Relationships between Culture and Health Status: A Multi-Site Study of the Older Chinese in Canada* Daniel W.L. Lai, 1 Ka Tat Tsang, 2 Neena Chappell, 3 David C.Y. Lai 3 , and Shirley B.Y. Chau 4 RE ´ SUME ´ La pre ´sente e ´tude examine les relations entre la culture et l’e ´tat de sante ´ des aı ˆne ´s chinois au Canada. Les donne ´es ont e ´te ´ recueillies lors d’entretiens face a ` face avec un e ´chantillon transversal de 2 272 aı ˆne ´s chinois de 55 a ` 101 ans se ´lectionne ´s au hasard dans sept villes canadiennes. Leur e ´tat de sante ´ae ´te ´e ´value ´ en fonction du nombre de maladies chroniques, des limites de l’AVQ et de l’AIVQ, et de la Medical Outcome Study Short Form SF-36. Bien que les variables culturelles n’expliquent qu’une petite partie de la variance dans l’e ´tat de sante ´, e ˆtre davantage au courant des mode `les traditionnels de croyance a ` la sante ´ des Chinois est important si l’on veut pre ´voir la sante ´ physique, le nombre de maladies, et les limites associe ´es aux activite ´s instrumentales de la vie quotidienne. D’autres variables culturelles, notamment la religion, le pays d’origine, et la pe ´riode de re ´sidence au Canada e ´taient aussi importantes afin de pre ´voir certaines variables associe ´es a ` la sante ´. Les interventions visant a ` ame ´liorer la sante ´ devraient porter sur des strate ´gies permettant d’ame ´liorer la compatibilite ´ culturelle entre les utilisateurs et le syste `me de distribution des soins. ABSTRACT This study examined the relationships between culture and the health status of older Chinese in Canada. Data were collected through face-to-face interviews with a cross-sectional, randomly selected sample of 2,272 older Chinese between 55 and 101 years of age in seven Canadian cities. Health status was assessed by the number of chronic illnesses, by limitations in ADL and IADL, and by information on the Medical Outcome Study Short Form SF-36. Although cultural variables explained only a small proportion of variance in health status, having a stronger level of identification with traditional Chinese health beliefs was significant in predicting physical health, number of illnesses, and limitations on IADL. Other cultural variables, including religion, country of origin, and length of residence in Canada, were also significant in predicting some health variables. Interventions to improve health should focus on strategies to enhance cultural compatibility between users and the health delivery system. 1 Faculty of Social Work, University of Calgary 2 Faculty of Social Work, University of Toronto 3 Centre on Aging, University of Victoria 4 Faculty of Health and Social Development, School of Social Work, University of British Columbia–Okanagan * This research was funded by the Social Sciences and Humanities Research Council of Canada under the strategic theme Society, Culture and Health of Canadians (Grant No: 828-1999-1032). Manuscript received: / manuscrit rec ¸u : 18/08/04 Manuscript accepted: / manuscrit accepte ´ : 29/03/07 Mots cle ´s : vieillissement, aı ˆne ´s chinois, personnes a ˆge ´es, culture, sante ´ Keywords: aging, Chinese elderly, older people, culture, health Requests for offprints should be sent to:/Les demandes de tire ´s-a `-part doivent e ˆtre adresse ´es a `: Daniel W.L. Lai, Ph.D. Professor & Alberta Heritage Health Scholar Faculty of Social Work, University of Calgary 2500 University Drive NW Calgary, AB T2N1N4 ([email protected]) Canadian Journal on Aging / La Revue canadienne du vieillissement 26 (3) : 171 - 184 (2007) 171 doi: 10.3138/cja.26.3.171

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Relationships between Culture and HealthStatus: A Multi-Site Study of the OlderChinese in Canada*
Daniel W.L. Lai,1 Ka Tat Tsang,2 Neena Chappell,3 David C.Y. Lai3, and Shirley B.Y. Chau4
RESUMELa presente etude examine les relations entre la culture et l’etat de sante des aınes chinois au Canada. Les donnees ontete recueillies lors d’entretiens face a face avec un echantillon transversal de 2 272 aınes chinois de 55 a 101 ansselectionnes au hasard dans sept villes canadiennes. Leur etat de sante a ete evalue en fonction du nombre de maladieschroniques, des limites de l’AVQ et de l’AIVQ, et de la Medical Outcome Study Short Form SF-36. Bien que les variablesculturelles n’expliquent qu’une petite partie de la variance dans l’etat de sante, etre davantage au courant desmodeles traditionnels de croyance a la sante des Chinois est important si l’on veut prevoir la sante physique, le nombrede maladies, et les limites associees aux activites instrumentales de la vie quotidienne. D’autres variables culturelles,notamment la religion, le pays d’origine, et la periode de residence au Canada etaient aussi importantes afin deprevoir certaines variables associees a la sante. Les interventions visant a ameliorer la sante devraient porter surdes strategies permettant d’ameliorer la compatibilite culturelle entre les utilisateurs et le systeme de distribution dessoins.
ABSTRACTThis study examined the relationships between culture and the health status of older Chinese in Canada. Data werecollected through face-to-face interviews with a cross-sectional, randomly selected sample of 2,272 older Chinesebetween 55 and 101 years of age in seven Canadian cities. Health status was assessed by the number of chronicillnesses, by limitations in ADL and IADL, and by information on the Medical Outcome Study Short Form SF-36.Although cultural variables explained only a small proportion of variance in health status, having a stronger level ofidentification with traditional Chinese health beliefs was significant in predicting physical health, number of illnesses,and limitations on IADL. Other cultural variables, including religion, country of origin, and length of residence inCanada, were also significant in predicting some health variables. Interventions to improve health should focus onstrategies to enhance cultural compatibility between users and the health delivery system.
1 Faculty of Social Work, University of Calgary2 Faculty of Social Work, University of Toronto3 Centre on Aging, University of Victoria4 Faculty of Health and Social Development, School of Social Work, University of British Columbia–Okanagan
* This research was funded by the Social Sciences and Humanities Research Council of Canada under the strategic themeSociety, Culture and Health of Canadians (Grant No: 828-1999-1032).
Manuscript received: / manuscrit recu : 18/08/04
Manuscript accepted: / manuscrit accepte : 29/03/07
Mots cles : vieillissement, aınes chinois, personnes agees, culture, sante
Keywords: aging, Chinese elderly, older people, culture, health
Requests for offprints should be sent to:/Les demandes de tires-a-part doivent etre adressees a:Daniel W.L. Lai, Ph.D.Professor & Alberta Heritage Health ScholarFaculty of Social Work, University of Calgary2500 University Drive NWCalgary, AB T2N1N4([email protected])
Canadian Journal on Aging / La Revue canadienne du vieillissement 26 (3) : 171 - 184 (2007) 171doi: 10.3138/cja.26.3.171

IntroductionCultural diversity is a reality facing the populationof Canada. The increase in the aging population ofculturally diverse groups adds to the importance ofunderstanding the unique health needs of variousgroups, particularly from a service provider andpractitioner point of view. This study examines theeffects of culture and related variables on the healthof the older Chinese in Canada.
Cultural Diversity and the ChinesePopulation in CanadaIn 2001, 13.4 per cent of the Canadian population wascomposed of visible minorities, a major increasefrom 8.8 per cent in 1991 (Statistics Canada, 2003).With these changes in the population, an increasingnumber of the clients that service providers work withdaily are members of ethnic minorities, includingthose who are new to Canada and may speak differentlanguages or have different cultural values andbeliefs. Yet relatively little research on the healthstatus of ethnic minority groups, particularly theelderly sub-population, is available in Canada. Thismakes it difficult for service providers to understandthe health status of this aging population. Theprevailing myth that all members of an ethnic groupare the same perpetuates the assumption that‘‘one-size-fits-all’’ in health care, resulting in a poorfit between available services and the needs ofparticular sub-groups of users, especially those fromethnic minority sub-groups.
