Renal replacement therapy Dr . Ashish Moderator : Dr. Muralidhar www.anaesthesia.co.in [email protected]

Renal replacement therapy Dr. Ashish Moderator : Dr. Muralidhar [email protected]@gmail.com.
Dec 11, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Renal replacement therapy
Dr . Ashish
Moderator : Dr. Muralidhar
www.anaesthesia.co.in [email protected]

Epidemiology of AKI • Prospective epidemiology survey of AKI was
conducted in ICU patient who were either treated with RRT or had ARF(U.O< 200ml /12hr or BUN>30mmol/l)
• Of 29269 critical ill pts. 5.7% pt. had AKI during ICU stay including 4.3% who were t/t with RRT
BEST study(Beginning and ending supportive therapy for the kidney investigators Acute renal failure in critically ill patients JAMA 294;813-818,2005)
• Overall hospital mortality was 60.3%
• Most common contributing factor was septic shock in 47.5%
• At hospital discharge 86.2% survivors were independent from dialysis
BEST study(Beginning and ending supportive therapy for the kidney investigators Acute renal failure in critically ill patients JAMA 294;813-818,2005)
Introduction
• Term RRT is used to describe all the currently available approaches to artificial mechanical support of renal function
• Includes traditional intermittent hemodialysis,peritoneal dialysis and variety of other intermittent and continuous therapy, and renal transplant

Indications to start and stop RRT
• There is no consensus as to indication for initiation of RRT
• Common indications are azotemia , anuria, and complications of AKI , including pulmonary edema, severe fluid overload ,hyperkalemia and uncontrolled metabolic acidosis
• Routine clinical practice is to adequately control fluid balance and to maintain a serum urea <30 mg/dl, creatinine < 2mg/dl and normal electrolyte values
Indications of RRT
• Anuria – oliguria(diuresis <200 ml in 12 hr)
• Severe metabolic acidosis(pH<7.10)
• Hyperazotemia(BUN> 80mg/dl) or creatinine >4mg/dl
• Hyperkalemia K >6.5mEq/l
• Clinical signs of uremic toxicity
Indications of RRT
• Severe dysnatremia Na<115 or Na>160mEq/l
• Hyperthermia (>40 deg.C without response to medical therapy)
• Anasarca or severe fluid overload
• Multiple organ failure with renal dysfunction and /SIRS, sepsis, or septic shock with renal dysfunction

Technique and modalities
• All RRT consist of blood purification by having the blood flow through SPM.
• Blood flow into hollow fibers composed by porous biocompatible synthetic materials
Technique and modalities
• Wide range of substances( water , urea,and low, middle and high mol.wt. solutes)allow the blood across such membranes by diffusion (solutes) and by convection(solute and water)
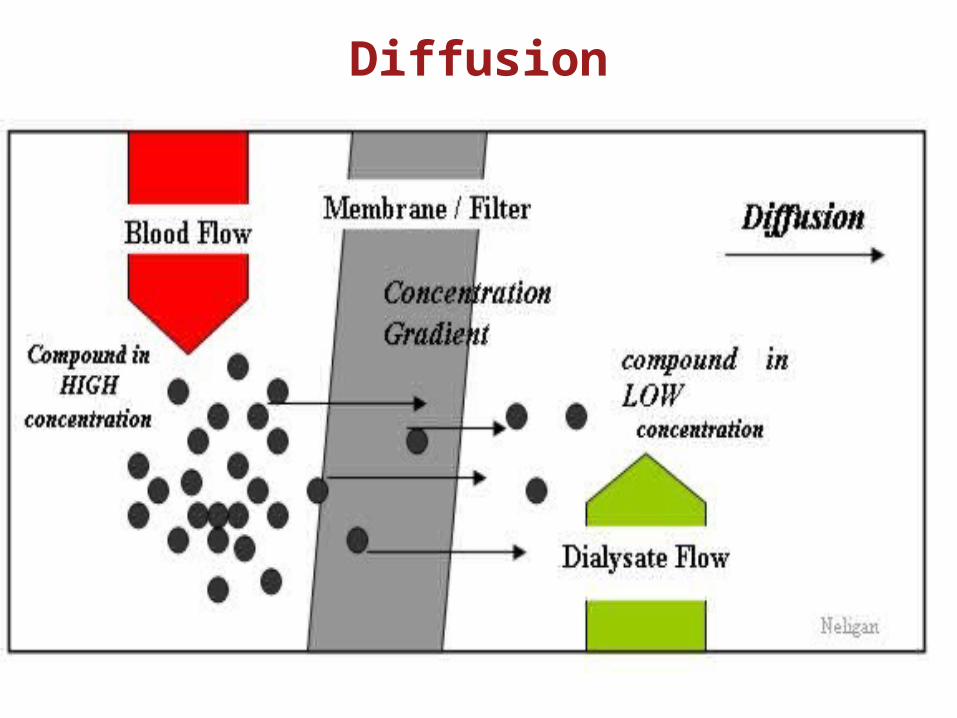
Diffusion
• Solute move from blood across membrane to reach same concentration on each side of membrane
• Leads to passage of solute from compartment with highest conc. to lower compartment with lowest conc.

