RETROGRADE MEMORY DEFICITS IN SEVERE CLOSED- HEAD INJURY PATIENTS Giovanni A. Carlesimo 1 , Maurizio Sabbadini 1 , Patrizia Bombardi 2 , Ester Di Porto 2 , Antonella Loasses 1 and Carlo Caltagirone 1, 3 ( 1 I.R.C.C.S. S. Lucia, Roma; 2 Anni Verdi, Roma; 3 Clinica Neurologica, Università di Roma “Tor Vergata”) ABSTRACT A battery of tests evaluating different aspects of retrograde memory (autobiographical, public events, semantic knowledge) was administered to a group of 20 patients who had suffered from a severe closed-head injury (CHI) and who had recovered from the post- traumatic amnesia period and to a group of sex-, age- and education-matched normal controls. Results document a high prevalence of retrograde memory deficits among CHI individuals. The deficit involves both autobiographical and public events memories and extends to early acquired basic and cultural knowledge. The severity of the deficit does not vary according to some kind of temporal gradient or according to a presumed hierarchical or modality organization of the semantic system. However, in the domain of basic knowledge it more severely affects information pertaining to living than nonliving categories of objects. With the exception of a more severe deficit in retrieving autobiographical events occurred in the last year before trauma in a subgroup of patients with focal lesions restricted to the right hemisphere as compared to left lesioned patients, no clear relationship emerges between severity of the retrograde memory deficit and locus of focal cerebral lesions as demonstrated by neuroradiological exams. Key words: memory, head trauma, semantic system INTRODUCTION A memory disorder is likely the most frequent cognitive deficit in persons who have recovered from the acute phase of a severe closed-head injury (CHI) (e.g., Brooks, McKinlay, Simington et al., 1987). The difficulty in storing new information (anterograde amnesia) has been extensively investigated in both clinical (e.g., Russell, 1971) and neuropsychological studies (e.g., Carlesimo, Sabbadini, Loasses et al., 1997; Levin and Goldstein, 1986; for a review, see Levin, 1989). The impairment in recalling autobiographical and public events which occurred before the head trauma and general semantic information acquired early in life (retrograde amnesia) has been far less investigated. Indeed, in the only group study devoted to this topic, Levin, High, Meyers et al. (1985) compared groups of severe CHI patients who were still experiencing the post-traumatic amnesia period, severe CHI patients following resolution of post-traumatic amnesia and age-matched normal controls on a recognition memory task for titles of television programs broadcasted for a single season in a period ranging from 1 to 13 years prior to the head trauma (Squire and Slater, 1978). In this task, post-traumatic amnesia patients obtained the lowest scores and Cortex, (1998) 34, 1-23

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

RETROGRADE MEMORY DEFICITS IN SEVERE CLOSED-HEAD INJURY PATIENTS
Giovanni A. Carlesimo1, Maurizio Sabbadini1, Patrizia Bombardi2, Ester Di Porto2,Antonella Loasses1 and Carlo Caltagirone1, 3
(1I.R.C.C.S. S. Lucia, Roma; 2Anni Verdi, Roma; 3Clinica Neurologica, Università di Roma “Tor Vergata”)
ABSTRACT
A battery of tests evaluating different aspects of retrograde memory (autobiographical,public events, semantic knowledge) was administered to a group of 20 patients who hadsuffered from a severe closed-head injury (CHI) and who had recovered from the post-traumatic amnesia period and to a group of sex-, age- and education-matched normalcontrols. Results document a high prevalence of retrograde memory deficits among CHIindividuals. The deficit involves both autobiographical and public events memories andextends to early acquired basic and cultural knowledge. The severity of the deficit does notvary according to some kind of temporal gradient or according to a presumed hierarchicalor modality organization of the semantic system. However, in the domain of basicknowledge it more severely affects information pertaining to living than nonliving categoriesof objects. With the exception of a more severe deficit in retrieving autobiographical eventsoccurred in the last year before trauma in a subgroup of patients with focal lesions restrictedto the right hemisphere as compared to left lesioned patients, no clear relationship emergesbetween severity of the retrograde memory deficit and locus of focal cerebral lesions asdemonstrated by neuroradiological exams.
Key words: memory, head trauma, semantic system
INTRODUCTION
A memory disorder is likely the most frequent cognitive deficit in personswho have recovered from the acute phase of a severe closed-head injury (CHI)(e.g., Brooks, McKinlay, Simington et al., 1987). The difficulty in storing newinformation (anterograde amnesia) has been extensively investigated in bothclinical (e.g., Russell, 1971) and neuropsychological studies (e.g., Carlesimo,Sabbadini, Loasses et al., 1997; Levin and Goldstein, 1986; for a review, seeLevin, 1989). The impairment in recalling autobiographical and public eventswhich occurred before the head trauma and general semantic informationacquired early in life (retrograde amnesia) has been far less investigated.
Indeed, in the only group study devoted to this topic, Levin, High, Meyers etal. (1985) compared groups of severe CHI patients who were still experiencingthe post-traumatic amnesia period, severe CHI patients following resolution ofpost-traumatic amnesia and age-matched normal controls on a recognitionmemory task for titles of television programs broadcasted for a single season in aperiod ranging from 1 to 13 years prior to the head trauma (Squire and Slater,1978). In this task, post-traumatic amnesia patients obtained the lowest scores and
Cortex, (1998) 34, 1-23

their memory performance declined the closer to the head trauma date the TVprogram had been broadcasted (negative temporal gradient). The chronic CHIgroup, instead, performed lower than the age-matched controls, but theirperformance profile, compared to that exhibited by normal subjects, did not varyappreciably as a function of the time elapsed since the TV program broadcast. Ina second experiment, accuracy of memory for personal episodes that occurredprior to the head trauma was investigated in the chronic and post-traumaticamnesia CHI groups. Also in this case, post-traumatic amnesia patients performedworse than chronic CHI patients and their memory for autobiographical eventswas progressively poorer the more recently the events occurred. Unfortunately,since a group of normals was not included in this experiment, no conclusion canbe reached about the severity and the qualitative characteristics of theautobiographical memory deficit in the CHI patients following the resolution ofpost-traumatic amnesia.
In contrast to the paucity of group studies, the literature is relatively richwith single case reports describing in detail the characteristics of the retrogradememory impairment in single individuals who had recovered from the acutephase of a severe CHI. Whereas most of these patients suffered from a pervasivememory impairment involving both anterograde and retrograde periods (e.g.,Laiacona, Barbarotto and Capitani, 1993a; Markowitsch, Calabrese, Liess et al.,1993), in some cases a selective deficit for retrograde memories is described,delineating the syndrome picture defined by Kapur (1993) as Focal RetrogradeAmnesia (e.g., Goldberg, Antin, Bilder et al., 1981; Rousseaux, Delafgosse,Cabaret et al., 1984; Stracciari, Ghidoni, Guarino et al., 1994). A negativetemporal gradient of the retrograde memory deficit was only observedsporadically in these patients (Markowitsch et al., 1993; Mattioli, Grassi, Peraniet al., 1996). Moreover, while in most cases the retrograde memory impairmentinvolved both autobiographical and semantic knowledge (Laiacona et al., 1993a;Markowitsch et al., 1993; Mattioli et al., 1996), cases with a memory deficitcircumscribed to autobiographical events (De Renzi, Lucchelli, Muggia et al.,1995) or semantic knowledge (Grossi, Trojano, Grasso et al., 1988) have alsobeen recorded.
The abundance of reports describing single CHI patients with a prevalent orexclusive deficit of retrograde memory suggests that a difficulty in accessingmemory records formed prior to a severe head trauma is likely to occur morefrequently than generally believed. Presumably, the fact that routineneuropsychological investigation is mostly or exclusively concerned with thedifficulty in storing new memories leaves the retrograde memory deficitundetected most of the times.
The aim of this study was to evaluate the frequency of occurrence, theseverity and the qualitative characteristics of the retrograde memory impairmentin an unselected group of severe CHI patients who had recovered from the post-traumatic amnesia period. Performances of these patients were compared tothose of a group of age-matched normal controls on a neuropsychological testbattery investigating autobiographical memory, memory for public events andgeneral semantic knowledge. We were particularly interested in evaluating:
(a) whether the retrograde memory deficit in chronic CHI survivors, relative
2 Giovanni A.Carlesimo and Others

to the remote memory performance exhibited by age-matched normal controls, ishomogeneous across different lifetime periods or whether it varies according tosome kind of temporal gradient;
(b) the level of information processing at which the retrograde memoryimpairment occurs in these patients; in particular, whether it involves lexicalrepresentations of knowledge, or whether it involves more “central” semanticrepresentations;
(c) possible dissociations in the content of semantic memory impairment. Inparticular, following previous suggestions deriving from single CHI case reports(e.g., Laiacona et al., 1993a), we looked for a category-specific dissociationbetween knowledge of living versus nonliving things, a dissociation linked torepresentation modality (visual versus verbal knowledge) and, finally, a gradientof the deficit based on the presumed hierarchical organization of knowledge inthe semantic memory system.
(d) possible dissociations between different aspects of the long-term memoryimpairment. In particular, we looked for patients with selective anterograde orretrograde memory impairment and, in the context of retrograde memory, forpatients with a deficit circumscribed to the autobiographical or semantic aspectsof knowledge.
MATERIALS AND METHODS
Subjects
Twenty consecutive chronic survivors of severe CHI, participating in the Physical andCognitive Rehabilitation Program of the S. Lucia Hospital in Rome, and 20 normalcontrols (NC) matched one-to-one to the CHI patients for age, sex and education took partin this study. CHI individuals had suffered a closed-head trauma at least 3 months before(Glasgow Coma Scale at hospital admission consistently < 8). All patients had recoveredfrom a period of coma ranging from 5 to 60 days and were out of the subsequent post-traumatic amnesia period as revealed by a score > 75 on the Galveston OrientationAmnesia test (Levin, O’Donnel and Grossman, 1979). Excluded from the experimentalsample were patients with a history of alcohol or drug abuse, psychiatric or neurologicalsymptoms preceding the head trauma, patients with coma duration of less than 3 days andpatients who were unable to attend the experimental procedures because of too severelanguage or attentional deficits. Personal and clinical data as well as performance scores onsome neuropsychological tests of CHI patients included in the study are summarized inTable I.