With a total population of over one million, theChinese are the largest visible minority group inCanada, followed by South Asians and Filipinos, and,in 2001, accounted for 25.8 per cent of all visibleminorities (Statistics Canada, 2003). The proportionof older Chinese people is greater than for othervisible minority groups. In 2001, 9.9 per cent ofChinese-Canadians were 65 years or older, while theelderly population among most other visible minoritygroups ranged around 6 per cent. Aside from thesignificant size of the Chinese-Canadian elderlypopulation, cultural uniqueness, particularly as tohealth beliefs, suggests that health professionalsshould have adequate knowledge to serve better thisgrowing sub-population. This is particularly the casefor many older Chinese, who often retain traditionalChinese cultural values and health beliefs that mayinfluence their health outcomes.
Culture as a Determinant of HealthA culture is the set of values, beliefs, and behaviouralnorms common to a given group of individuals; it
forms the context and creates the guidelines for thelives and world-views of individuals within thatparticular group. Thus members of a cultural groupgenerally have similar values, beliefs, ideas, knowl-edge, morals, rules, and customs (Singh, 1995). Healthbeliefs, attitudes, outcomes, and other health-relatedbehaviours are also related to culture.
Culture is an important factor in determining healthcare use and health outcomes among older adults(Day & Cohen, 2000). For example, its significance inthe lives of older immigrants was emphasized in astudy on Russian Jewish immigrants (Day & Cohen,2000). In that case, culture acted as a crucial self-identifying component for older adults with or with-out dementia, serving both as a therapeutic barrier aswell as a therapeutic resource and problem-solvingtool (Day & Cohen, 2000).
In spite of assimilation and acculturation, immigrants’main cultural beliefs generally remain unchanged(Henderson, 1996). For instance, beliefs and viewsabout aging, health, illness, and religion do notchange significantly. In addition, patients sufferingfrom serious illness and stress often move towardstreatment based on the cultural ideas and beliefs theylearned in early life (Evan & Cunningham, 1996).In the case of elderly immigrants from a differentculture, cultural values and beliefs are particularlyrelevant to their health status. Previous research hasshown that a higher level of migratory grief isassociated with a higher level of depression (Casado& Leung, 2001). Shapiro et al. (1999) reported thatimmigrants who were the most acculturated or mostbicultural were the healthiest and least depressed.
Chinese Culture and HealthTraditionally speaking, Chinese culture places strongemphasis on the values of family, kin, and communitynetwork (Wu & Tseng, 1985). The cultural view ofhealth is more holistic, ecological, and dynamic, whencompared with that of Western medicine. TraditionalChinese culture generally defines health and illnessaccording to a unifying world-view (Gaw, 1993).Human beings are envisioned as components of thelarger universe. Health exists when there is a finebalance of the energy (Qi) within the body andbetween the body and its physical environment.The traditional cultural values and health beliefs ofChinese people affect their perception of and compli-ance with Western medical aetiology and healthpractices. The health beliefs and values of theChinese often result in health practices that arereflective of the cultural uniqueness of this ethnicgroup (e.g., a belief in the balance of energy within thebody explains the reason for the use of T’ai Chi and
172 Canadian Journal on Aging 26 (3) Daniel W.L. Lai et al.

qi qong, traditional Chinese physical exercises focus-ing on harmonizing the energies (qi) within thehuman body). Traditional health beliefs about certainfoods or herbal supplements also result in a holisticand preventive approach to dealing with illnessesand diseases.
When individuals adhere to Chinese cultural valuesand health beliefs, they may face additional incom-patibilities in a society where the health systemoperates with Western concepts and delivery methods(Gelfand, 2003). On the other hand, traditional cul-tural values and health beliefs can serve as resources,enabling someone to retain and maintain her/hisethnic identity and ethnic networks as a way to copewith the adjustments and challenges of having differ-ent values and beliefs than the dominant culture(Gee, 1999; Sokolovsky, 1985). The former view isconsistent with ethnicity as deprivation, while thelatter reflects ethnicity as compensation (Gee, 1999;Sokolovksy, 1985).
Most of the published research studies of olderChinese were conducted in the home countries ofthe participants, such as Hong Kong (Boey & Chi,1998; Ho et al., 1995), mainland China (Boey, 1997),or Taiwan (Hwu, Chang, Yeh, Chang, & Yeh, 1996).The focus of these research studies is usually onphysiological or mental health status and theirpredictors. Little attention has been paid to cultureas a variable.
A few other studies have examined the health ofChinese seniors living in non-Chinese societies andhave explored their adjustment to those cultures.One conducted in Liverpool assessed the prevalenceof dementia and depression among Chinese and otherethnic minority seniors (McCracken, Boneham,Copeland, Williams, & Wilson, 1997). In the UnitedStates, there have been studies of Chinese seniorswith respect to various social and health concerns,including depression and its predictors (Lam, Pacala,& Smith, 1997), suicide rate (Baker, 1994), death rate(Yu, 1986), attitude toward death (Craine, 1996), andsocial support networks/service use (Tsai & Lopez,1997). Once again, cultural values and beliefs werenot a key focus in these studies.
In Canada, studies of older Chinese-Canadians havetended to use small, non-random, and/or localizedsamples (Bagley, 1993; Lai & McDonald, 1995) and toexamine issues such as life satisfaction (Lai &McDonald, 1995), adjustment (Chan, 1983), oralhistory (Li, 1985), social support (Li, 1990), healthstatus, and psychological and social adjustment(Bagley, 1993). Some studies have involved the useof cross-cultural comparison (Bagley, 1993) toidentify the cultural differences between the elderly
Chinese and other elderly groups. However, thisapproach further perpetuates the assumption thatculture is a constant (Li, 1977) and the myth thateveryone in the same ethnic or cultural group isessentially the same. Most importantly, the influenceof cultural factors on health outcomes was inade-quately addressed in these studies, despite the factthat understanding the relationship between cultureand health is crucial to providing good health care.
In addition, many researchers in the past haveequated culture with membership in a particularethnic group. This results in cross-cultural compara-tive studies in which members from the same ethnicbackground are clustered into the same group andcompared with members from another group. Whilemembers of the same ethnic group may still considerthemselves to be similar to each other, the assumptionthat everyone in an ethnic group adheres to the samecultural views and practices is questionable.
To bridge the knowledge gap, this current study asksthe research question: ‘‘What is the effect of cultureon the health status of the older Chinese in Canada?’’We hypothesize that, even within the same ethnicgroup, differences in cultural values and health beliefsexist and are significant in predicting health status.The world-views, values, and beliefs of individualscontinue to evolve, particularly in the context of anongoing interaction with other cultures. This isparticularly the case in a multicultural society whereindividuals live their lives in a pluralistic culturalcontext.
Theoretical Perspectives on Cultureand HealthThe conceptualization of the research question inthis study was based on three major theoreticalframeworks. First,’’the mandala of health’’ (Hancock& Perkins, 1985) concept defines human ecology asthe constant interaction of culture and environment.The interactions among culture, community, andfamily result in variations in lifestyle with specialreference to an individual’s interrelated biological,spiritual, and psychological experiences. An indivi-dual’s perspective on illness, health, health beliefs,and health practices is shaped by cultural andcommunity contexts. Therefore, the cultural perspec-tive of ethnic minority older adults, particularlyamong immigrant populations, is shaped andnurtured in a bicultural or even multicultural milieu.
Second, Kleinman’s (1980) explanatory modelprovided the foundation for the hypothesized rela-tionship between culture and related health variables.According to Kleinman, every culture has its own
The Culture and Health of the Older Chinese La Revue canadienne du vieillissement 26 (3) 173

ideas and beliefs about illness and methods of health-related treatment. Each culture has a health care systemand the symbolic meanings, values, and behaviouralnorms associated with different illnesses and theirconcomitant methods of treatment are culturallyunique. The health care system consists of threesocial arenas: the popular arena, the professionalarena, and the folk arena. The popular arena is anon-professional cultural arena where illness is firstencountered. The professional arena includes medicaland other health professionals. The Western medicalsystem is the most commonly used in Canada, but insome cultures, like Chinese or Indian, the indigenoussystem co-exists with the Western system. The folkarena consists of traditional approaches to healinglike shamanism, recourse to faith healers, or rituals.This model focuses on explanations for the cause ofillness and on how symptoms are explained andtreated in a given cultural context. This explanatoryapproach is a cognitive model, focusing on whatillness and health mean to individuals and on howattitudes and actions towards treatment are formedand (probably) result in different health outcomes.
