J Med Syst (2007) 31:185–196 DOI 10.1007/s10916-007-9054-3 ORIGINAL PAPER Research-Based-Decision-Making in Canadian Health Organizations: A Behavioural Approach Jalila Jbilou · Nabil Amara · R´ ejean Landry Received: 27 November 2006 / Accepted: 22 January 2007 / Published online: 1 May 2007 C Springer Science+Business Media, LLC 2007 Abstract Decision making in Health sector is affected by a several elements such as economic constraints, political agendas, epidemiologic events, managers’ values and environment ... These competing elements create a complex environment for decision making. Research- Based-Decision-Making (RBDM) offers an opportunity to reduce the generated uncertainty and to ensure efficacy and efficiency in health administrations. We assume that RBDM is dependant on decision makers’ behaviour and the identification of the determinants of this behaviour can help to enhance research results utilization in health sector decision making. This paper explores the determinants of RBDM as a personal behaviour among managers and professionals in health administrations in Canada. From the behavioural theories and the existing literature, we build a model measuring “RBDM” as an index based on five items. These items refer to the steps accomplished by a decision maker while developing a decision which is based on evi- dence. The determinants of RBDM behaviour are identified using data collected from 942 health care decision makers in Canadian health organizations. Linear regression is used to model the behaviour RBDM. Determinants of this behaviour are derived from Triandis Theory and Bandura’s construct “self-efficacy.” The results suggest that to improve research use among managers in Canadian governmental health orga- nizations, strategies should focus on enhancing exposition to evidence through facilitating communication networks, part- nerships and links between researchers and decision makers, with the key long-term objective of developing a culture that supports and values the contribution that research can make J. Jbilou () · N. Amara · R. Landry Universit´ e Laval, Qu´ ebec, Canada e-mail: [email protected] to decision making in governmental health organizations. Nevertheless, depending on the organizational level, deter- minants of RBDM are different. This difference has to be taken into account if RBDM adoption is desired. Decision makers in Canadian health organizations (CHO) can help to build networks, develop partnerships between professionals locally, regionally and nationally, and also act as change agents in the dissemination and adoption of knowledge and innovations in health services. However, the research focused on knowledge use as a support to decision-making, further research is needed to identify and evaluate effective incentives and strategies to implement so as to enhance RBDM adoption among health decision makers and more theoretical development are to complete in this perspective. Keywords Research-Based-Decision-Making . Healthcare decision-makers . Behavioural theories . Research utilization . Empirical . Canada Introduction Research is developed to generate new knowledge and estab- lish evidences to provide information for decision makers to use to enhance efficacy and efficiency in the decision-making process [1]. However, literature suggests that a gap between research and practice still exists [2]. The major part of factors enumerated in literature are related to organizational dimen- sions for example uncertainty of evidence, competing results [3], trialability of evidence [4], researchers failure to commu- nicate with practitioners [5] complexity of decision making context [6], lack of integration of theory into health services research [7], lack of relevant and timely evidence and lack of culture of research in health organizations [8]... , but none Springer

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

J Med Syst (2007) 31:185–196DOI 10.1007/s10916-007-9054-3
ORIGINAL PAPER
Research-Based-Decision-Making in Canadian HealthOrganizations: A Behavioural ApproachJalila Jbilou · Nabil Amara · Rejean Landry
Received: 27 November 2006 / Accepted: 22 January 2007 / Published online: 1 May 2007C© Springer Science+Business Media, LLC 2007
Abstract Decision making in Health sector is affectedby a several elements such as economic constraints,political agendas, epidemiologic events, managers’ valuesand environment . . . These competing elements create acomplex environment for decision making. Research-Based-Decision-Making (RBDM) offers an opportunityto reduce the generated uncertainty and to ensure efficacyand efficiency in health administrations. We assume thatRBDM is dependant on decision makers’ behaviour andthe identification of the determinants of this behaviour canhelp to enhance research results utilization in health sectordecision making. This paper explores the determinantsof RBDM as a personal behaviour among managers andprofessionals in health administrations in Canada. From thebehavioural theories and the existing literature, we build amodel measuring “RBDM” as an index based on five items.These items refer to the steps accomplished by a decisionmaker while developing a decision which is based on evi-dence. The determinants of RBDM behaviour are identifiedusing data collected from 942 health care decision makers inCanadian health organizations. Linear regression is used tomodel the behaviour RBDM. Determinants of this behaviourare derived from Triandis Theory and Bandura’s construct“self-efficacy.” The results suggest that to improve researchuse among managers in Canadian governmental health orga-nizations, strategies should focus on enhancing exposition toevidence through facilitating communication networks, part-nerships and links between researchers and decision makers,with the key long-term objective of developing a culture thatsupports and values the contribution that research can make
J. Jbilou (�) · N. Amara · R. LandryUniversite Laval,Quebec, Canadae-mail: [email protected]
to decision making in governmental health organizations.Nevertheless, depending on the organizational level, deter-minants of RBDM are different. This difference has to betaken into account if RBDM adoption is desired. Decisionmakers in Canadian health organizations (CHO) can help tobuild networks, develop partnerships between professionalslocally, regionally and nationally, and also act as changeagents in the dissemination and adoption of knowledgeand innovations in health services. However, the researchfocused on knowledge use as a support to decision-making,further research is needed to identify and evaluate effectiveincentives and strategies to implement so as to enhanceRBDM adoption among health decision makers and moretheoretical development are to complete in this perspective.
Keywords Research-Based-Decision-Making . Healthcaredecision-makers . Behavioural theories . Researchutilization . Empirical . Canada
Introduction
Research is developed to generate new knowledge and estab-lish evidences to provide information for decision makers touse to enhance efficacy and efficiency in the decision-makingprocess [1]. However, literature suggests that a gap betweenresearch and practice still exists [2]. The major part of factorsenumerated in literature are related to organizational dimen-sions for example uncertainty of evidence, competing results[3], trialability of evidence [4], researchers failure to commu-nicate with practitioners [5] complexity of decision makingcontext [6], lack of integration of theory into health servicesresearch [7], lack of relevant and timely evidence and lack ofculture of research in health organizations [8]. . . , but none
Springer

186 J Med Syst (2007) 31:185–196
has explored research utilisation by decision makers throughbehavioural theories.
The early part of the 1990s ushered in evidence-basedmedicine. Presently, there is resurgence in evidence-baseddecision making within health organizations and evidence-based management [4]. Evidence-based decision making in-volves a wide range of individuals from different organi-zational levels with different skills and different level ofpower on decisions they should take to achieve objectives.In the field of health care, turbulences are explored from twoangles: the structural reforms taking place within a givenhealth care system, and the crisis affecting public health, ofwhich epidemics- such as SARS and Avian Influenza—areof particular concern. In both cases, however, the recourseto scientific proofs remains the best option that would en-sure the most effective decision. In addition, decision mak-ing in public health care organizations confronts two typesof challenges which are intrinsically related to the system’sguiding principles. Essentially, each health care system’s de-cision must take into consideration three values: equity, effi-ciency, and autonomy. These three—at times oppositional—values could put the decision-making process into a cumber-some situation [9]. Likewise, studies effected in the field ofknowledge transfer have shown that there is a wide gap be-tween the existent knowledge, the taken decision, and prac-tice as well for clinic as for management [2, 4, 10]. Thevery fact that the decision-maker is a human being, it isour strong postulation, that he/she must be influenced byhis/her own subjective values, beliefs, and norms. In orderto explore the subjective factors affecting decision makers inthe Canadian health care system, we shall explore ResearchBased Decision Making (RBDM) through behaviouraltheories.
It has to be noted that in this study, the term decisionmakers will be used to designate individuals who work in alltype of Canadian Health organizations. The decision makerstargeted in this study are not mainly health care practitioners.Some of them are in charge, directly (managers) or indirectly(professionals), of developing decisions in Canadian healthorganizations. Professionals here are administrative profes-sionals not clinicians (MD, nurses . . .). The decisions thatare targeted in this study are managerial decisions (organiza-tional, financial, structural . . .) but not clinical or therapeuticones.
