Med, & bioL Engng, Vol. 6, pp. 53-69. Pergamon Press, 1968. Printed in Great Britain RENAL ARTERIAL COMPLIANCE AND CONDUCTANCE MEASUREMENT USING ON-LINE SELF-ADAPTIVE ANALOG COMPUTATION OF MODEL PARAMETERS* CARL F. ROTHE'I" and FRANKLIN D. NASH Department of Physiology, Indiana University School of Medicine, Indianapolis, Indiana 46207 Abstract--Dynamic renal arterial flow pattern, arterial compliance, and pre-glomerular conductance were predicted from the measured canine renal arterial pressure pulse pattern using on-line analog computer simulation of renal arterial parameters. The flow was accurately predicted not only under steady-state conditions but also in the presence of marked fluctuations in arterial pressure pattern, mean level, and heart rate. The model has five parameters: large- artery resistance, inertance, and compliance; a pre-glomerular arteriolar conductance; and a non-pulsatile glomerular pressure. The first two were set manually while the last three were automatically adjusted by the method of steepest descents to minimize the absolute error expressed as the instantaneous difference between the measured flow in the artery and the flow predicted by the computer. 1. INTRODUCTION FEW MEASURESof renal arterial compliance have been available under normal conditions or in response to autonomic nervous system trans-- mitters (SPENCER and DENISON, 1963). It has not been possible to measure dynamic changes in the volume of a vascular bed as complex as that of the branching arterial tree with termina- tions in thousands of capillaries. Because of the importance of changes in vascular wall charac- teristics in certain disease states, e.g. athero- sclerosis, a technique for the measurement of compliance of small vessel beds might provide valuable knowledge about the pathophysiology of these conditions. The method described used on-line analog computation to provide an estimate of renal pre-giomerular conductance, large-artery resist- ance, arterial compliance, effective inertance of the blood accelerated in the large arteries, and the glomerular pressure. The system auto- matically followed, in real-time, changes of pre-glomerular arteriolar conductance, arterial compliance, and glomerular pressure resulting from changes in the state of the living organism. The pulsatile flow pattern was predicted by driving the analog computer model with the scaled pattern of the arterial pressure pulse. The difference between the predicted flow and the flow measured at the same site as the pressure provided an error signal which, using the method of steepest descents, minimized the absolute error by automatically optimizing the para- meters. Early application to biological systems of techniques for automatic determination of parameter values were made by CLYMER (1959) and DONALDSON (1960). Other studies of vascular characteristics (ATT]NGER et al., 1966; McDONALD, 1964; and O'RouRgE and TAYLOR, I966) have provided estimates of the magnitude of vascular impedance and phase angle at the harmonics of the heart rate by use of Fourier analysis of the pressure and flow patterns. Even these have not included * First received 1 February, 1967 andin revised form 2 May, 1967. These studies were supported in part by United States Public Health Service Grants HE 07723, HE 08055, and H 6308. A preliminary report was presented at the FASEB meetings, Chicago, 19 April 1967. t This work was done during the tenure of an Established Investigatorship of the American Heart Association. 53

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Med, & bioL Engng, Vol. 6, pp. 53-69. Pergamon Press, 1968. Printed in Great Britain
RENAL ARTERIAL COMPLIANCE AND CONDUCTANCE MEASUREMENT USING ON-LINE SELF-ADAPTIVE ANALOG
COMPUTATION OF MODEL PARAMETERS*
CARL F. ROTHE'I" and FRANKLIN D. NASH
Department of Physiology, Indiana University School of Medicine, Indianapolis, Indiana 46207
Abstract--Dynamic renal arterial flow pattern, arterial compliance, and pre-glomerular conductance were predicted from the measured canine renal arterial pressure pulse pattern using on-line analog computer simulation of renal arterial parameters. The flow was accurately predicted not only under steady-state conditions but also in the presence of marked fluctuations in arterial pressure pattern, mean level, and heart rate. The model has five parameters: large- artery resistance, inertance, and compliance; a pre-glomerular arteriolar conductance; and a non-pulsatile glomerular pressure. The first two were set manually while the last three were automatically adjusted by the method of steepest descents to minimize the absolute error expressed as the instantaneous difference between the measured flow in the artery and the flow predicted by the computer.
1. INTRODUCTION
FEW MEASURES of renal arterial compliance have been available under normal conditions or in response to autonomic nervous system trans-- mitters (SPENCER and DENISON, 1963). I t has not been possible to measure dynamic changes in the volume of a vascular bed as complex as that of the branching arterial tree with termina- tions in thousands of capillaries. Because of the importance of changes in vascular wall charac- teristics in certain disease states, e.g. athero- sclerosis, a technique for the measurement of compliance of small vessel beds might provide valuable knowledge about the pathophysiology of these conditions.
The method described used on-line analog computation to provide an estimate of renal pre-giomerular conductance, large-artery resist- ance, arterial compliance, effective inertance of the blood accelerated in the large arteries, and the glomerular pressure. The system auto- matically followed, in real-time, changes of
pre-glomerular arteriolar conductance, arterial compliance, and glomerular pressure resulting f rom changes in the state of the living organism. The pulsatile flow pattern was predicted by driving the analog computer model with the scaled pattern of the arterial pressure pulse. The difference between the predicted flow and the flow measured at the same site as the pressure provided an error signal which, using the method of steepest descents, minimized the absolute error by automatically optimizing the para- meters. Early application to biological systems of techniques for automatic determination of parameter values were made by CLYMER (1959) and DONALDSON (1960).
Other studies of vascular characteristics (ATT]NGER et al., 1966; McDONALD, 1964; and O'RouRgE and TAYLOR, I966) have provided estimates of the magnitude of vascular impedance and phase angle at the harmonics of the heart rate by use of Fourier analysis of the pressure and flow patterns. Even these have not included
* First received 1 February, 1967 andin revised form 2 May, 1967. These studies were supported in part by United States Public Health Service Grants HE 07723, HE 08055, and H 6308. A preliminary report was presented at the FASEB meetings, Chicago, 19 April 1967. t This work was done during the tenure of an Established Investigatorship of the American Heart Association.
53
54 CARL F. ROTHE and FRANKLIN D. NASH
the renal artery, probably because of its short- ness, difficulty of surgical approach, and the problem of obtaining simultaneous dynamic pressure and flow estimates. Furthermore, impedance and phase angle have less direct biological significance than compliance, con- ductance, and inertance. Since the same data, instantaneous flow and pressure at the renal artery, are used by both the method described here and those using Fourier analysis, it should be possible, using assumptions similar to ours, to estimate compliance from impedance data. The studies of ATTINGER et al. (1966) provide estimates of vascular compliance for larger vessels but are based on assumed values of wall elasticity or differential pressure measurements along the arterial segment. Direct measurement of the dynamic downstream pressure at the arterioles or capillaries is not readily available.
This model and parameter-optimizing tech- nique were developed, in part, as a tool in the search for an explanation for the increases in mean renal blood flow and flow pulse amplitude which occur during ureteral pressure elevation (NASH and SELKURT, 1964; SELKURT, 1963; and THURAU and HENNE, 1964). These studies will be described in a separate paper.
