North West LHIN Rehabilitation and Complex Continuing Care Capacity Plan May 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

North West LHIN
Rehabilitation and Complex Continuing Care Capacity Plan May 2017

3
Table of Contents
....................................................................................................................................................................................... 1
Acronym List ............................................................................................................................................... 6
Executive Summary .................................................................................................................................... 7
Background .................................................................................................................................................................... 7
Goal ............................................................................................................................................................................... 7
Alignment ...................................................................................................................................................................... 7
Methodology .................................................................................................................................................................. 8
Findings ......................................................................................................................................................................... 8
Desired Future State ...................................................................................................................................................... 9
Recommendations ....................................................................................................................................................... 12
Conclusions ................................................................................................................................................ 18
Background and Context ......................................................................................................................... 19
Project Rationale.......................................................................................................................................................... 19
Goal ............................................................................................................................................................................. 20
Alignment with Regional and Provincial Priorities ..................................................................................................... 20
Methodology ................................................................................................................................................................ 22
Limitations ................................................................................................................................................................... 25
Current State Analysis ............................................................................................................................. 26
Demographics, Population Characteristics, Health Status and Behavioural Factors ................................................... 26
Inpatient Rehabilitation ............................................................................................................................................... 30
Recommendation #1: ................................................................................................................................................... 35
Strengths, Gaps, and Recommendations ...................................................................................................................... 48
Recommendation #4: ................................................................................................................................................... 49
4
Recommendation #3: ................................................................................................................................................... 49
Recommendation #2: ................................................................................................................................................... 49
Recommendation #2: ................................................................................................................................................... 52
Recommendation #4: ................................................................................................................................................... 61
Recommendation #2: ................................................................................................................................................... 61
Recommendation #3: ................................................................................................................................................... 61
Outpatient and Community Services ........................................................................................................................... 61
Recommendation #5: ................................................................................................................................................... 65
Health Human Resources ............................................................................................................................................ 85
Special Consideration for Northern and Remote Issues in North West LHIN ............................................................ 86
Desired Future State ................................................................................................................................. 91
Regional Rehabilitative Care Lead Organization ........................................................................................................ 93
Care Streams ................................................................................................................................................................ 96
Flexible Inpatient Beds at the DHC and LHH Levels ............................................................................................... 102
Use of Technology in Care Provision ........................................................................................................................ 103
Remote North Access to Care .................................................................................................................................... 105
Francophone Access to Care ..................................................................................................................................... 107
Performance Measurement ........................................................................................................................................ 107
Recommendations ................................................................................................................................... 108
Next Steps ................................................................................................................................................ 114
Stakeholder Engagement ........................................................................................................................................... 114
Timelines ................................................................................................................................................................... 115
Conclusions .............................................................................................................................................. 117
Works Cited ............................................................................................................................................. 118
Appendix A – Rehabilitative Care Alliance Bedded Levels of Rehabilitative Care Definitions Framework ........... 124
Appendix B – Rehabilitative Care Alliance: Definitions for Community-Based Levels of Rehabilitative Care ...... 137
Appendix C – Rehabilitative Care Alliance Capacity Planning Framework ............................................................. 146

5
Appendix D – Rehabilitation Care Alliance Planning Considerations for Reclassification of Rehabilitation/CCC
beds ............................................................................................................................................................................ 147
Appendix D – Project Charter ................................................................................................................................... 148
Appendix E – Project Roles and Responsibilities ...................................................................................................... 193
Appendix F – Operationalization and Impact of RCA Deliverables ......................................................................... 196
Appendix G – Methodology Quantitative Data Sources ........................................................................................... 197
Appendix H – Physical Rehabilitation Advisory Committee Rehabilitative Care Review Guiding Principles ........ 198
Appendix I – Community Engagement Stakeholders ................................................................................................ 206
Appendix J – RCA Bedded Levels of Rehabilitative Care Mapping Tool ................................................................ 207
Appendix K – RCA Community-Based Levels of Rehabilitative Care Mapping Tool ............................................. 208
Appendix L – System Strengths and Gaps ................................................................................................................ 209
Appendix M – Regional Population breakdowns by IDN: ........................................................................................ 217
Appendix M – Current Estimated Beds ..................................................................................................................... 219
Appendix N – Hip Fracture Process Map .................................................................................................................. 220
Appendix O – North Western Ontario Community Physiotherapy Referral Decision Tree ...................................... 221
Appendix P – Rehabilitation Resources in the North West LHIN ............................................................................. 222
Appendix Q – Geriatric Assessment & Rehabilitative Care Stream .......................................................................... 225
Appendix R – Stroke/Neuro Care Stream .................................................................................................................. 227
Appendix S – Musculoskeletal Care Stream ............................................................................................................. 229
Appendix T – Medically Complex Care Stream........................................................................................................ 231

6
Acronym List
Acronym Meaning
ALC Alternative Level of Care
AR Activation/Restoration
CCAC Community Care Access Center
CCB Convalescent Care Bed
CCC Complex Continuing Care
CCRS Continuing Care Reporting System
CHF Congestive Heart Failure
COPD Chronic Obstructive Pulmonary Disorder
DPC Designated Physiotherapy Clinic
EOC Episode of Care
ER Emergency Room
FIM Functional Independence Measure
FTE Full Time Equivalent
HBAM Health Based Allocation Model
HCCP Home and Community Care Program
IDN Integrated District Network
IHCO Integrated Health Care Organization
IHSP Integrated Health Service Plan
ISAEC IntraSpinal Assessment and Education Centre
LHH Local Health Hub
LHIN Local Health Integration Network
LOS Length of Stay
LTC Long Term Care
MOH Ministry of Health
MOHLTC Ministry of Health and Long-Term Care
MOST Moving on After Stroke
MSK Musculoskeletal
NIHB Non-Insured Health Benefits
NP Nurse Practitioner
NRS National Rehabilitation Reporting System
NWO North Western Ontario
OT Occupational Therapist
OTN Ontario Telemedicine Network
PCVC Personal Computer Virtual Conferencing
PRAC Physical Rehabilitation Advisory Committee
PSW Personal Support Worker
PT Physiotherapist
QBP Quality Based Procedures
RCA Rehabilitative Care Alliance
RJAC Regional Joint Assessment Center
SJCG St. Joseph’s Care Group
SJH St. Joseph’s Hospital
SLP Speech and Language Pathologist
SW Social Worker
TBRHSC Thunder Bay Regional Health Sciences Center
VON Victoria Order of Nurses

7
Executive Summary
Background
Rehabilitative care is defined as “a broad range of interventions that result in the improved physical,
mental and social wellbeing of those suffering from injury, illness or chronic disease.” The importance of
rehabilitation within the global context of healthcare has been well documented. In light of the ongoing
changes and increased demand placed on the healthcare system, it has become increasingly important to
identify optimal care practices and efficiencies. In the North West Local Health Integration Network
(LHIN), the above average burden of chronic diseases and musculoskeletal disorders, combined with a
widely dispersed population, present a unique challenge to providing equitable access to high quality
rehabilitative care. In order to meet this challenge, the North West LHIN is committed to ensuring all
aspects of rehabilitative care within the region are delivered within an integrated system, including care
provided as close to home as possible. In 2014, the LHIN initiated a capacity-planning project to create an
integrated model of rehabilitative care for the North West LHIN.
The following plan represents a culmination of this work and presents recommendations to support an
integrated service delivery model of inpatient and outpatient rehabilitative care services for the residents
of Northwestern Ontario (NWO). The term rehabilitation is used throughout this report and is inclusive of
complex continuing care (CCC).
Goal
To examine the current state of rehabilitative care services and develop a future state model of
rehabilitative care in NWO to improve access to safe, comprehensive and high quality rehabilitative care
for all residents of NWO.
Alignment
All recommendations and strategic directions contained within this report are consistent and aligned with
strategy at the provincial and LHIN level. Provincially, the plan aligns with Patients First: Action Plan
for Health Care, the recommendations from the 2013 Annual Report from the Ontario Auditor General
for Provincial Standardization of Rehabilitative Care, Ontario’s Seniors Strategy, as well as Health
System Funding Reform initiatives including Quality Based Procedure (QBP) implementation. Locally,
the plan aligns with the North West LHIN Strategic Directions, Integrated Health Service Plan (IHSP)
2016-2019, and Health Services Blueprint. The proposed model is based on the North West LHIN Health
Services Blueprint recommendations of a model of services and care delivered at the local, district and
regional levels, specifically known as the Local Health Hub (LHH), Integrated District Network (IDN) or
LHIN sub-region, and Regional or LHIN-wide levels.
8
Throughout this capacity-planning exercise, tools developed by the Rehabilitative Care Alliance (RCA)
were utilized to ensure the review process and all recommendations support the ongoing efforts to
increase standardization of rehabilitative care in Ontario.
Methodology
The North West LHIN Rehabilitative Care Capacity Plan and integrated service delivery model
recommendations and actions plans were created through the analysis and synthesis of qualitative and
quantitative information. In addition, extensive community engagement was conducted with key
stakeholders throughout the North West LHIN including health service providers, administrators, clients,
and families. Finally, a literature review and consultations with subject matter experts and a number of
other LHINs was conducted.
The RCA capacity-planning framework formed the foundation of this review. This framework guided the
evaluation of bedded levels of rehabilitative care, community/ambulatory care, and bedded, long stays
services. An evaluation of acute care was not included in the scope of this review and is only discussed in
relation to the demand and provision of inpatient rehabilitative care.
Findings
This review provides current data for populations receiving and requiring rehabilitative care, the available
resources within each local LHH and, to a more limited extent, the ability to access and receive care.
The following strengths and gaps were identified in the current system of rehabilitative care in the North
West LHIN:
Strengths Gaps
• High degree of satisfaction with rehabilitation
services throughout NWO and appreciation of
the services available in their home
communities by clients and families
• Existing provincial (Rehabilitation Care
Alliance) and regional networks (Regional
Stroke Network and Regional Orthopaedic
program) with common “mandates”
• Access to specialized services within the
region
• Health service providers (HSPs) willing to
work together; informal collaboration is key
tenet of providing care in the North West
LHIN
• Rehabilitation care experts willing to provide
consultation and support to providers across
the region and across disciplines
• Lack of a regional approach to rehabilitative
care planning and delivery in the North West
LHIN making it difficult to coordinate care
across settings and communities
• Variability in the availability of rehabilitative
care at the LHH and IDN levels (ie. OT, SLP
and SW); timely access to care is a challenge
• Limited access to ongoing clinical education,
experiential learning, and mentorship for
providers at all levels of care, *especially for
support workers in Aboriginal communities
• Individuals who may benefit from a
rehabilitative approach to care are not able to
consistently access the appropriate level of
care
• Timely access to home safety and equipment
assessments

9
• Providers from all disciplines and care
settings desire to enhance capacity to deliver
rehabilitative care closer to home through
participation in ongoing education, skill
development, and using innovative
technologies to facilitate communication,
education, and increased access to care.
• Many existing programs can be leveraged to
support individuals and caregivers in the
community
• Existing, extensive secure videoconference
and Personal Computer Virtual Conferencing
(PCVC) infrastructure and processes in place
in the North West LHIN
• Willingness to explore partnerships to assist
with service provision, and human resource
recruitment and retention
• Limited supportive housing and social
supports throughout the region
• Lack of communication, shared medical
record and coordination at times of transition
along the care continuum, especially between
Aboriginal community providers and other
health care services; Family Health Teams
and hospital services; and between hospitals
and Community Care Access Centre
contracted service providers
• There is a loss of rehabilitation education at
the graduate level locally in NWO, through
partnerships with NOSM and McMaster
which will potentially impact recruitment and
retention
• Limited monitoring, reporting, and evaluation
of outpatient rehabilitation activities and
services at the system level
Desired Future State
The vision for NWO is to create an integrated system of care across the full continuum, from inpatient
rehabilitation to outpatient rehabilitation and reintegration to the community, which will serve all
individuals who could benefit from rehabilitative care. Regardless of the care setting, individuals will
receive care that is client-centred, sensitive to diversity and culture, delivered by an interprofessional
team, and close to home.
Within an integrated model of care, healthcare providers across the region will work together to organize
services and the delivery of care across the 14 LHHs and 5 IDNs, including specialized regional
programs, which serve all of NWO. This model has been developed in alignment with the North West
LHIN health services delivery model; within existing resources; building on the existing strengths of the
current system; and addressing the gaps in care delivery identified within the current state analysis.
The future state model will include the following key elements: a Rehabilitative Care Lead Organization,
Regional Rehabilitative Care Streams, flexibility in local LHHs to meet care needs, partnerships with the
LHHs and Integrated Health Care Organizations (IHCO), identification of specialized regional programs,
and improved regional access to all rehabilitative care services.

10
The Regional Rehabilitation Program is structured with two objectives in mind:
1. Leading regional level initiatives that will result in a standardized, evidenced-based, integrated approach to care across NWO.
2. Supporting work at the IDN, LHH, and HSP levels to implement best practices and deliver
standardized rehabilitative care programs and services to all populations across the North West
LHIN.
The Rehabilitative Care Lead Organization will provide the required leadership for coordination and
planning, monitoring and evaluation, evidence-based practice knowledge translation, communication,
education, research, capacity-building, and advocacy, over and above actual service delivery. Each Care
Stream will have identified leaders as consistent contacts and knowledge exchange experts for a specific
area of rehabilitation, and teams of rehabilitation professionals who will be available to provide
assessments and consultation with regional providers as required. Under the guidance of the Regional
Program, community facilitators will be identified at the LHH or IDN level to lead the development of
rehabilitative care in every LHH. The Rehabilitative Care Lead organization, Care Stream Leads, and
community facilitators will provide leadership to implement recommendations from the Regional
Program at the LHH level.
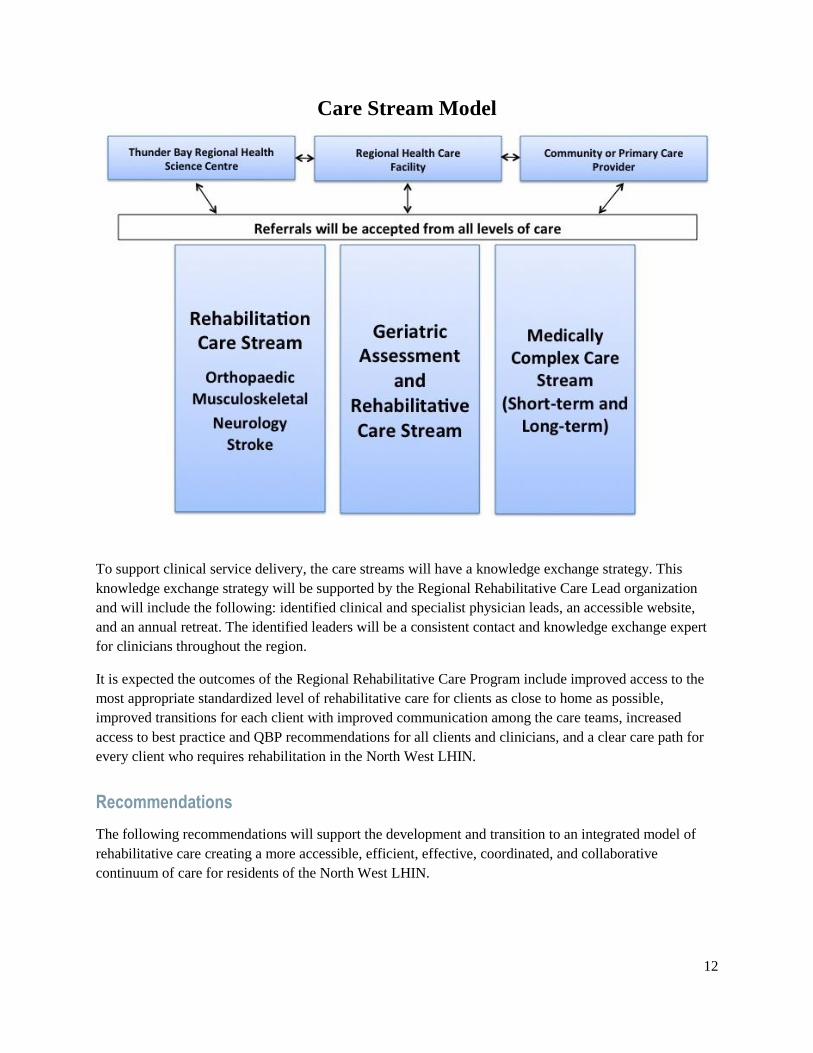
Based on RCA bedded levels of rehabilitative care definitions, existing care pathways, and client care
needs, the following care streams will meet the specialized care needs of NWO:
• Geriatric Assessment and Rehabilitative Care.
• Specialized Rehabilitation (Neurological, Stroke; Orthopaedic and Musculoskeletal) Services
Stream.
• Medically Complex Services (Wound, Lymphedema, Pulmonary, and Chronic Disease).

11
The following figure depicts the structure of this integrated system.
North West LHIN Regional Rehabilitative Care Program - Integrated Systems of Care
The model aims to coordinate rehabilitation services across the region by leveraging existing services and
expertise from a larger regional centre with more specialized and comprehensive services, to enhance and
support existing services in each smaller, remote community where population, economies of scale,
recruitment, and retention do not support the same level of care. Collaboration between specialized
rehabilitative care services delivered at the regional level and rehabilitative care delivered at the LHH will
ensure client needs are met as close to home as possible. This model will promote improved access and
better transitions in care by encouraging integration within each level, and across all levels of care. The
overall goal of an integrated system is to provide excellence in care, built on a vision of improved access
and flow, standardization, coordination, and the use of evidence-based care to improve the client journey.
12
Care Stream Model
To support clinical service delivery, the care streams will have a knowledge exchange strategy. This
knowledge exchange strategy will be supported by the Regional Rehabilitative Care Lead organization
and will include the following: identified clinical and specialist physician leads, an accessible website,
and an annual retreat. The identified leaders will be a consistent contact and knowledge exchange expert
for clinicians throughout the region.
It is expected the outcomes of the Regional Rehabilitative Care Program include improved access to the
most appropriate standardized level of rehabilitative care for clients as close to home as possible,
improved transitions for each client with improved communication among the care teams, increased
access to best practice and QBP recommendations for all clients and clinicians, and a clear care path for
every client who requires rehabilitation in the North West LHIN.
Recommendations
The following recommendations will support the development and transition to an integrated model of
rehabilitative care creating a more accessible, efficient, effective, coordinated, and collaborative
continuum of care for residents of the North West LHIN.

13
Action Items Healthcare
Level Deliverables Outcomes
Recommendation #1
Improve client experience and outcomes through the implementation of the RCA definitions framework to align rehabilitative care in the North West LHIN
with the provincial framework.
1.1 Ensure there is regional alignment
with the RCA definitions frameworks
for bedded and community-based
levels of rehabilitative care
• Provincial
• Regional
• RCA Bedded and Community Mapping
Tool results
• Full alignment with approved exceptions
• Plan for any alignment issues
1.2 Educate service providers regarding
the definitions
• Regional
• IDN
• LHH
• Education module on rehabilitative
levels of care
• Education module delivered in all
hospitals throughout North West LHIN
• Increased knowledge & understanding of
rehabilitative levels of care
1.3 Create an implementation schedule to
achieve alignment by March 2017
• LHIN
• IDN
• LHH
• Implementation Plan • Full alignment by March 31, 2017
• Plan for any alignment issues
1.4 Upon referral, establish a process to
determine the appropriate level of
rehabilitative care for each client and
the appropriate location of
rehabilitative care i.e. LHH, IDN and
the region
• Regional
• IDN
• LHH
• Care stream process map developed and
shared throughout the LHIN
• Regional Rehab referral system piloted
in 2 IDNs
• Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
1.5 Confirm the required health human
resources to provide each level of care
and the capacity of each health hub
and integrated network to provide the
level of care
• LHIN • Capacity Plan • Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
1.6 Establish a process to gather
information regarding the
rehabilitative care provided by
regional hospitals on their inpatient
units
• LHIN • RCA Bedded & Community Mapping
Tool
• Completed community engagement
profile
• Regional Rehabilitation Health Human
Resources Table
• Improved access to care
• Care as close to home as possible
• Capacity planning completed at the LHH and
IDN levels

14
Action Items Healthcare
Level Deliverables Outcomes
1.7 Maximize Convalescent Care Bed use
to align with Activation/ Restoration
Bedded Levels of Care by addressing
process issues related to barriers such
as IV medications, staffing resources,
and discharge location determination.
• LHIN
• IDN
• LHH
• Committee established between
stakeholders to identify and address
barriers
• Process map developed and shared
throughout the LHIN
• Full alignment with Activation/Restoration
Level of Care in IDNs with CCB
• Improved access to care
• Care as close to home as possible
Recommendation #2
Develop a LHIN-wide strategy to improve client access and client transitions across the continuum of rehabilitative care.
2.1 Review current or create
appropriate diagnosis-specific
client care pathways based on best
practices to support the access and
transition between inpatient and
outpatient services across the entire
North West region
• Regional
• Care Pathways
• QBP Heat Map for stroke, TKR, THR,
Hip Fracture, COPD, CHR, etc.
• Care stream Leads established
• Appropriate LOS
• QBP optimization
• Improved access to care
• Improved client/care transitions
• Improved quality of care
• Care close to home
2.2 Develop a plan and implementation
strategy to improve transitions
between specialized rehabilitation
services and local services at either
the IDN or LHH level and
transitions home
• Regional • Discharge process map
• Discharge checklist
• Standardized documentation
• Standardized referral form across
regional/IDN/LHH
• Standardized process for accessing OT
Home visits post discharge from
hospitals
• Improved client care transitions
• Improved quality of care
• Clear documentation
• Enhanced communication among providers
2.3 Improve direct access from primary
care and community care providers
to both inpatient and
outpatient/community-based
rehabilitation programs throughout
the region
• LHIN
• IDN
• LHH
• Care pathways established: community-
hospital-community
• Coordinated referral management
system for rehabilitative care
• Memorandum of agreement with FHTs
• Frail Senior/Medically Complex Care
stream Lead
• Improved access to care
• Decrease unnecessary ER/acute care visits
• Improved quality of care
• Decrease ALC for LTC
• Care close to home as soon as possible

15
Action Items Healthcare
Level Deliverables Outcomes
2.4 Evaluate opportunities for the
development specialized outpatient
programs to be delivered closer to
home, building on successful
regional models
• Regional
• IDN
• LHH
• Care Stream Leads
• Specialized OP programs delivered at
IDN/LHH
• Provision of local temporary housing as
necessary
• Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
2.5 Strengthen connections between
local service providers and regional
care networks to provide support
for LHH provision of rehabilitative
care
• Regional
• IDN
• LHH
• Annual Retreat
• Care Leads
• Health Human Resources Contact List
• Enhanced communication amongst providers
• Improved client care transitions
• Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
2.6 Develop a mechanism to share
information regarding and access to
visiting specialists programs to
support an integrated regional
model of specialized client care
• LHIN
• FHT
• IDN
• LHH
• Visiting specialist program integration
• Care Leads/Care Streams
• Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
Recommendation #3
Facilitate adherence to best practices for rehabilitative care to improve client-centred care.
3.1 Build capacity to meet best practice
and QBP expectations at a local
level though knowledge-sharing
across the region
• Regional
• IDN
• LHH
• Annual Retreat
• Care Leads/Care Streams
• Website
• Communication with Physicians
• Full QBP funding
• Quality, evidence-based care
• Improved quality of care
• Improved access to care
• Care as close to home as possible
3.2 Strengthen and expand existing
clinical practice networks for
rehabilitative care providers to
ensure an integrated model exists
across the Northwest
• Regional
• IDN
• LHH
• Annual Retreat
• Care Leads/Care Streams
• Website
• Quality, evidence-based care
• Improved quality of care
• Enhanced communication amongst providers
• Improved access to care
• Care as close to home as possible
16
Action Items Healthcare
Level Deliverables Outcomes
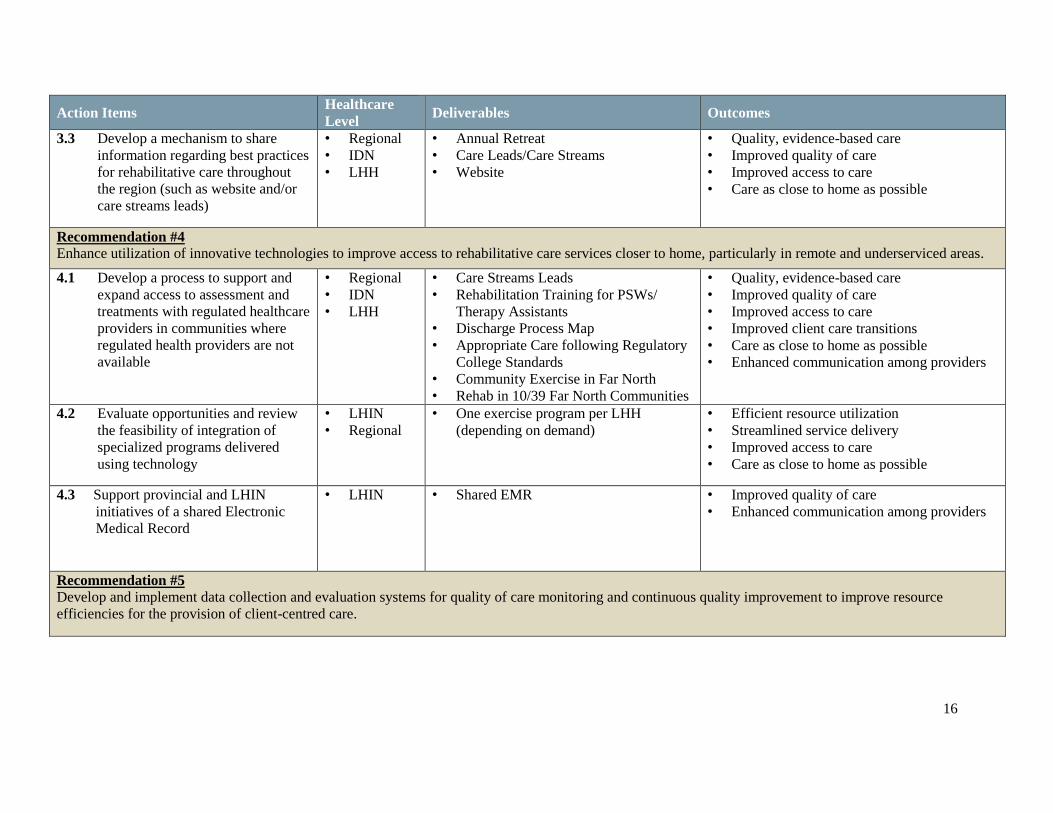
3.3 Develop a mechanism to share
information regarding best practices
for rehabilitative care throughout
the region (such as website and/or
care streams leads)
• Regional
• IDN
• LHH
• Annual Retreat
• Care Leads/Care Streams
• Website
• Quality, evidence-based care
• Improved quality of care
• Improved access to care
• Care as close to home as possible
Recommendation #4
Enhance utilization of innovative technologies to improve access to rehabilitative care services closer to home, particularly in remote and underserviced areas.
4.1 Develop a process to support and
expand access to assessment and
treatments with regulated healthcare
providers in communities where
regulated health providers are not
available
• Regional
• IDN
• LHH
• Care Streams Leads
• Rehabilitation Training for PSWs/
Therapy Assistants
• Discharge Process Map
• Appropriate Care following Regulatory
College Standards
• Community Exercise in Far North
• Rehab in 10/39 Far North Communities
• Quality, evidence-based care
• Improved quality of care
• Improved access to care
• Improved client care transitions
• Care as close to home as possible
• Enhanced communication among providers
4.2 Evaluate opportunities and review
the feasibility of integration of
specialized programs delivered
using technology
• LHIN
• Regional
• One exercise program per LHH
(depending on demand)
• Efficient resource utilization
• Streamlined service delivery
• Improved access to care
• Care as close to home as possible
4.3 Support provincial and LHIN
initiatives of a shared Electronic
Medical Record
• LHIN • Shared EMR • Improved quality of care
• Enhanced communication among providers
Recommendation #5
Develop and implement data collection and evaluation systems for quality of care monitoring and continuous quality improvement to improve resource
efficiencies for the provision of client-centred care.

17
Action Items Healthcare
Level Deliverables Outcomes
5.1 Review existing reporting
mechanisms and provide advice
regarding how to improve data
accuracy and quality to support
future decision-making regarding
rehabilitative care services.
• Provincial
• LHIN
• Adopt RCA recommendations
regarding key indicators; collect and
monitor key indicators
• OP Minimal Data Set
• Accurate quality data
• Improved decision making regarding
rehabilitative care needs
5.2 Provide training and assist in the
implementation of data collection
systems for outpatient programs to
align with RCA minimum data set
recommendations, including care
outcomes, experience and cost.
• Provincial
• Regional
• Adopt RCA recommendations
regarding key indicators; collect and
monitor key indicators
• OP Minimal Data Set Tool kit
• Accurate quality data to inform decision
making
5.3 Monitor and measure overall
system performance
• Provincial
• LHIN
• Rehabilitation Score Card
• Evaluation of referral management
system
• Improved quality of care
• Improved client experience
• Improved access to care
• Efficient resource use
5.4 Using RCA tools, measure the
client progress and care experience
in each rehabilitative care setting
• Provincial
• LHIN
• Regional
• Key indicator data sets • Quality, evidence-based care
• Improved quality of care
• Improved client experience
• Improved access to care

18
Conclusions
Implementation of the identified recommendations and action plans will result in a coordinated regional
model of rehabilitative care. The use of technology, development of care networks, and partnerships with
our remote communities will continue to enhance our care provision, and in turn assist to develop a
strong, lasting, equitable, integrated system of rehabilitative care. By building on the existing passion and
commitment to meet the unique rehabilitation needs of our clients, the integrated system will provide
excellence in care, built on a vision of improved access and flow, standardization, coordination, and the
use of evidence-based care to improve the client journey.
A Rehabilitative Care Lead Organization will be announced followed by the establishment of a
Rehabilitative Care Advisory Committee which will include regional stakeholders and participation
across all levels of rehabilitative care including client and family representation, clinician representation,
and administration representation. At the same time, Regional Rehabilitative Care Streams will be
implemented to support best practices, QBP adherence, and availability of rehabilitation for all clients
across the continuum and across the region. Each care stream will have interprofessional teams to provide
assessments, triage, and consultation with regional providers as required, as well as an identified Care
Stream Lead to facilitate knowledge exchange for clinicians and appropriate, efficient, and effective client
transitions.

19
Background and Context
Project Rationale
Rehabilitative care is defined as “a broad range of interventions that result in the improved physical,
mental and social wellbeing of those suffering from injury, illness or chronic disease.” The importance of
rehabilitation within the global context of healthcare has been well documented. Rehabilitation is
“instrumental in enabling people with limitations in functioning to remain in or return to their home or
community, live independently, and to participate in education, the labour market and civic life”. In light
of the ongoing changes and increased demand placed on the healthcare system due to the aging
population, it has become increasingly important to identify optimal care practices and efficiencies. In
response to the 2013 Annual Report of the Office of the Auditor General of Ontario, the Rehabilitation
Care Alliance (RCA) was created to standardize the provision of rehabilitative services (inpatient and
outpatient) across the province, with the goal that all Ontarians can expect the same standard range of
rehabilitative services to be provided anywhere in the province, within certain geographic and population
limitations. The challenges to providing access to healthcare in NWO are long-standing: sparsely-
populated, vast geographical area; a healthcare budget which is population-focused; and attracting and
retaining qualified healthcare professionals. In recent years, the North West Local Health Integrated
Network (LHIN) has conducted ongoing evaluations of healthcare practices in order to develop a strategy
to meet changing needs.
In the North West LHIN, there is a strong demand for rehabilitative care services and the demand is
expected to increase significantly as the population continues to age. Over the next ten years, the
population aged 65 to 79 will increase by 42 percent in the region and as a result, an age-related increase
in chronicity and complexity of medical conditions. Based on these factors, it is expected there will be an
even greater demand for rehabilitation and restorative care services, prevention, and the need for
programs to support health maintenance to prevent the premature decline in health status. The term
rehabilitation is used throughout this report and is inclusive of complex continuing care (CCC).
Historically, these services were primarily based out of the City of Thunder Bay, with over 65% of the
allotted CCC bed capacity and 100% of the designated rehabilitation beds located in the City of Thunder
Bay. While these services have met the needs of many residents of Northwestern Ontario (NWO), gaps
remain within the current system, which limit access to quality rehabilitative care for some residents. As
outlined in the 2013 North West LHIN Health Services Blueprint, there is a need for integrated, post-
acute rehabilitative care, which improves client outcomes and client experiences along the entire
continuum of rehabilitative care services.

20
Figure 1. The Patient Journey
In 2012-2013, a detailed review of Rehabilitation and CCC in NWO was completed to help inform the
development of the North West LHIN Health Service Blueprint. In 2014, the North West LHIN funded
St. Joseph’s Care Group (SJCG) to complete the first phase of the post-acute rehabilitative care services
review by consolidating existing information to inform future planning and this capacity-planning
exercise.
Goal
The overall goal of this plan is develop an integrated rehabilitative care model to improve access to safe,
comprehensive and high quality rehabilitative care for all residents of NWO. The plan provides a
comprehensive analysis of the current and future state needs for rehabilitative care in the North West
LHIN which when implemented will facilitate improved quality, efficiency, and cost-effectiveness with
the benefit of services delivered as close to home as possible.
Alignment with Regional and Provincial Priorities
Alignment with Provincial Priorities
The development of the North West LHIN rehabilitation capacity-planning review was informed by and
advances the strategic directions found in a number of Ministry of Health and Long-Term Care’s
(MOHLTC) and North West LHIN reports including: Patients First: Action Plan for Health Care;

21
Ontario’s Seniors Strategy; Living Longer, Living Well; North West LHIN’s Health Services Blueprint:
Building our Future; as well as the Integrated Health Services Plan (IHSP) 2016-2019. All of these
reports include the themes of:
• Providing the right care, at the right time, in the right place, as close to home as possible.
• Delivering coordinated and integrated care in the community.
• Ensuring access to the same high-quality standard of care for all.
• Providing care as close to home as possible.
• Promoting use of evidence-based solutions and continuous quality improvement.
• Increasing the use of virtual care tools and innovative approaches to care.
• Increasing the utilization of the most appropriate resource through interprofessional care teams.
• Enhancing chronic disease management.
• Improving the client care experience.
• Ensuring health system accountability and sustainability.
This review also recognizes the financial context of rehabilitative care reform. Health System Funding
Reform is challenging large and medium-sized hospitals and the Community Care Access Centres
(CCAC) to review who accesses service and how to best provide care. In the North West LHIN, the three
hospitals affected by the Health-Based Allocation Model are Thunder Bay Regional Health Sciences
Centre (TBRHSC), SJCG in Thunder Bay, and Lake of the Woods Hospital in Kenora. The rest of the
hospitals in the North West LHIN are considered small hospitals and receive global funding. Health
System Funding Reform has an effect on all hospitals, but significantly impacts how the three hospitals
operate inpatient and outpatient services and will be examined in more detail in the findings section of
this report.
Rehabilitative Care Alliance (RCA) Background
The RCA is a provincial, task-oriented, collaborative group created to effect positive changes in
rehabilitative care across Ontario. It was created in 2013 by Ontario’s 14 LHINs in response to the need
to develop standardization across Ontario’s rehabilitative care system. The RCA utilizes several task and
advisory groups, with broad stakeholder engagement, to develop tools and definitions to help service
providers improve system integration and ensure the quality and sustainability of rehabilitative care
services.
Within the first mandate (April 2013-April 2015), the following key priorities were addressed:
• Definitions – the development of standardized definitions and standards of practice for all levels
of rehabilitative care (Appendix A and B).
• Capacity Planning & System Evaluation – the development of a standard rehabilitative care
capacity-planning and evaluation toolkit (C).

22
• Frail Senior/Medically Complex – the development of an approach for frail senior and medically
complex populations to support the Assess and Restore framework.
• Outpatient/Ambulatory – the development of a standardized minimum data set for outpatient/
ambulatory rehabilitation to inform evaluation and planning at all levels of care.
• Re-classification of Rehabilitation/CCC beds – development of a standardized provincial process
to evaluate the need to re-classify CCC to inpatient rehabilitation beds (Appendix D).
These five mandates provide the foundation of this rehabilitative care review, with the utilization of the
RCA capacity-planning toolkit as a guiding document to create the report. Capacity planning exercises
are taking place throughout Ontario in order to align with the RCA work and the need to standardize
rehabilitative care across the province. The RCA has been extended for a second mandate (April 2015-
April 2017) to support the LHINs in the implementation of the above standardized tools, processes, and
frameworks and develop tools and frameworks for implementation of Quality Based Procedures (QBPs)
for Hip Fracture and Total Joint Replacement. This report also considered other local, provincial and
federal initiatives as outlined in the Project Charter (Appendix E).
Overall, this capacity planning exercise aligns with the strategic initiative of building an integrated
healthcare system. The anticipated outcomes of an integrated model for rehabilitative care will improve
access to care as close to home as possible for all clients, while promoting best care practices. Significant
strategies to achieve this include defining which basket of rehabilitation services will be available at the
Local Health Hub (LHH), Integrated District Network (IDN) and Regional levels; the use of technology
for system integration and service provider networking; and referral management.
Methodology
The North West LHIN Rehabilitative Care Capacity Plan and integrated service delivery model were
created through the analysis and synthesis of qualitative and quantitative information including:
• Community engagement across the North West LHIN.
• Existing reports of the North West LHIN and Ministry of Health and Long-Term Care.
• Provincial initiatives led by the provincial RCA and Greater Toronto Area Rehabilitation Network.
• A literature review focused on integrated models of care and rural and remote communities.
• Consultations with neighbouring LHINs.
• Quantitative data from multiple sources (Appendix F).
A review of the current state of inpatient, outpatient and community-based rehabilitative service, both
CCC and Rehabilitation, was completed in order to identify current practices within the region. A desired
future state model of care was developed based on current best practices, aligning with identified
provincial standards of care, and stakeholder engagement. Subsequently, current system strengths and

23
gaps were identified within the region in order to leverage regional strengths and develop a
comprehensive regional care model.
The RCA capacity-planning framework (Appendix C) formed the foundation of this review using the
definition of restorative potential as outlined by the RCA: “there is reason to believe the client’s condition
is likely to undergo functional improvement and benefit from rehabilitative care”. This framework guided
the evaluation of bedded levels of rehabilitative care, community/ambulatory care, and bedded, long stays
services and identified limitations of rehabilitative care in NWO across the continuum of rehabilitative
care to inform the development of an integrated model of care. Within this process both the siting
(location) and sizing of rehabilitative-bedded levels of care were reviewed in order to inform where
inpatient services should be located. The opportunity to use technology and mobile service delivery was
also examined within the model of rehabilitative care.
Outside the scope of this review are clients seen within dedicated acute care, hospice/palliative care,
mental health, or long-term care beds and pediatric clients. Acute care is discussed in relation to the
demand and provision of inpatient rehabilitative care. The review does include clients in acute care who
could be served in “post-acute” care or were alternative level of care within this resource. This capacity
planning exercise does not provide a detailed analysis of specific medical conditions, and/or condition
prevalence. Rehabilitative care in other parts of the province was not examined except to explore
comparative data or approaches in regions similar to NWO.
The local review process had oversight by a project-specific governance structure. This included North
West LHIN and SJCG executive sponsorship and the use of the SJCG Physical Rehabilitation Advisory
Committee (PRAC) to vet the process and recommendations. The PRAC is an existing quarterly advisory
committee with the purpose of providing advice regarding the rehabilitation programs and services at St.
Joseph’s Hospital (SJH). Project-specific terms of reference were developed and the membership of the
advisory committee was augmented to ensure cross-continuum regional representation. Ex-officio
members included SJCG administrative staff and LHIN representation (Appendix G). A data-analysis
working group provided support to the PRAC to review and confirm accuracy of data developed to
inform the rehabilitative review process. The working group included representation from regions east
and west of Thunder Bay, the North West LHIN, acute and rehabilitative cares organizations, and the
North West Health Alliance.
Literature Search
A literature review was conducted on ‘integrated models for rehabilitative care’ and ‘rehabilitation in
rural and remote areas’ and ‘rehabilitation and indigenous populations’. Relevant evidence-based models
of care such as the integrated models of care, the “Hub and Spoke” model of care, and the primary care
approach were identified along with a model for community capacity-building approach. Components of
these models will be incorporated into the regional care model for the North West LHIN. Elements of the
literature review will serve as evidence throughout this plan.

24
Quantitative Data
A detailed analysis of available quantitative data was conducted in order to inform decision making and
illustrate demand for varying types of rehabilitative care across the North West LHIN. Data collection and
analysis for inpatient care used provincial databases for CCC and designated rehabilitation beds and was
completed by Preyra Solutions consulting firm (contracted through the North West LHIN) and the SJCG
Planning and Performance team.
Community Engagement
Extensive community engagement was conducted with key stakeholders including frontline providers,
leadership teams, clients and families. (Appendix H) Input was obtained, directly through individual and
group discussion and indirectly through members of the advisory committee.
The first phase of community engagement took place in the summer of 2015 and aimed to engage
regional administrators throughout the continuum of care, professional advisory committees, Aboriginal
agency stakeholders, and key informants. The primary purpose of these engagement sessions was to
provide an opportunity for discussion and input on the current state of access to rehabilitative services in
the North West LHIN and gaps to be addressed in an ideal future state.
The second phase of community engagement occurred between November 2015 and December 2015. A
mapping exercise, using the RCA definitions framework of bedded and community rehabilitation,
determined alignment with the RCA standardized definition frameworks for inpatient and outpatient care
within all publicly-funded healthcare organizations in the North West LHIN (Appendix I and J). These
results helped to inform the capacity-planning process.

25
The final phase of community engagement was carried out during the fall of 2016. Videos were prepared
and pre-circulated one week prior to site visits to rehabilitation care providers and managers at the
regional hospitals throughout the North West LHIN. Video content included: the proposed integrated
model of care and preliminary recommendations, the RCA levels of care definitions for both inpatient and
outpatient including fictitious case studies, the impending care streams changes at SJH to align with the
RCA rehabilitative care definitions, and information on hip fracture, primary joint replacement and stroke
QBPs. Site visits to rehabilitative care providers, clients and families at all regional hospitals within the
North West LHIN were conducted to inform the current state, verify the recommendations and secure
feedback regarding the integration of rehabilitative care. Identified system strengths and gaps are
embedded throughout the Current State section of the report and details can be found in Appendix K.
Further Aboriginal stakeholder engagement was completed to clarify identified gaps for this population
and to seek feedback on the recommendations and implementation.
Limitations
Throughout the rehabilitative care capacity-planning exercise for NWO, limitations became apparent. The
primary limitation encountered was the quality of available data. Through the capacity-planning exercise,
it was determined organizations do not report data consistently, particularly within designated CCC beds.
Data were also limited to the use of rehabilitative care services within the North West LHIN for both
residents and non-residents of the North West LHIN but did not capture the use of rehabilitative care
services outside the North West LHIN for residents of the North West LHIN. Further information is
required on the use of rehabilitative care services in Manitoba for residents of the North West LHIN. With
respect to data analysis, the capacity-planning exercise was also limited by the applicability of forecasted
data. Data projections are based on provincial normative values and information reported through the
Continuing Care Reporting System (CCRS) for designated CCC beds and National Rehabilitation
Reporting System (NRS) for designated rehabilitation beds. Since most regional hospitals do not report in
the CCRS system, clients receiving rehabilitative care are not represented in the data.

26
Current State Analysis
Demographics, Population Characteristics, Health Status and Behavioural Factors
North West LHIN Context for Planning
The North West LHIN has the smallest population of all Ontario LHINs, with approximately 235, 900
residents. It also serves the largest geographic area of all Ontario LHINs, covering 47% of the province’s
land mass. According to the Integrated Health Service Plan 2016-2019 Common Environmental Scan,
46% of the residents in the North West LHIN live in Thunder Bay, the only large urban population centre
in the region, while 34% of the population lives in rural areas with more than two-thirds of communities
only accessible seasonally, or by air. Among this population, seniors (aged 65+) account for 17% of the
population. The North West LHIN is home to the greatest proportion of people who identify as
Aboriginal provincially; of the total population in the North West LHIN, 21.5% self-report as Aboriginal.
Between 2010 and 2015, the population of North West LHIN has declined by 0.5% in comparison to the
provincial population, which has grown by 5.1%. It is anticipated over the next five to ten years, the
population of the North West LHIN will remain relatively stable, while the overall provincial population
will continue to increase. However, in comparison to the rest of the province, the North West LHIN’s
proportion of seniors is projected to have higher growth. Over the next 20 years, in the North West LHIN,
the proportion of those aged 65 and over is projected to increase from the current 15-16% to 27-28%.
Provincially, the proportion is expected to increase from the current 14-15% to 22-23%. As the
population ages, the demand for high quality rehabilitative care will increase.
To guide the planning and delivery of healthcare services, while acknowledging the unique needs
across the region, the North West LHIN has been divided into five DNs, as shown in figure 2.

27
Figure 2. North West LHIN Integrated District Networks Map
Many of the IDNs are experiencing an overall decline in total population and an increase in the number of
people aged 65 and over. The following table and Appendix L illustrate these differences in population
size, age, language, and Aboriginal identity and the need to consider the unique characteristics of each
IDN when planning for the regional delivery of rehabilitative care.

28
Table 1. 2011 Census Population Characteristics
IDN Total Population % Age 65+ % Aboriginal Identity % Francophone
Northern 21 815 5.5 81.3 0.5
Kenora 43 130 15.6 25.5 2.9
Rainy River 20 370 17.2 22.3 1.8
City of Thunder Bay 127 975 17.1 9.9 2.7
District of Thunder Bay 17 830 13.9 32.4 13.0
North West LHIN 231 120 15.5 21.5 3.4
IDN Minimum 17 830 5.5 9.9 0.5
IDN Maximum 127 975 17.2 81.3 13.0
Sources: 1 . Sta t i s t i cs Canada. 2011 Census. 2 . Sta t is t i cs Canada. 2011 Nat iona l Household Survey. The non -response
ra te for the Abor ig ina l ident i ty quest ion in the NHS was approximate ly 30% for the North West LHIN res idents wi th
s ign i f icant var ia t ion between communi t ies .
In the Northern IDN, for example, there is a smaller proportion of seniors and a large Aboriginal
population (81.3%) spread out across a number of small, remote communities. While the overall
population of the North West LHIN is decreasing slightly, within the Northern IDN the growth of the
younger population is outpacing that of the older population (40.6% vs. 5.5%). This is significant when
planning for future rehabilitative services as this younger population will likely present different
rehabilitative care needs, for potentially an increased frequency of traumatic injury and early onset
chronic diseases. In addition, specific cultural and geographical needs must be taken into consideration
while planning for rehabilitative care in the Northern IDN. Alternatively, the City of Thunder Bay IDN
has a higher number of seniors living in an urban setting, within close proximity to a range of healthcare
services. It is important to consider the unique needs of each community of the North West LHIN in the
development of a regional model of rehabilitative care in order to meet the local healthcare needs of the
population, while leveraging the existing strengths of each IDN.
North West LHIN Health Status and Behavioural Factors
In addition to a widely dispersed geography, the health status and behavioral factors observed in the
North West LHIN lead to increased prevalence of rehabilitative care needs and subsequently a significant
demand on the healthcare system. Compared to the rest of Ontario, the North West LHIN is below
average in relation to:
• Life Expectancy (78.5 years vs. 81.5 years)
• Self-Perceived Health as Very Good or Excellent (58.8% vs. 60.0%)
• Avoidable Death Rate (258 vs. 171 deaths/100,000)

29
• Percentage of the population with a regular doctor (82.7% vs. 91.2%)
According to the North West LHIN Integrated Health Services Plan, the greatest post-acute and
rehabilitation-related health limitations in the region, as compared to the rest of the province, include:
• Greater number of residents with multiple chronic conditions (20%),
• Higher use of acute care for the management of chronic conditions (26%),
• Higher hospitalization rates for Diabetes (228.5 vs. 99.3 per 100 000), Chronic Obstructive
Pulmonary Disease (COPD) (371.1 vs. 182.4 per 100 000) and Congestive Heart Failure (CHF) (278.4 vs.183.8 per 100 000),
• Higher level of frailty for those aged 75+ (by 45-55%)
• Higher smoking rates (23.6% vs. 18.0%)
• Higher alcohol consumption rates (25.2% vs. 17.2%)
• Higher obesity rates (65.2 %vs. 53.5%)
• Third lowest labour force participation rate in the province
• Largest proportion of residents without a certificate/degree or diploma and a lower proportion
without completed post-secondary education, which contributes to lower literacy levels in the
population.
The health status of Aboriginal people in Canada is poorer than non-Aboriginal people on most
measureable health indicators. Within the North West LHIN, Aboriginal adults are more than twice as
likely as the non-Aboriginal population to die of preventable causes. This represents a decrease in life
expectancy of on average five to seven years as compared to non-Aboriginal people. Remote populations,
large geographic areas, language and cultural barriers, low literacy rates, and inter-generational historical
traumas all impact the challenges in timely access to rehabilitation services for this population.
Factors Affecting Health Status and Access
The large geography and relatively small, dispersed population of the North West LHIN represents one of
the most significant challenges in providing rehabilitative care. These factors create challenges in terms of
service delivery, access and travel to care, recruiting and retaining healthcare professionals and support
workers, and healthcare costs per capita. Further impeding the delivery of rehabilitative care in the North
West LHIN is the lack of road access to one third of communities.
Utilizing population-based growth research, projections indicate an increase in demand for rehabilitation
due to population characteristics and an aging population. However, the overall population of the North
West LHIN is decreasing relative to the rest of the province. Since funding formulas are population- and
volume-based, this presents additional challenges to rehabilitative care service delivery. As such, it is
essential to identify how the North West LHIN differs from other provincial districts. Specifically, due to
the cultural and societal differences described above, the population in the North West demonstrates a
higher degree of frailty and the typical medical concerns related with aging frequently occur at a younger
age, making it difficult to draw comparisons to provincial norms. It is anticipated services associated with

30
the frail elderly, including rehabilitative care, will represent the area highest need due to the sharp rise in
the number of seniors.
Inpatient Rehabilitation
This section of the review includes a detailed evaluation of the current and expected rehabilitative care
needs across the region, including the utilization of Rehabilitation, Convalescent Care and Complex
Continuing Care beds across the region. This includes a comparison of the number of clients reported in
each facility, the number of clients from each community who are receiving care, and identification of
potential limitations in the accuracy of reported number including the impact of Alternative Level of Care
(ALC).
According to the North West LHIN population health profiles, Table 2 outlines the breakdown of
inpatient beds across NWO for all bed types.
Table 2. Summary of current bed allotment in NWO
Hospital Acute* Inpatient
Rehabilitation CCC CCB Total Beds
Thunder Bay Regional Health Sciences Centre 375 375
St. Joseph’s Care Group 50 174 224
Lakehead Manor 9 9
City of Thunder Bay IDN Total 375 50 174 9 608
Lake of the Woods District Hospital 71 71
Dryden Regional Hospital 31 10 41
Red Lake Margaret Cochenour Memorial Hospital 14 4 18
Kenora IDN Total 116 14 130
Atikokan General Hospital 11 8 19
Riverside Health Care Facilities Inc. –
Emo Health Centre 3 4 7
Riverside Health Care Facilities Inc. –
La Verendrye Hospital (Fort Frances) 40 20 60
Riverside Health Care Facilities Inc. – Rainy River Health Centre
3 3
Rainy River IDN Total 57 28 89
Geraldton District Hospital 23 7 30
Manitouwadge General Hospital 9 9
Wilson Memorial General Hospital 9 12 21
Nipigon District Memorial Hospital 15 7 22
The McCausland Hospital 10 13 23
Thunder Bay District IDN Total 66 39 105
Sioux Lookout Meno Ya Win Health Centre 41 8 41
Northern IDN Total 41 8 41
TOTAL 655 50 263 13 981
Includes Medica l /Surg ica l Beds, Obste tr i ca l , Menta l Hea l th , In tens ive Care Uni ts and Acute ped ia tr i cs beds in reg iona l
hosp i ta ls ; Does not include Obste tr i ca l Bassinets
The Auditor General Report identifies inpatient rehabilitation to include both regular (frequent sessions
for a short term) and restorative (slower-paced and over a longer term) with regular rehabilitation being
delivered in a designated rehabilitation bed and restorative rehabilitation being delivered in a CCC

31
designated bed. Designated rehabilitation beds deliver programs that are short-term with frequent
rehabilitation sessions. They are also known as high-tolerance, short-duration rehabilitation. Nationally,
data for these beds are reported using the National Rehabilitation Reporting System (NRS) at either a
general rehabilitation or special (more extensive) rehabilitation level.
The MOHLTC defines CCC as “[the provision of] continuing, medically complex and specialized
services to both young and old, sometimes over extended periods of time. CCC is provided in hospitals
for people who have long-term illnesses or disabilities typically requiring skilled, technology-based care
not available at home or in long-term care facilities”. Within the North West LHIN, the expectation is all
designated CCC beds will be utilized for clients who fall within this definition. Currently, the definition
utilized for CCC varies between facilities provincially.
As a result, the RCA has recently standardized inpatient rehabilitative care definitions. It has been
provincially mandated these definitions be adopted by April 2017, supporting the need to accept a
common definition across the region for the care provided. According to the RCA, there are four
definitions of rehabilitative care, any of which may apply to clients admitted to a CCC or rehabilitation
unit. These definitions outline the client characteristics; medical, nursing and allied health resources; and
reporting tools for each level of client needs. Implementation of bedded levels of care (standardized
inpatient rehabilitative care definitions) must ensure these common definitions are utilized by all facilities
within the region.
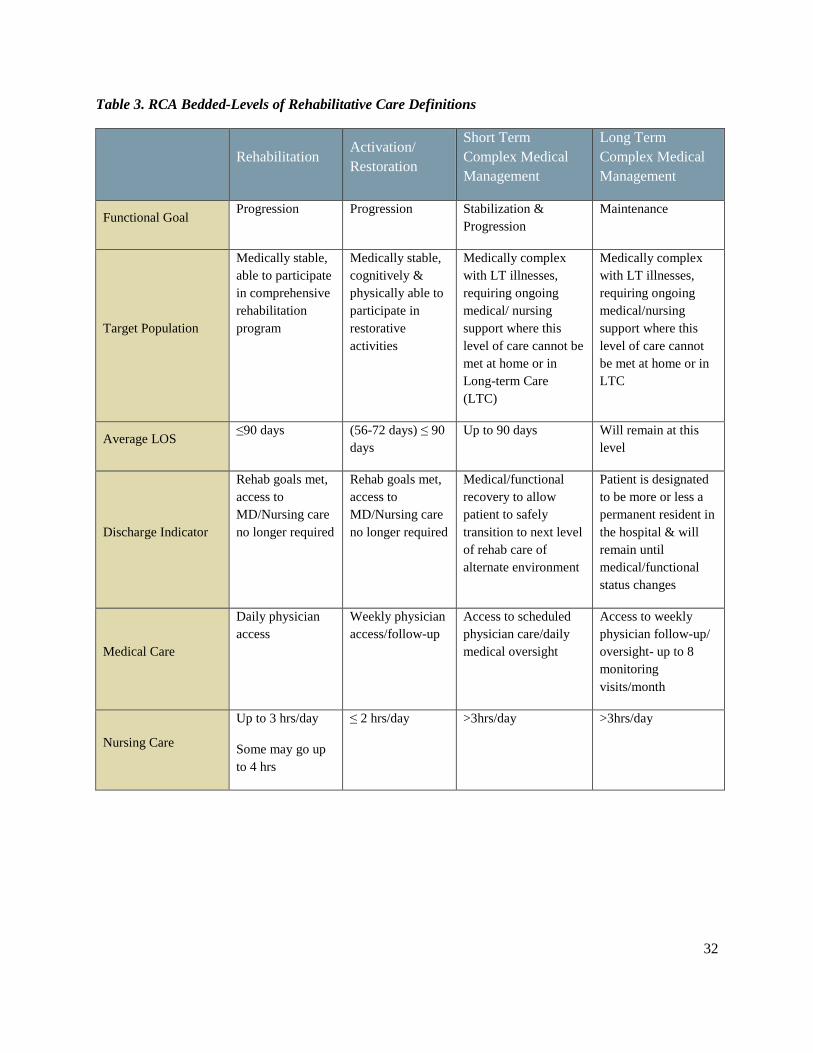
The categories of bedded-levels of care expected in Rehabilitation or CCC designated beds include:
Rehabilitation, Activation/Restoration, Short-term Complex Medical Management, and Long-term
Complex Medical Management. Key characteristics of each of the categories are described in Table 3 and
are detailed in Appendix A.
32
Table 3. RCA Bedded-Levels of Rehabilitative Care Definitions
Rehabilitation Activation/
Restoration
Short Term
Complex Medical
Management
Long Term
Complex Medical
Management
Functional Goal Progression Progression Stabilization &
Progression
Maintenance
Target Population
Medically stable,
able to participate
in comprehensive
rehabilitation
program
Medically stable,
cognitively &
physically able to
participate in
restorative
activities
Medically complex
with LT illnesses,
requiring ongoing
medical/ nursing
support where this
level of care cannot be
met at home or in
Long-term Care
(LTC)
Medically complex
with LT illnesses,
requiring ongoing
medical/nursing
support where this
level of care cannot
be met at home or in
LTC
Average LOS ≤90 days (56-72 days) ≤ 90
days
Up to 90 days Will remain at this
level
Discharge Indicator
Rehab goals met,
access to
MD/Nursing care
no longer required
Rehab goals met,
access to
MD/Nursing care
no longer required
Medical/functional
recovery to allow
patient to safely
transition to next level
of rehab care of
alternate environment
Patient is designated
to be more or less a
permanent resident in
the hospital & will
remain until
medical/functional
status changes
Medical Care
Daily physician
access
Weekly physician
access/follow-up
Access to scheduled
physician care/daily
medical oversight
Access to weekly
physician follow-up/
oversight- up to 8
monitoring
visits/month
Nursing Care
Up to 3 hrs/day
Some may go up
to 4 hrs
≤ 2 hrs/day >3hrs/day >3hrs/day
33
Rehabilitation Activation/
Restoration
Short Term
Complex Medical
Management
Long Term
Complex Medical
Management
Therapy Care
Direct care by
regulated health
professionals and
as assigned to
non-regulated
professionals
Consulted by
regulated health
professionals,
delivered by non-
regulated
professional as
assigned
Regulated health
professionals to
maintain/maximize
cognitive, physical,
emotional, functional
abilities. Supported by
non-regulated
professionals as
assigned
Regulated health
professionals to
maintain/maximize
cognitive, physical,
emotional, functional
abilities. Supported
by non-regulated
professionals as
assigned
Therapy Intensity
15-30 min of
therapy 3X/day up
to 3 hrs/day based
on patient
tolerance
Group or 1:1
setting throughout
day. 30min or up
to 2 hrs/day, 5-7
days/week
Up to 1 hr as tolerated
by the patient
Regulated health
professionals
available to maintain
and optimize
functional activities
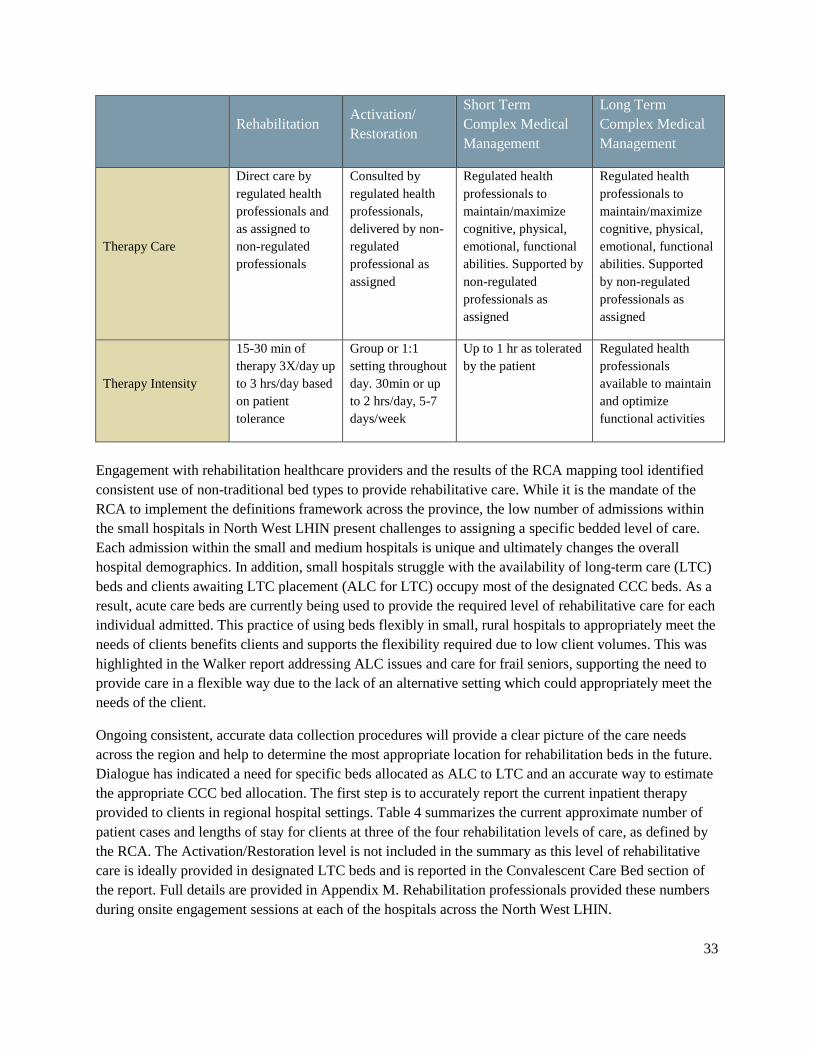
Engagement with rehabilitation healthcare providers and the results of the RCA mapping tool identified
consistent use of non-traditional bed types to provide rehabilitative care. While it is the mandate of the
RCA to implement the definitions framework across the province, the low number of admissions within
the small hospitals in North West LHIN present challenges to assigning a specific bedded level of care.
Each admission within the small and medium hospitals is unique and ultimately changes the overall
hospital demographics. In addition, small hospitals struggle with the availability of long-term care (LTC)
beds and clients awaiting LTC placement (ALC for LTC) occupy most of the designated CCC beds. As a
result, acute care beds are currently being used to provide the required level of rehabilitative care for each
individual admitted. This practice of using beds flexibly in small, rural hospitals to appropriately meet the
needs of clients benefits clients and supports the flexibility required due to low client volumes. This was
highlighted in the Walker report addressing ALC issues and care for frail seniors, supporting the need to
provide care in a flexible way due to the lack of an alternative setting which could appropriately meet the
needs of the client.
Ongoing consistent, accurate data collection procedures will provide a clear picture of the care needs
across the region and help to determine the most appropriate location for rehabilitation beds in the future.
Dialogue has indicated a need for specific beds allocated as ALC to LTC and an accurate way to estimate
the appropriate CCC bed allocation. The first step is to accurately report the current inpatient therapy
provided to clients in regional hospital settings. Table 4 summarizes the current approximate number of
patient cases and lengths of stay for clients at three of the four rehabilitation levels of care, as defined by
the RCA. The Activation/Restoration level is not included in the summary as this level of rehabilitative
care is ideally provided in designated LTC beds and is reported in the Convalescent Care Bed section of
the report. Full details are provided in Appendix M. Rehabilitation professionals provided these numbers
during onsite engagement sessions at each of the hospitals across the North West LHIN.

