–80 mg of prednisone
for various periods in this study. As a result, about 10% of
patients developed perioperative hypotension, but only 3
patients showed low blood cortisol levels, and most of
them were treated by fluid administration. They also mea-
sured cortisol concentration in patients undergoing major
Table 1. Signs of Adrenal Crisis [15]
Signs of adrenal crisis
Dehydration, hypotension
Nausea and vomiting with a history of weight loss and anorexia
Abdominal pain (“acute abdomen”)
Unexplained hypoglycemia
Unexplained fever
Hyponatremia, hyperkalemia, azotemia, hypercalcemia, eosinophilia
Hyperpigmentation or vitiligo
Other autoimmune endocrine deficiencies (hypothyroidism or gonad-al failure)
10 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
KS
AP
abdominal surgery and minor procedures such as hand
surgery or uterine curettage, and estimated cortisol secre-
tion due to surgical stress was found to be 75–150 mg/day
and 50 mg/day for major and minor surgeries, respectively.
The results of this study formed the rationale for subse-
quent recommendations of perioperative glucocorticoid
supplementation [7,20].
De Lange and Kars [5] and Khazen and El-Hussuna [6]
investigated the incidence of AI following administration of
stress-doses or conventional maintenance doses of gluco-
corticoids based on prospective and retrospective studies.
The randomized controlled trials included in their me-
ta-analysis mostly targeted minor to moderate surgery with
a limited number of patients, and both meta-analyses con-
cluded that the incidence of perioperative AI was very low
[5,6]. These studies reported that patients taking less than
5–10 mg/day of prednisone did not have adverse side effect
of AI, even if only the daily dose was maintained during
relatively less invasive surgery [21–23].
PHYSIOLOGICAL RATIONALE FOR PERIOPERATIVE GLUCOCORTICOID
SUPPLEMENTATION
Despite the low incidence of surgery-induced AI, several
major pathophysiologic mechanisms support the necessity
of glucocorticoid administration in the perioperative period.
Vascular tone and maintenance of blood pressure
Glucocorticoids have a permissive effect on vascular
tone and maintenance of blood pressure [24]. Glucocorti-
coids alone do not increase blood pressure, but when ad-
ministered with a vasopressor, glucocorticoids enhance
vascular reactivity to vasopressors. The effect of glucocorti-
coid on vascular tone is exerted by inhibition of the synthe-
sis of prostacyclin I2 (PGI2), a potent vasodilator, in the vas-
cular endothelium [25]. If the inhibitory effect on vascular
tone disappears due to a decrease in cortisol response, it
may lead to increased production of PGI2, vasodilation,
and hypotension.
Catecholamine synthesis and secretion
Cortisol is involved in catecholamine synthesis and me-
diates the release of catecholamine from sympathetic
nerve cells by directly regulating the activity of phenyletha-
nolamine N-methyltransferase, an enzyme that catalyzes
the conversion of norepinephrine to epinephrine in the
adrenal medulla [26]. Cortisol also mediates catechol-
amine release from sympathetic cells [27].
Myocardial contractility
Cortisol helps the myocardium adapt to perioperative
stress [28]. In animal studies, acute adrenal failure caused
reduced myocardial contractility due to a decrease in the
activity of myofibrillar adenosine triphosphatase, which is
directly dependent on glucocorticoids [29]. In patients with
hemodynamically unstable secondary AI, bolus intrave-
nous hydrocortisone increases the stroke work index of the
left ventricle [30].
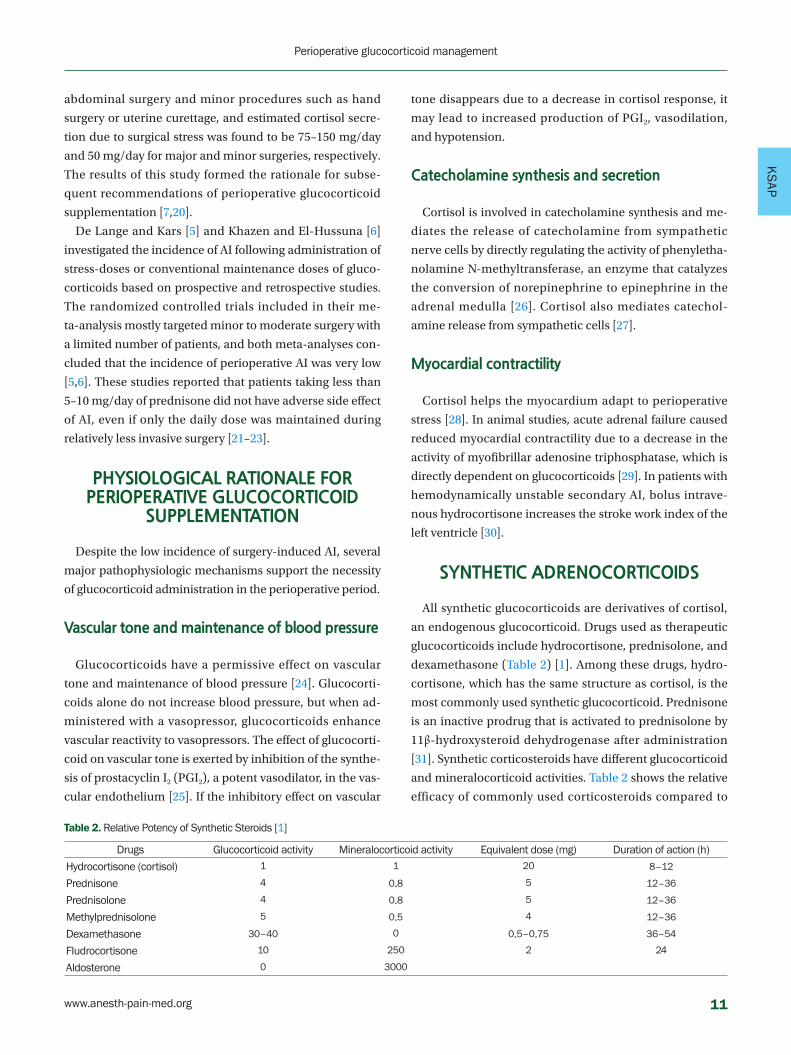
SYNTHETIC ADRENOCORTICOIDS
All synthetic glucocorticoids are derivatives of cortisol,
an endogenous glucocorticoid. Drugs used as therapeutic
glucocorticoids include hydrocortisone, prednisolone, and
dexamethasone (Table 2) [1]. Among these drugs, hydro-
cortisone, which has the same structure as cortisol, is the
most commonly used synthetic glucocorticoid. Prednisone
is an inactive prodrug that is activated to prednisolone by
11β-hydroxysteroid dehydrogenase after administration
[31]. Synthetic corticosteroids have different glucocorticoid
and mineralocorticoid activities. Table 2 shows the relative
efficacy of commonly used corticosteroids compared to
Table 2. Relative Potency of Synthetic Steroids [1]
Drugs Glucocorticoid activity Mineralocorticoid activity Equivalent dose (mg) Duration of action (h)
Hydrocortisone (cortisol) 1 1 20 8–12
Prednisone 4 0.8 5 12–36
Prednisolone 4 0.8 5 12–36
Methylprednisolone 5 0.5 4 12–36
Dexamethasone 30–40 0 0.5–0.75 36–54
Fludrocortisone 10 250 2 24
Aldosterone 0 3000
www.anesth-pain-med.org 11
Perioperative glucocorticoid management

that of hydrocortisone [1]. When adrenal gland function is
reduced, corticosteroids are used to replace both glucocor-
ticoids and mineralocorticoids. Therefore, in patients with
primary AI in which mineralocorticoids are not secreted,
dexamethasone is not appropriate and synthetic mineralo-
corticoids, fludrocortisone, and hydrocortisone should be
administered [7]. Secondary and tertiary AI are caused by a
lack of glucocorticoids, so the administration of drugs with
mineralocorticoid activity may cause side effects such as
dose-dependent edema, fluid retention, and hypokalemia
[7]. Therefore, when a high dose of hydrocortisone of 100
mg or more is required in patients with secondary and ter-
tiary AI, switching to a drug with a higher glucocorticoid
activity ratio than that of mineralocorticoid such as meth-
ylprednisolone should be considered [24].
Side effects of prolonged administration of high dose of glucocorticoid
Continuous administration of high doses of glucocorti-
coids after surgery can cause unwanted side effects [31].
Glucocorticoids promote gluconeogenesis in the liver and
proteolysis and adipolysis in muscles, resulting in hyper-
glycemia. In addition, continuous glucocorticoid adminis-
tration results in sodium retention, subsequent plasma
volume increase, and intensifies vasopressor response to
angiotensin II and catecholamines, leading to hyperten-
sion [32]. Glucocorticoids inhibit cytokine signaling and
the synthesis of matrix metalloproteinases and collagen,
which play an important role in wound healing [33]. In ad-
dition, it can cause gastrointestinal bleeding and various
psychiatric symptoms [7]. However, most side effects occur
in proportion to the duration of glucocorticoid administra-
tion, therefore, the incidence of side effects after short-
term treatment is low even with high doses.
PERIOPERATIVE STRESS-DOSE GLUCOCORTICOID
Glucocorticoids should be administered during the
perioperative period because cortisol secretion in response
to surgical stress may fail, resulting in AI, hemodynamic
instability, and adrenal crisis. Therefore, the dose of gluco-
corticoid should be administered at the same level as that
of normal physiological response to the surgical stress after
evaluating the invasiveness of surgery and inhibition of the
HPA axis [24]. If there is no suppression of the HPA axis or
the requirement due to surgical stress does not exceed the
maintenance dose of glucocorticoids already being taken,
a perioperative stress-dose of glucocorticoid is not re-
quired unless the patient shows signs of AI [7]. However,
when glucocorticoid requirement increases rapidly due to
surgical stress, and the inhibition of the HPA axis is clini-
cally important, the administration of stress doses should
be considered [7,8].
Approach according to HPA axis suppression
1. Nonsuppressed HPA axis
Steroid dose and duration affect HPA axis suppression.
Regardless of duration, the risk of HPA axis suppression is
low if the prednisone dose taken in the morning does not
exceed 5 mg/day (≈ methylprednisolone 4 mg/day, dexa-
methasone 0.5 mg/day, hydrocortisone 20 mg/day) or 10
mg of prednisone every other day. In addition, if any dose
of glucocorticoid is administered for less than three weeks,
the HPA axis is less likely to be suppressed. These patients
do not require additional administration of glucocorticoids
or tests to assess the HPA axis [7].
2. Patients with suppressed HPA axis
Patients on daily dose of prednisone exceeding 20 mg for
a period of more than three weeks and patients with symp-
toms of Cushing syndrome who are taking glucocorticoids
are at high risk of HPA axis suppression [7]. These patients
should be administered perioperative supplemental gluco-
corticoids according to the invasiveness of surgery [7].
3. Unknown HPA axis suppression
Besides these patients, patients taking prednisone at
5–20 mg/day or equivalent doses over a period of three or
more weeks may experience various ranges of HPA axis
suppression depending on their age, and dosage and dura-
tion of administration [34]. Even in cases with discontin-
ued exposure of steroids, patients who inhaled high-dose
steroids or high-potency topical steroids should be tested
for adrenal function preoperatively and supplemental glu-
cocorticoids should be administered based on the results
of the test. There is a risk of HPA axis inhibition when in-
haled glucocorticoid fluticasone ≥ 750 μg/day (or beclo-
methasone ≥ 1,500 μg/day ≈ prednisolone ≥ 10 mg/day) is
administered for more than 3 weeks before surgery [35,36].
The absorption rate of topical steroids varies depending on
the period of use, strength, and application site, but when
12 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
AP
topical steroids with high potency are used for > 2 g/day
for more than 2 weeks, suppression of the HPA axis may
occur [37]. In addition, patients who have received three or
more intra-articular or spinal glucocorticoid injections
within three months prior to surgery, have symptoms of AI,
or Cushing's syndrome, the HPA axis needs to be evaluated
[38].
Assessment of HPA axis suppression
1. Morning serum cortisol
Measurement of morning serum cortisol concentrations
before 8 am after stopping glucocorticoids for 24 h is a
good screening test for assessing secondary and tertiary AI
symptoms [39]. If the morning serum cortisol concentra-
tion is lower than 5 μg/dl, suppression of the HPA axis may
be suspected and the administration of additional gluco-
corticoids is required [7]. If the morning cortisol concen-
tration is greater than 10 μg/dl, it can be considered that
there is no inhibition of the HPA axis, and the usual dose of
glucocorticoid is taken until the day of surgery and no ad-
ditional administration is required [7]. If the morning corti-
sol concentration is 5 to 10 μg/dl, ACTH stimulation tests
are conducted, or glucocorticoids are administered based
on experience.
2. Short ACTH stimulation tests
The ACTH stimulation test determines whether adrenal
function is inhibited by administering synthetic ACTH (co-
syntropin 250 μg); the concentration of serum cortisol are
measured 30 min after the administration of ACTH [24]. If
cortisol concentration is higher than 18 μg/dl, it can be deter-
mined that proper adrenal function is maintained and addi-
tional administration of glucocorticoid is not required [7].
RECOMMENDED DOSE OF GLUCOCORTICOID ACCORDING TO
SURGICAL STRESS
Based on recent studies, recommendations were pub-
lished in Anesthesiology in 2017 and Anaesthesia in 2020
[7,8]. As presented in Table 3, Liu et al. proposed recom-
mendations based on estimated daily cortisol secretions
according to the invasiveness of surgery [7,16,17].
Recently, the Royal College of Anaesthetists and the En-
docrinology Society of the United Kingdom also published
guidelines in Anaesthesia [8], but they are different from
those of Liu et al. [7]. They have similarity in that they rec-
ommend administering stress-dose steroids to patients
with primary and secondary AI and HPA axis suppression.
However, they recommended 100 mg of hydrocortisone for
all patients undergoing minor procedures as well as major
surgeries [8]. After the publication of this recommendation,
when questions arose about administering the same dose
for a relatively simple operation [40], the authors respond-
ed that this dose may not be appropriate for simple proce-
Table 3. Surgical Stress according to Procedures and Recommended Dosing of Glucocorticoid [7]
Type of surgery Estimated cortisol secretion rate Examples Recommended dosing
Superficial 8–10 mg/day Dental surgery Usual daily dose
Biopsy
Minor 50 mg/day Inguinal hernia repair Usual daily dose plus
Colonoscopy
Uterine curettage Hydrocortisone 50 mg IV before incision
Hand surgery Hydrocortisone 25 mg IV every 8 h × 24 h
Moderate 75–150 mg/day Lower extremity revascularization Then usual daily dose
Total joint replacement
Cholecystectomy
Colon resection
Abdominal hysterectomy
Major 75–150 mg/day Esophagectomy Usual daily dose plus
Total proctocolectomy Hydrocortisone 100 mg IV before incision
Major cardiac/vascular surgery Followed by continuous IV hydrocortisone 200 mg (> 24 h)
Hepaticojejunostomy or
Delivery Hydrocortisone 50 mg IV every 8 h × 24 h
Trauma Taper dose by half per day until usual daily dose reached
IV: intravenously.
www.anesth-pain-med.org 13
Perioperative glucocorticoid management

dures [41]. Therefore, we can only refer to their recommen-
dations for major surgery. According to this guideline, for
patients undergoing major surgery, hydrocortisone 100 mg
or dexamethasone 6–8 mg should be administered at time
of induction of anesthesia, followed by immediate initia-
tion of a continuous infusion of hydrocortisone 200 mg/
day until the patients can be administered double the
pre-surgical oral dose [8].
CONCLUSION
Cortisol has a variety of critical physiological actions,
and an increase in concentration due to surgical stress is
important for maintaining hemodynamic stability during
surgery. Although studies with more appropriate evidence
are still required, evaluation of patients with possible AI
and glucocorticoid administration according to surgical
stress is crucial and can improve prognosis.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
ORCID
Kwon Hui Seo, https://orcid.org/0000-0003-4397-9207
REFERENCES
1. Keegan MT. Endocrine Pharmacology. In: Pharmacology and
physiology for anesthesia: foundations and clinical applica-
tion. 2nd ed. Edited by Hemmings HC Jr, Egan TD: Philadel-
phia, Elsevier. 2019, pp 708-31.
2. Fraser CG, Preuss FS, Bigford WD. Adrenal atrophy and irre-
versible shock associated with cortisone therapy. J Am Med
Assoc 1952; 149: 1542-3.
3. Lewis L, Robinson RF, Yee J, Hacker LA, Eisen G. Fatal adrenal
cortical insufficiency precipitated by surgery during prolonged
continuous cortisone treatment. Ann Intern Med 1953; 39:
116-26.
4. Marik PE, Varon J. Requirement of perioperative stress doses of
corticosteroids: a systematic review of the literature. Arch Surg
2008; 143: 1222-6.
5. de Lange DW, Kars M. Perioperative glucocorticosteroid sup-
plementation is not supported by evidence. Eur J Intern Med
2008; 19: 461-7.
6. Khazen BF, El-Hussuna A. The use of a perioperative su-
pra-physiological dose of glucocorticoid is not supported by
evidence - a systematic review. Dan Med J 2018; 65: A5488.
7. Liu MM, Reidy AB, Saatee S, Collard CD. Perioperative steroid
management: approaches based on current evidence. Anes-
thesiology 2017; 127: 166-72.
8. Woodcock T, Barker P, Daniel S, Fletcher S, Wass JAH, Tomlin-
son JW, et al. Guidelines for the management of glucocorti-
coids during the peri-operative period for patients with adre-
nal insufficiency: guidelines from the Association of Anaesthe-
tists, the Royal College of Physicians and the Society for Endo-
crinology UK. Anaesthesia 2020; 75: 654-63.
9. Debono M, Ghobadi C, Rostami-Hodjegan A, Huatan H,
Campbell MJ, Newell-Price J, et al. Modified-release hydrocor-
tisone to provide circadian cortisol profiles. J Clin Endocrinol
Metab 2009; 94: 1548-54.
10. Esteban NV, Loughlin T, Yergey AL, Zawadzki JK, Booth JD,
Winterer JC, et al. Daily cortisol production rate in man deter-
mined by stable isotope dilution/mass spectrometry. J Clin
Endocrinol Metab 1991; 72: 39-45.
11. Coursin DB, Wood KE. Corticosteroid supplementation for ad-
renal insufficiency. JAMA 2002; 287: 236-40.
12. Chrousos GP. Chapter 39: adrenocorticosteroids & adrenocorti-
cal antagonists. In: Basic & clinical pharmacology. 14th ed. Ed-
ited by Katzung BG: New York, McGraw-Hill. 2018.
13. MacKenzie CR, Goodman SM. Stress dose steroids: myths and
perioperative medicine. Curr Rheumatol Rep 2016; 18: 47.
14. Woods CP, Argese N, Chapman M, Boot C, Webster R, Dabhi V,
et al. Adrenal suppression in patients taking inhaled glucocor-
ticoids is highly prevalent and management can be guided by
morning cortisol. Eur J Endocrinol 2015; 173: 633-42.
15. Garcia JEL, Hill GE, Joshi GP. Perioperative stress dose steroids:
is it really necessary? ASA Newsl 2013; 77: 32-5.
16. Kehlet H, Binder C. Adrenocortical function and clinical course
during and after surgery in unsupplemented glucocorti-
coid-treated patients. Br J Anaesth 1973; 45: 1043-8.
17. Salem M, Tainsh RE Jr, Bromberg J, Loriaux DL, Chernow B.
Perioperative glucocorticoid coverage. A reassessment 42 years
after emergence of a problem. Ann Surg 1994; 219: 416-25.
18. Prete A, Yan Q, Al-Tarrah K, Akturk HK, Prokop LJ, Alahdab F, et
al. The cortisol stress response induced by surgery: a systemat-
ic review and meta-analysis. Clin Endocrinol (Oxf ) 2018; 89:
554-67.
19. Donati A, Ruzzi M, Adrario E, Pelaia P, Coluzzi F, Gabbanelli V,
et al. A new and feasible model for predicting operative risk. Br
J Anaesth 2004; 93: 393-9.
20. Lamberts SW, Bruining HA, de Jong FH. Corticosteroid therapy
14 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
AP
in severe illness. N Engl J Med 1997; 337: 1285-92.
21. Glowniak JV, Loriaux DL. A double-blind study of perioperative
steroid requirements in secondary adrenal insufficiency. Sur-
gery 1997; 121: 123-9.
22. Thomason JM, Girdler NM, Kendall-Taylor P, Wastell H, Weddel
A, Seymour RA. An investigation into the need for supplemen-
tary steroids in organ transplant patients undergoing gingival
surgery. A double-blind, split-mouth, cross-over study. J Clin
Periodontol 1999; 26: 577-82.
23. Zaghiyan K, Melmed GY, Berel D, Ovsepyan G, Murrell Z,
Fleshner P. A prospective, randomized, noninferiority trial of
steroid dosing after major colorectal surgery. Ann Surg 2014;
259: 32-7.
24. Axelrod L. Perioperative management of patients treated with
glucocorticoids. Endocrinol Metab Clin North Am 2003; 32:
367-83.
25. Axelrod L. Inhibition of prostacyclin production mediates per-
missive effect of glucocorticoids on vascular tone. Perturba-
tions of this mechanism contribute to pathogenesis of Cush-
ing's syndrome and Addison's disease. Lancet 1983; 1: 904-6.
26. Wong DL, Siddall B, Wang W. Hormonal control of rat adrenal
phenylethanolamine N-methyltransferase. Enzyme activity,
the final critical pathway. Neuropsychopharmacology 1995; 13:
223-34.
27. Shi LJ, He HY, Liu LA, Wang CA. Rapid nongenomic effect of
corticosterone on neuronal nicotinic acetylcholine receptor in
PC12 cells. Arch Biochem Biophys 2001; 394: 145-50.
28. Sabourdin N. Steroids: the evidence. The rationale for periop-
erative glucocorticoid supplementation for patients under
chronic steroid treatment. Curr Anesthesiol Rep 2015; 5: 140-6.
29. Bhaskar M, Stith RD, Brackett DJ, Wilson MF, Lerner MR, Reddy
YS. Changes in myocardial contractile protein ATPases in
chronically adrenalectomized rats with and without glucocor-
ticoid replacement. Biochem Med Metab Biol 1989; 42: 118-24.
30. Bouachour G, Tirot P, Varache N, Gouello JP, Harry P, Alquier P.
Hemodynamic changes in acute adrenal insufficiency. Inten-
sive Care Med 1994; 20: 138-41.
31. Czock D, Keller F, Rasche FM, Häussler U. Pharmacokinetics
and pharmacodynamics of systemically administered gluco-
corticoids. Clin Pharmacokinet 2005; 44: 61-98.
32. Rhen T, Cidlowski JA. Antiinflammatory action of glucocorti-
coids--new mechanisms for old drugs. N Engl J Med 2005; 353:
1711-23.
33. Sato S, Kim T, Arai T, Maruyama S, Tajima M, Utsumi N. Com-
parison between the effects of dexamethasone and indometh-
acin on bone wound healing. Jpn J Pharmacol 1986; 42: 71-8.
34. Freudzon L. Perioperative steroid therapy: where's the evi-
dence? Curr Opin Anaesthesiol 2018; 31: 39-42.
35. Todd GR, Acerini CL, Ross-Russell R, Zahra S, Warner JT, Mc-
Cance D. Survey of adrenal crisis associated with inhaled corti-
costeroids in the United Kingdom. Arch Dis Child 2002; 87:
457-61.
36. Lipworth BJ. Systemic adverse effects of inhaled corticosteroid
therapy: a systematic review and meta-analysis. Arch Intern
Med 1999; 159: 941-55.
37. Hengge UR, Ruzicka T, Schwartz RA, Cork MJ. Adverse effects
of topical glucocorticosteroids. J Am Acad Dermatol 2006; 54:
1-15.
38. Lansang MC, Farmer T, Kennedy L. Diagnosing the unrecog-
nized systemic absorption of intra-articular and epidural ste-
roid injections. Endocr Pract 2009; 15: 225-8.
39. Hägg E, Asplund K, Lithner F. Value of basal plasma cortisol as-
says in the assessment of pituitary-adrenal insufficiency. Clin
Endocrinol (Oxf) 1987; 26: 221-6.
40. McConachie I. Peri-operative glucocorticoid guidelines. Anaes-
thesia 2020; 75: 1394.
41. Vercueil A; Working Party. Guidelines for the management of
glucocorticoids during the peri-operative period for patients
with adrenal insufficiency: a reply. Anaesthesia 2020; 75: 1398-
9.
www.anesth-pain-med.org 15
Perioperative glucocorticoid management
INTRODUCTION
Corticosteroids are very attractive as drugs for many
musculoskeletal diseases because of their potent anti-in-
flammatory effect. Epidural steroid injection (ESI) is widely
used to treat various back pain conditions such as herniat-
ed intervertebral disc and spinal stenosis. Corticosteroids
have been used to treat spinal diseases for a long time. Ini-
tially, they were delivered into intrathecal space in 1954 [1].
However, because of the transient pharmacological effect,
the injection route of corticosteroids was changed into epi-
dural space. Several studies have supported the efficacy of
ESI in spinal disease [2–4]. Transforaminal epidural steroid
injection (TFESI) is used to relieve pain and reduce the po-
tential need for surgery [5,6]. Radicular pain is caused not
only by mechanical compression but also due to inflam-
Corresponding author Ho Sik Moon, M.D., Ph.D. Department of Anesthesiology and Pain Medicine, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 1021 Tongil-ro, Eunpyeong-gu, Seoul 03312, Korea Tel: 82-2-2030-3864Fax: 82-2-2030-3861E-mail: [email protected]
Spine disease is one of the most common musculoskeletal diseases, especially in an aging society. An epidural steroid injection (ESI) is a highly effective treatment that can be used to bridge the gap between physical therapy and surgery. Recently, it has been increasingly used clinically. The purpose of this article is to review the complications of corticosteroids administered epidurally. Common complications include: hypothalamic-pituitary-adrenal (HPA) axis suppression, adrenal insufficiency, iatrogenic Cushing’s syndrome, hyperglyce-mia, osteoporosis, and immunological or infectious diseases. Other less common complica-tions include psychiatric problems and ocular ailments. However, the incidence of complica-tions related to epidural steroids is not high, and most of them are not serious. The use of nonparticulate steroids is recommended to minimize the complications associated with epi-dural steroids. The appropriate interval and dosage of ESI are disputed. We recommend that the selection of appropriate ESI protocol should be based on the suppression of HPA axis, which reflects the systemic absorption of the corticosteroid.
Keywords: Drug-related side effects and adverse reactions; Epidural injections; Glucocorti-coids; Guideline; Review; Safety.
Safety of epidural steroids: a review
Min Soo Lee and Ho Sik Moon
Department of Anesthesiology and Pain Medicine, College of Medicine, The Catholic
University of Korea, Seoul, Korea
Received January 1, 2021Revised January 18, 2021 Accepted January 18, 2021
ReviewAnesth Pain Med 2021;16:16-27https://doi.org/10.17085/apm.21002pISSN 1975-5171 • eISSN 2383-7977
mation of the affected nerve roots because the nucleus
pulposus of the intervertebral disc evokes an immune re-
action mediated via inflammatory molecules [7]. Thus the
rationale for using corticosteroids in epidural block is es-
tablished [8].
The complications associated with corticosteroid use are
as many as their therapeutic effects. However, most com-
plications related to ESI are not serious. Lee et al. [9] ana-
lyzed 52,935 ESI procedures performed in 22,059 patients
and found no major adverse events. Similarly, no major
adverse events were detected in another single-center
study of 1,300 lumbar transforaminal epidural injections.
Kang et al. [10] surveyed complications of 825 patients who
were treated with dexamethasone epidurally. Forty pa-
tients (4.8%) showed systemic but minor and transient side
effects of corticosteroids including facial flushing (1.5%),
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
16

KS
PS
urticaria (0.8%), and insomnia (0.8%). Serious complica-
tions such as adrenal insufficiency (AI), Cushing's syn-
drome, neurological accidents, and osteonecrosis have
been reported rarely [11,12]. Because these complications
cause irreversible sequelae, pain physicians need to be
cognizant of the side effects of corticosteroids and their
prevention.
ESI is a valuable procedure used to treat spinal pain. Al-
though systemic side effects of treatment with long-term
oral administration of steroids are well established, the
pharmacology and side effects associated with ESI are
poorly understood. This review summarizes the complica-
tions of epidural steroids and techniques as well as related
mechanical injury.
PHARMACOLOGIC PROPERTIES OF EPIDURAL STEROIDS
Pathophysiology of radiculopathy
Radiculopathy is caused by inflammation and the me-
chanical compression of the nerve root. Inflammation
plays a major role in the evolution of radiculopathy [13].
Clinically, a large herniation of an intervertebral disc asso-
ciated with significant neural compression may be asymp-
tomatic, whereas severe radicular pain may exist without
detectable root compression. Also, the size or shape of her-
niation, and eventual change in size or shape does not cor-
relate with clinical presentation or course [14,15]. This
shows the importance of inflammation in the pathophysi-
ology of radiculopathy. The damaged structures release
various inflammatory mediators, which trigger inflamma-
tory reaction in the spine. For instance, the damaged facet
joints release bradykinin, serotonin, norepinephrine, and
interleukin (IL)-1. Also, the nerve endings of the posterior
longitudinal ligament, outer annulus, facet capsule, or
periosteum release substance P, vasoactive intestinal pep-
tide, and calcitonin gene-related peptide. The nucleus pul-
posus generates inflammatory mediators, including phos-
pholipase A2 (PLA2), prostaglandin E2, IL-1α, IL-1β, IL-6,
tumor necrosis factor, and nitric oxide, and it is well known
that discogenic pain is mediated by these inflammatory
mediators and neovascularization induced by chemical
signaling [8,16]. PLA2 is the rate-limiting factor involved in
the synthesis of arachidonic acid, which is the principal
substrate in the cyclo-oxygenase and lipo-oxygenase path-
ways. Prostaglandins, along with other arachidonic acid
byproducts, can cause or exacerbate pain mediated via in-
flammatory mechanisms and sensitization of peripheral
nociceptors [17,18]. Among the inflamed structures, the
dorsal root ganglion is more sensitive to mechanical pres-
sure than the nerve root [16].
Rationale for the use of epidural corticosteroids in radiculopathy
The therapeutic effects of corticosteroids in radiculopa-
thy are yet to be fully understood. Until now, several mech-
anisms have been proposed: inhibition of leukocyte func-
tion; alleviation of inflammatory events such as edema, fi-
brin deposition, capillary dilatation, leukocyte aggregation,
phagocytosis, capillary and fibroblast proliferation, colla-
gen deposition and cicatrization; inhibition of the synthe-
sis of pro-inflammatory substances like PLA2; inhibition of
the activity of lymphokines; inhibition of the display of
chemotactic molecules on the surface of the endothelial
cells; and minimization of endothelial injury [16]. In addi-
tion to their anti-inflammatory effects, corticosteroids may
inhibit pain via suppression of ectopic discharges from in-
jured nerves and decreased conduction in normal unmy-
elinated C fibers [19].
Pharmacokinetics of epidural steroids
The elimination half-life of triamcinolone acetonide 80
mg following interlaminar epidural injection is 506 ± 255
h, and the time to maximum concentration (Tmax) is 37.5 ±
37.5 h [20]. These pharmacokinetic properties of epidural
steroids vary depending on the route of administration.
The elimination half-life after oral, intravenous, intraartic-
ular, and intravitreal injection of triamcinolone varies: oral,
2.6 h [21]; intravenous, 2.0 h [21]; intraarticular knee injec-
tion, 77–154 h [22]; and intravitreal, 446 h [23]. The differ-
ences between oral/intravenous and intraarticular/intrav-
itreal/epidural administration of triamcinolone appear to
be due to its particulate form. Interestingly, in the case of
cervical interlaminar epidural injection with triamcinolone
acetonide 80 mg, the elimination half-life was 310 ± 212 h
and Tmax was 22.8 ± 13.1 h, which was shorter than that of
lumbar ESI due to the cervical epidural vasculature [24].
Current evidence suggests that more soluble glucocorti-
coids have shorter duration of systemic effect than less sol-
uble glucocorticoids [25]. Intramuscular administration of
dexamethasone is followed by partial absorption into the
www.anesth-pain-med.org 17
Safety of epidural steroid injection

systemic circulation and the biological half-life of dexa-
methasone is 5.2 ± 0.4 h [26]. Unfortunately, there has
been no study on the pharmacokinetic features of epidural
dexamethasone, and further research is required.
ENDOCRINOLOGICAL COMPLICATIONS
HPA axis suppression, AI, and iatrogenic Cushing’s syndrome
Glucocorticoids are synthesized in the adrenal cortex
under the regulation of the HPA axis. They are produced on
demand and not stored in body. The glucocorticoid syn-
thesis is inhibited by three mechanisms. First, the rapid
feedback (less than 10 min) is sensitive to changes in circu-
lating glucocorticoids and not to the absolute levels of ste-
roid. Second, early delayed feedback (30 min to 2 h) is as-
sociated with the suppression of adrenocorticotropic hor-
mone (ACTH) synthesis, which is affected by the concen-
tration of circulating glucocorticoids. Third, late delayed
feedback (about a day) is related to high concentration of
glucocorticoids, persisting for days or weeks [27].
HPA axis suppression occurs in most of the patients who
receive ESI, and most of them recover within 2–4 weeks
[28–32]. This complication is likely to be asymptomatic and
does not require treatment in most cases. Studies involving
orally administered corticosteroids have shown that the
treatment dose or duration is not correlated with the sever-
ity of HPA axis suppression and reported substantial indi-
vidual variation in clinical effects depending on age and
co-existing disease [33]. However, the results of ESI differed
from the effects of oral corticosteroid intake. Sim et al. [30]
conducted a randomized controlled trial comparing the
HPA axis suppression under different dosages of epidural
triamcinolone (40 mg vs. 20 mg) and showed that the HPA
suppression in the triamcinolone 40 mg group (19.7 ± 3.1
days) was longer than in the group treated with triamcino-
lone 20 mg (8.0 ± 2.4 days), and the recovery rate of the tri-
amcinolone 40 mg group was lower than in the triamcino-
lone 20 mg group (P = 0.015). However, the extent of HPA
axis reduction, i.e., the difference between salivary cortisol
(SC) concentration before ESI and SC concentration on
day 1 after ESI was not affected by the dosage of corticoste-
roid [30]. The type of corticosteroid also affects the HPA
axis suppression. Friedly et al. [25] reported that HPA axis
suppression was more likely with longer-acting insoluble
corticosteroid formulations such as methylprednisolone or
triamcinolone than betamethasone and dexamethasone.
However, patient demographics did not influence the du-
ration of HPA axis suppression [25].
Secondary AI is known as a rare disease (0.00015–
0.00028%) [34]. Its mortality is two-fold higher than in gen-
eral population, which is associated with infection or adre-
nal crisis [34]. The common symptoms of AI are fatigue,
loss of appetite, weight loss, nausea, vomiting, abdominal
pain, and muscle and joint pain, which are nonspecific and
therefore do not facilitate easy diagnosis. Moreover, specif-
ic symptoms such as hyperpigmentation, salt craving, and
postural hypotension are uncommon in AI induced with
exogenous glucocorticoids because of intact mineralocor-
ticoid axis [35]. Therefore, an early diagnosis of iatrogenic
AI is challenging for physicians. Park et al. reported that
11.8% of patients who were treated with long-term ESI be-
yond 6 months developed secondary AI, although they did
not show AI symptoms [28]. The average number of ESIs
per year in the AI group was 7.7 ± 1.3/yr and in the Non-AI
group was 7.4 ± 3.3/yr.
The risk of iatrogenic Cushing's syndrome after ESI is
unknown. No well-controlled study about its incidence af-
ter ESI is available, and only several cases have been re-
ported [36–38]. Interestingly, a few cases were associated
with ritonavir treatment of patients with human immuno-
deficiency virus [37,38]. Park et al. [28] reported that none
of the 18 subjects who were treated long-term with ESI be-
yond 6 months manifested iatrogenic Cushing's syndrome.
The authors used the late-night salivary cortisol (LNSC)
test, which is usually performed between 23:00 and 24:00,
and is known to be very sensitive and specific for the diag-
nosis of Cushing's syndrome [39]. Sim et al. [30] also con-
ducted an LNSC test in 30 subjects who received triamcin-
olone acetate 40 mg or 20 mg and showed the absence of
iatrogenic Cushing's syndrome in either group.
Effects on glucose metabolism & hyperglycemia
Glucocorticoids decrease insulin sensitivity and periph-
eral glucose uptake as well as hepatic gluconeogenesis.
Hyperglycemia may be one of the annoying side effects af-
ter ESI, especially in patients with diabetes.
In a study by Ward et al. [40], 10 healthy volunteers were
administered 80 mg of triamcinolone (equivalent to dexa-
methasone 16 mg) via caudal ESI. Fasting insulin and glu-
cose levels rose significantly one day after ESI and returned
to normal by 1 week. In a study of patients receiving ESI or
18 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
glenohumeral joint injection, serum glucose was elevated
for approximately 1 day [41]. Maillefert et al. [42] followed
nine healthy subjects for 21 days after a single epidural in-
jection of dexamethasone 15 mg and found no changes in
fasting glucose. These studies dispute the hypoglycemic ef-
fect of ESIs in healthy individuals.
ESIs appear to have a greater effect on glucose control in
diabetics. Diabetic patients may have significantly reduced
cytochrome p450 3A4 expression and activity [43]. There-
by, a decreased clearance of glucocorticoids and increased
duration of systemic side effects are observed. Gonzalez et
al. [44] followed 12 patients with diabetes after epidural in-
jection of betamethasone 12–18 mg via transforaminal and
caudal route and reported statistically significant eleva-
tions in blood glucose levels in diabetic subjects. This ef-
fect peaked on the day of the injection and lasted approxi-
mately 2 days. A study of 100 patients with pre-existing dia-
betes by Kim et al. [45] reported that ESIs were associated
with significant elevations in postprandial blood glucose in
diabetic patients for up to 4 days after the procedure. The
higher dose of triamcinolone increased the glucose levels
greater than the lower dose regardless of pain control, em-
ployment status, or clinical outcome. Thus, they recom-
mended lower doses in patients with diabetes [45]. Based
on the above studies, the elevation in blood glucose among
diabetic subjects was observed for two to three days fol-
lowing ESI, and therefore diabetic patients are advised to
control their blood sugar levels tightly until three days after
the procedure.
Effects on bone metabolism & osteoporosis
In general, corticosteroid therapy results in bone loss
and osteoporosis, which could be a challenge, especially in
postmenopausal women. Corticosteroids affect bone re-
modeling by increasing bone resorption via apoptosis of
osteocytes and enhanced osteoclast activity. Many studies
have investigated bone mineral density (BMD) in patients
taking oral corticosteroids. However, orally administered
corticosteroids exhibit different absorption characteristics
and effects compared with those associated with epidural
injections. Therefore, a direct comparison between the two
is difficult.
Dubois et al. [46] reported the absence of a relationship
between cumulative epidural steroid dose and BMD in
healthy men and women pretreated with at least 3 g of
methylprednisolone. However, in postmenopausal wom-
en, an ESI with triamcinolone 80 mg induced a significant
decrease in hip BMD at 6 months compared with baseline
(P = 0.002) and an age-matched control group (P = 0.007)
[47]. Similarly, Kim and Hwang [48] reported a retrospec-
tive study in which multiple ESIs with an approximate cu-
mulative dose of triamcinolone 400 mg reduced hip BMD
in postmenopausal women. The average duration between
the first and last ESIs was 34.4 ± 2.6 months. The risk of os-
teoporotic fracture appears to increase due to ESI. Mandel
et al. [49] conducted a large retrospective cohort study
comparing 3,415 patients who received at least one ESI
with 3,000 patients who did not receive any ESI. ESI in-
creased the risk of fractures by a factor of 1.21 (95% confi-
dence interval, 1.08–1.30) after adjustment for covariates (P
= 0.003). Therefore, physicians should keep in mind that
ESI increases the risk of osteoporosis and fracture in post-
menopausal women.
Abnormal uterine bleeding
Abnormal uterine bleeding (AUB) is not infrequent in
women treated with ESI. The incidence of AUB in women
(70% premenopausal and 30% postmenopausal) who re-
ceived ESI was 2.5% of 8,166 ESIs [50]. However, the exact
relationship between AUB and ESI was not revealed exactly
and sex hormone levels after ESI have yet to be measured.
In the case of intra-articular injection, corticosteroid thera-
py induces a temporary, but considerable suppression of
sex hormone secretion [51].
IMMUNOLOGICAL/INFECTIOUS COMPLICATIONS
Immunosuppression and infection
Immunosuppression is one of the most serious side ef-
fects associated with iatrogenic corticosteroid use. Cortico-
steroids suppress inflammatory genes, upregulate anti-in-
flammatory genes, decrease the production of proinflam-
matory cytokines, and inhibit phagocyte function [52]. Pre-
operative intra-articular corticosteroid injection is associ-
ated with an increased risk of postoperative periprosthetic
infection [53]. Preoperative ESI also appears to be related
to infection after spine surgery. The overall rate of postop-
erative infection related to single-level lumbar decompres-
sion after ESI was reported to vary between 0.8% and 1.7%,
which was more common within 1 month and 1–3 months
www.anesth-pain-med.org 19
Safety of epidural steroid injection

before surgery than within 3–6 months and 6–12 months
before surgery [54]. Therefore, the optimal interval be-
tween the last preoperative ESI and surgery should be at
least 3 months to prevent postoperative infection. Singla et
al. [55] also reported similar results suggesting that preop-
erative ESI within 3 months of lumbar fusion was associat-
ed with an increased rate (1.6%) of postoperative infection
in a retrospective cohort of 88,540 patients.
Allergic reaction & anaphylaxis
Despite the anti-inflammatory and anti-allergic effects of
corticosteroids, no systemic hypersensitivity was detected,
paradoxically [56]. The allergic reactions or hypersensitivi-
ty usually occur due to exposure to preservatives or ste-
roids. The incidence of anaphylaxis was 0.5% in the study
of patients injected with intravenous corticosteroids [57].
However, no study analyzed the incidence of anaphylaxis
in patients using epidural corticosteroids except in a few
cases. Most of the cases are associated with triamcinolone
or methylprednisolone treatment and symptoms include
sneezing, angioedema, tachycardia, marked hypotension,
itching, redness, and peri-orbital edema [58–60].
Facial flushing is a common side effect of ESI, and is as-
sociated immunoglobulin E and histamine-mediated reac-
tion [61]. Most types of corticosteroids used in ESI cause
facial flushing. Cicala et al. [61] reported that 9.3% of pa-
tients who received cervical ESI with methylprednisolone
acetate manifested facial flushing. In the retrospective co-
hort study of Kim et al. [62], the overall incidence of facial
flushing was 28% among 150 subjects who received ESI
with 16 mg of dexamethasone. In this study, the female
subjects were vulnerable to facial flushing (64%) and all
cases of flushing were resolved within 48 h.
MISCELLANEOUS COMPLICATIONS
Psychiatric complications
Corticosteroid-induced psychiatric complications are
not infrequent. Wada et al. [63] reported that corticoste-
roid-induced psychiatric syndrome including depression,
mania, psychosis, and delirium occurred in 0.87% of 2,069
patients (15 patients with a mood disorder and 3 patients
with a psychotic disorder), who showed a relatively good
outcome with full remission within 1–3 months. However,
the pathophysiology of this complication was not clear.
Corticosteroid is suggested to affect dopaminergic or cho-
linergic systems, reduce serotonin release, and induce tox-
ic effects in the hippocampus or other brain regions [64].
Most of the studies involved oral or intravenous adminis-
tration of corticosteroid, but not ESI. Benyamin et al re-
ported a case of a 67-year-old male who received multiple
corticosteroid injections including ESI, and developed psy-
chotic symptoms such as racing thoughts, anger, agitation,
pressured hyper-verbal speech, and paranoia, which spon-
taneously resolved in 7–10 days [65].
Ocular complications
Corticosteroid therapy can increase intraocular pressure
(IOP), which is known as steroid-induced ocular hyperten-
sion, steroid-induced glaucoma (SIG), and at worst blind-
ness. The prevalence of SIG is not reported yet, but non-re-
sponders to corticosteroid was accounted for 61–63% (IOP
elevation < 5 mmHg), moderate responders 33% (IOP ele-
vation ranging 6 to 15 mmHg), and high responders consti-
tuted 4–6% (IOP elevation > 15 mmHg) [66]. However,
these results are based on corticosteroid administration
through the topical, intraocular, periocular, oral, intrave-
nous, inhaled, nasal, and transcutaneous routes. A single
case report involved a patient who experienced sudden bi-
lateral blurred vision due to increased IOP after ESI, war-
ranting immediate ophthalmic intervention. The symptom
resolved within three and one half months [67]. In addi-
tion, a few case reports involved other ophthalmological
complications such as retinal venous hemorrhage, ambly-
opia, transient bilateral vision defect, central serous cho-
rioretinopathy, and subcapsular cataracts after ESI [68,69].
Steroid-induced myopathy
Steroid-induced myopathy is a rare complication charac-
terized clinically by proximal lower extremity weakness,
normal creatine kinase, normal electromyogram, and loss
of type IIa fibers [52]. There is no research or case report on
steroid-induced myopathy associated with ESI. Therefore,
further research is needed to address this problem.
Epidural lipomatosis
A few case reports suggest epidural lipomatosis, which is
characterized by excessive accumulation of unencapsulat-
ed fat in the spinal canal [70–72]. This complication is usu-
20 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
ally associated with long-term ESI and can cause symp-
toms of spinal cord or nerve root compression. The prog-
nosis of epidural lipomatosis is not good. Two of the cases
required spine surgery [71,72].
MISCELLANEOUS ISSUES FOR SAFE ESI
Corticosteroids: particulate vs. nonparticulate steroids
The corticosteroids for ESI are divided into particulate
(triamcinolone and methylprednisolone) and nonparticu-
late (dexamethasone and betamethasone) formulations.
Several cases of spinal cord ischemia after ESI have been
reported since they were first described in 2002 by Houten
and Errico [73]. Reports of spinal cord ischemia, paralysis,
permanent blindness, and death after ESI have raised con-
cerns about the potential embolization of particulate corti-
costeroids. Proposed mechanisms include direct injury to
the spinal arteries and embolization. Specifically, the
transforaminal approach entails needle insertion in close
proximity to the spinal cord arteries. Inadvertent arterial
injection of a particulate corticosteroid may result in em-
bolic infarction and subsequent permanent neurologic
compromise. Recent investigations demonstrate an alter-
native mechanism of injury. Several particulate steroids
have been shown to exert immediate and massive effect on
microvascular perfusion in a mouse model via formation
of red blood cell (RBC) aggregates associated with the
transformation of RBCs into spiculated RBCs [74,75].
However, dexamethasone does not form particles or ag-
gregates large enough to cause an embolism, based on
published case reports of paraplegia, quadriplegia, or
stroke following ESI [74]. However, a mixture of dexameth-
asone or betamethasone and ropivacaine induced a
pH-dependent crystallization in vitro [76,77]. In 2011, the
Food and Drug Administration (FDA) required a label
change for triamcinolone, stating that it should not be used
for ESI. Nonetheless, particulate steroids continue to be
used because of a theoretical advantage of pain relief sec-
ondary to delayed clearance from the spinal canal [78].
Three randomized studies investigated the effectiveness of
different steroid preparations. Two studies reported no evi-
dence that nonparticulate steroids such as dexamethasone
at 10 mg were less effective than particulate steroids such
as methylprednisolone, triamcinolone, or betamethasone
in lumbar TFESI [79,80]. Conversely, Park et al. [81] report-
ed that the nonparticulate steroid dexamethasone was sta-
tistically less effective than the particulate steroid in terms
of pain relief. In 2020, Donohue et al. [82] reported that
there was no significant difference in pain relief at any
point between nonparticulate and particulate steroids and
recommended the use of nonparticulate corticosteroids in
ESI given the safety concerns associated with particulate
corticosteroids. Considering the potential risk of cata-
strophic complications, nonparticulate steroid prepara-
tions should be considered as first-line agents when per-
forming ESI. Further studies are necessary to compare cor-
ticosteroid preparations.
Optimal interval and dosage of ESI
Unfortunately, there is no definite consensus on what
constitutes the appropriate regimen of ESIs, and little in-
formation concerning recommendations or practice guide-
lines is available to date. A significant variation in dose, fre-
quency, and ESI interval was attributed to physician pref-
erence. In a survey conducted by Vydra et al. [2], most phy-
sicians (56.0%) preferred 10 mg of dexamethasone for ESI,
followed by 8 mg (12%), 4 mg (9%), 15 mg (8%), 20 mg
(6%), 6 mg (6%), and 12 mg (3%). Also, many of the doctors
(40%) allowed 4 ESIs annually, followed by 3 (29%), 6
(17%), 5 (6%), 2 (3%), 8 (2%), 10 (2%), 9 (1%), and > 10 in-
jections (1%) [2]. Kim et al. [83] published a survey of 122
pain centers adopting the current ESI regimen. More than
half (55%) of Korean pain physicians used dexamethasone
for ESIs. The minimum interval of subsequent ESIs is 3.1
weeks at academic institutions and 2.1 weeks at private
pain clinics [83].
Determining the optimal steroid dose, duration, and in-
terval for ESIs is essential to develop a treatment protocol
with minimal complications without compromising the
treatment effectiveness. Above all, a consensus is needed
to determine the major complications associated with ste-
roids indicating limited corticosteroid use. Rare complica-
tions, such as epidural lipomatosis, steroid-induced myop-
athy, and iatrogenic Cushing’s syndrome or complications
that are patient-specific such as allergic reactions cannot
be used as a criterion for limited ESI use. Most epidural
steroid complications are associated with systemic absorp-
tion of corticosteroids, which is reflected by HPA axis sup-
pression. The HPA axis suppression as an indicator of a ESI
limitation has several advantages. First, it is observed in all
patients who receive ESI [28,30–32]. Second, the recovery
www.anesth-pain-med.org 21
Safety of epidural steroid injection

curve of HPA function after ESI is similar to that of the
elimination of epidurally injected steroid [20,24]. Third, it
represents a dose-response relationship, which provides
important information about minimal dosage of epidural
steroids [30]. Finally, the recovery of HPA axis function is
closely related to AI, one of the serious complications of
ESI [28].
Before discussing appropriate ESI interval, physicians
should consider the need to repeat ESI multiple times. Re-
peated ESIs within 3 months provide cumulative benefit
[84]. If multiple ESIs are considered, an appropriate inter-
val between ESIs should be decided based on the average
duration of HPA axis suppression after ESI without affect-
ing the physiological restoration. Another rationale for an
appropriate interval is to wait until the peak effects of epi-
dural steroid treatment are detected to avoid needless ad-
ditional ESI [85]. Chon and Moon [31] reported that the
HPA axis suppression period after ESI with triamcinolone
40 mg was 19.9 ± 6.8 days, which was similar to that of Sim
et al. [30] (19.7 ± 3.1 days). Accordingly, the minimum rec-
ommended interval between ESIs using triamcinolone 40
mg might be 3 to 4 weeks for safety. The HPA axis suppres-
sion period is affected by the dose of epidural steroid ad-
ministered. In the study of Sim et al. [30], the HPA suppres-
sion period after the epidural injection of triamcinolone 20
mg was 8.0 ± 2.4 days. Therefore, the smaller the dose of
epidural steroid, the closer is the ESI minimum interval.
The type of corticosteroid also affects the duration of HPA
axis suppression. Friedly et al. [25] reported that particu-
late corticosteroids such as methylprednisolone and triam-
cinolone showed relatively longer HPA axis suppression
than the non-particulate forms like betamethasone and
dexamethasone. In the case of methylprednisolone and
triamcinolone, the HPA suppression lasted an average of 3
weeks; however, the serum cortisol concentrations follow-
ing 3-week treatment with betamethasone and dexameth-
asone was not significantly different from the control
group. Similarly, Chutatape et al. [86] reported that epidur-
al dexamethasone 8 mg decreased both ACTH and serum
cortisol concentrations below 7 days. These results may be
associated with the characteristics of the particulate steroid
formulations, suggesting that long-acting and insoluble
types can cause sustained systemic absorption of the corti-
costeroid. In summary, multiple ESIs using particulate ste-
roid require sufficient interval of about 3–4 weeks because
of long-lasting HPA axis suppression, while non-particulate
steroids require shorter periods.
The types of corticosteroids, treatment effectiveness and
duration, and the incidence of complications should be
considered to determine the optimal dosage of ESI. In the
case of oral corticosteroid intake, a multidisciplinary Euro-
pean League Against Rheumatism (EULAR) task force
group of experts recommended that the risk of long-term
corticosteroid therapy depended on dosage: treatment
with less than 5 mg prednisone equivalent per day had low
risk, whereas patient-specific characteristics should be
considered between 5 mg and 10 mg/day, and levels great-
er than 10 mg/day could increase the risk of harm [87].
However, in the case of ESI, it is controversial whether
there is a relationship between systemic complications and
the dosage of corticosteroids. Habib et al. [88] conducted a
randomized, single-blind, controlled trial that showed no
significant difference between the two ESI doses of methyl-
prednisolone (80 mg and 40 mg) in terms of the rate of sec-
ondary AI (P = 0.715) at 3 weeks, except for the visual ana-
log scale (VAS) (P = 0.049) at 3 weeks. However, in the
double-blind, randomized controlled trial of Sim et al. [30],
there was a significant difference between ESIs with 40 mg
and 20 mg doses of triamcinolone in terms of HPA sup-
pression period (19.7 ± 3.1 days vs. 8.0 ± 2.4 days, P =
0.0005) and the slope in the linear mixed-effects model de-
noting the recovery rate of HPA axis (0.00431 ± 0.00043 vs.
0.00647 ± 0.00069, P = 0.015) at 4 weeks. However, there
were no differences in VAS (P > 0.99) and AI incidence (P
= 0.220) at 4 weeks between the two groups in Sim's study.
The World Institute of Pain (WIP) Benelux working group
recommended that the number of ESIs should be adjusted
according to the clinical response, suggesting that a 2-week
interval for additional ESI may be appropriate for proper
evaluation and minimization of endocrine side effects, and
the lowest effective dose should be used for ESI (40 mg for
methylprednisolone, 10 to 20 mg for triamcinolone acetate,
and 10 mg for dexamethasone phosphate) [68].
ESI for a pregnant or breastfeeding patient
Approximately 50% of pregnant women experience low
back pain. Despite its prevalence, low-back pain (LBP) in
pregnancy is considered normal by many patients and
physicians. Also, safe treatment options in pregnancy are
still disputed. Concerns regarding maternal and fetal
well-being restrict the use of interventional treatment regi-
mens by pain physicians, resulting in a higher incidence of
obstetric complications.
22 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
Sehmbi et al. [89] reviewed 56 studies investigating man-
agement strategies for LBP in pregnancy. According to this
review, three case reports involved ESI to alleviate symp-
toms of LBP, but all pregnant patients eventually required
operative intervention due to recurrence or progression of
neurological symptoms. In brief, there is weak evidence
supporting the analgesic and surgery-delaying effect of ESI
in pregnant patients with LBP, which is consistent with ob-
servations involving non-pregnant patients. Although a
single dose of epidural steroid appears to be associated
with a low risk to the fetus, it is recommended that ESI
should be reserved for pregnant patients with new onset of
signs or severe symptoms of lumbar nerve root compres-
sion before surgery.
The use of ESI during breastfeeding has yet to be investi-
gated comprehensively. The secretory function of prolactin
in humans is sensitive to changes in the activity of the HPA
axis in a dose-dependent manner [90]. McGuire reported a
case of 35-year-old mother treated with ESI and facet joint
injection with triamcinolone 80–120 mg resulting in tem-
porary reduction of lactation [91]. Although a detailed
study is needed, patients should be informed that the
amount of breast milk may decrease from day 3 to day 9 af-
ter ESI. Karahan et al. [92] reported that methylpredniso-
lone concentrations in breast milk and maternal serum fol-
lowing high-dose (1,000 mg) methylprednisolone IV pulse
therapy showed a similar trend at all time points. Eight
hours after the injection, the concentrations of methyl-
prednisolone in the milk and maternal serum were low; the
transfer of methylprednisolone into breast milk is low.
They recommended that mothers need to wait for 2–4 h to
further limit the level of exposure although the risk to the
infant seems low. Currently, no information on the effect of
epidural steroids on breast milk or breastfed infants is
available.
CONCLUSIONS
The complications caused by epidural corticosteroids
are relatively rare and rarely serious. However, pain physi-
cians should be aware of the complications because a
growing number of patients with various diseases are treat-
ed with ESI. Although the relationship between the degree
of systemic absorption and the side effects of ESI are not
well known, and most ESI-related complications appear to
be associated with systemic absorption of corticosteroids.
Thus, the complications of ESI differ from those adminis-
tered via oral or venous routes and depend on the type of
steroids used. The duration of HPA axis suppression ade-
quately reflects the systemic absorption of epidural corti-
costeroids. In terms of safety, non-particulate steroids are
preferred over particulate steroids. The ESI interval should
be at least 3–4 weeks for a particulate steroid, but non-par-
ticulate steroids may be administered more frequently. The
ESI dosage is controversial and should be designed to min-
imize HPA axis suppression for each drug.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Min Soo Lee, Ho Sik Moon. Formal
analysis: Min Soo Lee. Writing - original draft: Min Soo
Lee, Ho Sik Moon. Writing - review & editing: Ho Sik Moon.
Supervision: Ho Sik Moon.
ORCID
Min Soo Lee, https://orcid.org/0000-0002-9968-1998
Ho Sik Moon, https://orcid.org/0000-0003-2298-7734
REFERENCES
1. Lucherini T. [First findings in the use of hydrocortisone by en-
dospinal route]. Policlinico Prat 1954 61: 841-6. Italian.
2. Vydra D, McCormick Z, Clements N, Nagpal A, Julia J, Cush-
man D. Current trends in steroid dose choice and frequency of
administration of epidural steroid injections: a survey study.
PM R 2020; 12: 49-54.
3. Mordhorst TR, McCormick ZL, Presson AP, Collier WH, Spiker
WR. Examining the relationship between epidural steroid in-
jections and patient satisfaction. Spine J 2020; 20: 207-12.
4. Sabbaghan S, Mirzamohammadi E, Ameri Mahabadi M, Nik-
ouei F, Rahbarian F, Ahmadichaboki S, et al. Short-term effica-
cy of epidural injection of triamcinolone through translaminar
approach for the treatment of lumbar canal stenosis. Anesth
Pain Med 2020; 10: e99764.
5. Manson NA, McKeon MD, Abraham EP. Transforaminal epi-
dural steroid injections prevent the need for surgery in patients
with sciatica secondary to lumbar disc herniation: a retrospec-
tive case series. Can J Surg 2013; 56: 89-96.
www.anesth-pain-med.org 23
Safety of epidural steroid injection