2. RENAL VASCULAR MODEL
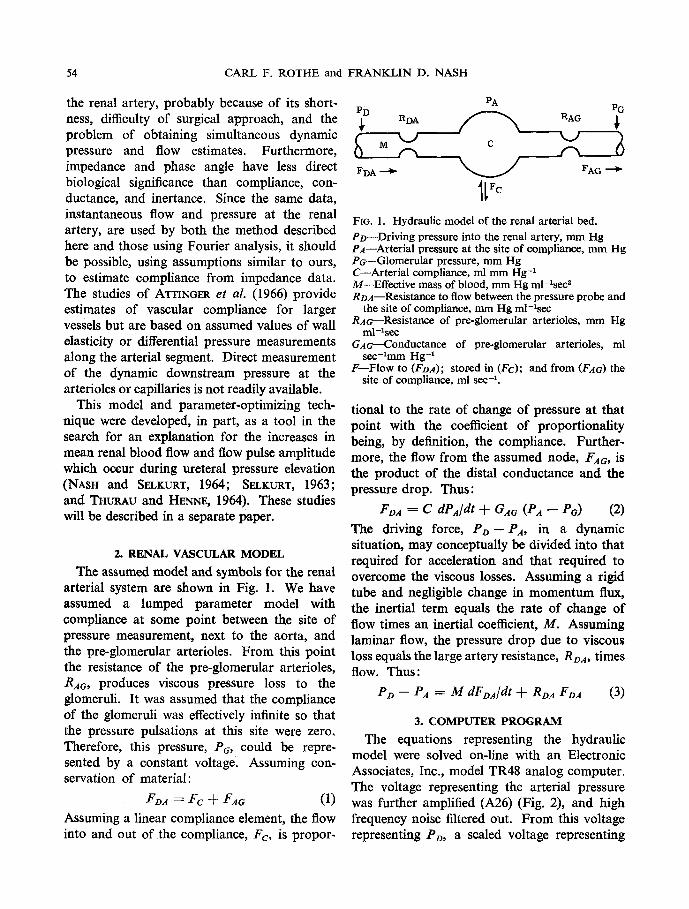
The assumed model and symbols for the renal arterial system are shown in Fig. 1. We have assumed a lumped parameter model with compliance at some point between the site of pressure measurement, next to the aorta, and the pre-glomerular arterioles. From this point the resistance of the pre-glomerular arterioles, RAG, produces viscous pressure loss to the giomeruli. It was assumed that the compliance of the glomeruli was effectively infinite so that the pressure pulsations at this site were zero. Therefore, this pressure, Pc, could be repre- sented by a constant voltage. Assuming con- servation of material:
FDA = F C + Fa6 (1)
Assuming a linear compliance element, the flow into and out of the compliance, F o is propor-
PA PD PG
RDA ~ RAG ;
'L I
FD A ~ ~ FAG --~
FIo. 1. Hydraulic model of the renal arterial bed. PD--Driving pressure into the renal artery, mm Hg PA--Arterial pressure at the site of compliance, mm Hg Pr---Glomerular pressure, mm Hg C--Arterial compliance, ml mm Hg -1 M--Effective mass of blood, mm Hg ml-lsec ~ RDA--Resistance to flow between the pressure probe and
the site of compliance, mm Hg ml-Xsec RAo--Resistance of pre-glomerular arterioles, mm Hg
m l - - l spJ~
G.46---Conductance of pre-glomerular arterioles, ml sec-lmm Hg -1
F--Flow to (FD,4); stored in (Fc); and from (FAo) the site of compliance, ml sec-L
tional to the rate of change of pressure at that point with the coefficient of proportionality being, by definition, the compliance. Further- more, the flow from the assumed node, Far , is the product of the distal conductance and the pressure drop. Thus:
FD. 1 = C dPa/d t + GA~ (Pa ~ Po) (2)
The driving force, P o - Pa, in a dynamic situation, may conceptually be divided into that required for acceleration and that required to overcome the viscous losses. Assuming a rigid tube and negligible change in momentum flux, the inertial term equals the rate of change of flow times an inertial coefficient, M. Assuming laminar flow, the pressure drop due to viscous loss equals the large artery resistance, RDa, times flow. Thus:
PD -- PA = M dFDA/dt + RDa FDa (3)
3. COMPUTER PROGRAM
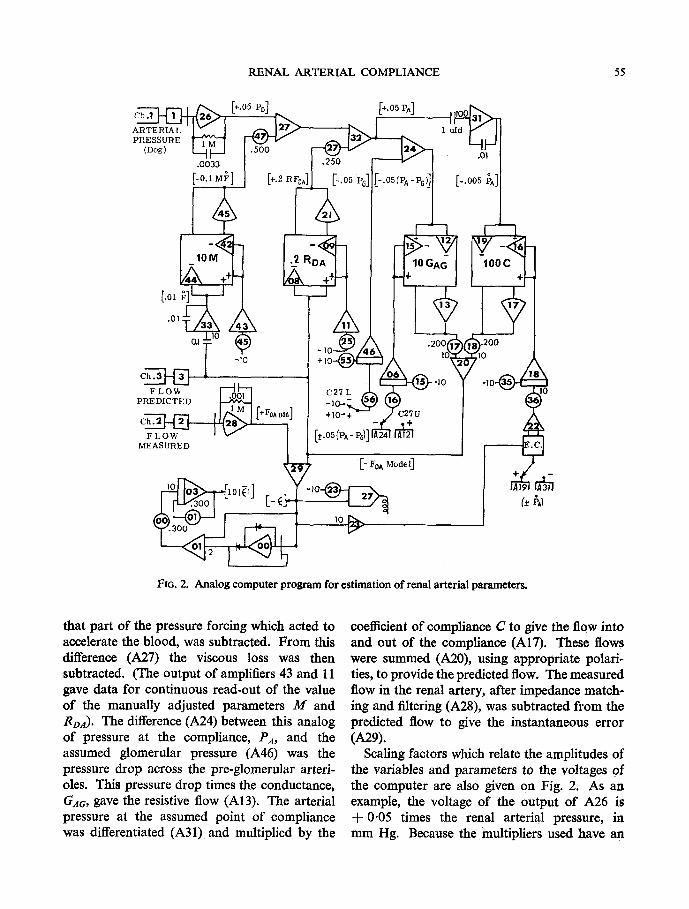
The equations representing the hydraulic model were solved on-line with an Electronic Associates, Inc., model TR48 analog computer. The voltage representing the arterial pressure was further amplified (A26) (Fig. 2), and high frequency noise filtered out. From this voltage representing PD, a scaled voltage representing
Ch .1
ARTERIAL PRESSURE
(Dog)
+.05 PD]
RENAL ARTERIAL COMPLIANCE
[+.OS PA]
~ ~ ] .5oo .oo33
[-0.1M1 ~ ] [+.2 .250 I _ P o ]
1 ufd
.01
[-.005 ~]
55
[oi ~]~I-- .01
-I0 Ch .3
A uREOW " ]
L-E~
- , o - ~ "W +10-+ / C27U
(_* hal
FIG. 2. Analog computer program for estimation of renal arterial parameters.
that part of the pressure forcing which acted to accelerate the blood, was subtracted. From this difference (A27) the viscous loss was then subtracted. (The output of amplifiers 43 and l l gave data for continuous read-out of the value of the manually adjusted parameters M and gDA). The difference (A24) between this analog of pressure at the compliance, PA, and the assumed glomerular pressure (A46) was the pressure drop across the pre-glomerular arteri- oles. This pressure drop times the conductance, GAa, gave the resistive flow (A13). The arterial pressure at the assumed point of compliance was differentiated (A31) and multiplied by the
coefficient of compliance C to give the flow into and out of the compliance (A17). These flows were summed (A20), using appropriate polari- ties, to provide the predicted flow. The measured flow in the renal artery, after impedance match- ing and filtering (A28), was subtracted from the predicted flow to give the instantaneous error (A29).
Scaling factors which relate the amplitudes of the variables and parameters to the voltages of the computer are also given on Fig. 2. As an example, the voltage of the output of A26 is + 0.05 times the renal arterial pressure, in mm Hg. Because the multipliers used have an
56 CARL F. ROTHE and FRANKLIN D. NASH
inherent attenuation of one-tenth, the voltages of amphfiers 43, 11, 06 and 18 represent the coefficients or vascular parameters which are scaled as indicated with each multiplier. As an example, the output of integrator 18 is 1000 C and after attenuation in the multiplier is 100 C. Amplifiers 00, 01, and 03 were used to provide an estimate of the average of 10 times the absolute error using a 3.3 sec time constant.
The automatic adjustment of parameters used the method of steepest descents. Fn~Ex (1961), LEVlNn (1964), KORN and KORN (1964), and Electronic Associates (1964), among others, have provided a review of the mathematical bases of this optimizing technique which can follow, on-hne, changes in system parameters by automatic, self-adaptive adjustments in model parameters. It is based on the fact that an error will result if the coefficients of the mathematical model are not of the correct values. This error is the instantaneous difference between the measured response of the bio- physical system and the predicted or computed response.
The method can be described most simply in the case of conductance. If, for example, the predicted flow was greater than the actual flow, the error was positive. This caused the relay of comparator 27 to be at the positive terminal, and so the output of amplifier 12 (a positive value representing the pressure drop across the segment ( P a - Pc)) was applied to potentio- meter 16 and thence to integrator 06 causing its output, the analog of the pre-glomerutar con- ductance, to decrease in value, and thus led to a smaller predicted flow. The process continued until the average error approached zero. If the predicted flow had been less than the measured flow, the calculated conductance would increase. The rate of convergence to the optimal value was determined by the potentiometer setting (P16).
If the mathematical model is not adequate, the error can be minimized but not eliminated by this technique. Furthermore, with some models, e.g. those with polynomial terms, more than one root may exist, and so judicious choices of parameter values must be made
initially to obtain the correct roots. In the simulation of a biological system one hopes to find the unique set of parameter values repre- senting the system, but one must realize that simulation, by its nature, can lead to different sets of parameters, each set giving a relatively good fit, but not being the true set. Only with near-zero error under a wide variety of input forcings can one attain a reasonable degree of confidence that the proper set is being obtained.
