Responsibility, metacognition and unrealistic pessimism in obsessive–compulsive disorder Helen Niemeyer a,n,1 , Steffen Moritz b,1 , Reinhard Pietrowsky a a Heinrich-Heine-University, Institute for Experimental Psychology, Department of Clinical Psychology, Universit¨ atsstraße 1, 40225 D¨ usseldorf, Germany b University Medical Center Hamburg-Eppendorf, Department of Psychiatry and Psychotherapy, Martinistraße 52, 20246 Hamburg, Germany article info Article history: Received 8 June 2012 Received in revised form 15 December 2012 Accepted 2 January 2013 Available online 11 January 2013 Keywords: Obsessive–compulsive disorder Responsibility Metacognition Overestimation of threat Unrealistic optimism abstract Cognitive models stress the importance of cognitive belief domains (CBD) for the pathogenesis of obsessive–compulsive disorder (OCD). However, the relative contribution of responsibility and metacognition – core aspects of CBD – to OC symptoms is not fully understood yet. Furthermore, two subcomponents of overestimation of threat (OET), overestimation of the personal probability (unrealistic pessimism) and overestimation of the general risk of negative events, require clarification. First, we investigated the relative contribution of responsibility and metacognition to OC symptoms. Second, we hypothesized that OCD patients overestimate the personal risk and display unrealistic pessimism. Thirty-four OCD patients and 34 healthy controls completed the Obsessive Beliefs Ques- tionnaire (OBQ) and the Unrealistic Optimism Questionnaire (UO). Responsibility significantly predicted obsessive symptoms after controlling for metacognition. In contrast to previous findings, responsibility is not fully explained by metacognition. Finally, our results confirm unrealistic pessimism in OCD, even after controlling for depression. & 2013 Elsevier Inc. All rights reserved. 1. Introduction Cognitive theories of obsessive–compulsive disorder (OCD) stress the importance of cognitive and metacognitive belief domains (Rachman, 1997; Salkovskis, 1985, 1989; Wells, 2009). A large body of literature have demonstrated the importance of an inflated sense of responsibility (Salkovskis et al., 2000; Shafran, Thordarson, & Rachman, 1996; Smari & Holmsteinsson, 2001; Steketee, Frost, & Cohen, 1998) as well as the relevance of metacognition (Amir, Cashman, & Foa, 1997; Emmelkamp & Aardema, 1999; Solem, Myers, Fisher, Vogel, & Wells, 2010; Wells & Papageorgiou, 1998). In recent studies metacognition significantly predicted inflated responsibility (Gwilliam, Wells, & Cartwright-Hatton, 2004; Myers & Wells, 2005) but not vice versa. It is currently unresolved whether responsibility is merely a by-product of metacognition with no additional contribution to OC symptoms (Wells, 1997, 2009), or has predictive value in its own right. Overestimation of threat (OET) is another prominent cognitive bias discussed as being relevant for OCD. It is closely related to responsibility: both load on the same factor in the Obsessive Beliefs Questionnaire (OBQ-44; Obsessive–Compulsive Cognitions Working Group (OCCWG, 2005). OET is a complex construct comprising a number of independent components, which require systematic study of their individual contributions to obsessive symptoms. Recently, our group (Moritz & Jelinek, 2009; Moritz & Pohl, 2006, 2009) applied the unrealistic optimism paradigm (Weinstein, 1982) to OCD to shed light on the relevance of two subcomponents for OCD, namely the overestimation of the personal and the objective incidence probability of negative events. This paradigm is well suited to help to clarify whether OCD patients are especially prone to a biased perception of their personal incidence probability. It can be used to investigate whether subjects display a bias towards enhanced subjective vulnerability, whether they have indeed experienced negative events in the past more often, or whether they merely or additionally overestimate the severity of harm (Moritz & Jelinek, 2009; Moritz & Pohl, 2009). Unrealistic optimism arises from the overestimation of the subjective likelihood for positive events to happen to oneself, while at the same time the personal risk for negative events is underestimated. The reverse response pattern, labeled as unrealistic pessimism, might be an important compo- nent of OET. The UO paradigm goes beyond present question- naires for OET which do not differentiate between these important components. Our group (Moritz & Jelinek, 2009; Moritz & Pohl, 2006, 2009) found that patients with OCD over- estimated their personal risk for negative events compared to healthy controls, but not the objective probability of threat. Since results are not fully consistent across studies, further clarification Contents lists available at SciVerse ScienceDirect journal homepage: www.elsevier.com/locate/jocrd Journal of Obsessive-Compulsive and Related Disorders 2211-3649/$ - see front matter & 2013 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jocrd.2013.01.001 n Corresponding author. Tel.: þ49 211 81 12272; fax: þ49 211 81 14261. E-mail address: [email protected] (H. Niemeyer). 1 HN and SM have equally contributed and split first authorship. Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129 Author's Personal Copy

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Responsibility, metacognition and unrealistic pessimism
in obsessive–compulsive disorder
Helen Niemeyer a,n,1, Steffen Moritz b,1, Reinhard Pietrowsky a
a Heinrich-Heine-University, Institute for Experimental Psychology, Department of Clinical Psychology, Universitatsstraße 1, 40225 Dusseldorf, Germanyb University Medical Center Hamburg-Eppendorf, Department of Psychiatry and Psychotherapy, Martinistraße 52, 20246 Hamburg, Germany
a r t i c l e i n f o
Article history:
Received 8 June 2012
Received in revised form
15 December 2012
Accepted 2 January 2013
Available online 11 January 2013
Keywords:
Obsessive–compulsive disorder
Responsibility
Metacognition
Overestimation of threat
Unrealistic optimism
a b s t r a c t
Cognitive models stress the importance of cognitive belief domains (CBD) for the pathogenesis of
obsessive–compulsive disorder (OCD). However, the relative contribution of responsibility and
metacognition – core aspects of CBD – to OC symptoms is not fully understood yet. Furthermore,
two subcomponents of overestimation of threat (OET), overestimation of the personal probability
(unrealistic pessimism) and overestimation of the general risk of negative events, require clarification.
First, we investigated the relative contribution of responsibility and metacognition to OC symptoms.
Second, we hypothesized that OCD patients overestimate the personal risk and display unrealistic
pessimism. Thirty-four OCD patients and 34 healthy controls completed the Obsessive Beliefs Ques-
tionnaire (OBQ) and the Unrealistic Optimism Questionnaire (UO). Responsibility significantly predicted
obsessive symptoms after controlling for metacognition. In contrast to previous findings, responsibility
is not fully explained by metacognition. Finally, our results confirm unrealistic pessimism in OCD, even
after controlling for depression.
& 2013 Elsevier Inc. All rights reserved.
1. Introduction
Cognitive theories of obsessive–compulsive disorder (OCD)
stress the importance of cognitive and metacognitive belief
domains (Rachman, 1997; Salkovskis, 1985, 1989; Wells, 2009).
A large body of literature have demonstrated the importance of an
inflated sense of responsibility (Salkovskis et al., 2000; Shafran,
Thordarson, & Rachman, 1996; Smari & Holmsteinsson, 2001;
Steketee, Frost, & Cohen, 1998) as well as the relevance of
metacognition (Amir, Cashman, & Foa, 1997; Emmelkamp &
Aardema, 1999; Solem, Myers, Fisher, Vogel, & Wells, 2010;
Wells & Papageorgiou, 1998). In recent studies metacognition
significantly predicted inflated responsibility (Gwilliam, Wells, &
Cartwright-Hatton, 2004; Myers & Wells, 2005) but not vice
versa. It is currently unresolved whether responsibility is merely
a by-product of metacognition with no additional contribution to
OC symptoms (Wells, 1997, 2009), or has predictive value in its
own right.
Overestimation of threat (OET) is another prominent cognitive
bias discussed as being relevant for OCD. It is closely related to
responsibility: both load on the same factor in the Obsessive
Beliefs Questionnaire (OBQ-44; Obsessive–Compulsive Cognitions
Working Group (OCCWG, 2005). OET is a complex construct
comprising a number of independent components, which require
systematic study of their individual contributions to obsessive
symptoms. Recently, our group (Moritz & Jelinek, 2009; Moritz &
Pohl, 2006, 2009) applied the unrealistic optimism paradigm
(Weinstein, 1982) to OCD to shed light on the relevance of two
subcomponents for OCD, namely the overestimation of the
personal and the objective incidence probability of negative
events. This paradigm is well suited to help to clarify whether
OCD patients are especially prone to a biased perception of their
personal incidence probability. It can be used to investigate
whether subjects display a bias towards enhanced subjective
vulnerability, whether they have indeed experienced negative
events in the past more often, or whether they merely or
additionally overestimate the severity of harm (Moritz & Jelinek,
2009; Moritz & Pohl, 2009). Unrealistic optimism arises from the
overestimation of the subjective likelihood for positive events to
happen to oneself, while at the same time the personal risk for
negative events is underestimated. The reverse response pattern,
labeled as unrealistic pessimism, might be an important compo-
nent of OET. The UO paradigm goes beyond present question-
naires for OET which do not differentiate between these
important components. Our group (Moritz & Jelinek, 2009;
Moritz & Pohl, 2006, 2009) found that patients with OCD over-
estimated their personal risk for negative events compared to
healthy controls, but not the objective probability of threat. Since
results are not fully consistent across studies, further clarification
Contents lists available at SciVerse ScienceDirect
journal homepage: www.elsevier.com/locate/jocrd
Journal of Obsessive-Compulsive and Related Disorders
2211-3649/$ - see front matter & 2013 Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.jocrd.2013.01.001
n Corresponding author. Tel.: þ49 211 81 12272; fax: þ49 211 81 14261.
E-mail address: [email protected] (H. Niemeyer).1 HN and SM have equally contributed and split first authorship.
Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129
Author's Personal Copy

of unrealistic pessimism in OCD is necessary. Furthermore, its
relationship with responsibility and metacognition awaits
examination.
1.1. Inflated responsibility and metacognition
Responsibility is considered to be a core cognitive belief domain
for the development and maintenance of OCD (Salkovskis &
Forrester, 2002). It has been defined by Salkovskis, Forrester, and
Richards (1998, p. 285) as ‘‘the belief that one has power which is
pivotal to bring about or prevent subjectively crucial negative
outcomes. These outcomes are perceived as essential to prevent.
They may be actual, that is having consequences in the real world,
and/or at a more moral level’’. Cognitive models, predicated on
Beck’s (1976) cognitive theory, posit that obsessions and compul-
sions arise from specific dysfunctional beliefs. Individuals with OCD
interpret intrusions, which are common phenomena (Rachman &
De Silva, 1978; Salkovskis & Harrison, 1984), misleadingly as
indicating an inflated responsibility for preventing the harm the
intrusive thought implied. This responsibility appraisal leads to
intense fear and tension and urges the individual to conduct
neutralizing behavior with the aim of averting the negative con-
sequences. A reduction of discomfort after neutralizing and the
ascribed importance lead to the maintenance of compulsions and
avoidance, thus consolidating the dysfunctional belief of an inflated
responsibility (Salkovskis, 1991, 1996; Salkovskis & Forrester,
2002).
