Retrospective Study of Bone Grafting Procedures Before Implant Placement Gustavo Davi Rabelo, DDS,* Priscila Marani de Paula, DDS,† Flaviana Soares Rocha, DDS,‡ Cla ´ udia Jorda ˜ o Silva, DDS, MSc, PhD,§ and Darceny Zanetta-Barbosa, DDS, MSc, PhD D ental rehabilitation of partially or totally edentulous patients with oral implants has become common practice with reliable long- term results. 1 However, unfavorable lo- cal conditions of the alveolar ridge, because of atrophy, periodontal disease, and trauma sequelae, may cause insuf- ficient bone volume, which may render implant placement impossible. 2 When the alveolar ridges lack the appropriate bone volume, additional surgical recon- structive procedures are required. Researchers continuously strive to improve on current bone grafting tech- niques and provide faster and denser bone regeneration. A variety of autoge- nous, 3 allogenous, 4 xenogenous, 5 and al- loplastic 6,7 grafts, alone or in different combinations, have been used to pro- vide sufficient ridge width or high for proper positioning of endosseous im- plants. 8–10 Additionally, the use of platelet-rich plasma (PRP) offers a po- tentially useful adjunct to bone grafts 11 due to osteoinductive properties of PRP. 12,13 The use of autogenous bone grafts from intra- 14 or extraoral 15 donor sites has been considered to be the gold stan- dard in comparison with new bone graft materials due to their biological proper- ties and the lack of possibility of disease transmission or host rejection. 14,16,17 Complications after grafting proce- dures are relatively rare 11 ; however, every surgical procedure presents ad- vantages and disadvantages, which must be carefully evaluated before surgery. The clinician must make the appropriate selection of the graft material and tech- nique based on the size, shape, and di- mensions of the defect and its location in the mouth. 18 A guideline for surgical decision in reconstruction for oral reha- bilitation with implants may help pre- vention of possible failures. The aim of this retrospective study was to evaluate morbidity and possible complications in augmentation proce- dures before implant placement. PATIENTS AND METHODS The records of all patients submit- ted to implant-supported rehabilitation at Department of Oral and Maxillofa- *Master Student, School of Dentistry, Uberla ˆ ndia Federal University, Minas Gerais, Brazil. †Dental Surgeon, School of Dentistry, Uberla ˆ ndia Federal University, Minas Gerais, Brazil. ‡Master Student, School of Dentistry, Uberla ˆ ndia Federal University, Minas Gerais, Brazil. §Assistant Professor, Oral & Maxillofacial Surgery and Implantology Department, Uberla ˆ ndia Federal University, Minas Gerais, Brazil. Full Professor, Oral & Maxillofacial Surgery and Implantology Department, Uberla ˆ ndia Federal University, Minas Gerais, Brazil. Reprint requests and correspondence to: Darceny Zanetta- Barbosa, DDS, MSc, PhD, Avenida Para ´ s/n°, Campus Umuarama, Bloco 4T, Departamento de Cirurgia e Traumatologia Buco-Maxilo-Facial, Bairro Umuarama, Uberla ˆndia, Minas Gerais, Brazil, CEP: 38.400 –902, Fax and Telephone: 55-34-3218-2636, E-mail: ctbmf@ umuarama.ufu.br or [email protected] ISSN 1056-6163/10/01904-342 Implant Dentistry Volume 19 • Number 4 Copyright © 2010 by Lippincott Williams & Wilkins DOI: 10.1097/ID.0b013e3181e416f9 Aim: The aim of this retrospec- tive study was to evaluate morbidity and possible complications in aug- mentation procedures before im- plant placement. Methods: Records from 93 con- secutive patients with indication for autogenous bone grafting before im- plant placement, treated at Depart- ment of Oral and Maxillofacial Surgery and Implantology of Uberla ˆndia Fed- eral University, in a 7-year period (July 2000 until July 2007), were re- viewed. The need for bone grafting was defined by the impossibility of in- stalling implants of adequate length or diameter to fulfill prosthetic require- ments or for aesthetic reasons. Results: A total of 136 bone graft- ing procedures were performed. The mandibular external oblique line and ascending ramus were the most fre- quently used donor areas (59.64%) and block grafts (67.64%) were the most frequently used type of graft, frequently from the mandibular external oblique line/ascending ramus (52.18%). Platelet-rich plasma was used in 20.1% of all procedures, usually associated with particulate bone grafts. Maxillary procedures represented the majority of surgeries (75%), but with fewer compli- cations compared with the mandible. Si- nus mucosa perforation was the most frequent complication in maxillary procedures, whereas graft expo- sure was the most common compli- cation in mandible. Conclusions: Alveolar recon- struction using autogenous bone followed by implant placement is a reliable treatment for patients with in- sufficient bone. Complications and morbidity were frequently observed. However, in only 6.6% of all proce- dures, the final rehabilitation with dental implants was not possible. (Implant Dent 2010;19:342–350) Key Words: bone graft, implant, sur- gery, complications 342 BONE GRAFTING PROCEDURES BEFORE IMPLANT PLACEMENT •RABELO ET AL

Retrospective Study of Bone Grafting Procedures Before ... · Retrospective Study of Bone Grafting Procedures Before Implant Placement ... E-mail: ctbmf@ umuarama.ufu.br or [email protected]
Dec 03, 2018
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Retrospective Study of Bone GraftingProcedures Before Implant Placement
Gustavo Davi Rabelo, DDS,* Priscila Marani de Paula, DDS,† Flaviana Soares Rocha, DDS,‡Claudia Jordao Silva, DDS, MSc, PhD,§ and Darceny Zanetta-Barbosa, DDS, MSc, PhD�
Dental rehabilitation of partiallyor totally edentulous patientswith oral implants has become
common practice with reliable long-term results.1 However, unfavorable lo-cal conditions of the alveolar ridge,because of atrophy, periodontal disease,and trauma sequelae, may cause insuf-ficient bone volume, which may renderimplant placement impossible.2 Whenthe alveolar ridges lack the appropriatebone volume, additional surgical recon-structive procedures are required.
