This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Neuropsychologia 48 (2010) 2903–2911
Contents lists available at ScienceDirect
Neuropsychologia
journa l homepage: www.e lsev ier .com/ locate /neuropsychologia
Representation and disconnection in imaginal neglect�
G. Rodea,b,∗, F. Cottonc, P. Revola,b, S. Jacquin-Courtoisa,b, Y. Rossetti a,b, P. Bartolomeod,e
a Université de Lyon, Université Lyon 1, INSERM-UMRS 534, Bron, Franceb Hospices Civils de Lyon, Service de médecine physique et réadaptation neurologique, Hôpital Henry Gabrielle, Lyon, Francec Université de Lyon, Université Lyon 1, service de radiologie, Centre Hospitalier Lyon Sud, Hospices Civils de Lyon, Lyon, Franced INSERM-UPMC UMRS 975, and Fédération de Neurologie, AP-HP, Hôpital de la Salpêtrière, Paris, Francee Department of Psychology, Catholic University, Milan, Italy
a r t i c l e i n f o
Article history:Received 13 July 2009Received in revised form 1 May 2010Accepted 28 May 2010Available online 4 June 2010
Keywords:Visual neglectRepresentational neglectSpatial imageryTop-down mechanisms
a b s t r a c t
Patients with neglect failure to detect, orient, or respond to stimuli from a spatially confined region,usually on their left side. Often, the presence of perceptual input increases left omissions, while sensorydeprivation decreases them, possibly by removing attention-catching right-sided stimuli (Bartolomeo,2007). However, such an influence of visual deprivation on representational neglect was not observedin patients while they were imagining a map of France (Rode et al., 2007). Therefore, these patientswith imaginal neglect either failed to generate the left side of mental images (Bisiach & Luzzatti, 1978),or suffered from a co-occurrence of deficits in automatic (bottom-up) and voluntary (top-down) ori-enting of attention. However, in Rode et al.’s experiment visual input was not directly relevant to thetask; moreover, distraction from visual input might primarily manifest itself when representation guidessomatomotor actions, beyond those involved in the generation and mental exploration of an internal map(Thomas, 1999). To explore these possibilities, we asked a patient with right hemisphere damage, R.D.,to explore visual and imagined versions of a map of France in three conditions: (1) ‘imagine the map inyour mind’ (imaginal); (2) ‘describe a real map’ (visual); and (3) ‘list the names of French towns’ (propo-sitional). For the imaginal and visual conditions, verbal and manual pointing responses were collected;the task was also given before and after mental rotation of the map by 180◦. R.D. mentioned more townson the right side of the map in the imaginal and visual conditions, but showed no representational deficitin the propositional condition. The rightward inner exploration bias in the imaginal and visual conditionswas similar in magnitude and was not influenced by mental rotation or response type (verbal responsesor manual pointing to locations on a map), thus suggesting that the representational deficit was robustand independent of perceptual input in R.D. Structural and diffusion MRI demonstrated damage to severalwhite matter tracts in the right hemisphere and to the splenium of corpus callosum. A second right-braindamaged patient (P.P.), who showed signs of visual but not imaginal neglect, had damage to the sameintra-hemispheric tracts, but the callosal connections were spared. Imaginal neglect in R.D. may resultfrom fronto-parietal dysfunction impairing orientation towards left-sided items and posterior callosaldisconnection preventing the symmetrical processing of spatial information from long-term memory.
© 2010 Elsevier Ltd. All rights reserved.
Introduction
Patients with right hemisphere damage and left visual neglectare sometimes unable to describe the left part of internally gener-ated images. This representational, or imaginal, neglect has beenascribed to a failure to generate or maintain a normal represen-
� A preliminary version of this work was presented at the European CognitiveNeurosciences meeting held in Bressanone, Italy (27–31 January 2009).
∗ Corresponding author at: Service de médecine physique et réadaptation neu-rologique, Hôpital Henry Gabrielle, route de Vourles, F-69230 Saint-Genis-Laval,France. Tel.: +33 478865066.
E-mail address: [email protected] (G. Rode).
tation of the contralesional side of mental images (Berti, 2004;Bisiach & Berti, 1987; Bisiach & Luzzatti, 1978; Bisiach, Luzzatti,& Perani, 1979). Representational neglect is commonly assessed byrequiring subjects to draw objects from memory (Chokron, Colliot,& Bartolomeo, 2004; Critchley, 1953) or to name the towns or thecountries on an imagined map (Bartolomeo, D’Erme, & Gainotti,1994; Rode & Perenin, 1994).
The presence or absence of visual input may influence neglectpatients’ performance in drawing from memory. Perceptual inputincreases left omissions, while the absence of visual feedback maydecrease them. For example, Anderson (1993) reported on a patientwith neglect who displayed an object-centered neglect with theeyes open, which disappeared with the eyes closed. Chokron etal. (2004) described a similar pattern of performance in 3 out of
0028-3932/$ – see front matter © 2010 Elsevier Ltd. All rights reserved.doi:10.1016/j.neuropsychologia.2010.05.032

Author's personal copy
2904 G. Rode et al. / Neuropsychologia 48 (2010) 2903–2911
6 right-brain damaged patients with neglect. In the same study,5 patients also showed improved drawing symmetry when blind-folded, reflecting an increase in the extent and the number of detailson the left side of the drawing and a reduction of the extent of theright. These results suggest that the attentional capture exerted bythe right-sided details of drawings that subjects were producingmay be reduced in the absence of visual input, thus facilitating aleftward orienting of attention (Bartolomeo, 2007).
Does visual input exert a similar influence on representationalneglect when assessed by description from memory? Such a possi-bility might suggest that similar attentional systems are impaired inperceptual and in imaginal neglect (Bartolomeo & Chokron, 2002a).However, evidence contrary to this hypothesis emerged from arecent study (Rode, Revol, Rossetti, Boisson, & Bartolomeo, 2007),in which 8 normal participants and 8 brain-damaged patients withleft representational neglect were invited to imagine the map ofFrance and to name as many towns as possible within 2 min, eitherwith their eyes open or while blindfolded. Patients’ representa-tional neglect remained unchanged by the presence/absence ofvisual input. The defective retrieval and generation from long-termmemory of topographic information about towns on the westernpart of the map was the same in both conditions, while perfor-mance on mental evocation of towns on the middle and easternparts of the map was similar in both conditions and not differ-ent from healthy controls. These findings suggested that visualinput did not influence the mental representation of space in a taskrequiring only visual mental imagery (Rode et al., 2007), and thatsuch representational deficit may result from either a failure to gen-erate the left side of mental images (Bisiach & Luzzatti, 1978), orthe co-occurrence of distinct deficits in orienting of attention, per-haps involving automatic (bottom-up) and voluntary (top-down)orienting (Bartolomeo et al., 1994).
