Renal Biopsy Findings in Children and Adolescents With Fabry Disease and Minimal Albuminuria Camilla Tøndel, MD, 1 Leif Bostad, MD, 2,3 Asle Hirth, MD, 4,5 and Einar Svarstad, MD, PhD 6,7 Background: Information concerning renal pathological characteristics in Fabry disease in childhood is limited. Our objective is to define renal morphological abnormalities in children and adolescents with Fabry disease and minimal proteinuria. Study Design: Case series. Setting & Participants: 9 symptomatic patients (7 males, 2 females; age range, 7 to 18 years); 2 patients had received enzyme replacement therapy for 2 years. Outcomes & Measurements: Renal morphological changes assessed by using light and electron microscopy. Results: All patients had acroparesthesia and typical eye changes, 7 showed hypohidrosis, 7 had gastrointestinal problems, and 2 had typical angiokeratomas. Mean albumin-creatinine ratio was 38 mg/mg (range, 5.3 to 104.3 mg/mg). Measured glomerular filtration rate was normal in all patients. Light microscopy showed changes in glomerular, tubulointerstitial, or vascular compartments alone or in combination in 7 patients. Electron microscopy showed lesions in all patients. Limitations: Small sample size. Conclusions: Glomerular and vascular changes are present before progression to overt proteinuria and decreased glomerular filtration rate. The combination of acroparesthesia and mild albuminuria, glomerular endothelial cell deposits, and arteriopathy may constitute a clinical and morphological combination heralding a potentially progressive renal disease. Am J Kidney Dis 51:767-776. © 2008 by the National Kidney Foundation, Inc. INDEX WORDS: Fabry disease; children; kidney biopsy; glomerular filtration rate. F abry disease is an X-linked glycosphingolipi- dosis caused by deficient synthesis of the enzyme -galactosidase A. Lysosomal accumula- tion of mostly globotriaosylceramide in cells from various organs appears at different ages and rates in individual patients, usually far ahead of clinical manifestations of the renal disease. 1 How- ever, the large individual variation and often progressive nature of these changes with result- ant organ failure raises questions concerning the appropriate timing of the initiation of enzyme replacement therapy (ERT). There is an obvious need for a more systematic approach in address- ing these issues. The first clinical presentation of Fabry disease is mainly episodic neuropathic pain, presenting with burning pain in the hands and feet (acroparesthesia). Gastrointestinal symp- toms and hypohidrosis also are common in the early stage of the disease. Clinical onset of Fabry disease is reported as early as 3 years in boys and 6 years in girls, and mean age at symptom presentation was shown to be 10 years in boys and 15 years in girls. 2-5 In children with Fabry disease, ERT largely has been given to improve such clinical symp- toms as acroparesthesia and gastrointestinal symptoms when symptomatic treatment is inad- equate. Enzyme substitution is believed to pre- vent later organ damage of the kidneys, heart, and brain. 3,6 Information concerning renal mor- phological changes is limited in young patients with Fabry disease. This is in contrast to the well-described renal changes in adult patients showing glycolipid accumulation in glomerular, vascular, interstitial, and distal tubular cells and various degrees of ischemic damage, and progres- sive disease usually is accompanied by protein- uria and decreased renal function. 1,7-9 Further- more, recent data showed a limited effect of ERT on progressive organ damage when treatment was initiated at a late stage. 10 As a consequence, From the Departments of 1 Pediatrics and 2 Pathology, Haukeland University Hospital; 3 Institute of Gade and 4 In- stitute of Clinical Medicine, University of Bergen; 5 Depart- ment of Heart Disease and 6 Medical Department, Hauke- land University Hospital; and 7 Institute of Medicine, University of Bergen, Bergen, Norway. Received August 1, 2007. Accepted in revised form December 11, 2007. Originally published online as doi: 10.1053/j.ajkd.2007.12.032 on March 20, 2008. Address correspondence to Camilla Tøndel, MD, Depart- ment of Pediatrics, Haukeland University Hospital, N-5021 Bergen, Norway. E-mail: [email protected] © 2008 by the National Kidney Foundation, Inc. 0272-6386/08/5105-0009$34.00/0 doi:10.1053/j.ajkd.2007.12.032 American Journal of Kidney Diseases, Vol 51, No 5 (May), 2008: pp 767-776 767

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

FetfrcepaarniFpated6pa
htse
A
Renal Biopsy Findings in Children and Adolescents With Fabry Diseaseand Minimal Albuminuria
Camilla Tøndel, MD,1 Leif Bostad, MD,2,3 Asle Hirth, MD,4,5 and Einar Svarstad, MD, PhD6,7
Background: Information concerning renal pathological characteristics in Fabry disease in childhoodis limited. Our objective is to define renal morphological abnormalities in children and adolescents withFabry disease and minimal proteinuria.
Study Design: Case series.Setting & Participants: 9 symptomatic patients (7 males, 2 females; age range, 7 to 18 years); 2
patients had received enzyme replacement therapy for 2 years.Outcomes & Measurements: Renal morphological changes assessed by using light and electron
microscopy.Results: All patients had acroparesthesia and typical eye changes, 7 showed hypohidrosis, 7 had
gastrointestinal problems, and 2 had typical angiokeratomas. Mean albumin-creatinine ratio was 38mg/mg (range, 5.3 to 104.3 mg/mg). Measured glomerular filtration rate was normal in all patients. Lightmicroscopy showed changes in glomerular, tubulointerstitial, or vascular compartments alone or incombination in 7 patients. Electron microscopy showed lesions in all patients.
Limitations: Small sample size.Conclusions: Glomerular and vascular changes are present before progression to overt proteinuria
and decreased glomerular filtration rate. The combination of acroparesthesia and mild albuminuria,glomerular endothelial cell deposits, and arteriopathy may constitute a clinical and morphologicalcombination heralding a potentially progressive renal disease.Am J Kidney Dis 51:767-776. © 2008 by the National Kidney Foundation, Inc.
