Brief Communications Response of Cluster Headache to Kudzu R. Andrew Sewell, MD Objective.—To describe the self-treatment of cluster headache with kudzu. Background.—Many cluster headache patients take over-the-counter (OTC) kudzu extract in the belief that it helps their cluster attacks. Kudzu’s actual efficacy has not been studied. Methods.—A database of cluster headache patients was questioned about their use of various alternative remedies to treat their cluster headache. Of 235 patients identified, 16 had used kudzu, consented to interviews, and provided medical records. Results.—In total, 11 (69%) experienced decreased intensity of attacks, 9 (56%) decreased frequency, and 5 (31%) decreased duration, with minimal side effects. Conclusion.—Anecdotal evidence suggests that a component in OTC products labeled as kudzu may prove useful in managing cluster headache. This hypothesis should be tested with a randomized clinical trial. Key words: cluster headache, case series, kudzu (Headache 2009;49:98-105) Cluster headache is a rare disorder, generally considered to be the most painful of all types of head- ache. 1 It occurs predominantly in men (0.4% vs 0.08% of women), typically beginning in the third decade, and is categorized as either episodic, occurring for periods interspersed with pain-free remissions, or chronic, in which the headaches occur constantly for more than a year with no remission longer than one month. 2 Ten percent of episodic cluster headaches ultimately evolve into the chronic form, and these are termed secondary chronic. In standard descriptions of cluster headache, an “attack” refers to the actual paroxysm of pain, a “cluster period” to a period of time when attacks occur regularly, and a “remission period” to an interval during which no attacks occur. 3 Cluster periods tend to recur at fixed intervals ranging from several months to several years, often occurring at the same time each year, and are marked by recurrent stabbing attacks that increase in inten- sity over 5 to 10 minutes, last 15 minutes to 3 hours, and then fade away. Attacks typically occur 1 to 3 times a day, usually at strikingly predictable times (often 2 hours after the patient falls asleep) but can sometimes occur as often as every 2 hours.The inten- sity of the pain is severe enough that patients have been known to commit suicide. 4 Standard care for cluster headache includes acute treatments such as triptans or high-flow oxygen taken at the onset of an attack, supplemented with prophy- lactic treatments such as verapamil or lithium, which are taken on a continuous basis once a cluster period has begun, or before sleep in order to prevent noctur- nal attacks in the case of ergotamine. 1 Unfortunately, From the VA Connecticut Healthcare/Yale University School of Medicine—Psychiatry, West Haven, CT, USA. Address all correspondence to R.A. Sewell, VA Connecticut Healthcare/Yale University School of Medicine—Psychiatry, West Haven, CT 06516, USA. Accepted for publication August 2, 2008. Conflict of Interest: None ISSN 0017-8748 doi: 10.1111/j.1526-4610.2008.01268.x Published by Wiley Periodicals, Inc. Headache © 2008 the Author Journal compilation © 2008 American Headache Society 98

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Brief Communications
Response of Cluster Headache to Kudzu
R. Andrew Sewell, MD
Objective.—To describe the self-treatment of cluster headache with kudzu.Background.—Many cluster headache patients take over-the-counter (OTC) kudzu extract in the belief that it helps their
cluster attacks. Kudzu’s actual efficacy has not been studied.Methods.—A database of cluster headache patients was questioned about their use of various alternative remedies to treat
their cluster headache. Of 235 patients identified, 16 had used kudzu, consented to interviews, and provided medical records.Results.—In total, 11 (69%) experienced decreased intensity of attacks, 9 (56%) decreased frequency, and 5 (31%)
decreased duration, with minimal side effects.Conclusion.—Anecdotal evidence suggests that a component in OTC products labeled as kudzu may prove useful in
managing cluster headache. This hypothesis should be tested with a randomized clinical trial.
Key words: cluster headache, case series, kudzu
(Headache 2009;49:98-105)
Cluster headache is a rare disorder, generallyconsidered to be the most painful of all types of head-ache.1 It occurs predominantly in men (0.4% vs 0.08%of women), typically beginning in the third decade,and is categorized as either episodic, occurring forperiods interspersed with pain-free remissions, orchronic, in which the headaches occur constantly formore than a year with no remission longer than onemonth.2 Ten percent of episodic cluster headachesultimately evolve into the chronic form, and these aretermed secondary chronic. In standard descriptionsof cluster headache, an “attack” refers to the actualparoxysm of pain, a “cluster period” to a period oftime when attacks occur regularly, and a “remission
period” to an interval during which no attacks occur.3
Cluster periods tend to recur at fixed intervalsranging from several months to several years, oftenoccurring at the same time each year, and are markedby recurrent stabbing attacks that increase in inten-sity over 5 to 10 minutes, last 15 minutes to 3 hours,and then fade away. Attacks typically occur 1 to 3times a day, usually at strikingly predictable times(often 2 hours after the patient falls asleep) but cansometimes occur as often as every 2 hours. The inten-sity of the pain is severe enough that patients havebeen known to commit suicide.4
Standard care for cluster headache includes acutetreatments such as triptans or high-flow oxygen takenat the onset of an attack, supplemented with prophy-lactic treatments such as verapamil or lithium, whichare taken on a continuous basis once a cluster periodhas begun, or before sleep in order to prevent noctur-nal attacks in the case of ergotamine.1 Unfortunately,
From the VA Connecticut Healthcare/Yale University Schoolof Medicine—Psychiatry, West Haven, CT, USA.
Address all correspondence to R.A. Sewell, VA ConnecticutHealthcare/Yale University School of Medicine—Psychiatry,West Haven, CT 06516, USA.
Accepted for publication August 2, 2008. Conflict of Interest: None
ISSN 0017-8748doi: 10.1111/j.1526-4610.2008.01268.xPublished by Wiley Periodicals, Inc.
Headache© 2008 the AuthorJournal compilation © 2008 American Headache Society
98