The large artery resistance and inertanee terms, R~a and M, were manually adjusted to minimize the amplitude of the peak-to-peak error which was viewed on an oscilloscope with the pressure signal used to drive the horizontal axis. In later experiments a dual-beam oscillo- scope was used to provide simultaneous displays of the predicted and actual flows. Adjustments of parameters were made to produce super- imposition of these traces.
In response to a step change in parameters of a simulated model set up on another computer, the pre-glomerular arteriolar conductance had a response time of less than 1 see and that of the arterial compliance about 3 see. The responses were linear with time rather than exponential.
4. DATA ACQUISITION
Mongrel dogs, 23.4 4- 2.8 SD kg in weight, were used. They were anesthetized with sodium pentobarbital (about 30 mg/kg); shivering was suppressed with about 2 mg/hr of chlorpro- mazine, intravenously. In most of the experi- ments the dogs were suspended upright with their limbs dependent, and the left renal artery was approached through an extraperitoneal flank incision. By suspending a dog in this manner, the weight of the kidney slightly stretched the artery, providing sufficient length for placement of transducers near the origin of a renal artery without necessitating mechanical traction. In some cases the artery branched within 1 cm of the aorta; in these cases, the right renal artery was used.
A Carolina Medical Electronics Model 321 electromagnetic flowmeter was used with cuff- type probes (Model EMP400, Electromagnetic
RENAL ARTERIAL COMPLIANCE 57
Probe Co.). Usually a 10 mm (internal circum- ference) probe was used, although in some cases an 8 or 12 mm probe fitted better. Static cali- bration was made by cannulating the artery distal to the probe at the end of the experiment and making timed collections of blood. The frequency response was uniform to about 10 I-Iz and was down 16 per cent at 35 Hz. These values were provided by the manufacturer and were verified by using a multiplier of the analog computer to modulate the voltage obtained by applying the magnet current across a 2 ohm resistor and then attenuating the modulated signal through a I00,000 to 1 attenuator to provide a signal to the flowmeter input. A lag of approximately 7 msec was present at all frequencies. This produced an equivalent phase lag of 25 ~ at 10 Hz and 84 ~ at 35 Hz. An RC circuit with a 3.3 msec time constant, placed in the arterial pressure measuring system, provided s o m e compensation for this phase shift, but the delay undoubtedly modified the results of these experiments, especially the value for inertance.
Pressure was measured within I cm of the flow probe using a Statham P23Db transducer coupled with 3 cm of thick-wail vinyl tubing (0.58 mm i.d. and 2.2ram o.d.) to a special 20 ga. or 23 ga. thin-wall needle shaped like a question mark. The needle had a taper point and two lateral holes of approximately the same diameter as the lumen 3 mm from the tip (Beeton- Dickinson Sketch SH1086). Since clotting of blood in the needle occurred within about 5 min even when high concentrations of heparin were used, a 30 ga. needle 1 cm long (0.15 mm i.d.) was soldered into a hole in the side of the 20 ga. transducer-to-probe adapter needle, and a constant 250 mm Hg pressure was applied to a bottle of sterile 0.9 per cent sodium chloride which was filtered through a �89 diameter 0.2 micron filter (Type GM-8, Gelman Instru- ment Co., (Ann Arbor, Michigan)) in a Swinny- type adapter. The resulting flow of 1 ml/min produced an indicated pressure of 2 mm Hg when using the 20 ga. needle and 10 mm Hg when using the 23 ga. needle. Because the net perfusion pressure was about half of the
reservoir pressure when the needle was intro- duced into the artery, the zero of the transducer was set 1 or 5 mm Hg below zero, respectively, when the transducer was positioned for record- ing, saline running, and the needle not yet placed in the artery. The frequency response of the system was checked by using a signal generator (Model 105, Wavetek (San Diego, California)) driving a d.c. amplifier (Hewlett- Packard Model 6823A) which energized a loud- speaker coil coupled through a thin-wall (0.0012 in.), 0.312 in. o.d. electro-formed nickel bellows (Servometer Corp., Clifton, New Jersey.) The pressure generator was monitored using a P23Db pressure transducer mounted so that its diaphragm was flush with the wall of the pressure chamber; the needle of the pressure transducer system was introduced into the pressure chamber through a 3 mm diameter rubber serum cap. With the 20 ga. needle, the response was uniform to 15 Hz with a resonant peak of about 165 per cent of the 10 Hz response at about 40 Hz; with the 23 ga. needle, the response was uniform to I0 Hz with a 130 per cent resonant peak at about 35 Hz. The pressure signal system was checked at the beginning of each experiment by occluding the needle side holes with two fingers and then rapidly releasing the fingers. At high paper speeds, small oscillations at the resonant frequency were seen, and the transducer was flushed until the resonant frequency was above 30 Hz. Analog signals were recorded with a Beckman 6-channel Type S recorder. Multi- plexing was used on one channel for additional recording of parameter and mean variable values.
The pressure needle was introduced into the artery about 1 cm below the flow probe with the tip pointing upstream to position the side holes as close to the probe as possible. The pressure in the aorta was not used because of the likeli- hood of pressure distortion produced by the arterial branch and the mass of blood between aortic catheter tip and flow probe. A No. 1 silk snare was placed between the flow probe and the pressure transducer needle for occlusion and
58
RENAL ARTERIAL PRESSURE (ram Hg)
MEASURED FLOW
( m l / s e c )
PREDICTED FLOW
(ml/sec)
CARL F. ROTHE and FRANKLIN D. NASH
18o]- 120T\ E
6
4
2
0
8
ERROR :t (ml/sec) 2
0
! 1 sec. I
mm Hg. sec
ml mm Hg )
NORE PINE PHRINE ACE TYLCHOLINE (25 jugm I .V. ) C O N T R O L (100 ~ugm I .V . )
�9 056
�9
�9 064
.0021 CA
M (mmHg'sec2) ml 0.0 0.0 0.0
[mm Hg. see) RDA k ml 0.0 0.0 0.0
PG (mm Hg ) 42. 41. 36.
PART ( mm Hg ) 92. 94. 58.
( ml/sec ) 2.8 3.4 2.2
ERRORI ( m l / s e c ) �9 12 �9 10
. 1 0 0
.0031
. 10
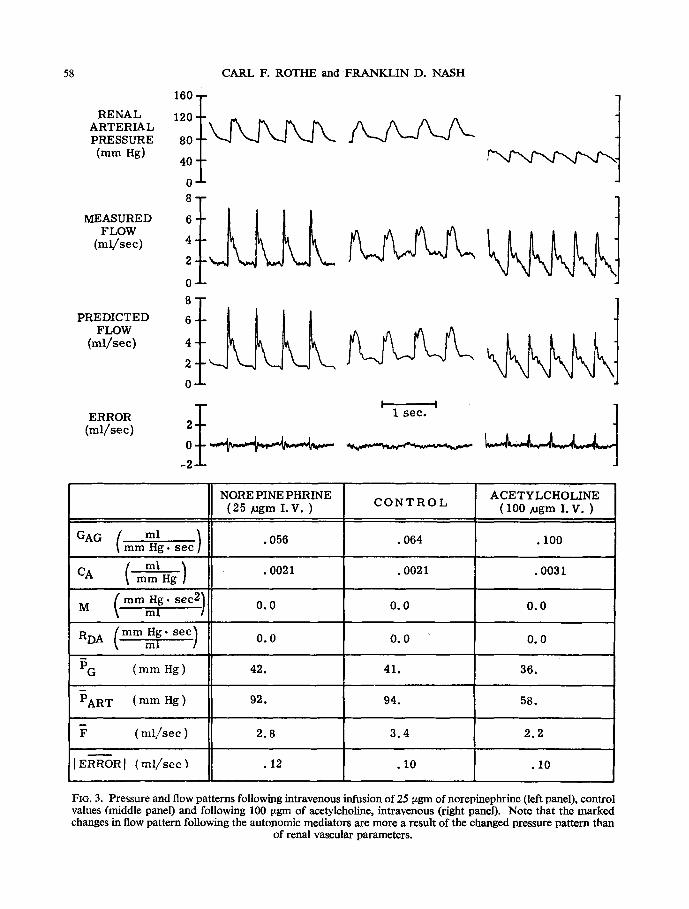
FIG. 3. Pressure and flow patterns following intravenous infusion of 25 tzgm of norepinephrine (left panel), control values (middle panel) and following 100 ~gm of acetylcholine, intravenous (right panel). Note that the marked changes in flow pattern following the autonomic mediators are more a result of the changed pressure pattern than
of renal vascular parameters.
