Reperfusion of Acute Myocardial Infarction in Carolina Emergency Departments (RACE) Project

Reperfusion of Acute Myocardial Infarction in Carolina Emergency Departments (RACE) Project.
Dec 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Reperfusion of Acute Myocardial Infarction in Carolina Emergency Departments (RACE)
Project
• Research grants/contracts from – Sanofi Aventis, AstraZeneca, Novartis, Boehringer
Ingelheim, Genentech, Procter and Gamble, Alexion, GlaxoSmithKline, BMS, Medicines Company, BlueCross BlueShield
• Consulting fees/honoraria from– Sanofi Aventis, AstraZeneca, Genentech,
GlaxoSmithKline, Medicines Company
COI Disclosure Related to This Presentation:
Complete listing available at:http://www.dcri.duke.edu/research/coi.jsp

Death from heart attack is 3 times more common than death from motor vehicle crashes.
Rapid reperfusion is the most important way to improve early survival.
rapid PCI (or fibrinolysis if not available)
Before the RACE project, 1st door-to-balloon for patients transferred for PCI from non-PCI center was nearly 3 hours.
Lack of “systems” and coordination to rapidly and effectively treat heart attacks.
The Problem
Background
Transfer for PCI shown to be possible and effective in Europe
While RACE project was ongoing, we collaborated with other programs (Minneapolis, Boston, Maine, Los Angeles, D2B)
None in US had reported a comprehensive approach involving multiple PCI centers and multiple EMS systems in a statewide program