Researchers continuously strive toimprove on current bone grafting tech-niques and provide faster and denserbone regeneration. A variety of autoge-nous,3 allogenous,4 xenogenous,5 and al-loplastic6,7 grafts, alone or in differentcombinations, have been used to pro-vide sufficient ridge width or high forproper positioning of endosseous im-plants.8 –10 Additionally, the use ofplatelet-rich plasma (PRP) offers a po-tentially useful adjunct to bone grafts11
due to osteoinductive properties ofPRP.12,13
The use of autogenous bone graftsfrom intra-14 or extraoral15 donor siteshas been considered to be the gold stan-dard in comparison with new bone graftmaterials due to their biological proper-ties and the lack of possibility of diseasetransmission or host rejection.14,16,17
Complications after grafting proce-dures are relatively rare11; however,every surgical procedure presents ad-vantages and disadvantages, which mustbe carefully evaluated before surgery.The clinician must make the appropriateselection of the graft material and tech-nique based on the size, shape, and di-
mensions of the defect and its locationin the mouth.18 A guideline for surgicaldecision in reconstruction for oral reha-bilitation with implants may help pre-vention of possible failures.
The aim of this retrospective studywas to evaluate morbidity and possiblecomplications in augmentation proce-dures before implant placement.
PATIENTS AND METHODS
The records of all patients submit-ted to implant-supported rehabilitationat Department of Oral and Maxillofa-
*Master Student, School of Dentistry, Uberlandia FederalUniversity, Minas Gerais, Brazil.†Dental Surgeon, School of Dentistry, Uberlandia FederalUniversity, Minas Gerais, Brazil.‡Master Student, School of Dentistry, Uberlandia FederalUniversity, Minas Gerais, Brazil.§Assistant Professor, Oral & Maxillofacial Surgery andImplantology Department, Uberlandia Federal University, MinasGerais, Brazil.�Full Professor, Oral & Maxillofacial Surgery and ImplantologyDepartment, Uberlandia Federal University, Minas Gerais, Brazil.
Reprint requests and correspondence to: Darceny Zanetta-Barbosa, DDS, MSc, PhD, Avenida Para s/n°, CampusUmuarama, Bloco 4T, Departamento de Cirurgia eTraumatologia Buco-Maxilo-Facial, Bairro Umuarama,Uberlandia, Minas Gerais, Brazil, CEP: 38.400–902, Faxand Telephone: 55-34-3218-2636, E-mail: [email protected] or [email protected]
ISSN 1056-6163/10/01904-342Implant DentistryVolume 19 • Number 4Copyright © 2010 by Lippincott Williams & Wilkins
DOI: 10.1097/ID.0b013e3181e416f9
Aim: The aim of this retrospec-tive study was to evaluate morbidityand possible complications in aug-mentation procedures before im-plant placement.
Methods: Records from 93 con-secutive patients with indication forautogenous bone grafting before im-plant placement, treated at Depart-ment of Oral and Maxillofacial Surgeryand Implantology of Uberlandia Fed-eral University, in a 7-year period(July 2000 until July 2007), were re-viewed. The need for bone graftingwas defined by the impossibility of in-stalling implants of adequate length ordiameter to fulfill prosthetic require-ments or for aesthetic reasons.
Results: A total of 136 bone graft-ing procedures were performed. Themandibular external oblique line andascending ramus were the most fre-quently used donor areas (59.64%)and block grafts (67.64%) were themost frequently used type of graft,
frequently from the mandibular externaloblique line/ascending ramus (52.18%).Platelet-rich plasma was used in 20.1%of all procedures, usually associatedwith particulate bone grafts. Maxillaryprocedures represented the majority ofsurgeries (75%), but with fewer compli-cations compared with the mandible. Si-nus mucosa perforation was the mostfrequent complication in maxillaryprocedures, whereas graft expo-sure was the most common compli-cation in mandible.
Conclusions: Alveolar recon-struction using autogenous bonefollowed by implant placement is areliable treatment for patients with in-sufficient bone. Complications andmorbidity were frequently observed.However, in only 6.6% of all proce-dures, the final rehabilitation withdental implants was not possible.(Implant Dent 2010;19:342–350)Key Words: bone graft, implant, sur-gery, complications
342 BONE GRAFTING PROCEDURES BEFORE IMPLANT PLACEMENT • RABELO ET AL
cial Surgery and Implantology of Fed-eral University of Uberlandia, fromJuly 2000 to July 2007, were reviewedand those who underwent bone recon-struction procedures were included inthe current retrospective study.
The need for bone grafting was de-fined by the impossibility of installingimplants of adequate length or diameterto fulfill prosthetic requirements or byaesthetic reasons. The following situa-tions were considered for augmentationprocedures:
1. Less than 5 mm of bone bellowmaxillary sinus.
2. Less than 4 mm of width in poste-rior areas.
3 Vertical defects of more than 3 mmin aesthetic area.
All patients should be in goodhealthy conditions, without any diseasethat would contraindicate surgery. Allsurgeries were performed by trainee im-plantologists and supervised by a Pro-fessor of Oral and Maxillofacial Surgeryand Implantology Department.
