Report of the 2nd ad hoc Committee on the TB epidemic Jaap F. Broekmans STOP TB Partner’s Forum NEW DELHI 22 - 26 June 2004

Report of the 2nd ad hoc Committee on the TB epidemic Jaap F. Broekmans STOP TB Partner’s Forum
Dec 30, 2015
Report of the 2nd ad hoc Committee on the TB epidemic Jaap F. Broekmans STOP TB Partner’s Forum NEW DELHI 22 - 26 June 2004. 2nd ad hoc C ommittee on the TB epidemic. 19981st ad hoc Committee, London 2000Ministerial Conference for 20 HBCs, Amsterdam 2001Global Plan to Stop TB - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Report of the 2nd ad hoc Committee
on the TB epidemic
Jaap F. Broekmans
STOP TB Partner’s Forum
NEW DELHI
22 - 26 June 2004

2nd 2nd ad hoc Cad hoc Committee on the TB epidemicommittee on the TB epidemic
1998 1st ad hoc Committee, London
2000 Ministerial Conference for 20 HBCs, Amsterdam
2001 Global Plan to Stop TB
2003 2nd ad hoc Committee, Montreux
2005 WHA targets
2010 G8 Okinawa targets
2015 Millennium Development Goals

Objectives of 2nd Objectives of 2nd ad hoc Cad hoc Committeeommittee
(1) review status of TB epidemic and of TB control efforts
(2) review progress in implementing the 1st ad hoc Committee recommendations (London, 1998)
(3) analyse constraints in HBCs (DEWG)
(4) make recommendations in defining a mid-term strategic direction for the DOTS expansion movement
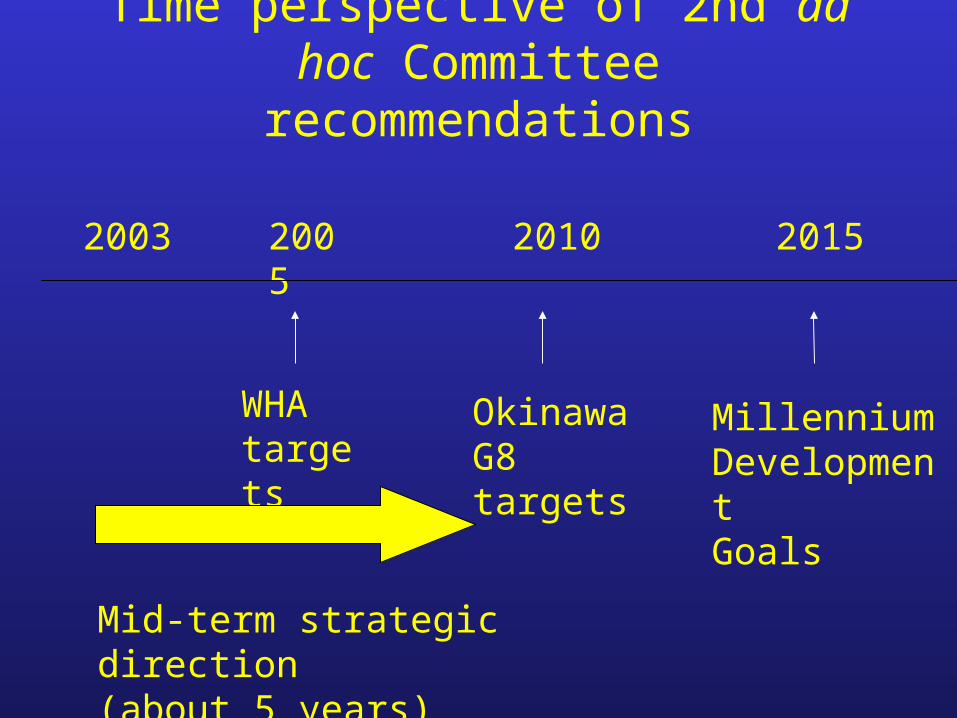
Time perspective of 2nd ad hoc Committee recommendations
WHA targets
MillenniumDevelopmentGoals
2003 2005 2015
Mid-term strategic direction(about 5 years)
2010
OkinawaG8 targets
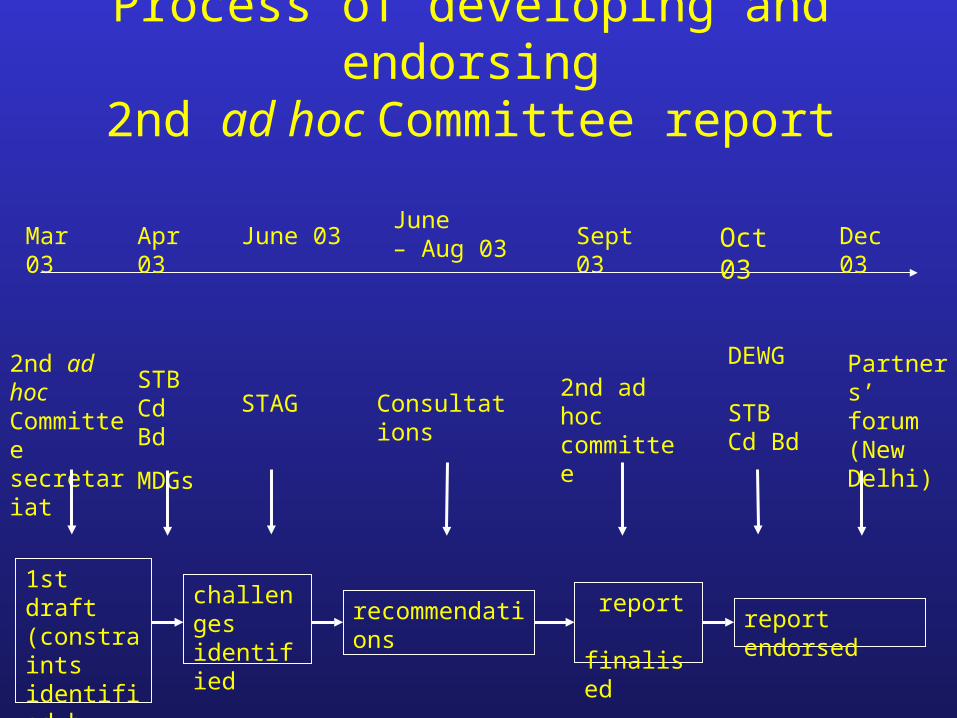
Process of developing and endorsing2nd ad hoc Committee report
2nd ad hoc Committeesecretariat
Consultations
1st draft (constraints identified by DEWG)
challenges identified
report finalised
recommendations
DEWG
STB Cd Bd
Sept 03Mar 03 June 03June – Aug 03 Dec 03
Partners’ forum(New Delhi)
report endorsed
Apr 03
STAGSTB Cd Bd
MDGs
Oct 03
2nd ad hoc committee

