Australian Health System Decentralisation – A Comparison of Organisational Changes in the Primary and Acute Health Care Settings A report for Strategic Policy Unit Department of Health Renata Filtrin Pessanha An Intern with the Australian National Internships Program 21 st October 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Australian Health System Decentralisation –
A Comparison of Organisational Changes in the Primary and
Acute Health Care Settings
A report for
Strategic Policy Unit
Department of Health
Renata Filtrin Pessanha
An Intern with the Australian National Internships Program
21st October 2013
ii
Executive Summary
The Australian health care system has been evolving since its creation, in
terms of health services, workforce, funding and governance. This paper
focuses on governance changes in primary and acute care.
Chapter one will introduce the importance of the topic decentralisation in
international and Australian contexts.
Chapter two will outline governance trends, particularly focusing on
decentralisation. It will discuss definitions, typologies and central issues of
decentralisation.
The third chapter will outline the potential benefits, risks, enablers and
barriers of a decentralisation policy.
Chapter four will detail the Australian health system. It will provide the
context for the next section that outlines the governance changes in primary
and acute health care, notably changes from Divisions of General Practice to
Medicare Locals and from Hospital Districts to Local Hospital Networks.
The chapter five will then analyse the key features of governance.
It is expected that explaining these changes in the context of
decentralisation‟s definitions, typologies, benefits, risks, enablers and barriers
will help to inform decision-makers when setting future health policy.
iii
Acknowledgements
First, I am thankful for the National Council for Scientific and
Technological Development (CNPq) for giving me the chance to come to
Australia and paying my scholarship during the program Science without
Borders (CsF).
I would like to thank the Australian National University (ANU) for receiving
so many Brazilians students (including me) during a year. Thanks for the
Australian National Internships Program (ANIP) for accepting and placing me
at Department of Health which taught me so many things about health reform,
politics and Australia. Thanks to Dr Marshall Clark, who placed, lead and
helped all the students during the internships. Thanks for Cheryl Wilson and
Patricia Oxborrow, two patient women who always help the interns.
I am thankful for all the Strategic Policy Unit (SPU). Specially Professor
David Cullen who believed I was able to complete this important project; Miss
Barbara Whitlock, my supervisor, who helped me and advised me so many
times; Miss Rita Raizis, for the comforting smiles and the insights; Mr Richard
Juckes, for the advices; Miss Libby Gonsalves, who helped me to understand
the project, the health system and presented me to the department.
Thanks for Lizzie Moore, who was an important friend when I most
needed one and helped me with my English.
I am thankful for my parents and my family (especially Fábio and Mônica
Filtrin) for the support in this new journey called Australia.
Thanks for my friends, Carolina Azevedo, Erika Cunha, Ernesto Junior,
Julia Coelho, Priscila Shibao and Thamires Mirolli for staying by my side
during this trip and helping not to get depressed.
Thanks for Iara Araujo and Juliana Fuzati, those who introduced me to
ANIP, and helped me to enrol in this course. Thanks for my friends: Giullia
Kurt, Luiz Moreira and Thiago Melo de Oliveira, those who became my family
and showed me Australia.
Last but not least, thanks for Mariana Sacco. An unforgettable friend that
spent hours listening my problems and helped me here to find a way to be
happy.
iv
Table of Contents
Executive Summary ......................................................................................... ii
Acknowledgements ..........................................................................................iii
Table of Contexts ............................................................................................ iv
List of Figures and Illustrations ........................................................................ v
List of Symbols, Abbreviations and Nomenclature .......................................... vi
CHAPTER 1: INTRODUCTION ....................................................................... 1
CHAPTER 2: DECENTRALISATION ............................................................... 2
Definition ................................................................................................. 2
Typologies ............................................................................................... 4
Decentralisation in Practice: Central Issues ............................................ 7
CHAPTER 3: DECENTRALISATION‟S RISKS, BENEFITS,
ENABLERS AND BARRIERS ................................................... 9
Risks and Benefits ................................................................................. 10
Enablers and Barriers ............................................................................ 12
CHAPTER 4: AUSTRALIA ............................................................................. 13
Geographic Profile ................................................................................. 13
Health Care Profile ................................................................................ 16
Primary Health Care Governance Arrangements ............................ 18
Divisions of General Practice .................................................... 18
Medicare Locals ........................................................................ 19
Evaluation ................................................................................. 22
Hospital Governance Arrangements ............................................... 23
Queensland Health ................................................................... 24
Local Hospital Networks ........................................................... 25
Evaluation ................................................................................. 26
CHAPTER 5: ANALYSIS OF DECENTRALIZATION..................................... 27
REFERENCE LIST ........................................................................................ 29
v
List of Figures and Illustrations
Figure 2.1: Types of network structure ............................................................. 3
Figure 2.2: Summary of decentralisation typologies ........................................ 4
Figure 4.1: Australian population density ....................................................... 14
Figure 4.2: Indigenous population clusters .................................................... 15
Figure 4.3: Projected Australian population ................................................... 16
Figure 4.4: Waiting time for an „urgent‟ appointment with a GP ..................... 22
vi
List of Symbols, Abbreviations and Nomenclature
Symbol Definition
$ Australian Dollar
AIHW Australian Institute of Health and Welfare
AMA Australian Medical Association
AMLA Australian Medicare Local Alliance
ANIP Australian National Internships Program
ANU Australian National University
ASGC Australian Standard Geographical Classification
CHERE Centre for Health Economics Research Evaluation
CNPq National Council for Scientific and Technological Development
COAG Council of Australian Governments
CsF Science without Borders
DGPs Divisions of General Practice
DoHA Department of Health and Ageing
GP General Practitioner
LHNs Local Hospital Networks
MRSA Methicillin-Resistant Staphylococcus Aureus
NCCSDO National Co-ordinating Centre for Service Delivery and Organisation
NHA National Healthcare Agreement
PHI Private Health Insurance
PIP Practice Incentive Program
PSD Portfolio Strategies Division
SBOs State-based Organisations
SCoH Ministerial Standing Council on Health
SPU Strategic Policy Unit
UNDP United States Development Programme
USA United States of America
WHO World Health Organization
1
CHAPTER ONE – INTRODUCTION
In 1993, the World Bank released the World Development Report,
encouraging a decentralisation policy in developing countries aiming to
improve the quality and efficiency of government health services. As a result,
not only developing countries, but developed countries, such as France, Italy,
Portugal and Switzerland, also decentralised their health systems (Saltman &
Bankauskaite 2006; Wyss & Lorenz 2000).
In general, the most desired effects of decentralisation are strengthening
community participation in decision making and increasing coverage (Taal
1993); enhancing cost-consciousness (Bergman 1998); implementing health
care based on need (Jervis & Plowden 2003); and improving efficiency,
management and responsiveness of public health service (WHO 1995).
However, in other central European countries, important elements have
been recentralised as a result of concerns raised about inequity and
ineffectiveness of some health delivery services due to decentralisation
(Saltman, Bankauskaite & Vrangbæk 2007).
In addition, some different classifications of decentralisation are
demonstrated in the literature. This divergence may be the result of the
differing contexts when the term is applied (Bankauskaite & Saltman 2007).
In terms of decentralisation in Australia, some characteristics of the
Australian primary acute health care have been recently modified. Divisions of
General Practice (DGPs) have become Medicare Locals and State-run
hospital districts have become Local Hospital Networks (LHNs).
This work starts with presenting a broad definition of decentralisation, in
order to achieve clarity. Then, it will discuss three different approaches to
classifying and the points to consider when implementing decentralisation.
The third chapter will discuss the enablers, barriers, risks and benefits of
decentralisation. Finally, this report will examine the structural changes
implemented in the Australian primary and acute health care: Medicare Locals
and LHNs.
2
It is expected to provide principles and set explanations about the
possible gains from decentralisation. So, this work can inform decision-
makers when setting health policy.
CHAPTER TWO – DECENTRALISATION
Decentralisation is a complex and difficult term to be defined. Applying
decentralisation policy is also not easy, mainly because there are different
aspects of the health system that can be decentralised and there are many
issues around its practice. For this reason, this chapter will explore different
definitions of decentralisation towards a better understand of it, hence
analysing its different components. Thus, decentralisation will be classified
using the widespread points of view in the literature. The central issues will
also be discussed.
Definition
The following extract made by Furniss (1974) shows just one
unsuccessful attempt at transparency of the meaning of decentralisation:
“Decentralization may mean the transfer of authority over public
enterprises from political officials to a relatively autonomous board; the
development of regional economic inputs into national planning efforts; the
transfer of administrative functions either downward in the hierarchy, spatially,
or by problem; the establishment of legislative units of smaller size; or the
transfer of responsibility to subnational legislative bodies, the assumption of
control by more people within an economically productive enterprise, the hope
for a better world to be achieved by more individual participation.”
In another way, Vrangbæk clarifies decentralisation (2007b) as:
“The transfer of formal responsibility and power to make decisions
regarding the management, production, distribution and/or financing of health
services, usually from a smaller to a larger number of geographically or
organizationally separate actors.”
3
Following this reasoning, decentralisation suggests transference in formal
accountability and decision-making structures (Vrangbæk 2007b). The author
explains decentralisation is done “usually from a smaller to a larger number”
of entities, i.e., these can happen in the same or in a different organisational
structure (political and administrative). Also, the term “geographically or
organizationally” refers to creating spatial or functional boundaries,
respectively, to the actors‟ action.
Despite this broad meaning of decentralisation, some authors may not
have used the term appropriately. For example, relocating acute services from
hospitals to home care was termed as decentralisation, which is not a shift in
the structure of power or authority (Bankauskaite & Saltman 2007). Therefore,
understanding the meaning of decentralisation is important to avoid erroneous
conclusions.
