Retinopati Diabetika Abstrak Retinopati diabetika merupakan suatu gangguan pada mata yang disebabkan akibat penyakit diabetes mellitus yang diderita dalam waktu yang relatif lama . Jumlah insidens penderitanya yang cukup tinggi ditambah pula dengan manifestasi klinis tahap akhir berupa kebutaan ; keduanya merupakan tantangan tersendiri bagi para klinisi untuk mengoptimalkan penatalaksanaan bagi penderita diabetes mellitus sebelum mereka kehilangan daya penglihatannya . Terapi yang dilakukan hingga saat ini adalah mengontrol faktor penyebab dan laser terapi . Diperlukan telaah yang lebih dalam , agar dapat ditemukan suatu cara yang lebih optimal guna menghindari terjadinya retinopati diabetika ini pada penderita deabetes mellitus . Kata kunci : retinopati diabetika – diabetes mellitus – neuro oftalmologi Abstract Diabetic retinopathy is visual disorder cause by hiperglycemi and depend by time . Incidens for diabetic retinopathy is high, and its end stage clinical manifestation ( blind ) made this situation must become a caution for clinician to find the optimize way to prevent . So far, how to manage hiperglycemi and laser therapy are the best way that we could done . We need more courage and curious to find the better way to prevent hyperglycemi cause diabetic retinopathy . Keywords : diabetic retinopathy – diabetes mellitus – neuro ophthalmology Pendahuluan Diabetes mellitus merupakan gangguan dari metabolisme karbohidrat , dimana tepung dan gula tidak disimpan atau

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Retinopati Diabetika
Abstrak Retinopati diabetika merupakan suatu gangguan pada mata yang disebabkan akibat penyakit diabetes mellitus yang diderita dalam waktu yang relatif lama . Jumlah insidens penderitanya yang cukup tinggi ditambah pula dengan manifestasi klinis tahap akhir berupa kebutaan ; keduanya merupakan tantangan tersendiri bagi para klinisi untuk mengoptimalkan penatalaksanaan bagi penderita diabetes mellitus sebelum mereka kehilangan daya penglihatannya . Terapi yang dilakukan hingga saat ini adalah mengontrol faktor penyebab dan laser terapi .Diperlukan telaah yang lebih dalam , agar dapat ditemukan suatu cara yang lebih optimal guna menghindari terjadinya retinopati diabetika ini pada penderita deabetes mellitus . Kata kunci : retinopati diabetika – diabetes mellitus – neuro oftalmologi Abstract Diabetic retinopathy is visual disorder cause by hiperglycemi and depend by time . Incidens for diabetic retinopathy is high, and its end stage clinical manifestation ( blind ) made this situation must become a caution for clinician to find the optimize way to prevent . So far, how to manage hiperglycemi and laser therapy are the best way that we could done . We need more courage and curious to find the better way to prevent hyperglycemi cause diabetic retinopathy . Keywords : diabetic retinopathy – diabetes mellitus – neuro ophthalmology Pendahuluan
Diabetes mellitus merupakan gangguan dari metabolisme karbohidrat , dimana
tepung dan gula tidak disimpan atau dipakai dengan semestinya . Hal ini menimbulkan
gangguan pula pada nutrisi jaringan diseluruh tubuh, termasuk mata . Pengobatannya
dengan diit dan insulin , dapat memperpanjang umur penderita diabetes mellitus ,
sehingga proses degenerasi dimata menjadi bertambah penting . Yang paling khas adalah
penyulitnya di retina . (1,2)
Retinopati diabetika biasanya timbul setelah penderita menderita diabetes
mellitus selama 5 – 15 tahun. Dimana angka kejadian pada wanita lebih banyak daripada
pria . Umur yang terbanyak menderita retinopati diabetika adalah 50 – 65 tahun .(3)
Walaupun demikian Watkins memberikan batasan rentang umur yang lebih panjang lagi
yaitu berkisar antara 30 – 69 tahun .(9) Retinopati ini merupakan penyulit yang paling
penting dari diabetes mellitus , dengan frekuensi 40 – 50% dari penderita diabetes .
Prognosanya kurang baik untuk penglihatan. Di Amerika Serikat , 5000 orang
pertahunnya menjadi buta oleh retinopati diabetika, sedang di Inggris , keadaan ini
merupakan penyebab kebutaan nomor 4 dari seluruh penyebab kebutaan . Selain oleh
karena kelainan endokrin, stresspun dapat menimbulkan diabetes mellitus .(3)
Patogenesa
Beberapa teori dikatakan dapat menyebabkan terjadinya retinopati diabetika .
Namun terdapat 2 buah teori yang paling banyak menarik perhatian para pakar , yaitu (10)
1. Teori Enzim katalisis aldose reduktase .
Enzim ini akan mengkatalisa perubahan glukosa menjadi sorbitol . Bila kadar
glukosa intraselular meningkat , hal ini akan meningkatkan pula kadar sorbitor
intraselular, yang kemudian akan menghambat sintesis mio-inositol yang terdapat
pada glomerular dan jaringan saraf . Penurunan kadar mio-inositol ini akan
menurunkan metabolisme fosfo-inositidin, yang kemudian akan menurunkan
aktivitas dari Na-K-ATPase dan memperburuk kerusakan mikrovaskular .
2. Teori protein Aminoguanidin .
Aminoguanidin ( suatu fraksi dari protein esensial ) , melalui mekanisme yang
masih terus diselidiki , pada tikus tikus percobaan ternyata dapat memperlambat
pertambahan mikroaneurisma dan penumpukan deposit protein pada kapiler
kapiler di retina .
Retinopati diabetika merupakan mikroangiopati , sebagai akibat dari gangguan
metabolik , yaitu defisiensi insulin dan hiperglikemi . Peningkatan gula darah sampai
ketinggian tertentu , mengakibatkan keracunan sel sel tubuh , terutama darah dan dinding
pembuluh darah , yang disebut glikotoksisitas. Peristiwa ini merupakan penggabungan
irreversibel dari molekul glukosa dengan protein yang disebut proses glikosilase protein .(1,2,3)
Dalam keadaan normal , proses glikosilase ini hanya sekitar 4-9% , sedang pada
penderita diabetes mencapai 20% .(4) Glikosilase ini dapat mengenai isi dan dinding
pembuluh darah , yang secara keseluruhan dapat menyebabkan meningkatnya viskositas
darah , gangguan aliran darah , yang dimulai pada aliran didaerah sirkulasi kecil ,
kemudian disusul dengan gangguan pada daerah sirkulasi besar dan menyebabkan
hipoksia jaringan yang diurusnya . Kelainan kelainan ini didapatkan juga didalam
pembuluh pembuluh darah retina , yang dapat diamati dengan melakukan (2)
1. fundus fluorescein angiography
2. pemotretan dengan menggunakan film berwarna
3. oftalmoskop langsung dan tak langsung
4. biomikroskop dengan lensa kontak dari goldman
Mula mula didapatkan kelainan pada kapiler vena, yang dindingnya menebal dan
mempunyai affinitas yang besar terhadap fluoresein . Keadaan ini menetap untuk waktu
yang lama tanpa mengganggu penglihatan . Dengan melemahnya dinding kapiler , maka
akan menonjol membentuk mikroaneurisma . Mula mula keadaan ini terlihat pada daerah
kapiler vena sekitar makula, yang tampak sebagai titik titik merah pada oftalmoskop .
Adanya 1-2 mikroaneurisma sudah cukup mendiagnosa adanya retinopati diabetika .(2)
Pada keadaan lanjut , mikroaneurisma didapatkan sama banyaknya pada kapiler vena
maupun arteri . Baik kapiler yang abnormal maupun aneurisma menibulkan kebocoran ,
yang tampak sebagai edema, eksudat, perdarahan, di sekitar kapiler dan mikroaneurisma . (8)
Adanya edema dapat mengancam ketajaman penglihatan bila terdapat di daerah
makula, edema yang ringan dapat diabsorbsi, tetapi yang hebat dan berlangsung dalam
waktu relatif lama akan menyebabkan degenerasi kistoid . Bila hal ini terjadi di daerah
makula , ketajaman penglihatan yang terganggu, tak dapat dikembalikan kepada keadaan
semula meskipun dilakukan fotokoagulasi pada pengobatan . (4,5)
Perdarahan selain akibat kebocoran juga dapat disebabkan oleh karena pecahnya
mikroaneurisma . Kebocoran lipoprotein , tampak sebagai eksudat keras , menyerupai
lilin berkelompok yang berbentuk lingkaran di daerah makula, yang disebut bentuk
sirsiner berwarna putih kekuning kuningan . Eksudat lemak ini didapatkan pada penderita
yang gemuk dengan kadar lemak darah yang tinggi . (2,3 )
Akibat perubahan isi dan dinding pembuluh darah , dapat menimbulkan
penyumbatan yang dimulai di kapiler, kearteriola, dan pembuluh darah besar ; karenanya
timbul hipoksi, disusul dengan daerah iskemik kecil dan timbulnya kolateral kolateral .
Hipoksi mempercepat timbulnya kebocoran, neovaskularisasi, dan mikroaneurisma yang
baru . Akibat hipoksi timbul eksudat lunat yang disebut cotton wool patch , yang
merupakan bercak nekrose .(7,8)
Pembuluh darah vena melebar dengan lumen dan diameter yang tidak teratur.
Juga disini terjadi kebocoran dan penyumbatan, sehingga didapatkan perdarahan
sepanjang pembuluh darah vena . Gangguan aliran darah vena juga merangsang
timbulnya pembuluh darah baru yang dapat timbul dari pembuluh darah yang ada di papil
atau dimana saja . Bentuknya dapat berupa gulungan atau rete mirabile . Letaknya
intraretina dan menjalar menjadi preretina . Neovaskularisasi ini diikuti kemudian diikuti
dengan jaringan proliferasi .(5) Bila jaringan fibrivaskular ini mengkerut dapat
menimbulkan perdarahan dan tarikan pada retina sehingga menyebabkan ablasi retina
dengan atau tanpa robekan . Hal ini dapat menimbulkan penurunan ketajaman
penglihatan sampai kebutaan . Perdarahan yang timbul didalam badan kaca dapat
menyebabkan glaukoma hemoragik , yang sangat sakit dan menimbulkan kebutaan . (7)
Perdarahan di dalam badan kaca juga diikuti dengan pembentukan jaringan fibrotik yang
disertai neovaskularisasi , yang juga dapat mengkerut dan menyebabkan ablasi retina dan
kebutaan . Dengan demikian, bila tidak diambil tindakan , retinopati diabetika cepat atau
lambat akan berakhir dengan kebutaan . (2)
Neovaskularisasi juga timbul pada permukaan iris yang disebut rubeosis iris, yang
dapat menimbulkan glaukoma akibat tertutupnya sudut bilik mata oleh pembuluh darah
baru tersebut dan juga akibat perdarahan , karena pecahnya rubeosis iris . (8)
Manifestasi klinis
Penurunan ketajaman pada penglihatan sentral berlangsung secara perlahan
lahan , tergantung dari lokalisasi, luas dan beratnya kelainan .(7)
Timbulnya gangguan visus, pada masa sebelum dibentuk jaringan fibrovaskuler,
tergantung dari besar dan lokasi kelainan. Edema, eksudat, perdarahan yang terdapat di
daerah makula, yang disebut makulopati, cepat menimbulkan gangguan penglihatan.
Pada umumnya visus pada stadium ini masih baik, tetapi bila sudah terjadi pembentukan
jaringan fibrovaskuler , gangguan visus pasti menyusul .(9)
Kelainan kelainan yang didapat pada retinopati diabetika : (2)
1. Obstruksi kapiler , yang menyebabkan berkurangnya aliran darah dalam kapiler
retina.
2. Mikroaneurisma, berupa tonjolan dinding kapiler. Merupakan tanda awal dari
retinopati diabetika
3. Eksudat berupa :
a. hard eksudat : berwarna kuning karena eksudasi plasma yang lama . Pada
angiografi fluoresin tampak sebagai kebocoran fluoresin diluar pembuluh
darah . Terutama terdiri dari lipid yang didapatkan pada
hiperlipoproteinemia .
b. cotton wool patch : berwarna putih , tidak berbatas tegas, dihubungkan
dengan iskemik retina .
4. Shunt arteri vena , akibat pengurangan aliran darah arteri karena obstruksi kapiler
5. Pelebaran vena , lumennya tidak teratur, berkelok kelok, terjadi akibat kelainan
sirkulasi . Dapat disertai kelainan endotel dan eksudasi plasma .
6. Perdarahan bintik atau perdarahan bercak, akibat gangguan permeabilitas
mikroaneurisma atau karena pecahnya kapiler .
7. Akibat proliferasi sel sel endotel , timbul neovaskularisasi , tampak sebagai
pembuluh darah yang berkelok kelok , yang merupakan tanda awal dari penyakit
yang berat . Mula mula terdapat pada retina, kemudian menjalar ke preretina
untuk kemudian masuk kedalam badan kaca. Bila neovaskularisasi ini pecah
dapat menimbulkan perdarahan di retina, preretina, dan juga didalam badan kaca .
8. Neovaskularisasi preretina diikuti pula dengan proliferasi sel glia .
9. Edema makula , kondisi ini merupakan penyebab utama dari gangguan
penglihatan pada pasien pasien diabetes . Dalam setahunnya di Amerika ,
didapatkan 75.000 kasus baru .
Berdasarkan kelainan diatas . Daniel Vaughan membagi retinopati diabetes menjadi
stadium : (2)
I. Mikroaneurisma , yang merupakan tanda khas, tampak sebagai perdarahan
bulat kecil didaerah papil dan makula ; dengan vena sedikit melebar dan
secara histologis didapatkan mikroaneurisma di kapiler bagian vena dilapisan
nuklear luar .
II. Vena melebar ; tampak eksudat kecil kecil seperti lilin , tersebar , dan
terletak dilapisan pleksiform luar .
III. Stadium II + cotton wool patches, sebagai akibar iskemik pada arteriola
terminal .
IV. Vena vena melebar, sianosis, disertai sheating pembuluh darah . Perdarahan
nyata besar dan kecil, terdapat pada semua lapisan retina dan preretina .
V. Perdarahan besar di retina dan preretina, juga infiltrasi ke badan kaca .
Disusul dengan terjadinya retinitis proliferans , yang diakibarkan timbulnya
jaringan fibrotik dan neovaskularisasi .
Derajat retinopati ini berhubungan erat dengan lamanya diabetes melitus diderita .
