This article was published in an Elsevier journal. The attached copy is furnished to the author for non-commercial research and education use, including for instruction at the author’s institution, sharing with colleagues and providing to institution administration. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
This article was published in an Elsevier journal. The attached copyis furnished to the author for non-commercial research and
education use, including for instruction at the author’s institution,sharing with colleagues and providing to institution administration.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Manual Therapy 13 (2008) 132–138
Original Article
Rehabilitative ultrasound measurement of select trunk muscleactivation during induced pain
Kyle B. Kiesela,�, Tim Uhlb, Frank B. Underwoodc, Arthur J. Nitzd,e
aRehabilitation Sciences Doctoral Program, University of Kentucky, USAbDepartment of Rehabilitation Sciences, Division of Athletic Training, University of Kentucky, USA
cDepartment of Physical Therapy, University of Evansville, USAdDepartment of Rehabilitation Sciences, Division of Physical Therapy, University of Kentucky, USA
eDepartment of Rehabilitation Sciences, Rehabilitation Sciences Doctoral Program, University of Kentucky College of Health Sciences,
900 South Limestone, CHS 126, Lexington, KY 40536-0200, USA
Received 16 February 2006; received in revised form 11 September 2006; accepted 9 October 2006
Abstract
Rehabilitative ultrasound imaging (RUSI) is considered a valid method to measure muscle activation in key spinal muscles in
asymptomatic subjects. Research measuring muscle activation with RUSI in painful subjects is limited. The aim of this study was to
determine if changes in muscle activation from experimentally induced pain can be measured by RUSI.
Six male subjects performed tasks known to activate the transverse abdominis (TrA) and lumbar multifidus (LM) while RUSI
measurements of muscle thickness were obtained during control and hypertonic saline conditions. The abdominal draw-in maneuver
was used to volitionally activate the TrA and a series of upper extremity lifting tasks were used to automatically activate the LM.
Pain was induced by injecting 5% hypertonic saline into the longissimus muscle adjacent to the LM at the L4 level. The percent
change in muscle thickness from rest to contraction represented muscle activation.
Activation was significantly less (po0.01) during the painful condition on 4 of the 5 tasks performed for the LM and on the task
performed for the TrA.
These results indicate that RUSI can be used to measure pain-related changes in deep trunk muscle activation. Future research
should include a larger sample size and women.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Rehabilitative ultrasound imaging; Transverse abdominis; Lumbar multifidus
1. Introduction
Contemporary rehabilitation for patients with lowback pain (LBP) includes specific exercise aimed atrestoring motor control of key stabilizing musclesincluding the transverse abdominis (TrA) and thelumbar multifidus (LM) (O’Sullivan et al., 1997;Richardson and Jull, 2000; Hides et al., 2001; Moseley,2002; Niemisto et al., 2003). Surface electromyography
does not accurately measure activation characteristics ofthese deep spinal muscles (McGill et al., 1996; Stokeset al., 2003), requiring invasive techniques for measure-ment which are not routinely used in the clinical setting(Teyhen et al., 2005). Rehabilitative ultrasound imaging(RUSI) can be used to assess muscle activation bymeasuring change in muscle geometry during contrac-tion. The most common measurement utilized to assessmuscle activation is change in muscle thickness (Hodges,2005). Muscle thickness change has been shown torepresent muscle activation by simultaneous EMGrecording in the TrA muscle (Hodges et al., 2003b;McMeeken et al., 2004) and the LM muscle (Kieselet al., 2006) in normal subjects.
ARTICLE IN PRESS
www.elsevier.com/locate/math
1356-689X/$ - see front matter r 2006 Elsevier Ltd. All rights reserved.
doi:10.1016/j.math.2006.10.003
�Corresponding author. Department of Physical Therapy, Univer-
sity of Evansville, Evansville, IN 47714, USA. Tel.: +1812479 2646;
fax: +18124792717.
E-mail address: [email protected] (K.B. Kiesel).

Author's personal copy
Few studies have been conducted to measure musclethickness change with RUSI in LBP subjects. Ferreiraet al. (2004) demonstrated thickness change of the TrAis less in asymptomatic subjects with a history of LBP.This study utilized a loaded lower extremity task, similarto recumbent biking, to measured automatic recruit-ment of TrA over the course of the task. Critchley andCoutts (2002) used RUSI to measure thickness changein the TrA on chronic LBP subjects performing theabdominal draw-in maneuver. The magnitude of thick-ness change in the LBP subjects was significantly lessthan asymptomatic age matched control subjects.Thickness change of the LM has not been measuredwith RUSI in the LBP population. RUSI has been usedas biofeedback during intervention in an acute LBPpopulation where thickness change was thought torepresent activation (Hides et al., 1996).