RENAL ARTERIAL COMPLIANCE 59
checking flow zero. In most experiments the flow probe was placed on the renal artery in such a way that it was not immersed in saline; nevertheless, the ,maximum zero drift of the system throughout each experiment was less than 0.5 ml per sec and was usually less than 5 per cent of the average flow.
Acetylcholine chloride (MERCK) was dissolved in 0.85 per cent sodium chloride at a concentra- tion of 100 tzg/ml. Norepinephrine (Levophed bitartrate, Winthrop) was diluted to 50 ~tg/ml in 5 per cent dextrose in saline. Injections of 0.1 ml were made into the saline-flush line of the pressure transducer tap. The high resistance of the 30 ga. needle, with respect to the low com- pliance of the pressure transducer, led to no detectable changes in pressure pattern due to the injection procedure per se. The retrograde movement of the drug into the flush line on injection recluired about 1 min to clear.
5. EXPERIMENTAL RESULTS
An estimate of the quality of match between predicted and measured flow may be seen from
iso T ~ I RENAL 120 T ARTERIAL
PRESSURE 80 ~ (ram Hg) 40
0
FLOW 4 (hal/see)
(rnl/see)
ERROR 2~ (ml/sec) 0 ~ : - _ - :-= ~,-'---.': ::~-J
-2 A.
.06 t
-o;2 I ' I I I , , I I I 0 1 2 3 4 5 6
TIME IN SECONDS
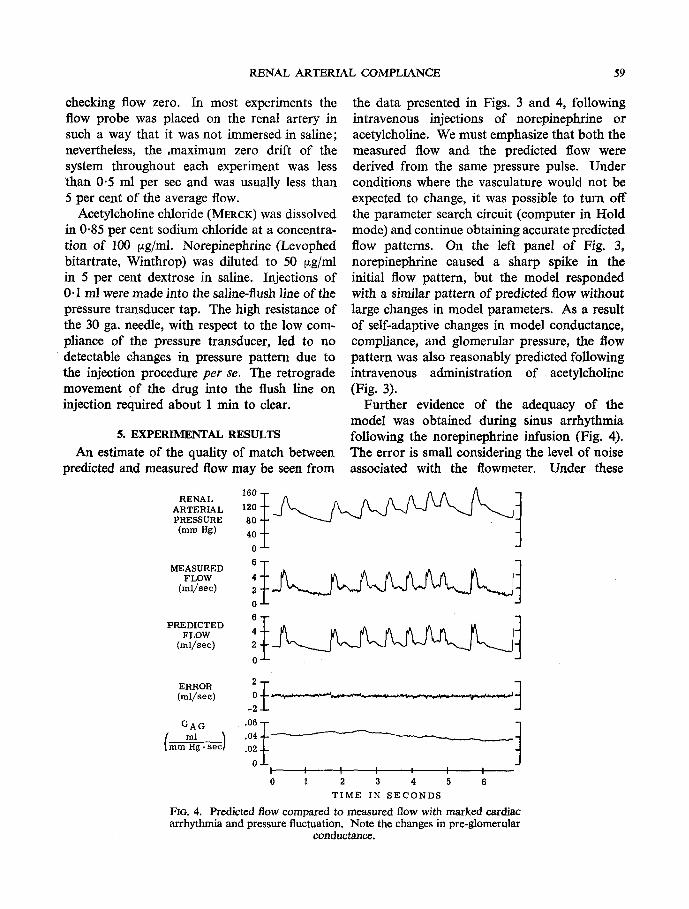
Fro. 4. Predicted flow compared to measured flow with marked cardiac arrhythmia and pressure fluctuation. Note the changes in pre-glomerular
conductance.
the data presented in Figs. 3 and 4, following intravenous injections of norepinephrine or acetylcholine. We must emphasize that both the measured flow and the predicted flow were derived from the same pressure pulse. Under conditions where the vasculature would not be expected to change, it was possible to turn off the parameter search circuit (computer in Hold mode) and continue obtaining accurate predicted flow patterns. On the left panel of Fig. 3, norepinephrine caused a sharp spike in the initial flow pattern, but the model responded with a similar pattern of predicted flow without large changes in model parameters. As a result of self-adaptive changes in model conductance, compliance, and glomerular pressure, the flow pattern was also reasonably predicted following intravenous administration of acetylcholine (Fig. 3).
Further evidence of the adequacy of the model was obtained during sinus arrhythmia following the norepinephrine infusion (Fig. 4). The error is small considering the level of noise associated with the flowmeter. Under these
60 CARL F. ROTHE and FRANKLIN D. NASH
conditions, pre-glomerular arteriolar conduct- ance, G,~c, decreased during the increase in heart rate and blood pressure suggesting effec- tive, rapid renal autoregulation.
The following control values were obtained from 38 observations in the last 10 experiments. Indices of dispersion are the standard deviations about the means. The mean flow was 4.2 4- 1.0 ml/sec with the maximum instantneous flow averaging 6.4 ml/sec and the minimum 3.1 ml/sec. The average absolute error between the measured and predicted flow was 0.11 4-0.03 ml/sec while the peak-to-peak error was 1-0 -4- 0.3 ml/sec. Of this error, random noise from the flowmeter, with the artery occluded, averaged 0.07 ml/sec and did not exceed 0.5 ml/sec peak to peak.
The renal arterial pressure was 104 4- 15 mm Hg and the indicated glomerular pressure was 42 4- 10 mm Hg. This estimate of glomerular pressure is unphysiologically low. Because manual changes of this parameter had little effect on the magnitude of the error, it is doubt- ful whether this technique gives a reasonable estimate of glomerular pressure, especially under changing physiological conditions.
"Ihe compliance of the renal artery was 0.0028 :k 0.0011 ml/mm Hg. This suggests that 0.29 ml of blood was stored at the mean pressure of 104 mm Hg in addition to the volume present in the undistended arteries. The total blood volume of the dog kidney has been estimated at 0.081 ml/gm tissue (ALTMAN et al., 1959, p. 70). The left kidney weight of 18 dogs weighing 23.5 to 24.5 kg averaged 59 gm in comparable experiments. Thus, about 4.8 ml of blood was present. Assuming that 30 per cent of this volume was pre-glomerular, then the 0-29 ml increase due to distension suggests that the normal arterial pressure increased the volume of these intermediate-sized arteries by about one fifth.
The pre-glomerular arteriolar conductance, GAa, was 0.070-4-0.016 ml/mm Hg.sec. The total resistance between the pressure probe and the glomeruli was 15.5 4-4"4 mm Hg-sec/ml (20.6 • 103 4- 5.9 • 108 dyne-sec/cm'). To
provide an acceptable prediction of flow, only 0.28 4-0.60 mm Hg-sec/ml of large-artery resistance was needed. Although it would be impossible for this resistance to be zero, our data suggest that it is insignificant.
The inertial term, as suggested by SPENCER' and DENmON (1963), is also insignificant, averaging only 0"010 4-0-011 mm Hg-sec*/ml. Assuming a lumped mass and plug-flow in a non-tapering 2 mm i.d. artery, this is equivalent to a mass of only 0.013 gm.
