Endourology and Stones Relationships Between Carbonation Rate of Carbapatite and Morphologic Characteristics of Calcium Phosphate Stones and Etiology Xavier Carpentier, Michel Daudon, Olivier Traxer, Paul Jungers, Aurélie Mazouyes, Guy Matzen, Emmanuel Véron, and Dominique Bazin OBJECTIVES To examine the significance of the carbonation rate (CR) in carbonated apatite (carbapatite [CA]) stones and its relationships with the morphologic characteristics of CA and etiology. CA stones without struvite can result from metabolic disorders or urinary tract infection, but the latter etiology is still debated. Infection stones caused by urea-splitting bacteria are made of CA admixed with struvite and exhibit a high CO 3 2 /PO 4 3 ratio (CR). However, little is known as to the significance of the CR of CA in the absence of struvite in idiopathic calcium phosphate stones. METHODS We studied 39 urinary calculi mainly composed of CA without struvite. Of the 39 patients, 13 had a past or present history of urinary tract infection, 24 had hypercalciuria, and 2 had medullary sponge kidney. The stones were examined by Fourier transform infrared spectroscopy and scanning electron microscopy. The presence of amorphous carbonated calcium phosphate or whitlockite was also considered. RESULTS The CR of CA was 14% 9%. On scanning electron microscopy, the CA particles appeared as spherules of 4.5 3.0 m in diameter and were significantly larger in females than in males. In 16 cases, scanning electron microscopy showed bacterial imprints. In these calculi, the CR was significantly greater (22% 7%) than in those without a visible bacterial imprint (8% 5%, P .0001). Amorphous carbonated calcium phosphate was found in 15 of 16 stones (93.8%) with imprints and in none of the 23 stones without imprints (P .0001). CONCLUSIONS A close relationship was observed between the presence of bacterial imprints, indicative of past or current urinary tract infection, and both the presence of amorphous carbonated calcium phosphate (or whitlockite) and a high CR of CA. UROLOGY 73: 968 –975, 2009. © 2009 Elsevier Inc. C alculi made of apatite as the main component represent about 10% of urinary stones in West- ern countries, with a greater prevalence in women than in men. 1-3 They are observed in patients with hypercalciuria, anomalies of urine pH, or distal tubular acidosis. 4,5 A possible relationship with urinary tract infection (UTI) has been suggested, but this has been questioned for stones devoid of struvite. 6 As shown by Fourier transform infrared (FTIR) spectroscopy anal- ysis, apatite is always found as carbonated apatite (car- bapatite [CA]), which contains variable amounts of car- bonate (CO 3 2 ) ions. 2 It is well established that stones resulting from UTI due to urea-splitting bacteria consist of CA admixed with struvite, 7–9 and exhibit a high CO 3 2 content. 7 However, little is known regarding the etiopathogenic significance of the CO 3 2 content of CA in the absence of struvite in idiopathic calcium phos- phate stones. The present investigation sought to examine the CO 3 2 /PO 4 3 ratio (carbonation rate [CR]) in CA, the morphology at the mesoscopic scale of calcium phosphate stones devoid of struvite, and the possible relationships between the CR, stone composition, and morphologic characteristics of CA as observed by scanning electron microscopy (SEM) and the etiology. MATERIAL AND METHODS The study material consisted of 39 urinary calcium phosphate calculi predominantly composed of CA without any struvite, as determined by routine FTIR spectroscopy and stereomicroscopy From the Department of Urology, Tenon Hospital, Assistance Publique–Hôpitaux de Paris, Paris, France; Departments of Biochemistry A and Nephrology, Necker Hospital, Assistance Publique–Hôpitaux de Paris, Paris, France; Solid State Laboratory, Paris XI University, Orsay, France; and Research Unit on Conditions Extrêmes et Matériaux: Hautes Températures et Irradiation UPR3079, Centre National de la Recherche Scientifique, Orléans, France Reprint requests: Michel Daudon, Ph.D., Laboratoire de Biochimie A, Hôpital Necker, 149 Rue de Sèvres, Paris 75743 Cedex15 France. E-mail: michel.daudon@ nck.aphp.fr Submitted: August 31, 2008, accepted (with revisions): December 22, 2008 968 © 2009 Elsevier Inc. 0090-4295/09/$34.00 All Rights Reserved doi:10.1016/j.urology.2008.12.049

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

E
RCaCXG
O
M
R
C
Cwwttbbyb
FPAUHS
Nn
9
ndourology and Stones
elationships Betweenarbonation Rate of Carbapatitend Morphologic Characteristics ofalcium Phosphate Stones and Etiology
avier Carpentier, Michel Daudon, Olivier Traxer, Paul Jungers, Aurélie Mazouyes,uy Matzen, Emmanuel Véron, and Dominique Bazin
BJECTIVES To examine the significance of the carbonation rate (CR) in carbonated apatite (carbapatite [CA])stones and its relationships with the morphologic characteristics of CA and etiology. CA stoneswithout struvite can result from metabolic disorders or urinary tract infection, but the latter etiologyis still debated. Infection stones caused by urea-splitting bacteria are made of CA admixed withstruvite and exhibit a high CO3
2�/PO43� ratio (CR). However, little is known as to the significance
of the CR of CA in the absence of struvite in idiopathic calcium phosphate stones.ETHODS We studied 39 urinary calculi mainly composed of CA without struvite. Of the 39 patients, 13
had a past or present history of urinary tract infection, 24 had hypercalciuria, and 2 hadmedullary sponge kidney. The stones were examined by Fourier transform infrared spectroscopyand scanning electron microscopy. The presence of amorphous carbonated calcium phosphate orwhitlockite was also considered.