Beliefs about thoughts and thinking processes are referred to
as metacognitive beliefs (Purdon & Clark, 2002). Metacognition is
defined as any knowledge or cognitive process that is involved in
the appraisal, monitoring or control of cognition (Flavell, 1979). A
closely related concept that can also be defined as a subset of the
general concept of metacognition is thought-action fusion (TAF;
Rachman, 1997; Shafran, Thordarson, & Rachman, 1996). It
denotes that thoughts can cause events or are equivalent to the
actions they concern. In patients with OCD, intrusions activate
certain dysfunctional metacognitions, for example ‘‘If I think
about something, bad it will happen’’ (thought-action fusion).
Subjects with OCD interpret intrusions as overly important and
dangerous or threatening. Wells explicit metacognitive theory of
OCD (Wells & Matthews, 1994) was built on this earlier meta-
cognitive perspective by Rachman and Shafran and is part of his
generic metacognitive Self-Regulatory Executive Function Model
(S-REF; Wells, 2009; Wells & Matthews, 1994). According to Wells
(2009), metacognition can be subdivided into three domains:
beliefs about the uncontrollability of thoughts, beliefs about their
meaning and importance, and beliefs about the need to perform
rituals. This metacognitive appraisal activates metacognitive
beliefs about rituals, and as a consequence compulsions and
neutralizing behavior are implemented as attempts to control
one�s thoughts. The negative appraisal of the intrusions and the
dysfunctional control strategies invoked in turn enhance their re-
occurrence. Thus, the appraisal of one�s own thoughts determines
the focus of attention as well as the personal reaction to the
thoughts (Wells, 2009).
The exact relationship between responsibility and metacogni-
tion is controversial and unclear. In Wells�S-REF-model metacog-
nition is explicitly elaborated and distinguished from
responsibility. According to this model, metacognition causes
inflated responsibility (Wells, 2009; Wells & Matthews, 1994).
However, in Salkovskis� cognitive model of OCD, metacognitions
are not explicitly mentioned, but are rather defined as subtypes of
responsibility (Salkovskis, 1989, 1996; Salkovskis & Forrester,
2002; Salkovskis, Shafran, Rachman, & Freeston, 1999). It is
important to note that responsibility within the context of the
appraisal model shows much resemblance to the construct of
metacognition, as the interpretation of intrusive cognitions is a
central part of the appraisal model of OCD. Due to this concep-
tualization the Responsibility Interpretations Questionnaire (RIQ;
Salkovskis et al., 2000), for example, assesses interpretations of
inflated responsibility regarding intrusive thoughts through items
about thought control (e.g., ‘‘I must regain control of my
thoughts’’) and items about responsibility.
Whether inflated responsibility is a contributing or causal factor
in dysfunctional metacognitions, or whether it is itself a conse-
quence or by-product of metacognition is an unresolved question.
Experimental designs used the manipulation of metacognitive
beliefs (thought-action fusion; Rassin, Merckelbach, Muris, &
Spaan, 1999) and cognitive beliefs about responsibility and danger
(Arntz, Voncken, & Goosen, 2007), all of which evoked intrusions
and neutralizing behavior. However, Coles, Pietrefesa, Schofield,
and Cook (2008) found only a modest prediction of metacognition
for distress caused by obsessive symptoms. Myers, Fisher, and
Wells (2009a, 2009b) could show in two studies that only TAF
predicted OC symptoms significantly, but not the responsibility/
overestimation of threat and the importance of thoughts/control of
thoughts subscales (Myers et al., 2009b) of the Obsessive Beliefs
Questionnaire (OBQ-44; OCCWG, 2003). Gwilliam et al. (2004),
Myers and Wells (2005) and Myers, Fisher, and Wells (2008) found
that metacognition significantly predicted OCD when responsibil-
ity was controlled, whereas the association between responsibility
and obsessive symptoms was not significant after controlling for
metacognition. However, some of the questionnaires aimed to
measure responsibility like the Responsibility Appraisal Question-
naire (RAQ2; Rachman, Thordarson, Shafran, & Woody, 1995) or
the Responsibility Attitude Scale (RAS; Salkovskis et al., 2000)
include items measuring TAF and thus might overlap with
metacognition.
1.2. Unrealistic pessimism as component of OET
A related cognitive belief domain to responsibility and meta-
cognition is OET. Responsibility and OET both loaded on the same
factor in a factor analytic study (OCCWG, 2005). Furthermore,
Rachman (2002) argued that high perceived responsibility in
combination with high perceived probability of harm and per-
ceived seriousness of harm might determine the intensity and
duration of compulsive checking. Moreover, he states that ele-
vated responsibility leads to increased perception of danger, and
that intense checking will enhance responsibility in turn. Also,
metacognitive dimensions are likely to be implicated in threat
monitoring, as they may be responsible for predisposing indivi-
duals to engage in monitoring for negative stimuli (Sica, Steketee,
Ghisi, Chiri, & Franceschini, 2007). Responsibility concerns and
metacognitions might be particularly related to personal vulner-
ability and overestimation of the severity of the consequences of
events. Both might increase subjective vulnerability, and vice
versa. However, no studies about possible associations to respon-
sibility and metacognition have been conducted yet, and further
research is necessary to shed light on this.
OET is a multidimensional construct, according to Salkovskis�
cognitive model for OCD (Salkovskis & Wahl, 2003; Sookman &
Pinard, 2002). It consists of several components, including over-
estimation of the objective risk, a perceived enhanced personal
vulnerability, and dysfunctional coping strategies. Most of the
questionnaires tapping OET do not contain subscales for its
different components. As our group (Moritz & Jelinek, 2009)
pointed out, the overestimation of threat subscale of the OBQ-44
(OCCWG, 2003) covers a variety of different components: general
overestimation of threat, overestimation due to prior experiences and
overestimation of the personal vulnerability. A more detailed
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129120
Author's Personal Copy

investigation of the relevance of each of these subfacettes is
required in order to elucidate the core distortion involved in OCD.
Moritz and Pohl (2006) began to analyze the aforementioned
components separately and found that OCD patients did not differ
from healthy controls in their estimation of the incidence fre-
quency of both OCD-related and OCD-unrelated negative events in
general. In two recent studies the paradigm of unrealistic optimism
was applied to investigate whether subjects with OCD show a
biased perception of their personal incidence probability of the
occurrence of negative and positive events (Moritz & Jelinek, 2009;
Moritz & Pohl, 2009). As mentioned, unrealistic optimism means
that people overestimate the probability of positive events hap-
pening to them, whereas they think that negative events happen
more likely to other people. This bias is almost universal and has
been found in both healthy and high risk samples for severe bodily
diseases (Weinstein, 1982; Weinstein & Klein, 1996; Weinstein,
Marcus, & Moser, 2005). As opposed to unrealistic optimism,
unrealistic pessimism refers to overestimating the probability of
negative events happening to oneself, while assuming that positive
events happen more likely to other people. Moritz and Jelinek
(2009) and Moritz and Pohl (2009) administered the Unrealistic
Optimism Questionnaire (UO), which is described in detail in the
methods section, to OCD patients and healthy controls.
Unrealistic pessimism concerning negative events is connected
to vulnerable self-themes and sensitive self-domains in OCD, as
the results of Moritz and Pohl (2009) and Moritz and Jelinek
(2009) suggest. Moritz and Jelinek (2009) found that in a
comparison of self versus others the healthy sample displayed
an unrealistic optimism bias, whereas the OCD sample, as
expected, showed the opposite bias, unrealistic pessimism, espe-
cially for negative events that were related to washing and
checking. The bias is investigated with paradigms tapping implicit
and explicit comparisons. The explicit comparison entails that the
person directly compares oneself to others regarding probability
estimates for positive and negative events, whereas the implicit
comparison contrasts two separate estimates, one for oneself and
one for others (first versus second block). The results of the two
blocks are compared post-hoc (Moritz & Jelinek, 2009; Moritz &
Pohl, 2009). Moritz and Jelinek (2009) found evidence for an
implicit but not an explicit bias in an OCD sample. This pattern of
results is consistent with former studies on smokers which found
that implicit measures are more sensitive to capture unrealistic
optimism (Weinstein et al., 2005). Moritz and Pohl (2009) did not
apply an implicit, but only an explicit comparison, to investigate
this component in detail. They found that OCD patients felt less
safe to experience negative and especially OCD-related events,
but could not confirm an unrealistic pessimism bias, as partici-
pants with OCD rather showed an attenuated unrealistic opti-
mism regarding negative events in an explicit comparison. In
contrast to unrealistic optimism, which means that persons think
that positive events are more likely to happen to themselves than
to others, whereas negative events are less likely, the term
‘‘attenuated unrealistic optimism’’ is used to refer to the pattern
that the usual unrealistic optimism bias is present (and not
reversed) but less strong.
Thus, in their OCD sample Moritz and Pohl (2009) did not find
unrealistic pessimism in the explicit comparison, but rather less
unrealistic optimism, whereas Moritz and Jelinek (2009) found no
bias in the explicit comparison, but an unrealistic pessimism (i.e.,
the unrealistic optimism bias was reversed) in the implicit
comparison. To summarize, the results of the two studies differ
with respect to the explicit comparison, whereas an implicit
comparison was not implemented in the study by Moritz and
Pohl (2009). Thus, it is not yet resolved whether participants with
OCD are more prone to unrealistic pessimism or instead tend to
show attenuated unrealistic optimism.
OC symptoms correlated with the personal risk for washing-
and checking-related events, also pointing to the relevance of the
subjective personal vulnerability in OCD (Moritz & Jelinek, 2009).
In addition, the UO captures the valence of negative and positive
events, and the OCD sample saw graver consequences of negative
events than did the control sample, indicating an overestimation
of harm severity (Moritz & Jelinek, 2009). According to self-report,
OCD patients had not actually experienced the relevant events
more often in the past than the healthy controls, thus making it
unlikely that the pessimism arises from prior experience.
1.3. Present study
Three aims were pursued in the present investigation: First,
we wanted to clarify the relevance of responsibility and meta-
cognition for obsessive symptoms by examining the relative
contribution of each belief domain to OC symptoms using
hierarchical regression. While some previous research obtained
mixed results, the studies by Wells and colleagues showed a
greater influence of metacognition on OC symptoms compared to
responsibility. The interpretation of these findings is complicated
by the fact that there is an overlap in the operationalization of
metacognition and responsibility in some of the studies. For the
present study, responsibility was operationalized with as little
overlap with metacognition as possible, thus leading us to expect
that both metacognition and responsibility would predict OC
symptoms. To our knowledge, it is the first study investigating
the relative contribution of responsibility and metacognition to
OC symptoms in a German sample. We think that our results
can be generalized to other patient samples in industrialized
countries.