these treatments are rarely entirely effective andoften have serious disadvantages. Triptans and ergotalkaloids often cannot be given frequently enough,and oxygen tanks are unwieldy and inconvenient.Many herbal remedies have been proposed to treatheadache; of these, feverfew5 and cannabis6 have themost empirical support, but neither has been specifi-cally evaluated for cluster headache.
Kudzu refers to any one of a number of vinespecies of the genus Pueraria that is indigenous toAsian countries, was imported to the USA in 1876,and has subsequently been used for green manureand fodder and as ground cover to prevent soil ero-sion.7 The use of Ge-gen (kudzu root) was describedin the Chinese medical book Shang Han Lun – “Trea-tise on Fever” – 1800 years ago,8 and today its rhizomeis a traditionally used component in Chinese medicalpolyprescriptions for liver diseases, strokes, and aller-gies. Kudzu contains antioxidants,9 has antipyreticand anesthetic effects,10 treats hypertension,11 dilatescerebral blood vessels, increases cerebral blood flow,and improves brain acetylcholine in a mouse Al-zheimer model.12 Historically, it has had use in thetreatment of alcohol-related problems since AD600.13 Its use in the treatment of cluster headache hasnot previously been described.
METHODSThe study was approved by the McLean Hospital/
Harvard Medical School IRB. A database of 235cluster headache patients was surveyed via email ontheir use of a number of complementary and alterna-tive remedies, including kudzu root. The subjects hadbeen previously recruited for a study unrelated tokudzu14 and came from 3 sources – members of theClusterbusters patient advocacy group (37), respon-dents to an online survey about quality of life issuesaffecting cluster headache patients who had checkeda box agreeing to be contacted for future researchstudies (189), and people who had heard on the Inter-net that we were studying cluster headache and inde-pendently emailed us asking to participate (9). As ofOctober 10, 2006, 159 (68%) had responded; of these,22 (14%) endorsed using kudzu root or extract toself-treat their cluster headache. Questions wereasked on a variety of complementary and alternative
treatments for cluster headache and phrased in such away that kudzu did not appear to be a topic of undueinterest. We restricted our analysis to the 16 (73%)individuals who (1) agreed to be contacted for evalu-ation by telephone or email; (2) met InternationalClassification of Headache Disorders, 2nd edition, cri-teria for cluster headache; (3) allowed us to obtaincopies of medical records documenting a diagnosis ofcluster headache by an MD or DO. If the medicalrecords did not support the diagnosis, the subject wasexcluded from further analysis.
RESULTSResults are summarized in the Table. Of the
11 subjects with episodic cluster headache, 8 (73%)experienced a decrease in the intensity of theirattacks, 7 (64%) experienced a decrease in frequency,4 (36%) experienced decreased attack length, and 2(18%) experienced a truncated cluster period. Onesubject experienced increased attack intensity, fre-quency, and duration. Of the 5 subjects with chroniccluster headache, 3 (60%) experienced decreasedattack intensity, 2 (40%) decreased frequency, and 1(20%) decreased attack duration, while 1 (20%) hadincreased attack intensity.
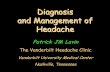
Efficacy for cluster attack in this group showed aclear dose–response relationship: 3 of the 4 treatmentnonresponders were taking less than 1000 mg a day(total pill weight; actual dose of kudzu is substantiallyless), and only 3 of 7 (43%) patients taking kudzu lessthan 3 times a day showed benefit. Of the 6 whoreported no effects or worse effects from kudzu, allwere taking it less than 3 times a day, whereas 8 of 10(80%) taking the more frequent dose benefitted(Fig. 1). Side effects were mild and infrequent, themost common being gastrointestinal effects experi-enced by 4 (25%). Measured by total dose per day, theeffect of kudzu on cluster attack intensity, frequency,and duration also showed a dose–response relation-ship, whereas its effect on cluster period length didnot.
In comparison, of the 36 (13%) respondents fromthe cohort of 285 in the database who endorsed usingacupuncture, 4 (11%) felt it made their cluster head-ache worse, 7 (20%) felt it improved their clusterheadache, and 21 (58%) reported no effect. Of the 58
Headache 99

Tabl
e.—
Eff
ect
ofK
udzu
onC
lust
erH
eada
che
No.
Age
(yea
rs)
Sex
Hea
dach
ety
peK
udzu
bran
dD
ose
(mg)
Freq
.Tr
iall
engt
h
Eff
ect
onat
tack
Peri
odle
ngth
Side
effe
cts
Inte
ns.
Freq
.D
ur.
159
F2°
chro
nic
NW
613
Tid
2m
onth
sØ
ØØ
N/A
Ø2
36M
Epi
sodi
cro
ot?
Bid
6w
eeks
!!
ØØ
CN
S3
35M
Epi
sodi
cPF
1500
Tid
7w
eeks
!!
!!
Ø4
47F
2°ch
roni
cPF
1500
Tid
12m
onth
s!
!!
N/A
GI
536
F2°
chro
nic
NW
1226
Qd
2w
eeks
"Ø
ØN
/AØ
657
ME
piso
dic
PF15
00Q
hs1
day
!!
Ø?
GI
757
FE
piso
dic
NW
1226
Tid
12m
onth
s!
!!
ØØ
832
ME
piso
dic
PF15
00Ti
d12
mon
ths
ØØ
ØØ
GI
948
ME
piso
dic
PF15
00Ti
d8
mon
ths
!!
!Ø
GI,
MS
1048
M2°
chro
nic
PF15
00Ti
d2
mon
ths
!Ø
ØN
/AØ
1143
FE
piso
dic
NW
613
Bid
3w
eeks
""
"?
Ø12
42M
Epi
sodi
cN
W12
26Ti
d12
mon
ths
!!
?Ø
Ø12
PF15
00B
id3
wee
ks!
!!
ØØ
1340
F1°
chro
nic
NW
1226
Tid
13w
eeks
!!
?N
/AØ
1431
FE
piso
dic
NSI
650
Qd-
tid5
wee
ks!
!Ø
ØØ
1549
ME
piso
dic
SW80
0Q
hs3
wee
ksØ
ØØ
!Ø
1632
FE
piso
dic
NH
100
Qd
ØØ
ØØ
Ø
Ø=
noef
fect
;C
NS=
cent
ral
nerv
ous
syst
em;
Dur
.=du
ratio
n;F=
fem
ale;
Freq
.=fr
eque
ncy;
GI=
gast
roin
test
inal
;In
tens
.=in
tens
ity;
M=
mal
e;M
S=
mus
culo
skel
etal
;N
/A=
chro
nic
clus
terh
eada
che
ther
efor
eno
clus
terp
erio
ds;N
SI=
Neu
trac
eutic
alsS
cien
ceIn
stitu
te;N
W=
Nat
ure’
sWay
;PF=
Plan
etar
yFo
rmul
a;SW
=St
arW
estB
otan
ical
s;N
H=
Nat
ure’
sH
erb;
1°=
prim
ary;
2°=
seco
ndar
y.
100 January 2009

(20%) respondents who endorsed using the “watermethod” – drinking a glass of water every half an hourduring the cluster period – 3 (5%) felt it made theircluster headache worse, 16 (28%) felt it improvedtheir cluster headache, and 37 (64%) reported noeffect (Fig. 2). These data should not be construed asevidence of lack of efficacy of these 2 methods; rather,assuming that the effects of acupuncture and polydip-sia on cluster headache are no different than placebo,then the reported efficacy of kudzu in this cohort ismore than twice as great as would be expected fromchance alone.
REPRESENTATIVE CASES (ALL OTHERSARE INCLUDED IN APPENDIX A,AVAILABLE ONLINE ONLY)
Case No. 2.—A 36-year-old man with no othermedical conditions had suffered from episodic clusterheadache since age 16 years, characterized by 6 weeksof one or two 2-hour attacks per day separated by a 4-or 5-month remission period.The attacks consisted ofa boring pain in his temple and a knot in his neck,along with lacrimation, ptosis, meiosis, conjunctivalinjection, flushing, diaphoresis, and restlessness. Fre-quent absences caused problems at work, and thesecondary depression and fatigue caused strain in hisinterpersonal relationships.
He finds oxygen and sumatriptan to be effectiveabortive medications, and as prophylactic medication,he has tried propanolol and amitriptyline, which areineffective, verapamil and psilocybin, which decreasethe frequency and intensity of attacks, and pred-nisone, which stops the attacks only while he is takingit.
When his last cluster period began, in June of2005, he read on an Internet forum that kudzu treatedcluster headache, so he decided to boil 1.5 ounces ofdried kudzu root and drink it as a tea twice a day.Even though he was using no other medication, hesuffered only 4 attacks during the entire 6-weekcluster period, all mild. The cluster period wasunchanged in length. He also had approximately 10“phantom attacks,” a phenomenon he had experi-enced previously on verapamil. He was able to avoidtaking all conventional prophylactic medication, andsuffered no side effects from the kudzu other thanvivid dreams. He does not smoke or use illicit drugs,but drinks 3 or 4 glasses of wine a week and 2 cups ofgreen tea a day.
Case No. 3.—A 36-year-old man with no significantmedical conditions except for a history of benignfamilial infantile convulsions, which he had outgrownby age 3 years, started to have episodic cluster head-aches at age 28 years and was correctly diagnosed atage 33 years. Each cluster period lasted 8 to 10 weeksseparated by a remission period of 7 or 8 months,occurred usually in autumn or late February, and con-sisted of as many as 6 cluster attacks a day, at all timesof day and night. Each attack was characterized by a
Fig 1.—Percent of patients reporting improvement in clusterattack intensity, frequency, and duration and cluster periodlength, stratified by total daily dose of unstandardized extractconsumed. A dose–response relationship is apparent in kudzu’seffects on cluster attacks, but not on cluster period length.
Fig 2.—Subjective global effect of different “alternative” treat-ment modalities on cluster headache symptoms. There is noevidence to suggest that either acupuncture or polydipsia ismore effective for cluster headache than placebo.
Headache 101

