Results of a Randomized Phase III Trial (MPACT) of Weekly nab- Paclitaxel Plus Gemcitabine vs Gemcitabine Alone for Patients With Metastatic Adenocarcinoma of the Pancreas With PET and CA19-9 Correlates Daniel D. Von Hoff, 1 Thomas Ervin, 2 Francis P. Arena, 3 E. Gabriela Chiorean, 4 Jeffrey Infante, 5 Malcolm Moore, 6 Thomas Seay, 7 Sergey A. Tjulandin, 8 WenWee Ma, 9 Mansoor N. Saleh, 10 Marion Harris, 11 Michele Reni, 12 Ramesh K. Ramanathan, 1 Josep Tabernero, 13 Manuel Hidalgo, 14 Eric Van Cutsem, 15 David Goldstein, 16 Xinyu Wei, 17 Jose Iglesias, 18 Markus F. Renschler 17 1 TGen, Scottsdale Healthcare, AZ, USA; 2 Florida Cancer Specialists/Sarah Cannon Research Institute, Englewood, FL; 3 Arena Oncology Associates, Lake Success, NY, USA; 4 University of Washington, Seattle, WA, USA; 5 Sarah Cannon Research Institute/Tennessee Oncology, PLLC, Nashville, TN; 6 Princess Margaret Hospital, Toronto, Canada; 7 Atlanta Cancer Care, GA, USA; 8 Blokhin Cancer Research Center, Moscow, Russia; 9 Roswell Park Cancer Institute, Buffalo, NY, USA; 10 Cancer Specialists, Atlanta, GA, USA; 11 Southern Health, East Bentleigh, VIC, Australia; 12 San Raffaele Scientific Institute, Milan, Italy; 13 Vall d'Hebron University Hospital, Barcelona, Spain; 14 Centro Integral Oncológico Clara Campal, Madrid, Spain; 15 Leuven University, Belgium; 16 Prince of Wales Hospital, Sydney, NSW, Australia; 17 Celgene Corporation, Summit, NJ, USA; 18 Bionomics, Thebarton, Australia

Results of a Randomized Phase III Trial (MPACT) of Weekly nab-Paclitaxel Plus Gemcitabine vs Gemcitabine Alone for Patients With Metastatic Adenocarcinoma.
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Results of a Randomized Phase III Trial (MPACT) of Weekly nab-Paclitaxel PlusGemcitabine vs Gemcitabine Alone for
Patients With Metastatic Adenocarcinoma of the Pancreas With PET and CA19-9
Correlates
Daniel D. Von Hoff,1 Thomas Ervin,2 Francis P. Arena,3 E. Gabriela Chiorean,4 Jeffrey Infante,5 Malcolm Moore,6 Thomas Seay,7 Sergey A. Tjulandin,8 WenWee Ma,9 Mansoor N. Saleh,10 Marion Harris,11 Michele Reni,12 Ramesh K. Ramanathan,1 Josep Tabernero,13 Manuel Hidalgo,14 Eric Van
Cutsem,15 David Goldstein,16 Xinyu Wei,17 Jose Iglesias,18 Markus F. Renschler 17
1TGen, Scottsdale Healthcare, AZ, USA; 2Florida Cancer Specialists/Sarah Cannon Research Institute, Englewood, FL; 3Arena Oncology Associates, Lake Success, NY, USA; 4University of Washington, Seattle, WA, USA; 5Sarah Cannon Research Institute/Tennessee Oncology,
PLLC, Nashville, TN; 6Princess Margaret Hospital, Toronto, Canada; 7Atlanta Cancer Care, GA, USA; 8Blokhin Cancer Research Center, Moscow, Russia; 9Roswell Park Cancer Institute, Buffalo, NY, USA; 10Cancer Specialists, Atlanta, GA, USA; 11Southern Health, East Bentleigh,
VIC, Australia; 12San Raffaele Scientific Institute, Milan, Italy; 13Vall d'Hebron University Hospital, Barcelona, Spain; 14Centro Integral Oncológico Clara Campal, Madrid, Spain; 15Leuven University, Belgium; 16Prince of Wales Hospital, Sydney, NSW, Australia; 17Celgene
Corporation, Summit, NJ, USA; 18Bionomics, Thebarton, Australia

Disclosures
2Von Hoff et al. ASCO 2013.