Many researchers have reported changes in muscleactivation in LBP subjects as compared to asympto-matic control subjects (van Dieen et al., 2003). Themajority of studies have utilized surface EMG to assessthe response to pain in superficial muscles. Results varywidely and are in part dependent on the task studied,with some demonstrating hyperactivity while otherstudies demonstrating hypoactivity in the presence ofpain. These results have been used to support and refutethe two main theories of how pain affects motor control:(1) pain-spasm-pain model (predicts pain increasesactivity) and (2) the pain-adaptive model (predicts painwill cause an increase in muscle activity when themuscles act as antagonist and decreases activity whenthe muscle is active as an agonist). van Dieen et al.(2003) concluded that ‘‘lumbar erector spinae EMGactivity in LBP subjects is highly variable and thought todepend upon the task studied.’’
Researchers demonstrating the effects of induced painon trunk muscle activation also offer no consistentfindings, with results appearing to vary depending onthe task. Arendt-Nielsen et al. (1996) induced pain withhypertonic saline and demonstrated an increase inerector spinae activity during walking. Zedka et al.(1999) measured erector spinae activity during trunkflexion and extension before and after hypertonic saline-induced pain and found an increase in activity whenEMG activity is normally silent and a decrease or nochange when EMG activity is normally high.
More recent work has focused on deep muscleactivation, in particular on the timing of activation inthe presence of pain. Delays in activation of the TrA, inresponse to rapid limb movement, have consistentlybeen demonstrated in subjects with LBP (Hodges andRichardson, 1996), subjects with a history of LBP inremission at the time of testing (Hodges and Richard-son, 1998, 1999) and in asymptomatic subjects whenpain is experimentally induced (Hodges et al., 2003a).There are several studies demonstrating various impair-
ments of the LM in subject with LBP including selectivemorphologic changes such as decreased girth and fattyinfiltrate development (Hides et al., 1994, 1996; Dan-neels et al., 2000; Kader et al., 2000; Yoshihara et al.,2003). Despite these consistent findings, muscle activa-tion deficits of the LM have not been consistentlyidentified. Hodges et al. (2003a) failed to show recruit-ment differences in the deep portions of the LM inresponse to rapid limb movements during induced pain.Other studies have shown diminished EMG activity inthe LM during forward and backward bending (Sihvo-nen et al., 1997) and a reduction in fatigue resistance(Roy et al., 1989). Measurement of changes in muscleactivation associated with LBP may be beneficial to theclinician in development of select intervention to reversethe identified impairment.
Experimental pain can be induced by many methods,but hypertonic saline-induced pain has been usedextensively to test the effects of pain on various aspectsof motor control (Graven-Nielsen et al., 2000) andutilized specifically to study the effects of pain on motorcontrol of spinal muscles (Arendt-Nielsen et al., 1996;Zedka et al., 1999; Hodges et al., 2003a). Intramuscularinjection of hypertonic saline is thought to produce painby primarily exciting nociceptive fibers. Other possiblecontributors to the pain response are increases inintramuscular pressure and a nonspecific excitation ofnon-nociceptive afferents (Graven-Nielsen et al., 2000),but it has been shown that injection of isotonic salinedoes not produce pain beyond that associated with theinjection itself (Hodges et al., 2003a). Using intramus-cular injection of hypertonic saline to produce pain isconsidered safe, reliable and comparable to clinical pain(Graven-Nielsen et al., 2000). The advantage of usingexperimental pain applied to healthy subjects overpatients in clinical studies is the control obtained forpain intensities and duration. Such control may beimportant when measuring the LM because of itstendency to become inhibited quickly in those withacute LBP (Hides et al., 1996) and because of knownmorphological changes in chronic LBP subjects (Kaderet al., 2000; Yoshihara et al., 2001, 2003) which mayaffect measurement accuracy. To our knowledge, nostudy has demonstrated if RUSI can detect change inmuscle activation in those with acute pain at the time oftesting. Therefore, the aim of this study was todetermine if changes in muscle activation from experi-mentally induced pain can be measured with RUSI.
2. Methods
2.1. Subjects
A convenience sample of 7 healthy male subjects(mean age ¼ 26.0 years SD 7.3, mean height ¼ 176.9 cm
ARTICLE IN PRESSK.B. Kiesel et al. / Manual Therapy 13 (2008) 132–138 133

Author's personal copy
SD 10.7, mean weight ¼ 83.0 kg SD 11.7) volunteeredfor this study. Females were not included because ofknown differences in LM activation levels (Arokoskiet al., 2001). Potential subjects were also excluded if theyhad a history of LBP or hip pain, spondylolithesis, or acongenital lumbar/sacral condition such as spina bifida.All volunteering subjects signed an institutional-review-board-approved consent form following verbal instruc-tions of the procedure.
