Reversal strategies for NOACs Namur Thrombosis Haemostasis Center April 28th Peter Verhamme Vascular Medicine and Haemostasis University of Leuven Belgium

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Reversal strategies for NOACs
Namur Thrombosis Haemostasis Center
April 28th
Peter Verhamme
Vascular Medicine and Haemostasis
University of Leuven
Belgium
Honoraria for lectures and advisory boards
• Boehringer Ingelheim• Bayer • Daiichi Sankyo• Pfizer• Sanofi• Ionis Pharmaceuticals• Portola
Research Support • Boehringer Ingelheim• Bayer• Leo Pharma
Disclosures

A real-life patient…
URGENT SURGERY
Needs urgent ERCP

Does your hospital have a
protocol for bleeding and emergencies?

• NOACs provide effective treatment NOACs cause less serious bleeding than warfarin
Weitz et al. Circulation (2012); Majeed et al. Circulation (2013); Graham et al. Circulation (2015)
Do we need reversal agents for NOACs ?

• NOACs provide effective treatment NOACs cause less serious bleeding than warfarin
• However:- Emergencies (bleeding, urgent procedures) are not infrequent
- Fear of bleeding and the lack of an antidote are barriers for the use of NOACs
Weitz et al. Circulation (2012); Majeed et al. Circulation (2013); Graham et al. Circulation (2015)
Do we need reversal agents for NOACs ?

Meta-analysis: ARISTOTLE, ENGAGE-AF, RE-LY and ROCKET AF
VKAs versus NOACs:
organ-specific patterns of bleeding
Relative risk difference (%) (95% CI)
Intracranial bleeding
Other major bleeding
Gastrointestinal bleeding
Vanassche et al, Thrombosis and Haemostasis, 2014
Favours novel OAC Favours warfarin–100 –50 0 50 100
84,540 patients and 4781 bleeding events

– General measures and supportive care
• Interrupt treatment• Identify and control source of bleeding
• Volume replacement
• Transfusion (packed cells, platelets, FFP)
Weitz et al. Circulation (2012); Majeed et al. Circulation (2013); Graham et al. Circulation (2015)
Management of serious bleeding

– General measures and supportive care
• Interrupt treatment• Identify and control source of bleeding
• Volume replacement
• Transfusion (packed cells, platelets, FFP)
– Non-specific measures to support haemostasis
• Factor concentrates (PCCs, aPCCs, FVIIa)
Weitz et al. Circulation (2012); Majeed et al. Circulation (2013); Graham et al. Circulation (2015)
Management of serious bleeding

PCC or aPCC to reverse the anticoagulant effect of NOACs?
Dabigatran 1–14 Rivaroxaban 1-3,15–18 Apixaban 1-3,14,19–21 Edoxaban 1
PCC
Animal models
Preclinical studies
Human volunteers
Case reports
aPCC
Animal models
Preclinical studies
Human volunteers
Case reports �
�
����
�
?
�
�
�
?
�
�
�
�
�
�
?
�
�
?
�
����
?
?
?
�
�
?
?
?
?
?
?
� . Siegal DM. J Thromb Thrombolysis 2015;39:395–402; 2. Babilonia K, Trujillo T. Thromb J 2014;12:8; 3. Lazo-Langner A et al. Crit Care 2013;17:230; 4. Honickel M et al. Thromb Haemost 2015;113:728–40; 5. Herzog E et al. Thromb Res 2014;134:729–36; 6. Grottke O et al. Crit Care 2014;18:R27; 7. Masotti L et al. J Thromb Thrombolysis 2015;39:427–33; 8. Plener I et al. Can J Hosp Pharm 2014;67:43–7; 9. Diaz MQ et al. Haematologica 2013;98:e144; 10. Lillo-Le Louet A et al. Thromb Haemost 2012;108:583–5; 11. Dumkow LE et al. Am J Health Syst Pharm 2012;69:1646–50; 12. Wychowski M, Kouides P. Ann Pharmacother 2012;46:e10; 13. Lindahl TL et al. Thromb Res 2015;135:544–7; 14. Dinkelaar J et al. Clin Chem Lab Med 2014;52:1615–2; 15. Herzog E et al. Thromb Res 2015;135:554–60; 16. Zhou W et al. Stroke 2013;44:771–778; 17. Beyer-Westendorf J et al. Blood 2014;124:955–962; 18. Piccini JP et al. Eur Heart J 2014;35:1873–80; 19. Martin AC et al. J Thromb Haemost 2015;13:426–36; 20. Escolar G et al. PLoS One 2013;8:e78696; 21. Perlstein I et al. Presented at ASH 2014; abstr 345

