PRESENTED BY: DR DIVYA RANA PG 2 nd YEAR MGDCH

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PRESENTED BY:
DR DIVYA RANA
PG 2nd YEAR
MGDCH

Bones can break, muscles can atrophy, glands can loaf, even the brain can go to sleep without immediate danger to survival. But -- should kidneys fail.... neither bone, muscle, nor brain could carry on.
Homer Smith, Ph.D.

Renal circulation receives 20 - 25 % of cardiac output under normal physiologic conditions.
The bodies blood volume circulates through the kidney every 6 minutes (12 times/hour).

Renin secretion and the regulation of volume and composition of extracellular fluid.
Excretion Blood pressure control
Vitamin D activation Acid-base balance
regulation. Erythropoietin
production Urine formation

Renin is important in the regulation of blood pressure.
It is released from the granular cells of the efferent arteriole in response to decreased arteriole blood pressure, renal ischemia, extracellular fluid depletion, increased norepinephrine, and increased urinary Na+ concentration.

4 mechanisms are involved Volume control Aldosterone effect Renin-angiotensin-aldosterone Renal prostaglandin

Prostoglandins (PGs)- synthesized by most body tissues. In the kidney, PGs are synthesized in the medulla and have a vasodilating action and promote Na+ excretion. PGs counteract the vasoconstrictor effect of angiotensin and norepinephrine. Renal PGs systemically lower blood pressure by decreasing systemic vascular resistance.

Acquired by the body through diet or through synthesis by ultraviolet radiation on the cholesterol in the skin.
The liver and the kidney make the vitamin active in the body.

Erythropoietin is produced and released by the kidneys in response to decreased oxygen tension in the renal blood supply that is created by the loss of red blood cells.
Erythropoietin stimulates the production of RBCs in the bone marrow.
Erythropoietin deficiency leads to anemia in renal failure.

Kidney secrete Erythropoietin, it stimulates the bone marrow to produce RBC’s
in oxygen delivery simulates release in response the RBC count rises in 3 - 5 days speeds the maturation of RBC’s

Kidneys regulate acid-base balance by stabilizing body fluid volume & flow rate to enhance the reabsorption or excretion of bicarbonate & hydrogen ions

Sodium Potassium Calcium Need to Know: Phosphate Normal Values Magnesium Functions Chloride Factors affect

Over 200 waste products excreted Only 2 are used for clinical assessment
BUN Creatinine
Over 200 waste products excreted Only 2 are used for clinical assessment
BUN Creatinine

Normal 8 - 20 mg/dl Nitrogenous waste product of protein
metabolism Unreliable in measurement of renal function
Relevance is assessed in conjunction with Creatinine

Urine flow low renal perfusion Volume depletion Metabolic rate Protein metabolism Drugs

A waste product of muscle metabolism Normal value 0.6 - 1.2 mg/dl 2 times normal = 50% damage 8 times normal = 75% damage 10 times normal = 90% damage Exception - severe muscular disease can
greatly Creatinine levels

Blood TestsBUN elevated (norm 10-20)Creatinine elevated (norm 0.6 - 1.2)K elevatedPO4 elevatedCa decreased
UrinalysisSpecific gravityProteinCreatinine clearance

Biopsy Ultrasound X-Rays

Sudden onset - hours to days Often reversible Severe - 50% mortality rate overall; generally
related to infection.
Homeostatic functions affected most Electrolyte imbalances Volume regulation Blood pressure control
Endocrine functions affected lease Require time to evolve
Renal size is preserved Evidence of acute illness or insult exists

Sudden fall in glomerular filtration rate (GFR) Retention of nitrogenous (BUN and creatinine)
and other wastes Hours to days
About 5% of all hospitalizations About 20% of ICU admissions
Mortality 50 – 80% Independent risk factor for death – 5x
increase risk

Slow progressive renal disorder related to nephron loss, occurring over months to years
Culminates in End Stage Renal Disease

Cause & onset often unknown Loss of function precedes lab abnormalities Lab abnormalities precede symptoms Symptoms (usually) evolve in orderly
sequence Renal size is usually decreased