However, it must be noted that visual input was not relevantin the map description task used in this study, in contrast to visualfeedback in the drawing task, where the already drawn details wereobviously important to the progression of the task. Task-relevantvisual details might be more effective in capturing patients’ atten-tion (Ptak & Schnider, 2006). Also, visual input might influenceperformance on spatial representation tasks only when these tasksrequire a manual response, i.e. an interaction between neural pro-cesses supporting visual representation and action. Even withoutvisual input, such tasks incorporate a major intentional compo-nent that underlies the act of drawing itself as well as the ongoingdynamic process involved in repeatedly comparing what is imag-ined to have been drawn with the original mental image template.This intentional component could also help patients with imag-inal neglect to obtain more symmetrical levels of performance(Cristinzio et al., 2009).
In order to explore these issues, we asked a patient withright hemisphere damage and signs of robust left representationalneglect to recall topographic knowledge about towns of France indifferent conditions: when imaging the map of France, when view-ing a map presented in front of him and without any imaginal orperceptual requirements. Moreover, for imagery and perceptualconditions, two types of answer were noted (verbal and motor)and tasks were also applied before and after a mental rotation ofthe map by 180◦.
A further important issue concerns the lesional correlates ofimaginal neglect. There is currently an intense debate aboutthe anatomy of perceptual neglect, whose typical lesional corre-lates were classically identified with the inferior parietal gyrus(Mort et al., 2003; Vallar, 2001) or, more recently, with thecentral/rostral portions of the superior temporal gyrus (Karnath,Ferber, & Himmelbach, 2001). Other results stress the importanceof white matter disconnections (Bartolomeo, Thiebaut de Schotten,& Doricchi, 2007), especially in the fronto-parietal components of
the superior longitudinal fasciculus (SLF) (Thiebaut de Schottenet al., 2005). Fronto-parietal networks are important for spatialorienting and other attentional processes. Dysfunction of thesenetworks in neglect is broadly consistent with the prominent atten-tional problems in these patients. In a similar way, the study ofthe lesional correlates of imaginal neglect can provide evidencerelevant to its functional mechanisms. Imaginal neglect has notbeen thoroughly explored in this respect. Many cases have largeright-hemisphere lesions similar to those observed in patientswith perceptual neglect (Bartolomeo et al., 1994; Bisiach, Capitani,Luzzatti, & Perani, 1981). Single cases with isolated imaginalneglect had lesions in the dorsolateral prefrontal cortex (Guariglia,Padovani, Pantano, & Pizzamiglio, 1993) or the thalamus (Ortigue etal., 2001). However, anatomical studies on imaginal neglect did notaddress the possibility that disconnection factors may contributeto this deficit. For the present patient, high-definition anatomi-cal MRI was obtained, as well as diffusion sequences employedfor subsequent DTI-based reconstruction of relevant white mattertracts. Neuroimaging results were compared with those of a secondright-brain damaged patient, who had signs of visual neglect in theabsence of representational impairment.
Patients
Two right-handed patients with unilateral lesions in the righthemisphere participated in the study after having signed a writteninformed consent form.
Patient R.D., a 75-year-old man, with 10 years of schooling, whohad been working as a craftsman, was admitted to a neurologi-cal unit for the sudden onset of left-sided weakness, confusion,left homonymous hemianopia, and left spatial neglect, consec-utive to a vascular infarct in the territory of the right middlecerebral artery. This stroke was secondary to a thrombosis of theright internal carotid artery due to cardiac embolism in a contextof cardiac arrhythmia. One month after stroke onset, the patientshowed a mild left upper limb paresis with somatosensory andproprioceptive deficits. Goldmann’s perimetry demonstrated a lefthomonymous hemianopia. Visual acuity was corrected-to-normal(10/10) with lenses for the two eyes. The patient also showedleft auditory and somatosensory extinction to double simultane-ous stimulation. Neither motor neglect nor motor extinction waspresent.
Neuropsychological examination one month post-onsetrevealed a persistent left-sided neglect. On the Bell’s cancellationtask (Gauthier, Dehaut, & Joanette, 1989), the patient crossed out23/35 targets, with 11 omissions on the left half of the sheet andone omission on the right half. In a letter cancellation task (Diller& Weinberg, 1977), the patient crossed out 8/25 targets on theleft half, and 24/25 targets on the right half of the sheet. On a linebisection task (Schenkenberg, Bradford, & Ajax, 1980), the patientdisplaced the subjective center rightwards by 31% of the total linelength on average. The patient showed evidence of object-centeredneglect in a drawing copy task (Gainotti et al., 1972), with left-sided omissions of 3 items. He also omitted left-sided items whenasked to complete a clock-face from memory, or to draw or copy adaisy or a tree. The patient also had signs of constructional apraxiawhen drawing figures such as a cube or a house. Verbal descriptionfrom memory of objects or animals was flawless. There was noimpairment on verbal fluency tasks: Patient R.D. gave respectively17, 14 and 10 correct responses for the letters /P/, /R/and /V/ ina verbal fluency alphabetic test (normal values: 19.28 ± 7.05 for/P/; 16.78 ± 6.04 for /R/ and 14.5 ± 6.46 for /V/) and 23, 12 and 10correct responses for the items /animal/, /fruit/ and /furniture/ ina verbal fluency categorical test (normal values: 27.14 ± 8.53 for/animals/; 15.42 ± 3.85 for /fruits/ and 11.71 ± 3.53 for/furniture/)within 2 min (Cardebat, Doyon, Puel, Goulet, & Joanette, 1990).

Author's personal copy
G. Rode et al. / Neuropsychologia 48 (2010) 2903–2911 2905
The second patient (P.P.) was a 70-year-old woman, with 15years of schooling, who was admitted to a neurological unit forthe sudden onset of left-sided neglect with a left somatosen-sory deficit of his left upper limb, confusion, left homonymoushemianopia, and left spatial neglect, consecutive to a right occipito-parietal haematoma. Cerebral angiography was normal. One monthafter stroke onset, when neuropsychological tests were given,the patient showed a minor upper limb paresis with a reductionof dexterity associated to a motor neglect component. Examina-tion revealed persistent incomplete somatosensory deficit of thearm. She had no anosognosia, nor sensory extinction; Goldmann’sperimetry demonstrated a left inferior homonymous quadran-tanopia. Visual acuity was corrected-to-normal (10/10) with lensesfor the two eyes. Neuropsychological examination one monthpost-onset revealed a persistent left-sided visual neglect withoutimaginal neglect. Perceptual neglect was present on cancellationtasks, with 28/35 crossed targets (7 omissions on the left half ofthe sheet) in the Bell’s cancellation task (Gauthier et al., 1989),8/25 crossed targets on the left half, and 25/25 crossed targetson the right half of the sheet in a letter cancellation task (Diller& Weinberg, 1977). Line bisection (Schenkenberg et al., 1980) wasalso impaired; on average, P.P. displaced the subjective center right-wards by 27% of the total line length.