Pengobatan yang baik dapat memperlambat timbulnya retinopati , namun sekali timbul ,
tampaknya tidak ada satu obatpun yang mampu mempengaruhi jalannya keadaan ini .(5)
Diabetes pada orang muda , dapat menyebabkan retinopati diabetes yang hebat
dalam 20 tahun meskipun dikontrol dengan baik .(7)
Beberapa keadaan yang dapat memperberat retinopati diabetes adalah (2,3)
1. arteriosklerosis dan hipertensi arteri
2. hipoglikemi
3. hiperlipoproteinemi
4. kehamilan pada penderita diabetes juvenilis.
Terapi
Pengobatan dari diabetes melitusnya sendiri dengan diit dan pemberian obat obat
anti diabetik . Kontrol gula yang ketat dapat menurunkan insidens dan perbutukan dari
retinopati diabetika ini , terutama pada penderita diabetes IDDM .(6)
Fotokoagulasi dengan Xenon Arc Fotokoagulator atau Argon Laserphoto Koagulator .
Dimana sinar dari alat tersebut ditembakan secara tidak langsung sehingga menimbulkan
jaringan parut di khorioretina, sehingga mengurangi kebutuhan metabolisme dan
berakibat regresinya neovaskularisasi . Tujuan dari fotokoagulasi ini adalah menutup

kebocoran , merangsang penyerapan cairan , mengurangi neovaskularisasi, mencegah
timbulnya ablasi retina , dengan harapan dapat menghambat menurunnya visus.(7)
Kesimpulan :
1. Retinopati diabetika merupakan salah satu penyulit yang paling penting pada
penderita diabetes melitus , dan sangat berpotensi menyebabkan kecacatan
berupa kebutaan .
2. Perjalanan penyakit akan semakin memberat bila faktor penyebabnya yaitu
diabetes melitus tidak diatasi .
3. Penatalaksaan diabetes yang tepat , akan memperlambat perjalanan retinopati
diabetika
4. Terapi yang digunakan hingga saat ini adalah kontrol yang ketat dari diabetes
melitus dan fotokoagulasi .
5. Pembetian aspirin pada keadaan retinopati diabetika hingga saat ini masih
mengundang berbagai pendapat , baik yang setuju ataupun tidak .
Daftar Pustaka 1. Kline LB, Bajandas FJ . Neuro-ophthalmology Review Mannual 5th ed. Slack
Incorporated New Jersey 2001; 155-6
2. Sudiana N . Ilmu Penyakit Mata. Trisakti Press , Jakarta 1990;
3. Valero SO, Droilhet JH . Background of retinopathy Diabetic . E medicine 2004
4. Harding S, Kohner E. Clinical Evidence of Retinopathy Diabetic : Virectomy in
people with maculopathy . E-medicine 2005
5. Ryder B . Screening for diabetic retinopathy . BMJ 1995;311:207-208
6. Kohner EM .Aspirin for diabetic retinopathy . BMJ 2003;327:1060-1061 7. Christie B . Scotland to start screening programme for diabetic retinopathy. BMJ
April 2002;324:871
8. Feman SS . Ocular Problem in Diabetes Mellitus . NEJM July 329: 286-287
9. Watkins PJ . ABC of diabetes retinopathy . NEJM April BMJ 2003;326:924-926
10.Clark CM, Lee DA . Prevention and treatment of the complication of Diabetes Mellitus. NEJM
1995;333(12): 810
http://www.freewebs.com/fsumantri/retinopatidiabetika.htm
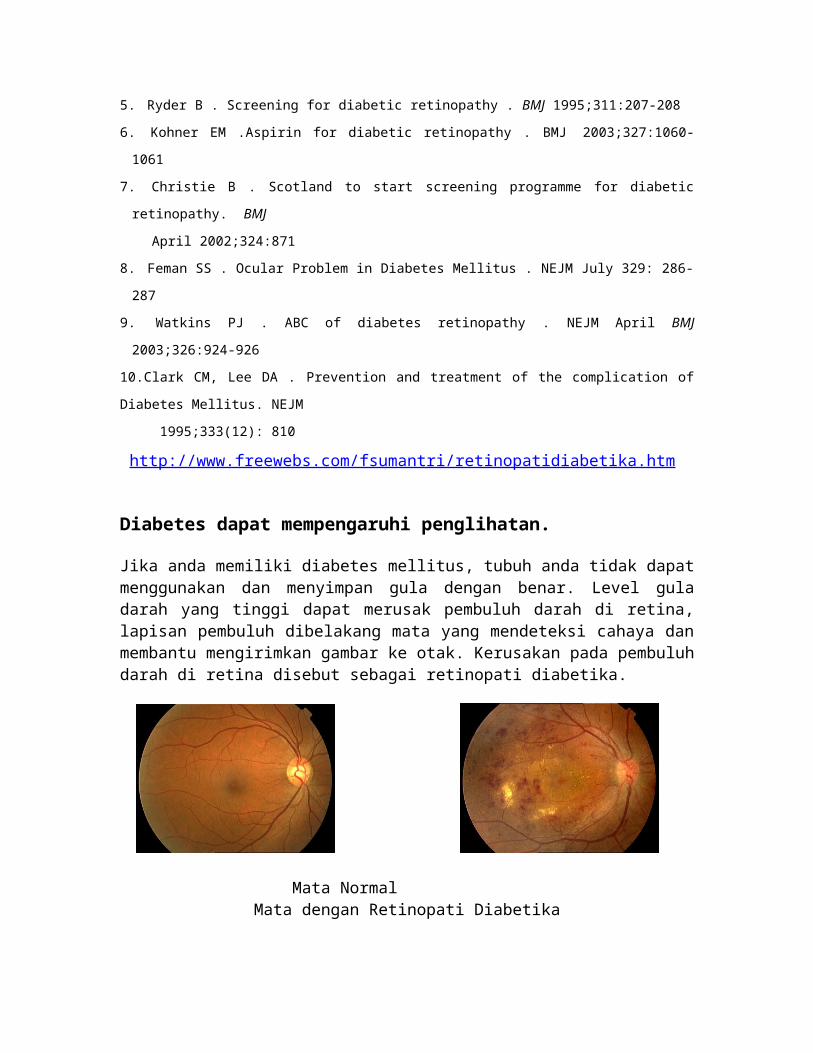
Diabetes dapat mempengaruhi penglihatan.
Jika anda memiliki diabetes mellitus, tubuh anda tidak dapat menggunakan dan menyimpan gula dengan benar. Level gula darah yang tinggi dapat merusak pembuluh darah di retina, lapisan pembuluh dibelakang mata yang mendeteksi cahaya dan membantu mengirimkan gambar ke otak. Kerusakan pada pembuluh darah di retina disebut sebagai retinopati diabetika.
Mata Normal Mata dengan Retinopati Diabetika
Jenis-jenis Retinopati Diabetika
Terdapat 2 jenis diabetic retinopathy:
Nonprofile(NPDR) dan PDR
NPDR dikenal sebagai retinopathy latar belakang, adalah tahap awal dari retinopati diabetika. Dalam tahap ini, pembuluh darah kecil di dalam retina mengalami kebocoran darah atau cairan. Cairan tersebut menyebabkan kebengkakan pada retina atau menyebabkan penyumbatan yang disebut exudates.
Banyak orang dengan diabetes memiliki NPDR ringan, yang biasanya tidak mempengaruhi penglihatan mereka. Ketika penglihatan terpengaruh itu adalah hasil dari edema macular.
Edema macular adalah pembengkakan atau penebalan pada macula, area kecil di tengah retina yang membuat kita melihat secara lebih detil. Pembengkakan disebabkan oleh kebocoran cairan pada pembuluh darah retina. Ini adalah penyebab yang paling umum berkurangnya penglihatan karena diabetes. Hilangnya penglihatan bisa ringan atau parah, akan tetapi dalam kasus terburuk penglihatan periperal masih dapat berfungsi.
Iscemia macula terjadi apabila pembuluh darah kecil (kapiler) menutup. Penglihatan menjadi rabun dikarenakan macula tidak mendapat asupan darah yang cukup untuk bekerja dengan sempurna.
PDR muncul ketika pembuluh darah baru yang abnormal (neovascularization) mulai tumbuh pada permukaan retina atau saraf optik. Penyebab utama dari PDR adalah banyaknya pembuluh darah retina yang tertutup sehingga aliran darah menjadi tidak lancar. Retina merespon dengan menumbuhkan pembuluh darah baru dengan maksud untuk menyuplai darah pada area dimana pembuluh darah asli tidak mampu lagi untuk berfungsi.
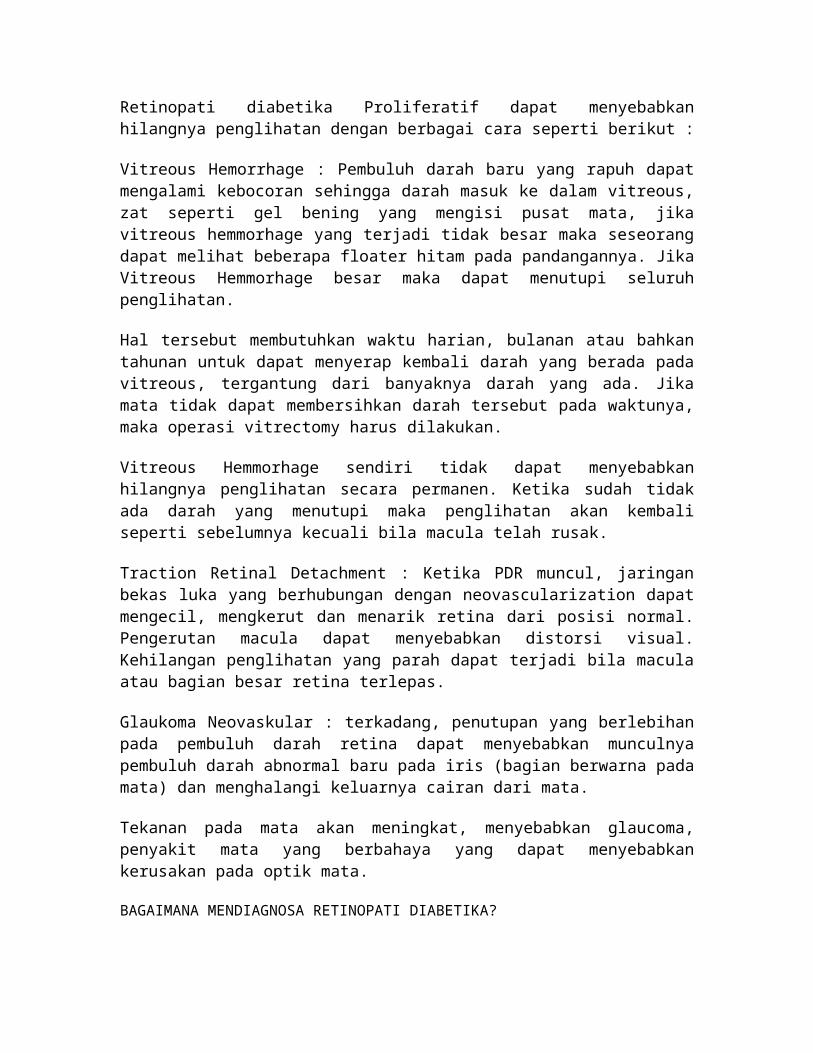
Retinopati diabetika Proliferatif dapat menyebabkan hilangnya penglihatan dengan berbagai cara seperti berikut :
Vitreous Hemorrhage : Pembuluh darah baru yang rapuh dapat mengalami kebocoran sehingga darah masuk ke dalam vitreous, zat seperti gel bening yang mengisi pusat mata, jika vitreous hemmorhage yang terjadi tidak besar maka seseorang dapat melihat beberapa floater hitam pada pandangannya. Jika Vitreous Hemmorhage besar maka dapat menutupi seluruh penglihatan.
Hal tersebut membutuhkan waktu harian, bulanan atau bahkan tahunan untuk dapat menyerap kembali darah yang berada pada vitreous, tergantung dari banyaknya darah yang ada. Jika mata tidak dapat membersihkan darah tersebut pada waktunya, maka operasi vitrectomy harus dilakukan.
Vitreous Hemmorhage sendiri tidak dapat menyebabkan hilangnya penglihatan secara permanen. Ketika sudah tidak ada darah yang menutupi maka penglihatan akan kembali seperti sebelumnya kecuali bila macula telah rusak.
Traction Retinal Detachment : Ketika PDR muncul, jaringan bekas luka yang berhubungan dengan neovascularization dapat mengecil, mengkerut dan menarik retina dari posisi normal. Pengerutan macula dapat menyebabkan distorsi visual. Kehilangan penglihatan yang parah dapat terjadi bila macula atau bagian besar retina terlepas.
Glaukoma Neovaskular : terkadang, penutupan yang berlebihan pada pembuluh darah retina dapat menyebabkan munculnya pembuluh darah abnormal baru pada iris (bagian berwarna pada mata) dan menghalangi keluarnya cairan dari mata.
Tekanan pada mata akan meningkat, menyebabkan glaucoma, penyakit mata yang berbahaya yang dapat menyebabkan kerusakan pada optik mata.
BAGAIMANA MENDIAGNOSA RETINOPATI DIABETIKA?
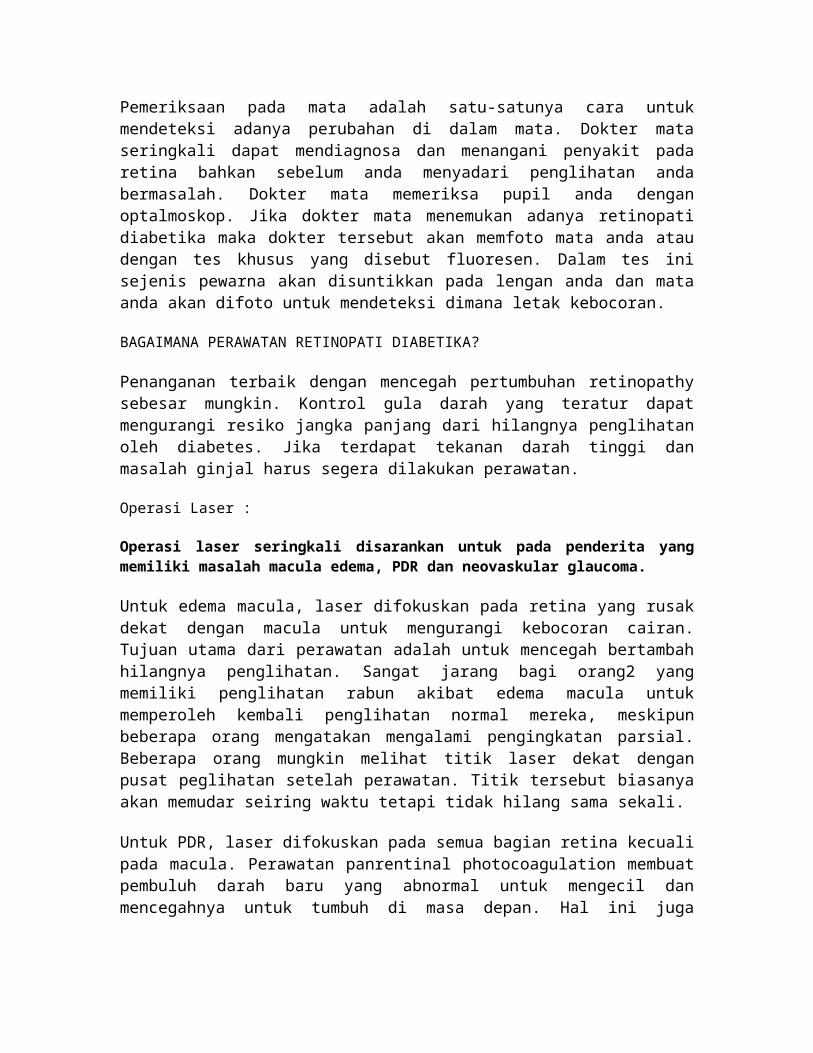
Pemeriksaan pada mata adalah satu-satunya cara untuk mendeteksi adanya perubahan di dalam mata. Dokter mata seringkali dapat mendiagnosa dan menangani penyakit pada retina bahkan sebelum anda menyadari penglihatan anda bermasalah. Dokter mata memeriksa pupil anda dengan optalmoskop. Jika dokter mata menemukan adanya retinopati diabetika maka dokter tersebut akan memfoto mata anda atau dengan tes khusus yang disebut fluoresen. Dalam tes ini sejenis pewarna akan disuntikkan pada lengan anda dan mata anda akan difoto untuk mendeteksi dimana letak kebocoran.
