Responding to the Zika Epidemic: Working with Partners Allyn K. Nakashima, MD State Epidemiologist October 13, 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Responding to the ZikaEpidemic: Working with
PartnersAllyn K. Nakashima, MDState EpidemiologistOctober 13, 2016

Welcome!
Acknowledgements and Disclaimer• Sources:
– Centers for Disease Control and Prevention (CDC)
– Other global and national public health agencies, e.g., WHO and PAHO
– published literature ‐ citations provided– news media ‐ citations provided– This is a rapidly changing area and the information has been updated through October 4, 2016

10 Essential Public Health Services1. Monitor Disease2. Diagnose and Investigate3. Inform, Educate, Empower4. Mobilize Community Partnerships5. Develop Policies6. Enforce Laws7. Link to Personal Health Services and Care8. Assure a Competent Workforce9. Evaluate10. Research for New and Innovative Solutions
One Health Approach Is Needed to Accomplish Essential Public Health Services
Objectives• Review of Zika virus infection• How the Utah public health
community has responded to the Zika epidemic
• Role of partnerships in that response

Zika Virus
• Single‐stranded RNA virus isolated from a monkey in 1947 in Uganda
• Flavivirus (related to other Flaviridaeviruses: dengue, West Nile virus, Japanese B encephalitis, and yellow fever)
• Transmitted by Aedes spp. mosquitoes

Zika Vectors in Humans• Aedes aegypti is the primary vector
• Aedes albopictusmay also be a vector
• Eggs are laid in water containers around households
• Peak feeding during daytime, but also bites at night
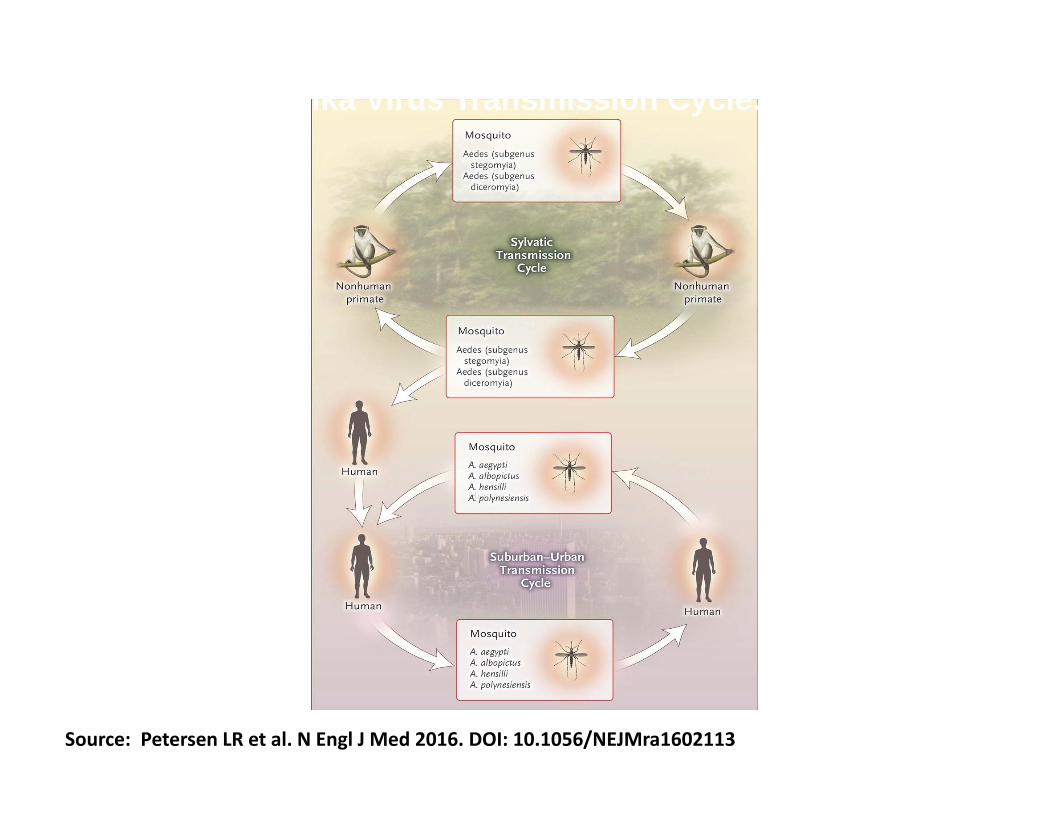
Source: Petersen LR et al. N Engl J Med 2016. DOI: 10.1056/NEJMra1602113
Zika Virus Transmission Cycle.

