SMIJAL GM PSM DENTAL COLLEGE

Regressive alterations of teeth
Aug 22, 2014
NON CARIOUS LESIONS & MANAGEMENT
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

SMIJAL GMPSM DENTAL COLLEGE
CONTENTS• Attrition• Abrasion• Erosion• Abfraction• Fractures• Localized Nonhereditory
Enamel Hypoplasia• Localized Non Hereditary
Enamel Hypocalcification
• Localized Non Hereditary Dentin Hypoplasia
• Localized Non Hereditary Dentin Hypocalcification
• Discoloration• Malformation• Amelogenesis Imperfecta• Dentinogenesis Imperfecta
ATTRITION• Attrition is mechanical wear of the incisal
or occlusal surface as a result of functional or parafunctional movements of mandible ( tooth- to- tooth contact .
• Is a continuous, age dependentprocess, which is usually physiologic.
• Seen in both deciduous and permanent dentition.(rare in decidous not retained for a longer period of time).
• Seen in children those who have Dentinogenesis and Amelogenesis imperfecta.
• Men exhibit more severe attrition than women.

2 TYPESa) Proximal surface attritionb) Occluding surface attritionProximal surface attrition :• Widening of proximal contact areas.• Decreased mesio-distal width of teeth.• Interproximal space will be decreased in
dimension.Occluding surface attrition :• Loss, flattening, faceting and /or reverse
cusping of occluding elements.• Loss of vertical dimension of tooth.• Cheek biting and gingival irritation occurs.

.Predisposing factors; • coarseness of diet ,chewing tobacco or
bruxism, occupation –person exposed to an atmosphere of abrasive dust.
Clinical manifestation • Appearance of small polished facet on a
cusp tip or ridge or a slight flattening of incisal edge.
• Gradual reduction of cusp height & flattening of occlusal inclined plane with aging.
• Tooth sesitivity• TMJ problem elicited especially in the
overclosure situation.
• In some older patients, the enamel of the cusp tips or incisal edges is worn off, resulting in cupped-out areas because the exposed, softer dentin wears faster than surrounding enamel.
• Sometimes these areas are an annoyance because of food retention or the presence of peripheral, ragged, sharp enamel edges.
• Advanced attrition – enamel may worn away results in an extrinsic yellow or brown staining of exposed dentin from food or tobacco.
• May progress to complete loss of cuspal interdigitation.





ABRASION• Abrasion is an abnormal tooth surface loss
resulting from direct friction forces between the teeth and external objects or from frictional forces between contacting teeth components in the presence of an abrasive medium.
• It is the pathologic wearing away of tooth substance through some abnormal mechanical process .
Mainly due to :Tooth brushingAbnormal habits
•