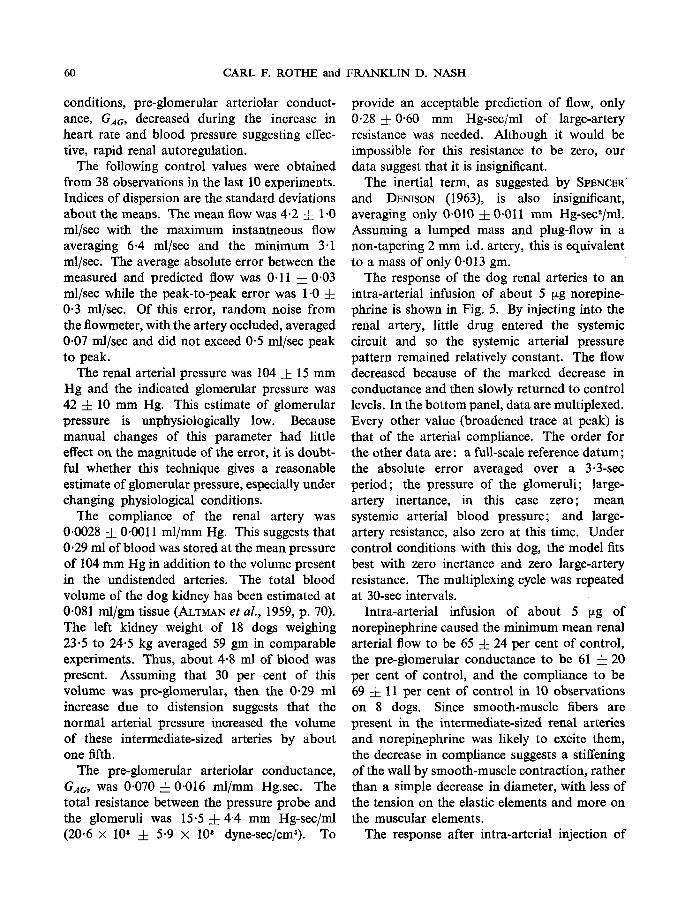
"[he response of the dog renal arteries to an intra-arterial infusion of about 5 ~tg norepine- phrine is shown in Fig. 5. By injecting into the renal artery, little drug entered the systemic circuit and so the systemic arterial pressure pattern remained relatively constant. The flow decreased because of the marked decrease in conductance and then slowly returned to control levels. In the bottom panel, data are multiplexed. Every other value (broadened trace at peak) is that of the arterial compliance. The order for the other data are: a full-scale reference datum; the absolute error averaged over a 3.3-sec period; the pressure of the glomeruli; large- artery inertance, in this case zero; mean systemic arterial blood pressure; and large- artery resistance, also zero at this time. Under control conditions with this dog, the model fits best with zero inertance and zero large-artery resistance. The multiplexing cycle was repeated at 30-sec intervals.
Intra-arterial infusion of about 5 ~g of norepinephrine caused the minimum mean renal arterial flow to be 65 -4- 24 per cent of control, the pre-glomerular conductance to be 61 -4-20 per cent of control, and the compliance to be 69 4- 11 per cent of control in 10 observations on 8 dogs. Since smooth-muscle fibers are present in the intermediate-sized renal arteries and norepinephrine was likely to excite them, the decrease in compliance suggests a stiffening of the wall by smooth-muscle contraction, rather than a simple decrease in diameter, with less of the tension on the elastic elements and more on the muscular elements.
The response after intra-arterial injection of
RENAL ARTERIAL COMPLIANCE 61
RENAL ARTERIAL PRESSURE (ram Hg)
MEASURED FLOW
(ml/sec)
PREDICTED FLOW
(mI/sec)
ERROR (ml/sec)
GAG
C ml
160
120
80
40
0 8
6
4
2 0
6
4
2
0
2
0 -2
-4
.08
.06
.04
.02
0 O01 .004 .003
.001 0
M -RE FERENCE PART ' -- RDA
. . . . . . . . . . . , N F ? 1 . . . . . . . . . . . .
1 Minute
FIG. 5. Renal arterial parameter changes following intra-arterial norepine- phrine. Full scale values for the multiplexed data, line 6, are: Reference, 10 V; C, 0.005 ml mm Hg-1; Error (average), 1.0 ml see-*; P6, 200 mm Hg; M, 0'1 mm Hg m1-1 sect; PART, 200 mm Hg; and RDA, 5 mm Hg m1-1 sec.
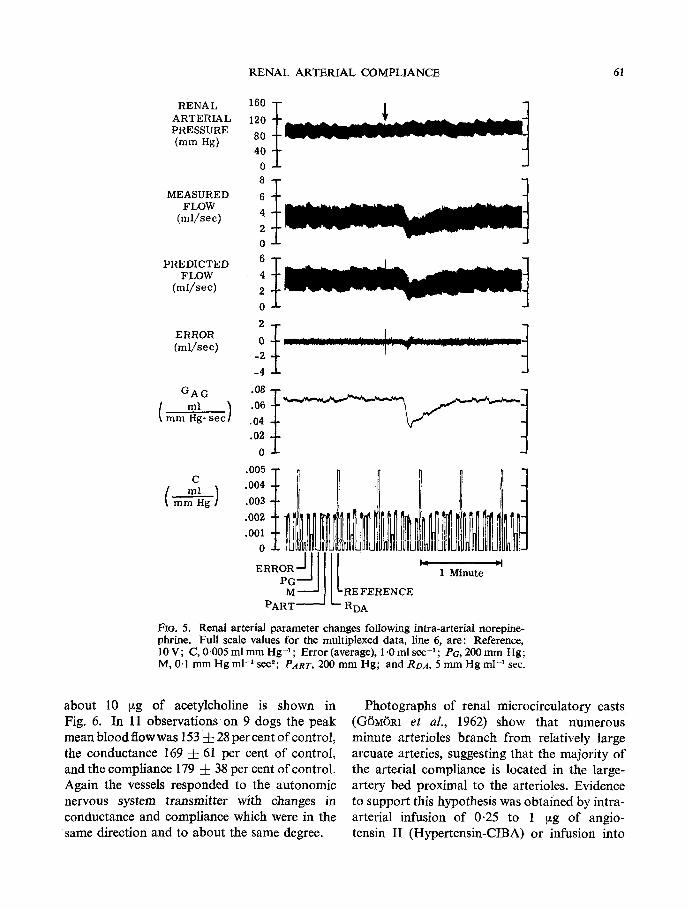
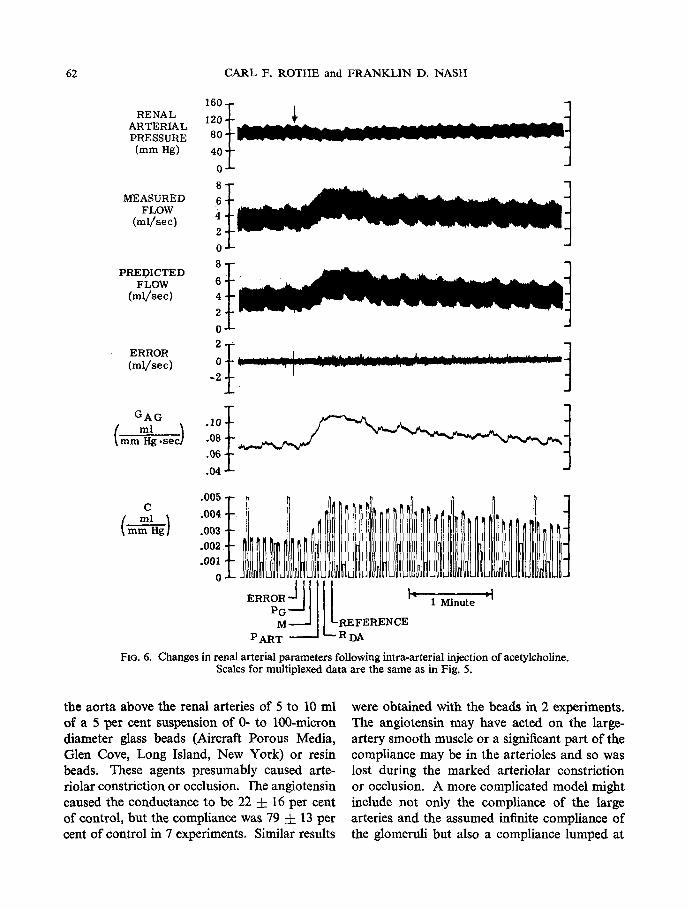
about 10 ~g of acetylcholine is shown in Fig. 6. In 11 observations on 9 dogs the peak mean blood flowwas 153-4- 28 percent of control, the conductance 169 • 61 per cent of control, and the compliance 179 • 38 per cent of control. Again the vessels responded to the autonomic nervous system transmitter with changes in conductance and compliance which were in the same direction and to about the same degree.
Photographs of renal microcirculatory casts (G6M6RI et aL, 1962) show that numerous minute arterioles branch from relatively large arcuate arteries, suggesting that the majority of the arterial compliance is located in the large- artery bed proximal to the arterioles. Evidence to support this hypothesis was obtained by intra- arterial infusion of 0.25 to 1 ~g of angio- tensin II (Hypertensin-CIBA) or infusion into
62 CARL F. ROTHE and F R A N K L I N D. NASH
RENAL ARTERIAL PRESSURE (ram Hg)
MEASURED FLOW
(ml /sec)
PREDICTED FLOW
(ml /sec)
ERROR (ml/sec)
GAG
160 - 1
-~ I 80
40 -
0 "
8
6 4 2 0 8
6
4 2
0
0 l ~ , , , i J t ' . [t . . . . . . . . . . . . . . . . . _ . . . . . . . . . . . . . . . . . . . . . . . .