Evidence of Sylvatic Transmission
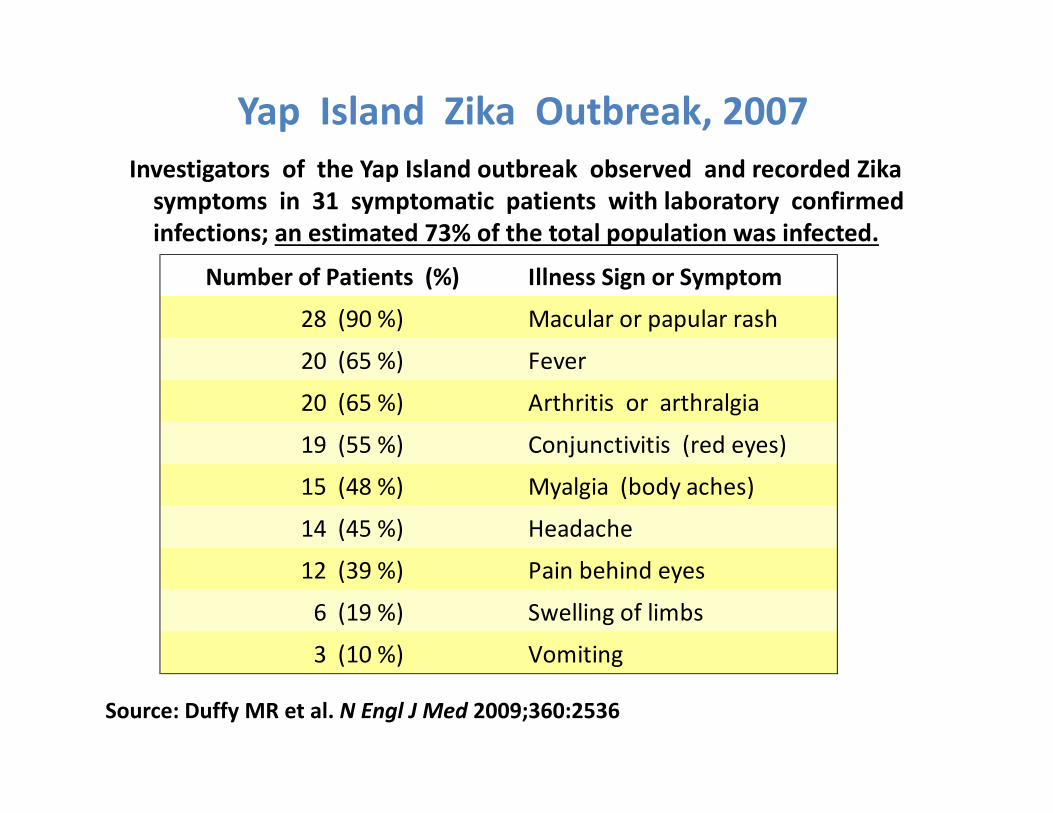
Yap Island Zika Outbreak, 2007Investigators of the Yap Island outbreak observed and recorded Zikasymptoms in 31 symptomatic patients with laboratory confirmed infections; an estimated 73% of the total population was infected.
Number of Patients (%) Illness Sign or Symptom
28 (90 %) Macular or papular rash
20 (65 %) Fever
20 (65 %) Arthritis or arthralgia
19 (55 %) Conjunctivitis (red eyes)
15 (48 %) Myalgia (body aches)
14 (45 %) Headache
12 (39 %) Pain behind eyes
6 (19 %) Swelling of limbs
3 (10 %) Vomiting
Source: Duffy MR et al. N Engl J Med 2009;360:2536
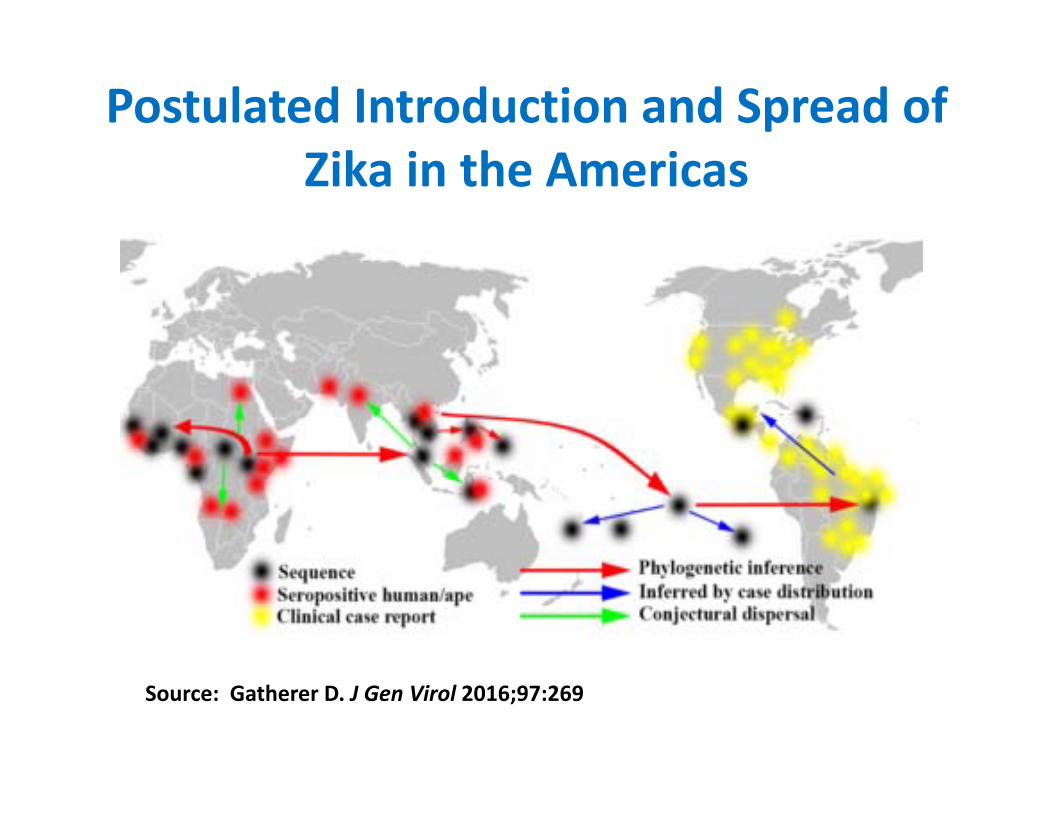
Postulated Introduction and Spread of Zika in the Americas
Source: Gatherer D. J Gen Virol 2016;97:269
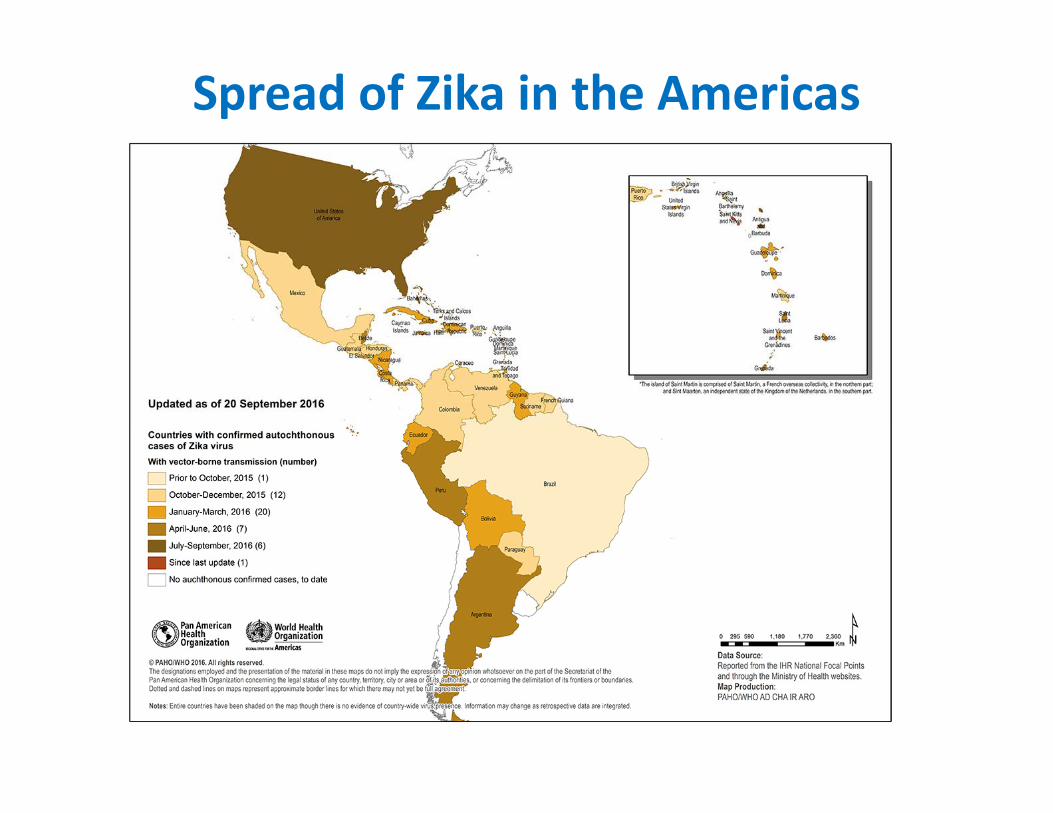
Spread of Zika in the Americas
. . .”the [Zika] outbreak was triggered by‘a perfect storm’ of biological, economic,and climatic events.”
Laurie GarrettSenior Fellow for Global Health