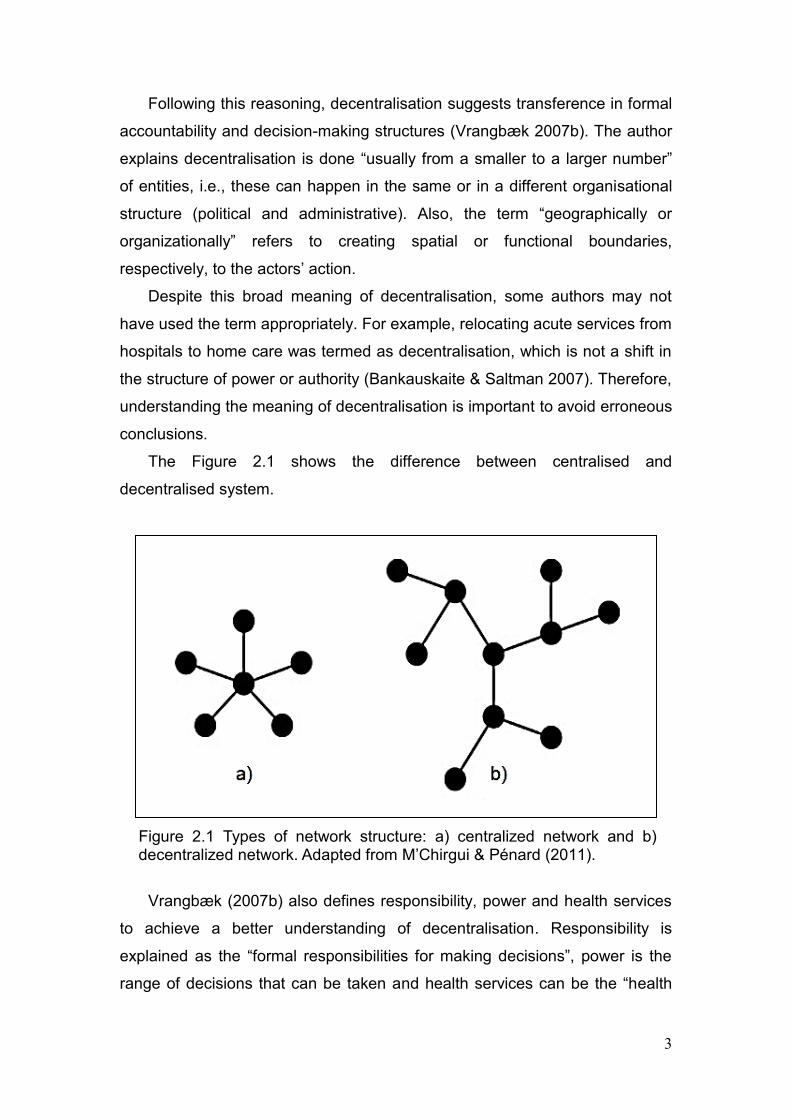
The Figure 2.1 shows the difference between centralised and
decentralised system.
Figure 2.1 Types of network structure: a) centralized network and b) decentralized network. Adapted from M‟Chirgui & Pénard (2011).
Vrangbæk (2007b) also defines responsibility, power and health services
to achieve a better understanding of decentralisation. Responsibility is
explained as the “formal responsibilities for making decisions”, power is the
range of decisions that can be taken and health services can be the “health
4
care services, management, production, distribution and/or financing of public
goods”.
Typologies
Different typologies of decentralisation are found in the literature. Authors
present divergent opinions even within the same approach of decentralisation.
Also, different approaches often overlap. For example, a differentiation made
by Sherwood (cited in Bankauskaite & Saltman 2007) shows decentralisation
and devolution as the first term refers to intra-organisational structure and the
second as an inter-organisational pattern of power relationships. Collins and
Green (cited in Bankauskaite & Saltman 2007) discern decentralisation and
privatisation. They explain decentralisation as a transfer of power,
responsibilities, and/or resources from the centre to periphery and
privatisation from the public to the private. Meanwhile, the World Bank (1983)
allocates privatisation and devolution as two categories of decentralisation.
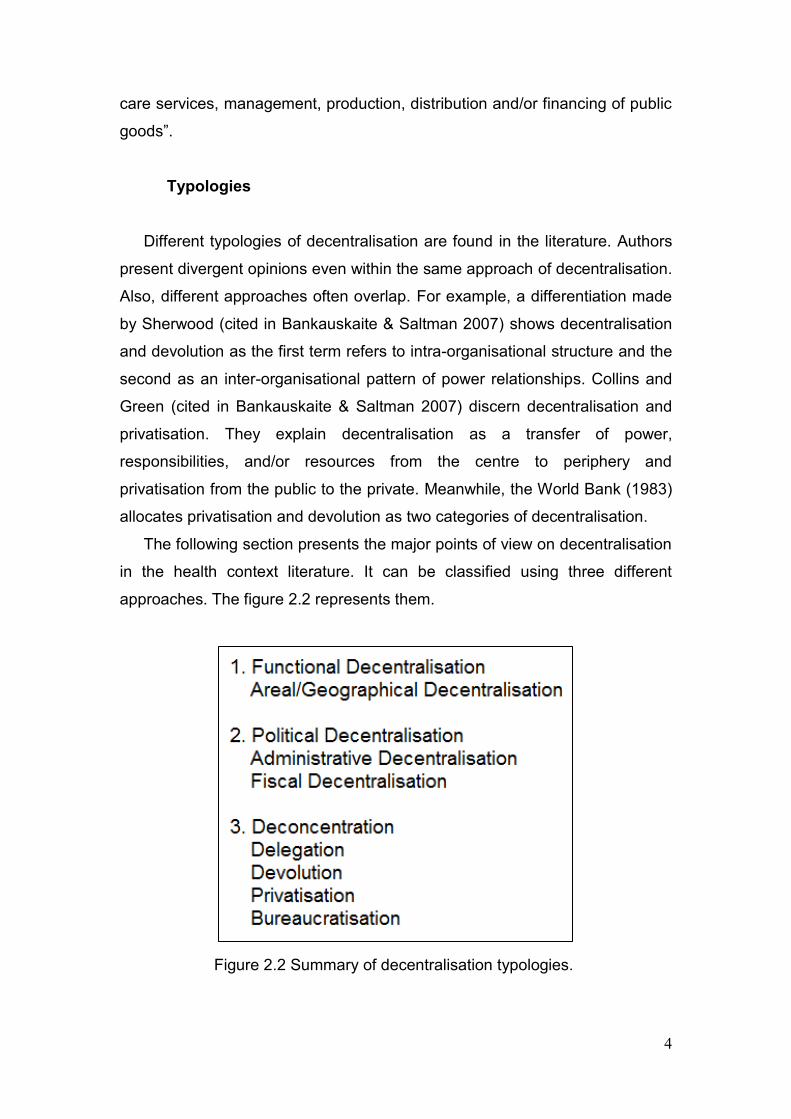
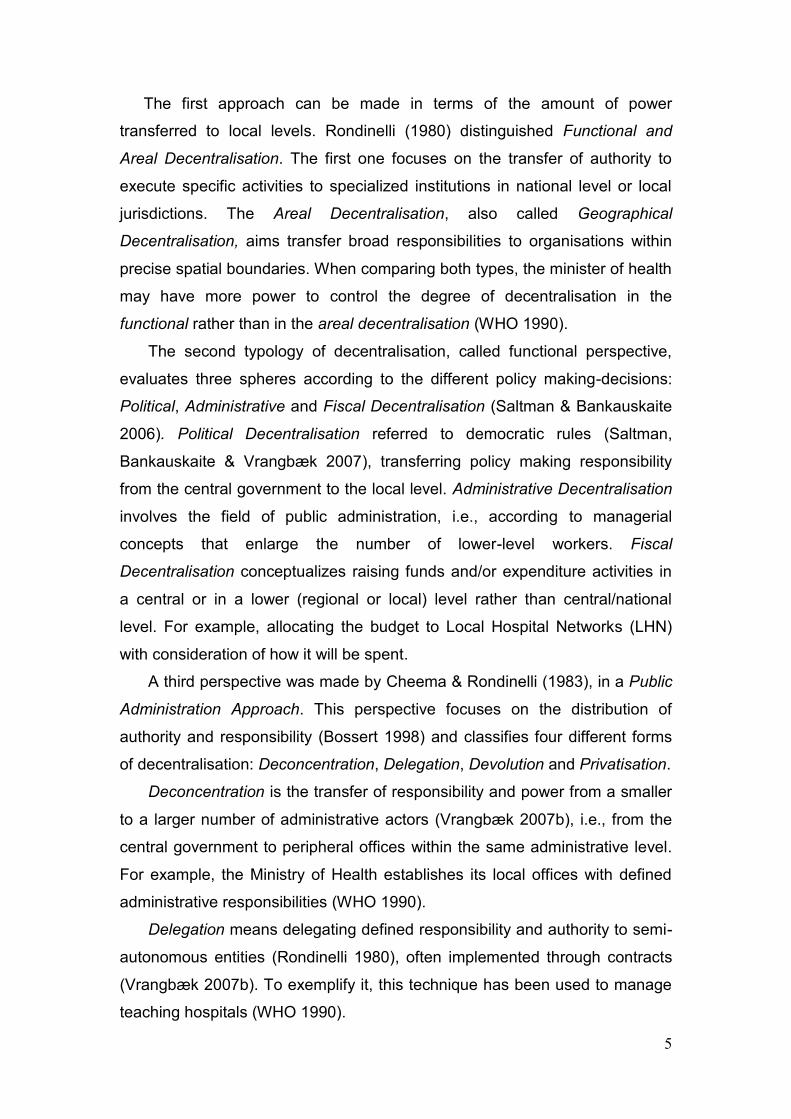
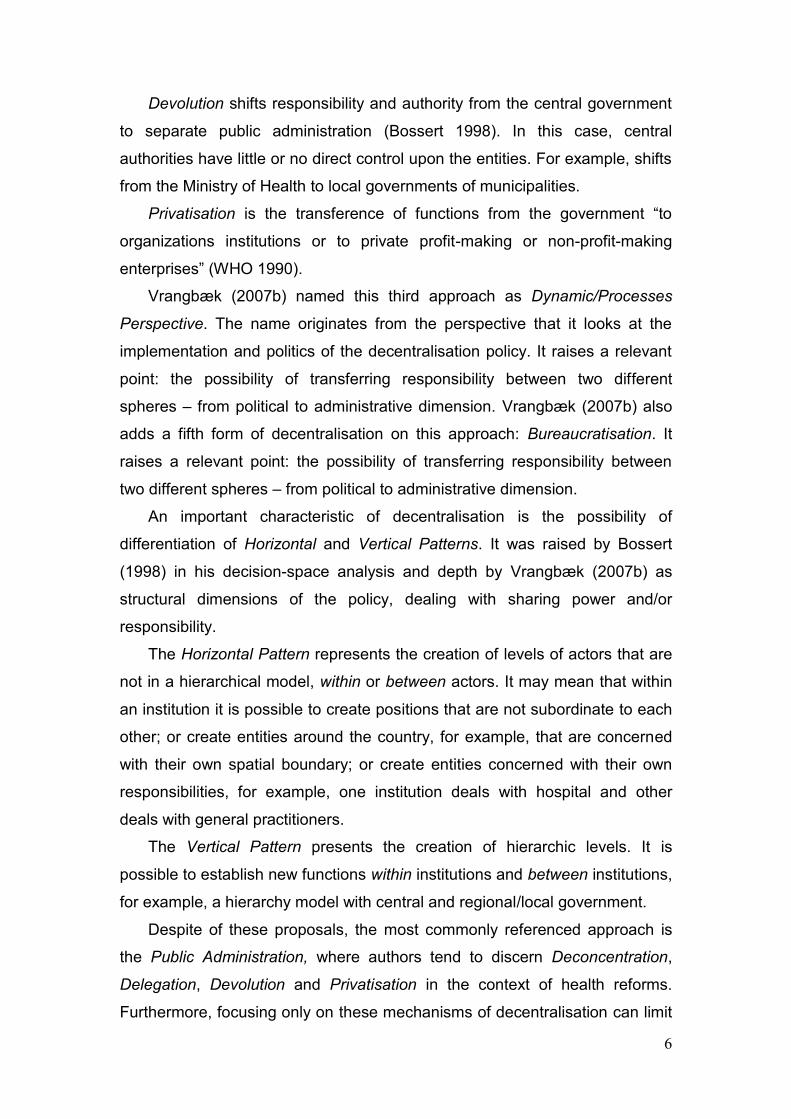
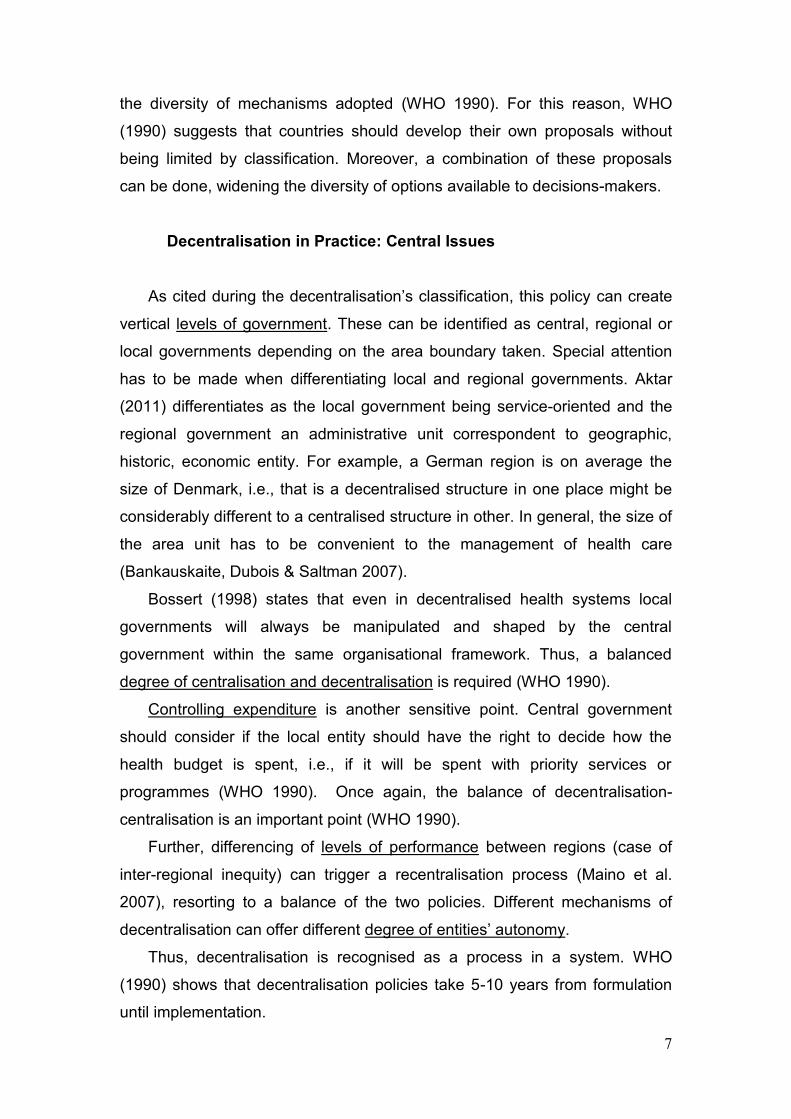
The following section presents the major points of view on decentralisation
in the health context literature. It can be classified using three different
approaches. The figure 2.2 represents them.
Figure 2.2 Summary of decentralisation typologies.
5
The first approach can be made in terms of the amount of power
transferred to local levels. Rondinelli (1980) distinguished Functional and
Areal Decentralisation. The first one focuses on the transfer of authority to
execute specific activities to specialized institutions in national level or local
jurisdictions. The Areal Decentralisation, also called Geographical
Decentralisation, aims transfer broad responsibilities to organisations within
precise spatial boundaries. When comparing both types, the minister of health
may have more power to control the degree of decentralisation in the
functional rather than in the areal decentralisation (WHO 1990).
The second typology of decentralisation, called functional perspective,
evaluates three spheres according to the different policy making-decisions:
Political, Administrative and Fiscal Decentralisation (Saltman & Bankauskaite
2006). Political Decentralisation referred to democratic rules (Saltman,
Bankauskaite & Vrangbæk 2007), transferring policy making responsibility
from the central government to the local level. Administrative Decentralisation
involves the field of public administration, i.e., according to managerial
concepts that enlarge the number of lower-level workers. Fiscal
Decentralisation conceptualizes raising funds and/or expenditure activities in
a central or in a lower (regional or local) level rather than central/national
level. For example, allocating the budget to Local Hospital Networks (LHN)
with consideration of how it will be spent.
A third perspective was made by Cheema & Rondinelli (1983), in a Public
Administration Approach. This perspective focuses on the distribution of
authority and responsibility (Bossert 1998) and classifies four different forms
of decentralisation: Deconcentration, Delegation, Devolution and Privatisation.
Deconcentration is the transfer of responsibility and power from a smaller
to a larger number of administrative actors (Vrangbæk 2007b), i.e., from the
central government to peripheral offices within the same administrative level.
For example, the Ministry of Health establishes its local offices with defined
administrative responsibilities (WHO 1990).
Delegation means delegating defined responsibility and authority to semi-
autonomous entities (Rondinelli 1980), often implemented through contracts
(Vrangbæk 2007b). To exemplify it, this technique has been used to manage
teaching hospitals (WHO 1990).
6
Devolution shifts responsibility and authority from the central government
to separate public administration (Bossert 1998). In this case, central