.08
.06
. 04
001 1 C ml .004 I ~ , , I
FIG. 6. Changes in renal arterial parameters following intra-arterial injection of acetylcholine. Scales for multiplexed data are the same as in Fig. 5.
the aorta above the renal arteries of 5 to 10 ml of a 5 per cent suspension of 0- to 100-micron diameter glass beads (Aircraft Porous Media, Glen Cove, Long Island, New York) or resin beads. These agents presumably caused arte- riolar constriction or occlusion, l'he angiotensin caused the conductance to be 22 :k 16 per cent of control, but the compliance was 79 ~: 13 per cent of control in 7 experiments. Similar results
were obtained with the beads in 2 experiments. The angiotensin may have acted on the large- artery smooth muscle or a significant part of the compliance may be in the arterioles and so was lost during the marked arteriolar constriction or occlusion. A more complicated model might include not only the compliance of the large arteries and the assumed infinite compliance of the glomeruli but also a compliance lumped at
RENAL ARTERIAL COMPLIANCE 63
about the middle of the arterioles. Whether such a model would provide a better fit than one using a non-linear compliance based on static data from large arteries is open to question.
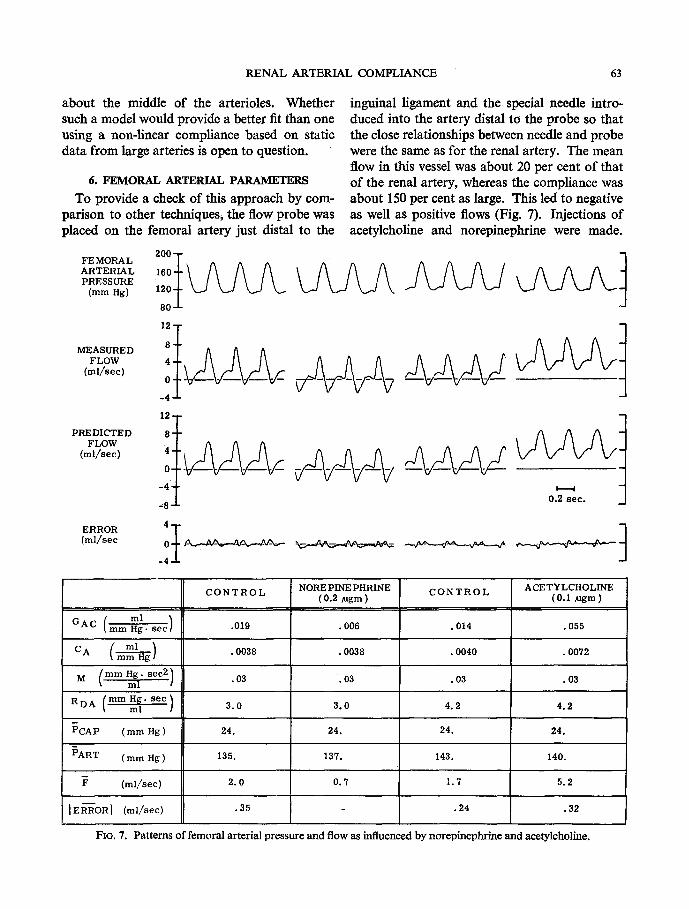
6. FEMORAL ARTERIAL PARAMETERS
To provide a check of this approach by com- parison to other techniques, the flow probe was placed on the femoral artery just distal to the
FEMORAL 2 ~ 1 7 6 ,oot- \ s s 1 6 3 PRESSURE(ram Hg) 120 t k_J k.~ ~ k.~
80-J-
MEASURED FLOW
(ml/sec)
PREDICTED FLOW
(ml/sec)
inguinal ligament and the special needle intro: duced into the artery distal to the probe so that the close relationships between needle and probe were the same as for the renal artery. The mean flow in this vessel was about 20 per cent of that of the renal artery, whereas the compliance was about 150 per cent as large. This led to negative as well as positive flows (Fig. 7). Injections of acetylcholine and norepinephrine were made.
O. see-- 1 (ml/sec ~ _ _ _ ~
GAC (mm ml Hg. Se~)
C O N T R O L
PART ( mm Hg )
NOREPINEPHRINE (0.2 ~gm ) C O N T R O L ACETYLCHOLINE
(0.1 ~gm )
(ml/sec) 2.0 I. 7 5.2
I E ~'-6OR I (ml/sec) .35 - .24 .32
FIG. 7. Patterns offcmoral artcrialprcssurc and flow as influenced bynorepincphrinc and acetylcholinc.
m
0.7
.019 .006 .014 .055
ml CA ( ~ ) .0038 .0038 .0040 .0072
M ( mm Hg. sec 2) .03 .03 .03 .03 ml /
(ram Hg. s ec ) 3.0 3.0 4.2 4.2 RDA / ml
PCAP ( mm Hg ) 24. 24. 24. 24.
135. 137. 143. 140.
64 CARL F. ROTHE and FRANKLIN D. NASH
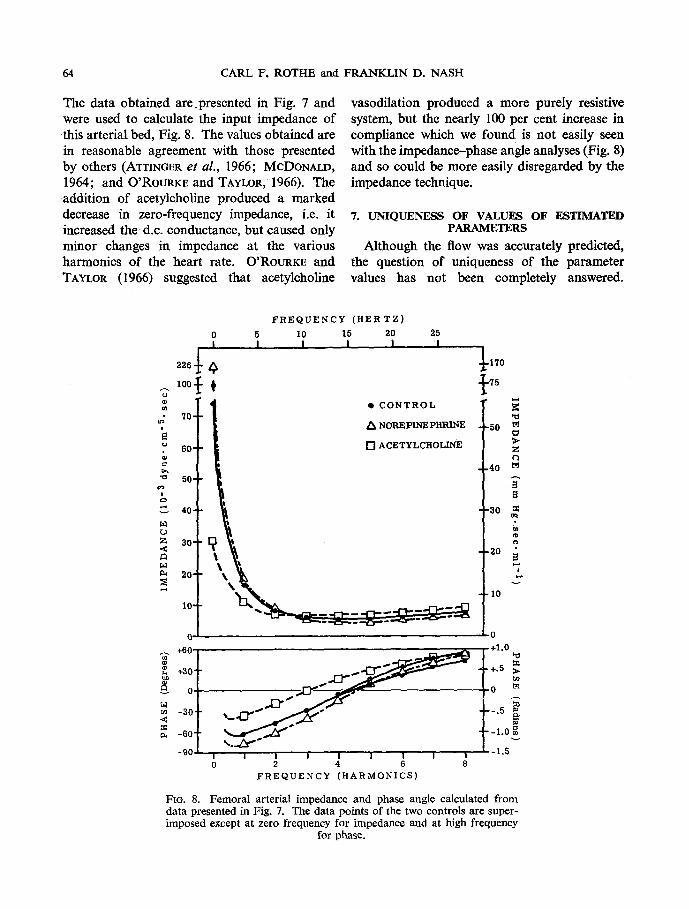
The data obtained are.presented in Fig. 7 and were used to calculate the input impedance of this arterial bed, Fig. 8. The values obtained are in reasonable agreement with those presented by others (ATTINGER et aL, 1966; MCDONALO, 1964; and O'RoURKE and TAYLOR, 1966), The addition of acetylcholine produced a marked decrease in zero-frequency impedance, i.e. it increased the d.c. conductance, but caused only minor changes in impedance at the various harmonics of the heart rate. O'RoURKE and TAYLOR (1966) suggested that acetylcholine
vasodilation produced a more purely resistive system, but the nearly 100 per cent increase in compliance which we found is not easily seen with the impedance-phase angle analyses (Fig. 8) and so could be more easily disregarded by the impedance technique.
7. UNIQUENESS OF VALUES OF ESTIMATED PARAMETERS
Although the flow was accurately predicted, the question of uniqueness of the parameter values has not been completely answered.
FREQUENCY (HERTZ) 0 5 10 15 20 25 I I, I I I I ,
2 2 6 ~ , ~L170
lOO} r {,5
I| "NORE,IN ,H."E 5o;
r, ,
- o I , j..[::~-~--~- . . . .
-901 I "I I I I . . . . . . I I I I ~-I 5~ 0 2 4 6 8
FREQUENCY (HARMONICS)
FIO, 8. Femoral arterial impedance and phase angle calculated from data presented in Fig. 7. The data points of the two controls are super- imposed except at zero frequency for impedance and at high frequency
for phase.
RENAL ARTERIAL COMPLIANCE 65
Indeed, with the simplicity of the hydraulic model a perfect match is impossible.
