INTRODUCTION The Ospital ng Maynila (OMMC) has been established to provide city residents, 80 of whom have been classified as indigents, a better standard of medical care. As hospital operated and maintained through taxes paid by Manila residents, Ospital ng Maynila will have for its primary concern the admission and treatment of patients who are bona-fide residents of the city. The Ospital ng Maynila Medical Center is a 300-bed non-profit tertiary, general and training hospital in Malate, Manila, Philippines. It is the laboratory hospital of health science students (students of medicine, nursing and physical therapy) enrolled at the Pamantasan ng Lungsod ng Maynila, one of the Philippines' most prestigious universities. As hospital operated and maintained through taxes paid by Manila residents, OMMC has for its primary concern the admission and treatment of patients who are actual residents of the city. Furthermore, it is responsible for the provision of an integrated community health program and in the promotion of scientific excellence through research activities. BRIEF HISTORY Studies reveal that an alarming number of city residents die without medical attendance. During the year 1967, 16.45% of the total deaths in the city occurred without medical attendance, and 14.43% with incomplete medical attendance. Added to this problem was the fact all the four national hospitals located in the city cannot accommodate all needy patients and even refuse some 8,000 patients a month. The enactment on June 22, 1957, or Republic Act 1939, otherwise known as the Hospital Financing Act, spurred the City of Manila to establish its own hospital. The law required Manila to contribute 1% of its annual income for the operation and maintenance of national hospitals in the city. Events leading to the establishment of the city hospital followed rapidly:

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
INTRODUCTION
The Ospital ng Maynila (OMMC) has been established to provide city residents, 80 of whom have been classified as indigents, a better standard of medical care.
As hospital operated and maintained through taxes paid by Manila residents, Ospital ng Maynila will have for its primary concern the admission and treatment of patients who are bona-fide residents of thecity. The Ospital ng Maynila Medical Center is a 300-bed non-profit tertiary, general and training hospital in Malate, Manila, Philippines. It is the laboratory hospital of health science students (students of medicine, nursing and physical therapy) enrolled at the Pamantasan ng Lungsod ng Maynila, one of the Philippines' most prestigious universities.
As hospital operated and maintained through taxes paid by Manila residents, OMMC has for its primary concern the admission and treatment of patients who are actual residents of the city. Furthermore, it is responsible for the provision of an integrated community health program and in the promotion of scientific excellencethrough research activities.
BRIEF HISTORY
Studies reveal that an alarming number of city residents die without medical attendance. During the year 1967, 16.45% of the total deaths in the city occurred without medical attendance, and 14.43% with incomplete medical attendance. Added to this problem was the fact all the four national hospitals located in the city cannot accommodate allneedy patients and even refuse some 8,000 patients a month.
The enactment on June 22, 1957, or Republic Act 1939, otherwise known as the Hospital Financing Act, spurred the City of Manila to establishits own hospital. The law required Manila to contribute 1% of its annual income for the operation and maintenance of national hospitals in the city.
Events leading to the establishment of the city hospital followed rapidly:
December 30, 1959– Then Councilor Eriberto A. Remigio sponsors, and the municipal board enacts, Ordinance No. 4201 appropriating the amount of PHP 1 million for the construction of the city hospital.
January 11, 1960– In his inaugural address before the municipal board, the late Mayor Arsenio H. Lacson endorsed the hospital project which he said would cost PHP 6 million.
October 11, 1960– Mayor Lacson issues Executive Order No. 39 creating a city general hospital advisory committee.
May 23, 1961– The municipal board, presided over by then Vice Mayor Antonio J. Villegas, passes Ordinance No. 4363 appropriating in additional amount of PHP 1.5 million, as requested by Mayor Lacson.
April 11, 1962– Then President Diosdado Macapagal issues Presidential Proclamation No. 31 turning over to the City of Manila for hospital purposes the national government property at the corner of Harrison and Roxas Boulevard.
April 15, 1962– Immediately upon assumption to office, Mayor Villegas pushes through the construction of the city hospital in theconsonance with his program of “Libreng Pilipino” which hold, among other tings, that the right to medical care is part of the larger and more basic right of the individual to life, liberty and the pursuit of happiness.