34
Table 4. Current Estimated Number of Beds for Rehabilitative Levels of Care in Regional
Hospitals (Sept-Oct 2016)
IDN Facility # of
Beds
Bed
Type # Pts
Avg.
LOS
Est
Avg
Bed
Days/
Mth
Est
Bed
Req
%
Acute
Care
Beds
District of
Thunder
Bay
Geraldton District Hospital 23 Acute 2 1-3
mths 60 2.00 8.7%
Manitouwadge District
Hospital 9 Acute 2
1-4
wks 33 1.10 12.2%
Nipigon District Memorial
Hospital 15 Acute 7
2 wks-
yrs 170.5 5.68 37.9%
McCausland Hospital
(Terrace Bay) 10 Acute 9
3 wks-
yrs 216 7.20 72.0%
Wilson Memorial General
Hospital
(Marathon)
9 Acute 5 3 wks-
yrs 145 4.82 53.6%
Northern Sioux Lookout Meno Ya Win
Health Centre 41 Acute 15
1 wk-
yrs 450 15.00 36.6%
Kenora
Lake of the Woods District
Hospital 71 Acute 13 2d-yrs 278 9.27 13.0%
Dryden Regional Health
Centre 31 Acute 10
2 wks-
yrs 255 8.50 27.4%
Margaret Cochenour
Memorial Hospital (Red
Lake)
14 Acute 4 1 wk-
yrs 88 2.93 20.9%
Rainy
River
Fort Frances LaVerendrye
Hospital 40
Acute 18 2d-yrs 540 18.00 45.0%
Atikokan General Hospital 11 Acute 3 3d-yrs 79 2.63 23.9%
Total 274 78 2,314 77.13 28.1%
#=number;Pts=Pat ients;Avg=average; LOS=Length o f Stay, Req=Required; Est .=est imated; wk=wee ks; d=days; m th=months;
yr=year

35
Inpatient Rehabilitation Beds
The only place to receive extensive, specialized inpatient rehabilitative care in NWO is within a
designated inpatient rehabilitation bed. The corresponding RCA-defined level of rehabilitative care in
these beds is the rehabilitation level. Care is focused on the trajectory of progression and provides a time-
limited, coordinated, interprofessional plan of care “to promote reach and maintain optimal physical,
sensory, intellectual, psychological and social functional levels.” Achievement of client-identified goals
requires frequent or daily reassessment by rehabilitation professionals to create the treatment plan.
Typically, rehabilitation clients require up to three hours of daily nursing care, and rehabilitation 15-30
minutes three times daily up to three hours daily for up to seven days a week. These beds are designed to
support adherence to best practice standards for rehabilitation and are essential in the provision of
specialized inpatient care associated with the delivery of QBPs for stroke, hip fractures and primary joint
replacements. See page 33 for details.
In the North West LHIN, SJH is the only facility with designated inpatient rehabilitation beds.
Rehabilitation inpatient services are located at SJH due to the population and rehabilitative care needs of
the City of Thunder Bay and proximity to the tertiary acute care provider, TBRHSC, which provides
specialized acute care services to many client populations, including those on QBP pathways, those with
spinal cord injuries (both traumatic and non-traumatic), acquired brain injuries, multiple traumas,
amputees, and those who require specialized inpatient or outpatient post-acute care. The
recommendations for designated rehabilitation beds within the QBP framework outline the need for care
by an interdisciplinary team with specialized knowledge of the QBPs and adherence to condition-specific
best practices. In addition, it is recommended clients at the rehabilitation-level of care receive a minimum
of twice daily therapy by the team. Quality-based Procedure care requirements indicate a need for
specialized services within designated rehabilitation beds.
St. Joseph’s Hospital in Thunder Bay has an allocation of 50 rehabilitation beds across two units of care:
a general rehabilitation unit and a special rehabilitation unit. Both programs are designed to provide high
intensity, time-limited, interprofessional, coordinated inpatient rehabilitation care for medically stable
clients. General rehabilitation is specifically designed to provide rehabilitative care for clients with the
primary diagnoses of hip and/or knee replacement (complicated cases), amputation (prosthetic training
stage), hip fractures, spinal cord injury, neurosurgical conditions, and other orthopaedic injuries. Special
rehabilitation provides rehabilitation for client’s who have experienced a stroke and/or acquired brain
injury.
Rehabilitation Bed Utilization
In order determine utilization of rehabilitation beds, an exploration of the fiscal years 2013 to 2015 was
completed. Key elements reviewed included: wait times, percent occupancy, patient days, average length
Recommendation #1: Improve client experience and outcomes through the implementation of
the RCA definitions framework to align rehabilitative care in the North West LHIN within the
provincial framework

36
of stay (LOS), admission rates, and discharge rates. This evaluation identified some differences between
the two rehabilitation units at SJH. General rehabilitation demonstrated a greater client turnover and
lower total occupancy rate until 2015/16, when occupancy in general rehabilitation surpassed special
rehabilitation (Table 5). As indicated in table 5, special rehabilitation exhibited a significantly longer
client LOS, contributing to the high wait time in 2013/14, but as LOS decreased, wait time and ALC for
rehabilitation days at TBRHSC also decreased significantly (see Table 6), and both units have an average
wait time of two days to admission. Wait times will continue to decrease as LOS targets, based on
provincial averages, QBPs, and best practices are implemented at SJH, resulting in shorter LOS and
therefore improved access.
Table 5. SJCG Inpatient Rehabilitation Beds Utilization Data
Service Year Admissions Discharges Expired Patient
Days
Average
Length of
Stay
Percent
Occupancy
Average
Wait
for
Admission
(days)
General
Rehabilitation
2013/14 282 280 0 8196 28.7 89.82 2.4
2014/15 265 266 0 8567 32.8 93.88 2.0
2015/16 291 295 0 8609 29.7 94.09 2.0
Special
Rehabilitation
2013/14 200 201 2 8842 42.9 96.90 7.0
2014/15 206 206 1 8739 42.8 95.77 3.0
2015/16 222 223 1 8468 38.6 92.55 2.0 Source: Medi tech

37
Table 6. TBRHSC Inpatient ALC Cases by Discharge Disposition 2013/14 and 2015/16
FY 2013/14 FY 2015/16
DISCHARGE DISPOSITION TOTAL
CASES
ALC
Days as
Beds/
Day
% of
Total ALC
Days
TOTAL
CASES
ALC Days
as
Beds/Day
% of
Total
ALC
Days
Discharged to Home/Home Setting with
Support 14,891 11.7 18.80% 15,327 14.1 23.5%
Transferred to Continuing Care - SJCG
SJCG-CCC 706 18.8 30.20% 789 13.7 22.9%
SJCG-Special Rehabilitation 152 1.6 2.60% 176 1.8 3.0%
SJCG-General Rehabilitation 217 1.7 2.70% 229 2.0 3.4%
SJCG-Subtotal 1,075 22.1 35.50% 1,194 17.5 29.3%
Transferred to Continuing Care - Other 2,318 28.4 45.7% 2,302 25.0 47.2%
GRAND TOTAL 18,284 62.2 100.00% 18,823 56.6 100.0%
Table 7 presents the rehabilitation bed use (discharge case volumes) by Rehabilitation Patient Group
(RPG), as reported through NRS. During 2015/16, 498 episodes of care (EOC) were served within these
two units with an average LOS of approximately 35 days (Table 8).
Table 7. SJCG Rehabilitation Discharged Case Mix Volume 2011-2016
SJCG Cases
2010-
2011
2011-
2012
2012-
2013
2013-
2014
2014-
2015
2015-
2016
Amputation, Lower Extremity 18 20 17 23 34 15
Amputation, Not Lower Extremity 1 0 1 0 0 0
Fracture of Lower Extremity 68 71 103 95 103 103
Maj Mult Trauma with Brain or
Spinal Cord Injury 1 1 2 3 9 1
Maj Mult Trauma, Oth Mult Trauma
& Maj Mult Frac 5 3 7 6 9 8
Neurological 12 14 12 13 10 15
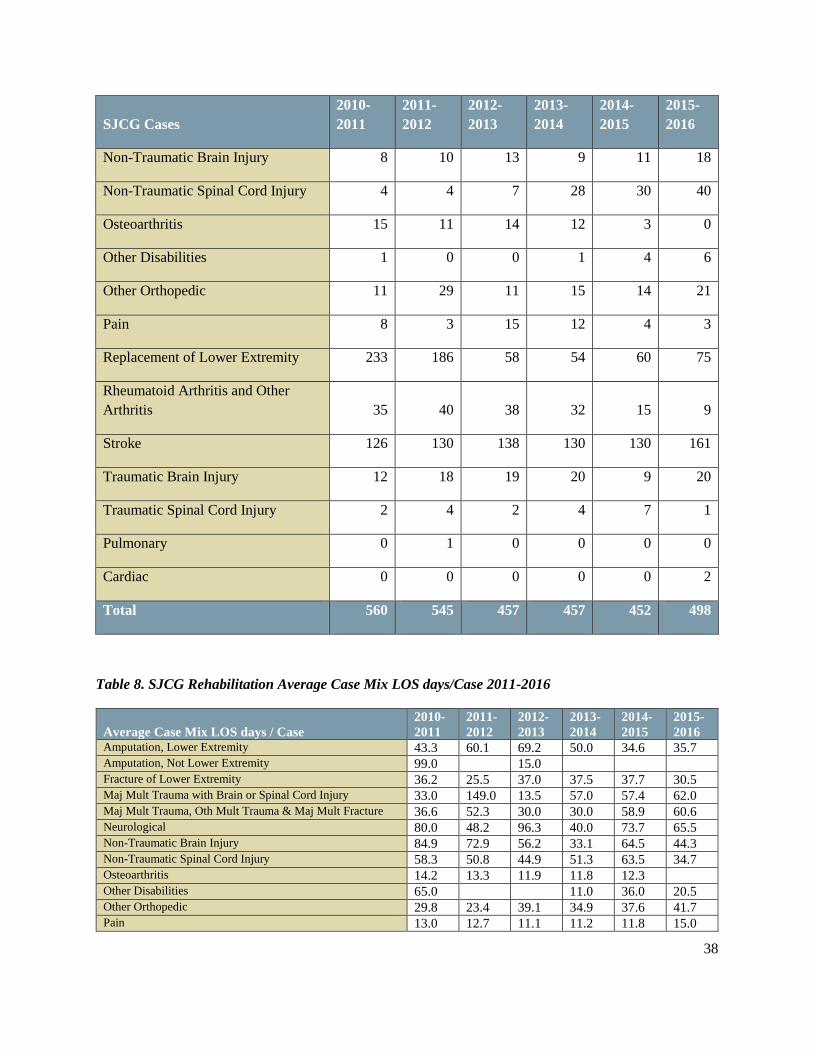
38
SJCG Cases
2010-
2011
2011-
2012
2012-
2013
2013-
2014
2014-
2015
2015-
2016
Non-Traumatic Brain Injury 8 10 13 9 11 18
Non-Traumatic Spinal Cord Injury 4 4 7 28 30 40
Osteoarthritis 15 11 14 12 3 0
Other Disabilities 1 0 0 1 4 6
Other Orthopedic 11 29 11 15 14 21
Pain 8 3 15 12 4 3
Replacement of Lower Extremity 233 186 58 54 60 75
Rheumatoid Arthritis and Other
Arthritis 35 40 38 32 15 9
Stroke 126 130 138 130 130 161
Traumatic Brain Injury 12 18 19 20 9 20
Traumatic Spinal Cord Injury 2 4 2 4 7 1
Pulmonary 0 1 0 0 0 0
Cardiac 0 0 0 0 0 2
Total 560 545 457 457 452 498
Table 8. SJCG Rehabilitation Average Case Mix LOS days/Case 2011-2016
Average Case Mix LOS days / Case
2010-
2011
2011-
2012
2012-
2013
2013-
2014
2014-
2015
2015-
2016 Amputation, Lower Extremity 43.3 60.1 69.2 50.0 34.6 35.7 Amputation, Not Lower Extremity 99.0 15.0 Fracture of Lower Extremity 36.2 25.5 37.0 37.5 37.7 30.5 Maj Mult Trauma with Brain or Spinal Cord Injury 33.0 149.0 13.5 57.0 57.4 62.0 Maj Mult Trauma, Oth Mult Trauma & Maj Mult Fracture 36.6 52.3 30.0 30.0 58.9 60.6 Neurological 80.0 48.2 96.3 40.0 73.7 65.5 Non-Traumatic Brain Injury 84.9 72.9 56.2 33.1 64.5 44.3 Non-Traumatic Spinal Cord Injury 58.3 50.8 44.9 51.3 63.5 34.7 Osteoarthritis 14.2 13.3 11.9 11.8 12.3 Other Disabilities 65.0 11.0 36.0 20.5 Other Orthopedic 29.8 23.4 39.1 34.9 37.6 41.7 Pain 13.0 12.7 11.1 11.2 11.8 15.0
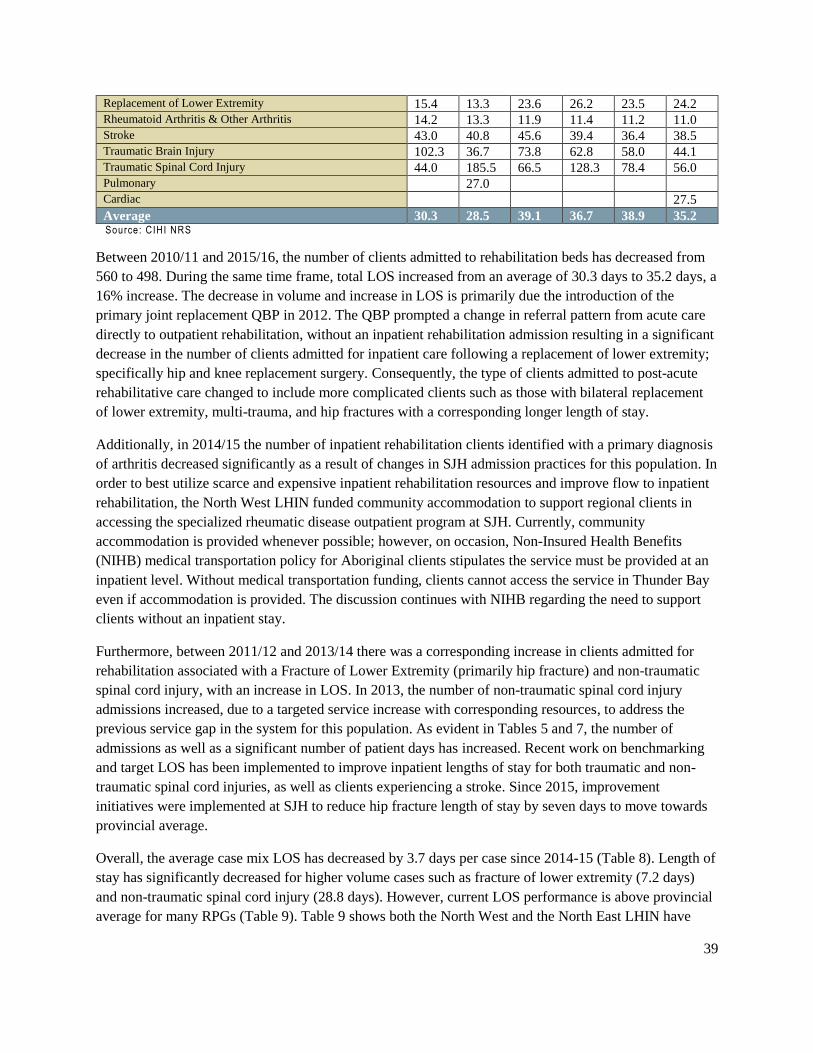
39
Replacement of Lower Extremity 15.4 13.3 23.6 26.2 23.5 24.2 Rheumatoid Arthritis & Other Arthritis 14.2 13.3 11.9 11.4 11.2 11.0 Stroke 43.0 40.8 45.6 39.4 36.4 38.5 Traumatic Brain Injury 102.3 36.7 73.8 62.8 58.0 44.1 Traumatic Spinal Cord Injury 44.0 185.5 66.5 128.3 78.4 56.0 Pulmonary 27.0 Cardiac 27.5
Average 30.3 28.5 39.1 36.7 38.9 35.2 Source: CIHI NRS
Between 2010/11 and 2015/16, the number of clients admitted to rehabilitation beds has decreased from
560 to 498. During the same time frame, total LOS increased from an average of 30.3 days to 35.2 days, a
16% increase. The decrease in volume and increase in LOS is primarily due the introduction of the
primary joint replacement QBP in 2012. The QBP prompted a change in referral pattern from acute care
directly to outpatient rehabilitation, without an inpatient rehabilitation admission resulting in a significant
decrease in the number of clients admitted for inpatient care following a replacement of lower extremity;
specifically hip and knee replacement surgery. Consequently, the type of clients admitted to post-acute
rehabilitative care changed to include more complicated clients such as those with bilateral replacement
of lower extremity, multi-trauma, and hip fractures with a corresponding longer length of stay.
Additionally, in 2014/15 the number of inpatient rehabilitation clients identified with a primary diagnosis
of arthritis decreased significantly as a result of changes in SJH admission practices for this population. In
order to best utilize scarce and expensive inpatient rehabilitation resources and improve flow to inpatient
rehabilitation, the North West LHIN funded community accommodation to support regional clients in
accessing the specialized rheumatic disease outpatient program at SJH. Currently, community
accommodation is provided whenever possible; however, on occasion, Non-Insured Health Benefits
(NIHB) medical transportation policy for Aboriginal clients stipulates the service must be provided at an
inpatient level. Without medical transportation funding, clients cannot access the service in Thunder Bay
even if accommodation is provided. The discussion continues with NIHB regarding the need to support
clients without an inpatient stay.
Furthermore, between 2011/12 and 2013/14 there was a corresponding increase in clients admitted for
rehabilitation associated with a Fracture of Lower Extremity (primarily hip fracture) and non-traumatic
spinal cord injury, with an increase in LOS. In 2013, the number of non-traumatic spinal cord injury
admissions increased, due to a targeted service increase with corresponding resources, to address the
previous service gap in the system for this population. As evident in Tables 5 and 7, the number of
admissions as well as a significant number of patient days has increased. Recent work on benchmarking
and target LOS has been implemented to improve inpatient lengths of stay for both traumatic and non-
traumatic spinal cord injuries, as well as clients experiencing a stroke. Since 2015, improvement
initiatives were implemented at SJH to reduce hip fracture length of stay by seven days to move towards
provincial average.
Overall, the average case mix LOS has decreased by 3.7 days per case since 2014-15 (Table 8). Length of
stay has significantly decreased for higher volume cases such as fracture of lower extremity (7.2 days)
and non-traumatic spinal cord injury (28.8 days). However, current LOS performance is above provincial
average for many RPGs (Table 9). Table 9 shows both the North West and the North East LHIN have

40
significantly longer average lengths of stay compared to the rest of Ontario. It is that hypothesized rural
and remote discharge destinations and limited access to outpatient services may have a role in the
increased LOS for these LHINs. To increase access to inpatient rehabilitation and reduce cost per case,
SJH is continuing to focus on reducing LOS. A LOS target has been set for all RPG-based on provincial
average or best practice and QBPs, when available. Individual case reviews occur at SJH when actual
LOS is expected to exceed the target, in order to identify and remove barriers to discharge. As noted in
Table 10, these strategies have resulted in improved FIM change score (22.1 in 2013 to 24.2 in 2015) and
the North West LHIN change scores are now higher than ten other LHINs, and slightly above the
provincial average.
Table 9. Ontario Case Mix Volumes and Average LOS days by LHIN, 2015-2016
Facility Region
Case Mix
Clients
(COUNT)
Case Mix
Avg LOS
Erie St. Clair 1,958 22
South West 2,010 28
Waterloo Wellington 1,092 24
Hamilton Niagara Haldimand Brant 2,811 27
Central West 1,156 26
Mississauga Halton 2,602 24
Toronto Central 7,032 28
Central 3,899 23
Central East 2,961 25
South East 943 28
Champlain 3,628 23
North Simcoe Muskoka 394 25
North East 915 35
North West 498 35
Source: CIHI NRS

41
Table 10. Inpatient Rehabilitation Average Admit, Discharge, and FIM Change Scores /LHIN
FY 2013 FY 2014 FY 2015
LHIN
Avg.
Admit
FIM
Avg.
D/C
FIM
Avg.
FIM
Change
Avg.
Admit
FIM
Avg.
D/C
FIM
Avg.
FIM
Change
Avg.
Admit
FIM
Avg.
D/C
FIM
Avg.
FIM
Change
Central 73.2 91.8 18.3 71.1 91.0 19.8 73.1 92.8 19.5
Central East 73.8 97.5 23.0 70.2 94.0 23.4 70.7 93.6 22.9
Central West 80.5 100.8 19.0 76.0 100.3 22.1 75.1 98.2 21.7
Champlain 80.9 101.1 19.9 81.0 99.2 17.7 78.6 98.5 19.5
Erie St. Clair 77.6 97.3 19.1 72.4 92.9 20.1 71.5 92.7 20.7
Hamilton Niagara Hald.
Brant 79.7 100.8 20.5 78.4 99.8 21.1 79.4 100.7 21.0
Mississauga Halton 68.9 91.5 22.5 67.7 89.5 21.6 64.4 88.5 24.1
North Simcoe Muskoka 75.6 103.4 26.1 74.7 104.5 29.0 75.1 101.6 25.7
North -East 77.4 98.5 20.8 78.1 97.9 19.5 78.6 99.4 20.3
North - West 80.2 103.2 22.1 75.5 99.1 22.8 75.4 101.2 24.2
South East 74.8 94.4 19.2 74.4 93.6 19.1 74.1 91.8 17.7
South West 77.1 97.9 20.7 75.0 95.0 19.9 75.9 96.5 20.5
Toronto Central 82.4 106.4 23.8 80.0 104.5 24.2 78.2 104.0 25.6
Waterloo Wellington 78.1 100.1 21.8 70.7 96.1 25.6 70.6 96.9 26.0
PROVINCE-
ONTARIO 78.3 100.2 21.9 76.1 98.3 21.9 75.2 98.0 22.6
Quality Based Procedures (QBP) and Best Practices
One of the key factors in the provision of care in rehabilitation is the recent introduction of QBPs for
several of the most common medical conditions requiring care. The goal of QBPs is to promote
innovation in healthcare delivery. In June 2010, the Excellent Care for All Act was legislated, formally
mandating improvements in quality and value of client experiences within the healthcare system.
Specifically, the Act directs the provision of the right evidence-informed healthcare, at the right time, and

42
in the right place, throughout the continuum of care: acute to post-acute to in-home, and
outpatient/community services.
Quality-based procedures play a key role in linking high quality care delivery and fiscal responsibility
within the Act. This evidence-informed pricing strategy encourages providers to adopt best practice
standards, modify clinical processes to improve client outcomes, and develop innovative care delivery
models to enhance the client care experience. Through the full implementation of QBPs, improvements in
discharge planning, elimination of unnecessary assessments, and closer attention to post-operative
complications will be realized.
In the development of any future state of rehabilitative care, it is important to consider the role of existing
and proposed QBP’s. It is recommended that enhanced post-acute rehabilitative care be adhered to as
identified in the QBP handbooks. These documents were developed to help support the implementation of
QBPs in clinical practice in consultation from the MOHLTC, Health Quality Ontario, and diagnosis-
specific expert panels. The RCA is currently reviewing the Total Joint Replacement and Hip Fracture
Handbooks to ensure outpatient recommendations are based on best practices for optimal outcomes and
attempt to measure the impact of implementation on client outcomes. An advantage of QBP
implementation is the development of client-centred pathways, reflecting the full continuum of care a
client needs from acute inpatient to post-acute inpatient to outpatient/community services.
Quality-based procedures are developed for clinically-related diagnoses or treatments. Among the
conditions with developed QBPs requiring rehabilitative care are: Primary Joint (Hip and Knee)
Replacement (implemented), Hip Fracture (not yet implemented), Stroke (not yet fully implemented), and
to a lesser extent Chronic Obstructive Pulmonary Disease (COPD) and Congestive Heart Failure (CHF).
Please refer to Table 7 for rehabilitation trending for these populations.
Stroke
Clients with a stroke are a large client population in need of rehabilitation services. From 2010/11 to
2015/16, the number of people with a stroke, as a percentage of all rehabilitation clients, increased from
126 cases (22.5%) to 161 cases (32.3%). Of all clients with a stroke, 65-75% are seniors (65+ years) but
the number of clients within this age range has decreased over the past five years. This may indicate an
increased prevalence of people with a stroke who are less than 65 years. Approximately 50% of all
rehabilitation clients with a stroke were female, and 55% were seniors.
Clients with a stroke with an alphaFIM (Functional Independence Measure) score of 40-80 (minimum
score of 18 indicating lowest function to maximum score 126 indicating highest function) are admitted to
the Special Rehabilitation Unit at SJH in accordance with the stroke pathway protocol (currently being
updated). The alphaFIM is a standardized assessment to determine the care needs for clients following
stroke and other medical events. Clients are considered for admission to a rehabilitation bed if they
demonstrate restorative potential and the ability to tolerate a high intensity level of rehabilitation, up to
three hours daily.

43
Hip Fracture
Hip fracture rehabilitation cases have shown substantial growth in the past six years, from 57 cases in
2010/2011 (10%) to 89 cases in 2015/16 (18%). The majority of these clients were seniors (93%-96%)
and 70% were female. Clients with hip fractures are seen on the General Rehabilitation Unit if they are
from the City of Thunder Bay or if their care needs are unable to be met in their IDN or LHH. Most
components of the hip fracture QBP are initiated in acute care at Thunder Bay Regional Health Sciences
Centre (ie. Orthopaedic consult, bone density testing, geriatric assessment) and their rehabilitative care
needs can usually be met locally. As such, following surgery and stabilization at the Thunder Bay
Regional Health Sciences Centre, clients are repatriated to their home hospital for rehabilitation. This was
confirmed during community engagement sessions with both healthcare providers and clients and
families. On occasion, there are reported difficulties in nursing rehabilitative care knowledge and skills
and health human resources in the smaller LHHs, which may necessitate admission to the regional
rehabilitation unit. See Appendix N for the current implemented hip fracture care pathway for the North
West LHIN.
Joint Replacement
The number of joint replacement (unilateral hip and unilateral knee) rehabilitation cases decreased
considerably between the years 2010/11 and 2015/16, as a result of two potential causes:
3. A change in practice and referral pattern from acute care.
4. The increased availability of rehabilitation service delivery in the community.
44
In 2010/2011, joint replacement rehabilitation comprised 191 (42%) of all rehabilitation cases. This
number decreased to 47 (13%) by 2015/16. The majority of cases were seniors, ranging from 72%-87%
over the past six years. Female clients represented 70% of all the cases in both senior and non-senior
cases in 2010/2011 to 2011/2012. By 2014/2015, the female and male ratios became 55% and 45%
respectively. Those referred to inpatient rehabilitation are more complicated clients, including those with
bilateral replacements.
COPD and CHF
Quality-based procedures have been developed for COPD & CHF, with the primary focus on the acute
episodes of care. Both handbooks refer to pulmonary rehabilitation, however the handbooks do not clearly
indicate if this rehabilitation is to be done in acute care, post-acute care, or as an outpatient service. There
is a reference to a transitional care pathway, which has not been defined or confirmed by the expert panel.
The transitional care pathway for CHF refers to community support partners, avoiding inpatient
rehabilitative care unless associated with a co-morbid condition. Overall for CHF, the majority of
discharges is home with or without services (54.21%), followed by discharged to LTC (12.73%), with the
final significant disposition being death in acute care (9.01%). Transfers to another facility providing
inpatient hospital care (including rehabilitation) account for only 4.3% of discharges. Until these
transitional care pathways are reviewed and clarified, the role of rehabilitative care in the pathway
remains unclear. This being said, there is cooperation by service providers (SJH, TBRHSC and CCAC)
underway to establish a central point of access for pre- and post-pulmonary services (including COPD,
CHF), the co-location of services in the City of Thunder Bay, and a model to support clients regionally
through a network of services.
Throughout the North West LHIN, it is imperative that rehabilitative care is coordinated and reflective of
the QBPs. As part of an integrated rehabilitation model, care pathways need to be created or reviewed to
align with the QBPs from pre-operative care, inpatient, outpatient, and to community care for the entire
North West LHIN region. It is essential that the existing Regional Orthopaedic Program and Regional
Stroke Network are collaborative partners in the development, implementation, and sustainability of an
integrated rehabilitation model.
Alternative Level of Care (ALC) Impact on Rehabilitation and Discharge Disposition
In 2015/16 both rehabilitation units experienced bed days attributed to clients designated ALC. Sixty-two
(62) clients were discharged from rehabilitation with a total accumulation of 826 alternate level of care
days (Table 11). These clients completed active rehabilitation and were waiting for a LTC home, other
housing, and/or services in another sector. It is important to also recognize although some regional clients
have completed their rehabilitation needs at SJH; they require local rehabilitation services, such as a home
visit and community support planning. The current process involves repatriation to their LHH, so clients
are not coded as ALC as they transfer to the “acute care” facility in order to arrange for these services.
This results in the reported ALC numbers being lower than they actually are. While these ALC numbers
remain low, they must be accounted for as they can reduce the unit capacity by up to 16% (4 of 25 beds)
at any given time and ultimately limit access to care. Ideally, there should be no ALC days on the
rehabilitation units.

45
Table 11. 2011/12 to 2015/16 Alternative Level of Care Data- SJCG Rehabilitation
Number of Discharges ALC Days
Discharge
Destination
2011-
12
2012-
13
2013-
14
2014-
15
2015-
16
2011-
12
2012-
13
2013-
14
2014-
15
2015-
16
CCC 30 40 38 33 54 893 1478 796 469 728
Home 5 1 4 12 5 39 56 106 149 105
LTC 5 7 4 3 5 142 190 169 47 103
Supportive Housing 5 5 1 5 2 114 210 22 138 36
Other 5 7 3 3 6 61 161 4 1 36
Total 50 60 50 56 72 1249 2095 1097 804 1008
As discussed, improvement initiatives are currently underway at SJH to reduce LOS and ALC rates to
improve flow. This includes designating CCC beds on both rehabilitation units. Clients more appropriate
for CCC-level services will be able to access this care without having to be physically moved to another
unit. The corresponding number of rehabilitation beds will be created on the SJH Geriatric Assessment
and Rehabilitation Care units. This should help eliminate ALC to CCC, except when beds are not
available.
Regional Rehabilitation Needs
As all North West LHIN rehabilitation beds are currently located in the City of Thunder Bay, it is
important to evaluate the regional utilization of these services. Evaluation of all clients admitted to
designated rehabilitation beds for the years 2013-15 was completed using home postal code search. Table
12 outlines the case mix LOS days during the fiscal years 2013-2015 by client’s home IDN. In 2015/16,
the percentage of days relating to clients from the City of Thunder Bay has declined from 74% to 69%,
with remaining 30% of days related to clients from other North West LHIN IDNs and less than 1% of
days from out of province.
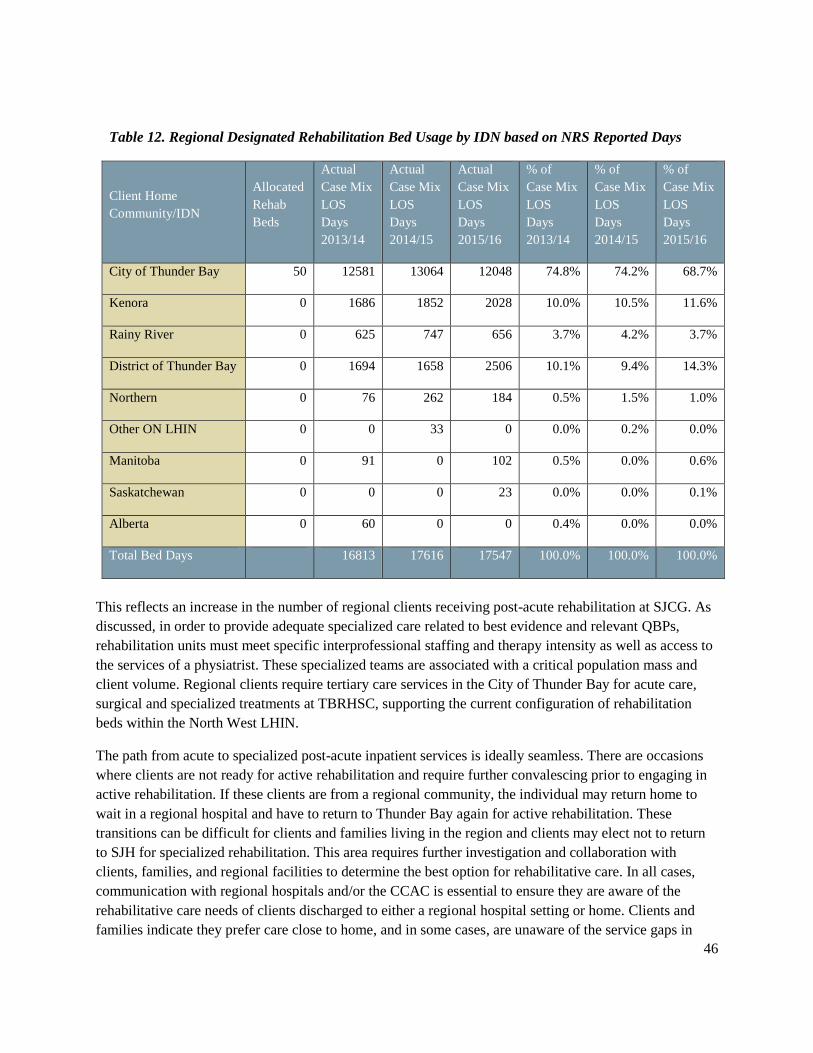
46
Table 12. Regional Designated Rehabilitation Bed Usage by IDN based on NRS Reported Days
Client Home
Community/IDN
Allocated
Rehab
Beds
Actual
Case Mix
LOS
Days
2013/14
Actual
Case Mix
LOS
Days
2014/15
Actual
Case Mix
LOS
Days
2015/16
% of
Case Mix
LOS
Days
2013/14
% of
Case Mix
LOS
Days
2014/15
% of
Case Mix
LOS
Days
2015/16
City of Thunder Bay 50 12581 13064 12048 74.8% 74.2% 68.7%
Kenora 0 1686 1852 2028 10.0% 10.5% 11.6%
Rainy River 0 625 747 656 3.7% 4.2% 3.7%
District of Thunder Bay 0 1694 1658 2506 10.1% 9.4% 14.3%
Northern 0 76 262 184 0.5% 1.5% 1.0%
Other ON LHIN 0 0 33 0 0.0% 0.2% 0.0%
Manitoba 0 91 0 102 0.5% 0.0% 0.6%
Saskatchewan 0 0 0 23 0.0% 0.0% 0.1%
Alberta 0 60 0 0 0.4% 0.0% 0.0%
Total Bed Days 16813 17616 17547 100.0% 100.0% 100.0%
This reflects an increase in the number of regional clients receiving post-acute rehabilitation at SJCG. As
discussed, in order to provide adequate specialized care related to best evidence and relevant QBPs,
rehabilitation units must meet specific interprofessional staffing and therapy intensity as well as access to
the services of a physiatrist. These specialized teams are associated with a critical population mass and
client volume. Regional clients require tertiary care services in the City of Thunder Bay for acute care,
surgical and specialized treatments at TBRHSC, supporting the current configuration of rehabilitation
beds within the North West LHIN.
The path from acute to specialized post-acute inpatient services is ideally seamless. There are occasions
where clients are not ready for active rehabilitation and require further convalescing prior to engaging in
active rehabilitation. If these clients are from a regional community, the individual may return home to
wait in a regional hospital and have to return to Thunder Bay again for active rehabilitation. These
transitions can be difficult for clients and families living in the region and clients may elect not to return
to SJH for specialized rehabilitation. This area requires further investigation and collaboration with
clients, families, and regional facilities to determine the best option for rehabilitative care. In all cases,
communication with regional hospitals and/or the CCAC is essential to ensure they are aware of the
rehabilitative care needs of clients discharged to either a regional hospital setting or home. Clients and
families indicate they prefer care close to home, and in some cases, are unaware of the service gaps in
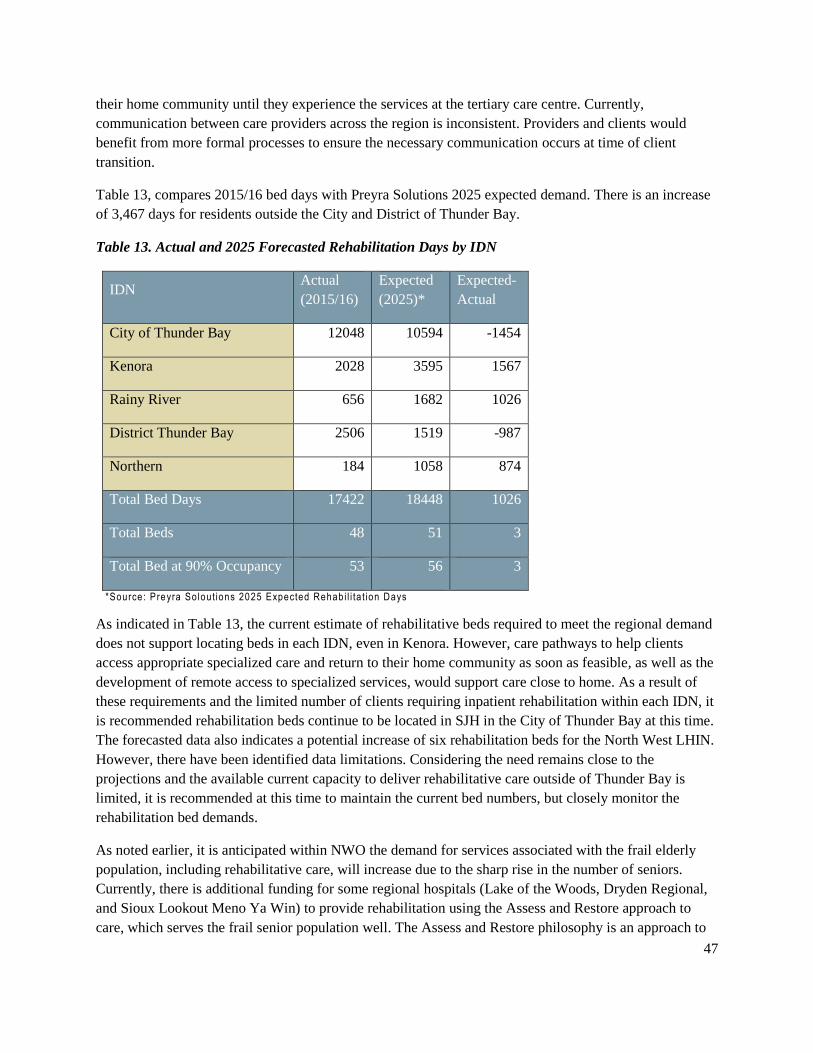
47
their home community until they experience the services at the tertiary care centre. Currently,
communication between care providers across the region is inconsistent. Providers and clients would
benefit from more formal processes to ensure the necessary communication occurs at time of client
transition.
Table 13, compares 2015/16 bed days with Preyra Solutions 2025 expected demand. There is an increase
of 3,467 days for residents outside the City and District of Thunder Bay.
Table 13. Actual and 2025 Forecasted Rehabilitation Days by IDN
IDN Actual
(2015/16)
Expected
(2025)*
Expected-
Actual
City of Thunder Bay 12048 10594 -1454
Kenora 2028 3595 1567
Rainy River 656 1682 1026
District Thunder Bay 2506 1519 -987
Northern 184 1058 874
Total Bed Days 17422 18448 1026
Total Beds 48 51 3
Total Bed at 90% Occupancy 53 56 3
*Source: Preyra So lout ions 2025 Expected Rehabi l i ta t ion Days
As indicated in Table 13, the current estimate of rehabilitative beds required to meet the regional demand
does not support locating beds in each IDN, even in Kenora. However, care pathways to help clients
access appropriate specialized care and return to their home community as soon as feasible, as well as the
development of remote access to specialized services, would support care close to home. As a result of
these requirements and the limited number of clients requiring inpatient rehabilitation within each IDN, it
is recommended rehabilitation beds continue to be located in SJH in the City of Thunder Bay at this time.
The forecasted data also indicates a potential increase of six rehabilitation beds for the North West LHIN.
However, there have been identified data limitations. Considering the need remains close to the
projections and the available current capacity to deliver rehabilitative care outside of Thunder Bay is
limited, it is recommended at this time to maintain the current bed numbers, but closely monitor the
rehabilitation bed demands.
As noted earlier, it is anticipated within NWO the demand for services associated with the frail elderly
population, including rehabilitative care, will increase due to the sharp rise in the number of seniors.
Currently, there is additional funding for some regional hospitals (Lake of the Woods, Dryden Regional,
and Sioux Lookout Meno Ya Win) to provide rehabilitation using the Assess and Restore approach to
care, which serves the frail senior population well. The Assess and Restore philosophy is an approach to

48
care, rather than a bed designation. The MOHLTC defines this philosophy as individualized bundles of
short-term rehabilitative and other restorative care services delivered by integrated teams, which include
regulated health professionals with expertise in geriatrics. Care is directed towards increasing strength,
mobility, and functional ability and is targeted to frail seniors and other persons who have experienced a
recent loss of functional ability following a medical event or decline in health; are at high risk for
imminent hospitalization or admission into a long-stay LTC home bed as a result of functional loss ('high-
risk’); and have the potential to regain functional loss so they are no longer at high risk (‘restorative
potential’). At present, this level of care is happening in CCC or acute care beds throughout NWO, but
meets the criteria for rehabilitation level of care as defined by the RCA bedded-levels of care. The RCA
rehabilitation definition at present indicates the need for data reporting through NRS, which is only done
in designated rehabilitation beds. The RCA is exploring the development of a new category within NRS
to capture these types of clients. A toolkit has been developed by the RCA to help hospitals determine if a
case should be made to their LHIN to convert beds to rehabilitation beds.
Currently, between the designated rehabilitation beds and the level of rehabilitation provided in current
CCC and acute care beds, the majority of rehabilitative care needs is provided within our LHIN.
Strategies are being developed by SJH to decrease hospital LOS, and improve care transitions and the
availability of rehabilitation in regional communities.
Strengths, Gaps, and Recommendations
The quality of care is clearly identified as a strength of the rehabilitation level of care in the North West
LHIN. Clients note staff is always professional, kind, and exceptionally knowledgeable. One family
member noted: “Staff truly cared about my dad and his progress.”
The centralization of designated rehabilitative care beds in Thunder Bay continues to have a negative
impact on clients and families who must remain far from home to receive post-acute services. These
clients already required travel to Thunder Bay to access appropriate specialized acute care at the tertiary
care centre. One client noted: “I wished I could have been home sooner.” Families identified the need for
affordable lodging with kitchenettes or a hostel environment such as Tamarack House for clients with
cancer. Rehabilitative care is always delivered as close to home as possible but in some cases, the most
appropriate location is Thunder Bay to access specialized rehabilitation knowledge, skills, equipment and
intensity. It has been identified during rehabilitation professional engagement sessions that some clients
will elect to receive a different level of care locally versus travelling several hours to a specialized
program. Unfortunately, due to current data limitations, it is difficult to determine the number of clients
affected. These clients will receive the best care possible within their LHHs available resources.
In addition, there were issues noted in communication and collaboration at times of client transitions.
Assumptions were often made regarding the availability of inpatient, outpatient, and/or community
resources when clients moved from Thunder Bay to their LHH. The variability of these services and
availability of rental medical equipment such as walkers and wheelchairs impacted the length of time
clients needed at their LHH before finally returning home. Regional healthcare providers noted a lack of
relevant client information despite a regional electronic medical record.
49
The lack of critical mass and specialized services indicate it is not feasible to reallocate rehabilitative care
beds at this time. It is recommended a system of support be developed for regional rehabilitative clients
who may seek alternate levels of care close to home. Opportunities and recommendations will be
developed within the future state model of care.
Rehabilitation in Convalescent Care – Activation/Restoration (AR)
The RCA has defined an Activation/Restoration (AR) level of care with a progression trajectory like
rehabilitation. However, this level of care differs from rehabilitation with respect to the goal “to promote
activity, increase strength, endurance, independence and ability to manage activities of daily living…with
a focus on restoring function”. The primary focus of rehabilitative care within AR is to provide
opportunities for functional practice, wellness, and self-care activities. This level of care takes place in
Convalescent Care Beds (CCBs). CCB were established to improve patient flow. They are a short stay
program in LTC homes for persons who need time to recover strength, endurance or functioning and are
anticipated to return home. Currently, clients can access a CCB while their weight-bearing restrictions or
healing wounds limit their ability to participate in active rehabilitation or until they have gained strength
and endurance in order to participate in active rehabilitation. Occasionally, clients may also access a CCB
after they have completed active rehabilitation but need additional time to gain strength or endurance to
be able to safely return home. The ultimate objective is to support the return of clients to their previous
living environment.
In order to qualify following an acute episode, clients must be medically stable and cognitively able to
participate in restorative activities designed to enable a return home or progress to a rehabilitative level of
care. Clients are expected to have a discharge location, typically home, and cannot be waiting for
placement in a LTC facility. Clients should not require daily access to a comprehensive interprofessional
rehabilitation team, and should be able to have their needs addressed through exercise and recreational
activities provided primarily by unregulated healthcare providers, such as personal support workers, life
enrichment staff, or rehabilitation assistants, in a group setting. Less than two hours of nursing care per
day is required. Typically, an average length of stay is 56-72 days to a maximum of 90 days.
Recommendation #2: Develop a LHIN-wide strategy to improve client access and
client transitions across the continuum of rehabilitative care
Recommendation #3: Facilitate adherence to best practices for rehabilitative care to
improve client-centred care
Recommendation #4: Enhance utilization of innovative technologies to improve access
to rehabilitative care services closer to home, particularly in remote and underserviced
areas

50
Convalescent Care Bed Utilization
Convalescent care beds in the North West (13 in total) are a small proportion (1.8%) of the total volume
available in Ontario and sited in Fort Frances (4) and Thunder Bay (9). The average LOS ranged from
50.7 days in 2011/12 to 64.3 days in 2014/15. The primary discharge destination is the community at
69.6% for the North West LHIN in 2014/15.
The small number of beds makes occupancy comparisons difficult, as a single bed has a greater impact on
the measure (Table 14).
Table 14. Convalescent Care Program Occupancy rates in the North West LHIN
June 2014 (Q1) Sept 2014 (Q2) Dec 2014 (Q3) March 2015 (Q4) June 2015 (Q1)
Discharge
Destination # Beds
Occ.
Rate # Beds
Occ.
Rate # Beds
Occ.
Rate # Beds
Occ.
Rate # Beds
Occ.
Rate
Lakehead
Manor 9 77.8% 9 100.0% 9 33.3% 9 55.6% 9 100.0%
Rainycrest 4 50.0% 4 100.0% 4 75.0% 4 100.0% 4 75.0%
Ontario 729 88.2% 738 89.0% 755 82.3% 755 86.9% 723 90.7%
Table 2(a) – Source: MOHLTC - CCP Survey, 2016 ; #=number; Occ=Occupancy
Alternative Level of Care (ALC) Impact on CCB
As with other services, CCB are under increasing pressure from ALC clients. The North West LHIN has
the second highest rate of increase in the percentage of ALC days as well as the second highest rate of
increase in ALC days (Table 15).
Table 15. Convalescent Care Program Percentage of ALC Days in Ontario by LHIN 2012/13 to
2014/15
% ALC Days Change in % ALC Days
LHIN 2012/13 2013/14 2014/15 12/13 vs.
13/14 13/14 vs.
14/15 12/13 vs.
14/15
04 HNHB 13.80% 15.16% 18.23% 9.86% 20.25% 32.10%
09 Central East 14.39% 16.14% 16.84% 12.16% 4.34% 17.03%
10 South East 13.58% 13.19% 15.40% -2.87% 16.76% 13.40%
12 North Simcoe Muskoka 23.22% 21.41% 21.02% -7.80% -1.82% -9.47%
13 North East 23.81% 23.67% 23.17% -0.59% -2.11% -2.69%
14 North West 16.52% 17.79% 21.72% 7.69% 22.09% 31.48%
Ontario 14.09% 14.03% 14.35% -0.43% 2.28% 1.85%
Table 2(b) – Source: MOHLTC - CCP Survey, 2016

51
Regional Needs
Table 16 summarizes a snapshot of the number of cases and length of stay for clients at the
Activation/Restoration level of rehabilitative care as defined by the RCA. Rehabilitation professionals
provided these numbers during onsite engagement sessions at each of the hospitals across the North West
LHIN. The staff in Fort Frances indicated an unusually high number of clients requiring AR level of care
for wound healing. It is unknown if this is due to a demographic population need or if this is the result of
the wound expertise developed within this IDN, increasing awareness, and use of inpatient resources to
promote wound care best practices. Further investigation is warranted to determine if these clients could
be managed at a community level of care.
Table 16. Snapshot of the Estimated Number of Beds for Activation/Restoration Level of Care in
Regional Hospitals (Fall 2016)
IDN Facility #
Existing
Beds
Bed
Type
# A/R
Pts
Avg.
LOS
Est. Avg.
A/R Bed
D/ Yr
Est A/R
Beds
Req’d
% of
Acute
Care
Beds
District
of
Thunder
Bay
Geraldton District Hospital 23 Acute 4/yr 4-8 wks 168 0.46 2.0%
Manitouwadge District Hospital 9 Acute 5/yr 3-6 wks 158 0.43 4.8%
Nipigon District Memorial
Hospital
15 Acute 3-5/yr 6-12 wks 252 0.69 4.6%
McCausland Hospital 10 Acute 1-2 6-8 wks 548 1.50 15.0%
Wilson Memorial General
Hospital
9 Acute 6-8/yr 6-8 wks 343 0.94 10.4%
Northern Sioux Lookout Meno Ya Win
Health Centre
41 Acute 6-7 4-8 wks 2,190 6.00 14.6%
Kenora Lake of the Woods District
Hospital
71 Acute 5-6 6-8 wks 1,825 5.00 7.0%
Dryden Regional Health Centre 31 Acute 1-3 6-8 wks 730 2.00 6.4%
Margaret Cochenour Memorial
Hospital
14 Acute 4/yr 4-8 wks 168 0.46 3.3%
Rainy
River
Fort Frances LaVerendrye
Hospital
4 CCB 1 90 days 365 1.00 25.0%
40 Acute 9-12 4-26 wks 3,833 10.50 26.3%
Atikokan General Hospital 11 Acute 1-2/yr 4-8 wks 84 0.23 2.1%
Total 278
10,663 29.21 10.5%
#=number; Est=Est imated; A/R= Act i va t ion /Resto ra t ion ; Avg=Average; LOS=Length o f Stay, wk=weeks; d=days; mth=months;
yr=year;