Experimental Investigation
Autobiographical Memory Interview
A modified version of the Autobiographical Memory Interview devised by Kopelman,Wilson and Baddeley (1989) was used to test retrograde memory for personal events. Thistest, originally created for assessing remote memories in aged amnesic patients (mainlydemented patients), was adapted for people from 18 to 35 years of age. Subjects wererequired to produce a memory of a specific incident from their past, relating it to each ofthe items specified (Table II). They were encouraged to produce a specific memory in itsspecific temporal and spatial context rather than a general memory. When the subject failedto produce any memory, he or she was prompted using the cues indicated in Table II. Eachsubject’s response was scored by at least two independent raters on a 0-3 scale based on
Retrograde memory in severe closed-head trauma 3

the descriptive richness of the account of the incident and its specificity in time and place(see Kopelman et al., 1989). For both CHI and normal control subjects, the interview wasdivided into three main time blocks with three items in each: early childhood (before 10years of age), adolescence (11-18 years), twenties (19-29 years). For CHI patients only, afinal block of questions regarded the last year before the head trauma.
4 Giovanni A.Carlesimo and Others
TABLE IPersonal and Clinical Data and Performance Scores on Some Neuropsychological Tests of the
CHI Patients
Pt. Age Sex EducationInjury-test Duration GOS CT/MRI finding PM ’47 Delayed Rey’s (years) (years) Interval of coma (Raven, Prose 15 words
(months) (days) 1949) Recall learning(Spinnler task:
and 15’ delayedTognoni, recall
1987) (Rey, 1958)
1 23 M 8 8 30 4 Negative 35 6.0 142 18 M 12 10 50 4 Cortical-subcortical 35 2* 4*
atrophy3 26 F 13 24 18 5 Right fronto-temporal 30 4 10
hypodensity4 24 F 14 16 33 5 Bilateral frontal 36 1* 4*
hygroma; rightparietal hypodensity
5 28 M 8 35 20 5 Bilateral frontal 36 1.1* 3*hygroma
6 30 M 13 36 22 4 Subdural right 36 6.9 14fronto-temporo-
parietal hematoma7 19 M 11 28 60 4 Small right parietal 33 3* 1*
hypodensity8 20 M 12 24 20 3 Multiple small 33 5.5 9
contusions; left fronto-temporo-parietal hygroma
9 20 F 7 15 45 5 Left frontal contusion 26 3* 5*10 18 M 8 3 5 5 Right frontal 24 2* 4*
subdural hematoma11 34 F 13 7 30 4 Left temporo- 31 4 8
parietal hypodensity12 25 M 13 26 21 5 Left temporal 33 2.3* 7*
hypodensity13 19 M 8 17 57 4 Left temporal, bilateral25 6.4 4*
frontal hypodensities14 20 M 13 11 10 5 Left temporal, bilateral36 6.9 10
frontal hypodensities15 25 M 8 3 18 5 Right frontal 36 5.5 9
hypodensity16 23 M 11 9 Negative 30 3.3 6*17 34 M 13 22 30 4 Left parieto-occipital 20* 3.6 12
and frontal hypodensities
18 36 M 6 16 35 4 Left fronto-temporal 33 6.4 5*hypodensities
19 34 M 13 4 5 5 Bilateral parieto- 33 3.3 9occipital hypodensities
20 26 M 13 46 25 5 Left fronto-temporo- 34 3* 15parietal hypodensity
* Performance score below the lower limit of the 95% tolerance interval
Famous Events Recognition Test
The Famous Events Recognition test was a modified version of the test devised byCosta, De Renzi and Faglioni (1989). For each of 6 two-year periods from 1982-83 to1992-93, eight events were selected which had been extensively covered by newspapersand TV news programs in the period they occurred. Further, eight events which occurred in1994 with the same characteristics as the previous ones were also selected. For each testitem, the subject was questioned about a detail concerning a single event (e.g., “July 12,1986, a 16 year-old girl was condemned to capital punishment in the U.S.A. What was hername?”) and requested to indicate the correct response on a 4-choice array of alternatives(e.g., Jessie Neel, Geraldine Adler, Janet Ross, Paula Cooper). The questions and theresponse alternatives were proposed orally by the examiner based on the chronologicalorder in which the events occurred.
Naming and Questionnaire of Living and Non-living Things
This test, devised by Laiacona, Barbarotto, Trivelli et al. (1993b), consists of a PictureNaming task and a multiple-choice format Questionnaire. For the Naming test, 60 lineardrawings (10 from each of 6 categories) were selected from Snodgrass and Vanderwart’s(1980) series. Six categories were investigated, three of living things (animals, fruits andvegetables) and three of nonliving things (tools, furniture, vehicles). Subjects were requestedto name all 60 pictures, presented individually in random order. The Verbal Questionnaireinvolved six questions for each of the 60 items (e.g., butterfly), the first two pertained toSuperordinate information [one general superordinate (e.g., Is it an animal, a vegetable or
Retrograde memory in severe closed-head trauma 5
TABLE II
Autobiographical Memory Interview Schedule
Time period Incident to be recalled Suggested prompts
I. Childhood (1-10 years) 1. Before school - first memory?(9 points) - involving brother or sister?
2. At primary school - involving a friend? a teacher? a journey?3. A ceremony, a vacation or a - involving a marriage? a baptism? a funeral?
hospital - a vacation with your parents? with a friend?- in a hospital for an illness?an illness of a friend? a relative?
II. Adolescence (11-18 years)1. Middle school - involving a friend?a teacher? a journey?(9 points) 2. Secondary school, professional- involving a friend? a teacher?a journey
course or first job3. A ceremony, a vacation or a - involving a marriage? a baptism? a funeral?
hospital - a vacation with your parents? with a friend?- in a hospital for an illness?an illness of a friend? a relative?
III. Twenties 1. University or job - involving a friend?a teacher? the employer?(9 points) 2. Marriage - your wedding?the wedding of some friend?
of a relative?3. A ceremony, a vacation or a - involving a marriage? a baptism? a funeral?
hospital - a vacation with your parents? with a friend?- in a hospital for an illness?an illness of a friend? a relative?
IV. Last year before trauma 1. School or job - involving a friend?a teacher? the employer?(9 points) 2. A holiday - Involving you?a friend?a relative?
3. A ceremony, a vacation or a - involving a marriage? a baptism? a funeral?hospital - a vacation with your parents? with a friend?
- in a hospital for an illness?an illness of a friend? a relative?
an object?) and one same-category superordinate (e.g., Is it a four-legged animal, a bird oran insect?)], two concerned Subordinate Perceptual attributes (e.g., Has it transparentwings, multicolored wings or no wings?) and the last two were about Subordinate Functionalattributes (e.g., Does it jump, run or fly?). The probes were presented orally in standardizedrandom order, first providing the name of the item and then asking the six questions alwaysin the same order.
Both the Picture Naming and the Questionnaire tasks are potentially able to revealperformance dissociations across taxonomic categories, particularly related to the living-nonliving distinction. Moreover, by distinguishing a superordinate from a subordinate levelof knowledge, the Questionnaire provides insights into the presumed hierarchical structureof memory in the semantic system. Finally, the distinction between Subordinate Perceptualand Functional can show possible dissociations between a visually- and a language-basedsystem of knowledge.
Since Naming and response to Questionnaire performance can be influenced by anumber of intrinsic variables pertaining to the specific items, Laiacona and coworkers(Barbarotto, Capitani and Laiacona, 1996; Capitani, Laiacona and Barbarotto, 1993;Laiacona et al., 1993a, 1993b) suggest analyzing performance scores by means of regressionanalyses in which Naming or Questionnaire response for single items is covaried for anumber of intrinsic properties of words or images.
The following word properties are taken into account:(i) Frequency of the stimulus words in the Italian lexicon (Bortolini, Tagliavini and
Zampulli, 1971) after logarithmic transformation.(ii) Prototypicality of the stimulus word according to Battig and Montague (1969). In
their study, 442 normal controls were given a limited amount of time to name as manyitems as possible belonging to a given category. The frequency of each item was recordedas a measure of its prototypicality.
(iii) Familiarity of the stimulus according to Snodgrass and Vanderwart (1980). Subjectswere asked to rate how usual or unusual the concept of the given item was in their realmof experience on a 5-point scale (1 = very familiar).
The following intrinsic properties of the pictures are considered:(i) Name agreement, i.e. the percentage of times each name was given by the Italian
control sample (Laiacona et al., 1993b).(ii) Image agreement according to Snodgrass and Vanderwart (1980). Subjects were
asked to indicate how closely each picture corresponded to their own mental image of theitem on a 5-point scale (1 = low agreement).
(iii) Visual complexity according to Snodgrass and Vanderwart (1980). The amount ofdetail or intricacy of lines in the picture was judged on a 5-point scale (1 = very simple).
Finally, since the difficulty of single questions on the Questionnaire can vary in anunpredictable way, thus representing another variable potentially able to influence responseaccuracy on single items, a final intrinsic property of items in this task is a difficulty indexobtained with 10 young, well-educated subjects who were asked to rate the difficulty ofeach question on a 5-point scale (1 = very difficult).
Famous Personalities Test
This test explores semantic knowledge for famous personalities. The personalities inquestion were not contemporaries of the patients and their knowledge about them waspresumably acquired during the schooling period. In order to investigate separately thelexical and semantic levels of representation and the supposed hierarchical structure ofsemantic knowledge, questions regarding single personalities were organized in order toexplore a familiarity lexical level (lst question), a semantic superordinate level (questions2-3) and a semantic subordinate level (questions 4-5) of knowledge.
For each of 30 items, 5 four-choice questions were posed. The 1st question was alexical familiarity judgment in which the subjects were requested to indicate, from fouralternatives, the proper name of a famous personality (e.g., Gioacchino Rossini, LorenzoManescalchi, Fiorenzo Sebastianelli, Ugo Piepoli). The 2nd question (intercategorysuperordinate) regarded the main occupation of the famous personality (e.g., archeologist,
6 Giovanni A.Carlesimo and Others
scientist, musician, politician). The 3rd question (intracategory superordinate) investigatedthe specific field of activity of the personality (e.g., did he mainly compose symphonies,madrigals, music for piano, operas). The 4th question (functional context) specificallyinvolved some achievement of the person (e.g., did he compose Aida, The Barber ofSeville, Boheme, Parsifal). The final question (temporal context) was about the historicalperiod in which the personality lived (e.g., 13th century, our century, 16th century, 18thcentury).