This study was sponsored by Celgene Corporation
Von Hoff: consultant or advisory role, honoraria, and research funding, Celgene; Ervin: research funding, Celgene; Arena: research funding, Clinical Research Alliance and Celgene; Chiorean: research funding, Celgene; Moore: consultant or advisory role and research funding, Celgene; Seay: research funding, Celgene; Tjulandin: research funding, Celgene; Ma: research funding, Celgene; Saleh: research funding, Celgene; Reni: consultant or advisory role, honoraria, and research funding, Celgene; Ramanathan: consultant or advisory role, honoraria, and research funding, Celgene; Tabernero: consultant or advisory role and honoraria, Celgene; Hidalgo: consultant or advisory role, honoraria, and research funding, Celgene; Van Cutsem: research funding, Celgene; Goldstein: consultant or advisory role and research funding, Celgene; Wei: employment or leadership position and stock ownership, Celgene; Iglesias: employment or leadership position at Bionomics and stock ownership, Celgene; Renschler: employment or leadership position and stock ownership, Celgene; Infante, Harris: nothing to disclose.

nab-Paclitaxel + Gemcitabine in Pancreatic Cancer
1. Preclinical models1,2:• nab-Paclitaxel (nab-P) active as single agent• Synergizes with gemcitabine (Gem)
2. In a 67-patient phase I/II trial of nab-P + Gem1
• MTD: nab-P 125 mg/m2 + Gem 1000 mg/m2 on days 1, 8, and 15 every 28 days
• Promising activity at MTD• ORR: 48%• Median PFS: 7.9 months• Median OS: 12.2 months
1. Von Hoff DD, et al. J Clin Oncol. 2011;29:4548-4554. 2. Frese KK, et al. Cancer Discov. 2012;2:260-269. 3Von Hoff et al. ASCO 2013.

Study Design
1:1, stratified by KPS, region, liver metastasis
Planned N = 842
• Stage IV• No prior treatment for
metastatic disease• KPS ≥ 70 • Measurable disease• Total bilirubin ≤ ULN• No age limitation
nab-P125 mg/m2 IV qw 3/4
+
Gem1000 mg/m2 IV qw 3/4
Gem1000 mg/m2 IV qw 7/8
then qw 3/4
4
Primary endpoint– OS
Secondary endpoints– PFS and ORR by
independent review (RECIST)
Safety and tolerability– By NCI CTCAE v3.0
• With 608 events, 90% power to detect OS; HR = 0.769 (2-sided α = 0.049)
• Treat until progression• CT scans every 8 weeks• PET scans in an initial cohort of
patients at baseline and weeks 8 and 16• CA19-9 measurements at baseline and
every 8 weeks
Von Hoff et al. ASCO 2013.
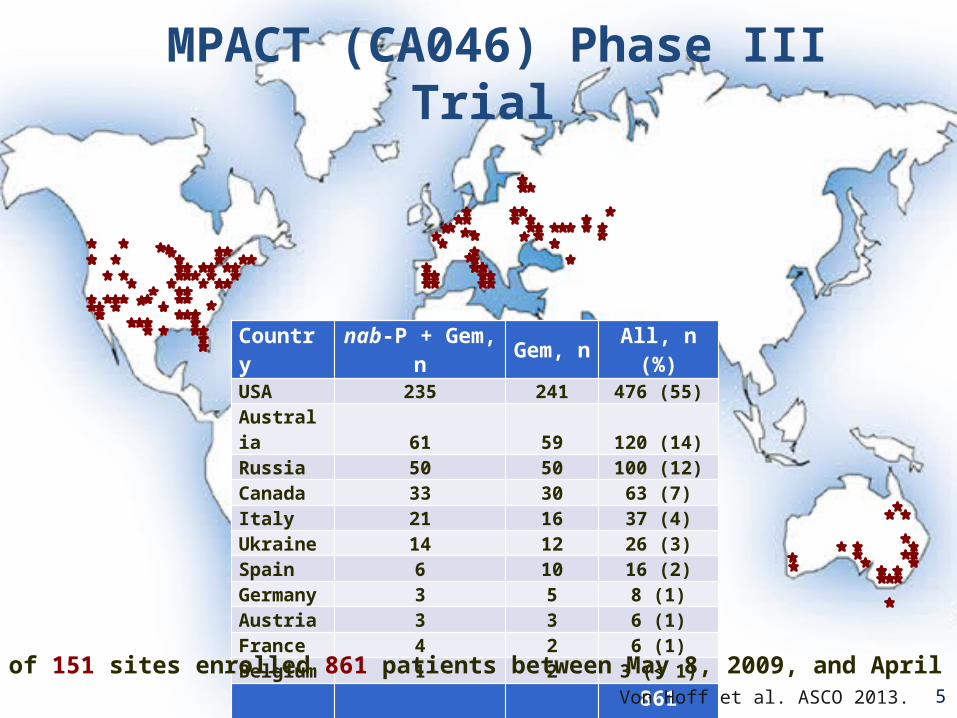
Country nab-P + Gem, n Gem, n All, n (%)
USA 235 241 476 (55)Australia 61 59 120 (14)Russia 50 50 100 (12)Canada 33 30 63 (7)Italy 21 16 37 (4)Ukraine 14 12 26 (3)Spain 6 10 16 (2)Germany 3 5 8 (1)Austria 3 3 6 (1)France 4 2 6 (1)Belgium 1 2 3 (< 1)Total 431 430 861 (100)
MPACT (CA046) Phase III Trial
Total of 151 sites enrolled 861 patients between May 8, 2009, and April 17, 20125Von Hoff et al. ASCO 2013.
