Results of Surgery in Patients with Refractory Extratemporal Epilepsy with Normal or Nonlocalizing Magnetic Resonance Findings Investigated with Subdural Grids Arthur Cukiert, Jose A. Buratini, Elcio Machado, Alcione Sousa, Joaquim O. Vieira, Meire Argentoni, Cassio Forster, and Cristine Baldauf Epilepsy Surgery Program, Hospital Brigadeiro, São Paulo, Brazil Summary: Purpose: To study the efficacy of extensive cov- erage of the brain surface with subdural grids in defining ex- tratemporal cortical areas amenable for resection in patients with refractory extratemporal epilepy (R-ExTE) and normal or nonlocalizing magnetic resonance imaging (MRI) scans. Methods: Sixteen patients with R-ExTE were studied. Eleven patients had simple partial, eight had complex partial, and three had supplementary motor area seizures. Seizure fre- quency ranged from three per month to daily episodes. Interic- tal EEG showed large focal spiking areas in 11 patients, secondary bilateral synchrony in four, and was normal in one patient. Surface ictal recordings were nonlocalizing in six pa- tients, and in 10, they disclosed large ictal focal spiking areas. MRI was normal in 10 patients, and in six patients, focal non- localizing potentially epileptogenic lesions were found. All pa- tients were given an extensive coverage of the cortical convexity with subdural electrodes through large unilateral (n 4 13) or bilateral (n 4 3) craniotomies. Bipolar cortical stimu- lation was carried out through the implanted electrodes. Results: Interictal invasive recording findings showed wide- spread spiking areas in 13 patients and secondary bilateral syn- chrony in three. Ictal invasive recordings showed focal seizure onset in all patients. There were six frontal, two parietal, one temporooccipital, four rolandic, and three posterior quadrant resections. Thirteen patients had been rendered seizure free after surgery, and three had ø90% of seizure-frequency reduc- tion. Pathologic findings included gliosis (n 4 10), cortical dysplasia (n 4 5), or no abnormalities (n 4 1). Six patients had transient postoperative neurologic morbidity. Conclusions: Extensive subdural electrodes coverage seems to be an effective way to investigate patients with R-ExTE and normal or nonlocalizing MRI findings. Key Words: Epi- lepsy—Surgery—Subdural electrodes—MRI—Results. The surgical treatment of refractory extratemporal epi- lepsy (R-ExTE) has always represented a challenge. The surgical results that have been published in the pre– magnetic resonance imaging (MRI) era were poorer then those obtained in the treatment of patients with temporal lobe epilepsy (1–3). After the appearance of MRI, it has been possible to detect potentially epileptogenic lesions preoperatively, and the surgical results obtained in pa- tients with R-ExTE have improved considerably (4–6). Conversely, patients with R-ExTE and normal or nonlo- calizing MR scans still represent the most difficult pa- tients to handle, and they frequently need invasive recordings. The paradigms for invasive electrode placement vary from one center to the other, including the use of depth, subdural, epidural, and foramen ovale electrodes (7–10). Subdural grids and strips have been used to cover the cortical convexity and mesial surfaces. Subdural strips are easier to implant, usually through a burr-hole or small craniotomy, but the cortical coverage is not extensive. Subdural grids cover a larger cortical area but need large craniotomies to be inserted. We studied the efficacy of an extensive coverage of the brain surface with subdural grids in defining extratemporal cortical areas amenable for resection in patients with R-ExTE. METHODS Sixteen patients with R-ExTE were studied. All pa- tients were studied from 1997 to 2000. These patients represented all the group of patients with refractory ex- tratemporal epilepsy and nonlocalizing MRI investigated with subdural electrodes during that period. They were given prolonged video-EEG monitoring and had high- resolution MR scanning before invasive recordings. In Revision accepted May 7, 2001. Address correspondence and reprint requests to Dr. A. Cukiert at R Dr. Alceu Campos Rodrigues 247, 12 andar, 121, São Paulo SP, Brazil CEP 04544-000. E-mail: [email protected] Epilepsia, 42(7):889–894, 2001 Blackwell Science, Inc. © International League Against Epilepsy 889

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Results of Surgery in Patients with Refractory ExtratemporalEpilepsy with Normal or Nonlocalizing Magnetic Resonance
Findings Investigated with Subdural Grids
Arthur Cukiert, Jose A. Buratini, Elcio Machado, Alcione Sousa, Joaquim O. Vieira,Meire Argentoni, Cassio Forster, and Cristine Baldauf
Epilepsy Surgery Program, Hospital Brigadeiro, São Paulo, Brazil
Summary: Purpose:To study the efficacy of extensive cov-erage of the brain surface with subdural grids in defining ex-tratemporal cortical areas amenable for resection in patientswith refractory extratemporal epilepy (R-ExTE) and normal ornonlocalizing magnetic resonance imaging (MRI) scans.
