21026 May 2000 Reproductive Health and WORLD Health Sector Reform BANK Linking Outcomes to Action INSTITUTE Kdtherine Krasovec and R. Paul Shaw WBI WorkirlgPapers WBFWrIrLEapr Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
21026May 2000
Reproductive Health and WORLDHealth Sector Reform BANKLinking Outcomes to Action INSTITUTEKdtherine Krasovec and R. Paul Shaw WBI Workirlg Papers
WBFWrIrLEapr
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Recent Books from WBI
Case Studies in Participatory Irrigation ManagementDavid Groenfeldt and Mark Svendsen, editors1999. 169 pages. ISBN 0-8213-4540-0. Stock No. 14540. Price code 522
Chile: Recent Policy Lessons and Emerging ChallengesGuillermo Pery and Danny M. Leipziqer, editors1999. 437 pages. ISBN 0-8213-4500-1. Stock No. 14500. Price code 535
Curbing Corruption: Toward a Model for Building National IntegrityRick Stapenhurst and Sahr Kpundeh, editors1998. 264 pages. 15SN 0-8213-4Q57-6. Stock No. 14257. Price code 525
Economic Development and Environmental SustainabilityJose I. dos R. Furtado and Tamara Belt with Ramachandra Jammi, editors2000. 123 pages. ISBN 0-8213-4573-7. Stock No. 14573, Price code 522
Implementing Health Sector Reform in Central AsiaPapers from the EDI Health Policy Seminar in Ashgabat, Turkmenistan, June 1996Zuzana Feachem, Martin Hensher, and Laura Rose, editors1999. 162 pages. ISBN 0-8213-4337-8. Stock No. 14337, Price code 525
Preventing Bank Crises: Lessons from Recent Global Bank FailuresGerard Caprio, Jr., William C. Hunter, George G. Kaufman, and Danny M. Leipzlger, editors1998. 392 pages. ISBN 0-8213-4202-9. Stock No. 14202. Price code 540
Principles of Health Economics for Developing CountriesWilliam Jack1999. 305 pages. ISBN 0-8213-4571-0. Stock No. 14571. Price Code 530
Resetting Price Controls for Privatized Utilities: A Manual for RegulatorsRichard Green and Martin Rodriguez Pardina1999. 116 pages. ISBN 0-8213-4338-6. Stock No. 14338. Price code 535
Social Funds and Reaching the Poor: Experiences and Future DirectionsAnthony G. Bigio, editor1998. 258 pages. ISBN 0-8213-4209-6. Stock No, 14209. Price code S95
Strategic Reforms for Agricultural Growth in PakistanRashid Faruqee, editor1999. 162 pages. ISBN 0-8213-4336-X. Stock No. 14336. Price code S30
Working Together for a Change: Government, Business, and Civic Partnershipsfor Poverty Reduction in Latin America and the CaribbeanAriel Fiszbein and Pamela Lowden1999. 176 pages. ISBN 0-8213-4339-4. Stock No. 14339. Price code 525
The complete list of Institute publications is available in theWBI Publications Catalog 2000. Stock No. 31708
Order World Bank Institute publications
by phone or fax; Phone: 1-800-645-7247 or (703) 661 -1580; Fax: (703) 661-1501
bymail.:Write to The World Bank, P.O. Box 960, Herndon, VA 20172-0960, U.S.A.
by e-mail:[email protected]
through the World Wide Web at; http://www.worldbank.org/publications
or visit the W81 website at: http://www.worldbank.org/wbi
Reproductive Health and Health Sector ReformLinking Outcomes to Action
Katherine KrasovecPartnershipsfor Health Reform, Abt Associates Inc
R. Paul ShawWorld Bank Institute
AcknowledgementsThe authors wish to acknowledge helpful comments and contributions by Arlette M.Campbell White, Carlos Cueller, A. Edward Elmendorf, Francoise Decaillet, Edna Jonas,Susan Harmeling, Marilyn Lauglo, Charlotte Leighton, Susannah Mayhew, JulieMcLaughlin, Thomas Merrick, Marc Mitchell, Mary Paterson, Pamela Putney, BenitoReverente, Awadu Tinorgah, and Caroline Zwicker
World Bank Institute
Copyright C 2000The International Bank for Reconstructionand Development/The World Bank1818 H Street, N.W.Washington, D.C. 20433, U.S.A.
First printing May 2000
The World Bank enjoys copyright under protocol 2 of the Universal Copyright Convention. Thismaterial may nonetheless be copied for research, educational, or scholarly purposes only in themember countries of The World Bank. Material in this series is subject to revision. The findings,interpretations, and conclusions expressed in this document are entirely those of the author(s)and should not be attributed in any manner to the World Bank, to its affiliated organizations, orthe members of its Board of Executive Directors or the countries they represent.
Stock Number: 37159
Abstract
In 1999, the World Bank Institute (WBI) launched a major learning program for Bankclient countries and Bank staff on "Population, Reproductive Health and Health SectorReform". It aims to complement the Bank's extensive lending activities for populationand reproductive health (about $500 million annually) by providing information aboutoptions, interventions and best practices to advance the reproductive health agenda incountries undergoing reform.
An important part of the learning program is to identify sector-wide changes in healthsystems that are required to combat deeply entrenched, systemic performance problemsthat currently undermine desired reproductive health outcomes. This is a dauntingchallenge especially for those who have been associated with more narrowly managedfamily planning and reproductive health projects, and must now champion the integrationof population and reproductive health concerns in overall health sector development. Todo so, new skills will be required including knowledge about how different forms offinancing, provider payments, organizational arrangements, regulation, and ways ofpromoting healthy behaviors can be brought to bear to improve reproductive health.
Acknowledging the immense challenge ahead, this paper does not pretend to offer anexhaustive review of all problems involved or ways of dealing with them. Its purposerather is to:
* explain why health sector reform prevails in many countries and why reproductivehealth advocates cannot ignore it;
n propose a diagnostic approach for 'thinking about' reproductive health that linksundesirable outcomes to their causes, as well as five categories of health reforminterventions or "levers" than can be employed to remedy them;
* illustrate the application of the reforrn categories or "levers" in countries where aconcerted effort is underway to improve reproductive health outcomes; and
* contribute to a common language and understanding of reform options that can helpempower advocates of reproductive health in their dialogue and negotiations withMinistries of Health, Ministries of Finance, and the international donor community.
iii
Contents
Part I: Linking Reproductive Health and Health Reform IIntroduction IWhy is Health Sector Reform Important for Reproductive Health? 3Motivations for Health Sector Reform 5A Diagnostic Approach to Using Health Sector Reform to Improve
Reproductive Health 12The Five Reform Levers 14
Scope of the Reform Levers 15Financing and Resource Allocation 16Provider Payments, Incentives and Motivation 19Organizational Change 24Regulation 30Promoting Healthy Behaviors 35
Combining the Five Reform Levers 38
Part II: Country Level Examples 39
Reforms in Different Types of Health Systems 39Trends in Public Sector Reform 41
New Public Management 41
Ghana 45Background to Reform 45
The Reform Levers 47
Lessons Learned 50Trends in Public/Private Service Delivery Models 51Egypt 52
Background to Reform 52
The Reform Levers 53
Lessons Learned 57Trends in Private Service Delivery Model 58Bolivia 59
Background to Reform 59
The Reform Levers 60
Lessons Learned 64Philippines 64
Background to Reform 64
The Reform Levers 65
Lessons Learned 70
Conclusion 70

Part I: Linking Reproductive Health and Health Reform
"Reproductive health is a state of complete physical, mental andsocial well-being and not merely the absence of disease orinfirmity, in all matters relating to the reproductive system and toits functions and processes. Reproductive health thereforeimplies that people are able to have a satisfying and safe sex lifeand that they have the capability to reproduce and the freedom todecide if, when and how often to do so. Implicit in this lastcondition are the right of men and women to be informed and tohave access to safe, effective, affordable and acceptable methodsof family planning of their choice, as well as other methods oftheir choice for the regulation of fertility which are not againstthe law, and the right of access to appropriate health careservices that will enable women to go safely through pregnancyand childbirth and provide couples with the best chance ofhaving a healthy infant. In line with the above definition ofreproductive health, reproductive health care is defined as theconstellation of methods, techniques and services that contributeto reproductive health and well-being by preventing and solvingreproductive health problems. It also includes sexual health, thepurpose of which is the enhancement of life and personalrelations, and not merely counseling and care related toreproduction and sexually transmitted diseases."
(ICPD Programme of Action, Paragraph 7.2 )i
Introduction
The ICPD agenda poses a formidable challenge to those concerned with population andreproductive health because it reaches far beyond the scope of traditional projects toembrace entire national health systems, as well as other sectors that have significantimpacts on health. It calls for a more comprehensive and integrated approach toreproductive health and principles of equity, with the implication that allstakeholders-government, NGOs, other private sector actors, and households-need tobe engaged to achieve the vision.
There is growing recognition that implementation of ICPD recommendations and thereproductive health approach already is (in some cases) and needs to be (in other cases)grounded in a broader context of health sector reform efforts that are simultaneouslytaking place in many developing countries. Health sector reform can be described assustained purposeful change to improve the performance of the health sector. It is aninherently political process, initiated by public or political action, motivated bydissatisfaction caused by the failure to deliver outcomes deemed important by society andimplemented on a sector wide level.
The ICPD was held in Cairo, Egypt in 1994. 178 countries have adopted the Programme of Action of theICPD, or what is commonly referred to as the "Cairo Agenda".
I
The process of health reform significantly alters the ways in which health services arefinanced and delivered; this in turn largely determines the extent and way in whichreproductive health care is financed and delivered. In some countries, reproductive healthand health sector reform efforts are complementary and compatible. In other countries,there are conflicts between the goals and means of health sector reform and those ofreproductive health.
Compared to concerns about equity, quality or accountability, many on-going healthreform efforts are primarily implemented in response to resource constraints as well aswidespread perceptions that available resources are being used inefficiently. Addressingall of the many reproductive health conditions and providing better and morereproductive health services to all men and women is a difficult - if not impossible - taskfor an already financially strapped health system. The reproductive health approachexplicitly puts rights, equity, and empowerment as key goals; health reform efforts insome countries may not. In these instances, health reforms may be both incompatiblewith reproductive health goals/values and inconsistent with a particular society's viewsand values.
In other cases, health reforms may be consistent with societal values that reproductivehealth advocates would argue need to be changed.2 Badly designed, poorly implementedand rigid health reform efforts that are not evaluated and adjusted in light of whether theyare achieving positive intended effects or resulting in unintended negative consequencesare not successful from any perspective -- whether one is primarily interested in healthsector reform or reproductive health. Deciding upon the goals and strategies of healthsector reformn and reproductive health which balance goals of quality, equity, andaccountability with efficiency concerns and effectively implementing these interventionsare major challenges for both reproductive health advocates and health sector reformers.
Clearly, to effectively advance the reproductive health agenda, one needs at least a basicunderstanding of the motivations behind and the building blocks of health sector reform.This paper is designed to assist in building that knowledge base. It is not intended to bean exhaustive review of health reform, rather it is an attempt to demystify some of themain concepts and techniques of health reform for those with a background inreproductive health. Our objective is not simply to argue that health reforn is importantfor reproductive health. It is also to illustrate how health reform can be used to tackleobstacles that undermine the capacity of health systems to deliver good qualityreproductive health services in an efficient, equitable and sustainable manner.
In Section I of this paper, we present a rationale for why health reform is important forthose involved in reproductive health efforts, a review and discussion of the motivationsfor health sector reform, and a diagnostic approach for using health reform to improvereproductive health. In Section II, we examine how health reform is being implementedin three countries-Ghana, Egypt and the Philippines-to make improvements in healthin general, and in reproductive health in particular.
2 Many individuals involved in health sector reform would be in agreement with reproductive healthadvocates and make the same arguments that certain societal values need to be change, but either they werenot involved in the reform decisions or they were overruled.
2
Why is Health Sector Reform Important for Reproductive Health?
Why should reproductive health advocates care about health sector reform? Can and dohealth sector reform efforts help reproductive health efforts? If so, how? What doreproductive health advocates lose by ignoring or fighting against health reform efforts?What do they gain by a better understanding of reform efforts taking place on the groundor active participation in health reform? These are critical questions which set the stagefor a closer look at the motivations for health sector reform, areas of compatibility withreproductive health goals, and means of harnessing reform options to advance thereproductive health agenda.
Perhaps the main reason that health reform is important for reproductive health is thatdeficiencies that characterize the financing and provision of reproductive healthservices are closely linked to those that characterize health services in general andtend to be system wide. Recognition of this problem in the past often resulted in theestablishment of vertical programs that by-passed inefficiencies in national healthsystems by creating more efficient, donor-funded parallel systems. A foundation stone ofthe Cairo Conference and ICPD + 5 is that commitments to revitalizing national systemsof health care must include a more integrated approach to the delivery of population andreproductive health services in well functioning national health systems. This implies theneed to resolve deficiencies that characterize system-wide financing and provision ofhealth services in general, and reproductive health care more specifically.
Another fundamental reason that health reform is critical to reproductive health is thatthe Cairo agenda cannot be effectively implemented without the existence of well-functioning services at several levels of the health system and beyond. Consider, forexample, one of the conditions that appears on nearly every country's list of majorreproductive health problems-high levels of maternal mortality. It is clear that broaderhealth sector capacities need to be engaged to effectively deal with maternal deaths and todeliver appropriate services. In order to remedy the most direct causes of maternal deathsin developing countries-hemorrhage, sepsis, obstructed labor, eclampsia, and theconsequences of unsafe abortions-a country must have an effective system for handlingobstetric emergencies. It is impossible to effectively manage obstetrical emergencieswithout: 1) improving the quality of care provided in secondary and tertiary care(hospital) facilities as well as primary care facilities; and 2) insuring a functioningreferral and transport (emergency evacuation) system. This latter requirement in itselfrequires an effective communication between different levels of the health system as wellas effective communication and understanding of needs and capacities between thecommunity and the health system.
The centrality of improving the quality of care as well as communications and referrals inefforts to reduce maternal mortality ratios is illustrated in Grenada. Training anddelegation of additional obstetric responsibilities to nurse-midwives, complemented withimprovements in interactions and telephone communication between levels of the healthcare system were essential to bring the maternal mortality ratio by half, to levels of 120
3
deaths per 1 00,000 live births by the early 1 990s. 3 In Matlab, Bangladesh a program thattrained midwives, posted them in remote health centers near the population to assist inhome births and supported referrals to a higher level maternity center from the trainedmidwives in cases of obstetrical complications reduced the maternal mortality ratio by68% in only 3 years. An evaluation of EOC pilot programs in Mali, Burkina Faso,Senegal and Benin found that the most successful approaches to reducing maternalmortality: 1) improved the technical quality of care at both the health center and referencelevels, 2) established and maintained an effective referral and transport system, 3)improved physical access to services, 4) lowered the costs to the population due todeliberate cost sharing mechanisms, 5) improved collaboration between clients and healthcenter personnel, 6) involved strong community participation and community inclusion indecision making and problem solving at the health facility,5'
These causal factors that together influence the magnitude of maternal deaths cannot beremedied by making small changes 'at the margin' of the health system. Instead, theyrequire major changes in the way health services are financed and delivered, often increative, new ways.
A third reason that health reform is critical to reproductive health and vice versa is thathealth reform and reproductive health advocates share common concerns. The mostobvious of these is Cairo's concern for equity and client empowerment. The language ofICPD and country implementation since 1994 refers to reproductive health as conditionsand interventions, but also as an approach:
"Reproductive health is also an approach. When we use the language of ICPD,we talk about health needs, but we also talk about rights, equity, dignity,empowerment, self-determination and responsibility in relationships.Reproductive health is an approach to analyzing and then respondingcomprehensively to the needs of women and men in their sexual relationshipsand reproduction." (ICPD +5, WHO, 1999)
The reproductive health approach represents a major paradigm shift from previousthinking on population and development. While the commitment to slowing populationgrowth as a goal remains, there has been a significant shift in the strategies to achieve thisgoal - an emphasis on meeting the needs of individual women and men rather than onachieving demographic targets. This emphasis is clearly consistent with the ultimategoals and strategies of health systems and health reform; in fact, it fits much better than amore narrowly focused "demographic targets approach". The results of a health systemand health sector reform are ideally measured in terms of health and reproductive healthoutcomes such as morbidity, mortality and malnutrition, client measures of quality, and abalance of equity and efficiency concerns.
3Laukeran V and Bahattacharya A Maternity Care in Grenada, West Indies: A Comprehensive Study.Paper presented at the 1 8 th Annual NCIH Conference, Arlington, VA, 1991 in Timyan J et al, 1993.4Faveau V, Stewart K, khan SA, Chakraborty J Effect on mortality of community-based maternity careprogramme in rural Bangladesh. Lancet 338: 1183-1186, 1991.
Sall,F and Krasovec K Cost and Financing of Projects to Improve Essential Obstetrical Care in 4 West
African Countries, in press.
4

Since the reproductive health approach is a move away from demographic targets tomeeting the reproductive health needs of individual women and men, it would seempreferable to defend certain reproductive health priorities in equity terms, such asdecreasing unmet need for contraceptives or other reproductive health services in pooreror under-served households or for adolescents, than in termns of declines in fertility rates -AND this equity argument is likely to carry more weight with those designing andimplementing health reform. Furthermnore, by insisting that the range of reproductivehealth services is provided through the primary health care system, reproductive healthefforts are deliberately linked with efforts to improve the health system in general, whichis also consistent with health sector reform goals.
A final reason that health sector reform is important for reproductive health advocates is apractical one. Simply put,,health sector reform is happening and the most powerfulstakeholders in health systems are involved. Policy makers and implementersconcerned with reproductive health need to take part in diagnosing system-wideproblems and selecting among competing strategic options if they want topreserve/achieve reproductive health goals. Moreover, those implementing healthsector reform may not have a good understanding of reproductive health needs or howhealth sector reform efforts might unintentionally hinder reproductive health goals. Thismight happen, for example, where health sector reform is inappropriately tipping thebalance too far away from quality and equity of reproductive health services in efforts toincrease overall efficiencies. Health sector reform can have both positive or negativeimpacts on reproductive health, whether deliberately or not. Provisions will, therefore, beneeded in health sector reform to protect reproductive health goals and reproductivehealth proponents will need to become effective advocates for these goals. In order to doso, reproductive health people need to understand and learn the language of health sectorreform and how to use these tools to effectively to achieve reproductive health goals.6
Motivations for Health Sector Reform
Health sector reform is motivated by the need to address fundamental deficiencies inhealth care systems that affect all health care services, including reproductive healthservices. The most common reasons for developing countries to undertake significanthealth sector reform efforts are to address the problems of:
* poor quality of care,* inequities and limited access to health services,* insufficient funding for health,* inefficiencies in delivery of services,* lack of accountability, and/or* insufficient responsiveness to client needs.
6 An important distinction needs to be made between 1) protecting reproductive health GOALS orSERVICES and 2) protecting vertical reproductive health PROGRAMS. Health reform efforts can and
should be helpful in the former, but not the latter.
5
Reform tends to be contentious and difficult because (i) systemic deficiencies are oftendeeply entrenched, with historical and political underpinnings, (ii) some groups in societywill invariably resist change, and (iii) to be successful, health reform efforts usually needseek to tackle some combination of these deficiencies simultaneously.
A fundamental motivating factor for health reform in most developing countries is toimprove the quality of health care outcomes provided by the health system. Most healthsector managers, providers and patients would agree that providing good quality care isan essential, if not THE essential, role of the health system. However, not all would agreeon just what constitutes good quality care. In addition, not all would agree on whosepoint of view -- patients or providers (technicians) -- is most important in assessingquality when market failures such as asymmetries of information between provider andclient are involved.
The determination of what constitutes good quality health care is difficult and has beenthe subject of much research and programmatic effort. Research and evaluations ofquality of health care in the US, other industrialized countries and, increasingly,developing countries is inspired by and based on the extensive work of ArvedisDonabedian, who created the structure - process - outcome framework for describing andevaluating quality of care in the health field. Donabedian defines quality of care as "thatkind of care which is expected to maximize an inclusive measure of patient welfare, afterone has taken account of the balance of expected gains and losses that attend the processof care in all its parts."'
In the Donabedian framework, quality improvements are contingent on 'structure','process' and 'outcome':
* structure refers to all aspects of the health system that support the patient-healthsystem interaction (among others, this includes things like facilities, personnel,training, commodities, equipment, management and supervision);
* process refers to all that happens during the patient-health system interaction(including technical and interpersonal aspects of the patient-provider interaction andother aspects of the service delivery setting that directly impact the patient, such ascheck-in, patient flow, handling confidentiality or privacy concerns, referrals, IEC,etc.); and
* outcome refers to changes in health status (morbidity, mortality, malnutrition, casefatality) as well as patient variables (perceptions of and satisfaction with health care,health-related knowledge acquired and behavior change) that can be attributed to thehealth care that the patient received. Outcomes of the health system are influenced byprocesses, which themselves are the results of structure - two key points are that theprocess of care is critical in determining outcomes, and that structure can onlyinfluence outcomes by changing process, not directly.
7Donabedian, 1980.
6
Determining and improving essential or minimal elements of structure has been thetraditional focus of most quality of care work in health in developing countnres. Yet, asimportant and necessary as structural elements of quality are, they do not automaticallylead to better process quality or, in turn, higher quality outcomes. Thus, quality of careefforts that have focused exclusively on structure can only be expected to "go so far" inimproving health care processes and subsequently, health outcomes.8 Determining andimproving essential elements of process aspects of quality are much more difficult,particularly since both medicine and management of medical care are both as much art asscience.
On the other hand, most health professionals and patients can come to some sort ofagreement on what good quality outcomes of a health system are - less morbidity, lessmortality, less malnutrition, lower case fatality; more satisfied, more knowledgeable andbetter behaved patients (who follow prescnrption and medical advice to the letter, andpractice better life-style habits, more exercise (or reduced workloads in the case of under-nourished pregnant women), better nutritional practices, use of preventive care serviceslike antenatal care, family planning, immunizations, STI prevention, less abuse of alcoholand other drugs, less smoking or exposure to household smoke).
Limitations of focusing on structure or process aspects of quality as a way of improvingperformance have prompted greater use of outcome aspects of quality to monitor andevaluate quality of health care .9 The challenge for health reform efforts is to determineand manipulate the mix of major levers of health reform (financing, organization,provider motivation, regulation and promotion of healthy behaviors) that most effectivelyand efficiently influence improvements in the process of health care and, in turn, healthoutcomes. These levers are examined in more detail in the next Section.
A second important reason for health reform in many countries is to make the health caresystem more equitable in the form of access to care as well as financing and funding ofcare. In health care, under-served population groups are often defined by income (e.g.poor), socio-economic status (e.g. less educated), age (e.g. adolescents), ethnicity (e.g.minority groups) or gender (e.g. females, young girls). Although equity in health may bedefined as equity of health status (self or professionally assessed) or equity of access,most health sector reforns are concerned with equity in terms of equity of access tohealth care.
Access itself has physical, economic and cultural dimensions.10 Physical access refers tothe availability of or distance away from health facilities, specific services or providers.Some common indicators used to measure physical access include: percentage of the
8A caveat to this argument is that certain minimal elements of quality are necessary to providing healthcare and do not universally exist in many developing country settings. These include: availability of drugs,essential obstetric care, etc. For example, providing drugs to primary care facilities has been shown to be anecessary, if not sufficient, element of quality improvement, as well important as a patient perception of agood quality outcomes. (Health Policy and Planning, Vol. 10 No.3, Special Issue: Improving quality, equityand access to health services through health financing reform in Africa, September 1995).9 Grundmann, C, The Association between Structure, Process and Outcome in the Rwandan Public HealthCare System. PhD Thesis, Johns Hopkins University School of Hygiene and Public Health, May 1997.10 Knowles, J, Leighton C and Stinson, W Measuring Results of HSR for Systems Performance: AHandbook of Indicators, PHR: Special Initiatives Report No. 1, September 1997.
7
population residing within 3-5 kilometers of a primary care health facility (or 10-15kilometers from a hospital), percent of the population residing within 30 minutes of ahospital that provides 24 hour EOC care, or population per doctor.
Economic or financial access refers to factors related to the cost of seeking care,obtaining care and following through with treatment. Economic access includestransportation costs, direct fees paid for care at health facilities, and medications andother consumables. It is important to note that for poor populations in many developingcountries, the cost of medicines and transportation often account for the majority of thetotal cost for health care, compared to direct fees for services. Common indicators ofeconomic access include: average cost of an outpatient illness episode, average cost of ahospital stay, average fee paid per outpatient visit, or average cost per day ofhospitalization.
Economic costs of health care that people face can lead to inappropriate and sometimesdangerous health practices, particularly for the poor. There are many examples ofcountries where it is common practice for the poor, when they are ill, to bypass treatmentor prescription from a medical provider/facility to avoid paying direct fees and transportcosts and go directly to pharmacies for medications. In other cases, poor, sick individualswill seek medical care but then only partially fill prescriptions for medicines. In bothcases, the poor cannot afford both medical care and medicines, so they choose one or partof one over the other. In worse case scenarios, the poor or certain subgroups, like womenwho may have less access to household financial resources, forgo care completely.
Because of equity concerns, indicators of economic access are often measured andreported in relation to individual or household income. Common discussions about"willingness and ability" of patients to pay for a particular health service are goodexamples of this approach. Some economists, most notably the Nobel laureate Sen, insistthat the economic impact of health care or health reforms be evaluated not only inrelation to client or household income, but also in relation to individual or householdspending patterns (how and what people spend their money on, social choice).' l
Cultural dimensions of access are most easily thought of as social or cultural barriers thatinhibit utilization of health services. Cultural barriers may include such things as:inappropriate gender, age, ethnicity, social class or language competencies of healthproviders in general or providers of specific services; health care service hours that arenot convenient for the population or subgroups of the population; not allowing relativesor culturally appropriate "helpers" to accompany inpatients or women in labor to healthservices; or special treatment (hours, entrances, etc.) for sensitive services or subgroupsof the population.
