ARF/AKI Definition Workgroup

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ARF/AKI Definition
Workgroup

• To develop standard clinical definitions on select
diagnoses & categories to be used consistently across
all hospitals in Maryland Definitions will be informed by published criteria, existing hospital-
developed definitions and supported by industry consensus and
comments from the field
Definitions will not conflict with federal inpatient coding guidelines and
will be applied to any occurrence of the diagnosis, not only in scenarios
that might trigger a PPC
• Our goal is that these definitions will be considered and
adopted by hospitals’ Medical Executive Committees
Purpose
2

• Under the state’s waiver agreement, hospitals must meet reduction
targets for Potentially Preventable Complications (PPCs)
Additionally, the Health Services Cost Review Commission
(HSCRC) incorporates reduction targets into payment policy
• Having a uniform set of clinically defined criteria may facilitate care
improvement
Consistency allows for both a performance comparison among
hospitals and for a measurement of an individual hospital’s
performance improvement over time
Consistency helps demonstrate that Maryland hospitals have
put in time and effort to achieve clinically significant
performance improvement in addition to improvement achieved
through revised documentation and coding practices
Background
3

Participants
4
HOSPITALS
Greater Baltimore Medical Center
Rekha Motagi, MD, Assistant Director of Hospitalists, GBMC
John Saunders, MD, Chief Medical Officer, GBMC
Johns Hopkins
Carol Morris, Senior Coding Compliance Auditor, Johns Hopkins Health System
Paul Segal, MD, Assistant Professor, Nephrology, Johns Hopkins Bayview
Carol Ware, RN, QI Team Leader for Special Projects, Johns Hopkins Hospital
MedStar
Eskandar Yazaji, MD, Chief Quality Officer, MedStar Health
University of Maryland
Lisa Aiken, RN, BWMC
Mangla Gulati, MD, Assistant Chief Medical Officer, Assistant Professor of Medicine, UMMC
Cindy Knott, Director, Quality Improvement, BWMC
Jason Marx, MD, Chair, Department of Medicine, UM St. Joseph Medical Center
Kevin Rossiter, MD, Nephrologist, UM St. Joseph Medical Center
Adam Weinstein, MD, Nephrologist, UM Shore Regional Health
STAFF
Maryland Hospital Association
Nicole Stallings, Vice President
Justin Ziombra, RN, Analyst
Berkeley Research Group
Joni Dion, Associate Director
Kristen Geissler, Managing Director
Brenda Watson, Senior Managing Consultant

Phase 1 Meeting Calendar
5
All meetings will be held from 8:30 – 11:30 at MHA
UTIPPCs 65, 66
January 13
January 28
February 17
RenalPPCs 24, 25
January 20
February 2
February 23
OBPPCs 55, 56, 57, 58
January 29
February 18
March 5
Respiratory
PPCs 3, 4, 5, 6
February 5
February 19
March 10

• Meeting 1, January 20:
Review coding rules, query rules and how clinical definitions can and cannot be
used
Review existing definitions to eliminate non-starters, identify similarities and
develop an initial consensus
• Homework prior to Meeting 2:
Participants will review initial consensus with appropriate clinical and
administrative stakeholders for input
• Meeting 2, February 2:
Review feedback from stakeholders and update draft definitions
• Homework prior to Meeting 3:
Draft definitions will be submitted to hospital field for comment
• Meeting 3, February 23:
Review comments
Finalize definitions
Meeting Workflow Schedule
6