INDEX WORDS: Fabry disease; children; kidney biopsy; glomerular filtration rate.
vapwwsvvsumow
HsmlU
D1
mB
abry disease is an X-linked glycosphingolipi-dosis caused by deficient synthesis of the
nzyme �-galactosidase A. Lysosomal accumula-ion of mostly globotriaosylceramide in cellsrom various organs appears at different ages andates in individual patients, usually far ahead oflinical manifestations of the renal disease.1 How-ver, the large individual variation and oftenrogressive nature of these changes with result-nt organ failure raises questions concerning theppropriate timing of the initiation of enzymeeplacement therapy (ERT). There is an obviouseed for a more systematic approach in address-ng these issues. The first clinical presentation ofabry disease is mainly episodic neuropathicain, presenting with burning pain in the handsnd feet (acroparesthesia). Gastrointestinal symp-oms and hypohidrosis also are common in thearly stage of the disease. Clinical onset of Fabryisease is reported as early as 3 years in boys and
years in girls, and mean age at symptomresentation was shown to be 10 years in boysnd 15 years in girls.2-5
In children with Fabry disease, ERT largelyas been given to improve such clinical symp-oms as acroparesthesia and gastrointestinalymptoms when symptomatic treatment is inad-
quate. Enzyme substitution is believed to pre-merican Journal of Kidney Diseases, Vol 51, No 5 (May), 2008: p
ent later organ damage of the kidneys, heart,nd brain.3,6 Information concerning renal mor-hological changes is limited in young patientsith Fabry disease. This is in contrast to theell-described renal changes in adult patients
howing glycolipid accumulation in glomerular,ascular, interstitial, and distal tubular cells andarious degrees of ischemic damage, and progres-ive disease usually is accompanied by protein-ria and decreased renal function.1,7-9 Further-ore, recent data showed a limited effect of ERT
n progressive organ damage when treatmentas initiated at a late stage.10 As a consequence,
From the Departments of 1Pediatrics and 2Pathology,aukeland University Hospital; 3Institute of Gade and 4In-
titute of Clinical Medicine, University of Bergen; 5Depart-ent of Heart Disease and 6Medical Department, Hauke-
and University Hospital; and 7Institute of Medicine,niversity of Bergen, Bergen, Norway.Received August 1, 2007. Accepted in revised form
ecember 11, 2007. Originally published online as doi:0.1053/j.ajkd.2007.12.032 on March 20, 2008.
Address correspondence to Camilla Tøndel, MD, Depart-ent of Pediatrics, Haukeland University Hospital, N-5021ergen, Norway. E-mail: [email protected]© 2008 by the National Kidney Foundation, Inc.0272-6386/08/5105-0009$34.00/0
doi:10.1053/j.ajkd.2007.12.032p 767-776 767

tiBvdTmlmmb
pFdmAta
pfoaTtah02mcpmctaANmPRom5
lpta
R
ri
fiSemcihmliimClggipaaso
C
oddEbpavalwtltIat
C
wycasll(tv
Tøndel et al768
he issue of timely initiation of enzyme treatmentn childhood is an increasingly important debate.aseline renal morphological findings may pro-ide important information supporting treatmentecisions and also may have a prognostic impact.he purpose of our study is to define renalorphological abnormalities in children and ado-
escents with Fabry disease with minimal albu-inuria or proteinuria and establish a baselineorphological diagnosis of the renal disease
efore ERT.
METHODSWe performed renal biopsies in 9 (7 male and 2 female
atients) of a total of 16 patients 18 years or younger in ourabry-patient cohort. One patient (patient 4) received aiagnosis because of severe acroparesthesia,11 and the re-aining patients were identified based on family history.croparesthesia was present in 81%; gastrointestinal symp-
oms, in 56%; hypohidrosis, in 50%; eye changes, in 94%;nd angiokeratomas, in 13% of our patients.
Based on the general concept that albuminuria usuallyrecedes manifest proteinuria and later progressive kidneyailure, a renal biopsy was performed after informed consentn a consecutive basis in all patients for whom albuminuriand/or proteinuria became evident in repeated urine samples.he protocol was approved by the Regional Ethics Commit-
ee. Until 2005, urinary protein estimation was measured aslbumin-creatinine ratio and protein-creatinine ratio in 24-our urine samples, and protein concentration less than.015 mg/L (0.15 g/L) were not routinely measured. Since005, we have used overnight urine samples, recorded as theedian value of 3 consecutive morning samples. Albumin-
reatinine ratio less than 22 mg/mg (�2.5 mg/mmol) androtein-creatinine ratio less than 177 mg/mg (�20 mg/mol) are considered normal in our laboratory, and mi-
roalbuminuria is defined as albumin-creatinine ratio of 22o 265 mg/mg (2.5 to 30 mg/mmol). Urine albumin wasnalyzed by using nephelometry (Behring Nephelometernalyser II; Siemans Healthcare Diagnostics, Tarrytown,Y). Urine protein was analyzed by using a turbidometricethod based on benzethonium chloride (Modular Analytics800; Roche Diagnostics GmbH, Mannheim, Germany).
enal biopsies were performed before the start of ERT in 7f 9 patients and after 2 years of ERT (agalsidase alfa, 0.2g/kg every second week) in 2 of 9 patients (patients 4 and
) with microalbuminuria before the biopsy.Renal function was measured by using serum creatinine
evel, an iohexol glomerular filtration rate (GFR) single-oint method after 4 hours (high-performance liquid chroma-ography analysis), and estimated GFR (Schwartz formula)nd corrected to 1.73 m2 of body surface.
enalMorphological Characteristics
After stereomicroscopic verification, representative mate-ial for electron microscopy was sectioned from the core and
mmediately fixed in McDowell solution. Tissue was post- ixed in 1% osmium tetroxide and embedded in Epon.emithin sections were stained with toluidine blue andxamined by using light microscopy. A representative glo-erulus was processed for transmission electron micros-
opy. For standard light microscopy, biopsy tissue was fixedn 10% formalin, embedded in paraffin, and stained withematoxylin and eosin, periodic acid–Schiff, silver-methena-ine (Jones stain), and Congo red. Sections from the forma-
in-fixed paraffin-embedded material were examined by us-ng the immunoperoxidase method for the demonstration ofmmune deposits. The following antibodies were used: im-unoglobulin G, immunoglobulin A, immunoglobulin M,3, and C1q. Biopsy specimens were scored by means of
ight microscopy according to changes in glomeruli (globallomerular sclerosis, focal segmental glomerulosclerosis,lomerular hyaline, arteriopathy and arteriolopathy, andnterstitial fibrosis). The finding of periodic acid–Schiff–ositive hyaline-like material in media of small and largerteries was defined and registered as arteriopathy. Globotri-osylceramide inclusions in various cell types were scoredemiquantitatively (� to ���) by using light microscopyf the semi-thin sections and electron microscopy.
ardiacMeasurements
Cardiac evaluation was undertaken in all patients as partf our Fabry protocol. M-Mode and 2-dimensional echocar-iography were performed by the same operator in accor-ance with recommendations of the American Society ofchocardiography.12 Left ventricular mass was calculatedy using the Devereux cube formula and indexed by the 2.7ower of height (grams/meter2.7). Transmitral flow patternnd the Simpson biplane method were used to estimate leftentricular systolic and diastolic performance. Mitral andortic regurgitation was assessed indirectly by using Dopp-er echocardiography. Furthermore, all participants under-ent standard 12-lead electrocardiography and Holter moni-
oring. Left ventricular hypertrophy (LVH) was defined aseft ventricular mass greater than 51 g/m2.7, and relative wallhickness greater than 0.45 was considered pathological.12,13
t was also registered as a cardiac finding if the patient hadn age-dependent pathological electrocardiogram or morehan mild aortic or mitral regurgitation.
