Reinvigorating Continuing Medical Education: Meeting the Challenges of the Digital Age Michael W. Cullen, MD; Jeffrey B. Geske, MD; Nandan S. Anavekar, MBBCh; Julie A. McAdams, MBA; Mary Ellen Beliveau, MEd; Steve R. Ommen, MD; and Rick A. Nishimura, MD Abstract Clinicians in today’s health care environment face an overwhelming quantity of knowledge that re- quires continued education and lifelong learning. However, traditional continuing medical education (CME) courses cannot meet these educational needs, particularly given the proliferation of knowledge and increasing demands on clinicians’ time and resources. CME courses that previously offered only in-person, face-to-face education must evolve in a learner-centric manner founded on principles of adult learning theory to remain relevant in the current era. In this article, we describe the transition of the Mayo Clinic Cardiovascular Review for Cardiology Boards and Recertification (CVBR) from a traditional course with only live content to a course integrating live, online, and enduring materials. This evolution has required leveraging technology to maximize learner engagement, offering faculty development to ensure content alignment with learner needs, and strong leadership dedicated to providing learners an unparalleled educational experience. Despite stagnation in growth of the traditional live course, these changes have increased the overall reach of the Mayo Clinic CVBR. Learners engaging with digital content have demonstrated larger increases in knowledge with less educational time commitment. Courses seeking to implement similar changes must develop formal learning objectives focused on learner needs, build an online presence that includes an assessment of learner knowledge, enlist a cohort of dedicated faculty who teach based on principles of adult learning theory, and perpetually refresh educational content based on learner feedback and performance. Following these principles will allow traditional CME courses to thrive despite learners’ resource constraints and alternative means to access information. ª 2019 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2019;94(12):2501-2509 C ontinuing medical education (CME) in the 21st century is evolving rapidly. 1-6 Advances in technology now permit multiple points of learner contact. Busy clinicians can access educational material through a variety of digital recordings and online platforms. In this setting, an explosion of clinical knowl- edge underscores an ongoing need for continuing education. These changes have shifted the paradigm of CME. Live courses are no longer neces- sary to deliver knowledge. In addition, clini- cians are less able to leave their practices because of productivity, financial, and administrative expectations, and fewer are willing to spend nonworking time away from their families. Ubiquitous access to in- formation makes live didactic knowledge de- livery, a stalwart of traditional continuing medical education, less necessary in the cur- rent era. Learners now expect easily acces- sible activities that facilitate knowledge synthesis and prioritize clinically relevant problem solving. 1 Finally, evolving proof of competence requirements from medical spe- cialty boards oblige continuous rather than periodic learning. 7-9 All these factors have negatively affected attendance at and engage- ment with traditional live CME meetings. To meet the needs of learners in this changing environment, CME courses must themselves evolve. Courses can no longer consist of a series of loosely related content From the Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN (M.W.C., J.B.G., N.S.A., J.A.M., S.O., R.A.N.) and Chief Executive Offi- cer, Knowledge to Prac- tice, Bethesda, MD (M.E.B.). SPECIAL ARTICLE Mayo Clin Proc. n December 2019;94(12):2501-2509 n https://doi.org/10.1016/j.mayocp.2019.07.004 www.mayoclinicproceedings.org n ª 2019 Mayo Foundation for Medical Education and Research 2501

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SPECIAL ARTICLE
Reinvigorating Continuing Medical Education:Meeting the Challenges of the Digital AgeMichael W. Cullen, MD; Jeffrey B. Geske, MD; Nandan S. Anavekar, MBBCh;Julie A. McAdams, MBA; Mary Ellen Beliveau, MEd; Steve R. Ommen, MD;and Rick A. Nishimura, MD
Abstract
Clinicians in today’s health care environment face an overwhelming quantity of knowledge that re-quires continued education and lifelong learning. However, traditional continuing medical education(CME) courses cannot meet these educational needs, particularly given the proliferation of knowledgeand increasing demands on clinicians’ time and resources. CME courses that previously offered onlyin-person, face-to-face education must evolve in a learner-centric manner founded on principles ofadult learning theory to remain relevant in the current era. In this article, we describe the transition ofthe Mayo Clinic Cardiovascular Review for Cardiology Boards and Recertification (CVBR) from atraditional course with only live content to a course integrating live, online, and enduring materials.This evolution has required leveraging technology to maximize learner engagement, offering facultydevelopment to ensure content alignment with learner needs, and strong leadership dedicated toproviding learners an unparalleled educational experience. Despite stagnation in growth of thetraditional live course, these changes have increased the overall reach of the Mayo Clinic CVBR.Learners engaging with digital content have demonstrated larger increases in knowledge with lesseducational time commitment. Courses seeking to implement similar changes must develop formallearning objectives focused on learner needs, build an online presence that includes an assessment oflearner knowledge, enlist a cohort of dedicated faculty who teach based on principles of adult learningtheory, and perpetually refresh educational content based on learner feedback and performance.Following these principles will allow traditional CME courses to thrive despite learners’ resourceconstraints and alternative means to access information.
ª 2019 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2019;94(12):2501-2509
From the Department ofCardiovascular Medicine,Mayo Clinic, Rochester,MN (M.W.C., J.B.G.,N.S.A., J.A.M., S.O., R.A.N.)and Chief Executive Offi-cer, Knowledge to Prac-tice, Bethesda, MD(M.E.B.).
C ontinuing medical education(CME) in the 21st century isevolving rapidly.1-6 Advances in
technology now permit multiple points oflearner contact. Busy clinicians can accesseducational material through a variety ofdigital recordings and online platforms. Inthis setting, an explosion of clinical knowl-edge underscores an ongoing need forcontinuing education.