We hypothesized that such an approach could provide an umbrella to manage barriers of competing practices and hospitals and encourage broad participation
RACE Objectives
Establish a state-wide system for reperfusion, as exits for trauma care, to overcome systematic barriers to:
1) Increase speed of reperfusion
2) Increase reperfusion rate
Organizeregions
Baselinedata
Intervention Postdata
2005 Q3 2005 2006 Q1 2007
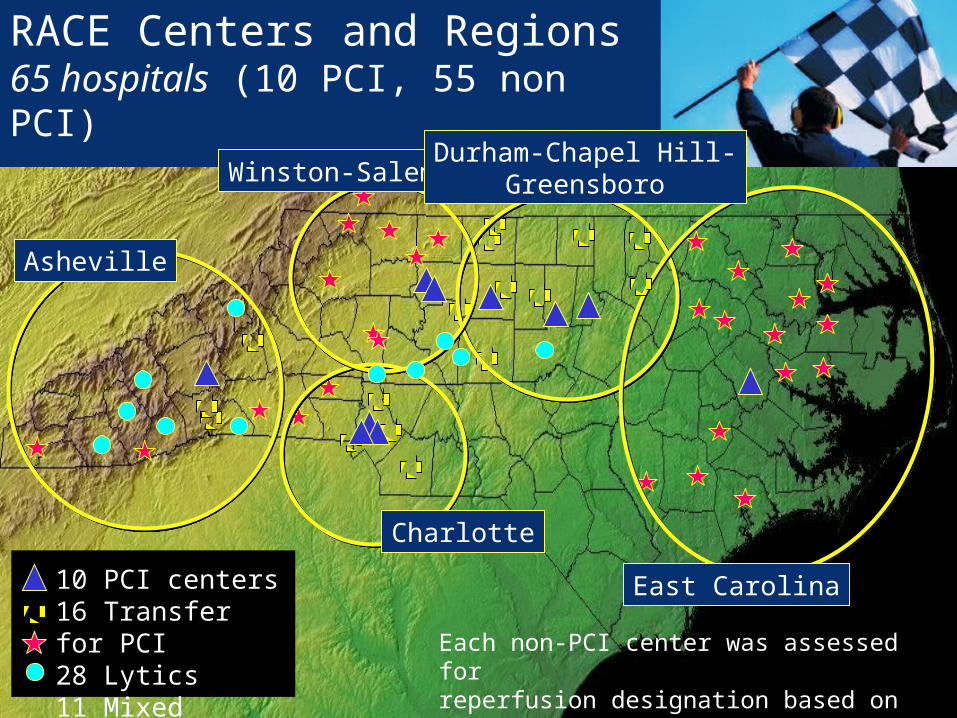
10 PCI centers16 Transfer for PCI28 Lytics11 Mixed
RACE Centers and Regions65 hospitals (10 PCI, 55 non PCI)
Asheville
Winston-SalemDurham-Chapel Hill-
Greensboro
Charlotte
East Carolina
Each non-PCI center was assessed forreperfusion designation based on resources, transfer ability, and transfer time to PCI center

RACE Participating Hospitals by Region 5 Regions, 65 hospitals
Asheville: Mission Hospitals, Asheville (PCI)Angel Medical Center, FranklinHarris Regional Hospital, SylvaHaywood Regional Medical Center, WaynesvilleHighlands-Cashiers, HighlandsMc Dowell Hospital, MarionMurphy Medical Center, MurphyPardee Hospital, HendersonvillePark Ridge Hospital, FletcherRutherford Hospital, RutherfordtonSpruce Pine Community Hospital, Spruce PineSt. Luke's Hospital, ColumbusTransylvania Community Hospital, Brevard
Charlotte: Carolinas Medical Center (CMC) (PCI)CMC-Mercy (PCI)Presbyterian Hospital (PCI), CharlotteCMC- Lincoln, LincolntonCMC- Pineville, Charlotte CMC-Union, MonroeCMC-University, Charlotte Cleveland Medical Center, ShelbyLake Norman Regional Hospital, MooresvillePresbyterian Hospital, Huntersville Presbyterian Hospital, Matthews Rowan Regional Medical Center, Salisbury