The second aim was to investigate the relevance of the
components overestimation of the personal vulnerability and over-
estimation of the objective likelihood of the incidence of events (for
other persons) in both an implicit and an explicit comparison, and
in addition to investigate the overvaluation of the valence of
negative and positive events. We hypothesized that participants
with OCD will be prone to a subjective personal vulnerability, but
not to a general overestimation, thus showing an unrealistic
pessimism. Furthermore, we expected that they appraise the
consequences of negative events as more grave. To determine
whether unrealistic pessimism occurs depending on OCD we
controlled for depression in subsidiary analyses, as depression
has been shown to correlate with OC symptoms (Moritz, Meier,
Hand, Schick, & Jahn, 2004) and to induce a negative view of
events (Clark, 2001). Finally, exploratory correlational analyses
were conducted to examine the interrelationships between the
components of an unrealistic pessimism to inflated responsibility
and metacognition.
2. Methods
2.1. Participants
Sixty-eight participants, all at least 18 years old, took part in the study. The 34
participants in the OCD group were recruited in the psychotherapeutic out-patient
clinic of the Psychology Department at the University Duesseldorf and from
therapists in private practice. This group had (1) a total score in Obsessive–
Compulsive Inventory-Revised (OCI-R; Foa et al., 2002, German Version: Goenner,
Ecker, & Leonhart, 2009) of Z18, constituting the German cut-off, as well as (2) a
self-report Yale-Brown Obsessive–Compulsive Scale (Y-BOCS-SR; Goodman et al.,
1989, German Version: Baer, 1993) total score ofZ10 in case of either mental or
behavioral obsessions, orZ16 if it both occurred; and (3) the OCD diagnosis was
verified with the Structured Clinical Interview for DSM-IV (Wittchen, Zaudig, &
Fydrich, 1997) or confirmed by the clinicians who were treating the patients for OCD.
In the latter case, clinicians applied DSM-IV criteria for diagnosis, but without
applying a structured interview. Exclusion criteria for the OCD sample were current
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129 121
Author's Personal Copy

or previous diagnoses of (1) psychosis or schizophrenia, (2) bipolar disorder,
(3) substance dependence, or (4) neurological disorders.
The healthy participants were recruited via an established subject pool and
word-of-mouth advertisement and consisted of students enrolled at the university
as well as non-student participants recruited from the community, who were
mainly prior study participants. In a questionnaire, they were asked about current
or former psychological disorders and whether they had ever undergone psy-
chotherapeutic or pharmacological treatment. Furthermore, they had to (1) score
below both the OCI-R cut-off, (2) also the Y-BOCS-SR cut-off, (3) score low on
depressive symptoms (score lower than 14 in the BDI-II; Beck, Steer, & Brown,
1996, German Version: Hautzinger, Keller, & Kuehner, 2009), and (4) as described
above, have no current or previous psychiatric diagnoses.
2.2. Measures
OCD symptom severity was assessed using the OCI-R and the Y-BOCS-SR. The
psychometric properties of both the original and the German versions are good
(Goodman et al., 1989; Schaible, Armbrust, & Nutzinger, 2001; Steketee, Frost, &
Bogart, 1996; Goenner et al., 2009). The OCI-R consists of 18 items inquiring the
extent of distress caused by OC symptoms during the last month. The Y-BOCS-SR
comprises 10 items and demonstrated a good convergent validity with the Y-BOCS
clinical interview (Schaible et al., 2001; Steketee et al., 1996).
Participants also completed the Beck Depression Inventory-II to assess the
comorbid depression symptom severity (BDI-II; Beck et al., 1996, German Version:
Hautzinger et al., 2009), which also has good psychometric properties.
2.2.1. Obsessive Beliefs Questionnaire (OBQ)
We administered three self-report inventories to assess the cognitive variables
and considered the particular subscales that covered the belief domains of interest
for our statistical analysis. To assess metacognition beliefs, the German version of
the OBQ (Ertle et al., 2008) was applied, which contains 24 items from the English
version that loaded on the designated factor with a minimum alpha of a ¼ .30. Due
to this reduction of the number of items the subscales of the German OBQ cover
mainly the domains importance of thoughts, perfectionism and OET. All subscales
share good reliability and validity. For the present study the subscale importance of
thoughts was used.
2.2.2. Responsibility and Interpersonal Behaviors and Attitudes Questionnaire
(RIBAQ)
The RIBAQ is an inventory designed to assess pro-social (one subscale) and
anti-social (two subscales) attitudes associated to responsibility, aimed to capture
interpersonal ambivalence. An initial long form of 60 items developed by clinical
experts on OCD was shortened to 32 items following a factor analysis (Moritz
et al., 2009). The questionnaire consists of three subscales (excessive worry and
responsibility, latent aggression, and suspiciousness/distrust); only those items
were included that had loadings greater than .4 and differed from the loadings on
the two other factors by at least .2 (absolute value) in order to ensure
independence of subscales. Only the responsibility subscale was used for our
statistical analyses. This scale of 17 items shows good reliability (Cronbach’s
alpha: a¼ .87) and convergent validity with the respective subscale of the OBQ
(r¼ .64, p o .001; Moritz et al., 2009). Furthermore, the scale correlated with the
Y-BOCS (r¼ .17, p¼ .02) and the MOCI total score (r¼ .29, p o .001; Moritz et al.,
2009).
Participants were asked to rate how well the following behaviors, attitudes
and habits apply to them using a 4-point scale with response categories ranging
from ‘‘does not apply’’ (¼0) to ‘‘applies only slightly’’ (¼1), ‘‘mostly applies’’ (¼2)
and ‘‘applies completely’’ (¼4). Example items of the subscale ‘‘excessive worry
and responsibility’’ employed in the present study are ‘‘To save the life of a
relative, I would donate an organ’’, ‘‘I suffer from a strict conscience concerning my
relatives’’, or ‘‘I fear that people at work do not think that I am 100% reliable’’.
2.2.3. Unrealistic Optimism Questionnaire (UO)
To assess unrealistic pessimism we administered a self-report questionnaire
that allows contrasting an implicit and an explicit comparison (Moritz & Jelinek,
2009). It consists of five blocks in which the same negative and positive events are
presented. In block 1, participants estimated the likelihood that the depicted event
would happen to themselves in the future (personal vulnerability), without direct
comparison with other persons, while block 2 in turn requested an estimate of the
likelihood that an average person of the same sex and age would experience such
an event in the future (general vulnerability). For both blocks a 7-point Likert scale
with response categories from ‘‘very unlikely’’ (1) until ‘‘highly probable’’ (7) with
‘‘medium’’ (4) as midpoint was applied. Contrasting block 1 and 2 allows for an
implicit comparison, resulting in four dependent measures (self-positive, self-
negative, others positive and others negative).
Block 3 required participants to compare the relative probability that the
event would happen to them in the future versus an average person of the same
age and sex, using a 7-point scale ranging from ‘‘much less compared to others’’
(1) to ‘‘much higher compared to others’’ (7), with ‘‘equally high’’ (4) representing
the midpoint. Thus, block 3 asks in direct comparison how likely negative and
positive events might happen to oneself versus to another person (comparative
vulnerability).
Block 4 requested participants to appraise the consequences of each event
(appraisal or valence): Each person appraised the subjective negativity of the
negative and the subjective positivity of the positive events for him or herself.
Endpoints were ‘‘extremely negative’’ (1) and ‘‘extremely positive’’ (7), the
midpoint was ‘‘neutral’’ (4).
In block 5, participants indicated how often the respective events had occurred
to either themselves or to a friend, relative or acquaintance (prior experience) using
the three rating options ‘‘never’’ (1), ‘‘once’’ (2), and ‘‘several times’’ (3).
Except for the different instructions, the events to be rated were the same for
all five blocks. Examples are ‘‘y to become 90 years old‘‘ for positive events,
and’’y to transmit a disease to someone because of inattentiveness or insufficient
hygiene’’ for the OCD-related events or ‘‘y to directly or indirectly cause a fire
(e.g. oven or candle left burning)’’ for negative events. For the present study blocks
1, 2, 3 and 4 were statistically analyzed.
All questionnaires were delivered in paper–pencil format. The healthy parti-
cipants received them in personal contact or by mail. The participants in the OCD
group received the questionnaire from their therapists and returned the anon-
ymized questionnaires to the out-patient department via mail. The therapists in
turn were given the questionnaire in person. Participants were informed about the
study and gave written consent to participate. They were offered the option of
generating an anonymous code, which allowed them to access their test results
anonymously at the end of the study.
2.3. Overview of statistical analyses
T-tests for independent samples were conducted comparing the samples with
respect to the clinical measures. Univariate analyses of variance (ANOVAs) with
group as factor (OCD and control sample) were conducted to test for significant
differences between the dependent variables responsibility, metacognition and
the two investigated subcomponents of OET. Two hierarchical regression analyses
were conducted to investigate how much variance in OC symptoms was explained
by either responsibility or metacognition. In the first regression responsibility was
entered on step 1 and metacognition on step 2, whereas in the second regression
analysis we reversed the sequence. Three-way mixed ANOVAs and post-hoc
univariate ANOVAs were calculated to investigate unrealistic pessimism in the
implicit comparison. To control for the influence of depression on unrealistic
pessimism we applied a median split: We divided the OCD sample into two groups
with BDI larger or smaller than the median. We then conducted subsidiary
analyses with the subsample of low level depression patients (n¼17). This
approach has been adopted before (Moritz, Kloss, Jahn, Schick, & Hand, 2003).
In addition, we conducted a second, more stringent subsidiary analysis with all
patients below the BDI-cut-off of 19 for moderate depression (Hautzinger et al.,
2009; Kuehner, Buerger, Keller, & Hautzinger, 2007). One-sample t-tests were
used to test the explicit comparison of unrealistic pessimism against the neutral
midpoint (4) of the UO scale. Pearson correlations (r) or, if the variables were not
normally distributed, non-parametric Spearman’s rho coefficients (rs) were calcu-
lated to investigate the relationships between all variables. To compensate for an
inflation of the alpha error the p-value was adjusted, when necessary, that is in
calculations with the OCI-R and the Y-BOCS-SR, which both measure OC symp-
toms. All correlations and the regression analyses were calculated using the
complete sample (n¼68), assuming the quasi-dimensionality of non-clinical and
clinical obsessions and compulsions (Rachman, 1997; Salkovskis, 1991). Subclini-
cal symptoms of OCD are assumed to differ only gradually from clinical obses-
sions, but not qualitatively (Gibbs, 1996). Missing data occurred only for the use of
psychotropic drugs, but not in the questionnaires.