In terms of sensitivity of the model response to changes in parameter values, small changes in the pre-glomerular conductance caused the entire error term to be either dearly positive or negative. Small changes in the compliance term produced a widening or narrowing of an oscilloscope display of the pressure vs. predicted-flow loop. With the pre-glomerular conductance, compliance, and the glomerular pressure under automatic control, the effects of changes in the coefficient for large artery resistance were seen mostly in changes in the shape of the systolic peak flow and the early down-sweep features of the pattern associated with intermediate frequency components. There was interaction between the compliance and the large artery resistance in determining the width of the pressure-flow loop. The inertial term had the greatest effect on the rapid changes seen during the initial part of systole where the rate-of-change of flow was maximum. The effect of changes in the glomerular pressure coefficient was best seen during the diastolic run-off period of the cycle. Since the auto- optimization system changed the pre-glomerular conductance in response to changes in glomerular pressure so that the mean error approached zero, only small changes in absolute error occurred with i 10 mm Hg changes in estimated glomerular pressure.
With the relatively noisy data available, the computer would not stabilize to a solution when all 5 parameters were set for automatic control. We, therefore, set the three most sensitive parameters for automatic control and manually adjusted the inertial and large artery resistance to minimize the peak absolute error. The latter two parameters were then held constant during drug-induced changes in the biological system since it seemed reasonable to assume that they would not change appreciably in response to changes in systemic arterial pressure, drugs, or neural influences. During the experiments the values of RDA and M were periodically checked in an attempt to reduce the error still further. E
As a further check of the validity of the parameters obtained, the mean flows over 3 cycles were estimated by planimetry of the flow data using chart speeds of 50 mm/see. These data were compared to the mean flows calcu- lated by dividing the difference between the mean renal arterial pressure and the computed glomerular pressure by the sum of the com- puted large artery resistance and the pre- glomerular resistance (i.e. ( P o - P~)/(Roa + 1~GAB)). Ten observations from 7 experiments averaged 3.49 ml/sec by planimetry compared to 3.62 ml/sec by computation. The difference of + 0.129 + 0.060 ml/sec represented an average error of only 3.7 per cent of the mean and was comparable to the average absolute error.
Improvements in the estimation of the para- meters could be made in several ways:
(1) More accurate pressure and flow data Transducers to provide completely accurate
measurements are not available. To measure pressure at the same location as the flow probe requires a compromise, since the pressure probe should be as large in diameter as possible for complete dynamic fidelity, but any size will tend to reduce flow, either by restriction or by induc- tion of turbulence. Likewise, the pressure probe should be in the plane of the electrodes of the flowmeter, but if this is realized, it would prob- ably distort the electrical field and produce errors in the flow estimation. The 0-5 to 1.0 cm dis- tance between flow and pressure measurement sites probably did not cause significant error (ATTINGER et al., 1966). Electromagnetic probes must have firm contact with the vessel wall, but this produces restriction of flow. In addition, noise associated with the microvolt signals from the flowmeter probes is significant, as are phase shifts and deviations in frequency response.
The high-frequency filter with 3-3 msec time constant on the driving pressure amplifier (A26) in part compensated for the 7 msec flow signal delay; a 7 msec delay line would be better but hard to obtain, although a second order Pade
66 CARL F. ROTHE and FRANKLIN D. NASH
circuit might provide a good compromise (CARLSON and HA~rr~Atn~R, 1964).
(2) More accurate computation In most of the experiments, the series resistor
in the differentiator o f P a was 10k instead of lk ohm. This limited the peak rate-of-change and so probably accounted for some of the error spikes seen. When another computer (an EAI TR-20) was set up as an artificial dog, using a diode function generator and repetitive timing circuit to generate the pressure wave- form, and the main computer was run to optimize the parameters, this differentiating error caused the calculated compliance to be about 75 per cent of the true value. An even greater effect was seen in the calculated value of RDa, and this may account for the use of zero RDA in several experiments. High frequency noise from the pressure and flow signals caused a 'perfect' differentiator to saturate, so some high frequency limitation was necessary. State variable filters using Paynter filter coefficients (Korm, 1967) would give more useful deriva- tives.
Other computer programs could have been used which would have eliminated the need for differentiation. BENEr~N (1965) obtained com- puted pressure by integrating the sum of inflow and outflow to a segment and multiplying this distending volume by the reciprocal of com- pliance. This approach, however, requires that finite values of large artery resistance and inertanee be used. After trying both approaches, we felt that being able to set RD~ and M to zero outweighed the problems of differentiation.
f3) A more realistic model The model chosen assumes lumped para-
meters, whereas it is obvious that the compliance, inertance, and conductance are distributed along the length of the arterial tree. A more complex model with additional resistance-compliance elements could be used, but the uncertainty in the data because of noise, non-uniform fre- quency response and phase shift of the trans- ducers would make it unlikely that such addi-
tional parameters could be fitted unambiguously. In addition, the model used implies a single channel, whereas branching from one to over two hundred thousand parallel channels occurs in the canine kidney with a large widening in effective cross-sectional area.
The present model assumes linear differential equations to describe the pressure-flow relation- ship, whereas a more realistic model would at least use a non-linear relationship between pressure and vascular volume. The arterial compliance or elasticity in general depends on pressure (ALTMAN et al., 1959, p. 60), for as the pressure is increased the compliance decreases; the wall becomes stiffer as the connective tissue in the wall is stretched. As a next step towards improvement of the model, compliance could be made a linear function of pressure. To add such refinements, however, presents problems because of the relative uncertainty of the raw data avilable in relation to the wide variety of possible non-linearities.
(4) A more accurate auto-optimization procedure Another potential source of error is the relay
eomparator throw-time (less than 10 msec in the EAI units) and uncompensated zero offset (adjusted by P23 for each experiment). An electronic comparator was used for the com- pliance. These time-delay or phase errors contributed to the error spikes seen and, especially, to the uncertainty in the inertanee value. Because the full value of the variable is applied to the integrator generating the value of the parameter, no matter what the magnitude of the total error, fluctuations of the parameter occur. This requires relatively low gains on the integrator to reduce the fluctuation to an acceptable value. If the gain is inordinately low, the model will not follow changes in parameters which are occurring rapidly. For these reasons, compromise was required, and, as seen in Figs. 5 and 6, there were fluctuations in both com- pliance and pre-glomerular conductance with each pressure pulse. These fluctuations are a reflection, in part, of the inadequacies of the model and data, for with a better model and a
RENAL ARTERIAL COMPLIANCE 67
noise-free transducer system, they would be reduced, and the gain of the integrator could then be increased to shorten the response time. With the model used, the time course of change of model compliance to a step-input was of the same order of magnitude as that of the com- pliance changes following arterial occlusion or the beginning of drug influences; changes in conductance were followed more accurately.
A substantial improvement would be to minimize the error squared rather than the absolute error so that with small errors the drive signal to the parameter-setting integrators would be reduced. Although minimization of the absolute value of the error is better than mini- mization of the squared error for computer solution of the roots of polynomials and similar mathematical equations, because the rate of change of parameters is faster near zero error (L~vIN~, 1964), in an adaptive parameter-search technique with significant noise it would appear that the minimization of the sum of squared deviations would be more effective. Higher integrator gain could be used for more rapid optimization of parameters seriously in error or rapidly changing, and then, as low errors are approached, the fluctuations of the parameter with each heart beat would be relatively less. The need for another multiplier for each para- meter makes this approach less attractive unless a large computer is available.
8. DISCUSSION An easily-justified purpose for simulating a
biological system is to improve our under- standing of that system. Unfortunately for the theoretician, (1) biological systems have distri- buted rather than lumped characteristics, (2) they are highly variable between individuals, (3) biological systems are disconcertingly non- linear, and (4) many parameters are continuously changing as part of the neural and humoral control of homeostasis.
With the complexity and variability of bio- logical systems, many mathematical systems (white boxes) might be adjusted to describe, at least over a limited range, the biological systems
(black boxes). Unless the accuracy of the measurements of the biological systems is sufficient to provide clear choices between various details of a model, it is difficult to justify any but the simplest. Without proof by biological experimentation, the complex theoretical model remains relatively sterile, though still provoca- tive. Thus, the philosophy of using the simplest model which fits the known anatomical and physiological characteristics of the organ mini- mizes ambiguity and continues to be an appro- priate criterion of simulation quality. It also seems reasonable to express models in terms of clearly physical counterparts in t h e biological system, such as inertance, compliance, and resistance, so that comparisons to anatomical features are possible.