The present study was also built upon a populationhealth framework (Health Canada, 2001) that iden-tified 11 additional social determinants of health,including income and social status, social supportnetworks, education, employment/working condi-tions, social environments, physical environments,personal health practices and coping skills, healthychild development, biology and genetic endowment,health services, and gender. Previous research studieshave shown that being female (Roberts & Fawcett,1998), having a lower level of education (Winkleby,Darius, Frank, & Fortmann, 1992), living alone(Latimer & Sheahan, 1998), having a lower income(Nelson, 1994), and having a lower level of socialsupport (Krause, 1990) are predictors of poorer healthstatus among older adults. Although these same socialdeterminants are likely to have a similar impact on thehealth of older Chinese-Canadians, this has yet to beshown.
MethodThe data were collected as part of a cross-sectionalsurvey on the health and well-being of older Chinesein Canada (Lai, Tsang, Chappell, Lai, & Chau, 2003).The data were collected between summer 2001 andspring 2002 in seven major Canadian cities with asubstantial concentration of Canadian-Chinese popu-lation (89 per cent of the entire Chinese-Canadianpopulation of Canada [Statistics Canada, 2003]). Thetarget population was ethnic Chinese aged 55 yearsand older. Identifying Chinese surnames from
telephone directories in each site was the samplingframe, a method used in previous studies (Lauderdale& Kestenbaum, 2000; Rosenwaike, 1994; Tjam, 2001).From the local telephone directories, 297,064 Chinesesurname listings were identified. Using the SPSSVersion 11 random cases selection function, a sub-sample of telephone numbers was randomly selected,based upon the size of the Chinese-Canadian popu-lation at a given site and the estimated proportion ofthat population 55 years of age and older. As a result,a total of 40,654 numbers listed under 876 Chinesesurnames were randomly selected.
Trained telephone interviewers who were proficient inEnglish and at least one major Chinese dialect—suchas Cantonese, Mandarin, or Toishanese—madetelephone contact to identify eligible participants(ethnic Chinese aged 55 years or older). The inter-viewers were mainly graduate students in socialscience or human service disciplines or communityinterviewers who had experience in conductingsurvey interviews in the Chinese community. Allinterviewers participated in a one-day structuredtraining session conducted by the research teammembers. Eligible participants were then invited totake part in a face-to-face interview, either at theparticipant’s home or at the premises of one of thecommunity organizations that collaborated withthe research project at the local site. For householdswith more than one eligible participant, only one wasrandomly selected through a roll of the dice. Bilingualinterviewers, using either English or a Chinese dialectspoken by the participants, conducted the interviews.In the original study, a total of 2,949 eligibleparticipants were identified and a total of 2,272completed the face-to-face interview, a response rateof 77 per cent.
Such a high response rate was probably the positiveresult of a partnership between research teammembers and the Chinese community at each of thedata collection sites. To facilitate the implementationof this study, an advisory committee was formed toconnect the research team with local service provi-ders, particularly those working closely with the localChinese community. In addition to providing inputfor the research planning and implementation pro-cess, the community partners in the advisory com-mittees were involved in informing older Chineseadults about this research. Chinese-language televi-sion, radio, and print media were contacted so thatawareness was built among older adults as well asamong their family members. A national Chinesetelevision network was also involved in publicizingthe launch of the study. Many of the local communitypartners involved in this study also helped to informtheir Chinese clients and local communities about
174 Canadian Journal on Aging 26 (3) Daniel W.L. Lai et al.

this study through their regular newsletters orpublicity materials.
An orally administered, structured questionnaire wasused for data collection. Because most of the olderChinese people in Canada are able to speak a Chinesedialect, the questions were initially constructed inwritten Chinese, except for the standardized instru-ments that have a Chinese-language version. Toattend to the language needs of participants,an English version of the questionnaire was alsoprepared. A standard forward–backward translationprocess was used. The original questions in Chinesewere translated into English and then translated backinto Chinese. This process ensured that the Englishversion was consistent with the Chinese version.In the interview, the participants could choose toanswer either the Chinese or the English version ofthe questionnaire.
As a large-scale study, the original questionnairecovered a wide range of health-related topics, includ-ing physical and mental health status, Chinese healthbeliefs, Chinese cultural values, and service utiliza-tion. The full questionnaire took about 45 minutes to1 hour to complete. For the purpose of this study,only selected variables relevant to culture and healthstatus were used for the analysis.
Measures
The dependent variable, health status, was representedby number of chronic illnesses, functioning capacity,and general physical and mental health status.The number of chronic illnesses was measured byasking the participants to answer either yes (1) or no(0) to each item on a list of 24 health problems,including allergies, high blood pressure, cancer,diabetes, and stroke. The participants could also addadditional health problems to the others category. Ahigher score represented more illnesses. Functioningcapacity was measured by a list of four basic (ADL)and eight instrumental (IADL) activities of dailyliving (Ikegami, 1995). Examples of the ADL andIADL included dressing, grooming, toileting, bathing,ambulation (i.e., walking, climbing stairs), transfer(i.e., chair to bed, chair to toilet), eating, medicationadministration, meal preparation, housework, useof telephone, shopping, money management, use oftransportation, and interpretation and translation.Participants were asked to indicate the level ofassistance they needed; responses ranged from none(0) to a lot (3). The responses were summed to givescores for ADL and IADL. Each of the final scores wasaveraged across the total number of items measured,resulting in a score that ranged between 0 and 3, witha higher score representing a higher level of limitation
in this functioning area. For the participants in thisstudy, a Cronbach’s alpha of 0.84 and 0.83 wasreported for ADL and IADL.
General physical health and mental health weremeasured using the Medical Outcomes Study36-item Short Form (SF-36), a well-established, stan-dardized health assessment instrument that has beenused with people from various cultural backgrounds(Ware & Gandek, 1998; Ware & Kosinski, 2001; Wareet al., 1998; Ware, Kosinski, & Keller, 1994; Ware &Sherbourne, 1992). This scale has also been adaptedand translated for Chinese respondents. Psychometricevaluation confirms the reliability and validity of theinstrument (Ren, Amick, Zhou, & Gandek, 1998; Ren& Chang, 1998). This 36-item scale yielded scores fortwo dimensions, the physical component summary (PCS)and the mental component summary (MCS), represent-ing physical and mental health, with higher scoresmeaning better health status. When the instrumentwas used with the older Chinese in this study, aCronbach’s alpha of 0.9 was reported for the PCS andof 0.8 for the MCS.
Cultural factors, the key independent variablesexamined in this study, were measured by countryof origin, length of residence in Canada, religion,Chinese health beliefs, and Chinese cultural values.Country of origin referred to the place where theparticipants were born. Countries of origin includedCanada, mainland China, Hong Kong, Taiwan,Vietnam, Southeast Asia, and others. Length of resi-dence was measured by asking the participants toindicate the total number of years they had resided inCanada. Religions of the participants were groupedinto three categories—not having a religion, having aWestern religion, such as Christianity or Catholicism,and having a non-Western religion, such as Buddhism,Taoism, or ancestor worship.