52
Strengths, Gaps, and Recommendations
During engagement sessions, healthcare providers indicated some reasons why CCB are not utilized to
their full capacity. Firstly, it was indicated many clients requiring the AR level of rehabilitation are not
able to have their needs met in CCB due to the current criteria of a one-person (not two) assist for all
transfers and mobility; funding limitations for intravenous medications and pumps required for wound
healing; and a limited skill set of LTC nurses for intravenous pumps. As such, in the City of Thunder
Bay, these clients are often admitted to SJG and in Fort Frances to the acute care hospital La Verendrye.
Secondly, clinicians indicated the current process of CCAC managing the CCB admissions is lengthy. For
short lengths of stay of one to two weeks, it is perceived to be easier and more client-centred to have the
client remain where they are until they are able to go home or can access rehabilitation, as CCBs are in a
different physical location. Finally, the criteria indicating the need for a discharge destination of home or
another location (e.g. confirmed rehabilitation bed) also limits availability of this service.
This feedback differs from the recent results of a provincial survey in which barriers to access were
identified as distribution/location of beds, concerns about the ability of the LTC home to meet the
person’s care needs, concerns about the likelihood the client would be ready for discharge within 90 days,
CCAC concerns they were asked to take clients who were inappropriate and would likely end up on the
crisis list, and client/family concerns about leaving hospital and the location or condition of the LTC
home offering CCBs.
Currently, the care needs of these clients are provided primarily in acute care beds throughout the North
West LHIN. Rehabilitation professionals indicated that at hospitals where unregulated health
professionals (PSWs, rehabilitation or physiotherapy assistants) are unavailable, clients receive care
provided by regulated health professionals. This would indicate partial alignment with the rehabilitation
care definitions, but essentially “over treating” the clients, as the appropriate level of service is currently
unavailable. This can only be alleviated by improved utilization of the current CCB capacity, recognizing
the need for additional CCB throughout the NW LHIN, and adding unregulated health professional
resources in facilities offering this level of care.
Inpatient Complex Continuing Care Beds
In contrast to the designated inpatient rehabilitation beds, CCC beds in the North West LHIN are located
throughout the region in regional hospitals (Table 17). With the exception of Manitouwadge General
Hospital, and Lake of the Woods District Hospital who no longer operates CCC beds, all regional
hospitals have allotted CCC beds. The current breakdown of designated CCC beds is as follows:
Recommendation #2: Develop a LHIN-wide strategy to improve client access and
client transitions across the continuum of rehabilitative care
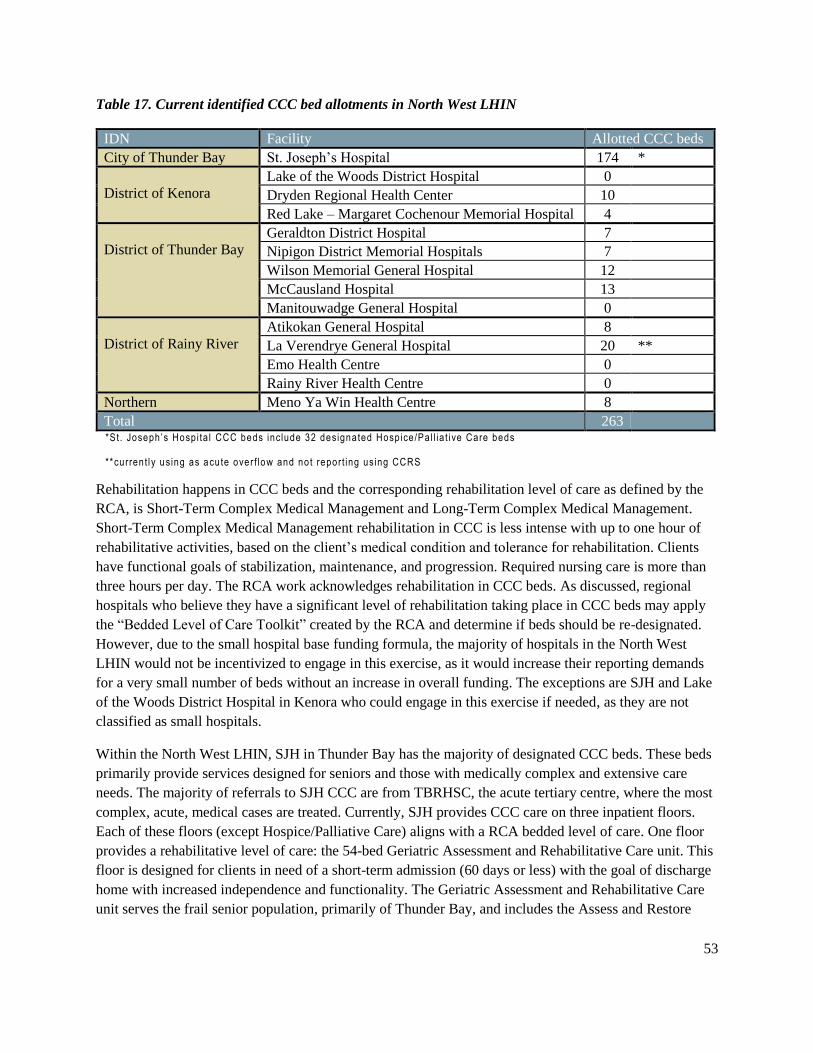
53
Table 17. Current identified CCC bed allotments in North West LHIN
IDN Facility Allotted CCC beds
City of Thunder Bay St. Joseph’s Hospital 174 *
District of Kenora
Lake of the Woods District Hospital 0
Dryden Regional Health Center 10
Red Lake – Margaret Cochenour Memorial Hospital 4
District of Thunder Bay
Geraldton District Hospital 7
Nipigon District Memorial Hospitals 7
Wilson Memorial General Hospital 12
McCausland Hospital 13
Manitouwadge General Hospital 0
District of Rainy River
Atikokan General Hospital 8
La Verendrye General Hospital 20 **
Emo Health Centre 0
Rainy River Health Centre 0
Northern Meno Ya Win Health Centre 8
Total 263 *St. Joseph ’s Hosp i ta l CCC beds include 32 designated Hosp ice/Pa l l ia t i ve Care beds
**current l y using as acute over f low and not report ing using CCRS
Rehabilitation happens in CCC beds and the corresponding rehabilitation level of care as defined by the
RCA, is Short-Term Complex Medical Management and Long-Term Complex Medical Management.
Short-Term Complex Medical Management rehabilitation in CCC is less intense with up to one hour of
rehabilitative activities, based on the client’s medical condition and tolerance for rehabilitation. Clients
have functional goals of stabilization, maintenance, and progression. Required nursing care is more than
three hours per day. The RCA work acknowledges rehabilitation in CCC beds. As discussed, regional
hospitals who believe they have a significant level of rehabilitation taking place in CCC beds may apply
the “Bedded Level of Care Toolkit” created by the RCA and determine if beds should be re-designated.
However, due to the small hospital base funding formula, the majority of hospitals in the North West
LHIN would not be incentivized to engage in this exercise, as it would increase their reporting demands
for a very small number of beds without an increase in overall funding. The exceptions are SJH and Lake
of the Woods District Hospital in Kenora who could engage in this exercise if needed, as they are not
classified as small hospitals.
Within the North West LHIN, SJH in Thunder Bay has the majority of designated CCC beds. These beds
primarily provide services designed for seniors and those with medically complex and extensive care
needs. The majority of referrals to SJH CCC are from TBRHSC, the acute tertiary centre, where the most
complex, acute, medical cases are treated. Currently, SJH provides CCC care on three inpatient floors.
Each of these floors (except Hospice/Palliative Care) aligns with a RCA bedded level of care. One floor
provides a rehabilitative level of care: the 54-bed Geriatric Assessment and Rehabilitative Care unit. This
floor is designed for clients in need of a short-term admission (60 days or less) with the goal of discharge
home with increased independence and functionality. The Geriatric Assessment and Rehabilitative Care
unit serves the frail senior population, primarily of Thunder Bay, and includes the Assess and Restore
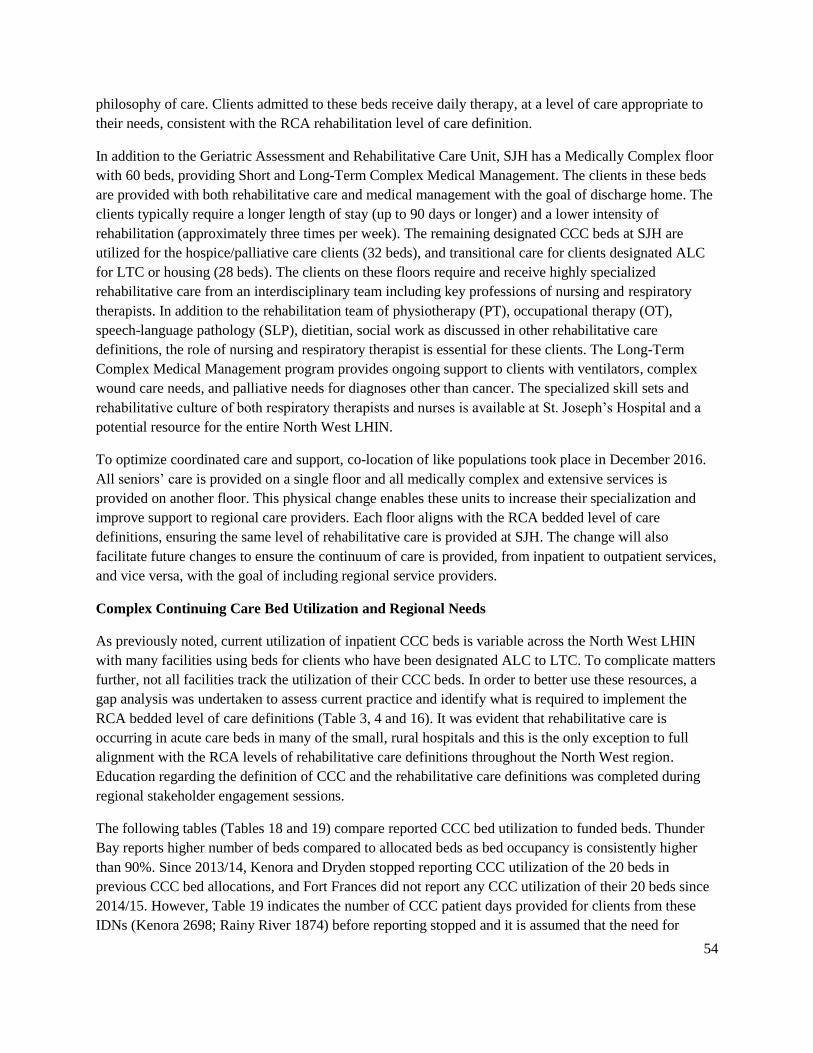
54
philosophy of care. Clients admitted to these beds receive daily therapy, at a level of care appropriate to
their needs, consistent with the RCA rehabilitation level of care definition.
In addition to the Geriatric Assessment and Rehabilitative Care Unit, SJH has a Medically Complex floor
with 60 beds, providing Short and Long-Term Complex Medical Management. The clients in these beds
are provided with both rehabilitative care and medical management with the goal of discharge home. The
clients typically require a longer length of stay (up to 90 days or longer) and a lower intensity of
rehabilitation (approximately three times per week). The remaining designated CCC beds at SJH are
utilized for the hospice/palliative care clients (32 beds), and transitional care for clients designated ALC
for LTC or housing (28 beds). The clients on these floors require and receive highly specialized
rehabilitative care from an interdisciplinary team including key professions of nursing and respiratory
therapists. In addition to the rehabilitation team of physiotherapy (PT), occupational therapy (OT),
speech-language pathology (SLP), dietitian, social work as discussed in other rehabilitative care
definitions, the role of nursing and respiratory therapist is essential for these clients. The Long-Term
Complex Medical Management program provides ongoing support to clients with ventilators, complex
wound care needs, and palliative needs for diagnoses other than cancer. The specialized skill sets and
rehabilitative culture of both respiratory therapists and nurses is available at St. Joseph’s Hospital and a
potential resource for the entire North West LHIN.
To optimize coordinated care and support, co-location of like populations took place in December 2016.
All seniors’ care is provided on a single floor and all medically complex and extensive services is
provided on another floor. This physical change enables these units to increase their specialization and
improve support to regional care providers. Each floor aligns with the RCA bedded level of care
definitions, ensuring the same level of rehabilitative care is provided at SJH. The change will also
facilitate future changes to ensure the continuum of care is provided, from inpatient to outpatient services,
and vice versa, with the goal of including regional service providers.
Complex Continuing Care Bed Utilization and Regional Needs
As previously noted, current utilization of inpatient CCC beds is variable across the North West LHIN
with many facilities using beds for clients who have been designated ALC to LTC. To complicate matters
further, not all facilities track the utilization of their CCC beds. In order to better use these resources, a
gap analysis was undertaken to assess current practice and identify what is required to implement the
RCA bedded level of care definitions (Table 3, 4 and 16). It was evident that rehabilitative care is
occurring in acute care beds in many of the small, rural hospitals and this is the only exception to full
alignment with the RCA levels of rehabilitative care definitions throughout the North West region.
Education regarding the definition of CCC and the rehabilitative care definitions was completed during
regional stakeholder engagement sessions.
The following tables (Tables 18 and 19) compare reported CCC bed utilization to funded beds. Thunder
Bay reports higher number of beds compared to allocated beds as bed occupancy is consistently higher
than 90%. Since 2013/14, Kenora and Dryden stopped reporting CCC utilization of the 20 beds in
previous CCC bed allocations, and Fort Frances did not report any CCC utilization of their 20 beds since
2014/15. However, Table 19 indicates the number of CCC patient days provided for clients from these
IDNs (Kenora 2698; Rainy River 1874) before reporting stopped and it is assumed that the need for

55
rehabilitative care at this level continues. These facilities now use acute care beds to treat clients requiring
this level of care and/or their clients are treated in other IDNs such as the City of Thunder Bay. The City
of Thunder Bay also provides this CCC-level rehabilitative care to people throughout the North West
LHIN. There was also a significant increase in CCC patient days since 2014 for clients from the City of
Thunder Bay, District of Thunder Bay and the Northern IDN.
It is important to note that within this data set, CCC patient days are calculated for clients admitted and
discharged within the year, which under-represents the actual usage. In small communities such as the
District of Thunder Bay with only 28 discharges in 2013 and LOS from 365 to 2872 days, the low
volumes of actual clients will have a greater effect on the apparent accuracy of the data and may explain
the low volumes noted in 2012 and 2013.
Table 18. CCC Bed Utilization Data 2013-2015 by IDN
CCC Patient Days 15-16
Actual
Beds**
Bed
Variance
*** IDN Community Allocated Beds 2013/14 2014/15 2015/16
City of Thunder Bay Thunder Bay 142 50846 50917 50012 151 9
Kenora
Kenora 0 0 0 0 0 0
Dryden 10 0 0 0 0 -10
Red Lake 4 1457 1362 1460 4 0
Rainy River
Atikokan 8 1995 2410 2262 7 -1
Fort Frances 20 182 0 0 0 -20
Emo 0 0 0 0 0 0
Rainy River 0 0 0 0 0 0
District Thunder Bay
Marathon 12 2082 2403 2892 9 -3
Terrace Bay 13 1416 2694 1690 5 -8
Geraldton 7 2544 2453 2474 7 0
Nipigon 7 2544 2520 2541 8 1
Manitouwadge 0 0 0 0 0 0
Northern Sioux Lookout 8 1491 2000 2044 6 -2
Total Bed Days 231 64557 66759 65375 197 -34
*Source: CIHI CCRS, Thunder Bay excludes Hosp ice/Pa l l ia t i ve Care and Temporary Transi t iona l Care
**90% Occupancy; ** * Actua l f rom Funded

56
Table 19. CCC LOS (in days) on Discharge with Home IDN based on Postal Code
IDN 2011 2012 2013 2014 2015
City of Thunder Bay 57,089 54,326 51,945 69,666 72,943
District of Kenora 2,698 441 37 124 577
District of Rainy River 2,232 1,874 360 605 186
District of Thunder Bay 37,279 13,123 6,797 22,424 22,460
Northern 3,591 3,613 3,522 8,133 5,471
Out of North West LHIN or Unknown 480 91 702 434 17
North West LHIN 103,369 73,468 63,363 101,386 101,654
Source: In te l l ihea l th , Ontar io , 2016
Table 20 compares current bed use with expected bed use by 2025. Based on expected, it is forecasted
CCC bed requirements will decrease by 96 beds for the North West LHIN, with the most significant
decrease in the City of Thunder Bay. The expected bed use includes bedded levels of care for
Activation/Restoration and Complex Medical Management (Short-Term/Long-Term) but does not take
into account current ALC for LTC use of CCC beds and excludes palliative care.
Table 20. Current and 2025 Forecast of CCC Days by IDN
IDN Community
15-16 Actual
Beds 90%
Occupancy
2025
Expected
Days *
Expected
Beds @ 90%
Occupancy
Variance
Expected
from
Actual
City of Thunder Bay Thunder Bay 151 19,350 58 -92
District of Kenora
Kenora 0 4,152 13 13
Dryden 0 1,656 5 5
Red Lake 4 725 2 -2
District of Rainy
River
Atikokan 7 532 2 -5
Fort Frances 0 1,743 5 5
Emo 0 312 1 1
Rainy River 0 493 1 1
Marathon 9 523 2 -7

57
IDN Community
15-16 Actual
Beds 90%
Occupancy
2025
Expected
Days *
Expected
Beds @ 90%
Occupancy
Variance
Expected
from
Actual
District of Thunder
Bay
Terrace Bay 5 451 1 -4
Geraldton 7 817 2 -5
Nipigon 8 568 2 -6
Manitouwadge 0 366 1 1
Northern District Sioux Lookout 6 1,825 6 -1
Total 197 33,513 101 -96
*Preyra So lu t ions Expected Days
The following table includes the addition of ALC to rehabilitation and CCC from TBRHSC for fiscal
years 2013/14, 2014/15, and 2015/16. Adding this data to the actual SJH data gives a more accurate
prediction of the CCC needs and confirms reports that SJH is over bedded for CCC.
Table 21. SJH – 2013-2016 Summary of Current CCC and Rehab Patient days and Beds (excluding
Palliative Care and ALC)
Bed Type Allott
ed
Actual Reported 2013/14 Actual Reported 2014/15 Actual Reported 2015/16
Patient
Days
Bed
#
Bed # at
95%
occupancy
Patient
Days
Bed
#
Bed # at
95%
occupancy
Patient
Days
Bed
#
Bed # at
95%
occupancy
CCC 142 27,541 76 80 32,374 89 94 36,702 101 106
Rehab 50 15,783 43 46 16,766 46 48 16,098 44 46
Total 192 43,324 119 126 49,140 135 142 52,800 145 152
TBR ALC to CCC 3,402 9.3 9.8 6,847 18.8 19.8 5,002 13.7 14.4
TBR ALC- Rehab 1,814 5.0 5.3 1,208 3.3 3.5 1,400 3.8 4.0
Total CCC 30,943 85.3 89.8 39,221 108 114 41,704 115 120
Total Rehab 15,597 48 51.3 17,974 49.3 51.5 17,498 47.8 50
Grand Total 48,540 133 141 57,195 157 165.5 59,202 162 170
Note 1 : Al l Actua l pat ien t days and beds exclude hosp ice/pa l l ia t i ve care and ALC days as reported in access to care reports
The various data sources present inconsistent information related to regional use of CCC beds in the
North West LHIN. The service delivery by specific health service providers (HSP) has changed over the
years making interpretation of the results very difficult.
The number of rehabilitation beds required in the North West LHIN will remain relatively stable at 50
beds, and with predictions (Table 13) indicating the need for an increase of approximately 5 beds in 2025.
The actual number of CCC beds required in the City of Thunder Bay appears to be 120 taking into
consideration ALC days to CCC at TBRHSC. The current number of beds at SJH less Palliative Care
beds is 142. It would appear that SJH is overbedded by 22 beds if the ALC to LTC and ALC to other
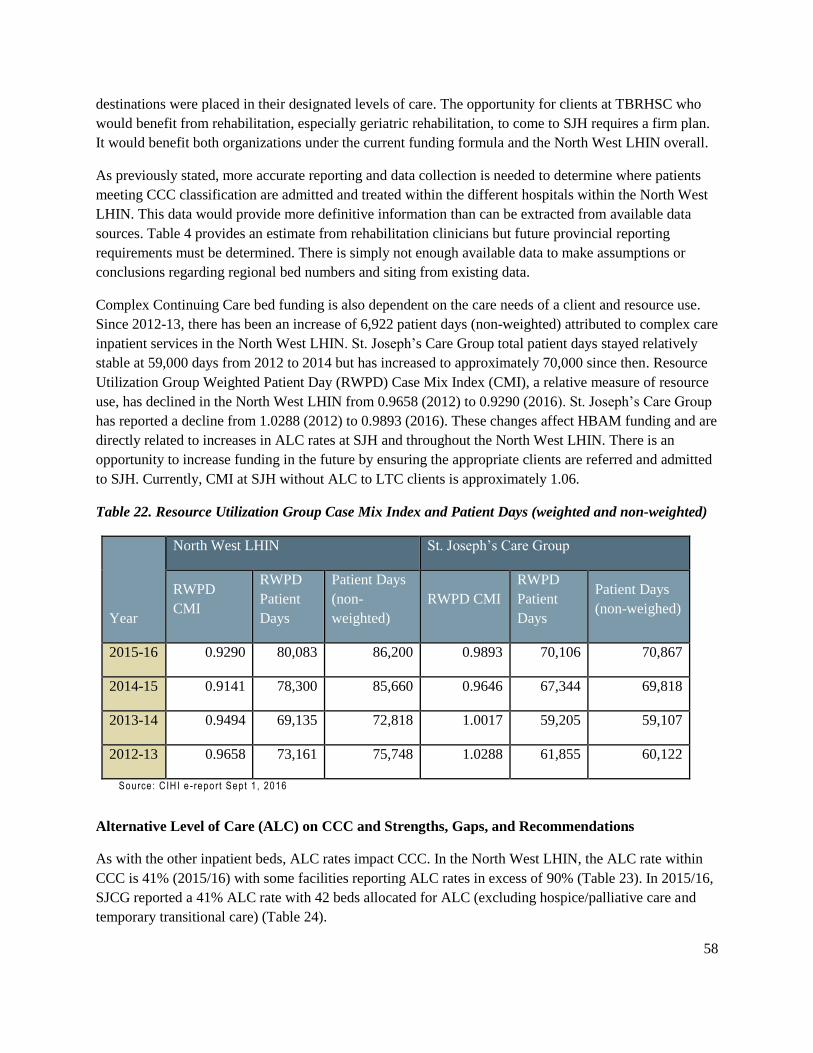
58
destinations were placed in their designated levels of care. The opportunity for clients at TBRHSC who
would benefit from rehabilitation, especially geriatric rehabilitation, to come to SJH requires a firm plan.
It would benefit both organizations under the current funding formula and the North West LHIN overall.
As previously stated, more accurate reporting and data collection is needed to determine where patients
meeting CCC classification are admitted and treated within the different hospitals within the North West
LHIN. This data would provide more definitive information than can be extracted from available data
sources. Table 4 provides an estimate from rehabilitation clinicians but future provincial reporting
requirements must be determined. There is simply not enough available data to make assumptions or
conclusions regarding regional bed numbers and siting from existing data.
Complex Continuing Care bed funding is also dependent on the care needs of a client and resource use.
Since 2012-13, there has been an increase of 6,922 patient days (non-weighted) attributed to complex care
inpatient services in the North West LHIN. St. Joseph’s Care Group total patient days stayed relatively
stable at 59,000 days from 2012 to 2014 but has increased to approximately 70,000 since then. Resource
Utilization Group Weighted Patient Day (RWPD) Case Mix Index (CMI), a relative measure of resource
use, has declined in the North West LHIN from 0.9658 (2012) to 0.9290 (2016). St. Joseph’s Care Group
has reported a decline from 1.0288 (2012) to 0.9893 (2016). These changes affect HBAM funding and are
directly related to increases in ALC rates at SJH and throughout the North West LHIN. There is an
opportunity to increase funding in the future by ensuring the appropriate clients are referred and admitted
to SJH. Currently, CMI at SJH without ALC to LTC clients is approximately 1.06.
Table 22. Resource Utilization Group Case Mix Index and Patient Days (weighted and non-weighted)
Year
North West LHIN St. Joseph’s Care Group
RWPD
CMI
RWPD
Patient
Days
Patient Days
(non-
weighted)
RWPD CMI
RWPD
Patient
Days
Patient Days
(non-weighed)
2015-16 0.9290 80,083 86,200 0.9893 70,106 70,867
2014-15 0.9141 78,300 85,660 0.9646 67,344 69,818
2013-14 0.9494 69,135 72,818 1.0017 59,205 59,107
2012-13 0.9658 73,161 75,748 1.0288 61,855 60,122
Source: CIHI e -report Sept 1 , 2016
Alternative Level of Care (ALC) on CCC and Strengths, Gaps, and Recommendations
As with the other inpatient beds, ALC rates impact CCC. In the North West LHIN, the ALC rate within
CCC is 41% (2015/16) with some facilities reporting ALC rates in excess of 90% (Table 23). In 2015/16,
SJCG reported a 41% ALC rate with 42 beds allocated for ALC (excluding hospice/palliative care and
temporary transitional care) (Table 24).

59
Table 23. North West LHIN CCC ALC Rate
IDN Facility 2013/14 2014/15 2015/16
City of Thunder Bay St. Joseph's Hospital 46.0% 45.0% 41.0%
District of Kenora Red Lake 0.0% 0.0% 0.0%
District of Rainy River Atikokan 77.8% 61.0% 91.8%
District of Thunder Bay
Geraldton 75.5% 77.7% 79.3%
Wilson Memorial 35.6% 37.8% 21.3%
McCausland 0.0% 0.0% 14.7%
Northern District Sioux Lookout 93.3% 98.7% 90.4%
North West LHIN 44.8% 44.0% 40.8%
Source: WTIS Access to Care
Table 24. St. Joseph’s Care Group CCC ALC Rate
2014/15 2015/16
CCC ALC Days* 18,051 14,063
ALC Beds (90% occupancy) 54 42
Source: SJCG; *excl . Hosp ice/Pa l l ia t i ve Care and Temp. Transi t iona l Care
In all of the IDNs, the majority of ALC clients are waiting for LTC. There has been a recent increase in
the number of Extended Care beds in Atikokan but the issue continues throughout the region. Within the
City of Thunder Bay, the expectation is the number of clients waiting for LTC will temporarily decrease
with the Hogarth Riverview Manor expansion opening in 2017 and the announcement that Bethammi
Nursing Home will remain open providing a net increase of 148 LTC beds to the system. However, the
demand for LTC homes continues to grow.
However, there will continue to be clients waiting for supportive and accessible housing units in Complex
Continuing Care. This has been identified as a concern in all IDNs. In the City of Thunder Bay, clients are
ALC for supportive housing at both SJH and TBRHSC. The wait lists remain lengthy for Sister Leila
Greco, PR Cook, Jasper Place, HAGI, and BISNO as well as direct funding opportunities for support and
accessible, affordable housing with The District of Thunder Bay Social Services Administration Board.
Little movement occurs for years. Initiatives in the North West region to combine clients needing
supportive housing with individuals requiring low-income housing needs have been challenged by low
volumes and safety concerns. Client and healthcare professional stakeholders indicate vulnerable clients
60
do not feel safe in this mixed environment. The North West LHIN will be required to develop a plan to
provide more supportive housing opportunities for the clients affected by the lack of an affordable,
accessible housing supply. There is also an opportunity to provide a higher level of support to those in the
community as well as in the current supportive housing programs to support aging in place and reduce the
reliance on LTC when care needs increase.
In addition to causing issues with client flow, ALC clients impact funding formulas. Clients who are
awaiting any alternate level of care impact the RWPD CMI significantly, as they require and receive less
extensive medical services and/or rehabilitation than CCC clients.
The ALC issue presents itself differently across the province, and one solution will not meet the needs of
all LHINs. The North East and North West LHINs experienced similar rates in 2014/15 but the North
East LHIN rate has remained steady, whereas the North West LHIN has seen rapid growth. North Simcoe
Muskoka had a similar rate to North West LHIN in 2104/15, yet is experiencing a decline in the ALC
rate, year over year. The Hamilton, Niagara, Haldimand, Brant LHIN is experiencing the same trend as
the North West LHIN, where the ALC rate is increasing. Solutions at the community and environment-
level will be needed in each LHIN and is beyond the scope of a single HSP. The high rate of ALC within
CCC beds makes current evaluation more challenging, as it is difficult to get an accurate view of
appropriate use and need of CCC beds in each location. As each LHIN develops strategies to address
ALC rates, it would be helpful to share ideas on how to stop the continual increase of clients being
designated as requiring LTC, since these clients make up the majority of ALC clients in any given LHIN.
The Ontario healthcare system strives to provide the right care, in the right place, at the right time. The
ALC issue exemplifies, at times, the lack of early intervention or delay in accessing rehabilitative care for
those in need, which results in clients presenting in the emergency department requiring acute care when
other preventative strategies may have helped avoid this presentation and/or admission to acute care.
Summary
The goal to provide the right care, in the right place (as close to home as possible), at the right time is
limited in the North West LHIN by the relatively small population over a vast geography. The delivery of
inpatient rehabilitative care is challenged by the sheer economies of scale, which impact the availability
of rehabilitation beds, LTC homes, supportive housing, and health human resources. Despite these issues,
the current recommendation is to maintain the number and location of rehabilitation and CCC beds
throughout the North West LHIN, while making efforts to improve the appropriate use of these beds
through strategies to address the ALC issues with all stakeholders and partners; continue efforts to
achieve efficiencies regarding lengths of stay, and develop a strategy to build capacity to provide
rehabilitative care as close to home as possible. Within the North West LHIN, there is potential for
improved care with the implementation of an integrated system.
61
Outpatient and Community Services
In order to support and improve utilization of resources at all levels of rehabilitative care, it is essential to
identify outpatient and community-level services as an essential part of the continuum of care. The term
outpatient and community services will be used interchangeably to describe care clients receive in private
clinics, community-based facilities, and hospital-based outpatient services. The term home care will
specifically refer to care provided in the home through CCAC services.
Outpatient/ambulatory rehabilitative care is not a universally insured service under the Canada Health
Act, and in the past few years, there has been an erosion of the number and scope of hospital-based
outpatient rehabilitation programs and associated NIHB services for Aboriginal people, in an effort to
achieve cost containment. Existing outpatient services require a review to accurately identify current
utilization trends and opportunities for enhanced service delivery. The RCA is currently developing and
piloting a process to implement a provincial minimum data set for outpatient services. This data collection
system aims to ensure care provision across the province meets minimum standards for clinical outcomes,
client satisfaction, access and transition, and financial responsibility.
In addition to the minimum data set, the RCA has standardized progression and maintenance definitions
for community-based rehabilitative care (Appendix B). Adherence to these definitions will ensure future
service delivery in outpatient/community settings will be consistent, with all clients being treated
according to a defined progression or maintenance level of care, providing clarity for clients, families, and
referring professionals regarding expectations of care. The RCA definitions framework outlines what
resources should be available within each level of community-based rehabilitative care. The definitions
developed by the RCA, are specifically designed to characterize care for clients with restorative potential;
Recommendation #2: Develop a LHIN-wide strategy to improve client access and
client transitions across the continuum of rehabilitative care
Recommendation #3: Facilitate adherence to best practices for rehabilitative care to
improve client-centred care
Recommendation #4: Enhance utilization of innovative technologies to improve access
to rehabilitative care services closer to home, particularly in remote and underserviced
areas

62
described by the RCA as “reason to believe that the clients condition is likely to undergo functional
improvements and benefit from rehabilitative care”.
Community-based rehabilitative care can be provided in an individual or group format, in a hospital-
based or community clinic or within the client’s home. In order to meet the eligibility criteria for
outpatient/community therapy as defined by the RCA, care must be overseen by a regulated healthcare
professional. Wellness-focused health promotion and prevention programs not supervised by regulated
health professionals are beyond the scope of the definitions framework for community levels of
rehabilitative care. Although these programs play an important role preventing health decline and
maintaining the health of clients on a rehabilitative care journey, they are not included within the
definitions framework, or the rehabilitative care review. Those programs will be considered when
reviewing the continuum of care required to support clients.
The community-based levels of care include:
• Progression: Within a progression level of care, the goal of therapy is to provide assessment and
time-limited treatment through a single service of coordinated interprofessional approach. This
may include restoring or maximizing function, adapting the home environment to support
reintegration to the community, supporting transitions from and preventing admission to acute
care, and providing opportunities to learn and practice in a familiar environment. Progression
level of therapy is typically for clients following acute episodes or worsening of symptoms. The
overall target of a progression level of therapy is to improve, develop, or restore function that has
been lost or impaired.
• Maintenance: A maintenance-level of community care is designed to prevent functional decline
or injury and to maintain functional performance. Typically, clients who are seen in a
maintenance level of care require an individual assessment and treatment program with periodic
assessment and oversight of care plan. Clients in this level of care generally have a prolonged
condition requiring intervention to prevent a decline in functional status and/or allow them to
remain at home. Individuals within this level of care frequently participate in community-based
group interventions such as falls prevention exercise classes to promote ongoing maintenance.
Presently, publicly-funded outpatient and community services in the North West LHIN are primarily
provided through the North West CCAC, hospital outpatient facilities, Victoria Order of Nurses (VON),
and a few private physiotherapy (PT) clinics in some IDNs. All clinics operate using specific service
eligibility criteria; however, an examination of how to best utilize services to enhance overall system flow
is required. There are six primary publicly-funded platforms through which clients receive
outpatient/community rehabilitative care services. These platforms include:
5. CCAC for in home therapy.
6. Hospital-based outpatient programs.
7. Specialized outpatient service programs (e.g. Neurology, Regional Joint Assessment Centre, Asthma Clinic, etc.).
8. Designated Community Physiotherapy Clinics (CPC).

63
9. Community Health Clinics (CHCs) and Family Health Teams (FHTs).
10. Alternative Payment Plan/Ontario Health Insurance Program (OHIP) - funded Physiotherapy Clinics. (Note these clinics are not included in the table below).
The following table (Table 25) defines the different platforms as outlined in the “Physiotherapy Reforms
in the North West LHIN”. It is noted however, this table does not include hospital-based outpatient
programs or the Alternative Payment Plan/OHIP funded programs.
Table 25. Overview of the Physiotherapy Reform in the North West LHIN (updated June 2014)
Stream 1
Exercise & Falls
Prevention Classes
Stream 2
In-Home PT Service
Stream 3
Long Term Care Homes
Stream 4
Publically Funded PT
Clinics
Stream 5
Primary Care Settings
• No cost to
participants
• No MD referral
needed
• No cap on number
of classes a participant can
attend • Screening by lead
agency
• Combination of in-
person and v/c
programming • Per/LHIN
allocating based on
population
distribution (seniors)
• Locations:
• Dryden
• Patricia
Region Senior Services
Incorporated
• All other
communities in North West
LHIN
• Victorian
Order of Nurses (VON)
• NW CCAC as central
intake
• New clients assessed
for and provided with
PT services as per CCAC criteria
• For previous clients
receiving DPC support:
• All clients
previously
receiving 1:1 PT services in
retirement homes
and supportive housing were
assessed for
ongoing care • Clients meeting
CCAC criteria for
PT continue to
receive; others d/c and/or transitioned
to exercise and
falls classes.
• LTCHs went through
RFP process and/or
retained previous
providers • Change in service
delivery with PT focus
on 1:1 care
• $750/patient bed for PT services (global
allocation)
• ADP included in PT
funding envelope • Additional funding for
exercise classes under
alternate funding
envelope.
• Previously no DPCs in
North West LHIN
• Funding based on episode
of care (patient-based
funding) • $312/episode of care
(EOC)
• MD referral required
• No lower/upper limit on
number of visits • No cap on number of
EOCs/person/year
• Each EOC must be a new
client concern with new
referral • Assessment/goals/
discharge plans must be
submitted including
resources
recommended/referred to
on discharge
• Contact with MOHLTC with reporting criteria
detailed
• Per/LHIN allocation based
on population distribution (seniors).
• Locations
• Thunder Bay
• Fairway
Physiotherapy
• Closing the Gap
• Outside Thunder Bay
• Wilson Memorial General Hospital
• Lake of the Woods
District Hospital
• Red Lake Margaret
Cochenour Memorial Hospital
• Dryden Regional
Health Centre
• Atikokan General
Hospital • Sioux Lookout Meno
Ya Win Health
Centre
• Not yet announced
• Priority is under-
served population
• Requirement to
intake ‘un-rostered’
patients • Direct administration
by MOHLTC

64
Table 26 demonstrates the relatively small number of community-based rehabilitation program options in
the North West LHIN. It is important to note although only two exercise programs and two Falls
Prevention programs are reported, the VON Exercise and Falls Prevention program services 14 sites
across the North West LHIN. It is also important to note although three CPCs are reported in this table,
there are actually eight CPCs in the North West LHIN, as well as one Community Health Clinic which
offers PT services and two publicly-funded clinics with OHIP alternative payment plans not noted on this
table. In addition to these programs, some family health teams offer community-based exercise and
chronic disease management programs. However, these programs are not within the scope of
rehabilitative care as they do not require service provision from a regulated healthcare provider.
Table 26. Number of Community-Based Rehabilitation Programs by LHIN
LHIN
# Community Based CHC
CHC – In
home
Exercise
Program
Community Physio
Clinic
Community
Program
Community
Rehab
Falls
Prevention Total
1 Erie-St. Clair 13
2 South West 9 1 31 2 7 50
3 Waterloo Wellington 12 12
4 Hamilton Niagara Haldimand Brant 5 2 1 30 1 40 79
5 Central West 4 4
6 Missisauga Halton 2 11 1 5 19
7 Toronto Central 18 24 14 56
8 Central 25 27
9 Central East 26 27
10 South East 2 2
11 Champlain 14 10 24
12 North Simcoe Muskoka 10 10 2 22
13 North East 3 13 1 20
14 North West 2 3 2 7
Total 52 2 6 214 13 2 73 362
Source : RCA Al ignment Report

65
Throughout Ontario, there has been a demonstrated lack of available data regarding outpatient services.
This limitation impacts the quality and reliability of data obtained for community rehabilitation programs
in NWO. In order to determine the amount of care provided in the community, programs funded by the
North West LHIN or Ministry of Health and Long-Term Care were surveyed using the RCA
Community Levels of Care Mapping Tool (Appendix J). This tool summarized the amount of
care for both RCA defined levels: progression and maintenance. Table 27 provides a list of the
rehabilitation programs reported in mapping exercise. Table 28 provides a summary of the
number of visits provided by each of the different programs. All the programs report full
alignment with the RCA community levels of care definitions. The data should be viewed as an
estimate of current services, recognizing a standardized data collection system is still outstanding
for outpatient services. This specific limitation is the second focus of the RCA outpatient-
working group. A proof of concept for a minimum data set for outpatient services is currently
underway. This minimum data set will include measurements in four domains: Client/Caregiver
Experience, Clinical Outcomes, Access and Transition, and Financial Performance.
Recommendation #5: Develop and implement data collection and evaluation systems for
quality of care monitoring and continuous quality improvement to improve resource
efficiencies for the provision of client-centred care
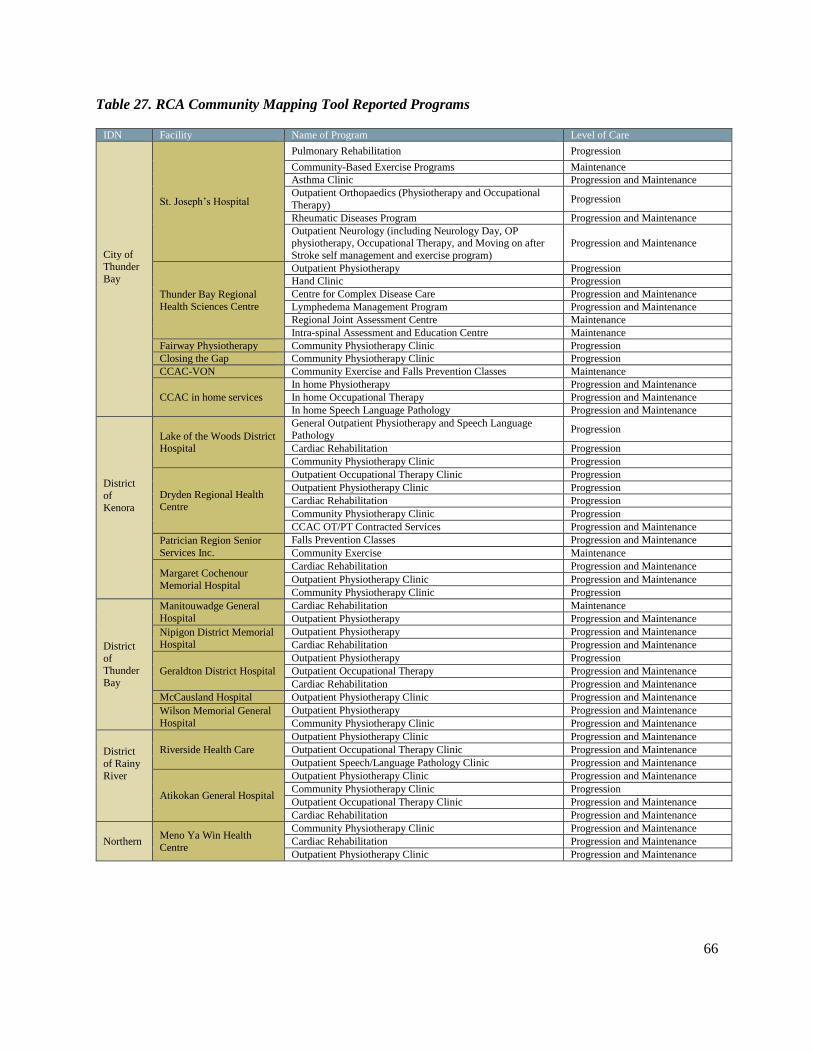
66
Table 27. RCA Community Mapping Tool Reported Programs
IDN Facility Name of Program Level of Care
City of Thunder
Bay
St. Joseph’s Hospital
Pulmonary Rehabilitation Progression
Community-Based Exercise Programs Maintenance
Asthma Clinic Progression and Maintenance
Outpatient Orthopaedics (Physiotherapy and Occupational
Therapy) Progression
Rheumatic Diseases Program Progression and Maintenance
Outpatient Neurology (including Neurology Day, OP physiotherapy, Occupational Therapy, and Moving on after
Stroke self management and exercise program)
Progression and Maintenance
Thunder Bay Regional
Health Sciences Centre
Outpatient Physiotherapy Progression
Hand Clinic Progression
Centre for Complex Disease Care Progression and Maintenance
Lymphedema Management Program Progression and Maintenance
Regional Joint Assessment Centre Maintenance
Intra-spinal Assessment and Education Centre Maintenance
Fairway Physiotherapy Community Physiotherapy Clinic Progression
Closing the Gap Community Physiotherapy Clinic Progression
CCAC-VON Community Exercise and Falls Prevention Classes Maintenance
CCAC in home services
In home Physiotherapy Progression and Maintenance
In home Occupational Therapy Progression and Maintenance
In home Speech Language Pathology Progression and Maintenance
District
of Kenora
Lake of the Woods District Hospital
General Outpatient Physiotherapy and Speech Language Pathology
Progression
Cardiac Rehabilitation Progression
Community Physiotherapy Clinic Progression
Dryden Regional Health Centre
Outpatient Occupational Therapy Clinic Progression
Outpatient Physiotherapy Clinic Progression
Cardiac Rehabilitation Progression
Community Physiotherapy Clinic Progression
CCAC OT/PT Contracted Services Progression and Maintenance
Patrician Region Senior
Services Inc.
Falls Prevention Classes Progression and Maintenance
Community Exercise Maintenance
Margaret Cochenour
Memorial Hospital
Cardiac Rehabilitation Progression and Maintenance
Outpatient Physiotherapy Clinic Progression and Maintenance
Community Physiotherapy Clinic Progression
District
of Thunder
Bay
Manitouwadge General
Hospital
Cardiac Rehabilitation Maintenance
Outpatient Physiotherapy Progression and Maintenance
Nipigon District Memorial Hospital
Outpatient Physiotherapy Progression and Maintenance
Cardiac Rehabilitation Progression and Maintenance
Geraldton District Hospital
Outpatient Physiotherapy Progression
Outpatient Occupational Therapy Progression and Maintenance
Cardiac Rehabilitation Progression and Maintenance
McCausland Hospital Outpatient Physiotherapy Clinic Progression and Maintenance
Wilson Memorial General
Hospital
Outpatient Physiotherapy Progression and Maintenance
Community Physiotherapy Clinic Progression and Maintenance
District
of Rainy
River
Riverside Health Care
Outpatient Physiotherapy Clinic Progression and Maintenance
Outpatient Occupational Therapy Clinic Progression and Maintenance
Outpatient Speech/Language Pathology Clinic Progression and Maintenance
Atikokan General Hospital
Outpatient Physiotherapy Clinic Progression and Maintenance
Community Physiotherapy Clinic Progression
Outpatient Occupational Therapy Clinic Progression and Maintenance
Cardiac Rehabilitation Progression and Maintenance
Northern Meno Ya Win Health
Centre
Community Physiotherapy Clinic Progression and Maintenance
Cardiac Rehabilitation Progression and Maintenance
Outpatient Physiotherapy Clinic Progression and Maintenance
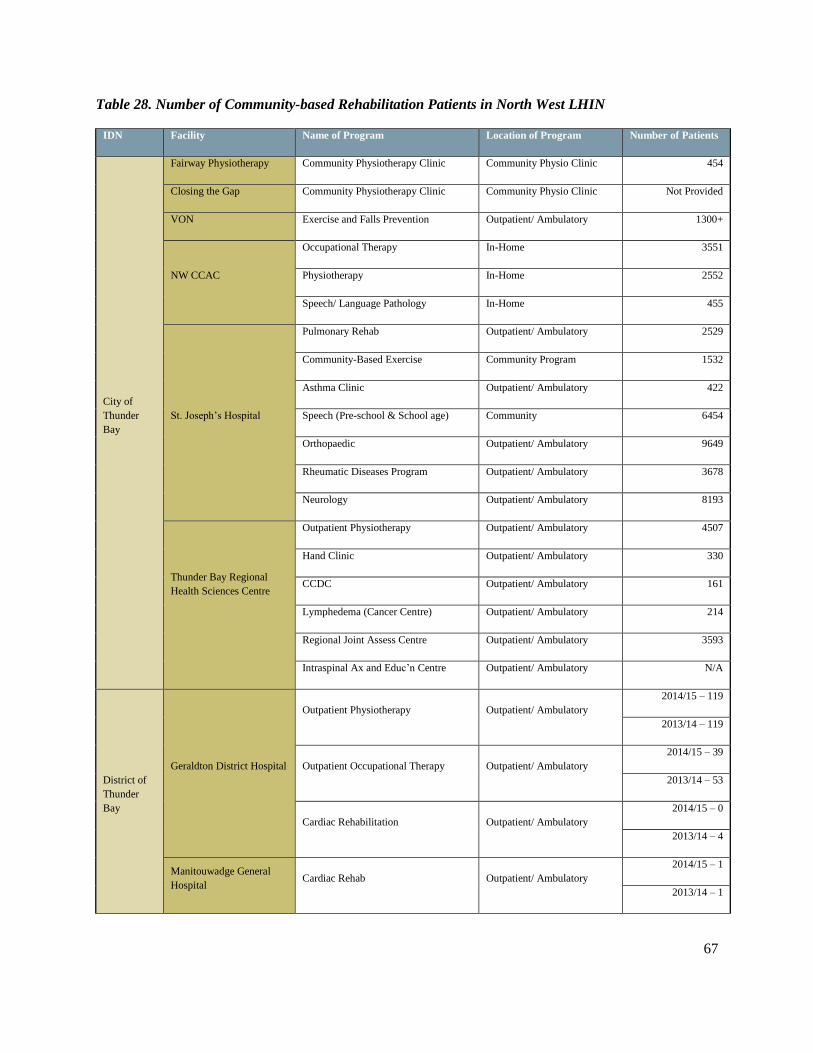
67
Table 28. Number of Community-based Rehabilitation Patients in North West LHIN
IDN Facility Name of Program Location of Program Number of Patients
City of
Thunder
Bay
Fairway Physiotherapy Community Physiotherapy Clinic Community Physio Clinic 454
Closing the Gap Community Physiotherapy Clinic Community Physio Clinic Not Provided
VON Exercise and Falls Prevention Outpatient/ Ambulatory 1300+
NW CCAC
Occupational Therapy In-Home 3551
Physiotherapy In-Home 2552
Speech/ Language Pathology In-Home 455
St. Joseph’s Hospital
Pulmonary Rehab Outpatient/ Ambulatory 2529
Community-Based Exercise Community Program 1532
Asthma Clinic Outpatient/ Ambulatory 422
Speech (Pre-school & School age) Community 6454
Orthopaedic Outpatient/ Ambulatory 9649
Rheumatic Diseases Program Outpatient/ Ambulatory 3678
Neurology Outpatient/ Ambulatory 8193
Thunder Bay Regional
Health Sciences Centre
Outpatient Physiotherapy Outpatient/ Ambulatory 4507
Hand Clinic Outpatient/ Ambulatory 330
CCDC Outpatient/ Ambulatory 161
Lymphedema (Cancer Centre) Outpatient/ Ambulatory 214
Regional Joint Assess Centre Outpatient/ Ambulatory 3593
Intraspinal Ax and Educ’n Centre Outpatient/ Ambulatory N/A
District of
Thunder
Bay
Geraldton District Hospital
Outpatient Physiotherapy Outpatient/ Ambulatory
2014/15 – 119
2013/14 – 119
Outpatient Occupational Therapy Outpatient/ Ambulatory
2014/15 – 39
2013/14 – 53
Cardiac Rehabilitation Outpatient/ Ambulatory
2014/15 – 0
2013/14 – 4
Manitouwadge General
Hospital Cardiac Rehab Outpatient/ Ambulatory
2014/15 – 1
2013/14 – 1

68
IDN Facility Name of Program Location of Program Number of Patients
Outpatient Physiotherapy Outpatient/ Ambulatory
2014/15 – 174
2013/14 – 190
Nipigon District Memorial
Hospital
Outpatient Physiotherapy (Adult) Outpatient/ Ambulatory
2014/15 – 167
2013/14 – 224
Outpatient Physiotherapy (Pediatric) Outpatient/ Ambulatory
2014-2015 – 10
2013-2014 – 19
Cardiac Rehabilitation Outpatient/ Ambulatory
2014-2015 – 8
2013-2014 – 7
McCausland Hospital Outpatient Physiotherapy Outpatient/ Ambulatory 320
Wilson Memorial General
Hospital
Outpatient Physiotherapy Outpatient/ Ambulatory 208
Community Physiotherapy Clinic Community Physio Clinic 262
Northern Meno Ya Win Health
Centre
Community Physiotherapy Clinic Community Physio Clinic 72
Cardiac Rehabilitation Outpatient/ Ambulatory 26
Outpatient Physiotherapy Outpatient/ Ambulatory 61
Kenora
Lake of the Woods District
Hospital
General Outpatient Outpatient/ Ambulatory 700
Cardiac Rehabilitation Outpatient/ Ambulatory 12
WSIB/Staff Outpatient/ Ambulatory 180
Community Physiotherapy Clinic Community Physio Clinic 342
Dryden Regional Hospital
Outpatient Occupational Therapy Outpatient/ Ambulatory
2014/15 - 70
2013/14 - 118
Outpatient Physiotherapy Outpatient/ Ambulatory
2014/15 – 470
2013/14 – 514
Cardiac Rehabilitation Outpatient/ Ambulatory
2014/15 – 12
2013/14 – 13
CCAC Home Care Contracted OT/PT
service In-Home
2014/15 – 467
2013/14 – 460
Community Physiotherapy Clinic Community Physio Clinic
2014/15 – 180
2013/14 – 13
Falls Prevention Patricia Gardens 5

69
IDN Facility Name of Program Location of Program Number of Patients
Patricia Region Senior
Service Exercise Program Patricia Gardens/10 Victoria 59
Margaret Cochenour Mem.
Hospital
Cardiac Rehabilitation Outpatient/ Ambulatory 8
Outpatient Physiotherapy Outpatient/ Ambulatory 563
Community Physiotherapy Clinic Community Physio Clinic 247
Rainy River
Riverside Health Care
Physiotherapy Outpatient/ Ambulatory 2050
Occupational Therapy Outpatient/ Ambulatory 246
Speech/ Language Pathology Outpatient/ Ambulatory 341
Atikokan General Hospital
Cardiac Rehabilitation Outpatient/ Ambulatory 166 (visits)
Outpatient Physiotherapy Outpatient/ Ambulatory 3352 (visits)
Community Physiotherapy Clinic Community Physio Clinic 1460 (visits)
PT CCAC In-Home 32 (visits)
Outpatient OT Outpatient/ Ambulatory 1110 (visits)
OT CCAC In-Home 107 (visits)
In addition to the lack of standardized data for outpatient services, referral patterns are non-standardized.
Most referrals are generated by primary care practitioners who may base referrals on their experience and
familiarity with a specific program, rather than matching the individual client need with the optimal
service or available publicly-funded resource. Community rehabilitation may require private payment or
extended health benefits when publicly funded options are not available. Occasionally, publicly-funded,
specialized clinics are inappropriately used when community-based outpatient programs are not available
locally. In addition, as a result of poor timely access to needed services, clients are often referred to
several programs simultaneously, with the anticipation of being admitted to the most appropriate
program. This referral method results in over-representation and inaccurate projections of the need for
services, inefficient use of resources, and ultimately leads to poor access to services due to inflated wait
lists.
In order to gain a better understanding of the publicly-funded programs available and their impact on the
regional rehabilitative care model, the six platforms of care provision were examined.
Community Care Access Centres (CCAC)
Within Ontario, publicly-funded therapy provided in the home is coordinated by CCAC. Within the North
West LHIN, CCAC services are coordinated by the North West CCAC. From a rehabilitative care
perspective, CCAC uses contracted service providers within each LHH to provide PT, OT, and SLP
assessment and treatment for clients who cannot access outpatient services as well as other in-home
support services such as personal care provided by PSWs and nursing care. There are also Nurse
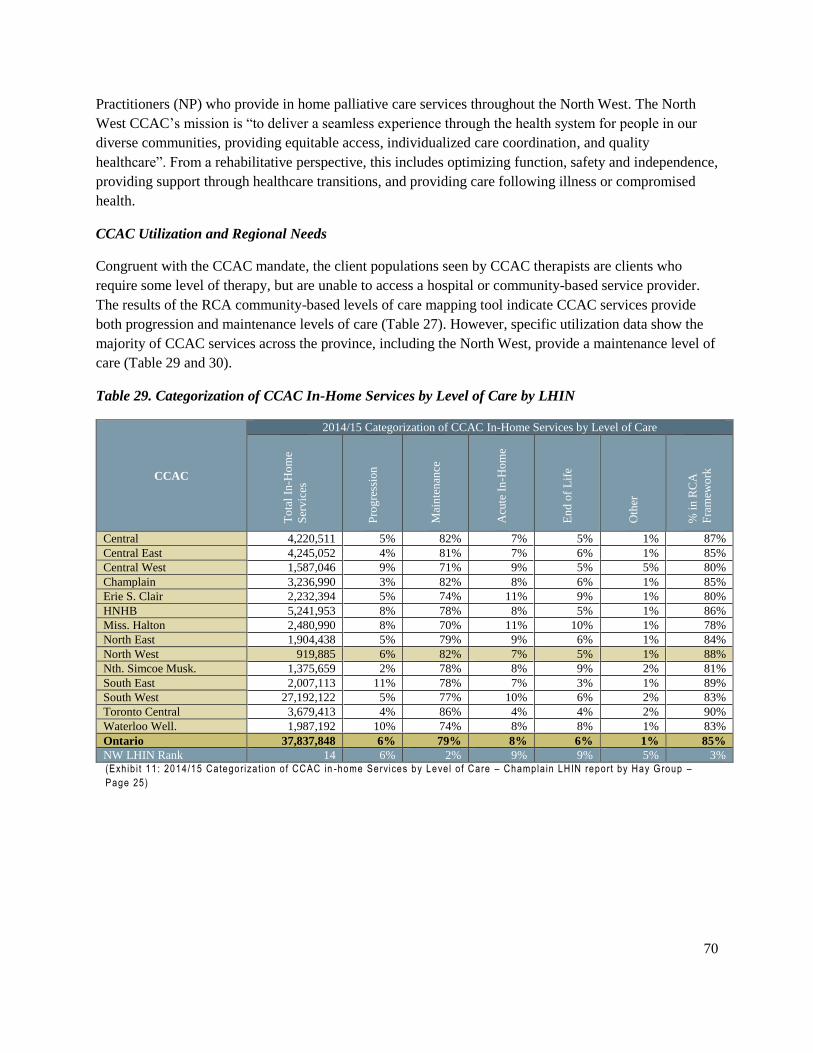
70
Practitioners (NP) who provide in home palliative care services throughout the North West. The North
West CCAC’s mission is “to deliver a seamless experience through the health system for people in our
diverse communities, providing equitable access, individualized care coordination, and quality
healthcare”. From a rehabilitative perspective, this includes optimizing function, safety and independence,
providing support through healthcare transitions, and providing care following illness or compromised
health.
CCAC Utilization and Regional Needs
Congruent with the CCAC mandate, the client populations seen by CCAC therapists are clients who
require some level of therapy, but are unable to access a hospital or community-based service provider.
The results of the RCA community-based levels of care mapping tool indicate CCAC services provide
both progression and maintenance levels of care (Table 27). However, specific utilization data show the
majority of CCAC services across the province, including the North West, provide a maintenance level of
care (Table 29 and 30).
Table 29. Categorization of CCAC In-Home Services by Level of Care by LHIN
CCAC
2014/15 Categorization of CCAC In-Home Services by Level of Care
To
tal
In-H
om
e
Ser
vic
es
Pro
gre
ssio
n
Mai
nte
nan
ce
Acu
te I
n-H
om
e
En
d o
f L
ife
Oth
er
% i
n R
CA
Fra
mew
ork
Central 4,220,511 5% 82% 7% 5% 1% 87%
Central East 4,245,052 4% 81% 7% 6% 1% 85%
Central West 1,587,046 9% 71% 9% 5% 5% 80%
Champlain 3,236,990 3% 82% 8% 6% 1% 85%
Erie S. Clair 2,232,394 5% 74% 11% 9% 1% 80%
HNHB 5,241,953 8% 78% 8% 5% 1% 86%
Miss. Halton 2,480,990 8% 70% 11% 10% 1% 78%
North East 1,904,438 5% 79% 9% 6% 1% 84%
North West 919,885 6% 82% 7% 5% 1% 88%
Nth. Simcoe Musk. 1,375,659 2% 78% 8% 9% 2% 81%
South East 2,007,113 11% 78% 7% 3% 1% 89%
South West 27,192,122 5% 77% 10% 6% 2% 83%
Toronto Central 3,679,413 4% 86% 4% 4% 2% 90%
Waterloo Well. 1,987,192 10% 74% 8% 8% 1% 83%
Ontario 37,837,848 6% 79% 8% 6% 1% 85%
NW LHIN Rank 14 6% 2% 9% 9% 5% 3% (Exh ib i t 11 : 2014/15 Categor iza t ion o f CCAC in -home Services by Leve l o f Care – Champla in LHIN report by Hay Group –
Page 25)
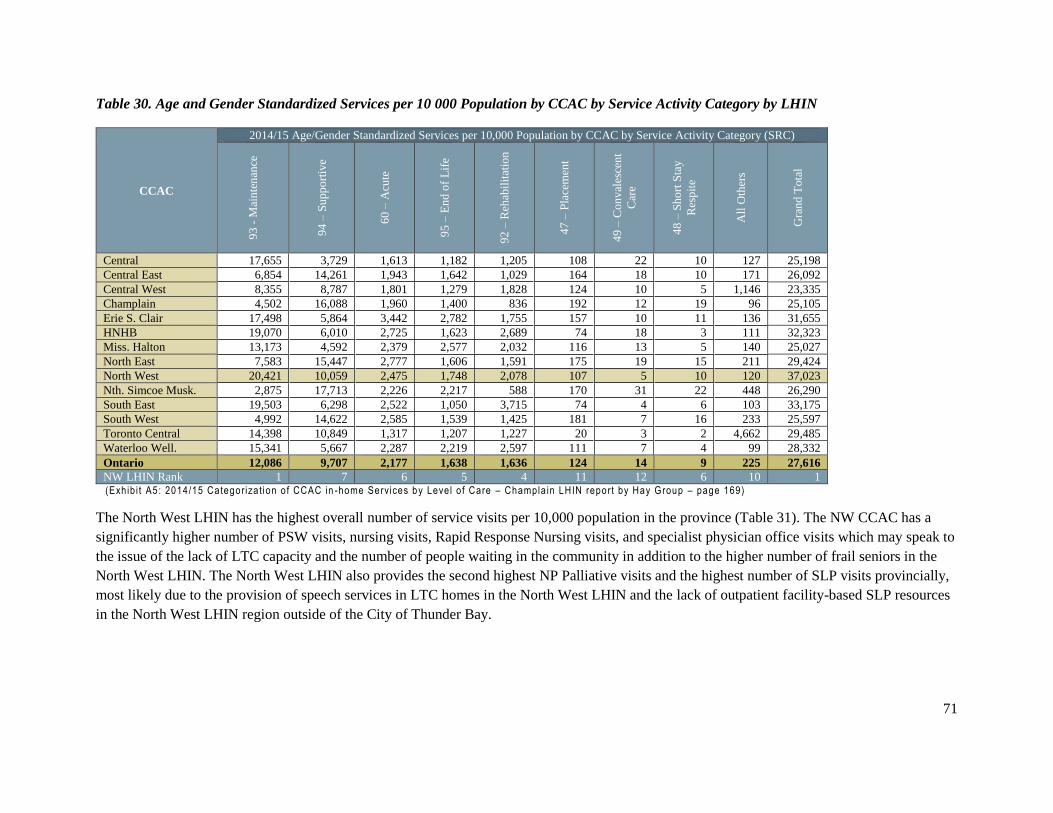
71
Table 30. Age and Gender Standardized Services per 10 000 Population by CCAC by Service Activity Category by LHIN
CCAC
2014/15 Age/Gender Standardized Services per 10,000 Population by CCAC by Service Activity Category (SRC)
93
- M
ain
ten
ance
94
– S
upp
ort
ive
60
– A
cute
95
– E
nd
of
Lif
e
92
– R
ehab
ilit
atio
n
47
– P
lace
men
t
49
– C
on
val
esce
nt
Car
e
48
– S
ho
rt S
tay
Res
pit
e
All
Oth
ers
Gra
nd
Tota
l
Central 17,655 3,729 1,613 1,182 1,205 108 22 10 127 25,198
Central East 6,854 14,261 1,943 1,642 1,029 164 18 10 171 26,092
Central West 8,355 8,787 1,801 1,279 1,828 124 10 5 1,146 23,335
Champlain 4,502 16,088 1,960 1,400 836 192 12 19 96 25,105
Erie S. Clair 17,498 5,864 3,442 2,782 1,755 157 10 11 136 31,655
HNHB 19,070 6,010 2,725 1,623 2,689 74 18 3 111 32,323
Miss. Halton 13,173 4,592 2,379 2,577 2,032 116 13 5 140 25,027
North East 7,583 15,447 2,777 1,606 1,591 175 19 15 211 29,424
North West 20,421 10,059 2,475 1,748 2,078 107 5 10 120 37,023
Nth. Simcoe Musk. 2,875 17,713 2,226 2,217 588 170 31 22 448 26,290
South East 19,503 6,298 2,522 1,050 3,715 74 4 6 103 33,175
South West 4,992 14,622 2,585 1,539 1,425 181 7 16 233 25,597
Toronto Central 14,398 10,849 1,317 1,207 1,227 20 3 2 4,662 29,485
Waterloo Well. 15,341 5,667 2,287 2,219 2,597 111 7 4 99 28,332
Ontario 12,086 9,707 2,177 1,638 1,636 124 14 9 225 27,616
NW LHIN Rank 1 7 6 5 4 11 12 6 10 1 (Exh ib i t A5: 2014/15 Categor iza t ion o f CCAC in -home Services by Leve l o f Care – Champla in LHIN report by Hay Group – page 169)
The North West LHIN has the highest overall number of service visits per 10,000 population in the province (Table 31). The NW CCAC has a
significantly higher number of PSW visits, nursing visits, Rapid Response Nursing visits, and specialist physician office visits which may speak to
the issue of the lack of LTC capacity and the number of people waiting in the community in addition to the higher number of frail seniors in the
North West LHIN. The North West LHIN also provides the second highest NP Palliative visits and the highest number of SLP visits provincially,
most likely due to the provision of speech services in LTC homes in the North West LHIN and the lack of outpatient facility-based SLP resources
in the North West LHIN region outside of the City of Thunder Bay.
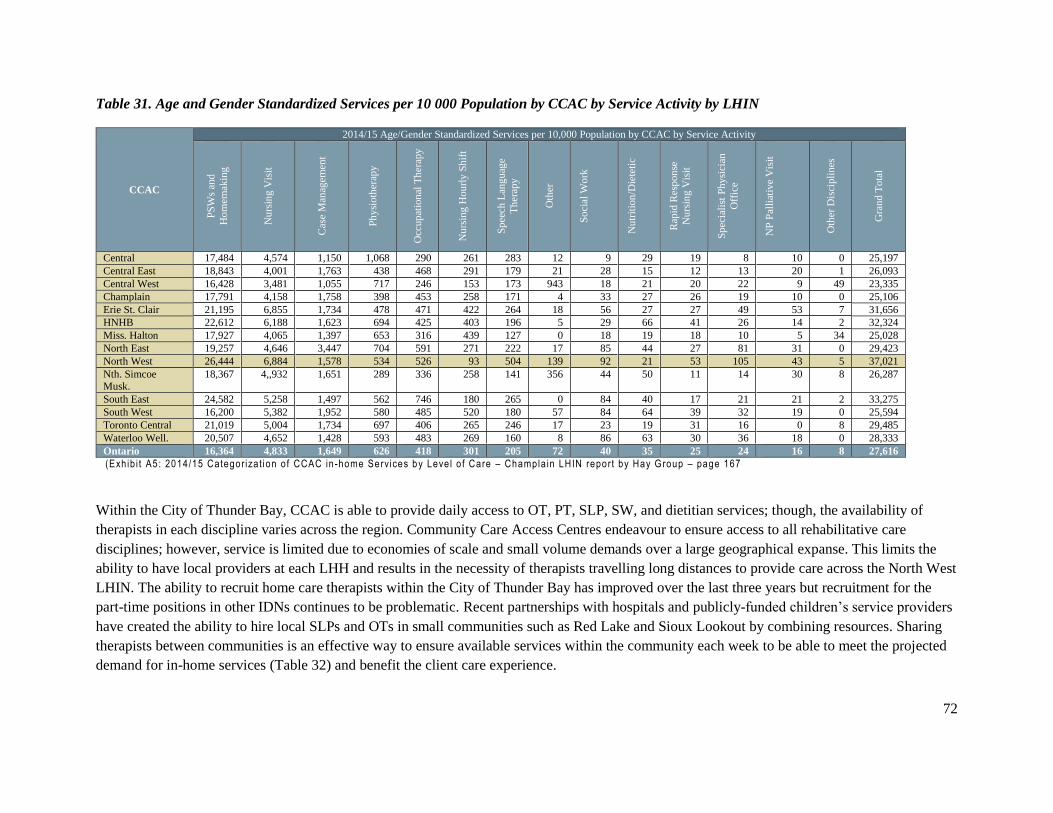
72
Table 31. Age and Gender Standardized Services per 10 000 Population by CCAC by Service Activity by LHIN
CCAC
2014/15 Age/Gender Standardized Services per 10,000 Population by CCAC by Service Activity
PS
Ws
and
Ho
mem
akin
g
Nu
rsin
g V
isit
Cas
e M
anag
emen
t
Ph
ysi
oth
erap
y
Occ
up
atio
nal
Th
erap
y
Nu
rsin
g H
ou
rly
Sh
ift
Sp
eech
Lan
guag
e
Th
erap
y
Oth
er
So
cial
Wo
rk
Nu
trit
ion
/Die
teti
c
Rap
id R
esp
on
se
Nu
rsin
g V
isit
Sp
ecia
list
Ph
ysi
cian
Off
ice
NP
Pal
liat
ive
Vis
it
Oth
er D
isci
pli
nes
Gra
nd T
ota
l
Central 17,484 4,574 1,150 1,068 290 261 283 12 9 29 19 8 10 0 25,197
Central East 18,843 4,001 1,763 438 468 291 179 21 28 15 12 13 20 1 26,093
Central West 16,428 3,481 1,055 717 246 153 173 943 18 21 20 22 9 49 23,335
Champlain 17,791 4,158 1,758 398 453 258 171 4 33 27 26 19 10 0 25,106
Erie St. Clair 21,195 6,855 1,734 478 471 422 264 18 56 27 27 49 53 7 31,656
HNHB 22,612 6,188 1,623 694 425 403 196 5 29 66 41 26 14 2 32,324
Miss. Halton 17,927 4,065 1,397 653 316 439 127 0 18 19 18 10 5 34 25,028
North East 19,257 4,646 3,447 704 591 271 222 17 85 44 27 81 31 0 29,423
North West 26,444 6,884 1,578 534 526 93 504 139 92 21 53 105 43 5 37,021
Nth. Simcoe Musk.
18,367 4,,932 1,651 289 336 258 141 356 44 50 11 14 30 8 26,287
South East 24,582 5,258 1,497 562 746 180 265 0 84 40 17 21 21 2 33,275
South West 16,200 5,382 1,952 580 485 520 180 57 84 64 39 32 19 0 25,594
Toronto Central 21,019 5,004 1,734 697 406 265 246 17 23 19 31 16 0 8 29,485
Waterloo Well. 20,507 4,652 1,428 593 483 269 160 8 86 63 30 36 18 0 28,333
Ontario 16,364 4,833 1,649 626 418 301 205 72 40 35 25 24 16 8 27,616
(Exh ib i t A5: 2014/15 Categor iza t ion o f CCAC in -home Services by Leve l o f Care – Champla in LHIN report by Hay Group – page 167
Within the City of Thunder Bay, CCAC is able to provide daily access to OT, PT, SLP, SW, and dietitian services; though, the availability of
therapists in each discipline varies across the region. Community Care Access Centres endeavour to ensure access to all rehabilitative care
disciplines; however, service is limited due to economies of scale and small volume demands over a large geographical expanse. This limits the
ability to have local providers at each LHH and results in the necessity of therapists travelling long distances to provide care across the North West
LHIN. The ability to recruit home care therapists within the City of Thunder Bay has improved over the last three years but recruitment for the
part-time positions in other IDNs continues to be problematic. Recent partnerships with hospitals and publicly-funded children’s service providers
have created the ability to hire local SLPs and OTs in small communities such as Red Lake and Sioux Lookout by combining resources. Sharing
therapists between communities is an effective way to ensure available services within the community each week to be able to meet the projected
demand for in-home services (Table 32) and benefit the client care experience.