• Factors affecting rate of diffusion –
1. Thickness and surface of membrane,
2. Temperature of blood
3. Diffusion coefficient
• Dialysis occur when solution flows through semi- permeable conduit countercurrent to blood, allowing maximal solute diffusion, because solute conc. is lower in solution than blood
Diffusion
Diffusion
• During diffusion , solute flux (Jx) is function of
solute concentration gradient(dc)between two sides of SPM, temp(T), diffusivity coefficient(D), membrane thickness(dx)and surface area(A)
Jx=D.T.A(dc/dt)
Convection
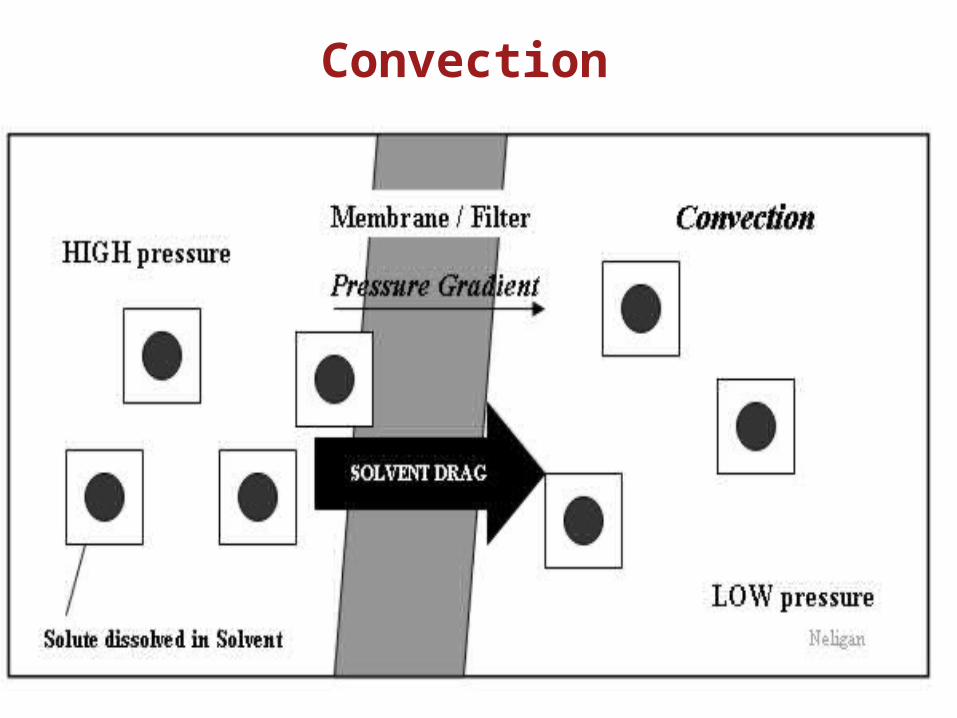
• During convection , movement of solute across a SPM occurs with significant amount of ultrafiltration( water transferring across the membrane)
Convection
• As the solvent (water in plasma) is pushed across the SPM in response to TMP(transmembrane pressure) by UF, solutes are carried with it, as long as porosity of membrane allows the molecules to be sieved from blood
Convection
• The process of ultrafiltration is governed by UF rate (Qf), membrane UF coefficient(Km) and TMP gradient generated by pressure on both sides of hollow fiber
Qf= Km.TMP
• TMP= Pb-Pd-Blood oncotic pressure
Pb: Blood hydrostatic pressure
Pd:Hydrostatic pressure on UF side of SPM
• Hydrostatic pressure in blood compartment dependent on blood flow(Qb)
• Greater the Qb , greater the TMP
• Modern RRT machine , UF is maximised by applying a pump, which generates control of UF rate