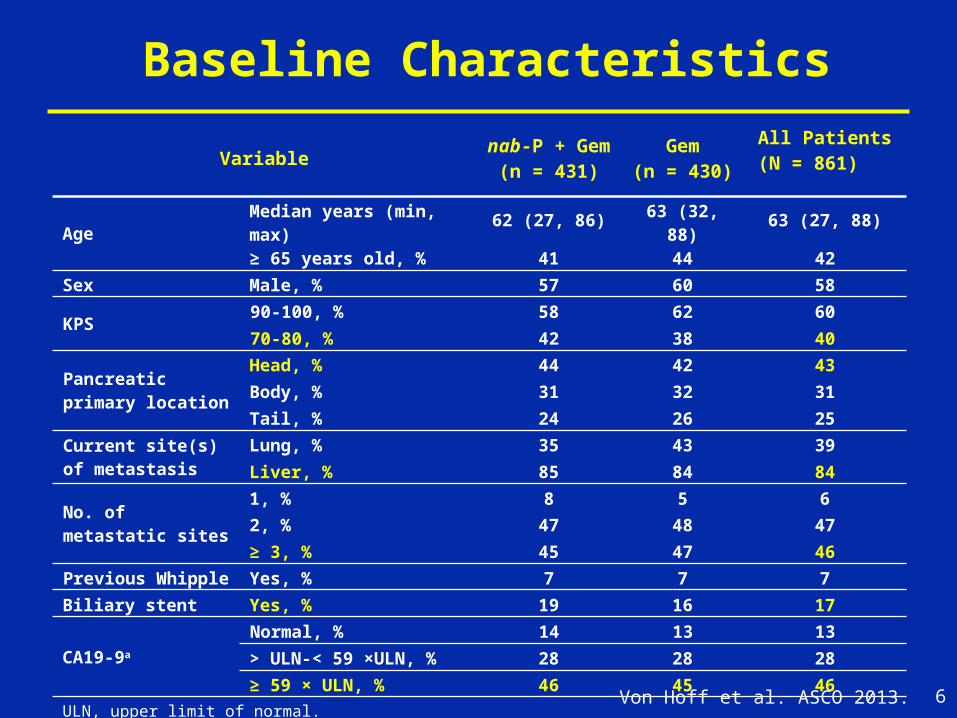
Baseline Characteristics
Variablenab-P + Gem
(n = 431)Gem
(n = 430)
All Patients(N = 861)
AgeMedian years (min, max) 62 (27, 86) 63 (32, 88) 63 (27, 88)
≥ 65 years old, % 41 44 42
Sex Male, % 57 60 58
KPS90-100, % 58 62 60
70-80, % 42 38 40
Pancreatic primary location
Head, % 44 42 43
Body, % 31 32 31
Tail, % 24 26 25
Current site(s) of metastasis
Lung, % 35 43 39
Liver, % 85 84 84
No. of metastatic sites
1, % 8 5 6
2, % 47 48 47
≥ 3, % 45 47 46
Previous Whipple Yes, % 7 7 7
Biliary stent Yes, % 19 16 17
CA19-9a
Normal, % 14 13 13
> ULN-< 59 ×ULN, % 28 28 28
≥ 59 × ULN, % 46 45 46
ULN, upper limit of normal.a CA19-9 at baseline was unknown in 13% of patients. 6Von Hoff et al. ASCO 2013.