right-sided sharp boring pain radiating into his jawand neck, sweating, ptosis and eyelid edema, conjunc-tival injection, rhinorrhea, phono- and osmophobialasting 45 to 90 minutes. He coped well, suffering nojob or relationship difficulties as a result, but grappledwith persistent fears that there was “somethingdeeply wrong” with his brain.
For 5 years he remained untreated, assuming thathe had a sinus problem or simply trying not to thinkabout it, and then started medication. Verapamil120 mg a day decreased his attack frequency to onceor twice daily, but did not decrease the attack inten-sity and caused him memory and coordination diffi-culties. Valproate triggered 2 of the most painful andprolonged attacks he had ever experienced, so hediscontinued it. Sumatriptan was an effective abor-tive, but side effects that included intensification andprolongation of subsequent attacks as well as a dullpersistent ache at the site of the attacks the next dayprompted him to discontinue it.
In February 2005, he started to experience“twinges” in his right eye, heralding the beginning ofa cluster period, and with his first full-blown attack,he started on Planetary Formulas kudzu extract1500 mg 3 times a day as well as a twice-daily mul-tivitamin. To his surprise, he found that he experi-enced only 8 attacks for the remainder of the clusterperiod, which was half its usual length (only 7weeks), no attack lasting longer than 30 minutes. Theattacks differed from the usual – although they stillcaused agitation and pacing, there were no associ-ated autonomic symptoms, only pain, and the inten-sity of the pain was attenuated – and these occurredonly when he decreased the dose of kudzu to twicea day, forgot, or delayed a dose. He experienced noside effects.
His next cluster period began with 4 times dailyattacks in late November 2005, but he delayed takingkudzu until the intensity of the attacks became excru-ciating, in the second week of December, for fear thathe would develop tachyphylaxis. Restarting a dose ofPlanetary Formulas 1500 mg 3 times a day, he foundthat his attacks diminished in both frequency andintensity to zero over the next 2 weeks, and theremainder of the cluster period passed asymptomati-cally until it ended in January.
He smokes a pack of cigarettes every day, drinksone drink of alcohol every few months, and smokescannabis roughly twice a year. He uses no other illicitdrugs but drinks 4 to 5 cups of coffee a day.
DISCUSSIONThe putative mechanism of action by which
kudzu might affect cluster headache should theseresults be verified is unclear. It is thought that theother therapeutic benefits of kudzu are due to phy-toestrogens, particularly isoflavones, which possessboth estrogenic and antiestrogenic properties, can actas selective estrogen receptor modulators,15 and havea long pedigree in the treatment of a number of dis-orders.16 Flavonoids are phenolic compounds widelydistributed in plants, with over 4000 currentlyknown.17 Their astringency probably repels insects,making isoflavonoids the most important group ofplant-protective phytoalexins.18 The isoflavone puer-arin, which is the principal component in kudzu,19
has hypoglycemic properties and increases coronaryblood flow, reducing the frequency of acute anginaevents20 and normalizing endothelin, renin, angio-tensin II post-myocardial infarction in 3 days.21 Puer-arin attenuates mecamylamine-induced deficits ininhibitory avoidance performance in rats, presumablythrough nicotinic-receptor agonism and N-methyl-D-aspartic acid (NMDA) agonism and serotonindecrease.22 It does not act as a beta-blocker or calciumantagonist, however.23 The 3 times daily dosing ofkudzu that appears necessary to ameliorate clusterheadache is consistent with puerarin’s pharmacoki-netic profile.24 Daidzein is a metabolite of puerarinand daidzin, another isoflavone in kudzu. Unlikedaidzin and puerarin, daidzein scavenges free radi-cals25 and is estrogenic,26 albeit thousands of times lesspotent than the synthetic estrogen diethylstilbestrol.
Estrogen and progesterone levels are normal incluster headache, but the dramatically higher preva-lence of the disorder in males, the increase in inci-dence around menopause,27 and the tendency ofcluster headache to remit during pregnancy28 arguefor a protective effect of female reproductive hor-mones that may be replicated by the phytoestrogensin kudzu.
102 January 2009

Kudzu has been reported to decrease alcoholintake in both preclinical29 and clinical trials. Inves-tigators found that over-the-counter (OTC) prepara-tions of kudzu that contain less than 1% or 2%isoflavones are not effective in limiting alcoholintake, but a concentrated (25% isoflavone) form ofkudzu was effective in reducing alcohol intake bybinge drinkers.30 The rate of alcoholism is high incluster headache patients,31 which is surprising asalcohol is a reliable trigger of a cluster attack duringa cluster period, although it may be consumedwithout consequence during a remission period. Inone sample, 91% of cluster headache patients drankalcohol, with 61% falling into the category of mod-erate to excessive drinkers,32 and in another, morethan 90% drank alcohol, with a significant propor-tion being “heavy drinkers.”31 Levi found that 67%of his sample assessed with the Mm-MAST (Michi-gan Alcoholism Screening Test) had scores indica-tive of alcoholism.33 Other studies have found lowerrates of alcohol consumption, but still far higherthan those of noncluster headache controls – 61% vs41% in one sample,34 with daily use reported by36% of cluster headache patients vs 14% of con-trols. However, as alcohol triggers cluster attacks,79% of cluster headache patients dramaticallydecrease their alcohol consumption during a clusterperiod,33 in contrast with smoking, the rate of whichdoes not change. It is thus conceivable that theisoflavones in kudzu are treating a common factorunderlying both alcoholism and cluster attacks.
The use of kudzu to treat cluster headache wasunknown before December 2005, when reports of itstherapeutic effects appeared on the Internet andpropagated rapidly through the cluster headachepatient population. A number of studies have foundthat approximately 50% of patients use the Internetto obtain medical information, and 60% in one studyreported that they felt that information on the Inter-net was the “same as” or “better than” informationfrom their doctors.35 Although Internet medicaladvice is frequently characterized as inaccurate,incomplete, or inconsistent,36 the rapid and wide-spread dissemination of unverified medical informa-tion also permits the trial-and-error discovery of newtreatments by enthusiastic patient groups.
Caution should be applied in interpreting thesefindings, as case series are by their very nature subjectto selection bias, recall bias, and the placebo response.However, several factors mitigate these limitations inthis case series. Recruitment over the Internet selectsfor younger, more educated, and more motivated sub-jects,37 likely leading to increased reported efficacy.This group was not, however, otherwise selected forpositive response to kudzu or alternative medica-tions, and this group did not report a comparablepositive response to acupuncture and other alterna-tive medications.Although it has not been establishedthat acupuncture and polydipsia are ineffective intreating cluster headache, if these methods are actu-ally effective, then that would strengthen, not weaken,our conclusions.
Although there was no placebo arm, clusterheadache is known to respond poorly to placebo; con-trolled trials have shown a placebo response of 0% toprophylactic medications such as verapamil,38 capsai-cin,39 and melatonin.40 As cluster attacks typicallywax and wane over the course of a cluster period,improvement in symptoms can be difficult to attributeto medication effect. However, each cluster period isgenerally very similar in pattern and length for agiven patient, making differences noticeable, and 2patients (no. 4 and no. 12, see supplemental cases)used a challenge–rechallenge test to verify that thekudzu was having an effect on their headaches. Fur-thermore, 6 (38%) of the subjects had maintaineddetailed headache diaries corroborating their retro-spective recall of efficacy.
Finally, the concentration of isoflavones in OTCkudzu preparations is unstandardized, and variesfrom 0.5% to 3% (Lukas, personal communication),making it difficult to quantify the actual amount ofactive ingredient ingested by the subjects. However,this variability should attenuate rather than exag-gerate any dose–response relationship, and the factthat such a relationship was still identifiable despitethe variable concentrations of isoflavones present,further argues for therapeutic effect.
CONCLUSIONAlthough few subjects were able to completely
discontinue conventional medications, a substantial
Headache 103