Methods: Sixteen patients with R-ExTE were studied.Eleven patients had simple partial, eight had complex partial,and three had supplementary motor area seizures. Seizure fre-quency ranged from three per month to daily episodes. Interic-tal EEG showed large focal spiking areas in 11 patients,secondary bilateral synchrony in four, and was normal in onepatient. Surface ictal recordings were nonlocalizing in six pa-tients, and in 10, they disclosed large ictal focal spiking areas.MRI was normal in 10 patients, and in six patients, focal non-localizing potentially epileptogenic lesions were found. All pa-tients were given an extensive coverage of the corticalconvexity with subdural electrodes through large unilateral (n
4 13) or bilateral (n4 3) craniotomies. Bipolar cortical stimu-lation was carried out through the implanted electrodes.
Results:Interictal invasive recording findings showed wide-spread spiking areas in 13 patients and secondary bilateral syn-chrony in three. Ictal invasive recordings showed focal seizureonset in all patients. There were six frontal, two parietal, onetemporooccipital, four rolandic, and three posterior quadrantresections. Thirteen patients had been rendered seizure freeafter surgery, and three hadù90% of seizure-frequency reduc-tion. Pathologic findings included gliosis (n4 10), corticaldysplasia (n4 5), or no abnormalities (n4 1). Six patientshad transient postoperative neurologic morbidity.
Conclusions:Extensive subdural electrodes coverage seemsto be an effective way to investigate patients with R-ExTE andnormal or nonlocalizing MRI findings.Key Words: Epi-lepsy—Surgery—Subdural electrodes—MRI—Results.
The surgical treatment of refractory extratemporal epi-lepsy (R-ExTE) has always represented a challenge. Thesurgical results that have been published in the pre–magnetic resonance imaging (MRI) era were poorer thenthose obtained in the treatment of patients with temporallobe epilepsy (1–3). After the appearance of MRI, it hasbeen possible to detect potentially epileptogenic lesionspreoperatively, and the surgical results obtained in pa-tients with R-ExTE have improved considerably (4–6).Conversely, patients with R-ExTE and normal or nonlo-calizing MR scans still represent the most difficult pa-tients to handle, and they frequently need invasiverecordings.
The paradigms for invasive electrode placement varyfrom one center to the other, including the use of depth,
subdural, epidural, and foramen ovale electrodes (7–10).Subdural grids and strips have been used to cover thecortical convexity and mesial surfaces. Subdural stripsare easier to implant, usually through a burr-hole or smallcraniotomy, but the cortical coverage is not extensive.Subdural grids cover a larger cortical area but need largecraniotomies to be inserted. We studied the efficacy of anextensive coverage of the brain surface with subduralgrids in defining extratemporal cortical areas amenablefor resection in patients with R-ExTE.
METHODS
Sixteen patients with R-ExTE were studied. All pa-tients were studied from 1997 to 2000. These patientsrepresented all the group of patients with refractory ex-tratemporal epilepsy and nonlocalizing MRI investigatedwith subdural electrodes during that period. They weregiven prolonged video-EEG monitoring and had high-resolution MR scanning before invasive recordings. In
Revision accepted May 7, 2001.Address correspondence and reprint requests to Dr. A. Cukiert at
R Dr. Alceu Campos Rodrigues 247, 12 andar, 121, São Paulo SP,Brazil CEP 04544-000. E-mail: [email protected]
Epilepsia,42(7):889–894, 2001Blackwell Science, Inc.© International League Against Epilepsy
889

all patients, cortical resection was performed after sub-dural grids implantation. The clinical summary and pre-implantation findings of these patients are shown inTable 1.