There was no evidence of object-centered neglect when thepatient was asked to draw or to copy from memory a daisy, abutterfly or a tree. She did not omit left-sided items when askedto complete a clock-face from memory or in a 5 items drawingcopy task (Gainotti, Messerli, & Tissot, 1972). When asked to men-tally visualize a geographic space as a city square or the map ofFrance, P.P. did not show any evidence of imaginal neglect (see theResults section below). Patient P.P. had no impairment on a ver-bal semantic and alphabetic fluency task: she gave respectively 34,20 and 19, correct responses within 2 min for the items /animals/,/fruits/ and /furniture/ (normal values: 32.64 ± 7.9 for /animals/;19.35 ± 3.24 for /fruits/ and 17 ± 4.64 for /furniture/) and 22, 20and 17 for the letter /P/, /R/ and /V/ (normal values: 23.78 ± 8.35for /P/; 21.14 ± 7.16 for /R/ and 17.71 ± 5.91 for /V/) (Cardebat etal., 1990).
Methods
MRI
Brain MRIs were obtained six months post-onset for patientR.D. (for whom a CT scan performed at the time of the neuropsy-chological test gave identical results) and one year post-onset forpatient P.P. Both MRIs were performed on a Philips Achivea 1.5 TMR system (Philips Medical Systems, Erlangen, The Netherlands)with an 8-channel head coil. Morphological acquisition includedspin echo and Gradient-Echo axial T2-weighted images and 3DT1-weighted images with an isotropic voxel of 0.9 mm. DiffusionTensor Imaging was acquired with 32 directions and a b valueof 1000 s/mm2 [FOV: 240 cm; voxel size: 2.5 cm; slice thickness:2.5 cm; gap: 0; slice number: 60; Sense: no; stacks: 1; Fast imag-ing mode: EPI, single-shot; TE: 115 ms; flip angle: 90◦; TR: 15 ms;Motion: cardiac synchronization with PPU; NSA: 1] then the auto-mated Philips 3-dimensional fiber tracking tool was used on anextended MR workspace to determine white matter pathway trackspassing through ROIs. Neuroanatomy of brain damage, includinggyri and white matter pathways, was assessed by the same neu-roanatomist and neuroradiologist (F.C.).
Mental imagery conditions
Patients were asked to mentally visualize the map of France asif ‘they could see the map in front of them in their mind’. In order
to help them, they were asked to remember the map of Francethat they had learned during their primary school period or toremember the ‘weather forecast map featured on television or inthe newspapers’. They had to list all the towns that they could ‘see’,within 2 min. No instruction was given concerning the directionof mental scanning (Rode, Perenin, & Boisson, 1995). Patient R.D.was asked to perform the imagery task either with eyes closed oropen (see details in Rode et al., 2007). When R.D. imagined themap with eyes closed, the patient answered in naming the citiesthat he imagined to see on the map. When required to imagine themap with eyes open, R.D. had to provide responses either orallyor, in separate sessions, by writing the responses on an A4 sheetof paper with the major axis aligned with the patient’s body axis.A further imagery condition required the mental inversion of theimagined map (Bisiach & Luzzatti, 1978; Rode & Perenin, 1994). Thepatient first had to imagine the map in front of him in the normalorientation and then in the reverse orientation (i.e. after a men-tal rotation of 180◦). In each condition, the patient had to nameas many towns as possible he could see on the map within 2 min.Patient P.P. performed the imaginal test with her eyes closed.
Visual perceptual conditions
Patient R.D. was asked to look at the contour of a map of France(scale: 1/5,000,000; 1 cm = 50 km) drawn on an A4 sheet. The mapwas presented on a table with its major axis aligned with thepatient’s body axis. No instruction was given concerning the direc-tion of visual scanning. The patient had to name as many townsas possible he could locate on the map within 2 min. Similarly tothe imagery conditions, a real map turned upside-down was alsopresented to the patient. The patient first had to explore the map infront of him, which was presented with a normal orientation andthen in the reverse orientation (i.e. after a 180◦ rotation of map).In each condition, the patient had to point on the map to as manylocations as possible corresponding to French towns, within 2 min.
“Propositional” town listing
Patient R.D. was instructed to remember and name as manytowns as possible within 2 min, without building a visual mentalimage of the map of France (see details in Rode, Rossetti, Perenin,& Boisson, 2004).
For patient R.D., the experimental procedure included 7 differ-ent sessions, which took place over a period of three weeks, with aninterval of 2–3 days between conditions. The order of presentationof the different conditions is indicated in the Table 1. For patient P.P.,the experimental procedure included 1 session of mental imagerycondition. For all conditions, both patients were assessed in thesame location and by the same investigators (GR, PR).
Analysis
Following Rode et al. (2007) responses were recorded in twoways: (i) mean total scores, indicating the number of towns named;(ii) mean left and right-sided scores defined by the position ofreported towns on the two halves of the map. Towns located insidea 75 km stripe centered on a vertical meridian line (linking Lille toPerpignan) were not taken into account (middle score). The numberof repetition was also noted for each condition.
Results
Neuroimaging results
For patient R.D., MRI scan showed an unilateral ischaemic lesionin the right hemisphere. The lesion involved the temporal lobe (T1,
Author's personal copy
2906 G. Rode et al. / Neuropsychologia 48 (2010) 2903–2911
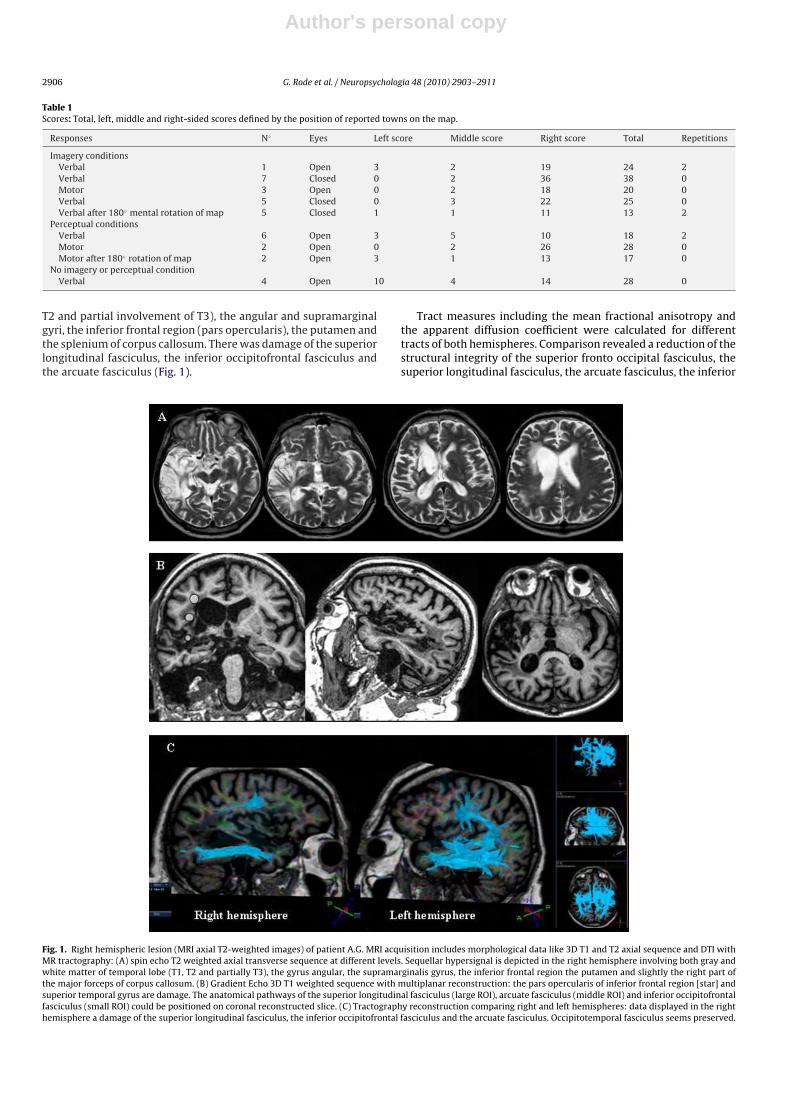
Table 1Scores: Total, left, middle and right-sided scores defined by the position of reported towns on the map.