proportion found that kudzu extract in a variety oflow-concentration OTC preparations ameliorated theintensity, frequency, and duration of their clusterattacks, with minimal side effects, although kudzu hadno effect on the length of the cluster period. Shouldthese results be confirmed with a randomized clinicaltrial of standardized extracts, kudzu may prove tohave a role in the management of cluster headache.
Acknowledgments: The author thanks Earth andFire Erowid, Robert Wold and the Clusterbusters, forassistance with data collection; Harrison Pope, ScottLukas, Mehmet Sofuoglu, and Bruce Price for their com-ments on an earlier draft of this article, and JonathanByron for bringing kudzu to the attention of the clusterheadache community. Funding was provided by NIDA,NIH T32-DA07252. No funding source had any role instudy design, collection, analysis, or interpretation of data,writing of the report, or submission of the manuscript.
REFERENCES1. Silberstein S, Lipton R, Goadsby P. Headache in
Clinical Practice, 2nd edn. London: Martin DuniyzLtd.; 2002:147.
2. Headache Classification Subcommittee of the Inter-national Headache Society. The international classi-fication of headache disorders. Cephalalgia. 2004;24(Suppl. 1):44-48.
3. Ekbom K. Some remarks on the terminology ofcluster headache. Cephalalgia. 1988;8:59-60.
4. Dodick DW, Rozen TD, Goadsby PJ, SilbersteinSD. Cluster headache. Cephalalgia. 2000;20:787-803.
5. Vogler BK, Pittler MH, Ernst E. Feverfew as a pre-ventive treatment for migraine:A systematic review.Cephalalgia. 1998;18:704-708.
6. Russo E. Cannabis for migraine treatment:The onceand future prescription? An historical and scientificreview. Pain. 1998;76:3-8.
7. Roecklein J, Leung P. A Profile of Economic Plants.New Brunswick: Transaction Book; 1987:467.
8. Zhang Z. Shang Han Lun: On Cold Damage, Trans-lation & Commentaries. Taos, NM: Paradigm Publi-cations; 1999:273.
9. Guerra MC, Speroni E, Broccoli M, et al. Compari-son between Chinese medical herb Pueraria lobatacrude extract and its main isoflavone puerarinantioxidant properties and effects on rat liver
CYP-catalysed drug metabolism. Life Sci.2000;67:2997-3006.
10. Havsteen BH. The biochemistry and medical signifi-cance of the flavonoids. Pharmacol Ther. 2002;96:67-202.
11. Qicheng F. Some current study and researchapproaches relating to the use of plants in thetraditional Chinese medicine. J Ethnopharmacol.1980;2:57-63.
12. Chen K, Chan K. Preliminary basic science researchinto the treatment of dementia using Chinese herbalmedicine [in Chinese]. Tradit Chin Med West Med.1995;15:120-123.
13. Sun S. Beji-Quianjin-Yaofang. Circa ad 600.14. Sewell R, Halpern J, Pope H. Response of cluster
headache to psilocybin and LSD. Neurology. 2006;66:1920-1922.
15. Fitzpatrick LA. Selective estrogen receptor modula-tors and phytoestrogens: New therapies for the post-menopausal women. Mayo Clin Proc. 1999;74:601-607.
16. Tham DM, Gardner CD, Haskell WL. Clinicalreview 97: Potential health benefits of dietary phy-toestrogens: A review of the clinical, epidemiologi-cal, and mechanistic evidence. J Clin EndocrinolMetab. 1998;83:2223-2235.
17. Cody V, Middleton E, Harborne JB. Plant Fla-vonoids in Biology and Medicine, Biochemical,Pharmacological, and Structure-Activity Relation-ships. Symposium Proceedings, Buffalo, NY, July22–24, 1985. New York: Alan R. Liss; 1986: 15.
18. Smith D, Banks S. Biosynthesis, elicitation and bio-logical activity of isoflavonoid phytoalexins. Phy-tochemisty. 1986;25:979-995.
19. Harada M, Ueno K. Pharmacological studies onpueraria root. I. Fractional extraction of puerariaroot and identification of its pharmacologicaleffects. Chem Pharm Bull (Tokyo). 1975;23:1798-1805.
20. Zhao Z, Yang X, Zhang Y. [Clinical study of puer-arin in treatment of patients with unstable angina].Zhongguo Zhong Xi Yi Jie He Za Zhi. 1998;18:282-284.
21. Li SM, Liu B, Chen HF. [Effect of puerarin onplasma endothelin, renin activity and angiotensin IIin patients with acute myocardial infarction]. Zhong-guo Zhong Xi Yi Jie He Za Zhi. 1997;17:339-341.
22. Hsieh MT, Kuo LH, Tsai FH, Wang WH, WuCR. Effects of puerarin on scopolamine-,
104 January 2009