Ages ranged from 8 to 28 years (m4 20.5 years), andthe age at onset of the epileptic syndrome ranged from 1to 7 years (m4 3.5 years). Eleven patients had simplepartial (somatosensitive in three, motor in six, versive inone, visual in one, and aphasic blockage in three), eighthad complex partial, and three had supplementary motorarea (SMA) seizures. Seizure frequency ranged fromthree per month to daily episodes. Interictal EEG showedlarge focal spiking areas in 11 patients, secondary bilat-eral synchrony in four, and normal in one patient. Sur-face ictal recordings were nonlocalizing in six patients,and in 10, it disclosed large ictal focal spiking areas.MRI was normal in 10 patients, and in six patients, focalnonlocalizing potentially epileptogenic lesions werefound: congenital porencephaly (n4 3), hemisphericatrophy (n4 1), multifocal areas of cortical dysplasia (n4 1), and bioccipital anoxic lesions (n4 1) .
At least two ictal single-photon emission computedtomography (SPECT) scans were available in seven pa-tients (VI, VII, IX, XI, XII, XIII, and XIV). All patientswith SMA-type seizures (VI, VII, IX) and two patients(XII and XIV) with somatomotor seizures had normal
ictal SPECT scans; patient XI and XIII had right and leftfrontal hyperperfusion, respectively.
All patients were given an extensive coverage of thecortical convexity with subdural electrodes through largeunilateral (n4 13) or bilateral (n4 3) craniotomies.The number of implanted electrodes ranged from 64 to160 contacts. Bipolar cortical stimulation was carried outthrough the implanted electrodes using squares pulseswith current varying from 3 to 8 mA, 0.1 ms in duration,and 100 Hz. Follow-up time ranged from 1 to 4 years (m4 1.9 years).
RESULTS
Interictal invasive recording findings showed wide-spread spiking areas in 13 patients and secondary bilat-eral synchrony in three (Table 2). Ictal invasiverecordings showed focal seizure onset in all patients. Allpatients underwent cortical resections that included theentire ictal zone and the most active interictal areas aswell, whenever possible, sparing eloquent cortical re-gions defined by means of preresection cortical stimula-tion. There were six frontal (Fig. 1), two parietal, onetemporooccipital, four rolandic (Fig. 2), and three pos-terior quadrant resections. Posterior quadrant resectionsincluded the removal of the occipital, parietal, and pos-
TABLE 1. Summary of preimplantation clinical data
PatientAge(yr)
Age szonset(yr) Sz types
Szfrequency Interictal EEG Ictal EEG MRI
Implantationparadigm
I 16 2 SS SPS RH/CPS 2×/wk Left hemisphere Left post quadrant Left P porencephaly 96 cts; left postquadrant
II 8 4 CPS 3×/wk Left FT Left FT Left FT porencephaly 64 cts; left FTIII 21 4 SS SPS RH/CPS 2×/wk Left hemisphere Left post quadrant Left P porencephaly 96 cts; left post
quadrantIV 21 1 SM SPS LH/CPS Daily Right hemisphere Nonlocalizing Right cingulum/
premotor dysplasia96 cts; right FP
V 16 2 Versive SPS/CPS 3×/wk FP SBS Nonlocalizing Left hemisphericatrophy
128 cts; left FTPO
VI 16 5 SMA Daily FP SBS Nonlocalizing Normal 160 cts; bilateral FMVII 24 3 SMA Daily FP SBS Nonlocalizing Normal 160 cts; bilateral FMVIII 19 4 Visual SPS/CPS 3×/mo Left hemisphere Left postquadrant Normal 96 cts; left post
quadrantIX 28 2 SMA Daily FP SBS Nonlocalizing Normal 160 cts; bilateral FMX 22 2 SS SPS LH/CPS 4×/wk Right hemisphere Right hemisphere Bioccipital
demyelination96 cts; right FPO
XI 28 4 SM SPS LF Daily Right hemisphere Right hemisphere Normal 96 cts; right FPOXII 23 5 SM RF +
Aphasic SPSDaily Left hemisphere Left hemisphere Normal 96 cts; left FTO
XIII 24 3 SM RF +Aphasic SPS
Daily Left hemisphere Left FP Normal 96 cts; left FTO
XIV 23 7 SM SPS LL Daily Normal Normal Normal 102 cts; right FPMXV 20 6 SM RF +
Aphasic SPSDaily Left FP Left FP Normal 96 cts; left FP
XVI 19 2 CPS 3×/wk Left hemisphere Left post quadrant Normal 96 cts; left FPO
Sz, seizure; SS, somatosensory; SM, somatomotor; SPS, simple partial seizure; CPS, complex partial seizure; RH, right hand; LH, left hand; LF,left face; RF, right face; LL, left leg; SMA, supplementary motor area; FT, frontotemporal; FP, frontoparietal; FTPO, frontotemporoparietooccipital;FM, frontomesial; FPO, frontoparietooccipital; FTO, frontotemporooccipital; FPM, frontoparieto–mesial; post, posterior; cts, contacts; SBS,second-ary bilateral synchrony.