The pertinent data of the surgicalprocedure were organized as follows:
1. Donor areas: symphysis, mandibu-lar external oblique line/ascendingramus, implant area, calvaria, andiliac crest.
2. Use or not of PRP.3. Type of graft: block graft and par-
ticulate bone graft.4. Transsurgical complications: graft
fracture, sinus mucosa perforation,insufficient bone at time of implantinstallation, graft displacement, im-plant instability, and fracture of fix-ation screw.
5. Postsurgical complications: pain,bleeding, infection, graft or implantexposure, graft or implant loss, si-nusitis, paresthesia, and hematoma.
All patients with transsurgical orpostsurgical complications receivedappropriate treatment. The data of allpatients were analyzed and presentedin tables.
RESULTS
In the 7-year period of the currentstudy, 136 bone grafting procedureswere performed in 93 patients and the
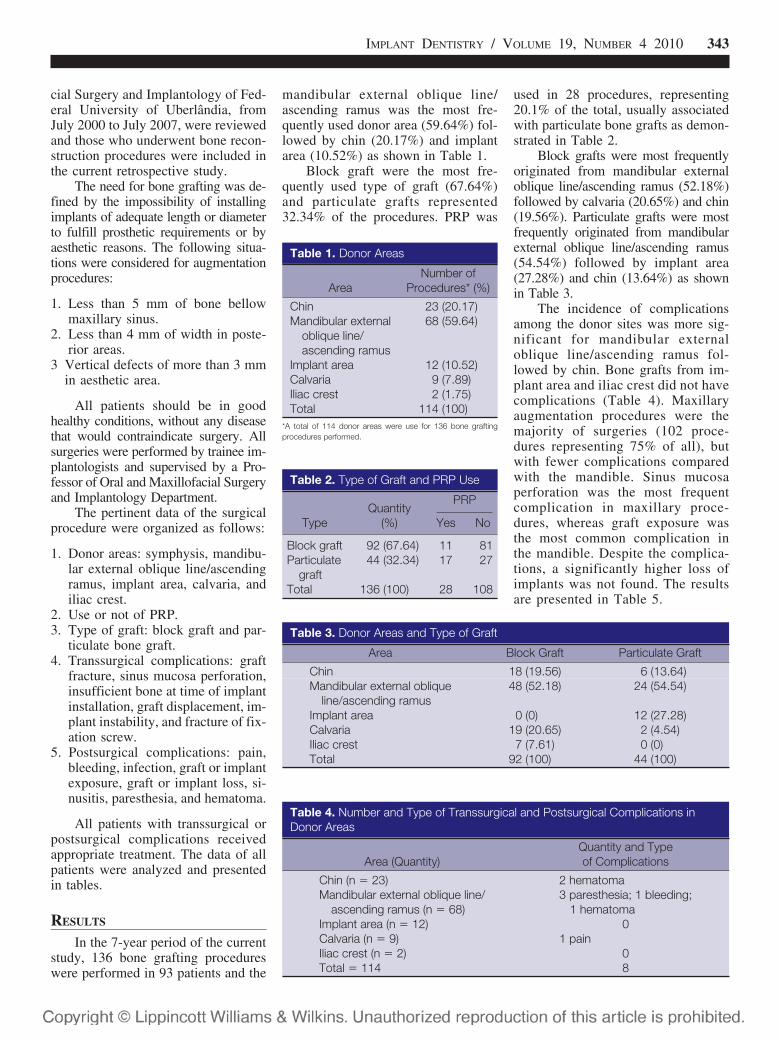
mandibular external oblique line/ascending ramus was the most fre-quently used donor area (59.64%) fol-lowed by chin (20.17%) and implantarea (10.52%) as shown in Table 1.
Block graft were the most fre-quently used type of graft (67.64%)and particulate grafts represented32.34% of the procedures. PRP was
used in 28 procedures, representing20.1% of the total, usually associatedwith particulate bone grafts as demon-strated in Table 2.
Block grafts were most frequentlyoriginated from mandibular externaloblique line/ascending ramus (52.18%)followed by calvaria (20.65%) and chin(19.56%). Particulate grafts were mostfrequently originated from mandibularexternal oblique line/ascending ramus(54.54%) followed by implant area(27.28%) and chin (13.64%) as shownin Table 3.
The incidence of complicationsamong the donor sites was more sig-nificant for mandibular externaloblique line/ascending ramus fol-lowed by chin. Bone grafts from im-plant area and iliac crest did not havecomplications (Table 4). Maxillaryaugmentation procedures were themajority of surgeries (102 proce-dures representing 75% of all), butwith fewer complications comparedwith the mandible. Sinus mucosaperforation was the most frequentcomplication in maxillary proce-dures, whereas graft exposure wasthe most common complication inthe mandible. Despite the complica-tions, a significantly higher loss ofimplants was not found. The resultsare presented in Table 5.
Table 1. Donor Areas
AreaNumber of
Procedures* (%)
Chin 23 (20.17)Mandibular external
oblique line/ascending ramus
68 (59.64)
Implant area 12 (10.52)Calvaria 9 (7.89)Iliac crest 2 (1.75)Total 114 (100)
*A total of 114 donor areas were use for 136 bone graftingprocedures performed.