Responses N◦ Eyes Left score Middle score Right score Total Repetitions
Imagery conditionsVerbal 1 Open 3 2 19 24 2Verbal 7 Closed 0 2 36 38 0Motor 3 Open 0 2 18 20 0Verbal 5 Closed 0 3 22 25 0Verbal after 180◦ mental rotation of map 5 Closed 1 1 11 13 2
Perceptual conditionsVerbal 6 Open 3 5 10 18 2Motor 2 Open 0 2 26 28 0Motor after 180◦ rotation of map 2 Open 3 1 13 17 0
No imagery or perceptual conditionVerbal 4 Open 10 4 14 28 0
T2 and partial involvement of T3), the angular and supramarginalgyri, the inferior frontal region (pars opercularis), the putamen andthe splenium of corpus callosum. There was damage of the superiorlongitudinal fasciculus, the inferior occipitofrontal fasciculus andthe arcuate fasciculus (Fig. 1).
Tract measures including the mean fractional anisotropy andthe apparent diffusion coefficient were calculated for differenttracts of both hemispheres. Comparison revealed a reduction of thestructural integrity of the superior fronto occipital fasciculus, thesuperior longitudinal fasciculus, the arcuate fasciculus, the inferior
Fig. 1. Right hemispheric lesion (MRI axial T2-weighted images) of patient A.G. MRI acquisition includes morphological data like 3D T1 and T2 axial sequence and DTI withMR tractography: (A) spin echo T2 weighted axial transverse sequence at different levels. Sequellar hypersignal is depicted in the right hemisphere involving both gray andwhite matter of temporal lobe (T1, T2 and partially T3), the gyrus angular, the supramarginalis gyrus, the inferior frontal region the putamen and slightly the right part ofthe major forceps of corpus callosum. (B) Gradient Echo 3D T1 weighted sequence with multiplanar reconstruction: the pars opercularis of inferior frontal region [star] andsuperior temporal gyrus are damage. The anatomical pathways of the superior longitudinal fasciculus (large ROI), arcuate fasciculus (middle ROI) and inferior occipitofrontalfasciculus (small ROI) could be positioned on coronal reconstructed slice. (C) Tractography reconstruction comparing right and left hemispheres: data displayed in the righthemisphere a damage of the superior longitudinal fasciculus, the inferior occipitofrontal fasciculus and the arcuate fasciculus. Occipitotemporal fasciculus seems preserved.

Author's personal copy
G. Rode et al. / Neuropsychologia 48 (2010) 2903–2911 2907
occipitofrontal fasciculus and the splenium of corpus callosum ofthe right hemisphere compared to the left, except for the inferiorlongitudinal fasciculus (ILF) which was spared (Fig. 2).
For patient P.P., MRI scan showed an unilateral hypo-intenselesion in the right hemisphere. The lesion involved the superior andinferior parietal lobules, including the intraparietal sulcus. Tractmeasures including the mean fractional anisotropy and the appar-ent diffusion coefficient were calculated for different tracts of eachhemisphere. Comparison revealed a reduction of the structuralintegrity of the superior longitudinal fasciculus while the inferiorlongitudinal fasciculus, the inferior occipitofrontal fasciculus, thearcuate fasciculus and the splenium of corpus callosum were spared(Fig. 3).
Behavioural results
Table 1 reports the number of responses of patient R.D. foreach test condition, as a function of spatial position (left, middleor right). Inspection of the table suggests that, for all the conditionsexcept the propositional town listing, patient R.D. had a dramati-cally asymmetrical performance, with many more towns reportedon the right side than on the left side (see also Figs. 4 and 5). Theabsence of visual input was clearly unable to decrease the asym-metry.
Statistical control confirmed that patient R.D.’s performancechanged as a function of the different conditions, �2 (16) = 44.71,p = 0.0002. The table of post-hoc cell contributions indicatedthat the cells which significantly contributed to this result(with ˛ = 0.05) were the following: (1) the decreased number ofleft-sided responses and (2) the increased number right-sidedresponses in the blindfolded condition with oral responses; (3)the decrease of right-sided responses in the perceptual-verbalcondition; (4) the increase of left-sided response and (5) thedecrease of right-sided responses (i.e., the lack of left–rightasymmetry) in the propositional town listing condition. Frequen-
Fig. 2. Mean Fractional Anisotropy (FA; a) and Apparent Diffusion Coefficient (ADC;b) for different analyzed tracts in the right hemisphere (RH) and the left hemisphere(LH). Abbreviations: SFOF: superior fronto occipital fasciculus; SLF: superior longi-tudinal fasciculus; AF: arcuate fasciculus; IFOF: inferior occipitofrontal fasciculusand ILF: inferior longitudinal fasciculus. Error bars indicate SDs.
Fig. 3. Right hemispheric lesion (MRI axial T2-weighted images) of patient P.P. MRI acquisition includes morphological data like 3D T1 axial sequence and DTI with MRtractography: (A) Gradient Echo 3D T1 weighted sequence with multiplanar reconstruction: sequellar hyposignal is depicted in the right hemisphere involving the superior andinferior lobules. (B) Tractography reconstruction comparing right and left hemispheres: data displayed a damage of the right superior longitudinal fasciculus [Mean FractionalAnisotropy (FA) = 0.345 ± 0.12; Apparent Diffusion Coefficient (ADC) = 0.935 ± 0.17 × 10−3 mm2/s] compared to the left [FA = 0.444 ± 0.13; ADC = 0.766 ± 0.14 × 10−3 mm2/s].The inferior longitudinal fasciculus, the inferior occipitofrontal fasciculus, the arcuate fasciculus and the splenium of corpus callosum were preserved.
