Renal Transplantation Cherelle Fitzclarence 6.2009

Renal Transplantation Cherelle Fitzclarence 6.2009.
Dec 21, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Renal Transplantation
Cherelle Fitzclarence
6.2009
Kidney Transplantation
Why Transplant? Figures Cadaveric/Live donors Donor Criteria Recipient criteria Post Op management Medications Issues to consider Workup
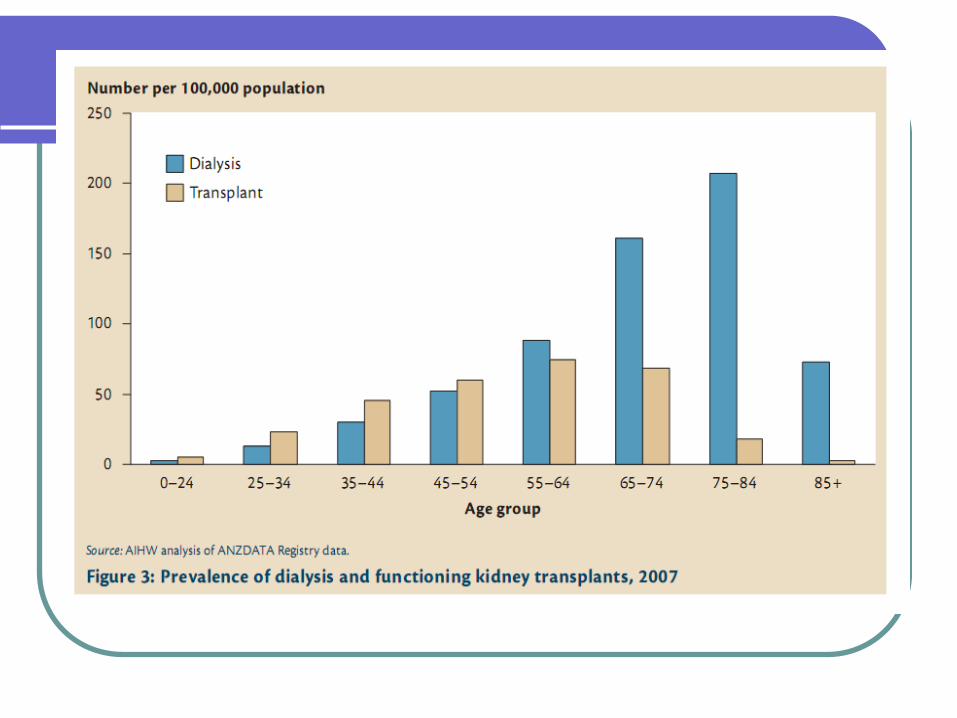
Why Transplant?
Quality of lifeLower long term mortality riskFiscally responsible – vastly decreased
costs
Transplant Options
Cadaver
Living related
Living non related
Preparation for transplant
Stop smokingOptimal dialysisDon’t be fatBP controlDental care Exercise
Cadaver
Kidney donated by someone who is deceased – either by there pre death will or from family
Different team look after donor’s family and recipient’s family
Problem with ‘down’ time – ischaemic time

Cadaver kidney source

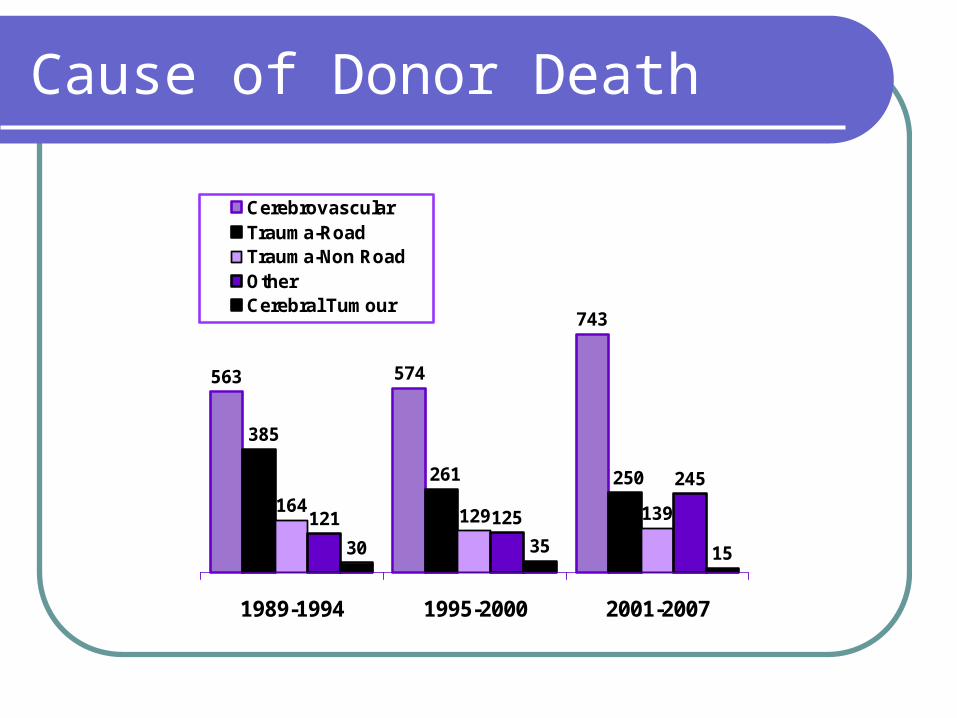
Cause of Donor Death
563 574
743
164129 139121 125
245
30 35 15
250261
385
1989-1994 1995-2000 2001-2007