Table 2. Type of Graft and PRP Use
TypeQuantity
(%)
PRP
Yes No
Block graft 92 (67.64) 11 81Particulate
graft44 (32.34) 17 27
Total 136 (100) 28 108
Table 3. Donor Areas and Type of Graft
Area Block Graft Particulate Graft
Chin 18 (19.56) 6 (13.64)Mandibular external oblique
line/ascending ramus48 (52.18) 24 (54.54)
Implant area 0 (0) 12 (27.28)Calvaria 19 (20.65) 2 (4.54)Iliac crest 7 (7.61) 0 (0)Total 92 (100) 44 (100)
Table 4. Number and Type of Transsurgical and Postsurgical Complications inDonor Areas
Area (Quantity)Quantity and Typeof Complications
Chin (n � 23) 2 hematomaMandibular external oblique line/
ascending ramus (n � 68)3 paresthesia; 1 bleeding;
1 hematomaImplant area (n � 12) 0Calvaria (n � 9) 1 painIliac crest (n � 2) 0Total � 114 8
IMPLANT DENTISTRY / VOLUME 19, NUMBER 4 2010 343

Cases where installation of theimplants and rehabilitation were notpossible, even with bone grafting pro-cedures and appropriate treatment forall complications are presented in Ta-ble 6. In 6.61% of all cases, implantinstallation was not possible due toinsufficient bone after augmentationprocedures.
DISCUSSION
Implant-supported fixed or re-movable prostheses provide a propertreatment modality.1 Nevertheless, theuse of endosseous implants may belimited by insufficient quality andquantity of available bone. Severalgrafting procedures have been de-scribed to create sufficient volume ofbone for implant placement.19 Autog-enous grafts still remain the “goldstandard” in reconstructive surgeriesdue to their osteoinductive, osteocon-ductive, and osteogenic potential14,16,17
essential for bone morphogenesis.16,17
Serra e Silva et al14 conclude that au-togenous bone grafts are the best op-tion compared with allografts and
xenografts due to its properties andconstitute a viable form of treatmentfor patients with alveolar bone loss.19
Autogenous bone can be har-vested from intra- or extraoral donorsites. Schwartz-Arad and Levin20 con-cluded that the intraoral bone blockgrafting is a predictable operation witha high success rate for long-span aug-mentation. In this study, the predilectionfor intraoral donor areas was based onadvantages like lower morbidity, loweroperatory cost, and easier access duringsurgery.20 Other advantages include theuse of local anesthesia instead of generalanesthesia, relatively short operatingtime and no need of postoperative hos-pitalization.19 Nevertheless, complica-tions with intraoral donor sites canoccasionally occur14 and include alteredsensation of teeth, mucosa and skin, lim-ited mouth opening, bleeding, swelling,pain, contour changes in donor areas,and postoperative infections.21,22 When alarge amount of autologous bone is re-quired for reconstruction, other areassuch as the calvaria or iliac crest, shouldbe considered as an alternative.15
Studies to determine which donorsites provide sufficient bone with theleast patient discomfort and risk ofcomplications are needed.23 The risksand morbidity of harvesting autoge-nous bone from intraoral sites can beassociated with some complications,14
which do not significantly compro-mise rehabilitation when appropriatetreatment is established. The same au-thors also revealed that mandibularsymphysis is the intraoral donor sitewith the highest prevalence of compli-cations compared with other intraoral
donor sites. This was not confirmed inour study. According to Freihofer etal,24 the mandibular symphysis is anattractive donor site as the patients arereported to have lesser pain and dis-comfort. The main criticism for theuse of mandibular symphysis as a graftis the limited volume of bone availablefor grafting,25 thus they are not suit-able for larger bone defects.
The mandibular external obliqueline/ascending ramus are common sitesfor cortical bone harvesting21 but therisk of damaging the inferior alveolarnerve is of great concern when usingthis technique. In our study, 3 cases oftemporary nerve paresthesia werefound. However, the number of proce-dures in this area was high (68), and theincidence of this complication (4.4%)may be considered to be low evenamong the trainee implantologists.
Small amounts of particulatebone grafts may be collected fromthe implant area during implant sitepreparation, and the resulting bonechips can then be used to fill smalldefects or be mixed with other graftmaterials. Collection of bone chipsduring drilling for implant place-ment is done under copious irriga-tion. The main disadvantage of thistechnique is the contamination withoral bacteria. Therefore, it is sug-gested to use 2 surgical aspirators:one of them only for saliva and an-other directly applied to the drillingsite, collecting only bone and salinesolution, thus reducing the risk ofexcessive bacterial contamination.26
In accordance with Chiapasco etal,2 we found that the block graft wasused in the majority of cases. Particu-lated bone was associated with boneblocks in case of simultaneous sinusgrafting procedures or as a filling ma-terial around or between bone blocks.Only bone blocks maintain the archi-tecture of bone and appear to adapteasily to the receptor area, whereasparticulate bone grafts must be placedinto cavities or associated with blockgrafts, which limits its use for specificclinical situations.
Higher implant failure rates havebeen reported when implants areplaced into grafted sites.27 However,in this study, despite the number of
Table 5. Number and Type of Transsurgical and Postsurgical Complications inReceptor Areas After Bone Grafting Procedures
Area (Quantity) Specific Area (Quantity) Quantity and Type of Complications
Mandible(n � 34)
Anterior mandible (n � 5) 0Posterior mandible
(n � 29)5 graft exposure; 2 graft loss; 1 break of
fixation screw; 2 implant exposure; 1graft displacement; 1 infection
Maxila (n � 102) Anterior maxila (n � 40) 2 graft displacement; 2 implant loss;1 infection
Posterior maxila(n � 62)
4 sinus mucosa perforation; 2 insufficientbone during implant placement; 2implant exposure; 1 fracture; 2implant loss; 1 pain
Total 136 29
Table 6. Reconstructed AreasWhere Rehabilitation Was NotPossible (n � 136)
Reason of theNoninstallation of
the Implant Quantity (%)
Personal/financial/other reasons
10 (7.35)
Referred to orthodontist 3 (2.20)Nonrehabilitation due to
insufficient bone9 (6.61)
Total 22 (16.17)
344 BONE GRAFTING PROCEDURES BEFORE IMPLANT PLACEMENT • RABELO ET AL

complications, rehabilitation with oralimplants was not possible in only6.6% of all bone grafting procedures.Aghaloo and Moy18 have already indi-cated similar success rates betweenimplants placed into grafted sitedcompared with implants placed intonative bone.