BAGAIMANA PERAWATAN RETINOPATI DIABETIKA?
Penanganan terbaik dengan mencegah pertumbuhan retinopathy sebesar mungkin. Kontrol gula darah yang teratur dapat mengurangi resiko jangka panjang dari hilangnya penglihatan oleh diabetes. Jika terdapat tekanan darah tinggi dan masalah ginjal harus segera dilakukan perawatan.
Operasi Laser :
Operasi laser seringkali disarankan untuk pada penderita yang memiliki masalah macula edema, PDR dan neovaskular glaucoma.
Untuk edema macula, laser difokuskan pada retina yang rusak dekat dengan macula untuk mengurangi kebocoran cairan. Tujuan utama dari perawatan adalah untuk mencegah bertambah hilangnya penglihatan. Sangat jarang bagi orang2 yang memiliki penglihatan rabun akibat edema macula untuk memperoleh kembali penglihatan normal mereka, meskipun beberapa orang mengatakan mengalami pengingkatan parsial. Beberapa orang mungkin melihat titik laser dekat dengan pusat peglihatan setelah perawatan. Titik tersebut biasanya akan memudar seiring waktu tetapi tidak hilang sama sekali.
Untuk PDR, laser difokuskan pada semua bagian retina kecuali pada macula. Perawatan panrentinal photocoagulation membuat pembuluh darah baru yang abnormal untuk mengecil dan mencegahnya untuk tumbuh di masa depan. Hal ini juga mengurangi kemungkinan pendarahan pada vitreous atau distorsi retina akan timbul.
Perawatan laser berkala terkadang dibutuhkan. Operasi laser tidak dapat menyembuhkan Diabetic retinopathy dan tidak selalu dapat mencegah berkurangnya penglihatan.
Vitrectomy : Pada PDR tingkat lanjut, Dokter mata boleh menyarankan untuk vitrectomy. Selama prosedur operasi ini, yang dilakukan di dalam ruang operasi, vitreous yang dipenuhi dengan darah akan dibuang dan diganti dengan larutan bening. Dokter mata akan menunggu selama beberapa bulan sampai dengan setahun untuk melihat apakah darah tersebut akan menghilang dengan sendirinya atau harus dilakukan Vitrectomy.
Vitrectomy dapat mencegah pendarahan lanjutan dengan membuang pembuluh abnormal yang menyebabkan pendarahan tersebut. Jika retina terlepas, dapat diperbaiki pada saat operasi Vitrectomy. Operasi harus dilakukan lebih awal karena distorsi macular atau lepasnya retina dapat menyebabkan hilangnya penglihatan secara permanen. Semakin lama terjadi distorsi macular semakin serius kurangnya penglihatan.
KAPAN UNTUK MENJADWALKAN PEMERIKSAAN?
Orang dengan diabetes harus menjadwalkan pemeriksaan setidaknya setahun sekali. Kunjungan lebih sering harus dilakukan apabila didiagnosis mengidap Retinopati Diabetika.
Wanita hamil dengan diabetes harus menjadwalkan kunjungan pada tiga bulan pertama. Karena retinopathy dapat menyebar dengan cepat pada masa kehamilan.
Jika anda ingin diperiksa untuk kacamata, sangat penting untuk mengontrol kadar gula darah anda terlebih dahulu sebelum menemui dokter mata. Kacamata tidak akan berfungsi dengan baik ketika gula darah kita tidak stabil.
Perubahan yang cepat pada kadar gula darah dapat menyebabkan fluktuasi penglihatan di kedua mata bahkan jika tidak terdapat Retinopati Diabetika.
Jika anda didiagnosa diabetes anda harus memeriksakan mata anda :
dalam jangka waktu lima tahun dari diagnosis jika berusia 29 tahun atau kurang.
dalam jangka waktu beberapa bulan dari diagnosis jika berusia 30 tahun atau lebih.
http://www.jec-online.com/index.php?option=com_content&view=article&id=126&Itemid=124
Retinopathy, Diabetic, ProliferativeAbdhish R Bhavsar, MD, Adjunct Assistant Professor, Department of Ophthalmology, University of Minnesota; Director of Clinical Research, Retina Center, PA; Past Chair, Consulting Staff, Department of Ophthalmology, Phillips Eye InstituteNeal H Atebara, MD, Clinical Assistant Professor, Department of Surgery, Division of Ophthalmology, University of Hawaii School of Medicine; John H Drouilhet, MD, FACS, Clinical Associate Professor, Department of Surgery, Section of Ophthalmology, University of Hawaii, John A Burns School of MedicineContributor Information and Disclosures
Updated: Sep 7, 2006
Print This Email This
Overview Differential Diagnoses & Workup Treatment & Medication Follow-up Multimedia
References Keywords
Introduction
BackgroundDiabetes mellitus (DM) is a major medical problem throughout the world. Diabetes causes an array of long-term systemic complications, which have considerable impact on both the patient and the society because it typically affects individuals in their most productive years. Ophthalmic complications of diabetes include corneal abnormalities, glaucoma, iris neovascularization, cataracts, and neuropathies. However, the most common and potentially most blinding of these complications is diabetic retinopathy.
PathophysiologyThe exact mechanism by which diabetes causes retinopathy remains unclear, but several theories have been postulated to explain the typical course and history of the disease.
Growth hormone
Growth hormone appears to play a causative role in the development and progression of diabetic retinopathy. It was noted that diabetic retinopathy was reversed in women who had postpartum hemorrhagic necrosis of the pituitary gland (Sheehan syndrome). This led to the controversial practice of pituitary ablation to treat or prevent diabetic retinopathy in the 1950s. This technique has been
abandoned because of numerous systemic complications and the discovery of the effectiveness of laser treatment.
Platelets and blood viscosity
Several hematologic abnormalities in diabetes, such as increased erythrocyte aggregation, decreased RBC deformability, increased platelet aggregation, and adhesion, predispose to sluggish circulation, endothelial damage, and focal capillary occlusion. This leads to retinal ischemia, which, in turn, contributes to the development of diabetic retinopathy.
Aldose reductase and vasoproliferative factors
Fundamentally, DM causes abnormal glucose metabolism as a result of decreased levels or activity of insulin. Increased levels of blood glucose are thought to have a structural and physiologic effect on retinal capillaries causing them to be both functionally and anatomically incompetent.
A persistent increase in blood glucose levels shunts excess glucose into the aldose reductase pathway in certain tissues, which converts sugars into alcohol (eg, glucose into sorbitol, galactose to dulcitol). Intramural pericytes of retinal capillaries seem to be particularly affected by this increased level of glucose because of its high aldose reductase content, eventually leading to the loss of its primary function (ie, autoregulation of retinal capillaries).
Loss of function of pericytes results in weakness and eventual saccular outpouching of capillary walls. These microaneurysms are the earliest detectable signs of DM retinopathy.
Ruptured microaneurysms (MA) result in retinal hemorrhages either superficially (flame-shaped hemorrhages) or in deeper layers of the retina (blot and dot hemorrhages).
Increased permeability of these vessels results in leakage of fluid and proteinaceous material, which clinically appears as retinal thickening and exudates. If the swelling and exudation would happen to involve the macula, a diminution in central vision may be experienced. Macular edema is the most common cause of vision loss in patients with nonproliferative diabetic retinopathy (NPDR). However, it is not exclusively seen only in patients with NPDR, but it also may complicate cases of proliferative diabetic retinopathy (PDR).
As the disease progresses, eventual closure of the retinal capillaries occurs, leading to hypoxia. Infarction of the nerve fiber layer leads to the formation of cotton-wool spots (CWS) with associated stasis in axoplasmic flow.
More extensive retinal hypoxia triggers compensatory mechanisms within the eye to provide enough oxygen to tissues. Venous caliber abnormalities, such as venous beading, loops, and dilation, signify increasing hypoxia and almost always are seen bordering the areas of capillary nonperfusion.
Intraretinal microvascular abnormalities (IRMA) represent either new vessel growth or remodeling of preexisting vessels through endothelial cell proliferation within the retinal tissues that act as shunts through areas of nonperfusion.
Further increases in retinal ischemia trigger the production of vasoproliferative factors, such as vascular endothelial growth factor (VEGF), that stimulate new vessel formation. The extracellular matrix is broken down first by proteases, and new vessels arising mainly from the retinal venules penetrate the internal limiting membrane and form capillary networks between the inner surface of the retina and the posterior hyaloid face.
Neovascularization most commonly is observed at the borders of perfused and nonperfused retina and most commonly occur along the vascular arcades and at the optic nerve head. New vessels break through and grow along the surface of the retina and into the scaffold of the posterior hyaloid face. By themselves, these vessels rarely cause visual compromise. However, they are fragile and highly permeable. These delicate vessels are disrupted easily by vitreous traction, which leads to hemorrhage into the vitreous cavity or the preretinal space.
These new blood vessels initially are associated with a small amount of fibroglial tissue formation. However, as the density of the neovascular frond increases, so does the fibrous tissue formation. In later stages, the vessels may regress leaving only networks of avascular fibrous tissue adherent to both the retina and the posterior hyaloid face. As the vitreous contracts, it may exert tractional forces on the retina via these fibroglial connections. Traction may cause retinal edema, retinal heterotropia, and both tractional retinal detachments and retinal tear formation with subsequent detachment.
FrequencyUnited States
Approximately 700,000 Americans have PDR with an annual incidence of 65,000. Approximately 500,000 persons have clinically significant macular edema (CSME) with an annual incidence of 75,000.
Mortality/MorbidityApproximately 16 million Americans have diabetes, with 50% of them not even aware that they have it. Of these, only one half receives appropriate eye care. Thus, it is not surprising that diabetic retinopathy is the leading cause of new blindness in persons aged 25-74 years in the United States.
Approximately 8,000 eyes become blind yearly because of diabetes. The treatment of diabetic retinopathy entails tremendous costs, but it has been estimated that this represents only one eighth of the costs of social security payments for vision loss. This cost does not compare to the cost in terms of loss of productivity and quality of life.
Clinical
History
In the initial stages, patients are generally asymptomatic; however, in the advanced stages of the disease, patients may experience floaters, blurred vision, or progressive visual acuity loss.
PhysicalThese findings occur in addition to all the findings that can be seen in nonproliferative or background diabetic retinopathy. See Retinopathy, Diabetic, Background.