General bleeding management algorithms are available to guide clinical decisions
Consider:
•PCC 50 IU/kg;
•aPCC 50 U/kg; max 200 U/kg/day
• rFVIIa* 90 µg/kg
Supportive measures•Control Source of Bleeding•Fluid replacement •RBC transfusion •FFP (as plasma expander)•Platelet transfusion (if platelet count ≤60×109/L or on long-acting antiplatelet drugs)
Additional options for dabigatran•Consider haemodialysis
+ +
• Delay or discontinue next dose
• Reconsider concomitant medication
Mild bleeding Moderate/severe bleeding Life-threatening bleeding
Heidbuchel H et al. Europace 2013 & 2015;
Bleeding while using a NOAC
NOAC reversal agents in development
Greinacher A et al. Thromb Haemost 2015;113:931–42;
Approved by EMA/FDA
Phase IIIPatients requiring urgent surgery/with major bleeding; started May 20142,3
Phase IIPhase IIdarucizumabTarget: dabigatran

NOAC reversal agents in development
Greinacher A et al. Thromb Haemost 2015;113:931–42;
Approved by EMA/FDA
Phase IIIPatients requiring urgent surgery/with major bleeding; started May 20142,3
Phase IIIPatients with major bleeding; started Jan 20154
Phase II
Phase II
Phase I
Phase I
IdarucizumabTarget: dabigatran
Andexanet alfa (PRT064445)Target: FXa inhibitors