73
Table 32. Actual and Expected Home Care Services by IDN
2013/14 2025 Forecast
Long stay Home Care Clients* Other Home Care Clients† Long Stay Home Care Clients* Other Home Care Clients†
NW LHIN Integrated District
Networks and Local Health Hubs Actual Expected
Actual-
Expected Actual Expected
Actual-
Expected Actual Expected
Actual-
Expected Actual Expected
Actual-
Expected
LSHCC
Expected
%
OHCC
Expected
%
District of Kenora Total 59,108 89,137 -30,029 33,123 41,906 -8,783 75,731 113,853 -38,122 40,436 51,673 -11,237 27.7% 23.3%
District of Rainy River Total 35,329 47,145 -11,816 13,546 21,306 -7,760 39,100 53,730 -14,631 15,895 23,959 -8,064 14.0% 12.5%
District of Thunder Bay Total 26,296 32,565 -6,269 14,033 16,221 -2,188 43,750 47,306 -3,556 18,170 21,556 -3,386 45.3% 32.9%
City of thunder Bay Total 459,505 294,405 165,100 181,307 133,523 47,784 517,412 335,739 181,673 205,384 150,914 54,470 14.0% 13.0%
Northern Total 4,612 24,653 -20,041 4,153 13,109 -8,956 7,152 33,124 -25,972 5,341 17,037 -11,696 34.4% 30.0%
Grand Total 584,850 487,904 96,946 246,462 226,064 20,098 683,145 583,753 99,392 285,227 265,139 20,088 19.9% 17.3%
Sources: HCD 2013/14, NW LHIN Popula t ion Data
Note : Expected se rv ices are ca lcu la ted a t provinc ia l average use per cap i ta , ad justed for age.
*c l ien ts whose in i t ia l service goa l was “ in home main tenance” or “ in home long stay”
†cl ien ts whose in i t ia l service goa l was “ in home acute”, “ in home rehab i l i ta t ion” or “ in home end o f l i fe ” . Excludes cl ien ts whose in i t ia l se rv ice goa l set t ing was not in home.

74
Strengths, Gaps, and Recommendations
Within the rehabilitative care journey, CCAC plays an important role in the recovery and return to
independent functioning. It has become essential CCAC services are connected directly to inpatient care
facilities in order to ensure a smooth transition between care providers and service delivery. Presently,
there are challenges when clients transition between facility-based service providers and CCAC
community service providers, similar to the identified challenges when clients transition between
hospitals. During stakeholder consultation (outside the City of Thunder Bay), the need for improvement
in client transitions were identified in the following areas: communication between service providers at
handover, process and timeliness of home safety assessments, availability of rental equipment at the LHH
level, and knowledge of available community services across the region and across the rehabilitative care
spectrum.
Despite challenges, current strategies for better transitions were identified. Many stakeholders identified
the addition of a CCAC care coordinator at team rounds and discharge conferences has had a positive
influence on these transitions. Currently, hospitals have access to the CCAC client information portal to
confirm if a client was receiving CCAC services prior to admission. This helps ensure clients are
reconnected with CCAC in-home service at discharge. In addition, in some smaller communities, the
same department or even the same therapist provides care at the inpatient, home care, and outpatient
phases. In these communities, issues with handover and communication are non-existent, resulting in
seamless care. This was clear in Dryden, where the Dryden Regional Health Centre is the service provider
contract for CCAC OT, PT, and SLP services. Therapists are able to access Meditech, the same electronic
medical record for inpatient hospital stays, to obtain background medical and care information; are able to
easily communicate with the inpatient therapist who has cared for the client; and, in turn, are able to
easily communicate with the therapist they are transitioning the client to in outpatient services.
Furthermore, there is no barrier to transition the client to the appropriate level of service. Clients are
transitioned to the most appropriate level of service for their care when they are ready.

75
The issue of client home safety assessments was a recurrent and frequent theme with a variety of
contributing factors. Firstly, a lack of local OTs, especially within the District of Thunder Bay, limits the
timeliness of the safety assessments and equipment recommendations. Despite the fact that it is the
responsibility of the “owner” of the patient at the time of discharge to ensure safe discharge, CCAC is
often filling the gap and completing these safety assessments. The CCAC service provider for the District
of Thunder Bay communities is based in Thunder Bay and visits every two weeks. This may result in
longer than required hospital stays, if clients are unable to return home until the safety of their home can
be assessed. Consequently, PTs complete many components of the home assessment such as stairs, toilet
and tub transfers, car transfers, and in-home mobility with the client and make temporary equipment
recommendations until such time a formal and complete home safety assessment can be completed by the
OT. In some low risk cases, this results in earlier discharge and good use of available resources. If a client
is deemed to be very high priority and needs to get home in a hurry, CCAC indicates additional therapist
visits can be arranged before the two weeks.
Secondly, the process of home safety assessments needs to be outlined and clarified. Stakeholders
acknowledged their local processes, but these were inconsistent across the region. The need for an
electronic referral initiated at the hospital for the CCAC assessment and rental equipment was clear and,
although the actual person completing this process varied from site to site, this was not the issue. It was
also identified either healthcare professionals or CCAC hospital case managers could initiate this in
Thunder Bay before repatriation back to the local LHH. The concern raised was how a client could attend
a home safety assessment with a CCAC service provider while being a hospital inpatient. If the client
safety risk is low to medium, the client’s discharge was coordinated between the hospital and CCAC to
occur at the time of the home safety assessment. There is an understanding if the environment is not safe,
the client would need to return to the hospital to await home renovations, equipment or further functional
ability. This process was identified, but the timing, coordination, and assessment of client risk between
the three facilities involved (sending, receiving, and CCAC) varied. In many cases, clients are discharged
to their LHH for a home safety assessment with the understanding this process would occur prior to their
discharge home. However, occasionally local providers assess the client’s risk level to be low and the
client is discharged home to await the formal home assessment. This is frustrating for both sending and
receiving service providers and perceived as risky and inefficient use of resources respectively. The gaps
for home safety assessments in the North West LHIN are the cases where clients are medium to high risk
for safe discharge home or where an assessment is required to determine appropriate equipment to access
the home such as a porch lift, ramp, or bathroom renovations. In these cases, the client may be permitted a
leave of absence from the hospital to attend the home safety assessment with the CCAC service provider.
These situations are much more complicated when clients do not have family support to transport them to
the home assessment or for clients who live outside the immediate area of the hospital but still within the
hospital catchment area, such as Rossport for Terrace Bay, Ignace for Dryden, and Kakebeka Falls for
Thunder Bay. Clients are encouraged to use available transportation options such as Handi-transit, taxis,
or Ambutrans, as appropriate, and these complicated situations require discussion and planning with all
parties involved, including the discharge planning team and the CCAC coordinator. It is recommended
that the involved facilities within the North West LHIN have further communication and clarification of
processes in these uncommon situations.

76
Thirdly, the availability of local equipment impacts the home safety assessments. Often, different types of
equipment need to be trialed with a client in their home environment to determine appropriateness. Some
hospital departments have limited rental equipment. The current vendors for rental equipment are based
in Thunder Bay, Fort Frances, Kenora, and Dryden and in these communities equipment is available each
day of the week. However, in small communities such as Red Lake, Atikokan, Nipigon, Terrace Bay,
Marathon, Geraldton and Manitouwadge, equipment delivery is only twice a week. As a result, “best
guess” equipment is often arranged prior to the client discharge. For these communities, it was identified
this could often be done in Thunder Bay before the client transitions back to their LHH. If a client is
deemed to be very high priority and needs to get home in a hurry, rush equipment rental can be arranged.
In addition, home care therapists often arrange to meet with the vendor in the community at the time of
the visit to assist with complicated equipment. These scenarios exemplify the need for communication
between service providers at the time of client transitions.
Lastly, similar to hospital-to-hospital transitions and inpatient-to-outpatient transitions, there is room for
improved communication between providers at time of transition from hospital to CCAC, especially in
IDNs outside the City of Thunder Bay and between IDNs. At times, medical information such as
diagnosis, weight-bearing status, physician orders, and surgical reports are missing, requiring in-home
therapists to take extra time to ensure effective service efficiently on first contact with the client. Other
identified areas of concern regarding communication include: the reason for the referral or safety
assessment, specific concerns, and availability of local resources. Home care direct service providers
receive a therapy report with the referral provided by the CCAC case manager. Direct service providers
do not currently have access to the electronic medical record from the hospitals unless they also work for
the hospital and are within the client circle of care. Case managers at CCAC have access to the EMR but
do not always provide the service provider with the profession-specific level of details required, such as
recently completed assessments, physical status on discharge, equipment trialed and recommended,

77
splinting trialed and recommended, and continence. These gaps in information and duplication of
assessments result in inefficiencies in the system. Planning for successful client discharge and community
reintegration requires knowledge of local community resources, which varies significantly throughout the
North West LHIN. Local resources should be understood and clarified at the time of these transitions in
order to ensure consistent messaging, ultimately improving the client experience. One major CCAC
service provider recently underwent a series of prospective safety analyses to improve the completeness
of relevant rehabilitation information required for quality, efficient client care at this time of transition.
Administrative staff screened referrals to ensure relevant information was complete and retrieved missing
information prior to the therapist receiving the referral. This was also an opportunity for education with
CCAC case managers. This cycle of continuous quality improvement resulted in improved information
transfer completeness and efficiency, confirmed by a recent random chart audit. Improvements in
documentation accuracy and consistency within the hospital EMR and targeted training with CCAC case
managers, have potential to improve the efficiencies at client transitions.
In order to solve some of these issues and to improve client transitions home, the North West LHIN
recently conducted a time-limited pilot project to support high-risk geriatric clients for two weeks
following discharge from rehabilitation by the same team of OT, PT and rehabilitation assistants. The
model proved to be an effective way to support discharging high risk geriatric clients as soon as possible
to their home and eliminated the issues with transitions and communication identified above. Especially
for time-limited OT services, it is client centred and efficient to have the same professional follow the
client home to ensure the home environment meets the needs of the client. The same is true for short-term
PT services. This model already occurs in some regional communities since the hospital and the
contracted CCAC provider employ the same OT and PT. Eliminating an additional healthcare provider
team involved with the client and the associated assessments and documentation for such a short period of
time gains efficiencies and minimizes client care transitions. It is recommended this program model be
further investigated by the North West LHIN to track specific outcomes to determine cost effectiveness
and reduced ER visits.
In addition, a follow-up phone call to CCC and Rehabilitation discharged clients was implemented by
SJH. Clients very much appreciated the follow-up phone call. The major concern expressed was related to
PSW’s not arriving to provide care. In follow-up with CCAC, clients were given information to contact
the CCAC directly.
Hospital-based Outpatient Programs
Within the North West LHIN, the majority of outpatient services are delivered in hospital-based
programs. In addition, as indicated in Table 27, hospital-based outpatient departments are the only
publicly-funded PT services available in all communities except Thunder Bay, and the only available PT
services in all communities except Thunder Bay, Dryden, Kenora, and Fort Frances where private PT
clinics are also available. As outlined in the mapping tool exercise, hospital-based outpatient PT services
are available at each of the hospitals across the North West LHIN providing both progression and
maintenance levels of community rehabilitation. The ability to identify current and future needs for
outpatient services is difficult and an area where the RCA is working to further inform each LHIN and the
province.

78
Hospital-based Outpatient Utilization
As noted above, within most LHHs, hospital-based programs represent the only available outpatient
rehabilitation option, as most communities are too small to support private clinics. Table 28 indicates the
number of patients and visits served in the North West LHIN.
Strengths, Gaps, and Recommendations
All hospitals in the North West LHIN have dedicated resources for outpatient PT, with varying wait time
lengths, but very few have outpatient OT and SLP services. The availability of local PT services was
identified as a system strength. The lack of OT and SLP was clearly identified as a gap during stakeholder
consultation with both healthcare providers and clients and families. In particular, services for cognitive
deficits, return to driving, and speech and language deficits were identified. Innovative solutions to
address the issues noted include sharing an OT resource with the Dryden Family Health Team to provide
more community-based OT services for driving, community reintegration and cognition; and using
Personal Computer Virtual Conferencing (PCVC) connections to address the gap in adult SLP services.
Facilities that do offer these services have variable wait times to access these services. As such, it is
evident that the current services are insufficient but the determination of exact need is difficult at this
time. It is recommended that each LHH has the local services of an OT to serve both inpatient and
outpatient levels of care and facilitate transitions home.
Specialized Programs
Supporting CCAC and hospital-based outpatient services are several specialized programs. These
programs are designed to meet the needs of specific populations who require ongoing therapy not
otherwise available within a community. In general, the specialized programs in the North West LHIN
provide direct therapy locally in Thunder Bay and some provide access regionally. Others provide
informal consultation and subject matter expertise as requested. Many of the specialized programs
incorporate chronic disease self-management into client treatment plans. Presently, there is no formal
knowledge exchange system for all specialized programs. It is recommended regional access to
specialized services be made available to encourage the opportunity for clients to receive outpatient
services as close to home as possible, or within their home environment.
Currently, specialized outpatient programs are primarily available in Thunder Bay, with the majority of
services being provided through SJH, TBRHSC, and CCAC services. Among the specialized programs
are:
• Rheumatic Disease Program*
• Neurology Services*
• Amputee Clinic*
• Moving On After Stroke (MOST)*
• Pulmonary Rehabilitation, COPD, CHF Program
• Cardiac Rehabilitation*

79
• VON Falls Prevention Program*
• Lymphedema Management*
• Regional Joint Assessment Centre (RJAC)*
• Intra-spinal Assessment and Education Centre (ISAEC)*
• Regional Wound Care Program*
*Denotes programs that provide a regional service through consultation, regional block admissions, or
technology-based regional service delivery platforms
Regional access to specialized programs currently ranges from consultation, when requested, to regularly
schedule telemedicine-connected exercise and education programs. Many specialized programs are able
to meet the needs of regional and remote clients; however, current outpatient service delivery models are
often insufficient to provide adequate specialized care outside the City of Thunder Bay. This results in
limiting access to only those clients who are able to attend programming outside their home community.
Strengths, Gaps, and Recommendations
During regional stakeholder engagement, both strengths and gaps were noted in particular for the
following programs: Cardiac Rehabilitation/Healthy Lifestyles, Chronic Pain, Rheumatic Diseases, and
Neurology Services. The programs are noted to be specialized, client-centred, well-resourced, and
evidence-based; however regional access is limited due to wait lists, accommodations, and transportation.
The former Cardiac Rehabilitation Program, now called Healthy Lifestyles, is a well-established program
throughout the North West LHIN, at multiple LHHs. The program uses a central referral process with
physical assessment and exercise prescription completed at the TBRHSC site and local provision of
exercise and monitoring. The program supports regional service providers with initial training and
ongoing access to the coordinator for any questions or concerns. In addition, participants of the program
are able to access the monthly education session using videoconference platform. The program has a wait
list and some challenges accessing timely support with recent program staffing changes. To compensate,
some larger regional IDNs have continued to provide the program locally without any support from the
Healthy Lifestyles program. The program recently expanded to meet this identified gap and increased
opportunities for people with other diagnoses such as stroke and diabetes, to participate in ongoing
exercise and chronic disease self-management. This model of care provides a good opportunity to
leverage support for a variety of clients with chronic diseases throughout the North West LHIN.
The Chronic Pain program has adapted programming intensity and the overall length of the program;
however, continues to have challenges providing regional service. The program identifies it is difficult to
establish connections for ongoing local programming, with high staff turnover. The need for this program
is evident throughout the region and many LHH providers feel as though the referrals to this program
“fall into a black hole”. Recent increase in funding is hoped to address this gap.
The Rheumatic Diseases program is another well-respected program. St. Joseph’s Care Group
successfully delivered the Arthritis Care Network project using the Hub and Spoke model 12 years ago.
Ongoing tele-rheumatology services conducted by the rheumatologist with local rehabilitation support,
80
and regular polyarthritis education workshops conducted by the Rheumatic Diseases team are examples
of sustainable initiatives developed from this project.
The Rheumatic Diseases Program continues to develop alternative models of care to meet the needs of the
ongoing need and recent reduction of local rheumatologists. The regional stakeholders noted this program
“works well for patients that get in!” Service providers at the LHH level appreciate the specialized
training provided to support the delivery of the program assessments using videoconferencing technology
but note ongoing “refreshers” of the polyarthritis workshops are beneficial and currently needed. They
also noted local physicians have recently been accessing visiting specialists programs and telehealth to
access rheumatologists throughout the province. Physiotherapists and OTs are appropriately skilled to
support these assessments; however, this has impacted their service delivery for other programming. This
is also an opportunity for coordination with the specialized service in Thunder Bay through integrated
triaging processes. Clients could then access specialized physician and support services in order of
priority.
The Neurology Day program is another program highlighted to fill a gap regionally due to challenges in
transportation and accommodation. Some clients are able to stay with family in Thunder Bay or access
accommodations and their experience with the program is very positive as noted by this family member:
“Without the physiotherapy that Dad received at SJG, Neurology Day and continues to
receive in Kenora, he wouldn’t have the quality of life that he does and the movement and
progress he has continued to make. We appreciated the option to continue in Neuro Day at a
more frequent intensity than was available in our own community.”
The Stroke Best Practice Guidelines indicate community-based therapy should be delivered at an intensity
of two to three times weekly for eight to twelve weeks following discharge from acute care or inpatient
rehabilitation. This is currently only available in the Neurology Day program in Thunder Bay. The
Ontario Stroke Network notes “patients living within 30 minutes’ drive were identified as outpatient
candidates and patients living beyond were identified as community-based rehab.” Accessibility to
community services following stroke should be less than 60 minutes from home. The Northwestern
Ontario Regional Stroke program is investigating a geo-mapping project to identify the 30-minute, 60-
minute, and 120-minute radius of each LHH in the North West LHIN. This will assist in identifying
where services are required throughout the expansive North West LHIN.
These three programs have made use of local, funded accommodations whenever possible, such as
Wequedong Lodge for Aboriginal clients and PR Cook bedsitter apartments funded by the North West
LHIN until December 2016. To access transportation, clients are encouraged to use the provincial travel
grant funding program and NIHB. However, there continues to be ongoing challenges with consistent
access to NIHB funding for medical transportation for rehabilitation.
Another identified gap is the lack of community-based respiratory therapy outside the pulmonary
rehabilitation program and asthma clinic in the City of Thunder Bay. Specifically there is an identified
gap to support clients with long-term palliative care and ventilation needs such as Amyotrophic Lateral
Sclerosis in the community.

81
Models continue to be developed and programs expanded to work with regional service providers and
incorporate regional treatment and triage platforms, throughout the North West LHIN.
Community Physiotherapy Clinics
The primary rehabilitative care discipline provided in an outpatient setting is PT. The role of community-
based PT clinics has traditionally been divided between private care providers and publicly-funded PT
services. Private providers typically serve clients who have the financial ability to pay or access to
insurance coverage (extended health benefits, accident, or workplace injury-related). Publicly-funded PT
services are typically based within hospital settings or provided in-home through CCAC services.
Recently, the provision of publicly-funded PT services was reviewed and changes were made in August,
2013. A lack of access to community PT services was acknowledged across Ontario. The review
identified Designated Physiotherapy Clinics (DPC), introduced to increase access to publicly-funded PT
services, were primarily serving the Greater Toronto Area. As a result of this finding, clinic-based PT
services were expanded to include some publicly-funded services. These services were established to
ensure adequate access to PT services for underserviced populations in cities across the province. Within
NWO, eight clinics were allocated funding to provide a defined number of episodes of care (EOC) to
identified client populations. These allocations were distributed between hospital-based programs and
private clinic settings throughout the region, with the City of Thunder Bay clinics being funded by and
reporting directly to the MOH, and the regional programs accountable to the North West LHIN.
Table 33. Designated Physiotherapy Clinic Episode of Care Allocations for NWO
Community Physiotherapy Clinic City Allotted
EOC
Fairway Physiotherapy Clinic Thunder Bay 706
Closing the Gap Thunder Bay 707
Lake of the Woods District Hospital Kenora 342
Dryden Regional Hospital Dryden 183
Red Lake Margaret Cochenour Memorial Hospital Red Lake 48
Atikokan General Hospital Atikokan 200
Wilson Memorial Hospital Marathon 308
Meno Ya Win Health Centre Sioux Lookout 124
Total 2,618
In order to qualify for publicly-funded PT services through the CPCs, clients must have a valid Ontario
health card, a referral from their physician or NP, and meet one of the following criteria:
• Age 65 or older.
• Age 19 or younger.
• Any age after overnight hospitalization for a condition which requires PT (and for which they are
not otherwise eligible through other publicly-funded programs).
• A recipient of Ontario Works or Ontario Disability Support Program (with or without a valid
health card).
82
Services provided within the designated CPC include assessment, diagnosis, and treatment; with the goal
of improving or developing physical function; and promoting mobility when function and/or mobility has
been lost or impaired as a result of a debilitating event or disease, pain, injury or surgical procedure.
Discharge is dependent upon client achievement of therapeutic objectives identified in their treatment
plan; or when equivalent gains could be achieved through an exercise, falls prevention, activation, or
similar program; or when no further gains are likely to result from ongoing PT. Current evaluation of
these CPCs indicates services are utilized in all identified programs. Presently, all clinics but one
provided either a measure of EOC or volume of clients seen within 2014/2015 or 2015/2016 with all
clinics reporting at or near their allotted volumes. Consistent measures of EOC volumes by all community
clinics will enable ongoing comparison and adjustment of service funding according to regional demand.
It is an expectation clients will be treated according to recommended guidelines and therapeutic goals;
however, through this review it has become evident differences exist with respect to treatment philosophy
among designated clinics. Due to the limited funding available for each EOC, some clinics provide
primarily consultative services to clients, while others provide more direct “hands on” treatment
approaches. It is recommended a standardized treatment approach, and clearer expectations regarding the
intended use of the funding be developed and monitored. Participation in the RCA minimum data set will
help to ensure the appropriate levels of care and EOC allotment are in place for each clinic.
In addition, provincially there is variation whether CPCs provide PT services to clients following post-
joint replacement surgeries at CPCs. The current Primary Joint Replacement QBP clinical handbook
indicates these clients should not be seen under the EOC payment model in CPCs as funding is provided
within the QBP framework; however, these handbooks are being reviewed provincially and parameters
need to be confirmed and further discussed as regional rehabilitation models are implemented.
Strengths, Gaps, and Recommendations
Ongoing evaluation of the PT needs within communities that do not currently have allocated CPC funding
is required. An initial review of outpatient PT volumes in these communities is available from the RCA
mapping tools for community levels of care. According to these surveys, among the communities without
a designated PT clinic, Fort Frances reported the greatest volume of clients seen in their outpatient PT
clinic. A more detailed evaluation of the client demographics within outpatient PT clinics and monitoring
of the CPCs to ensure there is an increase in outpatient service volumes will help to inform ongoing
decisions regarding the need for further designated CPCs across the North West LHIN.
In addition to the new CPCs, there are three other PT clinics providing publicly-funded PT services
within the North West LHIN. Two clinics in Thunder Bay, Victoriaville Physiotherapy Centre and
Thunder Bay Physiotherapy Centre, provide services with special funding directly from the Ministry of
Health and Long-Term Care and the Mary Berglund Community Health Centre in Ignace provides PT
services through their Ministry of Health-funded global budget. Although these clinics do not receive
funding from the North West LHIN, their services are similar to those offered at the CPCs. In Ignace
however, the PT services provided include cardio-respiratory, neurological, and wound management in
addition to the typical orthopaedic caseload. The clinic uses an interprofessional team model with nurses,
physicians, and PTs to ensure appropriate care for clients. At present, a PT is contracted from Thunder
Bay and provides direct services in the clinic one day a week and uses OTN videoconference services a
83
second day a week to do initial assessments and initiate treatment as appropriate, maximizing the use of
the time in person. In addition, the Mary Berglund clinic offers cardiac rehabilitation using
videoconference access for the twice-weekly exercise program and the monthly education component.
Joint assessments with rheumatology specialized clinics are also provided locally using videoconference
allowing the clients to remain in their home community. There are currently no PT services provided at
the other Community Health Centre sites in Thunder Bay, Armstrong, and Longlac. There is opportunity
to provide PT services through Family Health Teams and the NorWest Community Health Centre similar
to the Mary Berglund Community Health Centre.
Community Exercise Programs
Rehabilitation services include the entire continuum of care from inpatient to outpatient services to home
care to ongoing community exercise. As described earlier, only exercise programs requiring service
provision from a regulated healthcare provider are included in the scope of this report. For the North West
LHIN, this includes the Community Exercise and Falls Prevention Classes delivered by Dryden Regional
Social Services in Dryden and throughout NWO (Thunder Bay, Atikokan, Emo, Fort Frances, Ignace,
Kenora, Sioux Lookout, Marathon, Manitouwadge, and Nipigon, Rainy River, Red Lake, Red Rock,
Schreiber, Terrace Bay) by VON. In addition to the exercise programs mentioned, SJH also delivers
disease-specific exercise classes for people in the City of Thunder Bay in the community, in partnership
with the Canada Games Complex and the 55+ Centre. Trained fitness instructors, not healthcare
professionals, deliver these classes and participants are all assessed and monitored by a PT. The
partnership also outlines the ability for the instructors to consult with the PT at any time. This model has
potential for ongoing exercise programming throughout NWO, in particular the remote communities in
the Far North.
Strengths, Gaps, and Limitations
Health service providers identified the availability of ongoing, supervised exercise programs as a strength
of the healthcare system within NWO; however, they suggested better marketing of the programs, better
integration with rehabilitation services at the hospitals and any private clinics, and better availability to
the remote, northern communities. In Dryden, PTs working in-home assist clients to transition to these
programs as part of their care.
Summary
Similar to inpatient rehabilitative care, outpatient rehabilitation provided within the community and
outpatient facilities in NWO will be standardized according to provincial norms. At present, outpatient
and community-based rehabilitative care programs in the North West LHIN are fully aligned with
provincial definitions.
Currently, there are several outpatient programs providing rehabilitative services in the region. These
programs provide examples of regional group-based service delivery, including OTN opportunities,
allowing clients to access specialized education and exercises within their home community, and remote
access to assessment and triage. Learning from the existing strategies, all specialized rehabilitation
programs should evaluate their service delivery for opportunities to provide regional assessment, triage,

84
and treatment services. In addition, it would be beneficial to integrate access to the visiting specialist
programs throughout the North West LHIN.
As a result of the many avenues to access outpatient services, there are frequent difficulties in
determining the most appropriate service for clients. Further complicating the referral process for
outpatient services is the requirement of a physician referral to access many programs. Wait times for
non-urgent appointments with primary care physicians range from weeks to months and thus the
requirement for a physician referral to access publicly-funded rehabilitation services is an added delay.
The combination of these factors has led to a system in which clients are often referred to multiple
programs, or inappropriate services. To help alleviate some of the difficulty surrounding eligibility
criteria for PT services, a detailed referral flow chart was developed by all stakeholders throughout the
North West LHIN led by SJH. This chart was designed to help guide clients to the most appropriate
service, while at the same time increasing awareness of the available services across the region (Appendix
O). It was also intended as a tool for primary care providers to assist them in referring directly to the most
appropriate service provider within the North West LHIN and was made available to outpatient service
providers for distribution to primary care referring partners. The dissemination and reinforcement of these
tools should be part of the implementation plan of the regional rehabilitation program. It is also
recommended the need for a physician referral should be eliminated whenever possible, especially when
clients are transitioning between levels of care for the same issue.
In order to integrate services and improve access across the region and the care continuum, it is
imperative all services are aligned, from regional providers to LHH providers, and inpatient teams,
specialized services, and outpatient services. This connection and ongoing communication will ensure all
clients are able to easily access regional specialized programs and local rehabilitation services in their
home community or as close to home as possible. In addition, this connection will ensure as client
demographics and available programs change, clients will continue to receive the care they require in a
timely, coordinated manner.
85
Health Human Resources
The provision of rehabilitative care services is largely dependent on regulated healthcare providers within
each facility. Direct service providers are a significant strength within rehabilitative care in NWO.
Through the capacity planning process, it is clear client needs are placed at the highest priority within
each care facility. Further, the clinicians providing care have demonstrated the tenacity to work with
limited resources, ongoing staffing challenges and, at times, minimal supports.
Throughout these challenges, the strength of individual care providers and collective creativity in care
provision has developed. This creativity is a significant strength and, with some encouragement, can be
directed into a collective rehabilitative care system to serve the entire region. Currently, collaboration
occurs on a localized scale within rehabilitation networks formed in the District of Thunder Bay and west
of Thunder Bay including District of Kenora, District of Rainy River, and Northern IDNs. These groups
meet on a quarterly basis to support care provision, education needs, and collaborate as providers. Further
coordination of these groups into a regular LHIN-wide collaboration will serve to strengthen the
connections and knowledge sharing across our entire region.
One of the primary challenges in providing care within NWO is the ability to maintain a steady
compliment of allied healthcare providers within each facility. The HSPs throughout the North West
LHIN have partnerships with academic rehabilitation facilities, in particular McMaster University and the
Northern Ontario School of Medicine (NOSM), to facilitate clinical teaching for students. This is a source
of recruitment as well as a retention strategy for rehabilitation professionals. The Northern Studies Stream
academic portion of McMaster University for both OT and PT was recently discontinued. This eight-
week academic block followed by a six-week clinical placement program was highlighted as a key
recruitment and retention strategy for rehabilitation staff throughout NWO. The program was
discontinued in a cost-savings measure, as it was determined recruitment is no longer an issue in the
North. The loss of this program was reported as a concern for future recruitment and retention during
engagement sessions.
Due to the low volumes in smaller facilities, there is not always a need for full time professionals.
Healthcare providers in NWO are often working in multiple locations or across a variety of services,
which further challenges the already difficult process of recruiting and retaining healthcare professionals
to remote and northern regions. A specific examination of OT, PT, and SLP availability is necessary in
the review of rehabilitative care. The current allotment of allied healthcare providers is provided in
Appendix P. This information is based on a current snapshot and frequently fluctuates. In the region,
allied health staff is generally shared between inpatient and outpatient programs and will at times work
within Family Health Teams, and/or provide care through the CCAC, in order to maintain a full time
equivalent (FTE) position. The CCAC contracted rehabilitative services may have to travel to a number of
communities in order to provide service and provide service across age groups, from children to adults.
The low population density and large geography make it difficult for clients to access care and for
providers to meet the needs of clients in the region.
One unintentional benefit of service providers working across the continuum of care is the continuity of
care for clients. The inpatient PT may also be the outpatient as well as the CCAC contracted provider.
Therapists noted client transitions were smooth, coordinated, and efficient as client rapport is already

86
established and access to information and communication is easily facilitated. There are occasions when a
sole service provider negatively influences client provider choice while accessing care. However, the
same therapist is most often advantageous for both clients and healthcare providers, especially if it allows
the service providers to pool resources and offer a full-time position.
Staffing considerations are important when evaluating the opportunity to provide rehabilitative care. All
four definitions of rehabilitative levels of care require some degree of interprofessional care, but the
rehabilitation level requires a coordinated, interprofessional rehabilitation plan of care with a team which
should include: dietitian, discharge planner, nurse, OT, pharmacist, PT, physiatrist and/or geriatrician,
social worker, and SLP. The gap in OTs in the District of Thunder Bay and lack of SLPs throughout the
North West impacts the provision of rehabilitation. The recent addition of funding for Assess and Restore
programming by the North West LHIN has supported positive increases in service provision such as an
OT in Kenora, a SLP in Dryden, and a Kinesiologist in Sioux Lookout. Best practice guidelines for Spinal
Cord Injury and Acquired Brain Injury and QBP guidelines for stroke and hip fracture specify the needs
for adequate interprofessional staffing and sufficient client volumes in order to provide the prescribed
level of care. In order to maintain adequate staffing to provide the required levels of rehabilitative care,
consideration must be given to providing full-time, permanent positions to attract the required
rehabilitative professionals.
Where it is virtually impossible to recruit regulated health professional rehabilitative staff, it is worth
exploring creative use of rehabilitation assistants or extended role personal support workers to provide a
minimum level of care under the guidance of the regulated health professional. Professional Regulator
College standards need to be carefully considered when exploring these models of care; appropriate
training, supervision and maintenance of skills needs to be implemented; and appropriate funding is
required to match the increase in service provision for both volume and skill. It is important an integrated
rehabilitation system across the region is nimble enough to provide the appropriate care for the client in
times of health human resource shortages.
Special Consideration for Northern and Remote Issues in North West LHIN
As noted in the demographics and population health section on page 21, a large geographical area, small
population numbers, and poor social determinants of health when compared with the rest of the province
of Ontario, challenge the North West LHIN. Furthermore, the North West LHIN services 32 Northern,
remote Aboriginal communities with the same challenges, only amplified. These communities are
accessible only by air. The communities vary in size from less than 100 people to approximately 3,000
people. Issues related to access, intergenerational trauma, and racism further challenge the social
determinants of health. To complicate matters further, healthcare and related rehabilitation care in these
communities is funded by multiple agencies including Health Canada, NIHB, and OHIP, which must be
navigated. While each community is unique, there are some commonalities.
The federal government is the primary provider of health services on reserves. The Home and Community
Care Program (HCCP) is funded by the First Nations and Inuit Health Branch (FNIHB) of Health Canada
to assist people who have chronic and acute illnesses or disease to receive the care they need in their
home or community. The amount of funding allocated to each community through Health Canada’s
87
Primary Care or HCCP budgets is population-dependent based on 1997 Indigenous and Northern Affairs
Canada population statistics. Rehabilitation services are not funded as an essential service under the
HCCP and therefore are only provided if budget and staff capacity allow, making it difficult for small
communities to provide most of the required rehabilitation services. There are some communities within
Ontario who have partnered within their treaty organizations or tribal councils to share resources and are
therefore able to provide more services. An example of this is Dilico, an in-home service provider for
nine communities. With amalgamated funding, Dilico is able to provide a nurse to multiple communities,
contract PT, OT and SLP services, and are even piloting a part-time care coordinator in the TBRHSC to
assist with discharges from this facility. The combination of multiple funding sources and different
providers make it difficult to coordinate care for the rest of the Aboriginal communities in the North
West.
Throughout most of the far north, access to rehabilitation is relatively non-existent. There are currently
only three PTs (no OTs or SLPs) servicing only 10 of the 32 communities, every two to three months. To
be effective and provide service for both in-home and outpatients, teaching family, clients, and existing
staff to carry out programs and providing general exercises throughout the community is required.
Unfortunately, the inconsistent presence of rehabilitation service providers presents the same challenges
to care transitions and communication outlined in the inpatient section of this report.

88
Communication between health service providers has been identified as a major issue impacting the
continuity of care for all residents of the North West LHIN, but is exemplified in the remote Aboriginal
communities. There is often a gap in communication when an Aboriginal community member is
discharged from a hospital to return to their home on reserve. One stakeholder noted: “when our clients
are discharged from the hospital, the tie is severed.” Another noted: “There is an information void!” They
are often not informed when one of their community members is set to return home from the hospital.
These communities have no access to the common electronic medical record. There is no clear transition
or formal hand-off from the hospital to the providers on-reserve as there is often no appropriate follow-up
provider with which to connect. To complicate matters further, each community is unique in their
relationship between the nursing station and the HCCP. Rehabilitation providers at the hospitals often do
not know who the appropriate contact is for each Aboriginal community regarding making arrangements
for home care and any possible ongoing rehabilitation once the individual is discharged. In some
communities, there may be multiple service providers who each play a role in coordinating home and
community care. There is also a concern for respecting the individual’s privacy and maintaining
confidentiality. Home and Community Care Program staff and workers in the Band’s Heath Department
are often inappropriately not included in the Circle of Care communication. There is currently a “patient
portal” project in Thunder Bay for clients identified with high healthcare needs. This portal provides a
secure system for providers and the client to upload and have “read only” access to information such as
discharge plans, lab results, etc. This portal system has the potential to improve communication and client
care in Northern and remote communities. Communication with all appropriate parties takes time, but is
essential to have accurate, complete information.
It is current practice to transfer clients to Meno Ya Win Health Centre in Sioux Lookout for a short time
prior to final discharge home. Meno Ya Win Health Centre is unique in that it provides medical services
to approximately 32 Northern Aboriginal communities. Meno Ya Win has a hostel, traditional healing
room, and available interpreters, in addition to traditional hospital services which are helpful to support
more complicated discharges. When discharging to northern communities, it can be challenging to
coordinate services and equipment as each community operates independently and NW CCAC does not
provide service on First Nations. Follow up PT can be arranged in some communities but not all, and OT
follow up services are not available. Clients who no longer require acute hospital services are transferred
to the hostel attached the hospital; this way, the client can continue with the Assess and Restore
interventions twice a day and maximize their gains prior to returning home. A social worker coordinating
discharge planning is aware of the community services available.
Issues with accessing equipment for clients and having clients and families access rehabilitation at the
appropriate location challenge rehabilitation staff. Consultation with stakeholders from various service
providers, funding agencies, tribal councils, and Aboriginal liaisons at the North West LHIN confirmed
these identified areas of concern and ongoing inconsistent interpretation of legislation. Examples include
the NIHB medical travel and medical equipment policies; and the lack of provision of services by CCAC
to Aboriginal communities, both rural and remote.
Currently, Assembly of First Nations and FNIHB are jointly reviewing NIHB nationally. Of relevance are
the medical transportation benefit and medical supplies and equipment benefit policies. Input from
rehabilitation agencies across the North West LHIN have been submitted (including submissions from
89
SJH) expressing concern and recommendations regarding access to services. The concerns outlined in the
submission were also highlighted during this stakeholder engagement session. As noted earlier, there are
often no, and at best very limited, local rehabilitation services in most of the Aboriginal communities in
the Northern IDN. Access to any of the aforementioned publicly-funded programs at the hospital or CPCs
require transportation by plane and local accommodations. At present, most outpatient appointments for
rehabilitation do not qualify for NIHB travel and accommodation funding due to a lack of OHIP billing
code. As stated, most outpatient rehabilitation services and specialized regional services are provided
within a hospital global budget. Without funding for travel and accommodation, these services are not
accessible to the community members due to the sheer cost of travel. While it is acknowledged there is a
process in place for clients to make appeals regarding NIHB decision, this process results in further
delays in accessing service and the inefficient use of scarce health human resources to navigate the
system. Medical Transportation is essential to access rehabilitation services for most Aboriginal people in
the North West LHIN.
In addition to access for the client, the Medical Transportation Benefit also provides transportation and
accommodation for family members as medical escorts. Healthcare providers rely on informal family
caregivers to assist with rehabilitation recommendations throughout the continuum of care at home. It is
essential these family members be recognized as a part of the rehabilitation team, with the client and
healthcare providers. Their involvement also helps improve communication.

90
The second benefit under review is the Medical Equipment and Supplies Benefit. Equipment needs are
also highlighted as a particular challenge. Other LHHs in the North West LHIN noted difficulties with
vendors delivering equipment twice a week; however, for these northern Aboriginal communities there is
no availability of rental equipment at all. Home and Community Care programs are required to provide
the necessary short-term equipment, but the budget is very limited. Healthcare providers (when available)
complete prescriptions for personal equipment, but the approval process for the necessary equipment is
time-consuming. Provincial and personal funding programs are accessed first, often with a four to six
week approval process, before being submitted to NIHB for approval, which involves another four to six-
week approval process in many cases. In addition, NIHB equipment prescriptions require extensive
personal information and medical justification, which is not congruent with current privacy legislation.
Furthermore, the Northern and remote environment requires the appropriate equipment with more regular
maintenance (which is unavailable) or replacement sooner. Recommendations to streamline the
equipment approval process have been outlined in the review submission.
Over recent years, there have been funded pilot projects to improve access to rehabilitation services in
Aboriginal communities. Initiatives such as the Moving on After Stroke (MOST) program connection
with Sandy Lake First Nation, the Sandy Lake Community-based Primary Stroke Prevention Program,
and the Rheumatic Diseases visiting therapist program in Fort Hope are examples of outpatient services
with extended access to remote communities in a limited capacity. While these programs have
demonstrated success in partnering with a specific community, several initiatives to increase the
availability of local service provision within remote northern communities have failed to have long-term
sustainability.
Trials to provide tele-rehabilitation consultations were successful from the telehealth studios in the local
nursing station but not without challenges. Challenges included the bandwidth required and availability
for some communities, the availability of consistent and reliable staff to manage the program as well as
support the client appointments, ongoing training requirements due to staff turnover, and in some
communities, access to operational equipment. Trials with an in-home camera were more challenging due
to the complicated technology and extra security measures required. Barring these issues, there is a huge
potential to provide telemedicine follow-up appointments with rehabilitation staff after hospital
admissions, visits to outpatient clinics, or after local therapist visits, to improve access to rehabilitative
care.
The need for ongoing communication and development of relationships with each of the unique
communities, although essential, takes time. Everyone has a right to culturally safe care in their own
language and access to their traditional healing practices. Regardless of improvements in the processes
around rehabilitative care provision, there is a lack of access to these services for the Aboriginal
population in the North West LHIN. The provision of rehabilitation services is an essential part of the
healthcare continuum and this gap needs to be addressed.

91
Desired Future State
The vision for NWO is to create a system of care which will serve all individuals who could benefit from
rehabilitative care. The system will respond to the needs of the individual and their family and caregivers
as well. A full continuum, of care will be available from inpatient rehabilitation to outpatient
rehabilitation and community reintegration all within a chronic disease management framework. All
individuals, regardless of their care setting, will receive care that is client-centred, culturally safe, focused
on enhancing quality of life, delivered by an interdisciplinary team, and close to home. Individual and
family needs will be identified early to engage them as partners in all care planning and decision-making.
A model for rehabilitative care cannot be developed in isolation from the system as a whole. The desired
future state of rehabilitative care described here has been developed in alignment with the North West
LHIN Blueprint integrated health service delivery model and within existing resources. As noted earlier,
the province’s healthcare allocation model is primarily population-based. It is anticipated the North West
LHIN growth rate will remain below provincial averages and, as such, no funding increase is anticipated,
except for provincial initiatives, such as Palliative Care. The North West LHIN Blueprint recommends
identifying opportunities to meet increased demands for health services within existing resources. Within
an integrated model of care, healthcare providers across the region work together to organize services and
delivery of care.
Within NWO, delivery of services is organized across the following levels:
11. Fourteen Local Health Hubs (LHH) which provide services based on unique needs of their communities.
12. Five Integrated District Networks (IDNs) with District Health Campuses which provide specialist care to clients within the district.
13. Specialized regional programs that serve all of NWO.
Figure 3. North West LHIN Health Services Blueprint Integrated Services Delivery Model

92
Each LHH, in conjunction with the Regional Rehabilitative Care Program, will arrange for the provision
of a coordinated continuum of rehabilitative care services. Specialized regional programs focus on high
cost, high complexity, and high impact services to ensure the provision of specialized care throughout the
North West LHIN. These programs may be delivered at the local level, or in a regional centre. Regional
programs are determined largely on the ability to deliver care based on best practices, including
provincially recognized QBPs. Figure 4 visualizes the structure of this integrated system.
Figure 4. North West LHIN Regional Rehabilitative Care Program Model – Integrated System of Care
The Hub and Spoke model of care is not new to healthcare and is typically implemented in rural and
remote areas where larger centres have more specialized and comprehensive services (the hub) than the
smaller, remote communities (spokes) where population, economies of scale, recruitment, and retention
do not support the same level of care. The model aims to formally integrate rehabilitation services across
the region by leveraging existing services and expertise from a hub centre to enhance and support existing
services in each spoke community. Northwestern Ontario fits the profile with a large area and many rural
and remote communities, and therefore would benefit from this model of rehabilitation service delivery.
Within the current state evaluation of rehabilitative care in NWO, the need was identified for an
integrated delivery model to increase coordination within and across all levels of care. The North West
LHIN is currently in the demonstration phase of implementing Integrated Health Care Organizations
(IHCO) who will provide end-to-end integrated services at the local level. Within rehabilitative care, this
will include inpatient, outpatient, and community rehabilitative care in addition to local chronic disease
93
management. Each IHCO will be responsible for coordinating local services and ensuring appropriate
care provision is available within each LHH. Collaboration between specialized rehabilitative care
services and the described regional service delivery model will ensure client needs are met as close to
home as possible.
This model will promote improved access and better transitions in care by encouraging integration within
each level, and across all levels of care. The overall goal of an integrated system is to provide excellence
in care, built on a vision of improved access and flow, standardization, coordination, and the use of
evidence-based care to improve the client journey.
The following information provides an overview of the key elements included in the future state of
rehabilitative care in the North West LHIN. The future state model has been developed to build on the
existing strengths of the current system, and help to overcome the gaps in care delivery identified within
the current state analysis. Overall, the future-state model of rehabilitative care will align with the future
state of healthcare within the North West LHIN. This will include defining the rehabilitative care lead
organization, implementing regional rehabilitative care streams roles, specific focus on enabling
flexibility in local hospitals to meet care needs, establishing partnerships with the IHCO’s, identification
of regional programs, and improving regional access to all rehabilitative care services.
Regional Rehabilitative Care Lead Organization
Within the integrated health system model, leadership is critical for coordination and planning, over and
above of service delivery. Lead organizations require the necessary human and capital resources to
develop a sustainable system for rehabilitative care throughout the region, facilitating access to
specialized programs and services for the residents of the North West LHIN within the Chronic Disease
Management framework. In addition, the Regional Rehabilitative Care Lead is intended to provide
support to both clients and clinicians throughout the five IDN’s. The foundation for successful integration
of rehabilitative care will be largely dependent on collaboration and joint planning between the Regional
Rehabilitative Care Lead Organization, LHHs, and IHCOs. Formal structures to support communication
between these organizations will be required to ensure a seamless journey through the various stages of
rehabilitative care, ensuring each client has access to the right care, at the right time, and in the right
place.
The Regional Rehabilitative Care Lead Organization will:
• Be recognized as leaders in enabling evidence-based care throughout the North West LHIN.
• Be recognized in the LHIN and provincially as demonstrating innovation and leading practice.
• Be able to change and embrace new thinking and successfully fulfill the role of early adopters.
• Work with the North West LHIN to implement the recommendations of this plan.
• Work with the North West LHIN to implement the plan to align with provincially mandated
definitions of rehabilitative care.
• Ensure care is based on evidence and leading practice throughout the North West LHIN.

94
• Support collaboration and capacity building at the HSP, LHH, IDN, and Regional levels.
• Provide advice and advocacy to the North West LHIN on identified local and regional service
gaps, strengths, and priorities.
• Demonstrate strong partnerships and involvement in healthcare education and research.
• Lead the development of a standardized, quality, and integrated approach to rehabilitative care
across the continuum of care for the North West LHIN.
• Monitor, evaluate, and report on system performance and client and caregiver outcomes.
• Have the demonstrated ability to establish effective partnerships with both LHIN funded and non-
LHIN funded providers.
• Have the capacity to deliver LHIN-wide mandates for standardization, quality, and integration
across the continuum of care.
Within the North West LHIN, a primary role of the Rehabilitative Care Lead will be to facilitate
information and knowledge sharing across all health disciplines, and to ensure a minimum level of service
is available for all clients regardless of human resource limitations. In order to provide this level of
support, the Rehabilitative Care Lead organization will identify interprofessional care teams for each of
the Care Streams (see page 99) that consist of rehabilitation professionals who will be available to provide
assessments and consultation with regional providers as required. In addition, each care stream will have
identified leaders, a consistent contact and knowledge exchange expert for clinicians throughout the
region. This role will also help to develop regional communication networks for clinicians. As noted in
the Health Human Resources Section, rehabilitation networks already exist within and between IDNs to
support care provision, education needs, and collaborate as providers. Further expansion of these groups
into regular LHIN-wide collaboration opportunities will serve to strengthen the connections and
knowledge sharing across our entire region.
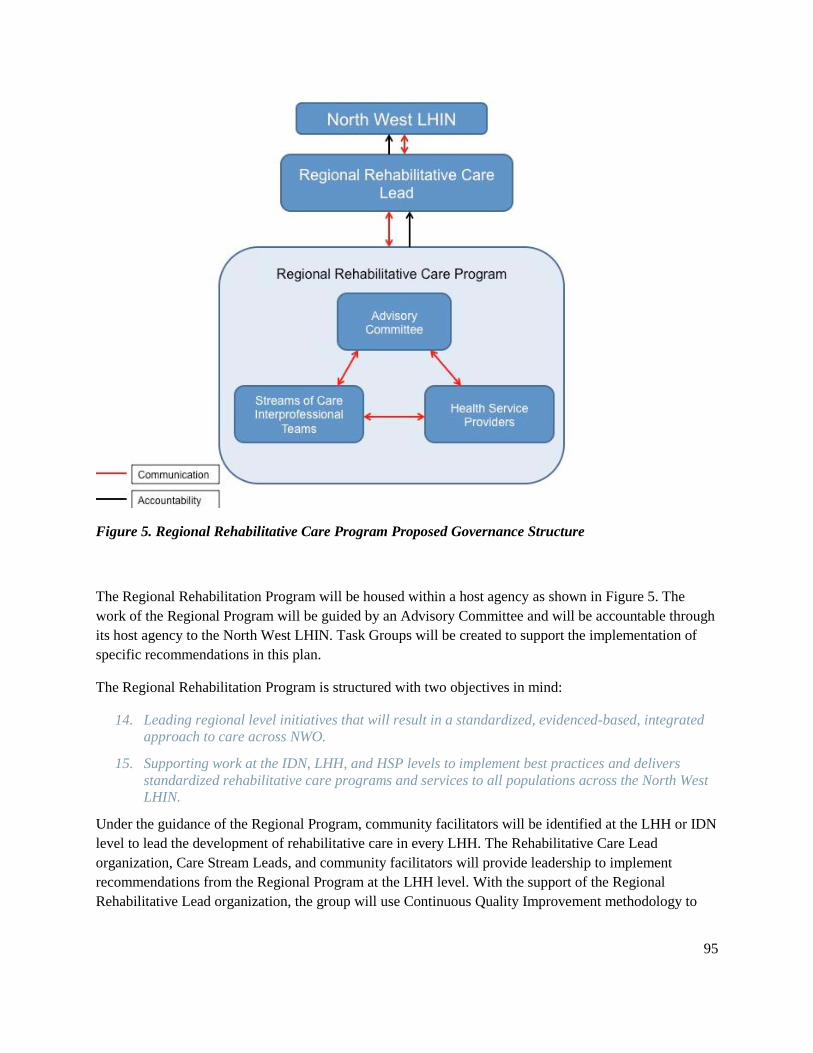
95
Figure 5. Regional Rehabilitative Care Program Proposed Governance Structure
The Regional Rehabilitation Program will be housed within a host agency as shown in Figure 5. The
work of the Regional Program will be guided by an Advisory Committee and will be accountable through
its host agency to the North West LHIN. Task Groups will be created to support the implementation of
specific recommendations in this plan.
The Regional Rehabilitation Program is structured with two objectives in mind:
14. Leading regional level initiatives that will result in a standardized, evidenced-based, integrated
approach to care across NWO.
15. Supporting work at the IDN, LHH, and HSP levels to implement best practices and delivers
standardized rehabilitative care programs and services to all populations across the North West LHIN.
Under the guidance of the Regional Program, community facilitators will be identified at the LHH or IDN
level to lead the development of rehabilitative care in every LHH. The Rehabilitative Care Lead
organization, Care Stream Leads, and community facilitators will provide leadership to implement
recommendations from the Regional Program at the LHH level. With the support of the Regional
Rehabilitative Lead organization, the group will use Continuous Quality Improvement methodology to

96
plan, implement, and evaluate initiatives to address specific gaps in their communities and then spread the
initiatives across the North West LHIN.
It is essential the Rehabilitative Care Lead organization help to facilitate access to rehabilitative care
resources and facilitate the future development of regional resources as required. Due to the ever-
changing state of rehabilitative care and availability of services in the region, it is essential the
Rehabilitative Care Lead organization remain aware of changes in the state of rehabilitation across the
region. This organization will additionally act as an advocate for rehabilitative care in the North West
LHIN among provincial stakeholders and be active in the RCA to ensure the needs of NWO residents are
being met.
Care Streams
As outlined above, examination of the current rehabilitative care system in NWO has indicated the need
for a formalized, integrated, and coordinated system to support specialized care across the region between
the three levels of care. This type of system will provide support to local healthcare providers and clients,
thus enabling clients to receive specialized care as close to home as possible. Due to the large geographic
areas, distances between service locations, and scarcity of resources, a single therapist is often responsible
for all clients requiring care within their community. These healthcare providers function as generalists,
so the ability for clients to receive specialized care within their community is often limited. In order to
support care as close to home as possible, three regional care streams will be implemented within NWO.
These care streams will support best practices, QBP adherence, and availability of specialized
rehabilitation for all clients. In addition, the care streams will provide opportunities for interprofessional
care teams consisting of rehabilitation professionals with detailed knowledge of diagnosis-specific
resources available within the region to provide assessments, triage, and consultation with regional
providers as required. Based on RCA bedded levels of rehabilitative care definitions, existing care
pathways, and client care needs, the following primary care streams will meet the specialized care needs
of NWO:
• Geriatric Assessment and Rehabilitative Care.
• Specialized Rehabilitation (Neurological, Stroke; Orthopaedic and Musculoskeletal) Services
Stream.
• Medically Complex Services (Wound, Lymphedema, Pulmonary, and Chronic Disease).
These care streams will maximize current high priority areas of rehabilitative care and available local
specializations. See Appendices Q-T for details. While clients may present with multiple medical
conditions, it is anticipated each client requiring ongoing rehabilitative care will align with one of these
streams for their primary condition.