These changes have shifted the paradigmof CME. Live courses are no longer neces-sary to deliver knowledge. In addition, clini-cians are less able to leave their practicesbecause of productivity, financial, andadministrative expectations, and fewer arewilling to spend nonworking time away
Mayo Clin Proc. n December 2019;94(12):2501-2509 n https://doi.owww.mayoclinicproceedings.org n ª 2019 Mayo Foundation for M
from their families. Ubiquitous access to in-formation makes live didactic knowledge de-livery, a stalwart of traditional continuingmedical education, less necessary in the cur-rent era. Learners now expect easily acces-sible activities that facilitate knowledgesynthesis and prioritize clinically relevantproblem solving.1 Finally, evolving proof ofcompetence requirements from medical spe-cialty boards oblige continuous rather thanperiodic learning.7-9 All these factors havenegatively affected attendance at and engage-ment with traditional live CME meetings.
To meet the needs of learners in thischanging environment, CME courses mustthemselves evolve. Courses can no longerconsist of a series of loosely related content
rg/10.1016/j.mayocp.2019.07.004edical Education and Research
2501

MAYO CLINIC PROCEEDINGS
2502
experts lecturing to the audience about theirown field of expertise. Instead, traditionallydidactic courses must shift from a teacher-centered to a student-centered model, designcurriculum to meet the specific needs oftheir learners, and build a team of facultymembers who cohesively deliver broad anddeep content without gaps or redundancies.This evolution of CME needs to remaingrounded in established, evidence-basedprinciples of lifelong continuing education.
This article describes our experiencecontemporizing a live CME course with ablend of both online and live learning. Thisevolution has been made possible by 3important factors: (1) learner engagementthrough technology, (2) faculty develop-ment, and (3) visionary leadership and men-toring for the next generation of educators.These changes have improved learner perfor-mance and increased longitudinal involve-ment with educational materials while stillmaintaining relevance of the live CMEcourse despite challenges from the externalenvironment.
THE MAYO CLINIC CARDIOVASCULARREVIEW FOR CARDIOLOGY BOARDS ANDRECERTIFICATION COURSE AND ADULTLEARNING THEORYThe Mayo Clinic Cardiovascular Review forCardiology Boards and Recertification(ie, Mayo Clinic Cardiovascular Review forCardiology Boards and Recertification[CVBR]) began in 1995. The course wasinitially structured as a traditional CME pro-gram, with didactic lectures spread over 5-6days. Sessions covered the gamut of topics ingeneral and subspecialty cardiology, with afocus on preparing first-time certifiers andrecertifiers to pass their American Board ofInternal Medicine (ABIM) CardiovascularBoard Examination. Given its comprehen-sive content, the course also attracted prac-ticing cardiologists seeking to refresh theirknowledge from a comprehensive,evidence-based curriculum. At its peak in2008, 850 participants attended the liveannual course.
As the environment surrounding CMEevolved, the course directors recognized
Mayo Clin Proc. n December 2019;9
the need to grow the course beyond thetraditional didactic format. In 2013, theypartnered with a third party consultinggroup, Knowledge to Practice (K2P). K2Pprovided unique services compared withother third-party CME vendors, such Oak-stone’s Practical Reviews or WoltersKluwer’s Audio Digest, that offer digital con-tent delivery without comprehensive inte-gration into existing live programming. Thepartnership between the Mayo Clinic CVBRand K2P sought to integrate curriculumdesign, faculty development, course manage-ment, and learner analysis to deliver person-alized, competency-based learning. Both K2Pand course leaders understood that changesof this magnitude required a strong theoret-ical basis. Therefore, they founded the evolu-tion of the Mayo Clinic CVBR on establishedprinciples of adult learning theory.
The concept of adult learning theorydates to the 1970s, when educational expertMalcolm Knowles outlined his principles ofandragogy, also known as adult learning the-ory.10-13 These principles contrast with peda-gogy, which takes a teacher-centeredapproach to education. The curriculum inandragogy is learner defined rather thanteacher defined. Teachers must focus onconcepts relevant to a learner’s specific goals.Concepts build on learner experience asopposed to an instructor’s area of expertise,because learners must integrate their priorexperiences into new knowledge to feelcomfortable changing their behavior. Objec-tive self-assessments shift motivation fromextrinsic to intrinsic sources. Therefore,learning in andragogic theory is directlyapplicable to a learner’s knowledge gapsinstead of predefined subjects or tasks.