Durham-Greensboro-Chapel-Hill:Duke University Medical Center, Durham (PCI)Moses H. Cone Memorial Hospital, Greensboro (PCI)North Carolina Memorial Hospital, Chapel-Hill (PCI)Alamance Regional Medical Center, BurlingtonAnnie Penn Hospital, Reidsville Chatham Hospital, Siler City Franklin Regional Medical Center, LouisburgMaria Parham Medical Center, Henderson
Durham-Greensboro-Chapel-Hill (continued)Morehead Memorial Hospital, EdenPerson Memorial Hospital, RoxboroRandolph Hospital, AsheboroSampson Regional Medical Center, ClintonWesley Long Community Hospital, Greensboro
East North Carolina:Pitt County Memorial Hospital, Greenville (PCI)Beaufort County Hospital, WashingtonBertie Memorial Hospital, WindsorChowan Hospital, EdentonDuplin General Hospital, KenansvilleHalifax Regional Medical Center, Roanoke RapidsHeritage Hospital, TarboroLenoir Memorial Hospital, KinstonMartin General Hospital, WilliamstonNash General Hospital, Rocky MountOnslow Memorial, JacksonvilleOur Community Hospital, Scotland NeckPungo District Hospital, BelhavenRoanoke-Chowan hospital, AhoskieWashington County Hospital, Plymouth
Winston-Salem: Forsyth Medical Center, Winston-Salem (PCI)Wake Forest University/Baptist Medical Center, Winston-Salem (PCI) Alleghany Memorial Hospital, SpartaAshe Memorial Hospital, JeffersonDavis Regional Medical Center, StatesvilleHugh Chatham Memorial