ESULTS The CR of CA was 14% � 9%. On scanning electron microscopy, the CA particles appeared asspherules of 4.5 � 3.0 �m in diameter and were significantly larger in females than in males. In16 cases, scanning electron microscopy showed bacterial imprints. In these calculi, the CR wassignificantly greater (22% � 7%) than in those without a visible bacterial imprint (8% � 5%,P � .0001). Amorphous carbonated calcium phosphate was found in 15 of 16 stones (93.8%)with imprints and in none of the 23 stones without imprints (P � .0001).
ONCLUSIONS A close relationship was observed between the presence of bacterial imprints, indicative of past orcurrent urinary tract infection, and both the presence of amorphous carbonated calcium phosphate
(or whitlockite) and a high CR of CA. UROLOGY 73: 968–975, 2009. © 2009 Elsevier Inc.broCeip
Cmsbcm
M
Tc
alculi made of apatite as the main componentrepresent about 10% of urinary stones in West-ern countries, with a greater prevalence in
omen than in men.1-3 They are observed in patientsith hypercalciuria, anomalies of urine pH, or distal
ubular acidosis.4,5 A possible relationship with urinaryract infection (UTI) has been suggested, but this haseen questioned for stones devoid of struvite.6 As showny Fourier transform infrared (FTIR) spectroscopy anal-sis, apatite is always found as carbonated apatite (car-apatite [CA]), which contains variable amounts of car-
rom the Department of Urology, Tenon Hospital, Assistance Publique–Hôpitaux dearis, Paris, France; Departments of Biochemistry A and Nephrology, Necker Hospital,ssistance Publique–Hôpitaux de Paris, Paris, France; Solid State Laboratory, Paris XIniversity, Orsay, France; and Research Unit on Conditions Extrêmes et Matériaux:autes Températures et Irradiation UPR3079, Centre National de la Recherche
cientifique, Orléans, FranceReprint requests: Michel Daudon, Ph.D., Laboratoire de Biochimie A, Hôpitalecker, 149 Rue de Sèvres, Paris 75743 Cedex15 France. E-mail: michel.daudon@
dck.aphp.frSubmitted: August 31, 2008, accepted (with revisions): December 22, 2008
68 © 2009 Elsevier Inc.All Rights Reserved
onate (CO32�) ions.2 It is well established that stones
esulting from UTI due to urea-splitting bacteria consistf CA admixed with struvite,7–9 and exhibit a highO3
2� content.7 However, little is known regarding thetiopathogenic significance of the CO3
2� content of CAn the absence of struvite in idiopathic calcium phos-hate stones.The present investigation sought to examine the
O32�/PO4
3� ratio (carbonation rate [CR]) in CA, theorphology at the mesoscopic scale of calcium phosphate
tones devoid of struvite, and the possible relationshipsetween the CR, stone composition, and morphologicharacteristics of CA as observed by scanning electronicroscopy (SEM) and the etiology.
ATERIAL AND METHODS
he study material consisted of 39 urinary calcium phosphatealculi predominantly composed of CA without any struvite, as
etermined by routine FTIR spectroscopy and stereomicroscopy0090-4295/09/$34.00doi:10.1016/j.urology.2008.12.049

fotiscqsaio
walstw
FwiU ned concentric layers. (E) Carbapatite morphology resemblinga les of carbapatite grouped as spherules.
F1
U
or morphologic typing.10 The stones were selected on the basisf 4 criteria. The first requirement was the presence of CA ashe main component (ie, the most abundant crystalline phasedentified in the stone). The total calcium phosphate content oftones was 62%-94%, with a CA content of 44%-90%; otheralcium phosphates accounted for 0%-42%. The second re-uirement was the absence of struvite as determined by theecond derivative of infrared spectra. The third requirement wasn infrared spectrum profile allowing the determination graph-cally of the CR on the spectrum. Finally, a sufficient quantityf material was required for both infrared and SEM analysis.The studied calculi came from 39 patients (20 men and 19