3. Results
3.1. Sociodemographic variables
The group of OCD patients did not differ from the healthy
control subjects with respect to age and gender on a minimum
significance level of p 4 .9 (see Table 1). The mean age of patients
was 36.94 years (SD¼12.25, range 18–65), that of the control
group was 37.12 years (SD¼12.53, range 18–63). Both groups
consisted of 20 women and 14 men. The highest level of educa-
tion was also identical (w2 (4)¼ .00, p 4 .9). 97.1% of OCD subjects
were currently in treatment due to OCD, and 61.8% had been in
treatment in the past. The mean age of patients in the subsample
with low depression was 37.5 years (SD¼12.93, range 21–65),
and the group consisted of eight women and nine men. The
subsample of patients below the cut-off for moderate depression
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129122
Author's Personal Copy

(five men and five women) had a mean age of 42.3 (SD¼12.32,
range 27–65).
3.2. Clinical measures
As expected, OCD subjects scored higher on OCI-R than the
controls, t (66)¼14.57, p o .001. Likewise, the mean Y-BOCS-SR
score was higher in the OCD group, t (66)¼20.03, p o .001. The
mean BDI-score was M¼25.59 in the OCD group, and M¼5.03 in
the control group; t (66)¼9.08, p o .001. Twenty-nine patients
met the criteria of a comorbid major depression episode. In the
OCD group 19 subjects (55.90%) were unmedicated, nine (26.50%)
were medicated, and six (17.60%) did not state their medication
status. These omissions were treated as missing data. All 34
subjects in the control group were unmedicated (100%). Detailed
information about the sociodemographic, clinical and cognitive
variables is given in Table 1.
3.3. Metacognition and responsibility
3.3.1. Group differences
Subjects with OCD exceeded controls significantly on respon-
sibility, F (1, 66)¼49.29, p o .001, and on metacognition, F (1,
66)¼21.62, p o .001 (see Table 1).
3.3.2. Hierarchical regression analyses
Two hierarchical regression analyses with responsibility and
metacognition as predictor variables for obsessive symptoms
were conducted. Because the OCI-R and the Y-BOCS-SR were
highly correlated, while the Y-BOCS-SR scores were not normally
distributed, we restricted these analyses to the OCI-R. Due to the
high intercorrelations between responsibility and metacognition
we tested for multicollinearity, but the test showed an acceptable
tolerance of .69 (see Tabachnik & Fidell, 2007). The normality of
the scores was assessed and verified for both variables. Homo-
scedasticity of the standardized residuals, assessed by examining
the scatterplots of all variables, was also confirmed.
The results of the regression are shown in Table 2. In a first
step, responsibility was entered into the analysis. It explained a
significant amount of variance (42%). On step 2 metacognition
was included, giving an additional 3.9% of explained variance;
DF (1, 65)¼4.67, p o .05; b¼ .24, p o .05; B¼1.84. With both
variables as significant predictors, we obtained an R2 of .46 and an
adjusted R2 (adj.) of .45 for the final model.
In the second analysis, metacognition was entered on step
1 and responsibility on step 2. Metacognition entered on step
1 explained 28% of variance in obsessive symptoms. Additional
19% of the variance was significantly explained by responsibility
on step 2 (DF (1, 65)¼22.58, p o .01; b¼ .52, p o .01; B¼15.07).
In the final equation the R2 was .46 and the adjusted R2 (adj.)¼ .45.
3.4. Unrealistic optimism
3.4.1. Implicit comparison
In order to assess an unrealistic pessimism in the implicit
comparison, a three-way mixed ANOVA was conducted. Locus
(self versus comparable other) and event type (positive versus
negative) were entered as within-subject factors and group as
between-subject factor. The event probability, on a rating scale
from 1 (‘‘very unlikely’’) to 7 (‘‘highly probable’’), was defined as
dependent variable. The main effect of locus was significant, F
(1,66)¼23.47, p o .001, and so was the main effect of event type F
(1,66)¼33.55, p o .001, as was the interaction between group
and event, F (1,66)¼15.26, p o .001. The main effects of locus and
event type arise from significant differences in pair wise
comparisons between all levels, except for one non-significant
difference between the levels self-positive and others negative.
The interaction between group and locus was not significant,
F (1,66)¼ .87, p 4 .05, but the three-way interaction was,
F (1,66)¼8.71, p o .01. The three-way interaction effect indicates
that the incidence probability of positive and negative events for
oneself versus others differed significantly between the two
groups. Univariate ANOVAs, conducted post-hoc with group as
factor and locus/event type as dependent variable, confirmed that
the estimate of the OCD sample of the likelihood of positive
events happening to them was lower than that of the healthy
control sample, F (1,66)¼15.45, p o .001, while they thought that
their personal likelihood to experience negative events was
higher than did the controls, F (1,66)¼8.01, p o .01. There was
no difference in the estimate of the probability for other persons,
neither for positive events, F (1,66)¼2.21, p 4 .05, nor for
negative events, F (1,66)¼ .84, p 4 .05. The results of this implicit
comparison are displayed in Table 1.
Furthermore, we controlled for the influence of depression by
conducting two subsidiary analyses. First, we included all OCD
patients with a BDI-score below the median of the patient group
(n¼17, cut-off¼24.5) and repeated the above three-way mixed
Table 1
Sociodemographic, psychopathological und cognitive variables and between-
group comparisons. Means and standard deviations (in parentheses).
Variable OCD (n¼34) Healthy
(n¼34)
Statistics
Sociodemographic variables:
Age 36.94
(12.25)
37.12 (12.53) t(66)¼ .00, p 4 .9
Sex (male/female) 14/20 14/20 w2(1)¼ .00, p 4 .9
Psychopathology:
OCI-R 30.71 (7.93) 7.53 (4.82) t(66)¼14.57, p o .001
Y-BOCS-SR 23.03 (5.95) 1.12 (2.31) t(66)¼20.03, p o .001
BDI-II 25.59
(12.45)
5.03 (4.4) t(66)¼9.08, p o .001
Cognitive variables:
Responsibility 2.54 (.37) 1.94 (.34) F(1,66)¼49.29, p
o .001
Metacognition 3.96 (1.73) 2.27 (1.23) F(1,66)¼21.62, p
o .001
Unrealistic optimism
Implicit, self (þ) 2.90 (.97) 3.81 (.94) F(1,66)¼15.45, p
o .001
Implicit, self (�) 2.93 (.78) 2.43 (.67) F(1,66)¼8.01, p o .01
Implicit, others (þ) 3.69 (.84) 3.97 (.74) F(1,66)¼2.21, p 4 .05
Implicit, others (�) 3.20 (.95) 2.99 (.97) F(1,66)¼ .84, p 4 .05
Explicit (þ) 3.24 (.76) 3.95 (.59) F(1,66)¼18.65, p
o .001
Explicit (�) 3.71 (.64) 3.38 (.58) F(1,66)¼4.99, p o .05
Valence (þ) 5.07 (1.82) 5.97 (.79) F(1,66)¼7.04, p o .05
Valence (�) 1.86 (.84) 1.62 (.66) F(1,66)¼1.70, p 4 .05
Note: OCD¼Obsessive–compulsive disorder; OCI- R¼Obsessive–Compulsive
Inventory-Revised; Y-BOCS-SR¼Yale-Brown Obsessive–Compulsive Scale self-
report; BDI-II¼Beck Depression Inventory-II; (þ)¼ likelihood of positive events;
(�)¼ likelihood of negative events.
Table 2
Hierarchical regression.
Variable df1 df2 DF p b p B R2 R2adj.
Regression 1
Step 1 Responsibility 1 66 48.54 o .001 .65 o .001 18.87 .42 .42
Step 2 Metacognition 1 65 4.67 o .05 .24 o .05 1.84 .46 .45
Regression 2
Step 1 Metacognition 1 66 25.11 o .001 .53 o .001 4.09 .28 .27
Step 2 Responsibility 1 65 22.58 o .01 .52 o .01 15.07 .46 .45
Note: R2adj.¼R2 adjusted.
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129 123
Author's Personal Copy

ANOVA. Results remained essentially unchanged. Again, the main
effect of locus was significant, F (1,49)¼15.70, p o .001, as was
the main effect of event type F (1,49)¼28.56, p o .001. Compar-
able to the analysis with the full sample, the interaction between
group and locus, F (1,49)¼ .47, p 4 .05, was non-significant,
whereas the interaction between group and event was significant,
F (1,49)¼6.33, p o .05. The three-way interaction was also
significant, F (1,49)¼6.17, p o .05. Univariate ANOVAs confirmed
that the estimate of the OCD sample of the likelihood of positive
events happening to them was lower than that of the healthy
control sample, F (1,49)¼6.70, p o .05. However, there was no
difference between the groups regarding their personal likelihood
to experience negative events, F (1,49)¼3.90, p 4 .05. As in the
full sample, there was also no difference in the estimate of the
probability for other persons, neither for positive events, F
(1,49)¼ .88, p 4 .05, nor for negative events, F (1,49)¼ .41, p
4 .05. The results of this subsidiary analysis to control for
depression are displayed in Table 3.
Second, we conducted a more stringent subsidiary analysis
considering all OCD patients with a BDI-score below the cut-off
for moderate depression (BDI score of 19, n¼10). The three-way
mixed ANOVA was repeated and yielded much the same results as
before. The main effect of locus was significant, F (1,42)¼7.79, p
o .01, as was the main effect of event type, F (1,42)¼17.79, p
o .001. The interaction between group and locus, F (1,42)¼ .002, p
4 .05, was non-significant, whereas the interaction between
group and event was significant, F (1,42)¼6.04, p o .05. One
result did change, however: the three-way interaction was no
longer significant, F (1,42)¼2.67, p o .05, perhaps owing to the
smaller sample size. For the estimated likelihood of positive
events happening to themselves the univariate ANOVA resulted
in a non-significant difference, F (1,42)¼3.65, p 4 .05, which
deviates from the results in the full sample and in the subsample
below the median for depression. However, we found a difference
between the groups regarding the subjective likelihood to experi-
ence negative events, F (1,42)¼4.44, p o .05. This result was
found for the full sample, as well. Finally, no difference occurred
for the judgments for other persons, neither for positive events, F
(1,42)¼1.85, p 4 .05, nor for negative events, F (1,42)¼ .42, p
4 .05 (see Table 4).