September 11, 1962– The cornerstone of the city hospital is laid under the auspices of Mayor Antonio J. Villegas.
October 20, 1962– At the instance of Mayor Villegas, the municipal board passes Ordinance No. 4636 naming the proposed city general hospital as the Arsenio H. Lacson Memorial Hospital.
December 18, 1963– Actual construction work on the hospital buildingbegins.
December 5, 1968– Upon the insistent representations of Mayor Lacson’s widow, the municipal board passes Ordinanace No. 6807 renaming the hospital as the Ospital ng Maynila.

OMMC was established on January 31, 1969 by the government of the Cityof Manila. The primary motivation in establishing the Medical Center was to provide city residents, 80% of who are classified as indigents,a better standard of medical care. It was originally planned to provide a total in-patient capacity of 300 beds and 60–90 nursery cribs. In addition, an outpatient department was included to provide medical care to ambulatory patients.
In May 2005, OMMC renovated its Emergency Department, Infirmary Ward and Neonatal Intensive Care Unit (Nursery). Moreover, it also acquired250 new hospital beds, two incubators, two respirators, and Computed Tomography (CT) Scan services that is free for all legitimate residents of Manila.
On December 23, 2008, the hospital integrated the anthroposophic framework beginning with the institutionalization of integrative and complimentary alternative medicinethrough the help of Dr. Michaela Glocker, who is the leader of the Medical Section at the Goetheanum, the School of Spiritual Science in Dornach, Switzerland since 1988.
ORGANIZATIONAL SET-UP OF THE HOSPITAL
OMMC ORGANIZATIONALSTRUCTURE
ADMINISTRATIONDEPARMENTALORGANIZATION
ADMINISTRATIVESERVICES
MEDICALSERVICES
NURSING ANDALLIED
SERVICES
Family Medicine SurgeryPediatrics Obstetrics &
GynecologyAnesthesia OphthalmologyOtorhinolaryngol Dermatology
BOARD OF TRUSTEES
CEO or HospitalAdministrator

Administration
The Board of Trustees, the governing bodyof the hospital, formulates all the generalpolicies regarding the operation of thehospital, and recommended, for the Mayor’sconsideration, the appointment of hospital staff and personnel, as well as assist in securing additional financial support for the hospital. The members, who are appointees of the mayor, serve on a voluntary basis and not entitled to any remuneration.
The Chief Executive Officer or Hospital Administrator, the actual authority for the administration of the hospital, is in direct charge of its management and responsible for the smooth functioning of hospital activities. The administrator is guided by policies determined by the Board and shall coordinate effectively medical, nursing, and administrative services, in order to attain the objectives or goals of the hospitals.
Departmental organization
The various departments, including both in-patient and out-patient services, are grouped under 3 major services:
Administrative services
A hospital volunteer service will soon be established by the Board. This shall assist the hospital in project like promotion of community interest, fund-raising, and other equally important undertakings.
Dental Services
PLM-OMMC Medical Library
Psychiatry Service
Medical Social Service
Medical Records and Library
Hemodialysis
Children’s Cancer
Homeward Haven:
Family Medicine SurgeryPediatrics Obstetrics &
GynecologyAnesthesia OphthalmologyOtorhinolaryngol Dermatology

Medical services
Departments
Apart from the Outpatient Services, Medical Services Division is sub-divided into the different departments.
Residency Training Program
The Department of Family and Community Medicine in the Ospital ng Maynila has a distinguished history of excellence in its medical services, training education and research program. Our accredited residency program ensures the department's legacy of developing 5-star physicians and community leaderscontinues. The training is a three-year program fully accredited by the Philippine Academy of Family Physicians. It uses as curriculum the highly effective spiral rotation for the holistic training of its residents that ensures theywill always remember and practice what they have learned.
The mentors and consultants of the Family Medicine are respected and well-known Family Physicians in the country. This includes Family Physician of the Year, Dr. Isabelita Samaniego, fellow for life and examiner, Dra. Cecilia Cuaresma, and distinguished members and authors of the different boards and review committees of medical textbooks and practice guidelines like Dr. Paolo de Castro and Dra Alyssa Calderon. Graduates from this institution have had successful practices in their own hometowns. They have also become catalyst of change in their localities and leaders inthe communities.