omen). Of the studied calculi, 13 were spontaneously passed,nd 20 kidney stones were removed by percutaneous nephro-ithotomy (n � 15), open surgery (n � 3), or extracorporealhock wave lithotripsy (n � 2). Four stones were removed fromhe ureter by ureteroscopy (n � 2) or extracorporeal shock
igure 1. Scanning electron microscopy photographs of caith rod-like bacterial imprints on surface suggesting infect
mprints on surface suggesting infection by cocci species.nusual morphology of carbapatite spherules with well-defiggregated needles without special organization. (F) Need
rbapatite stones without struvite. (A) Spherules of carbapatiteion by bacilli. (B) Spherules of carbapatite with round bacterial(C) Spherules of carbapatite without any bacterial imprint. (D)
ave lithotripsy (n � 2), and 2 stones were extracted from the c
ROLOGY 73 (5), 2009
%
5,0
12,5
20,0
27,5
35,0
0,0 6,3 12,5 18,8 25,0Bacterial_prints
Car
bona
tion_
rate
Nb/100 µm2
R = 0.86, p < 0.0001
igure 2. Correlation between number of bacterial imprints/00 �m2 and carbonation rate of carbapatite. Slope � 0.9. R,
orrelation coefficient.969
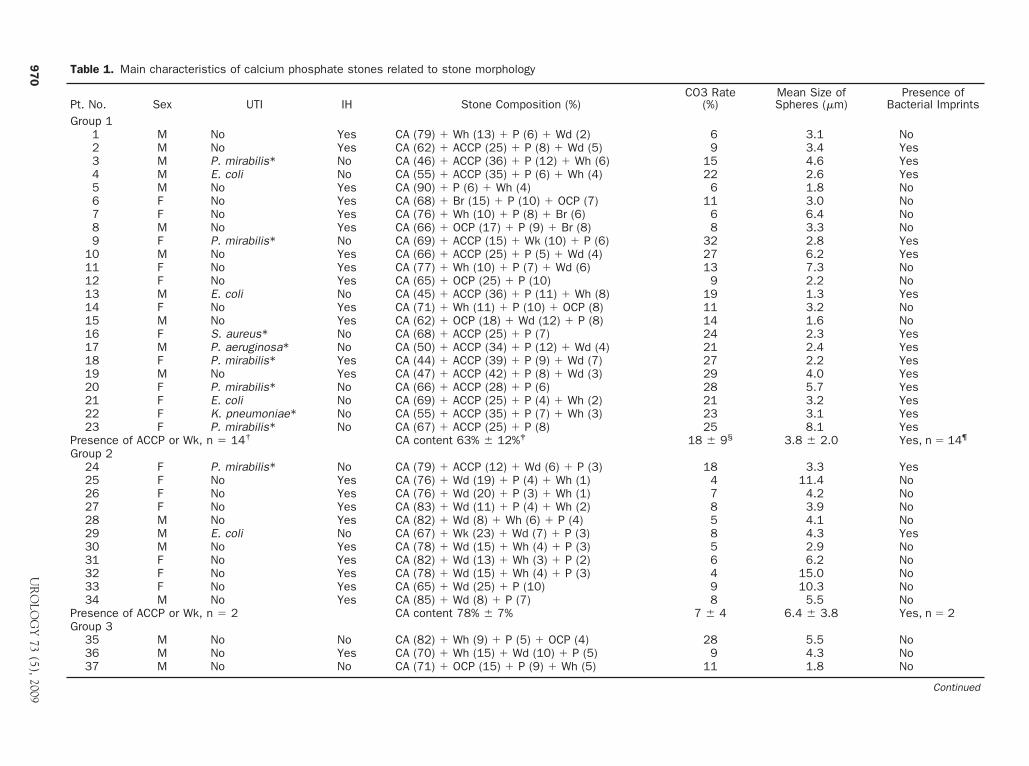
Table 1. Main characteristics of calcium phosphate stones related to stone morphology
Pt. No. Sex UTI IH Stone Composition (%)CO3 Rate
(%)Mean Size ofSpheres (�m)
Presence ofBacterial Imprints
Group 11 M No Yes CA (79) � Wh (13) � P (6) � Wd (2) 6 3.1 No2 M No Yes CA (62) � ACCP (25) � P (8) � Wd (5) 9 3.4 Yes3 M P. mirabilis* No CA (46) � ACCP (36) � P (12) � Wh (6) 15 4.6 Yes4 M E. coli No CA (55) � ACCP (35) � P (6) � Wh (4) 22 2.6 Yes5 M No Yes CA (90) � P (6) � Wh (4) 6 1.8 No6 F No Yes CA (68) � Br (15) � P (10) � OCP (7) 11 3.0 No7 F No Yes CA (76) � Wh (10) � P (8) � Br (6) 6 6.4 No8 M No Yes CA (66) � OCP (17) � P (9) � Br (8) 8 3.3 No9 F P. mirabilis* No CA (69) � ACCP (15) � Wk (10) � P (6) 32 2.8 Yes
10 M No Yes CA (66) � ACCP (25) � P (5) � Wd (4) 27 6.2 Yes11 F No Yes CA (77) � Wh (10) � P (7) � Wd (6) 13 7.3 No12 F No Yes CA (65) � OCP (25) � P (10) 9 2.2 No13 M E. coli No CA (45) � ACCP (36) � P (11) � Wh (8) 19 1.3 Yes14 F No Yes CA (71) � Wh (11) � P (10) � OCP (8) 11 3.2 No15 M No Yes CA (62) � OCP (18) � Wd (12) � P (8) 14 1.6 No16 F S. aureus* No CA (68) � ACCP (25) � P (7) 24 2.3 Yes17 M P. aeruginosa* No CA (50) � ACCP (34) � P (12) � Wd (4) 21 2.4 Yes18 F P. mirabilis* Yes CA (44) � ACCP (39) � P (9) � Wd (7) 27 2.2 Yes19 M No Yes CA (47) � ACCP (42) � P (8) � Wd (3) 29 4.0 Yes20 F P. mirabilis* No CA (66) � ACCP (28) � P (6) 28 5.7 Yes21 F E. coli No CA (69) � ACCP (25) � P (4) � Wh (2) 21 3.2 Yes22 F K. pneumoniae* No CA (55) � ACCP (35) � P (7) � Wh (3) 23 3.1 Yes23 F P. mirabilis* No CA (67) � ACCP (25) � P (8) 25 8.1 Yes
Presence of ACCP or Wk, n � 14† CA content 63% � 12%‡ 18 � 9§ 3.8 � 2.0 Yes, n � 14¶
Group 224 F P. mirabilis* No CA (79) � ACCP (12) � Wd (6) � P (3) 18 3.3 Yes25 F No Yes CA (76) � Wd (19) � P (4) � Wh (1) 4 11.4 No26 F No Yes CA (76) � Wd (20) � P (3) � Wh (1) 7 4.2 No27 F No Yes CA (83) � Wd (11) � P (4) � Wh (2) 8 3.9 No28 M No Yes CA (82) � Wd (8) � Wh (6) � P (4) 5 4.1 No29 M E. coli No CA (67) � Wk (23) � Wd (7) � P (3) 8 4.3 Yes30 M No Yes CA (78) � Wd (15) � Wh (4) � P (3) 5 2.9 No31 F No Yes CA (82) � Wd (13) � Wh (3) � P (2) 6 6.2 No32 F No Yes CA (78) � Wd (15) � Wh (4) � P (3) 4 15.0 No33 F No Yes CA (65) � Wd (25) � P (10) 9 10.3 No34 M No Yes CA (85) � Wd (8) � P (7) 8 5.5 No
Presence of ACCP or Wk, n � 2 CA content 78% � 7% 7 � 4 6.4 � 3.8 Yes, n � 2Group 3
35 M No No CA (82) � Wh (9) � P (5) � OCP (4) 28 5.5 No36 M No Yes CA (70) � Wh (15) � Wd (10) � P (5) 9 4.3 No37 M No No CA (71) � OCP (15) � P (9) � Wh (5) 11 1.8 No
Continued
97
0U
RO
LOG
Y73
(5),2009
b5
menmudph
pitTs(aipw
eemtwvwvcrt
v
RTTwsdt1itpwsiwwt
swi(bl
e1
.C
ontin
ued
.N
o.S
exU
TIIH
Sto
neC
ompo
sitio
n(%
)C
O3
Rat
e(%
)M
ean
Siz
eof
Sph
eres
(�m
)Pr
esen
ceof
Bac
teria
lIm
prin
ts
38
MN
oYe
sC
A(5
1)
�W
d(2
5)
�B
r(1
1)
�W
h(9
)�
P(4
)1
02
.2N
o3
9M
No
No
CA
(47)
�P
(28)
�O
CP
(15)
�W
h(1
0)
81
.3N
oes
ence
ofAC
CP
orW
k�
1C
Aco
nten
t64%
�15%
13
�8
3.9
�3
.0Ye
s,n
�0
eral
lmea
n�
SD
CA
cont
ent
68%
�13%
14
�9
4.5
�3
.0
.No.