Causes• Improper brushing technique• Abrasive dentrifices & Hard tooth brush• Habits such as holding a pipe stem by the
teeth, opening of bobby pins with the teeth (resulting notching of incisal edges of maxillary CI )
• In carpenters, tailors, shoe makers who holds nail, tacks and pins between the teeth
• Improper use of tooth picks and dental floss• Pipe smokers, Chewing tobacco
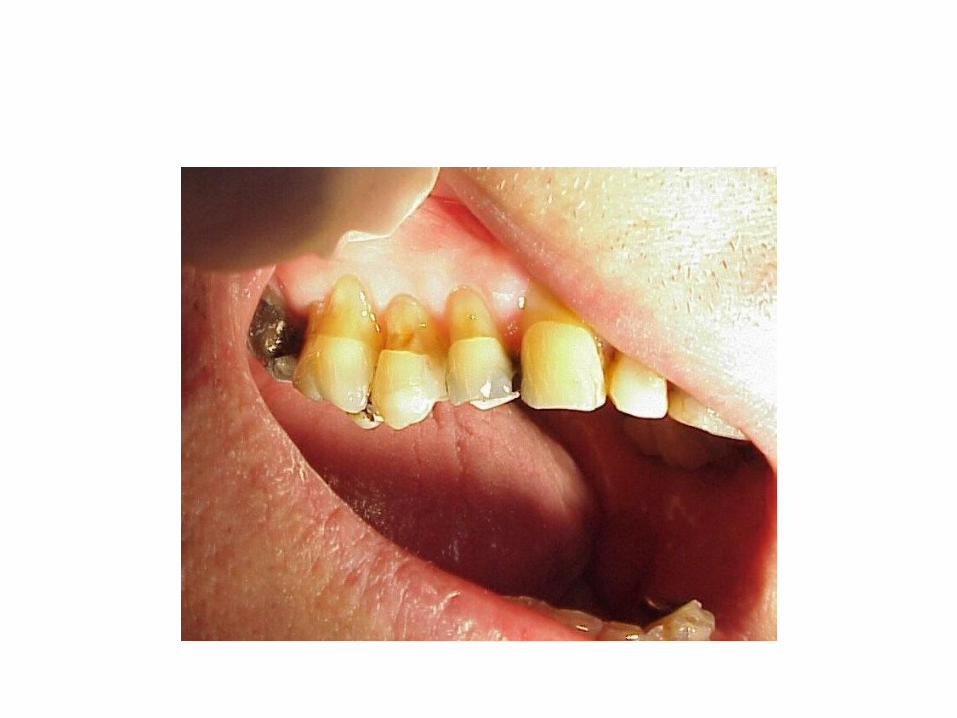
Clinical features• Tooth brush abrasion is more common, occuring
cervically.• Usually occurs on exposed root surfaces of teeth
and in sometimes incisal and occlusal surfaces.• Abrasion caused by dentrifices appears as “v”
shaped or wedge shaped ditch on the root side of CEJ in teeth with gingival recession.It also involving cervical enamel and dentin.
• Abrasion more common on left side of mouth in right handed people.
• Canines and premolars are most affected.• Exhibit sharp margins and sharp internal angles.• Exposed surface appears smooth and polished.• Sometimes the surface may show scratches.
• Many teeth are affected.Usually on the facial surfaces of maxillary left canine to molar region in right handed person and vice versa