In some cases, offering all services at all hours is more culturally appropriate thanseparate service hours for sensitive services, such as family planning or STD services,and leads to increased access for sensitive groups. PROSALUD (a not-for profit privateservice provider) services in Bolivia, for example, are specifically organized so thatpatients can receive a variety of adult and pediatric curative and preventive services
Sen, A. NIH Lecture, June 1999.
8
during clinic hours, so that it is impossible for any waiting patients to know what servicesother patients are waiting for.'2
Ensuring equity by reducing physical barriers to access might mean, for example, thatmore providers who can insert IUDs need to be assigned to rural health clinics, but not tourban areas where households already live within close proximity to providers who canprovide this service.
Ensuring equity by reducing economic access barriers may mean that fees for specifichospital services are lower for women than for men (even in households which do notmeet income cutoffs), since women may not have access to enough household resourcesto cover the total cost of fees, transportation and medicines.
Ensuring equity by reducing cultural barriers may also mean that female health providersmust be available to clients so as not to discourage use of certain reproductive healthservices or components of services (i.e. pelvic exams). It may also mean that partners andfamily members are encouraged to be with women during labor and birth and that babiesare kept with their mothers, in the same bed. after delivery.
A third reason for health sector reform is insufficient funding. Insufficient funding forhealth services is a nearly universal problem in developing (and developed) countries.Historically, the public health sector in most countries has not been particularlysuccessful in competing with other sectors for scarce government resources. In manylower income countries, the percentage of government revenue that has gone intofinancing health care has declined since the early 1980's.'3
In some countries, like Indonesia, Mexico and Tanzania, economic upheavals haveresulted in significant reductions in government tax revenues, and subsequently forMinistry of Finance allocations to the Ministry of Health.'4 Moreover, new demands arebeing placed on the limited resources of the health sector:
* the population continues to increase, which means that the health system has to meetthe needs of additional clients with fewer resources;
* with increased communications and educational levels, expectations and demand forhealth care on the part of developing country populations are also increasing;
* competing challenges posed by the changing epidemiological profile of developingcountries - rising levels of (expensive to treat) chronic diseases in primarily urbanpopulations on the one hand, and continued high levels of infectious disease relatedmorbidity and mortality in the primarily rural populations on the other hand.Together, this results in even greater demands on old and still necessary types of careby less politically powerful and more vulnerable groups (who governments aresupposed to protect) and very vocal demands for new kinds of health care to meet thechanging health needs of more politically powerful groups.
12 Putney, Pamela and Carlos Cuellar, Expanding Women's Access to Health Services in Bolivia, A CaseStudy of PROSALUD, Draft report to the World Bank, 1999.1 Hsiao, 1995.14 Forman, Shepard and Romita Ghosh. The Reproductive Health Approach to Population andDevelopment, 1999.
9
Funds for health care can be mobilized through four main sources: direct governmentfinancing, donor financing, private user charges and third party payments (healthinsurance, community financing or mutuelle schemes). Some analysts reduce thesesources into 3 categories, by combining donor and government financing as a singlesource since, in most instances, donor financing either flows through government coffersor is included in government budget and expenditure reports.'5
In the last decade, faced with decreases in both direct government financing and reduceddonor assistance, many developing countries have attempted to raise additional funds forhealth by instituting private user charges, cost-sharing or user fees for services that hadpreviously been provided free of charge by public sector health facilities. User feestrategies have been employed fairly extensively throughout the developing world. Feesfor hospital inpatient services have been on the books for a long time in most developingcountries; "newer" user fee initiatives have applied fees to primary health care services.Experience shows, however, that user fees (for primary care) cannot be counted on as theprimary solution to make up for funding shortfalls for the health sector. A review of userfees in Africa revealed that, on average, user fees in poor countries only covered 10 to
1 615% of total recurrent costs of publicly operated facilities
However, even if user fees cannot be expected to be a major source of revenue for theoverall health system in developing countries, this does not mean that user fees arewithout merit. Fees often provide 60% or more of non-personnel recurrent costs inprimary health care facilities. Fees have been shown to be useful in improving somestructural aspects of quality (drug availability, financial book-keeping) at primary carefacilities. They can also be useful in improving patient perceptions of care (an outcomeaspect of quality) or providing financial incentives to health workers when fees werereserved for use at the facility where the fees were collected. These improvements areimportant in financially strapped systems, particularly since very small levels ofunrestricted revenue can go a long way in primary care facilities, where directgovernment resources are scarce. Moreover, without user fees, many NGO providers, aswell as private providers, would not be able to sustain themselves, thus forcinggovernment to satisfy all health needs and demands.
The important point to stress is that since the simple user fee structures used in mostdeveloping countries are inherently regressive, efforts to ensure that the poor or othervulnerable groups are protected should be implemented in conjunction with user feesystems. This is an illustration of how efforts to remedy the problem of insufficient
funding in many countries need to be closely linked to efforts to ensure equity. Thistension in user fee systems has also led many countries to begin to experiment withprepayment or insurance reforms (which require their own different mechanisms tosubsidize or protect the poor.)
A fourth motivating factor for health sector reform is to decrease current inefficiencies inthe current health financing or delivery system. Improving efficiency is an important way
15 Dunlop and Martins, World Bank, EDI, 1995.16 Shaw and Ainsworth, 1995.
10
to maximize scarce resources and one that is more directly under the control of healthmanagers. Efficiency is the concept of getting "the most bang for your buck", getting agood rate of return on your investment and expenditures, or making the most out of yourinputs or resources; be they human, financial or material (equipment and supplies), whileat the same time ensuring quality.'7
Efficiency is often discussed in terms of the use of funds or inputs, but also in terms ofthe use of services by clients. A compelling example of this is provided in a World Bankstudy, Better Health in Africa, where it is claimed that for every $100 spent by the publicsector on drugs, 80% is lost due to inefficiency and waste-through inadequate buyingpractices (10%), procurement and quantification problems (41%), inefficient distribution(10%), irrational prescription (15%), and non-compliance by patients in taking the drugsproperly (3%). 18
In quality of care termns, efficiency refers to the patient-health system interaction(process) using the available structure in such as way as to maximize quality outcomes. Itis important to recognize that efficiency and quality should not be treated separately sinceefficient, poor quality health care is never a desirable outcome of a health system.
Some common complaints of inefficiencies in health systems are: "too much money isbeing spent on hospitals, rather than primary care;" "public funds are being spent oninappropriate or cost-ineffective services;" "too much of the health care budget is spenton salaries, compared to operating costs;" "too much of the health budget is spent at thecentral or regional level, not at the periphery and not on service delivery;" "maternitywards in large referral hospitals are overcrowded, women are delivering in the hallways;"and/or "maternity wards in district hospitals or health centers are underutilized; midwivesor doctors only deliver 1 baby per week." Some common solutions employed with thegoal of making health services more efficient are: designing and delivering of essentialpackages of services which are based primarily on cost-effectiveness considerations orintegration of various health services (MCH and FP, FP and STI services) at a specificservice delivery point (health center or hospital).
Finally, an increasingly explicit motivating factor for many health reform efforts is toincrease accountability of the health sector (providers) to the client and otherstakeholders. Accountability takes many forms; in some countries the concern isprimarily for greater accountability in terms of providing good quality care as judged byhealth professionals, in others it is accountability for responding to client needs, in stillothers it is primarily accountability for use of funds or to reduce levels of corruption.Integration of services is also often cited as a way for health services to better respond toclient needs, by instituting "one stop shopping," making it easier for clients to accessmultiple health services for themselves or for multiple family members (usually a motherand her young child or children) at a single health facility visit. Decentralization isanother form of organizational change that is often instigated on the assumption thatdecentralized services are inherently more accountable to local populations, although this
17 For a more detailed discussion of the concepts of technical, economic and allocative efficiency, seeBehrman, Jere and James Knowles, Population and Reproductive Health: An Economnic Framework forPolicy Evaluation, Pop and Dev Review 24 (4), December 1998., World Bank, 1994, Better Health in Africa, (Washington DC: World Bank)
* S~~~II

is not automatic and there is little empirical evidence to suggest that decentralization, initself, leads to increased accountability.
Lack of responsiveness to client needs (in terms of what services are provided, how theyare provided and at what cost) is sometimes referred to as lack of client empowerment.People are willing to and do spend their own money for privately provided health care,whether through direct fees for service, under-the-table payments, for medicines andsupplies, or through traditional or modern/formal system. Out of pocket expenditures byindividuals and families account for greater than 50% of health care funding in mostcountries, even poor countries.19 Enhancing people's ability to "vote with their feet" byintroducing different forms of provider payments, such as capitation (discussed later), isan important method of client empowerment that is emerging in many reforns.
A Diagnostic Approach to Using Health Sector Reform to Improve ReproductiveHealth
At this juncture, it is useful to introduce a diagnostic framework to clarify relationshipsbetween desired reproductive health outcomes, motivations for health sector reform, andpolicy levers that are available to bring about change. This is presented in Figure 1.2°For reasons explained in the balance of this paper, we believe that the components ofFigure 1 provide a useful way of thinking about (i) linkages between reproductive healthand health sector reform, as well as (ii) broad, operationally-oriented policy levers thatare available to improve reproductive health outcomes.
The starting point, or initial emphasis in Figure 1, is on OUTCOMES desired by society.This mirrors a shift in emphasis by policy makers and implementers over the last tenyears, from an input-oriented approach to one that stresses improving performnance interms of achieving measurable OUTCOMES. It is no longer sufficient, for example, toclaim that a country's health sector is performing better simply because it has built morehospitals, deployed more personnel (i.e., inputs), increased hospital bed occupancy rates(outputs), or increased dissemination of FP commodities or IEC. Rather, theperformance of health systems is increasingly being judged nationally and internationallyby how well resources are being used to achieve outcomes that impact more directly onthe well-being of households.
In the case of reproductive health, the desirable outcomes might include: low or reducedlevels of maternal mortality (MM), low or reduced levels of infant mortality (IMR), lowor decreasing prevalence of HIV/AIDS in men of reproductive ages, or reduced unmetneed for family planning services. From a reform perspective, it is only when failure toachieve desired outcomes is placed on the 'societal radar map' and stakeholders reachconsensus on their importance that motivation for real reforrn begins to build. In turn, it isonly when improved outcomes are demonstrated that reform efforts are said to enjoy ameasure of success. What is new or different in the sequence of thinking in Figure 1 is
19 NHA documents, Berman, Peter.20 Figure I has been adapted from the diagnostic framework of the World Bank Institute's FlagshipProgram on Health Sector Reform and Sustainable Financing. It has also benefited from contributions byCharlotte Leighton, PHR Project, Abt Associates.
12
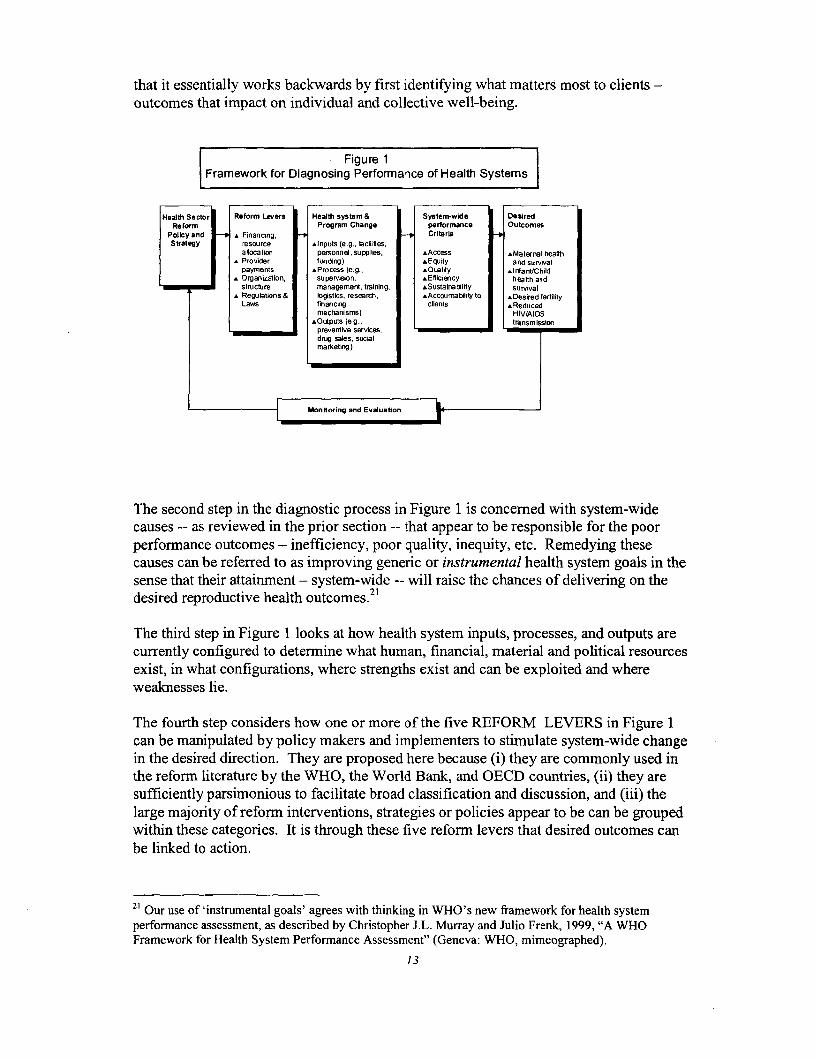
that it essentially works backwards by first identifying what matters most to clients -outcomes that impact on individual and collective well-being.
Figure 1Framework for Diagnosing Performrance of Health Systems
Healh sectorn Reform Levers Healdg system & System1wide DesiredReform a Prograo e Chancqe performance Outco.ies
Policy and be AFinancing, t CritLr n hStrategy arsoutre sInputs (emgi, wcilites,
S allocation personnel, su pp lies, AAccess A Maternal heafthrProed ider fund ng) Equity and surival
S payments sProcess (e. D Cualfty .Irant/nChildT A Organ izguron, su peNision, h Eel ici ency heas th and
cu_rently configustructre mai waement, training, aSustancabil,ty survivale Regulat ions & gistics, research, eAccointabilia y to bDesired fertility
Laws financig clients Reducedmechanisms) HIV/AIDS
cltyputs (egr, transmissionin thedesireddirection.Theypreventive services, h br
dnrg sales, socialmarketing)
The second step in the diagnostic process in Figure is concened with system-widecauses -- as reviewed in the prior section -- that appear to be responsible for the poorperforwi ance outcomes - inefficiency, poor quality, inequity, etc. Remedying thesecauses can be referred to as improving generic or insteumental health system goals in thesense that their attai,nent - system-wide -- will raise the chances of delivering on thedesired reproductive health outcomes.2
The third step in Figure m looks at how health system inputs, processes, and outputs arecurrently configured to determine what human, financial, material and political resourcesexist, in what configurations, where strengths exist and can be exploited and whereweaknesses lie.
The fourth step considers how one or more of the five REFORM LEVERS in Figure Ican be manipulated by policy makers and implementers to stimulate system-wide changein the desired direction. They are proposed here because (i) they are commonly used inthe reform literature by the WHO, the World Banlk, and OECD countries, (ii) they aresufficiently parsimonious to facilitate broad classification and discussion, and (iii) thelarge majority of reform interventions, strategies or policies appear to be can be groupedwithin these categories. It is through these five reform levers that desired outcomes canbe linked to action.
21 Our use of 'instrumental goals' agrees with thinking in WHO's new framework for health systemperforrnance assessment, as described by Christopher J.L. Murray and Julio Frenk, 1999, "A WHOFramework for Health System Performance Assessmenf '(Geneva: WHO, mimeographed).
1 3
This diagnostic framework has been developed and discussed widely in the context of theWorld Bank Institute Flagship Program on Health Sector Reform and SustainableFinancing.22 We have found that its appeal to policy makers lies in its action-orientedfocus on change agents or reform levers -- within which policies, strategies, andinterventions can be organized in mutually reinforcing ways. Clearly, this way ofthinking about health sector refonn stands in sharp contrast to discussions of reform inmany developing countries that tend to be more narrowly focused on of 'structuraladjustment', decentralization policies, application of user fees, privatization, etc.
The Five Reform Levers
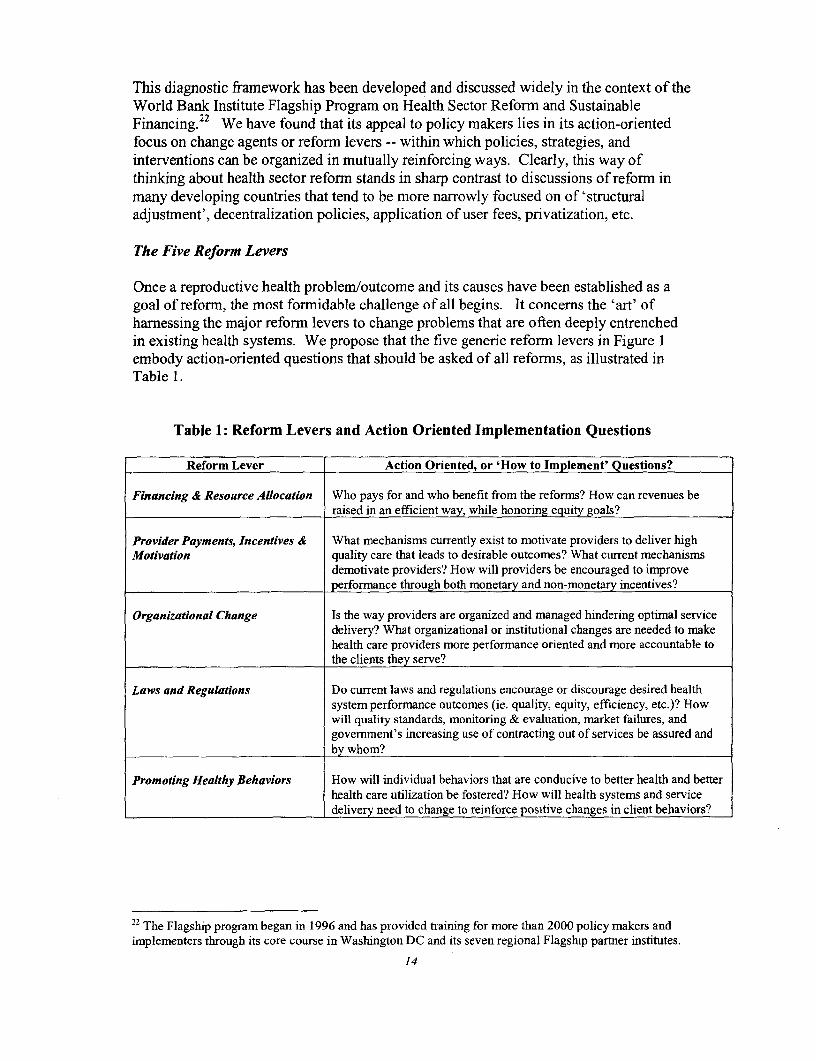
Once a reproductive health problem/outcome and its causes have been established as agoal of reform, the most formidable challenge of all begins. It concerns the 'art' ofharnessing the major reform levers to change problems that are often deeply entrenchedin existing health systems. We propose that the five generic reforrn levers in Figure 1embody action-oriented questions that should be asked of all reforms, as illustrated inTable 1.
Table 1: Reform Levers and Action Oriented Implementation Questions
Reform Lever Action Oriented, or 'How to Implement' Questions?
Financing & Resource Allocation Who pays for and who benefit from the reforns? How can revenues be
raised in an efficient way, while honoring equity goals?
Provider Payments, Incentives & What mechanisms currently exist to motivate providers to deliver highMotivation quality care that leads to desirable outcomes? What current mechanisms
demotivate providers? How will providers be encouraged to improve
performance through both monetary and non-monetary incentives?
Organizational Change Is the way providers are organized and managed hindering optimal service
delivery? What organizational or institutional changes are needed to make
health care providers more perforrance oriented and more accountable to
the clients they serve?
Laws and Regulations Do current laws and regulations encourage or discourage desired healthsystem performance outcomes (ie. quality, equity, efficiency, etc.)? Howwill quality standards, monitoring & evaluation, market failures, and
government's increasing use of contracting out of services be assured and
by whom?
Promoting Healthy Behaviors How will individual behaviors that are conducive to better health and betterhealth care utilization be fostered? How will health systems and service
delivery need to change to reinforce positive changes in client behaviors?
22 The Flagship program began in 1996 and has provided training for more than 2000 policy makers and
implementers through its core course in Washington DC and its seven regional Flagship partner institutes.
14
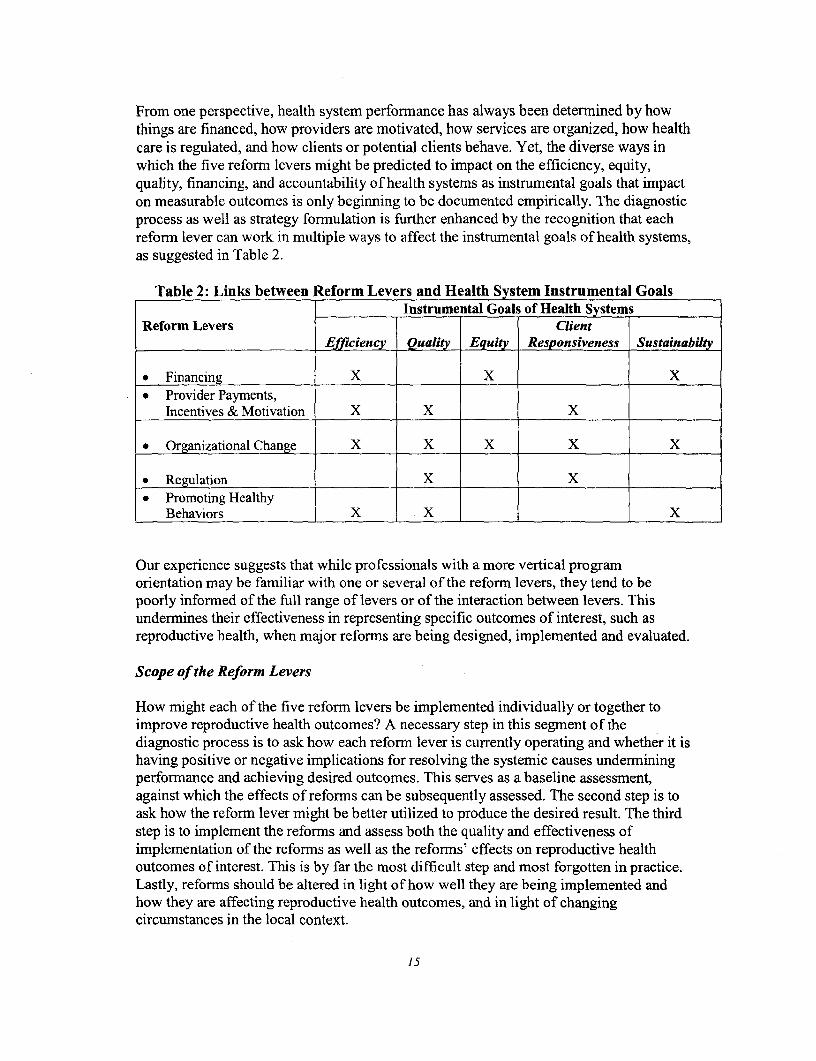
From one perspective, health system perfornance has always been determined by howthings are financed, how providers are motivated, how services are organized, how healthcare is regulated, and how clients or potential clients behave. Yet, the diverse ways inwhich the five reform levers might be predicted to impact on the efficiency, equity,quality, financing, and accountability of health systems as instrumental goals that impacton measurable outcomes is only beginning to be documented empirically. The diagnosticprocess as well as strategy formulation is further enhanced by the recognition that eachreform lever can work in multiple ways to affect the instrumental goals of health systems,as suggested in Table 2.
Table 2: Links between Reform Levers and Health System Instrumental GoalsInstrumental Goals of Health Systems
Reform Levers ClientEfficiency Quality Equity Responsiveness Sustainabilty
* Financing X X X* Provider Payments,
hicentives & Motivation X X X
* Organizational Change X X X X X
* Regulation X X* Promoting Healthy
Behaviors X X x
Our experience suggests that while professionals with a more vertical programorientation may be familiar with one or several of the reform levers, they tend to bepoorly informed of the full range of levers or of the interaction between levers. Thisundermines their effectiveness in representing specific outcomes of interest, such asreproductive health, when major reforms are being designed, implemented and evaluated.
Scope of the Reform Levers
How might each of the five reform levers be implemented individually or together toimprove reproductive health outcomes? A necessary step in this segment of thediagnostic process is to ask how each reform lever is currently operating and whether it ishaving positive or negative implications for resolving the systemic causes underminingperformance and achieving desired outcomes. This serves as a baseline assessment,against which the effects of reforms can be subsequently assessed. The second step is toask how the reform lever might be better utilized to produce the desired result. The thirdstep is to implement the reforms and assess both the quality and effectiveness ofimplementation of the reforms as well as the reforms' effects on reproductive healthoutcomes of interest. This is by far the most difficult step and most forgotten in practice.Lastly, reforms should be altered in light of how well they are being implemented andhow they are affecting reproductive health outcomes, and in light of changingcircumstances in the local context.
15
These steps sound logical and simple in theory, but are rarely simple and straightforwardin practice. Clearly, in the space of this short paper, we cannot possibly conduct anexhaustive treatment of each of these steps. Our aim, rather, is to characterize andillustrate aspects of each of the reform levers, leaving applied analysis and the experienceof real country applications to later sections.