CerebrovascularTrauma-RoadTrauma-Non RoadOtherCerebral Tumour
Donation after Cardiac Death
ICU Following cessation
treatment On Registry Pre family consent
Living
Higher success rate 5-10%May need fewer anti-rejection drugsCan plan the operation at a suitable timeNo ‘down’ time
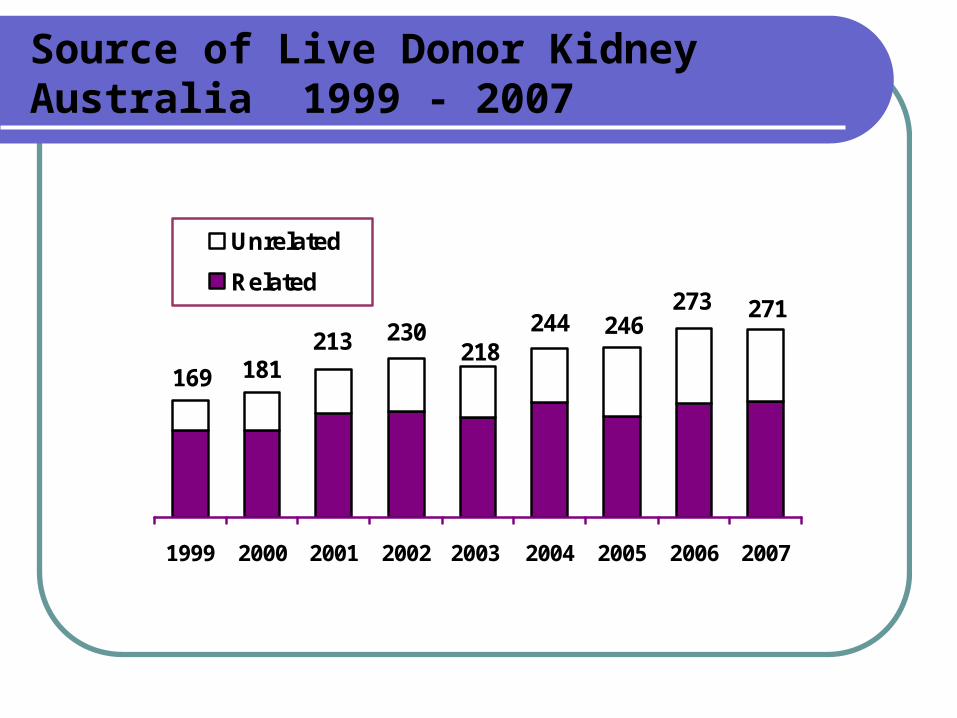
Source of Live Donor KidneyAustralia 1999 - 2007
169 181213 230
218244 246
273 271
1999 2000 2001 2002 2003 2004 2005 2006 2007
Unrelated
Related
Advantages of living donor Transplant
Better resultsLong wait for cadaveric kidneyRelieves stress on cadaveric donor
supplyEmotional gain to donorPlanning convenience
Donor complications
PnemothoraxBlood transfusionThrombosis – DVT, PEPneumoniaInfections – wound, urineKidney failure – laterOther – AMI, Bowel obstructinRisk of dying 3 in 10,000
Complications for recipient
RejectionInfectionCancerHypertension
Disadvantages of live donor Transplant
Operative mortality 3 in 10 000Major post op complications 2%Minor post op complications 50%Risk of traumatic injury to single kidneyMinimise risk factors to prevent future
health problems