97
The identified care streams will leverage existing knowledge within NWO and will be linked directly to
the Rehabilitative Care Lead organization in order to ensure ongoing access to rehabilitative care from
anywhere in the region. Each stream will serve the following primary functions:
• Identification and triaging of all rehabilitative care needs through the use of a single point of
access and updated care pathways to determine the most appropriate location and level of care required.
• Assessment of individual clients to determine rehabilitative care needs and the most appropriate
location and level of care required.
• System navigation to allow clients and families to access the most appropriate rehabilitative care
program regardless of their referral location for the entire care continuum.
• Access to specialized physician services including assessment and treatment in the most appropriate location including technology-based support and outreach.
• Provision of rehabilitative care interventions at appropriate intensity, duration, and mode, by
appropriate professional team, in appropriate location including technology-based support and outreach.
• Development of resources and provision of education to clients and clinicians in order to provide
specialized evidence based practice.
• Support to regional care providers for complex, specialized clients.
• Support transitions between care locations to ensure clients access the most appropriate services,
including a designated inpatient rehabilitation program if required and transitions to primary care,
home, or community programs.
• Development of partnerships locally and provincially to support evidence-based care, innovation, and research.

98
Figure 6. Roles of Care Streams with an Integrated Regional Rehabilitative Program
Screening Assessment Intervention Transition Navigation
Identification of
Clients with
Rehabilitation
Needs
Primary Care
Providers
ER/ Hospitals
Community and
Regional Agencies
Rural and Remote
Communities
Central Intake
Triaging and
information
gathering by phone
Determine most
appropriate care
stream
Within care stream,
determine required
services and
availability in LHH
vs. IDN vs. regional
program
considering
inpatient vs.
outpatient and use
of telehealth
Determine those not
requiring service;
referrals back to
Primary Care or
onto other
community
programs
Basket of
Services
Group or individual
rehabilitation at
appropriate
intensity, duration,
by appropriate
professionals
Inpatient or
outpatient care
In-home rehab and
health support
(RPN/CCAC)
Appropriate location
with use of
technology as
appropriate
Provision of
education, supports,
and resources as
needed for ongoing
care needs to both
client/family and
rehabilitation care
providers at LHHs
Planning for
Care
The team works
with client/family to
review needs and
options along the
continuum of care
Reevaluate Level of
care (Inpatient,
Outpatient, and
Community) and
availability of
required services in
LHH vs. IDN or
Regional program
Ongoing support at
time of transitions
between locations
and levels of care
CCAC involvement
for home service
coordination as
required
Decision
Guidance
The team identifies
a main contact for
client and family
until services end
Clients and
caregivers can call
back to Central
Intake if they
require service if
service ends
Comprehensive
Assessment
Single service
rehabilitation
professional OR
Specialized team of
rehabilitation
professionals
including:
Geriatrician,
Psychiatrist,
physiatrist, PT, OT,
SLP, nurse, social
worker, pastoral
care, dietitian and/or
therapeutic
recreationist
Transition to
Home
Short-term follow
up by individual or
team service
CCAC in-home
rehab service if
required
Transition to
Primary Care
Primary care
provider to follow
If client does not
have a provider,
team to assist that
link
Specialist may
follow in the interim
Transition to
Community
Programs
Other community
programs (Falls
Prevention, Keep
Moving with
Stroke, Parkinson’s,
Day Centres,
Alzheimer’s
Society, etc.)
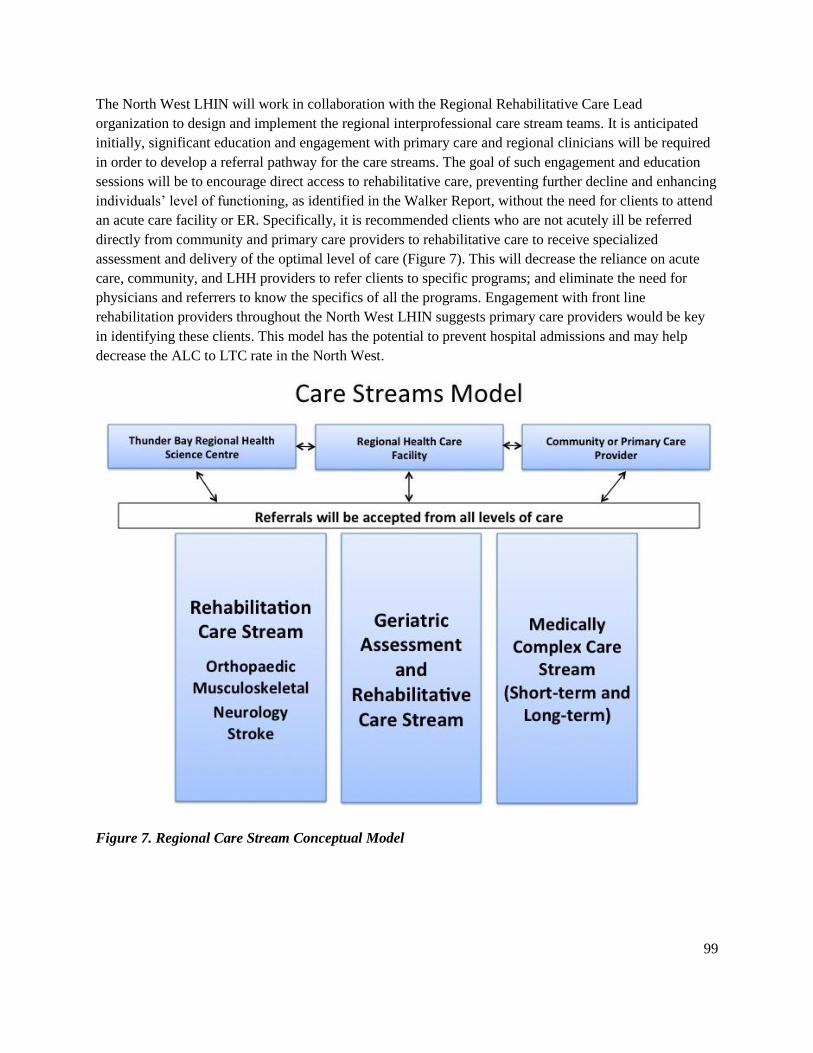
99
The North West LHIN will work in collaboration with the Regional Rehabilitative Care Lead
organization to design and implement the regional interprofessional care stream teams. It is anticipated
initially, significant education and engagement with primary care and regional clinicians will be required
in order to develop a referral pathway for the care streams. The goal of such engagement and education
sessions will be to encourage direct access to rehabilitative care, preventing further decline and enhancing
individuals’ level of functioning, as identified in the Walker Report, without the need for clients to attend
an acute care facility or ER. Specifically, it is recommended clients who are not acutely ill be referred
directly from community and primary care providers to rehabilitative care to receive specialized
assessment and delivery of the optimal level of care (Figure 7). This will decrease the reliance on acute
care, community, and LHH providers to refer clients to specific programs; and eliminate the need for
physicians and referrers to know the specifics of all the programs. Engagement with front line
rehabilitation providers throughout the North West LHIN suggests primary care providers would be key
in identifying these clients. This model has the potential to prevent hospital admissions and may help
decrease the ALC to LTC rate in the North West.
Figure 7. Regional Care Stream Conceptual Model

100
Figure 8. St. Joseph’s Hospital Care Stream Model

101
When it is determined a client requires rehabilitative care, they will be referred to the most appropriate
care stream using a central intake or single point of access. A screening process will determine the
appropriate location and level of care for assessment and care planning. For specialized or complex
rehabilitation needs, clients would access an assessment by an interprofessional care stream team at St.
Joseph’s Hospital using specialized knowledge of their primary rehabilitative care area and a foundation
in Chronic Disease Self-Management. Given the client’s rehabilitation needs, goals, and home
community, the most appropriate level of care and program will be determined. Interprofessional care
within each stream will include access to a team including (as required): OT, PT, SLP, Social Worker
(SW), Dietitian, nursing, specialized physician/Nurse Practitioner (NP), and any other condition-specific
disciplines. Through the use of standardized assessments, communication tools, and care practices, each
team will be able to support client care across the continuum of rehabilitative care including inpatient,
outpatient, and community settings.
To support service delivery, the care streams will have a knowledge exchange strategy. This knowledge
exchange strategy will be supported by the Regional Rehabilitative Care Lead Organization and will
include the following: identified clinical and specialist physician leads, an accessible website, and an
annual retreat. The identified leaders will be a consistent contact and knowledge exchange expert for
clinicians throughout the region. Using the Rapid Access to Consultative Expertise (RACE) model,
clinicians throughout the North West LHIN will be able to connect via telephone for urgent questions and
consultations and use e-consultation for non-urgent questions and consultations. The care stream leads
will also have rapid access to professionals within the team such as physiatrists, rheumatologists, and
geriatricians, should the consultation require a more profession-specific focus. A model similar to this is
in place for the North West LHIN Regional Palliative Care Program, providing access to clinical expertise
on a 24/7 basis using SJH Palliative Care Unit as a resource. This model supports provincial and local
values including access, decision-making, clinical judgment, education, knowledge transfer, and practice
efficiencies, as well as alignment with the Triple Aim Principles of enhancing the care experience,
improving population health, and controlling per capita costs of healthcare.
A website is another platform for referrals (healthcare provider only portal) and information sharing
regarding best practices, program descriptions, community resources, contact information, and self-
management resources for clients, families, and healthcare providers. It is essential the website be
accessible in both English and French languages due to the demographics of our region. This will require
significant time and investment and therefore a phased in approach is recommended.
The final component of the knowledge exchange platform is an in-person annual retreat hosted by the
Rehabilitative Care Lead organization. This forum will build capacity and provide an opportunity for best
practice updates, case study discussion, clinical skills training, and practical advice about data collection,
assessment, and treatment updates for each of the care streams. The hands on education components of
this forum will be helpful in addressing the knowledge, skill, and rehabilitation culture gap for nurses
throughout the North West LHIN as identified during stakeholder engagement. An additional component
of this annual retreat should be clinical education, an opportunity to leverage existing partnerships with
NOSM and provide assistance with long-term planning recruitment and retention. Most importantly, the
retreat will provide an opportunity to network and connect with one another in person, which will
improve future communications required for effective client transitions and an integrated system.
102
Within the broader scope of rehabilitative care, the care stream teams/leads will communicate with the
Regional Rehabilitative Care Lead organization and district IHCO’s and LHHs to continually monitor
available inpatient, outpatient, and community programs, and to establish regional programs to increase
access to evidence-based care via outreach as per the Regional Rehabilitative Care Program governance
structure.
It is expected the outcomes of the care stream model will be improved access to the most appropriate
rehabilitative care program for each client as close to home as possible, improved transitions for each
client with improved communication among the care team, increased access to best practice and QBP
recommendations for all clients and clinicians, and a clear care path for every client who requires
rehabilitation in the North West LHIN.
Flexible Inpatient Beds at the DHC and LHH Levels
In order to meet the continually changing needs of regional facilities, the future state model of
rehabilitative care will be flexible. It is essential the care system within the DHC and LHH levels be
designed to allow flexibility of care for each individual client. As identified in the Walker Report, instead
of aligning specific levels of care to pre-determined beds, facilities will adapt their resources to meet the
needs of the population. Rehabilitative levels of care will be determined on an individual basis and the
appropriate level of rehabilitative care will be provided to the client, regardless of the “bed” definition.
At present, the majority of rehabilitative care provided outside of the City of Thunder Bay occurs within
designated acute care beds; beds allotted for CCC are being utilized for clients designated ALC to LTC.
Care providers throughout NWO indicate the appropriate level of rehabilitative care is being provided,
regardless of the bed definition. Tables 4 and 16 describe the current estimated bed days required for each
of the levels of inpatient rehabilitative levels of care. Interestingly, many of the estimates appropriately
match the current number of designated CCC beds.
Aligning with this approach, the proposed future system supports the independent assessment of each
individual requiring inpatient rehabilitative care. Clients will be identified as being “rehabilitative” once
they become medically stable and are no longer accessing care for acute medical management. At this
time, their medical, nursing, and therapeutic care needs will be evaluated and the level of care determined
according to the standardized bedded levels of care definitions (Appendix A). Identification of the most
appropriate level of care for each client will inform the amount of therapy each client will receive. For
example, if a client’s care needs align with the definition for Short-Term Complex Medical Management
level of care, the corresponding therapy provision will be based on the Short-Term Complex Medical
Management level of care therapy recommendations. This includes recommendations for therapy
frequency, discharges indicators, expected LOS, and required involvement of an interprofessional team. It
is essential each client receiving rehabilitative care be informed of the frequency of rehabilitation they
will receive in order to improve, according to provincial standards.
Adherence to this strategy will ensure regional facilities and the North West LHIN align with the
provincial standards for the provision of rehabilitative care. Overall, clients will receive the same care
regardless of where they reside within Ontario, as recommended by the Auditor General in 2013. It will
103
also assist in improved communication between clients, families, and caregivers regarding expected care
provision and create clear expectations for both clients and service providers.
Use of Technology in Care Provision
The care system in NWO has developed to provide service in innovative ways given the geographic
challenges. One of the biggest strengths of the North West LHIN is the availability and utilization of
technology to enhance care provision. While opportunities for utilization of technology continue to be
explored for rehabilitation, the availability of virtual care constitutes a significant strength. It is
recommended the use of technology to enhance care provision continue and be expanded where
appropriate. It is also recommended partnerships between Ontario Telemedicine Network (OTN),
Keewaytinook Okimakanak Telemedicine (KOTM), rural and remote northern locations and regional
partners, and care providers be utilized and nurtured to ensure the platform is used to its full capacity.
Using this available technology, several specialized programs are currently delivered throughout NWO,
providing care otherwise unavailable for many clients. Current programs and associated videoconference
processes are in place to support regional self-management education and exercise groups such as the
MOST program for stroke survivors and the Healthy Lifestyles program for specialized cardiac
rehabilitation. Both programs are delivered locally in Thunder Bay and available within most healthcare
facilities across the region via videoconference access. The desired future state will explore further
opportunities to deliver specialized programming locally with videoconferencing support and evaluate the
potential amalgamation of components of this programming, as appropriate.

104
Other technological platforms currently in place include OTN PCVC and “guest link”, which allow direct,
face-to-face video access between clients and clinicians who may be hundreds of kilometers apart. The
PCVC platform enables individual assessment and treatment through secure online connections from any
network connection: at home or in regional healthcare facilities, including nursing stations. Currently,
these technologies are being utilized to provide regional access to speech language therapy, wound care
consultations, fracture clinic appointments, and occasionally other assessments.
The PCVC technology supports a regional aphasia strategy. In response to limited availability of adult
outpatient SLP, a program was recently implemented at SJH to enable an outpatient SLP in Thunder Bay
to provide services to clients within remote communities through the guest-link system. This now permits
clients to return home and still access the care needed in the appropriate environment rather than being in
hospital. In fact, the opportunity to remain in a home environment while acquiring the necessary skills for
ongoing recovery allows people to practice speech skills on a daily basis.
Regional wound care consultations are another service provided at SJH using the PCVC technology. The
specialized wound care team includes: the client and a local health service provider to provide the
recommended care such as dressing changes, a registered nurse, a physician, and access to an OT, PT,
Social Worker and Chiropodist as required. The program leverages client appointments in Thunder Bay to
see the client in person but most of the care recommendations are conducted in the LHH with the
telemedicine nurse or using a secure OTN portal to upload pictures of the wound. Some clients are not
even required to leave their own home.
Another significant strength in NWO is the utilization of telemedicine visits for fracture clinic
appointments, health promotion, and follow-up. The use of telemedicine for these services prevents
inconvenient, time-consuming, expensive, and often difficult trips. With increased access for regional
clients, this service allows people to return to their home communities with the confidence their needs
will be met. Utilization of technology and the telemedicine infrastructure will continue to enhance the
ability of clients to remain in their homes or in their local community while receiving more specialized
care.
In order for individual video assessment and treatments to occur, there must be coordination of equipment
and the availability of dedicated, trained staff (ideally rehabilitation assistant) within each community to
assist with assessment and intervention being recommended by the offsite, treating therapist. These local
needs are one of the primary barriers to increased uptake of technology-based service provision at this
time. In order to increase the utilization of technology-based service provision, dedicated clinical and
clerical resources to provide remote care provision are required. Utilization of technology in conjunction
with the Rehabilitative Care Lead organization and Care Stream approach will enhance the access to
specialized care across the region and ensure every client in NWO has access to a minimum level of
rehabilitative care services.

105
Remote North Access to Care
In addition to the recommendations made throughout the described future state of rehabilitative care in
NWO, special consideration must be made to ensure equitable access to care is made available to clients
who live in remote and rural areas who do not currently have access to rehabilitative care within their
community. Despite small successful initiatives and several attempts to implement rehabilitative care
within Northern remote communities, there is ongoing difficulty with the development of a sustainable
model for rehabilitative care. At present, provision of rehabilitation services in remote communities range
from non-existent to very limited and funding for transportation is not available through the NIHB
program for clients who require assessment and intervention from an allied healthcare provider.
The inability to sustain consistent service provision within remote and rural communities is due to several
factors. One factor is the availability of local, trained, skilled service providers, as demonstrated by the
VON exercise programs. VON currently has a mandate of providing strength, balance, and falls
prevention programs to seniors within NWO. In 2014-2016, these programs have been unavailable in
remote Aboriginal communities due to inability to hire local employees. The VON program has the
capacity to provide fall prevention classes in remote communities using laptops and videos prepared by a
registered healthcare professional, but without adequate local support of an exercise lead, implementation
of this program has not been possible.
A similar finding was observed through the Assess and Restore First Nations Capacity Building project
completed in April 2015. The primary focus of this project was the development of a community-based
model to maintain activity for seniors and others living with chronic health conditions. The pilot project
included the development and implementation of a holistic, health-based afternoon program including an
exercise session with support from workers with the North Caribou Lake Home and Community Care
program. The afternoon provided an example of an effective rehabilitative care program within the North
Caribou Lake community. Presently, no further care has been provided in follow-up to this program;
however, a series of recommendations were developed. In order to build a sustainable program, the First
Nations Capacity Building project recommended development of partnerships with current service
providers within remote communities using the HCCP in order to increase their role in delivering exercise
programming.

106
The role of utilizing existing home care providers within local communities is well established in other
parts of Canada. Currently, this model of care is used in Nunavut and involves training community
therapists through the University of Winnipeg. These trained service providers are able to assist with the
implementation of exercises, facilitation of remote assessments, and provision of personal care services.
Through stakeholder engagement sessions, the utilization of local service providers to facilitate access to
rehabilitative care was further supported. It was recommended local service providers, with training as
personal support workers, would enable a sense of trust between the client and regulated healthcare
provider. This would facilitate participation in the assessment and treatment as well as bridging cultural
differences including language.
First and foremost, it must be confirmed that provision of rehabilitative care to remote and rural
communities is a Northern IDN objective. Current infrastructure and cultural services at Meno Ya Win
attest to their experience and expertise working in partnership with the Aboriginal communities in the
Northern IDN. Training and staff development for community care providers need to involve regulated
healthcare providers for rehabilitative care assessment and exercise prescription. It is recommended the
identified Rehabilitative Care Lead organization and Care Streams interprofessional teams partner with
Meno Ya Win to provide the necessary training and education for community healthcare providers.
Prior to the implementation of any training or service delivery model, an in-person engagement session
with each remote and rural community is required. It has been identified the adaptation of regional care
models to provide care in remote northern communities is often unsuccessful. In order to gain the trust,
commitment, and ongoing partnership with each community, a service delivery model must be developed
to meet the needs of individual communities. Community involvement in the development and delivery is
key to the success and sustainability of the model of care.
First, a detailed inventory of available resources within each community is required in order to attain the
benefits identified using existing community resources. In addition, it is important to ensure adequate
resources are available to provide rehabilitative care. It is anticipated additional Personal Support Worker
(PSW) or HCCP trained staff would be required. It is recommended rehabilitative care training be
provided for new and existing support care workers to enable their participation in rehabilitative care-
based assessments and interventions. To complement this initial training, it is recommended these
individuals have ongoing education and training with respect to best practices in care, and the
fundamentals of providing rehabilitative care exercises.
The long-term sustainability of any model of service delivery in NWO is dependent on the utilization of
technology-based care platforms. Through services such as OTN, KOTM, PCVC, and ‘guestlink’, service
providers will be able to provide assessment and treatment from a remote location, preventing the need
for extensive travel. This system of remote assessment and treatment is similar to the recommended
system to support access to specialized care within LHHs, and will require the use of a trained
rehabilitative assistant or service provider to provide on-site assistance for client assessments.
107
Overall, the recommended service delivery model for rehabilitative care in the rural and remote areas of
NWO will require significant communication, coordination, stable human resources, and reliance on
technology. Once rehabilitative care service delivery has been confirmed as a priority in the rural and
remote areas of NWO, there is an opportunity for the Regional Rehabilitation Lead organization to
partner with the rural and remote communities and Health Canada’s FNIHB. This equal partnership
throughout development is essential for the success of any program. Finally, funding agencies must
recognize and approve rehabilitative care, resources must be shared across care models, and
communication between care provision and funding organizations will be required.
Francophone Access to Care
Every person deserves healthcare to be provided in a culturally safe way. The North West LHIN has a
multi-cultural population and every attempt should be made to provide care, documentation, and
information in the person’s first language. Specific to the North West LHIN, there is a significant
Aboriginal population noted above and although not as large, there is a sizable Francophone population,
especially in the District of Thunder Bay (13%). Engagement with this population has demonstrated they
are accustomed to service not being provided in their own language and consequently don’t often
complain. Therefore, it is recommended clients, whose first language is French, be identified as French
speaking and actively offered health service delivery in their first language. Health service providers
should self-identify their own staff who are Francophone or who have the ability to provide service using
the French language and every effort should be made to match the resources appropriately with clients.
As with all clients, care must be taken at times of transitions along the care continuum to ensure
information is accurately transferred in both languages to the next stage of rehabilitative care.
Francophone clients often prefer any documentation be provided in both English and French as they may
often only know the English word for healthcare terms. In addition, it is recommended any forms or
website information are accessible in both English and French. When internal healthcare providers are
unable to meet the needs of a Francophone client, it is recommended providers access the free healthcare
interpretation service L’accueil francophone for both accompaniment and translation services. These
services are available either in person or via telemedicine platforms.
It is recommended to continue working in partnership with the French Language Services Health
Planning at the North West LHIN to build capacity and disseminate the resources for the needs of this
population in order to provide accessible rehabilitative care throughout the North West LHIN.
Performance Measurement
The RCA and the MOHLTC have collectively identified outcomes that are to be achieved through
rehabilitation restructuring. The work of the Rehabilitative Care Regional Program will contribute to the
achievement of these outcomes for the North West LHIN. It is recognized progress toward these system
level outcomes will be slow but deliberate. Process and outcome measures will be identified to track
overall progress on the implementation of this plan. At the time of writing this plan, significant work on
data and performance indicators was still underway at the provincial level. These indicators will be
incorporated into the plan as they are developed.

108
Recommendations
Throughout the planning process, the complexity of moving from a current state to a future state delivery
model was discussed by committee members, care providers, and subject matter experts. It was
recommended that an incremental approach to implementation be adopted, first, addressing current
challenges and then build on current outreach programs. It was also recommended the model be scalable
and incremental, starting with the use of early adopter sites and initiatives where activity could slowly be
increased and evaluated in order to ensure changes are producing desired results.
In order to facilitate the transition to an integrated rehabilitative care model, a series of recommendations
have been developed. These recommendations are designed to meet the overall strategic priorities
required to improve rehabilitative care across the North West LHIN. With each recommendation, a series
of action items have been outlined to guide the specific changes required. Each action plan is
accompanied by a timeline within a three-year period. Within each action plan, the healthcare level
directly involved, as well as the specific deliverables and expected outcomes, have been identified (Table
34). Overall, the list of outcomes will demonstrate the key elements to be represented within the future
state model of rehabilitative care.
The following recommendations were developed to support the transition to an integrated model of
rehabilitative care. Through the implementation of the recommendations, it is anticipated clients across
the region will experience improved access to rehabilitative care services and flow through the
rehabilitative care system. In addition, access to specialized care, coordination, collaboration and
knowledge will improve for both clients and clinicians across the region.

109
Table 34. Implementation Plan
Action Items Healthcare
Level Deliverables Outcomes Status
Recommendation #1
Improve client experience and outcomes through the implementation of the RCA definitions framework to align rehabilitative care in the North West LHIN with the
provincial framework
1.1 Ensure there is regional alignment with
the RCA definitions frameworks for
bedded and community-based levels of
rehabilitative care
• Provincial
• Regional
• RCA Bedded and Community
Mapping Tool results
• Full alignment with approved
exceptions
• Plan for any alignment issues
1.2 Educate service providers regarding the
definitions
• Regional
• IDN
• LHH
• Education module on
rehabilitative levels of care
• Education module delivered in all
hospitals throughout North West
LHIN
• Increased knowledge &
understanding of rehabilitative levels
of care
1.3 Create an implementation schedule to
achieve alignment with RCA definitions
by March 2017
• LHIN
• IDN
• LHH
• Implementation Plan • Full alignment by March 31, 2017
• Plan for any alignment issues
1.4 Upon referral, establish a process to
determine the appropriate level of
rehabilitative care for each client and
the appropriate location of rehabilitative
care i.e. LHH, IDN and the region
• Regional
• IDN
• LHH
• Care stream process map
developed and shared throughout
the LHIN
• Regional Rehab referral system
piloted in 2 IDNs
• Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
1.5 Confirm the required health human
resources to provide each level of care
and the capacity of each health hub and
integrated network to provide the level
of care
• LHIN • Capacity Plan • Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
1.6 Establish a process to gather
information regarding the rehabilitative
• LHIN • RCA Bedded and Community
Mapping Tool
• Improved access to care
• Care as close to home as possible

110
Action Items Healthcare
Level Deliverables Outcomes Status
care provided by regional hospitals on
their inpatient unit.
• Completed community
engagement profile
• Regional Rehabilitation Health
Human Resources Table
• Capacity planning completed at the
LHH and IDN levels
1.7 Maximize Convalescent Care Bed use
to align with Activation/Restoration
Bedded Levels of Care by addressing
process issues related to barriers such as
IV medications, staffing resources, and
discharge location determination
• LHIN
• IDN
• LHH
• Working group established
between stakeholders to identify
and address barriers
• Process map developed and
shared throughout region
• Full alignment with
Activation/Restoration Level of Care
in IDNs with CCB
• Improved access to care
• Care as close to home as possible
Recommendation #2
Develop a LHIN-wide strategy to improve client access and client transitions across the continuum of rehabilitative care
2.1. Review current or create appropriate
diagnosis-specific client care pathways
based on best practices to support the
access and transition between inpatient
and outpatient services across the entire
North West region
• Regional
• Care Pathways
• QBP Heat Map for stroke, TKR,
THR, Hip #
• Care stream Leads established
• Appropriate LOS
• QBP optimization
• Improved access to care
• Improved client/care transitions
• Improved quality of care
• Care close to home
2.2 Develop a plan and implementation
strategy to improve transitions between
specialized rehabilitation services and
local services at either the IDN or LHH
level and transitions home
• Regional • Discharge process map
• Discharge checklist
• Standardized documentation
• Standardized referral form across
regional/IDN/LHH
• Standardized process for
accessing OT home visits post
discharge from hospitals
• Improved client care transitions
• Improved quality of care
• Clear documentation
• Enhanced communication among
providers
2.3 Improve direct access from primary care
and community care providers to both
inpatient and outpatient/community-
based rehabilitation programs
throughout the region
• LHIN
• IDN
• LHH
• Care pathways established:
community-hospital-community
• Coordinated referral management
system for rehabilitative care
• Improved access to care
• Decrease unnecessary ER/acute care
visits
• Improved quality of care
• Decrease ALC for LTC

111
Action Items Healthcare
Level Deliverables Outcomes Status
• Memorandum of agreement with
FHTs
• Frail Senior/Medically Complex
Care stream Lead
• Care close to home as soon as
possible
2.4 Evaluate opportunities for the
development specialized outpatient
programs to be delivered closer to home,
building on successful regional models
• Regional
• IDN
• LHH
• Care Stream Leads
• Specialized OP programs
delivered at IDN/LHH
• Provision of local temporary
housing as necessary
• Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
2.5 Strengthen connections between local
service providers and regional care
networks to provide support for LHH
provision of rehabilitative care
• Regional
• IDN
• LHH
• Annual Retreat
• Care Leads
• Health Human Resources Contact
List
• Enhanced communication amongst
providers
• Improved client care transitions
• Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
2.6 Develop a mechanism to share
information regarding and access to
visiting specialists programs to support
an integrated regional model of
specialized client care
• LHIN
• FHT
• IDN
• LHH
• Visiting specialist program
integration
• Care Leads/Care Streams
• Quality, evidence-based care
• Improved access to care
• Care as close to home as possible
Recommendation #3
Facilitate adherence to best practices for rehabilitative care to improve client-centred care
3.1 Build capacity to meet best practice and
QBP expectations at a local level though
knowledge-sharing across the region
• Regional
• IDN
• LHH
• Annual Retreat
• Care Leads/Care Streams
• Website
• Full QBP funding
• Quality, evidence-based care
• Improved quality of care
• Improved access to care
• Care as close to home as possible

112
Action Items Healthcare
Level Deliverables Outcomes Status
3.2 Strengthen and expand existing clinical
practice networks for rehabilitative care
providers to ensure an integrated model
exists across the Northwest
• Regional
• IDN
• LHH
• Annual Retreat
• Care Leads/Care Streams
• Website
• Quality, evidence-based care
• Improved quality of care
• Enhanced communication amongst
providers
• Improved access to care
• Care as close to home as possible
3.3 Develop a mechanism to share
information regarding best practices for
rehabilitative care throughout the region
(such as website and/or care streams
leads)
• Regional
• IDN
• LHH
• Annual Retreat
• Care Leads/Care Streams
• Website
• Quality, evidence-based care
• Improved quality of care
• Improved access to care
• Care as close to home as possible
Recommendation #4
Enhance utilization of innovative technologies to improve access to rehabilitative care services closer to home, particularly in remote and underserviced areas
4.1 Develop a process to support and
expand access to assessment and
treatments with regulated healthcare
providers in communities where
regulated health providers are not
available
• Regional
• IDN
• LHH
• Care Streams Leads
• Rehabilitation Training for PSWs/
Therapy Assistants
• Discharge Process Map
• Appropriate Care following
Regulatory College Standards
• Community Exercise in Far North
• Rehabilitation in 10/39 Far North
Communities
• Quality, evidence-based care
• Improved quality of care
• Improved access to care
• Improved client care transitions
• Care as close to home as possible
• Enhanced communication among
providers
4.2 Evaluate opportunities and review the
feasibility of integration of specialized
programs delivered using technology
• LHIN
• Regional
• One exercise program per LHH
(depending on demand)
• Efficient resource utilization
• Streamlined service delivery
• Improved access to care
• Care as close to home as possible
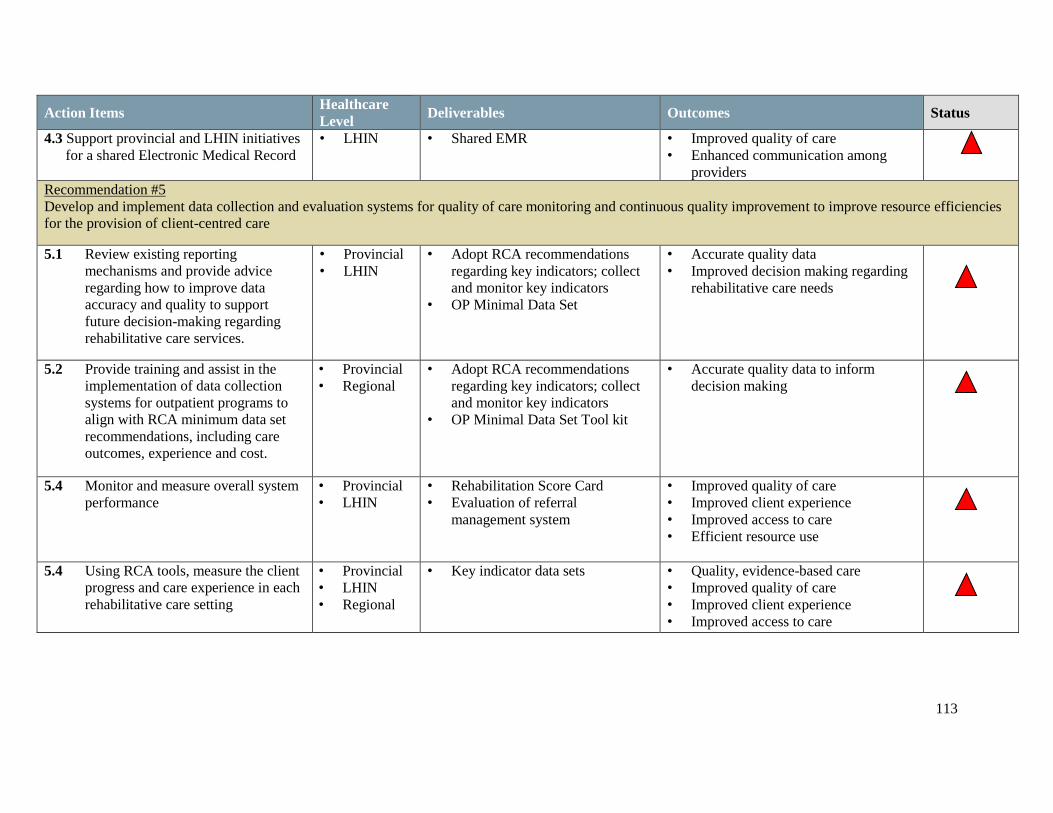
113
Action Items Healthcare
Level Deliverables Outcomes Status
4.3 Support provincial and LHIN initiatives
for a shared Electronic Medical Record
• LHIN • Shared EMR • Improved quality of care
• Enhanced communication among
providers
Recommendation #5
Develop and implement data collection and evaluation systems for quality of care monitoring and continuous quality improvement to improve resource efficiencies
for the provision of client-centred care
5.1 Review existing reporting
mechanisms and provide advice
regarding how to improve data
accuracy and quality to support
future decision-making regarding
rehabilitative care services.
• Provincial
• LHIN
• Adopt RCA recommendations
regarding key indicators; collect
and monitor key indicators
• OP Minimal Data Set
• Accurate quality data
• Improved decision making regarding
rehabilitative care needs
5.2 Provide training and assist in the
implementation of data collection
systems for outpatient programs to
align with RCA minimum data set
recommendations, including care
outcomes, experience and cost.
• Provincial
• Regional
• Adopt RCA recommendations
regarding key indicators; collect
and monitor key indicators
• OP Minimal Data Set Tool kit
• Accurate quality data to inform
decision making
5.4 Monitor and measure overall system
performance
• Provincial
• LHIN
• Rehabilitation Score Card
• Evaluation of referral
management system
• Improved quality of care
• Improved client experience
• Improved access to care
• Efficient resource use
5.4 Using RCA tools, measure the client
progress and care experience in each
rehabilitative care setting
• Provincial
• LHIN
• Regional
• Key indicator data sets • Quality, evidence-based care
• Improved quality of care
• Improved client experience
• Improved access to care

114
Next Steps
The implementation of the integrated model of rehabilitative care in NWO and recommendations
identified in this report will be led by the Regional Rehabilitative Care Lead Organization in partnership
with the North West LHIN. It is essential the lead organization is clearly identified and has an
accountability agreement with the North West LHIN. Following announcement of the Rehabilitative Care
Lead Organization, engagement of the Chief Executive Officers of the North West LHIN hospitals will be
essential, and a Rehabilitative Care Advisory Committee will be established. This committee will include
regional stakeholders and participation across all levels of rehabilitative care including client and family
representation, clinician representation, and administration representation. The advisory committee will
be established in conjunction with the Rehabilitative Care Lead Organization in order to drive an
implementation plan for each recommendation and outlined action plan. It is expected the Rehabilitative
Care Lead Organization and Rehabilitative Care Advisory group will be established in 2017. The
membership requirements and terms of reference will provide a foundation for the establishment of this
specific rehabilitative care advisory group.
Between 2017 and 2020, all publicly-funded rehabilitation providers will be expected to participate in the
implementation phase of the rehabilitative care review. It is essential all organizations identify a
rehabilitation champion who will assist with the ongoing development of rehabilitative care and adoption
of recommended changes within their organization.
Stakeholder Engagement
Throughout the implementation of the recommendations and action plans, it is imperative there is
ongoing stakeholder engagement. In order for the recommendations to be successfully implemented, and
the overall rehabilitative care system in NWO to improve, every level of stakeholder must be involved.
Recommended stakeholder sessions will be provided within each LHH throughout the implementation
with specific focus groups held for care recipients/local citizens, clinicians, supporting agencies, primary
healthcare providers, and administration. In addition, region-specific engagement will be required to
focus on the challenges of access for the most remote locations within the North West LHIN.
Members of the Rehabilitative Care Advisory Committee and designated rehabilitative care champions
within each facility will be expected to participate in ongoing stakeholder engagement. These individuals
will be responsible for communicating any changes and expectations identified by the Rehabilitative Care
Advisory group, as well as bringing forward recommendations to support further integration and
improvement identified by front line staff, clients, and families.
115
Timelines
A three-year timeline has been established for implementation of the identified recommendations. This
timeframe will ensure the accuracy of information obtained during this review and allow for an
incremental implementation, reflecting the complex nature of the healthcare system and the requirement
to evaluate progress and adjust development accordingly. It is anticipated some changes will be required
due to ongoing healthcare developments in the province; however, a three-year timeline to initiate all
identified action plans will provide a strong momentum for change and development of a foundation from
which to continue to monitor and evaluate ongoing needs.
As discussed, a phased approach will be used throughout the implementation of the integrated
rehabilitation system. This will allow opportunity to initiate small components using Plan-Do-Study-Act
cycles, or Continuous Quality Improvement to spread the initiatives across the region, evaluate the
implementation progress, and adjust the timelines and action plans as required. Within the first year of
implementation, it is expected the advisory committee will evaluate the recommended year one action
plans and work to develop required working groups with resources outside of the committee, and action
plans for the execution of the priority projects. The Gantt chart depicted in Figure 8 presents a proposed
implementation schedule through to the end of the 2019-2020 fiscal year.
Within the Phase I Post-acute Care report, several recommendations were developed to help guide the
development of the integrated model of rehabilitative care. This review focused on priority rehabilitative
care areas, but additional recommendations will be important to the overall success of implementing an
integrated model of rehabilitative care. Specifically, the Rehabilitative Care Advisory Committee should
address the following recommendations:
• The examination of utilization/reallocation of LTC/EldCap/CCC beds located outside the City of
Thunder Bay.
• Examine activity that is by definition “rehabilitative care” currently being provided by acute care
facilities and make recommendations regarding appropriate sponsorship of these services.

116
Figure 9. Gantt Chart of Proposed Implementation of Rehabilitative Care Regional Program
May
-16
Jun
-16
Au
g-1
6
Sep
-16
No
v-1
6
Jan
-17
Feb
-17
Ap
r-1
7
Jun
-17
Jul-
17
Sep
-17
No
v-1
7
Dec
-17
Feb
-18
Ap
r-1
8
May
-18
Jul-
18
Au
g-1
8
Oct
-18
Dec
-18
Jan
-19
Mar
-19
May
-19
Jun
-19
Au
g-1
9
Oct
-19
No
v-1
9
Jan
-20
Mar
-20
Ap
r-2
0
Educate Stakeholders on RCA Definitions Frameworks
Review ability of each facility to provide identified therapy intensities
Implement care stream and applicable flow maps
Develop a communication system between clinicians to improve transitions between regional sites
Review current diagnosis specific client care pathways based on best practices across NOW
Develop specialized Interprofessional care teams and leads within each care stream
Establish connections between service providers and regional care networks
Identify and facilitate access to a minimum basket of services including equipment
Develop a process to determine individual levels of care
Build capacity to meet best practice and QBP expectations at a local level
Deliver rehabilitation professionals annual retreat/forum
Expand the role of care stream teams to increase regional access to specialized care
Improve direct access from primary care and community care provider to rehab programs
Participate within LHH and regional forums to address ALC, supportive housing and community supports
Support provision of shared EMR
Refinement of roles within Care Stream Model
Establish the delivery of one community-based exercise program per LHH
Evaluate clients who were referred to streams of care
Implement electronic referal management system
Implement rehabilitative Care delivery model to remote North communities
Develop and share Rehabilitation Score Card

117
Conclusions
The regional rehabilitative care plan is the result of years of ongoing discussion and evaluations. This
plan has been developed with the insight from both local and provincial rehabilitative care capacity-
planning exercises. Using these findings and building on the Post-Acute Review Phase I Report, the
recommendations developed within this capacity planning exercise will provide strategic direction to the
overall re-design of an integrated rehabilitative care system in NWO. By aligning the 2016-2019 IHSP
and Health Services Blueprint in the North West LHIN, the recommended integrated model of
rehabilitative care will flow seamlessly within the overall integrated health system network in the North
West LHIN.
The high level recommendations identified within this capacity planning review will not only advance the
effectiveness of rehabilitative care within NWO, but will ultimately improve the overall quality of
rehabilitative care and client experience within the rehabilitative care system.
Rehabilitative care is currently provided within a variety of inpatient, outpatient, and community care
settings, often with little support and coordination between facilities. While each organization endeavours
to provide the best care possible for their clients, gaps remain with respect to ensuring equal service is
available to all residents in the region. As such, there are identified areas of concern with respect to
accessing best practices and adhering to QBP’s, client transitions between locations and levels of care,
and collecting and interpreting quantitative data to evaluate care provision across the region.
Implementation of the identified recommendations and action plans will result in a coordinated regional
model of rehabilitative care. Through individual organization contributions and collaborative regional
efforts, the North West LHIN will be well positioned to align with provincial standards for rehabilitative
care and improve the care journey for clients requiring rehabilitation. Through ongoing partnerships with
the RCA, the North West LHIN will continue to ensure the unique needs of our region are addressed on a
provincial level, and our successes continue to be showcased as a leader in remote/regional rehabilitative
care provision.
By building on the existing passion and commitment to meet the unique rehabilitation needs of our
clients, the North West LHIN will continue to demonstrate excellence in care provision. The use of
technology, development of care networks, and partnerships with our remote communities will continue
to enhance our care provision, and in turn assist to develop a strong, lasting, integrated system of
rehabilitative care.
Works Cited
Government of Ontario. (September 2015). Get Physiotherapy (Online). Available:
https://www.ontario.ca/page/get-physiotherapy#section-0
Government of Ontario. Health Services Branch. (December 2013). Changes to Publicly Funded
Physiotherapy Services: Questions & Answers (Online). Available:
http://www.health.gov.on.ca/en/pro/programs/ohip/bulletins/4000/bul4620_2.pdf
Government of Ontario. Ministry of Health and Long-Term Care, Health Analytics Branch.
Integrated Health Services Plan 2016-2019 Common Environmental Scan: A Review of Selected
Information about Ontario’s Local Health Integration Networks. Queen’s Printer for Ontario,
June 2015.
Government of Ontario. Ministry of Health and Long-Term Care. Complex Continuing Care Co-
Payment (Online). Queens Printer for Ontario, 2016. Available:
http://www.health.gov.on.ca/en/public/publications/chronic/chronic.aspx.
Government of Ontario. Ministry of Health and Long-Term Care. Patients First: Action Plan for
Health Care (Online). Queens Printer for Ontario: February, 2015. Available:
http://health.gov.on.ca/en/ms/ecfa/healthy_change/docs/rep_patientsfirst.pdf
Government of Ontario. North West Community Care Access Centre. Strategic Priorities 2014-
2016 (Online). Thunder Bay, 2014. Available:
http://healthcareathome.ca/northwest/en/Documents/14%2010%2031%20Strategic%20Priorities
%20Final.pdf
Government of Ontario. North West Local Health Integration Network. Health Services
Blueprint: Building Our Future. PwC. Thunder Bay: February 2012.

119
Government of Ontario. North West Local Health Integration Network. IHSP IV Integrated
Health Service Plan 2016-2019. Thunder Bay: 2016
Government of Ontario: North West Local Health Integration Network. Integrated District
Network Map (Ontario). Thunder Bay, 2016. Available:
file:///C:/Users/clackj/Downloads/NorthWestLHIN_IDNmap%20(1).pdf
Government of Ontario. North West Local Health Integration Network. Local Environmental
Scan. Thunder Bay: 2015
Government of Ontario. Waterloo Wellington Local Health Integration Network. Rural Health
Care Review Final Report (Online). Waterloo, January 2010. Available:
file:///C:/Users/clackj/Downloads/RPT_20100110_WWLHIN_RuralHealthReportFinal.pdf
Institute for Healthcare Improvement. The IHI Triple Aim (Online). 2016. Available:
http://www.ihi.org/Engage/Initiatives/TripleAim/Pages/default.aspx.
Health Quality Ontario; Ministry of Health and Long-Term Care. Quality-Based Procedures:
Clinical Handbook for Hip and Knee Replacement. Toronto, ON: Health Quality Ontario; 2014
February. 94 p. Available from: http://www.hqontario.ca/evidence/publications-and-ohtac-
recommendations/clinical-handbooks.
Health Quality Ontario; Ministry of Health and Long-Term Care. Quality-Based Procedures:
Clinical Handbook for Hip Fracture. Toronto, ON: Health Quality Ontario; 2013 May. 97 p.
Available from: http://www.hqontario.ca/evidence/publications-and-ohtac-
recommendations/clinical-handbooks
Health Quality Ontario; Ministry of Health and Long-Term Care. Quality-Based Procedures:
Clinical Handbook for Stroke. Toronto, ON: Health Quality Ontario; 2013 September. 59 p.
Available from: http://www.hqontario.ca/evidence/publications-and-ohtac-
recommendations/clinical-handbooks

120
Office of the Auditor General of Ontario. 2013. 2013 Annual Report (Online). Queens Printer for
Ontario, 2013. Available:
http://www.auditor.on.ca/en/content/annualreports/arreports/en13/2013ar_en_web.pdf
Ontario Hospital Association. (2012). Local Health Hubs for Rural and Northern Communities:
An Integrated Service Delivery Model Whose Time Has Come. Toronto, 2012.
Ontario Hospital Association. Optimizing the Role of Complex Continuing Care and
Rehabilitation in the Transformation of the Health Care Delivery System. Toronto, May 2006.
Ontario Hospital Association. (May 2013). Toolkit to Support the Implementation of Quality-
Based Procedures. Toronto, 2013.
Preyra Solutions. 2013/14 Actual Less Expected Rehabilitation Days by Bedded Levels of
Rehabilitation Care. Unpublished Raw Data.
Rehabilitative Care Alliance. Definitions Framework for Bedded Levels of Rehabilitative Care
(Online). Toronto, 2014. Available:
http://www.rehabilitationcarealliance.ca/uploads/File/Toolbox/Definitions/Definitions_Framewo
rk_for_Bedded_Levels_of_Rehabilitative_Care__FINAL_Dec_2014_.pdf
Rehabilitative Care Alliance. Definitions Framework for Community Based Levels of
Rehabilitative Care (Online). Toronto, March 2015. Available:
http://www.rehabilitationcarealliance.ca/uploads/File/Final_Report_2013-
15/Definitions/Def_Framework_for_Community_Based_Levels_of_Rehabilitative_Care__Final
_March_2015_.pdf
Rehabilitative Care Alliance. Inspiring New Directions in Rehabilitative Care (Online).
[Toronto], 2015. Available: www.rehabilitationcarealliance.ca/mandate-1-final-report

121
Rehabilitative Care Alliance. Outpatient/Ambulatory Task Group. Outpatient Data Collection
Technical Report (Online). Toronto: March 2015. Available:
http://www.rehabilitationcarealliance.ca/uploads/File/Final_Report_2013-
15/OPAMB/Technical_Report_describing_the_data_elements_within_the_Access_and_Transiti
on_and_Financial_Quadrants_of_the_MDS.pdf
Sinha, SK. (2012). Living Longer, Living Well. Toronto (December, 2012).
St. Joseph’s Care Group. Review of Post-Acute Rehabilitative Care Services in the North West
LHIN. Unpublished Document. August, 2014.
Reinikka KJ, Taylor DM, Daniel S, Burns-Hogan S, DePass B, McGill L, McLeod M, Safadi S,
Veit S. Hip fracture, hip and knee replacement quality-based procedures: Physiotherapist
perceptions of adherence, barriers and facilitator. Physiotherapy Canada in press. Impact
Factor: 0.77.
Yahn J., Farrell S. (2012). North West LHIN Regional Rehabilitation and Complex Continuing
Care Final Report and Recommendations. Thunder Bay: 2012.
Canadian Health Services Research Foundation. CHSRF Series on Cost Drivers and Health
System Efficiency: Paper 4 (Online). Ottawa: March 2011. Available:
http://www.cfhi-fcass.ca/Libraries/Hospital_Funding_docs/CHSRF-Sutherland-
HospitalFundingENG.sflb.ashx
Fricke M., Achtemichuk, M., Cooper J., Martin B., Macaulay A., Durcan A., Development of a
community-based medical rehabilitation programme in the Kivalliq Region of Nunavut, Canada.
(Online) 2003. Available:
http://www.circumpolarhealthjournal.net/index.php/ijch/article/viewFile/17867/20344
CCC/Rehab Expert Panel – Definitions Working Group, 2011.
122
World Health Organization, 2016(a). Rehabilitation. Retrieved November 11, 2016.
http://www.who.int/topics/rehabilitation/en/
World Health Organization, 2016(b). Disability and Rehabilitation. Retrieved November 11,
2016. http://www.who.int/disabilities/care/en/
Ontario Ministry of Health and Long-Term Care, 2015. Health System Funding Reform.
Retrieved November 11, 2016.
http://www.health.gov.on.ca/en/pro/programs/ecfa/funding/hs_funding.aspx
North West LHIN. Population Health Profile. December 2012.
Ontario Ministry of Finance, 2016. Ontario Populations Projections Update (page 10).
http://www.fin.gov.on.ca/en/economy/demographics/projections/projections2015-2041.pdf
Government of Ontario. North West Local Health Integration Network. Health Profiles for the
five Integrated District Networks. Thunder Bay, 2015.
Ontario Ministry of Health and Long Term Care, 2015. About the Excellent Care for All Act.
Retrieved November 11, 2016.
http://www.health.gov.on.ca/en/pro/programs/ecfa/legislation/act.aspx
Data Source: DAD 2010/11 – QBP CHF Handbook, Page 32.
Ontario Ministry of Health and Long Term Care, 2014. Assess and Restore guideline. Retrieved
October 19 at: http://www.health.gov.on.ca/en/pro/programs/assessrestore/docs/ar_guideline.pdf
123
Assess and Restore. North West LHIN Small Hospital Review and Capacity-Building Project
Final Report. April 2015.
Levy, C., Balogh, S., Perkins, E., Rehabilitative Care Alliance, 2016. Realizing the Potential of
Rehabilitative Care for People with Complex Health Conditions: the Time is Now (page 2).
Retrieved November 11, 2016.
http://www.rehabcarealliance.ca/uploads/File/Reports_and_Presentations/HQ_Vol19_No2-
Levy.pdf
Meyer M., et al, 2012. The Impact of Moving to Stroke Rehab Best Practices in Ontario.
Ontario Stroke Network.
Rapid Access to Consultative Expertise: An innovative Program to Provide Telephone Advice,
August 2016. Retrieved November 11, 2016 at: http://www.raceconnect.ca/what-is-race/
Walker D, 2011. Caring for our aging population and addressing alternate level of care. Report
submitted to the Ministry of Health and Long-term Care. Retrieved Oct 15, 2016 at:
www.health.gov.on.ca/en/common/ministry/publications/reports/walker_2011/walker_2011.aspx
St. Joseph’s Care Group. Assess and Restore First Nations Capacity Building. Unpublished
Document. April 2015.
Government of Ontario. North West Local Health Integration Network. Health Profiles for the
five Integrated District Networks. Thunder Bay, 2015

124
Appendix A – Rehabilitative Care Alliance Bedded Levels of Rehabilitative Care Definitions Framework
125
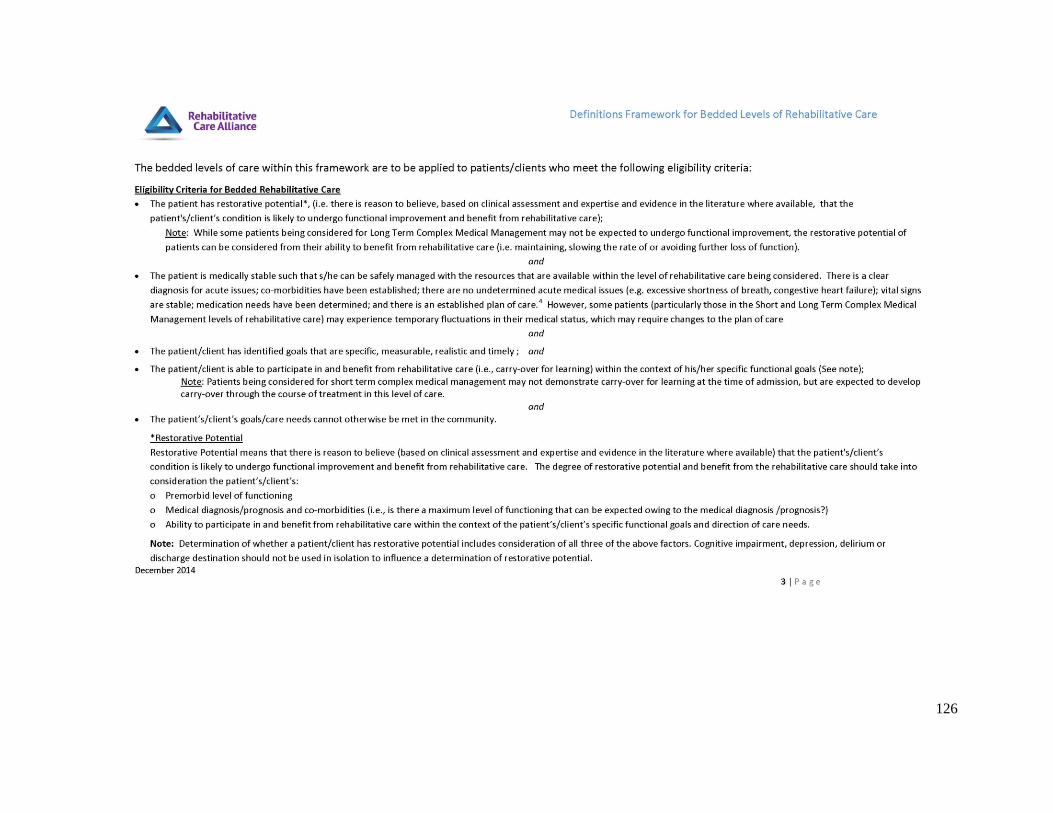
126
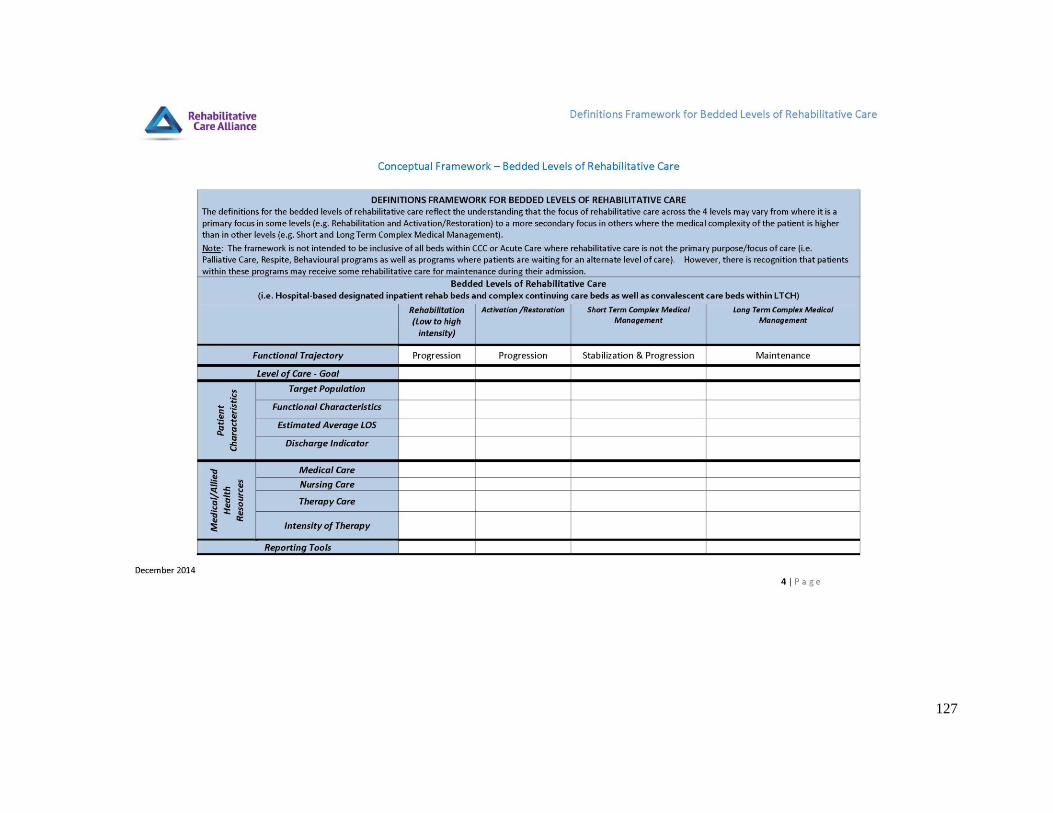
127
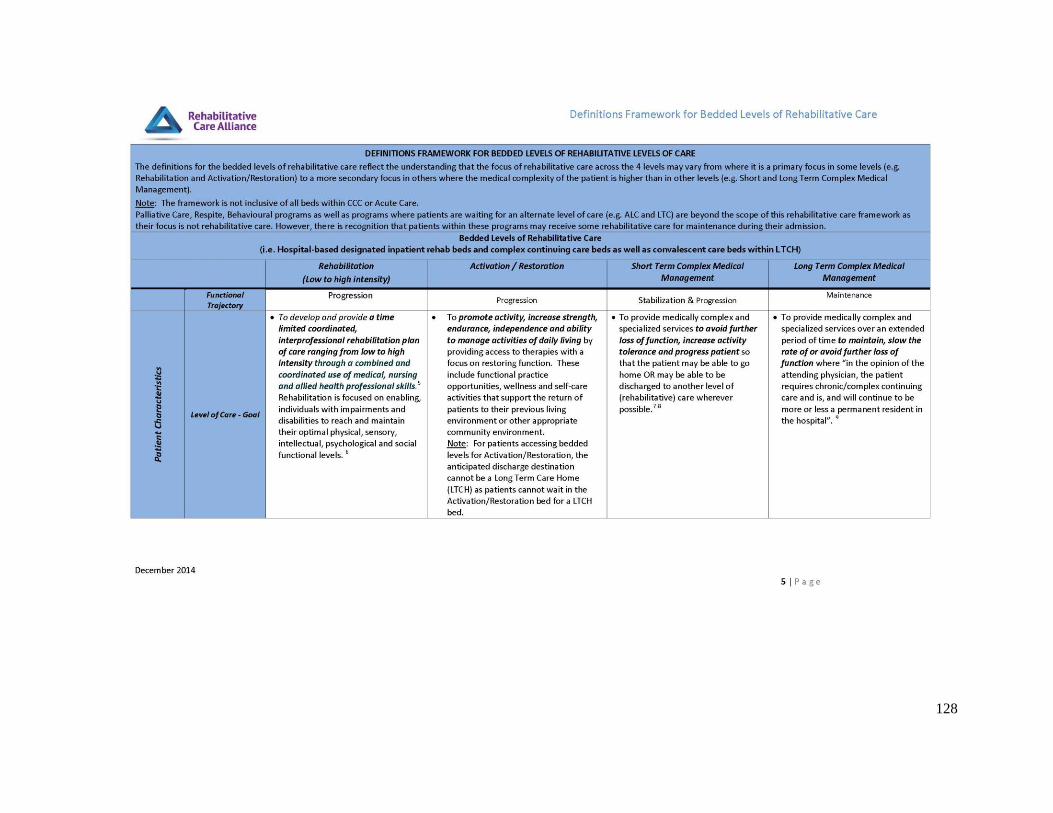
128