authorities have little or no direct control upon the entities. For example, shifts
from the Ministry of Health to local governments of municipalities.
Privatisation is the transference of functions from the government “to
organizations institutions or to private profit-making or non-profit-making
enterprises” (WHO 1990).
Vrangbæk (2007b) named this third approach as Dynamic/Processes
Perspective. The name originates from the perspective that it looks at the
implementation and politics of the decentralisation policy. It raises a relevant
point: the possibility of transferring responsibility between two different
spheres – from political to administrative dimension. Vrangbæk (2007b) also
adds a fifth form of decentralisation on this approach: Bureaucratisation. It
raises a relevant point: the possibility of transferring responsibility between
two different spheres – from political to administrative dimension.
An important characteristic of decentralisation is the possibility of
differentiation of Horizontal and Vertical Patterns. It was raised by Bossert
(1998) in his decision-space analysis and depth by Vrangbæk (2007b) as
structural dimensions of the policy, dealing with sharing power and/or
responsibility.
The Horizontal Pattern represents the creation of levels of actors that are
not in a hierarchical model, within or between actors. It may mean that within
an institution it is possible to create positions that are not subordinate to each
other; or create entities around the country, for example, that are concerned
with their own spatial boundary; or create entities concerned with their own
responsibilities, for example, one institution deals with hospital and other
deals with general practitioners.
The Vertical Pattern presents the creation of hierarchic levels. It is
possible to establish new functions within institutions and between institutions,
for example, a hierarchy model with central and regional/local government.
Despite of these proposals, the most commonly referenced approach is
the Public Administration, where authors tend to discern Deconcentration,
Delegation, Devolution and Privatisation in the context of health reforms.
Furthermore, focusing only on these mechanisms of decentralisation can limit
7
the diversity of mechanisms adopted (WHO 1990). For this reason, WHO
(1990) suggests that countries should develop their own proposals without
being limited by classification. Moreover, a combination of these proposals
can be done, widening the diversity of options available to decisions-makers.
Decentralisation in Practice: Central Issues
As cited during the decentralisation‟s classification, this policy can create
vertical levels of government. These can be identified as central, regional or
local governments depending on the area boundary taken. Special attention
has to be made when differentiating local and regional governments. Aktar
(2011) differentiates as the local government being service-oriented and the
regional government an administrative unit correspondent to geographic,
historic, economic entity. For example, a German region is on average the
size of Denmark, i.e., that is a decentralised structure in one place might be
considerably different to a centralised structure in other. In general, the size of
the area unit has to be convenient to the management of health care
(Bankauskaite, Dubois & Saltman 2007).
Bossert (1998) states that even in decentralised health systems local
governments will always be manipulated and shaped by the central
government within the same organisational framework. Thus, a balanced
degree of centralisation and decentralisation is required (WHO 1990).
Controlling expenditure is another sensitive point. Central government
should consider if the local entity should have the right to decide how the
health budget is spent, i.e., if it will be spent with priority services or
programmes (WHO 1990). Once again, the balance of decentralisation-
centralisation is an important point (WHO 1990).
Further, differencing of levels of performance between regions (case of
inter-regional inequity) can trigger a recentralisation process (Maino et al.
2007), resorting to a balance of the two policies. Different mechanisms of
decentralisation can offer different degree of entities‟ autonomy.
Thus, decentralisation is recognised as a process in a system. WHO
(1990) shows that decentralisation policies take 5-10 years from formulation
until implementation.
8
The context where decentralisation is undertaken is also important.