A. CUKIERT ET AL.890
Epilepsia, Vol. 42, No. 7, 2001

terior temporal cortex. Additionally, a posterior trans-ventricular hippocampectomy was performed.
EEG seizure onset preceded or was concomitant withthe clinical manifestations in all patients. Seizures initi-ated simultaneously in up to three contiguous electrodesin eight patients; in four to six electrodes in four patients,and in more than six electrodes in four patients. No pa-tient had seizures starting simultaneously in differentnoncontiguous cortical areas. Seizure-onset patterns in-cluded low-amplitude fast activity evolving into a re-cruiting rhythm (n4 9), rhythmic theta activity (n4 4),and high-amplitude spiking (n4 3).
Only one patient had SMA seizures originating fromthe SMA proper. The other two patients had epilepto-genic zones outside this region. Interestingly, in one ofthese patients, the same typical SMA seizures could betriggered by the stimulation of both SMA cortex. Patientswith simple partial motor or somatosensitive seizuresalso disclosed epileptogenic areas well beyond theboundaries of the rolandic cortex. In only one of eightpatients with such seizures was the epileptogenic arearestricted to the rolandic gyri, whereas in the other seven,ictally spiking areas anterior or posterior to the rolandiccortex were present.
The ability to reproduce stimuli during cortical stimu-lation helped patients to define further their simple par-tial seizures, and in 68% of them, the typical partialseizures were obtained. Only one of 11 patients in whomcortical stimulation effectively reproduced the typicalsimple partial seizure has not been rendered seizure freeafter surgery. Conversely, no simple partial seizures
could be elicited by cortical stimulation in two of threepatients who have not been rendered seizure free aftersurgery.
Thirteen patients had been rendered seizure free aftersurgery, and three hadù90% seizure-frequency reduc-tion. Pathological findings included gliosis (with loss ofgray matter; n4 10), cortical dysplasia (n4 5), or noabnormalities (n4 1). Six patients had transient post-operative neurologic morbidity: hemiparesis (n4 1; 4days), facial paresis with dysphasia (n4 3; 1 week, 1week, and 2 weeks, respectively), facial paresis only (n4 1; 2 weeks), and unilateral crural paresis (n4 1; 1month). All patients given posterior quadrant resections(I, III, and X) were hemianoptic preoperatively.