RESULTS
Autobiographical Memory Interview
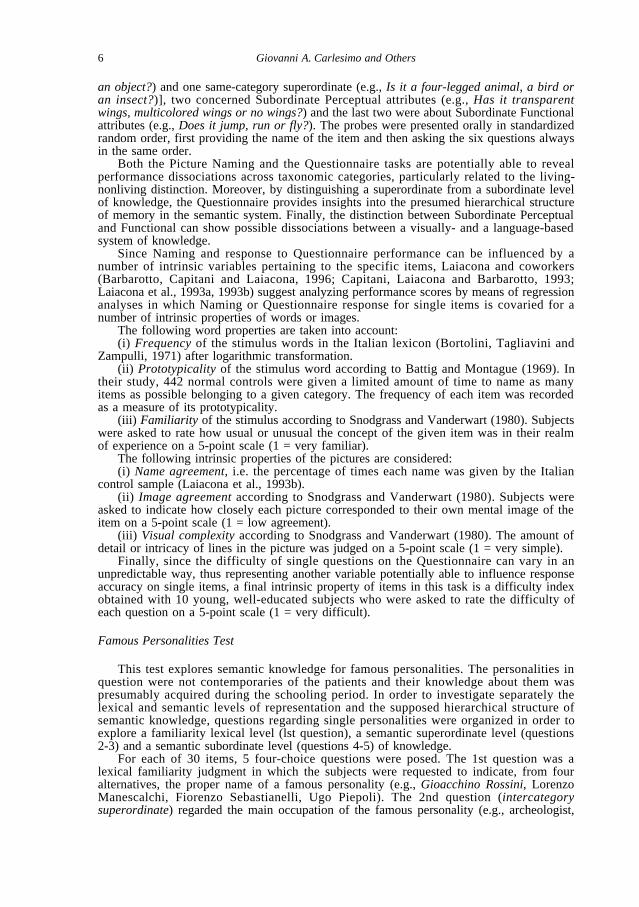
The overall interview, comprehending all four time blocks for CHI patientsand the first three for NCs, was only applicable to individuals over 23 years ofage (n = 11 in both CHI and NC groups). The time block relative to twentieswas not administered to younger individuals. As shown in Figure 1,autobiographical memory of NCs was consistently better than that of CHIpatients. In both groups, memories relative to the early childhood period wererecalled less accurately than those coming from successive lifetime periods.Moreover, the CHI group displayed a mild decline in recall accuracy formemories relative to the last year before the trauma.
A first two-way mixed ANOVA was performed to compare autobiographicalrecall scores of the whole CHI and NC groups from the early childhood andadolescence periods. Results of this analysis documented significantly higherrecall scores in the NC (8.0) as compared to the CHI (5.7) group (F = 22.6; p<.001 with 1, 38 d.f.) and, in the overall sample, better recall from theadolescent (7.0) than the childhood (6.7) period (F = 5.6; p <.05 with 1, 38 d.f.),but no Group × Lifetime Period interaction (F = 0.4; p = n.s. with 1, 38 d.f.). Asecond two-way ANOVA considered only CHI and NC subjects over 23 yearsof age. Also in this case, CHI patients (6.3) on the whole recalled less than age-matched NCs (7.9) (F=12.7; p <.01 with 1, 20 d.f.). However, no difference wasdetected between the three lifetime periods examined (6.8, 7.3 and 7.3 for earlychildhood, adolescence and the twenties respectively) (F = 1.4; p = n.s. with 2,40 d.f.) and no Group × Lifetime Period interaction emerged (F = 0.3; p = n.s.with 2, 40 d.f.).
In order to assess whether CHI patients presented a significant decline intheir autobiographical recall scores for the last year preceding the head traumacompared to previous lifetime periods, two one-way within ANOVAs, the firstcomparing memory scores relative to childhood, adolescence and the last yearbefore trauma in the whole CHI group, the second one comparing memoryscores relative to all the time blocks in CHI patients over 23 years of age wereperformed. No significant difference between autobiographical memory scoresemerged relative to the different lifetime periods for either case (F = 0.5 with 2,38 d.f. and F = 0.3 with 3, 30 d.f. respectively).
Retrograde memory in severe closed-head trauma 7
Famous Events Recognition Test
In order to restrict the analysis exclusively to truly retrograde memories,performance of each CHI patient was scored only for events that occurred beforehis/her head trauma. Moreover, to be reasonably sure that the single patient hadbeen exposed to the information in the period the event occurred, only events thatoccurred when the subject was more than 10 years old were considered. In thisway, since the youngest patient in our sample had suffered the head trauma whenhe was 18 years old, the minimum period covered by the test in our patients was7 or 8 years (4 two-year periods or 3 two-year periods plus 1994). Each NCsubject was scored for the same time period considered for his CHI match.
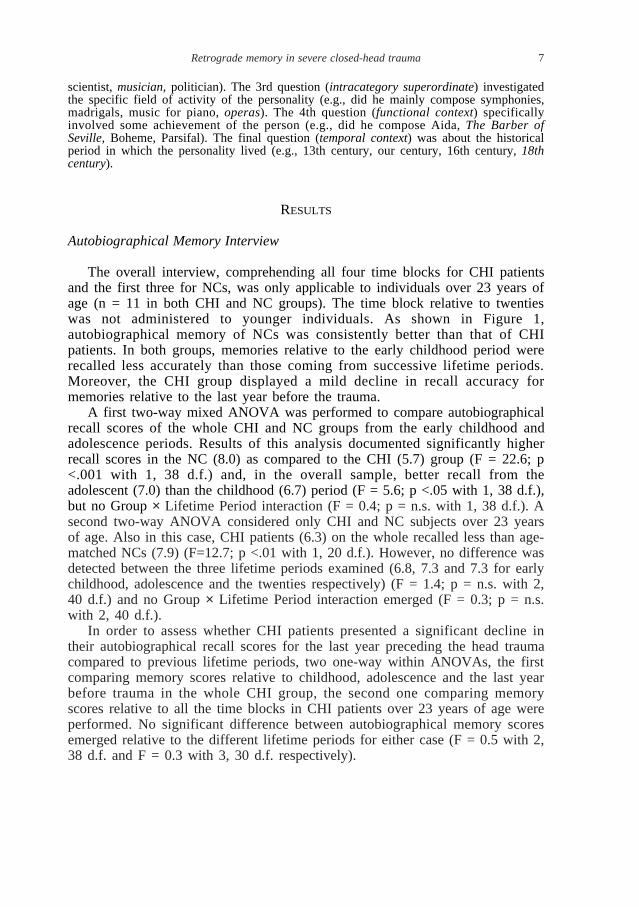
As shown in Figure 2, when considering the whole sample of CHI and NCsubjects, normal controls recognized consistently more events than head traumapatients. Moreover, while a temporal gradient can be shown in the NC group,with events relative to more recent years better recalled, the same trend is notobservable in the CHI group, which has a coarsely flat temporal profile. A two-way mixed ANOVA applied to these data confirmed a significant differencebetween the overall recognition of NC (6.3) and CHI (4.5) patients (F = 22.6; p<.001 with 1, 38 d.f.). Moreover, in the whole group the Time Period effect wassignificant (F = 3.5; p <.05 with 3, 114 d.f.), thus confirming better recognitionfor events that occurred more recently. However, the Group × Time Periodinteraction did not approach significance (F = 1.0 with 3, 114 d.f.), thus not
Fig. 1 – Average performance scores of CHIand NCsubjects on the Autobiographical MemoryInterview as a function of lifetime period considered.For each period, the average score is calculatedon all subjects administered questions for that period: all CHI and NC subjects for Childhood andAdolescent periods, 11 CHI and 11 NCsubjects over 23 years of age for the twenties period, all CHIpatients for the last year before trauma period.
CHI
9
8
7
6
5
Lifetime periods
Childhood Adolescence Twenties Last year
Controls
8 Giovanni A.Carlesimo and Others
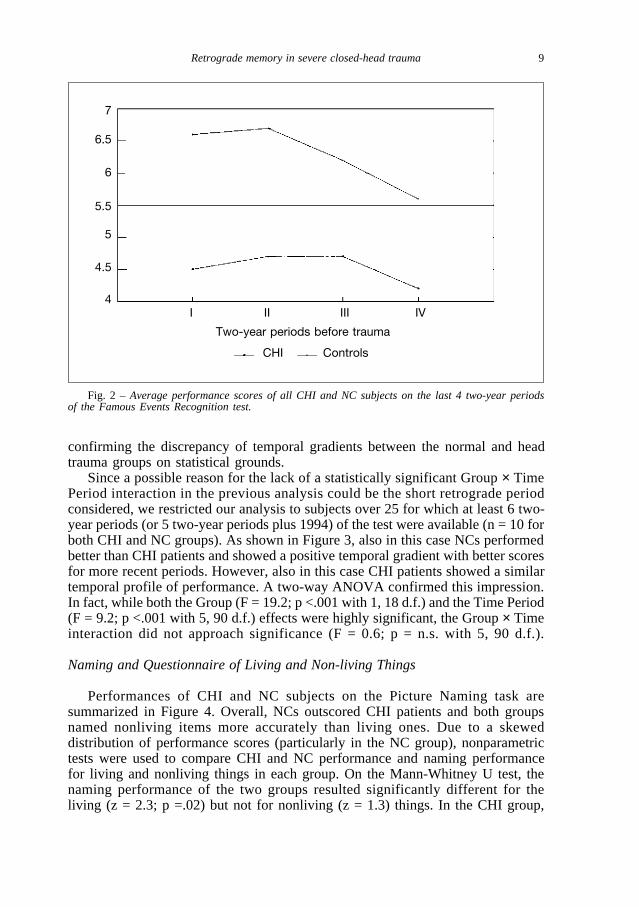
confirming the discrepancy of temporal gradients between the normal and headtrauma groups on statistical grounds.