• Modern dentrifices are not sufficiently abrasive to damage intact enamel severely, can cause wear cementum & dentin,particularly in horizontal direction rather than vertical direction .
• Pipesmoking “depression abrasion” which is an abraded depression on the occluding surfaces of teeth at a latero-anterior of arch coinciding with intraoral location of pipestem.
• Results from intrusion and abrasion of the tooth.• Chewing tobacco cause generalized occlusal surface
abrasion.• Pica-syndrome, which is due to the habit chewing
clay(mud) has a specific occlusal abrasion.• Iatrogenic tooth abasion.



PATHOGENESIS SIMILAR TO ATTRITION.
EROSION• Erosion is the wear or loss of tooth
surface by chemicomechanical action.• It is the irreversible loss of dental hard
tissue that does not involves bacteria.• Dissolution of mineralised tooth structures
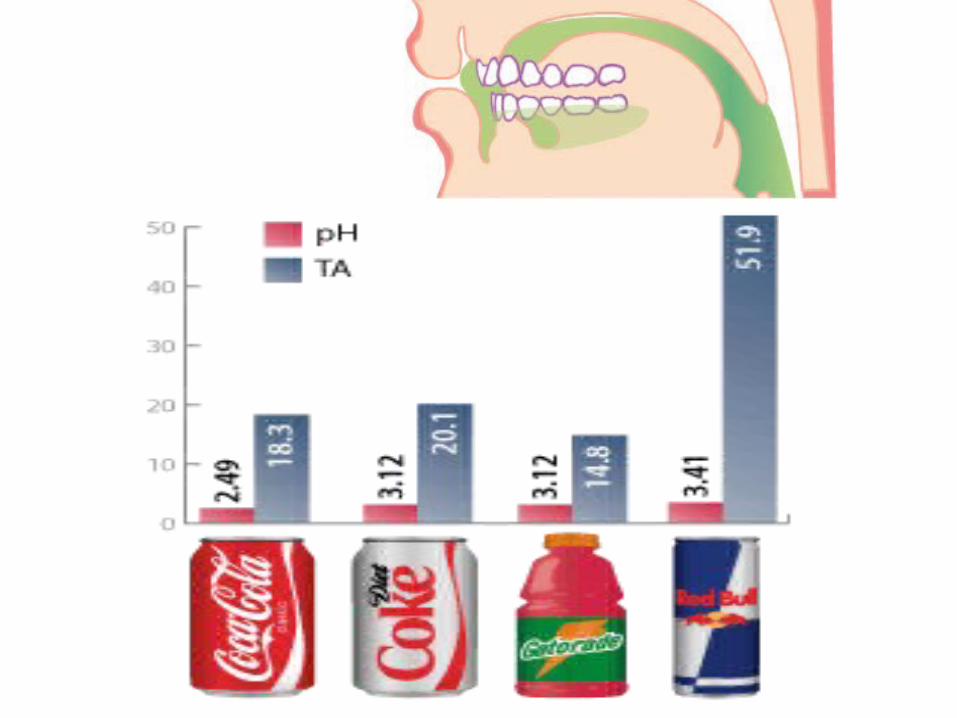
occurs upon contact with acids that are introduced in to oral cavity from intrinsic (eg , gastroesophageal reflux ,vomiting ) or extrinsic sources (eg,acidic beverages , citrus fruits)