Hospital, ElkinIredell Memorial Hospital, StatesvilleNorthern Hospital of Surry County, Mount AiryLexington Memorial Hospital, LexingtonThomasville Medical Center, ThomasvilleTwin County Regional Hospital, GalaxWilkes Regional Medical Center, N. Wilkesboro
Organization
Supported by grant from Blue Cross Blue Shield of North Carolina
Nurse coordinator and steering committee (EMS, ED, nursing, hospital administration, QI experts, cardiology) for each region
Buy-in from all PCI centers in each region
Co-funded RACE Regional Coordinators
Co-sponsored by NC Chapter of ACC with focus on the patient by promoting ACC/AHA STEMI guidelines
Data systems support from Genentech
Organization
Physician leaders (continued) Joseph Shiber Greg Tarleton F. Scott Valeri Bradley Watling Hadley Wilson
Oversight Board Robert M. Califf Pamela Douglas Robert Harris Greg Mears William O’Neill
Regional Coordinators Marla Jordan, RN Lourdes Lorenz, RN, MSN Lisa Monk, RN, MSN Mary Printz, RN, FNP-C Stephanie Starling-Edwards, RN Jenny Underwood, RN
Central Steering Committee and Statistics
James Jollis, MD Chris Granger, MD Mayme Roettig, RN, MSN Kevin Anstrom, PhD
Physician leaders Akinyele Aluko Robert Applegate Joseph Babb Peter Berger David Bohle Sidney Fletcher J. Lee Garvey Robert Hathaway James Hoekstra Robert Kelly William Maddox
RACEInterventions
OPERATIONS MANUALOptimal system specifications
by point of care– EMS
– Non-PCI and PCI ED
– Transfer
– Catheterization lab
– Other system issues – payers, regulations