129
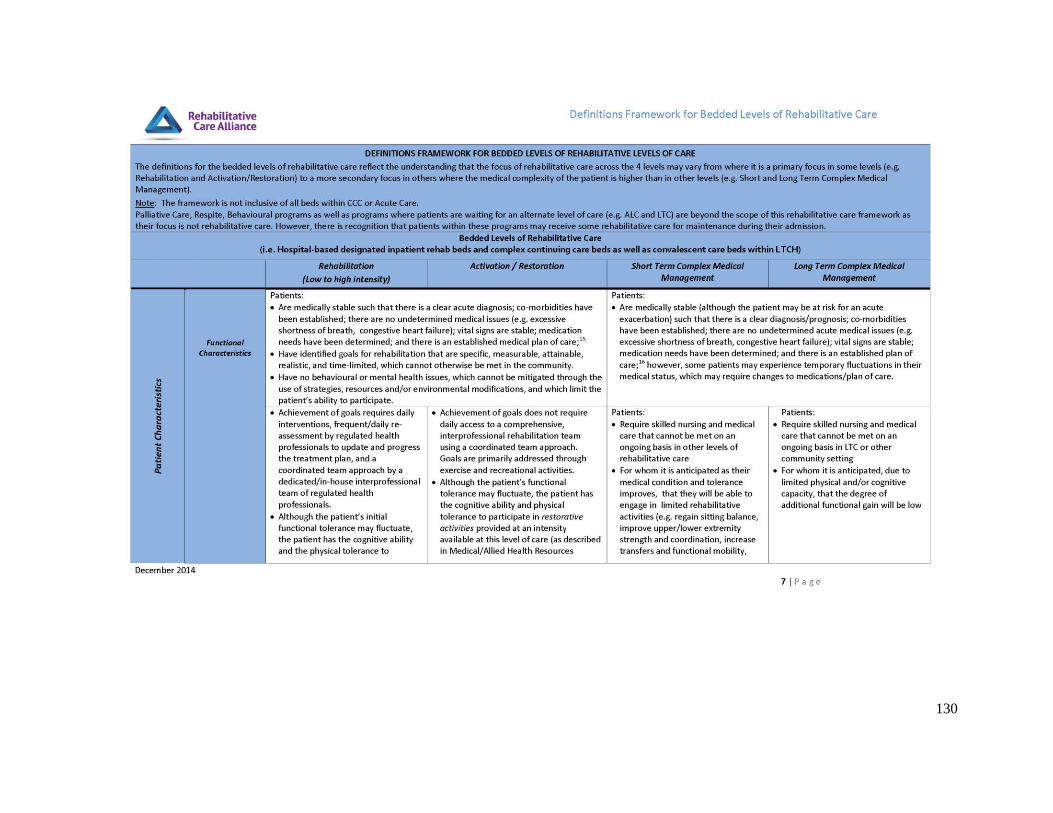
130

131
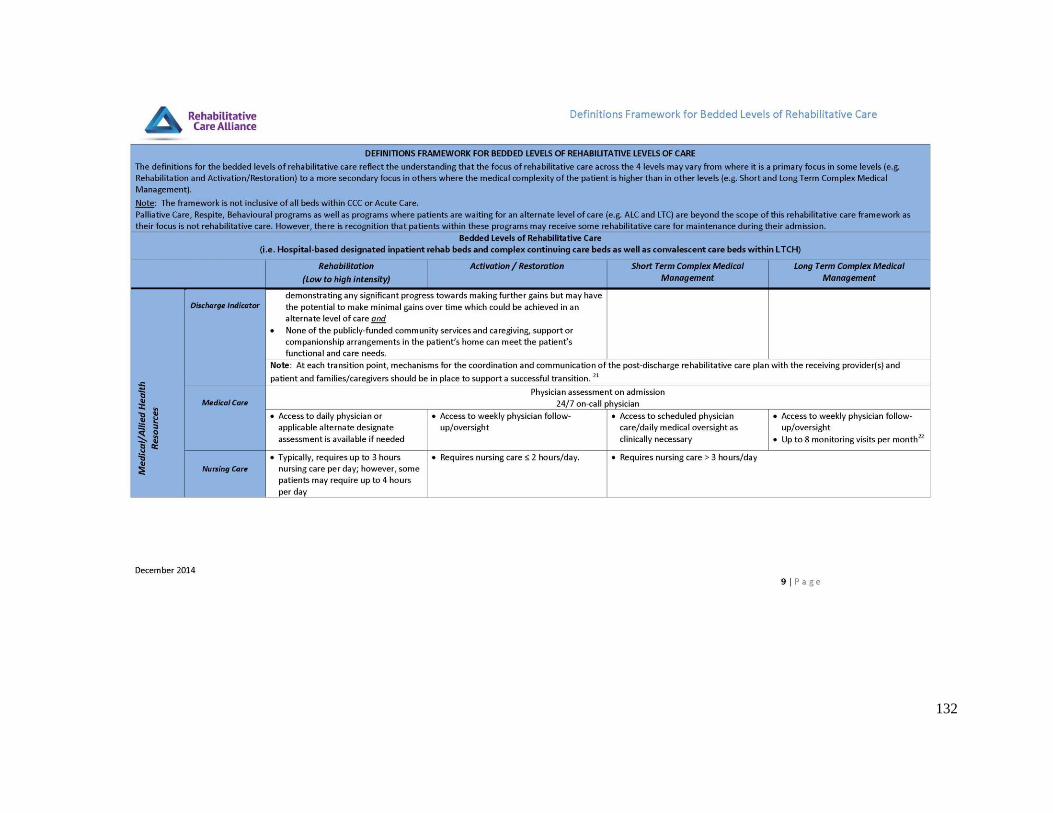
132

133
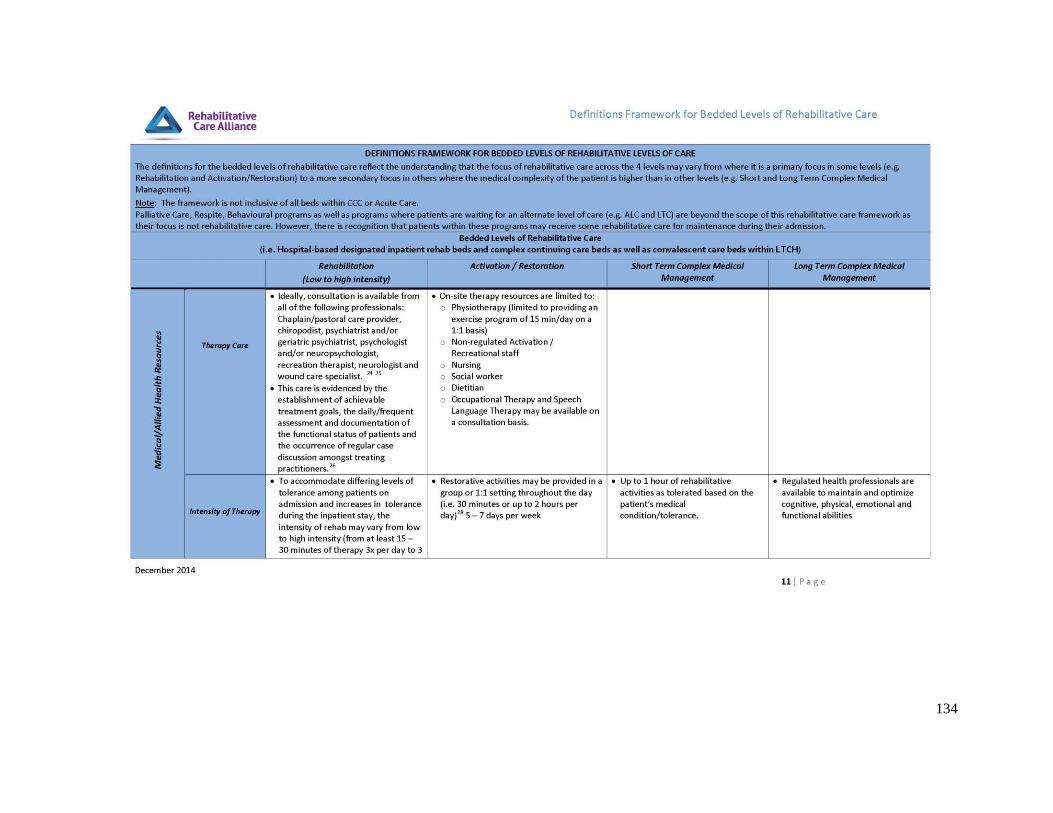
134
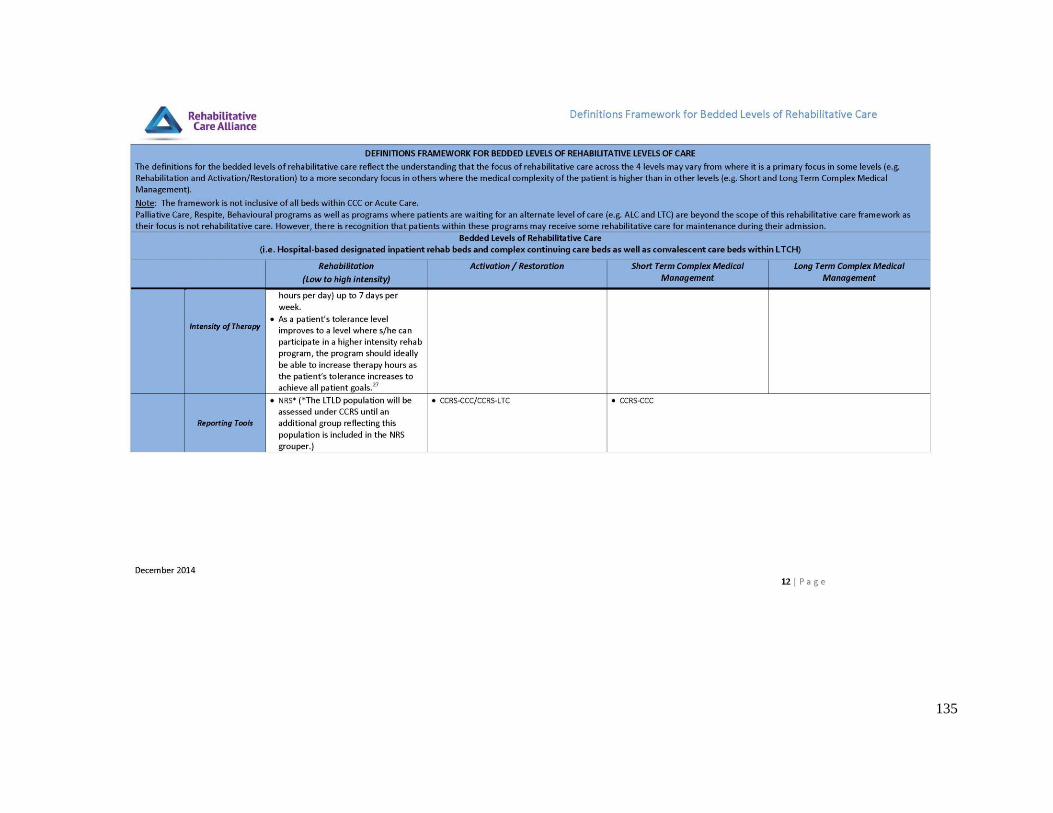
135

136
137
Appendix B – Rehabilitative Care Alliance: Definitions for Community-Based Levels of Rehabilitative Care
138
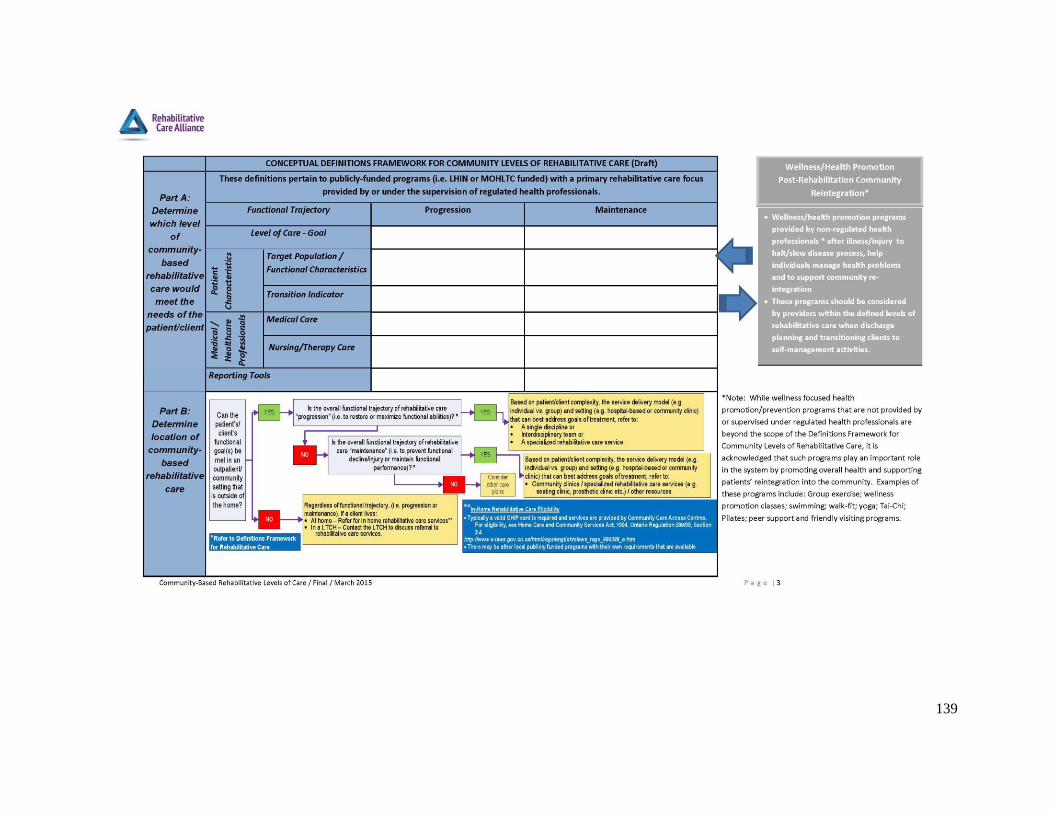
139
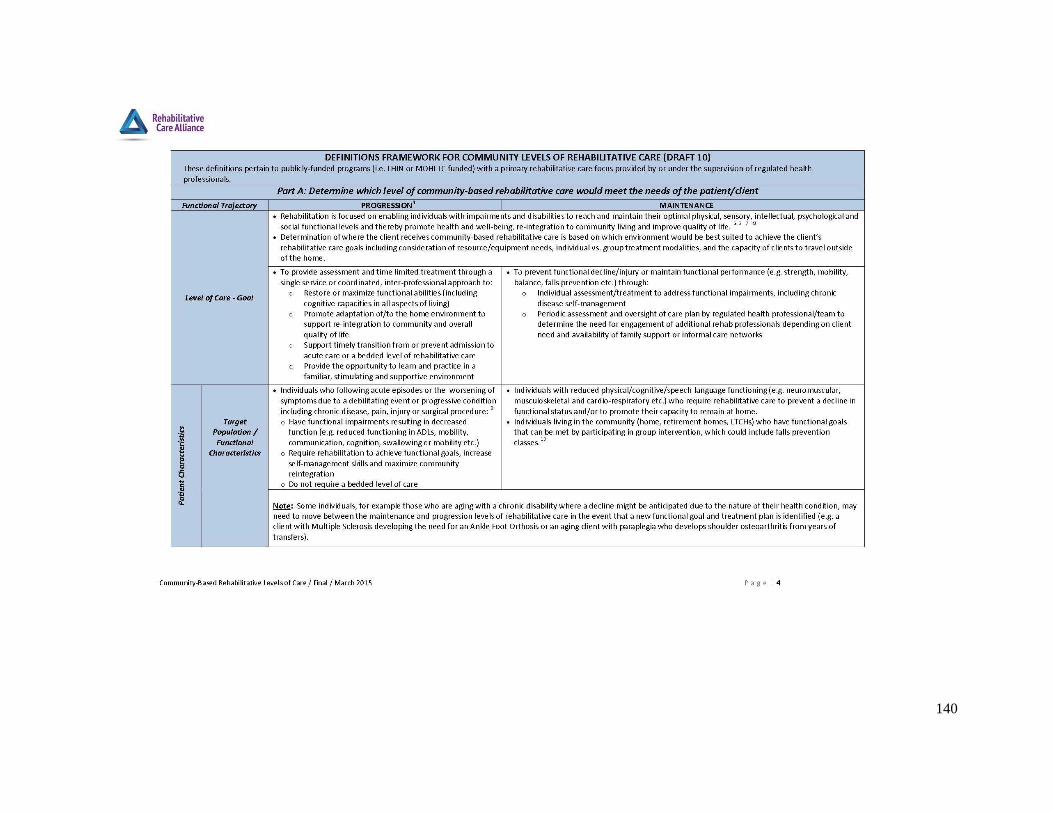
140
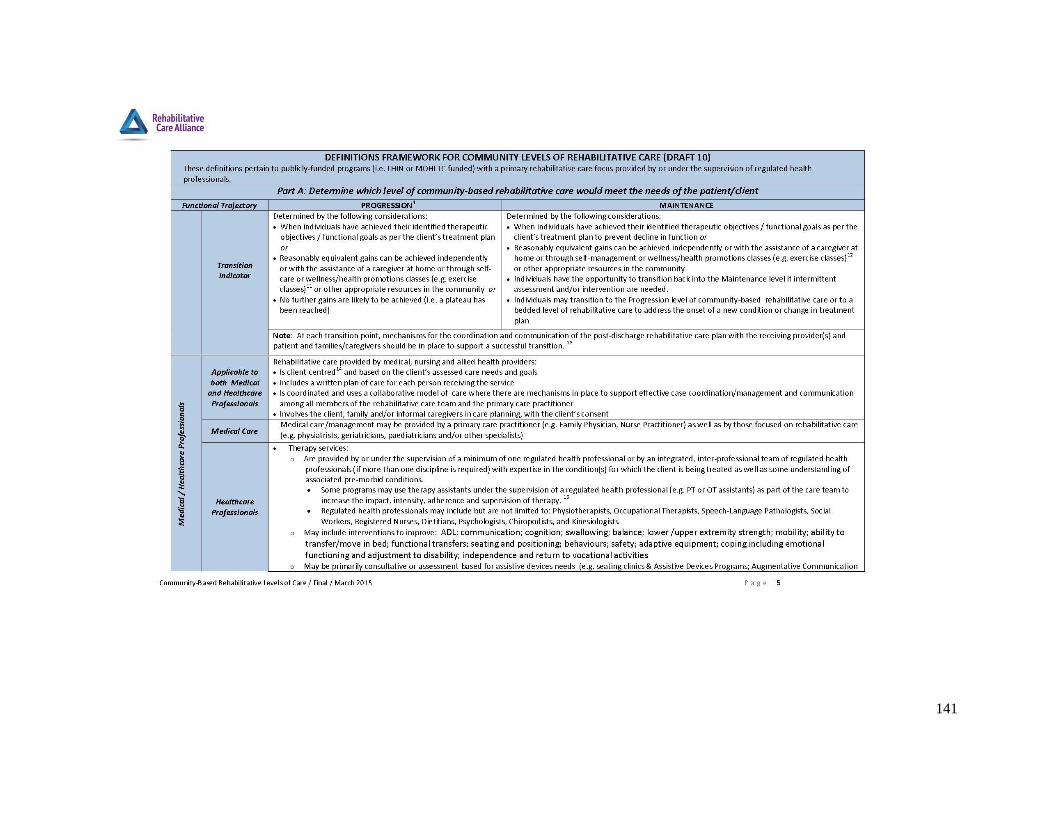
141

142
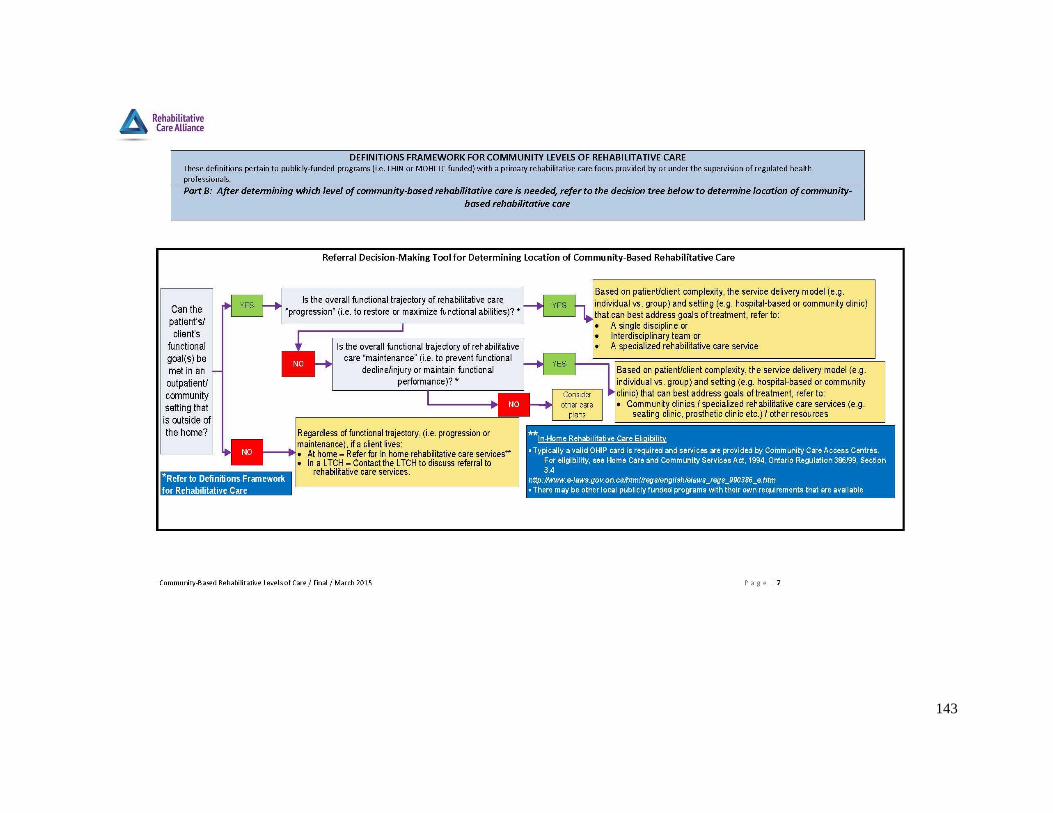
143

144

145

146
Appendix C – Rehabilitative Care Alliance Capacity Planning Framework

147
Appendix D – Rehabilitation Care Alliance Planning Considerations for Reclassification of Rehabilitation/CCC beds

Project Charter
148
Appendix D – Project Charter
Project Charter
North West LHIN: Post-Acute Review (Integrated Model of
Rehabilitative Care)
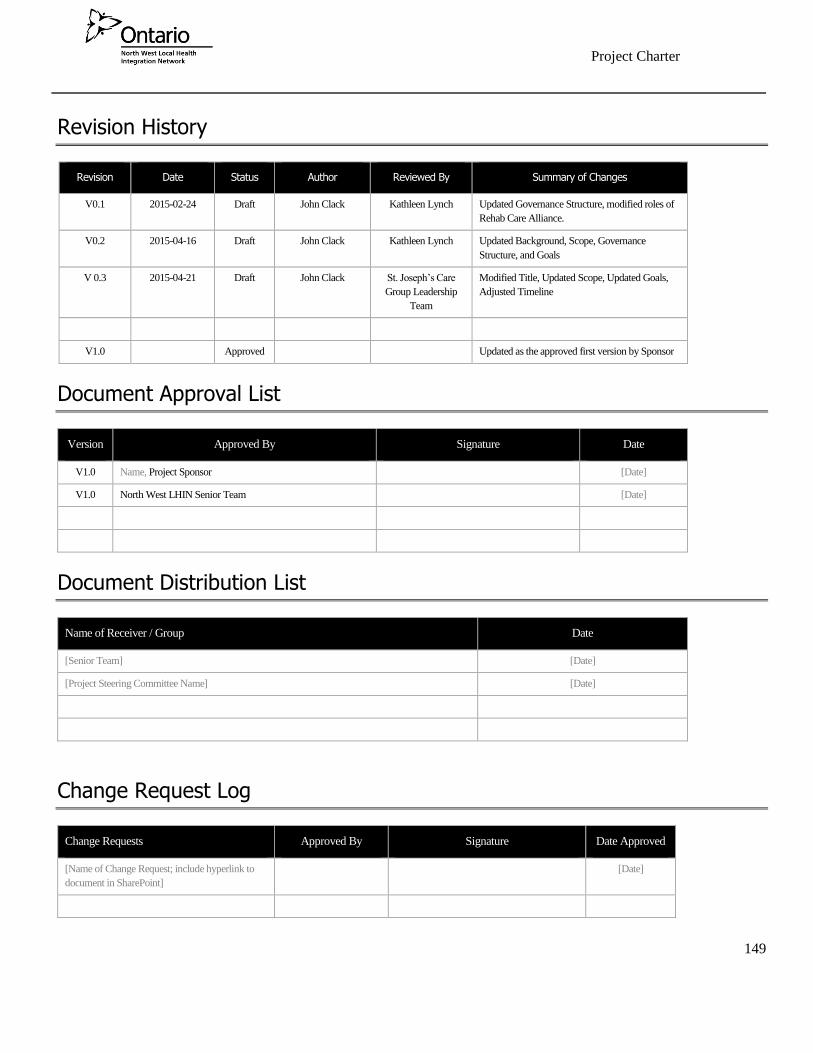
Project Charter
149
Revision History
Revision Date Status Author Reviewed By Summary of Changes
V0.1 2015-02-24 Draft John Clack Kathleen Lynch Updated Governance Structure, modified roles of
Rehab Care Alliance.
V0.2 2015-04-16 Draft John Clack Kathleen Lynch Updated Background, Scope, Governance
Structure, and Goals
V 0.3 2015-04-21 Draft John Clack St. Joseph’s Care
Group Leadership
Team
Modified Title, Updated Scope, Updated Goals,
Adjusted Timeline
V1.0 Approved Updated as the approved first version by Sponsor
Document Approval List
Version Approved By Signature Date
V1.0 Name, Project Sponsor [Date]
V1.0 North West LHIN Senior Team [Date]
Document Distribution List
Name of Receiver / Group Date
[Senior Team] [Date]
[Project Steering Committee Name] [Date]
Change Request Log
Change Requests Approved By Signature Date Approved
[Name of Change Request; include hyperlink to
document in SharePoint]
[Date]
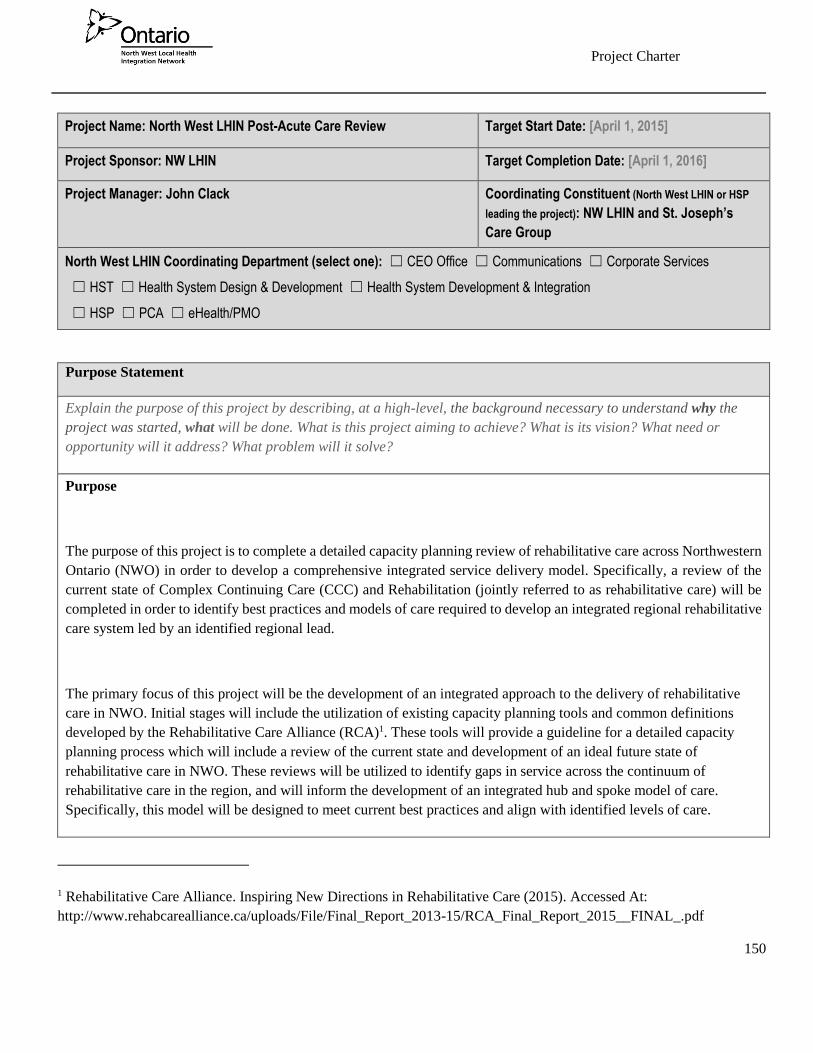
Project Charter
150
Project Name: North West LHIN Post-Acute Care Review Target Start Date: [April 1, 2015]
Project Sponsor: NW LHIN Target Completion Date: [April 1, 2016]
Project Manager: John Clack Coordinating Constituent (North West LHIN or HSP
leading the project): NW LHIN and St. Joseph’s
Care Group
North West LHIN Coordinating Department (select one): ☐ CEO Office ☐ Communications ☐ Corporate Services
☐ HST ☐ Health System Design & Development ☐ Health System Development & Integration
☐ HSP ☐ PCA ☐ eHealth/PMO
Purpose Statement
Explain the purpose of this project by describing, at a high-level, the background necessary to understand why the
project was started, what will be done. What is this project aiming to achieve? What is its vision? What need or
opportunity will it address? What problem will it solve?
Purpose
The purpose of this project is to complete a detailed capacity planning review of rehabilitative care across Northwestern
Ontario (NWO) in order to develop a comprehensive integrated service delivery model. Specifically, a review of the
current state of Complex Continuing Care (CCC) and Rehabilitation (jointly referred to as rehabilitative care) will be
completed in order to identify best practices and models of care required to develop an integrated regional rehabilitative
care system led by an identified regional lead.
The primary focus of this project will be the development of an integrated approach to the delivery of rehabilitative
care in NWO. Initial stages will include the utilization of existing capacity planning tools and common definitions
developed by the Rehabilitative Care Alliance (RCA)1. These tools will provide a guideline for a detailed capacity
planning process which will include a review of the current state and development of an ideal future state of
rehabilitative care in NWO. These reviews will be utilized to identify gaps in service across the continuum of
rehabilitative care in the region, and will inform the development of an integrated hub and spoke model of care.
Specifically, this model will be designed to meet current best practices and align with identified levels of care.
1 Rehabilitative Care Alliance. Inspiring New Directions in Rehabilitative Care (2015). Accessed At:
http://www.rehabcarealliance.ca/uploads/File/Final_Report_2013-15/RCA_Final_Report_2015__FINAL_.pdf

Project Charter
151
Through the identification of gaps in current services, elimination of service duplication and streamlining of referrals, a
more efficient use of available resources will be achieved. Collaboration between the North West LHIN, St. Joseph’s
Care Group (SJCG), Thunder Bay Regional Health Sciences Center (TBRHSC), North West Community Care Access
Center (CCAC), and regional health care providers will be integral in the optimal utilization of services and ultimate
improvement in patient/client experience. Through an integrated service delivery model, the region will experience
improved efficiency, quality, and cost-effective health care with the benefit of services delivered as close to home as
possible.
Within the development of an integrated service model, based on best practice guidelines, this review will examine
bedded levels of care, outpatient and ambulatory rehabilitative care, and community based programs across the region.
Further, it will identify strengths in current care provision in order to reach remote communities across the region, and
ensure provision of services as close to home as possible.
Background
The importance of rehabilitation within the global context of health care has been well documented2. In light of the
ongoing changes and increased demand placed on the health care system, it has become increasingly important to
identify optimal care practices and efficiencies. In recent years, the NW LHIN has conducted ongoing evaluations of
health care practices in order to develop a strategy to meet changing needs3.
Within the NW LHIN, there is a strong demand for rehabilitative care services and programs. Historically, these services
have primarily been based out of the City of Thunder Bay with 60% of the CCC bed capacity and 100% of the
rehabilitative care bed capacity located in within the City of Thunder Bay. While these services have met the needs of
many residents of NWO, it has been identified that gaps remain within the current system that limit access to quality
rehabilitative care for some residents in NWO.
Demand for rehabilitation services in NWO is expected to increase significantly as our population continues to age. It
2 Office of the Auditor General of Ontario. 2013 Annual Report. (2013). Accessed at:
http://www.auditor.on.ca/en/reports_en.en13/2013ar_en_web.pdf
3 Yahn J., FarrellS. (2012). North West LHIN Regional Rehabilitation and Complex Continuing Care Final Report and
Recommendations.
Project Charter
152
is expected that over the next 10 years, the population aged 65 to 79 will increase by 42 percent in the region4. In
addition, it has been demonstrated that with increased average age of care recipients, there is a related increase in
chronicity and complexity of medical conditions and a disproportionate increase in demand for healthcare. Based on
these factors, it is expected that there will be an even greater demand placed on rehabilitation and restoration services,
prevention, and maintenance of health as a means of stability within the health care system.
In 2012 a detailed review of Rehabilitation and CCC in NWO was completed. This review included both quantitative
and qualitative evaluations of rehabilitative care from 2009-2011. Further evaluation was completed prior to the 2013
development of the NW LHIN health service blueprint, which outlined a need for increased integration across the region
with respect to care provision. From these documents, the LHIN and SJCG completed a phase one review of post-acute
rehabilitative care services which was submitted to the LHIN in August 2014. This document provided an initial
evaluation of services across the NW LHIN and a starting point for this review.
Literature Review:
Recent literature on innovative rehabilitative care models has largely focused on the concept of vertical integration and
the utilization of health hub models. Across Canada, and internationally, there has been an increased emphasis on the
utilization of a hub model for health care provision in rural and remote communities5. To date, these models have
primarily been utilized in broad healthcare systems that include the full spectrum of care from primary and
acute/emergency through rehabilitative care. Such models however can also be directly utilized in a more defined scope
such as within a rehabilitative care model. Specifically, the utilization of vertical integration defined as the “integration
of different inter-related or inter-dependent health sector elements on the continuum of care” and may include primary,
secondary and tertiary care6.
A review of current health care practices in remote and rural regions indicates several innovative strategies that have
demonstrated some level of success. Among the most commonly identified strategies are increased utilization of
4 North West LHIN: Health Services Blueprint: Building Our Future. (2012). Accessed at:
http://www.northwestlhin.on.ca/goalsandachievements/Health%20Services%20Blueprint/BlueprintReport.aspx
5 Ontario Hospital Association. Local Health Hubs for Rural and Northern Communities (2012). Accessed at:
http://www.oha.com/KnowledgeCentre/Library/Documents/Local%20Health%20Hubs%20for%20Rural%20and%20No
rthern%20Communities.pdf.
6 Ministry of Health and Long Term Care. The Health Planner’s Toolkit: Module 4 (2006). Accessed at:
http://www.health.gov.on.ca/transformation/providers/information/resources/health_planner/module_4.pdf
Project Charter
153
telemedicine and e-learning for clients and staff, expanded health care provider roles, and utilization of educational
models for disease management and prevention. The most commonly used and well established of these innovative
strategies is the utilization of telemedicine. At present, this service is primarily being used to allow clients access to
physician follow-up from their home community. Research however has indicated a potential for this service to enable
at home rehabilitative care with the support of personal service workers and caregivers allowing them to provide
exercises within the home environment. Further, this system has been utilized in NWO for ongoing community
education and support through programs such as Moving on After Stroke (MOST) and geriatrics consultation. Building
on these successes will create opportunities for specialized rehabilitative consultation and education for remote health
care workers, and the development of a coordinated care network to ensure best practices despite geographic challenges.
Rationale
As outlined in the 2013 NW LHIN Health Services Blueprint, a primary goal is integrated health care services by 2021.
The plan has identified the need for integrated post-acute rehabilitative care services focusing on improving the patient
experience within the healthcare system through a coordinated continuum of services.
A specific focus at this time has been placed on post-acute care services (including Rehabilitative Care,
Ambulatory/outpatient care, and community services). In NWO, regional residents have less access to inpatient
rehabilitation, home care services, post-acute CCC and Long-Term Care (LTC) services in comparison to City of
Thunder Bay residents. As such, it is essential that these services are reviewed and modified such that increased
equitability is available across the region.
Within NWO, the LHIN provides funding for 96 health service providers (HSP). To date, the region has relied as much
as possible on the use of innovative approaches to care, however health provider input has acknowledged duplication,
inconsistencies, and gaps in healthcare services across the region. More significantly, a lack of vision for integration
and communication across levels of care with respect to equitable, system wide access has been identified. These
findings highlight the importance of evaluating current services and creating an integrated systems approach to care
across the region.
These challenges are long-standing and current solutions have failed to meet the needs of communities. The challenges
of providing access to health care have been hindered by several factors such as geographic remoteness, long distances,
low population densities and limited qualified health care providers. The need for a review of the entire system of post-
acute rehabilitative care is required as opposed to a piecemeal approach of trying to meet individual needs of each
community in isolation.
Project Charter
154
Expected Outcomes
It is anticipated that this project will result in the development of an integrated system for rehabilitative care in NWOo.
Within this process both the siting and sizing of rehabilitative programs/services will be examined.
The identified rehabilitative care model will be designed to meet the unique needs of the NW Region specifically,
accounting for the lack of critical mass to implement best practice care in many locations, and the challenge of service
provision in remote parts of the region. The opportunity to use technology and mobile service delivery will be examined
within the model of rehabilitative care.
An integrated system of service delivery will address as appropriate the LHIN blueprint recommendations of7:
- [a model to] organize services and delivery of care at three levels within the NW LHIN: the local, district, and
regional or LHIN-wide (Health Hubs, Integrated District Networks, and Regional Rehabilitative Care Lead)
- The development of networks that provide or arrange to provide a coordinated continuum of services to a target
population.
Fiscally, this review will recommend services across the rehabilitative care continuum throughout the region. It will
additionally inform necessary adjustments to avoid duplication and increase effectiveness in care provision across the
spectrum of rehabilitative care.
Project Scope
Summarize the scope of this project. Then describe ‘what is’ and ‘what is not’ included as part of the work to be
performed on this project. Consider specific features, functions, quality needs or other “must have” requirements and
7 North West LHIN: Health Services Blueprint: Building Our Future. (2012). Accessed at:
http://www.northwestlhin.on.ca/goalsandachievements/Health%20Services%20Blueprint/BlueprintReport.aspx
Project Charter
155
place them in the “IN” scope section. Spell out any exclusions i.e. work that will not be performed, in the “OUT” of
scope section.
“IN” Scope “OUT” of Scope
Describe specific items that WILL be included as part of
the work performed by this project.
Describe specific items that WILL NOT be included as part
of the work performed by this project.
Use of the SJCG Physical Rehabilitation Advisory
Committee as a project governance committee to
provide guidance regarding recommendations for post
acute care in NWO. Additions to the membership as
required will be made to ensure a balanced
representation of members from key stakeholders.
Form sub committees as needed to complete the
work of the Post Acute Review.
Create a clearly defined decision making
process to support the development of a future
state rehabilitation delivery model
Carry out a Current State Analysis: Detailed list of
current service providers across all levels of care:
A detailed environmental scan of current
rehabilitation resources and capacity (including
all inpatient, community based outpatient,
community based services, and outpatient
rehabilitation provided by acute care facilities)
Current referral resources and resources
Current process for transition from pediatric to
adult rehabilitative care
Client demographics
The impact of Quality Based Procedure (QBP)
implementation
Wait times and timeframe to access
rehabilitative care (time from acute admission to
Completion of a detailed current state analysis or
recommendations for acute care provision. Acute care
review will be limited to identifying the number of
clients and length of stay related to these clients who
could be served in a post acute setting.
Inclusion of acute care services within the scope of
this project will be limited to development of
standardized referral processes to rehabilitative care.
This may impact acute care LOS and utilization but
will not impact current rehabilitation care practices.
This project will be limited to a review of physical
rehabilitative care and will not include a detailed
review of mental health care availability and needs in
the region. While it is recognized that there is a role
for mental health care provision within physical
rehabilitation, this will not be the primary focus of
this project. It will however be accounted for in the
assessment of co-morbidities.
Evaluation of the current and future state of palliative
care in NWO will be limited to the current state of
bed allocations, and the impact this has on availability
of rehabilitative care beds. The scope of care provided
for palliative care is beyond the scope of this project.
Focus will remain on rehabilitative care within the
NW LHIN. Evaluation beyond the Northwestern
region will be limited to comparative data in similar
regions and provincial averages.
Project Charter
156
referral and time from referral to rehabilitative
care admission)
Innovative practices currently being utilized
Current capacity and opportunities to achieve
system efficiencies
Current utilization by location and projected
demand for rehabilitative care across the
continuum
Review of current barriers to accessing
rehabilitative care
Volume of service delivered per provider
Review of care being provided outside of the
NW LHIN (including out of province)
Create a Future State and Gap Analysis: Present a
recommended future state of rehabilitative care in the
NW LHIN identifying how to address gaps in service
provision.
A Model of service provision applying the
Health Services Blueprint service delivery
model decision making framework and
definition of basket of services available at the
local Health Hub, District Health campus and
Regional Levels.
Alignment of NWO rehabilitative care services
within levels of care identified through RCA
definitions framework
Future volumes/utilization of services
Identification of opportunities for service
integration
Identification of potential services that can be
carried out at regional locations

Project Charter
157
Identification of opportunities to shift care to
community and identification of the impact
including changes to roles and responsibilities
of care providers
Identification of a plan to address unmet service
needs
Best practice principles applied to decisions
regarding location of service provision
The development of a model for remote
community access
Introduction of innovative practices including
care close to home philosophy
Complete community consultation through Physical
Rehabilitation Advisory Committee
Engage and consult stakeholders throughout the
process in broad geographic regions (Eastern,
Western, Central) and across continuum of
rehabilitative care in order to validate findings
and analyze gaps
Include progress updates to clinicians,
management, leadership and hospital boards as
appropriate.
Develop a LHIN-wide strategy for smooth transition
from Acute Care and across the continuum of
rehabilitative care aligned with other initiatives and
reforms.
Align with work on the Orthopaedic Capacity
Plan, Assess and Restore principles, QBPs for
stroke, hip fracture, and hip/knee replacement,
Physiotherapy reform, Ontario Special Needs
Strategy, and Seniors Health Strategy.
Project Charter
158
Identify/develop clearly defined protocols and
standardized assessments for referrals to and transfers
within rehabilitative care
Apply standardized definitions for levels of
bedded care (utilize RCA Bedded Levels of
Care toolkit)
Explore the benefits and risks of a coordinated
referral and placement process for all
rehabilitative care across the region
Build in strategies to mitigate impacts of
staffing limitations in regional care centers
Identify standardized referral processes across
all facilities (including acute care)
Develop an implementation plan outlining processes
required to reach ideal future state
Identify bed designations (rehabilitation, CCC,
convalescent care) for all facilities
Review patient critical mass and optimal
staffing to provide best quality care
Identify opportunities for innovative care across
region
Confirm the role of Rehabilitative Care
Regional Lead
Ensure cultural appropriateness of programs and
services is accounted for at individual facility
levels
Review progress and plan at small hospital level
for input as needed

Project Charter
159
Carry out a risk assessment including financial
considerations to identify potential impact and barriers
to the successful implementation of the rehabilitative
care integrated service model
Evaluate the impact of HSFR including QBPs
Analyze financial impact on service providers
Identify potential environmental/physical
changes required based on recommended
changes
Establish a detailed evaluation process to monitor
ongoing success and respond to challenges
Appropriateness of referrals
Availability/access to inpatient and outpatient
services across all levels of care
Timeliness of referrals and causes of any
delays/waits
Develop a detailed implementation plan outlining
necessary considerations and steps over 3-5 year
timeframe
Identification of changes in staffing and service
provision for each site
Pilot of small scale versions of recommended
changes at various sites
Consideration of necessary steps for
implementation including staffing changes,
environmental changes, financial impacts
Work with existing review processes to ensure
coordination of post acute services with the Orthopaedic
Project Charter
160
Steering committee, Small Hospitals working group,
Informing Care for seniors, and other current initiatives
Goals, Objectives & Performance Measures
Provide the details of what this project aims to accomplish by listing its specific goals, objectives and deliverables.
State the goals in terms of high-level outcomes to be achieved. Identify specific objectives and deliverables for each
goal listed (reference those identified in your Business Case).
Goals Objectives/Deliverables Performance Measures
List all goals to be achieved by
the project – ensure alignment
with project purpose.
For each goal, list specific objectives
and/or deliverables that will signify
achievement of goal when finished.
Objectives should be the ‘how’ the goal
will be achieved; Deliverables are
concrete products/services/structures
that are produced.
For each objective/deliverable, list the
measures that will be used to evaluate
success of results achieved. Use the
numbering convention shown to link
performance measures to objectives/
deliverables (adjust as needed).
1. Develop guiding principles to
be utilized throughout the
project
A. Work with Physical Rehab
Advisory Committee to develop a
set of guiding principles that will be
followed by all parties involved in
the project
Guiding principles will be
agreed upon by stakeholders
and utilized throughout the
project
All regional care providers
will commit to participating in
a process to develop an
integrated system approach
B. Communication with all regional
partners that an integrated
rehabilitative system, according to
recommended best practices for
care is required
2. Utilize the RCA Capacity
Planning Toolkit to complete
an analysis of the current state
of rehabilitative care in NWO
A. Develop a list of current
rehabilitative care services available
and where clients are being referred
(inpatient rehabilitation, CCC,
Convalescent Care, community and
A detailed list will be
developed including all
regional inpatient, outpatient
and community programs
Project Charter
161
hospital based outpatient programs
and community programs)
A system will be implemented
to ensure the list is updated
according to staffing and
availability changes in
programs over time
B. Evaluate utilization of existing
rehabilitative care system
Comprehensive review of
current service utilization
completed and reviewed for
accuracy by involved
stakeholders
C. Review current referral processes
for rehabilitative care
D. Identify gaps in current service
provision
E. Evaluate current performance of
rehabilitative care (LOS,
readmission rates, client
satisfaction, and recovery rates)
F. Highlight current innovative and
best practices
G. Consult with stakeholders to
validate current state analysis
3. Identify a future state delivery
model for rehabilitative care
A. Complete and validate 2014 survey
results for bedded levels of
rehabilitative care by the RCA
Comparison of
recommendations for best
practices and current practices
utilized to develop ideal future
state projections B. Identify projected rehabilitative
care needs in NWO over the next 5-
10 years
C. Utilize current best practice models
to forecast necessary resources to
meet rehabilitative care needs
D. Confirm the process to access
rehabilitative care (Assess and
Restore) beds directly from the
community/ED

Project Charter
162
E. Develop/identify a referral
management system to ensure
ongoing integration across all levels
of rehabilitative care (Process to
begin in the inpatient care settings)
Development of a coordinated
referral management system
for rehabilitative care
Development/utilization of a
standardized referral form
across all levels of care in
NWO
Identification of
comprehensive evaluation
metrics to evaluate and
monitor effectiveness and
breakdowns of
referral/utilization system
F. Review care structures and
resources/ programs that are needed
to support recommended best
practices
G. Build on the Assess and Restore
process for accessing rehabilitative
care from acute and community
programs (including access to
bedded care, outpatient care,
community care and home based
care)
H. Identify costs strategies to support
required resourcing and geographic
distribution of care as applicable
Development of clear role
definitions for the provision of
rehabilitative care through
Local Health Hubs, Integrated
District Networks, District
Health Campuses, and
Regional lead
Identify innovative strategies
to meet regional care needs
Identify the costs and
environmental changes
required to complete the
proposed plan and adjust the
future model accordingly
based on feedback.
I. Consult with stakeholders to
validate future state model and
ensure accuracy for NW LHIN
4. Develop an action plan for the
implementation of the
integrated model for
rehabilitative care using the
local health hub, IDN and
A. Identify ideal sizing of each level of
the integrated service network
Identification of critical mass
necessary to meet best
practices at each level of care
B. Identification of siting/ designation
of each level of care within the
integrated service network
Determination of the siting of
Regional Rehabilitative Care
lead, care provision levels
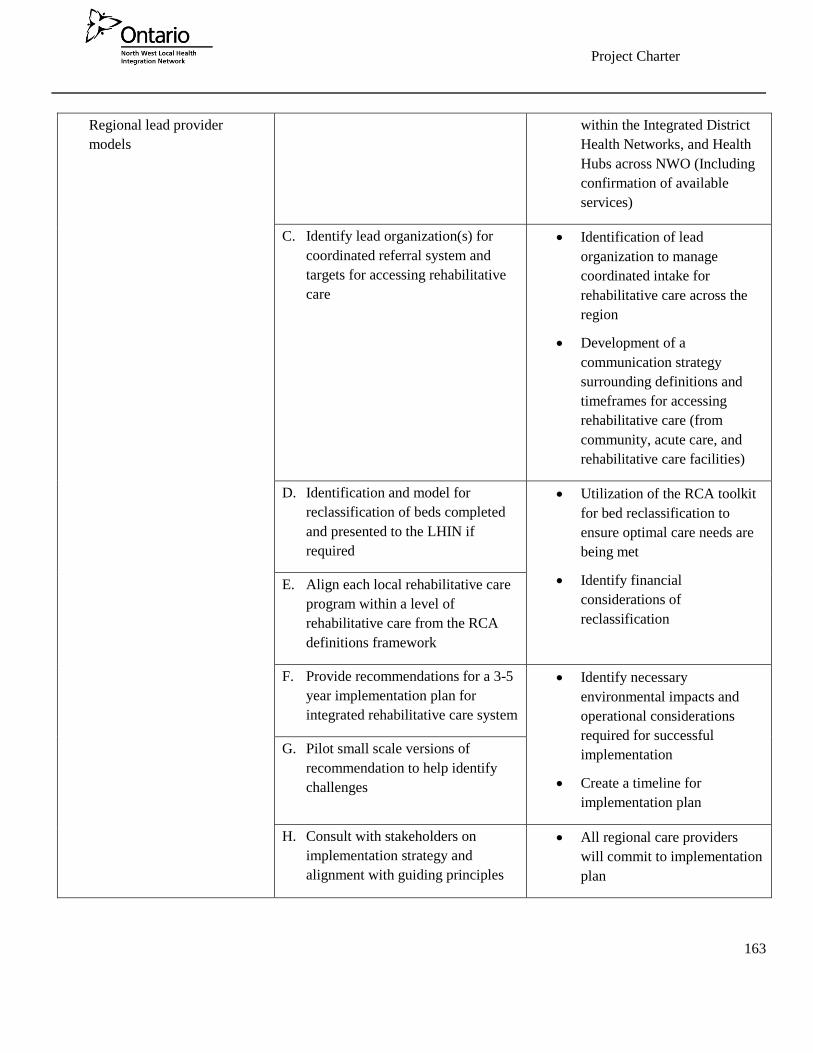
Project Charter
163
Regional lead provider
models
within the Integrated District
Health Networks, and Health
Hubs across NWO (Including
confirmation of available
services)
C. Identify lead organization(s) for
coordinated referral system and
targets for accessing rehabilitative
care
Identification of lead
organization to manage
coordinated intake for
rehabilitative care across the
region
Development of a
communication strategy
surrounding definitions and
timeframes for accessing
rehabilitative care (from
community, acute care, and
rehabilitative care facilities)
D. Identification and model for
reclassification of beds completed
and presented to the LHIN if
required
Utilization of the RCA toolkit
for bed reclassification to
ensure optimal care needs are
being met
Identify financial
considerations of
reclassification
E. Align each local rehabilitative care
program within a level of
rehabilitative care from the RCA
definitions framework
F. Provide recommendations for a 3-5
year implementation plan for
integrated rehabilitative care system
Identify necessary
environmental impacts and
operational considerations
required for successful
implementation
Create a timeline for
implementation plan
G. Pilot small scale versions of
recommendation to help identify
challenges
H. Consult with stakeholders on
implementation strategy and
alignment with guiding principles
All regional care providers
will commit to implementation
plan
Project Charter
164
Alignment with Strategic Directions and Priorities
Identify the project’s strategic alignment with the North West LHIN Strategic Directions, Integrated Health Services
Plan (IHSP) priorities, and eHealth Service Plan priorities. Provide an explanation below if needed.
Strategic Directions:
x Improved health outcomes, resulting in healthier people
x Access to health care that people need, as close to home as possible
x Continuous quality improvement
x A system-wide culture of accountability
Integrated Health Services Plan (2013-2016) Priorities:
x Building an integrated health care system
x Building an integrated eHealth framework
eHealth Service Plan Priorities (2013 – 2016):
x Integrate regional electronic health records (EHRs) to improve patient-centred care
x Build regional capacity to accelerate adoption of eHealth systems and technologies to gain system-wide
efficiencies, as rapidly as possible
x Provide innovative technology solutions to improve access to care and health outcomes, resulting in
healthier people
x Improving access to care
x Enhancing chronic disease prevention and management
Description of Alignment (if needed)
This project has been developed in alignment with the strategic initiative of building an integrated health care system.
The anticipated outcomes of an integrated model for rehabilitative care include improved access as close to home as
possible for all patients, while maintaining best practices for care provision. Incorporated in this will be increased
utilization of technology in both service provision for remote communities and in adoption of technologies to improve
communication and reduce duplication of service delivery in the rehabilitative care sector.