• Topographically, the extent of erosive lesion can range from a fine unnoticeable line at CEJ to substancial tooth substance loss making an hour-glass shape out ofa tooth.

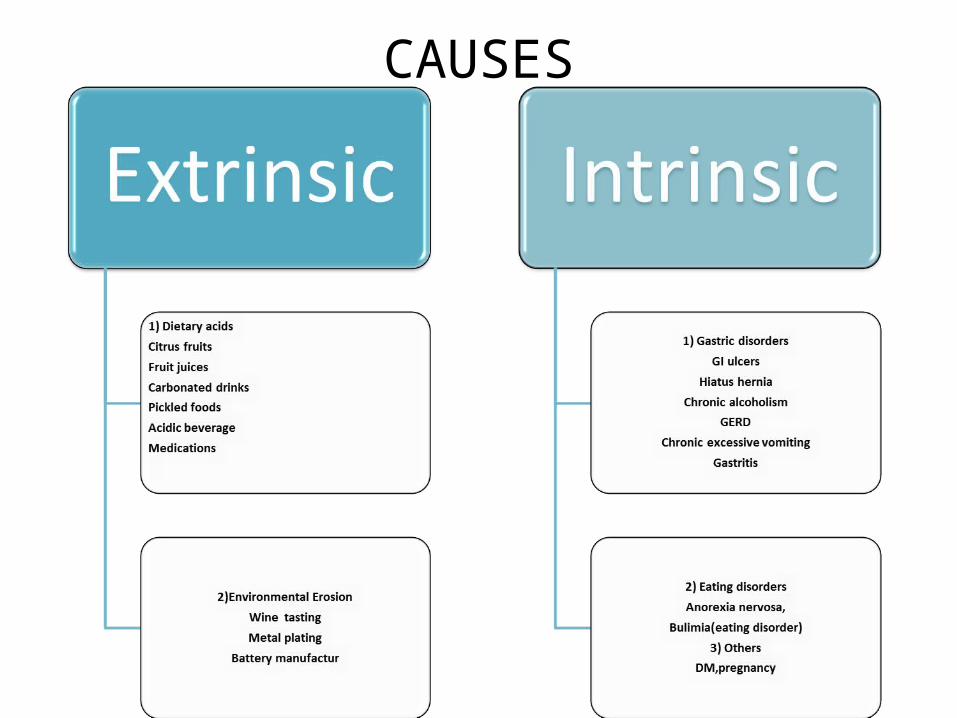
CAUSES
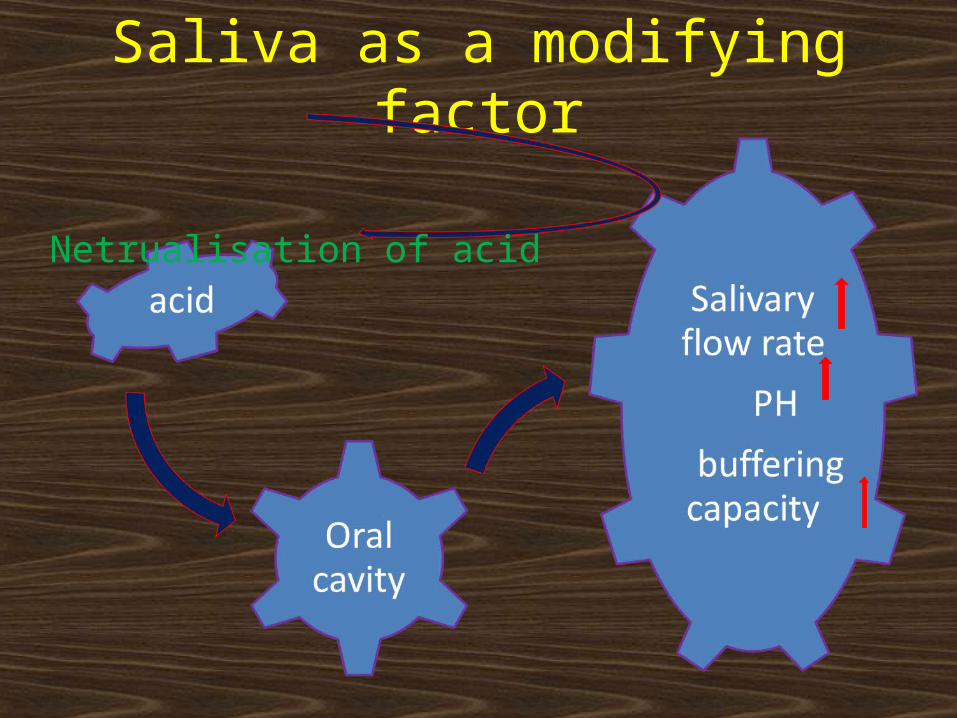
Saliva as a modifying factor
Netrualisation of acid
Clinical features:• Erosion lesion generally present as broad,
shallow, saucer- shaped defects involving enamel and dentin.
• No sharp line angles and the margins of the defects are not well defined.
• Surface appears smooth and polished• Occurs on facial or lingual surfaces.But usually
on the lingual surfaces of maxillary anteriors.• Exogeneous agents such as lemon juice (by
lemon sucking) , cause crescent or dished defects ( rounded as opposed to angular) on the surfaces of exposed teeth.
• Endogenous agents cause generalized erosion on the lingual, incisal and occlusal surfaces.
Erosive lesion is pathognoic in following situations :• No demarcation between lesion & adjacent
tooth surface..• Erosion usually does not affect occluding
surface, except in advanced situations.• Erosion rate is similar for enamel, dentin,
cemetum & sometimes for restorative materials.
• Adacent periodontium and gingiva are sound and healthy.
• Tooth sensitivity to physical, chemical & mechanical stimuli .
• No carious lesion present.Rate of erosion in active lesion was esteemed
to be 1micron per day.• Affects upper teeth especially on the facial
aspect of cuspids & premolas.


