Retention of urine HAMAD EMAD HAMAD DHUHAYR 10110067

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Retention of urine HAMAD EMAD HAMAD DHUHAYR
10110067

Definition
Urinary retention is defined as the inability to completely or partially empty the bladder.
It is a sudden painful inability to urinate inspite of a full bladderUrinary retention, also known as ischuria, is a lack of ability to urinate
Suffering from urinary retention means you may be unable to start urination, or if you are able to start, you can’t fully empty your bladder.
Normal micturition cycle:
A. Filling: Impulses from the CNS to sympathetic and pudendal nerves relax the bladder and close the outlet.
B. Voiding: Inhibition of sympathetic and pudendal impulses. Stimulation of parasympathetic (S2-4) leads to detrusor contraction → voiding in the absence of obstruction

Acute Urinary retention Painful inability to void, with relief of pain following drainage of the bladder by catheterization. Pathophysiology:
◦ Increased urethral resistance, i.e., bladder outlet obstruction (BOO)
◦Low bladder pressure, i.e., impaired bladder contractility◦ Interruption of sensory or motor innervations of the bladder.

Differential diagnosis of acute retention and obstructive / anuria
Acute retention obstuctive AnuriaDesire to urinate + - -Suprapubic pain + - -Renal pain - - +General exam. Good May be uremicAbdominal exam. Tender Full bladder Empty Loin bladder

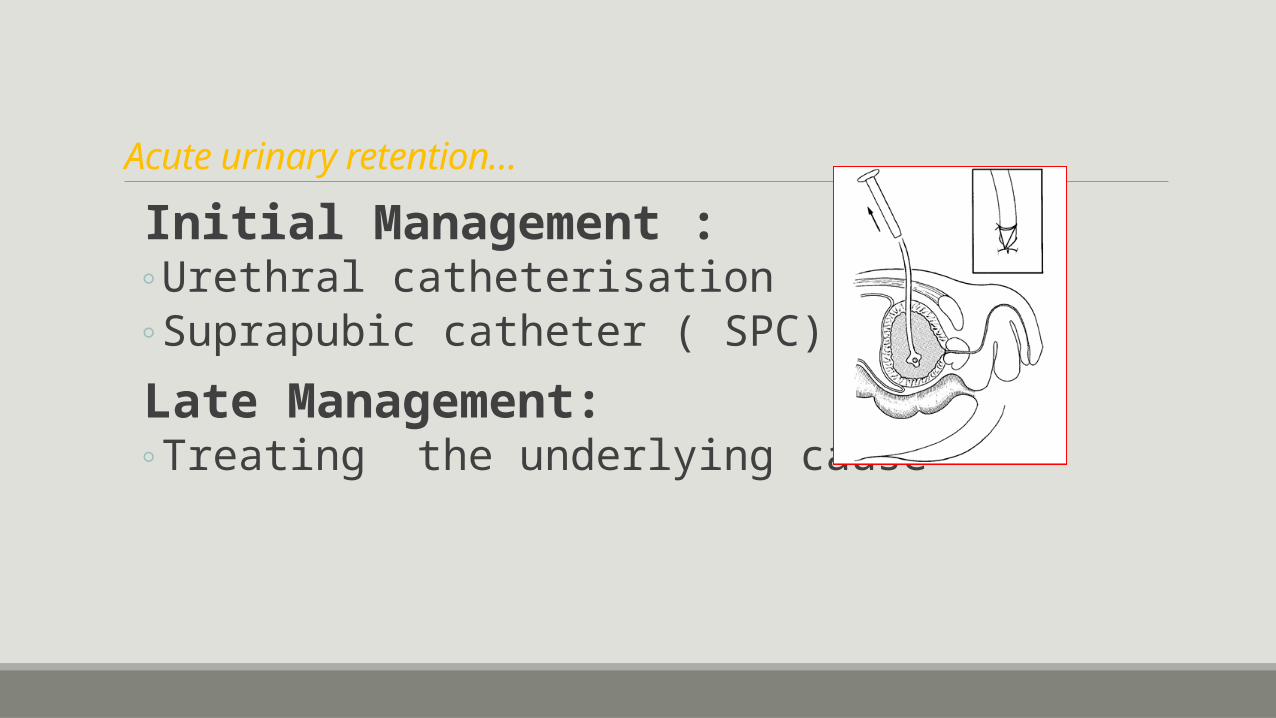
Acute urinary retention…
Causes :◦ Men:
◦ Benign prostatic enlargement (BPE) due to BPH ◦ Carcinoma of the prostate◦ Urethral stricture◦ Prostatic abscess
◦ Women ◦ Pelvic prolapse (cystocoele, rectocoele, uterine)◦ Urethral stricture;◦ Urethral diverticulum; ◦ Post surgery for ‘stress’ incontinence ◦ pelvic masses (e.g., ovarian masses)