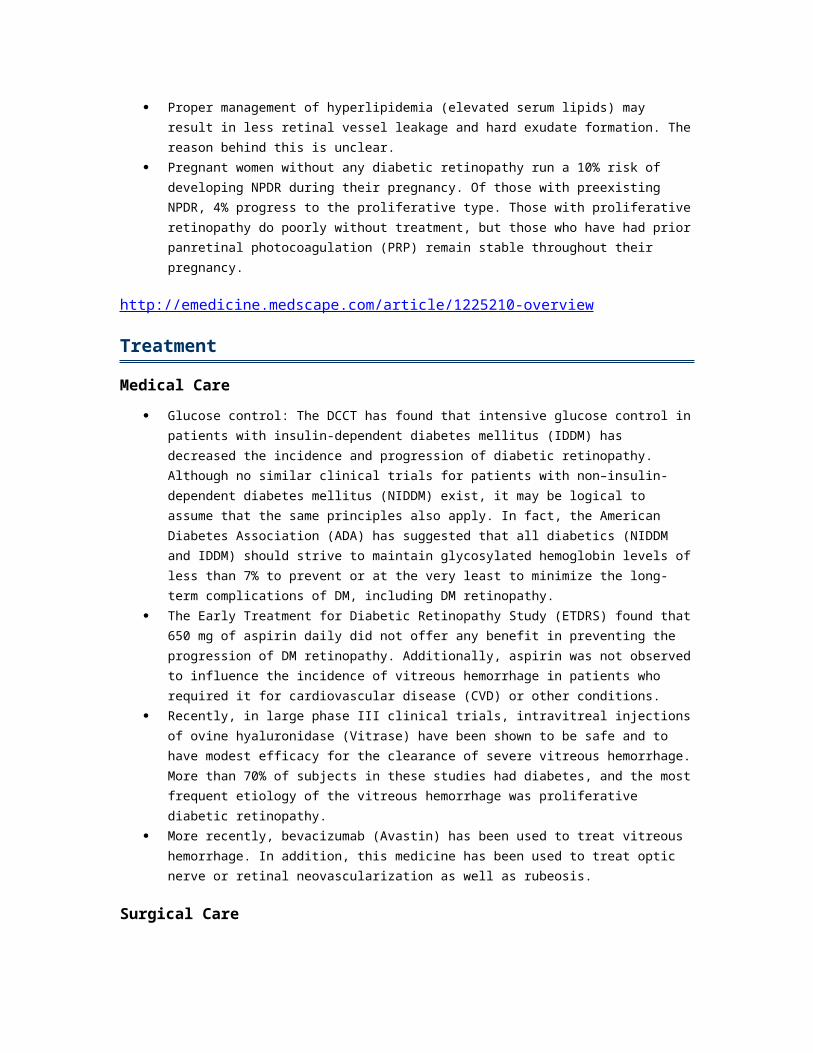
Neovascularization o Hallmark of PDR o Most often occurs near the optic disc (neovascularization of the disc [NVD]) or within
3 disc diameters of the major retinal vessels (neovascularization elsewhere [NVE]) Preretinal or vitreous hemorrhage
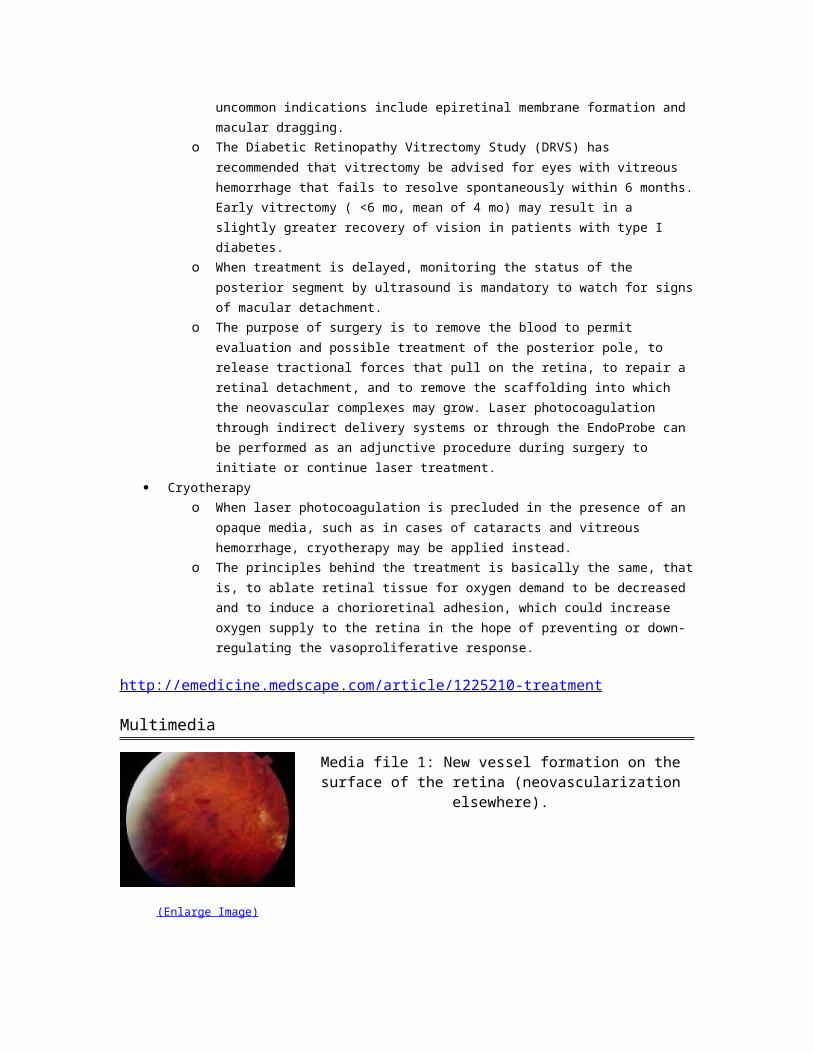
o Preretinal hemorrhages appear as pockets of blood within the potential space
between the retina and the posterior hyaloid face. As the blood pools within this space, they may appear boat shaped.
o Hemorrhage into the vitreous may appear as a diffuse haze or as clumps of blood
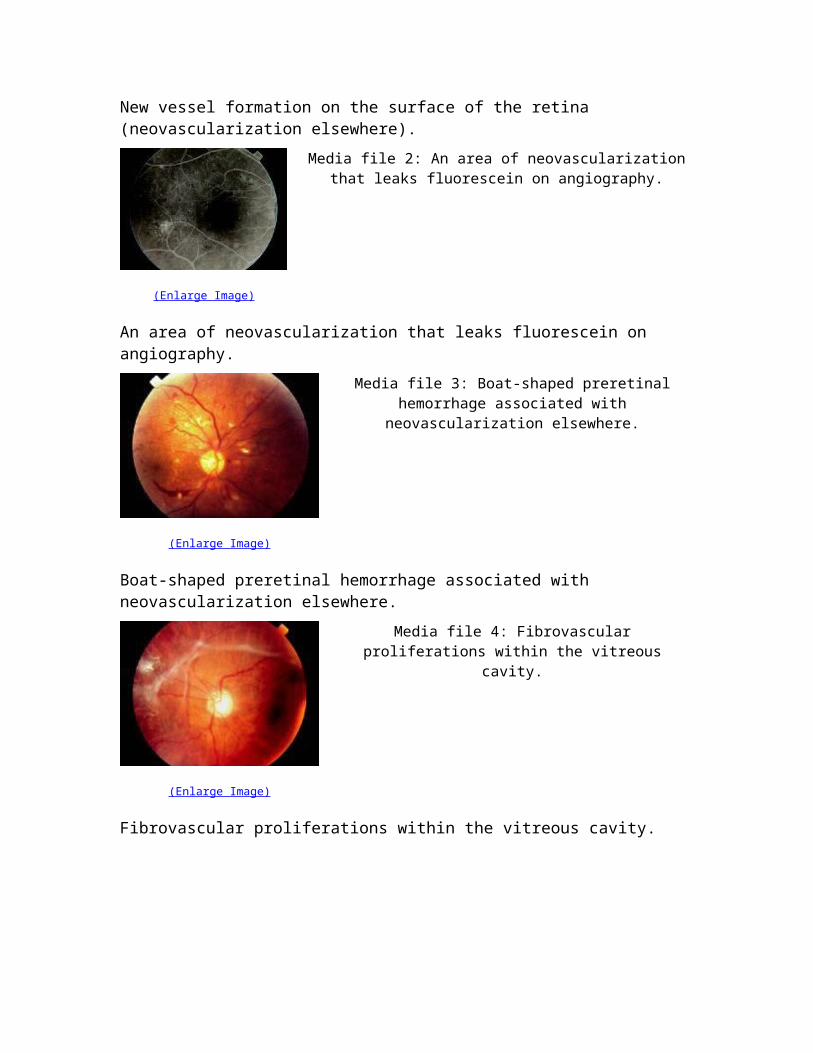
clots within the gel. Fibrovascular tissue proliferation is usually seen associated with the neovascular complex and
also may appear avascular when the vessels have already regressed. Traction retinal detachments usually appear tented up, immobile, and concave compared to
rhegmatogenous retinal detachments, which are bullous, mobile, and convex. However, a combination of both mechanisms is not an uncommon finding.
Macular edema o Leading cause of visual impairment in patients with diabetes o Possibly due to functional damage and necrosis of retinal capillaries o In cases of PDR, edema also may be caused by retinal traction if the retina is
sufficiently elevated away from the retinal pigment epithelium (RPE). o CSME is defined as any of the following:
Retinal thickening located 500 µm or less from the center of the foveal avascular zone (FAZ)
Hard exudates with retinal thickening 500 µm or less from the center of the FAZ
Retinal thickening 1 disc area or larger in size located within 1 disc diameter of the FAZ
Classification of proliferative diabetic retinopathy o Early proliferative diabetic retinopathy - Presence of new vessels but not meeting the
criteria for high-risk PDR o High-risk proliferative diabetic retinopathy
NVD greater than or equal to one-third to one-half disc area (DA) Any amount of NVD with vitreous or preretinal hemorrhage NVE greater than or equal to one-half DA with preretinal or vitreous
hemorrhage
CausesRisk factors
Duration of the diabetes o In patients with type I diabetes, no clinically significant retinopathy can be seen in the
first 5 years after the initial diagnosis of diabetes. In 10-15 years, 25-50% of patients show some signs of retinopathy. This prevalence increases to 75-95% after 15 years and approaches 100% after 30 years of diabetes. PDR is rare within the first decade of diagnosis but increases to 14-17% by 15 years, rising steadily thereafter.
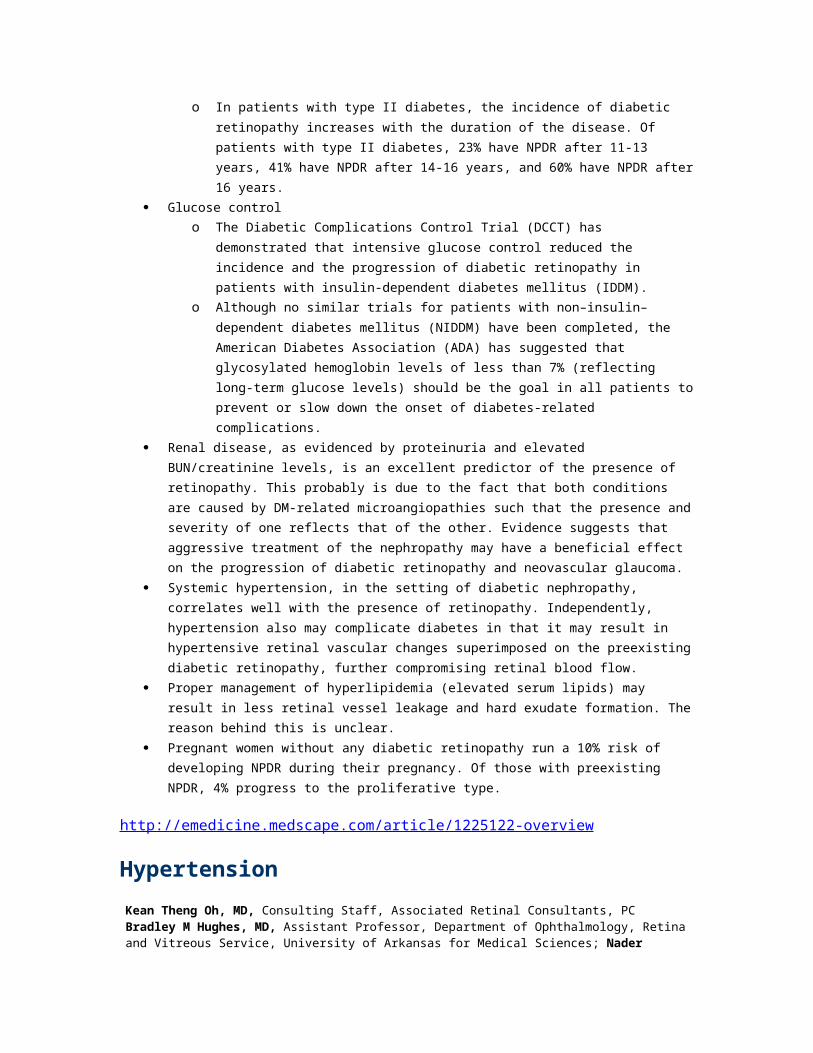
o In patients with type II diabetes, the incidence of diabetic retinopathy likewise
increases with the duration of the disease. Of patients with type II diabetes, 23% have NPDR after 11-13 years, 41% have NPDR after 14-16 years, and 60% have NPDR after 16 years. PDR was found in 3% of patients 11 or more years after the diagnosis.
Renal disease, as evidenced by proteinuria and elevated BUN/creatinine levels, is an excellent predictor of the presence of retinopathy. This is probably because of the fact that both conditions are caused by DM-related microangiopathies such that the presence and severity of one reflects that of the other. Evidence suggests that aggressive treatment of the nephropathy may have a beneficial effect on the progression of diabetic retinopathy and neovascular glaucoma.
Systemic hypertension, in the setting of diabetic nephropathy, correlates well with the presence of retinopathy. Independently, hypertension also may complicate diabetes in that it may result in hypertensive retinal vascular changes superimposed on the preexisting diabetic retinopathy, further compromising retinal blood flow.
Proper management of hyperlipidemia (elevated serum lipids) may result in less retinal vessel leakage and hard exudate formation. The reason behind this is unclear.
Pregnant women without any diabetic retinopathy run a 10% risk of developing NPDR during their pregnancy. Of those with preexisting NPDR, 4% progress to the proliferative type. Those with proliferative retinopathy do poorly without treatment, but those who have had prior panretinal photocoagulation (PRP) remain stable throughout their pregnancy.
http://emedicine.medscape.com/article/1225210-overview
Treatment
Medical Care Glucose control: The DCCT has found that intensive glucose control in patients with insulin-
dependent diabetes mellitus (IDDM) has decreased the incidence and progression of diabetic retinopathy. Although no similar clinical trials for patients with non–insulin-dependent diabetes mellitus (NIDDM) exist, it may be logical to assume that the same principles also apply. In fact, the American Diabetes Association (ADA) has suggested that all diabetics (NIDDM and
IDDM) should strive to maintain glycosylated hemoglobin levels of less than 7% to prevent or at the very least to minimize the long-term complications of DM, including DM retinopathy.
The Early Treatment for Diabetic Retinopathy Study (ETDRS) found that 650 mg of aspirin daily did not offer any benefit in preventing the progression of DM retinopathy. Additionally, aspirin was not observed to influence the incidence of vitreous hemorrhage in patients who required it for cardiovascular disease (CVD) or other conditions.
Recently, in large phase III clinical trials, intravitreal injections of ovine hyaluronidase (Vitrase) have been shown to be safe and to have modest efficacy for the clearance of severe vitreous hemorrhage. More than 70% of subjects in these studies had diabetes, and the most frequent etiology of the vitreous hemorrhage was proliferative diabetic retinopathy.
More recently, bevacizumab (Avastin) has been used to treat vitreous hemorrhage. In addition, this medicine has been used to treat optic nerve or retinal neovascularization as well as rubeosis.
Surgical CareThe advent of laser photocoagulation in the 1960s and early 1970s provided a noninvasive treatment modality, which has a relatively low complication rate and a significant degree of success.
PRP is the preferred form of treatment of PDR. This involves applying laser burns over the entire retina sparing the central macular area. This may be performed using a variety of delivery systems, including the slit lamp, an indirect ophthalmoscope, and the EndoProbe.
o Application starts in a circumference of 500 µm from the disc and 2 disc diameters
from the fovea to wall off the central retina. Moderate intensity burns of 200-500 µm (gray-white burns) are placed 1 spot size apart, except in areas of neovascularization where the entire frond is treated. This procedure is continued peripherally to achieve a total of 1200-1600 applications over 2-3 sessions.
o The presence of high-risk PDR is an indication for immediate treatment. o In cases where macular edema and PDR coexist, laser treatments are performed,
first for the macular edema, and then the PRP is spread over 3-4 sessions. If it is necessary to complete both procedures at the same time, the PRP is applied initially to the nasal third of the retina.
o The strategy for treating macular edema depends on the type and extent of vessel
leakage. If the edema is due to focal leakage, microaneurysms are treated directly with laser photocoagulation. In cases where the foci of leakage are nonspecific, a grid pattern of laser burns is applied. Burns (100-200 µm) are placed 1 burn size apart covering the affected area.
o The exact mechanism by which PRP works is not entirely understood. One theory is
that destroying the hypoxic retina presumably decreases the production of vasoproliferative factors, such as VEGF, which, in turn, reduces the rate of neovascularization. Another theory is that PRP allows increased diffusion of oxygen from the choroid, supplementing retinal circulation. The enhanced oxygen delivery
also down-regulates vasoproliferative factor production and subsequent neovascularization.