�pa
tient
num
ber;
UTI
�ur
inar
ytr
acti
nfec
tion;
IH�
idio
path
ichy
perc
alci
uria
;M�
mal
e;F
�fe
mal
e;C
A�
carb
apat
ite(c
arbo
nate
dap
atite
);W
h�
whe
wel
lite
(cal
cium
oxal
ate
mon
ohyd
rate
);�
prot
ein;
Wd
�w
edde
llite
(cal
cium
oxal
ate
dihy
drat
e);
Br
�br
ushi
te(d
ical
cium
phos
phat
edi
hydr
ate)
;O
CP
�oc
taca
lciu
mph
osph
ate
pent
ahyd
rate
;AC
CP
�am
orph
ous
carb
onat
edca
lciu
mos
phat
e;W
k�
whi
tlock
ite.
Dat
apr
esen
ted
asm
ean
�S
Dor
num
bers
ofpa
tient
s;da
tain
pare
nthe
ses
are
perc
enta
ges.
Gro
up1
cons
iste
dof
type
IV(c
alci
umph
osph
ate
ston
es);
grou
p2
cons
iste
dof
mix
edty
peIV
�II
ston
es(m
ixtu
res
ofca
lciu
mph
osph
ate
and
wed
delli
te);
and
grou
p3
cons
iste
dof
hete
roge
neou
sor
phol
ogie
san
dco
mpo
sitio
ns.
Ure
ase-
prod
ucin
gm
icro
orga
nism
s.�
.01
vsgr
oup
2.
�.0
01
vsgr
oup
2.
�0
.00
01
vsgr
oup
2.
�.0
2vs
grou
p2
.
UROL
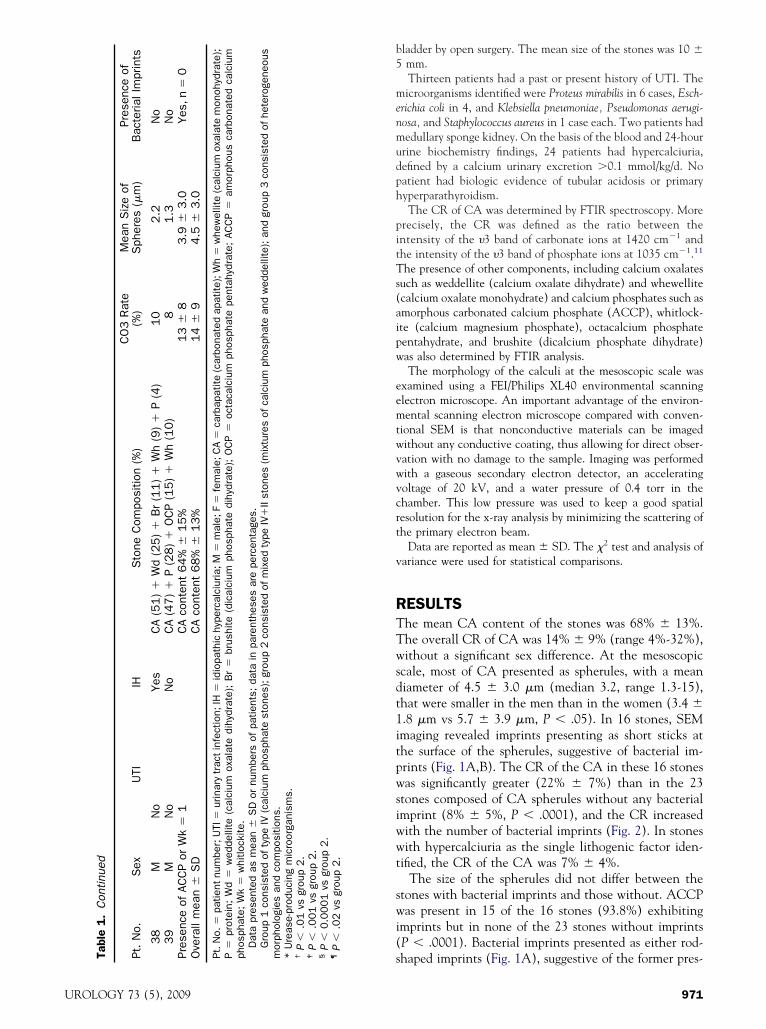
ladder by open surgery. The mean size of the stones was 10 �mm.Thirteen patients had a past or present history of UTI. Theicroorganisms identified were Proteus mirabilis in 6 cases, Esch-
richia coli in 4, and Klebsiella pneumoniae, Pseudomonas aerugi-osa, and Staphylococcus aureus in 1 case each. Two patients hadedullary sponge kidney. On the basis of the blood and 24-hour
rine biochemistry findings, 24 patients had hypercalciuria,efined by a calcium urinary excretion �0.1 mmol/kg/d. Noatient had biologic evidence of tubular acidosis or primaryyperparathyroidism.The CR of CA was determined by FTIR spectroscopy. More
recisely, the CR was defined as the ratio between thentensity of the �3 band of carbonate ions at 1420 cm�1 andhe intensity of the �3 band of phosphate ions at 1035 cm�1.11
he presence of other components, including calcium oxalatesuch as weddellite (calcium oxalate dihydrate) and whewellitecalcium oxalate monohydrate) and calcium phosphates such asmorphous carbonated calcium phosphate (ACCP), whitlock-te (calcium magnesium phosphate), octacalcium phosphateentahydrate, and brushite (dicalcium phosphate dihydrate)as also determined by FTIR analysis.The morphology of the calculi at the mesoscopic scale was
xamined using a FEI/Philips XL40 environmental scanninglectron microscope. An important advantage of the environ-ental scanning electron microscope compared with conven-
ional SEM is that nonconductive materials can be imagedithout any conductive coating, thus allowing for direct obser-ation with no damage to the sample. Imaging was performedith a gaseous secondary electron detector, an acceleratingoltage of 20 kV, and a water pressure of 0.4 torr in thehamber. This low pressure was used to keep a good spatialesolution for the x-ray analysis by minimizing the scattering ofhe primary electron beam.