2.2. Procedures
2.2.1. Ultrasound measurements
Rest and activation measures (control and hypertonicsaline conditions) of thickness of the TrA and LM wereobtained using the Sonosite 180 Plus sonography unit(Sonosite Inc, Bothell, WA, USA) with a 70mm2–5MHz curvilinear transducer. The TrA measure-ments as described by Richardson et al. were takenwith the subjects in the supine hook lying position withthe transducer placed just superior to the iliac crestalong the axillary line (Richardson et al., 2004). Toensure measurements were taken at similar points alongthe TrA, the transducer was adjusted until the medialmost portion of the TrA was visualized in the farleft portion of the screen (Henry and Westervelt, 2005)(Fig. 1). Subjects were then taught to preferentiallyactivate their TrA by performing the abdominal draw-inmaneuver with visual feedback from the ultrasound.
Once the skill had been adequately learned (isolated TrAactivation as determined by the tester viewing the RUSI)the resting measure was captured at the end of quietexpiration followed by the activation measure.
The LM measurements were taken with the subjectspositioned prone on a standard plinth. An inclinometerwas placed longitudinally over the lumbo/sacral junc-tion and pillows were used to flatten the lumbar curve toless than 101. The L4 spinous process was identified bypalpation and marked for reference. Then the transdu-cer was placed longitudinally along the spine, movedlaterally, and then angled slightly medial until the L4/5facet joint could be identified. This scan point wasdirectly over the LM. A measurement from this land-mark to the plane between the muscle and subcutaneoustissue was used for the thickness measurement of LM atrest and during activation (Fig. 2) (Stokes et al., 2005).
To activate the LM, 2 trials each of 5 increasinglydemanding contralateral upper extremity lifting taskswere performed while ultrasound images were obtained.The first level had resistance of only the limb with theshoulder adducted and the elbow fully flexed; next theshoulder was abducted to 1201 and lifted with justresistance from the limb, then graded resistance wasadded for the next 3 lifts based on the subject’s bodyweight (see Table 1). The average of the two trials foreach task was used for analysis. A percent change fromrest was calculated [(activity�rest)/rest*100] for musclethickness measures obtained during each task. This
ARTICLE IN PRESS
Fig. 1. Sonogram of the anterior abdominal wall demonstrating measurement of the TrA at rest (left panel) and during volitional abdominal draw-in
(right panel).
Fig. 2. Sonogram of a parasagital view of lumbar spine with the L4/5 facet joint in the center. Measurement of the LM at rest (left panel) and during
automatic recruitment (right panel) via contralateral arm lifting while in prone position.
K.B. Kiesel et al. / Manual Therapy 13 (2008) 132–138134
Author's personal copy
percent change in muscle thickness represented muscleactivation as measured by RUSI. Resting and all TrAmeasurements were performed with the on-screencalipers. The intratester reliability of these measureswas established in a pilot study (TrA ICC3,1 ¼ 0.95, LMICC3,1 ¼ 0.85) performed on 8 asymptomatic subjects.LM images captured during the UE lifting tasks weresaved and printed for off screen manual measurement.The intraimage reliability of this measurement is(ICC3,1 ¼ 0.95). The off screen LM activation measure-ments were taken by a researcher who was blind to bothtask and condition.
2.2.2. Induced pain
After completion of the measurements during thecontrol condition, subjects remained positioned on theplinth. To induce acute pain, a 1.5ml bolus ofhypertonic saline (5%) was injected into the longissimusmuscle 6 cm lateral to the L4 spinous process at a depthof approximately 3.5 cm as described by Hodges et al.(2003a). Pain was measured on a 0–10 point visualanalog scale at 60 s post injection and every 60 sthereafter. Reported pain scores had to reach X4/10and maintain that level throughout the hypertoniccondition data collection. If reported pain droppedbelow the pre-determined threshold of 4/10, an addi-tional 0.5ml bolus was administered. Subjects wereoffered a 0.5ml subcutaneous injection of 1% lidocaineto diminish the superficial pain associated with thesubsequent saline injection.
2.3. Statistical analysis
Paired t-tests were used to determine if muscleactivation was different between the two conditions oneach of the 5 activation tasks for the LM and on thevolitional TrA contraction. The alpha level was set atp0.05 and a Bonferroni correction was performed onthe LM data to diminish the risk of committing a Type Ierror due to multiple comparisons. The correction wasdone by dividing the alpha level of 0.05 by the numberof comparisons which was five. Therefore, the alphalevel for acceptance for the LM was p0.01 andremained at p0.05 for the TrA.