Vitrectomy o Vitrectomy may be necessary in cases of long-standing vitreous hemorrhage (where
visualization of the status of the posterior pole is too difficult), tractional retinal detachment, and combined tractional and rhegmatogenous retinal detachment. More uncommon indications include epiretinal membrane formation and macular dragging.
o The Diabetic Retinopathy Vitrectomy Study (DRVS) has recommended that
vitrectomy be advised for eyes with vitreous hemorrhage that fails to resolve spontaneously within 6 months. Early vitrectomy ( <6 mo, mean of 4 mo) may result in a slightly greater recovery of vision in patients with type I diabetes.
o When treatment is delayed, monitoring the status of the posterior segment by
ultrasound is mandatory to watch for signs of macular detachment. o The purpose of surgery is to remove the blood to permit evaluation and possible
treatment of the posterior pole, to release tractional forces that pull on the retina, to repair a retinal detachment, and to remove the scaffolding into which the neovascular complexes may grow. Laser photocoagulation through indirect delivery systems or through the EndoProbe can be performed as an adjunctive procedure during surgery to initiate or continue laser treatment.
Cryotherapy o When laser photocoagulation is precluded in the presence of an opaque media, such
as in cases of cataracts and vitreous hemorrhage, cryotherapy may be applied instead.
o The principles behind the treatment is basically the same, that is, to ablate retinal
tissue for oxygen demand to be decreased and to induce a chorioretinal adhesion, which could increase oxygen supply to the retina in the hope of preventing or down-regulating the vasoproliferative response.
http://emedicine.medscape.com/article/1225210-treatment
Multimedia
(Enlarge Image)
Media file 1: New vessel formation on the surface of the retina (neovascularization elsewhere).
New vessel formation on the surface of the retina (neovascularization elsewhere).
(Enlarge Image)
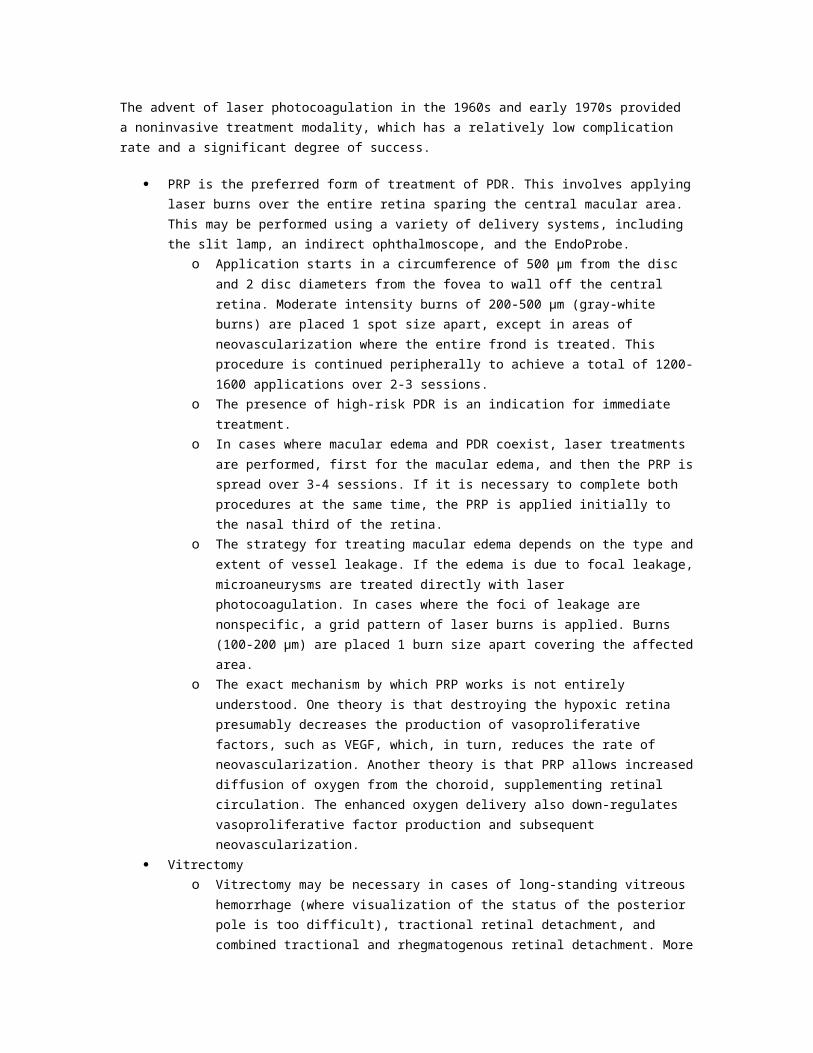
Media file 2: An area of neovascularization that leaks fluorescein on angiography.
An area of neovascularization that leaks fluorescein on angiography.
(Enlarge Image)
Media file 3: Boat-shaped preretinal hemorrhage associated with neovascularization elsewhere.
Boat-shaped preretinal hemorrhage associated with neovascularization elsewhere.
(Enlarge Image)
Media file 4: Fibrovascular proliferations within the vitreous cavity.
Fibrovascular proliferations within the vitreous cavity.
(Enlarge Image)
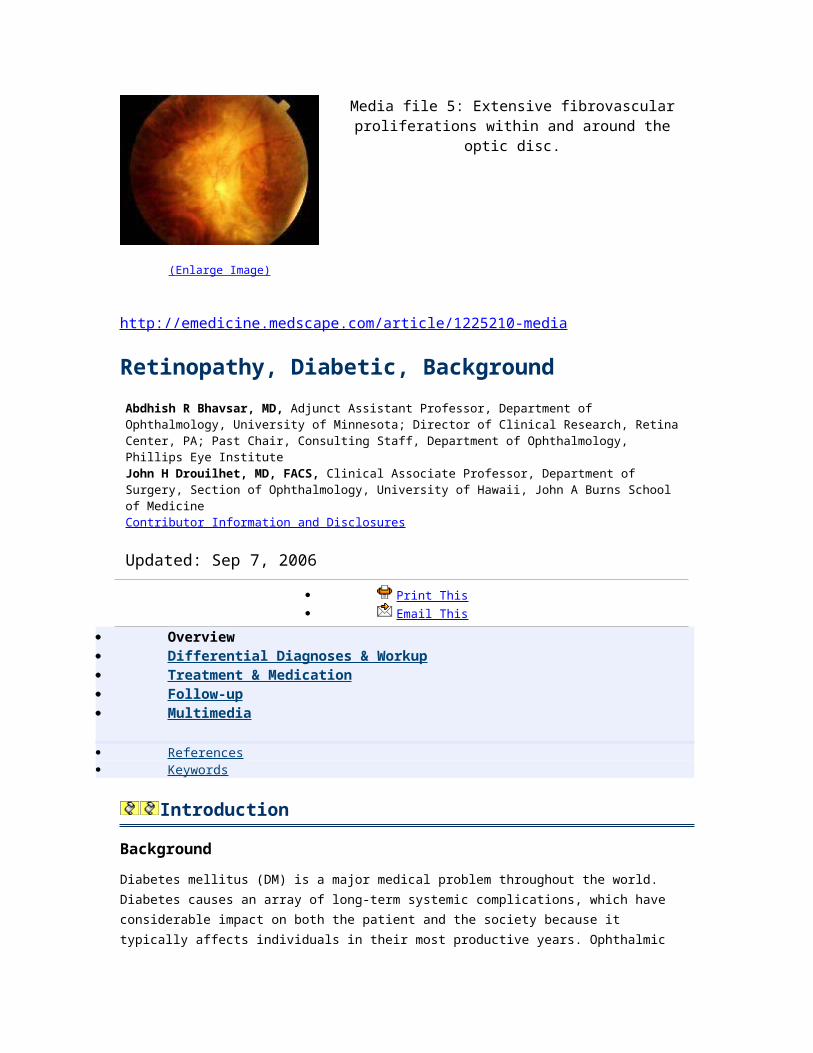
Media file 5: Extensive fibrovascular proliferations within and around the optic disc.
http://emedicine.medscape.com/article/1225210-media
Retinopathy, Diabetic, BackgroundAbdhish R Bhavsar, MD, Adjunct Assistant Professor, Department of Ophthalmology, University of Minnesota; Director of Clinical Research, Retina Center, PA; Past Chair, Consulting Staff, Department of Ophthalmology, Phillips Eye InstituteJohn H Drouilhet, MD, FACS, Clinical Associate Professor, Department of Surgery, Section of Ophthalmology, University of Hawaii, John A Burns School of MedicineContributor Information and Disclosures
Updated: Sep 7, 2006
Print This Email This
Overview Differential Diagnoses & Workup Treatment & Medication Follow-up Multimedia
References Keywords
Introduction
BackgroundDiabetes mellitus (DM) is a major medical problem throughout the world. Diabetes causes an array of long-term systemic complications, which have considerable impact on both the patient and the society because it typically affects individuals in their most productive years. Ophthalmic complications of diabetes include corneal abnormalities, glaucoma, iris neovascularization, cataracts, and neuropathies. However, the most common and potentially most blinding of these complications is diabetic retinopathy.
PathophysiologyThe exact mechanism by which diabetes causes retinopathy remains unclear, but several theories have been postulated to explain the typical course and history of the disease.
Growth hormone
Growth hormone appears to play a causative role in the development and progression of diabetic retinopathy. It was noted that diabetic retinopathy was reversed in women who had postpartum hemorrhagic necrosis of the pituitary gland (Sheehan syndrome). This led to the controversial practice of pituitary ablation to treat or prevent diabetic retinopathy in the 1950s. This technique has been abandoned because of numerous systemic complications and the discovery of the effectiveness of laser treatment.

Platelets and blood viscosity
The variety of hematologic abnormalities seen in diabetes, such as increased erythrocyte aggregation, decreased RBC deformability, increased platelet aggregation, and adhesion, predispose to sluggish circulation, endothelial damage, and focal capillary occlusion. This leads to retinal ischemia, which, in turn, contributes to the development of diabetic retinopathy.
Aldose reductase and vasoproliferative factors
Fundamentally, DM causes abnormal glucose metabolism as a result of decreased levels or activity of insulin. Increased levels of blood glucose are thought to have a structural and physiologic effect on retinal capillaries causing them to be both functionally and anatomically incompetent.
A persistent increase in blood glucose levels shunts excess glucose into the aldose reductase pathway in certain tissues, which converts sugars into alcohol (eg, glucose into sorbitol, galactose to dulcitol). Intramural pericytes of retinal capillaries seem to be affected by this increased level of sorbitol, eventually leading to the loss of its primary function (ie, autoregulation of retinal capillaries).
Loss of function of pericytes results in weakness and eventual saccular outpouching of capillary walls. These microaneurysms are the earliest detectable signs of DM retinopathy.
Ruptured microaneurysms (MA) result in retinal hemorrhages either superficially (flame-shaped hemorrhages) or in deeper layers of the retina (blot and dot hemorrhages).
Increased permeability of these vessels results in leakage of fluid and proteinaceous material, which clinically appears as retinal thickening and exudates. If the swelling and exudation would happen to involve the macula, a diminution in central vision may be experienced. Macular edema is the most common cause of vision loss in patients with nonproliferative diabetic retinopathy (NPDR). However, it is not exclusively seen only in patients with NPDR, but it also may complicate cases of proliferative diabetic retinopathy (PDR).
Another theory to explain the development of macular edema deals with the increased levels of diacylglycerol (DAG) from the shunting of excess glucose. This is thought to activate protein kinase C (PKC), which, in turn, affects retinal blood dynamics, especially permeability and flow, leading to fluid leakage and retinal thickening.
As the disease progresses, eventual closure of the retinal capillaries occurs, leading to hypoxia. Infarction of the nerve fiber layer leads to the formation of cotton-wool spots (CWS) with associated stasis in axoplasmic flow.
More extensive retinal hypoxia triggers compensatory mechanisms within the eye to provide enough oxygen to tissues. Venous caliber abnormalities, such as venous beading, loops, and dilation, signify increasing hypoxia and almost always are seen bordering the areas of capillary nonperfusion. Intraretinal microvascular abnormalities (IRMA) represent either new vessel growth or remodeling of
preexisting vessels through endothelial cell proliferation within the retinal tissues to act as shunts through areas of nonperfusion.
Further increases in retinal ischemia trigger the production of vasoproliferative factors that stimulate new vessel formation. The extracellular matrix is broken down first by proteases, and new vessels arising mainly from the retinal venules penetrate the internal limiting membrane and form capillary networks between the inner surface of the retina and the posterior hyaloid face.
Neovascularization most commonly is observed at the borders of perfused and nonperfused retina and most commonly occur along the vascular arcades and at the optic nerve head. The new vessels break through and grow along the surface of the retina and into the scaffold of the posterior hyaloid face. By themselves, these vessels rarely cause visual compromise. However, they are fragile and highly permeable. These delicate vessels are disrupted easily by vitreous traction, which leads to hemorrhage into the vitreous cavity or the preretinal space.
These new blood vessels initially are associated with a small amount of fibroglial tissue formation. However, as the density of the neovascular frond increases, so does the degree of fibrous tissue formation. In later stages, the vessels may regress leaving only networks of avascular fibrous tissue adherent to both the retina and the posterior hyaloid face. As the vitreous contracts, it may exert tractional forces on the retina via these fibroglial connections. Traction may cause retinal edema, retinal heterotropia, and both tractional retinal detachments and retinal tear formation with subsequent detachment.
FrequencyUnited States
Approximately 16 million Americans have diabetes, with 50% of them not even aware that they have it. Of those that know, only one half receives appropriate eye care. Thus, it is not surprising that diabetic retinopathy is the leading cause of new blindness in persons aged 25-74 years in the United States, responsible for more than 8000 cases of new blindness each year. This means that diabetes is responsible for 12% of blindness; the rate is even higher among certain ethnic groups.
International
The incidence of diabetes appears to be increasing throughout the world, at least in part due to the increasing incidence of obesity and sedentary lifestyle. Dietary changes involving diets with higher fat and carbohydrate intake as well as the increasing size of portions of food and drinks over the past several decades may also be responsible.
Mortality/MorbidityThe treatment of diabetic retinopathy entails tremendous costs, but it has been estimated that this represents only one eighth of the costs of social security payments for vision loss. This cost does not compare to the cost in terms of loss of productivity and quality of life.