Coding Guidelines

• ICD-9-CM Official Guidelines for Coding and Reporting have been approved by the four
cooperating parties:
The American Hospital Association (AHA)
The American Health Information Management Association (AHIMA)
The Centers for Medicare and Medicaid Services (CMS)
The National Center for Health Statistics (NCHS)
• The inpatient coding process is based on the documentation provided by licensed providers
who are treating the patient
Generally, the provider treating the patient will be the “attending physician”
− The use of attending physician documentation is the “gold standard,” however,
sometimes it may not be practical or optimal to only accept documentation from
the attending physician
EXAMPLE
The consultant documents acute renal failure, but the attending physician does not; If there is no
conflicting documentation, then the renal failure would be coded; If there is conflicting
documentation (i.e., acute renal failure vs. acute renal insufficiency), then the attending physician
would be queried for clarification
Documentation for Coding Purposes
8
References:
1. AHIMA Standards of Ethical Coding
2. Coding Clinic – 3Q/2006, Page 10
3. Centers for Medicare and Medicaid Services
4. Federal Register 42 cfr 412.46
5. ICD-9-CM Official Guidelines for Coding and Reporting

ICD-9-CM Official Guidelines for Coding and Reporting
• Selection of Principal Diagnosis
The principal diagnosis is “the condition established after study to be chiefly
responsible for occasioning the admission of the patient to the hospital for care”
• General Rules for Other (Additional) Diagnoses
For reporting purposes the definition for “other diagnoses” is interpreted as
additional conditions that affect patient care in terms of requiring:
− clinical evaluation; or
− therapeutic treatment; or
− diagnostic procedures; or
− extended length of hospital stay; or
− increased nursing care and/or monitoring
• Each case has one principal diagnosis, and in Maryland, up to 29 reportable
additional conditions
Guidelines for Coding and Reporting*
9
1 of 2
*See Appendix for Coding Guidelines Specific to Renal Failure

ICD-9-CM Official Guidelines for Coding and Reporting
• Abnormal findings
Abnormal findings (laboratory, x-ray, pathologic, and other diagnostic results) are
not coded and reported unless the provider indicates their clinical significance
− If the findings are outside the normal range and the attending provider has
ordered other tests to evaluate the condition or prescribed treatment, then
it is appropriate to ask the provider whether the abnormal findings should
be added
• Uncertain Diagnosis
If the diagnosis documented at the time of discharge is qualified as “probable,”
“suspected,” “likely,” “questionable,” “possible,” or “still to be ruled out” or other
similar terms indicating uncertainty, then code the condition as if it existed or
was established
Note: This guideline is applicable only to inpatient billing (not to physician billing)
Guidelines for Coding and Reporting*
10
2 of 2
*See Appendix for Coding Guidelines Specific to Renal Failure

Criteria Currently In Use

• Among those hospitals that submitted definitions, some reported using the AKIN* criteria to
diagnose Acute Renal Failure (ARF)/Acute Kidney Injury (AKI), while others reported using
the KDIGO* and RIFLE* criteria
More hospitals have adopted KDIGO criteria than either RIFLE or AKIN
One hospital did not endorse a definition, citing a lack of professional consensus
One hospital doesn’t use either AKIN, RIFLE, OR KDIGO but instead uses criteria
requiring a higher threshold for urinary output decline and creatinine escalation
− This hospital suggested that cases that fail to meet its high threshold be
diagnosed as “Acute Renal Insufficiency” instead of ARF/AKI
• There was little consensus regarding terminology
• Some hospitals used ARF and AKI or ‘Renal Failure’ and AKI interchangeably (one
reported that these terms are “synonymous”)
• One hospital explicitly stated that ARF is not the same as AKI
• One hospital stated that ‘Renal Failure’ and AKI are synonymous, but that Acute
Renal Failure was a separate diagnosis
• Two hospitals made specific mention that ‘renal insufficiency’ is a separate diagnosis from
either ARF or AKI
• Some hospitals state that patients must have their volume restored before ARF/AKI can be
diagnosed
Criteria Used By Hospitals
12*Note: AKIN = Acute Kidney Injury Network KDIGO = Kidney Disease: Improving Global
Outcomes RIFLE = Risk, Injury, Failure, Loss of Kidney Function, and End-Stage Kidney
Disease