We also investigated the unrealistic biases separately for the
OCD group and the healthy controls. Comparing for each sample
separately the estimation of the personal probability to the
estimation of the probability for others (implicit self versus
implicit others), we found that the OCD sample estimated that
positive events were less likely to happen to themselves than to
another comparable person (p o .001, see Table 5). Thus, patients
are unrealistically pessimistic regarding positive events. The
estimation of the incidence of negative events did not differ
significantly. The healthy sample showed the opposite pattern:
the estimation of positive events did not differ significantly, but
they estimated the incidence of negative events for themselves as
significantly lower (p o .001). To summarize, the OCD sample
demonstrates halfway unrealistic pessimism, while the control
subjects are unrealistically optimistic (see Table 5; Fig. 1).
3.4.2. Explicit comparison
Univariate ANOVAs showed that for the explicit comparison
(block 3) groups differed in the estimated incidence probability of
positive events, F (1,66)¼18.65, p o .001. The OCD sample rated
the incidence probability for positive events as significantly
lower. The incidence probability rating of negative events like-
wise differed, with the OCD sample judging personal probability
as significantly higher, F (1,66)¼4.99, p o .05. To conclude, in
comparison to healthy controls the OCD group displays an
unrealistic pessimism (see Table 1). In the subsidiary analysis
with low level depressed patients, the groups also differed in the
estimated probability of positive events, F (1,49)¼9.76, p o .01,
but not of negative events, F (1,49)¼1.03, p 4 .05 (see Table 3).
However, results changed in the second subsidiary analysis with
OCD patients below the cut-off for moderate depression: there
was a significant difference for negative events, F (1,42)¼5.72, p
o .05, but none for positive events, F (1,42)¼3.26, p 4 .05 (see
Table 4).
To compare the rating of each full sample against the neutral
score of the scale (4), we conducted one-sample t-tests for each
group. The OCD sample differed significantly from the neutral
score for both positive, t (33)¼�5.84, p o .001, and negative
event probabilities, t (33)¼�2.68, p o .05, but the healthy
control sample differed merely for the rating of negative events,
t (33)¼�6.28, p o .001. All groups scored lower than the neutral
center point of the scale, which means that they all under-
estimated the incidence probability for both positive and negative
events (see Table 6).
Participants with OCD and healthy controls rated the personal
valence of negative events (block 4) equally (see Table 1). The
valence of positive events was rated significantly lower by the
OCD sample than the control group, F (1,66)¼7.04, p o .05. In a
subsidiary analysis with all OCD patients below the median of the
depression score of the experimental group, there was no longer a
difference between the two groups in the valence of positive
events, F (1,49)¼ .24, p 4 .05. The rating of the valence of negative
events was equal across samples, F (1,49)¼ .43, p 4 .05 (see
Table 3
Subsidiary analyses for unrealistic optimism with low level depression patients.
Means and standard deviations (in parentheses).
Variable OCD (n¼17) Healthy (n¼34) Statistics
Unrealistic optimism
Implicit, self (þ) 3.08 (.98) 3.81 (.94) F(1,49)¼6.70, p o .05
Implicit, self (�) 2.83 (.72) 2.43 (.67) F(1,49)¼3.90, p 4 .05
Implicit, others (þ) 3.76 (.74) 3.97 (.74) F(1,49)¼ .88, p 4 .05
Implicit, others (�) 3.16 (.75) 2.99 (.97) F(1,49)¼ .41, p 4 .05
Explicit (þ) 3.35 (.74) 3.95 (.59) F(1,49)¼9.76, p o .01
Explicit (�) 3.56 (.71) 3.38 (.58) F(1,49)¼1.03, p 4 .05
Valence (þ) 5.82 (1.37) 5.97 (.79) F(1,49)¼ .24, p 4 .05
Valence (�) 1.5 (.53) 1.62 (.66) F(1,49)¼ .96, p 4 .05
Note: OCD¼Obsessive–compulsive disorder; OCI-R¼Obsessive–Compulsive
Inventory-Revised; Y-BOCS-SR¼Yale-Brown Obsessive–Compulsive Scale self-
report; BDI-II¼Beck Depression Inventory-II; (þ)¼ likelihood of positive events;
(�)¼ likelihood of negative events.
Table 4
Subsidiary analyses for unrealistic optimism with patients below the cut-off for
moderate depression (BDI scoreo19). Means and standard deviations (in
parentheses).
Variable OCD (n¼10) Healthy (n¼34) Statistics
Unrealistic optimism
Implicit, self (þ) 3.17 (.93) 3.81 (.94) F(1,42)¼3.65, p 4 .05
Implicit, self (�) 2.98 (.87) 2.43 (.67) F(1,42)¼4.44, p o .05
Implicit, others (þ) 3.63 (.48) 3.97 (.74) F(1,42)¼1.85, p 4 .05
Implicit, others (�) 3.20 (.71) 2.99 (.97) F(1,42)¼ .42, p 4 .05
Explicit (þ) 3.57 (.59) 3.95 (.59) F(1,42)¼3.26, p 4 .01
Explicit (�) 3.85 (.43) 3.38 (.58) F(1,42)¼5.72, p o .05
Valence (þ) 6.33 (.57) 5.97 (.79) F(1,42)¼1.81, p 4 .05
Valence (�) 1.41 (.30) 1.62 (.66) F(1,42)¼ .96, p 4 .05
Note: OCD¼Obsessive–compulsive disorder; OCI-R¼Obsessive–Compulsive
Inventory-Revised; Y-BOCS-SR¼Yale-Brown Obsessive–Compulsive Scale self-
report; BDI-II¼Beck Depression Inventory-II; (þ)¼ likelihood of positive events;
(�)¼ likelihood of negative events.
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129124
Author's Personal Copy

Table 3). The same significances were found for the subsample
below the cut-off for moderate depression (see Table 4).
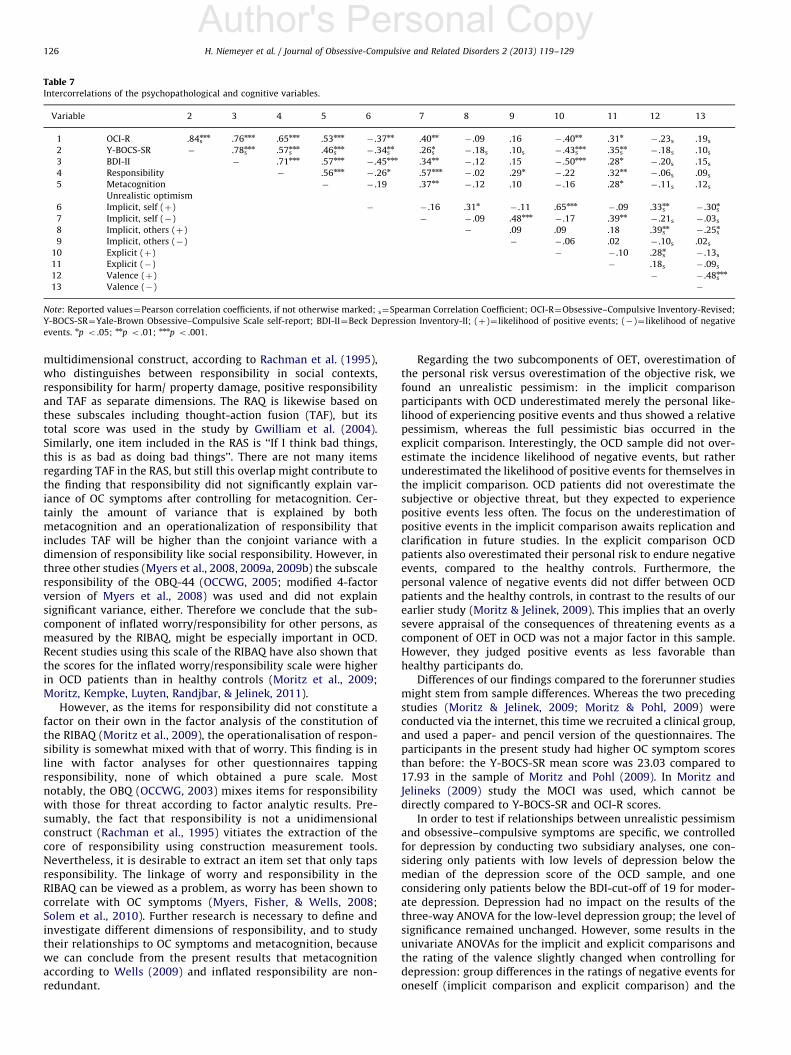
3.5. Correlational analyses
3.5.1. Associations between cognitive variables and obsessive
symptoms
The two questionnaires for symptom assessment, OCI-R and
Y-BOCS-SR were significantly correlated. Moreover, responsibility
and metacognition were both significantly associated with the
OCI-R and the Y-BOCS-SR scores. All intercorrelations are dis-
played in Table 7.
3.5.2. Intercorrelations between the belief domains
Responsibility and metacognition were significantly associated
(r¼ .56, p o .001). For all correlations of the components of the
implicit and explicit comparison with each other and with the
valences of positive and negative events, see Table 7.
Responsibility was positively associated with the subjective
likelihood of negative events for self and others in the implicit
comparison and in the explicit comparison, and negatively with
the personal incidence likelihood of positive events. Metacogni-
tion correlated with the personal incidence probability rating of
negative events in the implicit comparison, and with negative
events in the explicit comparison, but not with any other
components. There was no correlation between the evaluation
of positive and negative events (valence) and either metacogni-
tion or responsibility.
3.5.3. Intercorrelations between depression and unrealistic
pessimism
The BDI score in the OCD sample correlated negatively with
the personal valence of positive (rs¼� .49, p o .01) and positively
with the valence of negative (rs¼ .40, p o .05) events, but not with
any of the components of implicit and explicit comparison for an
unrealistic pessimism. In the control group, the BDI score corre-
lated negatively with the self positive component of the implicit
comparison (r¼� .34, p o .05), and positively with the personal
valence of positive events (rs¼ .48, p o .01).
4. Discussion
Our study first aimed to investigate the relative contribution of
responsibility and metacognition to the severity of OC symptoms,
and second to assess a possible overestimation of personal risk
and thus an unrealistic pessimism in OCD patients. We turn first
to the results pertaining to metacognition and responsibility and
then proceed with the data on unrealistic optimism.
Previous studies (Gwilliam et al., 2004; Myers & Wells, 2005)
found that responsibility did not significantly contribute to OC
symptoms when metacognition was controlled for, whereas
metacognition made a significant contribution after controlling
for responsibility. To clarify the relevance of each of these
constructs for OCD, our study aimed to reinvestigate this con-
troversial issue. To this end, we took care to operationalize
responsibility with as little overlap to metacognition as possible,
and used a scale that operationalizes a dimension of social
responsibility, namely inflated worry/responsibility. As expected,
both metacognition and responsibility where highly correlated
with OCD. Conducting two hierarchical regression analyses,
entering the two constructs in reverse order, we found that
metacognition indeed contributed significantly but modestly to
obsessive–compulsive symptoms after responsibility was con-
trolled for, and conversely responsibility made a significant
contribution after controlling for metacognition. The amount of
variance explained by responsibility on step two was even about
four times that explained by metacognition on step two in the
corresponding regression analysis.