Disadvantages of live donor transplant
Psychological Stress
Exclusion Criteria - For Donation
Hypertensive Diabetic proteinuria, haematuria Hx recurrent kidney stones Significant medical illness Hx thrombosis, thromboembolism Strong family Hx renal disease, diabetes, high
BP Healthy weight
Exclusion Criteria - For Donation
<18
>65
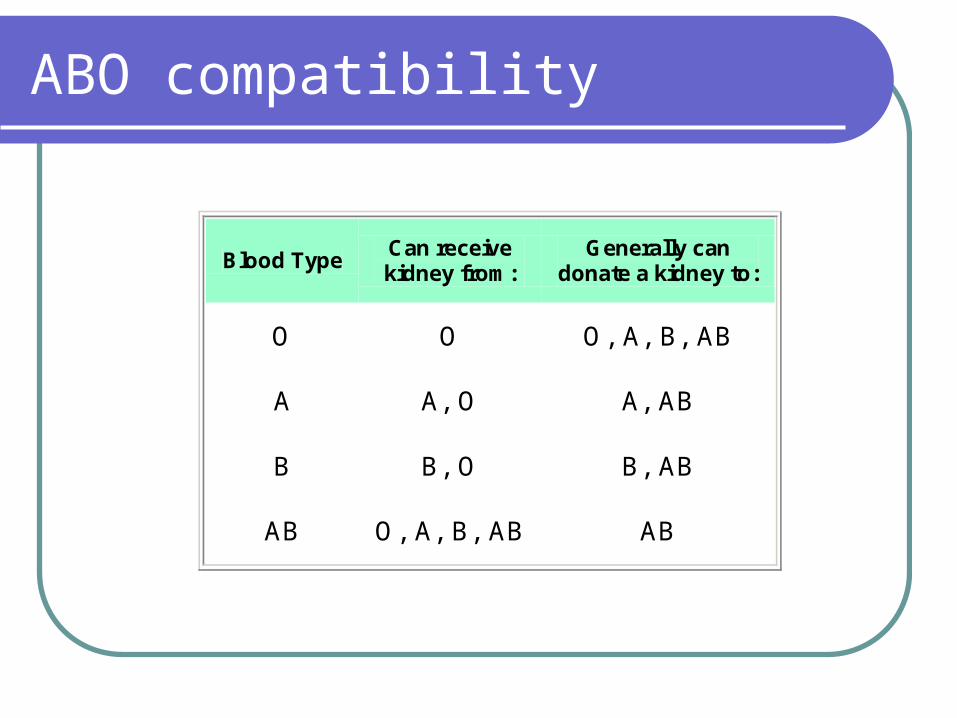
ABO compatibility
Blood Type Can receive kidney from:
Generally can donate a kidney to:
O O O, A, B, AB
A A, O A, AB
B B, O B, AB
AB O, A, B, AB AB
Cadaveric Donor Matching
Blood Group CompatibleTissue Typing - A, B, AB, OAntibodiesTime on Dialysis CrossmatchLong term waiters
Other option
Who?
Pt must be eligible for a kidney transplant. Recipient must have a living donor(s) who are
willing but unable to donate because of ABO incompatibility or a positive crossmatch.
Donors must be willing to take part and willing to donate their kidney to another person.
Cadaver organ available Common blood groups with low sensitisation
have greater chance.
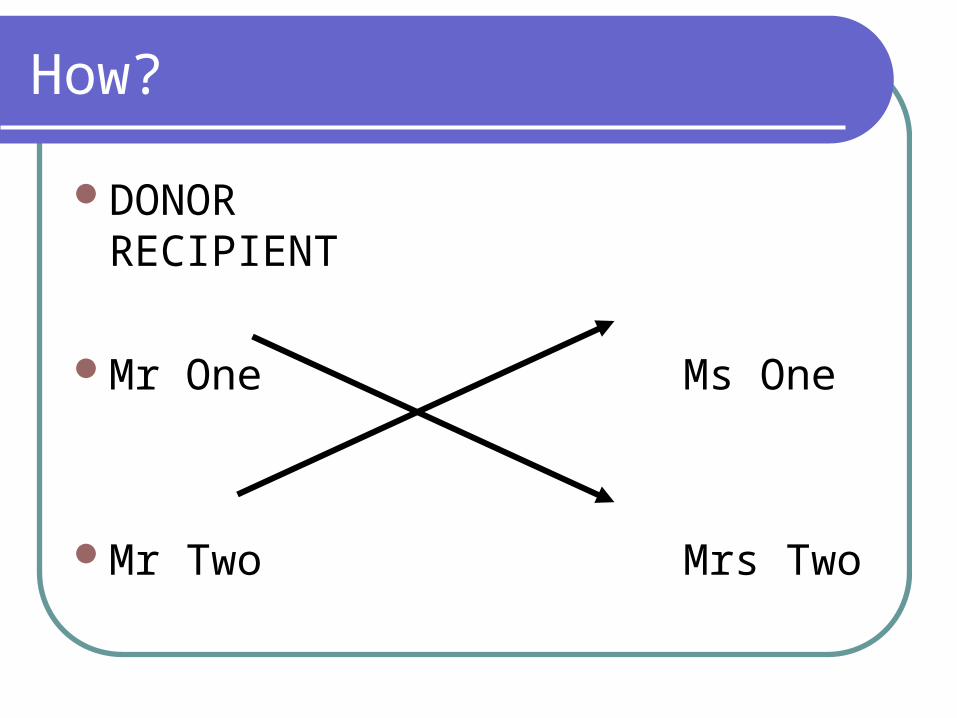
How?