6. Bicket MC, Horowitz JM, Benzon HT, Cohen SP. Epidural injec-
tions in prevention of surgery for spinal pain: systematic review
and meta-analysis of randomized controlled trials. Spine J
2015; 15: 348-62.
7. Maus TP, Bogduk N. Epidural steroid injections. In: Bonica's
management of pain. 5th ed. Edited by Ballantyne JC, Fishman
SM, Rathmell JP: Philadelphia, Wolters Kluwer. 2019, pp 1611-
22.
8. Cohen SP, Bicket MC, Jamison D, Wilkinson I, Rathmell JP. Epi-
dural steroids: a comprehensive, evidence-based review. Reg
Anesth Pain Med 2013; 38: 175-200.
9. Lee JW, Lee E, Lee GY, Kang Y, Ahn JM, Kang HS. Epidural ste-
roid injection-related events requiring hospitalisation or emer-
gency room visits among 52,935 procedures performed at a
single centre. Eur Radiol 2018; 28: 418-27.
10. Kang WY, Lee JW, Lee E, Kang Y, Ahn JM, Kang HS. Systemic ef-
fects of fluoroscopically guided epidural steroid injection with
dexamethasone. Korean J Pain 2019; 32: 178-86.
11. McGrath JM, Schaefer MP, Malkamaki DM. Incidence and
characteristics of complications from epidural steroid injec-
tions. Pain Med 2011; 12: 726-31.
12. Berthelot JM, Le Goff B, Maugars Y. Side effects of corticoste-
roid injections: what's new? Joint Bone Spine 2013; 80: 363-7.
13. Mulleman D, Mammou S, Griffoul I, Watier H, Goupille P.
Pathophysiology of disk-related sciatica. I.--Evidence support-
ing a chemical component. Joint Bone Spine 2006; 73: 151-8.
14. Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW. Abnor-
mal magnetic-resonance scans of the lumbar spine in asymp-
tomatic subjects. A prospective investigation. J Bone Joint Surg
Am 1990; 72: 403-8.
15. Boos N, Rieder R, Schade V, Spratt KF, Semmer N, Aebi M. 1995
Volvo Award in clinical sciences. The diagnostic accuracy of
magnetic resonance imaging, work perception, and psychoso-
cial factors in identifying symptomatic disc herniations. Spine
(Phila Pa 1976) 1995; 20: 2613-25.
16. McLain RF, Kapural L, Mekhail NA. Epidural steroid therapy for
back and leg pain: mechanisms of action and efficacy. Spine J
2005; 5: 191-201.
17. Kuslich SD, Ulstrom CL, Michael CJ. The tissue origin of low
back pain and sciatica: a report of pain response to tissue stim-
ulation during operations on the lumbar spine using local an-
esthesia. Orthop Clin North Am 1991; 22: 181-7.
18. Olmarker K, Størkson R, Berge OG. Pathogenesis of sciatic pain:
a study of spontaneous behavior in rats exposed to experimen-
tal disc herniation. Spine (Phila Pa 1976) 2002; 27: 1312-7.
19. Johansson A, Hao J, Sjölund B. Local corticosteroid application
blocks transmission in normal nociceptive C-fibres. Acta An-
aesthesiol Scand 1990; 34: 335-8.
20. Hooten WM, Nicholson WT, Gazelka HM, Reid JM, Moeschler
SM, Lamer TJ. Serum triamcinolone levels following interlami-
nar epidural injection. Reg Anesth Pain Med 2016; 41: 75-9.
21. Derendorf H, Hochhaus G, Rohatagi S, Möllmann H, Barth J,
Sourgens H, et al. Pharmacokinetics of triamcinolone aceton-
ide after intravenous, oral, and inhaled administration. J Clin
Pharmacol 1995; 35: 302-5.
22. Derendorf H, Möllmann H, Grüner A, Haack D, Gyselby G.
Pharmacokinetics and pharmacodynamics of glucocorticoid
suspensions after intra-articular administration. Clin Pharma-
col Ther 1986; 39: 313-7.
23. Beer PM, Bakri SJ, Singh RJ, Liu W, Peters GB 3rd, Miller M. In-
traocular concentration and pharmacokinetics of triamcino-
lone acetonide after a single intravitreal injection. Ophthal-
mology 2003; 110: 681-6.
24. Lamer TJ, Dickson RR, Gazelka HM, Nicholson WT, Reid JM,
Moeschler SM, et al. Serum triamcinolone levels following cer-
vical interlaminar epidural injection. Pain Res Manag 2018;
2018: 8474127.
25. Friedly JL, Comstock BA, Heagerty PJ, Bauer Z, Rothman MS,
Suri P, et al. Systemic effects of epidural steroid injections for
spinal stenosis. Pain 2018; 159: 876-83.
26. Jobe AH, Milad MA, Peppard T, Jusko WJ. Pharmacokinetics
and pharmacodynamics of intramuscular and oral betametha-
sone and dexamethasone in reproductive age women in India.
Clin Transl Sci 2020; 13: 391-9.
27. Scherer J, Rainsford KD, Kean CA, Kean WF. Pharmacology of
intra-articular triamcinolone. Inflammopharmacology 2014;
22: 201-17.
28. Park J, Kwak J, Chung S, Hong HJ, Chon JY, Moon HS. Incidence
of adrenal insufficiency and Cushing's syndrome after long-
term epidural steroid injections over six months or longer: a
preliminary study. J Pain Res 2020; 13: 1505-14.
29. Stout A, Friedly J, Standaert CJ. Systemic absorption and side
effects of locally injected glucocorticoids. PM R 2019; 11: 409-
19.
30. Sim SE, Hong HJ, Roh K, Seo J, Moon HS. Relationship between
epidural steroid dose and suppression of hypothalamus-pitu-
itary-adrenal axis. Pain Physician 2020; 23(4S): S283-94.
31. Chon JY, Moon HS. Salivary cortisol concentration changes af-
ter epidural steroid injection. Pain Physician 2012; 15: 461-6.
32. Abdul AJ, Ghai B, Bansal D, Sachdeva N, Bhansali A, Dhatt SS.
Hypothalamic pituitary adrenocortical axis suppression fol-
lowing a single epidural injection of methylprednisolone ace-
tate. Pain Physician 2017; 20: E991-1001.
33. Liu D, Ahmet A, Ward L, Krishnamoorthy P, Mandelcorn ED,
24 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
KS
PS
Leigh R, et al. A practical guide to the monitoring and manage-
ment of the complications of systemic corticosteroid therapy.
Allergy Asthma Clin Immunol 2013; 9: 30.
34. Chabre O, Goichot B, Zenaty D, Bertherat J. Group 1. Epidemi-
ology of primary and secondary adrenal insufficiency: preva-
lence and incidence, acute adrenal insufficiency, long-term
morbidity and mortality. Ann Endocrinol (Paris) 2017; 78: 490-
4.
35. Bancos I, Hahner S, Tomlinson J, Arlt W. Diagnosis and man-
agement of adrenal insufficiency. Lancet Diabetes Endocrinol
2015; 3: 216-26.
36. Leary J, Swislocki A. Hypothalamic-pituitary-adrenal suppres-
sion and iatrogenic Cushing's syndrome as a complication of
epidural steroid injections. Case Rep Endocrinol 2013; 2013:
617042.
37. Grierson MJ, Harrast MA. Iatrogenic Cushing syndrome after
epidural steroid injections for lumbar radiculopathy in an
HIV-infected patient treated with ritonavir: a case report high-
lighting drug interactions for spine interventionalists. PM R
2012; 4: 234-7.
38. Albert NE, Kazi S, Santoro J, Dougherty R. Ritonavir and epidur-
al triamcinolone as a cause of iatrogenic Cushing's syndrome.
Am J Med Sci 2012; 344: 72-4.
39. Elias PC, Martinez EZ, Barone BF, Mermejo LM, Castro M,
Moreira AC. Late-night salivary cortisol has a better perfor-
mance than urinary free cortisol in the diagnosis of Cushing's
syndrome. J Clin Endocrinol Metab 2014; 99: 2045-51.
40. Ward A, Watson J, Wood P, Dunne C, Kerr D. Glucocorticoid
epidural for sciatica: metabolic and endocrine sequelae. Rheu-
matology (Oxford) 2002; 41: 68-71.
41. Younes M, Neffati F, Touzi M, Hassen-Zrour S, Fendri Y, Béjia I,
et al. Systemic effects of epidural and intra-articular glucocor-
ticoid injections in diabetic and non-diabetic patients. Joint
Bone Spine 2007; 74: 472-6.
42. Maillefert JF, Aho S, Huguenin MC, Chatard C, Peere T, Mar-
quignon MF, et al. Systemic effects of epidural dexamethasone
injections. Rev Rhum Engl Ed 1995; 62: 429-32.
43. Dostalek M, Court MH, Yan B, Akhlaghi F. Significantly reduced
cytochrome P450 3A4 expression and activity in liver from hu-
mans with diabetes mellitus. Br J Pharmacol 2011; 163: 937-47.
44. Gonzalez P, Laker SR, Sullivan W, Harwood JE, Akuthota V. The
effects of epidural betamethasone on blood glucose in patients
with diabetes mellitus. PM R 2009; 1: 340-5.
45. Kim WH, Sim WS, Shin BS, Lee CJ, Jin HS, Lee JY, et al. Effects of
two different doses of epidural steroid on blood glucose levels
and pain control in patients with diabetes mellitus. Pain Physi-
cian 2013; 16: 557-68.
46. Dubois EF, Wagemans MF, Verdouw BC, Zwinderman AH, Van
Boxtel CJ, Dekhuijzen PN, et al. Lack of relationships between
cumulative methylprednisolone dose and bone mineral densi-
ty in healthy men and postmenopausal women with chronic
low back pain. Clin Rheumatol 2003; 22: 12-7.
47. Al-Shoha A, Rao DS, Schilling J, Peterson E, Mandel S. Effect of
epidural steroid injection on bone mineral density and mark-
ers of bone turnover in postmenopausal women. Spine (Phila
Pa 1976) 2012; 37: E1567-71.
48. Kim S, Hwang B. Relationship between bone mineral density
and the frequent administration of epidural steroid injections
in postmenopausal women with low back pain. Pain Res
Manag 2014; 19: 30-4.
49. Mandel S, Schilling J, Peterson E, Rao DS, Sanders W. A retro-
spective analysis of vertebral body fractures following epidural
steroid injections. J Bone Joint Surg Am 2013; 95: 961-4.
50. Suh-Burgmann E, Hung YY, Mura J. Abnormal vaginal bleeding
after epidural steroid injection: a paired observation cohort
study. Am J Obstet Gynecol 2013 209: 206.e1-6.
51. Weitoft T, Larsson A, Rönnblom L. Serum levels of sex steroid
hormones and matrix metalloproteinases after intra-articular
glucocorticoid treatment in female patients with rheumatoid
arthritis. Ann Rheum Dis 2008; 67: 422-4.
52. Gensler LS. Glucocorticoids: complications to anticipate and
prevent. Neurohospitalist 2013; 3: 92-7.
53. Schairer WW, Nwachukwu BU, Mayman DJ, Lyman S, Jerabek
SA. Preoperative hip injections increase the rate of peripros-
thetic infection after total hip arthroplasty. J Arthroplasty 2016;
31(9 Suppl): 166-9.e1.
54. Yang S, Werner BC, Cancienne JM, Hassanzadeh H, Shimer AL,
Shen FH, et al. Preoperative epidural injections are associated
with increased risk of infection after single-level lumbar de-
compression. Spine J 2016; 16: 191-6.
55. Singla A, Yang S, Werner BC, Cancienne JM, Nourbakhsh A,
Shimer AL, et al. The impact of preoperative epidural injec-
tions on postoperative infection in lumbar fusion surgery. J
Neurosurg Spine 2017; 26: 645-9.
56. Barbaud A, Waton J. Systemic allergy to corticosteroids: clinical
features and cross reactivity. Curr Pharm Des 2016; 22: 6825-
31.
57. Klein-Gitelman MS, Pachman LM. Intravenous corticosteroids:
adverse reactions are more variable than expected in children.
J Rheumatol 1998; 25: 1995-2002.
58. Mace S, Vadas P, Pruzanski W. Anaphylactic shock induced by
intraarticular injection of methylprednisolone acetate. J Rheu-
matol 1997; 24: 1191-4.
59. Amin N, Brancaccio R, Cohen D. Cutaneous reactions to inject-
www.anesth-pain-med.org 25
Safety of epidural steroid injection
able corticosteroids. Dermatitis 2006; 17: 143-6.
60. Moran DE, Moynagh MR, Alzanki M, Chan VO, Eustace SJ.
Anaphylaxis at image-guided epidural pain block secondary to
corticosteroid compound. Skeletal Radiol 2012; 41: 1317-8.
61. Cicala RS, Westbrook L, Angel JJ. Side effects and complications
of cervical epidural steroid injections. J Pain Symptom Manage
1989; 4: 64-6.
62. Kim CH, Issa MA, Vaglienti RM. Flushing following interlami-
nar lumbar epidural steroid injection with dexamethasone.
Pain Physician 2010; 13: 481-4.
63. Wada K, Yamada N, Sato T, Suzuki H, Miki M, Lee Y, et al. Corti-
costeroid-induced psychotic and mood disorders: diagnosis
defined by DSM-IV and clinical pictures. Psychosomatics 2001;
42: 461-6.
64. Kenna HA, Poon AW, de los Angeles CP, Koran LM. Psychiatric
complications of treatment with corticosteroids: review with
case report. Psychiatry Clin Neurosci 2011; 65: 549-60.
65. Benyamin RM, Vallejo R, Kramer J, Rafeyan R. Corticosteroid
induced psychosis in the pain management setting. Pain Phy-
sician 2008; 11: 917-20.
66. Roberti G, Oddone F, Agnifili L, Katsanos A, Michelessi M, Mas-
tropasqua L, et al. Steroid-induced glaucoma: epidemiology,
pathophysiology, and clinical management. Surv Ophthalmol
2020; 65: 458-72.
67. Manjiani D, Said S, Kaye AD. Transient glaucoma after an epi-
dural steroid injection: a case report. Ochsner J 2015; 15: 79-82.
68. Van Boxem K, Rijsdijk M, Hans G, de Jong J, Kallewaard JW,
Vissers K, et al. Safe use of epidural corticosteroid injections:
recommendations of the WIP Benelux work group. Pain Pract
2019; 19: 61-92.
69. Chen YC, Gajraj NM, Clavo A, Joshi GP. Posterior subcapsular
cataract formation associated with multiple lumbar epidural
corticosteroid injections. Anesth Analg 1998; 86: 1054-5.
70. Tok CH, Kaur S, Gangi A. Symptomatic spinal epidural lipoma-
tosis after a single local epidural steroid injection. Cardiovasc
Intervent Radiol 2011; 34 Suppl 2: S250-5.
71. Danielson KD, Harrast MA. Focal spinal epidural lipomatosis
after a single epidural steroid injection. PM R 2011; 3: 590-3.
72. Sandberg DI, Lavyne MH. Symptomatic spinal epidural lipo-
matosis after local epidural corticosteroid injections: case re-
port. Neurosurgery 1999; 45: 162-5.
73. Houten JK, Errico TJ. Paraplegia after lumbosacral nerve root
block: report of three cases. Spine J 2002; 2: 70-5.
74. Derby R, Lee SH, Date ES, Lee JH, Lee CH. Size and aggregation
of corticosteroids used for epidural injections. Pain Med 2008;
9: 227-34.
75. Laemmel E, Segal N, Mirshahi M, Azzazene D, Le Marchand S,
Wybier M, et al. Deleterious effects of intra-arterial administra-
tion of particulate steroids on microvascular perfusion in a
mouse model. Radiology 2016; 279: 731-40.
76. Watkins TW, Dupre S, Coucher JR. Ropivacaine and dexameth-
asone: a potentially dangerous combination for therapeutic
pain injections. J Med Imaging Radiat Oncol 2015; 59: 571-7.
77. Hwang H, Park J, Lee WK, Lee WH, Leigh JH, Lee JJ, et al. Crys-
tallization of local anesthetics when mixed with corticosteroid
solutions. Ann Rehabil Med 2016; 40: 21-7.
78. Benzon HT, Chew TL, McCarthy RJ, Benzon HA, Walega DR.
Comparison of the particle sizes of different steroids and the
effect of dilution: a review of the relative neurotoxicities of the
steroids. Anesthesiology 2007; 106: 331-8.
79. Dreyfuss P, Baker R, Bogduk N. Comparative effectiveness of
cervical transforaminal injections with particulate and non-
particulate corticosteroid preparations for cervical radicular
pain. Pain Med 2006; 7: 237-42.
80. Kim D, Brown J. Efficacy and safety of lumbar epidural dexa-
methasone versus methylprednisolone in the treatment of
lumbar radiculopathy: a comparison of soluble versus particu-
late steroids. Clin J Pain 2011; 27: 518-22.
81. Park CH, Lee SH, Kim BI. Comparison of the effectiveness of
lumbar transforaminal epidural injection with particulate and
nonparticulate corticosteroids in lumbar radiating pain. Pain
Med 2010; 11: 1654-8.
82. Donohue NK, Tarima SS, Durand MJ, Wu H. Comparing pain
relief and functional improvement between methylpredniso-
lone and dexamethasone lumbosacral transforaminal epidural
steroid injections: a self-controlled study. Korean J Pain 2020;
33: 192-8.
83. Kim EJ, Moon JY, Park KS, Yoo da H, Kim YC, Sim WS, et al. Epi-
dural steroid injection in Korean pain physicians: a national
survey. Korean J Pain 2014; 27: 35-42.
84. Murthy NS, Geske JR, Shelerud RA, Wald JT, Diehn FE, Thielen
KR, et al. The effectiveness of repeat lumbar transforaminal
epidural steroid injections. Pain Med 2014; 15: 1686-94.
85. Mattie R, Schneider BJ, Smith C. Frequency of epidural steroid
injections. Pain Med 2020; 21: 1078-9.
86. Chutatape A, Menon M, Fook-Chong S, George JM. Metabolic
and endocrinal effects of epidural glucocorticoid injections.
Singapore Med J 2019; 60: 140-4.
87. Strehl C, Bijlsma JW, de Wit M, Boers M, Caeyers N, Cutolo M,
et al. Defining conditions where long-term glucocorticoid
treatment has an acceptably low level of harm to facilitate im-
plementation of existing recommendations: viewpoints from
an EULAR task force. Ann Rheum Dis 2016; 75: 952-7.
88. Habib G, Jabbour A, Salman J, Hakim G, Haddad H. The effect
26 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
of epidural methylprednisolone acetate injection on the hypo-
thalamic-pituitary-adrenal axis. J Clin Anesth 2013; 25: 629-33.
89. Sehmbi H, D'Souza R, Bhatia A. Low back pain in pregnancy:
investigations, management, and role of neuraxial analgesia
and anaesthesia: a systematic review. Gynecol Obstet Invest
2017; 82: 417-36.
90. Hubina E, Nagy GM, Tóth BE, Iván G, Görömbey Z, Szabolcs I,
et al. Dexamethasone and adrenocorticotropin suppress pro-
lactin secretion in humans. Endocrine 2002; 18: 215-9.
91. McGuire E. Sudden loss of milk supply following high-dose tri-
amcinolone (Kenacort) injection. Breastfeed Rev 2012; 20: 32-4.
92. Zengin Karahan S, Boz C, Terzi M, Aktoz G, Sen S, Ozbudun B,
et al. Methylprednisolone concentrations in breast milk and
serum of patients with multiple sclerosis treated with IV pulse
methylprednisolone. Clin Neurol Neurosurg 2020; 197: 106118.
www.anesth-pain-med.org 27
Safety of epidural steroid injection

Corresponding author Hyun Kang, M.D., Ph.D.Department of Anesthesiology and Pain Medicine, Chung-Ang University College of Medicine, 84 Heukseok-ro, Dongjak-gu, Seoul 06974, Korea Tel: 82-2-6299-2586 Fax: 82-2-6299-2585 E-mail: [email protected]
Background: Postoperative delirium (POD) is a condition of cerebral dysfunction and a com-mon complication after surgery. This study aimed to compare and determine the relative ef-ficacy of pharmacological interventions for preventing POD using a network meta-analysis.
Methods: We performed a systematic and comprehensive search to identify and analyze all randomized controlled trials until June 29, 2020, comparing two or more pharmacological interventions, including placebo, to prevent or reduce POD. The primary outcome was the in-cidence of POD. We performed a network meta-analysis and used the surface under the cu-mulative ranking curve (SUCRA) values and rankograms to present the hierarchy of the pharmacological interventions evaluated.
Results: According to the SUCRA value, the incidence of POD decreased in the following or-der: the combination of propofol and acetaminophen (86.1%), combination of ketamine and dexmedetomidine (86.0%), combination of diazepam, flunitrazepam, and pethidine (84.8%), and olanzapine (75.6%) after all types of anesthesia; combination of propofol and acetamin-ophen (85.9%), combination of ketamine and dexmedetomidine (83.2%), gabapentin (82.2%), and combination of diazepam, flunitrazepam, and pethidine (79.7%) after general anesthesia; and ketamine (87.1%), combination of propofol and acetaminophen (86.0%), and combination of dexmedetomidine and acetaminophen (66.3%) after cardiac surgery. However, only the dexmedetomidine group showed a lower incidence of POD than the con-trol group after all types of anesthesia and after general anesthesia.
Conclusions: Dexmedetomidine reduced POD compared with the control group. The combi-nation of propofol and acetaminophen and the combination of ketamine and dexmedetomi-dine seemed to be effective in preventing POD. However, further studies are needed to de-termine the optimal pharmacological intervention to prevent POD.
Keywords: Delirium; Network meta-analysis; Pharmacology; Surgical procedures, operative.
Pharmacological strategies to prevent postoperative delirium: a systematic review and network meta-analysis
Jun Mo Lee1, Ye Jin Cho1, Eun Jin Ahn1, Geun Joo Choi1,2, and Hyun Kang1,2
1Department of Anesthesiology and Pain Medicine, Chung-Ang University College
of Medicine, 2The Institute of Evidence Based Clinical Medicine, Chung-Ang University,
Seoul, Korea
Received September 25, 2020 Revised October 15, 2020 Accepted October 16, 2020
Clinical ResearchAnesth Pain Med 2021;16:28-48https://doi.org/10.17085/apm.20079pISSN 1975-5171 • eISSN 2383-7977
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
28

KS
NAC
CINTRODUCTION
Postoperative delirium (POD) is a condition of cerebral
dysfunction and a common complication after surgery that
occurs in 15–35% patients [1]. Old age, a history of stroke,
use of narcotic analgesics, poor physical condition, alco-
holism, preexisting cognitive impairment, and type of sur-
gery are known risk factors for POD [2,3]. Especially pa-
tients undergoing major surgery, including cardiac surgery,
are at increased risk of developing POD because of the
complexity of the surgical procedure, the administration of
intraoperative and postoperative anesthetic and other
pharmacological agents. For this reason, POD is reported
to affect up to 57% of cardiac-surgery patients [4].
POD is characterized by altered consciousness, disorien-
tation, impaired memory, perceptual disturbance, altered
psychomotor activity, and altered sleep-wake cycles after
surgery. POD increases the rate of mortality, length of hos-
pital stay, risk of placement to long-term care institutions,
or functional disability, thus increasing hospitalization
costs [2,5]. Therefore, appropriate prevention and treat-
ment of POD is important for enhancing postoperative re-
covery and quality of life in elderly patients [6].
The treatment strategies for POD are well organized
compared to the prevention strategies. The treatment for
POD includes treating the underlying cause; correcting flu-
id and electrolyte imbalance or hypoxia; removing cathe-
ters if present, and treating patients who are restless, ag-
gressive, agitative, and harm to themself or others with an-
tipsychotics such as haloperidol, chlorpromazine, olanzap-
ine, and risperidone [7,8].
However, it is unclear which strategies are effective for
preventing POD. Therefore, various strategies to prevent
POD, especially variable pharmacological interventions,
such as dexmedetomidine, propofol, midazolam, ket-
amine, and acetaminophen, have been applied and com-
pared. However, each study only compared two or three
drugs and reported diverse results.
Recently, a few systematic reviews and meta-analyses
have demonstrated and integrated the preventive effect of
various interventions [9–14]. However, each study was lim-
ited to pair-wise meta-analysis and examined only two
pharmacological interventions. No previous network me-
ta-analysis (NMA) has compared the effectiveness of all
available pharmacological interventions. Further, the
aforementioned studies included studies conducted prior
to 2017.
NMA complements traditional pair-wise meta-analysis
by combining direct and indirect comparisons of treat-
ments and provides objective ranking of various treatments
based on the corresponding surface under the cumulative
ranking curve (SUCRA) [15].
Thus, we reviewed all articles that investigated the effec-
tiveness of pharmacological interventions to prevent POD
and performed NMA to compare and quantify the rank or-
der of the effectiveness of pharmacological interventions to
prevent POD.
MATERIALS AND METHODS
Protocol and registration
We developed the protocol for this systematic review and
NMA according to the preferred reporting requirements for
systematic review and meta-analysis protocol (PRISMA-P)
statement [16]. We registered the review protocol at the
International Prospective Register of Systematic Reviews
(registration no. CRD42020189363; www.crd.york.ac.uk/
prospero) on May 7, 2020.
This systematic review and NMA of pharmacological in-
terventions for preventing POD were performed according
to the protocol recommended by the Cochrane Collabora-
tion [17] and reported according to the PRISMA extension
for NMA guidelines [18].
Search strategy
We searched MEDLINE, EMBASE, Cochrane Central
Register of Controlled Trials (CENTRAL), and Google
Scholar from inception to June 29, 2020 using the search
terms related to pharmacological interventions for pre-
venting POD. The search terms used for MEDLINE and
EMBASE are presented in Supplementary Material. Two
investigators (GJC and HK) screened the titles and ab-
stracts of the retrieved articles. Reference lists were import-
ed to Endnote software 8.1 (Thompson Reuters, USA), and
duplicate articles were removed. Additionally, the refer-
ences of articles obtained from the original search were re-
viewed to identify relevant articles.
Inclusion criteria and exclusion criteria
We included only randomized controlled trials (RCTs)
that compared two or more pharmacological interventions
www.anesth-pain-med.org 29
Pharmacological strategies for POD

to prevent POD.
The PICO-SD information included the following:
1. Patients (P): all patients receiving surgery under gen-
eral or regional anesthesia
2. Intervention (I): pharmacological interventions to pre-
vent POD
3. Comparison (C): other pharmacological interventions
to prevent POD, placebo, or no treatment
4. Outcome measurements (O): the incidence of POD
5. Study design (SD): RCTs
6. Subgroup analysis: general anesthesia and cardiac sur-
gery
Exclusion criteria contained the following features:
1. Review articles, case reports, case-series, letters to the
editor, commentaries, proceedings, laboratory science
studies, and all other non-relevant studies
2. Studies that failed to report the outcomes of interest
3. Studies that investigated the effect of inhalational an-
esthetics or patient-controlled analgesia (PCA) regi-
mens
There was on language limitations or date restrictions in
our study.
Study selection
Two reviewers (JML and YJC) independently screened
the titles and abstracts of the studies to identify trials that
met the inclusion criteria outlined above. For articles de-
termined to be eligible based on the title and/or abstract,
the full paper was retrieved. Potentially relevant studies
chosen by at least one author were retrieved, and the full
text was evaluated. Full-text articles were assessed sepa-
rately by two authors (JML and YJC), and any disagree-
ments were resolved through discussion. In cases where
agreement could not be reached, the dispute was resolved
with the help of a third investigator (HK). To minimize data
duplication owing to multiple reporting, articles from the
same author, organization, or country were compared.
Data extraction
Using a standardized extraction form, the following data
were extracted independently by two investigators (JML
and YJC): 1) title, 2) name of the first author, 3) name of the
journal, 4) year of publication, 5) study design, 6) type of
pharmacological interventions, 7) dose of pharmacological
agents, 8) country, 9) risk of bias, 10) inclusion criteria, 11)
exclusion criteria, 12) age, 13) number of subjects, and 14)
incidence of POD.
If the information was inadequate, attempts were made
to contact the study authors, and additional information
was requested. If unsuccessful, missing information was
calculated from the available data, if possible, or was ex-
tracted from the figure using the open source software Plot
Digitizer (version 2.6.8; http://plotdigitizer.sourceforge.
net).
The reference lists were divided into two halves. Two in-
vestigators completed data extraction, one for each half of
the reference list. Data extraction forms were cross-
checked to verify the accuracy and consistency of the ex-
tracted data.
The degree of agreement between the two independent
data extractors was computed using kappa statistics to
measure the difference between the observed and expect-
ed agreements, i.e., whether they were random or by
chance. Kappa values were interpreted as: 1) less than 0:
less than chance agreement; 2) 0.01 to 0.20: slight agree-
ment; 3) 0.21 to 0.40: fair agreement; 4) 0.41 to 0.60: mod-
erate agreement; 5) 0.61 to 0.80: substantial agreement;
and 6) 0.8 to 0.99: almost perfect agreement [19].
Risk of bias assessment
The quality of the studies was independently assessed by
two investigators (JML and YJC) using the Revised Co-
chrane risk of bias tool for randomized trials (RoB 2.0). Risk
of bias judgment was assessed in the following domains:
bias arising from the randomization process, bias due to
deviations from intended intervention, bias due to missing
outcome data, bias in measurement of the outcome, and
bias in selection of the reported results. Based on the re-
sults of risk of bias judgment, formal overall risk of bias
judgment was categorized as “low risk of bias,” “some con-
cern,” and “high risk of bias” [20].
Statistical analysis
Ad-hoc tables were designed to summarize data from the
included studies by showing their key characteristics and
any important questions related to the review objectives.
After extracting the data, the reviewers determined the fea-
sibility of a meta-analysis.
A multiple treatment comparison NMA is a meta-analy-
sis generalization method that includes both direct and in-
30 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
NAC
Cdirect RCT comparison of treatments. A random-effects
NMA based on a frequentist framework was performed us-
ing STATA software (version 15, StataCorp LP, USA) based
on mvmeta with NMA graphical tools developed by
Chaimani et al. [21].
Before conducting the NMA, we evaluated the transitivi-
ty assumption by examining the comparability of the risk
of bias (all versus removing high risks of bias from the ran-
domization process and overall risk of bias), demograph-
ics, and types of pharmacological interventions as poten-
tial treatment-effect modifiers across comparisons.
A network plot linking the included pharmacological in-
terventions to prevent POD and their combination with
other pharmacological agents was formed to indicate the
types of agents, number of patients on different agents, and
the level of pair-wise comparisons. The nodes show com-
parisons of pharmacological agents being compared, and
the edges show the available direct comparisons among
the pharmacological agents. The nodes and edges are
weighed on the basis of the weights applied in NMA and
the inverse of the standard error of effect.
We evaluated the consistency assumption for the entire
network using the design-by-treatment interaction model.
We also evaluated each closed loop in the network to eval-
uate local inconsistencies between the direct and indirect
effect estimates for the same comparison. For each loop,
we estimated the inconsistency factor (IF) as the absolute
difference between the direct and indirect estimates and
95% confidence interval (CI) for each paired comparison in
the loop [22]. When the IF value with 95% CI started at 0, it
indicated that the direct evidence and the indirect evi-
dence were consistent.
Mean summary effects with CI were presented together
with their predictive intervals (PrIs) to facilitate interpreta-
tion of the results considering the magnitude of heteroge-
neity. PrIs provide an interval that is expected to encom-
pass the estimate of a future study.
A rankogram and a cumulative ranking curve were
drawn for each pharmacological intervention. Rankogram
plots are the probabilities for treatments to assume a possi-
ble rank. We used surface under the cumulative ranking
curve (SUCRA) values to present the hierarchy of pharma-
cological interventions to prevent the incidence of POD.
The SUCRA is a relative ranking measure that accounts for
the uncertainty in the treatment order, that is, accounts for
both the location and the variance of all relative treatment
effects. A higher SUCRA value is regarded as a more posi-
tive result for individual interventions [23].
We performed subgroup analysis based on all types of
anesthesia, general anesthesia, and cardiac surgery, be-
cause the incidence of POD is expected to be different ac-
cording to the type of anesthesia, and increase after cardiac
surgery.
Quality of evidence
The evidence grade was determined using the Grading of
Recommendations, Assessment, Development, and Evalu-
ation (GRADE) system, which uses a sequential assessment
of the evidence quality, followed by an assessment of the
risk-benefit balance and a subsequent judgment on the
strength of the recommendations [24].
RESULTS
Study selection
We initially retrieved 235 articles from MEDLINE, EM-
BASE, CENTRAL, and Google Scholar databases and 17 ar-
ticles through a manual search. After adjusting for dupli-
cates, 245 studies remained. Of these, 182 studies were dis-
carded after reviewing the title and abstracts for the follow-
ing reasons: related to other topics, designed as systematic
reviews, reviews or retrospective studies, and conference
abstracts. The full texts of the 63 remaining studies were re-
viewed in detail; 12 studies were excluded for the following
reasons: three were study protocols [25–27], two were edi-
torials [13,28], four were systematic reviews, [9–12] and
three did not report the outcome of our interest (two com-
pared an inhalational agent [13,29] and one was compared
in the PCA regimen [30]). Thus, 51 studies with a total of
22,565 patients that included 18 different pharmacological
interventions were included in this NMA (Fig. 1). The kap-
pa value for the selected articles between the two reviewers
was 0.844.
Characteristics of the included studies
The characteristics of the 51 studies are summarized in
Table 1. All the studies were performed on adults with
American Society of Anesthesiologists physical status clas-
sifications I, II, and III. The 51 studies were conducted in
various countries, such as Australia [31,32], Canada [33,34],
China [1,2,6,35–47], Denmark [48], Greece [49], India
www.anesth-pain-med.org 31
Pharmacological strategies for POD

[50,51], Iran [52,53], Japan [54–57], the Netherlands [58–
61], South Korea [62,63], Switzerland [64], Taiwan [65,66],
Thailand [67], the United Kingdom [68], the United States
of America [4,69–76], and Saudi arabia [77].
Twenty-seven types of pharmacological agents, includ-
ing dexmedetomidine (Dexm) [2,4,6,31,33,35,36,38–45,47,
50,51,62,63,65,66,69,70], propofol (Prop) [4,33,42–44,
47,51,66,70], acetaminophen (AAP) [70], midazolam
(Mida) [4,6,77], remifentanil (Remi) [62], morphine (Morp)
[31], methylprednisolone (MPDL) [32,34,48], melatonin
(Mela) [58,77], dexamethasone (Dexa) [52,59,61], haloperi-
dol (Halo) [37,54,55,60], rivastigmine (Riva) [64], ketamine
(Keta) [39,71], olanzapine (Olan) [72], gabapentin (Gaba)
[73,76], nimodipine (Nimo) [1], cyproheptadine (Cypr)
[53], ondansetron (Onda) [49], risperoidone (Risp) [67],
L-tryptophan(L-tyr) [74], donepezil (Done) [68,75], Yoku-
kansan (TJ-54) [56], diazepam (Diaz) [57], flunitrazepam
(Flun) [57] and pethidine (Peth) [57], parecoxib (Pare) [46],
and clonidine (Clon) [77] were evaluated.
The types of surgery investigated included cardiovascular
surgery [4,31–35,42,43,47,50–52,59,61,62,64,67,70,71], ortho-
pedic surgery [1,2,6,39,40,44,46,48,49,54,58,60,68,72,73,75–
77], thoracoscopic and pulmonary surgery [41,56,65,74], ab-
dominal and laparoscopic surgery [54–57,63,66], vascular
and urology surgery [74], free flap [38], oral cancer surgery
[45], and non-cardiac surgery [36,37,53,69]. The anesthesia
method in the studies included only general anesthesia [1,
2,4,6,31–35,38,39,41–43,45,47,49–52,55–57,59,61–67,69–
71,76], general anesthesia + regional anesthesia [36,37,48,
54,72-74], type of anesthesia were not decribed [40,53,58,
60,68,75], and only regional anesthesia [44,46,77].
Study quality assessment
The risk of bias assessment in the included studies using
the Cochrane tool is presented in Table 2.
All types of anesthesia
A total of 51 studies (22,565 patients) measured the inci-
dence of POD. The pooled overall incidence of POD after
all types of anesthesia was 18.5% (95% CI: 16.2% to 21.0%,
Pchi2 < 0.001, I2 = 92.0%). The network plot of all eligible
comparisons for this endpoint is depicted in Fig. 2A.
Although all 27 management modalities (nodes) were
connected to the network, two comparisons (Control [Cont],
Dexm) were compared directly to the other 25 nodes.
The evaluation of the network inconsistency using the
design-by-treatment interaction model suggested no sig-
nificant inconsistency (χ2 [8] = 13.37, P = 0.100). Of the 14
closed loops in the network for the comparison of postop-
erative delirium, four loops (Dexm-Dexm + AAP-pro + AAP
[01-04-05] [70], Dexm-Keta-Keta + Dexm [01-09-22] [39],
Pro-Dexm + AAP-Prop + AAP [03-04-05] [70], Mida-Me-
la-Clon [06-11-25] [77]) were formed only by multi-arm tri-
als. Thus, local inconsistency was evaluated in 10 loops. Al-
though most loops showed no relevance in the local incon-
sistency between the direct and indirect point estimates,
235 records identified through database searching
245 records screened with titles and abstracts 182 records excluded
Excluded (n = 12):
• Study protocol (n = 3)• Editorial (n = 2)• Systematic review (n = 4)• Not report the outcome of interest (n = 3)
63 full-text articles assessed for eligibility
51 studies included in NMA (n = 22,565)
17 records identified through hand searching
Fig. 1. PRISMA flowchart of included and excluded trials. PRISMA: preferred reporting requirements for systematic review and meta-analysis, NMA: network meta-analysis.
245 records after 7 duplicates removed
32 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
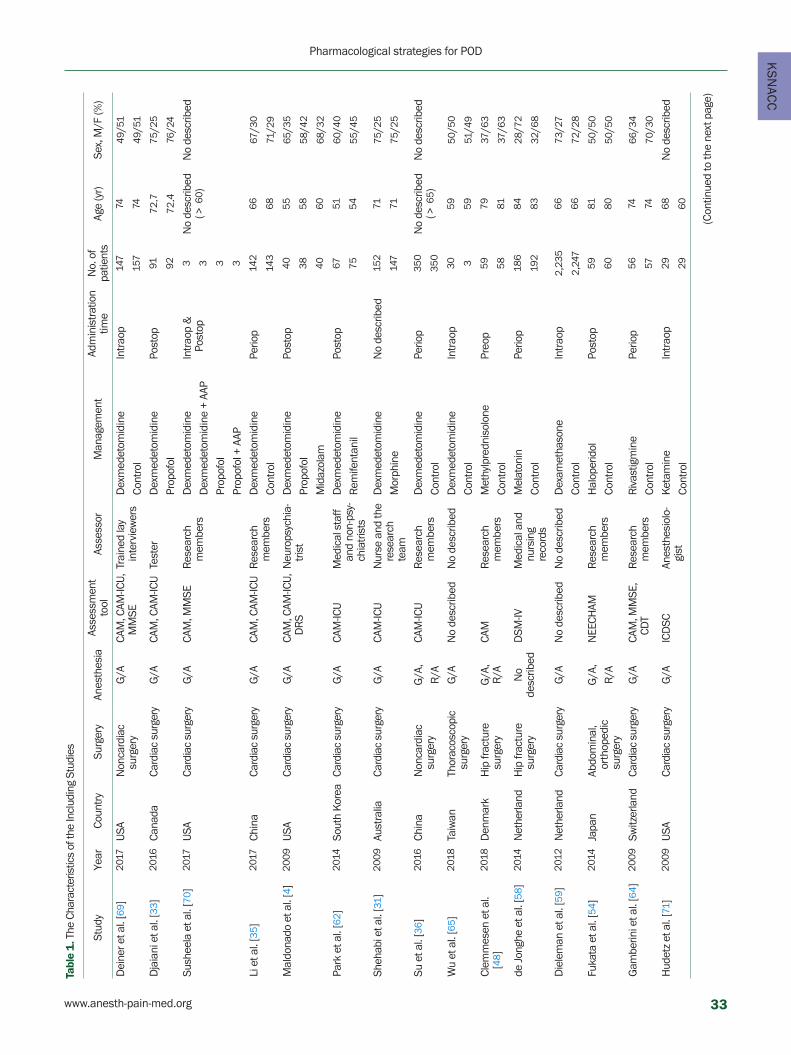
KS
NAC
C
Tabl
e 1
. The
Cha
ract
eris
tics
of th
e In
clud
ing
Stud
ies
Stud
yYe
arCo
untr
ySu
rger
yAn
esth
esia
Asse
ssm
ent
tool
Asse
ssor
Man
agem
ent
Adm
inis
trat
ion
time
No.
of
patie
nts
Age
(yr)
Sex,
M/F
(%)
Dei
ner e
t al.
[69 ]
2017
USA
Non
card
iac
surg
ery
G/A
CAM
, CAM
-ICU,
M
MSE
Trai
ned
lay
in
terv
iew
ers
Dex
med
etom
idin
eIn
trao
p14
774
49/5
1
Cont
rol
157
7449
/51
Dja
iani
et a
l. [3
3 ]20
16Ca
nada
Card
iac
surg
ery
G/A
CAM
, CAM
-ICU
Test
erD
exm
edet
omid
ine
Post
op91
72.7
75/2
5
Prop
ofol
9272
.476
/24
Sush
eela
et a
l. [7
0 ]20
17U
SACa
rdia
c su
rger
yG
/ACA
M, M
MSE
Res
earc
h m
embe
rsD
exm
edet
omid
ine
Intr
aop
&
Post
op3
No
desc
ribed
(>
60 )
No
desc
ribed
Dex
med
etom
idin
e +
AAP
3
Prop
ofol
3
Prop
ofol
+ A
AP3
Li e
t al.
[35 ]
2017
Chin
aCa
rdia
c su
rger
yG
/ACA
M, C
AM-IC
UR
esea
rch
mem
bers
Dex
med
etom
idin
ePe
riop
142
6667
/30
Cont
rol
143
6871
/29
Mal
dona
do e
t al.
[4]
2009
USA
Card
iac
surg
ery
G/A
CAM
, CAM
-ICU,
D
RS
Neu
rops
ychi
a-tr
ist
Dex
med
etom
idin
ePo
stop
4055
65/3
5
Prop
ofol
3858
58/4
2
Mid
azol
am40
6068
/32
Park
et a
l. [6
2 ]20
14So
uth
Kor
eaCa
rdia
c su
rger
yG
/ACA
M-IC
UM
edic
al s
taff
and
non-
psy-
chia
tris
ts
Dex
med
etom
idin
ePo
stop
6751
60/4
0
Rem
ifent
anil
7554
55/4
5
Sheh
abi e
t al.
[31 ]
2009
Aust
ralia
Card
iac
surg
ery
G/A
CAM
-ICU
Nur
se a
nd th
e re
sear
ch
team
Dex
med
etom
idin
eN
o de
scrib
ed15
271
75/2
5
Mor
phin
e14
771
75/2
5
Su e
t al.
[36 ]
2016
Chin
aN
onca
rdia
c su
rger
yG
/A,
CAM
-ICU
Res
earc
h m
embe
rsD
exm
edet
omid
ine
Perio
p35
0N
o de
scrib
ed
(> 6
5 )N
o de
scrib
ed
R/A
Cont
rol
350
Wu
et a
l. [6
5 ]20
18Ta
iwan
Thor
acos
copi
c su
rger
yG
/AN
o de
scrib
edN
o de
scrib
edD
exm
edet
omid
ine
Intr
aop
3059
50/5
0
Cont
rol
359
51/4
9
Clem
mes
en e
t al.
[48 ]
2018
Den
mar
kH
ip fr
actu
re
surg
ery
G/A
,R
/ACA
MR
esea
rch
mem
bers
Met
hylp
redn
isol
one
Preo
p59
7937
/63
Cont
rol
5881
37/6
3
de J
ongh
e et
al.
[58 ]
2014
Net
herla
ndH
ip fr
actu
re
surg
ery
No
de
scrib
edD
SM-IV
Med
ical
and
nu
rsin
g
reco
rds
Mel
aton
inPe
riop
186
8428
/72
Cont
rol
192
8332
/68
Die
lem
an e
t al.
[59 ]
2012
Net
herla
ndCa
rdia
c su
rger
yG
/AN
o de
scrib
edN
o de
scrib
edD
exam
etha
sone
Intr
aop
2 ,23
566
73/2
7
Cont
rol
2 ,24
766
72/2
8
Fuka
ta e
t al.
[54 ]
2014
Japa
nAb
dom
inal
, or
thop
edic
su
rger
y
G/A
,N
EECH
AMR
esea
rch
mem
bers
Hal
oper
idol
Post
op59
8150
/50
R/A
Cont
rol
6080
50/5
0
Gam
berin
i et a
l. [6
4 ]20
09Sw
itzer
land
Card
iac
surg
ery
G/A
CAM
, MM
SE,
CDT
Res
earc
h m
embe
rsR
ivas
tigm
ine
Perio
p56
7466
/34
Cont
rol
5774
70/3
0
Hud
etz
et a
l. [7
1 ]20
09U
SACa
rdia
c su
rger
yG
/AIC
DSC
Anes
thes
iolo
-gi
stK
etam
ine
Intr
aop
2968
No
desc
ribed
Cont
rol
2960
(Con
tinue
d to
the
next
pag
e)
www.anesth-pain-med.org 33
Pharmacological strategies for POD
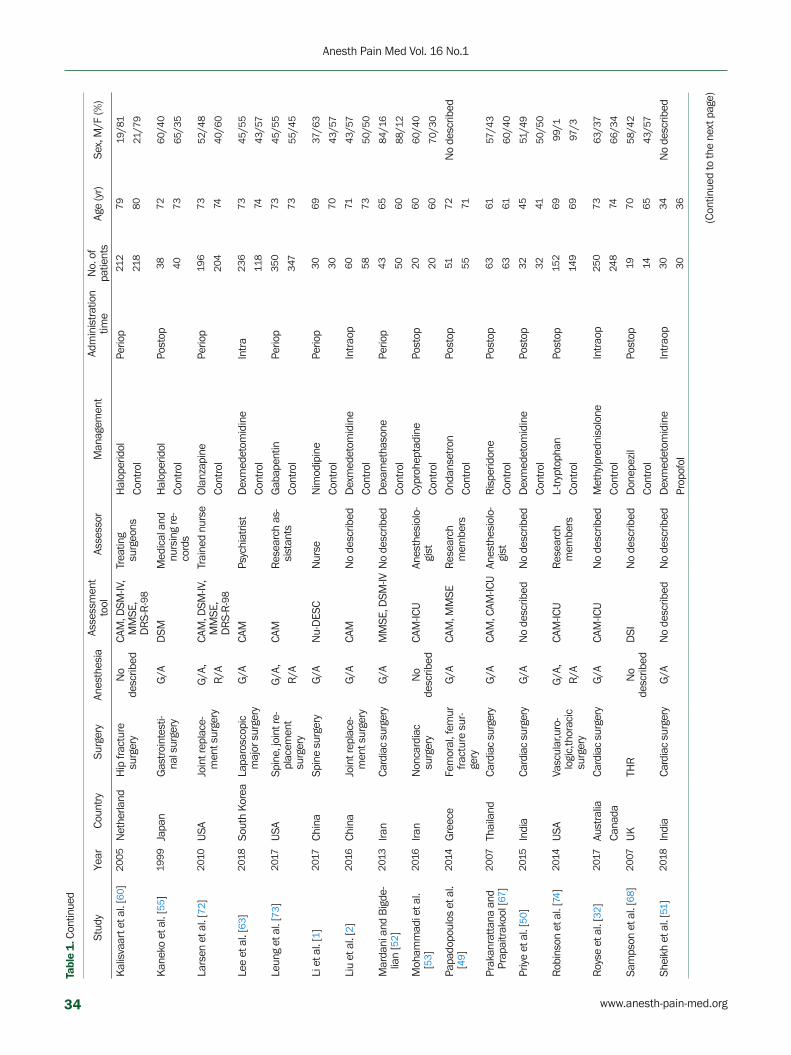
Kal
isva
art e
t al.
[60 ]
2005
Net
herla
ndH
ip fr
actu
re
surg
ery
No
de
scrib
edCA
M, D
SM-IV
, M
MSE
, D
RS-
R-9
8
Trea
ting
su
rgeo
nsH
alop
erid
olPe
riop
212
7919
/81
Cont
rol
218
8021
/79
Kan
eko
et a
l. [5
5 ]19
99Ja
pan
Gas
troi
ntes
ti-na
l sur
gery
G/A
DSM
Med
ical
and
nu
rsin
g re
-co
rds
Hal
oper
idol
Post
op38
7260
/40
Cont
rol
4073
65/3
5
Lars
en e
t al.
[72 ]
2010
USA
Join
t rep
lace
-m
ent s
urge
ryG
/A,
CAM
, DSM
-IV,
MM
SE,
DR
S-R
-98
Trai
ned
nurs
eO
lanz
apin
ePe
riop
196
7352
/48
R/A
Cont
rol
204
7440
/60
Lee
et a
l. [6
3 ]20
18So
uth
Kor
eaLa
paro
scop
ic
maj
or s
urge
ryG
/ACA
MPs
ychi
atris
tD
exm
edet
omid
ine
Intr
a23
673
45/5
5
Cont
rol
118
7443
/57
Leun
g et
al.
[73 ]
2017
USA
Spin
e, jo
int r
e-pl
acem
ent
surg
ery
G/A
,CA
MR
esea
rch
as-
sist
ants
Gab
apen
tinPe
riop
350
7345
/55
R/A
Cont
rol
347
7355
/45
Li e
t al.
[1]
2017
Chin
aSp
ine
surg
ery
G/A
Nu-
DES
CN
urse
Nim
odip
ine
Perio
p30
6937
/63
Cont
rol
3070
43/5
7
Liu
et a
l. [2
]20
16Ch
ina
Join
t rep
lace
-m
ent s
urge
ryG
/ACA
MN
o de
scrib
edD
exm
edet
omid
ine
Intr
aop
6071
43/5
7
Cont
rol
5873
50/5
0
Mar
dani
and
Big
de-
lian
[52 ]
2013
Iran
Card
iac
surg
ery
G/A
MM
SE, D
SM-IV
No
desc
ribed
Dex
amet
haso
nePe
riop
4365
84/1
6
Cont
rol
5060
88/1
2
Moh
amm
adi e
t al.
[53 ]
2016
Iran
Non
card
iac
surg
ery
No
de
scrib
edCA
M-IC
UAn
esth
esio
lo-
gist
Cypr
ohep
tadi
nePo
stop
2060
60/4
0
Cont
rol
2060
70/3
0
Papa
dopo
ulos
et a
l. [4
9 ]20
14G
reec
eFe
mor
al, f
emur
fr
actu
re s
ur-
gery
G/A
CAM
, MM
SER
esea
rch
mem
bers
Ond
anse
tron
Post
op51
72N
o de
scrib
ed
Cont
rol
5571
Prak
anra
ttan
a an
d Pr
apai
trak
ool [
67]
2007
Thai
land
Card
iac
surg
ery
G/A
CAM
, CAM
-ICU
Anes
thes
iolo
-gi
stR
ispe
ridon
ePo
stop
6361
57/4
3
Cont
rol
6361
60/4
0
Priy
e et
al.
[50 ]
2015
Indi
aCa
rdia
c su
rger
yG
/AN
o de
scrib
edN
o de
scrib
edD
exm
edet
omid
ine
Post
op32
4551
/49
Cont
rol
3241
50/5
0
Rob
inso
n et
al.
[74 ]
2014
USA
Vasc
ular
,uro
-lo
gic,
thor
acic
su
rger
y
G/A
,CA
M-IC
UR
esea
rch
mem
bers
L-tr
ypto
phan
Post
op15
269
99/1
R/A
Cont
rol
149
6997
/3
Roy
se e
t al.
[32 ]
2017
Aust
ralia
Card
iac
surg
ery
G/A
CAM
-ICU
No
desc
ribed
Met
hylp
redn
isol
one
Intr
aop
250
7363
/37
Cana
daCo
ntro
l24
874
66/3
4
Sam
pson
et a
l. [6
8 ]20
07U
KTH
RN
o
desc
ribed
DSI
No
desc
ribed
Don
epez
ilPo
stop
1970
58/4
2
Cont
rol
1465
43/5
7
Shei
kh e
t al.
[51 ]
2018
Indi
aCa
rdia
c su
rger
yG
/AN
o de
scrib
edN
o de
scrib
edD
exm
edet
omid
ine
Intr
aop
3034
No
desc
ribed
Prop
ofol
3036
Tabl
e 1
. Con
tinue
d
Stud
yYe
arCo
untr
ySu
rger
yAn
esth
esia
Asse
ssm
ent
tool
Asse
ssor
Man
agem
ent
Adm
inis
trat
ion
time
No.
of
patie
nts
Age
(yr)
Sex,
M/F
(%)
(Con
tinue
d to
the
next
pag
e)
34 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
NAC
C
Suga
no e
t al.
[56 ]
2017
Japa
nG
I, lu
ng c
ance
r su
rger
yG
/AD
SM-IV
Phys
icia
nsTJ
-54
Perio
p93
7665
/35
Cont
rol
9377
65/3
5
Wan
g et
al.
[37 ]
2012
Chin
aN
onca
rdia
c su
rger
yG
/A,
CAM
-ICU
Res
earc
h m
embe
rsH
alop
erid
olPo
stop
229
7463
/37
R/A
Cont
rol
228
7463
/37
Whi
tlock
et a
l. [3
4 ]20
15Ca
nada
Card
iac
surg
ery
G/A
CAM
Out
com
e
adju
dica
tors
Met
hylp
redn
isol
one
Intr
aop
3 ,75
568
60/4
0
Cont
rol
3 ,75
267
61/3
9
Yang
et a
l. [3
8 ]20
15Ch
ina
Free
flap
sur
-ge
ryG
/ACA
M-IC
UIn
vest
igat
orD
exm
edet
omid
ine
Perio
p39
5050
/50
Cont
rol
4050
50/5
0
He
et a
l. [6
]20
18Ch
ina
Vert
ebra
l ost
e-ot
omy
G/A
CAM
No
desc
ribed
Dex
med
etom
idin
ePe
riop
3083
53/4
7
Mid
azol
am30
8263
/37
Cont
rol
3083
56/4
4
Ma
et a
l. [3
9 ]20
13Ch
ina
Ort
hope
dic
surg
ery
G/A
CAM
Res
earc
h m
embe
rsK
etam
ine
Perio
p30
6653
/47
Dex
med
etom
idin
e30
6934
/66
Keta
min
e +
Dex
emet
omid
ine
3066
40/6
0
Cont
rol
3068
60/4
0
Xuan
et a
l. [4
0 ]20
18Ch
ina
Join
t rep
lace
-m
ent s
urge
ryN
o
desc
ribed
CAM
, CAM
-ICU
Res
earc
h m
embe
rsD
exm
edet
omid
ine
Post
op22
767
42/5
8
Cont
rol
226
6745
/55
Sauë
r et a
l. [6
1 ]20
14N
ethe
rland
Card
iac
surg
ery
G/A
CAM
, CAM
-ICU
Res
earc
h nu
rse
Dex
amet
haso
neIn
trao
p36
767
70/3
0
Cont
rol
370
6669
/31
Huy
an e
t al.
[41 ]
2019
Chin
aRa
dica
l pul
mo-
nary
rese
ctio
nG
/AIC
DSC
No
desc
ribed
Dex
med
etom
idin
ePe
riop
173
7151
/49
Cont
rol
173
7254
/46
Shi e
t al.
[42 ]
2019
Chin
aCa
rdia
c su
rger
yG
/ACA
MR
esea
rch
mem
bers
Dex
med
etom
idin
eIn
trao
p84
7575
/25
Prop
ofol
8074
70/3
0
Liu
et a
l. [4
3 ]20
16Ch
ina
Card
iac
surg
ery
G/A
CAM
No
desc
ribed
Dex
med
etom
idin
ePo
stop
4453
52/4
8
Prop
ofol
4457
68/3
2
Mei
et a
l. [4
4 ]20
18Ch
ina
Hip
art
hrop
last
yR
/ACA
MR
esea
rch
mem
bers
Dex
med
etom
idin
eIn
trao
p14
876
43/5
7
Prop
ofol
148
7448
/52
Guo
et a
l. [4
5 ]20
15Ch
ina
Ora
l can
cer
surg
ery
G/A
CAM
-ICU
No
desc
ribed
Dex
med
etom
idin
ePo
stop
7872
53/4
7
Cont
rol
7871
50/5
0
Aiza
wa
et a
l. [5
7 ]20
02Ja
pan
GI s
urge
ryG
/AD
SM-IV
Psyc
hiat
rist
Dia
zepa
m +
Flu
nitr
azep
am
+ Pe
thid
ine
(DFP
)Po
stop
2076
75/2
5
Cont
rol
20
7655
/45
Mu
et a
l. [4
6 ]20
17Ch
ina
Join
t rep
lace
-m
ent s
urge
ryR
/ACA
M, C
AM-IC
UR
esea
rch
mem
bers
Pare
coxi
bN
o de
scrib
ed31
070
26/7
4
Cont
rol
310
7127
/73
Tabl
e 1
. Con
tinue
d
Stud
yYe
arCo
untr
ySu
rger
yAn
esth
esia
Asse
ssm
ent
tool
Asse
ssor
Man
agem
ent
Adm
inis
trat
ion
time
No.
of
patie
nts
Age
(yr)
Sex,
M/F
(%)
(Con
tinue
d to
the
next
pag
e)
www.anesth-pain-med.org 35
Pharmacological strategies for POD

Tabl
e 2.
Ris
k of
Bia
s As
sess
men
t
Stud
yB
ias
aris
ing
from
the
ra
ndom
izat
ion
proc
ess
Bia
s du
e to
dev
iatio
ns fr
om
inte
nded
inte
rven
tions
Bia
s du
e to
mis
sing
ou
tcom
e da
taB
ias
in m
easu
rem
ent
of th
e ou
tcom
eB
ias
in s
elec
tion
of
the
repo
rted
resu
ltO
vera
ll ris
k of
bia
s ju
dgem
ent
Dei
ner e
t al.,
201
7 [6
9 ]Lo
w ri
skSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Som
e co
ncer
ns
Dja
iani
et a
l., 2
016
[33 ]
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Sush
eela
et a
l., 2
017
[70 ]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Li e
t al.,
201
7 [3
5 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Mal
dona
do e
t al.,
200
9 [4
]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Park
et a
l., 2
014
[62 ]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Sheh
abi e
t al.,
200
9 [3
1 ]So
me
conc
erns
Low
risk
Low
risk
Low
risk
Low
risk
Som
e co
ncer
ns
Su e
t al.,
201
6 [3
6 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Wu
et a
l., 2
018
[65 ]
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
Clem
mes
en e
t al.,
201
8 [4
8 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
de J
ongh
e et
al.,
201
4 [5
8 ]So
me
conc
erns
Low
risk
Low
risk
Low
risk
Low
risk
Som
e co
ncer
ns
Die
lem
an e
t al.,
201
2 [5
9 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Fuka
ta e
t al.,
201
4 [5
4 ]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Gam
berin
i et a
l., 2
009
[64 ]
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
Hud
etz
et a
l., 2
009
[71 ]
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
(Con
tinue
d to
the
next
pag
e)
Sulta
n [7
7 ]20
10Sa
udi A
rabi
aH
ip a
rthr
opla
s-ty
R/A
AMT
Res
iden
t an
esth
etis
tM
elat
onin
Preo
p53
7045
/55
Mid
azol
am50
7052
/48
Clon
idin
e51
7253
/47
Cont
rol
4972
45/5
5
Lipt
zin
et a
l. [7
5 ]20
05U
SAJo
int r
epla
ce-
men
t sur
gery
No
de-
scrib
edCA
M, D
SM-IV
, D
SIR
esea
rch
mem
bers
Don
epez
ilPe
riop
3967
36/6
4
Cont
rol
4168
49/5
1
Leun
g et
al.
[76 ]
2006
USA
Spin
e su
rger
yG
/ACA
MR
esea
rch
mem
bers
Gab
apen
tinPe
riop
957
44/5
6
Cont
rol
1261
58/4
2
Liu
et a
l. [4
7 ]20
16Ch
ina
Card
iac
surg
ery
G/A
CAM
No
desc
ribed
Dex
med
etom
idin
ePe
riop
2953
34/6
6
Prop
ofol
3255
47/5
3
Chan
g et
al.
[66 ]
2018
Taiw
anG
I sur
gery
G/A
CAM
No
desc
ribed
Dex
med
etom
idin
ePe
riop
3171
61/3
9
Prop
ofol
2970
55/4
5
CAM
: con
fusi
on a
sses
smen
t met
hod,
CAM
-ICU
: con
fusi
on a
sses
smen
t met
hod
for i
nten
sive
car
e un
it, M
MSE
: min
i-men
tal s
tate
exa
min
atio
n, D
RS:
del
irium
ratin
g sc
ale,
DSM
-IV: d
iagn
ostic
and
st
atis
tical
man
ual o
f m
enta
l dis
orde
rs-IV
, NEE
CHAM
: nee
lon
and
cham
pagn
e co
nfus
ion
scal
e, C
DT:
clo
ck d
raw
ing
test
, ICD
SC: i
nten
sive
car
e de
liriu
m s
cree
ning
che
cklis
t, D
RS-
R-9
8: d
eliri
um
ratin
g sc
ale-
revi
sed-
98, N
u-D
ESC:
nur
sing
del
irium
scr
eeni
ng s
core
, DSI
: del
irium
sym
ptom
inte
rvie
w, A
MT:
app
revi
ated
men
tal t
est,
Intr
aop:
intr
a-op
erat
ive,
Per
iop:
per
i-ope
rativ
e, P
reop
: pre
-op
erat
ive,
G/A
: gen
eral
ane
sthe
sia,
R/A
: reg
iona
l ane
sthe
sia,
TH
R: t
otal
hip
repl
acem
ent,
GI:
gast
ro-in
test
inal
.
Tabl
e 1
. Con
tinue
d
Stud
yYe
arCo
untr
ySu
rger
yAn
esth
esia
Asse
ssm
ent
tool
Asse
ssor
Man
agem
ent
Adm
inis
trat
ion
time
No.
of
patie
nts
Age
(yr)
Sex,
M/F
(%)
36 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
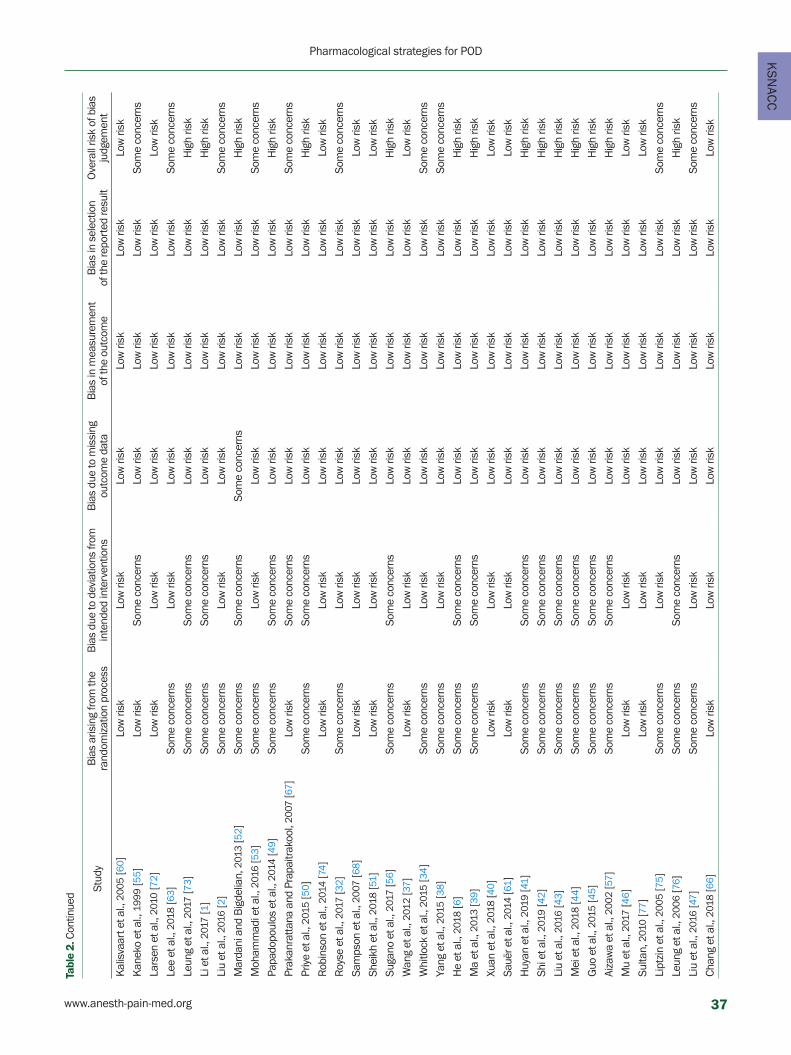
KS
NAC
C
Kal
isva
art e
t al.,
200
5 [6
0 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Kan
eko
et a
l., 1
999
[55 ]
Low
risk
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
Lars
en e
t al.,
201
0 [7
2 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Lee
et a
l., 2
018
[63 ]
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
Leun
g et
al.,
201
7 [7
3 ]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Li e
t al.,
201
7 [1
]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Liu
et a
l., 2
016
[2]
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
Mar
dani
and
Big
delia
n, 2
013
[52 ]
Som
e co
ncer
nsSo
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skH
igh
risk
Moh
amm
adi e
t al.,
201
6 [5
3 ]So
me
conc
erns
Low
risk
Low
risk
Low
risk
Low
risk
Som
e co
ncer
ns
Papa
dopo
ulos
et a
l., 2
014
[49 ]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Prak
anra
ttana
and
Pra
paitr
akoo
l, 20
07 [6
7 ]Lo
w ri
skSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Som
e co
ncer
ns
Priy
e et
al.,
201
5 [5
0 ]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Rob
inso
n et
al.,
201
4 [7
4 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Roy
se e
t al.,
201
7 [3
2 ]So
me
conc
erns
Low
risk
Low
risk
Low
risk
Low
risk
Som
e co
ncer
ns
Sam
pson
et a
l., 2
007
[68 ]
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Shei
kh e
t al.,
201
8 [5
1 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Suga
no e
t al.,
201
7 [5
6 ]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Wan
g et
al.,
201
2 [3
7 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Whi
tlock
et a
l., 2
015
[34 ]
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
Yang
et a
l., 2
015
[38 ]
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
He
et a
l., 2
018
[6]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Ma
et a
l., 2
013
[39 ]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Xuan
et a
l., 2
018
[40 ]
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Sauë
r et a
l., 2
014
[61 ]
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Huy
an e
t al.,
201
9 [4
1 ]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Shi e
t al.,
201
9 [4
2 ]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Liu
et a
l., 2
016
[43 ]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Mei
et a
l., 2
018
[44 ]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Guo
et a
l., 2
015
[45 ]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Aiza
wa
et a
l., 2
002
[57 ]
Som
e co
ncer
nsSo
me
conc
erns
Low
risk
Low
risk
Low
risk
Hig
h ris
k
Mu
et a
l., 2
017
[46 ]
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Sulta
n, 2
010
[77 ]
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Low
risk
Lipt
zin
et a
l., 2
005
[75 ]
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
Leun
g et
al.,
200
6 [7
6 ]So
me
conc
erns
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skH
igh
risk
Liu
et a
l., 2
016
[47 ]
Som
e co
ncer
nsLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skSo
me
conc
erns
Chan
g et
al.,
201
8 [6
6 ]Lo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
skLo
w ri
sk
Tabl
e 2.
Con
tinue
d
Stud
yB
ias
aris
ing
from
the
ra
ndom
izat
ion
proc
ess
Bia
s du
e to
dev
iatio
ns fr
om
inte
nded
inte
rven
tions
Bia
s du
e to
mis
sing
ou
tcom
e da
taB
ias
in m
easu
rem
ent
of th
e ou
tcom
eB
ias
in s
elec
tion
of
the
repo
rted
resu
ltO
vera
ll ris
k of
bia
s ju
dgem
ent
www.anesth-pain-med.org 37
Pharmacological strategies for POD