National context and history (Vrangbæk 2007a), sets of institutions within the
country, values and missions, social and cultural values (Bankauskaite &
Saltman 2007), financial situation (WHO 1990) and particular political
interests (UNDP & Government of Germany 1999) are important in deciding
the way to take on the issue of decentralisation. Financial situation is
important, as the cost of the policy may increase immediately through the
need of building new edifices and contracting more people. If there are
insufficient resources, patient outcomes are more likely to be poor that will
indicate a sense that decentralisation does not solve all the problems.
As the methods of implementing decentralisation, national contexts and
aspects of health care are different among countries, cross-national analysis
is restricted (Smith 1985). For this reason, Smith (1985) suggests analysing
the changes during the process of decentralisation.
Along with decentralisation comes a loss of regulatory tools by the central
government (Smith & Häkkinen 2007), at the same time the central authority
empowers the regional/local levels. However, regulatory supervision will
always be needed (Smith & Häkkinen 2007). Thus, there are some concerns
in collecting and verifying good quality of data. For example, regional/local
government could distort unverifiable data, in order to achieve the goals
asked by the central government or to gain benefits.
Ham (1998) discusses another point that a failure over centralist policy
may rebound against politicians, for this reason they may decide to
decentralisation. However, at the same time, if problems arise after
implementing decentralisation policy, the central government may be also
blamed.
A different term appears when discussing decentralisation:
regionalisation. Some public sectors and providers use regionalisation to
explain the health reform started in 1970 in Canada (Lewis & Kouri 2004) or
the recent changes made in Australia since 2010 (DoHA 2011b). Lewis and
Kouri (2004) argue there is no consensus about the definition of
regionalisation and the complexity to define it. Marchildon (2005) defines it as
devolution of funding from the central government to regional authorities,
based on regional needs, which implies set boundaries. The term also
9
requires a centralisation of delivery management from individual facilities to
the regional authorities. As discussed, devolution can be classified as one
type of decentralisation, in this case devolution of funding. It is also required a
centralisation of some health delivery elements. On the other hand,
decentralisation does not mean excluding centralisation, but a balance of both
policies. For this reason, regionalisation can be exemplified as a specific type
of decentralisation.
The World Health Organization (1990) argues the “top-down”
implementation of decentralisation is likely to fail because of the possible wide
gap between the purpose of the policy and the real situation. As the local and
regional authorities/organizations are empowered to make decisions, they
need to accept the new work. Hence, consultations are necessary, using “top-
down” and “bottom-up” interactions.
Changes during the process of decentralisation happen to achieve the
outcomes. Also, country health profiles vary along time requiring structural
changes. For example, recentralising and decentralising different aspects of
health system. As Bossert (1998) pronounced decentralisation is “a means
toward the ends of broad health reform, rather than an end in itself”. Thus,
depending on the circumstances, it may be vigorously pursued at times and
less so at other times.
CHAPTER THREE – DECENTRALISATION’S RISKS, BENEFITS,
ENABLERS AND BARRIERS
As discussed, decentralisation is an evolution and occurs over time. This
policy is a process and does not occur alone but is balanced with
centralisation. To implement it and decrease risks, a number of points should
be considered before making decisions. Consequently this section will outline
the risks, benefits, enablers and barriers of decentralisation.
10
Risks and Benefits
One major reason for adopting decentralisation is based on its malleability
which allows coexistence of different local agendas and national priorities.
(Saltman, Bankauskaite & Vrangbæk 2007). Nevertheless, a decentralised
government, which tries to conciliate national and local priorities, may have
problems when intervening without local support (Wyss & Lorenz 2000).
The promotion of democracy and accountability are important outcomes
of decentralisation to the local population (Bossert 1998). Moreover, public
participation is strongly correlated as a key factor to improve allocative
efficiency (Bankauskaite & Saltman 2007). The principle is that smaller
organisations are able to perform better than bigger entities, because they are
closer to the population (NCCSDO 2005) and can understand and solve
problems of a defined framework. It means empowering the local government.
However, despite the correlation between decentralisation and increased
accountability, the former does not imply causation of the latter (NCCSDO
2005). Innovation may be a benefit of decentralisation as well, due to a more
production of approaches, solutions and products in decentralised
jurisdictions.
Decentralisation can alert the local workforce about the costs in health
services, encouraging a more careful understanding of costs and benefits
(Vrangbæk 2007a), which would lead to the most cost-effective service.
Reducing costs is another major goal on health system given to „explosion of
costs in the health sector‟ (Wyss & Lorenz 2000). Nevertheless, a
decentralised system does not necessarily provide the most cost-effective
service. In fact, implementing this policy increased administration costs and
bureaucracy in some countries (Saltman, Bankauskaite & Vrangbæk 2007;
WHO 1995).
There are contradictory views about staff satisfaction in a decentralised
model. NCCSDO (2005) argues that despite some articles associating
decentralisation with staff satisfaction, there is little empirical evidence related
to support this argument.
The most frequent concern amongst decision-makers is the possibility of
inequity arising from decentralisation (Bankauskaite & Saltman 2007). This
11
policy has the potential to increase equity, if looks local authorities seem to be
better at answering local needs (WHO 1995). Decentralisation may also
increases inequity, by creating variation between groups or geographical
areas (NCCSDO 2005).
Attempts are frequently made to reduce inter-regional inequity. Due to
differences in wealth among regions of a country, central government often
creates formulas to equalize budgets across a nation, such as, special funds,
resource allocation and national subsidies (Saltman & Bankauskaite 2006).
The adjustment is important to ensure inter-regional equity of funding
(Saltman & Bankauskaite 2006). However, the studies do not differentiate
between the various forms of inequity, such as, geographical, class, age and
gender inequity which makes the analysis difficult (NCCSDO 2005).
Koivusalo, Wyss & Santana (2007) argue inequalities are associated with
the different decentralisation policies, local decisions and previous health care
organisations. The authors mention inequity also exists in centralised
systems. For Kutzin (in WHO 1995), equity primarily depends on the resource
allocation of decentralised units. Applying cross-subsidies between population
groups and geographical areas and considering previous inequities and
special needs may avoid this result (Bankauskaite & Saltman 2007;
Koivusalo, Wyss & Santana 2007; WHO 1995). Other actions, such as social
protection (Wyss & Lorenz 2000), regulation, standard setting and
performance criteria (Koivusalo, Wyss & Santana 2007), could also be
implemented.
Decentralisation may also result in “fragmented” documentation, i.e., the
same information being found in multiple places. That can result in confusion
and duplication of data (United States Environmental Agency 2012).
Rondinelli (1980) argues that the failures of decentralised systems are
often related to two reasons: first, the lack of a concise conception of its
meaning; second, the variety of forms that decentralisation can take. The
potential problems of this policy can also be due to a lack of attention to the
political and economic context (WHO 1995).
12
Enablers and Barriers
There are a number of enablers and barriers which can affect how well
decentralisation works.
One enabler is to have sufficient data to analyse each area or institution
performance, for example, aged care beds numbers, immunisation levels,
waiting time, etc. The clarity of performance targets along with well-developed
performance indicators and transparency though annual reports may assist
decision-makers.
A sector regulator, as used in the United Kingdom, may assist and advise
the central government decision-makers along the decentralisation process.
This function would have the ability to monitor the system based on risk
ratings; create and apply contingency strategies when services became
problematic; develop payment systems rewarding quality and efficiency; and
ensure that choice and competition are operating in the best interests of
patients.
Appointing expertise-based boards, rather than representative-based
boards may also improve performance. Alternatively local decision makers
should use the information provided by expert planners, as well as the
community values to set priorities (WHO 1995).
To avoid duplicated actions, the new roles should be clear with a tightly
defined scope of practice. This allows staff and institutions to understand their
functions. Constitutional and legal changes may be required to ensure
responsibility is vested in an appropriate body (WHO 1990). These changes
avoid duplicated roles and lack of responsibility to a defined role.
The geographical boundaries must be well planned. That is considering
the legally recognized areas (Rondinelli 1980), the absolute and relative size
of the units, population density, country size, homogeneity of population
(Bankauskaite, Dubois & Saltman 2007), the cultural difference and proximity
of services-community.
As discussed previously, context is important. For example, an economic
recession may create a barrier to success. The transition to decentralised
situation may require some extras payments, such as additional training, new
buildings or new equipment (WHO 1995). Political context is also important.
13
The powerful interest groups need to understand the meaning of
decentralisation and the central government‟s intention. They also need to be
actively willing its implementation, because they will receive the
responsibilities associated with serving the local community (WHO 1995).
If the local autonomy does not support decentralisation, tension between
it and the central control may occur (WHO 1995). Tensions may also arise
between the central and decentralised bodies if the goals set by the central
government are perceived as too high (Bankauskaite & Saltman 2007).
All these enablers added to good governance processes and systems
delineate the policy to achieve the best outcomes.
CHAPTER FOUR – AUSTRALIA
As discussed previously in this work, there are a number of potential
benefits and risks of decentralisation. It has also been discussed that the
particularities of a country determine the policy context for structural changes.
This section will first explain Australia‟s health and geographic profile.
Understanding the health care profile is important to analyse how the health
system is set out. Understanding the geographic population is important to
plan and analyse provision of services, in particular tailoring them to where
people live and work (AIHW 2013). Second, it will examine the structural
changes within primary and acute health care respectively namely: Divisions
of General Practice/ Medicare Locals and Hospital Boards and Districts/Local
Hospital Networks.
Geographic Profile
Australia is the sixth largest country in the world in geographic area
(Australian Government c. 2013) with around 23 million people in April 2013
(AIHW 2013). Australia‟s population is concentrated along the Australian
coastline, from Adelaide to Cairns with a small concentration around Perth
and sparse population in the centre (Australian Government c. 2013).