– Choice of PCI or lytic reperfusion regimens
available at www.nccacc.org
RACEInterventions
Focus on SYSTEMATIC BARRIERS to care
STEMI team – hospital administration, ED, EMS,
nursing, cardiology
Prespecified reperfusion plan for hospital and region
Prehospital ECGs, interpretation, and earliest
activation
Emergency physician (or paramedic) able to activate
the cath lab
Intense education with focus on EMS and EDs
RACEInterventions
PCI Hospitals
Single number cath lab activation
Accept all STEMI patients regardless of bed
availability
Ongoing QI and data feedback– NRMI database
RACE Regional Coordinator
Responsible for improving process in every
hospital - EMS system in the region
Data CollectionDistinct but overlapping databases
• Non-PCI hospital data – Regional coordinators abstracted data from (10) consecutive
charts from STEMI reperfusion candidates in non-PCI EDs
– Emergency Department data only
– Feedback to all stakeholders
– Not linked to PCI hospital data to satisfy HIPPA restrictions
• PCI hospital data – RACE NRMI 5 system report
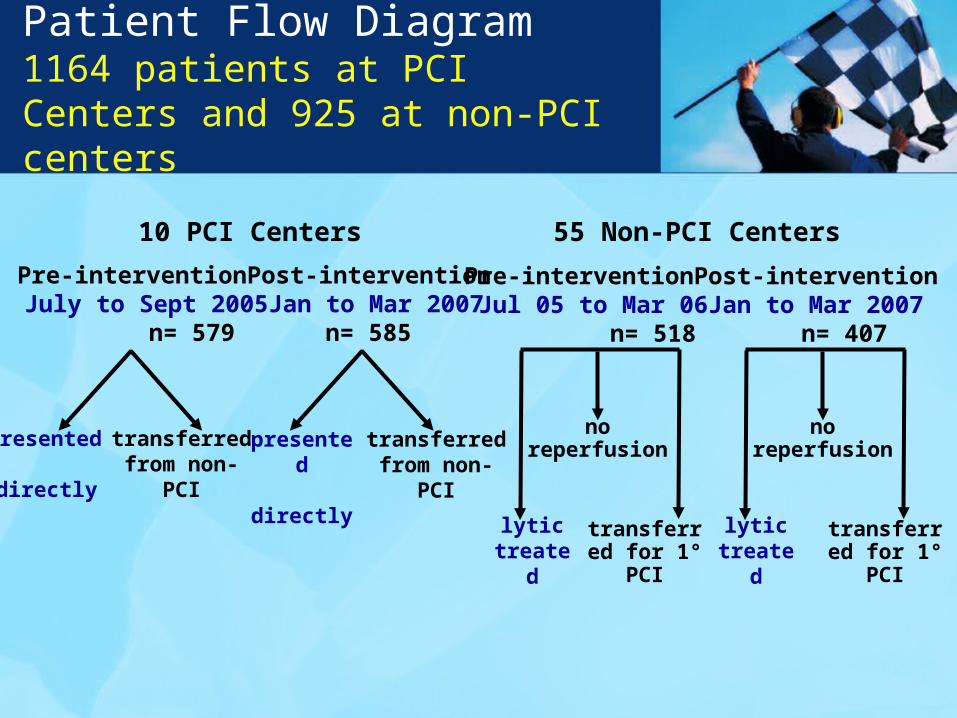
Pre-intervention Post-interventionJuly to Sept 2005 Jan to Mar 2007 n= 579 n= 585
10 PCI Centers
presented directly
transferred from non-PCI
presented directly
transferred from non-PCI
55 Non-PCI Centers
Pre-intervention Post-interventionJul 05 to Mar 06 Jan to Mar 2007 n= 518 n= 407
lytictreated
transferred for 1° PCI
no reperfusion
lytictreated
transferred for 1° PCI
no reperfusion