Chinese health beliefs referred to conceptual views,beliefs, and attitudes toward various health conceptsin Chinese culture. As no existing standardized scalewas available, one was constructed by the researchteam of the original study, based on previous litera-ture on Chinese health beliefs and norms (Lau, Leung,& Tsui, 2001; Satia et al., 2000; Spector, 2000).Two independent traditional Chinese medicine practi-tioners were also consulted before finalizing thequestions for the scale developed for measuringChinese health beliefs in this study. A Chinesehealth belief scale was developed, with 12 statementsmeasuring level of agreement with health beliefsrelated to healthy eating habits, health maintenance,and the use of traditional Chinese medicine. Samplestatements included, ‘‘[e]ating too much deep-friedfood will cause Re Qi’’; ‘‘[t]raditional Chinese herbal
The Culture and Health of the Older Chinese La Revue canadienne du vieillissement 26 (3) 175

medicine could balance yin and yang in the body’’;‘‘[t]raditional Chinese herbal medicine could cure theroot of the disease; whereas Western medicationsonly cure the symptoms’’. Participants were asked toindicate their level of agreement with each statementas disagree (1), neither agree nor disagree (2), or agree (3).Responses from the 12 statements were summed andweighted by the total number of items in the scaleto give a score ranging between 1 and 3, with a higherscore representing higher agreement with Chinesehealth beliefs. A Cronbach’s alpha of 0.85 wasreported for the older Chinese in this study.
Chinese cultural values referred to traditional Chinesecultural beliefs and values with respect to languageuse, gender roles, interracial marriage, food and diet,and parent–child relationships. They were measuredby a list of 11 statements, using a 5-point scale,ranging from strongly disagree (1) to strongly agree (5),with higher scores indicating a higher level of iden-tification with Chinese cultural values. Responsesfrom the 11 statements were summed and weightedby the total number of items in the scale to give ascore ranging between 1 and 5, with a higher scorerepresenting higher agreement with Chinese culturalvalues. These items were constructed by the researchteam of the original research study, based on previousliterature on typical Chinese cultural values (Bond &Hwang, 1986; Ho, 1986; Tsuei, 1992), and on inputfrom community research partners who were expertsin working with various Chinese communities inCanada. Examples of the statements included, ‘‘[i]tshould be the responsibility of adult children to takecare of aging parents’’; ‘‘[t]aking care of children’sdaily routines should be a woman’s major responsi-bility at home’’; ‘‘[a] Chinese person should showmore appreciation of Chinese food than Westernfood’’. A Cronbach’s alpha of 0.82 was reported forolder Chinese in this study.
In addition to the cultural variables, other socio-demographic variables, including age, gender, maritalstatus, living arrangement, education, self-ratedEnglish competency, self-rated financial adequacy,and personal monthly income, were included in theanalysis. It is commonly accepted that being elderlyis associated with poorer health (Deimling, Sterns,Bowman, & Kahana, 2005; Femia, Zarit, & Johansson,2001; Gijsen et al., 2001); older women are in poorerhealth than older men (Roberts & Fawcett, 1998);older people who are married are in better health thanthose who are single (Pettee et al., 2006); and olderpeople living alone are more likely to be in poorhealth than those living with someone (Gee, 2000;Kasper & Pearson, 1995). Finally, higher socio-economic status, such as higher education level or
better financial status, is positively related to betterhealth status (Plouffe, 2003).
In this study, age referred to the chronological age ofthe participants. Gender was grouped as male (1) andfemale (0). Marital status was grouped into married(1) and single (0), which included those who reportedbeing widowed, divorced, separated, or never married.Living arrangement was grouped as living alone andliving with someone. Education level was treated asan ordinal variable, with values ranging from 1 to 4,representing no formal education, elementary, secondary,and post-secondary and above, respectively. Self-ratedcompetency was assessed by two questions askingparticipants whether or not they were able to under-stand English and whether or not they were ableto speak English. The participants would choosethe answer to each question from choices of not at all(1), a little (2), and very well (3). The sum of thescores for the two questions gave the self-ratedEnglish competency score, ranging from 2 to 6, withhigher scores representing a higher level of Englishcompetency. Self-rated financial adequacy wasmeasured by how well income and investmentssatisfied financial needs, using an ordinal scaleranging from 1 to 4, representing very inadequate,not very well, adequate, and very well, respectively.Personal monthly income of the participants wasalso measured as a 4-point ordinal variable, withvalues ranging from 1 to 4, representing less than $500,$500 to $999, $1,000 to $1,499, and $1,500 and above,respectively.
Data Analysis
SPSS Version 14.0.1 was the statistical software usedfor data analysis. Frequency distribution and meanswere used to present the descriptive findings on thebackground information of the participants. Bivariateanalysis, including t tests and �2 tests, was performedto examine the association between health outcomeand the predicting factors. Hierarchical multipleregression using the stepwise method was performedusing each of the health status variables as thedependent variable. The statistical assumptions ofmultiple regression analysis were checked and bivari-ate correlation coefficients were calculated to checkfor potential multi-collinearity problems among theindependent variables. Missing values were minimalin the variables with a maximum of only 1 or 2 percent of the cases. They were replaced using theexpectation-maximization (EM) method of SPSS, inwhich an EM-algorithm method was used to estimatemissing values by an iterative process. In the regres-sion models, the socio-demographic variableswere entered first, followed by the cultural variables.
176 Canadian Journal on Aging 26 (3) Daniel W.L. Lai et al.

This strategy identified the changes in the proportionof variance in the health variables explained, whenthe cultural variables were added to the regressionmodels.
ResultsDetailed demographic information on the olderChinese in this study is presented in Table 1.
A diverse group, they vary by age, gender, maritalstatus, education, and other socio-economic factors.
When compared with 2001 census data, the partici-pants in this study were similar, in age and genderdistribution, to the general Canadian and Chinesepopulations. The proportion of older Chinese parti-cipants in this study who reported their maritalstatus as single was lower than for the general
Table 1: Socio-demographic, culture, and health variables
All Cases 55–64 Years Old 65–74 Years Old 75 Years & Older Test Statistics
Socio-Demographic VariablesAge (mean%) 69.8 (100) 59.9 (30.5) 69.5 (40.7) 80.7 (28.7)Gender—Male (%) 44.2 43.9 50.2 36.0 �2
¼31.2**Being married (%) 66.0 85.9 68.2 41.7 �2
¼296.6**Living alone (%) 13.8 4.3 10.4 28.6 �2
¼182.6**Education (%)No formal education (%) 12.7 2.4 13.3 22.8 �2
¼259.5**Elementary 28.3 16.4 31.9 36.0Secondary 37.8 51.2 34.8 27.9Post-sec. & above 21.1 30.0 20.0 13.3Self-rated English competency 4.1 4.1 4.1 4.0 F¼2.1ns
Financial adequacy, mean 2.8 2.7 2.8 2.8 F¼8.5**Personal monthly income (%)
Less than $500 16.4 19.6 17.4 11.6 �2¼170.1**
$500–$999 38.0 23.6 40.8 49.3$1000–$1499 34.2 35.4 32.9 34.8$1,500 & above 11.4 21.3 9.0 4.3
Culture VariablesCountry of origin (%)
Born in Canada 1.6 1.3 1.1 2.8 �2¼34.7*
Mainland China 27.1 24.2 31.0 24.7Hong Kong 51.1 50.3 48.9 55.0Taiwan 4.4 5.1 4.7 3.1Vietnam 7.9 8.5 8.1 7.1Southeast Asia 4.0 5.1 3.0 4.3Other countries 3.9 5.5 3.3 3.1
Length of residence, mean 19.0 18.0 18.3 21.1 F¼10.7**Length of residence (%)
0–5 years 9.0 35.6 48.7 15.6 �2¼66.8**
6–10 years 24.1 34.4 45.6 20.111–20 years 30.6 24.3 41.4 34.2Over 20 years 36.3 32.0 34.8 33.1
Religion (%)No religion 42.1 46.1 44.2 34.9 �2
¼22.9**Western religion 26.9 25.4 24.4 32.1Non-Western religion 30.9 28.5 31.3 33.1
Chinese cultural values, mean 3.7 3.6 3.7 3.8 F¼31.1***Chinese health beliefs, mean 2.5 2.4 2.5 2.5 F¼5.1**Health Variables
Physical health, mean 51.1 51.7 51.2 50.5 F¼3.1*Mental health, mean 48.4 48.7 48.9 47.4 F¼4.3*Chronic illnesses, mean 3.3 2.7 3.3 4.0 F¼45.9***ADL, mean 0.0 0.0 0.0 0.1 F¼17.1***IADL, mean 0.5 0.3 0.5 0.9 F¼165.9***
* p < 0.05; ** p < 0.01; *** p < 0.001ns¼not significant
The Culture and Health of the Older Chinese La Revue canadienne du vieillissement 26 (3) 177

Canadian population within the same age range buthigher than for the Chinese population in Canada.The proportion of participants living alone was alsolower than for the general Canadian population buthigher than for the older Chinese population. Theeducation level of the older Chinese in this study waslower than for the general Canadian population aswell as for the Chinese population, with fewer of themreporting a post-secondary education level. Whencompared with the general Canadian population,a smaller population of older Chinese participantsreported a Western religion. However, a higherpercentage in the sample reported having a Westernreligion than for the Chinese population in the census.