Project Charter
165
This project is also aligned with:
Health System Funding Reform – Including Quality Based Procedures Recommendations
Health Quality Ontario Initiatives
Ontario Stroke Network directions
Ontario Renal Network directions
Provincial Palliative Care Planning
Ontario’s Seniors Strategy (Dr. Sinha Report)
Rehabilitative Care Alliance work
Physiotherapy Reform
Provincial Assess and Restore Guidelines
Provincial and North West LHIN - Orthopaedic Capacity Planning
Provincial Resource Matching and Referral Initiative
Health Links
North West LHIN Regional Rehabilitation and Complex Continuing Care Report
2013 Ontario Auditor General Report – Rehabilitative Services at Hospitals
Ontario Seniors Friendly Hospital Initiative
Ontario Special Needs Strategy
Project Benefits
Complete the Benefits Realization in the ‘Benefits Realization, Change Management, Communications Workbook
file’ (in Operations>eHealth>eHealth>Templates>PMO). Identify specific results-based benefits that can be
expected as a result of completing this project.
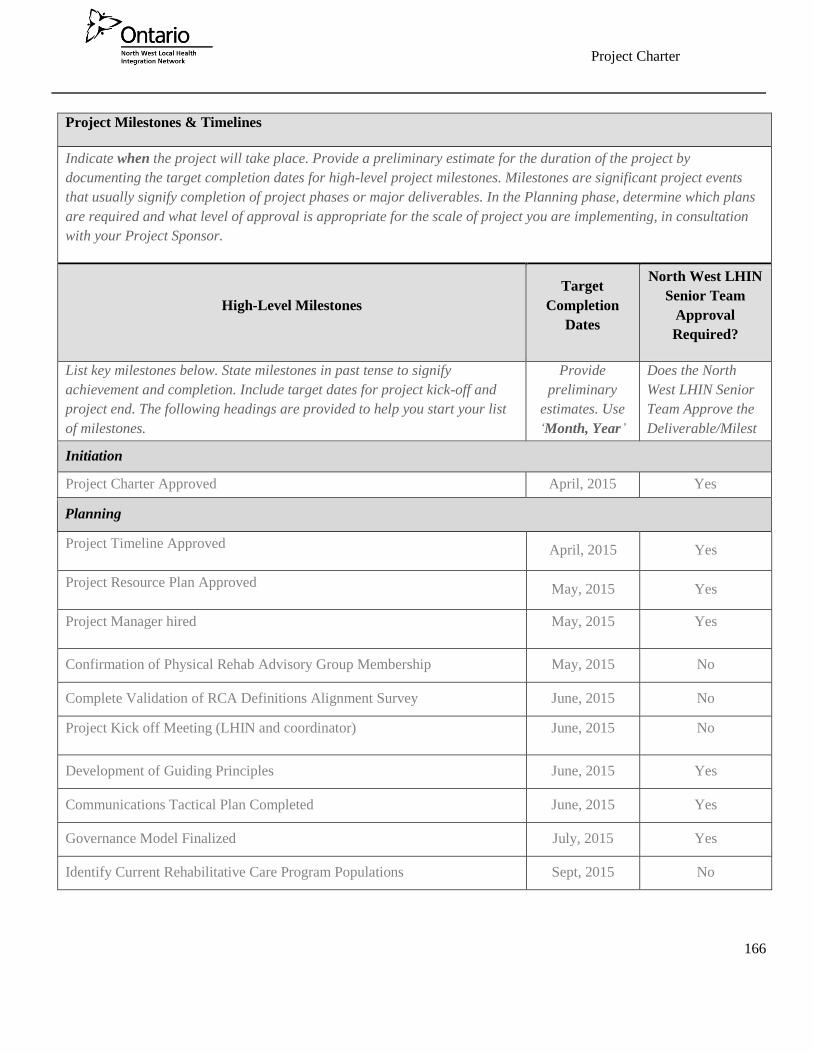
Project Charter
166
Project Milestones & Timelines
Indicate when the project will take place. Provide a preliminary estimate for the duration of the project by
documenting the target completion dates for high-level project milestones. Milestones are significant project events
that usually signify completion of project phases or major deliverables. In the Planning phase, determine which plans
are required and what level of approval is appropriate for the scale of project you are implementing, in consultation
with your Project Sponsor.
High-Level Milestones
Target
Completion
Dates
North West LHIN
Senior Team
Approval
Required?
List key milestones below. State milestones in past tense to signify
achievement and completion. Include target dates for project kick-off and
project end. The following headings are provided to help you start your list
of milestones.
Provide
preliminary
estimates. Use
‘Month, Year’
format.
Does the North
West LHIN Senior
Team Approve the
Deliverable/Milest
one Completion? Initiation
Project Charter Approved April, 2015 Yes
Planning
Project Timeline Approved April, 2015 Yes
Project Resource Plan Approved May, 2015 Yes
Project Manager hired May, 2015 Yes
Confirmation of Physical Rehab Advisory Group Membership May, 2015 No
Complete Validation of RCA Definitions Alignment Survey June, 2015 No
Project Kick off Meeting (LHIN and coordinator) June, 2015 No
Development of Guiding Principles June, 2015 Yes
Communications Tactical Plan Completed June, 2015 Yes
Governance Model Finalized July, 2015 Yes
Identify Current Rehabilitative Care Program Populations Sept, 2015 No

Project Charter
167
Establish Working Groups/Terms of Reference June - Sept,
2015 No
Develop a 3-5 year projected implementation plan Dec 2016 Yes
Executing
Project Team Members Acquired May, 2015 No
Obtain Data on Program Utilization June, 2015 No
Evaluate Data in Comparison to Current State Aug, 2015 No
Complete Current State Analysis Sept, 2015 No
Complete Future State Analysis Oct, 2015 No
Identification of Ideal Population and critical Mass levels to meet best
practices
Jan, 2016 No
Identification of ideal location for Rehabilitative care LEAD, IDNs, Hubs Feb, 2016 Yes
Finalize proposed changes to current bedded care levels/locations Mar, 2016 Yes
Finalize plan for coordinated referral system Mar, 2016 Yes
Finalize a common referral form for all rehabilitative care Mar, 2016 No
Pilot recommended integrations plan at various sites June, 2016 No
Complete stakeholder feedback session and evaluation following pilot Sept, 2016 No
Monitoring & Controlling
Monthly Project Status Reporting (ongoing throughout project) Ongoing No
Benefits Realization Reconciliation Report Complete [Month, Year] No
Development of an evaluation Metric for coordinated referrals Mar, 2016 No
Evaluate Coordinated referral process Ongoing No
Complete evaluation of proposed integrated system and central referral
process
Sept, 2016 Yes
Closing

Project Charter
168
Lessons Learned Complete Dec, 2016 No
Project Close-Out Report and final recommendations complete
(Senior Team Approval consists of a debrief of the Close-Out report with
Lessons Learned to Senior Team, by Project Sponsor)
Jan, 2017 Yes
Funding Sources
Identify source of funding for this project. Indicate whether project costs will be absorbed by an existing organization
or if separate source of funding is required. Refer to your Business Case to summarize funding sources.
[North West LHIN staff covered by North West LHIN operational budget.]
Project Governance
Show the Governance Structure for the project. Identify the North West LHIN Senior Team, the Project Sponsor, and
Project Manager roles, including the composition of a Steering Committee (if needed), and any other related
governing bodies associated with the project.
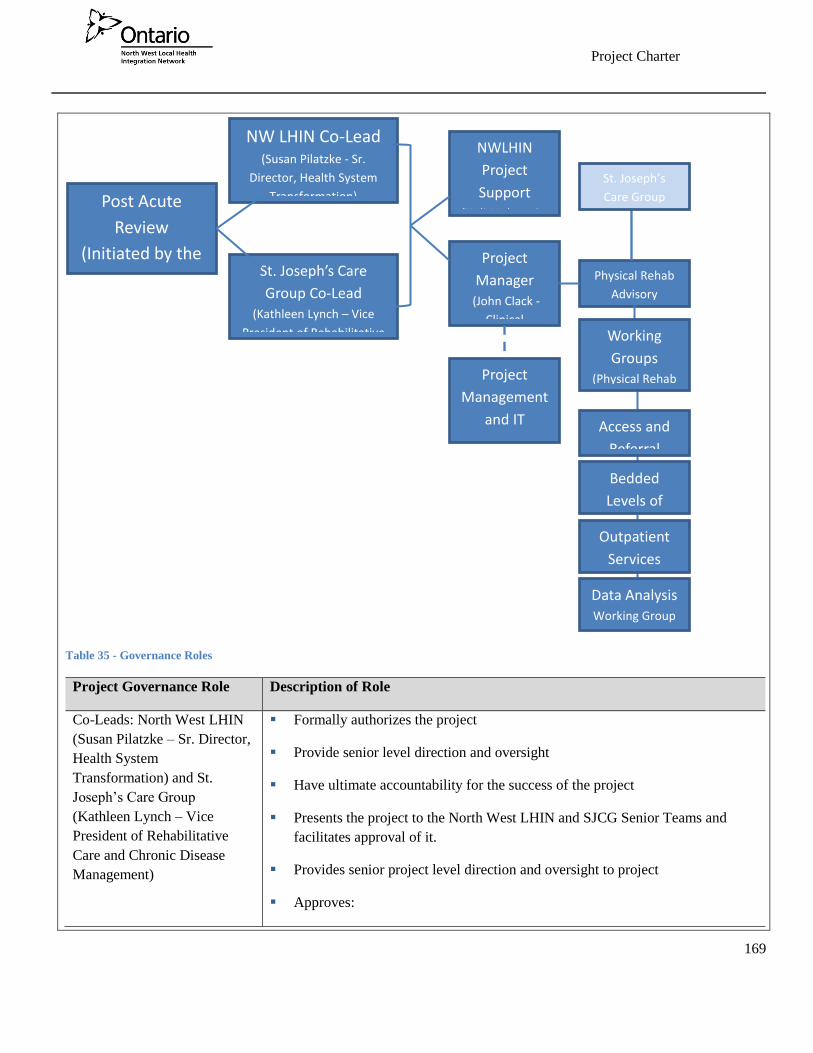
Project Charter
169
Table 35 - Governance Roles
Project Governance Role Description of Role
Co-Leads: North West LHIN
(Susan Pilatzke – Sr. Director,
Health System
Transformation) and St.
Joseph’s Care Group
(Kathleen Lynch – Vice
President of Rehabilitative
Care and Chronic Disease
Management)
Formally authorizes the project
Provide senior level direction and oversight
Have ultimate accountability for the success of the project
Presents the project to the North West LHIN and SJCG Senior Teams and
facilitates approval of it.
Provides senior project level direction and oversight to project
Approves:
Post Acute
Review
(Initiated by the
NWLHIN) Project
Manager (John Clack -
Clinical
St. Joseph’s Care
Group Co-Lead
(Kathleen Lynch – Vice
President of Rehabilitative
NW LHIN Co-Lead (Susan Pilatzke - Sr.
Director, Health System
Transformation)
NWLHIN
Project
Support (Heli Mehta , Sr.
Project
Management
and IT
support
Physical Rehab
Advisory
St. Joseph’s
Care Group
Working
Groups (Physical Rehab
Access and
Referral
Bedded
Levels of
Outpatient
Services
Data Analysis Working Group

Project Charter
170
Project Charter
Material/significant changes to Project Scope or Budget
Material/significant increases to Project Resource Requirements
Material/significant increases to Project Schedule (extension to the Project
End Date or extension to Milestone/Deliverable dates that are identified as
requiring Senior Team approval in the Project Charter)
Changes to Senior Team approvals, as identified in Project Charter
Key project milestones/deliverables (identified in the Project Charter as
requiring Senior Team approval)
Project resources, on behalf of their respective organization (i.e. commits
resources)
Budget expenditures beyond sponsor’s signing authority
Project Manager (John Clack,
Clinical Manager - St.
Joseph’s Care Group)
Project Lead (Heli Mehta, Sr.
Planning and Integration
Consultant - NW LHIN)
Presents the project to the NW LHIN and SJCG co-leads, via project charter
Responsible for the successful planning, execution and delivery of the project
within the approved constraints
Active and visible project champion, advocates for its success
Identifies key risks and issues to the project, manages issues to ensure
resolution and mitigates risks to the acceptable risk tolerance levels; escalates
to the Project Sponsor when necessary
Coordinates overall delivery of the project team
Controls the day-to-day activities of the project
Completes regular organizational status reporting, keeping Project Sponsor
informed of project status
Resolves issues and makes decisions in a timely manner
Is the liaison with the Physical Rehabilitation Advisory Committee
Approves:
Project Charter
171
Non-significant changes to Project Scope, Budget, Resource
Requirements,
Non-significant increases to Project Schedule (those that do not extend the
Project End Date or the Milestone/Deliverable dates that are identified as
requiring Senior Team approval in the Project Charter)
Milestones/deliverables, and recommends/endorses approval of key
milestones/deliverables that require Senior Team approval (as identified in
the Project Charter)
Project expenditures within budget and within signing authority
Lessons Learned and Project Close Out Report (provides a debrief to
Senior Team)
Physical Rehabilitation
Advisory Committee
Represents the stakeholders across all sectors of rehabilitative care and regions
throughout Northwestern Ontario.
Formally advises the project on behalf of their region as a whole
Responsible for sharing perspectives and providing direction to project
Engages regional input and perspectives to inform the project
Informally authorizes the project on behalf of their respective organizations
Recommends/endorses changes to project scope and/or timelines
Garners input from stakeholders and represents the interests of all parties
impacted by the project
Provides project updates to relevant stakeholders as deemed appropriate by the
committee and project team
Project and IT support (North
West Health Alliance)
Formally advises the project on behalf of their region as a whole
Responsible for sharing perspectives and providing direction to project
Provides subject matter expertise to the Project Manager and Project Sponsor
in terms of best practices for project delivery
Active and visible project champion, advocates for its success
Identifies key risks and issues to the project and helps mitigate risks to the
acceptable risk tolerance levels

Project Charter
172
Provides technical support and guidance throughout the project planning,
implementation, and evaluation stages
Working Groups (Physical
Rehab Working group and
relevant stakeholders as
required)
Access and Referral Working Group
o Evaluate current referral system for inpatient and outpatient care
o Identify strategies to ensure equitable access to care across the region
Bedded Levels of Care Working Group
o Review RCA definitions for bedded levels of care
o Review validation survey completed by RCA
o Determine utilization of definitions within integrated system
Outpatient Services Working Group
o Review RCA work on minimum data set
o Review current outpatient services and service delivery models
o Identify optimal outpatient service delivery model to meet best
practices
Data Analysis working group
o Review all relevant data to inform current and future state analysis
o Work with other working groups to determine data requirements
o Participate in RCA outpatient minimum data set
implementation/evaluation
Project Team
Identify who is needed on the core project team to complete project deliverables and achieve its goals and objectives.
What skills, knowledge and experiences are required? Consider the need for special expertise to deal with people and
organization change challenges. Use table below to indicate who will be part of the core project team and who will be
brought-in as required. Include resources from partnering organizations as appropriate. Please consider policy,
architecture, and privacy and security domains for resource requirements.
Role on the Project Required Involvement
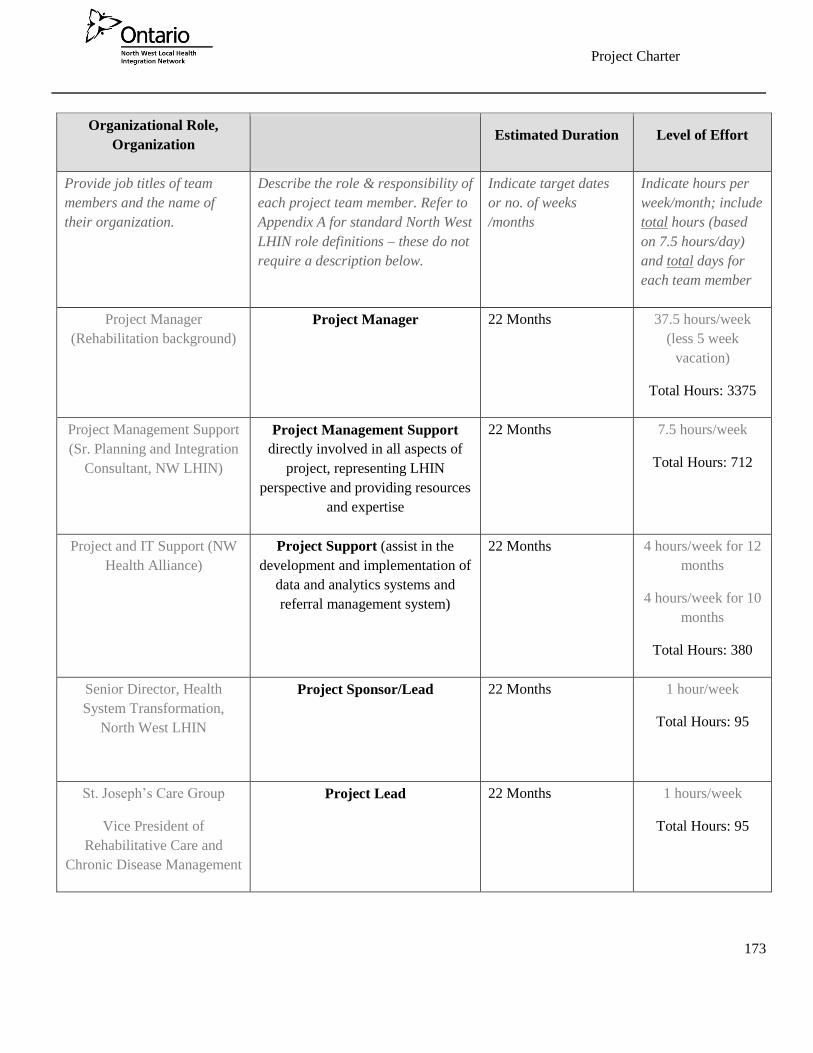
Project Charter
173
Organizational Role,
Organization Estimated Duration Level of Effort
Provide job titles of team
members and the name of
their organization.
Describe the role & responsibility of
each project team member. Refer to
Appendix A for standard North West
LHIN role definitions – these do not
require a description below.
Indicate target dates
or no. of weeks
/months
Indicate hours per
week/month; include
total hours (based
on 7.5 hours/day)
and total days for
each team member
Project Manager
(Rehabilitation background)
Project Manager
22 Months 37.5 hours/week
(less 5 week
vacation)
Total Hours: 3375
Project Management Support
(Sr. Planning and Integration
Consultant, NW LHIN)
Project Management Support
directly involved in all aspects of
project, representing LHIN
perspective and providing resources
and expertise
22 Months 7.5 hours/week
Total Hours: 712
Project and IT Support (NW
Health Alliance)
Project Support (assist in the
development and implementation of
data and analytics systems and
referral management system)
22 Months 4 hours/week for 12
months
4 hours/week for 10
months
Total Hours: 380
Senior Director, Health
System Transformation,
North West LHIN
Project Sponsor/Lead 22 Months 1 hour/week
Total Hours: 95
St. Joseph’s Care Group
Vice President of
Rehabilitative Care and
Chronic Disease Management
Project Lead 22 Months 1 hours/week
Total Hours: 95

Project Charter
174
Epidemiologist, North West
LHIN
Project Team Member 22 Months 0.5 Day/Month
Total Hours: 88
Communications, North West
LHIN
Project Team Member 22 Months 0.5 hours/Week
Total Hours: 48
Physical Rehabilitation
Advisory Committee
Advisory Committee 22 Months 3 hours/Quarter and
Working Group
Participation as
needed
Total Hours: 35+
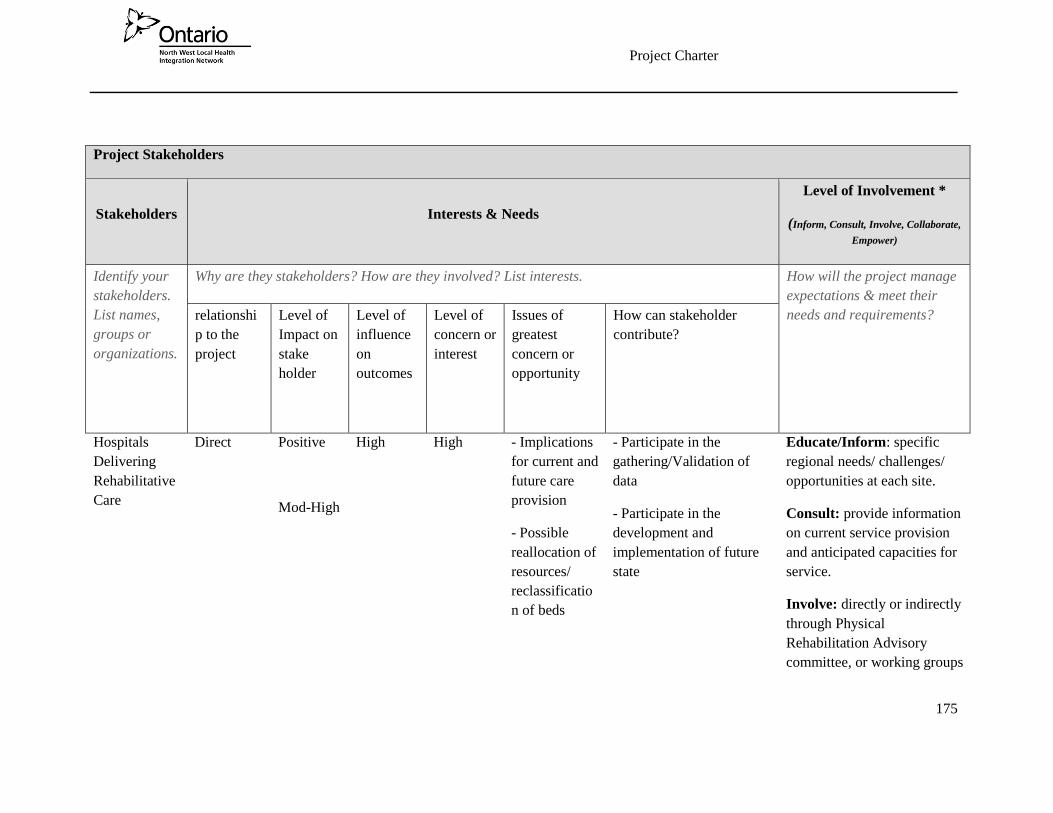
Project Charter
175
Project Stakeholders
Stakeholders Interests & Needs
Level of Involvement *
(Inform, Consult, Involve, Collaborate,
Empower)
Identify your
stakeholders.
List names,
groups or
organizations.
Why are they stakeholders? How are they involved? List interests. How will the project manage
expectations & meet their
needs and requirements? relationshi
p to the
project
Level of
Impact on
stake
holder
Level of
influence
on
outcomes
Level of
concern or
interest
Issues of
greatest
concern or
opportunity
How can stakeholder
contribute?
Hospitals
Delivering
Rehabilitative
Care
Direct Positive
Mod-High
High High - Implications
for current and
future care
provision
- Possible
reallocation of
resources/
reclassificatio
n of beds
- Participate in the
gathering/Validation of
data
- Participate in the
development and
implementation of future
state
Educate/Inform: specific
regional needs/ challenges/
opportunities at each site.
Consult: provide information
on current service provision
and anticipated capacities for
service.
Involve: directly or indirectly
through Physical
Rehabilitation Advisory
committee, or working groups

Project Charter
176
Collaborate: provide input
on referral design and
evaluation
North West
Community
Care Access
Centers
Direct Positive
High
Mod High -Increased
involvement
in referral
management
system
- Changes in
community
service
provision
- Participate in the
gathering/validation of
data
- Participate in the
development and
implementation of the
future state
Educate/Inform: Provide
insight on regional needs,
limitations and system
improvements
Consult: provide information
on current service provision
and anticipated capacities for
service.
Involve: through Physical
Rehabilitation Advisory
committee and working
groups.
Collaborate: provide input
on referral design and
evaluation methods
Physical
Rehabilitation
Advisory
Committee
Direct Neutral
Mod
High High - Represent
various
stakeholders
- Change in
overall
mandate of
- Represent and provide
recommendations from
various stakeholders
- Participate in
development and
evaluation of future state
Educate/Inform: Provide
information and updates to
stakeholders across the
region.
Ensure that all perspectives
are represented.
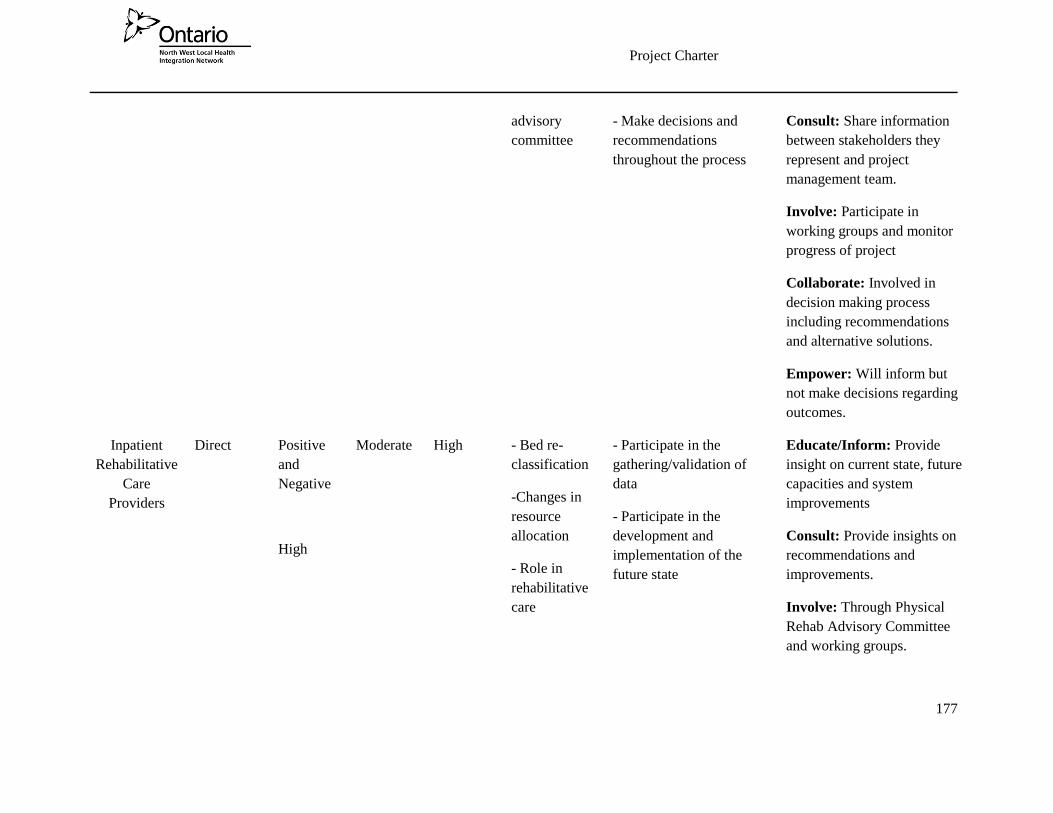
Project Charter
177
advisory
committee
- Make decisions and
recommendations
throughout the process
Consult: Share information
between stakeholders they
represent and project
management team.
Involve: Participate in
working groups and monitor
progress of project
Collaborate: Involved in
decision making process
including recommendations
and alternative solutions.
Empower: Will inform but
not make decisions regarding
outcomes.
Inpatient
Rehabilitative
Care
Providers
Direct Positive
and
Negative
High
Moderate High - Bed re-
classification
-Changes in
resource
allocation
- Role in
rehabilitative
care
- Participate in the
gathering/validation of
data
- Participate in the
development and
implementation of the
future state
Educate/Inform: Provide
insight on current state, future
capacities and system
improvements
Consult: Provide insights on
recommendations and
improvements.
Involve: Through Physical
Rehab Advisory Committee
and working groups.
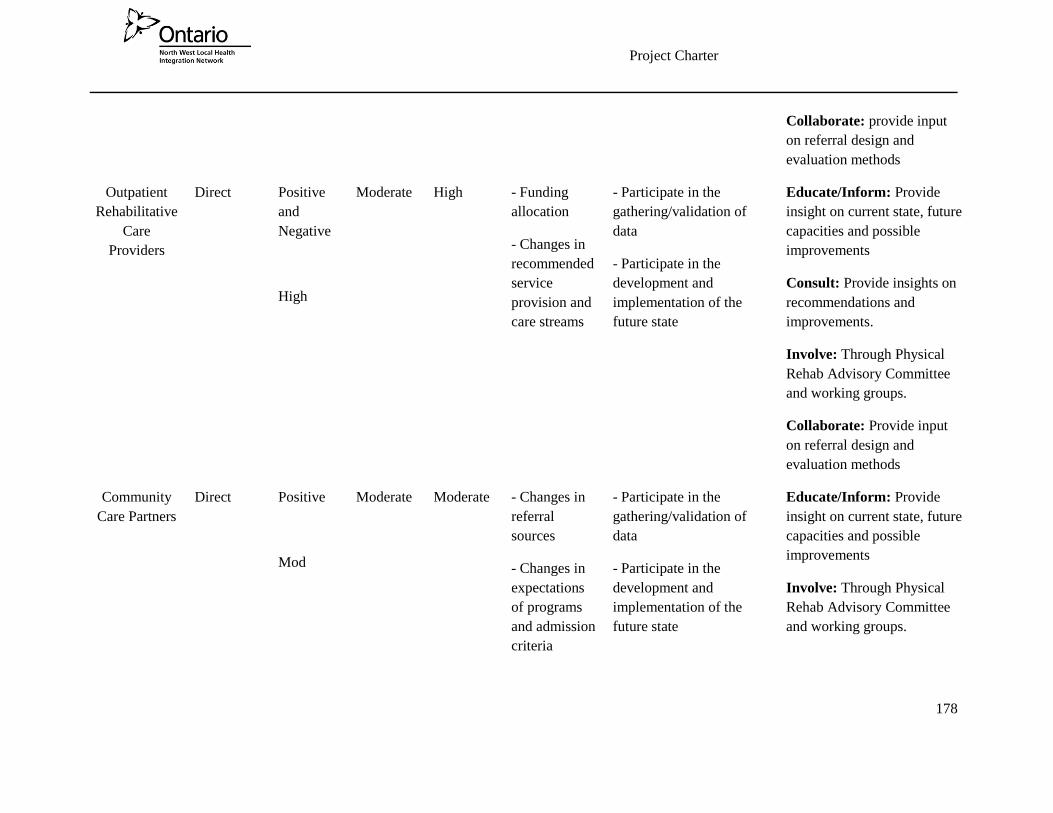
Project Charter
178
Collaborate: provide input
on referral design and
evaluation methods
Outpatient
Rehabilitative
Care
Providers
Direct Positive
and
Negative
High
Moderate High - Funding
allocation
- Changes in
recommended
service
provision and
care streams
- Participate in the
gathering/validation of
data
- Participate in the
development and
implementation of the
future state
Educate/Inform: Provide
insight on current state, future
capacities and possible
improvements
Consult: Provide insights on
recommendations and
improvements.
Involve: Through Physical
Rehab Advisory Committee
and working groups.
Collaborate: Provide input
on referral design and
evaluation methods
Community
Care Partners
Direct Positive
Mod
Moderate Moderate - Changes in
referral
sources
- Changes in
expectations
of programs
and admission
criteria
- Participate in the
gathering/validation of
data
- Participate in the
development and
implementation of the
future state
Educate/Inform: Provide
insight on current state, future
capacities and possible
improvements
Involve: Through Physical
Rehab Advisory Committee
and working groups.
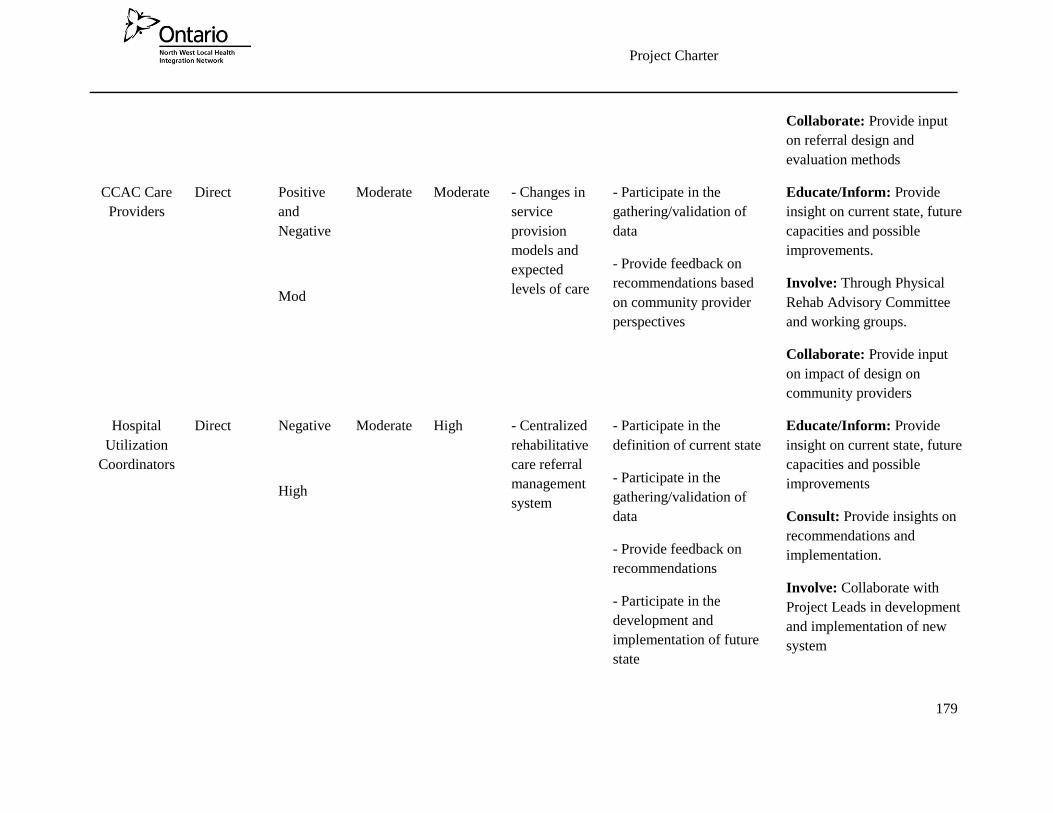
Project Charter
179
Collaborate: Provide input
on referral design and
evaluation methods
CCAC Care
Providers
Direct Positive
and
Negative
Mod
Moderate Moderate - Changes in
service
provision
models and
expected
levels of care
- Participate in the
gathering/validation of
data
- Provide feedback on
recommendations based
on community provider
perspectives
Educate/Inform: Provide
insight on current state, future
capacities and possible
improvements.
Involve: Through Physical
Rehab Advisory Committee
and working groups.
Collaborate: Provide input
on impact of design on
community providers
Hospital
Utilization
Coordinators
Direct Negative
High
Moderate High - Centralized
rehabilitative
care referral
management
system
- Participate in the
definition of current state
- Participate in the
gathering/validation of
data
- Provide feedback on
recommendations
- Participate in the
development and
implementation of future
state
Educate/Inform: Provide
insight on current state, future
capacities and possible
improvements
Consult: Provide insights on
recommendations and
implementation.
Involve: Collaborate with
Project Leads in development
and implementation of new
system

Project Charter
180
Physicians
referring to
rehabilitative
care
Direct Positive
and
Negative
High
Moderate High - Changes in
referral
processes
- Participate in the
definition of current state
- Participate in the
gathering/validation of
data
- Provide feedback on
recommendations
- Participate in the
development and
implementation of future
state
Educate/Inform: Provide
insight on current state, future
capacities and possible
improvements.
Consult: Provide feedback on
Physician utilization of
system.
Collaborate: Provide input
regarding physician
acceptance
Empower: Will advise and
endorse final
recommendations
MOHLTC Indirect Positive
Min
High High - Increased
integration of
care
- Changes in
resource
allocation
- Contribute data from
peer processes
- Participate in support of
recommendations and
implementation plan
Educate/Inform: Provide
information on similar
projects
Consult: Voice concerns
throughout project
Empower: Will review final
recommendations and endorse
all final decisions
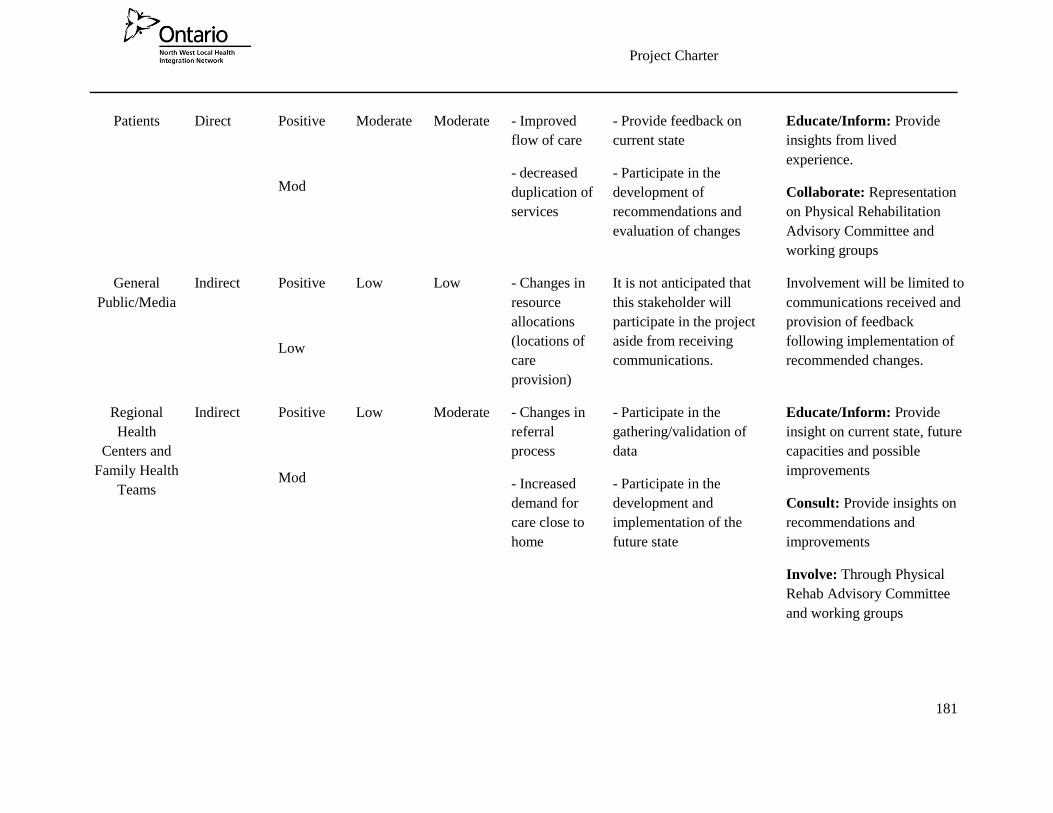
Project Charter
181
Patients Direct Positive
Mod
Moderate Moderate - Improved
flow of care
- decreased
duplication of
services
- Provide feedback on
current state
- Participate in the
development of
recommendations and
evaluation of changes
Educate/Inform: Provide
insights from lived
experience.
Collaborate: Representation
on Physical Rehabilitation
Advisory Committee and
working groups
General
Public/Media
Indirect Positive
Low
Low Low - Changes in
resource
allocations
(locations of
care
provision)
It is not anticipated that
this stakeholder will
participate in the project
aside from receiving
communications.
Involvement will be limited to
communications received and
provision of feedback
following implementation of
recommended changes.
Regional
Health
Centers and
Family Health
Teams
Indirect Positive
Mod
Low Moderate - Changes in
referral
process
- Increased
demand for
care close to
home
- Participate in the
gathering/validation of
data
- Participate in the
development and
implementation of the
future state
Educate/Inform: Provide
insight on current state, future
capacities and possible
improvements
Consult: Provide insights on
recommendations and
improvements
Involve: Through Physical
Rehab Advisory Committee
and working groups

Project Charter
182
Collaborate: Provide input
on referral design and
evaluation methods
Ontario
Telemedicine
Network
Direct Positive
Mod
Low Moderate - Increased
reliance on
innovative
strategies
- Participate in the
gathering/validation of
data
- Participate in the
capacity and future state
planning
Educate/Inform: Provide
information on available
services
MPP’s Indirect Positive
Low
Low Low - Public
Response to
changes
- Help to disseminate
information to the public
in alignment with
communication strategy.
Will be limited to
communication with
necessary stakeholders as
required throughout the
project
North West
LHIN
Direct Positive
Low
High High - Increased
integration of
care and
decreased
duplication of
services
- Alignment
with health
services
blueprint
- Participate in the
gathering/validation of
data
- Participate in the
gathering/validation of
input
- Provide communication
to external stakeholders
- Support/endorse final
project recommendations
Educate/Inform: Provide
strategic directions and
leadership
Consult: Review all
recommendations and
approve all decisions.
Involve: Represent collective
interests of the region as a
whole
Collaborate: Participate in
the Physical Rehabilitation
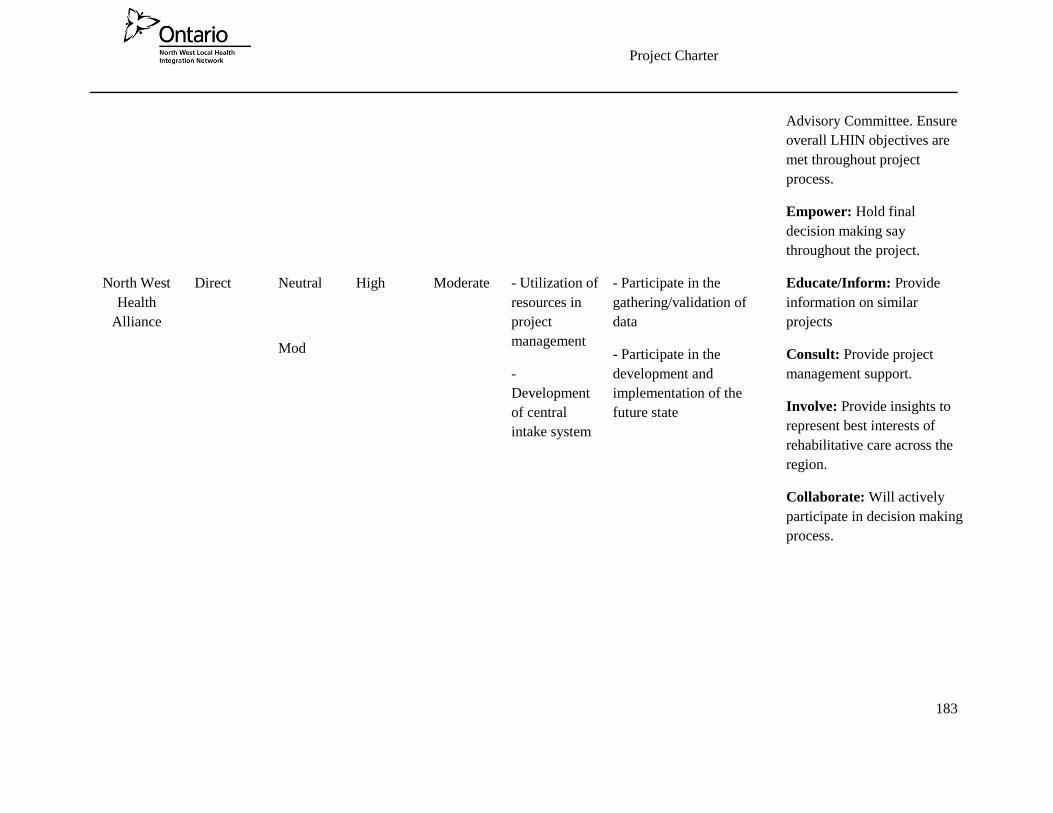
Project Charter
183
Advisory Committee. Ensure
overall LHIN objectives are
met throughout project
process.
Empower: Hold final
decision making say
throughout the project.
North West
Health
Alliance
Direct Neutral
Mod
High Moderate - Utilization of
resources in
project
management
-
Development
of central
intake system
- Participate in the
gathering/validation of
data
- Participate in the
development and
implementation of the
future state
Educate/Inform: Provide
information on similar
projects
Consult: Provide project
management support.
Involve: Provide insights to
represent best interests of
rehabilitative care across the
region.
Collaborate: Will actively
participate in decision making
process.
Project Charter
184
Change Management
Identify the amount of change that will result from the implementation of this project. Rate the expected amount of
change as Low, Medium, or High. Consider things such as: the breadth/scope of the project, the magnitude of the
change, the degree of automation that the implemented solution will result in, the amount of change required to
existing business processes, and the impact on individuals with regards to how they currently perform their jobs.
Amount of change expected: ☐ Low x Medium ☐ High
Identify the areas impacted by the change - both the people and structures of the affected organizations. Who will be
impacted, either positively or negatively, as a result of the change that will result from implementing this project? Are
there any security, legal or privacy implications that need to be considered? What will the project do to ensure end-
user/client uptake of the new product, service or solution?
Description of Impact Impact Management Strategies
List the change impacts this project will have on people
and organizations. Identify who/what will be impacted
and provide a description of that impact.
List the strategies that will be adopted on this project to
minimize the negative and maximize the positive change
impacts of this project.
- All rehabilitative care will utilize a common
referral form and a coordinated referral
management system
- Agreement by hospital CEO’s for global adoption
of a new system
- Involvement of allied health, physicians, CCAC
and utilization coordinators in referral form
development
- Utilization of NorthWest Health Alliance in
implementation of referral management system
- Adoption of common definitions for levels of
rehabilitative care
* Level of Involvement:
Educate/Inform (i.e. provide balanced and objective information to assist
with understanding the problem, alternatives, opportunities and/or
solutions)
Consult (i.e. obtain feedback on analysis, alternatives and/or decisions)
Involve (i.e. work directly throughout the project to ensure that concerns
and aspirations are consistently understood and considered)
Collaborate (i.e. partner in the decision process including the
development of alternatives and identification of preferred
solutions)
Empower (i.e. to allow final decision-making)

Project Charter
185
- Built-in regular evaluation metrics
- Potential redefinition of bed allocation and
outpatient/community program utilization
- Involve input from all organizations providing
rehabilitative care
- Ensure client needs are best met by any changes
- Follow best-practices guidelines for service
provisions
- Mitigate staffing changes and focus on resource
allocation within each location/service
- Designation of roles for each organization
within hub and spoke model
- Provide clear definitions of expectations for ; local
health hubs, district integrated networks and
rehabilitative care lead organization
- Outline how each level can collaborate to promote
integrated and close to home care
Procurements
Identify any procurements (e.g. project personnel, equipment, computer system) needed for the project.
Are procurements required? x Yes ☐ No If Yes, identify the type(s) of procurements needed.
Personnel:
- Dedicated project management support for the capacity planning, system re-design and implementation of an
integrated health system for rehabilitative care (1.0 Project manager position for 24 months)
- Dedicated technology support for the identification and implementation of a centralized referral system
(Support to be provided by the North West Health Alliance)
Equipment:
- Dedicated office, computer and telephone access for Project Manager
Computer System:
- In conjunction with CCAC, an electronic computer system to enable centralized referrals and ongoing
utilization support for all levels of rehabilitative care in the region. This will include an ongoing database of
Project Charter
186
available beds, staffing, and anticipated discharges across the region (inpatient, outpatient and community
programs).
Note: If Yes, the Procurement Plan is to be completed during the Planning phase of the project. Refer to PMO
template directory on SharePoint.
Community Engagement
Determine if any Community Engagement (CE) is needed for the project.
Note: CE is both a legislated responsibility and a core function of the LHINs. Local decision making is the model that
the LHINs are built on, and one that values the input of community members, health care professionals, and
stakeholders to inform our planning and decision making processes.
Is Community Engagement required? x Yes ☐ No
Note If Yes, the Community Engagement Plan is to be completed during the Planning phase of the project. Refer to
PMO template directory on SharePoint.
Project Risks
Consider what if… Document high-level project risks, apparent at this point, that could either positively or negatively
impact the achievement of project goals and objectives. Risks are uncertain events that may take place. Indicate the
risk, your response to manage it i.e. the Treatment and Response, the residual likelihood of it occurring, and its
anticipated residual impact. Focus on risks that are likely to happen and those that could have significant effect on
project success. Be sure to consider risks associated with people & organizational change, knowledge management,
and transition to operations.
Risk Treatment* Response Likelihood*
*
Impact**
*

Project Charter
187
List high-level risks i.e.
uncertain events that
pose threats or
opportunities to the
project.
Accept
Avoid
Mitigate
Transfer
Explain what will be done to accept, avoid,
mitigate or transfer the risk.
(Refer to
legend
below)
(Refer to
legend
below)
Not all stakeholders
agree on future state of
Rehabilitative Care
Mitigate - Involve representation of all
stakeholders throughout the project
- Utilize best practice guidelines to
support/facilitate recommendations
- Utilize Rehabilitative Care
Alliance decision making
frameworks to ensure objective
decision making
Likely Moderate
Not all organizations
willing to participate
Mitigate - Ensure commitment and support of
LHIN and CEO’s for full
participation
- Base recommendation on best
practices for client care
- Utilize available resources to
develop common definitions across
all organizations/levels of care
Possible Major
Insufficient financial
support to ensure success
of the project
Mitigate - Develop clear financial expectations
for the duration of the project
- Ensure ongoing communication
between LHIN and project leads
Unlikely Major
Capacity planning
exercise indicates need
for bed reductions
Mitigate - Evaluate entire system to identify
opportunities to offset potential bed
reductions (ie. alternate bed
allocations)
Possible Minor
Resource Matching and
Referral implementation
process not in alignment
with project
Mitigate - Continue to communicate with
MOHLTC and LHIN regarding
progression of RM&R
Possible Minor
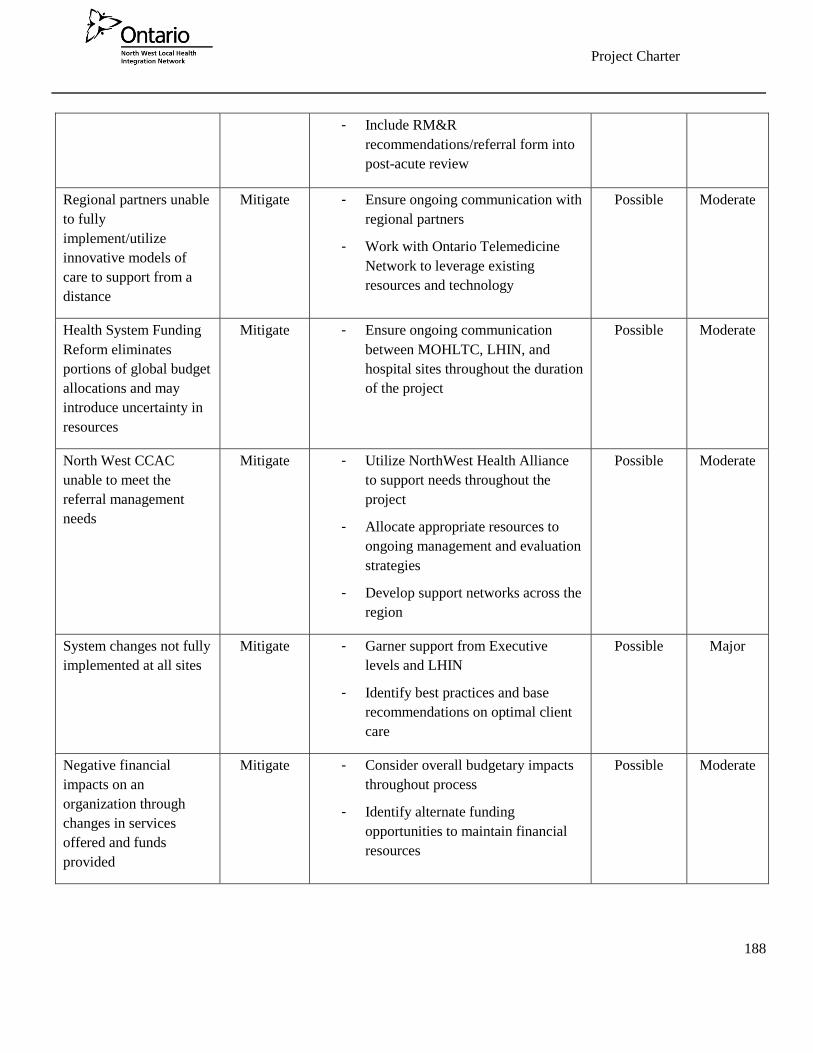
Project Charter
188
- Include RM&R
recommendations/referral form into
post-acute review
Regional partners unable
to fully
implement/utilize
innovative models of
care to support from a
distance
Mitigate - Ensure ongoing communication with
regional partners
- Work with Ontario Telemedicine
Network to leverage existing
resources and technology
Possible Moderate
Health System Funding
Reform eliminates
portions of global budget
allocations and may
introduce uncertainty in
resources
Mitigate - Ensure ongoing communication
between MOHLTC, LHIN, and
hospital sites throughout the duration
of the project
Possible Moderate
North West CCAC
unable to meet the
referral management
needs
Mitigate - Utilize NorthWest Health Alliance
to support needs throughout the
project
- Allocate appropriate resources to
ongoing management and evaluation
strategies
- Develop support networks across the
region
Possible Moderate
System changes not fully
implemented at all sites
Mitigate - Garner support from Executive
levels and LHIN
- Identify best practices and base
recommendations on optimal client
care
Possible Major
Negative financial
impacts on an
organization through
changes in services
offered and funds
provided
Mitigate - Consider overall budgetary impacts
throughout process
- Identify alternate funding
opportunities to maintain financial
resources
Possible Moderate

Project Charter
189
Failure to recruit
sufficient human
resources to support
recommendations
Accept - Develop strategies to manage with
varying staffing availability within
the recommendations
Likely Minor
**Likelihood – The likelihood or probability that the risk/issue will occur.
Rare – Extremely unlikely. <2%
Unlikely– Could occur but unlikely. 10%
Possible – Might occur sometime. 25%
Likely – Will probably occur sometime. 50%
Almost Certain – Expected to occur in most circumstances. >75%
***Impact – The impact to the project the risk will have.
Insignificant – Can be dealt with or taken advantage of
easily/routinely.
Minor – Threat will threaten efficiency or effectiveness of some aspect
of the project but can be dealt with internally.
Moderate – Threat will significantly affect the project but not threaten
its survival.
Major – Threat could threaten the survival of the project as presently
defined.
Critical – Threat will almost certainly stop the project.
*Treatment – How you will manage the risk.
Accept – Acknowledge the risk and not take any action unless the risk occurs
Avoid – Eliminate the threat or protect the project from its impact
Mitigate – Reduce the probability of occurrence or impact
Transfer – Shift the impact of a threat to a third party along with the
ownership of the response e.g. buying insurance

Project Charter
190
Critical Success Factors
Define key factors that are critical to success of the project. These conditions must be satisfied to enable successful
completion of project objectives and deliverables. Include significant events or decisions that need to take place.
Successful development of guiding principles and adherence to principles by all organizations involved in the
review.
Full commitment and ongoing input from all stakeholders and support of CEO’s. This will be achieved through
advisory committee and working group involvement, and broad community forums as required.
Ongoing effective communication occurs to ensure engagement at all levels of care (front line providers, clients,
management, and administration) and across all stages of rehabilitative care (inpatient, outpatient, and
community).
Identification and development of an implementation plan for a system to manage all referrals and program
placement throughout the region.
Development of an evaluation system to monitor effectiveness and identify system breakdowns in order to
maintain ongoing utilization and commitment to system use.
Assumptions & Constraints
Assumptions are external factors that, at the time of writing the charter, are considered true, real or certain for
purposes of planning. Certain unverified or unknown aspects that are likely to happen must be assumed as facts to
proceed. Constraints are factors that are external to the project (i.e. outside the control of the project team), that
restrict or regulate the project. They limit available options and affect performance of the project e.g. an imposed
deadline, a specific budget, etc.
Assumptions Constraints
List the assumptions made to date. What did you
have to assume to be true to complete the charter?
List project constraints. Consider time, budget, scope, quality,
availability/skills of resources, priorities, etc.
All parties involved adhere to guiding
principles throughout the project
All organizations will commit to participate in
the capacity planning exercise in a timely
fashion
Continually changing staffing needs and care demands will
necessitate ongoing communication throughout the project
Limited data is available to inform certain areas of capacity
planning and may impact the overall results. This will
require some reliance on subjective data reporting creating
a risk of misrepresentation.

Project Charter
191
All rehabilitative care facilities/programs will
accept the recommendations and participate
fully in an integrated system
Sufficient resources are made available through
capacity planning, system development, and
recommendation phases
Full support of CCAC to increase role and
manage central intake of rehabilitative care
Availability of an appropriate electronic referral
management system that can accept referrals
and monitor ongoing program and staff
availabilities across the region
Time and resources are limited (all organizations may be
participating in several initiatives simultaneously and will
have competing demands due to internal operational
responsibilities).
Senior Team Representative
Sign-off by a member of Senior Team signifies that there is clear commitment on behalf of Senior Team to: provide
the necessary guidance and support, contribute necessary resources and budget, make decisions (approvals) and
resolve escalated issues in a timely manner, and, remove barriers to facilitate timely project completion, as outlined
in the charter. By approving the project charter, Senior Team has understood what will be delivered.
Name Signature Date
Project Sponsor
Sign-off by Project Sponsor signifies that there is clear accountability for the project by the sponsor, and a
commitment to: provide guidance and support, obtain necessary resources and budget, facilitate timely resolution of
escalated issues, ensure timely decisions are made and obtained, and confirm that all deliverables produced
contribute to achieving the project goals and objectives outlined in the charter. By approving the project charter,
Sign-Off
Project Charter must be approved & signed-off by the Project Manager, Project Sponsor and the North West
LHIN’s Senior Team before Planning can be begin. Once completed & signed-off, the charter forms the basis for
detailed planning and future decision-making. It cannot be modified without securing the sponsor’s approval and
possibly Senior Team’s approval. Any changes to information contained in the charter must be documented using a
formal Project Change Request and the associated process.

Project Charter
192
the sponsor has understood what will be delivered to achieve the identified business goals/benefits, and is in
agreement with the performance measures and success factors identified.
Name Signature Date
Project Manager
Sign-off by Project Manager signifies that there is clear commitment to adhere to the terms of the charter and
ensure that the project proceeds to meet the objectives defined in it.
Name Signature Date
Steering Committee Chair/Co-Chair [delete this section if not using a Steering Committee]
Sign-off by Steering Committee Chair/Co-Chair signifies that there is clear commitment to adhere to the terms of the
charter and to: provide guidance and support, obtain necessary resources and budget, facilitate timely resolution of
escalated issues, ensure timely decisions are made and obtained, and confirm that all deliverables produced
contribute to achieving the project goals and objectives outlined in the charter. By approving the project charter,
the Steering Committee members have understood what will be delivered to achieve the identified business goals/
benefits, and are in agreement with the performance measures and success factors identified.
Name Signature Date
Project Charter
193
Appendix E – Project Roles and Responsibilities
The following identifies the standardized project roles and responsibilities for North West LHIN projects.

Project Charter
194

Project Charter
195
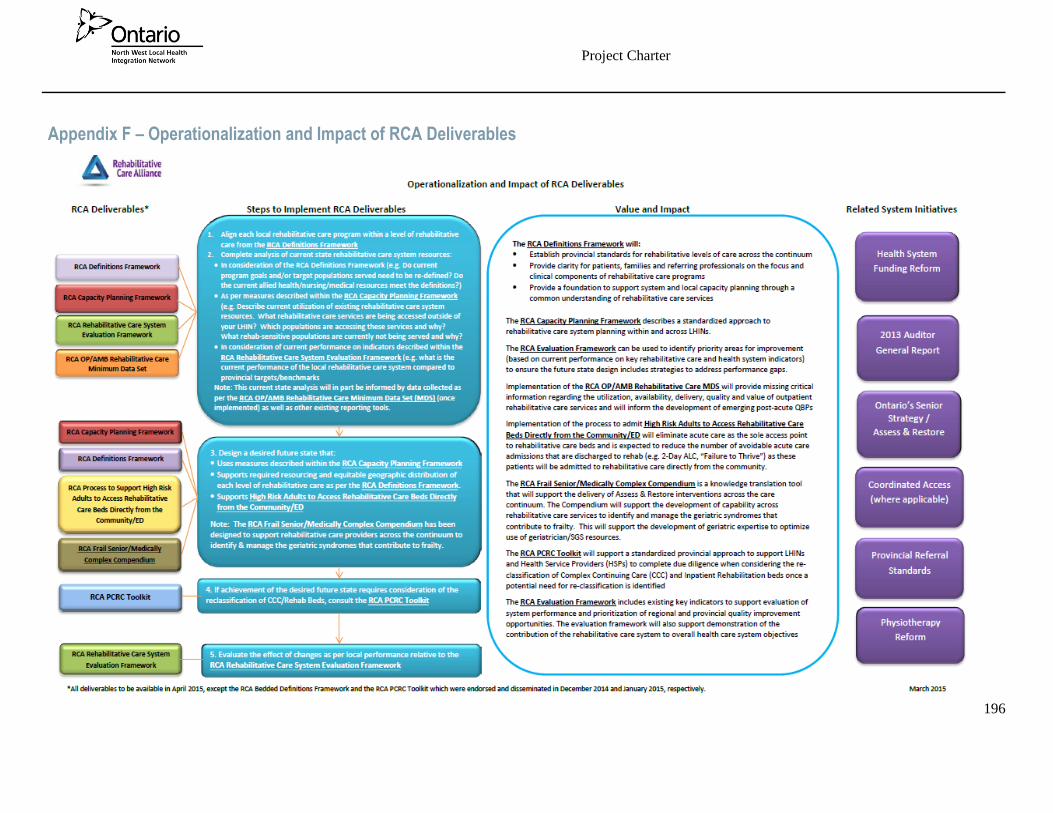
Project Charter
196
Appendix F – Operationalization and Impact of RCA Deliverables

197
Appendix G – Methodology Quantitative Data Sources
Continuing Care Reporting System (CCRS),
National Rehabilitation Reporting System (NRS),
Cancer Care Ontario Access to Care reports,
Meditech Data,
Intellihealth Data collection system,
North West Health Alliance (NWHA) data collection systems,
Analysis provided by Preyra Solutions and the Central West LHIN.

198
Appendix H – Physical Rehabilitation Advisory Committee Rehabilitative Care Review
Guiding Principles
Guiding Principles:
Post-Acute Review - Physical Rehabilitation Advisory Committee 2015-16
1) The committee will share a common vision for creating an integrated rehabilitative care system
that is sustainable and meets the needs of consumers and families.
2) Discussions will begin from a position of trust: in preparation for the discussions, mutual
expectations will clearly be articulated. Members of the committee will work together to resolve
issues within the scope of the terms of reference (see attached).
3) Staff will readily share available data, information, knowledge, and wisdom to inform advisory
committee members so they may provide feedback and advice in the best interest of the
integrated rehabilitative care system as a whole. This will be conducted in a safe environment
for all members.
4) Members will work collaboratively, striving to reach optimal outcomes to meet the shared vision
of local health system planning including; equitable access for all as close to home as possible;
equitable access to appropriately resourced care regardless of ability to pay; a rehabilitative
care model with linkages between hospitals and community services supported by system-wide
support for access and navigation. Clinical best practices, metrics and standards will be utilized
and based on best available scientific evidence and updated as necessary by content expert
panels (eg. Orthopaedic review, Ontario Stroke Network, Quality Based Procedures, etc.).
5) Members will focus on achieving system wide transformations in the delivery of quality,
integrated patient-centered, sustainable rehabilitative care services.
6) Every rural region and community is unique in its history and development, and therefore in its
needs and aspirations.
7) The value of a service to the population must be considered to accurately assess performance of
rehabilitative care delivery in more sparsely populated rural areas.