3. Results
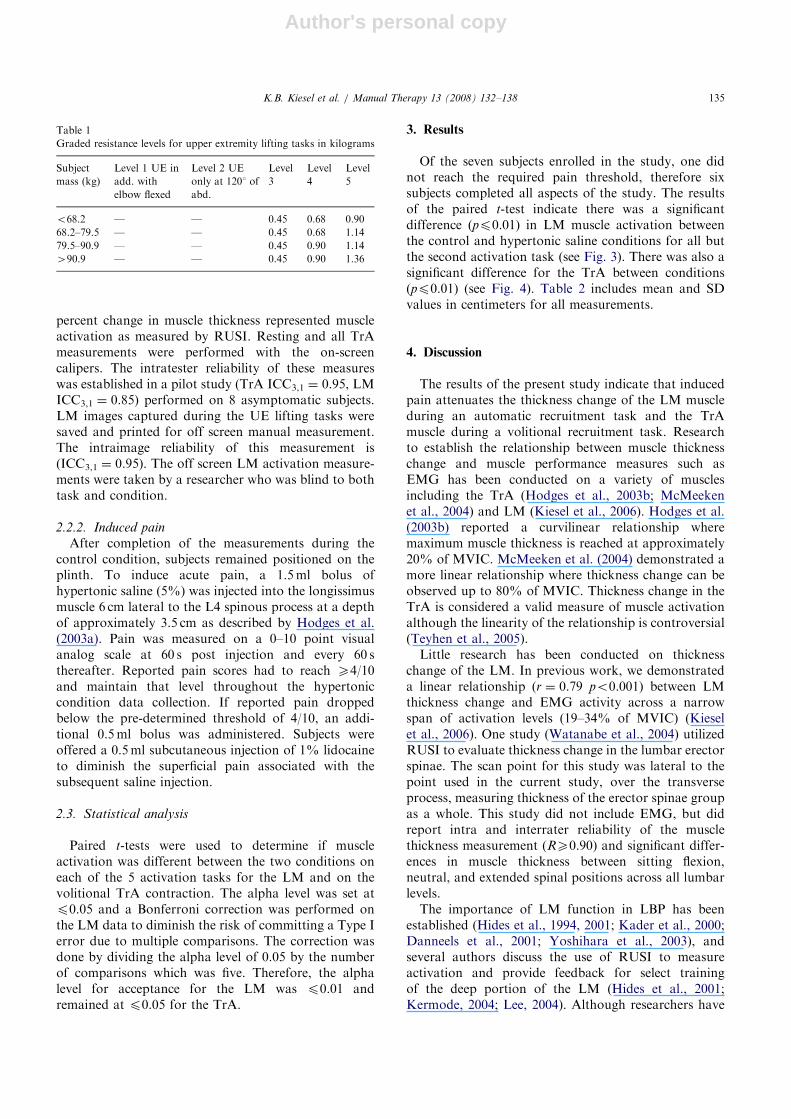
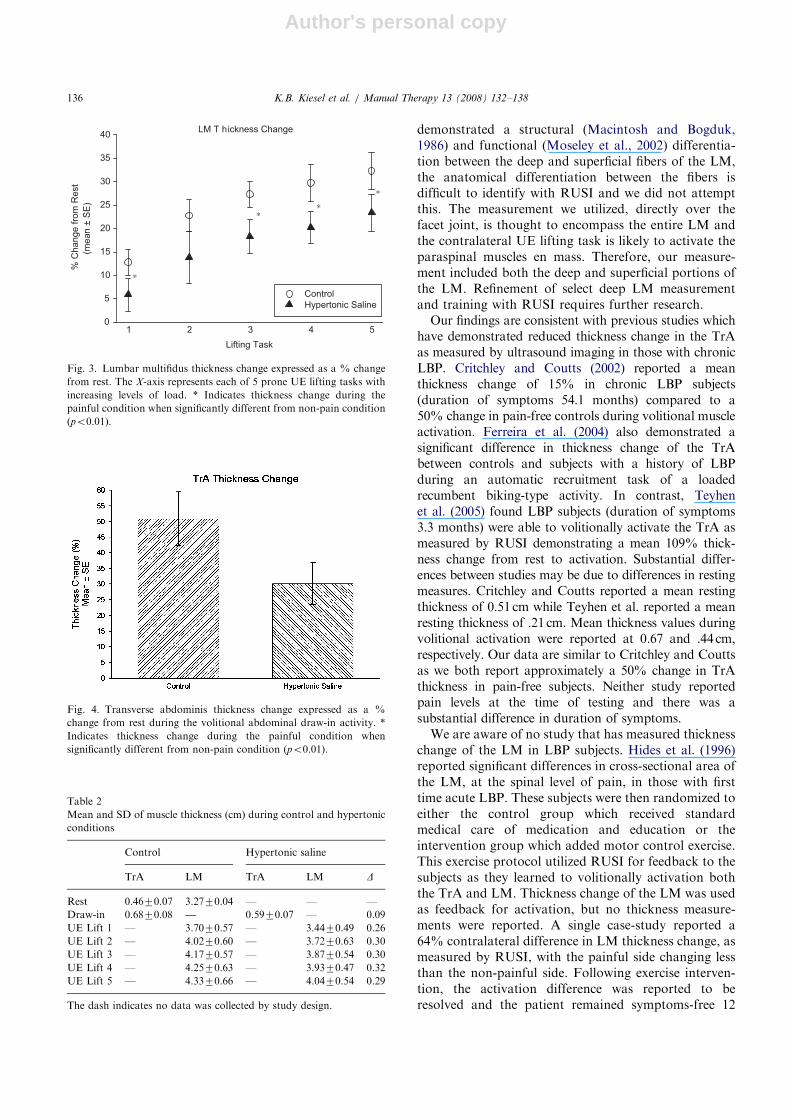
Of the seven subjects enrolled in the study, one didnot reach the required pain threshold, therefore sixsubjects completed all aspects of the study. The resultsof the paired t-test indicate there was a significantdifference (pp0.01) in LM muscle activation betweenthe control and hypertonic saline conditions for all butthe second activation task (see Fig. 3). There was also asignificant difference for the TrA between conditions(pp0.01) (see Fig. 4). Table 2 includes mean and SDvalues in centimeters for all measurements.
4. Discussion
The results of the present study indicate that inducedpain attenuates the thickness change of the LM muscleduring an automatic recruitment task and the TrAmuscle during a volitional recruitment task. Researchto establish the relationship between muscle thicknesschange and muscle performance measures such asEMG has been conducted on a variety of musclesincluding the TrA (Hodges et al., 2003b; McMeekenet al., 2004) and LM (Kiesel et al., 2006). Hodges et al.(2003b) reported a curvilinear relationship wheremaximum muscle thickness is reached at approximately20% of MVIC. McMeeken et al. (2004) demonstrated amore linear relationship where thickness change can beobserved up to 80% of MVIC. Thickness change in theTrA is considered a valid measure of muscle activationalthough the linearity of the relationship is controversial(Teyhen et al., 2005).
Little research has been conducted on thicknesschange of the LM. In previous work, we demonstrateda linear relationship (r ¼ 0.79 po0.001) between LMthickness change and EMG activity across a narrowspan of activation levels (19–34% of MVIC) (Kieselet al., 2006). One study (Watanabe et al., 2004) utilizedRUSI to evaluate thickness change in the lumbar