The General Surgery Residency Training Program of the hospital is a five-year program fully accredited by the Philippine Societyof General Surgeons. It is highly structured and has a well-defined general surgery curriculum in which the philosophy, learning objectives, content, teaching-learning activities, and assessment methods are clearly described, implemented asplanned, regularly monitored and evaluated annually for improvements.

The teaching-learning activities are formulated always with effectiveness, efficiency, and humaneness in mind. These consist of active and self-directed learning activities; community-oriented, competency-based, and problem-based learning approaches; and, a variety of innovative and student-friendly learning methods such as simulated learning, debates, computer-aided and internet-aided studies.
The program also provides career assistance such as preparation for the Philippine Board of Surgery examinations, privilege to have private practice in OMMC while preparing for the certifying examinations, and placement through the Surgeon to Surgeonless Community Program andfellowship programs in other hospitals.
Nursing and Allied servicesThe Nursing Services is responsible for the provision of an organized program of nursing care to patients; the provision of education and training to its staff; the establishment of a positive program of selection and recruitment of nursing personnel; programming nursing budgetary needs; conducting of periodic standardization program in nursing; and conducting nursing research and studies. Other departments are engineering and dietary services.
PLANS AND PROGRAMS
GUIDELINES IN THE PLANNING AND DESIGN OF A HOSPITAL AND OTHER HEALTHFACILITIES
A hospital and other health facilities shall be planned and designed to observe appropriate architectural practices, to meet prescribed functional programs, and to conform to applicable codes as part of normal professional practice
1. Environment: A hospital and other health facilities shall beso located that it is readily accessible to the community and reasonably free from undue noise, smoke, dust, foul odor, flood, and shall not be located adjacent to railroads,
freight yards, children's playgrounds, airports, industrial plants, disposal plants
2. Occupancy: A building designed for other purpose shall not be converted into a hospital. The location of a hospital shall comply with all local zoning ordinances.
3. Safety: A hospital and other health facilities shall provideand maintain a safe environment for patients, personnel and public. The building shall be of such construction so that no hazards to the life and safety of patients, personnel andpublic exist. It shall be capable of withstanding weight andelements to which they may be subjected.3.1 Exits shall be restricted to the following types: door leading directly outside the building, interior stair, ramp,and exterior stair.3.2 A minimum of two (2) exits, remote from each other, shall be provided for each floor of the building.3.3 Exits shall terminate directly at an open space to the outside of the building.
4. Security: A hospital and other health facilities shall ensure thesecurity of person and property within the facility.
5. Patient Movement: Spaces shall be wide enough for free movement ofpatients, whether they are on beds, stretchers, or wheelchairs. Circulation routes for transferring patients from one area to another shall be available and free at all times.
5.1 Corridors for access by patient and equipment shall havea minimum width of2.44 meters.5.2 Corridors in areas not commonly used for bed, stretcher and equipment transport may be reduced in width to 1.83 meters.
5.3 A ramp or elevator shall be provided for ancillary, clinical and nursing areas located on the upper floor.
5.4 A ramp shall be provided as access to the entrance of the hospital not on the same level of the site.
6. Lighting: All areas in a hospital and other health facilities shall be provided with sufficient illumination to promote
comfort, healing and recovery of patients and to enable personnelin the performance of work.
7. Ventilation: Adequate ventilation shall be provided to ensure comfort of patients, personnel and public.
8. Auditory and Visual Privacy: A hospital and other health facilities shall observe acceptable sound level and adequate visual seclusion to achieve the acoustical and privacy requirements in designated areas allowing the unhampered conduct of activities.
9. Water Supply: A hospital and other health facilities shall use anapproved public water supply system whenever available. The watersupply shall be potable, safe for drinking and adequate, and shall be brought into the building free of cross connections.
10. Waste Disposal: Liquid waste shall be discharged into an approvedpublic sewerage system whenever available, and solid waste shall be collected, treated and disposed of in accordance with applicable codes, laws or ordinances.