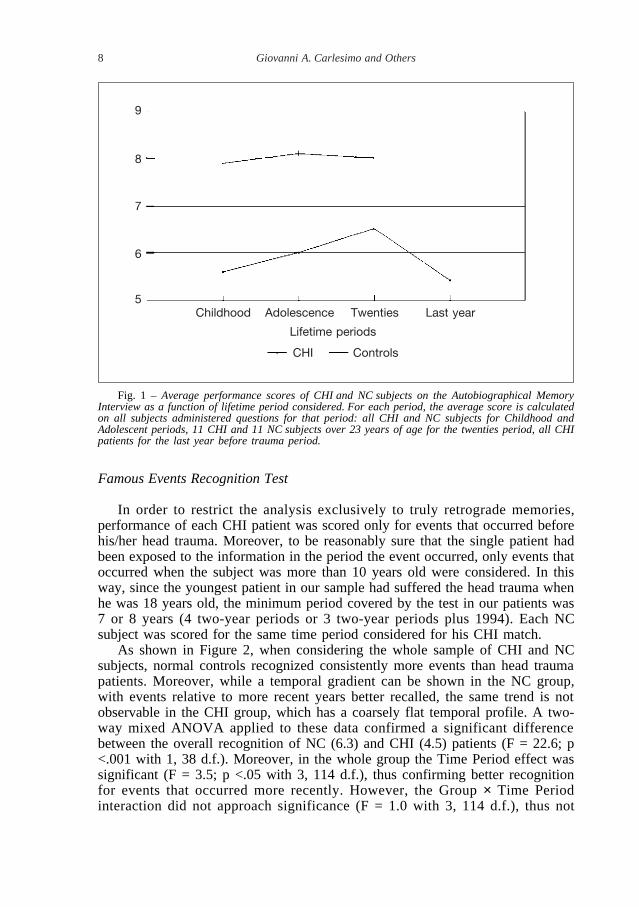
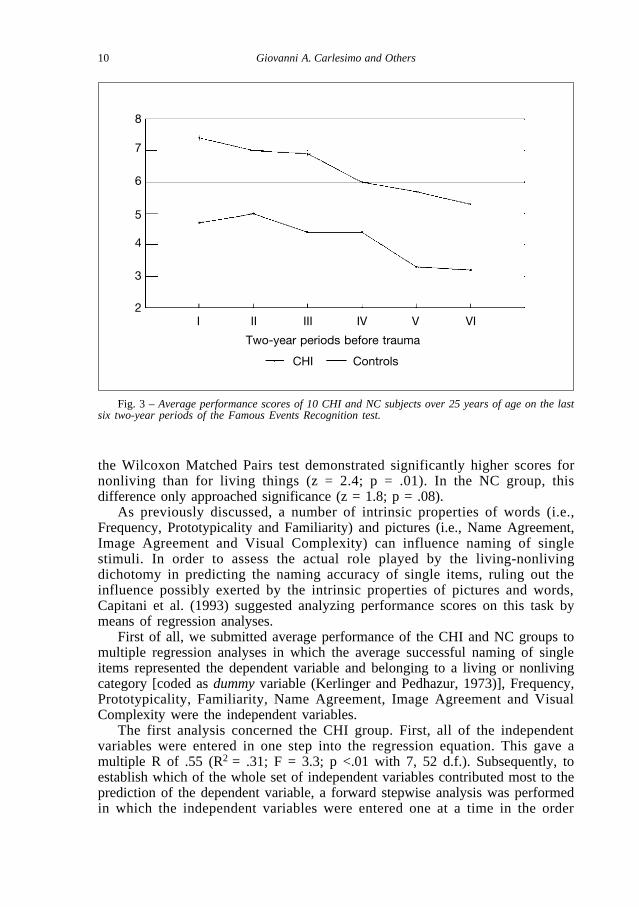
Since a possible reason for the lack of a statistically significant Group × TimePeriod interaction in the previous analysis could be the short retrograde periodconsidered, we restricted our analysis to subjects over 25 for which at least 6 two-year periods (or 5 two-year periods plus 1994) of the test were available (n = 10 forboth CHI and NC groups). As shown in Figure 3, also in this case NCs performedbetter than CHI patients and showed a positive temporal gradient with better scoresfor more recent periods. However, also in this case CHI patients showed a similartemporal profile of performance. A two-way ANOVA confirmed this impression.In fact, while both the Group (F = 19.2; p <.001 with 1, 18 d.f.) and the Time Period(F = 9.2; p <.001 with 5, 90 d.f.) effects were highly significant, the Group × Timeinteraction did not approach significance (F = 0.6; p = n.s. with 5, 90 d.f.).
Naming and Questionnaire of Living and Non-living Things
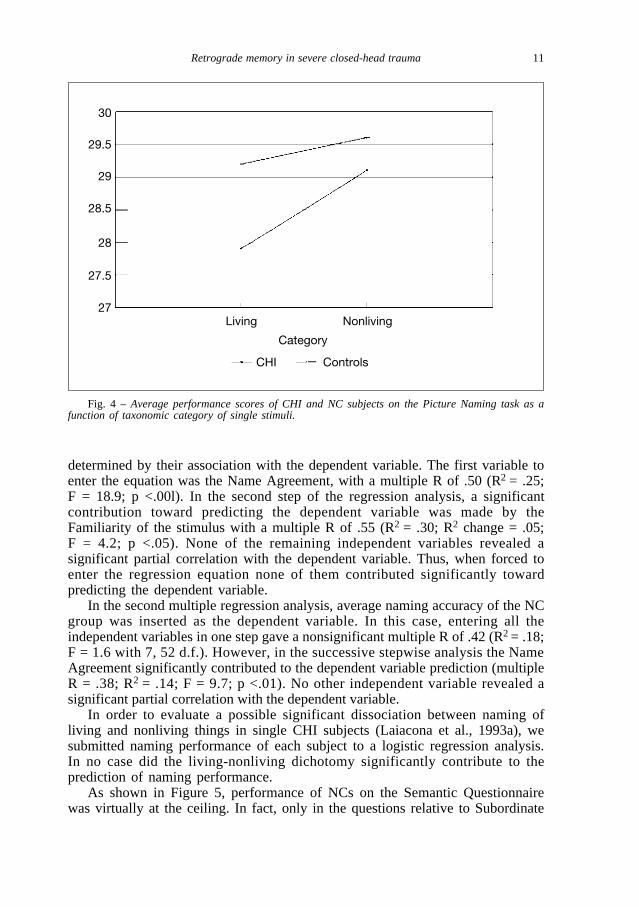
Performances of CHI and NC subjects on the Picture Naming task aresummarized in Figure 4. Overall, NCs outscored CHI patients and both groupsnamed nonliving items more accurately than living ones. Due to a skeweddistribution of performance scores (particularly in the NC group), nonparametrictests were used to compare CHI and NC performance and naming performancefor living and nonliving things in each group. On the Mann-Whitney U test, thenaming performance of the two groups resulted significantly different for theliving (z = 2.3; p =.02) but not for nonliving (z = 1.3) things. In the CHI group,
Retrograde memory in severe closed-head trauma 9
Fig. 2 – Average performance scores of all CHI and NC subjects on the last 4 two-year periodsof the Famous Events Recognition test.
CHI
7
6.5
6
5.5
5
4.5
4
Two-year periods before trauma
I II III IV
Controls
the Wilcoxon Matched Pairs test demonstrated significantly higher scores fornonliving than for living things (z = 2.4; p = .01). In the NC group, thisdifference only approached significance (z = 1.8; p = .08).
As previously discussed, a number of intrinsic properties of words (i.e.,Frequency, Prototypicality and Familiarity) and pictures (i.e., Name Agreement,Image Agreement and Visual Complexity) can influence naming of singlestimuli. In order to assess the actual role played by the living-nonlivingdichotomy in predicting the naming accuracy of single items, ruling out theinfluence possibly exerted by the intrinsic properties of pictures and words,Capitani et al. (1993) suggested analyzing performance scores on this task bymeans of regression analyses.
First of all, we submitted average performance of the CHI and NC groups tomultiple regression analyses in which the average successful naming of singleitems represented the dependent variable and belonging to a living or nonlivingcategory [coded as dummy variable (Kerlinger and Pedhazur, 1973)], Frequency,Prototypicality, Familiarity, Name Agreement, Image Agreement and VisualComplexity were the independent variables.
The first analysis concerned the CHI group. First, all of the independentvariables were entered in one step into the regression equation. This gave amultiple R of .55 (R2 = .31; F = 3.3; p <.01 with 7, 52 d.f.). Subsequently, toestablish which of the whole set of independent variables contributed most to theprediction of the dependent variable, a forward stepwise analysis was performedin which the independent variables were entered one at a time in the order
10 Giovanni A.Carlesimo and Others
Fig. 3 – Average performance scores of 10 CHI and NC subjects over 25 years of age on the lastsix two-year periods of the Famous Events Recognition test.
CHI
8
7
6
5
4
3
2
Two-year periods before trauma
I II III IV V VI
Controls
determined by their association with the dependent variable. The first variable toenter the equation was the Name Agreement, with a multiple R of .50 (R2 = .25;F = 18.9; p <.00l). In the second step of the regression analysis, a significantcontribution toward predicting the dependent variable was made by theFamiliarity of the stimulus with a multiple R of .55 (R2 = .30; R2 change = .05;F = 4.2; p <.05). None of the remaining independent variables revealed asignificant partial correlation with the dependent variable. Thus, when forced toenter the regression equation none of them contributed significantly towardpredicting the dependent variable.
In the second multiple regression analysis, average naming accuracy of the NCgroup was inserted as the dependent variable. In this case, entering all theindependent variables in one step gave a nonsignificant multiple R of .42 (R2 = .18;F = 1.6 with 7, 52 d.f.). However, in the successive stepwise analysis the NameAgreement significantly contributed to the dependent variable prediction (multipleR = .38; R2 = .14; F = 9.7; p <.01). No other independent variable revealed asignificant partial correlation with the dependent variable.
In order to evaluate a possible significant dissociation between naming ofliving and nonliving things in single CHI subjects (Laiacona et al., 1993a), wesubmitted naming performance of each subject to a logistic regression analysis.In no case did the living-nonliving dichotomy significantly contribute to theprediction of naming performance.