erectorspinae. The scan point for this study was lateral to thepoint used in the current study, over the transverseprocess, measuring thickness of the erector spinae groupas a whole. This study did not include EMG, but didreport intra and interrater reliability of the musclethickness measurement (RX0.90) and significant differ-ences in muscle thickness between sitting flexion,neutral, and extended spinal positions across all lumbarlevels.
The importance of LM function in LBP has beenestablished (Hides et al., 1994, 2001; Kader et al., 2000;Danneels et al., 2001; Yoshihara et al., 2003), andseveral authors discuss the use of RUSI to measureactivation and provide feedback for select trainingof the deep portion of the LM (Hides et al., 2001;Kermode, 2004; Lee, 2004). Although researchers have
ARTICLE IN PRESS
Table 1
Graded resistance levels for upper extremity lifting tasks in kilograms
Subject
mass (kg)
Level 1 UE in
add. with
elbow flexed
Level 2 UE
only at 1201 of
abd.
Level
3
Level
4
Level
5
o68.2 — — 0.45 0.68 0.90
68.2–79.5 — — 0.45 0.68 1.14
79.5–90.9 — — 0.45 0.90 1.14
490.9 — — 0.45 0.90 1.36
K.B. Kiesel et al. / Manual Therapy 13 (2008) 132–138 135
Author's personal copy
demonstrated a structural (Macintosh and Bogduk,1986) and functional (Moseley et al., 2002) differentia-tion between the deep and superficial fibers of the LM,the anatomical differentiation between the fibers isdifficult to identify with RUSI and we did not attemptthis. The measurement we utilized, directly over thefacet joint, is thought to encompass the entire LM andthe contralateral UE lifting task is likely to activate theparaspinal muscles en mass. Therefore, our measure-ment included both the deep and superficial portions ofthe LM. Refinement of select deep LM measurementand training with RUSI requires further research.