11. Sanitation: Utilities for the maintenance of sanitary system, including approved water supply and sewerage system, shall be provided through the buildings and premises to ensure a clean andhealthy environment.12. Housekeeping: A hospital and other health facilities shall provide and maintain a healthy and aesthetic environment for patients, personnel and public.
13. Maintenance: There shall be an effective building maintenance program in place. The buildings and equipment shall be kept in a state of good repair. Proper maintenance shall be provided to prevent untimely breakdown of buildings and equipment.
14. Material Specification: Floors, walls and ceilings shall be of sturdy materials that shall allow durability, ease of cleaning and fire resistance
15. Segregation: Wards shall observe segregation of sexes. Separate toilet shall be maintained for patients and personnel, male and female, with a ratio of one (1) toilet for every eight (8) patients or personnel.
16 Fire Protection: There shall be measures for detecting fire such asfire alarms in walls, peepholes in doors or smoke detectors in ceilings. There shall be devices for quenching fire such as fire extinguishers or fire hoses that are easily visible and accessible in strategic areas.
17 Signage. There shall be an effective graphic system composed ofa number ofindividual visual aids and devices arranged to provide information, orientation, direction, identification, prohibition,warning and official notice considered essential to the optimum operation of a hospital and other health facilities.
18 Parking. A hospital and other health facilities shall provide a minimum of one (1) parking space for every twenty-five (25) beds.
19 Zoning: The different areas of a hospital shall be grouped according to zones as follows:
19.1 Outer Zone – areas that are immediately accessible to the public: emergency service, outpatient service, and administrative service. They shall be located near the entrance of the hospital.
19.2 Second Zone – areas that receive workload from the outer zone: laboratory, pharmacy, and radiology. They shall be located near the outer zone.
19.3 Inner Zone – areas that provide nursing care and management of patients: nursing service. They shall be located in private areas but accessible to guests.19.4 Deep Zone – areas that require asepsis to perform the prescribed services: surgical service, delivery service, nursery, and intensive care. They shall be segregated19.5 Service Zone – areas that provide support to hospital activities: dietary service, housekeeping service, maintenance and motorpool service, and mortuary. They shall be located in areas away from normal traffic.
20 Function: The different areas of a hospital shall be functionallyrelated with each other.
20.1 The emergency service shall be located in the ground floor to ensure immediate access. A separate entrance to theemergency room shall be provided.
20.2 The administrative service, particularly admitting office and business office, shall be located near the main entrance of the hospital. Offices for hospital management can be located in private areas.
20.3 The surgical service shall be located and arranged to prevent non-related traffic. The operating room shall be as remote as practicable from the entrance to provide asepsis. The dressing room shall be located to avoid exposure to dirty areas after changing to surgical garments. The nurse station shall be located to permit visual observation of patient movement.
20.4 The delivery service shall be located and arranged to prevent non-related traffic. The delivery room shall be as remote as practicable from the entrance to provide asepsis. The dressing room shall be located to avoid exposure to dirty areas after changing to surgical garments. The nurse station shall be located to permit visual observation of patient movement. The nursery shall be separate but immediately accessible from the delivery room.20.5 The nursing service shall be segregated from public areas. The nurse station shall be located to permit visual observation of patients. Nurse stations shall be provided inall inpatient units of the hospital with a ratio of at leastone (1) nurse station for every thirty-five (35) beds. Roomsand wards shall be of sufficient size to allow for work flowand patient movement. Toilets shall be immediately accessible from rooms and wards.