DONORRECIPIENT
Mr One Ms One
Mr Two Mrs Two
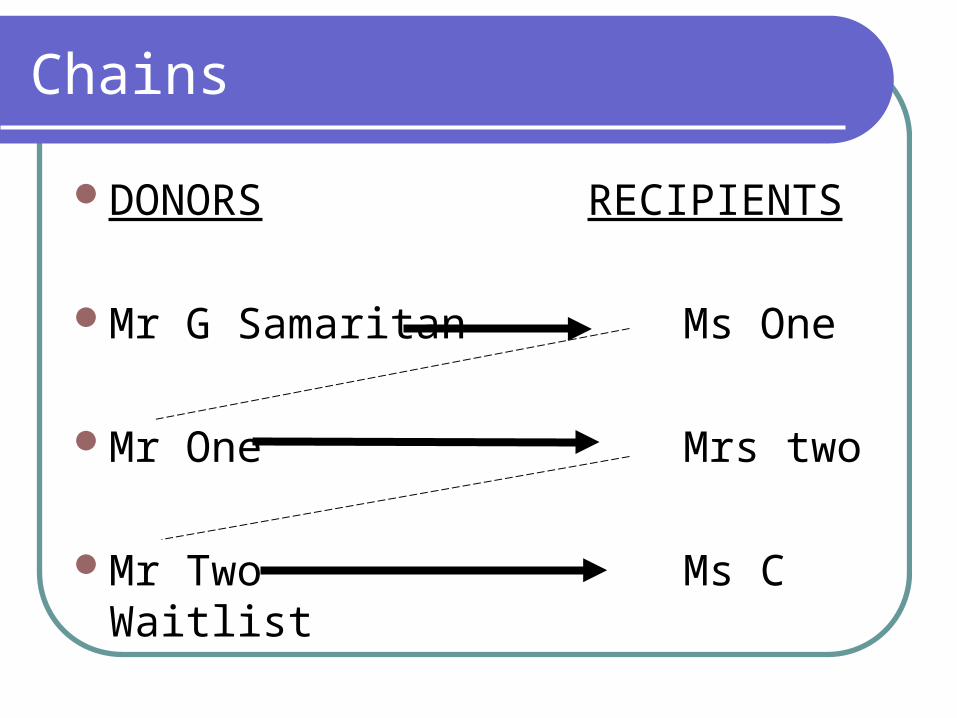
Chains
DONORS RECIPIENTS
Mr G Samaritan Ms One
Mr One Mrs two
Mr Two Ms C Waitlist
What…does the future hold?
Altruistic donors to make a chainDutch experience.US experience, how far can it go?More states involved…even nationwide.
Kidney Transplant
First one in 1954 in BostonIdentical twinsMore than 600 in Australia last year
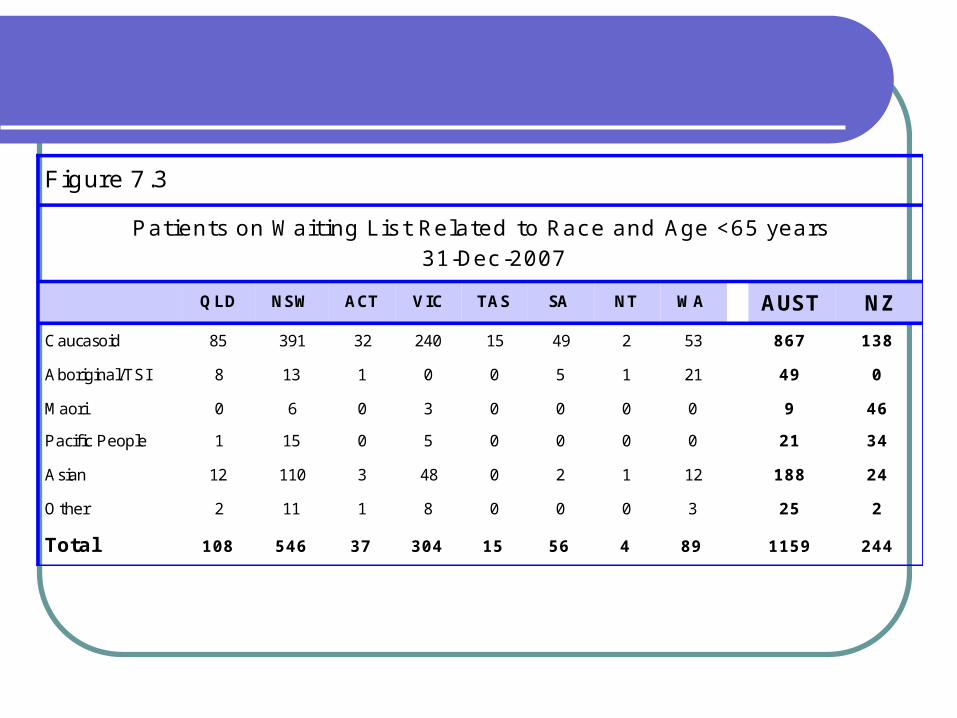
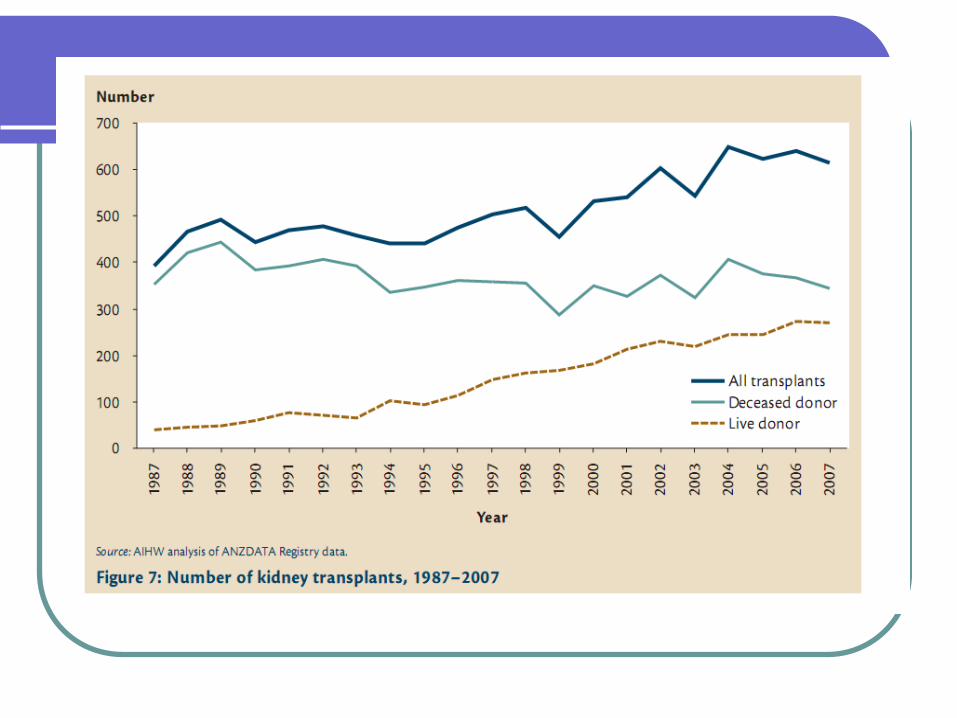
Figure 7.3
Patients on Waiting Lis t Related to Race and Age <65 years 31-Dec-2007
QLD NSW ACT VIC TAS SA NT WA AUST NZ
Caucasoid 85 391 32 240 15 49 2 53 867 138
Aboriginal/TSI 8 13 1 0 0 5 1 21 49 0
Maori 0 6 0 3 0 0 0 0 9 46
Pacific People 1 15 0 5 0 0 0 0 21 34
Asian 12 110 3 48 0 2 1 12 188 24
Other 2 11 1 8 0 0 0 3 25 2
Total 108 546 37 304 15 56 4 89 1159 244
Waitlist
1800 on national organ transplant waiting lists – half for kidneys
Average wait 3-4 years
Medications used
Cyclosporine TacrolimusSirolimusAzathioprineMycophenolate Mofetil Prednisone OKT3 Antithymocyte Ig (ATGAM)
Cyclosporin (Neoral)
1980’sVast improvement in graft successBlocksSide effects; hirsutism, gum hypertrophy,
liver impairment, fatigue, hyperlipidaemia, nausea, hypertension
Tacrolimus (Prograf)
Tacrolimus is a macrolide lactone with potent in vitro and in vivo immunosuppressive activity.
Studies suggest that tacrolimus inhibits the formation of cytotoxic lymphocytes which are regarded as being primarily responsible for graft rejection.
Tacrolimus suppresses T cell activation and T helper cell dependent B cell proliferation, as well as the formation of lymphokines such as interleukins-2 and 3 and gamma-interferon and the expression of the interleukin-2 receptor.
At the molecular level, the effects of tacrolimus appear to be mediated by binding to a cytosolic protein (FKBP) which is responsible for the intracellular accumulation of the compound. A complex of tacrolimus-FKBP-12, calcium, calmodulin and calcineurin is formed and the phosphatase activity of calcineurin inhibited.
Side Effects; Tremor, hypertension, nausea, renal impairment, diabetes
Tacrolimus
Higher rate of diabetes, gastro symptoms and neurological symptoms
Similar risk rate to cyclosporin for infection and post transplant malignancy
Sirolimus (Rapamune)
Sirolimus inhibits T cell activation induced by most stimuli by blocking calcium dependent and calcium independent intracellular signal transduction.
Studies demonstrated that its effects are mediated by a mechanism that is different from that of cyclosporin, tacrolimus and other immunosuppressive agents.