Maxillary procedures representedthe majority of surgeries and presentedfew complications, which could be re-lated to the best donor site irrigation.Sinus mucosa perforations occurredduring sinus floor elevation proce-dures, mainly due to technical difficul-ties. However, they were not related tosignificantly higher loss of implants.The morbidity and complication rateof maxillary sinus augmentation re-ported in the literature is very low.28
Raghoebar et al22 concluded that max-illary sinus bone grafting with autog-enous bone for the insertion ofimplants is a reliable treatment modal-ity with good long-term results.
The highest incidence of compli-cations occurred in the mandible.Temporary sensory disturbances andgraft exposures were the most com-mon complications. None of themsignificantly influenced the successof rehabilitation.
When grafts are loaded andstimulated, significant resorptionduring the initial 6 months of healingis relatively common.9 One-stagesurgery reduces the number of sur-gical interventions and the healingtime. However, some authors havereported better results with the2-stage than with the 1-stage ap-proach.8,29 In this study, all caseswere treated by 2-staged surgeries,allowing revascularization and in-corporation of the graft22 in a firstmoment, followed by osseointegra-tion of the implant before prostheticrehabilitation, which could havecontributed to the high success ratesfound. Delayed placement also per-mits proper angulation and precisepositioning compared with implantsplaced at the time of bone grafting.30
CONCLUSION
Reconstruction using autoge-nous bone followed by implantplacement is a reliable treatment
with high success rates. Complica-tions and morbidity were noted inmany cases. In 6.61% of all cases,implant installation was not possi-ble. This retrospective study of bonegrafting surgeries can serve as aguide in the prevention of possiblefailures and consequently improvethe quality of future procedures.
ACKNOWLEDGMENT
The authors claim to have nofinancial interest in any company orany of the products mentioned in thisarticle.
REFERENCES
1. Lang NP, Berglundh T, Heitz-Mayfield LJ, et al. Consensus statementsand recommended clinical procedures re-garding implant survival and complica-tions. Int J Oral Maxillofac Implants. 2004;19(suppl):150-154.
2. Chiapasco M, Zaniboni M, BoiscoM. Augmentation procedures for the reha-bilitation of deficient edentulous ridges withoral implants. Clin Oral Implants Res.2006;17(Suppl 2):136-159.
3. Simion M, Jovanovic SA, Tinti C, etal. Long-term evaluation of osseointe-grated implants inserted at the time or aftervertical ridge augmentation. A retrospec-tive study on 123 implants with 1–5 yearfollow-up. Clin Oral Implants Res. 2001;12:35-45.
4. Friedmann A, Strietzel FP, MaretzkiB, et al. Histological assessment of aug-mented jaw bone utilizing a new collagenbarrier membrane compared to a standardbarrier membrane to protect a granularbone substitute material. Clin Oral ImplantsRes. 2002;13:587-594.
5. Araujo MG, Sonohara M, Hay-acibara R, et al. Lateral ridge augmentationby the use of grafts comprised of autolo-gous bone or a biomaterial. An experimen-tal in the dog. J Clin Periodontol. 2002;29:1122-1131.
6. Barone A, Crespi R, Aldini NN, etal. Maxillary sinus augmentation: Histo-logic and histomorphometric analysis. IntJ Oral Maxillofac Implants. 2005;20:519-525.
7. Meyer C, Chatelain B, Benarroch M,et al. Massive sinus-lift procedures withbeta-tricalcium phosphate: Long-term re-sults. Rev Stomatol Chir Maxillofac. 2009;110:69-75.
8. Barone A, Covani U. Maxillary alve-olar ridge reconstruction with nonvascu-larized autogenous block bone: Clinicalresults. J Oral Maxillofac Surg. 2007;65:2039-2046.
9. Block MS, Kent JN, Kallukaran FU,et al. Bone maintenance 5 to 10 years aftersinus grafting. J Oral Maxillofac Surg.1998;56:706-715.
10. Chiapasco M, Colletti G, Romeo E,et al. Long-term results of mandibular re-construction with autogenous bone graftsand oral implants after tumor resection.Clin Oral Implants Res. 2008;19:1074-1080.
11. Meraw SJ, Eckert SE, YacyshynCE, et al. Retrospective review of graftingtechniques utilized in conjunction withendosseous implant placement. IntJ Oral Maxillofac Implants. 1999;14:744-747.
12. Kim E, Park E, Choung P. Plateletconcentrates and its effect on bone forma-tion in calvarial defects: An experimentalstudy in rabbits. J Prosth Den. 2001;86:428-433.
13. Kim SG, Kim WK, Park JC, et al. Acomparative study of osseointegration ofAvana implants in a demineralized freeze-dried bone alone or with platelet-richplasma. J Oral Maxillofac Surg. 2002;60:1018-1025.
14. Serra e Silva FM, Cortez ALV,Moreira RWF, et al. Complications of in-traoral donor site for bone grafting prior toimplant placement. Implant Dentistry.2006;15:420-426.
15. Smolka W, Bosshardt DD,Mericske-Stern R, et al. Reconstruction ofthe severely atrophic mandible using cal-varial split bone grafts for implant-supported oral rehabilitation. Oral SurgOral Med Oral Pathol Oral Radiol Endod.2006;101:35-42.
16. Lohmann H, Grass G, Rangger C,et al. Economic impact of cancellous bonegrafting in trauma surgery. Arch OrthopTrauma Surg. 2007;127:345-348.
