International Journal of Dermatology 2002, 41 , 44–45 © 2002 The International Society of Dermatology 44 A 56-year-old-man who had refractory anemia with an excess of blasts underwent an allogeneic peripheral blood stem cell transplantation (PBSCT) from his brother after preparation with melphalan and fludarabin. He received GvHD (graft-vs.-host disease) prophylaxis with cyclosporine from day –1 at a daily dose of 5 mg/kg of body weight. The daily dosage was tapered gradually from day +20. On post-PBSCT day 68 he developed acute cutaneous GvHD grade 3 and acute gastrointestinal GvHD grade 2–3, which was resolved with a daily dose of 1 mg/kg of body weight of prednisone. The patient was discharged in good clinical condition and without signs of GvHD, and he started tapering his immunosuppressive treatment. By day 160 he developed oral lichen planus-like changes, with several reticulate white lesions on the oral mucosa. A biopsy specimen was microscopically consistent with lichenoid GvHD (Fig. 1). By day 150 after PBSCT, when he was being treated with CsA 100 mg once daily and prednisone 10 mg once daily, his fingernails started to grow abnormally and gradually became dystrophic and painful. Two months later his toenails became similarly affected. Although affecting all finger and toe nails, the lesions were especially important in both thumbs. Physical examination revealed multiple findings on his nails (Fig. 2): thickening, fragility, onycholysis, longitudinal striations, and even pterygium. The micological cultures were negative. A biopsy specimen showed an sparse papillary dermis lymphoid infiltrate with focal exocytosis and presence of isolated multiple necrotic keratinocytes (Fig. 3). These findings were interpreted as a lichenoid GvHD with oral and nail involvement. The patient did not have other associated cutaneous lesions. He did not develop signs or symptoms consistent with hepatic GvHD. In May 2000 thalidomide was added to the immunosuppressive therapy, at a daily dose from 100 to 300 mg according to tolerance (constipation, sedation, ...). The lesions on the oral mucous showed a substantial improvement, but the nail changes remained more or less stable. Thalidomide was discontinued after 7 months because the patient displayed numbness and tingling in the hands and feet consistent with a peripheral neuropathy. Twenty days later he stopped taking thalidomide and the oral lichenoid lesions worsened, resulting in difficulty in eating. He also developed periungueal erythema, swelling and intense pain after minimal trauma. The daily dose of prednisone increased to 20–30 mg with moderate improvement. However, the dose could not be increased because of the secondary immunosuppressive effects. Twenty-three months post-PBSCT the patient remains with intense oral and nail lichenoid lesions. Blackwell Science Ltd Oxford, UK IJD International Journal of Dermatology 0011-9059 Blackwell Science, 2001 January 2001 000 000 Cameo Nail changes in graft vs. host disease Palencia et al. January 2001 000 000 Cameo Nail changes in graft vs. host disease Palencia et al. Lichenoid nail changes as sole external manifestation of graft vs. host disease Sara Isabel Palencia, MD , Jose Luis Rodríguez-Peralto, MD , Esther Castaño, MD , Francisco Vanaclocha, MD , and Luis Iglesias, MD From the Departments of Dermatology and Pathology, Hospital Universitario 12 de Octubre, Madrid, Spain Correspondence Jose Luis Rodríguez-Peralto, MD Departamento de Anatomía Patológica Hospital Universitario 12 de Octubre Ctra Andalucía km 5,400, 28041 Madrid E-mail: [email protected] Discussion GvHD is a frequent complication of allogeneic bone marrow transplantation (BMT). GvHD occurs when immunocompetent cells from a donor recognize and react against “foreign” tis- sue antigens in an immunocompromised host, and BMT is the commonest stimulus for such reactions. GvHD is divided into two forms: acute GvHD, which occurs during the first 3 months following BMT, and chronic GvHD, which includes all the manifestations that develop after the third month following transplantation. Chronic GvHD develops in 10% of all patient undergoing allogeneic BMT and may develop de novo, a gradual progression from acute GvHD, or following resolu- tion of acute GvHD, as in our patient. Traditionally, chronic GvHD includes lichenoid and sclerodermoid forms. 1 Lichen planus-like GvHD can affect the skin, the oral mucosa 2 and the genital organs. Nail manifestations of chronic GvHD are rare, nonspecific 3,4 and include atrophy, dystrophy, thickening,

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

International Journal of Dermatology
2002,
41
, 44–45 © 2002
The International Society of Dermatology
44
A 56-year-old-man who had refractory anemia with an excess of blasts underwent an allogeneic
peripheral blood stem cell transplantation (PBSCT) from his brother after preparation with
melphalan and fludarabin. He received GvHD (graft-vs.-host disease) prophylaxis with
cyclosporine from day –1 at a daily dose of 5 mg/kg of body weight. The daily dosage was
tapered gradually from day +20. On post-PBSCT day 68 he developed acute cutaneous GvHD
grade 3 and acute gastrointestinal GvHD grade 2–3, which was resolved with a daily dose of
1 mg/kg of body weight of prednisone. The patient was discharged in good clinical condition and
without signs of GvHD, and he started tapering his immunosuppressive treatment. By day 160
he developed oral lichen planus-like changes, with several reticulate white lesions on the oral
mucosa. A biopsy specimen was microscopically consistent with lichenoid GvHD (Fig. 1). By
day 150 after PBSCT, when he was being treated with CsA 100 mg once daily and prednisone