Patient Flow Diagram1164 patients at PCI Centers and 925 at non-PCI centers

RACE resultsPatient features
PCI hospital Non-PCI hospitalPre Post Pre Post
n 579 585 518 407
Age (years, median) 60 61 62 61 ≥ 75 years 20% 19% 22% 20%
Female 33% 28% 33% 30%
Chest pain at presentation 93% 96% 90% 89%
Killip III/IV 4.7% 4.3% 2.7% 5.5%
Initial reperfusion strategy No reperfusion 23% 11% 15% 15% Fibrinolysis (pre transfer) 28% 25% 45% 39% Primary PCI 48% 63% 40% 46% CABG 1.7% 1.5% -- --
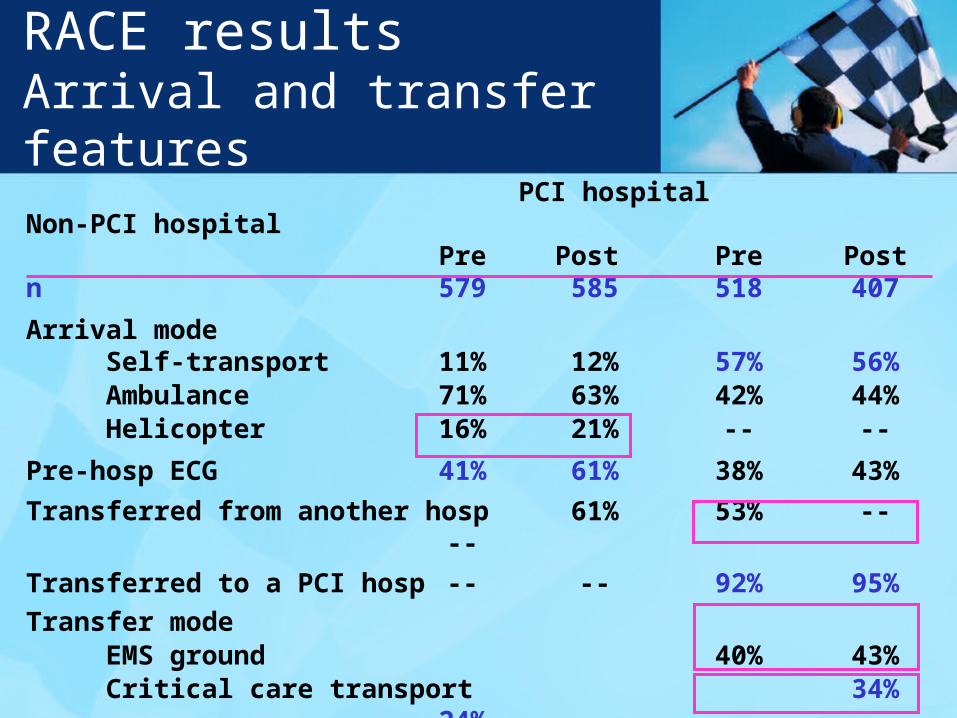
RACE resultsArrival and transfer features PCI hospital Non-PCI hospital
Pre Post Pre Postn 579 585 518 407
Arrival mode Self-transport 11% 12% 57% 56% Ambulance 71% 63% 42% 44% Helicopter 16% 21% -- --
Pre-hosp ECG 41% 61% 38% 43%
Transferred from another hosp 61% 53% -- --
Transferred to a PCI hosp -- -- 92% 95%
Transfer mode EMS ground 40% 43% Critical care transport 34% 24% Helicopter 25% 43%AMI Hotline used 32% 85%
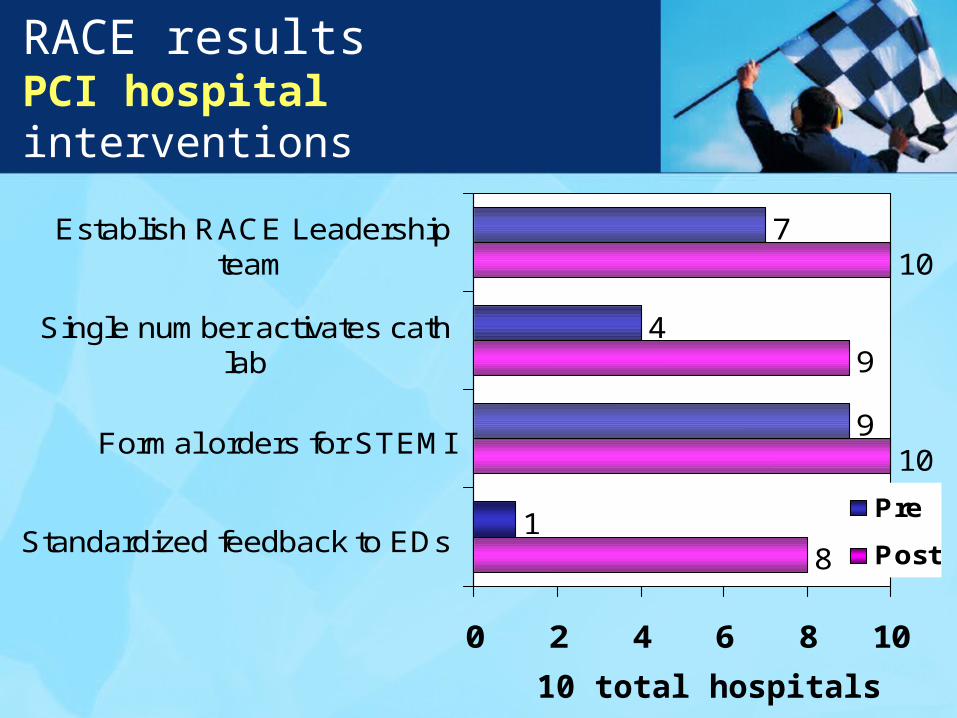
RACE resultsPCI hospital interventions
8
10
9
10
1
9
4
7
0 2 4 6 8 10
Standardized feedback to EDs
Formal orders for STEMI
Single number activates cathlab
Establish RACE Leadershipteam
Pre
Post
10 total hospitals
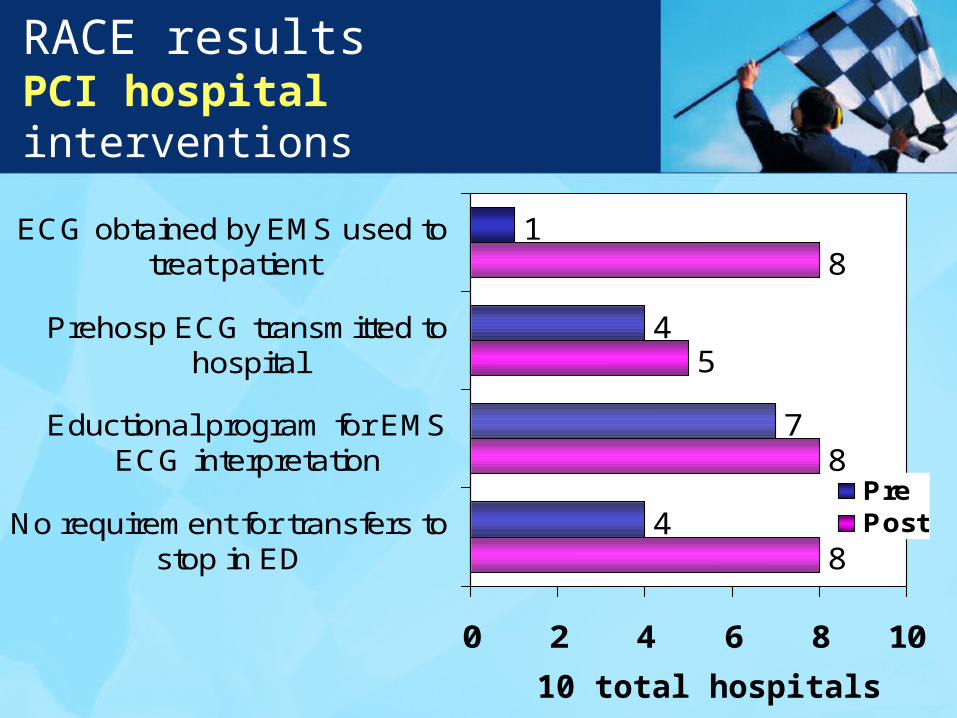
RACE resultsPCI hospital interventions
8
8
5
8
4
7
4
1
0 2 4 6 8 10
No requirement for transfers tostop in ED
Eductional program for EMSECG interpretation
Prehosp ECG transmitted tohospital
ECG obtained by EMS used totreat patient
PrePost
10 total hospitals