For more than 25 years, studies havedocumented that approaches that use princi-ples of adult learning theory improve theeffectiveness of CME. For instance, multiplesystematic reviews have demonstrated thatdidactic sessions alone are less effective forimproving performance or affecting patientcare.14,15 In contrast, workshops and casediscussions, which are more interactive,learner-centered, and engaging, demonstratehigher degrees of effectiveness.14,16
4(12):2501-2509 n https://doi.org/10.1016/j.mayocp.2019.07.004www.mayoclinicproceedings.org
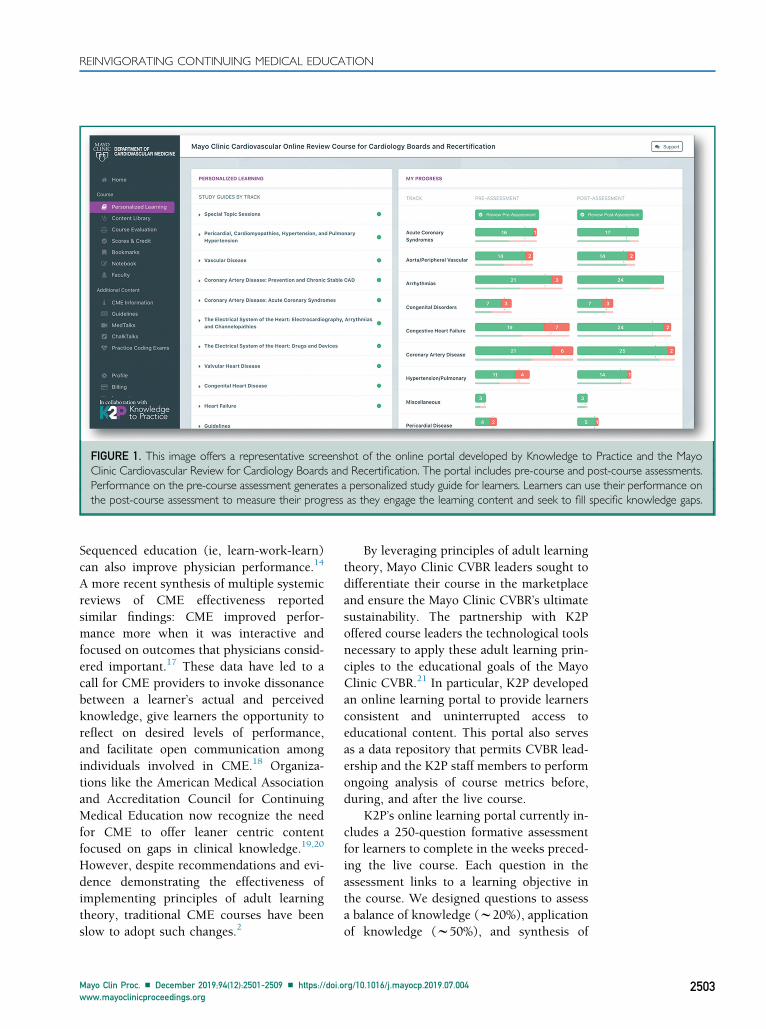
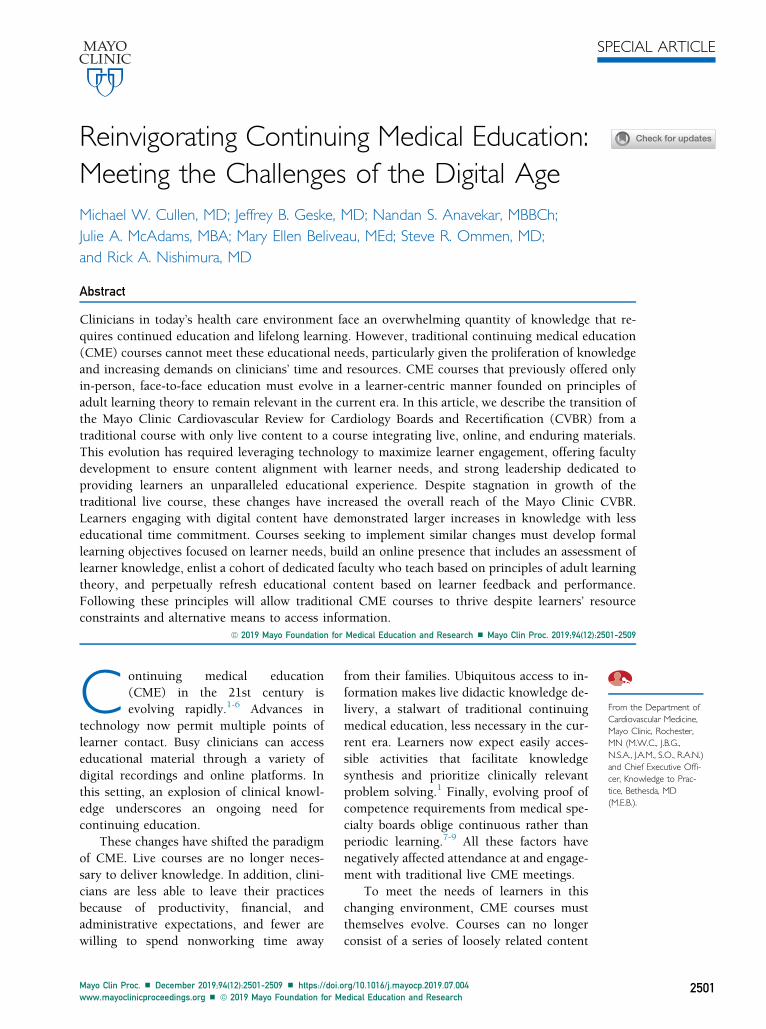
FIGURE 1. This image offers a representative screenshot of the online portal developed by Knowledge to Practice and the MayoClinic Cardiovascular Review for Cardiology Boards and Recertification. The portal includes pre-course and post-course assessments.Performance on the pre-course assessment generates a personalized study guide for learners. Learners can use their performance onthe post-course assessment to measure their progress as they engage the learning content and seek to fill specific knowledge gaps.
REINVIGORATING CONTINUING MEDICAL EDUCATION
Sequenced education (ie, learn-work-learn)can also improve physician performance.14
A more recent synthesis of multiple systemicreviews of CME effectiveness reportedsimilar findings: CME improved perfor-mance more when it was interactive andfocused on outcomes that physicians consid-ered important.17 These data have led to acall for CME providers to invoke dissonancebetween a learner’s actual and perceivedknowledge, give learners the opportunity toreflect on desired levels of performance,and facilitate open communication amongindividuals involved in CME.18 Organiza-tions like the American Medical Associationand Accreditation Council for ContinuingMedical Education now recognize the needfor CME to offer leaner centric contentfocused on gaps in clinical knowledge.19,20
However, despite recommendations and evi-dence demonstrating the effectiveness ofimplementing principles of adult learningtheory, traditional CME courses have beenslow to adopt such changes.2
Mayo Clin Proc. n December 2019;94(12):2501-2509 n https://doi.owww.mayoclinicproceedings.org
By leveraging principles of adult learningtheory, Mayo Clinic CVBR leaders sought todifferentiate their course in the marketplaceand ensure the Mayo Clinic CVBR’s ultimatesustainability. The partnership with K2Poffered course leaders the technological toolsnecessary to apply these adult learning prin-ciples to the educational goals of the MayoClinic CVBR.21 In particular, K2P developedan online learning portal to provide learnersconsistent and uninterrupted access toeducational content. This portal also servesas a data repository that permits CVBR lead-ership and the K2P staff members to performongoing analysis of course metrics before,during, and after the live course.