Q1: What scientific and other partners are needed to help us understand the Zika epidemic?

• March 2015 – Brazil reports to WHO the first cases of a new illness characterized by a skin rash
• April 2015 – laboratory confirmation of Zika
• May 2015 – PAHO issues an Epidemiological Alert of Zika infection in Brazil
• July 2015 – Brazil reports laboratory‐confirmed local transmission of Zika in 12 states
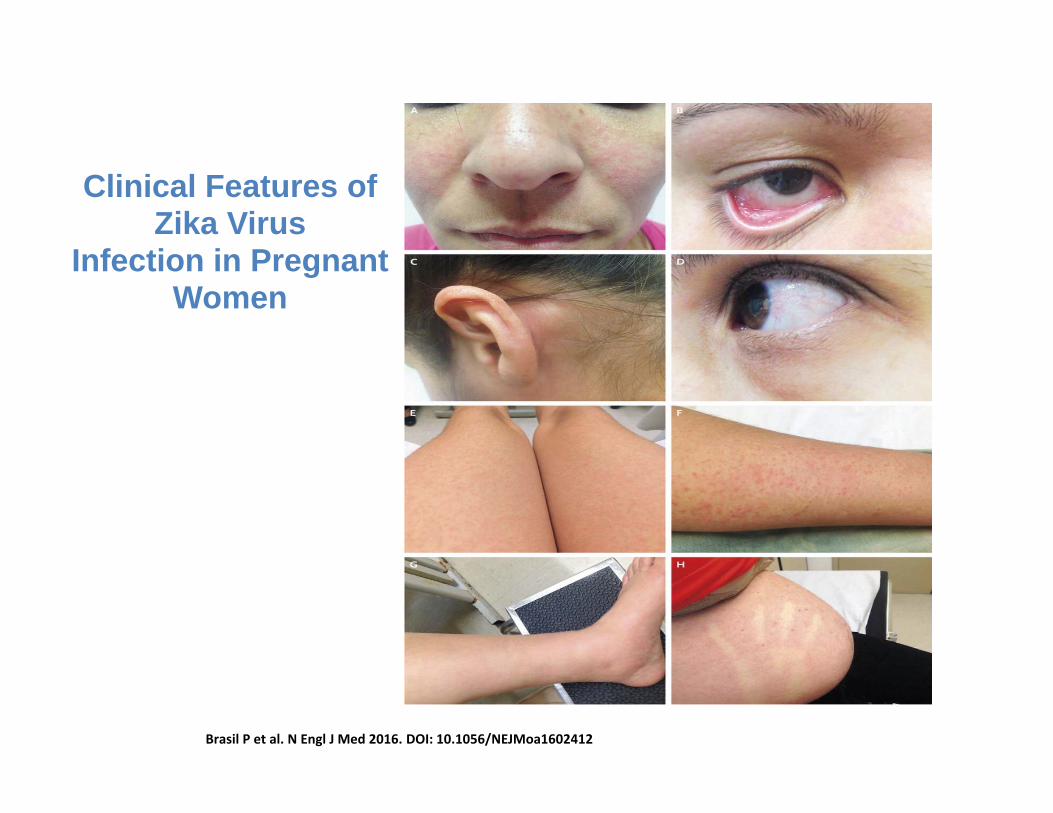
Brasil P et al. N Engl J Med 2016. DOI: 10.1056/NEJMoa1602412
Clinical Features of Zika Virus
Infection in Pregnant Women