RESULTS
linical Findings
Renal biopsies were performed in 9 patientsith a mean age of 13.5 years (range, 7 to 18ears; Table 1, patients 1 to 9). No biopsy compli-ations were seen in our patients. All patients hadcroparesthesia and typical eye changes, 7howed hypohidrosis, 7 had gastrointestinal prob-ems, and 2 had typical angiokeratomas. Table 2ists laboratory data. �-Galactosidase A levelsnormal reference, 63.7 to 95.0 nmol/h/mg pro-ein [17.7 to 26.4 �kat/kg protein]) were se-erely depressed in boys and slightly decreased
n the 2 girls (patients 2 and 3). Mean albumin-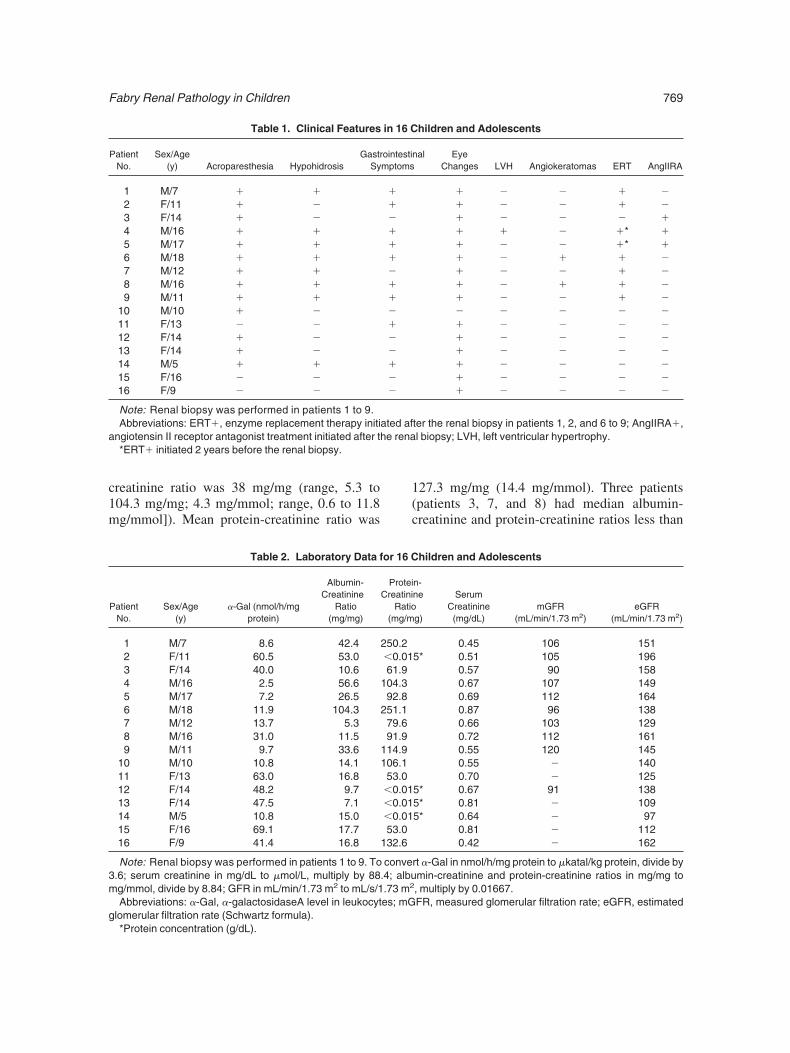
c1m
1(c
a
3m
g
Fabry Renal Pathology in Children 769
reatinine ratio was 38 mg/mg (range, 5.3 to04.3 mg/mg; 4.3 mg/mmol; range, 0.6 to 11.8g/mmol]). Mean protein-creatinine ratio was
Table 1. Clinical Features
PatientNo.
Sex/Age(y) Acroparesthesia Hypohidrosis
GastrSy
1 M/7 � �2 F/11 � �3 F/14 � �4 M/16 � �5 M/17 � �6 M/18 � �7 M/12 � �8 M/16 � �9 M/11 � �
10 M/10 � �11 F/13 � �12 F/14 � �13 F/14 � �14 M/5 � �15 F/16 � �16 F/9 � �
Note: Renal biopsy was performed in patients 1 to 9.Abbreviations: ERT�, enzyme replacement therapy initi
ngiotensin II receptor antagonist treatment initiated after th*ERT� initiated 2 years before the renal biopsy.
Table 2. Laboratory Data f
PatientNo.
Sex/Age(y)
�-Gal (nmol/h/mgprotein)
Albumin-Creatinine
Ratio(mg/mg)
1 M/7 8.6 42.42 F/11 60.5 53.03 F/14 40.0 10.64 M/16 2.5 56.65 M/17 7.2 26.56 M/18 11.9 104.37 M/12 13.7 5.38 M/16 31.0 11.59 M/11 9.7 33.6
10 M/10 10.8 14.111 F/13 63.0 16.812 F/14 48.2 9.713 F/14 47.5 7.114 M/5 10.8 15.015 F/16 69.1 17.716 F/9 41.4 16.8
Note: Renal biopsy was performed in patients 1 to 9. To.6; serum creatinine in mg/dL to �mol/L, multiply by 88g/mmol, divide by 8.84; GFR in mL/min/1.73 m2 to mL/s/1Abbreviations: �-Gal, �-galactosidaseA level in leukocyt
lomerular filtration rate (Schwartz formula).