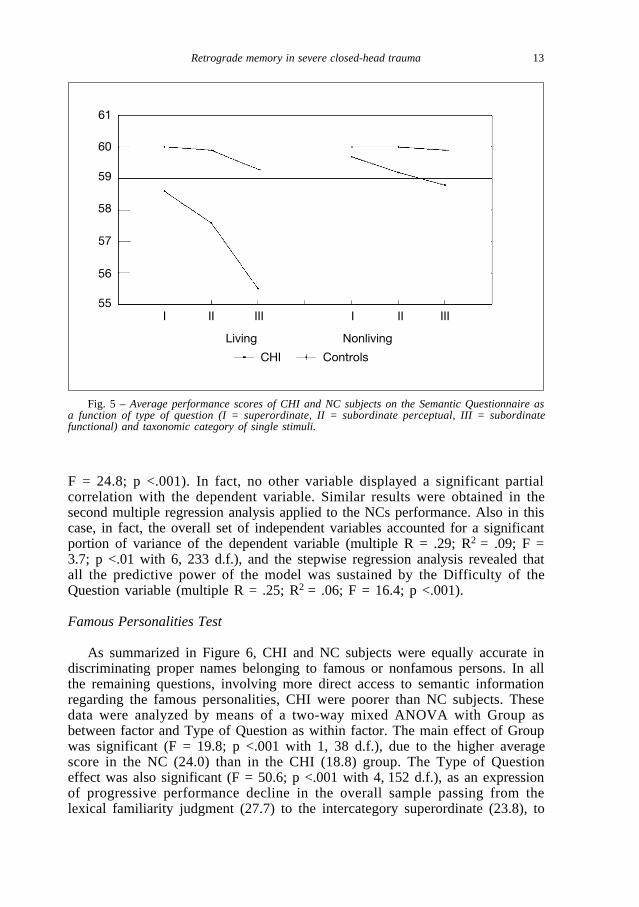
As shown in Figure 5, performance of NCs on the Semantic Questionnairewas virtually at the ceiling. In fact, only in the questions relative to Subordinate
Fig. 4 – Average performance scores of CHI and NC subjects on the Picture Naming task as afunction of taxonomic category of single stimuli.
CHI
30
29.5
29
28.5
28
27.5
27
Category
Living Nonliving
Controls
Retrograde memory in severe closed-head trauma 11
Functional were some errors observed, somewhat more on living then nonlivingthings. CHI patients, instead, performed worse on the questions relative to livingthan nonliving things and performed progressively worse passing fromSuperordinate to Subordinate Perceptual to Subordinate Functional questions.Also in this case, due to the particularly skewed distribution of the NCs’performance scores, we used nonparametric tests for the statistical analyses.Analogously to the Naming task, CHI patients performed worse than NCs onliving (z = 5.2; p <.001) than nonliving (z = 1.0) items. However, in this case,both CHI and NC subjects answered questions relative to living things moreaccurately than nonliving things (z = 3.9 and 3.7 respectively; p <.001 in bothcases).
As noted above, variables concomitant to the living-nonliving dichotomy, inthe case of the Questionnaire, are the intrinsic properties of words (i.e.,Frequency, Prototypicality and Familiarity), a Difficulty Index for singlequestions and the Type of Question (Superordinate, Subordinate Functional andSubordinate Perceptual). In this case, two multiple regression analyses wereperformed for each group. In the first one, comprehending all 360 questions, theType of Question variable contrasted Superordinate and Subordinate questions.In the second regression analysis, restricted to the 240 questions relative tosubordinate attributes, the Type of Question variable contrasted Functional andPerceptual questions.
The first of the multiple regression analyses, applied to performance scores ofthe CHI group, gave an overall multiple R of .47 (R2 = .22; F = 17.1; p <.001 with 6,353 d.f.). In the forward stepwise analysis, the first variable to enter the equationwas the difficulty of the question, with a multiple R of .40 (R2 = .16; F = 69.9; p<.001). In the second step of the regression analysis, a significant contributiontoward predicting the dependent variable was made by the living-nonlivingdichotomy with a multiple R of .46 (R2 = .21; R2 change = .05; F = 22.7; p <.001).When forced to enter the regression equation, none of the remaining independentvariables contributed significantly toward predicting the dependent variable. Similarresults were provided by the second multiple regression analysis applied toperformance scores of the CHI group. In fact, also in this case inserting all of theindependent variables in one step into the regression equation gave a multiple R of.45 (R2 = .20; F = 10.0; p <.001 with 6, 323 d.f.) and the only variables thatindividually contributed to the prediction of the dependent variable in the stepwiseregression were the difficulty of the question and the taxonomic category (multiple R= .35 and .43; R2 = .13 and .19; F = 35.0 and 17.7 respectively; p <.001 in both cases).
It is worthy of note that when performances of single CHI patients wereevaluated by means of logistic regression analyses, two patients revealed asignificant effect of category (p <.05) and in three other cases this effectapproached significance (p <.10). In all of these cases, performance on livingitems was disproportionately worse than on nonliving items.
The first of the multiple regression analyses applied to Questionnaire resultsof the NC group provided an overall multiple R of .26 (R2 = .07; F = 4.4; p<.001 with 6, 353 d.f.). In this case, the stepwise regression analysis indicatedthe Difficulty of the Question as the independent variable alone able to accountfor all the predictive value of the regression model (multiple R = .25; R2 = .06;
12 Giovanni A.Carlesimo and Others
F = 24.8; p <.001). In fact, no other variable displayed a significant partialcorrelation with the dependent variable. Similar results were obtained in thesecond multiple regression analysis applied to the NCs performance. Also in thiscase, in fact, the overall set of independent variables accounted for a significantportion of variance of the dependent variable (multiple R = .29; R2 = .09; F =3.7; p <.01 with 6, 233 d.f.), and the stepwise regression analysis revealed thatall the predictive power of the model was sustained by the Difficulty of theQuestion variable (multiple R = .25; R2 = .06; F = 16.4; p <.001).
Famous Personalities Test
As summarized in Figure 6, CHI and NC subjects were equally accurate indiscriminating proper names belonging to famous or nonfamous persons. In allthe remaining questions, involving more direct access to semantic informationregarding the famous personalities, CHI were poorer than NC subjects. Thesedata were analyzed by means of a two-way mixed ANOVA with Group asbetween factor and Type of Question as within factor. The main effect of Groupwas significant (F = 19.8; p <.001 with 1, 38 d.f.), due to the higher averagescore in the NC (24.0) than in the CHI (18.8) group. The Type of Questioneffect was also significant (F = 50.6; p <.001 with 4,152 d.f.), as an expressionof progressive performance decline in the overall sample passing from thelexical familiarity judgment (27.7) to the intercategory superordinate (23.8), to
Retrograde memory in severe closed-head trauma 13
Fig. 5 – Average performance scores of CHI and NC subjects on the Semantic Questionnaire asa function of type of question (I = superordinate, II = subordinate perceptual, III = subordinatefunctional) and taxonomic category of single stimuli.
CHI
61
60
59
58
57
56
55I II III I II III
Living Nonliving
Controls
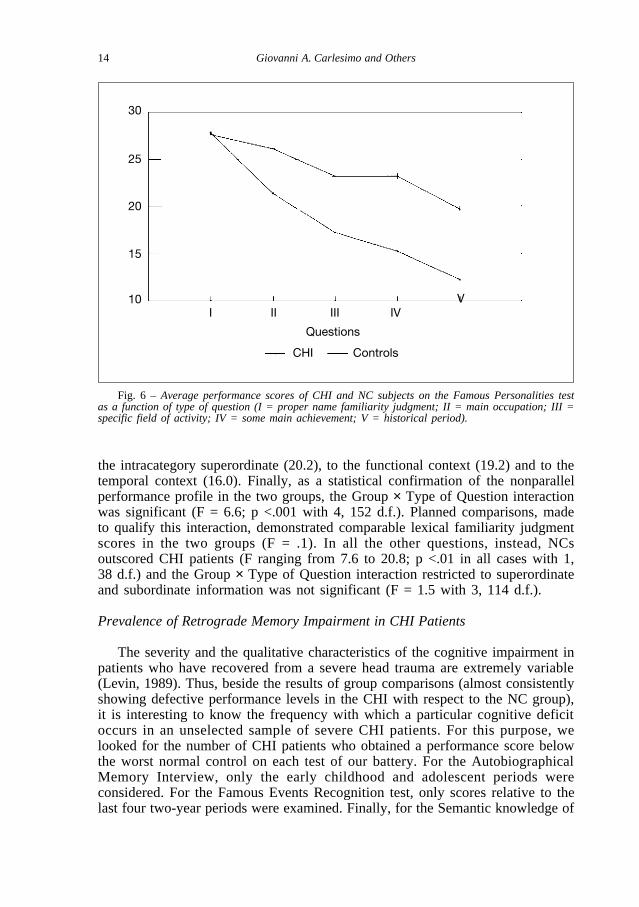
the intracategory superordinate (20.2), to the functional context (19.2) and to thetemporal context (16.0). Finally, as a statistical confirmation of the nonparallelperformance profile in the two groups, the Group × Type of Question interactionwas significant (F = 6.6; p <.001 with 4, 152 d.f.). Planned comparisons, madeto qualify this interaction, demonstrated comparable lexical familiarity judgmentscores in the two groups (F = .1). In all the other questions, instead, NCsoutscored CHI patients (F ranging from 7.6 to 20.8; p <.01 in all cases with 1,38 d.f.) and the Group × Type of Question interaction restricted to superordinateand subordinate information was not significant (F = 1.5 with 3, 114 d.f.).
Prevalence of Retrograde Memory Impairment in CHI Patients
The severity and the qualitative characteristics of the cognitive impairment inpatients who have recovered from a severe head trauma are extremely variable(Levin, 1989). Thus, beside the results of group comparisons (almost consistentlyshowing defective performance levels in the CHI with respect to the NC group),it is interesting to know the frequency with which a particular cognitive deficitoccurs in an unselected sample of severe CHI patients. For this purpose, welooked for the number of CHI patients who obtained a performance score belowthe worst normal control on each test of our battery. For the AutobiographicalMemory Interview, only the early childhood and adolescent periods wereconsidered. For the Famous Events Recognition test, only scores relative to thelast four two-year periods were examined. Finally, for the Semantic knowledge of
Fig. 6 – Average performance scores of CHI and NC subjects on the Famous Personalities testas a function of type of question (I = proper name familiarity judgment; II = main occupation; III =specific field of activity; IV = some main achievement; V = historical period).
CHI
30
25
20
15
10
Questions
I II III IVV
Controls
14 Giovanni A.Carlesimo and Others

famous personalities test, only questions regarding superordinate and subordinateinformation (thus, with the exclusion of the lexical familiarity judgement) wereanalyzed. As shown in Table III, percentage of CHI subjects falling below theworst NC subject varied as a function of test examined, ranging from a minimumof 10% in the Picture Naming task to a maximum of 85% in the SemanticQuestionnaire.