10 mg once daily, his fingernails started to grow abnormally and gradually became dystrophic
and painful. Two months later his toenails became similarly affected. Although affecting all finger
and toe nails, the lesions were especially important in both thumbs. Physical examination
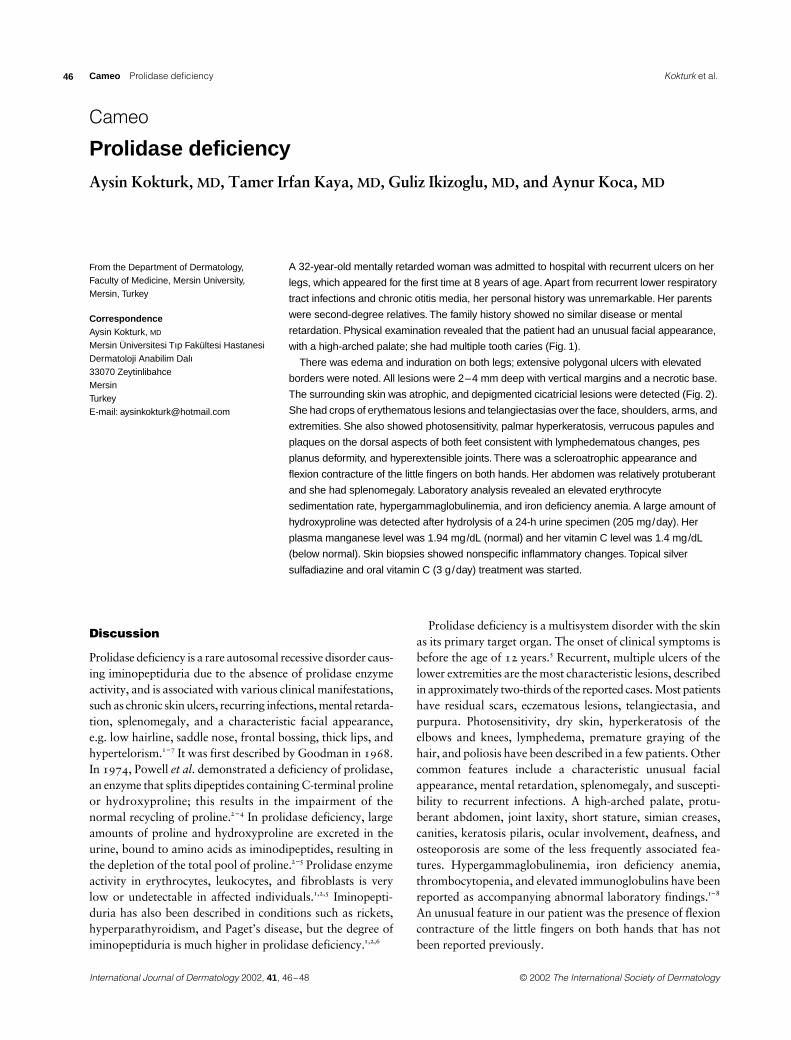
revealed multiple findings on his nails (Fig. 2): thickening, fragility, onycholysis, longitudinal
striations, and even pterygium. The micological cultures were negative. A biopsy specimen
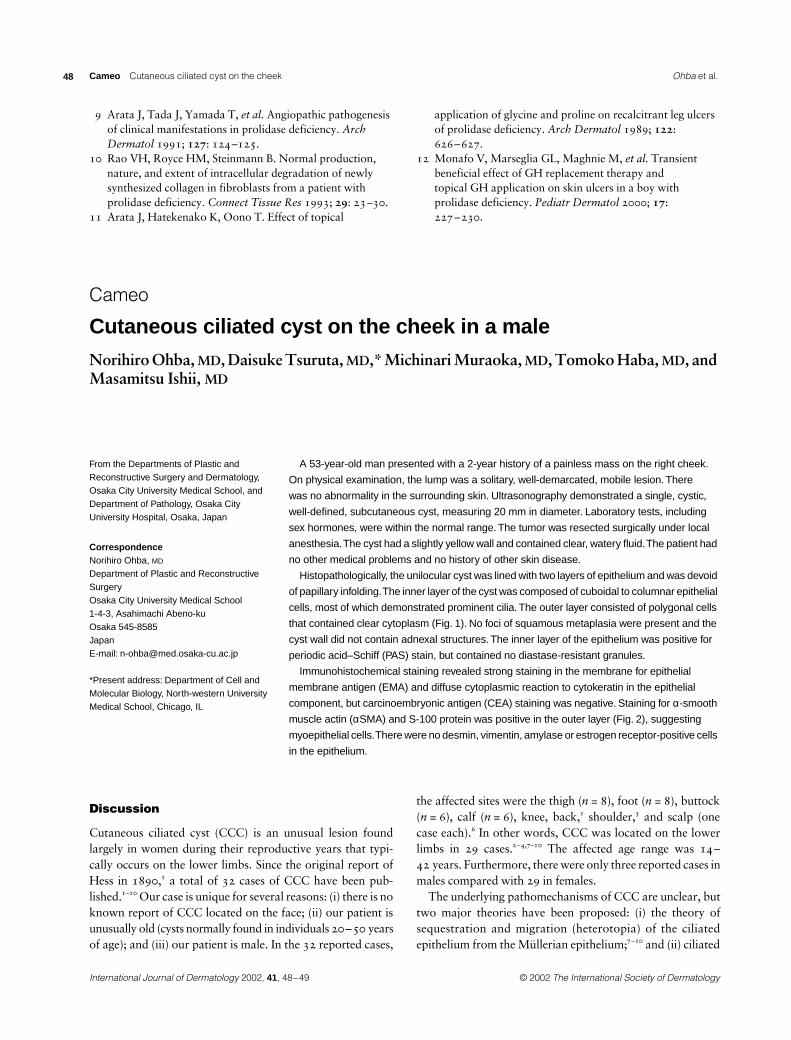
showed an sparse papillary dermis lymphoid infiltrate with focal exocytosis and presence of
isolated multiple necrotic keratinocytes (Fig. 3). These findings were interpreted as a lichenoid
GvHD with oral and nail involvement. The patient did not have other associated cutaneous
lesions. He did not develop signs or symptoms consistent with hepatic GvHD. In May 2000
thalidomide was added to the immunosuppressive therapy, at a daily dose from 100 to 300 mg
according to tolerance (constipation, sedation, ...). The lesions on the oral mucous showed a
substantial improvement, but the nail changes remained more or less stable. Thalidomide
was discontinued after 7 months because the patient displayed numbness and tingling in
the hands and feet consistent with a peripheral neuropathy. Twenty days later he stopped
taking thalidomide and the oral lichenoid lesions worsened, resulting in difficulty in eating. He
also developed periungueal erythema, swelling and intense pain after minimal trauma. The daily
dose of prednisone increased to 20–30 mg with moderate improvement. However, the dose
could not be increased because of the secondary immunosuppressive effects. Twenty-three
months post-PBSCT the patient remains with intense oral and nail lichenoid lesions.
Blackwell Science LtdOxford, UKIJDInternational Journal of Dermatology0011-9059Blackwell Science, 2001January 2001000000CameoNail changes in graft vs. host diseasePalencia et al.January 2001000000
Cameo
Nail changes in graft vs. host diseasePalencia et al.
Lichenoid nail changes as sole external manifestation of graft vs. host disease
Sara Isabel Palencia,
MD
, Jose Luis Rodríguez-Peralto,
MD
, Esther Castaño,
MD
, Francisco Vanaclocha,
MD
, and Luis Iglesias,
MD
From the Departments of Dermatology and Pathology, Hospital Universitario 12 de Octubre, Madrid, Spain
Correspondence
Jose Luis Rodríguez-Peralto,
MD
Departamento de Anatomía Patológica Hospital Universitario 12 de Octubre Ctra Andalucía km 5,400, 28041 Madrid E-mail: [email protected]
Discussion
GvHD is a frequent complication of allogeneic bone marrowtransplantation (BMT). GvHD occurs when immunocompetentcells from a donor recognize and react against “foreign” tis-sue antigens in an immunocompromised host, and BMT is thecommonest stimulus for such reactions. GvHD is divided intotwo forms: acute GvHD, which occurs during the first 3 monthsfollowing BMT, and chronic GvHD, which includes all the
manifestations that develop after the third month followingtransplantation. Chronic GvHD develops in 10% of all patientundergoing allogeneic BMT and may develop de novo, agradual progression from acute GvHD, or following resolu-tion of acute GvHD, as in our patient. Traditionally, chronicGvHD includes lichenoid and sclerodermoid forms.
1
Lichenplanus-like GvHD can affect the skin, the oral mucosa
2
and thegenital organs. Nail manifestations of chronic GvHD are rare,nonspecific
3,4
and include atrophy, dystrophy, thickening,
IJD_1399.fm Page 44 Saturday, February 9, 2002 5:14 PM
© 2002
The International Society of Dermatology International Journal of Dermatology
2002,
41
, 44–45
45
Palencia
et al. Nail changes in graft vs. host disease
Cameo
fragility, onycholysis, periungueal erythema, swelling, whitesuperficial onychomycosis.
5
The typical nail changes of lichenplanus in GvHD are extremely uncommon. Although thesechanges are named in some articles
6,7
there are few publica-tions which describe in detail these lesions. Liddle
et al
. in1990
8
reported a case of pterygium developing in a patientwith chronic GvHD. We describe a patient who developednail manifestations characteristic of lichen planus withpterygium formation as a manifestation of chronic GvHD.This manifestation enhances the spectrum of GvHD. Over-all, nail changes are usually not of concern to the patientbut, as they may be a very early manifestation, detailedclinical examination of the nails should be included in theassessment of a patient for GvHD.
4
References
1 Black MM. Graft-versus-host disease. In: Rook A, Wilkinson DS, Ebling FJG, eds.
Textbook of Dermatology
, 6th edn. Oxford: Blackwell Science, 1998 pp 1919–1921.
2 Schubert MM, Sullivan KM, Morton TH,
et al
. Oral manifestations of chronic graft-versus-host disease.
Arch Intern Med
1984;
144
: 1591–1595.3 De Berker DAR, Baran R, Dawber RPR. The nail in
dermatological diseases. In:
Handbook of Diseases of the Nails and Their Management (de Berker DAR, Baran R. Dawber RPR)
, 2nd edn. Oxford: Blackwell Science Limited 1994; pp 175–176.
4 Andrews ML, Robertson I, Weedon D. Cutaneous manifestations of chronic graft-vs.-host disease.
Australas J Dermatol
1997;
38
: 53–62.5 Basuk PJ, Scher BK. Onichomycosis in graft-versus-host
disease.
Cutis
1987;
40
: 237–241.6 Saurat JH, Gluckman E. Lichen planus-like eruption
following bone marrow transplantation. a manifestations of the graft-versus-host disease.
Clin Exp Dermatol
1977;
2
: 335–344.
7 Shulman HM, Sale GE, Lerner KG,
et al
. Chronic cutaneous graft-versus-host disease in man.
Am J Pathol
1978;
92
: 545–570.
8 Liddle BJ, Cowan MA. Lichen planus-like eruption and nail changes in a patient with graft-versus-host disease.
Br J Dermatol
1990;
122
: 841–843.