NOAC reversal agents in development
Greinacher A et al. Thromb Haemost 2015;113:931–42;
Approved by EMA/FDA
Phase IIIPatients requiring urgent surgery/with major bleeding; started May 20142,3
Phase IIIPatients with major bleeding; started Jan 20154
Phase II
Phase II
Phase I
Phase I
IdarucizumabTarget: dabigatran
Andexanet alfa (PRT064445)Target: FXa inhibitors
Ciraparantag(PER977)Target: universal?
Phase I
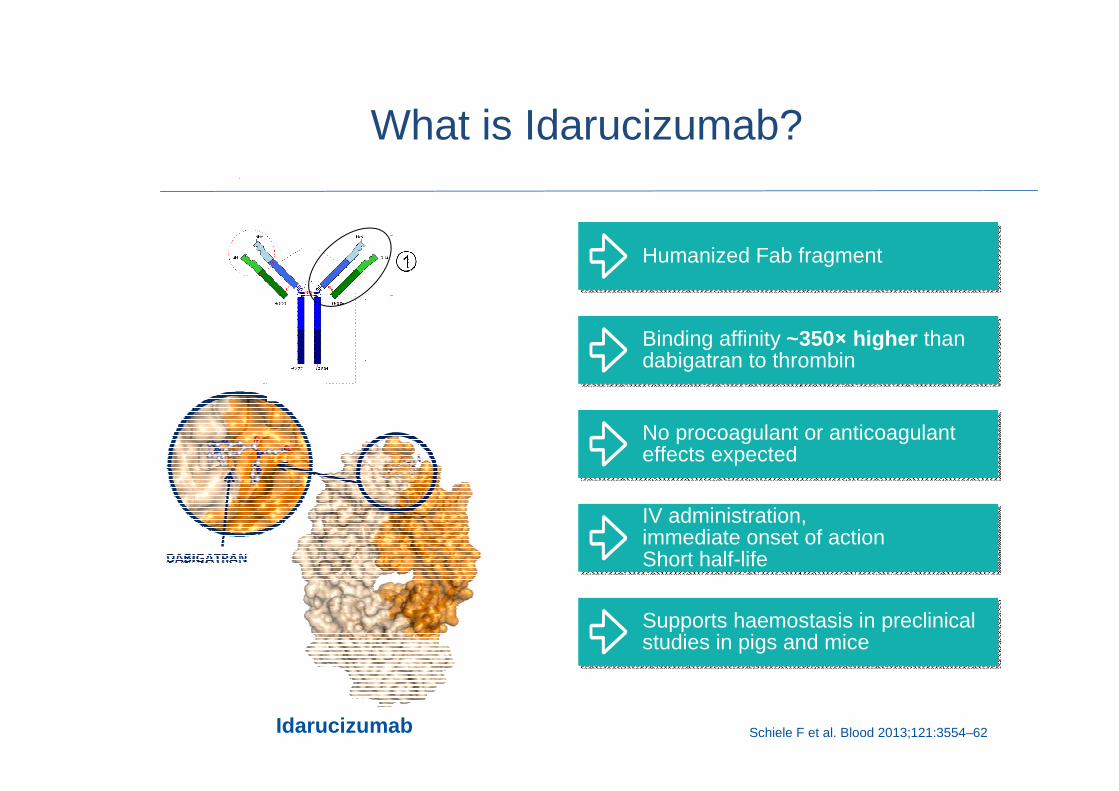
Schiele F et al. Blood 2013;121:3554–62
What is Idarucizumab?
Idarucizumab
Humanized Fab fragmentHumanized Fab fragment
IV administration,immediate onset of action Short half-life
IV administration,immediate onset of action Short half-life
Binding affinity ~350×××× higher than dabigatran to thrombinBinding affinity ~350×××× higher than dabigatran to thrombin
No procoagulant or anticoagulant effects expectedNo procoagulant or anticoagulant effects expected
Supports haemostasis in preclinical studies in pigs and miceSupports haemostasis in preclinical studies in pigs and mice
•Glund et al. Lancet 2015
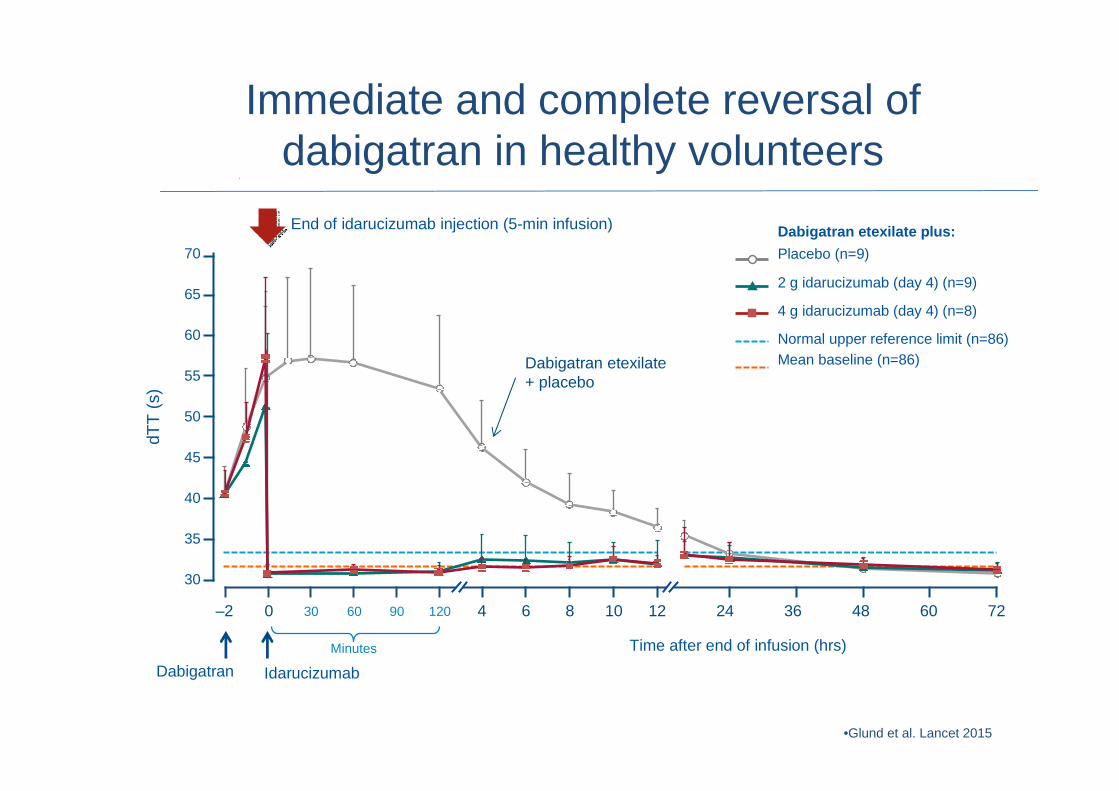
Immediate and complete reversal of dabigatran in healthy volunteers
16
End of idarucizumab injection (5-min infusion)
Dabigatran etexilate + placebo
dTT
(s)
70
65
60
55
50
45
40
35
30
Dabigatran Idarucizumab
Time after end of infusion (hrs)Minutes
72–2 0 120906030 36241264 8 10 48 60
Dabigatran etexilate plus:
Placebo (n=9)
Internal use only – strictly confidential
2 g idarucizumab (day 4) (n=9)
4 g idarucizumab (day 4) (n=8)
Normal upper reference limit (n=86)Mean baseline (n=86)