It is now universally accepted that anterograde and retrograde memory canbe, at least partially, dissociable, with some amnesic patients suffering almostexclusively from an inability to store new information but showing normalaccess to information acquired before the amnesia onset (Kapur, Ellison, Smithet al., 1992; Zola-Morgan, Squire and Amaral, 1986) and patients with thereverse pattern of dissociation (Kapur, 1993). Moreover, in the context ofretrograde memory, patients with impaired memory for autobiographical eventsbut normal access to semantic information (De Renzi et al., 1995) and, on thecontrary, patients with preserved memory for personal events but reducedpatrimony of semantic knowledge (Grossi et al., 1988) have been described. Inorder to evaluate the possible presence of these dissociations in our CHI sample,we looked for single patients with pathological scores only on anterograde(Rey’s 15-word learning task and Short story recall) or only on retrogradememory tests and, in the context of the latter, only on the autobiographical orsemantic tests. As previously described, performance scores below the worst NCsubject were considered pathological for the retrograde memory tests. For theanterograde memory tests, instead, since performance scores for the age-matchedcontrol group were not available, normality cut-off scores were derived frompublished normative studies (Carlesimo, Caltagirone and Gainotti, 1996;Spinnler and Tognoni, 1987). In this way, we were able to individuate onepatient (case nr. 12) with deficient anterograde memory but normal performanceon at least three out of four retrograde memory tests, one patient (nr. 17) withnormal performance on anterograde memory tests but deficient scores on at leastthree retrograde tests, one patient (nr. 15) with a deficient autobiographicalmemory but normal scores on all the semantic memory tests and a last patient(nr. 16) with preserved autobiographical memory but deficient performance onall of the semantic tests.
Retrograde memory in severe closed-head trauma 15
TABLE III
Number of CHIPatients Whose Performance Score on the Various Tests of the Battery Fell below theWorst Normal Control
Test Worst control’s score CHI patients falling below the worst control score
Autobiographical Memory Interview 6 10/20Famous Events Recognition test 4 10/20Picture Naming task 55 2/20Semantic Questionnaire 356 17/20Famous Personalities test 14 7/20

Role of Focal Cerebral Lesions
Cortical areas whose lesion has been most frequently implicated in the genesisof retrograde amnesia are the poles and the infero-lateral surfaces of the temporallobes (Damasio, Eslinger, Damasio et al., 1985; Kapur et al., 1992; Markowitschet al., 1993). In order to investigate a possible relationship between the retrogradememory impairment demonstrated by our CHI group and the locus of focalcerebral lesions documented by neuroradiological exams, we comparedperformances of the 9 CHI patients with temporal focal lesions with those of theremaining 11 CHI patients free of temporal focal lesions on the various tasks ofour battery. Performance patterns of the two subgroups substantially overlappedand in no case did a significant Group effect emerge (F consistently < 2.0).
Recent metabolic studies on normal subjects have suggested a functionalasymmetry between cerebral hemispheres in the retrieval of remote memories,with the right hemisphere more largely involved in the ecphory ofautobiographical episodes (Fink, Markowitsch, Reinkemeier et al., 1996) and theleft hemisphere more implicated in the access to non-autobiographicalinformation (Fletcher, Frith, Grasby et al., 1995; Tulving, Markowitsch, Craik etal., 1996). We tested a possible differential impairment of autobiographical andsemantic memories as a function of laterality of lesion in our CHI group bycomparing performance scores of the 5 patients with neuroradiological evidenceof focal lesion involving only the right hemisphere with those of the 6 patientswith lesions confined to the left hemisphere. With the exception of theAutobiographical Memory Interview, statistical comparisons did not reveal anysignificant group effect or group × test condition interaction. On theAutobiographical Memory Interview, a significant Group × Lifetime periodinteraction emerged (F = 4.1; p <.05 with 2, 18 d.f.). In effect, while right andleft hemispheric groups did not differ in the recall scores relative to thechildhood (5.0 vs. 5.2) and adolescence (5.4 vs. 5.7) periods, right hemispherepatients were much poorer than left hemisphere patients in the retrieval ofautobiographical episodes from the last year before trauma (4.6 vs. 7.4).
DISCUSSION
Results of the present study document the high prevalence of retrogradememory disorders in CHI patients also following resolution of the post-traumaticamnesia period. With the exception of the Picture Naming task (in which only10% of CHI patients scored lower than the worst control subject), on all othertasks the prevalence of pathological performances in our CHI sample was morethan 30%, reaching 85% on the Semantic Questionnaire. Most of the time, CHIpatients suffered from a pervasive memory impairment, affecting bothautobiographical and semantic information. In sporadic cases, however, singlepatients demonstrated a selective impairment of anterograde memory with asubstantial sparing of retrograde memory or, in contrast, a relevant difficulty inaccessing pre-trauma memories with normal storage of new information. Thesedata give further support to the well-documented dissociability of anterogradeand retrograde memory deficits in brain damaged patients (for reviews, see
16 Giovanni A.Carlesimo and Others
Kapur, 1993; Kapur et al., 1992). Moreover, two CHI patients in our groupdisplayed a specular impairment of retrograde memory; one was selectivelycompromised in the retrieval of personal memories but with normal access tosemantic, nonpersonal information; the other one had the reverse pattern ofcognitive deficit and sparing. Neuropsychological evidence supporting adissociability of autobiographical and semantic memory impairment in thedomain of retrograde amnesia has also been provided (De Renzi et al., 1987,1995; Grossi et al., 1988).
The impairment in recovering both autobiographical and public events in ourCHI group did not vary as a function of time elapsed between trauma onset andthe date of event occurrence. Indeed, both in the Autobiographical Interview andin the Famous Events test, the lack of a significant Group × Time Periodinteraction documented a homogeneous decline of retrograde memory in the CHIgroup across the whole time interval covered by the tests (the entire lifespan inthe autobiographical test, the period starting from adolescence in the publicevents test). These data substantially confirm previous results obtained by Levinet al. (1985) for public events and extend to the autobiographical domain theclaim of a lack of negative temporal gradient in the retrograde memoryimpairment exhibited by chronic CHI patients. This conclusion [even iftempered by the report of single CHI patients presenting with a negativetemporal gradient in their retrograde memory deficit (Markowitsch et al., 1993;Mattioli et al., 1996)] is quite surprising if one considers that a positiverelationship between accuracy of event recall and time elapsed since eventoccurrence is a consistent finding in amnesic syndromes subsumed by a varietyof etiologies, such as Korsakoff disease (Albert, Butters and Levin, 1979;Kopelman, 1989), Herpes virus encephalitis (Cermak and O’Connor, 1983),electroshock treatment for the relief of mood disorders (Cohen and Squire, 1981;Squire, 1975) and Alzheimer’s disease (Beatty, Salmon, Butters et al., 1988;Kopelman, 1989; Sagar, Cohen, Sullivan et al., 1988; but see Wilson, Kaszniakand Fox, 1981, for discordant results).
One possible reason for the lack of a negative temporal gradient in theretrograde memory impairment exhibited by the majority of CHI patients is thatthe young age of most of these subjects (and, accordingly, the short time intervalexaminable) precludes a possible dishomogeneity of memory accuracy acrossdifferent lifetime periods from emerging. We tested this hypothesis by focusingthe analysis on the temporal gradient displayed by the over-23 CHI patients inthe autobiographical test and by the over-25 patients in the Famous Events test.Results were clearly negative: on both tests, performance profiles of the olderCHI subgroup were lower than, but substantially parallel to, that exhibited bynormal matches. It should be considered, however, that the oldest CHI patientsrecruited in the present study were 36, probably making the lifetime periodexaminable still too restricted to permit a possible temporal gradient to emerge.In the future, evaluation of samples of CHI patients older than those consideredin the present study could answer the question of whether the lack of negativetemporal gradient is a genuine characteristic of the retrograde memoryimpairment in severe head-trauma patients or whether it is just anepiphenomenon resulting from the young age of most of these patients.
Retrograde memory in severe closed-head trauma 17

Basic knowledge about the external world, presumably acquired early in life,and cultural information learned during the period of formal education wereevaluated by means of Picture naming, Semantic Questionnaire and FamousPersonalities tests.
The performance discrepancy in our CHI group between relatively goodnaming of visual items in the Picture Naming task and the poor access toencyclopedic knowledge about the same items in the Semantic Questionnaire isstriking. In our opinion, it reflects the different involvement of the semanticsystem while performing the two tasks. In the naming task, a discrete node inthe semantic system is directly activated by the visual stimulus and, in turn,evokes the corresponding phonological referent in the speech output lexicon.The mild impairment exhibited by CHI patients on this task documents therelative sparing of this simple linear relationship between visual, semantic andlexical representations. In contrast, CHI patients’ poor performances on theSemantic Questionnaire indicate a deterioration of or a difficulty in accessing thesemantic network underlying the encyclopedic knowledge about the same itemsproficiently named in the previous task.
In the Semantic Questionnaire, CHI patients performed better on thequestions pertaining to nonliving than to living categories of objects. Moreover,they were more accurate in responding to questions regarding superordinate thansubordinate information and among subordinate questions, those about functionalrather than perceptual attributes of items. However, when performance wascovaried for intrinsic properties of words and, above all, for the difficulty rate ofquestions, the only single characteristic still contributing to predict the responseaccuracy of CHI patients was the living-nonliving dichotomy, with access tosemantic information regarding living things disproportionately more affectedthan nonliving things.
In the Famous Personalities test, CHI patients disclosed a straightforwarddissociation between fully normal identification of names belonging to famouspeople and deficient recovery of semantic information about the same persons.However, in the domain of semantic knowledge, they were similarly impaired inaccess to superordinate and subordinate levels of information.
To summarize, the CHI patients examined in the present study had nodifficulty in accessing the phonological input lexicon (as demonstrated by theirnormal familiarity judgment about the names of famous personalities) anddisplayed a relatively preserved access to the output lexicon (as revealed by theirmild deficit in the Picture Naming task). So, their deficit in basic and culturalknowledge seems to be circumscribed to the semantic level of processing. In thiscontext, the deficit does not dissociate according to a presumed hierarchicalorganization of knowledge (Collins and Quillian, 1969, 1970) (both in theSemantic Questionnaire and Famous Personalities tests, superordinate andsubordinate levels of knowledge were similarly affected) nor according to apresumed bipartitionning of the semantic system into functional and structuralsubtypes of knowledge (Shallice, 1987) (functional and perceptual attributes inthe Questionnaire were similarly disrupted). Rather, the taxonomic category ofstimuli seems to be the critical variable along which the semantic impairment ofCHI patients dissociates.