K2P’s online learning portal currently in-cludes a 250-question formative assessmentfor learners to complete in the weeks preced-ing the live course. Each question in theassessment links to a learning objective inthe course. We designed questions to assessa balance of knowledge (w20%), applicationof knowledge (w50%), and synthesis of
rg/10.1016/j.mayocp.2019.07.004 2503
Live course
2010 2011 2012 2013 2014 2015 2016 2017
Online course DVD sales Total participant reach
Num
ber
of p
artic
ipan
ts
0
200
400
600
800
1000
1200
1400
1600
1800
2000
FIGURE 2. The number of participants in the traditional live course has remained stagnant and slightlydecreased. However, the course has expanded its total participant reach through distribution of enduringmaterials, particularly online content.
MAYO CLINIC PROCEEDINGS
2504
knowledge (w30%). Learners do not typi-cally complete the pretest in a single setting,which distributes the burden of answering250 questions. Despite the large number ofquestions, over the last 3 years, 58% of at-tendees have completed the formative assess-ment. The formative assessment helpslearners to evaluate their current knowledge,identify knowledge gaps, and focus theirattention while they attend the live course.When learners complete their formativeassessment, the online portal generates alist of personalized learning recommenda-tions. These recommendations highlight ses-sions in the upcoming course that address agiven learner’s knowledge gaps. During thelive course, learners use the portal to followlecture content, ask faculty questions, accesssupplemental reference material such asguidelines important publications, completefaculty evaluations, and review supplemen-tary online-only presentations that are notpart of the live course. The Mayo ClinicCVBR first integrated K2P’s online learningportal as part of the 2014 course. Figure 1displays a representative screenshot ofK2P’s portal.
These tools from K2P have allowed theMayo Clinic CVBR to expand beyond a
Mayo Clin Proc. n December 2019;9
traditional live course. Digital recordings ofthe course have been available for purchaseas DVDs for several years and remain a pop-ular method through which learners asyn-chronously engage with the content.However, DVD technology is becoming lessaccessible, and simple viewing of recordedlectures remains a passive form of learning.Therefore, in 2015, the course began offeringan option for online-only registration, givinglearners access to content through the onlinelearning portal without attending the livecourse. These offerings expanded in 2016,when content from the Mayo Clinic CVBRbecame available as a segmented onlinecourse, giving learners access to content insmaller, 5-10-minute segments targeted tospecific learning objectives and knowledgegaps. Those participating in this segmentedonline course do not have the benefit ofdirect interaction with faculty and peers ordedicated time away from other personaland professional demands that attendingthe live course offers. Rather, the segmentedapproach facilitates “learning-on-the-go,”allowing learners to access small pieces ofknowledge without requiring them to investlarge segments of time. Over the past severalyears, the Mayo Clinic CVBR has increased
4(12):2501-2509 n https://doi.org/10.1016/j.mayocp.2019.07.004www.mayoclinicproceedings.org

Live course Complete onlinecourse
Segmented onlinecourse
62
3021
47
20
40
60
80
100
27
89
Hours of engagement (annualized) % Increase in knowledge
FIGURE 3. Data from the Mayo Clinic Cardiovascular Review for Cardi-ology Boards and Recertification demonstrates that, while hours ofengagement decreases, knowledge lift can actually increase with a movefrom traditional live learning formats to online learning.
REINVIGORATING CONTINUING MEDICAL EDUCATION
its reach by more than 2000 total partici-pants, driven largely through an increase inonline access to the course. In contrast, livecourse participation has stabilized whilegrowth of DVD sales has slowed(Figure 2). Moving forward, these trendswill likely accelerate, as resources for livelearning become more limited and technol-ogy increasingly permit online and digitalaccess to information and medicalknowledge.
LEARNER ENGAGEMENT AND IMPACT OFTECHNOLOGYA key component underlying the evolutionof the Mayo Clinic CVBR has been the focuson learner engagement through technolog-ical innovation. This engagement hasoccurred on several levels, all of which arefounded on principles of adult learningtheory.
Learner engagement begins severalmonths before the live CVBR course, whenregistrants receive access to the online pre-test. The online pretest drives engagementthrough multiple mechanisms. For example,literature demonstrates that physicians’ abil-ity to self-evaluate their competence in rela-tion to their peers is notoriously poor.22,23
After completing the pretest, learners receivean objective assessment of their own perfor-mance in relation to competency and theperformance of their peers. These resultsidentify knowledge gaps and create discor-dance between actual and perceived compe-tence, which can drive intrinsic motivationand engagement. During the 2017 MayoClinic CVBR, learners who completed thepretest had 28% more online portal viewsthan did learners who did not complete thepretest. This result demonstrates thatengagement before the course is associatedwith subsequent engagement during and af-ter the course.
Learner engagement continues duringthe live course as well. Learners can takeand store lecture notes directly in the onlineportal. They can post online questions thatfaculty members answer immediately aftertheir lecture. Course directors use analyticdata from audience response questions in
Mayo Clin Proc. n December 2019;94(12):2501-2509 n https://doi.owww.mayoclinicproceedings.org
the lectures to formulate “sprint tests” atthe end of each day that reinforce teachingdirected toward the audience’s learninggaps for that day’s content. Finally, a largeportion of the ABIM’s certification examina-tion in cardiovascular diseases includesinterpretation of coronary angiograms, echo-cardiograms, and electrocardiograms. Theonline portal provides sample cases in whichlearners can practice their interpretation ofthese critical imaging modalities throughan interface that simulates the environmentof the ABIM Cardiovascular BoardExamination.