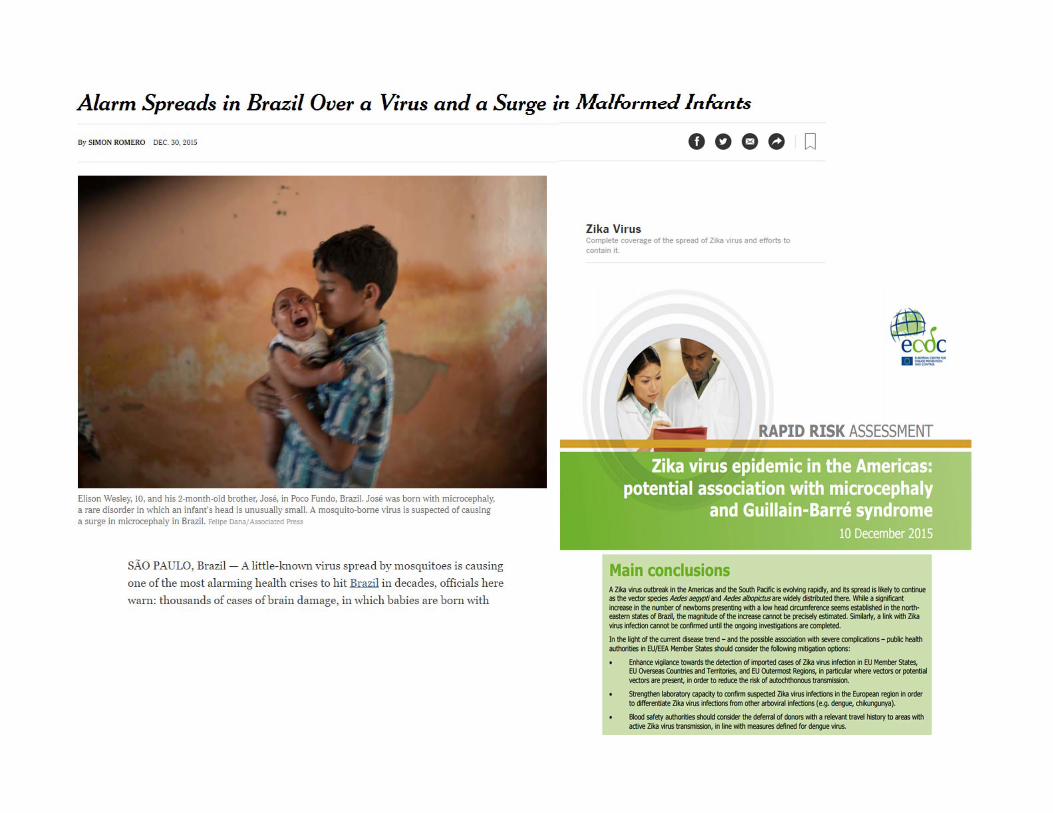
Early Alert of Increase in Microcephaly in Infants in Brazil

Q2: At this point, what should public health in Utah do and what partners should be involved?

Source: CDC/AMA webinar at https://www.youtube.com/watch?v=L1csVKfquoM
Treatment• No antivirals• Supportive treatment only• Use of aspirin and NSAIDs should be avoided until dengue is ruled out
• Differential diagnosis: other Flavivirusinfections, tickborne diseases, other viral infections that present with rash, malaria

Sequelae of Zika Infection• Disease is mild and self‐limited for most people with complete recovery.
• Guillain‐Barré syndrome and other neurologic manifestations may follow infection, but the incidence is unknown.
• Adverse pregnancy outcomes, e.g., microcephaly or still birth, may occur in pregnant women. The incidence is unknown, but has been estimated at 1‐10% for women infected during the first trimester.