RaceAn increased risk of diabetic retinopathy appears to exist in patients with Native American, Hispanic, and African American heritage.
Clinical
HistoryIn the initial stages, patients are generally asymptomatic; however, in the more advanced stages of the disease, patients may experience symptoms, including blurred vision, distortion, or visual acuity loss.
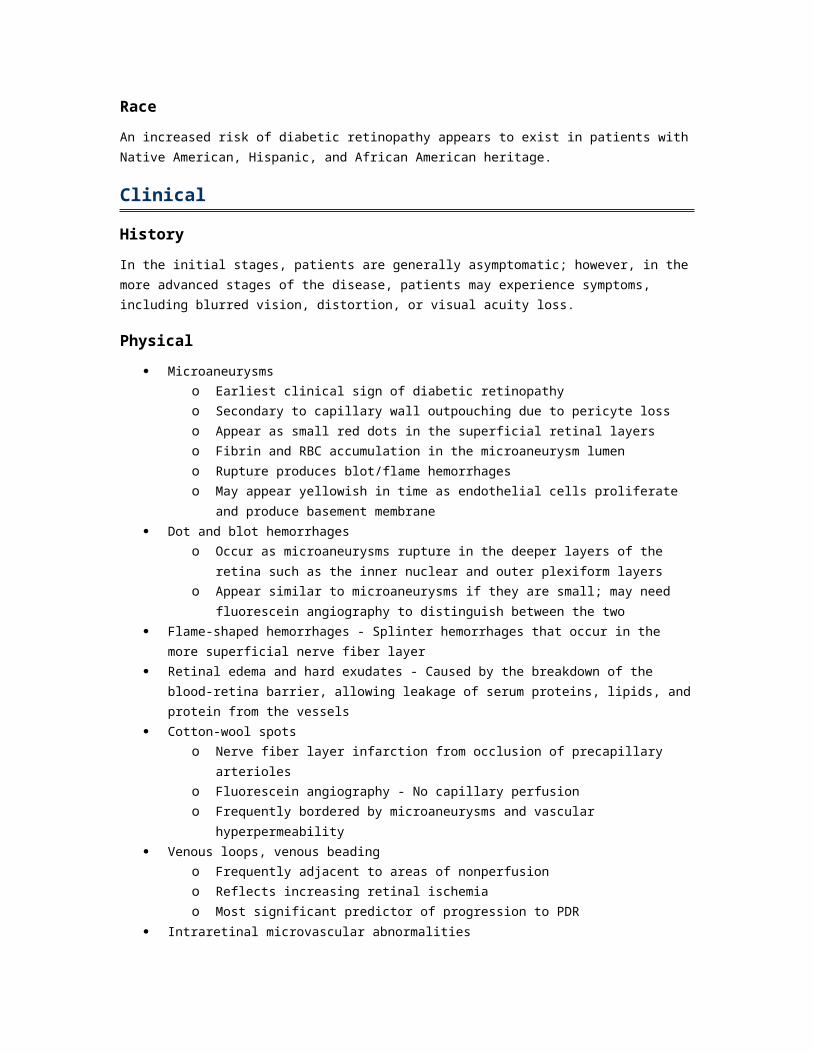
Physical Microaneurysms
o Earliest clinical sign of diabetic retinopathy o Secondary to capillary wall outpouching due to pericyte loss o Appear as small red dots in the superficial retinal layers o Fibrin and RBC accumulation in the microaneurysm lumen o Rupture produces blot/flame hemorrhages o May appear yellowish in time as endothelial cells proliferate and produce basement
membrane Dot and blot hemorrhages
o Occur as microaneurysms rupture in the deeper layers of the retina such as the inner
nuclear and outer plexiform layers o Appear similar to microaneurysms if they are small; may need fluorescein
angiography to distinguish between the two Flame-shaped hemorrhages - Splinter hemorrhages that occur in the more superficial nerve
fiber layer Retinal edema and hard exudates - Caused by the breakdown of the blood-retina barrier,
allowing leakage of serum proteins, lipids, and protein from the vessels Cotton-wool spots
o Nerve fiber layer infarction from occlusion of precapillary arterioles o Fluorescein angiography - No capillary perfusion o Frequently bordered by microaneurysms and vascular hyperpermeability
Venous loops, venous beading o Frequently adjacent to areas of nonperfusion o Reflects increasing retinal ischemia o Most significant predictor of progression to PDR
Intraretinal microvascular abnormalities o Remodeled capillary beds without proliferative changes o Collateral vessels that do not leak on fluorescein angiography o Usually can be found on the borders of the nonperfused retina
Macular edema
o This condition is the leading cause of visual impairment in patients with diabetes. A
reported 75,000 new cases of macular edema are diagnosed annually. o Possibly due to functional damage and necrosis of retinal capillaries o Clinically significant macular edema (CSME) is defined as any of the following:
Retinal thickening located 500 µm or less from the center of the foveal avascular zone (FAZ)
Hard exudates with retinal thickening 500 µm or less from the center of the FAZ
Retinal thickening 1 disc area or larger in size located within 1 disc diameter of the FAZ
Mild nonproliferative diabetic retinopathy - Presence of at least 1 microaneurysm Moderate nonproliferative diabetic retinopathy
o Presence of hemorrhages, microaneurysms, and hard exudates o Soft exudates, venous beading, and IRMA less than that of severe NPDR
Severe nonproliferative diabetic retinopathy (4-2-1) o Hemorrhages and microaneurysms in 4 quadrants o Venous beading in at least 2 quadrants o IRMA in at least 1 quadrant
Mild NPDR reflects structural changes in the retina caused by the physiological and anatomical effects of diabetes. On the other hand, the more advanced stages of NPDR reflect the increasing retinal ischemia setting up the stage for proliferative changes.
CausesRisk factors
Duration of the diabetes o In patients with type I diabetes, no clinically significant retinopathy can be seen in the
first 5 years after the initial diagnosis of diabetes is made. After 10-15 years, 25-50% of patients show some signs of retinopathy. This prevalence increases to 75-95% after 15 years and approaches 100% after 30 years of diabetes.
o In patients with type II diabetes, the incidence of diabetic retinopathy increases with
the duration of the disease. Of patients with type II diabetes, 23% have NPDR after 11-13 years, 41% have NPDR after 14-16 years, and 60% have NPDR after 16 years.
Glucose control o The Diabetic Complications Control Trial (DCCT) has demonstrated that intensive
glucose control reduced the incidence and the progression of diabetic retinopathy in patients with insulin-dependent diabetes mellitus (IDDM).
o Although no similar trials for patients with non–insulin–dependent diabetes mellitus
(NIDDM) have been completed, the American Diabetes Association (ADA) has suggested that glycosylated hemoglobin levels of less than 7% (reflecting long-term
glucose levels) should be the goal in all patients to prevent or slow down the onset of diabetes-related complications.
Renal disease, as evidenced by proteinuria and elevated BUN/creatinine levels, is an excellent predictor of the presence of retinopathy. This probably is due to the fact that both conditions are caused by DM-related microangiopathies such that the presence and severity of one reflects that of the other. Evidence suggests that aggressive treatment of the nephropathy may have a beneficial effect on the progression of diabetic retinopathy and neovascular glaucoma.
Systemic hypertension, in the setting of diabetic nephropathy, correlates well with the presence of retinopathy. Independently, hypertension also may complicate diabetes in that it may result in hypertensive retinal vascular changes superimposed on the preexisting diabetic retinopathy, further compromising retinal blood flow.
Proper management of hyperlipidemia (elevated serum lipids) may result in less retinal vessel leakage and hard exudate formation. The reason behind this is unclear.
Pregnant women without any diabetic retinopathy run a 10% risk of developing NPDR during their pregnancy. Of those with preexisting NPDR, 4% progress to the proliferative type.
http://emedicine.medscape.com/article/1225122-overview
HypertensionKean Theng Oh, MD, Consulting Staff, Associated Retinal Consultants, PCBradley M Hughes, MD, Assistant Professor, Department of Ophthalmology, Retina and Vitreous Service, University of Arkansas for Medical Sciences; Nader Moinfar, MD, Consulting Staff, Vitreoretinal Department, Magruder Eye InstituteContributor Information and Disclosures
Updated: Nov 17, 2008
Print This Email This
Overview Differential Diagnoses & Workup Treatment & Medication Follow-up
References Keywords
Introduction
BackgroundHypertension is a leading cause of morbidity and mortality worldwide. This vascular condition involves every organ system.
Ocular involvement was first described in 1859 by Liebreich in the setting of malignant hypertension. Hayreh, over the course of the 1970s and 1980s, elucidated pathophysiologic mechanisms and described clinical findings through direct patient management observations and animal models. Fundamentally, ocular effects of hypertension are based on its effects on the ocular vasculature and consequences therefrom.
Ocular blood vessels have different characteristics based on their anatomical location that, subsequently, dictate their response to elevated blood pressure. Retinal arterioles and capillaries are similar in anatomy to cerebral vessels in that they exhibit autoregulatory mechanisms and tight junctions to maintain the blood ocular barrier. Choroidal arterioles and capillaries have fenestrations (ie, no blood ocular barrier) and do not exhibit autoregulation. Optic nerve head vessels exhibit intermediary characteristics with autoregulation but an incompetent blood-ocular barrier as a result of the peripapillary choroidal vessels.
Ocular changes can be the initial finding in an asymptomatic patient necessitating a primary care referral. Both acute and chronic changes may manifest in the eyes. On the other side, a symptomatic patient may be referred to the ophthalmologist for visual changes due to hypertensive changes. The mechanisms and physical findings of hypertensive changes in the eye are discussed in this article.
PathophysiologyThe pathophysiology of hypertensive ocular changes can be subdivided into acute changes from malignant hypertension and chronic changes from long-term systemic hypertension. Because of the vascular differences between the retina, choroid, and optic nerve, each of these anatomical regions respond differently, but together represent the clinical picture of the ocular response to systemic hypertension.
Malignant arterial hypertension
Hypertensive retinal changes (hypertensive retinopathy) o Changes in the retinal circulation in the acute phase of hypertension primarily involve
the terminal arterioles rather than the main retinal arterioles. Main retinal arteriole changes are seen and recognized as a response to chronic systemic hypertension.
o Focal intraretinal periarteriolar transudates (FIPTs)
First described by Hayreh Only observed in malignant arterial hypertension One of the earliest lesions seen in the retina as a consequence of malignant
hypertension Focal, oval, small white lesions deep in the retina, associated with major
arteriole vessels Not associated with capillary obliteration; hyperfluoresce and leak on
fluorescein angiography May be related to dilation of terminal arterioles and breakdown of
autoregulatory mechanisms due to acute, malignant increase in blood
pressure. This results in breakdown of the blood retinal barrier allowing transudation and accumulation of macromolecules.
Specifically, FIPTs are not cotton-wool spots.o Inner retinal ischemic spots (cotton-wool spots)
Hayreh used the term inner retinal ischemic as a more descriptive term than cotton-wool spots.
Fluffy white lesion at the level of the nerve fiber layer found more commonly in the posterior pole, related to the distribution of the radial peripapillary capillaries.
Fluorescein angiography appearance is hypofluorescence due to nonperfusion and capillary dropout.
Last approximately 3-6 weeks before fading awayo Other acute retinal changes
Capillary obliteration results in development of microaneurysms, shunt vessels, and collaterals.
Retinal hemorrhages: Hayreh noted that the development of blot retinal hemorrhages are neither an early nor a conspicuous finding associated with malignant hypertension.
Macular edema can develop as a consequence of hypertensive choroidopathy.
Hypertensive choroidopathy o Related to the anatomical and functional differences found in the choroidal
vasculature as compared to the retinal vasculature Sympathetic innervation makes terminal arterioles more susceptible to
vasoconstriction. Fenestrations in the capillaries and the consequent lack of a blood ocular
barrier allow free passage of macromolecules. No autoregulation increases susceptibility to elevated perfusion pressures.
o Retinal pigment epithelial changes
Acute ischemic changes in the choriocapillaris and overlying retinal pigment epithelium results in acute focal retinal pigment epithelium lesions.
Focal white spots at the level of retinal pigment epithelium similar to FIPTso Serous retinal detachments
Preferentially affects the macular region causing neurosensory retinal detachments (NSRD) and cystoid macular edema
Ischemic damage to the retinal pigment epithelium leads to breakdown of the blood retinal barrier.
Hayreh observed that the presence of a NSRD was correlated to the degree of choroidal circulation disruption.
Hypertensive optic neuropathy o Anatomical differences in optic nerve head blood supply
Optic disc vessels possess autoregulation.
Lacks a competent blood retinal barrier due to peripapillary choroidal perfusion
o Optic disc edema is a primary manifestation of hypertensive optic neuropathy.
Ischemic cause for optic disc edema Blood supply to the optic nerve is via posterior ciliary arteries and
peripapillary choroidal vessels. Vasoconstriction and choroidal ischemia in the setting of malignant hypertension result in optic disc edema and axoplasmic flow stasis.
Chronic hypertensive changes
Retina o Arteriolosclerosis: Localized or generalized narrowing of vessels
Copper wiring and silver wiring of arterioles Arteriovenous-nicking
o Retinal hemorrhages o Nerve fiber layer losses o Increased vascular tortuosity o Remodeling changes due to capillary nonperfusion, such as shunt vessels and
microaneurysms Choroid
o Retinal pigment epithelial changes
Diffuse pigmentary granularity and moth-eaten appearance Elschnig spots: Areas of retinal pigment epithelium clumping and atrophy
that form from the focal acute white retinal pigment epithelium lesions Triangular patches of atrophy as a result of occlusion of a larger caliber
choroidal vessel Optic nerve: Optic disc pallor
FrequencyUnited States
According to the Centers for Disease Control and Prevention and National Center for Health Statistics, 23.1% of the US population is estimated to have hypertension. According to Ryan, 58 million adults in the United States have elevated blood pressure or are taking antihypertensive medications.
International
Worldwide, hypertension has been rated the fourth largest mortality risk in the world, accounting for 6% of all deaths.
Mortality/Morbidity
Cardiac, neurologic, renal, and ophthalmic sequelae lead to morbidity and mortality. Systemic hypertension accelerates progression of diabetic retinopathy and increases the risk of arterial and venous occlusion. Of affected individuals, 30% will have early cardiovascular damage, and acceleration in atherosclerosis will contribute to increased morbidity and mortality.
RaceHypertension is more common in the African American population. Approximately 30% of the African American population is estimated to have hypertension as opposed to 20% of Caucasians. However, no racial predilection for hypertensive retinopathy has been noted.
SexAccording to the Centers for Disease Control and Prevention and National Center for Health Statistics, 25.3% of men and 20.8% of women have hypertension.
AgeAccording to the Centers for Disease Control and Prevention and National Center for Health Statistics, 64.2% of men older than 75 years and 77.3% of women older than 75 years had hypertension.