About two-fifths of the older Chinese in this studyreported an income level between CAN$500 and $999.However, 16 per cent reported a personal monthlyincome of less than $500, and 34 per cent reported anincome between $1,000 and $1,499. Only 11 per centreported an income of $1,500 and above. In termsof self-rated financial adequacy, the participantsreported a mean score of 2.8 (SD ¼ 0.6) along a4-point scale. Over half of the participants (51%) hadmigrated from Hong Kong, followed by those frommainland China (27.1%), Vietnam (7.9%), SoutheastAsia (4%), Taiwan (4.4%), and other countries (3.9%).The average length of residence in Canada for thissample was 19 years (SD¼ 13.7).
Findings on health variables are presented in Table 1.On average, participants reported having 3.3 illnesses,which is higher than the 2 health conditions reportedby older adults in the general Canadian population(Statistics Canada, 2005). Participants reported a lowlevel of limitation in ADL but a slightly higher level oflimitation in IADL. As indicated in an earlier study(Lai, 2004), the PCS (51.1) score of the older ChineseCanadians in this study was actually higher than theone reported by older Canadians in general, while theMCS (48.4) score was lower (Hopman et al., 2000).
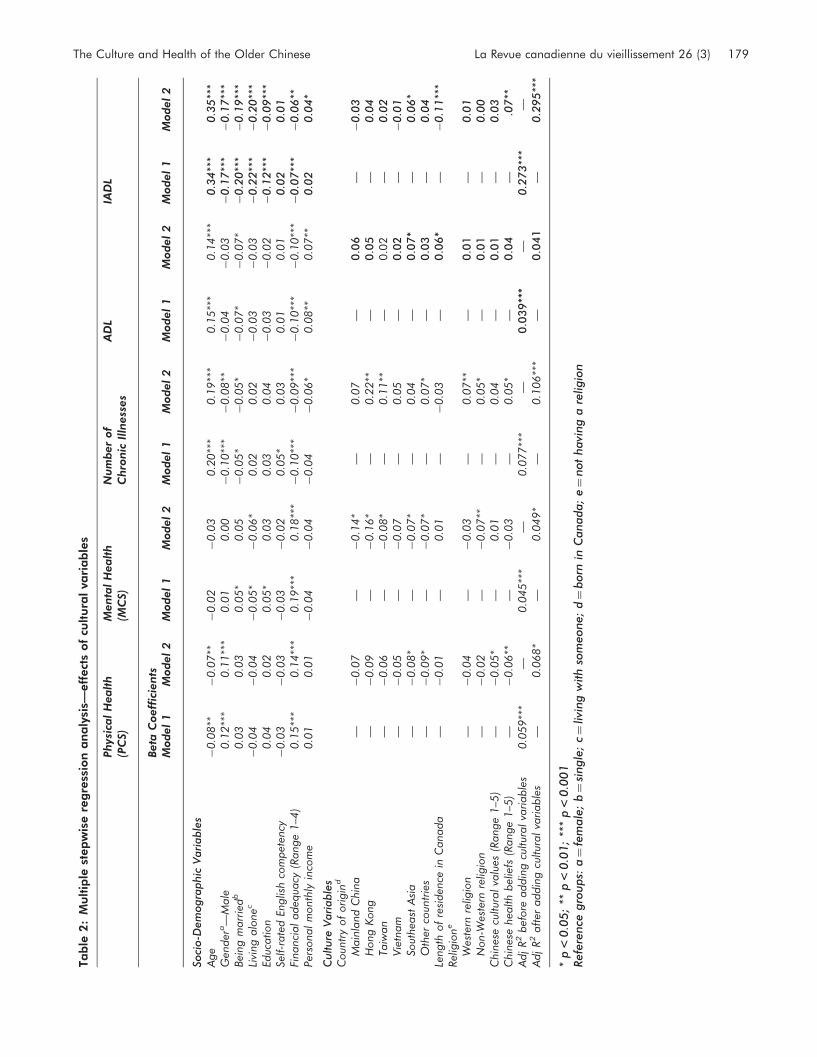
Hierarchical multiple regression analysis wasperformed using the stepwise method, with each ofthe health variables treated as the dependent variablerespectively. The socio-demographic variables werefirst entered as a block, followed by the culturalvariables. The results in Table 2 report the betacoefficient for each of the significant predictors.The results listed under Model 1 for each dependentvariable indicate the effect of the socio-demographicvariables, before the cultural variables were addedto the model. The findings listed under Model2 demonstrate the effects of the predictor variableswhen the cultural variables were added.
The findings in Table 2 indicate that some of the socio-demographic variables were significant in predicting
most of the health variables. Being older was apredictor of poorer physical health, more chronicillnesses, and more limitations in ADL and IADL.When compared with the females, males reportedbetter physical health, fewer chronic illnesses, and alower level of limitation in IADL. The marriedreported fewer chronic illnesses and a higher levelof limitation in ADL and IADL than did singleparticipants. The positive effect on mental health ofbeing married disappeared after the cultural variableswere added, indicating a potential relationshipbetween marital status and the cultural factors.
Although those who reported living alone had a lowerlevel of limitation in IADL, they reported poorermental health than those who lived with someone.A higher level of education was originally significantin predicting better mental health status. But its effectwas not significant after adding the cultural variables.Participants with a higher level of education reporteda lower level of limitation in IADL. Participants’self-perceived English competency was significant inpredicting the number of chronic illnesses but itseffect disappeared after adding the cultural variables.Financial adequacy was the one predictor that wassignificant in predicting all health variables: A higherlevel of financial adequacy was associated with betterphysical and mental health, fewer illnesses, and alower level of limitation in ADL and IADL. Personalmonthly income was mainly significant in predictingnumber of illnesses and limitations in personalfunctioning capacities. Participants reporting higherincomes also reported fewer illnesses and a lowerlevel of limitations in ADL and IADL. The significanteffect of personal monthly income on number ofillnesses and IADL only surfaced after the culturalvariables were added to the regression models.