DISCUSSION
Eighty-one percent of the patients in this series wererendered seizure free after surgery. This might be con-sidered a good surgical outcome rate compared with pre-viously published data (11–15). Some aspects of theresections performed in this series may be emphasized.The extent of the resections was larger than those per-formed in patients with temporal lobe epilepsy. Theywere maximized to include the ictal and prevailing in-terictal areas and were limited basically by the presenceof eloquent cortex, or most frequently, by dominantdraining veins. Special attention was paid to keep thesurrounding arteries and veins intact when performingsubpial resections near or inside eloquent cortex (i.e.,rolandic or perirolandic). All transient neurologic mor-
TABLE 2. Summary of postimplantation clinical data
Patient Interictal ECoG Ictal ECoG Resection Outcome PathologyComplications/
durationFollow-up
(mo)
SPSafterCS
I Left post quadrant Left TP Left post quadrant Seizure free Gliosis None 48 NoII Left FT Left FT Left FT 90%
improvementGliosis None 46 No
III Left post quadrant Left TPO Left post quadrant Seizure free Gliosis None 36 NoIV Right FP Right premotor Right F Seizure free Dysplasia None 18 YesV Left hemisphere Left area 6 Left premotor/
callosotomy90%
improvementGliosis None 18 No
VI SBS right 4left
Right F mesial Right F 90%improvement
Dysplasia Left hemiparesis/4 days
20 Yes
VII SBS right 4 left Right inferior F Right F Seizure free Gliosis None 16 YesVIII Left post quadrant Left OT Left OT Seizure free Dysplasia None 18 YesIX SBS right 4 left Left F mesial Left F Seizure free Gliosis None 16 YesX Right hemisphere Right post quadrant Right post quadrant Seizure free Gliosis None 18 YesXI Right hemisphere Right rolandic/
perirolandicRight rolandic face/
tongue + perirolandicSeizure free Gliosis Left facial paresis/
2 wk24 Yes
XII Left hemisphere Left rolandic Left rolandic face/tongue
Seizure free Gliosis Right facial paresis+ dysphasia/2 wk
18 Yes
XIII Left FP Left rolandic/perirolandic
Left rolandic face/tongue + perirolandic
Seizure free Dysplasia Right facial paresis+ dysphasia/1 wk
18 Yes
XIV Right mesial FP Right mesialrolandic
Right SMA + mesial P Seizure free Normal Left crural paresis/1 mo
18 Yes
XV Left FP Left rolandic/perirolandic
Left rolandic face/tongue + left F
Seizure free Gliosis Right facial paresis+ dysphasia/2 wk
20 Yes
XVI Left post quadrant Left P Left P Seizure free Dysplasia None 12 No
EcoG, electrocorticography; SPS, simple partial seizure; CS, cortical stimulation; post, posterior; FT, frontotemporal; FP, frontoparietal; SBS, secondary bilateralsynchrony; TP, temporoparietal; TPO, temporoparietoocciptal; F, frontal; OT, occipitotemporal; P, parietal; SMA, supplementary motor area.
SURGERY FOR EXTRATEMPORAL EPILEPSY 891
Epilepsia, Vol. 42, No. 7, 2001
bidity seen in these patients was expected preoperativelyand was directly related to the cortical areas defined astargets for removal (i.e., facial paresis after lower rolan-dic resections) (16). Contrary to others’ findings (17),our preliminary experience with multiple subpial tran-sections alone in eloquent extratemporal cortex has beenvery poor (personal communication). We prefer to resectrelatively eloquent cortex (i.e., face area cortex) andleave absolutely eloquent cortex intact.
Four patients had areas of microdysgenesis not de-tected preoperatively by MRI. Conversely, the mainpathological finding was gliosis with loss of gray matter,mostly compatible with the normal preoperative MRscans. In contrast to patients with subpial gliotic changesalone, the patients with gliosis and gray matter loss seemto have a better surgical outcome. In these four patientswith preoperatively undetected cortical dysplasia, there
was no alteration of the gyral pattern, which was alsotrue for the patients in whom gliosis was found. It isunlikely that improvement in anatomic MR techniqueswould allow us to detect further abnormalities in thesetypes of patients.