Data are reported as mean � SD. The �2 test and analysis ofariance were used for statistical comparisons.
ESULTShe mean CA content of the stones was 68% � 13%.he overall CR of CA was 14% � 9% (range 4%-32%),ithout a significant sex difference. At the mesoscopic
cale, most of CA presented as spherules, with a meaniameter of 4.5 � 3.0 �m (median 3.2, range 1.3-15),hat were smaller in the men than in the women (3.4 �.8 �m vs 5.7 � 3.9 �m, P � .05). In 16 stones, SEMmaging revealed imprints presenting as short sticks athe surface of the spherules, suggestive of bacterial im-rints (Fig. 1A,B). The CR of the CA in these 16 stonesas significantly greater (22% � 7%) than in the 23
tones composed of CA spherules without any bacterialmprint (8% � 5%, P � .0001), and the CR increasedith the number of bacterial imprints (Fig. 2). In stonesith hypercalciuria as the single lithogenic factor iden-
ified, the CR of the CA was 7% � 4%.The size of the spherules did not differ between the
tones with bacterial imprints and those without. ACCPas present in 15 of the 16 stones (93.8%) exhibiting
mprints but in none of the 23 stones without imprintsP � .0001). Bacterial imprints presented as either rod-
shaped imprints (Fig. 1A), suggestive of the former pres-Ta Pt Pr Ov
Pt P ph m * †P
‡P
§P
¶P
OGY 73 (5), 2009 971

et1Aprrh
ctaswwofispsww
6mpcoaOrfAaIwU
77tTwAtp
kpow
CAosg
Fu1ttstppvaas
lftiurhaEcsiacpcpaniuracitimtcuurepscilps
9
nce of bacilli, or round imprints (Fig. 1B), suggestive ofhe former presence of cocci. Whitlockite was present instone with bacterial rod imprints that did not containCCP. As listed in Table 1, all stones from the 13
atients with a reported history of UTI contained bacte-ial imprints. However, 3 other stones contained bacte-ial imprints in the absence of a reported present or pastistory of UTI.CA stones can be classified according to morphologic
riteria, as previously reported.10 Among the 6 mainypes of this classification, type IV includes all calciumnd magnesium phosphate stones, and type II includestones mainly composed of weddellite. Because CA andeddellite often coexist in stones, especially in patientsith hypercalciuria, a mixed type IV�II is frequentlybserved. According to the morphologic examinationndings, 3 groups could be distinguished in our series oftones: group 1 included 23 stones composed of nearlyure calcium phosphate (type IV); group 2 included 11tones composed of a mixture of calcium phosphate andeddellite (type IV�II), and group 3 included 5 stonesith a complex heterogeneous structure.In the group 1 stones, the mean CA content was
3% � 12%, the CR of the CA was 18% � 9%, and theean size of the spherules was 3.8 � 2 �m. ACCP was
resent in 14 of these stones (60.9%), all of whichontained bacterial imprints (Table 1). Eleven (47.8%)f these 23 patients had a past or present history of UTI,nd hypercalciuria was present in 13 patients (56.5%).ne patient had both hypercalciuria and a history of
ecurrent UTI. In 3 other cases, bacterial imprints wereound in the stones of patients who had hypercalciuria.mong the patients with a past or present history of UTI,
ll but 1 produced stones with a CR of the CA of �15%.n 2 cases in which the CR of the CA was high, E. colias identified as the microorganism responsible for theTI.In the group 2 stones, the mean CA content was
8% � 7% (P � .001 vs group 1), the CR of CA was% � 4% (P � .0001 vs group 1), and the mean size ofhe spherules was 6.4 � 3.8 �m (P � .05 vs group 1).wo stones (18.2%, P � .02 vs group 1) from patientsith a history of UTI exhibited bacterial imprints.CCP was present in 1 and whitlockite in the other of
hese stones. Hypercalciuria was diagnosed in 9 of the 11atients (81.8%).Group 3 included the 2 patients with medullary sponge
idney and 2 patients with hypercalciuria. None of theatients had a history of UTI. No bacterial imprint wasbserved on SEM. The mean CA content of the stonesas 64% � 15%, and the CR of CA was 13% � 8%.