Calcineurin Inhibitors
Tacrolimus FK506Cyclosporin
Complications
Tacrolimus and cyclosporin both can be associated with chronic allograft nephropathy (CAN)
Acute rejection on cyclosporin may be able to be salvaged with a switch to tacrolimus
Complications
Interleukin 2 mediated activation of lymphocytes is a critical factor in the cellular immune response of acute kidney transplant rejection
Decreased loss of allograft at 12 months in pts treated with tacrolimus as opposed to cyclosporin
Calcineurin Inhibitor Nephrotoxicity
Gold standard for diagnosis is renal allograft biopsy
Acute calcineurin nephrotoxicity
Related to haemodynamic changes on the afferent arteriole which are dose dependent and reversible

Chronic calcineurin nephrotoxicity
Focal or striped tubulo-interstitial fibrosisHyaline arteriolopathyFocal collapsing glomerulosclerosis
Diltiazem
Antihypertensive Increases available levels of anti rejection drugs via
the hepatic metabolism pathway Inhibit the influx of calcium ions during membrane
depolarisation of cardiac and vascular smooth muscle Produces its antihypertensive effects primarily by
relaxation of vascular smooth muscle and the resultant decrease in peripheral vascular resistance. The magnitude of blood pressure reduction is related to the degree of hypertension
Azathioprine
Used in combination with cyclosporin or tacrolimus or sirolimus
Side effects; skin rash , myalgias, fever, headache, vomiting
Mycophenolate (Cellcept)
Can be used instead of Azathioprine1995Side effects; diarrhoea,constipation,
nausea, indigestion, fluid retention
Prednisolone
SteroidHigh doses initially and then weaned
Side effects; weight gain, increased appetite, high blood sugars, diabetes, delayed wound healing, muscle wasting, osteoporosis
Bactrim
Antibacterial
Meds and pregnancy
Trough levels of cyclosporin tend to drop in later pregnancy
Acute rejection – decreased risk despite lower levels
High level of 2 year post pregnancy graft loss Miscarriage, prematurity, low birth weight,