Pregnancy Outcomes of 9 U.S. Women Infected with Zika
• 257 pregnant women tested during August 2015‐February 2016– 151 (59%) had symptoms compatible with Zika– 9 (3.5%) were positive for Zika
• Characteristics of 9 pregnant women positive for Zika– All had rash; 8/9 had one other symptom of infection– No hospitalizations or deaths
• Pregnancy outcomes:– 2 miscarriages– 2 terminations due to severe defects seen on ultrasound– 1 infant born microcephaly– 2 apparently normal infants– 2 pregnancies continuing without complications
• All women with adverse outcomes thought they were infected during the first trimester of pregnancy
Source: Meaney‐Delman D. MMWR Morbid Mortal Wkly Rep 2016;65:215


Main Discussion Points for the UDOH ZikaIncident Command System (ICS)
• Improved communication to pregnant women, travelers, healthcare providers, etc.
• Surveillance of travelers returning from Zika‐affected countries
• Laboratory testing updates• Vector surveillance and control activities• Follow‐up of pregnant women and infants• Activities and budgets to support activities hat may be needed in ELC, PHEP and other grants

Q3: Who should be invited to participate in the UDOH Zika ICS?
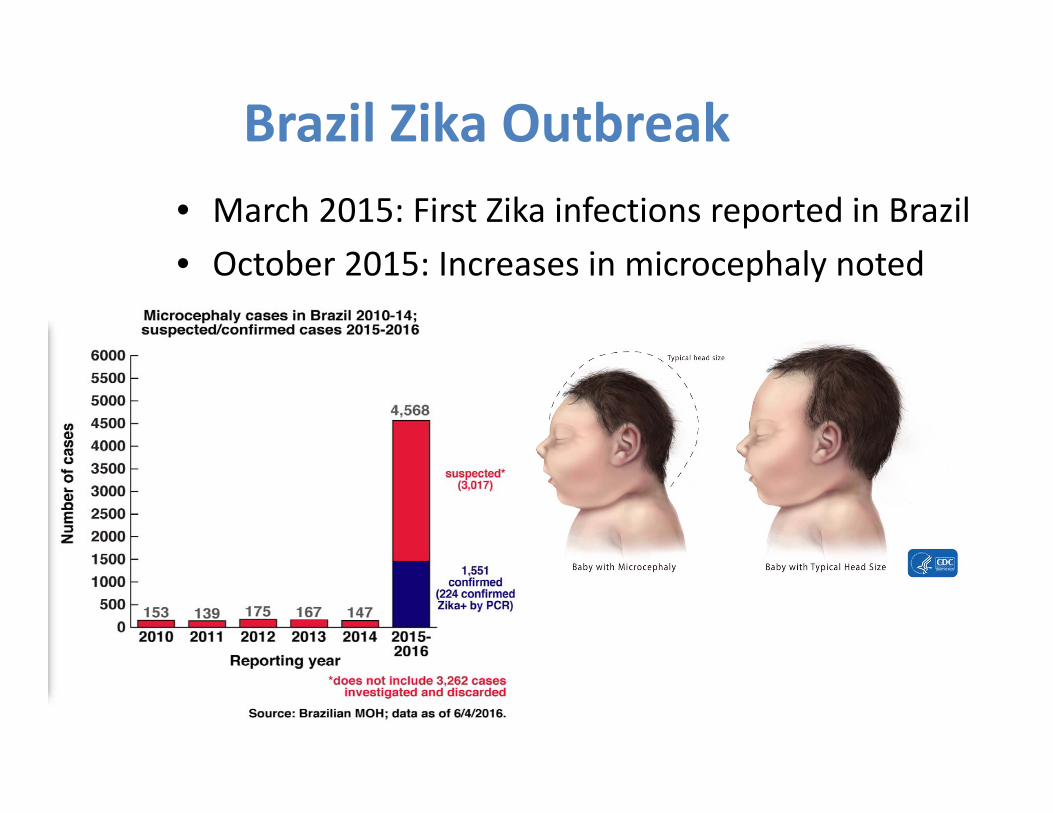
Brazil Zika Outbreak• March 2015: First Zika infections reported in Brazil • October 2015: Increases in microcephaly noted

The TORCH ConceptThe concept of congenital viral infection emerged in 1947 with the observations of Gregg. In the 1970s scientists at the CDC and Emory University coined the term “TORCH” to signify that certain symptoms and signs were common to congenital infections due to:
– Toxoplasma gondii– Other: Varicella zoster virus, lymphocytic
choriomeningitis virus, Zika virus– Rubella virus– Cytomegalovirus (CMV)– Herpes simplex virus
Source: Gregg NM. Congenital defects associated with maternal rubella. Aust Hosp 1947;14:7-9.