Diabetes Hypertension Glomerulonephritis Cystic disorders Developmental - Congenital Infectious Disease

Neoplasms Obstructive disorders Autoimmune diseases
Lupus Hepatorenal failure Scleroderma Amyloidosis Drug toxicity

24 hour urine for creatinine clearance
Can estimate creatinine clearance by:140 – {age x weight (kg)} 72 x serum creatinine

Reduced Renal Reserve
Renal Insufficiency
End Stage Renal Disease (ESRD)

Stage 1: GFR > 90 ml/min despite kidney damage

Stage 2: Mild reduction (GFR 60 – 89 ml/min)
1. GFR of 60 may represent 50% loss in function.2. Parathyroid hormones starts to increase.

No symptoms
Serum creatinine doubles
Up to 50% nephron loss

Stage 3: Moderate reduction (GFR 30 – 59 ml/min)1. Calcium absorption decreases2. Malnutrition onset3. Anemia secondary to Erythropoietin deficiency4. Left ventricular hypertrophy

Stage 4: Sever reduction (GFR 15 – 29 ml/min)1. Serum triglycerides increase2. Hyperphosphatemia3. Metabolic acidosis4. Hyperkalemia

Signs and symptoms worsen if kidneys are stressed
Decreased ability to maintain homeostasis

75% nephron loss Decreased: glomerular filtration rate, solute
clearance, ability to concentrate urine and hormone secretion
Symptoms: elevated BUN & Creatinine, mild azotemia, anemia

Stage 5: Kidney failure (GFR < 15 ml/min)1. Azotemia

Residual function < 15% of normal Excretory, regulatory and hormonal functions
severely impaired. metabolic acidosis Marked increase in: BUN, Creatinine,
Phosphorous Marked decrease in: Hemoglobin,
Hematocrit, Calcium Fluid overload

Uremic syndrome develops affecting all body systems can be diminished with early diagnosis &
treatment
Last stage of progressive CRF Fatal if no treatment


Mood swings Impaired judgment Inability to concentrate and perform simple
math functions Tremors, twitching, convulsions Peripheral Neuropathy
restless legs foot drop

Pale, grayish-bronze color Dry scaly Severe itching Bruise easily Uremic frost

Visual blurring Occasional blindness
Volume expansion and fluid overload Metabolic Acidosis Electrolyte Imbalances
Hyperkalemia

Uremic fetor Anorexia, nausea, vomiting GI bleeding

Anemia Platelet dysfunction

Muscle cramps Soft tissue calcifications Weakness Related to calcium phosphorous imbalances


Hypertension Congestive heart failure Pericarditis Pulmonary edema Pleural effusions

Erythropoietin production decreased Hypothyroidism Insulin resistance Growth hormone decreased Gonadal dysfunction Parathyroid hormone and Vitamin D3
Hyperlipidemia

Oral manifestations Enlarged (asymptomatic) salivary glands Decreased salivary flow Dry mouth Odor of urea on breath Metallic taste Increased calculus formation Low caries rate Enamel hypoplasia Dark brown stains on crowns Extrinsic (secondary to liquid ferrous sulfate therapy) Intrinsic (secondary to tetracycline staining)

Dental malocclusions Pale mucosa with diminished color demarcation between
attached gingiva and alveolar mucosa Low-grade gingival inflammation Petechiae and ecchymosis Bleeding from gingiva Prolonged bleeding Candidal infections Burning and tenderness of mucosa Erosive glossitis Tooth erosion (secondary to regurgitation associated with
dialysis) Dehiscence of wounds