14
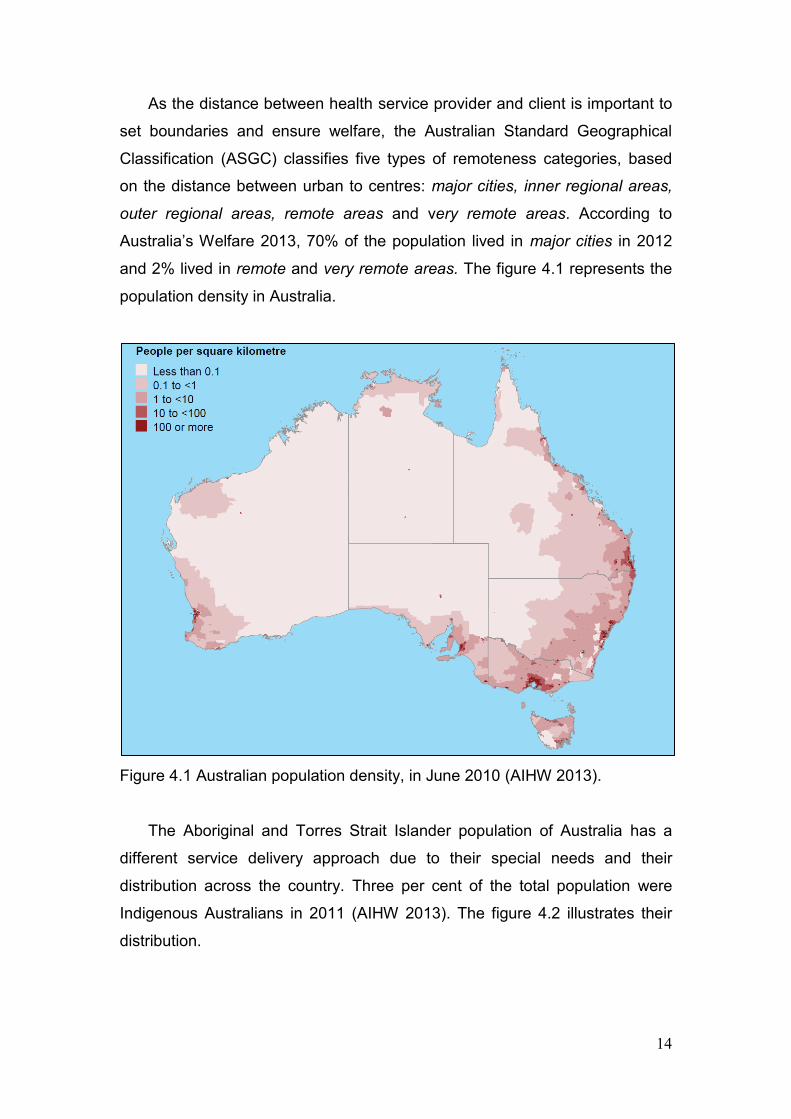
As the distance between health service provider and client is important to
set boundaries and ensure welfare, the Australian Standard Geographical
Classification (ASGC) classifies five types of remoteness categories, based
on the distance between urban to centres: major cities, inner regional areas,
outer regional areas, remote areas and very remote areas. According to
Australia‟s Welfare 2013, 70% of the population lived in major cities in 2012
and 2% lived in remote and very remote areas. The figure 4.1 represents the
population density in Australia.
Figure 4.1 Australian population density, in June 2010 (AIHW 2013).
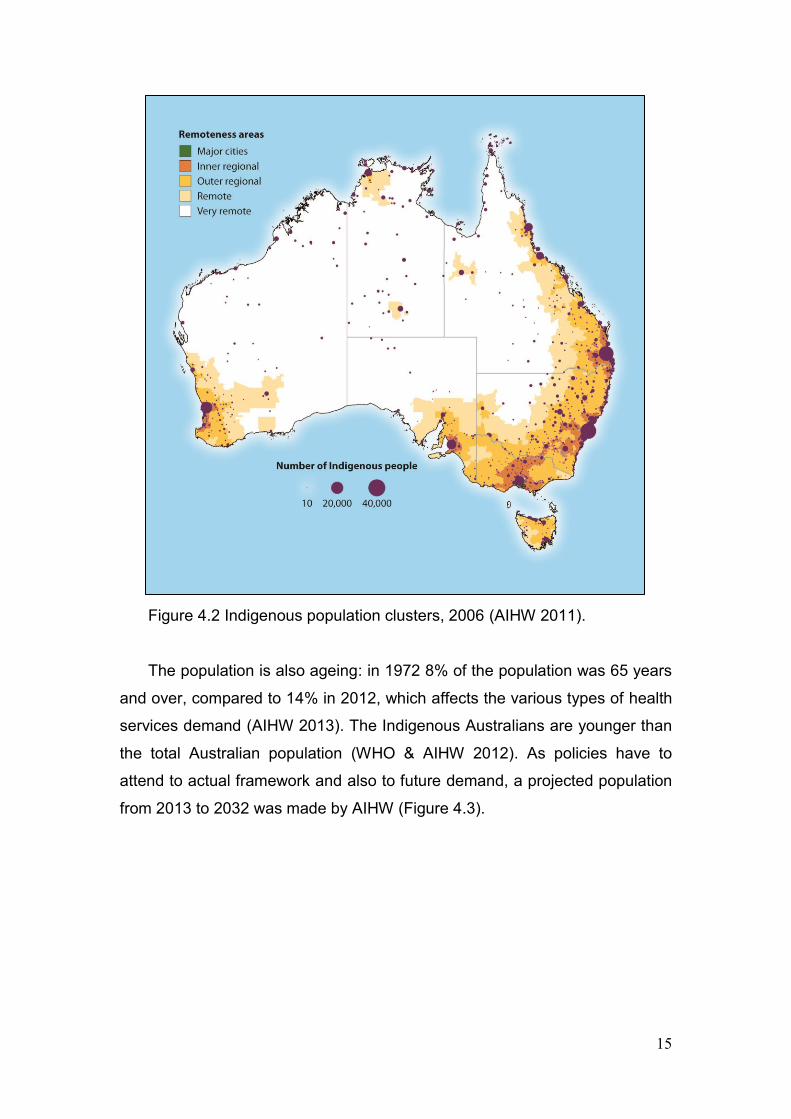
The Aboriginal and Torres Strait Islander population of Australia has a
different service delivery approach due to their special needs and their
distribution across the country. Three per cent of the total population were
Indigenous Australians in 2011 (AIHW 2013). The figure 4.2 illustrates their
distribution.
15
Figure 4.2 Indigenous population clusters, 2006 (AIHW 2011).
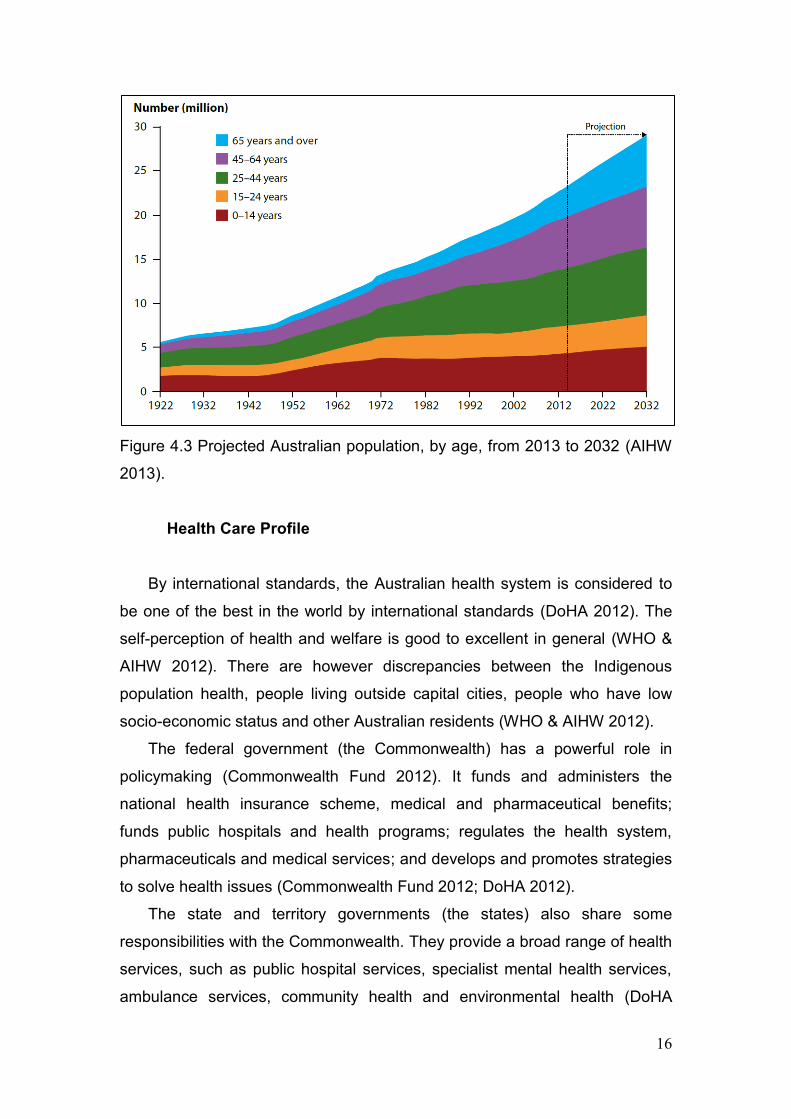
The population is also ageing: in 1972 8% of the population was 65 years
and over, compared to 14% in 2012, which affects the various types of health
services demand (AIHW 2013). The Indigenous Australians are younger than
the total Australian population (WHO & AIHW 2012). As policies have to
attend to actual framework and also to future demand, a projected population
from 2013 to 2032 was made by AIHW (Figure 4.3).
16
Figure 4.3 Projected Australian population, by age, from 2013 to 2032 (AIHW
2013).
Health Care Profile
By international standards, the Australian health system is considered to
be one of the best in the world by international standards (DoHA 2012). The
self-perception of health and welfare is good to excellent in general (WHO &
AIHW 2012). There are however discrepancies between the Indigenous
population health, people living outside capital cities, people who have low
socio-economic status and other Australian residents (WHO & AIHW 2012).
The federal government (the Commonwealth) has a powerful role in
policymaking (Commonwealth Fund 2012). It funds and administers the
national health insurance scheme, medical and pharmaceutical benefits;
funds public hospitals and health programs; regulates the health system,
pharmaceuticals and medical services; and develops and promotes strategies
to solve health issues (Commonwealth Fund 2012; DoHA 2012).
The state and territory governments (the states) also share some
responsibilities with the Commonwealth. They provide a broad range of health
services, such as public hospital services, specialist mental health services,
ambulance services, community health and environmental health (DoHA
17
2012). They assist the federal government in training health workers and
regulating the health professionals and private hospitals (DoHA 2012).
The shared responsibilities are made between the states and the
Commonwealth through National Healthcare Agreement (NHA) which focuses
on improving the health care outcomes for all Australians and sustainability of
the health care system (COAG 2012). It was first signed in 2008 by the
Council of Australian Governments (COAG) (DoHA 2012) that jointly with the
Ministerial Standing Council on Health (SCoH) sets goals for health services
with specific roles.