mecamylamine-, p-chloroamphetamine- anddizocilpine-induced inhibitory avoidance perfor-mance impairment in rats. Planta Med. 2002;68:901-905.
23. Feng YP, Zhang LY, Zeng GY. [Effect of puerarinand analogues of daidzein on adrenoceptors].Zhongguo Yao Li Xue Bao. 1984;5:238-241.
24. Penetar D, Teter C, Ma Z, Tracy M, Lee D, LukasSE. Pharmacokinetic profule of the isoflavone puer-arin after acute and repeated administration of anovel kudzu extract to human volunteers. J AlternComplement Med. 2006;12:543-548.
25. Choo MK, Park EK, Yoon HK, Kim DH. Anti-thrombotic and antiallergic activities of daidzein, ametabolite of puerarin and daidzin produced byhuman intestinal microflora. Biol Pharm Bull.2002;25:1328-1332.
26. Cheng EW, Yoder L, Story CD, Burroughs W.Estrogenic activity of some naturally occurringisoflavones. Ann N Y Acad Sci. 1955;61:652-658. dis-cussion, 8-9.
27. Ekbom K, Svensson DA, Traff H, Waldenlind E. Ageat onset and sex ratio in cluster headache: Observa-tions over three decades. Cephalalgia. 2002;22:94-100.
28. Ekbom K, Waldenlind E. Cluster headache inwomen: Evidence of hypofertility? Headaches inrelation to menstruation and pregnancy. Cephalal-gia. 1981;1:167-174.
29. Keung WM, Vallee BL. Daidzin and daidzein sup-press free-choice ethanol intake by Syrian goldenhamsters. Proc Natl Acad Sci USA. 1993;90:10008-10012.
30. Lukas SE, Penetar D, Berko J, et al. An extract ofthe Chinese herbal root kudzu reduces alcoholdrinking by heavy drinkers in a naturalistic setting.Alcohol Clin Exp Res. 2005;29:756-762.
31. Manzoni GC, Terzano MG, Bono G, Micieli G, Mar-tucci N, Nappi G. Cluster headache – clinical find-ings in 180 patients. Cephalalgia. 1983;3:21-30.
32. Kudrow L. Physical and personality characteristicsin cluster headache. Headache. 1974;13:197-202.
33. Levi R, Edman GV, Ekbom K, Waldenlind E.Episodic cluster headache. II: High tobacco and
alcohol consumption in males. Headache. 1992;32:184-187.
34. Saper J. Nonheadache disorders and characteristicsof cluster headache patients. In: Mathew N, ed.Cluster Headache. New York: Spectrum Publica-tions, Inc.; 1984:31-44.
35. Diaz JA, Griffith RA, Ng JJ, Reinert SE, FriedmannPD, Moulton AW. Patients’ use of the Internet formedical information. J Gen Intern Med. 2002;17:180-185.
36. Griffiths KM, Christensen H. Quality of web basedinformation on treatment of depression: Cross sec-tional survey. BMJ. 2000;321:1511-1515.
37. Etter JF, Perneger TV. A comparison of cigarettesmokers recruited through the Internet or by mail.Int J Epidemiol. 2001;30:521-525.
38. Leone M, D’Amico D, Frediani F, et al. Verapamilin the prophylaxis of episodic cluster headache: Adouble-blind study versus placebo. Neurology. 2000;54:1382-1385.
39. Marks DR, Rapoport A, Padla D, et al. A double-blind placebo-controlled trial of intranasal capsaicinfor cluster headache. Cephalalgia. 1993;13:114-116.
40. Leone M, D’Amico D, Moschiano F, Fraschini F,Bussone G. Melatonin versus placebo in the prophy-laxis of cluster headache: A double-blind pilot studywith parallel groups. Cephalalgia. 1996;16:494-496.
SUPPORTING INFORMATION
Additional Supporting Information may be found inthe online version of this article:
SUPPLEMENTAL CASE REPORTS FOR“Response of Cluster Headache to Kudzu” (Case no. 1,4-16).
Please note: Blackwell Publishing is not responsiblefor the content or functionality of any supporting mate-rials supplied by the authors. Any queries (other thanmissing material) should be directed to the correspond-ing author for the article.
Headache 105

Headache ISSN 0017-8748
! 2008 the Author doi: 10.111/j.1526-4610.2008.01268.x
Journal compilation ! 2008 American Headache Society Published by Wiley Periodicals, Inc.
S1
SUPPLEMENTAL CASE REPORTS FOR
Response of Cluster Headache to Kudzu (Case no. 1, 4-16)
CASE #1
A 60-year old woman with no other medical
conditions was diagnosed with episodic chronic
cluster headaches at age 42 that became chronic at
age 43. She usually suffered three but could have as
many as eight attacks per day lasting 90 minutes
each, following no pattern that she could discern. The
attacks consisted of lacrimation, miosis, ptosis,
rhinorrhea, injected sclera, flushing, diaphoresis,
restlessness, and a boring pain in her temple. Her
social life and marriage deteriorated as a result, and
she became chronically depressed.
Propanolol, verapamil, lithium, and amitriptyline
had no effect on the frequency or intensity of her
attacks, but she found oxygen and sumatriptan to be
effective abortives. In February of 2005, she read on
an Internet cluster-headache forum that kudzu extract
could control cluster headache, so she started taking
Nature’s Way 613 mg capsules three times a day.
After two months, she noted no difference in the
frequency or intensity of her attacks—albeit no side
effects, either—so discontinued the kudzu. She
drinks a glass of red wine two or three times a week,
smokes half a pack of cigarettes a day, drinks 3 or 4
cups of coffee a day, but uses no other drugs.
CASE #4
A 47-year old woman with hypertension, asthma,
and a history of ruptured MCA aneurysm had her
first cluster attack in October 1973 at age 16 but was
not diagnosed until May 2000, when she transformed
to secondary chronic following years of misdiagnosis
with migraine, sinus infection, and
temporomandibular joint syndrome. Attacks were
left-sided, could last for as long as an hour, occurred
two to six times a day, and consisted of injected
sclera, ptosis, lacrimation, rhinorrhea, pressure from
nose to temple, neck spasms, and a feeling of having
a hot poker driven into her eyeball combined with an
urge to bang her head into a wall. These attacks made
it difficult for her to care for her newborn and were a
contributing factor in two divorces.
Propanolol, lithium, and verapamil were partially
effective in treating her CH, although she found the
lithium hard to tolerate, and oxygen was effective as
an abortive only 50% of the time. She initially gained
relief with rizatriptan but had to discontinue it
because of concerns following her cerebral
hemorrhage.
In February of 2005, while taking 360 mg
verapamil, 1800 mg gabapentin and 150 mg lithium
carbonate daily, and still suffering attacks three times
a day at 10 am, 2 pm and 10:30 pm, she read on an
Internet site that kudzu had been used in Chinese
medicine to treat migraines, so decided to self-
administer it. Starting with a 750 mg tablet of
Planetary Formulas kudzu extract she noticed that
within 24 hours her attacks ceased, and the residual
pain that she had suffered for several hours a day was
also cut in intensity and duration. Over several weeks
she increased her dose to 4500 mg a day, and found
that her attacks decreased in intensity and frequency
to one every three or four days. She also began to
experience “phantom attacks”—autonomic attacks
consisting of lacrimation, rhinorrhea, hidrosis, ptosis,
eyelid edema, flushing, photo- and phonophobia, but
no pain—roughly three times a day. She found the
kudzu most effective when taken two hours prior to
an expected attack. She was able to taper and
discontinue both the lithium and gabapentin, but
remained on verapamil at a reduced dose of 240 mg
daily for her hypertension. In May she experienced
six pain-free days in a row, and assuming that she
had cured her disease, began to taper the kudzu by
750 mg daily to 1500 mg daily. Within four days, her
daily attacks resumed, but were different in nature,
lasting only ten minutes each and lacking the usual
autonomic symptoms. She returned to her prior dose