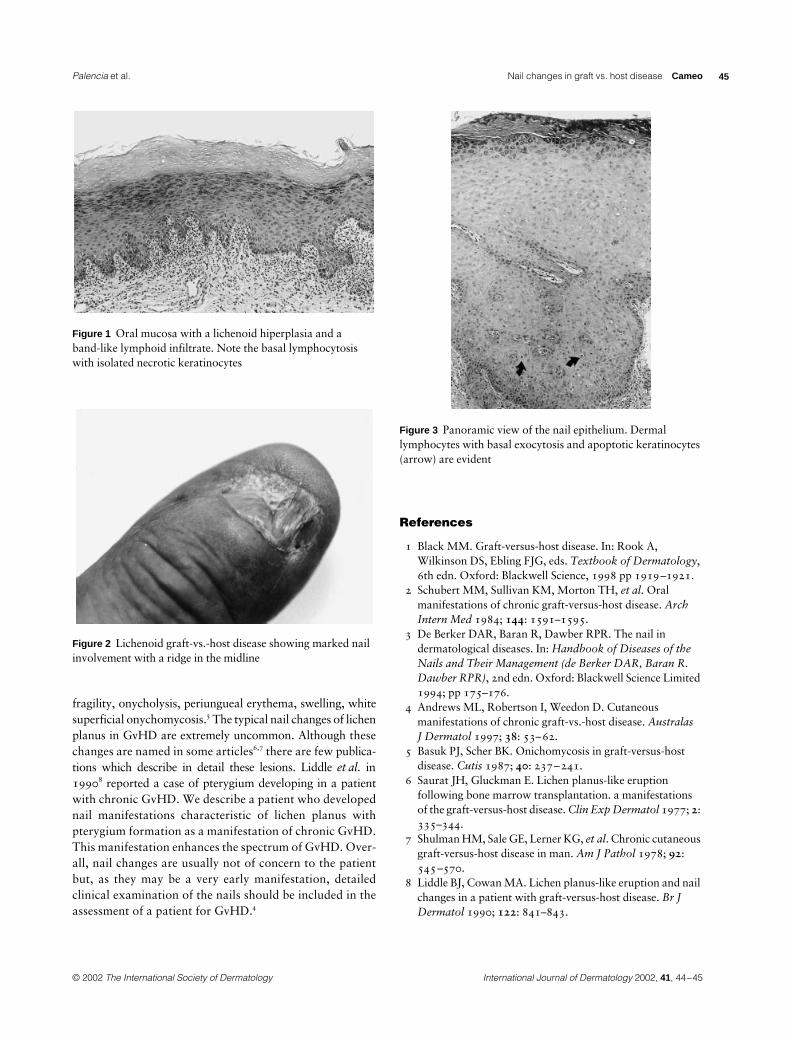
Figure 1 Oral mucosa with a lichenoid hiperplasia and a band-like lymphoid infiltrate. Note the basal lymphocytosis with isolated necrotic keratinocytes
Figure 2 Lichenoid graft-vs.-host disease showing marked nail involvement with a ridge in the midline
Figure 3 Panoramic view of the nail epithelium. Dermal lymphocytes with basal exocytosis and apoptotic keratinocytes (arrow) are evident
IJD_1399.fm Page 45 Saturday, February 9, 2002 5:14 PM
International Journal of Dermatology
2002,
41
, 44–45 © 2002
The International Society of Dermatology
46 Cameo
Prolidase deficiency
Palencia
et al.
Cameo
Prolidase deficiency
Prolidase deficiency
Aysin Kokturk,
MD
, Tamer Irfan Kaya,
MD
, Guliz Ikizoglu,
MD
, and Aynur Koca,
MD
From the Department of Dermatology, Faculty of Medicine, Mersin University, Mersin, Turkey
Correspondence
Aysin Kokturk,
MD
Mersin Üniversitesi Tıp Fakültesi Hastanesi Dermatoloji Anabilim Dalı 33070 Zeytinlibahce Mersin Turkey E-mail: [email protected]
A 32-year-old mentally retarded woman was admitted to hospital with recurrent ulcers on her
legs, which appeared for the first time at 8 years of age. Apart from recurrent lower respiratory
tract infections and chronic otitis media, her personal history was unremarkable. Her parents
were second-degree relatives. The family history showed no similar disease or mental
retardation. Physical examination revealed that the patient had an unusual facial appearance,
with a high-arched palate; she had multiple tooth caries (Fig. 1).
There was edema and induration on both legs; extensive polygonal ulcers with elevated
borders were noted. All lesions were 2–4 mm deep with vertical margins and a necrotic base.
The surrounding skin was atrophic, and depigmented cicatricial lesions were detected (Fig. 2).
She had crops of erythematous lesions and telangiectasias over the face, shoulders, arms, and
extremities. She also showed photosensitivity, palmar hyperkeratosis, verrucous papules and
plaques on the dorsal aspects of both feet consistent with lymphedematous changes, pes
planus deformity, and hyperextensible joints. There was a scleroatrophic appearance and
flexion contracture of the little fingers on both hands. Her abdomen was relatively protuberant
and she had splenomegaly. Laboratory analysis revealed an elevated erythrocyte
sedimentation rate, hypergammaglobulinemia, and iron deficiency anemia. A large amount of
hydroxyproline was detected after hydrolysis of a 24-h urine specimen (205 mg/day). Her
plasma manganese level was 1.94 mg/dL (normal) and her vitamin C level was 1.4 mg/dL
(below normal). Skin biopsies showed nonspecific inflammatory changes. Topical silver
sulfadiazine and oral vitamin C (3 g/day) treatment was started.
Discussion
Prolidase deficiency is a rare autosomal recessive disorder caus-ing iminopeptiduria due to the absence of prolidase enzymeactivity, and is associated with various clinical manifestations,such as chronic skin ulcers, recurring infections, mental retarda-tion, splenomegaly, and a characteristic facial appearance,e.g. low hairline, saddle nose, frontal bossing, thick lips, andhypertelorism.
1–7
It was first described by Goodman in 1968.In 1974, Powell
et al
. demonstrated a deficiency of prolidase,an enzyme that splits dipeptides containing C-terminal prolineor hydroxyproline; this results in the impairment of thenormal recycling of proline.
2 –4
In prolidase deficiency, largeamounts of proline and hydroxyproline are excreted in theurine, bound to amino acids as iminodipeptides, resulting inthe depletion of the total pool of proline.
2–5
Prolidase enzymeactivity in erythrocytes, leukocytes, and fibroblasts is verylow or undetectable in affected individuals.
1,2,5
Iminopepti-duria has also been described in conditions such as rickets,hyperparathyroidism, and Paget’s disease, but the degree ofiminopeptiduria is much higher in prolidase deficiency.
1,2,6
Prolidase deficiency is a multisystem disorder with the skinas its primary target organ. The onset of clinical symptoms isbefore the age of 12 years.
5
Recurrent, multiple ulcers of thelower extremities are the most characteristic lesions, describedin approximately two-thirds of the reported cases. Most patientshave residual scars, eczematous lesions, telangiectasia, andpurpura. Photosensitivity, dry skin, hyperkeratosis of theelbows and knees, lymphedema, premature graying of thehair, and poliosis have been described in a few patients. Othercommon features include a characteristic unusual facialappearance, mental retardation, splenomegaly, and suscepti-bility to recurrent infections. A high-arched palate, protu-berant abdomen, joint laxity, short stature, simian creases,canities, keratosis pilaris, ocular involvement, deafness, andosteoporosis are some of the less frequently associated fea-tures. Hypergammaglobulinemia, iron deficiency anemia,thrombocytopenia, and elevated immunoglobulins have beenreported as accompanying abnormal laboratory findings.
1–8
An unusual feature in our patient was the presence of flexioncontracture of the little fingers on both hands that has notbeen reported previously.
Kokturk
et al.
International Journal of Dermatology
2002,
41
, 46–48
IJD_1399.fm Page 46 Saturday, February 9, 2002 5:14 PM

© 2002
The International Society of Dermatology International Journal of Dermatology
2002,
41
, 44–45
47
Palencia
et al. Prolidase deficiency
Cameo
The pathophysiology of the biochemical defect in prolidasedeficiency still remains to be elucidated. Proline and hydroxy-proline are among the major constituents of collagen. In theabsence of prolidase, the recycling of proline, necessary for
the synthesis of new collagen, is blocked and the result is dis-turbed connective tissue metabolism of the skin and vessels.
1,2
Amorphous vascular deposits, often Congo red-positive,and ultrastructural changes in collagen molecules have beenreported.
1–3,9
Although the pathogenic mechanisms leading tothe skin changes are poorly understood, the induction of therelease of histamine from isolated mast cells and of collagenasefrom polymorphonuclear leukocytes by dipeptides contain-ing proline and hydroxyproline, resulting in an inflammatoryreaction and ulceration, is a plausible explanation.
10
Impairment of the immune system leads to recurrent infec-tions, and the coexistence of prolidase deficiency and lupuserythematosus has been described, suggesting that prolidasedeficiency might be a risk factor for the development of sys-temic lupus erythematosus.
3,6
Effective treatment of prolidase deficiency is still not avail-able. Bed rest, occlusive dressings, topical antiseptics andskin grafting, large doses of oral proline supplements, topicalapplication of glycine and proline, topical application ofgrowth hormone and growth hormone replacement, oral dapsoneat 75 mg/day, the transfusion of normal erythrocytes, and oralsupplements of manganese and ascorbic acid, both modulatorsof prolidase activity, are among the treatment modalities, allwith limited and temporary effects.