As noted by others (18), there was no localizing clini-cal sign in our three patients with SMA-type seizures.Neither the direction of head rotation nor the asymmetricposturing was able to predict the SMA involved in thegeneration of seizures. The only way to localize fociadequately in patients with SMA seizures, secondary bi-lateral synchrony, and normal MRI was extensive inva-sive coverage of the frontal mesial surface andconvexity. Even using this paradigm, a bilateral and syn-chronous sentinel spike was seen immediately or a fewseconds before the ictal recruiting pattern could be seenover one of the mesial surfaces. This might be related to
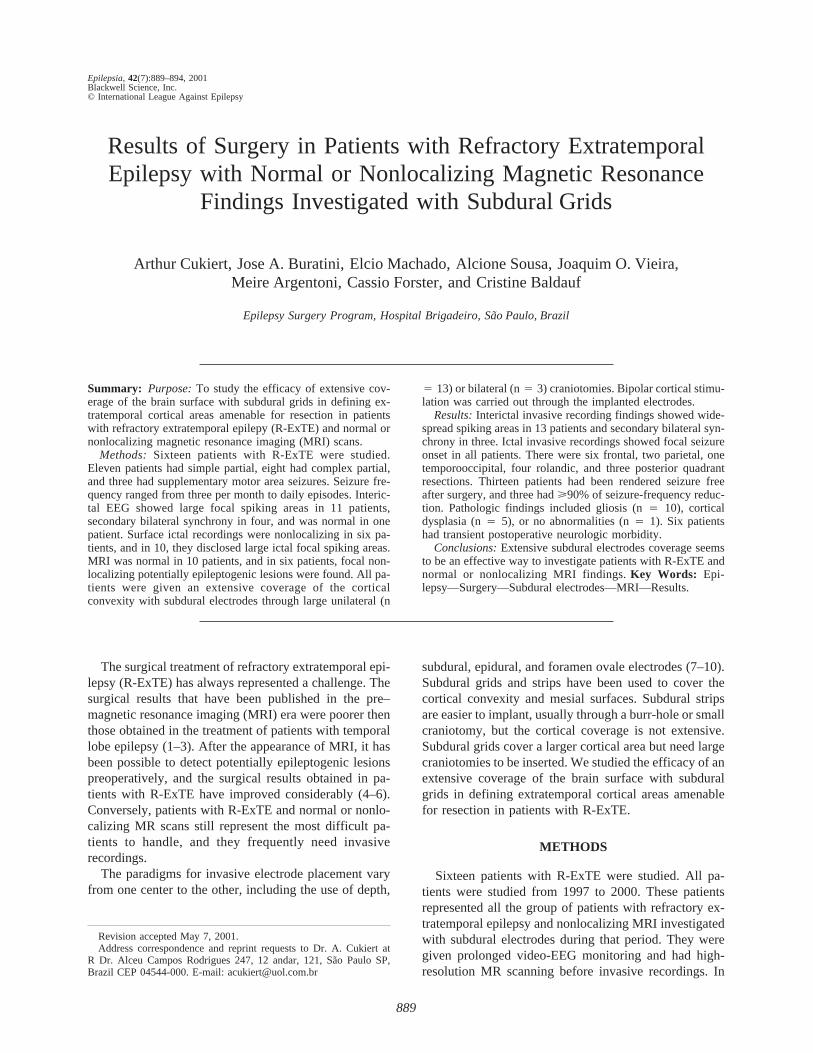
FIG. 1. Patient IX, who showed a largefrontomesial focus and secondary bilat-eral synchrony. A: Skull radiographshowing the extensive bilateral front-omesial subdural electrodes coverage.B: Intraoperative view of the left hemi-sphere with superimposed invasive neu-rophysiologic data. The frontal pole is onthe left side, the parietal lobe is on theright, and the mesial surface is seen su-periorly. Pink tags, epileptogenic area;green tags, motor strip; blue tag, Broca’sarea; double line, extent of resection.
A. CUKIERT ET AL.892
Epilepsia, Vol. 42, No. 7, 2001
a more widespread epileptogenesis in these patients. Ourfindings showed that patients with SMA and somatomo-tor seizures often have extra-SMA and extrarolandic epi-leptogenic zones. These findings further emphasized theneed for adequately defining epileptogenic and sympto-matogenic zones in these patients.
Complex partial seizures were seen arising from allcerebral lobes. As compared with those originating fromthe temporal lobes, extratemporal complex partial sei-zures originated from a much larger cortical surface, andin five of eight patients, the epileptogenic area was mul-tilobar. There was a better surgical outcome in patients inwhom cortical stimulation was able to reproduce the pa-tient’s typical seizure.