199
2015-16 PRAC Representation
NAME REPRESENTATION NOTES
Esme French (Chair) Public Representative Voting
Lauri Moffat-Zawacki Local Services Provider (BISNO) Voting
Jason Taddeo Local Services Provider (Family Physio) Voting
Dr. Hanan El Sherif Professional Staff Voting
Kathryn Hughes Local Services Provider (CCAC) Voting
Karen Pontello Local Services Provider Voting
Maria Lassonde Public Representative Voting
Stephen Mangoff (Vice Chair) Regional Hospital (East) Voting
Judy Mostow Public Representative Voting
Laura-Lee Barrie Local Hospital (TBRHSC) Voting
Lucy Venne-Fecho Regional Hospital (West) Voting
Sister Cecily Hewitt SJCG Board Representative Voting
Nancy Bouchard First Nation Representative Voting
Jocelyn Bourgoin
Angie Bishop
Susan Pilatzke
Heather Gray
STAFF RESOURCES
Kathleen Lynch VP, Rehabilitative Care & Chronic Disease Management Non-voting
Janine Black Director, Inpatient Complex Care & Rehabilitative Care Non-Voting
Susan Franchi Director, Outpatient Rehabilitative Care & Chronic Disease
Management
Non-Voting
John Clack Post-Acute Review Coordinator Non-Voting
200
ST. JOSEPH’S CARE GROUP
THUNDER BAY, ON
APPROVED: SEPTEMBER 2014
PHYSICAL REHABILITATION ADVISORY COMMITTEE
TERMS OF REFERENCE
MISSION STATEMENT
St. Joseph’s Care Group is a Catholic organization that identifies and responds to the unmet needs of the
people of Northwestern Ontario, as a way of continuing the healing mission of Jesus in the tradition of the
Sisters of St. Joseph of Sault Ste. Marie.
VISION STATEMENT
A leader in client-centred care.
PREAMBLE
Rehabilitation is a dynamic, goal-oriented, time-limited process which allows an individual with
impairment to identify and reach his/her optimal mental, physical, cognitive and social levels.

201
Rehabilitation provides opportunities for the individual, the family and the community to accommodate a
limitation or loss of function and aims to facilitate social integration and independence.8
St. Joseph's Care Group is committed to high quality rehabilitation programs and services that meet the
needs of individuals and their families within the region of Northwestern Ontario. Interdisciplinary teams
of care providers work with clients and families within a variety of inpatient and outpatient programs.
PURPOSE OF THE ADVISORY COMMITTEE
The Advisory Committee for Physical Rehabilitation Services is established by the Board of Directors of
St. Joseph’s Care Group to provide advice regarding the Rehabilitation programs and services within the
Hospital. The primary responsibilities of this advisory committee are as follows:
1. To make recommendations to the Board of Directors regarding policy issues related to the
rehabilitation programs.
2. To assist with the development and maintenance of co-operative relationships with other agencies
providing rehabilitation services in the community and region.
3. To advise the Board of Directors of needs and concerns to which the rehabilitation programs
should respond.
4. To participate in the development and ongoing evaluation of the programs and make
recommendations for the achievement of the program objectives.
COMMITTEE MEMBERSHIP:
8Ministry of Health, Rehabilitation Strategy, 1993; Adapted from the World Health Organization.

202
1. The Committee will consist of representatives from a variety of identified key stakeholder groups
from the community and region.
2. Membership on the Committee will reflect the makeup of our community.
3. The Committee will consist of 14 members from the community and region and one member
representing Care Group Administration. Representation shall be as follows:
four (4) representatives from local service providers
one (1) representative from Thunder Bay Regional Health Sciences Centre
two (2) representatives from regional hospitals or service providers (1 representative
from the east and 1 representative from the west)
one (1) member of the Professional Staff
three (3) public representatives
one (1) representative from the First Nations
one (1) representative from the Board of Directors, St. Joseph’s Care Group
one (1) representative from Administration, St. Joseph’s Care Group (non-voting)
4. Participation will be on a voluntary basis and the term of service will be a renewable three year
term. Members may be re-nominated, but may only serve three consecutive three year terms.
5. The Advisory Committee will make recommendations to the Board of Directors of St. Joseph's
Care Group for its own replacements.
6. The Chairperson and the Vice-chairperson will be selected by the Advisory Committee and will
serve a one year renewable term. The Vice-chairperson will become the Chairperson subsequent to
the completion of the Chairperson's term. No Committee member may serve as Chairperson or
Vice-chairperson for more than three (3) consecutive annual terms in one office; however,
203
following a break of at least one annual term in the continuous service, the same person may be re-
elected in either office.
7. Every effort will be made to rotate up to 25% of the membership each year.
8. Each Committee member should attend at least 75% of the scheduled meetings.
9. When a member resigns his or her seat on the Committee, or is unable to complete the term for any
reason, then the Committee shall decide whether to fill the vacancy or leave the position vacant
until the beginning of the next calendar year.
MEETINGS
The Advisory Committee for Physical Rehabilitation Services shall meet a minimum of four times a year,
with additional meetings as required. In June, the dates and time for the meetings will be established for the
entire year. The Care Group will provide the secretarial support for the year.
QUORUM
There shall be a requirement of a minimum for fifty percent (50%) plus one attendance to constitute a
working quorum.

204
VOTING
There shall be a requirement of a minimum of fifty percent (50%) plus one favourable vote of those member
representatives in attendance to resolve or approve any issue requiring a vote.
In the development and/or research of issues to be discussed, the Advisory Committee may establish a
format and structure to ensure appropriate input. In addition, program staff and other identified "experts"
may be requested by the membership to comment on issues as the need arises, to assist members in
providing an informed vote. Guests may be invited to meetings with the prior approval of the chairperson.
AGENDA
The agenda will be developed by the Chairperson and program staff and by specific request from committee
members. Every effort will be made to have all material in the hands of the committee members no later
than one week prior to the meeting.
ORIENTATION
All new committee members will receive an orientation to the committee. This is the responsibility of the
Chairperson and program staff. Ongoing orientation and continuing education for committee members will
be provided as needed.
AD HOC COMMITTEES
Ad hoc committees should be formed to deal with one time issues, have a limited time span, and can draw
on any number of persons who are experts, have interest in, or are neutral to but knowledgeable of the issue.
This type of committee is to report to the Advisory Committee for Physical Rehabilitation Services on

205
findings and recommendations, in order that the Advisory Committee for Physical Rehabilitation Services
can conduct a factual discussion and subsequent vote on the issue.
ONGOING COMMITTEES
Ongoing committees should be formed for the purpose of planning, implementing, monitoring, co-
ordinating, evaluating and maintaining a regionally designated or agreed programs and services, and
reporting on progress and related matters to the Advisory Committee for Physical Rehabilitation Services
at prescribed intervals. Such a committee should function as an advisory and information body to the
Advisory Committee for Physical Rehabilitation Services.
Recommended to the Board of Directors: September 20, 2012

206
Appendix I – Community Engagement Stakeholders
Atikokan General Hospital- rehabilitation providers, manager, and clients/families
Dryden Regional Hospital- rehabilitation providers, manager, and clients/families
Geraldton District Hospital- rehabilitation providers, manager, and clients/families
Lake of the Woods District Hospital- rehabilitation providers, manager, and clients/families
La Verendrye Hospital- rehabilitation providers, managers, and clients/families
Manitouwadge General Hospital- rehabilitation provider
Margaret Cochenour Memorial Hospital- rehabilitation providers
McCausland Hospital- rehabilitation providers, clients/families
Nipigon Memorial District Hospital- rehabilitation providers
Sioux Lookout Meno Ya Win Health Centre- rehabilitation providers, manager
St. Joseph's Hospital- rehabilitation providers, managers, and clients/families
Wilson Memorial General Hospital- rehabilitation providers, clients/families
Bayshore Therapy and Rehab
North West CCAC
Partners in Rehabilitation
Aboriginal Advisors North West LHIN
Chiefs of Ontario
Dilico
Home and Community Care Program, Ontario Region; First Nation Inuit Health Branch Health
Canada
Public Health Unit, Ontario Region; First Nation Inuit Health Branch Health Canada
Le Réseau du mieux-être francophone du Nord de l’Ontario

207
Appendix J – RCA Bedded Levels of Rehabilitative Care Mapping Tool

208
Appendix K – RCA Community-Based Levels of Rehabilitative Care Mapping Tool
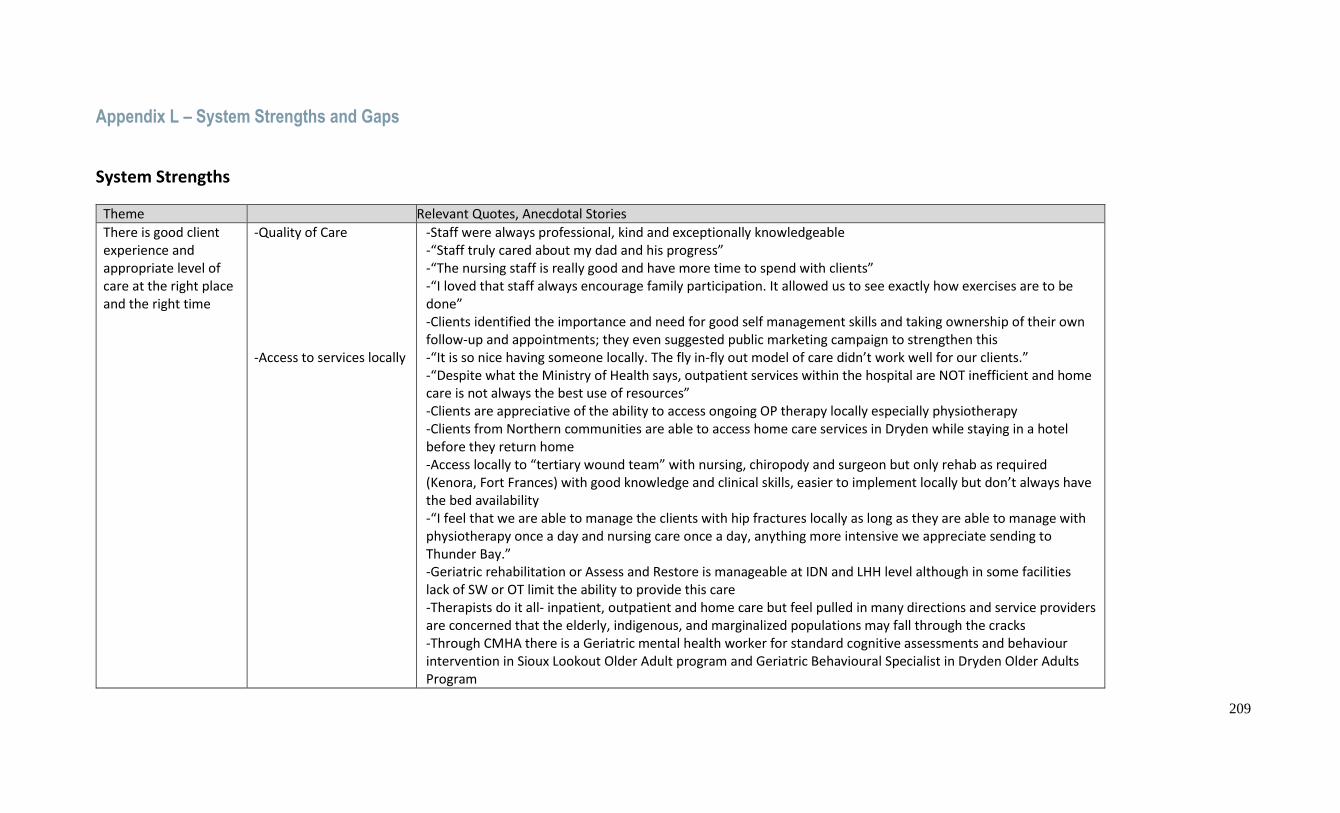
209
Appendix L – System Strengths and Gaps
System Strengths
Theme Relevant Quotes, Anecdotal Stories
There is good client experience and appropriate level of care at the right place and the right time
-Quality of Care -Access to services locally
-Staff were always professional, kind and exceptionally knowledgeable -“Staff truly cared about my dad and his progress” -“The nursing staff is really good and have more time to spend with clients” -“I loved that staff always encourage family participation. It allowed us to see exactly how exercises are to be done” -Clients identified the importance and need for good self management skills and taking ownership of their own follow-up and appointments; they even suggested public marketing campaign to strengthen this -“It is so nice having someone locally. The fly in-fly out model of care didn’t work well for our clients.” -“Despite what the Ministry of Health says, outpatient services within the hospital are NOT inefficient and home care is not always the best use of resources” -Clients are appreciative of the ability to access ongoing OP therapy locally especially physiotherapy -Clients from Northern communities are able to access home care services in Dryden while staying in a hotel before they return home -Access locally to “tertiary wound team” with nursing, chiropody and surgeon but only rehab as required (Kenora, Fort Frances) with good knowledge and clinical skills, easier to implement locally but don’t always have the bed availability -“I feel that we are able to manage the clients with hip fractures locally as long as they are able to manage with physiotherapy once a day and nursing care once a day, anything more intensive we appreciate sending to Thunder Bay.” -Geriatric rehabilitation or Assess and Restore is manageable at IDN and LHH level although in some facilities lack of SW or OT limit the ability to provide this care -Therapists do it all- inpatient, outpatient and home care but feel pulled in many directions and service providers are concerned that the elderly, indigenous, and marginalized populations may fall through the cracks -Through CMHA there is a Geriatric mental health worker for standard cognitive assessments and behaviour intervention in Sioux Lookout Older Adult program and Geriatric Behavioural Specialist in Dryden Older Adults Program

210
Theme Relevant Quotes, Anecdotal Stories
-Infrastructure to support Indigenous culturally appropriate care in Sioux Lookout
-Clients are appreciative of local physiotherapy services and identify local OP OT and SLP resources as a gap -Creative partnerships for funding shared position has resulted in more services locally including: OT with Dryden FHT and hospital, OT with Firefly and Red Lake Hospital, SLP with Meno Ya Win and Dryden Hospital -The Sioux Lookout Meno Ya Win hospital has excellent infrastructure in place to provide culturally appropriate care for indigenous population such as on site hostel, healing rooms, interpreters -Due to the proximity and access to resources, families/escorts are able to come to Sioux Lookout for teaching two days prior to discharge home
Access to specialized services regionally is invaluable
-Neurology services
-“Without the physiotherapy that Dad received at St. Joseph’s Hospital, Neuro Day and continues to receive in Kenora, he wouldn’t have the quality of life that he does and the movement and progress he has an continue to make” -“We appreciated the option to continue in Neuro Day at a more frequent intensity that was available in our own community” -“It was nice to know a physiatrist was just a phone call away “ -Specialized wheelchair prescription and training is provided appropriately in Thunder Bay -Specialized stroke rehabilitation is provided appropriately in Thunder Bay due to interprofessional team, intensity, knowledge and skills
There is smooth transitions and communication along the continuum of care
-Electronic Medical Record infrastructure -Connections with other rehabilitation professionals in NWO -Integration of CCAC services within hospital infrastructure
-The common electronic medical record throughout NWO makes information and communication much easier, this is very apparent when there are clients who have had care elsewhere in Sudbury, Sault Ste. Marie or Manitoba -“It is always easier to call and communicate with the next care provider when I already know them as a person” -Having a contact list of other rehabilitation providers through NOSM was great but difficult to keep updated, it would be beneficial to have added areas of specialty included -Formal meetings with other therapists and managers in the West and the North Shore group in the east are very valued but “there is a disconnect between Thunder Bay and the region.” -Communication with the CCAC provider locally is smooth as we are so small we know each other well -Hospital having CCAC contract in the region makes client transitions easier, seamless, and more appropriate and more efficient with the added benefit of accessing the shared EMR -Clients in a small community noted that when there are personality differences, they have no choice, it is the same therapist for inpatients, outpatients and home care -Where this isn’t in place, it was suggested there be better communication with local SW when CCAC contract providers will be in town -Integration of FHT and CCAC nursing in Manitouwadge is working well

211
Theme Relevant Quotes, Anecdotal Stories
Use of technology to access services close to home
-Cardiac Rehabilitation/ Healthy Lifestyles -Moving on after Stroke -Rheumatology Services -Psychiatry services -OP Physiotherapy Services -Nursing
-The cardiac rehabilitation model works really well with frequent communication to specialists in Thunder Bay; cardiac rehab is sometimes limited for people on shift work; one client noted that he had a 9 month wait to get his stress test for cardiac rehab and another month to actually get started on the program from a rural site; -Other facilities noted this is a gap and clients are repatriated with NO cardiology follow up or referral to cardiac rehab- some facilities have started their own programming locally -Service providers suggest similar systems to cardiac rehab for pulmonary rehab -Great to have access to this and it worked well but not timely -Access to Rheumatologist via telehealth is great but a refresher on assisting with joint counts would be good; “works really well for patients that get in!” -Coordination with local resources is necessary as impacts ie. OT in Geraldton -Recent access to visiting specialist Dr. Aubrey in Kenora -Access to psychiatry services working well but service providers locally need to remember there is access -Provision of initial assessment and self management initial treatment for physiotherapy in Ignace, could be expanded to other areas ie. Nipigon to Beardmore -good use of CCAC Diabetes and BP phone call and telegeriatric nursing
Evidence based care, client centered care
-Family Health Teams -The Family Health Team in Dryden supports return to driving screening assessments and triaging for their clients by providing OT resource within FHT model -FHTs are providing exercise opportunities (Zumba, nordic pole walking, walk and talk and resistance bands) in some communities targeting clients with Diabetes, high risk factors for stroke, and cardiac issues -FHTs providing Chronic disease self management 6 week program and pre-op behavior changes such as weight loss and smoking cessation
System Gaps
Theme Suggestions, Relevant Quotes, Anecdotal Stories
The client experience is limited by geographical distance
-Preferred location -Access to temporary accommodations
-Thunder Bay is so far away- families and clients often would rather go to Winnipeg for services such as prosthetics -“I wished could have been home sooner” -Temporary accommodations similar to Tamarack house for Cancer patients or better hospital rates at hotels in Thunder Bay would be beneficial -Provide a list of housing and hotel options with kitchenettes for regional families

212
Theme Suggestions, Relevant Quotes, Anecdotal Stories
-NIHB medical travel policies
-Having family in Thunder Bay makes it manageable for many -NIHB medical transportation policies limits service to many Indigenous clients to Neuro Day; there is very inconsistent approval and ability to extend stay beyond 4 weeks
Clients are lacking appropriate level of care at the right place and the right time
-Inpatient Occupational Therapy -Inpatient SLP services -Outpatient OT services -Nursing culture -Use of support personnel in rehab -Social Supports -Medical Equipment:
-The lack of OT inpatient services was noted in hospitals in the District of Thunder Bay (except Geraldton) and would assist with home visits, discharge assessments and cognitive assessments and treatments and support the ability to provide Assess and Restore interventions and driving screens -Without a local SLP, facilities needing a swallowing assessment for inpatients need to refer to the next level of health service (ie. IDN) -“In a perfect world there would be outpatient OT services within the hospital like there is physio” -This would assist in earlier discharge and decreased LOS -There is a large gap in cognitive, community reintegration, and arm and hand interventions as CCAC OT services focus on home safety and equipment -Integration with the FHT in Dryden has allowed for access to OP OT services with good results -There is no “rehab culture” in the nursing departments of small hospitals and as a result rehab staff continue to provide care that is defined by RCA to be delivered by nursing or non-regulated providers; this is due to the shared roles for many nurses who are the charge nurses, the discharge planners and the chemotherapy nurse at the same time - There are many new grad nurses in rural hospitals with minimal skill experience -“There would need to be a cultural shift- historically our hospital uses professional staff rather than support -personnel” but this would support alignment with use of regulated professionals -There may be some possibilities using rehab assistant model to support OT services in smaller LHHs -There is an identified need for more supportive housing options throughout the North West LHIN -There is limited ongoing social support programs in many of the local health hubs for people still in their own homes such as communal dining, accessible public transportation, ongoing exercise classes resulting in premature need for LTC -There needs to be homemaking after 6 pm and more accessibility on weekends in the small communities -Identified need for ongoing social support for people with stroke following OP and MOST in the region like Stroke Recovery Network in Thunder Bay -“The system doesn’t currently account for the profound sense of loneliness in the ‘home first’ program” -Loan equipment is not available at all hospitals and there are not local rentals available in all LHH; this equipment is difficult to track and maintain -Anticipated equipment needs in advance of transitions and advance of home visits are helpful

213
Theme Suggestions, Relevant Quotes, Anecdotal Stories
-Delivery and servicing of equipment twice a week (some only every 7 weeks) to LHH is limiting especially with recent changes in vendor -Strong relationships with vendors is helpful -Most vendors won’t provide rental equipment to northern communities or other First Nation communities such as Aroland who aren’t serviced by CCAC; although they can rent while staying in Thunder Bay or Dryden -Pediatric equipment availability is very limited in LHHs -Clients need to come to LHH with appropriate braces as there is nothing locally even while waiting for custom
Accessibility to specialized inpatient rehabilitation is limited and criteria for program admission would benefit from clarification [from service providers]
-Wound Beds -Inpatient admission to SJH -Weekend therapy
-“There are never any wound beds available” -Acceptance decisions are made with little explanation just “she doesn’t qualify” -It would be nice to talk to the other therapist directly and explain the situation and recommendation for access to regional rehabilitation bed -Many service providers were unaware of potential for direct access to specialized senior rehab to avoid readmissions and felt this would be appropriate and the Family Health Team would be a good referral source, in some cases in the District of Thunder Bay referrals were denied admission; the perception is that if someone is ambulatory, they don’t get in -Sometimes local physicians are a barrier if things didn’t go well for another client, they won’t refer again -The process for referring to inpatient programming needs to be clarified (?STRATA referral rather that physician to physician contact) -Limited access to therapy on the weekend -“Weekends were long. There needs to be more staff”
There are identified gaps in Specialized outpatient services
-Chronic Pain services -Geriatric/Psychogeriatric and Wound Care services
-Access to Chronic pain programming in Thunder Bay is identified as a gap and sites have started to use 6 week chronic disease management program for these clients at the local FHT -“Hub and Spoke? Feels more like a desert island. If you can swim to us you can stay but most can’t get to the island!” regarding physical access, need to be well enough to stay in Thunder Bay for 6 weeks on own but not too well that you aren’t already back to work as then it is difficult to access a 6 week program; have started a 2-3 day program; there is also potential to work with LHHs to develop their own programs with support; there is potential to VC exercise/movement session to the region and do follow up through PCVC -It is difficult to establish connections for ongoing programming using Hub and Spoke Model with staff turnover in the region. It takes time to develop relationships and find a champion -Consultations are provided but not implemented [wound care; geriatric services] -Access to psychogeriatric services are not timely *accessing Dr. Conn? From Baycrest in Sioux Lookout; suggested that psychogeriatric assessment should be in person first and follow up via telehealth
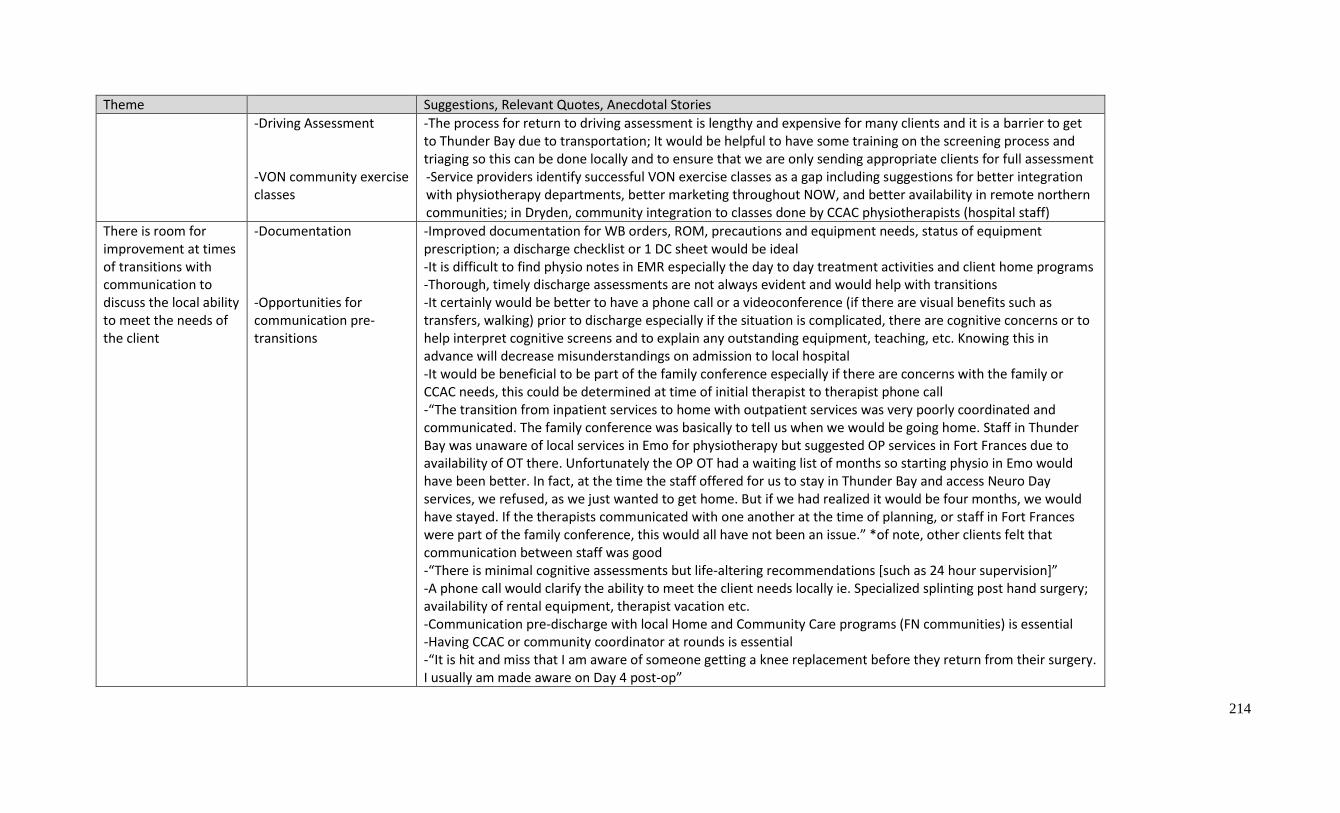
214
Theme Suggestions, Relevant Quotes, Anecdotal Stories
-Driving Assessment -VON community exercise classes
-The process for return to driving assessment is lengthy and expensive for many clients and it is a barrier to get to Thunder Bay due to transportation; It would be helpful to have some training on the screening process and triaging so this can be done locally and to ensure that we are only sending appropriate clients for full assessment -Service providers identify successful VON exercise classes as a gap including suggestions for better integration with physiotherapy departments, better marketing throughout NOW, and better availability in remote northern communities; in Dryden, community integration to classes done by CCAC physiotherapists (hospital staff)
There is room for improvement at times of transitions with communication to discuss the local ability to meet the needs of the client
-Documentation -Opportunities for communication pre- transitions
-Improved documentation for WB orders, ROM, precautions and equipment needs, status of equipment prescription; a discharge checklist or 1 DC sheet would be ideal -It is difficult to find physio notes in EMR especially the day to day treatment activities and client home programs -Thorough, timely discharge assessments are not always evident and would help with transitions -It certainly would be better to have a phone call or a videoconference (if there are visual benefits such as transfers, walking) prior to discharge especially if the situation is complicated, there are cognitive concerns or to help interpret cognitive screens and to explain any outstanding equipment, teaching, etc. Knowing this in advance will decrease misunderstandings on admission to local hospital -It would be beneficial to be part of the family conference especially if there are concerns with the family or CCAC needs, this could be determined at time of initial therapist to therapist phone call -“The transition from inpatient services to home with outpatient services was very poorly coordinated and communicated. The family conference was basically to tell us when we would be going home. Staff in Thunder Bay was unaware of local services in Emo for physiotherapy but suggested OP services in Fort Frances due to availability of OT there. Unfortunately the OP OT had a waiting list of months so starting physio in Emo would have been better. In fact, at the time the staff offered for us to stay in Thunder Bay and access Neuro Day services, we refused, as we just wanted to get home. But if we had realized it would be four months, we would have stayed. If the therapists communicated with one another at the time of planning, or staff in Fort Frances were part of the family conference, this would all have not been an issue.” *of note, other clients felt that communication between staff was good -“There is minimal cognitive assessments but life-altering recommendations [such as 24 hour supervision]” -A phone call would clarify the ability to meet the client needs locally ie. Specialized splinting post hand surgery; availability of rental equipment, therapist vacation etc. -Communication pre-discharge with local Home and Community Care programs (FN communities) is essential -Having CCAC or community coordinator at rounds is essential -“It is hit and miss that I am aware of someone getting a knee replacement before they return from their surgery. I usually am made aware on Day 4 post-op”
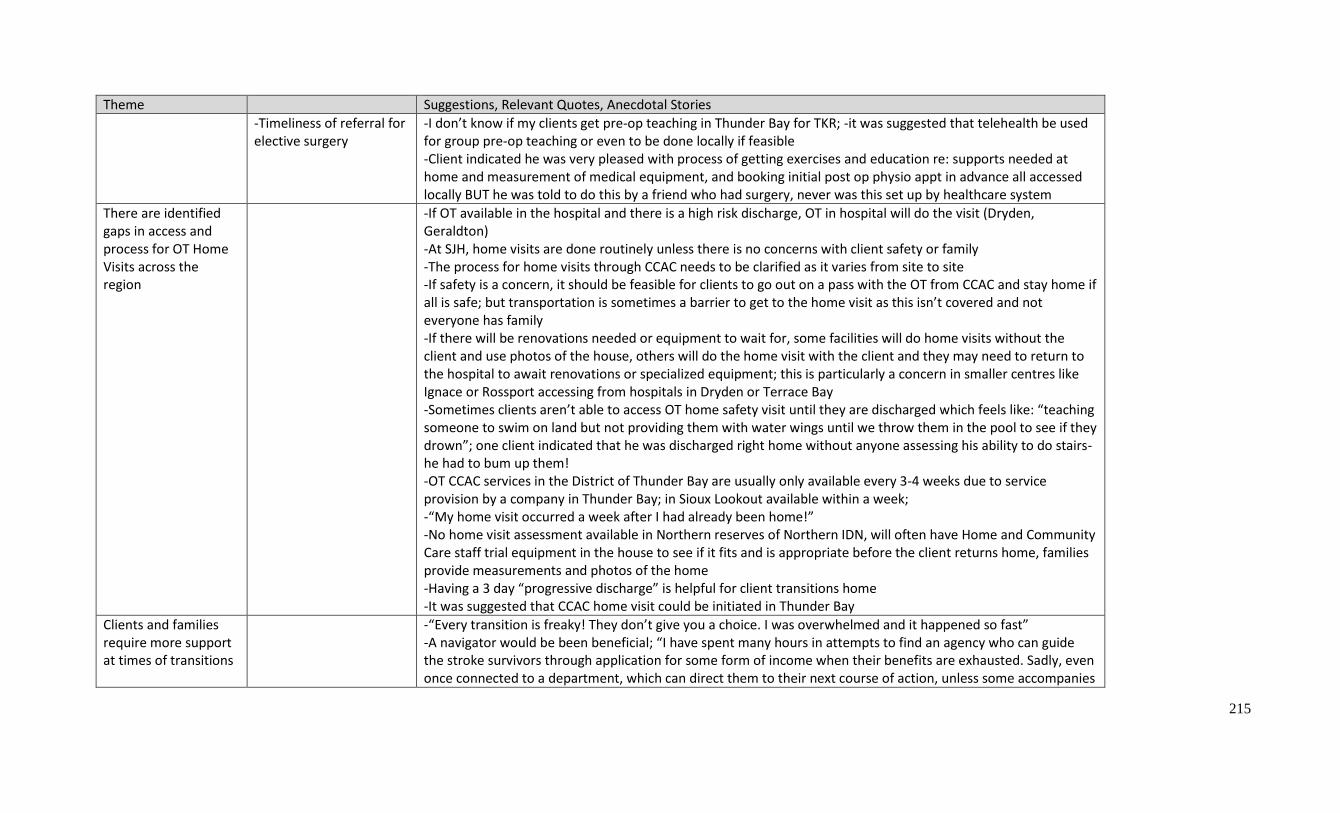
215
Theme Suggestions, Relevant Quotes, Anecdotal Stories
-Timeliness of referral for elective surgery
-I don’t know if my clients get pre-op teaching in Thunder Bay for TKR; -it was suggested that telehealth be used for group pre-op teaching or even to be done locally if feasible -Client indicated he was very pleased with process of getting exercises and education re: supports needed at home and measurement of medical equipment, and booking initial post op physio appt in advance all accessed locally BUT he was told to do this by a friend who had surgery, never was this set up by healthcare system
There are identified gaps in access and process for OT Home Visits across the region
-If OT available in the hospital and there is a high risk discharge, OT in hospital will do the visit (Dryden, Geraldton) -At SJH, home visits are done routinely unless there is no concerns with client safety or family -The process for home visits through CCAC needs to be clarified as it varies from site to site -If safety is a concern, it should be feasible for clients to go out on a pass with the OT from CCAC and stay home if all is safe; but transportation is sometimes a barrier to get to the home visit as this isn’t covered and not everyone has family -If there will be renovations needed or equipment to wait for, some facilities will do home visits without the client and use photos of the house, others will do the home visit with the client and they may need to return to the hospital to await renovations or specialized equipment; this is particularly a concern in smaller centres like Ignace or Rossport accessing from hospitals in Dryden or Terrace Bay -Sometimes clients aren’t able to access OT home safety visit until they are discharged which feels like: “teaching someone to swim on land but not providing them with water wings until we throw them in the pool to see if they drown”; one client indicated that he was discharged right home without anyone assessing his ability to do stairs- he had to bum up them! -OT CCAC services in the District of Thunder Bay are usually only available every 3-4 weeks due to service provision by a company in Thunder Bay; in Sioux Lookout available within a week; -“My home visit occurred a week after I had already been home!” -No home visit assessment available in Northern reserves of Northern IDN, will often have Home and Community Care staff trial equipment in the house to see if it fits and is appropriate before the client returns home, families provide measurements and photos of the home -Having a 3 day “progressive discharge” is helpful for client transitions home -It was suggested that CCAC home visit could be initiated in Thunder Bay
Clients and families require more support at times of transitions
-“Every transition is freaky! They don’t give you a choice. I was overwhelmed and it happened so fast” -A navigator would be been beneficial; “I have spent many hours in attempts to find an agency who can guide the stroke survivors through application for some form of income when their benefits are exhausted. Sadly, even once connected to a department, which can direct them to their next course of action, unless some accompanies
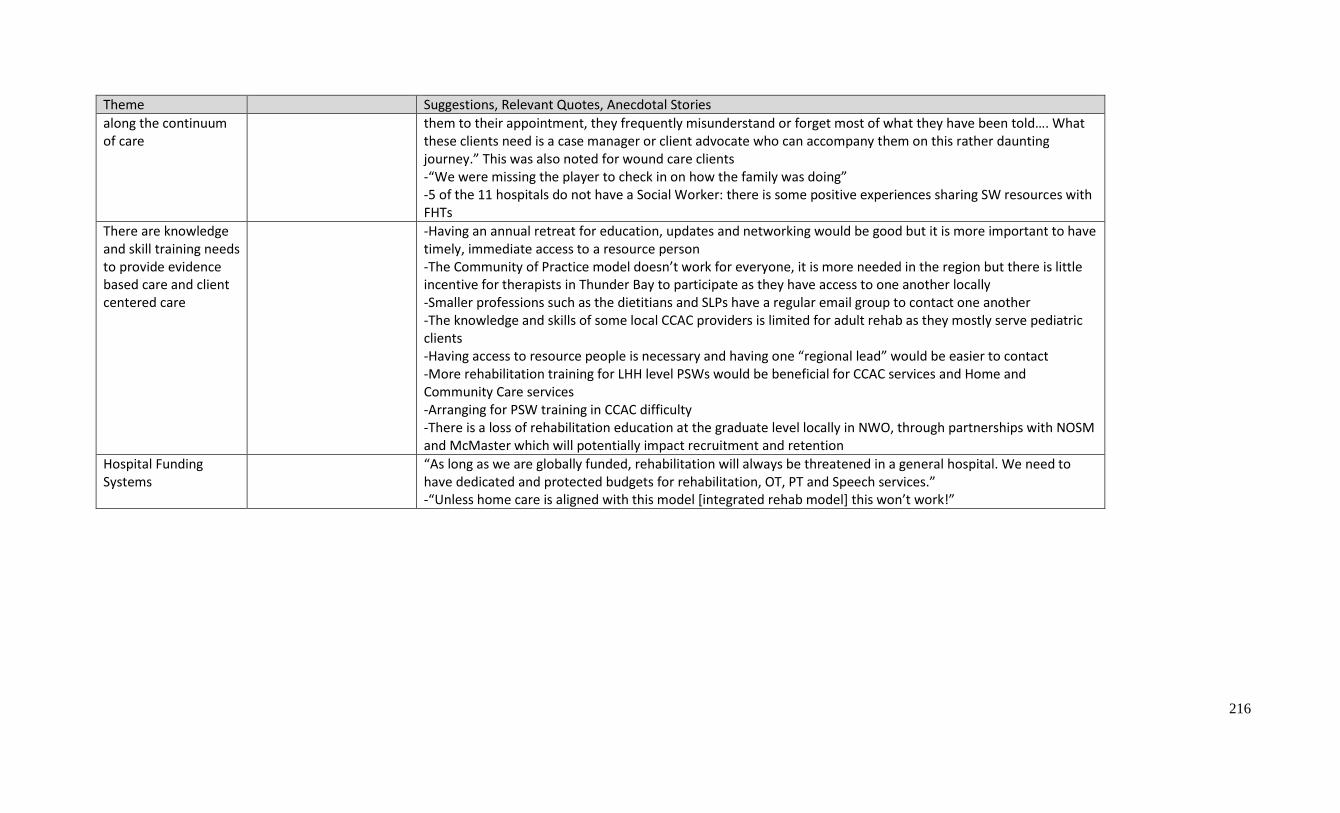
216
Theme Suggestions, Relevant Quotes, Anecdotal Stories
along the continuum of care
them to their appointment, they frequently misunderstand or forget most of what they have been told…. What these clients need is a case manager or client advocate who can accompany them on this rather daunting journey.” This was also noted for wound care clients -“We were missing the player to check in on how the family was doing” -5 of the 11 hospitals do not have a Social Worker: there is some positive experiences sharing SW resources with FHTs
There are knowledge and skill training needs to provide evidence based care and client centered care
-Having an annual retreat for education, updates and networking would be good but it is more important to have timely, immediate access to a resource person -The Community of Practice model doesn’t work for everyone, it is more needed in the region but there is little incentive for therapists in Thunder Bay to participate as they have access to one another locally -Smaller professions such as the dietitians and SLPs have a regular email group to contact one another -The knowledge and skills of some local CCAC providers is limited for adult rehab as they mostly serve pediatric clients -Having access to resource people is necessary and having one “regional lead” would be easier to contact -More rehabilitation training for LHH level PSWs would be beneficial for CCAC services and Home and Community Care services -Arranging for PSW training in CCAC difficulty -There is a loss of rehabilitation education at the graduate level locally in NWO, through partnerships with NOSM and McMaster which will potentially impact recruitment and retention
Hospital Funding Systems
“As long as we are globally funded, rehabilitation will always be threatened in a general hospital. We need to have dedicated and protected budgets for rehabilitation, OT, PT and Speech services.” -“Unless home care is aligned with this model [integrated rehab model] this won’t work!”

217
Appendix M – Regional Population breakdowns by IDN:
City of Thunder Bay IDN:
The City of Thunder Bay IDN is comprised of one Local Health Hub serving twelve communities and a
total population of 127,975. This IDN accounts for 55.3% of the North West LHIN’s population over a
geographic area of 37,100 square KM. The median age of residents within the City of Thunder Bay is 44
years of age. Additionally, 17.2% of residents in the District of the City of Thunder Bay are over 65 years
of age. There are 26 unique health service providers offering 41 LHIN funded programs within this
district. Additionally, there are two primary hospital facilities within the City of Thunder Bay IDN;
Thunder Bay Regional Health Sciences Centre (Tertiary) and St. Joseph’s Hospital (Post-Acute Care).
District of Kenora IDN:
The District of Kenora is comprised of three Local Health Hubs, Kenora, Dryden, and Red Lake that
serve 21 communities. The population of the District of Kenora IDN is 43,133 representing the second
largest IDN in the North West LHIN (18.7% of the total population). The Kenora IDN has an
approximate total area of 54,108 square Km with 53.5% of the population living in rural areas.
Approximately one-quarter of the population in this district self-identify as Indigenous. Within the
District of Kenora IDN there are three primary health care facilities; Dryden Regional Health Centre
(Dryden), Lake of the Woods District Hospital (Kenora), and Red Lake Margaret Cochenour Memorial
Hospital (Red Lake). In addition, the District of Kenora IDN has 37 unique health service providers
offering 51 LHIN funded programs. Due to their proximity to Manitoba, clients in the District of Kenora
IDN often seek complex/tertiary medical services in Winnipeg as opposed to travelling to Thunder Bay
in order to remain close to home.
District of Rainy River IDN:
The District of Rainy River IDN is comprised of four local health hubs, Rainy River, Fort Frances, Emo,
and Atikokan that serve 19 communities. This IDN is the fourth most populated district in the North
West LHIN with a total population of 20,370 accounting for approximately 8.8% of the total LHIN
population. The District of Rainy River IDN has an approximate total area of 15,474 square Km and
21.8% of the population lives in rural areas. In addition, the District of Rainy River IDN is home to the
greatest proportion of adults over the age of sixty-five, comprising approximately 20.5% of the districts
population. Within The district of Rainy River IDN, there are 19 unique health service providers offering
31 LHIN funded programs. The primary care facilities include LaVerendrye Hospital (Fort Frances) and
Atikokan General Hospital (Atikokan) with additional health centers in Rainy River and Emo.
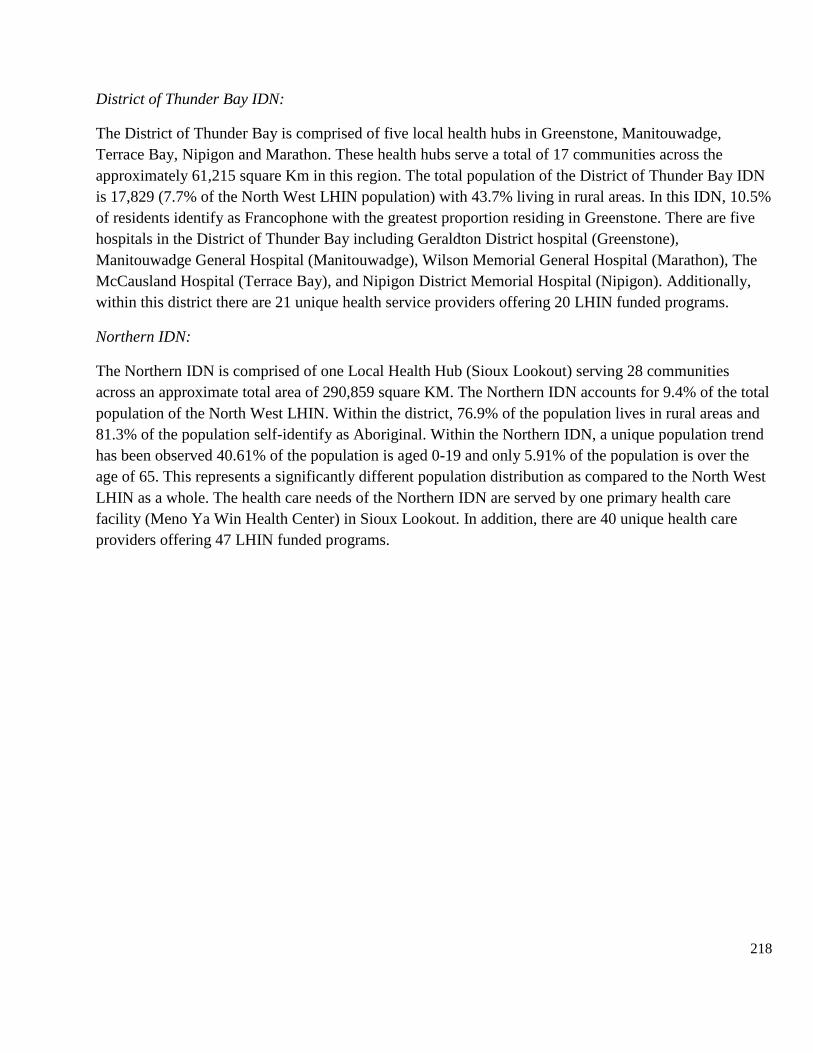
218
District of Thunder Bay IDN:
The District of Thunder Bay is comprised of five local health hubs in Greenstone, Manitouwadge,
Terrace Bay, Nipigon and Marathon. These health hubs serve a total of 17 communities across the
approximately 61,215 square Km in this region. The total population of the District of Thunder Bay IDN
is 17,829 (7.7% of the North West LHIN population) with 43.7% living in rural areas. In this IDN, 10.5%
of residents identify as Francophone with the greatest proportion residing in Greenstone. There are five
hospitals in the District of Thunder Bay including Geraldton District hospital (Greenstone),
Manitouwadge General Hospital (Manitouwadge), Wilson Memorial General Hospital (Marathon), The
McCausland Hospital (Terrace Bay), and Nipigon District Memorial Hospital (Nipigon). Additionally,
within this district there are 21 unique health service providers offering 20 LHIN funded programs.
Northern IDN:
The Northern IDN is comprised of one Local Health Hub (Sioux Lookout) serving 28 communities
across an approximate total area of 290,859 square KM. The Northern IDN accounts for 9.4% of the total
population of the North West LHIN. Within the district, 76.9% of the population lives in rural areas and
81.3% of the population self-identify as Aboriginal. Within the Northern IDN, a unique population trend
has been observed 40.61% of the population is aged 0-19 and only 5.91% of the population is over the
age of 65. This represents a significantly different population distribution as compared to the North West
LHIN as a whole. The health care needs of the Northern IDN are served by one primary health care
facility (Meno Ya Win Health Center) in Sioux Lookout. In addition, there are 40 unique health care
providers offering 47 LHIN funded programs.

219
Appendix M – Current Estimated Beds

220
Appendix N – Hip Fracture Process Map
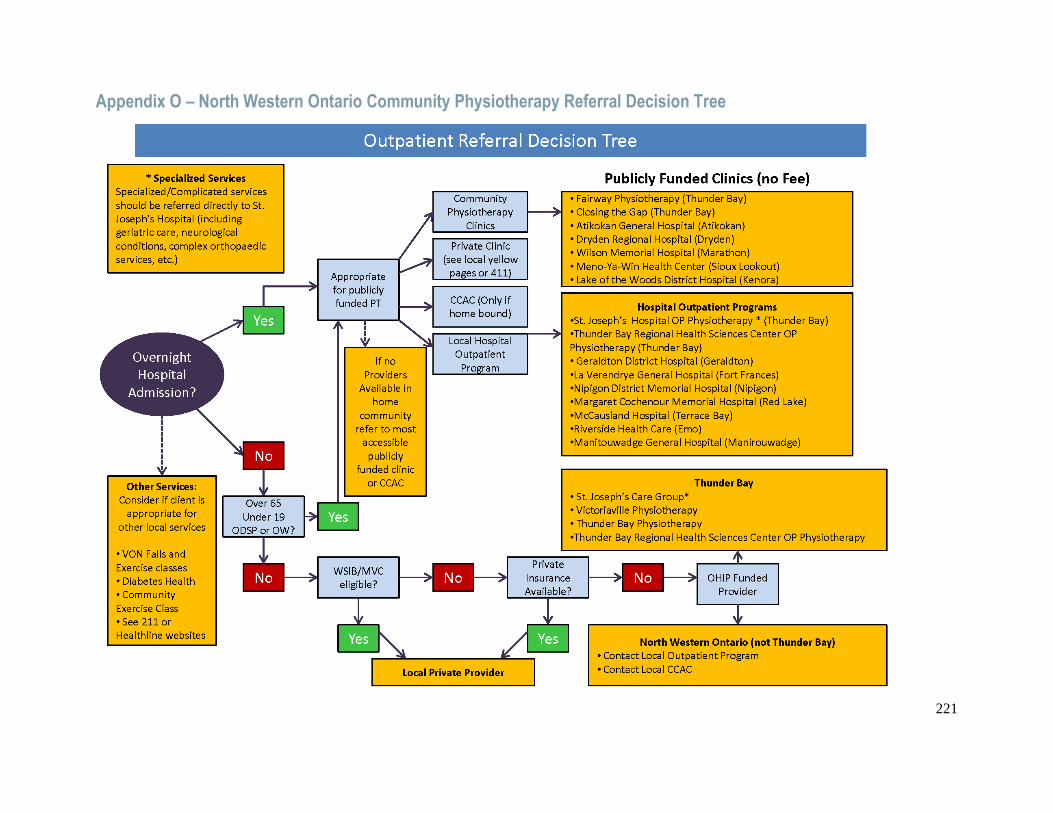
221
Appendix O – North Western Ontario Community Physiotherapy Referral Decision Tree
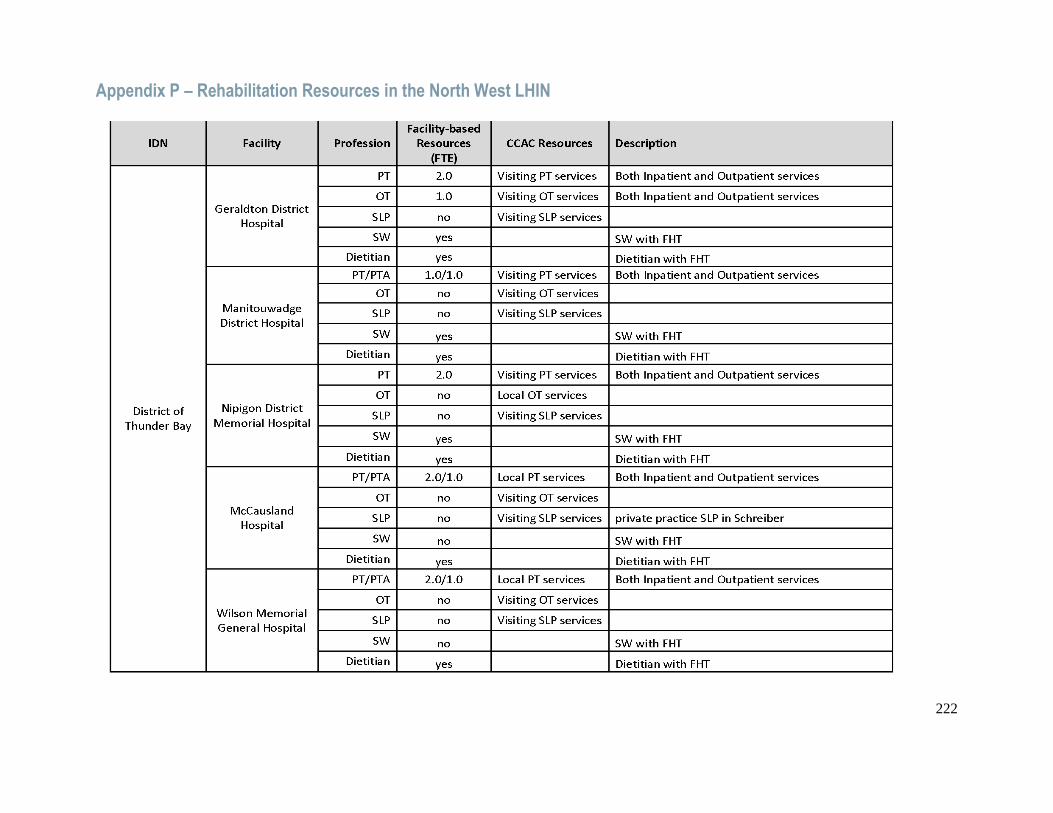
222
Appendix P – Rehabilitation Resources in the North West LHIN
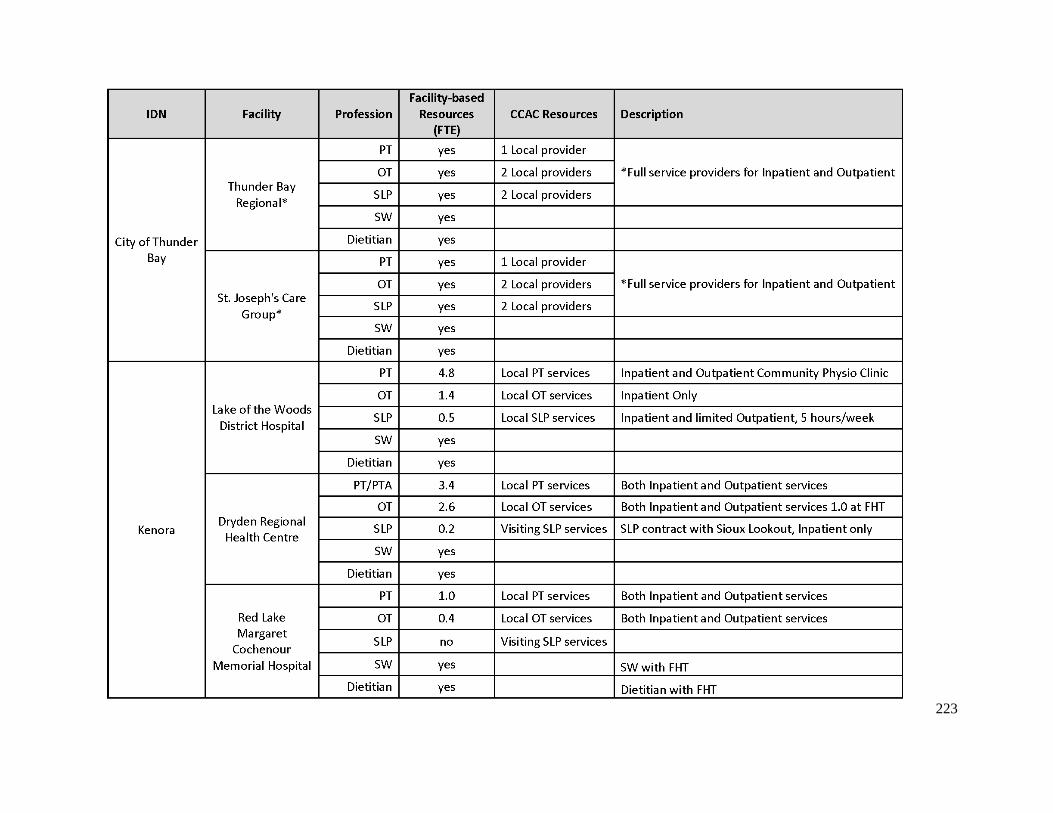
223
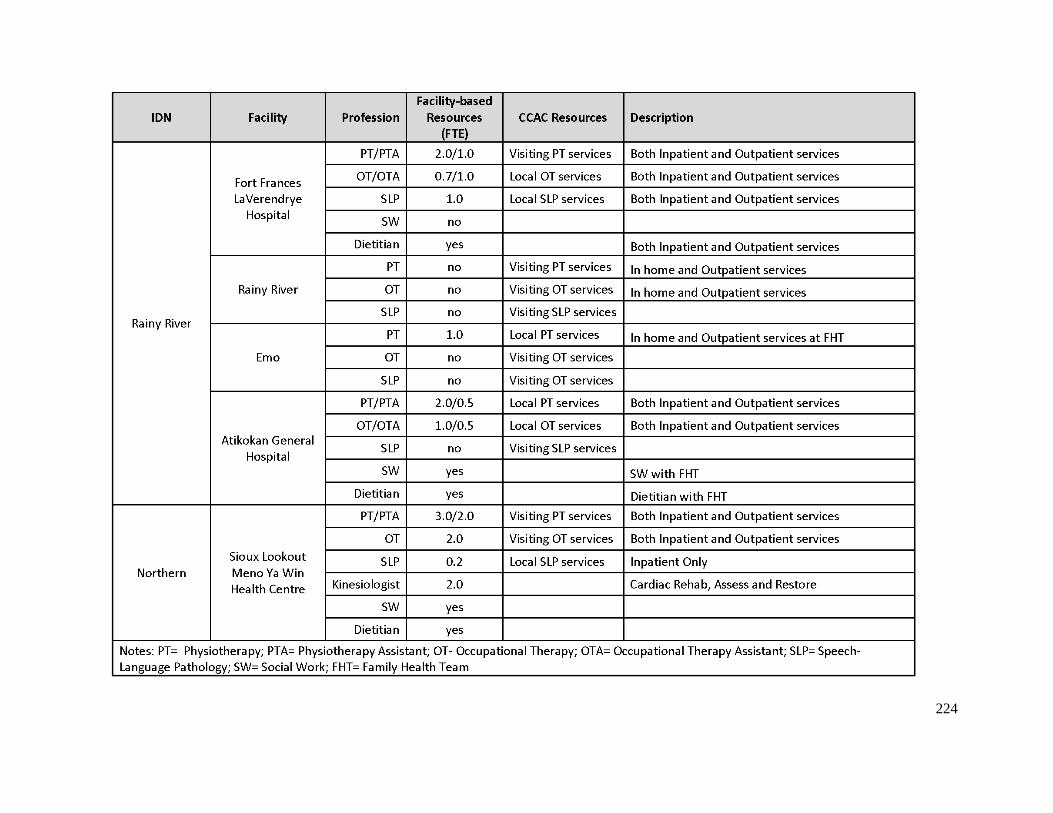
224

225
Appendix Q – Geriatric Assessment & Rehabilitative Care Stream

226

227
Appendix R – Stroke/Neuro Care Stream

228

229
Appendix S – Musculoskeletal Care Stream

230
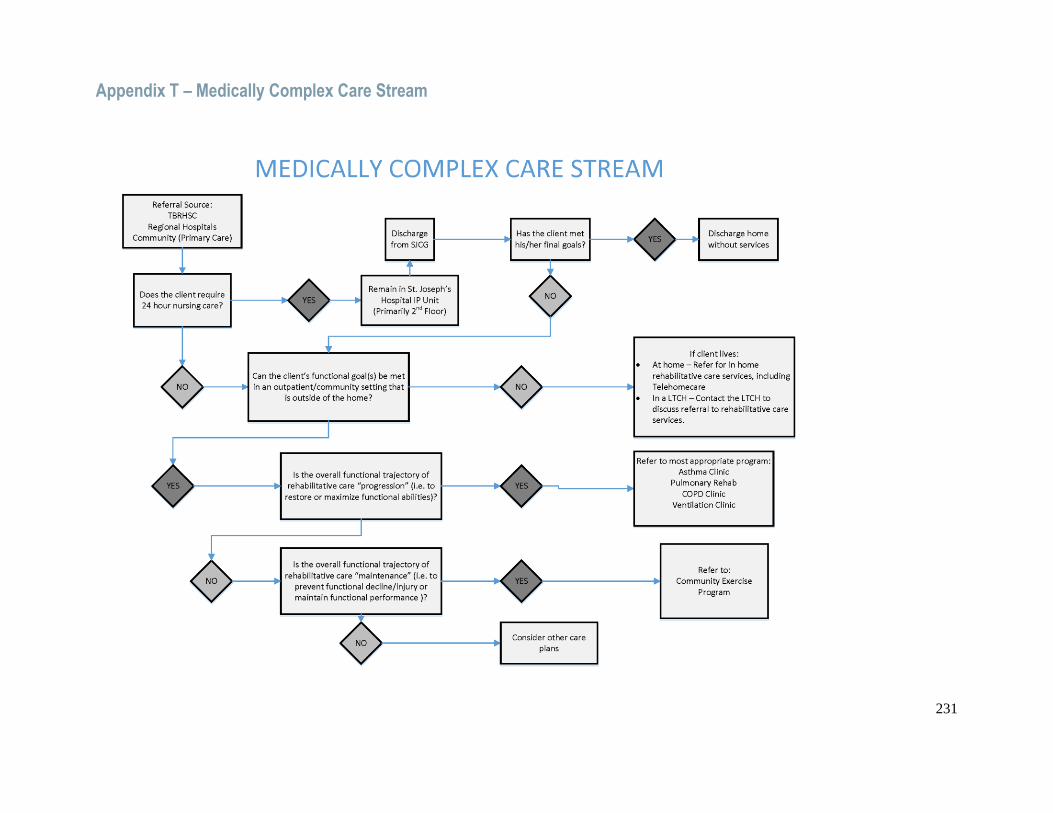
231
Appendix T – Medically Complex Care Stream

232
Related Documents