• As blood is processed , membrane fiber get soiled and a negative pressure become necessary to maintain a constant Qf
• Molecules cleared during convection are physically dragged to UF side , but this function is limited by protein layer that progressively develops and closes fiber pores during convective treatments
• As UF proceeds over time, plasma water and solutes are filtered from blood, hydrostatic pressure within filter is lost
• And oncotic pressure is gained as blood concentrates and Hct rise

• The fraction of plasma water that is removed from blood during UF is called Filtration Fraction
• F.F. is kept ~20-25% to prevent hemoconcentration within filtering membrane
• Replacing plasma water with a substitution solution completes the hemofiltration(HF) and returns the purified blood to patient
• Post dilution HF - Replacement fluid infused after the filter
• Pre dilution HF - Replacement fluid infused before the filter
• Post dilution HF allow urea clearance equivalent to therapy delivery(2L/hr)
• While pre dilution l/t prolonged circuit lifespan by reducing hemoconcentration and protein caking effect
• Conventional HF is performed with highly permeable membrane with surface area of about 1sq.mt, steam sterlized with cutoff point 30kD
• Difference b/n volume of ultra filtered plasma water and reinfused substitution solution is Net UF
• Net UF is fluid finally removed from patient

• Prescriptions for net UF are based on individual patient need
• Range from >1L/hr(pulmonary edema pt. with CHF who is resistant to diuretic)
• To zero net UF ( sepsis with catabolic state with increased creatinine levels)

• Net UF rate must be added to dialysis to achieve fluid balance during diffusion that do not allow water movement
IHD
• Most common techniqe utilised for CRF
• Diffusive t/t in which blood & dialysate are circulated in countercurrent manner & usually low permeability,cellulose membrane is employed
• Dialysate must be pyrogen free but not necessarily sterile, as blood contact does not occur
IHD
• UF rate is equal to scheduled weight loss
• This t/t can be typically performed 4 hrs thrice weekly or daily
• Qb :150-300ml/min , Qd:300-500ml/min

PD
• Diffusive t/t in which blood circulating along capillaries of peritoneal membrane , is exposed to a dialysate
• Peritoneal catheter allows abdominal instillation of dialysate
PD
• Solute & water movement achieved by means of variable concentration and tonicity gradients generated by dialysate
• Can be done continuously or intermittently
Dose and prescription for RRT
• During continuous t/t in ICU goal – deliver urea clearance of 2 l/hr
• Evaluation of chronic dialysis in ESRD described by fractional clearance of given solute = Kt/v
K: dialysis clearance
t: time for dialysis treatment
v : solute marker volume of distribution
• Kt/v urea of 1.2 currently recommended

Dose reciept of more dialysis improve patient outcome?

Effects of different doses in CVVH on outcome of ARF - Ronco & Bellomo study. Lancet . july 00
• Prospective study on 425 patients - 3 groups:
• Study: –survival after 15 days of HF stop–recovery of renal function

100
90
80
70
60
50
40
30
20
10
0
Group 1(n=146)
((Uf = = 20 ml/h/Kg)
Group 2 (n=139)
(Uf = 35 ml/h/Kg)
Group 3 (n=140)
(Uf = 45 ml/h/Kg)
41 % 57 % 58 %
p < 0.001 p n..s.
p < 0.001
Sur
viva
l (%
)S
urvi
val (
%)
Effects of different doses in CVVH on outcome of ARF - Ronco & Bellomo study. Lancet . july 00
•Is an extracorporeal blood purification therapy intended to substitute for impaired renal function over an extended period of time and applied for or aimed at being applied for 24 hours a day.
* Bellomo R., Ronco C., Mehta R, Nomenclature for Continuous Renal
Replacement Therapies, AJKD, Vol 28, No. 5, Suppl 3, November 1996
Continuous Renal Replacement Therapy (CRRT)
Requirements for CRRT
• CRRT requires:– A central double-lumen veno-venous
hemodialysis catheter– An extracorporeal circuit and a
hemofilter– A blood pump and a effluent pump. – With specific CRRT therapies
dialysate and/or replacement pumps are required.