20.6 The dietary service shall be away from morgue with at least 25-meter distance.
21 Space: Adequate area shall be provided for the people, activity, furniture, equipment and utility.

Guiding Principles, Standards and Criteria:1. The standards of excellence and quality for structure and services shall not be different from that of the government and private facilities.2. Access to care must be a function of a person’s health needs ratherthan ability to pay.3. Regardless of the nature or purpose of the clinic, the highest priority shall be to achieve the best quality service that can be offered to a high coverage of the population served.4. Services provided in each category shall be cognizant of their appropriate roles and respective strengths, ever mindful however, of its complementary and supportive roles in the overallhealth care delivery system. In order to promote and enhance the acceptability of performance and structure of these facilities to a certain degree of quality, the standards and criteria were developed in consideration of the following: (Chart is on the Next Page)
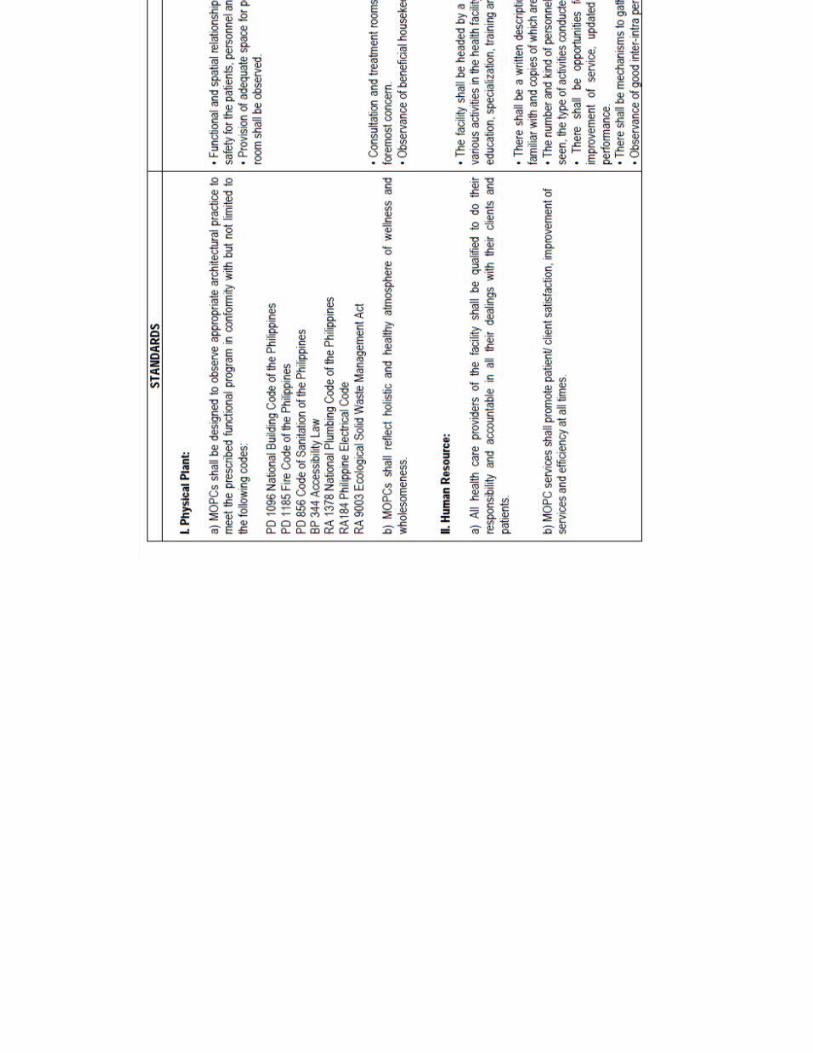
Guidelines in the Planning and Design of Medical Out-Patient Clinics:MOPCs shall be planned and designed to observe appropriate architectural practices, to meet prescribed functional programs, and to conform to applicable codes as part of normal professional practice.
1. Safety: MOPCs shall provide and maintain a safe environment for clients/ patients, personnel and the public. The facility shall be of such construction so that no hazards to the life and safety of clients/ patients, personnel and public exist. It shall be capable of withstanding weight and elements to which they may be subjected.
1.1 Exits shall be restricted to the following types: door leading directly outside the building, interior stair, ramp, and exterior stair.1.2 A minimum of two (2) exits, remote from each other, shall be provided for each floor of the building.1.3 Exits shall terminate directly at an open space to the outside of the building.
2. Patient Movement: Spaces shall be wide enough for free movement of clients/ patients, personnel and other guests.
3. Lighting: All areas in a MOPC-HCF shall be provided with sufficient illumination to enable personnel to properly perform procedures and tasks.
4. Ventilation: Adequate ventilation shall be provided to ensure comfort ofclients/ patients, personnel and public.
5. Water Supply: All MOPCs shall use an approved public water supply system whenever available. The water supply shall be adequate and shall be brought into the building free of cross connections.