OMMENTll biologic apatites appear to be uniformly composed
f similar elementary anisotropic nanocrystals, with aize of 10-15 nm.12 However, they exhibit a much
reater diversity at the mesoscopic scale. As shown in 672
igure 1, CA crystallites presented essentially as spher-les of various sizes ranging from 1.3 to 15 �m (Fig.A-D) but also as less-organized structures (Fig. 1E)hat sometimes coexisted with spherulitic structures inhe same stone (Fig. 1F). The mean size of the CApherules was significantly larger in the women than inhe men and had no significant correlation with theresence or absence of either ACCP or bacterial im-rints. In other biologic materials such as bone, sali-ary calculi, or Randall’s plaques,13 CA crystallitesppear as nonspherulitic structures, probably owing tohigh protein content, which orients the tridimen-
ional organization of CA.Our results suggest that UTI was involved in the
ithogenic process in �16 cases, and a history of UTI wasound in 13 instances. The relationship between UTI andhe formation of kidney stones is firmly established innfection stones made of struvite and CA induced byrea-splitting enterobacteria.7-9 However, a lithogenicole of UTI in calcium-phosphate stones devoid of struviteas also been suggested. Edin-Liljegren et al.14 reported thatlthough E. coli strains are usually not urease-producing,. coli is often cultured in phosphate-containing urinaryalculi. In an in vitro study, they showed that E. colitrongly reduced urinary citrate and increased urease-nduced calcium phosphate crystallization. Leusmannnd Sabinski15 observed a matrix effect of bacterial gly-oproteins, inducing the initial precipitation of calciumhosphate, which might subsequently be coated by cal-ium oxalate. Cohen et al.16 reported that both urease-roducing and nonurease-producing microorganisms canccumulate calcium crystals intracellularly, thus formingidi for calculus formation. In addition, they showed that
n vitro inoculation of urease-negative E. coli in sterilerine samples from a nonstone-forming healthy volunteeresulted some days later in the formation of hydroxyap-tite crystals, apart from any urease activity.17 Thus, E.oli, even devoid of urea-splitting activity, is able tonduce the formation of calcium phosphate crystals. Inhis respect, we have previously reported that whitlock-te, an infrequent component of stones, was associated inost cases with UTI involving nonurease-splitting bac-
eria, and E. coli was identified in �25% of patients.2 Itan therefore be hypothesized that bacterial imprints inrinary stones are likely to reflect the past presence ofrea-splitting or nonurea-splitting bacteria that played aole in stone formation. In the 1970s and 1980s, Cifu-ntes Delatte and Santos18 and Cifuentes Delatte19 re-orted the presence of such bacterial imprints in renaltones using transmission and scanning electron micros-opy, and similar observations have been made by othernvestigators as well.20 These findings might explain, ateast in part, the well-known greater prevalence of phos-hate stones in women than in men,6,21 because of thetrikingly greater incidence of UTI episodes in women.22
In our study, bacterial imprints were observed in only
.2% of CA stones without ACCP. In contrast, theyUROLOGY 73 (5), 2009
wptpaoCCUOft
idwicsisbAr
Fmapsc obs
U
ere present in all CA stones that contained any pro-ortion of ACCP, evidence of a close correlation be-ween the presence of UTI and the presence of ACCP inhosphate stones. UTI caused by urea-splitting bacteria isn established condition inducing the co-crystallizationf struvite and CA phosphate.23 Accordingly, the CR ofA is especially high in these stones, and therefore aR �15% appears to be indicative of the contribution ofTI by urea-splitting bacteria in the lithogenic process.2
ur present findings suggest that the same might be trueor calcium phosphate calculi without struvite, because
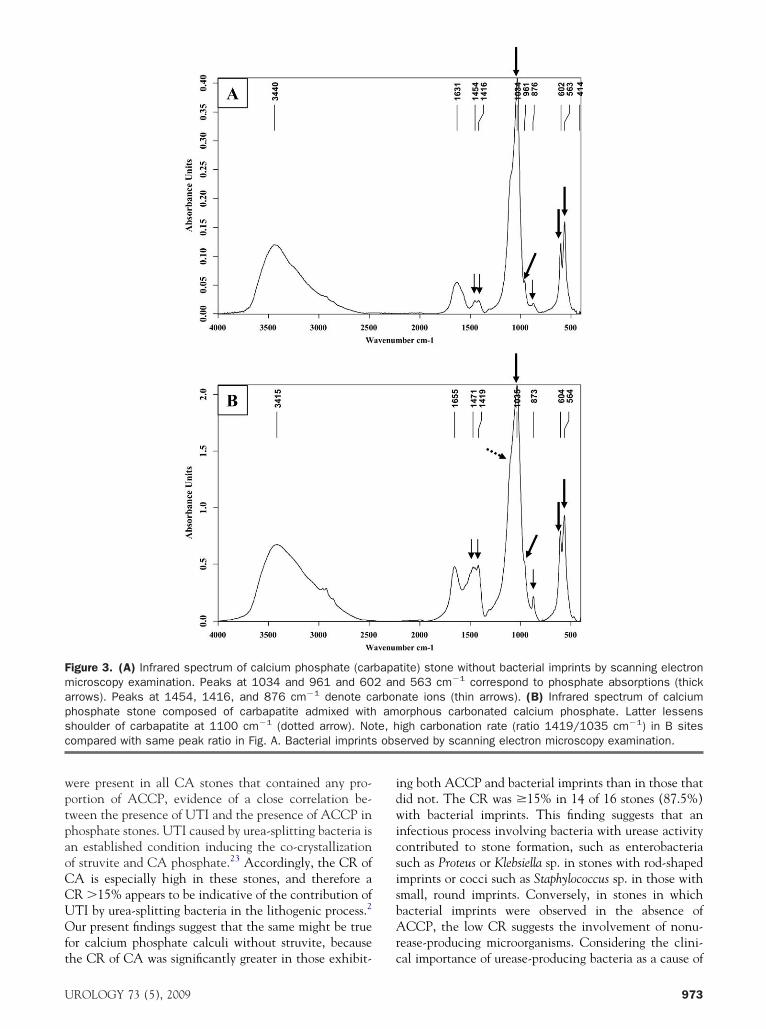
igure 3. (A) Infrared spectrum of calcium phosphate (caricroscopy examination. Peaks at 1034 and 961 and 60rrows). Peaks at 1454, 1416, and 876 cm�1 denote cahosphate stone composed of carbapatite admixed withhoulder of carbapatite at 1100 cm�1 (dotted arrow). Noompared with same peak ratio in Fig. A. Bacterial imprints
he CR of CA was significantly greater in those exhibit- c
ROLOGY 73 (5), 2009
ng both ACCP and bacterial imprints than in those thatid not. The CR was �15% in 14 of 16 stones (87.5%)ith bacterial imprints. This finding suggests that an
nfectious process involving bacteria with urease activityontributed to stone formation, such as enterobacteriauch as Proteus or Klebsiella sp. in stones with rod-shapedmprints or cocci such as Staphylococcus sp. in those withmall, round imprints. Conversely, in stones in whichacterial imprints were observed in the absence ofCCP, the low CR suggests the involvement of nonu-
ease-producing microorganisms. Considering the clini-
tite) stone without bacterial imprints by scanning electrond 563 cm�1 correspond to phosphate absorptions (thickate ions (thin arrows). (B) Infrared spectrum of calciumorphous carbonated calcium phosphate. Latter lessensigh carbonation rate (ratio 1419/1035 cm�1) in B siteserved by scanning electron microscopy examination.