Author's personal copy
2908 G. Rode et al. / Neuropsychologia 48 (2010) 2903–2911
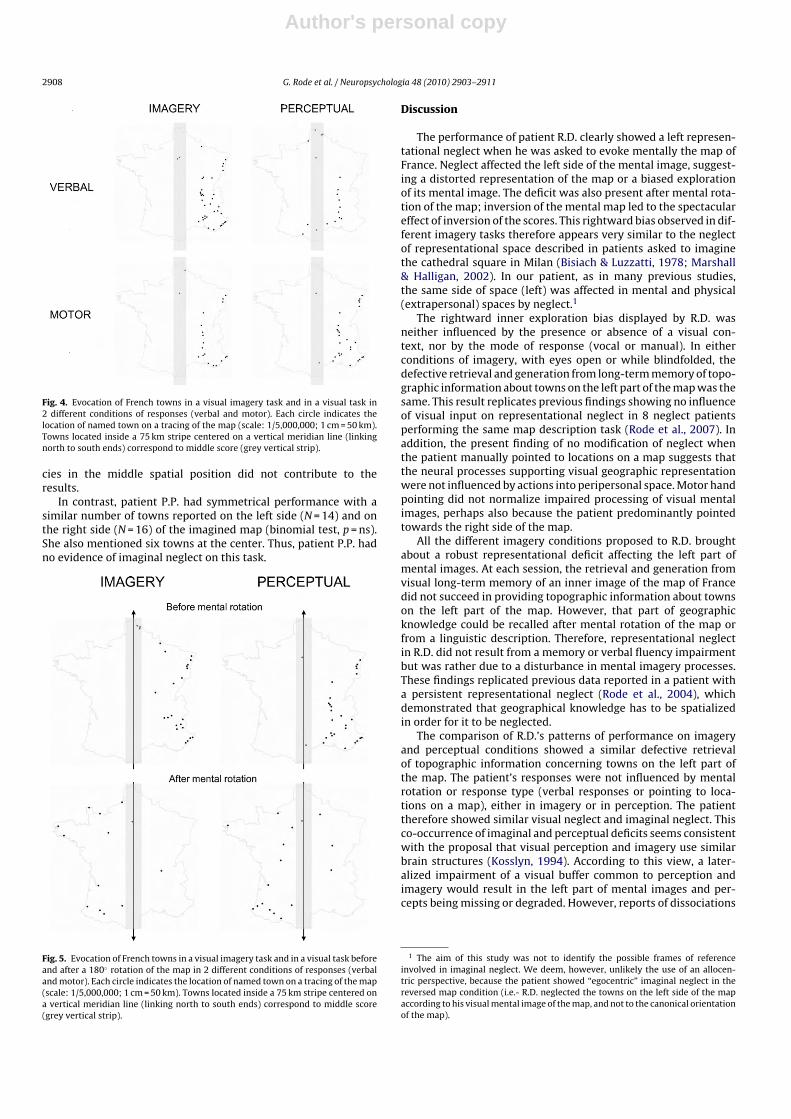
Fig. 4. Evocation of French towns in a visual imagery task and in a visual task in2 different conditions of responses (verbal and motor). Each circle indicates thelocation of named town on a tracing of the map (scale: 1/5,000,000; 1 cm = 50 km).Towns located inside a 75 km stripe centered on a vertical meridian line (linkingnorth to south ends) correspond to middle score (grey vertical strip).
cies in the middle spatial position did not contribute to theresults.
In contrast, patient P.P. had symmetrical performance with asimilar number of towns reported on the left side (N = 14) and onthe right side (N = 16) of the imagined map (binomial test, p = ns).She also mentioned six towns at the center. Thus, patient P.P. hadno evidence of imaginal neglect on this task.
Fig. 5. Evocation of French towns in a visual imagery task and in a visual task beforeand after a 180◦ rotation of the map in 2 different conditions of responses (verbaland motor). Each circle indicates the location of named town on a tracing of the map(scale: 1/5,000,000; 1 cm = 50 km). Towns located inside a 75 km stripe centered ona vertical meridian line (linking north to south ends) correspond to middle score(grey vertical strip).
Discussion
The performance of patient R.D. clearly showed a left represen-tational neglect when he was asked to evoke mentally the map ofFrance. Neglect affected the left side of the mental image, suggest-ing a distorted representation of the map or a biased explorationof its mental image. The deficit was also present after mental rota-tion of the map; inversion of the mental map led to the spectaculareffect of inversion of the scores. This rightward bias observed in dif-ferent imagery tasks therefore appears very similar to the neglectof representational space described in patients asked to imaginethe cathedral square in Milan (Bisiach & Luzzatti, 1978; Marshall& Halligan, 2002). In our patient, as in many previous studies,the same side of space (left) was affected in mental and physical(extrapersonal) spaces by neglect.1
The rightward inner exploration bias displayed by R.D. wasneither influenced by the presence or absence of a visual con-text, nor by the mode of response (vocal or manual). In eitherconditions of imagery, with eyes open or while blindfolded, thedefective retrieval and generation from long-term memory of topo-graphic information about towns on the left part of the map was thesame. This result replicates previous findings showing no influenceof visual input on representational neglect in 8 neglect patientsperforming the same map description task (Rode et al., 2007). Inaddition, the present finding of no modification of neglect whenthe patient manually pointed to locations on a map suggests thatthe neural processes supporting visual geographic representationwere not influenced by actions into peripersonal space. Motor handpointing did not normalize impaired processing of visual mentalimages, perhaps also because the patient predominantly pointedtowards the right side of the map.
All the different imagery conditions proposed to R.D. broughtabout a robust representational deficit affecting the left part ofmental images. At each session, the retrieval and generation fromvisual long-term memory of an inner image of the map of Francedid not succeed in providing topographic information about townson the left part of the map. However, that part of geographicknowledge could be recalled after mental rotation of the map orfrom a linguistic description. Therefore, representational neglectin R.D. did not result from a memory or verbal fluency impairmentbut was rather due to a disturbance in mental imagery processes.These findings replicated previous data reported in a patient witha persistent representational neglect (Rode et al., 2004), whichdemonstrated that geographical knowledge has to be spatializedin order for it to be neglected.
The comparison of R.D.’s patterns of performance on imageryand perceptual conditions showed a similar defective retrievalof topographic information concerning towns on the left part ofthe map. The patient’s responses were not influenced by mentalrotation or response type (verbal responses or pointing to loca-tions on a map), either in imagery or in perception. The patienttherefore showed similar visual neglect and imaginal neglect. Thisco-occurrence of imaginal and perceptual deficits seems consistentwith the proposal that visual perception and imagery use similarbrain structures (Kosslyn, 1994). According to this view, a later-alized impairment of a visual buffer common to perception andimagery would result in the left part of mental images and per-cepts being missing or degraded. However, reports of dissociations
1 The aim of this study was not to identify the possible frames of referenceinvolved in imaginal neglect. We deem, however, unlikely the use of an allocen-tric perspective, because the patient showed “egocentric” imaginal neglect in thereversed map condition (i.e.- R.D. neglected the towns on the left side of the mapaccording to his visual mental image of the map, and not to the canonical orientationof the map).

Author's personal copy
G. Rode et al. / Neuropsychologia 48 (2010) 2903–2911 2909
between visual and imaginal neglect (Anderson, 1993; Bartolomeoet al., 1994; Beschin, Cocchini, Della Sala, & Logie, 1997; Coslett,1997; Guariglia et al., 1993) suggest that visual spatial perceptionand imagery depend on partly distinct neural processes.