S2 2008
of 4500 mg kudzu, but never achieved the same level
of relief again. The only side effect she noted was
excessive flatulence. She rarely drinks, continues to
smoke two packs a day of cigarettes and cannabis
three times a month, but uses no other illicit drugs.
CASE #5
A 38-year old woman with “severe sinus
headaches” from her teen years had her first clearly
identifiable six-week cluster period at age 28. At first
her remission periods lasted for two years, but her
cluster periods lengthened over time and she became
secondarily chronic in July of 2003, and has
experienced no more than seven pain-free days
between attacks since. Attacks last between 25
minutes and three hours, average five a day, and
consist of excruciating pain behind her right eye and
temple radiating to the jaw, lacrimation, nasal
congestion and rhinorrhea, conjunctival injection,
forehead and facial sweating, miosis, flushing,
phonophobia, tachycardia, anxiety, rocking, pacing,
and inability to concentrate. They occur reliably at
noon, 2 pm, 10 pm, 4:20 am and between 7 and 9 am,
with additional attacks at 5 pm and 8 pm at peak, and
have adversely affected her marriage, education, and
social life.
Propanolol and amitriptyline were ineffective,
and verapamil caused unacceptable hypotension.
Prednisone was effective but caused weight gain and
extreme mood swings, and she became toxic on
lithium before its efficacy could be determined.
Sumatriptan was effective but caused her attack
pattern to become irregular, and she had to
discontinue it in May 2004 after she developed
Prinzmetal angina. Oxygen initially worked
“miraculously” but decreased in effectiveness as time
went by and currently only works 50% of the time if
used immediately at the beginning of an attack. She
has tried over 50 medications in the last five years.
In February 2005, while on a regimen of fentanyl
200 µg twice daily and Tylox (acetamenophen/
oxycodone) 500/5 mg three times a day, she started
taking kudzu as an adjunctive. After ten days of
Nature’s Way 1226 mg in the morning she realized
that her afternoon attacks had doubled in intensity.
She stopped the kudzu but restarted it in the summer
of 2005 without concurrent opiates, and again found
that her afternoon attacks were much more painful.
Taking kudzu before bed caused her to experience
multiple nocturnal attacks—midnight, 2 am, and 4
am—for the first time. She discontinued it and
continues to take fentanyl and Tylox with oxygen for
breakthrough attacks. She smokes 1/2 pack a day,
drinks rarely, and uses no other drugs except topical
steroids for psoriasis.
CASE #6
A 57-year old man with no other medical
problems suffered episodic cluster headaches since
age 20, each cluster period lasting from six to eight
weeks, separated by a remission period of two years,
although his most recent remission period was six
years. Attacks occur up to four times a day, last one
to two hours, and consist of lacrimation, ptosis,
rhinorrhea, pacing, and chills. They cause him
irritability but no serious problems in jobs or
relationships.
Neither methysergide, lithium, indomethacin,
verapamil, prednisone, chlorpromazine, amitriptyline,
melatonin, topiramate, nor naratriptan have had any
effect on the frequency or intensity of his attacks.
Sumatriptan was effective as an acute abortive, but he
was forced to discontinue use after a myocardial
infarction in 1998. Oxygen has been only partially
effective, but he has not used a non-rebreather mask.
A month following the end of his last cluster
period in February 2005, and still experiencing heavy
“shadows” every other day, he read that kudzu was
reputed to treat cluster headache, so he took one dose
of Planetary Formulas Kudzu Recovery 1500 mg at
night. He noticed immediate “jabs and jolts”—a
phenomenon he had never experienced before—for
the rest of the evening but no shadows the following
day. The kudzu gave him an upset stomach. The next
day he began to experience shadows again, at which
point he ingested Hawaiian baby woodrose seeds.
The pain then stopped and did not return.
He drinks a glass of wine on the weekend but
does not smoke, use caffeine or illicit drugs. He
remains on atenolol, pravastatin, and aspirin.

S3 2008
CASE #7
A 57-year old woman without other medical
conditions has suffered from two years of chronic
cluster headaches consisting of an irregular pattern of
nocturnal right-sided forty-minute cluster attacks that
occur once a day within an hour and half of going to
sleep, with no remission period longer than three
weeks, with the exception of an interval on
prednisone. These attacks consist of ptosis, nasal
congestion, flushing, sweating, shivering,
osmophobia, and severe pain in her right teeth and
jaw. The pain has severely affected her social life,
and interfered with her and her husband’s sleep and
peace of mind.
Prednisone tapers have twice provided her with a
pain-free period, and sumatriptan is partially effective
in controlling her attacks. Reading that some people
had found relief with kudzu, on February 24, 2005
she began taking Nature’s Way kudzu extract 1226
three times a day, and noticed that the attacks
immediately shortened to five to ten minutes,
occurred twice a week rather than every day, and
became so much less intense that she no longer
needed abortive medication. Her use of triptans
declined from twice a week to none. On kudzu 1226
mg three times a day, a multivitamin, B-50 complex
and B-12, she can now be pain-free for as long as two
weeks between consecutive attacks. She notices no
side effects from the kudzu, smokes one pack a day
but does not drink or use illicit drugs.
CASE #8
A 32-year old man without other medical
conditions has suffered episodic cluster headache
since age 26, consisting of eight-week cluster periods
separated by four-month remission periods. During a
cluster period, he will experience four to six 90-
minute mostly nocturnal cluster attacks that feel “like
an ice-cream headache only worse”. The attacks start
with a dull ache behind the right eye, slowly increase
in intensity over five minutes to a constant boring
pain that spreads to the upper teeth, and is associated
with ptosis, conjunctival injection, tearing,
photophobia, and a compulsion to press his right
temple. These can be triggered by alcohol or odors of
gasoline, diesel fumes, nail polish, and perfume.
Until he was finally diagnosed in February 2005, he
underwent two courses of antibiotics a year for
presumed sinus infections, and had three healthy
teeth removed. He had to stop working as a train
conductor after he almost caused a derailment during
a cluster attack. During a cluster period, he will get
only two or three hours of sleep a night for weeks,
causing him to be irritable and adversely affecting his
relationship with his wife. Sleep deprivation also
impaired his ability to study and forced him to drop
out of college.
As a prophylactic, prednisone was ineffective,
and valproate doubled the frequency of his attacks,
but verapamil 480 mg reduced both the intensity of
the attacks by a third and the frequency by 20%.
Sumatriptan is effective, and oxygen is completely
effective 75% of the time and reduces the intensity of
remaining attacks the remainder of the time.
Melatonin causes the attacks to shift from diurnal to
nocturnal.
An extended cluster period began in February
2005 that lasted for nine months. In April he tried
Planetary Formulas kudzu extract 1500 mg twice a
day, increasing to three times a day after two months.
After three months of co-administration with
verapamil, melatonin, sumatriptan and oxygen, he
noted no change in the frequency or intensity of his
attacks, but suffered from gastrointestinal distress, so
discontinued it. Subsequently, there was no
noticeable difference in his cluster attacks, which
were occurring three to five times a day. He took
psilocybin mushrooms in October 2005 and the
cluster period stopped. He has been pain-free since.
He smokes a pack and a half and drinks up to two
pots of coffee a day, but does not drink alcohol or use
illicit drugs.
CASE #9
A 49-year old man with no other medical
conditions has endured episodic cluster headache
since age 20, diagnosed at age 35. Every 10 to 13
months he will experience nine months of hour-long
attacks that occur up to four times daily, consisting of
intense non-throbbing pain centered in his right eye,
associated with lacrimation, rhinorrhea, pacing,
irritability, and rocking back and forth. These attacks