18 Giovanni A.Carlesimo and Others
A categorical performance asymmetry in semantic memory tasks withknowledge regarding living or nonliving things differentially affected has beenrepeatedly reported in the neuropsychological literature in the last few years. Inthe great majority of cases, knowledge of living things is more severely (or alsoselectively) impaired. This performance pattern has been reported in single caseanalyses of Herpes virus encephalitis (Sartori and Job, 1988; Silveri andGainotti, 1988), CHI (Farah, Hammond, Mehta et al., 1989; Hills andCaramazza, 1991) and degenerative (Basso, Capitani and Laiacona, 1988)patients, in multiple single-case reports of encephalitis (Barbarotto et al., 1996;Warrington and Shallice, 1984) and CHI (Laiacona et al., 1993b) patients and,finally, in a group study involving Alzheimer’s disease patients (Silveri, Daniele,Giustolisi et al., 1991). The reverse pattern of dissociation, namely theknowledge of nonliving things disproportionately more affected than livingthings, has been much more sporadically described (Hills and Caramazza, 1991;Warrington and McCarthy, 1987).
One possible account of the category asymmetry in semantic memoryimpairment, in terms of different familiarity of items belonging to the living andnonliving categories (Funnel and Sheridan, 1992; Stewart, Parkin and Hunkin,1992), was ruled out in the present study by the utilization of a statisticalapproach to data analysis that covaried performance on single questions for anumber of intrinsic properties of items such as familiarity and difficulty.
An alternative hypothesis attributes the category effect to a differentialinvolvement of the visually-based and verbally-based subsystems in which thesemantic system is presumably articulated (Shallice, 1987). Damage to thevisually-based subsystem will result in a prevalent impairment of knowledge forthose categories, such as living things, in which individuals are hardlycharacterized on the basis of function and are mostly distinguishable by theirphysical appearance. In contrast, a lesion in the verbally-based subsystem mainlydisrupts knowledge of nonliving objects whose visual aspect is scarcelyexpressive of their use and whose identification is mainly based on the verbaldescription of function (Silveri and Gainotti, 1988). In our CHI patients, thiskind of explanation of the category effect is not supported. If somewhat, theywere more impaired in responding to questions about the functional than theperceptual attributes of items and, in any case, after covarying for the difficultyindex of questions, no significant difference between subordinate functional andperceptual questions held.
A last theory accounting for the living/nonliving dissociation in semanticmemory is one that assumes the existence of distinct cerebral cortical sitesstoring information for living and nonliving categories of items. Based onmetabolic data from normal subjects and morphological data from brain-lesionedpatients, Damasio, Grabowski, Tranel et al. (1996) proposed the anterior sectorof the inferotemporal region of the left hemisphere as the critical region forsemantic information pertaining to living things and more posterior sectors ofthe same cortical region as the brain areas that store information regardingnonliving things. Indeed, a possible account of the category discrepancy in thesemantic memory impairment exhibited by CHI patients as due to a differentialinvolvement of the neural substrates underlying knowledge of living and
Retrograde memory in severe closed-head trauma 19
nonliving categories of objects needs to be considered within the broaderquestion of localizing focal cerebral lesions determining retrograde memoryimpairment.
As previously noted, most authors agree in attributing an eminent role in thestorage and retrieval of remote memories to the cortical areas of the temporallobes. In particular, the substantial sparing of retrograde memory in deepanterograde amnesic patients with lesions confined to the hippocampalformations (Zola-Morgan et al., 1986) and, in contrast, a selective difficulty inaccessing remote memories in patients with lesions encroaching upon thetemporal lobes but sparing hippocampi (Kapur et al., 1992; Markowitsch et al.,1993) suggests that, in the context of temporal lobes, the areas mostly involvedin the retrieval of old memories are the poles and infero-lateral surfaces.
In our CHI group, the presence of a focal lesion in the temporal lobes wasnot predictive of retrograde memory impairment. Indeed, retrograde memoryperformances of a subgroup of temporal lobe-lesioned patients did not differfrom those of the remaining patients. It is worth noting that a lack of associationbetween memory deficits and locus of focal cerebral lesions in groups of CHIpatients is not a novelty. A failure to detect a significant association betweenperformance on anterograde memory tests and temporal lobe sufferance hasresulted both from MRI (Wilson, Wiedmann, Hadley et al., 1988; Wilson,Wiedmann, Hadley and Brooks, 1989) and SPECT (Goldenberg, Oder, Spatt etal., 1992) investigations. Among possible explanations for this lack ofcorrelation, a first one refers to the limited resolution power of neuroradiologicalexams. Small post-traumatic contusive lesions in the grey and white matter ofthe cerebral lobes can remain undetected also on MRI, thus preventing a reliableidentification of cortical and subcortical structures lesioned by the traumaticevent. An alternative account refers to the fact that functional deficits consequentto severe CHI are more likely related to the diffuse axonal damage destroyingneural pathways connecting cortical areas than to a direct involvement of thecritical cortical regions. Further studies, possibly relying on PET and SPECTtechnologies for the detection of regional metabolic and blood flowabnormalities, are needed to reach more founded conclusions about the neuralsubstrate underlying retrograde memory deficits in CHI patients. It worthsnoting, however, that the comparison of small groups of CHI patients with focallesions confined to one of the two hemispheres (generally involving frontal andtemporal lobes) revealed significantly poorer retrieval of autobiographicalmemories pertaining to the last year before trauma in the right hemispheregroup. As above noted, PET data on normal subjects have been recentlyprovided suggesting a dominance of frontotemporal regions of the righthemisphere in the ecphory of old autobiographical memories (Fink,Markowitsch, Reinkemeier et al., 1996). The small size of our unilateral lesionedpatient groups and the fact the intergroup difference was limited to the very lastperiod preceding trauma make hazardous drawing conclusions from these data.Further investigations conducted on larger groups of patients are necessary inorder to discovery possible neuropsychological dissociations between semanticand autobiographical retrograde memory deficits as a function of laterality oflesion.
20 Giovanni A.Carlesimo and Others
In conclusion, results of the present study document the high prevalence ofthe retrograde memory impairment in severe CHI patients also following theresolution of the post-traumatic amnesia period. This deficit is more frequentlyaccompanied by a difficulty in storing new information, but it can besporadically observed in isolation. It generally encompasses both personal eventsand basic semantic knowledge but, in some cases, affects selectively personal orsemantic types of knowledge. Up until now, the role of memory deficits indetermining poor social adjustment and failure in resuming pre-trauma job hasbeen investigated only with regard to the impairment of anterograde memory(e.g., Vilkki, Ahola, Holst et al., 1994). Indeed, a severe loss of memory forpersonal events and semantic information acquired during the entire lifetime canbe equally, if not more, disrupting to the subject’s suitability to resume hisprevious social and familiar role. In our opinion, results of the present studygive strong indications of the need to pay more attention to the possiblepresence of retrograde memory deficits both in the neuropsychologicalevaluation and rehabilitation treatment of severe CHI patients.
REFERENCES
ALBERT, M.S., BUTTERS, N., andLEVIN, Temporal gradients in the retrograde amnesia of patients withalcoholic Korsakoff’s disease.Archives of Neurology, 36:211-216, 1979.
BARBAROTTO, R., CAPITANI; E., and LAIACONA, M. Naming deficit in herpes simplex encephalitis.ActaNeurologica Scandinavica, 93: 272-280, 1996.
BASSO, A., CAPITANI, E., andLAIACONA, M. Progressive language impairment without dementia: Acasewith isolated category specific semantic defect.Journal of Neurology, Neurosurgery and Psychiatry,51: 1201-1207, 1988.
BATTIG, W.F., andMONTAGUE, W.E.Category norms for verbal items in 56 categories: A replication andextension of the Connecticut category norms.Journal of Experimental Psychology Monography, 80,part 2, 1969.
BEATTY, W.W., SALMON, D.P., BUTTERS, N., HEINDEL, W.C., andGRANHOLM, E.L. Retrograde amnesiain patients with Alzheimer’s disease or Huntington’s disease.Neurobiology of Aging, 9: 181-186,1988.
BORTOLINI, V. TAGLIAVINI , C., and ZAMPOLLI , A. Lessico di frequenze della lingua italianacontemporanea. Milano: Garzanti, 1971.
BROOKS, N. MCKINLAY , W., SIMINGTON, C., BEATTIE, A., and CAMPSIE, L. Return to work within the firstseven years of severe head injury.Brain Injury, 1: 5-19, 1987.
CAPITANI, E. LAIACONA, M., AND BARBAROTTO R. Dissociazioni semantiche intercategoriali. Parte II:procedura automatica di analisi di una batteria standardizzata.Archivio di Psicologia, Neurologia ePsichiatria, 54: 457-476, 1993.
CARLESIMO, G.A., CALTAGIRONE, C. GAINOTTI, G., and the group for the standardization of the MentalDeterioration Battery.The Mental Deterioration Battery: Normative data, diagnostic reliability andqualitative analyses of cognitive impairment.European Neurology, 36: 378-384, 1996.
CARLESIMO, G.A., SABBADINI , M. LOASSES, A., and CALTAGIRONE., C.Forgetting from long term memoryin severe closed-head injury patients: Effect of retrieval conditions and semantic organization.Cortex, 33: 131-142, 1997.
CERMAK, L.S., and O’CONNOR, M. The anterograde and retrograde retrieval ability of a patient withamnesia due to encephalitis. Neuropsychologia, 21: 213-234, 1983.
COHEN, N.J., and SQUIRE, L.R. Retrograde amnesia and remote memory impairment.Neuropsychologia,19: 337-356, 1981.
COLLINS, A.M., andQUILLIAN , M.R. Retrieval time from semantic memory.Journal of Verbal Learningand Verbal Behaviour, 8: 240-247, 1969.
COLLINS, A.M., and QUILLIAN , M.R. Experiments on semantic memory and language comprehension.InL.W. Gregg (Ed.), Cognition in Learning and Memory. New York: John Wiley & Sons Inc., 1970.
COSTA, M., DE RENZI, E., and FAGLIONI , P. Un questionario italiano per lo studio della memoriaretrograda.Archivio di Psicologia, Neurologia e Psichiatria, 50:735-755, 1989.