Fig. 2. Network plot of included studies comparing different pharmacological interventions. The nodes show a comparison of pharmacological interventions to prevent postoperative delirium, and the edges show the available direct comparisons among the pharmacological interventions. The nodes and edges are weighed on the basis of the weights applied in the network meta-analysis and the inverse of the standard error of effect. (A) All types of anesthesia, (B) general anesthesia, (C) cardiac surgery.
inconsistencies were observed between the direct and in-
direct point estimates in the Cont-Mela-Clon (02-11-25)
and Cont-Mida-Mela (02-06-11) loops (Fig. 3A).
Dexm showed a lower incidence of POD than Cont only
in terms of 95% CI. Olan showed marginal significance
compared with Cont in terms of 95% CI (Fig. 4A). Insignifi-
cance in the 95% PrIs suggests that any future RCT could
change the significance of the effectiveness of these com-
parisons.
The rankograms showed that Prop+AAP and Keta+Dexm
had the lowest incidence of POD (Fig. 5A). The cumulative
ranking plot was drawn, and the SUCRA probabilities of the
different pharmacological agents for POD were calculated
(Fig. 6A). The expected mean rankings and SUCRA values of
each pharmacological intervention are presented in Fig. 7A.
According to the SUCRA value, the incidence of POD was
lower in the order of the Prop + AAP (86.1%), followed by
Keta + Dexm (86.0%), Diaz + Flun + Pethi (84.8%), and Olan
(75.6%). The comparison-adjusted funnel plots showed that
the funnel plots were symmetrical around the zero line,
which suggested a less likely publication bias (Fig. 8A).
General anesthesia
A total of 35 studies (17,241 patients) were analyzed. The
pooled overall incidence of POD after general anesthesia
was 16.5% (95% CI: 14.2% to 19.2%, Pchi2 < 0.001, I2 =
89.3%).
The network plot of all eligible comparisons for this end-
point is depicted in Fig. 2B. Although all 20 management
modalities (nodes) were connected to the network, two
comparisons (Cont, Dexm) were directly compared to the
other 18 nodes.
The evaluation of the network inconsistency using the
design-by-treatment interaction model suggested no sig-
nificant inconsistency (χ2 [6] = 11.50, P = 0.074). Of the 10
closed loops in the network for the comparison of postop-
erative delirium, three loops (Dexm-Dexm + AAP-Prop +
AAP [01-04-05] [70], Pro-Dexm + AAP-Prop + AAP [01-09-
19] [70], Dexm-Keta-Dexm + Keta [03-04-05] [39]) were
formed only by multi-arm trials. Thus, local inconsistency
was evaluated in seven loops. There was no significance in
the local inconsistency between the direct and indirect
point estimates (Fig. 3B).
Dexm showed a lower incidence of POD than Cont only
in terms of 95% CI (Fig. 4B). Insignificance in the 95% PrIs
suggests that any future RCT could change the significance
Keta Morp Remi
B
A
C
38 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
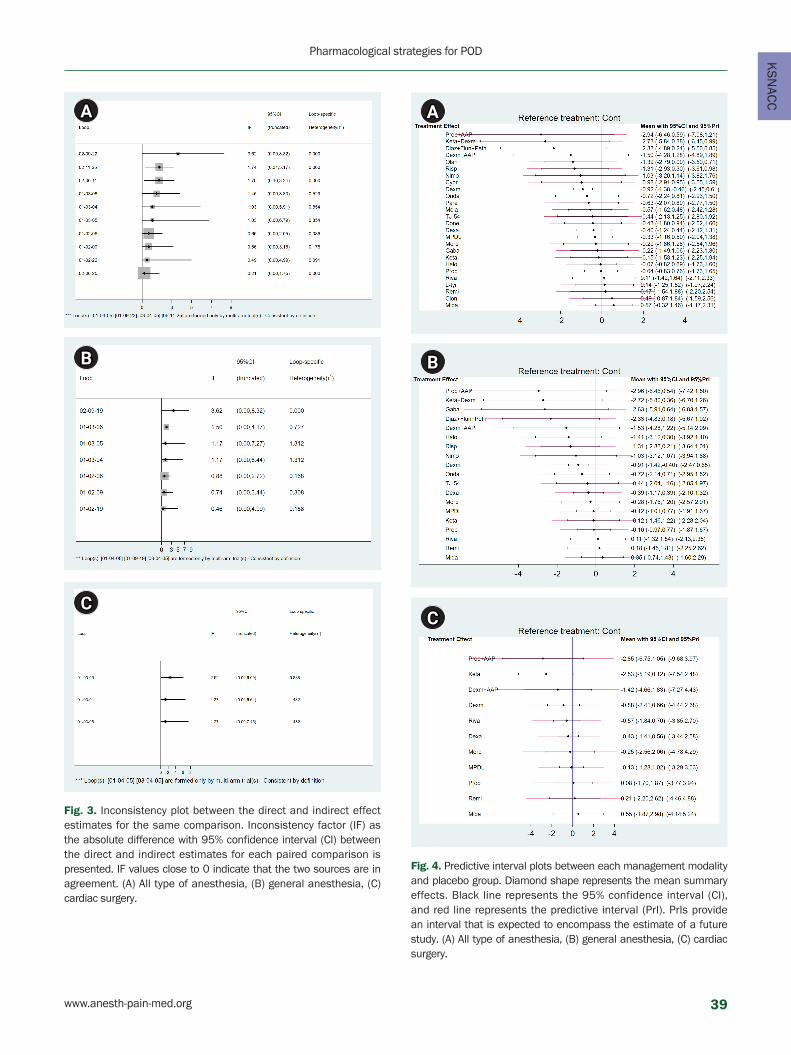
KS
NAC
C
Fig. 4. Predictive interval plots between each management modality and placebo group. Diamond shape represents the mean summary effects. Black line represents the 95% confidence interval (CI), and red line represents the predictive interval (PrI). PrIs provide an interval that is expected to encompass the estimate of a future study. (A) All type of anesthesia, (B) general anesthesia, (C) cardiac surgery.
Fig. 3. Inconsistency plot between the direct and indirect effect estimates for the same comparison. Inconsistency factor (IF) as the absolute difference with 95% confidence interval (CI) between the direct and indirect estimates for each paired comparison is presented. IF values close to 0 indicate that the two sources are in agreement. (A) All type of anesthesia, (B) general anesthesia, (C) cardiac surgery.
B
A
C
B
A
C
www.anesth-pain-med.org 39
Pharmacological strategies for POD

Fig. 5. Rankogram. Profiles indicate the probabilities for treatments to assume any of the possible ranks. It is the probability that a given treatment ranks first, second, third, and so on, among all of the treatments evaluated in the NMA. (A) All type of anesthesia, (B) general anesthesia, (C) cardiac surgery. NMA: network meta-analysis.
Fig. 6. Cumulative ranking curve plot. The profile indicates the sum of the probabilities from those ranked first, second, third, and so on. A higher cumulative ranking curve (surface of under cumulative ranking curve [SUCRA]) value is regarded as an improved result for an individual’s intervention. When ranking treatments, the closer the SUCRA value is to 100%, the higher the treatment ranking is relative to all other treatments. (A) All type of anesthesia, (B) general anesthesia, (C) cardiac surgery.
B
A
C
B
A
C
40 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
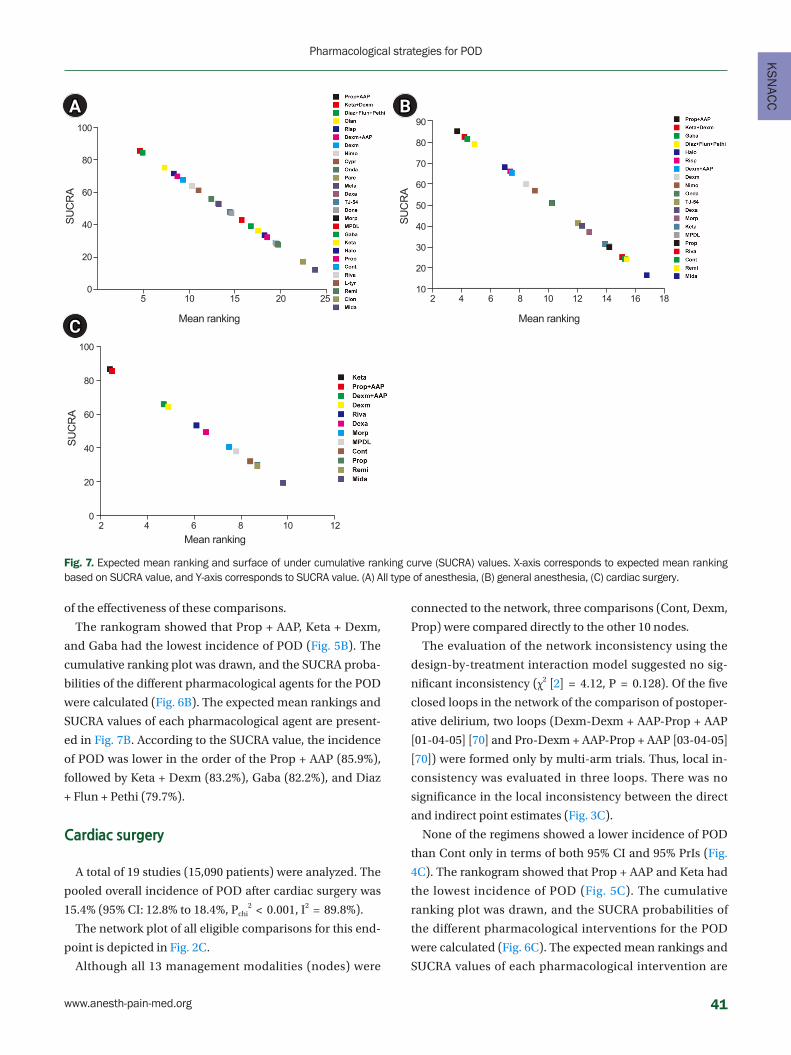
KS
NAC
C
SUC
RA
SUC
RA
SUC
RA
Mean ranking
Mean ranking
Mean ranking
5 10 15 20 25 2
2
4
4
6
6
8
8
10
10
12
12
14 16 18
100
80
60
40
20
0
100
80
60
40
20
0
90
80
70
60
50
40
30
20
10
BA
C
Fig. 7. Expected mean ranking and surface of under cumulative ranking curve (SUCRA) values. X-axis corresponds to expected mean ranking based on SUCRA value, and Y-axis corresponds to SUCRA value. (A) All type of anesthesia, (B) general anesthesia, (C) cardiac surgery.
of the effectiveness of these comparisons.
The rankogram showed that Prop + AAP, Keta + Dexm,
and Gaba had the lowest incidence of POD (Fig. 5B). The
cumulative ranking plot was drawn, and the SUCRA proba-
bilities of the different pharmacological agents for the POD
were calculated (Fig. 6B). The expected mean rankings and
SUCRA values of each pharmacological agent are present-
ed in Fig. 7B. According to the SUCRA value, the incidence
of POD was lower in the order of the Prop + AAP (85.9%),
followed by Keta + Dexm (83.2%), Gaba (82.2%), and Diaz
+ Flun + Pethi (79.7%).
Cardiac surgery
A total of 19 studies (15,090 patients) were analyzed. The
pooled overall incidence of POD after cardiac surgery was
15.4% (95% CI: 12.8% to 18.4%, Pchi2 < 0.001, I2 = 89.8%).
The network plot of all eligible comparisons for this end-
point is depicted in Fig. 2C.
Although all 13 management modalities (nodes) were
connected to the network, three comparisons (Cont, Dexm,
Prop) were compared directly to the other 10 nodes.
The evaluation of the network inconsistency using the
design-by-treatment interaction model suggested no sig-
nificant inconsistency (χ2 [2] = 4.12, P = 0.128). Of the five
closed loops in the network of the comparison of postoper-
ative delirium, two loops (Dexm-Dexm + AAP-Prop + AAP
[01-04-05] [70] and Pro-Dexm + AAP-Prop + AAP [03-04-05]
[70]) were formed only by multi-arm trials. Thus, local in-
consistency was evaluated in three loops. There was no
significance in the local inconsistency between the direct
and indirect point estimates (Fig. 3C).
None of the regimens showed a lower incidence of POD
than Cont only in terms of both 95% CI and 95% PrIs (Fig.
4C). The rankogram showed that Prop + AAP and Keta had
the lowest incidence of POD (Fig. 5C). The cumulative
ranking plot was drawn, and the SUCRA probabilities of
the different pharmacological interventions for the POD
were calculated (Fig. 6C). The expected mean rankings and
SUCRA values of each pharmacological intervention are
www.anesth-pain-med.org 41
Pharmacological strategies for POD

Fig. 8. Comparison-adjusted funnel plot.
presented in Fig. 7C. According to the SUCRA value, the in-
cidence of POD was lower in the order of Keta (87.1%),
Prop + AAP (86.0%), followed by Dexm + AAP (66.3%). The
comparison-adjusted funnel plots showed that the funnel
plots were symmetrical around the zero line, which sug-
gested a less likely publication bias (Fig. 8C).
Quality of evidence
Three outcomes were evaluated using the GRADE sys-
tem. For each outcome, the qualities of inconsistency, in-
directness, imprecision and publication bias were assessed
as not serious, but qualities of risk of bias were assessed as
serious. Thus, the overall quality of evidence for each out-
come was downgraded and rated as moderate (Table 3).
DISCUSSION
There are various pharmacological interventions to pre-
vent POD. We performed a network meta-analysis to com-
pare the effectiveness of reported pharmacological inter-
ventions. In our study, the incidence of POD was decreased
in the following order: Prop + AAP, Keta + Dexm, Gaba, and
Diaz + Flun + Pethi after all types of anesthesia; Prop + AAP,
Keta +Dexm, Gaba, and Diaz + Flun + Pethi after general
anesthesia; and Keta, Prop + AAP, and Dexm + AAP after
cardiac surgery. However, only the Dexm group showed a
statistically lower incidence of POD compared with the
control group after all types of anesthesia and after general
anesthesia.
In our study, there was a synergistic effect when Prop
was added to AAP. Although Prop + AAP failed to show sta-
tistical significance, Prop + AAP was ranked the most effec-
tive pharmacological intervention with a low incidence of
POD after all types of anesthesia and after general anesthe-
sia. Prop is a short-acting, intravenous sedative-hypnotic
agent commonly used for general anesthesia and sedation.
It has also been used to control other conditions such as
chemotherapy-induced emesis, as an antipruritic in pa-
tients with intractable pruritus due to liver disease, as an
adjuvant in alcohol withdrawal syndrome, and to treat sta-
tus epilepticus and severe refractory delirium. Prop has
been recently shown to have a long-term neuroprotective
effect and CNS inhibition effect [78–80]. AAP is commonly
used as an adjuvant analgesic. Some prior studies have in-
dicated that AAP reduces opioid consumption and inflam-
mation. Recently, AAP has been shown to confer central
B
A
C
42 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
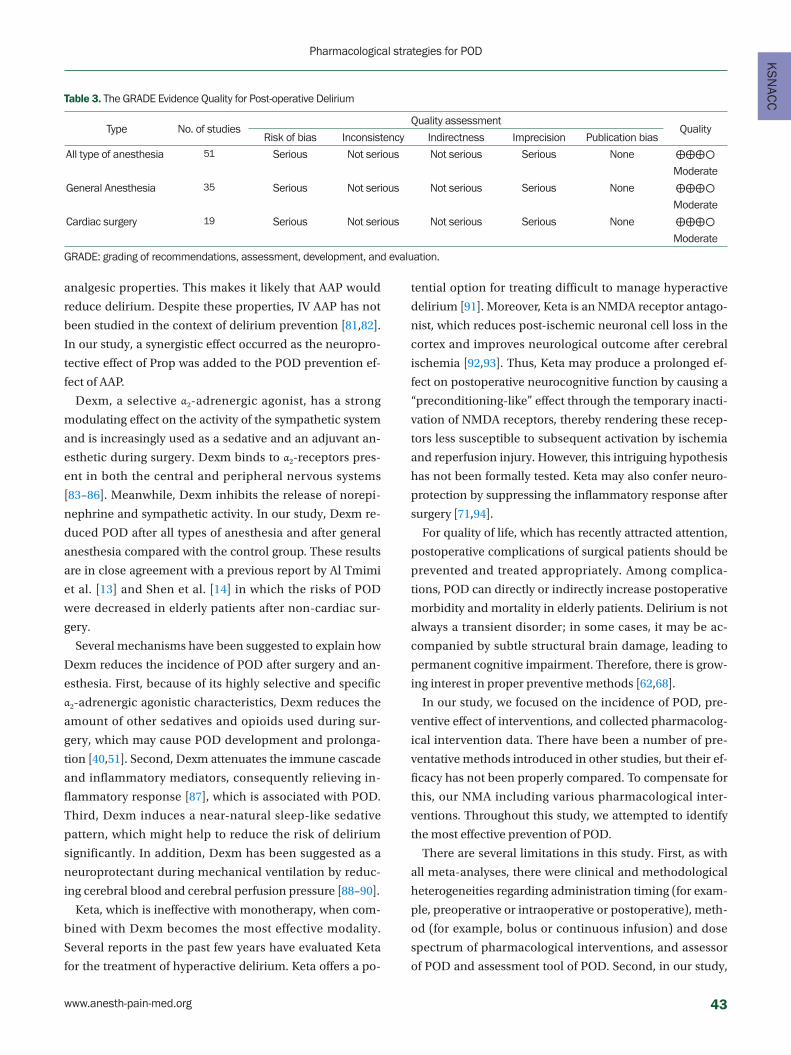
KS
NAC
C
analgesic properties. This makes it likely that AAP would
reduce delirium. Despite these properties, IV AAP has not
been studied in the context of delirium prevention [81,82].
In our study, a synergistic effect occurred as the neuropro-
tective effect of Prop was added to the POD prevention ef-
fect of AAP.
Dexm, a selective α2-adrenergic agonist, has a strong
modulating effect on the activity of the sympathetic system
and is increasingly used as a sedative and an adjuvant an-
esthetic during surgery. Dexm binds to α2-receptors pres-
ent in both the central and peripheral nervous systems
[83–86]. Meanwhile, Dexm inhibits the release of norepi-
nephrine and sympathetic activity. In our study, Dexm re-
duced POD after all types of anesthesia and after general
anesthesia compared with the control group. These results
are in close agreement with a previous report by Al Tmimi
et al. [13] and Shen et al. [14] in which the risks of POD
were decreased in elderly patients after non-cardiac sur-
gery.
Several mechanisms have been suggested to explain how
Dexm reduces the incidence of POD after surgery and an-
esthesia. First, because of its highly selective and specific
α2-adrenergic agonistic characteristics, Dexm reduces the
amount of other sedatives and opioids used during sur-
gery, which may cause POD development and prolonga-
tion [40,51]. Second, Dexm attenuates the immune cascade
and inflammatory mediators, consequently relieving in-
flammatory response [87], which is associated with POD.
Third, Dexm induces a near-natural sleep-like sedative
pattern, which might help to reduce the risk of delirium
significantly. In addition, Dexm has been suggested as a
neuroprotectant during mechanical ventilation by reduc-
ing cerebral blood and cerebral perfusion pressure [88–90].
Keta, which is ineffective with monotherapy, when com-
bined with Dexm becomes the most effective modality.
Several reports in the past few years have evaluated Keta
for the treatment of hyperactive delirium. Keta offers a po-
tential option for treating difficult to manage hyperactive
delirium [91]. Moreover, Keta is an NMDA receptor antago-
nist, which reduces post-ischemic neuronal cell loss in the
cortex and improves neurological outcome after cerebral
ischemia [92,93]. Thus, Keta may produce a prolonged ef-
fect on postoperative neurocognitive function by causing a
“preconditioning-like” effect through the temporary inacti-
vation of NMDA receptors, thereby rendering these recep-
tors less susceptible to subsequent activation by ischemia
and reperfusion injury. However, this intriguing hypothesis
has not been formally tested. Keta may also confer neuro-
protection by suppressing the inflammatory response after
surgery [71,94].
For quality of life, which has recently attracted attention,
postoperative complications of surgical patients should be
prevented and treated appropriately. Among complica-
tions, POD can directly or indirectly increase postoperative
morbidity and mortality in elderly patients. Delirium is not
always a transient disorder; in some cases, it may be ac-
companied by subtle structural brain damage, leading to
permanent cognitive impairment. Therefore, there is grow-
ing interest in proper preventive methods [62,68].
In our study, we focused on the incidence of POD, pre-
ventive effect of interventions, and collected pharmacolog-
ical intervention data. There have been a number of pre-
ventative methods introduced in other studies, but their ef-
ficacy has not been properly compared. To compensate for
this, our NMA including various pharmacological inter-
ventions. Throughout this study, we attempted to identify
the most effective prevention of POD.
There are several limitations in this study. First, as with
all meta-analyses, there were clinical and methodological
heterogeneities regarding administration timing (for exam-
ple, preoperative or intraoperative or postoperative), meth-
od (for example, bolus or continuous infusion) and dose
spectrum of pharmacological interventions, and assessor
of POD and assessment tool of POD. Second, in our study,
Table 3. The GRADE Evidence Quality for Post-operative Delirium
Type No. of studiesQuality assessment
QualityRisk of bias Inconsistency Indirectness Imprecision Publication bias
All type of anesthesia 51 Serious Not serious Not serious Serious None ⨁⨁⨁○
Moderate
General Anesthesia 35 Serious Not serious Not serious Serious None ⨁⨁⨁○
Moderate
Cardiac surgery 19 Serious Not serious Not serious Serious None ⨁⨁⨁○
Moderate
GRADE: grading of recommendations, assessment, development, and evaluation.
www.anesth-pain-med.org 43
Pharmacological strategies for POD

incidence of POD was used as an indicator of prevention.
However, to reduce morbidity and mortality associated
with POD, it is also important to reduce the severity and
duration of POD. Therefore, further studies should be con-
ducted to evaluate the effects on the severity and duration
of POD. Third, the most efficacious modalities determined
in the current NMA were documented to be effective in a
limited number of clinical trials. Further, as our NMA was
based on various single-center small-scale trials, a risk of
overestimation or underestimation of true treatment ef-
fects or lack of power to discriminate the effectiveness of
pharmacological interventions may be present. Therefore,
further large-scale RCTs with the qualified protocol should
be conducted in the future to encompass different phar-
macological interventions and substantiate our findings.
Despite these limitations, the current NMA has several
strengths compared to previous NMAs. First, a rigorous
methodology based on a published, pre-planned protocol
to provide evidence of pharmacological interventions to
prevent POD was used. Second, inconsistencies among the
enrolled studies were not significant, and publication bias
of the enrolled studies was minimal. Third, most enrolled
studies exhibited a low risk of bias, except for bias from the
randomization process and bias due to deviations from in-
tended intervention domains.
In conclusion, the NMA performed in this study has
strength and meaning for comparing pharmacological in-
terventions in the clinical efficacy of preventing POD.
Dexm showed a significant decrease in the incidence of
POD compared with the control group. The combination of
Prop and AAP and the combination of Keta and Dexm
seemed to be effective in preventing POD. However, fur-
ther studies are needed to determine the optimal pharma-
cological intervention to prevent POD.
SUPPLEMENTARY MATERIALS
Supplementary data including search terms used for
MEDLINE and EMBASE can be found online at https://doi.
org/10.17085/apm.20079
ACKNOWLEDGEMENTS
This research was supported by the Basic Science Re-
search Program through the National Research Foundation
of Korea (NRF) funded by the Ministry of Education, Sci-
ence and Technology (2018R1A2A2A05021467).
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Jun Mo Lee, Eun Jin Ahn, Geun Joo
Choi, Hyun Kang. Data curation: Jun Mo Lee, Hyun Kang.
Formal analysis: Ye Jin Cho, Hyun Kang. Funding acquisi-
tion: Hyun Kang. Methodology: Geun Joo Choi, Hyun
Kang. Project administration: Jun Mo Lee, Ye Jin Cho, Hyun
Kang. Visualization: Ye Jin Cho, Geun Joo Choi, Hyun Kang.
Writing - original draft: Jun Mo Lee, Ye Jin Cho, Geun Joo
Choi, Hyun Kang. Writing - review & editing: Jun Mo Lee,
Eun Jin Ahn, Hyun Kang. Investigation: Jun Mo Lee, Ye Jin
Cho, Eun Jin Ahn, Hyun Kang. Resources: Jun Mo Lee,
Hyun Kang. Software: Hyun Kang. Supervision: Eun Jin
Ahn, Geun Joo Choi, Hyun Kang. Validation: Jun Mo Lee,
Ye Jin Cho, Eun Jin Ahn, Hyun Kang.
ORCID
Jun Mo Lee, https://orcid.org/0000-0001-5607-7232
Ye Jin Cho, https://orcid.org/0000-0002-9138-6126
Eun Jin Ahn, https://orcid.org/0000-0001-6321-5285
Geun Joo Choi, https://orcid.org/0000-0002-4653-4193
Hyun Kang, https://orcid.org/0000-0003-2844-5880
REFERENCES
1. Li YN, Zhang Q, Yin CP, Guo YY, Huo SP, Wang L, et al. Effects
of nimodipine on postoperative delirium in elderly under gen-
eral anesthesia: a prospective, randomized, controlled clinical
trial. Medicine (Baltimore) 2017; 96: e6849.
2. Liu Y, Ma L, Gao M, Guo W, Ma Y. Dexmedetomidine reduces
postoperative delirium after joint replacement in elderly pa-
tients with mild cognitive impairment. Aging Clin Exp Res
2016; 28: 729-36.
3. American Geriatrics Society Expert Panel on Postoperative De-
lirium in Older Adults. Postoperative delirium in older adults:
best practice statement from the American Geriatrics Society. J
Am Coll Surg 2015 220: 136-48.e1.
4. Maldonado JR, Wysong A, van der Starre PJ, Block T, Miller C,
Reitz BA. Dexmedetomidine and the reduction of postopera-
tive delirium after cardiac surgery. Psychosomatics 2009; 50:
206-17.
44 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
NAC
C5. Parikh SS, Chung F. Postoperative delirium in the elderly.
Anesth Analg 1995; 80: 1223-32.
6. He F, Shen L, Zhong J. A study of dexmedetomidine in the pre-
vention of postoperative delirium in elderly patients after ver-
tebral osteotomy. Int J Clin Exp Med 2018; 11: 4984-90.
7. Whitlock EL, Vannucci A, Avidan MS. Postoperative delirium.
Minerva Anestesiol 2011; 77: 448-56.
8. Reddy SV, Irkal JN, Srinivasamurthy A. Postoperative delirium
in elderly citizens and current practice. J Anaesthesiol Clin
Pharmacol 2017; 33: 291-9.
9. Janssen TL, Alberts AR, Hooft L, Mattace-Raso F, Mosk CA, van
der Laan L. Prevention of postoperative delirium in elderly pa-
tients planned for elective surgery: systematic review and me-
ta-analysis. Clin Interv Aging 2019; 14: 1095-117.
10. Liu Y, Li XJ, Liang Y, Kang Y. Pharmacological prevention of
postoperative delirium: a systematic review and meta-analysis
of randomized controlled trials. Evid Based Complement Al-
ternat Med 2019; 2019: 9607129.
11. Nazemi AK, Gowd AK, Carmouche JJ, Kates SL, Albert TJ, Beh-
rend CJ. Prevention and management of postoperative deliri-
um in elderly patients following elective spinal surgery. Clin
Spine Surg 2017; 30: 112-9.
12. Zhang H, Lu Y, Liu M, Zou Z, Wang L, Xu FY, et al. Strategies for
prevention of postoperative delirium: a systematic review and
meta-analysis of randomized trials. Crit Care 2013; 17: R47.
13. Al Tmimi L, Verbrugghe P, Van de Velde M, Meuris B, Meyfroidt
G, Milisen K, et al. Intraoperative xenon for prevention of delir-
ium after on-pump cardiac surgery: a randomised, observ-
er-blind, controlled clinical trial. Br J Anaesth. 2020. doi: 10.
1016/j.bja.2019.11.037. [Epub ahead of print].
14. Shen QH, Li HF, Zhou XY, Yuan XZ. Dexmedetomidine in the
prevention of postoperative delirium in elderly patients follow-
ing non-cardiac surgery: a systematic review and meta-analy-
sis. Clin Exp Pharmacol Physiol 2020; 47: 1333-41.
15. Cui Y, Li G, Cao R, Luan L, Kla KM. The effect of perioperative
anesthetics for prevention of postoperative delirium on gener-
al anesthesia: a network meta-analysis. J Clin Anesth 2020; 59:
89-98.
16.; PRISMA-P Group. Preferred reporting items for systematic re-
view and meta-analysis protocols (PRISMA-P) 2015: elabora-
tion and explanation. BMJ 2015; 350: g7647.
17. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page M,
et al. Cochrane handbook for systematic reviews of interven-
tions. 2nd ed. Hoboken, Wiley-Blackwell. 2019.
18. Cornell JE. The PRISMA extension for network meta-analysis:
bringing clarity and guidance to the reporting of systematic re-
views incorporating network meta-analyses. Ann Intern Med
2015; 162: 797-8.
19. Viera AJ, Garrett JM. Understanding interobserver agreement:
the kappa statistic. Fam Med 2005; 37: 360-3.
20. Higgins JPT, Savović J, Page MJ, Elbers RG, Sterne JAC. Assess-
ing risk of bias in a randomized trial. In: Cochrane handbook
for systematic reviews of interventions. 2nd ed. Edited by Hig-
gins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page M, et
al.: Hoboken, Wiley-Blackwell. 2019.
21. Chaimani A, Higgins JP, Mavridis D, Spyridonos P, Salanti G.
Graphical tools for network meta-analysis in STATA. PLoS One
2013; 8: e76654.
22. White IR, Barrett JK, Jackson D, Higgins JP. Consistency and in-
consistency in network meta-analysis: model estimation using
multivariate meta-regression. Res Synth Methods 2012; 3: 111-
25.
23. Salanti G, Ades AE, Ioannidis JP. Graphical methods and nu-
merical summaries for presenting results from multiple-treat-
ment meta-analysis: an overview and tutorial. J Clin Epidemiol
2011; 64: 163-71.
24. Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et
al.; GRADE Working Group. Grading quality of evidence and
strength of recommendations. BMJ 2004; 328: 1490.
25. O'Gara B, Marcantonio ER, Pascual-Leone A, Shaefi S, Mueller
A, Banner-Goodspeed V, et al. Prevention of early postopera-
tive decline (PEaPoD): protocol for a randomized, controlled
feasibility trial. Trials 2018; 19: 676.
26. Shankar P, Mueller A, Packiasabapathy S, Gasangwa D, Patxot
M, O'Gara B, et al. Dexmedetomidine and intravenous acet-
aminophen for the prevention of postoperative delirium fol-
lowing cardiac surgery (DEXACET trial): protocol for a pro-
spective randomized controlled trial. Trials 2018; 19: 326.
27. Sánchez A, Thomas C, Deeken F, Wagner S, Klöppel S,
Kentischer F, et al.; PAWEL Study group. Patient safety, cost-ef-
fectiveness, and quality of life: reduction of delirium risk and
postoperative cognitive dysfunction after elective procedures
in older adults-study protocol for a stepped-wedge cluster ran-
domized trial (PAWEL Study). Trials 2019; 20: 71.
28. Farlinger C, Clarke H, Wong CL. Perioperative pregabalin and
delirium following total hip arthroplasty: a post hoc analysis of
a double-blind randomized placebo-controlled trial. Can J An-
aesth 2018; 65: 1269-70.
29. Joys S, Samra T, Kumar V, Mohanty M, Sodhi HBS, Mahajan S,
et al. Comparison of postoperative delirium in patients anes-
thetized with isoflurane versus desflurane during spinal sur-
gery: a prospective randomized controlled trial. Surg Neurol
Int 2019; 10: 226.
30. Wang X, Wang Y, Hu Y, Wang L, Zhao W, Wei L, et al. Effect of
www.anesth-pain-med.org 45
Pharmacological strategies for POD

flurbiprofen axetil on postoperative delirium for elderly pa-
tients. Brain Behav 2019; 9: e01290.
31. Shehabi Y, Grant P, Wolfenden H, Hammond N, Bass F, Camp-
bell M, et al. Prevalence of delirium with dexmedetomidine
compared with morphine based therapy after cardiac surgery:
a randomized controlled trial (DEXmedetomidine COmpared
to Morphine-DEXCOM Study). Anesthesiology 2009; 111:
1075-84.
32. Royse CF, Saager L, Whitlock R, Ou-Young J, Royse A, Vincent J,
et al. Impact of methylprednisolone on postoperative quality
of recovery and delirium in the steroids in cardiac surgery trial:
a randomized, double-blind, placebo-controlled substudy.
Anesthesiology 2017; 126: 223-33.
33. Djaiani G, Silverton N, Fedorko L, Carroll J, Styra R, Rao V, et al.
Dexmedetomidine versus propofol sedation reduces delirium
after cardiac surgery: a randomized controlled trial. Anesthesi-
ology 2016; 124: 362-8.
34. Whitlock RP, Devereaux PJ, Teoh KH, Lamy A, Vincent J, Pogue
J, et al.; SIRS Investigators. Methylprednisolone in patients un-
dergoing cardiopulmonary bypass (SIRS): a randomised, dou-
ble-blind, placebo-controlled trial. Lancet 2015; 386: 1243-53.
35. Li X, Yang J, Nie XL, Zhang Y, Li XY, Li LH, et al. Impact of dex-
medetomidine on the incidence of delirium in elderly patients
after cardiac surgery: a randomized controlled trial. PLoS One
2017; 12: e0170757.
36. Su X, Meng ZT, Wu XH, Cui F, Li HL, Wang DX, et al. Dexmede-
tomidine for prevention of delirium in elderly patients after
non-cardiac surgery: a randomised, double-blind, place-
bo-controlled trial. Lancet 2016; 388: 1893-902.
37. Wang W, Li HL, Wang DX, Zhu X, Li SL, Yao GQ, et al. Haloperi-
dol prophylaxis decreases delirium incidence in elderly pa-
tients after noncardiac surgery: a randomized controlled trial*.
Crit Care Med 2012; 40: 731-9.
38. Yang X, Li Z, Gao C, Liu R. Effect of dexmedetomidine on pre-
venting agitation and delirium after microvascular free flap
surgery: a randomized, double-blind, control study. J Oral
Maxillofac Surg 2015; 73: 1065-72.
39. Ma P, Piao M, Wang Y, Ma H, Feng C. Influence of dexmedeto-
midine and sub-anesthetic dose of ketamine on postoperative
delirium in elderly orthopedic patients under total intravenous
anesthesia. J Jilin Univ Med Ed 2013; 39: 128–32.
40. Xuan Y, Fan R, Chen J, Wang Y, Wu J, Yang J, et al. Effects of dex-
medetomidine for postoperative delirium after joint replace-
ment in elderly patients: a randomized, double-blind, and pla-
cebo-controlled trial. Int J Clin Exp Med 2018; 11: 13147-57.
41. Huyan T, Hu X, Peng H, Zhu Z, Li Q, Zhang W. Perioperative
dexmedetomidine reduces delirium in elderly patients after
lung cancer surgery. Psychiatr Danub 2019; 31: 95-101.
42. Shi C, Jin J, Qiao L, Li T, Ma J, Ma Z. Effect of perioperative ad-
ministration of dexmedetomidine on delirium after cardiac
surgery in elderly patients: a double-blinded, multi-center,
randomized study. Clin Interv Aging 2019; 14: 571-5.
43. Liu X, Zhang K, Wang W, Xie G, Fang X. Dexmedetomidine se-
dation reduces atrial fibrillation after cardiac surgery com-
pared to propofol: a randomized controlled trial. Crit Care
2016; 20: 298.
44. Mei B, Meng G, Xu G, Cheng X, Chen S, Zhang Y, et al. Intraop-
erative sedation with dexmedetomidine is superior to propofol
for elderly patients undergoing hip arthroplasty: a prospective
randomized controlled study. Clin J Pain 2018; 34: 811-7.
45. Guo Y, Sun LL, Chen ZF, Li QF, Jiang H. [Preventive effect of
dexmedetomidine on postoperative delirium in elderly pa-
tients with oral cancer]. Shanghai Kou Qiang Yi Xue 2015; 24:
236-9. Chinese.
46. Mu DL, Zhang DZ, Wang DX, Wang G, Li CJ, Meng ZT, et al.
Parecoxib supplementation to morphine analgesia decreases
incidence of delirium in elderly patients after hip or knee re-
placement surgery: a randomized controlled trial. Anesth An-
alg 2017; 124: 1992-2000.
47. Liu X, Zhang K, Wang W, Xie G, Cheng B, Wang Y, et al. Dexme-
detomidine versus propofol sedation improves sublingual mi-
crocirculation after cardiac surgery: a randomized controlled
trial. J Cardiothorac Vasc Anesth 2016; 30: 1509-15.
48. Clemmesen CG, Lunn TH, Kristensen MT, Palm H, Foss NB. Ef-
fect of a single pre-operative 125 mg dose of methylpredniso-
lone on postoperative delirium in hip fracture patients; a ran-
domised, double-blind, placebo-controlled trial. Anaesthesia
2018; 73: 1353-60.
49. Papadopoulos G, Pouangare M, Papathanakos G, Arnaoutoglou
E, Petrou A, Tzimas P. The effect of ondansetron on postopera-
tive delirium and cognitive function in aged orthopedic pa-
tients. Minerva Anestesiol 2014; 80: 444-51.
50. Priye S, Jagannath S, Singh D, Shivaprakash S, Reddy DP. Dex-
medetomidine as an adjunct in postoperative analgesia follow-
ing cardiac surgery: a randomized, double-blind study. Saudi J
Anaesth 2015; 9: 353-8.
51. Sheikh TA, Dar BA, Akhter N, Ahmad N. A comparative study
evaluating effects of intravenous sedation by dexmedetomi-
dine and propofol on patient hemodynamics and postopera-
tive outcomes in cardiac surgery. Anesth Essays Res 2018; 12:
555-60.
52. Mardani D, Bigdelian H. Prophylaxis of dexamethasone pro-
tects patients from further post-operative delirium after cardi-
ac surgery: a randomized trial. J Res Med Sci 2013; 18: 137-43.
46 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
KS
NAC
C53. Mohammadi M, Ahmadi M, Khalili H, Cheraghchi H, Arbabi M.
Cyproheptadine for the prevention of postoperative delirium:
a pilot study. Ann Pharmacother 2016; 50: 180-7.
54. Fukata S, Kawabata Y, Fujisiro K, Katagawa Y, Kuroiwa K, Akiya-
ma H, et al. Haloperidol prophylaxis does not prevent postop-
erative delirium in elderly patients: a randomized, open-label
prospective trial. Surg Today 2014; 44: 2305-13.
55. Kaneko T, Cai J, Ishikura T, Kobayashi M, Naka T, Kaibara N.
Prophylactic consecutive administration of haloperidol can re-
duce the occurrence of postoperative delirium in gastrointesti-
nal surgery. Yonago Acta Medica 1999; 42: 179-84.
56. Sugano N, Aoyama T, Sato T, Kamiya M, Amano S, Yamamoto
N, et al. Randomized phase II study of TJ-54 (Yokukansan) for
postoperative delirium in gastrointestinal and lung malignan-
cy patients. Mol Clin Oncol 2017; 7: 569-73.
57. Aizawa K, Kanai T, Saikawa Y, Takabayashi T, Kawano Y, Mi-
yazawa N, et al. A novel approach to the prevention of postop-
erative delirium in the elderly after gastrointestinal surgery.
Surg Today 2002; 32: 310-4.
58. de Jonghe A, van Munster BC, Goslings JC, Kloen P, van Rees C,
Wolvius R, et al; Amsterdam Delirium Study Group. Effect of
melatonin on incidence of delirium among patients with hip
fracture: a multicentre, double-blind randomized controlled
trial. CMAJ 2014; 186: E547-56.
59. Dieleman JM, Nierich AP, Rosseel PM, van der Maaten JM, Ho-
fland J, Diephuis JC, et al.; Dexamethasone for Cardiac Surgery
(DECS) Study Group. Intraoperative high-dose dexametha-
sone for cardiac surgery: a randomized controlled trial. JAMA
2012; 308: 1761-7.
60. Kalisvaart KJ, de Jonghe JF, Bogaards MJ, Vreeswijk R, Egberts
TC, Burger BJ, et al. Haloperidol prophylaxis for elderly
hip-surgery patients at risk for delirium: a randomized place-
bo-controlled study. J Am Geriatr Soc 2005; 53: 1658-66.
61. Sauër AM, Slooter AJ, Veldhuijzen DS, van Eijk MM, Devlin JW,
van Dijk D. Intraoperative dexamethasone and delirium after
cardiac surgery: a randomized clinical trial. Anesth Analg 2014;
119: 1046-52.
62. Park JB, Bang SH, Chee HK, Kim JS, Lee SA, Shin JK. Efficacy
and safety of dexmedetomidine for postoperative delirium in
adult cardiac surgery on cardiopulmonary bypass. Korean J
Thorac Cardiovasc Surg 2014; 47: 249-54.
63. Lee C, Lee CH, Lee G, Lee M, Hwang J. The effect of the timing
and dose of dexmedetomidine on postoperative delirium in el-
derly patients after laparoscopic major non-cardiac surgery: a
double blind randomized controlled study. J Clin Anesth 2018;
47: 27-32.
64. Gamberini M, Bolliger D, Lurati Buse GA, Burkhart CS, Grapow
M, Gagneux A, et al. Rivastigmine for the prevention of postop-
erative delirium in elderly patients undergoing elective cardiac
surgery--a randomized controlled trial. Crit Care Med 2009; 37:
1762-8.
65. Wu CY, Lu YF, Wang ML, Chen JS, Hsu YC, Yang FS, et al. Effects
of dexmedetomidine infusion on inflammatory responses and
injury of lung tidal volume changes during one-lung ventila-
tion in thoracoscopic surgery: a randomized controlled trial.
Mediators Inflamm 2018; 2018: 2575910.
66. Chang YF, Chao A, Shih PY, Hsu YC, Lee CT, Tien YW, et al.;
NTUH Center of Microcirculation Medical Research (NCM-
MR). Comparison of dexmedetomidine versus propofol on he-
modynamics in surgical critically ill patients. J Surg Res 2018;
228: 194-200.
67. Prakanrattana U, Prapaitrakool S. Efficacy of risperidone for
prevention of postoperative delirium in cardiac surgery. An-
aesth Intensive Care 2007; 35: 714-9.
68. Sampson EL, Raven PR, Ndhlovu PN, Vallance A, Garlick N,
Watts J, et al. A randomized, double-blind, placebo-controlled
trial of donepezil hydrochloride (Aricept) for reducing the inci-
dence of postoperative delirium after elective total hip replace-
ment. Int J Geriatr Psychiatry 2007; 22: 343-9.
69. Deiner S, Luo X, Lin HM, Sessler DI, Saager L, Sieber FE, et al.
Intraoperative infusion of dexmedetomidine for prevention of
postoperative delirium and cognitive dysfunction in elderly
patients undergoing major elective noncardiac surgery: a ran-
domized clinical trial. JAMA Surg 2017; 152: e171505.
70. Susheela AT, Packiasabapathy S, Gasangwa DV, Patxot M, O'Ne-
al J, Marcantonio E, et al. The use of dexmedetomidine and in-
travenous acetaminophen for the prevention of postoperative
delirium in cardiac surgery patients over 60 years of age: a pilot
study. F1000Res 2017; 6: 1842.
71. Hudetz JA, Patterson KM, Iqbal Z, Gandhi SD, Byrne AJ, Hudetz
AG, et al. Ketamine attenuates delirium after cardiac surgery
with cardiopulmonary bypass. J Cardiothorac Vasc Anesth
2009; 23: 651-7.
72. Larsen KA, Kelly SE, Stern TA, Bode RH Jr, Price LL, Hunter DJ,
et al. Administration of olanzapine to prevent postoperative
delirium in elderly joint-replacement patients: a randomized,
controlled trial. Psychosomatics 2010; 51: 409-18.
73. Leung JM, Sands LP, Chen N, Ames C, Berven S, Bozic K, et al.;
Perioperative Medicine Research Group. Perioperative gab-
apentin does not reduce postoperative delirium in older surgi-
cal patients: a randomized clinical trial. Anesthesiology 2017;
127: 633-44.
74. Robinson TN, Dunn CL, Adams JC, Hawkins CL, Tran ZV, Rae-
burn CD, et al. Tryptophan supplementation and postopera-
www.anesth-pain-med.org 47
Pharmacological strategies for POD
tive delirium--a randomized controlled trial. J Am Geriatr Soc
2014; 62: 1764-71.
75. Liptzin B, Laki A, Garb JL, Fingeroth R, Krushell R. Donepezil in
the prevention and treatment of post-surgical delirium. Am J
Geriatr Psychiatry 2005; 13: 1100-6.
76. Leung JM, Sands LP, Rico M, Petersen KL, Rowbotham MC,
Dahl JB, et al. Pilot clinical trial of gabapentin to decrease post-
operative delirium in older patients. Neurology 2006; 67: 1251-
3.
77. Sultan SS. Assessment of role of perioperative melatonin in pre-
vention and treatment of postoperative delirium after hip ar-
throplasty under spinal anesthesia in the elderly. Saudi J An-
aesth 2010; 4: 169-73.
78. Saporito A, Sturini E. Incidence of postoperative delirium is
high even in a population without known risk factors. J Anesth
2014; 28: 198-201.
79. Brown KE, Mirrakhimov AE, Yeddula K, Kwatra MM. Propofol
and the risk of delirium: exploring the anticholinergic proper-
ties of propofol. Med Hypotheses 2013; 81: 536-9.
80. Covarrubias-Gómez A, López Collada-Estrada M. Propo-
fol-based palliative sedation to treat antipsychotic-resistant
agitated delirium. J Pain Palliat Care Pharmacother 2017; 31:
190-4.
81. Subramaniam B, Shankar P, Shaefi S, Mueller A, O'Gara B, Ban-
ner-Goodspeed V, et al. Effect of intravenous acetaminophen
vs placebo combined with propofol or dexmedetomidine on
postoperative delirium among older patients following cardiac
surgery: the DEXACET randomized clinical trial. JAMA 2019;
321: 686-96.
82. Farkas J. PULMCrit- DEXACET: four grams of acetaminophen a
day keeps the delirium away? PULMCrit [serial on the Inter-
net]. 2019 Mar [cited 2020 Apr]. Available from https://emcrit.
org/pulmcrit/dexacet/.
83. Cai Y, Xu H, Yan J, Zhang L, Lu Y. Molecular targets and mecha-
nism of action of dexmedetomidine in treatment of ischemia/
reperfusion injury. Mol Med Rep 2014; 9: 1542-50.
84. Sottas CE, Anderson BJ. Dexmedetomidine: the new all-in-one
drug in paediatric anaesthesia? Curr Opin Anaesthesiol 2017;
30: 441-51.
85. Fan H, Zhao Y, Sun M, Ye JH, Chen GD, Zhu JH. Dexmedetomi-
dine based sedation for post-surgery critically ill adults: a me-
ta-analysis of randomized controlled trials. Iran J Public Health
2017; 46: 1611-22.
86. Yu X, Franks NP, Wisden W. Sleep and sedative states induced
by targeting the histamine and noradrenergic systems. Front
Neural Circuits 2018; 12: 4.
87. Sanders RD, Hussell T, Maze M. Sedation & immunomodula-
tion. Crit Care Clin 2009; 25: 551-70.
88. Bekker A, Haile M, Kline R, Didehvar S, Babu R, Martiniuk F, et
al. The effect of intraoperative infusion of dexmedetomidine
on the quality of recovery after major spinal surgery. J Neuro-
surg Anesthesiol 2013; 25: 16-24.
89. Zhang X, Wang J, Qian W, Zhao J, Sun L, Qian Y, et al. Dexme-
detomidine inhibits tumor necrosis factor-alpha and interleu-
kin 6 in lipopolysaccharide-stimulated astrocytes by suppres-
sion of c-Jun N-terminal kinases. Inflammation 2014; 37: 942-9.
90. Chen J, Yan J, Han X. Dexmedetomidine may benefit cognitive
function after laparoscopic cholecystectomy in elderly pa-
tients. Exp Ther Med 2013; 5: 489-94.
91. Hayes BD. Ketamine for excited delirium syndrome. ALiEM
[serial on the Internet]. 2015 May [cited 2020 Apr]. Available
from https://www.aliem.com/ketamine-for-excited-deliri-
um-syndrome/.
92. Reeker W, Werner C, Möllenberg O, Mielke L, Kochs E. High-
dose S(+)-ketamine improves neurological outcome following
incomplete cerebral ischemia in rats. Can J Anaesth 2000; 47:
572-8.
93. Proescholdt M, Heimann A, Kempski O. Neuroprotection of
S(+) ketamine isomer in global forebrain ischemia. Brain Res
2001; 904: 245-51.
94. Avidan MS, Maybrier HR, Abdallah AB, Jacobsohn E, Vlisides
PE, Pryor KO, et al.; PODCAST Research Group. Intraoperative
ketamine for prevention of postoperative delirium or pain after
major surgery in older adults: an international, multicentre,
double-blind, randomised clinical trial. Lancet 2017; 390: 267-
75.
48 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
OA
Comparison of the effect of general and spinal anesthesia for elective cesarean section on maternal and fetal outcomes: a retrospective cohort study
Tae-Yun Sung1,2, Young Seok Jee1, Hwang-Ju You1, and Choon-Kyu Cho1
1Department of Anesthesiology and Pain Medicine, 2Myunggok Medical Research
Center, Konyang University Hospital, Konyang University College of Medicine,
Daejeon, Korea
Received September 2, 2020Revised October 12, 2020 Accepted October 15, 2020
Corresponding author Young Seok Jee, M.D., Ph.D. Department of Anesthesiology and Pain Medicine, Konyang University Hospital, Konyang University College of Medicine, 158 Gwanjeodong-ro, Seo-gu, Daejeon 35365, Korea Tel: 82-42-600-9319 Fax: 82-42-545-2132 E-mail: [email protected]
Background: Anesthesia is needed to ensure both maternal and fetal safety during cesare-an sections. This retrospective cohort study compared maternal and fetal outcomes be-tween general and spinal anesthesia for cesarean section based on perioperative hemody-namic parameters (pre- and postoperative systolic blood pressure, heart rate), mean differ-ence of hematocrit and estimated blood loss, and neonatal Apgar scores at 1 and 5 min.
Methods: Data from electronic medical records of 331 singleton pregnancies between Jan-uary 2016 and December 2018 were analyzed retrospectively; 44 cases were excluded, and 287 cases were assigned to the general group (n = 141) or spinal group (n = 146).
Results: Postoperative hemodynamic parameters were significantly higher in the general group than the spinal group (systolic blood pressure: 136.8 ± 16.7 vs. 119.3 ± 12.7 mmHg, heart rate: 93.2 ± 16.8 vs. 71.0 ± 12.7 beats/min, respectively, P < 0.001). The mean dif-ference between the pre- and postoperative hematocrit was also significantly greater in the general than spinal group (4.8 ± 3.4% vs. 2.3 ± 3.9%, respectively, P < 0.001). The estimat-ed blood loss was significantly lower in the spinal than general group (819.9 ± 81.9 vs. 856.7 ± 117.9 ml, P < 0.001). There was a significantly larger proportion of newborns with 5-min Apgar scores < 7 in the general than spinal group (6/141 [4.3%] vs. 0/146 [0%], re-spectively, P = 0.012).
Conclusions: General group is associated with more maternal blood loss and a larger pro-portion of newborns with 5-min Apgar scores < 7 than spinal group during cesarean sec-tions.
Keywords: Cesarean section; General anesthesia; Outcome measures; Spinal anesthesia.
Clinical ResearchAnesth Pain Med 2021;16:49-55https://doi.org/10.17085/apm.20072pISSN 1975-5171 • eISSN 2383-7977
INTRODUCTION
Anesthesia used for cesarean section is either general or
regional. The advantages of general anesthesia include the
facilitation of a rapid procedure in obstetric emergencies
and loss of consciousness, which ensures less distress to
parturient women. The disadvantages of general anesthe-
sia include the possibility of aspiration pneumonia, mater-
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
49
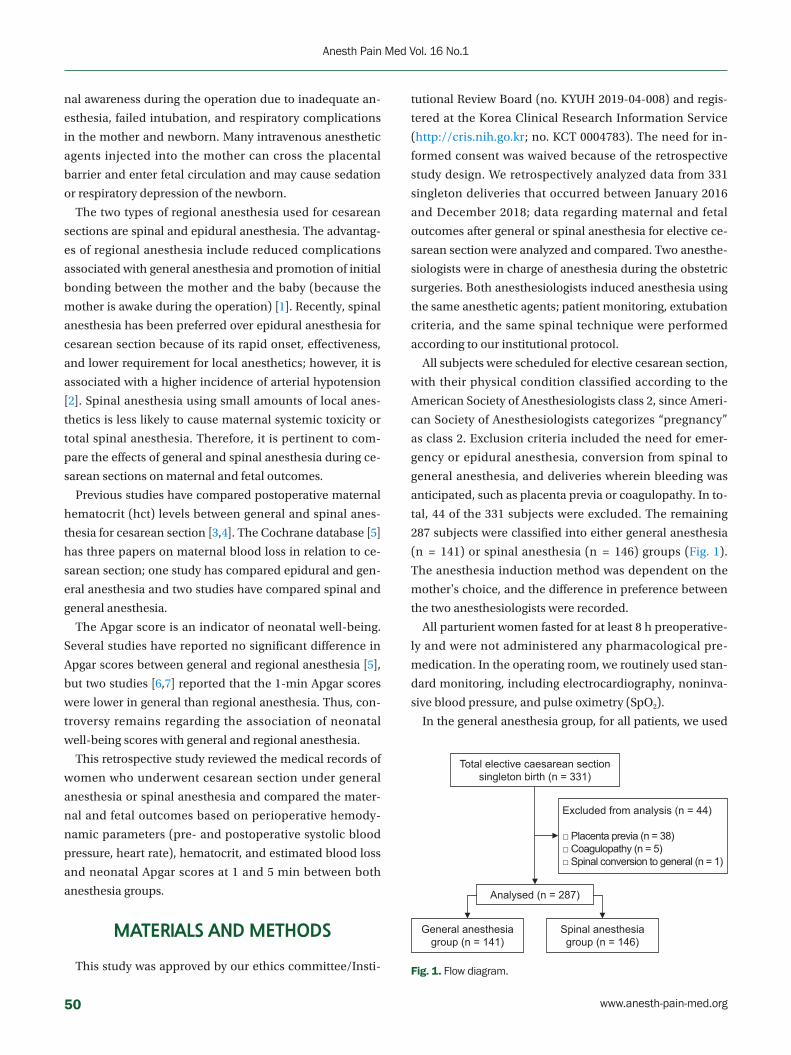
nal awareness during the operation due to inadequate an-
esthesia, failed intubation, and respiratory complications
in the mother and newborn. Many intravenous anesthetic
agents injected into the mother can cross the placental
barrier and enter fetal circulation and may cause sedation
or respiratory depression of the newborn.
The two types of regional anesthesia used for cesarean
sections are spinal and epidural anesthesia. The advantag-
es of regional anesthesia include reduced complications
associated with general anesthesia and promotion of initial
bonding between the mother and the baby (because the
mother is awake during the operation) [1]. Recently, spinal
anesthesia has been preferred over epidural anesthesia for
cesarean section because of its rapid onset, effectiveness,
and lower requirement for local anesthetics; however, it is
associated with a higher incidence of arterial hypotension
[2]. Spinal anesthesia using small amounts of local anes-
thetics is less likely to cause maternal systemic toxicity or
total spinal anesthesia. Therefore, it is pertinent to com-
pare the effects of general and spinal anesthesia during ce-
sarean sections on maternal and fetal outcomes.
Previous studies have compared postoperative maternal
hematocrit (hct) levels between general and spinal anes-
thesia for cesarean section [3,4]. The Cochrane database [5]
has three papers on maternal blood loss in relation to ce-
sarean section; one study has compared epidural and gen-
eral anesthesia and two studies have compared spinal and
general anesthesia.
The Apgar score is an indicator of neonatal well-being.
Several studies have reported no significant difference in
Apgar scores between general and regional anesthesia [5],
but two studies [6,7] reported that the 1-min Apgar scores
were lower in general than regional anesthesia. Thus, con-
troversy remains regarding the association of neonatal
well-being scores with general and regional anesthesia.
This retrospective study reviewed the medical records of
women who underwent cesarean section under general
anesthesia or spinal anesthesia and compared the mater-
nal and fetal outcomes based on perioperative hemody-
namic parameters (pre- and postoperative systolic blood
pressure, heart rate), hematocrit, and estimated blood loss
and neonatal Apgar scores at 1 and 5 min between both
anesthesia groups.
MATERIALS AND METHODS
This study was approved by our ethics committee/Insti-
tutional Review Board (no. KYUH 2019-04-008) and regis-
tered at the Korea Clinical Research Information Service
(http://cris.nih.go.kr; no. KCT 0004783). The need for in-
formed consent was waived because of the retrospective
study design. We retrospectively analyzed data from 331
singleton deliveries that occurred between January 2016
and December 2018; data regarding maternal and fetal
outcomes after general or spinal anesthesia for elective ce-
sarean section were analyzed and compared. Two anesthe-
siologists were in charge of anesthesia during the obstetric
surgeries. Both anesthesiologists induced anesthesia using
the same anesthetic agents; patient monitoring, extubation
criteria, and the same spinal technique were performed
according to our institutional protocol.
All subjects were scheduled for elective cesarean section,
with their physical condition classified according to the
American Society of Anesthesiologists class 2, since Ameri-
can Society of Anesthesiologists categorizes “pregnancy”
as class 2. Exclusion criteria included the need for emer-
gency or epidural anesthesia, conversion from spinal to
general anesthesia, and deliveries wherein bleeding was
anticipated, such as placenta previa or coagulopathy. In to-
tal, 44 of the 331 subjects were excluded. The remaining
287 subjects were classified into either general anesthesia
(n = 141) or spinal anesthesia (n = 146) groups (Fig. 1).
The anesthesia induction method was dependent on the
mother's choice, and the difference in preference between
the two anesthesiologists were recorded.
All parturient women fasted for at least 8 h preoperative-
ly and were not administered any pharmacological pre-
medication. In the operating room, we routinely used stan-
dard monitoring, including electrocardiography, noninva-
sive blood pressure, and pulse oximetry (SpO2).
In the general anesthesia group, for all patients, we used
Total elective caesarean sectionsingleton birth (n = 331)
Excluded from analysis (n = 44)
□ Placenta previa (n = 38)□ Coagulopathy (n = 5)□ Spinal conversion to general (n = 1)
General anesthesia group (n = 141)
Spinal anesthesia group (n = 146)
Analysed (n = 287)
Fig. 1. Flow diagram.
50 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
OA
the bispectral index (BIS) and preoxygenation using 100%
oxygen delivered over 3–5 min. Subsequently, anesthesia
was induced with 5 mg/kg of thiopental. Intravenous injec-
tion of 0.5 mg/kg rocuronium facilitated endotracheal in-
tubation, with the Sellick maneuver applied to prevent as-
piration. In all cases, we established controlled ventilation
with a tidal volume of 8 ml/kg and a respiration rate of 12–
14 breaths per minute. Anesthesia was maintained with a
mixture of 1.5–2.0 vol% sevoflurane and 50% nitrous oxide
in oxygen. If a maintenance dose was required, 0.15 mg/kg
of rocuronium was added intravenously. At the end of the
surgery, the residual neuromuscular block was reversed
with pyridostigmine (0.2 mg/kg) and glycopyrrolate (4 μg/
kg). Patients were extubated once they were fully awake to
prevent aspiration.
Spinal anesthesia was introduced at L2/3 or L3/4 level
with a 25-G pencil-point needle (Sprotte, Pajunk, Germa-
ny), with patients in a left lateral decubitus position; O2 was
supplied at a rate of 6 L/min via an oxygen mask. After con-
firming a clear, free flow of cerebrospinal fluid, 9–10 mg of
0.5% bupivacaine (Marcaine Heavy, Astra Zeneca, UK) with
10 μg fentanyl was injected slowly. Patients were then
placed in a fully supine position and tilted 15° downward
and leftward to prevent the supine hypotensive syndrome.
The sensory block level was determined using a cold test.
The operation was initiated when the sensory block had
reached an adequate level (T4–T5). Phenylephrine (1 mg/
h) was continuously infused to prevent arterial hypoten-
sion. If hypotension persisted, 0.1 mg phenylephrine was
injected by IV bolus, or the continuous injection rate was
increased up to 2 mg/h. If hypertension occurred, the con-
tinuous injection rate was decreased to 0.5 mg/h or discon-
tinued. We defined hypotension as systolic blood pressure
below 90 mmHg or below 70% of the baseline blood pres-
sure. After the newborn had been delivered, mothers were
sedated with intravenous midazolam as required if she
wanted.
Cesarean section was performed via a standard lower
segment transverse uterine incision with basic monitoring,
including heart rate and blood pressure. After the baby had
been delivered, carbetocin (Inj. Hanlim, Korea) was rou-
tinely administered to induce uterine contraction.
Measurements
Data on gestational age, parity, height, body weight, pre
and postoperative systolic blood pressure (mmHg), heart
rates (beats/min), hct (%), duration of hospital stay (day),
surgical time, anesthesia time, time between skin incision
and delivery, estimated blood loss (EBL), and transfusions
were collected from medical records. EBL was measured
by a visual estimation and a gravimetric method that in-
volves weighing of soiled sponges and measurement of flu-
id in suction canisters. Newborns were evaluated by a pe-
diatrician in terms of their sex, weight, and 1- and 5-min
Apgar scores. Pediatricians were randomly assigned for the
cesarean delivery.
We defined our primary outcome as the mean difference
between the pre- and postoperative hematocrit, and the
secondary outcome as the 1- and 5-min Apgar scores.
Statistical analysis
The sample size required to detect a statistically signifi-
cant difference between the pre- and postoperative hema-
tocrit was determined using R software (version 3.5.3, R
Development Core Team, Austria). The differences be-
tween the pre- and postoperative hematocrit were mea-
sured in a preliminary study (n = 10 for each), and the av-
erage difference of hematocrit in the general anesthesia
and spinal groups was 5.06 (SD, 3.31) and 2.13 (SD, 4.02),
respectively. Sample size was calculated with an effect size
of 0.796, power of 80%, and an α-value of 0.05; accordingly,
26 subjects were needed in each group.
All statistical analyses were performed using R software
(version 3.5.3). The normality of the distribution of contin-
uous variables was analyzed using the Shapiro–Wilk test.
We used independent t-tests to analyze continuous, nor-
mally distributed variables and the Wilcoxon rank-sum test
to analyze continuous, non-normally distributed variables.
Categorical variables were compared using the χ2 test or
Fisher’s exact test. Descriptive statistics are presented as
mean ± standard deviation, median (1Q, 3Q), or percent-
age. Perioperative change in hct (%) was compared be-
tween the two anesthesia groups using repeated-measures
analysis of variance, followed by Student’s t-test. A P value
of less than 0.05 was considered statistically significant.
RESULTS
Between January 2016 and December 2018, a total of 331
women (singleton pregnancies) underwent elective cesar-
ean section at our hospital. In total, 44 patients were ex-
cluded owing to failed spinal anesthesia, placenta previa,
www.anesth-pain-med.org 51
General vs. spinal for cesarean section
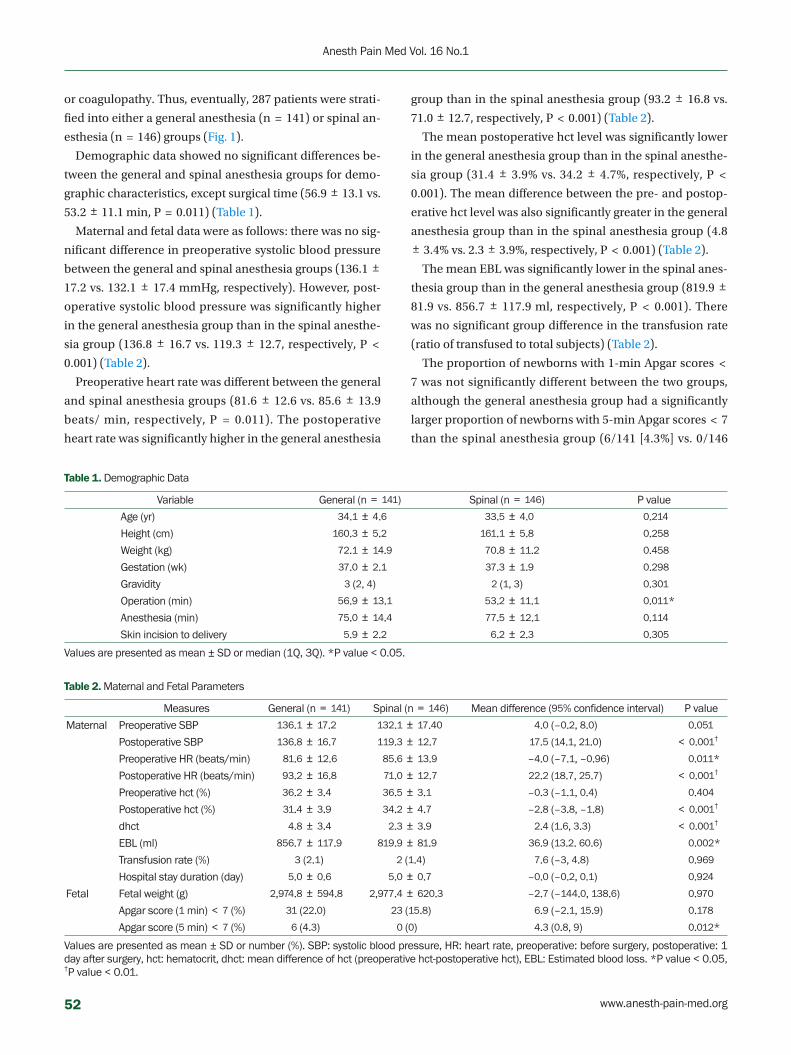
Table 1. Demographic Data
Variable General (n = 141) Spinal (n = 146) P value
Age (yr) 34.1 ± 4.6 33.5 ± 4.0 0.214
Height (cm) 160.3 ± 5.2 161.1 ± 5.8 0.258
Weight (kg) 72.1 ± 14.9 70.8 ± 11.2 0.458
Gestation (wk) 37.0 ± 2.1 37.3 ± 1.9 0.298
Gravidity 3 (2, 4) 2 (1, 3) 0.301
Operation (min) 56.9 ± 13.1 53.2 ± 11.1 0.011*
Anesthesia (min) 75.0 ± 14.4 77.5 ± 12.1 0.114
Skin incision to delivery 5.9 ± 2.2 6.2 ± 2.3 0.305
Values are presented as mean ± SD or median (1Q, 3Q). *P value < 0.05.
Table 2. Maternal and Fetal Parameters
Measures General (n = 141) Spinal (n = 146) Mean difference (95% confidence interval) P value
Maternal Preoperative SBP 136.1 ± 17.2 132.1 ± 17.40 4.0 (–0.2, 8.0) 0.051
Postoperative SBP 136.8 ± 16.7 119.3 ± 12.7 17.5 (14.1, 21.0) < 0.001†
Preoperative HR (beats/min) 81.6 ± 12.6 85.6 ± 13.9 –4.0 (–7.1, –0.96) 0.011*
Postoperative HR (beats/min) 93.2 ± 16.8 71.0 ± 12.7 22.2 (18.7, 25.7) < 0.001†
Preoperative hct (%) 36.2 ± 3.4 36.5 ± 3.1 –0.3 (–1.1, 0.4) 0.404
Postoperative hct (%) 31.4 ± 3.9 34.2 ± 4.7 –2.8 (–3.8, –1.8) < 0.001†
dhct 4.8 ± 3.4 2.3 ± 3.9 2.4 (1.6, 3.3) < 0.001†
EBL (ml) 856.7 ± 117.9 819.9 ± 81.9 36.9 (13.2. 60.6) 0.002*
Transfusion rate (%) 3 (2.1) 2 (1.4) 7.6 (–3, 4.8) 0.969
Hospital stay duration (day) 5.0 ± 0.6 5.0 ± 0.7 –0.0 (–0.2, 0.1) 0.924
Fetal Fetal weight (g) 2,974.8 ± 594.8 2,977.4 ± 620.3 –2.7 (–144.0, 138.6) 0.970
Apgar score (1 min) < 7 (%) 31 (22.0) 23 (15.8) 6.9 (–2.1, 15.9) 0.178
Apgar score (5 min) < 7 (%) 6 (4.3) 0 (0) 4.3 (0.8, 9) 0.012*
Values are presented as mean ± SD or number (%). SBP: systolic blood pressure, HR: heart rate, preoperative: before surgery, postoperative: 1 day after surgery, hct: hematocrit, dhct: mean difference of hct (preoperative hct-postoperative hct), EBL: Estimated blood loss. *P value < 0.05, †P value < 0.01.
or coagulopathy. Thus, eventually, 287 patients were strati-
fied into either a general anesthesia (n = 141) or spinal an-
esthesia (n = 146) groups (Fig. 1).
Demographic data showed no significant differences be-
tween the general and spinal anesthesia groups for demo-
graphic characteristics, except surgical time (56.9 ± 13.1 vs.
53.2 ± 11.1 min, P = 0.011) (Table 1).
Maternal and fetal data were as follows: there was no sig-
nificant difference in preoperative systolic blood pressure
between the general and spinal anesthesia groups (136.1 ±
17.2 vs. 132.1 ± 17.4 mmHg, respectively). However, post-
operative systolic blood pressure was significantly higher
in the general anesthesia group than in the spinal anesthe-
sia group (136.8 ± 16.7 vs. 119.3 ± 12.7, respectively, P <
0.001) (Table 2).
Preoperative heart rate was different between the general
and spinal anesthesia groups (81.6 ± 12.6 vs. 85.6 ± 13.9
beats/ min, respectively, P = 0.011). The postoperative
heart rate was significantly higher in the general anesthesia
group than in the spinal anesthesia group (93.2 ± 16.8 vs.
71.0 ± 12.7, respectively, P < 0.001) (Table 2).
The mean postoperative hct level was significantly lower
in the general anesthesia group than in the spinal anesthe-
sia group (31.4 ± 3.9% vs. 34.2 ± 4.7%, respectively, P <
0.001). The mean difference between the pre- and postop-
erative hct level was also significantly greater in the general
anesthesia group than in the spinal anesthesia group (4.8 ± 3.4% vs. 2.3 ± 3.9%, respectively, P < 0.001) (Table 2).
The mean EBL was significantly lower in the spinal anes-
thesia group than in the general anesthesia group (819.9 ±
81.9 vs. 856.7 ± 117.9 ml, respectively, P < 0.001). There
was no significant group difference in the transfusion rate
(ratio of transfused to total subjects) (Table 2).
The proportion of newborns with 1-min Apgar scores <
7 was not significantly different between the two groups,
although the general anesthesia group had a significantly
larger proportion of newborns with 5-min Apgar scores < 7
than the spinal anesthesia group (6/141 [4.3%] vs. 0/146
52 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
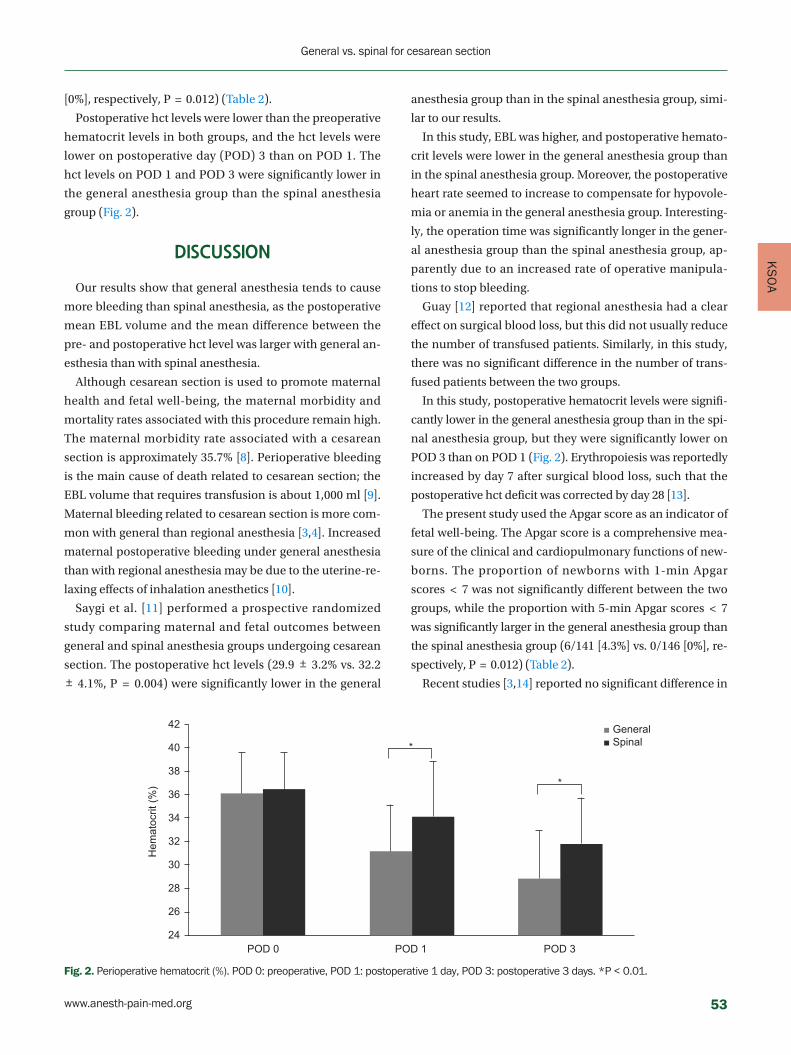
KS
OA
[0%], respectively, P = 0.012) (Table 2).
Postoperative hct levels were lower than the preoperative
hematocrit levels in both groups, and the hct levels were
lower on postoperative day (POD) 3 than on POD 1. The
hct levels on POD 1 and POD 3 were significantly lower in
the general anesthesia group than the spinal anesthesia
group (Fig. 2).
DISCUSSION
Our results show that general anesthesia tends to cause
more bleeding than spinal anesthesia, as the postoperative
mean EBL volume and the mean difference between the
pre- and postoperative hct level was larger with general an-
esthesia than with spinal anesthesia.
Although cesarean section is used to promote maternal
health and fetal well-being, the maternal morbidity and
mortality rates associated with this procedure remain high.
The maternal morbidity rate associated with a cesarean
section is approximately 35.7% [8]. Perioperative bleeding
is the main cause of death related to cesarean section; the
EBL volume that requires transfusion is about 1,000 ml [9].
Maternal bleeding related to cesarean section is more com-
mon with general than regional anesthesia [3,4]. Increased
maternal postoperative bleeding under general anesthesia
than with regional anesthesia may be due to the uterine-re-
laxing effects of inhalation anesthetics [10].
Saygi et al. [11] performed a prospective randomized
study comparing maternal and fetal outcomes between
general and spinal anesthesia groups undergoing cesarean
section. The postoperative hct levels (29.9 ± 3.2% vs. 32.2 ± 4.1%, P = 0.004) were significantly lower in the general
anesthesia group than in the spinal anesthesia group, simi-
lar to our results.
In this study, EBL was higher, and postoperative hemato-
crit levels were lower in the general anesthesia group than
in the spinal anesthesia group. Moreover, the postoperative
heart rate seemed to increase to compensate for hypovole-
mia or anemia in the general anesthesia group. Interesting-
ly, the operation time was significantly longer in the gener-
al anesthesia group than the spinal anesthesia group, ap-
parently due to an increased rate of operative manipula-
tions to stop bleeding.
Guay [12] reported that regional anesthesia had a clear
effect on surgical blood loss, but this did not usually reduce
the number of transfused patients. Similarly, in this study,
there was no significant difference in the number of trans-
fused patients between the two groups.
In this study, postoperative hematocrit levels were signifi-
cantly lower in the general anesthesia group than in the spi-
nal anesthesia group, but they were significantly lower on
POD 3 than on POD 1 (Fig. 2). Erythropoiesis was reportedly
increased by day 7 after surgical blood loss, such that the
postoperative hct deficit was corrected by day 28 [13].
The present study used the Apgar score as an indicator of
fetal well-being. The Apgar score is a comprehensive mea-
sure of the clinical and cardiopulmonary functions of new-
borns. The proportion of newborns with 1-min Apgar
scores < 7 was not significantly different between the two
groups, while the proportion with 5-min Apgar scores < 7
was significantly larger in the general anesthesia group than
the spinal anesthesia group (6/141 [4.3%] vs. 0/146 [0%], re-
spectively, P = 0.012) (Table 2).
Recent studies [3,14] reported no significant difference in
42
40
38
36
34
32
30
28
26
24POD 0
Hem
atoc
rit (%
)
POD 1
*
*
POD 3
■ General■ Spinal
Fig. 2. Perioperative hematocrit (%). POD 0: preoperative, POD 1: postoperative 1 day, POD 3: postoperative 3 days. *P < 0.01.
www.anesth-pain-med.org 53
General vs. spinal for cesarean section