Our findings are consistent with previous studies whichhave demonstrated reduced thickness change in the TrAas measured by ultrasound imaging in those with chronicLBP. Critchley and Coutts (2002) reported a meanthickness change of 15% in chronic LBP subjects(duration of symptoms 54.1 months) compared to a50% change in pain-free controls during volitional muscleactivation. Ferreira et al. (2004) also demonstrated asignificant difference in thickness change of the TrAbetween controls and subjects with a history of LBPduring an automatic recruitment task of a loadedrecumbent biking-type activity. In contrast, Teyhenet al. (2005) found LBP subjects (duration of symptoms3.3 months) were able to volitionally activate the TrA asmeasured by RUSI demonstrating a mean 109% thick-ness change from rest to activation. Substantial differ-ences between studies may be due to differences in restingmeasures. Critchley and Coutts reported a mean restingthickness of 0.51 cm while Teyhen et al. reported a meanresting thickness of .21 cm. Mean thickness values duringvolitional activation were reported at 0.67 and .44 cm,respectively. Our data are similar to Critchley and Couttsas we both report approximately a 50% change in TrAthickness in pain-free subjects. Neither study reportedpain levels at the time of testing and there was asubstantial difference in duration of symptoms.
We are aware of no study that has measured thicknesschange of the LM in LBP subjects. Hides et al. (1996)reported significant differences in cross-sectional area ofthe LM, at the spinal level of pain, in those with firsttime acute LBP. These subjects were then randomized toeither the control group which received standardmedical care of medication and education or theintervention group which added motor control exercise.This exercise protocol utilized RUSI for feedback to thesubjects as they learned to volitionally activation boththe TrA and LM. Thickness change of the LM was usedas feedback for activation, but no thickness measure-ments were reported. A single case-study reported a64% contralateral difference in LM thickness change, asmeasured by RUSI, with the painful side changing lessthan the non-painful side. Following exercise interven-tion, the activation difference was reported to beresolved and the patient remained symptoms-free 12
ARTICLE IN PRESS
Table 2
Mean and SD of muscle thickness (cm) during control and hypertonic
conditions
Control Hypertonic saline
TrA LM TrA LM D
Rest 0.4670.07 3.2770.04 — — —
Draw-in 0.6870.08 — 0.5970.07 — 0.09
UE Lift 1 — 3.7070.57 — 3.4470.49 0.26
UE Lift 2 — 4.0270.60 — 3.7270.63 0.30
UE Lift 3 — 4.1770.57 — 3.8770.54 0.30
UE Lift 4 — 4.2570.63 — 3.9370.47 0.32
UE Lift 5 — 4.3370.66 — 4.0470.54 0.29
The dash indicates no data was collected by study design.
Fig. 4. Transverse abdominis thickness change expressed as a %
change from rest during the volitional abdominal draw-in activity. *
Indicates thickness change during the painful condition when
significantly different from non-pain condition (po0.01).
LM T hickness Change
Lifting Task
1 2 3 4 5
% C
ha
ng
e f
rom
Re
st
0
5
10
15
20
25
30
35
40
Control
Hypertonic Saline
∗
∗ ∗
∗
*
(mean ±
SE
)
Fig. 3. Lumbar multifidus thickness change expressed as a % change
from rest. The X-axis represents each of 5 prone UE lifting tasks with
increasing levels of load. * Indicates thickness change during the
painful condition when significantly different from non-pain condition
(po0.01).
K.B. Kiesel et al. / Manual Therapy 13 (2008) 132–138136

Author's personal copy
months following intervention (Kiesel and Malone,2004).
Previous research demonstrates experimentally in-duced pain alters muscle activity, including delays in thetiming of TrA activation (Hodges et al., 2003a) andeither an increase or decrease in erector spinae activitydependent upon the phase of the movement task tested(Zedka et al., 1999). The pain-adaptation model (Lundet al., 1991) predicts pain will alter muscle activitydepending on a given muscle’s role as an agonist orantagonist to control movement for protection. Thismodel is described by Graven-Nielsen et al. (2000) in areview article as the current best explanation of howpain likely alters motor control. It is difficult tocategorize the role of LM in the prone UE lifting taskused in this study as either agonistic or antagonistic, butthe pain-adaptation model predicts increased activitywhen a muscle would normally be silent and decreasedactivity when a muscle would normally be active,therefore a decrease in LM activity could be expected.Hodges et al. (2003a) reported an initial increase in deepLM EMG amplitude following saline injection duringrapid arm lifting. Differences may be related to theposition of subjects. The authors postulate that becausesubjects were in the standing position, an initial increasein activity of the LM may have been part of a protectivetrunk splinting response.
Limitations of this study include the small sample sizeas well as the lack of EMG data. Measuring if EMGalso changes during the painful condition would addvalidity to the study as well as to the use of thicknesschange as a measure of muscle activation. Additionally,the strength of contraction was not measurable andmaximal contraction could not be confirmed in eithermuscle tested. This may not be relevant from a clinicalperspective as high force contractions are not functionalin that the stabilizing role of deep muscles is thought tooccur at relatively low forces.