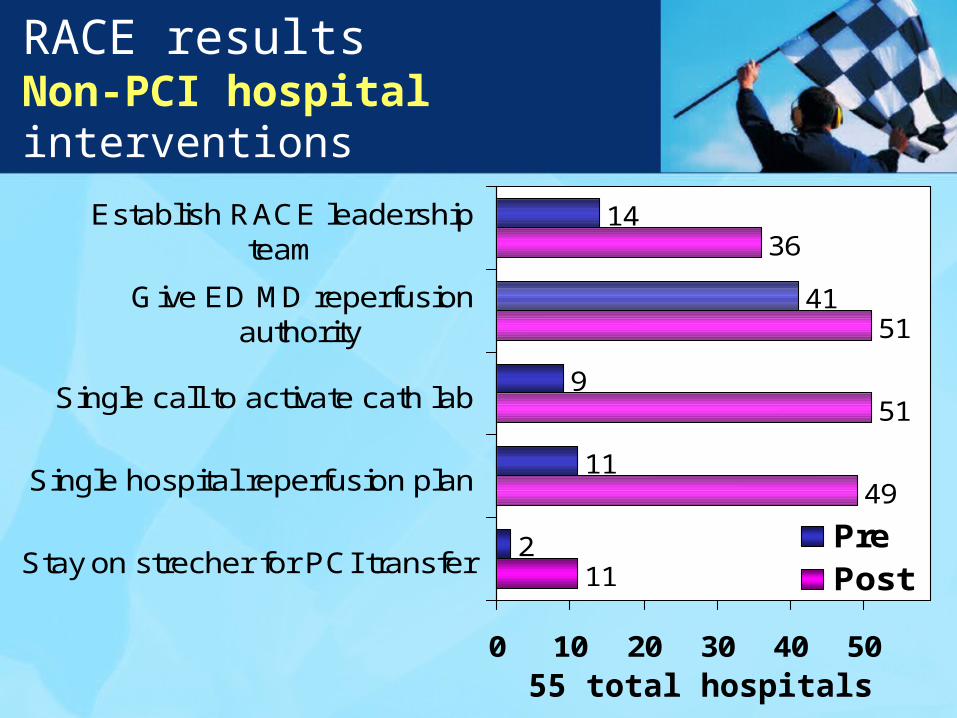
RACE resultsNon-PCI hospital interventions
11
49
51
51
36
2
11
9
41
14
0 10 20 30 40 50
Stay on strecher for PCI transfer
Single hospital reperfusion plan
Single call to activate cath lab
Give ED MD reperfusionauthority
Establish RACE leadershipteam
PrePost
55 total hospitals
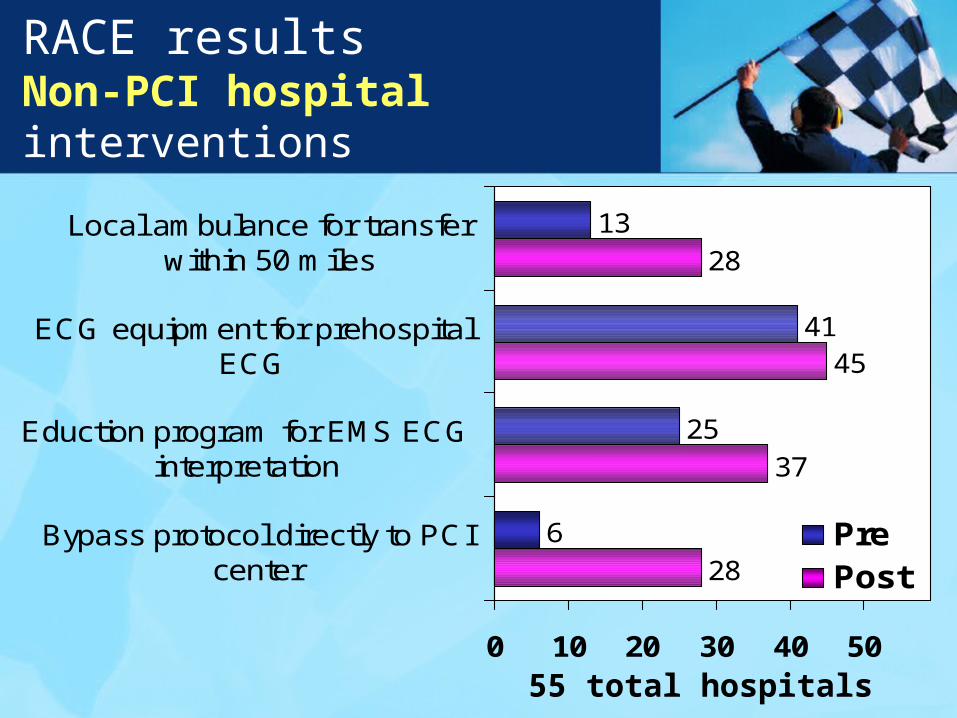
RACE resultsNon-PCI hospital interventions
28
37
45
28
6
25
41
13
0 10 20 30 40 50
Bypass protocol directly to PCIcenter
Eduction program for EMS ECGinterpretation
ECG equipment for prehospitalECG
Local ambulance for transferwithin 50 miles
PrePost
55 total hospitals
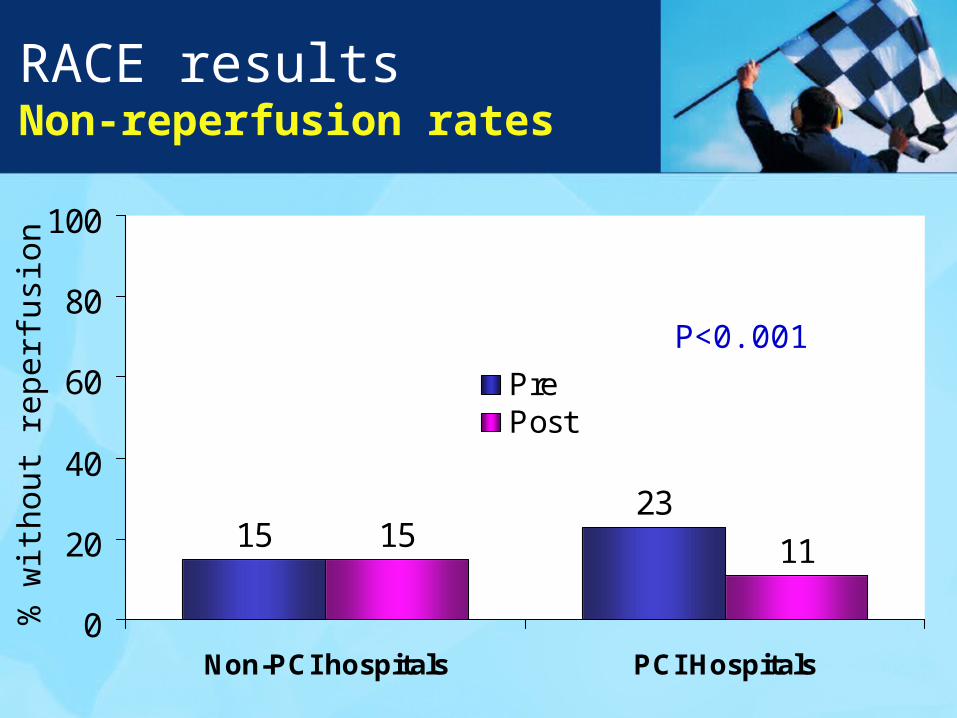
RACE resultsNon-reperfusion rates
1523
15 11
0
20
40
60
80
100
Non-PCI hospitals PCI Hospitals
PrePost
% w
ithou
t re
perf
usio
n
P<0.001
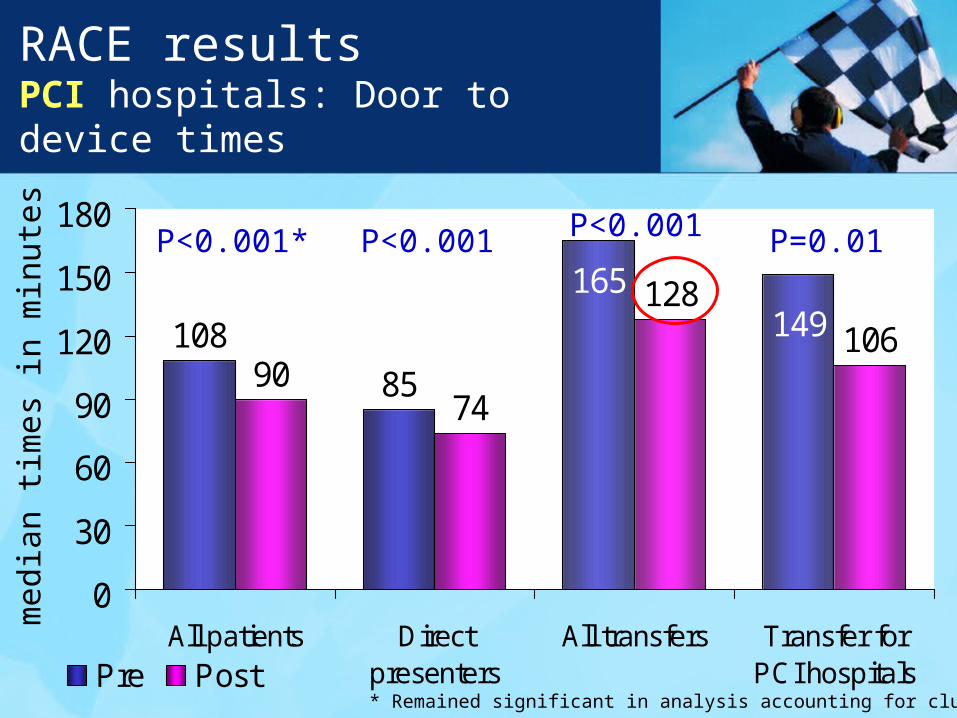
RACE resultsPCI hospitals: Door to device times
108
859074
128106149
165
0
30
60
90
120
150
180
All patients Directpresenters
All transfers Transfer forPCI hospitalsPre Post
P<0.001* P<0.001
med
ian
times
in m
inut
es
P<0.001 P=0.01
* Remained significant in analysis accounting for clustering
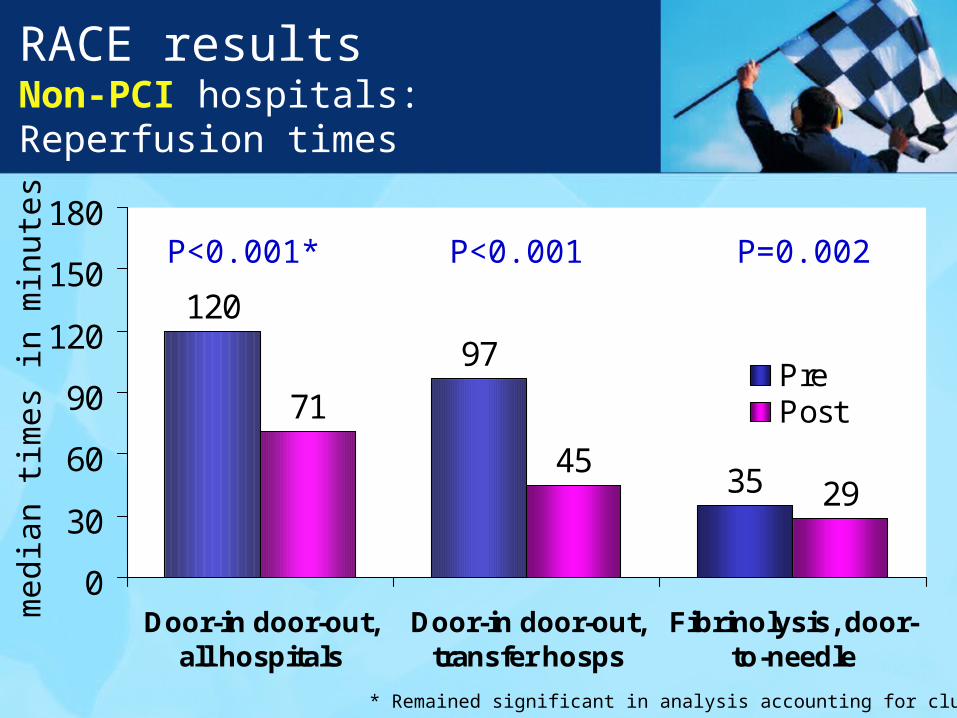
RACE resultsNon-PCI hospitals: Reperfusion times
120
97
71
452935
0
30
60
90
120
150
180
Door-in door-out,all hospitals
Door-in door-out,transfer hosps
Fibrinolysis, door-to-needle
PrePost
P<0.001* P<0.001
med
ian
times
in m
inut
es P=0.002
* Remained significant in analysis accounting for clustering
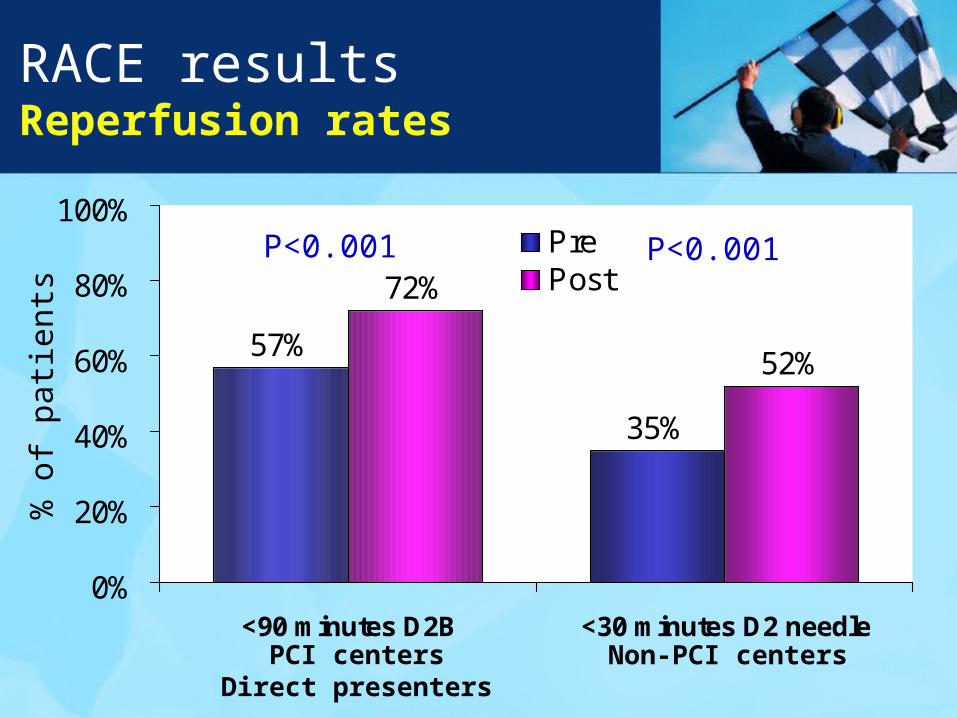