In the literature, the idea of evidence encompass, amongothers, different concepts such as experience, beliefs, val-ues, abilities, resources, legislations, and researches results[2, 11–14]. In the present study, we will focus solely on theconcept of “research results” as scientific evidence. Indeed,in the specialized literature, RBDM is defined as “ . . . theuse of the best possible evidence when dealing with “reallife” circumstances . . . ” [2, 15–17]. In this study, we do ex-
tend the definition of the concept of research results so asto include five stages: 1. the reception of the research result,2. the reading and understanding of the research result, 3.the citation of the research result, 4. the adaptation of theresearch result, 5. the efforts exerted in order to promotethe research result. The usage of the research result dependsgreatly on decision maker’s willing to, the benefits it providesto him/her, and the risks he/she is ready to take [18]. Thestudies of managers’ behaviours within health care presentbig challenges to the different actors in the public system(population, academics, and institutions). Through a betterunderstanding and prediction of the managers’ behaviours,such a research prospective provides an unmatched oppor-tunity for the development of strategies in favour of RBDM.Important to mention that several researches have exploredthis issue [19–24]. Accordingly, it is conspicuous that theseresearchers and because they have concentrated their re-searches on processes—information systems, developmentof capacities, structural reorganisation, organisational de-terminants, type of use · · · —they have not given the dueattention to the individuals’ behaviour [19, 25].
Important to mention that the results aimed at by thisresearch are inscribed within two different, but very com-plimentary, perspectives: 1. A conceptual perspective whoseobjective lies in the elaboration and the validation of anexplanatory model stemming from behavioural theories. 2.A practical perspective that consists in profiling a numberof specific strategies indispensable to the improvement ofthe use of research results in times of decision making inCanadian Health Organisations (CHO).
Theoretical framework
In the field of psychology, the bulk of theoretical works real-ized for the benefit of health care and whose main objectiveis behavioural prediction, has resulted in the developmentof a plethora of theories that make up what is commonlyknown as the Behavioural Approach. From the latter, wehave chosen two theories for two reasons: 1. since healthis a highly individual value, the concerned decision-makermust be unconsciously influenced by this fact while con-cerned making a decision. 2. In the behaviour in favour forhealth, the psychological weight of decision making in rela-tion to the environmental factors is comparable to the weighta decision-maker has to confront in relation to researchresults.
The Theory of Planned Behaviour (TPB) was proposedin 1975 by Fishbein and Ajzen [26]. It postulates that thebehavioural choices are well-thought of, reasoned, and actedupon. The intention of adopting such or such behaviourremains the most crucial factor. This model, it is to benoted, takes into consideration the enormous pressure of the
Springer

J Med Syst (2007) 31:185–196 187
Fig. 1 Theoretical modelassociating Triandis’ theory ofinterpersonal behaviours (1979)and Bandura’s perceivedeffectiveness (1986)
social environment in the adoption of particular behaviours.In the elaboration of intention, several factors are combined:1. cognitive (evaluating the advantages and the disadvantagesof the potential behaviours). 2. Affective (likes and dislikes).3. Social. 4. Moral. In order to elaborate his theory on inter-personal behaviours (TIB), Triandis [27] has relied heavilyon the researches of Ajzen and Fishbein. Triandis ‘start-ing point was that several behaviours manifest themselvesunconsciously. To consolidate this, he has integrated theconcept of habits and extrinsic—facilitating or inhibiting—factors to the TPB model. In addition, Trandis is credited withsetting the distinction between the beliefs linking emotionsto behaviour and those linking the identified consequencesand the intention of acting. This theoretical approach, it isto be noted, has been used to study the behaviour of indi-viduals in several fields. This is significantly true when itcomes to the adoption of the use of information and commu-nication technologies [28], enterprise creation [29] . . . Thebehavioural approach, however, has not been exploited inthe filed of the utilisation of research results as a support tothe decision- making process of managers in the health caresector.
Similar to other authors, and by introducing dimensionsrelatives to the individuals’ psychological characteristics, wewanted to give a larger perspective to our model [30]. There-fore, we have opted to use the concept of the perceivedself-efficacy developed by Bandura during his research onsocial and cognitive theory [31]. This concept refers to theperception that an individual has in relation to the controlthat he or she is able to exert in order to adopt the desired be-haviour. This concept possesses a double action [31, 32]. Infact, it acts not only through the arbitration of intention, butalso through direct action on behaviour. The perceived effec-tiveness has been used in several fields of research in generaland in the field of the study of behaviours in the health care
sector in particular [33–40]. Important to mention that thetheoretical articulation with Triandis’ TIB concepts was pre-viously tested and validated by other authors such as Caronand Coll [41].
In the present study, we have been inspired by the conceptsdeveloped by Triandis and Bandura in order to elaborate apredictive model of the adoption of the RBDM behaviour bythe managers and the professionals in the health care sector.Our contribution at this level is not only limited to the utili-sation of the concepts proposed by Triandis and Bandura inthe filed of knowledge transfer, but it includes also testingtheir direct impact on the RBDM behaviour without usingmotivation as a mediating variable. The underlying hypoth-esis is that the organisational behaviour in this context isdifferent from that in the health care sector. This is true sincemotivation is an independent component in which a directaction could be exerted without being obliged to go throughthe pressures of social/personal norms, cognition or attitude.The model (Fig. 1) which we propose to test, will allow us,in the first place, to identify the determinants of the RBDMbehaviour, and in the second place, to validate our theoreticalhypothesis.
The operational hypotheses—discerned from the previousmodel—which we will try to verify and are as follows, themeasures are derived from a review of the literature.
H.1 the perceived value of the research positively influencesthe RBDM adoption by health care decision makers(cognitive component) [4].
H.2 the personal convictions of the individual positively in-fluence the RBDM adoption by health care decisionmakers (personal normative component) [4, 10].
H.3 the beliefs in the existence of specific social roles andthe felt pressures positively influence the adoption ofthe RBDM behaviour by health care decision makers(social normative component) [42]
Springer

188 J Med Syst (2007) 31:185–196
Table 1 Dependant variable composing items’ distribution
Very Does notNever Rarely Sometimes Often often apply Average on 1–5(1) (2) (3) (4) (5) (6) Total scale (S.D.)a
During the last five years, on a Likert scale where 1 = never . . .
(in % of respondents)I have received research results concerning the
area for which I’m responsible3.5 8.6 29.8 36.6 20.3 1.2 100.0 3.62 (1.01)
I have read and understood the research reportsthat I have received
1.1 2.9 20.6 42.6 30.6 2.3 100.0 4.01 (0.86)
I have cited research evidence to colleagues orpatients as a reference in my work
4.8 6.5 29.2 38.7 19.1 1.7 100.0 3.62 (1.02)
I have adapted the format of the research resultsto provide information useful to our decision
5.8 11.0 35.4 31.0 14.5 2.2 100.0 3.38 (1.05)
I have made efforts to promote the adoption ofresearch evidence in my field
5.6 9.7 30.9 34.4 17.2 2.2 100.0 3.49 (1.07)
a(S.D.) refer to standard deviation.
H.4 the valuing of the RBDM by health care decision makers(emotional component) [42]
H.5 an organisational context favourable to research and tothe use of the research results positively influence theadoption of the RBDM behaviour by health care deci-sion makers (conditions facilitation adoption) [43, 44]
H.6 the recurrence of the behaviour positively influence theadoption of the RBDM behaviour by health care deci-sion makers (habit component) [44]
H.7 the intention positively influences the adoption of theRBDM behaviour by health care decision makers (mo-tivation component) [4, 10, 45]
H.8 the perceived effectiveness positively influences theadoption of the RBDM behaviour by health care de-cision makers [45]
H.9 the socio-demographic characteristics positively influ-ence the adoption of the RBDM behaviour by healthcare decision makers [44].
The aforementioned limitations of this behavioural ap-proach lie mainly in the fact that this theory “ . . . tended tobe particularly interested in understanding people’s motiva-tion to change behaviour rather than ability to change . . . ”[30]. In the present study, we aim at determining the ex-planatory factors of behaviours and it is important to men-tion that we are not interested in exploring the developmentof capacities supporting them. Indeed, the latter will be thesubject of a future work devoted to the subject we that weare developing about the use of research results from theperspective of individual behaviour. Form the latter, we willproceed to the study of the prediction of behaviour adoptionwhile taking into account the mediation of motivation andthrough which we will we use the methodology of the struc-
tural equations in order to determine the mediating effect ofmotivation.