Acute urinary retention…Causes…
Both Sex◦ Haematuria leading to clot retention◦ Drugs◦ Pain◦ Sacral nerve compression or damage(cauda equina compression )◦ Radical pelvic surgery◦ Pelvic fracture rupturing the urethra ◦ Neurotropic viruses involving the sensory dorsal root ganglia of S2–S4 (herpes simplex or
zoster);◦ Multiple sclerosis◦ Transverse myelitis ◦ Diabetic cystopathy ◦ Damage to dorsal columns of spinal cord causing loss of bladder sensation (tabes dorsalis,
pernicious anaemia).
Acute urinary retention…
Initial Management :◦Urethral catheterisation◦Suprapubic catheter ( SPC)
Late Management:◦Treating the underlying cause

Chronic urinary retention
Obstruction develops slowly, the bladder is distended (stretched) very gradually over weeks/months, so pain is not a feature . Presentation:
◦ Urinary dribbling ◦Overflow incontinence ◦Palpable lower suprapubic mass

Chronic Retention of Urine
Causes: Long standing incomplete obstruction
A) Mechanical : BPH, prostate cancer
B) Functional: Neuropathic flaccid bladder.- Large amounts of residual urine exist.- When the vesical pressure exceeds the urethral resistance, the patient can pass some urine or dribble continuously. This is called false or overflow incontinence.
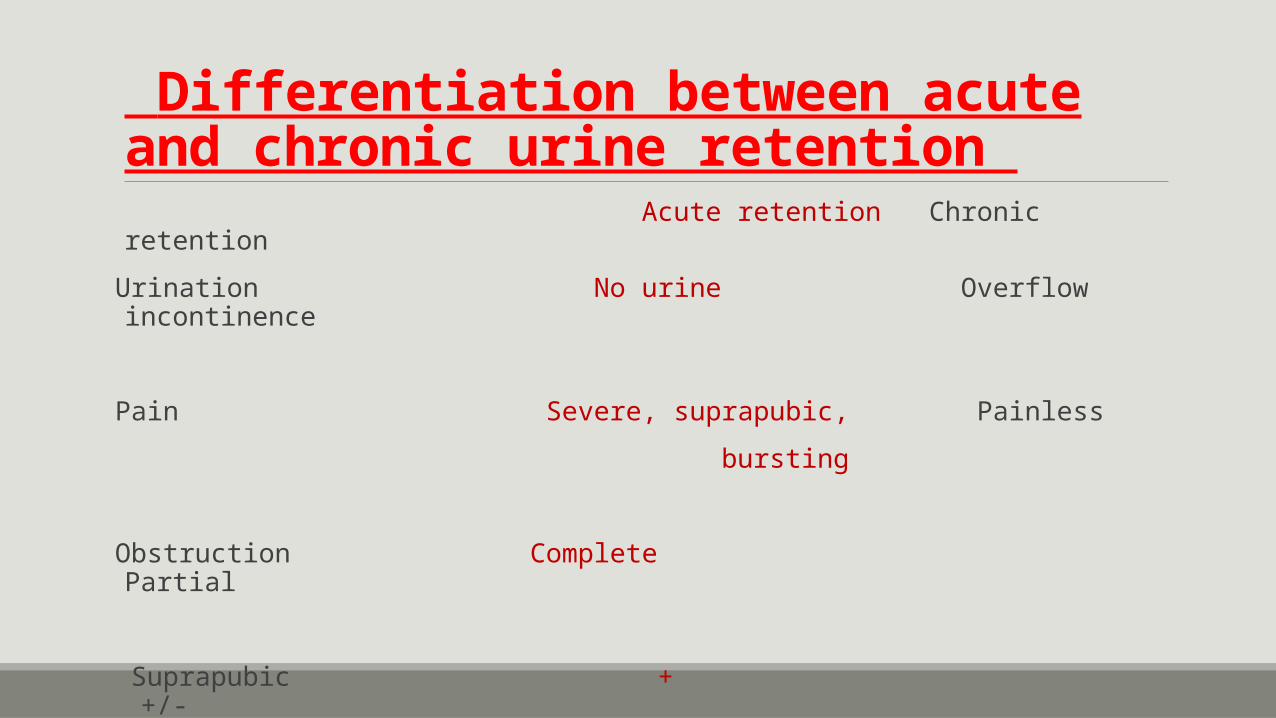
Differentiation between acute and chronic urine retention
Acute retention Chronic retention
Urination No urine Overflow incontinence
Pain Severe, suprapubic, Painless
bursting
Obstruction Complete Partial
Suprapubic + +/-
tenderness
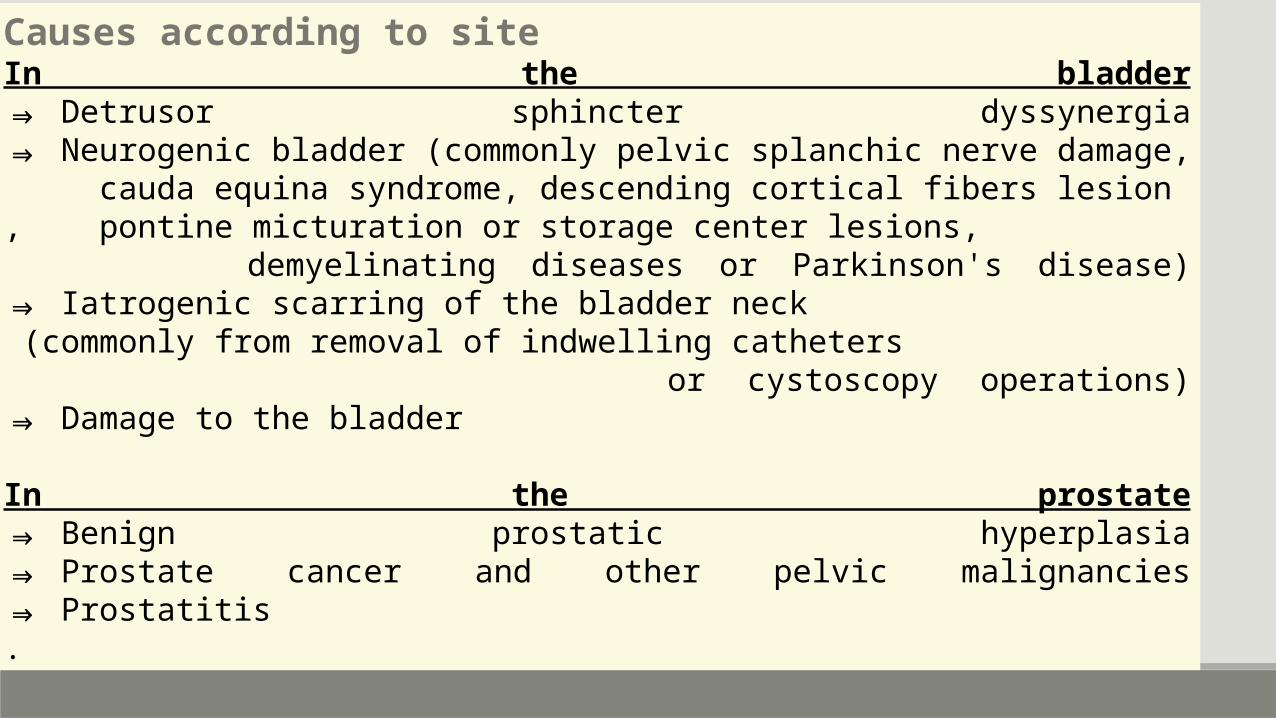
Causes according to siteIn the bladder⇒ Detrusor sphincter dyssynergia⇒ Neurogenic bladder (commonly pelvic splanchic nerve damage, cauda equina syndrome, descending cortical fibers lesion, pontine micturation or storage center lesions, demyelinating diseases or Parkinson's disease)⇒ Iatrogenic scarring of the bladder neck (commonly from removal of indwelling catheters or cystoscopy operations)⇒ Damage to the bladder
In the prostate⇒ Benign prostatic hyperplasia⇒ Prostate cancer and other pelvic malignancies⇒ Prostatitis.