Defining & Staging Criteria For
ARF/AKI1
13
Serum Creatinine
Urine Output
RIFLE AKIN KDIGO
Increase in serum
creatinine of >50%
developing over <7
days
Increase in serum
creatinine of 0.3 mg/dL
or >50% developing
over <48 hrs
Increase in serum
creatinine of 0.3 mg/dL
developing within 48
hrs or >50%
developing over 7 days
Urine output of <0.5
mL/kg/hr for >6 hours
RIFLE - Risk Increase in serum
creatinine of >50%
Increase in serum
creatinine of 0.3 mg/dL
or >50%
Increase in serum
creatinine of 0.3 mg/dL
or >50%
Urine output of <0.5
mL/kg/hr for >6 hoursAKIN / KDIGO stage 1
RIFLE – Injury Increase in serum
creatinine of >100%
Increase in serum
creatinine of >100%
Increase in serum
creatinine of >100%
Urine output of <0.5
mL/kg/hr for >12 hrsAKIN / KDIGO stage 2
RIFLE – Failure Increase in serum
creatinine of >200%
Increase in serum
creatinine of >200%
Increase in serum
creatinine of >200%
Urine output of <0.3
mL/kg/hr for >12 hrs or
anuria for >12 hrsAKING / KDIGO stage 3
RIFLE – Loss Need for renal
replacement therapy
for >4 weeks
RIFLE – End Stage Need for renal
replacement therapy
for >3 months
Defining Criteria
Staging
1. Definition of Acute Kidney Injury (Acute Renal Failure) – UpToDate; last updated Sept
11, 2014

Workgroup Discussion
14
• What is our initial consensus?

Homework
15
• Review the consensus we developed today with the
appropriate clinical and administrative staff at your
hospitals
• Come to our next meeting prepared to discuss their
feedback as well as any additional thoughts or research
that you may have
• Our next meeting is here, on February 2nd at 830am
Thank You!!

Appendix

Renal Failure Related ICD-9-CM
Codes
17
Documented Diagnosis ICD-9 Diagnosis
Description ICD-9-CM Code
Acute renal failure Acute kidney
failure, unspecified
584.9
Acute kidney injury Acute kidney
failure, unspecified
584.9
Acute kidney failure with
lesion of tubular necrosis
(ATN)
Acute kidney
failure with lesion
of tubular necrosis
584.5
Acute renal insufficiency Disorder of kidney
& ureter
593.9
1 of 2

Renal Failure Related ICD-9-CM
Codes
18
Other Specific Types of Acute Renal Failure ICD-9-CM Code
Acute kidney failure with lesion of renal cortical
necrosis
584.6
Acute kidney failure with lesion of renal medullary
(papillary) necrosis
584.7
Acute kidney failure with pathological lesion in kidney 584.8
2 of 2
Other Renal Conditions ICD-9-CM Code
Prerenal / postrenal / extrarenal azotemia (symptoms
involving urinary system)
788.99
Azotemia (abnormal blood chemistry) 790.6
Elevated creatinine (nonspecific abnormal results of
function study of kidney)
794.4
Dehydration (often associated with acute renal
failure)
276.51