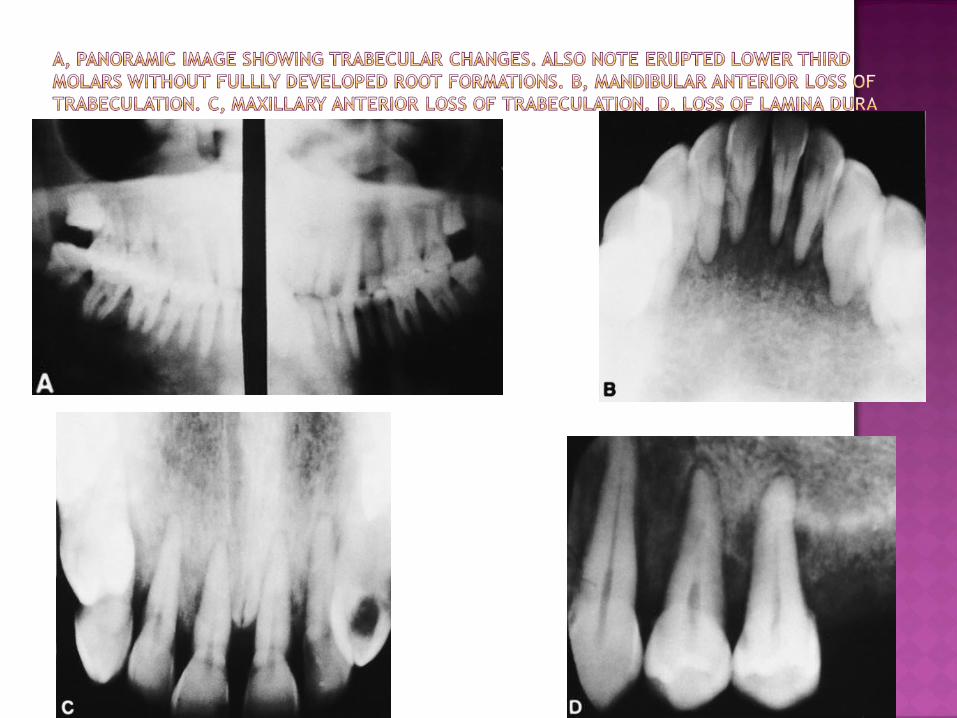
Radiographic manifestations Demineralization of bone Loss of bony trabeculation Ground-glass appearance Loss of lamina dura Giant cell lesions, “brown tumors” Socket sclerosis Pulpal narrowing and calcification Tooth mobility Arterial and oral calcifications

Hemodialysis Peritoneal Dialysis Transplant

Removal of soluble substances and water from the blood by diffusion through a semi-permeable membrane.

Blood removed from patient into the extracorporeal circuit.
Diffusion and ultrafiltration take place in the dialyzer.
Cleaned blood returned to patient.



Arterio-venous shunt (Scribner External Shunt)
Arterio-venous (AV) Fistula PTFE Graft Temporary catheters “Permanent” catheters

External- one end into artery, one into vein.
Advantagesplace at bedsideuse immediately
Disadvantages infectionskin erosionaccidental separation limits use of extremity

Patients own artery and vein surgically anastomosed.
Advantagespatients own veinlongevitylow infection and thrombosis rates
Disadvantageslong time to mature, 1- 6 months“steal” syndromerequires needle sticks

Synthetic “vessel” anastomosed into an artery and vein.
Advantages for people with inadequate vesselscan be used in 7-14 daysprominent vessels
Disadvantagesclots easily“steal” syndrome more frequentrequires needle sticks infection may necessitate removal of graft

Dual lumen catheter placed into a central vein-subclavian, jugular or femoral.
Advantagesimmediate useno needle sticks
Disadvantageshigh incidence of infectionsubclavian vein stenosispoor flow-inadequate dialysisclotting

NO BP’s, needle sticks to arm with vascular access. This includes finger sticks.
Place ID bands on other arm whenever possible.
Palpate thrill and listen for bruit. Teach patient nothing constrictive, feel for
thrill.

During dialysisFluid and electrolyte related
hypotensionCardiovascular
arrythmiasAssociated with the extracorporeal circuit
exsanguinationNeurologic
seizuresother
fever

Between treatments Hypertension/Hypotension Edema Pulmonary edema Hyperkalemia Bleeding Clotting of access

Long termMetabolic
hyperparathyroidism diabetic complications
Cardiovascular CHF AV access failure
Respiratory pulmonary edema
Neuromuscular neuropathy

Long term cont’d Hematologic
anemia GI
bleeding dermatologic
calcium phosphorous deposits Rheumatologic
amyloid deposits

Long term cont’d Genitourinary
infection sexual dysfunction
Psychiatric depression
Infection bloodborne pathogens

Fluid restrictions Phosphorous restrictions Potassium restrictions Sodium restrictions Protein to maintain nitrogen balance
too high - waste products too low - decreased albumin, increased mortality
Calories to maintain or reach ideal weight
Removal of soluble substances and water from the blood by diffusion through a semi-permeable membrane that is intracorporeal (inside the body).