*Protein concentration (g/dL).27.3 mg/mg (14.4 mg/mmol). Three patientspatients 3, 7, and 8) had median albumin-reatinine and protein-creatinine ratios less than
hildren and Adolescents
nal EyeChanges LVH Angiokeratomas ERT AngIIRA
� � � � �� � � � �� � � � �� � � �* �� � � �* �� � � � �� � � � �� � � � �� � � � �� � � � �� � � � �� � � � �� � � � �� � � � �� � � � �� � � � �
ter the renal biopsy in patients 1, 2, and 6 to 9; AngIIRA�,l biopsy; LVH, left ventricular hypertrophy.
hildren and Adolescents
n-ne
g)
SerumCreatinine(mg/dL)
mGFR(mL/min/1.73 m2)
eGFR(mL/min/1.73 m2)
0.45 106 1515* 0.51 105 196
0.57 90 1580.67 107 1490.69 112 1640.87 96 1380.66 103 1290.72 112 1610.55 120 1450.55 � 1400.70 � 125
5* 0.67 91 1385* 0.81 � 1095* 0.64 � 97
0.81 � 1120.42 � 162
rt �-Gal in nmol/h/mg protein to �katal/kg protein, divide bymin-creatinine and protein-creatinine ratios in mg/mg to, multiply by 0.01667.FR, measured glomerular filtration rate; eGFR, estimated
in 16 C
ointestimptoms
����������������
ated afe rena
or 16 C
ProteiCreatini
Ratio(mg/m
250.2�0.0161.9
104.392.8
251.179.691.9
114.9106.153.0�0.01�0.01�0.0153.0
132.6
conve.4; albu.73 m2
es; mG
tms9m
smmerm
aGm
R
ioipsuttSliot1hf1spsl
r
f
Tøndel et al770
he lower reference levels of 22 mg/mg (2.5g/mmol) and 177 mg/mg (20 mg/mmol), re-
pectively. Five patients (patients 1, 4, 5, 6, and) had combined abnormal proteinuria and albu-inuria (Table 2).Iohexol-GFR was normal in all renal biopsy
tudy patients (n � 9; mean, 106 mL/min/1.732; range, 90 to 120 mL/min/1.73 m2). Esti-ated GFR by using the Schwartz formula over-
stimated GFR (mean, 155 mL/min/1.73 m2;ange, 129 to 196 mL/min/1.73 m2 [2.15 to 3.27L/s/1.73 m2]) compared with iohexol-GFR in
Figure 1. Renal biopsy specimen from patient 1: ste-eomicroscopy shows white-looking glomeruli.
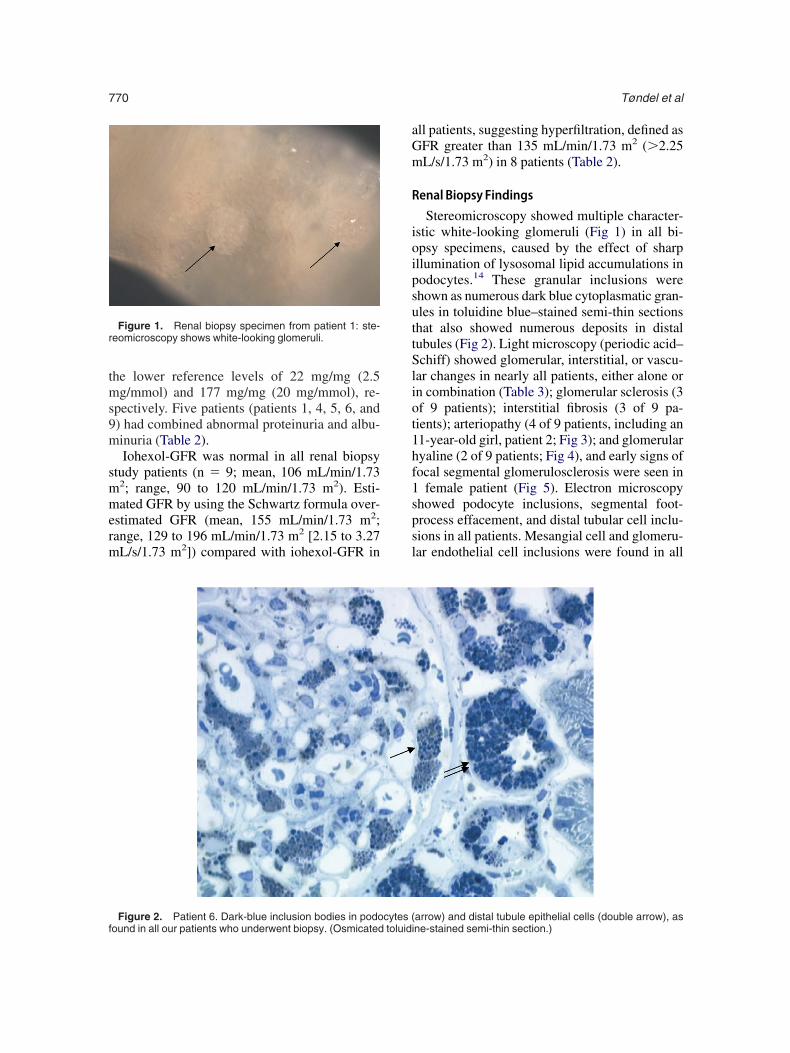
Figure 2. Patient 6. Dark-blue inclusion bodies in podocytes (ound in all our patients who underwent biopsy. (Osmicated toluidi
ll patients, suggesting hyperfiltration, defined asFR greater than 135 mL/min/1.73 m2 (�2.25L/s/1.73 m2) in 8 patients (Table 2).