CRRT Modalities
• SCUF- Slow Continuous Ultrafiltration
– Ultrafiltration
• CVVH- Continuous Veno-Venous Hemofiltration
– Convection
• CVVHD- Continuous Veno-Venous Hemodialysis
– Diffusion
• CVVHDF- Continuous Veno-Venous Hemodiafiltration
– Diffusion and Convection
SCUF
• Blood driven through highly permeable filter via extracorporeal circuit in venovenous mode
• UF produced during membrane transit is not replaced so it correspond to wt. loss
• Used only for fluid control in overloaded pt. (CHF pt not responding to diuretic t/t)
• Qb :100-250 ml/min &Quf:5-15ml/min

SCUF-Ultrafiltration
• Slow continuous ultrafiltration:
– Requires a blood and an effluent pump.
– No dialysate or replacement solution.
– Solute control is not goal of this therapy
– Fluid removal up to 2 liters/hr can be achieved.
• Primary Goal
– Safe management of fluid removal
– Large fluid removal via ultrafiltration

SCUF
Syringe pump
Return Pressure Air Detector
Blood Pump
Access Pressure Filter Pressure
BLD
Hemofilter
Patient
Effluent Pump
Return Clamp
Pre Blood Pump
Effluent Pressure
CVVH(Continuous venovenous
hemofiltration)
• Blood driven through highly permeable membrane via extracorporeal circuit in venovenous mode
• UF produced during membrane transit is replaced in part or completely to achieve blood purification & volume control
• Pre or post dilution hemofiltration based on replacement fluid delivery before or after filter
CVVH-Convection
• Continuous veno-venous hemofiltration–Requires blood, effluent and
replacement pumps.–Dialysate is not required.–Plasma water and solutes are removed
by convection and ultrafiltration.

CVVHReturn Pressure Air Detector
Return Clamp Patient
Access Pressure
Effluent Pump
Syringe Pump
Filter Pressure
Hemofilter
Pre Post
Post
Replacement Pump Replacement Pump Pre Blood Pump
Effluent Pressure
CVVHD Continuous venovenous hemodialysis
• Blood driven through low permeability dialyzer via extracorporeal circuit in venovenous mode and countercurrent flow of dialysate delivered in dialysis compartment
• UF produced during membrane transit correspond to wt. loss
• Solute clearance is mainly diffusive & efficiency limited to small solutes only
• Qb :100-250ml/min & Qd :15- 60ml/min
CVVHD-Diffusion
• Continuous veno-venous hemodialysis
–Requires the use of blood, effluent and dialysis pumps.
–Replacement solution is not required.
–Plasma water and solutes are removed by diffusion and ultrafiltration.

CVVHDReturn Pressure Air Detector
Return Clamp
Access Pressure
Blood Pump Syringe Pump
Filter Pressure
Hemofilter
Patient
Effluent Pump Dialysate Pump Pre Blood Pump
BLD
Effluent Pressure
CVVHDF Continuous venovenous hemodiafiltration
• Blood driven through highly permeable dialyzer via extracorporeal circuit in venovenous mode and countercurrent flow of dialysate is delivered in dialysate compartment
• UF produced during membrane transit is in excess of pt. desired wt. loss
CVVHDF• Continuous veno-venous hemodiafiltration
–Requires the use of a blood, effluent, dialysate and replacement pumps.
–Both dialysate and replacement solutions are used.
–Plasma water and solutes are removed by diffusion, convection and ultrafiltration.
CVVHDF
• Removal of small molecules by diffusion through the addition of dialysate solution.
• Removal of middle to large molecules by convection through the addition of replacement solution.
SLEDD(Slow low efficiency daily dialysis)
• Hybrid therapy that try to match physiological advantage of CRRT
• Involves use of blood & dialysate flows less than in IHD
• Qb : 100-200ml/min & Qd :< 300ml/min
• T/t time extended to 6-12hr every day
SLEDD(Slow low efficiency daily dialysis)
• Result slower solute clearance & fluid removal & result in hemodynamic stability comparable to CRRT.
• Removal of sodium & water cannot be dissociated when using diuretic & some RRT
• Diuretics l/t natriuresis whereas dialysis may result in hypotonia or hypertonia
• Depending on effect of dialysis on diffusion & on removal of molecules , including urea & other electrolyte