Ictal SPECT would be able to define the quadrant
(anterior, posterior; left or right) in∼50% of the patientswith extratemporal refractory epilepsy and normal MRI,but it lacks the spatial and anatomic resolution needed toobviate the need for invasive recordings. Conversely, inthe majority of the patients, intensive video-EEG moni-toring is able to guide adequately the establishment of asubdural grid implantation pattern. All patients with re-fractory extratemporal epilepsy and normal MRI havebeen ultimately given invasive recordings in our series ifcortical resection is being contemplated. Subdural gridcoverage should be extensive in such patients; limitedcoverage of the cortical surface with subdural strips orepidural electrodes may very likely lead to inadequatelocalization or mapping.
Our series included a set of patients whose preopera-
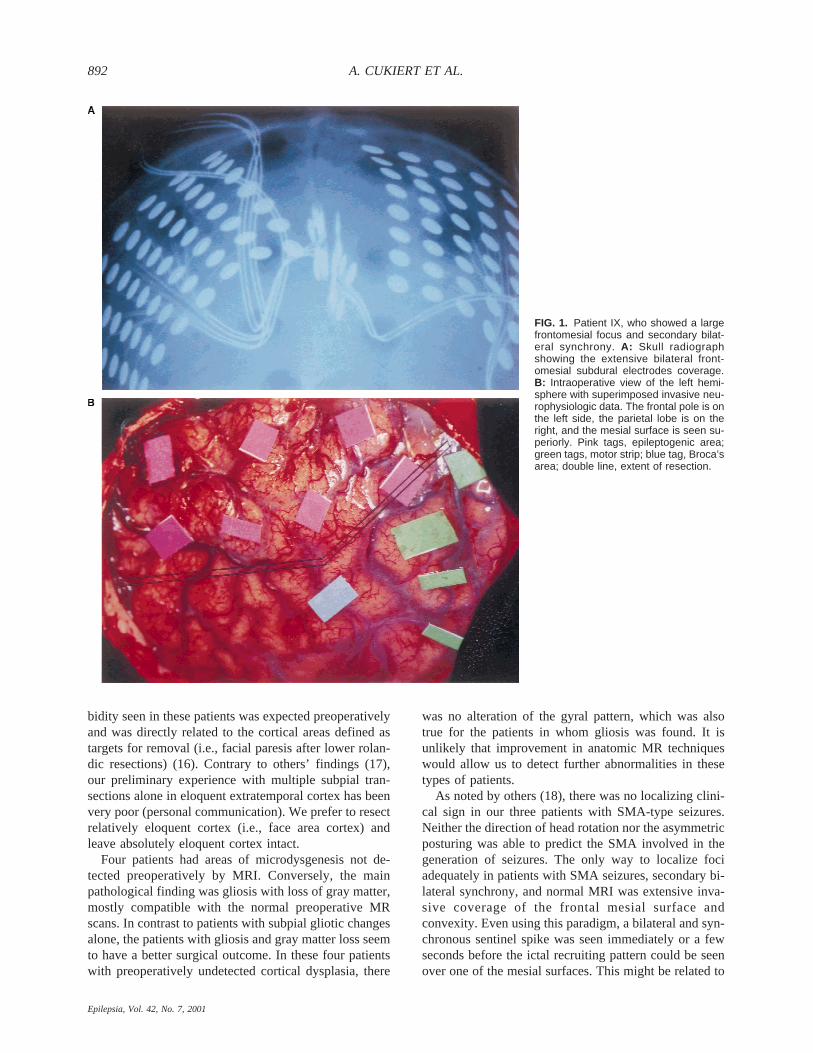
FIG. 2. Patient XII, who disclosed a fo-cus restricted to the dominant rolandicareas. A: Skull radiograph showing cov-erage of almost all the left hemisphere.B: Intraoperative view of the left hemi-sphere with superimposed invasive neu-rophysiologic data. The frontal pole is onthe right side, the parietal lobe is on theleft, and the sylvian fissure is seen supe-riorly. Ruler in centimeters. White tag,Broca’s area; dark blue tags, motor strip;light blue tags, epileptogenic area; yel-low tag, site from which the patient’s typi-cal simple partial seizure was obtainedafter cortical stimulation; double line, ex-tent of resection.