There are some important differences between our study and
previous studies conducted by other groups. First, Myers, Wells
and colleagues used non-clinical samples in all their studies,
whereas our sample consisted of 34 clinical and 34 healthy
participants. Second, we chose to operationalize a different
dimension of responsibility: whereas some of the forerunner
studies used questionnaires such as the RAS (Myers & Wells,
2005; Salkovskis et al., 2000) or the RAQ (Gwilliam et al., 2004;
Rachman et al., 1995), we employed the inflated worry/responsi-
bility scale of the RIBAQ which measures social responsibility.
Responsibility should be defined and operationalized as a
Table 5
Implicit comparison of unrealistic optimism. Means and standard deviations (in
parentheses).
Group and valence Implicit, self Implicit, others F (df¼33)
OCD
(þ) 2.90 (.97) 3.69 (.84) 15.23, p o .001
(�) 2.93 (.78) 3.20 (.95) 2.66, p 4 .05
Healthy controls
(þ) 3.81 (.94) 3.97 (.74) .91, p 4 .05
(�) 2.43 (.67) 2.99 (.97) 15.66, p o .001
Note: OCD¼Obsessive–compulsive disorder; (þ)¼ likelihood of positive events;
(�)¼ likelihood of negative events.
Fig. 1. Unrealistic optimism in the implicit comparison. Probability that a positive
or negative event will happen to oneself (block 1) and to a person with the same
age and sex (block 2), respectively. Scores ranged from ‘‘highly unlikely’’ (¼2) over
‘‘unlikely’’ (¼3) to ‘‘fifty–fifty’’ (¼4).
Table 6
Comparison of explicit ratings in OCD and healthy control group against neutral
score of the unrealistic optimism scale. Means and standard deviations (in
parentheses).
Group and valence Explicit Neutral score t (df¼33)
OCD
(þ) 3.24 (.76) 4 �5.84, p o .001
(�) 3.71 (.64) 4 �2.68, p o .05
Healthy controls
(þ) 3.95 (.59) 4 � .48, p 4 .05
(�) 3.38 (.58) 4 �6.28, p o .001
Note: OCD¼Obsessive–compulsive disorder; (þ)¼ likelihood of positive events;
(�)¼ likelihood of negative events.
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129 125
Author's Personal Copy
multidimensional construct, according to Rachman et al. (1995),
who distinguishes between responsibility in social contexts,
responsibility for harm/ property damage, positive responsibility
and TAF as separate dimensions. The RAQ is likewise based on
these subscales including thought-action fusion (TAF), but its
total score was used in the study by Gwilliam et al. (2004).
Similarly, one item included in the RAS is ‘‘If I think bad things,
this is as bad as doing bad things’’. There are not many items
regarding TAF in the RAS, but still this overlap might contribute to
the finding that responsibility did not significantly explain var-
iance of OC symptoms after controlling for metacognition. Cer-
tainly the amount of variance that is explained by both
metacognition and an operationalization of responsibility that
includes TAF will be higher than the conjoint variance with a
dimension of responsibility like social responsibility. However, in
three other studies (Myers et al., 2008, 2009a, 2009b) the subscale
responsibility of the OBQ-44 (OCCWG, 2005; modified 4-factor
version of Myers et al., 2008) was used and did not explain
significant variance, either. Therefore we conclude that the sub-
component of inflated worry/responsibility for other persons, as
measured by the RIBAQ, might be especially important in OCD.
Recent studies using this scale of the RIBAQ have also shown that
the scores for the inflated worry/responsibility scale were higher
in OCD patients than in healthy controls (Moritz et al., 2009;
Moritz, Kempke, Luyten, Randjbar, & Jelinek, 2011).
However, as the items for responsibility did not constitute a
factor on their own in the factor analysis of the constitution of
the RIBAQ (Moritz et al., 2009), the operationalisation of respon-
sibility is somewhat mixed with that of worry. This finding is in
line with factor analyses for other questionnaires tapping
responsibility, none of which obtained a pure scale. Most
notably, the OBQ (OCCWG, 2003) mixes items for responsibility
with those for threat according to factor analytic results. Pre-
sumably, the fact that responsibility is not a unidimensional
construct (Rachman et al., 1995) vitiates the extraction of the
core of responsibility using construction measurement tools.
Nevertheless, it is desirable to extract an item set that only taps
responsibility. The linkage of worry and responsibility in the
RIBAQ can be viewed as a problem, as worry has been shown to
correlate with OC symptoms (Myers, Fisher, & Wells, 2008;
Solem et al., 2010). Further research is necessary to define and
investigate different dimensions of responsibility, and to study
their relationships to OC symptoms and metacognition, because
we can conclude from the present results that metacognition
according to Wells (2009) and inflated responsibility are non-
redundant.
Regarding the two subcomponents of OET, overestimation of
the personal risk versus overestimation of the objective risk, we
found an unrealistic pessimism: in the implicit comparison
participants with OCD underestimated merely the personal like-
lihood of experiencing positive events and thus showed a relative
pessimism, whereas the full pessimistic bias occurred in the
explicit comparison. Interestingly, the OCD sample did not over-
estimate the incidence likelihood of negative events, but rather
underestimated the likelihood of positive events for themselves in
the implicit comparison. OCD patients did not overestimate the
subjective or objective threat, but they expected to experience
positive events less often. The focus on the underestimation of
positive events in the implicit comparison awaits replication and
clarification in future studies. In the explicit comparison OCD
patients also overestimated their personal risk to endure negative
events, compared to the healthy controls. Furthermore, the
personal valence of negative events did not differ between OCD
patients and the healthy controls, in contrast to the results of our
earlier study (Moritz & Jelinek, 2009). This implies that an overly
severe appraisal of the consequences of threatening events as a
component of OET in OCD was not a major factor in this sample.
However, they judged positive events as less favorable than
healthy participants do.
Differences of our findings compared to the forerunner studies
might stem from sample differences. Whereas the two preceding
studies (Moritz & Jelinek, 2009; Moritz & Pohl, 2009) were
conducted via the internet, this time we recruited a clinical group,
and used a paper- and pencil version of the questionnaires. The
participants in the present study had higher OC symptom scores
than before: the Y-BOCS-SR mean score was 23.03 compared to
17.93 in the sample of Moritz and Pohl (2009). In Moritz and
Jelineks (2009) study the MOCI was used, which cannot be
directly compared to Y-BOCS-SR and OCI-R scores.
In order to test if relationships between unrealistic pessimism
and obsessive–compulsive symptoms are specific, we controlled
for depression by conducting two subsidiary analyses, one con-
sidering only patients with low levels of depression below the
median of the depression score of the OCD sample, and one
considering only patients below the BDI-cut-off of 19 for moder-
ate depression. Depression had no impact on the results of the
three-way ANOVA for the low-level depression group; the level of
significance remained unchanged. However, some results in the
univariate ANOVAs for the implicit and explicit comparisons and
the rating of the valence slightly changed when controlling for
depression: group differences in the ratings of negative events for
oneself (implicit comparison and explicit comparison) and the
Table 7
Intercorrelations of the psychopathological and cognitive variables.
Variable 2 3 4 5 6 7 8 9 10 11 12 13
1 OCI-R .84snnn .76nnn .65nnn .53nnn
� .37nn .40nn� .09 .16 � .40nn .31n
� .23s .19s2 Y-BOCS-SR � .78s
nnn .57snnn .46s
nnn� .34s
nn .26sn
� .18s .10s � .43snnn .35s
nn� .18s .10s
3 BDI-II � .71nnn .57nnn� .45nnn .34nn
� .12 .15 � .50nnn .28n� .20s .15s
4 Responsibility � .56nnn� .26n .57nnn
� .02 .29n� .22 .32nn
� .06s .09s5 Metacognition � � .19 .37nn
� .12 .10 � .16 .28n� .11s .12s
Unrealistic optimism
6 Implicit, self (þ) � � .16 .31n� .11 .65nnn
� .09 .33snn
� .30sn
7 Implicit, self (�) � � .09 .48nnn� .17 .39nn
� .21s � .03s8 Implicit, others (þ) � .09 .09 .18 .39s
nn� .25s
n
9 Implicit, others (�) � � .06 .02 � .10s .02s10 Explicit (þ) � � .10 .28s
n� .13s
11 Explicit (�) � .18s � .09s12 Valence (þ) � � .48s
nnn
13 Valence (�) �
Note: Reported values¼Pearson correlation coefficients, if not otherwise marked; s¼Spearman Correlation Coefficient; OCI-R¼Obsessive–Compulsive Inventory-Revised;
Y-BOCS-SR¼Yale-Brown Obsessive–Compulsive Scale self-report; BDI-II¼Beck Depression Inventory-II; (þ)¼ likelihood of positive events; (�)¼ likelihood of negative
events. np o .05; nnp o .01; nnnp o .001.
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129126
Author's Personal Copy

evaluation of positive events disappeared. Thus, the estimation of
the incidence rates for negative events is affected by depression,
as is the personal valence of events. Nevertheless, even OCD
patients with low levels of depression display elevated levels of
unrealistic pessimism for positive events. In addition, when
analyses were confined to patients below the cut-off for moderate
depression most of the results remained unchanged. However,
the three-way interaction was no longer significant, and in the
post-hoc univariate ANOVA the difference between the groups for
the estimated likelihood of positive events happening to oneself
disappeared. While results in the explicit comparison differed, the
personal valence of events remained the same as in the low-level
depression group. We attribute the changes to the relatively small
sample size in the subgroup (n¼10). To conclude, we found that
controlling for depression somewhat attenuated but did not
abolish unrealistic pessimism in OCD.
Furthermore, in separately calculating correlations between
depression and unrealistic pessimism, we found that both in the
healthy sample and in the OCD sample the two variables were
hardly associated with each other. In the OCD sample, depression
correlated only with the personal valence of positive and negative
events, but not with implicit and explicit comparison for unrea-
listic pessimism. In the healthy sample, depression correlated
only minimally with unrealistic pessimism: only with the self
positive component of implicit comparison. Furthermore, as for
the OCD sample, it was associated with the personal valence of
positive events. We can conclude from these results that depres-
sion and unrealistic pessimism are not closely intertwined.