Clinical
HistoryMost patients are asymptomatic. However, symptomatic patients most commonly present with headaches and blurred vision.
Physical Arteriosclerosis
o Arteriosclerotic changes are chronic changes as a result of systemic hypertension. o According to Duane's Ophthalmology, arteriosclerosis is defined as hardening and
thickening of arteries. It is composed of atherosclerosis (changes in the intima), medial sclerosis, and arteriolosclerosis (changes in the intima with or without media). In the retina, atherosclerosis and arteriolosclerosis predominate. The former is characterized by an atheroma, which evolves from the accumulation of fat-laden cells between the intimal elastic lamella and the endothelium of the vessel wall. The latter is characterized by intimal hyalinization, medial hypertrophy, and endothelial hyperplasia.
Light reflex change o According to Spencer, the normal light reflex of the retinal vasculature is formed by
the reflection from the interface between the blood column and vessel wall.1 Initially, the increased thickness of the vessel walls causes the reflex to be more diffuse and less bright. Progression of sclerosis and hyalinization causes the reflex to be more
diffuse and the retinal arterioles to become red-brown. This is known as copper wiring.
o Advanced sclerosis leads to increased optical density of the vessel wall, visible on
ophthalmoscopy as a phenomenon known as sheathing of the vessels. When the anterior surface becomes involved, the entire vessel appears opaque (pipe stem sheathing). The patency of such vessels has been demonstrated by fluorescein angiography. When sheathing encircles the wall, it produces a silver-wire vessel.
Attenuation o Generalized attenuation of the arterioles occurs as a result of diffuse vasospasm,
which occurs when a significant elevation of blood pressure has persisted for an appreciable period. A relationship has been noted between the narrowing of the caliber of the arteriole and the height of the diastolic pressure. Increased intraluminal pressure either in the retinal arterioles or in the central artery of the retina causes narrowing of the arterioles.
o Focal narrowing occurs from spasm of local areas of the vascular musculature.
Spencer speculates that either edema in and around the vessel wall, or vascular spasm leads to focal narrowing, which can become permanent with fibrosis.
o These are chronic changes due to systemic hypertension.
AV nicking (the Gunn sign): Impeded circulation results in a dilated or swollen vein peripheral to the crossing, causing hourglass constrictions on both sides of the crossing and aneurysmal-like swellings. Histologically, Spencer notes findings of various authors, to include the following:1
o Ikui noted that arteriole and venous basement membranes are adherent with shared
collagen fibers at the crossing points. Thickening of the basement membrane and the media of the arteriole in hypertension impinge on the vein and cause the crossing phenomenon.
o Mimatsu asserts that the crossing changes were due to sclerotic thickening of the
wall of the venule and not by compression by the arteriole. o Seitz attributed the crossing phenomenon to vascular sclerosis and perivascular glial
cell proliferation and not to venous compression. Arterial narrowing and straightening: Sclerosis may shorten or elongate retinal arterioles with
the branches coming off at right angles. This change in length deflects the veins at the common sheath and changes the course of the vein (Salus sign). According to Albert and Jakobiec, the original crossing angle, the degree of vascular thickening, and the pressure differential influence this phenomenon.2
Extravascular retinal lesions o Microaneurysms: Postulated to occur at localized areas of capillary wall weakness,
microaneurysms are most visible by angiography. Stasis engorgement of the capillaries may lead to anoxia and poor nutrition, which contributes to microaneurysm formation.
o Retinal hemorrhages: In addition to microaneurysms, loss of endothelial integrity
leads to extravasation of plasma, which leads to retinal hemorrhages. Streak
hemorrhages located in the nerve fiber layer predominate over the blot hemorrhages located deeper in the outer plexiform layer.
o Retinal and macular edema o Retinal lipid deposits: Absorption of the plasma component of retinal edema leads to
protein accumulation. Histologically, there is accumulation of edema residue and lipid-containing macrophages. Although the deposits assume many shapes and appear in many parts of the retina, the macular star is the most predominant appearance, and this appearance is due to the radially oriented nerve fiber layer of Henle.
Inner retinal ischemic spots (cotton-wool spots): See Pathophysiology. Focal intraretinal periarteriolar transudate (FIPT): See Pathophysiology.
CausesIn general, the degree and the duration of hypertension are the primary determinants of hypertensive retinopathy. However, the changes described above are not unique for hypertension. These changes may be seen in other diseases with vascular risk factors, such as diabetes. The retinopathy may also be more severe and more progressive when diabetes and hypertension are associated. Other factors, such as hyperlipidemia, may make the retinopathy worse as well
http://emedicine.medscape.com/article/1201779-overview
Diabetes Mellitus, Type 1Aneela Naureen Hussain, MD, FAAFM, Assistant Professor, Department of Family Medicine, State University of New York Downstate Medical Center; Consulting Staff, Department of Family Medicine, University Hospital of BrooklynMiriam T Vincent, MD, PhD, Professor and Chair, Department of Family Practice, State University of New York Downstate Medical CenterContributor Information and Disclosures
Updated: Nov 2, 2007
Print This Email This
Overview Differential Diagnoses & Workup Treatment & Medication Follow-up
References Keywords
Introduction
Background

Diabetes mellitus (DM) is a multisystem disease with both biochemical and anatomical consequences. It is a chronic disease of carbohydrate, fat, and protein metabolism caused by the lack of insulin. In type 1 diabetes, insulin is functionally absent because of the destruction of the beta cells of the pancreas. Type 1 DM occurs most commonly in juveniles but can occur in adults, especially in those in their late 30s and early 40s. Unlike people with type 2 DM, those with type 1 DM generally are not obese and may present initially with diabetic ketoacidosis (DKA).
PathophysiologyType 1 DM is a catabolic disorder in which circulating insulin is very low or absent, plasma glucagon is elevated, and the pancreatic beta cells fail to respond to all insulin-secretory stimuli. Patients need exogenous insulin to reverse this catabolic condition, prevent ketosis, decrease hyperglucagonemia, and normalize lipid and protein metabolism.
Type 1 DM is an autoimmune disease. The pancreas shows lymphocytic infiltration and destruction of insulin-secreting cells of the islets of Langerhans, causing insulin deficiency. Approximately 85% of patients have circulating islet cell antibodies, and the majority also have detectable anti-insulin antibodies before receiving insulin therapy. Most islet cell antibodies are directed against glutamic acid decarboxylase (GAD) within pancreatic B cells.
One theory regarding the etiology of type 1 DM is that it results from damage to pancreatic beta cells from an infectious or environmental agent. It triggers the immune system in a genetically susceptible individual to develop an autoimmune response against altered pancreatic beta cell antigens or molecules in beta cells that resemble a viral protein. Currently, autoimmunity is considered the major factor in the pathophysiology of type 1 DM. Prevalence is increased in patients with other autoimmune diseases, such as Graves disease, Hashimoto thyroiditis, and Addison disease. Approximately 95% of patients with type 1 DM have either human leukocyte antigen (HLA)-DR3 or HLA-DR4. HLA-DQs are considered specific markers of type 1 DM susceptibility.
Environmental agents that have been hypothesized to induce an attack on beta cell function include viruses (eg, mumps, rubella, Coxsackie B4), toxic chemicals, exposure to cow's milk in infancy, and cytotoxins.
Recent evidence suggests a role for vitamin D in the pathogenesis and prevention of diabetes mellitus.
FrequencyUnited States
Roughly 5-15% of all cases of diabetes are type 1 DM. It is the most common metabolic disease of childhood, with a yearly incidence of 15 cases per 100,000 people younger than 18 years. Approximately 1 million Americans have type 1 DM, and physicians diagnose 10,000 new cases every year.
According to the American Diabetes Association, there are 20.8 million children and adults in the United States, or 7% of the population, who have diabetes. While an estimated 14.6 million have been diagnosed, unfortunately, 6.2 million people (or nearly one-third) are undiagnosed. Fifty-four million people are prediabetes status. In people younger than 20 years, 176,500 cases, or 0.22% of all people in this age group, have diabetes. About one in every 400-600 children and adolescents has type 1 DM. Two million adolescents (or 1 in 6 overweight adolescents) aged 12-19 years have prediabetes status. In people aged 20 years or older, 1.5 million new cases of diabetes were diagnosed in 2005.
International
Scandinavia has the highest prevalence rates for type 1 DM (ie, approximately 20% of the total number of people with DM), while China and Japan have the lowest prevalence rates, with less than 1% of all people with diabetes. Some of these differences may relate to definitional issues and the completeness of reporting.
Mortality/MorbidityType 1 DM is associated with a high morbidity and premature mortality due to complications. The annual financial cost from diabetes overall exceeds $100 billion, almost $1 of every $7 dollars of US health expenditures in terms of medical care and loss of productivity. Advances in treatment that permit tight glycemic control and control of comorbidities (hyperlipidemia) can greatly reduce the incidence of microvascular and macrovascular complications.
As a result of these complications, people with diabetes have an increased risk of developing ischemic heart disease, cerebral vascular disease, peripheral vascular disease with gangrene of lower limbs, chronic renal disease, reduced visual acuity and blindness, and autonomic and peripheral neuropathy.
RaceType 1 DM is more common among non-Hispanic whites, followed by African Americans and Hispanic Americans. It is comparatively uncommon among Asians.
SexType 1 DM is more common in men than in women.
AgeType 1 DM usually starts in children aged 4 years or older, with the peak incidence of onset at age 11-13 years, coinciding with early adolescence and puberty. Also, a relatively high incidence exists in people in their late 30s and early 40s, when it tends to present in a less aggressive manner, ie, early hyperglycemia without ketoacidosis and gradual onset of ketosis.
Clinical
History
The most common symptoms of type 1 diabetes mellitus (DM) are polyuria, polydipsia, and polyphagia, along with lassitude, nausea, and blurred vision, all of which are due to the hyperglycemia itself. The disease onset may be sudden, with the presentation of an infection. It is not unusual for type 1 DM to present with ketoacidosis; it may occur de novo or develop with the stress of illness or surgery. An explosive onset of symptoms in a young lean patient with ketoacidosis always has been considered diagnostic of type 1 DM.
Polyuria and thirst: Polyuria is due to osmotic diuresis secondary to hyperglycemia. Thirst is due to the hyperosmolar state and dehydration.
Polyphagia with weight loss: The weight loss with a normal or increased appetite is due to depletion of water and a catabolic state with reduced glycogen, proteins, and triglycerides.
Fatigue and weakness: This may be due to muscle wasting from the catabolic state of insulin deficiency, hypovolemia, and hypokalemia.
Muscle cramps: This is due to electrolyte imbalance. Nocturnal enuresis: Severe enuresis secondary to polyuria can be an indication of onset of
diabetes in young children. Blurred vision: This also is due to the effect of the hyperosmolar state on the lens and vitreous
humor. Glucose and its metabolites cause dilation of the lens, altering its normal focal length. Gastrointestinal symptoms: Nausea, abdominal discomfort or pain, and change in bowel
movements may accompany acute DKA. Acute fatty liver may lead to distention of the hepatic capsule, causing right upper quadrant pain. Persistent abdominal pain may indicate another serious abdominal cause of DKA, eg, pancreatitis. Chronic gastrointestinal symptoms in the later stage of diabetes are due to visceral autonomic neuropathy.
Patients may maintain their normal weight or exhibit wasting, depending on the interval between the onset of the disease and initiation of treatment.
Peripheral neuropathy: This presents as numbness and tingling in both hands and feet, in a glove and stocking pattern. It is bilateral, symmetric, and ascending neuropathy, which results from many factors, including the accumulation of sorbitol in peripheral sensory nerves due to sustained hyperglycemia.
Symptoms at the time of the first clinical presentation can usually be traced back several days to several weeks; however, beta cell destruction may have started months, or even years, before the onset of clinical symptoms.
PhysicalIn new cases of diabetes, physical examination findings are usually normal, except in DKA, wherein signs of Kussmaul respiration, dehydration, hypotension, and, in some cases, altered mental status are present.
In established cases, patients should be examined every 3 months for macrovascular and microvascular complications. They should have funduscopic examination for retinopathy and monofilament testing for peripheral neuropathy.
Causes
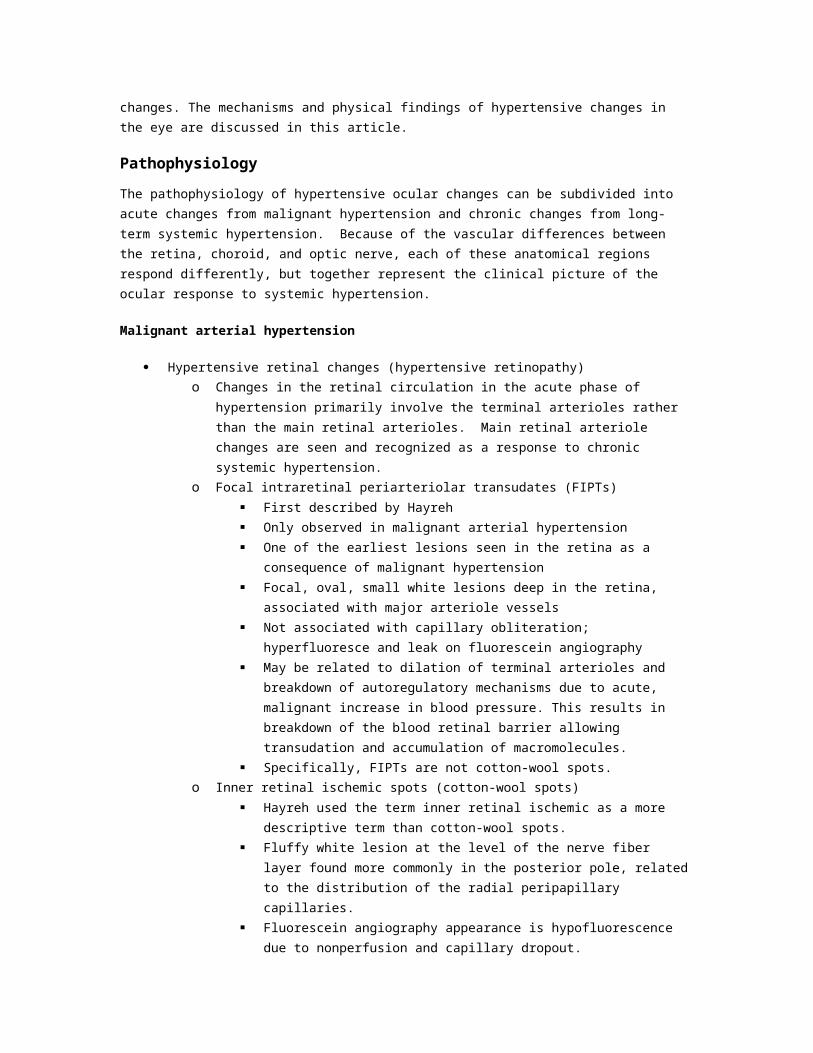
The etiology of type 1 DM has a strong genetic component. Nevertheless, identical twins have a concordance rate for type 1 DM of less than 50%. Extragenetic factors also may contribute
http://emedicine.medscape.com/article/117739-overview
Growth Hormone DeficiencyMohsen S Eledrisi, MD, FACP, FACE, Consultant, Department of Internal Medicine, Division of Endocrinology and Metabolism, King Abdulaziz National Guard Medical Center, Saudi ArabiaContributor Information and Disclosures
Updated: Jun 2, 2008
Introduction
BackgroundThe somatotroph cells of the anterior pituitary gland produce growth hormone. The hormone's secretion is stimulated by growth hormone – releasing hormone (GHRH) and is inhibited by somatostatin, both of which are produced by the hypothalamus.