1–3,8,11,12
The case reported here is, to our knowledge, the first reportfrom Turkey of a patient with prolidase deficiency, suffering fromchronic and recurrent leg ulceration. We suggest that patientspresenting with chronic and recurrent leg ulcers and suggest-ive signs of the disease should have urine analyses performedin order to reveal a possible underlying prolidase deficiency.
References
1 Bishara JF, Kaloustian VMD. Prolidase deficiency.
Int J Dermatol
1986;
7
: 431–433.2 Milligan A, Graham-Brown RAC, Burns DA, Anderson I.
Prolidase deficiency: a case report and literature review.
Br J Dermatol
1989;
121
: 405–409.3 Bissonette R, Friedmann D, Giroux JM,
et al.
Prolidase deficiency: a multisystemic hereditary disorder.
J Am Acad Dermatol
1993;
29
: 818–821.4 Goodman SI, Solomons CC, Muschenheim F,
et al.
A syndrome resembling lathyrism associated with iminopeptiduria.
Am J Med
1968;
45
: 152–159.5 Leoni A, Cetta G, Tenni R,
et al.
Prolidase deficiency in two siblings with chronic leg ulcerations.
Arch Dermatol
1987;
123
: 493–499.6 Shrinath M, Walter JH, Haeney M,
et al.
Prolidase deficiency and systemic lupus erythematosus.
Arch Dis Child
1997;
76
: 441–444.7 Powell GF, Rasco MA, Maniscalo RM. A prolidase
deficiency in man with iminopeptiduria.
Metabolism
1974;
23
: 505–513.8 Ogata A, Tanaka S, Tomoda T,
et al.
Autosomal recessive prolidase deficiency.
Arch Dermatol
1981;
117
: 689–694.
Figure 1 Facial appearance of the patient
Figure 2 Ulcers and depigmented cicatricial lesions on the legs
Kokturk
et al.
International Journal of Dermatology
2002,
41
, 46–48
IJD_1399.fm Page 47 Saturday, February 9, 2002 5:14 PM
International Journal of Dermatology
2002,
41
, 44–45 © 2002
The International Society of Dermatology
48 Cameo
Cutaneous ciliated cyst on the cheek
Palencia
et al.
9 Arata J, Tada J, Yamada T,
et al.
Angiopathic pathogenesis of clinical manifestations in prolidase deficiency.
Arch Dermatol
1991;
127
: 124–125.10 Rao VH, Royce HM, Steinmann B. Normal production,
nature, and extent of intracellular degradation of newly synthesized collagen in fibroblasts from a patient with prolidase deficiency.
Connect Tissue Res
1993;
29
: 23–30.11 Arata J, Hatekenako K, Oono T. Effect of topical
application of glycine and proline on recalcitrant leg ulcers of prolidase deficiency.
Arch Dermatol
1989;
122
: 626–627.
12 Monafo V, Marseglia GL, Maghnie M,
et al.
Transient beneficial effect of GH replacement therapy and topical GH application on skin ulcers in a boy with prolidase deficiency.
Pediatr Dermatol
2000;
17
: 227–230.
Cameo
Cutaneous ciliated cyst on the cheek
Cutaneous ciliated cyst on the cheek in a male
Norihiro Ohba,
MD
, Daisuke Tsuruta,
MD
,*
Michinari Muraoka,
MD
, Tomoko Haba,
MD
, and Masamitsu Ishii,
MD
From the Departments of Plastic and Reconstructive Surgery and Dermatology, Osaka City University Medical School, and Department of Pathology, Osaka City University Hospital, Osaka, Japan
Correspondence
Norihiro Ohba,
MD
Department of Plastic and Reconstructive Surgery Osaka City University Medical School 1-4-3, Asahimachi Abeno-ku Osaka 545-8585 Japan E-mail: [email protected]
*Present address: Department of Cell and Molecular Biology, North-western University Medical School, Chicago, IL
A 53-year-old man presented with a 2-year history of a painless mass on the right cheek.
On physical examination, the lump was a solitary, well-demarcated, mobile lesion. There
was no abnormality in the surrounding skin. Ultrasonography demonstrated a single, cystic,
well-defined, subcutaneous cyst, measuring 20 mm in diameter. Laboratory tests, including
sex hormones, were within the normal range. The tumor was resected surgically under local
anesthesia. The cyst had a slightly yellow wall and contained clear, watery fluid. The patient had
no other medical problems and no history of other skin disease.
Histopathologically, the unilocular cyst was lined with two layers of epithelium and was devoid
of papillary infolding. The inner layer of the cyst was composed of cuboidal to columnar epithelial
cells, most of which demonstrated prominent cilia. The outer layer consisted of polygonal cells
that contained clear cytoplasm (Fig. 1). No foci of squamous metaplasia were present and the
cyst wall did not contain adnexal structures. The inner layer of the epithelium was positive for
periodic acid–Schiff (PAS) stain, but contained no diastase-resistant granules.
Immunohistochemical staining revealed strong staining in the membrane for epithelial
membrane antigen (EMA) and diffuse cytoplasmic reaction to cytokeratin in the epithelial
component, but carcinoembryonic antigen (CEA) staining was negative. Staining for
α
-smooth
muscle actin (
α
SMA) and S-100 protein was positive in the outer layer (Fig. 2), suggesting
myoepithelial cells. There were no desmin, vimentin, amylase or estrogen receptor-positive cells
in the epithelium.
Discussion
Cutaneous ciliated cyst (CCC) is an unusual lesion foundlargely in women during their reproductive years that typi-cally occurs on the lower limbs. Since the original report ofHess in 1890,
1
a total of 32 cases of CCC have been pub-lished.
1–10
Our case is unique for several reasons: (i) there is noknown report of CCC located on the face; (ii) our patient isunusually old (cysts normally found in individuals 20–50 yearsof age); and (iii) our patient is male. In the 32 reported cases,
the affected sites were the thigh (
n
= 8), foot (
n
= 8), buttock(
n
= 6), calf (
n
= 6), knee, back,
1
shoulder,
5
and scalp (onecase each).
6
In other words, CCC was located on the lowerlimbs in 29 cases.
2–4,7–10
The affected age range was 14–42 years. Furthermore, there were only three reported cases inmales compared with 29 in females.
The underlying pathomechanisms of CCC are unclear, buttwo major theories have been proposed: (i) the theory ofsequestration and migration (heterotopia) of the ciliatedepithelium from the Müllerian epithelium;
7–10
and (ii) ciliated
Ohba
et al.
International Journal of Dermatology
2002,
41
, 48–49
IJD_1399.fm Page 48 Saturday, February 9, 2002 5:14 PM
© 2002
The International Society of Dermatology International Journal of Dermatology
2002,
41
, 44–45
49
Palencia
et al. Cutaneous ciliated cyst on the cheek
Cameo
metaplasia of the eccrine glands.
2–4,6
In support of the formertheory, several groups have reported that the ciliated cells ofCCC are morphologically similar to the epithelium of thefallopian tube and show positive staining for various fallo-pian tube markers, such as amylase,
9
S-100 protein,
10
and sexsteroid receptors.
6
Furthermore, the anatomical proximity ofthe fallopian tube and lower limb buds further explains theanatomical predilection of CCC for the lower extremities.This theory is quite intriguing and plausible in most cases of
CCC, but cannot explain the following three points: (i) themolecular markers that are relatively specific to the fallopiantube are not consistently expressed in all CCC;
4
(ii) threeknown male cases have been reported; and (iii) three of thereported cases of CCC were not located on the lower limbs.
The latter explanation of metaplasia or preservation ofembryonal remnants is based on the presence of embryonaleccrine glands containing cilia in their secretory and ductalepithelia. This theory is reinforced by the presence of remnantsof cilia in eccrine and apocrine spiradenoma. This theory,however, cannot explain the predominant localization ofCCC on the lower extremities and immunoreactivity forcarcinoembryonic antigen (CEA). Strong immunoreactivityfor
α
-smooth muscle actin (
α
SMA) and S-100 protein in theouter layer suggests the existence of myoepithelial cells, whichsupports the eccrine origin of CCC. Further studies arerequired to determine whether the immunohistochemicalfindings in our case resemble those of the eccrine gland and toestablish the eccrine origin of CCC.
References
1 Hess K. Ueber eine subcutane flimmerzyste.
Beitr Pathol
1890;
8
: 98–109 (in German).2 Leonforte JF. Cutaneous ciliated cystadenoma in a man.
Arch Dermatol
1982;
118
: 1010–1012.3 Trotter SE, Rassl DM, Saad M,
et al. Cutaneous ciliated cyst occurring in a male. Histopathology 1994; 25: 492–493.