Financing and Resource Allocation
Financing and resource allocation refers to the mechanisms for raising money to supporthealth sector activities or pay for health care. Financing usually tops the list of reformlevers because money is widely perceived to 'make the wheels go round'. Broadly,sources of financing for health and reproductive health come from taxes, social healthinsurance, private insurance, or direct payments to providers - as well as some financingmodalities such as community health financing. Most country's health systems contain amixture of these financing sources, so it is impossible to put a country purely in any onebox.
Commonly cited weaknesses in financing of developing country health systems that mayhinder achievement of reproductive health goals include:2 3
o Financial resources are simply inadequate to enable the public sector to providereproductive health services for everyone in low- and middle-income countries. Allgovernments face tough financing decisions related to the provision of healthservices-what services to finance or provide, to whom, and at what level. Theeconomic crisis affecting many developing countries, economic restructuringaffecting others and severe debt burdens in yet others place substantial constraints onthe public sector's ability to provide current health services, let alone "new"reproductive health services. A review of post ICPD implementation in Bangladesh,Egypt, Indonesia, Mexico, South Africa and Thailand, found that sources and levelsof overall health sector financing were a major concern in all countries.2 4
* Scarce public resources for reproductive health are often allocated in ways thatbenefit relatively rich households more than relatively poor ones: In El Salvador,benefit-incidence analysis reveals that 65% of women using subsidized hospitalbirthing care are from high and middle-income households.25 In Vietnam, the poorest20% of the population receives only 15% of public subsidies for family planningwhereas the richest 20% receives almost 30%.26 In Tanzania, the poorest 20% of thepopulation accounts for only 9% of hospital outpatients and 16% of inpatients,
23 It is important to note that these health system weaknesses are not exclusive to reproductive healthservices, but affect other health interventions as well Thus, tackling these weaknesses should improve thequality of health services in general and improve client satisfaction with health services overall. Irnprovinggeneral health service quality and client satisfaction are ultimately responsive to the ICPD goals and shouldhave the additional benefit of increasing utilization of all services, including reproductive health services.This connment holds for the examples provided here and in the next 3 sections on reform levers.24 Forman, Shepard and Ghosh, Romita, The Reproductive Health Approach to Population andDevelopment, 1999.25 Farrell et al: 199426 Behrman and Knowles: 1998.
16
compared with 37% and 35%, respectively, for the highest expenditure quintile.27 InIndonesia, 54% of high-income households obtain family planning services fromsubsidized sources, along with 80% of low-income households who are intentionallytargeted.
* Cost sharing arrangements are poorly designed or poorly implemented, thusdiscouraging use of reproductive health services or increasing inequities (poor,adolescents, rural areas, etc.). User fees for preventive and primary care often deteruse of services by those needing them most, whereas more desirable prepayment andother community risk pooling schemes remain underdeveloped, especially in lowincome countries in Africa and South Asia.
* Risk sharing arrangements are inadequately developed to the extent that poorhouseholds risk huge financial loss at times of serious reproductive healthcomplications. In China, for example, approximately one-third of all households gointo debt due to the need to pay for expensive curative care at times of serious illnessor injury. In some cases, it takes decades to pay off the debt.
According to two World Bank studies - the 1993 World Development Report and BetterHealth in Africa-about $12 per person per year is required to provide an essentialpackage of health services to the poor in less developed countries, of which about $6.75is directly or indirectly related to reproductive health.28 The good news is that theseamounts need not be prohibitive for most countries, assuming that governments targetscarce public revenues effectively towards the poor, and service needs can be jointlyfinanced from both public and private sources. That is, total revenues for health in lowincome countries that represented 3.5 billion people were about $20, on average--$7 percapita from public sources and $13 per capita from private sources.29
What are the prevailing patterns of resource allocation in developing countries? In mostcountries, scarce public funds are seldom targeted effectively to help those suffering mostfrom poor reproductive health, and/or those least able to afford care. In addition, largeshares of resources have traditionally gone to 'bricks and mortar' projects, resulting inconcentrations of spending at secondary and tertiary level hospitals in and around largeurban areas, rather than on preventive and primary health services in and around ruralareas where the majority of the population lives. Crude estimates of these concentrationssuggest that 70-85% of all health spending in low and middle-income countries goes tocurative level care, 10-20% to preventive level care, and 5-10% to community level care.
Weak government revenues can be expected to prevail in many poor countries becausetheir tax base is comprised of a large share of relatively low income, rural and/oragricultural households where systems of collecting taxes tend to be inefficient andunderdeveloped. This underscores the importance of stimulating new forms ofcollaborative financing involving both public and private collaboration and cost-sharing.Such forms will include a mixture of government revenues from general revenue taxes(income, import/export, sales taxes), social insurance revenues from earmarked
27 Shaw and Griffin: 1995.28 World Bank, World Development Report 'Investing in Health' 1993. World Bank, Better Health inAfrica, 1994.29 ICPD +5, WHO, 1999.
17
employer/employee taxes, out-of-pocket payments or user fees, community health funds,and donor contributions. Without such collaboration, or without massive infusions ofdonor aid (which is unlikely), it is difficult to imagine how 2.4 billion of the world'spopulation in relatively poor countries will ever enjoy equitable access to reproductivehealth services.
How might the financing reform lever work better to advance the reproductive healthagenda in developing countries? Examples include:
* Public health expenditures by governments and multiple donors might be bettercoordinated, combined and allocated to finance an affordable, basic set of services,and sustain the delivery of the set of services to low income households in both ruraland urban areas?30 The 'sector wide approaches' underway in Bangladesh, Pakistan,Ghana and Zambia provide examples. Sector wide approaches aim to reduce technicalinefficiencies and costs associated with multiple, parallel projects and activities, andto better target scarce public funds to subsidize provision of a basic package ofreproductive health and other services.
* Government can play a more active role in stimulating public-private collaboration toincrease both financing and provision of reproductive health services. In manycountries, representatives of NGO church or 'mission' health facilities are excludedfrom or marginalized in MOH policy formulation, planning, and donor meetings,even though these NGOs may play an important role in providing specificreproductive health services, general health services to specific geographical areas orhealth and reproductive health services to the poor. An exception to this rule is foundin Malawi, where the government works closely with the Christian Health MedicalAssociation (CHAM), subsidizing about 15% of the recurrent costs of the missionfacilities (NGOs) in return for collaborating in providing a range of FP services andIEC. Indonesia provides another example where the government provides support forprivate health insurance that includes coverage for FP.
a Government revenues can be complemented by other earmarked sources of funds forhealth, such as social health insurance, to finance a benefit package of services thatfeature reproductive health services. Egypt provides an example as it aims to poolcontributions from social health insurance funds with government revenues to providea benefit package to households in Alexandria. This is described in more detail in PartII of this paper.
* Government can allocate revenues in ways that correct gender imbalances in access toservices, such as in Bolivia, where local governments are required to use 6% of thefederal tax dollars they receive to support a maternal and child health 'insurancefund' that provides basic entitlements to primary and curative care.
* Governments under tight resource constraints and deficit financing can encourageforms of cost sharing that are more sensitive to the needs and capacities of the poor topay. Tanzania provides an example in its Community Health Fund in Igunga District
30 Note: In many contexts the "set of services" we are referring to may be called a "package" of services.
18
where cost-sharing by households combines with government subsidies to sustain ahealth card that entitles households to basic reproductive health and other health careservices at rural health centers. Piloting of the scheme in a poor rural district, Igunga,has fired enthusiasm country-wide to the extent that expansion is now taking place inan adjacent six districts. In Kolokani, Mali, an emergency referral and evacuationsystem for obstetric care has been set up with 1/3 financing from the district level, 1/3from the community, and 1/3 from evacuees who pay user fees.3 1 In Uganda, severaldistricts are creating insurance schemes to finance ambulances in a public sectoremergency obstetric care system. In Rwanda, a prepayment scheme that coverspreventive and basic curative care provided by nurses in health centers, essentialdrugs, and coverage for hospitalization and ambulance transfer to the district hospitalin the case of obstetric emergencies is being pilot tested in 3 districts. One of the mainreasons for offering a prepayment plan, as opposed to a fee for service system, wasthat rural Rwandan farmers often forgo medical care in times of need because theylack the resources to pay, except at specific times of the year (primarily following the2 post-harvest periods). As one satisfied patient who was successfully referred andreceived a caesarian-section at the district hospital said, "if I were not a member, Iwould not have had enough money to pay for my treatment".3 2
Providers Payments, Incentives and Motivation
An efficient, motivated work force -- doctors, nurses, midwives and others-areobviously central to providing good quality reproductive health services. Professionalism,occupational standards and protocols, altruism, as well as compliance to the Hippocraticoath are traditionally invoked by governments and the medical establishment asmotivating factors for health providers.
Commonly cited weaknesses that underscore the importance of provider incentives inquality and access to reproductive health services include:
* Lack of incentives for providers to deliver good quality care: The way in whichproviders are paid and/or offered opportunities for advancement in their careers canprovide strong incentives for them to deliver good services. Public providers in mostdeveloping countries are paid a salary, which provides no incentive to deliver morecare or higher quality carc-especially when salaries are low and payment isunpredictable. A frequently observed pattern in many poor countries, such as Egypt,is that doctors employed by the public sector maintain private sector clinics, wherethey allocate considerable time in response to more lucrative user fees. Fee for servicepayments to private providers can also result in perverse outcomes. In Brazil, forexample, a study of 7000 births in one region in 1982 found that C-section rates were54% for private patients, who tended to be covered by private health insurance whichwould reimburse doctors for C-sections, as opposed to only 13% for indigent women,
31 Sall, Farba. La prise en charge des urgences obstetricales au Mali: L'experience de Kolokani.Partnerships for Health Reform, Abt Associates Inc. November 1998.32 George Phara, 1999, "Prepayment Programs in Rwanda: More than 12,000 Members in Two Months",Quarterly Highlights (Bethesda: Maryland, Partnerships for Health Reform, Abt Assocates).
19
who might not be able to pay for more complicated procedures.3 3 In this case, boththe private and the indigent patients suffered in terns of receiving poorer qualitycare-the private patients being more likely to receive unnecessary C-sections andthe indigent less likely to receive necessary C-sections.
* Lack of disincentives or sanctions for providers who deliver poor quality care: This isthe converse of the first point. Not only are providers not rewarded for giving goodcare, there also tend to be little or no disincentives or sanctions for health providers inmost countries who deliver poor quality care, are rude to clients or are inattentive toclient needs and circumstances.
* Lack of accountability ofproviders to clients/users: Clients currently are notempowered in relation to public health providers. In many countries, the absence oflinkages with the community power structure and lack of understanding ofcommunity needs and desires hinders access to and use of services. Salaried providersare paid regardless of the number of clients they serve or client satisfaction. Altematepayment methods such as 'capitation' have been designed to change this overlysupply-side orientation to a demand-side focus with 'money following patients'. Thiswill be elaborated in the Egypt case later.
Provider payments can be particularly important for motivating providers to behave in acertain manner, especially when they are contained in contractual arrangements, linked toperformance of duties and outcomes. Contractual arrangements and obligations take onan increasing role in contexts where 'purchasers' of health care services-such as aDistrict Health Authority, a Social Health Insurance Fund, a Community HealthFund-pay or reimburse public, NGO and private providers for serving serve clients.Other incentive schemes utilize non-pecuniary awards such as staff holidays for goodperformance, employee of the month awards, and so on. On the other hand, innovativeapproaches to empower clients are contained in national or even private 'client charters',such as in the UK and Malaysia, where promises to the public are announced regardingservices available, quality of care, and waiting times. In view of space limitations, theremainder of this section will discuss provider payments as a means to motivate healthproviders to improve performance and reproductive health outcomes.3 4
Provider payments refer to the means by which the money raised for financing istransferred to individuals and organizations within the health sector. Institutions (e.g.hospitals or health clinics) can be paid in many different ways: per admission, per day,per service, or on an overall budget. Practitioners can also be paid per capita fees forthose under their care, or per case or per service, or by salary. Each of these forns ofpayment has its own incentive effects.
Empirical evidence shows that different provider payment mechanisms can incentivizehealth personnel in both positive and negative ways. Depending on the forrn of payment,
33 Barros FC, Baughan JP and Vicotra C Why so many Caesarean sections? The need for a future policychange in Brazil. Health Policy and Planning, 1 (1): 19-29, 1986.34 R. Paul Shaw, 1999, "New Trends in Public Sector Management in Heal6th: Applications in Developedand Developing Countries" World Bank Institute Working Paper, (Washington DC).
20
health care workers may focus more on quality (than volume), take more time to betterunderstand client needs and prescribe effective action, and treat poor clients with morerespect. Negative effects of inappropriate provider payments on reproductive health indeveloping countries have been seen where, for example, providers are given bonuses forattracting new contraceptive clients or methods, without controls on quality. For example,in Indonesia, previous incentive payments to village midwives that stressed quantity-inthe form of greater supplies of contraceptive methods - resulted in oversupply, non-useand waste by households. In Indonesia, these incentive payments have been recentlyreplaced by performance-based contracts to compensate midwives for providing a clearlydefined package of services to the poor (a targeted intervention), as well as a morelimited set of public health services to the entire village.35
An important underlying rationale for enlisting NEW formns of provider payments toimprove outcomes is to 'transfer the financial risk' of poor performance from the PAYERof services (e.g., government, insurance funds) to the PROVIDER of services. As we willsee below, some forms of provider payments specifically aim to make providers moreresponsive and accountable for the work they do, with reimbursement tied more directlyto desired performance.
What are the prevailing patterns regarding provider payments in developing countriesconcerned with improving reproductive health? To a large extent, payment of salaries todoctors, nurses or midwives in public hospitals and clinics has been the dominant form ofprovider payment, with line-item budgeting for other health workers at district level? Insuch cases, payment of salaries takes place on a regular, pre-deterrmined basis and islargely divorced from what the recipient has or has not accomplished in his or her work.There are no monetary incentives if a salaried provider sees more clients than usual, andno monetary disincentives if the provider fails to be polite, considerate, thorough, andclient-oriented. This scenario applies particularly to the provision of reproductive healthservices by MOH employees in many countries.
In other contexts, for example, where significant numbers of doctors, nurses or midwiveswork in private clinics or hospitals, remuneration is in the form of fee-for-service. In thiscase, the payers of services may be the individuals who receive the service (i.e., out-of-pocket payments), by governments who are contracting with the private sector, or byhealth insurance funds. Empirical studies show that fee-for-service payments provideincentives to providers to deliver more expensive services (and technology) and to seemore clients. This is because their total income derives from the VOLUME of servicesthey provide TIMES the FEE per service, with more volume leading to rapid increases inprovider incomes. This not only leads to cost-escalation in the health sector but can resultin oversupply of services which carry high reimbursement rates. It also motivatesproviders to see those who are able and willing to pay fees-the relatively rich.
The negative effects of fee-for-service can be illustrated with respect to the oversupply ofcostly C-section deliveries in several Latin America countries. In Brazil, for example,higher rates of fecs paid by the social security system to physicians for C-sections as
35 Patricia Daly and Fadia Saadah, 1999, "Indonesia: Facing the Challenge to Reduce Maternal Mortality",East Asia and the Pacific Region 'Watching Brief (Washington DC: World Bank).
21
compared to fees for vaginal deliveries resulted in a doubling of the C-section rate from15% to 30% between 1970 and 1980. Even after social security payments were changedand made equivalent for the two procedures in 1980 in response to this problem, financialincentives continued to favor C-sections and high rates remained. Physicians continued togain higher remuneration for C-sections due to their ability to collect fees for extracharges like longer hospital stays and higher use of medications.36
Even when PAYERS seek to control costs by modifying payments, providers tend to becrafty in finding ways of protecting or insuring their earnings growth. In Australia, forexample, the government repeatedly placed controls on the level of fees paid to privatedoctors in efforts to keep national health costs down. Physicians responded to eachcontrol measure however by increasing utilization levels to the point that their earningscontinued to grow each year ahead of inflation.
How might provider payments work better to advance reproductive health services? Arelatively simple approach relies on continuation of salary payments for public or privateproviders, with the addition of a bonus for the provision of a set of selected or targetedservices. In the case of reproductive health, bonuses might be paid for targeted servicesthat include pre- and post-natal care, family planning consultations, nutritionalsupplements for mothers, and HIV/AIDS or STI testing and counseling. Bonuses can alsobe applied to redress gender imbalances in utilization of services, such as screening ofmales for STDs. An important rationale behind the bonus is that increased provision ofpreventive services will improve health, reduce the need for more costly curativeservices, and therefore be self-financing over the long run. This approach is beingimplemented by Health Maintenance Organizations in the US, Chile and the Philippineswhere physicians, on salary, are given incentives to provide preventive services such asfamily planning consultations, pre- and post-natal screening, and immunizations, inreturn for service-related bonus payments.
A more complicated forrn of payment that is growing in popularity to motivate providersto be attentive of preventive care and reproductive health needs is called 'capitation'.Under a capitation scheme, a provider is prepaid a pre-determined amount of money foreach person s/he agrees to care for over a specified period of time. This requiresagreement on the prepayment amount, the number of clients enrolled in the provider'spractice, and the range of service entitlements to be provided. For example, a doctor,nurse or midwife paid by capitation with a practice serving 1,000 people (all enrolled atthe practice) might receive $20 per capita per year for each of the 1,000 people s/he isresponsible for. The provider could therefore count on receiving $20,000 per year, inreturn for which s/he agrees to provide care to enrolled members seeking it. Under'capitation' payment schemes, the provider is motivated to emphasize preventive care soas to keep their enrolled population as healthy as possible, with reduced need forexpensive curative care. This is because providers under capitation are allowed to keepsavings resulting from reduced health expenditures on their enrollees.
36 Barros FC, Baughan JP and Vicotra C Why so many Caesarean sections? The need for a future policychange in Brazil. Health Policy and Planning, I (1): 19-29, 1986.
22
Capitation can also be used as a form of payment to a group of providers working out of asingle facility, such as a hospital and a network of clinics serving an enrolled population,or a district responsible for, say, 100,000 people.
Capitation is now the major form of payment to providers who are reimbursed by theU.S. government (for Medicare and Medicaid enrollees), and is growing rapidly in manydeveloping countries such as Chile, the Philippines, Brazil and Nicaragua. Purchasers ofhealth services-governments, health insurance funds, HMOs-are increasingly favoringcapitation as a method of payment because:
* It is relatively simple to administer (enrolled population times per capita amount)
* It involves negotiations between the purchaser (e.g., government or insurance fund)and the provider (e.g., public or private doctor, nurse or midwife; clinic or hospital)on what services are to be provided at what cost; and it records agreements in theform of a contract.
* Contracts usually stipulate that patients can switch providers-and take theircapitated payment "with them"-should they be dissatisfied with the quality ofservice they receive. This gives and incentive to providers to be more accountable totheir clients.
* Since providers are allowed to keep money from the capitated payments they don'tuse in providing services, they are strongly motivated to feature timely preventivecare which will keep down the need and demand for more expensive curative care fortheir clients.
* Capitation is compatible with an integrated approach to reproductive health becausecapitated payments are almost always linked to client entitlements to a clearlyspecified menu of integrated services.
On the negative side, capitation requires precautions because it tends to provideincentives to providers to limit treatment, especially more expensive treatments, so as toprotect their overall budget envelope and earnings levels. Also, the notion that clients canswitch providers-thus taking their capitated payment with them-assumes a relativelybroad provider base to choose from. If clients have little or no choice in switchingproviders if service is not to their standards, then the incentive for providers to beresponsive to their clients is effectively removed.
As noted previously, the single most important feature of enlisting new forms of providerpayments - from a health reform perspective -- is to transfer the 'financial risk' forperformnance from the PURCHASER or PAYER of services to the provider. This is notpossible under more traditional forms of salary payments in the public sector, where thepurchaser of services (government making use of tax money on behalf of taxpayers) paysa regular salary to workers in government owned health facilities. If these workers fail toproduce the outputs needed to improve reproductive health outcomes, it is thegovernment-the PURCHASER-rather than the provider - who must absorb thenegative consequences of poor value for money. Alternatively, under capitation, if the
23
provider or facility fails to deliver the goods, the goods are of poor quality, or theprovider or facility is inefficient and overspends the total capitation payment it receives,it is the PROVIDER-NOT the purchaser-who must bear the financial risk of loss. Theprovider's losses will be exacerbated as disgruntled patients switch to higher qualityproviders, because the poorly performing provider's enrolled population will be depletedand his/her capitation payments will decline. Moreover, if the provider fails to deliverhigh quality preventive services, s/he will be forced to absorb the costs of serving anenrolled population that is less healthy, and more in need of expensive curative services.
Organizational Change
Our use of organizational change refers to how providers-Ministries, hospitals, healthcenters, clinics -- are organized in termns of arrangements affecting inputs, processes andoutputs of health care provision. If government and the Ministry of Health in a particularcountry are responsible for the financing and provision of all reproductive health care,then our analysis of organizational change could be content on focusing solely onperfonnance of the public sector. Were we to satisfactorily re-organize the public sectorin such a context, we might reasonably assume relatively direct impacts on desiredreproductive health outcomes. In reality, however, public sector providers share the stagewith NGO and private-for-profit providers. To the extent that reforms do notacknowledge the importance of "public-private collaboration", they are sure to fall shortin achieving national reproductive health outcomes.
The significance of the private sector in overall financing and provision of health care canbe illustrated from National Health Accounts in several low income Asian countries. InViet Nam, 68% of total financing for health derived from private sources in 1993, whilethe private sector's share in provision amounted to about 50% of all health expenditures.In Bangladesh, about 47% of total financing for health derived from private sources(households) in 1994/95, while the private sector's share in provision accounted for 46%of all health expenditures. In Sri Lanka, non-governnental sources of finance accountedfor just over 50% of total financing for health in 1990, while the private sector's share inprovision accounted for 53% of health expenditures. Finally, in Nepal, the privatesector's share in financing accounted for 71% of total health expenditures in 1984/85.
More specific to reproductive health, the proportion of women using for-profit sources offamily planning is about 46%, on average, in countries of Latin American and theCaribbean, 44% in the Middle East and North Africa, 27% in sub-Saharan Africa, and26% in Asia (excluding China and India).37 Other examples of private provisioninclude: 3 8
* In Morocco and Tunisia, 48% and 25% of women 15-49 years, respectively use theprivate sector for prenatal care.39
* In the Philippines, 23% of women 15-49 years, use private facilities for their firstprenatal Visit.40
37 James E. Rosen and Shanti R. Conly, 1999, Ibid.38 See Rosen and Conly, 1999, Ibid.3 9 Berman and Rose, 199640 East-West Center, 1996
24
* In South Africa, 35% of nearly 5,000 STD patients in a rural health district soughttreatment from private doctors.41
* In Nigeria, 60% of 120 women receiving treatment for abortion complications in alarge public hospital had the initial procedure performed at a private hospital orclinic. 4 2
Organizations have both macro and micro components. Macrostructure refers to the legaland market conditions that impact on the organization's production function from"outside". If an organization is a monopoly, with no competitors, then it is likely to havea big say in what it produces, how it ascertains quality, and the cost to produce itsproduct. But if the organization has competitors and is exposed to market forces, then theway it does business will be very much influenced by how others are doing business andhow successful they are at it.
Microstructure refers to what happens inside an organization that affects its perfornance.How are staff and other resources managed, what kinds of incentive structures can beused to mobilize staff to be more efficient, stress quality and be responsive to clients;who sets performance targets; and to whom are managers accountable? The importanceof microstructure can be illustrated by comparing the management of two hypotheticalhospitals. In hospital #1, the directors/managers do not have authority to hire or fire staff,build new structures, change the profile of services, or decide on user charge policies.Rather, an outside body, in this case the Ministry of Health, sets organizational protocolsthat determine what can and cannot be done. Hospital #1 is typical of public, non-autonomous hospitals in many developing countries. In the case of Hospital #2, however,directors or managers can hire and fire staff, determine who will provide drugs and non-clinical supplies to the hospital, spend resources on construction and determine feecharging policies (to cover costs). This degree of management autonomy is often seen inNGO or mission facilities, private for profit hospitals and in some autonomous publichospitals. It is also often credited as a major reason for superior performance of NGOfacilities over government facilities in providing reproductive health and other services.43
Commonly cited weaknesses related to organizational and institutional capacity thatunderscore the importance of organizational change in health sector reform include:
Reproductive health services are poorly managed: Effective planning andimplementation of reproductive health programs and activities in many countries arehindered by weak technical and administrative capacities at the national, regional andservice delivery levels. Often, responsibility within Ministries of Health forpopulation and reproductive health services is located in relatively unempoweredoffices-in terms of budget, authority, and staff skills. Decentralization policiesincrease concerns among reproductive health proponents, because greater numbers ofactors with more variable technical and administrative expertise need to be engagedto ensure effective implementation.
41 Wilkinson et al, 199842 Konje and Obiseasan, 199143 See R. Paul Shaw, 1999, 'New Trends in Public Sector Management in Health: Applications inDeveloped and Developing Countries', (Washington DC: World Bank Institute, WBI Working Papers).
25
* Monitoring and evaluation is weak: Monitoring and evaluation is seldom linked tohealth outcome improvements or responsiveness to client needs or desires. In manycountries, disparate and parallel MIS systems exist and new programs insert newrequirements on an already overburdened and redundant system.
* Referral systems are non-existent orfunction poorly; there is a lack of linkagebetween levels of care: This is a particularly important problem for services toprevent maternal mortality. 'Women experiencing an obstetric emergency willalways need a functioning health system, one that recognizes the gravity of theirsituation, and refers and then provides them with the appropriate care. " ICPD +5,WHO, 1999.