enal Biopsy Findings
Stereomicroscopy showed multiple character-stic white-looking glomeruli (Fig 1) in all bi-psy specimens, caused by the effect of sharpllumination of lysosomal lipid accumulations inodocytes.14 These granular inclusions werehown as numerous dark blue cytoplasmatic gran-les in toluidine blue–stained semi-thin sectionshat also showed numerous deposits in distalubules (Fig 2). Light microscopy (periodic acid–chiff) showed glomerular, interstitial, or vascu-
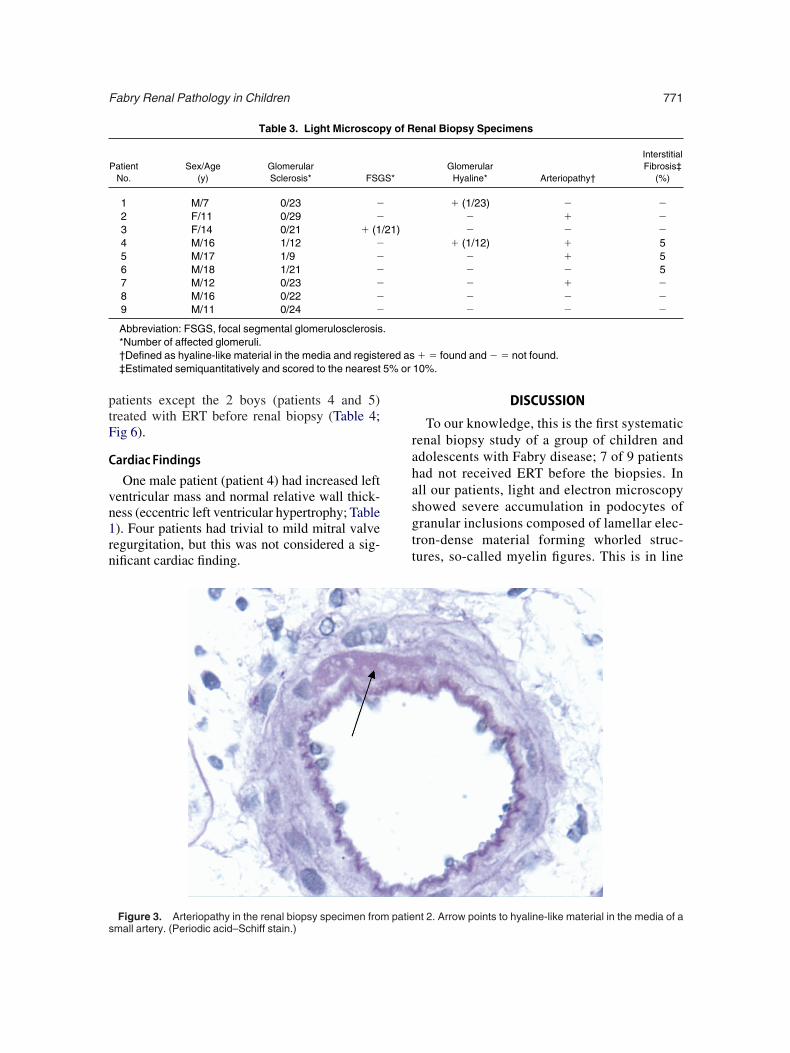
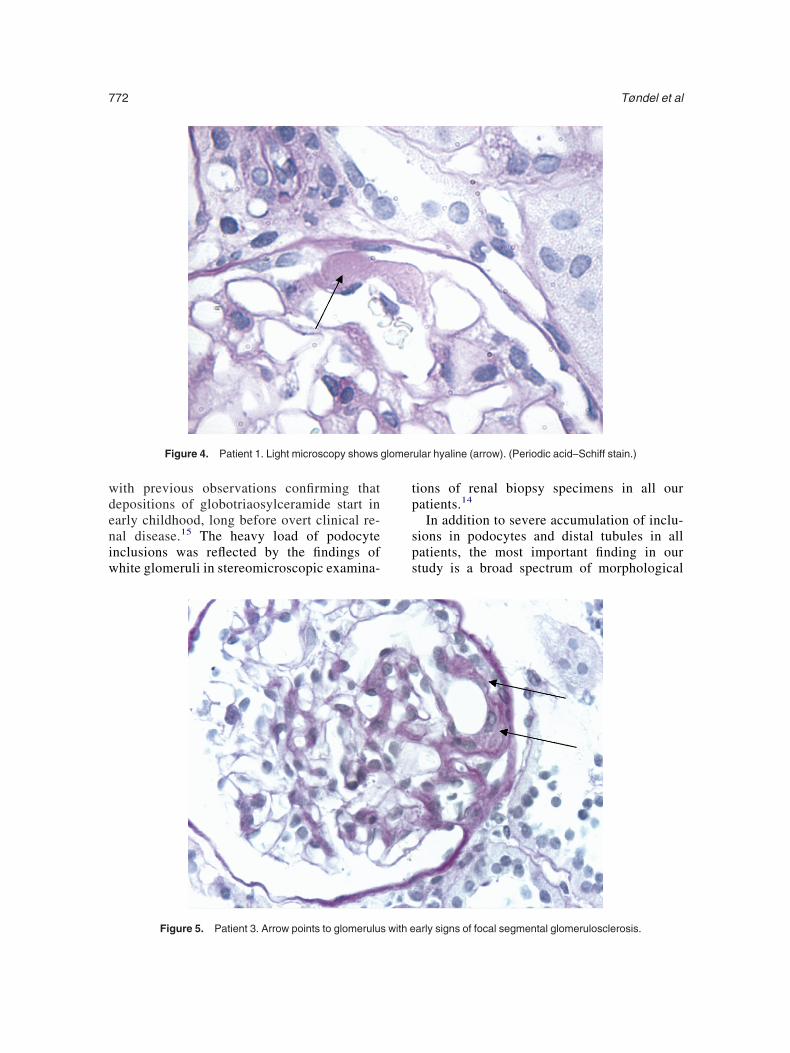
ar changes in nearly all patients, either alone orn combination (Table 3); glomerular sclerosis (3f 9 patients); interstitial fibrosis (3 of 9 pa-ients); arteriopathy (4 of 9 patients, including an1-year-old girl, patient 2; Fig 3); and glomerularyaline (2 of 9 patients; Fig 4), and early signs ofocal segmental glomerulosclerosis were seen in
female patient (Fig 5). Electron microscopyhowed podocyte inclusions, segmental foot-rocess effacement, and distal tubular cell inclu-ions in all patients. Mesangial cell and glomeru-ar endothelial cell inclusions were found in all
arrow) and distal tubule epithelial cells (double arrow), asne-stained semi-thin section.)
ptF
C
vn1rn
rahasgtt
5% or
s
Fabry Renal Pathology in Children 771
atients except the 2 boys (patients 4 and 5)reated with ERT before renal biopsy (Table 4;ig 6).
ardiac Findings
One male patient (patient 4) had increased leftentricular mass and normal relative wall thick-ess (eccentric left ventricular hypertrophy; Table). Four patients had trivial to mild mitral valveegurgitation, but this was not considered a sig-ificant cardiac finding.
Table 3. Light Microscop
PatientNo.
Sex/Age(y)
GlomerularSclerosis* FSG
1 M/7 0/23 �2 F/11 0/29 �3 F/14 0/21 � (14 M/16 1/12 �5 M/17 1/9 �6 M/18 1/21 �7 M/12 0/23 �8 M/16 0/22 �9 M/11 0/24 �
Abbreviation: FSGS, focal segmental glomerulosclerosis*Number of affected glomeruli.†Defined as hyaline-like material in the media and registe‡Estimated semiquantitatively and scored to the nearest
Figure 3. Arteriopathy in the renal biopsy specimen from patiemall artery. (Periodic acid–Schiff stain.)