A possible account is that R.D. failed to pay attention to theleft sides of his mental map in a similar way as he failed to payattention to the left side of visual map (see Bartolomeo et al.,2007; Meador, Loring, Bowers, & Heilman, 1987).2 Support to thishypothesis comes from the beneficial effects on imaginal neglect ofmanoeuvres, such as vestibular stimulation (Rode & Perenin, 1994)and prism adaptation (Rode, Rossetti, & Boisson, 2001), which mayinfluence orienting of visuospatial attention (Chokron, Dupierrix,Tabert, & Bartolomeo, 2007). Also consistent with this hypothe-sis are the results of Bartolomeo, Bachoud-Levi, Azouvi, & Chokron(2005), who devised a response time test in which patients had toindicate whether towns or regions of France presented auditorilywere situated left or right of Paris. Two patients with visual neglecthad a response time asymmetry suggesting imaginal neglect, butwith symmetrical accuracy. This dissociation between responsetimes and accuracy suggested that, in these patients, the left sideof the mental map of space was not lost, but only “explored” lessefficiently. However, using a similar paradigm Bourlon, Pradat-Diehl, Duret, Azouvi, & Bartolomeo (2008) subsequently describeda patient with fewer correct responses on the left than on theright side of the imagined scene (see also Bourlon et al., in press).Loetscher and Brugger (2007) reported a patient showing a dis-engagement deficit in visuo-motor and representational space.Interestingly, their patient scanned first the right side of a mentalimage before he turned his attention towards the left. In the currentstudy, R.D.’s time to recall towns was limited to 2 min per condi-tion. This leaves open the possibility that R.D. would have startedto recall left-sided towns if he had more time, consistent with anattentional bias in imagery activity.
In a multiple single-case study which explored the relationshipsbetween perceptual and imaginal neglect, Bartolomeo et al. (1994)observed that one of their patients, who initially showed both per-ceptual and imaginal neglect, eight months after initial testing hadrecovered from perceptual but not from imaginal neglect. This pat-tern of selective recovery led the authors to speculate that patientsmight learn with time (and rehabilitation) to compensate for theirneglect in the visuospatial domain, but not in the imaginal domain,where feedback from the external world is not available. In thesame study, it was found that patients (in the acute and subacutestage) often showed signs of perceptual neglect in isolation, with-out imaginal neglect. On the basis of this finding, Bartolomeo et al.(1994) further proposed that a single underlying mechanisms (i.e.a biased orienting of exogenous attention) might contribute to thetwo forms of neglect, but that real stimuli would be more capableto capture patients’ attention than imagined ones.
The present evidence, however, suggests that, if attentionalmechanisms are implicated in imaginal neglect, they do not com-pletely overlap with those used in visual exploratory behaviour,because manoeuvres known to modulate visual attention, such asthe presence/absence of visual input (see Chokron et al., 2004), didnot influence imaginal neglect in R.D. (see also Rode et al., 2007).
Important differences between imagery tasks such as thedescription of a map and their perceptual counterpart are a greaterimplication in imaginal performance of active building/explorationcapacities and of “rehearsing” mechanisms associated with spatialworking memory. It might thus be that deficits of more endoge-nous components of attention, or interactions between attentional
2 In their seminal paper, Bisiach and Luzzatti (1978) already evoked the possibilityof a defective exploration of an otherwise intact imagined scene, but rejected thishypothesis on grounds of parsimony.
deficits and deficits of spatial working memory (Della Sala, Logie,Beschin, & Denis, 2004), contribute to imaginal neglect, whereas itis well known that perceptual neglect entails substantial deficitsof exogenous, or stimulus-based, attention (see Bartolomeo &Chokron, 2002b, for review).3
In healthy individuals, spatial working memory does interactwith mechanisms of visual attention (Awh & Jonides, 2001). Inparticular, spatial orienting to perceptual targets and to itemsrehearsed in spatial working memory relies on similar fronto-parietal networks, with the exception that some early activityin prefrontal regions seems to be selective for mnemonic items(Lepsien & Nobre, 2006). Importantly, fronto-parietal activity dur-ing attention to remembered items seems to be lateralized in asimilar way as it is for perceptual items, with each hemisphere tak-ing care of opposite-side objects (Lepsien & Nobre, 2006). Recently,the respective roles of the left and right parietal lobes in spa-tial mental imagery have been investigated in normal participantsusing TMS (Sack, Camprodon, Pascual-Leone, & Goebel, 2005).Results showed that the left parietal lobe might be important dur-ing the early stages of generation of spatial images, whereas theright parietal lobe could later carry out spatial operations on theseimages.
The substantial but partial overlap of functional and neuralmechanisms of spatial orienting in the perceptual and in the imag-inal domains seems consistent with the patterns of performance ofpatients with visuospatial and imaginal neglect, and suggest thatsimilar orienting problems, resulting from dysfunction of fronto-parietal networks (see Bartolomeo et al., 2007), may contributeto neglect signs in both domains (Bartolomeo & Chokron, 2002a).However, the present results showing that imaginal neglect may beindependent of visual input, as well as the dissociations betweenvisuospatial and imaginal neglect described in the literature, sug-gest that processes specific to perception or to imagery may beinfluenced to a different extent by brain damage. In order totackle this issue, precise anatomical descriptions of brain lesionsin patients with or without imaginal neglect are mandatory.
As mentioned in the introduction, several cortical loci of damagein the right hemisphere have been described in patients with imag-inal neglect. These include lesions in temporo-parietal (Bartolomeoet al., 1994), frontal (Guariglia et al., 1993) and thalamic (Ortigue etal., 2001) regions. Network-based models of neglect (e.g., Mesulam,1999) have recently received support from results from animal andpatient studies (reviewed by Bartolomeo et al., 2007). Accordingto this perspective, neglect may depend not only on focal corticaldamage, but also from disconnection among distant cortical mod-ules resulting in large-scale network dysfunction. For the presentpatients, we could obtain not only high-definition anatomical MRI,but also diffusion sequences that can be used to test the anatomicalintegrity of long-range white matter pathways. White matter tractswhose disconnection might contribute to neglect are the supe-rior longitudinal fasciculus, the inferior fronto-occipital fasciculusand the callosal commissure (Bartolomeo et al., 2007; Doricchi,Thiebaut de Schotten, Tomaiuolo, & Bartolomeo, 2008). DTI tractog-raphy demonstrated damage to that all these pathways in R.D., andto the intra-hemispheric pathways in P.P. The inferior longitudinalfasciculus, on the other hand, was intact and symmetrical in the twohemispheres of both patients. This result is consistent with previ-ous reports on neglect patients (but see Bird et al., 2006; Shinoura etal., 2009; Urbanski et al., 2008), and provides a control of the validityof the procedure. Thus, lesions in the present patients are compati-ble with an intra-hemispheric disconnection interpretation of their
3 Note that spatial working memory deficits can also contribute to perceptualneglect, by impairing the patient’s ability of keeping track of already explored objectsor locations (Malhotra et al., 2005; Cristinzio et al., 2009).