After the live course, learner engagementcontinues. Learners retain access to the on-line portal for 1 year after the live course.This access allows them to review contentfrom the live course lectures along with sup-plemental online-only content in a variety offormats, including videos, slide sets, tran-scripts, and audio files. They complete aboard-style assessment after the course,which contains the same questions as thepretest. Learners who do not participate inthe live course maintain access to digital re-cordings of the live course and the dedicatedonline only content. This approach has notadversely affected knowledge gain. Incontrast, learners who engage through thecomplete or segmented online courses have
rg/10.1016/j.mayocp.2019.07.004 2505
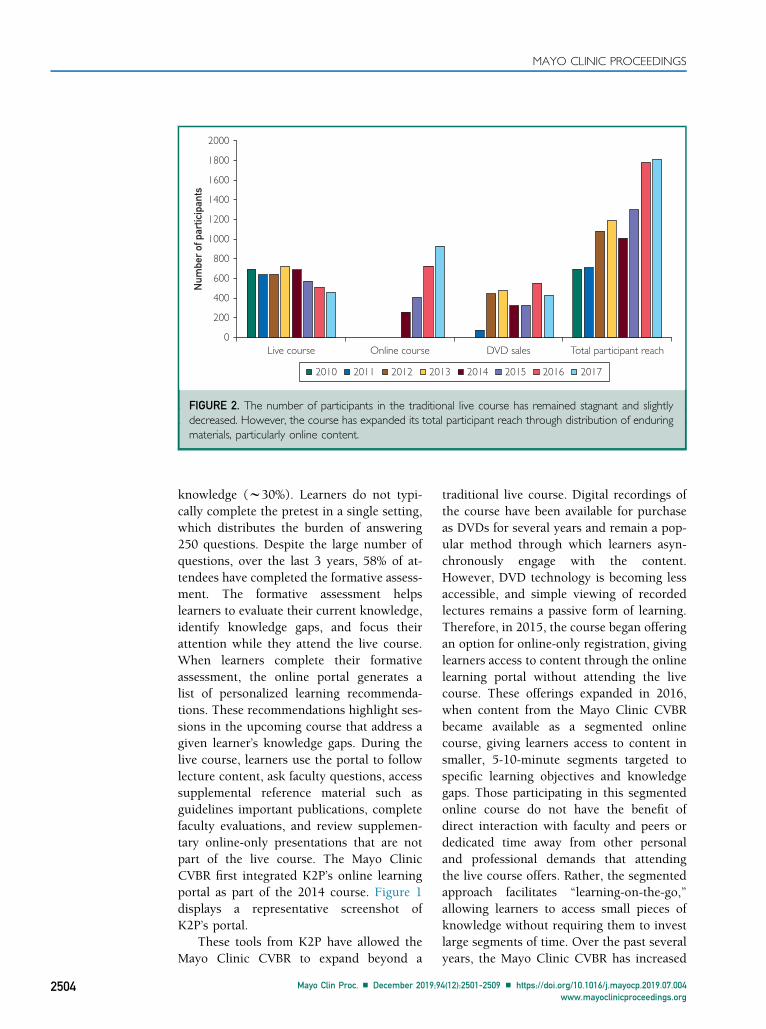
Before the live course During the live course After the live course
Online pretest assessment Digital note taking Online posttest assessment
Moderated question-and-answersessions with faculty members
using submitted online questions
Portal access for online contentreview in multiple formats,
including learning session videos,slide sets, transcripts, and
audio files
Daily sprint tests focused on the audience’s learning gaps
Sample coding examinations for angiograms, echocardiograms,
and electrocardiograms
Access to animated faculty slides
FIGURE 4. Methods of learner engagement that leverage digital technology before, during, and after thelive Mayo Clinic Cardiovascular Review for Cardiology Boards and Recertification.
MAYO CLINIC PROCEEDINGS
2506
demonstrated 3-fold increases in knowledgefrom pretest to posttest, with 50% less timededicated to content engagement(Figure 3). This finding suggests that novelapproaches to learner engagement canaugment knowledge in a more time- andresource-efficient manner. Although itwould be impossible to isolate the influenceof education from our course relative toother continuing professional education en-deavors in which our attendees participate,future efforts must still attempt to assessthe impact of this increased knowledge onpractice behaviors and patient-leveloutcomes.
Figure 4 outlines these tools for opti-mizing learner engagement that movebeyond the traditional model of CME.The tools emphasize longitudinal interac-tion with content for continuous knowl-edge and skill development targeted atlearner specific practice gaps rather thanisolated lectures based on areas of facultyexpertise. This learner engagement canoccur through blended engagement at alive course and digital interactions outsidethe bounds of traditional live destinationmeetings.
Mayo Clin Proc. n December 2019;9
FACULTY DEVELOPMENTThe cardiology community has placedincreasing value on the role of educatordevelopment24,25 and presentation design26
in the delivery of educational content. Akey aspect in the evolution of the MayoClinic CVBR has been faculty developmenttoward a learner centric model. This evolu-tion has involved developing content basedon learning objectives, improving presenta-tion design and delivery, and sharing exper-tise with learners through traditional andnovel means.