DISCUSSION
To our knowledge, this is the first systematicenal biopsy study of a group of children anddolescents with Fabry disease; 7 of 9 patientsad not received ERT before the biopsies. Inll our patients, light and electron microscopyhowed severe accumulation in podocytes ofranular inclusions composed of lamellar elec-ron-dense material forming whorled struc-ures, so-called myelin figures. This is in line
enal Biopsy Specimens
GlomerularHyaline* Arteriopathy†
InterstitialFibrosis‡
(%)
� (1/23) � �� � �� � �
� (1/12) � 5� � 5� � 5� � �� � �� � �
� � found and � � not found.10%.
y of R
S*
/21)
.
red as
nt 2. Arrow points to hyaline-like material in the media of a
wdeniw
tp
sps
glomer
Tøndel et al772
ith previous observations confirming thatepositions of globotriaosylceramide start inarly childhood, long before overt clinical re-al disease.15 The heavy load of podocytenclusions was reflected by the findings ofhite glomeruli in stereomicroscopic examina-
Figure 4. Patient 1. Light microscopy shows
Figure 5. Patient 3. Arrow points to glomerulus with e
ions of renal biopsy specimens in all ouratients.14
In addition to severe accumulation of inclu-ions in podocytes and distal tubules in allatients, the most important finding in ourtudy is a broad spectrum of morphological
ular hyaline (arrow). (Periodic acid–Schiff stain.)
arly signs of focal segmental glomerulosclerosis.
cvc(((gmdtep
depasdnesbcn
matrix
(
Fabry Renal Pathology in Children 773
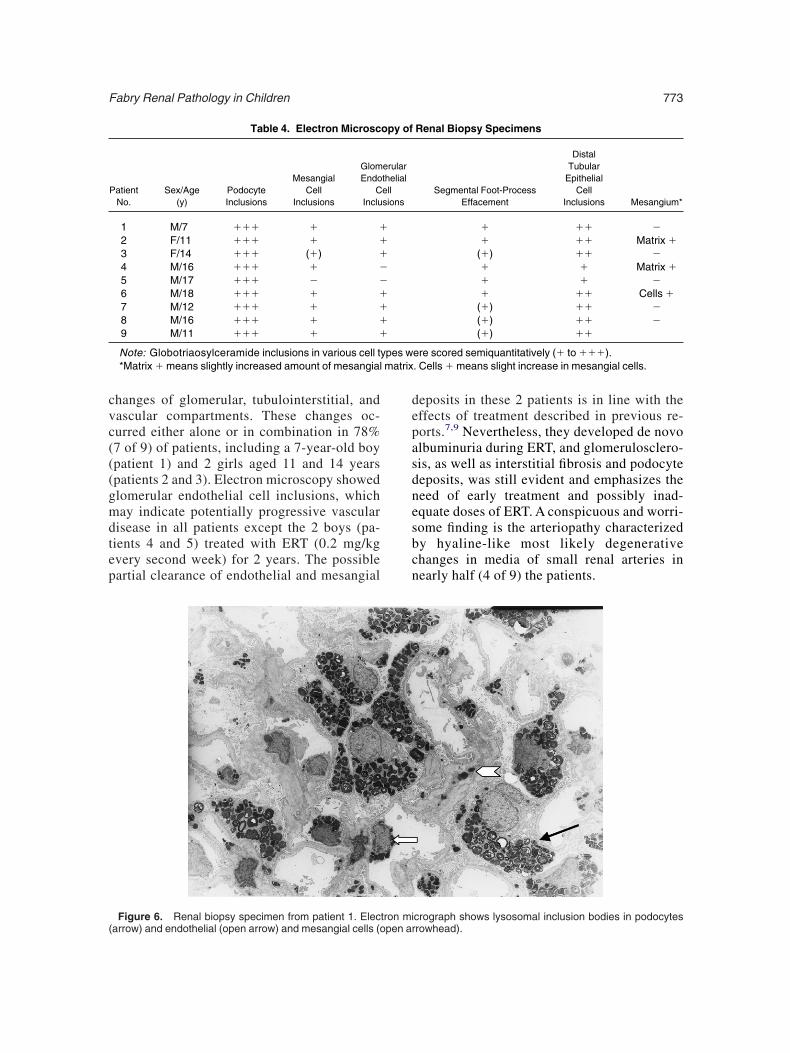
hanges of glomerular, tubulointerstitial, andascular compartments. These changes oc-urred either alone or in combination in 78%7 of 9) of patients, including a 7-year-old boypatient 1) and 2 girls aged 11 and 14 yearspatients 2 and 3). Electron microscopy showedlomerular endothelial cell inclusions, whichay indicate potentially progressive vascular
isease in all patients except the 2 boys (pa-ients 4 and 5) treated with ERT (0.2 mg/kgvery second week) for 2 years. The possibleartial clearance of endothelial and mesangial
Table 4. Electron Microsc
PatientNo.
Sex/Age(y)
PodocyteInclusions
MesangialCell
Inclusions
GlomEndo
CInclu
1 M/7 ��� � �2 F/11 ��� � �3 F/14 ��� (�) �4 M/16 ��� � �5 M/17 ��� � �6 M/18 ��� � �7 M/12 ��� � �8 M/16 ��� � �9 M/11 ��� � �
Note: Globotriaosylceramide inclusions in various cell t*Matrix � means slightly increased amount of mesangial
Figure 6. Renal biopsy specimen from patient 1. Electron miarrow) and endothelial (open arrow) and mesangial cells (open ar
eposits in these 2 patients is in line with theffects of treatment described in previous re-orts.7,9 Nevertheless, they developed de novolbuminuria during ERT, and glomerulosclero-is, as well as interstitial fibrosis and podocyteeposits, was still evident and emphasizes theeed of early treatment and possibly inad-quate doses of ERT. A conspicuous and worri-ome finding is the arteriopathy characterizedy hyaline-like most likely degenerativehanges in media of small renal arteries inearly half (4 of 9) the patients.
Renal Biopsy Specimens
Segmental Foot-ProcessEffacement
DistalTubular
EpithelialCell
Inclusions Mesangium*
� �� �� �� Matrix �
(�) �� �� � Matrix �� � �� �� Cells �
(�) �� �(�) �� �(�) ��
ere scored semiquantitatively (� to ���).. Cells � means slight increase in mesangial cells.
opy of
erularthelialellsions
ypes w
crograph shows lysosomal inclusion bodies in podocytesrowhead).