Renal Failure Related ICD-10-CM
Codes
19
1 of 2
ICD-10 Diagnosis Description ICD-10-CM Code
Acute renal failure N179
Acute kidney injury N179
Acute kidney failure with lesion of tubular necrosis
(ATN)
N170
Acute renal insufficiency (disorder of kidney & ureter
unspecified)
N289
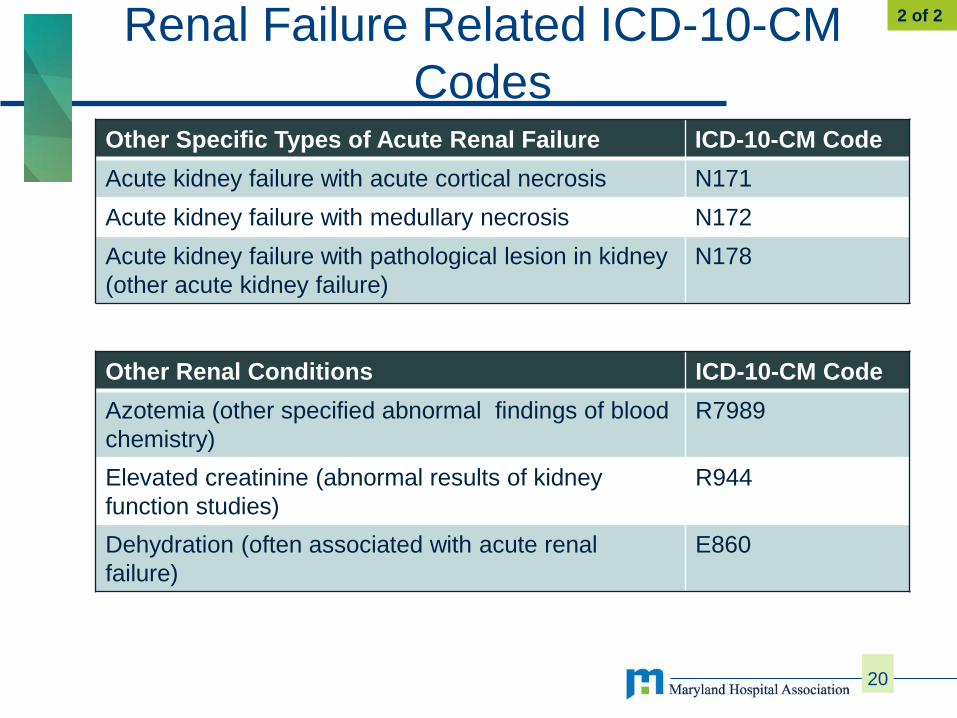
Renal Failure Related ICD-10-CM
Codes
20
Other Specific Types of Acute Renal Failure ICD-10-CM Code
Acute kidney failure with acute cortical necrosis N171
Acute kidney failure with medullary necrosis N172
Acute kidney failure with pathological lesion in kidney
(other acute kidney failure)
N178
2 of 2
Other Renal Conditions ICD-10-CM Code
Azotemia (other specified abnormal findings of blood
chemistry)
R7989
Elevated creatinine (abnormal results of kidney
function studies)
R944
Dehydration (often associated with acute renal
failure)
E860

Renal Failure Guidelines
Coding Clinic, First Quarter 1992
• Renal failure (code 584, Acute renal failure, code 585, Chronic renal failure, code 586, Renal
failure, unspecified) is a progression of renal insufficiency where renal function is further impaired
and overt clinical consequences, such as anemia, have developed
In essence, renal insufficiency is more of an abnormal laboratory assessment, while renal
failure incorporates both abnormal laboratory and clinical findings.
• If irreversible chronic renal failure is present, the treatment of choice may be either dialysis or
transplantation; Acute renal failure may be temporary and the patient's renal function may recover
after certain interventions, including dialysis
The coder should not arbitrarily add an additional diagnosis to the final diagnostic statement
on the basis of an abnormal laboratory finding alone. Remember to always query the physician
regarding the specific diagnosis being treated if it is not clearly stated in the medical record.
Coding Guidelines For Renal Failure
21
1 of 2

• Documentation in the medical record which might indicate the presence of renal failure could
include:
(a) Markedly abnormal elevated values of serum creatinine or BUN, or diminished creatinine
clearance
(b) Specific clinical and laboratory manifestations of the degree of renal impairment (mostly
seen as renal failure progresses)
− Examples:
o Anemia
o Hyperphosphatemia
o Hypocalcemia
o Hyperkalemia
o Acidemia
o Renal Osteodystrophy
o Uremic symptoms: nausea, vomiting,
o Itching, hemorrhagic conditions,
o Hypertension, edema, dyspnea,
o Lethargy, coma, etc.
Coding Guidelines For Renal Failure
22
2 of 2
Related Documents