Theoretical model
The objective of the present study is to identify the deter-minants of RBDM behaviour for health care managers. Assuch, we have chosen to use the quantitative methodologybased on a questionnaire elaborated at the end of a 1998study on the use of the university research results by healthcare managers and professionals in Canadian health careadministrations. The RBDM behaviour represents the de-pendent variable measured by an index of 5 items. In thefollowing lines, we will provide more precise informationon both the data that we have used and the characteristics ofthe studied sample. After that, we will delineate the processof the construction and present the validation of the indicesand the results of the realised analyses. Finally, we will fo-cus on the discussions and the implications of the presentwork.
Data
The data used in this research were collected during a pan-Canadian survey administered in 2001 by Infras.Inc de Que-bec. The target population was made up of managers andprofessionals belonging to the Canadian public administra-tions with a quota per province in proportion to the popu-lation. Three information sources were identified in orderto identify and match up the target population. Firstly, inthe case of the regional board of Quebec and the OntarianDistrict Health Council, it is the Health Evidence Appli-cations and Linkage Network (HEALNet). As for similar
Springer

J Med Syst (2007) 31:185–196 189
Table 2 Descriptive statistics
Variables Type of variables Minimum Maximum Mean Standard deviation Cronbach’s α
Continuous variableAcquisition effort Index: 6 items 1 5 3.40 0.82 0.8958Contributions of users Index: 4 items 1 5 3.12 0.66 0.7611Impact of research findings Index: 2 items 1 5 3.39 0.83 0.7460Relational capital Index: 5 items 1 5 2.81 0.75 0.7393Radicalness of research findings Index: 4 items 1.33 5 3.64 0.20 0.6387Log% of work time spent on research Continue: numeric 0 4.62 2.58 0.34
activitiesLog of size of the organization Continue: numeric 0 11.51 6.62 0.70Log% of time spent on acquisition of Continue: numeric 0 5 2.58 1.02
research evidence
Binary variablesPertinence of research in daily practice 69.7% has respond that research evidence is important or very important in their daily practiceCollaborative research 61.8% (YES)Most advanced university degree PhD = 10.1%, MSc = 46.9%, BSc = 25.7% = , college = 9.2% et autre = 9.2%Research culture 65.5% (YES)Gender 44.4% (Male)Status in the organization Manager = 45.1%, Professional = 54.6%, other = 0.3%
information on the decision makers working in the min-istries (chief executive officer, manager or division boss ineach ministry or governmental agency), were collected byconsulting the Scott’s Government Index [46]. Thirdly, in-formation on the addresses and telephone numbers of pro-fessionals and managers in the hospitals was provided by theCanadian Health Facilities Directory (2001).
The survey firm had as an objective of collecting 340usable questionnaires provided from each of these 3 groupsof decision makers targeted by the study. The number ofvalid questionnaire was 942. The rate of answer generated ishigher than 100%, what could be explained by the use of the“snow-ball” sampling procedure.
Results
Decriptive statistics
Among the 942 participants who replied to the questionnaire,10.1% had a PhD, 46.9% a MSc, 25.7% a BSc, 9.2% a colle-gial diploma and 8.1% other certificates. However, 44.4% ofthe respondents were men. Among the respondents, 45.1%are managers, 54.6% are professionals and 0.3% occupiesanother position in the organisation. On average, there re-spondents possess an occupational seniority of 11.96 yearsin a position while realising the interviews, with a stan-dard deviation of 14.52 years. The population repartition ofthe study by fields of activity reveals that 24.7% work inhospital or intensive care, 6.7% community care (1rst line,home care, . . .), 18.9% in public health or population health,6.5% in long-term care and 43.2% other organisations. How-
ever, the repartition by organisational level shows that 39%work in a ministry or provincial agency, 30.8% in a regionalboard (RHA for Anglophone Canada), 23.6% in a unit healthcare, 0.4% in a ministry or federal agency and 5.4% in an-other type of organisations. The geographic repartition of thissample, however, indicates that 24.5% are in Quebec, 16.7%in Ontario, 10.6% in Alberta, 5.2% in Nova Scotia, 9.2% inSaskatchewan, 9.8% in British Colombia, 7.5% in Manitoba,5.1% in New-Brunswick, 5.9% in Newfoundland, 3.5% inPrince Edward Island and 1.9% in Yukon/north Territories.
The dterminants of the RBDM behaviour
In order to study the impact of the explicatory variables on theadoption of the RBDM behaviour by managers and profes-sionals in the health care sector in Canada, we have estimatedby the linear regression method the following model:
RBDM = β0 + β1 PERTRE + β2 RECUL + β3 CONTU
+β4 LnTSA + β5 ACQEF + β6 RELAK
+β7 COLREC + β8 IMPRES + β9 GEND
+β10 MOSDEG + β11 STATOR
+β12 LnTRA + β13 LnUNS
+β14 NOVEL + ε (1)
where,β i (i = 0, . . . , 14) are the coefficients to estimate;ε is the error term.
Springer

190 J Med Syst (2007) 31:185–196
Tabl
e3
Cor
rela
tion
mat
rix
LnO
RS
GE
ND
PER
TR
EST
AT
OL
nTSA
RE
CU
LM
OSD
EG
IMPR
ES
CO
LR
EC
NO
VE
LA
CQ
EF
RE
LA
KC
ON
TU
LnT
RA
LnO
RS
1−
.056
.027
−.02
9−.
010
−.08
8−.
018
.053
.043
−.00
8.0
57.1
27.0
49.0
32G
EN
D1
−.03
6.0
36.0
92−.
053
.129
−.00
8.0
89.0
11−.
096
.046
−.07
8−.
069
PER
TR
E1
−.10
1.1
99.4
29.1
13.3
19.1
51.0
33.3
39.2
58.3
35.3
10ST
AT
O1
−.16
1−.
107
−.08
8−.
058
−.03
4−.
022
−.10
1−.
015
−.05
5−.
148
LnT
SA1
.165
.132
.168
.276
.044
.243
.270
.141
.465
RE
CU
L1
.136
.320
.204
.017
.394
.225
.302
.322
MO
SDE
G1
.108
.227
−.05
8.1
94.2
13.1
19.2
00IM
PRE
S1
.260
.077
.465
.364
.401
.364
CO
LR
EC
1.0
21.3
03.3
03.1
71.2
47N
OV
EL
1.1
23.0
85.1
16.0
87A
CQ
EF
1.4
31.3
71.4
83R
EL
AK
1.3
89.4
32C
ON
TU
1.3
30L
nTR
A1
This model has been elaborated by using information col-lected from 943 respondents from different organisationallevels in the health care sector in Canada. The dependentvariable RBDM is an index elaborated from 5 items whichcome from the definition that we have retained: 1) evidencereception, 2) reading and comprehension of the evidence, 3)citation of the evidence, 4) adaptation of the evidence and5) conceded efforts in order to promote the evidence adop-tion. For each of the steps, the respondents had to give theirbehaviour, by using a scale of 5 levels, ranging between 1(never) to 5 (very often). The attributed value to this indexvaries between 1 and 5 with an average of 3.6142 and a stan-dard deviation of 0.8194. Among the 942 individuals of thesample, 937 individuals have used the research results to sup-port the decision. The results of Table 1 revealed that nearlyhalf of the individuals have replied � often � or � veryoften, � during the 5 last years, for each of the 5 items. Thedependent variable RBDM is therefore the weighted aver-age of the different responses and can take the value rangingfrom 1 to 5. in order to evaluate the validity of the index,we have proceeded at a factorial analysis (principal compo-nents factorial analysis (PCFA)) with VARIMAX rotation,in order to evaluate the unidimensionality [47]. The resultsshow that one factor explains 61.95% of the initial varianceof the RBDM behaviour with an initial Eigenvalue of 3.098.Hence, we are able to confirm that the items constituting thedependent variable are associated and constitute a uniformand homogeneous concept.