•Idarucizumab is currently in development and is not approved for use in any country. The information presented here is intended for medical education pu rposes only. The information contained herein does not necessarily reflect the content of the approved Can adian product monograph dTT, diluted thrombin time•Glund et al. ASH 2014
Reversal in elderly and volunteers with moderate renal impairment
17
End of bolus
dTT
(s)
90
80
70
55
50
45
40
35
25
Time after end of infusion (hrs)Minutes
30
24–2 0 120906030 20161284
85
75
65
60
Dabigatran Idarucizumab
Mild renal impairment
5-g dose calculated to reverse total body load of dabigatran
associated with 99th percentile in RE-LY®

RE-VERSE AD: multicentre, ongoing, open-label, single-arm Phase III study
dTT, diluted thrombin time; ECT, ecarin clotting time
Pollack CV et al. Thromb Haemost 2015;114:198–205
N=300
0–15 minutes 90 days follow-up
0–24 hours
Hospital arrival
5 g idarucizumab (two infusions of 2.5 g)
Pre-2nd vial 2 h 4 h 12 h 24 h 30 d 90 dPre-1st vial 1 hBlood
samples10–30 min
Primary endpoint: dabigatran reversal within 4 hours
(dTT or ECT)
7 d

RE-VERSE AD: multicentre, ongoing, open-label, single-arm Phase III study
dTT, diluted thrombin time; ECT, ecarin clotting time
Pollack CV et al. Thromb Haemost 2015;114:198–205
N=300
0–15 minutes 90 days follow-up
0–24 hours
Hospital arrival
5 g idarucizumab (two infusions of 2.5 g)
Pre-2nd vial 2 h 4 h 12 h 24 h 30 d 90 dPre-1st vial 1 hBlood
samples10–30 min
Primary endpoint: dabigatran reversal within 4 hours
(dTT or ECT)
7 d
Reverses up to the 99th percentile of dabigatran levels
measured in RE-LY