Evidence That Zika Causes Birth Defects
• French Polynesia outbreak re‐analysis: estimated baseline prevalence of microcephaly was 2/100,000 births; during Zikaepidemic, 95/100,000 births
• Epidemiologic data from Brazil• Zika isolated from variety of fetal tissues and amniotic fluid• Prospective follow‐up of symptomatic pregnant women
infected with Zika show a high incidence of fetal demise and birth defects
• In vitro studies show Zika virus has a predilection for infecting neural stem cells and destroying them
• April 13, 2016: CDC confirms the association between Zikainfection and microcephaly and reinforces travel recommendations
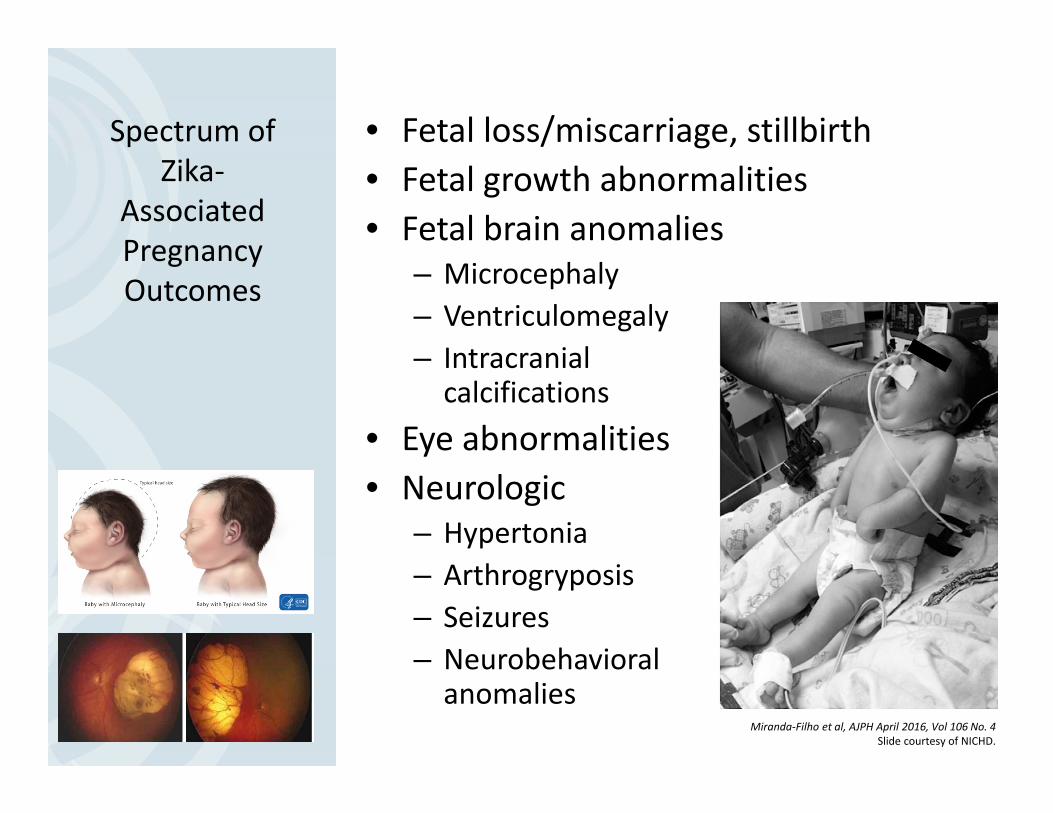
Spectrum of Zika‐
AssociatedPregnancy Outcomes
• Fetal loss/miscarriage, stillbirth• Fetal growth abnormalities• Fetal brain anomalies
– Microcephaly– Ventriculomegaly– Intracranial calcifications
• Eye abnormalities• Neurologic
– Hypertonia– Arthrogryposis– Seizures– Neurobehavioral anomalies
Miranda‐Filho et al, AJPH April 2016, Vol 106 No. 4Slide courtesy of NICHD.

Fetal ultrasounds at 20 weeks’ gestation
Marko Culjat et al. Clin Infect Dis. 2016;63:805-811
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail [email protected].

Photograph of the side head (A) shows severe microcephaly with occipital keel‐like prominence, and normally developed face
Marko Culjat et al. Clin Infect Dis. 2016;63:805-811
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail [email protected].

Prospective Study in Brazil• 88 pregnant women with rash in previous 5 days enrolled
– 72 (82%) tested positive for Zika– Timing of infection was 6 to 38 weeks of gestation
• 42 of the Zika‐positive women agreed to have ultrasound; of these, 12 (29%) had fetal abnormalities. Findings:– 5 with in utero growth retardation including microcephaly– 7 with ventricular calcifications or other CNS lesions– 7 with abnormal amniotic fluid volume or cerebral or umbilical
artery flow • Outcomes to publication date:
– 2 fetal deaths at 36 and 38 weeks gestation– 8 who have delivered have confirmed abnormalities seen on
ultrasound
Source: Brasil P etal. N Engl J Med March 4, 2016
Numerous Unanswered Questions• What is the relationship between the timing
and severity of maternal infection and fetal outcome?
• How long is the period of fetal vulnerability?• Do infants shed virus postnatally? If so, is
there ongoing damage to the developing brain?
• What are the long term neurodevelopmental outcomes for infants with congenital Zika?
• What are the potential neurological complications of Zika virus infections in children and adults?

Hope for a Vaccine• Rhesus macaque model demonstrating that once infected, re‐challenges with Zika virus results in no detectable virus replication.– Source: Dudley D, et al. Nature June 28, 2016
• Three different candidate vaccines induced Zika‐specific neutralizing antibodies that protect rhesus monkeys from re‐infection.
• NIH announces phase 1 clinical trial on VRC319 vaccine on August 3– Source: Abbink P, et al. Science August 4, 2016