Achievable learning objectives representa key element of lifelong learning.27 Theyfacilitate transitions between lectures, reducecontent gaps and redundancies, improvecurricular organization, and facilitate knowl-edge assimilation. Many courses offerlearning objectives only as an obligatoryresponse to accreditation requirements;however, learning objectives serve severalimportant roles. First of all, they focuslearner attention on key aspects of their cur-riculum. Perhaps more importantly, learningobjectives provide an organizational frame-work for faculty to structure their contentand presentations. To facilitate the shift to
4(12):2501-2509 n https://doi.org/10.1016/j.mayocp.2019.07.004www.mayoclinicproceedings.org
40%
Lear
ner
ratin
g
50% 60% 70%
Expert observer rating80% 90% 100%
94%
95%
96%
97%
98%
99%
100%
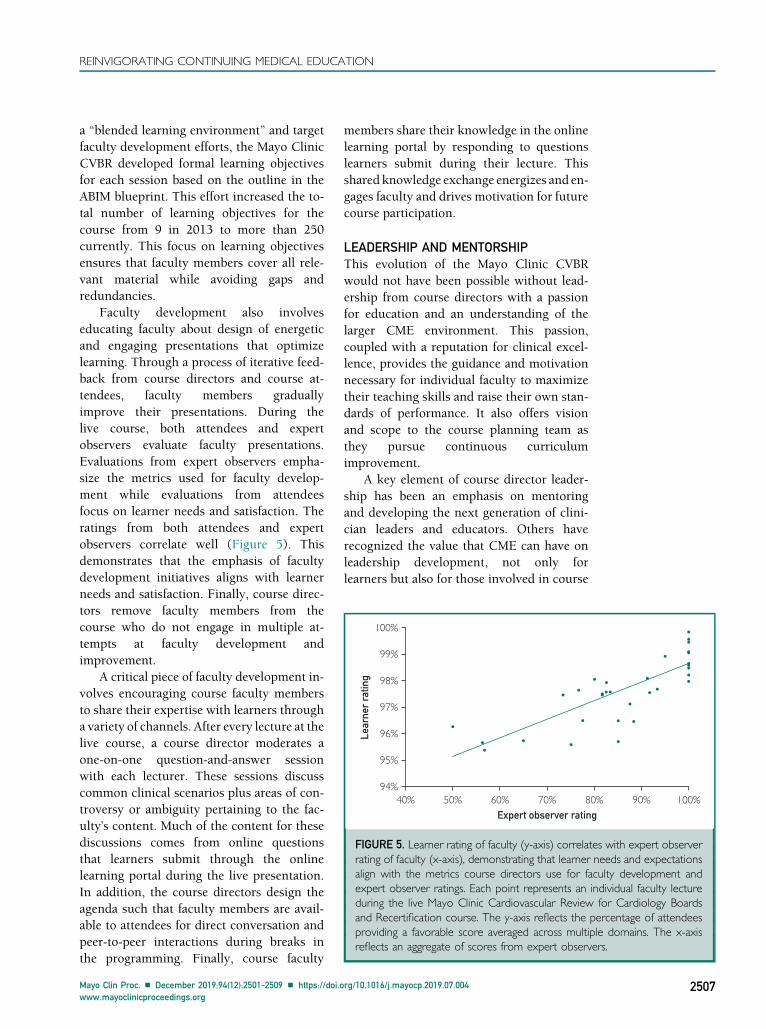
FIGURE 5. Learner rating of faculty (y-axis) correlates with expert observerrating of faculty (x-axis), demonstrating that learner needs and expectationsalign with the metrics course directors use for faculty development andexpert observer ratings. Each point represents an individual faculty lectureduring the live Mayo Clinic Cardiovascular Review for Cardiology Boardsand Recertification course. The y-axis reflects the percentage of attendeesproviding a favorable score averaged across multiple domains. The x-axisreflects an aggregate of scores from expert observers.
REINVIGORATING CONTINUING MEDICAL EDUCATION
a “blended learning environment” and targetfaculty development efforts, the Mayo ClinicCVBR developed formal learning objectivesfor each session based on the outline in theABIM blueprint. This effort increased the to-tal number of learning objectives for thecourse from 9 in 2013 to more than 250currently. This focus on learning objectivesensures that faculty members cover all rele-vant material while avoiding gaps andredundancies.
Faculty development also involveseducating faculty about design of energeticand engaging presentations that optimizelearning. Through a process of iterative feed-back from course directors and course at-tendees, faculty members graduallyimprove their presentations. During thelive course, both attendees and expertobservers evaluate faculty presentations.Evaluations from expert observers empha-size the metrics used for faculty develop-ment while evaluations from attendeesfocus on learner needs and satisfaction. Theratings from both attendees and expertobservers correlate well (Figure 5). Thisdemonstrates that the emphasis of facultydevelopment initiatives aligns with learnerneeds and satisfaction. Finally, course direc-tors remove faculty members from thecourse who do not engage in multiple at-tempts at faculty development andimprovement.
A critical piece of faculty development in-volves encouraging course faculty membersto share their expertise with learners througha variety of channels. After every lecture at thelive course, a course director moderates aone-on-one question-and-answer sessionwith each lecturer. These sessions discusscommon clinical scenarios plus areas of con-troversy or ambiguity pertaining to the fac-ulty’s content. Much of the content for thesediscussions comes from online questionsthat learners submit through the onlinelearning portal during the live presentation.In addition, the course directors design theagenda such that faculty members are avail-able to attendees for direct conversation andpeer-to-peer interactions during breaks inthe programming. Finally, course faculty
Mayo Clin Proc. n December 2019;94(12):2501-2509 n https://doi.owww.mayoclinicproceedings.org
members share their knowledge in the onlinelearning portal by responding to questionslearners submit during their lecture. Thisshared knowledge exchange energizes and en-gages faculty and drives motivation for futurecourse participation.
LEADERSHIP AND MENTORSHIPThis evolution of the Mayo Clinic CVBRwould not have been possible without lead-ership from course directors with a passionfor education and an understanding of thelarger CME environment. This passion,coupled with a reputation for clinical excel-lence, provides the guidance and motivationnecessary for individual faculty to maximizetheir teaching skills and raise their own stan-dards of performance. It also offers visionand scope to the course planning team asthey pursue continuous curriculumimprovement.
A key element of course director leader-ship has been an emphasis on mentoringand developing the next generation of clini-cian leaders and educators. Others haverecognized the value that CME can have onleadership development, not only forlearners but also for those involved in course
rg/10.1016/j.mayocp.2019.07.004 2507
Build an online presence, including a bank of digital questions used for formative and summative assessments.
Engage faculty members through direct and novel approaches to audience interactions.
Formalize learning objectives.
Continually reassess needs of learners through survey data and responses to preassessment and postassessment questions.