After taking into account the socio-demographicvariables, the effect of country of origin was signifi-cant in predicting the health variables but variedaccording to the country of origin reported by theparticipants. When compared with participants whowere born in Canada, immigrants from SoutheastAsian and countries in the other category reportedlower levels of physical health. Immigrants in thesetwo groups as well as those from China, Hong Kong,and Taiwan also reported lower levels of mentalhealth than those who were born in Canada.Immigrants from Hong Kong, Taiwan, and countriesin the other category reported more chronic illnesses,while immigrants from Southeast Asia reportedgreater limitation in both ADL and IADL. Length ofresidence in Canada was significant in predictingone’s limitation in ADL and IADL. Participants whohad resided in Canada for a longer time reporteda higher level of limitation in ADL but a lower level of
178 Canadian Journal on Aging 26 (3) Daniel W.L. Lai et al.
Ta
ble
2:
Mu
ltip
lest
ep
wis
ere
gre
ssio
na
na
lysi
s—eff
ect
sof
cultu
ral
vari
ab
les
Phys
ical
Healt
h(P
CS)
Menta
lH
ealt
h(M
CS)
Num
ber
of
Chro
nic
Illn
ess
es
AD
LIA
DL
Beta
Coeff
icie
nts
Model
1M
odel
2M
odel
1M
odel
2M
odel
1M
odel
2M
odel
1M
odel
2M
odel
1M
odel
2
Soci
o-D
em
ogra
phic
Vari
able
sA
ge
�0.0
8**
�0.0
7**
�0.0
2�
0.0
30.2
0**
*0.1
9**
*0.1
5**
*0.1
4**
*0
.34
***
0.3
5**
*G
ender
a—
Male
0.1
2**
*0.1
1**
*0.0
10.0
0�
0.1
0**
*�
0.0
8**
�0.0
4�
0.0
3�
0.1
7**
*�
0.1
7**
*Bei
ng
marr
ied
b0.0
30.0
30.0
5*
0.0
5�
0.0
5*
�0.0
5*
�0.0
7*
�0.0
7*
�0
.20
***
�0
.19
***
Livi
ng
alo
nec
�0.0
4�
0.0
4�
0.0
5*
�0.0
6*
0.0
20.0
2�
0.0
3�
0.0
3�
0.2
2**
*�
0.2
0**
*Ed
ucation
0.0
40.0
20.0
5*
0.0
30.0
30.0
4�
0.0
3�
0.0
2�
0.1
2**
*�
0.0
9**
*Se
lf-r
ate
dEn
glis
hco
mpet
ency
�0.0
3�
0.0
3�
0.0
3�
0.0
20.0
5*
0.0
30.0
10.0
10
.02
0.0
1Fi
nanci
al
adeq
uacy
(Range
1–4
)0.1
5**
*0.1
4**
*0.1
9**
*0.1
8**
*�
0.1
0**
*�
0.0
9**
*�
0.1
0**
*�
0.1
0**
*�
0.0
7**
*�
0.0
6**
Per
sonalm
onth
lyin
com
e0.0
10.0
1�
0.0
4�
0.0
4�
0.0
4�
0.0
6*
0.0
8**
0.0
7**
0.0
20
.04
*
Culture
Vari
able
sC
oun
try
of
origin
d
Main
land
Chin
a—
�0.0
7—
�0.1
4*
—0.0
7—
0.0
6—
�0
.03
Hong
Kong
—�
0.0
9—
�0.1
6*
—0.2
2**
—0.0
5—
0.0
4Ta
iwan
—�
0.0
6—
�0.0
8*
—0.1
1**
—0
.02
—0
.02
Vie
tnam
—�
0.0
5—
�0.0
7—
0.0
5—
0.0
2—
�0
.01
Sout
hea
stA
sia
—�
0.0
8*
—�
0.0
7*
—0.0
4—
0.0
7*
—0
.06
*O
ther
coun
trie
s—
�0.0
9*
—�
0.0
7*
—0.0
7*
—0.0
3—
0.0
4Le
ngth
of
resi
den
cein
Canada
—�
0.0
1—
0.0
1—
�0.0
3—
0.0
6*
—�
0.1
1**
*Rel
igio
ne
Wes
tern
relig
ion
—�
0.0
4—
�0.0
3—
0.0
7**
—0.0
1—
0.0
1N
on-W
este
rnre
ligio
n—
�0.0
2—
�0.0
7**
—0.0
5*
—0.0
1—
0.0
0C
hin
ese
cultur
alva
lues
(Range
1–5
)—
�0.0
5*
—0.0
1—
0.0
4—
0.0
1—
0.0
3C
hin
ese
hea
lth
bel
iefs
(Range
1–5
)—
�0.0
6**
—�
0.0
3—
0.0
5*
—0.0
4—
.07
**A
djR
2bef
ore
addin
gcu
ltur
alva
riable
s0.0
59**
*—
0.0
45**
*—
0.0
77**
*—
0.0
39**
*—
0.2
73
***
—A
djR
2aft
eraddin
gcu
ltur
alva
riable
s—
0.0
68*
—0.0
49*
—0.1
06**
*—
0.0
41
—0
.29
5**
*
*p
<0
.05
;**
p<
0.0
1;
***
p<
0.0
01
Refe
rence
gro
ups:
a¼
fem
ale
;b¼
single
;c¼
livi
ng
with
som
eone;
d¼
born
inC
anada;
e¼
not
havi
ng
are
ligio
n
The Culture and Health of the Older Chinese La Revue canadienne du vieillissement 26 (3) 179

limitation in IADL. However, one should note thatthe effect on ADL was quite small, with a regressioncoefficient of only 0.06. Religion was significant inpredicting mental health and number of illnesses.Participants with a non-Western religion reportedpoorer mental health than did participants who didnot have a religion. Those with a Western or a non-Western religion reported more illnesses than didthose who did not have a religion. Finally, partici-pants reporting a higher level of identification withChinese health beliefs were less healthy physically,having more illnesses and a higher level of limitationin IADL.
As a group, the cultural variables were significant inexplaining variance in four of the five healthvariables, including physical health, mental health,number of illnesses, and limitation in IADL. Yet,although the cultural variables did have significanteffects on some health outcomes, the proportion ofvariance they explained was relatively small. Amongthe various health variables, the cultural variablescontributed the most (3%) to the variance in thenumber of illnesses reported by the participants.When compared with the effect of other socio-demographic variables, their influence in terms ofbeta coefficients was quite sizeable.
DiscussionThe findings show that, although many Chinesepeople share some values and beliefs, intra-groupvariations do exist and indicate that caution is neededwhen making generalizations about a visible minoritygroup. Health- and service-delivery professionalsworking with culturally diverse groups need torecognize the importance of not over-generalizingindividual characteristics and behaviours withingroups. Research that groups the aging popula-tion according to ethnicity may underestimatewithin-group differences and diversity.
The finding that there is a negative impact onhealth of being older, female, unmarried, and poor isconsistent with previous research. Contrary to thebelief that language may be a factor affecting thehealth of cultural minority groups (Miller & Chandler,2002), the findings do not indicate any significanteffect on health of the participants’ self-rated Englishcompetency. This may be because competency inEnglish affects access to services rather than healthstatus directly (Persidsky & Kelly, 1992). Futurestudies should examine how the limited Englishcompetency of this ethnic minority population affectsaccess to services and, consequently, affects healthoutcomes.
Surprisingly, living alone was not a predictor of poorhealth, possibly because those who choose to livealone are healthier and more capable of self-care thanthose who live with others. This is especially true inthe Chinese culture, where a strong sense of respectfor elders often results in families’ taking care of anelderly relative at home when the individual is toofrail to live alone.
Our finding that participants who identified morestrongly with traditional Chinese cultural values andbeliefs also reported less favourable health outcomessupports the view that ethnicity is related to depri-vation in old age for some groups (Gee, 1999;Sokolovksy, 1985). There are two possible explana-tions for this. First, those with stronger Chinesecultural values and beliefs may face a greaterchallenge in adapting socially to a Western system ofvalues and beliefs regarding health, health practices,and service access. The cultural shock and dissonanceexperienced by older Chinese individuals may havedirect negative effects on their health status and onrelated health outcomes. Second, the cultural gapbetween the older Chinese and mainstream societymay result in service barriers for the older Chinesewhen they try to access the health services needed tomaintain health. These barriers include languagedifficulties and discomfort with discussing one’scultural health practices with health service providers.Because this study did not measure the specificincompatibilities experienced by older Chinese inthe existing Western health care system and did notexamine the level of cultural shock and stress relatedto the adjustment to Western culture, further researchis needed to validate this finding.
Health disparities reported between Canadian-bornolder Chinese and immigrant Chinese may be due tothe cultural barriers and adjustment challenges facingimmigrants from different countries of origin. On theother hand, a poorer pre-migration health statuscould also be a reason for such health disparities.Further research is, however, required to examine thevalidity of this argument because no data werecollected on the pre-migration health status of theseimmigrants.