Besides that, we have realised an evaluation of internalconsistence of the index, which has revealed a Cronbachalpha of 0.8457. We have, then, did in the same manner for allthe explicatory variables having necessity the constructionof an index for their measure namely ACQUEF, CONTU,IMPRES, NOVEL and RECAPO (Table 2).
In addition, we have tested the correlations betweenthe different independent variables retained in our model(Table 3). The highest coefficient of correlation is 0.483,improved for ACQUEF and LogTSA. This allows us to con-clude that there are no multi-colinearity problems betweenthe explicatory variables.
The results of the regression that correspond to the ex-plicatory model of the adoption of the RBDM behaviourby health care managers and professionals are delineated inTable 4. We can deduce that all of the independent vari-ables introduced in the model explain in a statistically il-lustrative manner the RBDM adoption behaviour. This issuggestive at levels varying between 1% and 5%. The totalvariance explained by this model is represented by an R2
adjusted by 0.58. Table 4 reveals that the adoption of theRBDM behaviour is favoured by: the positive evaluation ofthe pertinence of research results in daily practice, the adop-tion of a research culture that refers to the preference of
Springer

J Med Syst (2007) 31:185–196 191
Tabl
e4
Reg
ress
ion
mod
els
estim
atin
gde
term
inan
tsof
RB
DM
byde
cisi
onm
aker
sin
Can
adia
nhe
alth
orga
niza
tions
:Glo
bala
ndfo
rea
chor
gani
zatio
nall
evel
Dep
enda
ntva
riab
le:R
BD
Mby
deci
sion
mak
ers
inC
anad
ian
heal
thad
min
istr
atio
nsG
loba
lmod
elM
acro
leve
lM
ediu
mle
vel
Mic
role
vel
Inde
pend
entv
aria
ble
Coe
ffici
ents
(p-v
alue
)aT
ratio
sC
oeffi
cien
ts(p
-val
ue)a
Tra
tios
Coe
ffici
ents
(p-v
alue
)aT
ratio
sC
oeffi
cien
ts(p
-val
ue)a
Tra
tios
Inte
rcep
tR
esea
rch
Bas
edD
ecis
ion
Mak
ing
[RB
DM
].9
31(.
000)
∗∗∗
5.63
1.9
35(.
000)
∗∗∗
3.56
1.6
92(.
010)
∗∗∗
2.31
51.
179
(.00
0)∗∗
∗4.
089
Cog
nitiv
epe
rson
alco
mpo
nent
Res
earc
his
pert
inen
tfor
my
prof
essi
onal
prac
tice
[PE
RT
RE
].1
57(.
000)
∗∗∗
3.45
3.1
18(.
058)
∗1.
576
.172
(.01
7)∗∗
2.13
3.1
77(.
018)
∗∗2.
106
Aff
ectiv
eco
mpo
nent
Res
earc
hcu
lture
[RE
CU
L]
.100
(.01
4)∗∗
∗2.
205
.131
(.04
3)∗∗
1.72
4.1
23(.
052)
∗1.
630
.068
(.21
6)N
S.7
89Pe
rson
alno
rmat
ive
com
pone
ntC
olla
bora
tive
rese
arch
[CO
LR
EC
].1
25(.
001)
∗∗∗
3.05
0.2
29(.
000)
∗∗∗
3.30
7.0
64(.
186)
NS
.896
−.04
6(.
226)
NS
−.59
7So
cial
norm
ativ
eco
mpo
nent
Invo
lvem
ento
fre
sear
ch’
user
s[C
ON
TU
].0
52(.
049)
∗∗∗
1.65
2.0
41(.
217)
NS
.784
.095
(.05
9)∗
1.57
4−.
020
(358
)NS
−.36
6H
abits
Lnb
Tim
esp
ento
nre
sear
chac
tiviti
es[L
nTR
A]
.018
(.00
0)∗∗
∗3.
449
.020
(.00
7)∗∗
∗2.
482
.023
(.01
4)∗∗
2.22
9.0
12(.
101)
NS
1.28
3L
nbT
ime
spen
ton
evid
ence
acqu
isiti
on[L
nTSA
].1
20(.
000)
∗∗∗
6.52
4.1
15(.
001)
∗∗∗
2.95
5.1
27(.
001)
∗∗∗
3.16
8.1
09(.
013)
∗∗2.
243
Mot
ivat
ion
Acq
uisi
tion
effo
rts[
AC
QE
F]
.048
(.00
0)∗∗
∗5.
114
−.00
8(.
432)
NS
−.17
3.1
87(.
000)
∗∗∗
3.62
4.0
98(.
036)
∗∗1.
777
Faci
litat
ing
cond
ition
sN
ovel
tyof
evid
ence
[NO
VE
L]
−.06
1(.
020)
∗∗∗
−2.0
47−.
043
(.19
3)N
S−.
867
−.10
1(.
023)
∗∗−2
.006
−.06
9(1
25)N
S−1
.156
Lnb
Size
ofth
eor
gani
zatio
n[L
nOR
S].0
03(.
381)
NS
.303
.036
(.07
2)∗
1.46
4.0
11(.
228)
NS
.748
.008
(.31
2)N
S.4
90R
elat
iona
lcap
ital[
RE
LA
K]
.097
(.00
0)∗∗
∗3.
188
.166
(.00
1)∗∗
∗3.
148
.036
(.25
0)N
S.6
76.0
94(.
043)
∗∗1.
717
Perc
eive
dse
lf-e
ffica
cyIm
pact
ofre
sear
chon
prac
tice
[IM
PR
ES]
.384
(.00
0)∗∗
∗14
.704
.368
(.00
0)∗∗
∗8.
767
.386
(.00
0)∗∗
∗7.
539
.402
(.00
0)∗∗
∗8.
782
Soci
o-de
mog
raph
icch
arac
teri
stic
sG
ende
r[G
EN
DE
R]
.103
(.00
2)∗∗
∗2.
787
.031
(.30
1)N
S.5
21.1
95(.
001)
∗∗∗
2.97
2.0
67(.
173)
NS
.947
Stat
usin
the
orga
niza
tion
[STA
TO
]−.
060
(.05
2)∗∗
−1.6
28−.
060
(.16
1)N
S−.
993
−.07
6(.
116)
NS
−1.1
95−.
050
(.23
4)N
S−.
727
Uni
vers
ityde
gree
[MO
SDE
G]
.144
(.00
0)∗∗
∗3.
781
.074
(.12
1)N
S1.
175
.132
(.02
4)∗∗
1.99
9.2
71(.
000)
∗∗∗
3.64
4N
umbe
rof
resp
onde
nts
942
382
302
244
Adj
uste
dR
20.
560.
520.
560.
64C
alcu
late
dF
=75
.526
;T
heor
etic
alF
(13;
942)
=2.
05at
1%
Cal
cula
ted
F=
26.0
80;
The
oret
ical
F(1
3;38
2)=
2.15
at1%
Cal
cula
ted
F=
25.3
81;
The
oret
ical
F(1
3;30
2)=
2.16
at1%
Cal
cula
ted
F=
27.5
63;
The
oret
ical
F(1
3;24
4)=
2.17
at1%
Not
e.N
umbe
rsbe
twee
nbr
acke
tsin
dica
tep-
valu
e.a∗
;∗∗an
d∗∗
∗in
dica
teth
atva
riab
leis
sign
ifica
ntre
spec
tivel
yat
10%
,5%
and
1%.
NSno
nsi
gnifi
ant.
bL
nin
dica
tes
alo
gari
thm
ictr
ansf
orm
atio
nof
the
vari
able
.