CAPD: Continuous ambulatory peritoneal dialysis
CCPD: Continuous cycling peritoneal dialysis IPD: Intermittent peritoneal dialysis

Catheter into peritoneal cavity Exchanges 4 - 5 times per day Treatment 24 hours; 7 days a week Solution remains in peritoneal cavity except
during drain time Independent treatment


Fill: fluid infused into peritoneal cavity Dwell: time fluid remains in peritoneal cavity Drain: time fluid drains from peritoneal
cavity

Infectionperitonitistunnel infectionscatheter exit site
Hypervolemiahypertensionpulmonary edema
Hypovolemiahypotension
Hyperglycemia Malnutrition

Obesity Hypokalemia Hernia Cuff erosion

Independence for patient No needle sticks Better blood pressure control Some diabetics add insulin to solution Fewer dietary restrictions
protein loses in dialysate generally need increased potassium less fluid restrictions



Vitamins - water soluble Phosphate binder - (Phoslo, Renagel,
Calcium, Aluminum hydroxide) Give with meals
Iron Supplements - don’t give with phosphate binder or calcium
Antihypertensives - hold prior to dialysis

Erythropoietin Calcium Supplements - Between meals, not
with iron Activated Vitamin D3 - aids in calcium
absorption Antibiotics - hold dose prior to dialysis if it
dialyzes out

Many drugs or their metabolites are excreted by the kidney
Dosages - many change when used in renal failure patients
Dialyzability - many removed by dialysis varies between HD and PD

Alleviate fear Dialysis process Fistula/catheter care Diet and fluid restrictions Medication Diabetic teaching




Restoration of “normal” renal function Freedom from dialysis Return to “normal” life

Life long medications Multiple side effects from medication Increased risk of tumor Increased risk of infection Major surgery

Major surgery with general anesthesia Assessment of renal function Assessment of fluid and electrolyte balance Prevention of infection Prevention and management of rejection

ATN? (acute tubular necrosis) 50% experience
Urine output >100 <500 cc/hr BUN, creatinine, creatinine clearance Fluid Balance Ultrasound Renal scans Renal biopsy

Accurate I & OCRITICAL TO AVOID DEHYDRATIONOutput normal - >100 <500 cc/hr, could be
1-2 L/hrPotential for volume overload/deficit
Daily weights Hyper/Hypokalemia potential Hyponatremia Hyperglycemia

Major complication of transplantation due to immunosuppression
HANDWASHING Crowds, Kids Patient Education

Hyperacute - preformed antibodies to donor antigen function ceases within 24 hours Rx = removal
Accelerated - same as hyperacute but slower, 1st week to month Rx = removal

Acute - generally after 1st 10 days to end of 2nd month 50% experience must differentiate between rejection and
cyclosporine toxicity Rx = steroids, monoclonal (OKT3), or polyclonal
(HTG) antibodies

Chronic - gradual process of graft dysfunction Repeated rejection episodes that have not been
completely resolved with treatment Rx = return to dialysis or re-transplantation

Prednisone Prevents infiltration of T lymphocytes
Side effects cushnoid changes Avascular Necrosis GI disturbances Diabetes infection risk of tumor

Azathioprine (Imuran) Prevents rapid growing lymphocytes
Side Effects bone marrow toxicity hepatotoxicity hair loss infection risk of tumor

Cyclosporin Interferes with production of interleukin 2 which
is necessary for growth and activation of T lymphocytes.
• Side Effects– Nephrotoxicity– HTN– Hepatotoxicity– Gingival hyperplasia– Infection

Cytoxan - in place of Imuran less toxic FK506 - 100 x more potent than Cyclosporin Prograf Cellcept