Author's personal copy
2910 G. Rode et al. / Neuropsychologia 48 (2010) 2903–2911
neglect signs. In particular, fronto-parietal disconnection mightdisrupt the co-ordinated activity of right-hemisphere networksimportant for spatial orienting and arousal (Bartolomeo, 2006). Thepresence of posterior callosal disconnection in R.D. further sug-gests that left-hemisphere systems important for the generationof visual mental images (see, e.g., Formisano et al., 2002; Sack et al.,2005) might receive inadequate input from the right hemisphere,resulting in incomplete exploration of the left part of the imagegenerated by the left hemisphere. Interestingly, the present patientP.P., who showed perceptual but not imaginal neglect, had signs ofSLF damage but not splenial disconnection. On the other hand, sple-nial disconnection per se does not seem a sufficient condition forimaginal neglect to emerge, as shown by two patients with splenialdisconnection and lesions of the visual pathways or of the visualcortex leading to hemianopia, who had signs of perceptual neglectbut no imaginal neglect (Tomaiuolo et al., in press). Manoeuvreswhich ameliorate spatial exploration in neglect, such as vestibu-lar or proprioceptive stimulation and prism adaptation (Rossetti &Rode, 2002; Vallar, Guariglia, & Rusconi, 1997) might act on imagi-nal neglect by improving the left hemisphere capacities to deal withleft-sided information. For example, prism adaptation might recruitintact left hemisphere areas (Luaute et al., 2009), whose activationcorrelates with improvement of visuospatial neglect (Luaute et al.,2006). Also optokinetic stimulation may promote a compensatoryrecruitment of left hemisphere areas (Thimm et al., 2009). Furtherdetailed anatomical studies of patients with perceptual or imagi-nal forms of neglect are necessary to explore the viability of thesehypotheses and test the possible contributions of posterior callosaldisconnection to representational neglect.
References
Anderson, B. (1993). Spared awareness for the left side of internal visual images inpatients with leftsided extrapersonal neglect. Neurology, 43, 213–216.
Awh, E., & Jonides, J. (2001). Overlapping mechanisms of attention and spatial work-ing memory. Trends in Cognitive Sciences, 5, 119–126.
Bartolomeo, P., D’Erme, P., & Gainotti, G. (1994). The relationship between visuospa-tial and representational neglect. Neurology, 44, 1710–1714.
Bartolomeo, P., & Chokron, S. (2002a). Can we change our vantage point to exploreimaginal neglect? (Commentary on Pylyshyn: Mental imagery: In search of atheory). Behavioral and Brain Sciences, 25, 184–185.
Bartolomeo, P., & Chokron, S. (2002b). Orienting of attention in left unilateral neglect.Neuroscience and Biobehavioral Reviews, 26, 217–234.
Bartolomeo, P., Bachoud-Levi, A. C., Azouvi, P., & Chokron, S. (2005). Time to imaginespace: A chronometric exploration of representational neglect. Neuropsycholo-gia, 43, 1249–1257.
Bartolomeo, P. (2006). A parieto-frontal network for spatial awareness in the righthemisphere of the human brain. Archives of Neurology, 63, 1238–1241.
Bartolomeo, P. (2007). Visual neglect. Current Opinion in Neurology, 20, 381–386.Bartolomeo, P., Thiebaut de Schotten, M., & Doricchi, F. (2007). Left unilateral neglect
as a disconnection syndrome. Cerebral Cortex, 45, 3127–3148.Berti, A. (2004). Cognition in dyschiria: Edoardo Bisiach’s theory on misconception
of space and consciousness. Cortex, 24, 275–280.Beschin, N., Cocchini, G., Della Sala, S., & Logie, R. (1997). What the eyes perceive,
the brain ignores: A case of pure unilateral representational neglect. Cortex, 33,3–26.
Bisiach, E., & Luzzatti, C. (1978). Unilateral neglect of representational space. Cortex,14, 129–133.
Bisiach, E., Luzzatti, C., & Perani, D. (1979). Unilateral neglect, representationalschema and consciousness. Brain, 102, 609–618.
Bisiach, E., Capitani, E., Luzzatti, C., & Perani, D. (1981). Brain and conscious repre-sentation of outside reality. Neuropsychologia, 19, 543–551.
Bisiach, E., & Berti, A. (1987). Dyschiria: An attempt at its systemic explanation. InM. Jeannerod (Ed.), Neurophysiological and neuropsychological aspects of spatialneglect (pp. 183–201).
Bird, C. M., Malhotra, P., Parton, A., Coulthard, E., Rushworth, M. F. S., & Husain, M.(2006). Visual neglect after right posterior cerebral artery infarction. Journal ofNeurology, Neurosurgery and Psychiatry, 77, 1008–1012.
Bourlon, C., Pradat-Diehl, P., Duret, C., Azouvi, P., & Bartolomeo, P. (2008). Seeingand imagining the « same » objects in unilateral neglect. Neuropsychologia, 46,2602–2606.
Bourlon, C., Duret, C., Pradat-Diehl, P., Azouvi, P., Loeper-Jény, C., Merat-Blanchard,M., Levy, C., Chokron, S., & Bartolomeo, P. (2009). Vocal response times to realand imagined stimuli in spatial neglect: A group study and single-case report.Cortex, in press.
Cardebat, D., Doyon, B., Puel, M., Goulet, P., & Joanette, Y. (1990). Evocation lexicaleformelle et sémantique chez des sujets normaux: performances et dynamiquesde production en fonction du sexe, de l’âge et du niveau d’étude. Acta NeurologicaBelgica, 90, 207–217.
Chokron, S., Colliot, P., & Bartolomeo, P. (2004). The role of vision on spatial repre-sentations. Cortex, 40, 281–290.
Chokron, S., Dupierrix, E., Tabert, M., & Bartolomeo, P. (2007). Experimental remis-sion of unilateral spatial neglect. Neuropsychologia, 45, 3127–3148.
Coslett, H. B. (1997). Neglect in vision and visual imagery: A double dissociation.Brain, 120, 1163–1171.
Cristinzio, C., Bourlon, C., Pradat-Diehl, P., Trojano, L., Grossi, D., Chokron, S., &Bartolomeo, P. (2009). Representational neglect in “invisible” drawing frommemory. Cortex, 45, 313–317.
Critchley, M. (1953). The parietal lobes. New York: Hafner.Della Sala, S., Logie, R. H., Beschin, N., & Denis, M. (2004). Preserved visuo-spatial
transformations in representational neglect. Neuropsychologia, 42, 1358–1364.Diller, L., & Weinberg, J. (1977). Hemi-inattention in rehabilitation: The evolution
of a rational remediation program. In E. A. Weinstein, & R. P. Friedland (Eds.),Hemi-inattention and hemisphere specialization (pp. 62–82). New York: RavenPress.
Doricchi, F., Thiebaut de Schotten, M., Tomaiuolo, F., & Bartolomeo, P. (2008). Whitematter (dis)connections and gray matter (dys)functions in visual neglect: Gain-ing insights into the brain networks of spatial awareness. Cortex, 44, 983–995.
Formisano, E., Linden, D. E. J., Di Salle, F., Trojano, L., Esposito, F., Sack, A. T., Grossi,D., Zanella, F. E., & Goebel, R. (2002). Tracking the Mind’s image in the brain. I:Time-resolved fMRI during visuospatial mental imagery. Neuron, 35, 185–194.
Gainotti, G., Messerli, P., & Tissot, R. (1972). Qualitative analysis of unilateral spatialneglect in relation to laterality of cerebral lesions. Journal of Neurology, Neuro-surgery and Psychiatry, 35, 545–550.