preeclampsia risks are increased Bubs have suppressed innate immunity Excreted in breast milk – same level as
maternal blood levels
Live Donation Steps
ID of suitable recipient. Medical and surgical history, blood group, FBP,
renal function, LFT, chol, coags, urine tests. Immunological and viral tests Establish compatibility CXR, ECG, psych review
Surgical review/ Surgery
Usually left kidney b/o longer renal vein.
Assessed post Spiral CT scan
Lap or Open. 2-3 hrs Inpatient 3 to 7 days Annual reviews of renal
function
Recipient Criteria
1/3 ESRF pts suitable65 - 70 yearsScreening ProtocolCardiac and Medical Risk Categories
High Cardiac Risk
Cardio, cerebro or peripheral vascular disease
DMage >55significant smoking historyIndigenous
High Medical Risk
Severe chronic lung diseaseHistory malignancyActive infection PUDMental illness/ poor complianceObesityPrior transplants
Pre op Care
IsolationImmunosuppression- quadruple or tripleSteroidsIV FluidsECG, ? Dialysis
Intra op/ Recovery
CVC and IDCIVAB prophylaxis- cefazolin 1GIV Frusemide 80mg at cross clamp
releaseMannitol and albuminMinimise ischaemic timePink + output
Immediate Post Op
PCA, redivac, CVC, IV access, IDC, wound Monitor blood loss- drain, swelling, wound
dressing, hypotension Urine output + fluid balance hourly, CVP 12-
15 Pain, nausea, resp, vital signs U&E, K+,Hb, BSL Renal ultrasound and doppler
Ward Care
Immunosuppression- daily levelsDiltiazem, AB proph, famotidine, statin,
+/- lasix, CMV prophRemoval of IV, CVC, IDC day 2-3Biopsy if signs of rejectionDischarge 5 -7 days
Long Term Management
Education Daily clinic visits 2 weeks “ First 3 months are Hell!” Monitor for signs of rejection JJ stent removal 5-6 weeks BP, Chol, BSL, CMV Cancer screenings- skin checks, pap smears,
mammograms Dental, weight, diet
Options to consider?
Kidney Exchange
‘Pool’ of Recipients/Donors
Consent Going national in
July
ABO incompatible donation
PlasmapharesisImmunoadsorption columnTitresRituximabHigher riskMade in Japan