Preservation of enamel at gingival crevice B

ABFRACTION• Abfraction is the pathological loss of tooth substance
due to biomechanical loading forces that result in flexure and ultimate fatigue of enamel and dentin at a location away from loading.
• It has been proposed that the predominant causative factor of some cervical, wedge- shaped is a strong(heavy) eccentric occlusal force resulting in microfractures or abfractures.
• Such microfractures occurs as the cervical areas of the tooth flexes under such loads.
• This defect is termed idiopathic erosion or abfraction.• Mainly confined to gingival third of clinical crown was
thought to the result of tooth brush abrasion.

• With each bite , occlusal forces causes teeth to flex.
• Constant flexing ; enamel to break from the crown usually on the buccal surface.
• Parafunctional habits such as bruxism and clenching is also a cause of abfraction.
• Forces could be static ,such as produced by swallowing & clenching or cyclic as those generated during chewing action.
• Abrasive lesions were caused by flexure & ultimate material fatigue of susceptible teeth at locations away from the point of loading. The breakdown was dependent on the magnitude , duration ,direction , frequency & location of the forces.
• Having sharp margins , even be seen in a single tooth.
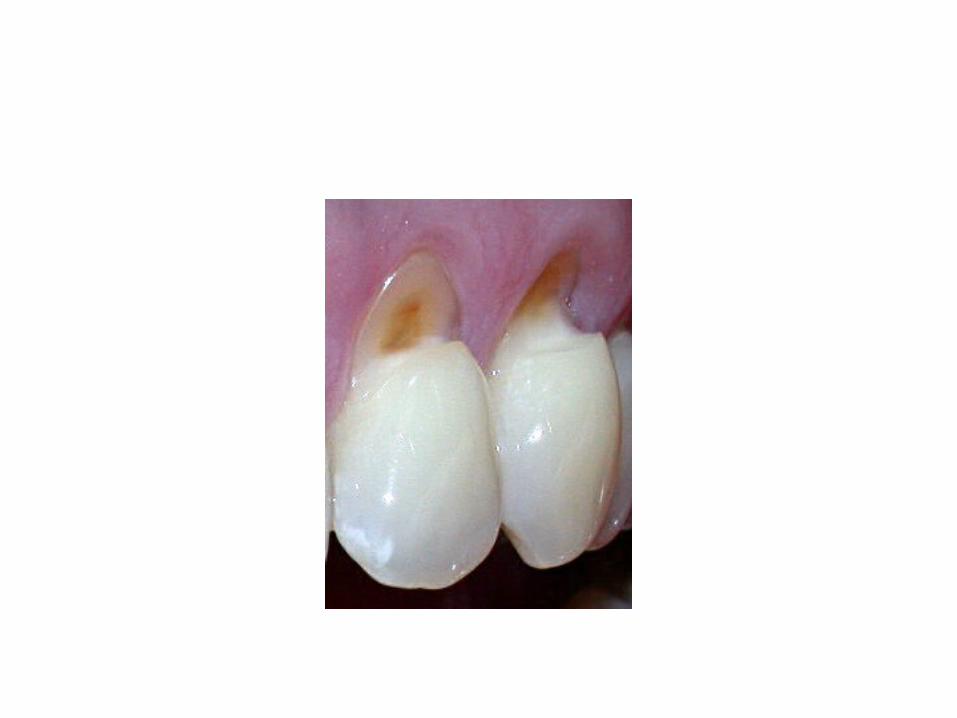
Clinical features :• Appears as wedge-shaped defects on the
facial aspects.• With sharp margins and internal line
angles.• In the initial stages the enamel surface is
rough and shows striations or grooves.• Later stages the defects progresses
deeper in dentin two or more grooves may be visible on the surface.
FRACTURESa)Incomplete Fracture Not Directly Involving Vital Pulp• Also called Greenstick fracture.• This condition is very sensitive, yet the patient can
specify only which side of the mouth rather than the specific tooth.
a)Complete Fracture Not Involving (Not into) Vital Pulp
• Not associated with pain, unless the gingival border of the fractured segment is still held by periodontal tissue
• Restorative treatment is indicated.

c)Fracture Involving (into) Vital Pulp• Always result in pulpal infection and
severe pain.• If tooth is restorabe, immediate root
canal therapy is indicated, otherwise it must be extracted.
• Ellis classification :• Class 1 : Fracture of enamel, involving little
or no dentin.• Class 2 : Fracture of enamel and dentin, but
no pulp.• Class 3 : Fracture of enamel, dentin and pulp.• Class 4 : Tooth becomes non-vital with or
without loss of crown.• Class 5 : Traumatically avulsed tooth.• Class 6 : Frature of root wit or withot crown
fracture.• Class 7 : Displacement of tooth without
fracture of crown or root.• Class 8 : Cervical crown fracture• Class 9 : Fracture of deciduous teeth



NON HEREDITORY ENAMEL HYPOPLASIA
• Occurs when ameloblasts are injured during enamel formation, resulting in defective enamel formation (diminished form or calcification or both ).
• Usually seen on anterior teeth and first molars in the form of opaque white or light brown areas with smooth, intact, hard surface or of pitted or grooved enamel, which is usually hard & discoloured.
Causes :• Nutritional deficiencies (vit.A,C & D)• Exanthematous diseases (Measels,chicken pox,Scarlet
fever)• Congenital syphilis

• Hypocalcaemia• Fluorides• Birth injury,prematurity, Rh hemolytic disease• Local infection or trauma• IdiopathicClinical features :• In mild condition, few small grooves, pits,or
fissures on the enamel surface.• In severe condition, rows of deep pits arranged
horizontally across the surface of tooth.• Enamel hypoplasia due to congenital syphilis is
not of pitting variety, instead almost pathognomic appearance.It involves maxillary & mandibular permanent incisors and first molars.

