Renovascular Disease Daniel Shoskes MD, MSc, FRCSC Professor of Surgery/Urology Glickman Urological and Kidney Institute Cleveland Clinic

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Renovascular Disease
Daniel Shoskes MD, MSc, FRCSC
Professor of Surgery/Urology
Glickman Urological and Kidney Institute
Cleveland Clinic

• Pathophysiology
• Classification of Lesions
• Clinical Evaluation
• Medical and Surgical Management
• Renal Artery Aneurysm
Overview
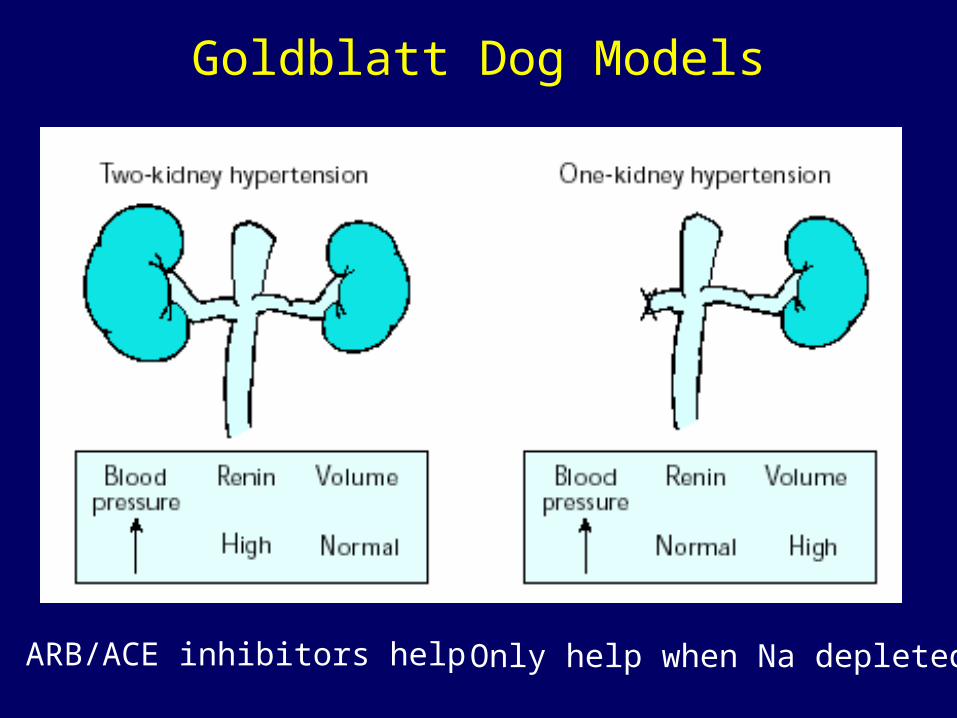
Goldblatt Dog Models
ARB/ACE inhibitors help Only help when Na depleted

Ischemic Nephropathy
• Does not correlate with hypertension
• Progressive azotemia in pt with risk factors
for atherosclerotic disease
• Progresses through nephrosclerosis and
atheroemboli
• Treatment of hypertension will not improve
renal function, may actually exacerbate

Diameter and Blood Flow

• Atherosclerotic (70%)
• Fibromuscular Disease (30%)
Classification

Fibromuscular Disease
Medial Fibroplasia: 77%
Perimedial Fibroplasia: 10%
Intimal Fibroplasia: 10%
Fibromuscular Hyperplasia: 3%

Atherosclerosis
• typically a systemic disease
• involves proximal 2 cm of artery
• may only be seen on oblique views
• progression common, at least 50% in 2 years
• 10-15% progress to occlusion
• can cause hypertension and Renal Failure

Medial Fibroplasia
• most common fibrous
• women 25-50
• commonly bilateral
• "string of beads"
• involves distal 2/3 and
branches
• progression less
common

Clinical Clues to RVH
• HTN onset < 30 yrs or > 55
• sudden onset, short duration
• lack of family history
• difficult to control
• malignant crisis
• bruits
• disseminated atherosclerotic disease
• renal size disparity

Key Diagnostic Points• Captopril provocation
– reduction of GFR detected by nuclear scan• best predictor of surgical cure (spec 93-98%)
– increased PRA (off most drugs)• Renal Vein Renins
– ipsilateral hypersecretion, contralateral suppression– best for bilateral disease
• Ultrasound– operator dependent, independent of renal function
• MRA – poor images beyond main renal artery

Investigation of Ischemic Nephropathy
• High suspicion
– straight to angiography
• Mild to Moderate suspicion
– non-invasive imaging (local preference)
– if significant azotemia, US rather than MRA or
spiral CT

Investigation of RVH
• High suspicion– angiography and Renal Vein Renins if bilateral
• Moderate suspicion– captopril nuclear renography (can do "post"
study first)– positive -> angio– equivocal -> non-invasive imaging– negative -> stop
Treatment of RVH
• Select medical management based on risk of ischemic nephropathy and lesion progression
– medial fibroplasia and atherosclerotic (without ischemic nephropathy) best for medical
• angioplasty +/- stents usually procedure of choice unless
– branch vessel disease
– renal artery aneurysm
• Nephrectomy if small and non-functioning

Treatment of Ischemic Nephropathy
• No benefit with unilateral disease• Signs of reversibility
– progressive occlusion– collaterals– retrograde arterial filling– size > 9 cm– Cr < 4.0– preservation of glomeruli on biopsy

Surgical Approaches
• Hepatorenal
• Splenorenal
• Ileorenal
• Autotransplant
• Arteriotomy
• Aortorenal
• Thoracic aorta - renal

Renal Artery Aneurysms
• most small and asymptomatic• pathology
– saccular (most common), fusiform, dissecting, intrarenal
• risk of rupture– absent/incomplete calcification, >2cm diameter,
expanding, hypertension, pregnancy
• other complications– pain, hematuria, dissection, emboli
Related Documents