Springer
192 J Med Syst (2007) 31:185–196
Table 5 Elasticities of determinants of RBDM by decision makers in Canadian health organizations: global and for each organizational level
Partial elasticity
% Global modelMacroorganizational level
Mediumorganizational level
Microorganizational level
(A) Continuous variablesAcquisition efforts (ACQEF) 0.47 NS 1.84 0.92Users’ contribution (CONTU) 0.46 NS 0.84 NSImpact of research (IMPRES) 3.67 −0.08 3.73 3.86Relational capital (RELAK) 0.78 −0.45 NS 0.73Novelty of research (NOVEL) −0.01 NS −1.08 NSLn Size of organization (LnORS) NS 1.34 NS NSLn%Time spent on evidence acquisition (LnTSA) 0.85 0.378 0.90 0.76Ln%Time spent on research activities (LnTRA) 0.1 3.45 0.02 NS
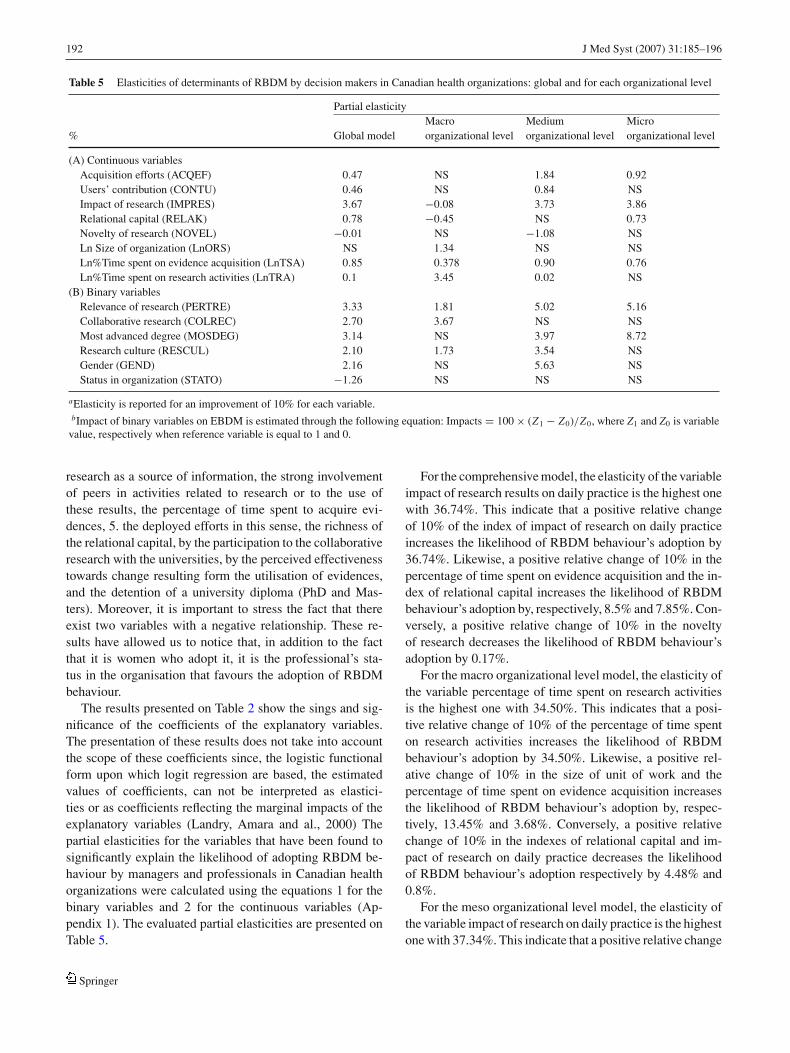
(B) Binary variablesRelevance of research (PERTRE) 3.33 1.81 5.02 5.16Collaborative research (COLREC) 2.70 3.67 NS NSMost advanced degree (MOSDEG) 3.14 NS 3.97 8.72Research culture (RESCUL) 2.10 1.73 3.54 NSGender (GEND) 2.16 NS 5.63 NSStatus in organization (STATO) −1.26 NS NS NS
aElasticity is reported for an improvement of 10% for each variable.bImpact of binary variables on EBDM is estimated through the following equation: Impacts = 100 × (Z1 − Z0)/Z0, where Z1 and Z0 is variablevalue, respectively when reference variable is equal to 1 and 0.
research as a source of information, the strong involvementof peers in activities related to research or to the use ofthese results, the percentage of time spent to acquire evi-dences, 5. the deployed efforts in this sense, the richness ofthe relational capital, by the participation to the collaborativeresearch with the universities, by the perceived effectivenesstowards change resulting form the utilisation of evidences,and the detention of a university diploma (PhD and Mas-ters). Moreover, it is important to stress the fact that thereexist two variables with a negative relationship. These re-sults have allowed us to notice that, in addition to the factthat it is women who adopt it, it is the professional’s sta-tus in the organisation that favours the adoption of RBDMbehaviour.
The results presented on Table 2 show the sings and sig-nificance of the coefficients of the explanatory variables.The presentation of these results does not take into accountthe scope of these coefficients since, the logistic functionalform upon which logit regression are based, the estimatedvalues of coefficients, can not be interpreted as elastici-ties or as coefficients reflecting the marginal impacts of theexplanatory variables (Landry, Amara and al., 2000) Thepartial elasticities for the variables that have been found tosignificantly explain the likelihood of adopting RBDM be-haviour by managers and professionals in Canadian healthorganizations were calculated using the equations 1 for thebinary variables and 2 for the continuous variables (Ap-pendix 1). The evaluated partial elasticities are presented onTable 5.
For the comprehensive model, the elasticity of the variableimpact of research results on daily practice is the highest onewith 36.74%. This indicate that a positive relative changeof 10% of the index of impact of research on daily practiceincreases the likelihood of RBDM behaviour’s adoption by36.74%. Likewise, a positive relative change of 10% in thepercentage of time spent on evidence acquisition and the in-dex of relational capital increases the likelihood of RBDMbehaviour’s adoption by, respectively, 8.5% and 7.85%. Con-versely, a positive relative change of 10% in the noveltyof research decreases the likelihood of RBDM behaviour’sadoption by 0.17%.
For the macro organizational level model, the elasticity ofthe variable percentage of time spent on research activitiesis the highest one with 34.50%. This indicates that a posi-tive relative change of 10% of the percentage of time spenton research activities increases the likelihood of RBDMbehaviour’s adoption by 34.50%. Likewise, a positive rel-ative change of 10% in the size of unit of work and thepercentage of time spent on evidence acquisition increasesthe likelihood of RBDM behaviour’s adoption by, respec-tively, 13.45% and 3.68%. Conversely, a positive relativechange of 10% in the indexes of relational capital and im-pact of research on daily practice decreases the likelihoodof RBDM behaviour’s adoption respectively by 4.48% and0.8%.
For the meso organizational level model, the elasticity ofthe variable impact of research on daily practice is the highestone with 37.34%. This indicate that a positive relative change
Springer

J Med Syst (2007) 31:185–196 193
of 10% of the percentage of time spent on research activi-ties increases the likelihood of RBDM behaviour’s adoptionby 37.34%. Likewise, a positive relative change of 10% inthe index of acquisition efforts, users’ contribution, and per-centage of time spent on evidence acquisition increases thelikelihood of RBDM behaviour’s adoption by, respectively,18.37%, 8.38% and 8.99%. Conversely, a positive relativechange of 10% in the variable degree of novelty of researchdecreases the likelihood of RBDM behaviour’s adoption by10.82%.
For the micro organizational level model, the elasticity ofthe variable impact of research on daily practice is the high-est one with 38.64%. This indicate that a positive relativechange of 10% of the percentage of impact of research ondaily practice increases the likelihood of RBDM behaviour’sadoption by 38.64%. Likewise, a positive relative change of10% in the variables acquisition efforts, percentage of timespent on evidence acquisition and relational capital increasethe likelihood of RBDM behaviour’s adoption by, respec-tively, 9.17%, 7.58% and 7.28%.
Conclusion and implications
The objectives of the present study were of two types: 1. con-ceptual to test the validity of the behavioural theory in orderto explain RBDM. 2. Operational in order to determine thekey factors favouring or hindering the adoption of this be-haviour by health care decision makers in Canada. In order toelaborate our RBDM explanatory model, we have opted forTriandis’s theory of interpersonal behaviour in associationwith Bandura’s concept of the perceived self-efficacy. Wehave assumed that RBDM for health care decision makers isa processual behavior that includes 5 phases: 1. the receptionof the evidence, 2. the reading and the understanding of theevidence, 3. the citation of the evidence, 4. the adaptationof the evidence, 5. the efforts exerted to promote the adop-tion of the evidence. These components have been the basisfor the elaboration of an RBDM index. Also, the data thatwe have used reveal that among the 943 respondents, morethan 50% have answered 4 (often) or 5 (very often) to eachitem constituting the index measuring the dependent variableRBDM.