RE-VERSE AD: multicentre, ongoing, open-label, single-arm Phase III study
dTT, diluted thrombin time; ECT, ecarin clotting time
Pollack CV et al. Thromb Haemost 2015;114:198–205
N=300
0–15 minutes 90 days follow-up
0–24 hours
Hospital arrival
5 g idarucizumab (two infusions of 2.5 g)
Pre-2nd vial 2 h 4 h 12 h 24 h 30 d 90 dPre-1st vial 1 hBlood
samples10–30 min
Primary endpoint: dabigatran reversal within 4 hours
(dTT or ECT)
7 d
Reverses up o the 99th percentile of dabigatran levels
measured in RE-LY
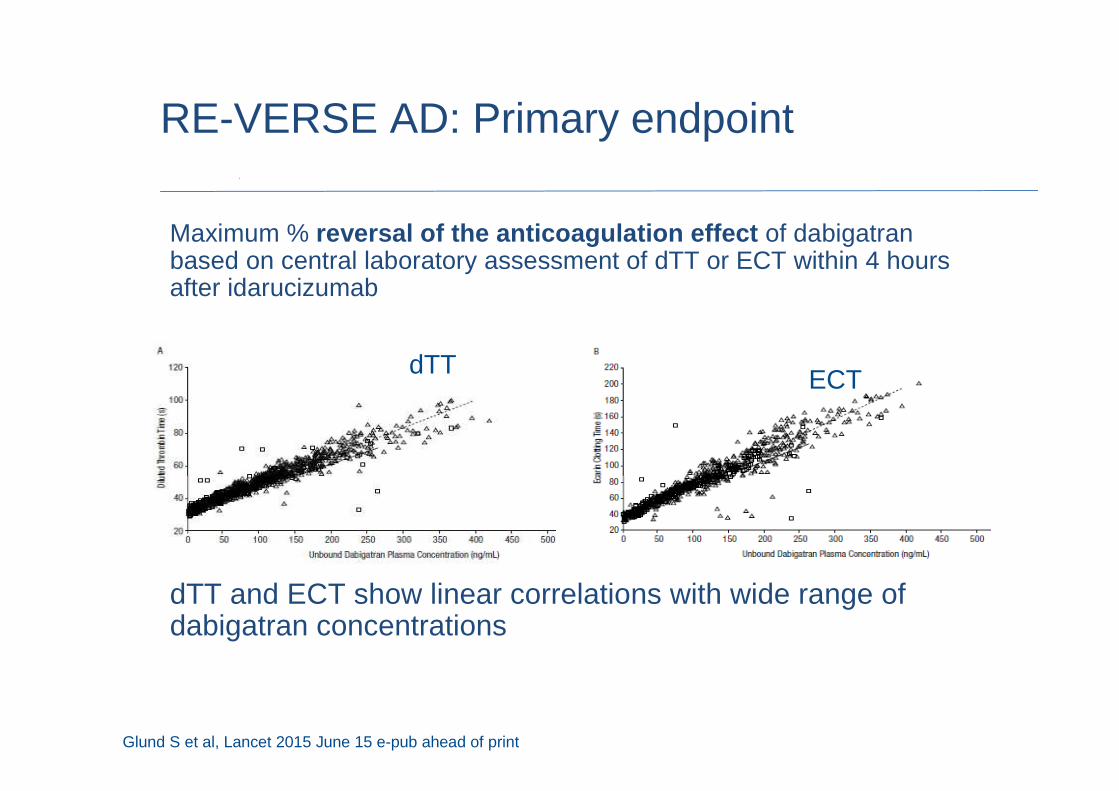
Maximum % reversal of the anticoagulation effect of dabigatran based on central laboratory assessment of dTT or ECT within 4 hours after idarucizumab
dTT and ECT show linear correlations with wide range of dabigatran concentrations
Glund S et al, Lancet 2015 June 15 e-pub ahead of print
RE-VERSE AD: Primary endpoint
dTT ECT

RE-VERSE AD: Baseline characteristics
Characteristic Group A Group B Total
Number n=51 n=39 N = 90
Indication for dabigatran
stroke prevention in A Fib47/51 39/39 86/90
Age median,
range (years)
77
(48–93)
76
(56–93)
76.5
(48–93)
Creatinine clearance median,
range (mL/min)
51.5
(15.8–186.8)
60.1
(11.5–171)
57.6
(11.5–186.8)
Patient-reported time since last
dose, median (hours)15.2 16.6 15.4
Elevated dTT or ECT at baseline 47/51 34/39 81/90
Pollack CV, et al. N Engl J Med 2015Pollack CV et al. N Engl J Med 2015:373:511–20