the 1- or 5-min Apgar scores of newborn babies under gen-
eral versus spinal anesthesia for cesarean section. Howev-
er, Tonni et al. [15] reported that, although the mother's ox-
ygen partial pressure and saturation were higher with gen-
eral anesthesia than with regional anesthesia, the partial
pressure of oxygen and umbilical cord blood pH in the
general anesthesia group were lower than in the spinal and
epidural groups. They hypothesized that newborns deliv-
ered under general anesthesia experience transient respi-
ratory depression because anesthetics given to the mother
cross the placental barrier and enter fetal circulation.
In this study, the proportion with 5-min Apgar scores < 7
was significantly larger in the general anesthesia group
than the spinal anesthesia group. We supposed that anes-
thetic agents crossing the placenta might influence the fe-
tus to some degree, although the fetus well tolerated them.
Regional anesthesia can minimize the exposure of new-
borns to anesthetics and improve placental perfusion and
oxygenation of the fetus due to sympathetic blockade.
Therefore, regional anesthesia is preferable to general an-
esthesia during the cesarean section for both maternal and
fetal safety.
Usually, the administration of general anesthesia is inev-
itable in cases of maternal coagulopathy or fetal distress.
Neonatal respiratory depression accompanied by low Ap-
gar scores and umbilical arterial and venous pH changes
associated with general anesthesia is often transient. How-
ever, careful and appropriately administered general anes-
thetic has no significant adverse effects on fetuses or neo-
nates [16].
Although many reports have shown that regional and
general anesthesia are almost identical in terms of neona-
tal well-being, regional anesthesia, especially spinal, is rec-
ommended for elective cesarean section to avoid neonatal
depression, especially for preterm delivery.
This study had some limitations. First, it was retrospec-
tive study, and we could not control all confounding vari-
ables that may have affected the outcomes. Second, the P
values of some major results (Apgar scores) are relatively
large; the sample size is relatively small. Therefore, the sig-
nificant results might be purely by chance (random error).
The sample size was based on the number of participants
required to detect a statistically significant difference in the
hct level, but not the Apgar score between the groups.
Since spinal anesthesia for cesarean section was only intro-
duced in our hospital two years ago, the maximum possi-
ble sample size for the spinal anesthesia group was 146.
According to the power calculation, 232 subjects were
needed in each group to detect statistically significant dif-
ferences in Apgar scores. Thus, our findings regarding the
Apgar scores should be interpreted with caution, and fu-
ture research should include adequate sample sizes.
During cesarean section, general anesthesia group is as-
sociated with more maternal blood loss and a larger pro-
portion of newborns with 5-min Apgar scores < 7 than spi-
nal anesthesia.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Young Seok Jee. Data curation: Hwang-
Ju You. Writing - original draft: Young Seok Jee. Statistical
analysis: Tae-Yun Sung, Young Seok Jee. Writing - review &
editing: Tae-Yun Sung, Young Seok Jee, Choon-Kyu Cho.
ORCID
Tae-Yun Sung, https://orcid.org/0000-0002-0714-1477
Young Seok Jee, https://orcid.org/0000-0001-9154-0691
Hwang-Ju You, https://orcid.org/0000-0001-9921-4241
Choon-Kyu Cho, https://orcid.org/0000-0001-9906-1396
REFERENCES
1. Enkin M, Keirse MJ, Neilson J, Crowther C, Duley L, Hodnett E,
et al. Effective care in pregnancy and childbirth: a synopsis.
Birth 2001; 28: 41-51.
2. Ng K, Parsons J, Cyna AM, Middleton P. Spinal versus epidural
anaesthesia for caesarean section. Cochrane Database Syst Rev
2004; (2): CD003765.
3. Dyer RA, Els I, Farbas J, Torr GJ, Schoeman LK, James MF. Pro-
spective, randomized trial comparing general with spinal an-
esthesia for cesarean delivery in preeclamptic patients with a
nonreassuring fetal heart trace. Anesthesiology 2003; 99: 561-9;
discussion 5A-6A.
4. Hong JY, Jee YS, Yoon HJ, Kim SM. Comparison of general and
epidural anesthesia in elective cesarean section for placenta
previa totalis: maternal hemodynamics, blood loss and neona-
tal outcome. Int J Obstet Anesth 2003; 12: 12-6.
5. Afolabi BB, Lesi FE. Regional versus general anaesthesia for
54 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
KS
OA
caesarean section. Cochrane Database Syst Rev 2012; (10):
CD004350.
6. Mancuso A, De Vivo A, Giacobbe A, Priola V, Maggio Savasta L,
et al. General versus spinal anaesthesia for elective caesarean
sections: effects on neonatal short-term outcome. A prospec-
tive randomised study. J Matern Fetal Neonatal Med 2010; 23:
1114-8.
7. Sener EB, Guldogus F, Karakaya D, Baris S, Kocamanoglu S, Tur
A. Comparison of neonatal effects of epidural and general an-
esthesia for cesarean section. Gynecol Obstet Invest 2003; 55:
41-5.
8. Ronsmans C, Graham WJ; Lancet Maternal Survival Series
steering group. Maternal mortality: who, when, where, and
why. Lancet 2006; 368: 1189-200.
9. Bergholt T, Stenderup JK, Vedsted-Jakobsen A, Helm P, Len-
strup C. Intraoperative surgical complication during cesarean
section: an observational study of the incidence and risk fac-
tors. Acta Obstet Gynecol Scand 2003; 82: 251-6.
10. Wong CA. General anesthesia is unacceptable for elective ce-
sarean section. Int J Obstet Anesth 2010; 19: 209-12.
11. Saygı Aİ, Özdamar Ö, Gün İ, Emirkadı H, Müngen E, Akpak YK.
Comparison of maternal and fetal outcomes among patients
undergoing cesarean section under general and spinal anes-
thesia: a randomized clinical trial. Sao Paulo Med J 2015; 133:
227-34.
12. Guay J. The effect of neuraxial blocks on surgical blood loss and
blood transfusion requirements: a meta-analysis. J Clin Anesth
2006; 18: 124-8.
13. Wallis JP, Wells AW, Whitehead S, Brewster N. Recovery from
post-operative anaemia. Transfus Med 2005; 15: 413-8.
14. Kavak ZN, Başgül A, Ceyhan N. Short-term outcome of new-
born infants: spinal versus general anesthesia for elective ce-
sarean section. A prospective randomized study. Eur J Obstet
Gynecol Reprod Biol 2001; 100: 50-4.
15. Tonni G, Ferrari B, De Felice C, Ventura A. Fetal acid-base and
neonatal status after general and neuraxial anesthesia for elec-
tive cesarean section. Int J Gynaecol Obstet 2007; 97: 143-6.
16. Mattingly JE, D'Alessio J, Ramanathan J. Effects of obstetric an-
algesics and anesthetics on the neonate: a review. Paediatr
Drugs 2003; 5: 615-27.
www.anesth-pain-med.org 55
General vs. spinal for cesarean section

Anaphylaxis is defined as a serious, life-threatening, gen-
eralized or systemic hypersensitivity reaction with a rapid
onset [1].
Although anaphylaxis during anesthesia induction oc-
curs only in approximately 1 of 20,000 cases, it can be
life-threatening. Neuromuscular blocking agents, particu-
larly, rocuronium and succinylcholine, are the most com-
mon pharmacologic causes in approximately 60% to 70%
of cases [2–4]. The first choice of treatment for anaphylaxis
during anesthesia is immediate discontinuation of the ana-
phylactic agent and the use of drugs that improve the he-
modynamic status of the patient [3]. Sugammadex is a se-
lective antagonist of rocuronium and rapidly reverses ro-
curonium-induced neuromuscular blockade [5]. This
Corresponding author Seung-Ah Ryu, M.D.Department of Anesthesiology and Pain Medicine, Seoul Medical Center, 156 Sinnae-ro, Jungnang-gu, Seoul 02053, Korea Tel: 82-2-2276-7659 Fax: 82-2-8876-7658 E-mail: [email protected]
Background: Perioperative anaphylaxis is a life-threatening clinical condition characterized by severe respiratory and cardiovascular manifestations. Neuromuscular blocking agents are the most common cause of anaphylaxis during anesthesia.
Case: We report a case of rocuronium-induced anaphylaxis treated with sugammadex. A 75-year-old female was scheduled to undergo spinal surgery. She had no history of allergies. After the injection of rocuronium, she developed hypotension and tachycardia, and skin rashes and urticaria appeared. The patient received sugammadex to delay the operation, and her vital signs were stabilized. On the 76th postoperative day, we performed intrader-mal tests for rocuronium, propofol, and cefazolin. Diluted rocuronium alone induced 14 mm of flare and 8 mm of wheal within 5 min, both of which disappeared within 15 min after the intradermal injection.
Conclusions: Sugammadex is a useful rocuronium antagonist that can be used to treat ro-curonium-induced anaphylaxis.
Keywords: Anaphylaxis; Anesthesia; Rocuronium; Sugammadex; Shock; Treatment.
Treatment of rocuronium-induced anaphylaxis using sugammadex - A case report -
Sun-Min Kim, Sei-hoon Oh, and Seung-Ah Ryu
Department of Anesthesiology and Pain Medicine, Seoul Medical Center, Seoul,
Korea
Received September 11, 2020 Revised October 28, 2020 Accepted October 28, 2020
Case ReportAnesth Pain Med 2021;16:56-59https://doi.org/10.17085/apm.20074pISSN 1975-5171 • eISSN 2383-7977
pharmacological characteristic of sugammadex favors its
use in the treatment of rocuronium-induced anaphylaxis
[6]. We report a case of rocuronium-induced anaphylaxis
treated with sugammadex.
CASE REPORT
A written informed consent form was obtained for publi-
cation of this report. A 75-year-old female (weight, 51 kg;
height, 146 cm) was scheduled to undergo a decompres-
sive lumbar laminectomy and interbody fusion (lumbar
level, 3-4 and 4-5) under general anesthesia. She had
well-controlled hypertension. Five years earlier, she under-
went an uneventful procedure under general anesthesia
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
56

KN
RS
(transobturator vaginal tape operation). She reported no
known allergy to medication, food, or latex. Results of pre-
operative laboratory examinations, chest radiography,
electrocardiography, transthoracic echocardiography, thal-
lium scan, and pulmonary function tests were normal.
On arrival in the operating room, she had a noninvasive
blood pressure of 102/63 mmHg, a heart rate of 98 beats/
min, and an oxygen saturation (SpO2) at room air of 100%.
After starting pre-oxygenation anesthesia induction, the
patient received propofol (100 mg) for anesthesia induc-
tion and rocuronium bromide (50 mg) to facilitate tracheal
intubation. Anesthesia was maintained with 4–8 vol% des-
flurane and target-controlled infusion of remifentanil (2
mg; 2 ng/ml). Thereafter, endotracheal intubation was per-
formed. A 16-gauge peripheral intravenous cannula and a
20-gauge arterial line were placed. The results of the first
arterial blood gas analysis were within the normal range
(pH, 7.43; pCO2, 37; pO2, 168). The patient was placed in
the prone position after administration of prophylactic an-
tibiotics (cefazoline, 2 g).
Five minutes after the position change, which was per-
formed 10 min after induction, an arterial blood pressure
of 68/43 mmHg and sinus tachycardia of 113 beats/min
were noted. Even though the skin test for sensitivity to ce-
fazoline was negative, the prophylactic antibiotics were
discontinued immediately and ephedrine (10 mg), phenyl-
ephrine (200 mg), 1,100 ml of crystalloid, and 500 ml of
colloid were administered. The follow-up arterial blood
analysis results remained unchanged. Despite these inter-
ventions, the blood pressure decreased further to 35/25
mmHg and the heart rate was 130 beats/min. Subsequent-
ly, dexamethasone (5 mg) and pheniramine (4 mg) were
administered. However, the patient’s skin symptoms con-
tinued to worsen and spread from her trunk to her head.
We strongly suspected an anaphylactic reaction, and epi-
nephrine infusion (0.1 μg/kg/min) was started after ad-
ministration of an intravenous epinephrine bolus. Despite
appropriate traditional management, the skin symptoms
worsened, and the situation was still critical. The epineph-
rine infusion dose was increased every minute and bolus
drugs were needed to restore the blood pressure. A deci-
sion was made to delay the surgery and sugammadex (200
mg; 4 mg/kg) was administered to reverse the neuromus-
cular blockade because her train-of-four ratio was 0.2 [7].
Shortly thereafter, the patient’s arterial blood pressure re-
covered to the pre-induction level. Hemodynamic data af-
ter sugammadex injection were as follows: heart rate, 102
beats/min; blood pressure, 95/48 mmHg; and oxygen satu-
ration, 100%. The patient was sedated with a bolus of mid-
azolam and transferred to the intensive care unit for further
observation. She was extubated within 30 min of arrival in
the intensive care unit, and no further vasopressor support
was required (Fig. 1).
The patient was discharged without any complications.
One month later, she visited the Department of Allergy
Medicine for the identification of the agent that caused her
intraoperative anaphylaxis. Intradermal skin tests were
performed four weeks later with rocuronium and cefazo-
line. A marked positive, persistent, wheal-and-flair re-
sponse was recorded at the site of rocuronium injection,
comparable to that of the positive control (histamine), with
negative responses at the other sites. Three months later,
she decided to undergo surgery again. In the operating
room, the patient received an induction dose of propofol
and cisatracurium instead of rocuronium. Thereafter, en-
dotracheal intubation was performed, and the surgery was
conducted successfully in the prone position. No adverse
events occurred intraoperatively, and the patient was dis-
charged without any complications.
DISCUSSION
This case report describes the usefulness of intraopera-
tive sugammadex administration in treating an episode of
confirmed rocuronium-induced anaphylaxis, which was
temporally associated with a marked improvement in the
160
140
120
100
80
60
40
20
0
SBP/DBP/HR
Operation time
SBP (mmHg)
DBP (mmHg)
HR (beat/min)
0 10 20 30 40 Min
†*
‡
Fig. 1. Chart showing the vital sign changes. HR: heart rate, SBP: systolic arterial blood pressure, DBP: diastolic arterial blood pressure. *Rocuronium injection and intubation. †Epinephrine. ‡Sugammadex intravenous injection.
www.anesth-pain-med.org 57
Rocuronium-induced anaphylaxis

patient’s critical hemodynamic status. This case report pro-
vides evidence to support the role of sugammadex in the
management of rocuronium-induced anaphylaxis.
The reported incidence of anaphylaxis induced during
anesthesia has varied from 1:3,500 to 1:20,000 [8,9]. Most
cases have been reported in women and during the use of
muscle relaxants. Neuromuscular blocking agents
(NMBAs) account for most IgE-mediated anaphylactic re-
actions that occur during general anesthesia induction
[8,10]. Among the muscle relaxants that induce anaphylax-
is, rocuronium is the most common causative drug [11].
NMBAs induce the release of tryptase and histamine from
mast cells, both of which have direct vasodilatory effects on
the blood vessels and induce changes in capillary permea-
bility, urticaria, erythema, angioedema, hypotension, and
bronchospasm [12]. Independent risk factors associated
with death were male sex, emergency setting, history of hy-
pertension or other cardiovascular diseases, ongoing be-
ta-blocker treatment, and obesity [13].
According to the World Allergy Organization (WAO), the
diagnosis of anaphylaxis depends on the recognition of
characteristic symptoms and signs that occur minutes to
hours after exposure to a known or potential trigger [1]. Al-
though the intradermal skin test or skin prick test are the
gold- standard methods for identifying a potential anaphy-
lactogen, they are indicators of the procedure and test con-
centrations used for most drugs. The optimal interval be-
tween the time of anaphylactic shock and the skin test is
controversial. The test is commonly recommended in a
minimum time interval of three weeks and no more than
three months after the anaphylactic episode. In our case,
intradermal skin test to identify the anaphylactogen was
performed four weeks after the episode of anaphylactic
shock.
When a patient is experiencing an anaphylactic shock,
prompt acknowledgement as well as rapid and specific
management is essential, including intravenous fluid re-
placement and the use of cardiovascular drugs. Epinephrine
is the first-choice drug used to treat anaphylaxis [1]. Once an
agent has been administered intravenously, it is difficult to
eliminate it from the body. Sugammadex is a γ-cyclodextrin
derivative with a truncated cone-like shape and a hydropho-
bic cavity. The molecular cavity of sugammadex encapsu-
lates the steroid backbone of rocuronium with high affinity.
Once enveloped within the sugammadex molecule, rocuro-
nium cannot bind to acetylcholine receptors. This mecha-
nism of sugammadex has a positive effect during the treat-
ment of rocuronium-induced anaphylaxis [5].
Cases of sugammadex-induced anaphylaxis have been
reported in countries that frequently use the drug. These
cases of anaphylactic reactions appear to be more frequent
at higher clinical doses [6]. Although sugammadex-in-
duced anaphylaxis has been reported, sugammadex is a
great antagonist of rocuronium. The optimal dose of
sugammadex in such cases is unknown. Theoretically, it
has been suggested that large doses (up to 16 mg/kg) may
be required to encapsulate all circulating rocuronium mol-
ecules in a patient’s body [5]. This dose is dependent on
the initial dose of rocuronium administered and the time
elapsed since its administration. In our case, 200 mg of
sugammadex was administered because it was readily
available. In the present case, this dose appeared to fully
reverse the underlying neuromuscular block, as expected
given that 80 min had elapsed since rocuronium adminis-
tration [14,15].
In conclusion, although cases of sugammadex-induced
anaphylaxis have been reported, sugammadex is a useful
rocuronium antagonist. It is noteworthy that sugammadex
adequately reversed the adverse effects of rocuronium-in-
duced anaphylaxis; however, the optimal dose to prevent
anaphylaxis has not been reported yet. Therefore, further
studies should be conducted to identify the optimal dose.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Seung-Ah Ryu. Data curation: Sun-
Min Kim. Formal analysis: Sun-Min Kim, Sei-hoon Oh,
Seung-Ah Ryu. Writing - original draft: Sun-Min Kim. Writ-
ing - review & editing: Sei-hoon Oh, Seung-Ah Ryu. Investi-
gation: Sun-Min Kim, Sei-hoon Oh. Supervision: Seung-Ah
Ryu. Validation: Seung-Ah Ryu.
ORCID
Sun-Min Kim, https://orcid.org/0000-0002-1022-7781
Sei-hoon Oh, https://orcid.org/0000-0002-9476-5594
Seung-Ah Ryu, https://orcid.org/0000-0002-5544-3445
58 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
KN
RS
REFERENCES
1. Simons FE, Ardusso LR, Bilò MB, El-Gamal YM, Ledford DK,
Ring J, et al. World Allergy Organization. World Allergy Organi-
zation guidelines for the assessment and management of ana-
phylaxis. World Allergy Organ J 2011; 4: 13-37.
2. Harper NJ, Dixon T, Dugué P, Edgar DM, Fay A, Gooi HC, et al.
Working Party of the Association of Anaesthetists of Great Brit-
ain and Ireland. Suspected anaphylactic reactions associated
with anaesthesia. Anaesthesia 2009; 64: 199-211.
3. McDonnell NJ, Pavy TJ, Green LK, Platt PR. Sugammadex in
the management of rocuronium-induced anaphylaxis. Br J An-
aesth 2011; 106: 199-201.
4. Mertes PM, Laxenaire MC; GERAP. [Anaphylactic and anaphy-
lactoid reactions occurring during anaesthesia in France. Sev-
enth epidemiologic survey (January 2001-December 2002)].
Ann Fr Anesth Reanim 2004 23: 1133-43. French.
5. Jones PM, Turkstra TP. Mitigation of rocuronium-induced ana-
phylaxis by sugammadex: the great unknown. Anaesthesia
2010; 65: 89-90; author reply 90.
6. Peeters PA, van den Heuvel MW, van Heumen E, Passier PC,
Smeets JM, van Iersel T, et al. Safety, tolerability and pharma-
cokinetics of sugammadex using single high doses (up to
96 mg/kg) in healthy adult subjects: a randomized, dou-
ble-blind, crossover, placebo-controlled, single-centre study.
Clin Drug Investig 2010; 30: 867-74.
7. Kim KS. Clinical use of sugammadex. Anesth Pain Med 2011; 6:
307-13.
8. Fisher MM, Baldo BA. The incidence and clinical features of
anaphylactic reactions during anesthesia in Australia. Ann Fr
Anesth Reanim 1993; 12: 97-104.
9. Hepner DL, Castells MC. Anaphylaxis during the perioperative
period. Anesth Analg 2003; 97: 1381-95.
10. Mertes PM, Laxenaire MC, Alla F; Groupe d'Etudes des Réac-
tions Anaphylactoïdes Peranesthésiques. Anaphylactic and
anaphylactoid reactions occurring during anesthesia in France
in 1999-2000. Anesthesiology 2003; 99: 536-45.
11. Axon AD, Hunter JM. Editorial III: anaphylaxis and anaesthe-
sia--all clear now? Br J Anaesth 2004; 93: 501-4.
12. Mertes PM, Moneret-Vautrin DA, Leynadier F, Laxenaire MC.
Skin reactions to intradermal neuromuscular blocking agent
injections: a randomized multicenter trial in healthy volun-
teers. Anesthesiology 2007; 107: 245-52.
13. Reitter M, Petitpain N, Latarche C, Cottin J, Massy N, Demoly P,
et al. French Network of Regional Pharmacovigilance Centres.
Fatal anaphylaxis with neuromuscular blocking agents: a risk
factor and management analysis. Allergy 2014; 69: 954-9.
14. Gijsenbergh F, Ramael S, Houwing N, van Iersel T. First human
exposure of Org 25969, a novel agent to reverse the action of
rocuronium bromide. Anesthesiology 2005; 103: 695-703.
15. Jones RK, Caldwell JE, Brull SJ, Soto RG. Reversal of profound
rocuronium-induced blockade with sugammadex: a random-
ized comparison with neostigmine. Anesthesiology 2008; 109:
816-24.
www.anesth-pain-med.org 59
Rocuronium-induced anaphylaxis

Comparison of postoperative pulmonary complications between sugammadex and neostigmine in lung cancer patients undergoing video-assisted thoracoscopic lobectomy: a prospective double-blinded randomized trial
Tae Young Lee, Seong Yeop Jeong, Joon Ho Jeong, Jeong Ho Kim, and So Ron Choi
Department of Anesthesiology and Pain Medicine, Dong-A University Hospital,
Dong-A University College of Medicine, Busan, Korea
Received June 23, 2020Revised September 10, 2020 Accepted October 7, 2020
Corresponding author Tae Young Lee, M.D. Department of Anesthesiology and Pain Medicine, Dong-A University Hospital, Dong-A University College of Medicine, 26 Daesingongwon-ro, Seo-gu, Busan 49201, Korea Tel: 82-51-240-5390Fax: 82-51-247-7819E-mail: [email protected]
Background: Reversal of neuromuscular blockade (NMB) at the end of surgery is important for reducing postoperative residual NMB; this is associated with an increased risk of postop-erative pulmonary complications (PPCs). Moreover, PPCs are associated with poor prognosis after video-assisted thoracoscopic surgery (VATS) for lobectomy. We compared the effects of two reversal agents, sugammadex and neostigmine, on the incidence of PPCs and duration of hospital stay in patients undergoing VATS lobectomy.
Methods: After VATS lobectomy was completed under neuromuscular monitoring, the sugammadex group (n = 46) received sugammadex 2 mg/kg, while the neostigmine group (n = 47) received neostigmine 0.05 mg/kg with atropine 0.02 mg/kg after at least the third twitch in response to the train of four stimulation. The primary outcome was incidence of PPCs. The secondary outcomes were duration of hospital stay and intensive care unit (ICU) admission.
Results: There was no significant difference in the incidence of PPCs for both the sugamma-dex and neostigmine groups (32.6% and 40.4%, respectively; risk difference = 0.08; 95% confidence interval = [−0.12, 0.27]; P = 0.434). The lengths of hospital (P = 0.431) and ICU (P = 0.964) stays were not significantly different between the two groups.
Conclusions: The clinical use of sugammadex and neostigmine in NMB reversal for patients undergoing VATS lobectomy was not significantly different in the incidence of PPCs and du-ration of hospital and ICU stay.
Keywords: Enhanced recovery after surgery; Neostigmine; Neuromuscular blockade; Post-operative complications; Sugammadex; Thoracic surgery, video-assisted.
Clinical ResearchAnesth Pain Med 2021;16:60-67https://doi.org/10.17085/apm.20056pISSN 1975-5171 • eISSN 2383-7977
INTRODUCTION
The primary goal of enhanced recovery after surgery
(ERAS) in lung surgery is to optimize perioperative and in-
traoperative management to reduce postoperative compli-
cations and decrease the length of hospital stay [1,2]. Par-
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
60

KS
CVA
ticularly, in the field of anesthesia management, neuro-
muscular blockade (NMB) and its reversal are important
because deep NMB is necessary during thoracoscopic lung
surgery to secure a good field of view and operating space
for the surgeon. Additionally, the choice of reversal agent
used to reverse NMB after surgery is important for proper
recovery by reducing postoperative residual NMB
(PRNMB) [1,3]; this is important for patient safety in the
early postoperative period because PRNMB increases the
incidence of adverse respiratory events, such as impaired
upper airway function, increased risk of aspiration, and re-
spiratory insufficiency [4–6].
As a cholinesterase inhibitor, neostigmine mainly inhib-
its acetylcholine breakdown, increases acetylcholine levels
in the neuromuscular junction, and enhances the ability of
acetylcholine to compete with non-depolarized muscle re-
laxants at the receptor [3,7]. However, in several studies on
the routine use of neostigmine, the incidence of PRNMB
on arrival to the post-anesthesia care unit did not change.
Furthermore, because it is not a direct neuromuscular
blocking agent antagonist, the reversal of NMB using
neostigmine is associated with an increased incidence of
postoperative atelectasis, desaturation, postoperative pul-
monary complications (PPCs), and longer hospital stay
[7,8]. In addition, PRNMB is associated with an increased
risk of PPCs [7–10].
In contrast, de Menezes et al. [11] reported that under
neuromuscular monitoring, sugammadex led to a com-
plete reversal of NMB after incomplete reversal by neostig-
mine. Similarly, sugammadex is a selective relaxant bind-
ing agent that rapidly reverses moderate or deep NMB. It is
a synthetically modified gamma-cyclodextrin with a hydro-
philic exterior and a hydrophobic core, specifically de-
signed to encapsulate steroidal neuromuscular blocking
agents [3,6,7]. Sugammadex reverses NMB more rapidly
and effectively than cholinesterase inhibitors, even at deep
block levels, by directly binding to steroidal neuromuscular
blocking agents without residual muscle relaxation [3,8].
Therefore, in the reversal of NMB at the end of surgery, it
is thought that sugammadex would contribute to reducing
PPCs by reducing PRNMB. However, few studies have as-
sessed the reversal of NMB in video-assisted thoracoscopic
(VATS) lobectomy. Thus, we hypothesized that sugamma-
dex would reduce PPCs and the length of hospital stay in
patients undergoing VATS lobectomy, compared with the
traditionally and widely used neostigmine.
MATERIALS AND METHODS
The study was approved by the Institutional Review
Board (no. DAUHIRB-18-047) and was conducted between
April 2018 and May 2020. Informed written consent was
obtained from patients who were scheduled for elective
surgery before enrollment and who voluntarily agreed to
participate. One hundred and two patients were enrolled,
who underwent VATS lobectomy, had an American Society
of Anesthesiologists physical status of I–III, and were over
18 years old. Cases with open conversion during the opera-
tion were excluded. This randomized and double-blinded
prospective study was registered at the Korea Clinical Re-
search Information Service (no. KCT 0003891).
Using a computer-generated random number, 102 par-
ticipants were randomly allocated to the neostigmine
group (n = 51) or sugammadex group (n = 51) in parallel;
this was performed by the main researcher (1:1 assignment
ratio), who did not participate in anesthesia and was not
involved in data collection. Ten milliliters of study drug
solution was prepared in normal saline by the main re-
searcher, based on the patient’s body weight. The sugam-
madex group was administered sugammadex 2 mg/kg,
while the neostigmine group was administered neostig-
mine 0.05 mg/kg (maximum 5 mg) with atropine 0.02 mg/
kg. The study drug was labeled as reverse after being
shielded with a silver foil, and it was delivered to the anes-
thesia nurse.
All patients were administered 0.2 mg glycopyrrolate in-
tramuscularly and 20 mg famotidine intravenously as pre-
medication. Non-invasive blood pressure, electrocardiog-
raphy, pulse oximetry, bispectral index (BIS) (Aspect Med-
ical Systems, USA), and neuromuscular monitoring (TOFs-
can®, Dräger, France) were performed when the patients
arrived at the operating room.
Anesthesia was induced by two blinded anesthesiolo-
gists, each of whom had experience with over 50 cases of
one-lung ventilation, using propofol 2 mg/kg and rocuro-
nium 0.6 mg/kg for NMB. We performed bag-mask ventila-
tion with 100% oxygen. After confirming muscle relaxation
(no reaction in response to the train of four [TOF] stimula-
tion), we performed endotracheal intubation using a dou-
ble lumen endobronchial tube (DLT) (ShileyTM, Covidien,
USA). An arterial catheter and a central venous catheter
were inserted. Anesthesia was maintained with sevoflurane
1.5–2.5 vol% to maintain a BIS of 40–60; remifentanil infu-
sions (0.05–2 μg/kg/min) were administered for pain con-
www.anesth-pain-med.org 61
Sugammadex or neostigmine for lobectomy

trol. To maintain a deep block, vecuronium (0.01 mg/kg)
was administered as required (first twitch of the TOF re-
sponse) [12]. Oxygen concentration in an air/oxygen mix-
ture was adjusted to 100% according to arterial blood gas
analysis (ABGA) results. During severe hypoxemia, contin-
uous positive airway pressure was applied to the non-de-
pendent lung [13]. The end-tidal CO2 concentration was
maintained between 35 and 40 cmH2O, and the following
lung-protective ventilation strategies were implemented
[2,13]: low tidal volume (4–6 ml/ kg), positive end-expira-
tory pressure, and lung recruitment. Flexible fiber-optic
bronchoscopy (ED 3.1 mm, Olympus Optical, Japan) was
used at least twice to confirm correct placement of the DLT
immediately following intubation and repositioning.
The intra-cuff pressure was maintained between 10 and
20 cmH2O using a cuff pressure manometer (Cuff Pressure
Gauge, VBM Medizintechnik, Germany).
When one-lung ventilation was complete, administra-
tion of vecuronium was terminated, and a patient-con-
trolled analgesia device (GemStarTM Infusion System, Hos-
pira, Inc., USA) was connected to the intravenous line. It
contained fentanyl 30 µg/kg and ramosetron 0.6 mg in nor-
mal saline with a total volume of 100 ml, and it was deliv-
ered at 1 ml/h as a background infusion with a 1 ml bolus
dose (10 min lock-out time). To reduce opioid consump-
tion, 0.5% ropivacaine was infused at 5 ml/h through a pain
buster (Pain Relief System, Halyard Health, Inc., USA) in-
tercostally before the end of surgery [2].
At the end of surgery, the labeled NMB reversing agent
was administered at the reappearance of the third twitch in
response to the TOF stimulation. Tracheal and oral secre-
tions were gently suctioned once. After suction was ap-
plied, lung recruitment was performed. Neuromuscular
monitoring continued until the end of anesthesia, and the
DLT was removed when the recovering TOF ratios (TOFR)
reached 0.9, which is considered adequate recovery from
NMB [7].
Postoperative care included chest tube use, intensive
care unit (ICU) stay, intubation, and ventilation; postoper-
ative hospital stay was routinely implemented according to
VATS lobectomy guidelines at the department of thoracic
surgery. Intraoperative ABGA, operation time, and dura-
tion of anesthesia were recorded.
The primary outcome was the incidence of PPCs includ-
ing prolonged air leak, pneumonia and atelectasis, desatu-
ration, and reintubation as confirmed from progress and
discharge records. Prolonged air leakage was defined as an
air leak present on day 6 after surgery. Pneumonia and at-
electasis were diagnosed based on radiologic findings of
the postoperative chest radiograph. Desaturation was de-
fined as saturation levels less than 95% after removing the
oxygen mask. Reintubation was performed when respira-
tory failure occurred. Atrial fibrillation was diagnosed
based on electrocardiography findings, when the patient
complained of symptoms, such as dyspnea, palpitation,
and fatigue. Pulmonary thromboembolism was diagnosed
based on computed tomography and D-dimer test results.
The secondary outcomes were the length of hospital stay
and duration of ICU stay.
Statistical analyses
Based on the results of Cho et al. [3], in which the overall
incidence of PPCs was 54.8% in the control group and
26.3% in the experimental group, 46 subjects were needed
in each group to detect statistically significant differences (α
= 0.05, power = 0.80). Thus, 51 patients per group were
enrolled to compensate for potential dropouts (drop rate =
10%).
Data were presented as means ± SD, number of patients
(%) or medians (1Q, 3Q). Categorical variables were ana-
lyzed using the chi-squared or Fisher’s exact test. Continu-
ous variables were analyzed using Student’s t-test. All re-
ported P values were two sided, and P values less than 0.05
were considered statistically significant. Data were ana-
lyzed using SPSS version 26 software (IBM Corp., USA).
RESULTS
Of the 102 patients, nine were excluded due to conver-
sion to open surgery (four in the neostigmine group and
five in the sugammadex group) (Fig. 1). Table 1 shows the
patient characteristics of both groups. There were no sig-
nificant differences between the two groups in factors that
could affect postoperative complications, such as smoking
history, body mass index, American Society of Anesthesiol-
ogists physical status classification , lobectomy site, or
medical history. Predictive postoperative forced expiratory
volume in 1 s was statistically significant (P = 0.016); how-
ever, there is no clinical significance to this, since the abso-
lute values were not low in either group.
In addition, there was no significant difference in anes-
thesia management during surgery in terms of the opera-
tion time, anesthetic time, ABGA results, and total vecuro-
62 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
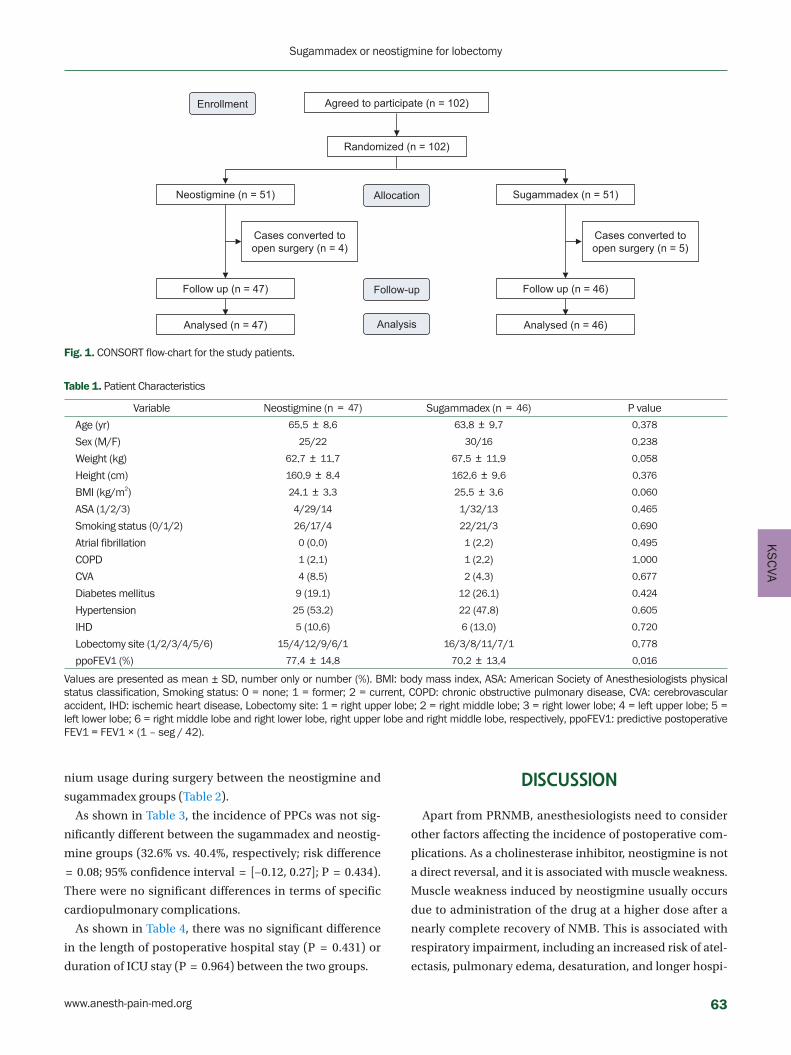
KS
CVA
nium usage during surgery between the neostigmine and
sugammadex groups (Table 2).
As shown in Table 3, the incidence of PPCs was not sig-
nificantly different between the sugammadex and neostig-
mine groups (32.6% vs. 40.4%, respectively; risk difference
= 0.08; 95% confidence interval = [−0.12, 0.27]; P = 0.434).
There were no significant differences in terms of specific
cardiopulmonary complications.
As shown in Table 4, there was no significant difference
in the length of postoperative hospital stay (P = 0.431) or
duration of ICU stay (P = 0.964) between the two groups.
DISCUSSION
Apart from PRNMB, anesthesiologists need to consider
other factors affecting the incidence of postoperative com-
plications. As a cholinesterase inhibitor, neostigmine is not
a direct reversal, and it is associated with muscle weakness.
Muscle weakness induced by neostigmine usually occurs
due to administration of the drug at a higher dose after a
nearly complete recovery of NMB. This is associated with
respiratory impairment, including an increased risk of atel-
ectasis, pulmonary edema, desaturation, and longer hospi-
Agreed to participate (n = 102)
Neostigmine (n = 51) Allocation
Follow-up
Enrollment
Analysis
Cases converted to open surgery (n = 4)
Cases converted to open surgery (n = 5)
Analysed (n = 47)
Sugammadex (n = 51)
Analysed (n = 46)
Randomized (n = 102)
Follow up (n = 47) Follow up (n = 46)
Fig. 1. CONSORT flow-chart for the study patients.
Table 1. Patient Characteristics
Variable Neostigmine (n = 47) Sugammadex (n = 46) P value
Age (yr) 65.5 ± 8.6 63.8 ± 9.7 0.378
Sex (M/F) 25/22 30/16 0.238
Weight (kg) 62.7 ± 11.7 67.5 ± 11.9 0.058
Height (cm) 160.9 ± 8.4 162.6 ± 9.6 0.376
BMI (kg/m2) 24.1 ± 3.3 25.5 ± 3.6 0.060
ASA (1/2/3) 4/29/14 1/32/13 0.465
Smoking status (0/1/2) 26/17/4 22/21/3 0.690
Atrial fibrillation 0 (0.0) 1 (2.2) 0.495
COPD 1 (2.1) 1 (2.2) 1.000
CVA 4 (8.5) 2 (4.3) 0.677
Diabetes mellitus 9 (19.1) 12 (26.1) 0.424
Hypertension 25 (53.2) 22 (47.8) 0.605
IHD 5 (10.6) 6 (13.0) 0.720
Lobectomy site (1/2/3/4/5/6) 15/4/12/9/6/1 16/3/8/11/7/1 0.778
ppoFEV1 (%) 77.4 ± 14.8 70.2 ± 13.4 0.016
Values are presented as mean ± SD, number only or number (%). BMI: body mass index, ASA: American Society of Anesthesiologists physical status classification, Smoking status: 0 = none; 1 = former; 2 = current, COPD: chronic obstructive pulmonary disease, CVA: cerebrovascular accident, IHD: ischemic heart disease, Lobectomy site: 1 = right upper lobe; 2 = right middle lobe; 3 = right lower lobe; 4 = left upper lobe; 5 = left lower lobe; 6 = right middle lobe and right lower lobe, right upper lobe and right middle lobe, respectively, ppoFEV1: predictive postoperative FEV1 = FEV1 × (1 – seg / 42).
www.anesth-pain-med.org 63
Sugammadex or neostigmine for lobectomy

tal stay [7,14]. Moreover, Abad-Gurumeta et al. [8] reported
in a review article that even when extubation was achieved
under high doses of neostigmine ( > 0.6 mg/kg), at TOFR
greater than 0.9, neostigmine administration was associat-
ed with atelectasis, pulmonary edema, tracheal re-intuba-
tion, and prolonged hospital stay. In addition, Schepens et
al. [15] obtained computed tomography scans during the
spontaneous breathing cycle (TOFR > 0.9) after adminis-
tering neostigmine (0.06 mg/kg), sugammadex (15 mg/kg),
or saline at a TOFR of 0.5 in rats. They found that rats being
administered neostigmine exhibited a smaller relative con-
tribution of diaphragm movement to the total change in
Table 2. Perioperative Management
Neostigmine (n = 47) Sugammadex (n = 46) P value
Preoperative ABGA
pH (mmHg) 7.4 ± 0.0 7.4 ± 0.0 0.269
PaO2 (mmHg) 91.6 ± 16.6 92.8 ± 18.7 0.742
PaCO2 (mmHg) 39.1 ± 4.3 37.3 ± 3.6 0.028
O2 saturation (%) 96.4 ± 3.0 96.5 ± 2.1 0.853
One lung ABGA
pH (mmHg) 7.4 ± 0.1 7.4 ± 0.1 0.078
PaO2 (mmHg) 114.6 ± 66.4 111.3 ± 61.8 0.805
PaCO2 (mmHg) 38.9 ± 4.1 39.0 ± 5.5 0.900
O2 saturation (%) 96.0 ± 3.9 96.0 ± 3.5 0.912
Two lung ABGA
pH (mmHg) 7.4 ± 0.0 7.4 ± 0.1 0.142
PaO2 (mmHg) 269.8 ± 118.4 257 ± 113.5 0.539
PaCO2 (mmHg) 36.4 ± 4.4 36.2 ± 5.0 0.993
O2 saturation (%) 99.7 ± 0.7 99.6 ± 0.8 0.686
Total vecuronium usage (mg/kg) 0.158 ± 0.063 0.156 ± 0.054 0.899
Anesthetic time (min) 320 (285, 350) 333 (295, 371) 0.102
Operation time (min) 245 (210, 275) 238 (210, 304) 0.361
Values are presented as mean ± SD or median (1Q, 3Q). ABGA: arterial blood gas analysis.
Table 3. Postoperative Complications
Neostigmine (n = 47) Sugammadex (n = 46) RD (95% CI) P value
Incidence of PPCs 19 (40.4) 15 (32.6) 0.08 (−0.12, 0.27) 0.434
Prolonged air leakage 5 (10.6) 2 (4.3) 0.06 (−0.04, 0.17) 0.435
Pneumonia 2 (4.3) 1 (2.2) 0.02 (−0.05, 0.09) 1.000
Atelectasis 14 (29.8) 8 (17.4) 0.12 (−0.05, 0.29) 0.160
Desaturation 5 (10.6) 6 (15.0) –0.07 (−0.21, 0.07) 0.348
Reintubation 1 (2.1) 0 (0.0) 0.02 (−0.02, 0.06) 1.000
Number of complications per patient (1/2/3) 13/4/2 11/4/0 0.379
Atrial fibrillation 3 (6.4) 1 (2.2) 0.04 (−0.04, 0.12) 0.617
Values are presented as number (%) or number only. RD: risk difference, 95% CI: 95% confidence interval, PPCs: postoperative pulmonary complications, PTE: pulmonary thromboembolism.
Table 4. Postoperative Care
Neostigmine (n = 47) Sugammadex (n = 46) P value
Duration of oxygen mask use (min) 210 (120, 370) 225 (120, 375) 0.913
Oxygen saturation 24 h after surgery (%) 99.2 ± 1.2 98.6 ± 1.9 0.062
Chest tube removal (d) 2.0 (2.0, 3.0) 2.0 (2.0, 3.0) 0.994
ICU LOS (d) 1.0 (1.0, 1.0) 1.0 (1.0, 1.3) 0.964
Postoperative hospital LOS (d) 7.0 (6.0, 10.0) 8.0 (7.0, 10.0) 0.431
Values are expressed as median (1Q, 3Q) or mean ± SD. ICU: intensive care unit, LOS: length of stay.
64 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
CVA
lung volume compared with sugammadex or saline. This
may be due to the effect of neostigmine on neuromuscular
transmission because the residually occupied acetylcho-
line receptors may decrease the efficiency of neuromuscu-
lar coupling at the diaphragm. In our research, the dose of
neostigmine was predetermined; a dose of 0.5 mg/kg above
the light block (TOFR > 0.4) may cause muscle weakness
in high-risk patients and may be associated with the occur-
rence of complications. Furthermore, the risk of cardiovas-
cular complications is also relatively high with neostigmine
because of hemodynamic changes caused by bradycardia
and cardiac arrhythmias [7]. However, theoretically,
sugammadex is a selective relaxant-binding agent and has
a lower risk of cardiopulmonary complications than a com-
bination of neostigmine and atropine [3,6,7,16]. Moreover,
sugammadex possibly reduces the time required for com-
plete recovery from NMB without increasing the incidence
of hypersensitivity or anaphylactic reactions, even in deep
blocks [16–18]. Furthermore, in a systematic review by Pa-
ton et al. [16], sugammadex was found to be more cost ef-
fective and potentially time-saving intraoperatively than
neostigmine. Thus, we theorized that sugammadex was ef-
fective in reducing the incidence of PPCs compared with
neostigmine, thereby helping to reduce the length of hos-
pital stay.
Nevertheless, the primary outcome of this study showed
no statistical significance regarding the effect of sugamma-
dex and neostigmine in the reversal of moderate to light
NMB after VATS lobectomy. In the present study, neuro-
muscular monitoring was performed until the end of anes-
thesia, as the drug dose was predetermined, owing to the
double-blind method. Administration of the reversal agent
was performed at the moderate to light block (over TOF
count 3) and observed when TOFR reached 0.9, which is
considered adequate recovery from NMB; this was fol-
lowed by tracheal extubation because tracheal extubation
at TOFR less than 0.9 was associated with more complica-
tions, including hypoxia, upper airway obstruction, oxygen
desaturation, micro-aspiration, and reintubation, than ex-
tubation at TOFR greater than 0.9 [8]. This would have con-
tributed to reducing the incidence of PRNMB after reversal
in the neostigmine group, resulting in reduced incidence of
PPCs. In addition, Togioka et al. [19] recently reported that
among the 200 older adults undergoing prolonged surgery
(high-risk subjects), there was no significant difference in
the incidence of PPCs between the sugammadex and
neostigmine groups (33% vs. 40%, respectively; odds ratio
= 0.74; 95% confidence interval = [0.40, 1.37]; P = 0.30).
They found that the contribution of reversal agent to de-
creased incidence of PPCs can be masked in the high-risk
population through the impact of the disease on the inci-
dence of complications. In the present study, the average
age of the patient group was 64 years, and the average op-
eration time was more than 3 h. In addition, the incidence
of PPCs in patients undergoing VATS lobectomy is as high
as 10–40% [20]. For these reasons, it is thought that the
contribution of sugammadex to the reduction of PPCs may
have been obscured by the high incidence of complica-
tions. Therefore, sugammadex did not show a statistical
difference in reducing the incidence of PPCs compared
with neostigmine (32.6% vs. 40.4%, respectively; risk differ-
ence = 0.08; 95% confidence interval = [−0.12, 0.27]; P =
0.434).
The secondary outcomes of this study showed no signifi-
cant differences between the two groups in terms of the
length of hospital stay, ICU admission, and chest tube re-
moval. This suggests that there was no significant differ-
ence between the effect of neostigmine and sugammadex
on the incidence of critical complications affecting the
length of hospital stay and ICU stay. In addition, the de-
partment of thoracic surgery at our hospital routinely per-
forms early chest tube removal to reduce pain and encour-
age early ambulation in order to reduce hospital stay, un-
less serious complications occur according to the ERAS,
which may have also affected our results [1,7].
There were a few limitations in our study. First, it was not
possible to confirm whether PRNMB was actually reduced
because neuromuscular monitoring was not performed in
the ICU after extubation. In addition, PRNMB and muscle
weakness were not evaluated; therefore, it was not possible
to confirm their correlation with PPCs.
In conclusion, in clinical use, the use of sugammadex in
reversing NMB at a minimum TOF count of 3 did not re-
duce the incidence of PPCs in patients undergoing VATS
lung lobectomy compared with neostigmine under quanti-
tative neuromuscular monitoring. In addition, there was
no difference in the duration of hospital and ICU stay be-
tween both groups. Therefore, more quantitative and large-
scale studies in patient groups or surgeries with high inci-
dence of complications are needed to demonstrate the
benefits of sugammadex as a NMB reversal agent in the
correlation between preoperative risk factors and PPCs.
www.anesth-pain-med.org 65
Sugammadex or neostigmine for lobectomy

ACKNOWLEDGEMENTS
This study was supported by Dong-A University.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: So Ron Choi. Data curation: Tae
Young Lee, Seong Yeop Jeong, Joon Ho Jeong. Formal anal-
ysis: Seong Yeop Jeong. Methodology: So Ron Choi. Project
administration: Joon Ho Jeong. Writing - original draft:
Seong Yeop Jeong. Writing - review & editing: Tae Young
Lee, Jeong Ho Kim. Investigation: Tae Young Lee. Resourc-
es: Jeong Ho Kim. Supervision: So Ron Choi.
ORCID
Tae Young Lee, https://orcid.org/0000-0002-9241-9735
Seong Yeop Jeong, https://orcid.org/0000-0002-9579-9278
Joon Ho Jeong, https://orcid.org/0000-0001-7586-5592
Jeong Ho Kim, https://orcid.org/0000-0003-4447-2838
So Ron Choi, https://orcid.org/0000-0002-4173-8939
REFERENCES
1. D'Andrilli A, Rendina EA. Enhanced recovery after surgery
(ERAS) and fast-track in video-assisted thoracic surgery (VATS)
lobectomy: preoperative optimisation and care-plans. J Vis
Surg 2018; 4: 4.
2. Gao S, Barello S, Chen L, Chen C, Che G, Cai K, et al. Clinical
guidelines on perioperative management strategies for en-
hanced recovery after lung surgery. Transl Lung Cancer Res
2019; 8: 1174-87.
3. Cho HC, Lee JH, Lee SC, Park SY, Rim JC, Choi SR. Use of
sugammadex in lung cancer patients undergoing video-assist-
ed thoracoscopic lobectomy. Korean J Anesthesiol 2017; 70:
420-5.
4. Schepens T, Cammu G. Neuromuscular blockade: what was, is
and will be. Acta Anaesthesiol Belg 2014; 65: 151-9.
5. Martinez-Ubieto J, Ortega-Lucea S, Pascual-Bellosta A, Ara-
zo-Iglesias I, Gil-Bona J, Jimenez-Bernardó T, et al. Prospective
study of residual neuromuscular block and postoperative re-
spiratory complications in patients reversed with neostigmine
versus sugammadex. Minerva Anestesiol 2016; 82: 735-42.
6. Hristovska AM, Duch P, Allingstrup M, Afshari A. The compar-
ative efficacy and safety of sugammadex and neostigmine in
reversing neuromuscular blockade in adults. A Cochrane sys-
tematic review with meta-analysis and trial sequential analysis.
Anaesthesia 2018; 73: 631-41.
7. Luo J, Chen S, Min S, Peng L. Reevaluation and update on effi-
cacy and safety of neostigmine for reversal of neuromuscular
blockade. Ther Clin Risk Manag 2018; 14: 2397-406.
8. Abad-Gurumeta A, Ripollés-Melchor J, Casans-Francés R, Es-
pinosa A, Martínez-Hurtado E, Fernández-Pérez C, et al. Evi-
dence Anaesthesia Review Group. A systematic review of
sugammadex vs neostigmine for reversal of neuromuscular
blockade. Anaesthesia 2015; 70: 1441-52.
9. Paech MJ, Kaye R, Baber C, Nathan EA. Recovery characteris-
tics of patients receiving either sugammadex or neostigmine
and glycopyrrolate for reversal of neuromuscular block: a ran-
domised controlled trial. Anaesthesia 2018; 73: 340-7.
10. Oh TK, Ryu JH, Nam S, Oh AY. Association of neuromuscular
reversal by sugammadex and neostigmine with 90-day mortal-
ity after non-cardiac surgery. BMC Anesthesiol 2020; 20: 41.
11. de Menezes CC, Peceguini LA, Silva ED, Simões CM. Use of
sugammadex after neostigmine incomplete reversal of rocuro-
nium-induced neuromuscular blockade. Rev Bras Anestesiol
2012; 62: 543-7.
12. Pühringer FK, Gordon M, Demeyer I, Sparr HJ, Ingimarsson J,
Klarin B, et al. Sugammadex rapidly reverses moderate rocuro-
nium- or vecuronium-induced neuromuscular block during
sevoflurane anaesthesia: a dose-response relationship. Br J
Anaesth 2010; 105: 610-9.
13. Şentürk M, Slinger P, Cohen E. Intraoperative mechanical ven-
tilation strategies for one-lung ventilation. Best Pract Res Clin
Anaesthesiol 2015; 29: 357-69.
14. Sasaki N, Meyer MJ, Malviya SA, Stanislaus AB, MacDonald T,
Doran ME, et al. Effects of neostigmine reversal of nondepolar-
izing neuromuscular blocking agents on postoperative respira-
tory outcomes: a prospective study. Anesthesiology 2014; 121:
959-68.
15. Schepens T, Cammu G, Maes S, Desmedt B, Vos W, Deseure K.
[Functional respiratory imaging after neostigmine- or sugam-
madex-enhanced recovery from neuromuscular blockade in
the anesthetised rat: a randomised controlled pilot study]. Rev
Bras Anestesiol 2017 67: 443-9. Portuguese.
16. Paton F, Paulden M, Chambers D, Heirs M, Duffy S, Hunter JM,
et al. Sugammadex compared with neostigmine/glycopyrro-
late for routine reversal of neuromuscular block: a systematic
review and economic evaluation. Br J Anaesth 2010; 105: 558-
66 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
CVA
67.
17. Min KC, Woo T, Assaid C, McCrea J, Gurner DM, Sisk CM, et al.
Incidence of hypersensitivity and anaphylaxis with sugamma-
dex. J Clin Anesth 2018; 47: 67-73.
18. An J, Kim E, Lee J, Kim H, Son J, Huh J, et al. Comparison of
sugammadex and pyridostigmine bromide for reversal of rocu-
ronium-induced neuromuscular blockade in short-term pedi-
atric surgery: a prospective randomized study. Anesth Pain
Med 2019; 14: 288-93.
19. Togioka BM, Yanez D, Aziz MF, Higgins JR, Tekkali P, Treggiari
MM. Randomised controlled trial of sugammadex or neostig-
mine for reversal of neuromuscular block on the incidence of
pulmonary complications in older adults undergoing pro-
longed surgery. Br J Anaesth 2020; 124: 553-61.
20. Agostini PJ, Lugg ST, Adams K, Smith T, Kalkat MS, Rajesh PB,
et al. Risk factors and short-term outcomes of postoperative
pulmonary complications after VATS lobectomy. J Cardiotho-
rac Surg 2018; 13: 28.
www.anesth-pain-med.org 67
Sugammadex or neostigmine for lobectomy