Overall Survival
Months
Pro
po
rtio
n o
f S
urv
ival
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
1.0
0.00 3 6 9 12 15 18 21 24 27 30 33 36 39
Pts at risknab-P + Gem:
Gem:
431
430
357
340
269
220
169
124
108
69
67
40
40
26
27
15
16
7
9
3
4
1
1
0
1
0
0
0
nab-P + Gem
Gem
OS, months
Events/n (%) Median (95% CI)75th
Percentile
333/431 (77) 8.5 (7.89-9.53) 14.8
359/430 (83) 6.7 (6.01-7.23) 11.4
HR = 0.7295% CI (0.617-0.835)P = 0.000015
7Von Hoff et al. ASCO 2013.
• Subsequent therapy: 38% for nab-P + Gem and 42% for Gem• OS censored at time of secondary therapy: 9.4 vs 6.8 months; HR 0.68; P = 0.00007• Trial conclusions not impacted by secondary therapies
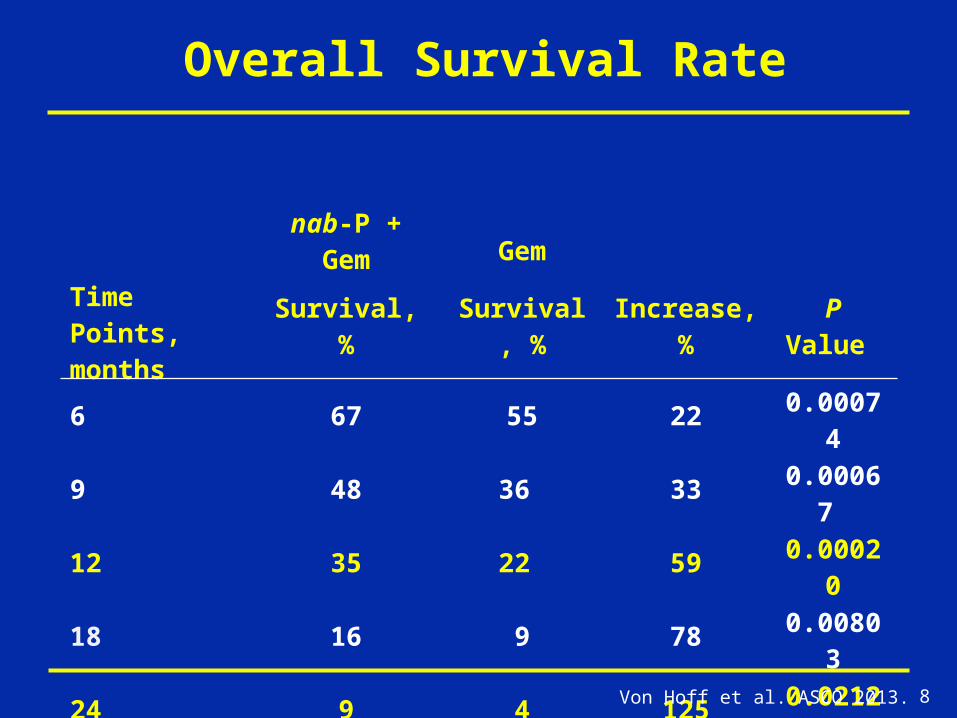
Overall Survival Rate
nab-P + Gem Gem
Time Points,months Survival, % Survival, % Increase, % P Value
6 67 55 22 0.00074
9 48 36 33 0.00067
12 35 22 59 0.00020
18 16 9 78 0.00803
24 9 4 125 0.02123
8Von Hoff et al. ASCO 2013.