Establish a succession plan.
Rigorously analyze presentations and learner performance on multiple-choice assessments.
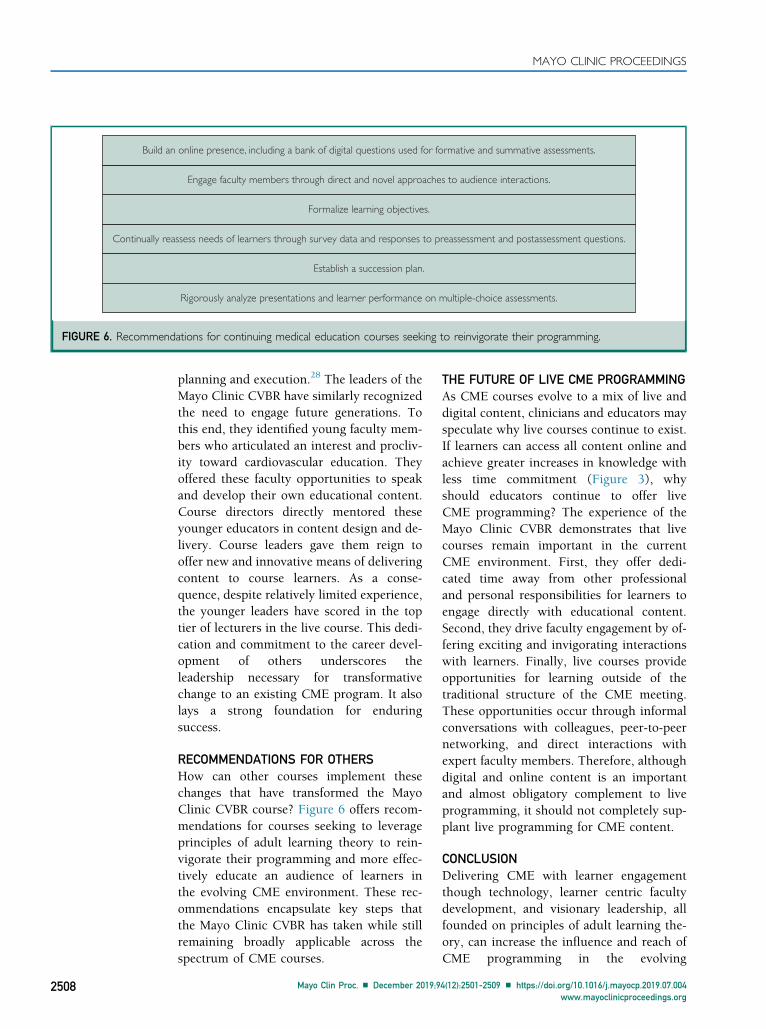
FIGURE 6. Recommendations for continuing medical education courses seeking to reinvigorate their programming.
MAYO CLINIC PROCEEDINGS
2508
planning and execution.28 The leaders of theMayo Clinic CVBR have similarly recognizedthe need to engage future generations. Tothis end, they identified young faculty mem-bers who articulated an interest and procliv-ity toward cardiovascular education. Theyoffered these faculty opportunities to speakand develop their own educational content.Course directors directly mentored theseyounger educators in content design and de-livery. Course leaders gave them reign tooffer new and innovative means of deliveringcontent to course learners. As a conse-quence, despite relatively limited experience,the younger leaders have scored in the toptier of lecturers in the live course. This dedi-cation and commitment to the career devel-opment of others underscores theleadership necessary for transformativechange to an existing CME program. It alsolays a strong foundation for enduringsuccess.
RECOMMENDATIONS FOR OTHERSHow can other courses implement thesechanges that have transformed the MayoClinic CVBR course? Figure 6 offers recom-mendations for courses seeking to leverageprinciples of adult learning theory to rein-vigorate their programming and more effec-tively educate an audience of learners inthe evolving CME environment. These rec-ommendations encapsulate key steps thatthe Mayo Clinic CVBR has taken while stillremaining broadly applicable across thespectrum of CME courses.
Mayo Clin Proc. n December 2019;9
THE FUTURE OF LIVE CME PROGRAMMINGAs CME courses evolve to a mix of live anddigital content, clinicians and educators mayspeculate why live courses continue to exist.If learners can access all content online andachieve greater increases in knowledge withless time commitment (Figure 3), whyshould educators continue to offer liveCME programming? The experience of theMayo Clinic CVBR demonstrates that livecourses remain important in the currentCME environment. First, they offer dedi-cated time away from other professionaland personal responsibilities for learners toengage directly with educational content.Second, they drive faculty engagement by of-fering exciting and invigorating interactionswith learners. Finally, live courses provideopportunities for learning outside of thetraditional structure of the CME meeting.These opportunities occur through informalconversations with colleagues, peer-to-peernetworking, and direct interactions withexpert faculty members. Therefore, althoughdigital and online content is an importantand almost obligatory complement to liveprogramming, it should not completely sup-plant live programming for CME content.
CONCLUSIONDelivering CME with learner engagementthough technology, learner centric facultydevelopment, and visionary leadership, allfounded on principles of adult learning the-ory, can increase the influence and reach ofCME programming in the evolving
4(12):2501-2509 n https://doi.org/10.1016/j.mayocp.2019.07.004www.mayoclinicproceedings.org
REINVIGORATING CONTINUING MEDICAL EDUCATION
educational environment. Learner engage-ment occurs through both traditional anddigital means. Digital content adds intrinsicvalue but does not substitute for traditionalin-person learning. Courses seeking toimplement similar changes must proceedwith a firm understanding of adult learningtheory. Identifying learners’ knowledgegaps, creating dissonance between actualand perceived knowledge, facilitating opencommunication between learners and fac-ulty, and using learning objectives andfocused scenarios relevant to learners’ dailypractice and professional scope are criticalfor CME courses to evolve. Ultimately, thismultifaceted approach can serve as anenduring model for CME in the 21stcentury.