S4 2008
have disrupted his social life, because he often cannot
risk attending social events, and his professional life
as a University administrator, because he lives in fear
of a cluster attack removing his ability to successfully
think through problems.
Propanolol was ineffective in ameliorating his
attacks, while verapamil was effective for about three
years then ceased to work. Prednisone was effective
but caused him unpleasant mood changes, excessive
weight gain and edema, and topiramate caused him
paresthesias and hallucinations. He can reliably abort
acute attacks with sumatriptan and occasionally with
oxygen.
Frustrated with what he considered to be
unacceptable side effects from the prophylactic
agents he had tried, when his current cluster period
began on May 29, 2005, he decided to take kudzu
instead, which he had read about on an online cluster
headache forum. On June 7, he started taking 1500
mg Planetary Formula kudzu three times a day,
and noted a slight decrease in the intensity and
duration of his attacks and an immediate decrease in
their frequency from four a day to two or fewer.
Skipping a dose of kudzu or even changing the
timing of a dose results in an immediate increase in
the frequency but not the intensity of the attacks. The
only side effects he suffered were indigestion and a
“looser neck”. He drinks alcohol once or twice a
week when in a remission period, smokes cigarettes
when he drinks, but uses no illegal drugs. He has one
or two cups of coffee a day. He can continue to have
one or two mild attacks a day on kudzu, ergotamine
tartrate 2 mg at night, and melatonin 9 mg at night.
CASE #10
A 49 year old right-handed man has had cluster
headache since age 13, becoming secondarily chronic
at age 25. He had been run over by a car at age 4,
resulting in persistent cognitive deficits from his
brain injury, and also suffers from migraines and
depression. He can have up to 6 attacks a day that are
mostly right-sided but that can alternate within
the same cluster period, consisting of 30 minutes of
lancinating pain, eyelid edema, and ptosis that cause
him to scream, sob, and punch himself in the head
and that have left him with a permanent right eyelid
droop. Attacks occur night and day, making it
difficult for him to keep a job, as he has frequently
quit impulsively while in a cluster period. His mood
is frequently so foul during his worst periods that his
family has to walk around “on eggshells”.
He found amitriptyline and methadone, which he
started in his 30s, to be partially effective at
controlling his attacks, but did not like the mental
dullness or difficulties with orgasm that they gave
him. Lithium was ineffective, and sumatriptan was
effective in controlling his attacks, but becoming less
so with time and eventually causing increased
intensity attacks, anxiety, and confusion that stopped
when he discontinued it. At this time he was forced
to go on permanent disability.
In April 2005 he read on the Internet about the
kudzu treatment for cluster headache. He
discontinued his methadone and alprazolam, but not
his melatonin, suffering five days of withdrawal
symptoms, then started kudzu extract (Planetary
Formulas, Kudzu Recovery) 750 mg three times
daily, noticing no effect. Upon increasing this to
1500 mg three times daily, he noticed an immediate
50% decrease in the intensity of his pain, although
the frequency of the attacks remained unchanged.
After two months on kudzu, he decided that although
it was more effective for him than sumatriptan or
morphine, the discontinuation of his other
medications had caused his insomnia, restless leg
syndrome, and chronic pain to worsen. He therefore
discontinued the kudzu and instead took Hawaiian
baby woodrose seeds for prophylaxis, finding them to
be more effective than kudzu, and sumatriptan for
breakthrough attacks. He remains on morphine SR 60
mg for chronic pain and alprazolam 1 mg. He does
not smoke, drink, or use recreational drugs.
CASE #11
A 43-year old right-handed woman in Louisiana
with no other medical conditions except for
gastroesophageal reflux disease has had episodic
cluster headache since age 12. Each cluster period
lasts six to eight weeks separated by a remission
period of 7 to 18 months. At worst, she will suffer
three two-hour attacks per day, mostly nocturnal,
consisting of lacrimation, ptosis, conjunctival

S5 2008
injection, rhinorrhea, diaphoresis, restlessness, neck
stiffness, and severe, boring pain in her eye, ear, and
temple. These have deprived her of sleep and made
her irritable, embarrassed for repeated cancelling
social plans, guilty over her inability to be industrious
during a cluster period, and resigned to remaining in
a bad marriage for fear that her condition will make it
impossible for her to find another partner.
She has found propanolol ineffective, and
verapamil and prednisone partially effective in
decreasing the frequency and severity of attacks.
Oxygen lessens the intensity of attacks but does not
truncate them; triptans abort an attack about a quarter
of the time.
In July 2005, her fiancé read an article that said
that kudzu could potentially help her cluster
headache. When her most recent cluster period
started that month, she started taking Nature’s Way
613 mg twice a day for the next three weeks, but
found that her attacks were worse—more intense,
more frequent during daylight hours, and longer, and
the cluster period itself was also longer than normal.
This coincided with hurricane Katrina’s landfall,
however, and with it a month of increased stress, 95-
degree temperatures, and no electricity or air
conditioning. She stopped taking the kudzu when it
ran out. She experienced no side effects from the
kudzu. She currently smokes one pack per day of
cigarettes, drinks one or two servings of alcohol
several times a week and three to five cups of coffee
a day, but uses no illegal drugs.
CASE #12
A 42-year old man without any other medical
problems has had episodic cluster headaches since his
late twenties. For four to six weeks, twice a year, he
suffers one or two right-sided cluster attacks daily or
every other day, lasting one to three hours each.
These are characterized by rhinorrhea, ptosis,
mydriasis, and severe orbital pain that often leaves
him unable to do anything but rock back and forth or
writhe around on the floor. During these periods, he
is forced to schedule his personal and professional
life around anticipated attacks, which is disruptive
and anxiety-provoking for him and his family.
He had used no medication prior to his most
recent cluster period, which began in February 2005,
after which he used both oxygen and intramuscular
sumatriptan and found them effective in terminating
his cluster attacks in less than 15 minutes.
Finding a reference online to kudzu in February
2005, he started taking 1226 mg Nature’s Way kudzu
extract three times a day and found that the frequency
and intensity of his attacks dropped almost to zero.
He had only two more attacks during that cluster
period. In July 2005, he started to suffer cluster
attacks that were provoked by vigorous exercise,
heralding the beginning of another cluster period, so
he restarted kudzu at the same dose. He experienced
only five or six half-strength attacks for the
remainder of the cluster period—four weeks—and
these attacks did not occur spontaneously, but rather
were triggered by aerobic exercise or alcohol, and
responded promptly to oxygen. This scenario
repeated almost exactly during his next cluster
period, which began in January of 2006. Despite the
infrequency of attacks, he is able to tell that he
remains in the cluster period by a subtle heaviness in
his head and “tickle” behind his eyeball, and in a
remission period he is able to consume alcohol and
run a marathon once or twice a year without
triggering an attack. He notices no side effects from
the kudzu.
When his most recent cluster period started on
March 12th
, 2006, he began taking Planetary
Formulas 1500 mg twice a day and found it less
effective than Nature’s Way but better than
nothing—although his cluster attacks were only 10 to
15 minutes in length and aborted by oxygen, and
much less painful in intensity, he continued to have
an attack almost every day. Discontinuing kudzu
increased the frequency to two or three a night.
His father is his only relative known to have
cluster headache. Neither he nor his father has a
history of head injury, although his father’s brother
had a seizure disorder. He drinks one or two beers or
glasses of wine a day, stopped smoking nine years
ago, and uses no illicit drugs.