SURGERY FOR EXTRATEMPORAL EPILEPSY 893
Epilepsia, Vol. 42, No. 7, 2001

tive workup is time and effort consuming. Extensive sub-dural electrode coverage seems to be an effective way toinvestigate these patients.
REFERENCES
1. Fish DR, Smith SJ, Quesnay LF, et al. Surgical treatment of chil-dren with medically intractable frontal or temporal lobe epilepsy:results and highlights of 40 years’ experience.Epilepsia1993;34:244–7.
2. Hajek M, Wieser HG. Extratemporal, mainly frontal lobe, epilep-sies: surgical results.J Epilepsy1988;1:103–19.
3. Rasmussen T. Tailoring of cortical excisions for frontal lobe epi-lepsy.Can J Neurol Sci1991;18:606–10.
4. Fish D, Andermann F, Olivier A. Complex partial seizures andsmall posterior temporal or extratemporal structural lesions: sur-gical management.Neurology1991;41:1781–4.
5. Cascino GD, Jack CR, Parisi JE, et al. MRI in the presurgicalevaluation of patients with frontal lobe epilepsy and children withtemporal lobe epilepsy: pathologic correlation and prognostic im-portance.Epilepsy Res1992;11:51–9.
6. Olivier A, Awad I. Extratemporal resection. In: Engel J Jr, ed.Surgical treatment of the epilepsies.New York: Raven Press,1993:489–500.
7. Lee SA, Spencer DD, Spencer SS. Intracranial EEG seizure-onsetpatterns in neocortical epilepsy.Epilepsia2000;41:297–307.
8. Spencer SS, Spencer DD, Williamson PD, et al. Combined depthand subdural electrode investigation in uncontrolled epilepsy.Neu-rology 1990;40:74–9.
9. Adelson PD, O’Rourke DK, Albright AL. Chronic invasive moni-toring for identifying seizure foci in children.Neurosurg ClinNorth Am1995;6:491–504.
10. Ludwig BI, Marsan CA, van Buren J. Depth and direct corticalrecording in seizure disorders of extratemporal origin.Neurology1976;26:1085–99.
11. Haglund NM, Ojemann GA. Extratemporal resective surgery forepilepsy. Neurosurg Clin North Am1993;4:283–92.
12. Davies KG, Weeks RD. Cortical resections for intractable epilepsyof extra-temporal origin: experience with seventeen cases overeleven years.Br J Neurosurg1993;7:343–53.
13. Prats AR, Morrison G, Wolf AL. Focal cortical resections for thetreatment of extratemporal epilepsy in children.Neurosurg ClinNorth Am1995;6:533–40.
14. Adler J, Erba G, Winston KR, et al. Results of surgery for extra-temporal partial epilepsy that began in childhood.Arch Neurol1991;48:133–40.
15. Palmini A, Andermann F, Olivier A, et al. Neuronal migrationdisorders (NMD): extent of lesion removal is the main predictor ofseizure control in the surgical treatment of epilepsy.Neurology1991;41(suppl 1):403.
16. Cascino GD, Sharbrough FW, Trenerry MR, et al. Extratemporalcortical resections and lesionectomies for partial epilepsy: compli-cations of surgical treatment.Epilepsia1994;35:1085–90.
17. Smith MC. Multiple subpial transection in patients with extratem-poral epilepsy.Epilepsia1998;39(suppl 4):S81–9.
18. Bleasel A, Kotagal P, Kankirawatana P, et al. Lateralizing valueand semiology of ictal limb posturing and version in temporal lobeand extra-temporal epilepsy.Epilepsia1997;38:168–74.
A. CUKIERT ET AL.894
Epilepsia, Vol. 42, No. 7, 2001
Related Documents


![A Case of Benign Meningioma Presented with Subdural Hemorrhage · Meningioma with Subdural Hemorrhage Martínez-Lage et al. [4] studied 57 cases of meningioma with hemorrhagic onset](https://static.cupdf.com/doc/110x72/5eca99262fcc5c7ee06897d3/a-case-of-benign-meningioma-presented-with-subdural-hemorrhage-meningioma-with-subdural.jpg)