Gauthier, L., Dehaut, F., & Joanette, Y. (1989). The bells test: A quantitative and qual-itative test for visual neglect. International Journal of Clinical Neuropsychology,11, 49–53.
Guariglia, C., Padovani, A., Pantano, P., & Pizzamiglio, L. (1993). Unilateral neglectrestricted to visual imagery. Nature, 364, 235–237.
Karnath, H.-O., Ferber, S., & Himmelbach, M. (2001). Spatial awareness is a functionof the temporal not the posterior parietal lobe. Nature, 411, 950–963.
Kosslyn, S. M. (1994). Image and brain: The resolution of the imagery debate. Cam-bridge, MA: The MIT Press.
Lepsien, J., & Nobre, A. C. (2006). Cognitive control of attention in the human brain:Insights from orienting attention to mental representations. Brain Research,1105, 20–31.
Loetscher, T., & Brugger, P. (2007). A disengagement deficit in representational space.Neuropsychologia, 45, 1299–1304.
Luaute, J., Michel, C., Rode, G., Pisella, L., Jacquin-Courtois, S., Costes, N., Cotton, F.,le Bars, D., Boisson, D., Halligan, P., & Rossetti, Y. (2006). Functional anatomyof the therapeutic effects of prism adaptation on left neglect. Neurology, 66,1859–1867.
Luaute, J., Schwartz, S., Rossetti, Y., Spiridon, M., Rode, G., Boisson, D., & Vuilleumier,P. (2009). Dynamic changes in brain activity during prism adaptation. Journal ofNeuroscience, 29, 169–178.
Malhotra, P., Jäger, H. R., Parton, A., Greenwood, R., Playford, E. D., Brown, M. M.,Driver, J., & Husain, M. (2005). Spatial working memory capacity in unilateralneglect. Brain, 128, 424–435.
Marshall, J. C., & Halligan, P. W. (2002). Whoever would have imagined it? Bisiachand Luzzatti (1978) on representational neglect in patient IG and NV. In C. Code,C. W. Wallesh, & Y. Joanette (Eds.), Classic cases in neuropsychology (pp. 257–279).New York: Psychology Press.
Meador, K. J., Loring, D. W., Bowers, D., & Heilman, K. M. (1987). Remote memoryand neglect syndrome. Neurology, 37, 522–526.
Mesulam, M. M. (1999). Spatial attention and neglect: Parietal, frontal and cingulatecontributions to the mental representation and attentional targeting of salientextrapersonal events. Philosophical Transactions of the Royal Society of London,Series B, 354, 1325–1346.
Mort, D. J., Malhotra, P., Mannan, S. K., Rorden, C., Pambakian, A., Kennard, C., &Husain, M. (2003). The anatomy of visual neglect. Brain, 126, 1986–1997.
Ortigue, S., Viaud-Delmon, I., Annoni, J. M., Landis, T., Michel, C., Blanke, O., Vuiller-mier, P., & Mayer, E. (2001). Pure representational neglect after right thalamiclesion. Annals of Neurology, 50, 401–404.
Ptak, R., & Schnider, A. (2006). Reflexive orienting in spatial neglect is biased towardsbehaviourally salient stimuli. Cerebral Cortex, 16, 337–345.
Rode, G., Perenin, M. T., & Boisson, D. (1995). Négligence de l’espace représenté: miseen évidence par l’évocation mentale de la carte de France. Revista de Neurologia,151, 161–164.
Rode, G., & Perenin, M. T. (1994). Temporary remission of representational hemine-glect through vestibular stimulation. Neuroreport, 5, 869–872.
Rode, G., Rossetti, Y., & Boisson, D. (2001). Prism adaptation improves representa-tional neglect. Neuropsychologia, 39, 1250–1254.
Rode, G., Rossetti, Y., Perenin, M. T., & Boisson, D. (2004). Geographic informationhas to be spatialised to be neglected: A representational neglect case. Cortex, 40,391–397.
Rode, G., Revol, P., Rossetti, Y., Boisson, D., & Bartolomeo, P. (2007). Looking whileimaging. The influence of visual input on representational neglect. Neurology,68, 432–437.
Rossetti, Y., & Rode, G. (2002). Reducing spatial neglect by visual and other sensorymanipulations: Non-cognitive (physiological) routes to the rehabilitation of acognitive disorder. In H.-O. Karnath, D. Milner, & G. Vallar (Eds.), The cognitive

Author's personal copy
G. Rode et al. / Neuropsychologia 48 (2010) 2903–2911 2911
and neural bases of spatial neglect (pp. 375–396). New York: Oxford UniversityPress.
Sack, A. T., Camprodon, J. A., Pascual-Leone, A., & Goebel, R. (2005). The dynamicsof interhemispheric compensatory processes in mental imagery. Science, 5722,702–704.
Schenkenberg, T., Bradford, D. C., & Ajax, E. T. (1980). Line bisection and unilateralvisual neglect in patients with neurologic impairment. Neurology, 30, 509–517.
Shinoura, N., Suzuki, Y., Yamada, R., Tabei, Y., Saito, K., & Yagi, K. (2009). Damage tothe right superior longitudinal fasciculus in the inferior parietal lobe plays a rolein spatial neglect. Neuropsychologia, 47, 2600–2603.
Thiebaut de Schotten, M., Urbanski, M., Duffau, H., Volle, E., Lévy, R., Dubois, B., &Bartolomeo, P. (2005). Direct evidence for a parietal–frontal pathway subservingspatial awareness in humans. Science, 309, 2226–2228.
Thimm, M., Fink, G. R., Küst, J., Karbe, H., Willmes, K., & Sturm, W. (2009). Recoveryfrom hemineglect: Differential neurobiological effects of optokinetic stimula-tion and alertness training. Cortex, 45, 850–862.
Thomas, N. J. T. (1999). Are theories of imagery theories of imagination? Anactive perception approach to conscious mental content. Cognitive Science, 23,207–245.
Tomaiuolo, F., Voci, L., Bresci, M., Cozza, S., Posteraro, F., Oliva, M. & Dorrichi, F.Selective visual neglect in right brain damaged patients with splenial interhemi-spheric disconnection. Experimental Brain Research, in press.
Urbanski, M., Thiebaut de Schotten, M., Rodrigo, S., Catani, M., Oppenheim, C.,Touzé, E., Chokron, S., Méder, J.-F., Lévy, R., Dubois, B., & Bartolomeo, P. (2008).Brain networks of spatial awareness: Evidence from diffusion tensor imag-ing tractography. Journal of Neurology, Neurosurgery and Psychiatry, 79, 598–601.
Vallar, G. (2001). Extrapersonal visual unilateral spatial neglect and its neu-roanatomy. Neuroimage, 14, 552–558.
Vallar, G., Guariglia, C., & Rusconi, M. L. (1997). Modulation of the neglect syndromeby sensory stimulation. In P. Their, & H.-O. Karnath (Eds.), Parietal lobe contribu-tions to orientation in 3D space (pp. 555–578). Heidelberg: Springer-Verlag.
Related Documents