RE-VERSE AD interim results: primary endpoint by dTT reversal
Assay upper limit of normal
Idarucizumab 2x 2.5 g
dTT
(s)
130
110
70
60
50
40
30
20
120
100
90
80
1h 2h 4h 12h 24hBaseline Betweenvials
10–30min
Time post idarucizumab
Uncontrolled bleeding
Interim analysis includes data for the first 90 patients.
Pollack CV et al. N Engl J Med 2015:373:511–20
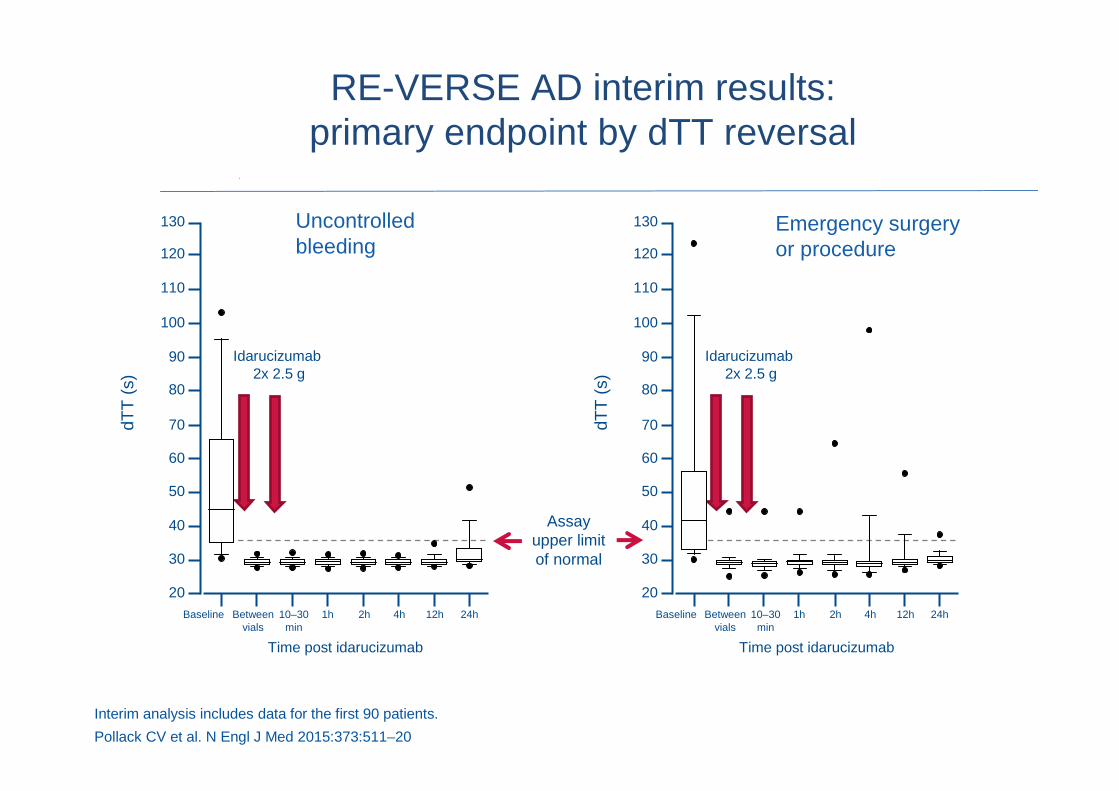
RE-VERSE AD interim results: primary endpoint by dTT reversal
Emergency surgery or procedure
Idarucizumab 2x 2.5 g
dTT
(s)
130
110
70
60
50
40
30
20
120
100
90
80
1h 2h 4h 12h 24hBaseline Betweenvials
10–30min
Time post idarucizumab
Assay upper limit of normal
Idarucizumab 2x 2.5 g
dTT
(s)
130
110
70
60
50
40