The states have flexibility to provide and use funding, but the NHA
identifies priority areas for reform, assessed by the COAG Reform Council
annually. Despite the clear objectives of the NHA, the issues are complex
(DoHA 2012).
The health insurance scheme can basically be divided in two forms: public
and private. The Australian national public health insurance scheme,
Medicare, is provided to all Australian citizens and permanents residents
(Commonwealth Fund 2012). It can however be complemented with the
private health system that is subsidized by the federal government through
private health insurance (PHI). It allows individuals to pay less for PHI with a
greater choice of care delivered (DoHA 2012). With this policy, the
government aims to attract people to buy private insurance, avoiding an
overcrowded public system.
The primary health care is usually provided in community-based settings,
such as general practices, state-run Community Health Centres and
Aboriginal Community-Controlled Health Services. Primary health service is
largest provided and co-ordinated by General Practitioners (GPs), with about
85% of the Australia population seeing a GP at least once a year. On the
other hand, the hospital services are delivered currently via LHNs. Both
aspects and changes made by the government during the last few years will
be discussed separately.
18
Primary Health Care Governance Arrangements
Divisions of General Practice
Divisions of General Practice (DGPs) were introduced in Australia in 1992
with $17 million of federal funding. They were separate legally incorporated
entities aiming to improve integration and to provide a mechanism for GPs to
become involved in local health planning and priority setting (Clark 2003).
Over time, their goals were broadened, including care co-ordination,
information managements systems, public health initiatives, continuing
medical education, after-hours service delivery and other programs
(Department of Health 2010).
Membership of DGPs was voluntary and consisted of legal entities with
eight boards of directors on average. The boards of directors usually had
members with different expertise, such as accounting skills and community
representatives. They also had on average 10 full-time staff per Division
(mainly non-GPs).
From 1992 to 1998, defined geographic boundaries emerged in the
country. By 1998, all Australia territory was completely covered by DGPs.
State-based organisations were designed to build the capacity of DGPs, help
co-ordinate national programs and link to the state governments. Australian
General Practice Network, on the other hand, helped to co-ordinate the
network, supported the national programs delivery, advised on performance
standards, collaborated with academic organisations and provided input into
submissions.
In 1998, the Divisions were reviewed by the General Practice Strategy
Review Group and funding changes were made. The changes provided
stability associated with enhanced planning and reporting requirements
moving from a short-term infrastructure subsidy to outcome-based funding for
three years (the „block funding‟). Moreover, the Practice Incentive Program
(PIP) was introduced to reward practices with minimum standards for
infrastructure, access to care and evidence-based activity in chronic disease,
mental health and prevention. PIP was funded by Medicare Australia, but the
GPs payments were facilitated by DGPs.
19
In 2003, the Phillips Review was released, with a government response in
April 2004. It concluded there was too much diversity of Divisions, which
needed a set of common objectives. It included changing priorities, a new
National and Quality Performance System and improving governance and
accountability arrangements. The performance indicators were then agreed
between DGPs and the Department of Health and Ageing (DoHA, nowadays
Department of Health). They included governance, prevention, access,
integration, chronic disease management, practice, quality and workforce
support, and consumer focus.
By 2005, there were 120 DGPs based on area (local governance), eight
state-based organisations (regional governance) and one national
organisation (Australian General Practice Network, central governance).
More than 94% of GPs were members of divisions. The DGPs received
$140.6 million, which nearly 50% was core funding. Additional funds were
made by specific federal government programs as well as a small amount of
funding from other public and private sources.
In 2007, an evaluation of DGPs found them engaged in a broad range of
activities, with non-quantitate data. The priorities varied across area, with rural
areas focusing on attracting doctors and providing locum relief, while regional
cities focused on after-hours services. Over time, all these different priorities
ended in inter-regional inequities. The evaluation also found a statistically
significant effect of the DGPs on health care performance, in which the largest
effects were in areas of improving GP infrastructure. It also showed the strong
effect of Divisions on accessing PIP payments, which culminated in a larger
number of staff associated and higher proportion of GPs enrolled to receive
PIP payments (Australian General Practice Network 2007).
Medicare Locals
In June 2009, „A healthier future for all Australians: final report’ was
delivered to the Kevin Rudd Government (2007-2010). It presented 123
recommendations about changes in the Australian health system, focused on
primary health care, centralising and integrating governance arrangements
20
(as the Commonwealth funding the entire primary health care) and creating
Comprehensive Primary Health Care Organisations to replace DGPs.
The government responded to it producing a report titled A National
Health and Hospitals Network for Australia’s Future in 2010. It created the
Medicare Locals to reduce service gaps, improve the service delivery in local
level and access to integrated care. The Medicare Locals, then, would play a
role in delivery services funded by the federal government. They also would
be drawn from existing DGPs which had the capacity to take on the roles and
functions expected under new arrangements.
In late 2010, the Julia Gillard Government (2010-2013) provided a more
developed view of Medicare Locals, as independent legal entities, providing
more co-ordinated care and accountability to the Commonwealth and their
local community. Their objectives also included identifying local health needs
and operating as health system planners, focusing on prevention; improving
co-ordination; supporting clinicians through prevention and management of
chronic disease; helping to implement primary health care programs; and
improving efficiency and accountability with strong governance and effective
management.
To establish the initial operations of Medicare Locals, DoHA release
guidelines in 2011 to implement them in three stages. From July 2011 to July
2012, 61 Medicare Locals were created. They work with local primary health
care, Local Hospital Networks, aged care providers and communities. In some
instances, Medicare Locals deliver services themselves or they can sub-
contract other organisations to do it (for example after hours clinical services).
They have a skills-based governance structure, where the Board member
selection varies between seven to nine people, being sometimes also
members of LHNs. They are selected based on the range of professional,
industry and personal skills required to achieve the strategic objectives.
The governance arrangements were determined with each Medicare
Locals individually, that is, they have different approaches to governance
across the country.
On 30 June 2012, all core funding under the DGPs, under state-based
organisations (SBOs) and under Australian General Practice Network would
have been ceased. However, on 19 July 2011, Minister Butler (Minister of
21
Health and Ageing) announced that funding provided to SBOs not forming a
Medicare Local would be extended until 31 December 2012, enabling to
continue their transition work.
On the first July 2012, the Australian Medicare Local Alliance (AMLA) was
established to co-ordinate and support the Medicare Local network and
engage primary health care providers. It facilitates stakeholder consultation at
the national level and, since January 2013, has some co-ordination by state
level.
The expenditure on Medicare Locals is made by the Department of Health
and can be classified into three major types: core funding, flexible funding and
program funding.
The first one is distributed to meet the required governance arrangements
with more responsiveness to the local population needs on strategic
objectives. It is allocated on weighted-population basis which considers health
inequalities for people living in rural and remote areas, the Indigenous
population, English-language proficiency in overseas-born population, socio-
economic status and age profiles. It is also attentive to relative cost
differences associated with staffing and operating Medicare Locals across the
country, and the travel costs in remote areas.
The non-core funding (flexible funding) considers the similar parameters
as the core funding.
The third funding type is provided for specific programs, such as face to
face after-hours care, mental health, rural health, immunisation and
Indigenous health. It is calculated through individual Program Schedules
under a Deed, managed by program areas through the Department of Health.
The Medicare Locals provide reports to the Department of Health
including Needs Assessment Report, Annual Plans and Budgets, Strategic
Plans and six and twelve Month Reports, including financial reports. Another
Department‟s responsibility is monitoring the performance of each Medicare
Local, addressing five strategic objectives. The Health Communities Reports,
which are about access to services, quality of service delivery, financial
responsibility and patient experience in Medicare Locals are monitored and
produced by the National Health Performance Authority. They provide
22
nationally consistent and locally relevant information about the primary health
care system and Medicare Locals.
Evaluation
A review of primary care performance between 1991 and 2003 showed a
significantly improvement practising GP population (Charles, Britt & Valenti
2004). In 2007, an evaluation found that DGPs were engaged on the area,
with statistically significant effect (Australian General Practice Network 2007).
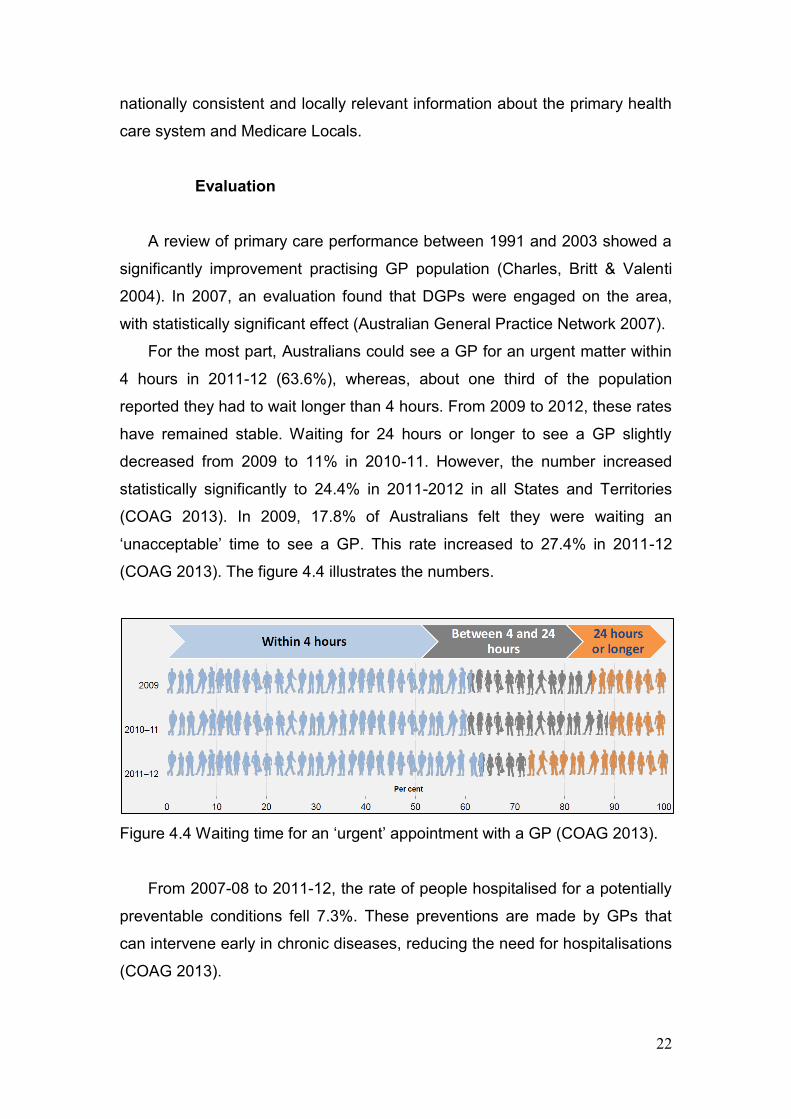
For the most part, Australians could see a GP for an urgent matter within
4 hours in 2011-12 (63.6%), whereas, about one third of the population
reported they had to wait longer than 4 hours. From 2009 to 2012, these rates
have remained stable. Waiting for 24 hours or longer to see a GP slightly
decreased from 2009 to 11% in 2010-11. However, the number increased
statistically significantly to 24.4% in 2011-2012 in all States and Territories
(COAG 2013). In 2009, 17.8% of Australians felt they were waiting an
„unacceptable‟ time to see a GP. This rate increased to 27.4% in 2011-12
(COAG 2013). The figure 4.4 illustrates the numbers.