Penile urethra⇒ Congenital urethral valves⇒ Phimosis or pinhole meatus⇒ Circumcision⇒ Obstruction in the urethra, for example a metastasis or a precipitated pseudogout crystal in the urine⇒ STD lesions (gonorrhoea causes numerous strictures, leading to a rosary bead appearance, whereas chlamydia usually causes a single stricture)
Other⇒ Paruresis ( shy bladder syndrome )-, urinary retention can result
⇒ Consumption of some psychoactive substances, mainly stimulants, such as amphetamine.
⇒ Use of NSAIDs or drugs with anticholinergic properties.
⇒ Stones or metastases can theoretically appear anywhere along the urinary tract, but vary in frequency depending on anatomy
History Duration Painfull? Precipitating factors Preceding LUTS Other urinary complaints Differential diagnosis Medical illnesses - D/D, co-morbidity
Catheterization ◦Easy◦Caliber◦Urine quantity / color◦Where / by whom◦ TWOC

Examination Meatus Urethra Bladder DRE Hernia Neurological ex
◦ Higer mental functions◦ Cranial nerves◦ Lower limb◦ perineum - sensations

Investigations Urine RFTS US X ray KUB Urodynamics study Cystoscopy

Treatment Urethral catheterization
◦Technique ◦ Explain / consent ( need / discomfort)◦ Keep Items ready◦ Theatre / dressing room / bed◦ Supine posture legs separated◦ Female – knee bent & separated, feet together◦ Gloves
Referrences Matary
Baily
Website
Related Documents