30
20
120
100
90
80
1h 2h 4h 12h 24hBaseline Betweenvials
10–30min
Time post idarucizumab
Uncontrolled bleeding
Interim analysis includes data for the first 90 patients.
Pollack CV et al. N Engl J Med 2015:373:511–20
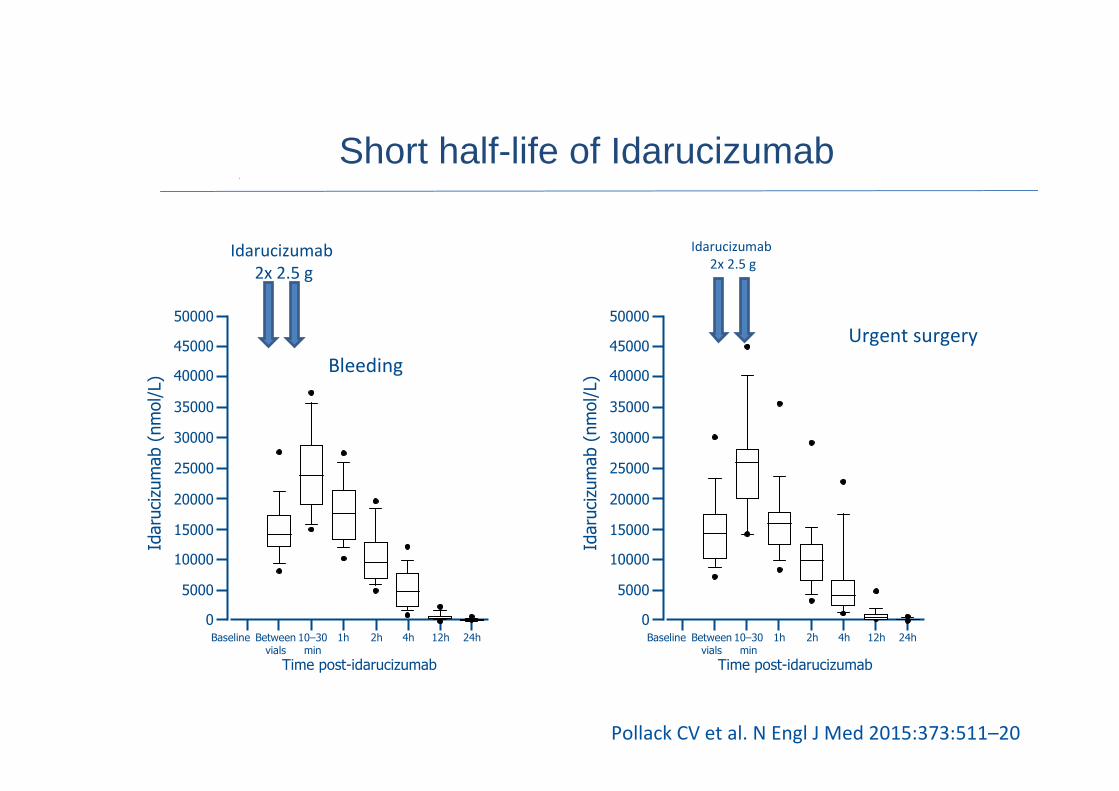
Short half-life of Idarucizumab Idarucizumab (nmol/L)
50000
40000
20000
15000
10000
5000
0
45000
35000
30000
25000
1h 2h 4h 12h 24hBaseline Betweenvials
10–30min
Time post-idarucizumab
1h 2h 4h 12h 24hBaseline Betweenvials
10–30min
Time post-idarucizumab
Idarucizumab (nmol/L)
50000
40000
20000
15000
10000
5000
0
45000
35000
30000
25000
Idarucizumab
2x 2.5 g
Idarucizumab
2x 2.5 g
Urgent surgery
Bleeding
Pollack CV et al. N Engl J Med 2015:373:511–20