17. Lye KW, Deatherage JR, Waite PD.The use of demineralized bone matrix forgrafting during Le Fort I and chinosteotomies: Techniques and complica-tions. J Oral Maxillofac Surg. 2008;66:1580-1585.
18. Aghaloo TL, Moy PK. Which hardtissue augmentation techniques are themost successful in furnishing bony sup-port for implant placement? Int J OralMaxillofac Implants. 2007;22(Suppl):49-70.
19. Sant’Ana E. Short-term survival ofosseointegrated implants installed in alve-olar ridge reconstructed with autogenousgraft (Thesis submitted to obtain PhD).Bauru School of Dentistry, Sao Paulo Uni-versity, 1997.
20. Schwartz-Arad D, Levin L. Intraoralautogenous block onlay bone grafting forextensive reconstruction of atrophic maxil-lary alveolar ridges. J Periodontol. 2005;76:636-641.
21. Misch CM. Comparison of intraoral
IMPLANT DENTISTRY / VOLUME 19, NUMBER 4 2010 345

donor sites for onlay grafting prior to im-plant placement. Int J Oral Maxillofac Im-plants. 1997;12:767-776.
22. Raghoebar GM, Timmenga NM,Reintsema H, et al. Maxillary bone graftingfor insertion of endosseous implants: Re-sults after 12–124 months. Clin Oral ImplRes. 2001;12:279-286.
23. Esposito M, Grusovin MG,Coulthard P, et al. The efficacy of variousbone augmentation procedures for dentalimplants: A Cochrane systematic review ofrandomized controlled clinical trials. Int J OralMaxillofac Implants. 2006;21:696-710.
24. Freihofer HP, Borstlap WA, Kuijpers-Jagtman AM, et al. Timing and transplantmaterials for closure of alveolar clefts. A clin-
ical comparison of 296 cases. J Craniomax-illofac Surg. 1993;21:143-148.
25. Booij A, Raghoebar GM, Jansma J,et al. Morbidity of chin bone transplantsused for reconstructing alveolar defects incleft patients. Cleft Palate Craniofac J.2005;42:533-538.
26. Blay A, Tunchel S, Sendyk WR. Vi-ability of autogenous bone grafts obtainedby using bone collectors: Histological andmicrobiological study. Pesqui OdontolBras. 2003;17:234-240.
27. Lorenzoni M, Pertl C, WegscheiderW, et al. Retrospective analysis of Frialit-2implants in the augmented sinus. Int J Peri-odontics Restorative Dent. 2000;20:255-267.
28. Ardekian L, Oved-Peleg E, MacteiEE, et al. The clinical significance of sinusmembrane perforation during augmenta-tion of the maxillary sinus. J Oral MaxillofacSurg. 2006;64:277-282.
29. Sjostrom M, Lundgren S, Sen-nerby L. A histomorphometric comparisonof the bone graft-titanium interface be-tween interpositional and onlay/inlay bonegrafting techniques. Int J Oral MaxillofacImplants. 2006;21:52-62.
30. Bell RB, Blakey GH, White RP,et al. Staged reconstruction of the se-verely atrophic mandible with autoge-nous bone graft and endosteal implants.J Oral Maxillofac Surg. 2002;60:1135-1141.
Abstract Translations
GERMAN / DEUTSCHAUTOR(EN): Gustavo Davi Rabelo, DDS, Priscila Marani dePaula, DDS, Flaviana Soares Rocha, DDS, Claudia Jordao Silva,DDS, MSc, PhD, Darceny Zanetta-Barbosa, DDS, MSc, PhDRetrospektive Studie von Knochentransplantierungsa-blaufen vor Einsetzung von Implantaten
ZUSAMMENFASSUNG: Zielsetzungen: Diese retrospe-ktive Studie zielte darauf ab, die Sterblichkeit und moglichenKomplikationen bei Augmentation vor Implantateinpflan-zung zu beurteilen. Materialien und Methoden: Es wurdendie Aufzeichnungen von 93 aufeinander folgenden Patientenmit einer Indikation fur die Transplantierung von autologemKnochengewebe vor Implantatsetzung untersucht, die inder Abteilung fur Gesichts- und Kieferchirurgie und-implantologie an der staatlichen Universitat Uberlandia in-nerhalb eines Zeitraums von 7 Jahren (Juli 2000 bis Juli2007) behandelt wurden. Die Notwendigkeit fur eineKnochentransplantation wurde durch die fehlenden Moglich-keiten bestimmt, Implantate von ausreichender Lange oderausreichendem Durchmesser zur Erfullung der prothetischenErfordernisse einsetzen zu konnen, oder aber durch asthe-tische Grunde. Ergebnisse: Insgesamt wurden 136 Knochen-transplantierungsbehandlungen durchgefuhrt. Die externeabgeschragte Linie im Unterkiefer sowie der aufsteigende Astwurden am haufigsten als Spendebereich (59,64%) eingesetztund Blocktransplantate (67,64%) waren die am meisten eing-esetzten Arten von Transplantaten und dies haufig von derexternen schragen Linie im Unterkiefer / aufsteigendem Ast(52,18%). Thrombozytreiches Plasma wurde in 20,1% allerFalle verwendet, normalerweise in Verbindung mit partikel-formigem Knochentransplantat. Die meisten chirurgischenEingriffe wurden im Oberkiefer abgewickelt (75%). Hierbeigab es insgesamt trotzdem weniger Komplikationen zu ver-
zeichnen, als bei Eingriffen im Unterkiefer. Bei den Ein-griffen im Oberkiefer war als haufigste Komplikation einePerforation der Sinusschleimhaut festzustellen, wahrenddie Aufdeckung des Transplantats beim Unterkieferdie am haufigsten auftretende Komplikation darste-llte. Schlussfolgerungen: Eine alveolare Rekonstruktionunter Verwendung von autogenem Knochengewebe mitanschließender Implantateinpflanzung stellt eine zuverlas-sige Behandlungsalternative fur Patienten mit unzu-reichendem Knochengewebe dar. Es wurden sehr haufigKomplikationen und Sterblichkeit beobachtet. Allerdingswas in nur 6,6% aller Falle die abschließende Wiederher-stellung mit Zahnimplantaten uberhaupt nicht moglich.