INTRODUCTION
Since establishment of the Korean Network for Organ
Sharing (KONOS) in 2000, allocation of deceased donor
livers had been performed according to patient status us-
ing Child-Turcotte-Pugh (CTP) score [1]. This system is
based on that of the United Network for Organ Sharing
(UNOS). Since 2002, UNOS has maintained an allocation
policy that relies on Model for End-stage Liver Disease
Corresponding author Gaab Soo Kim, M.D., Ph.D. Department of Anesthesiology and Pain Medicine, Samsung Medical Centre, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: 82-2-3410-0360Fax: 82-2-3410-0361E-mail: [email protected]
Background: The allocation policy for deceased donor livers in Korea was changed in June 2016 from Child-Turcotte-Pugh (CTP) scoring system-based to Model for End-stage Liver Dis-ease (MELD) scoring system-based. Thus, it is necessary to review the effect of allocation policy changes on anesthetic management.
Methods: Medical records of deceased donor liver transplantation (DDLT) from December 2014 to May 2017 were reviewed. We compared the perioperative parameters before and after the change in allocation policy.
Results: Thirty-seven patients underwent DDLT from December 2014 to May 2016 (CTP group), and 42 patients underwent DDLT from June 2016 to May 2017 (MELD group). The MELD score was significantly higher in the MELD group than in the CTP group (36.5 ± 4.6 vs. 26.5 ± 9.4, P < 0.001). The incidence of hepatorenal syndrome was higher in the MELD group than in the CTP group (26 vs. 7, P < 0.001). Packed red blood cell transfusion oc-curred more frequently in the MELD group than in the CTP group (5.0 ± 3.6 units vs. 3.4 ± 2.2 units, P = 0.025). However, intraoperative bleeding, vasopressor support, and postoper-ative outcomes were not different between the two groups.
Conclusions: Even though the patient’s objective condition deteriorated, perioperative pa-rameters did not change significantly.
Keywords: Liver transplant; Perioperative care; Tissue and oragan procurement; Unrelated donors.
Changes in the allocation policy for deceased donor livers in Korea: perspectives from anesthesiologists
Seung Yeon Yoo and Gaab Soo Kim
Department of Anesthesiology and Pain Medicine, Samsung Medical Center,
Sungkyunkwan University School of Medicine, Seoul, Korea
Received May 14, 2020Revised October 23, 2020 Accepted October 26, 2020
Clinical ResearchAnesth Pain Med 2021;16:68-74https://doi.org/10.17085/apm.20035pISSN 1975-5171 • eISSN 2383-7977
(MELD) score, and this practice has been adopted in many
countries to distribute deceased donor livers [2,3]. After
several years of research and simulation, the allocation
policy based on MELD score was implemented in Korea in
June 2016 [3].
Although debates remain on the association between
MELD score and surgical outcomes, the MELD score-
based allocation policy has led to a reduction in the num-
ber of new registrations on waiting lists, lower mortality,
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
68

KS
TA
shorter listing time, and an increase in the number of liver
transplantation (LT) without altering the overall graft and
patient survival rates after LT. As prioritization of recipients
has switched from time on the waiting list to the principle
of “sickest first”, the medical severity of recipient status has
increased [4,5]. Obviously, MELD score-based allocation
brings sicker patients to the operating room, and anesthet-
ic management of these patients might be more challeng-
ing. Therefore, it is necessary to review the effect of the al-
location policy change on anesthetic management of
transplant recipients.
The aim of the present study was to analyze and report
changes in patient status and anesthetic management be-
fore and after implementation of the MELD scoring system
at a single institution.
MATERIALS AND METHODS
After obtaining approval from the Institutional Review
Board (no. 2020-04-155), we retrospectively investigated
adult patients who underwent deceased donor liver trans-
plantation (DDLT) from September 2014 to May 2017. In-
cluded patients were divided into two groups according to
allocation policy. Multiple organ transplantation, pediatric
patients, and re-transplant cases were excluded. Thir-
ty-seven patients underwent transplantation before the
new allocation policy was adopted (CTP group) while 42
patients had surgery after the new allocation policy was
implemented (MELD group).
According to the overall surgical policy at our institution,
anastomosis of the liver graft was performed using a piggy-
back technique without a veno-venous bypass, and intra-
operative continuous renal replacement therapy (CRRT)
was not administered. A cell salvage device was used rou-
tinely during LT. Transfusion guidelines for the hospital
were hemoglobin 8 g/dl for packed red blood cells (RBCs),
hemoglobin 9 g/dl for cell salvage blood, prothrombin time
(PT) expressed as an international normalized ratio (INR)
3 for fresh frozen plasma (FFP), platelet count 30 K/μl for
platelet concentrate, and fibrinogen 80 mg/dl for cryopre-
cipitate.
Patient age, sex, MELD and CTP scores at the time of al-
location, prevalence of hepatorenal syndrome (HRS), pre-
operative use of CRRT, and primary liver disease were in-
vestigated. For intraoperative parameters, incidence of po-
tassium level > 4.5 mEq/L before reperfusion and base ex-
cess < –10 mEq/L during surgery, blood loss, transfusion
amount, operation time, and maximal vasoactive-inotropic
score (VISmax) were analyzed. Lengths of pre- and postop-
erative stays in intensive care units (ICU), postoperative
mechanical ventilation, and total hospital stay, along with
the one-year patient and graft survival rates were analyzed.
And the same parameters were analyzed by subdividing
each group into high ( > 30) and low MELD scores ( ≤ 30).
The amount of intraoperative blood loss was calculated
using the concept of red cell mass (RCM). Lost RCM (ml) =
estimated blood volume (ml) × (preoperative hematocrit
in % – postoperative hematocrit in %) + (transfused packed
RBCs in units × 213 × 70%) + (transfused cell salvage
blood in ml × 55%) [6]. The VISmax was calculated using the
following equation:
VISmax = dopamine dose (μg/kg/min) + dobutamine
dose (μg/kg/min) + 100 × epinephrine (μg/kg/min) + 10 ×
milrinone dose (μg/kg/min) + 10,000 × vasopressin dose
(U/kg/min) + 100 × norepinephrine dose (μg/kg/min) [7].
Continuous variables showing normality were analyzed
using Student t-test and are expressed as mean ± standard
deviation. Continuous variables that did not show normal-
ity were analyzed using Mann–Whitney U test and are ex-
pressed as median (1Q, 3Q). Categorical variables were
presented as number and frequency and were compared
using chi-square test or Fisher’s exact test. For all analyses,
a P value < 0.05 was considered statistically significant.
Statistical analyses were performed using IBM SPSS Statis-
tics software, version 25.0 (IBM Co., Armonk, NY, USA).
RESULTS
Table 1 summarizes the demographic characteristics of
the patients. Although there was no difference in CTP score
between the two groups, the MELD score was significantly
higher in the MELD group than in the CTP group (36.5 ±
4.6 vs. 26.5 ± 9.4, P < 0.001). The incidence of HRS also
was higher in the MELD group than in the CTP group (26
vs. 7, P < 0.001).
Intraoperative profiles are summarized in Table 2. Al-
though preoperative hemoglobin concentration was not
different between the two groups, the amount of packed
RBC transfusion was higher in the MELD group than in the
CTP group (5.0 ± 3.6 units vs. 3.4 ± 2.2 units, P = 0.025).
Only one case in the CTP group received transfusion-free
transplantation. The amount of blood loss, operation time,
and VISmax were not significantly different between the two
groups.
www.anesth-pain-med.org 69
Allocation policy changes and anesthesia

Pre- and postoperative ICU stay, total hospital stay, and
patient and graft survival rates are presented in Table 3; no
variables showed significant difference between the two
groups.
In subgroup analysis, MELD score was significantly high-
er in the MELD group with score both ≤ 30 (median value:
29 vs. 19.9 ± 5.7, P = 0.005) and > 31 (median value: 40 vs.
36 ± 2.3, P = 0.048). Patients with a MELD score less than
30 numbered 5 patients in the MELD group while 22 in the
CTP group (Fig. 1). Length of postoperative ICU stay was
significantly shorter in the MELD group with low MELD
score compared to the CTP group with low MELD score
(median: 4 days vs. 5.5 days, P = 0.023). All other variables
showed no significant difference (Tables 4, 5).
Table 1. Demographic Characteristics of the Patients
Variable MELD group (n = 42) CTP group (n = 37) P value
Age (yr) 50.8 ± 11.6 53.1 ± 1.3 0.377
Sex (M/F) 30/12 22/15 0.177
MELD score 36.5 ± 4.6 26.5 ± 9.4 < 0.001
CTP score 11.2 ± 1.8 10.7 ± 1.9 0.615
HRS 26 7 < 0.001
Preoperative CRRT 13 3 < 0.001
Primary liver disease
HBV-related 18 10
HCV-related 5 4
Alcohol-related 14 15
Others* 6 9
Values are presented as mean ± SD or number. MELD: Model for End-stage Liver Disease, CTP: Child-Turcotte-Pugh, HRS: hepatorenal syndrome, CRRT: continuous renal replacement therapy, HBV: hepatitis B virus, HCV: hepatitis C virus, NBNC: non-B, non-C, HCC: hepatocellular carcinoma. *Others include NBNC liver cirrhosis or HCC or autoimmune, unknown etc.
Table 2. Intraoperative Profiles of the Patients
Variable MELD group (n = 42) CTP group (n = 37) P value
Lost RCM (ml) 1,573.9 ± 1,400.1 1,472.2 ± 879.8 0.708
Transfused blood products
Packed RBC (units) 5.0 ± 3.6 3.4 ± 2.2 0.025
Fresh Frozen Plasma (units) 4 (2, 8) 4 (2, 6) 0.159
Platelet concentrate (units) 1 (0, 1) 1 (0.25, 1) 0.133
Cryoprecipitate (units) 6 (0, 6) 6 (0, 6) 0.990
Cell Saver (ml) 985.5 (686.5, 1,438.8) 1,179.5 (552.3, 2,102.3) 0.682
Operation time (min) 399.4 ± 92.5 388.9 ± 61.7 0.566
VISmax 38.0 ± 14.1 33.5 ± 14.3 0.170
Potassium > 4.5 mEq/L before reperfusion (%) 10 (23.8) 8 (21.6) 0.823
Base excess < –10 mEq/L during LT (%) 20 (47.6) 14 (37.8) 0.381
Values are presented as mean ± SD, median (1Q, 3Q), or number (%). MELD: Model for End-stage Liver Disease, CTP: Child-Turcotte-Pugh, RCM: red cell mass, RBC: red blood cell, VISmax: maximal vasoactive-inotropic score, LT: liver transplantation.
Table 3. Postoperative Profiles of the Patients
Variable MELD group (n = 42) CTP group (n = 37) P valuePreoperative ICU stay (d) 0 (0, 2.3) 0 (0, 2.8) 0.769
Postop ICU stay (d) 6 (4, 7.5) 6 (5, 7) 0.729
Postop MV (h) 36.9 ± 37.1 29.7 ± 41.8 0.451
Total hospital stay (d) 25.5 (19, 42.8) 23 (17.3, 33.5) 0.834
Graft loss 6 (14.3) 5 (13.5) 0.841
Patient survival, 1 year (%) 75.0 73.7 0.810
Values are presented as median (1Q, 3Q), mean ± SD, or number (%). MELD: Model for End-stage Liver Disease, CTP: Child-Turcotte-Pugh, ICU: Intensive care unit, MV: mechanical ventilation.
70 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
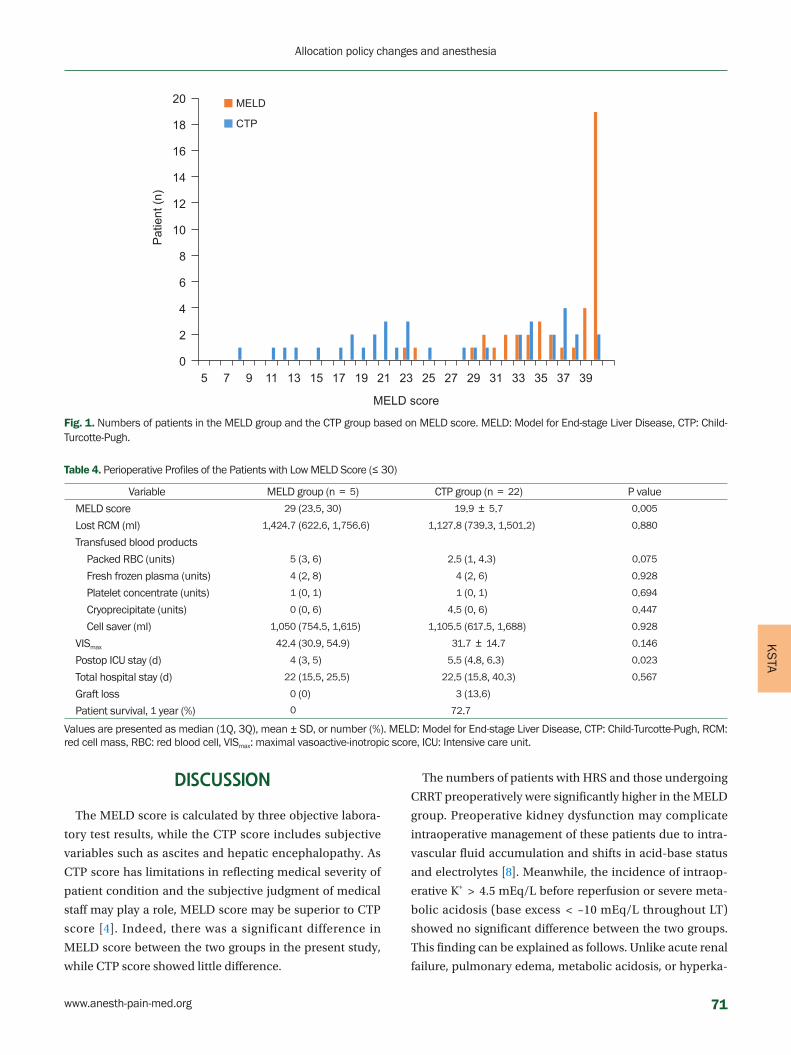
KS
TA
20
18
16
14
12
10
8
6
4
2
05 7 9 11 13 15 17 19
MELD score
Patie
nt (n
)
■ MELD
■ CTP
21 23 25 27 29 31 33 35 37 39
Fig. 1. Numbers of patients in the MELD group and the CTP group based on MELD score. MELD: Model for End-stage Liver Disease, CTP: Child-Turcotte-Pugh.
Table 4. Perioperative Profiles of the Patients with Low MELD Score (≤ 30)
Variable MELD group (n = 5) CTP group (n = 22) P value
MELD score 29 (23.5, 30) 19.9 ± 5.7 0.005
Lost RCM (ml) 1,424.7 (622.6, 1,756.6) 1,127.8 (739.3, 1,501.2) 0.880
Transfused blood products
Packed RBC (units) 5 (3, 6) 2.5 (1, 4.3) 0.075
Fresh frozen plasma (units) 4 (2, 8) 4 (2, 6) 0.928
Platelet concentrate (units) 1 (0, 1) 1 (0, 1) 0.694
Cryoprecipitate (units) 0 (0, 6) 4.5 (0, 6) 0.447
Cell saver (ml) 1,050 (754.5, 1,615) 1,105.5 (617.5, 1,688) 0.928
VISmax 42.4 (30.9, 54.9) 31.7 ± 14.7 0.146
Postop ICU stay (d) 4 (3, 5) 5.5 (4.8, 6.3) 0.023
Total hospital stay (d) 22 (15.5, 25.5) 22.5 (15.8, 40.3) 0.567
Graft loss 0 (0) 3 (13.6)
Patient survival, 1 year (%) 0 72.7
Values are presented as median (1Q, 3Q), mean ± SD, or number (%). MELD: Model for End-stage Liver Disease, CTP: Child-Turcotte-Pugh, RCM: red cell mass, RBC: red blood cell, VISmax: maximal vasoactive-inotropic score, ICU: Intensive care unit.
DISCUSSION
The MELD score is calculated by three objective labora-
tory test results, while the CTP score includes subjective
variables such as ascites and hepatic encephalopathy. As
CTP score has limitations in reflecting medical severity of
patient condition and the subjective judgment of medical
staff may play a role, MELD score may be superior to CTP
score [4]. Indeed, there was a significant difference in
MELD score between the two groups in the present study,
while CTP score showed little difference.
The numbers of patients with HRS and those undergoing
CRRT preoperatively were significantly higher in the MELD
group. Preoperative kidney dysfunction may complicate
intraoperative management of these patients due to intra-
vascular fluid accumulation and shifts in acid-base status
and electrolytes [8]. Meanwhile, the incidence of intraop-
erative K+ > 4.5 mEq/L before reperfusion or severe meta-
bolic acidosis (base excess < –10 mEq/L throughout LT)
showed no significant difference between the two groups.
This finding can be explained as follows. Unlike acute renal
failure, pulmonary edema, metabolic acidosis, or hyperka-
www.anesth-pain-med.org 71
Allocation policy changes and anesthesia

lemia is not common in HRS, except in cases of excessive
fluid therapy [9,10]. Any CRRT performed immediately be-
fore LT would partially adjust the acid-base balance and
electrolytes. Also, in line with another report from our in-
stitution, serum potassium level and metabolic acidosis
can be well controlled medically in recipients managed
with preoperative CRRT [11]. However, the presence of
HRS prior to transplantation is a strong predictor of mor-
tality after LT [12]. The prognosis for patients with cirrhosis
and renal failure is poor, and HRS is associated with the
worst prognosis [9]. Further study of the long-term out-
comes after the allocation policy change is required.
Prioritizing the sickest patients raises concerns, such as
increased risk of intraoperative bleeding and increased fre-
quency of transfusion. However, except for packed RBC
transfusion, this study found no significant difference in
patients following the allocation policy change. This result
is similar to those of another study in which MELD score
did not predict blood loss or blood product requirement
during LT [13]. In a study that evaluated the effect of the
MELD score-based allocation system in LT, increased
blood loss and transfusion rates were noted [14]. However,
consistent with our results, Varotti et al. [15] suggested that
MELD score is an independent variable associated with in-
creased perioperative packed RBC transfusion. In a study
by Frasco et al. [16], MELD score and preoperative fibrino-
gen concentration were independent predictors of transfu-
sion exposure. They detected significant differences in se-
verity of disease at the time of transplantation (as indicated
by a higher MELD score), degree of impairment of coagu-
lation function, and need for transfusion of RBCs and com-
ponent therapy by comparing living donor LT and cadaver-
ic donor LT [16]. This outcome may explain our findings of
increased packed RBC transfusion in the MELD group. The
causes of bleeding during LT can be multifactorial, and
there is a limit to predicting the amount of bleeding or
transfusion using only MELD score. Despite these limita-
tions and the relatively small sample size of this study, a
larger amount of packed RBC transfusion in the MELD
group may be a notable finding.
Preoperative INR in the MELD group was significantly
higher than that in the CTP group (3.45 ± 2.87 vs. 2.30 ±
0.83, P = 0.020). This result was not unexpected because
MELD score is calculated based on total bilirubin, INR, and
creatinine. However, surprisingly, there was no significant
difference in FFP transfusion rate between the two groups,
which may be partly explained by rebalanced hemostasis.
Multiple studies have shown that patients with cirrhosis
have deficiencies in both the pro-coagulant and anticoagu-
lant pathways, leading to a “rebalanced” coagulation sys-
tem [17–19]. The extent of coagulopathy as measured by PT
or INR does not appear predictive of bleeding complica-
tions, and the observed derangements in hemostatic vari-
ables might not translate to a diffuse bleeding risk during
LT [17,20]. However, prediction, prevention, and monitor-
ing of bleeding in patients with liver disease are complicat-
ed as a result of their extensive baseline changes and a
more precarious hemostatic system in these patients
[17,18]. Although some studies have reported no differenc-
es in bleeding or blood transfusion rates before or after us-
ing this coagulation testing [21], application of a viscoelas-
tic coagulation test for liver transplantation may be recom-
Table 5. Perioperative Profiles of the Patients with High MELD Score (> 30)
Variable MELD group (n = 37) CTP group (n = 15) P value
MELD score 40 (35, 40) 36 ± 2.3 0.048
Lost RCM (ml) 1,198.5 (907.5, 1,713.9) 1,730.9 (1,153.6, 2,482.6) 0.164
Transfused blood products
Packed RBC (units) 4 (3, 6.5) 4.5 (2, 6) 0.848
Fresh frozen plasma (units) 4 (2, 8) 6 (4, 6.5) 0.699
Platelet concentrate (units) 1 (0, 1) 1 (1, 1) 0.060
Cryoprecipitate (units) 6 (0, 6) 6 (3, 6.3) 0.473
Cell saver (ml) 965 (686, 1,440) 1,478 (292.5, 3,723.8) 0.473
VISmax 37.3 ± 14.2 36.3 ± 13.6 0.825
Postop ICU stay (d) 6 (5, 9.5) 6 (5, 8.8) 0.543
Total hospital stay (d) 28 (19, 45) 26 (18, 32.5) 0.627
Graft loss 6 (16.2) 2 (13.3) 0.891
Patient survival, 1 year (%) 64.9 66.7 0.443
Values are presented as median (1Q, 3Q), mean ± SD, or number (%). MELD: Model for End-stage Liver Disease, CTP: Child-Turcotte-Pugh, RCM: red cell mass, RBC: red blood cell, VISmax: maximal vasoactive-inotropic score, ICU: intensive care unit.
72 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
TA
mended to reduce the incidence of bleeding and blood
transfusion. This test has the advantage of reflecting the
overall process of coagulation, and it is more sensitive and
accurate at diagnosing coagulopathy than conventional
coagulation test performed during the surgery [22].
The VIS is a scale showing the amounts of vasoactive and
inotropic support [7]. We analyzed VISmax to identify any
change in vasopressor support during LT and found no sta-
tistically significant difference. However, Xia et al. [23] re-
ported that patients with a high ( > 30) MELD score re-
quired more vasopressors both before and during LT, al-
though they only indicated whether a vasopressor was ad-
ministered and did not specify the amount. VISmax was
higher in the high-MELD score patients in the CTP group
than in the low-MELD score patients, although the differ-
ence was not statistically significant (31.7 ± 14.7 vs. 36.3 ±
13.6, P = 0.071). Only five patients in MELD group had a
low MELD score, and the VISmax analysis in the MELD
group was limited. Further exploration with a larger sam-
ple size is necessary.
Giving priority to the sickest patient has the potential to
create other concerns such as longer ICU stay. Oberkofler
et al. [12] reported that MELD score greater than 23 was an
independent risk factor for morbidity represented by ICU
stay longer than 10 days. Oberkofler et al. [12] also found
that transfusion of more than seven units of packed RBCs
was an independent risk factor for mortality and prolonged
ICU stay. Otherwise, there was no significant difference in
duration of ICU stay in the present study. A similar group
of patients reported by our institution showed no signifi-
cant difference in six-month survival rate or in-hospital
stay, but complication and readmission rates within the
first three months were higher in the MELD group [24]. The
one-year survival rate analyzed in this study did not differ
significantly between the two groups. This finding is con-
sistent with the results of other studies that overall patient
survival after change to MELD scoring was not worse than
that based on the pre-MELD criteria [9,25,26].
This study had certain limitations. It utilized a retrospec-
tive study design based on single-center data and a small
sample size. Temporal changes in clinical practice would
have influenced the results beyond a change in allocation
system. In addition, demographics and underlying physi-
cal status of the donor and quality of the graft, which may
influence the need for transfusions and vasopressors, were
not addressed in the study. Also, the data included only
DDLT, so the results may differ in LDLT recipients.
Contrary to our expectations, although the patient’s ob-
jective condition worsened, perioperative parameters did
not change significantly. This outcome may be attributed
to advances in perioperative monitoring skills, improved
proficiency of surgeons, or more sophisticated ICU man-
agement. Our finding can also be explained by the shorter
postoperative ICU stay of the MELD group than that of the
CTP group in participants with low MELD score. Despite
these limitations, this topic is important, especially from
the anesthesiologist’s perspective. The parameters were
compared immediately before and after conversion to the
MELD score-based allocation system, and also were com-
pared by dividing the patients into groups according to
MELD score. In addition to the results shown by the pa-
rameters, it was clear that objective patient condition had
deteriorated, and that it is difficult to predict the patient
progress during LT. As a result, more detailed perioperative
care is required in the MELD era.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Gaab Soo Kim. Data acquisition:
Seung Yeon Yoo, Gaab Soo Kim. Data analysis: Seung Yeon
Yoo. Writing-original draft: Seung Yeon Yoo. Writing-re-
view & editing: Seung Yeon Yoo, Gaab Soo Kim.
ORCID
Seung Yeon Yoo, https://orcid.org/0000-0002-7226-4238
Gaab Soo Kim, https://orcid.org/0000-0002-1563-4482
REFERENCES
1. Korean Network for Organ Sharing (KONOS). Korean law and
regulation related with organ donation and transplantation.
Ministry of Health and Welfare [serial on the Internet]. 2013
[cited 2014 Nov 5]. Available from http://www.konos.go.kr.
2. Wiesner RH, McDiarmid SV, Kamath PS, Edwards EB, Malin-
choc M, Kremers WK, et al. MELD and PELD: application of
survival models to liver allocation. Liver Transpl 2001; 7: 567-
80.
3. Kim MS. Modification of emergency status in deceased donor
www.anesth-pain-med.org 73
Allocation policy changes and anesthesia

liver allocation: evidence for Korean Model of End-stage Liver
Disease (MELD) system. J Korean Soc Transplant 2016; 30: 51-
8.
4. Dutkowski P, Oberkofler CE, Béchir M, Müllhaupt B, Geier A,
Raptis DA, et al. The model for end-stage liver disease alloca-
tion system for liver transplantation saves lives, but increases
morbidity and cost: a prospective outcome analysis. Liver
Transpl 2011; 17: 674-84.
5. Bernardi M, Gitto S, Biselli M. The MELD score in patients
awaiting liver transplant: strengths and weaknesses. J Hepatol
2011; 54: 1297-306.
6. Bang SR, Ahn HJ, Kim GS, Yang M, Gwak MS, Ko JS, et al. Pre-
dictors of high intraoperative blood loss derived by simple and
objective method in adult living donor liver transplantation.
Transplant Proc 2010; 42: 4148-50.
7. Gaies MG, Gurney JG, Yen AH, Napoli ML, Gajarski RJ, Ohye
RG, et al. Vasoactive-inotropic score as a predictor of morbidity
and mortality in infants after cardiopulmonary bypass. Pediatr
Crit Care Med 2010; 11: 234-8.
8. Angeli P, Bezinover D, Biancofiore G, Bienholz A, Findlay J,
Paugam Burtz C, et al. Acute kidney injury in liver transplant
candidates: a position paper on behalf of the Liver Intensive
Care Group of Europe. Minerva Anestesiol 2017; 83: 88-101.
9. Ginès P, Schrier RW. Renal failure in cirrhosis. N Engl J Med
2009; 361: 1279-90.
10. Kwon S. Hepatorenal syndrome. Clin Mol Hepatol 2004; 10(3
Suppl): S57-66.
11. Kim HY, Lee JE, Ko JS, Gwak MS, Lee SK, Kim GS. Intraopera-
tive management of liver transplant recipients having severe
renal dysfunction: results of 42 cases. Ann Surg Treat Res 2018;
95: 45-53.
12. Oberkofler CE, Dutkowski P, Stocker R, Schuepbach RA, Stover
JF, Clavien PA, et al. Model of end stage liver disease (MELD)
score greater than 23 predicts length of stay in the ICU but not
mortality in liver transplant recipients. Crit Care 2010; 14:
R117.
13. Massicotte L, Beaulieu D, Roy JD, Marleau D, Vandenbroucke F,
Dagenais M, et al. MELD score and blood product require-
ments during liver transplantation: no link. Transplantation
2009; 87: 1689-94.
14. Massicotte L, Carrier FM, Karakiewicz P, Hevesi Z, Thibeault L,
Nozza A, et al. Impact of MELD score-based organ allocation
on mortality, bleeding, and transfusion in liver transplantation:
a before-and-after observational cohort study. J Cardiothorac
Vasc Anesth 2019; 33: 2719-25.
15. Varotti G, Santori G, Andorno E, Morelli N, Ertreo M, Strada P,
et al. Impact of Model for End-Stage Liver Disease score on
transfusion rates in liver transplantation. Transplant Proc 2013;
45: 2684-8.
16. Frasco PE, Poterack KA, Hentz JG, Mulligan DC. A comparison
of transfusion requirements between living donation and ca-
daveric donation liver transplantation: relationship to model
of end-stage liver disease score and baseline coagulation sta-
tus. Anesth Analg 2005; 101: 30-7.
17. Lisman T, Porte RJ. Rebalanced hemostasis in patients with liv-
er disease: evidence and clinical consequences. Blood 2010;
116: 878-85.
18. Lisman T, Porte RJ. Pathogenesis, prevention, and management
of bleeding and thrombosis in patients with liver diseases. Res
Pract Thromb Haemost 2017; 1: 150-61.
19. Henry Z, Northup PG. The rebalanced hemostasis system in
end-stage liver disease and its impact on liver transplantation.
Int Anesthesiol Clin 2017; 55: 107-20.
20. Hartmann M, Szalai C, Saner FH. Hemostasis in liver trans-
plantation: pathophysiology, monitoring, and treatment.
World J Gastroenterol 2016; 22: 1541-50.
21. Roullet S, Freyburger G, Cruc M, Quinart A, Stecken L, Audy M,
et al. Management of bleeding and transfusion during liver
transplantation before and after the introduction of a rotation-
al thromboelastometry-based algorithm. Liver Transpl 2015;
21: 169-79.
22. Park SY. Viscoelastic coagulation test for liver transplantation.
Anesth Pain Med (Seoul) 2020; 15: 143-51.
23. Xia VW, Du B, Braunfeld M, Neelakanta G, Hu KQ, Nourmand
H, et al. Preoperative characteristics and intraoperative trans-
fusion and vasopressor requirements in patients with low vs.
high MELD scores. Liver Transpl 2006; 12: 614-20.
24. Lee JA, Choi G, Kim JM, David Kwon CH, Joh JW. Comparison
study of outcomes of deceased donor liver transplantation be-
fore and after Korean Model for End-Stage Liver Disease
(MELD) system: single center experience. J Korean Soc Trans-
plant 2018; 32: 7-11.
25. Gonwa TA, McBride MA, Anderson K, Mai ML, Wadei H, Ahsan
N. Continued influence of preoperative renal function on out-
come of orthotopic liver transplant (OLTX) in the US: where
will MELD lead us? Am J Transplant 2006; 6: 2651-9.
26. Yadav SK, Saraf N, Saigal S, Choudhary NS, Goja S, Rastogi A, et
al. High MELD score does not adversely affect outcome of liv-
ing donor liver transplantation: experience in 1000 recipients.
Clin Transplant 2017; 31: e13009.
74 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
KS
TA
Hereditary angioedema (HAE) is a rare, life-threatening
autosomal dominant disorder caused by a deficiency of C1
esterase inhibitor (C1-INH), with an estimated prevalence
of 1:50,000 [1,2]. HAE can be classified by the levels of C1-
INH. Type I is diagnosed by low levels of C1-INH and C,
and type II is diagnosed by normal levels but dysfunctional
C1-INH [1,2]. HAE is potentially fatal because it may pres-
ent with sudden life-threatening edema of the skin and
Corresponding author Ki Tae Jung, M.D. Department of Anesthesiology and Pain Medicine, Chosun University Hospital, 365 Pilmun-daero, Dong-gu, Gwangju 61453, Korea Tel: 82-62-220 3223 Fax: 82-62-223-2333 E-mail: [email protected]
Background: Hereditary angioedema (HAE) is a rare disease caused by the deficiency of C1 esterase inhibitor. HAE has a risk of life-threatening complications such as capillary leak syn-drome (CLS) and disseminated intravascular coagulation (DIC).
Case: A 42-year-old male patient with HAE presented for deceased-donor kidney transplan-tation. Prophylactic fresh frozen plasma (FFP) was given before surgery because of the risk of edema development. With careful management during anesthesia, there were no prob-lems during surgery. However, generalized edema, hypotension, hypoalbuminemia, massive drainage of serosanguineous fluids from the intraabdominal space, and DIC occurred on the day after surgery. CLS was suspected and sustained hypotension with generalized edema became worse despite treatment with albumin, danazol, FFP, and vasoactive drugs. The pa-tient’s condition worsened despite intensive care and he died due to shock.
Conclusions: The anesthesiologist should prepare for the critical complications of HAE and prepare the appropriate treatment options.
Keywords: Capillary leak syndrome; Complement C1 inhibitor protein; Complement C1s; Disseminated intravascular coagulation; Hereditary angioedema; Kidney transplantation.
Capillary leak syndrome and disseminated intravascular coagulation after kidney transplantation in a patient with hereditary angioedema - A case report -
Jeong Wook Park1,2, Jinyoung Seo1, Sang Hun Kim1,3, and Ki Tae Jung1,3
1Department of Anesthesiology and Pain Medicine, Chosun University Hospital, 2Department of Medicine, Graduate School, Chosun University, 3Department of
Anesthesiology and Pain Medicine, School of Medicine, Chosun University,
Gwangju, Korea
Received December 22, 2020Revised January 10, 2021 Accepted January 12, 2021
Case ReportAnesth Pain Med 2021;16:75-80https://doi.org/10.17085/apm.20098pISSN 1975-5171 • eISSN 2383-7977
aerodigestive tract (face, extremities, larynx, genitals, and
trunk) recurrently or spontaneously [2,3]. Thus, patients
are recommended to avoid general anesthesia with endo-
tracheal intubation, or careful prophylactic therapies be-
fore surgery are required if surgery with general anesthesia
is unavoidable. Besides the well-known clinical presenta-
tions, HAE may also produce hypovolemic shock due to
the tissue leakage of fluids [4] and may lead to potentially
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
75

life-threatening conditions such as capillary leak syndrome
(CLS) and disseminated intravascular coagulation (DIC)
[5,6]. Here, we report a case of suspected CLS and DIC after
kidney transplantation in a patient with HAE. The Institu-
tional Review Board approved the study (CHOSUN 2020-
05-005) to publish in a case report and granted a waiver of
consent from the patient.
CASE REPORT
A 42-year-old male patient (height: 165 cm, weight: 61.7
kg) was admitted due to acute kidney injury with dyspnea.
He complained of swelling in the face and upper arms,
which occurred once or twice per year for 30 years. He
could not remember his familial history. During admis-
sion, the patient’s facial swelling got worse and HAE was
suspected. According to the laboratory results, the level of
C4 and C1-INH were 7.15 mg/dl (normal range: 10–40 mg/
dl) and 5.0 mg/dl (normal range: 21–39 mg/dl), respective-
ly. The patient was treated with high doses of androgen
therapy (Danazol, Young Poong Pharma, Korea; 600 mg
daily) as prophylactic maintenance therapy for the swelling
due to HAE. However, his kidney injury worsened and pro-
gressed to chronic kidney disease. A decision for kidney
transplant surgery was made, and he received hemodialy-
sis until surgery.
Seven months later, the patient was selected as the recip-
ient of a kidney from a deceased donor and emergency
surgery was planned. However, his level of C1-INH was still
low (15.7 mg/dl), and there was a risk of edema developing
during surgery. Thus, three units of fresh frozen plasma
(FFP) were administered about one hour before surgery
because C1-INH concentrate was not available due to the
suspension of imports in Korea, although it was designated
as an orphan drug. Anesthesia was induced with thiopen-
tal sodium (5 mg/kg) and cisatracurium (0.17 mg/kg).
Careful intubation by video-laryngoscopy was performed
with a 7.5 mm microcuffed endotracheal tube (Taper
Guard®, Mallinckrodt, Ireland). The cuff pressure was ad-
justed to 20 cmH2O using a cuff manometer (Mallinckrodt)
and confirmed air leakage at an airway pressure of more
than 20 cmH2O. Anesthesia was maintained with desflu-
rane and remifentanil, and mechanical ventilation was
done with a fresh gas flow of 3 L/min of an oxygen/air mix-
ture. His vital signs were maintained within 30% of the
baseline during surgery. The surgery took about four
hours. The administered fluid and estimated blood loss
were 1,000 ml and 400 ml, respectively. At the end of the
surgery, neuromuscular blockade was confirmed (train-of-
four > 99%) after the administration of reversal agents (10
mg of pyridostigmine and 0.4 mg of glycopyrrolate). After
confirming the absence of edema in the larynx by video-la-
ryngoscopy, early extubation with mask ventilation before
restoration of consciousness of the patient was done to
avoid irritation of the larynx. The patient recovered con-
sciousness and adequate respiration and was transferred
to the aseptic intensive care unit (ICU). Immunosuppres-
sants (tacrolimus and thymoglobulin), ganciclovir, and
prostaglandin E1 were administered according to the hos-
pital protocol. After surgery, his vital signs remained stable
and urine output was about 190 ml after reperfusion during
the hour in the ICU. During the night, his hemoglobin level
remained at 9.4 g/dl and there were no abnormalities in
the laboratory coagulation tests (platelet count, 202,000;
prothrombin time [PT], 11.5 s; activated partial thrombo-
plastin time [aPTT], 20.7 s; and international normalized
ratio [INR], 1.04).
The next morning, the patient complained of dyspnea
with abdominal discomfort. Then, hypotension (60/30
mmHg) and tachycardia (130 beats/min) developed, and
he lost consciousness (Fig. 1). He was intubated and me-
chanical ventilation was applied, and norepinephrine and
dobutamine were administered for the treatment of hypo-
tension. At that time, abdominal distension with massive
serosanguineous fluids ( > 1,000 ml) in the drainage was
found and generalized edema with low urine output (10 ml
over eight hours) was also observed. He showed a low he-
moglobin level (7.3 g/dl) with coagulopathy (PT, 22.8 s;
aPTT, 44.1 s: and INR, 2.04), and DIC was diagnosed (fi-
brinogen < 100 mg/dl; fibrin degradation product, FDP
221 μg/ml: and D-dimer, 27,699 ng/ml). Thus, transfusion
was performed (red blood cells six units; FFP, three units;
cryoprecipitate 10 units: and apheresis platelets, one unit),
and continuous renal replacement therapy (CRRT) was ap-
plied. Despite the treatments, there was no improvement
in his conditions, and an emergency second-look opera-
tion was performed with the suspicion of leakage at the
anastomosis site. However, there was no anastomosis leak-
age and normal blood flow to the kidney was confirmed by
Doppler. Thus, the operation ended without specific treat-
ment.
However, severe generalized edema with hypoalbumin-
emia (2.5 g/dl) was sustained after surgery, although the
C1-INH level had increased to 22.9 mg/dl after the contin-
76 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
TA
Preparing emergency kidney transplantation
- Danazol 400 mg PO- FFP 3U transfusionEmergency Operation - DDKT
Treatment
Diagnosed hereditary angioedema- Danazol 400 mg oral medication
Generalized edemaUrine output (−)Disseminated intravascular coagulationLoss of consciousness
Hypotension (60/30 mmHg)Tachycardia (130 beats/min)Serosanguineous drainage
(> 1,000 ml/day)
PneumoniaPulmonary edemaRejection of transplanted kidneySustained severe hypotension- No responese to hemodynamic drugs
DNARDeath
CRRT started Intubation - Mechanical ventilationTransfusion
Emergency second look operation- No anastomosis leakage- Normal blood flow to kidney
(Doppler)
6 months before
operationOperation POD #1 POD #2 POD #3 POD #4 POD #5
C1-INH (mg/dl) 5.0 15.7 22.9
Hb (g/dl) 12.9 7.3 10.6 10.5 9.4 7.8
WBC (x103/μl) 6.55 6.36 19.31 12.85 12.1 0.52
Albumin (g/dl) 4.26 2.5 2.82 2.79 2.43 2.31
BUN (mg/dl) 64.5 26.6 35.6 19.5 20.1 18.7
Creatinine (mg/dl) 14.42 7.76 9.64 3.41 3.2 2.01
Coagulation test
PT 11.5 22.8 25.3 25.4 29.3
INR 1.04 2.04 2.26 2.27 2.61
a-PTT 20.7 44.1 30.7 37.1 54.2
Fibrinogen (mg/dl) < 100 169 131 126 123
FDP (μl/ml) 221 216 230 105 33.5
D-dimer (ng/ml) 27,699 26,626 12,983 3,855
Input
Crystalloid (ml) 2,000 3,130 10,820 8,980 13,230
FFP (unit) 4 3 2 2
RBC (unit) 6 4 2
20% Albumin 2 2 2 2 2
Output 1,049 3,017 5,815 6,364 4,725
Urine output (ml) 190 10 30 30 15
Drainage (ml) 859 > 1,000 1,305 1,506 1,394
CRRT (ml) 2,007 4,480 4,828 3,316
Danazol 400 mg PO
Ganciclovir, Tacrolimus, Prostaglandin E1, Thymoglobulin
CRRT, Mechanical ventilation
Hypotension management with norepinephrine, dobutamine
Transfusion (RBC, FFP, Platelet, Cryoprecipitate)
20% Albumin x2/day
Fig. 1. Course and treatment of the patient after surgery. A patient with hereditary angioedema who was treated with danazol presented for deceased-donor kidney transplantation. Generalized edema with hypoalbuminemia developed the day after surgery and severe hypotension occurred. Despite intensive care, the patient died due to shock. DDKT: deceased-donor kidney transplantation, FFP: fresh frozen plasma, CRRT: continuous renal replacement therapy, DNAR: Do-Not-Attempt-Resuscitation, C1-INH: C1 esterase inhibitor, Hb: hemoglobin, WBC: white blood cells: BUN: blood urine nitrogen, PT: prothrombin time, INR: international normalized ratio, aPTT: activated partial thromboplastin time, FDP: fibrinogen degradation products, RBC: red blood cell, POD: postoperative day.
www.anesth-pain-med.org 77
HAE attack after kidney transplantation

uous administration of 20% albumin, danazol at 400 mg via
a Levin tube, and FFP transfusions. We thought that the
worsening of the patient’s condition despite increases in
the C1-INH level was due to harmful substrate proteins in
the FFP, and would be transient. The laboratory blood cul-
ture results showed no evidence of bacterial growth. De-
spite intensive care with hypotensive drugs, transfusions,
and CRRT, his condition worsened because of sustained
generalized edema with hypoalbuminemia, coagulopathy,
and DIC. On the fourth day after the surgery, pulmonary
edema, pneumonia, and rejection of the transplanted kid-
ney developed and sustained severe hypotension without
response to hemodynamic drugs was seen. The patient's
guardians did not want any additional treatment and the
patient died because of shock after a day.
DISCUSSION
The complement system contributes to the immunologi-
cal defense mechanism of the body. HAE is caused by a
SERPING1 gene (Serine Protease Inhibitor Gene 1 present
on the Long Arm of Chromosome 11 [11q]) defect, which
results in decreased or dysfunctional C1-INH [1–3]. Al-
though HAE attacks are unpredictable and the triggering
factors are unclear, numerous physical stimuli such as den-
tal and surgical procedures, emotional stress, infections,
and medications can be triggering factors of life-threaten-
ing angioedema [1–3]. Still, there are no definite periopera-
tive guidelines for the prophylaxis of an HAE attack. How-
ever, the following prophylactic therapy is usually suggest-
ed: C1-INH concentrate, 1,000 units before surgery; andro-
gens such as danazol (400 to 600 mg/day), five days before
and five days after surgery or a procedure; and FFP (two
units for adults, 10 ml/kg in children), one to two hours be-
fore surgery [1–3]. Among those treatments, C1-INH con-
centrate or androgens is known to have the best effect.
Tranexamic acid can also be used for long-term prophylax-
is, especially in children, but it has not been recommended
recently because it has little benefit as short-term prophy-
laxis or for the acute treatment of HAE attacks due to its
delayed onset of action [7]. However, some patients under-
go HAE attacks after surgical procedures despite prophy-
laxis. Thus, careful approaches to the patient with rescue
management are required [3].
The patient in our case was diagnosed with type I HAE
with low levels of C1-INH and C4, and we used the prophy-
lactic administration of FFP instead of C1-INH concentrate
before surgery because it was not available in Korea. De-
spite prophylactic treatment with FFP, generalized edema
developed in the patient, and the catastrophic outcome of
DIC developed. We will discuss the possible causes of the
deterioration of the patient's condition.
C1-INH plays an important role in the regulation of not
only the classical pathway of the immune system but also
the plasminogen-plasmin and kallikrein-kinin systems
(contact system), and coagulation/fibrinolysis [8]. The de-
ficiency or dysfunction of C1-INH in patients with HAE
predominantly results in the increased activation of brady-
kinin by kallikrein, which leads to vasodilation, an increase
in vascular permeability, and the typical angioedema of
HAE. In patients with HAE, C3 and C1/C1-inhibitor com-
plexes are easily activated by physical stress [9]. Especially,
complement activation is associated with ischemia/reper-
fusion injury during cold storage of the organ and rejec-
tion, and is considered the major factor in graft failure after
transplantation by triggering tissue damage and interfering
with the anticoagulant and fibrinolytic capacity of the vas-
cular endothelium [10]. Our patient was a kidney trans-
plant recipient with the possibility of increased activation
of the immune system. Therefore, it is thought that the reg-
ulation of complement activation would not be achieved
after major surgery because of C1-INH deficiency in our
patient, resulting in the acute rejection of the transplanted
kidney by excessive complement activation.
CLS is one of the common complications associated with
low C1-INH activity [10]. CLS is characterized by hypoten-
sion or multi-organ failure by massive third-space loss of
fluids due to increased capillary permeability, which is ac-
companied by extravasation and diffuse edema. We con-
sidered CLS as the cause of the sustained hypotension be-
cause of the distinguishing features such as generalized
edema with hypoalbuminemia despite albumin treatment,
massive drainage of serosanguineous fluids from the in-
traabdominal space without anastomosis leakage, and the
absence of anaphylaxis or sepsis, which should be ruled
out due to similar characteristics [11]. Treatment for the
prevention of antibody-mediated rejection after kidney
transplantation has the potential risk for developing CLS
[3].
C1-INH also plays a significant role in both coagulation
and fibrinolysis [8]. The activation of C1-INH leads to
thrombin generation and plasmin inhibition, which ac-
counts for about 15% of the fibrinolysis. Hence C1-INH de-
ficiency can lead to pathologic thrombosis. Generally, HAE
78 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
TA
is not associated with coagulation properties clinically.
However, there is a possibility that C1-INH deficiency
might affect the coagulation system in the pathologic con-
dition. Kodama et al. [12] revealed that the symptom of an
HAE attack in older adults was hypercoagulation because
activation of the complement system mainly activates the
tissue factor pathway instead of the kallikrein-kinin system.
Such physiologic changes with aging lead to the generation
of thrombin and the activation of antithrombin-III during
an HAE attack, which precipitates DIC. The hypercoagula-
bility of pregnancy and intravascular fluid depletion due to
increased vascular permeability during an HAE attack may
also contribute to the development of DIC [6]. In our pa-
tient, DIC developed simultaneously from the severe intra-
vascular volume depletion in the HAE attack. The de-
creased hemoglobin level due to DIC was misinterpreted
as anastomosis leakage and interfered with the diagnosis
of CLS.
In the treatment of acute HAE attacks, C1-INH concen-
trate, ecallantide (a kallikrein inhibitor) and icatibant (a
bradykinin B2-receptor antagonist) are recommended as
the first-line drugs [7]. However, as mentioned above, none
of those drugs were available in Korea at that time, and it
was very regrettable that they could not be administered to
the patient. The administration of C1-INH concentrate re-
stores the inhibitory action of complement system by cor-
recting the C1-INH deficiency or dysfunction. Also, C1-
INH concentrate is generally well-tolerated in the treat-
ment of CLS after kidney transplantation caused by the
preventive treatment of antibody-mediated rejection [11].
Daily intravenous infusions of C1-INH concentrate also
showed effectiveness in patients with HAE accompanied
by ascites, hypovolemic shock, and renal and respiratory
failure who did not tolerate conventional ICU treatment [5].
Moreover, C1-INH concentrate is considered a multifunc-
tional regulator of the cascade systems, which were recent-
ly shown to improve graft function by inhibiting comple-
ment activation and reducing the postoperative inflamma-
tion [10]. Our patient would have been better if he was
treated with C1-INH concentrate. Fortunately, icatibant
has recently become available in Korea and is thought to
help severe HAE attacks like that of our patient because it
can mediate vasodilatation and increase capillary permea-
bility by preventing the receptor binding of bradykinin [7].
The use of FFP should only be considered when the first-
line drugs are not available in an HAE attack. FFP is known
as an effective substitute for C1-INH concentrate during
HAE because it contains C1-INH. However, FFP may wors-
en the symptoms paradoxically because it contains not
only C1-INH but also other substrates such as kininogens
[3]. Therefore, the anesthesiologist should monitor the pa-
tient’s condition during an HAE attack treated with FFP.
There is a possibility that the poor outcome of our patient
despite the increase in C1-INH levels after the massive
transfusion of FFP was due to the increase in harmful sub-
strates administered in the FFP. Unfortunately, our patient
had no option for treatment except FFP.
In conclusion, HAE is a disease with a decrease or dys-
function of C1-INH, which may lead to life-threatening
complications such as CLS and DIC. Careful prophylactic
therapy with androgen, FFP, and C1-INH concentrates is
essential before surgery. However, in stressful conditions
such as organ transplantation, HAE attacks may occur de-
spite prophylactic treatment and produce fatal complica-
tions such as hypovolemic shock due to CLS and DIC. C1-
INH concentrate may be an important option for severe
HAE attacks. We experienced a case of suspected CLS and
DIC after kidney transplantation in a patient with HAE.
Unfortunately, we could not use C1-INH concentrate for
the patient at the appropriate time. In Korea, C1-INH con-
centrate is not available. However, the use of recently
proved icatibant might help treat a severe HAE attack. If
those first-line drugs are not available, FFP should be used
with careful monitoring. The anesthesiologist should un-
derstand the critical complications of HAE and prepare the
appropriate treatment options.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Ki Tae Jung. Data acquisition: Jeong
Wook Park, Jinyoung Seo. Supervision: Ki Tae Jung. Writ-
ing—original draft: Jeong Wook Park, Jinyoung Seo, Ki Tae
Jung. Writing—review & editing: Sang Hun Kim, Ki Tae
Jung.
ORCID
Jeong Wook Park, https://orcid.org/0000-0002-3990-4715
Jinyoung Seo, https://orcid.org/0000-0002-5256-6132
www.anesth-pain-med.org 79
HAE attack after kidney transplantation

Sang Hun Kim, https://orcid.org/0000-0003-3869-9470
Ki Tae Jung, https://orcid.org/0000-0002-2486-9961
REFERENCES
1. Zuraw BL. Clinical practice. Hereditary angioedema. N Engl J
Med 2008; 359: 1027-36.
2. Vilaça MJL, Coelho FM, Faísco A, Carmona C. [Anesthetic con-
siderations for a patient with hereditary angioedema - a clini-
cal case]. Rev Bras Anestesiol 2017 67: 541-3. Portuguese.
3. Williams AH, Craig TJ. Perioperative management for patients
with hereditary angioedema. Allergy Rhinol (Providence) 2015;
6: 50-5.
4. Cohen N, Sharon A, Golik A, Zaidenstein R, Modai D. Heredi-
tary angioneurotic edema with severe hypovolemic shock. J
Clin Gastroenterol 1993; 16: 237-9.
5. Pham H, Santucci S, Yang WH. Successful use of daily intrave-
nous infusion of C1 esterase inhibitor concentrate in the treat-
ment of a hereditary angioedema patient with ascites, hypovo-
lemic shock, sepsis, renal and respiratory failure. Allergy Asth-
ma Clin Immunol 2014; 10: 62.
6. Oguma K, Suzuki T, Mano S, Takeuchi S, Takeda J, Maruyama Y,
et al. Hereditary angioedema with deep vein thrombosis and
pulmonary thromboembolism during pregnancy. Taiwan J
Obstet Gynecol 2019; 58: 895-6.
7. Maurer M, Magerl M, Ansotegui I, Aygören-Pürsün E, Betschel
S, Bork K, et al. The international WAO/EAACI guideline for
the management of hereditary angioedema-the 2017 revision
and update. Allergy 2018; 73: 1575-96.
8. Levi M, Cohn DM, Zeerleder S. Hereditary angioedema: link-
ing complement regulation to the coagulation system. Res
Pract Thromb Haemost 2018; 3: 38-43.
9. Nielsen EW, Johansen HT, Gaudesen O, Osterud B, Olsen JO,
Høgåsen K, et al. C3 is activated in hereditary angioedema,
and C1/C1-inhibitor complexes rise during physical stress in
untreated patients. Scand J Immunol 1995; 42: 679-85.
10. Kirschfink M. C1-inhibitor and transplantation. Immunobiolo-
gy 2002; 205: 534-41.
11. Ramirez-Sandoval JC, Varela-Jimenez R, Morales-Buenrostro
LE. Capillary leak syndrome as a complication of anti-
body-mediated rejection treatment: a case report. CEN Case
Rep 2018; 7: 110-3.
12. Kodama J, Uchida K, Kushiro H, Murakami N, Yutani C. Hered-
itary angioneurotic edema and thromboembolic diseases: I:
how symptoms of acute attacks change with aging. Intern Med
1998; 37: 440-3.
80 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
INTRODUCTION
Chronic musculoskeletal pain is defined as pain that
lasts for three to six months or beyond the time of normal
healing [1]. Musculoskeletal disorders are the most com-
mon source of chronic musculoskeletal pain, and their in-
Corresponding author Yunhee Lim, M.D., Ph.D. Department of Anesthesiology and Pain Medicine, Sanggye Paik Hospital, Inje University College of Medicine, 1342 Dongil-ro, Nowon-gu, Seoul 01757, Korea Tel: 82-2-350-1176Fax: 82-2-950-1323 E-mail: [email protected]
Background: Prolotherapy, which stimulates the healing of loosened ligaments and ten-dons, is a cost-effective and safe treatment modality for chronic musculoskeletal pain. Its benefits may be affected by injection protocols, comparative regimens, and evaluation scales. The aim of this study was to determine the effectiveness of dextrose prolotherapy as a long-term treatment for chronic musculoskeletal pain.
Methods: Medline, Embase, Cochrane Central, KoreaMed, and KMbase databases were searched for studies published up to March 2019. We included randomized controlled trials which compared the effect of dextrose prolotherapy with that of other therapies such as ex-ercise, saline, platelet-rich plasma, and steroid injection. The primary outcome was pain score change during daily life.
Results: Ten studies involving 750 participants were included in the final analysis. Pain scores from 6 months to 1 year after dextrose prolotherapy were significantly reduced com-pared to saline injection (standardized mean difference [SMD] –0.44; 95% confidence inter-val [CI] –0.76 to –0.11, P = 0.008) and exercise (SMD –0.42; 95% CI –0.77 to –0.07, P = 0.02). Prolotherapy yielded results similar to platelet-rich plasma or steroid injection, that it showed no significant difference in pain score.
Conclusions: Dextrose prolotherapy is more effective in the treatment of chronic pain com-pared to saline injection or exercise. Its effect was comparable to that of platelet-rich plasma or steroid injection. Adequately powered, homogeneous, and longer-term trials are needed to better elucidate the efficacy of prolotherapy.
Keywords: Musculoskeletal pain; Platelet-rich plasma; Prolotherapy; Steroids.
Prolotherapy for the patients with chronic musculoskeletal pain: systematic review and meta-analysis
Geonhyeong Bae, Suyeon Kim, Sangseok Lee, Woo Yong Lee, and Yunhee Lim
Department of Anesthesiology and Pain Medicine, Sanggye Paik Hospital, Inje University
College of Medicine, Seoul, Korea
Received September 23, 2020Revised October 14, 2020 Accepted October 16, 2020
Clinical ResearchAnesth Pain Med 2021;16:81-95https://doi.org/10.17085/apm.20078pISSN 1975-5171 • eISSN 2383-7977
creasing prevalence has led to a need for effective non-sur-
gical solutions, such as physical therapy, pharmacologic
treatment, and injection-based treatment [2]. Injection
therapies can be introduced when pain or functional lim-
itations are significant despite oral medication or exercise
[3]. Corticosteroid injections are the most common regi-
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
81

men for musculoskeletal disorders; they provide short-
term symptomatic improvement, but aggravate cartilage
damage, thus increasing the risk of tissue atrophy [4].
Therefore, physicians have become interested in alterna-
tive injectants, such as prolotherapy or platelet-rich plasma
(PRP) [5].
Prolotherapy is a nonsurgical regenerative injection
technique that administers small amounts of an irritant
solution to the degenerated tendon insertions (entheses),
joints, ligaments, and adjacent joint spaces over a series of
several treatment sessions [6–8]. The mechanism of action
behind prolotherapy is not completely understood, but the
current theory is that the injected proliferate causes a heal-
ing process that is similar to the body’s natural healing pro-
cess, whereby a local inflammatory cascade is initiated,
which triggers the release of growth factors and collagen
deposition [2]. To date, many studies which support the
benefits of the use of prolotherapy in patients with chronic
musculoskeletal pain have been reported [9,10]. However,
few meta-analyses have analyzed the effect of prolotherapy
in patients with chronic musculoskeletal pain. Therefore,
we designed a meta-analysis to evaluate the effect of pro-
lotherapy in the treatment of chronic musculoskeletal pain
and compare the effect of prolotherapy with other treat-
ments.
MATERIALS AND METHODS
Study design
This meta-analysis was performed according to the rec-
ommendations of the PRISMA and Cochrane Collabora-
tion. The protocol was registered with PROSPERO (no.
CRD42019130609).
Information sources and search strategy
Two reviewers (WL, YL) systematically searched elec-
tronic databases such as Medline, Embase, and the Co-
chrane Library (CENTRAL) with no limitations on the year
of publication. Additionally, KoreaMed (https://koreamed.
org) and KMbase (http://kmbase.medric.or.kr) were used
to search for manually relevant domestic articles. Broad
search terms such as “prolotherapy”, “chronic osteoarthri-
tis”, and “randomized controlled trials”, were included to
achieve higher sensitivity, and Medical Subject Heading
(MeSH) terms were used. The languages of the articles
were limited to Korean and English. The last search was
conducted on March 10, 2019.
We did not search grey literature, despite its important
contribution to a systematic review, because we wanted to
present an effective basis for treatment to clinicians with as
little bias as possible, based on the results of RCTs.
Study selection and eligibility criteria
All relevant studies were independently screened by two
reviewers (WL and YL). Selection of relevant articles was
done primarily at the title and abstract level, then after at
the full-text level. Studies for the final assessment were se-
lected based on the agreement of the two reviewers. Any
disagreement was resolved by discussion with a third re-
viewer (SL).
Studies were included in the meta-analysis if they satis-
fied the following criteria: (1) patients with chronic muscu-
loskeletal pain lasting for more than 3 months; (2) pro-
lotherapy using dextrose for any joints, tendon, and/or lig-
aments; (3) results of the non-prolotherapy group were re-
ported; and (4) the post-injection pain score was reported
as the primary outcome.
Studies were excluded for the following reasons: (1) use
of prolotherapy solutions containing anything other than
glucose (polidocanol, manganese, zinc, human growth
hormone, phenol-glucose-glycerine, pumice, ozone, glyc-
erin, phenol, PRP, bone marrow, lipoaspirate, stem cells, or
sodium morrhuate); (2) injection into the epidural space;
(3) did not report appropriate outcomes or outcome mea-
surements as mentioned; (4) non-randomized controlled
trials; (5) non-human studies; (6) articles not in English or
Korean.
Risk of bias in individual studies
Two independent authors (WL and YL) reviewed the ar-
ticles to assess the risk of bias (ROB) using the ROB tool
provided in the Review Manager software version 5.3 (The
Cochrane Collaboration, UK) based on Cochrane’s assess-
ment of the risk of bias [11]. If necessary, a third reviewer
(SL) was included in the discussion to sort out the dis-
agreements. The following eight domains were used to as-
sess the risk of bias in each trial: random sequence genera-
tion (selection bias), allocation concealment (selection
bias), blinding of participants and personnel (performance
bias), blinding of outcome assessment (detection bias), in-
82 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
complete outcome data (attrition bias), selective reporting
(reporting bias), and other bias. The methodology for each
trial was graded as “high”, “low”, or “unclear” to reflect a
high risk of bias, low risk of bias, or uncertainty of bias, re-
spectively. The agreement between the two independent
reviewers for the level of risk of bias regarding the eight do-
mains was assessed using Cohen’s kappa. Kappa values
were interpreted as follows: 1) less than 0: less than chance
agreement, 2) 0.01 to 0.20: slight agreement, 3) 0.21 to 0.40:
fair agreement, 4) 0.41 to 0.60: moderate agreement, 5) 0.61
to 0.80: substantial agreement, and 6) 0.8 to 0.99: almost
perfect agreement.
Data collection process and extracted items
Two authors (WL and YL) extracted data from the origi-
nal articles, and another author (SL) independently con-
firmed all of the extracted data. The general characteristics
(i.e., the study design, publication year, and name of the
first author), intervention types and methods, and out-
comes were extracted for each study based on the inclu-
sion criteria. Each method of the intervention, such as the
prolotherapy regimen, interval, and duration, was extract-
ed. The measured outcomes included the number of pa-
tients analyzed in each group, tools for pain assessment,
and pain scores.
The main outcome was determined by the severity of the
pain, derived from the results of the pain scale. The first
priority of pain measurement extraction was the pain score
for 6 months to 1 year. To assess the effectiveness of dex-
trose prolotherapy, we used the standardized mean differ-
ence of pain scores between the prolotherapy group and
other comparator groups using exercise, saline, PRP, and
steroid injection.
Subgroup analysis
We grouped the analyses of VAS for pain into less than
three months, three to six months, and more than six
months while registering our review in PROSPERO. How-
ever, we were unable to classify the subgroups as originally
planned because not all the individual studies followed the
patients and reported the resulting variables on these crite-
ria. Using the common denominator of the results of the
individual studies, we were able to synthesize results that
could be divided into three subgroups: baseline to 1
month, 1 month to 3 months, and 6 months to 1 year.
Statistical analysis
Continuous data (e.g., post-injection pain scores) were
pooled as standardized mean differences (SMDs) because
different outcome measurement scaling was expected
across trials. We also calculated the 95% confidence inter-
vals (CIs) for all estimates. A random-effect model was
used to pool the study results, taking into account possible
variations in effect sizes across trials. The heterogeneity
statistic Cochrane Q and its corresponding degrees of free-
dom (df) and P value, as well as Higgins’ I2 as a measure of
heterogeneity were calculated. P values < 0.05 were con-
sidered to be representative of statistically significant het-
erogeneity, and I2 values > 50% were considered to repre-
sent significant heterogeneity. Post-hoc subgroup analyses
were performed where possible for each outcome to ex-
plore heterogeneity based on the different sites of injec-
tion. Chi-squared tests for heterogeneity were performed
to identify differences between subgroups. Publication bias
was not evaluated because only a few ( < 10) studies were
included in this meta-analysis. We conducted a sensitivity
analysis to evaluate the influence of each study on the
long-term (six months to one year) therapeutic effect of
prolotherapy compared with saline by excluding one trial
at a time from the pooled effects. All analyses were per-
formed using R 3.51 (R Foundation for Statistical Comput-
ing, Austria) and Review Manager (RevMan, version 5.3,
The Cochrane Collaboration).
RESULTS
Study selection and characteristics
We retrieved 680 articles after the initial database search:
Medline (n = 250), EMBASE (n = 64), CENTRAL (n = 168),
and Korean databases (n = 198).
After excluding 567 duplicate articles, primary selection
was performed on 131 articles. First, we excluded 66 unre-
lated articles based on titles and abstracts. Second, we ex-
cluded 27 articles that only included abstracts. Thereafter,
full-text reviews were conducted for 38 articles. Of these 38
full-text articles, 28 were excluded for the following rea-
sons: not controlled with placebo or other treatment (n =
14), patients’ pain period not clearly described or less than
three months (n = 9), duplication (n = 4), and articles not
in English or Korean (n = 1). The reasons for exclusion of
these papers are given in detail in Table 1. Finally, ROB
www.anesth-pain-med.org 83
Dextrose prolotherapy and chronic pain