DAMASIO, A.R., ESLINGER, P.J., DAMASIO, H., VAN HOESEN, G.W., and CORNELL, S. Multimodal amnesicsyndrome following bilateral temporal and basal forebrain damage.Archives of Neurology, 42: 252-259, 1985.
Retrograde memory in severe closed-head trauma 21

DAMASIO, H., GRABOWSKI, T.J., TRANEL, D., HICHWA, R.D., and DAMASIO, A.R. A neural basis forlexical retrieval.Nature, 380:499-505, 1996.
DE RENZI, E., LIOTTI, M., and NICHELLI , P.Semantic amnesia with preservation of autobiographicmemory.A case report.Cortex, 23: 575-597, 1987.
DE RENZI, E.,LUCCHELLI, F., MUGGIA, S., AND SPINNLER, H. Persistent retrograde amnesia following aminor trauma.Cortex, 31: 531-542, 1995.
FARAH, M.J., HAMMOND, K.M., MEHTA, Z., and RATCLIFF, G. Category-specificity and modality-specificity in semantic memory.Neuropsychologia, 27: 193-200, 1989.
FINK, G.R., MARKOWITSCH, H.J., REINKEMEIER, M., BRUCKBAUER, T., KESSLER, J., and HEISS, W.Cerebral representation of one’s own past: Neural networks involved in autobiographical memory.Journal of Neuroscience, 16:4275-4282, 1996.
FLETCHER, P.C. FRITH, C.D., GRASBY, P.M., SHALLICE, T., FRACKOWIACK, R.S.J., andDOLAN, R.J. Brainsystems for encoding and retrieval of auditory-verbal memory: An in vivo study in humans.Brain,118: 401-416, 1995.
FUNNELL, E., and SHERIDAN, J.Categories of knowledge? Unfamiliar aspects of living and nonlivingthings.Cognitive Neuropsychology, 9:135-153, 1992.
GOLDBERG, E., ANTIN, S.P., BILDER, R.M., GERSTMAN, L.J., HUGHES, J.E.O., andMATTIS, S. Retrogradeamnesia: Possible role of mesencephalic reticular activation in long-term memory.Science, 213:1392-1394, 1981.
GOLDENBERG, G., ODER, W., SPATT, J., and PODREKA, I. Cerebral correlates of disturbed executivefunction and memory in survivors of severe closed head injury: A SPECT study.Journal ofNeurology, Neurosurgery and Psychiatry, 55: 362-368, 1992.
GROSSI, D., TROJANO, L., GRASSO, A., and ORSINI, A. Selective “semantic amnesia” after closed-headinjury. A case report.Cortex, 24: 457-464, 1988.
HILLIS, A.E., and CARAMAZZA , A. Category-specific naming and comprehension impairment: A doubledissociation.Brain, 114: 2081-2094, 1991.
KAPUR, N. Focal retrograde amnesia in neurological disease: Acritical review.Cortex, 29:217-234,1993.
KAPUR, N., ELLISON, D., SMITH, M.P., MCLELLAN, D.L., and BURROWS, E.H. Focal retrograde amnesiafollowing bilateral temporal lobe pathology.Brain, 115:73-85, 1992.
KERLINGER, F.N., AND PEDHAZUR, E.J. Multiple Regression in behavioral Research. New York: Holt,Rinehart and Winston, 1973.
KOPELMAN, M.D. Remote and autobiographical memory, temporal context memory, and frontal atrophyin Korsakoff and Alzheimer patients.Neuropsychologia, 27: 437-460, 1989.
KOPELMAN, M.D., WILSON, B.A., and BADDELEY, A.D. The autobiographical memory interview: Anewassessment of autobiographical and personal semantic memory in amnesic patients. Journal ofClinical and Experimental Neuropsychology, 11: 724-744, 1989.
LAIACONA, M., BARBAROTTO, R., and CAPITANI, E.Perceptual and associative knowledge in categoryspecific impairment of semantic memory: Astudy of two cases.Cortex, 29:727-740, 1993a.
LAIACONA, M., BARBAROTTO, R., TRIVELLI , C., and CAPITANI , E. Dissociazioni semanticheintercategoriali: Descrizione di una batteria standardizzata e dati normativi. Archivio di Psicologia,Neurologia e Psichiatria, 54:209-248, 1993b.
LEVIN, H.S. Memory deficit after closed-head injury.Journal of Clinical and ExperimentalNeuropsychology, 12: 129-153, 1989.
LEVIN, H.S., and Goldstein, F.C. Organization of verbal memory after severe closed-head injury.Journalof Clinical and Experimental Neuropsychology, 8: 643-656, 1986.
LEVIN, H.S., HIGH, W.M., MEYERS, C.A., VON LAUGEN, A., HAYDEN, M.E., and EIDENBERG, H.M.Impairment of retrograde memory after closed head injury.Journal of Neurology, Neurosurgery andPsychiatry, 48:556-563, 1985.
LEVIN, H.S., O’DONNEL, V.M., and GROSSMAN, R.G. The Galveston Orientation and Amnesia test.Journal of Nervous and Mental Disease, 167: 675-684, 1979.
MARKOWITSCH, H.J., CALABRESE, P., LIESS, J., HAUPTS, M., DURWEN, H.F., and GEHLEN, W. Retrogradeamnesia after traumatic injury of the fronto-temporal cortex.Journal of Neurology, Neurosurgeryand Psychiatry, 56: 988-992, 1993.
MATTIOLI , F., GRASSI, F., PERANI, D., CAPPA, S.F., MIOZZO, A., and FAZIO, F. Persistent post-traumaticretrograde amnesia: Aneuropsychological and (18F)FDG PET study.Cortex, 32:121-129, 1996.
ROUSSEAUX, M., DELAFGOSSE, A., CABARET, M., LESOIN, F., and JOMIN, M. Amnesie retrograde posttraumatique.Cortex, 20:575-583, 1984.
RUSSELL, W.R. The Traumatic Amnesia. New York: Oxford University Press, 1971.SAGAR, H.J., COHEN, N.J., SULLIVAN , E.V., CORKIN, S., and GROWDON, J.H. Remote memory function in
Alzheimer’s disease and Parkinson’s disease. Brain, 111: 525-539, 1988.SARTORI, G., and JOB, R. The oyster with four legs: Aneuropsychological study on the interaction of
visual and semantic information.Cognitive Neuropsychology, 5: 105-132, 1988.
22 Giovanni A.Carlesimo and Others

SHALLICE, T. Impairment of semantic processing: Multiple dissociations.In M. Coltheart, R. Job and G.Sartori (Eds.), The Cognitive Neuropsychology of Language. London: Lawrence Erlbaum AssociatesLtd., 1987.
SILVERI, M.C., DANIELE, A., GIUSTOLISI, L., and GAINOTTI, G. Dissociation between knowledge of livingand nonliving things in dementia of the Alzheimer type.Neurology, 41:545-546, 1991.
SILVERI, M.C., and GAINOTTI, G. Interaction between vision and language in category-specific semanticimpairment.Cognitive Neuropsychology, 5: 677-709, 1988.
SNODGRASS, J.G., and VANDERWART, M. A standardized set of 260 pictures: Norms for name agreement,image agreement, familiarity, and visual complexity.Journal of Experimental Psychology: HumanLearning and Memory, 6: 174-215, 1980.
SPINNLER, H., and TOGNONI, P. Standardizzazione e taratura italiana di test neuropsicologici.ItalianJournal of Neurological Sciences, suppl. 6:44-46, 1987.
SQUIRE, L.R. A stable impairment in remote memory following electroconvulsive therapy.Neuropsychologia, 13: 51-58, 1975.
SQUIRE, L.R., and SLATER, P.C. Anterograde and retrograde memory impairment in chronic amnesia.Neuropsychologia, 16:313-322, 1978.
STEWART, F., PARKIN, A.J., and HUNKIN, N.M. Naming impairments following recovery from HerpesSimplex encephalitis: category-specific?The Quarterly Journal of Experimental Psychology, 44A:261-284, 1992.
STRACCIARI, A., GHIDONI, E., GUARINO, M. POLETTI, M., and PAZZAGLIA , P.Post-traumatic retrogradeamnesia with selective impairment of autobiographical memory.Cortex 30:459-468, 1994.
TULVING, E., MARKOWITSCH, H.J., CRAIK, F.I.M., HABIB, R., and HOULE, S.Functional neuroanatomy ofencoding and retrieval of pictorial information in memory.Cerebral Cortex, 3: 79-94, 1996.
VILKKI , J., AHOLA, K. HOLST, P., OHMAN, J., SERVO, A., and HEISKAPEN, O. Prediction of psychosocialrecovery after head injury with cognitive tests and neurobehavioral ratings.Journal of Clinical andExperimental Neuropsychology, 16: 325-338, 1994.
WARRINGTON, E.K., and MCCARTHY, R. Categories of knowledge.Further fractionation and an attemptedintegration, Brain, 110: 1273-1296, 1987.
WARRINGTON, E.K., and SHALLICE, T. Category specific semantic impairments.Brain, 107: 829-854,1984.
WILSON, R.S., KASZNAIK, A.W., and FOX, J.H. Remote memory in senile dementia.Cortex, 17: 41-48,1981.
WILSON, J.T.L., WIEDMANN, K.D., HADLEY, D.M., CONDON, B., and TEASDALE, G. Early and latemagnetic resonance imaging and neuropsychological outcome after head injury. Journal ofNeurology, Neurosurgery and Psychiatry, 51: 391-396, 1988.
WILSON, J.T.L., WIEDMANN, K.D., HADLEY, D.M., and BROOKS, D.N. The relationship between visualmemory function and lesions detected by magnetic resonance imaging after closed head jnjury.Neuropsychology, 3: 255-256, 1989.
ZOLA-MORGAN, S., SQUIRE, L.R., and AMARAL , D.G.Human amnesia and the medial temporal region:Enduring memory impairment following a bilateral lesion limited to field CA1 of the hippocampus.Journal of Neuroscience, 6: 1950-1967, 1986.
Giovanni A.Carlesimo, IRCCSS.Lucia, V.Ardeatina, 306, 00179 Roma, Italy.
(Received 4 March 1997; accepted 15 July 1997)
Retrograde memory in severe closed-head trauma 23
Related Documents