Zika Cases in the United States• As of September 29: 3,813 cases in US states and 24,201 in US territories reported to CDC.– Pregnant women infected with Zika: 837 in US states and 1,638 in US territories
– 13 cases of Guillian‐Barré in US states• Number of locally‐acquired Zika infections in US states: 105 (all in Florida)
• So far 22 live‐born infants in US states have been documented with birth defects; 5 stillbirths with birth defects
• Regular updates: http://www.cdc.gov/zika/
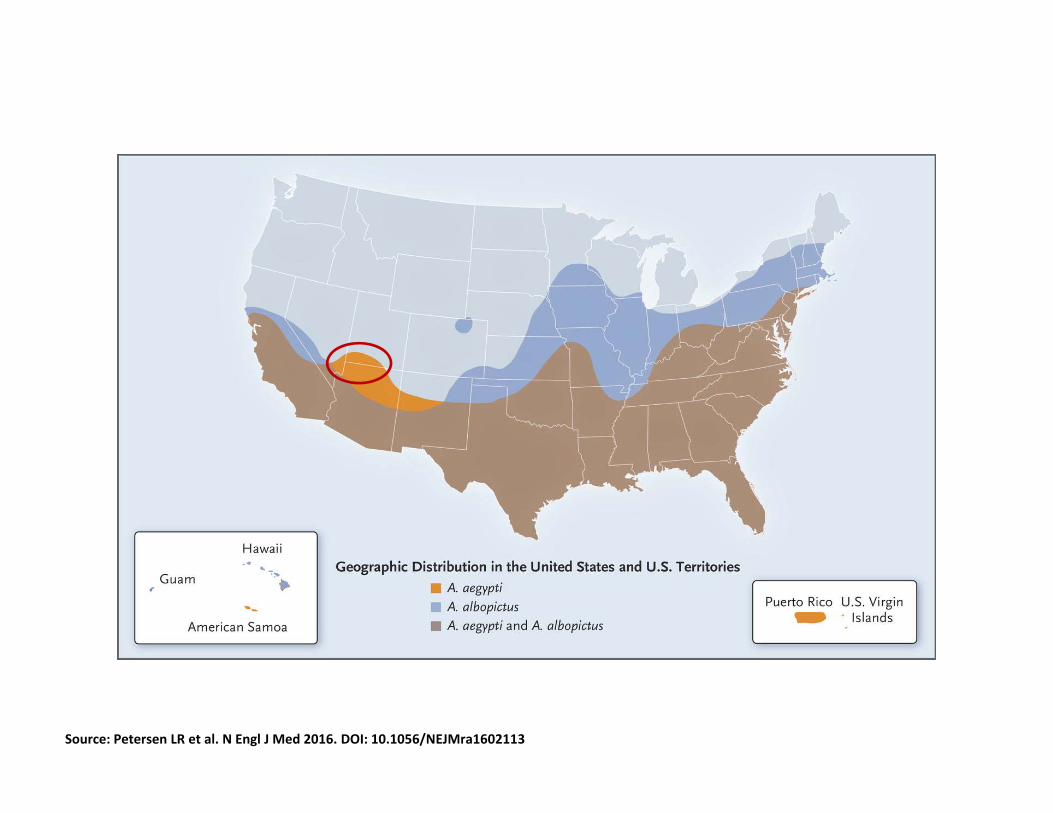
Source: Petersen LR et al. N Engl J Med 2016. DOI: 10.1056/NEJMra1602113
Approximate Ranges of A. aegypti and A. albopictus in the United States (as of March 2016).
Utah Zika SituationAs of October 11, 2016:• 545 persons have been tested for Zika; of these, 305 (56%)
were pregnant women.• 18 persons have tested positive for Zika; of these, 8 are
pregnant women. The delivery status of the pregnant women:– 4 have delivered apparently normal infants, and infants are being
followed– 2 miscarried in the first trimester– 1 are still pregnant and being followed– 1 lost‐to‐follow‐up
• One individual (‘Index Case’) has died, probably due to Zika as indicated by high levels of Zika viremia. A close contact (Patient A) to this individual developed Zika. The contact had no travel history or other risk exposures for Zika. (Swaminathan S. N EnglJ Med;September 28, 2016)

Utah Zika Investigation• Objective: to identify the most likely cause of transmission to Patient A who had no history of travel to an area with active Zika transmission
• Studies conducted:– Family and close contact study– Healthcare worker serosurvey– Community serosurvey
• To date, the only risk identified is close contact with the Index Case without using personal protective equipment or other standard precautions. (See Notes to the Field in September 14, 2016, issue of the Morbidity Mortality Weekly Report)
• Stay informed:– https://www.cdc.gov/zika/– https://emergency.cdc.gov/coca/calls/zikaresources.asp
• Collaborate with your public health partners: Local County Health Deptand UDOH
What Can Providers Do?
• UDOH is responsible for conducting surveillance of Zika infections in Utah and sending this information to CDC
• Investigations of suspect cases are conducted by LHDs and UDOH– They will contact your office for information about these cases
• UDOH is constantly updating our local guidance as the national recommendations from CDC and other experts change– http://health.utah.gov/epi/diseases/zika/
Working with Your Public Health Partners