5. Conclusion
The results of this study provide preliminary dataindicating RUSI can be used to measure pain-relatedchanges in select trunk muscle activation. This adds to thevalidity of using RUSI in the clinical setting and may helpto expand its use beyond that of feedback and measure-ment for the TrA. Additionally, the decreased activationas measured by RUSI supports the pain model describedby previous authors Lund and Graves-Nielsen.
Acknowledgments
The authors would like to thank Daniel Underwoodand Joshua McCormack for their assistance with thisresearch.
References
Arendt-Nielsen L, Graven-Nielsen T, Svarrer H, et al. The influence of
low back pain on muscle activity and coordination during gait: a
clinical and experimental study. Pain 1996;64(2):231–40.
Arokoski JP, Valta T, Airaksinen O, et al. Back and abdominal muscle
function during stabilization exercises. Archives of Physical
Medicine and Rehabilitation 2001;82(8):1089–98.
Critchley D, Coutts F. Abdominal muscle function in chronic low back
pain patients; measurement with real-time ultrasound scanning.
Physiotherapy 2002;88(6):322–32.
Danneels LA, Vanderstraeten GG, Cambier DC, et al. CT imaging of
trunk muscles in chronic low back pain patients and healthy
control subjects. European Spine Journal 2000;9(4):266–72.
Danneels LA, Vanderstraeten GG, Cambier DC, et al. Effects of three
different training modalities on the cross sectional area of the
lumbar multifidus muscle in patients with chronic low back pain.
British Journal of Sports Medicine 2001;35(3):186–91.
Ferreira PH, Ferreira ML, Hodges PW. Changes in recruitment of the
abdominal muscles in people with low back pain: ultrasound
measurement of muscle activity. Spine 2004;29(22):2560–6.
Graven-Nielsen T, Svensson P, Arendt-Nielsen L. Effect of muscle
pain on motor control: a human experimental approach. Advances
in Physiotherapy 2000;2:26–38.
Henry SM, Westervelt KC. The use of real-time ultrasound feedback
in teaching abdominal hollowing exercises to healthy subjects.
Journal of Orthopaedic & Sports Physical Therapy 2005;35(6):
338–45.
Hides JA, Stokes MJ, Saide M, et al. Evidence of lumbar multifidus
muscle wasting ipsilateral to symptoms in patients with acute/
subacute low back pain. Spine 1994;19(2):165–72.
Hides JA, Richardson CA, Jull GA. Multifidus muscle recovery is not
automatic after resolution of acute, first-episode low back pain.
Spine 1996;21(23):2763–9.
Hides JA, Jull GA, Richardson CA. Long-term effects of specific
stabilizing exercises for first-episode low back pain. Spine 2001;
26(11):E243–8.
Hodges P. Ultrasound imaging in rehabilitation: just a fad? Journal of
Orthopaedic & Sports Physical Therapy 2005;35(6):333–7.
Hodges PW, Richardson CA. Inefficient muscular stabilization of
the lumbar spine associated with low back pain. A motor
control evaluation of transversus abdominis. Spine 1996;21(22):
2640–50.
Hodges PW, Richardson CA. Delayed postural contraction of
transversus abdominis in low back pain associated with movement
of the lower limb. Journal of Spinal Disorders 1998;11(1):46–56.
Hodges PW, Richardson CA. Altered trunk muscle recruitment in
people with low back pain with upper limb movement at different
speeds. Archives of Physical Medicine and Rehabilitation 1999;
80(9):1005–12.
Hodges PW, Moseley GL, Gabrielsson A, et al. Experimental muscle
pain changes feed forward postural responses of the trunk muscles.
Experimental Brain Research 2003a;151(2):262–71.
Hodges PW, Pengel LH, Herbert RD, et al. Measurement of muscle
contraction with ultrasound imaging. Muscle & Nerve 2003b;27(6):
682–92.
Kader DF, Wardlaw D, Smith FW. Correlation between the MRI
changes in the lumbar multifidus muscles and leg pain. Clinical
Radiology 2000;55(2):145–9.
Kermode F. Benefits of utilzing real-time ultrasound imaging in the
rehabilitation of the lumbar spine stabilising muscles following low
back injury in the elite athlete; a single case study. Physical Therapy
in Sport 2004;5:13–6.
Kiesel KB, Malone TR. Use of ultrasound imaging to measure
muscular impairment and guide intervention of a patient with
recurring low back pain (Poster Presentation). In American
ARTICLE IN PRESSK.B. Kiesel et al. / Manual Therapy 13 (2008) 132–138 137
Author's personal copy
Physical Therapy Association Combined Sections Meeting,
Nashville, TN, 2004.