* Administration and delivery of services is inefficient: Services that are delivered oradministered vertically, for example, are often inefficient from both the client andprovider perspectives. Clients find the hours for preventive services limited and arenot willing to make special visits for each of the different services they or their familymembers may need. Integrating services or offering all services at all hours that afacility is open may encourage clients to seek a wider variety of preventive andcurative services than they otherwise might. In Bangladesh and Egypt, integrationresulted in cost savings both in the administration of programs and delivery ofservices. Mexico reported a fifty percent savings in staff time when three serviceswere provided at a single consultation rather than one.44
* Services are organized to meet the needs or convenience ofproviders, not necessarilyto respond to client need or desires: Services offered may be too expensive, offeredin inappropriate manners and at inconvenient times, with no provisions for privacy.Antenatal care or family planning may be offered only at specific times of the week,rather than whenever clients show up. Facilities often do not have personnel on call oron guard 24 hours a day to respond to emergencies-this is particularly essential forobstetrical emergencies.
* The range of services or options offered to clients are limited: In most countries,women lack access to the total range of reproductive health services. This is not just amatter of lack of resources, it is also a due to a lack of understanding and respect forclient choice. In some countries, the majority of reproductive health services are notavailable or are only available to better off women in urban areas.
* Drug supply (essential drug) systems are weak and accountability is inadequate: Inresponse to weak drug systems many countries have adopted a vertical drug supplysystem for contraceptives which, in many cases, function well. However, thesevertical systems often rely on donor financing and technical assistance and may beunable to function as separate systems without donor support.
The push for change in the organization of the health sector has been motivated bywidespread impressions that overly centralized Ministries of Health lackentrepreneurship, are not accountable to the clients they serve, and provide poor quality
44 RHA to Population and Development, Forman and Ghosh, 1999.
26
service. For example, a survey conducted for the World Bank's 1997 WorldDevelopment Report on the role of the state in the financing and provision of social andother services found that only 6% of domestic private managers in 58 developingcountries rated public service delivery as efficient. Health services scored lowest. Sixtypercent of the business managers rated the efficiency of health services as low, 33% asmoderate, and only 7% as high.
In response to these complaints, decentralization is perhaps the most common, visible,reform option being implemented in developing countries-the explicit goal being toimprove performance by increasing the involvement and entrepreneurial talents of localactors and establishing greater accountability to the communities served. The frameworkby Rondinelli has become widely accepted in public health.4 5 Rondinelli describes four"pure" types of decentralization: deconcentration, devolution, delegation andprivatization.46 Broadly,
* with deconcentration, authority is transferred from a central ministry to lower levelswithin the same ministry. An example of this is the introduction of MOH districtbased planning and resource allocation by District Health Management Teams incontexts where planning and resource allocation were previously centralized.
* Devolution involves transferring authority away from a line ministry (e.g. the MOH)to local government units who are not part of the line ministry. These localgovernment units are usually elected officials representing regions, districts,municipalities or rural communities.
* Delegation involves transferring authority from the government to parastatal or somesimilar organization created by the government but lying outside of governmentcontrol. While common in the electrical and telephone sectors in developingcountries, delegation has not been widely used to date in the health sector.
* Under privatization, functions held by the government are "handed over" to theprivate sector.
Decentralization reforms in developing countries tend to be deconcentration ordevolution, or a combination of the two. In some countries, decentralization (in the formof deconcentration) is confined to the health sector and pursued as a deliberate healthreform strategy. A common form of deconcentration in the health sector is the WHOdistrict model, in which a district hospital (and its staff) are handed over responsibility fora group of geographically clustered satellite health clinics. In other instances, countriesthat are considering or undergoing health reform are simultaneously undergoingdecentralization (devolution or deconcentration) as a national development strategy,which extends beyond the health sector. The different forms of decentralization changethe incentives for organization and provider behavior in different ways. For example,decentralized decision-making without devolved control over finances often results inlittle new implementation.
41 WHO, 1997.46 Rondinelli, 1981 and 1983.
27
A second major type of organizational reform taking place in developing countries-onethat focuses on improving the way public institutions are managed - is the "New PublicSector Management" approach. New Public Sector Management has grown out ofconsensus that public sector organizations can benefit by identifying, mimicking, andimporting business-like practices from the private sector that appear responsible for betterperformance. It stresses accountability for performance among government employees byadding considerable clout in the form of (i) annual personnel performance agreementsbetween employer and employee, (ii) performance-related budgeting that linksexpenditures to achieved outcomes, and (iii) performance monitoring and evaluation toassure outcomes are achieved. Often, this involves giving greater autonomy andmanagement of publicly owned agencies such as central procurement agencies, publicworks, and hospitals.
A third organizational change strategy being introduced in some developing countriesaims to reshape EXTERNAL forces impacting on performance through a 'separation ofpublic finance from public provision'. The rationale for separating public finance frompublic provision is to get government out of the business of providing services, so as toconcentrate more on policy development, public health goods and services, and subsidiesfor the poor. This approach envisions (i) making greater use of the efficiencies of privatesector provision, financed through government contracting, and (ii) more value formoney by requiring competition for government contracts. Trinidad and Tobago,Nicaragua, and Mongolia, to name just a few country examples, are progressivelyintroducing these kinds of changes.
A key organizational feature associated with the separation of public finance andprovision is the emergence of PURCHASING agencies in systems of 'managedcompetition'. The underlying rationale is to establish organizational intermediaries thathave an arms length relationship to the policy roles of government (leaving that toMOH), and concentrate on the function of getting best value for money for the clients itrepresents. This is precisely what social health insurance organizations try to do whenthey contract a health maintenance organization (HMO) to provide high qualityreproductive health services for members of the social insurance plan. This organizationchange has also been referred to as a 'purchaser-provider split' and is defined, along withtypical functions of the purchaser vs. provider in Box 1.
For example, in the UK, the new purchasers are District Health Authorities who purchaseservices from public and private hospitals as well as clinics. Zambia has adopted a similarapproach and Ghana plans to do so. In Nicaragua, the purchasers are social healthinsurance funds that purchase services from public or private providers. In the UnitedStates, the purchasers are large employer groups (called sponsors) that purchase servicesfrom health maintenance organizations, like Kaiser Permanente, that owns its ownhospitals and clinics, as well as contracts from others. In Lebanon, the purchasers areprivate sector entities (e.g., MEDNET), that act on behalf of several private insurancefunds to get the best deal they can from public and private hospitals and other providers.
The organizational significance of the new purchasers is that they can have considerableclout in (i) getting providers to comply with the services they want their members to get,
28
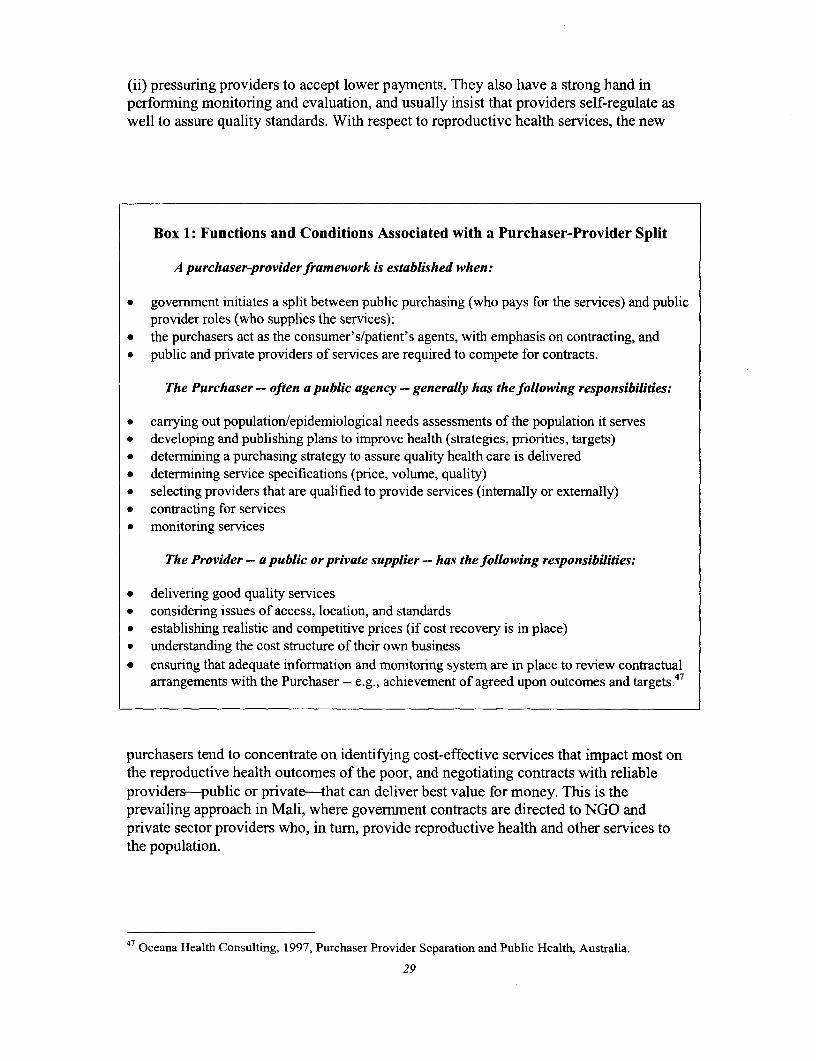
(ii) pressuring providers to accept lower payments. They also have a strong hand inperforning monitoring and evaluation, and usually insist that providers self-regulate aswell to assure quality standards. With respect to reproductive health services, the new
Box 1: Functions and Conditions Associated with a Purchaser-Provider Split
A purchaser-provider framework is established when:
* government initiates a split between public purchasing (who pays for the services) and publicprovider roles (who supplies the services):
* the purchasers act as the consumer's/patient's agents, with emphasis on contracting, and* public and private providers of services are required to compete for contracts.
The Purchaser - often a public agency - generally has the following responsibilities:
* carrying out population/epidemiological needs assessments of the population it serves* developing and publishing plans to improve health (strategies, priorities, targets)* determining a purchasing strategy to assure quality health care is delivered* determining service specifications (price, volume, quality)* selecting providers that are qualified to provide services (intemally or externally)* contracting for services* monitoring services
The Provider - a public or private supplier - has the following responsibilities:
* delivering good quality services* considering issues of access, location, and standards* establishing realistic and competitive prices (if cost recovery is in place)* understanding the cost structure of their own business* ensuring that adequate information and monitoring system are in place to review contractual
arrangements with the Purchaser -- e.g., achievement of agreed upon outcomes and targets.47
purchasers tend to concentrate on identifying cost-effective services that impact most onthe reproductive health outcomes of the poor, and negotiating contracts with reliableproviders-public or private-that can deliver best value for money. This is theprevailing approach in Mali, where government contracts are directed to NGO andprivate sector providers who, in turn, provide reproductive health and other services tothe population.
47 Oceana Health Consulting, 1997, Purchaser Provider Separation and Public Health, Australia.
29
Needless to say, organizational changes of this scope have been strongly resisted by thestatus quo. A legitimate complaint concerns the skills required to prepare, negotiate,monitor and evaluate contracts. Trial and error suggests that considerable training ofpublic sector officials, as well as 'learning-by-doing', is required to establish effectivecontracting. It is also clear that contracting of some kinds of services, such as non-clinicalservices (e.g., laundry, food, maintenance) is easier than clinical services (e.g.,operations).48 Nevertheless, the momentum to separate finance and provision, and to usecontracting as a means of fostering public-private collaboration to increase efficiency andgreater access is picking up and is sure to prevail in low and middle income countriesalike over the next decade.
Regulation
Regulation embodies various mechanisms that have been designed to constrain thebehavior of organizations in the health sector as well as direct them in societally desireddirections. It is perhaps the most important lever government has at its disposal to assurequality, protect client needs, and promote access, if not equity. Regulation becomesparticularly important in contexts where NGOs and private-for-profit providers are activein health systems, as a means of insuring quality, responsiveness to clients, and standardsand protocols related to individual safety. As summarized in Box 2, regulatory measureshave wide scope and can affect conditions affecting entry, price, quality, and buyer-sellerrelationships.
Commonly cited weaknesses related to regulatory issues in developing country healthsystems that hinder achievement of reproductive health goals include:
• Lack of experience and capacities for a government regulatory role in assuringquality ofpublic health goals: In most developing countries, government workershave little experience or expertise in regulation, and it has not in the past been animportant part of their jobs. Service standards and norTns for various healthprofessionals or for different services and procedures may be non-existent, not up todate or poorly disseminated. Procedures for enforcement of standards may need to beestablished and maintained. In some countries, the problem may be confined tojointly establishing, disseminating or enforcing standards with private sectorproviders, so that the public and private sectors follow similar standards and norms.
* Lack of a legal or regulatory framework to help facilitate and guide NGO action inreproductive health: Legal frameworks which provide NGOs with freedom of actionin reproductive health, still do not exist or require revision in many countries. Yet,NGOs tend to be key actors in developing and delivering reproductive healthapproaches and services in many countries. They have been instrumental inestablishing policies, setting priorities, developing and testing innovative programs,translating client needs and demands, and holding governments accountable for theiractions.
48 Anne Mills, 1998, "To Contract or Not to Contract? Issues for Low and Middle Income Countries",Health Policy and Planning, Vol. 13, no. 1, pp. 32-40.
30
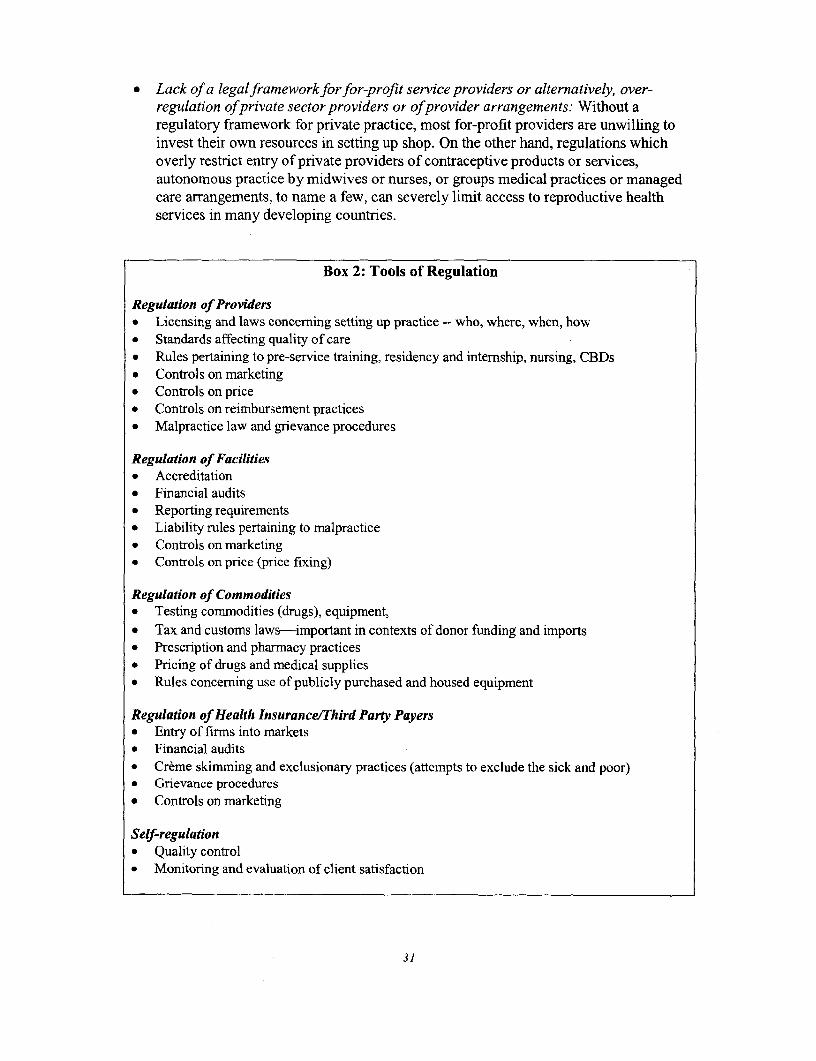
* Lack of a legalframeworkforfor-profit service providers or alternatively, over-regulation ofprivate sector providers or ofprovider arrangements: Without aregulatory framework for private practice, most for-profit providers are unwilling toinvest their own resources in setting up shop. On the other hand, regulations whichoverly restrict entry of private providers of contraceptive products or services,autonomous practice by midwives or nurses, or groups medical practices or managedcare arrangements, to name a few, can severely limit access to reproductive healthservices in many developing countries.
Box 2: Tools of Regulation
Regulation of Providers* Licensing and laws concerning setting up practice -- who, where, when, how* Standards affecting quality of care* Rules pertaining to pre-service training, residency and internship, nursing, CBDs* Controls on marketing* Controls on price* Controls on reimbursement practices* Malpractice law and grievance procedures
Regulation of Facilities* Accreditation* Financial audits* Reporting requirements* Liability rules pertaining to malpractice* Controls on marketing* Controls on price (price fixing)
Regulation of Commodities* Testing commodities (drugs), equipment,* Tax and customs laws-important in contexts of donor funding and imports* Prescription and pharmacy practices* Pricing of drugs and medical supplies* Rules concerning use of publicly purchased and housed equipment
Regulation of Health Insurance/Third Party Payers* Entry of firms into markets* Financial audits* Creme skimming and exclusionary practices (attempts to exclude the sick and poor)* Grievance procedures* Controls on marketing
Self-regulation* Quality control* Monitoring and evaluation of client satisfaction
31
* Tax policies that are unfavorable to reproductive health goals: Imposing heavyimport or value added taxes and customs charges on certain public healthcommodities, such as contraceptives, can substantially increase their prices toconsumers. This can, in turn have negative implications for the use of thesecommodities by economically disadvantaged individuals. In almost all developingcountries, when donors purchase and import these commodities, the products aregranted a tax free status. However, taxes are imposed on these same products whenthe government, private providers, pharmaceutical distributors or NGOs purchasethem. A recent survey on the tax treatment of 3 pubic health commodities (vaccines,ORS and contraceptives) in 22 responding countries found that specific taxarrangements for the three products varied greatly between countries, but wereseldom implemented with public health goals in mind. Vaccines tended receive themost favorable tax treatment (i.e. exoneration of most types of taxes for the greatestnumber of purchasers), while contraceptives receive the least favorable treatment.49
* Lack of a supportive legalframework beyond the health sector to supportreproductive health goals: For reproductive health, this includes: laws on the legalage of sexual consent and marriage which allow men to marry young girls oradolescents; poor legal protection of women in areas such as marriage (includingviolence against women by their husbands), divorce and polygamy; restrictions onabortion in some countries and stigmatization of abortion in others; laws or policiesthat prohibit sexuality education for young people; laws that restrict free andinformed choices of people related to sexual and reproductive health.
Regulation takes on priority as a health sector 'reform lever' because it can be used to'operationalize' a vision of what selected inputs, structures, and outputs should be inplace to achieve desired reproductive health outcomes. It seeks compliance fromfinanciers and providers that they will honor the standards and protocols mandated bygovernment. And it aims to protect the public in cases where informnation is imperfect(e.g., comnmodities and procedures that may involve risks to one's health) and whereproviders may not act in the best interest of clients (e.g., when insurers reject people withhealth conditions from membership in health insurance plans).
Two issues concerning regulation are: to what extent will compliance with existingstandards/norms improve outcomes, and to what extent might changes in existing lawsand regulations or new regulations improve reproductive health outcomes?
Compliance with existing reproductive health standards and norms is a major issuebecause governments tend to be weak in carrying out their regulatory functions-weak inlimited numbers of regulators, weak in enforcement, weak in levying penalties for non-compliance. If government is the only financier and provider of reproductive health then,in a sense, there is no formal regulation because government itself sets and complies withits own standards and protocols. Regulation is almost always important however becauseNGOs, not-for-profit and for profit organizations tend to be heavily involved in thefinancing and provision of reproductive health as well. Moreover, many governments are
49 Katherine Krasovec and Catherine Connor, "Survey on tax treatment of public health commodities,"PHR Technical Report #17. Bethesda, MD January, 1998.
32
trying to expand the size of the private health care sector, as well as its role in assuringdelivery of quality reproductive health services.
Many countries' existing laws or regulations limit the population's access to reproductivehealth services. For example, access to family planning products and services arerestricted in some countries because pharmacies are not allowed to distributecontraceptive products without a prescription from a health provider (usually aphysician). In many cases, clients, particularly poorer clients, would prefer to get aprescription directly from a pharmacy or pharmacist, so that they do not have to maketwo separate trips to separate facilities and incur additional financial costs. Limiting IUDinsertion to physicians or certain specialist physicians, when midwives or nurses can anddo provide these same services safely and effectively in other countries, hinders thepopulation's access-geographically, financially and often socially-to this method ofcontraception. Constraints on autonomous paramedical practice limits access toimportant, good quality services that these providers can and are willing to deliver inrural or poorer areas where physicians are unwilling and unable (for financial, social andcultural reasons) to practice. Limiting group medical practices, managed carearrangements, or other arrangements in which the financial burden and risk for a medicalpractice can be shared between providers, also constrains possibilities for expandingservice availability.
Some ways that regulation has been used in developing countries to improve healthsector performance and reproductive health include:
* requiring medical graduates to serve time in remote areas where health andreproductive health are substandard. In Thailand, for example, the government starteda program in 1995 to produce 300 doctors annually, specifically for rural areas,whereby students must spend at least one year providing rural services and threeyears of their training at a regional hospital, networking with district hospitals.5 0
* requiring that medical, nursing, midwifery and other paramedical schools providetraining in selected reproductive health topics of concern to society.
* providing a legal framework for midwives to deliver reproductive health servicespreviously restricted to physicians. In some countries, midwives now have the legalframework to insert UJDs or provide other contraceptive products. In others,midwives or nurses can be registered as private autonomous providers of midwiferyservices. In others midwives can now perform certain obstetrical functions previouslylimited to physicians. Tunisia, Turkey, Morocco and Chile, to name a few, all have orare investigating reforms of this nature.
* requiring that NGOs contribute to public health goals. For example, the governmentof Malawi subsidizes about 15% of the recurrent costs of facilities managed by theChristian Health Medical Association-a group of mission clinics and hospitals-in
50 Suwit Wibulpolpersert, "Strategies to Solve Inequitable Distribution of Doctors: A Review of Experiencefrom Thailand", (case study prepared for World Bank Institute Flagship Program on 'Health Sector Reformand Sustainable Financing'), 1997.
33
return for their compliance to population, FP and reproductive health norms andprovision of specified services to poor households.
* requiring that insurance programs do not creme skim clients (reject the sick andneedy in favor of the healthy and wealthy); requiring regular auditing of healthinsurance funds.
* requiring that gender issues are featured as an explicit part of policy formulation, andthat gender neutrality takes place in the quantity, quality and access to servicesdelivered.
In what new ways might regulation be employed to advance reproductive healthoutcomes? As governments increasingly advocate the provision of basic packages ofhealth services (which include reproductive health), and increasingly contract with publicand private providers to offer the basic package, there will be a major role for theregulator to play in assuring the reproductive health services are indeed available. In thiscontext, the regulation can be built into contracts in the formn of services that must beprovided, as well as agreed procedures to monitor and evaluate compliance. The sameapplies to benefit packages offered to paying clients of social health insurance and privateinsurance funds. In this context, regulatory functions can be jointly undertaken by thepublic and private sector, possibly under the umbrella of an NGO that takes the lead inperforming 'rating' and 'watchdog' functions.
Another important way of harnessing regulation as a reform lever to advancereproductive health outcomes is to encourage self-regulation among competing entities.In markets where large NGO and private providers are competing for clients (for exampleunder capitation payments) they are inclined to self-regulate for quality, motivated by thedesire to satisfy and retain their client base. Governments can tap this propensity for self-regulation by influencing the standards and norms that must be met and possiblysubsidizing the technical training and data systems involved. In Germany, for example,where financing and funding of health services is performed by German Sickness Funds,the funds self-regulate for quality. Government itself is only responsible for about 10% ofregulatory tasks in the country.
The 'flip side' of regulation is that government regulations might be overly stringent tothe extent they crowd out private sector entrepreneurs. We have already cited examplesof regulations that may restrict direct provision of reproductive health services. Otherregulations-on prices, patents, and commercial markets for products, can have negativerepercussions as well. For example, in Egypt, Jordan and elsewhere, government controlson the price of oral contraceptives that were intended to make products more affordablehave discouraged commercial sector interest. Furthermore, government policymakerstypically know little about the commercial sector and may unintentionally inhibit thegrowth of commercial markets, thus hampering the achievement of public health goals. InSouth Africa, for example, a major U.S.-based pharmaceutical company suspended plans
34

to set up production facilities over concerns that govenment neglect of weak patentprotections would make it unprofitable to manufacture products in the country.5
Promoting Healthy Behaviors52
Promoting healthy behaviors refers to interventions that can be taken to influence careseeking behaviors-that is, the demand side of health care. This is an important reformlever because individual behaviors -- rooted in habits, values, perceptions and ideas -- canwork both for and against optimal reproductive health. The role of healthy behaviorpromotion is to mobilize individuals to adopt healthy behaviors by (i) identifying,clarifying and communicating the benefits he or she will gain by adopting thesebehaviors and, (ii) providing information on how and where to access assistance whenproblems or concerns arise. For example, a healthy behavior objective among consentingindividuals show decide to engage in sexual activity is to get them to practice 'safe sex'.A healthy behavior objective for individuals who drive cars with seat belts is to get themto use the seat belts. A healthy behavior objective regarding pregnant women in ruralvillage households is to motivate them to use skilled providers as birth attendants.