The clinical manifestations of growth hormone deficiency (GHD) are variable, depending on the age of onset.1 Children usually present with short stature, while adults have reduced physical performance and impaired psychological well-being.
The goals of growth hormone therapy differ in children and adults. In children, therapy promotes linear growth and restores body composition; in adults, the goals are to improve conditioning and strength, to restore normal body composition, and to improve the quality of life.2, 3
Related eMedicine topics:Growth Failure Growth Hormone Deficiency [Pediatrics: General Medicine]Growth Hormone Replacement in Older Men Short Stature
PathophysiologyGrowth hormone promotes linear growth by regulating the endocrine and paracrine production of insulinlike growth factor 1 (IGF-1), which is produced by the liver and other target tissues, including the epiphyseal growth plate. Growth hormone's diverse metabolic actions also include anabolic, lipolytic, and diabetogenic effects.4, 5
GHD results in alterations in the physiology of different systems of the body, manifesting in increased subcutaneous visceral fat and decreased muscle mass, bone density, and exercise performance.4, 5
Frequency
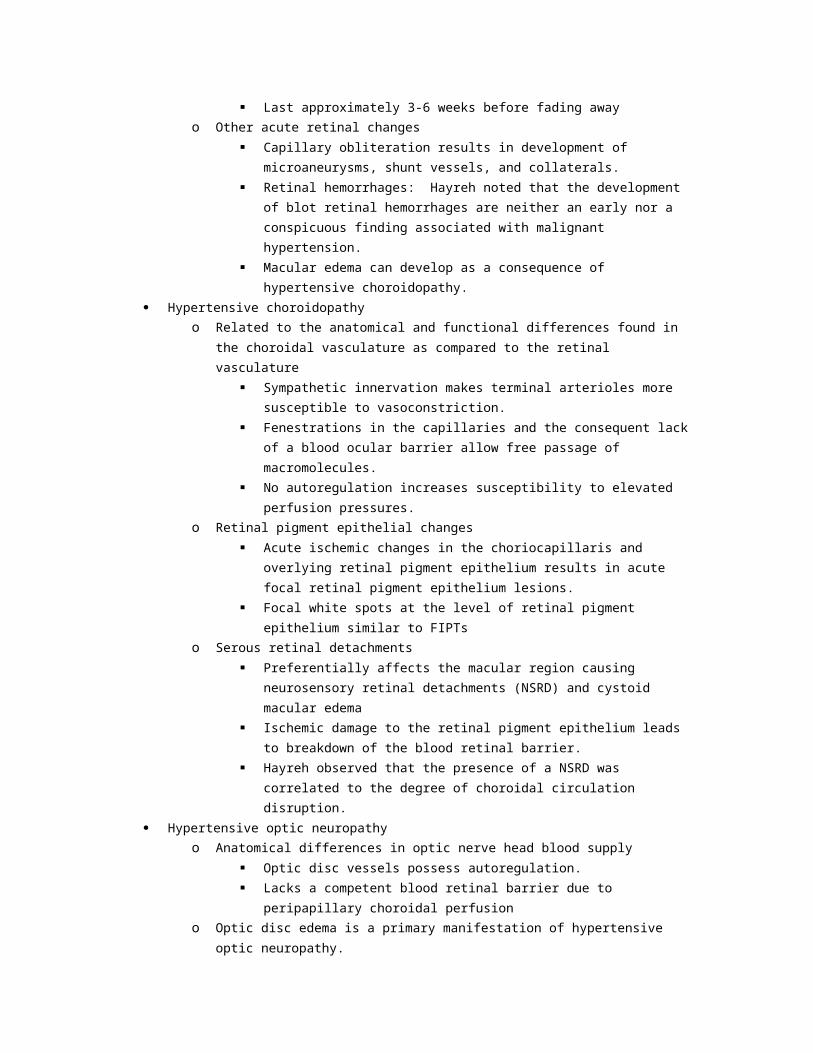
United States
The incidence of short stature associated with severe childhood GHD has been estimated in several studies to range between 1 per 4,000 to 1 per 10,000 live children. About 20,000 children per year receive growth hormone therapy, and approximately 4,000 new children are diagnosed annually as candidates for this treatment.
The exact prevalence of adult-onset GHD is not known. Approximately 35,000 adults have GHD, and about 6,000 new adult patients are diagnosed annually.
International
No data are available.
Mortality/Morbidity Adult GHD is associated with the following problems2, 3:
o Reduced bone mineral density and increased risk of osteoporotic bone fractures o Impaired cardiac function o Central obesity o Increased insulin sensitivity o Reduced exercise capacity o Emotional disturbances o Decreased quality of life
Epidemiologic data suggest that adults with GHD have reduced life expectancy. This increased mortality is probably attributable to premature cardiovascular disease.6, 7
Age In children, the age of presentation varies with respect to the time of onset and the degree of
GHD. Children with complete absence of growth hormone secretion usually present before reaching the age of 3 years, whereas those with lesser degrees of deficiency present at older ages.
In adults, the age of presentation often coincides with the discovery of pituitary tumors, usually between the fourth and fifth decades of life.
Related eMedicine topic: Pituitary Tumors
Clinical
History Children
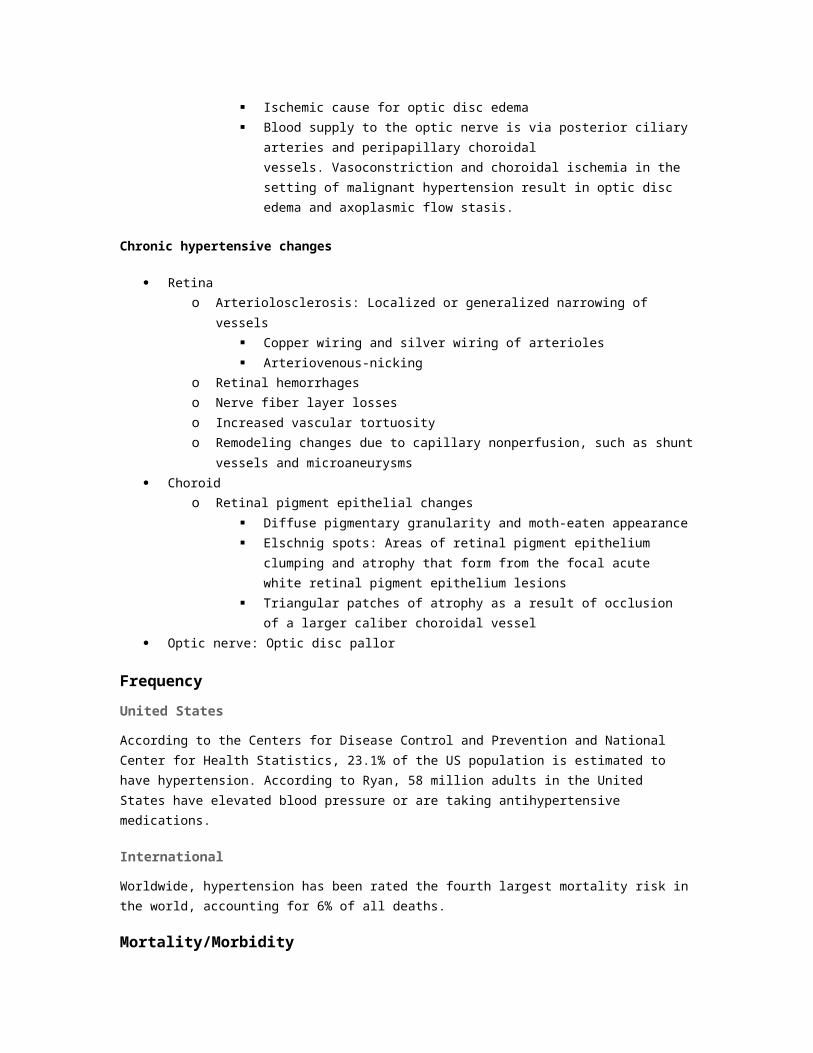
o Growth failure after a period of normal growth is a characteristic feature of GHD that
presents during childhood. Children present with short stature and low growth velocity for age and pubertal stage.8
o Consider the possibility of hypopituitarism in patients with neonatal hypoglycemia,
prolonged jaundice, septo-optic dysplasia, midline facial defects (eg, cleft palate, solitary central incisor), male micropenis (not necessarily related to gonadotropin deficiency), histiocytosis X, previous cranial irradiation, and symptoms of a mass lesion in the hypothalamic-pituitary region (eg, headaches, visual disturbances).
Adults9 o Adults with GHD usually have a history of pituitary tumors that may have been
treated with surgery or radiation, or they may have previously suffered a head trauma.
o Some patients will also have manifestations of deficiency of other pituitary hormones,
such as thyroid, adrenal, and gonadal hormones o The symptoms of GHD in adults are often nonspecific. Reported symptoms may
include low energy level, decreased strength and exercise tolerance, increased weight or difficulty losing weight, emotional lability, anxiety, social isolation, decreased libido, and impaired sleep. Some persons with GHD are entirely asymptomatic.4
Related eMedicine topics: Hypopituitarism [Emergency Medicine]Hypopituitarism [Pediatrics: General Medicine]Hypopituitarism (Panhypopituitarism)
Physical Children
o The standing height standard deviation score is usually below -2. o Growth velocity is below the 10-25th percentile, which reflects growth deceleration. o Increased subcutaneous fat is present, especially around the trunk. o The face is immature, with a prominent forehead and depressed midfacial
development. o Dentition is delayed. o The average age of pubertal onset is delayed in males and females. o In males, the phallus may be small.
Adults o Reduced lean body mass and increased weight, with body fat mass predominantly in
the abdominal region o Thin and dry skin o Cool peripheries o Poor venous access o Reduced muscle mass and strength and reduced exercise performance
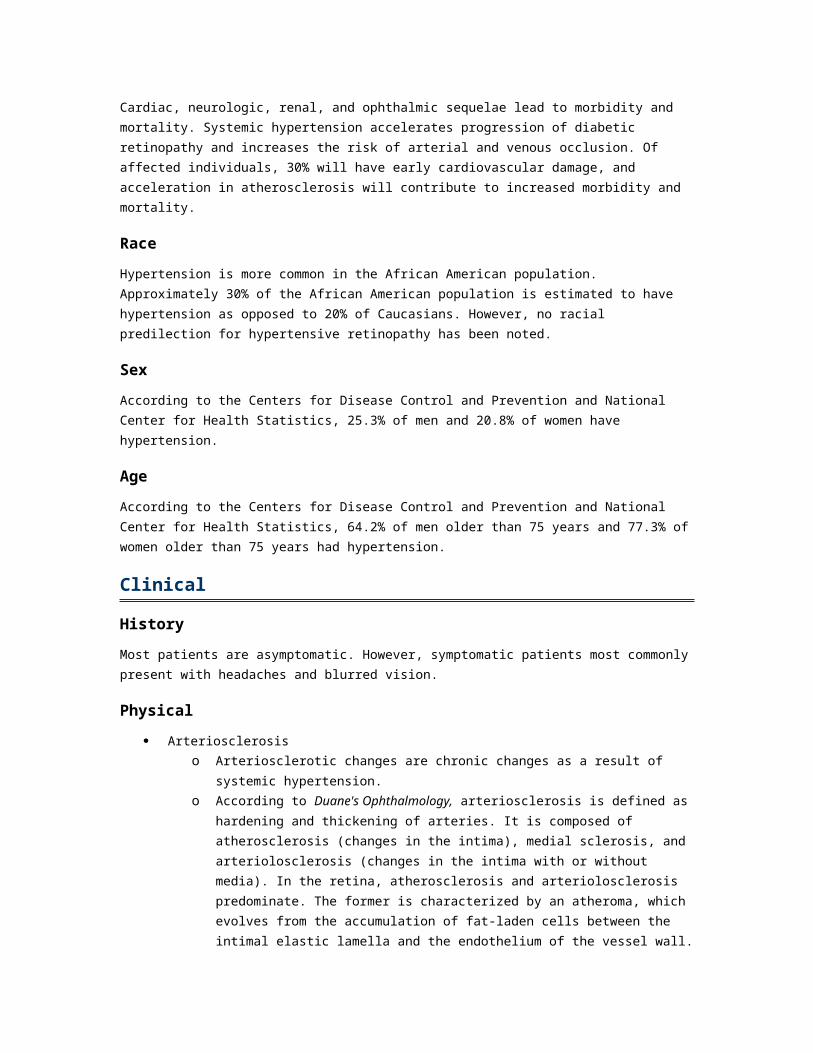
o Depressed affect o Labile emotions
Causes Causes of GHD in children can be divided into 3 categories.
o Congenital conditions
Defective pituitary development that leads to pituitary aplasia Empty sella Encephalocele Midline defects Septo-optic dysplasia Panhypopituitarism Genetic abnormalities, including autosomal-recessive, autosomal-dominant,
or X-linked defects or a mutation or deletion in the growth hormone gene or in the GHRH.
o Acquired conditions
Tumors of the hypothalamic-pituitary region - Craniopharyngioma is the most common tumor.
Cranial irradiation Infiltrative diseases, including sarcoidosis, tuberculosis, histiocytosis X,
hemochromatosis, and lymphocytic hypophysitis Trauma Hypoxic insult
o Idiopathic - In many cases, no clear etiology can be identified.
Causes of GHD in adults o Pituitary disease - More than 90% of patients have pituitary disease, which is usually
caused by a pituitary tumor, by surgery, or by radiation therapy for the tumor. o Other causes - These include trauma, tuberculosis, histiocytosis X,
hemochromatosis, lymphocytic hypophysitis, and infiltrative diseases, such as sarcoidosis.
o Idiopathic - In rare instances, no cause can be found
http://emedicine.medscape.com/article/120767-overview
Related Documents