OS—Prespecified SubgroupsGroup
0.125 0.25 0.5 1.0 2.0
HR
All patients
nab-P + GemEvents/n
GemEvents/n HR
333/431 359/430 0.72
188/254 209/242 0.65
145/177 150/188 0.81
138/186 141/173 0.72
195/245 218/257 0.72
142/179 146/161 0.61
187/248 212/268 0.75
142/191 155/180 0.59188/237 201/246 0.80
290/365 309/360 0.69
43/66 50/70 0.86
21/33 16/21 0.41
159/202 163/206 0.75
104/136 121/140 0.79
49/60 59/63 0.50
47/60 43/56 1.07
96/122 95/120 0.83
151/197 171/195 0.6150/61 53/59 0.6762/64 59/62 0.8414/38 17/38 0.72
207/268 230/271 0.68
Age < 65 yearsAge ≥ 65 years
FemaleMale
KPS 70-80KPS 90-100
Australia
Western EuropeNorth America
Eastern Europe
Primary tumor location: head Primary tumor location: other
No liver metastases
Liver metastases
Normal CA19-9
CA19-9 ULN to < 59 x ULNCA19-9 ≥ 59 x ULN
> 3 metastatic sites
1 metastatic site
3 metastatic sites
2 metastatic sites
9Favors GemFavors nab-P + Gem Von Hoff et al. ASCO 2013.

PFS by Independent Review
Months
Pro
po
rtio
n o
f P
rog
ress
ion
-Fre
e S
urv
ival
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
1.0
0.00 3 6 9 12 15 18 21 24
Pts at Risknab-P + Gem:
Gem:
431
430
281
209
122
51
62
23
24
10
8
6
4
4
2
0
0
0
nab-P + Gem
Gem
PFS, months
Events/n (%) Median (95% CI)75th
Percentile
277/431 (64) 5.5 (4.47-5.95) 9.2
265/430 (62) 3.7 (3.61-4.04) 5.9
HR = 0.6995% CI (0.581-0.821)P = 0.000024
10
PFS Rate at nab-P + Gem Gem Increase
6 months 44% 25% 76%
12 months 16% 9% 78%Von Hoff et al. ASCO 2013.

Response Rates
Variable nab-P + Gem(n = 431)
Gem(n = 430)
P Value
Overall response rate Independent review, % (95% CI) Investigator assessment, % (95% CI)
23 (19.1-27.2)
29 (25.0-33.8)
7 (5.0-10.1)
8 (5.3-10.6)
1.1 x 10−10
3.3 x 10−16
Disease control rate by independent review,a % (95% CI)
48(43.0-52.6)
33(28.4-37.5)
7.2 x 10−6
11
a Includes CR + PR + SD ≥ 16 weeks.
Von Hoff et al. ASCO 2013.
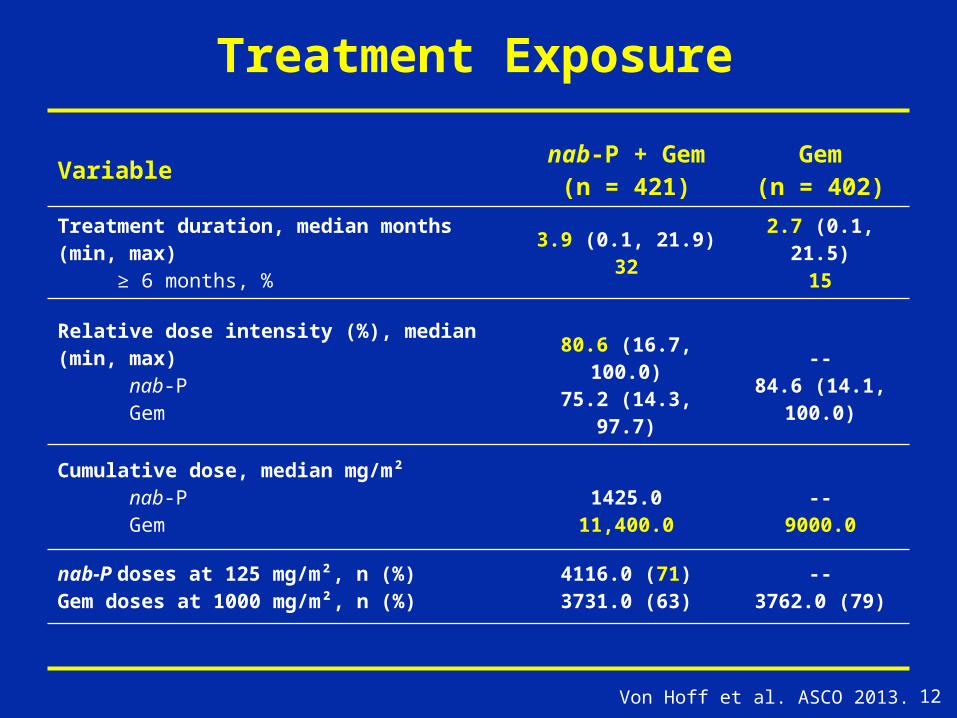
Variablenab-P + Gem
(n = 421)Gem
(n = 402)
Treatment duration, median months (min, max) ≥ 6 months, %
3.9 (0.1, 21.9)32
2.7 (0.1, 21.5)15
Relative dose intensity (%), median (min, max) nab-P Gem
80.6 (16.7, 100.0)75.2 (14.3, 97.7)
--84.6 (14.1, 100.0)
Cumulative dose, median mg/m² nab-P Gem
1425.011,400.0
--9000.0
nab-P doses at 125 mg/m², n (%)Gem doses at 1000 mg/m², n (%)
4116.0 (71)3731.0 (63)
--3762.0 (79)
Treatment Exposure
12Von Hoff et al. ASCO 2013.