Some commonly cited weakness in developing country health systems related topromoting healthy behaviors for better reproductive health are:
* Low levels of contraceptive use in high risk situations. UNFPA estimates that at least350 million couples worldwide lack access to infonnation about contraceptives and arange of modern contraceptive methods.53 This is particularly problematic in poorcountries where the incidence and prevalence of HIV is high, such as in countries ofsub-saharan Africa and South Asia. Moreover, between 120 and 150 million marriedwomen who desire to limit or space future pregnancies are not using contraceptivesand have an unmet need for family planning infonnation and services. This is asmuch a matter of educating men and women about their reproductive health rights,needs and choices, and confronting biases regarding contraceptive use, as it is aboutmaking more services and commodities available and affordable.
* Lack of effective use of available health professionals: Lack of appropriate demandfor maternity care services: only 65% of women in developing countries make use ofantenatal care, compared to 97% of their counterparts in developed countries. Evenfewer women -- less than 30% -- receive postpartum care, compared to 90% ofwomen in developed countries. Only slightly more than half (53%) of all developingcountry deliveries take place with the assistance of a skilled doctor or midwife. Thistranslates into 60 million unskilled deliveries per year in developing countries inwhich a woman either delivers alone, with a family member or with an unskilledattendant.54 Service use is low for a variety of reasons, including physical and
51 James E. Rosen and Shanti R. Conly, "Getting Down to Business: Expanding the Private CommercialSector's Role in Meeting Reproductive Health Needs" (Washington DC: Population Action International),1999.52 This section borrows from presentations by Michael Reich, Harvard School of Public Health, to theWorld Bank Institute Flagship Program on Health Sector Reform and Sustainable Financing.3 UNFPA, The State of the World's Population, New York, 1997.
54 WHO, Coverage of Maternal Care: a Listing of Available Information, Fourth Edition, Geneva, 1997.
35
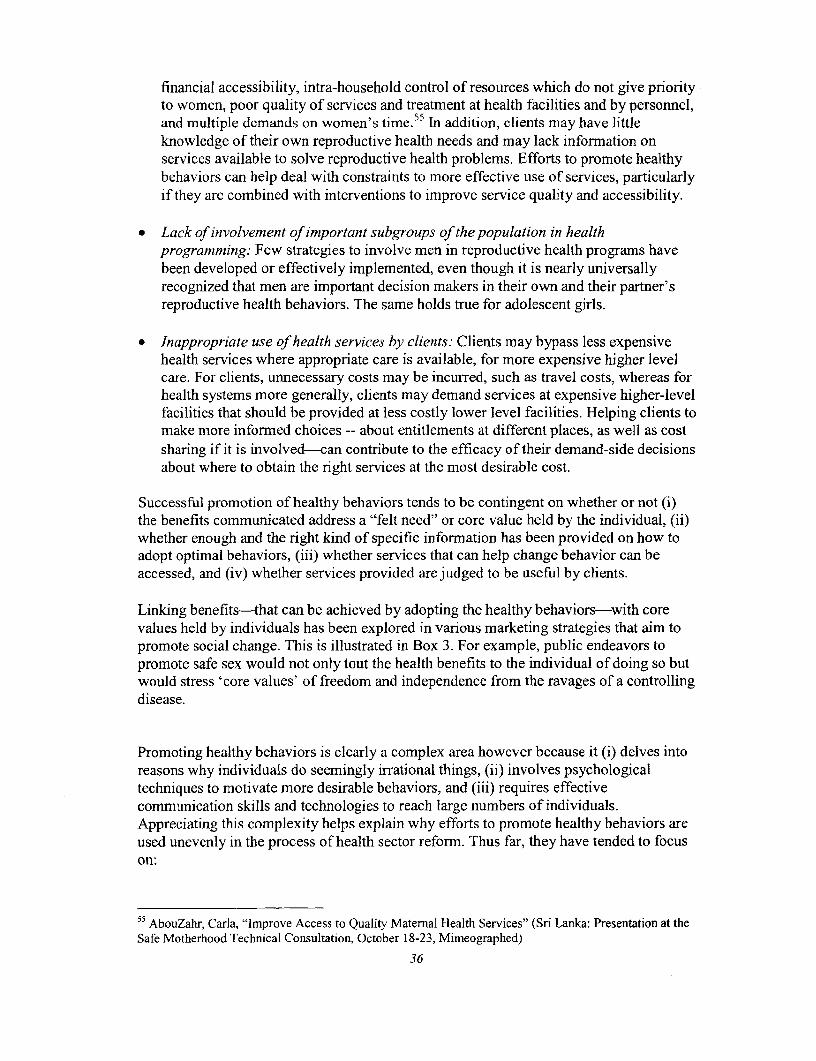
financial accessibility, intra-household control of resources which do not give priorityto women, poor quality of services and treatment at health facilities and by personnel,and multiple demands on women's time.55 In addition, clients may have littleknowledge of their own reproductive health needs and may lack information onservices available to solve reproductive health problems. Efforts to promote healthybehaviors can help deal with constraints to more effective use of services, particularlyif they are combined with interventions to improve service quality and accessibility.
* Lack of involvement of important subgroups of the population in healthprogramming: Few strategies to involve men in reproductive health prograrns havebeen developed or effectively implemented, even though it is nearly universallyrecognized that men are important decision makers in their own and their partner'sreproductive health behaviors. The same holds true for adolescent girls.
* Inappropriate use of health services by clients: Clients may bypass less expensivehealth services where appropriate care is available, for more expensive higher levelcare. For clients, unnecessary costs may be incurred, such as travel costs, whereas forhealth systems more generally, clients may demand services at expensive higher-levelfacilities that should be provided at less costly lower level facilities. Helping clients tomake more informed choices -- about entitlements at different places, as well as costsharing if it is involved-can contribute to the efficacy of their demand-side decisionsabout where to obtain the right services at the most desirable cost.
Successful promotion of healthy behaviors tends to be contingent on whether or not (i)the benefits communicated address a "felt need" or core value held by the individual, (ii)whether enough and the right kind of specific information has been provided on how toadopt optimal behaviors, (iii) whether services that can help change behavior can beaccessed, and (iv) whether services provided are judged to be useful by clients.
Linking benefits-that can be achieved by adopting the healthy behaviors-with corevalues held by individuals has been explored in various marketing strategies that aim topromote social change. This is illustrated in Box 3. For example, public endeavors topromote safe sex would not only tout the health benefits to the individual of doing so butwould stress 'core values' of freedom and independence from the ravages of a controllingdisease.
Promoting healthy behaviors is clearly a complex area however because it (i) delves intoreasons why individuals do seemingly irrational things, (ii) involves psychologicaltechniques to motivate more desirable behaviors, and (iii) requires effectivecommunication skills and technologies to reach large numbers of individuals.Appreciating this complexity helps explain why efforts to promote healthy behaviors areused unevenly in the process of health sector reform. Thus far, they have tended to focuson:
55 AbouZahr, Carla, "Improve Access to Quality Maternal Health Services" (Sri Lanka: Presentation at theSafe Motherhood Technical Consultation, October 18-23, Mimeographed)
36
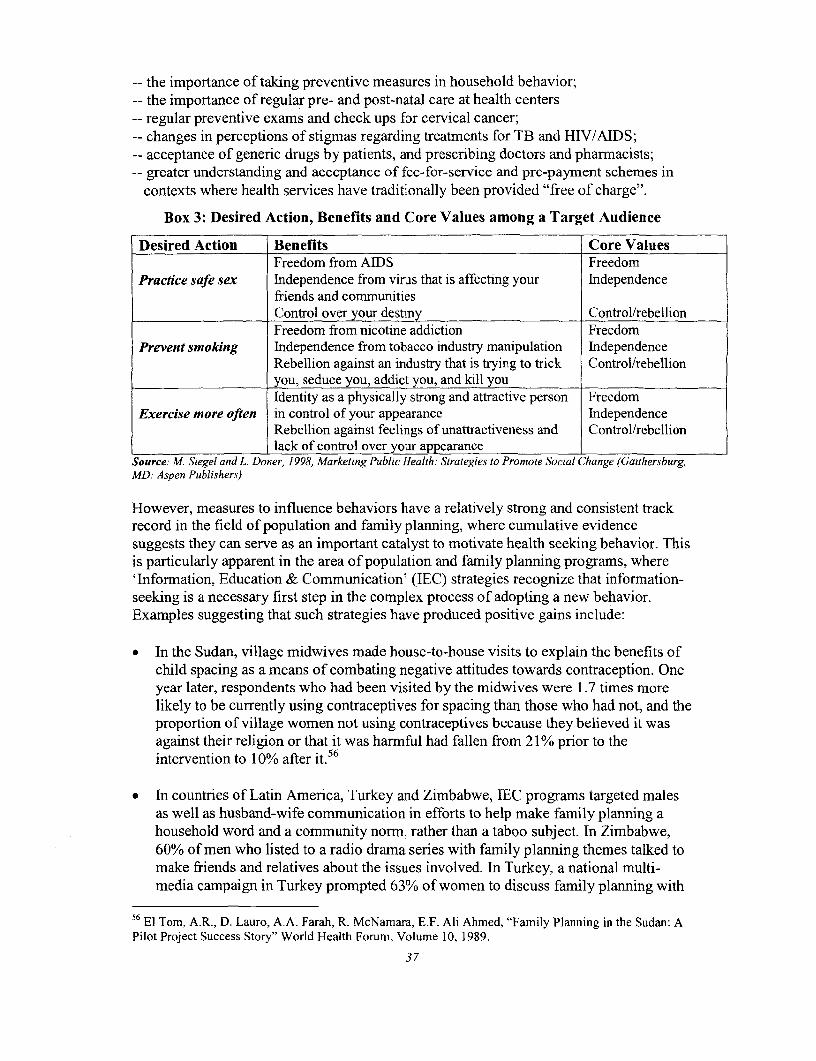
-- the importance of taking preventive measures in household behavior;-- the importance of regular pre- and post-natal care at health centers-- regular preventive exams and check ups for cervical cancer;-- changes in perceptions of stigmas regarding treatments for TB and HIV/AIDS;-- acceptance of generic drugs by patients, and prescribing doctors and pharmacists;-- greater understanding and acceptance of fee-for-service and pre-payment schemes in
contexts where health services have traditionally been provided "free of charge".
Box 3: Desired Action, Benefits and Core Values among a Target Audience
Desired Action Benefits Core ValuesFreedom from AIDS Freedom
Practice safe sex Independence from virus that is affecting your Independencefriends and communitiesControl over your destiny Control/rebellionFreedom from nicotine addiction Freedom
Prevent smoking Independence from tobacco industry manipulation IndependenceRebellion against an industry that is trying to trick Control/rebellionyou, seduce you, addict you, and kill youIdentity as a physically strong and attractive person Freedom
Exercise more often in control of your appearance IndependenceRebellion against feelings of unattractiveness and Control/rebellionlack of control over your appearance
Source: M. Siegel and L. Doner, 1998, Marketing Public Health: Strategies to Promote Social Change (Gaithersburg,MD: Aspen Publishers)
However, measures to influence behaviors have a relatively strong and consistent trackrecord in the field of population and family planning, where cumulative evidencesuggests they can serve as an important catalyst to motivate health seeking behavior. Thisis particularly apparent in the area of population and family planning programs, where'Information, Education & Communication' (IEC) strategies recognize that information-seeking is a necessary first step in the complex process of adopting a new behavior.Examples suggesting that such strategies have produced positive gains include:
- In the Sudan, village midwives made house-to-house visits to explain the benefits ofchild spacing as a means of combating negative attitudes towards contraception. Oneyear later, respondents who had been visited by the midwives were 1.7 times morelikely to be currently using contraceptives for spacing than those who had not, and theproportion of village women not using contraceptives because they believed it wasagainst their religion or that it was harmful had fallen from 21% prior to theintervention to 10% after it.56
* In countries of Latin America, Turkey and Zimbabwe, IEC programs targeted malesas well as husband-wife communication in efforts to help make family planning ahousehold word and a community norm, rather than a taboo subject. In Zimbabwe,60% of men who listed to a radio drama series with family planning themes talked tomake friends and relatives about the issues involved. In Turkey, a national multi-media campaign in Turkey prompted 63% of women to discuss family planning with
56 El Tom, A.R., D. Lauro, A.A. Farah, R. McNamara, E.F. Ali Ahmed, "Family Planning in the Sudan: APilot Project Success Story" World Health Forum, Volume 10, 1989.
37

their husbands. Studies in Latin America, Niger and India, reveal that interventionsthat improved communication between both men and women contributed to jointdecision makers in family planning and had a significant, positive impact on bothacceptance and continuation of family planning.5 7
* In Indonesia, the government launched a "Blue Circle Campaign" that aimed toimprove the image and status of private doctors and trained midwives as high-qualityproviders of family planning services. After a five month campaign, the averageweekly family planning caseload increased by 28% for doctors and 36% for nurses.5 8
* In Kenya, a project aimed to change behavior of male truck drivers through aworkplace intervention that combined IEC about unsafe/unprotected sex, STItreatment, and access to condoms. After one year, there was a 13% decrease inextramarital sex (49% to 36%), and a 6% decrease in visits to commercial sexworkers (12% to 6%). There was also a decline in STIs.59
Combining the Reform Levers
Each of the five reform levers can be invoked to inject change into the health system.What makes health sector reformn so complex and demanding, however, is that majorimprovements in system-wide performance and outcomes are unlikely to take place ifonly one reform lever is manipulated at a time. In fact, changes in one of the reformlevers almost always leads to changes in one of the others, making it impossible to workon one lever without affecting changes in the others. Lack of understanding of how thefour reformn levers interact can be expected to result in situations where well-intentionedchanges in one reform lever may be undermined or sabotaged by neglect of others.Moreover, simultaneous action on all five levers will probably need to be orchestrated toremedy deeply entrenched performance problems in health systems.
In some contexts, the changes brought about by manipulating the reformn levers have beenintentionally rapid, and so sweeping that the resulting policies have been called 'BigBang' reforms. This applies to developed countries like the UK and New Zealand wherea separation of finance and provision, and the creation of internal markets was introducedby political fiat, then bulldozed through the health system by the govemment in power.Such reforms encountered considerable political risk because inadequate efforts weredevoted to building consensus among different stakeholders. In the UK, for example, themedical establishment fought endlessly against the separation of financing and provision,the establishment of internal markets, and contracting. Even though the arguments infavor of the reformns gradually won increasing favor and support across the country, theconflicts along the way resulted in a certain amount of backtracking.
57 Phyllis T. Potrow, K.A. Treiman, J.G. Rimon II, S.Hee Yun, B.V. Lzare, and R-C. Meyer, 1990,"Strategies for Family Planning Information, Education, and Communication" (Baltimore, MD: School ofHygiene and Public Health, The Johns Hopkins University).58 Ibid., 199059 Jackson, D., J. Rakwar, el al, 1997, "Decreased Incidence of Sexually Transmitted Diseases amongTrucking Company Workers in Kenya: Results of a Behavior Risk-Reduction Programme", AIDS, Vol. 11,pp. 903-909.
38
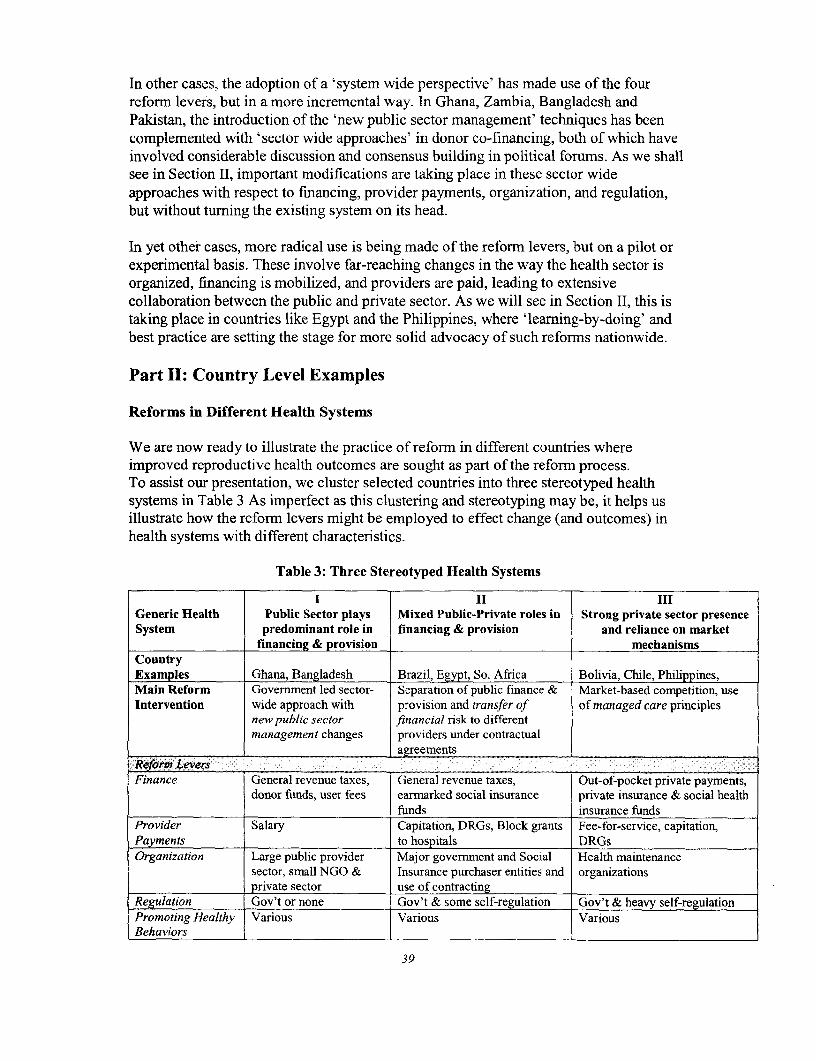
In other cases, the adoption of a 'system wide perspective' has made use of the fourreform levers, but in a more incremental way. In Ghana, Zambia, Bangladesh andPakistan, the introduction of the 'new public sector management' techniques has beencomplemented with 'sector wide approaches' in donor co-financing, both of which haveinvolved considerable discussion and consensus building in political forums. As we shallsee in Section II, important modifications are taking place in these sector wideapproaches with respect to financing, provider payments, organization, and regulation,but without turning the existing system on its head.
In yet other cases, more radical use is being made of the reform levers, but on a pilot orexperimental basis. These involve far-reaching changes in the way the health sector isorganized, financing is mobilized, and providers are paid, leading to extensivecollaboration between the public and private sector. As we will see in Section II, this istaking place in countries like Egypt and the Philippines, where 'learning-by-doing' andbest practice are setting the stage for more solid advocacy of such refonns nationwide.
Part II: Country Level Examples
Reforms in Different Health Systems
We are now ready to illustrate the practice of reform in different countries whereimproved reproductive health outcomes are sought as part of the reform process.To assist our presentation, we cluster selected countries into three stereotyped healthsystems in Table 3 As imperfect as this clustering and stereotyping may be, it helps usillustrate how the reform levers might be employed to effect change (and outcomes) inhealth systems with different characteristics.
Table 3: Three Stereotyped Health Systems
I II IIIGeneric Health Public Sector plays Mixed Public-Private roles in Strong private sector presenceSystem predominant role in financing & provision and reliance on market
financing & provision mechanismsCountryExamples Ghana, Bangladesh Brazil, Egypt, So. Africa Bolivia, Chile, Philippines,Main Reform Government led sector- Separation of public finance & Market-based competition, useIntervention wide approach with provision and transfer of of managed care principles
new public sector financial risk to differentmanagement changes providers under contractual
agreementsRefornm LeversFinance General revenue taxes, General revenue taxes, Out-of-pocket private payments,
donor funds, user fees earmarked social insurance private insurance & social healthfunds insurance funds
Provider Salary Capitation, DRGs, Block grants Fee-for-service, capitation,Payments to hospitals DRGsOrganization Large public provider Major government and Social Health maintenance
sector, small NGO & Insurance purchaser entities and organizationsprivate sector use of contracting
Regulation Gov't or none Gov't & some self-regulation Gov't & heavy self-regulationPromoting Healthy Various Various VariousBehaviors
39
The first stereotyped system represents a country where government plays a dominantrole in financing and provision of health services and sees itself as largely responsible forimproving reproductive health outcomes in the country.6 0 Historically, this kind ofsystem is referred to as a 'Beveridge-type' system after Lord Beveridge of England, andprevails in the historical development of Commonwealth countries. It applies to mostcountries of Anglophone and Francophone Africa, as well as countries of South Asia. Insuch contexts, a strong role of government and donors in financing and providing healthservices tends to be advocated. This tends to be justified by the absence of a wellorganized private sector, weak resource mobilization capacities, and highly politicizedpublic commitments to subsidize the poor. We will focus almost exclusively on GHANAas an example to illustrate how government is using the reform levers to revitalize itspublic service delivery model to achieve improved reproductive health and other healthoutcomes.
The second stereotyped system represents a country where government continues to playan important role in both health financing and provision of services, but is increasinglyrecasting itself as a purchaser of health care services -- on behalf of citizens -- fromprivate voluntary and private-for profit providers. In these contexts, markets and privatesector capacities tend to be considerably more developed, more choice of public versusprivate providers exists, and higher household incomes are more conducive to client'sability and willingness to pay. Moreover, many countries in this category haveestablished social insurance funds (SHI), thus earmarking funds to cover health care ofemployees in the formal sector. Such changes introduce greater autonomy in themanagement of health resources by autonomous funds, and often creates powerful new'purchasers' of services that may or may not adequately feature reproductive healthservices. Private insurance companies may also be mobilizing resources for health insuch contexts, and may compete to serve clients or may offer complementary insuranceto 'top up' services provided by government or social insurance. This kind of systemprevails in many middle income countries, particularly in Latin America. We will focuson EGYPT to illustrate how government is using the reform levers to create a new publicand private service delivery model.
The third stereotyped system is characterized by a relatively large private sector in thesense that large shares of the population pay out-of-pocket for the health services theyreceive, and a significant share of providers are Egos or not-for-profit as well as for-profit. In many of these contexts, the philosophy that market forces and competitionshould play a strong role in financing and providing health care prevails as well. On theone hand, we will examine an NGO in Bolivia that aims to compete with MOH and
60 The strong link between government finance and government-owned health facilities can be traced backto British influence and the formation of a 'national health service'. This kind of system-historicallycalled a called a 'Beveridge' system (after Lord Beveridge)-is sharply differentiated from the Germanmodel which mobilizes funds for health through mandated social health insurance contributions (fromemployers and employees) that is historically called a 'Bismark' system. An important difference betweenthe two systems is that public funds for health in a Beveridge-type system can be usurped and used forother purposes (e.g., fight a war), whereas funds for health in a Bismark-type system are earmarked forhealth and cannot be reallocated to other ends by political whim.
40
private-for-profit providers by providing an integrated approach to reproductive healthand other services while, at the same time, sustaining itself through cost recovery. On theother hand, we will focus on the Philippines to illustrate how government has encouragedprivate entities to pilot a new private service delivery model, making use of the principlesof managed.
At this juncture, we caution that the countries examined below should not be viewed ascontrolled experiments where the reforms are solely concerned with improvingreproductive health. Indeed, we know of NO such countries. Rather, the health sectorreforms we will examine typically involve changes and tradeoffs in a broad constellationof health sector inputs, processes and structures that aim to improve a broad constellationof health sector outputs. This is quite different from a more traditional project approachwhere reproductive health per se might be the target of intervention. Accordingly,expectations need to be tempered that reproductive health alone matters in a world ofserious budget constraints, limited national capacities, and competing priorities.
Trends in Public Sector Reform
In developing countries where the public sector plays a prominent role in both thefinancing and delivery of health services, governments are increasingly experimentingwith new modes of organization to improve performance. Many such countries sufferfrom widespread poverty and have relatively limited private sector capacities, thuselevating the importance of government roles in health as well as the stakes associatedwith reformns.
Table 4 identifies four important trends in developing countries that have beenimplemented in varying degrees during the 1980's and 90's. These include (i) new publicmanagement changes, (ii) sector-wide perspectives, (iii) private sector development, and(iv) cost recovery. Each trend is further described in terms of reform levers involved,expected impacts and lessons learned regarding implementation.
In view of space limitations and our desire to illustrate reforms that benefit reproductivehealth outcomes, we focus here on changes involving new public management (NPM),combined with a sector-wide perspective in Ghana. Both practices or strategies arelargely illustrative of the organizational reforrn lever, though we will also comment onuse of the remaining reform levers in this context as well.
New Public Management
The new public management (NPM) grew out of efforts in several OECD countries, suchas the UK and New Zealand, to 'revitalize' if not 'reinvent' practices that shape publicsector perfornance. Acknowledging widespread dissatisfaction with public sectorperformance, it advocates serious study of private sector practices that have provenefficient and identification of those that might benefit the public sector as well. In anutshell, it aims to (i) identify business-like practices in the private sector that havereduced costs and improved quality in the private sector and (ii) mimic or import thesepractices into the public sector towards enhancing performance.
41

Thus far, general practices in the private sector that have been identified as valuableinclude greater emphasis on (I) achieving measurable outcomes desired by society (i.e.,clients, taxpayers, voters, NGOs, etc.), (ii) monitoring and evaluating progress relative tobaseline estimates, (iii) linking performance-based incentives for public sector workersand contractors to job performance, and (iv) performance related budgeting that linksexpenditures to the attainment of measurable products. Contracting is used as a keymechanism to formalize such performance agreements, both within and betweeninstitutions. Underlying the new public management philosophy is an explicitacknowledgement that clients are the ultimate target and beneficiary of investments.6'
61 See R. Paul Shaw, 1999, 'New Trends in Public Sector Management in Health: Applications inDeveloped and Developing Countries', (Washington DC: World Bank Institute, WBI Working Papers).