bapa2 anrbonam
te, h
al importance of urease-producing bacteria as a cause of
973

amtccbuocepnpwpAtttAp
tfafpb
Ctdhras�lya
eaatpsspcCekcrafebIw(thciopCFhcAciipanCu
CIsbaSssiidAm
Fus
9
significant proportion of calcium phosphate stones, itight be of interest for physicians that the urease-posi-
ive property of a microorganism identified after urineulture should be mentioned with the bacterial identifi-ation. In our series, 2 stones contained both ACCP andacterial imprints with a CR of CA �15%, suggesting arease activity. Also, E. coli was identified as the micro-rganism present in the urine. Perhaps these strains of E.oli were weakly urease-positive. However, a possibilityxists that another bacterium, producing urease, wasresent in the urine and not recognized. FTIR determi-ation of the degree of carbonation of CA in calciumhosphate stones and the identification of ACCP orhitlockite could be a simple method to identify theossible implication of UTI in the lithogenic process.CCP is not easily identified by x-ray diffraction, and
he CR of calcium phosphate cannot be determined usinghis technique. In contrast, infrared spectroscopy offershe advantage of reliably detecting the presence ofCCP admixed with CA and assessing its CR, thus
roviding more complete information.As suggested by the stone morphology and composi-
ion, hypercalciuria was an active promoter of stoneormation found in 61.5% of cases. However, UTI waslso a factor of lithogenesis in 35.9% of cases, and bothactors were associated in �4 cases. Thus, stone analysisrovided more accurate information than the clinical andiologic data in identifying the cause of the stones.Of clinical interest is the site of carbonate ions in the
A crystals. From a chemical point of view, CA can formhrough a carbonate ion substitution for either the hy-roxyl group (A type) or the phosphate group (B type) ofydroxyapatite.24,25 Carbonate ions can also be incorpo-ated at the surface of the apatite crystals (labile carbon-te). A-type and B-type carbonate are, respectively, as-essed by the 878 cm�1 and 872 cm�1 components of2CO3; a third peak at 866 cm�1 is associated with theabile carbonate.26 There has been controversy for manyears regarding the location of carbonate (CO3) in the
Epithelium damage NH3 CO2
Bacteria adhesion
Mg2+ Struvite Carbapatite and Ca2+
(Magnesium ammonium ACCP (Carbonatedphosphate) calcium phosphates)
UreaH2N-CO-NH2
Urease
pH > 8 NH4+ HCO3
- CO32-
+ PO43- + PO4
3-
+ hyperuricosuria Ammonium urate
+ H2O
igure 4. Schematic representation of urea breakdown byrease-producing microorganisms inducing formation oftruvite and/or of highly carbonated calcium phosphates.
patite lattice.27 Several investigators examining differ- w
74
nt carbonate substitution mechanisms in bulk hydroxy-patite recently showed that B (or PO4) site substitutionsre energetically preferred to A (or OH) site substitu-ions.28-30 In urinary stones, the constant presence ofroteins, sometimes in high proportion, makes the mea-urement of the �3 CO3 band for carbonate ions in the Aite difficult. Therefore, we evaluated the carbonate/hosphate ratio at 1420 cm�1, which corresponds toarbonate ions in the B site. The finding that the averageR of CA was 2-fold greater (19% � 8%) in the pres-
nce of ACCP than in its absence (8% � 4%), is ineeping with the fact that an environment with a higharbonate content is a condition needed for carbonate-ich apatites to crystallize in urine.27 The increased rel-tive absorbance and the slight shift of the �2CO3 bandrom 876 (Fig. 3A) to 873 cm�1 (Fig. 3B) reflect thenrichment of carbonate ions of CA associated withacterial imprints mainly involving B sites of the lattice.n parallel, the alteration of the �3 PO4 peak of CA,hich reflects a poorly crystallized calcium phosphate
presence of ACCP) suggests a relationship between bac-eria and enrichment of carbonate ions in B sites. Inuman urine, the unique condition able to induce a higharbon dioxide content is the local formation of theseons through urea breakdown (Fig. 4). Thus, the presencef ACCP could be a marker for chronic UTI by urease-roducing microorganisms. The detection of both a highR of calcium phosphate and presence of ACCP byTIR stone analysis might alert the physician as to theypothesis of UTI as the cause of the stone and toonsider the possible indication of antibacterial therapy.s deduced from Figure 4, struvite should be present with
alcium phosphate in the case of UTI by urease-produc-ng bacteria. However, calcium phosphate crystallizations more sensitive than struvite to weak changes of urineH. Struvite crystallization requires a high magnesiummmonium phosphate molar product, a condition that isot always found in infected urine, thus explaining howA stones without struvite might be the result of UTI byrea-splitting bacteria.