Tabl
e 1
. Rea
sons
for E
xclu
sion
of t
he 2
8 Fu
ll Te
xt A
rtic
les
Title
Auth
orR
easo
n fo
r exc
lusi
onJo
urna
l/So
urce
Hyp
erto
nic
dext
rose
inje
ctio
n (p
rolo
ther
apy)
for k
nee
oste
oart
hriti
s: lo
ng
term
out
com
es (2
015 )
Rab
ago
DN
ot R
CTCo
mpl
emen
tary
The
rapi
es in
Med
icin
e
The
effic
acy
of p
rolo
ther
apy
for l
ater
al e
pico
ndyl
osis
: a p
ilot s
tudy
(200
8 )Sc
arpo
ne M
Use
of p
rolo
ther
apy
solu
tions
con
tain
ing
any-
thin
g ot
her t
han
gluc
ose
Clin
ical
Jou
rnal
of S
port
Med
icin
e
The
effe
cts
of p
rolo
ther
apy
in p
atie
nts
with
sub
acro
mia
l im
ping
emen
t syn
-dr
ome
(201
3 )H
anna
n EA
Not
RCT
Arth
ritis
and
Rhe
umat
ism
The
effe
cts
of in
ject
ing
intr
a-ar
ticul
ar p
late
let-r
ich
plas
ma
or p
rolo
ther
apy
on p
ain
scor
e an
d fu
nctio
n in
kne
e os
teoa
rthr
itis
(201
8 )R
ahim
zade
h P
Unc
erta
in p
ain
perio
dCl
inic
al In
terv
entio
ns in
Agi
ng
A ra
ndom
ized
cont
rolle
d tr
ial o
f int
ra-a
rtic
ular
pro
loth
erap
y ve
rsus
ste
roid
in
ject
ion
for s
acro
iliac
join
t pai
n (2
010 )
Kim
WM
Insu
ffici
ent p
ain
perio
dJo
urna
l of A
ltern
ativ
e an
d Co
mpl
emen
tary
Med
-ic
ine
(New
Yor
k, N
Y)Q
ualit
ativ
e as
sess
men
t of p
atie
nts
rece
ivin
g pr
olot
hera
py fo
r kne
e os
teo-
arth
ritis
in a
mul
timet
hod
stud
y (2
016 )
Rab
ago
DN
o co
ntro
lled
grou
pJo
urna
l of A
ltern
ativ
e an
d Co
mpl
emen
tary
Med
-ic
ine
(New
Yor
k, N
Y)Ef
fect
of r
ehab
ilita
tion
and
prol
othe
rapy
on
pain
and
func
tiona
l per
for-
man
ce in
pat
ient
s w
ith c
hron
ic p
atel
lar t
endi
nopa
thy
(201
7 )Ch
o SI
No
evid
ence
of r
ando
mize
d co
ntro
lled
tria
lG
azze
tta
Med
ica
Italia
na A
rchi
vio
per L
E Sc
ien-
ze M
edic
hePr
olot
hera
py in
ject
ions
and
ecc
entr
ic lo
adin
g ex
erci
ses
for p
ainf
ul A
chill
es
tend
inos
is: a
rand
omis
ed tr
ial (
2011
)Ye
lland
MJ
Insu
ffici
ent p
ain
perio
dB
ritis
h Jo
urna
l of S
port
s M
edic
ine
Prol
othe
rapy
inje
ctio
ns fo
r chr
onic
low
bac
k pa
in: r
esul
ts o
f a p
ilot c
ompa
r-at
ive
stud
y (2
000 )
Yella
nd M
Unc
erta
in ra
ndom
izat
ion
Aust
rala
s M
uscu
losk
elet
Med
Eval
uatio
n of
the
effic
acy
of d
iffer
ent c
once
ntra
tions
of d
extr
ose
prol
othe
r-ap
y in
tem
poro
man
dibu
lar j
oint
hyp
erm
obili
ty tr
eatm
ent (
2018
)M
usta
fa R
Unc
erta
in p
ain
perio
dJo
urna
l of C
rani
ofac
ial S
urge
ryN
o ev
iden
ce o
f mas
king
Prol
othe
rapy
ver
sus
cort
icos
tero
id in
ject
ions
and
pho
noph
ores
is fo
r the
tr
eatm
ent o
f pla
ntar
fasc
iitis
: a ra
ndom
ized
cont
rolle
d tr
ial (
2015
)D
emir
GU
ncer
tain
pai
n pe
riod
Arth
ritis
and
Rhe
umat
olog
yN
o ev
iden
ce o
f mas
king
Prol
othe
rapy
ver
sus
cort
icos
tero
id in
ject
ions
for t
he tr
eatm
ent o
f lat
eral
ep
icon
dylo
sis:
a ra
ndom
ized
cont
rolle
d tr
ial (
2011
)Ca
raya
nnop
oulo
s A
Use
of p
rolo
ther
apy
solu
tions
PM &
R: t
he J
ourn
al o
f Inj
ury,
Fun
ctio
n, a
nd R
e-ha
bilit
atio
nco
ntai
ning
any
thin
g ot
her t
han
gluc
ose
Intr
a-ar
ticul
ar h
yalu
roni
c ac
id in
ject
ions
vs.
dex
tros
e pr
olot
hera
py in
the
trea
tmen
t of o
steo
arth
ritic
kne
e pa
in (2
012 )
Has
hem
i SM
Turk
ish
text
Tehr
an U
nive
rsity
Med
ical
Jou
rnal
The
effe
cts
of p
rolo
ther
apy
with
hyp
erto
nic
dext
rose
ver
sus
prol
ozon
e (in
-tr
aart
icul
ar o
zone
) in
patie
nts
with
kne
e os
teoa
rthr
itis
(201
5 )H
ashe
mi M
Use
of p
rolo
ther
apy
solu
tions
con
tain
ing
any-
thin
g ot
her t
han
gluc
ose
Anes
thes
iolo
gy a
nd P
ain
Med
icin
e
Prol
othe
rapy
inje
ctio
ns, s
alin
e in
ject
ions
, and
exe
rcis
es fo
r chr
onic
low
ba
ck p
ain:
a ra
ndom
ized
tria
l (20
03)
Yella
nd M
JD
uplic
ated
stu
dySp
ine
Dex
tros
e pr
olot
hera
py fo
r kne
e os
teoa
rthr
itis:
resu
lts o
f a ra
ndom
ized
con-
trol
led
tria
l (20
11)
Rab
ago
DP
Dup
licat
ed s
tudy
Ost
eoar
thrit
is a
nd C
artil
age
Is d
extr
ose
prol
othe
rapy
sup
erio
r to
plac
ebo
for t
he tr
eatm
ent o
f tem
poro
-m
andi
bula
r joi
nt h
yper
mob
ility
? A
rand
omize
d cl
inic
al tr
ial (
2016
)Cö
mer
t Kili
ç S
Unc
erta
in p
ain
perio
dIn
tern
atio
nal J
ourn
al o
f Ora
l and
Max
illof
acia
l Su
rger
yB
enef
it of
dex
tros
e pr
olot
hera
py in
pai
nful
rota
tor c
uff t
endi
nopa
thy
case
s re
ceiv
ing
phys
ical
ther
apy:
a ra
ndom
ized
cont
rolle
d tr
ial (
2015
)B
ertr
and
HD
uplic
ated
stu
dyPa
in R
esea
rch
and
Man
agem
ent
The
effic
acy
of d
extr
ose
prol
othe
rapy
for t
empo
rom
andi
bula
r joi
nt h
yper
-m
obili
ty: a
pre
limin
ary
pros
pect
ive,
rand
omize
d, d
oubl
e-bl
ind,
pla
ce-
bo-c
ontr
olle
d cl
inic
al tr
ial (
2011
)
Ref
ai H
Unc
erta
in p
ain
perio
dJo
urna
l of O
ral a
nd M
axill
ofac
ial S
urge
ry
Effic
acy
of in
tra-
artic
ular
hyp
erto
nic
dext
rose
pro
loth
erap
y ve
rsus
nor
mal
sa
line
for k
nee
oste
oart
hriti
s: a
pro
toco
l for
a tr
iple
-blin
ded
rand
omize
d co
ntro
lled
tria
l (20
18)
Sit R
WS
Dup
licat
ed s
tudy
BM
C Co
mpl
emen
tary
and
Alte
rnat
ive
Med
icin
e
(Con
tinue
d to
the
next
pag
e)
84 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
Asso
ciat
ion
betw
een
dise
ase-
spec
ific
qual
ity o
f life
and
mag
netic
reso
-na
nce
imag
ing
outc
omes
in a
clin
ical
tria
l of p
rolo
ther
apy
for k
nee
oste
o-ar
thrit
is (2
013 )
Rab
ago
DU
se o
f pro
loth
erap
y so
lutio
ns c
onta
inin
g an
y-th
ing
othe
r tha
n gl
ucos
eAr
chiv
es o
f Phy
sica
l Med
icin
e an
d R
ehab
ilita
-tio
n
Hyp
erto
nic
dext
rose
and
mor
rhua
te s
odiu
m in
ject
ions
(pro
loth
erap
y) fo
r la
tera
l epi
cond
ylos
is (t
enni
s el
bow
): re
sults
of a
sin
gle-
blin
d, p
ilot-l
evel
, ra
ndom
ized
cont
rolle
d tr
ial (
2013
)
Rab
ago
DU
se o
f pro
loth
erap
y so
lutio
ns c
onta
inin
g an
y-th
ing
othe
r tha
n gl
ucos
eAm
eric
an J
ourn
al o
f Phy
sica
l Med
icin
e &
Reh
a-bi
litat
ion
Inve
stig
atio
n th
e ef
ficac
y of
intr
a-ar
ticul
ar p
rolo
ther
apy
with
ery
thro
poie
tin
and
dext
rose
and
intr
a-ar
ticul
ar p
ulse
d ra
diof
requ
ency
on
pain
leve
l re-
duct
ion
and
rang
e of
mot
ion
impr
ovem
ent i
n pr
imar
y os
teoa
rthr
itis
of
knee
(201
4 )
Rah
imza
deh
PU
ncer
tain
pai
n pe
riod
Jour
nal o
f Res
earc
h in
Med
ical
Sci
ence
s
Shor
t ter
m a
nalg
esic
effe
cts
of 5
% d
extr
ose
epid
ural
inje
ctio
ns fo
r chr
onic
lo
w b
ack
pain
: a ra
ndom
ized
cont
rolle
d tr
ial (
2017
)M
aniq
uis-
Smig
el L
Epid
ural
inje
ctio
nAn
esth
esio
logy
and
Pai
n M
edic
ine
Chan
ge o
f site
of i
ntra
-art
icul
ar in
ject
ion
of h
yper
toni
c de
xtro
se re
sulte
d in
di
ffere
nt e
ffect
s of
trea
tmen
t (20
18)
Foud
a AA
Unc
erta
in p
ain
perio
dB
ritis
h Jo
urna
l of O
ral a
nd M
axill
ofac
ial S
urge
ry
Peria
rtic
ular
dex
tros
e pr
olot
hera
py in
stea
d of
intr
a-ar
ticul
ar in
ject
ion
for
pain
and
func
tiona
l im
prov
emen
t in
knee
ost
eoar
thrit
is (2
017 )
Rez
asol
tani
ZN
o co
ntro
lled
grou
pJo
urna
l of P
ain
Res
earc
h
Prol
othe
rapy
: an
effe
ctiv
e th
erap
y fo
r Tie
tze
synd
rom
e (2
017 )
Sent
urk
EN
o ra
ndom
ized
cont
rolle
d tr
ial
Jour
nal o
f Bac
k an
d M
uscu
losk
elet
al R
ehab
ili-
tatio
nEf
fect
of r
egen
erat
ive
inje
ctio
n th
erap
y on
func
tion
and
pain
in p
atie
nts
with
kne
e os
teoa
rthr
itis:
a ra
ndom
ized
cros
sove
r stu
dy (2
012 )
Dum
ais
RCr
osso
ver s
tudy
Pain
Med
icin
e (U
nite
d St
ates
)
RCT
: Ran
dom
ized
Cont
rolle
d Tr
ial.
Tabl
e 1
. Con
tinue
d
Title
Auth
orR
easo
n fo
r exc
lusi
onJo
urna
l/So
urce
evaluation and data extraction were performed on 10 arti-
cles (Fig. 1).
All studies were randomized controlled trials. Various
injection sites, including large joints such as the knee
and small joints such as finger joints and carpometacar-
pal joints were investigated. The comparator groups were
saline injection, exercise, steroid injection, PRP injec-
tion, and extracorporeal shock wave therapy. The severi-
ty of pain as the primary outcome was measured using
the Visual Analog Scale (VAS), the Western Ontario and
McMaster Universities Osteoarthritis Index, the Karnof-
sky Performance Score, and Foot Function Index. The
concentration, volume of dextrose solution, and interval
between injection sessions were different between stud-
ies. The dextrose concentration ranged from 5% to 25%,
and the injection interval ranged from weeks to months
(Table 2).
Quality assessment of the included studies (risk of bias within studies)
ROB evaluation revealed an overall low risk for selection
and reporting bias, while almost half of the studies showed
a high risk of performance bias because they could not be
blinded to the differences in procedures (Figs. 2, 3). All
studies reported detailed information regarding the ran-
domization techniques that were used, such as manual
random number selection or a computer-generated ran-
dom number table. Allocation concealment was unclear in
five studies which did not mention the specific allocation
concealment method.
For performance bias, four studies [12–15] were unable
to blind the participants and five studies [12–14,16,17]
could not blind the physicians because the injection site
was different or because exercise was included in a control
group. These studies were considered “high” bias. Two
studies had high detection bias [15,17].
The risk of incomplete outcome data was “high” in four
studies that did not mention a minimal sample size
[15,16,18,19]. Four other studies did not meet a minimal
sample size, resulting in an unclear risk of bias [14,17,20,21].
Reporting bias was low because there was no selective
reporting in any of the studies. Regarding the potential
bias, four studies were rated as unclear because there was
no detailed description of the sample size calculation, and
one study was high risk because the number of samples
was very small [17].
www.anesth-pain-med.org 85
Dextrose prolotherapy and chronic pain
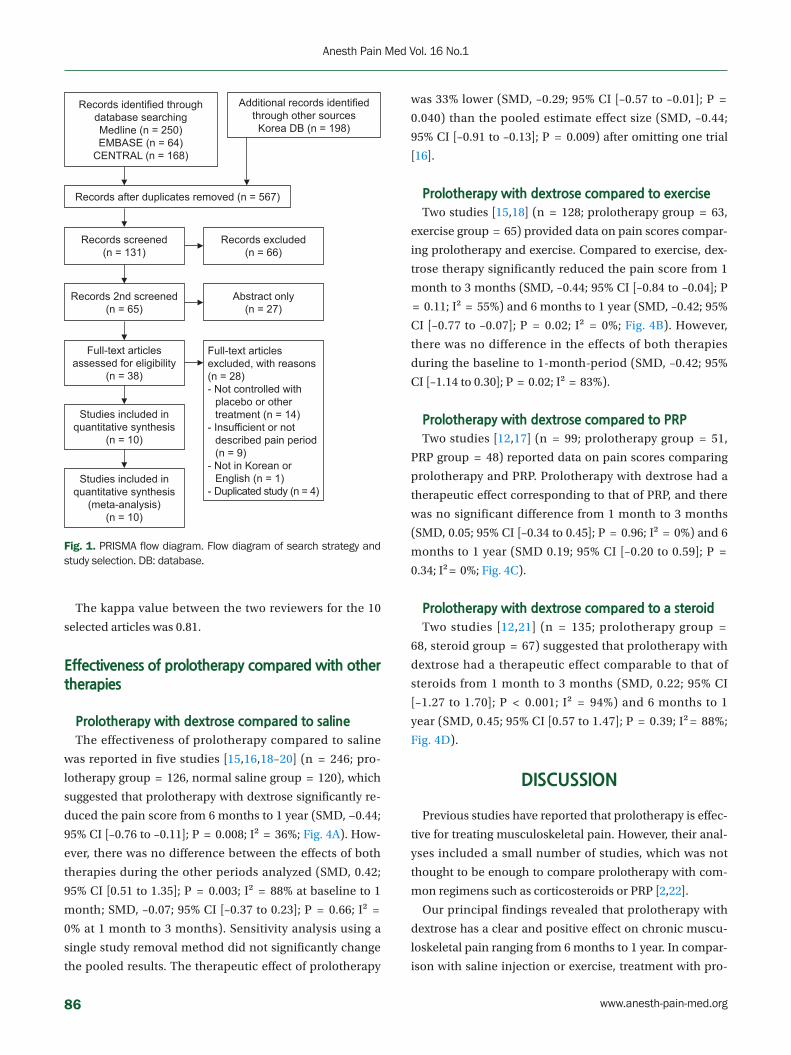
Records identified through database searchingMedline (n = 250)EMBASE (n = 64)
CENTRAL (n = 168)
Records after duplicates removed (n = 567)
Records screened(n = 131)
Records 2nd screened(n = 65)
Full-text articles assessed for eligibility
(n = 38)
Studies included in quantitative synthesis
(n = 10)
Studies included in quantitative synthesis
(meta-analysis)(n = 10)
Records excluded(n = 66)
Abstract only(n = 27)
Full-text articles excluded, with reasons (n = 28)- Not controlled with
placebo or other treatment (n = 14)
- Insufficient or not described pain period (n = 9)
- Not in Korean or English (n = 1)
- Duplicated study (n = 4)
Additional records identified through other sources Korea DB (n = 198)
Fig. 1. PRISMA flow diagram. Flow diagram of search strategy and study selection. DB: database.
The kappa value between the two reviewers for the 10
selected articles was 0.81.
Effectiveness of prolotherapy compared with other therapies
Prolotherapy with dextrose compared to saline
The effectiveness of prolotherapy compared to saline
was reported in five studies [15,16,18–20] (n = 246; pro-
lotherapy group = 126, normal saline group = 120), which
suggested that prolotherapy with dextrose significantly re-
duced the pain score from 6 months to 1 year (SMD, −0.44;
95% CI [–0.76 to –0.11]; P = 0.008; I² = 36%; Fig. 4A). How-
ever, there was no difference between the effects of both
therapies during the other periods analyzed (SMD, 0.42;
95% CI [0.51 to 1.35]; P = 0.003; I² = 88% at baseline to 1
month; SMD, –0.07; 95% CI [–0.37 to 0.23]; P = 0.66; I² =
0% at 1 month to 3 months). Sensitivity analysis using a
single study removal method did not significantly change
the pooled results. The therapeutic effect of prolotherapy
was 33% lower (SMD, –0.29; 95% CI [–0.57 to –0.01]; P =
0.040) than the pooled estimate effect size (SMD, –0.44;
95% CI [–0.91 to –0.13]; P = 0.009) after omitting one trial
[16].
Prolotherapy with dextrose compared to exercise
Two studies [15,18] (n = 128; prolotherapy group = 63,
exercise group = 65) provided data on pain scores compar-
ing prolotherapy and exercise. Compared to exercise, dex-
trose therapy significantly reduced the pain score from 1
month to 3 months (SMD, –0.44; 95% CI [–0.84 to –0.04]; P
= 0.11; I² = 55%) and 6 months to 1 year (SMD, –0.42; 95%
CI [–0.77 to –0.07]; P = 0.02; I² = 0%; Fig. 4B). However,
there was no difference in the effects of both therapies
during the baseline to 1-month-period (SMD, –0.42; 95%
CI [–1.14 to 0.30]; P = 0.02; I² = 83%).
Prolotherapy with dextrose compared to PRP
Two studies [12,17] (n = 99; prolotherapy group = 51,
PRP group = 48) reported data on pain scores comparing
prolotherapy and PRP. Prolotherapy with dextrose had a
therapeutic effect corresponding to that of PRP, and there
was no significant difference from 1 month to 3 months
(SMD, 0.05; 95% CI [–0.34 to 0.45]; P = 0.96; I² = 0%) and 6
months to 1 year (SMD 0.19; 95% CI [–0.20 to 0.59]; P =
0.34; I² = 0%; Fig. 4C).
Prolotherapy with dextrose compared to a steroid
Two studies [12,21] (n = 135; prolotherapy group =
68, steroid group = 67) suggested that prolotherapy with
dextrose had a therapeutic effect comparable to that of
steroids from 1 month to 3 months (SMD, 0.22; 95% CI
[–1.27 to 1.70]; P < 0.001; I² = 94%) and 6 months to 1
year (SMD, 0.45; 95% CI [0.57 to 1.47]; P = 0.39; I² = 88%;
Fig. 4D).
DISCUSSION
Previous studies have reported that prolotherapy is effec-
tive for treating musculoskeletal pain. However, their anal-
yses included a small number of studies, which was not
thought to be enough to compare prolotherapy with com-
mon regimens such as corticosteroids or PRP [2,22].
Our principal findings revealed that prolotherapy with
dextrose has a clear and positive effect on chronic muscu-
loskeletal pain ranging from 6 months to 1 year. In compar-
ison with saline injection or exercise, treatment with pro-
86 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
Tabl
e 2.
Cha
ract
eris
tics
of th
e In
clud
ed S
tudi
es a
nd S
umm
ary
of th
e Pr
epar
atio
ns a
nd In
ject
ion
Det
ails
of P
rolo
ther
apy
in th
e Re
trie
ved
Tria
ls
Stud
yD
isea
seIn
terv
entio
n
(num
ber o
f pa
tient
s)Av
erag
e ag
e (y
r)O
utco
me
m
easu
re (s
)Fo
llow
-up
tim
ing
Tota
l num
ber o
f pro
loth
erap
y in
ject
ion
& in
terv
alPr
olot
hera
py
regi
men
Prol
othe
rapy
vo
lum
e pe
r dos
ePr
olot
hera
py
inje
ctio
n te
chni
que
Rab
ago
et a
l.,
2013
[15 ]
Kne
e O
AD
extr
ose
(30 )
Salin
e (2
9 )Ex
erci
se (3
1 )
Dex
tros
e 56
.8 ±
7 .
9
Salin
e 56
.8 ±
6.7
Exer
cise
56 .
4 ±
7 .
0
WO
MAC
KPS
Bas
elin
e, 5
, 9,
12, 2
4 , 5
2 w
eeks
3 (1
, 5, 9
wee
ks. 3
bas
ic
dose
s bu
t add
ition
al in
jec-
tions
wer
e al
low
ed a
t 13 ,
17
wee
ks)
Intr
a-ar
ticul
ar 2
5 %
dext
rose
10
ml:
5 m
l 50 %
dex
tros
e +
5 m
l 1%
lido
-ca
ine
6 m
l6 .
0 m
l was
inje
cted
us
ing
an in
fero
med
i-al
app
roac
h
Extr
a-ar
ticul
ar 1
5 %
dext
rose
22 .
5 m
l: 6 .
75 m
l 50 %
dex
-tro
se +
4.5
ml 1
%
lidoc
aine
+ 1
1 .25
m
l sal
ine
per 0
.5 m
l, up
to
22.5
ml
Palp
atio
n at
maj
or
tend
er te
ndon
and
lig
amen
t ins
ertio
ns
thro
ugh
up to
15
skin
pun
ctur
es u
s-in
g a
pepp
erin
g te
chni
que,
pla
cing
a
poss
ible
tota
l 22 .
5 m
l of s
olut
ion
Ber
tran
d et
al.,
20
16 [1
6 ]R
otat
or c
uff
tend
inop
a-th
y
Enth
esis
dex
tros
e (2
7 )En
thes
is s
alin
e (2
7 )Su
perf
icia
l sal
ine
(27 )
Enth
esis
dex
tros
e 53
.8 ±
13 .
5
Enth
esis
sal
ine
51.1
± 9
.2Su
perf
ic s
alin
e 49
.0 ±
11 .
9
VAS
USP
RS
Satis
fact
ion
mea
sure
(0–
10 s
cale
)
For V
AS a
t ba
selin
e, 3
, 9
mon
ths
For U
SPR
S &
Sa
tisfa
ctio
n m
easu
re a
t ba
selin
e, 9
m
onth
s
3 (0
, 1, 2
mon
ths)
25%
dex
tros
e/
0 .1 %
lido
cain
e/sa
line
1 to
3 m
l at p
rima-
ry in
ject
ion
site
0 .5
ml a
t adj
acen
t to
prim
ary
inje
c-tio
n ar
ea a
t 1
cm in
terv
als
The
supr
aspi
natu
s,
infra
spin
atus
, and
te
res
min
or in
ser-
tions
, ins
ertio
ns o
n th
e co
raco
id p
ro-
cess
, wer
e in
ject
ed
with
the
shou
lder
in
neut
ral r
otat
ion.
The
bice
ps lo
ng h
ead,
su
bsca
pula
ris in
ser-
tion,
and
infe
rior g
le-
nohu
mer
al li
gam
ent
wer
e in
ject
ed w
ith
the
shou
lder
in v
ari-
ous
degr
ees
of e
x-te
rnal
rota
tion
and
abdu
ctio
n/ad
duc-
tion.
Orig
ins
of th
e te
res
min
or, t
eres
maj
or,
and
the
post
erio
r in-
ferio
r gle
nohu
mer
al
ligam
ent w
ere
inje
ct-
ed p
oste
riorly
(Con
tinue
d to
the
next
pag
e)
www.anesth-pain-med.org 87
Dextrose prolotherapy and chronic pain
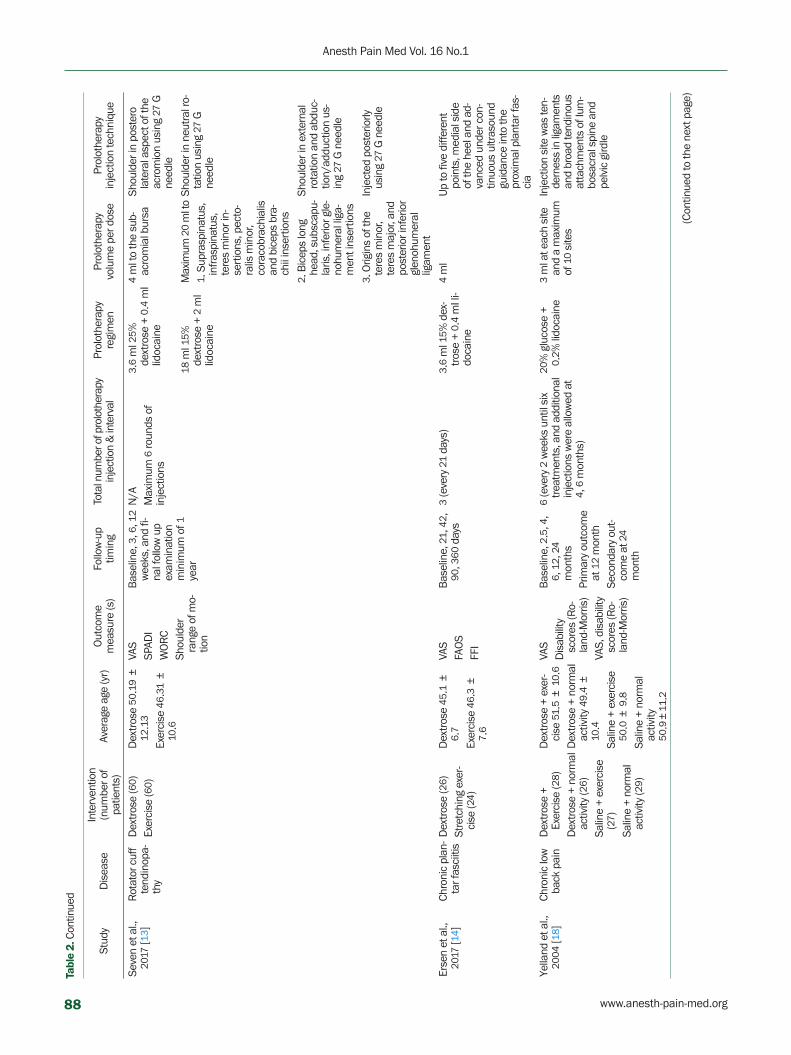
Seve
n et
al.,
20
17 [1
3 ]R
otat
or c
uff
tend
inop
a-th
y
Dex
tros
e (6
0 )Ex
erci
se (6
0 )D
extr
ose
50.1
9 ±
12
.13
Exer
cise
46 .
31 ±
10
.6
VAS
SPAD
IW
OR
CSh
ould
er
rang
e of
mo-
tion
Bas
elin
e, 3
, 6, 1
2 w
eeks
, and
fi-
nal f
ollo
w u
p ex
amin
atio
n m
inim
um o
f 1
year
N/A
Max
imum
6 ro
unds
of
inje
ctio
ns
3 .6
ml 2
5 %
dext
rose
+ 0
.4 m
l lid
ocai
ne
4 m
l to
the
sub-
acro
mia
l bur
saSh
ould
er in
pos
tero
la
tera
l asp
ect o
f the
ac
rom
ion
usin
g 27
G
need
le18
ml 1
5 %
dext
rose
+ 2
ml
lidoc
aine
Max
imum
20
ml t
o1 .
Sup
rasp
inat
us,
infra
spin
atus
, te
res
min
or in
-se
rtio
ns, p
ecto
-ra
lis m
inor
, co
raco
brac
hial
is
and
bice
ps b
ra-
chii
inse
rtio
ns
Shou
lder
in n
eutr
al ro
-ta
tion
usin
g 27
G
need
le
2 . B
icep
s lo
ng
head
, sub
scap
u-la
ris, i
nfer
ior g
le-
nohu
mer
al li
ga-
men
t ins
ertio
ns
Shou
lder
in e
xter
nal
rota
tion
and
abdu
c-tio
n/ad
duct
ion
us-
ing
27 G
nee
dle
3 . O
rigin
s of
the
tere
s m
inor
, te
res
maj
or, a
nd
post
erio
r inf
erio
r gl
enoh
umer
al
ligam
ent
Inje
cted
pos
terio
rly
usin
g 27
G n
eedl
e
Erse
n et
al.,
20
17 [1
4 ]Ch
roni
c pl
an-
tar f
asci
itis
Dex
tros
e (2
6 )St
retc
hing
exe
r-ci
se (2
4 )
Dex
tros
e 45
.1 ±
6 .
7
Exer
cise
46 .
3 ±
7 .
6
VAS
FAO
SFF
I
Bas
elin
e, 2
1 , 4
2 ,
90, 3
60 d
ays
3 (e
very
21
days
)3 .
6 m
l 15 %
dex
-tr
ose
+ 0 .
4 m
l li-
doca
ine
4 m
lU
p to
five
diff
eren
t po
ints
, med
ial s
ide
of th
e he
el a
nd a
d-va
nced
und
er c
on-
tinuo
us u
ltras
ound
gu
idan
ce in
to th
e pr
oxim
al p
lant
ar fa
s-ci
a
Yella
nd e
t al.,
20
04 [1
8 ]Ch
roni
c lo
w
back
pai
nD
extr
ose
+
Exer
cise
(28 )
Dex
tros
e +
norm
al
activ
ity (2
6 )Sa
line
+ ex
erci
se
(27 )
Salin
e +
norm
al
activ
ity (2
9 )
Dex
tros
e +
exer
-ci
se 5
1 .5
± 1
0 .6
Dex
tros
e +
norm
al
activ
ity 4
9 .4
±
10.4
Salin
e +
exer
cise
50
.0 ±
9.8
Salin
e +
norm
al
activ
ity
50.9
±11
.2
VAS
Dis
abili
ty
scor
es (R
o-la
nd-M
orris
)VA
S, d
isab
ility
sc
ores
(Ro-
land
-Mor
ris)
Bas
elin
e, 2
.5, 4
, 6 ,
12 ,
24
mon
ths
Prim
ary
outc
ome
at 1
2 m
onth
Seco
ndar
y ou
t-co
me
at 2
4 m
onth
6 (e
very
2 w
eeks
unt
il si
x tre
atm
ents
, and
add
ition
al
inje
ctio
ns w
ere
allo
wed
at
4 , 6
mon
ths)
20%
glu
cose
+
0 .2 %
lido
cain
e3
ml a
t eac
h si
te
and
a m
axim
um
of 1
0 si
tes
Inje
ctio
n si
te w
as te
n-de
rnes
s in
liga
men
ts
and
broa
d te
ndin
ous
atta
chm
ents
of l
um-
bosa
cral
spi
ne a
nd
pelv
ic g
irdle
Tabl
e 2.
Con
tinue
d
Stud
yD
isea
seIn
terv
entio
n
(num
ber o
f pa
tient
s)Av
erag
e ag
e (y
r)O
utco
me
m
easu
re (s
)Fo
llow
-up
tim
ing
Tota
l num
ber o
f pro
loth
erap
y in
ject
ion
& in
terv
alPr
olot
hera
py
regi
men
Prol
othe
rapy
vo
lum
e pe
r dos
ePr
olot
hera
py
inje
ctio
n te
chni
que
(Con
tinue
d to
the
next
pag
e)
88 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1
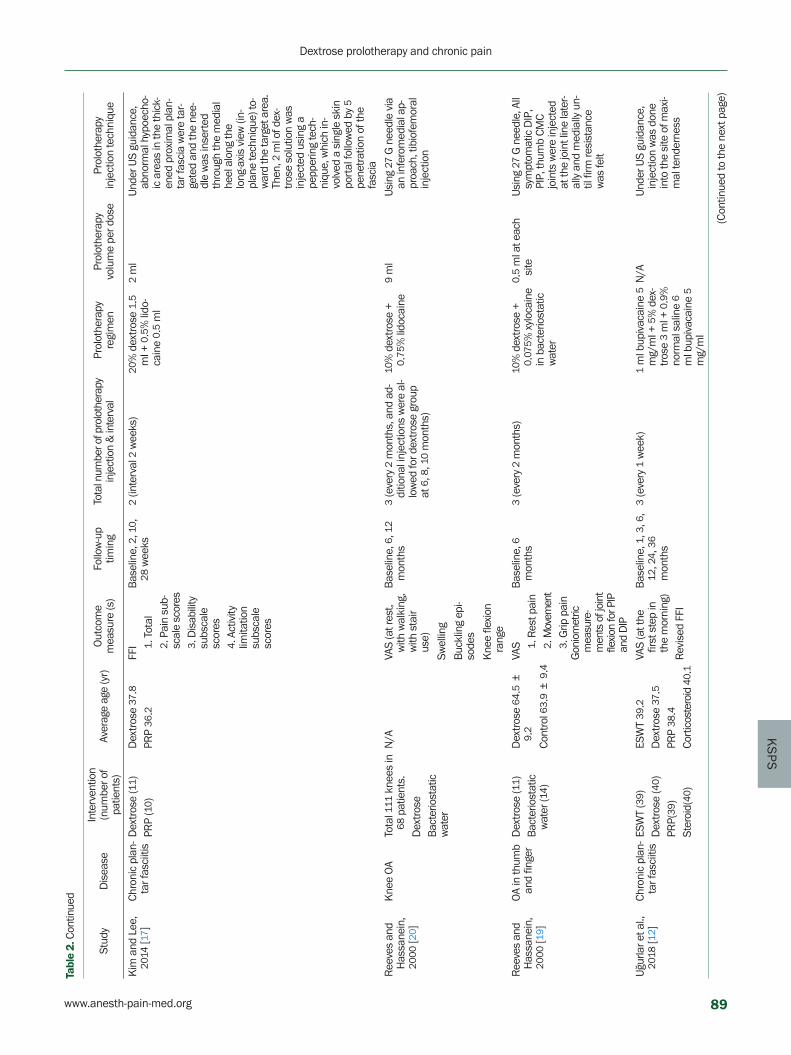
KS
PS
Kim
and
Lee
, 20
14 [1
7 ]Ch
roni
c pl
an-
tar f
asci
itis
Dex
tros
e (1
1 )PR
P (1
0 )D
extr
ose
37.8
PRP
36.2
FFI
1 .
Tot
al
2 . P
ain
sub-
scal
e sc
ores
3 .
Dis
abili
ty
subs
cale
sc
ores
4 .
Act
ivity
lim
itatio
n su
bsca
le
scor
es
Bas
elin
e, 2
, 10 ,
28
wee
ks2
(inte
rval
2 w
eeks
)20
% d
extr
ose
1 .5
ml +
0.5
% li
do-
cain
e 0 .
5 m
l
2 m
lU
nder
US
guid
ance
, ab
norm
al h
ypoe
cho-
ic a
reas
in th
e th
ick-
ened
pro
xim
al p
lan-
tar f
asci
a w
ere
tar-
gete
d an
d th
e ne
e-dl
e w
as in
sert
ed
thro
ugh
the
med
ial
heel
alo
ng th
e lo
ng-a
xis
view
(in-
plan
e te
chni
que)
to-
war
d th
e ta
rget
are
a.
Then
, 2 m
l of d
ex-
tros
e so
lutio
n w
as
inje
cted
usi
ng a
pe
pper
ing
tech
-ni
que,
whi
ch in
-vo
lved
a s
ingl
e sk
in
port
al fo
llow
ed b
y 5
pene
trat
ion
of th
e fa
scia
Ree
ves
and
Has
sane
in,
2000
[20 ]
Kne
e O
ATo
tal 1
11 k
nees
in
68 p
atie
nts.
Dex
tros
eB
acte
riost
atic
w
ater
N/A
VAS
(at r
est,
with
wal
king
, w
ith s
tair
use)
Bas
elin
e, 6
, 12
mon
ths
3 (e
very
2 m
onth
s, a
nd a
d-di
tiona
l inj
ectio
ns w
ere
al-
low
ed fo
r dex
tros
e gr
oup
at 6
, 8, 1
0 m
onth
s)
10%
dex
tros
e +
0 .75
% li
doca
ine
9 m
lU
sing
27
G n
eedl
e vi
a an
infe
rom
edia
l ap-
proa
ch, t
ibio
fem
oral
in
ject
ion
Swel
ling
Buc
klin
g ep
i-so
des
Kne
e fle
xion
ra
nge
Ree
ves
and
Has
sane
in,
2000
[19 ]
OA
in th
umb
and
finge
rD
extr
ose
(11 )
Bac
terio
stat
ic
wat
er (1
4 )
Dex
tros
e 64
.5 ±
9 .
2
Cont
rol 6
3 .9
± 9
.4
VAS
1 .
Res
t pai
n
2 . M
ovem
ent
3 .
Grip
pai
nG
onio
met
ric
mea
sure
-m
ents
of j
oint
fle
xion
for P
IP
and
DIP
Bas
elin
e, 6
m
onth
s3
(eve
ry 2
mon
ths)
10%
dex
tros
e +
0 .07
5 % x
yloc
aine
in
bac
terio
stat
ic
wat
er
0 .5
ml a
t eac
h si
teU
sing
27
G n
eedl
e, A
ll sy
mpt
omat
ic D
IP,
PIP,
thum
b CM
C jo
ints
wer
e in
ject
ed
at th
e jo
int l
ine
late
r-al
ly a
nd m
edia
lly u
n-til
firm
resi
stan
ce
was
felt
Uğu
rlar e
t al.,
20
18 [1
2 ]Ch
roni
c pl
an-
tar f
asci
itis
ESW
T (3
9 )D
extr
ose
(40 )
PRP(
39)
Ster
oid(
40)
ESW
T 39
.2D
extr
ose
37.5
PRP
38.4
Cort
icos
tero
id 4
0 .1
VAS
(at t
he
first
ste
p in
th
e m
orni
ng)
Rev
ised
FFI
Bas
elin
e, 1
, 3, 6
, 12
, 24 ,
36
mon
ths
3 (e
very
1 w
eek)
1 m
l bup
ivac
aine
5
mg/
ml +
5%
dex
-tro
se 3
ml +
0.9
%
norm
al s
alin
e 6
ml b
upiv
acai
ne 5
m
g/m
l
N/A
Und
er U
S gu
idan
ce,
inje
ctio
n w
as d
one
into
the
site
of m
axi-
mal
tend
erne
ss
Tabl
e 2.
Con
tinue
d
Stud
yD
isea
seIn
terv
entio
n
(num
ber o
f pa
tient
s)Av
erag
e ag
e (y
r)O
utco
me
m
easu
re (s
)Fo
llow
-up
tim
ing
Tota
l num
ber o
f pro
loth
erap
y in
ject
ion
& in
terv
alPr
olot
hera
py
regi
men
Prol
othe
rapy
vo
lum
e pe
r dos
ePr
olot
hera
py
inje
ctio
n te
chni
que
(Con
tinue
d to
the
next
pag
e)
www.anesth-pain-med.org 89
Dextrose prolotherapy and chronic pain

Jaha
ngiri
et a
l.,
2014
[21 ]
OA
in th
e fir
st c
arpo
-m
etac
arpa
l
Dex
tros
e (3
0 )Co
rtic
oste
roid
(30 )
Dex
tros
e 63
.9 ±
9 .
4
Cort
icos
tero
id
63.3
± 1
0 .1
VAS
(pai
n in
-te
nsity
of
tend
erne
ss,
pain
on
join
t m
ovem
ent)
Han
d fu
nctio
n (s
elf-a
dmin
-is
tere
d qu
es-
tionn
aire
H
AQ-D
I ab
out e
atin
g,
grip
ping
, dr
essi
ng)
Stre
ngth
(lat
er-
al p
inch
grip
)
Bas
elin
e, 1
, 2, 6
m
onth
s3
(eve
ry 1
mon
ths)
20%
dex
tros
e 0 .
5 m
l + 2
% li
do-
cain
e 0 .
5 m
l
1 m
lA
25 G
nee
dle
was
in-
sert
ed to
war
d th
e ul
nar s
ide
of th
e ex
-te
nsor
pol
licis
bre
vis
and
just
pro
xim
al to
th
e ba
se o
f the
firs
t m
etac
arpa
l in
the
snuf
fbox
Valu
es a
re p
rese
nted
as
mea
n ±
SD
. O
A: o
steo
arth
ritis
, PR
P: p
late
let-r
ich
plas
ma,
N/A
: no
t av
aila
ble
, ES
WT:
ext
raco
rpor
eal s
hock
wav
e th
erap
y, W
OM
AC:
Wes
tern
Ont
ario
McM
aste
r U
nive
rsiti
es O
steo
arth
ritis
Inde
x, K
PS: k
nee
pain
sca
le, V
AS: V
isua
l Ana
log
Scal
e, U
SPR
S: u
ltras
ound
sho
ulde
r pa
thol
ogy
ratin
g sc
ale,
SPA
DI:
shou
lder
pai
n an
d di
sabi
lity,
WO
RC:
Wes
tern
O
ntar
io R
otat
or C
uff,
FAO
S: F
oot
and
Ankl
e O
utco
me
Scor
e, F
FI:
foot
fun
ctio
n in
dex,
PIP
: pr
oxim
al in
terp
hala
ngea
l joi
nts,
DIP
: dis
tal i
nter
phal
ange
al jo
ints
, HAQ
-DI:
Hea
lth A
sses
smen
t Q
uest
ionn
aire
Dis
abili
ty In
dex,
CM
C: c
arpo
met
acar
pal.
Tabl
e 2.
Con
tinue
d
Stud
yD
isea
seIn
terv
entio
n
(num
ber o
f pa
tient
s)Av
erag
e ag
e (y
r)O
utco
me
m
easu
re (s
)Fo
llow
-up
tim
ing
Tota
l num
ber o
f pro
loth
erap
y in
ject
ion
& in
terv
alPr
olot
hera
py
regi
men
Prol
othe
rapy
vo
lum
e pe
r dos
ePr
olot
hera
py
inje
ctio
n te
chni
que after treatment.
Corticosteroid injection has been widely used as it is
known to be effective in the treatment of musculoskeletal
disorders. In vitro studies have shown that corticosteroids
have therapeutic effects on the tendon and the surround-
ing connective tissues by inhibiting collagen, extracellular
matrix molecules, and granulation tissue production, in
addition to inflammatory suppression [23]. However, such
positive therapeutic effects of corticosteroids may exist
only in the short term [24]. Uğurlar et al. [12] reported that
corticosteroid injection was an effective treatment in the
first 6 months, but lost its effectiveness after the first 6
months. The effect of pain relief in prolotherapy was seen
within 3 to 12 months. In another study, Jahangiri et al. [21]
compared the effects of corticosteroid injection and pro-
lotherapy in patients with first carpometacarpal osteoar-
thritis and reported that the corticosteroid injection group
had better results of pain score at 1 month. However, after
2 months, prolotherapy had a more favorable outcome
than corticosteroid injection. Although not shown in our
study, another concern of corticosteroids is adverse effects,
such as focal inflammation, necrosis, fragmentation of col-
lagen bundles in the subacromial space, tendon/ligament
weakening or rupture, and worsening osteoarthritic chang-
es [25–27]. In contrast, prolotherapy has no serious side ef-
fects and is effective, safe, and sustainable [10]. In this
study, three RCTs reported only minor transient complica-
tions such as mild to moderate pain and self-limiting
bruising after prolotherapy.
We found that PRP and dextrose prolotherapy were
shown to be effective for treating degenerative conditions
and injuries. Both PRP therapy and prolotherapy common-
ly have regenerative therapeutic properties, but the central
mechanisms of prolotherapy and PRP are different. In pro-
lotherapy, hyperosmolar dextrose triggers an inflammatory
response, increases platelet-derived growth factor expres-
sion, and upregulates several mitogenic factors that may
act as signaling mechanisms in tendon repair [28–30]. In
PRP therapy, it aims to augment the natural healing pro-
cess of tendon repair and regeneration by delivering high
concentrations of growth factors directly to a lesion [31].
For preparation, following the extraction of autologous ve-
nous blood with a large-gauge needle to prevent premature
platelet activation [32], platelets are separated from other
blood components and further concentrated [33]. This oc-
curs through a centrifuge process, in which platelets can be
isolated from the other cell components of blood based on
90 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
their physiological size [33]. Further concentration of plate-
lets occurs with subsequent centrifuge cycles [34]. As such,
several steps are needed to prepare PRP, whereas the
preparation of the prolotherapy is simple. And PRP in-
volves an invasive procedure (i.e., blood drawing) and
lacks an optimized standardized protocol. In this regard,
prolotherapy can provide more convenience to both pa-
tients and treatment providers.
Of the ten papers included in the study, nine papers
showed generally positive results of achieving pain relief
and patient satisfaction regardless of the injection site. Yel-
land et al. [18] reported that prolotherapy was not more ef-
fective than injections of normal saline for low back pain.
Nevertheless, participants exhibited marked and sustained
improvements in their pain and disability, even with saline
injections. They assumed that these therapeutic effects
could be achieved by other factors such as patients were
enrolled in a trial during severe pain and then sponta-
neously recovered naturally, or by the therapeutic effect by
direct needling of entheses, or the placebo effect by clinical
visits.
In the case of using physiotherapy as a control group
[13,14], the positive result from the comparison with pro-
lotherapy was within expectations because injection car-
ries a strong placebo effect, which usually leads to a superi-
or response to the noninvasive treatment.
The present study mainly analyzed the pain measure-
ment outcomes, and functional improvement measure-
ments were not considered. Among the RCTs, investiga-
tions of functional improvements were conducted in eight
studies. Six studies reported that the prolotherapy group
Bertand et al., 2016 [16]
Ran
dom
seq
uenc
e ge
nera
tion
(sel
ectio
n bi
as)
Allo
catio
n co
ncea
lmen
t (se
lect
ion
bias
)
Blin
ding
of p
artic
ipan
ts (p
erfo
rman
ce b
ias)
Blin
ding
of p
erso
nnel
(per
form
ance
bia
s)
Blin
ding
of o
utco
me
asse
ssm
ent (
dete
ctio
n bi
as)
Inco
mpl
ete
outc
ome
data
(attr
ition
bias
)
Sele
ctive
repo
rting
(rep
ortin
g bi
as)
Oth
er b
ias
Ersen et al., 2017 [14]
Reeves and Hassanein, 2000 [20]
Kim and Lee, 2014 [17]
Jahangiri et al., 2014 [21]
Rabago et al., 2013 [15]
Reeves and Hassanein, 2000 [19]
Seven et al., 2017 [13]
Uğurlar et al., 2018 [12]
Yelland et al., 2004 [18]
Fig. 3. Risk of bias summary. Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
lotherapy showed a moderately superior therapeutic effect.
In particular, prolotherapy was found to be more effective
than exercise from one month after treatment. It was also
found to have a similar effect to steroids or PRP one month
Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of participants (performance bias)
Blinding of personnel (performance bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome date (attrition bias)
Selective reporting (reporting bias)
Other bias
0% 25%
Low risk of bias Unclear risk of bias High risk of bias
50% 75% 100%
Fig. 2. Risk of bias graph. Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
www.anesth-pain-med.org 91
Dextrose prolotherapy and chronic pain

Fig. 4. Forest Plot; (A) saline (B) exercise (C) PRP (D) steroid. Forest plot diagram showing comparisons of VAS for Pain Composite between dextrose prolotherapy and the reference treatments 6 months-1 year. (A) Dextrose vs. Saline on VAS for pain composite 6 months-1 year. (B) Dextrose vs. Exercise on VAS for pain composite 6 months-1 year. (C) Dextrose vs. PRP on VAS for pain composite 6 months-1 year. (D) Dextrose vs. Steroid on VAS for pain composite 6 months-1 year. PRP: platelet-rich plasma, VAS: Visual Analog Scale, Std. Mean difference: standardized mean difference, IV: weighted mean difference, CI: confidence interval, SD: standard deviation.
had a significant improvement in function compared to the
control group [13,15,17,19–21]. One study showed func-
tional improvement at 90 days after treatment, but after
360 days, both the prolotherapy and control groups showed
similar results [14]. In one study, no significant improve-
ment was noted in any of the groups at the end of the fol-
low-up period [12]. However, unlike other studies which
used a dextrose concentration of 10% or higher, this study
only used a 5% concentration. When used clinically, dex-
trose concentrations higher than 10% are partly affected by
inflammatory mechanisms, while concentrations less than
10% are considered noninflammatory [35,36]. Considering
this, it is possible that a low concentration of dextrose
could have affected the therapeutic effect. Although the
degree of pain reduction and functional improvement is
not completely consistent, there seems to be a correlation
A. Dextose vs. Saline on VAS for Pain Composite 6 months–1 year (SMD)
B. Dextose vs. Exercise on VAS for Pain Composite 6 months–1 year (SMD)
C. Dextose vs. Platelet-rich plasma on VAS for Pain Composite 6 months–1 year (SMD)
D. Dextose vs. Steroid on VAS for Pain Composite 6 months–1 year (SMD)
92 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
between the two in the studies that were included in this
meta-analysis.
Although there were several positive aspects of our study,
there are some limitations. First, despite recent studies be-
ing added, the number of trials eligible for inclusion in the
meta-analysis was limited. Since the results regarding pro-
lotherapy corresponding to the effects of corticosteroids
and PRP were derived by analyzing only two studies, addi-
tional studies are needed. Second, there is heterogeneity in
the pooled analyses; this is likely attributable to multiple
factors, including differences in patient characteristics,
control treatment, study design, injection protocol meth-
ods, dextrose concentrations, follow-up duration, and out-
come assessment methods. A limited number of studies
and heterogeneity have inhibited more detailed meta-anal-
yses of subgroups. Third, due to a lack of a uniform lon-
ger-term follow-up duration across the studies, pooling of
results could only be done with data collected between 6
months and one year of follow-up. Considering that pro-
lotherapy is hypothesized to work by healing and regenera-
tion over several months, reported results of effects may
underestimate long-term benefits. Therefore, further stud-
ies (including cohort studies) are needed to evaluate the
long-term effects. Fourth, since prolotherapy has been
shown to have comparable effects to steroid injection and
PRP, further studies should be conducted regarding cost
effectiveness. Jahangiri et al. [21] compared prolotherapy
and corticosteroids and mentioned that there was no sig-
nificant difference in cost. In previous study, prolotherapy
was more effective [14], and has a better cost advantage
compared to PRP [37].
In the future, subgroup analysis should be performed to
identify patients who respond most favorably to prolother-
apy. There are several ways in which treatment strategies
can vary; for example, dextrose concentrations/volumes
may differ, the interval and total duration of treatment may
differ, and the site of injection (intra- or extra-articular ar-
eas) may differ. Since there are no clear criteria or standard
treatment, this should be discussed in the future. Reducing
pain, improving functionality, and increasing patient satis-
faction provide a solid foundation for further research in
attempt of treatment standardization.
In conclusion, dextrose-based prolotherapy has been
shown to have a positive and significantly beneficial effect
for patients with chronic musculoskeletal pain, ranging from
6 months to 1 year. There is evidence that dextrose-based
prolotherapy has a better therapeutic effect than exercise,
and that it has a similar effect compared to PRP and steroid
injection. Adequately powered, longer-term trials with uni-
form endpoints are needed to better elucidate the efficacy
of prolotherapy.
ACKNOWLEDGEMENTS
Special thanks to Jiyeon Ju, and Joonho Cho in contribu-
tion to writing this article.
This work was supported by grant from Inje University,
2019.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Geonhyeong Bae, Yunhee Lim. Data
curation: Geonhyeong Bae, Sangseok Lee, Woo Yong Lee,
Yunhee Lim. Formal analysis: Geonhyeong Bae, Yunhee
Lim. Funding acquisition: Yunhee Lim. Writing - original
draft: Geonhyeong Bae, Yunhee Lim. Writing - review &
editing: Suyeon Kim, Sangseok Lee, Woo Yong Lee, Yunhee
Lim. Supervision: Yunhee Lim.
ORCID
Geonhyeong Bae, https://orcid.org/0000-0002-8527-0004
Suyeon Kim, https://orcid.org/0000-0002-6167-4952
Sangseok Lee, https://orcid.org/0000-0001-7023-3668
Woo Yong Lee, https://orcid.org/0000-0002-1632-1314
Yunhee Lim, https://orcid.org/0000-0003-2399-4768
REFERENCES
1. Institute of Medicine of the National Academies. Relieving pain
in America: a blueprint for transforming prevention, care, edu-
cation, and research. Washington, D.C., National Academies
Press. 2011. p. 382.
2. Hung CY, Hsiao MY, Chang KV, Han DS, Wang TG. Compara-
tive effectiveness of dextrose prolotherapy versus control injec-
tions and exercise in the management of osteoarthritis pain: a
systematic review and meta-analysis. J Pain Res 2016; 9: 847-
57.
3. Ayhan E, Kesmezacar H, Akgun I. Intraarticular injections (cor-
www.anesth-pain-med.org 93
Dextrose prolotherapy and chronic pain

ticosteroid, hyaluronic acid, platelet rich plasma) for the knee
osteoarthritis. World J Orthop 2014; 5: 351-61.
4. Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, Wells G.
Intraarticular corticosteroid for treatment of osteoarthritis of
the knee. Cochrane Database Syst Rev 2006; (2): CD005328.
5. Aufiero D, Vincent H, Sampson S, Bodor M. Regenerative in-
jection treatment in the spine: review and case series with
platelet rich plasma. J Stem Cells Res Rev Rep 2015; 2: 1019.
6. Linetsky FS, Manchikanti L. Regenerative injection therapy for
axial pain. Tech Reg Anesth Pain Manag 2005; 9: 40-9.
7. Adams E. Bibliography: prolotherapy for musculoskeletal pain.
Boston, Veterans. 2008.
8. Goswami A. Prolotherapy. J Pain Palliat Care Pharmacother
2012; 26: 376-8.
9. Nair LS. Prolotherapy for tissue repair. Transl Res 2011; 158:
129-31.
10. Rabago D, Best TM, Beamsley M, Patterson J. A systematic re-
view of prolotherapy for chronic musculoskeletal pain. Clin J
Sport Med 2005; 15: 376-80.
11. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman
AD, et al.; Cochrane Bias Methods Group; Cochrane Statistical
Methods Group. The Cochrane Collaboration's tool for assess-
ing risk of bias in randomised trials. BMJ 2011; 343: d5928.
12. Uğurlar M, Sönmez MM, Uğurlar ÖY, Adıyeke L, Yıldırım H,
Eren OT. Effectiveness of four different treatment modalities in
the treatment of chronic plantar fasciitis during a 36-month
follow-up period: a randomized controlled trial. J Foot Ankle
Surg 2018; 57: 913-8.
13. Seven MM, Ersen O, Akpancar S, Ozkan H, Turkkan S, Yıldız Y,
et al. Effectiveness of prolotherapy in the treatment of chronic
rotator cuff lesions. Orthop Traumatol Surg Res 2017; 103: 427-
33.
14. Ersen Ö, Koca K, Akpancar S, Seven MM, Akyıldız F, Yıldız Y, et
al. A randomized-controlled trial of prolotherapy injections in
the treatment of plantar fasciitis. Turk J Phys Med Rehabil
2017; 64: 59-65.
15. Rabago D, Patterson JJ, Mundt M, Kijowski R, Grettie J, Segal
NA, et al. Dextrose prolotherapy for knee osteoarthritis: a ran-
domized controlled trial. Ann Fam Med 2013; 11: 229-37.
16. Bertrand H, Reeves KD, Bennett CJ, Bicknell S, Cheng AL. Dex-
trose prolotherapy versus control injections in painful rotator
cuff tendinopathy. Arch Phys Med Rehabil 2016; 97: 17-25.
17. Kim E, Lee JH. Autologous platelet-rich plasma versus dextrose
prolotherapy for the treatment of chronic recalcitrant plantar
fasciitis. PM R 2014; 6: 152-8.
18. Yelland MJ, Glasziou PP, Bogduk N, Schluter PJ, McKernon M.
Prolotherapy injections, saline injections, and exercises for
chronic low-back pain: a randomized trial. Spine (Phila Pa
1976) 2004; 29: 9-16.
19. Reeves KD, Hassanein K. Randomized, prospective, place-
bo-controlled double-blind study of dextrose prolotherapy for
osteoarthritic thumb and finger (DIP, PIP, and trapeziometa-
carpal) joints: evidence of clinical efficacy. J Altern Comple-
ment Med 2000; 6: 311-20.
20. Reeves KD, Hassanein K. Randomized prospective dou-
ble-blind placebo-controlled study of dextrose prolotherapy
for knee osteoarthritis with or without ACL laxity. Altern Ther
Health Med 2000 6: 68-74, 77-80.
21. Jahangiri A, Moghaddam FR, Najafi S. Hypertonic dextrose ver-
sus corticosteroid local injection for the treatment of osteoar-
thritis in the first carpometacarpal joint: a double-blind ran-
domized clinical trial. J Orthop Sci 2014; 19: 737-43.
22. Sit RW, Chung VC, Reeves KD, Rabago D, Chan KK, Chan DC,
et al. Hypertonic dextrose injections (prolotherapy) in the
treatment of symptomatic knee osteoarthritis: a systematic re-
view and meta-analysis. Sci Rep 2016; 6: 25247.
23. Paavola M, Kannus P, Järvinen TA, Järvinen TL, Józsa L, Järvin-
en M. Treatment of tendon disorders. Is there a role for corti-
costeroid injection? Foot Ankle Clin 2002; 7: 501-13.
24. Dean BJ, Lostis E, Oakley T, Rombach I, Morrey ME, Carr AJ.
The risks and benefits of glucocorticoid treatment for tendi-
nopathy: a systematic review of the effects of local glucocorti-
coid on tendon. Semin Arthritis Rheum 2014; 43: 570-6.
25. Tempfer H, Gehwolf R, Lehner C, Wagner A, Mtsariashvili M,
Bauer HC, et al. Effects of crystalline glucocorticoid triamcino-
lone acetonide on cultered human supraspinatus tendon cells.
Acta Orthop 2009; 80: 357-62.
26. Stannard JP, Bucknell AL. Rupture of the triceps tendon associ-
ated with steroid injections. Am J Sports Med 1993; 21: 482-5.
27. Scarpone M, Rabago DP, Zgierska A, Arbogast G, Snell E. The
efficacy of prolotherapy for lateral epicondylosis: a pilot study.
Clin J Sport Med 2008; 18: 248-54.
28. Okuda Y, Adrogue HJ, Nakajima T, Mizutani M, Asano M, Tachi
Y, et al. Increased production of PDGF by angiotensin and high
glucose in human vascular endothelium. Life Sci 1996; 59:
1455-61.
29. Oh JH, Ha H, Yu MR, Lee HB. Sequential effects of high glucose
on mesangial cell transforming growth factor-beta 1 and fi-
bronectin synthesis. Kidney Int 1998; 54: 1872-8.
30. Di Paolo S, Gesualdo L, Ranieri E, Grandaliano G, Schena FP.
High glucose concentration induces the overexpression of
transforming growth factor-beta through the activation of a
platelet-derived growth factor loop in human mesangial cells.
Am J Pathol 1996; 149: 2095-106.
94 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
31. Kampa RJ, Connell DA. Treatment of tendinopathy: is there a
role for autologous whole blood and platelet rich plasma injec-
tion? Int J Clin Pract 2010; 64: 1813-23.
32. Sampson S, Gerhardt M, Mandelbaum B. Platelet rich plasma
injection grafts for musculoskeletal injuries: a review. Curr Rev
Musculoskelet Med 2008; 1: 165-74.
33. Foster TE, Puskas BL, Mandelbaum BR, Gerhardt MB, Rodeo
SA. Platelet-rich plasma: from basic science to clinical applica-
tions. Am J Sports Med 2009; 37: 2259-72.
34. de Mos M, van der Windt AE, Jahr H, van Schie HT, Weinans H,
Verhaar JA, et al. Can platelet-rich plasma enhance tendon re-
pair? A cell culture study. Am J Sports Med 2008; 36: 1171-8.
35. Jensen KT, Rabago DP, Best TM, Patterson JJ, Vanderby R Jr.
Early inflammatory response of knee ligaments to prolothera-
py in a rat model. J Orthop Res 2008; 26: 816-23.
36. Jensen KT, Rabago DP, Best TM, Patterson JJ, Vanderby R Jr. Re-
sponse of knee ligaments to prolotherapy in a rat injury model.
Am J Sports Med 2008; 36: 1347-57.
37. Mei-Dan O, Mann G, Maffulli N. Platelet-rich plasma: any sub-
stance into it? Br J Sports Med 2010; 44: 618-9.
www.anesth-pain-med.org 95
Dextrose prolotherapy and chronic pain