• Focus on pregnant women and women who could become pregnant
• Ask these women about upcoming travel plans for themselves and their partners
• Refer to CDC travel website: http://www.cdc.gov/zika/geo/index.html
Providers, you are in the best position to give these women advice not to travel to countries where Zika is being transmitted!
Need for More Effective Implementation of Prevention Messages
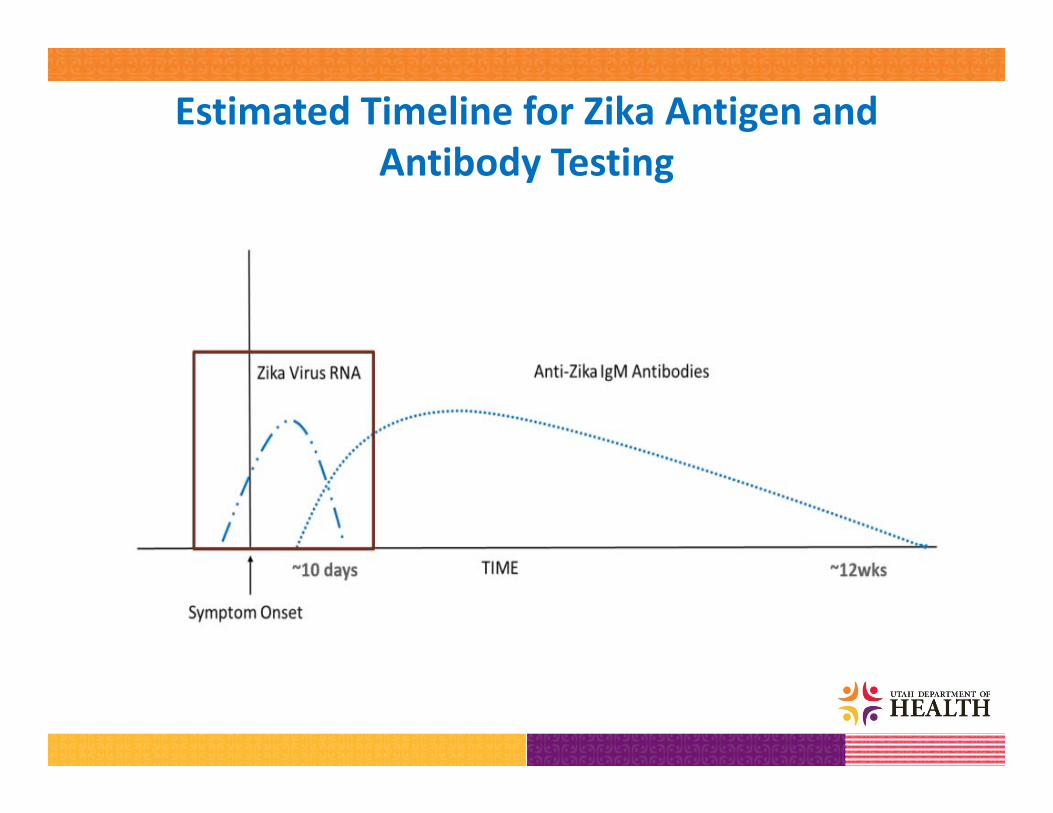
Estimated Timeline for Zika Antigen and Antibody Testing

• Zika tests:– rtPCR for serum, urine, CSF, amniotic fluid
oUPHL performs the Trioplex rtPCR test from CDC. This tests for dengue and chikungunya to rule these out
o Several other commercial rtPCR tests are available but these only test for Zika and need confirmation
– IgM antibody test (MAC ELISA): UPHL performs this test
– Plaque reduction neutralization test (PRNT): available only at CDC
Zika Testing

• Symptomatic patients with an exposure history (i.e., travel or sexual)
• All pregnant women with an exposure history
• Do not test asymptomatic:– Men– Children– Women who are not
pregnant
Who Should Be Tested for Zika?

• Sex partners of pregnant women, who are returning from Zika affected areas should abstain or use condoms for the duration of the pregnancy, regardless of test results.
• For couples trying to get pregnant:– Wait 8 weeks if the female partner has traveled to a Zika‐
affected area regardless of symptoms– Wait 8 weeks if the male partner has traveled to a Zika‐affected
area and is asymptomatic– Wait 6 months if the male partner is symptomatic
• WHO has simplified the recommendations: couples where one or both partners have traveled to a Zika‐affected area should postpone pregnancy for 6 months regardless of symptoms. CDC may be adopting this recommendation soon.
Recommendations to Prevent Sexual Transmission

• UPHL has Trioplex rtPCR and IgM tests, free of charge
• UPHL will also refer specimens (including placenta and umbilical cord) for testing to CDC as appropriate (Do not send specimens directly to CDC!)
• All testing done by UPHL must be approved by UDOH Epidemiology. To request testing, contact:– Davis County Health Department at 801‐525‐5220– UDOH Epidemiology at 801‐538‐6191 (24/7)
Requesting Zika Testing from Public Health

Laboratory Testing for Zika
http://health.utah.gov/epi/diseases/zika/Zika_Virus_Testing_Guidance.pdf

• Follow‐up of Zika‐infected pregnant women by OB providers:– Get consultation from a high risk pregnancy expert– Repeat PCR testing on serum and urine– Serial ultrasounds
• Labor and delivery:– OB providers work with public health to collect specimens (e.g., placenta, cord) at delivery and transport these to UPHL
– Pediatric providers should evaluate the infant and collect a serum specimen for Zika testing before discharge
Follow‐Up of Zika‐Infected Pregnant Women
https://emergency.cdc.gov/coca/calls/2016/callinfo_080916.asp

Follow‐Up of Infants
http://www.cdc.gov/zika/hc‐providers/infants‐children.html
Post‐natal follow‐up of infant for at least one year:
Pediatric providers work with UDOH Birth Defects to conduct regular follow‐up exams and collect data for CDC

Q4: Are there additional partners you would add to the Zika response as our knowledge has increased?

Partners Responding to Zika• Public health – local, state,
federal, international– Applied epidemiologists– Public health educators– Public health laboratory– Public information officers– Emergency responders
• Policymakers and Funders• Research scientists –
epidemiologists, laboratory scientists, entomologists, veterinarians, climate ecologists, vaccine development researchers, mathematical modelers
• Mosquito abatement programs
• Pregnancy program providers, e.g., Baby‐Your Baby
• Birth defects programs• Clinical providers – general
(obstetricians, family practice, pediatricians) and experts in fetal developmental medicine, high risk pregnancy, and early childhood development

Summary• Zika is a rapidly emerging infectious disease in the Americas that causes birth defects and possibly other neurologic problems
• Response to the Zika epidemic requires a One Health approach that involves many partners
Thanks for Listening! Questions?
Related Documents