The conceptual model that we have built has allowedus to confirm the fact that the RBDM behaviour could bemeasured within a behavioural perspective. This work hasstrongly approved the impact of the organizational and theindividual characteristics on the use of research results byCanadian health care managers. In the first place, this hasindeed allowed us to know the profile of the potential userof the evidences—let’ say a professional woman holding aPhD or a master’s degree (MSc) with a diversified network
and activity (research and administrative tasks). Also, andmore importantly, it has permitted us to confirm the fact thatin order to promote an individual RBDM behaviour, effortsmust be exerted to assure both individual and peer valuing ofresearch findings utilisation, to strive to create interfaces andopportunities so as to improve collaborative research withthe universities,to provide a modality of work organisationwhich leaves a room to the manager to manage his or hertime in order to be able to both collect and study the neces-sary evidences. These assertions show the importance of thedevelopment of a global strategy for favouring the RBDM inhealth care managers and professionals. This strategy targetsthe organisational structures (work time organisation and thedevelopment of collaborative research) as well as the be-liefs and values of the decision makers (individual and peervaluing of the RBDM). It is unquestionable that the RBDMbehaviour is intrinsically linked to the beliefs and values ofthe actors. In fact, this does strongly suggest the incumbentnecessity of profound reflection on the strategies to be devel-oped in order to reach a real paradigmatic change in favourof RBDM before even thinking on the structures and theprocesses. RBDM is an individual behavior that has to besupported by organizational structure and culture of KT/KU.More, determinants of RBDM are different depending onorganizational level; specific strategies and incentives haveto be developed for each level.
Moreover, the current context of crisis does strongly evokea state of emergency especially when it comes to the proac-tive organizations. Strategically speaking, the health caresector organisations should favour the recruitment of pivotalprofessionals adopting RBDM behaviour in order to dissem-inate such behaviour in the first place and, in the secondplace, to exert their full efforts in times of crises. However,the present work presents a limitation that is intrinsicallylinked to the administrative context of health care managersand professionals in Canada. This is particularly true dueto the fact that the Canadian health care system is publiclyfinanced and it is known for its hierarchic and bureaucraticmanagement which makes decision making extremely cen-tralized. These realities require us to assert the fact that re-sults generalization must be taken with precaution. In orderto enhance the knowledge and strength then the actions infavour of RBDM behaviour in health care, it is of paramountimportance to investigate a number of research issues andexplore other research avenues: 1) What are the strategieswhich are judged to be effective and efficient in order toachieve a pragmatic change in favour of RBDM ? 2) Whatare the effective and efficient organisational modalities to im-plement in order to provide a framework favouring RBDMin health care? 3) What are the challenges that are to beconfronted while striving to enhance the RBDM behaviourhealth care?
Springer
194 J Med Syst (2007) 31:185–196
Take
Hom
em
essa
ges
RB
DM
isa
beha
vior
that
isde
term
ined
bySe
lf-e
ffica
cyan
dT
IBco
mpo
nent
sIn
divi
dual
char
acte
rist
ics
•Edu
catio
nPh
D/M
Sc
•Gen
der
(Fem
ale)
•Res
earc
hac
tivity
and
cultu
re
•Net
wor
king
(div
ersi
fied)
Asu
ppor
tive
orga
niza
tion
with
Agl
obal
stra
tegy
for
RB
DM
impr
ovem
enta
mon
gD
ecis
ion
Mak
ers:
•An
inte
grat
ive
cultu
rals
trat
egy
(ind
ivid
uala
ndpe
ers
valu
atio
nof
rese
arch
and
RB
DM
,res
earc
hcu
lture
)•A
stru
ctur
alst
rate
gy(W
ork
time
man
agem
ent,
colla
bora
tive
rese
arch
,res
ourc
esfo
rK
T,im
pact
s’as
sess
men
t)T
rans
vers
alde
term
inan
tsT
ime
spen
ton
rese
arch
findi
ngs
acqu
isiti
onR
elev
ance
ofre
sear
chfo
rda
ilypr
actic
e(a
dequ
acy
and
read
ines
sto
use)
Perc
eive
dim
pact
ofre
sear
chon
prac
tice,
serv
ices
...
App
endi
x1
Var
iabl
eV
aria
ble
Des
crip
tion
Var
iabl
em
easu
re
PER
TR
ER
esea
rch
pert
inen
cefo
rda
ilypr
actic
e.It
mea
sure
sth
eco
gniti
veco
mpo
nent
ofth
ebe
havi
our
ofth
em
anag
erfa
cing
the
RB
DM
beha
viou
r.
Con
tinuo
usva
riab
lem
easu
red
byth
equ
estio
n“O
vera
ll,i
nth
efie
ldof
my
prof
essi
onal
prac
tice
,res
earc
his
pert
inen
tfor
my
prof
essi
onal
prac
tice
”co
ded
ona
Lik
erts
cale
betw
een
1(n
ever
)an
d5
(ver
yof
ten)
.
RE
CU
LR
esea
rch
cultu
re.I
tmea
sure
sth
eaf
fect
ive
com
pone
ntof
the
man
ager
’sat
titud
eto
war
dsth
ead
optio
nof
the
RB
DM
beha
viou
r.
Var
iabl
em
easu
red
byth
equ
estio
n“O
vera
ll,i
nth
efie
ldof
my
prof
essi
onal
prac
tice
,res
earc
his
my
pref
erre
dso
urce
ofin
form
atio
n,in
itial
lyco
ded
ona
Lik
erts
cale
betw
een
1(n
ever
)an
d5
(ver
yof
ten)
,the
ntr
ansf
orm
edin
tobi
nary
vari
able
or1
corr
espo
ndin
gto
the
choi
ceof
resp
onse
4an
d5
and
0w
hen
choo
sing
1,2,
3).
CO
NT
UIm
plic
atio
nof
rese
arch
user
s.It
mea
sure
sth
eno
rmat
ive
soci
alco
mpo
nent
cont
inuo
usva
riab
lere
pres
ente
dby
anin
dex
com
pose
dof
4ite
mm
easu
red
byth
equ
estio
ns1)
Inm
ypr
ofes
sion
alfie
ld,u
sers
ofre
sear
ch,c
reat
eev
ents
for
tran
sfer
ofre
sear
ch,2
)In
my
prof
essi
onal
field
,use
rsof
rese
arch
,org
aniz
etr
aini
ngac
tivi
ties
whi
chin
tegr
ate
rese
arch
resu
lts,
3)In
my
prof
essi
onal
field
,use
rsof
rese
arch
,inv
estm
ater
ialo
rfin
anci
alre
sour
ces
inkn
owle
dge
tran
sfer
et4)
Inm
ypr
ofes
sion
alfie
ld,u
sers
ofre
sear
ch,d
evel
opne
wap
proa
ches
,new
inte
rven
tion
sor
new
deli
very
syst
ems
base
don
rese
arch
resu
lts.
The
resp
onse
sar
eco
ded
ona
Lik
erts
cale
betw
een
1(n
ever
)an
d5
(ver
yof
ten)
ofea
chite
m.
Log
TSA
Perc
enta
geof
wor
ktim
esp
enti
nac
quir
ing
scie
ntifi
cev
iden
ces.
Itm
easu
res
the
habi
tof
real
isin
gth
eR
BD
Mbe
havi
our.
Con
tinuo
usva
riab
lem
easu
red
byth
equ
estio
n“W
hatp
erce
ntag
eof
your
wor
kti
me
doyo
usp
end
onac
quis
itio
nof
rese
arch
evid
ence
?”th
ere
spon
ses
vary
betw
een
0an
d10
0%.I
twas
cate
gori
sed
in5
quin
tiles
.Alo
gari
thm
ictr
ansf
orm
atio
nw
asre
alis
edin
orde
rto
besu
reof
ano
rmal
dist
ribu
tion.