42
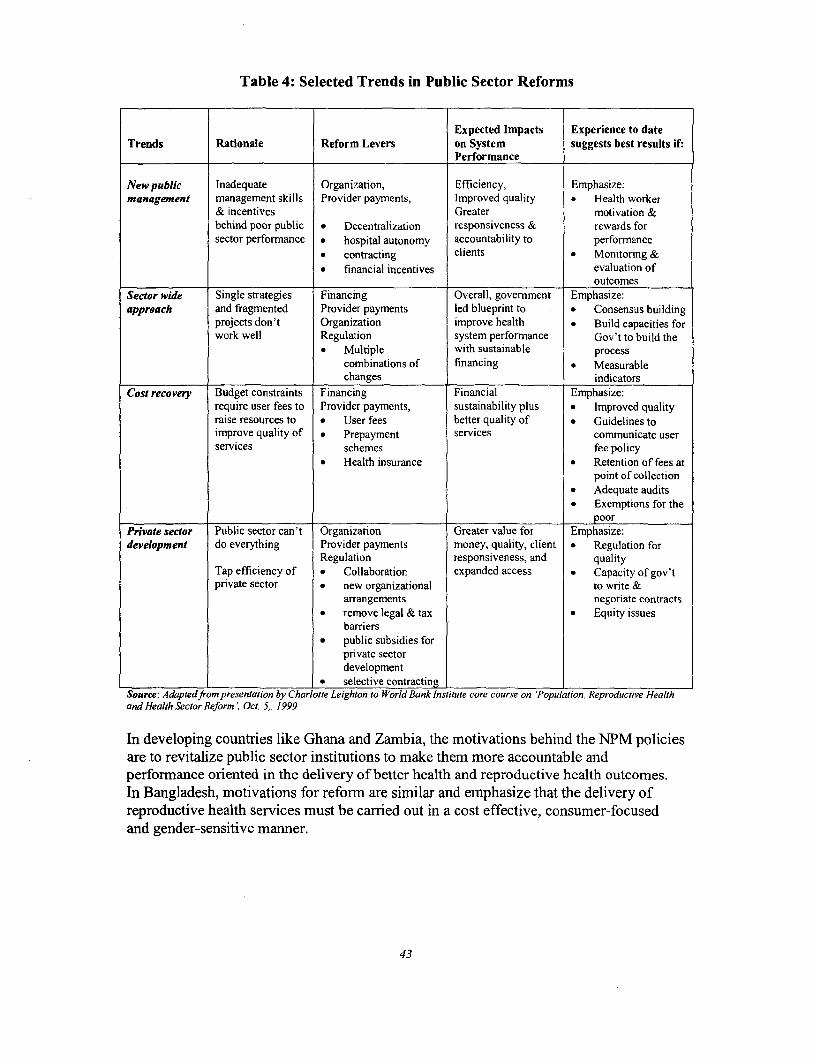
Table 4: Selected Trends in Public Sector Reforms
Expected Impacts Experience to dateTrends Rationale Reform Levers on System suggests best results if:
Performance
New public Inadequate Organization, Efficiency, Emphasize:management management skills Provider payments, Improved quality * Health worker
& incentives Greater motivation &behind poor public * Decentralization responsiveness & rewards forsector performance * hospital autonomy accountability to performance
* contracting clients * Monitoring &* financial incentives evaluation of
outcomesSector wide Single strategies Financing Overall, government Emphasize:approach and fragmented Provider payments led blueprint to * Consensus building
projects don't Organization improve health . Build capacities forwork well Regulation system performance Gov't to build the
* Multiple with sustainable processcombinations of financing * Measurablechanges indicators
Cost recovery Budget constraints Financing Financial Emphasize:require user fees to Provider payments, sustainability plus * Improved qualityraise resources to * User fees better quality of * Guidelines toimprove quality of * Prepayment services communicate userservices schemes fee policy
* Health insurance * Retention of fees atpoint of collection
* Adequate audits* Exemptions for the
______________.________ poorPrivate sector Public sector can't Organization Greater value for Emphasize:development do everything Provider payments money, quality, client * Regulation for
Regulation responsiveness, and qualityTap efficiency of * Collaboration expanded access * Capacity of gov'tprivate sector * new organizational to write &
arrangements negotiate contracts* remove legal & tax * Equity issues
barriers* public subsidies for
private sectordevelopment
* selective contractingSource: Adaptedfrom presentation by Charlotte Leighton to World Bank Institute core course on 'Population, Reproductive Healthand Health Sector Reform', Oct. 5,. 1999
In developing countries like Ghana and Zambia, the motivations behind the NPM policiesare to revitalize public sector institutions to make them more accountable andperformance oriented in the delivery of better health and reproductive health outcomes.In Bangladesh, motivations for reform are similar and emphasize that the delivery ofreproductive health services must be carried out in a cost effective, consumer-focusedand gender-sensitive manner.
43
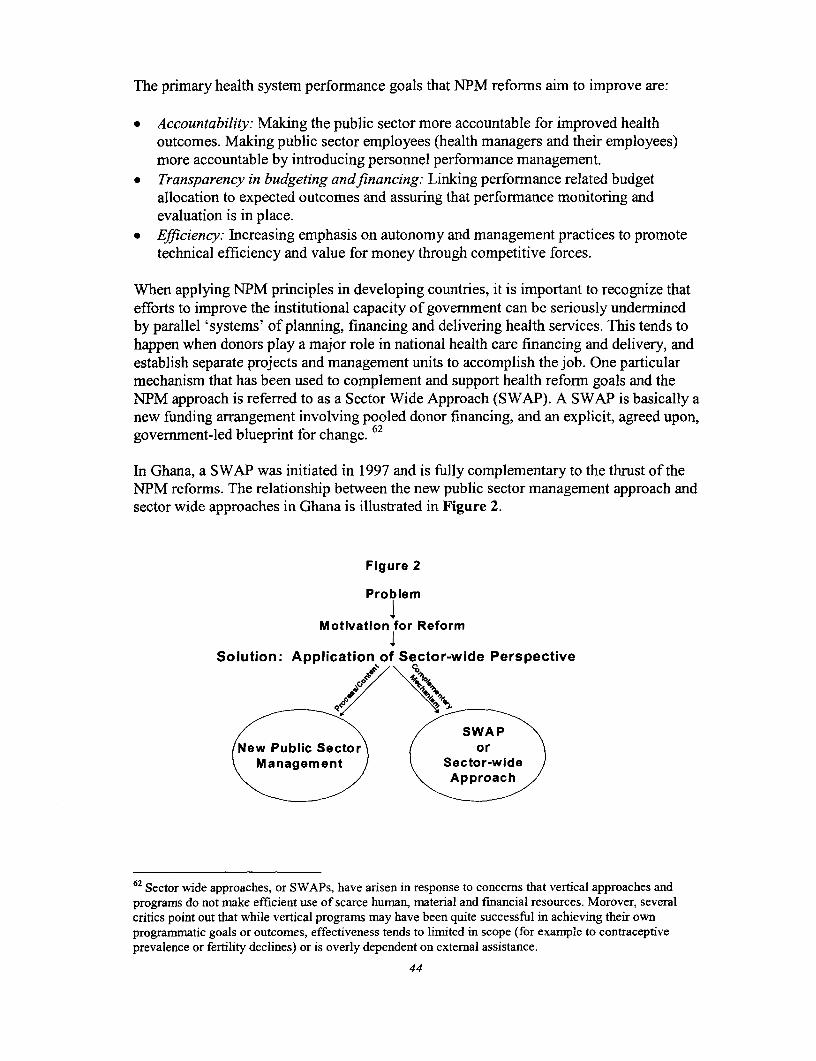
The primary health system performance goals that NPM reforrms aim to improve are:
* Accountability: Making the public sector more accountable for improved healthoutcomes. Making public sector employees (health managers and their employees)more accountable by introducing personnel performance management.
* Transparency in budgeting andfinancing: Linking performance related budgetallocation to expected outcomes and assuring that performance monitoring andevaluation is in place.
* Efficiency: Increasing emphasis on autonomy and management practices to promotetechnical efficiency and value for money through competitive forces.
When applying NPM principles in developing countries, it is important to recognize thatefforts to improve the institutional capacity of government can be seriously underminedby parallel 'systems' of planning, financing and delivering health services. This tends tohappen when donors play a major role in national health care financing and delivery, andestablish separate projects and management units to accomplish the job. One particularmechanism that has been used to complement and support health reform goals and theNPM approach is referred to as a Sector Wide Approach (SWAP). A SWAP is basically anew funding arrangement involving pooled donor financing, and an explicit, agreed upon,government-led blueprint for change. 62
In Ghana, a SWAP was initiated in 1997 and is fully complementary to the thrust of theNPM reforms. The relationship between the new public sector management approach andsector wide approaches in Ghana is illustrated in Figure 2.
Figure 2
Problem
Motivation for Reform
Solution: Application of Sector-wide Perspective
/ \ / ~~~SWA PXNew Public Sector or
Management Sector-wideApproach
62 Sector wide approaches, or SWAPs, have arisen in response to concerns that vertical approaches andprograms do not make efficient use of scarce human, material and financial resources. Morover, severalcritics point out that while vertical programs may have been quite successful in achieving their ownprogrammatic goals or outcomes, effectiveness tends to limited in scope (for example to contraceptiveprevalence or fertility declines) or is overly dependent on external assistance.
44
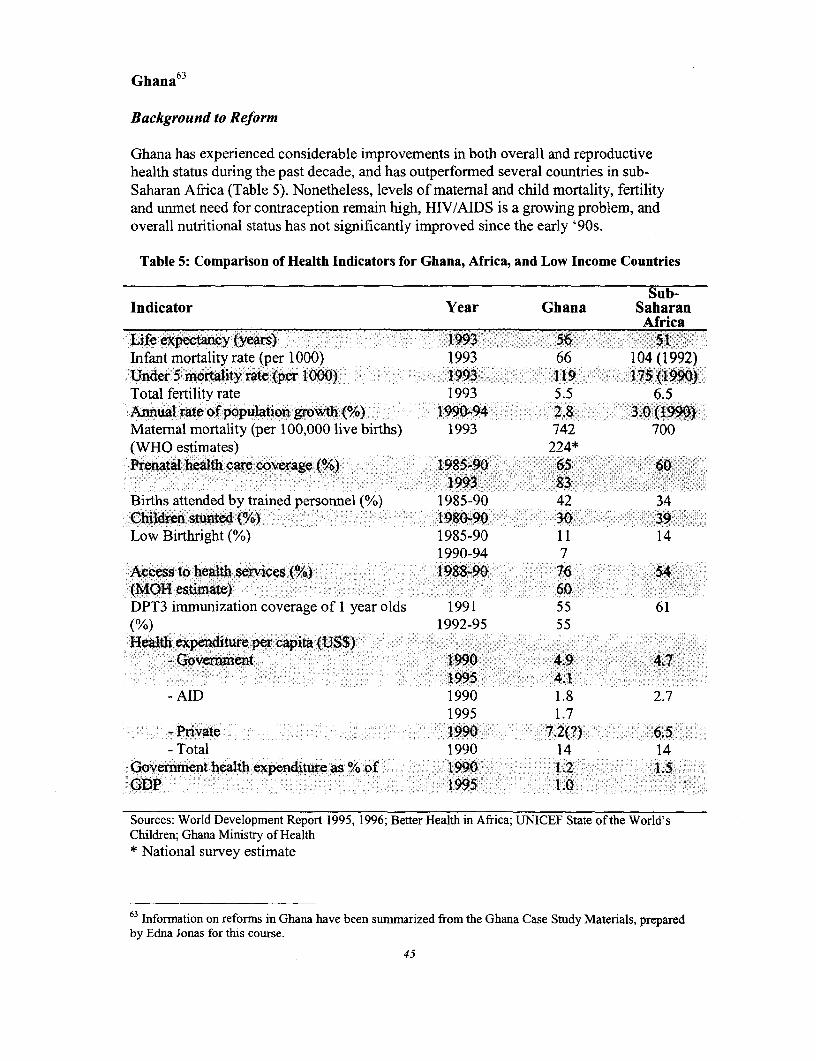
Ghana 6 3
Background to Reform
Ghana has experienced considerable improvements in both overall and reproductivehealth status during the past decade, and has outperformed several countries in sub-Saharan Africa (Table 5). Nonetheless, levels of matemal and child mortality, fertilityand unmet need for contraception remain high, HIV/AIDS is a growing problem, andoverall nutritional status has not significantly improved since the early '90s.
Table 5: Comparison of Health Indicators for Ghana, Africa, and Low Income Countries
Sub-Indicator Year Ghana Saharan
AfricaLife expectancy (years) 1993 56 51Infant mortality rate (per 1000) 1993 66 104 (1992)Under 5 mortality rate (per 1000) 1993 119 175 (1990)Total fertility rate 1993 5.5 6.5Annual rate of population growth (%) 1990-94 2.8 3.0(1990)Maternal mortality (per 100,000 live births) 1993 742 700(WHO estimates) 224*Prenatal health care coverage (%) 1985-90 65 60
1993 83Births attended by trained personnel (%) 1985-90 42 34Children stunted (%) 1980-90 30 39Low Birthright(°) 1985-90 11 14
1990-94 7Access to health services(%) 1988-90 76 54(MOH estimate) 60DPT3 immunization coverage of 1 year olds 1991 55 61(%) 1992-95 55Health expernditure pe capita (US$)
- Government 1990 4.9 4.71995 4.1
-AID 1990 1.8 2.71995 1.7
- Private 1990 7.2(?) 6.5- Total 1990 14 14
Goverrnent health expenditure as % of 1990 1.2 1.5GDP 1995 1.0
Sources: World Development Report 1995, 1996; Better Health in Africa; UNICEF State of the World'sChildren; Ghana Ministry of Health* National survey estimate
63 Information on reforms in Ghana have been sumiarized from the Ghana Case Study Materials, preparedby Edna Jonas for this course.
45
The main issues faced by the health system, as identified in the Ministry of Health'smedium term strategy, are poor access and poor quality of health and reproductivehealth services. Approximately, 30 percent to 40 percent of the Ghanaian population,mostly in rural areas, do not have access to health services and utilization of publiclyprovided outpatient services is quite low, at 0.35 visits per capita. Limited economicaccess on the part of the poor is assumed to have particularly negative implications forreproductive health since (1) maternity care and treatment for sexually transmitteddiseases are not exempted from fees at health facilities and (2) women have relativelyless access to financial resources than men. Numerous studies having identified the costof care as a major reason that the poor delay or avoid seeking appropriate care.
Ghana's health system faces major financing constraints, which have increased overtime. The government's recurrent health expenditures decreased from 14 percent to 9percent of total government spending between 1990-95'. Government spending is lessthan $5 per capita (about average for sub-Saharan Africa). Complicating the problemlimited public resources is the equity of public financing. The poorest quintile of thepopulation received onlyl2 percent of public expenditures on health in 1992-93, whereasthe richest quintile "captured" 33 percent of public expenditures.
In addition to government expenditures for health care, out-of-pocket health expendituresare estimated to be about equal to government expenditures. Combined, these twosources of financing are still less than the estimated $12 needed to finance a basicpackage of health services.64
User fees at public health facilities have been introduced to help shore up revenues, buthave not been administered equitably or efficiently in the past, and cost-recovery throughpatient fees continues to be a politically sensitive issue. After the introduction of user feesin public health facilities in 1985, utilization of public facilities fell, although utilizationhas since recovered. Currently, user fees finance about 10 percent of recurrent costs andhave been the major source of funds for non-wage recurrent costs at the district level. Toprotect the poor, user fees have been accompanied by an exemption policy and agovernment-financed fund for facilities to use to compensate them for loss of revenue.
Although the public sector is the dominant provider of health services, the private sector(both NGO and for-profit) plays a significant role in service delivery, providingapproximately 35 percent of outpatient services. Mission hospitals fill gaps for inpatientcare in rural areas and urban slums. For-profit providers, particularly clinics that targetwealthier segments of the population, are prevalent in cities in the southern part of thecountry.
We have selected Ghana for closer study because it faces immense budget constraints inits endeavor to reform deeply entrenched health system problems, government hasdecided to take the lead in launching ambitious reforms, and improved reproductivehealth outcomes are targeted by the reforms. How might such a country proceed, whatexpectations is it reasonable to aim for?
64 World Bank, 1995, Better Health in Africa, (Washington, DC)
46
The Reform Levers
Strengthening the health sector is a central focus of Ghana's development vision and isreflected in the government's 1993 Medium Term Health Strategy. By the year 2001,government aims to achieve the following outcomes:
* Increase life expectancy from 58 to 60 years* Decrease infant mortality from 66/1000 live births to 50/1000* Decrease under 5 mortality from 132/1000 live births to 100/1000* Decrease maternal mortality from 214/100,000 live births to 100/100,000* Decrease the annual rate of population growth from 2.8 percent to 2.75* Decrease total fertility from 5.5 children per woman to 5.0
To achieve these outcomes, govermment has identified a number of health systemperformance goals (i.e., instrumental goals), including:
* Improve efficiency of the public sector in delivering services, providing a basicpackage of services and integration of services.
* Improve equity by increasing physical and economic access to health andreproductive health services and providing higher quality services.
* Increase the availability offunds for service delivery, particularly at the district leveland below, and increase efficiency of collection and reimbursement through pooledfunds.
* Increase accountability, through increased transparency of funding sources and usesand periodic review of sector budgets, plans, and government performance, usercharges and external assistance.
• Increase efficiency through pooled funding,* Foster linkages with other sectors in order to decrease population growth and
malnutrition, increase female education, increase access to water and sanitation, anddecrease poverty.
To achieve these results, the Ghana reforrns employ several of the reform levers asfollows:
Financing
The Ghana reforms include major changes in the financing of health services. Financingof the sector has been reorganized and streamlined at a national level in order to increasetechnical efficiencies and costs associated with multiple, parallel projects and activities,and to better concentrate public subsidies on the funding and provision of a basic packageof reproductive health and other services. Pooled donor funding through a SWAPmechanism is complementing and strengthening government resources. In this sense, thefinancing lever serves improved efficiency goals -- efficiency in terms of minimizingduplication, reducing costs, and achieving greater value for money.
47
Efforts are also in place to improve the equity of financing and resource allocation bychanneling increased resources to the primary and secondary level within districts. Theseefforts include:
* deconcentration of resources from the central MOH to local Budget and ManagementCenters (BMCs): Since 1995, both planning and the authority to handle budgets forrecurrent expenses have been transferred from the central MOH to certified Budgetand Management Centers (BMC). BMCs can be District Health Management Teams,hospitals or other institutions that meet certain criteria. Currently, approximately 350of the more than 1,000 BMCs in the country have been certified and haveresponsibility to handle funds for recurrent expenses. Over time, responsibility forglobal budgets will be deconcentrated to BMCs.
* improvements in the user fee and exemption system to (i) make fees more transparentto the public, (ii) exempt vulnerable groups, (iii) build systems to regularly reviewand change payment rates, and (iv) incorporate incentives for patients to use primarycare services, rather than more expensive services.
Performance related budgeting is another important feature of the Ghanaian reforms.Funding allocations from the central MOH to the districts are now determined annuallyafter annual performance reviews, which assess progress at the district level towardreaching 20 sector-wide process and output indicators. Among these, for example, areimnmunization and couple years of protection targets, increased access to providers ofreproductive health services, and indicators of client satisfaction.
Organizational Change
Decentralization is a key organizational feature of Ghana's reform process. In Ghana,decentralization takes the form of deconcentration of responsibility for planning andbudgeting. Reorganization of the Ministry of Health and decentralization of responsibilityto District Health Management Teams (DHMTs) began in the late 1980s. As describedabove, BMCs (which include, but are not limited to DHMTs) are now responsible forrecurrent budgets and will evolve over time to have global budget responsibility. Reformplans also call for regional plans that will no longer be separate from the national plan;each regional office will be expected to prepare a strategy to guide the district's planningprocess. Under these reforms, the role of central MOH will change. Its functions willinclude policy oversight, resource allocation and financing, regulation, and advocacy,rather than the direct provision of inputs and services.
The reform process also involves new relationships between the governrment and non-profit and for-profit private providers. Historically, the government provided salarysupport and other operating expenses to mission hospitals that filled the gap in publicservice provision in under-served areas. An important reform just getting underway inGhana is the introduction of performance based contracting between the government andprivate not-for-profit mission hospitals. Eventually, the responsibility for these contractswill to shift from the national level to the districts, thus resulting in a clearer separation ofpublic finance and provision. For example, contracts with NGOs will specify the type andfrequency of reproductive services to be provided, along with monitoring guidelines.
48
Ghana also plans to pilot new arrangements between the government and private for-profit providers. These initiatives will link payment to performance and use financing toleverage and influence the distribution of services. Groups of private providers,physicians and ancillary providers will be encouraged to bid on contracts for providingreproductive health and other services in remote rural areas. The contracts will specifythe range of services to be provided and standards of care.
Regulation
Performnance-based monitoring and evaluation is not only being stressed in themanagement of public agencies and institutions (like hospitals) but is being incorporated,formally, in performance based contracts as noted above. Contracting is thereforeemerging as a more visible and powerfal tool for government-as purchaser of servicesfrom private or NGO providers-to assure quality, timeliness, compliance with treatmentprotocols, and provision of key reproductive health services.
Promoting Healthy Behaviors
The sector wide perspective in Ghana is guided by overarching development plans aswell as the government's Vision 2020, both of which identify selected social and culturalbehaviors that may be at odds with best practices in family planning, STD's/AIDSprevention, safe motherhood, and a more wholistic, gender sensitive approach toreproductive health.
Government has noted widespread pro-natallist values, conservative attitudes towardscontraception, lack of information and education on responsible sexual behavior andparenthood, and harmnful traditional practices that can affect the reproductive health ofmen and women, such as female genital mutilation.
To combat these influences, national health policy and health sector reformstrategies-relevant to reproductive health-have underscored the importance ofactivities to;
* promote birth spacing, breast feeding, immunization and other child survivalstrategies;
* educate and motivate men to accept and practice family planning;* create awareness of, and educate the public on the causes, consequences and
prevention of HIV/AIDS and other STDs;* discouragement of harmful traditional practices such as female genital mutilation;* information and counseling on responsible sexual behavior.
49
In addition, the 1994 ICPD conference, followed by the 1995 Fourth InternationalWomen's Conference have resulted in greater advocacy for women's rights and genderequity.65
Beyond advocacy, however, on-the-ground interventions to combat social and culturalbehaviors that are 'hostile' to better reproductive health have been limited and largely adhoc, with most socio-cultural interventions undertaken by NGOs and researchers. Forexample, the University of Ghana-Legon has done some interesting work on sexualbehaviors, but has had difficulties in influencing and inforning government policy.66
Research has also been undertaken on cultural perceptions of family planning andreproductive health interventions by the Navrongo Health Research Centre, resulting insome small scale interventions to encourage community engagement with health workersand targeting of male and elder opinion leaders.67 Some small scale initiatives have alsobeen conducted by a small private practitioner, aimed at village elders about theimportance of contraception and the need to cater to pregnant women.6 8
Lessons Learned
Slowly, but incrementally, the reforns being implemented in Ghana are demonstratingsome positive, measurable results. For example, Table 6 shows progress indicatorsrelated to reproductive health outcomes over the period 1996-98, showing gains in childimmunizations, couple years of protection, and attended deliveries.
Contrary to common expectations, little direct evidence was found of a donor-drivenpolicy agenda for reproductive health or for its integration but, rather, a government ledprocess located within the wider context of ongoing health reforms.69 Though manybottlenecks and challenges remain as the reforn process proceeds, it is also reassuring tonote positive process indicators including:
3 Increased Transparency: Independent financial and management audits of the MOHwere conducted in 1997 and 1998, and will continue to be conducted annually.
v Pooled Funding: Pooling of donor and govemrnment resources is progressing well.* Reproductive Health: Knowledge and support for reproductive health are high, and
Ghana introduced National Reproductive Health Service Policy and Standards in1996. However, national service standards remain largely unimplemented.
* Quality Assurance: Quality assurance teams are functional in five of the nine regionalhospitals and partially functional in one other. Quarterly monitoring of qualityassurance indicators was carried out in several regions.
65 65 Joe Annan and Helen Dzikunu, 1998, "A Study of Barriers and Opportunities for Integration ofReproductive Health Services in Ghana", (London: London School of Hygiene and Tropical Medicine,Mimeographed).
66 This refers to research by J. Anarfi and K. Awusabo-Asare in the Faculty of Social Science.67 This refers to work headed by Dr. Fred Binka and Dr. Alex Nazzar, with funding by the PopulationCouncil, Rockefeller and Ford Foundations.68 This refers to work by Dr. Odoi-Agyarko in the rural Upper East Region, with funding by UNFPA.69 Ibid.