sduiwmtmbcafitaeoEAd2cp(uzei
otrtispsdfiGa
emcfpwefi
awmbasgaiwtfitmmfa1b1ocgm
vwaiitfahFaaMtraarskiwvpe
Tøndel et al774
The surprising rather uniform electron micro-copic distribution of distinct glomerular andistal tubular cell inclusions in slightly albumin-ric children adds important information concern-ng the natural history of renal disease in patientsith Fabry disease. Our findings of prevalentorphological changes in glomeruli, as well as
he tubulointerstitial and vascular renal compart-ents, further strengthen the indication for ERT
efore progression to overt proteinuria, de-reased GFR, and irreversible renal damage. Inddition, until valid prognostic parameters areound, our biopsy findings also raise the intrigu-ng question of whether a renal biopsy at someime should be part of the diagnostic workup inll children with clinical symptoms for whichnzyme treatment is a matter of discussion. Basedn clinical symptoms and renal biopsy findings,RT was initiated in all except 1 of our patients.n angiotensin II receptor antagonist was intro-uced as adjunctive renoprotective therapy in thepatients with the most extensive renal pathologi-al findings (patients 4 and 5) and the femaleatient (patient 3) who did not receive ERTTable 1). A recent study showed that antiprotein-ric therapy with angiotensin-converting en-yme inhibitors and angiotensin receptor block-rs may stabilize the progression of renal diseasen patients with manifest proteinuria.16
Uncertainty concerning correct measurementsf GFR in these patients increases the impor-ance of a renal biopsy in the diagnosis of earlyenal disease. Overestimation of GFR by usinghe Schwartz formula compared with inulin andohexol methods, as well as cystatin C, wasuggested in pediatric patients in several re-orts17,18 and may lead to an erroneous conclu-ion of hyperfiltration as a sign of early renalamage. This observation is supported by ourndings of significantly increased estimatedFRs compared with normal iohexol-GFRs in
ll patients in the present group.In contrast to adult patients with Fabry dis-
ase, there are few previous reports of renalorphological pathological characteristics in
hildhood. Kidney involvement was described inetal life,19 and renal changes showing foamy cyto-lasm in enlarged podocytes in a 12-year-old girlith Fabry disease recently were presented.20 An
arly study by Gubler et al1 showed renal biopsy
ndings for 12 patients, including 3 children pged 8 (female), 11, and 12 years (males), allithout proteinuria. However, low levels of albu-inuria cannot be ruled out in these patients
ecause only manifest proteinuria was reportednd methods of protein measurements were nottated. The investigators found that glycosphin-olipid deposits were fully developed at an earlyge and were prevalent in vessels and glomerulin hemizygous patients, whereas the distributionas more irregular in heterozygotes. Moreover,
hey found that age-related degenerative changesrst involved the vessels. Our findings add fur-
her information concerning the early develop-ent of potentially progressive vascular involve-ent. Arteriopathy and/or interstitial fibrosis were
ound in more than half (5 of 9) our patients, allged 11 to 17 years, and the youngest was an1-year-old girl. Interstitial fibrosis was seen iniopsy specimens from the oldest patients aged6 to 18 years. Our findings also support thebservation of Gubler et al1 that the naturalourse of lipid depositions often is rapidly pro-ressive in the early teenage period, showingore widespread changes with increasing age.The pathogenesis of the progressive renal in-
olvement in patients with Fabry disease is notell understood. Although overt proteinuria usu-
lly is a late sign, it should be borne in mind thatndividual progression of glomerulosclerosis andnterstitial fibrosis may differ depending on varia-ions in disease phenotype and cause. Renalailure developed as early as 16 years of age.2 Instudy of 35 children and adolescents, 6 patientsad proteinuria, all older than 14 years.4 In theabry Outcome Survey database, 8 patients hadlbuminuria and 12 patients had proteinuria fromtotal of 82 patients younger than 18 years.21
ean age and amounts of albuminuria and pro-einuria in our patients were similar to thoseeported in the study of 25 children by Ries etl.22 The recognition of increasing albuminuriand proteinuria as a hallmark of progressiveenal disease in patients with Fabry disease isimilar to that found in patients with many otheridney diseases.23 This was confirmed recentlyn the phase 4 study in which these parametersere associated with increased renal and cardio-ascular risk.24 Our findings therefore may im-ly that albuminuria in children with Fabry dis-ase should be considered a marker of potentially
rogressive vascular damage, as in other ne-
psusa
sRoacltcismvo
edasarsipoAnwshmttptf
etvaiptlm
pwtualspnnw
Dg1
J
md
cc
Fi7
zw
lbN
m2
sfK
Wi
ee
dc
Fabry Renal Pathology in Children 775
hropathies, preceding chronic renal failure byeveral years. Consequently, in our view, albumin-ria in a child or adolescent with Fabry diseasehould lead to a prompt renal biopsy to evaluatend characterize the extent of renal damage.
The majority of our patients did not showignificant cardiac disease. This is in contrast toies et al,22 who found that approximately 50%f their patients had cardiac involvement by thege of 15 years. The discrepancy is probablyaused by different definitions of cardiac patho-ogical states12,13 and emphasizes the impor-ance of agreement on adequate criteria for bothardiac and renal evaluation at an early age. Thiss especially relevant because recent studies de-cribed the association of double-organ involve-ent in adults and potential regression of left
entricular hypertrophy after timely introductionf ERT.10,25,26
There are few studies of ERT in children. Riest al3 conducted a prospective study with agalsi-ase alfa during 6 months in 24 children (meange, 11.8 years; range, 6.5 to 18 years) andhowed that treatment was safe and well toler-ted. Furthermore, renal hyperfiltration was cor-ected, microalbuminuria decreased in 3 of 4ubjects, and heart rate variability increased,ndicating that early treatment in children mayrove a “window of opportunity” to correct earlyrgan damage and prevent progressive disease.3
part from severely symptomatic patients witheuropathic pain in Fabry disease, the time athich ERT should be initiated to prevent progres-
ive organ damage is an important question thatas not yet been settled. Because organ involve-ent usually is asymptomatic for a long time and
he speed of progression is individual, earlyreatment may be of greater benefit in someatients, and renal biopsies may be an importantool in providing potential indicators of organailure in some patients.