4 Ashton MA. Cutaneous ciliated cyst of the lower limb in a male. Histopathology 1995; 26: 467–469.
5 Sabourin JC, Grossin M, Potet F. Cutaneous ciliated cyst of the scapular area. Ann Dermatol Venereol 1993; 120: 383–385.
6 Sickel JZ. Cutaneous ciliated cyst of the scalp: a case report with immunohistochemical evidence for estrogen and progesterone receptors. Am J Dermatopathol 1994; 16: 76–79.
7 Farmer ER, Helwig EB. Cutaneous ciliated cysts. Arch Dermatol 1978; 114: 70–73.
8 Park CH, Grisoni E, Reid JD. Cutaneous ciliated cyst: case report and discussion of pathogenesis. J Pediatr Surg 1982; 17: 410–411.
9 Varma SK, Rayner SS, Brown LJ. Cutaneous ciliated cyst: case report and literature review. Plast Reconstr Surg 1990; 86: 344–346.
10 Al Nafussi A, Carder P. Cutaneous ciliated cyst: a case report and immunohistochemical comparison with fallopian tube. Histopathology 1990; 16: 595–598.
Figure 1 Hematoxylin and eosin staining. A unilocular cyst lined with two layers of epithelium (original magnification, × 200)
Figure 2 α-Smooth muscle actin (αSMA) staining was positive in the outer layer (original magnification, × 100)
Ohba et al.
International Journal of Dermatology 2002, 41, 48–49
IJD_1399.fm Page 49 Saturday, February 9, 2002 5:14 PM
International Journal of Dermatology 2002, 41, 44–45 © 2002 The International Society of Dermatology
50 Cameo Stingray injury in a domestic aquarium Palencia et al.
CameoStingray injury in a domestic aquariumStingray injury in a domestic aquarium
Alberto Schiera, MD, Maria Luisa Battifoglio, MD, Gabriele Scarabelli, MD, and Dario Crippa, MD
From the Department of Dermatology, San Gerardo Hospital, Monza, Italy
Correspondence Alberto Schiera, MD Department of Dermatovenereology San Gerardo Hospital Via Donizetti, 106 20052 Monza (MI) Italy E-mail: [email protected]
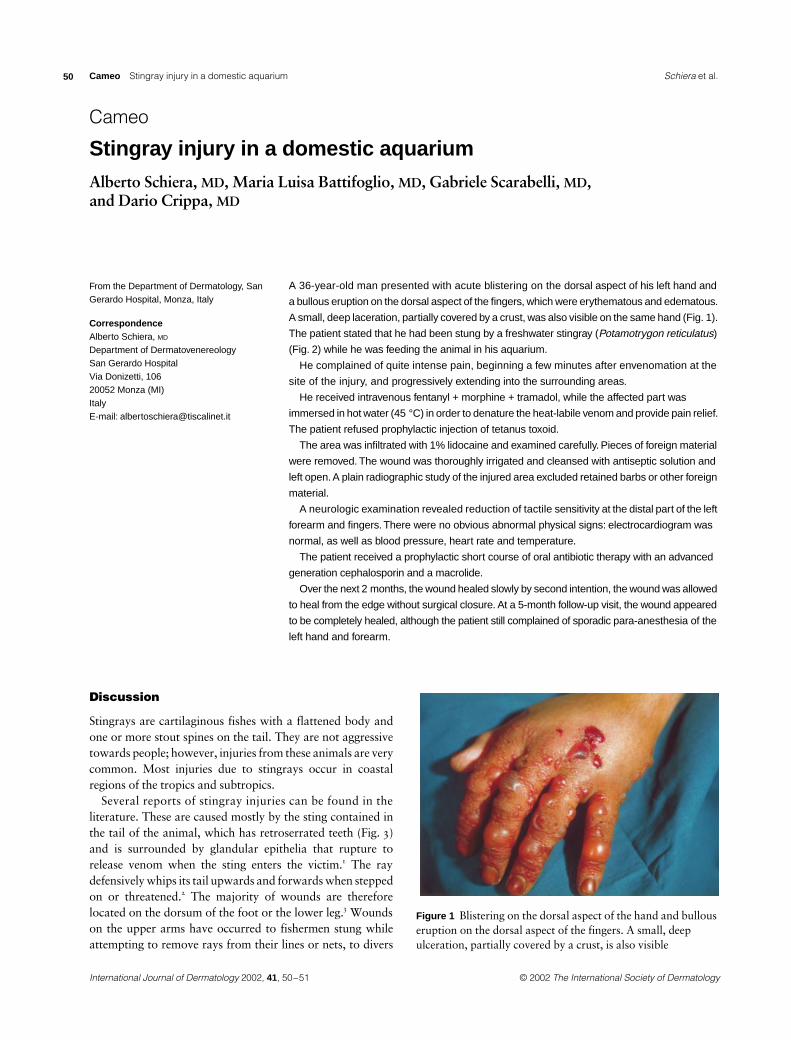
A 36-year-old man presented with acute blistering on the dorsal aspect of his left hand and
a bullous eruption on the dorsal aspect of the fingers, which were erythematous and edematous.
A small, deep laceration, partially covered by a crust, was also visible on the same hand (Fig. 1).
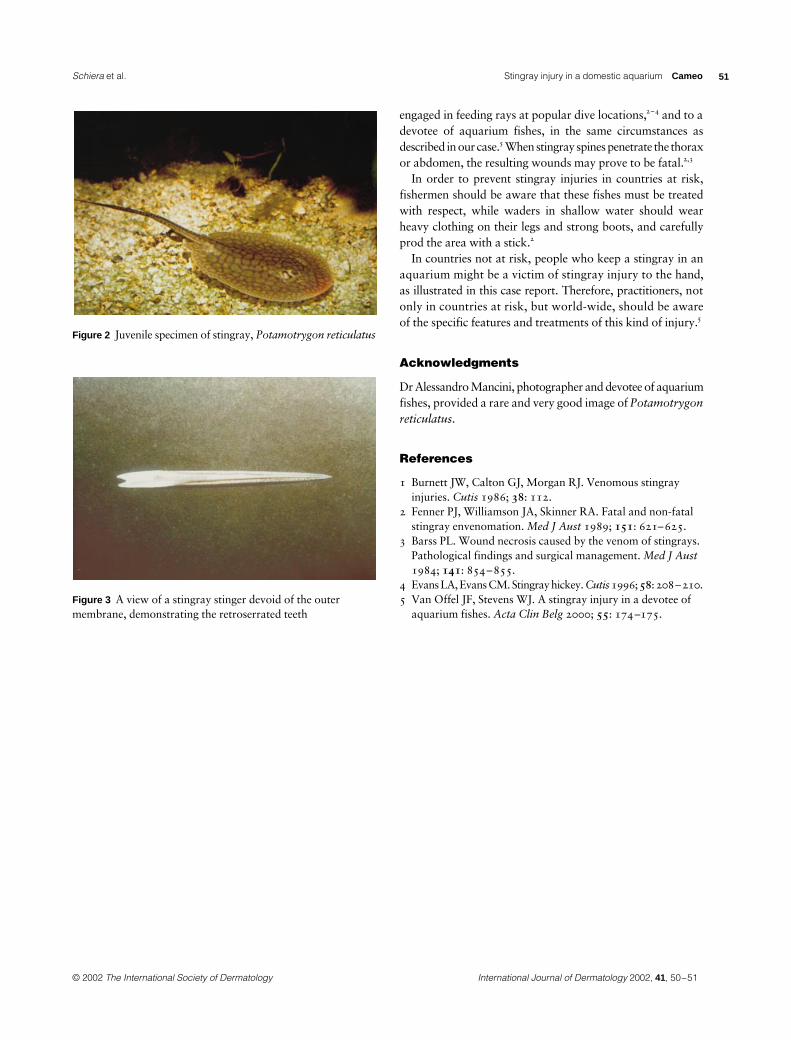
The patient stated that he had been stung by a freshwater stingray (Potamotrygon reticulatus)
(Fig. 2) while he was feeding the animal in his aquarium.
He complained of quite intense pain, beginning a few minutes after envenomation at the
site of the injury, and progressively extending into the surrounding areas.
He received intravenous fentanyl + morphine + tramadol, while the affected part was
immersed in hot water (45 °C) in order to denature the heat-labile venom and provide pain relief.
The patient refused prophylactic injection of tetanus toxoid.
The area was infiltrated with 1% lidocaine and examined carefully. Pieces of foreign material
were removed. The wound was thoroughly irrigated and cleansed with antiseptic solution and
left open. A plain radiographic study of the injured area excluded retained barbs or other foreign
material.