SCHLUSSELWORTER: Knochentransplantat, Implantat,Chirurgie, Komplikationen
SPANISH / ESPAÑOLAUTOR(ES): Gustavo Davi Rabelo, DDS, Priscila Marani dePaula, DDS, Flaviana Soares Rocha, DDS, Claudia JordaoSilva, DDS, MSc, PhD, Darceny Zanetta-Barbosa, DDS,MSc, PhDEstudio retrospectivo de procedimientos de injerto de huesoantes de la colocacion del implante
ABSTRACTO: Objetivos: El objetivo de este estudio retro-spectivo fue evaluar la morbosidad y posibles complicacionesen los procedimientos de aumentacion antes de la colocaciondel implante. Materiales y metodos: Se evaluaron los regis-tros de 93 pacientes consecutivos con indicacion de injertoautogeno de hueso antes de la colocacion del implante, trata-dos en el Departamento de Cirugía Oral y Maxilofacial eImplantología de la Universidad Federal Uberlandia, en unperíodo de 7 anos (Julio/2000 hasta Julio/2007). La necesidad
346 BONE GRAFTING PROCEDURES BEFORE IMPLANT PLACEMENT • RABELO ET AL

del injerto de hueso se definio segun la imposibilidad decolocar implantes de longitud o diametro adecuado paracumplir los requisitos prosteticos o por razones esteticas.Resultados: Se realizaron un total de 136 procedimientos deinjerto de hueso. La zonas de donacion usadas con mayorfrecuencia fueron la línea oblicua externa de la mandíbula yel ramo ascendente (59,64%) y los injertos de bloque(67,64%) fueron el tipo de injerto usado con mayor frecuen-cia, con frecuencia desde la línea oblicua externa de lamandíbula/ramo ascendente (52,18%). Se uso plasma rico enplaquetas en un 20,1% de todos los procedimientos, general-mente asociados con injertos de partículas de hueso. Losprocedimientos en el maxilar representaron la mayoría de lasoperaciones (75%), pero con menos complicaciones com-parado con la mandíbula. La perforacion de la mucosa delseno fue la complicacion mas frecuente en los procedimientosdel maxilar mientras que el contacto con el injerto fue lacomplicacion mas comun en la mandíbula. Conclusiones: Lareconstruccion alveolar usando un hueso autogeno seguidopor la colocacion del implante es un tratamiento confiablepara los pacientes con hueso insuficiente. Se observaron confrecuencia complicaciones y morbosidad. Sin embargo, ensolamente un 6,6% de todos los procedimientos, la rehabil-itacion final con los implantes dentales no fue posible.
PALABRAS CLAVES: Injerto de hueso, implante, cirugía,complicaciones
PORTUGUESE / PORTUGUÊSAUTOR(ES): Gustavo Davi Rabelo, Cirurgiao-Dentista,Priscila Marani de Paula, Cirurgia-Dentista, Flaviana SoaresRocha, Cirurgia-Dentista, Claudia Jordao Silva, Cirurgia-Dentista, Mestre em Ciencia, PhD, Darceny Zanetta-Barbosa,Cirurgia-Dentista, Mestre em Ciencia, PhDEstudo retrospectivo de procedimentos de enxertamento deosso antes da colocacao de implante
RESUMO: Objetivos: O objetivo deste estudo retrospectivofoi avaliar a morbidade e possíveis complicacoes em procedi-mentos de aumento antes da colocacao de implante. Materi-ais e Metodos: Registros de 93 pacientes consecutivos comindicacao de enxertamento de osso autogeno antes da colo-cacao de implante, tratados no Departamento de CirurgiaOral e Maxilofacial e Implantologia da Universidade Federalde Uberlandia, num período de 7 anos (julho/2000 ate julho/2007), foram revisados. A necessidade de enxertamento os-seo foi definida pela impossibilidade de instalar implantes decomprimento ou diametro adequado para preencher requisitosproteticos ou por razoes esteticas. Resultados: Um total de136 procedimentos de enxertamento de osso foi realizado. Alinha mandibular externa oblíqua e o ramo ascendente foramas areas doadoras mais frequentemente usadas (59,64%) e osenxertos em bloco (67,64%) foram o tipo de enxerto maisfrequentemente usado, frequentemente da linha mandibularexterna oblíqua/ramo ascendente (52,18%). Foi usado plasma
rico em plaquetas em 20,1% de todos os procedimentos,normalmente associado a enxertos de osso particulado. Osprocedimentos maxilares representaram a maioria das cirurg-ias (75%), mas com menos complicacoes em comparacaocom a mandíbula. A perfuracao da mucosa da cavidade foi acomplicacao mais frequente em procedimentos maxilares,enquanto a exposicao do enxerto foi a complicacao maiscomum na mandíbula. Conclusoes: A reconstrucao alveolarusando osso autogeno seguida por colocacao de implante eum tratamento confiavel para pacientes com osso insufici-ente. Complicacoes e morbidade foram frequentementeobservadas. Contudo, a reabilitacao final com implantesdentarios nao foi possível em apenas 6,6% de todos osprocedimentos.