• The anterior teeth affected are called “Hutchisons teeth”& molar are called “Mulberry Molars” (Moon’s molars,Fournier’s molars).
• Enamel Hypoplasia due to local infection or truama seen in single tooth, commonly permanent max. incisors or max. or mand. Premolars called Turner’s teeth and the condition is called Turner’s Hypoplasia.
• Occurs as mild brownish discolouration of the enamel to a sever pitting and irregularity of the crown.
• Due fluoride ingestion during the time of tooth formation result in mottled enamel.

• Depending upon the level of fluoride in the water supply,
1)Questionable changes charecterizd by white flecking or spotting of enamel.
2)Mild changes manifested by white opaque areas involving more of tooth surface area.
3) Moderate & severe changes showing pitting and brownish staining of the surface
4) Corroded appearance of the teethModerately or severly affected teeth may
show wear & even fracture of the enamel

Non Hereditary Enamel Hypocalcification
• Destruction of ameloblast interfere the formation of enamel.
• Also interfere with mineralization of matrix.• Clinical features :• Affected area will not be defective.• Chalky and soft to indendation and will be stainable.• If extensive it changed to attrition & abrasion.• Enamel can be chipped if the lesion involves the
entire surface.

Non Hereditary Dentin Hypoplasia
• Odntoblast are disturbed by enironmental irritation.
• Result in defective dentin deposition.

Non Hereditary Dentin Hypocalcification
• Have same cases as Hypoplasia.• Dentin is softer, more penetrable, and less
resilient. Eg. Interglobular dentin• Mostly the lesion is unnoticed.

DiscolourationClassified as• Extrinsic : Surface staining due calculus.• Intrinsic : Changes in one or more of tooth
tissues• 1)Discolouration in enamel –Hypoplasia &
Hypocalcification• 2) Discolouration in dentin – Due to non
vitality resulting in disintegration of dentinal tubules or from pigmentation or staining.
• 3) Tetracycline discolouration• 4) Discolouration in pulp

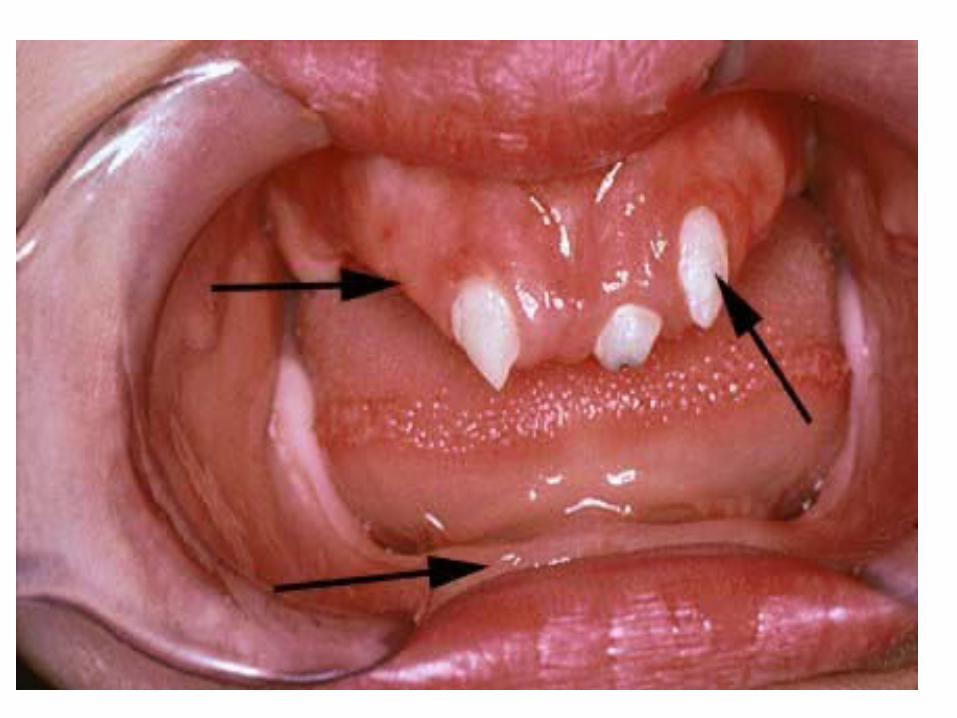
Malformation
• Either in micro or macro forms.• Usually hereditary in origin.• Most common type is one or two teeth
become smaller called peg teeth.• Commonly upper laterals are involved