ONCLUSIONSn phosphate stones without struvite, a significant as-ociation was observed between a high CR of CA andoth the presence of ACCP as determined by FTIR,nd the presence of bacterial imprints as shown byEM. Thus, the finding of both a high CR and ACCPpherules in a phosphate stone, in the absence oftruvite, is highly suggestive of the past or currentmplication of microorganisms with weak urease activ-ty. The reason the structural characteristics of CAiffer among calcium phosphate stones is not yet clear.dditional studies are needed to better correlate suchorphologic characteristics at the mesoscopic scale
ith stone etiology.UROLOGY 73 (5), 2009

R
1
1
1
1
1
1
1
1
1
1
2
2
2
22
2
2
2
2
2
3
U
eferences1. Daudon M, Donsimoni R, Hennequin C, et al. Sex- and age-related
composition of 10 617 calculi analyzed by infrared spectroscopy.Urol Res. 1995;23:319-326.
2. Maurice-Estepa L, Levillain P, Lacour B, et al. Crystalline phasedifferentiation in urinary calcium phosphate and magnesium phos-phate calculi. Scand J Urol Nephrol. 1999;33:299-305.
3. Parks JH, Worcester EM, Coe FL, et al. Clinical implications ofabundant calcium phosphate in routinely analyzed kidney stones.Kidney Int. 2004;66:777-785.
4. Coe FL, Parks JH. Stone disease in hereditary distal renal tubularacidosis. Ann Intern Med. 1980;93:60-61.
5. Pak CYC, Adams-Huet B. Elucidation of factors determining for-mation of calcium phosphate stones. J Urol. 2004;172:2267-2270.
6. Gault MH, Paul MD, Longerich L. Comparison of urinary tractinfection in calcium oxalate and calcium phosphate stone formers.Nephron. 1990;55:408-413.
7. Griffith DP. Infection-induced renal calculi. Kidney Int. 1982;21:422-430.
8. Cohen TD, Preminger GM. Struvite calculi. Semin Nephrol. 1996;16:425-434.
9. Bichler KH, Eipper E, Naber K, et al. Urinary infection stones. IntJ Antimicrob Agents. 2002;19:488-498.
0. Daudon M, Bader C, Jungers P. Urinary calculi: review of classifi-cation methods and correlations with aetiology. Scan Microsc. 1993;7:1081-1106.
1. Nguyen Q, Dao, Daudon M. Infrared and Raman Spectra of Calculi.Paris: Elsevier; 1997.
2. Becker A, Epple M, Muller KM, et al. A comparative study ofclinically well-characterized human atherosclerotic plaques withhistological, chemical, and ultrastructural methods. J Inorg Bio-chem. 2004;98:2032-2038.
3. Daudon M, Traxer O, Jungers P, et al. Stone morphology suggestiveof Randall’s plaque. In: Evan AP, Lingeman JE, Williams JC Jr eds.Renal Stone Disease. Am Inst Phys Conf Proc. 2007;900:26-34.
4. Edin-Liljegren A, Hedelin HH, Grenabo L, et al. Impact of Esch-erichia coli on urine citrate and urease-induced crystallization. Scan
Microsc. 1995;9:901-905.ROLOGY 73 (5), 2009
5. Leusmann DB, Sabinski F. Potential contribution of optional ure-ase-positive bacteria to idiopathic urinary calcium stone formation.Urol Res. 1996;24:73-78.
6. Cohen MS, Warren MM, Bauer P, et al. Intracellular crystalformation in bacteria from human urines: a contributing factor inurinary calculi. Urol Res. 1981;9:55-61.
7. Cohen MS, Davis CP, Czerwinski EW, et al. Calcium phosphatecrystal formation in Escherichia coli from human urine: an in-vitrostudy. J Urol. 1982;127:184-185.
8. Cifuentes Delatte L, Santos M. Calcified bacteria in renal stones:electron microscopic aspects. Eur Urol. 1977;3:96-99.
9. Cifuentes Delatte L. Composicion y estructura de los calculos renales.Barcelona: Salvat; 1984.
0. Leusmann DB. Erste Zusammenfassende Ergenbisse der kombini-erten Phasen-und gefügeanalyse von Harnsteinen mittels Roent-genbeugung Rasterelektronen Mikroskopie. Pathog Klin Harnsteine.1982;8:275-280.
1. Daudon M. Epidemiology of nephrolithiasis in France. Ann Urol.2005;39:209-231.
2. Harrington RD, Hooton TM. Urinary tract infection risk factorsand gender. J Gend Specif Med. 2000;3:27-34.
3. Griffith DP. Struvite stones. Kidney Int. 1978;13:372-382.4. Santos M, Gonzalez-Diaz PF. A model for B carbonate apatite.
Inorg Chem. 1977;16:2131-2134.5. McConnell D, Foreman DW Jr. Model for carbonate apatite. Inorg
Chem. 1978;17:2039-2040.6. Elliott JC, Bonel G, Trombe JC. Space group and lattice constants
of Ca10 (PO4)6 CO3. J Appl Crystallogr. 1980;13:618-621.7. Elliott JC. Structure and Chemistry of the Apatites and Other Calcium
Orthophosphates. Amsterdam: Elsevier; 1994.8. Astala R, Stott MJ. First principles investigation of mineral com-
ponent of bone: CO3 substitutions in hydroxyapatite. Chem Mater.2005;17:4125-4133.
9. Wilson RM, Dowker SE, Elliott JC. Rietveld refinements andspectroscopic structural studies of a Na-free carbonate apatite madeby hydrolysis of monetite. Biomaterials. 2006;27:4682-4692.
0. Antonakos A, Liarokapis E, Leventouri T. Micro-raman and FTIRstudies of synthetic and natural apatites. Biomaterials. 2007;28:
3043-3054.975
Related Documents