In conclusion, standard light microscopic andlectron microscopic examinations showed poten-ially progressive glomerular and vascular in-olvement in renal biopsy specimens in nearlyll albuminuric male and female patients, includ-ng worrisome arteriopathy in nearly half theatients. This emphasizes the importance of sys-ematic urine examinations in the routine fol-ow-up of children with Fabry disease. Further-
ore, appropriately timed renal biopsies may drove an important diagnostic tool in patientsith signs of early renal disease. The combina-
ion of acroparesthesia, mild albuminuria/protein-ria, glomerular endothelial cell deposits, andrteriopathy may constitute a clinical and morpho-ogical combination heralding potentially progres-ive disease and timely initiation of ERT torevent later manifest organ damage. The prog-ostic value of such a combination of findingseeds to be confirmed in additional clinical trialsith renal biopsies.
ACKNOWLEDGEMENTSSupport: None.Financial Disclosure: None.
REFERENCES1. Gubler MC, Lenoir G, Grunfeld JP, Ulmann A, Droz
, Habib R: Early renal changes in hemizygous and heterozy-ous patients with Fabry’s disease. Kidney Int 13:223-235,9782. Desnick RJ, Brady RO: Fabry disease in childhood.
Pediatr 144:S20-S26, 2004 (suppl 5)3. Ries M, Clarke JT, Whybra C, et al: Enzyme-replace-ent therapy with agalsidase alfa in children with Fabry
isease. Pediatrics 118:924-932, 20064. Ries M, Ramaswami U, Parini R, et al: The early
linical phenotype of Fabry disease: A study on 35 Europeanhildren and adolescents. Eur J Pediatr 162:767-772, 2003
5. MacDermot KD, Holmes A, Miners AH: Anderson-abry disease: Clinical manifestations and impact of disease
n a cohort of 98 hemizygous males. J Med Genet 38:750-60, 20016. Ramaswami U, Wendt S, Pintos-Morell G, et al: En-
yme replacement therapy with agalsidase alfa in childrenith Fabry disease. Acta Paediatr 96:122-127, 20077. Germain D, Waldek S, Banikazemi M, et al: Sustained,
ong-term renal stabilization after 54 months of agalsidaseeta therapy in patients with Fabry disease. J Am Socephrol 18:1368-1370, 20078. Sessa A, Meroni M, Battini G, et al: Renal involve-ent in Anderson-Fabry disease. J Nephrol 16:310-313,
0039. Thurberg BL, Rennke H, Colvin RB, et al: Globotriao-
ylceramide accumulation in the Fabry kidney is clearedrom multiple cell types after enzyme replacement therapy.idney Int 62:1933-1946, 200210. Breunig F, Weidemann F, Strotmann J, Knoll A,anner C: Clinical benefit of enzyme replacement therapy
n Fabry disease. Kidney Int 69:1216-1221, 200611. Tøndel C, Laegreid LM, Hirth A, et al: Intravenous
nzyme substitution therapy in children with Fabry’s dis-ase. Tidsskr Nor Laegeforen 123:3388-3390, 2003
12. Lang RM, Bierig M, Devereux RB, et al: Recommen-ations for chamber quantification: A report from the Ameri-an Society of Echocardiography’s Guidelines and Stan-
ards Committee and the Chamber Quantification Writing
GAS2
Mvar
cF2
Pd2
tpw2
GGf
Ccp
CC
iP
e2
mF
d
Bpf
bA
eAc1
mi
Tøndel et al776
roup, developed in conjunction with the Europeanssociation of Echocardiography, a branch of the Europeanociety of Cardiology. J Am Soc Echocardiogr 18:1440-1463,00513. de Simone G, Devereux RB, Daniels SR, Koren MJ,eyer RA, Laragh JH: Effect of growth on variability of left
entricular mass: Assessment of allometric signals in adultsnd children and their capacity to predict cardiovascularisk. J Am Coll Cardiol 25:1056-1062, 1995
14. Svarstad E, Iversen BM, Bostad L: Bedside stereomi-roscopy of renal biopsies may lead to a rapid diagnosis ofabry’s disease. Nephrol Dial Transplant 19:3202-3203,00415. Elleder M: Sequelae of storage in Fabry disease—
athology and comparison with other lysosomal storageiseases. Acta Paediatr Suppl 92:S46-S53; discussion, S45,00316. Tahir H, Jackson LL, Warnock DG: Antiproteinuric
herapy and Fabry nephropathy: Sustained reduction ofroteinuria in patients receiving enzyme replacement therapyith agalsidase-beta. J Am Soc Nephrol 18:2426-2428,00717. Pierrat A, Gravier E, Saunders C, et al: Predicting
FR in children and adults: A comparison of the Cockcroft-ault, Schwartz, and Modification of Diet in Renal Disease
ormulas. Kidney Int 64:1425-1436, 200318. Grubb A, Nyman U, Bjork J, et al: Simple cystatin
-based prediction equations for glomerular filtration rateompared with the Modification of Diet in Renal Disease
rediction equation for adults and the Schwartz and the 1ounahan-Barratt prediction equations for children. Clinhem 51:1420-1431, 200519. Elleder M, Poupetova H, Kozich V: [Fetal pathology
n Fabry’s disease and mucopolysaccharidosis type I]. Ceskatol 34:7-12, 199820. Raas-Rothschild A, Friedlaender MM, Pizov G, Back-
nroth R: The kidney in Fabry disease. J Pediatr 146:148,00521. Ramaswami U, Whybra C, Parini R, et al: Clinicalanifestations of Fabry disease in children: Data from theabry Outcome Survey. Acta Paediatr 95:86-92, 200622. Ries M, Gupta S, Moore DF, et al: Pediatric Fabry
isease. Pediatrics 115:e344-e355, 200523. Shahinfar S, Dickson T, Zhang Z, Keane WF, Brenner
M: Baseline predictors of end-stage renal disease risk inatients with type 2 diabetes and nephropathy: New lessonsrom the RENAAL Study. Kidney Int Suppl S48-S51, 2005
24. Banikazemi M, Bultas J, Waldek S, et al: Agalsidase-eta therapy for advanced Fabry disease: A randomized trial.nn Intern Med 146:77-86, 200725. Hughes DA, Elliott PM, Shah J, et al: Effects of
nzyme replacement therapy on the cardiomyopathy ofnderson-Fabry disease: A randomized, double-blind, pla-
ebo-controlled clinical trial of agalsidase-alfa. Heart 94:153-58, 200826. Linhart A, Kampmann C, Zamorano JL, et al: Cardiacanifestations of Anderson-Fabry disease: Results from the
nternational Fabry Outcome Survey. Eur Heart J 28:1228-
235, 2007
Related Documents