Springer
J Med Syst (2007) 31:185–196 195
Con
tinue
d
Var
iabl
eV
aria
ble
Des
crip
tion
Var
iabl
em
easu
re
AC
QU
EF
Con
cede
def
fort
sin
acqu
irin
gth
ere
sear
chre
sults
.Itm
easu
res
the
mot
ivat
ion
toad
optt
heR
BD
Mbe
havi
our
cont
inuo
usva
riab
lere
pres
ente
dby
anin
dex
com
pose
dof
6ite
ms,
mea
sure
dby
the
ques
tions
:1)
Inte
rms
ofyo
urpr
ofes
sion
alin
volv
emen
t,w
hati
sth
eim
port
ance
ofac
tive
invo
lvem
enti
nre
sear
chpr
ojec
ts,2
)In
term
sof
your
prof
essi
onal
invo
lvem
ent,
wha
tis
the
impo
rtan
ceof
part
icip
atio
nin
prof
essi
onal
conf
eren
ces
and
wor
ksho
psin
volv
ing
rese
arch
ers,
3)In
term
sof
your
prof
essi
onal
invo
lvem
ent,
wha
tis
the
impo
rtan
ceof
mem
bers
hip
onex
pert
-pan
els
and
com
mit
tees
invo
lvin
gre
sear
cher
s,4)
Inte
rms
ofyo
urpr
ofes
sion
alin
volv
emen
t,w
hati
sth
eim
port
ance
ofne
wsl
ette
rsan
dre
sear
chin
form
atio
nde
live
red
dire
ctly
tom
e,5)
Inte
rms
ofyo
urpr
ofes
sion
alin
volv
emen
t,w
hati
sth
eim
port
ance
ofre
sear
chre
port
sse
ntto
me
byE
-mai
l,6)
Inte
rms
ofyo
urpr
ofes
sion
alin
volv
emen
t,w
hati
sth
eim
port
ance
ofre
sear
chof
evid
ence
avai
labl
eon
the
Inte
rnet
.The
resp
onse
sar
eco
ded
ona
Lik
erts
cale
betw
een
1(n
otim
port
ant)
and
5(v
ery
impo
rtan
t)fo
rea
chite
m.
RE
CA
POR
elat
iona
lcap
italw
ithre
sear
cher
s.It
mea
sure
sth
eco
nditi
ons
faci
litat
ing
the
adop
tion
ofth
eR
BD
Mbe
havi
our
Con
tinuo
usva
riab
lere
pres
ente
dby
the
inde
xco
mpo
sed
of5
item
sm
easu
red
byth
equ
estio
n.1)
how
freq
uent
lydo
you
have
pers
on-t
o-pe
rson
cont
actw
ith
rese
arch
ers
inun
iver
sity
,2)
how
freq
uent
lydo
you
have
pers
on-t
o-pe
rson
cont
actw
ith
rese
arch
ers
hosp
ital
s,3)
how
freq
uent
lydo
you
have
pers
on-t
o-pe
rson
cont
actw
ith
rese
arch
ers
inre
gion
alhe
alth
care
auth
orit
ies,
4)ho
wfr
eque
ntly
doyo
uha
vepe
rson
-to-
pers
onco
ntac
twit
hre
sear
cher
sin
gove
rnm
enta
genc
ies,
5)ho
wfr
eque
ntly
doyo
uha
vepe
rson
-to-
pers
onco
ntac
twit
hre
sear
cher
sin
priv
ate
firm
s.T
here
spon
ses
are
code
don
aL
iker
tsca
lebe
twee
n1
(nev
er)
and
5(v
ery
ofte
n)fo
rea
chite
m.
CO
LR
EC
Col
labo
rativ
ere
sear
chw
ithth
eun
iver
sitie
s.It
mea
sure
sth
epe
rson
alno
rmat
ive
com
pone
ntvi
s-a-
vis
the
RB
DM
beha
viou
r:di
chot
omou
sva
riab
lem
easu
red
byth
equ
estio
n“I
nth
ela
stfiv
eye
ars,
have
you
been
invo
lved
ina
rese
arch
stud
yth
atco
mbi
neun
iver
sity
and
non-
univ
ersi
tyin
vest
igat
ors?
”co
ded
1(y
es)
and
0(n
o).
IMPR
ES
Res
earc
him
pact
onth
epr
actic
e.It
mea
sure
the
perc
eive
def
fect
iven
ess
whe
nit
com
esto
the
real
isat
ion
ofth
eR
BD
Mbe
havi
our
cont
inuo
usva
riab
lere
pres
ente
dby
the
anin
dex
com
pose
dof
2ite
ms
mea
sure
dby
the
ques
tions
:1)
duri
ngth
ela
stfiv
eye
ars
rese
arch
evid
ence
has
led
me
tom
ake
prof
essi
onal
choi
ces
and
deci
sion
sth
atI
wou
ldno
thav
em
ade
othe
rwis
e,2)
duri
ngth
ela
stfiv
eye
ars
the
util
izat
ion
ofre
sear
chev
iden
ceha
sle
dto
conc
rete
chan
ges
inth
epr
ogra
ms
orse
rvic
espr
ovid
edby
my
orga
niza
tion
.The
resp
onse
sar
eco
ded
ona
Lik
erts
cale
betw
een
1(n
ever
)an
d5
(ver
yof
ten)
for
each
item
.G
EN
Dre
spon
dent
’sge
nder
Bin
ary
vari
able
code
d1
for
Man
and
0fo
rW
oman
.ST
AT
Oth
ere
spon
dent
’sst
atus
inth
eor
gani
satio
nB
inar
yva
riab
leco
ded
1fo
rm
anag
ers
and
0fo
rth
epr
ofes
sion
als.
MO
SDE
Ghi
ghes
tedu
catio
nald
egre
eB
inar
yva
riab
leco
ded
1fo
rth
ose
havi
nga
PhD
ora
mas
ters
(MSc
)an
d0
for
othe
rL
nTR
APe
rcen
tage
oftim
eof
wor
ksp
ento
nre
sear
chac
tiviti
es.I
tmea
sure
sth
eha
bitt
ore
aliz
eth
ebe
havi
orR
BD
M.I
tre
flect
sth
ero
utin
isat
ion
ofth
ere
sear
chac
tiviti
es.
Con
tinuo
usva
riab
lem
easu
red
byth
equ
estio
n“W
hatp
erce
ntag
eof
your
wor
kti
me
doyo
usp
end
one
rese
arch
acti
viti
es?”
the
answ
ers
vary
from
0to
100%
.Alo
gari
thm
ictr
ansf
orm
atio
nw
asre
aliz
edto
mak
esu
reof
ano
rmal
dist
ribu
tion.
LnO
RS
Num
ber
ofpe
rson
sw
orki
ngin
the
orga
niza
tion
whe
rere
spon
dent
wor
ks.
Itre
flect
sth
esi
zeof
the
orga
niza
tion
whe
reth
ere
spon
dent
wor
ks.
Con
tinuo
usva
riab
lem
easu
red
byth
equ
estio
n“W
hati
sth
eap
prox
imat
enu
mbe
rof
empl
oyee
sin
your
adm
inis
trat
ive
orga
niza
tion
?”th
ean
swer
sva
ryfr
om0
to65
00.A
loga
rith
mic
tran
sfor
mat
ion
was
real
ized
tom
ake
sure
ofa
norm
aldi
stri
butio
n.
NO
VE
LT
here
quir
edef
fort
san
dre
sour
ces
tous
eev
iden
ce.I
tmea
sure
sth
eef
fort
san
dre
sour
ces
that
resp
onde
ntha
sto
inve
stto
use
evid
ence
sw
hen
head
opts
RB
DM
;ext
ensi
vely
itre
fers
toth
eno
velty
ofev
iden
ce.
Con
tinuo
usva
riab
lere
pres
ente
dby
anin
dex
cons
titut
edof
4ite
ms,
mea
sure
dby
the
ques
tions
:In
your
field
ofpr
ofes
sion
alpr
actic
e,th
eut
iliz
atio
nof
rese
arch
resu
lts
tode
velo
pne
wor
impr
oved
heal
thse
rvic
esw
ould
requ
ire:
1)th
ecu
stom
izat
ion
ofre
sear
chre
sult
sfo
rea
chse
rvic
e,2)
the
deve
lopm
ento
fane
wte
chno
logy
,3)
sign
ifica
ntfin
anci
alin
vest
men
ts,4
)si
gnifi
cant
inve
stm
ents
inth
etr
aini
ngof
pers
onne
l.T
hean
swer
sar
eco
ded
ona
Lik
erts
cale
rang
ing
betw
een
1(s
tron
gly
disa
gree
)an
d5
(str
ongl
yag
ree)
for
each
ofth
eite
ms.