Lumbar disc herniation (LDH) commonly causes low
back pain (LBP) and radiculopathy. LDH often resolves
over time with a spontaneous resorption rate of 60% or
above [1]. Therefore, the consensus for treating patients
with LDH is to offer conservative treatment first and then
surgical intervention for non-responders [2].
One conservative treatment used for LDH is transforam-
inal epidural steroid injection (TFESI). TFESI is a method
used to deliver steroids and local anesthetics into the epi-
dural space through the spinal neural foramen. Numerous
reports and extensive reviews have demonstrated the diag-
Corresponding author Yong-Hyun Cho, M.D. Department of Anesthesiology and Pain Medicine, Seoul Sungsim General Hospital, 259 Wangsan-ro, Dongdaemun-gu, Seoul 02488, Korea Tel: 82-2-966-1616 Fax: 82-2-968-2394 E-mail: [email protected]
Background: Transforaminal epidural steroid injection (TFESI) is a conservative treatment for patients with lumbar disc herniation (LDH). However, there are reports of various compli-cations that can occur after TFESI; among these, paraplegia is a serious complication.
Case: A 70-year-old woman who was unable to lie supine due to low back pain exacerbation during back extension underwent TFESI. After injection, there was pain relief and the patient was able to lie supine; however, paraplegia developed immediately. Magnetic resonance im-aging confirmed cauda equina syndrome (CES) due to nerve compression from L1–2 LDH. We determined that the patient’s LDH was already severe enough to be considered CES and that the TFESI procedure performed without an accurate understanding of the patient’s con-dition aggravated the disease.
Conclusions: It is important to accurately determine the cause of pain and disease state of a patient to establish a correct treatment plan before TFESI is performed.
Keywords: Cauda equina syndrome; Epidural injection; Intervertebral disc displacement; Paraplegia.
Paraplegia after transforaminal epidural steroid injection in a patient with severe lumbar disc herniation - A case report -
Seok Ho Jeon, Won Jang, Sun-Hee Kim, Yong-Hyun Cho, Hyun Seok Lee, and Hyun Cheol Ko
Department of Anesthesiology and Pain Medicine, Seoul Sungsim General Hospital,
Seoul, Korea
Received August 27, 2020Revised November 4, 2020 Accepted November 4, 2020
Case ReportAnesth Pain Med 2021;16:96-102https://doi.org/10.17085/apm.20068pISSN 1975-5171 • eISSN 2383-7977
nostic efficacy of TFESI as well as its effectiveness in LBP
and relief from radiculopathy pain [3]. However, various
complications have been reported as the use of TFESI has
increased. Some classic complications of TFESI include in-
travascular injections, vascular trauma, epidural hemato-
ma, and neural damage [4]. There are also case reports
documenting paraplegia—a serious complication—follow-
ing TFESI. Most of the reported paraplegia cases were due
to spinal cord ischemia from a vascular injury or a particu-
late steroid embolism [5].
We encountered a patient whose severe LBP and radiating
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
96

KS
PS
pain induced by postural changes prevented the assessment
with imaging modalities. Thus, TFESI was performed to re-
lieve the patient's pain. Here, we report this case as the pa-
tient developed paraplegia immediately after TFESI.
CASE REPORT
The patient has provided written informed consent for
publication of the case and associated images. This case
report follows the CARE (CAse REport) guidelines [6].
A 70-year-old woman came to the emergency room (ER)
complaining of severe LBP. The patient was not able to
walk, and she was in the left lateral decubitus position with
lumbar flexion. The patient's numerical rating scale (NRS,
0 being no pain and 10 being the worst pain imaginable)
score for LBP was 6/10, but when asked to perform lumbar
extension or move to a supine position, the NRS score for
LBP increased to 9/10, with development of left buttock
pain and radiating pain in the left thigh. The patient had
undergone a posterior lumbar interbody fusion at L2–S1
for a herniated nucleus pulposus 2 years prior to the ER
visit. The pain dissipated after the surgery; however, the
patient started to experience intermittent recurrences of
LBP 1 year after. Three days prior to hospitalization, the
patient was unable to lie in the supine position even when
sleeping owing to severe LBP and buttock pain.
The patient’s height was 154 cm, and her weight was 65
kg. The vital signs included blood pressure 150/90 mmHg,
body temperature 36.5°C, pulse rate 86/min, and respirato-
ry rate 20/min. Due to the complaint of extreme pain with
any change in position, it was necessary to perform a neu-
rological examination on the patient; therefore, the ortho-
pedic surgeon quickly performed the possible tests in the
left lateral decubitus position as desired by the patient.
However, during the neurological examination, the patient
continued to complain of pain. A neurological examination
to assess the motor power revealed left ankle dorsiflexion
grade 4/5, left big toe dorsiflexion 4/5, left knee extension
4/5, and left hip flexion 4/5, indicating motor weakness.
The patient also had a sensory deficit throughout the left
leg and complained of numbness in the left thigh. The pa-
tient showed an absence of the Babinski reflex, an ankle
jerk reflex scale measurement of 2+, and a knee jerk scale
measurement of 3+. The right leg did not show any motor
weakness or sensory deficit. The patient did not have uri-
nary incontinence or saddle anesthesia, and the anal
sphincter tone was retained.
However, we recognized that the patient’s spinal disease
may be serious due to the patient’s history of previous sur-
gery, complaint of severe pain, and abnormal findings on
neurological examination of the left lower limb. Conse-
quently, the orthopedic surgeon explained that the disease
was severe, and that the patient may require surgery, and
additional imaging tests. In our hospital, magnetic reso-
nance imaging (MRI) can only be performed in the supine
position; however, as the patient was in a very nervous
state due to pain and complained of pain even when mov-
ing on the bed or changing position for examination, it was
determined that pain control was necessary for additional
examination; 100 μg of fentanyl (50 μg/ml) was then ad-
ministered intravenously. However, the pain relief was in-
adequate and the patient was unable to change position.
Since additional examinations could not be performed, the
patient strongly requested priority pain relief before addi-
tional imaging examinations.
Our anesthesia and pain medicine department was
asked to control this patient’s pain. We also considered that
the patient may be at high risk for complications with a
nerve block because the type of spinal disease was not
clearly identified, the state of the nerves could not be as-
certained, and abnormal findings were already observed in
the neurological examination. However, we understood the
urgency of the imaging test; hence, we explained the risk of
the procedure and the possibility of side effects to the pa-
tient and then planned the pain relief procedure. Given the
patient’s L2–S1 vertebral body fusion with possible adja-
cent segment disease, we chose to perform a TFESI
through the left L1–2 neural foramen.
The procedure was conducted 3 h after the patient ar-
rived at the ER, with the patient kept in her preferred left
lateral decubitus position with lumbar flexion. C-arm fluo-
roscopy was performed, and the typical lateral view angle
was used in order to obtain the anteroposterior view. A flu-
oroscopic lateral image indicated a kyphotic deformity at
the L1 vertebral body, likely caused by osteonecrosis.
After the skin had been sterilized, 2 ml of 1% lidocaine
was administered for local anesthesia. To create an oblique
view in order to visualize the left L1–2 neural foramen, the
C-arm angle was turned 20º to the left from the anteropos-
terior view. A 20-gauge short bevel nerve block needle was
inserted until the needle tip reached the inferior margin of
the L1 lumbar pedicle, and the lateral view was checked af-
ter the needle tip reached the middle of the pedicle. In the
lateral view, the needle tip was located immediately before
www.anesth-pain-med.org 97
Paraplegia after TFESI

reaching the dorsal periosteum of the L1 vertebral body; 2
ml of contrasting agent was used to confirm that the loca-
tion of the needle tip was appropriate for the epidural in-
jection (Fig. 1). No blood vessel contrasting was observed.
During the procedure, the contrast agent did not disappear
rapidly due to blood or cerebrospinal fluid flow. The con-
trast agent showed a pattern of spreading along the epidur-
al space.
A 6 ml mixture containing 10 mg of 0.5% bupivacaine (5
mg/ml), 3 ml of normal saline, and 5 mg of dexamethasone
(5 mg/ml) was injected slowly.
Five minutes after the injection, the patient’s LBP NRS
score decreased to 2/10. A neurological examination
showed no change in motor or sensory functions com-
pared to pre-injection. Her vital signs were as follows:
blood pressure, 124/68 mmHg; body temperature, 36.5°C;
pulse rate, 70/min; and respiratory rate, 16/min. Although
the blood pressure was lower than that before the proce-
dure, it was within the normal range, and this was judged
to be due to the reduction in pain. When epidural nerve
block is performed, neurological changes and changes in
vital signs may occur slowly, and thus additional patient
monitoring was necessary. However, after further discus-
sions with an orthopedic surgeon, it was decided that the
imaging test should be performed quickly. The patient was
able to lie supine with reduced pain and was sent for an
MRI. During the MRI scan, the patient reported acute para-
plegia and a complete loss of motor and sensory functions
in both legs including the sensation around the anus. The
patient also lost the anal reflex and bulbocavernosus reflex.
The vital signs were as follows: blood pressure, 118/70
mmHg; body temperature, 36.6°C; pulse rate, 70/min; and
respiratory rate, 18/min.
We assessed the situation at the time of the procedure,
and contrasted images were reviewed to determine the
cause of paraplegia. The operator who had performed TFE-
SI judged that the contrast medium had spread to the epi-
dural space. The possibility of intrathecal injection could
not be completely ruled out. However, we injected bupiva-
caine at a low concentration, so the complete loss of motor
sensory function as seen in this patient was determined to
be unlikely. We also speculated that the progress of cauda
equina syndrome (CES) may have been accelerated due to
the effect of the pressure or volume when the drug was in-
jected. It was also impossible to completely rule out the
possibility of a hematoma being produced due to blood
vessel damage caused by the needle. We could obtain the
patient’s MRI results. Upon assessing the MR images, we
found that the patient’s conus medullaris was located
above the L1 body and CES occurred due to L1–2 LDH.
There was no indication of any cord injury (Fig. 2).
An emergency decompression surgery was performed 1
h after the paraplegia developed. The L1 lamina was ex-
cised, and decompression and discectomy on both sides
were performed. In order to resolve the kyphotic deformi-
ty, posterior lumbar fusion was also performed at T11–L1
(Fig. 3). The surgeon confirmed that the dural sac was
strongly compressed by the disc at the L1–2 level during
surgery. In addition, there was slight bleeding around the
disc at L1–2. The situation was determined to be inconsis-
tent with nerve compression due to bleeding. However, it
was difficult to clearly identify the cause of this bleeding. It
was not possible to specify whether bleeding occurred due
to the TFESI procedure, or whether blood vessel damage
occurred due to pressure applied to the inner portion of
the spinal canal by the disc.
The patient’s paralysis did not resolve after the surgery.
B
A
Fig. 1. (A) Anteroposterior view fluoroscopy shows the needle, which was inserted under the L1 lumbar pedicle. (B) Lateral view fluoroscopy shows the contrasting agent spreading from the L1–2 neural foramen into the epidural space.
98 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
The patient was hospitalized for 6 weeks, and repeated
neurological examinations were conducted to assess signs
of recovery. At week 6, no change in motor function, and
only a mild recovery of sensory function were observed.
There was a recovery of fine touch and proprioception in
both thighs, but the bladder function did not recover. The
patient was transferred to a rehabilitation hospital at her
request, and she agreed to come in for a 6-month fol-
low-up. At the follow-up visit, the patient had a 3/5 of mus-
cle strength grade and did not have any voiding difficulties.
However, numbness throughout both legs persisted.
DISCUSSION
Recently, TFESI has been widely used in patients with
various spinal diseases. TFESI is particularly useful for pain
relief in patients with LDH. However, several complications
caused by TFESI, including infection, vascular injury, he-
matoma, intravascular drug injection, nerve damage, em-
bolism, and paraplegia, have been reported. To prevent the
occurrence of these complications, we need to understand
the patient's disease state as early as possible and decide
on the most appropriate treatment plan. The process of
making this judgment is facilitated by the patient's medical
history, neurological examination, and imaging tests.
Among these, the most helpful information is provided by
the MRI examination [2].
It is very rare to encounter a patient whose posture
change is completely impossible due to extreme pain, as
was the case with our patient. As a result, the patient was
unable to lie in a supine position, making imaging tests
completely impossible. In general, if a patient's symptoms
are severe and neurologic deficit is involved, imaging tests
are performed first. TFESI is then performed to facilitate
the diagnosis and treatment of the patient. However, we
were asked to perform a TFESI for the purpose of perform-
ing an imaging test without being provided with any imag-
ing test results prior to the procedure. The patient's pain
was not controlled even with narcotic analgesics. The ini-
tial neurological examination did not prompt us to suspect
CES. Under the opinion that the MRI was necessary even
for surgery, we proceeded with TFESI. At that time, the pa-
tient complained of extreme pain and had abnormal neu-
rological examination findings. If a patient shows CES or
neurological symptoms are progressing rapidly, surgical
treatment should be selected [2].
According to the results of the MRI, which was per-
Fig. 2. (A) Lumbar sagittal T2-weighted magnetic resonance imaging shows compression of the cauda equina due to L1–2 lumbar disc herniation (white arrow). Conus medullaris (black arrow). (B) Lumbar axial T2-weighted magnetic resonance image showing compression of the cauda equina due to L1–2 lumbar disc herniation.
Fig. 3. Anteroposterior view (A) and lateral view (B) lumbar X-ray images taken after surgery.
B
A
BA
www.anesth-pain-med.org 99
Paraplegia after TFESI

formed after TFESI and the patient's pain had been allevi-
ated, it was presumed that the patient had already had
Kümmell’s disease or spondylodiscitis. Further, a kyphotic
deformity due to osteonecrosis was progressing at the L1–2
level. In addition, severe LDH of L1–2 could cause severe
pain and paralysis. It was presumed that the patient was
avoiding paralysis by keeping the spinal canal wide via
lumbar flexion [7]. So, it seems that the patient felt severe
pain and refused to adopt a position of back extension.
This patient developed paraplegia after TFESI, as the dis-
ease rapidly worsened. The relationship between CES and
TFESI in this patient is not clear. However, there are several
possible causes that may have led to CES in this patient.
First, CES may have occurred due to a rapid increase in
pressure within the epidural space as the drug was injected
during the procedure. According to a study by Usubiaga et
al. [8], pressure in the epidural space can increase from –10
cmH2O to a maximum of 65 cmH2O when 10 ml of 2% lido-
caine is injected. In particular, pressure in the epidural
space was higher in elderly patients, and high levels of
pressure could be maintained up to 2 min after injection of
the drug. The patient in our case had an epidural space
volume that was too small for her to tolerate pain without
adopting the lumbar flexion position. For this reason, it
was thought that the pressure created by drug injection
into the epidural space acted more strongly. If such an el-
derly patient is expected to have high pressure in the epi-
dural space due to severe LDH, a small amount of the drug
should be injected as slowly as possible.
Alternatively, it is possible that blood vessel damage oc-
curred. The radicular artery enters the intervertebral fora-
men along the nerve root. The probability of the radicular
artery being in the upper portion of the intervertebral fora-
men is twice as high as that of it being in the lower portion
[9]. The patient in our case had undergone posterior lum-
bar interbody fusion surgery at the L2–S1 level, and it was
assumed that severe LDH occurred at the L1–2 level. We
predicted that it would be difficult for the needle to enter
the lower portion of the foramen while performing TFESI
at the L1–2 level and instead inserted the needle into the
upper portion of the foramen. Although the blood vessels
were not imaged using a contrast agent, the possibility that
blood vessel damage occurred cannot be excluded. In ad-
dition, the radicular artery or internal vertebral venous
plexus may have been damaged as the pressure in the epi-
dural space increased as mentioned previously [10]. It is
possible that this vascular injury contributed to the occur-
rence of CES.
A third reason, post-procedural changes in posture due
to pain relief may have exacerbated the disease. The lum-
bar flexion posture can exacerbate LDH by applying pres-
sure within the disc. However, the lumbar flexion position
increases the capacity of the spinal canal [7]. As mentioned
previously, the patient had already experienced a serious
LDH condition that caused CES, but her position may have
reduced the pressure applied to the dural sac by increasing
the diameter of the spinal canal with lumbar flexion. How-
ever, after TFESI, the patient was able to lie in the supine
position because back extension was possible. At this time,
the capacity of the spinal canal would have decreased. As a
result, it is expected that the dural sac was strongly pressed
and CES occurred immediately. There is an existing case
report of CES that progressed according to a similar mech-
anism [11]. In the reported case, the patient was diagnosed
with spinal stenosis, and an MRI scan was difficult due to
the severe pain experienced by the patient when in the su-
pine and back extension position. Hence, to proceed with
the examination, the patient was sedated with propofol
while lying in the supine position. Subsequently, an MRI
scan was performed and CES occurred.
Before TFESI is performed, it is important to determine
the patient's neurological condition, disease, and cause of
pain via MRI. However, as was observed in our case, if a
posture change is impossible and the imaging test cannot
be performed, it can be challenging to effectively treat the
patient. Recently, MRI equipment capable of performing
examinations in various postures such as sitting or stand-
ing has been developed and used [12]. The use of such
equipment is thought to be helpful for imaging tests in pa-
tients who are unable to maintain a supine position due to
pain.
However, if such equipment is unavailable, the cause
and severity of pain, as well as the risk of the procedure,
should be determined by reviewing the patient's medical
history and performing a neurological examination. In pa-
tients with LDH, lumbar motion limitation, resting pain,
and deformity are red flags [13]. In addition, patients who
experience leg pain during lumbar extension have a poor
prognosis [14]. When TFESI is performed on high-risk LDH
patients, a thorough assessment of position- and mo-
tion-based pain characteristics, including a neurological
examination, is necessary. Patients should be informed
and educated about the risks of exacerbation of their exist-
ing disease with positional changes after pain relief from
100 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
TFESI. In addition, when performing TFESI on high-risk
LDH patients, physicians should be prepared for any emer-
gency.
In our case, the patient developed CES due to L1–2 level
LDH. Fortunately, the patient’s conus medullaris was lo-
cated above the L1 body; however, the conus medullaris is
usually located between T12 and L2. Conventionally, if the
dural sac of the L1–2 level is compressed, not only CES but
also conus medullaris syndrome (CMS) can occur. In both
CES and CMS, radiating pain, as well as motor and sensory
dysfunction of the lower extremities, can occur, and blad-
der dysfunction and saddle anesthesia may be seen. Since
both syndromes show similar symptoms, it is difficult to
distinguish them based on clinical features alone; however,
they are easily distinguishable via MRI. Additionally, treat-
ment of both syndromes commonly requires emergency
decompression surgery [15]. If CMS would have occurred,
recovery would have been more difficult even if emergency
decompression surgery had been performed.
We performed TFESI without an accurate initial assess-
ment of the patient's disease state and observed paraplegia
in this patient after TFESI had been performed. It is im-
portant to accurately evaluate the patient before this pro-
cedure, establish a correct treatment plan, and safely per-
form the procedure using methods designed to reduce the
occurrence of complications. In addition, it is important to
explain the risks and possible complications of the proce-
dure to the patient, so that they are able to prepare for the
possibility of experiencing serious complications. Even
when extreme care is taken, complications may occur after
the procedure. If such a complication occurs, the rapid
identification of its cause and a prompt response greatly
affect patient recovery.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Seok Ho Jeon, Yong-Hyun Cho. Data
curation: Hyun Seok Lee, Hyun Cheol Ko. Writing - original
draft: Won Jang, Yong-Hyun Cho. Writing - review & edit-
ing: Seok Ho Jeon, Sun-Hee Kim, Yong-Hyun Cho.
ORCID
Seok Ho Jeon, https://orcid.org/0000-0003-3351-1627
Won Jang, https://orcid.org/0000-0001-8275-9317
Sun-Hee Kim, https://orcid.org/0000-0002-9110-6462
Yong-Hyun Cho, https://orcid.org/0000-0002-8323-1933
Hyun Seok Lee, https://orcid.org/0000-0002-7809-5914
Hyun Cheol Ko, https://orcid.org/0000-0002-8479-2871
REFERENCES
1. Zhong M, Liu JT, Jiang H, Mo W, Yu PF, Li XC, et al. Incidence
of spontaneous resorption of lumbar disc herniation: a me-
ta-analysis. Pain Physician 2017; 20: E45-52.
2. Andersson GB, Brown MD, Dvorak J, Herzog RJ, Kambin P,
Malter A, et al. Consensus summary of the diagnosis and treat-
ment of lumbar disc herniation. Spine (Phila Pa 1976) 1996;
21(24 Suppl): 75S-8S.
3. Vad VB, Bhat AL, Lutz GE, Cammisa F. Transforaminal epidural
steroid injections in lumbosacral radiculopathy: a prospective
randomized study. Spine (Phila Pa 1976) 2002; 27: 11-6.
4. Boswell MV, Shah RV, Everett CR, Sehgal N, McKenzie Brown
AM, Abdi S, et al. Interventional techniques in the manage-
ment of chronic spinal pain: evidence-based practice guide-
lines. Pain Physician 2005; 8: 1-47.
5. Kennedy DJ, Dreyfuss P, Aprill CN, Bogduk N. Paraplegia fol-
lowing image-guided transforaminal lumbar spine epidural
steroid injection: two case reports. Pain Med 2009; 10: 1389-94.
6. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D;
CARE Group. The CARE guidelines: consensus-based clinical
case report guideline development. J Clin Epidemiol 2014; 67:
46-51.
7. Dai LY, Xu YK, Zhang WM, Zhou ZH. The effect of flexion-ex-
tension motion of the lumbar spine on the capacity of the spi-
nal canal. An experimental study. Spine (Phila Pa 1976) 1989;
14: 523-5.
8. Usubiaga JE, Wikinski JA, Usubiaga LE. Epidural pressure and
its relation to spread of anesthetic solutions in epidural space.
Anesth Analg 1967; 46: 440-6.
9. Melissano G, Chiesa R. Advances in imaging of the spinal cord
vascular supply and its relationship with paraplegia after aortic
interventions. A review. Eur J Vasc Endovasc Surg 2009; 38:
567-77.
10. Desai MJ, Dua S. Perineural hematoma following lumbar trans-
foraminal steroid injection causing acute-on-chronic lumbar
radiculopathy: a case report. Pain Pract 2014; 14: 271-7.
11. Kuramoto A, Chang L, Graham J, Holmes S. Lumbar spinal ste-
www.anesth-pain-med.org 101
Paraplegia after TFESI

nosis with exacerbation of back pain with extension: a poten-
tial contraindication for supine MRI with sedation. J Neuroim-
aging 2011; 21: 92-4.
12. Jinkins JR, Dworkin JS, Damadian RV. Upright, weight-bearing,
dynamic-kinetic MRI of the spine: initial results. Eur Radiol
2005; 15: 1815-25.
13. Verhagen AP, Downie A, Popal N, Maher C, Koes BW. Red flags
presented in current low back pain guidelines: a review. Eur
Spine J 2016; 25: 2788-802.
14. Saal JA. Natural history and nonoperative treatment of lumbar
disc herniation. Spine (Phila Pa 1976) 1996; 21(24 Suppl): 2S-9S.
15. Brouwers E, van de Meent H, Curt A, Starremans B, Hosman A,
Bartels R. Definitions of traumatic conus medullaris and cauda
equina syndrome: a systematic literature review. Spinal Cord
2017; 55: 886-90.
102 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
Spinal cord stimulation (SCS) has been used to treat var-
ious chronic neuropathic pain conditions for many de-
cades [1]. SCS has been reported to be a relatively safe and
reversible procedure with several complications due to
minimally invasive properties. Common complications as-
sociated with SCS include lead migration, connection fail-
ure, lead breakage, pain at the implant site, seroma forma-
tion, and infection [2]. Catastrophic complications, includ-
ing breakdown of the tissue overlaying implant site and ex-
trusion of the device through the skin are possible, but very
Corresponding author Gyeong-Jo Byeon, M.D., Ph.D. Department of Anesthesia and Pain Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Geumoro 20, Mulgeumeup, Yangsan 50612, Korea Tel: 82-55-360-2758 Fax: 82-55-360-2149 E-mail: [email protected]
Background: Despite significant technological advances in the implantable pulse generator (IPG), complications can still occur. We report a case that unexpected extrusion of the IPG of spinal cord stimulation (SCS) was promptly identified and successfully removed without any complications.
Case: After a car accident 4 years ago, a 55-year-old male who was diagnosed with complex local pain syndrome in his right leg. The SCS was inserted with 2 leads, with the IPG being implanted in the right lower abdomen region. Four years later, he developed extrusion of the IPG from his abdominal region. This unexpected extrusion may have been related to pres-sure necrosis caused by continued compression of pocket site where a belt was frequently tied. The IPG and the leads were successfully removed without infection occurring.
Conclusions: To prevent unexpected extrusion of IPG, it is necessary to consider in advance whether the pocket site is pressed against the belt.
Keywords: Complex regional pain syndrome; Devices; Necrosis; Neuropathic pain; Spinal cord stimulation.
Unexpected extrusion of the implantable pulse generator of the spinal cord stimulator - A case report -
Eun-Ji Choi1,2, Hyun-Su Ri1,2, Hyeonsoo Park1, Hye-Jin Kim1,2, Ji-Uk Yoon1,2, and Gyeong-Jo Byeon1,2
1Department of Anesthesia and Pain Medicine, Pusan National University Yangsan
Hospital, Pusan National University School of Medicine, 2Research Institute for
Convergence of Biomedical Science and Technology, Pusan National University
Yangsan Hospital, Yangsan, Korea
Received June 23, 2020Revised October 4, 2020Accepted November 26, 2020
Case ReportAnesth Pain Med 2021;16:103-107https://doi.org/10.17085/apm.20054pISSN 1975-5171 • eISSN 2383-7977
rare [3]. Pacemakers, which have a structure similar to that
of the implantable pulse generator (IPG) component, have
been reported to extrude out of the chest [4].
We report a case that unexpected extrusion of the IPG of
SCS was promptly identified and successfully removed
without any further adverse complications. Prior to this re-
port, we received prior written informed consent for publi-
cation from the patient.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
103
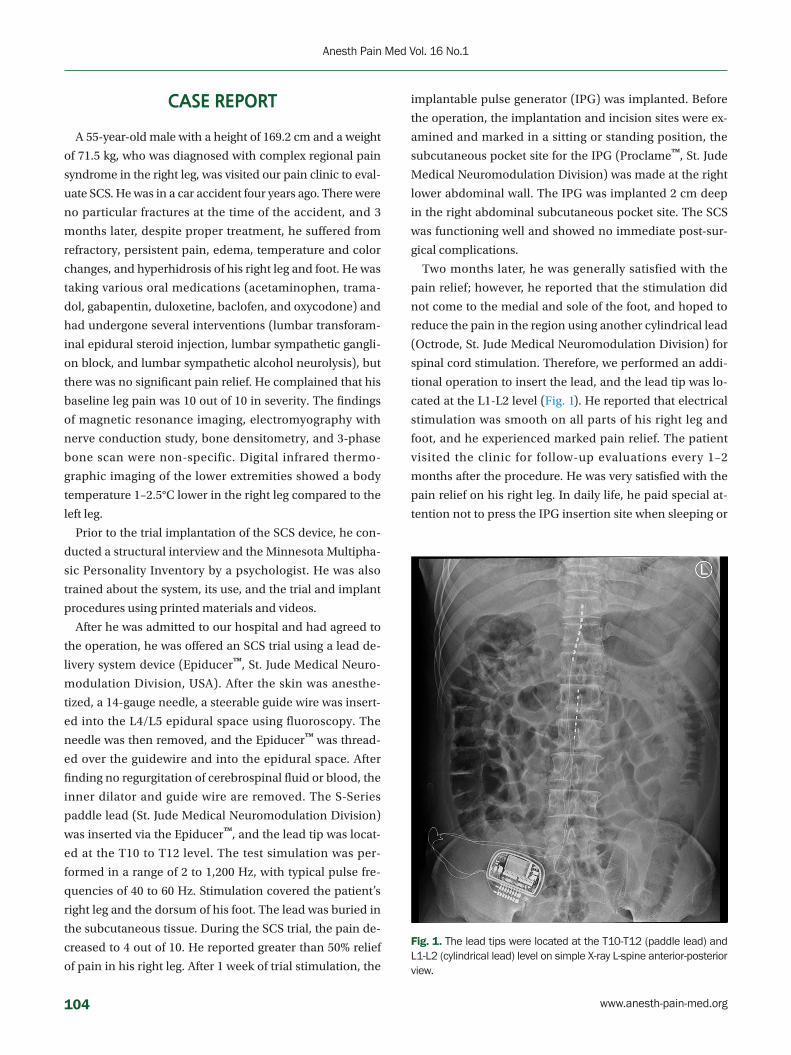
CASE REPORT
A 55-year-old male with a height of 169.2 cm and a weight
of 71.5 kg, who was diagnosed with complex regional pain
syndrome in the right leg, was visited our pain clinic to eval-
uate SCS. He was in a car accident four years ago. There were
no particular fractures at the time of the accident, and 3
months later, despite proper treatment, he suffered from
refractory, persistent pain, edema, temperature and color
changes, and hyperhidrosis of his right leg and foot. He was
taking various oral medications (acetaminophen, trama-
dol, gabapentin, duloxetine, baclofen, and oxycodone) and
had undergone several interventions (lumbar transforam-
inal epidural steroid injection, lumbar sympathetic gangli-
on block, and lumbar sympathetic alcohol neurolysis), but
there was no significant pain relief. He complained that his
baseline leg pain was 10 out of 10 in severity. The findings
of magnetic resonance imaging, electromyography with
nerve conduction study, bone densitometry, and 3-phase
bone scan were non-specific. Digital infrared thermo-
graphic imaging of the lower extremities showed a body
temperature 1–2.5°C lower in the right leg compared to the
left leg.
Prior to the trial implantation of the SCS device, he con-
ducted a structural interview and the Minnesota Multipha-
sic Personality Inventory by a psychologist. He was also
trained about the system, its use, and the trial and implant
procedures using printed materials and videos.
After he was admitted to our hospital and had agreed to
the operation, he was offered an SCS trial using a lead de-
livery system device (Epiducer™, St. Jude Medical Neuro-
modulation Division, USA). After the skin was anesthe-
tized, a 14-gauge needle, a steerable guide wire was insert-
ed into the L4/L5 epidural space using fluoroscopy. The
needle was then removed, and the Epiducer™ was thread-
ed over the guidewire and into the epidural space. After
finding no regurgitation of cerebrospinal fluid or blood, the
inner dilator and guide wire are removed. The S-Series
paddle lead (St. Jude Medical Neuromodulation Division)
was inserted via the Epiducer™, and the lead tip was locat-
ed at the T10 to T12 level. The test simulation was per-
formed in a range of 2 to 1,200 Hz, with typical pulse fre-
quencies of 40 to 60 Hz. Stimulation covered the patient’s
right leg and the dorsum of his foot. The lead was buried in
the subcutaneous tissue. During the SCS trial, the pain de-
creased to 4 out of 10. He reported greater than 50% relief
of pain in his right leg. After 1 week of trial stimulation, the
implantable pulse generator (IPG) was implanted. Before
the operation, the implantation and incision sites were ex-
amined and marked in a sitting or standing position, the
subcutaneous pocket site for the IPG (Proclame™, St. Jude
Medical Neuromodulation Division) was made at the right
lower abdominal wall. The IPG was implanted 2 cm deep
in the right abdominal subcutaneous pocket site. The SCS
was functioning well and showed no immediate post-sur-
gical complications.
Two months later, he was generally satisfied with the
pain relief; however, he reported that the stimulation did
not come to the medial and sole of the foot, and hoped to
reduce the pain in the region using another cylindrical lead
(Octrode, St. Jude Medical Neuromodulation Division) for
spinal cord stimulation. Therefore, we performed an addi-
tional operation to insert the lead, and the lead tip was lo-
cated at the L1-L2 level (Fig. 1). He reported that electrical
stimulation was smooth on all parts of his right leg and
foot, and he experienced marked pain relief. The patient
visited the clinic for follow-up evaluations every 1–2
months after the procedure. He was very satisfied with the
pain relief on his right leg. In daily life, he paid special at-
tention not to press the IPG insertion site when sleeping or
Fig. 1. The lead tips were located at the T10-T12 (paddle lead) and L1-L2 (cylindrical lead) level on simple X-ray L-spine anterior-posterior view.
104 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
during activities, however, he was engaged in agriculture
and was always doing hard work with his body bent in a
sitting position. He occasionally noted a foreign body sen-
sation in the IPG pocket site when wearing a belt. Some-
times, when he tightened his belt, he complained that the
skin of the IPG site felt under pressure.
At a routine follow-up, he complained of wound site ero-
sion, and a metal piece was exposed from his lower ab-
dominal wall for 2 days. He denied having fevers and chills.
On examination, the IPG had moved approximately 3cm
below the pocket, and a 0.5 cm area of metal part was ex-
truding from his right lower abdominal wall. There was
erosion around the entry and exit points of the IPG, with
apparent healing of the tissue beneath. There was no dis-
charge from the extrusion site from the eroded areas, and
microbiological cultures were taken from several points
around that region (Fig. 2). The pocket did not show any
signs of active inflammation or infection. The IPG test re-
vealed that the device’s functional values were completely
within normal ranges. After obtaining written informed
consent, the patient had the stimulator leads and the IPG
removed. The lower abdominal pocket site was thoroughly
cleaned and debrided after the IPG removal, and the
wound was sutured (Fig. 3). After surgery, the patient re-
covered uneventfully. The stimulator leads and the IPG re-
moved during surgery were sent for aerobic and anaerobic
culture, which returned back negative. The patient was
prescribed cefazoline as postoperative antibiotic for 14
days. After removal of IPG, his right leg pain was 8-9 out of
10 in severity, as the pain was managed with only oral
medication and several conservative interventions. With
all the risk of infection removed and stable, we decided to
perform re-implantation of the SCS device later.
DISCUSSION
SCS has been an effective surgical procedure for improv-
ing suffering among patients with chronic neuropathic
pain. However, several complications can occur despite
significant technological advances in the IPG, with signifi-
cant decreases in both size and weight, and rechargeable
capabilities.
Complications of SCS have been reported to have an in-
cidence of 30–40% in several studies [5,6]. Its complications
are divided into three main categories: hardware-related,
biological, and programming or therapy-related. Hard-
ware-related complications include lead fracture or dis-
connection reported incidence of 5–9%, lead migration re-
ported incidence of 0– 27%, and IPG failure in around 1.7%
[1,7]. Biological complications include pain at the implant
site, allergic reaction, IPG seroma, infection, epidural fi-
brosis, epidural hematoma, dura puncture-related head-
aches and more serious nerve damage, including spinal
cord injury and paralysis [8,9]. Programming or therapy-re-
lated complications include loss of paresthesia and painful
Fig. 2. The implantable pulse generator was extruded at the lower abdominal pocket site.
Fig. 3. The lower abdominal pocket site was thoroughly cleaned and debrided after implantable pulse generator removal, and the wound was sutured.
www.anesth-pain-med.org 105
Extrusion of implantable pulse generator

or unpleasant paresthesia. These are less threatening and
can usually be resolved through programming, although
on rare occasions can be removed due to therapy failure
[10].
Among the several complications mentioned above, IPG
extrusion is a hardware-related complication, and it is a
very rare complication of SCS. In two cases, IPG extrusion
was reported after implantation in the gluteal area [3,11].
In one of these cases, the patient was a truck driver who
had been driving for a long time for three months, causing
skin erosion in the buttocks and extruding the IPG. In the
other case, an extrusion of the IPG in a sacral stimulator
was due to rapid weight loss after the patient underwent
gastric bypass surgery. Our report is the first case of extru-
sion after implantation of the IPG of a spinal cord stimula-
tor into the abdominal wall. In a case similar to our report,
there are multiple case reports of pulse generator extrusion
of a pacemaker [4,12]. They were caused by the skin erod-
ing around the IPG insertion. The incidence of skin erosion
due to the underlying pacemaker generator has been esti-
mated to be approximately 0.8%. Factors predisposing skin
erosion are the presence of a thin subcutaneous fat layer,
tissue fragility in old-age patients, abrasive action exerted
on the skin from external agents, pressure exercised from
the device on the subcutaneous tissue and possible infec-
tions of the site [13].
The patient had been doing well after the operation. Oc-
casionally the patient complained of the discomfort of the
IPG insertion when wearing a belt. The IPG were sutured
to the subcutaneous fat layer of the abdominal wall to fix at
the initial insertion site, but it seems that a tear occurred at
the suture site. As a result, the IPG migrated downward
from the initial insertion site, and it seems that the down-
ward migration was a little worse due to the compression
of the belt. Skin erosion occurred due to compression of
the belt, and the IPG was extruded through this area.
Whenever the patient wore a belt, he complained of dis-
comfort due to the constant pressure on the IPG pocket
site. We should have carefully observed skin erosion during
follow-up. The early stages of skin erosion can develop ex-
posure of the pocket site, and even IPG migration and ex-
trusion. If the IPG size and configuration are not appropri-
ate, excessive pressure can be placed on the subcutaneous
tissue, and improperly sized pockets may result in the de-
velopment of infection and dysfunction of the IPG [14].
With a careful follow-up as well as a clear understanding of
potential complications and a careful approach to device
selection can minimize the incidence of complications. It
is important to identify early signs of erosion before the de-
vice damages the skin. If the skin is not damaged, surgical
modification of the pocket is often necessary to prevent
contamination and infection of the device. However, if the
hardware is exposed, it should be assumed that the device
is contaminated, and treatments generally involve a much
more complicated procedure to remove all devices, includ-
ing IPG and leads [15].
In conclusion, extrusion of the IPG from the pocket site
is very rare. In order to prevent this rare complication, pri-
or to permanent SCS insertion, the clinicians should fully
consider the patient's age, occupational hazards, and daily
life habits that could cause excessive pressure on the IPG.
And the skin of abdominal wall should be inspected care-
fully at the site of the intended pocket, and the belt-tight-
ening area should be examined in advance to see if all the
SCS components, such as the IPG, will not be pressed by
the belt. A deep pocket (about 2–3 cm depth), instead of
just a pocket under the skin, should be considered. In ad-
dition, it is necessary to educate the patient not to habitu-
ally touch the IPG insertion site with a sense of foreign
body.
ACKNOWLEDGEMENTS
This work was supported by clinical research grant from
Pusan National University Yangsan Hospital in 2019.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: Eun-Ji Choi, Gyeong-Jo Byeon. Writ-
ing - original draft: Eun-Ji Choi, Gyeong-Jo Byeon. Writing
- review & editing: Ji-Uk Yoon, Gyeong-Jo Byeon. Investiga-
tion: Hyun-Su Ri, Hyeonsoo Park, Hye-Jin Kim. Supervi-
sion: Ji-Uk Yoon.
ORCID
Eun-Ji Choi, https://orcid.org/0000-0003-3731-0785
Hyun-Su Ri, https://orcid.org/0000-0002-7305-4144
Hyeonsoo Park, https://orcid.org/0000-0002-3376-3691
106 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

KS
PS
Hye-Jin Kim, https://orcid.org/0000-0003-1630-0422
Ji-Uk Yoon, https://orcid.org/0000-0002-3971-2502
Gyeong-Jo Byeon, https://orcid.org/0000-0001-5333-3894
REFERENCES
1. Deer TR, Mekhail N, Provenzano D, Pope J, Krames E, Leong
M, et al. Neuromodulation Appropriateness Consensus Com-
mittee. The appropriate use of neurostimulation of the spinal
cord and peripheral nervous system for the treatment of
chronic pain and ischemic diseases: the Neuromodulation
Appropriateness Consensus Committee. Neuromodulation
2014; 17: 515-50.
2. Mekhail NA, Mathews M, Nageeb F, Guirguis M, Mekhail MN,
Cheng J. Retrospective review of 707 cases of spinal cord stim-
ulation: indications and complications. Pain Pract 2011; 11:
148-53.
3. Rabi J, Anitescu M. Late extrusion of an implantable pulse
generator of a spinal cord stimulator. Pain Physician 2016; 19:
E671-4.
4. Yuksel S, Demir S, Sahin M. Total extrusion of a normally
functioning pacemaker. Tex Heart Inst J 2012; 39: 156-7.
5. Kumar K, Taylor RS, Jacques L, Eldabe S, Meglio M, Molet J, et
al. Spinal cord stimulation versus conventional medical
management for neuropathic pain: a multicentre ran-
domised controlled trial in patients with failed back surgery
syndrome. Pain 2007; 132: 179-88.
6. Kemler MA, Barendse GA, van Kleef M, de Vet HC, Rijks CP,
Furnée CA, et al. Spinal cord stimulation in patients with
chronic reflex sympathetic dystrophy. N Engl J Med 2000;
343: 618-24.
7. Cameron T. Safety and efficacy of spinal cord stimulation for
the treatment of chronic pain: a 20-year literature review. J
Neurosurg 2004; 100: 254-67.
8. Levy R, Henderson J, Slavin K, Simpson BA, Barolat G, Ship-
ley J, et al. Incidence and avoidance of neurologic complica-
tions with paddle type spinal cord stimulation leads. Neuro-
modulation 2011; 14: 412-22.
9. Barolat G. Experience with 509 plate electrodes implanted
epidurally from C1 to L1. Stereotact Funct Neurosurg 1993;
61: 60-79.
10. Kumar K, Wilson JR, Taylor RS, Gupta S. Complications of
spinal cord stimulation, suggestions to improve outcome,
and financial impact. J Neurosurg Spine 2006; 5: 191-203.
11. Nold CJ, McLennan MT. Spontaneous extrusion of sacral
nerve implant secondary to massive weight loss. Int Urogy-
necol J Pelvic Floor Dysfunct 2007; 18: 105-7.
12. Santarpia G, Sarubbi B, D'Alto M, Romeo E, Calabro R. Extru-
sion of the device: a rare complication of the pacemaker im-
plantation. J Cardiovasc Med (Hagerstown) 2009; 10: 330-2.
13. Harcombe AA, Newell SA, Ludman PF, Wistow TE, Sharples
LD, Schofield PM, et al. Late complications following perma-
nent pacemaker implantation or elective unit replacement.
Heart 1998; 80: 240-4.
14. Pavia S, Wilkoff B. The management of surgical complica-
tions of pacemaker and implantable cardioverter-defibrilla-
tors. Curr Opin Cardiol 2001; 16: 66-71.
15. Sohail MR, Uslan DZ, Khan AH, Friedman PA, Hayes DL, Wil-
son WR, et al. Management and outcome of permanent pace-
maker and implantable cardioverter-defibrillator infections.
J Am Coll Cardiol 2007; 49: 1851-9.
www.anesth-pain-med.org 107
Extrusion of implantable pulse generator

INTRODUCTION
Pressure injury, also called pressure ulcer or pressure
sore, is defined as localized cellular necrosis caused by
constant compression between external materials and
Corresponding author Sangseok Lee, M.D.Department of Anesthesiology and Pain Medicine, Sanggye Paik Hospital, Inje University College of Medicine, 1342 Dongil-ro, Nowon-gu, Seoul 01757, Korea Tel: 82-2-950-1989 Fax: 82-2-950-1323 E-mail : [email protected]
Background: Perioperative patients are potentially at risk for pressure injuries due to anes-thetic agents and surgical positioning. Pressure injury increases discomfort and pain in pa-tients and causes complications, which lead to an increase in mortality and hospitalization duration. Most previous studies did not focus on specific types of surgery or surgical posi-tioning. We tried to identify the incidence of perioperative pressure injury during spinal sur-gery and perioperative risk factors that contribute to pressure injury.
Methods: We retrospectively analyzed electronic medical records of 663 patients who un-derwent spinal surgery between March 2016 and May 2018. The primary outcome was oc-currence of pressure injury. Potential risk factors of pressure injury were selected based on previous studies and expert opinion, and divided into two sub-categories: preoperative and intraoperative risk factors. We compared the clinical characteristics of patients in the pres-sure injury and non-injury groups. Perioperative risk factors for pressure injury were analyzed by logistic regression.
Results: Among 663 patients, the incidence of all stages of pressure injury was 5.9%. The face and inguinal regions were the most injured sites (both 28.6%). The pressure injury group showed a 13% longer hospitalization period. Preoperative plasma concentration of protein was associated with 0.5-fold lower pressure injury (OR: 0.50; 95% CI: 0.27 to 0.95; P = 0.034).
Conclusions: The incidence of pressure injury was similar to that previously reported and occurred in the direct weight-bearing areas, which led to longer hospitalization. We found that a lower preoperative serum protein level is significantly associated with intraoperative pressure injury occurrence during spinal surgery.
Keywords: Anesthesia; Neoplasm; Orthopedics; Pressure ulcer; Protein; Risk factors; Skin ulcer.
An exploratory study of risk factors for pressure injury in patients undergoing spine surgery
DaeHee Suh, Su Yeon Kim, Byunghoon Yoo, and Sangseok Lee
Department of Anesthesiology and Pain Medicine, Sanggye Paik Hospital, Inje
University College of Medicine, Seoul, Korea
Received September 29, 2020Revised October 21, 2020 Accepted October 23, 2020
Clinical ResearchAnesth Pain Med 2021;16:108-115https://doi.org/10.17085/apm.20081pISSN 1975-5171 • eISSN 2383-7977
bony prominences. The severity of pressure injury varies
from erythema to tissue destruction. The National Pressure
Injury Advisory Panel (NPUAP) defines a 4-stage classifica-
tion system as follows: Stage 1, non-blanchable erythema
of intact skin; Stage 2, partial-thickness skin loss involving
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
108

General
epidermis or dermis, such as abrasion, blister, or shallow
crater; Stage 3, full-thickness skin loss involving damage or
necrosis of subcutaneous tissue; and Stage 4, full-thickness
skin loss with extensive destruction, tissue necrosis, and
damage to muscle, bone, and supporting structures [1].
Perioperative patients are at risk of developing pressure
injuries since anesthetic agents interrupt normal relaxation
and contraction of blood vessels and reduce perfusion at
the site of the bony prominence. The patient’s surgical po-
sition is another factor that increases incidence of pressure
injury, as anatomical structures such as nerves, muscles,
and tendons are extended or compressed for a long period,
which interferes with capillary perfusion. The incidence
varies from 3.7% to 23.8% [2,3] in surgical patients, which
may depend on the patients’ characteristics (age, comor-
bidities, etc.), type of surgery, injury stage, and time after
surgery when the injury was discovered .
Previous literature have typically reported stage 2 pres-
sure injuries or higher as these injuries are associated with
bacterial infections, osteomyelitis, and squamous cell car-
cinoma and contribute to increased mortality [4]. However,
stage 1 pressure injury should not be overlooked as it may
lead to patient discomfort, pain, prolonged hospital stay,
and subsequent pressure ulcer development [5,6]. Al-
though surgical factors, such as type of procedure and po-
sitioning, are important factors associated with pressure
injury, most previous studies did not focus on a specific
type of surgery or surgical position. In our clinical experi-
ence, pressure injuries more frequently occurred in pa-
tients undergoing spinal surgery than in patients undergo-
ing other surgeries. Spinal surgeries are mostly performed
in a prone position, and many of them are for spinal fusion,
which usually cause a considerable amount of bleeding
and are associated with prolonged surgery duration, which
are associated with the known perioperative risk factors for
pressure injury, To date, very few studies have been con-
ducted on pressure injury in spinal surgery; additionally,
analysis of the risk factors associated with pressure injury
have shown inconclusive results.
Moreover, previous studies have mostly included the in-
jury found immediately after surgery as well as the injuries
that were discovered during the postoperative period of 24
h to several months. To minimize the postoperative effect
and analyze only the intraoperative factors, it is necessary
to limit the study to injuries found immediately after sur-
gery.
The relatively high incidence of pressure injury reported
so far indicates that risk assessment and the use of protec-
tive measures should be improved [7]. Additionally, the lit-
erature shows that approximately 95% of all pressure inju-
ries in perioperative patients can be prevented with early
risk assessment and appropriate interventions [8]. There-
fore, it is important to particularly target reversible factors
through prior risk assessment for the patient group with a
high risk of pressure injury. This study aimed to identify
the incidence of perioperative pressure injury during spi-
nal surgery and explore the perioperative risk factors that
may potentially contribute to pressure injury.
MATERIALS AND METHODS
This study analyzed the data of 692 patients who under-
went spinal surgery from March 2016 to May 2018 at a sin-
gle university teaching hospital. Ethical approval from the
Institutional Review Board (IRB no. 2019-08-004) was re-
ceived. Data were retrospectively analyzed from the data-
base of the institution's electronic medical records (EMR).
There were 20 duplicate cases in the initial data prepara-
tion stage, which were duplicated due to reoperation two
(18 patients) and three times (1 patient) in the same pa-
tient, and repeat surgery by the same person may intro-
duce a bias against the risk of pressure injury. In all cases,
only the first spinal surgery was included in the analysis.
Patients aged 18 years and older, of both sexes, undergo-
ing elective or emergency spinal surgeries were included in
the study. We excluded 9 cases of cervical spine operation,
supine/lateral position, simple short procedures such as
‘wound debridement’ or ‘incision & drain.’ Ultimately, 663
patients were included in the study (Fig. 1).
Outcome and risk factor evaluation
The primary outcome was the occurrence of pressure in-
jury. Attending anesthesiologists, surgeons, and scrub
nurses examined the patient’s whole body before and after
the surgery. The injury site, size, and characteristics of the
pressure injury were obtained from the description in the
EMR. We categorized the pressure injuries into 4 stages ac-
cording to the NPUAP classification system [1].
Potential risk factors for pressure injury were selected
based on previous studies and expert opinions. The au-
thors first considered the common and known risk factors,
obtained from previous studies of risk assessment for pres-
sure injury [2,3,9–11]. These commonly known risk factors
www.anesth-pain-med.org 109
Risk factors for pressure injury

can classified into three categories: preoperative, intraop-
erative, and postoperative factors. We focused on the pre-
operative and intraoperative factors that might be mediat-
ed by an anesthesiologist to prevent pressure injury.
We explored the following characteristics as preoperative
risk factors for pressure injury: demographic data (age, sex,
body mass index), current status regarding smoking/alco-
hol consumption, history or presence of various comorbid-
ities (cardiovascular, respiratory, renal, hepatic, diabetes,
malignancy, and neurologic disease), preoperative labora-
tory test results (hemoglobin, hematocrit, protein, albu-
min, glucose, blood urea nitrogen, creatinine, sodium, po-
tassium, etc.), and American Society of Anesthesiologists
classification.
Additionally, intraoperative risk factors consisted of an-
esthesia duration, total amount of intraoperative fluid ad-
ministration, total amount of all intraoperative blood prod-
uct transfusion, total amount of intraoperative bleeding,
average body temperature during surgery, and the total
dose of vasopressor agent administered. These risk factors
were selected based on consensus among experts and sur-
geons on the likelihood of these factors affecting the devel-
opment of a pressure injury [10].
Statistical analysis
All statistical analyses were performed using R software
(version 3.6.1, R Foundation for Statistical Computing,
Austria; https://www.R-project.org/). We compared the
clinical characteristics between the pressure injury group
and the non-injury group using a Student’s t-test or Mann–
Whitney U test for continuous variables based on the re-
sults of a Shapiro-Wilk normality test, and we used a Fish-
er’s exact test or chi-square test for categorical or propor-
tional variables.
A multivariable logistic regression analysis based on a
binomial generalized linear model was performed to iden-
tify the risk factors associated with perioperative pressure
injury. We explored the relationship between each variable
and the pressure injury through a univariate logistic regres-
sion analysis, and then performed multivariable logistic re-
gression, which consisted of variables with P < 0.1 from
the univariate logistic regression. Independent risk factors
with P < 0.05 in the multivariable analysis were considered
statistically significant. To produce the final logistic regres-
sion model, the risk factors were selected by weighting
their clinical implications and statistical values (e.g., Akaike
Records identified from electronic medical records (EMR)
(n = 692)
Records included in study finally(n = 663)
Records excluded(2 repetitive surgeries in 18 patients,
3 repetitive surgeries in 1 patient)(n = 20)
Records excluded(n = 9)
Iden
tifica
tion
Scre
enin
gIn
clud
ed
Records after duplicate cases removed (If repetitive spinal surgeries were performed on the same patient during the period, only the first surgery was included in the study)
(n = 672)
Records screened(excluded cases of cervical spine operation, supine/lateral, simple short procedures such as 'wound debridement' or 'Incision & drain')
(n = 663)
Fig. 1. CONSORT flow diagram of study. CONSORT: consolidated standards of reporting trials.
110 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

General
Information Criterion). Hosmer–Lemeshow goodness-of-
fit tests were used to assess the fitness of the logistic regres-
sion model. The optimal cut-off point of the explored risk
factor was determined by maximizing the sum of sensitivi-
ty and specificity using a receiver operating characteristic
(ROC) curve to measure association and evaluate the pre-
diction accuracy of a significant risk factor for the occur-
rence of pressure injury.
RESULTS
All results are expressed as mean ± standard deviation
or median (interquartile range; 1Q, 3Q) as appropriate. The
incidence of all stages of pressure injury was 5.9% (39/663).
All patients had a relatively low stage of pressure injury;
nine patients (18%) had stage-1 and 40 patients (82%) had
stage-2 injuries, while none had a stage-3 injury or higher.
Eight patients had two different sites of injuries, and one
patient had three different sites of injuries. The face and in-
guinal regions were the most injured sites (both 28.6%).
Other sites, in order of frequency of injury occurrence, in-
cluded the following: chest (24.5%), anterior superior iliac
spine (6.1%), abdomen (6.1%), arm (4.1%), and femur
(2.1%) (Table 1).
Table 2 shows a comparison of the general characteris-
tics of patients from the pressure injury and non-pressure
injury groups. These characteristics include factors that
could potentially be considered as risk factors for pressure
injury, general physiological information of the patient,
and the characteristics related to the patient's surgical out-
come, such as total duration of hospital stay.
The pressure injury group showed a 13% longer hospital-
ization period and a 3% lower protein plasma concentra-
tion than the non-pressure injury group. There were a total
of 3 (7.7%) cases of malignancy in the pressure injury
group, which included solid tumors in organs such as the
prostate, uterus, and lung. They also had 25% longer sur-
gery time and larger volumes of fluid and blood product
than the other group. Intraoperative bleeding was also 20%
higher than that of the non-pressure injury group (Table 2).
Table 3 presents the results of the univariate and base-
line/final multivariable logistic regression analyses for the
perioperative risk factors of pressure injury. All previously
known and clinically estimated risk factor candidates were
explored using univariate analyses. Through univariate
analysis, the following seven independent variables with a
cut-off value of P < 0.1 were included in the multivariate
analysis: preoperative plasma concentration of protein,
surgery time, total infused volume of fluids, total adminis-
tered volume of blood product, total volume of intraopera-
tive bleeding, total administered amounts of vasopressor,
and comorbidity of malignancy. The final reduced model
indicated that a preoperative plasma concentration of pro-
tein was associated with a 0.5-fold lower pressure injury
(adjusted odds ratio: 0.502; 95% confidence interval, 0.267–
0.953; P = 0.034) (Table 3).
The Hosmer-Lemeshow goodness-of-fit test showed that
the fitted values of the multivariable logistic regression
model (final reduced model) showed chi-squared =
9.3867, df = 8, and P value = 0.311 and, therefore, was a
valid model. All variables in our final reduced regression
model had a variance inflation factor value below 10,
which showed no collinearity. In the ROC analysis, the fi-
nal reduced model showed an area under the curve of
0.711 in pressure injury, with an optimal cut-off value of
5.17, and 68.6% sensitivity and 65.2% specificity.
DISCUSSION
The incidence of pressure injury in this study was approxi-
Table 1. Sites and Grades of Pressure Injury Founded Right after Surgery
Injury area Stage-1 Stage-2 Stage-3 or higher Total
Face 3 11 0 14 (28.6)
Inguinal region 3 11 0 14 (28.6)
Chest 0 12 0 12 (24.5)
ASIS 1 2 0 3 (6.1)
Abdomen 1 2 0 3 (6.1)
Forearm 0 2 0 2 (4.1)
Femur 1 0 0 1 (2.0)
Total 9 (18) 40 (82) 0 49 (100)*
Values are presented as number (%). ASIS: anterior superior iliac spine. *Pressure injury occurred in 39 patients, with 2 regional injuries in 8 patients, and 3 regional injuries in 1 patient, resulting in a total of 49 regional injuries.
www.anesth-pain-med.org 111
Risk factors for pressure injury
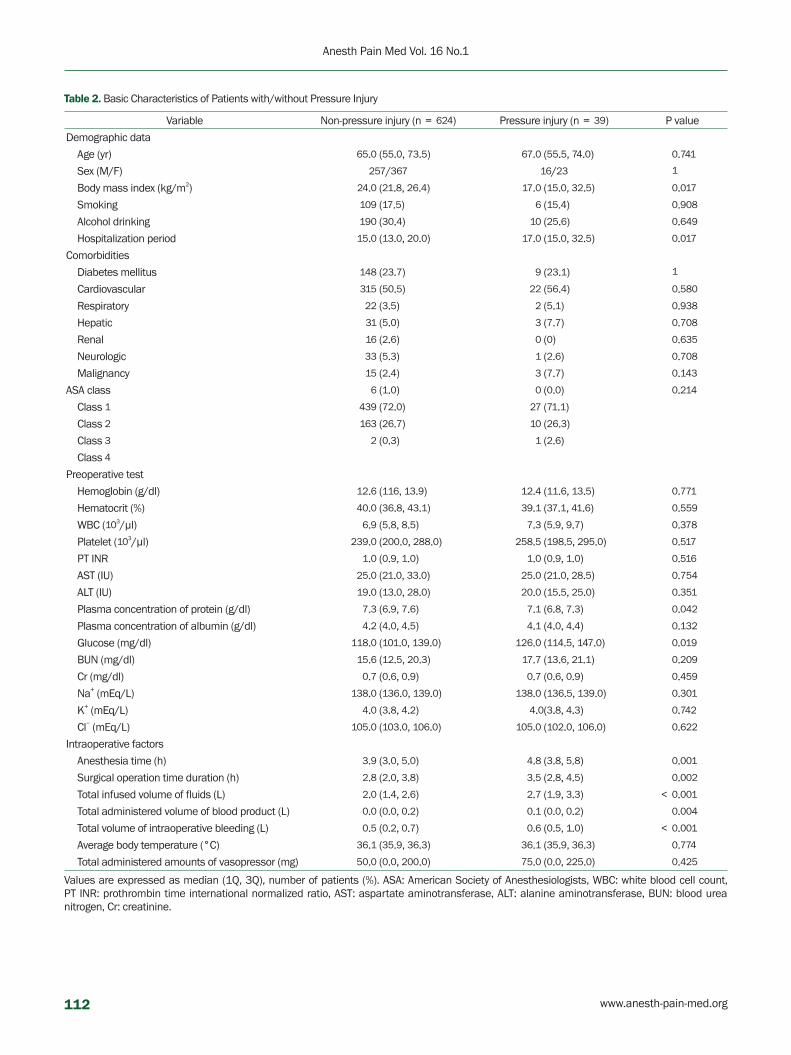
Table 2. Basic Characteristics of Patients with/without Pressure Injury
Variable Non-pressure injury (n = 624) Pressure injury (n = 39) P value
Demographic data
Age (yr) 65.0 (55.0, 73.5) 67.0 (55.5, 74.0) 0.741
Sex (M/F) 257/367 16/23 1
Body mass index (kg/m2) 24.0 (21.8, 26.4) 17.0 (15.0, 32.5) 0.017
Smoking 109 (17.5) 6 (15.4) 0.908
Alcohol drinking 190 (30.4) 10 (25.6) 0.649
Hospitalization period 15.0 (13.0, 20.0) 17.0 (15.0, 32.5) 0.017
Comorbidities
Diabetes mellitus 148 (23.7) 9 (23.1) 1
Cardiovascular 315 (50.5) 22 (56.4) 0.580
Respiratory 22 (3.5) 2 (5.1) 0.938
Hepatic 31 (5.0) 3 (7.7) 0.708
Renal 16 (2.6) 0 (0) 0.635
Neurologic 33 (5.3) 1 (2.6) 0.708
Malignancy 15 (2.4) 3 (7.7) 0.143
ASA class 6 (1.0) 0 (0.0) 0.214
Class 1 439 (72.0) 27 (71.1)
Class 2 163 (26.7) 10 (26.3)
Class 3 2 (0.3) 1 (2.6)
Class 4
Preoperative test
Hemoglobin (g/dl) 12.6 (116, 13.9) 12.4 (11.6, 13.5) 0.771
Hematocrit (%) 40.0 (36.8, 43.1) 39.1 (37.1, 41.6) 0.559
WBC (103/μl) 6.9 (5.8, 8.5) 7.3 (5.9, 9.7) 0.378
Platelet (103/μl) 239.0 (200.0, 288.0) 258.5 (198.5, 295.0) 0.517
PT INR 1.0 (0.9, 1.0) 1.0 (0.9, 1.0) 0.516
AST (IU) 25.0 (21.0, 33.0) 25.0 (21.0, 28.5) 0.754
ALT (IU) 19.0 (13.0, 28.0) 20.0 (15.5, 25.0) 0.351
Plasma concentration of protein (g/dl) 7.3 (6.9, 7.6) 7.1 (6.8, 7.3) 0.042
Plasma concentration of albumin (g/dl) 4.2 (4.0, 4.5) 4.1 (4.0, 4.4) 0.132
Glucose (mg/dl) 118.0 (101.0, 139.0) 126.0 (114.5, 147.0) 0.019
BUN (mg/dl) 15.6 (12.5, 20.3) 17.7 (13.6, 21.1) 0.209
Cr (mg/dl) 0.7 (0.6, 0.9) 0.7 (0.6, 0.9) 0.459
Na+ (mEq/L) 138.0 (136.0, 139.0) 138.0 (136.5, 139.0) 0.301
K+ (mEq/L) 4.0 (3.8, 4.2) 4.0(3.8, 4.3) 0.742
Cl− (mEq/L) 105.0 (103.0, 106.0) 105.0 (102.0, 106.0) 0.622
Intraoperative factors
Anesthesia time (h) 3.9 (3.0, 5.0) 4.8 (3.8, 5.8) 0.001
Surgical operation time duration (h) 2.8 (2.0, 3.8) 3.5 (2.8, 4.5) 0.002
Total infused volume of fluids (L) 2.0 (1.4, 2.6) 2.7 (1.9, 3.3) < 0.001
Total administered volume of blood product (L) 0.0 (0.0, 0.2) 0.1 (0.0, 0.2) 0.004
Total volume of intraoperative bleeding (L) 0.5 (0.2, 0.7) 0.6 (0.5, 1.0) < 0.001
Average body temperature (°C) 36.1 (35.9, 36.3) 36.1 (35.9, 36.3) 0.774
Total administered amounts of vasopressor (mg) 50.0 (0.0, 200.0) 75.0 (0.0, 225.0) 0.425
Values are expressed as median (1Q, 3Q), number of patients (%). ASA: American Society of Anesthesiologists, WBC: white blood cell count, PT INR: prothrombin time international normalized ratio, AST: aspartate aminotransferase, ALT: alanine aminotransferase, BUN: blood urea nitrogen, Cr: creatinine.
112 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