Preferred Termnab-P + Gem
(n = 421)Gem
(n = 402)Pts with at least 1 AE leading to death, % 4 4
Grade ≥ 3 hematologic AEs,a % Neutropenia Thrombocytopenia Anemia
381313
279
12
Pts who received growth factors, % 26 15
Febrile neutropenia,b % 3 1
Grade ≥ 3 nonhematologic AEsb in > 5% pts, % Fatigue Peripheral neuropathyc
Diarrhea
17176
7< 11
Grade ≥ 3 neuropathy Time to onset, median days Time to improvement by 1 grade, median days Time to improvement to grade ≤ 1, median days Pts who resumed nab-P, %
140212944
11329----
Safety
a Based on laboratory values; b Based on investigator assessment of treatment-related events; c Grouped term.
13Von Hoff et al. ASCO 2013.
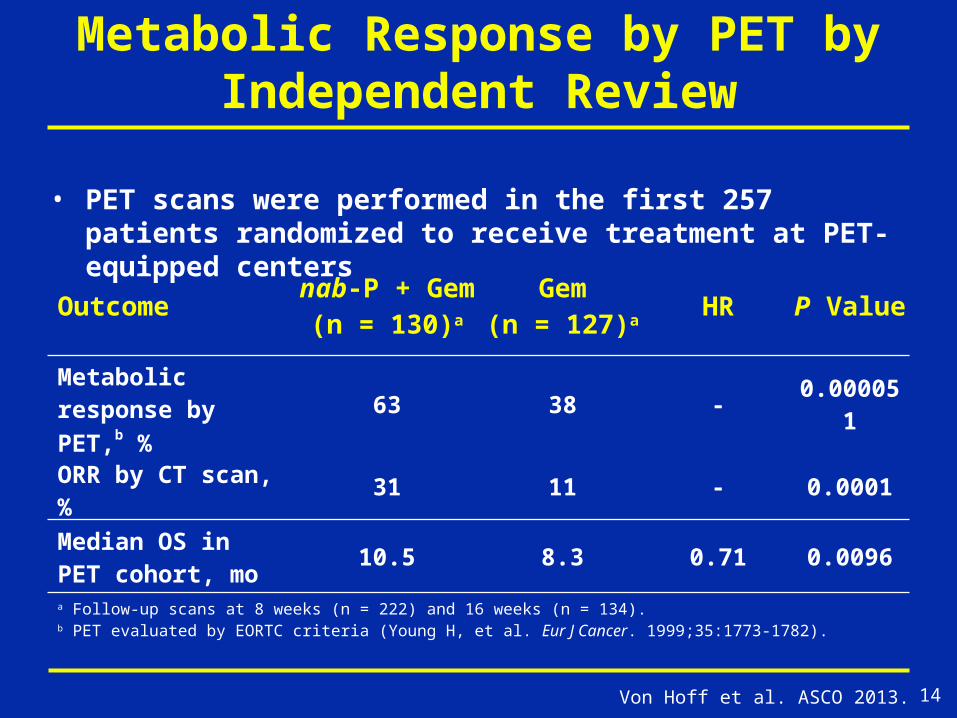
Metabolic Response by PET by Independent Review
• PET scans were performed in the first 257 patients randomized to receive treatment at PET-equipped centers
14
Outcome nab-P + Gem(n = 130)a
Gem(n = 127)a HR P Value
Metabolic response by PET,b %
63 38 - 0.000051
ORR by CT scan, % 31 11 - 0.0001
Median OS in PET cohort, mo
10.5 8.3 0.71 0.0096
a Follow-up scans at 8 weeks (n = 222) and 16 weeks (n = 134).b PET evaluated by EORTC criteria (Young H, et al. Eur J Cancer. 1999;35:1773-1782).