Kiesel KB, Underwood FB, Rodd DW, Uhl T, Nitz AJ. Measurement
of lumbar multifidus muscle contraction with ultrasound imaging.
Manual Therapy 2006; September 12, Epub ahead of print.
Lee D. The pelvic girdle. 3rd ed. St. Louis: Churchill Livingstone;
2004.
Lund JP, Donga R, Widmer CG, et al. The pain-adaptation model: a
discussion of the relationship between chronic musculoskeletal pain
and motor activity. Canadian Journal of Physiology and Pharma-
cology 1991;69(5):683–94.
Macintosh J, Bogduk N. The morphology of the human lumbar
multifidus. Clinical Biomechanics 1986;1:205–31.
McGill S, Juker D, Kroof P. Appropriately placed surface EMG
electrodes reflect deep muscle activity (psoas, quadratus lumborum,
abdominal wall) in the lumbar spine. Journal of Biomechanics
1996;29:1503–7.
McMeeken JM, Beith ID, Newham DJ, et al. The relationship between
EMG and change in thickness of transversus abdominis. Clinical
Biomechanics (Bristol, Avon) 2004;19(4):337–42.
Moseley G. Combined physiotherapy and education is efficacious for
chronic for back pain. Australian Journal of Physiotherapy
2002;48:297–302.
Moseley GL, Hodges PW, Gandevia SC. Deep and superficial fibers of
the lumbar multifidus muscle are differentially active during
voluntary arm movements. Spine 2002;27(2):E29–36.
Niemisto L, Lahtinen-Suopanki T, Rissanen P, et al. A randomized
trial of combined manipulation, stabilizing exercises, and physician
consultation compared to physician consultation alone for chronic
low back pain. Spine 2003;28(19):2185–91.
O’Sullivan PB, Phyty GD, Twomey LT, et al. Evaluation of specific
stabilizing exercise in the treatment of chronic low back pain with
radiologic diagnosis of spondylolysis or spondylolisthesis. Spine
1997;22(24):2959–67.
Richardson CA, Jull GA. Muscle control-pain control. What exercises
would you prescribe? Manual Therapy 2000;1(1):2–10.
Richardson CA, Hodges PW, Hides JA. Therapeutic exercise for
lumbopelvic stabilization; a motor control approach for the
treatment and prevention of low back pain. 2nd ed. Edinburgh:
Churchill Linvingstone; 2004.
Roy SH, De Luca CJ, Casavant DA. Lumbar muscle fatigue and
chronic lower back pain. Spine 1989;14(9):992–1001.
Sihvonen T, Lindgren KA, Airaksinen O, et al. Movement dis-
turbances of the lumbar spine and abnormal back muscle
electromyographic findings in recurrent low back pain. Spine 1997;
22(3):289–95.
Stokes IA, Henry SM, Single RM. Surface EMG electrodes do not
accurately record from lumbar multifidus muscles. Clinical
Biomechanics (Bristol, Avon) 2003;18(1):9–13.
Stokes M, Rankin G, Newham DJ. Ultrasound imaging of lumbar
multifidus muscle: normal reference ranges for measurements and
practical guidance on the technique. Manual Therapy 2005;10(2):
116–26.
Teyhen DS, Miltenberger CE, Deiters HM, Del Toro YM, Pulliam JN,
Childs JD, et al. The use of ultrasound imaging of the abdominal
drawing-in maneuver in subjets with low back pain. Journal of
Orthopaedics & Sports Physical Therapy 2005;35(6):346–55.
van Dieen JH, Selen LP, Cholewicki J. Trunk muscle activation in low-
back pain patients, an analysis of the literature. Journal of
Electromyography and Kinesiology 2003;13(4):333–51.
Watanabe K, Miyamoto K, Masuda T, et al. Use of ultrasonography to
evaluate thickness of the erector spinae muscle in maximum flexion
and extension of the lumbar spine. Spine 2004;29(13):1472–7.
Yoshihara K, Shirai Y, Nakayama Y, et al. Histochemical changes in
the multifidus muscle in patients with lumbar intervertebral disc
herniation. Spine 2001;26(6):622–6.
Yoshihara K, Nakayama Y, Fujii N, et al. Atrophy of the multifidus
muscle in patients with lumbar disk herniation: histochemical and
electromyographic study. Orthopedics 2003;26(5):493–5.
Zedka M, Prochazka A, Knight B, et al. Voluntary and reflex control
of human back muscles during induced pain. Journal of Physiology
1999;520(2):591–604.
ARTICLE IN PRESSK.B. Kiesel et al. / Manual Therapy 13 (2008) 132–138138
Related Documents