Our findings indicate that the impact on health ofbeing married, of education, and of personal monthlyincome may be related to some of the culturalvariables. Specifically, the predictive effects of educa-tion level and of marital status disappeared, while theeffect of personal income surfaced, after the culturalvariables were added. Future research should payattention to the potential moderating and interactioneffects of these socio-demographic and culturalvariables.
180 Canadian Journal on Aging 26 (3) Daniel W.L. Lai et al.

Generally, the predictor variables explained smallproportions of the variance in health variables. Onereason may be that other factors were not included inthis study; for example, factors related to lifestyle,diet, exercise, and pre-migration health status. Thecross-sectional design of this study limits our capacityto draw conclusions regarding the causal relation-ships between the cultural variables and the healthvariables. Future researchers should consider usinga longitudinal design to track health changes, theaging process, and changes in sociocultural situationof the older Chinese in Canada. This includes know-ing the original health status of the participants beforethey migrated to Canada. Future research shouldconsider measuring the baseline health status ofimmigrants upon their arrival and integrating thisinformation into a longitudinal research design.
Most of the cultural variables, such as Chinesecultural values, Chinese health beliefs, and non-Western religion, have relatively weak and insignifi-cant effects on health variables, particularly whencompared with the effects reported for the socio-demographic predictors. Based on the strong impactof socio-demographic factors, programs and policiesshould focus on strategies to enhance the healthof vulnerable individuals by providing financialresources and strengthening social support for thosewho are older, female, unmarried, and have a poorfinancial status.
Although the effects of the cultural variables arerelatively weak, they do indicate the challenges thatolder Chinese in Canada face within a Western societyin which cultural values and beliefs differ signifi-cantly from their own values and beliefs. Negativehealth outcomes can be addressed by a proactiveapproach to providing culturally competent andculturally appropriate health services and facilitatingaccess to these services. Previous research has shownthat understanding health differences among ethnicgroups, targeting specific cultural groups for healthpromotion, and providing a concrete knowledge baseabout the outcomes of such endeavours is needed(Yee & Weaver, 1994). The findings reported here addto our knowledge about the practice sector byilluminating the need for health professionals toaddress within-group variations, not just in healthstatus and health outcomes, but also in culture-relatedvalues, beliefs, and norms. Health care professionalscan take an approach to providing services thatinvolves negotiating differences by attempting to under-stand health practices that are not Western in origin(Moody, 1998). In particular, during service delivery,health service providers can ask clients specificallyabout their cultural health practices using anapproach that is respectful and non-judgemental.
As well, service providers need to be challenged toanalyse carefully and change the structures thatrestrict minorities from receiving care in a way thatis equitable across cultures (Brotman, 2003).
ReferencesBagley, C.R. (1993). Social psychological adjustments of
migrant and non-migrant elderly in Canada and HongKong. Asia Pacific Journal of Social Work, 3, 67–76.
Baker, F.M. (1994). Suicide among ethnic minority elderly:A statistical and psychosocial perspective. Journal ofGeriatric Psychiatry, 27(2), 241–264.
Boey, K.W. (1997). Paths to psychiatric care: A study ofthe elderly in urban China. Clinical Gerontologist, 18(2),65–80.
Boey, K.W., & Chi, I. (1998). A study of life events andpsychological well-being of the older adults in HongKong. Journal of Clinical Geropsychology, 4(1), 55–64.
Bond, M.H., & Hwang, K.K. (1986). The social psychology ofthe Chinese people. In M.H. Bond (Ed.), The psychologyof the Chinese people (pp. 213–266). Hong Kong: OxfordUniversity Press.
Brotman, S. (2003). The limits of multiculturalism in elderlycare services. Journal of Aging Studies, 17, 209–229.
Casado, B.L, & Leung, P. (2001). Migratory grief anddepression among elderly Chinese American immig-rants. Journal of Gerontological Social Work, 36(1), 5–26.
Chan, K.B. (1983). Coping with aging and managing self-identity: The social world of the elderly Chinesewomen. Canadian Ethnic Studies, 15(3), 36–50.
Craine, M. (1996). A cross-cultural study of beliefs, attitudesand values in Chinese-born American and non-Chinesefrail homebound elderly. Journal of Long Term HomeHealth Care, 15(1), 9–18.
Day, K., & Cohen, U. (2000). The role of culture in designingenvironments for people with dementia: A study ofRussian Jewish immigrants. Environment and Behavior,32(3), 361–399.
Deimling, G.T., Sterns, S., Bowman, K.F., & Kahana, B.(2005). The health of older-adult, long-term cancersurvivors. Cancer Nursing, 28(6), 415–424.
Evan, C.A., & Cunningham, B.A. (1996). Caring for theethnic elder. Geriatric Nursing, 17(3), 105–110.
Femia, E., Zarit, S., & Johansson, B. (2001). The disablementprocess in very late life: A study of the oldest-old inSweden. Journal of Gerontology: Psychological Science,56B, 12–13.
Gaw, A.C. (1993). Psychiatric care of Chinese Americans. InA.C. Gaw (Ed.), Culture, ethnicity, and mental illness(pp. 245–280). Washington, DC: American PsychiatricPress.
The Culture and Health of the Older Chinese La Revue canadienne du vieillissement 26 (3) 181

Gee, E.M. (1999). Ethnic identity among foreign-bornChinese Canadian elders. Canadian Journal on Aging,18(4), 415–429.
Gee, E.M. (2000). Living arrangements and quality of lifeamong Chinese Canadian elders. Social IndicatorsResearch, 51(3), 309–329.
Gelfand, D.E. (2003). Aging and ethnicity: Knowledge andservices. (2nd ed.) New York: Springer.
Gijsen, R., Hoeymans, N., Schellevis, E., Ruwaard, D.,Satariano, W., & Van den Bos, G. (2001). Causes andconsequences of comorbidity: A review. Journal ofClinical Epidemiology, 54, 661–674.
Hancock, T., & Perkins, F. (1985). The mandala of health: Aconceptual model and teaching tool. Health Promotion,24, 8–10.
Health Canada. (2001). The population health template workingtool. Ottawa, ON: Author. Retrieved 25 September2006 from http://www.hc-sc.gc.ca/hppb/phdd/pdf/template_tool.pdf
Henderson, J.N. (1996). Cultural dynamics of dementia ina Cuban and Puerto Rican population in the UnitedStates. In G. Yeo, & D. Gallagher-Thompson (Eds.),Ethnicity and the dementias (pp. 153–166). Washington,DC: Taylor and Francis.
Ho, D.Y.F. (1986). Chinese patterns of socialization: Acritical review. In M.H. Bond (Ed.), The psychology ofthe Chinese people (pp. 1–37). Hong Kong: OxfordUniversity Press.
Ho, S.C., Woo, J., Lau, J., Chan, S.G., Yuen, Y.K., &Chan, Y.K. (1995). Life satisfaction and associatedfactors in older Hong Kong Chinese. Journal of theAmerican Geriatric Society, 43(3), 252–255.
Hopman, W.M., Towheed, T., Anastassiades, T.,Tenenhouse., A., Poliquin, S., & Berger, C. et al.(2000). Canadian normative data for the SF-36health survey. Canadian Medical Association Journal,163(3), 265–271.
Hwu, H.G., Chang, I.H., Yeh, E.K., Chang, C.J., & Yeh, L.L.(1996). Major depressive disorder in Taiwan defined bythe Chinese diagnostic interview schedule. Journal ofNervous and Mental Disease, 184(8), 497–502.
Ikegami, N. (1995). Functional assessment and its place inhealth care. New England Journal of Medicine, 332(9),598–599.
Kasper, J., & Pearson, J.L. (1995). Living arrangements,social integration, and personal control: Correlates oflife satisfaction among older people. Journal of MentalHealth and Aging, 1(1), 21–34.