OKT3 - monoclonal antibody used to treat rejection or induce immunosuppressiondecreases CD3 cells within 1 hour
Side effectsanaphylaxis fever/chillspulmonary edemarisk of infectiontumors
1st dose reaction expected & wanted, pre-treat with Benadryl, Tylenol, Solumedrol

Atgam - polyclonal antibody used to treat rejection or induce immunosuppressiondecreased number of T lymphocytes
Side effectsanaphylaxisfever chillsleukopeniathrombocytopeniarisk of infectiontumor

Signs of infection Prevention of infection Signs of rejection
decreased urine output increased weight gain tenderness over kidney fever > 100 degrees F
Medications time, dose, side effects

Indication Drug Magnesium content Antacids (Maalox, milk of
magnesia) Laxatives
Potassium content IV fluids Salt substitutes Massive penicillin therapy (1.7
mEq/million U)
Sodium content Carbenicillin (4.7 mEq/g) Alka Seltzer (23 mEq tablet) IV fluid
Acidifying effects Ascorbic acid Ammonium chloride (in cough syrup) Nonsteroidal anti-inflammatory
agents

Catabolic effects Tetracyclines
Steroids
Nephrotoxicity Phenacetin Ketorolac
Cephalosporins*
Alkalosis effect Absorbed antacids
Carbenicillin (large doses
Penicillin (large doses

Before treatment
Determine dialysis schedule and treat on day after dialysis. Consult with patient’s nephrologist for recent laboratory tests and discussion of antibiotic prophylaxis. Identify arm with vascular access and type; notate in chart and avoid taking blood pressure measurement/injection of medication on this arm. Evaluate patient for hypertension/hypotension. Institute preoperative hemostatic aids (DDAVP, conjugated estrogen) when appropriate. Determine underlying cause of renal failure (underlying disease may affect provision of care). Obtain routine annual dental radiographs to establish presence and follow manifestations of renal osteodystrophy. Consider routine serology for HBV, HCV, and HIV antibody. Consider antibiotic prophylaxis when appropriate. Consider sedative premedication for patients with hypertension

During treatment
Perform a thorough history and physical examination for presence of oral
manifestations. Aggressively eliminate potential sources of infection/bacteremia. Use adjunctive hemostatic aids during oral/periodontal surgical
procedures. Maintain patient in a comfortable uncramped position in the
dental chair. Allow patient to walk or stand intermittently during long
procedures

After treatment
Use postsurgical hemostatic agents. Encourage meticulous home care. Institute therapy for xerostomia when appropriate. Consider use of postoperative antibiotics for traumatic
procedures. Avoid use of respiratory-depressant drugs in presence of severe
anemia. Adjust dosages of postoperative medications according to extent
of renal failure. Ensure routine recall maintenance.



Recurrent herpes labialis in an immunocompromised patient
Recurrent herpes labialis

Recurrent intraoral herpes in a cardiac transplant recipient.
Chronic herpes simplex in a chronically immunosuppressed transplant recipient

Pseudomembranous candidiasisHyperplastic candidiasis in a kidney transplant recipient. This infection did not respond to fluconazole

Graft-versus-host disease in a patient who had undergone HCT. Note the clinical resemblance to erosive lichen planus

Pre-transplantation considerations
Significantly ill patient with end-organ damage Medical consultation required Consider postponing elective treatment Dental consultation prior to anticipated transplant: Rule out dental infectious sources, definitively Perform necessary treatment; this will require consultation with
transplantation physician to determine medical risk-to-benefit ratio Obtain laboratory information/supplemental information as
needed Become acquainted with specific management issues (eg, blood
products, prophylactic antibiotics) that may need to be employed if
treatment is rendered.

Post-transplantation considerations Immediate post-transplantation period No elective dental treatment performed Emergency treatment only with medical consultation and consideration of specific management needs Stable post-transplantation period Elective treatment may be performed after medical consultation with the transplantation physician Issues of immunosuppression must be recognized Oral mucosal disease must be diagnosed and treated Supplemental corticosteroids (steroid boost) may be necessary Consideration of antibiotic prophylaxis needed Consideration of specific management needs Post-transplantation chronic rejection period Only emergency treatment Patients are very ill as they are immunosuppressed and have organ failure

Thank you.
Related Documents