Main recommendationsMain recommendations
(1) Consolidate, sustain and advance achievements
(2) Enhance political commitment
(3) Address the health workforce crisis
(4) Strengthen health systems, particularly primary care delivery
(5) Accelerate response to the HIV/AIDS emergency
(6) Mobilise communities and the private sector
(7) Invest in research and development to shape the future
(1) Consolidate, sustain and advance achievements The Stop TB Partnership should
(1) demonstrate the effectiveness and added value of the Partnership, GDF, GLC and its collaboration with the GFATM;
(2) involve a wider range of stakeholders at all levels;
(3) use existing mechanisms at national level, e.g. NICCs, Sector-Wide committees, CCMs;
(4) strengthen its relationship with the GFATM;
(5) seek enhanced and sustained donor support for GDF;
(6) advocate for support for TB activities based on success stories of TB as pathfinder for health system reform.

(2) Enhance political commitment
The Stop TB Partnership should
(1) explore complementary “top-down” (e.g. lobbying by high- level missions, political mapping and analysis) and “bottom-up” approaches (social mobilisation and communications);
(2) seek financial support from a broader donor base;
(3) argue the case for increased donor budget commensurate with global TB burden, e.g. GFATM;
(4) adopt the 2015 MDGs relevant to TB as impact targets while retaining WHA 2005 targets as process targets.

(3) Address the health workforce crisis The Stop TB Partnership should collaborate with governments and international bodies to:
(1) develop policies to remove administrative barriers to creating and filling posts;
(2) develop policies to promote terms and conditions of service attractive to employees;
(3) promote assessment of human resource needs;
(4) support human resource planning and training;
(5) explore strategies for mobilising human resources from the full
range of primary care providers, especially community groups.

(4) Strengthen health systems, particularly primary care deliveryThe Stop TB Partnership should(1) promote reflection of TB control needs in design and implementation of health reform strategies;
(2) ensure that TB programmes contribute to broader health system strengthening;
(3) foster NTP stewardship capacity;
(4) explore strategies for harnessing the contribution of the full range of health care providers;
(5) encourage partners in Global TB Monitoring and Surveillance Project to intensify collaboration with other programmes and improvements in accuracy of estimates of progress towards targets.
(6)

(5) Accelerate response to the HIV/AIDS emergency The Stop TB Partnership should
(1) urgently step up collaboration with HIV/AIDS partnerships to implement strategy of expanded scope to control HIV-related TB;
(2) support countries in delivering TB care as part of the HIV/AIDS care package;
(3) support countries in making progress towards the “3 by 5” goal, by promoting HIV testing among TB patients and referral for ART;
(4) support ART programmes in making use of lessons learned from TB programmes in applying public health principles to large scale diagnosis and treatment of a chronic communicable disease.

(7) Invest in research and development to shape the future
The Stop TB Partnership should
(1) ensure a framework to support interaction between the WGs on
new tools and the WGs on implementation;
(2) work with the research community on advocacy for new tools, funding and preparation of trial sites;
(3) promote operational research;
(4) develop and articulate arguments in favour of increased research capacity building to encourage OECD countries to increase funding for this.

Main implications for Stop TB PartnershipMain implications for Stop TB Partnership
(1) Speed of progress in reaching WHA 2005 targets now
depends on collaboration with other programmes and other constituencies.
(2) Need to reach out to other programmes within the health sector, in addressing the key health system issues, e.g. human resources, general health infrastructure, primary care providers, health system reform.
(3) Need to reach out to other sectors beyond health, in enhancing political commitment, expanding the resource base, and mobilising communities.
Related Documents