A neurologic examination revealed reduction of tactile sensitivity at the distal part of the left
forearm and fingers. There were no obvious abnormal physical signs: electrocardiogram was
normal, as well as blood pressure, heart rate and temperature.
The patient received a prophylactic short course of oral antibiotic therapy with an advanced
generation cephalosporin and a macrolide.
Over the next 2 months, the wound healed slowly by second intention, the wound was allowed
to heal from the edge without surgical closure. At a 5-month follow-up visit, the wound appeared
to be completely healed, although the patient still complained of sporadic para-anesthesia of the
left hand and forearm.
Discussion
Stingrays are cartilaginous fishes with a flattened body andone or more stout spines on the tail. They are not aggressivetowards people; however, injuries from these animals are verycommon. Most injuries due to stingrays occur in coastalregions of the tropics and subtropics.
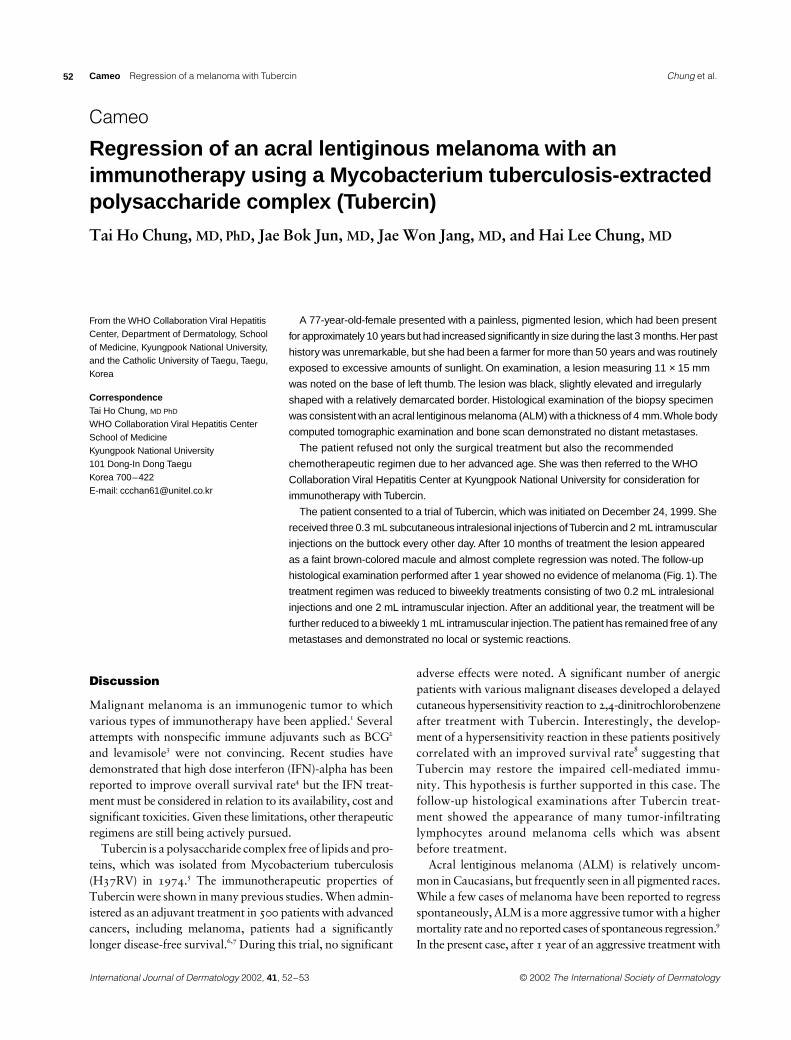
Several reports of stingray injuries can be found in theliterature. These are caused mostly by the sting contained inthe tail of the animal, which has retroserrated teeth (Fig. 3)and is surrounded by glandular epithelia that rupture torelease venom when the sting enters the victim.1 The raydefensively whips its tail upwards and forwards when steppedon or threatened.2 The majority of wounds are thereforelocated on the dorsum of the foot or the lower leg.3 Woundson the upper arms have occurred to fishermen stung whileattempting to remove rays from their lines or nets, to divers
Figure 1 Blistering on the dorsal aspect of the hand and bullous eruption on the dorsal aspect of the fingers. A small, deep ulceration, partially covered by a crust, is also visible
Schiera et al.
International Journal of Dermatology 2002, 41, 50–51
IJD_1399.fm Page 50 Saturday, February 9, 2002 5:14 PM
© 2002 The International Society of Dermatology International Journal of Dermatology 2002, 41, 44–45
51Palencia et al. Stingray injury in a domestic aquarium Cameo
engaged in feeding rays at popular dive locations,2–4 and to adevotee of aquarium fishes, in the same circumstances asdescribed in our case.5 When stingray spines penetrate the thoraxor abdomen, the resulting wounds may prove to be fatal.2,3
In order to prevent stingray injuries in countries at risk,fishermen should be aware that these fishes must be treatedwith respect, while waders in shallow water should wearheavy clothing on their legs and strong boots, and carefullyprod the area with a stick.2
In countries not at risk, people who keep a stingray in anaquarium might be a victim of stingray injury to the hand,as illustrated in this case report. Therefore, practitioners, notonly in countries at risk, but world-wide, should be awareof the specific features and treatments of this kind of injury.5
Acknowledgments
Dr Alessandro Mancini, photographer and devotee of aquariumfishes, provided a rare and very good image of Potamotrygonreticulatus.
References
1 Burnett JW, Calton GJ, Morgan RJ. Venomous stingray injuries. Cutis 1986; 38: 112.
2 Fenner PJ, Williamson JA, Skinner RA. Fatal and non-fatal stingray envenomation. Med J Aust 1989; 151: 621–625.
3 Barss PL. Wound necrosis caused by the venom of stingrays. Pathological findings and surgical management. Med J Aust 1984; 141: 854–855.
4 Evans LA, Evans CM. Stingray hickey. Cutis 1996; 58: 208–210.5 Van Offel JF, Stevens WJ. A stingray injury in a devotee of
aquarium fishes. Acta Clin Belg 2000; 55: 174–175.January 2001000000
Figure 2 Juvenile specimen of stingray, Potamotrygon reticulatus
Figure 3 A view of a stingray stinger devoid of the outer membrane, demonstrating the retroserrated teeth
Schiera et al.
International Journal of Dermatology 2002, 41, 50–51
IJD_1399.fm Page 51 Saturday, February 9, 2002 5:14 PM
International Journal of Dermatology 2002, 41, 44–45 © 2002 The International Society of Dermatology
52 Cameo Regression of a melanoma with Tubercin Palencia et al.
CameoRegression of a melanoma with TubercinRegression of an acral lentiginous melanoma with an immunotherapy using a Mycobacterium tuberculosis-extracted polysaccharide complex (Tubercin)
Tai Ho Chung, MD, PhD, Jae Bok Jun, MD, Jae Won Jang, MD, and Hai Lee Chung, MD
From the WHO Collaboration Viral Hepatitis Center, Department of Dermatology, School of Medicine, Kyungpook National University, and the Catholic University of Taegu, Taegu, Korea
Correspondence Tai Ho Chung, MD PhD WHO Collaboration Viral Hepatitis Center School of Medicine Kyungpook National University 101 Dong-In Dong Taegu Korea 700–422 E-mail: [email protected]
A 77-year-old-female presented with a painless, pigmented lesion, which had been present
for approximately 10 years but had increased significantly in size during the last 3 months. Her past
history was unremarkable, but she had been a farmer for more than 50 years and was routinely
exposed to excessive amounts of sunlight. On examination, a lesion measuring 11 × 15 mm
was noted on the base of left thumb. The lesion was black, slightly elevated and irregularly
shaped with a relatively demarcated border. Histological examination of the biopsy specimen
was consistent with an acral lentiginous melanoma (ALM) with a thickness of 4 mm. Whole body
computed tomographic examination and bone scan demonstrated no distant metastases.
The patient refused not only the surgical treatment but also the recommended
chemotherapeutic regimen due to her advanced age. She was then referred to the WHO
Collaboration Viral Hepatitis Center at Kyungpook National University for consideration for
immunotherapy with Tubercin.