RACE resultsReperfusion rates
57%
35%
72%
52%
0%
20%
40%
60%
80%
100%
<90 minutes D2B <30 minutes D2 needle
PrePost
% o
f pa
tient
s
PCI centersDirect presenters
Non-PCI centers
P<0.001 P<0.001
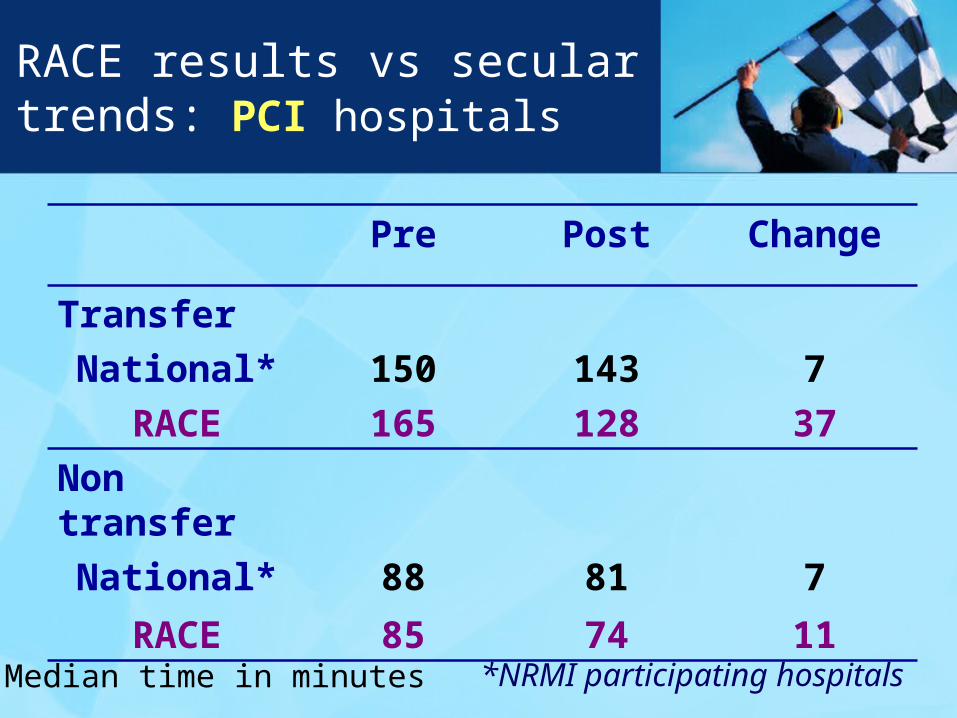
RACE results vs secular trends: PCI hospitals
Pre Post Change
Transfer
National* 150 143 7
RACE 165 128 37
Non transfer
National* 88 81 7
RACE 85 74 11
Median time in minutes *NRMI participating hospitals
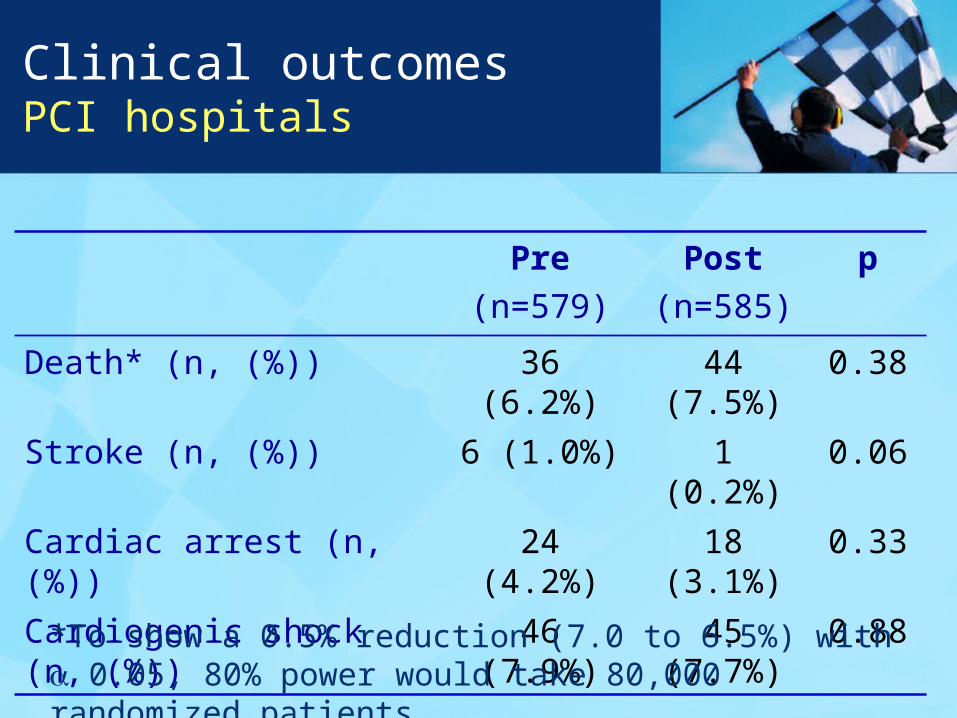
Clinical outcomes PCI hospitals
Pre
(n=579)
Post
(n=585)
p
Death* (n, (%)) 36 (6.2%) 44 (7.5%) 0.38
Stroke (n, (%)) 6 (1.0%) 1 (0.2%) 0.06
Cardiac arrest (n, (%)) 24 (4.2%) 18 (3.1%) 0.33
Cardiogenic shock (n, (%)) 46 (7.9%) 45 (7.7%) 0.88
*To show a 0.5% reduction (7.0 to 6.5%) with 0.05, 80% power would take 80,000 randomized patients
Summary and Conclusions
RACE represents the largest regional STEMI reperfusion system in the United States.
We focused on moving care forward: enabling EMS to diagnose and ED personnel to initiate treatment, with improved communication, integration, and data feedback.
All times – door-to-balloon at PCI centers, door-in to door out in non-PCI centers, 1st door-to-balloon in transfer patients, and door-to-needle for fibrinolysis – were significantly improved.
Improved application of reperfusion care on a broad scale is possible and should be a high national priority.

RACE Regional Coordinators
Now available online at http://jama.ama-assn.org/
Related Documents