PALAVRAS-CHAVE: Enxerto Osseo, Implante, Cirurgia,Complicacoes
RUSSIAN /������: Gustavo Davi Rabelo, ������ ���������� �����������, Priscila Marani de Paula, ���������������� �����������, Flaviana Soares Rocha,������ ���������� �����������, Cláudia JordãoSilva, ������ ���������� �����������, ������������������ ���� � ������� ��������, ���������������, Darceny Zanetta-Barbosa, ���������������� �����������, ������ ���������������� � ������� ��������, ������ ��������������� ����� ����������� ����� ����-��������� ���� � ��� ���� ������ � ��-��������
������. ����. ����� ������ ��������������������������� �������� ������ ������������������������ � ��������� ��������� � ������������������ ����������� ������ �����, ��������������� ��������� ����������. �������� � ����.���� ������ ������ 93 ����������� ������������������� � ����������� � �������� ���������-����� ������ ����� ����� ��������� ����������,�������� �� ������ � ��������� ���������� �����������, �������-������ ������� � ��-���������� (Department of Oral and Maxillofacial Sur-gery and Implantology) ������������ Uberlândia FederalUniversity, � ������ 7-������ ������� (� ���� 2000 .�� ���� 2007 .). !������������ � �������������������� ����� ���� ����������� ����������������������� ����������� ��������� ����� ����������� � ����� ������������ ������������������������ ��� �� "���������� �������. ��������. # ���� ��������� ���� ��������� 136�������� �������������� ������ �����. !������������ ����� � ���������� ����� ����� ���������� �������� ���� ������������� ������������������� (59,64 %), � ������ ������������ (67,64
IMPLANT DENTISTRY / VOLUME 19, NUMBER 4 2010 347

%) ���� �������� ���� ������������ ����� �����-��������� � ��� ���� ������� �� ������� ������� ���� ����� / ��������� ����� ����� ������(52,18 %). ������ ������������ �������������������� � 20,1 % ���� ��������, �������������� � ��������������� �������� ���������-������. $�������� � ������� ������������� ��-���� ���������� ���� ������ ������������������ (75 %), �� � ���� �� ������������������� �� ��������� � ����������� � ������������ ������. %���� ����� ����������� ������������� �������� � ������� ������ ���������� ���������� �������� ������� ������, ������ ���������������� ����������� ������������� �������� � ������� ����� ���������� ��������� �������������. ����.&������������ ������������ ����� ��������������� �������� ����� � ���������� ��������� ������������� �������� ��������������� ������ ��������� � ��������������'���� ������ �����. (��������� �������������� ���������� ����������� ����.(����� ������ � 6,6 % ���� �������� ������������������ ��������� � ������� ���������������� ���������� .
�������� �����: ������ ������������, ��-�������, ����������� ��������, ����������
TURKISH / TURKCEYAZARLAR: Gustavo Davi Rabelo, DDS, Priscila Marani dePaula, DDS, Flaviana Soares Rocha, DDS, Claudia JordaoSilva, DDS, MSc, PhD, Darceny Zanetta-Barbosa, DDS,MSc, PhD
Implant yerlestirme oncesinde kemik greftleme prosedurl-erinin retrospektif bir calısması
OZET: Amaclar: Bu retrospektif calısmanın amacı, implantyerlestirme oncesinde yapılan ogmantasyon prosedurlerininolası komplikasyonlarını ve morbiditesini degerlendirmekti.Gerec ve Yontem: Uberlandia Federal Universitesinin Oralve Maksilofasiyal Cerrahi ve Implantoloji Anabilim Dalında7 yıllık bir donemde (Temmuz 2000�den Temmuz 2007�yekadar) tedavi edilen ve implant yerlestirme islemi oncesindeotojen kemik greftleme endikasyonu olan art ardına 93 has-tanın kayıtları incelendi. Protez kosullarını karsılamak ya daestetik nedenlere cevap vermek icin yeterli uzunluk ve captaimplant yerlestirmenin imkansız olması kemik greftlemegereksinimi olarak tanımlandı. Bulgular: Toplam 136 kemikgreftleme proseduru yapıldı. En sık kullanılan (%59.64) do-nor yerler mandibuler eksternal oblik hat ve asendan ramusolup, blok greft (%67.64) en sık kullanılan greft turu idi. Bugreft sıklıkla mandibuler eksternal oblik hat / asendan ramus-tan (%52.18) alındı. Prosedurlerin %20.1�inde genellikle par-tikulat kemik greftleri ile baglantılı olan trombositten zenginplazma kullanıldı. Maksiller prosedurler cerrahi islemlerinincogunlugunu olusturdu (%75) ve alt ceneye kıyasla daha azkomplikasyona neden oldu. Maksiller prosedurlerde en sıkkomplikasyon sinus mukozasının perforasyonu iken, altcenede en yaygın komplikasyonun greftin acıga cıkmasıoldugu goruldu. Sonuc: Kemik yetersizligi olan hastalardaotojen kemik kullanarak alveoler rekonstruksiyon yapılmasıve ardından implant yerlestirilmesi guvenilir bir tedavi sek-lidir. Komplikasyonlar ve morbidite sık bir sekilde gozlendi.Ancak, tum prosedurlerin sadece %6.6’sında dental implantile nihai rehabilitasyon saglanamadı.
ANAHTAR KELIMELER: Kemik grefti, Implant, Cerrahi,Komplikasyon
348 BONE GRAFTING PROCEDURES BEFORE IMPLANT PLACEMENT • RABELO ET AL

JAPANESE /
CHINESE /
IMPLANT DENTISTRY / VOLUME 19, NUMBER 4 2010 349

KOREAN /
350 BONE GRAFTING PROCEDURES BEFORE IMPLANT PLACEMENT • RABELO ET AL
Related Documents