AMELOGENESIS IMPERFECTA
• Enamel is defective in form or calcification as a result of hereditary and has an appearance ranging from essentially normal to extremely unsightly.
• Also called Hereditary enamel dysplasia or Hereditary brown enamel or Hereditary brown opalescent teeth.
• 3 types• Hypoplastic • Hypocalcified• Hypomaturation

• In radiographically, the overall shape of the teeth may or may not be normal depending upon the amount of enamel present on the tooth and the amount of occlusal & incisal wear.
• Enamel appear totally absent or when present appear as thin layer, chiefly over the tips of cusp and on interproximal surface.
• No treatment except for the improvement of cosmetic.


DENTINOGENESIS IMPERFECTA• Is a hereditary condition in which only the dentin is
defective.• Normal enamel is weakly attached and lost early.• Affecting both decidous and permanent detition.• Affected teeth are gray to yellowish brown and
have broad crowns with constriction of cervical area resulting a ‘tulip’shape
• Radiographically, teeth appear solid, lacking pulp champers and root canals.
• Enamel is easily broken leading to exposure of dentin that undergo accelerated attrition.

• 2 types• Dentinogenesis imperfecta 1• Dentinogenesis imperfecta 2
Dentinogenesis imperfecta type 1• Also called Opalescent dentin or
Capdepont teeth or Den. Imperfecta with out Osteogenesis imperfecta. Or Shields type II.
• Affects only the teeth, no bone fractures.• Blue grey or amber brown or opalescent.• On X-rays teeth as bulbous crowns, roots

are narrow and pulp champers and root canals are smaller than normal or completely obliterated.
• Enamel split from dentin when subjected to occlusal stress.
Dentinogenesis imperfecta 2• Also called Shields type III or Brandywine type• Crowns of the deciduos and permanent teeth wear
rapidly after eruption.• Multiple pulp exposure may occur.• X-rays of decidous teeth show large pulp
Champers and root canals & reduced in size as age advances.
• Permanent teeth have pulpal spaces that are either smaller than normal or completely obliterated.
• Appearance of shell teeth.


CLINICAL MANAGEMENT OF NON-CARIOUS LESIONS

• Non-carious lesions require clinical attention if any of the following factors exist :
1)Tooth sensitivity2)Compromised esthetic3)Risk of tooth fracture4)Pulpal damage5)Caries6)Poor periodontal health
Treatment options
• Dentin desensitization• Restorations• Endodontic therapy• Periodontal therapy
• 1) Dentin desensitization
• Used in situations where minimal amount of dentin is exposed (less than 1mm) & patient experiences hypersesitivity.
• This managed by any of the method suggested for dentin desensitization such as :
• Fluoride varnishes or fluride iontophoresis• Dentin bonding agents• Use of desensitization tooth pastes

2) RestortionsIndicated in following situations• Considerable loss enamel and dentin• Esthetic is compromised• Deep lesion affecting the strength of the tooth and
pulpal integrity• Caries beginning in the cervical lesion• Significant sensitivity of the exposed dentinChoice of restorative material :• Class v non carious lesion with any of the
permanent restorative material presently available.• Of these, Amalgam, direct gold, cast gold inlays
and ceramic inlays are no longer preffered as they require some amount of cavity preparation to make the restoration retentive.