Abbreviations and Acronyms: ABIM = American Board ofInternal Medicine; CME = continuing medical education;CVBR = Cardiovascular Review for Cardiology Boards andRecertification; K2P = Knowledge to Practice
Potential Competing Interests: Ms Beliveau is the ChiefExecutive Officer of Knowledge to Practice. Neither MsBeliveau nor Knowledge to Practice have any additional re-lationships with industry related to this work.
Correspondence: Address to Michael W. Cullen, MD,FACC, Department of Cardiovascular Medicine, MayoClinic, 200 First St SW, Rochester, MN 55905 ([email protected]).
REFERENCES1. McMahon GT. What do I need to learn today?d The evolution
of CME. N Engl J Med. 2016;374(15):1403-1406.2. Beliveau ME, Warnes CA, Harrington RA, et al. Organizational
change, leadership, and the transformation of continuing pro-fessional development: lessons learned from the AmericanCollege of Cardiology. J Contin Educ Health Prof. 2015;35(3):201-210.
3. Olson CA. Twenty predictions for the future of CPD: Implica-tions of the shift from the update model to improving clinicalpractice. J Contin Educ Health Prof. 2012;32(3):151-152.
4. Institute of Medicine of the National Academy. RedesigningContinuing Education in the Health Professions. Washington,DC: The National Academies Press; 2010.
5. McMahon GT. Advancing continuing medical education. JAMA.2015;314(6):561-562.
6. Kates AM, Morris P, Poppas A, Kuvin JT. Impact of live, scientificannual meetings in today’s cardiovascular world. J Am Coll Car-diol. 2018;72(17):2082-2085.
7. Baron RJ. Professional self-regulation in a changing world:Old problems need new approaches. JAMA. 2015;313(18):1807-1808.
Mayo Clin Proc. n December 2019;94(12):2501-2509 n https://doi.owww.mayoclinicproceedings.org
8. Baron RJ, Braddock CHI. Knowing what we don’t know d
improving maintenance of certification. N Engl J Med. 2016;375(26):2516-2517.
9. Baron RJ, Johnson D. The American Board of Internal Medicine:evolving professional self-regulation. Ann Int Med. 2014;161(3):221-223.
10. Norman GR. The adult learner: a mythical species. Acad Med.1999;74(8):886-889.
11. Taylor DCM, Hamdy H. Adult learning theories: Implicationsfor learning and teaching in medical education: AMEE GuideNo. 83. Med Teach. 2013;35(11):e1561-e1572.
12. Knowles MS. The Adult Learner: A Neglected Species. Houston,TX: Gulf Publishing Company; 1973.
13. Cooper AZ, Richards JB. Lectures for adult learners: breakingold habits in graduate medical education. Am J Med. 2017;130(3):376-381.
14. Davis D, O’Brien M, Freemantle N, Wolf FM, Mazmanian P,Taylor-Vaisey A. Impact of formal continuing medical educa-tion: Do conferences, workshops, rounds, and other traditionalcontinuing education activities change physician behavior orhealth care outcomes? JAMA. 1999;282(9):867-874.
15. Davis DA, Thomson M, Oxman AD, Haynes R. Evidence forthe effectiveness of CME: a review of 50 randomizedcontrolled trials. JAMA. 1992;268(9):1111-1117.
16. Davis DA, Thomson M, Oxman AD, Haynes R. Changingphysician performance: a systematic review of the effect ofcontinuing medical education strategies. JAMA. 1995;274(9):700-705.
17. Cervero RM, Gaines JK. The impact of CME on physicianperformance and patient health outcomes: an updated syn-thesis of systematic reviews. J Contin Educ Health Prof. 2015;35(2):131-138.
18. Mazmanian PE, Davis DA. Continuing medical education andthe physician as a learner: Guide to the evidence. JAMA.2002;288(9):1057-1060.
19. Accreditation Council for Continuing Medical Education.Accreditation criteria. Available at: http://www.accme.org/requirements/accreditation-requirements-cme-providers/accreditation-criteria 2018. Accessed February 28, 2018.
20. AccreditationCouncil forContinuingMedical Education.AMAandACCME announce simplification and alignment of credit andaccreditation systems. Available at: http://www.accme.org/news-releases/ama-and-accme-announce-simplification-and-alignment-credit-and-accreditation-systems. Accessed February 28, 2018.
21. Cook DA, McDonald FS. E-learning: is there anything specialabout the “E”? Perspect Biol Med. 2008;51(1):5-21.
22. Davis DA, Mazmanian PE, Fordis M, Van Harrison RR,Thorpe KE, Perrier L. Accuracy of physician self-assessmentcompared with observed measures of competence: a system-atic review. JAMA. 2006;296(9):1094-1102.
23. Duffy F, Holmboe ES. Self-assessment in lifelong learning andimproving performance in practice: physician know thyself.JAMA. 2006;296(9):1137-1139.
24. Auseon AJ, O’Gara PT, Klodas E, et al. The essential role ofeducator development: 10 years of the ACC Emerging FacultyProgram. J Am Coll Cardiol. 2016;67(18):2177-2182.
25. Nishimura R, Warnes C. Educating cardiovascular fellows in thecomtemporary era: developing competent cardiologists. JAMACardiol. 2017;2(2):119-120.
26. El Sabbagh A, Killu AM. The art of presentation: a valuableskill in a contemporary era. J Am Coll Cardiol. 2015;65(13):1373-1376.
27. Narang A, Velagapudi P, Rajagopalan B, et al. A new educa-tional framework to improve lifelong learning for cardiologists.J Am Coll Cardiol. 2018;71(4):454-462.
28. McMahon GT. The leadership case for investing in continuingprofessional development. Acad Med. 2017;92(8):1075-1077.
rg/10.1016/j.mayocp.2019.07.004 2509
Related Documents