The patient consented to a trial of Tubercin, which was initiated on December 24, 1999. She
received three 0.3 mL subcutaneous intralesional injections of Tubercin and 2 mL intramuscular
injections on the buttock every other day. After 10 months of treatment the lesion appeared
as a faint brown-colored macule and almost complete regression was noted. The follow-up
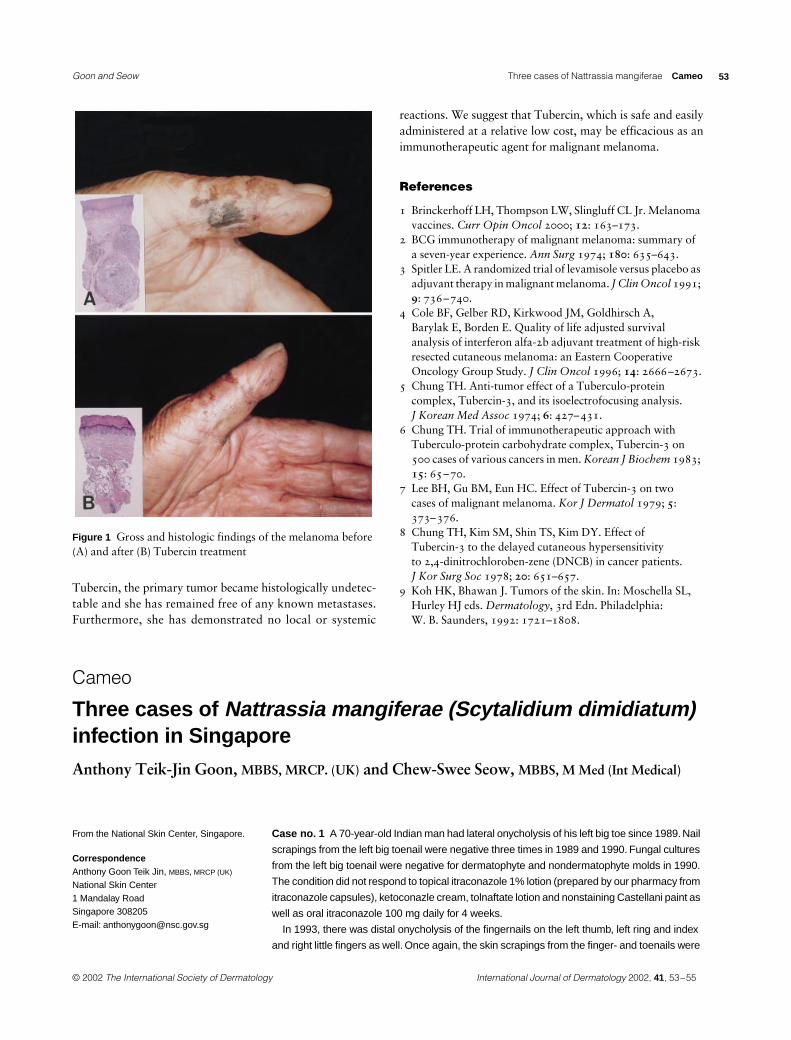
histological examination performed after 1 year showed no evidence of melanoma (Fig. 1). The
treatment regimen was reduced to biweekly treatments consisting of two 0.2 mL intralesional
injections and one 2 mL intramuscular injection. After an additional year, the treatment will be
further reduced to a biweekly 1 mL intramuscular injection. The patient has remained free of any
metastases and demonstrated no local or systemic reactions.
Discussion
Malignant melanoma is an immunogenic tumor to whichvarious types of immunotherapy have been applied.1 Severalattempts with nonspecific immune adjuvants such as BCG2
and levamisole3 were not convincing. Recent studies havedemonstrated that high dose interferon (IFN)-alpha has beenreported to improve overall survival rate4 but the IFN treat-ment must be considered in relation to its availability, cost andsignificant toxicities. Given these limitations, other therapeuticregimens are still being actively pursued.
Tubercin is a polysaccharide complex free of lipids and pro-teins, which was isolated from Mycobacterium tuberculosis(H37RV) in 1974.5 The immunotherapeutic properties ofTubercin were shown in many previous studies. When admin-istered as an adjuvant treatment in 500 patients with advancedcancers, including melanoma, patients had a significantlylonger disease-free survival.6,7 During this trial, no significant
adverse effects were noted. A significant number of anergicpatients with various malignant diseases developed a delayedcutaneous hypersensitivity reaction to 2,4-dinitrochlorobenzeneafter treatment with Tubercin. Interestingly, the develop-ment of a hypersensitivity reaction in these patients positivelycorrelated with an improved survival rate8 suggesting thatTubercin may restore the impaired cell-mediated immu-nity. This hypothesis is further supported in this case. Thefollow-up histological examinations after Tubercin treat-ment showed the appearance of many tumor-infiltratinglymphocytes around melanoma cells which was absentbefore treatment.
Acral lentiginous melanoma (ALM) is relatively uncom-mon in Caucasians, but frequently seen in all pigmented races.While a few cases of melanoma have been reported to regressspontaneously, ALM is a more aggressive tumor with a highermortality rate and no reported cases of spontaneous regression.9
In the present case, after 1 year of an aggressive treatment with
Chung et al.
International Journal of Dermatology 2002, 41, 52–53
IJD_1399.fm Page 52 Saturday, February 9, 2002 5:14 PM
© 2002 The International Society of Dermatology International Journal of Dermatology 2002, 41, 44–45
53Palencia et al. Three cases of Nattrassia mangiferae Cameo
Tubercin, the primary tumor became histologically undetec-table and she has remained free of any known metastases.Furthermore, she has demonstrated no local or systemic
reactions. We suggest that Tubercin, which is safe and easilyadministered at a relative low cost, may be efficacious as animmunotherapeutic agent for malignant melanoma.
References
1 Brinckerhoff LH, Thompson LW, Slingluff CL Jr. Melanoma vaccines. Curr Opin Oncol 2000; 12: 163–173.
2 BCG immunotherapy of malignant melanoma: summary of a seven-year experience. Ann Surg 1974; 180: 635–643.
3 Spitler LE. A randomized trial of levamisole versus placebo as adjuvant therapy in malignant melanoma. J Clin Oncol 1991; 9: 736–740.
4 Cole BF, Gelber RD, Kirkwood JM, Goldhirsch A, Barylak E, Borden E. Quality of life adjusted survival analysis of interferon alfa-2b adjuvant treatment of high-risk resected cutaneous melanoma: an Eastern Cooperative Oncology Group Study. J Clin Oncol 1996; 14: 2666–2673.
5 Chung TH. Anti-tumor effect of a Tuberculo-protein complex, Tubercin-3, and its isoelectrofocusing analysis. J Korean Med Assoc 1974; 6: 427–431.
6 Chung TH. Trial of immunotherapeutic approach with Tuberculo-protein carbohydrate complex, Tubercin-3 on 500 cases of various cancers in men. Korean J Biochem 1983; 15: 65–70.
7 Lee BH, Gu BM, Eun HC. Effect of Tubercin-3 on two cases of malignant melanoma. Kor J Dermatol 1979; 5: 373–376.
8 Chung TH, Kim SM, Shin TS, Kim DY. Effect of Tubercin-3 to the delayed cutaneous hypersensitivity to 2,4-dinitrochloroben-zene (DNCB) in cancer patients. J Kor Surg Soc 1978; 20: 651–657.
9 Koh HK, Bhawan J. Tumors of the skin. In: Moschella SL, Hurley HJ eds. Dermatology, 3rd Edn. Philadelphia: W. B. Saunders, 1992: 1721–1808.
Figure 1 Gross and histologic findings of the melanoma before (A) and after (B) Tubercin treatment
CameoThree cases of Nattrassia mangiferaeThree cases of Nattrassia mangiferae (Scytalidium dimidiatum)
infection in Singapore
Anthony Teik-Jin Goon, MBBS, MRCP. (UK) and Chew-Swee Seow, MBBS, M Med (Int Medical)
From the National Skin Center, Singapore.
Correspondence Anthony Goon Teik Jin, MBBS, MRCP (UK) National Skin Center 1 Mandalay Road Singapore 308205 E-mail: [email protected]
Case no. 1 A 70-year-old Indian man had lateral onycholysis of his left big toe since 1989. Nail
scrapings from the left big toenail were negative three times in 1989 and 1990. Fungal cultures
from the left big toenail were negative for dermatophyte and nondermatophyte molds in 1990.
The condition did not respond to topical itraconazole 1% lotion (prepared by our pharmacy from
itraconazole capsules), ketoconazle cream, tolnaftate lotion and nonstaining Castellani paint as
well as oral itraconazole 100 mg daily for 4 weeks.
In 1993, there was distal onycholysis of the fingernails on the left thumb, left ring and index
and right little fingers as well. Once again, the skin scrapings from the finger- and toenails were
Goon and Seow
International Journal of Dermatology 2002, 41, 53–55
IJD_1399.fm Page 53 Saturday, February 9, 2002 5:14 PM

International Journal of Dermatology 2002, 41, 44–45 © 2002 The International Society of Dermatology
54 Cameo Three cases of Nattrassia mangiferae Palencia et al.
negative. The condition did not respond to topical tolnaftate lotion, clotrimazole 1% lotion,
miconazole 1% lotion, thiabendazole 10% lotion and nonstaining Castellani paint.