General
Tabl
e 3.
The
Uni
varia
te a
nd M
ultiv
aria
ble
Logi
stic
Reg
ress
ion
Anal
ysis
for P
ress
ure
Inju
ry
Fact
ors
Uni
varia
te lo
gist
ic a
naly
sis
Mul
tivar
iabl
e lo
gist
ic a
naly
sis
(B
asel
ine
Full
Mod
el)
Mul
tivar
iabl
e lo
gist
ic a
naly
sis
(F
inal
Red
uced
Mod
el)
Odd
s ra
tio95
% C
IP
valu
eAO
R95
% C
IP
valu
eAO
R95
% C
IP
valu
e
Preo
pera
tive
plas
ma
conc
entr
atio
n of
pro
tein
(g/d
l)0 .
532
0 .29
5 –0 .
973
0 .03
80 .
493
0 .26
0 –0 .
942
0 .03
10 .
502
0 .26
7 –0 .
953
0 .03
4
Surg
ical
ope
ratio
n tim
e du
ratio
n (h
)1 .
417
1 .18
5 –1 .
693
< 0
.001
1 .04
90 .
733 –
1 .46
70 .
785
NA
NA
NA
Tota
l inf
used
vol
ume
of fl
uids
(L)
1 .58
1 .26
8 –1 .
972
< 0
.001
1 .51
50 .
821 –
2 .73
80 .
175
1 .53
50 .
929 –
2 .45
60 .
083
Tota
l adm
inis
tere
d vo
lum
e of
blo
od p
rodu
ct (L
)2 .
644
1 .46
3 –5 .
111
0 .00
30 .
262
0 .03
7 –1 .
430
0 .16
30 .
241
0 .03
5 –1 .
257
0 .13
2
Tota
l vol
ume
of In
trao
pera
tive
blee
ding
(L)
2 .12
51 .
429 –
3 .28
5<
0.0
012 .
094
0 .91
0 –6 .
062
0 .13
32 .
137
0 .93
8 –6 .
144
0 .11
9
Tota
l adm
inis
tere
d am
ount
s of
vas
opre
ssor
(mg)
1 .00
21 .
000 –
1 .00
30 .
010
0 .99
90 .
997 –
1 .00
20 .
574
NA
NA
NA
Com
orbi
dity
of m
alig
nanc
y3 .
383
0 .75
9 –10
.841
0 .06
33 .
428
0 .70
5 –12
.243
0 .08
13 .
364
0 .69
2 –11
.901
0 .08
5
CI: c
onfid
ence
inte
rval
, AO
R: a
djus
ted
odds
ratio
, NA:
not
ava
ilabl
e.
mately 5.9%, with stage-1 and stage-2 injuries accounting for
18% and 82% of all injuries, respectively (Table 1). The dif-
ference in incidence among studies may be based on the
patients’ characteristics, type of surgery, surgical position,
injury stage, and follow-up time after surgery. Hwang et al.
[9] reported a pressure injury incidence of 4.3% in all surgi-
cal positions and 30% in the prone position. Choi et al. [3]
reported a higher incidence of 23.8% in all surgical posi-
tions and 63.9% in the prone position. In the prone posi-
tion, decreased venous return and inferior vena cava com-
pression were associated with decreased tissue perfusion
[12]. Weight-bearing areas are at risk of pressure injury oc-
currence. We used the Jackson Spinal & Imaging Table (JST
2000, Mizuhosi OSI, USA). The most injured regions in-
cluded the face (28.6%), inguinal region (28.6%), and chest
(24.5%), whereas Luo et al. [13] reported that the most in-
jured region was the ischium (85.8%). However, the types
of operating tables and weight-supporting areas used in
the two studies may be different. Since the detailed design
of the weight-supporting area is different for each frame of
the operation table, the injury site also depends on the
frame. In addition, the type of face pillows and the prophy-
lactic dressings used can also affect these results [14,15].
A stage-1 injury could be a potential risk factor for a
more severe form of pressure injury [5,6]. The criteria for
stage-1 injuries, such as redness and erythema, may be
subjective and could be missed in an physical examination
for pressure injury. Non-blanching erythema must be dis-
tinguished from blanching erythema since it may lead to
pressure ulcer development [5]. Another reason for the
high incidences reported by Hwang et al. [9] and Choi et al.
[3] was that they included injuries that occurred until the
24th hour. The pressure injuries could have been caused by
the excessive friction or shearing forces applied during the
transfer of patients from the surgical table to a stretcher or
hospital bed.
Proteins are generally known as indicators of a patient’s
nutritional status and play an important role in healing
damaged skin by affecting collagen synthesis, activation of
the immune system, and fibroblast proliferation [16].
Among all plasma proteins, albumin has the largest pro-
portion. Previous studies often used albumin levels instead
of proteins to demonstrate a correlation between pressure
injury and serum protein levels [2,5]. However, the results
are unclear [2,3,5,14,17]. Albumin has a short half-life;
thus, it may not reflect the patient’s nutritional status at the
time of surgery. Various proteins, such as α-, β-, and γ-glob-
www.anesth-pain-med.org 113
Risk factors for pressure injury

ulin and fibrinogen exist in plasma, and the colloid oncotic
pressure (COP) is determined by the total amount of pro-
teins present in plasma. When a specific protein in the
plasma decreases, COP may also decrease, resulting in in-
terstitial edema, which is a major cause of pressure injury
[10].
Choi et al. [3] reported that the risk increased 4.5 times in
surgeries with a duration greater than 4 h, and Hicks [18]
reported twice the incidence in surgeries that lasted longer
than 4 h. In this study, the average surgery time was 3.5 h,
which may have contributed to the low association be-
tween this factor and pressure injury occurrence. Large in-
traoperative bleeding can cause both hypotension and low
hemoglobin levels, which may decrease tissue perfusion
and oxygenation. Consequently, it may increase the risk of
pressure injury. In this study as well as previous studies,
the intraoperative total amount of fluid and blood prod-
ucts, the total volume of bleeding, and the total amount of
vasopressor, showed a positive correlation with pressure
injury occurrence (Table 3) [3,11,19]. Nutritional deficits,
such as cachexia and low activity levels due to fatigue, are
usually accompanied by malignancy [20]. These factors are
highly related to the previously known risk factors of pres-
sure ulcers, and Ranzani et al. showed its correlation [21].
However, although some patients have completed chemo-
therapy and radiation therapy and are in a complete remis-
sion state, it is still difficult to explain why pressure injury
occurred in these patients.
Pressure injury can cause prolonged hospitalization.
Han et al. [22] reported that pressure injuries influenced
mortality (OR 2.18) and increased the risk of increased
hospital stay (OR 5.55), along with increased risk of read-
mission (OR 1.30) and emergency department visits after
discharge (OR 1.70). Analysis of the association between
pressure injury and medical costs requires further research
using substantial data.
There are a few limitations to this study. Since this is a
study performed with patients from a single institution
with a relatively small number of patients, differences in
surgery time, operating tables, protective equipment, and
comorbidities of patient groups may have affected the re-
sults. There may have been other potential confounders.
The area under the curve value of 0.711 may indicate that
the model used was not optimal. Therefore, our model may
not fully explain the risk factors for intraoperative pressure
injury, and it is expected that there are more potential risk
factors that we were unable to identify.
In conclusion, the incidence of pressure injury was con-
siderable and mainly lower-stage injuries occurred. Pres-
sure injury mainly occurred in the region directly receiving
weight load during spinal surgery. In the cases of pressure
injuries occurred within a relatively short period of time as
like as intraoperative period, preoperative risk factors such
as plsma protein level rather than intraoperative factors
may be more closely related to the pressure injury. Al-
though further follow-up studies are needed to prove this
assumption, it is believed that the patient's nutritional sta-
tus and fluid status related to colloid oncotic pressure have
a substantial influence on the incidence of pressure injury
[10,16]. Therefore, proper correction of plasma protein lev-
el before surgery is very important in preventing pressure
injuries.
ACKNOWLEDGEMENTS
This work was supported by the 2019 Inje University re-
search grant.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS
Conceptualization: DaeHee Suh, Byunghoon Yoo,
Sangseok Lee. Data curation: DaeHee Suh, Sangseok Lee.
Formal analysis: Sangseok Lee. Funding acquisition:
Sangseok Lee. Methodology: DaeHee Suh, Byunghoon Yoo,
Sangseok Lee. Project administration: Sangseok Lee. Writ-
ing - original draft: DaeHee Suh, Byunghoon Yoo, Sangseok
Lee. Writing - review & editing: Su Yeon Kim, Byunghoon
Yoo, Sangseok Lee. Investigation: Su Yeon Kim, Byunghoon
Yoo, Sangseok Lee. Software: Sangseok Lee. Supervision:
Byunghoon Yoo, Sangseok Lee. Validation: Sangseok Lee.
ORCID
DaeHee Suh, https://orcid.org/0000-0003-4191-0708
Su Yeon Kim, https://orcid.org/0000-0002-6167-4952
Byunghoon Yoo, https://orcid.org/0000-0002-1958-8380
Sangseok Lee, https://orcid.org/0000-0001-7023-3668
114 www.anesth-pain-med.org
Anesth Pain Med Vol. 16 No.1

General
REFERENCES
1. Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieg-
green M. Revised National Pressure Ulcer Advisory Panel pres-
sure injury staging system: revised pressure injury staging sys-
tem. J Wound Ostomy Continence Nurs 2016; 43: 585-97.
2. Kim JM, Lee H, Ha T, Na S. Perioperative factors associated
with pressure ulcer development after major surgery. Korean J
Anesthesiol 2018; 71: 48-56.
3. Choi SJ, Kim DW, Chung HS, Ahn HJ, Gwak MS, Yang M, et al.
The incidence rate and risk factors of pressure-induced skin
breakdown during operation. Korean J Anesthesiol 2006; 50:
525-9.
4. Edlich RF, Winters KL, Woodard CR, Buschbacher RM, Long
WB, Gebhart JH, et al. Pressure ulcer prevention. J Long Term
Eff Med Implants 2004; 14: 285-304.
5. Nixon J, Cranny G, Bond S. Skin alterations of intact skin and
risk factors associated with pressure ulcer development in sur-
gical patients: a cohort study. Int J NursStud 2007; 44: 655-63.
6. Allman RM, Goode PS, Patrick MM, Burst N, Bartolucci AA.
Pressure ulcer risk factors among hospitalized patients with
activity limitation. JAMA 1995; 273: 865-70.
7. Munro CA. The development of a pressure ulcer risk-assess-
ment scale for perioperative patients. AORN J 2010; 92: 272-87.
8. Peixoto CA, Ferreira MBG, Felix MMDS, Pires PDS, Barichello
E, Barbosa MH. Risk assessment for perioperative pressure in-
juries. Rev Lat Am Enfermagem 2019; 27: e3117.
9. Hwang HY, Shin YS, Cho HS, Yeo JS. Risk factors of pressure
sore in patients undergoing general anesthesia. Korean J Anes-
thesiol 2007; 53: 79-84.
10. Jesurum J, Joseph K, Davis JM, Suki R. Balloons, beds, and
breakdown. Effects of low-air loss therapy on the development
of pressure ulcers in cardiovascular surgical patients with in-
tra-aortic balloon pump support. Crit Care Nurs Clin North
Am 1996; 8: 423-40.
11. O'Brien DD, Shanks AM, Talsma A, Brenner PS, Ramachandran
SK. Intraoperative risk factors associated with postoperative
pressure ulcers in critically ill patients: a retrospective observa-
tional study. Crit Care Med 2014; 42: 40-7.
12. Dharmavaram S, Jellish WS, Nockels RP, Shea J, Mehmood R,
Ghanayem A, et al. Effect of prone positioning systems on he-
modynamic and cardiac function during lumbar spine surgery:
an echocardiographic study. Spine (Phila Pa 1976) 2006; 31:
1388-93; discussion 1394.
13. Luo M, Long XH, Wu JL, Huang SZ, Zeng Y. Incidence and risk
factors of pressure injuries in surgical spinal patients: a retro-
spective study. J Wound Ostomy Continence Nurs 2019; 46:
397-400.
14. Yoshimura M, Ohura N, Tanaka J, Ichimura S, Kasuya Y, Hotta
O, et al. Soft silicone foam dressing is more effective than poly-
urethane film dressing for preventing intraoperatively acquired
pressure ulcers in spinal surgery patients: the Border Operat-
ing room Spinal Surgery (BOSS) trial in Japan. Int Wound J
2018; 15: 188-97.
15. Wu T, Wang ST, Lin PC, Liu CL, Chao YF. Effects of using a
high-density foam pad versus a viscoelastic polymer pad on
the incidence of pressure ulcer development during spinal sur-
gery. Biol Res Nurs 2011; 13: 419-24.
16. Saghaleini SH, Dehghan K, Shadvar K, Sanaie S, Mahmoodpoor
A, Ostadi Z. Pressure ulcer and nutrition. Indian J Crit Care
Med 2018; 22: 283-9.
17. Mistrík E, Dusilová-Sulková S, Bláha V, Sobotka L. Plasma albu-
min levels correlate with decreased microcirculation and the
development of skin defects in hemodialyzed patients. Nutri-
tion 2010; 26: 880-5.
18. Hicks DJ. An incidence study of pressure sores following sur-
gery. ANA Clin Sess 1970; 49-54.
19. Tschannen D, Bates O, Talsma A, Guo Y. Patient-specific and
surgical characteristics in the development of pressure ulcers.
Am J Crit Care 2012; 21: 116-25.
20. Lyder CH. Assessing risk and preventing pressure ulcers in pa-
tients with cancer. Semin Oncol Nurs 2006; 22: 178-84.
21. Ranzani OT, Simpson ES, Japiassú AM, Noritomi DT; Amil Crit-
ical Care Group. The challenge of predicting pressure ulcers in
critically ill patients. A multicenter cohort study. Ann Am Tho-
rac Soc 2016; 13: 1775-83.
22. Han Y, Jin Y, Jin T, Lee SM, Lee JY. Impact of pressure injuries on
patient outcomes in a Korean hospital: a case-control study. J
Wound Ostomy Continence Nurs 2019; 46: 194-200.
www.anesth-pain-med.org 115
Risk factors for pressure injury

TO THE EDITOR: For low-flow anesthesia, the anesthe-
sia workstation, monitoring technology and desflurane,
sevoflurane, which were a low blood-gas partition coeffi-
cient, have gradually been adopted. Low-flow anesthesia is
considered effective in maintaining the heat and the mois-
ture of the breathing circuit and preserving the mucociliary
function of the respiratory tract. In addition, it is safer and
more effective at lowering the economic burden and global
warming potential [1,2]. We read, with interest, your paper
on “Change of inspired oxygen concentration in low flow
anesthesia” (Anesth Pain Med 2020; 15: 434-40). We appre-
ciate your results and have some questions to discuss.
We have a few questions about the monitoring and the
maintenance of body temperature. How did you maintain
and monitor the temperature of the operating room? Was
the patient's temperature measured only in the esophagus?
What was the depth of the esophageal temperature probe?
Depending on the room temperature and the depth of in-
sertion, the body temperature can change with ambient in-
fluences, such as blood flow of venous return and inhaled
gas temperature [3]. Therefore, the authors used a heated
breathing system and a heat moisture exchanger (HME) to
heat the breathing circuit. During anesthetic care, the pa-
tient’s temperature did not show a statistically significant
change after 60–75 min of low flow. However, it started in-
creasing significantly after 120 min of low flow.
In this study, soda lime (CO2 absorber) and a standard
circular rebreathing circuit with a heated breathing circuit
were used. Did you use the HME in the heated breathing
circuit? One CO2 molecule, exhaled by the patient, produc-
es two water (H2O) molecules and generates approximately
40°C of heat during its reaction with soda lime. The mois-
ture and heat generated by the reaction are sufficient for
the patient's humidification and warmth during anesthesia
30 min after induction [1,4]. Therefore, if a low-flow system
is used, there is no reason to use a heated breathing circuit
and HME, sufficient heat and moisture can be maintained
without a heated breathing circuit and HME [1–5]. We
Letter to the EditorAnesth Pain Med 2021;16:116-117pISSN 1975-5171 • eISSN 2383-7977
Change of inspired oxygen concentration and temperature in low flow anesthesia
think that the increased temperature within the circuit is not
an advantage but a problem caused by adding the heated
breathing circuit and HME during low flow rather than high
flow. What do you expect to get if you do not attach either of
or both the heating breathing circuit and HME?
Hong Seuk Yang, Dong Ho Park, and Chang Young Jeong
Department of Anesthesiology and Pain Medicine, Daejeon Eulji Medical Center, Medical College, Eulji University, Daejeon, Korea
Corresponding author: Hong Seuk Yang, M.D., Ph.D.
E-mail: [email protected]
Received December 8, 2020; Accepted: January 13, 2021
https://doi.org/10.17085/apm.20095
CONFLICTS OF INTEREST No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS Methodology: Hong Seuk Yang. Writing - review & edit-
ing: Dong Ho Park. Supervision: Chang Young Jeong.
ORCID Hong Seuk Yang, https://orcid.org/0000-0003-2023-8705
Dong Ho Park, https://orcid.org/0000-0002-6587-3756
Chang Young Jeong, https://orcid.org/0000-0002-8830-3406
REFERENCES 1. Baxter AD. Low and minimal flow inhalational anaesthesia.
Can J Anaesth 1997; 44: 643-52; quiz 652-3.
2. Baum JA, Aitkenhead AR. Low-flow anaesthesia. Anaesthesia
1995; 50 Suppl: 37-44.
3. Lenhardt R. Monitoring and thermal management. Best Pract
Res Clin Anaesthesiol 2003; 17: 569-81.
4. Parthasarathy S. The closed circuit and the low flow systems.
Indian J Anaesth 2013; 57: 516-24.
5. Braz JRC, Braz MG, Hayashi Y, Martins RHG, Betini M, Braz LG,
et al. Effects of different fresh gas flows with or without a heat
and moisture exchanger on inhaled gas humidity in adults un-
dergoing general anaesthesia: A systematic review and me-
ta-analysis of randomised controlled trials. Eur J Anaesthesiol
2017; 34: 515-25.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.Copyright © the Korean Society of Anesthesiologists, 2021
116

General
IN REPLY: We would like to thank the letter for their pos-
itive comments on our paper. The response to the letter
gave us the opportunity to supplement methodology of the
paper. We agree with the author of the letter that use of a
heated circuit or heat moisture exchanger (HME) for low-
flow anesthesia is not required. In low flow anesthesia, the
heating and humidification effect of the anesthesia circuit
is well known. Humidifying and warming effect of low flow
anesthesia has been reported to be sufficient to replace the
effect of HME and heating circuits at high flow anesthesia
[1]. We focused on oxygen concentration during low and
high flow anesthesia, therefore we used the same heating
circuit and HME in both groups for variable control.
In our hospital, the ambient temperature of the operat-
ing room was maintained at 20–23°C [2]. The patients in
this study were anesthetized under these room tempera-
ture conditions. If the patient's body temperature is not
stable, it is natural to control the room temperature outside
the range, and this did not happen in the study.
Esophageal temperature was not measured for all pa-
tients, but either the axillary or esophageal temperature
may be measured depending on the situation. In this study,
only the esophageal temperature was measured to mini-
mize the deviation due to the measurement method. The
esophageal temperature sensor used in this study was an
Esophageal Stethoscope with Temperature Sensor 18
French (DeRoyal, USA). The temperature sensor is mount-
ed at the depth where heart sounds are best heard using a
stethoscope.
We focused on oxygen concentration during low and
high flow anesthesia. Therefore, we studied patients un-
dergoing thyroidectomy. Since temperature management
was not challenging for these patients, this study could not
examine the detailed effects of low-flow anesthesia on
temperature management. Further research may be need-
ed to clarify this aspect.
Jiwook Kim, Hochul Lee, Sungwon Ryu, Donghee Kang,
Siejeong Ryu, and Doosik Kim
Department of Anesthesiology and Pain Medicine, Kosin University Gospel
Hospital, Kosin University College of Medicine, Busan, Korea
Corresponding author: Doosik Kim, M.D., Ph,D.
E-mail: [email protected]
Received January 6, 2021; Accepted: January 13, 2021
https://doi.org/10.17085/apm.21005
CONFLICTS OF INTEREST No potential conflict of interest relevant to this article
was reported.
AUTHOR CONTRIBUTIONS Conceptualization: Doosik Kim. Data curation: Hochul
Lee, Sungwon Ryu. Formal analysis: Siejeoung Ryu. Meth-
odology: Jiwook Kim. Visualization: Donghee Kang. Writ-
ing - original draft: Jiwook Kim. Writing - review & editing:
Donghee Kang, Siejeong Ryu. Supervision: Siejeong Ryu,
Doosik Kim.
ORCID
Jiwook Kim, https://orcid.org/0000-0001-9944-2113
Hochul Lee, https://orcid.org/0000-0002-9486-3135
Sungwon Ryu, https://orcid.org/0000-0001-6450-197X
Donghee Kang, https://orcid.org/0000-0001-6614-9244
Siejeong Ryu, https://orcid.org/0000-0002-0677-4168
Doosik Kim, https://orcid.org/0000-0003-3809-0139
REFERENCES
1. Johansson A, Lundberg D, Luttropp HH. The effect of heat and
moisture exchanger on humidity and body temperature in a
low-flow anaesthesia system. Acta Anaesthesiol Scand 2003;
47: 564-8.
2. Katz JD. Control of the environment in the operating room.
Anesth Analg 2017; 125: 1214-8.
Letter to the Editor
www.anesth-pain-med.org 117

www.anesth-pain-med.org
1. Online manuscript review process and guidelines for submission
1) All manuscripts must be submitted through the online
submission system (available at http://submit.anesth-
pain-med.org). Any inquiries about the manuscripts
should be posted on the “Contacting Author” page,
which is available to the right upon logging in. Specify
the manuscript number, author, and corresponding au-
thor when posting an inquiry.
2) The corresponding author should be a faculty. The cor-
responding author will be notified by e-mail whenever
there is any change in the status of a submitted manu-
script, and any resubmission can only be made by the
corresponding author.
3) Once the manuscript has been submitted and placed
under review, the content or author information can-
not be changed.
4) Before submitting the reviewed manuscripts, please en-
sure that the title page contains the author names, affil-
iations, and corresponding author information.
APM Notices
5) Failure to submit responses to comments by reviewers
and editors, along with the revised manuscript, within
60 days will be considered as “no intention to publish,”
and the review process will be terminated.
2. Mandatory English editing for Korean authors
APM has made English editing mandatory for manu-
scripts submitted on or after September 1, 2013. Authors are
responsible for the cost of editing. For English manuscripts,
please submit them to a professional editing service after
acceptance and upload the edited file and certificate of edit-
ing in the manuscript submission system. Manuscripts edit-
ed by an individual and not through a professional editing
service will not be accepted. Manuscripts submitted in Ko-
rean will be translated into English by the Society after ac-
ceptance, and Korean version will be published only on the
website (www.anesth-pain-med.org).

Anesthesia and Pain Medicine (APM) is the official scientific
journal of Korean Society of Neuroscience in Anesthesiology
and Critical Care (KSNACC), The Korean Society for Anesthetic
Pharmacology (KSAP), The Korean Society of Obstetric Anes-
thesiologists (KSOA), The Korean Society of Pediatric Anesthe-
siologists (KSPA), Korean Neuromuscular Research Society
(KNRS), Korean Society of Cardiothoracic and Vascular Anes-
thesiologists (KSCVA), Korean Society of Transplantation Anes-
thesiologists (KSTA), and The Korean Spinal Pain Society (KSPS)
and Korean Society of Regional Anesthesia (KSRA), and Korean
Society for Airway Management (KSAM). The abbreviated title
is “Anesth Pain Med”. It is published four times a year on the last
day of January, April, July, and October in English.
I. Editorial Policy
The Editor assumes that all authors listed in a manuscript
have agreed with the following policy of the APM on submis-
sion of manuscript. Except for the negotiated secondary pub-
lication, manuscript submitted to the APM must be previously
unpublished and not be under consideration for publication
elsewhere. Under any circumstances, the identities of the ref-
erees will not be revealed. Minimum publication charges and
additional fee for reprints will due on every manuscript. All
published manuscripts become the permanent property of the
Korean Society of Anesthesiologists (KSA) and may not be
published elsewhere without written permission. APM ad-
heres completely to guidelines and best practices published
by professional organizations, including Recommendations
for the Conduct, Reporting, Editing, and Publication of Schol-
arly Work in Medical Journals (http://www.icmje.org/icm-
je-recommendations.pdf ) from ICMJE and Principles of
Transparency and Best Practice in Scholarly Publishing (joint
statement by COPE, DOAJ, WAME, and OASPA; http://doaj.
org/bestpractice) if otherwise not described below.
II. General Information
1. Publication types
APM focuses on clinical research, experimental research,
case reports, reviews, and letters to the editor, online images
Enacted: May 15, 2006
Recently revised (13th): August 4, 2020
and various introductions.
2. Language
APM publishes articles in English. Manuscript submitted in
Korean will be translated into English by the society after accep-
tance, Korean version will be published only on the website
(www.anesth-pain-med.org).
Spellings should abide by American spellings. Medical termi-
nology should be written based on the most recent edition of
Dorland’s Illustrated Medical Dictionary. Accepted manuscripts
are requested to be proofread by professional English editors.
3. Submission of manuscripts
In addition to members of the Korean Society of Anesthesiol-
ogists, any researcher throughout the world can submit a man-
uscript if the scope of the manuscript is appropriate. Authors
are requested to submit their papers electronically by using the
online manuscript submission system, available at: http://sub-
mit.anesth-pain-med.org. Authors, reviewers, and editors send
and receive all correspondences through this system. Final revi-
sions by authors should be submitted within 1 week of the re-
quest.
4. Data Availability Statement
Data sharing is encouraged by the APM, but a Data Availabili-
ty Statement will be required and published with the manu-
script. Authors will be provided the following options during
submission or may use draft their own.
• The datasets generated during and/or analyzed during the
current study are available in the [NAME] repository, [PER-
SISTENT WEB LINK TO DATASETS]
• The datasets generated during and/or analyzed during the
current study are not publicly available due [REASON WHY
DATA ARE NOT PUBLIC] but are available from the corre-
sponding author on reasonable request.
• The datasets generated during and/or analyzed during the
current study are available from the corresponding author
on reasonable request.
Instructions for Authors
www.anesth-pain-med.org

• Data sharing not applicable to this article as no datasets
were generated or analyzed during the current study.
• All data generated or analyzed during this study are includ-
ed in this published article [and its supplementary infor-
mation files].
• The data that support the findings of this study are available
from [third party name] but restrictions apply to the avail-
ability of these data, which were used under license for the
current study, and so are not publicly available. Data are
however available from the authors upon reasonable re-
quest and with permission of [third party name].
5. Peer review process
APM uses double-blind review, which means that both the
reviewer and author identities are concealed from the review-
ers, and vice versa, throughout the review process. To facilitate
this, authors need to ensure that their manuscripts are pre-
pared in a way that does not give away their identity. If one or
more of edtors are involved as authors, the editor(s) should
not be involved in the peer reviewer selection, evaluation, or
decision process. Submitted manuscripts will be reviewed by
2 or more experts in the corresponding field. The Editorial
Board may request authors to revise the manuscripts accord-
ing to the reviewer’s opinion. After revising the manuscript,
the author should upload the revised files with a reply to each
item of the reviewer’s opinion. Additions and amendments to
the revised manuscript should be highlighted in red. The au-
thor’s revisions should be completed within 60 days after the
request. If it is not received by the due date, the Editorial
Board will not consider it for publication. To extend the revi-
sion period to more than 60 days, the author should negotiate
with the Editorial Board. The manuscript review process
should be finished the second review. If the reviewers wish
further review, the Editorial Board may consider it. The Edito-
rial Board will make a final decision on the approval for publi-
cation of the submitted manuscripts and can request any fur-
ther corrections, revisions, and deletions of the article text if
necessary. Statistical editing is also performed if the data need
professional statistical review by a statistician. The review and
publication processes that are not described in the Instruc-
tions for Authors will be incorporated into the Editorial Policy
Statements approved by the Council of Science Editors Board
of Directors, available at: www.councilscienceeditors.org/.
6. Article processing charge and publication fee
There is no submission-related fee. Article processing charge
(APC) of KRW 300,000 (USD 250) per article will be issued to the
corresponding author. APC is waived if the affiliations of the first
and corresponding authors are outside Korea. APC for invited
articles is also waived.
7. Copyrights and secondary publication
Copyrights of all published materials are owned by the APM.
On behalf of co-author(s), corresponding author must complete
and submit the journal’s copyright transfer agreement, which in-
cludes a section on the disclosure of potential conflicts of interest
based on the recommendations of the International Committee
of Medical Journal Editors, “Uniform Requirements for Manu-
scripts Submitted to Biomedical Journals”. A copy of the form is
made available to the submitting author within the online manu-
script submission process. It is possible to republish manuscripts
if ONLY the manuscripts satisfy the condition of secondary publi-
cation of the Uniform Requirements for Manuscripts Submitted
to Biomedical Journals, available at: http://www.icmje.org
8. Open access
APM is an Open Access journal accessible for free on the In-
ternet. Accepted peer-reviewed articles are freely available on
the journal website for any user, worldwide, immediately upon
publication without additional charge.
III. Research and Publication Ethics Guidelines
For the policies on research and publication ethics, the “Good
Publication Practice Guidelines for Medical Journals” (https://
www.kamje.or.kr/board/view?b_name = bo_publication&bo_
id = 13) or the “Ethical Guidelines on Good Publication” (http://
publicationethics.org/resources/guidelines) or “Ethical Consid-
erations in the International Committee of Medical Journal Edi-
tors” (http://www.icmje.org/recommendations) are applied.
1. Conflict-of-interest statement
The corresponding author is required to summarize all au-
thors’ conflict of interest disclosures. Disclosure form shall be
same with ICMJE Uniform Disclosure Form for Potential Con-
flicts of Interest (www.icmje.org/conflicts-of-interest). A conflict
of interest may exist when an author (or the author’s institution
or employer) has financial or personal relationships or affilia-
tions that could influence (or bias) the author’s decisions, work,
or manuscript. All authors should disclose their conflicts of in-
www.anesth-pain-med.org

www.anesth-pain-med.org
terest, i.e., (1) financial relationships (such as employment,
consultancies, stock ownership, honoraria, paid expert testimo-
ny), (2) personal relationships, (3) academic competition, and
(4) intellectual passion. These conflicts of interest must be in-
cluded as a footnote on the title page or in the Acknowledge-
ments section.
All sources of funding should be declared on the title page or in
the Acknowledgements section at the end of the text. If an au-
thor’s disclosure of potential conflicts of interest is determined to
be inaccurate or incomplete after publication, a correction will be
published to rectify the original published disclosure statement,
and additional action may be taken as necessary.
If one or more of editors are involved as authors, the authors
should declare conflict of interests.
Ex) AAA has been an editor of the Anesthesia and Pain Medi-
cine since 2017; however, he was not involved in the peer re-
viewer selection, evaluation, or decision process of this arti-
cle. No other potential conflicts of interest relevant to this ar-
ticle were reported.
2. Statement of informed consent
Copies of written informed consents and Institutional Review
Board (IRB) approval for clinical research are recommended
kept. The editor or reviewers may request copies of these docu-
ments to make potential ethical issues clear.
3. Protection of privacy, confidentiality, and written informed consent
Identifying details should not be published in written descrip-
tions, photographs, or pedigrees unless it is essential for scientific
purposes and the patient (or his/her parents or guardian) pro-
vides written informed consent for publication. Additionally, in-
formed consent should be obtained in the event that anonymity
of the patient is not assured. For example, masking the eye region
of patients in photographs is not adequate to ensure anonymity.
If identifying characteristics are changed to protect anonymity,
authors should provide assurance that alterations do not distort
scientific meaning. When informed consent has been obtained,
this should be indicated in the published article.
4. Protection of human and animal rights
In the reporting of experiments that involve human subjects, it
should be stated that the study was performed according to the
Helsinki Declaration of 1975 (revised 2013) (Available from https://
www.wma.net/policies-post/wma-declaration-of-helsinki-ethi-
cal-principles-for-medical-research-involving-human-subjects/)
and approved by the Institutional Review Board (IRB) of the insti-
tution where the experiment was performed. Clinical studies that
do not meet the Helsinki Declaration will not be considered for
publication. Identifying details should not be published (such as
name, initial of name, ID numbers, or date of birth).
In the case of an animal study, a statement should be provid-
ed indicating that the experimental processes, such as the
breeding and the use of laboratory animals, were approved by
the Research Ethics Committee (REC) of the institution where
the experiment was performed or that they did not violate the
rules of the REC of the institution or the NIH Guide for the Care
and Use of Laboratory Animals (Institute of Laboratory Animal
Resources, Commission on Life Sciences, National Research
Council, https://www.nap.edu/catalog/5140/guide-for-the-
care-and-use-oflaboratory-animals). The authors should pre-
serve raw experimental study data for at least 1 year after the
publication of the paper and should present this data if required
by the Editorial Board.
5. Registration of the clinical research
It is recommended that all clinical trials be registered in the
primary registry before submission. APM accepts registration in
any of the primary registries that participate in the World Health
Organization (WHO) International Clinical Trials Portal (http://
www.who.int/ictrp/en), NIH ClinicalTrials.gov (http://www.
clinicaltrials.gov), or Korea Clinical Research Information Ser-
vice (CRiS, http://cris.nih.go.kr).
6. Reporting guidelines
The APM recommends a submitted manuscript to follow re-
porting guidelines appropriate for various study types. Good
sources for reporting guidelines are the EQUATOR Network
(www.equatornetwork.org) and the NLM’s Research Reporting
Guidelines and Initiatives (www.nlm.nih.gov/services/re-
search_report_guide.html).
7. Author and authorship
An author is considered as an individual who has made
substantive intellectual contributions to a published study and
whose authorship continues to have important academic, so-
cial, and financial implications.
Authorship credit should be based on: (1) substantial contri-
butions to the conception or design of the work, or to the acqui-
sition, analysis, or interpretation of data for the work; (2) the
www.anesth-pain-med.org
drafting of the article or revising it critically for important intel-
lectual content; (3) final approval of the version to be published;
and (4) agreement on taking accountability for the accuracy or
integrity of the work. Authors should meet these four criteria.
These criteria distinguish the authors from other contributors.
When a large, multicenter group has conducted the work,
the group should identify the individuals who accept direct re-
sponsibility for the manuscript. When submitting a manu-
script authored by a group, the corresponding author should
clearly indicate the preferred citation and identify all individu-
al authors as well as the group name. Acquisition of funding,
collection of data, or general supervision of the research group
alone does not constitute authorship. Journals generally list
other members of the group in the Acknowledgments section.
8. Plagiarism and duplicate publication
Plagiarism is the use of previously published material without
attribution. Prior to peer review, all manuscripts are screened
for plagiarism by the Editor-in-Chief using iThenticate. When
plagiarism is detected at any time before publication, the APM
editorial office will take appropriate action as directed by the
standards set forth by the Committee on Publication Ethics
(COPE). For additional information, please visit http://www.
publicationethics.org. Text copied from previously published
work is interpreted using the following taxonomy:
1) Intellectual theft
Deliberate copying of large blocks of text without attribution
2) Intellectual sloth
Copying of “generic” text, e.g., a description of a standard
technique, without clear attribution
3) Plagiarism for scientific English
Copying of verbatim text, often from multiple sources
4) Technical plagiarism
Use of verbatim text without identifying it as a direct quota-
tion but citing the source
5) Self-“plagiarism”
Manuscripts are only accepted for publication if they have
not been published elsewhere. Manuscripts published in this
journal should not be submitted for publication elsewhere. Du-
plicate submissions identified during peer review will be imme-
diately rejected. Duplicate submissions that are discovered after
publication will be retracted. It is mandatory for all authors to
resolve any copyright issues when citing a figure or table from a
different journal that is not open access.
When duplicate publication is detected, the APM editorial of-
fice will notify the counterpart journal on this violation. Addi-
tionally, it will be notified to the authors’ affiliation and penal-
ties will be imposed on the authors. It is possible to republish
manuscripts if the manuscripts satisfy the condition of second-
ary publication of the Uniform Requirements for Manuscripts
Submitted to Biomedical Journals, available at: www.icmje.org.
If the author or authors wish to obtain a duplicate or secondary
publication for reasons such as publication for readers of a dif-
ferent language, the author(s) should obtain approval from the
Editors-in-Chief of both the first and second journal.
IV. Manuscript Preparation
APM recommends compliance with some or all of the follow-
ing guidelines (www.equatornetwork.org/library).
CONSORT for reporting of randomized controlled trials
(http://www.consort-statement.org)
STARD for reporting of diagnostic accuracy studies (http://
www.stard-statement.org)
STROBE for reporting of observational studies in epidemiolo-
gy (http://www.strobe-statement.org)
PRISMA for reporting of systematic reviews (http://www.pris-
ma-statement.org)
MOOSE for reporting of observational studies (http://www.
emgo.nl/kc/reporting-your-study-results-in-a-scientific-article)
GLOBAL ADVANCES in Health and Medicine for reporting of
clinical cases (http://www.gahmj.com)
1. Word processors and format of manuscripts
A manuscript must be written in proper and clear English or
Korean. Our preferred file format is DOCX or DOC. Manuscripts
should be typed double-spaced on A4-sized paper, using 12
point font in English, using 10 point font in Korean.
2. Abbreviation of terminology
Abbreviations should be avoided as much as possible. When
they are used, full expression of the abbreviated words should
be provided at the first use, with the abbreviation following in
parentheses.
Ex) target controlled infusion (TCI)
After that, “TCI” can be used instead of “target controlled infu-
sion.” Common abbreviations may be used, however, such as
DNA. Abbreviations can be used if they are listed as a MeSH
subject heading (https://www.ncbi.nlm.nih.gov/mesh).

www.anesth-pain-med.org
3. Word spacing
1) Leave 1 space on each side when using arithmetic marks
such as +,–, × , etc.
Ex) 24 ± 2.5
Leave no space when using hyphen between words.
Ex) intra-operative
2) When using parentheses, leave 1 space on each side in En-
glish, and leave no space in the Korean manuscript.
3) When using brackets in parentheses, apply square brackets.
Ex) ([ ])
4) Manuscripts in Korean should obey the rules of Korean
spelling (www.korean.go.kr).
4. Citations
1) If a citation has 2 authors, write as “Hirota and Lambert”. If
there are more than 3 authors, apply “et al.” at the end of
the first author’s surname.
Ex) Kim et al. [1]
2) Citations should be applied after the last word.
Ex) It is said that hypertension can be induced [1] and the
way to injure the brain [2] is…
Ex) Choi and Kim [1] reported…
3) Apply citations before a comma or period.
Ex) ....is reported [1],
4) Several or coupled superscripts can be written as [1–5] or
[1,3,5].
5. Arrangement of manuscript
The manuscript should be organized in the order of title, ab-
stract, introduction, materials and methods, results, discussion,
acknowledgments, references, tables, figures, and figure leg-
ends. Figures should be uploaded as separate files. The title of
each new section should begin on a new page. The conclusion
should be included in the discussion section. Number pages
consecutively, beginning with the first page of the manuscript.
Page numbers should be placed at the middle of the bottom of
the page. For survey-based clinical studies, the original survey
document does not need to be included in the body of the man-
uscript but may be included as a supplement in an appendix.
6. Organization of manuscript
1) Clinical or experimental research
(1) Cover page (upload separately)
① Title
Title should be concise and precise. The first word
should be capitalized. Drug names in the title should be
written with generic names, not brand names. For the
title, only the first letter of the first word should be capi-
talized.
Ex) Effect of smoking on bronchial mucus transport
velocity under total intravenous anesthesia ··········
[○]
Ex) Effect of Smoking on Bronchial Mucus Transport
Velocity under Total Intravenous Anesthesia ········ [ × ]
Provide drug names as generic names, not product
names.
Ex) In CPR, Isosorbide Dinitrate is, ·········· [○]
Ex) In CPR, Isosorbide Dinitrate (Isoket®) is, ········ [ × ]
Ex) In CPR, Isoket® is, ·········· [ × ]
② Running title
A running title of no more than 40 characters, includ-
ing letters and spaces in Korean, or 10 words in En-
glish, should be provided. If this title is inappropriate,
the Editorial Board may revise it.
Ex) Kim et al. [1]
③ Author information
First name, middle initial, and last name of each author,
with their highest academic degree(s) (M.D., Ph.D.,
etc.), and institutional affiliations; make sure the names
of and the order of authors as they appear on the Title
Page and entered in the system match exactly.
④ Previous presentation in conferences
Title of the conference, date of presentation, and the
location of the conference may be described.
⑤ Funding statement
Disclosure of all financial support for the work, in-
cluding departmental or institutional funding/sup-
port.
⑥ Conflicts of interest
Any conflicts of interest for any or all authors within
the 36 months of submission. If no competing inter-
ests, please add the following statement: “The au-
thors declare no competing interests.” If any of these
elements are not applicable to your submission,
write “not applicable” after thenumber and topic; for
example, “Prior Presentations: Not applicable.”
(2) Manuscript
① Title and Running title (without author information)
It should be the same as the Cover page.
② Abstract
All manuscripts should contain a structured abstract
that is written only in English. Authors should pro-

www.anesth-pain-med.org
vide an abstract of no more than 250 words. It should
contain 4 subsections: Background, Methods, Re-
sults, and Conclusions. Citation of references is not
permitted in the abstract. A list of key words at least 4,
with a maximum of 10 items, should be included at
the end of the abstract. Key words should be selected
from MeSH (https://www.ncbi.nlm.nih.gov/mesh),
and these should be written in small letters with the
first letter capitalized. Separate each word with a
semicolon (;), and include a period (.) at the end of
the last word. Ex) Keywords: Carbon dioxide; Cere-
bral vessels; Oxygen; Spinal analgesia.
③ Introduction
The introduction should address the purpose of the
article concisely and include background informa-
tion that is relevant to the purpose of the paper.
④ Materials and Methods
The materials and methods section should include
sufficient details regarding the design, subjects, and
methods of the research in order, as well as methods
used for data analysis and control of bias in the study.
Sufficient details must be provided in the methodol-
ogy section of an experimental study so that it can be
further replicated by others.
Institute and author names should be avoided.
When reporting experiments with human or animal
subjects, the authors should indicate whether they
received approval from the Institutional Review
Board for the study. When reporting experiments
with animal subjects, the authors should indicate
whether the handling of the animals was supervised
by the Institutional Board for the Care and Use of
Laboratory Animals. Demographic data should be
included in the materials and methods section if ap-
plicable. As a rule, subsection titles are not recom-
mended. If several study designs were used, then
subtitles can be used without assigning numbers.
Ensure correct use of the terms sex (when reporting bi-
ological factors) and gender (identity, psychosocial or
cultural factors), and, unless inappropriate, report the
sex and/or gender of study participants, the sex of ani-
mals or cells, and describe the methods used to deter-
mine sex and gender. If the study was done involving an
exclusive population, for example in only one sex, au-
thors should justify why, except in obvious cases (e.g.,
prostate cancer). Authors should define how they deter-
mined race or ethnicity and justify their relevance.● Units Laboratory information should be reported
using the International System of Units [SI], available
at : https://www.nist.gov/pml/special-publica-
tion-811
< Exceptions >
A. The unit for volume is “L”, while others should be
written as “dl, ml, μl”.
Ex) 1 L, 5 ml
B. The units for pressure are mmHg or cmH2O.
instead of Pascal.
C. Use Celsius for temperature. °C
D. Units for concentration are M, mM, μM.
Ex) μmol/L; [ × ]
E. When more than 2 items are presented, diago-
nal slashes are acceptable for simple units.
Negative exponents should not be used.
Ex) mg/kg/min [O], mgㆍkg-1ㆍmin-1 [ × ]
F. Leave 1 space between number and units, except
%, oC.
Ex) 5 mmHg
Ex) 5%, 36oC
G. Units of time
Ex) hour: 1 h = 60 min = 3,600 s, day: 1 d = 24 h
= 86,400 s● Machines and equipment
Provide model name and manufacturer’s name, and
country. Do not put “.” between words when writing
the names of countries.
Ex) U.S.A. [ × ], USA [O]
For drug names, use generic names. If a brand name
should be used, insert it in parentheses after the ge-
neric name. Provide® or TM as a superscript and the
manufacturer’s name and country.● Ions
Ex) Na+[○], Mg2+[O], Mg++[ × ], Mg+2[ × ]
Ex) Premedicated magnesium [O]
Ex) Premedicated Mg2+ [O]
⑤ Results
Results should be presented in a logical sequence in
the text, tables, and figures, giving the main or most
important findings first. Do not repeat all of the data
provided in the tables or figures in the text; empha-
size or summarize only the most important observa-
tions. Results can be sectioned by subsection titles
but should not be numbered. Citation of tables and
figures should be provided as Table 1 and Fig. 1.
Type or print each table on a separate page. Figures
should be uploaded as separate tif, jpg, pdf, gif, ppt
files.

www.anesth-pain-med.org
⑥ Statistics
Precisely describe the methods of statistical analysis
and computer programs used. Mean and standard
deviation should be described as mean ± SD, and
mean and standard error should be written as mean
± SEM. Median and interquartile should be de-
scribed as median (1Q, 3Q). When displaying P val-
ues, use a capital P and do not put a “-” between “P”
and “value”.
A. Describe the statistical tests employed in the study
with enough detail so that readers can reproduce
the same results if the original data are available.
The name and version of the statistical package
should be provided.
B. Authors should describe the objective of the study
and hypothesis appropriately. The primary/sec-
ondary endpoints are predetermined sensibly ac-
cording to the objective of the study.
C. The characteristics of measured variables should
determine the use of a parametric or nonpara-
metric statistical method. When a parametric
method is used, the authors should describe
whether the basic statistical assumptions are met.
For an analysis of a continuous variable, the nor-
mality of data should be examined. Describe the
name and result of the particular method to test
normality.
D. When analyzing a categorical variable, if the num-
ber of events and sample is small, exact test or as-
ymptotic method with appropriate adjustments
should be used. The standard chi-squared test or
difference-in-proportions test may be performed
only when the sample size and number of events
are sufficiently large.
E. The APM strongly encourages authors to show
confidence intervals. It is not recommended to
present the P value without showing the confi-
dence interval. In addition, the uncertainty of esti-
mated values, such as the confidence interval,
should be described consistently in figures and
tables.
F. Except for study designs that require a one-tailed
test, for example, non-inferiority trials, the P val-
ues should be two-tailed. A P value should be ex-
pressed up to three decimal places (ex. P = 0.160
not as P = 0.16 or P < 0.05). If the value is less
than 0.001, it should be described as “P < 0.001”
but never as “P = 0.000.” For large P value greater
than 0.1, the values can be rounded off to one
decimal place, for example, P = 0.1, P = 0.9.
G. A priori sample size calculation should be de-
scribed in detail. Sample size calculation must
aim at preventing false negative results pertain-
ing to the primary, instead of secondary, end-
point. Usually, the mean difference and standard
deviation (SD) are typical parameters in estimat-
ing the effect size. The power must be equal to or
greater than 80 percent. In the case of multiple
comparisons, an adjusted level of significance is
acceptable.
H. When reporting a randomized clinical study, a
CONSORT type flow diagram, as well as all the
items in the CONSORT checklist, should be in-
cluded. If limited in terms of the space of the
manuscript, this information should be submitted
as a separate file along with the manuscript.
I. Results must be written in significant figures. The
measured and derived numbers should be round-
ed off to reflect the original degree of precision.
Calculated or estimated numbers (such as mean
and SD) should be expressed in no more than one
significant digit beyond the measured accuracy.
Therefore, the mean (SD) of cardiac indices in pa-
tients measured on a scale that is accurate to 0.1
L/min/m2 should be expressed as 2.42 (0.31) L/
min/m2.
J. Except when otherwise stated herein, authors
should conform to the most recent edition of the
American Medical Association Manual of Style.
⑦ Discussion
The discussion should be described to emphasize
the new and important aspects of the study, includ-
ing the conclusions. Do not repeat in detail the re-
sults or other information that is provided in the in-
troduction or the results section. Describe the con-
clusions according to the purpose of the study but
avoid unqualified statements that are not adequately
supported by the data. Conclusions may be stated
briefly in the last paragraph of the discussion section.
⑧ Acknowledgments
Persons or institutes that contributed to the manu-
script but not sufficiently to be coauthors may be rec-
ognized. Financial support, including foundations,
institutions, pharmaceutical and device manufactur-
ers, private companies, or intramural departmental
sources, or any other support, should be described.
www.anesth-pain-med.org
⑨ References● References should be obviously related to docu-
ments and should not exceed 30. References should
be numbered consecutively in the order in which
they are first mentioned in the text. Provide cita-
tions in the body text. All references should be list-
ed in English, including author, title, name of jour-
nal, etc.● The format for references follows the descriptions
below. Otherwise, it follows the NLM Style Guide
for Authors, Editors, and Publishers (Patrias, K. Cit-
ing medicine: the NLM style guide for authors, edi-
tors, and publishers [Internet]. 2nd ed. Wendling,
DL, technical editor. Bethesda (MD): National Li-
brary of Medicine (US); 2007 [updated 2015 Oct 2;
cited Year Month Day]. Available at: www.ncbi.nlm.
nih.gov/books/NBK7256/).● If necessary, the Editorial Board may request origi-
nal documents for the references.● The journal title should be listed according to the
List of Journals Indexed for MEDLINE, available at:
https://www.nlm.nih.gov/archive/20130415/tsd/
serials/lji.html, or the List of KoreaMed Journals
(journal browser of KoreaMed Services), available
at: http://koreamed.org/JournalBrowserNew.php.● Six authors can be listed. If there are more than 6
authors, only list 6 names with “et al.”.● Provide the start and final page numbers of the cit-
ed reference.● Abstracts of conferences may not be included in the
references. The American Society of Anesthesiolo-
gists (ASA) refresher course lecture is not accept-
able as a reference.● Description format
A. Regular journal
Author name. Title of article. Name of journal pub-
lished year; volume: start page-final page. Ex) Ros-
enfeld BA, Faraday N, Campbell D, Dorman T,
Clarkson K, Siedler A, et al. Perioperative platelet
activity of the effects of clonidine. Anesthesiology
1992; 79: 256-61.
Ex) Hirota K, Lambert DG. Ketamine: its mecha-
nism(s) of action and unusual clinical uses. Br
J Anaesth 1996; 77: 741-4.
Ex) Kang JG, Lee SM, Lim SW, Chung IS, Hahm TS,
Kim JK, et al. Correlation of AEP, BIS, and OAA/
S scores under stepwise sedation using propo-
fol TCI in orthopedic patients undergoing total
knee replacement arthroplasty under spinal an-
esthesia. Korean J Anesthesiol 2004; 46: 284-92.
Ex) ‘2006; 7(Suppl 1): 64-96’ ‘2007; 76: H 232-8’
B. Monographs
- Author. Book name. Edition. Place, press. Pub-
lished year, pp (start page)-(End page).
- If reference page is only 1 page, mark ‘p’.
- Note if it is beyond the 2nd edition.
Ex) Nuwer MR. Evoked potential monitoring in the
operating room. 2nd ed. New York, Raven
Press. 1986, pp 136- 71.
- Translated documents cannot be used as refer-
ences. The original documents should be provided
as references.
C. Chapter
Any separate author of a chapter should be provid-
ed.
Ex) Blitt C. Monitoring the anesthetized patient. In:
Clinical Anesthesia. 3rd ed. Edited by Barash
PG, Cullen BF, Stoelting RK: Philadelphia, Lip-
pincott -Raven Publishers. 1997, pp 563-85.
D. Electronic documents
Ex) Grainge MJ, Seth R, Guo L, Neal KR, Coupland
C, Vryenhoef P, et al. Cervical human papillo-
mavirus screening among older women.
Emerg Infect Dis [serial on the Internet]. 2005
Nov [2005 Nov 25]. Available from wwwnc.cdc.
gov/eid/article/11/11/05-0575_article.
E. Online journal article
Ex) Sampson AL, Singer RF, Walters GD. Uric acid
lowering therapies for preventing or delaying
the progression of chronic kidney disease. Co-
chrane Database Syst Rev 2017; 10: CD009460.
F. Advance access article
Ex) Baumbach P, Gotz T, Gunther A, Weiss T, Meis-
sner W. Chronic intensive care-related pain:
Exploratory analysis on predictors and influ-
ence on health-related quality of life. Eur J Pain
2017. Advance Access published on Nov 5,
2017. doi:10.1002/ejp.1129.
⑩ Tables● Only one table is to be drawn per page in the order
cited in the text.● The title of the table is to be in English and written
at the top of the table in the form of a phrase.● Words in the table excluding the title should use
capital letters for the first word, and the following
words are to be written in small letters.

www.anesth-pain-med.org
● For demographic data, gender is recorded as M/F,
age as yr, (if necessary, use days or months in chil-
dren) without decimal point. The “ ± ” sign within the
table is to be aligned with the rows above and below.● Footnotes are to be written in the following order:
“Values are mean ± SD (or SEM) or median (1Q,
3Q)”, the explanations for the groups and the abbre-
viations in order of appearance, and statistics. Ab-
breviations apart from internationally recognized
abbreviations are to be explained with their full
spellings at the bottom of the table. Full spellings
are to be presented even for repeated abbreviations
for each table in order of appearance.● Significance marks are to conform to the Vancouver
style (Uniform Requirements for Manuscripts Sub-
mitted to Biomedical Journals. JAMA 1997; 227:
927-34). In other words, these must be in the order
of *, †, ‡, §, ∥, ¶, **, ††, ‡‡ and written as superscripts.
⑪ Legends for figures and photographs● All of the figures and photographs should be de-
scribed in the text separately.● The description order is the same as in the foot-
notes in tables and should be in recognizable sen-
tences.● Define all abbreviations every time they are repeated.
(3) Figures and Photographs
① APM encourages authors to use color to increase the
clarity of figures. Please note that color figures are
used without charge.
② Standard colors should be used (black, red, green,
blue, cyan, magenta, orange, and gray). Avoid colors
that are difficult to see on the printed page (e.g., yel-
low) or are visually distracting (e.g., pink). Figure back-
grounds and plot areas should be white, not gray. Axis
lines and ticks should be black and thick enough to
clearly frame the image. Axis labels should be large
enough to be easily readable, and printed in black.
③ Figures should be uploaded as separate tif, jpg, pdf,
gif, or ppt files. Width of figure should be 84 mm (one
column). Contrast of photos or graphs should be at
least 600 dpi. Contrast of line drawings should be at
least 1,200 dpi. Number figures as “Fig. (Arabic nu-
meral)” in the order of their citation (ex. Fig. 1).
④ Photographs should be submitted individually. If Fig.
1 is divided into A, B, C, and D, do not combine it
into 1, but submit each of them separately. Authors
should submit line drawings in black and white.
⑤ In horizontal and vertical legends, the letter of the
first English word should be capitalized.
⑥ Connections between numbers should be denoted
by “–”, not “~”. Do not space the numbers (ex. 2–4).
⑦ An individual should not be recognizable in photo-
graphs or X-ray films unless written consent has been
obtained from the subject and is provided at the time
of submission.
⑧ Pathological samples should be pictured with a mea-
suring stick.
(4) Video (movie) clip(s)
The APM publishes supplemental video (movie) clip(s)
that will be available online. Authors should submit vid-
eos according to our video submission guidelines.
① Each video clip should clearly illustrate the primary
findings within an adequate amount of viewing time
and should be discussed in the text. Authors should
provide appropriate labeling (e.g., arrows, abbrevia-
tions of anatomic structures, etc.) in the video clips.
However, all identifying information, including pa-
tient names and/or ID numbers, hospital names, and
dates of the procedures, should be removed.
② Video clips should contain succinct teaching points
that must be supported by the current literature or
standard reference texts, preferably those most ac-
cessible to the general reader. The adequacy of the
teaching points will be evaluated during the review
process and finally confirmed by the Editorial Board
at the end of the review process.
③ Video clips are uploaded as the last file(s) at the time
of manuscript submission and should be marked as
supplementary video files.
④ The video clip(s) should have simple file names (e.g.,
Video 1, Video 2) and should include the appropriate
extension (e.g., .mov, .mpg, .avi).
⑤ The maximum number of video clips is 20.
⑥ The video clip(s) should be playable on Microsoft
Windows OS. The video clip(s) should be tested for
playback before submission, preferably on comput-
ers not used for their creation, to check for any com-
patibility issues.
⑦ Individual video files should be a minimum of 480 ×
320 pixels (smaller clips will not be accepted) and a
maximum of 2 GB. Files of < 15 MB will be rejected
outright unless special arrangements have been
made with the editorial board prior to submission.
Approval of files of > 2 GB will be made at the end of
the review process.
⑧ Supplemental still images that correspond to the re-

www.anesth-pain-med.org
spective video clip(s) should be, but are not always
required to be, accompanied by legends. The video
clip file name(s) should refer to the corresponding
figure number(s).
⑨ The author will be able to find additional information
in the Figures and photographs section.
2) Case Reports
A case report is almost never a suitable means to describe
the efficacy of a treatment or a drug; instead, an adequately
powered and well-controlled clinical trial should be per-
formed to demonstrate such efficacy. The only context in
which a case report can be used to describe efficacy is in a
clinical scenario, or population, that is so unusual that a
clinical trial is not feasible. Case reports of humans must
state in the text that informed consent to publication was
obtained from the patient or guardian. Copies of written
informed consents should be kept. If necessary, the editor
or reviewers may request copies of these documents. If
these steps are impossible, Institutional Review Board ap-
proval should be obtained prior to submission. Rarity of a
disease condition is itself not an acceptable justification for
a case report.
(1) Cover page: Same as that for clinical and experimental
studies.
(2) Abstract: All case reports should contain a structured
abstract that is written only in English. Provide an ab-
stract of no more than 150 words. It should contain 3
subsections: Background, Case, and Conclusions. A list
of keywords, with a minimum of 3 and maximum of 10
items, should be included at the end of the abstract.
(3) Introduction: Should not be separately divided. Briefly
describe the case and background without a title.
(4) Case report: Describe only the clinical information that
is directly related to the diagnosis and anesthetic man-
agement.
(5) Discussion: Briefly discuss the case, and state conclu-
sions at the end of the case. Do not structure the con-
clusion section separately.
(6) References: The number of references should be less
than 15. However, if necessary, the number of reference
can be added in accordance with the decision of the
editorial committee.
(7) Tables and figures: Proportional to those for clinical and
experimental studies.
3) Reviews
Review articles synthesize previously published material
into an integrated presentation of our current understand-
ing of a topic. Review articles should describe aspects of a
topic in which scientific consensus exists, as well as aspects
that remain controversial and are the subject of ongoing
scientific disagreement and research. Review articles
should include unstructured abstracts written in English
equal to or less than 250 words. The organization should be
in order of abstract, introduction, text following each title,
conclusion and references. Figures and tables should be
provided in English. Body text should not exceed 30 A4-
sized pages, and the number of figures and tables should
each be less than 6. However, if necessary, the number of
pages, number of figures and tables can be added in accor-
dance with the decision of the editorial committee.
4) Letters to the Editor
Letters to the Editor should include brief constructive com-
ments that concern previously published articles and inter-
esting cases. Letters to the Editor should be submitted no
more than 3 months after the paper has been published.
(1) Cover pages should be formatted in the same way as
those of clinical research papers. The corresponding au-
thor should be the first author. A maximum of five au-
thors is allowable.
(2) The body text should not exceed 1,000 words and
should have no more than 5 references. A figure or a ta-
ble may be used.
(3) Letters may be edited by the Editorial Board, and if nec-
essary, responses by the author of the subject paper may
be provided.
5) Book reviews and announcements
Book reviews as well as news of scientific societies and sci-
entific meeting dates in Korea or abroad can be included.
Their formats will be same as those of Letters to the Editor.
6) Images and Videos in APM
This feature is intended to capture the sense of visual dis-
covery and variety that anesthesiologists experience.
(1) The title should contain no more than 8 words. No more
than 2 authors should be listed.
(2) The legend should contain no more than 250 words.
(3) If there is more than one panel, please label them Panel
A, Panel B, etc.
(4) The legends to the images and videos should briefly
present relevant clinical information, including a short
description of the patient’s history, relevant physical
and laboratory findings, clinical course, response to
treatment (if any), and condition at the last follow-up.

www.anesth-pain-med.org
□ Original Article □ Case Report □ Review Article □ Letter to the Editor □ Editorial □ Others
Article title:
Author(s):
(In identical order to the electronic submission and the corresponding author should be underlined)
Journal: Anesthesia and Pain Medicine
In the event that the above manuscript is accepted for publication in the Anesthesia and Pain Medicine, the copyright is trans-
ferred to the Korean Society of Anesthesiologists.
The author shall have the right to use all or part of the Work to revise, adapt, prepare derivative works, present orally, or distrib-
ute provided that such use is for the personal noncommercial benefit of the author. With written consent from the Anesthesia
and Pain Medicine, the author may use contents from the Work in other works provided that a full acknowledgment is made to
the original source of the material including the journal name, volume, issue, page numbers, year of publication, title of article.
All co-authors of the Work certify that they have participated sufficiently in the intellectual content, the analysis of data if appli-
cable, and the writing of the Work to take public responsibility for it. Each author of the Work certifies that none of the material in
the Work has been previously published, included in another work, or is currently under consideration for publication else-
where. Each author certifies that this Work has not been accepted for publication elsewhere, nor has assigned any right or inter-
est in the Work to any third party. All funding sources supporting the Work and all institutional or corporate affiliations of the au-
thors and commercial associations (e.g. consultancies, stock ownership, equity interests, patent-licensing arrangements, etc.)
that might pose a conflict of interest in connection with the Work should be acknowledged in a footnote on the front cover of the
Work.
I/we give consent to the above statements (It is THE RESPONSIBILITY of the Corresponding Author to collect the signatures
of all authors before sending the form to the Editorial Office).
Author’s Signature Date Author’s Signature Date
Author’s Signature Date Author’s Signature Date
Author’s Signature Date Author’s Signature Date
Author’s Signature Date Author’s Signature Date
Copyright transfer agreement

www.anesth-pain-med.org
Clinical Research
General instructions
1. Please note that it is unethical to submit the same manu-
script to two different journals simultaneously. The paper
should not have been submitted to the Anesthesia and
Pain Medicine either.
2. The Anesthesia and Pain Medicine holds the copyright of
published manuscripts.
3. The pages should be numbered, starting with the first
page.
4. Manuscripts should be written in 10 point or larger, dou-
ble-spaced, with a wide margin.
5. Should be a brief running title.
Abstract
6. The abstract should be in structured format (Background;
Methods; Results; and Conclusions)
7. Should only include less than 6 keywords.
8. Should be fewer than 250 words.
Contents: (Introduction-Discussion)
9. Background (referenced), objective. The introduction
should give a concise account of the background and pur-
pose of the investigation.
10. In a clinical study, written informed consent from the pa-
tients should be obtained and a statement concerning IRB
approval and informed consent procedures must appear
in the methods section of paper.
11. Figures and photographs should be submitted as jpg, gif or
tif files, separately from the text of the paper.
12. Legend of figure should be described on a separate page
following references in sentences of present tense.
13. Tables should be included in the text.
14. Follow the instructions for citing references.
15. Conclusion or summary should be the last section.
References
16. Follow the reference format.
17. Number references (as brackets; [ ]) in the sequence they
appear in the text.
18. If you cite accepted manuscripts “In Press” as references,
please provide one electronic copy.
Others
19. Raw data should be presented if the committee requests.
20. Please obtain permission from the copyright holder when
citing a graph, figure or table from a different journal or
book.
21. The names or affiliations of the authors should be con-
cealed in the manuscript and figures.
Experimental Research
General instructions
1. Please note that it is unethical to submit the same manu-
script to two different journals simultaneously. The paper
should not have been submitted to the Anesthesia and
Pain Medicine either.
2. The Anesthesia and Pain Medicine holds the copyright of
published manuscripts.
3. The pages should be numbered, starting with the first
page.
4. Manuscripts should be written in 10 point or larger, dou-
ble-spaced, with a wide margin.
5. Should be a brief running title.
Abstract
6. The abstract should be in structured format (Background;
Methods; Results; and Conclusions)
7. Should only include less than 6 keywords.
8. Should be fewer than 250 words.
Contents: (Introduction-Discussion)
9. Background (referenced), objective. The introduction
should give a concise account of the background and pur-
pose of the investigation.
10. Figures and photographs should be submitted as jpg, gif
or tif files, separately from the text of the paper.
11. Legend of figure should be described on a separate page
following references in sentences of present tense.
12. Tables should be included in the text.
Author’s checklist

www.anesth-pain-med.org
13. Follow the instructions for citing references.
14. Conclusion or summary should be the last section.
References
15. Follow the reference format.
16. Number references (as brackets; [ ]) in the sequence they
appear in the text.
17. If you cite accepted manuscripts “In Press” as references,
please provide one electronic copy.
Others
18. Raw data should be presented if the committee requests.
19. Please obtain permission from the copyright holder when
citing a graph, figure or table from a different journal or
book.
20. The names or affiliations of the authors should be con-
cealed in the manuscript and figures.
Related Documents