• Water removal is always a/w removal of other solutes & its amount depend on technique used
• UF from SCUF is iso-osmotic & and isonatremic because Na elimination is linked to Na conc. in plasma
• Best evidence to date support RRT dose of 35ml/kg/hr for CVVH, CVVHD, IHD

UNLOAD trial(UF versus i.v. diuretics for acute decompensated CHF)
First RCT comparing Diuretic versus HF in hypervolemic pt.
Principal Findings
1. Ultrafiltration l/t greater wt. & fluid loss
2. Reduction in rate & duration of subsequent hospitiliztions in pt with volume removal by UF
3. Benefits from short term use of UF over 90 days was achieved without significant adverse effects
Vascular Access
• A veno-venous double lumen hemodialysis catheter or two single lumen venous hemodialysis catheters may be used.

Access Location
• Internal Jugular Vein– Primary site of choice due to lower associated
risk of complication and simplicity of catheter insertion.
• Femoral Vein– Patient immobilized, the femoral vein is optimal
and constitutes the easiest site for insertion. • Subclavin Vein
– The least preferred site given its higher risk of pneumo/hemothorax

Anticoagulation
• Blood contact to circuit tubing in CCRT l/t activation of coagulation cascade
• Result in clotting of filter or circuit• Quantity & duration of anticoagulation
changes depending on schedule of RRT• Anticoagulation necessary for CRRT where
blood – artificial surface interaction is maximum
Circuit set up optimisation
• Vascular access adequate size
• Kinking of circuit tubing avoided
• Blood flow rate should exceed 100ml/min
• Plasma filtration fraction < 20%
• When possible predilution hemofiltration considered
Unfractionated heparin
• Dose 5-10 IU/kg/hr
• Regional heparinization in 1:1 ratio with protamine ( 150IU Of UFH per mg protamine)
• Problems :
1. Unpredictable bioavailibility
2. Necessity for AT III levels for optimal use
3. Heparin induced thrombocytopenia
LMWH
• Alternative to UFH• Prospective studies hav not shown it
superior to UFH in prolonging life of RRT circuit
• Better bioavailibility• Lower incidence of HIT• Cost 10% > than UFH
Prostacyclin (PGI2)
• Potent inhibitor of platelet aggregation with short half life
• Infusion dose 4-8ng/hr with or without addition of low dose UFH
• Problems:
Very short circuit life span
Hypotension
Citrate
• Citrate chelates calcium which prevents clot formation
Drawbacks :
1. Risk of hypoalcemia
2. Metabolic alkalosis
Complications as/w hemodialysis
• Hypotension – MC d/t osmolar shift & ultrafiltration- induced volume depletion
• Hypotensive episode may reflect myocardial ischemia,dysarrythmias or pericardial effusion with cardiac tamponade
• T/t – slowing rate of ultrafitration and/or i.v fluids
• Hypersensitivity reaction to ethylene oxide used to sterlize dialysis machine d/t specific membrane material polyacrylonitrile
• MC in pt. receiving ACE inhibitors
• This reaction d/t bradykinin release which is degraded by kinases but ACE inhibitors block this response

• Progressive renal failure,catabolism,&anorexia l/t loss of lean body mass but fluid retention mask this may l/t wt. gain
• Between t/t wt. gain of 3%-4% of body mass is appropriate
• Increased chances of ischemic heart disease in ESRD pt. on hemodialysis d/t
1. Systemic HTN
2. Anemia
3. Hyperlipidemia
4. Hyperhomocystemia
5. Accelerated atherosclerosis
6. Impaired oxygen delivery to myocardium d/t uremic toxin
• Pericarditis with pericardial effusion d/t inadequate hemodialysis
• T/t - Intensive heparin free dialysis
• Persistent effusion - pericardiocentesis
• Bleeding tendency d/t altered platelet function , partially correctable by hemodialysis
• Heparin free dialysis or administration of DDAVP , sufficient to correct bleeding tendency

• At risk of infection d/t impaired phagocytosis & chemotaxis
• T.B in pt on hemodialysis is extrapulmonary and atypical symptom mimicing inadequate dialysis
• Vaccinated against pneumococcal and hepatitis B
Summary
• Mechanism in RRT based on principles of water & solute transport via diffusion & convection
• These mechanism applied lead to different techniques & modalities
• Clinical effects on critically ill pt. depend on selected RRT strategy & on severity/ complexity of patients clinical picture
Related Documents