• Pollack CV et al. N Engl J Med 2015
Reversal was also evident on aPTT results
Patients with bleeding Patients with urgent procedures
Pollack CV et al. N Engl J Med 2015:373:511–20

• dTT normalized in 98% and 93% of Group A (Bleeding) and Group B (urgent surgery) patients, respectively*
• Clinical outcomes– cessation of bleeding: median time was <12 hours*– intraoperative haemostasis: normal in 92% of evaluable patients
Similar results with central laboratory aPTT, ECT an d TT, and unbound dagigatran
Endpoint vs. Outcomes
*calculated for patients with elevated levels at baseline Pollack CV et al. N Engl J Med 2015:373:511–20

• No idarucizumab related safety issues
• Five thrombotic events occurred– 1 early event (DVT + PE) within 72 hours of idarucizumab
administration
– 4 patients had events after 72 hours of idarucizumab administration (DVT, DVT+PE+LA thrombus, MI, ischemic stroke)
– None of these 5 patients was receiving any antithrombotic therapy when the events occurred
• 18 deaths occurred (9 in each Group)– Related to presenting index event and comorbidities
Safety
Pollack CV et al. N Engl J Med 2015:373:511–20
• Open label cohort study– no appropriate comparison
• Fixed dose based on anticipated dabigatran level– What in case of massive overdose?– What if acute renal failure with higher dabigatran
levels?– In this interim analysis, some patients show re-
appearance of low levels of dabigatran at 24 hrs
RE-VERSE AD: Discussion
Pollack CV et al. N Engl J Med 2015:373:511–20

Andexanet: Reversal of Anticoagulation by direct and indirect Factor Xa Inhibitors
Factor Xa andexanet
Catalytic DomainGla
Recombinant engineered version of human factor Xa
S S
S419
S S
A419Factor Xa inhibitor Factor Xa inhibitor
• No catalytic activity
• Binds Xa-inhibitors
Gla
Nature Medicine
(2013),19(4): 446-51

Andexanet in Helathy volunteers: Reversal of Anti-FXa Activity
• Within 2-5 mins, andexanet reversed anti-FXa activity from baseline by 92%-97% (p<0.0001 vs. placebo (21%-45%) for all comparisons)
• Bolus plus infusion of andexanet sustained reversal of anti-FXa activity (Fig.C,D) (Siegal, NEJM 2015)

Ciraparantag
• Binds heparin, rivaroxaban, edoxaban, apixaban, dabigatran (charge-charge and non-covalent hydrogen bonding)
Ansell J, et al. NEJM. 2014; 371: 2141-2142.

What could be the potential impact of the availability of NOAC reversal agents on
clinical practice?

What about the patient…
URGENT SURGERY
Needs urgent ERCP

22 patients / 24 months 8 bleeding / 14 urgent surgery
• ICH (intraparenchymal)• Intoxication• Gangrene Fournier• ICH (subdural 3x)• Cholangitis• Acute mesenteric
ischemia (2x)• Dialysis • Craniofacial trauma• Lower GI bleeding• Abscess drainage
• ‘Fausse route’ after urinary catheter
• Open Tibial Fracture• Visible vessel upper GI-
bleeding• Haematemesis• Hearttransplant (2x)• Colon bleeding • Urgent nephrostomy

Reversal of anticoagulation…
URGENT SURGERY
Heart Transplantation…

Introducing our patients…
MAJOR BLEEDING

• Reversal of anticoagulation ≠ improved clinical outcomes
• Institution wide protocol for emergencies
Implementing reversal agents in clinical practice

Updated bleeding management algorithm
• Idarucizumab 5g for dabigatran
Consider:
• PCC 50 IU/kg;
• aPCC 50 U/kg; max 200 U/kg/day
Supportive measures•Control Source of Bleeding•Fluid replacement •RBC transfusion •FFP (as plasma expander)•Platelet transfusion (if platelet count ≤60×109/L or on long-acting antiplatelet drugs)
Additional options for dabigatran•Consider haemodialysis
+ +
• Delay or discontinue next dose
• Reconsider concomitant medication
Mild bleeding Moderate/severe bleeding Life-threatening bleeding
Heidbuchel H et al. Europace 2013 & 2015;
Bleeding while using a NOAC
Conclusions
2Guidance is available to manage patients on NOACs who are bleeding, or undergoing emergency procedures
3Reversal agents will provide additional treatment options for patients undergoing emergency procedures, or with life-threatening bleeding
1NOACs have favourable safety and efficacy profiles vs warfarin
Related Documents