S6 2008
CASE #13
A 40-year-old woman with osteomalacia and
collagenous colitis has had chronic cluster headache
since age 38, when she tapered off the prednisone
that she had been taking for her celiac disease over
nine months. If unmedicated, she will have between
three and eight cluster attacks a day, lasting two
hours each, and consisting of a boring pain in her
temple accompanied by an urge to gouge out her eye,
lacrimation, ptosis, miosis, rhinorrhea, and sweating.
She was forced to stop working, and her marriage
ended.
Verapamil caused syncope, lithium was
ineffective, and topiramate caused hallucinations and
delusions, but oxygen will reliably end an attack in
five minutes. Triptans are also effective but
sumatriptan caused tachycardia, nausea, and
dysphoria, and frovatriptan caused the intensity of
her attacks to increase.
In December 2005, having read on the Internet
that kudzu was effective in treating cluster headache,
she started taking Natures Way 1226 mg three times
a day and noted that the intensity of her attacks
decreased by 50% and the frequency dropped to two
to three attacks per day. After 13 weeks, the
frequency slowly increased back to baseline, so she
stopped kudzu and switched to verapamil, then
topiramate, then lithium, hoping that they might be
more effective, which turned out not to be the case.
She suffered no side effects from the kudzu.
She does not smoke or use illegal drugs, drinks
alcohol twice a week, and drinks three coffees or
sodas a day. She currently takes only Rivea
corymbosa seeds and oxygen to treat her cluster
headache.
CASE #14
A 31-year old woman without other medical
conditions suffered from episodic cluster headaches
since age 16 that occurred for five week periods
separated by 11 month to 3-year remission periods.
At peak, she can have four 50-minute attacks per day,
consisting of severe boring pain, rhinorrhea, ptosis,
rocking, moaning, and compulsively rubbing or
hitting her temple. This leads to sleep-deprivation
and irritability, adversely affecting her relationship
with her husband. She was initially treated for sinus
infections every September during her regular cluster
period, until she finally received the correct diagnosis
in 2000.
Amitriptyline had no effect on the frequency or
intensity of her attacks, and prednisone rendered her
pain-free for only two days. Oxygen worked for half
of her cluster period in 2000, but not subsequent to
that. Injectable sumatriptan works 95% of the time.
In 2004, she read on an Internet forum that
kudzu extract could be used to treat cluster headache,
so at the anticipated beginning of her next cluster
period in September 2005, she began to take
Neutraceuticals Sciences Institute kudzu extract 650
mg daily. During that month, her cluster period did
not begin in its usual fashion; rather, she experienced
three “phantom attacks”, consisting of unilateral
nasal congestion, ptosis, and flushing but without any
pain. These were otherwise identical to her regular
attacks except that they lasted for only two or three
minutes.
In mid-October she discontinued the kudzu, but
when her cluster period began late in December, she
restarted kudzu at 650 mg one to three times a day
and for the remainder of the six weeks of her cluster
period noted that both the intensity and frequency of
subsequent attacks were lessened. By themselves, the
attacks were not shorter, but oxygen, which had
ceased to work, became effective again as an abortive
in combination with the kudzu. Her cluster period
remained the same length. She experienced no side
effects other than loose bowels. She remained on
duloxetine, alprazolam, and vitamins during this
period. She stopped smoking a pack a day a year ago,
and drinks two to four glasses of red wine four times
a week, but uses no illicit drugs or caffeine.
CASE #15
A 49-year old man with no medical history other
than a concussion from a motorcycle accident at age
16 started to have episodic cluster headache at age
23, consisting of two-month cluster periods every 18
to 24 months that often started during times of
relaxation following stressful periods such as a
deadline. At worst he will get two left-sided attacks a
day, lasting up to three hours each, characterized by a

S7 2008
boring pain in his temple with waves of more severe
pain approximately every ten minutes, a “hot knot” in
his neck and throat, miosis, lacrimation, conjunctival
injection, rhinorrhea, flushing, diaphoresis,
restlessness, photophobia, and a feeling “like an alien
in my head wants out”. During the attacks he is
completely incapacitated, and by the second week of
a cluster period, sleep deprivation renders him
irritable and unable to focus or make decisions at
home or at work. His neurologist has recommended
that he eliminate foods such as cheese, nuts,
chocolate, coconut, shellfish, tomatoes, alcohol and
just about anything "aged" from his diet, which
causes inconvenience when eating out or at social
gatherings. He also lost one five-year romantic
relationship in part because of his cluster headache.
Acupuncture has not helped his cluster headache,
nor has prednisone, which instead gave him anxiety,
depression, irritability, and mood swings. Oxygen
and rizatriptan, which he combines with a few drops
of “Bach Flower Rescue Remedy” and a cup of hot
coffee, are effective in aborting individual attacks. He
has also taken Cafergot, codeine, Vicodin, Dilaudid,
melatonin, Chinese herbal medicine and feverfew,
and tried homeopathy, craniosacral therapy, and
“Quantum Energetics” therapy. The Cafergot worked
only occasionally, and only if taken immediately at
the onset of a headache. Dilaudid helps early in the
cluster period, but increasing doses are required as
the cluster period continues.
In November 2005, one week into his most
recent cluster period, he read about kudzu on an
Internet forum, so started taking StarWest Botanicals
Inc. bulk kudzu root 800 mg to 1000 mg at night,
combined with drinking four to five liters of spring
water during the course of the day. He noted no
change in the intensity, frequency, or duration of
attacks, but his cluster period ended after only three
weeks. He experienced no side effects from the
kudzu.
He does not smoke, and while in a cluster period
does not drink alcohol or use illegal drugs, but will
drink coffee to help abort individual attacks. In a
remission period, he smokes prescribed medical
cannabis once or twice a day but uses no illegal
drugs, drinks 2.5 glasses of red wine daily, and drinks
a cup of coffee every morning.
CASE #16
A 33-year old right-handed woman with no other
medical conditions was diagnosed with episodic
cluster headache at age 22, consisting of
progressively longer—currently eight week—cluster
periods separated by nine- to twelve-month remission
periods. She experiences one or two 60-minute
attacks a day, characterized by ptosis, diaphoresis,
restlessness, photo- and osmophobia, and pain that
she describes as like a “lightning storm” or “worms
dipped in acid crawling through the right side of my
head.” She has suffered lost productivity in her job
from lingering headaches and medication side effects,
and since her triggers during a cluster period include
flickering lights and chemical smells, she cannot go
to bars, restaurants, grocery stores or movies,
severely impacting her social life.
Amitriptyline is ineffective as a prophylactic
agent, verapamil and duloxetine are partially
effective, and prednisone prevents attacks while she
takes it. Intranasal sumatriptan effectively aborts her
attacks.
In fall of 2005 she read on the Internet that
kudzu might be effective in treating cluster headache,
so she started taking Nature’s Herb 100 mg daily, but
noted no decrease in the frequency, intensity, or
duration of her cluster attacks and no effect on the
length of her cluster period. She suffered no side
effects from the kudzu, however. She currently
maintains herself on a combination of duloxetine,
verapamil, kudzu, magnesium, and melatonin. She
does not smoke or use illegal drugs, but drinks
occasional alcohol when in a remission period.
Related Documents