Figure 4.4 Waiting time for an „urgent‟ appointment with a GP (COAG 2013).
From 2007-08 to 2011-12, the rate of people hospitalised for a potentially
preventable conditions fell 7.3%. These preventions are made by GPs that
can intervene early in chronic diseases, reducing the need for hospitalisations
(COAG 2013).
23
The number of structures on the infrastructure to support GPs decreased
from 120 boundaries area in 2005 to 61 Medicare Locals currently. It shows
that a geographical centralisation happened on the primary health care
evolution in Australia.
In terms of funding, during DGPs, the central government funded the
divisions using the „block funding‟. DGPs were also funded by the state level
and were allowed to attract funding from other sources, such as membership
fees. The non-Commonwealth funding incomes had to be detailed to the
federal level, but the funding was not held accountable to the Commonwealth
for its use (AMA 2002). Nowadays, the federal government resources
Medicare Locals using three types of funding, but they are also allowed to
raise money by themselves. The flexible funding provided allows Medicare
Locals to inject money according to their local needs. Then, it could be
considered as a decentralisation policy due to providing a financial flexibility.
For these reasons, saying that a slightly fiscal decentralisation process
occurred is possible.
Moreover, according to DoHA (2013), the structural primary health care
changes reduced significantly administrative overhead and directed funding to
service provision.
Attributing the primary health performance changes solely to the operation
of the new system (Medicare Locals) is problematic. There are many factors
which influence health system performance such as workforce and population
health status. The federal government has also injected more money into
primary health care after The Health Reform. Isolating and evaluating the
Medicare Locals‟ impact is, therefore, difficult. It is likely they are instrumental
in ensuring the services are delivered appropriately. Proving this through
evaluations is difficult given the interdependencies and dynamic nature of the
health system.
Hospital Governance Arrangements
A National Health and Hospitals Network for Australia’s Future, a report
released in 2010, not only modified the primary health care but also the public
24
hospitals‟ management. After its released, the geographical boundaries, the
funding and some aspects of hospital management were changed.
To achieve a full context of policies driven in the whole country, an
analysis of the governance arrangements should be done in all eight
states/territories. In order to illustrate one of them, a review of Queensland
Health will be presented.
Queensland Health Changes
In 2005, a review of Queensland Health was undertaken by Peter Forster
(Department of the Premier and Cabinet 2005). It was written in a response to
the disquiet about safety following the practices of Dr Patel at the Bundaberg
Hospital. There were concerns about the excessive layers of decision making
and administrative staff with centralised formal structure at the hospital. This
structure included lack of responsiveness; decision-making bottlenecks;
fragmentation between policy development, governance, service delivery and
performance management; lack of accountability; lack of forward service
planning; inability to provide adequate statewide services; and limited
engagement with local communities in health decision making.
The review made a number of recommendations such as increasing
community engagement, devolving budgets, integrating health services and
increasing performance monitoring and management. Key recommendations
also included maintaining the 37 districts that covered 180 hospitals on the
state and setting three Area Health Services (according to population
number). They aimed to increase leadership, management, planning, policy,
responsibility and accountability.
In 2007, Queensland Health was restructured reducing the districts
numbers from 37 to 20, based on boundaries (Queensland Government
2008a). This change was made due to the belief that larger districts would
consolidate health services and improve integration within districts between
communities and hospitals. Developing District boundaries also considered
the boundaries of Divisions of general Practice.
In August 2008, Queensland Health was again changed. The Area Health
Services this time were abolished. Despite the Forster Review, these areas
25
didn‟t increase local decision making, but they “got in the way of decision
makers and the local communities they serve” (Queensland Government
2008b). In addition, the 20 districts were reduced to 15 Districts, based on
geographic boundaries, apart from Children‟s Health Services being
separated as a district.
Local Hospital Networks
The report titled „A healthier future for all Australians: final report' (2009)
focused on hospital governance, primarily leaning towards more centralised
governance arrangements. The report made by the Rudd Government
(2010a) outlined strategies to devolve governance and management of
hospital services to a local level called Local Hospital Networks (LHNs).
These networks "would be single or small groups of public hospitals with a
geographic or functional connection, large enough to operate efficiently and to
provide a reasonable range of hospital services" (Australian Government
2010a). It was also expected that LHNs would have common geographic
boundaries with Medicare Locals wherever possible. The decision making
would be devolved to LHNs "to give communities and clinicians a greater say
in how their hospital are run" (Australian Government 2010a).
LHNs would have a professional Governing Council and Chief Executive
Officer, responsible for delivering agreed services and performance standards
within an agreed budget. Governing Councils would include local health,
management and finance professionals, with an appropriate mix of skills,
expertise and backgrounds.
The state health departments would support LHNs by providing system-
side service planning, performance management, negotiate service
agreements, fund LHNs and transfer good practices. They would only
intervene in LHNs‟ daily operations when the performance was not meeting
standards.
The LHNs were responsible to set local activity targets (agreed with state
departments), receive funding for services under activity-based funding from
state and federal governments and managing the budget, corporate services
(for example human resources), implement clinical guidelines and pathways.
26
The state health departments would plan the workforce with the federal
government, provide funding to LHNs, plan capital and ownership, manage
and remediate performance and negotiate industrial relations.
The national health bodies would determine the efficient price for hospital
services (being done by the Independent Hospital Pricing Authority), fund
LHNs, set national governance arrangements, set the national performance
and accountability framework (being done by National Health Performance
Authority) and set guidelines, safety, quality and national clinical leadership
(being done by the Australian Commission on Safety and Quality Healthcare).
There are 123 geographically-based networks and 13 statewide networks
delivering specialised services. A total of 136 LHNs were established across
the country by first July 2012, all of them have governing councils (DoHA
2011a).
Evaluation
The creation of LHNs, in the most recent reforms, improved the data
collection and identified performance benchmarks and indicators to support
analysis. The performance benchmark achieved is related to a lower rate of a
resistant bacteria strain (MRSA). The indicators include waiting times for
elective surgery, emergency department care, health-care associated MRSA
(a resistant bacteria strain), unplanned hospital readmission rates; survival of
people diagnosed with notifiable cancers and rate of community follow-up
within first seven days of discharge from psychiatric admission.
Queensland health shows improvements. For example, the infection
benchmark and indicators such as shorter days in emergency departments
and shorter waits for elective surgery and specialist outpatient clinics have
been achieved.
Since 2005, in Queensland, there have been ongoing reforms aimed at
decentralising hospital administration. The changes included: clinician and
community involvement at the local level; devolving budgets to the local level;
setting performance agreements and monitoring them at the state level;
providing services required by all the hospitals (such as pathology and
27
recruitment) at the state level; and supporting local service provision by
gathering and distributing data about services at national level.
It is possible to say that accountability and transparency of health services
has improved. Much of the transparency improvement is from better data
collection and reporting done by central bodies such as AIHW and the
National Health Performance Authority. And, Queensland Health‟s LHNs have
been active participants in collecting and reporting data.
In terms of hospital management in Australia, a decentralisation policy
occurred (DoHA 2011a). Some functions also seem to be placed on the
appropriate level of governance. For example, pathology services and
standard setting were placed as statewide and national services. On the other
hand, boundaries placed around LHNs seem to be contentious due to some
pressure to redefine the boundaries combined to Medicare Locals and Aged
Care Planning Regions with the local government reference (CHERE 2013).
CHAPTER FIVE – ANALYSIS OF DECENTRALISATION
There have been few comprehensive empirically-based evaluations of the
governance arrangements for hospitals and DGPs. Government reviews,
academic studies and surveys provide some insights into their impact.
However, these reviews do not identify which aspects for governance
arrangements were responsible for improving outcomes. These analyses are
difficult because of the interdependencies and dynamic nature of factors
affecting health services.
Part of the difficulty with evaluating governance arrangements stems from
the lack of agreement among academics over which governance features will
ensure improvement in health outcomes. This is highlighted by the inability to
agree on definitions for key governance arrangements such as
decentralisation.
Governance arrangements exist in a nuanced realm. There are
dependent on the values of the country where they are implemented which
are designed to encourage innovation may be regarded as promoting inequity
28
in a different country. The method of implementing change may be just as
important to outcome as the change itself.
Governance arrangements may be described along a continuum, rather
than precise points. They are not an end itself, simply a means to an end. It is
also evident that there is no permanent solution with changes in design as
circumstances change.
The literature emphasizes:
regarded and desirable key features are more likely to occur under
particular governance arrangements and contexts;
some particular roles and responsibilities are better located at
certain points in the governance hierarchy.
The features consistently called for include:
clinician and community involvement at local levels;
devolving budgets to local level;
setting performance agreements and monitoring them
providing services required
supporting local service provisions by gathering and distributing
data about services at national level.
They also include accountability, efficiency, innovation, integration, co-
ordination, empowerment and responsiveness. There risks: duplication,
inefficiency, inequity, inability to maximise economies of scale and taking on
roles.
Factors which can enable good governance include data provision, role
clarity, agreed performance targets, adequate payment systems, regular
reporting and expertise-based boards rather the representative based-boards.