50
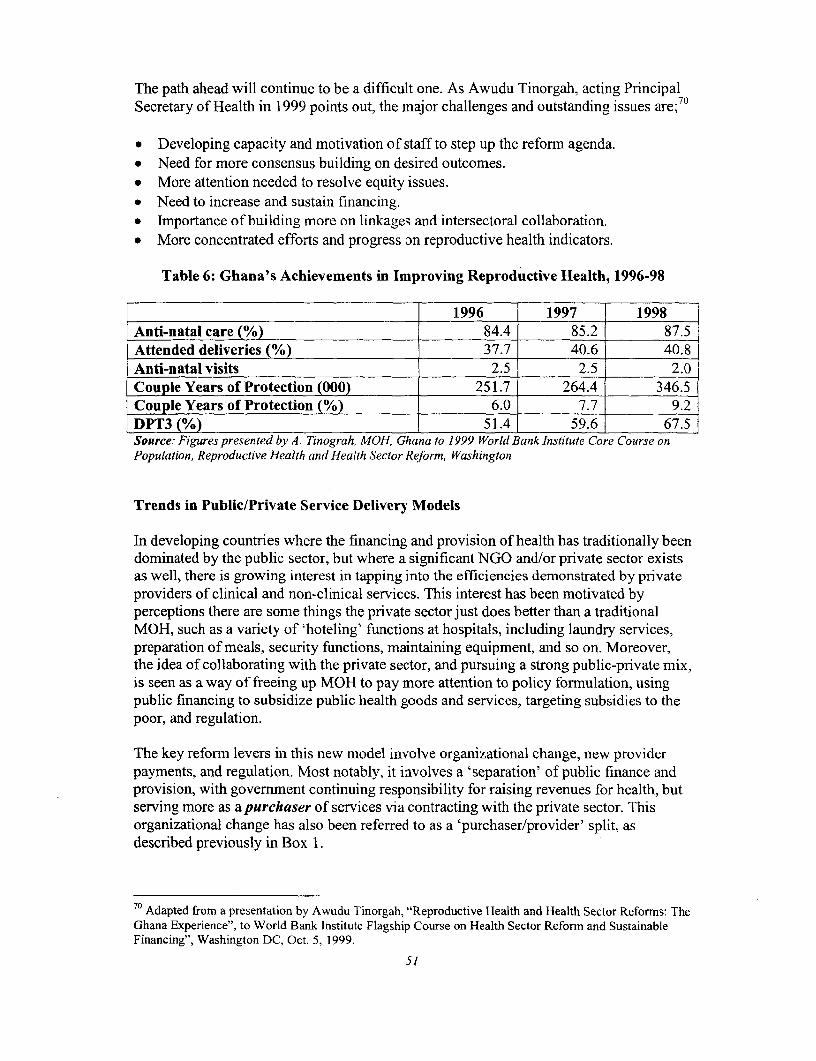
The path ahead will continue to be a difficult one. As Awudu Tinorgah, acting PrincipalSecretary of Health in 1999 points out, the major challenges and outstanding issues are;70
* Developing capacity and motivation of staff to step up the reformn agenda.* Need for more consensus building on desired outcomes.* More attention needed to resolve equity issues.* Need to increase and sustain financing.* Importance of building more on linkages and intersectoral collaboration.* More concentrated efforts and progress on reproductive health indicators.
Table 6: Ghana's Achievements in Improving Reproductive Health, 1996-98
1996 1997 1998Anti-natal care (%) 84.4 85.2 87.5Attended deliveries (%) 37.7 40.6 40.8Anti-natal visits 2.5 2.5 2.0Couple Years of Protection (000) 251.7 264.4 346.5Couple Years of Protection (%) 6.0 7.7 9.2DPT3 (%) 51.4 59.6 67.5Source: Figures presented by A. Tinograh, MOH, Ghana to 1999 World Bank Institute Core Course onPopulation, Reproductive Health and Health Sector Reform, Washington
Trends in Public/Private Service Delivery Models
In developing countries where the financing and provision of health has traditionally beendominated by the public sector, but where a significant NGO and/or private sector existsas well, there is growing interest in tapping into the efficiencies demonstrated by privateproviders of clinical and non-clinical services. This interest has been motivated byperceptions there are some things the private sector just does better than a traditionalMOH, such as a variety of 'hoteling' functions at hospitals, including laundry services,preparation of meals, security functions, maintaining equipment, and so on. Moreover,the idea of collaborating with the private sector, and pursuing a strong public-private mix,is seen as a way of freeing up MOH to pay more attention to policy formulation, usingpublic financing to subsidize public health goods and services, targeting subsidies to thepoor, and regulation.
The key reforrn levers in this new model involve organizational change, new providerpayments, and regulation. Most notably, it involves a 'separation' of public finance andprovision, with govermment continuing responsibility for raising revenues for health, butserving more as a purchaser of services via contracting with the private sector. Thisorganizational change has also been referred to as a 'purchaser/provider' split, asdescribed previously in Box 1.
70 Adapted from a presentation by Awudu Tinorgah, "Reproductive Health and Health Sector Reforms: TheGhana Experience", to World Bank Institute Flagship Course on Health Sector Reform and SustainableFinancing", Washington DC, Oct. 5, 1999.
51
The conditions alluded to above, as well as the sentiments regarding the private sector,characterize several developing countries, such as Egypt, Brazil, South Africa, Tanzania,Indonesia, that are currently experimenting with a purchaser/provider split. In Egypt, witha total population of 58 million, the new model was implemented in Alexandria in 1998,a city of 600,000, and in Menoufia, a city of 400,000. The Egyptian pilots are precursorsto nation-wide expansion assuming the pilots prove successful.
Egypt is also implementing major changes in the way they pay providers-switchingfrom salaries to capitation. Regulation is being tightened through licensing arrangements,negotiated contracts, and the monitoring and evaluation of client satisfaction. The Egyptpilot also pools tax revenues and social insurance contributions to enhance finicalsustainability of the new package of health services offered.
The motivation of the reformns is to:
* increase utilization of services (and access)* be more cost effective in the balance between preventive and curative services* get more value for money* increase client accountability* pool resources for health in a way that better cross-subsidizes the wealthy and poor,
the healthy and sick.
Improving reproductive health is a major preoccupation of the Egyptian pilot insofar asbasic packages of reproductive health and other services are provided in Family HealthUnits, with referrals for obstetric complications to nearby hospitals.
Egypt 71
Background to Reform
Egypt's health system has long suffered from four major structural weaknesses. First,while health care in Egypt is "free" to all citizens -- financed by general tax revenues andsocial insurance contributions -- resources have traditionally been lamented as inadequateto provide quality care, with glaring gaps in rural and poor areas. Total expenditures onhealth per capita were in the vicinity of $20 per capita in 1995, with public expendituresamounting to about $7 per capita and private expenditures of $13 per capita. Withouttapping private expenditures in an organized way, government has consistently fallenbehind its promises of providing wide access to a basic package of services.
Second, the delivery system is highly fragmented into many specialized programs,leading to inefficient coordination of care, relatively weak emphasis on primary andpreventive care, and lack of unifornity in records keeping. For example, there are 29uncoordinated government and public entities such as the Ministry of Health andPopulation, the Curative Care Organization, and the Health Insurance Organization,
71 Information on reforms in Egypt and Brazil has been summarized from the Egypt and Brazil CaseStudies, prepared by Susan Harmeling for this course.
52
along with numerous private, vertical programs in such areas as family planning,immunization, and control of parasitic diseases.
Third, the fragmented system of provision has given rise to relatively strongconstituencies for certain health issues, whereas other diseases and issues receive little orno attention to funding. This has created a maldistribution of resources and a very unevenhealth care system. For example, population and family planning have long beenrelatively large recipients of donor funding in Egypt, but with few links to otherreproductive health services.
Fourth, as most of the private verticalized programs are donor-financed, they aresomewhat unstable, subject to collapse if donors withdraw their funding.
In addition to the above, reviews of the health system in Egypt have traditionallylamented poor quality of governiment provided health services, inefficiencies in the formof low hospital occupancy rates (government owns most hospitals), and an oversupply ofpoorly paid physicians, with doctors usually having positions as an MOPH physician, aswell as maintaining a private practice. In 1995, 89% of physicians held multiple jobs.
Reproductive health indicators further suggest the country has major inequalities betweendifferent geographical and socio-economic groups. Infant and neonatal mortality were 51per 1,000 and 29 per 1,000 in rural areas, versus 87 per 1,000 and 42 per 1,000 in ruralareas. The infant and neonatal mortality rates were approximately three times higheramong women with no education and women who had completed secondary/highereducation. Overall, medical assistance at delivery was received by about 46 percent ofwomen in the mid-1990s, and about 39% had medical prenatal care. The CPR was about48%, signifying a positive effect of vertical FP programs. Overall, the maternal mortalityrate was about 174 per 100,000 live births.
We have selected Egypt for closer study because (i) the impetus to more away from anarrowly construed population and family planning programs to a reproductive healthapproach took place at the ICPD Conference in Cairo in 1994, and (ii) the government ofEgypt is highly motivated to translate the resolutions and rhetoric of the Cairo conferenceinto action. What approach has Egypt, with a per capita income of about $700 in 1995taken; what expectations have been realized?
The Reform Levers
The overall mission of health reform in Egypt is to improve health and reproductivehealth outcomes of the population by (i) making primary and preventive health care thefoundation of reform, (ii) integrating the provision of services in a system of community-focused providers (iii) assuring universal access to a basic benefits package to allmembers of the community, (iv) combining public and private health expenditures tofinance delivery of the package, and (v) create a more effective public-private partnershipin health care service provision.
53
With respect to reproductive health, the basic package of benefits includes three sets ofcost-effective services:
1. Maternal health care services, including selected safe motherhood interventions andfamily planning and
2. Child health services, including integrated management of childhood illnesses (acuterespiratory illness, diarrhea, malnutrition) and immunizations
3. Adult and all age group services, including treatment of TB, and management ofsexually transmitted diseases.
In view of the government's far reaching reform goals, it has commenced with pilots inthe urban and peri-urban areas of Alexandria, with a population of 600,000, followed byMenoufia, a medium sized urban area of about 400,000. These pilots are to set the stage
for nation-wide expansion over the next decade. The major reform levers in the Egyptianreforms are organizational change, financial and provider payments.72
Financing
The most important change in the financing of care involves (i) the separation publicfinance and provision of care, (ii) the creation of a Family Health Fund to purchase healthservices, and (iii) the adoption of a family practice model to provide a basic benefitspackage of integrated primary care services to patient rosters of 500-600 families (2,500-3,000 individuals).
With government endorsement and support of the new Family Health Fund, financing forservices derives from:
* government tax revenues* contributions for social health insurance (for those who pay into Egypt's Health
Insurance Organization)* a fee to join the roster of a family practice* co-payments for services obtained.
Out-of-pocket payments that were previously made in a haphazard way will now bechanneled into a more formal structure, namely a standard copayment and an annualenrollment fee. While subsidies will be provided for the poor, and fee levels will be keptlow, a major concern of the Egyptians is how to sustain provision of the basic packagefinancially.
During the pilot, the Family Health Fund has been designed to be a purchaser of healthservices on behalf of the citizens of Alexandria (or Menoufia). Its principal challenge isto attain much higher efficiency, value for money, and quality than had been attainedunder prior MOHP financed and provided health care. To this end, it enjoys a measure ofautonomy in its management, has control over earmarked revenues for health, and will bejudged on performance results.
72 Design and progress of the pilot is based on reviews and presentations during the fall of 1999 by MaryPatterson, Abt Associates, PHR project, Egypt, and Susan Harmeling, case study on Egypt, niimeo.
54
Organizational Change
The Family Health Fund contracts with various levels of care in the "family practicemodel" to provide health services to individuals and households on the roster. All public,not-for-profit or for-profit providers of services may compete for contracts, provided theysatisfy certain accreditation criteria.
Organizational reforms stress greater integration of primary, preventive and curative carethrough the family practice model's three levels of care, called the Family Health Unit(FHU) . The first level, the "Family Health Unit" provides the first level of preventiveand curative outpatient services. Families that join the roster are initially assigned to aunit, but they may change once a year to any unit of their choice. This responds to designelements in the pilot that aim to be client responsive. The second level, the "FamilyHealth Center" is the first level of referral for basic inpatient care including safeuncomplicated deliveries, essential obstetric care, uncomplicated neonatal services, andseverely ill children. The third level, the "District Hospital" is the second level of referralfor complicated deliveries and or/neonatal care, limited care for stabilization of diabetesand hypertension, severely ill children, etc. Additional organizational features of theFamily Health Unite are summarized in Box 4.
Box 4: What is a Family Health Unit (FHU)?
The central organizational features of a FHU are:* autonomous group practices with a 'management board' comprising an administrative
manager, as well as physician/nurse representation* 5 to 11 full-time qualified doctors (depending on size of the catchment area), that may be
MOHP or private sector physicians working in a new health facility, an existing facility, ahospital, or in rented or owned buildings
* an equal number of nurses (as doctors), staff for social work, reception, accounting andpatient education.
* viable economic entities to contract to provide health services and business functions
Provision of Services by an FHU includes:* entitlements by all enrollees to a basic package of health services, including RH
* 24 hour referral service by FHU doctors-who serve as gatekeepers-to Family HealthCenter (hospitals)
The philosophy behind the FHU:* a broader composition of health professionals in one place will promote better quality of care
than an individual practice* member doctors in each practice will have a vested interest and 'joint fate' in performance of
the overall group in the FHU* patients will be assured access to health services, even if one physician is away, sick, or on
vacation* pooling of resources, and application of business practices, will reduce administrative costs
and increase efficiency.
Note: Based on case material prepared by Susan Harmeling, World Bank Institute, 1999, and a presentation by AhsanSadiq, Partnerships for Health Reform Project (USAID) to the World Bank, Washington DC, 1998
55
Provider Payments
Payment reforms combine a base salary for both doctors and nurses, with a capitationpayment to the FHU for each person on the FHU enrollment roster. To prevent the FHUfrom enrolling more patients than it can accommodate, there is a cap on enrollees of2,500 per doctor/nurse combination. The capitation payment to the FHU is then used togive doctors and nurses incentive payments for quality. Penalties can also be levied ondoctors for over-referrals and over-prescribing. These arrangements, reviewed regularlyby the FHU 'management board' give leverage to the notion of 'joint fate' of allprofessionals in an FHU, as noted in Box 4.
Reimbursement of contracts is also performance based, meaning that if agreements andtargets explicitly built into the contract are not fulfilled, payment can be reduced orwithheld. This reflects new public management practices noted earlier, with contractingserving as a major vehicle for purchasers to specify, then monitor efficiency, quality, andvalue for money. Efficiency in contracts signed by the Family Health Fund is assessed interms of roster size (are enough or too many people on the roster), volume of visits perindividual, timeliness of encounters with providers, referral rates, and prescription costsper visit. Quality is assessed in terms of patient satisfaction, provider conformance withprotocols and guidelines, and overall outcome indicators.
Regulation
Regulation of this new approach is to being jointly shared by the MOHP and the FamilyHealth Fund, Family Health Units, and Family Health Centers (hospitals). Oversight isalso provided by the Ministry of Finance regarding past (or new) fixed investments ingovernment owned health infrastructure-such as approval of a new hospital.
Regulations are expected to be more enforceable in the new the new system because;
* physician groups seeking to qualify as a Family Health Unit must demonstrate to theFamily Health Fund they have meet licensing standards
* FHUs that contract with the Family Health Fund to provide services must agree toproviding a pre-determined benefit package to all enrollees, and must submit tomonitoring and evaluation of performance
* FHUs are expected to self-regulate physician and nurse performance, providingmonetary incentives for quality and penalties for over-prescribing and over-referrals.
* Client feedback, in the form of satisfaction surveys, will be used to reassessperformance of FHUs and modify behaviors as appropriate.
Promoting healthy behaviors
Promotion of healthy behaviors in the Egyptian context relies on two interventions: 1)proactive management of rosters by the family care team, and 2) cooperation between thehealth district and the family health unit to identify and manage health behaviors in thepopulation.
s6
The proactive management of the client registration rosters by the team includessurveying the roster to identify clients who are eligible for preventive services such asimmunization, well-baby care, and annual physical examination. Proactive rostermanagement also identifies targets for secondary prevention such as individuals withchronic disease or families with communicable diseases such as tuberculosis.
Cooperation between the family health unit and the health district means that healthpromotion can be affected either by the farnily health providers or by the public healthauthorities. Close cooperation between the family health unit and the district can result inrapid dissemination of information to the client since all families are rostered and knownto a primary health care team.
The pilot sites are using both interventions to promote healthy behaviors. For example,family health providers have identified all hypertensives and diabetics on their roster andare proactively managing their conditions according to agreed practice guidelines toprevent serious complications. The health district and the pilot sites have cooperated tocontrol several outbreaks of communicable disease among the school-age populationrepresented in the roster.
Lessons Learned
According to people involved in the Egyptian pilot, it was a wise decision to begin on apilot basis because a great deal of planning, learning-by-doing, and overcomingresistance is involved. While there is widespread agreement that major changes in theEgyptian health system are needed, and while policy makers and planners are rising tothe challenge, it is the deeply entrenched 'culture' of health care delivery in the countrythat is most difficult to change. That culture is characterized by:
* prevailing power structures in the organization financing and provision that resist thenew purchasing agents and focus on primary health care units
* a top-down management style -- where the top spots have traditionally been'rewarded' to physicians-that resists the new role of professionally trainedadministrators and business managers.
* modes of organizing and delivering services that corresponds more to theconvenience of providers than clients
* an economic class system that resists integration of both providers and clients ofhealth care
* a patient orientation that favors seeing specialists and receiving drugs* g prescriptions, rather than seeing more cost-effective providers of services at first-
referral centers.
As the Alexandria pilot only commenced in the spring of 1999, it is too early to ascertainimpacts on measurable outputs and health outcomes. However, process indicators revealthat:
* All pilot sites are rapidly filling their client registration rosters. The first facility toopen in the Montazah district completed their roster in three months for all familypractice teams and now has a waiting list of families. Preliminary results from
57
recently completed focus groups indicate that the care model is popular with mostfamilies, and the increased quality and responsiveness of care are recognized andvalued by all clients.
* The providers like the new care model, but they feel the current level ofreimbursement is not sufficient to support the increased productivity expectations.Additionally, all providers are requesting additional training to enable them to handlethe new integrated delivery of health and reproductive health services moreeffectively.
* More effective referral tracking is needed to assure continuity of care. The referralsystem does not always capture all information on the episode of care, and there areplans to improve both the organizational and cost information available on referrals.
* Preliminary accreditation visits have shown that the family practice model is not yetwell understood by clients. Many clients still do not understand the family practiceapproach with its emphasis on primary care and 'gatekeeper roles' to assure referralsare necessary, and want to see a specialist. More patient and community education isneeded to enhance understanding of the integrated care model.
• Further development of the concept depends on additional training, enhanced familyand community education, and careful analysis of provider payment strategies toassure a reasonable income for providers given the increased expectations forefficiency and effectiveness.
Trends in new Private Service Delivery Models
Reforms to improve reproductive health outcomes must extend beyond governmentcapacities to finance and provide services. NGOs and private-for-profit providers aremajor players in the provision of reproductive health services as well. A large portion ofhouseholds in many developing countries-up to 70 percent in India-make out-of-pocket payments for services that go directly to NGO or private providers. Are theserelationships and the kinds of services provided conducive to advancing the reproductivehealth agenda? In addition to satisfying immediate demands of clients, are NGO andprivate-for-profit providers also interested in promoting healthy behaviors, in tacklinggender-specific issues?
The prevailing motivation behind the provision of services in the private sector is tocover all production costs, make a faire rate of return, and be responsive to clientdemands. An appealing feature of private sector involvement in financing and providingreproductive health is that efficiency and quality of services are stressed. According tovarious sources, this is manifest in:
* Strong motivation to produce maximum output at minimum cost (technicalefficiency) and to allocate of resources in ways that respond to societal preferences,as expressed by individual's willingness to pay for different services (allocativeefficiency);
58
* Strong client orientation because inadequate attention to client preferences and poorquality will motivate clients to seek services elsewhere; and
* Motivation to spend money on research and development, as well as to communicateavailability goods and services to clients.
However, negative aspects of private sector involvement also tend to be widelydiscussed, particularly those that relate to equity concerns, as well as failure of privatemarkets to provide public health goods and services (positive externalities);
* lack of interest in providing preventive health goods and services to those unable topay;
* lack of interest in private financing or provision of "public" health goods andservices, meaning those goods and services with societal benefits that extend beyondwhat individuals are willing to pay for;
* motivation not to provide catastrophic insurance coverage to those who are poor, sick,or injured and are unable or unwilling to pay relatively high risk-rated insurancepremiums;
* supply-side 'moral hazard', whereby private providers may supply more costlyservices due to asymmetries of information between provider and client (the'principal-agent' problem), and therefore reap unfair profits;
* private insurance reimbursement patterns-especially fee-for-service -- that tends tofoster cost escalation and purchase of high tech equipment
* high administrative costs involved in competition among private insurers formembers, as well as high transaction cost (and investment of resources) in riskselection.
The challenge facing governments where private markets are thriving is to stimulate thecapacities of private health providers to get better value for money (efficiency and qualitygains), while requiring them to adopt practices that are in the best interests of clients andsociety. In the developing countries we review here-Bolivia and the Philippines-thegovernment or donors have played precisely this kind of nurturing role with the resultthat private sector entities have become allies in increasing financing and provision ofreproductive health services.
In Bolivia, we examine a self-sufficient NGO provider called PROSALUD (theAsociaci6n Protecci6n a la Salud), whereas in the Philippines we examine a ManagedCare HMO model to provide health and reproductive services to relatively low incomehouseholds. Both of these 'models' combine (i) efforts by government to guide privateentities to cater more for the needs of low income people, and (ii) innovations in privatesector health care delivery to provide highest quality care at lowest cost.
Bolivia
Background to Reform
Bolivia has a population of about 7 million people and a GNP per capita ofapproximately $500. The country has a long history of political instability, mediocreeconomic performance, and remains one of the poorest in Latin America (except for
59
Haiti). About half its population resides in urban and peri-urban areas. In recent years,hyperinflation has been brought under control (estimates ranging up to 30,000% in 1985)to less than 10% in 1995, and the country has experienced improved economic conditionssince market-oriented policies were introduced.
In 1993, the MOH provided services to about 43% of the population, while the privatesector-including traditional providers and private pharmacies - provided about 46% ofhealth services. Yet, overall, it has been estimated that only one-third of the Bolivianpopulation is receiving adequate medical attention, with even smaller proportions ofwomen receiving pre- or post-natal care.
Limited overall coverage, especially in peri-urban and rural areas, has prompted growthof NGOs as well as the practice of nontraditional medicine. In the past, the orientation ofprivate for profit providers has been largely curative, providing rather limited coverage tothose willing and able to pay. The private, not-for-profit sector on the other hand was notwell organized, has relied heavily on outside (donor) funding, and has involved littlecollaboration with the public sector in evolving standards, norms, priorities and practices.
The Reform Levers7 4
Reform of the Bolivian health system started in 1990 with emphasis on local govermnent,modernization of the social sector, opportunities for private sector development, newcriteria for external aid, and new health financing mechanisms. In addition, thegovernment had already paved the way for an integrated approach to delivering familyplanning in 1989, by deciding to incorporate family planning services into the nationalmother and child health program.
It is in this context that efforts to develop PROSALUD-beginning in 1987 with the helpof USAID-began to thrive. Legally, PROSALUD is a private, nonprofit Bolivian healthcare organization that serves low-income and lower-middle class populations in urbanand periurban areas. Between 1990 and 1998, growth of health services offered byPROSALUD grew fivefold from about 200,000 services in 1991 to more than a millionby 1998. By the end of 1999, it operated health facilities in nine cities throughout thecountry and offered services to about 500,000 people.
Initially, PROSALUD stressed primary and preventive services, while referring clients toexternal clinics and hospitals for more complicated curative care or hospital services.Finding the referral practice unsatisfactory to many clients, PROSALUD eventuallyadded referral facilities to its own network. It now provides a full package of preventiveand curative health and reproductive health services at its basic clinics, its polyclinics,and referrals to its hospital. Population and reproductive health services include:Basic clinics:
7 USAID, 1999, "Bolivia in Country Health Profile" (United States Agency for International Development,Latin American and the Caribbean Resources, ht:,/!www.info. usaid.gov/counitrieslbo.fbolipro.txt, Oct.19,1999.74 This section borrows from Carlos J. Cuellar, William Newbrander, and Gail Price, 2000, ExtendingAccess to Health Care Through Public-Private Partnerships: The Prosalud Experience, (Boston, MA:Management Sciences for Health).
60
* family planning-all reversible methods* reproductive health counseling* initial prenatal visit* follow-up prenatal care* deliveries* well-baby clinical services* immunizations* health education
Polyclinics:
* Pediatrician and gynecologist consulting time* Voluntary surgical contraception (in some)* immunizations* well-baby clinical services* reproductive health counseling* postpartum care* follow-up prenatal care* health education
Hospital:
* Cesarean section and other simple surgical procedures* Specialized laboratory services, including tests for HIV* Voluntary surgical contracept8ion* immunizations* well-baby clinical services* reproductive health counseling* postpartum care* follow-up prenatal care* health education
Financing
The management of PROSALUD aims to achieve self-sufficiency in financing, withouthaving to rely on external sources of donor funding clientele possible. PROSALUDcurrently finances its services by a fee-for-service structure that is designed to becompetitively priced with private health clinics by charging fees for consultations,laboratory tests, and drugs. The goal has been to provide high-quality services atreasonable prices, resulting in a high volume of services. This form of paymentrepresents 95% of all revenues.
For those patients who are truly unable to pay for the services needed, staff ofPROSALUD collaborate to determine a patient's ability to pay. Usually this results in anarrangement whereby the patient pays something at the time of service and some later.At the same time, PROSALUD cross-subsidizes the poor with revenues received by those
61
more able and willing to pay-especially for curative services -- so as to serve the widestpossible clientele. Through this approach, roughly 10% of all the curative servicesdelivered by PROSALUD are provided free to indigent clients. In addition, following theinitial consultation fees, PROSALUD tries to contain costs by pricing a completepackage of services for an episode of illness rather than set prices for individual services.
PROSALUD's health network recuperates over 70% of its costs from user fees. Thisrepresents one of the highest levels of self-sufficiency in the developing world, and anoteworthy achievement in a country considered the second poorest in Latin Amenrca.
As a means of strengthening its financial sustainability, PROSALUD is also offeringcompanies a deferred payment plan that consists of enrolling company employees in theirsystem and billing the companies at the end of each month for the services provided. Thisapproach, yet to be evaluated, replaces PROSALUD's attempt to initiate a prepaymentsystem, which resulted in overutilization (moral hazard in insurance terminology) andtremendously high drug costs.