Following Nephrectomy for Renal Cell Carcinoma
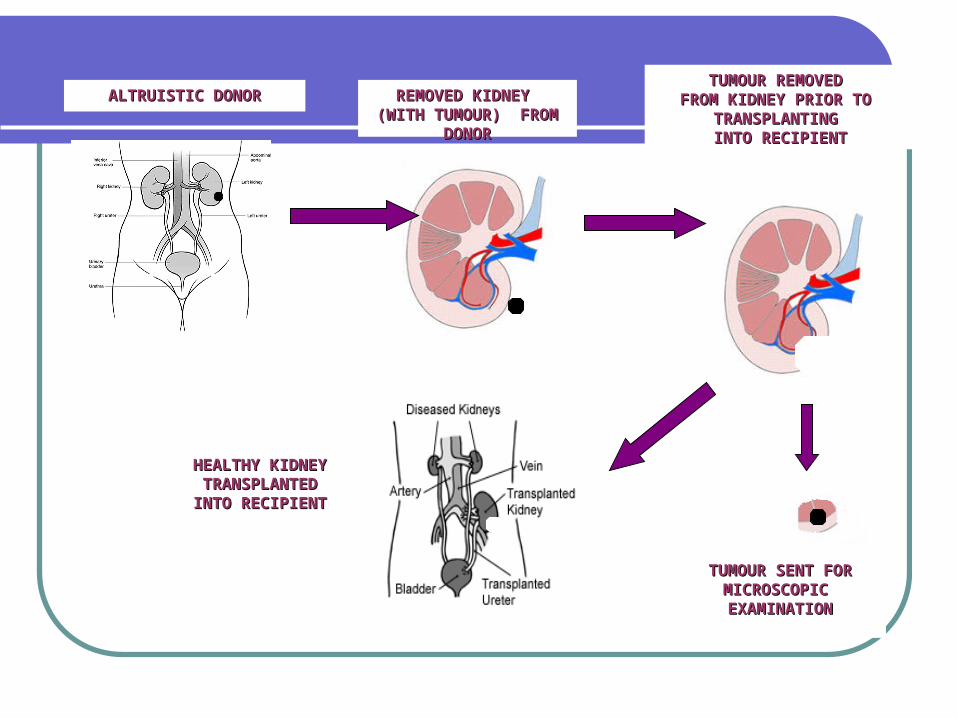
ALTRUISTIC DONORALTRUISTIC DONOR
REMOVED KIDNEY REMOVED KIDNEY (WITH TUMOUR) (WITH TUMOUR)
FROM DONORFROM DONOR
TUMOUR REMOVED TUMOUR REMOVED FROM KIDNEY PRIOR TO FROM KIDNEY PRIOR TO
TRANSPLANTING TRANSPLANTING INTO RECIPIENTINTO RECIPIENT
HEALTHY KIDNEY HEALTHY KIDNEY TRANSPLANTED TRANSPLANTED INTO RECIPIENTINTO RECIPIENT
TUMOUR SENT FOR TUMOUR SENT FOR MICROSCOPIC MICROSCOPIC EXAMINATIONEXAMINATION
2008 in WA
25 live donors – x2 ABOi6 tumour resected/altruistic1 altrustic7 Kidney exchange41 cadaveric.
Total of 80 transplants in WA.
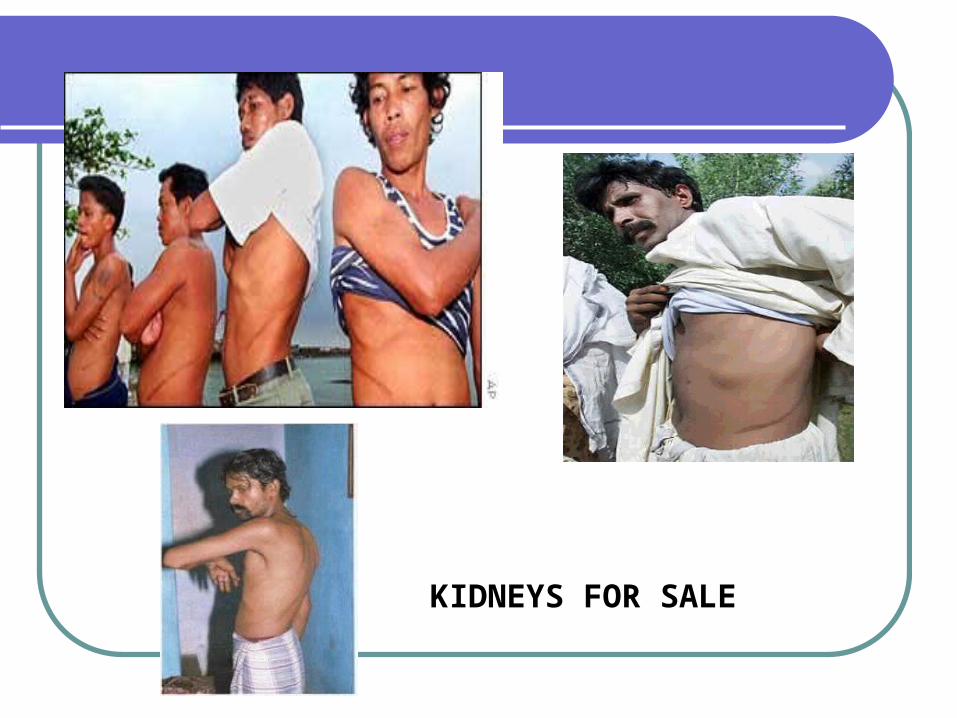
KIDNEYS FOR SALE
Internet
MatchingOrgans.Com
Xenotransplantation
Signs of rejection
FeverMalaiseTenderness over the kidneyHypertensionIncreased creatinine
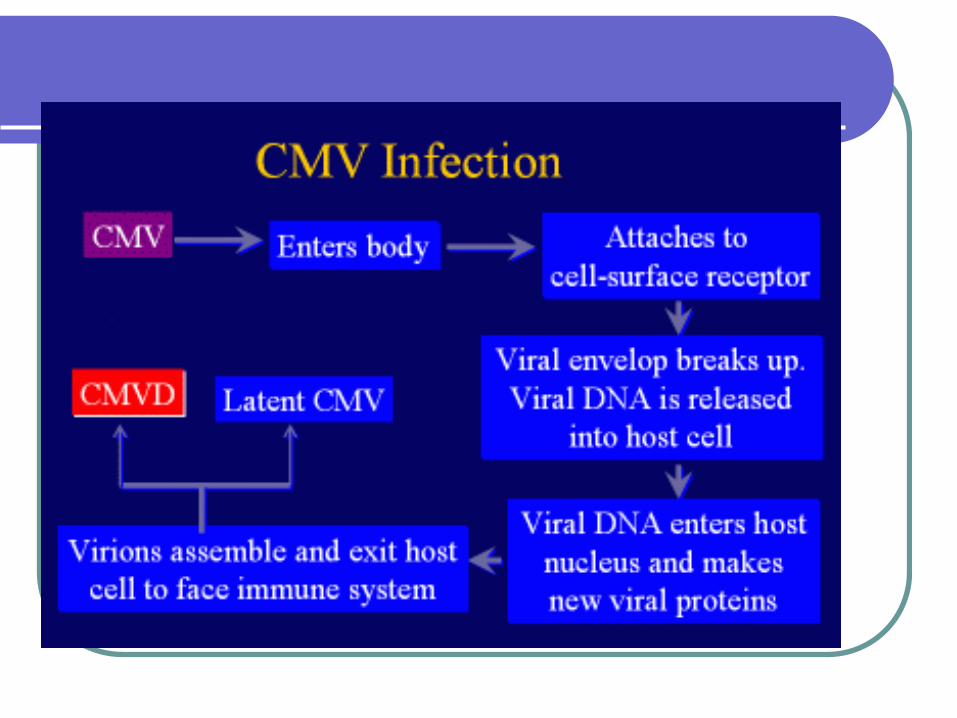
CMV
Belongs to a group of herpesvirusesCommon80% adults show seropositivity to
infectionMost common viral infection following
renal transplantCMV infection – detected without
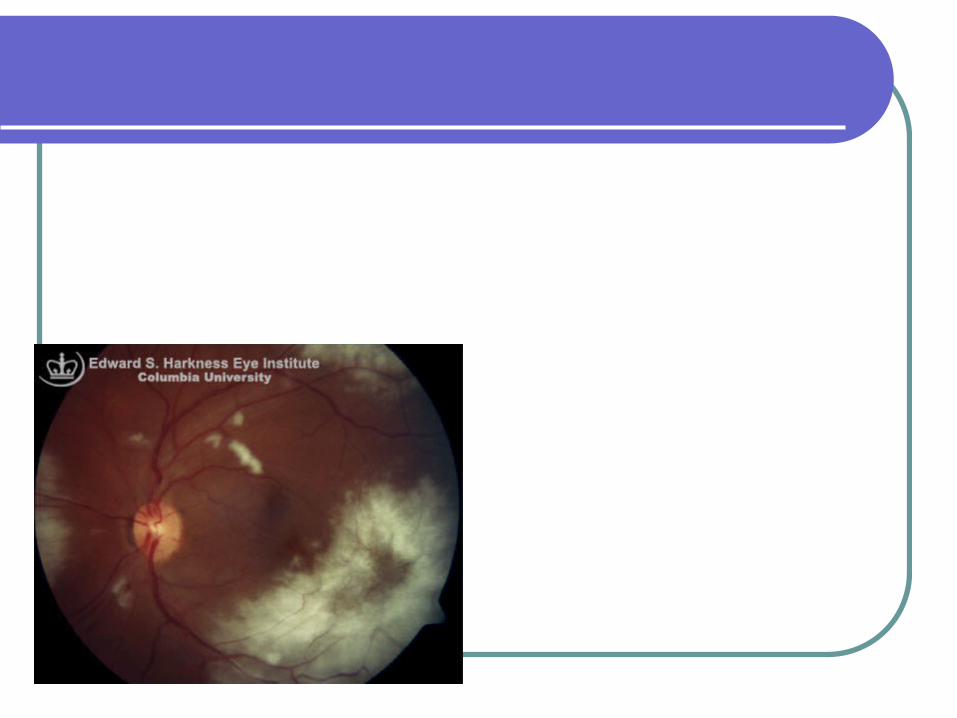
evidence of diseaseCMV disease – evidence of organ
damage
CMV
Disease characterised by fever, mononucleosis, leucopaenia, thrombocytopaenia
Pneumonitis, hepatitis, encephalitis, focal gastrointestinal disease
Ganciclovir is the treatment of choice for disease and should be given IV – at least 2 weeks
Alternative is valganciclovir orally – 10 times the bioavailablity
CMV
CMV disease associated with increased morbidity and mortality
CMV infection is associated with increased rejection and bacterial and fungal infection
Treatment is associated with better outcomes
CMV
Prophylactic treatment of CMV is recommended in solid organ transplant
Oral valaciclovir, oral or Iv ganciclovir or or valganciclovir – all equally effective
Indicated if donor positive and recipient positive or negative
CMV
Acknowledgements
Anne WargerCARI guidelinesRPH protocolsKidney Health AustraliaAIHW websiteChronic Kidney Disease in Australia
2009
Related Documents