6. Waste Segregation and Disposal: Liquid waste shall be discharged into an approved public sewerage system whenever available. Solid waste shall be collected, treated and disposed of in accordance with applicable codes, laws or ordinances.
7. Sanitation: Utilities for the maintenance of sanitary system, includingapproved water supply and sewerage system, shall be provided through the buildings and premises for insuring cleanliness.8. Maintenance: The building/ facility and equipment shall be kept in a state of good repair. Proper maintenance shall be provided to correct or prevent leaking roofs, loose plaster, uneven flooring, faulty equipment, or other undesirable conditions.
9. Material Specification: Floors, walls and ceilings shall be of sturdy materials that shall allow ease of cleaning.
10. Fire Protection: There shall be measures for detecting fire such as firealarms in walls, peepholes in doors or smoke detectors in ceilings. There shall be devices for quenching fire such as fire extinguishers or fire hoses that are easily visible and accessible in strategic areas.
11. Space: Adequate area shall be provided for the people, activity, furniture, equipment and utility.
Service Capability:1. General Administrative Service2. Clinical Service and/or any of the following as deemed appropriate with the specialty concerned:a) General Pediatrics e) ENT
b) General Obstetrics and Gynecology f) Ophthalmologyc) General Surgery g) Family Medicined) Internal Medicine h) Minor Surgery (when applicable)3. Health Education
Personnel:
1. General administrative servicea) Administrator and/or physician-administrator (1)2. Clinical servicea) Physician (1)b) Nurse or any other allied or health trained personnelc) Support staff as necessary
Equipment/Instrument:1. General Administrative Servicea) Bench (1) e) Desk (1/staff)b) Cabinet or open shelf (1) f) Fire extinguisher (1)c) Calculator (1) g) Color codedtrash containerd) Chair (1/staff)2. Clinical Servicea) Clinical weighing scale (1) h) Stethoscope (1)b) Examining table (if applicable) (1) i) Suturing set (if applicable) (1)c) Gooseneck lamp/examining light (1) j) EENT diagnostic set(if applicable) (1)
d) Instrument table (1) k) Nebulizer (if applicable) (1)
e) Minor surgery instrument set (if applicable) (1) l) Thermometerf) Sphygmomanometer (1) m) Emergency medicine cabinet and corresponding medicineg) Sterilizer (if applicable) (1) n) Consumable clinic supplies
Physical Facility:1. General Administrative Servicea) Waiting areab) Information and receiving areac) Access to toilet2. Clinical Servicea) Consultation area d) Sterilizing area (if applicable)b) Examination and treatment area with lavatory/sink e) Minoroperating room area ( if applicable)
c) Equipment and supply storage area/ appropriate cabinets
ACTIVITY/FUNCTIONAL SET-UP OF THE HOSPITAL
MEDICAL ROGRAMMING ANG PLANNING: A PROCESS PRESENTATION

1. Pre-programming Phase Post occupancy evaluation Existing space summaries Mission/vision statements Deficiency analysis Needs assessment Healthcare trends Staff flow and relationships
2. Programming Phase Circulation factor ranges from 15%-55%
Ex: NFA 4109sqm x CF 25% = GFA 5138sqm 3. Pre-schematic Design
Site Analysis Engineering Systems Orientation Circulation/Traffic Topography, Geology and Soil conditions Corporate and local culture (4B’s) Codes and Standards Review Local building codes, Uniform Building Codes – US, British Standards – EU, American Society for Heating, Refrigeration and Air Conditioning – US, AIA – Medical Planning Standards, Underwriter Laboratories – US, Japan Standards)
4. Schematic Design Phase Bubble Diagram/ Floor Plans Departmental Agencies and Proximities, Sizes Grid Analysis Structural Engineering, MEP Schematic Floor Plans/ Furniture layout
5. Design Development Phase Engineering Concepts Outline Materials Specifications Equipment Program Equipment Layout
6. Construction Documentation/ Tender/ Construction

Note: Attached here was the “Manual on Technical Guidelines For Hospitals and Health FacilitiesPlanning and Design form Department of Health (DOH), Manila, 1994
Related Documents