Barriers can include many existing bodies with undefined roles, inappropriate
geographical boundaries and inappropriate functions being selected for
decentralisation.

29
Reference List
Aktar, C 2011, The real issue: decentralization and regionalization, Hürriyet Daily News, viewed 10 October 2013, <http://www.hurriyetdailynews.com/default.aspx?pageid=438&n=the-real-issue-decentralization-and-regionalization-2011-01-07>. Australian General Practice Network 2007, The Value of the Divisions Network: An Evaluation of the Effect of Divisions of General Practice on Primary Care Performance, report prepared by A Scott & B Coote, Melbourne Institute of Economic and Social Research.
Australian Government 2010a, A national health and hospitals network for Australia’s future, Australian Government, Canberra. Australian Government 2010b, A national health and hospitals network for Australia’s future: delivering the reforms, Australian Government, Canberra. Australian Government c. 2013, Australian Government, viewed 4 October 2013, < http://australia.gov.au/about-australia/our-country>.
Australian Institute of Health and Welfare 2011, Australia’s welfare 2011, AIHW, Canberra. Australian Institute of Health and Welfare 2013, Australia’s welfare 2013, AIHW, Canberra.
Australian Medical Association 2002, Review of the role of divisions of general practice, AMA, viewed 18 October 2013, <https://www.google.com.au/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&ved=0CCsQFjAA&url=http%3A%2F%2Fwww.ama.com.au%2Fsystem%2Ffiles%2Fnode%2F3777%2FReview_of_Role_Divisions_in_GP.pdf&ei=AH1gUqqyE8avkAXru4DICw&usg=AFQjCNH2XItfsk2KwqO8WM6FWcBgoQWKsg&sig2=HgR8lXG5zF5AszGvDVNo1g&bvm=bv.54934254,d.dGI>.
Bankauskaite, V, Dubois, HFW, Saltman, RB 2007, „Patterns of decentralization across European health systems‟, in RB Saltman, V Bankauskaite & K Vrangbæk (eds), Decentralization in health care, Open University Press, Maidenhead.
Bankauskaite, V & Saltman RB 2007, „Central issues in the decentralization debate‟, in RB Saltman, V Bankauskaite & K Vrangbæk (eds), Decentralization in health care, Open University Press, Maidenhead.
Bergman, S 1998, „Swedish models of health care reform: a review and assessment‟, International Journal of Health Planning and Management, vol. 13, no. 2, pp. 91-106.
30
Bossert, T 1998, „Analyzing the decentralization of health systems in developing countries: a decision space, innovation and performance‟, Social Science & Medicine, vol. 47, no. 10, pp. 1513-1527. Centre for Health Economics Research and Evaluation 2013, Can we get there from here? Implementing health reform in Australia, University of Technology Sydney, viewed 18 October 2013, <http://www.chere.uts.edu.au/pdf/wp2013_02.pdf>. Charles, J, Britt, H & Valenti, L 2004, „The evolution of general practice workforce in Australia, 1991-2003‟, Medical Journal of Australia, vol. 181, no. 2, pp. 85-90. Cheema, GS & Rondinelli DA 1983, Decentralization and Development: Policy Implementation in Developing Countries, Sage Publications, Beverly Hills. Clark, S 2003, Consultation on the definition of a charity, email, Australian Divisions of General Practice Ltd, viewed 18 October 2013, <http://www.taxboard.gov.au/content/reviews_and_consultations/definition_of_a_charity/submissions/Australian_Divisions_of_General_Practice.pdf>. Commonwealth Fund 2012, International profiles of health care systems, 2012, eds. S Thomson, R Osborn, D Squires & M Jun, Commonwealth Fund, viewed 16 August 2013, <http://www.commonwealthfund.org/~/media/Files/Publications/Fund%20Report/2012/Nov/1645_Squires_intl_profiles_hlt_care_systems_2012.pdf>. Council of Australian Government 2012, National healthcare agreement 2012, Council of Australian Government, Canberra. Council of Australian Government 2013, Healthcare 2011-12: comparing performance across Australia, Council of Australian Government, Canberra. Department of Health 2010, Overview of divisions of general practice program, Department of Health, viewed 14 October 2013, <http://www.health.gov.au/internet/main/publishing.nsf/Content/health-pcd-programs-divisions-index.htm>. Department of Health and Ageing 2011a, Local hospital networks, DoHA, viewed 18 October 2013, <http://www.yourhealth.gov.au/internet/yourhealth/publishing.nsf/content/lochospnetwork#.UmCUSG_FUWs>. Department of Health and Ageing 2011b, Medicare Locals: guidelines for the establishment and initial operation of Medicare Locals & Information for applicants wishing to apply for funding to establish a Medicare Local, DoHA, Canberra.
31
Department of Health and Ageing (Portfolio Strategies Division) 2012, „Overview of the Australian Health System‟, Canberra. Department of Health and Ageing 2013, Portfolio budget statements, DoHA, viewed 18 October 2013, <http://www.health.gov.au/internet/budget/publishing.nsf/Content/2013-2014_Health_PBS/$File/2013-14_DoHA_PBS_1.04_Strategic_Direction_Statement.pdf>. Department of the Premier and Cabinet, Queensland Treasury, Queensland Police Service, Department of Public Works & Queensland Health 2005, Queensland Health Systems Review, report prepared by Peter Forster, The Consultancy Bureau, Brisbane. Furniss, N 1974, „The practical significance of decentralization‟, The Journal of Politics, vol. 36, no. 4, pp. 958-982. Ham, C 1998, „Elements of decentralization in plans to reform NHS may prevail‟, British Medical Journal, vol. 317, no. 7160, p. 753. Jervis, P & Plowden, W 2003, The impact of political devolution on the UK’s health services, Nuffield Trust, London. Koivusalo, M, Wyss, K, Santana, P 2007, „Effects of decentralization and recentralization on equity dimensions of health systems‟, in RB Saltman, V Bankauskaite & K Vrangbæk (eds), Decentralization in health care, Open University Press, Maidenhead.
Lewis, S, Kouri D 2004, „Regionalization: making sense of the Canadian experience‟, Healthcare Papers, vol. 5, no. 1, pp. 12-31. M‟Chirgui, Z & Pénard, T 2011, „How to provide Quality of Service guarantees in the Internet? Lessons learnt from the airline and card-based payment sectors‟, European Management Journal, vol. 29, pp. 306-318. Maino, F, Blomqvist, P, Bertinato, L, Santasusagna, LB, Garrido, RMU, Shishkin, S 2007, „Effects of decentralization and recentralization on political dimensions of health systems‟, in RB Saltman, V Bankauskaite & K Vrangbæk (eds), Decentralization in health care, Open University Press, Maidenhead. Marchildon, GP 2005, „Canadian health system reforms: lessons for Australia?‟, Australian Health Review, vol. 29, no. 1, pp. 105-119. Mills, A 1994, „Decentralization and accountability in the health sector from an international perspective: what are the choices?‟, Public Administration and Development, vol. 14, no. 3, pp. 281-292. National Co-ordinating Centre for Service Delivery and Organisation 2005, Decentralisation, centralisation and devolution in publicly funded health services: decentralisation as an organisational model for health care in
32
England, report prepared by S Peckham, M Exworthy, M Powell, I Greener, NCCSDO. National Health and Hospitals Reform Commission 2009, A healthier future for all Australians: final report, Commonwealth of Australia, Canberra. Queensland Government 2008a, Annual Report 2006–07 of the Director of Mental Health, Queensland Government, Brisbane. Queensland Government 2008b, Queensland Cabinet and Ministerial Directory, viewed 15 October 2013, <http://statements.qld.gov.au/Statement/Id/59712>. Rondinelli, DA 1980, „Government Decentralization in Comparative Perspective: Theory and Practice in Developing Countries‟, International Review of Administrative Sciences, vol. 47, pp. 133-145. Saltman, RB & Bankauskaite, V 2006, „Conceptualizing decentralization in European health systems: a functional perspective‟, Health, Economics, Policy and Law, vol. 1, no. 2, pp. 127-147. Saltman, RB, Bankauskaite, V & Vrangbæk, K 2007, Decentralization in health care, Open University Press, Maidenhead. Smith, BC 1985, Decentralization: the territorial dimension of the State, Allen & Unwin, London. Smith, PC & Häkkinen, U 2007, „Information strategies for decentralization‟, in RB Saltman, V Bankauskaite & K Vrangbæk (eds), Decentralization in health care, Open University Press, Maidenhead. Taal, H 1993, Decentralization and community participation for improving access to basic services: an empirical approach, report to UNICEF International Child Development Centre, Innocenti Occasional Papers Economic Policy, series 35, Florence. United States Environmental Protection Agency 2012, United States Environmental Protection Agency, viewed 25 September 2013, < http://www.epa.gov/records/tools/central.htm>. United States Development Programme & Government of Germany 1999, Decentralization: a sampling of definitions, viewed 17 September 2013, <http://web.undp.org/evaluation/documents/decentralization_working_report.PDF>. Vrangbæk K 2007a, „Key factors in assessing decentralization and recentralization in health systems‟ in RB Saltman, V Bankauskaite & K Vrangbæk (eds), Decentralization in health care, Open University Press, Maidenhead.
33
Vrangbæk K 2007b, „Towards a typology for decentralization in health care‟ in RB Saltman, V Bankauskaite & K Vrangbæk (eds), Decentralization in health care, Open University Press, Maidenhead.
Wyss, K & Lorenz, N 2000, „Decentralization and central and regional coordination of health services: the case of Switzerland‟, International Journal of Health Planning and Management, vol. 15, pp. 103-114. World Bank 1983, Decentralization in developing countries, report prepared by DA Rondinelli, JR Nellis & GS Cheema, World Bank, Washington. World Bank 1993, World development report 1993, Oxford University Press, New York. World Health Organization 1990, Health system decentralization: concepts issues and country experiences, report prepared by A Mills, JP Vaughan, DL Smith & I Tabibzadeh, World Health Organization, Geneva. World Health Organization 1995, Experience with organizational and financing reform of the health sector, report prepared by J Kutzin, Division of Strengthening of Health Services, World Health Organization, Geneva. World Health Organization & Australian Institute of Health and Welfare 2012, Australia Health service delivery profile, World Health Organization, viewed 4 October 2013, <http://www.wpro.who.int/health_services/service_delivery_profile_australia.pdf>.
Related Documents