In summary, similar to previous studies OCD patients showed
rather pessimistic evaluations (Moritz & Jelinek, 2009; Moritz &
Pohl, 2009). Moritz and Jelinek (2009) found an unrealistic
pessimism in the implicit, but not the explicit comparison, and
Moritz and Pohl (2009) found an attenuated unrealistic optimism
in the explicit comparison. The present study is the first in which
an unrealistic pessimism was found in both implicit and explicit
comparisons. The healthy controls in the present study displayed
a relative unrealistic optimism in the implicit comparison only
regarding the negative events, contrary to previous findings
where an optimistic bias was found in both cases (Moritz &
Jelinek, 2009; Weinstein et al., 2005).
It is important to note that in the explicit comparison the
estimated incidence rates were lower than the neutral baseline
(score¼4) in both the OCD as well as the healthy samples. This
indicates that both groups underestimated the incidence rates for
both positive and negative events for themselves compared to
others. It is difficult to explain the tendency that both groups
underestimated incidence probabilities. As not that many studies
on OCD samples and with the UO questionnaire have been
conducted yet, and as this finding has occurred for the first time,
it awaits replication by future studies.
Some components of the UO questionnaire show associations
with OC symptoms. We were able to replicate the relationship
between OC symptoms and personal vulnerability found earlier
(Moritz & Jelinek, 2009), which points to the importance of this
subcomponent of OET for OCD. Unlike in another foregoing study
(Moritz & Pohl, 2009) we found that the Y-BOCS-SR scores were
not inversely, but positively related to the subjective vulnerability
for negative events, in both explicit and implicit comparisons.
However, Moritz and Pohl (2009) found an attenuated optimism,
whereas we found an unrealistic pessimism in the explicit
comparison. Furthermore, we found inverse correlations between
OC symptoms and the personal incidence rating for positive
events in implicit and explicit comparisons, indicating that higher
OCD scores go along with more pronounced pessimistic attitudes.
The relationship between OCD and subjective vulnerability might
differ between subgroups of OCD, and probably certain subtypes
of OCD display differences in showing an attenuated optimism or
an unrealistic pessimism. Further studies differentiating between
the subtypes of OCD could shed light on different causal mechan-
isms of pessimistic biases.
This is the first study to investigate interrelationships between
unrealistic pessimism and responsibility and metacognition.
Responsibility is closely related to the personal vulnerability for
negative events judged in both implicit and explicit comparison.
Presumably, people who feel responsible for negative events will
experience more discomfort (Rassin et al., 1999). Furthermore,
responsibility is negatively correlated with implicit self positive
and positively correlated with implicit others negative. Like
responsibility, metacognition is closely associated with the per-
sonal vulnerability for negative events (implicit comparison).
However, the only other correlation besides this relationship is
with the estimation of negative events in explicit comparison.
None of the other components of unrealistic pessimism correlate
with metacognition. Surprisingly, neither construct was related to
the valence of positive and negative events.
The associations of metacognition with the vulnerability for
negative events are congruent with theoretical assumptions, as
people who believe that thinking about a threatening situation
makes it more likely that the situation actually occurs ought to be
more afraid. Accordingly, OET is regarded a consequence of
metacognition in the framework of Wells’ model (Myers &
Wells, 2005). Of interest, higher responsibility goes along with
less expectation to experience positive events, and is connected to
more pessimistic expectations for other persons to experience
negative events as well. However, more research is necessary
here. In particular, experimental study would be desirable, since
from the present results we cannot conclude whether responsi-
bility/worry or metacognition are causal for unrealistic pessimism
or vice versa.
4.1. Limitations of the present study
The present study has certain limitations. A limitation of the
screening procedure of the control group is that we relied only on
self-report to exclude the presence of psychological disorders.
Participants were not tested in a structured interview or accord-
ing to DSM-IV criteria by a clinician. Moreover, a limitation of our
study is the small sample size, with respect to the analyses we
conducted. Therefore, the results need to be interpreted with
caution. Confirmation of the present findings using larger samples
is desirable. For reasons of statistical power, the correlation and
regression analyses were calculated using both the clinical and
non-clinical sample. Some researchers agree in using non-clinical
samples because OC symptoms are quasi-dimensional in non-
clinical and clinical samples (Gibbs, 1996). Nevertheless, the
occurrence of cognitive and metacognitive biases might differ in
clinical and non-clinical samples, and further studies should use
entirely clinical samples to confirm the present findings regarding
the relations between the three constructs. However, in most of
the previous studies regarding responsibility and metacognition
non-clinical samples were used.
Furthermore, most of the patients who had undergone pre-
vious treatment had received CBT. Therefore, it cannot be fully
excluded that this affected their knowledge and judgment of the
cognitive variables and metacognitions addressed in our study.
However, as all of them still suffered from clinically relevant OC
symptoms and metacognition is not usually integrated into
standard CBT protocols. We thus consider it unlikely that a long
lasting modification of their cognitions had occurred that had a
major impact on our results.
To operationalize responsibility with as little overlap with
metacognition as possible we chose the Responsibility and
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129 127
Author's Personal Copy

Interpersonal Behaviors and Attitudes Questionnaire (RIBAQ,
Moritz et al., 2009) scale inflated worry/responsibility that does
not include items about TAF or thought control, but focuses on
social responsibility. However, as the appraisal of responsibility is
per se conceptually similar to the construct of metacognition, as
we have described above, any operationalization of responsibility
could also be considered an operationalization of metacognition
to some extent. From this point of view the present operationa-
lization of responsibility would still share some elements with
metacognition.
Moreover, we did not control for worry in the hierarchical
regression analyses, unlike the study by Myers et al. (2008), for
example. Additionally, we operationalized responsibility with
regard to its subcomponent inflated worry for other persons.
Worry as a general thinking style and inflated worry regarding
other persons might be highly correlated and future studies
should address it by controlling for worry.
Finally, one flaw of the UO is that its content is rather narrow,
as it captures 15 events only. Not all themes that are relevant for
OCD are covered, as for example the Y-BOCS checklist consists of
72 items. A further development of the instrument is in the
planning stage, including items about hitherto not covered
domains, such as compulsive orderliness and hoarding. In addi-
tion, items concerning the salience of the events asked for would
be advantageous, as well as items concerning further positive
events, in order to have a broader base and to be able to
generalize the results regarding an over- or underestimation of
positive events.
4.2. Conclusions
In conclusion, several implications can be drawn from our
results. First, it could be helpful to alter the underestimation of
positive events and the overestimation of negative events in
cognitive therapy with OCD patients, since obviously they reflect
a cognitive distortion. Not only the pessimistic bias, but also the
lack of the opposite bias of unrealistic optimism, which might
have a protective function in healthy persons, should be given
attention by therapists. The overestimation of subjective threat,
but not of objective risk can be well addressed by cognitive
restructuring. Second, responsibility and metacognition should
both be considered in OCD. Our findings did not completely
support the model of Wells, which proposes that responsibility
is merely a by-product of metacognition that does itself not
contribute to OCD after metacognition is taken into account.
The present findings support the role of both responsibility,
especially its social component, and metacognition in OCD. The
treatment of OCD should include interventions of both cognitive
therapy to address the cognitive biases responsibility and unrea-
listic pessimism as well as metacognitive therapy to address the
distortions regarding importance and control of thoughts.
Acknowledgment
The authors would like to thank Helen-Rose Cleveland, Daniela
Bertram and Annett Schmitz for their helpful technical assistance.
References
Amir, N., Cashman, L., & Foa, E. B. (1997). Strategies of thought control inobsessive–compulsive disorder. Behavior Research and Therapy, 33, 775–777.
Arntz, A., Voncken, M., & Goosen, A. C. A. (2007). Responsibility and obsessive–compulsive disorder: An experimental test. Behavior Research and Therapy, 45,425–435.
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York:International Universities Press.
Beck, A. T., Steer, R. A., & Brown, G. (1996). Manual for the Beck Depression
Inventory-II. San Antonio. TX: Psychology Corporation (German Version:Hautzinger, M., Keller, F. & Kuehner, Ch. (2009). Beck depressions-Inventar
Revision (BDI-II). Manual. (2. Auflage). Frankfurt am Main: Pearson Assessment& Information).
Clark, D. A. (2001). The persistent problem of negative cognition in anxiety anddepression: New perspectives and old controversies. Behavior Therapy, 32,3–12.
Coles, M. E., Pietrefesa, A. S., Schofield, C. A., & Cook, L. M. (2008). Predictingchanges in obsessive–compulsive symptoms over a six-month follow-up: Aprospective test of cognitive models of obsessive–compulsive disorder. Cog-nitive Therapy and Research, 32, 657–675.
Emmelkamp, P. M. G., & Aardema, A. (1999). Metacognition, specific obsessive–compulsive beliefs and obsessive–compulsive behavior. Clinical Psychology &
Psychotherapy, 6, 139–145.Ertle, A., Wahl, K., Bohne, A., Moritz, S., Kordon, A., & Schulte, D. (2008).
Dimensionen zwangsspezifischer Einstellungen. Der Obsessive-Beliefs Ques-tionnaire (OBQ) fur den deutschen Sprachraum analysiert [The dimensions ofobsessive beliefs. An analysis of the Obsessive-Beliefs Questionnaire (OBQ) forthe German language area]. Zeitschrift fur Klinische Psychologie und Psychother-
apie, 37, 263–271.Flavell, J. H. (1979). Meta-cognition and meta-cognitive monitoring: A new area of
cognitive developmental inquiry. American Psychologist, 34, 906–911.Foa, E. B., Huppert, J. D., Leiberg, S., Langner, R., Kichic, R., Hajcak, G., et al. (2002).
The Obsessive-Compulsive Inventory Development and validation of a shortversion. Psychological Assessment, 14, 485–496 (German Version: Goenner, S.,Ecker, W., & Leonhart, R. (Eds.) (2009). Obsessive Compulsive InventoryRevised (OCI-R). Deutsche Adaptation. Manual. Frankfurt am Main: PearsonAssessment & Information.).
Gibbs, N. A. (1996). Nonclinical populations in research on obsessive–compulsivedisorder: A critical review. Clinical Psychology Review, 16, 729–773.
Goenner, S., Ecker, W., & Leonhart, R. (Eds.). (2009). Obsessive–Compulsive Inven-
tory- Revised (OCI-R). Deutsche Adaptation. Manual. Frankfurt am Main: PearsonAssessment & Information.
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischman, R. L., & Hill,C. L. (1989). The Yale-Brown Obsessive Compulsive Scale: Development, use,and reliability. Archives of General Psychiatry, 46, 1006–1016 (German Version:Baer, L. (1993). Alles unter Kontrolle: Zwangsgedanken und Zwangshandlungen
uberwinden (2., uberarbeitete und erganzte Auflage). Bern: Huber).Gwilliam, P., Wells, A., & Cartwright-Hatton, S. (2004). Does meta-cognition or
responsibility predict obsessive–compulsive symptoms: A test of the meta-cognitive model. Clinical Psychology & Psychotherapy, 11, 137–144.