Springer
196 J Med Syst (2007) 31:185–196
References
1. Hemsley-Brown, J., Using research to support management de-cision making within the field of education. Manage. Decis.43(5):691–705, 2005.
2. Dobbins, M., et al., A framework for the dissemination and uti-lization of research for health-care policy and practice. Online J.Knowl. Synth. Nurs. 9:7, 2002.
3. Whynes, D., Policy forum: Health care reform: Towards anevidence-based national health service? Econ. J. 106(439):1702–1712, 1996.
4. Pfeffer, J., and Sutton, R., Evidence-based management. DecisionMaking, Harvard Business Review, pp. 63–74, 2006.
5. Kelemen, M., and Bansal, P., The conventions of management re-search and their relevance to management practice. Br. J. Manage.13:97–108, 2002.
6. Hewison, A., Evidence-based management in the NHS: Is it pos-sible? J. Health Org. Manage. 18(5):336–348, 2004.
7. Brazil, K., et al., From theory to practice: Improving the impact ofhealth services research. BMC Health Serv. Res. 5(1):1, 2005.
8. Kiefer, L., et al., Fostering evidence-based decision-making inCanada: examining the need for a Canadian population and publichealth evidence centre and research network. Can. J. Public Health96(3):I1–40, following 200, 2005.
9. Tavakoli, M., Davies, H. T., and Thomson, R., Decision analysisin evidence-based decision making. J. Eval. Clin. Pract. 6(2):111–120, 2000.
10. Learmonth, M., and Harding, N., Evidence-based management:The very idea. Public Administration 84(2):245–266, 2006.
11. Dobbins, M., et al., Use of systematic reviews in the developmentof new provincial public health policies in Ontario. Int. J. Technol.Assess. Health Care 20(4):399–404, 2004.
12. Estabrooks, C., et al., Decision aids: Are they worth it? A system-atic review. J. Health Serv. Res. Policy 6(3):170–182, 2001.
13. Estabrooks, C.A., Will evidence-based nursing practice make prac-tice perfect? Can. J. Nurs. Res. 30(1):15–36, 1998.
14. Sibbald, B., and Roland, M., Getting research into practice. J. Eval.Clin. Pract. 3(1):15–21, 1997.
15. Hayward, R. S., et al., Practice guidelines. What are internistslooking for? J. Gen. Intern. Med. 11(3):176–178, 1996.
16. Nutbeam, D., Improving the fit between research and practice inhealth promotion: Overcoming structural barriers. Can. J. PublicHealth 87(Suppl. 2):S18–23, 1996.
17. Sackett, D. L., et al., Evidence based medicine: What it is and whatit isn’t. BMJ 312(7023):71–72, 1996.
18. Walshe, K., and Rundall, T. G., Evidence-based management:From theory to practice in health care. Milbank Q. 79(3):429–457,IV–V, 2001.
19. Niedzwiedzka, B. M., Barriers to evidence-based decision makingamong Polish healthcare managers. Health Serv. Manage. Res.16(2):106–115, 2003.
20. Lindstrom, R. R., Evidence-based decision-making in healthcare:Exploring the issues though the lens of complex, adaptive systemstheory. Healthc. Pap. 3(3):29–35, 2003; discussion 66–71.
21. Mitton, C., and Donaldson, C., Health care priority setting: Prin-ciples, practice and challenges. Cost. Eff. Resour. Alloc. 2(1):3,2004.
22. Dobrow, M. J., et al., The impact of context on evidence utilization:A framework for expert groups developing health policy recom-mendations. Soc. Sci. Med., 2006.
23. Landry, R., Amara, N., and Lamari, M., Utilization of social scienceresearch knowledge in Canada. Res. Policy 30:333–349, 2001.
24. Amara, N., Ouimet, M., and Landry, R., New evidence on instru-mental, conceptual and symbolic utilization of university researchin government agencies. Sci. Commun. 26(1):75–106, 2003.
25. Holmberg, H., et al., Economic evaluation of screening for prostatecancer: A randomized population based programme during a 10-year period in Sweden. Health Policy 45(2):133–147, 1998.
26. Fishbein, M., and Ajzen, I., Belief, Attitude, Intention, and Be-havior: An Introduction to Theory and Research, Addison-Wesley,Reading, MA, 1975.
27. Triandis, H., The self and social behavior in differing culturalcontexts. Psychol. Rev. 96:506–520, 1989.
28. Gagnon, M. P., and Godin, G., An adaptation of the theory ofinterpersonal behaviour to the study of telemedicine adoption byphysicians. Int. J. Med. Inform. 71(2–3):103–115, 2003.
29. Emin, S., Les facteurs determinants la creation d’entreprise par leschercheurs publics: Application des modeles d’intension. Revue del’Entrepreunariat 3(1):1–19, 2004.
30. Jeffery, R. W., How can Health Behavior Theory be made moreuseful for intervention research? Int. J. Behav. Nutr. Phys. Act.1(1):10, 2004.
31. Bandura, A., Self-Efficacy: The Exercise of Control, Freeman, NewYork, WH, 1997.
32. Bandura, A., and A., L. E., Negative self-efficacy and goal effectsrevisited. J. Appl. Psychol. 88(1):87–99, 2003.
33. Beauchamp, M. R., Bray, S. R., et al. Pre-competition imagery,self-efficacy and performance in collegiate golfers. J. Sports Sci.20(9):697–705, 2002.
34. Benight, C. C., and Bandura, A., Social cognitive theory of post-traumatic recovery: The role of perceived self-efficacy. Behav. Res.Ther. 42(10):1129–1148, 2004.
35. Casey, L. M., Oei, T. P., et al., An integrated cognitive model ofpanic disorder: The role of positive and negative cognitions. Clin.Psychol. Rev. 24(5):529–555, 2004.
36. De Souza, G. A., Da Silva, A. M., et al., Self-efficacy as a mediatorfor improvement in oral health clinical indices. Pesqui. Odontol.Bras 16(1):57–62, 2002.
37. Lavelle, E., Smith, J., et al., The writing approaches of secondarystudents. Br. J. Educ. Psychol. 72(Pt 3):399–418, 2002.
38. Oetker-Black, S. L., et al., Preoperative teaching and hysterectomyoutcomes. Aorn J. 77(6):1215–1218, 1221–1231, 2003.
39. Shon, K. H., and Park, S. S., Medication and symptom managementeducation program for the rehabilitation of psychiatric patients inKorea: The effects of promoting schedule on self-efficacy theory.Yonsei. Med. J. 43(5):579–589, 2002.
40. 33(8), 2003.41. Caron, F., Godin, G., et al., Evaluation of a theoretically based
AIDS/STD peer education program on postponing sexual inter-course and on condom use among adolescents attending highschool. Health Educ. Res. 19(2):185–197, 2004.
42. Helfand, M., Using evidence reports: Progress and challengesin evidence-based decision making. Health Aff. (Millwood)24(1):123–127, 2005.
43. Nicklin, W., and Stipich, N., Enhancing skills for evidence-basedhealthcare leadership: The Executive Training for Research Ap-plication (EXTRA) program. Can. J. Nurs. Leadersh 18(3):35–44,2005.
44. Mitton, C., and Patten, S., Evidence-based priority-setting: whatdo the decision-makers think? J. Health Serv. Res. Policy 9(3):146–152, 2004.
45. Browman, G. P., Snider, A., and Ellis, P., Negotiating for change.The healthcare manager as catalyst for evidence-based practice:Changing the healthcare environment and sharing experience.Healthc. Pap. 3(3):10–22, 2003.
46. Scott’s Government, Index Scott’s Government Index, SouthamInformation Products Group, Don Mills, Ont., 2001.
47. Ahire, S., and Devaray, S., An empirical comparison of Statisti-cal Construct Validation Approaches. IEEE Trans. Eng. Manage.48(3):319–329, 2001.
Springer
Related Documents