Von Hoff et al. ASCO 2013.
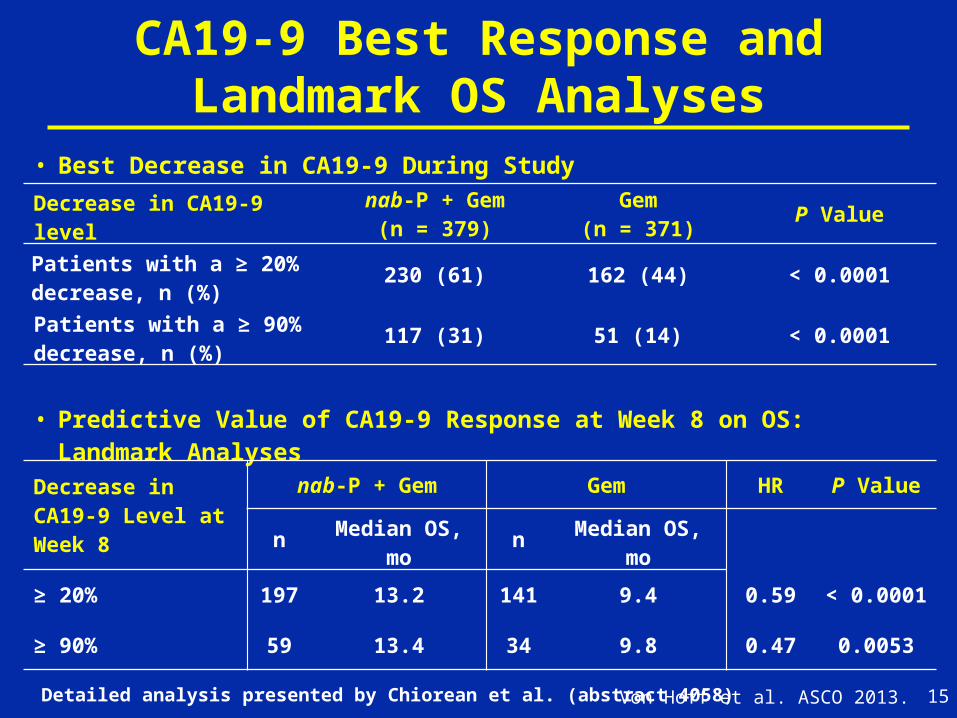
CA19-9 Best Response and Landmark OS Analyses
15Von Hoff et al. ASCO 2013.
• Best Decrease in CA19-9 During Study
Decrease in CA19-9 level nab-P + Gem(n = 379)
Gem(n = 371) P Value
Patients with a ≥ 20% decrease, n (%) 230 (61) 162 (44) < 0.0001
Patients with a ≥ 90% decrease, n (%) 117 (31) 51 (14) < 0.0001
• Predictive Value of CA19-9 Response at Week 8 on OS: Landmark Analyses
Decrease in CA19-9 Level at Week 8
nab-P + Gem Gem HR P Value
n Median OS, mo n Median OS, mo
≥ 20% 197 13.2 141 9.4 0.59 < 0.0001
≥ 90% 59 13.4 34 9.8 0.47 0.0053
Detailed analysis presented by Chiorean et al. (abstract 4058)
Conclusions from MPACT
1. MPACT study – a large, multi-center, international study performed at community and academic centers
2. OS, PFS, and ORR were superior for nab-P + Gem vs Gem
a) Improvement in OS across the entire curve, including median, 1-year, and 2-year survival rates
3. Metabolic response rate by PET and CA19-9 response rates were higher for nab-P + Gem vs Gem alone
a) Both were predictors for longer OS
16Von Hoff et al., ASCO 2013

Conclusions from MPACT (cont)
4. Serious life threatening toxicity not increased; AEs acceptable and manageable
5. nab-P + Gem, a new standard for the treatment of patients with metastatic pancreatic cancer, is superior to Gem alone and could become the backbone for new regimens
6. A phase III study of nab-P + Gem in the adjuvant setting is currently in development
17Von Hoff et al., ASCO 2013

MPACT Team
18Von Hoff et al. ASCO 2013.
Related Documents