In September 1999, both big toenails had crumbling nail plates and ragged distal edges. Nail
scrapings showed the presence of mycelium and the fungal culture result was reported
Scytalidium dimidiatum and Fusarium species. The Fusarium was thought to be a nonpathogenic
coloniser. He was treated with oral griseofulvin, thiabendazole 10% lotion and nonstaining
Castellani paint without much improvement.
He was last seen in January 2001. There was still destruction of the nail plate and separation
of the nail plate from the nail bed.
Case no. 2 A 45-year-old Chinese man who worked as a clerk in a cosmetic company was first
seen in July 1994 for scaly hyperkeratotic rashes on both soles for 10 years. He had tried using
miconazole cream but the problem persisted. Skin scrapings revealed the presence of mycelium
and fungal culture result war reported as Hendersonula toruloidea. He was born in Singapore
and had never lived overseas.
The condition persisted despite 9 weeks of oral griseofulvin 250 mg twice daily and miconazole
2% cream, 3 months of 10% thiabendazole lotion, 2 weeks of oral thiabendazole 500 mg twice
daily and ung Whitfield. He subsequently defaulted after the last visit in April 1995, when he was
prescribed amorolfine cream.
He was seen again in July 1998 for acne vulgaris. His soles were still hyperkeratotic but skin
scrapings were not taken. He defaulted again after 3 visits.
Case no. 3 A 33-year-old Indian man who had been working in a machine assembly line for
12 years presented with an itchy scaly rash on his feet for 3 years and on the hands for 1 year
in November 1996. The rash was especially prominent on the toewebs and occasionally formed
vesicles and became secondarily infected. He had been treated with antifungal creams, with the
addition of oral antibiotics for episodes of secondary infection, but the skin condition deteriorated.
He wore shoes at work and had been exposed to coolants for 3 years. There was no history of
atopy or allergies.
On examination, there was maceration and scaling between the right second and third toes.
Scaling was seen in the toewebs and near the thumbs bilaterally. The nails and groin were normal.
Skin scrapings were negative on the hands, but showed a few hyphae on the toewebs.
Fungal cultures from the toewebs were negative but bacterial cultures of the toewebs grew
Acinetobacter baumanii and Klebsiella species, both of which were sensitive to gentamicin.
The diagnoses of secondarily infected tinea pedis and hand dermatitis were made.
The infection settled with oral cloxacillin and topical gentamicin cream but the skin of the
hands and feet remained dry and fissured. He was then treated as for hand and foot dermatitis
with moderately potent topical corticosteroids with minimal improvement. Repeated skin
scrapings were negative in January and May 1997. He defaulted in September 1998.
He returned in March 2000 with an acute exacerbation of a dry itchy rash on his palms and soles.
He was treated as for dermatitis with cephalexin and a tapering course of prednisolone with
significant improvement. Due to the persistent rashs, a skin scraping of the feet was repeated
in May 2000 and this showed the presence of mycelium. He was treated with a course of oral
griseofulvin 250 mg twice daily for 4 weeks with no improvement. He was then treated
empirically with oral terbinafine 250 mg daily for 3 weeks and miconazole 2% cream,
as cultures were not available.
In June 2000 he had an infected exacerbation of his rash, which required treatment with oral
cephalexin followed by oral cotrimoxazole. The skin scraping of the toewebs was negative and
a diagnosis of acute dermatitis was made. He was given a tapering course of prednisolone with
improvement. A patch test was negative.
In November 2000, he still had a rash on the palms and soles. The fungal culture result was
reported as Scytalidum dimidiatum but fungal scrapes had not been done. He was treated with
oral itraconazole 200 mg daily for 4 weeks, oral cloxacillin and miconazole 2% cream.
Goon and Seow
International Journal of Dermatology 2002, 41, 53–55
IJD_1399.fm Page 54 Saturday, February 9, 2002 5:14 PM

© 2002 The International Society of Dermatology International Journal of Dermatology 2002, 41, 44–45
55Palencia et al. Three cases of Nattrassia mangiferae Cameo
Discussion
Nattrassia mangiferae has been increasingly reported as acause of human disease, which may be clinically impossibleto distinguish from dermatophytosis. It is common to havemixed infections with dermatophytes, where both organismsshould be considered as pathogens.1,2 The most commonlyaffected parts in immunocompetent hosts are the feet, palmsand nails. This mold is limited primarily to tissue containingkeratin, and may remain viable in dry skin scrapings at roomtemperature for 6 months.3 Infections are acquired by directcontact, especially in those individuals without protectiveclothing or footwear.4 It is difficult to prove anthropophilictransmission as infected individuals typically reside in or havevisited endemic areas. It is presumed that infection is a resultof direct contact with soil or plants. Proven transmission fromhuman to human or animal to human is not known.
A diagnostic clue is positive KOH but no growth oncycloheximide-containing agars. This combined with a historyof griseofulvin failure should alert the physician to a possiblenondermatophytic infection. Culture is diagnostic, and biopsyis not usually indicated.
It is important to keep in mind that these organisms do notgrow in the presence of cycloheximide. Since dermatophytosiscan coexist, both cycloheximide and noncycloheximide mediashould be used for isolation and identification of fungal agents.
There is no orally effective treatment. Griseofulvin andketoconazole are ineffective.5,6 Oral itraconazole7,8 and intra-venous amphotericin B9 have been reported to induce clinicaland mycological remission. Terbinafine and fluconazole havenot been shown to be effective against nondermatophytes.Topical antifungals including azoles are ineffective. In vitro,H toruloidea may be sensitive to clotrimazole but in vivo useof clotrimazole results in therapeutic failure.5 There has been acase report of successful treatment of Hendersonula toruloideaonychomycosis with nail avulsion followed by topicalciclopiroxolamine under occlusion nightly for 3–4 months,but the same patient’s palm and sole infection was resistant tociclopiroxolamine.10 Another report showed successful treat-ment of Scytalidium hyalinum onychomycosis with 5%amorolfine nail lacquer twice a week for 8 weeks.11 Terbinafineand amorolfine have been shown to have in vitro activityagainst Scytalidium species.12
As dermatophytosis and dermatomycosis often coexist,conventional antifungal therapy might result in resolution ofdermatophyte and overall apparent improvement, butcomplete mycological cure could only be verified by recultureon both cycloheximide and noncycloheximide media.
References
1 Moore MK. Hendersonula toruloidea and Scytalidium hyalinum infections in London, England. J Med Vet Mycol 1986; 24: 219–230.
2 Moore MK. Skin and nail infections by non-dermatophyte filamentous fungi. Mykosen Suppl 1978; 1: 128–132.
3 Kong BHP, Kapka L, Lee R. Keratin invasion by Hendersonula toruloidea; a tropical pathogenic fungus resistant to therapy. Int J Dermatol 1984; 23: 65–66.
4 Elewski B. “Phaeohyphomycosis” In: Demiss, J, eds. Clinical Dermatology, Philadelphia, Pa: JB Lippincott, 1991.
5 Moore MK, Palacio-Hernanz AD, Lopez-Gomez S. Scytalidium infection diagnosed in Spain. J Med Vet Mycol 1984; 22: 243–245.
6 Abramson C. Athlete’s foot and onychomycosis caused by Hendersonula toruloidea. Cutis 1990; 46: 128–132.
7 Gupta AK, Elewski BE. Nondermatophyte causes of onychomycosis and superficial mycoses. Curr Top Med Mycol 1996; 7: 87–97.
8 Romano C, Valenti L, Difonzo EM. Two cases of tinea pedis caused by Scytalidium hyalinum. J Eur Acad Dermatol Venereol 1999; 12: 38–42.
9 Sigler L, Summerbell RC, Poole L, et al. Invasive Nattrassia mangiferae infections. case report, literature review, and therapeutic and taxonomic appraisal. J Clin Microbiol 1997; 35: 433–440.
10 Rollman O, Johansson S. Hendersonula toruloidea infection. Successful response of onychomycosis to nail avulsion and topical ciclopiroxolamine. Acta Derm Venereol (Stockh) 1987; 67: 506–510.
11 Downs AMR, Lear AT, Archer CB. Scytalidium hyalinum onychomycosis successfully treated with 5% amorolfine nail lacquer. Br J Dermatol 1999; 140: 555.
12 Clayton YM. Relevance of broad-spectrum and fungicidal activity of antifungals in the treatment of dermatomycoses. Br J Dermatol 1994; 130 (Suppl. 43): 7–8.
Goon and Seow
International Journal of Dermatology 2002, 41, 53–55
IJD_1399.fm Page 55 Saturday, February 9, 2002 5:14 PM
Related Documents