Hautzinger, M., Keller, F., & Kuehner, Ch. (2009). Beck Depressions-Inventar Revision
(BDI-II). Manual. (2. Auflage). Frankfurt am Main: Pearson Assessment &Information.
Kuehner, C., Buerger, C., Keller, F., & Hautzinger, M. (2007). Reliabilitaet undValiditaet des revidierten Beck- Depressionsinventars (BDI-II): Befunde ausdeutschsprachigen Stichproben [Reliability and validity of the revised BeckDepression Inventory (BDI-II): Results form German Samples]. Nervenarzt, 78,651–656.
Moritz, S., & Jelinek, L. (2009). Inversion of the ‘‘Unrealistic Optimism’’ biascontributes to overestimation of threat in obsessive–compulsive disorder.Behavioural and Cognitive Psychotherapy, 37, 179–193.
Moritz, S., Kempke, S., Luyten, P., Randjbar, S., & Jelinek, L. (2011). Was Freudpartly right on obsessive–compulsive disorder (OCD)? Investigation of latentaggression in OCD. Psychiatry Research, 187, 180–184.
Moritz, S., Kloss, M., Jahn, H., Schick, M., & Hand, I. (2003). Impact of comorbiddepressive symptoms on nonverbal memory and visuospatial performance inobsessive–compulsive disorder. Cognitive Neuropsychiatry, 8, 261–272.
Moritz, S., Meier, B., Hand, I., Schick, M., & Jahn, H. (2004). Dimensional structureof the Hamilton Depression Rating Scale in patients with obsessive–compulsive disorder. Psychiatry Research, 125, 171–180.
Moritz, S., & Pohl, R. (2006). False beliefs maintenance for fear-related informationin obsessive–compulsive disorder: An investigation. Neuropsychology, 20,737–742.
Moritz, S., & Pohl, R. (2009). Biased processing of threat-related information ratherthan knowledge deficits contributes to overestimation of threat in obsessive–compulsive disorder. Behavior Modification, 33, 763–777.
Moritz, S., Wahl, K., Ertle, A., Jelinek, L., Hauschildt, M., Klinge, R., et al. (2009).Neither saints nor wolves in disguise. Ambivalent interpersonal attitudes andbehaviors in obsessive–compulsive disorder. Behavior Modification, 33,274–292.
Myers, S. G., Fisher, P. L., & Wells, A. (2008). Belief domains of the Obsessive BeliefsQuestionnaire-44 (OBQ-44) and their specific relationship with obsessive–compulsive symptoms. Journal of Anxiety Disorders, 22, 475–484.
Myers, S. G., Fisher, P. L., & Wells, A. (2009a). An empirical test of themetacognitive model of obsessive–compulsive symptoms: Fusion beliefs,beliefs about rituals, and stop signals. Journal of Anxiety Disorders, 19, 806–817.
Myers, S. G., Fisher, P. L., & Wells, A. (2009b). Metacognition and cognition aspredictors of obsessive–compulsive symptoms: A prospective study. Interna-tional Journal of Cognitive Therapy, 2, 132–142.
Myers, S. G., & Wells, A. (2005). Obsessive–compulsive symptoms: The contribu-tion of metacognitions and responsibility. Anxiety Disorders, 19, 806–817.
Obsessive Compulsive Cognitions Working Group (OCCWG) (2003). Psychometricvalidation of the Obsessive Beliefs Questionnaire and the Interpretation ofIntrusions Inventory: Part I. Behavior Research and Therapy, 41, 863–878.
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129128
Author's Personal Copy

OCCWG (2005). Psychometric validation of the Obsessive Beliefs Questionnaire
and Interpretation of Intrusions Inventory: Part 2: Factor analyses and testing
of a brief version. Behavior Research and Therapy, 43, 1527–1542.Purdon, C., & Clark, D. A. (2002). The need to control thoughts. In: R. O. Frost, &
G. Steketee (Eds.), Cognitive approaches to obsessions and compulsions – Theory,
assessment, and treatment (pp. 29–43). Boston: Pergamon.Rachman, S. (1997). A cognitive theory of obsessions. Behavior Research and
Therapy, 35, 793–802.Rachman, S. (2002). A cognitive theory of checking. Behavior Research and Therapy,
40, 625–639.Rachman, S. J., & De Silva, P. (1978). Abnormal and normal obsessions. Behavior
Research and Therapy, 16, 233–238.Rachman, S. J., Thordarson, D. S., Shafran, R., & Woody, S. R. (1995). Perceived
responsibility: Structure and significance. Behavior Research and Therapy, 33,
779–784.Rassin, E., Merckelbach, H., Muris, P., & Spaan, V. (1999). Thought-action fusion as
a causal factor in the development of intrusions. Behavior Research and
Therapy, 37, 231–237.Salkovskis, P. M. (1985). Obsessive–compulsive problems: a cognitive-behavioural
analysis. Behavior, Research and Therapy, 25, 571–583.Salkovskis, P. M. (1989). Cognitive behavioural factors and the persistence of
intrusive thoughts in obsessional problems. Behavior Research and Therapy, 27,
677–682.Salkovskis, P. M. (1991). The importance of behavior in the maintenance of anxiety
and panic: A cognitive account. Behavioural Psychotherapy, 79, 6–19.Salkovskis, P. M. (1996). Avoidance behavior is motivated by threat beliefs: A
possible resolution of the cognition-behavior debate. In: P. M. Salkovskis (Ed.),
Trends in Cognitive and Behavioural Therapies (pp. 25–41). Chichester: Wiley.Salkovskis, P. M., & Forrester, E. (2002). Responsibility. In: R. O. Frost, & G. Steketee
(Eds.), Cognitive approaches to obsessions and compulsions – Theory, assessment,
and treatment (pp. 45–61). Boston: Pergamon.Salkovskis, P. M., Forrester, E., & Richards, C. (1998). Cognitive-behavioral approach to
understanding obsessional thinking. British Journal of Psychiatry, 173, 53–63.Salkovskis, P. M., & Harrison, J. (1984). Abnormal and normal obsessions: A
replication. Behavior Research and Therapy, 22, 549–552.Salkovskis, P. M., Rachman, S., Ladouceur, R., Freeston, M., Taylor, S., Kyrios, M.,
et al. (1996). Defining responsibility in obsessional problems. In OC beliefs working
group. Northampton: Smith College.Salkovskis, P. M., Shafran, R., Rachman, S., & Freeston, M. H. (1999). Multiple
pathways to inflated responsibility beliefs in obsessional problems: possible
origins and implications for therapy and research. Behavior Research and
Therapy, 37, 1055–1072.Salkovskis, P. M., & Wahl, K. (2003). Treating obsessional problems using
cognitive-behavioural therapy. In: M. Reinecke, & D. A. Clark (Eds.), Cognitive
therapy across the lifespan: Theory, research and practice (pp. 138–171). Cam-
bridge, UK: Cambridge University Press.
Salkovskis, R. M., Wroe, A. L., Gledhill, A., Morrison, N., Forrester, E., Richards, C.,et al. (2000). Responsibility attitudes and interpretations are characteristic ofobsessive–compulsive disorder. Behavior Research and Therapy, 38, 347–372.
Schaible, R., Armbrust, M., & Nutzinger, D. O. (2001). Yale–Brown ObsessiveCompulsive Scale: Sind Selbst- und Fremdrating aequivalent? [The Yale–Brown Obsessive Compulsive Scale: are self-rating and interview equivalentmeasures?]. Verhaltenstherapie, 11, 298–303.
Shafran, R., Thordarson, D., & Rachman, S. (1996). Thought-action fusion inobsessive–compulsive disorder. Journal of Anxiety Disorders, 10, 379–392.
Sica, C., Steketee, G., Ghisi, M., Chiri, L. R., & Franceschini, S. (2007). Metacognitivebeliefs and strategies predict worry, obsessive–compulsive symptoms andcoping styles: a preliminary prospective study on an Italian non-clinicalsample. Clinical Psychology and Psychotherapy, 14, 258–268.
Smari, J., & Holmsteinsson, H. E. (2001). Intrusive thoughts responsibility attitudes,thought-action fusion, and chronic thought suppression in relation toobsessive–compulsive symptoms. Behavioural and Cognitive Psychotherapy,29, 13–20.
Solem, S., Myers, S. G., Fisher, P. L., Vogel, P. A., & Wells, A. (2010). An empirical testof the metacognitive model of obsessive–compulsive symptoms: Replicationand extension. Journal of Anxiety Disorders, 24, 79–86.
Sookman, D., & Pinard, G. (2002). Overestimation of threat and intolerance ofuncertainty in obsessive–compulsive disorder. In: R. O. Frost, & G. Steketee(Eds.), Cognitive approaches to obsessions and compulsions – Theory, assessment,
and treatment (pp. 63–89). Boston: Pergamon.Steketee, G., Frost, R., & Bogart, K. (1996). The Yale–Brown Obsessive Compulsive
Scale: Interview versus self-report. Behavior Research and Therapy, 34,675–684.
Steketee, G., Frost, R. O., & Cohen, I. (1998). Beliefs in obsessive–compulsivedisorder. Journal of Anxiety Disorders, 12, 525–537.
Tabachnik, B. G., & Fidell, L. S. (2007). Using multivariate statistics. New York:Pearson.
Weinstein, N. D. (1982). Unrealistic optimism about susceptibility to healthproblems. Journal of Behavioral Medicine, 5, 441–460.
Weinstein, N. D., & Klein, W. M. (1996). Unrealistic optimism: Present and future.Journal of Social and Clinical Psychology, 15, 1–8.
Weinstein, N. D., Marcus, S. E., & Moser, R. P. (2005). Smokers’ unrealistic optimismabout their risk. Tobacco Control, 14, 55–59.
Wells, A. (2009). Metacognitive therapy for anxiety and depression. New York:Guilford Press.
Wells, A., & Matthews, G. (1994). Attention and emotion: A clinical perspective. Hove,UK: Erlbaum.
Wells, A., & Papageorgiou, C. (1998). Relationships between worry, obsessive–compulsive symptoms and meta-cognitive beliefs. Behavior Research and
Therapy, 39, 899–913.Wittchen, H. U., Zaudig, M., & Fydrich, T. (1997). Strukturiertes Klinisches Interview
fuer DSM-IV [User’s guide for the Structured Clinical Interview for DSM–IV].Gottingen: Hogrefe.
H. Niemeyer et al. / Journal of Obsessive-Compulsive and Related Disorders 2 (2013) 119–129 129
Author's Personal Copy
Related Documents