The direct measurement of dynamic com- pliance, AV/AP, is probably not possible for the micro-vessels of the kidney. This approach would require simultaneous measurement of pressure and volume. With the kidney, and indeed with the microcirculation in general, it is manifestly impossible to instantaneously and reversibly occlude all of the distal ends of the arterial bed, since the renal artery branches so extensively into thousands of parallel pathways, each of different length, diameter, and, possibly, reactivity. Overall changes in arterial volume cannot be measured by total organ-volume measurements or inflow-minus-outflow tech- niques without untenable assumptions about constancy of volume of the other segments of the vasculature, and loss in the urine and lymph. Furthermore, measurement of the pressure in an assumed 'representative' segment under study is fraught with the likelihood that the pressure measured in a single small artery is not: a reasonable estimate of that in all other vessels; since the vessel would have been manipulated~ and so might have had induced in it changes in vascular smooth-muscle activity. In addition, the pressure-measuring probe or catheter in the vessel would likely be a significant fraction of the total cross-section and so would increase resistance to flow if flow were allowed to continue. If blood flow is reduced or stopped,
68 CARL F. ROTHE and FRANKLIN D. NASH
the metabolic processes soon change the system markedly. Externally applied pressure-measure- ment devices are difficult to calibrate, since the effective area is uncertain.
A shoulder on the up-stroke or notching at the apex of the pressure wave was often seen (e.g. Figs. 3 and 4). This shoulder or notch was real, for from this waveform a valid flow wave- form was predicted. This is particularly apparent in the left panel of Fig. 3, where norepinephrine, intra-arterial, led to an unusually sharp rise of pressure which in turn induced an initial spike of flow. O'ROUgKE and TAYLOR (1966) discussed the systolic shoulder and seem to conclude that it may be attributable to the vascular bed under study. Our data would suggest that t he pressure pattern results from the characteristics of the cardiac pulse and total arterial system and is little influenced by a single renal or femoral arterial bed. This pressure waveform, in conjunction with the parameters of the specific vascular bed, determines the flow waveform. The aortic pressure waveform is clearly a second-order process with a marked tendency toward oscillation and reflection, but the renal flow pattern, though complex, is primarily first-order with the complexities due to the driving pressure pattern. The renal
arterial bed, as suggested by SPENCEg and DENISON (1963), is primarily a combination of vascular resistance and compliance with negli- gible effective inertance.
Acknowledgements--We wish to acknowledge the technical assistance of JOHN DREES, JACK HARDIGO, THOMAS LESS, and THOMAS ROESENER, and the helpful suggestions of DRS. ROBERT FOX, KENNETH PURDY and ROBERT Korm of the Department of Mechanical Engin- eering, Purdue University.
REFERENCES ALTMAN, P. L., DxX'rME~, D. S. and GREBE, R. M. (1959)
Handbook of Circulation. Saunders, Philadelphia.
ATTINOER, E. O., SUOAWARA, H., NAVARRO, A., RXC~ETTO, A. and MARTIN, R. (1966) Pressure-flow relations in dog arteries. Circ. Res. 19, 230-246.
BENEKEN, J. E. W. (1965) A Mathematical Approach to Cardio-vascular Function. The Uncontrolled Human System. Institute of Medical Physics, Utrecht.
CARLSON, A. and HANNAUER, G. (1964) Handbook of Analog Computation. Electronic Associates, Inc., Long Branch, New Jersey.
CLYMER, A. B. (1959) Direct system synthesis by means of computers. AIEE Transactions (Communication and Electronics) pp. 798-806.
DONALDSON, P. E. K. (1960) Error decorrelation--a technique for matching a class of functions. Proc. 3rd Internat. Conf. med. Electron., LE.E., London, pp. 173-178.
ELECTRONIC ASSOCIATES, Inc. (1964) TR-48 Analog Computer Reference Handbook, pp. I30-136. Elec- tronic Associates, Inc., Long Branch, New Jersey.
FIVER, S. (1961) Analog Computation, Vol. 3, pp, 851- 855. MCGRAw-HILL, New York.
G6M6RI, P., MLrNKACSI, S., NAGY, Z., TAKACS, L. and KALLAY, K. (1962) Ischaemia and arteriovenous anastomoses of the kidney in shock, haemorrhage, dehydration and arterial hypoxia in dogs. Acta Med. Hung. 18, 119-125.
KO8R, R. H. (1967) On the identification of linear and non-linear systems. Simulation 8, 165-174.
KORN, G. A. and KORN, T. M. (1964) Electronic Analog and Hybrid Computers, pp. 510-518. McGraw-Hill, New York.
LEvn~, L. (1964) Methods for Solving Engineering Problems Using Analog Computers, pp, 217-244. McGraw-Hill, New York.
MCDONALD, D. A. (1964) Frequency dependence of vascular impedance. In Attinger, E. O. Pulsatile Blood Flow, pp. 115-133. McGraw-Hill, New York.
NASH, F. D. and SELKtrg~r, E. E. (1964) Effects of elevated ureteral pressure on renal blood flow. Circ. Res. 15, 1-142-I-147.
O'RouRKE, M. F. and TAYLOR, M. G. (1966) Vascular impedance of the femoral bed. Circ. Res. 18, 126-139.
SELKURT, E. E. (1963) Effect of ureteral blockade on renal blood flow and urinary concentrating ability. Am. J. Physiol. 205, 286-292.
SPENCER, M. P. and DENISON, A. B. JR. (1963) Pulsatile blood flow in the vascular system. In: Handbook of Physiology: Circulation. Edited by W. F. Hamilton, and P. Dow, Sec. 2, Vol. 2, pp. 839-864, American Physiological Society, Washington, D.C.
THURAU, K. and HENNE, G. (1964) Die transmurale Druckdifferenz der Widerstrands-gef~sse als Para- meter der Widerstandsregulation in der Niere. Pfliigers Arch. ges. Physiol. 279, 156-177.
RENAL ARTERIAL COMPLIANCE 69
M E S U R E D E LA C O N D U C T A N C E ET D E L ' I N D U C T A N C E M E C A N I Q U E DE L ' A R T E R E R E N A L E G R A C E A U C A L C U L
A N A L O G I Q U E EN TEMPS R E E L D E P A R A M E T E R S S I MU LES
Sommairc On a pu pr6voir l'allure dynamique du d6bit de l'art6re r6nale, rinductance m6canique de l'art6re, et la conductance pr6glom6rulaire, h l'aide d'un calculateur analogique traitant en temps r6el, h partir de param6tres simul6s, les impulsions issues d'une art6re r6nale de chien. Le d6bit a 6t6 tr6s exactement calcul6 non seulement darts le cas d'un 6tat stable, mais 6galement darts les conditions nettement fluctuantes de l'allure des impulsions de pression arterielle, du niveau moyen, et du rythme cardiaque. Le mod61e dispose de cinq param6tres: inertance, r6sistance et inductance m6canique des grandes attires; conductance des r~gions pr6glom6rulaires; et une pression glom6rulaire non puts6e. Les deux premiers param6tres sont affich6s manuellement, tandis que les trois autres sont automatiquement ajust6s par une m6thode appropri6e destin6e /t r6duire l'erreur absolue qui est l'expression de la diff6rence instantan6e entre le d6bit mesur6 et la d6bit calcul6.
M E S S U N G D E R D E H N B A R K E I T U N D D E R L E I T F , ~ H I G K E I T VON N I E R E N A R T E R I E N M I T S E L B S T A D A P T I E R E N D E R
O N - L I N E - A N A L O G R E C H N U N G V O N M O D E L L G R O S S E N
Zusammenfassung--Aus der Messung von Druckimpulsmustern der Nierenarterien von Hunden wurden mit Hilfe der on-line-Analogrechnersimulierung von Nierenarterienpara- metern der dynamische NierenarteriendurchfluB, die arterielle Dehnbarkeit und die pri~glomerul~tre Leitf~higkeit gemessen. Der Durchflu8 wurde genau vorausberechnet, nicht nur unter den Bedingungen des FlieBgleichgewichts, sondern auch bei betr/ichtlichen ,~nderungen im arteriellen Druckmuster, im mittleren Druck und in der Herzfrequenz. Das Modell enth/ilt ffinf Gr6Ben: Widerstand, Tr/igheit und Dehnbarkeit der groBen Arterie, pr/iglomerul~ire Arteriolenleitf/ihigkeit und ein nichtpulsierender Glomerulusdruck. Die beiden ersten Parameter wurden manuell festgesetzt, w~ihrend die iibrigen drei mit der Methode des steilsten Abfalls automatisch eingestellt wurden. Dadurch wurde der absolute Fehler auf ein Minimum gebracht; er ist ausgedriickt durch die Differenz zwischen gemessenen und vom Computer berechneten Durchflu~mengen zur Zeit.
Related Documents