Kleinman, A. (1980). Patients and healers in the context ofculture: An exploration of the borderland between anthro-pology, medicine and psychiatry. Los Angeles, CA:University of California Press.
Krause, N. (1990). Perceived health problems, formal/informal support, and life satisfaction among olderadults. Journal of Gerontology, 45(5), 193–205.
Lai, D.W.L. (2004). Health status of older Chinese in Canada.Canadian Journal of Public Health, 95(3), 193–197.
Lai, D.W.L., & McDonald, J.R. (1995). Life satisfaction ofChinese elderly immigrants in Calgary. Canadian Journalon Aging, 14(3), 536–552.
Lai, D.W.L., Tsang, K.T., Chappell, N.L., Lai, D.C.Y., &Chau, S.B.Y. (2003). Health and well-being of older Chinesein Canada. Calgary, AB: University of Calgary.
Lam, R.E., Pacala, J.T., & Smith, S.L. (1997). Factors related todepressive symptoms in an elderly Chinese Americansample. Clinical Gerontology, 17(4), 57–70.
Latimer, M., & Sheahan, S.L. (1998). Gender differencesin the causal factors affecting the health status of olderadults. American Journal of Health Behavior, 22(4),298–307.
Lau, J.T., Leung, E.M., & Tsui, H.Y. (2001). Predictingtraditional Chinese medicine’s use and the margin-alization of medical care in Hong Kong. AmericanJournal of Chinese Medicine, 29(3/4), 547–558.
Lauderdale, D.S., & Kestenbaum, B. (2000). Asian Americanethnic identification by surname. Population Researchand Policy Review, 19, 283–300.
Li, A.Y.H. (1990). Social support of Chinese elderly: Anexploratory study in Calgary. Master’s thesis, UniversityCalgary, National Library of Canada.
Li, P.S. (1977). Fictive kinship, conjugal tie and kinship chainamong Chinese immigrants in the United States. Journalof Comparative Family Studies, 8, 47–63.
Li, P.S. (1985). The use of oral history in studying elderlyChinese-Canadians. Canadian Ethnic Studies, 17(1),67–77.
McCracken, C.F.M., Boneham, M.A., Copeland, J.R.M.,Williams, K.E., & Wilson, K. (1997). Prevalence ofdementia and depressions among elderly people inblack and ethnic minorities. British Journal of Psychiatry,171, 269–273.
Miller, A.M., & Chandler, P.J. (2002). Acculturation,resilience, and depression in midlife women from theformer Soviet Union. Nursing Research, 51(1), 26–32.
Moody, H.R. (1998). Cross-cultural geriatric ethics:Negotiating our differences. Generations, 22(3), 32–39.
Nelson, M.A. (1994). Economic impoverishment as a healthrisk: Methodologic and conceptual issues. Advances inNursing Science, 16(3), 1–12.
Persidsky, I.V., & Kelly, J.J. (1992). Adjustment of Sovietelderly in the United States: An educationalapproach. Gerontology and Geriatrics Education,13(1/2), 129–140.
182 Canadian Journal on Aging 26 (3) Daniel W.L. Lai et al.

Pettee, K.K., Brach, J.S., Kriska, A.M., Boudreau, R.,Richardson, C.R., & Colbert, L.H. et al. (2006).Influence of marital status on physical activity levelsamong older adults. Medicine and Science in Sports andExercise, 38(3), 541–546.
Plouffe, L.A. (2003). Addressing social and gender inequal-ities in health among seniors in Canada. Canadian SaudePublica, 19(3), 855–860.
Ren, X.S., Amick, B., Zhou, L., & Gandek, B. (1998).Translation and psychometric evaluation of a Chineseversion of the SF-36 Health Survey in the United States.Journal of Clinical Epidemiology, 51, 1129–1138.
Ren, X.S., & Chang, K. (1998). Evaluating health statusof elderly Chinese in Boston. Journal of ClinicalEpidemiology, 51, 429–435.
Roberts, P., & Fawcett, G. (1998). At risk: A socio-economicanalysis of health and literacy among seniors. Ottawa:Statistics Canada.
Rosenwaike, I. (1994). Surname analysis as a means ofestimating minority of elderly, an application usingAsian surnames. Research on Aging, 16(2), 212–227.
Satia, J.A., Patterson, R.E., Taylor, V.M., Cheney, C.L.,Shiu-Thornton, S., & Chitnarong, K. et al. (2000).Perspectives in practice: Use of qualitative methods tostudy diet, acculturation, and health in Chinese-Amer-ican women. Journal of American Diet Association, 100(8),934–940.
Shapiro, J., Douglas, K., de la Rocha, O., Radecki, S., Vu, C.,& Dinh, T. (1999). Generational differences inpsychosocial adaptation and predictors of psychologi-cal distress in a population of recent Vietnameseimmigrants. Journal of Community Health, 24, 95–113.
Singh, N.N. (1995, November). Unity in diversity. Keynoteaddress presentation at 118th annual conference ofteacher education division of council for exceptionalchildren, Honolulu, HI.
Sokolovksy, J. (1985). Ethnicity, culture and aging:Do differences really make a difference? Journal ofApplied Gerontology, 4(1), 6–17.
Spector, R.E. (2000). Cultural diversity in health andillness. (5th ed., pp. 195–214). Upper Saddle River,NJ: Prentice Hall Health.
Statistics Canada. (2003). Canada’s ethnocultural portrait:The changing mosaic. Ottawa, ON: Author. Retrieved25 September 2006 from http://www12.statcan.ca/english/census01/products/highlight/Ethnicity/Index.cfm
Statistics Canada. (2005). Canadian Community Health Survey:Public use microdata file (Catalogue No. 82M0013XCB).Ottawa: Author.
Tjam, E.Y. (2001). How to find Chinese researchparticipants: Use of a phonologically based surnamesearch method. Canadian Journal of Public Health, 92,138–142.
Tsai, D.T., & Lopez, R.A. (1997). The use of social supportsby elderly Chinese immigrants. Journal of GerontologicalSocial Work, 29(1), 77–94.
Tsuei, W. (1992). Roots of Chinese culture and medicine. Jaya,Malaysia: Pelanduk.
Ware, J.E., & Gandek, B. (1998). Overview of SF-36 HealthSurvey and the international quality of life projectassessment (IQOLA) project. Journal of ClinicalEpidemiology, 51(11), 903–912.
Ware, J.E., & Kosinski, M. (2001). Interpreting SF-36summary health measures: A response. Quality of LifeResearch, 10, 405–413.
Ware, J.E., Kosinski, M., Gandek, B., Aaronson, N.K.,Apolone, G., & Bech, P. et al. (1998). The factorstructure of the SF-36 Health Survey in 10 countries:Results from the IQOLA Project. International Qualityof Life Assessment. Journal of Clinical Epidemiology,51(11), 1159–1165.
Ware, J.E., Kosinski, M., & Keller, S. D. (1994). SF-36 physicaland mental health summary scales: A user’s manual.Boston, MA: Health Institute, New England MedicalCentre.
Ware, J.E., & Sherbourne, C.D. (1992). The MOS 36-ItemShort-Form Health Survey (SF-36�): 1. Conceptualframework and item selection. Medical Care, 30(6),473–483.
Winkleby, M.A., Darius, E.J., Frank, E., & Fortmann, S.P.(1992). Socioeconomic status and health: How educa-tion, income, and occupation contribute to risk factorsfor cardiovascular disease. American Journal of PublicHealth, 82(6), 816–820.
Wu, D.Y.H., & Tseng, W.S. (1985). Introduction: Thecharacteristics of Chinese culture. Orlando, FL: AcademicPress.
Yee, B.W.K., & Weaver, G.D. (1994). Ethnic minorities andhealth promotion: Developing a culturally competentagenda. Generations, 18(1), 39–44.
Yu, E.SH. (1986). Health of the Chinese elderly in America.Research on Aging, 8(1), 84–109.
The Culture and Health of the Older Chinese La Revue canadienne du vieillissement 26 (3) 183
Related Documents