• Currently composite resins and glass ionomer cements are used.Because they are adhesive and do not require extensive cavity preparation.• Composite resin restorations :Stepsa) Tooth preparation : • No cavity preparation is necessary for class
v non carious lesions.Shape of the defect is amendable for filling .However enamel margin beveled to increase the surface area for bonding & to produce esthetic .
b) Pumice prophylaxis :• Clean the surface of any debris or plaque.
c)Shade selectiond) Isolatione)Acid etching & dentin bondingf)Composite resin placement g)Finishing & polishing
• Compomer Restoration :• New variety introduced in 1990s• Combines the durability of composite &
fluoride releasing ability of GIC.• Available as a single component light
curable material in a syringe. • Steps is same as that of composite
restoration

• Indicated for class V cavities.• Glass Ionomer Cements :• Chemically cured GIC have an excellent
track record for restoring class V noncarios defects.
• Nowadays resin-modified GIC are referred.
• ENDONTIC THERAPY :• When cervical tooth loss is extensive
reslting in pulpal involvement, endodontic therapy is necessary followed by post placement & full coverage in the form of crown
• PERIODONTAL THERAPY :• Required when non-carios cervical defects are associated
with gingival recession and mucogingival problems.
PREVENTION• Diet councilling• Use of sodium bicarbonate mouth rinse• Use of fluoride mouth rinse & xylitol gum• Psychiatric consultation• Correct brushing technique• Correct occlusal stresses• Provide mouth guards• Correct abnormal oral habits

Management of Attrition• Pulpally involved tooth should be
extracted or undergo endontic therapy.• Para-functional activities, notably bruxism,
controlled with proper discluding-protecting occlusal splints.
• Occlusal equilibration – by selective grinding of tooth surfaces (include rounding and smoothening the perepheries of occlusal tables.
• Restorative modalities- Metallic restoration in high stress concentrating areas

Management of Abrasion
• Remove the cause.• Treated with fluoride solution to improve
its caries resistance.• Lesion is exceeding 0.5mm into dentin, it
should be restored.• Tooth is sensitive then desensitize the
exposed dentin before starting restorative treatment. (Desensitization by 8-30% Na or Stannous fluoride for 4 to 8 min )
• Restoration by Direct tooth coloured materials(in anterior) & metallic restoration in posteriors.
Management of Erosion
• Remove the cause.• If restoration is the choice of treatment,
metallic restoration is ndicated because it is resistant to erosion.

Management of Fractures
• Restoration• Pulp therapy• Prosthesis

Management of Enamel Hypoplasia
• Bleach the affected teeth with an agent such as Hydrogen peroxide
• This carried out periodically,since the teeth continue to stain.
BLEACHING• Lightening of discolourations of teeth through
the application of chemical agents to oxidize the organic pigmentation of teeth
• Bleaching Agents :• Hydrogen peroxide • Sodium perborate• Carbamide peroxide

Mechansm of Action :• Low mol. Wt of H2O2 allows it to easily
diffuse through enamel & dentin.• Here it breaks down in to water and releases
perhydroxyl ions and nascent oxygen.• Due to its great oxidative power it breaks up
large macromolecule stains into smaller stains.
• These reflect less light and tooth appear lighter.The free oxygen opens the c-ring of pigment molecules converting them into colourless hydroxyl compound.

Non Hereditary Enamel Hypocalcification
• Mineralization of tooth enamel should be made using fluoride application, fluoride ionophoresis .
• Vital bleaching,laminated veneering,composite veneering, and porcelian fused to metal and cast ceramic crowns

Non heritary dentin hypoplasia and hypocalcification
• Intermediary basesCalcium HydroxideZinc phosphatePolycarboxylate
Management of Discolouration
• Extrinsic – Scaling & polishing• Intrinsic – Bleaching,laminated veneering,
composite veneering• Endodontic therapy

Management of Malformation
• Restoration• Malaligned teeth is repositioned
orthodontically.• Porcelain fusedto metal or cast ceramic
veneering restoration

Management of Dentinogenesis Imperfecta
• Cast metal crown or on posterior teeth and jacket crown on anterior teeth.
• Filling are not usually permanent because of softness of dentin.


CONCLUSION• With increasing dental awareness and
improved dental care, more and more people are retaining their teeth for a longer period of time.
• When loss of enamel and dentin at the CEJ becomes significant, resulting in loss of function and esthetic, restoration of these defects becomes necessary.
• Composite resins and GIC are used extensively for restoration of non-carious cervical defects.
Related Documents