Provider Payments, Incentives and Motivation
PROSALUD's doctors and specialists are paid by salary, as are medical workersemployed by the MOH. A problem with this means of payment is it contains noincentives to work beyond regular "office hours", or at times that might be moreconvenient for clients, such as evenings or weekends. Convinced that clients wantedaccess to PROSALUD facilities on weekends, PROSALUD's management took the riskof offering its doctors a considerably higher proportion of the patient revenues generatedon Saturdays than they could earn on weekdays. For PROSALUD specialists, a fee pervisit was established, with 50% of the fee going to the specialist.
These innovative payments had the effect of (i) increasing overall demand for patientservices, and (ii) motivating the physicians themselves to "bring in" additional patients toPROSALUD. This happened because wives (and children) who might ordinarily go toanother health center were more willing to come to centers that could also provide theirhusbands with care (men preferred to the facilities on weekend), and vice versa.
Organizational Change
PROSALUD functions under autonomous management, which oversees hiring, trainingand firing of personnel, purchasing and distribution of drugs and supplies, managingcommunity relations, overseeing the delivery of services and controlling quality, andmaintaining fiscal and financial structures. Reflecting commitments to decentralization inthe country, PROSALUD's central office is complemented by several decentralizedregional offices that manage health centers.
A fundamental understanding and application of basic market principles, such as supplyand demand and the promotion of services, has been key to PROSALUD's activities.During the planning, establishment, and management of the organization's cost-recoverystrategy, the analysis of market dynamics has consistently been utilized as a managerialtool. The centrality of these functions to sustaining the organization of PROSALUD's
62
activities-human resources, services rendered, configuration of facilities, monitoringand evaluation-can be appreciated in view of the reality that failure to attract clients andprovide high quality services would result in bankruptcy.
Use of basic market principles as well as rigorous application of performance-basedmanagement-including personnel recruitment and training-has resulted in;
* PROSALUD staff have been more productive than MOH staff in terms of servicesrendered;
* PROSALUD's unit costs have been lower than those of MOH clinics;* PROSALUD facilities were more efficient in their operation than MOH facilities;* PROSALUD's catchment population made greater use of services-nearly I visit per
person per year per PROSALUD member compared to .25 visits per year at MOHfacilities;
* Patient's perception of quality of care, as well as patient satisfaction are better than inMOH facilities;
* Cost-recovery percentages were higher in PROSALUD facilities than in MOHfacilities.
Regulation
PROSALUD's central management office has established working relationships withother service providers in the area, including the MOH. For example, PROSALUD'sstandard package of essential, curative, and specialty services was defined using thegovernment's guidelines and considering local community needs. All clinics providepreventive care and other priority public health interventions free of charge.
More important, PROSALUD self-regulates for quality, driven by its need to becompetitive, to attract clients with other choices. As part of its vision, it includes amongrights of its users, dignity, information, confidentiality, and quality.75 PROSALUD notonly attempts to abide by standards set by MOH, but has actually played a key role indemonstrating how to achieve those standards in its facilities, and therefore setting anexample for MOH clinics.
Promoting Healthy Behaviors
Each PROSALUJD clinic is staffed with community health workers who promoteservices, supply family planning, arrange for health education, and follow up with clientsto ensure that appropriate treatment has been provided. While motivated by 'good will',the real driving force behind such promotion is it serves as a key component ofPROSALUD's marketing strategy to reach more people and win more clients.PROSALUD staff members also collaborate with other local organizations to developand conduct large-scale IEC campaigns, using effective social marketing techniques toraise the public's awareness of the importance of preventive care and thus to generatedemand for these priority services. To bolster the accessibility of services and ties with
75 El libro azul de PROSALUD" (The 'Blue Book' for PROSALUD, an employees handbook.)
63
the local community, each PROSALUD clinic also includes a conference room for publicuse, as well as a community advisory committee.
Lessons Learned
Interest in replicating the PROSALUD model is growing in Bolivia and other developingcountries, based in part on successful replication in several Bolivian cities. It's experienceover more than a decade, lessons learned through trial and error, and extensivemonitoring and evaluation of performance provide a rich source of insights on what to doand not to do-far more than can be reviewed here. Briefly, some of the more importantlessons that emerge from this experience are:
* PROSALUD devoted considerable time and energy to refining multiple dimensionsof its organization-financing, incentivizing providers, management performance,self-regulation and monitoring, marketing strategies-in its attempt to build self-sufficiency and sustainability.
* Assuring financial sustainability was a key, if not the key building block, to assuringexpanded access to services (through cross-subsidization), quality of services, payingand incentivizing providers, and accommodating demands of clients. Costing andrealistic pricing of services was an essential ingredient to containing costs and livingwithin PROSALUD's budget envelope.
* The philosophy and practice of good marketing strategies-involving managerialoversight of products, identification of client target groups, dissemination ofIEC-involved a great deal of learning-by-doing, but emerged as a foundation stoneof PROSALUD's organizational efficiency.
* Decentralized management to regional and clinic level, as well as close collaborationand networking with community groups helped assure that PROSALUD's vision,facilities and services were relevant to client needs.
Philippines
Background to Reform
The Philippines has a population of about 74 million people and a GNP per capita ofabout $2,400 (1997). The country has a strong private sector, strong societal endorsementof market competition, and a public sector that has traditionally been plagued byshortages of revenues for health, poorly targeted subsidies for hospital care, and weakand ineffective local health spending on primary and reproductive health care.
Approximately 54% of personal health care in the Philippines was paid from privatesources in 1997 (including social insurance), with the remaining 39% paid bygovernment revenues and 7% by social insurance. Providers consist of HealthMaintenance Organizations in the larger cities, private polyclinics in the major cities,private practitioners and their clinics mostly in urban areas, and rural health units andclinics run by the government for out-patient primary care services.
64
The first HMO in the Philippines was established in 1978. Since then the industry hasgrown to 32 large, operating HMOs, most operating on a for-profit basis, and theremaining few run by NGOs and cooperatives. The HMO industry is entirely privatesector driven. It started without any specific govenmment regulatory mechanism and todate only an administrative order by the Department of Health regulates the operation ofHMOs.
In 1987, an Association of HMOs of the Philippines was formned by the private sectoragents involved to unite the industry, develop standards, and benchmark norms ofbusiness conduct. It consists of 18 HMOs that represent 95% of HMO clients. By 1997,their number had risen to 32, they provided coverage nationwide in major populationcenters, and they enrolled about 2 million or 10% of the population.
If and when the government launches a national health insurance program (as it hopes todo), it is expected that HMOs will be contracted by government to serve as majorproviders of households nationwide. However, concerns have been raised over the issueof affordability, especially in view of current HMO practices that cater to formal sectoremployers and their relatively well paid labor force.
With the above in mind, a USAID funded pilot project called Healthsaver hascollaborated with a major HMO PhilamCare to test the idea that low cost packages ofcare can be successfully provided to lower income workers. Success in this contextmeans that costs to the HMO can be recovered through premiums, and that a fair rate ofreturn on investments can be realized. Government's primary interest in expanding thismodel is not solely to reduce costs and improve efficiency-as in the US-but to increasefinancial access to quality service.
PhilamCare was first established in 1982, now serves about 300,000 members, includingover 650 corporate clients, owns clinics staffed by salaried physicians, and contracts in-patient services with mostly private tertiary hospitals. In 1996, it began to pilot three lowcost plans, aimed principally at employed males in factories and rural cooperatives.
The Reform Levers
Financing and Benefit Package7 6
Based on an assessment of unit costs, as well as market analysis of what clients werewilling and able to pay, Philamcare offered three different benefit packages to differentcategories of clients. An important guiding principal in the design of each package is thatprovision must be financially sustainable, otherwise bankruptcy would occur.
76 Source: Information derived from a presentation by Benito R. Reverente to the World Bank Institute Core Course onPopulation, Reproductive Health and Health Sector Reform, Washington DC, Oct. 7, 1999.
65
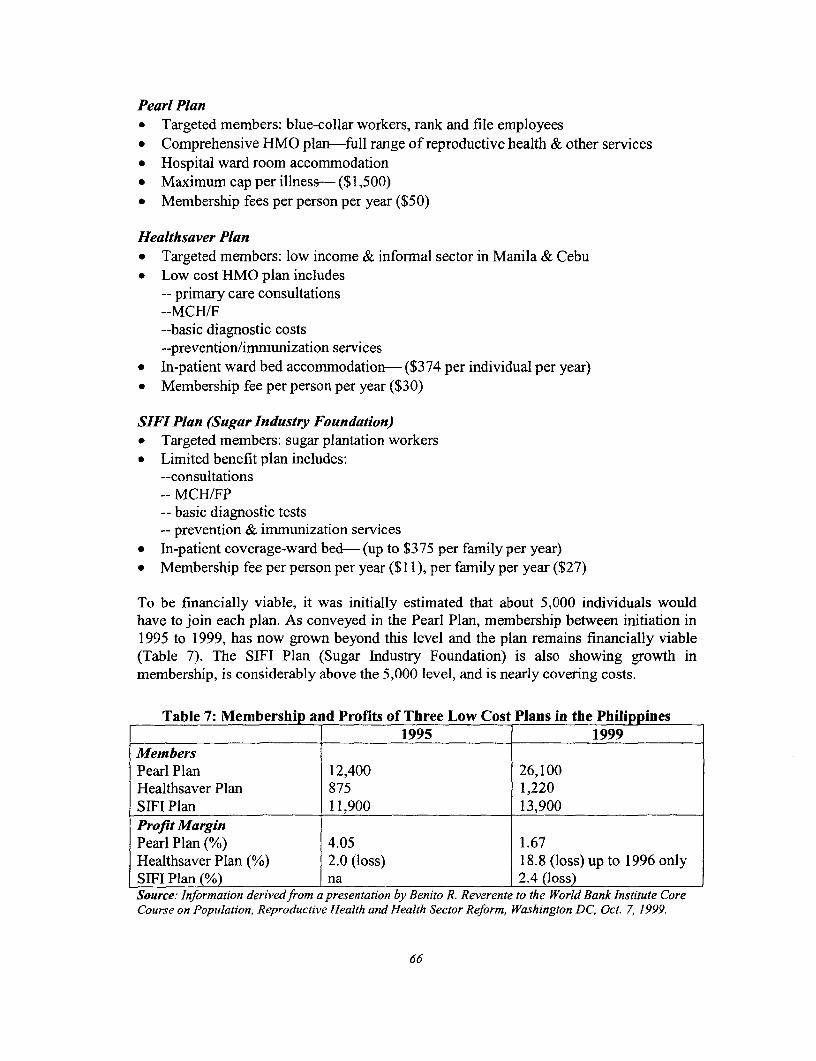
Pearl Plan* Targeted members: blue-collar workers, rank and file employees* Comprehensive HMO plan-full range of reproductive health & other services* Hospital ward room accommodation* Maximum cap per illness- ($1,500)* Membership fees per person per year ($50)
Healthsaver Plan* Targeted members: low income & informal sector in Manila & Cebu* Low cost HMO plan includes
-- primary care consultations--MCH/F--basic diagnostic costs--prevention/immunization services
* In-patient ward bed accommodation- ($374 per individual per year)* Membership fee per person per year ($30)
SIFI Plan (Sugar Industry Foundation)* Targeted members: sugar plantation workers* Limited benefit plan includes:
--consultations-- MCH/FP- basic diagnostic tests- prevention & immunization services
* in-patient coverage-ward bed- (up to $375 per family per year)* Membership fee per person per year ($1 1), per family per year ($27)
To be financially viable, it was initially estimated that about 5,000 individuals wouldhave to join each plan. As conveyed in the Pearl Plan, membership between initiation in1995 to 1999, has now grown beyond this level and the plan remains financially viable(Table 7). The SIFI Plan (Sugar Industry Foundation) is also showing growth inmembership, is considerably above the 5,000 level, and is nearly covering costs.
Table 7: Membership and Profilts of Three Low Cost Plans in the Philippines1995 1999
MembersPearl Plan 12,400 26,100Healthsaver Plan 875 1,220SIFI Plan 11,900 13,900Profit MarginPearl Plan (%) 4.05 1.67Healthsaver Plan (%) 2.0 (loss) 18.8 (loss) up to 1996 onlySIFI Plan (%) na 2.4 (loss)Source: Information derivedfrom a presentation by Benito R. Reverente to the World Bank Institute CoreCourse on Population, Reproductive Health and Health Sector Reforn, Washington DC, Oct. 7, 1999.
66
Greatest difficulty has been experienced in recruiting members and covering expenses inthe Healthsaver Plan-targeted to low income and informal sector workers inManila/Cebu. Philmeare has estimated the breakeven point to be 5,000 members, butonly if marketing costs are not included. With marketing costs, breakeven membership isestimated at 17,5000
Organizational Change
The low cost plans offered by Philamcare make use of five principles of managed care, assummarized in Table 8. These five principles derive from 'best practice' in the evolutionof HMOs in countries like the United States, Chile, and the Philippines, and are all ratherrecent. For the most part, each principle has appeal from a management and performanceviewpoint. The challenge is to get all five working together, and well, in oneorganization.
* The first principle of managed care-selective provider contracting-aims to get'best value for money' from providers and often pays providers through capitation.
* The second principle utilizes clinical protocols, case management, and cost effectiveprocedures to increase technical and allocative efficiency. Implementing this principlerequires a very effective health information system to track patients and procedures,as well as access to results of evidence-based medicine.
* The third principle employs utilization management so as to reduce demands oncostly in-patient services-by stressing preventive care, relying on primary caredoctors as 'gatekeepers' and shortening the length of stay in hospitals to acceptablemedical standards.
* The fourth principle stresses integrated care of the patient and his/her family, places alot of emphasis on educating the patient on how best to care for their own healthstatus, and monitors the performance of physicians.
* Finally, quality management is a key component of managed care which reliesprincipally on self-regulation and quality control the by HMO itself, as well ascollaboration with independent monitoring bodies, such as NGOs, or nationalaccreditation systems.
Provider Payments
Philmacare, as purchaser, pays providers of services contained in the three plans bycapitation. This method of payment was found to be financially viable as the hospitalsattained a modest surplus due to greater efficiencies and cost-savings in provision, andutilization was no higher than regular comprehensive HMO plans. Non-renewals anddrop-outs were relatively high however -up to 50% among individual enrollees, the mostcommon reason given being financial-with the implication that providers might not beso inclined to accept capitated payments, in view of high drop out rates and thepossibility of smaller populations to be served. .
67
Regulation
Regulation for quality was built into provider contracts and self-regulation played a majorrole through the principles and mechanisms of managed care. Only four percent of clientsexpressed dissatisfaction with the quality of services.
Promotion of Healthy Behaviors
Philamcare took a strong interest in promoting healthy behaviors among it's clients in theinterests of reducing their need for health services. Though Philamcare incurred costs topromote healthy behaviors among it's clients, the benefits outweighed the costs in thefonn of a healthier clientele that made fewer (expensive) demands on Philamcareproviders. In this case, the push to achieve cost-containment was complementary with thepush to promote healthy preventive behaviors, resulting in a win-win situation for bothPhilamcare and it's clients.
Philamcare initiatives to promote healthy behaviors include:
* Pre and post-natal care and well-baby care information, education, communication (aspart of all standard benefit packages,
* Family planning consultation and advice offered at out-patient clinics as part of thestandard benefit packages,
* Wellness seminars held at corporate client premises which focused on cessation ofsmoking, nutrition, and healthy lifestyles
* One-on-one health advisories given during primary care consultations rendered byclinic physicians,
* Cancer prevention and early detection programs, carried out from time to time,* A quarterly health newsletter with articles dealing mainly preventive health
68
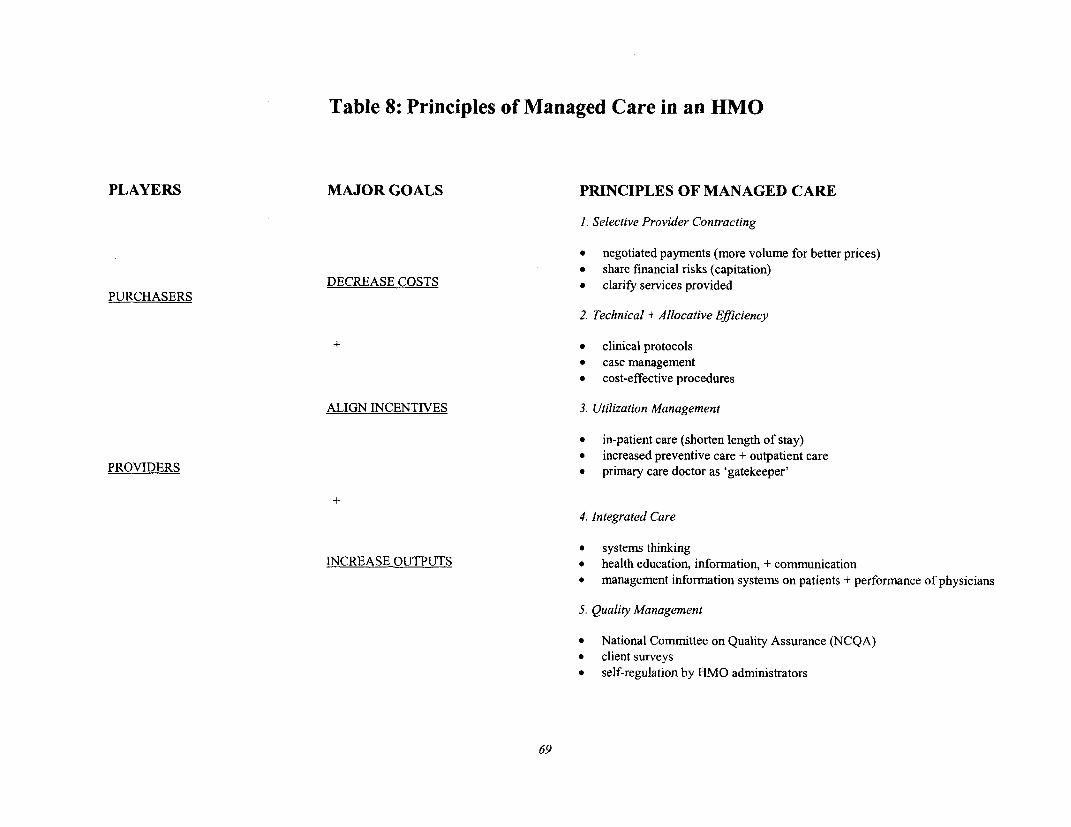
Table 8: Principles of Managed Care in an HMO
PLAYERS MAJOR GOALS PRINCIPLES OF MANAGED CARE
1 Selective Provider Contracting
* negotiated payments (more volume for better prices)* share financial risks (capitation)
DECREASE COSTS * clarify services providedPURCHASERS
2. Technical + Allocative Efficiency
+ * clinical protocols
* case management* cost-effective procedures
ALIGN INCENTIVES 3. Utilization Management
* in-patient care (shorten length of stay)* increased preventive care + outpatient care
PROVIDERS * primary care doctor as 'gatekeeper'
4. Integrated Care
* systems thinkingINCREASE OUTPUTS * health education, information, + communication
* management information systems on patients + performance of physicians
5. Quality Management
* National Committee on Quality Assurance (NCQA)* client surveys* self-regulation by HMO administrators
69

Lessons Learned
On the basis of these pilot plans, the past President of Philamcare, Dr. Benito Reverente,concludes that low cost HMO plans are financially feasible, and that managed care is aviable alternative for health care delivery in developing countries. The challenge facingsuch endeavors lies in building up membership in the risk pool to the extent that cross-subsidization of membership fees can cover costs of those experiencing illness or injuryas well as more expensive obstetric care, as well as generate a fair rate of return. Dr.Reverente is now serving as an adviser to government as it looks to tap the potential ofHMOs to serve a broader clientele.
A caveat in this positive scenario is that fee-charging benefit plans that includepopulation and reproductive health services are likely to exclude (i) some services thatare considered too expensive or unsustainable, as well as (ii) employers/employees thatcannot afford the fees. Such exclusions tend to be singled out as incompatible with broadpublic health advocacy goals to provide a complete, universally accessible package ofreproductive health services to all households. The answer to this dilemma is purported tolie in new forms of public-private collaboration whereby the excluded services, and theexcluded households are more effectively targeted by public subsidies. This responsepresumes, on the one hand, that more private sector involvement in the financing andprovision of reproductive health and other services -- as with Philamcare-will help freeup public resources for targeting to the poor, and that government will indeed reallocatethe freed up resources thus. This is precisely the spirit in which USAID collaborated withPhilamcare to launch low cost benefit packages for those willing and able to pay. Theextent to which such arrangements will jointly serve efficiency, equity, and sustainabilitygoals in the future remains, to date, and empirical question.
Conclusion
The Cairo Agenda poses a formidable challenge to those concerned with population andreproductive health because it reaches far beyond the scope of narrowly managed verticalprojects to embrace entire national health systems, as well as other sectors known to havesignificant impacts on health. It calls for a more comprehensive and integrated approachto reproductive health, with the implication that all stakeholders in health-government,NGOs, the private sector, and households - should be committed to achieving the vision.It advocates increases in overall funding for reproductive health, with potentially majorimplications for public and private financing and Ministries of Finance to re-allocatepublic resources. It implies significant changes in the way in which providers areincentivized to improve the quality of reproductive health services offered at bothprimary and secondary level facilities. It advocates significant changes in the way publicand private organizations should be monitored and evaluated for their work onreproductive health. And, it envisions the need for societal-level changes in awarenessand demand for reproductive and other health services at the household level.
How can all these priorities be effectively incorporated into the health systems of lowincome countries where (i) problems of inefficiency, inequity, and poor quality, tend tobe deeply entrenched, (ii) total expenditures on health from all sources may be less than
70
$10 per capita, and (iii) government failure to provide good services often co-existsalongside market failures in the private financing and provision of population andreproductive health services.
To what extent, how, and how fast can such deeply entrenched problems be transformedunder conditions of severe budget and human resource constraints? Our answer is'incrementally'. Big problems, such as high rates of maternal mortality, require big,system-wide changes to resolve them.
We have argued that the first step to advancing the reproductive health agenda in contextsof health sector reform is to identify OUTCOMES that are unsatisfactory to society, thenfocus on system-wide causes that underpin them. The second step is to determine the mixof inputs, processes and structure that would need to be in place to produce change in thedesired direction. The third step is to understand key reform levers and their scope ofinfluence, then put them to work to mobilize and reconfigure resources to move in thehealth system in the right direction.
The good news is that the focus on outcomes and reforn levers paves the way for a muchmore precise appreciation of cause and effect, where interventions in one or more areascan be classified, monitored and evaluated more precisely. Our experience suggests thatwhen armed with a broader understanding of major reform options and levers, advocatesfor better reproductive health will be far better prepared to make their case. The bad newsis that orchestrating the reform levers requires a much broader understanding of healthsystems and their determinants than are typically associated with well-managed familyplanning or other reproductive health projects. Indeed, our experience suggests that NOdeveloping country can yet claim to have reformed their health system in a way thatexemplifies the vision of better reproductive health advocated by Cairo. Rather, manyuneven and partial initiatives are underway, thus elevating the importance of diagnosingthe adequacy of various approaches, assessing impact, and communicating lessonslearned.
The case studies reviewed in this paper are therefore only indicative and illustrative ofnew ventures into vastly complicated territory. At the very least, they provide a baselineagainst which the nature of the challenges, differences of approach, and the need for moreconcentrated action can be better appreciated.
7]

Other WBI Working Papers
Acci6n Local, Mejores Vidas: Implementaci6n de Proyectos Participativosy DecentralizadosDaniel Sellen, editor1999. 77 pages. Stock No. 37140. Price code 000
Decentralization Briefing NotesJennie Litvack and Jessica Sedon, editors1999. 96 pages. Stock No. 37142. Price code 000
Empowering Civil Society to Monitor the Environment: Education for Students,Awareness for the Public, and Functional Literacy for Targeted GroupsDavid takshmanan Ariasingam1999. 40 pages. Stock No. 37141. Price code 000
Evaluating Digital Distance Learning Programs and ActivitiesMartin M. Valcke and Frans L. Leeuw with Albert Kamperman2000Q 83 pages. Stock No. 37155, Price code 000
Global Climate Change and BiodiversityJose I. dos Furtado and Nalin Kishor with G. V Rao and Catherine Wood1999. 54 pages. Stock No. 37151. Price code 000
New Trends in Public Sector Management in HealthR. Paul Shaw1999, 81 pages. Stock No. 37146. Price code 000
Patterns of Development: 1970-1994William H. Branson, Isabel Guerrero, and Bernhard G. Gunter1998. 49 pages. Stock No. 37132. Price code 000
Pillars of Integrity: The Importance of Supreme Audit Institutionsin Curbing CorruptionKenneth M. Dye and Rick Stapenhurst1998. 34 pages. Stock No. 37133. Price code 000
Population Economics, Demographic Transition, and DevelopmentAndrew Mason, Thomas Merrick, and R. Paul Shaw, editors1999. 250 pages. Stock No. 37154. Price code 000
Report on the Meeting of the Latin American and Caribbean Forumon Poverty, Inequality, and VulnerabilityBuenos Aires, October 19-2O, 19981999. 53 pages. Stock No. 37144. Price code 000
The complete list of Institute publications is available in theWBI Publications Catalog 2000. Stock No. 31708
Order World Bank Institute publicationsby phone or fax: Phone: 1 -800-645-7247 or (703) 661-1580; Fax: (703) 661-1501
bymail:Write to The World Bank, P.O. Box 960, Herndon, VA 20172-0960, U.S.A.
by e-mai/[email protected]
through the World Wide Web at.'http://www.worldbank.org/publications
or visit the WBI website at: http://www.worldbank.org/wbi
-e
- S
=~~U
StckNo 315
Related Documents